Embed Size (px)
Citation preview

Information needs of parents for acutechildhood illness: determining ‘what,how, where and when’ of safety nettingusing a qualitative exploration withparents and clinicians
Caroline H D Jones,1 Sarah Neill,2 Monica Lakhanpaul,3 Damian Roland,4
Hayley Singlehurst-Mooney,2 Matthew Thompson1
To cite: Jones CHD, Neill S,Lakhanpaul M, et al.Information needs of parentsfor acute childhood illness:determining ‘what, how,where and when’ of safetynetting using a qualitativeexploration with parents andclinicians. BMJ Open 2014;4:e003874. doi:10.1136/bmjopen-2013-003874
▸ Prepublication history forthis paper is available online.To view these files pleasevisit the journal online(http://dx.doi.org/10.1136/bmjopen-2013-003874).
Received 22 August 2013Revised 2 December 2013Accepted 4 December 2013
For numbered affiliations seeend of article.
Correspondence toDr Caroline H D Jones;[email protected]
ABSTRACTObjective: To explore the views of parents andclinicians regarding the optimal content, format anddelivery of safety netting information for acutechildhood illness.Design: Qualitative study including semistructuredfocus groups and interviews.Setting: First contact care settings, communitycentres, children’s centres and nurseries in theMidlands, UK.Participants: 27 parents from a travelling community,Asian British community and white British community.Sixteen clinicians including 10 doctors and 6 nursesfrom a general practice surgery, an out-of-hoursservice and two emergency departments (paediatricand combined adult and paediatric).Results: Participants described a need for safetynetting to contain information on signs and symptomsof serious and common illnesses, illness managementand where and when to seek help. Resources shouldbe basic, simple to use and contain simple symbols.A key criterion was professional endorsement ofresources. Internet-based information was desiredwhich is reliable, consistent and up-to-date.Participants described a need for different types ofinformation: that which could be delivered duringconsultations, as well as more general information forparents to access before consulting a healthcareprofessional. Face-to-face education, written materialsand digital media were suggested deliverymechanisms. Audiovisual material was preferred byfamilies with low literacy. Participants commonlysuggested internet-based and phone-based resources,but the travelling community was less comfortable withthese approaches.Conclusions: A multifaceted and tailored approach tosafety netting is needed so that effective resources areavailable for parents with varying information needs,literacy levels and ability to use informationtechnology. We have identified key aspects of content,quality criteria, format and delivery mechanisms forsafety netting information from the perspectives ofclinicians and parents. Resources should be
coproduced with parents and clinicians to ensure thatthey are valued and utilised by both groups.
INTRODUCTIONAcute childhood illness is a major contribu-tor to children’s presentation to primarycare, and to child mortality. Child and youngperson mortality has fallen in Europe, butchild death rates from treatable causesincluding asthma, pneumonia and meningi-tis are higher in the UK than elsewhere inEurope, highlighting a need to bettermanage acutely sick children.1 2 The vastmajority of children have minor, self-limitingillnesses requiring little or no medical inter-vention, and it is increasingly difficult forclinicians to identify the very few childrenwith serious illnesses, which often havenon-specific presentations and clinical fea-tures mimicking those of common, non-serious illness.3 Despite the prevalence of
Strengths and limitations of this study
▪ Parents and clinicians participated, and the find-ings could form the basis of truly coproducedresources.
▪ We included diverse groups of parents with dif-ferent information needs and abilities, and clini-cians from a range of first contact care settings,to ensure that the views of different groups wereincluded; however, the extent to which the find-ings are generalisable to other groups or popula-tions is not known.
▪ Data were collected and analysed by a team ofresearchers including clinical and non-clinical,some parents and some not, enabling a deeperunderstanding.
Jones CHD, Neill S, Lakhanpaul M, et al. BMJ Open 2014;4:e003874. doi:10.1136/bmjopen-2013-003874 1
Open Access Research
group.bmj.com on January 15, 2014 - Published by bmjopen.bmj.comDownloaded from

life-threatening acute childhood illness being at anall-time low, there has been an increase in children’semergency hospital admissions, many of which are forminor illnesses which could have been managed in thecommunity.4 5 Safety netting information given toparents during consultations advises them about whenand where to seek further help.6 As well as aiming toprevent misdiagnoses and avoidable child mortality,there is evidence that safety netting can reduce reatten-dances in febrile children.7 8
Safety netting was first described by Neighbour9 over20 years ago, who proposed it to be a core componentof general practice. More recently, safety netting hasbeen recommended in the management of acutely sickchildren by the National Institute for Health and CareExcellence (NICE),10 Scottish Intercollegiate GuidelinesNetwork (SIGN),11 other national groups,2 12 generalpractitioners6 13 and researchers,14 and has been intro-duced as a NICE quality standard.15 Despite theserecommendations, there are no set guidelines regardingthe optimal content, format and delivery of safetynetting.Anxiety and uncertainty surround parents’ decisions
about when to consult (and reconsult) healthcare pro-fessionals during acute childhood illness at home.16 17
Safety netting could potentially help to reduce these,and provide the more explicit and consistent advice thatparents seek.7 However, the most effective componentsand ways of delivering safety netting are yet to be identi-fied,18 19 and there is evidence that current safetynetting advice may be inadequate. For example, a studyof 220 feverish children making 570 contacts withurgent care services found that 19% of parents did notrecall being given any safety netting advice, and docu-mentation of safety netting advice regarding what tolook for was absent in nearly half (43%) of patients’records.8
As part of the Acutely Sick Kids—Safety NettingInterventions for Families (ASK SNIFF) project, thisstudy aimed to explore the opinions of parents and firstcontact clinicians regarding the optimal content, qualitycriteria, format and delivery of safety netting informa-tion. This is vital for the development of effective safetynetting materials to increase parental confidence, under-standing and satisfaction, decrease uncertainty andanxiety, as well as increase timely and appropriate pres-entation to primary care. Including and combining theopinions of clinicians and parents mirrors a key prin-ciple of the Children and Young People’s HealthOutcome’s Forum, that families must have a voice andbe engaged in the development of services.2
METHODSWe used a qualitative, exploratory approach due to thelack of prior knowledge on the topic. Maximum vari-ation sampling was used to recruit parents from a widerange of communities, and doctors and nurses working
in different first contact care settings in the Midlands,UK. Any parents with at least one child under the age of5 years and any clinicians treating children under 5 yearsof age at first contact, who were able to speak English,were eligible to participate. We conducted focus groupsand/or interviews in each parent community and ateach first contact care workplace.Recruitment was coordinated by email or in person
using the local Primary Care Research Network, theComprehensive Local Research Network for clinicians,community facilitators, health ambassadors and daynursery/children’s centre managers for parents. All par-ticipants gave written informed consent. The study wasapproved by the East Midlands—Nottingham 2 NHSResearch Ethics Committee (REC reference 12/EM/0076) —and the appropriate research and developmentoffices of each local Trust. Two experienced femaleresearchers (SN, a children’s nurse lecturer and HS, asocial scientist) facilitated focus groups and interviewsbetween May and December 2012, which were semistruc-tured and lasted around an hour. Participants wereasked a number of questions about provision of safetynetting information (see box 1), and the facilitatorsused prompts to elicit further details. One facilitatortook notes and gave a verbal summary at the end, askingthe participants to correct misinterpretations and givefurther comments. Focus groups and interviews wereaudio recorded, transcribed verbatim and anonymised.Data were analysed using the grounded theory
method of constant comparison. Three main themeswere predetermined by the research question and topicguide (content, quality criteria and format/delivery ofsafety netting). Codes and subthemes within each ofthese themes were developed according to the contentof focus groups/interviews. Separate coding schemeswere devised for parent and clinician data, with many ofthe same codes occurring in the parent and cliniciancoding schemes. Throughout the process of data
Box 1 Topic guide for focus groups and interviews
ParentsWhat information do you want/need to find when your childbecomes sick?Where would you like to find/be given this information?In what ways, if any, would you like to see access to informa-tion improved?In what ways, if any, do you think the information providedneeds to be improved?
CliniciansWhat safety netting information do you think parents of sickyoung children should be given?How do you think they should be given this information?In what ways, if any, do you feel the safety netting informationavailable needs to be improved?In what ways, if any, would you like to see access to informa-tion improved?
2 Jones CHD, Neill S, Lakhanpaul M, et al. BMJ Open 2014;4:e003874. doi:10.1136/bmjopen-2013-003874
Open Access
group.bmj.com on January 15, 2014 - Published by bmjopen.bmj.comDownloaded from

collection and analysis, codes were edited, combinedand new ones added, and codes were grouped togetheras subthemes were developed within each theme. Thecoding schemes were developed together by CJ (a non-clinical researcher) and SN (a children’s nurse lecturer),who allocated text to codes accordingly. CJ coded theclinician data and SN coded the parent data, and bothresearchers cross-checked the codings. Both researcherswere familiar with the content of all focus groups/inter-views and both coding schemes. Emerging subthemesand comparisons between parent and clinician datawere discussed and developed among the wider researchteam. The constant comparative method enabled us toidentify similarities and differences within the datacoded to the same and different subthemes fromparents and clinicians.
RESULTSParticipantsParticipants included 27 parents and 16 clinicians.Parents were from a travelling community (recruited via acommunity facilitator), Asian British community(recruited at a local community centre and a children’scentre) and white British community (recruited from achildren’s centre and a private nursery; see table 1).Clinicians were included from a general practice surgery,a District General Hospital (DGH) emergency depart-ment (ED) (treating adults and children), a paediatricED and an out-of-hours service (OOHS; see table 2).Below we present the three main themes—content,
quality criteria and format/delivery of safety netting—and the subthemes within them. Tables 3–5 display each
theme, respectively, and the subthemes within them,with quotes to illustrate aspects of our interpretation ofthe data within each of the subthemes.
Safety netting contentThere was consensus among the clinicians working inthe different settings that paediatric illness is broad, andsafety netting advice should focus on signs and symp-toms of the most serious and most common childhoodillnesses: “It’s the nasty ones that you want to catch andthe very common things that people will have neverseen before but are OK” (DGH ED doctor). Some clini-cians thought that in addition to specific advice givenduring consultations, there is a need for generic adviceor education: “perhaps there could be… more kind ofgeneric advice about unwell children” (OOHS GP);“instant access [to information] doesn’t really helpbecause you need to build up your knowledge longbefore the child becomes ill” (DGH ED doctor). Thisemphasises the potential need for two differentresources: a diagnosis or illness-related safety nettingresource for use during/postconsultation, and a moregeneral educational resource for use preconsultation.Clinicians described the importance of signposting
parents to different services according to illness severityand providing information on illness management.Primary care staff focused on the need to educateparents about when to care for their child at home orvisit the pharmacy, whereas ED staff focused more onthe need to communicate what signs and symptoms indi-cate that parents should attend an ED immediately.Parents’ need for information matched that of clini-
cians, namely what symptoms are associated with themost common and most serious illnesses (particularly
Table 1 Characteristics of participating parents
Characteristics of parents Number of parents
Community
Travelling families 6
Asian British 11
White British 10
Gender
Female 24
Male 3
Age (years)
Under 20 1
20–29 5
30–39 16
40–49 5
Adults in the household
Single parent household 5
Two parent household 18
More than two adult household 4
Number of children*
1 6
2 8
3 5
4 or more 6
*Data on the number of children missing for two parents.
Table 2 Characteristics of participating clinicians
Characteristics of cliniciansNumber ofclinicians
Setting
General practice 5
District general hospital emergency
department
5
Paediatric emergency department 4
Out-of-hours service 2
Profession
Doctor 10
Nurse 6
Gender
Female 6
Male 10
Ethnicity
Asian British 3
White British 13
Age (years)
30–39 7
40–49 7
50+ 2
Jones CHD, Neill S, Lakhanpaul M, et al. BMJ Open 2014;4:e003874. doi:10.1136/bmjopen-2013-003874 3
Open Access
group.bmj.com on January 15, 2014 - Published by bmjopen.bmj.comDownloaded from

meningitis), and when/where to access help. Afterreceiving a diagnosis, information is wanted on illnesscausation, management and trajectory: “Where I askevery question under the sun. What is it, why did theyget that, how many times will they get it again?” (travel-ling community mother).
Safety netting quality criteriaClinicians and parents similarly stated that safety nettingresources should be basic, simple to use, with simplemessages. Simple symbols and colour indicators weresuggested for presenting safety netting information visu-ally, which would be particularly useful for people whoare unable to easily understand written information.Suggestions included ticks and crosses, sad and happyfaces, traffic lights, red and green: “a picture with agreen smiley face, a meningococcal septicaemia rashwith a big upset blue light on top of it type face or some-thing like that” (DGH ED doctor). The parents and clin-icians felt that information should be provided in simplelanguage, as well as multiple languages; and that itshould be symptoms-based because parents would notalways know their child’s diagnosis when searching forinformation.
Importantly, it was commented that written information,including internet-based resources, should be easy andquick to access. However, one clinician raised a caveat:“you’ve got to be very careful with the information thatyou are putting out there, because you don’t want to drivethe paranoia more that there is” (paediatric ED doctor).A key quality criterion identified by parents and clini-
cians was professional endorsement: “I think if it wasNHS backed you’d kind of have a bit more trust” (whiteBritish mother). Publicity was also highlighted: “it needsto be publicised that patients know to access that site,whereas what’s happening now is that they’re accessingGoogle and getting a whole lot of symptoms which,y’know, lots of them are not necessarily useful and, erm,heightens the anxiety” (GP surgery doctor). These cri-teria were described particularly in relation to internet-based safety netting resources: currently, searching theinternet generates an ‘overload’ of information, some ofwhich are not useful, which creates uncertainty andanxiety among parents. Access to reliable, consistent,up-to-date internet-based information was commonlyrequested: “the problem is I think the information’sthere, it’s not all in one place, it’s all over different web-sites and if the Department of Health was able to
Table 3 Subthemes and illustrative quotes within the Safety Netting Content theme
Subtheme Illustrative quote
Most serious and most common
childhood illnesses
I don’t think it’s going to be possible to inform everybody about every
kind of conditions that are out there, but there may be some that we
can consider the common ones and more serious ones, you know
Asian British
father
Signposting to different services Is it phone, such and such, is it take to A&E, you know, is it wait till the
morning, see how it is?
White British
mother
Table 4 Subthemes and illustrative quotes within the Safety Netting Quality Criteria theme
Subtheme Illustrative quote
Basic It needs to be absolute almost so simple basic GP surgery
doctor
Simple symbols,
colours
Simple visual things like a tick and a cross. Lots of people know that a cross is not
a good thing or it’s a danger. Anything in red, anything green is good… or a sad
face or a happy face
Asian British
mother
Multiple languages The information that comes out actually needs to be in multiple languages as well DGH ED
doctor
Symptoms-based of course a lot of the time you don’t know the diagnosis so, yeah, so it’s important
it isn’t sort of restricted to a diagnosis really I think
OOHS GP
Professional
endorsement
Obviously it has to be audited and have involvement with the government Asian British
mother
Publicised half of it would be the media in letting the parents know that is out there, because
half of these things you don’t know that they exist and you don’t know what to trust
white British
mother
Easy and quick to
access
I think it’s just being able to access information very quickly white British
mother
Portable Nothing that adds to your weight of your bag white British
mother
I always tend to keep a lot of stuff like that in her bag so I always know where it is
and if I’m with her, her bag’s always around anyway, so I would prefer that
white British
mother
4 Jones CHD, Neill S, Lakhanpaul M, et al. BMJ Open 2014;4:e003874. doi:10.1136/bmjopen-2013-003874
Open Access
group.bmj.com on January 15, 2014 - Published by bmjopen.bmj.comDownloaded from

somehow streamline the advice nationally and set up aprocess of okaying national advice for parents… I thinkthat would be the way to do it” (paediatric ED doctor).
It was suggested that parents need resources whichare portable, particularly when caring for a distressedchild. Different methods were suggested for achieving
Table 5 Subthemes and illustrative quotes within the Format and Delivery of Safety Netting theme
Subtheme Illustrative quote
Consultation-based
Signs and symptoms
to look for
Simple things like tracheal recession that are quite easy to demonstrate…
just to show them if they come in with that presenting complaint and it’s
just talking through it isn’t it, if you see any of these signs then you need to
come straight back then
DGH ED nurse
Information sheets My doctor did give like an information leaflet… and I did read through it,
because like on the Internet, you can get into so many areas and then you
know you think, you need to feed your son, but when you’ve got a sheet at
least you can find time to do that
Asian British mother
Preconsultation education
Health visitors I think the information almost needs to come before your child’s ill at
health visitor level
DGH ED nurse
Peer education I think peer education with young parents would be good because the
thing is… they’re only actually learning when they actually come into you
GP surgery nurse
School, nursery, social
workers
Certainly social workers might be a valuable way of actually getting
information like this into these families… and teachers
DGH ED doctor
Books It’s easy to flick through a book when your breastfeeding or bottle feeding
or whatever
white British mother
I didn’t read the books, it was too much information. You don’t want to be
bombarded really I don’t think
white British mother
Posters They used to have a big resuscitation poster that they advised you to put
in your children’s bedroom… You could have your symptom checker thing
on there because you’re more likely to read it at the time you don’t need it,
than the time you do need it
DGH ED nurse
Information pack for
new parents
Because you read everything in that [information] pack because it’s your
first baby, so every leaflet is important in that [information] pack
DGH ED nurse
Adverts Like how many parents come forward and say, “Oh we found out our child
had meningitis because we did the glass roll test.” I actually think media
like that is one of the most powerful way of sort of getting to large groups
is to have like it on telly
white British mother
A lot of us can’t read or write… (parent 1). So I think they do pick up a lot,
travellers do rely on the adverts and that a lot more. They take more notice
of them kind of things (parent 2)
Travelling community
mothers
Centralised website if you’ve got an ill child and you’re wanting to find out what it could
possibly be, you don’t want to spend hours looking for that information,
you actually want to be able to go on a site
White British mother
Internet-based resources
If you’ve got a sick child at home and they’re maunging at you, you haven’t
got the time to go on the internet… you’ve got a child hanging off your leg
going, “Mummy I feel poorly, mummy I want this, mummy I want that,” or
you know, screaming or, I don’t think it’s that practical that often you don’t
have the chance to go on the internet
White British mother
Mobile-phone
accessible website
Yes the phone it’s easily accessible and especially when you’ve got a
baby. Rather than putting on the computer….I think the phone is a very
good source because you keep it all the time with you. That’s a very good
thing, yeah
White British mother
Audiovisual material
Pictures A picture says a thousand words but it helps. Pictures definitely help DGH ED doctor
Videos Mixed in with some kind of videos of things that you kind of click on to see
what it, or pictures to see what it looks like. Because they’re saying you’re
breathing faster, but as I said, that’s one thing for one person and you
know, it might mean something else to somebody else… And give patients
and parents that autonomy to say actually no, I’ve looked at this, this is
what it looks like and therefore my child is breathing fast
Paediatric ED doctor
Jones CHD, Neill S, Lakhanpaul M, et al. BMJ Open 2014;4:e003874. doi:10.1136/bmjopen-2013-003874 5
Open Access
group.bmj.com on January 15, 2014 - Published by bmjopen.bmj.comDownloaded from

this, including providing portable hard copy: “You’vegot them clung to you cause they’re unwell, you’re notgoing to sit at a computer” (GP surgery nurse); “I thinkthey sort of produce sort of credit card sized thingsthey can give out… so perhaps more of those sorts ofresources” (OOHS GP). Alternatively, phone-basedinternet access could provide a quick and easy access toinformation: “I would do it on my phone, oh yeah,yeah, yeah, very much so. And that I actually findeasier than picking up the phone because if you’ve gota crying child, trying to pick up the phone and talk tosomebody is actually a lot more difficult than having aquick look on the internet to see…” (white Britishmother).
Format and delivery of safety nettingAs described above, the participants described a needfor different types of safety netting resources includingthose delivered during consultations and those accessedprior to consultation. They also acknowledged that infor-mation should be provided in multiple formats: “It canbe on different forms of media, Internet. Obviously,Internet may not be accessible to many people and if itis accessible, they may not be able to go to the rightinformation, right section so having it in differentformats will be quite helpful” (Asian British father).
Consultation-based safety nettingClinicians described how verbal and written safetynetting information could be delivered during consulta-tions, and suggested demonstration of physical signsincluding tracheal tug, intercostal recession and slowcapillary refill time. Provision of written materialsduring consultations could be useful for parents: “Wellhalf the time when you’re taking your child to thedoctors they’re not very well, are they, so they’re clingy,you’ve had to probably strip them off… so they’recrying and they’re trying to tell you all this informationand getting them back dressed again really quickly…There is pressure to get out quickly, I think, so I thinkyou do forget what the doctor has said.” (white Britishmother).Another type of safety netting was referring children
to other services such as community children’s nurses.Some clinicians thought that written safety netting mate-rials should be tailored to the local area accordingly: “abit more specific to the area as well, that would be goodso it was, you know it takes into account sort of localpathways, what’s available locally including things likethe community children’s nurses” (OOHS GP).Conversely, one parent highlighted the need for standar-dised advice: “It should be across nationally and so on,so that everyone is getting the same message” (AsianBritish mother).
Preconsultation educationSafety netting resources for use prior to consultationincluded general preparatory educational information to
be accessed prior to illness occurring and more specificinformation for parents to access during acute child-hood illness, before they consult a healthcareprofessional.Educational methods suggested by the clinicians
included education by health visitors, and peer educa-tion so that parents can learn from the experiences ofothers—a caveat being that the information is correct:“actually learning by somebody else’s experience whathappened and what were you told and it’s getting thatbecause peer education, if it’s correct, ‘cause that’sanother reason why we get to see people, ‘causeanother relative has sent them in and said you must beseen, because advice has changed…” (GP surgerynurse). Other suggestions were delivery by school/nursery teachers and social workers. Parents hadsimilar suggestions to clinicians, namely education onchildhood illnesses by health visitors and schools/nur-series as well as novel suggestions including libraries,community centres and GP surgeries (in waiting roomsas well as during consultations). They also suggestedcommunity-based delivery systems including communitychampions, community educational programmes (suchas short courses in community centres) and communitysnowballing (whereby healthcare professionals provideinitial educational sessions, then peers provide thesesessions afterwards).Written materials were suggested for educating
parents prior to their child becoming ill. The parentsand clinicians mentioned posters, and suggested theinformation pack for new parents as a way to deliverwritten information (although parents did commentthat they did not use the information provided in thispack beyond the neonatal period). Other parental sug-gestions for written materials included booklets, leaflets,flash cards and small quizzes. The parents and GPs hada limited knowledge of the information on childhoodillness currently contained in the personal child healthrecord (‘red book’), and felt that it was not well used byparents or GPs. Building on the information containedin books, or introducing new books, may not be aneffective mechanism to educate parents about childhoodillness: “I think I possibly looked at it when I was a newmum with you know, so much enthusiasm, and thenabout a week in I was like… I’m far too tired to do this,there’s no way I’m reading through that book” (whiteBritish mother).Parents suggested a wide range of digital media which
could be used to deliver information, including internet,phone-based media, DVD, television programmes androlling displays on waiting room screens. Many parentsrecalled media campaigns for stroke, and the glass testfor non-blanching rash in meningitis. These campaignsappear to have reached all of the social groups in thesample. Parents felt that media campaigns could be suc-cessful for acute childhood illness. The GP surgery focusgroup acknowledged the success of media campaignsand suggested this could work for educating parents on
6 Jones CHD, Neill S, Lakhanpaul M, et al. BMJ Open 2014;4:e003874. doi:10.1136/bmjopen-2013-003874
Open Access
group.bmj.com on January 15, 2014 - Published by bmjopen.bmj.comDownloaded from

child illness, although it was acknowledged that mediacampaigns could create anxiety.
Internet-based resourcesInternet-based resources such as a centralised websitewere commonly mentioned by parents and cliniciansalike. One thing parents would like is a well-signpostedwebsite with NHS endorsement, which is easy to searchand appropriate for mobile phones. Parents were infavour of doctors giving out information about a reliablesite at the end of consultations. Clinicians indicated thatthey were happy to perform this; but it would need tobe simple to use: “you wouldn’t want to, yeah, be gettinginto huge conversations about how you do it… how youaccess it, so yeah, it would need to be sufficiently simpleand accessible” (OOHS GP).Similarly to parents, clinicians in all settings suggested
that a phone-based application could be successful inhelping parents of sick children assess whether/whereto seek help: “World and times are changing, everythingis about internet, everything is about apps and I think ifyou’ve got something well written and accessible, on theinternet with maybe an iPhone app, an android app,that people can download y’know, some sick kids guideor something like that with a bit of a symptom checkerand robust, this is what paediatricians, this is what GPs,this is what emergency physicians would advise you todo, then I think people will take that seriously and Isuspect it would cut down the attendance rate at all dif-ferent places plus make people a lot more happy” (DGHED doctor). However, the travelling community high-lighted that the current generation of parents are oftenunfamiliar with information technology: “But the newgeneration when they get a bit older, in a couple ofyears from now, cause all the children now they’re allpermanently at school that would help them but not forall us, not for this generation” (travelling communitymother).
Audiovisual materialA benefit of internet-based resources, highlighted byparents and clinicians, is that they could include shortvideo clips showing signs and symptoms, presentinginformation that is difficult to explain verbally or in dia-grams. Parents suggested clips of sounds of specificcoughs (croup, whooping cough), respiratory move-ments (recession) or the appearance of different rashes(chickenpox, meningitis). Conditions that were sug-gested for video format by clinicians, some of whichmatched those suggested by parents, were croup,wheeze, increased work of breathing, recession, bron-chiolitis, dehydrated child, floppy child, seizures andfainting, tracheal tug, capillary refill time and rashes.Parents highlighted that these could be viewed, forexample, on a mobile phone while holding a baby.Audiovisual material was the preferred option for fam-ilies with low literacy: the Asian British and travellingcommunities highlighted that some families would not
be able to read written language. Limitations of audiovi-sual material were however recognised: “[Doctor 1]Photos are very difficult because even if you look at thedifferent atlases we have for dermatology… [Doctor 2]and each book looks slightly different [Doctor 3] And itcan be falsely reassuring can’t it. ‘Cause you have menin-gococcal disease, you can have a blanching rash” (paedi-atric ED doctors).
It is important to note that in addition to discussinginformation resources, parents and clinicians alike high-lighted that for worried parents, nothing will replaceface-to-face reassurance from a healthcare professional:“only physical contact with somebody who you trust andfeel can answer your question will ever give you thereassurance with regards to a child that you’re lookingfor… ultimately you really just want to speak to someoneand show them your child, you want to speak tosomeone who you feel is experienced and knowledge-able about what you are talking about and can help youwith your child” (white British mother); “verbal advicecan reassure you, I don’t think any website or any infor-mation can reassure you” (DGH ED doctor). Thismessage came across particularly strongly from the AsianBritish community.
DISCUSSIONPrinciple findings and implicationsCoproductionParents and clinicians described a diverse range of desir-able attributes for safety netting advice, as well as techni-ques for its delivery. This highlights the need for truecoproduction of safety netting resources by parents andclinicians, throughout every stage of design and develop-ment of resources, to ensure that they meet the range ofcriteria identified as important by both groups. Thismirrors the key principle of the Children and YoungPeople’s Health Outcome’s Forum regarding familyinvolvement in the development of services.2 Safetynetting is a perfect example of where true coproductionby clinicians and parents could result in the develop-ment of effective resources which will be utilised andvalued by both groups.There were some important differences between
groups, for example, while clinicians in all settings, andmany parents, favoured the idea of internet-based andphone-based resources, the travelling community high-lighted that this would not be appropriate for thecurrent generation of parents; and the Asian British andtravelling communities highlighted that some familieswould not be able to read written English, thus particu-larly preferring audiovisual materials. However, generallyparents and clinicians from different communities/set-tings suggested a very similar range of content, qualitycriteria, format and delivery methods for safety nettingadvice, while acknowledging that multiple techniquesand resources are needed. (Note, however, that thenumber of participants from each community/setting
Jones CHD, Neill S, Lakhanpaul M, et al. BMJ Open 2014;4:e003874. doi:10.1136/bmjopen-2013-003874 7
Open Access
group.bmj.com on January 15, 2014 - Published by bmjopen.bmj.comDownloaded from
was small which limited our ability to draw compari-sons.) Previous research in the UK has also found com-monality of parental information needs across differentsocioeconomic groups regarding childhood illness.20
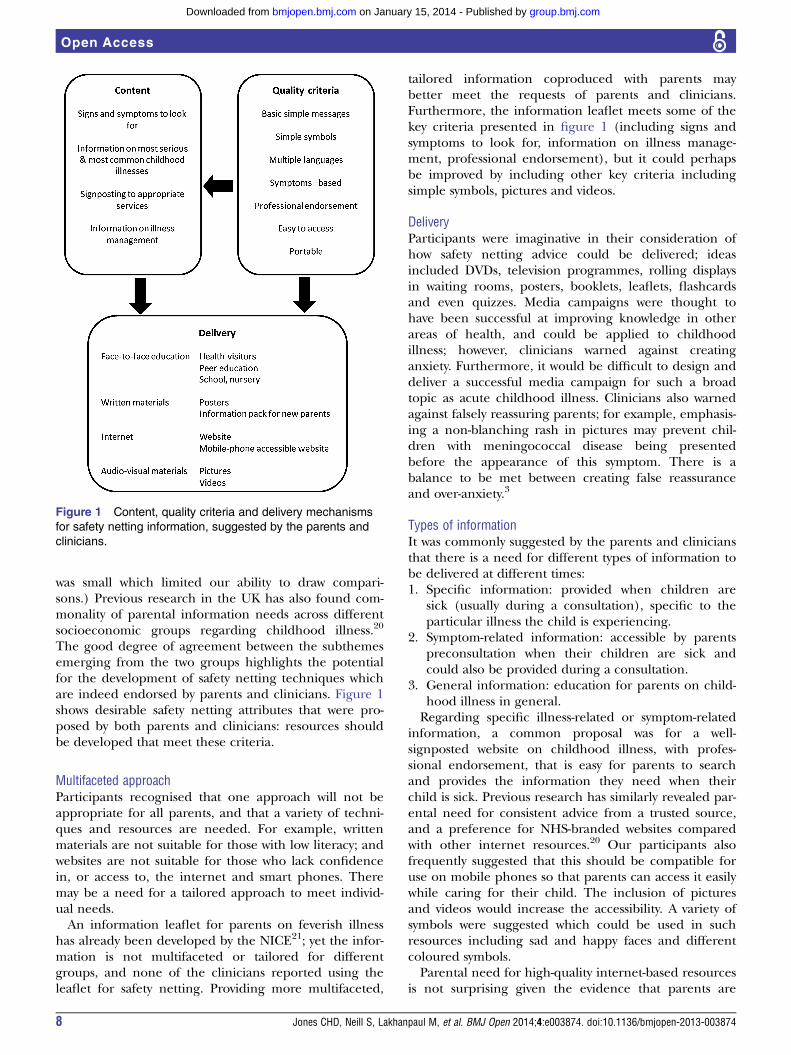
The good degree of agreement between the subthemesemerging from the two groups highlights the potentialfor the development of safety netting techniques whichare indeed endorsed by parents and clinicians. Figure 1shows desirable safety netting attributes that were pro-posed by both parents and clinicians: resources shouldbe developed that meet these criteria.
Multifaceted approachParticipants recognised that one approach will not beappropriate for all parents, and that a variety of techni-ques and resources are needed. For example, writtenmaterials are not suitable for those with low literacy; andwebsites are not suitable for those who lack confidencein, or access to, the internet and smart phones. Theremay be a need for a tailored approach to meet individ-ual needs.An information leaflet for parents on feverish illness
has already been developed by the NICE21; yet the infor-mation is not multifaceted or tailored for differentgroups, and none of the clinicians reported using theleaflet for safety netting. Providing more multifaceted,
tailored information coproduced with parents maybetter meet the requests of parents and clinicians.Furthermore, the information leaflet meets some of thekey criteria presented in figure 1 (including signs andsymptoms to look for, information on illness manage-ment, professional endorsement), but it could perhapsbe improved by including other key criteria includingsimple symbols, pictures and videos.
DeliveryParticipants were imaginative in their consideration ofhow safety netting advice could be delivered; ideasincluded DVDs, television programmes, rolling displaysin waiting rooms, posters, booklets, leaflets, flashcardsand even quizzes. Media campaigns were thought tohave been successful at improving knowledge in otherareas of health, and could be applied to childhoodillness; however, clinicians warned against creatinganxiety. Furthermore, it would be difficult to design anddeliver a successful media campaign for such a broadtopic as acute childhood illness. Clinicians also warnedagainst falsely reassuring parents; for example, emphasis-ing a non-blanching rash in pictures may prevent chil-dren with meningococcal disease being presentedbefore the appearance of this symptom. There is abalance to be met between creating false reassuranceand over-anxiety.3
Types of informationIt was commonly suggested by the parents and cliniciansthat there is a need for different types of information tobe delivered at different times:1. Specific information: provided when children are
sick (usually during a consultation), specific to theparticular illness the child is experiencing.
2. Symptom-related information: accessible by parentspreconsultation when their children are sick andcould also be provided during a consultation.
3. General information: education for parents on child-hood illness in general.Regarding specific illness-related or symptom-related
information, a common proposal was for a well-signposted website on childhood illness, with profes-sional endorsement, that is easy for parents to searchand provides the information they need when theirchild is sick. Previous research has similarly revealed par-ental need for consistent advice from a trusted source,and a preference for NHS-branded websites comparedwith other internet resources.20 Our participants alsofrequently suggested that this should be compatible foruse on mobile phones so that parents can access it easilywhile caring for their child. The inclusion of picturesand videos would increase the accessibility. A variety ofsymbols were suggested which could be used in suchresources including sad and happy faces and differentcoloured symbols.Parental need for high-quality internet-based resources
is not surprising given the evidence that parents are
Figure 1 Content, quality criteria and delivery mechanisms
for safety netting information, suggested by the parents and
clinicians.
8 Jones CHD, Neill S, Lakhanpaul M, et al. BMJ Open 2014;4:e003874. doi:10.1136/bmjopen-2013-003874
Open Access
group.bmj.com on January 15, 2014 - Published by bmjopen.bmj.comDownloaded from

increasingly using the internet to access health informa-tion. In two independent surveys, 52% of parents hadsought health information for their children on theinternet22 23; however, the quality and accuracy of inter-net advice are variable.24
Regarding general information, both groups suggestedthat education could be delivered by health visitors orby peers in the community, with the important caveat ofensuring that the information delivered is correct. Wehave recently completed a systematic review of the effect-iveness of interventions providing information on whento seek medical help for parents of acutely sick children(Neill et al, personal communication). Characteristics ofinterventions likely to be more effective included com-prehensive information, information on how to assessthe severity of their child’s illness as well as home man-agement advice and reinforcement from healthcare pro-fessionals. These match some key criteria summarised infigure 1. Interventions which were codesigned withparents were also more effective, again reinforcing theimportance of this approach.
Strengths and limitationsThis study has taken a first step at identifying the optimalcontent, format and delivery of information resources forparents of acutely sick young children, from the perspec-tives of parents and clinicians. Including parents and clin-icians strengthened our study because in order to beeffective, resources must be endorsed and valued by bothgroups. Indeed, we identified similar needs from bothgroups, indicating the possibility of developing resourceswhich are coproduced. Furthermore, we included diversegroups of parents with different literacy levels, informa-tion needs and ability to use information technology,ensuring that the views of different groups with diverseneeds are understood. A range of doctors and nursesfrom different settings were also included, allowing us toinclude the perspectives of the broad group of clinicianswho provide safety netting advice in different settings.However, while the maximum variation sampling pro-vided us with participants with a diverse range ofcharacteristics, the qualitative approach means that theextent to which the findings are generalisable to othersin the same or different groups and geographical loca-tions is not known. Data were collected and analysed by ateam of researchers with different backgrounds, so theirrange of perspectives helped to reduce bias and facili-tated a deeper understanding.
CONCLUSIONA multifaceted and tailored approach to safety netting isneeded, in which information is delivered in multipleways and is accessible to different groups of parents withvarying needs, resources and abilities. It is importantthat resources are coproduced with parents and clini-cians so that they are accessible to and understood byparents, as well as endorsed by clinicians. This study has
shown that it is possible to identify common prioritiesamong both groups regarding resource development.Research is needed to determine the effectiveness of
different components of safety netting resources and theimpact on parent knowledge, understanding, satisfac-tion, anxiety and reconsultation rates, among other out-comes. There is also a need for the development ofsafety netting quality standards to ensure that all clini-cians provide parents with appropriate advice, and sothat all parents receive the correct information in anefficient way. This study is a first step towards developingtestable safety netting interventions and developing anevidence base around safety netting on which to basequality standards.
Author affiliations1Department of Primary Care Health Sciences, University of Oxford, Oxford,UK2School of Health, University of Northampton, Northampton, UK3General and Adolescent Paediatrics Unit, Institute of Child Health, UniversityCollege London, London, UK4Paediatric Emergency medicine Leicester Academic Group, Department ofCardiovascular Sciences, Leicester University, Leicester, UK
Acknowledgements The authors would like to thank the participants fortaking part, and all those who coordinated the recruitment.
Contributors SN, ML, DR and MT conceptualised and designed the study. SNand HSM collected the data. CHDJ and SN analysed the data. CHDJ draftedthe manuscript. All the authors read and approved the final version.
Funding This publication presents independent research funded by theNational Institute for Health Research (NIHR) under its Programme Grants forApplied Research funding scheme (RP-PG-0407-10347) and arising from aCareer Development Fellowship supported by the NIHR (MT). The viewsexpressed in this publication are those of the author(s) and not necessarilythose of the NHS, the NIHR or the Department of Health.
Competing interests ML was the clinical director leading development for theNICE feverish illness guidelines, was a NICE fellow from 2010 to 2013 and ison the NHS evidence advisory board.
Ethics approval East Midlands—Nottingham 2 NHS Research EthicsCommittee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license,which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, providedthe original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
REFERENCES1. Wolfe I, Cass H, Thompson MJ, et al. Improving child health
services in the UK: insights from Europe and their implications forthe NHS reforms. BMJ 2011;342:d1277.
2. The Children and Young People’s Health Outcomes Forum. Reportof acutely ill children subgroup. 2012. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/216855/CYP-Acutely-Ill.pdf
3. Thompson MJ, Ninis N, Perera R, et al. Clinical recognition ofmeningococcal disease in children and adolescents. Lancet2006;367:397–403.
4. Gill PJ, Goldacre MJ, Mant D, et al. Increase in emergencyadmissions to hospital for children aged under 15 in England, 1999–2010: national database analysis. Arch Dis Child 2013;98:328–34.
Jones CHD, Neill S, Lakhanpaul M, et al. BMJ Open 2014;4:e003874. doi:10.1136/bmjopen-2013-003874 9
Open Access
group.bmj.com on January 15, 2014 - Published by bmjopen.bmj.comDownloaded from

5. Saxena S, Bottle A, Gilbert R, et al. Increasing short-stay unplannedhospital admissions among children in England; Time TrendsAnalysis’ 97–‘06. PLoS ONE 2009;4:e7484.
6. Almond S, Mant D, Thompson M. Diagnostic safety-netting. Br JGen Pract 2009;59:872–4.
7. Maguire S, Ranmal R, Komulainen S, et al. Which urgent careservices do febrile children use and why? Arch Dis Child2011;96:810–16.
8. Royal College of Paediatrics and Child Health, Royal College ofGeneral Practitioners, College of Emergency Medicine, et al. Tounderstand and improve the experience of parents and carers whoneed assessment when a child has a fever (high temperature).London: RCPCH, 2010.
9. Neighbour R. The inner consultation: how to develop an effectiveand intuitive consulting style. 2nd edn. Radcliffe Medical Press,2004.
10. National Institute for Health and Care Excellence. Feverish illness inchildren, assessment and initial management in children youngerthan 5 years. 2007. http://www.nice.org.uk/cg047
11. Scottish Intercollegiate Guidelines Network. Bronchiolitis in children;Quick reference guide. 2006. http://www.sign.ac.uk/pdf/qrg91.pdf
12. Royal College of General Practitioners. Out of Hours Clinical AuditToolkit. 2007. http://www.nhsalliance.org/publication/view/out-of-hours-clinical-audit-toolkit/
13. Gill PJ, Hislop J, Mant D, et al. General practitioners’ views onquality markers for children in UK primary care: a qualitative study.BMC Fam Pract 2012;13:92.
14. Van den Bruel A, Thompson M, Buntinx F, et al. Clinicians’ gutfeeling about serious infections in children: observational study. BMJ2012;345:e6144.
15. National Institute for Health and Care Excellence. Quality standardfor bacterial meningitis and meningococcal septicaemia in childrenand young people. 2012. http://publications.nice.org.uk/quality-standard-for-bacterial-meningitis-and-meningococcal-septicaemia-in-children-and-young-qs19/list-of-quality-statements
16. Houston AM, Pickering AJ. ‘Do I don’t I call the doctor’: a qualitativestudy of parental perceptions of calling the GP out-of-hours. HealthExpect 2000;3:234–42.
17. Neill SJ. Containing acute childhood illness within family life: asubstantive grounded theory. J Child Health Care 2010;14:327–44.
18. Buntinx F, Mant D, Van den Bruel A, et al. Dealing withlow-incidence serious diseases in general practice. Br J Gen Pract2011;61:43–6.
19. Oostenbrink R, Thompson M, Steyerberg EW. Barriers to translatingdiagnostic research in febrile children to clinical practice: a systematicreview. Arch Dis Child 2012;97:667–72.
20. Ingram J, Cabral C, Hay AD, et al. Parents’ information needs,self-efficacy and influences on consulting for childhood respiratorytract infections: a qualitative study. BMC Fam Pract 2013;14:106.
21. National Institute for Health and Care Excellence. Fever in childrenyounger than 5 years. 2013 [21 Nov 2013]; http://publications.nice.org.uk/ifp160
22. Khoo K, Bolt P, Babl FE, et al. Health information seeking byparents in the Internet age. J Paediatr Child Health 2008;44:419–23.
23. Bouche G, Migeot V. Parental use of the Internet to seek healthinformation and primary care utilisation for their child: across-sectional study. BMC Public Health 2008;8:300.
24. Scullard P, Peacock C, Davies P. Googling children’s health:reliability of medical advice on the internet. Arch Dis Childhood2010;95:580–2.
10 Jones CHD, Neill S, Lakhanpaul M, et al. BMJ Open 2014;4:e003874. doi:10.1136/bmjopen-2013-003874
Open Access
group.bmj.com on January 15, 2014 - Published by bmjopen.bmj.comDownloaded from

doi: 10.1136/bmjopen-2013-003874 2014 4: BMJ Open
Caroline H D Jones, Sarah Neill, Monica Lakhanpaul, et al. cliniciansqualitative exploration with parents and where and when' of safety netting using achildhood illness: determining 'what, how, Information needs of parents for acute
http://bmjopen.bmj.com/content/4/1/e003874.full.htmlUpdated information and services can be found at:
These include:
References http://bmjopen.bmj.com/content/4/1/e003874.full.html#ref-list-1
This article cites 16 articles, 9 of which can be accessed free at:
Open Access
non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/terms, provided the original work is properly cited and the use iswork non-commercially, and license their derivative works on different license, which permits others to distribute, remix, adapt, build upon thisCreative Commons Attribution Non Commercial (CC BY-NC 3.0) This is an Open Access article distributed in accordance with the
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on January 15, 2014 - Published by bmjopen.bmj.comDownloaded from





























