Embed Size (px)
Citation preview

www.elsevier.com/locate/ijcard
International Journal of Cardio
Impaired effect of endothelin-1 on coronary artery stiffness in
type 2 diabetes
Zenon S. Kyriakides a,*, Dimitrios Th. Kremastinos b, Athanasios E. Raptis b, Neil Johnston c,
Sotirios A. Raptis b, David J. Webb c, Stamatis Kyrzopoulos d, Eftichia Sbarouni d
a Red Cross Hospital, Athens, Greece, 2nd Cardiology Department, University of Athens, School of Medicine,
University General Hospital ‘‘Attikon’’, Athens, Greeceb 2nd Department of Internal Medicine- Propaedeutic, Research Institute and Diabetes Center, University of Athens, School of Medicine,
University General Hospital ‘‘Attikon’’, Athens, Greecec University of Edinburgh, Western General Hospital, UK
d Onassis Cardiac Center, Athens, Greece
Received 13 June 2005; received in revised form 4 August 2005; accepted 18 September 2005
Available online 2 December 2005
Abstract
Aim: We examined whether there is a differential effect of endothelin-A antagonism on coronary artery compliance in type 2 diabetes
mellitus compared to non-diabetic patients.
Patient and methods: We examined 32 patients, 11 type 2 diabetes mellitus and 21 non-diabetic patients, with atherosclerotic epicardial
arteries free of significant luminal stenoses. Intracoronary BQ-123 (6 Amol), an endothelin-A receptor antagonist, was infused over 20 min.
The artery lumen area in the proximal arterial segment was measured at end diastole and end systole before and after BQ-123 administration
using an intravascular ultrasound catheter. Calculations were made of normalized arterial compliance index, in mm Hg�1�103 and of arterialstiffness index h.Results: Pulse pressure and heart rate did not change after BQ-123. In type 2 diabetes mellitus, normalized compliance index decreased from
1.79T1.36 at baseline to 1.29T0.82 after BQ-123 administration, whereas in non-diabetic patients it increased from 2.10T1.36 to 3.00T2.07( p <0.05 versus baseline) (F =6.39, p =0.02). In type 2 diabetes mellitus, b index increased from 1.97T0.53 to 2.46T0.95, whereas in non-
diabetic patients it decreased from 1.83T0.95 to 1.63T0.84 (F =7.80, p =0.009). Big endothelin-1 at baseline was correlated with the
baseline b index ( p <0.0001, r =0.68).
Conclusions: Big endothelin-1 is correlated with the coronary artery stiffness. The effect of endogenous endothelin-1 on coronary artery
stiffness is impaired in type 2 diabetes mellitus. This may have important therapeutic implications with respect to the introduction of
endothelin receptor antagonists as cardiovascular therapeutic agents.
D 2005 Elsevier Ireland Ltd. All rights reserved.
Keywords: Endothelin; Artery elasticity; Catheterization; Type 2 diabetes mellitus
1. Introduction
Endogenous production of endothelin-1 contributes to
the maintenance of coronary vascular tone in coronary
0167-5273/$ - see front matter D 2005 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.ijcard.2005.09.018
* Corresponding author. B Cardiology Department Red Cross Hospital, 1
Erythrou Stavrou str., Athens 115 26, Greece. Tel.: +30 210 6414 705, 6414
587, 8104 554; fax: +30 210 6414 587.
E-mail address: [email protected] (Z.S. Kyriakides).
artery disease and healthy controls [1]. In animal models of
diabetes reduced responsiveness to endothelin-1 is seen in
both the large vessels and the microvasculature [2,3]. In
addition, exogenous as well as endogenous endothelin-1
exerts impaired vasoconstriction, in forearm arteries, in
patients with type 2 diabetes mellitus [4,5]. Compensatory
vessel enlargement occurs to a greater degree in patients
with unstable than with stable coronary syndromes, and is
associated with increased coronary artery distensibility
logy 112 (2006) 207 – 212

Table 1
Clinical features of the patients studied
Diabetic
patients
(n =11)
Non-diabetic
patients
(n =21)
Age, years 60T10 55T11Sex, M/F 10/1 17/4
Smoking, n 4 7
Systemic hypertension, n 6 8
Blood cholesterol, mg% 196T41 209T41Triglycerides, mg% 136T80 170T140
HDL-cholesterol, mg% 37T8 37T9
Patients on anti-diabetic diet, n 4 –
Patients taking anti-diabetic tablets, n 7 –
Blood glucose during catheterization, mg% 129T29 99T21*
HbA1c, % 7.4T1.6 5.5T0.6*
Studied artery, n
Left anterior descending artery 3 5
Right coronary artery 8 16
Medications, n
Z.S. Kyriakides et al. / International Journal of Cardiology 112 (2006) 207–212208
[6,7]. In diabetic patients coronary compliance is decreased
[8]. Recently, we showed that endothelin receptor antago-
nists improve coronary artery compliance in patients with
atherosclerotic vessels [9]. The role of endothelin-1 in the
regulation of vascular tone and coronary artery compliance
and the potential benefits of endothelin antagonists in
patients with type 2 diabetes mellitus are less clear.
Endothelin-1 binds to at least 2 receptors: the endothelin-A
receptor appears to be the major receptor causing vasocon-
striction in arteries, the endothelin-B receptor mediates
release of endothelium-dependent vasodilator substances
and is also present in some resistance and capacitance
arteries, where it contributes to vasoconstriction [10].
The aim of this study was to examine whether there is a
differential effect of endothelin-A antagonism on coronary
artery compliance in type 2 diabetes mellitus compared to
non-diabetic patients.
Beta blockers 3 8
Aspirin 10 20
Calcium channel blockers 6 7
Angiotensin converting enzyme
inhibitors or angiotensin receptor blockers
8 11
Statins 11 11
HbA1c: hemoglobin A1c; *p <0.05 versus diabetic patients.
2. Patients and methods
The Hospital Ethics Committee approved the study and
all patients gave written informed consent.
2.1. Study group
Forty patients with chest pain, on the waiting list for
diagnostic coronary angiography, were selected prospec-
tively on the basis of the following criteria: 1) atheroscle-
rotic epicardial arteries without significant coronary artery
stenoses and not calcified, 2) normal left ventricular ejection
fraction, and 3) coronary arteries eligible for intravascular
ultrasound studies [9].
Non diabetic patients underwent an oral glucose toler-
ance test in order the patients with impaired glucose
tolerance to be excluded.
2.2. Exclusion criteria
Acute or old myocardial infarction, unstable angina,
additional cardiac disease and severe non-cardiac disease.
All medications were discontinued at least 12 h before
the procedure.
Five patients were rejected for not having intravascular
ultrasound studies of sufficient quality, and 3 for having
impaired glucose tolerance tests. As a result, 32 patients
completed the study (Table 1).
2.3. Protocol
After the end of diagnostic coronary arteriography 2000
IU of heparin were administered.
Intravascular ultrasound studies were performed with an
Avanar, 2.9 French catheter of JoMed (Rijswijk, The
Netherlands) and image protocol was the same as indicated
earlier [9].
Maximal and minimal lumen areas at the selected sites
were identified during frame-by-frame playback analysis.
Vascular pulsatility, absolute compliance, normalized com-
pliance, and the stiffness index (h), which is considered to
be independent of the changes in blood pressure, were
obtained as indicated earlier [9]. Inter-observer variability
were very low [9].
Blood was obtained from the femoral artery sheath,
immediately before and after BQ-123 infusion for assay of
endothelin-1, big endothelin-1, renin and aldosterone
plasma levels.
2.4. Drug administration
After baseline recordings, while the catheter was in the
same site of the coronary artery, endothelin-A receptor
antagonist BQ-123 (Clinalfa, CH) was administered intra-
coronarily at a constant rate of 1 ml/min (300 nmol/min)
for 20 min. Before the initiation of BQ-123 infusion,
normal saline 0.9% was infused at a rate of 1 ml/min for 5
min and then the first baseline recordings were performed
(heart rate and arterial blood pressure—from the guiding
catheter—synchronously with intravascular ultrasound
recordings). The 2nd recordings were taken immediately
at the end of the 20 min infusion of BQ-123. The dose of
BQ-123 administered in this study (total dose of 6 Amol)
has been shown in other studies not to cause systemic
hemodynamic effects [10]. In the present study, this dose
was administered directly into the coronary circulation in
order to maximise delivery of the drug to the heart. The

Z.S. Kyriakides et al. / International Journal of Cardiology 112 (2006) 207–212 209
local concentrations achieved are likely to be greater than
the IC50 at the ETA receptor, but still selective for inhibition
of the ETA receptor, given the ¨2500-fold greater
selectivity of BQ-123 for this receptor, over the ETB
receptor [11].
2.5. Endothelin-1, big endothelin-1, aldosterone and renin
estimation
The very low levels of endothelin-1 and big endothelin-1
in plasma preclude the direct measurement of these peptides
by radioimmunoassay. Therefore endothelin-1 and big
endothelin-1 must first be extracted from plasma using a
sample preparation column, concentrated and the subse-
quent extract analyzed by radioimmunoassay. The extrac-
tion technique used is an acetic acid extraction and shown to
give the best recovery of endothelin-1 from plasma at 89%
[12]. Subsequent evaluation within our laboratory has also
shown this technique to give a recovery of big endothelin-1
of 91%.
The radioimmunoassays used were based on the com-
mercially available Bachem kits for the determination of
endothelin-1 and big endothelin-1 in plasma. (Bachem
(UK) Ltd, St. Helens, England). Intra assay (within day)
variation was 6.3% and inter assay (day to day) variation
was 7.2%.
Aldosterone was measured by ‘‘coat a count’’ radioim-
munoassay in serum. (Diagnostic Products Corporation, Los
Angeles, CA). Intra and inter assay variation were 3.5% and
6.5%, respectively.
Plasma Renin Activity in plasma was determined by
radioimmunoassay kit (Perkin-Elmer Life Sciences, Boston,
Table 2
The variables before and after BQ-123 administration
Pulse pressure, mm Hg Diabetic patients
Non-diabetic patients
Diastolic area, mm2 Diabetic patients
Non-diabetic patients
Arterial area change during systole, mm2 Diabetic patients
Non-diabetic patients
Pulsatility, % Diabetic patients
Non-diabetic patients
Absolute compliance index, mm2/mm Hg�1000 Diabetic patients
Non-diabetic patients
Normalized compliance index, mm Hg�1�1000 Diabetic patients
Non-diabetic patients
Index h Diabetic patients
Non-diabetic patients
Endothelin-1, pg/ml Diabetic patients
Non-diabetic patients
Big endothelin-1, pg/ml Diabetic patients
Non-diabetic patients
Aldosterone, pg/ml Diabetic patients
Non-diabetic patients
Renin, ng/ml Diabetic patients
Non-diabetic patients
* p <0.05 versus baseline.
MA). Intra and Inter assay variation were 5.2% and 8.6%,
respectively.
3. Statistical analysis
All data were expressed as mean valueT standarddeviation. Analysis of variance with repeated measures
was used for the statistical evaluation of the results,
followed by Tukey’s honestly significant difference test
for post-hoc comparisons. Linear regression analysis using
the least-square difference was used in order to examine
correlations between the different variables studied. A p
value of <0.05 was considered as statistically significant.
4. Results
Clinical characteristics, apart from the increased blood
glucose and hemoglobin A1c concentrations, which were
higher in type 2 diabetes mellitus, were similar in the two
groups (Table 1). Type 2 diabetes mellitus had systolic
hypertension more often, but this was not statistically
significant.
4.1. Intracoronary ultrasound and blood pressure
measurements
Heart rate at baseline was similar in the two groups
(69T9 beats/min in the type 2 diabetes mellitus and 74T16beats/min in the non-diabetic patients and did not change
after BQ-123 administration. Systolic blood pressure
Baseline After BQ-123 F p value
76T17 70T17 0.47 0.5
65T21 61T17
11.5T5.4 12.4T5.0 0.48 0.5
10.2T3.7 11.6T3.41.29T0.63 1.04T0.75 7.17 0.01
1.37T1.02 1.99T1.38*
13T9 9T7 8.07 0.008
13T8 18T12
18T10 15T8 6.31 0.02
23T18 35T27*
1.79T1.36 1.29T0.82 6.39 0.02
2.10T1.36 3.00T2.07*
1.97T0.53 2.46T0.95 7.80 0.009
1.83T0.95 1.63T0.84
1.87T0.71 1.51T0.75 0.05 0.8
1.94T1.44 1.43T0.96
46T22 39T23 1.28 0.3
76T121 188T32353T64 32T29 0.04 0.8
49T53 31T33
0.37T0.15 0.43T0.21 0.65 0.4
0.63T0.65 0.93T1.15
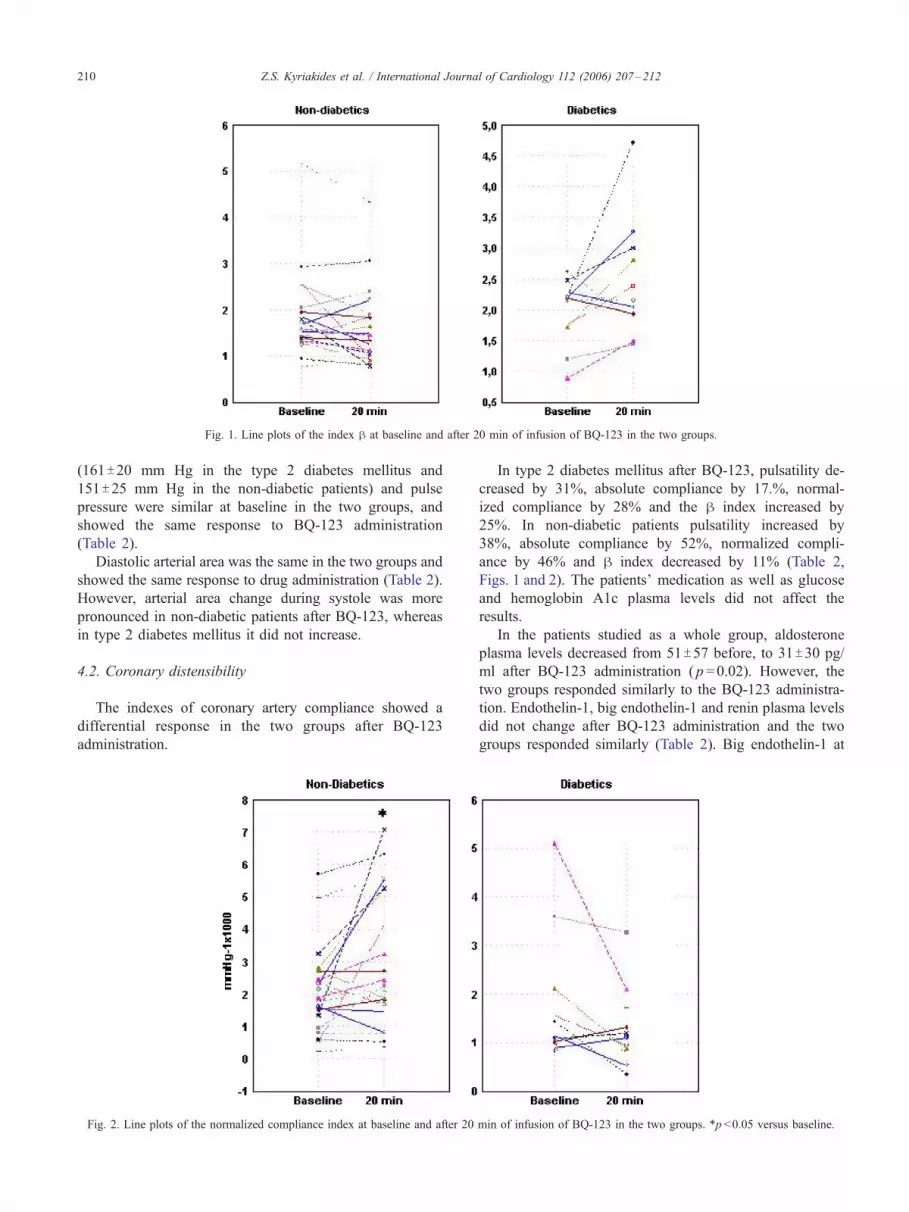
Fig. 1. Line plots of the index h at baseline and after 20 min of infusion of BQ-123 in the two groups.
Z.S. Kyriakides et al. / International Journal of Cardiology 112 (2006) 207–212210
(161T20 mm Hg in the type 2 diabetes mellitus and
151T25 mm Hg in the non-diabetic patients) and pulse
pressure were similar at baseline in the two groups, and
showed the same response to BQ-123 administration
(Table 2).
Diastolic arterial area was the same in the two groups and
showed the same response to drug administration (Table 2).
However, arterial area change during systole was more
pronounced in non-diabetic patients after BQ-123, whereas
in type 2 diabetes mellitus it did not increase.
4.2. Coronary distensibility
The indexes of coronary artery compliance showed a
differential response in the two groups after BQ-123
administration.
Fig. 2. Line plots of the normalized compliance index at baseline and after 20
In type 2 diabetes mellitus after BQ-123, pulsatility de-
creased by 31%, absolute compliance by 17.%, normal-
ized compliance by 28% and the h index increased by
25%. In non-diabetic patients pulsatility increased by
38%, absolute compliance by 52%, normalized compli-
ance by 46% and h index decreased by 11% (Table 2,
Figs. 1 and 2). The patients’ medication as well as glucose
and hemoglobin A1c plasma levels did not affect the
results.
In the patients studied as a whole group, aldosterone
plasma levels decreased from 51T57 before, to 31T30 pg/
ml after BQ-123 administration ( p =0.02). However, the
two groups responded similarly to the BQ-123 administra-
tion. Endothelin-1, big endothelin-1 and renin plasma levels
did not change after BQ-123 administration and the two
groups responded similarly (Table 2). Big endothelin-1 at
min of infusion of BQ-123 in the two groups. *p <0.05 versus baseline.

Fig. 3. Correlations between index h and baseline big endothelin-1.
Z.S. Kyriakides et al. / International Journal of Cardiology 112 (2006) 207–212 211
baseline was correlated to the baseline h index ( p <0.0001,
r =0.68), (Fig. 3).
5. Discussion
The present study demonstrates, for the first time, that
blockade of endothelin-A receptors results in an improve-
ment in coronary artery compliance in non-diabetic patients,
but not in type 2 diabetes mellitus patients, thereby
suggesting that endothelin-A-dependent activity is impaired
in the coronary arteries in type 2 diabetes mellitus patients.
It has been demonstrated that endothelin exerts a tonic
stiffening effect on the in vitro common carotid artery and that
this effect is mediated via the endothelin-A receptor [13]. In
the present study, big endothelin-1 plasma levels were
correlated to the stiffness of the coronary arteries, in
accordance with the above findings. However, in animal
models of diabetes and in patients with type 2 diabetes
mellitus, a reduced responsiveness to endothelin-1 is seen in
both the large peripheral vessels and themicrovasculature [2–
5]. Recently, a human study demonstrated that the effect of
endogenous endothelin-1 on endothelin-A receptors in the
periphery is enhanced in the resistance vessels of patients with
diabetes, whereas their sensitivity to exogenous endothelin-1
is blunted [14]. These discrepancies between the results of the
different studies could be ascribed to the following:
1) The patient’s quality of glucose control. It is possible that
a worse metabolic milieu may have affected the vaso-
dilatory mechanisms secondary to endothelin-A receptor
blockade, reducing the response to BQ-123;
2) The medications the patients were on and whether these
medications had been stopped before the study. Also, the
average duration of diabetes in the population may
contribute to the difference in the groups’ response;
3) Inter-individual variability, or to other unrecognised
factors; and
4) Gender issues.
In this study, we have extended, for the first time, these
observations concerning the effect of endothelin-1 in the
peripheral arteries of diabetic patients to the human
coronary circulation. We have demonstrated an improve-
ment in coronary artery compliance caused by endothelin-A
receptor antagonists in atherosclerotic arteries [9], which
was absent in type 2 diabetes mellitus patients.
BQ-123 has no inherent contractile action and has no
effect on the contractile response induced by various
agonists, indicating that the response to BQ-123 is due to
endothelin-1 antagonism rather than a non-specific action of
BQ-123 itself on the coronary vasculature [11].
There are several possible explanations to account for the
type 2 diabetes mellitus impaired response to endothelin-A
receptor antagonists as regards coronary artery compliance.
Hyperglycemia has been associated with increased basal
forearm blood flow [15] and hyperperfusion in the retinal
and glomerular microcirculation, which is reversible by
strict glycemic control [16]. Reduced contractility to
endothelin-1 of bovine pericytes in high concentrations of
glucose has been described [2]. It is possible that
hyperglycemia and insulin could cause endothelin-1 recep-
tor down-regulation. It is also possible that hyperglycemia
may result in glycosylation of the endothelin receptor and
impair receptor binding; alternatively, hyperglycemia may
impair intracellular events following binding to the endo-
thelin-A receptor. However, we detected no correlation
between the glucose blood levels and the coronary artery
compliance.
In our study we did not find higher endothelin-1 levels in
the type 2 diabetes mellitus than in non-diabetic patients as
in other studies [17]. It is possible, however, that tissue
rather than plasma endothelin-1 is important in determining
endothelin-A receptor down-regulation.
Finally, non-specific impairment of smooth muscle
constriction in diabetes is unlikely, as similar vasoconstric-
tion has been demonstrated in response to nonspecific
smooth muscle vasoconstrictors in diabetic patients and
control groups [18].

Z.S. Kyriakides et al. / International Journal of Cardiology 112 (2006) 207–212212
A consideration arising from our findings relates to their
possible clinical implications. These considerations may
become of practical significance as a result of the recent
introduction of non-peptidic endothelin receptor antagonists
as cardiovascular therapeutic agents.
5.1. Study limitations
Images of intravascular ultrasound represent a thin
tomographic cross-section of the artery and cannot be used
to evaluate changes simultaneously in adjacent regions or
the whole artery. A potential limitation of this study is that
measurement of coronary artery compliance may not reflect
changes in the microcirculation, which may also be
important. It would be valuable if similar findings could
be confirmed directly in the microcirculation itself. We did
not examine the effects of exogenous endothelin-1 on the
coronary artery compliance and the coronary circulation in
general, as this would not be so simple and would involve
risk for the patients studied.
In conclusion, the coronary artery stiffness effect of
endogenous endothelin-1 is impaired in type 2 diabetes
mellitus patients, and this may have important therapeutic
implications with respect to the introduction of endothelin
receptor antagonists as cardiovascular therapeutic agents.
This abnormality may participate in the pathophysiology of
vascular complications associated with diabetes. Further
studies in diabetic patients with systemic or pulmonary
hypertension are required to elucidate whether endothelin
antagonists will be of benefit in this group of patients.
References
[1] Kyriakides ZS, Kremastinos D, Bofilis E, Tousoulis D, Antoniadis A,
Webb DJ. Endogenous endothelin type A receptor stimulation in
patients undergoing coronary arteriography. Heart 2000;84:176–82.
[2] Chakravarthy U, McGinty A, McKillop J, Anderson P, Archer DB,
Trimble ER. Altered endothelin-1 induced contraction and second
messenger generation in bovine retinal microvascular pericytes
cultured in high glucose medium. Diabetologia 1994;37:36–42.
[3] Hodgson WC, King RG. Effects of glucose, insulin or aldose
reductase inhibition on responses to endothelin-1 of aortic rings
from streptozotocin-induced diabetic rats. Br J Pharmacol 1992;
106:644–9.
[4] Nugent AG, McGurk C, Hayes JR, Johnston GD. Impaired vasocon-
striction to endothelin 1 in patients with NIDDM. Diabetes 1996;
45:105–7.
[5] McAuley DF, McGurk C, Nugent AG, Hanratty C, Hayes JR,
Johnston GD. Vasoconstriction to endothelin-1 is blunted in non-
insulin-dependent diabetes: a dose– response study. J Cardiovasc
Pharmacol 2000;36:203–8.
[6] Jeremias A, Spies C, Herity NA, et al. Coronary artery compliance and
adaptive vessel remodeling in patients with stable and unstable
coronary artery disease. Heart 2000;84:314–9.
[7] Jeremias A, Spies C, Herity NA, et al. Coronary artery distensibility
and compensatory vessel enlargement—a novel parameter influencing
vascular remodeling? Basic Res Cardiol 2001;96:506–12.
[8] Vavuranakis M, Stefanadis C, Triandafyllidi E, Toutouzas K,
Toutouzas P. Coronary artery distensibility in diabetic patients with
simultaneous measurements of luminal area and intracoronary
pressure. Evidence of impaired reactivity to nitroglycerin. J Am Coll
Cardiol 1999;34:1075–81.
[9] Kyriakides ZS, Kremastinos DTh, Kolokathis F, Kostopoulou A,
Georgiadis M, Webb DJ. Acute endothelin A receptor antagonism
improves coronary artery compliance in coronary artery disease
patients. Clin Sci 2002;103:179S–83S.
[10] Haynes WG, Webb DJ. The endothelin family of peptides: local
hormones with diverse roles in health and disease? Clin Sci 1993;
84:485–500.
[11] Ihara M, Noguchi K, Saeki T, et al. Biological profiles of highly potent
endothelin antagonists selective for the endothelin A receptor. Life Sci
1992;50:247–55.
[12] Rolinski B, Sadri I, Bogner J, Goebel FD. Determination of
endothelin-1 immunoreactivity in plasma, cerebrospinal fluid and
urine. Res Exp Med (Berl) 1994;194:9–24.
[13] Marano G, Grigioni M, Palazzesi S, Ferrari AU. Endothelin and
mechanical properties of the carotid artery in Wistar–Kyoto and
spontaneously hypertensive rats. Cardiovasc Res 1999;41:701–7.
[14] Cardillo C, Campia U, Bryant MB, Panza JA. Increased activity of
endogenous endothelin in patients with type II diabetes mellitus.
Circulation 2002;106:1783–7.
[15] Halkin A, Benjamin N, Doktor HS, Todd SD, Viberti G, Ritter JM.
Vascular responsiveness and cation exchange in insulin-dependent
diabetes. Clin Sci 1994;81:223–32.
[16] Vora JP, Dolben J, Williams JD, Peters JR, Owens DR. Impact of
initial treatment on renal function in newly-diagnosed Type II (non-
insulin-dependent) diabetes mellitus. Diabetologia 1993;36:734–40.
[17] McAuley DF, Nugent AG, McGurk C, Maguire S, Hayes JR, Johnston
GD. Vasoconstriction to endogenous endothelin-1 is impaired in
patients with type II diabetes mellitus. Clin Sci 2000;99:175–9.
[18] Christlieb AR, Janka HU, Kraus B, et al. Vascular reactivity to
angiotensin II and nor epinephrine in diabetic subjects. Diabetes 1976;
25:268–74.





























