Embed Size (px)
Citation preview

Increased Nitric Oxide Radicals in PostmortemBrain From Patients With Schizophrenia
by Jeffrey K. Yao, Sherry Leonard, and Ravinder D. Reddy
Abstract
Alterations in antioxidant status in schizophrenia sug-gest free radical-mediated neurotoxicity; this findingcan be a consequence of increased free radical produc-tion. There are multiple pathways to excess free radi-cal generation and subsequent oxidative stress. Onesuch pathway is the formation of peroxynitrite by areaction of nitric oxide (NO) and superoxide radical.NO is formed from L-arginine by nitric oxide synthase(NOS). A constitutive cytosolic isoform, neuronal NOS(nNOS), appears to be fairly stable in the postmortembrain tissues. Utilizing a sensitive fluorometrie assay,NO levels were measured by its stable metabolites,nitrate and nitrite, in the caudate region of post-mortem brain tissues from patients and control sub-jects. In the human brain, NO is metabolized primar-ily in the form of nitrate. A significantly increased levelof NO was found in schizophrenia patients (241 ± 146pmol/mg dry weight, n = 18) than was found in thoseof normal (142 ± 65 pmol/mg dry weight, n = 20) andpsychiatric controls without schizophrenia (125 ± 83pmol/mg dry weight, n = 16) (analysis of covariance[ANCOVA], F = 6.446, df= 2,51,p = 0.003). These find-ings were independent of age, brain weight, post-mortem interval (PMI), sample storage time, or ciga-rette smoking. Elevated NO levels in the brains ofschizophrenia patients lend further support for thefree radical pathology in schizophrenia.
Keywords: Nitric oxide, caudate, postmortemchanges, schizophrenia.
Schizophrenia Bulletin, 30(4): 923-934, 2004.
Evidence suggests that free radicals are involved in mem-brane pathology and may play a role in schizophrenia(Cadet and Lohr 1987; Mahadik and Mukherjee 1996;Smythies 1997; Reddy and Yao 1999; Yao et al. 2001Z?).Free radicals are reactive chemical species generated dur-ing normal metabolic processes and, in excess, can dam-age lipids, proteins, and DNA. Regions of high oxygen
consumption, lipid content, and transition metals are atparticular risk (Smith 1992). Neuronal membranes aretherefore vulnerable to radical-mediated damage.Complex antioxidant defense systems exist to protectagainst oxidative stress. In schizophrenia, evidence for thedysregulation of free radical metabolism includes abnor-mal activities of critical antioxidant enzymes (Abdalla etal. 1986; Reddy et al. 1991; Yao et al. 1998a, 1999);reduced levels of antioxidants (Suboticanec et al. 1990;McCreadie et al. 1995; Brown et al. 1998; Yao et al.19986, 1998c; Yao et al. 2000); and other indices of lipidperoxidation in plasma, red blood cells, and cerebrospinalfluid (Prilipko 1992; Peet et al. 1993; McCreadie et al.1995; Mahadik et al. 1998). Such abnormalities have beenassociated with tardive dyskinesia, negative symptoms,neurological signs, poor premorbid function, and com-puted tomography scan abnormalities (Reddy and Yao1999). Studies to date have generally been exploratory.Further elucidation of the role of free radicals and antioxi-dants in schizophrenia and its treatment will require sys-tematic investigation.
Biological systems have evolved complex protectivestrategies against free radical toxicity. Under physiologi-cal conditions, the potential for free radical-mediateddamage is kept in check by the antioxidant defense sys-tem, which comprises several enzymatic and nonenzy-matic components. The critical antioxidant enzymesinclude superoxide dismutase, catalase, and glutathioneperoxidase (GSH-Px). These enzymes act cooperatively atdifferent sites in the metabolic pathway of free radicals.Superoxide dismutase catalyzes the conversion of super-oxide radicals to hydrogen peroxide. Catalase and glu-tathione peroxidase convert hydrogen peroxide to water.GSH-Px uses glutathione (GSH) to yield the oxidizedform of glutathione, which is converted back to GSH byglutathione reductase. Hydrogen peroxide is susceptible
Send reprint requests to Dr. J.K. Yao, VA Pittsburgh HealthcareSystem (Bldg. #13), 7180 Highland Drive, Pittsburgh, PA 15206; e-mail:[email protected].
923
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from

Schizophrenia Bulletin, Vol. 30, No. 4, 2004 J.K. Yao et al.
to autoxidation to form hydroxyl radicals, particularly inthe presence of metal catalysts such as iron.
In addition to superoxide and hydroxyl radicals, apathway to excess free radical generation and subse-quent oxidative stress is the formation of peroxynitriteby a reaction of nitric oxide radical and superoxide radi-cal (figure 1). NO can also produce hydroxyl radicals aswell as nitrogen dioxide radicals. NO is a free radicalbecause of its unpaired electron. Because NO radicalscannot produce initiation or propagation reactions, theydo not generate free radical chain reactions. However,NO is a unique second-messenger molecule that medi-ates a number of cellular functions including neurotrans-mission, neurotoxicity and plasticity, vasodilation, regu-lation of blood flow, and inhibition of plateletaggregation (Moncada et al. 1991; Bredt and Snyder1992; Ignarro et al. 1999; Krukoff 1999). Elevated NOproduction has been linked to various neurodegenerative
disorders including Alzheimer's disease (Norris et al.1996; Thorns et al. 1998), multiple sclerosis (Heales etal. 1999), and Parkinson's disease (Bockelmann et al.1994; Hunot et al. 1996; Gerlach et al. 1999). We under-took this investigation to determine whether increasedNO production is also present in schizophrenia. We mea-sured NO in the caudate region of postmortem brain tis-sues by its stable metabolites, nitrate and nitrite, using afluorometric assay.
MethodsPostmortem Brain Tissues. Tissues were collected atautopsy from several sources in the Denver area:University Hospital, Denver Veterans AdministrationHospital, the coroner's offices of Arapahoe and Denvercounties, and the Mile High Tissue Bank. Complete med-ical histories of the subjects, including their age, sex, race,
Figure 1. Production of nitric oxide radicals and decomposition of peroxynitrite pathways
NOS ArginaseL-Citrulline <-^ L-Arginine • Ornithine + Urea
NO SODH2O2
ONOO" ONOOH
•NO,
Radical scavengers
NO, Lipid Per oxidation
Note.— GSH = glutathione; GSSG = oxidized glutathione; H2O2 = hydrogen peroxide; NOS = nitric oxide synthase; NO = nitric oxide;NO2~ = nitrite; O2«~ = reactive oxygen species; »OH = hydroxy radical; ONOO" = peroxynitrite anion; ONOOH = peroxynitrous acid;SOD = superoxide dismutase.
924
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from

Increased Nitric Oxide Radicals in Postmortem Brain Schizophrenia Bulletin, Vol. 30, No. 4, 2004
cause of death, drug regimen, PMI, and detailed smokingand drinking histories, were taken from hospital charts,physicians, and family members. All patients with schizo-phrenia and other mental disorders (e.g., bipolar disorder,depression, alcoholism, and drug addiction) were onantipsychotic medications at the time of death. At the timeof autopsy, the brain was removed and hemisectioned inthe sagittal plane. One-half of the cerebrum, cerebellum,and brainstem was immersed in 10 percent formalin andfixed for 1 to 2 weeks for neuropathology evaluation. Theother hemisphere was sliced coronally and transported onaluminum plates, previously chilled on ice, to the labora-tory for dissection. To avoid hemispheric bias, alternate(left/right) hemispheres were collected. Immediately aftersample collection, tissue was dissected from approxi-mately 50 areas in 1-gram pieces and frozen on dry icesnow. The remainder of the hemisphere was also frozenon slabs of dry ice and stored with the dissected parts at-80 °C. In the present study, caudate regions from schizo-phrenia and control groups were used for NO analyses.Tissues were shipped on dry ice by Federal Express to Dr.Yao's laboratory at the Highland Drive VA PittsburghHealthcare System, Pittsburgh, PA.
Tissue Preparation. Approximately 0.2 g of brain sam-ple was first lyophilized before the dry weight was taken.Samples were then homogenized in 1.2 mL of 20 mMTris-HCl (pH = 7.4). Following centrifugation for 10 min-utes at 3,000 rpm, the cell-free homogenate was furtherdeproteinized by addition of 100 JJLL of 5 percentmetaphosphoric acid. The protein precipitates wereremoved by centrifugation for 10 minutes at 3,000 rpm.The resulting protein-free supernatant was used to per-form the NO assays.
Determination of Nitric Oxide Levels. Because nitricoxide is rapidly converted to nitrate and nitrite in vivo, wemeasured the sum of nitrate and nitrite (usingFluorometric Nitric Oxide kits by Calbiochem of La Jolla,CA) as an index of total NO produced. In brief, 20 (JLL ofeach protein-free homogenate was added to a 96-well flu-orometric detection plate. To each sample well we added80 (xL of assay buffer, 10 (JLL of enzyme cofactors, and 10|xL of nitrate reductase. The plates were covered and incu-bated at 24 °C for 2 hours. After incubation, 20 nL of 2,3-diaminonaphthalene (DAN) reagent and 10 (xL of sodiumhydroxide were added to each well. Detection was per-formed with a 1420 Victor2 multilabel counter using anexcitation wavelength of 375 nm and an emission wave-length of 415 nm. We calculated NO levels using a stan-dard curve generated by a nitrate standard. The assay islinear to 500 pmol. The sensitivity of this assay is lessthan 5 pmol.
Measurement of Nitrite and Nitrate Levels. Nitrite lev-els were determined using the same procedure describedabove, except that nitrate reductase and enzyme cofactorwere omitted in the incubation mixture. Nitrite contentswere determined using a standard curve generated by anitrite standard, whereas levels of nitrate were calculatedby subtraction of nitrite contents from the total NO pro-duced.
Statistical Analyses. We conducted multiple regressionanalyses to determine whether the brain collection andstorage variables (age, PMI, brain weight, and storagetime) were significantly associated with the biochemicalmeasures of interest. Separate regression analyses wereconducted for each of the biochemical measures. Thebrain collection and storage measures were entered intoeach of the regression analyses as predictor variables.We examined the distributions for all variables with nor-mality plots and the Kolmogorov-Smirnov test (Siegel1956), which quantifies the discrepancy between datadistribution and an ideal Gaussian distribution. We usedthe Dallal and Wilkinson approximation (Dallal andWilkinson 1986) to Lilliefors' test to compute the p val-ues. The data pass the normality test if p > 0.10. For nor-mally distributed data, we compared means and vari-ances with / tests and F tests. Fisher's exact test wasused to compare the frequency distributions of smokingand alcohol use between the schizophrenia and controlgroups.
We conducted one-way analysis of variance(ANOVA) to evaluate group differences for brain collec-tion and storage parameters among the schizophreniagroup and the two control groups: those with and with-out other mental disorders. We conducted analysis ofcovariance (ANCOVA) to control statistically for thepotential effects of the brain collection and storage vari-ables on the group differences for the biochemical mea-sures of interest. Group means for the NO measureswere compared using ANOVAs, with pairwise compar-isons (2-tailed unpaired t tests) following significantfindings.
Results
Brain Collection and Storage Parameters. We con-ducted ANOVAs to evaluate group differences in braincollection and storage parameters (table 1). Significantdifferences between the schizophrenia and control sam-ples were found in brain weights, PMI, and storage time.
The distribution of PMI among three groups is shownin figure 2. Only three samples from the schizophreniagroup have a PMI exceeding 40 hours; the PMI of theremaining samples are all within 30 hours.
925
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from

Schizophrenia Bulletin, Vol. 30, No. 4, 2004 J.K. Yao et al.
Table 1. Brain collection and storage parameters (mean ± SD)
Parameters
n
Age, yrs
Sex (male/female)
Smoker (yes/no)
Postmortem interval (hrs)
Brain weight (g)
Storage time (mos)
Schizophrenia
patients
18
55.4 ±15.3
16/2
14/4
24.2±12.61
1410 ±1692
39.7 ± 21.93
Without MD
20
55.7 ±14.5
13/7
14/6
14.4 ±7.5
1258 ±143
25.2 ±15.3
Controls
With other MD
16
47.3 ±13.3
16/0
13/3
16.4 ±6.6
1410 ±98
24.1 ±12.2
Note.—SD = standard deviation; ANOVA = analysis of variance; MD = mental disorders.1 Significantly higher than both control groups (ANOVA, F = 3.18, df= 2,51, p = 0.0058).2 Significantly higher than control group without MD (ANOVA, F = 3.18, df = 2,51; p= 0.0016).3 Significantly higher than both control groups (ANOVA, F = 3.18, d/=2,51, p = 0.0138).
Figure 2. Distribution of PMI between schizophrenia and control groups
40
30
20
10
0
• ••
• • " •• • • A
A *
• : ^
• A A A
• A
•• A AA A
A
• • T T T
T
• _•
TTT
Schizophrenia Patients Controls
GroupsControls - MD
Note.—MD = mental disorders; PMI = postmortem interval.
926
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from

Increased Nitric Oxide Radicals in Postmortem Brain Schizophrenia Bulletin, Vol. 30, No. 4, 2004
The distributions for all variables were examinedusing normality plots and the Kolmogorov-Smirnov test.The data pass the normality test if p > 0.10. Results didnot indicate that normality transformations of the datawere necessary. In addition, the frequency of smokingwas not significantly different between the schizophreniaand the control groups (Fisher's exact test).
Edema Measurement in Caudate Samples. Cerebraledema is commonly seen in various pathologicalprocesses in brain. To determine the water content incaudate samples, we measured both the fresh and dryweight of each sample and used the formula of Elliottand Jasper (1949) to calculate the percentage ofswelling (edema) or shrinkage. Water levels in the post-mortem caudate were significantly higher in the schizo-phrenia group than in the control groups (table 2).Samples from the schizophrenia group showed an aver-age of 15 percent swelling compared with the controlsamples. Therefore, we lyophilized our samples beforemeasuring NO.
Quantitative Determination of NO Levels. To mea-sure the distribution of NO metabolites, we measuredboth nitrate and nitrite levels. More than 90 percent ofNO metabolites in the human brain are in the form ofnitrates (figure 3).
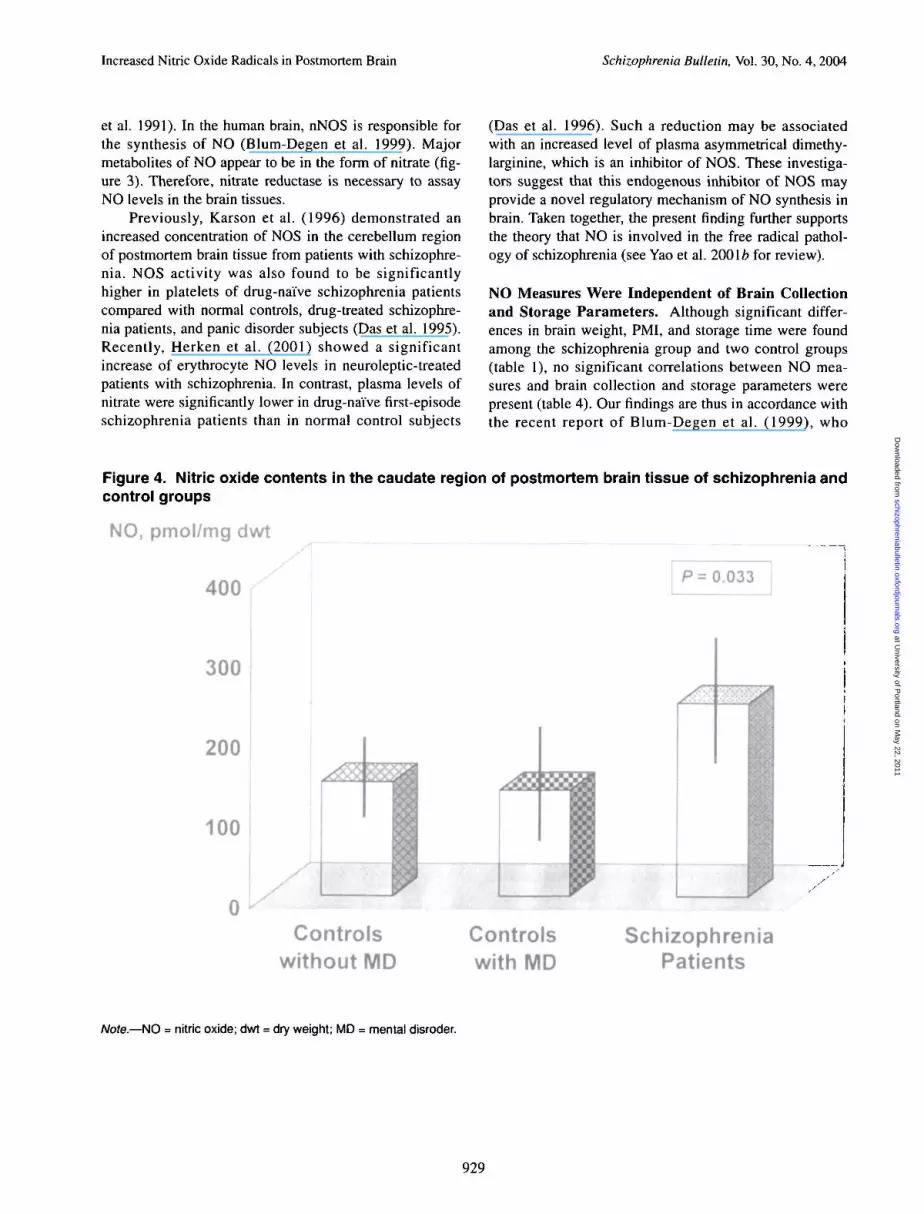
The mean levels of NO in the caudate region ofpostmortem brain tissue were significantly higher(ANCOVA, F = 6.446; df= 2,51; p = 0.003) in the schiz-ophrenia group than in the control groups (table 3). Toavoid the confounding effect of PMI, three samples withPMI greater than 30 hours in the schizophrenia group(figure 2) were omitted from the statistical analyses. Themean levels of NO in the caudate region of postmortembrain tissue were still significantly higher (ANCOVA,F = 5.481; df= 2,48; p = 0.007) in schizophrenia groupthan in the control groups (table 3 and figure 4).
Individual regression analyses were conducted todetermine whether age, PMI, brain weight, or storagetime were significantly associated with NO measures.None of these collection and storage parameters were sig-nificantly associated with NO measures (table 4).
Table 2. Measurement of edema in brain caudate region (mean ± SD)
Groups Fresh weight(mg) Dry weight (mg) Dry weight (%) Edema1 (%
ControlsWithout MDWith MD
Schizophrenia patients
159.7 ±32.2141.9 ±22.8
137.0 ±24.8
35.4 ±9.933.2 ±10.2
27.1 ±6.4
22.3 ± 3.822.6 ±4.0
18.9±2.4215.3
Note.—SD = standard deviation; MD = mental disorder.1 The percentage of swelling (edema) or shrinkage was calculated using the formula of Elliott and Jasper (1949).2 The dry weight of samples from schizophrenia subjects is significantly lower than that of control groups either with (p = 0.0033) or with-out (p = 0.0024) other mental disorders.
Table 3. Comparison of nitric oxide levels in the caudate region of postmortem brain tissue betweenschizophrenia patients and control groups
Controls(pmol/mg dry wt) ANCOVA
Methods
Schizophreniapatients
dry wt)Without MD(mean ± SD)
With other MD(mean ± SD) df
All samples
Samples1 withPMI < 30 hrs
241 ±146
209 ± 80
142 ±65
142 ±65
125 ±83
125 ±83
6.446 2,51
5.481 2,48
0.003
0.007
Note.— ANCOVA = one-way analysis of variance with covariates including age, postmortem interval (PMI), brain weight, and storagetime; MD = mental disorders; SD = standard deviation.1 Only three samples with PMI > 30 hours from the schizophrenia patients group were omitted from the comparison.
927
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from

Schizophrenia Bulletin, Vol. 30, No. 4, 2004 J.K. Yao et al.
Figure 3. Distribution of nitric oxide metabolites in brain caudate region
100
80
60-
40-
20
Nitric oxide Nitrite(pmol) (pmol)
Nitrate(pmol)
Nitrate
Table 4. Correlations between nitric oxide levels and brain collection and storage parameters
Groups
Schizophrenia patients
Controls without MD
Controls with other MD
n
18
20
16
Age
-0.0041
-0.0709
-0.1413
r (Correlation
Brain weight
0.1219
-0.1266
0.2508
Coefficient)
PMI
0.4486
0.3011
0.2107
Storage time
-0.2744
-0.1320
-0.2374
Note.— MD = mental disorder; PMI = postmortem interval.
Effect of Cigarette Smoking on NO Levels. Cigarettesmoke contains many pro-oxidants. To test whether NOlevels were affected by cigarette smoking, NO measureswere correlated with the number of cigarettes smoked byeach subject daily. Cigarette smoking data were available in81.5 percent of total samples examined. No significant cor-relations existed between NO levels and cigarette smokingin either total samples (r = 0.028, n = 44, p = 0.855) or theschizophrenia group (r = 0.078, n - \5,p- 0.782).
Discussion
Increased NO Production in Schizophrenia. The pre-sent study provides the first evidence of increased NOproduction in the postmortem brain tissue of patients withschizophrenia (figure 4). NO is the product of a five-elec-tron oxidation of the amino acid L-arginine by NOS(Palmer et al. 1988). The three isoforms of the NOS fam-ily are neuronal, inducible, and endothelial (Forstermann
928
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from
Increased Nitric Oxide Radicals in Postmortem Brain Schizophrenia Bulletin, Vol. 30, No. 4, 2004
et al. 1991). In the human brain, nNOS is responsible forthe synthesis of NO (Blum-Degen et al. 1999). Majormetabolites of NO appear to be in the form of nitrate (fig-ure 3). Therefore, nitrate reductase is necessary to assayNO levels in the brain tissues.
Previously, Karson et al. (1996) demonstrated anincreased concentration of NOS in the cerebellum regionof postmortem brain tissue from patients with schizophre-nia. NOS activity was also found to be significantlyhigher in platelets of drug-naive schizophrenia patientscompared with normal controls, drug-treated schizophre-nia patients, and panic disorder subjects (Das et al. 1995).Recently, Herken et al. (2001) showed a significantincrease of erythrocyte NO levels in neuroleptic-treatedpatients with schizophrenia. In contrast, plasma levels ofnitrate were significantly lower in drug-naive first-episodeschizophrenia patients than in normal control subjects
(Das et al. 1996). Such a reduction may be associatedwith an increased level of plasma asymmetrical dimethy-larginine, which is an inhibitor of NOS. These investiga-tors suggest that this endogenous inhibitor of NOS mayprovide a novel regulatory mechanism of NO synthesis inbrain. Taken together, the present finding further supportsthe theory that NO is involved in the free radical pathol-ogy of schizophrenia (see Yao et al. 200\b for review).
NO Measures Were Independent of Brain Collectionand Storage Parameters. Although significant differ-ences in brain weight, PMI, and storage time were foundamong the schizophrenia group and two control groups(table 1), no significant correlations between NO mea-sures and brain collection and storage parameters werepresent (table 4). Our findings are thus in accordance withthe recent report of Blum-Degen et al. (1999), who
Figure 4. Nitric oxide contents in the caudate region of postmortem brain tissue of schizophrenia andcontrol groups
NO, pmol/mg dwt
400
300
200
100
Controlswithout MD
Controlswith MD
SchizophreniaPatients
Note.—NO = nitric oxide; dwt = dry weight; MD = mental disroder.
929
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from

Schizophrenia Bulletin, Vol. 30, No. 4, 2004 J.K. Yao et al.
demonstrated that NOS activity remains unchanged dur-ing aging and is independent of PMI, gender, or samplestorage time.
Regional Distribution of NO Levels in the Brain.Nitric oxide is a highly diffusible cell-signaling mole-cule that is widely distributed in various regions of thebrain. Recently, Blum-Degen et al. (1999) found NOSactivity in 28 regions of the human brain, with the high-est levels of activity in the cerebellar cortex, nucleusaccumbens, substantia innominata, and subthalamicnucleus. They also demonstrated the presence of argi-nine and citrulline, precursor and product, respectively,of the NOS reaction, in these same regions of the brain.Although present data only show the increased NO pro-duction in the caudate region of the postmortem brainfrom patients with schizophrenia, elevated NO may alsoexist in other regions of the brain. We are currentlyexploring this possibility.
Possible Mechanisms Involving NO Production. Inaddition to the nNOS in the brain, various immunomodu-lators such as lipopolysaccharide and interferon caninduce NO production through the inducible NOS(Lorsbach et al. 1993; Lowenstein et al. 1993). A recentstudy on effects of bilateral infusion of interleukin-6 (IL-6) in the rat hippocampus indicated that IL-6 could induceNOS (Ma and Zhu 2000). Elevated levels of plasma IL-6have previously been reported in patients with schizo-phrenia (Shintani et al. 1991; Ganguli et al. 1994; Maes etal. 1995; Lin et al. 1998; van Kammen et al. 1999). Thus,increased NO production in the brains of schizophreniapatients may be mediated through an IL-6 induction.
Alternatively, NO levels can be regulated by theenzyme arginase, which is responsible for the hydrolysisof arginine to ornithine and urea. Reciprocal regulatorymechanisms exist between NOS and arginase pathways.Increased arginase activity leads to substrate depletionand thereby reduction of the NOS reaction (Corraliza etal. 1995), whereas inhibition of arginase by L-hydrox-yarginine (metabolite of NO pathway) may increase NOproduction (Daghigh et al. 1994).
Interaction Between NO Radicals and ThiolScavengers. Under physiological conditions, NO and itsmetabolites react with various thiols (e.g., GSH) to formstable S-nitrosothiols (Kharitonov et al. 1995fc). Thesethiol compounds play an important role in the suppressionof NO functions in cellular membranes. Recently, Gegg etal. (2003) demonstrated an increase of GSH in astrocytesexposed to NO. The present findings suggest that, to sup-press the NO radical function, the level of cytosolic thiolcompounds may be elevated in response to increased NO
production (Yao et al. 2001a). Thus, the reaction of NOwith free thiols may compete with a substrate such asGSH for decomposition of hydrogen peroxide by GSHperoxidase (figure 1).
NO-Induced Brain Edema. Previously, Brown et al.(1986) showed that the brains of patients with schizo-phrenia were 6 percent lighter and had lateral ventriclesthat were 19 percent larger in the anterior. They sug-gested that such enlargement is associated with tissueloss in the temporal lobe. The present study also demon-strated a decreased level of dry weight or increased watercontent in caudate region in patients with schizophreniacompared with the control groups (table 2), suggestingthe presence of brain edema in schizophrenia.Breakdown of the blood-brain barrier (BBB) is known tolead to vasogenic edema and secondary brain damage.Free radicals have long been considered contributors tothe alteration of BBB permeability that underlies brainedema (Demopoulous et al. 1972). Recent studies alsodemonstrated that NO can increase the permeability ofthe BBB that allows plasma constituents to enter thebrain (Schilling and Wahl 1997; Thiel and Audus 2001).Moreover, the association of brain edema with increasedNO production has been demonstrated in various experi-mental models for brain injury including hyperthermicbrain injury (Aim et al. 1998; Sharma et al. 2000), pneu-mococcal meningitis (Koedel et al. 1995), hyperammone-mia (Larsen et al. 2001), and cold injury (Gotoh et al.1998; Nag et al. 2000, 2001). On the other hand, inhibit-ing or deleting NOSs (Hara et al. 1996; Calapai et al.2000; Sharma et al. 2000; Takemori et al. 2000), free rad-ical scavengers (Petty et al. 1996), and antioxidants(Kawamata et al. 1997) could attenuate edema formation.Taken together, our present data further support thenotion that NO plays a pivotal role in the pathogenesis ofbrain damage.
Effect of Cigarette Smoking on NO Production.Cigarette smoking has long been associated with anincreased risk of cardiovascular and pulmonary diseases,which may be modulated by endogenous NO (Kharitonovet al. 1995a). Specifically, cigarette smoking reduces thelevels of exhaled (Kanazawa et al. 1996), nasal (Olin etal. 1998), and serum (Node et al. 1997) NO but increasesNO levels in breath condensate in healthy subjects (Balintet al. 2001). In addition, the platelet-derived NO release issignificantly impaired in long-term smokers, which leadsto an increase in platelet aggregability (Ichiki et al. 1996).On the other hand, smoking cessation is associated withan increased level of exhaled NO (Robbins et al. 1997).Thus, it appears that cigarette smoking may inhibit theenzyme NOS. In the present study, most samples were
930
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from

Increased Nitric Oxide Radicals in Postmortem Brain Schizophrenia Bulletin, Vol. 30, No. 4, 2004
obtained from subjects who smoked (table 1). No signifi-cant correlation between NO measures and cigarettesmoking was present. Therefore, the increased levels ofcaudate NO in the schizophrenia group appear to be inde-pendent of cigarette smoking.
Effect of Antipsychotic Drugs on NO Production.Arnaiz et al. (1999) recently demonstrated that haloperidolinhibits NO production in submitochondrial particles frommice, suggesting inhibited mitochondria] electron transferwith enhanced superoxide radical and hydrogen peroxideproduction. This finding is in accordance with that ofRengasamy and Johns (1993), which showed an inhibitionof NO synthase by a superoxide generating system.Moreover, Prince et al. (1997) reported that cytochromeoxidase enzyme activity increased in specific regions of therat brain following chronic neuroleptic treatment. Inhumans, platelet NOS was found to be significantly higherin drug-naive schizophrenia patients than in normal con-trols. Treatment with chlorpromazine, haloperidol, or cloza-pine appeared to normalize platelet NOS levels in patientswith schizophrenia (Das et al. 1995). In the present study,subjects with schizophrenia and those with other mentaldisorders were taking antipsychotic medications at the timeof death. However, no significant differences were detectedin caudate NO levels between control subjects with andwithout other mental disorders. Taken together, antipsy-chotic medications are unlikely to contribute significantlyto increased NO production in the caudate region of thebrains of schizophrenia patients.
Therapeutic Treatment. If NO does play a role in schiz-ophrenia, pursuing interventions against NO toxicity mayhave merit. Deutsch et al. (1997) showed a modest butstatistically significant decrease in the severity of psy-chopathology after patients were treated with methyleneblue (MB). Further studies are needed to illustrate thera-peutic efficacy of MB or other NOS inhibitors.
References
Abdalla, D.S.P.; Monteiro, H.P.; Oliviera, J.A.C.; andBechara, E.J. Activities of superoxide dismutase and glu-tathione peroxidase in schizophrenic and manic-depres-sive patients. Clinical Chemistry, 32:805-807, 1986.
Aim, P.; Sharma, H.S.; Hedlund, S.; Sjoquist, P.O.; andWestman, J. Nitric oxide in pathophysiology of hyperther-mic brain injury: Influence of a new anti-oxidant com-pound H-290/51; a pharmacological study using immuno-histochemistry in the rat. Amino Acids, 14:95-103, 1998.
Arnaiz, S.L.; Coronel, M.F.; Boveris, A. Nitric oxide,superoxide, and hydrogen peroxide production in brain
mitochondria after haloperidol treatment. Nitric Oxide,3:235-243, 1999.
Balint, B.; Donnelly, L.E.; Hanazawa, T; Kharitonov,S.A.; and Barnes, P.J. Increased nitric oxide metabolitesin exhaled breath condensate after exposure to tobaccosmoke. Thorax, 56:456-461, 2001.
Blum-Degen, D.; Heinemann, T.; Lan, J.; Pedersen, V.;Leblhuber, F.; Paulus, W.; Riederer, P.; and Gerlach, M.Characterization and regional distribution of nitric oxidesynthase in the human brain during normal ageing. BrainResearch, 834:128-135, 1999.
Bockelmann, R.; Wolf, G.; Ransmayr, G.; and Riederer, P.NADPH-diaphorase/nitric oxide synthase containing neu-rons in normal and Parkinson's disease putamen. Journalof Neural Transmission, Parkinson's Disease andDementia Section, 7:115-121, 1994.
Bredt, D.S., and Snyder, S.H. Nitric oxide, a novel neu-ronal messenger. Neuron, 8:3-11, 1992.
Brown, K.; Reid, A.; White, T; Henderson, T; Hukin, S.;Johnstone, C ; and Glen, A. Vitamin E, lipids, lipid perox-idation products and tardive dyskinesia. BiologicalPsychiatry, 43:863-867, 1998.
Brown, R.; Colter, N.; Corsellis, J.A.; Crow, T.J.; Frith,C D . ; Jagoe, R.; Johnstone, E.C.; and Marsh, L.Postmortem evidence of structural brain changes in schiz-ophrenia. Differences in brain weight, temporal horn area,and parahippocampal gyms compared with affective dis-order. Archives of General Psychiatry, 43:36—42, 1986.
Cadet, J.L., and Lohr, J.B. Free radicals and the develop-mental pathology of schizophrenic burnout. IntegrativePsychiatry, 5:40-48, 1987.
Calapai, G.; Marciano, M.C.; Corica, F.; Allegra, A.;Parisi, A.; Frisina, N.; Caputi, A.P.; and Buemi, M.Erythropoietin protects against brain ischemic injury byinhibition of nitric oxide formation. European Journal ofPharmacology, 401:349-356, 2000.
Corraliza, I.M.; Soler, G.; Eichmann, K.; and Modolell,M. Arginase induction by suppressors of nitric oxide syn-thesis (IL-4, IL-10 and PGE2) in murine bone-marrow-derived macrophages. Biochemical and BiophysicalResearch Communications, 206:667-673, 1995.
Daghigh, E; Fukuto, J.M.; and Ash, D.E. Inhibition of ratliver arginase by an intermediate in NO biosynthesis, NG-hydroxy-L-arginine: Implications for the regulation ofnitric oxide biosynthesis by arginase. Biochemical andBiophysical Research Communications, 202:174—180,1994.
Dallal, G.E., and Wilkinson, L. An analytic approximationto the distribution of Lilliefors's test statistic for normal-ity. The American Statistician, 40:294-296, 1986.
931
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from

Schizophrenia Bulletin, Vol. 30, No. 4, 2004 J.K. Yao et al.
Das, I.; Khan, N.S.; Puri, B.K.; and Hirsch, S.R. Elevatedendogenous nitric oxide synthase inhibitor in schizo-phrenic plasma may reflect abnormalities in brain nitricoxide production. Neuroscience Letters, 215:209-211,1996.
Das, I.; Khan, N.S.; Puri, B.K.; Sooranna, S.R.; deBelleroche, J.; and Hirsch, S.R. Elevated platelet calciummobilization and nitric oxide synthase activity may reflectabnormalities in schizophrenic brain. Biochemical andBiophysical Research Communications, 122:375-380,1995.
Demopoulous, H.B. Molecular aspects of membranestructure in cerebral edema. In: Reulen, H.J., ed. Steroidsand Brain Edema. Berlin, Germany: Springer-Verlag,1972. pp. 29-39.
Deutsch, S.I.; Rosse, R.B.; Schwartz, B.L.; Fay-McCarthy, M.; Rosenberg, P.B.; and Fearing, K.Methylene blue adjuvant therapy of schizophrenia.Clinical Neuropharmacology, 20:357-363, 1997.
Elliott, K.A.C., and Jasper, H. Measurement of experi-mentally induced brain swelling and shrinkage. AmericanJournal of Physiology, 157:122-129, 1949.
Forstermann, U.; Schmidt, H.H.; Pollock, J.S.; Sheng, H.;Mitchell, J.A.; Warner, T.D.; Nakane, M.; and Murad, F.Isoforms of nitric oxide synthase: Characterization andpurification from different cell types. BiochemicalPharmacology, 42:1849-1857, 1991.
Ganguli, R.; Yang, Z.; Shurin, G.; Chengappa, K.N.; Brar,J.S.; Gubbi, A.V.; and Rabin, B.S. Serum interleukin-6concentration in schizophrenia: Elevation associated withduration of illness. Psychiatry Research, 51:1-10, 1994.
Gegg, M.E.; Beltran, B.; Salas-Pino, S.; Bolanos, J.P.;Clark, J.B.; Moncada, S.; and Heales, S.J.R. Differentialeffect of nitric oxide on glutathione metabolism and mito-chondrial function in astrocytes and neurons: Implicationsfor neuroprotection/neurodegeneration? Journal ofNeurochemistry, 86:228-237, 2003.
Gerlach, M.; Blum-Degen, D.; Lan, J.; and Riederer, P.Nitric oxide in the pathogenesis of Parkinson's disease.Advanced Neurology, 80:239-245, 1999.
Gotoh, K.; Kikuchi, H.; Kataoka, H.; Nagata, I.; Nozaki,K.; Takahashi, J.C.; and Hazama, F. Nitric oxide synthaseimmunoreactivity related to cold-induced brain edema.Neurological Research, 20:637-642, 1998.
Hara, H.; Huang, PL.; Panahian, N.; Fishman, M.C.; andMoskowitz, M.A. Reduced brain edema and infarctionvolume in mice lacking the neuronal isoform of nitricoxide synthase after transient MCA occlusion. Journal ofCerebral Blood Flow and Metabolism, 14:605-611,1996.
Heales, S.J.R.; Bolanos, J.P; Stewart, V.C.; Brookes, P.S.;Land, J.M.; and Clark, J.B. Nitric oxide, mitochondriaand neurological disease. Biochimica et Biophysica Ada,1410:215-228, 1999.
Herken, H.; Uz, E.; Ozyurt, H.; and Akyol, O. Red bloodcell nitric oxide levels in patients with schizophrenia.[Letter]. Schizophrenia Research, 52:289-290, 2001.
Hunot, S.; Boissiere, F.; Faucheux, B.; Brugg, B.; Mouatt-Prigent, A.; Agid, Y.; and Hirsch, E.C. Nitric oxide syn-thase and neuronal vulnerability in Parkinson's disease.Neuroscience, 72:355-363, 1996.
Ichiki, K.; Ikeda, H.; Haramaki, N.; Ueno, T.; andImaizumi, T. Long-term smoking impairs platelet-derivednitric oxide release. Circulation, 94:3109-3114, 1996.
Ignarro, L.J.; Cirino, G.; Casini, A.; and Napoli, C. Nitricoxide as a signaling molecule in the vascular system: Anoverview. Journal of Cardiovascular Pharmacology,34:879-886, 1999.
Kanazawa, H.; Shoji, S.; Hirata, K.; Kurthara, N.; andYoshikawa, J. Role of endogenous nitric oxide in airflowobstruction in smokers. Chest, 110:927-929, 1996.
Karson, C.N.; Griffin, W.S.; Mrak, R.E.; Husain, M.;Dawson, T.M.; Snyder, S.H.; Moore, N.C.; and Sturner,W.Q. Nitric oxide synthase (NOS) in schizophrenia:Increases in cerebellar vermis. Molecular and ChemicalNeuropathology, 27:275-284, 1996.
Kawamata, T.; Katayama, Y.; Maeda, T.; Mori, T.;Aoyama, N.; Kikuchi, T.; and Uwahodo, Y. Antioxidant,OPC-14117, attenuates edema formation and behaviordeficits following cortical contusion in rats. AdaNeurochirurgica. Supplement, 70:191-193, 1997.
Kharitonov, S.A.; Robbins, R.A.; Yates, D.; Keatings, V.;and Barnes, P.J. Acute and chronic effects of cigarettesmoking on exhaled nitric oxide. American Journal ofRespiratory and Critical Care Medicine, 152:609-612,1995a.
Kharitonov, V.G.; Sundquist, A.R.; and Sharma,V.S.Kinetics of nitrosation of thiols by nitric oxide in the pres-ence of oxygen. Journal of Biological Chemistry,270:28158-28164, \995b.
Koedel, U.; Bernatowicz, A.; Paul, R.; Frei, K.; Fontana,A.; and Pfister, H.W. Experimental pneumococcal menin-gitis: Cerebrovascular alterations, brain edema, andmeningeal inflammation are linked to the production ofnitric oxide. Annals of Neurology, 37:313-323, 1995.
Krukoff, T.L. Central actions of nitric oxide in regulationof autonomic functions. Brain Research: Brain ResearchReviews, 30:52-65, 1999.
Larsen, F.S.; Gottstein, J.; and Blei, A.T. Cerebral hyper-emia and nitric oxide synthase in rats with ammonia-
932
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from

Increased Nitric Oxide Radicals in Postmortem Brain Schizophrenia Bulletin, Vol. 30, No. 4, 2004
induced brain edema. Journal of Hepatology, 34:548-554,2001.
Lin, A.; Kenis, G.; Bignotti, S.; Tura, G.J.; De Jong, R.;Bosnians, E.; Pioli, R.; Altamura, C ; Scharpe, S.; andMaes, M. The inflammatory response system in treatment-resistant schizophrenia: Increased serum interleukin-6.Schizophrenia Research, 32:9-15, 1998.
Lorsbach, R.B.; Murphy, W.J.; Lowenstein, C.J.; Snyder,S.H.; and Russell, S.W. Expression of the nitric oxidesynthase gene in mouse macrophages activated for tumorcell killing. Journal of Biological Chemistry,268:1908-1913, 1993.
Lowenstein, C.J.; Alley, E.W.; Raval, P.; Snowman,A.M.; Snyder, S.H.; Russell, S.W.; and Murphy, W.J.Macrophage nitric oxide synthase gene: Two upstreamregions mediate induction by interferon and lipopolysac-charide. Proceedings of the National Academy ofSciences of the United States of America, 90:9730-9734,1993.
Ma, T.C., and Zhu, X.Z. Effects of intrahippocampal infu-sion of interleukin-6 on passive avoidance and nitrite andprostaglandin levels in the hippocampus in rats.Arzneimittel-Forschung, 50:227-231, 2000.
Maes, M.; Bosmans, E.; Calabrese, J.; Smith, R.; andMeltzer, H.Y. Interleukin-2 and interleukin-6 in schizo-phrenia and mania: Effects of neuroleptics and mood sta-bilizers. Journal of Psychiatric Research, 29:141-152,1995.
Mahadik, S.P., and Mukherjee, S. Free radical pathologyand antioxidant defense in schizophrenia: A review.Schizophrenia Research, 19:1-17, 1996.
Mahadik, S.P.; Mukherjee, S.; Scheffer, R.E.; Correnti,E.E.; and Mahadik, J.S. Elevated plasma lipid peroxidesat the onset of nonaffective psychosis. BiologicalPsychiatry, 43:674-679, 1998.
McCreadie, R.G.; MacDonald, E.; Wiles, D.; Campbell,G.; and Paterson, J.R. The Nithsdale SchizophreniaSurveys: XIV. Plasma lipid peroxide and serum vitamin Elevels in patients with and without tardive dyskinesia, andnormal subjects. British Journal of Psychiatry,167:610-617, 1995.
Moncada, S.; Palmer, R.M.J.; and Higgs, E.A. Nitricoxide: Physiology, pathophysiology, and pharmacology.Pharmacology Review, 43:109-142, 1991.
Nag, S.; Picard, P.; and Stewart, D.J. Increasedimmunolocalization of nitric oxide synthases duringblood-brain barrier breakdown and cerebral edema. ActaNeurochirurgica. Supplement, 76:65-68, 2000.
Nag, S.; Picard, P.; and Stewart, D.J. Expression of oxidesynthases and nitrotyrosine during blood-brain barrier
breakdown and repair after cold injury. LaboratoryInvestigation, 81:41-49,2001.
Node, K.; Kitakaze, M.; Yoshikawa, H.; Kosaka, H.; andHori, M. Reversible reduction in plasma concentration ofnitric oxide induced by cigarette smoking in young adults.American Journal of Cardiology, 79:1538-1541, 1997.
Norris, P.J.; Faull, R.L.; and Emson, PC. Neuronal nitricoxide synthase (nNOS) mRNA expression and NADPH-diaphorase staining in the frontal cortex, visual cortex andhippocampus of control and Alzheimer's disease brains.Molecular Brain Research, 41:36-49, 1996.
Olin, A.C.; Hellgren, J.; Karlsson, G.; Ljungkvist, G.;Nolkrantz, K.; and Toren, K. Nasal nitric oxide and itsrelationship to nasal symptoms, smoking and nasalnitrate. Rhinology, 36:117-121, 1998.
Palmer, R.M.J.; Ashton, D.S.; and Moncada, S. Vascularendothelial cells synthesize nitric oxide from L-arginine.Nature, 333:664-666, 1988.
Peet, M.; Laugharne, J.; Rangarajan, N.; and Reynolds,G.P. Tardive dyskinesia, lipid peroxidation, and sustainedamelioration with vitamin E treatment. InternationalClinical Psychopharmacology, 8:151-153, 1993.
Petty, M.A.; Poulet, P.; Haas, A.; Namer, I.J.; and Wagner,J. Reduction of traumatic brain injury-induced cerebraloedema by a free radical scavenger. European Journal ofPharmacology, 307:149-155, 1996.
Prilipko, L.L. The possible role of lipid peroxidation inthe pathophysiology of mental disorders. In: Packer, L.;Prilipko, L.; and Christen, Y, eds. Free Radicals in theBrain. Berlin, Germany: Springer-Verlag, 1992. pp.146-152.
Prince, J.A.; Yassin, M.S.; and Oreland, L. Neuroleptic-induced mitochondrial enzyme alterations in the rat brain.Journal of Pharmacology and Experimental Therapeutics,280:261-267, 1997.
Reddy, R.; Sahebarao, M.P.; Mukherjee, S.; and Murthy,J.N. Enzymes of the antioxidant system in chronic schizo-phrenic patients. Biological Psychiatry, 30:409-412,1991.
Reddy, R.D., and Yao, J.K. Membrane protective strate-gies in schizophrenia: Conceptual and treatment issues.In: Peet, M.; Glen, I.; and Horrobin, D.F., eds.Phospholipid Spectrum Disorder in Psychiatry.Lancashire, U.K.: Marius Press, 1999. pp. 75-88.
Rengasamy, A., and Johns, R.A. Inhibition of nitric oxidesynthase by a superoxide generating system. Journal ofPharmacological and Experimental Therapeutics,267:1024-1027, 1993.
Robbins, R.A.; Millatmal, T; Lassi, K.; Rennard, S.; andDaughton, D. Smoking cessation is associated with an
933
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from

Schizophrenia Bulletin, Vol. 30, No. 4, 2004 J.K. Yao et al.
increase in exhaled nitric oxide. Chest, 112:313-318,1997.
Schilling, L., and Wahl, M. Brain edema: Pathogenesisand therapy. Review. Kidney International Supplement,59:S69-S75,1997.
Sharma, H.S.; Drieu, K.; Aim, P.; and Westman, J. Role ofnitric oxide in blood-brain barrier permeability, brainedema and cell damage following hyperthermic braininjury: An experimental study using EGB-761 andGingkolide B pretreatment in the rat. AdaNeurochirurgica Supplement, 76:81-86, 2000.
Shintani, F.; Kanba, S.; Maruo, N.; Nakaki, T.; Nibuya,M.; Suzuki, E.; Kinoshita, N.; and Yagi, G. Serum inter-leukin-6 in schizophrenic patients. Life Sciences,49:661-664, 1991.
Siegel, S. Nonparametric Statistics. New York, NY:McGraw-Hill, 1956.
Smith, C.V. Free radical mechanisms of tissue injury. In:Moslen, M.T., and Smith, C.V., eds. Free RadicalMechanisms of Tissue Injury. Boca Raton, FL: CRCPress, 1992. pp. 1-22.
Smythies, J. Oxidative reactions and schizophrenia: Areview-discussion. Schizophrenia Research, 24:357-364,1997.
Suboticanec, K.; Folnegovic-Smalc, V.; Korbar, M.;Mestrovic, B.; and Buzina, R. Vitamin C status in chronicschizophrenia. Biological Psychiatry, 28:959-966, 1990.
Takemori, K.; Ito, H.; Suzuki, T. Effects of induciblenitric oxide synthase inhibition on cerebral edema insevere hypertension. Acta Neurochirurgica Supplement,76:335-338, 2000.
Thiel, V.E., and Audus, K.L. Nitric oxide and blood-brainbarrier integrity: Review. Antioxidants and RedoxSignalling, 3:273-278, 2001.
Thorns, V.; Hansen, L.; and Masliah, E. nNOS expressingneurons in the entorhinal cortex and hippocampus areaffected in patients with Alzheimer's disease.Experimental Neurology, 150:14-20, 1998.
van Kammen, D.P.; McAllister-Sistilli, C.G.; Kelley,M.E.; Gurklis, J.A.; and Yao, J.K. Elevated interleukin-6in schizophrenia. Psychiatry Research, 87:129-136, 1999.
Yao, J.K.; Leonard, S.; and Reddy, R. Increased level ofmercaptans in postmortem brains from schizophrenicpatients. Biological Psychiatry, 49:172S, 2001a.
Yao, J.K.; Reddy, R.; McElhinny, L.G.; and vanKammen, D.P. Reduced status of plasma total antioxi-
dant capacity in schizophrenia. Schizophrenia Research,32:1-8, 1998a.
Yao, J.K.; Reddy, R.; McElhinny, L.G.; and van Kammen,D.P. Effects of haloperidol on antioxidant defense systemenzymes in schizophrenia. Journal of PsychiatricResearch, 32:385-391, 1998ft.
Yao, J.K.; Reddy, R.; and van Kammen, D.P. Reducedlevel of plasma antioxidant uric acid in schizophrenia.Psychiatric Research, 80:29-39, 1998c.
Yao, J.K.; Reddy, R.; and van Kammen, D.P. Humanplasma glutathione peroxidase and symptom severity inschizophrenia. Biological Psychiatry, 45:1512-1515,1999.
Yao, J.K.; Reddy, R.D.; and van Kammen, D.P. Abnormalage-related changes of plasma antioxidant proteins inschizophrenia. Psychiatry Research, 97:137-151, 2000.
Yao, J.K.; Reddy, R.D.; and van Kammen, D.P. Oxidativedamage and schizophrenia: An overview of the evidenceand its therapeutic implications. CNS Drugs, 15:287-310,200 \b.
Acknowledgments
This study was supported in part by Merit Review grants(J.K.Y., S.L.) and Research Career Scientist Awards(J.K.Y., S.L.) from the Office of Research andDevelopment, Department of Veterans Affairs, and theHighland Drive VA Pittsburgh Healthcare System. Theauthors are grateful to B. Bland and B. Sullivan for theirtechnical assistance.
The Authors
Jeffrey K. Yao, Ph.D., is Research Career Scientist, VAPittsburgh Healthcare System; Research Professor ofPsychiatry, Western Psychiatric Institute and Clinic,University of Pittsburgh Medical Center; and ResearchProfessor of Pharmaceutical Sciences, University ofPittsburgh School of Pharmacy, Pittsburgh, PA. SherryLeonard, Ph.D., is Research Career Scientist, DenverVA Medical Center, and Associate Professor,Departments of Psychiatry and Pharmacology,University of Colorado Health Sciences Center, Denver,CO. Ravinder D. Reddy, M.D., is Associate Professor ofPsychiatry, Western Psychiatric Institute and Clinic,University of Pittsburgh Medical Center, Pittsburgh,PA.
934
at University of P
ortland on May 22, 2011
schizophreniabulletin.oxfordjournals.orgD
ownloaded from





























