Embed Size (px)
Citation preview

10.1586/17434440.2013.811851 441ISSN 1743-4440© 2013 Informa UK Ltdwww.expert-reviews.com
Device Profile
More than 16 million people are currently diag-nosed with congestive heart failure (CHF) in Europe and the USA, where its prevalence aver-ages 2.5% of the normal population [101,102]. Left-ventricular assist devices (LVADs) offer very valuable therapeutic options for patients with end-stage heart failure, either as a short-term support, as bridge to transplant, bridge to recovery or as destination therapy [1,2]. Vast development has been seen in this field over last two decades and a new generation of small-size, durable, continuous-flow (CF) pumps are now a standard of care for patients with end-stage heart failure [3,4]. These devices, being small, quiet and durable with an acceptable quality of life, are increasingly used as an alternative to transplantation, especially in view of the shortage of donor organs [5]. The
new miniaturized centrifugal HVAD® Pump (HeartWare International, Inc., MA, USA) (Figure 1) is a novel third-generation ventricu-lar assist device (VAD). It uses a wide-blade impeller – the device’s only moving part – that is suspended by a hybrid magnetic and hydro-dynamic bearing system to avoid mechanical contact and wear to achieve optimal perfor-mance, hemocompatibility and long-term reli-ability (Figure 2) [6]. It has a displaced volume of just 50 cc, weighs 160 g and can deliver flows up to 10 l/min.
Similar to other commercially available VADs, the HVAD pump is designed for use as a bridge to cardiac transplantation and des-tination therapy in patients at risk of death from refractory end-stage CHF. The pump is implanted in the pericardial space (Figure 3) and
Anton Sabashnikov‡, Prashant N Mohite‡, André R Simon and Aron F Popov*Department of Cardiothoracic Transplantation & Mechanical Circulatory Support, Royal Brompton & Harefield NHS Foundation Trust, Harefield Hospital, Hill End Road, Harefield, Middlesex, UB9 6JH, UK *Author for correspondence:[email protected]
‡Authors contributed equally.
Increasing incidence of end-stage heart failure and limited availability of donor organs have led to longer waiting times for cardiac transplantation and subsequently increasing mortality. Ventricular assist device therapy is fast becoming an accepted alternative treatment to treat end-stage heart failure and is being implemented as a bridge to decision, bridge to myocardial recovery, bridge to heart transplantation or as a destination therapy. LVADs not only enable hemodynamic stabilization and recovery of secondary organ failure in severely ill patients, but have also been shown to reduce pulmonary vascular resistance in nontransplantable candidates. Technology of ventricular assist devices has evolved over several decades of time and generations of devices. The HVAD® Pump (HeartWare International, Inc., MA, USA) is a third-generation, miniaturized, continuous-flow ventricular assist device. Due to its miniaturized housing and intrapericardial placing, it can be used proficiently to support the right ventricle and has also demonstrated great utility in minimally invasive and off-pump implantation, exchange and explantation. It is favored for similar reasons in adolescents and in heart failure due to complex congenital heart disease. The purpose of this article is to review the clinical use of HeartWare® Ventricular Assist System (HeartWare System; HeartWare International, Inc.) with different strategies pertaining to its advantages and adverse events in comparison with contemporary devices.
Keywords: HeartWare • HVAD • ventricular assist device
HeartWare miniaturized intrapericardial ventricular assist device: advantages and adverse events in comparison to contemporary devicesExpert Rev. Med. Devices 10(4), 441–452 (2013)
Expert Review of Medical Devices
© 2013 Informa UK Ltd
10.1586/17434440.2013.811851
1743-4440
1745-2422
Device Profile

Expert Rev. Med. Devices 10(4), (2013)442
Device Profile
is designed both for in-hospital and out-of-hospital settings, including transportation via fixed-wing aircraft or helicopter [7]. The most common etiologies of CHF as an indication for assist device implantation are idiopathic (44–61%), ischemic (30–40%), familial (10%) or viral (6–9%) [8,9]. The contrain-dications for HVAD implantation include body surface area less than 1.2 m2, pregnancy and contraindications to anticoagulation therapy [7].
Device status in Europe & USAAfter satisfactory results in the initial trials, it was awarded CE Mark approval in January 2009 and is now commercially avail-able in Europe. In the USA, a premarket approval was obtained in November 2012 for the use of the HeartWare® system (HeartWare International, Inc.) as a bridge to transplant. Furthermore, the US FDA granted HeartWare approval for a randomized, con-trolled, multicenter clinical trial to evaluate the use of the device for destination therapy [10].
Clinical trialsThe first phase of a multicenter prospective clinical trial on evalua-tion of the safety and efficacy of the HVAD was performed at three European and two Australian centers between March 2006 and December 2007 and included 23 end-stage CHF patients. This initial clinical investigation was conducted as a bridge to trans-plant study with the combined primary end point of survival to heart transplant or survival to 180 days on device support, and demonstrated favorable results compared with those with other CF LVADs published at that time [11]. Following uneventful and uncomplicated intrapericardial HVAD Pump implantation in all patients, overall survival at 180 days and 1 year was 91 and 86%, respectively, while two patients underwent successful heart trans-plant within the first 180 days and another three between 180 and 365 days of implantation. The main limitations of this study were the small cohort and nonrandomized setting, which could have led to these ambitious results [8].
Although the primary end point was slightly modified in the second phase of this multicenter study after including 50 patients, the outcomes remained the same. The survival to heart transplant and device explantation following myocardial recovery or survival on device support at 180 days was 90, 84 and 79% at 6, 12 and 24 months after HVAD Pump implantation, respectively. The Seattle Heart Failure Model estimated survival (mean ± standard error of the mean) of this cohort if medical therapy was continued was 73 ± 3% at 180 days, 58 ± 4% at 1 year, and 40 ± 4% at 2 years (Figure 4). A total of 20 out of the 50 patients had a >50% estimated mortality at 1 year. The estimated hazard ratio for LVAD therapy, with the Seattle Heart Failure Model as a virtual control arm, was 0.33 at 180 days, 0.29 at 1 year and 0.26 at 2 years (all p-values ≤ 0.001) (Figure 4). However, the main limita-tions of this study were nonrandomized assignment of patients with noncontrolled and nonblinded conditions.
The most recent large multicenter study evaluating the HeartWare system as a bridge to transplantation was conducted at 30 centers in the USA and performed between August 2008 and August 2010. Although the study was nonrandomized, a significant advantage of this trial was the large patient population. Moreover, the results of the investigational pump were directly compared with those of the commercially available HeartMate®II (Thoratec Corp., CA, USA). The combined primary outcomes were survival to heart transplant, 180-day survival on device support or 60-day survival after pump explantation for myocar-dial recovery. Out of 140 patients supported with the HVAD enrolled in the trial, 92% reached the primary end point in the
Figure 1. The new miniaturized (50 cc) centrifugal HVAD® Pump (HeartWare International, Inc., MA, USA) with integrated inflow cannula allowing intrapericardial implantation. Reproduced with permission from HeartWare International, Inc.
Figure 2. HVAD® Pump (HeartWare Inc., MA, USA) showing the impeller, the only moving part, which is suspended by hybrid magnetic and hydrodynamic bearing system to avoid mechanical contact and wear. Reproduced with permission from HeartWare International, Inc.
Sabashnikov, Mohite, Simon & Popov

443www.expert-reviews.com
Device Profile
per-protocol study population and 90.7% in the safety study population, whereas 90.1% out of 499 control patients met these criteria. The HeartWare system was thus shown to be noninferior to commercially available controls [12].
Advantages of the HeartWare systemThe HVAD Pump, being a small and intra-pericardial device, has unique advantages over other contemporary devices available in the market.
Utilization as a biventricular assist deviceAlthough the HVAD was primarily designed for implantation in patients with advanced left-ventricular failure, it has been shown that this miniaturized pump can also be successfully used to support the right ventricle (RV) [13–19].
The possibility of the utilization of the HVAD system as an additional right ventricular support for patients with biventricular failure was evaluated in experimental conditions using mock circu-lation. The problem of low pulmonary vascular resistance (PVR) and low afterload, which might have led to high flow through the pulmonary circulation causing pulmonary edema, was resolved by artificially increasing PVR. This was achieved by adding an additional resistance as a serial connection at the HVAD outflow graft by simple reduction of the outflow graft diameter.
The HVAD implantation as biventricular support was first described by Strueber et al. in a patient with ischemic heart disease in 2010 [13]. The inflow cannula was only inserted approximately 1 cm from the anterior wall of the RV and no additional resist-ance element at the outflow graft was created. Despite irregular flow patterns after commencement of spontaneous breathing with very high pump flows during inhalation, there was no overloading of the pulmonary circulation noted and device function was appropriate for 180 days of follow-up [13]. However, outflow graft restriction demonstrated in further reports resulted in stable flow patterns and a reduced need for pump adjustments [14–17]. Echocardiographic analyses demonstrated the anterior free wall as the most optimal position of the HVAD in the RV, which provided sufficient distance between the inflow cannula and ventricular tissue. However, lower right-ventricular end diastolic pressure may require length reduction of the inflow cannula in order to avoid suction events within the RV [9], which can be achieved by using silicone rings or additional felt spacers placed under the sewing ring [14,15,17]. Furthermore, it was shown that the HVAD implantation can be also performed safely on the right diaphragmatic wall [14,17], or even in the right atrial position with placement of the pump in the right pleural cav-ity [19] if the space between the sternum and RV is not large enough for ‘classical’ device placement (Figure 5). In addition, Stulak et al. described the possibility of biventricular support with the right-sided HVAD and the left-sided HeartMate II [20]. The largest study
to date, with 17 patients, demonstrated that 30-day and 6-month survival was shown to be 82.4 and 50%, respectively, in patients with HVAD biventricular support [17]. Even though these results do not significantly differ from those with other assist devices used as a biventricular assist device, the advantages of the small size and weight of the HVAD, which eases the placement and implanta-tion of device and may significantly improve the quality of life on support, are persuasive. Moreover, contrary to expectations, it was shown that the degree of hemolysis on biventricular HVAD support compared with isolated left-ventricular support does not increase significantly. The most probable explanation for these results may be the advantage of HVAD Pump technology without mechanical wear and friction favoring it over extracorporeal devices commonly used for treatment of biventricular CHF [18].
Figure 3. 3D intrapericardial position of the HeartWare® System (HeartWare International, Inc., MA, USA) after implantation. (A) Frontal view; (B) fronto-lateral view. Reproduced with permission from HeartWare International, Inc.
A B
Figure 4. Outcomes in patients undergoing HVAD® Pump (HeartWare International, Inc., MA, USA) implantation from the time of implant to 24 months (solid line) compared with predicted survival rates based on the Seattle Heart Failure Model for optimal medical therapy (dashed line). SHFM: Seattle Heart Failure Model. Reproduced with permission from [9].
Follow-up (months)
Pat
ien
ts (
%)
00
20
40
60
80
100
6 12
73%
90%85%
58%
48%
40%
79%
p = 0.0001p = 0.0001p = 0.0001
0.330.290.26
180 days1 year2 years
HeartWare actuarial
18
Transplanted, recovery or ongoing
Estimated hazard ratio for HVAD
24
SHFM
HeartWare miniaturized intrapericardial ventricular assist device
Expert Rev. Med. Devices 10(4), (2013)444
Device Profile
Minimally invasive accessAlthough VAD implantation through median sternotomy and with establishment of cardiopulmonary bypass (CPB) remains the classical approach for device implantation, minimally invasive approaches may improve outcome in this high-risk patient collec-tive and remains as an attractive option for patient and surgeon. This possibility seems to be favorable, particularly for patients with pronounced comorbidities requiring an alter native access to classic median sternotomy, thus facilitating rapid postoperative recovery. Furthermore, VAD implantation using nonsternotomy incisions and preserving mediastinal integrity might be providential in reducing the risk of potential subsequent procedures requiring a full median sternotomy specifically after prolonged mechanical support, such as aortic valve replacement, mitral valve surgery, device exchange or heart transplantation. Finally, a minimally invasive approach might significantly reduce the risk of postoperative bleeding, re-explorations, massive transfusions and transfusion-related compli-cations that frequently occur after conventional VAD implantation in patients requiring strict postoperative anticoagulation.
In the last decade, there has been an increasing amount of literature on minimally invasive VAD implantation, exchange
and explantation, including Jarvik 2000 FlowMaker LVAS (Jarvik Heart, Inc., NY, USA) [21], HeartMate II [21–24], HeartMate XVE [25,26], HeartMate I [27] and Thoratec® (Thoratec Corp.) [26,28] with satisfactory outcome.
Due to its miniaturized housing, simple implantation through a ‘sewing ring’ – short inflow cannula and intrapericardial posi-tioning without necessity of pump pocket formation – minimally invasive HVAD implantation might enable uncomplicated surgery with a lower risk of infection. Currently, there are several reports on ele-gant and reproducible techniques of HVAD implantation, exchange and explantation available. In particular, bilateral anterior thoracotomy (Figure 6) [29] and upper minis-ternotomy [30] combined with left minithor-acotomy have been shown to be safe and reliable strategies of HVAD implantation with good clinical outcome in all cases.
HVAD explantation [31,32] due to success-ful myocardial recovery or device exchange [31] can also be performed using a single left anterolateral thoracotomy in a semi-lateral recumbent position. It can be done utilizing both a femoro–femoral CPB or off-pump technique. In this context, the outflow graft is ligated and transected, an individually manufactured titanium plug is inserted into the apical cannulation side and the driveline is divided close to the device and removed through the percutaneous drive-line exit site. The distal end of the outflow
graft remains in situ, and although it poses a theoretical risk for infection, no infection events have been reported so far. In the case of device exchange, a new outflow graft can be anastomosed to the remaining distal part of the previous outflow graft.
Despite sufficient exposure of the aorta and left ventricle (LV) for adequate surgical manipulation on outflow graft and the pump, minimally invasive LVAD implantations must be performed cautiously with constant observation of the patient’s hemodynamics and echocardiography, maintaining close commu-nication between surgeon and anesthetist. Furthermore, a care-ful assessment of candidates for such a challenging procedure is imperative to avoid possible intraoperative complications in severe heart failure patients.
Off-pump proceduresThe benefits of cardiac operations performed avoiding CPB still remains controversial. However, there are patient groups that are likely to benefit from off-pump procedures. In last few years, there has been a great deal of interest in the development of off-pump LVAD implantation and explantation in order to minimize
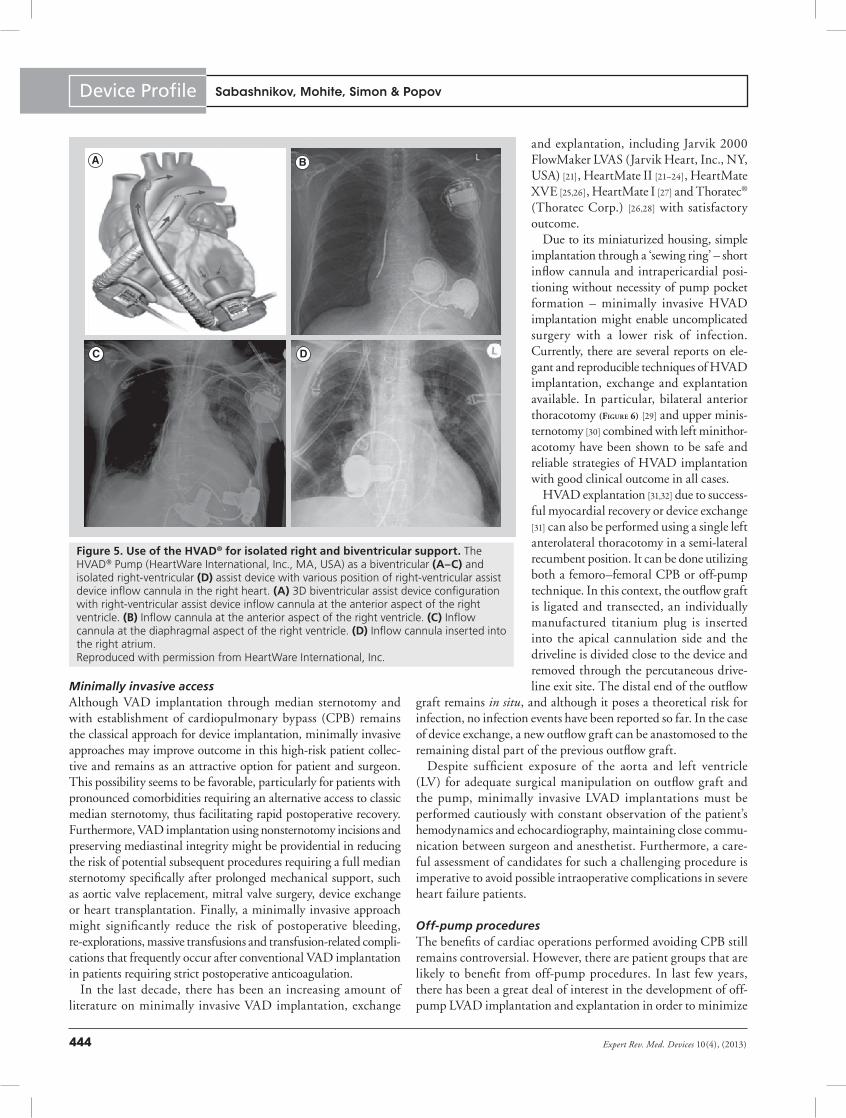
Figure 5. Use of the HVAD® for isolated right and biventricular support. The HVAD® Pump (HeartWare International, Inc., MA, USA) as a biventricular (A–C) and isolated right-ventricular (D) assist device with various position of right-ventricular assist device inflow cannula in the right heart. (A) 3D biventricular assist device configuration with right-ventricular assist device inflow cannula at the anterior aspect of the right ventricle. (B) Inflow cannula at the anterior aspect of the right ventricle. (C) Inflow cannula at the diaphragmal aspect of the right ventricle. (D) Inflow cannula inserted into the right atrium. Reproduced with permission from HeartWare International, Inc.
A
C D
B
Sabashnikov, Mohite, Simon & Popov

445www.expert-reviews.com
Device Profile
the adverse effects associated with the use of CPB, particularly right-ventricular fail-ure, exacerbation of end-organ dysfunc-tion and activation of the inflammatory and coagulation cascades, which may lead to severe coagulopathy and vasoplegia [29,30]. Currently, there are several reports on LVAD implantation and explantation without utilization of CPB using HVAD, through an upper ministernotomy and left minithoracotomy or left lateral thora-cotomy [21,22,29,30,32]. CPB and fibrillatory arrest can be avoided using an individu-ally manufactured titanium plug (Fittkau Metallbau GmbH, Berlin, Germany) for closure of the apical cannulation site.
Moreover, minimizing the surgical dis-section due to its small size and intrapericar-dial location, as well as avoiding extensive repair of the LV, such an HVAD explan-tation approach may significantly reduce the risk of intraoperative hemodynamic instability and postoperative bleeding with following consequences.
Pump size remains one of the crucial lim-iting factors for this approach due to diffi-culty in implanting larger VADs in patients with a low BMI. In this respect, HVAD as a miniaturized pump, with its favorable construction and accessible positioning, seems to be easier and safer in an off-pump setting compared with other conventional VADs.
Despite good results in this new field, further large studies on the comparison between on- and off-pump LVAD surgery, as well as possible utilization of alternative circuits (i.e., minimized extracor-poreal circuit) are warranted before the optimal strategy for these high-risk patients is clearly understood. One of the main limitations of minimally invasive access without CPB is the occasional need for urgent or emergent conversion to CPB support, in some cases requir-ing a full median sternotomy. Thus, such demanding procedures should be performed by specialists in experienced centers.
Stability after therapeutic radiation treatmentWith the increasing need for long-term LVAD support due to continuing rise of the number of heart failure patients and limited availability of donor organs, the prevalence of cancer patients on LVADs requiring radiation therapy will definitely increase. Instability in device function in patients undergoing radiation treatment implantation has already been described for permanent pacemakers and implantable cardioverter–defibrillator (ICDs). However, only limited information exists on the functional stability of LVADs after such radiation damage.
The HVAD Pump was investigated regarding changes in device functionality both in vitro and in vivo using high-energy thera-peutic proton beams. There were no significant changes in device functionality observed as well as no effect on external equipment
of HVAD after secondary neutron fluence in an in vitro study [33]. Furthermore, proton and neutron irradiation did not seem to cause HVAD battery depletion. Similar encouraging results were also achieved in an in vivo setting after repeated irradiation of the lung with the highest therapeutic intensity available (6 Gy/min, up to a cumulative dose of 74 Gy) on a radiation oncology particle accelerator [34].
Even though no adverse response of the Thoratec pneu-matic LVAD with TLC-II® Portable Driver (Thoratec) [35] and HeartMate II [36] systems to cancer radiation treatment have been reported in individual case reports, so far no evidence exists on device performance after cumulative radiation dose higher than 2000 cGy.
HVAD support in adolescenceAlthough there has been an increase in the number of pediatric cardiac transplants over the last decade, which comprise 14% of all cardiac transplants [37], this patient group also experiences a lack of available donor organs and faces the highest waiting-list mortality among all patients listed for solid-organ transplanta-tion in the USA [38]. However, although bridging to transplant is more common in adult patients, utilization of VADs and total artificial hearts in the pediatric population grown considerably. From 2005 to 2010, reported use of these devices has increased from 12.1 to 20.4% [37]. There are several reports on success-ful HVAD implantation in patients aged 6–16 years old with low morbidity and good outcome. A recent study by Miera et al. reported seven children with end-stage heart failure who received
Figure 6. HVAD® Pump (HeartWare International, Inc., MA, USA) implantation through bilateral anterior thoracotomy. (A) Implantation of the sewing ring through the left thoracotomy incision. (B) Establishment of cardiopulmonary bypass. (C) Tunneling of the outflow graft toward the right thoracotomy incision. (D) Postoperative result. Reproduced with permission from [29].
A B
C D
HeartWare miniaturized intrapericardial ventricular assist device

Expert Rev. Med. Devices 10(4), (2013)446
Device Profile
implantation of an HVAD as a bridge to transplantation, with six patients having been transplanted and one being on ongoing mechanical support [39]. D’Alessandro et al. and Kirklin et al. also independently reported on successful HVAD implantation as a bridge to transplantation in a 13- and a 9-year-old child. Both patients were successfully transplanted on postimplantation day 11 and 60, respectively [40,41]. No serious intra- or postopera-tive complications have been noticed in any of the reports. Owing to its small size, reasonable anatomical position in the pericardium and sufficient flow range up to 10 l/min, the HVAD offers a favorable alternative to other intra- and paracorporeal adult VAD systems approved for implantation in pediatric patients with a body surface area of at least 0.7 m2.
HVAD in the presence of atypical anatomy & with concomitant surgeryHVAD was shown to be a suitable device for systemic support in patients with heart failure and different types of surgically pretreated transposition of the great vessels. In such cases, the anatomical RV represents the functional LV and the LVAD implantation carries additional surgical risks due to complex unfamiliar anatomy and awkward implantation position. It was demonstrated that the morphological RV (functional LV) can be cannulated using either diaphragmatic surface or the free wall without significant changes in standard implantation technique with good outcome [42]. Furthermore, HVAD can be success-fully used in patients with heart failure requiring complex aortic pathologies [43].
Adverse events with use of HVADDevice thrombosisAlthough incidence of pump thrombosis has significantly decreased with the utilization of CF LVADs, the management of thromboembolic complications after implantation of these newer generation devices remains a major challenge. The incidence of device thrombosis after HVAD implantation in the 23 patients in the first multicenter trial was 26% [8]. A subsequent change in the impeller manufacturing process, including adjustments of the thrust bearing dimensions, led to a significant reduction to 8% [8,9,44]. The main trigger for development of HVAD thrombosis, as for other CF LVADs, remains the subtherapeutic international normalized ratio, which should be maintained between 2 and 3.
The clinical presentation of HVAD thrombosis is based on relatively limited evidence and depends on the origin of the thrombus. Abnormally increased power consumption and increased estimated pump flow were associated with thrombosis in most cases with HVAD support [45–47]; however, both a pro-gressive increase in flow with stable power resulting in reduction of the head pressure [48] and reduction in pump flow with gradual increase in power [49] have been shown in individual reports. Clinical symptoms are unspecific and can include dyspnea, fatigue, peripheral edema, ascites and worsening renal function. A further diagnostic characteristic of device thrombosis is hemol-ysis caused by turbulent flow patterns across the thrombus forma-tion and expressed as hematuria, increased lactate dehydrogenase,
bilirubin and free hemoglobin in blood serum. In the authors’ institution, with an audible rumbling sound from the HVAD was reported in several patients with device thrombosis, which may also be helpful in diagnosis. Echocardiography, the most common imaging technique for thrombosis diagnostics, is not always sufficient for adequate visualization of the inflow cannula and thrombus formation itself [50], but may provide information on consequences of pump obstruction, such as decompensation of left heart and frequent aortic valve opening and interven-tricular septal shift to the right due to insufficient unloading of the LV [45–49]. Further echocardiographic criteria of poten-tially dysfunctional devices, as could be seen from the example of HeartMate II LVAD, might be decreased basic diastolic CF velocity in inflow and outflow cannulas (up to 15–20 mm/s, whereas the normal range varies between 100 and 200 cm/s) with a pulsatile increase in flow velocity during ventricular con-traction, increased left-ventricular end-diastolic and end-systolic dimension, increased left-ventricular ejection time and aortic valve amplitude and higher grade of mitral regurgitation [51]. In addition, echocardiographic assessment of left-ventricular end-diastolic changes during pump speed increments (ramp test) was described as a useful diagnostic method of device thrombosis [52]. However, caution should be applied during echocardiographic direct visual assessment, particularly when the HVAD flow is high as suction events on the LV might lead to papillary muscles being misinterpreted as thrombi [53]. In case of doubt, computed tomography should be performed.
Few strategies are available to treat LVAD thrombosis – systemic or local thrombolytic therapy or surgical device exchange. Unfortunately, systemic thrombolysis, which represents the first-line and less elaborate treatment of device thrombosis, is not always successful. Another pitfall of such an approach is the higher risk of serious complications, such as systemic bleeding, hypercoagulo-pathy and possible thrombus rebuilding, which has been reported for HVAD [47]. However, a growing trend towards the targeted application of a reduced dose of the thrombolytic agent directly into the LV or the LVAD inflow cannula has significantly reduced this complication. This therapeutic option was successfully used in the treatment of HVAD thrombosis and was described in several reports [45,46,49]. The LV is usually accessed via the right or left radial artery using a 4-, 5- or 6-F pigtail catheter and recombi-nant tissue plasminogen activator (i.e., alteplase) is administered at a rate of 1 mg/min. The duration of injection to resolve the thrombotic formation and achieve normal energy consumption and device flow in HVAD ranges between 27 and 37 min. In all reported cases, this strategy was successful and no significant adverse events were reported.
Another, and usually the last, option in the management of LVAD thrombosis is surgical device exchange. This operation carries a significant risk of bleeding and is associated with higher morbidity and mortality [3]. HVAD Pump exchange can be per-formed either on- or off-pump [47] through a median sternotomy or using minimally invasive access [31], facilitating a wide range of techniques depending on risk stratification and anatomical characteristics in individual patients.
Sabashnikov, Mohite, Simon & Popov

447www.expert-reviews.com
Device Profile
Aortic insufficiencyAlong with recent advances in the development of CF LVADs and increased device durability, de novo aortic insufficiency (AI) is a frequent complication during long-term CF LVAD support. AI after LVAD implantation can result in progressive partial flow return from the outflow graft to the LV through the leaking aortic valve and adversely affect device perfor-mance. Currently, there are controversial data on the impact of less-frequent opening of the native aortic valve on AI devel-opment [54,55]. Although a considerable amount of literature has been published on AI in various CF LVADs, there is a lower incidence of this complication in patients supported with HVAD. The only report, by Soleimani, revealed no de novo AI in eight HVAD recipients during mean support time of 158.25 ± 107.1 days, providing no significant difference in AI prevalence between HeartMate II (six out of 55 patients, 10.9%) and HVAD recipients (p = 0.32) [54]. However, that was the only report with a small number of patients and it cannot be concluded that AI does not occur after HVAD implantation. That is why future studies with larger patient collectives should therefore concentrate on AI in HVAD patients.
Aortic valve replacement with a bioprosthesis or partial or complete surgical closure of the valve is the routine option for the management of AI with LVAD. Recently, percutaneous transcatheter aortic valve closure is being utilized with some success, particularly in patients with a high risk for conventional surgery [56].
Right heart failureElevated PVR and PVR refractory to medical therapy is one of the notable reasons for LVAD implantation. Many patients undergoing LVAD implantation have impaired right-ventricular function and there is reason to suspect at least a small RV improvement with long-term LVAD therapy. In their retrospec-tive study, Pauwaa et al. demonstrated that HVAD therapy can significantly improve hemodynamics in chronic heart failure patients, lowering pulmonary artery pressures, pulmo-nary capillary wedge pressure and PVR, as well as improving cardiac output and central venous saturation within 7 days following device implantation [57]. On the other hand, in real-ity, right-ventricular function can deteriorate significantly after LVAD implantation even if the preoperative condition of the RV is intact. Risk factors predictive of right-ventricular failure after LVAD implantation were reported in various studies and include greater preoperative presence of tricuspid valve regurgi-tation [58], central venous pressure:pulmonary capillary wedge pressure ratio more than 0.63, need for preoperative ventila-tor support and a blood–urea nitrogen level of >39 mg/dl [59], as well as preoperative need for intra-aortic balloon pump, increased PVR and destination therapy [60]. In HVAD, the overall event rate of RV failure requiring long-term intravenous inotropic support or short-term RVAD implantation amounts to 0.05–0.12 events per patient-year in multicenter trials [8,9] and 0.28–0.31 events per patient-year in single-center reports [44,58]. These results are comparable with other CF LVADs and
superior to PF LVADs [3,12]. The treatment of right heart failure ranges from optimization of intravascular volume, inotropic support and pulmonary vasodilators to RVAD implantation if the pharmacological therapy is not sufficient [57].
Device-related infectionsDespite perioperative antimicrobial prophylaxis and development of smaller-size LVADs, infections remain another important issue in patients undergoing support with foreign material VADs and also significantly affect morbidity and mortality [61]. However, most authors have used different definitions of VAD infections; Hannan et al. have recently provided a consensus-derived, stand-ard international classification of VAD infections, including major infections as well as details of all aspects of VAD-specific and VAD-related infections, taking into consideration clinical, micro-biologic, histopathological and radiological criteria [62]. Having a small size, intrapericardial location and a short integrated inflow cannula, HVAD is implanted in a less aggressive way, avoiding extended dissection compared with other LVADs. Despite that, according to the recent larger single- and multicenter HVAD trial outcomes, infection-related complications remain the most common adverse events, including sepsis (0.10–0.46 events per patient-year), localized non-device related infections (0.15–0.26 events per patient-year) and driveline infections (0.20–0.42 events per patient-year) [8,9,12,63].
Neurologic complicationsNeurologic complications are the major adverse events following LVAD surgery. Previous stroke, persistent malnutrition and inflammation, severity of heart failure and post-LVAD infections are key factors associated with development of neurologic compli-cations after LVAD implantation [64]. Patients with blood stream infections may have an eightfold risk of cerebrovascular accidents, particularly hemorrhagic stroke [65]. Lower body surface area is an independent risk factor for mortality due to stroke or systemic bleeding during the VAD support [66]. Also, the ability of von Willebrand factor to bind to collagen or the platelet receptor GP1b is impaired during VAD support, causing disturbance of primary hemostasis, possibly contributing to bleeding complications and hemorrhagic stroke [67,68].
Anticoagulation is an important part of LVAD therapy; it requires meticulous management and monitoring for preven-tion of thromboembolic and bleeding events. It is unclear which antithrombotic regimen should be used to reduce the risk of stroke. With HeartMate II support, a mild anticoagula-tion protocol (only coumarins and acetylsalicylic acid without dipyridamole) did not increase the risk of thrombotic events, but reduced the incidence of stroke from 0.17 to 0.07 per patient-year [69]. Also, it has been observed that mild anticoagulation is well tolerated after HVAD implantation, with an incidence of embolic complications of 0.04–0.05 events per patient-year and hemorrhagic strokes of 0.05–0.08 events per patient-year [8,9]. In a solitary case of excessive postoperative bleeding, no pump-related issues were observed after anticoagulation held for 5 days [70].
HeartWare miniaturized intrapericardial ventricular assist device

Expert Rev. Med. Devices 10(4), (2013)448
Device Profile
Surgical & gastrointestinal bleedingBesides infection and postoperative right-ventricular failure, bleeding is one of the most frequent complications after HVAD implantation. Apart from surgical wound bleeding (0.16–0.43 events per patient-year), gastrointestinal (GI) bleeding, with 0.16–0.43 events per patient-year in HVAD patients [8,9,12,63], has become a new field of particular interest. The rea-son for this increasing attention is obviously the fact that the frequency of GI bleeding events in patients on CF LVAD sup-port compared with those on PF LVAD is significantly higher than it could be expected only related to stricter anticoagulation regime. The pathophysiology of GI bleeding is still not clearly understood. Aside from anticoagulation and platelet inhibitors, factors such as deficiency of high-molecular-weight multimers of von Willebrand factor (acquired type IIA), GI angiodysplasia, increase in intraluminal pressure and dilation of mucosal veins as well as arteriovenous malformations might trigger GI bleed-ing predisposition and progression [70]. The treatment of this condition is limited to enhancement of ventricular pulsatility by pump speed reduction or intermittent local adrenaline adminis-tration, pharmacological treatment with octreotide, endoscopic obliteration and temporary interruption in anticoagulation [71]. Furthermore, recombinant factor VIIa (Novoseven®, Novo Nordisk, Inc., NJ, USA) was shown to be a safe and potent clotting factor for massive bleeding following HVAD implanta-tion, even combined with prolonged discontinuation of antico-agulation and antiplatelet therapy [70]. However, such treatment strategies should be applied cautiously due to the increasing risk of thromboembolic complications.
Other complicationsThere are a number of other various adverse events follow-ing HVAD implantation reported in large multi- and single-center studies that also can be associated with poor outcomes. These include arrhythmias (0.07–0.79 events per patient-year),
hemolysis (0.02–0.06 events per patient-year), respiratory failure ( 0.16–0.45 events per patient-year), renal dysfunc-tion (0.10–0.20 events per patient-year), hepatic dysfunc-tion (0–0.06 events per patient-year) and device replacement (0.04–0.15 events per patient-year) and cerebrovascular acci-dent (embolic 0.04–0.05 events per patient-year or hemorrhagic 0.05–0.08 events per patient-year) [8,9,12,63]. Twenty two percent of the patients after HVAD implantation did not experience any adverse event [5].
Five-year view & need for improvementContinuous increase in the incidence of heart failure and no sig-nificant improvement in organ availability will result in further demand for mechanical circulatory support as a bridge to trans-plantation and destination therapy in the coming years. The last decade saw a great deal of technological advance in the area of mechanical circulatory support; in particular, development of nonpulsatile assist devices and significant reduction in pump size represent the vital changes. Moreover, further size reduc-tion of newer generation VADs and subsequent development of less invasive surgical techniques will remain the current trend in this area. The HVAD represents one of the smallest LVADs, and can provide up to 10 l/min flow supporting left or RV. Although significantly smaller devices are increasingly used in clinical practice, their chief drawback is the limited flow, which is not always sufficient for support of patients with end-stage heart failure [72]. For this reason, we may anticipate that further improvements in LVAD technology in the next 5 years will not be particularly focused on size reduction but include develop-ment of transcutaneous energy transfer system and improvement of minimally invasive and off-pump techniques. This may avoid driveline infections and ascending pocket and pump infections, which is a jinx in the current LAVD therapy. Moreover, in view of the excellent results after biventricular HVAD support, devel-opment of a shorter inflow cannula would be an asset for closer placement of the pump housing to the heart, providing more optimal intrapericardial device localization and better right ventricular support.
Electromagnetic interference with ICDIn view of the increasing use of CF LVADs in patients with severe heart failure and ICD, the problem of electromagnetic inter-ference between the two devices may become an increasingly important area of research. To date, there are only a few reports on the interaction of HVAD and ICD and inappropriate shock therapy during VAD support. Mozes et al. published a case of an inadequate ICD shock in a patient with HVAD during an episode of tachyarrhythmia absoluta, which fell within the detec-tion zone of ventricular fibrillation. A possible explanation for this unexpected event might be the close proximity of the right-ventricular rate-sensing lead tip to the HVAD inflow cannula. With implantation of a new lead positioned far from the HVAD impeller in the right outflow tract, no further oversensing events could be detected [73]. Two similar cases of inappropriate inter-action of ICD with HVAD were reported in the ADVANCE
Figure 7. HVAD® Pump (HeartWare International, Inc., MA, USA) monitor with controller and batteries with capacity display. Reproduced with permission from HeartWare International, Inc.
Sabashnikov, Mohite, Simon & Popov

449www.expert-reviews.com
Device Profile
trial, again resulting in unexpected shocks. The sensing leads in these two patients were also replaced and secured at the mid-right septum with complete resolution of the electromagnetic interference [12]. Thus, the relevance of ICD rate-sensing lead placement as far as possible from the apex cordis in patients with heart failure and hypothetical indication for an LVAD represents an important practical implication. Moreover, further informa-tion on this topic would help us to establish a greater degree of accuracy on this matter.
Preload & afterload sensitivityThe HVAD pump is capable of providing moderate quantities of blood flow against moderate amounts of resistance, main-taining a constant motor speed that ranges between 1800 and 4000 RPM. The pump speed is determined and set by the clini-cian based on the hemodynamic status of the patient. However, compared to the human heart regulated by the Frank–Starling mechanism, the HVAD has significantly lower preload sensitiv-ity and three-times higher afterload sensitivity [74]. Thus, the ‘fixed’ mode used for HVAD may lead to ventricular suction events during low venous return and LV distension during high venous return. These findings may have an important implica-tion for the future development and design of VADs. Better hemodynamic performance of an LVAD and a greater physi-ological response to changes in preload and afterload could be achieved by implementation of a control system, which could automatically change the pump flow depending on the left atrial pressure and thereby provide physiological load of the ventricle.
External equipmentThe level of the overall patient satisfaction with external components of the HVAD is high, thus significantly contributing to their quality of life. In particular, the HVAD controller, which provides continu-ous information on blood pump parameters even if the display and power base are disconnected, the long battery run time of 6 h and the battery capacity display on batteries and system were shown as particular advantages of HVAD (Figure 7) [75,76]. These features might be the key factor contributing to the high and significantly better success rate compared with HeartMate II in addressing simulated common LVAD emergency issues, such as driveline disconnection or discharged or disconnected batteries. In particular, various cable and connector issues – that is, difficulties in reconnecting the cable to its connector – seem to be the matter of further development [76] before transcutaneous energy transfer becomes available. Moreover, the patient’s ability to disconnect the driveline from the controller can be limited in some cases of neurologic, orthopedic or cognitive dys-function as well as in elderly patients. For this reason, a cylindrical extraction tool with a flange for the driveline plug was developed at our institution and successfully put into clinical practice for patients with such disabilities [77].
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Key issues
• Over the last two decades, major advances have been made in the development of a new generation of small-size, continuous-flow and quiet VADs, which are increasingly being used as an alternative to heart transplantation.
• One of the most significant design advantages of the HVAD® Pump (HeartWare International, Inc., MA, USA) is its size, intrapericardial placement and versatility in terms of implant options. This has been confirmed by multiple case- and small-series reports of implants in children and patients with complex anatomies.
• The HVAD Pump can generate a flow of up to 10 l/min and its miniaturized housing and short inflow cannula allows intrapericardial placement.
• The overall survival to heart transplant, device explantation following myocardial recovery and survival on device support was 90, 84 and 79% at 6, 12 and 24 months after HVAD implantation, respectively, providing a 2-year survival rate similar to that of heart transplant.
• The HVAD can be successfully used as a biventricular assist device with excellent results and may significantly improve the quality of life on support due to its small size.
• Minimally invasive implantation, exchange and explantation, often in an off-pump setting, enables more uncomplicated and bloodless surgery with a lower risk of infection compared with other devices.
• Despite excellent results and improved quality of life, perioperative complications, such as device thrombosis, bleeding, right heart failure, infections and aortic valve regurgitation, remain significant issues, which need to be addressed in the near future.
ReferencesPapers of special note have been highlighted as:• of interest•• of considerable interest
1 Birks EJ, Yacoub MH, Banner NR, Khaghani A. The role of bridge to transplantation: should LVAD patients be
transplanted? Curr. Opin. Cardiol. 19(2), 148–153 (2004).
2 Goldstein DJ, Oz MC, Rose EA. Implant-able left ventricular assist devices. N. Engl. J. Med. 339(21), 1522–1533 (1998).
•• Representsabalancedandcomprehensiveoverviewonventricularassistdevices
(VADs)withthefocusontheirdevelopmentandtrendsinthefuture.
3 Slaughter MS, Rogers JG, Milano CA et al.; HeartMate II Investigators. Advanced heart failure treated with continuous-flow left ventricular assist device. N. Engl. J. Med. 361(23), 2241–2251 (2009).
HeartWare miniaturized intrapericardial ventricular assist device

Expert Rev. Med. Devices 10(4), (2013)450
Device Profile
4 Rogers JG, Aaronson KD, Boyle AJ et al.; HeartMate II Investigators. Continuous flow left ventricular assist device improves functional capacity and quality of life of advanced heart failure patients. J. Am. Coll. Cardiol. 55(17), 1826–1834 (2010).
5 Lahpor JR. State of the art: implantable ventricular assist devices. Curr. Opin. Organ Transplant. 14(5), 554–559 (2009).
6 Larose JA, Tamez D, Ashenuga M, Reyes C. Design concepts and principle of operation of the HeartWare ventricular assist system. ASAIO J. 56(4), 285–289 (2010).
7 HeartWare International, Inc. HeartWare® Ventricular Assist System. Instructions for Use. HeartWare International, Inc., MA, USA (2012).
8 Wieselthaler GM, O Driscoll G, Jansz P, Khaghani A, Strueber M; HVAD Clinical Investigators. Initial clinical experience with a novel left ventricular assist device with a magnetically levitated rotor in a multi-institutional trial. J. Heart Lung Transplant. 29(11), 1218–1225 (2010).
9 Strueber M, O’Driscoll G, Jansz P, Khaghani A, Levy WC, Wieselthaler GM; HeartWare Investigators. Multicenter evaluation of an intrapericardial left ventricular assist system. J. Am. Coll. Cardiol. 57(12), 1375–1382 (2011).
10 HeartWare International, Inc. US FDA Executive Summary. The Meeting of the Circulatory System Devices Panel P100047, April 25, 2012. HeartWare International, Inc., MA, USA (2013).
11 Miller LW, Pagani FD, Russell SD et al.; HeartMate II Clinical Investigators. Use of a continuous-flow device in patients awaiting heart transplantation. N. Engl. J. Med. 357(9), 885–896 (2007).
12 Aaronson KD, Slaughter MS, Miller LW et al.; HeartWare Ventricular Assist Device (HVAD) Bridge to Transplant ADVANCE Trial Investigators. Use of an intraperi-cardial, continuous-flow, centrifugal pump in patients awaiting heart transplantation. Circulation 125(25), 3191–3200 (2012).
•• Thisisuptodatethelargestmulticenter,prospectivetrialontheHVAD®Pump(HeartWareInternational,Inc.,MA,USA)asabridgetotransplantationcomparingsuccessandsurvivalagainstacontemporaneouscontrolgroup.
13 Strueber M, Meyer AL, Malehsa D, Haverich A. Successful use of the HeartWare HVAD rotary blood pump for biventricular support. J. Thorac. Cardiovasc. Surg. 140(4), 936–937 (2010).
14 Loforte A, Monica PL, Montalto A, Musumeci F. HeartWare third-generation implantable continuous flow pump as biventricular support: mid-term follow-up. Interact. Cardiovasc. Thorac. Surg. 12(3), 458–460 (2011).
15 Hetzer R, Krabatsch T, Stepanenko A, Hennig E, Potapov EV. Long-term biventricular support with the HeartWare implantable continuous flow pump. J. Heart Lung Transplant. 29(7), 822–824 (2010).
16 McGee EC Jr, Ahmad U, Tamez D et al. Biventricular continuous flow VADs demonstrate diurnal flow variation and lead to end-organ recovery. Ann. Thorac. Surg. 92(1), e1–e3 (2011).
17 Krabatsch T, Potapov E, Stepanenko A et al. Biventricular circulatory support with two miniaturized implantable assist devices. Circulation 124(11 Suppl.), S179–S186 (2011).
• TheauthorsofthismanuscriptpresentthelargestsinglecenterexperiencewiththeuseofHVADasbiventricularsupportemphasizingbetterqualityoflifeandmoremobilitythanwithusualbiventricularassistdevices.
18 Stepanenko A, Krabatsch T, Hennig E et al. Retrospective hemolysis comparison between patients with centrifugal biventricular assist and left ventricular assist devices. ASAIO J. 57(5), 382–387 (2011).
19 Krabatsch T, Stepanenko A, Schweiger M et al. Alternative technique for implanta-tion of biventricular support with HeartWare implantable continuous flow pump. ASAIO J. 57(4), 333–335 (2011).
20 Stulak JM, Griffith KE, Nicklas JM, Pagani FD. The use of the HeartWare HVAD for long-term right ventricular support after implantation of the Heart-Mate II device. J. Thorac. Cardiovasc. Surg. 142(3), e140–e142 (2011).
21 Gregoric ID, La Francesca S, Myers T et al. A less invasive approach to axial flow pump insertion. J. Heart Lung Transplant. 27(4), 423–426 (2008).
22 Cheung A, Bashir J, Kaan A, Kealy J, Moss R, Shayan H. Minimally invasive, off-pump explant of a continuous-flow left ventricular assist device. J. Heart Lung Transplant. 29(7), 808–810 (2010).
23 Haj-Yahia S, Birks EJ, Dreyfus G, Khaghani A. Limited surgical approach for explanting the HeartMate II left ventricu-lar assist device after myocardial recovery.
J. Thorac. Cardiovasc. Surg. 135(2), 453–454 (2008).
24 Tansley P, Yacoub M. Minimally invasive explantation of implantable left ventricular assist devices. J. Thorac. Cardiovasc. Surg. 124(1), 189–191 (2002).
25 Lodge AJ. Clinical experience with sternotomy versus subcostal approach for exchange of the HeartMate XVE to the HeartMate II ventricular assist device. Invited commentary. Ann. Thorac. Surg. 85(5), 1650 (2008).
26 Haj-Yahia SM, Birks EJ, Hardy J, Yacoub MH, Khaghani A. Minimally invasive technique for explantation of right ventricular assist devices. Ann. Thorac. Surg. 82(4), 1547–1548 (2006).
27 Gregoric ID, Bruckner BA, Jacob L et al. Clinical experience with sternotomy versus subcostal approach for exchange of the HeartMate XVE to the HeartMate II ventricular assist device. Ann. Thorac. Surg. 85(5), 1646–1649 (2008).
28 Hill JD, Avery GJ, Egrie G, Turley K, Reichenbach S. Less invasive Thoratec LVAD insertion: a surgical technique. Heart Surg. Forum 3(3), 218–223 (2000).
29 Popov AF, Hosseini MT, Zych B, Simon AR, Bahrami T. HeartWare left ventricular assist device implantation through bilateral anterior thoracotomy. Ann. Thorac. Surg. 93(2), 674–676 (2012).
30 Cheung A, Lamarche Y, Kaan A et al. Off-pump implantation of the HeartWare HVAD left ventricular assist device through minimally invasive incisions. Ann. Thorac. Surg. 91(4), 1294–1296 (2011).
31 Sajjad M, Butt T, Oezalp F et al. An alternative approach to explantation and exchange of the HeartWare left ventricular assist device. Eur. J. Cardiothorac. Surg. doi:10.1161/CIRCULATIONA-HA.109.933960 (2012) (Epub ahead of print).
32 Schweiger M, Potapov E, Vierecke J, Stepanenko A, Hetzer R, Krabatsch T. Expeditious and less traumatic explantation of a heartware LVAD after myocardial recovery. ASAIO J. 58(5), 542–544 (2012).
33 Gossman MS, Graham JD, Das IJ et al. Evaluation of a ventricular assist device system: stability in a proton beam therapy. ASAIO J. 58(6), 597–600 (2012).
34 Gossman MS, Graham JD, Tamez D, Voskoboynikov N, Larose JA. Evaluation of a ventricular assist device: stability under x-rays and therapeutic beam attenuation. ASAIO J. 58(3), 212–216 (2012).
Sabashnikov, Mohite, Simon & Popov

451www.expert-reviews.com
Device Profile
35 Lasher DE, Wojcicka JB, Malcom R, Shears LL. Case study of radiation therapy treatment of a patient with a cardiac ventricular assist device. J. Appl. Clin. Med. Phys. 9(4), 2851 (2008).
36 Chelikani NM, Masterson K, Down LA et al. Effects of γ radiation on a ventricular assist device and its percutaneous lead components. ASAIO J. 58(1), 19–24 (2012).
37 Kirk R, Dipchand AI, Edwards LB et al.; International Society for Heart and Lung Transplantation. The Registry of the International Society for Heart and Lung Transplantation: fifteenth pediatric heart transplantation report – 2012. J. Heart Lung Transplant. 31(10), 1065–1072 (2012).
38 Almond CS, Thiagarajan RR, Piercey GE et al. Waiting list mortality among children listed for heart transplantation in the United States. Circulation 119(5), 717–727 (2009).
39 Miera O, Potapov EV, Redlin M et al. First experiences with the HeartWare ventricular assist system in children. Ann. Thorac. Surg. 91(4), 1256–1260 (2011).
40 D’Alessandro D, Forest SJ, Lamour J, Hsu D, Weinstein S, Goldstein D. First reported use of the heartware HVAD in the US as bridge to transplant in an adolescent. Pediatr. Transplant. 16(8), E356–E359 (2012).
41 Kirklin JK, Pearce FB, Pamboukian SV et al. Implantation of the HeartWare HVAD in a child after a recent thrombo-embolic stroke. Ann. Thorac. Surg. 93(3), 977–978 (2012).
42 Huebler M, Stepanenko A, Krabatsch T, Potapov EV, Hetzer R. Mechanical circulatory support of systemic ventricle in adults with transposition of great arteries. ASAIO J. 58(1), 12–14 (2012).
43 Takeda K, Ahmad U, Malaisrie SC, Lee R, McCarthy PM, McGee EC Jr. Successful implantation of HeartWare HVAD left ventricular assist device with concomitant ascending and sinus of Valsalva aneurysms repair. J. Artif. Organs 15(2), 204–206 (2012).
44 Popov AF, Hosseini MT, Zych B et al. Clinical experience with HeartWare left ventricular assist device in patients with end-stage heart failure. Ann. Thorac. Surg. 93(3), 810–815 (2012).
• Thisreport(with[63])representsthelargestsingle-centerexperienceswiththeuseofHVADinpatientswithadvancedheartfailure.
45 Kamouh A, John R, Eckman P. Successful treatment of early thrombosis of HeartWare left ventricular assist device with intraven-tricular thrombolytics. Ann. Thorac. Surg. 94(1), 281–283 (2012).
46 Garbade J, Bittner HB, Mohr FW, Barten MJ. Fluoroscopy-guided resolution of ingested thrombus leading to functional disturbance of a continuous-flow left ventricular assist device. Case Rep. Surg. 2012, 791056 (2012).
47 Aissaoui N, Börgermann J, Gummert J, Morshuis M. HeartWare continuous-flow ventricular assist device thrombosis: the Bad Oeynhausen experience. J. Thorac. Cardiovasc. Surg. 143(4), e37–e39 (2012).
48 Santise G, Sciacca S, Baglini R, Clemenza F, Pilato M. Can learning to interpret pump messages help lead to an early diagnosis of HeartWare ventricular assist device thrombosis? ASAIO J. 58(6), 629–632 (2012).
49 Kiernan MS, Pham DT, DeNofrio D, Kapur NK. Management of HeartWare left ventricular assist device thrombosis using intracavitary thrombolytics. J. Thorac. Cardiovasc. Surg. 142(3), 712–714 (2011).
50 Shah NR, Cevik C, Hernandez A, Gregoric ID, Frazier OH, Stainback RF. Trans-thoracic echocardiography of the Heart-Ware left ventricular assist device. J. Card. Fail. 18(9), 745–748 (2012).
51 Paluszkiewicz L, Gürsoy D, Spiliopoulos S et al. HeartMate II ventricular assist device thrombosis-an echocardiographic approach to diagnosis: can Doppler evaluation of flow be useful? J. Am. Soc. Echocardiogr. 24(3), 350.e1–350.e4 (2011).
52 Uriel N, Morrison KA, Garan AR et al. Development of a novel echocardiography ramp test for speed optimization and diagnosis of device thrombosis in continuous-flow left ventricular assist devices: the Columbia ramp study. J. Am. Coll. Cardiol. 60(18), 1764–1775 (2012).
53 Aissaoui N, Paluszkiewicz L, Schulte-Eistrup S, Morshuis M, Gummert J. An atypical thrombus in the inflow cannula of the HeartWare left ventricular assist device. Ann. Thorac. Surg. 92(3), e57 (2011).
54 Soleimani B, Haouzi A, Manoskey A, Stephenson ER, El-Banayosy A, Pae WE. Development of aortic insufficiency in patients supported with continuous flow left ventricular assist devices. ASAIO J. 58(4), 326–329 (2012).
55 Hatano M, Kinugawa K, Shiga T et al. Less frequent opening of the aortic valve and a continuous flow pump are risk factors for postoperative onset of aortic insufficiency
in patients with a left ventricular assist device. Circ. J. 75(5), 1147–1155 (2011).
56 Parikh KS, Mehrotra AK, Russo MJ et al. Percutaneous transcatheter aortic valve closure successfully treats left ventricular assist device-associated aortic insufficiency and improves cardiac hemodynamics. JACC Cardiovasc. Interv. 6(1), 84–89 (2013).
57 Pauwaa S, Bhat G, Tatooles AJ et al. How effective are continuous flow left ventricu-lar assist devices in lowering high pulmonary artery pressures in heart transplant candidates? Cardiol. J. 19(2), 153–158 (2012).
58 Baumwol J, Macdonald PS, Keogh AM et al. Right heart failure and ‘failure to thrive’ after left ventricular assist device: clinical predictors and outcomes. J. Heart Lung Transplant. 30(8), 888–895 (2011).
59 Kormos RL, Teuteberg JJ, Pagani FD et al.; HeartMate II Clinical Investigators. Right ventricular failure in patients with the HeartMate II continuous-flow left ventricular assist device: incidence, risk factors, and effect on outcomes. J. Thorac. Cardiovasc. Surg. 139(5), 1316–1324 (2010).
60 Drakos SG, Janicki L, Horne BD et al. Risk factors predictive of right ventricular failure after left ventricular assist device implantation. Am. J. Cardiol. 105(7), 1030–1035 (2010).
61 Topkara VK, Kondareddy S, Malik F et al. Infectious complications in patients with left ventricular assist device: etiology and outcomes in the continuous-flow era. Ann. Thorac. Surg. 90(4), 1270–1277 (2010).
62 Hannan MM, Husain S, Mattner F et al.; International Society for Heart and Lung Transplantation. Working formulation for the standardization of definitions of infections in patients using ventricular assist devices. J. Heart Lung Transplant. 30(4), 375–384 (2011).
• Providesadetailed,consensusderived,standardinternationalclassificationofVADinfections.
63 Dell’Aquila AM, Schneider SR, Schlarb D et al. Initial clinical experience with the HeartWare left ventricular assist system: a single-center report. Ann. Thorac. Surg. 95(1), 170–177 (2013).
• Thisreport(with[44])representsthelargestsinglecenterexperienceswiththeuseofHVADinpatientswithadvancedheartfailure.
64 Kato TS, Schulze PC, Yang J et al. Pre-operative and post-operative risk
HeartWare miniaturized intrapericardial ventricular assist device

Expert Rev. Med. Devices 10(4), (2013)452
Device Profile
factors associated with neurologic complications in patients with advanced heart failure supported by a left ventricular assist device. J. Heart Lung Transplant. 31(1), 1–8 (2012).
65 Aggarwal A, Gupta A, Kumar S et al. Are blood stream infections associated with an increased risk of hemorrhagic stroke in patients with a left ventricular assist device? ASAIO J. 58(5), 509–513 (2012).
66 Komoda T, Drews T, Hetzer R, Lehmkuhl HB. Lower body surface area is highly related to mortality due to stroke or systemic bleeding in patients receiving an axial flow blood pump as a left ventricular assist device. Eur. J. Cardiothorac. Surg. 43(5), 1036–1042 (2013).
67 Meyer AL, Malehsa D, Bara C et al. Acquired von Willebrand syndrome in patients with an axial flow left ventricular assist device. Circ. Heart Fail. 3(6), 675–681 (2010).
68 Crow S, Chen D, Milano C et al. Acquired von Willebrand syndrome in continuous-flow ventricular assist device recipients. Ann. Thorac. Surg. 90(4), 1263–1269; discussion 1269 (2010).
69 Backes D, van den Bergh WM, van Duijn AL, Lahpor JR, van Dijk D, Slooter AJ.
Cerebrovascular complications of left ventricular assist devices. Eur. J. Cardiothorac. Surg. 42(4), 612–620 (2012).
70 Saeed D, Albert A, Kamiya H, Maxhera B, Westenfeld R, Lichtenberg A. Five days of no anticoagulation or antiplatelet therapy and NovoSeven administration in a HeartWare HVAD patient. Artif. Organs 36(8), 751–753 (2012).
71 Hayes HM, Dembo LG, Larbalestier R, O’Driscoll G. Management options to treat gastrointestinal bleeding in patients supported on rotary left ventricular assist devices: a single-center experience. Artif. Organs 34(9), 703–706 (2010).
72 Meyns BP, Simon A, Klotz S et al. Clinical benefits of partial circulatory support in New York Heart Association Class IIIB and Early Class IV patients. Eur. J. Cardiothorac. Surg. 39(5), 693–698 (2011).
73 Mozes A, DeNofrio D, Pham DT, Homoud MK. Inappropriate implantable cardioverter–defibrillator therapy due to electromagnetic interference in patient with a HeartWare HVAD left ventricular assist device. Heart Rhythm 8(5), 778–780 (2011).
74 Salamonsen RF, Mason DG, Ayre PJ. Response of rotary blood pumps to changes in preload and afterload at a fixed speed setting are unphysiological when compared with the natural heart. Artif. Organs 35(3), e47–e53 (2011).
75 Meyer AL, Kugler C, Malehsa D, Haverich A, Strueber M. Patient satisfaction with the external equipment of implantable left ventricular assist devices. Artif. Organs 34(9), 721–725 (2010).
76 Geidl L, Deckert Z, Zrunek P et al. Intuitive use and usability of ventricular assist device peripheral components in simulated emergency conditions. Artif. Organs 35(8), 773–780 (2011).
77 Mohite PN, Bowles CT, Simon AR. A novel drive-line handling tool for the HeartWare ventricular assist device in patients with a physical disability. J. Heart Lung Transplant. 31(12), 1323–1325 (2012).
Websites
101 Heart and stroke facts: 2006 update. www.americanheart.org
102 British Heart Foundation 2009. www.bhf.org.uk.
Sabashnikov, Mohite, Simon & Popov





























