Embed Size (px)
Citation preview
Leenen, Ho&well, and Cardella
heart transplantation: evidence for reversible right ventricu- lar dysfunction and myocardial edema. J Heart Transplant 1987;6:343-7.
27. Sagar KB, Hastillo A, Wolfgang TC, Lower RR, Hess ML. Left ventricular mass by M-mode echocardiography in cardiac transplant patients with acute rejection. Circulation 1981: 64jsuppl II):II-216-20.
28. Levy D, Anderson KM, Savage DD, Kannel WB, Christiansen JC, Castelli WP. Echocardiographically detected left ventric- ular hypertrophy: prevalence and risk factors. Ann Intern Med 1988;108:7-13.
29. Hammond IW, Devereux RB, Alderman MH, Lutas EM, Spitzer MC, Crowley JS, Laragh JH. The prevalence and cor- relates of echocardiographic left ventricular hypertrophy
October 1991
American Heart Journal
among employed patients with uncomplicated hypertension. J Am Co11 Cardiol 1986;7:639-50.
30. Sen S, Tarazi RC, Bumpus FM. Cardiac hypertrophy and an- tihypertensive therapy. Cardiovasc Res 1977;11:427-33.
31. Ostman-Smith I. Cardiac sympathetic nerves as the finai common pathway in the induction of adaptive cardiac hyper- trophy. Clin Sci 1981;61:265-72.
32. Stinson EB, Schroeder JS, Griepp RB, Shumway NE, Dong Jr E. Observations on the behavior of recipient atria after cardiac transplantation in man. Am d Cardiol 1972;30:615-22.
33. Pope SE, Stinson EB, Daughters GT, Schroeder JS, Ingel NB, Alderman EL. Exercise responses in the denervated heart in long term cardiac transplant recipients. Am J Cardiol 1980; 46:213-8.
Immediate blood pressure effects of the renin inhibitor enalkiren and the angiotensin-converting enzyme inhibitor enalaprilat
The antihypertensive effects of the renln inhibitor enaikiren were compared with those of the angiotenstn-converting enzyme inhibitor enaiapriiat in 17 hypertensive patients (14 white, 3 black; mean age 57 years), whose renin systems had been stimulated by diuretic pretreatment. Patients were studied on 3 separate in-hospital days. On the first study day patients received placebo alone. On day 2 they received intravenous boius doses of enaikiren (0.03 to 1.0 mg/kg), and on day 3, intravenous boius doses of enaiaprilat (0.626 to 1.25 mg). Each agent reduced systolic (p < 0.01) and diastolic (p < 0.01) blood pressures (BP) from baseline levels. The acute decrease in systolic BP of 16.5 t- 0.4 mm Hg during enaikiren tended to be greater (p < 0.01) than the decrease of 12.6 + 0.7 mm Hg durtng enaiapriiat. Decreases in diastolic BP during enaikiren (11.9 t 0.4 mm Hg) were also slightly greater (p < 0.1) than those during enaiapriiat (9.2 + 0.4 mm HQ). Based on prestudy plasma renin activity (PRA), patients were divided into “high” renin (PRA >3.5 ng angiotensin i/mi/hr; n = 6) and “low/normal” renin (<3.5 ng angiotensin i/mi/hr; n = 11) groups. Reductions in diastolic BP in the “high” renin group during enaikiren (30 2 5/20 + 3 mm Hg) tended to be greater (p < 0.07) than those during enaiapriiat (23 + 7/14 2 1 mm Hg); differences were not significant in the “low/normal” group (12 & 2/7 ? 2 and 7 k 2/6 & 1 mm Hg, respectively). Thus the renin inhibitor is at least as effective as the ACE inhibitor in Its immediate BP-lowering effects in hypertensive patients. (Am HEART J 1991;122:1094.)
Joel M. Neutel, MD, Robert R. Luther, MD, Robert S. Boger, MD, and Michael A. Weber, MD. Long Beach and Irvine, Calif.
From the Hypertension Center, Veterans Affairs Medical Center, Long Beach; and the University of California, Irvine. Supported in part by Department of Veterans Affairs Merit Review Fund- ing and hy a research grant from Abbott Laboratories. Received for publication Nov. 19, 1990; accepted April 8. 1991. Reprint requests: Michael A. Weber, MD, Hypertension Center (W130), VA Medical Center, 5901 East Seventh St., Long Beach, CA 90822. 4/l/31131
The renin-angiotensin system has been established as a regulator of cardiovascular homeostasis, and the clinical efficacy of angiotensin-converting enzyme inhibitors has underscored the role of this system in sustaining arterial hypertension. The development of highly specific, direct inhibitors of renin, the enzyme catalyzing rate-limiting step in the renin-angiotensin
1094

votums 122
Number 4, Part 1 Rerzin inhibitor enatkiren in hypertension 1095
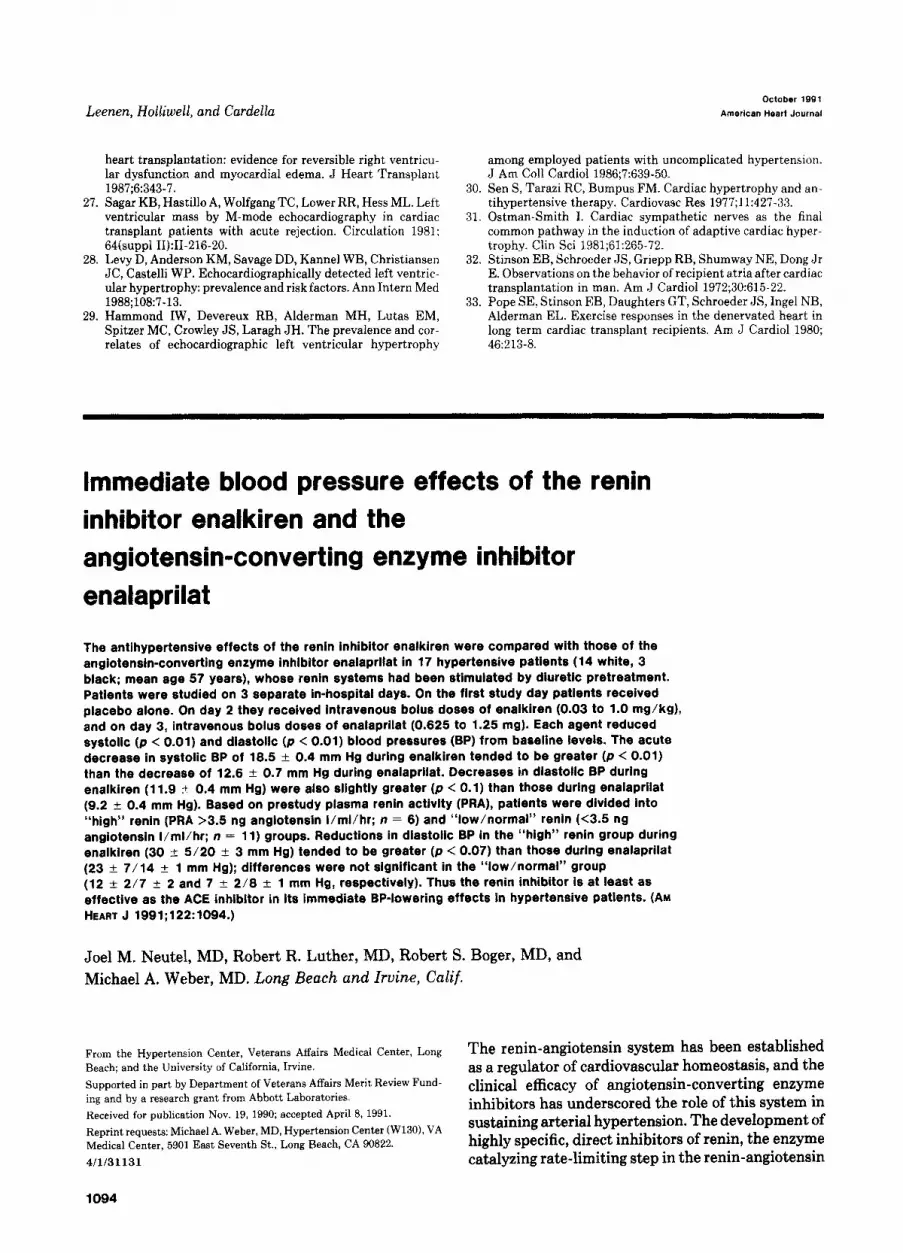
A--A Placebo *--a Enalapdat - Enalkiren
I I I
Baseline 5 10 15 20 25 30 35 40 45
Time After Maximum Dose (Mins.)
Fig. 1. Changes in systolic and diastolic blood pressures in hypertensive patients studied in the semire- cumbent position during the 45-minute period following the maximum doses of enalkiren, enalaprilat, or placebo.
pathway, has provided an additional probe for inves- tigating the relationship between renin mechanisms and systemic blood pressure.lW3 Differing types of re- nin inhibitors41 5 have been effective in decreasing both plasma renin activity and blood pressure in pri- mates. Most recently, dipeptides derived from the amino acid sequence of human angiotensinogen in the vicinity of its scissile bond have displayed high efficacy as inhibitors of renin.=t 3
We6 recently reported that the specific dipeptide renin inhibitor enalkiren produced significant and sustained decreases in plasma renin activity and in blood pressure when administered intravenously to hypertensive patients. The changes in blood pressure correlated with the baseline measurements of plasma renin activity. Furthermore, the blood pressure-low- ering effects of enalkiren were amplified in patients whose plasma renin activities were stimulated by pretreatment with a diuretic.6
Previous studies in nonhuman primates7-l5 have shown the blood pressure-lowering effects of differ-
ing renin inhibitors to be either equivalent to, greater than, or smaller than those produced by angiotensin- converting enzyme inhibitors. In the present study, we have compared the short-term effects on blood pressure of the intravenous administration of the re- nin inhibitor enalkiren and the angiotensin-convert- ing enzyme inhibitor enalaprilat. Enalkiren pro- duced immediate decreases in blood pressure that tended to be of greater amplitude than those pro- duced by enaiaprilat.
METHODS
The study was performed in 17 patients with mild to moderate essential hypertension (untreated diastolic blood pressure between 95 and 110 mm Hg measured with patients in the semirecumbent position). The patients were previously untreated or had been free of treatment for at least 3 weeks before the study. They were diagnosed as having essential hypertension after secondary forms of hy- pertension or other complicating conditions had been ex- cluded by standard clinical methods. The study group consisted of 15 men and 2 women; 14 patients were white

1096 Neutel et al. October 1991
American Heart Journal
p -15 1 53
% -20
g -25 .S
Lo
8
-35
Fig. 2. Mean change in systolic and diastolic blood pressures during the 45-minute period following max- imum doses of enalkiren and enalaprilat for the group as a whole (n = 17), for the “high” renin group (pa- tients with plasma renin activity >3.5 ng angiotensin I/ml hr; n = 6), and for the “low/normal” renin group (plasma renin activity <3.5 ng angiotensin I/ml/hr; n = 11). Values shown are the mean of nine blood pres- sure recordings taken 5 minutes apart during the 45-minute period following the maximum dose of each agent.
and 3 were black. Their ages ranged between 32 and 67 years (mean:57 years). Before entering the study, all patients signed an informed consent approved by the Hu- man Studies Subcommittee of the Veterans Affairs Med- ical Center, Long Beach, Calif.
Throughout the study, the patients consumed a normal diet with minimal restraints on sodium intake. Each patient was studied on three separate in-hospital days. The study days were separated by periods of between 3 and 7 days. To increase the sensitivity of the study, plasma renin activity was stimulated by treatment with 25 mg of hydro- chlorothiazide taken twice daily for 3 days prior to each study day. Patients were also instructed to take a dose of diuretic at 5 AM on the morning of each study day. Because enalkiren is an investigational drug, and because of reports of severe hypotension in nonhuman primates treated with the drug, the study was performed in an unblinded man- ner. To avoid observer bias, blood pressure and heart rates were measured and recorded by an automated device throughout the study.
The study protocols for day 1 and day 2 were identical. Each day was divided into the following consecutive peri- ods: an initial stabilizing period of 45 minutes to allow pa- tients to adapt to the semirecumbent posture, followed by a baseline period of 45 minutes during which a placebo (drug diluent alone) was administered intravenously. The baseline period was followed by four consecutive 4Bminute periods during which drug (or equivalent placebo) was ad- ministered in ascending doses of 0.03,0.1,0.3, and 1.0 mg/ kg given as intravenous boluses at the start of each 45-minute period. The renin inhibitor was administered as increasing bolus doses as a precaution to minimize the risk of excessive hypotensive responses in this early study with
an investigational drug. The patients were followed for a further 2 hours after the final dose of active drug had been administered. On day 1 the protocol was carried out with placebo being substituted for active drug during all four of the dosing periods. On day 2 the patients were given the renin inhibitor enalkiren (Abbott 64662; supplied by Ab- bott Laboratories Inc., North Chicago, Ill.) during each of the dosing periods. On the third day, following the initial stabilization and baseline periods, patients were given a bolus dose of 0.625 mg enalaprilat (the recommended maximum dose that has been shown to decrease circulat- ing angiotensin-converting enzyme to negligible level@) intravenously, followed by a second dose 1 hour later (if the diastolic blood pressure was >80 mm Hg) to ensure adequate inhibition of circulating angiotensin-converting enzyme. Patients were monitored for a further 2 hours af- ter the final dose of enalaprilat.
All 17 patients completed the 3 days of the study. Five patients did not receive the highest dose of enalkiren due to symptomatic hypotension after administration of the third dose; four patients did not receive the second dose of enalaprilat either because their diastolic blood pressures were less than 80 mm Hg or because they became symp- tomatic after the first dose. In each case the blood pressure values obtained during the 45-minute period following the maximum tolerated dose of each agent were used for anal- ysis. The mean decreases in blood pressures following in- travenous doses of drug or diluent were taken to be the difference between the average of the nine blood pressure values recorded at 5-minute intervals after drug (or pla- cebo) administration and the corresponding pretreatment blood pressure average (during the $&minute placebo pe- riod). Blood pressures and heart rates were measured at 5-

Volume122
Number 4, Part 1 Renin inhibitor enalkiren in hypertension 1097
minute intervals throughout each of the study days by an automated oscillometric device (Dinamap, Critikon, Inc., Tampa, Fla.), which had been calibrated for accuracy against a conventional mercury sphygmomanometer.
On day 1 and day 2 blood samples for the measurement of plasma renin activity were drawn 40 minutes after the administration of the placebo, 40 minutes after adminis- tration of each dose of enalkiren (or equivalent placebo on day l), and at 2 hours after the final dose of drug (or pla- cebo on day 1). On day 3 plasma renin activity was 6: -15-
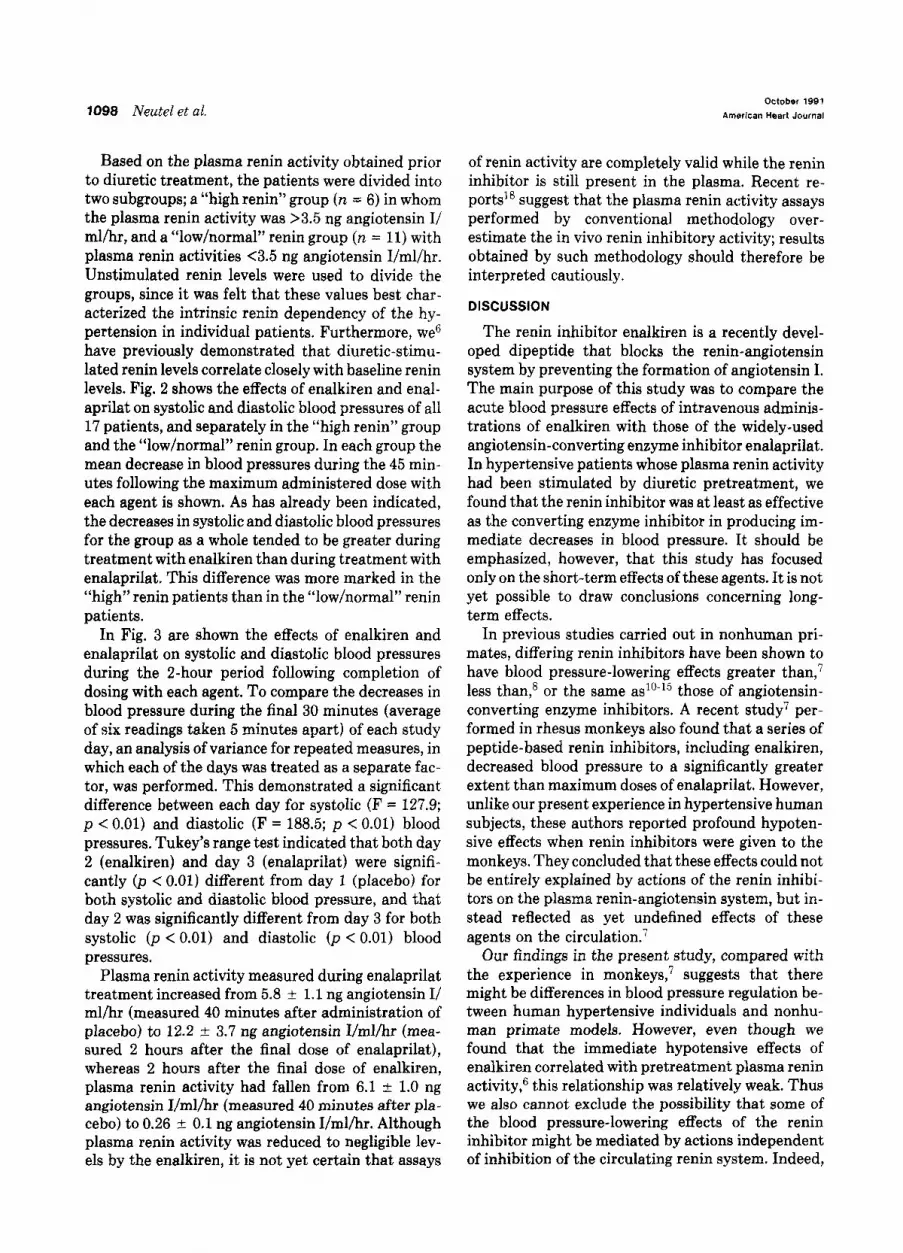
0
measured 5 minutes prior to the infusion of enalaprilat and m
again at 2 hours after the second dose of enalaprilat. In ad- ~-20 - dition, a baseline plasma renin activity level was obtained before the patients were started on diuretic treatment (prior to day 1). This was drawn after each patient had been in a semirecumbent position for 45 minutes. Plasma renin A--A Placebo
5 e-4 Enalapr~lat
activity was measured by radioimmunoassay. A pH of 7.4 - Enalktren
was used for the incubation step due to concern that the renin inhibitor might interfere with the assay at a pH of 5.7.17
Statistical analysis was by analysis of variance for repeated measures to compare the effects of placebo, enalkiren, and enalaprilat on blood pressure over time. A one-way analysis of variance was used to compare the de- creases in blood pressure produced by the two agents in the high and low renin groups. Pearson regression analysis was used to examine the relationship between changes in blood pressure and plasma renin activity. Values are given as mean -t SEM.
m -15
BaSelIne Maximum 1 15 2 dose
Time After Maximum Dose (hr)
RESULTS
There were no significant differences in baseline blood pressures measured on each of the 3 study days. Mean baseline blood pressures were 151 f 4.2/93 t- 2.0 mm Hg on day 1 (placebo), 142 f 4.2/92 + 2.4 mm Hg on day 2 (enalkiren), and 141 f 4.1/91 t- 2.0 mm Hg on day 3 (enalaprilat). The effects on systolic and diastolic blood pressures during the 45-minute period following the maximum doses of placebo, enalkiren, and enalaprilat are shown in Fig. 1. Analysis of variance for repeated measures, in which day 1, day 2, and day 3 were treated as separate factors, indicated a significant difference between each of the days for systolic (F = 219.7; p < 0.001) and diastolic (F = 245.7; p < 0.001) blood pressures. The average decreases in systolic and diastolic blood pressures were 0.6 +- 0.7/0.2 +- 0.4 mm Hg during placebo, 19 + 0.7/12 -t 0.4 mm Hg during enalkiren, and 13 +- 0.7/9 + 0.4 mm Hg during enalaprilat. A Tukey’s range test indicated that the decreases in systolic (p < 0.01) and diastolic (p < 0.01) blood pressures produced by both enalkiren (day 2) and enalaprilat (day 3) were significantly different from those that occurred with placebo (day 1). In addition, when comparing the two active drugs during the 45-
Fig. 3. Mean changes in systolic and diastolic blood pres- sure immediately after and for the 2-hour period after ad- ministration of the maximum dose of enalkiren, enalapri- lat, or placebo. Values shown represent the average of six blood pressure recordings measured 5 minutes apart at each time interval.
minute period following the maximum dose, the de- creases in systolic (p < 0.01) and diastolic (p < 0.01) blood pressures were greater in patients treated with enalkiren than in those treated with enalaprilat. There were no significant changes in heart rates on each of the 3 study days during the 45-minute period following administration of the maximum dose. The mean changes in heart rates were 3 beats/min on day 1, 0.7 beatslmin on day 2, and 0.4 beatslmin on day 3.
The decrease in diastolic blood pressure during enalkiren (F = 0.61; p < 0.01) and enalaprilat (r = 0.49; p < 0.02 j correlated significantly with base- line measurements of plasma renin activity (mea- sured 40 minutes after placebo administration on the respective days). Changes in systolic blood pressure correlated significantly with plasma renin activity in the enalkiren-treated (r = 0.55; p < 0.02) patients but not in the enalaprilat-treated patients.
1098 Neutel et al. October 199 1
American Heart Journal
Based on the plasma renin activity obtained prior to diuretic treatment, the patients were divided into two subgroups; a “high renin” group (n = 6) in whom the plasma renin activity was >3.5 ng angiotensin I/ ml/hr, and a “low/normal” renin group (n = 11) with plasma renin activities <3.5 ng angiotensin I/ml/hr. Unstimulated renin levels were used to divide the groups, since it was felt that these values best char- acterized the intrinsic renin dependency of the hy- pertension in individual patients. Furthermore, we6 have previously demonstrated that diuretic-stimu- lated renin levels correlate closely with baseline renin levels. Fig. 2 shows the effects of enalkiren and enal- aprilat on systolic and diastolic blood pressures of all 17 patients, and separately in the “high renin” group and the “low/normal” renin group. In each group the mean decrease in blood pressures during the 45 min- utes following the maximum administered dose with each agent is shown. As has already been indicated, the decreases in systolic and diastolic blood pressures for the group as a whole tended to be greater during treatment with enalkiren than during treatment with enalaprilat. This difference was more marked in the “high” renin patients than in the “low/normal” renin patients.
In Fig. 3 are shown the effects of enalkiren and enalaprilat on systolic and diastolic blood pressures during the 2-hour period following completion of dosing with each agent. To compare the decreases in blood pressure during the final 30 minutes (average of six readings taken 5 minutes apart) of each study day, an analysis of variance for repeated measures, in which each of the days was treated as a separate fac- tor, was performed. This demonstrated a significant difference between each day for systolic (F = 127.9; p < 0.01) and diastolic (F = 188.5; p < 0.01) blood pressures. Tukey’s range test indicated that both day 2 (enalkiren) and day 3 (enalaprilat) were signifi- cantly (p < 0.01) different from day 1 (placebo) for both systolic and diastolic blood pressure, and that day 2 was significantly different from day 3 for both systolic (p < 0.01) and diastolic (p < 0.01) blood pressures.
Plasma renin activity measured during enalaprilat treatment increased from 5.8 +- 1.1 ng angiotensin I/ ml/hr (measured 40 minutes after administration of placebo) to 12.2 + 3.7 ng angiotensin I/ml/hr (mea- sured 2 hours after the final dose of enalaprilat), whereas 2 hours after the final dose of enalkiren, plasma renin activity had fallen from 6.1 * 1.0 ng angiotensin I/ml/hr (measured 40 minutes after pla- cebo) to 0.26 -+ 0.1 ng angiotensin I/ml/hr. Although plasma renin activity was reduced to negligible lev- els by the enalkiren, it is not yet certain that assays
of renin activity are completely valid while the renin inhibitor is still present in the plasma. Recent re- ports18 suggest that the plasma renin activity assays performed by conventional methodology over- estimate the in vivo renin inhibitory activity; results obtained by such methodology should therefore be interpreted cautiously.
DISCUSSION
The renin inhibitor enalkiren is a recently devel- oped dipeptide that blocks the renin-angiotensin system by preventing the formation of angiotensin I. The main purpose of this study was to compare the acute blood pressure effects of intravenous adminis- trations of enalkiren with those of the widely-used angiotensin-converting enzyme inhibitor enalaprilat. In hypertensive patients whose plasma renin activity had been stimulated by diuretic pretreatment, we found that the renin inhibitor was at least as effective as the converting enzyme inhibitor in producing im- mediate decreases in blood pressure. It should be emphasized, however, that this study has focused only on the short-term effects of these agents. It is not yet possible to draw conclusions concerning long- term effects.
In previous studies carried out in nonhuman pri- mates, differing renin inhibitors have been shown to have blood pressure-lowering effects greater than,7 less than,8 or the same as1’-15 those of angiotensin- converting enzyme inhibitors. A recent study7 per- formed in rhesus monkeys also found that a series of peptide-based renin inhibitors, including enalkiren, decreased blood pressure to a significantly greater extent than maximum doses of enalaprilat. However, unlike our present experience in hypertensive human subjects, these authors reported profound hypoten- sive effects when renin inhibitors were given to the monkeys. They concluded that these effects could not be entirely explained by actions of the renin inhibi- tors on the plasma renin-angiotensin system, but in- stead reflected as yet undefined effects of these agents on the circulation.:
Our findings in the present study, compared with the experience in monkeys,7 suggests that there might be differences in blood pressure regulation be- tween human hypertensive individuals and nonhu- man primate models. However, even though we found that the immediate hypotensive effects of enalkiren correlated with pretreatment plasma renin activity,‘j this relationship was relatively weak. Thus we also cannot exclude the possibility that some of the blood pressure-lowering effects of the renin inhibitor might be mediated by actions independent of inhibition of the circulating renin system. Indeed,

Volume 122
Number 4, Part 1
we were unable to administer maximum doses of the renin inhibitor to some patients in whom initial lower doses produced blood pressure-lowering effects that were greater than predicted by pretreatment plasma renin values.
Blood pressure effects of the renin inhibitor that cannot be explained by its actions in the plasma might be due to effects on the tissue renin-angioten- sin system. Renin within vascular tissue sites has been shown previously to produce pressor effects, presumably through the local generation of angiotensin.18-22 Interruption of this system there- fore represents a possible mechanism by which such agents as renin inhibitors could produce antihyper- tensive effects. Additionally, it is possible that dif- fering access to the tissue renin-angiotensin system might explain our findings of greater blood pressure effects with the renin inhibitor than with the an- giotensin-converting enzyme inhibitor. Alternatively, in short-term studies such as the present one, it is possible that the angiotensin-converting enzyme in- hibitor was not given sufficient time in which to reach or work at sites of tissue converting enzyme. How- ever, there are no direct data in this study with which to test these possibilities.
Experience with renin inhibitors in hypertensive humans is limited. Contrary to our findings, a recent publication comparing the renin inhibitor CGP 38 560A with captopril demonstrated significantly greater reductions in blood pressure with captopril than with the renin inhibitor.‘* However, the blood pressure reductions obtained during treatment with CGP 38 560A were less than those seen in our own patients treated with enalkiren. These findings may be explained by a difference in efficacy between the renin inhibitors, or possibly that the doses of CGP 38 560A used were not sufficient to completely block the renin-angiotensin system. A further explanation for the observed blood pressure differences between the renin inhibitors might be related to their differing effects on nonrenin-mediated mechanisms.
The short-term blood pressure-lowering effects of the angiotensin-converting enzyme inhibitors result from blockade of angiotensin II formation in the plasma.23 During more chronic therapy, these agents have actions on other neurohumoral systems includ- ing kinin mechanisms, which could enhance their antihypertensive properties. It is possible that the inhibitory effects of angiotensin-converting enzyme inhibitors on the renin-angiotensin system may not be complete, especially in circumstances where accu- mulation of high angiotensin I concentrations might overwhelm the drug’s blockade of the converting enzyme.23 In the present study we found that the
Renin inhibitor endkiren in hypertension 1099
difference in blood pressure-lowering efficacy be- tween enalaprilat and enalkiren appeared to be greatest in high renin patients, a group in whom re- active increases in renin release (and presumably an- giotensin I) were greater than in other patients.
Since enalkiren is a new investigational drug with limited human experience, the study was performed unblinded and drug administration was not random. However, it is unlikely that the differences between enalkiren and enalaprilat were due to an ordering ef- fect. A period of at least 3 days was allowed between administration of the two agents in each patient to avoid any residual effects. Importantly, there was no difference between baseline plasma renin activity (6.0 + 1.0 ng angiotensin I/ml/hr before enalkiren administration and 5.8 k 1.1 ng angiotensin I/ml/hr before enalaprilat administration) on each of the study days. Moreover, the baseline blood pressures (142 ? 4.2192 + 2.4 mm Hg before enalkiren and 141 * 4.1191 + 2.0 mm Hg before enalaprilat) were virtually identical.
Additionally, it is possible that the difference be- tween the renin inhibitor and the angiotensin-con- verting enzyme inhibitor could be explained by actions of enalkiren unrelated to the renin system. Earlier studies with renin inhibitors explored the possibility of effects mediated through sympathetic nervous system mechanisms,5 although these could not be substantiated.24 Similarly, direct effects of re- nin inhibitors on the heart have been postulated, but again could not be confirmed.2” Peptide agents such as enalkiren might produce vasodilatory actions through as yet undefined mechanisms that affect the circulation. Assessment of this hypothesis will re- quire appropriately designed studies with nonpep- tide renin inhibitors when they become available.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
Delabays A, Nussberger J, Porchet M, Waeber B. Effects of a new renin inhibitor (Abbott 646621 in normal volunteers [Ab- stract]. Hypertension 1988;12:360. Sweet CS, Blaine EH. Angiotensin-converting enzyme and re- nin inhibitors. In: Anotonacccio M, ed. Cardiovascular phar- macolorrv. 2nd ed. New York: Raven Press. 1984;119-56. StreeteKDHP, Anderson GH, Freiberg JM, Dalakos T. Use of angiotensin II antagonist (saralasin) in recognition of “an- giotensinogenic” hypertension. N Engl J Med 1975;292:657- 62. Dzau VJ, Kopelman RI, Barger NC, Slater EE, Haber E. Re- nin-specific antibody for studv of cardiovascular homeostasis. Science 1980;207:1091-3. - Zusman RM. Christensen D. Burton J. Nussberger J, Dodds A, Haber E. ‘Hemodynamic effects-of a’ competit&e renin in- hibitory peptide in humans: evidence for multiple mechanisms of actions. Trans Assoc Am Physicians 1983;6:365-74. Weber MA, Neutel J, Essinger I, Glassman HN, Boger RS, Luther R. Assessment of renin dependency of hypertension with a dipeptide renin inhibitor. Circulation 1990;81:1768-74. Schaffer LW, &horn TW, Winquist RJ, Strouse JF, Payne L,

1100 Neutel et al.
8.
9.
10.
11.
12.
13.
14.
Chakravarty PK, De Laszlo SE, Tenbroeke J, Veber DF, Greenlee WJ, Siegl PKS. Acute hypotensive responses to peptide inhibitors of renin in conscious monkeys. An effect on blood pressure independent of plasma renin inhibition. J Hy- pertens 1990;8:251-9. Smith SG III, Seymour AA, Mazack EK, Boger J, Blaine EH. Comparison of a new renin inhibitor and enalaprilat in renal hypertensive dogs. Hypertension 1987;9:150-6. Wood JM. Jobber RA. Baum HP. Hofbauer KG. Comnarison of chronic’ inhibition of renin and converting enzyme in the marmoset. Clin Exp Hypertens 1987;A9:337-43. Sweet CS, Ludden CT, Frederick CM, Bush LR, Ribeiro LGT. Comparative hemodynamic effects of MK-422, enalaprilat, a converting enzyme inhibitor and a renin inhibitor in dogs with acute left ventricular failure. J Cardiovasc Pharmacol 1984; 6:1067-75. Szelke M, Tree M, Leckie BJ, Jones DM, Atrash B, Geattie S, Donovan B, Hallett A, Hughes M, Lever AF, Morton JJ, Suei- ras-Diaz J. A transition-state analogue inhibitor of human re- nin (H.261). Test in vitro and a comparison with captopril in the anesthetized baboon. J Hypertens 1985;3:13-8. Takori K, Hartley LH, Burton J. Hypotensive effects of the renin inhibitor (RI-78) and the converting enzyme inhibitor (teprotide) in conscious monkeys. Clin Exp Hypertens 1987; A9:387-90. Burton J, Cody RJ Jr, Herd JA, Haber E. Specific inhibition of renin by an angiotensinogen analog. Studies in sodium de- pletion and renin-dependent hypertension. Proc Nat1 Acad Sci USA 198&77:5476-g. Hofbauer KG, Menard J, Niche1 JB, Wood JM. Inhibition of
October lSQ1
Amerlcen Heart Journal
renin in the primate Callithrix jaccbus (common marmoset). Clin Exp Hypertens 1985;A5:1237-47.
15. Hofbauer KG, Wood JM, Gulati N, Heusser C, Menard J. In- creased plasma renin during renin inhibition. Studies with a novel immunoassay. Hypertension 1985;7:161-5.
16. Data on file with Merck, Sharp & Dohme; and Physicians’desk reference. 44th ed. Oradell, NJ: Medical Economics Co Inc, 1990:1461-4.
17. Sealy JE, Laragh JH. How to do a plasma renin assay. Cardio- vast Med 1977;2:1079-92.
18. Jeunemaitre X, Menard J, Nussberger, Guyene TT, Brunner HR, Corvol P. Plasma angiotensins, renin, and blood pressure during acute renin inhibition by CGP 38 560A in hypertensive patients. Am J Hypertens 1989;2:819-27.
19. Leckie B, Szelke M, Hallett A. Peptide inhibitors of renin. Clin Exp Hypertens 1983;A5:1221-36.
20. Dzau VJ. Significance of vascular renin-angiotensin pathway. Hypertension 1986;3:199-203.
21. Dzau VJ, Gibbons G, Levin D. Renovascular hypertension. An update on pathophysiology, diagnosis and treatment. Am J Nephrol 1986;3:172-6.
22. Dzau VJ. Circulating versus local renin-angiotensin system in cardiovascular homeostasis. Circulation 1988;77(suppl I):I4- 13.
23. Unger T, Scholkens BA, Ganten D, Lang RE. Tissue convert- ing enzyme inhibition and cardiovascular effects of converting enzyme inhibitors. Clin Exp Hypertens 1987;A9:417-26.
24. Brunner HR, Waeber B, Nussberger J. Angiotensin-convert- ing enzyme inhibition versus blockade of the renin angioten- sin system. Am J Med 1989;87(suppl 68):155-85.





























