Embed Size (px)
Citation preview

HHIITT
PPoolliiccyy CCoommmmiitttteeee
____________________
NNoovveemmbbeerr 77,, 22001122

#HITPolicy
AGENDA
HIT Policy Committee
November 7, 2012
9:30 a.m. to 2:45 p.m. [Eastern Time]
Omni Shoreham Hotel, 2500 Calvert Street, NW, Washington, DC 20008
9:30 a.m. CALL TO ORDER – MacKenzie Robertson, Office of the National Coordinator for
Health Information Technology
9:35 a.m. Remarks – Farzad Mostashari, National Coordinator
9:50 a.m. Review of the Agenda – Paul Tang, Vice Chair of the Committee
9:55 a.m. Update from CMS
– Robert Anthony, CMS
10:10 a.m. Final Walkthrough of Meaningful Use Stage 3 Request for Comment (RFC)
Meaningful Use – Paul Tang, Chair and George Hripcsak, Co Chair, MUWG
Quality Measures – David Lansky, Chair QMWG
Privacy and Security – Deven McGraw, Chair P&STT
ONC RFC – Farzad Mostashari, National Coordinator
12:10 p.m. Public Comment
12:25 p.m. LUNCH BREAK
1:15 p.m. Healtheway, Inc. and the eHealth Exchange
– Mariann Yeager, Interim Executive Director, Healtheway, Inc.
1:45 p.m. ONC Update
– Jodi Daniel, ONC
– Carol Bean, ONC
2:30 p.m. Public Comment
2:45 p.m. Adjourn


HIT Policy Committee
Members Organization
Chair
Farzad Mostashari HHS/ONC
Vice Chair
Paul Tang Palo Alto Medical Foundation
Members
David Bates Brigham and Women’s Hospital
Christine Bechtel National Partnership for Women & Families
Christopher Boone American Heart Association
Neil Calman The Institute for Family Health
Richard Chapman Kindred Healthcare
Arthur Davidson Denver Public Health Department
Connie Delaney University of Minnesota/School of Nursing
Paul Egerman Businessman/Entrepreneur
Judith Faulkner Epic Systems Corporation
Gayle Harrell Florida State Legislator
Charles Kennedy Aetna
David Lansky Pacific Business Group on Health
Deven McGraw Center for Democracy & Technology
Frank Nemec Gastroenterology Associates, Inc.
Marc Probst Intermountain Healthcare
Joshua Sharfstein Department of Health & Mental Hygiene, Maryland
Latanya Sweeney Harvard University
Scott White 1199 SEIU Training & Employment Fund
Federal Ex officios
Madhulika Agarwal Department of Veterans Affairs
Patrick Conway Centers for Medicare & Medicaid Services, HHS
Thomas Greig Department of Defense
Robert Tagalicod Centers for Medicare & Medicaid Services, HHS


HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 1
HIT Policy Committee
DRAFT
Summary of the October 3, 2012 Meeting
ATTENDANCE The following Committee members were in attendance at this meeting:
Farzad Mostashari
Paul Tang
Madhulika Agarwal
David Bates
Christine Bechtel
Christopher Boone
Neil Calman
Arthur Davidson
Connie White Delaney
Judith Faulkner
Thomas Greig
Gayle Harrell
Deven McGraw
Marc Probst
Joshua Sharfstein
Scott White
The following Committee members did not attend this meeting:
Richard Chapman
Patrick Conway
Paul Egerman
Charles Kennedy
David Lansky
Frank Nemec
Latanya Sweeney
Robert Tagalicod
KEY TOPICS
1. Call to Order
MacKenzie Robertson, Office of the National Coordinator (ONC), welcomed participants to the
41st Health Information Technology Policy Committee (HITPC) meeting. She reminded the
group that this was a Federal Advisory Committee (FACA) meeting being conducted with two
opportunities for public comment, and that a transcript will be posted on the ONC website. She
conducted roll call and reminded members to identify themselves for the transcript before
speaking. She turned the meeting over to HITPC Chair Farzad Mostashari.
2. Remarks

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 2
Farzad Mostashari, National Coordinator, gave extensive remarks on the recent news coverage of
HIT. He acknowledged that he was hurt by a Wall Street Journal opinion piece that referred to
ONC as a cheerleader. The piece reportedly referred to the few cost benefits and called HIT a
misguided effort and a waste of money, as well as criticized the government for not setting
standards for documentation of blood pressure and problem list. He reported that the academic
community and others had responded with evidence and opinions to the contrary. According to
Mostashari, 27 of the 31 published cost-benefit analyses show either cost reduction or health
benefits. Such studies have a narrow focus while HIT is an infrastructure and once in place can
do much with marginal costs. The real question should be how to implement HIT to maximize
health benefits and cost savings. He mentioned an article in the American Journal of Managed
Care that described a project in Minnesota to incorporate prior notification and authorization
requirements into clinical decision support. Findings showed improved health outcomes, savings
in providers’ time, and a decrease in unnecessary tests.
He continued his rebuttal, noting that although it was interesting that the WSJ encouraged more
regulation, its assertion about the lack of standards is untrue. In Stage 2, 42 distinct standards are
required. Next, he talked about a series of articles in The Washington Post and The New York
Times on billing. Data from the decade before the meaningful use program show an association
between the increase in severity of codes and their distribution across hospitals. According to
Mostashari, the articles imply that the incentive to adopt electronic health records (EHRs)
contributed to the increase in severity. He offered several alternative explanations, one being that
the more severe codes may have been the correct codes and not necessarily an indicator of fraud.
Only a few cost aspects were considered. Actually, the total costs for Medicare and Medicaid
were comparatively lower over the past few years. The purpose of EHRs is to refocus on
managing population costs. Coordination rather than documentation is the issue. There is a shift
away from payment on volume. Information is essential to manage care. Moreover, EHRs can be
useful tools for audit and enforcement. He pointed out that the Robert Wood Johnson
Foundation’s Open Notes project found that 99% of respondents wanted to continue to see their
providers’ notes. Patients can be made partners in detecting fraud.
He announced that for Stage 3, he wants the HITPC to look at policies around documentation of
patient care. There is lots of information being carried forward that may not be necessary. He
said that he wants to work with vendors and providers on functionality of EHRs to, for example,
look at audit logs and provider authentication and fraud. Stage 3 will focus on quality, outcomes
and population management. He referred to a recent article in the Annals of Internal Medicine
that describes increases in quality of care. He reminded the members that several years are
required for the results of change to be visible.
3. Review of the Agenda
Paul Tang, Vice Chairperson, reminded members that the meeting was dedicated to the request
for comment (RFC) for Stage 3 in which everything will be directed to improving outcomes. He
referred to the summary of the September 2012 meeting, which was circulated with the meeting
materials, and asked for a motion to approve the summary. The motion was made and seconded
and a voice vote resulted in unanimous approval.

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 3
Action item #1: The summary of the September 2012 HITPC meeting was
approved as circulated.
4. Meaningful Use Stage 3 Request for Comment (RFC) Input from the Meaningful Use
Workgroup
Tang, in his role as chair of the Meaningful Use Workgroup, explained that the workgroup
members and Michele Nelson, ONC, deliberated over the comments on the preliminary
recommendations presented to the HITPC in August and made a number of changes. He
reviewed the RFC schedule leading up to May 2013 when the HITPC is scheduled to transmit final Stage 3 recommendations to HHS. Once again, he reviewed the guiding principles:
• Supports new model of care (e.g., team-based, outcomes-oriented, population
management)
• Addresses national health priorities (e.g., NQS, Million Hearts)
• Broad applicability (since MU is a floor)
−Provider specialties (e.g., primary care, specialty care)
−Patient health needs
−Areas of the country
• Promotes advancement -- Not "topped out" or not already driven by market forces
• Achievable -- mature standards widely adopted or could be widely adopted by 2016
• Reasonableness/feasibility of products or organizational capacity
−Prefer to have standards available if not widely adopted
−Don’t want standards to be an excuse for not moving forward
Next, he referred members to the recommendations grid, which was both included in the
previously distributed meeting materials and shown on slides. The slides showed each objective
for Stages 1 and 2 and proposed for 3, as well as a recommended place holder for Stage 4. Red
items showed changes from Stage 1 to Stage 2, blue items from Stage 2 to Stage 3
recommendations and green items updates made following the August 1, 2012 HITPC meeting.
Beginning with the domain Improve Quality Safety, Efficiency and Reducing Health
Disparities, he methodically reviewed SGRP101 through SGRP121, concentrating on the
reasons for the most recent changes in Stage 3 recommendations (Stage 4 placeholders not listed
here):
101- CPOE for medications includes DDI checking for “never” combinations as
determined by an externally vetted list.
Certification Criteria: EHR must be able to consume an externally supplied list of
“never” DDIs, using RxNorm and NDF-RT standards along with a TBD DDI reactions
value set.
Certification Only for EPs
• EHRs must also have the ability to identify abnormal test results and track when
results are available.
• EHR must have the ability to transmit lab orders using the lab order and results
Interface guidelines produced by the S&I Framework Initiative.
RFC: Are the existing standards for laboratory orders adequate to support including this
certification criterion?
104 - Remove objective because topped out and ensure used in CQMs for disparities.

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 4
Certification criteria:
• Occupation and industry codes
• Sexual orientation, gender identity (optional fields)
• Disability status
Differentiate between patient reported and medically determined
Need to continue standards work
105 - Certification criteria only: Use of lab test results, medications, and vital signs (BP,
ht, wt, BMI), to support clinicians’ maintenance of up-to-date accurate problem lists.
Vendors utilize rules to help providers improve the problem list (e.g. Method for
Assigning Priority Levels ). System provides prompts about additions, edits, and
deletions for clinicians review and action.
RFC: How to incorporate into certification criteria for pilot testing?
106 - System provides prompts about additions, edits, and deletions for clinicians review.
RFC: How to incorporate into certification criteria for pilot testing
107 - System provides prompts about additions, edits, and deletions for clinicians review
and action.
113 - The 15 CDS interventions should include one or more interventions in each of the
following areas, as applicable to the EP's specialty:
• Preventative care (including immunizations)
• Chronic disease management (e.g., diabetes, hypertension, coronary artery
disease)
• Appropriateness of lab and radiology orders
• Advanced medication-related decision support* (e.g., renal drug dosing)
115 - EP Objective: Generate lists of patients for multiple specific conditions and present
near real-time (vs. retrospective reporting) patient-oriented dashboards to use for quality
improvement, reduction of disparities, research, or outreach reports. Dashboards are
incorporated into the EHR’s clinical workflow for the care coordinator or the provider. It
is actionable and not a retrospective report.
117 - 2) Mismatches (situations in which a provider dispenses a medication and/or dosing
that is not intended) are tracked and used for quality improvement.
Discussion of Revisions
Judy Faulkner asked about (slide 6) transitions with orders: What about transitions without
orders? Tang responded that the point is to encourage orders with all transitions and referrals; the
measure (denominator) is based on orders. Complaining about the difficult in reading the small
print, she inquired about (slide 11) maintaining the medication list. Tang explained, giving an
example that if an item appears on the problem list without a corresponding med (or vice versa),
an alert is generated. This is a spotting mechanism only. Faulkner said that (slide 14) the use of
the word “intervention” should be reconsidered. Tang replied that its use is consistent with the
NPRM language. Faulkner suggested “guidance.”

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 5
Gayle Harrell referred to slide 9 and proclaimed that some of the content in the placeholder could
be moved back to Stage 3. Most states have Prescription Drug Monitoring Programs (PDMP)
and all states have Medicaid formulary lists, both of which should be incorporated in and used in
Stage 3. Florida has been doing something similar since 2003, which resulted in very significant
cost savings. Available formularies should be used. Tang reported that according to the Health
Information Technology Standards Committee (HITSC), the necessary standards are not broadly
available. He agreed to investigate the suggestion about the Medicaid formularies.
Jodi Daniels, ONC, reported on a pilot project to make the Prescription Drug Monitoring
Program (PDMP) readily available to providers. Seven small pilots are underway. A toolkit will
be designed to make it easier to get to PDMP via EHRs. She invited members to send
suggestions to her.
Responding to a member’s concern about the absence of disability status on slide 10, Tang
pointed it out to her and said that the question is whether disability status should be patient
reported or medically reported or determined.
Marc Probst indicated that he was impressed with the detail of the recommendations. He
wondered whether the workgroup had categorized the requirements for the recommended
changes. Do we fully understand what we are asking? Tang referred to the principle of
reasonableness and feasibility and said that a matrix could be constructed to categorize the
objectives and criteria.
Tang moved to the domain Engage Patients and Families and explained each of the most recent
changes:
204A – MENU item: Automated Transmit: (builds on “Automated Blue Button Project”):
Before issue final recommendations in May, will review the result of Automated Blue
Button pilots.
204B - MENU: Provide 10% of patients with the ability to submit patient-generated
health information to improve performance on high priority health conditions, and/or to
improve patient engagement in care (e.g. patient experience, pre-visit information, patient
created health goals, etc.). This could be accomplished through semi-structured
questionnaires.
Based upon feedback from HITSC this can be a MENU item.
Need RFC language to describe the rational for this function (contributes to health
outcomes improvement, QI goals and care efficiency).
206 - Add language support: For the top 5 non-English languages spoken nationally,
provide 80% of patient-specific education materials in at least one of those languages
based on EP’s or EH’s local population, where publically available.
Discussion
Harrell talked about being concerned with the privacy and security of downloads. Is the goal for
the patient to be able to download a record and incorporate it into a PHR for transmission and if

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 6
so, what is the physician’s liability? Tang pointed out that provider-to-provider transmission is
covered under HIPAA. When a patient transmits her data to someone, she is responsible. Joy
Pritts, ONC, confirmed that once information is transmitted to the patient, it becomes the
responsibility of the patient. Discussion ensured. Someone commented on the distinction
between a patient giving directions on transmission once or at specific visits. Pritts reported that
she is working with others in HHS to determine the best approach to this new policy issue.
Considering HIPAA and HITECH, and the NPRM on the latter and based on the existing rule,
there is no restriction on the format in which the record is provided. In some states, laws may
restrict transmission. She indicated a lack of clarify as to whether the provider’s liability ends
with the receipt of permission to transmit. It is possible that the provider’s liability may extend to
the receipt of the transmitted information by the other party. Harrell said that people are very
concerned with the liability issue. Pritts noted that concerns commonly surface with the
introduction of new technology. Tang acknowledged that the issue should be explored in the
RFC. Christine Bechtel talked about a recommendation that patients receive a warning prior to
confirmation of a download. A pilot project is underway on auto-transmission of summaries.
Tang said that the RFC preamble will first describe what is known, followed by the questions.
Faulkner said that it is tricky to determine to what the patient has agreed. Difficulties include the
education of individual clinicians, the need for signature pads, paper overload and that too much
authorization impedes patient access to services. Pritts reported that a pilot on obtaining e-
consent will launch this month, using tablets and videos. Faulkner expressed concern about a
complicated process with unnecessary steps.
George Hripcsak, Co-Chair, Meaningful Use Workgroup, presented the most recent changes to
the recommendations for the Care Coordination domain in Stage 3.
302 - SC&C Recommendation: Standards work needs to be done to adapt and further
develop existing standards to define the nature of reactions for allergies (i.e. severity).
303 - Certification Criteria: Inclusion of data sets being defined by S&I Longitudinal
Coordination of Care WG, which are expected to complete HL7 balloting for
inclusion in the C-CDA by Summer 2013:
1) Consultation Request (Referral to a consultant or the ED)
2) Transfer of Care (Permanent or long-term transfer to a different facility, different
care team, or Home Health Agency)
304 - Certification Criteria: Develop standards for a shared care plan, as being
defined by S&I Longitudinal Coordination of Care WG. Some of the data elements
in the shared care plan overlap content represented in the CDA. Adopt standards for
the structured recording of other data elements, such as patient goals and related
interventions.
305 - Certification Criteria: Include data set defined by S&I Longitudinal
Coordination of Care WG and expected to complete HL7 balloting for inclusion in
the C-CDA by Summer 2013: Shared Care Encounter Summary (Consultation
Summary, Return from the ED to the referring facility, Office Visit)

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 7
\
3308 – 308 - IE workgroup recommendation (IF provider directories exist and are
operational):
EH OBJECTIVE: The EH/CAH will send electronic notification of a significant
healthcare event in a timely manner to key members of the patient’s care team, such
as the primary care provider, referring provider or care coordinator, with the
patient’s consent if required.
EH MEASURE: For 10% of patients with a significant healthcare event (arrival at
an Emergency Department (ED), admission to a hospital, admission to a long term
care facility, discharge from an ED or hospital, or death) , EH/CAH will send an
electronic notification to at least one key member of the patient’s care team, such as
the primary care provider, referring provider or care coordinator, with the patient’s
consent if required, within two hours of when the event occurs.
Discussion
Someone brought up the issue of what an EHR system can do for a practice beyond improving
care for the individual patient. Hripcsak acknowledged that the emphasis to date has been the
patient. But some functions, such as generating lists by conditions, can be used for population
management. Lists can be used for action. To do something such as examine a pattern of
unexpected ED visits or hospitals admissions will require more advanced analytics.
David Bates talked about a survey that his organization conducted for the National Quality
Forum (NQF). Currently, the use of EHRs is very primitive. Tools are needed to enable more
comprehensive analyses, but they have yet to be developed. Someone suggested adding a
question to the RFC to that effect. Tang indicated that a question on dashboards may cover it.
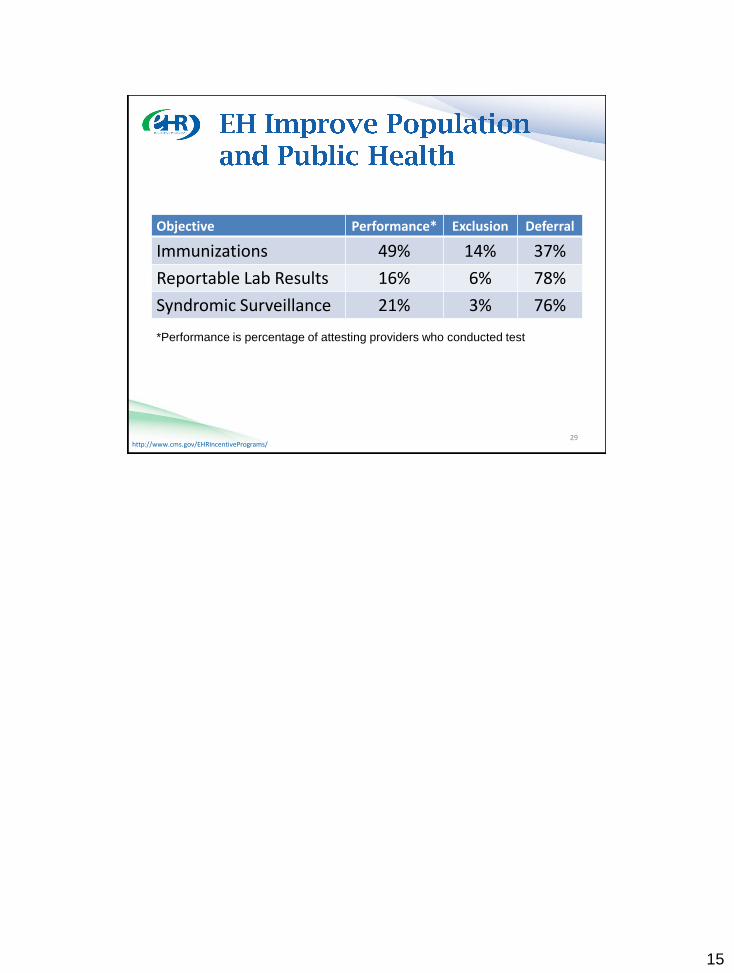
Hripcsak continued with the domain of Population Health. Only a minor change was made to
the threshold in 405.
Discussion
Joshua Sharfstein suggested having the capability to receive an urgent message from the state
health agency. He referred to a pilot project in Maryland in which this was successfully done.
Hripcsak replied that the workgroup examined ways to receive alerts for specific patients in stage
4. However, the workgroup members had not thought about a general message. Art Davidson
said that such a concept was embedded in slide 37. The Centers for Disease Control and
Prevention (CDC) sends health alert messages. Sharfstein pointed out a need for something
below the level of national messages. Davidson said standards for that function are not currently
available but that the Direct provider directory can possibly be used for messages.
Tang said that the recommendations will be revised per the comments.
5. Meaningful Use Stage 3 Request for Comment Input from the Information Exchange
Workgroup
Larry Garber, Member, Information Exchange Workgroup, presented three recommendations:
Query for Patient Information (EHR Certification Criteria) Proposed Criteria for the next
phase of EHR Certification:

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 8
1. The EHR must be able to query another entity* for outside records and respond to such
queries. This query may consist of three transactions:
• Patient query based on demographics and other available identifiers, as well as the
requestor and purpose of request.
• Query for a document list based for an identified patient
• Request a specific set of documents from the returned document list *the outside entity
may be another EHR system, a health information exchange, or an entity on the NwHIN,
for example.
2. When receiving in inbound patient query, the EHR must be able to:
• Tell the querying system whether patient authorization is required to retrieve the
patient’s records and where to obtain the authorization language**. (E.g. if authorization
is already on file at the record-holding institution it may not be required).
• At the direction of the record-holding institution, respond with a list of the patient’s
releasable documents based on patient’s authorization
• At the direction of the record-holding institution, release specific documents with
patient’s authorization
3. The EHR initiating the query must be able to query an outside entity** for the
authorization language to be presented to and signed by the patient or her proxy in order
to retrieve the patient’s records. Upon the patient signing the form, the EHR must be able
to send, based on the preference of the record-holding institution, either:
• A copy of the signed form to the entity requesting it
• An electronic notification attesting to the collection of the patient’s signature
Query Provider Directory (EHR Certification Criteria)
Proposed Criteria for the next phase of EHR Certification: The EHR must be able to
query a Provider Directory external to the EHR to obtain entity-level addressing
information (e.g. push or pull addresses).
Request for Comment for EHR Certification with these additional questions:
• Are there sufficiently mature standards in place to support this criteria? What
implementation of these standards are in place and what has the experience been?
Data Portability Between EHR Vendors (RFC) Request for Comment for EHR
Certification:
• What criteria should be added to the next phase of EHR Certification to further facilitate
healthcare providers’ ability to switch from using one EHR to another vendor’s EHR?
Discussion
Deven McGraw acknowledged her support for including the Information Exchange Workgroup’s
recommendations in the RFC. She assured the committee members that the Privacy and Security
Tiger Team will examine the use cases prior to the finalization of the recommendations.
6. Meaningful Use Stage 3 Request for Comment Input from the Privacy and Security
Tiger Team
McGraw, Co-Chair, Privacy and Security Tiger Team, presented questions in three areas:
The Health IT Policy Committee has already recommended that provider users of EHRs
be authenticated at National Institute for Standards and Technology (NIST) “Level of

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 9
Assurance” (LoA) 3 for remote access (e.g., more than user name and password required
to authenticate) by Stage 3 of MU.
1. Should the next phase of EHR certification criteria include capabilities to authenticate
provider users at LoA 3? If so, how would the criterion/criteria be described?
2. What is an appropriate MU measure for ensuring provider users authenticate at LoA 3
for remote access? Under what other circumstances (if any) should authentication at LoA
3 be required to meet MU?
3. NIST establishes guidance for authentication of individuals interacting remotely with
the federal government. What, if any, modifications to this guidance are recommended
for provider EHR users?
In Stages 1 and 2 of MU, EPs/EHs/CAHs are required to attest to completing a HIPAA
security risk assessment (and addressing deficiencies), and, in stage 2, attesting to
specifically addressing encryption of data at rest in CEHRT.
1.What, if any, security risk issues (or HIPAA Security Rule provisions) should be
subject to MU attestation in Stage 3?
2. For example, the requirement to make staff aware of the HIPAA Security Rule and to
train them on Security Rule provisions is one of the top 5 areas of Security Rule
noncompliance identified by the HHS Office for Civil Rights over the past 5 years. In
addition, entities covered by the Security Rule must also send periodic security reminders
to staff. The Tiger Team is considering requiring EPs/EHs/CAHs to attest to
implementing Security Rule provisions regarding staff outreach & training and sending
periodic security reminders; we seek feedback on this proposal.
Accounting for disclosures, surveillance for unauthorized access or disclosure and
incident investigation associated with alleged unauthorized access is a responsibility of
organizations that operate EHRs and other clinical systems. Currently the 2014 Edition
for Certified EHR Technology specifies the use of ASTM E-2147-01. This specification
describes the contents of audit file reports but does not specify a standard format to
support multiple-system analytics with respect to access. The Tiger Team requests
feedback on the following questions:
1. Is it feasible to certify the compliance of EHRs based on the prescribed standard?
2. Is it appropriate to require attestation by meaningful users that such logs are created
and maintained for a specific period of time?
3. Is there a requirement for a standard format for the log files of EHRs to support
analysis of access to health information access multiple EHRs or other clinical systems in
a healthcare enterprise?
4. Are there any specifications for audit log file formats that are currently in widespread
use to support such applications?
Discussion
Members had no comments. McGraw invited members to attend the virtual hearing on patient
identification and authentication on October 29.
7. Public Comment
Robertson announced that comments were limited to three minutes

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 10
Kelly Emerick of the Secure ID Coalition commented that she supported requiring LoA 3, but
that she preferred LoA 3 or higher. How do we know records are sent and received as intended?
She encouraged the HITPC to take a hard look at how to ensure secure transmission.
Joanne Lynn, Altarum Institute, complained about the movement of care plan from Stage 3 to
Stage 4 (slide 13) without explanation. A care plan is the most important aspect of care for the
seriously ill. She declared that care plan is not controversial and said that she had a similar issue
with slide 13 and advance care plan. Patients could carry a PDF with their advance directives.
Patients need mobility of this information. She probed for an explanation from Tang. Robertson
thanked her for her comments.
Amari, self-identified as both a patient and of the American Medical Association, thanked ONC
for providing two comment opportunities. Referring to p. 11, she acknowledged that as a
consumer she would not necessarily notice errors in her record. How would this happen? Would
the doctor ask, “Did I make an error?” HIPAA already allows for corrections. Regarding
certification, she asked for protection against misuse. She reported that she had previously
submitted comments to CMS requesting an evaluation of the meaningful use program. Providers
could be queried about the hardest measures to obtain. The requirements for meeting objectives
should be scaled back to allow more flexibility.
Diane Jones, American Hospital Association, commented on the timing of Stage 3. She
recommend a delay in the RFC release date, which is scheduled to occur at the same time that
many providers are focused on attestation for Stage 1 or implementing Stage 2. She
recommended extension of the comment period to 60 days.
Faulkner observed that it would be beneficial for the members themselves to have a time to
discuss public comments. Additionally, meeting materials should be distributed on a set schedule
in order to ensure sufficient preparation time. She also wondered about Stage 4: How would it be
funded and how would it work? She went on to say that a single national standard for
immunizations is needed. Robertson responded that she intended to institute administrative
meetings to deal with meeting issues.
Harrell had additional comments. She requested information on the outcomes of the many ONC
pilots mentioned during the meeting. Tang told her that the provision of such information was
the purpose of the monthly ONC updates. She declared that she wanted a list and summary of the
pilot projects. Neil Calman inquired about the criteria for applying for and selecting pilot sites.
Daniels responded that the pilots are often carried out via contracts. Contractors establish the
criteria (with ONC approval) and select the sites. She indicated that she is open to suggestions
for increasing transparency.
Robertson introduced new member Chris Boone, American Heart Association, who then
mentioned several consumer projects undertaken by his organization.
8. Meaningful Use Stage 3 Request for Comment Input from the Quality Measures
Workgroup

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 11
James Walker, member, Quality Measures Workgroup, prefaced his recommendations by
explaining that the workgroup had tried to rethink the purpose and form of quality measures. The
measures should leverage data routinely captured in the EHR and PHR during the process of
care. Support for clinical quality measure (CQM) calculations should be flexible and adaptive to
future requirements, which may include new measures or changes to measure definitions at
minimal cost. Providers should be able to configure the CQM calculation to use data elements
appropriate to local workflow. An end goal is to shift quality measurement and reporting from
sampled retrospective, human chart reviews and accounting records to concurrent, machine-
automated improvement support while recognizing that there will remain a place for human
abstracted quality measurement. He recommended the following questions for the RFC:
• Is a shift away from retooling legacy paper-based CQMs in exchange for designing e-
CQMs de novo a reasonable and desirable course of action?
• Is there an evidence basis for clinical population management platform use? Is there a
business case?
• What are the technological challenges to widespread release and adoption? Can the
HITPC encourage technology in this area without being prohibitively prescriptive?
Walker said that to leverage CQM innovation from health systems and professional societies, the
workgroup discussed a proposal to allow EPs or EHs to submit a locally developed CQM as a
menu item in partial fulfillment of requirements (in lieu of one of the existing measures specified
in the meaningful use program). Health care organizations choosing this optional menu track
would be required to use a brief submission form that describes some of the evidence that
supports their measure and how the measure was used in their organization to improve care. Two
non-mutually exclusive approaches are proposed. A conservative approach might allow
“Certified Development Organizations,” to develop, release and report proprietary CQMs. An
alternate approach might open the process to any EP or EH but constrain allowable e-CQMs via
measure design software (e.g., Measure Authoring Tool). The RFC question is what constraints
should be in place.
Discussion
Tang said that there is potential for better tools. The source of data can be reconsidered and the
burden of data collection reduced.
Harrell talked about making measures appropriate and meaningful to individual providers; the
specialties have not been addressed. She wondered who would vet new measures, a process that
would require the time and participation of many interest groups.
Jessie James, ONC, reported that ONC staff had located good measures used by DoD and VA
that did not go through the NQF process. Vendors have commented on their interest in making
measures relevant to specialties and subspecialties. A process for vetting has yet to be defined.
He suggested soliciting comments on a vetting structure. Walker said that both testing and
vetting must be done.
Kevin Larsen, ONC, pointed out that the need for a question on certification: How do products
enable development of new measures?

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 12
McGraw referred to a request by the Agency for Healthcare Research and Quality (AHRQ) for
comments on quality measures. An ONC staff member said that ONC and AHRC staffs were
working together. Comments are expected to be synthesized by January. A report will be made
available to the HITPC.
Harrell said that as the payment model changes, quality measures will become more important.
They need to be specific to the individual provider.
9. CMS Update Elizabeth Holland, CMS, presented the monthly update. September 2012 data are very
preliminary. Registration is up, the largest number to date. Forty-nine states are launched for
Medicaid and Puerto Rica recently launched. Hawaii is the 50th
state. CMS staff is trying to
educate providers on Stage 2 and conduct outreach for Stage 1. The latter has been much
affected by a restricted travel budget. The goal is for everyone to be a meaningful user. Twelve
hospitals came in October 1 for their second year. Regarding attestation, there was a slight
increase overall from August. 94,782 EPs have attested, 94,538 successfully. 1,895 hospitals
have successfully attested. Staff plans more webinars on Stage 2 and is working on FAQs and
with ONC for technical specification sheets for vendors. A guidance on how to apply for
payment adjustment hardship exceptions is forthcoming.
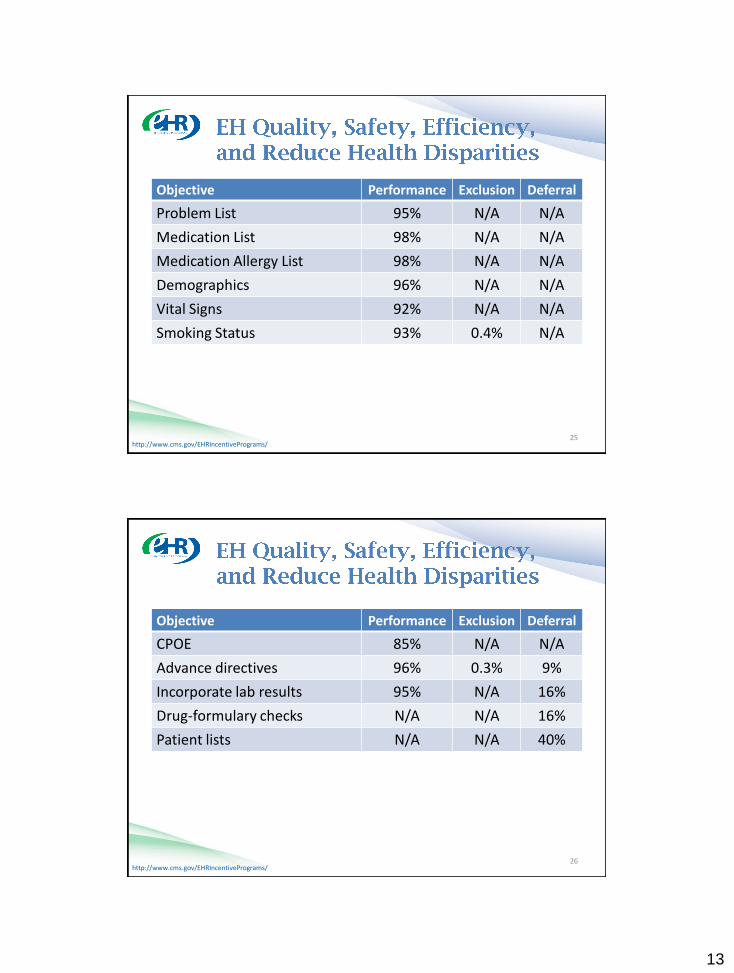
Regarding the objectives, on average all thresholds were greatly exceeded, but every threshold
has some providers on the borderline. Drug formulary, immunization registries and patient list
are the most frequently selected menu objectives for EPs. EHs most frequently select advance
directives, drug formulary and clinical lab test results. Least frequently selected menu objectives
for hospitals were transition of care and reportable lab results and for EPs transition of care
summary and patient reminders were the least frequently selected. There was little difference
among specialties in performance, but exclusions and deferrals varied.
Q&A
Harrell complained about the absence of percentages on penetration and participation in
Holland’s report. She emphasized that she wanted percentages, not simply pie charts.
10. ONC Update
Daniel informed the group that there is one vacancy on the HITPC and several on the HITSC.
She repeated an earlier comment that a website will be used to solicit members for new
workgroups on patient engagement. She hopes to get more diverse workgroup memberships.
Staff is updating the consumer health strategy, security and safety sections of the ONC strategic
plan. FCA, FCC and ONC staffs are preparing a congressionally mandated report on risk-based
management. Public hearings will be held. Their announcements will be published in Federal
Register. The Upcoming Health 2.0 conference will be another opportunity to obtain feedback on
that topic. ONC awarded a contract to RAND to evaluate risk management of HIT errors.
Another contract was awarded to design check lists. CQM specifications are in process.
Daniel repeated comments that she made earlier in the meeting (agenda item #4). ONC is
examining how HIT can contribute to the prevention of prescription drug abuse. PDMP are a

HIT Policy Committee 10-03-2012 DRAFT Meeting Summary Page 13
great resource at the state level, but providers do not routinely use them. ONC awarded a
contract to look at standards and policy to increase timely use by providers, emergency
departments and pharmacies. The contractor convened a workgroup, which generated
recommendations. The recommendations are being piloted in seven sites in Indiana, Michigan,
Washington and another state. A tool kit on the use of PDMP is being designed. ONC is open to
suggestions. She invited members to let her know on which projects they wish additional
information.
Q&A
Harrell expressed her support for the use of PDMP. She referred to a hearing on safety in 2011
and said that she wanted the hearing report. Daniels responded that ONC will publish its safety
and strategic plans and invite comments. She offered to make a presentation to the committee or
a workgroup upon request. She reminded Harrell that all hearings are open to the public. Tang
said that he wanted a report made to the HITPC on safety and the update to strategic plan.
11. Public Comment
Robin Raiford, The Advisory Board Company, reported that the CIO of a hospital in Joplin,
Missouri, told her that he qualified for meaningful use in spite of the tornado.
SUMMARY OF ACTION ITEMS:
Action item #1: The summary of the September 2012 HITPC meeting was
approved as circulated.
Meeting Materials
Agenda
Summary of September 2012 meeting
Presentations slides: Privacy and Security Tiger Team, Meaningful Use Workgroup, Information
Exchange Workgroup, Quality Measures Workgroup, ONC, CMS
Meaningful Use Workgroup RFC approach and questions


1
http://www.cms.gov/EHRIncentivePrograms/
HIT Policy Committee
October 2012
http://www.cms.gov/EHRIncentivePrograms/ 2

2
http://www.cms.gov/EHRIncentivePrograms/ 3
http://www.cms.gov/EHRIncentivePrograms/ 4

3
http://www.cms.gov/EHRIncentivePrograms/ 5
http://www.cms.gov/EHRIncentivePrograms/ 6 For final CMS reports, please visit:
http://www.cms.gov/EHRIncentivePrograms/56_DataAndReports.asp

4
http://www.cms.gov/EHRIncentivePrograms/ 7
http://www.cms.gov/EHRIncentivePrograms/ 8
For final CMS reports, please visit:
http://www.cms.gov/EHRIncentivePrograms/56_DataAndReports.asp

5
http://www.cms.gov/EHRIncentivePrograms/ 9
http://www.cms.gov/EHRIncentivePrograms/ 10

6
http://www.cms.gov/EHRIncentivePrograms/
19.04% 19.04%
60.75% 0.7979
Eligible Hospitals
5,011 Total
4,057 Total Registered
3,044 Paid
11
http://www.cms.gov/EHRIncentivePrograms/
41.90%
39.94%
18.16%
Registered Eligible Professionals
521,600 Total EPs
Registered Medicare EPs (208,331)
Registered Medicaid EPs (94,741)
12

7
http://www.cms.gov/EHRIncentivePrograms/
72.63%
15.82%
11.54%
Paid Eligible Professionals
521,600 Total EPs
Medicare EPs (82,535)
Medicaid EPs (60,208)
13
http://www.cms.gov/EHRIncentivePrograms/
• Over 60% of all eligible hospitals have received an
EHR incentive payment for either MU or AIU •Over 60% have made a financial commitment to put an EHR
in place
• Approximately 22% or 1 out of every 5 Medicare
EPs are meaningful users of EHRs
• Approximately 1 out of every 4 Medicare and
Medicaid EPs have made a financial commitment to an
EHR
• 58% of Medicare EPs receiving incentives are
specialists (non primary care) 14

8
http://www.cms.gov/EHRIncentivePrograms/ 15
Providers Paid Oct-12 LTD
Medicare EPs – [ESTIMATED] 5,250 87,750
Medicaid EPs (AIU + MU) [ESTIMATED] 3,800 64,000
Medicaid/Medicare Hospitals** [ESTIMATED] 400 4,600
Total Number of Providers Paid 9,450 156,350
http://www.cms.gov/EHRIncentivePrograms/ 16
Payments Oct-12 LTD
Medicare EPs [ESTIMATED] $95,000,000 $1,509,000,000
Medicaid EPs [ESTIMATED] $70,000,000 $1,313,000,000
Medicaid/Medicare Hospitals (Medicare Pymt) [ESTIMATED] $340,000,000 $2,905,000,000
Medicaid/Medicare Hospitals (Medicaid Pymt) [ESTIMATED] $140,000,000 $2,442,000,000
Total $645,000,000 $8,358,000,000

9
http://www.cms.gov/EHRIncentivePrograms/ 17
http://www.cms.gov/EHRIncentivePrograms/
• On average all thresholds were greatly exceeded, but
every threshold had some providers on the borderline
• Drug formulary, immunization registries and patient list
are the most popular menu objectives for EPs
• Advance Directives, Drug Formulary, and Clinical Lab Test
Results for hospitals
• Transition of care summary and patient reminders were
the least popular menu objectives for EPs
• Transition of Care and Reportable Lab Results for hospitals
• Little difference between EP and hospitals
• Little difference among specialties in performance, but
differences in exclusions and deferrals
18

10
http://www.cms.gov/EHRIncentivePrograms/
This data-only analysis shows our earliest
adopters who have attested, but does not inform
us on barriers to attestation.
At the time of the analysis
• 105,750 EPs had attested
• 105,514 Successfully
• 236 Unsuccessfully (208 EPs have resubmitted
successfully)
• 2,238 Hospital had attested
• All successfully
19
http://www.cms.gov/EHRIncentivePrograms/ 20
Objective Performance Exclusion Deferral
Problem List 97% N/A N/A
Medication List 97% N/A N/A
Medication Allergy List 97% N/A N/A
Demographics 91% N/A N/A
Vital Signs 91% 9% N/A
Smoking Status 90% 0.4% N/A

11
http://www.cms.gov/EHRIncentivePrograms/ 21
Objective Performance Exclusion Deferral
CPOE 83% 17% N/A
Electronic prescribing 81% 21% N/A
Incorporate lab results 92% 4% 36%
Drug-formulary checks N/A 14% 15%
Patient lists N/A N/A 25%
Send reminders to patients 61% 0.5% 81%
http://www.cms.gov/EHRIncentivePrograms/ 22
Objective Performance Exclusion Deferral
E – Copy of Health Information 97% 70% N/A
Office visit summaries 79% 2% N/A
Patient Education Resources 49% N/A 50%
Timely electronic access 72% 1% 67%

12
http://www.cms.gov/EHRIncentivePrograms/
23
Objective Performance Exclusion Deferral
Medication reconciliation 90% 3% 54%
Summary of care at transitions 90% 3% 84%
http://www.cms.gov/EHRIncentivePrograms/ 24
Objective Performance* Exclusion Deferral
Immunizations 35% 44% 20%
Syndromic Surveillance 6% 26% 69%
*Performance is percentage of attesting providers who conducted test
13
http://www.cms.gov/EHRIncentivePrograms/ 25
Objective Performance Exclusion Deferral
Problem List 95% N/A N/A
Medication List 98% N/A N/A
Medication Allergy List 98% N/A N/A
Demographics 96% N/A N/A
Vital Signs 92% N/A N/A
Smoking Status 93% 0.4% N/A
http://www.cms.gov/EHRIncentivePrograms/ 26
Objective Performance Exclusion Deferral
CPOE 85% N/A N/A
Advance directives 96% 0.3% 9%
Incorporate lab results 95% N/A 16%
Drug-formulary checks N/A N/A 16%
Patient lists N/A N/A 40%

14
http://www.cms.gov/EHRIncentivePrograms/
27
Objective Performance Exclusion Deferral
E – copy of health information 96% 69% N/A
E – copy of discharge Instructions
95% 65% N/A
Patient education resources 73% N/A 58%
http://www.cms.gov/EHRIncentivePrograms/
28
Objective Performance Deferral
Medication reconciliation 85% 72%
Summary of care at transitions 83% 91%
15
http://www.cms.gov/EHRIncentivePrograms/
Objective Performance* Exclusion Deferral
Immunizations 49% 14% 37%
Reportable Lab Results 16% 6% 78%
Syndromic Surveillance 21% 3% 76%
29
*Performance is percentage of attesting providers who conducted test


1
eHealth Exchange Update: HIT Policy Committee November 7, 2012
Mariann Yeager Interim Executive Director
Healtheway, Inc. 703-623-1924
1
Discussion Topics
• Context
• eHealth Exchange
• Transition
• Data Use and Reciprocal Support Agreement (DURSA)
• Healtheway
• Discussion
2

2
eHealth Exchange
• eHealth Exchange: A community of exchange partners who share information under a common trust agreement, common set of technical and policy requirements and testing process
• Based upon national standards, NwHIN and others
• Started as an NwHIN program initiative (NwHIN Exchange); production since 2009
• Transitioned to public-private partnership, operated by Healtheway and rebranded as eHealth Exchange
• Healtheway: Non-profit organization chartered to support the eHealth Exchange and focused on cross-industry collaboration to advance HIE implementation
3
eHealth Exchange Strategic Road Map
Initial Rollout
(2009 – 2011)
Mature, Grow, Scale
2012-2013
Sustainability
2014
Phase 1 Phase 2 Phase 3
• Early adopters • Federal business cases • Shared infrastructure • Early lessons learned • Success / viability • ONC program pilot
concludes • Production ramps up
• Transition to public-private model
• Grow participation and transactions
• Refine and scale • Expand value cases • Align with national
strategy • Implement
sustainability model
• Continued growth in participant and transactions
• Revenue model sustains operations
• Nationwide deployment
• Interoperable exchange among private entities
11/6/2012
4

3
eHealth Exchange Vision / Mission
• Vision
• To serve as a critical element of the nationwide health information infrastructure; and
• To improve the health and welfare of all Americans through health information exchange that is trusted, that scales, and enhances quality of care and health outcomes by supporting comprehensive longitudinal health records.
• Mission
• To expand trusted, secure and interoperable exchange of health information across the nation by providing shared governance and necessary shared service to public and private organizations who wish to interconnect as a network of networks.
5
• Alabama One Health Record
• Centers for Medicare and Medicaid Services (CMS)
• Childrens’ Hospital of Dallas
• Community Health Information Collaborative (CHIC)
• Conemaugh Health System
• Department of Defense (DOD)
• Department of Veterans Affairs
• Dignity Health
• Douglas County Individual Practice Association (DCIPA)
• Eastern Tennessee Health Information Network (etHIN)
• EHR Doctors
• HealthBridge
• HEALTHeLINK (Western New York)
• Idaho Health Data Exchange
• Inland Northwest Health Services (INHS)
• Kaiser Permanente
• Lancaster General Health
eHealth Exchange Participants • Marshfield Clinic
• Medical University of South Carolina (MUSC)
• MedVirginia
• MultiCare Health System
• National Renal Administrators Association (NRAA)
• New Mexico Health Information Collaborative (NMHIC)
• North Carolina Healthcare Information and Communications Alliance, Inc. (NCHICA)
• OCHIN
• Quality Health Network
• Regenstrief Institute
• Social Security Administration (SSA)
• South Carolina Health Information Exchange (SCHIEx)
• South East Michigan Health Information Exchange (SEMHIE)
• Strategic Health Intelligence
• University of California, San Diego
• Utah Health Information Network (UHIN)
• Wright State University 6

4
• Alere / Wellogic • ApeniMED • Aurion • Axolotl • CareEvolution • CGI • Cogon • CONNECT • CSC • Epic • Harris • K Force • MEDecision • MedFX
Technology Solution Providers who Support eHealth Exchange
• Medicity
• Mirth
• MobileMD
• Northrop Grumman
• OneHealthPort
• Orion Health
• SAIC
• Talis
• Thompson
• Vangent
• Wright State Research Institute 7
Value Proposition
Value Proposition
Implement once,
exchange with many
Recognition as part of trusted
community
Expanded connectivity
Cost effective and efficient
Enforced compliance
and accountability
Functional and scalable
shared services
11/6/2012
8

5
Transition Status
• Healtheway assumed responsibility for operations, effective 10/1/12
• Onboarding process (i.e. receipt / processing of applications)
• Participation Testing (facilitated by CCHIT as testing body)
• Digital certificates
• Service registry
• Coordinating Committee support
• DURSA and operating policies and procedures
• Implementation specifications
• Preparing to pilot and launch revamped testing program with CCHIT
• Implementing growth and sustainability strategy 9
Prior State / Current State
Previously
• ONC initiative - NwHIN Exchange
• Coordinating Committee*
• DURSA*
• Onboarding & testing facilitated by ONC
• Operations supported / funded by ONC
• Services provided to participants for free
Today
• Public-private initiative - eHealth Exchange
• Coordinating Committee*
• DURSA*
• Testing facilitated by testing body designated by CC
• Operations supported/ funded by Healtheway
• Participants begin paying for services in future 10
* Unchanged

6
Exchange Trust Framework Unchanged
• DURSA remains in full force and effect
• Coordinating Committee retains all authorities as specified in the DURSA
• Healtheway board does not have any oversight responsibilities with respect to Exchange, but will operate under an agreement with the Coordinating Committee
11
12
eHealth Exchange CC – Healtheway Board Functions
Federal Participants
State Participants
Private Participants
eHealth Exchange Coordinating Committee
Exec Director
Healtheway Board
3 CC Reps
Up to 9 Elected
Members
• Oversee eHealth Exchange participation • Approve specs, test guides, policies • Enforce DURSA • Handle disputes / breaches • Approve changes to DURSA • Designate Healtheway to support
Exchange operations
• Assure corporation is effectively supporting and providing value to its customers (e.g. Exchange, etc.)
• Make financial decisions (e.g. annual budget, membership program, funding, etc.)
• Engage & oversee Executive Director / staff • Guide business strategy and oversee business
(e.g. programs, marketing, partnerships, etc.) • Set strategic direction – HIE implementation
collaborative efforts
Appoint
• Any organization that wishes to be a part of Healtheway community collaboration (e.g. HIE, vendor, payer, non-profit, academic institution, etc.)
Government
Liaisons

7
Revamped eHealth Exchange Participation Testing Program • Moves testing from being an internal function of eHealth
Exchange to accrediting testing lab
• Consistent with national strategy
• Raised bar significantly – with focus on interoperability testing
• Streamlined, efficient and scalable
• Significantly less costly for eHealth Exchange to support
• Cost-effective for technology providers and applicants
• eHealth Exchange participating testing required as a condition of joining the eHealth Exchange
For more details regarding the strategy and test guides:
• http://exchange-iwg.wikispaces.com/
11/6/2012
13
Healtheway Mission
• To provide the infrastructure to support the safe and secure exchange of data which eHealth Exchange Participants use to further their respective missions to: • Improve clinical decision making and coordination, quality and
affordability of care;
• Support meaningful use;
• Enhance disease surveillance, support preparedness and routine public health missions to improve public health; and
• Realize efficiencies and expedite provision of funding and services to individuals to support their care and well-being.
• To support programs for Healtheway corporate members to advance implementation of HIE: • Testing program announced and will be launched with EHR HIE
Interoperability Workgroup 14

8
DATA USE AND RECIPROCAL SUPPORT AGREEMENT
Overview and Lessons Learned
15
Data Use and Reciprocal Support Agreement • A comprehensive, multi-party trust agreement that will be signed by
all eligible entities who wish to exchange data among eHealth Participants
• Eliminates the need for “point-to-point” agreements
• Requires signatories to abide by common set of terms and conditions that establish Participants’ obligations, responsibilities and expectations
• The obligations, responsibilities and expectations create a framework for safe and secure health information exchange, and are designed to promote trust among Participants and protect the privacy, confidentiality and security of the health data that is shared
• Assumes that each Participant has trust relationships in place with its agents, employees and data connections (end users, systems, data suppliers, networks, etc.)
• As a living document, the agreement will be modified over time 16

9
Key Provisions
• Participants in production • Applicable law • HIPAA privacy and security • Duty to respond • Future use of data • Autonomy principle • Breach notification • Mandatory, non-binding dispute resolution • Allocation of liability risk • Coordinating Committee composition, authority and duties • Permitted purposes • Identity proofing and truthful assertions • Disclosing participant required to meet its respective legal requirements before
releasing data • Authorization • Compliance with technical specifications and validation plan • Voluntary suspension • Change process for specifications, validation plan, operating policies and
procedures and DURSA
17
Lessons Learned
• Few questions / issues regarding the agreement itself
• Eliminates duplicative point-to-point agreements
• Realized return on investment to date
• Focus is on executing and implementing the agreement to assure “chain of trust”
• Determine who should sign
• Implement “flow-down” provisions via contracts or written policies with a participant’s agents, users, etc.
• Agreement has core elements needed for day-to-day exchange of health information
• DURSA and operating policies and procedures referenced by Coordinating Committee on routine basis
• Processes vetted and refined over time
18


1
ONC HIT Certification Program
Update
Carol Bean, Ph.D.
Director, Office of Certification
Office of the National Coordinator for Health IT
HIT Policy Committee
November 7, 2011
Overview
2
• ONC HIT Certification Program
• 2014 Test Method Development
• 2014 Test Method Public Review and Comment
• Technical Workshop
• 2014 Test Scenarios

2
ONC HIT Certification Program
3
ONC HIT Certification Program Transition
• Name Change: Permanent Certification Program = ONC HIT Certification
Program
• New Structure: ONC, NVLAP, ANSI, ATLs, and ACBs
• Separate testing and certification entities
• No impact on Temporary Program certifications
On October 4, 2012, the Temporary Certification Program
sunsetted and the ONC HIT Certification Program began.
ONC HIT Certification Program –
Participants
4
ONC Office of the National Coordinator (ONC), Office of Certification manages the
ONC HIT Certification Program.
NVLAP National Voluntary Laboratory Accreditation Program (NVLAP), administered by
the National Institute of Standards and Technology (NIST), accredits Accredited
Testing Laboratories (ATLs).
ONC–AA ONC-Approved Accreditor (ONC-AA) accredits and oversees ONC-Authorized
Certification Bodies (ONC-ACBs). Note: There is only one ONC-AA at a time.
ATL NVLAP Accredited Testing Laboratory (ATL) tests Health IT (HIT), including
Complete EHRs and/or EHR Modules. Note: There can be multiple ATLs.
ONC-ACB ONC-Authorized Certification Body (ONC-ACB) certifies HIT, including
Complete EHRs and/or EHR Modules. Note: There can be multiple ACBs.
Developer/Vendor Creator(s) of HIT, including Complete EHRs and/or EHR Modules.

3
ONC HIT Certification Program –
ATLs and ACBs
5
NVLAP – Accredits Testing Laboratories (ATLs)
• Certification Commission for HIT (CCHIT)
• Drummond Group, Inc.
• ICSA Laboratories, Inc.
• InfoGard Laboratories, Inc.
• SLI Global Solutions
ANSI – Accredits Certification Bodies (ACBs)
• Certification Commission for HIT (CCHIT)
• Drummond Group, Inc.
• ICSA Laboratories, Inc.
• InfoGard Laboratories, Inc.
• Orion Register, Inc.
ONC HIT Certification Program –
Office of the National Coordinator
6
ONC

4
ONC HIT Certification Program –
NVLAP and ONC-AA (ANSI)
7
ONC-AA Approved Accreditor
(ANSI)
ONC
accredits
approves
NIST NVLAP National Voluntary
Laboratory Accreditation Program
ISO/IEC 17011
ONC HIT Certification Program –
ONC-AA Accredits ONC-ACBs
8
ACB Authorized
Certification Body*
ACB Authorized
Certification Body*
ONC-ACB ONC-Authorized Certification Body
ONC-AA Approved Accreditor
(ANSI)
ONC
accredits
approves
accredits
NIST NVLAP National Voluntary
Laboratory Accreditation Program
ISO/IEC 17011
ISO/IEC Guide 65

5
ONC HIT Certification Program –
ONC Authorizes ONC-ACBs
9
ACB Authorized
Certification Body*
ACB Authorized
Certification Body*
ONC-ACB ONC-Authorized Certification Body
ONC-AA Approved Accreditor
(ANSI)
ONC
accredits
approves
accredits
NIST NVLAP National Voluntary
Laboratory Accreditation Program
auth
orize
s
ISO/IEC 17011
ISO/IEC Guide 65
ONC HIT Certification Program –
NVLAP Accredits ATLs
10
ACB Authorized
Certification Body*
Authorized Testing Body*
ACB Authorized
Certification Body*
ONC-ACB ONC-Authorized Certification Body
ONC-AA Approved Accreditor
(ANSI)
ONC
accredits
performs testing against criteria
approves
accredits
NIST NVLAP National Voluntary
Laboratory Accreditation Program
auth
orize
s
accredits
Authorized Testing Body*
ATL Accredited Testing
Laboratory
ISO/IEC 17011
ISO/IEC 17025
NIST 150
NIST 150-31
ISO/IEC Guide 65

6
ONC HIT Testing and Certification –
Developers and Vendors
11
ACB Authorized
Certification Body*
Authorized Testing Body*
ACB Authorized
Certification Body*
ONC-ACB ONC-Authorized Certification Body
performs testing against criteria
certifies tested products
Developer/Vendor
Authorized Testing Body*
ATL Accredited Testing
Laboratory
performs testing against criteria
ONC HIT Testing and Certification –
ATL Tests EHR Technology
12
ACB Authorized
Certification Body*
Authorized Testing Body*
ACB Authorized
Certification Body*
Product successfully passes testing
ONC-ACB ONC-Authorized Certification Body
performs testing against criteria
certifies tested products
Developer/Vendor
Authorized Testing Body*
ATL Accredited Testing
Laboratory
performs testing against criteria

7
ONC HIT Testing and Certification –
ONC-ACB Certifies EHR Technology
13
ACB Authorized
Certification Body*
Authorized Testing Body*
ACB Authorized
Certification Body*
Product successfully passes testing
ONC-ACB ONC-Authorized Certification Body
performs testing against criteria
certifies tested products
Developer/Vendor
Authorized Testing Body*
ATL Accredited Testing
Laboratory
performs testing against criteria
Product successfully achieves certification
ONC HIT Testing and Certification –
ONC Posts CEHRT to CHPL
14
ACB Authorized
Certification Body*
Authorized Testing Body*
ACB Authorized
Certification Body*
Product successfully passes testing
ONC reviews and posts certified
product to CHPL ONC-ACB
ONC-Authorized Certification Body
performs testing against criteria
certifies tested products
Developer/Vendor
Authorized Testing Body*
ATL Accredited Testing
Laboratory
performs testing against criteria
Product successfully achieves certification

8
15
0
500
1000
1500
2000
2500
3000
2/18
/201
1
3/18
/201
1
4/18
/201
1
5/18
/201
1
6/18
/201
1
7/18
/201
1
8/18
/201
1
9/18
/201
1
10/1
8/20
11
11/1
8/20
11
12/1
8/20
11
1/18
/201
2
2/18
/201
2
3/18
/201
2
4/18
/201
2
5/18
/201
2
6/18
/201
2
7/18
/201
2
8/18
/201
2
9/18
/201
2
10/1
8/20
12
Total Products
Total Unique Products
Total Unique Products Estimate
Total Vendors
Certified Health IT Product List –
Overview
2014 Test Method Timeline OCT NOV AUG SEPT DEC JAN
Public Comment Period
8/23/2012
9/7 11/15
W2 W3 W4 9/7 9/14 9/21 9/28
W5 10/18
W1
W1 9/7 9/21
W2 9/14 9/28
W3 9/21 10/5
W4 9/28 10/12
2014 Test Procedures Posted
12/14/2012
W6 11/2 11/14
W5 10/18 11/5
Test Procedures Revised 9/21 11/30
National Coordinator Approval
12/3 12/7
12/7 12/14
2014 Scope Expansion for ACBs and ATLs
Technical Workshop 12/14/2012
2014
Certification Begins
1/2/2012
Test Scenarios Reviewed/revised
12/7 On-going
11/1 CHPL 3.0
Development
CHPL 3.0 Release
12/1 CHPL 3.0
Testing Begins
10/1 CHPL 3.0
Requirements Gathering
11/2 W6
ACB / ATL setup operations
1/2/2012
W7 TBD TBD
TBD W7
DRAFT
Test Tool Demos (ATL/ACB)
10/2 10/4 10/31
Technical Workshop & Training
11/13 – 11/15

9
Test Method Development –
2014 Edition Technical Requirements
17
Final Rule
Publication
Final Rule Publication • September 4, 2012
• Published in the Federal Register
• Defines the 2014 Edition Certification Criteria
• Aligns with CMS’ Stage 2 MU
September 4, 2012
Test Method Development –
Test Method Draft Development
18
Final Rule
Publication
Draft Test
Method
Draft Test Method • September – November 2012
• Evaluates conformance to 2014
Edition Certification Criteria
• Overseen by ONC’s Office of
Certification
September 4, 2012 Sept. – Nov. 2012

10
Test Method Development –
Public Review and Feedback
19
Final Rule
Publication
Draft Test
Method
Public
Review
September 4, 2012 Sept. – Nov. 2012 Sept. 7 – Nov. 14, 2012
Public Review • September 7 – November 14, 2012
• Request feedback/input from the
public
• Draft Test Method posted on ONC’s
website in waves
Test Method Development –
Revision and Training
20
Final Rule
Publication
Draft Test
Method
Public
Review
Test Method
Update
September 4, 2012 Sept. – Nov. 2012 Sept. 7 – Nov. 14, 2012 Sept. – Nov. 2012
Test Method Update • September – November 2012
• Analyze public comments
• Update Test Method per public
review
• ATL and ACB training and
evaluation

11
Test Method Development –
Approval by National Coordinator
21
Final Rule
Publication
Draft Test
Method
Public
Review
Test Method
Update
Final Test
Method
September 4, 2012 Sept. – Nov. 2012 Sept. 7 – Nov. 14, 2012 Sept. – Nov. 2012 Mid-December 2012
Final Test Method • Mid-December 2012
• National Coordinator approves
final 2014 Edition Test Method
• Federal Register Notice
• Final Test Method posted on
ONC’s website
Test Method Development –
Implementation
22
Final Rule
Publication
Draft Test
Method
Public
Review
Test Method
Update
Final Test
Method Implementation
September 4, 2012 Sept. – Nov. 2012 Sept. 7 – Nov. 14, 2012 Sept. – Nov. 2012 Mid-December 2012 December 2012
Implementation • December 2012
• NVLAP and ANSI expand
scope to 2014 Ed.
• ONC authorizes ACBs
• ATLs and ACBs begin
operational implementation
• Testing and Certification
begins in January 2013

12
Draft Test Method Review Process –
Wave 1
23
Wave 1 (14 Test Procedures)
170.314(a)(1) Computerized provider order entry
170.314(a)(4) Vital signs, body mass index, and growth charts
170.314(a)(5) Problem list
170.314(a)(6) Medication list
170.314(a)(7) Medication allergy list
170.314(a)(10) Drug formulary checks
170.314(a)(11) Smoking status
170.314(a)(15) Patient-specific education resources
170.314(a)(17) Inpatient setting only—advance directives
170.314(d)(5) Automatic log-off
170.314(d)(8) Integrity
170.314(d)(9) Optional—accounting of disclosures
170.314(f)(1) Immunization Information
170.314(f)(2) Transmission to immunization registries
Wave 1
9/7/12 – 9/21/12
24
Wave 2 (7 Test Procedures)
170.314(a)(3) Demographics
170.314(a)(9) Electronic notes
170.314(a)(13) Family health history
170.314(a)(14) Patient list creation
170.314(d)(6) Emergency access
170.314(f)(5) Ambulatory setting only—cancer case information
170.314(f)(6) Ambulatory setting only—transmission to cancer registries
Wave 1
9/7/12 – 9/21/12
Wave 2
9/14/12 – 9/28/12
Draft Test Method Review Process –
Wave 2

13
25
170.314(a)(2) Drug-drug, drug-allergy interaction checks
170.314(a)(8) Clinical decision support
170.314(a)(12) Image Results
170.314(a)(16) Inpatient setting only—eMAR
170.314(b)(4) Clinical information reconciliation
170.314(e)(2) Ambulatory setting only—clinical summary
Wave 3 (6 Test Procedures)
Wave 1
9/7/12 – 9/21/12
Wave 2
9/14/12 – 9/28/12
Wave 3
9/21/12 – 10/5/12
Draft Test Method Review Process –
Wave 3
26
170.314(b)(7) Data portability
170.314(d)(1) Authentication, access control, and authorization
170.314(d)(2) Auditable events and tamper-resistance
170.314(d)(3) Audit reports
170.314(d)(4) Amendments
170.314(d)(7) End-user device encryption
170.314(e)(3) Ambulatory setting only—secure messaging
170.314(f)(3) Transmission to public health agencies—syndromic surveillance
170.314(g)(3) Safety-enhanced design
Wave 4 (9 Test Procedures)
Wave 1
9/7/12 – 9/21/12
Wave 2
9/14/12 – 9/28/12
Wave 3
9/21/12 – 10/5/12
Wave 4
9/28/12 – 10/12/12
Draft Test Method Review Process –
Wave 4

14
27
170.314(b)(2) Transitions of care—create and transmit transition of care/referral summaries
170.314(b)(3) Electronic prescribing
170.314(e)(1) View, download, and transmit to 3rd party
170.314(f)(4) Inpatient setting only—transmission of reportable lab tests and values/results
Wave 5 (4 Test Procedures)
Wave 1
9/7/12 – 9/21/12
Wave 2
9/14/12 – 9/28/12
Wave 3
9/21/12 – 10/5/12
Wave 4
9/28/12 – 10/12/12
Wave 5
10/18/12 – 11/1/12
Draft Test Method Review Process –
Wave 5
28
170.314(c)(1) Clinical quality measures—capture and export
170.314(c)(2) Clinical quality measures—import and calculate
170.314(c)(3) Clinical quality measures—electronic submission
170.314(g)(1) Automated numerator recording
170.314(g)(2) Automated measure calculation
Wave 6 (5 Test Procedures)
Wave 1
9/7/12 – 9/21/12
Wave 2
9/14/12 – 9/28/12
Wave 3
9/21/12 – 10/5/12
Wave 4
9/28/12 – 10/12/12
Wave 5
10/18/12 – 11/1/12
Wave 6
11/2/12 – 11/16/12
Draft Test Method Review Process –
Wave 6

15
29
Wave 1
9/7/12 – 9/21/12
Wave 2
9/14/12 – 9/28/12
Wave 3
9/21/12 – 10/5/12
Wave 4
9/28/12 – 10/12/12
Wave 5
10/18/12 – 11/1/12
Wave 6
11/2/12 – 11/16/12
Wave 7*
TBD
170.314(b)(1) Transitions of care—receive, display, and incorporate summary care records
170.314(b)(5) Incorporate lab tests and values/results
170.314(b)(6) Inpatient setting only—transmission of e-lab test and values/results to Amb provider
170.314(g)(4) Quality management system
Wave 7* (4 Test Procedures)
Draft Test Method Review Process –
Wave 7
*Represents the remaining Test Procedures. Wave number and content may change.
2014 Edition Test Tools
CCDA Validation Tool
via Direct and SOAP
Lab Results Interface
(LRI) Validation Tool Transport Testing Tool
Cypress Direct Certificate
Discovery Tool (DCDT)
HL7 v2 Validation Tool ePrescribing
Conformance Tool
HL7 Cancer Registry
Report Validation Tool
30

16
Technical Training & Workshop
31
Technical Workshop (public webinar)
• Presenters: ONC, NVLAP, ANSI, test and tool developers
• Date: November 13, 2012
Technical Training for ATLs and ACBs
• Participants: ONC, NVLAP, ANSI, ATLs, ACBs
• Date: November 14-15, 2012
• Location: DC
Topics
• Program timeline
• Test Procedures
• Overview of public review
• Test Tool demos
• CHPL 3.0
Test Scenario Development –
Unit Based Testing
32
• Minimum requirement
• Independent tests
• Individual test data and results
• Currently employed for 2011 Edition Test Procedures
Unit Based Testing

17
Test Scenario Development –
Scenario Based Testing
33
• Alternative to unit based testing
• Dependent tests
• Dependent test data and results
• Can remove individual test from sequence
Scenario Based Testing If test 1 is not applicable…
– Reflects a typical clinical workflow in multiple care settings
– Allows persistence of data elements (i.e. model for data threading)
– Maintains testing flexibility (e.g. add/remove ―unit test‖)
Test Scenario Development – Approach
34
Approach
Process
Types

18
– Reflects a typical clinical workflow in multiple care settings
– Allows persistence of data elements (i.e. model for data threading)
– Maintains testing flexibility (e.g. add/remove ―unit test‖)
Test Scenario Development – Process
35
– Develop clinically plausible workflow
– Initial development based on 2011 Edition Certification Criteria
– Reevaluate against the 2014 Edition Certification Criteria
Approach
Process
Types
– Reflects a typical clinical workflow in multiple care settings
– Allows persistence of data elements (i.e. model for data threading)
– Maintains testing flexibility (e.g. add/remove ―unit test‖)
Test Scenario Development – Types
36
– Develop clinically plausible workflow
– Initial development based on 2011 Edition Certification Criteria
– Reevaluate against the 2014 Edition Certification Criteria
– Medication Management
– Emergency Department
– Interoperability
– Outpatient
– Inpatient
Approach
Process
Types

19
ONC HIT Certification Program
37
Questions?






























