Embed Size (px)
Citation preview

Influence of chlorhexidine digluconate on theclinical performance of adhesive restorations:A 3-year follow-up
Neimar Sartori a,*, Sheila C. Stolf b, Silvana B. Silva b, Guilherme C. Lopes b,Marcela Carrilho c,d
aDivision of Restorative Science, Ostrow School of Dentistry, University of Southern California, Los Angeles, CA, USAbDepartment of Operative Dentistry, Federal University of Santa Catarina, Florianopolis, Santa Catarina, BrazilcGEO/UNIBAN, Health Institute, Bandeirante University of Sao Paulo (UNIBAN), Sao Paulo, BrazildDepartment of Restorative Dentistry, Piracicaba School of Dentistry, University of Campinas, Piracicaba, Brazil
j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 1 1 8 8 – 1 1 9 5
a r t i c l e i n f o
Article history:
Received 24 April 2013
Received in revised form
10 September 2013
Accepted 15 September 2013
Keywords:
Restorative dentistry
Clinical trial
Chlorhexidine
Dentine bonding agents
Composite resins
Non-carious cervical lesions
a b s t r a c t
Objectives: The aim of this clinical study was to evaluate the long-term clinical performance
of non-carious Class V restorations with and without application of chlorhexidine diglu-
conate to acid-etched dentine.
Methods: After the approval of the Ethics and Informed Consent Committee, 70 non-carious
cervical lesions were selected and randomly assigned into two groups, according to the
split mouth design. The control group was restored with a two-step etch-and-rinse
adhesive (Adper Single Bond 2) following manufacturer’s instructions; whereas in the
experimental group 2% chlorhexidine digluconate solution was applied to acid etched
dentine for 30 s after etching and prior to the adhesive application. All lesions were
restored with a nanofilled composite resin (Filtek Supreme XT) and polymerized with a
light-curing unit operating at 600 mW/cm2. Clinical performance was recorded after
1 week, 6, 12, and 36 months using modified Ryge/USPHS criteria in terms of retention,
marginal discoloration, marginal integrity, post-operative sensitivity, and secondary
caries incidence. Data were analyzed using Chi-Square, Fisher’s exact test and McNemar
tests (a = .05).
Results: After 36 months the control group showed a success rate of 88% in comparison to
76% of experimental group; however, no statistically difference between them was found
( p = .463). Moreover, no statistical differences were observed between groups in the criteria
post-operative sensitivity, marginal discoloration, marginal integrity, and secondary caries
incidence between the two groups.
Conclusion: The addition of 2% chlorhexidine digluconate conditioning step does not
improve the clinical durability of adhesive restorations.
# 2013 Elsevier Ltd. All rights reserved.
* Corresponding author at: Ostrow School of Dentistry of USC, Division of Restorative Sciences, Norris Dental Science Center, 925 West34th Street, DEN 4365, Los Angeles, CA 90089-064, USA. Tel.: +1 424 278 3041.
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.intl.elsevierhealth.com/journals/jden
E-mail address: [email protected] (N. Sartori).
0300-5712/$ – see front matter # 2013 Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.jdent.2013.09.004

1. Introduction
Since enamel etching technique introduction, by Buonocore in
1955, the adhesive systems have been extensively developed.1
The adhesion to the tooth tissues is normally based on
replacement of the tooth minerals, removed with acid-
etching, by resin monomers with low viscosity.2,3 The
heterogeneous composition of dentine tissue, its hydrophilic-
ity, low surface energy, variable permeability and the presence
of a smear layer, make the dentine a challenging substrate to
bond a resin composite restoration.1 Bonding to dentine has
become trustworthier since the introduction of hydrophilic
adhesive systems, which can infiltrate into the wet dentine
substrate, although bonding exclusively to dentine has shown
not to be as durable as expected when hydrophilic adhesive
systems are used.1
Several studies have been investigating the factors respon-
sible for the low durability of the resin–dentine bonds with
hydrophilic adhesives. One reason for this poor performance
is the slow hydrolysis of unprotected collagen fibrils within
and under the hybrid layer by host-derived enzymes in
incomplete resin-infiltrated zones of resin-bonded dentine.4,5
As a result nanoleakage occurs leading to the hydrolytic
breakdown of either the adhesive resin or collagen within the
hybrid layer, thereby compromising the durability of dentine6
Table 1 – Inclusion and exclusion criteria used in thisresearch.
Inclusion criteria
�Patients over the age of 18;
�Patients living in or near to the university;
�Patients with more than 20 natural teeth;
�Presence of two or four non-carious cervical lesions in
different hemiarches (1–3 mm of occluso-gingival height
and 1–2 mm depth);
�Non-retentive cavities, presenting �50% of margins in enamel
and �75% of total area in dentine;
�Presence of adjacent teeth (sound or restored);
�Cervical margins in dentine;
�Regular/good oral hygiene (bacterial plaque visible in <1/4 of
teeth).
Exclusion criteria
�Patients unable to attend follow-up appointments;
�Pregnant or breast-feeding patients;
�Patients using analgesics and/or anti-inflamatory medicine;
�Patients with severe systemic or psychologic disease;
�Patients under orthodontic therapy, using fluoride
supplements or desensitizing agents;
�Patients with bruxism;
�Patients with periodontal/gingival disease;
�Presence of caries, cracks, fractures, premature contact or
unsatisfactory restorations;
�Presence of sclerotic dentine (degree 4), according to the
classification of North Carolina University.25
j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 1 1 8 8 – 1 1 9 5 1189
bonding interface.
Dentine collagen fibrils degradation is managed by an
intrinsic proteolytic activity of dentine collagenases/gelati-
nases, which would be responsible to cause a progressive
disappearance of portions of hybrid layers over 6–12 months
in vivo.7 So far two kinds of endogenous proteolytic
enzymes with potential collagenolytic/gelatinolytic activi-
ties were identified in dentine: the metalloproteinases
(MMPs)8–11 and the cysteine-cathepsins.12–14 One strategy
to avoid the endogenous collagenolytic activity is the use of
protease inhibitors, such as chlorhexidine,5,15–17 galardin,18
or tetracycline.19 It has been demonstrated that when
chlorhexidine digluconate is used on demineralized den-
tine, after the acid etching and prior to the adhesive system
application, it significantly improves the hybrid layer
integrity, keeping a stronger bonding strength after short-
term clinical trials.7,20
The aim of this study was to evaluate if an additional
conditioning step, after etching and rinsing and prior to the
adhesive application, could improve the clinical performance
of adhesive restorations in non-carious cervical lesions. The
null hypothesis is that the addition of the chlorhexidine
digluconate conditioning step does improve the clinical
durability of composite resin restorations.
2. Materials and methods
After the approval from the Federal University of Santa
Catarina Internal Review Board, thirty patients with non-
carious cervical lesions were selected for this study. Ten
participants were excluded because they did not meet with all
inclusion criteria or they fit in one exclusion criterion
(Table 1).21 Seventy non-carious cervical lesions were selected
in 20 patients, 7 females and 13 males, with a mean age of 46.7
years (range 33–64).
All selected lesions were ‘‘V’’ or ‘‘U’’ shaped in the buccal
surface of teeth with incisal/occlusal margin in enamel and
gingival margin in dentine. The lesions were categorized in
terms of sensitivity (spontaneous or provoked), cervico-incisal
height (1.0–1.5 mm, 1.6–2.5 mm or 2.6–3.0 mm), depth
(�1.5 mm or >1.5 mm), degree of dentinal sclerosis (no
sclerosis, slight, moderate),22 and presence of wear facets
(present or absent). The data of pre-operative evaluation of
selected lesions are presented in Table 2.
2.1. Experimental design and restorative procedures
The best clinical trial to evaluate the effect of chlorhexidine
digluconate used under adhesive restorations is the split-
mouth design. This design was selected because all patients
receive restorations with both adhesive techniques, in differ-
ent quadrants, reducing the influence of patient individual
factors such as sensibility, diet, life style, occlusion, and habits
on results.23 Thus, after being randomly assigned, each patient
received the same number of restorations of both groups,
following the split-mouth design. Seventy lesions, 35 per
group, were restored in 20 patients. Five of them received 2
restorations, one each group, the others 15 patients received 4
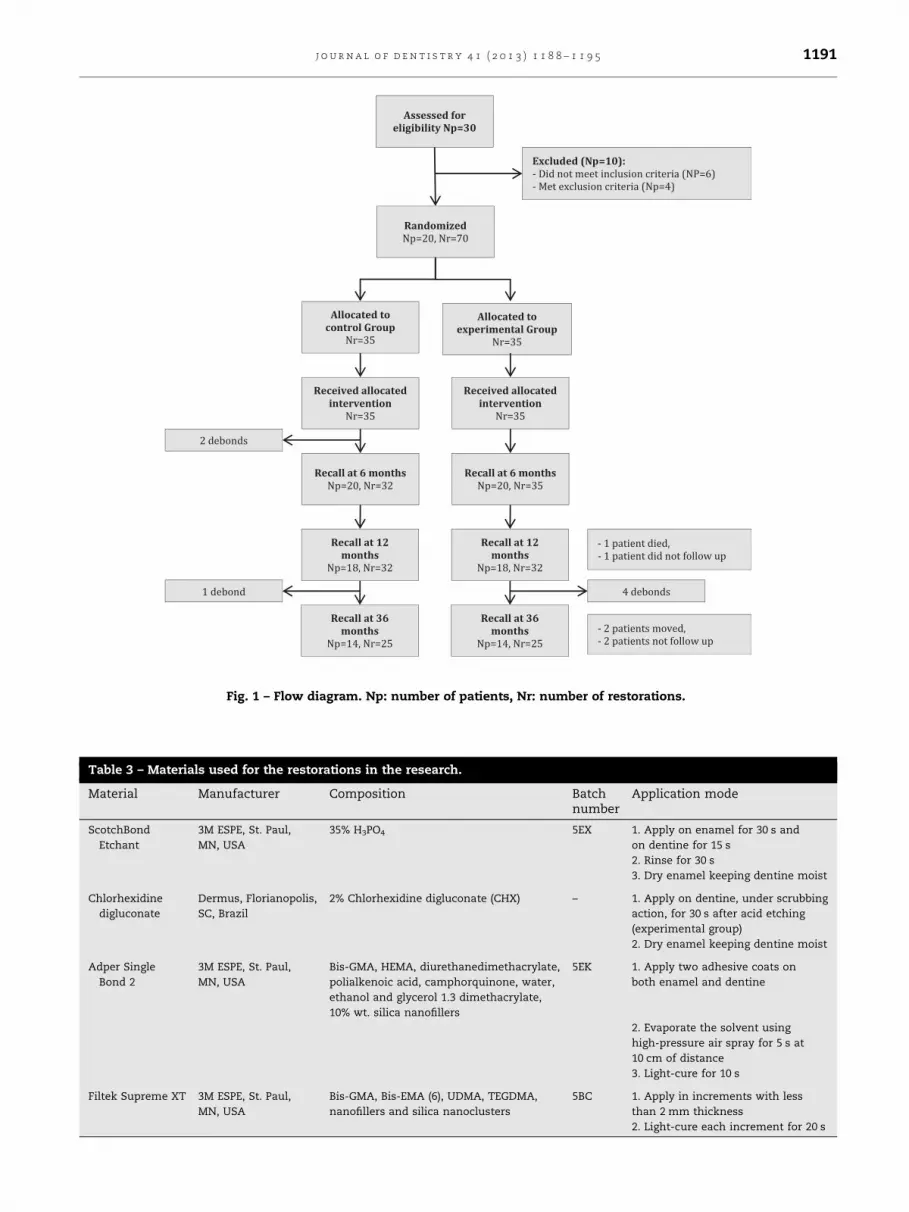
restorations, as it is showed in the flow diagram of patients
and restoration in this study (Fig. 1).
Before the adhesive procedures the teeth were cleaned
with pumice-water slurry using Robinson brushes with a
slow-speed handpiece to remove salivary pellicle and any
bacterial plaque. The tooth shade was selected using a shade
guide (VitaPan Classic, Vita Zahnfabrik, Bad Sackingen,
Germany) and the operative field isolation was accomplished

Table 2 – Evaluation methods and number of lesions according to their characteristics.
Evaluation method Number of lesions
Sensitivity Anamnesis and high-pressure air spray for 3 s at a distance of 3 cm
Provoked (non spontaneous) 43
Spontaneous (non provoked) 37
No sensitivity 27
Lesions’ shape Visual and tactil (probe)
‘‘U’’ shaped 25
‘‘V’’ shaped 45
Cervico-incisal height Periodontal probe
1.0–1.5 mm 25
1.6–2.4 mm 21
2.5–3.0 mm 24
Lesions’ depth Periodontal probe
�1.5 mm 39
>1.5 mm 31
Degree of sclerosis Visual and high-pressure air spray
No sclerosis Normal dentine with spontaneous or provoked sensitivity 37
Slightly sclerotic Opaque (or yellow) dentine with spontaneous or provoked sensitivity 6
Moderately sclerotic Yellow (or opaque) dentine without provoked sensitivity 27
Presence of wear facets Visual (after air drying)
Wear facets 70
No wear facets 0
Tooth distribution
Incisors 2
Canine 20
Premolar 40
Molar 8
j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 1 1 8 8 – 1 1 9 51190
by using labial retractors, cotton rolls and saliva aspirator. A
retraction cord (Knitted Retraction Cord, Pascal Company,
Bellevue, WA, USA) was used to retract the gingiva, exposing
the cervical margins and preventing contamination via
gingival fluid.
The same calibrated operator restored all non-cervical
lesions. Lesions of the experimental group were treated with
a 2% chlorhexidine digluconate (Dermus, Florianopolis, SC,
Brazil) after acid etching and prior to the application of the
adhesive system as describes below: (1) acid-etching with
phosphoric acid (Scotchbond Etchant, 3M ESPE, St Paul, MN,
USA) for 30 s in enamel and 15 s in dentine; (2) rinsing with
air/water spray for 30 s and removal of excess moisture
from dentine using sterilized cotton pellets and drying off
enamel with gentle air streams for 10 s at 2 cm of distance;
(3) application of 2% chlorhexidine digluconate, under
scrubbing action for 30 s using a disposable applicator just
on the experimental group lesions; (4) removal of excess
moisture from dentine and drying off enamel as described
at step 2; (5) application of the adhesive system (Adper
Single Bond 2, 3M ESPE) according to the manufacturer’s
instructions (Table 3); (6) light-curing for 10 s using a
halogen light-curing unit (VIP, Bisco Inc., Schamburg, IL,
USA), with measured light output (600 mW/cm2); (7) resto-
ration was build-up with a nanofilled composite (Filtek
Supreme XT, 3M ESPE) in three increments, beginning by the
gingival margin; (8) light-curing of each increment for 20 s.
Lesions of the control group were restored according to the
protocol described above without the steps 3 and 4.
Final contouring and polishing of the restorations were
performed at the same appointment, using a extra-fine grit
needle-shaped diamond bur (Komet, Lemgo, Germany), silicon
carbide points (Jiffy points, Ultradent Products, Inc., South
Jordan, UT, USA), aluminium oxide discs (Sof-Lex, 3M ESPE),
and polishing pastes (Diamond polish 1 mm and 0.5 mm,
Ultradent Products, Inc.).
2.2. Evaluation procedure
Two previously calibrated examiners who were fully blind to
the treatment carried out evaluated the restorations. The
examiners had Cohen’s Kappa index (K = .894) to inter-
examiner reliability and disagreements between evaluators
were resolved by consensus. The evaluations were performed
at four different periods: at baseline (7 day after restorations
placement), after 6, 12, and 36 months based on ADA’s
guidelines,24 and the USPHS modified criteria.25
The criteria evaluated were: retention, marginal discolor-
ation, marginal integrity, post-operative sensitivity, presence
of recurrent caries, and pulpal vitality. Retention, marginal
integrity, marginal discoloration and occurrence of caries
were used as key parameters determining the overall clinical
success. Post-operative sensitivity was measured subjectively
based on the patient’s response to an air stimulus (air stream,
1 cm distance for 1 s) and recorded according to the Verbal
Rating Scale (VRS).26 Pulpal vitality was assessed based on the
patient’s response to a cold stimulus. A cotton pellet saturated
with a refrigerant solution (ROEKO Endo-Frost, Coltene/
Asses sed for eligibility Np= 30
Excluded (Np=10):- Did not meet inc lusi on crit eria (N P=6)
- Met exclusion criteria (N p=4)
Random ized Np=20, Nr=70
All ocat ed to control Group
Nr=35
Allo cat ed to experimental Group
Nr=3 5
Rece ived al loca ted interv ention
Nr=35
Rece ived al loca ted interv ention
Nr=35
Recal l at 6 monthsNp=20, Nr=32
Recal l at 6 monthsNp=20, Nr=35
Recal l at 12 months
Np=18, Nr=32
Recal l at 12 months
Np=18, Nr =32
Recall at 36 month s
Np=14, Nr=25
Recall at 36 month s
Np=14, Nr=25
- 1 pa tie nt die d,
- 1 pa tien t did n ot follow up
- 2 pa tien ts m ove d,
- 2 pa tien ts n ot f oll ow u p
2 debonds
1 debond debonds 4
Fig. 1 – Flow diagram. Np: number of patients, Nr: number of restorations.
Table 3 – Materials used for the restorations in the research.
Material Manufacturer Composition Batchnumber
Application mode
ScotchBond
Etchant
3M ESPE, St. Paul,
MN, USA
35% H3PO4 5EX 1. Apply on enamel for 30 s and
on dentine for 15 s
2. Rinse for 30 s
3. Dry enamel keeping dentine moist
Chlorhexidine
digluconate
Dermus, Florianopolis,
SC, Brazil
2% Chlorhexidine digluconate (CHX) – 1. Apply on dentine, under scrubbing
action, for 30 s after acid etching
(experimental group)
2. Dry enamel keeping dentine moist
Adper Single
Bond 2
3M ESPE, St. Paul,
MN, USA
Bis-GMA, HEMA, diurethanedimethacrylate,
polialkenoic acid, camphorquinone, water,
ethanol and glycerol 1.3 dimethacrylate,
10% wt. silica nanofillers
5EK 1. Apply two adhesive coats on
both enamel and dentine
2. Evaporate the solvent using
high-pressure air spray for 5 s at
10 cm of distance
3. Light-cure for 10 s
Filtek Supreme XT 3M ESPE, St. Paul,
MN, USA
Bis-GMA, Bis-EMA (6), UDMA, TEGDMA,
nanofillers and silica nanoclusters
5BC 1. Apply in increments with less
than 2 mm thickness
2. Light-cure each increment for 20 s
j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 1 1 8 8 – 1 1 9 5 1191

Table 4 – Evaluation results in percentage of alpha at each evaluation period.
Recall period
Baseline 6 months 12 months 36 months
SB CHX SB CHX SB CHX SB CHX
Recall rate 100 100 100 100 91.4 91.4 71.4 71.4
Retention rate 100 100 94.3 100 93.5 100 88.0 76.0*
Marginal discoloration 100 100 93.9 97.1 93.1 93.5 72.7* 68.4*
Marginal integrity 100 100 100 100 100 96.8 90.9 78.9
Post-operative sensitivity 82.9 74.3 94.3 67.1 96.6 87.1 95.5 89.5
Absence of caries occurrence 100 100 100 100 100 100 100 100
Pulpal vitality 100 100 100 100 100 100 100 100
Overall clinical success rate 100 100 94.3 100 93.5 100 88.0 76.0*
SB, Control Group; CHX, Experimental Group; percentages of all parameters evaluated refer to retained restorations, except for recall rate,
retention rate and overall clinical success rate.
Baseline percentages for sensitivity refer to evaluation after the restoration. Number of lesions with sensitivity prior to restoration is shown in
Table 2.
There is no statistical difference between both groups at any evaluation. Percentage of Alpha followed by asterisk differs from baseline
evaluation (McNemar test).
j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 1 1 8 8 – 1 1 9 51192
Whaledent GMBH, Langenau, Germany) was placed on the
restored tooth. Once the patient responded to the cold
stimulation, the cotton pellet was removed and, for a normal
vital pulp, the pain should disappear in a few seconds.
2.3. Statistical analysis
The clinical bonding effectiveness was determined by the
percentage of debonded restorations during the evaluation
period. The data were processed using the Statistical Package
for Social Sciences IBM SPSS Statistics 19 (Chicago, IL, USA)
and descriptive statistic was used to present the results.
Cumulative retention failures were calculated by dividing the
number of lost restorations at the recalls by the total number
evaluated at each of the recalls. Chi-square and Fisher’s exact
tests were used to evaluate the presence of statistical
differences between groups at each recall and McNemar’s
test was used to verify the alpha ratings variation for each
evaluated criteria within the same group over time. For all
statistical analysis a 5% significant level was adopted (a = .05).
3. Results
The percentages of alpha scores, which represent the ideal
clinical situation, are compiled in Table 4. It was observed that
three restorations debonded from premolars of different
patients in the control group within 36-month follow-up.
Two restorations debonded at 6-month recall and another
debonding was observed at 36-month evaluation. These
restorations were placed in shallow lesions (�1.5 mm) with
slight moderate sclerosis level, two of them belonged to ‘‘V’’
shaped lesions and other one to ‘‘U’’ shaped lesions. In the
experimental group, it was noted that 4 restorations debonded
at 36-month recall, three restorations from premolars and one
from a molar. Two restorations were bonded to shallow
lesions (�1.5 mm) ‘‘V’’ shaped and two of them to deep lesions
(>1.5 mm) ‘‘U’’ shaped. The other restorations were bonded to
dentine with moderated sclerosis level, one to a slight
moderate and the other one to a lesion without any sclerosis
degree. Despite there was no statistical difference between the
two groups there is statistical difference between the baseline
and 36 months recalls for the experimental group ( p = .031).
Some clinical acceptable marginal discoloration was
observed in both groups after 36 months, without statistical
difference between them ( p = .763). However, there is statisti-
cal difference between the baseline and 36 months recalls for
both groups (control group, p = .031 and experimental group,
p = .013).
From the 61% of teeth with non-carious cervical lesions
that presented pre-operative sensitivity just 17.1% of the
restored teeth in the control group, and 25.7% in the
experimental group presented post-operative sensitivity after
one week. At 36 months recall the post-operative sensitivity
rate was 4.5% in the control group (one restoration) and 11.5%
in the experimental group (two restorations).
At 36 months recall none of the restored teeth became non-
vital due to the restoration placement and none of them
presented caries occurrence. Thereby, the clinical success
rates of these restorations were 88.0% for the control group
and 76.0% for the experimental group.
4. Discussion
Despite the addition of the chlorhexidine digluconate delayed
the period wherein the restorations started exhibiting unfa-
vourable clinical characteristics; its use did not improve the
clinical durability of adhesive restoration placed to non-
carious cervical lesions at 36-month follow-up. The null
hypothesis that chlorhexidine digluconate conditioning step
does improve clinical durability of composite resin restora-
tions was accepted because there is no statistical difference
between both groups in any criteria.
The durability of resin–dentine bonds can compromise the
lifespan of composite resin restorations, especially in restora-
tions where there is no macro mechanical retention, such as
Class V restorations of non-carious cervical lesions. Resin–
dentine bonds degradation probably occurs via hydrolysis of
suboptimally polymerized hydrophilic resin components and

j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 1 1 8 8 – 1 1 9 5 1193
degradation of resin-uncovered collagen matrices by matrix
metalloproteinases (MMPs) and cysteine cathepsins.13 Chlor-
hexidine has demonstrated being a potent inhibitor of MMPs
present in the dentine–pulp complex,11,27 such as, MMP-2,
MMP-8, and MMP-9.28 More recently, the inhibitory effect of
chlorhexidine on cysteine-cathepsins activity was also dem-
onstrated,29 indicating that chlorhexidine may have a wide
anti-proteolytic spectrum.
The experimental (treated with chlorhexidine) and control
groups showed similar clinical results at 36-month follow-up
in terms of retention rate. However, in the control group, the
restorations started debonding before 6 months of clinical
function, while in the experimental group none of the
restorations debonded until 12-month evaluation, just at 36-
month recall. Probably, the chlorhexidine treatment improved
mechanical and morphological stability of hybrid layers by
inhibiting the host-derived proteases over time.7 Despite
chlorhexidine could decelerate the rate of resin–dentine bonds
degradation by inhibition of host-derived proteases, chlor-
hexidine could not prevent the hydrolytic breakdown of
polymers that constitute those bonds,11 which could explain
why the restorations of chlorhexidine-treated cavities exhib-
ited a decrease of the rate of retention at 36-month recall.
The two-step etch-and-rinse adhesive used in the present
study consists of a BisGMA/HEMA-based system containing
13% polyalkenoic acid copolymer in an ethanol–water solvent.
This hydrophilic formulation is responsible for making the
material a permeable membrane after its polymerization.
Polyalkenoic acid copolymer can allow cured adhesives to
absorb an extensive amount of water over time,33 due to the
multiple pendent carboxylic acids along its linear backbone,
decreasing the cohesive strength of this adhesive layer.34
Many fundamental differences are found between the
present study and other previous in vivo studies that
employed chlorhexidine as an adjunctive resource to deceler-
ate the degradation of resin–dentine bonds. Apart from the
final evaluation time, factors such as cavity configuration and
type of testing analysis are listed as significant differences.
Hebling et al.,20 Carrilho et al.,7 and Brackett et al.,35 have
performed microscopic analyses of the hybrid layer integrity
formed between chlorhexidine-treated dentine and the etch-
and-rinse adhesive systems, the present protocol chose to
analyze the clinical, macro-response to chlorhexidine used as
a conditioning step. Thereby it was not possible to detect
microscopic differences between control and experimental
group that could show relevant differences in those treat-
ments. Another important aspect that cannot be detected with
the present study is the origin of the adhesive failures,
whether the recorded negative parameters were due to a
defect within the resin or the dentine matrix part of hybrid
layers. Carrilho et al.,7 has shown that, over time, in the
chlorhexidine-treated group, resin-bonded dentine had exhib-
ited a considerably reduction of the number of cohesive
failures within the bottom of hybrid layers. Furthermore
uncovered collagen would be more massively present, which
indicates the proactive effect of chlorhexidine against the
proteolytic enzyme activity.
It is also speculated that the interaction between chlorhex-
idine digluconate and hydroxyapatites on the enamel surface
can be responsible for the restorations debondings on the
experimental group. The chlorhexidine digluconate is a strong
base with cationic properties that can bind to the negatively
charges in trivalent phosphate in the hydroxyapatite crystal-
line lattice, creating a precipitation of needle-shaped birefrin-
gent crystals with the same refractive index as the phosphate
salt on the surface of the enamel.30–32 This precipitate could
act as a physical barrier, limiting the adhesive system
interaction with the hydroxyapatites, minimizing the poten-
tial of bonding.32
The causes of the diminished longevity of non-carious
Class V restorations are still poorly understood, in contrast
with other classes of restorations.36 Failure of cervical
adhesive restorations is often attributed to inadequate
moisture control and also to cuspal movement during
occlusion.37 Clinical studies also associate tooth flexure with
low retention in cervical restorations,38 showing that the para-
axial loading moment developed into the tooth has negative
effects at the cervical restorations interface.39 The repetitive
cyclic of para-functional loadings may induce a failure in the
cervical region of the restoration which undergoes strain
softening, generating micro-cracks at the restoration mar-
gin.36 If this hypothesis is true it can explain why there is a
statistical difference between the baseline and 36 months
recalls in marginal discoloration for both groups. Although it is
not possible correlate these clinical co-variables to retention
loss, the potential effect of excessive occlusal loading on
cervical stress concentration,40 can challenge the tooth–resin
interface.37,38
The results of sensitivity evaluation revealed no statistical
significant differences between groups in any recall, demon-
strating that chlorhexidine digluconate does not increase
post-operative sensitivity. After 36 months of clinical func-
tion, 3 restorations (one restoration in the control group and
two in the experimental group) presented clinical accepted
sensitivity when an air stimulus was applied. These three
restorations were placed to lesions with pre-operative
sensitivity and in the same patient, which may indicate that
patient factor, such as sensitivity, diet, life style, occlusion,
and habits, may influence the results.
Although this study was conducted with a small, well-
selected group of patients, the results suggest that the success
rate of control and chlorhexidine treated groups are similar, at
least within a 36-month follow-up. Other studies are indis-
pensable to evaluate the clinical performance of different
chlorhexidine concentrations applied in different teeth cavity
configurations, longer periods of clinical trials, and restored
using less hydrophilic materials.
5. Conclusion
From the results of this clinical study, chlorhexidine digluconate
conditioning step does not improve the clinical durability in
non-carious cervical restorations within 36-month follow-up.
Acknowledgements
We would like to thank Lais Dalmagro Peruchi and Dr. Sillas
Duarte Jr for editorial assistance. This study was partly

j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 1 1 8 8 – 1 1 9 51194
supported by the Brazilian Federal Agency for Support and
Evaluation of Graduate Education (CAPES).
r e f e r e n c e s
1. Van Dijken JW. Clinical evaluation of three adhesivesystems in class V non-carious lesions. Dental Materials2000;16:285–91.
2. Van Dijken JW. A prospective 8-year evaluation of a mildtwo-step self-etching adhesive and a heavily filled two-stepetch-and-rinse system in non-carious cervical lesions.Dental Materials 2010;26:940–6.
3. Pashley DH. Dentin: a dynamic substrate—a review.Scanning Microscopy 1989;3:161–74.
4. Breschi L, Mazzoni A, Ruggeri A, Cadenaro M, Di Lenarda R,De Stefano Dorigo E. Dental adhesion review: aging andstability of the bonded interface. Dental Materials 2008;24:90–101.
5. Pashley DH, Tay FR, Yiu C, Hashimoto M, Breschi L, CarvalhoRM, et al. Collagen degradation by host-derived enzymesduring aging. Journal of Dental Research 2004;83:216–21.
6. Eick JD, Gwinnett AJ, Pashley DH, Robinson SJ. Currentconcepts on adhesion to dentin. Critical Reviews in OralBiology & Medicine 1997;8:306–35.
7. Carrilho MR, Geraldeli S, Tay F, de Goes MF, Carvalho RM,Tjaderhane L, et al. In vivo preservation of the hybrid layerby chlorhexidine. Journal of Dental Research 2007;86:529–33.
8. Tjaderhane L, Larjava H, Sorsa T, Uitto VJ, Larmas M, Salo T.The activation and function of host matrixmetalloproteinases in dentin matrix breakdown in carieslesions. Journal of Dental Research 1998;77:1622–9.
9. Sulkala M, Larmas M, Sorsa T, Salo T, Tjaderhane L. Thelocalization of matrix metalloproteinase-20 (MMP-20,enamelysin) in mature human teeth. Journal of DentalResearch 2002;81:603–7.
10. Mazzoni A, Pashley DH, Tay FR, Gobbi P, Orsini G, Ruggeri JrA et al. Immunohistochemical identification of MMP-2 andMMP-9 in human dentin: correlative FEI-SEM/TEM analysis.Journal of Biomedical Materials Research Part A 2009;88:697–703.
11. Sulkala M, Tervahartiala T, Sorsa T, Larmas M, Salo T,Tjaderhane L. Matrix metalloproteinase-8 (MMP-8) is themajor collagenase in human dentin. Archives of Oral Biology2007;52:121–7.
12. Tersariol IL, Geraldeli S, Minciotti CL, Nascimento FD,Paakkonen V, Martins MT, et al. Cysteine cathepsins inhuman dentin–pulp complex. Journal of Endodontics2010;36:475–81.
13. Liu Y, Tjaderhane L, Breschi L, Mazzoni A, Li N, Mao J, et al.Limitations in bonding to dentin and experimentalstrategies to prevent bond degradation. Journal of DentalResearch 2011;90:953–68.
14. Nascimento FD, Minciotti CL, Geraldeli S, Carrilho MR,Pashley DH, Tay FR, et al. Cysteine cathepsins in humancarious dentin. Journal of Dental Research 2011;90:506–11.
15. Sano H, Takatsu T, Ciucchi B, Horner JA, Matthews WG,Pashley DH. Nanoleakage: leakage within the hybrid layer.Operative Dentistry 1995;20:18–25.
16. Leung D, Spratt DA, Pratten J, Gulabivala K, Mordan NJ,Young AM. Chlorhexidine-releasing methacrylate dentalcomposite materials. Biomaterials 2005;26:7145–53.
17. Hashimoto M, Ohno H, Sano H, Kaga M, Oguchi H. In vitrodegradation of resin–dentin bonds analyzed by microtensilebond test, scanning and transmission electron microscopy.Biomaterials 2003;24:3795–803.
18. Breschi L, Martin P, Mazzoni A, Nato F, Carrilho M,Tjaderhane L, et al. Use of a specific MMP-inhibitor (galardin)
for preservation of hybrid layer. Dental Materials2010;26:571–8.
19. Sorsa T, Tervahartiala T, Leppilahti J, Hernandez M,Gamonal J, Tuomainen AM, et al. Collagenase-2 (MMP-8) as apoint-of-care biomarker in periodontitis and cardiovasculardiseases. Therapeutic response to non-antimicrobialproperties of tetracyclines. Pharmacological Research2011;63:108–13.
20. Hebling J, Pashley DH, Tjaderhane L, Tay FR. Chlorhexidinearrests subclinical degradation of dentin hybrid layersin vivo. Journal of Dental Research 2005;84:741–6.
21. Hickel R, Roulet JF, Bayne S, Heintze SD, Mjor IA, Peters M,et al. Recommendations for conducting controlled clinicalstudies of dental restorative materials. Science CommitteeProject 2/98—FDI World Dental Federation study design(Part I) and criteria for evaluation (Part II) of direct andindirect restorations including onlays and partial crowns.The Journal of Adhesive Dentistry 2007;9(Suppl 1):121–47.
22. Swift Jr EJ, Perdigao J, Heymann HO, Wilder Jr AD, BayneSC, May Jr KN et al. Eighteen-month clinical evaluation ofa filled and unfilled dentin adhesive. Journal of Dentistry2001;29:1–6.
23. Van Landuyt K, Fieuws S, Van Meerbeek B. Sample sizeconsiderations for restoration-longevity randomizedcontrolled trials. The Journal of Adhesive Dentistry 2008;10:247.
24. American Dental Association Council on Scientific Affairs.Acceptance program guidelines: dentin and enameladhesive materials. Chicago: American Dental Association;2001.
25. Cvar JF, Ryge G. Reprint of criteria for the clinical evaluationof dental restorative materials. 1971. Clinical OralInvestigations 2005;9:215–32.
26. Holland GR, Narhi MN, Addy M, Gangarosa L, Orchardson R.Guidelines for the design and conduct of clinical trials ondentine hypersensitivity. Journal of Clinical Periodontology1997;24:808–13.
27. Mazzoni A, Mannello F, Tay FR, Tonti GA, Papa S, MazzottiG, et al. Zymographic analysis and characterization of MMP-2 and -9 forms in human sound dentin. Journal of DentalResearch 2007;86:436–40.
28. Gendron R, Grenier D, Sorsa T, Mayrand D. Inhibition of theactivities of matrix metalloproteinases 2, 8, and 9 bychlorhexidine. Clinical and Diagnostic Laboratory Immunology1999;6:437–9.
29. Carrilho M, Scaffa PMC, Vidal CMP, Barros NT, Ferreira TG,Pashley D, et al. Interaction between chlorhexidine andcysteine cathepsins B and K. Journal of Dental Research2011:90.
30. Misra DN. Interaction of chlorhexidine digluconate with andadsorption of chlorhexidine on hydroxyapatite. Journal ofBiomedical Materials Research 1994;28:1375–81.
31. Kim J, Uchiyama T, Carrilho M, Agee KA, Mazzoni A, BreschiL, et al. Chlorhexidine binding to mineralized versusdemineralized dentin powder. Dental Materials 2010;26:771–8.
32. Di Hipolito V, Rodrigues FP, Piveta FB, Azevedo Lda C,Bruschi Alonso RC, Silikas N, et al. Effectiveness of self-adhesive luting cements in bonding to chlorhexidine-treated dentin. Dental Materials 2012;28:495–501.
33. Sattabanasuk V, Vachiramon V, Qian F, Armstrong SR.Resin–dentin bond strength as related to differentsurface preparation methods. Journal of Dentistry2007;35:467–75.
34. Ferracane JL. Hygroscopic and hydrolytic effects in dentalpolymer networks. Dental Materials 2006;22:211–22.
35. Brackett MG, Tay FR, Brackett WW, Dib A, Dipp FA, Mai S,et al. In vivo chlorhexidine stabilization of hybrid layers ofan acetone-based dentin adhesive. Operative Dentistry2009;34:379–83.

j o u r n a l o f d e n t i s t r y 4 1 ( 2 0 1 3 ) 1 1 8 8 – 1 1 9 5 1195
36. Ichim I, Li Q, Loughran J, Swain MV, Kieser J. Restoration ofnon-carious cervical lesions. Part I. Modelling of restorativefracture. Dental Materials 2007;23:1553–61.
37. Rees JS, Jacobsen PH. The effect of cuspal flexure on a buccalClass V restoration: a finite element study. Journal ofDentistry 1998;26:361–7.
38. Heymann HO, Sturdevant JR, Bayne S, Wilder AD,Sluder TB, Brunson WD. Examining tooth flexureeffects on cervical restorations: a two-year clinical
study. The Journal of the American Dental Association1991;122:41–7.
39. Ichim I, Schmidlin PR, Kieser JA, Swain MV. Mechanicalevaluation of cervical glass-ionomer restorations: 3D finiteelement study. Journal of Dentistry 2007;35:28–35.
40. Takehara J, Takano T, Akhter R, Morita M. Correlations ofnoncarious cervical lesions and occlusal factors determinedby using pressure-detecting sheet. Journal of Dentistry2008;36:774–9.





























