Embed Size (px)
Citation preview

REVIEW ARTICLE
Histologic Evaluation of Ulcerative Colitis: A Systematic Reviewof Disease Activity IndicesMahmoud H. Mosli, MD,*,†,‡ Brian G. Feagan, MD,*,§,k William J. Sandborn, MD,§,¶
Geert D’Haens, MD, PhD,§,** Cynthia Behling, MD,†† Keith Kaplan, MD,‡‡ David K. Driman, MD,§§
Lisa M. Shackelton, PhD,§ Kenneth A. Baker, PhD,§ John K. MacDonald, MS,* Margaret K. Vandervoort, MS,§
Karel Geboes, MD, PhD,kk and Barrett G. Levesque, MD§,¶
Background: Ulcerative colitis (UC) is an idiopathic inflammatory disorder. Currently, the main goals of treatment are to induce and maintain clinicaland/or endoscopic remission. However, evidence indicates that persistent disease activity on colonic biopsies in the setting of clinical or endoscopicremission is an independent predictor of poor outcomes. A number of previous studies have proposed histologic indices for use in specific trials of UC.The aim of this study was to systematically review the existing histological indices for UC and assess their potential use in both patient management andclinical trials.
Methods: We performed a systematic review of histological indices evaluating disease activity in UC. MEDLINE (Ovid), EMBASE (Ovid), PubMed,the Cochrane Library (CENTRAL), and Digestive Diseases Week (DDW) abstracts of randomized and/or controlled trials clinical trials were searchedfrom inception to February 2013 for applicable studies. Data from these studies were reviewed and analyzed.
Results: After systematically applying inclusion criteria, we identified 108 scientific articles including 88 clinical studies and 21 related clinical reviews.Eighteen indices of histological activity in UC were identified and reviewed.
Conclusions: Although multiple histological scoring indices for assessment of UC disease activity currently exist, none of these instruments weredeveloped using a formal validation process and their operating properties remain poorly understood. Future studies are needed to address this deficiency.
(Inflamm Bowel Dis 2014;20:564–575)
Key Words: ulcerative colitis, histology, indices, outcome measures, disease activity
U lcerative colitis (UC) is a chronic inflammatory bowel diseaseof unknown etiology with a wide spectrum of disease severity.1
UC can be complicated by toxic megacolon and colorectal cancer.2
Pharmacologic management includes aminosalicylates, corticoste-roids, purine antimetabolites, and tumor necrosis factor antagonists,used sequentially or in combination.3–5 Induction and maintenanceof remission are important treatment goals; however, there is no
universally accepted definition of remission and no consensus onthe best way to assess disease activity.
In clinical practice, disease activity is assessed through theevaluation of symptoms and severity of colonic inflammation bysigmoidoscopy or colonoscopy.6 The imprecision in this approachlikely contributes to large variances in disease management andsuboptimal patient outcomes. Therefore, clinical investigatorsadvocate for the use of quantitative endoscopic indices as outcomemeasures in randomized controlled trials (RCTs).7,8 Mucosal healing(MH), evaluated by defined endoscopic criteria, confers greaterlong-term benefit than symptom control.9,10 Ardizzone et al10 pro-spectively evaluated a cohort of 157 newly diagnosed patients withmoderate-to-severely active UC who received corticosteroid therapyand were followed for up to 5 years. Patients without complete MHwere more likely to receive immunosuppressives (hazard ratio, 10.6;95% confidence interval [CI], 2.2–51.0), had greater rates of hospi-talization (hazard ratio, 3.6; 95% CI, 1.6–8.5), and were more likelyto undergo colectomy (hazard ratio, 8.4; 95% CI, 1.3–55.2) thanthose with complete MH. A population-based Norwegian cohortstudy had similar findings.11 The presence of an endoscopic scoreof 0 (normal mucosa), 1 (light erythema or granularity), or 2 (gran-ularity, friability, and bleeding, with or without ulcerations) 1 yearafter treatment initiation was associated with a significantly lowerrate of colectomy at 5 years than that observed in patients with more
Received for publication October 15, 2013; Accepted October 29, 2013.
From the *Department of Medicine, Western University, London, Ontario,Canada; †Department of Medicine, King Abdulaziz University, Jeddah, SaudiArabia; ‡Department of Epidemiology and Biostatistics, McGill University, Montreal,Canada; §Robarts Clinical Trials, Inc., Robarts Research Institute, Western University,London, Ontario, Canada; kDepartment of Epidemiology and Biostatistics, WesternUniversity, London, Ontario, Canada; ¶Division of Gastroenterology, University ofCalifornia San Diego, La Jolla, California; **Department of Gastroenterology, Aca-demic Medical Center, Amsterdam, The Netherlands; ††Pacific Rim Pathology MedicalCorporation, San Diego, California; ‡‡Carolinas Medical Center, Charlotte, NorthCarolina; §§Department of Pathology, Western University, London, Ontario, Canada;and kkDepartment of Pathology, University Hospital of KU Leuven, Leuven, Belgium.
The authors’ disclosure statement is available in the Acknowledgments.
Reprints: Barrett G. Levesque, MD, Division of Gastroenterology, Universityof California San Diego, 9500 Gilman Dr., La Jolla, CA 92093-0956 (e-mail:[email protected]).
Copyright © 2014 Crohn’s & Colitis Foundation of America, Inc.
DOI 10.1097/01.MIB.0000437986.00190.71
Published online 9 January 2014.
564 | www.ibdjournal.org Inflamm Bowel Dis � Volume 20, Number 3, March 2014

active endoscopic disease (relative risk, 0.22; 95% CI, 0.06–0.79).The Active Ulcerative Colitis Trials (ACT-1 and ACT-2) of inflix-imab showed that MH, defined as an absolute endoscopy subscoreof 0 (inactive) or 1 (mild disease [erythema, decreased vascularpattern, and mild friability]) at week 8, was associated with a lowerrate of colectomy after 54 weeks than that observed in patientswithout MH (P ¼ 0.0004).12 These observations suggest that treat-ments resulting in bowel healing might yield better long-term out-comes than those based on the symptom resolution.
Although bowel healing is associated with a favorable long-term outlook, endoscopy is a poor predictor of histologicallydefined healing.13,14 Truelove and Richards first reported that his-tological evidence of active inflammation was common in patientswith endoscopically normal mucosa after successful inductiontherapy.15 This is clinically relevant as histology may be usefulfor the prediction of relapse.16 Patients with chronic UC in symp-tomatic and endoscopic remission with histologic evidence ofacute inflammation had a 2- to 3-fold greater risk of relapse duringa 12-month follow-up period, which was positively correlatedwith the severity of the inflammatory infiltrate.17 Patients whoseinflammatory infiltrate was graded more severe had a 2-fold riskof relapse compared with those with lower scores. Bitton et al18
also found that the presence of residual histological inflammatoryactivity was an independent predictor of early clinical relapse in74 patients with clinically and endoscopically quiescent UC. Sim-ilarly, a retrospective analysis of 75 adult patients with endoscop-ically inactive UC showed that basal plasmacytosis and a Geboeshistologic score .3.119 was associated with a marked increase inrelapse rate.14 It is reasonable to speculate that a more stringentdefinition of remission incorporating both endoscopic healing andcomplete resolution of the inflammatory infiltrate might be a valu-able treatment goal, and that early assessment of microscopichealing may also predict response to treatment. Identification ofhistologic features of disease activity that can be accurately andreproducibly measured20 is a research priority.
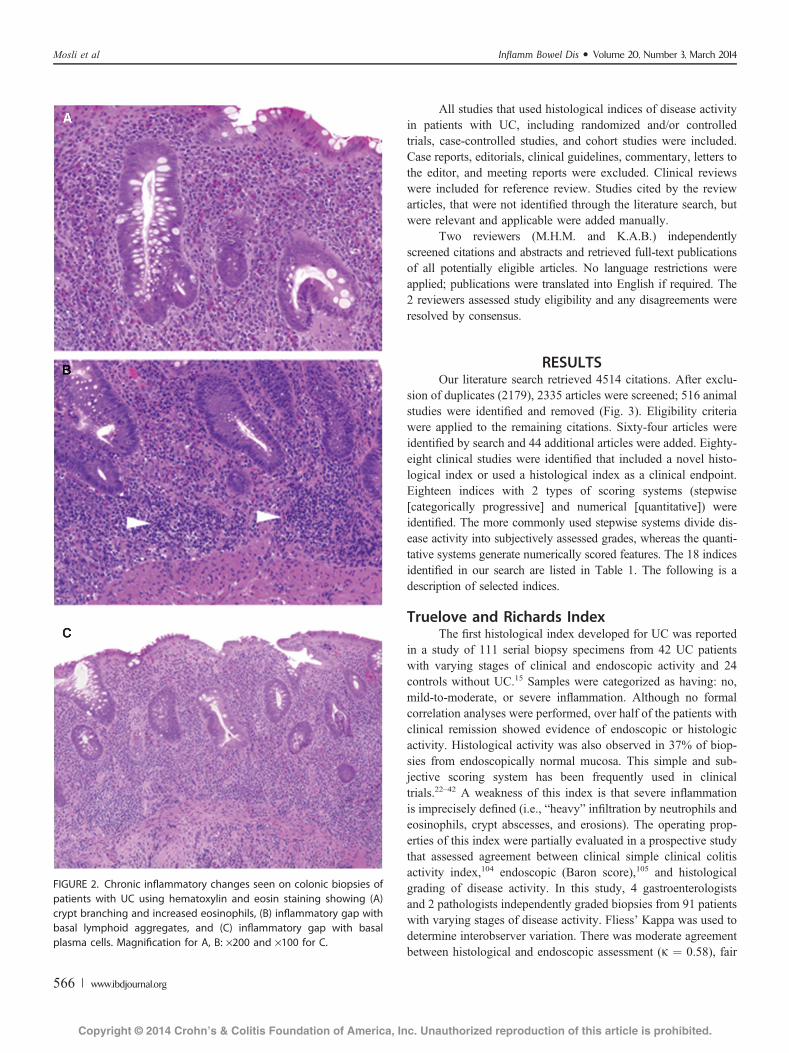
Multiple scoring systems have been developed to measurethe histologic features of UC including the degree of acute (Fig. 1)or chronic (Fig. 2) inflammatory cell infiltrates, the presence orabsence of architectural distortion of colonic crypts, and the integ-rity of the colonic epithelium.21 Although these indices havepotential value for informing clinical practice and as outcomemeasures in clinical trials, their operating properties have not beensystematically validated. We therefore reviewed the existing his-tological indices and assessed their potential utility in patientmanagement and as outcome measures in clinical trials.
MATERIALS AND METHODSMEDLINE, EMBASE, PubMed, the Cochrane Library
(CENTRAL), and DDW abstracts were electronically searchedfrom inception to February 2013 for histologic indices usedfor the evaluation of UC. Each database was searched for “ulcer-ative colitis” AND (“histology” OR “pathology” OR “immuno-histochemistry” OR “biopsy”) AND (“index” OR “indice” OR“scale” OR “score” OR “Riley” OR “Geboes”).
FIGURE 1. Acute inflammatory changes seen on colonic biopsies ofpatients with UC using hematoxylin and eosin staining showing (A)crypt abscess, (B) cryptitis, and (C) neutrophils in lamina propria.Magnification for A–C: ·400.
Inflamm Bowel Dis � Volume 20, Number 3, March 2014 Histologic Evaluation of Ulcerative Colitis
www.ibdjournal.org | 565
All studies that used histological indices of disease activityin patients with UC, including randomized and/or controlledtrials, case-controlled studies, and cohort studies were included.Case reports, editorials, clinical guidelines, commentary, letters tothe editor, and meeting reports were excluded. Clinical reviewswere included for reference review. Studies cited by the reviewarticles, that were not identified through the literature search, butwere relevant and applicable were added manually.
Two reviewers (M.H.M. and K.A.B.) independentlyscreened citations and abstracts and retrieved full-text publicationsof all potentially eligible articles. No language restrictions wereapplied; publications were translated into English if required. The2 reviewers assessed study eligibility and any disagreements wereresolved by consensus.
RESULTSOur literature search retrieved 4514 citations. After exclu-
sion of duplicates (2179), 2335 articles were screened; 516 animalstudies were identified and removed (Fig. 3). Eligibility criteriawere applied to the remaining citations. Sixty-four articles wereidentified by search and 44 additional articles were added. Eighty-eight clinical studies were identified that included a novel histo-logical index or used a histological index as a clinical endpoint.Eighteen indices with 2 types of scoring systems (stepwise[categorically progressive] and numerical [quantitative]) wereidentified. The more commonly used stepwise systems divide dis-ease activity into subjectively assessed grades, whereas the quanti-tative systems generate numerically scored features. The 18 indicesidentified in our search are listed in Table 1. The following is adescription of selected indices.
Truelove and Richards IndexThe first histological index developed for UC was reported
in a study of 111 serial biopsy specimens from 42 UC patientswith varying stages of clinical and endoscopic activity and 24controls without UC.15 Samples were categorized as having: no,mild-to-moderate, or severe inflammation. Although no formalcorrelation analyses were performed, over half of the patients withclinical remission showed evidence of endoscopic or histologicactivity. Histological activity was also observed in 37% of biop-sies from endoscopically normal mucosa. This simple and sub-jective scoring system has been frequently used in clinicaltrials.22–42 A weakness of this index is that severe inflammationis imprecisely defined (i.e., “heavy” infiltration by neutrophils andeosinophils, crypt abscesses, and erosions). The operating prop-erties of this index were partially evaluated in a prospective studythat assessed agreement between clinical simple clinical colitisactivity index,104 endoscopic (Baron score),105 and histologicalgrading of disease activity. In this study, 4 gastroenterologistsand 2 pathologists independently graded biopsies from 91 patientswith varying stages of disease activity. Fliess’ Kappa was used todetermine interobserver variation. There was moderate agreementbetween histological and endoscopic assessment (k ¼ 0.58), fair
FIGURE 2. Chronic inflammatory changes seen on colonic biopsies ofpatients with UC using hematoxylin and eosin staining showing (A)crypt branching and increased eosinophils, (B) inflammatory gap withbasal lymphoid aggregates, and (C) inflammatory gap with basalplasma cells. Magnification for A, B: ·200 and ·100 for C.
Mosli et al Inflamm Bowel Dis � Volume 20, Number 3, March 2014
566 | www.ibdjournal.org

agreement between clinical and endoscopic assessment (k ¼ 0.27),and moderate agreement between clinical and histological assess-ment (k ¼ 0.47), or between all 3 methods (k ¼ 0.44).42
Saverymuttu IndexThis index was first described in a prospective trial comparing
Indium-111 (111In) granulocyte scanning with endoscopy, histology,and fecal 111In-granulocyte excretion for the assessment of diseaseextent and severity in 52 patients with Crohn’s disease or UC.62 It isone of the most widely used histological scoring systems.63–70 Thisnumerical grading system generates a total score composed of4 subscores (Table 1). Excellent correlations between endoscopy,
histology, and 111In scans were shown (r ¼ 0.90 [endoscopy] andr ¼ 0.90 [histology] for extent; r ¼ 0.86 and r ¼ 0.91 for diseaseactivity). This index is simple and comprehensive, but has not beenvalidated.
Initial Riley Scoring SystemThe initial Riley score (Table 2) was described in a random-
ized, double-blind, parallel-group trial that compared delayed-release mesalamine and enteric-coated sulfasalazine maintenancetherapy for quiescent UC (endoscopically normal colonic mucosaor erythema).92
Biopsy sections were evaluated using a 5-point scale tomeasure the degree of chronic inflammatory cell infiltrate andtissue destruction. Relapse rates were not significantly differentbetween the treatment groups at the end of the 48-week trial, andRiley scores were low in patients who maintained remission inboth the treatment groups. This scoring system has not beenvalidated or used in clinical trials.
Riley and Modified Riley Scoring SystemsIn 1991, Riley et al17 prospectively examined the value of
histological inflammation to predict clinical recurrence overa 12-month period in 82 outpatients with asymptomatic UC inendoscopic remission. Unlike the initial Riley score, that gradedchronic inflammatory cell infiltration and tissue destruction exclu-sively, this study used a 4-point scale (none, mild, moderate, orsevere) to independently score 6 items: (1) presence of an acuteinflammatory cell infiltrate (neutrophils in the lamina propria),(2) crypt abscesses, (3) mucin depletion, (4) surface epithelialintegrity, (5) chronic inflammatory cell infiltrate (round cells inthe lamina propria), and (6) crypt architectural irregularities, by2 pathologists whose scores were averaged. These additional his-tologic features were included to better define and isolate featurescharacteristic of mucosal inflammation. The following frequen-cies of findings were noted: chronic inflammatory infiltrate(100%), crypt architectural irregularities (58%), acute inflamma-tory activity (32%), acute inflammatory cell infiltrate (28%), cryptabscesses (11%), and mucin depletion (22%). Interobserver agree-ment occurred in 90% to 98% of cases but was not adjusted forchance. The pathologists did not repeat the reading of slides tomeasure intraobserver agreement, and kappa’s were not calculatedas a measure of interobserver agreement; therefore, formal agree-ment estimates were not determinable. Twenty-seven patients(33%) relapsed after a median of 18 weeks (range, 3–44 weeks).Histologic, but not endoscopic, inflammation predicted relapse.Relapse occurred at similar rates in patients who had macroscop-ically normal mucosa or erythema at study entry (35% comparedwith 32%). Relapse rates were higher in the presence of an acuteinflammatory infiltrate (52% versus 25%, P ¼ 0.02), cryptabscesses (78% versus 27%, P , 0.0005), mucin depletion(56% versus 26%, P , 0.002), and any breach in the surfaceepithelium (75% versus 31%, P ¼ 0.10). The 4-point Riley scorehas been adopted as an endpoint in multiple RCTs.93–99
FIGURE 3. Algorithm undertaken in this systematic review.
Inflamm Bowel Dis � Volume 20, Number 3, March 2014 Histologic Evaluation of Ulcerative Colitis
www.ibdjournal.org | 567

TABLE 1. Histological Scoring Indices in UC
Index Setting Description of Scale Extent of Use
Level of
Validation
Truelove and Richardsindex (1956)15
Prospectivestudy
Stepwise 3-grade scale Multiple clinicalstudies andRCT22–41
Partiallyvalidated42(1) no inflammation
(2) mild to moderate inflammation
(3) severe inflammation
Matts Score (1961)43 Prospectivestudy
Stepwise 5-point grading system Multiple clinicalstudies andRCT44–47
Notvalidated(1) normal
(2) some infiltration of the mucosa or lamina propria, with eitherround cells or polymorphonuclear cells
(3) much cellular infiltration of the mucosa, lamina propria, andsub-mucosa
(4) presence of crypt abscesses, with much infiltration of all layers of themucosa
(5) ulceration, erosion, or necrosis of the mucosa, with cellular infiltrationof some or all of its layers
Watts Score (1966)48 Prospectivestudy
Stepwise 4-point grading scale One prospectivestudy48
Notvalidated(0) normal
(1) no significant epithelial changes but increased number of chronicinflammatory cells in the lamina propria
(2) mild epithelial changes, usually regenerative, leukocytes may be seenin the crypts or ducts along with paneth cells. Severe inflammatory cellscan be seen in the lamina propria
(3) severe inflammatory changes with evidence of crypt abscesses,inflammatory erosions, and frank ulceration, occasional multinucleatedgiant cells can be seen
Keren Score (1984)49 Prospectivestudy
Descriptive None Notvalidatedactive versus inactive
The Friedman Index(1985)50
RCT Stepwise 4-grade scale Multiple clinicalstudies andRCT51–58
Notvalidated(0) normal
(1) lamina propria inflammation
(2) crypt injury
(3) ulcerationGomes Score (1986)59 Prospective
studyNumerical 5-grade scale Clinical
studies60,61Notvalidated(0) normal
(1) mild edema and inflammation in the lamina propria
(2) crypt abscess formation and lamina propria involvement
(3) destructive crypt abscesses with or without granulomas
(4) active ulceration
Scores are summed to generate an overall total score (maximum score of 24).
Saverymuttu Index(1986)62
Prospectivestudy
Numerical grading system generating a total score composed of 4 differentvariable subscores:
Multiple clinicalstudies andRCT63–70
Notvalidated
a) Enterocyte damage: (0) Normal, (1) loss of single cells, (2) loss ofgroups of cells, and (3) frank ulcerations
b) Crypt abnormalities: (0) Normal, (1) single inflammatory cell, (2)cryptitis, and (3) crypt abscesses
c) Lamina propria involvement: (0) Normal, (1) slight increase inmononuclear cells, (2) moderate increase in mononuclear cells, and (3)marked increase in mononuclear cells
d) Acute inflammatory infiltration in the lamina propria: (0) normal, (1)mild increase, (2) moderate increase, and (3) marked increase
Mosli et al Inflamm Bowel Dis � Volume 20, Number 3, March 2014
568 | www.ibdjournal.org

TABLE 1 (Continued )
Index Setting Description of Scale Extent of Use
Level of
Validation
Floren Index (1987)71 Prospectivestudy
Stepwise 5-point grading system Multiple clinicalstudies andRCT72–79
Notvalidated(1) normal
(2) enhanced glands with intraepithelial granulocytes and stromalenhancement beyond normal of lymphoplasmacytic cells or eosinophilicgranulocytes (slight inflammation)
(3) goblet cell depletion, loss of tubular parallelism, and reduced mucinproduction in some glands with intraepithelial granulocytes, markedincrease of inflammatory cells in the stroma (intermediate inflammation)
(4) marked gland and mucosal atrophy, evident crypt abscesses and pus onthe surface, massive increase of acute inflammatory cells, and follicleformation in deeper cell layers (severe inflammation)
(5) Ulceration with pus, gland and mucosal atrophy, crypt abscesses,extensive stromal inflammation, and deep follicles (fulminantinflammation)
Hanauer Index (1993)80 RCT Stepwise 4-point grading system Few clinicalstudies andRCT81–83
Notvalidated(0) normal colonic mucosa, to
(3) high-grade active inflammatory bowel disease
Odze Index (1993)84 Prospectivestudy
Stepwise 4-point grading system None Notvalidated(a) normal
(b) active (ulcerations)
(c) chronically active (cryptitis, crypt abscesses, or surface erosions)
(d) chronically inactive (not defined)Categorized based on 6 parameters:
(1) crypt architecture, (2) villiform surface contour, (3) mixedinflammation in the lamina propria, (4) basal plasmacytosis, (5) basallylocated lymphoid aggregates, and (6) paneth cell metaplasia
Sandborn Index (1993)85 Prospectivestudy
Stepwise 4-point grading system Few clinicalstudies and RCT
Notvalidated(0) inactive chronic colitis (normocellular or hypercellular lamina propria;
PMNs absent)
(1) mild active chronic colitis (scant PMNs in lamina propria, occasionalcryptitis but few crypt abscesses, minimal glandular destruction orulceration)
(2) moderately active chronic colitis (moderate numbers of PMNs inlamina propria with cryptitis and crypt abscesses prominent, someglandular destruction)
(3) severely active chronic colitis (numerous PMNs with abundantcryptitis, crypt abscesses, extensive glandular destruction; ulcerationmay be prominent)
Scheppach/D’ArgenioScore (2001)86,87
Prospectivestudy
Numerical scoring system Few clinicalstudies86,88
NotvalidatedMeasures 6 variables (infiltration of the mucosa by lymphocytes and
plasma cells, infiltration of crypts by neutrophils, crypt abscesses,ulceration, mucous cell depletion, and crypt architectural distortion)each scored on a 0–2 scale according to the severity
Maximum overall score of 12
Harpaz Index (2003)89 Prospectivestudy
Stepwise grading system Two clinicalstudies90,91
Partiallyvalidated89Categorizes microscopic disease activity into:
a) inactive (no cryptitis)
b) mildly active colitis (cryptitis in ,50% of crypts)c) moderately active colitis (cryptitis in .50% of crypts)
d) severely active colitis (ulcerations or erosions)
Inflamm Bowel Dis � Volume 20, Number 3, March 2014 Histologic Evaluation of Ulcerative Colitis
www.ibdjournal.org | 569

The 4-point Riley score was empirically modified byFeagan et al100 (Table 3) to exclude items such as structural alter-ations (i.e., crypt branching), that are probably not responsive toclinically relevant changes in inflammation. This modified Rileyscore (MRS) ranks the degree of inflammation hierarchically,allowing for an unweighted aggregation of the scores that facili-tate the comparison of mean values. This instrument was used asan outcome measure in a RCT of the a4-b7 antagonist, vedolizu-mab (MLN02), for the treatment of active UC.100 The MRS wascalculated at baseline and at weeks 4 and 6. Mean histologyscores, endoscopically defined disease activity, and symptoms
significantly improved in patients assigned to vedolizumab.Although these results suggest that the MRS may be a usefuloutcome measure, the clinical relevance of the changes detectedby the MRS remains unknown.
Geboes ScoreGeboes et al19 developed a scoring system for microscopic
disease activity that incorporated a number of previously reportedhistological items. The score was generated with the premise thatthe major grades and subgrades are progressive and correlate withincreasing disease severity or activity (Table 4).
TABLE 1 (Continued )
Index Setting Description of Scale Extent of Use
Level of
Validation
Initial Riley Score(1988)92
RCT Stepwise 5-point scale None NotvalidatedMeasures the degree of chronic inflammatory cell infiltrate and tissue
destruction
Riley Score (1991)17 Prospectivestudy
Stepwise 4-point scale Multiple clinicalstudies andRCT93–99
NotvalidatedNone (0), mild (1), moderate, or (2) severe, and (3)
Independently scores 6 different features:a) presence of an acute inflammatory cell infiltrate (neutrophils in the
lamina propria)
b) crypt abscesses
c) mucin depletion
d) surface epithelial integrity
e) chronic inflammatory cell infiltrate (round cells in the lamina propria)
f) crypt architectural irregularitiesModified Riley score(2005)100
RCT Stepwise grading system None NotvalidatedConsists of select items from the original score that were believed to be
responsive to changes in acute inflammation
Geboes Score (2000)19 Prospectivestudy
Stepwise grading system Few clinicalstudies96,101,102
Partiallyvalidated19Categorizes patients into 7 grades based on:
(1) architectural changes
(2) chronic inflammatory infiltrate(3) lamina propria eosinophils
(4) lamina propria neutrophils
(5) epithelial neutrophils
(6) crypt destruction
(7) erosions or ulcerations
Chicago score (2007)103 Case-controlstudy
Stepwise 6-point scale One clinicalstudy77
Notvalidated(0) Normal (completely uninvolved, no architectural distortion, and no
infiltrates)
(1) Quiescent (architectural distortion, increased lamina proprialymphocytes, but no activity)
(2) Increased lamina propria granulocytes without definite intraepithelialgranulocytes
(3) Intraepithelial granulocytes (e.g., cryptitis) without crypt abscesses(4) Crypt abscesses in less than 50% of crypts
(5) Crypt abscesses in greater than 50% of crypts, or erosion/ulceration
PMN, polymorphonuclear leukocytes.
Mosli et al Inflamm Bowel Dis � Volume 20, Number 3, March 2014
570 | www.ibdjournal.org

To develop this index, 3 pathologists examined 99 biopsyslides obtained on 2 occasions from actively inflamed (n ¼ 68)and quiescent (n ¼ 31) colonic mucosa in patients with distal UC.Good agreement was noted between pathologists for biopsiesfrom endoscopically inflamed mucosa, but only moderate forthose obtained from noninflamed tissue. Recently, Lemmenset al106 examined the correlation between endoscopic activity,based on the Mayo score, and histological activity, based on boththe Riley and the Geboes score in 263 biopsy specimens from131 patients with UC. A significant correlation was found betweenthe endoscopic and histological grades (Kendall’s t ¼ 0.482, P ,0.0001) with more consistency seen between extremes of scores.
DISCUSSION
The Need for Validated ScoresFor histological indices for grading of UC disease severity
and activity to be clinically useful, their operating properties must beaccurately defined. Validity (extent to which an instrument measuresthe intended outcome); responsiveness (ability to detect a meaningfulchange in health status); reliability (consistency or reproducibility ofan instrument); and feasibility (ease with which an instrument can
be utilized), are essential properties of evaluative instruments. It isnotable that none of the indices currently used to evaluatehistopathology in clinical trials of UC have been fully validated.
Interobserver and intraobserver variability in histologicalscoring is a formidable problem. A statistical method that measuresagreement between observers and accounts for agreement becauseof chance should be used to assess reliability. The kappa statistic(or kappa coefficient) is most commonly used for this purpose.107 Akappa of 1 indicates perfect agreement, whereas a kappa of0 indicates agreement by chance.108 A limitation of the kappa sta-tistic is that it is affected by the prevalence of the finding underobservation. Interobserver agreement can be calculated by the intra-class coefficient, which is equivalent to weighted data in the case ofordinal scores.109 Other factors such as the number and quality ofsamples, and the feasibility of the scoring must also be consideredwhen assessing agreement between the readers.
The currently available scoring systems have been appliedto biopsy material that was collected under diverse protocols. Theoriginal Riley study used 1 biopsy from the anterior rectal wall,whereas 2 samples were used in the Geboes study. Histologicaldisease severity changes during the natural disease course andafter the administration of effective treatment.16,110 Therefore,although initially 1 biopsy sample may be reliable, histologicalactivity may differ among samples on follow-up. This differencemay be mitigated by collecting 2 or more samples.84
Sample quality is another potential confounder. In theGeboes study, fewer than one-third of the samples were consideredof good quality. Of 99 total samples, 31 were good, 36 substandard,and 22 were of poor quality (of which, 13 were not examined). Thisproblem has considerable implications for precision of scoring. Someindex items, such as basal plasmacytosis, require perpendicularsections of well-oriented samples for accurate interpretation. Sectionthickness may also affect the interpretation of results. In clinicaltrials, the operating characteristics of scores will vary depending onthe quality of samples obtained, and every effort should be made tostandardize and optimize the collection and processing of biopsysamples. It has been shown that local and systemic treatment has animpact on the microscopic activity in UC.16,84 Therefore, it is imper-ative to obtain at least 2 samples from the mucosa for evaluation,preferably from areas showing endoscopic involvement. In routinepractice for clinical trials, scoring is mostly performed on the sampleshowing maximum activity, as this may well be the most importantfor further evolution of the disease although this has not been stud-ied. The handling of the biopsy samples further influences the assess-ment of histological disease activity. Proper evaluation of basalplasmacytosis depends on the orientation of the specimens and avail-ability of perpendicular sections. The assessment of the compositionof the cellular infiltrate depends on the thickness of the sections,preferably 4 mm and the staining qualities. Epithelial integrity canbe damaged by the procedure of taking the biopsy sample with thebiopsy forceps and needs therefore to be defined properly.
Additional research is needed to define which, if any, of theexisting histopathologic indices are most reliable and valid inlarge clinical trials with heterogenous sample quality. The results
TABLE 2. Initial Riley Scoring System
Grade Microscopic Appearance
0 Normal
1 Mild increase in chronic inflammatory cell infiltrate, no tissuedestruction
2 Moderate increase in chronic inflammatory cell infiltrate, notissue destruction
3 Marked increase in chronic inflammatory cell infiltrate, mildtissue destruction
4 Marked increase in chronic inflammatory cell infiltrate, obvioustissue destruction
TABLE 3. Modified Riley Scoring System
Activity Histological Characteristics
None 0: Neutrophils in epithelium ¼ None (3.0)Mild 1: Neutrophils in epithelium ¼ ,25% crypts involved (3.1 or
3.2A)
2: Neutrophils in epithelium ¼ $25% to #75% cryptsinvolved (3.2B or 3.3A)
3: Neutrophils in epithelium ¼ .75% crypts involved (3.3B)
Moderate 4: Lamina propria neutrophils ¼ Mild but unequivocalincrease (2B.1)
5: Lamina propria neutrophils ¼ Moderate increase (2B.2)
6: Lamina propria neutrophils ¼ Marked increase (2B.3)
Severe 7: Erosion or ulceration ¼ Present (5.1 or 5.2 or 5.3 or 5.4)
Inflamm Bowel Dis � Volume 20, Number 3, March 2014 Histologic Evaluation of Ulcerative Colitis
www.ibdjournal.org | 571

obtained in these circumstances may differ from those frominterobserver and intraobserver studies performed on samples ofoptimal quality. Determining the relative merits of numerical versusstepwise scoring is also relevant. In some samples, for instancethose obtained from ulcers, granulation tissue may be the majorelement of the sample, making it difficult if not impossible toevaluate cryptitis or crypt abscesses. Similarly, basal plasmacytosismay be impossible to assess if a section is not correctly orientated.
Future DirectionsValid, reliable, responsive, and predictive histological
scoring systems are needed in UC. Validated scoring systems
used for both patient management and in clinical trials exist forother diseases, including the nonalcoholic fatty liver diseaseactivity score,111 the METAVIR or Ishak score for chronic hepa-titis,112 the Gleason score for prostate cancer,113 and the follicularlymphoma score.114 The score’s operative properties should beevaluated by a process of item selection through regression anal-ysis, conduct of an appropriately powered agreement study withcalculation of intraclass coefficient between the multiple centralreaders, and assessment of responsiveness to treatments of knownefficacy. Several methodological frameworks for the developmentand validation of evaluative instruments exist.115 Responsive indi-ces will facilitate early drug development by their efficiency indetecting a meaningful impact of therapies, and thus allow forsmaller samples sizes in early phase trials. In the future, use ofhistology should allow quantitation of specific features of a biopsysuch as number of plasma cells. In the clinical evaluation of UC,other modalities such as confocal endomicroscopy and opticalcoherence tomography have potential to augment biopsy-derivedinformation.116–118 Future trials are needed which examine the long-term outcomes, such as surgery and hospitalization, of patients whoachieve histologic remission compared with those who do not.These trials, including one or multiple histologic indices, wouldfurther define the predictive validity of histologic assessment in UC.
In summary, histopathology is an important component ofUC assessment both in clinical practice and for clinical trials, withpotential long-term implications for predicting remission rates,future surgery, and malignancy risk.90,103 Currently, the use ofa partially validated score such as the Geboes score or the MRSseems optimal for clinical research purposes, but requires furthervalidation. Ideally, improvements to current indices or develop-ment of new indices will lead to standardized methods of histo-logical assessment that can be employed in both clinical practiceand in clinical trials.
ACKNOWLEDGMENTSThe authors wish to thank Dr. David T. Rubin and
Dr. Noam Harpaz for providing us with valuable data regardingthe Chicago index and the Harpaz index, respectively.
Disclosures: M. H. Mosli has no financial disclosures.B.G. Feagan has received grant/research support from Millen-nium Pharmaceuticals, Merck, Tillotts Pharma AG, Abbott Labs,Novartis Pharmaceuticals, Centocor Inc., Elan/Biogen, UCBPharma, Bristol-Myers Squibb, Genentech, ActoGenix, WyethPharmaceuticals Inc.; Consulting fees from Millennium Pharma-ceuticals, Merck, Centocor Inc., Elan/Biogen, Janssen-Ortho,Teva Pharmaceuticals, Bristol-Myers Squibb, Celgene, UCBPharma, Abbott Labs, Astra Zeneca, Serono, Genentech, TillottsPharma AG, Unity Pharmaceuticals, Albireo Pharma, GivenImaging Inc., Salix Pharmaceuticals, Novonordisk, GSK, Actoge-nix, Prometheus Therapeutics and Diagnostics, Athersys, Axcan,Gilead, Pfizer, Shire, Wyeth, Zealand Pharma, Zyngenia, GiCarePharma Inc. Sigmoid Pharma; Speakers Bureau for UCB, Abbott,J&J/Janssen. W. J. Sandborn has received consulting fees from
TABLE 4. The Geboes Scoring System
Subscore Characteristics
Grade 0 Structural (architectural change)
0.0 No abnormality0.1 Mild abnormality
0.2 Mild or moderate diffuse or multifocal abnormalities
0.3 Severe diffuse or multifocal abnormalities
Grade 1 Chronic inflammatory infiltrate
1.0 No increase
1.1 Mild but unequivocal increase
1.2 Moderate increase
1.3 Marked increaseGrade 2A Lamina propria eosinophils
2A.0 No increase
2A.1 Mild but unequivocal increase
2A.2 Moderate increase
2A.3 Marked increase
Grade 2B Lamina propria neutrophils
2B.0 No increase
2B.1 Mild but unequivocal increase2B.2 Moderate increase
2B.3 Marked increase
Grade 3 Neutrophils in epithelium
3.0 None
3.1 ,5% crypts involved
3.2 ,50% crypts involved
3.3 .50% crypts involved
Grade 4 Crypt destruction4.0 None
4.1 Probable—local excess of neutrophils in part of crypt
4.2 Probable—marked attenuation
4.3 Unequivocal crypt destruction
Grade 5 Erosion or ulceration
5.0 No erosion, ulceration, or granulation tissue
5.1 Recovering epithelium + adjacent inflammation
5.2 Probable erosion 2 focally stripped5.3 Unequivocal erosion
5.4 Ulcer or granulation tissue
Mosli et al Inflamm Bowel Dis � Volume 20, Number 3, March 2014
572 | www.ibdjournal.org

Abbott, ActoGeniX NV, AGI Therapeutics Inc, Alba Therapeu-tics Corp, Albireo, Alfa Wasserman, Amgen, AM-Pharma BV,Anaphore, Astellas, Athersys Inc, Atlantic Healthcare Ltd, Apta-lis, BioBalance Corp, Boehringer-Ingelheim, Bristol-MyersSquibb, Celgene, Celek Pharmaceuticals, Cellerix SL, CerimonPharmaceuticals, ChemoCentryx, CoMentis, Cosmo Technolo-gies, Coronado Biosciences, Cytokine Pharmasciences, EaglePharmaceuticals, EnGene Inc, Eli Lilly, Enteromedics, ExagenDiagnostics Inc, Ferring Pharmaceuticals, Flexio TherapeuticsInc, Funxional Therapeutics Ltd, Genzyme Corp, Gilead Scien-ces, Given Imaging, GSK, Human Genome Sciences, IronwoodPharmaceuticals, KaloBios Pharmaceuticals, Lexicon Pharma-ceuticals, Lycera Corp, Meda Pharmaceuticals, Merck ResearchLaboratories, Merck Serono, Millenium Pharmaceuticals, NisshinKyorin Pharmaceuticals, Novo Nordisk, NPS Pharmaceuticals,Optimer Pharmaceuticals, Orexigen Therapeutics Inc, PDL Bio-pharma, Pfizer, Procter and Gamble, Prometheus Laboratories,ProtAb Ltd, Purgenesis Technologies Inc, Relypsa Inc, Roche,Salient Pharmaceuticals, Salix Pharmaceuticals, Santarus, Scher-ing Plough, Shire Pharmaceuticals, Sigmoid Pharma Ltd, SirtrisPharmaceuticals, SLA Pharma UK Ltd, Targacept, Teva Pharma-ceuticals, Therakos, Tillotts Pharma AG, TxCell SA, UCB Phar-ma, Viamet Pharmaceuticals, Vascular Biogenics Ltd, WarnerChilcott UK Ltd and Wyeth; research grants from Abbott,Bristol-Myers Squibb, Genentech, GSK, Janssen, MilenniumPharmaceuticals, Novartis, Pfizer, Procter and Gamble, ShirePharmaceuticals and UCB Pharma; payments for lectures/speak-ers bureaux from Abbott, Bristol-Myers Squibb and Janssen; andholds stock/stock options in Enteromedics. G. D’Haens hasreceived grant/research support from Merck, Abbott Labs, Cen-tocor Inc., Given Imaging, UCB Pharma, ActoGenix, Consultingfees from Boehringer-Ingelheim, Cosmo Technologies, EnGeneInc, Ferring Pharmaceuticals, Millennium Pharmaceuticals,Merck, Centocor Inc., Elan/Biogen, Janssen-Ortho, Teva Pharma-ceuticals, UCB Pharma, Abbott Labs, Astra Zeneca, Shire, TillottsPharma AG, Novonordisk, GSK, Actogenix, Pfizer, SigmoidPharma. C. Behling has received consulting fees from RobartsClinical Trials. K. Kaplan has no disclosures. D. Driman hasno disclosures. L. Shackelton has no disclosures. K. A. Bakerhad no disclosures. J.K. MacDonald has no disclosures. M. K.Vandervoort has no disclosures. K. Geboes has no disclosures.B. G. Levesque has received consulting fees from Santarus Inc.and Prometheus labs, Speakers bureau for Warner Chilcott, Salix,and UCB Pharma, and research grant support from Robarts Clin-ical Trials.
Author contributions: M. H. Mosli, B. G. Feagan, and B. G.Levesque contributed to the conception and design of the study,analysis and interpretation of data, and drafting the article;W. J. Sandborn, G. D’Haens, C. Behling, K. Kaplan, D. K. Driman,J. K. MacDonald, M. K. Vandervoort, K. Geboes, L. M Shackelton,and K. A. Baker contributed to the analysis and interpretation of thedata and revising the article for important intellectual content. Allauthors provided final approval of the version to be published.
REFERENCES1. Abraham C, Cho JH. Inflammatory bowel disease. N Engl J Med. 2009;
361:2066–2078.2. Baumgart DC, Sandborn WJ. Inflammatory bowel disease: clinical aspects
and established and evolving therapies. Lancet. 2007;369:1641–1657.3. Cohen RD. Evolving medical therapies for ulcerative colitis. Curr Gas-
troenterol Rep. 2002;4:497–505.4. Danese S, Fiocchi C. Ulcerative colitis. N Engl J Med. 2011;365:1713–1725.5. Hanauer SB. Medical therapy for ulcerative colitis 2004. Gastroenterol-
ogy. 2004;126:1582–1592.6. Truelove SC, Witts LJ. Cortisone in ulcerative colitis; final report on
a therapeutic trial. Br Med J. 1955;2:1041–1048.7. Travis SP, Schnell D, Krzeski P, et al. Developing an instrument to
assess the endoscopic severity of ulcerative colitis: the Ulcerative ColitisEndoscopic Index of Severity (UCEIS). Gut. 2012;61:535–542.
8. D’Haens G, Sandborn WJ, Feagan BG, et al. A review of activity indicesand efficacy end points for clinical trials of medical therapy in adultswith ulcerative colitis. Gastroenterology. 2007;132:763–786.
9. Pineton de Chambrun G, Peyrin-Biroulet L, Lémann M, et al. Clinicalimplications of mucosal healing for the management of IBD. Nat RevGastroenterol Hepatol. 2010;7:15–29.
10. Ardizzone S, Cassinotti A, Duca P, et al. Mucosal healing predicts lateoutcomes after the first course of corticosteroids for newly diagnosedulcerative colitis. Clin Gastroenterol Hepatol. 2011;9:483–489.
11. Froslie KF, Jahnsen J, Moum BA, et al. Mucosal healing in inflamma-tory bowel disease: results from a Norwegian population-based cohort.Gastroenterology. 2007;133:412–422.
12. Colombel JF, Rutgeerts P, Reinisch W, et al. Early mucosal healing withinfliximab is associated with improved long-term clinical outcomes inulcerative colitis. Gastroenterology. 2011;141:1194–1201.
13. Baars JE, Nuij VJ, Oldenburg B, et al. Majority of patients with inflam-matory bowel disease in clinical remission have mucosal inflammation.Inflamm Bowel Dis. 2012;18:1634–1640.
14. Bessissow T, Lemmens B, Ferrante M, et al. Prognostic value of serologicand histologic markers on clinical relapse in ulcerative colitis patients withmucosal healing. Am J Gastroenterol. 2012;107:1684–1692.
15. Truelove SC, Richards WC. Biopsy studies in ulcerative colitis. Br Med J.1956;1:1315–1318.
16. Geboes K, Dalle I. Influence of treatment on morphological features ofmucosal inflammation. Gut. 2002;50:iii37–iii42.
17. Riley SA, Mani V, Goodman MJ, et al. Microscopic activity in ulcerativecolitis: what does it mean? Gut. 1991;32:174–178.
18. Bitton A, Peppercorn MA, Antonioli DA, et al. Clinical, biological, andhistologic parameters as predictors of relapse in ulcerative colitis.Gastroenterology. 2001;120:13–20.
19. Geboes K, Riddell R, Ost A, et al. A reproducible grading scale forhistological assessment of inflammation in ulcerative colitis. Gut.2000;47:404–409.
20. Guyatt GH, Deyo RA, Charlson M, et al. Responsiveness and validity inhealth status measurement: a clarification. J Clin Epidemiol. 1989;42:403–408.
21. Travis SP, Higgins PD, Orchard T, et al. Review article: defining remis-sion in ulcerative colitis. Aliment Pharmacol Ther. 2011;34:113–124.
22. Sinha A, Nightingale JM, West KP, et al. Epidermal growth factorenemas are effective in the treatment of left-sided ulcerative colitis.Gastroenterology. 2001;120:A11–A12.
23. Ardizzone S, Petrillo M, Antonacci CM, et al. Sucralfate and hydrocorti-sone enemas in the treatment of active ulcerative proctitis—a randomizedsingle-blind comparative study. Aliment Pharmacol Ther. 1996;10:957–960.
24. Ardizzone S, Petrillo M, Imbesi V, et al. Is maintenance therapy alwaysnecessary for patients with ulcerative colitis in remission? Aliment Phar-macol Ther. 1999;13:373–379.
25. Bayles T, Sninsky C. Budesonide enema is an effective alternative tohydrocortisone enema in active distal ulcerative colitis. Gastroenterology.1995;108:A778.
26. Campieri M, Cottone M, Miglio F, et al. Beclomethasone dipropionateenemas versus prednisolone sodium phosphate enemas in the treatmentof distal ulcerative colitis. Aliment Pharmacol Ther. 1998;12:361–366.
27. Campieri M, Gionchetti P, Belluzzi A. Optimum dosage of 5-aminosalicylicacid as rectal enemas in active ulcerative colitis (UC). Gastroenterology.1989;96:A72.
Inflamm Bowel Dis � Volume 20, Number 3, March 2014 Histologic Evaluation of Ulcerative Colitis
www.ibdjournal.org | 573

28. Campieri M, Lanfranchi G, Bertoni F. 4-aminosalicylic acid (4-ASA)and 5-aminosalicylic acid (5-ASA) in topical treatment of ulcerativecolitis patients. Gastroenterology. 1984;86:A1039.
29. Chen QK, Yuan SZ, Wen ZF, et al. Characteristics and therapeuticefficacy of sulfasalazine in patients with mildly and moderately activeulcerative colitis. World J Gastroenterol. 2005;11:2462–2466.
30. D’Albasio G, Paoluzi P, Campieri M, et al. Maintenance treatment ofulcerative proctitis with mesalazine suppositories: a double-blindplacebo-controlled trial. Am J Gastroenterol. 1998;93:799–803.
31. Dong LF, Ouyang Q. The efficacy of azathiopurine in the treatment ofulcerative colitis. J Gastroenterol Hepatol. 2011;26:134.
32. Feurle G, Theuer D, Velasco S, et al. Olsalazine versus placebo in thetreatment of mild to moderate ulcerative colitis: a randomized double-blind trial. Gastroenterology. 1988;94:A126.
33. Gionchetti P, Rizzello F, Venturi A, et al. Comparison of oral with rectalmesalazine in the treatment of ulcerative proctitis. Dis Colon Rectum.1998;41:93–97.
34. Green JT, Thomas GAO, Rhodes J, et al. Nicotine enemas for activeulcerative colitis—a pilot study. Aliment Pharmacol Ther. 1997;11:859–863.
35. Ireland A, Mason CH, Jewell DP. Controlled trial comparing olsalazineand sulphasalazine for the maintenance treatment of ulcerative colitis.Gut. 1988;29:835–837.
36. Kruis W, Schreiber S, Theuer D, et al. Low dose balsalazide (1.5 g twicedaily) and mesalazine (0.5 g three times daily) maintained remission ofulcerative colitis but high dose balsalazide (3.0 g twice daily) was supe-rior in preventing relapses. Gut. 2001;49:783–789.
37. Liang HL, Ouyang Q. A clinical trial of combined use of rosiglitazoneand 5-aminosalicylate for ulcerative colitis. World J Gastroenterol.2008;14:114–119.
38. Merra G, Gasbarrini G, Laterza L, et al. Propionyl-L-carnitine hydro-chloride for treatment of mild to moderate colonic inflammatory boweldiseases. World J Gastroenterol. 2012;18:5065–5071.
39. Mikhailova TL, Sishkova E, Poniewierka E, et al. Randomised clinicaltrial: the efficacy and safety of propionyl-L-carnitine therapy in patientswith ulcerative colitis receiving stable oral treatment. Aliment PharmacolTher. 2011;34:1088–1097.
40. Rizzello F, Gionchetti P, D’Arienzo A, et al. Oral beclometasone dipropi-onate in the treatment of active ulcerative colitis: a double-blind placebo-controlled study. Aliment Pharmacol Ther. 2002;16:1109–1116.
41. Sinha A, Nightingale JM, West KP. A gradual dose reduction is neededafter 2 weeks of oral prednisolone treatment for ulcerative colitis.Gastroenterology. 2000;118:A782.
42. Thomas SJ, Walsh A, Von Herbay A, et al. How much agreement isthere between histological, endoscopic and clinical assessments of remis-sion in ulcerative colitis? Gut. 2009;58:A101–A102.
43. Matts SG. The value of rectal biopsy in the diagnosis of ulcerativecolitis. Q J Med. 1961;30:393–407.
44. Hurlstone DP, Sanders DS, McAlindon ME, et al. High-magnificationchromoscopic colonoscopy in ulcerative colitis: a valid tool for in vivooptical biopsy and assessment of disease extent. Endoscopy. 2006;38:1213–1217.
45. Kato K, Mizuno S, Umesaki Y, et al. Randomized placebo-controlledtrial assessing the effect of bifidobacteria-fermented milk on active ulcer-ative colitis. Aliment Pharmacol Ther. 2004;20:1133–1141.
46. Kimura K, Kanai T, Bessho R, et al. In vivo visualization and evaluationof colorectal inflammation in ulcerative colitis by a newly integratedendocytoscopy. Gastroenterology. 2011;1:S422.
47. Ohkusa T, Nomura T, Terai T, et al. Effectiveness of antibiotic combi-nation therapy in patients with active ulcerative colitis: a randomized,controlled pilot trial with long-term follow-up. Scand J Gastroenterol.2005;40:1334–1342.
48. Watts JM, Thompson H, Goligher JC. Sigmoidoscopy and cytology inthe detection of microscopic disease of the rectal mucosa in ulcerativecolitis. Gut. 1966;7:288–294.
49. Keren DF, Appelman HD, Dobbins WO III, et al. Correlation of histopath-ologic evidence of disease activity with the presence of immunoglobulin-containing cells in the colons of patients with inflammatory bowel disease.Hum Pathol. 1984;15:757–763.
50. Friedman L, Richter J, Kirkham S. 5-aminosalicylic acid (5-ASA) ene-mas in refractory distal ulcerative colitis (UC): a randomized, controlledtrial. Gastroenterology. 1985;88:A1388.
51. D’Arienzo A, Manguso F, Castiglione GN, et al. Beclomethasone dipro-pionate (3 mg) enemas combined with oral 5-ASA (2.4 g) in the treat-ment of ulcerative colitis not responsive to oral 5-ASA alone. Ital JGastroenterol Hepatol. 1998;30:254–257.
52. D’Arienzo A, Panarese A, Di Siervi P, et al. Low-dose 5-aminosalicylicacid (5-ASA) enemas in idiopathic distal proctocolitis therapy in patientsintolerant or unresponsive to salazopyrine. Clin Trials J. 1988;25:21–29.
53. D’Arienzo A, Panarese A, Talarico G, et al. 5-Aminosalicylic acid sup-positories in long- and short-term therapy for idiopathic distal proctoco-litis in patients intolerant or unresponsive to salazopyrine. Clin Trials J.1987;24:430–440.
54. Farup PG, Hovde O, Halvorsen FA, et al. Mesalazine suppositoriesversus hydrocortisone foam in patients with distal ulcerative colitis. Acomparison of the efficacy and practicality of two topical treatmentregimens. Scand J Gastroenterol. 1995;30:164–170.
55. Feagan BG, Sandborn WJ, D’Haens G, et al. The role of centralizedreading of endoscopy in a randomized controlled trial of mesalamine forulcerative colitis. Gastroenterology. 2013;145:149–157.
56. Friedman LS, Richter JM, Kirkham SE, et al. 5-aminosalicylic acidenemas in refractory distal ulcerative colitis: a randomized, controlledtrial. Am J Gastroenterol. 1986;81:412–418.
57. Kono T, Nomura M, Kasai S, et al. Effect of ecabet sodium enema onmildly to moderately active ulcerative proctosigmoiditis: an open-labelstudy. Am J Gastroenterol. 2001;96:793–797.
58. Roseth AG, Aadland E, Grzyb K. Normalization of faecal calprotectin:a predictor of mucosal healing in patients with inflammatory boweldisease. Scand J Gastroenterol. 2004;39:1017–1020.
59. Gomes P, du Boulay C, Smith CL, et al. Relationship between diseaseactivity indices and colonoscopic findings in patients with colonicinflammatory bowel disease. Gut. 1986;27:92–95.
60. Bennink R, Peeters M, D’Haens G, et al. Tc-99m HMPAO white bloodcell scintigraphy in the assessment of the extent and severity of an acuteexacerbation of ulcerative colitis. Clin Nucl Med. 2001;26:99–104.
61. Bennink RJ, Peeters M, Rutgeerts P, et al. Evaluation of early treatmentresponse and predicting the need for colectomy in active ulcerative coli-tis with 99mTc-HMPAO white blood cell scintigraphy. J Nucl Med.2004;45:1698–1704.
62. Saverymuttu SH, Camilleri M, Rees H, et al. Indium 111-granulocytescanning in the assessment of disease extent and disease activity ininflammatory bowel disease. A comparison with colonoscopy, histology,and fecal indium 111-granulocyte excretion. Gastroenterology. 1986;90:1121–1128.
63. Canani RB, Terrin G, Rapacciuolo L, et al. Faecal calprotectin as reliablenon-invasive marker to assess the severity of mucosal inflammation inchildren with inflammatory bowel disease. Dig Liver Dis. 2008;40:547–553.
64. Bunn SK, Bisset WM, Main MJ, et al. Fecal calprotectin: validation asa noninvasive measure of bowel inflammation in childhood inflamma-tory bowel disease. J Pediatr Gastroenterol Nutr. 2001;33:14–22.
65. Celasco G, Papa A, Jones R, et al. Clinical trial: oral colon-releaseparnaparin sodium tablets (CB-01-05 MMX) for active left-sided ulcer-ative colitis. Aliment Pharmacol Ther. 2010;31:375–386.
66. D’Haens GR, Kovacs A, Vergauwe P, et al. Clinical trial: preliminaryefficacy and safety study of a new Budesonide-MMX(R) 9 mg extended-release tablets in patients with active left-sided ulcerative colitis.J Crohns Colitis. 2010;4:153–160.
67. Dotan I, Hallak A, Arber N, et al. Low-dose low-molecular weightheparin (enoxaparin) is effective as adjuvant treatment in active ulcera-tive colitis: an open trial. Dig Dis Sci. 2001;46:2239–2244.
68. Langmead L, Feakins RM, Goldthorpe S, et al. Randomized, double-blind, placebo-controlled trial of oral aloe vera gel for active ulcerativecolitis. Aliment Pharmacol Ther. 2004;19:739–747.
69. Mahmud N, McDonald GSA, Kelleher D, et al. Microalbuminuria cor-relates with intestinal histopathological grading in patients with inflam-matory bowel disease. Gut. 1996;38:99–103.
70. Madsen SM, Schlichting P, Davidsen B, et al. An open-labeled, random-ized study comparing systemic interferon-alpha-2A and prednisoloneenemas in the treatment of left-sided ulcerative colitis. Am J Gastro-enterol. 2001;96:1807–1815.
71. Floren CH, Benoni C, Willen R. Histologic and colonoscopic assessmentof disease extension in ulcerative colitis. Scand J Gastroenterol. 1987;22:459–462.
Mosli et al Inflamm Bowel Dis � Volume 20, Number 3, March 2014
574 | www.ibdjournal.org

72. Cobden I, al-Mardini H, Zaitoun A, et al. Is topical therapy necessary inacute distal colitis? Double-blind comparison of high-dose oral mesala-zine versus steroid enemas in the treatment of active distal ulcerativecolitis. Aliment Pharmacol Ther. 1991;5:513–522.
73. Danielsson A, Hellers G, Lyrenas E, et al. A controlled randomized trialof budesonide versus prednisolone retention enemas in active distalulcerative colitis. Scand J Gastroenterol. 1987;22:987–992.
74. Danielsson A, Löfberg R, Persson T, et al. A steroid enema, budesonide,lacking systemic effects for the treatment of distal ulcerative colitis orproctitis. Scand J Gastroenterol. 1992;27:9–12.
75. Hartmann F, Stein J; BudMesa-Study G. Clinical trial: controlled, open,randomized multicentre study comparing the effects of treatment on qualityof life, safety and efficacy of budesonide or mesalazine enemas in activeleft-sided ulcerative colitis. Aliment Pharmacol Ther. 2010;32:368–376.
76. Lemann M, Galian A, Rutgeerts P, et al. Comparison of budesonide and5-aminosalicylic acid enemas in active distal ulcerative colitis. AlimentPharmacol Ther. 1995;9:557–562.
77. Lofberg R, Ostergaard Thomsen O, Langholz E, et al. Budesonide versusprednisolone retention enemas in active distal ulcerative colitis. AlimentPharmacol Ther. 1994;8:623–629.
78. Porro GB, Prantera C, Campieri M, et al. Comparative trial of methyl-prednisolone and budesonide enemas in active distal ulcerative colitis.Eur J Gastroenterol Hepatol. 1994;6:125–130.
79. Prantera C, Viscido A, Biancone L, et al. A new oral delivery system for5-ASA: preliminary clinical findings for MMx. Inflamm Bowel Dis.2005;11:421–427.
80. Hanauer S, Schwartz J, Robinson M, et al. Mesalamine capsules fortreatment of active ulcerative colitis: results of a controlled trial. PentasaStudy Group. Am J Gastroenterol. 1993;88:1188–1197.
81. Auwerda JJA, Zijlstra FJ, Tak CJAM, et al. Ridogrel enemas in distalulcerative colitis. Eur J Gastroenterol Hepatol. 2001;13:397–400.
82. Bariol C, Meagher AP, Vickers CR, et al. Early studies on the safety andefficacy of thalidomide for symptomatic inflammatory bowel disease.J Gastroenterol Hepatol. 2002;17:135–139.
83. Hanauer SB, Robinson M, Pruitt R, et al. Budesonide enema for the treat-ment of active, distal ulcerative colitis and proctitis: a dose-ranging study.U.S. Budesonide enema study group. Gastroenterology. 1998;115:525–532.
84. Odze R, Antonioli D, Peppercorn M, et al. Effect of topical5-aminosalicylic acid (5-ASA) therapy on rectal mucosal biopsy morphol-ogy in chronic ulcerative colitis. Am J Surg Pathol. 1993;17:869–875.
85. Sandborn WJ, Tremaine WJ, Schroeder KW, et al. Cyclosporine enemasfor treatment-resistant, mildly to moderately active, left-sided ulcerativecolitis. Am J Gastroenterol. 1993;88:640–645.
86. Scheppach W, Sommer H, Kirchner T, et al. Effect of butyrate enemas on thecolonic mucosa in distal ulcerative colitis.Gastroenterology. 1992;103:51–56.
87. D’Argenio G, Cosenza V, Riegler G, et al. Serum transglutaminasecorrelates with endoscopic and histopathologic grading in patients withulcerative colitis. Dig Dis Sci. 2001;46:649–657.
88. Girlich C, Schacherer D, Jung EM, et al. Comparison between quanti-tative assessment of bowel wall vascularization by contrast-enhancedultrasound and results of histopathological scoring in ulcerative colitis.Int J Colorectal Dis. 2012;27:193–198.
89. Fiel M, Qin L, Suriawinita A, et al. Histologic grading of disease activityin chronic IBD: inter- and intra-observer variation among pathologistswith different levels of experience. Mod Pathol. 2003;16:118A.
90. Hefti MM, Chessin DB, Harpaz NH, et al. Severity of inflammationas a predictor of colectomy in patients with chronic ulcerative colitis.Dis Colon Rectum. 2009;52:193–197.
91. Gupta RB, Harpaz N, Itzkowitz S, et al. Histologic inflammation is a riskfactor for progression to colorectal neoplasia in ulcerative colitis: a cohortstudy. Gastroenterology. 2007;133:1099–1105.
92. Riley SA, Mani V, Goodman MJ, et al. Comparison of delayed-release5-aminosalicylic acid (mesalazine) and sulfasalazine as maintenancetreatment for patients with ulcerative colitis. Gastroenterology. 1988;94:1383–1389.
93. Creed TJ, Probert CSJ, Norman MN, et al. Basiliximab for the treatmentof steroid-resistant ulcerative colitis: further experience in moderate andsevere disease. Aliment Pharmacol Ther. 2006;23:1435–1442.
94. Ando T, Watanabe O, Furuta R, et al. Predictors of a response to cyclo-sporine or leukocyte removal therapy in patients with refractory ulcera-tive colitis. Dig Endosc. 2005;17:153–158.
95. Fukunaga K, Ohda Y, Hida N, et al. Placebo controlled evaluation ofXilei San, a herbal preparation in patients with intractable ulcerativeproctitis. J Gastroenterol Hepatol. 2012;27:1808–1815.
96. Kruis W, Kiudelis G, Racz I, et al. Once daily versus three times dailymesalazine granules in active ulcerative colitis: a double-blind, double-dummy, randomised, non-inferiority trial. Gut. 2009;58:233–240.
97. Lemmens B, Arijs I, Van Assche GA, et al. Correlation between theendoscopic and histological score in assessing the activity of ulcerativecolitis. Gastroenterology. 2011;140:S421–S422.
98. Matsumoto T, Kuroki F, Mizuno M, et al. Application of magnifyingchromoscopy for the assessment of severity in patients with mild tomoderate ulcerative colitis. Gastrointest Endosc. 1997;46:400–405.
99. Creed TJ, Norman MR, Probert CSJ, et al. Basiliximab (anti-CD25)in combination with steroids may be an effective new treatment forsteroid-resistant ulcerative colitis. Aliment Pharmacol Ther. 2003;18:65–75.
100. Feagan BG, Greenberg GR, Wild G, et al. Treatment of ulcerative colitiswith a humanized antibody to the alpha4beta7 integrin. N Engl J Med.2005;352:2499–2507.
101. Di Nardo G, Oliva S, Aloi M, et al. Effectiveness of a rectal infusion ofLactobacillus Reuteri ATCC 55730 in children with distal active ulcer-ative colitis. Dig Liver Dis. 2009;41S:S233.
102. Travis S, Yap LM, Hawkey C, et al. RDP58 is a novel and potentiallyeffective oral therapy for ulcerative colitis. Inflamm Bowel Dis. 2005;11:713–719.
103. Rubin DTHD, Hetzel JT, et al. Increased degree of histological inflam-mation predicts colectomy and hospitalisation in patients with ulcerativecolitis. Gastroenterology. 2007;132:A19.
104. Walmsley RS, Ayres RC, Pounder RE, et al. A simple clinical colitisactivity index. Gut. 1998;43:29–32.
105. Baron JH, Connell AM, Lennard-Jones JE, et al. Sulphasalazine andsalicylazosulphadimidine in ulcerative colitis. Lancet. 1962;1:1094–1096.
106. Lemmens B, Arijs I, Van Assche G, et al. Correlation between theendoscopic and histologic score in assessing the activity of ulcerativecolitis. Inflamm Bowel Dis. 2013;19:1194–1201.
107. Viera AJ, Garrett JM. Understanding interobserver agreement: the kappastatistic. Fam Med. 2005;37:360–363.
108. Landis JR, Koch GG. The measurement of observer agreement for cat-egorical data. Biometrics. 1977;33:159–174.
109. Fleiss JL, Cohen J. The equivalence of weighted kappa and the intraclasscorrelation coefficient as measures of reliability. Educ Psychol Meas.1973;33:613–619.
110. Kleer CG, Appelman HD. Ulcerative colitis: patterns of involvement incolorectal biopsies and changes with time. Am J Surg Pathol. 1998;22:983–989.
111. Hjelkrem M, Stauch C, Shaw J, et al. Validation of the non-alcoholicfatty liver disease activity score. Aliment Pharmacol Ther. 2011;34:214–218.
112. Rozario R, Ramakrishna B. Histopathological study of chronic hepatitisB and C: a comparison of two scoring systems. J Hepatol. 2003;38:223–229.
113. King CR, McNeal JE, Gill H, et al. Extended prostate biopsy schemeimproves reliability of Gleason grading: implications for radiotherapypatients. Int J Radiat Oncol Biol Phys. 2004;59:386–391.
114. Matutes E, Owusu-Ankomah K, Morilla R, et al. The immunologicalprofile of B-cell disorders and proposal of a scoring system for thediagnosis of CLL. Leukemia. 1994;8:1640–1645.
115. Kirshner B, Guyatt G. A methodological framework for assessing healthindices. J Chronic Dis. 1985;38:27–36.
116. Bessho R, Kanai T, Hosoe N, et al. Correlation between endocytoscopyand conventional histopathology in microstructural features of ulcerativecolitis. J Gastroenterol. 2011;46:1197–1202.
117. Familiari L, Strangio G, Consolo P, et al. Optical coherence tomographyevaluation of ulcerative colitis: the patterns and the comparison withhistology. Am J Gastroenterol. 2006;101:2833–2840.
118. Li CQ, Xie XJ, Yu T, et al. Classification of inflammation activity inulcerative colitis by confocal laser endomicroscopy. Am J Gastroenterol.2010;105:1391–1396.
119. Rubin D, Keyashian K, Bunnag A, et al. Correlation between clinical,endoscopic, and histologic disease activity in ulcerative colitis. Am JGastroenterol. 2012;107:S694.
Inflamm Bowel Dis � Volume 20, Number 3, March 2014 Histologic Evaluation of Ulcerative Colitis
www.ibdjournal.org | 575





























