Embed Size (px)
Citation preview
Injection Temperature Significantly Affects In Vitro and In VivoPerformance of Collagen-Platelet Scaffolds
M.P. Palmer, E.L. Abreu, A. Mastrangelo, and M.M. MurrayDepartment of Orthopaedic Surgery, Children's Hospital Boston, 300 Longwood Avenue, Enders1022, Boston, Massachusetts 02115
AbstractCollagen-platelet composites have recently been successfully used as scaffolds to stimulate anteriorcruciate ligament (ACL) wound healing in large animal models. These materials are typically kepton ice until use to prevent premature gelation; however, with surgical use, placement of a coldsolution then requires up to an hour while the solution comes to body temperature (at which pointgelation occurs). Bringing the solution to a higher temperature before injection would likely decreasethis intra-operative wait; however, the effects of this on composite performance are not known. Thehypothesis tested here was that increasing the temperature of the gel at the time of injection wouldsignificantly decrease the time to gelation, but would not significantly alter the mechanical propertiesof the composite or its ability to support functional tissue repair. Primary outcome measures includedthe maximum elastic modulus (stiffness) of the composite in vitro and the in vivo yield load of anACL transection treated with an injected collagen-platelet composite. In vitro findings were thatinjection temperatures over 30°C resulted in a faster visco-elastic transition; however, the warmedcomposites had a 50% decrease in their maximum elastic modulus. In vivo studies found thatwarming the gels prior to injection also resulted in a decrease in the yield load of the healing ACLat 14 weeks. These studies suggest that increasing injection temperature of collagen-plateletcomposites results in a decrease in performance of the composite in vitro and in the strength of thehealing ligament in vivo and this technique should be used only with great caution.
Keywordscollagen; hydrogel; rheometry; ACL; tissue engineering
Recent studies have shown the efficacy of using collagen-platelet composites (CPCs) tostimulate anterior cruciate ligament (ACL) healing after partial and complete transection inanimal models.1–3 These composites are thought to serve as a scaffold in the ACL wound site,filling the gap between the ruptured ends of the ACL, releasing growth factors, and promotingcellular proliferation and migration into the scaffold.2,3 The use of collagen-based compositesis not limited to ACL repair. Collagen composites have also been used in the development oftissue analogues including vasculature,4 skin,5 nerve,6 and bone.7
Collagen composites typically undergo gelation via a visco-elastic transition when brought to37°C8,9 by nucleation of collagen monomers forming branched cross-linked networks.10
Therefore, these solutions are typically stored at 4°C until use to prevent premature networkformation. As a result, when these cold solutions are placed into the wound site at 4°C, it can
Correspondence to: M. M. Murray (T: 617-355-7132; F: 617-730-0170; E-mail: [email protected]).Disclosure. Since submission of this article, Martha Murray has become a shareholder and scientific advisory board member forConnective Orthopaedics.
NIH Public AccessAuthor ManuscriptJ Orthop Res. Author manuscript; available in PMC 2010 July 1.
Published in final edited form as:J Orthop Res. 2009 July ; 27(7): 964–971. doi:10.1002/jor.20804.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

take in excess of 60 min for complete gelation to occur.11 This extensive time requirementmakes the use of these materials prohibitive in the clinical arena. Therefore, there has beenmuch recent interest in a controlled heating of the gels to a temperature higher than 4°C beforeplacement in the wound site to lessen the gelation time and increase surgical efficiency.
A few researchers have examined visco-elastic properties (gelation time, elastic modulus [G′], and inelastic modulus [G″]) of collagen type I composites.10,12,13 Forgacs et al.10
investigated the visco-elastic properties of collagen composites correlating phase contrastmicroscopy and rheologic results, finding that the visco-elastic transition point occurs whencollagen nucleation clusters begin to interconnect forming a gel. Newman et al.12 reported thatthe time to gelation was inversely proportional to the time the neutralized collagen was kepton ice prior to testing. The work by Djabourov et al.13 correlated rheological properties ofcollagen gels with gelation mechanisms, and suggested that while collagen and gelatin aresimilar on a molecular level, their respective gelation processes occur though differentmechanisms. There has also been an investigation into how the collagen extracted from rats ofdifferent ages affects the collagen-composite visco-elastic properties.14 Furthermore, there hasbeen a reasonable amount of research using collagen composites as experimental scaffolds;4–7,15–17 however, few studies have examined their rheologic or visco-elastic properties as afunction of temperature. Some research has been completed comparing rheologic data for gelsmade of collagen to those made of fibrin. The work by Raeber et al.18 shows that cross-linkingdensity varies between the type of gels, and this leads to the differences in mechanical strength.He noted fibrin gels to have greater moduli than collagen gels. Furthermore, work completedby Weisel19 showed that for fibrin gels, increasing fiber diameter resulted in gels with greatermechanical properties. To our knowledge, there are no studies evaluating the mechanicalproperties of collagen-platelet-plasma composite materials in terms of rheologic behavior,although there have been several studies on the biologic consequences of creating thesecomposites.1–3,20,21
The hypothesis tested in this article was that increasing the temperature of the gel at the timeof injection would significantly decrease the time between injection and gelation (as measuredby time to the visco-elastic transition point), but would not significantly alter the mechanicalproperties of the composite or the subsequent repair tissue. To test this hypothesis, rheologicproperties of the composites as a function of temperature were measured in vitro, and thencomposites in a range of temperatures were placed in a healing wound and the mechanicalproperties of the resulting structure measured after 14 weeks in vivo. The primary outcomemeasures were the time to the visco-elastic transition point, the maximum elastic modulus ofthe composite, and the yield load of an ACL repair after 14 weeks in vivo. Secondary outcomemeasures included the maximum inelastic modulus and size of the in vivo scar mass asdetermined by magnetic resonance imaging (MRI).
Materials and MethodsIn Vitro Study: Experimental Design
To evaluate the effect of injection temperature on the final rheologic properties of the collagen-platelet gels, composites were manufactured under specified experimental conditions using aspecifically designed manufacturing device (Fig. 1) and then injected directly onto the plateof a small oscillation rheometer. Gelation was allowed to progress to completion as definedby a plateau in the elastic modulus values. Changes in elastic and inelastic modulus and timeto the visco-elastic transition and the plateau in elastic modulus were recorded for all samples(Fig. 2).
Palmer et al. Page 2
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Manufacturing of Acid-Soluble Collagen Used in CompositesThe collagen used in this study was derived from rat tails that were obtained from controlbreeder rats undergoing euthanasia for other Institutional Animal Care and Use Committeeapproved studies at our institution. The rat-tail tendons were sterilely harvested, minced, andsolubilized in 0.01 N hydrochloric acid. The collagen content in the resulting solution wasfound to be >5 mg/mL. Previous collagen slurries obtained using the same in-housemethodology were shown to be made mostly of type I collagen based on their amino acid profileand SDS-PAGE migration pattern. The same collagen solution was used in all experiments.
Prior to testing, the collagen solution was combined with HEPES Buffer (Cellgro; Mediatech,Inc., Herndon, VA), Ham's F-10 medium (MP Biomedicals, LCC, Aurora, OH), antibiotic-antimycotic solution (Cellgro), and sterile water. Sodium bicarbonate (7.5%; CambrexBioScience Walkersville, Inc., Walkersville, MD) was used to neutralize the acidic mixture toa pH of 7.4. The neutralized collagen solution was kept on ice until use.
Preparation of Platelet SolutionFive hundred milliliters of whole blood was drawn from each of two hematologically normalpigs undergoing other Institutional Animal Care and Use Committee approved studies for therheologic studies and autologously for each of the five animals in the in vivo studies. Bloodwas collected in a bag containing 10% by volume acid-citrate dextrose as an anticoagulant andtransferred to centrifuge tubes. The blood samples were centrifuged for 6 min at 150 ×g (GH3.8 rotor, Beckman GS-6 Centrifuge Beckman Coulter, Inc., Fullerton, CA). The supernatantwas collected as platelet concentrate. Complete blood counts (CBCs) were measured for thewhole blood and platelet concentrate. In vivo, the platelet solution was stored at roomtemperature for less then 30 min prior to addition to the neutralized collagen.
Preparation of GelsOne milliliter aliquots of the acid soluble collagen were vortexed with buffer to neutralize thesolution. This solution aspirated into a syringe containing a collapsible auguer. One milliliterof platelet concentrate was then aspirated into the same syringe. The syringe was affixed in thecradle and the auger engaged with the mixing motor and the gel heated and mixed accordingto the specified test conditions as detailed below. Mixing speed, mixing time, and heating ratewere controlled using a device made for this testing. (Fig. 1; TNCO, Inc., Whitman, MA). Anauger was designed to fit inside the 6 cc syringe held in the cradle. This allowed for mixing ofthe collagen composite components while simultaneously warming the composite. This devicehad a motor that was coupled to the auger to allow for control of mixing speed and time, anda heating pad under the syringe that allowed for control of heating rate. The device was drivenby a custom LabView (Austin, TX) application that allowed for control of the variables, andlogging of feedback data.
Composites were created using three different mixing speeds (50, 100, and 150 rpm), threedifferent mixing times (30, 60, and 120 s), and three different heating rates (0.05, 0.10, and0.15°/s). All combinations of those parameters were tested in triplicate (19 cases total). Controlgels were also tested, mixed for 30 s at 100 rpm, without heating. The final temperature of thegels was recorded for all mixing conditions. Additional triplicate gels having an injectiontemperature of 24°C–26°C, 26°C–28°C, 28°C–30°C, and 30°C–32°C were also tested. Theadditional gels were prepared by mixing at 100 rpm and heating at 0.10°/s for the time necessaryfor the gel to reach the specified final temperature.
Palmer et al. Page 3
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

In Vitro RheologyRheological properties of the gels were determined using Cone on Plate Small AmplitudeOscillatory Shear Rheometry using a TA Instruments AR 1000 Rheometer (New Castle, DE).The rheometer was fitted with a 60 mm 1° acrylic cone, and the base plate was maintained at25°C. For each test, 1 mL of the CPCs was dispensed onto the rheometer plate. The cone waslowered so that the composite was situated in a 38 μm layer between the cone and plate,subjected to a 1% oscillatory. Strain (γo) with an angular frequency of 6.3 rad/s, and theresultant stress (τ(τ)) were recorded. The stress waveform is broken down to one waveform inphase with the oscillatory strain (τ′), and one waveform 90° out of phase (τ″), with therelationship being: τ=τ′+τ′=τo'sinωt+τo″cosωt. The visco-elastic complex modulus (G*) of thegel can be derived from the relationship G*(t) = G′(t) + iG″(t), where G′(t) = τo′/γo and G″(t)= τo″/γo, with the elastic modulus representing the elastic portion of the scaffold, and theinelastic modulus representing the viscous component. Phase angle (δ), which represents thelag between the applied strain and the resultant stress, is determined by the geometricrelationship tan(δ) = G″/G′. A value of 45° represents the intersection of G′(t) and G″(t) andis defined as the visco-elastic transition point. Data points for elastic modulus, inelasticmodulus, and phase angle were collected at 0.1 Hz, until the rate of change of the increase inelastic modulus was less then 0.1% for three consecutive data points, which was themathematical definition of the plateau. A sample result is shown in Figure 2.
In Vivo Studies: Experimental DesignFive 30 kg female Yorkshire pigs were used to study the effect of injection temperature on thein vivo performance of the CPCs. Four animals had bilateral ACL transections and for each ofthese, one side was treated with a suture repair augmented with a collagen sponge containinga CPC injected at a temperature ranging from 28.9°C–32.4°C, while on the contralateral side,the transection was treated with suture repair with the collagen sponge carrier only. A CPCwas used because prior in vivo and in vitro studies have shown gradual platelet activation andplatelet growth factor release from these CPCs.20,21 In the remaining animal, unilateral surgerywas performed with the augmented repair and the contralateral side left as a contemporaryintact control. One of the animals developed a postoperative seroma. The seroma was treatedwith prophylactic antibiotics until complete wound closure was observed on the collagen-platelet side. This knee was excluded from the study. Therefore, there were a total of four kneesin the augmented repair group and four knees in the nonaugmented group. All animals weresurvived to 14 weeks and then underwent MRI evaluation and euthanasia. Knees wereimmediately harvested and frozen until biomechanical testing. Load to yield, load to failure,maximum linear stiffness, and displacement to failure were measured.
Surgical ProcedureInstitutional Animal Care and Use Committee approvals were obtained prior to beginning thestudy. Five 30 kg female Yorkshire pigs were used anesthetized per an approved protocol.After anesthesia had been obtained, the pigs were weighed and placed in the supine positionon the operating room table. Both hind limbs were shaved, prepared with chlorhexidinefollowed by betadyne paint, and sterilely draped. No tourniquet was used. To expose the ACL,a 4 cm incision was made over the medial border of the patellar tendon. The incision was carrieddown sharply through the synovium using electrocautery. The fat pad was released from itsproximal attachment and partially resected to expose the intermeniscal ligament. Theintermeniscal ligament was released to expose the tibial insertion of the ACL. The anteriorhorns of the medial and lateral menisci attach separately from the intermeniscal ligament andtherefore severing this ligament did not lead to gross meniscal instability. A Lachman maneuverwas performed prior to releasing the ACL to verify knee stability. Two #1 Vicryl sutures weresecured in the distal ACL stump at the middle and distal thirds of the ACL using a modified
Palmer et al. Page 4
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Kessler stitch. The ACL was transected completely at the junction of the middle and proximalthirds using a #12 blade. No medial collateral ligament (MCL) transection was performed.Complete transection was verified visually and a repeat Lachman maneuver was positive inall knees with no significant endpoint detected after complete transaction (knee was unstable).An absorbable suture anchor (TwinFix AB 5.0 Suture Anchor with DuraBraid Suture [USP#2];Smith and Nephew, Inc., Andover, MA) was placed at the back of the femoral notch. The kneewas irrigated with 500 cc of sterile normal saline to remove all synovial fluid. Once hemostasishad been achieved, a 1 cm ×1 cm collagen sponge was threaded onto the sutures of the sutureanchor and slid up into the intercondylar notch. In prior studies, the use of the collagen spongecombined with platelet-rich plasma showed enhanced healing using this technique at 4 weeks.1 The DuraBraid sutures were then tied to the Vicryl sutures previously placed in the ACLstump using maximum manual tension with the knees in resting flexion (approximately 70°,which is 40° short of full extension in these animals). A batch of CPC was mixed by sequentiallydrawing up equal aliquots of neutralized collagen solution and autologous platelet concentrateinto the mixing and heating device and mixing for 1 min at 50 rpm and 0.10°/s, which resultedin injection temperatures between 28.9°C and 32.4°C. The collagen-platelet mixture was theninjected to fill the notch and area around the ACL repair (Fig. 3). The knee was left in restingextension and allowed to gel while the identical technique of suture anchor repair wasperformed with an identical collagen sponge, but without the addition of the CPC. Gelationwas observed to have occurred within 10 min of gel injection by manual examination of thejoint and by opacification of the composite. In the knees treated with suture repair and collagenaponge only, blood clot was seen to soak the collagen sponge in situ after suture anchorplacement. The incisions were closed in multiple layers with absorbable sutures.
The animals were not restrained postoperatively, and were allowed ad lib activity. Once theanimals recovered from anesthesia, they were permitted to resume normal cage activity andnutrition ad lib. Buprenex 0.01 mg/kg IM once and a Fentanyl patch 1–4 mcg/kg transdermalwere provided for postoperative analgesia. All animals were weight bearing on their hind limbsby 24 h after surgery. After 14 weeks in vivo, the animals were again anesthetized andunderwent in vivo MR imaging using the protocol detailed below.
After the MR images had been obtained, the animals were euthanized using Fatal Plus at 1 cc/10 lbs. No animals had any surgical complications of difficulty walking normally, redness,warmth, and fever, or other signs of infection that would have necessitated early euthanasia.
Six intact control knees were obtained from age-, gender-, and weight-matched animals aftereuthanasia following surgical procedures to the chest. The hind limbs were frozen at −20°Cfor 3 months and thawed overnight at 4°C before mechanical testing. All other testingconditions for these knees were identical to those in the experimental groups.
MRIIn vivo MRI was performed at 1.5 Tesla (GE Medical Systems, Milwaukee, WI) with an eight-channel phased array coil at the specified time points. Scanning was performed with the kneesplaced maximum extension (between 30 and 45° of flexion). Conventional MR includedmultiplane T1, FSE PD, and T2 weighted images. Field of view (FOV), 16–18 cm matrix;256×256 (repetition time/echo time) TR/TE, 400/16, 2,500/32, 3,000/66 ms; echo train length(ETL), 8; bandwidth (BW), 15 kHz; slice thickness, 3; interslice gap, 1 mm.
Biomechanical TestingThe bone-ligament-bone ACL complex from both knees for each pig was tested in uniaxialtension as previously described.22 In brief, testing was performed with the knee flexed at 30°of flexion to align the ACL with the load axis. All tissue with the exception of the ACL was
Palmer et al. Page 5
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
resected. Testing was performed at room temperature. Immediately after preconditioning, eachspecimen was tested to failure in uniaxial tension at 20 mm/min.23,24 Close-range digitalimages were acquired at 3 Hz using a high resolution digital camera with a macro lens(PixeLINK PLA662 Megapixel Firewire camera; PixeLINK, Ottawa ON, Canada) todetermine failure mode. The yield load (defined as the point where the load-displacement curvebecomes nonlinear), displacement at yield, tangent modulus (maximum slope of force-displacement curve), maximum load at failure, displacement at failure, and total work to failure(area under force-displacement curve) were determined from the force-displacement curvemeasured for each bone-ligament-bone ACL complex. The yield load represented the pointalong the normalized force-displacement curve where the mechanical behavior of the ACLcomplex departed from “linear” behavior and for the purposes of this analysis was defined asthe point where the tangent modulus declined by at least 2% from its maximum value. Thedisplacement at yield was the displacement recorded at this same point. The maximum load isthe maximal normalized load sustained by the ACL complex prior to failure and thedisplacement at failure the displacement recorded at the maximum load. The energy to failurewas derived by integrating the total area under the force-displacement curve.
Histological AnalysisAfter mechanical testing, the knees were fixed in formalin for 1 week, decalcified, and 7 μmthick sagittal sections of the entire knee were stained using hematoxylin and eosin. Digitalphotographs were taken at 20× of the femoral and tibial insertion sites, and one photographwas taken midsubstanace.
Statistical AnalysisStatistical analysis was performed using SAS StatView 3.0 (SPS Institute, Cary, NC). For thein vitro studies, single factor analysis of variance (ANOVA) was used with the BonferroniDunn post-hoc test to compare between groups. A p value <0.05 was deemed statisticallysignificant. For the in vitro studies linear regression were performed, and r2 values and 95%confidence intervals were reported.
ResultsIn Vitro Results
Hematology—The centrifugation method used here resulted in a platelet enrichment factorof 2.05 ± 0.42× (mean ± SD). In the platelet solution, the red blood cell count averaged 3.50× 104 ± 0.70 × 104 cells/μL, and the white blood cell count averaged 2,450 ± 354 cells/μL.
Rheology—Increasing the mixing time from 30 to 120 s resulted in a 65% increase in theinjection temperature (20.29 ± 0.06°C to 33.08 ± 0.95°C, p < 0.001). The time to the visco-elastic transition point decreased 90% from 3.10 ± 0.00 min (30 s cycle) to 0.27 ± 0.03 min(120 s cycle) (p < 0. 001). Increasing the mixing time from 30 to 120 s also resulted in a 95%decrease in the maximum elastic modulus of the gels: 112.25 ± 34.04 Pa to 5.68 ± 1.92 Pa (p< 0.005) (Fig. 4A). Increasing the mixing time had no significant change on the time requiredto reach the maximum elastic modulus (16.20 ± 2.63 min [30 s cycle], 15.36 ± 2.56 min [60 scycle], 9.50 ± 5.20 min [120 s cycle], p > 0.01 for all comparisons); however, increasing themixing time from 60 to 120 s did significantly decrease the time to the maximum inelasticmodulus, 15.01 ± 2.62 min to 8.03 ± 6.83 min (p < 0.02).
Increasing the mixing speed from 50 to 200 rpm did not significantly affect the injectiontemperature of the gel (23.97 ± 1.00°C to 25.31 ± 0.65°C; p > 0.1). Time to the visco-elastictransition point, maximum elastic and inelastic moduli, and time to the maximum elastic andinelastic moduli were not affected by increasing the mixing speed (p > 0.1).
Palmer et al. Page 6
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Increasing the heating rate from 0.05°/s to either 0.10°/s or 0.15°/s significantly increased theinjection temperature of the gel: 22.03 ± 0.57°C to 23.97 ± 1.00°C or 25.33 ± 0.97°Crespectfully (p < 0.001). Increasing the heating rate from 0.05°/s to either 0.1°/s or 0.15°/ssignificantly decreased the time to the visco-elastic transition point: 3.63 ± 0.35 min to 2.47 ±0.42 min or 2.07 ± 0.50 min respectfully (p < 0.002). However, there was no statisticallysignificant change in the maximum elastic (105.90 ± 19.81 Pa, 124.47 ± 35.02 Pa, 88.60 ±55.82 Pa) or inelastic modulus (24.96 ± 4.18 Pa, 30.56 ± 22.16 Pa, 22.16 ± 15.77 Pa) or thetime required to reach these values (p > 0.1) (Fig. 4B).
Gels injected directly from the chilled chamber (average injection temperature 14.41 ± 0.1.24°C) took significantly longer to reach the visco-elastic time point (3.57 ± 0.25 min) comparedto the gels heated at 0.10°/s or 0.15°/s (p < 0.05) (average injection temperatures 23.97 ± 1.00°C or 25.33 ± 0.97°C respectively; p < 0.0001 for difference in injection temperature for bothcomparisons). The maximum elastic and inelastic modulus for the unheated gels injected at14°C were significantly greater than any of the heated gels (269.50 ± 41.02 Pa and 73.14 ±13.44 Pa, respectfully) (p < 0.0001), and the time required to reach these values was notsignificantly changed (12.50 ± 0.27 min for time to maximum elastic modulus and 12.37 ±0.31 min for time to maximum inelastic modulus) (p > 0.05).
The injection temperature had a significant effect on the gelation time (when defined as thetime to the visco-elastic transition point), with gels injected between 20°C and 25°C havingthe longest gelation time, and a steady decrease in gelation time noted as injection temperatureincreased (Fig. 5). Similar results were found for gelation time when defined as the time toreach maximum elastic and inelastic modulus.
Both the maximum elastic and maximum inelastic modulus were also affected by injectiontemperature. There was no significant change in either modulus when comparing the gelsinjected between 20°C–25°C (111.64 ± 31.08 Pa and 26.88 ± 7.76 Pa) and those injectedbetween 25°C–30°C (120.28 ± 37.51 Pa and 30.20 ± 9.94 Pa;p > 0.1). However, a significantdecrease in both moduli was noted when increasing the injection temperature above 30°C(50.18 ± 40.22 Pa and 12.78 ± 9.65 Pa;p < 0.001).
In Vivo ResultsHematology—The centrifugation method used here resulted in a platelet enrichment factorof 3.9 ± 2.1X (mean ± SD). In the platelet concentrate, the red blood cell count averaged3.5×104 ± 7.1×103 cells/μL, and the white blood cell count averaged 2,645 ± 115 cells/μL.
Gross Observations and Histology—Upon removal of the capsule and meniscal tissuefor mechanical testing of the ACL repair constructs, there was noted to be a fibrovascular bandbridging between femur and tibia in the location expected for the ACL in all specimens (Fig.6B). There was no sign of intact suture material, although in the majority of the specimens,broken remnants of the Durabraid suture were noted. There was no significant synovitis notedin any of the knees, and no gross cartilage or meniscal damage was seen in any of the animals.
Histology of the repair tissue noted in the region of the ACL revealed a fibrovascular scartissue, characterized by a densely packed collagenous matrix with varying degrees of fiberorganization. Near the insertion sites of the ACL, the collagen was in more parallel bundles,and this increased organization likely represented the original tibial and femoral ACLremnants. Bridging between these organized areas was a hypercellular tissue with moredisorganized collagen fibers (Fig. 6C) and blood vessels ranging from those with a single cellwall, consistent with capillaries, to those with a more cellular wall, consistent with largervessels. Red blood cells were observed in the lumen of the vessels, suggesting these vesselswere actively perfusing at the time of sacrifice.
Palmer et al. Page 7
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
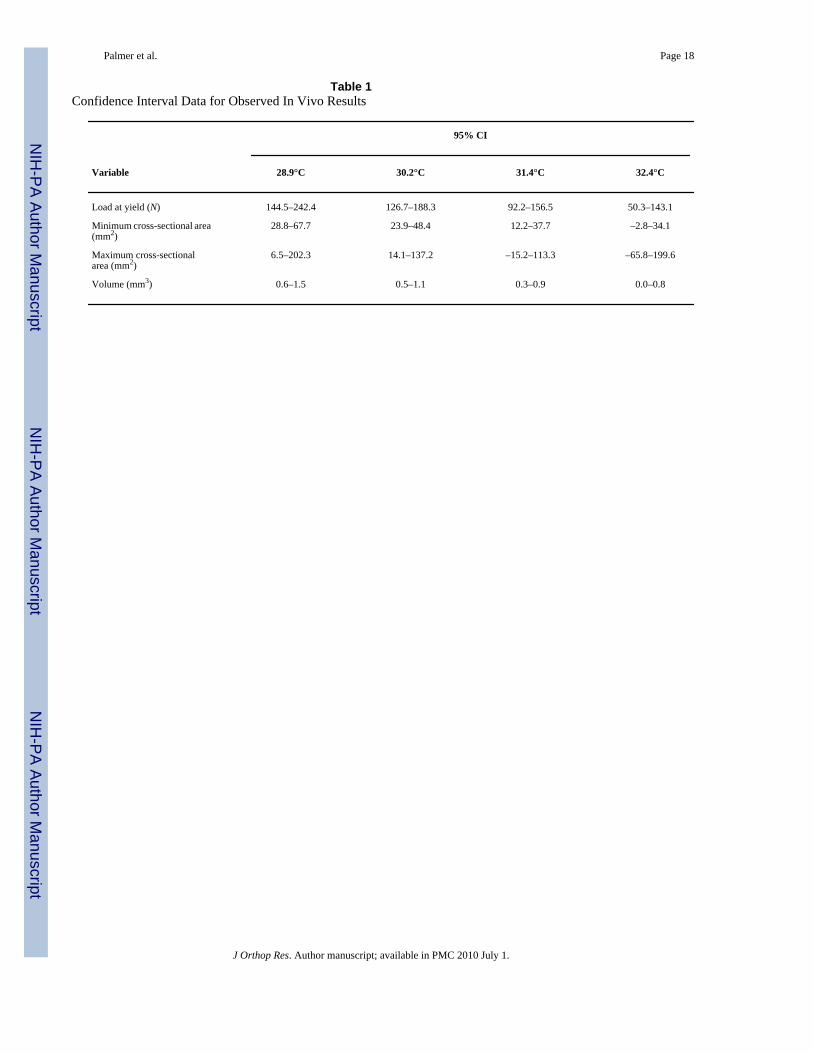
Mechanical Properties—Heating the collagen slurry to temperatures approaching bodytemperature resulted in a mechanically weaker repair tissue. For injection temperaturesbetween 28°C and 33°C, the yield load of the healing ACL was detrimentally affected byincreasing the injection temperature of the collagen. Injection temperature was inverselycorrelated with the strength of the healing ACL after 14 weeks in vivo (r2>0.94; Fig. 7). Thestrength of these repairs ranged from 88 to 184 N (Table 1, Supplemental Data). In thecontralateral knees treated with suture repair with a collagen sponge alone, and without theCPC, the strength of the repair averaged 206 ± 47 N.
MRI data were also analyzed and showed that the volume and maximum and minimum cross-sectional area of the resulting scar mass were inversely correlated with injection temperature.The scar volume measured 1.1, 0.77, 0.49, and 0.53 cm3 for injection temperatures rangingfrom 28°C to 33°C (r2 > 0.88) (Table 1, Supplemental Data). Maximum cross-sectional areaof the scar mass had areas of 122, 44, 57, and 33 mm2 for the injection temperatures rangingfrom 28°C to 33°C (r2 > 0.70) (Table 1, Supplemental Data). Minimal cross-sectional area ofthe scar mass had areas of 51, 34, 20, and 20 mm2 for the injection temperatures ranging from28°C to 33°C (r2 > 0.91) (Table 1, Supplemental Data). For reference, the cross sectional areaof the USP #2 Durabraid sutures was 0.2 mm2 and of the USP #1Vicryl sutures was 0.13mm2 at the time of surgical repair.
DiscussionThe temperature at the time of injection for CPCs has a significant effect on gel performancein vitro, and preliminary results suggest this is also reflected in the in vivo functionalperformance of the gel. In the in vitro studies here, injection temperatures of over 30°C resultedin gels with 50% lower stiffness than those with injection temperatures below 30°C. In the invivo studies, CPCs injected at a higher temperature resulted in a lower yield load of the healingligament—with a loss of 50% of the repair strength when the temperature increased from 29°C to 32.5°C.
One hypothesis to explain this phenomenon is that as the temperature of the CPC increases,networking of the collagen occurs during the gelation process, and the mechanical perturbationof this network during injection disrupts the nascent collagen quaternary structure. Whetherthese networks are formed of irreversible covalent crosslinks or the network is simply one ofphysical aggregation that is subsequently disrupted is unknown.
That at least some of this network may be due to covalent crosslinking is supported by findingsin previous studies where increasing the temperature of collagen in solution results in anincreased density of crosslink formation,25 as well as studies showing that these crosslinks areirreversible and once disrupted they do not re-form.26 Additional studies have demonstratedthat while collagen composites can be quite firm, when stress is applied to them the collagenassembly can easily be broken,11 thus if there is partial gelation in the syringe, the stress ofinjection through a needle may be enough to disrupt the collagen composite network.
In the in vivo arm of the study, the use of the warmed CPC resulted in an average maximumload of 154 ± 44 N (mean±SD, n=4), a value almost twice that previously reported in a groupof animals treated with an identical suture technique with suture alone where the maximumload was 81 ± 43 N (mean ± SD, n=5).27 However, despite this encouraging finding, the grouptreated with the collagen carrier alone had superior mechanical properties to the group treatedwith a warmed collagen gel. This suggests that use of gels at temperatures above 28°C mayactually be detrimental to wound healing. This may be because that with the elevatedtemperature of injection used in this study, the gels that form are weaker than the blood clotthat would form within the sponge, perhaps so weak that while they initially fill the wound
Palmer et al. Page 8
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
site, they prematurely break apart in the mechanical fluid flow of the synovial environment. Asecond possibility is that the warmed CPC causes an increased inflammatory response in theknee that leads to a more rapid degradation of the resorbable suture material. However, it mayalso be that the addition of the CPC at any temperature will also be detrimental. This appearsless likely given the encouraging data comparing cold CPC with suture repair alone thatreported a doubling of the repair strength with the addition of the cold CPC.1 Additional studiescomparing the use of a collagen sponge alone versus a cold CPC are planned and should beuseful for dissecting out the mechanism behind this observation.
One of the principal limitations of the in vivo studies is the small number of repairs studied.Only four animals were treated with the heated CPC. The small number of animals was studiedonly to detect if very large effects of heating the CPC on healing tissue mechanical propertieswere present. Interestingly enough, even with a sample of only four animals, the correlationcoefficient between the mechanical strength of the repairs at 15 weeks and the injectiontemperature of the composite was very high (r2=0.94). However, given the small number ofanimals treated with a heated CPC, these results must be considered only a trend, and futurestudies are required to adequately investigate the effects of heating CPCs on the healingproperties of the ACL.
In summary, while increasing the temperature of the CPCs did successfully decrease therequired in situ gelation time required for use of these materials clinically, detrimental resultsin rheologic properties of the gel, and more importantly, in the mechanical properties of thehealing tissue, were also observed. These studies suggest that increasing injection temperatureof collagen-platelet gels results in a decrease in performance of the gel in vitro and in vivo andthis technique should only be used with great caution.
AcknowledgmentsFunding received from CIMIT through DoD funding under cooperative agreement no. DAMD17-02-2-0006 and NIH/NIAMS grant AR049346 and AR052772 (M. M. M.).
References1. Murray MM, Spindler KP, Abreu E, et al. Collagen-platelet rich plasma hydrogel enhances primary
repair of the porcine anterior cruciate ligament. J Orthop Res 2007;25:81–91. [PubMed: 17031861]2. Murray MM, Spindler KP, Ballard P, et al. Enhanced histologic repair in a central wound in the anterior
cruciate ligament with a collagen-platelet-rich plasma scaffold. J Orthop Res 2007;25:1007–1017.[PubMed: 17415785]
3. Murray MM, Spindler KP, Devin C, et al. Use of a collagen-platelet rich plasma scaffold to stimulatehealing of a central defect in the canine ACL. J Orthop Res 2006;24:820–830. [PubMed: 16555312]
4. Brinkman WT, Nagapudi K, Thomas BS, et al. Photo-cross-linking of type I collagen gels in thepresence of smooth muscle cells: mechanical properties, cell viability, and function.Biomacromolecules 2003;4:890–895. [PubMed: 12857069]
5. van den Bogaerdt AJ, van Zuijlen PP, van Galen M, et al. The suitability of cells from different tissuesfor use in tissue-engineered skin substitutes. Arch Dermatol Res 2002;294:135–142. [PubMed:12029501]
6. Joosten EA, Bar PR, Gispen WH. Collagen implants and cortico-spinal axonal growth after mid-thoracic spinal cord lesion in the adult rat. J Neurosci Res 1995;41:481–490. [PubMed: 7473879]
7. Wiesmann HP, Nazer N, Klatt C, et al. Bone tissue engineering by primary osteoblast-like cells in amonolayer system and 3-dimensional collagen gel. J Oral Maxillofac Surg 2003;61:1455–1462.[PubMed: 14663811]
8. Kadler KE, Hulmes DJ, Hojima Y, et al. Assembly of type I collagen fibrils de novo by the specificenzymic cleavage of pC collagen. The fibrils formed at about 37 degrees C are similar in diameter,
Palmer et al. Page 9
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
roundness, and apparent flexibility to the collagen fibrils seen in connective tissue. Ann N Y Acad Sci1990;580:214–224. [PubMed: 2337298]
9. Sato K, Ebihara T, Adachi E, et al. Possible involvement of aminotelopeptide in self-assembly andthermal stability of collagen I as revealed by its removal with proteases. J Biol Chem 2000;275:25870–25875. [PubMed: 10851240]
10. Forgacs G, Newman SA, Hinner B, et al. Assembly of collagen matrices as a phase transition revealedby structural and rheologic studies. Biophys J 2003;84:1272–1280. [PubMed: 12547807]
11. Wallace DG, Rosenblatt J. Collagen gel systems for sustained delivery and tissue engineering. AdvDrug Deliv Rev 2003;55:1631–1649. [PubMed: 14623405]
12. Newman S, Cloitre M, Allain C, et al. Viscosity and elasticity during collagen assembly in vitro:relevance to matrix-driven translocation. Biopolymers 1997;41:337–347. [PubMed: 10917694]
13. Djabourov M, Lechaire JP, Gaill F. Structure and rheology of gelatin and collagen gels. Biorheology1993;30:191–205. [PubMed: 8286722]
14. Wu CC, Ding SJ, Wang YH, et al. Mechanical properties of collagen gels derived from rats of differentages. J Biomater Sci Polym Ed 2005;16:1261–1275. [PubMed: 16268252]
15. Mio T, Adachi Y, Romberger DJ, et al. Regulation of fibroblast proliferation in three-dimensionalcollagen gel matrix. In Vitro Cell Dev Biol Anim 1996;32:427–433. [PubMed: 8856343]
16. Lin PW, Wu CC, Chen CH, et al. Characterization of cortical neuron outgrowth in two- and three-dimensional culture systems. J Biomed Mater Res B Appl Biomater 2005;75:146–157. [PubMed:16001420]
17. Yang B, Cao DJ, Sainz I, et al. Different roles of ERK and p38 MAP kinases during tube formationfrom endothelial cells cultured in 3-dimensional collagen matrices. J Cell Physiol 2004;200:360–369. [PubMed: 15254963]
18. Raeber GP, Lutolf MP, Hubbell JA. Molecularly engineered PEG hydrogels: a novel model systemfor proteolytically mediated cell migration. Biophys J 2005;89:1374–1388. [PubMed: 15923238]
19. Weisel JW. The mechanical properties of fibrin for basic scientists and clinicians. Biophys Chem2004;112:267–276. [PubMed: 15572258]
20. Jacobson M, Fufa D, Abreu EL, et al. Platelets, but not erythrocytes, significantly affect cytokinerelease and scaffold contraction in a provisional scaffold model. Wound Repair Regen 2008;16:370–378. [PubMed: 18471255]
21. Fufa D, Shealy B, Jacobson M, et al. Activation of platelet-rich plasma using soluble type I collagen.J Oral Maxillofac Surg 2008;66:684–690. [PubMed: 18355591]
22. Spindler KP, Murray MM, Devin C, et al. The central ACL defect as a model for failure of intra-articular healing. J Orthop Res 2006;24:401–406. [PubMed: 16479574]
23. Katsuragi R, Yasuda K, Tsujino J, et al. The effect of nonphysiologically high initial tension on themechanical properties of in situ frozen anterior cruciate ligament in a canine model. Am J SportsMed 2000;28:47–56. [PubMed: 10653543]
24. Sakai T, Yasuda K, Tohyama H, et al. Effects of combined administration of transforming growthfactor-beta1 and epidermal growth factor on properties of the in situ frozen anterior cruciate ligamentin rabbits. J Orthop Res 2002;20:1345–1351. [PubMed: 12472251]
25. Nickerson MT, Patel J, Heyd DV, et al. Kinetic and mechanistic considerations in the gelation ofgenipin-crosslinked gelatin. Int J Biol Macromol 2006;39:298–302. [PubMed: 16797690]
26. Stenzel KH, Miyata T, Rubin AL. Collagen as a biomaterial. Annu Rev Biophys Bioeng 1974;3:231–253. [PubMed: 4607533]
27. Murray MM, Palmer M, Abreu E, et al. Platelet-rich plasma alone is not sufficient to enhance suturerepair of the ACL in skeletally immature animals: an in vivo study. J Orthop Res. in press
Palmer et al. Page 10
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
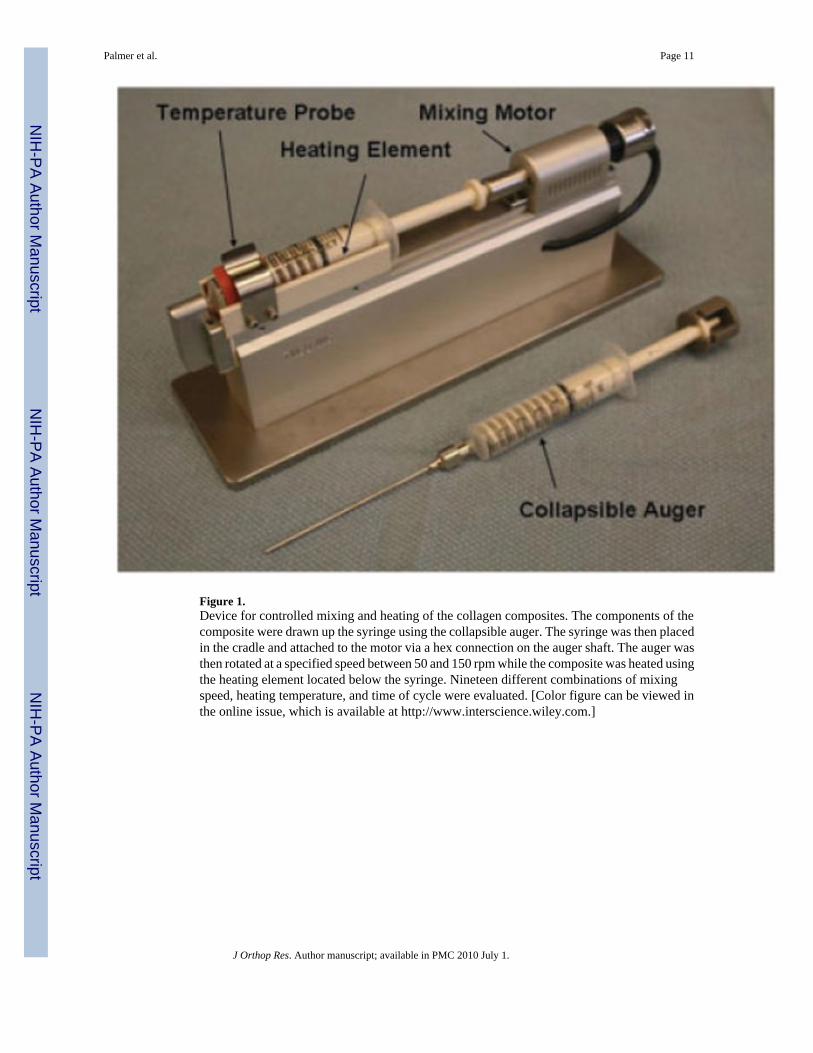
Figure 1.Device for controlled mixing and heating of the collagen composites. The components of thecomposite were drawn up the syringe using the collapsible auger. The syringe was then placedin the cradle and attached to the motor via a hex connection on the auger shaft. The auger wasthen rotated at a specified speed between 50 and 150 rpm while the composite was heated usingthe heating element located below the syringe. Nineteen different combinations of mixingspeed, heating temperature, and time of cycle were evaluated. [Color figure can be viewed inthe online issue, which is available at http://www.interscience.wiley.com.]
Palmer et al. Page 11
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
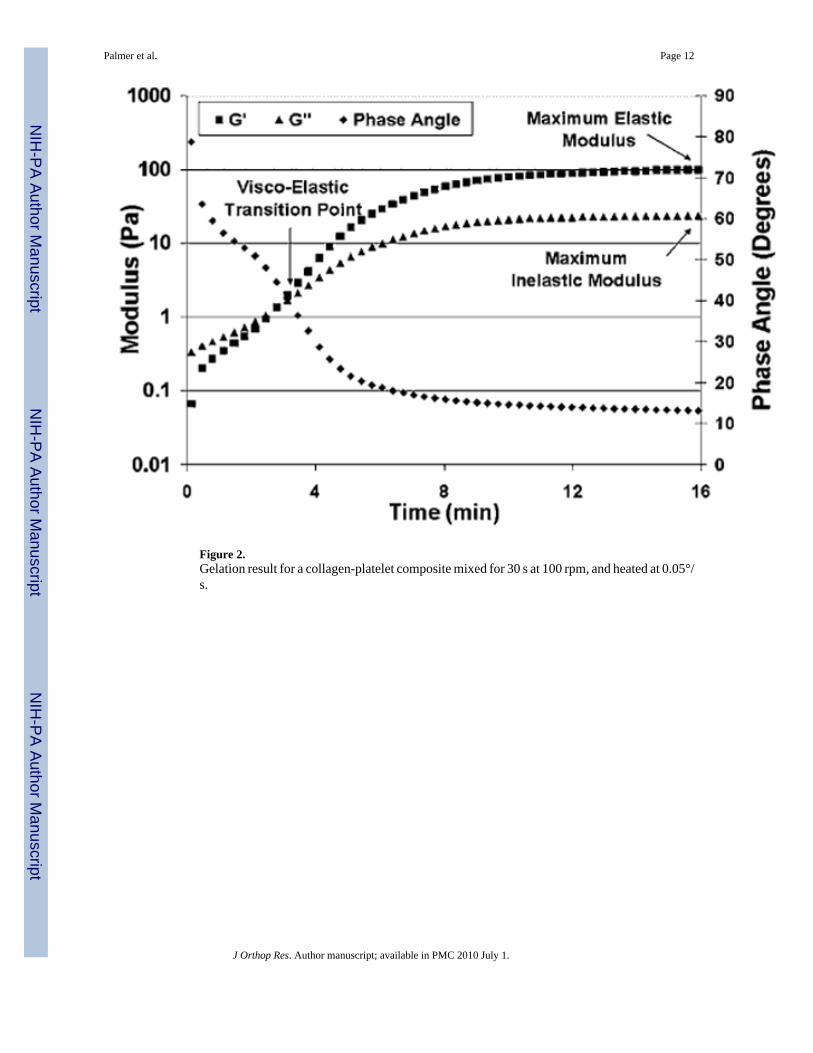
Figure 2.Gelation result for a collagen-platelet composite mixed for 30 s at 100 rpm, and heated at 0.05°/s.
Palmer et al. Page 12
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
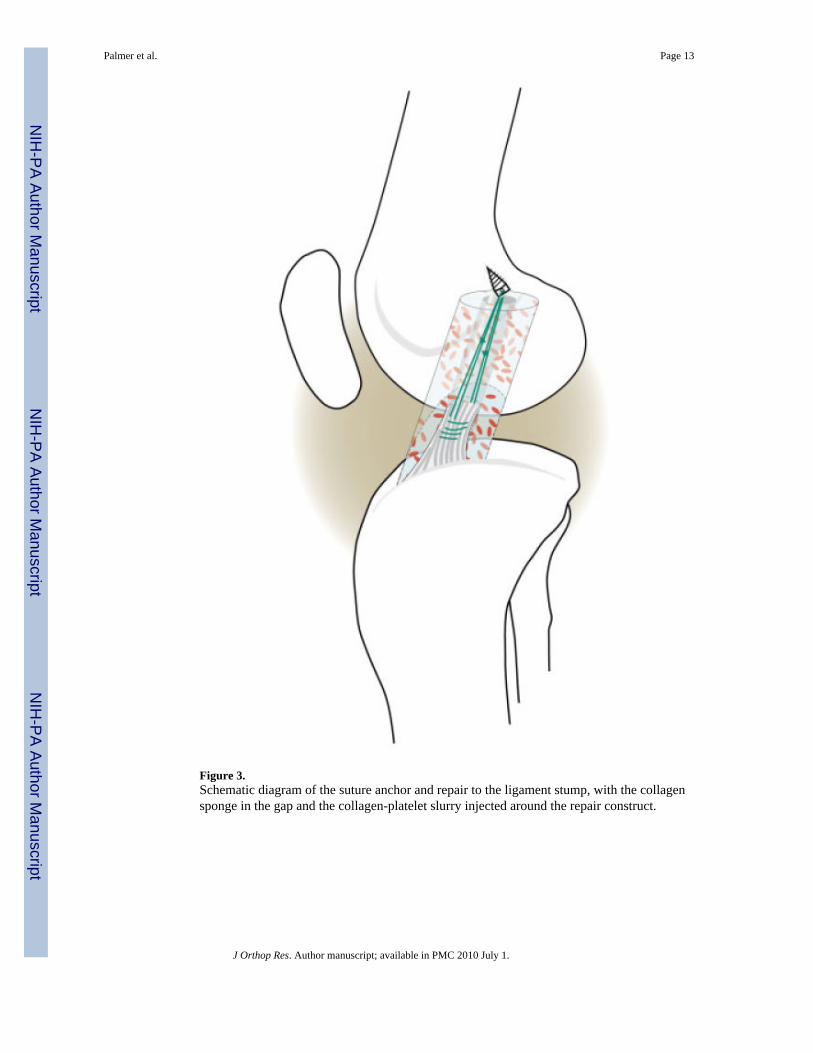
Figure 3.Schematic diagram of the suture anchor and repair to the ligament stump, with the collagensponge in the gap and the collagen-platelet slurry injected around the repair construct.
Palmer et al. Page 13
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
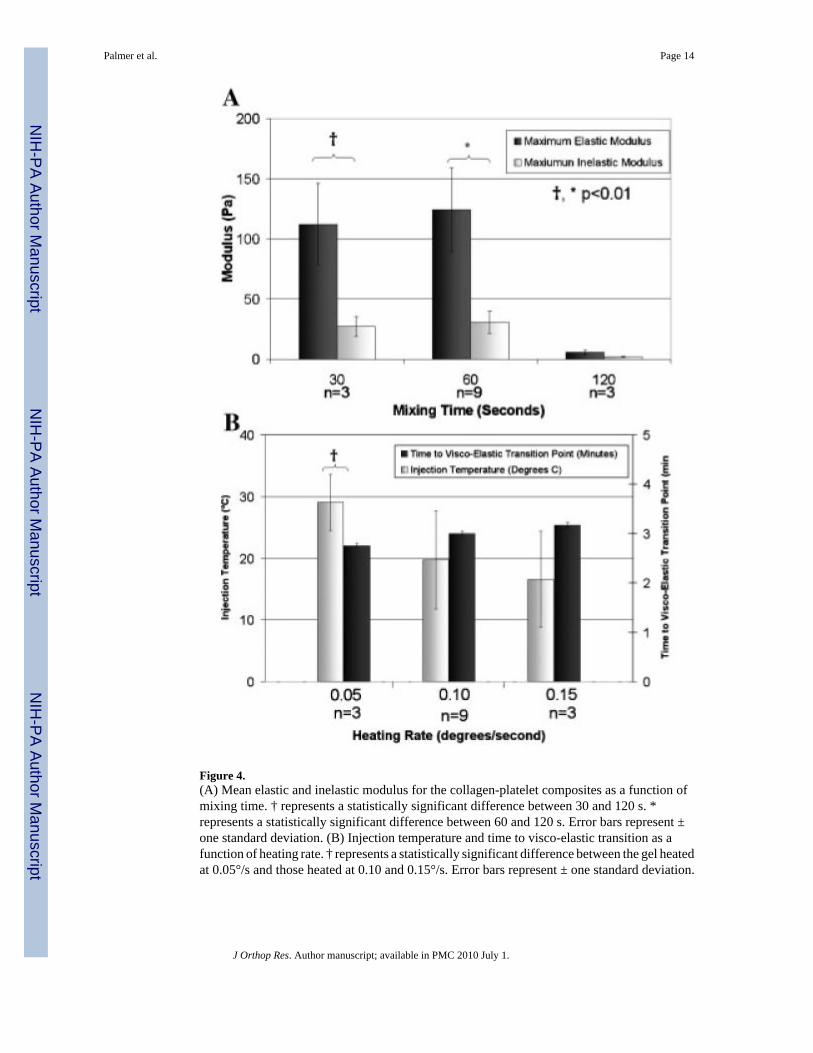
Figure 4.(A) Mean elastic and inelastic modulus for the collagen-platelet composites as a function ofmixing time. † represents a statistically significant difference between 30 and 120 s. *represents a statistically significant difference between 60 and 120 s. Error bars represent ±one standard deviation. (B) Injection temperature and time to visco-elastic transition as afunction of heating rate. † represents a statistically significant difference between the gel heatedat 0.05°/s and those heated at 0.10 and 0.15°/s. Error bars represent ± one standard deviation.
Palmer et al. Page 14
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
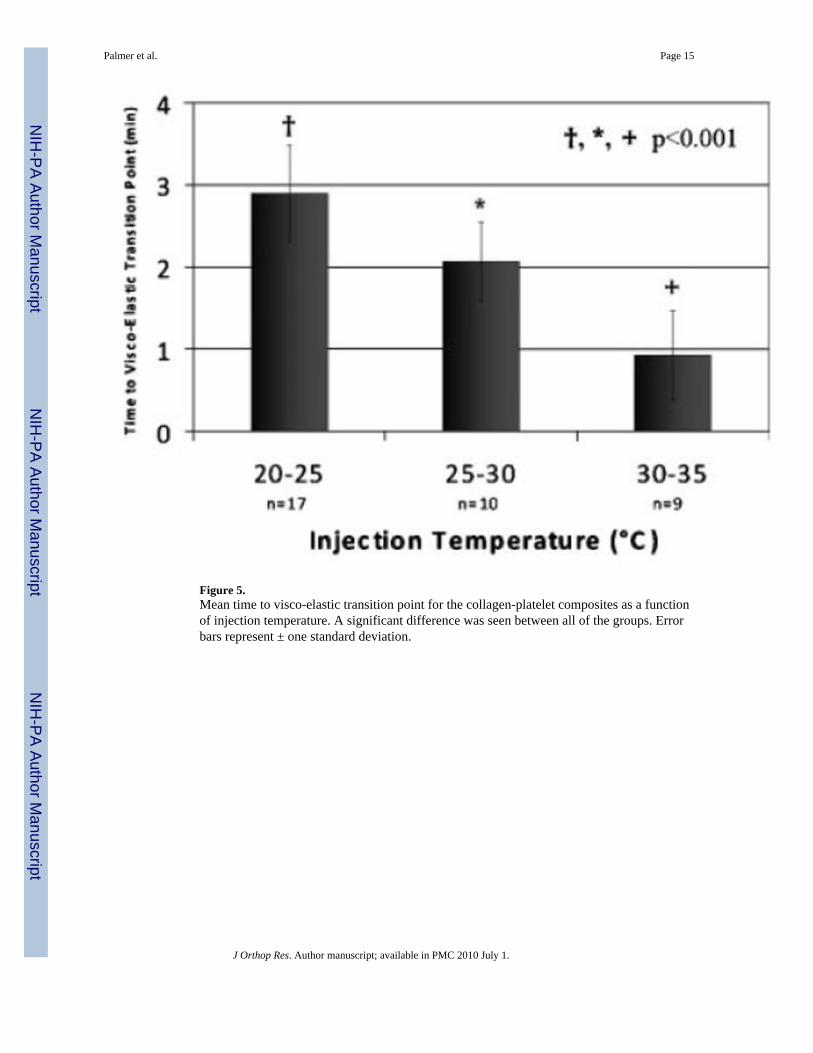
Figure 5.Mean time to visco-elastic transition point for the collagen-platelet composites as a functionof injection temperature. A significant difference was seen between all of the groups. Errorbars represent ± one standard deviation.
Palmer et al. Page 15
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
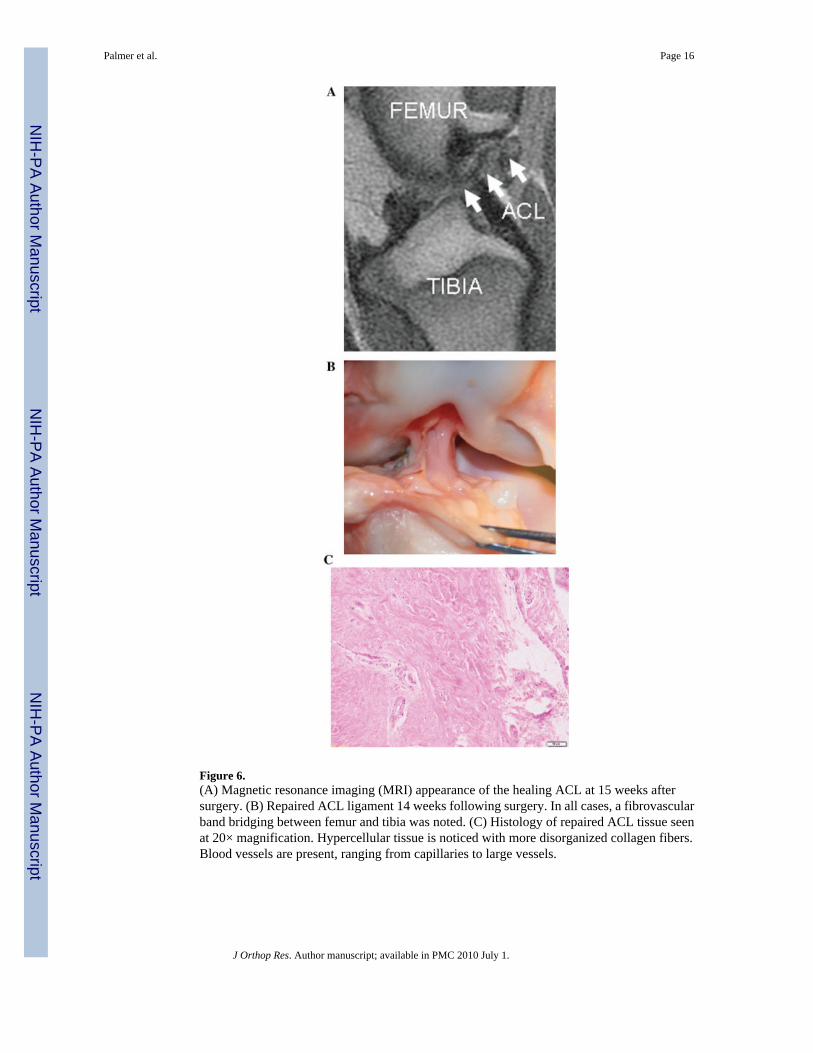
Figure 6.(A) Magnetic resonance imaging (MRI) appearance of the healing ACL at 15 weeks aftersurgery. (B) Repaired ACL ligament 14 weeks following surgery. In all cases, a fibrovascularband bridging between femur and tibia was noted. (C) Histology of repaired ACL tissue seenat 20× magnification. Hypercellular tissue is noticed with more disorganized collagen fibers.Blood vessels are present, ranging from capillaries to large vessels.
Palmer et al. Page 16
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
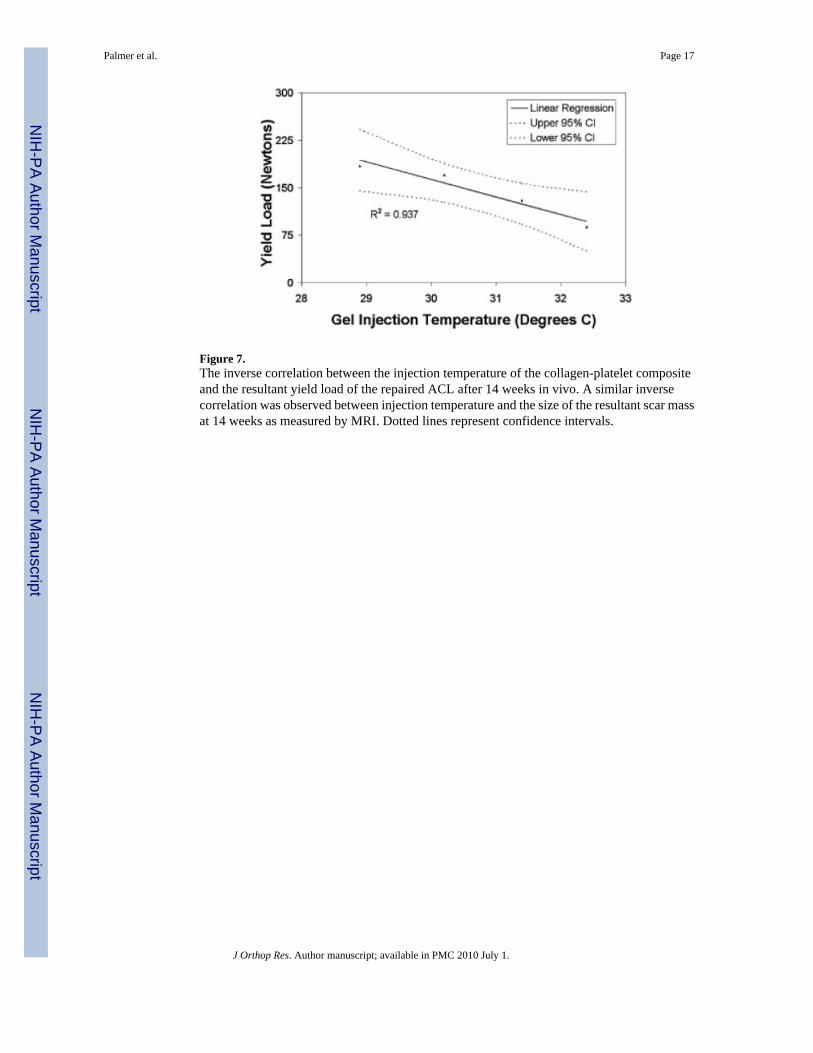
Figure 7.The inverse correlation between the injection temperature of the collagen-platelet compositeand the resultant yield load of the repaired ACL after 14 weeks in vivo. A similar inversecorrelation was observed between injection temperature and the size of the resultant scar massat 14 weeks as measured by MRI. Dotted lines represent confidence intervals.
Palmer et al. Page 17
J Orthop Res. Author manuscript; available in PMC 2010 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Palmer et al. Page 18
Table 1Confidence Interval Data for Observed In Vivo Results
Variable
95% CI
28.9°C 30.2°C 31.4°C 32.4°C
Load at yield (N) 144.5–242.4 126.7–188.3 92.2–156.5 50.3–143.1
Minimum cross-sectional area(mm2)
28.8–67.7 23.9–48.4 12.2–37.7 –2.8–34.1
Maximum cross-sectionalarea (mm2)
6.5–202.3 14.1–137.2 –15.2–113.3 –65.8–199.6
Volume (mm3) 0.6–1.5 0.5–1.1 0.3–0.9 0.0–0.8
J Orthop Res. Author manuscript; available in PMC 2010 July 1.





























