Embed Size (px)
Citation preview

Integrative Genetic Characterization and PhenotypeCorrelations in Pheochromocytoma and ParagangliomaTumoursJoakim Crona1, Margareta Nordling3, Rajani Maharjan1, Dan Granberg2, Peter Stalberg1, Per Hellman1,
Peyman Bjorklund1*
1 Department of Surgical Sciences, Uppsala University, Uppsala, Sweden, 2 Department of Medical Sciences, Uppsala University, Uppsala, Sweden, 3 Department of
Clinical Genetics, Sahlgrenska University Hospital, Goteborg, Sweden
Abstract
Background: About 60% of Pheochromocytoma (PCC) and Paraganglioma (PGL) patients have either germline or somaticmutations in one of the 12 proposed disease causing genes; SDHA, SDHB, SDHC, SDHD, SDHAF2, VHL, EPAS1, RET, NF1,TMEM127, MAX and H-RAS. Selective screening for germline mutations is routinely performed in clinical management ofthese diseases. Testing for somatic alterations is not performed on a regular basis because of limitations in interpreting theresults.
Aim: The purpose of the study was to investigate genetic events and phenotype correlations in a large cohort of PCC andPGL tumours.
Methods: A total of 101 tumours from 89 patients with PCC and PGL were re-sequenced for a panel of 10 disease causinggenes using automated Sanger sequencing. Selected samples were analysed with Multiplex Ligation-dependent ProbeAmplification and/or SNParray.
Results: Pathogenic genetic variants were found in tumours from 33 individual patients (37%), 14 (16%) were discovered inconstitutional DNA and 16 (18%) were confirmed as somatic. Loss of heterozygosity (LOH) was observed in 1/1 SDHB, 11/11VHL and 3/3 NF1-associated tumours. In patients with somatic mutations there were no recurrences in contrast to carriers ofgermline mutations (P = 0.022). SDHx/VHL/EPAS1 associated cases had higher norepinephrine output (P = 0.03) and lowerepinephrine output (P,0.001) compared to RET/NF1/H-RAS cases.
Conclusion: Somatic mutations are frequent events in PCC and PGL tumours. Tumour genotype may be further investigatedas prognostic factors in these diseases. Growing evidence suggest that analysis of tumour DNA could have an impact on themanagement of these patients.
Citation: Crona J, Nordling M, Maharjan R, Granberg D, Stalberg P, et al. (2014) Integrative Genetic Characterization and Phenotype Correlations inPheochromocytoma and Paraganglioma Tumours. PLoS ONE 9(1): e86756. doi:10.1371/journal.pone.0086756
Editor: Sadashiva Karnik, Cleveland Clinic Lerner Research Institute, United States of America
Received July 19, 2013; Accepted December 13, 2013; Published January 22, 2014
Copyright: ! 2014 Crona et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: The study was supported by grants from Swedish Cancer Society (PB), Selander Foundation (PB, PH, PS), Lions Cancer Foundation, Uppsala (JC, PH) andthe Swedish state under the LUA/ALF agreement concerning research and education of doctors, (MN, id no. 76310). The funders had no role in study design, datacollection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
Introduction
Pheochromocytoma (PCC) and paraganglioma (PGL) are rareneural crest-derived tumours arising in the adrenal medulla (PCC)or autonomic ganglia (PGL). A majority of patients present with afocal tumour lesion and may be cured with R0 resection [1–3].However, even following an apparently successful surgicalresection, there may be a risk of local or metastatic recurrencethat motivates a long follow up period [2,4,5]. Age, familial diseaseand tumour size correlate to increased risk of malignancy andrecurrence [2] and histologic criteria may also aid in predictingrisk for malignant disease [6,7]. Translational studies show thatapproximately 60% of PCC and PGL cases have either germlineor somatic mutations in one of 13 suggested disease causing loci;
SDH subunits A, B, C and D, SDHAF2, VHL, EPAS1, RET, NF1,TMEM127, MAX and H-RAS [8–20]. In the clinical setting,genetic screening of these genes by fragment prioritization ofgermline DNA is regarded as golden standard of care, and mayhave a substantial impact on patient management [21,22].Depending on the affected gene, the risk of local recurrenceand/or metastatic disease can be estimated and guide in theselection of appropriate preventive measures [22]. Screening fortumour specific genetic events is not recommended in clinicalpractice due to a lack of genotype-phenotype correlations thatcould justify the necessary resource allocation [8,23]. However, asmost genetic screening studies of PCC and PGL tumours havebeen performed on small cohorts, we hypothesized that acomprehensive genetic screening in a large clinically annotated
PLOS ONE | www.plosone.org 1 January 2014 | Volume 9 | Issue 1 | e86756

cohort could be informative. The aim of this study was, to describethe genetic landscape of PCC and PGL tumours and to correlatetumour genotype with patient characteristics and disease outcome.
Patients and Methods
PatientsThis is a single centre, retrospective study of 101 tumour
samples from 89 patients with PCC and PGL treated at theDepartment of Surgery, Uppsala university hospital, Sweden.Selected patients were previously screened for mutations in H-RASdescribing somatic genetic variants (n = 4) and MAX describing nopathogenic genetic variant [20,24]. Fourteen patients wereclinically diagnosed with hereditary syndromes; familial paragan-glioma type 4 (PGL4; n = 2), Von Hippel Lindau syndrome (VHL;n = 4) and Multiple Endocrine Neoplasia type 2 (MEN2; n = 8) bycertified genetic testing laboratories. Four additional patients hadbeen diagnosed with Neurofibromatosis type 1 (NF1) by presenceof clinical criteria. DNA samples from 195 healthy and unrelatedindividuals were utilized as a control to determine frequency ofgermline variants with unknown significance (VUS) in Swedishpopulation.
Ethical StatementEthical approval was obtained from the regional ethics committee
in Uppsala as well as written informed consent from the individualpatients. All patients were above 18 years of age at the time ofinclusion.
Clinical DataAge at diagnosis was set at the time for radiological diagnosis.
Tumour size was calculated as the mean of two diameters. Caseswere classified as metastatic by the presence of invasion intononchromaffin organs determined by histological examination orradiological/molecular imaging. Preoperative urinary catechol-amines measurements analysed in a clinical setting were includedfor evaluation. Norepinephrine assays had been performed with twodifferent reference intervals, ,350 nmol/24 h and ,400 nmol/24 h depending on utilized assays. Reference intervals for urinaryepinephrine was ,90 nmol/24 h, for plasma normetanephrine ,0,6 nmol/L and for plasma metanephrine ,0,3 nmol/L.
DNA Extraction & SequencingDNA was extracted from cryosections of tumour samples,
peripheral blood and/or normal tissue, using DNeasy Blood &Tissue Kit (Qiagen, Hilden, Germany) as previously described [25].Cryosections from included tumours were analysed for tissuemorphology and selected samples were macrodissected in order toreduce contamination of normal cells. Using a phenotype guidedfragment prioritization approach [1,26], exons and intron-exonboundaries of SDHB (NM_003000.2), SDHC (NM_003001.3),SDHD (NM_003002.2), SDHAF2 (NM_017841.2), VHL (NM_000551.3), EPAS1 (exons 9 and 12, NM_001430.4), RET (exons10–11 and 13–16, NM_020975.4), TMEM127 (NM_017849.3),MAX (NM_002382.3) and H-RAS (exons 2 and 3, NM_176795.3)were amplified by PCR and sequenced using automated Sangersequencing (Beckman Coulter Genomics, Takeley, UK). In patientswith pathogenic germline variants, all exons and intron-exonboundaries of the affected gene were sequenced in order toinvestigate a potentially inactivating variant on the 2nd allele.Ultimately, patients without detected pathogenic mutations in thisstudy had been screened for all ten above mentioned genes. Primersequences can be obtained by request.
Mutational AnalysisChromatograms generated by Sanger Sequencing were reviewed
using CLC genomics workbench 5.5 (CLC bio, Aarhus, Denmark).Genetic variants were annotated for overlapping informationavailable in public databases; Catalogue of Somatic Mutations inCancer (COSMIC) [27], the Single Nucleotide Polymorphismdatabase (dbSNP), Human Genome Mutation Database (HGMDpublic) [28] and Leiden Open source Variation Database (LOVD).In silico analysis was performed using Sorting Intolerant FromTolerant (SIFT) [29] and Polymorphism Phenotyping v2 (Poly-phen-2) [30].
Multiplex Ligation-dependent Probe AmplificationInclusion criteria for analysis were absence of a pathogenic
germline variant. Only DNA extracted from blood/normal tissuewas selected for Multiplex ligation-dependent probe amplification(MLPA). Included samples were analysed with SALSA MLPAP226 SDH and P016-B2 VHL probe mixes (MRC-Holland,Amsterdam, Netherlands) that have coverage of the SDHA, SDHB,SDHC, SDHD, SDHAF2 and VHL loci. Reactions were carried outas previously described [31] and an ABI3130xl Genetic Analyzer(Life Technologies, Carlsbad, CA) was used for fragmentseparation. The MLPA data were analyzed using GeneMapper4.0 genotyping software (Applied Biosystem) and SeqPilot version3.3.2 (JSI medical systems GmBH, Kippenheim, Germany). Theexperiments were carried out at a laboratory certified for clinicaluse and analysed by an experienced clinical investigator (MN).
Single Nucleotide Polymorphism ArrayInclusion criteria were presence of pathogenic or unknown
variants in SDHB, SDHC, VHL or clinical criteria of NF1. TumourDNA from the selected samples were subjected to SNParrayanalysis; using Illumina Omni1-Quad or Omni2,5-Quad chips(Illumina Inc, CA, USA), containing 1,140,419 and 2,379,855probes respectively. Hybridization and sequencing was performedby university core facilities, SNP&SEQ Technology Platform inUppsala, Sweden (http://molmed.medsci.uu.se/SNP+SEQ+Technology+Platform/). Generated data was imported into the Illumina BeadStudio(Illumina, CA, USA) software and analysed using Nexus Copy NumberVariation 7.0 Build 7887 (Biodiscovery Inc, CA, USA) to detect copynumber variation and allelic imbalance using default thresholds The fractionof DNA derived from tumour cells were estimated by analysing the B-allelefrequency in regions showing copy number alterations [32]. Samples withtumour cell purity ,70% were analysed with adjusted settings.
StatisticsSPSS 19 (IBM, Armonk NY, US) was used for statistical
calculations. Chi2 test was performed for analysis of nominalvariables. As age at diagnosis, tumour size and catecholamineoutput were not normally distributed, hence a non-parametric test(Mann-Whitney U test) was selected for analysis of these scaledvalues. Patients with variants of unknown significance (VUS) wereclassified as wild type. Multiple regression test of phenotypecorrelation to carrier status and genotypes were not possible toperform due to the low number of observations. P-values ,0.05were considered as significant and ,0.1 as borderline significant.
Results
Patient characteristics are described in table 1. The median ageat diagnosis was 49 years (range 15–85) and there were 35 malesand 53 females. Eighty patients had adrenal PCC (31 left adrenal,37 right adrenal, 10 bilateral), eight had thoracoabdominal PGLsand there were one head and neck PGL. The median tumour size
Genotype Phenotype Correlations in PCC and PGL
PLOS ONE | www.plosone.org 2 January 2014 | Volume 9 | Issue 1 | e86756

was 55 mm (range 8–170). There were wide discrepancies incatecholamine output; urinary norepinephrine range 112–19130 nmol/24 h (ref ,400/,350 nmol/24 h), urinary epineph-rine range 19–33322 nmol/24 h (ref ,90 nmol/24 h), plasmanormetanephrine range 1–37 nmol/L (ref ,0,6 nmol/L), andplasma metanephrine range 0–140 nmol/L (ref ,0,3 nmol/L).There were 13 patients with recurrent disease, eight of whomrecurred with distant metastases and five with local recurrences.One additional patient had distant metastases at the time ofdiagnosis. The median follow up time was 106 months (range 0–714 months).
Genetic ScreeningA total of 33 patients (37%) had a pathogenic genetic variant in
included disease causing loci. We could confirm 14 of thesemutations in constitutional DNA (Figure 1a) and 16 were confirmedas somatic by absence in constitutional DNA (Figures 1b and c).There was no constitutional DNA available for three of the patientswith pathogenic mutations. All genetic variants previously clinicallydiagnosed by the Department of Clinical Genetics (n = 14) wereverified in the present study. There were four additional patientswith clinical criteria of Neurofibromatosis type 1 but with no genetictesting. Cases with discovered mutations and corresponding clinicalcharacteristics are presented in Table 2.
Two related patients (mother and son) presented with multipleabdominal PGL. Both had several local recurrences that were notclassified as metastatic lesions. Re-sequencing revealed a patho-genic nonsense mutation in SDHB; c.268C.T, p.Arg90* [13] thatwas present in DNA from blood.
There were 12 cases with pathogenic mutations in the VHLgene. Patient number 9 with bilateral PCC (index case) had apathogenic germline missense mutation in VHL; c.482G.Ap.Arg161Gln. A family comprising of three siblings with bilateralor unilateral PCC had pathogenic germline missense mutation inVHL; c.499C.T, p.Arg167Trp [33]. Both p.Arg161Gln andp.Arg167Trp had previously been reported as pathogenic [33].Seven patients had somatic mutations in VHL. There were sixunique SNVs; c.193T.G, p.Ser65Ala; c.193T.A, p.Ser65Thr;c.238A.G, p.Ser80Gly; c.458T.A, p.Leu153Gln; c.475A.G,p.Lys159Glu and c.551T.A, p.Leu184His in one patient each.Patient number 4 had a 30 base pair deletion c.163_192del,p.Glu55_Arg64del that was absent in DNA from peripheral blood.All carriers of somatic VHL mutations had unilateral PCC,sporadic disease presentation and there were no apparent signs orsymptoms of VHL syndrome.
Two patients had mutations in EPAS1 which were absent inDNA from their blood; one c.1586T.C, p.Leu529Pro and onec.1589C.T, p.Ala530Val. These mutations are previouslydescribed as pathogenic [16,34]. Both patients had sporadicdisease presentation. Patient 16 had borderline polycytemia with ahaemoglobin level of 150 g/L (reference interval 120–150 g/L).
There were 13 patients with pathogenic mutations in RET.Eight had germline pathogenic mutations and clinical character-istics of MEN2 syndrome; c.1826G.C, p.Cys609Ser; c.1832G.A, p.Cys611Tyr; c.1900T.C, p.Cys634Arg; c.1900T.G,p.Cys634Gly; c.1901G.A, p. Cys634Tyr; c.2410G.A, p.Val804-Met in one patient each and c.2753T.C, p.Met918Thr in towdifferent patients. Two patients with unilateral PCC and sporadicdisease presentation had somatic mutation in RET; c.1900T.G,p.Cys634Gly and c.1900T.C, p.Cys634Arg. For three of thepatients with SNVs in RET there were no constitutional DNAavailable; c.1891G.T, p.Asp631Tyr in one patient andc.2753T.C, p.Met918Thr in two patients. All three cases hadsporadic disease presentation and there were no signs or symptoms
suggesting MEN2 syndrome. All these RET mutations aredescribed as pathogenic in the literature [8,33].
Four patients had previously been described with somatic H-RAS mutations [20]. One additional somatic mutation in H-RAS;c.181C.A, p.Gln61Lys; was detected in a male patient that hadsporadic disease presentation.
Variants of Unknown SignificanceFour patients had germline variants of unknown significance
(VUS). There were two VUS in SDHC; c.328C.T, Pro110Ser[35] and c.490A.T, Met164Leu in two different patients withunilateral PCC and sporadic disease presentation. Both mutationswere available in constitutional DNA. Succinate dehydrogenase subunitC Met164Leu has been reported to have impact in functionalmodels but was classified as benign in vivo [36]. The pathogenicityof Pro110Ser has not been investigated in detail [35]. Succinatedehydrogenase subunit C Codon 110 is conserved among vertebrateorthologs whereas codon 164 is not a conserved residue. In silicoanalysis determined the variants as benign, SIFT (0,93 and 0,96)and Polyphen2 (0,231 and 0,0).
Patient 36, a 28 year old male, was referred to the local hospitaldue to hypertension, headache and multiple episodes of syncope.Urinary norepinephrine was elevated, 1752 nmol/24 h (,350),but epinephrine was within reference margins 37 nmol/24 h (,90). A computed tomography revealed an abdominal mass locatedin close proximity to the left renal artery and vein. The lesion wassurgically resected and the pathology report showed a PGL,20 mm in size with a Ki67 index of ,1%. Genetic screening ofRET as well as Succinate Dehydrogenase subunits B and D was normal.The proband remains free of recurrence 21 months following theinitial diagnosis. There were no apparent signs or symptoms of vonHippel Lindau syndrome. Sanger sequencing revealed a singlenucleotide polymorphism in VHL; c.548C.T, p.Ser183Leu.Multiplex ligation-dependent probe amplification of constitutionalDNA did not show any pathological imbalances. In tumour tissue,loss of heterozogosity and copy number loss was observed on thewhole arm of chromosome 3p by Omni-1-quad SNP array(Illumina, CA, USA).VHL; c.548C.T, p.Ser183Leu has beenclassified as pathogenic in a functional model but the individualcontribution of the allele to patient phenotype is not fully described[37]. Screening of 190 healthy individuals revealed homozygous Callele in all cases. Codon 183 is conserved among mammalianorthologs and in silico analysis determined the variant as probablypathogenic: SIFT (0,18) and Polyphen2 (1,0).
Patient 37 was diagnosed with a unilateral PCC at 27 years of agehaving apparently sporadic presentation. Re-sequencing revealed aRET mutation c.2372A.T, p.Tyr791Phe that was found inconstitutional DNA. The pathogenicity of RET p.Tyr791Phe isdisputed [38,39].
There were no pathogenic variants discovered in SDHAF2,TMEM127 and MAX.
Structural VariationsMultiplex ligation-dependent probe amplification analysis did
not reveal any copy number gains or losses. Analysis of SNP arraydata showed loss of heterozygosity (LOH) located to the genomiccoordinates of the respective gene in 1/1 SDHB, 11/11 VHL and3/3 NF1-related tumours (table 3, figure 2). There were no LOHat coordinates corresponding to SDHC loci in tumours frompatients with germline SDHC Pro110Ser and Met164Leu variants.Patient 36 with a germline VHL p.Ser183Leu had LOH at theVHL loci. Analysis failed due to corrupted data in two cases, oneSDHB and one NF1-related tumour.
Genotype Phenotype Correlations in PCC and PGL
PLOS ONE | www.plosone.org 3 January 2014 | Volume 9 | Issue 1 | e86756

Ta
ble
1.
Clin
ical
char
acte
rist
ics
and
carr
ier
stat
us. C
oh
ort
(n=
89
)N
od
isco
ve
red
mu
tati
on
s(n
=5
2)*
Ge
rmli
ne
va
ria
nts
(n=
18
)**
So
ma
tic
va
ria
nts
(n=
16
)G
erm
lin
ea
nd
no
mu
tati
on
So
ma
tic
an
dn
om
uta
tio
n
Ge
rmli
ne
an
dS
om
ati
cm
uta
tio
n
Ra
ng
eR
an
ge
Ra
ng
eR
an
ge
P
Med
ian
age,
year
s49
,515
–85
5322
–85
29,5
15–6
648
25–8
10.
0021
0.62
210.
0251
Gen
der
,M
ale/
Fem
ale
35/5
319
/32
7/11
8/8
0.90
211
0.36
511
0.51
511
Tum
ou
rsp
ecifi
cati
on
s
Med
ian
size
,m
m55
8–17
060
20–1
4051
(n=
14)
20–1
7045
8–10
00.
1661
0.30
510.
7551
Loca
lizat
ion
,le
ftad
ren
al/r
igh
tad
ren
al31
/37
22/2
13/
55/
90.
4781
10.
3151
10.
9331
1
Ad
ren
al/e
xtra
adre
nal
tum
ou
r80
/947
/516
/214
/20.
8551
10.
7401
10.
9001
1
Mu
ltifo
cal
tum
ou
rs10
19
0,
0.00
111
0.56
111
,0.
0011
1
Bio
chem
istr
y
Med
ian
Uri
ne
No
rep
inep
hri
ne,
nm
ol/
24h
1687
112–
1913
021
81,5
230–
1913
083
611
2–45
4524
3922
5–14
244
0.03
310.
9621
0.04
91
Med
ian
Uri
ne
Epin
eph
rin
e,n
mo
l/24
h18
919
–333
2224
719
–333
2219
527
–641
9625
–116
640.
210.
5411
0.62
21
Med
ian
Pla
sma
No
rmet
anep
hri
ne,
nm
ol/
L6,
41–
377,
14–
161,
41–
211
,61–
370.
0041
0.64
010.
1361
Med
ian
Pla
sma
Met
aep
inep
hri
ne,
nm
ol/
L0,
50–
140
1,65
0–34
0,45
0–1
1,05
0–14
00.
5791
0.96
110.
3911
Rec
urr
ent
dis
ease
138
50
0.37
611
0.07
011
0.02
211
Met
asta
tic
dis
ease
***
97
20
0.79
711
0.12
111
0.16
911
Stat
isti
cal
corr
elat
ion
of
clin
ical
vari
able
san
dca
rrie
rsst
atu
s.M
ult
ifoca
ltu
mo
urs
was
def
ined
asb
ilate
ral
ph
eoch
rom
ocy
tom
ao
rm
ult
iple
par
agan
glio
ma
tum
ou
rs.
*Pat
ien
tsw
ith
no
avai
lab
leg
erm
line
DN
Aw
ere
excl
ud
ed.
**In
clu
ded
14g
erm
line
vari
ants
and
4p
atie
nts
wit
hcl
inic
alcr
iter
iao
fN
euro
fibro
mat
osi
sty
pe
1.**
*Nin
ep
atie
nts
had
met
asta
tic
dis
ease
,on
eo
fth
ese
had
met
asta
tic
dis
ease
atth
eti
me
of
dia
gn
osi
san
dth
ere
mai
nin
gh
adm
etas
tati
cre
curr
ence
sla
ter
on
inth
ed
isea
seco
urs
e.1
Man
n-W
hit
ney
UTe
stan
d11
Ch
iSq
uar
ete
st.
do
i:10.
1371
/jo
urn
al.p
on
e.00
8675
6.t0
01
Genotype Phenotype Correlations in PCC and PGL
PLOS ONE | www.plosone.org 4 January 2014 | Volume 9 | Issue 1 | e86756

Statistical CorrelationStatistical analyses of carrier status and genotype correlations to
phenotype are presented in Tables 1 and 4. Stratified into groupsaccordingly to mutation status, germline carriers had a age atdiagnosis that were significantly lower (median 29,5 years)compared to those with somatic aberrations (median 48 years,P = 0.025) as well as patients without known mutations (median 53years, P = 0.002). The frequency of mutifocal tumours were alsodifferent in germline carriers (53%) compared to patients withsomatic carrier status (0%, P,0.001) as well as those withoutknown mutations (2%, P,0.001).
No cases of recurrent disease were observed in somatic carriers(0%), in contrast to germline carriers (28%, P = 0.022) andborderline significant compared to patients without discoveredmutations (15%, P = 0.07). Preoperative levels of urine norepi-nephrine were lower in patients with germline carrier statuscompared to somatic carriers and those without mutation(P = 0.049 and P = 0.033 respectively). Gender, tumour size,tumour localization, metastatic disease as well as urine and plasmaepinephrine output were not different among the three carrierstatus groups.
Stratification according to genotype into cluster 1; SDHx/VHL/EPAS1 mutants and cluster 2; RET/NF1/H-RAS mutants, resultedin a difference in age at diagnosis between cluster 2 carriers(median 45) and patients without mutations (median 53,P = 0.036). A borderline significance difference was also notedfor PCC localization, there were one left adrenal and eight rightadrenals affected in cluster 1 compared to eight left and eightright-sided tumours in cluster 2 (P = 0.052). A difference in PCClateralization was also noted between cluster 1 patients and thosewithout discovered mutations (P = 0.028). In patients withoutmutation there were one case with multiple PGL and nonebilateral PCC, different than in cluster 1 (4 cases total, P,0.001)and cluster 2 (5 cases total, P = 0.004). Urine norepinephrine levels(Figures 3a and b) were higher in cluster 1 patients (median 2439/24 h, P = 0.03) and those without mutation (median 2181,5,P = 0.018) compared to cluster 2 (median 862). ReverselyEpinephrine levels were lower in cluster 1 (median 58/24 h, P,0.001) and in those without mutation (median 247 nmol/24 h,P = 0.002) compared to cluster 2 patients (median 520 nmol/24 h). Age at diagnosis, gender, plasma cathecolamines as well asrecurrent and metastatic disease were not different among thethree groups.
Discussion
GeneticsWe have analysed 101 PCC and PGL tumours for SNVs in nine
different genes, complemented by selective MLPA and SNP arrayanalysis. A total of 33 patients (37%) had pathogenic variants inSDHB, VHL, EPAS1, RET and H-RAS. Including patients withclinical criteria of Neurofibromatosis type 1 and loss of heterozy-gosity at the NF1 locus, 41% of the cohort could be associated withgenetic aberrations in known genes. We did not find anypathogenic germline mutations that had not been previouslydiscovered by clinical screening, this low frequency of germlinemutations in apparently sporadic patients have previously beendescribed in Swedish patients [40]. Considering the characteristicsof the cohort with a predominance of benign and unilateral PCChaving sporadic presentation, the frequencies of pathogenicgenetic variants and patient carrier status were similar to thosepreviously reported [8]. Loss of heterozygosity could be detected intumour DNA from 11/12 patients having somatic or germlinemutations in the SDHB or VHL genes. SNParray analysis oftumour DNA from patient 10 (VHL p.Arg161Gln) did not showLOH at any locus. This tumour sample will have to be carefullyreviewed for contaminating wild type cells and re-analysed.Patients with clinical criteria of NF1 syndrome did not have aclinical diagnostic genetic test performed, probably due to the sizeof the NF1 gene and the number of possible loci. Three of thesepatients tumours were analysed with SNParray that revealed lossof heterozygosity at the NF1 loci in tumour DNA in all investigatedcases. This strongly suggest that these patients do have a germlinemutation in NF1 [15,18]. The interpretation of clinical correla-tions in sporadic patients presented by this study is limited by theabsence of analysis of the NF1 gene that was recently found to becommonly affected in patients with sporadic PCC and PGL[15,18]. To analyse this extensive loci, further studies may utilizeNext Generation Sequencing or SNP arrays [35,41].
Multiplex ligation-dependent probe amplification analysis ofconstitutional DNA showed no copy number gains or losses in anyof the investigated cases. Both the MLPA laboratory workflow andresult analysis were performed using robust workflows byexperienced clinical investigators, ensuring high reliability of theseresults.
Figures 1. Chromatograms exported from CLC Genomics Workbench 5.5 displaying (A) Pathogenic genetic variants available inconstitutional DNA, (B) confirmed somatic variants and (C) 30 base pair somatic deletion in VHL.doi:10.1371/journal.pone.0086756.g001
Genotype Phenotype Correlations in PCC and PGL
PLOS ONE | www.plosone.org 5 January 2014 | Volume 9 | Issue 1 | e86756

Ta
ble
2.
Pat
ho
gen
ican
du
nkn
ow
ng
enet
icva
rain
tsan
dth
eir
corr
esp
on
din
gp
atie
nt
char
acte
rist
ics.
Pa
tie
nt
no
.D
iag
no
sis
Ge
nd
er
Ag
ea
td
iag
no
sis
He
red
ita
ryS
yn
dro
me
crit
eri
aS
ize
(mm
)U
nil
ate
ral/
mu
ltip
leR
ecu
rre
nt
Me
tast
ati
cG
en
eE
xo
nS
om
ati
c/G
erm
lin
ecD
NA
Am
ino
aci
dsu
bst
itu
tio
nC
on
clu
de
dP
ath
og
en
icit
y
1TA
PG
LM
15+
PG
L4-
Mu
ltip
le+
2SD
HB
3G
erm
line
c.26
8C.
Tp
.Arg
90*
Pat
ho
gen
ic
2TA
PG
LF
26+
PG
L4-
Mu
ltip
le+
2SD
HB
3G
erm
line
c.26
8C.
Tp
.Arg
90*
Pat
ho
gen
ic
3P
CC
M76
22
70U
ni
22
VH
L1
Som
atic
c.16
3_19
2del
p.G
lu55
_Arg
64d
elP
ath
og
enic
4P
CC
M58
22
90U
ni
22
VH
L1
Som
atic
c.19
3T.
Ap
.Ser
65Th
rP
ath
og
enic
5P
CC
F49
22
25U
ni
22
VH
L1
Som
atic
c.19
3T.
Gp
.Ser
65A
laP
ath
og
enic
6P
CC
F25
22
25U
ni
22
VH
L1
Som
atic
c.23
8A.
Gp
.Ser
80G
lyP
ath
og
enic
7P
CC
F47
22
8U
ni
22
VH
L2
Som
atic
c.45
8T.
Ap
.Leu
153G
lnP
ath
og
enic
8P
CC
M47
22
100
Un
i2
2V
HL
3So
mat
icc.
475A
.G
p.L
ys15
9Glu
Pat
ho
gen
ic
9P
CC
F66
NA
VH
L65
/60
Mu
ltip
le2
2V
HL
3G
erm
line
c.48
2G.
Ap
.Arg
161G
lnP
ath
og
enic
10P
CC
F25
+V
HL
60/4
0M
ult
iple
22
VH
L3
Ger
mlin
ec.
499C
.T
p.A
rg16
7Trp
Pat
ho
gen
ic
11P
CC
M21
+V
HL
40/3
0M
ult
iple
22
VH
L3
Ger
mlin
ec.
499C
.T
p.A
rg16
7Trp
Pat
ho
gen
ic
12P
CC
F25
+V
HL
30U
ni
22
VH
L3
Ger
mlin
ec.
499C
.T
p.A
rg16
7Trp
Pat
ho
gen
ic
13P
CC
F31
22
40U
ni
22
VH
L3
Som
atic
c.55
1T.
Ap
.Leu
184H
isP
ath
og
enic
14TA
PG
LF
642
220
Un
i2
2EP
AS1
12So
mat
icc.
1586
T.C
p.L
eu52
9Pro
Pat
ho
gen
ic
15P
CC
F81
22
45U
ni
22
EPA
S112
Som
atic
c.15
89C
.T
p.A
la53
0Val
Pat
ho
gen
ic
16P
CC
F27
+M
EN2A
100
Un
i2
2RE
T10
Ger
mlin
ec.
1826
G.
Cp
.Cys
609S
erP
ath
og
enic
17P
CC
F57
+M
EN2A
23M
ult
iple
+2
RET
10G
erm
line
c.18
32G
.A
p.C
ys61
1Tyr
Pat
ho
gen
ic
18P
CC
F61
22
15U
ni
22
RET
11N
Ac.
1891
G.
Tp
.Asp
631T
yrP
ath
og
enic
19P
CC
F29
+M
EN2A
30/4
7M
ult
iple
22
RET
11G
erm
line
c.19
00T.
Cp
.Cys
634A
rgP
ath
og
enic
20P
CC
F47
22
80U
ni
22
RET
11So
mat
icc.
1900
T.C
p.C
ys63
4Arg
Pat
ho
gen
ic
21P
CC
M29
+M
EN2A
20/N
AM
ult
iple
+2
RET
11G
erm
line
c.19
00T.
Gp
.Cys
634G
lyP
ath
og
enic
22P
CC
F57
22
60U
ni
22
RET
11So
mat
icc.
1900
T.G
p.C
ys63
4Gly
Pat
ho
gen
ic
23P
CC
F30
+M
EN2A
20/N
AM
ult
iple
22
RET
11G
erm
line
c.19
01G
.A
p.
Cys
634T
yrP
ath
og
enic
24P
CC
M65
-M
EN2A
95U
ni
++
RET
14G
erm
line
c.24
10G
.A
p.V
al80
4Met
Pat
ho
gen
ic
25P
CC
F18
2M
EN2B
25U
ni
+2
RET
16G
erm
line
c.27
53T.
Cp
.Met
918T
hr
Pat
ho
gen
ic
26P
CC
M34
2M
EN2B
60/6
0M
ult
iple
22
RET
16G
erm
line
c.27
53T.
Cp
.Met
918T
hr
Pat
ho
gen
ic
27P
CC
M45
22
30U
ni
NA
NA
RET
16N
Ac.
2753
T.C
p.M
et91
8Th
rP
ath
og
enic
28P
CC
F31
22
55U
ni
22
RET
16N
Ac.
2753
T.C
p.M
et91
8Th
rP
ath
og
enic
29P
CC
M54
22
45U
ni
22
H-R
AS
2So
mat
icc.
37G
.C
p.G
ly13
Arg
Pat
ho
gen
ic
30P
CC
M76
22
76U
ni
22
H-R
AS
3So
mat
icc.
181C
.A
p.G
ln61
Lys
Pat
ho
gen
ic
31P
CC
M36
22
30U
ni
22
H-R
AS
3So
mat
icc.
181C
.A
p.G
ln61
Lys
Pat
ho
gen
ic
32TA
PG
LM
312
210
0U
ni
22
H-R
AS
3So
mat
icc.
182A
.G
p.G
ln61
Arg
Pat
ho
gen
ic
33P
CC
M45
22
100
Un
i2
2H
-RA
S3
Som
atic
c.18
2A.
Gp
.Gln
61A
rgP
ath
og
enic
34P
CC
F61
22
25U
ni
22
SDH
C5
Ger
mlin
ec.
328C
.T
p.P
ro11
0Ser
Un
kno
wn
35P
CC
M55
22
65U
ni
22
SDH
C6
Ger
mlin
ec.
490A
.T
p.M
et16
4Val
Un
kno
wn
Genotype Phenotype Correlations in PCC and PGL
PLOS ONE | www.plosone.org 6 January 2014 | Volume 9 | Issue 1 | e86756
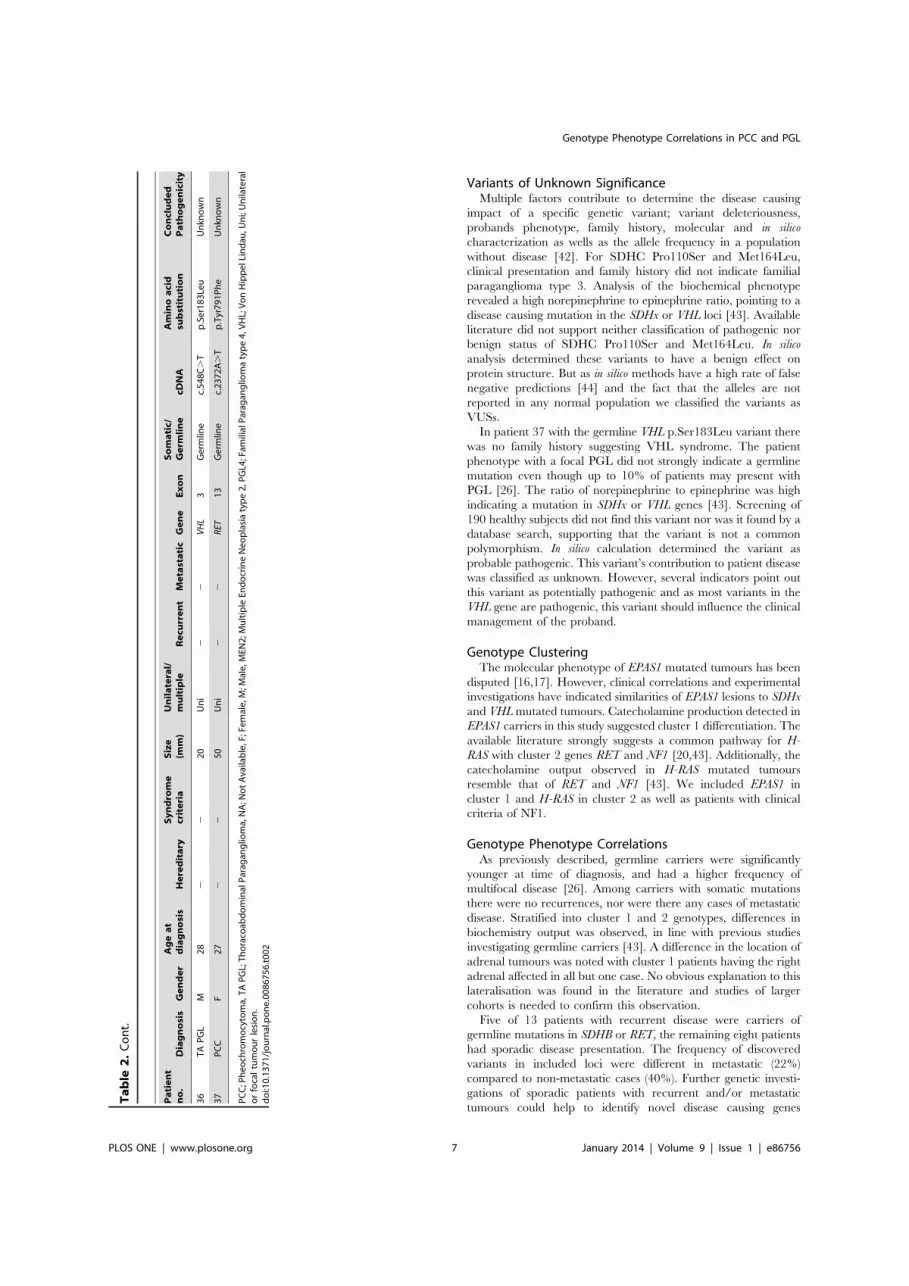
Variants of Unknown SignificanceMultiple factors contribute to determine the disease causing
impact of a specific genetic variant; variant deleteriousness,probands phenotype, family history, molecular and in silicocharacterization as wells as the allele frequency in a populationwithout disease [42]. For SDHC Pro110Ser and Met164Leu,clinical presentation and family history did not indicate familialparaganglioma type 3. Analysis of the biochemical phenotyperevealed a high norepinephrine to epinephrine ratio, pointing to adisease causing mutation in the SDHx or VHL loci [43]. Availableliterature did not support neither classification of pathogenic norbenign status of SDHC Pro110Ser and Met164Leu. In silicoanalysis determined these variants to have a benign effect onprotein structure. But as in silico methods have a high rate of falsenegative predictions [44] and the fact that the alleles are notreported in any normal population we classified the variants asVUSs.
In patient 37 with the germline VHL p.Ser183Leu variant therewas no family history suggesting VHL syndrome. The patientphenotype with a focal PGL did not strongly indicate a germlinemutation even though up to 10% of patients may present withPGL [26]. The ratio of norepinephrine to epinephrine was highindicating a mutation in SDHx or VHL genes [43]. Screening of190 healthy subjects did not find this variant nor was it found by adatabase search, supporting that the variant is not a commonpolymorphism. In silico calculation determined the variant asprobable pathogenic. This variant’s contribution to patient diseasewas classified as unknown. However, several indicators point outthis variant as potentially pathogenic and as most variants in theVHL gene are pathogenic, this variant should influence the clinicalmanagement of the proband.
Genotype ClusteringThe molecular phenotype of EPAS1 mutated tumours has been
disputed [16,17]. However, clinical correlations and experimentalinvestigations have indicated similarities of EPAS1 lesions to SDHxand VHL mutated tumours. Catecholamine production detected inEPAS1 carriers in this study suggested cluster 1 differentiation. Theavailable literature strongly suggests a common pathway for H-RAS with cluster 2 genes RET and NF1 [20,43]. Additionally, thecatecholamine output observed in H-RAS mutated tumoursresemble that of RET and NF1 [43]. We included EPAS1 incluster 1 and H-RAS in cluster 2 as well as patients with clinicalcriteria of NF1.
Genotype Phenotype CorrelationsAs previously described, germline carriers were significantly
younger at time of diagnosis, and had a higher frequency ofmultifocal disease [26]. Among carriers with somatic mutationsthere were no recurrences, nor were there any cases of metastaticdisease. Stratified into cluster 1 and 2 genotypes, differences inbiochemistry output was observed, in line with previous studiesinvestigating germline carriers [43]. A difference in the location ofadrenal tumours was noted with cluster 1 patients having the rightadrenal affected in all but one case. No obvious explanation to thislateralisation was found in the literature and studies of largercohorts is needed to confirm this observation.
Five of 13 patients with recurrent disease were carriers ofgermline mutations in SDHB or RET, the remaining eight patientshad sporadic disease presentation. The frequency of discoveredvariants in included loci were different in metastatic (22%)compared to non-metastatic cases (40%). Further genetic investi-gations of sporadic patients with recurrent and/or metastatictumours could help to identify novel disease causing genes
Ta
ble
2.
Co
nt.
Pa
tie
nt
no
.D
iag
no
sis
Ge
nd
er
Ag
ea
td
iag
no
sis
He
red
ita
ryS
yn
dro
me
crit
eri
aS
ize
(mm
)U
nil
ate
ral/
mu
ltip
leR
ecu
rre
nt
Me
tast
ati
cG
en
eE
xo
nS
om
ati
c/G
erm
lin
ecD
NA
Am
ino
aci
dsu
bst
itu
tio
nC
on
clu
de
dP
ath
og
en
icit
y
36TA
PG
LM
282
220
Un
i2
2V
HL
3G
erm
line
c.54
8C.
Tp
.Ser
183L
euU
nkn
ow
n
37P
CC
F27
22
50U
ni
22
RET
13G
erm
line
c.23
72A
.T
p.T
yr79
1Ph
eU
nkn
ow
n
PC
C;P
heo
chro
mo
cyto
ma,
TAP
GL;
Tho
raco
abd
om
inal
Par
agan
glio
ma,
NA
;No
tA
vaila
ble
,F;F
emal
e,M
;Mal
e,M
EN2;
Mu
ltip
leEn
do
crin
eN
eop
lasi
aty
pe
2,P
GL4
;Fam
ilial
Par
agan
glio
ma
typ
e4,
VH
L;V
on
Hip
pel
Lin
dau
,Un
i;U
nila
tera
lo
rfo
cal
tum
ou
rle
sio
n.
do
i:10.
1371
/jo
urn
al.p
on
e.00
8675
6.t0
02
Genotype Phenotype Correlations in PCC and PGL
PLOS ONE | www.plosone.org 7 January 2014 | Volume 9 | Issue 1 | e86756

associated with a high risk of recurrence. Genetic prognosticmarkers could potentially be of value in a clinical context in orderto personalize the extent of follow up [5,45]. Planned studiesaiming at identifying factors that might predict recurrent diseasewould favourably include tumour genotype characterization.
Tumour Genotype in Clinical ManagementThere is a growing rationale for analysing somatic events in
PCC and PGL tumours as a diagnostic test: (1) EPAS1 mutationsmay occur early in embryogenesis and these mosaic carriers arenot found by analysis of DNA in peripheral blood [16,46]; (2)Translational studies have suggested using genotype as predictive
markers for sensitivity to targeted therapy; SDHx/VHL mutationsmight benefit from antiangiogenic treatment whereas RET/NF1/TMEM127/MAX driven tumours could benefit from inhibitions ofkinase pathways [47,48]. The present study further suggests thattumour genotype might have additional prognostic implications.Even though methods for using formalin fixed archived tissue areevolving rapidly, analysis of tumour DNA is favourably performedusing high quality fresh frozen genetic material thus discussionsregarding the current routines, archiving only formalin fixedtissue, are warranted.
Figure 2. Detected copy number events from SNP array as displayed by Nexus copy number 7.0. Results are separated by chromosomeand presented for each individual tumour with patient id at the left margin. Presented data constitute cases harbouring pathogenic genetic variantsin VHL (n = 11) as well as patients with clinical criteria of NF1 (n = 3). Data is also presented for patient 36 that harboured a VHL mutation of unknownsignificance. Colour annotation indicates copy number loss (red), copy number gain (blue), loss of heterozygosity (yellow) and allelic imbalance(magenta). Arrows indicates VHL (chromosome 3) and NF1 (chromosome 17) loci. Loss of heterozygosity at VHL locus was detected in 11/11 tumourswith pathogenic VHL mutations and in 3/3 tumours from patients with clinical criteria of NF1.doi:10.1371/journal.pone.0086756.g002
Table 3. Copy number variation and loss of heterozygosity by SNP array.
Copy number variation Loss of heterozogozity
Patient no. GeneAmino acidsubstitution Chromosome Start position End position Start position End position
Nexus 7.0Quality score
3 VHL p.Glu55_Arg64del 3 Not detected 1 194000000 0,018
4 VHL p.Ser65Thr 3 1 85000000 1 194000000 0,046
5 VHL p.Ser65Ala 3 1 194000000 1 194000000 0,016
6 VHL p.Ser80Gly 3 1 85000000 1 85000000 0,017
7 VHL p.Leu153Gln 3 1 120000000 1 120000000 0,074
8 VHL p.Lys159Glu 3 1 194000000 1 194000000 0,028
9 VHL p.Arg161Gln 3 Not detected 1 194000000 0,024
10 VHL p.Arg167Trp 3 1 87000000 1 87000000 0,022
11 VHL p.Arg167Trp 3 1 194000000 1 194000000 0,025
12 VHL p.Arg167Trp 3 1 194000000 1 194000000 0,033
13 VHL p.Leu184His 3 9000000 13000000 1 194000000 0,022
36 VHL p.Ser183Leu 3 1 81000000 1 81000000 0,027
38 NF1 NA 17 1 39000000 1 39000000 0,026
39 NF1 NA 17 25000000 43000000 25000000 43000000 0,03
40 NF1 NA 17 Not detected 1 81000000 0,046
Tumours with loss of heterozygosity at loci of mutated tumour suppressor. Patients with diagnostic criteria of NF1 were considered as potential carriers of a pathogenicvariant in the NF1 gene. NA, Not Available.doi:10.1371/journal.pone.0086756.t003
Genotype Phenotype Correlations in PCC and PGL
PLOS ONE | www.plosone.org 8 January 2014 | Volume 9 | Issue 1 | e86756

Ta
ble
4.
Clin
ical
char
acte
rist
ics
and
gen
oty
pe.
No
dis
cov
ere
dm
uta
tio
ns
(n=
52
)
Clu
ste
r1
SDH
x/V
HL/
EPA
S1(n
=15
)C
lust
er
2R
ET/N
F1/H
-RA
S(n
=22
)C
lust
er
1a
nd
no
mu
tati
on
Clu
ste
r2
an
dn
om
uta
tio
nC
lust
er
1a
nd
Clu
ste
r2
Ra
ng
eR
an
ge
P
Med
ian
age,
year
s53
22–8
547
15–8
145
18–7
60.
0891
0.03
610.
6991
Gen
der
,M
ale/
Fem
ale
19/3
25/
1011
/11
0.78
111
0.31
011
0.31
511
Tum
ou
rsp
ecifi
cati
on
s
Med
ian
size
,m
m60
20–1
4040
8–10
051
15–1
700.
0861
0.21
310.
6581
Loca
lizat
ion
,le
ftad
ren
al/r
igh
tad
ren
al22
/21
1/8
8/8
0.02
811
0.93
711
0.05
211
Ad
ren
al/e
xtra
adre
nal
tum
ou
r47
/512
/321
/10.
2751
10.
4651
10.
1371
1
Mu
ltifo
cal
tum
ou
rs1
45
,0.
0011
10.
0041
10.
6931
1
Bio
chem
istr
y
Med
ian
Uri
ne
No
rep
inep
hri
ne,
nm
ol/
24h
2181
,523
0–19
130
2439
495–
1424
486
211
2–51
890.
9601
0.01
810.
031
Med
ian
Uri
ne
Epin
eph
rin
e,n
mo
l/24
h24
719
–333
2258
25–9
652
039
–116
640.
0021
0.23
21,
0.00
11
Med
ian
Pla
sma
No
rmet
anep
hri
ne,
nm
ol/
L7,
14–
1619
,32–
371,
51–
341.
010.
0761
0.32
71
Med
ian
Pla
sma
Met
aep
inep
hri
ne,
nm
ol/
L1,
650–
340,
250,
250,
70–
140
0.30
410.
9141
0.07
31
Rec
urr
ent
dis
ease
82
30.
6891
10.
7231
10.
9251
1
Met
asta
tic
dis
ease
70
20.
1331
10.
5991
10.
2301
1
Stat
isti
cal
anal
ysis
of
corr
elat
ion
bet
wee
ncl
inic
alch
arac
teri
stic
san
dg
eno
typ
e.1
Man
n-W
hit
ney
UTe
st,11
Ch
i-sq
uar
ete
st,
*P
atie
nts
wit
hcl
inic
alcr
iter
iao
fN
F1d
efin
edas
hav
ing
ger
mlin
eca
rrie
rst
atu
s.d
oi:1
0.13
71/j
ou
rnal
.po
ne.
0086
756.
t004
Genotype Phenotype Correlations in PCC and PGL
PLOS ONE | www.plosone.org 9 January 2014 | Volume 9 | Issue 1 | e86756

Conclusion
Somatic mutations are frequent events in PCC and PGLtumours. In patients with somatic carrier status there were nocases of recurrent nor metastatic disease. These findings suggestthat analysis of tumour DNA could have an impact on themanagement of PCC and PGL patients and should be furtherinvestigated as prognostic factors in these diseases.
Acknowledgments
We thank Prof. Gunnar Westin for generously sharing research facilitiesand express our gratitude to Mrs. Birgitta Bondesson and Mr. Johan
Tegerup for their excellent technical assistance. Bodil Svennblad andJohan Lindback at Uppsala Clinical Research Center (http://www.ucr.uu.se/) contributed excellent statistical support.
Author Contributions
Conceived and designed the experiments: JC PB. Performed theexperiments: JC MN RM. Analyzed the data: JC MN PB. Contributedreagents/materials/analysis tools: MN DG PS PH PB. Wrote the paper:JC PB.
References
1. Mannelli M, Castellano M, Schiavi F, Filetti S, Giacche M, et al. (2009)Clinically guided genetic screening in a large cohort of italian patients withpheochromocytomas and/or functional or nonfunctional paragangliomas. J ClinEndocrinol Metab 94: 1541–1547.
2. Amar L, Servais A, Gimenez-Roqueplo AP, Zinzindohoue F, Chatellier G, et al.(2005) Year of diagnosis, features at presentation, and risk of recurrence inpatients with pheochromocytoma or secreting paraganglioma. J Clin EndocrinolMetab 90: 2110–2116. Epub 2005 Jan 2111.
3. Darr R, Lenders JW, Hofbauer LC, Naumann B, Bornstein SR, et al. (2012)Pheochromocytoma - update on disease management. Ther Adv EndocrinolMetab 3: 11–26. doi: 10.1177/2042018812437356.
4. Scott HW, Jr., Halter SA (1984) Oncologic aspects of pheochromocytoma: theimportance of follow-up. Surgery 96: 1061–1066.
5. Van Slycke S, Caiazzo R, Pigny P, Cardot-Bauters C, Arnalsteen L, et al. (2009)Local-regional recurrence of sporadic or syndromic abdominal extra-adrenalparaganglioma: incidence, characteristics, and outcome. Surgery 146: 986–992.doi: 910.1016/j.surg.2009.1010.1055.
6. Agarwal A, Mehrotra PK, Jain M, Gupta SK, Mishra A, et al. (2010) Size of thetumor and pheochromocytoma of the adrenal gland scaled score (PASS): canthey predict malignancy? World J Surg 34: 3022–3028. doi: 3010.1007/s00268-00010-00744-00265.
7. Thompson LD (2002) Pheochromocytoma of the Adrenal gland Scaled Score(PASS) to separate benign from malignant neoplasms: a clinicopathologic andimmunophenotypic study of 100 cases. Am J Surg Pathol 26: 551–566.
8. Burnichon N, Vescovo L, Amar L, Libe R, de Reynies A, et al. (2011)Integrative genomic analysis reveals somatic mutations in pheochromocytomaand paraganglioma. Hum Mol Genet 20: 3974–3985.
9. Baysal BE, Ferrell RE, Willett-Brozick JE, Lawrence EC, Myssiorek D, et al.(2000) Mutations in SDHD, a mitochondrial complex II gene, in hereditaryparaganglioma. Science 287: 848–851.
10. Hao HX, Khalimonchuk O, Schraders M, Dephoure N, Bayley JP, et al. (2009)SDH5, a gene required for flavination of succinate dehydrogenase, is mutated inparaganglioma. Science 325: 1139–1142. Epub 2009 Jul 1123.
11. Qin Y, Yao L, King EE, Buddavarapu K, Lenci RE, et al. (2010) Germlinemutations in TMEM127 confer susceptibility to pheochromocytoma. Nat Genet42: 229–233. Epub 2010 Feb 2014.
12. Comino-Mendez I, Gracia-Aznarez FJ, Schiavi F, Landa I, Leandro-Garcia LJ,et al. (2011) Exome sequencing identifies MAX mutations as a cause ofhereditary pheochromocytoma. Nat Genet 43: 663–667.
13. Astuti D, Latif F, Dallol A, Dahia PL, Douglas F, et al. (2001) Gene mutations inthe succinate dehydrogenase subunit SDHB cause susceptibility to familial
pheochromocytoma and to familial paraganglioma. Am J Hum Genet 69: 49–54. Epub 2001 Jun 2012.
14. Niemann S, Muller U (2000) Mutations in SDHC cause autosomal dominantparaganglioma, type 3. Nat Genet 26: 268–270.
15. Welander J, Larsson C, Backdahl M, Hareni N, Sivler T, et al. (2012) Integrativegenomics reveals frequent somatic NF1 mutations in sporadic pheochromocy-tomas. Hum Mol Genet 24: 24.
16. Zhuang Z, Yang C, Lorenzo F, Merino M, Fojo T, et al. (2012) Somatic HIF2Again-of-function mutations in paraganglioma with polycythemia. N Engl J Med367: 922–930. doi: 910.1056/NEJMoa1205119.
17. Favier J, Buffet A, Gimenez-Roqueplo AP (2012) HIF2A mutations inparaganglioma with polycythemia. N Engl J Med 367: 2161; author reply2161–2162. doi: 2110.1056/NEJMc1211953#SA1211951.
18. Burnichon N, Buffet A, Parfait B, Letouze E, Laurendeau I, et al. (2012) SomaticNF1 Inactivation is a Frequent Event in Sporadic Pheochromocytoma. HumMol Genet 6: 6.
19. Ladroue C, Carcenac R, Leporrier M, Gad S, Le Hello C, et al. (2008) PHD2mutation and congenital erythrocytosis with paraganglioma. N Engl J Med 359:2685–2692.
20. Crona J, Delgado Verdugo A, Maharjan R, Stalberg P, Granberg D, et al.(2013) Somatic Mutations in H-RAS in Sporadic Pheochromocytoma andParaganglioma Identified by Exome Sequencing. Journal of Clinical Endocri-nology & Metabolism.
21. Amar L, Baudin E, Burnichon N, Peyrard S, Silvera S, et al. (2007) Succinatedehydrogenase B gene mutations predict survival in patients with malignantpheochromocytomas or paragangliomas. J Clin Endocrinol Metab 92: 3822–3828. Epub 2007 Jul 3824.
22. Buffet A, Venisse A, Nau V, Roncellin I, Boccio V, et al. (2012) A Decade(2001–2010) of Genetic Testing for Pheochromocytoma and Paraganglioma.Horm Metab Res 19: 19.
23. Weber A, Hoffmann MM, Neumann HP, Erlic Z (2012) Somatic MutationAnalysis of the SDHB, SDHC, SDHD, and RET Genes in the ClinicalAssessment of Sporadic and Hereditary Pheochromocytoma. Horm Cancer 3:187–192. Epub 2012 May 2010.
24. Crona J, Maharjan R, Delgado Verdugo A, Stalberg P, Granberg D, et al.(2013) MAX mutations status in Swedish patients with pheochromocytoma andparaganglioma tumours. Fam Cancer 7: 7.
25. Akerstrom T, Crona J, Delgado Verdugo A, Starker LF, Cupisti K, et al. (2012)Comprehensive re-sequencing of adrenal aldosterone producing lesions revealthree somatic mutations near the KCNJ5 potassium channel selectivity filter.PLoS One 7: e41926. Epub 42012 Jul 41927.
Figures 3. Box plots illustrating preoperative levels of urinary (A) norepinephrine and (B) epinephrine stratified accordingly togenotype clusters.doi:10.1371/journal.pone.0086756.g003
Genotype Phenotype Correlations in PCC and PGL
PLOS ONE | www.plosone.org 10 January 2014 | Volume 9 | Issue 1 | e86756

26. Welander J, Soderkvist P, Gimm O (2011) Genetics and clinical characteristicsof hereditary pheochromocytomas and paragangliomas. Endocr Relat Cancer18: R253–276.
27. Forbes SA, Bindal N, Bamford S, Cole C, Kok CY, et al. (2011) COSMIC:mining complete cancer genomes in the Catalogue of Somatic Mutations inCancer. Nucleic Acids Res 39: D945–950.
28. Stenson PD, Ball EV, Mort M, Phillips AD, Shiel JA, et al. (2003) Human GeneMutation Database (HGMD): 2003 update. Hum Mutat 21: 577–581.
29. Kumar P, Henikoff S, Ng PC (2009) Predicting the effects of coding non-synonymous variants on protein function using the SIFT algorithm. Nat Protoc4: 1073–1081. Epub 2009 Jun 1025.
30. Adzhubei IA, Schmidt S, Peshkin L, Ramensky VE, Gerasimova A, et al. (2010)A method and server for predicting damaging missense mutations. Nat Methods7: 248–249.
31. Arkblad EL, Darin N, Berg K, Kimber E, Brandberg G, et al. (2006) Multiplexligation-dependent probe amplification improves diagnostics in spinal muscularatrophy. Neuromuscul Disord 16: 830–838. Epub 2006 Oct 2017.
32. Banck MS, Kanwar R, Kulkarni AA, Boora GK, Metge F, et al. (2013) Thegenomic landscape of small intestine neuroendocrine tumors. J Clin Invest 15.
33. Neumann HP, Bausch B, McWhinney SR, Bender BU, Gimm O, et al. (2002)Germ-line mutations in nonsyndromic pheochromocytoma. N Engl J Med 346:1459–1466.
34. Yang C, Sun MG, Matro J, Huynh TT, Rahimpour S, et al. (2013) NovelHIF2A mutations disrupt oxygen sensing leading to polycythemia, paragangli-omas and somatostatinomas. Blood.
35. Crona J, Delgado Verdugo A, Granberg D, Welin S, Stalberg P, et al. (2013)Next generation sequencing in genetic screening of pheochromocytoma andparaganglioma. Endocrine Connections.
36. Panizza E, Ercolino T, Mori L, Rapizzi E, Castellano M, et al. (2013) Yeastmodel for evaluating the pathogenic significance of SDHB, SDHC and SDHDmutations in PHEO-PGL syndrome. Hum Mol Genet 22: 804–815. doi:810.1093/hmg/dds1487. Epub 2012 Nov 1021.
37. Bond J, Gale DP, Connor T, Adams S, de Boer J, et al. (2011) Dysregulation ofthe HIF pathway due to VHL mutation causing severe erythrocytosis andpulmonary arterial hypertension. Blood 117: 3699–3701. doi: 3610.1182/blood-2010-3612-327569.
38. Vaclavikova E, Dvorakova S, Sykorova V, Bilek R, Dvorakova K, et al. (2009)RET mutation Tyr791Phe: the genetic cause of different diseases derived fromneural crest. Endocrine 36: 419–424. Epub 2009 Oct 2014.
39. Erlic Z, Hoffmann MM, Sullivan M, Franke G, Peczkowska M, et al. (2010)Pathogenicity of DNA variants and double mutations in multiple endocrineneoplasia type 2 and von Hippel-Lindau syndrome. J Clin Endocrinol Metab 95:308–313. Epub 2009 Nov 2011.
40. Muth A, Abel F, Jansson S, Nilsson O, Ahlman H, et al. (2012) Prevalence ofgermline mutations in patients with pheochromocytoma or abdominalparaganglioma and sporadic presentation: a population-based study in Westernsweden. World J Surg 36: 1389–1394.
41. Comino-Mendez I, de Cubas AA, Bernal C, Alvarez-Escola C, Sanchez-MaloC, et al. (2013) Tumoral EPAS1 (HIF2A) mutations explain sporadicpheochromocytoma and paraganglioma in the absence of erythrocytosis. HumMol Genet 26: 26.
42. Easton DF, Deffenbaugh AM, Pruss D, Frye C, Wenstrup RJ, et al. (2007) Asystematic genetic assessment of 1,433 sequence variants of unknown clinicalsignificance in the BRCA1 and BRCA2 breast cancer-predisposition genes. AmJ Hum Genet 81: 873–883. Epub 2007 Sep 2006.
43. Eisenhofer G, Walther MM, Huynh TT, Li ST, Bornstein SR, et al. (2001)Pheochromocytomas in von Hippel-Lindau syndrome and multiple endocrineneoplasia type 2 display distinct biochemical and clinical phenotypes. J ClinEndocrinol Metab 86: 1999–2008.
44. Leslie EJ, Standley J, Compton J, Bale S, Schutte BC, et al. (2012) Comparativeanalysis of IRF6 variants in families with Van der Woude syndrome andpopliteal pterygium syndrome using public whole-exome databases. Genet Med15: 141.
45. van Heerden JA, Roland CF, Carney JA, Sheps SG, Grant CS (1990) Long-termevaluation following resection of apparently benign pheochromocytoma(s)/paraganglioma(s). World J Surg 14: 325–329.
46. Pacak K, Jochmanova I, Prodanov T, Yang C, Merino MJ, et al. (2013) NewSyndrome of Paraganglioma and Somatostatinoma Associated With Polycythe-mia. J Clin Oncol 18: 18.
47. Wells SA, Jr., Robinson BG, Gagel RF, Dralle H, Fagin JA, et al. (2012)Vandetanib in Patients With Locally Advanced or Metastatic MedullaryThyroid Cancer: A Randomized, Double-Blind Phase III Trial. J Clin Oncol30: 134–141. Epub 2011 Oct 2024.
48. Favier J, Igaz P, Burnichon N, Amar L, Libe R, et al. (2012) Rationale for Anti-angiogenic Therapy in Pheochromocytoma and Paraganglioma. Endocr Pathol23: 34–42.
Genotype Phenotype Correlations in PCC and PGL
PLOS ONE | www.plosone.org 11 January 2014 | Volume 9 | Issue 1 | e86756





















![[Pediatric pheochromocytoma and paraganglioma: an update]](https://img.pdfslide.net/doc/110x75/6335e909a1ced1126c0aff33/pediatric-pheochromocytoma-and-paraganglioma-an-update.jpg)







