Embed Size (px)
Citation preview

Bone Tumour Management
Dr Imran JavedAssociate Professor
SurgeryFiji National University
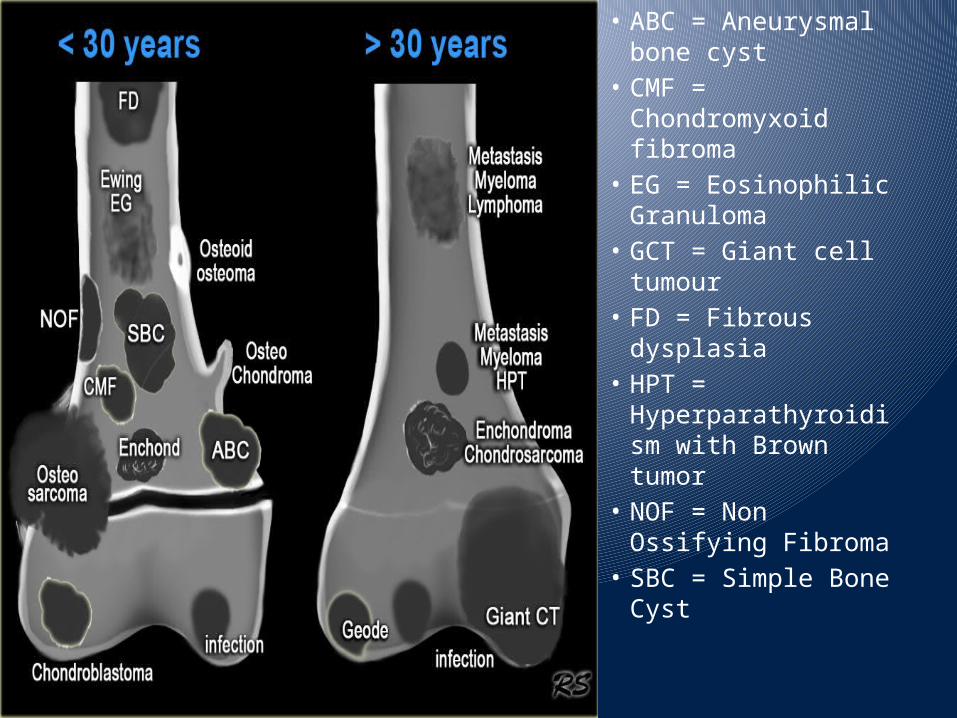
bull ABC = Aneurysmal bone cyst
bull CMF = Chondromyxoid fibroma
bull EG = Eosinophilic Granuloma
bull GCT = Giant cell tumour
bull FD = Fibrous dysplasia
bull HPT = Hyperparathyroidism with Brown tumor
bull NOF = Non Ossifying Fibroma
bull SBC = Simple Bone Cyst
CARTILAGE TUMOURSbull Osteochondroma bull Chondroma
ndash Enchondromandash Periosteal chondroma ndash Multiple chondromatosis
bull Chondroblastoma bull Chondromyxoid fibroma bull Chondrosarcoma
ndash Central primary and secondary ndash Peripheral ndash Dedifferentiated ndash Mesenchymal ndash Clear cell
OSTEOGENIC TUMOURSbull Osteoid osteoma bull Osteoblastoma bull Osteosarcoma
ndash Conventional bullchondroblastic bullfibroblasticbullosteoblastic
ndash Telangiectatic ndash Small cellndash Low grade central ndash Secondary ndash Parosteal ndash Periostealndash High grade surface
Continuedbull FIBROGENIC TUMOURS
ndash Desmoplastic fibroma ndash Fibrosarcoma
bull FIBROHISTIOCYTIC TUMOURSndash Benign fibrous histiocytoma ndash Malignant fibrous histiocytoma
bull EWING SARCOMAPRIMITIVE NEUROECTODERMAL TUMOURndash Ewing sarcoma
bull HAEMATOPOIETIC TUMOURSndash Plasma cell myeloma ndash Malignant lymphoma
Continuedbull GIANT CELL TUMOUR
ndash Giant cell tumour ndash Malignancy in giant cell tumour
bull NOTOCHORDAL TUMOURSndash Chordoma
bull VASCULAR TUMOURSndash Haemangioma ndash Angiosarcoma
bull SMOOTH MUSCLE TUMOURSndash Leiomyoma ndash Leiomyosarcoma
bull LIPOGENIC TUMOURSndash Lipoma ndash Liposarcoma
Continuedbull NEURAL TUMOURS
ndash Neurilemmoma bull MISCELLANEOUS TUMOURS
ndash Adamantinoma ndash Metastatic malignancy
bull MISCELLANEOUS LESIONSndash Aneurysmal bone cystndash Simple cystndash Fibrous dysplasiandash Osteofibrous dysplasiandash Langerhans cell histiocytosis ndash Erdheim-Chester diseasendash Chest wall hamartoma
bull JOINT LESIONSndash Synovial chondromatosis
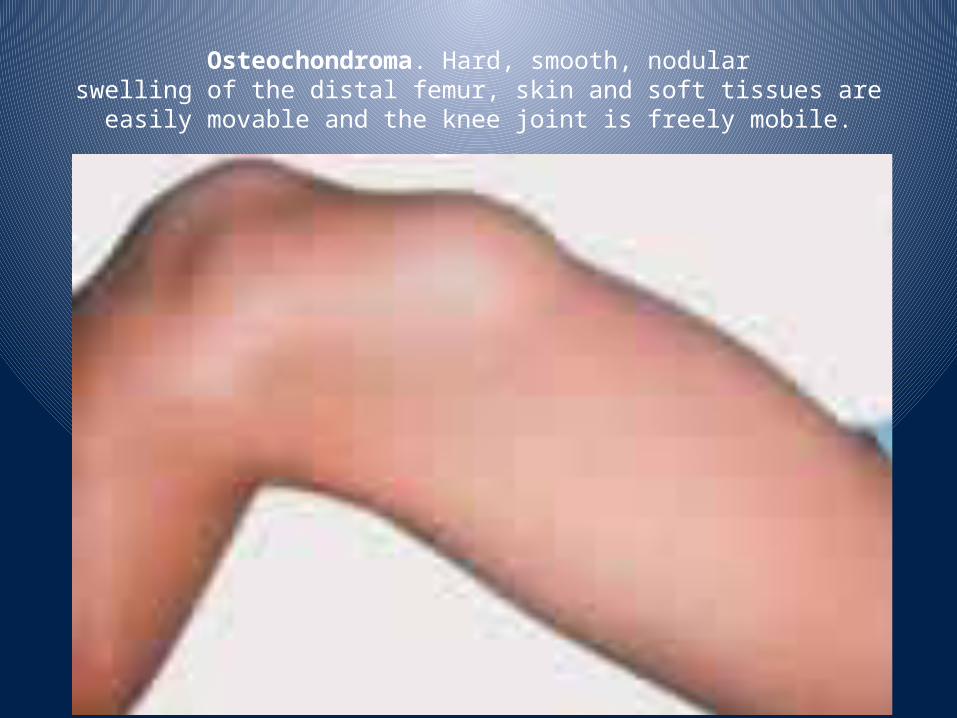
Osteochondroma Hard smooth nodularswelling of the distal femur skin and soft tissues are
easily movable and the knee joint is freely mobile
Osteosarcoma causing swelling in the distalfemur Soft tissues poorly movable consistency
ranging from tough to hard hyperthermia of the skinand marked veins
Ewing sarcoma of the proximal humeruspresenting as tightly elastic tense ulcerated
lesion with shining skin on a grey-white backgroundNote the marked veins and skin striation
The choice of the imaging technique
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
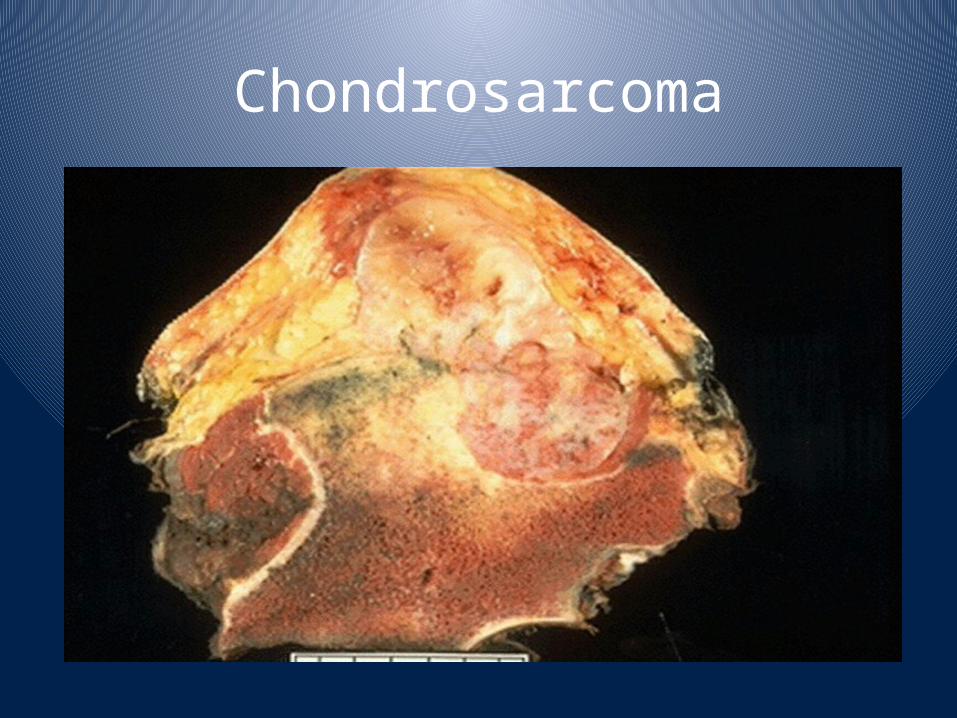
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
bull ABC = Aneurysmal bone cyst
bull CMF = Chondromyxoid fibroma
bull EG = Eosinophilic Granuloma
bull GCT = Giant cell tumour
bull FD = Fibrous dysplasia
bull HPT = Hyperparathyroidism with Brown tumor
bull NOF = Non Ossifying Fibroma
bull SBC = Simple Bone Cyst
CARTILAGE TUMOURSbull Osteochondroma bull Chondroma
ndash Enchondromandash Periosteal chondroma ndash Multiple chondromatosis
bull Chondroblastoma bull Chondromyxoid fibroma bull Chondrosarcoma
ndash Central primary and secondary ndash Peripheral ndash Dedifferentiated ndash Mesenchymal ndash Clear cell
OSTEOGENIC TUMOURSbull Osteoid osteoma bull Osteoblastoma bull Osteosarcoma
ndash Conventional bullchondroblastic bullfibroblasticbullosteoblastic
ndash Telangiectatic ndash Small cellndash Low grade central ndash Secondary ndash Parosteal ndash Periostealndash High grade surface
Continuedbull FIBROGENIC TUMOURS
ndash Desmoplastic fibroma ndash Fibrosarcoma
bull FIBROHISTIOCYTIC TUMOURSndash Benign fibrous histiocytoma ndash Malignant fibrous histiocytoma
bull EWING SARCOMAPRIMITIVE NEUROECTODERMAL TUMOURndash Ewing sarcoma
bull HAEMATOPOIETIC TUMOURSndash Plasma cell myeloma ndash Malignant lymphoma
Continuedbull GIANT CELL TUMOUR
ndash Giant cell tumour ndash Malignancy in giant cell tumour
bull NOTOCHORDAL TUMOURSndash Chordoma
bull VASCULAR TUMOURSndash Haemangioma ndash Angiosarcoma
bull SMOOTH MUSCLE TUMOURSndash Leiomyoma ndash Leiomyosarcoma
bull LIPOGENIC TUMOURSndash Lipoma ndash Liposarcoma
Continuedbull NEURAL TUMOURS
ndash Neurilemmoma bull MISCELLANEOUS TUMOURS
ndash Adamantinoma ndash Metastatic malignancy
bull MISCELLANEOUS LESIONSndash Aneurysmal bone cystndash Simple cystndash Fibrous dysplasiandash Osteofibrous dysplasiandash Langerhans cell histiocytosis ndash Erdheim-Chester diseasendash Chest wall hamartoma
bull JOINT LESIONSndash Synovial chondromatosis
Osteochondroma Hard smooth nodularswelling of the distal femur skin and soft tissues are
easily movable and the knee joint is freely mobile
Osteosarcoma causing swelling in the distalfemur Soft tissues poorly movable consistency
ranging from tough to hard hyperthermia of the skinand marked veins
Ewing sarcoma of the proximal humeruspresenting as tightly elastic tense ulcerated
lesion with shining skin on a grey-white backgroundNote the marked veins and skin striation
The choice of the imaging technique
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
CARTILAGE TUMOURSbull Osteochondroma bull Chondroma
ndash Enchondromandash Periosteal chondroma ndash Multiple chondromatosis
bull Chondroblastoma bull Chondromyxoid fibroma bull Chondrosarcoma
ndash Central primary and secondary ndash Peripheral ndash Dedifferentiated ndash Mesenchymal ndash Clear cell
OSTEOGENIC TUMOURSbull Osteoid osteoma bull Osteoblastoma bull Osteosarcoma
ndash Conventional bullchondroblastic bullfibroblasticbullosteoblastic
ndash Telangiectatic ndash Small cellndash Low grade central ndash Secondary ndash Parosteal ndash Periostealndash High grade surface
Continuedbull FIBROGENIC TUMOURS
ndash Desmoplastic fibroma ndash Fibrosarcoma
bull FIBROHISTIOCYTIC TUMOURSndash Benign fibrous histiocytoma ndash Malignant fibrous histiocytoma
bull EWING SARCOMAPRIMITIVE NEUROECTODERMAL TUMOURndash Ewing sarcoma
bull HAEMATOPOIETIC TUMOURSndash Plasma cell myeloma ndash Malignant lymphoma
Continuedbull GIANT CELL TUMOUR
ndash Giant cell tumour ndash Malignancy in giant cell tumour
bull NOTOCHORDAL TUMOURSndash Chordoma
bull VASCULAR TUMOURSndash Haemangioma ndash Angiosarcoma
bull SMOOTH MUSCLE TUMOURSndash Leiomyoma ndash Leiomyosarcoma
bull LIPOGENIC TUMOURSndash Lipoma ndash Liposarcoma
Continuedbull NEURAL TUMOURS
ndash Neurilemmoma bull MISCELLANEOUS TUMOURS
ndash Adamantinoma ndash Metastatic malignancy
bull MISCELLANEOUS LESIONSndash Aneurysmal bone cystndash Simple cystndash Fibrous dysplasiandash Osteofibrous dysplasiandash Langerhans cell histiocytosis ndash Erdheim-Chester diseasendash Chest wall hamartoma
bull JOINT LESIONSndash Synovial chondromatosis
Osteochondroma Hard smooth nodularswelling of the distal femur skin and soft tissues are
easily movable and the knee joint is freely mobile
Osteosarcoma causing swelling in the distalfemur Soft tissues poorly movable consistency
ranging from tough to hard hyperthermia of the skinand marked veins
Ewing sarcoma of the proximal humeruspresenting as tightly elastic tense ulcerated
lesion with shining skin on a grey-white backgroundNote the marked veins and skin striation
The choice of the imaging technique
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
OSTEOGENIC TUMOURSbull Osteoid osteoma bull Osteoblastoma bull Osteosarcoma
ndash Conventional bullchondroblastic bullfibroblasticbullosteoblastic
ndash Telangiectatic ndash Small cellndash Low grade central ndash Secondary ndash Parosteal ndash Periostealndash High grade surface
Continuedbull FIBROGENIC TUMOURS
ndash Desmoplastic fibroma ndash Fibrosarcoma
bull FIBROHISTIOCYTIC TUMOURSndash Benign fibrous histiocytoma ndash Malignant fibrous histiocytoma
bull EWING SARCOMAPRIMITIVE NEUROECTODERMAL TUMOURndash Ewing sarcoma
bull HAEMATOPOIETIC TUMOURSndash Plasma cell myeloma ndash Malignant lymphoma
Continuedbull GIANT CELL TUMOUR
ndash Giant cell tumour ndash Malignancy in giant cell tumour
bull NOTOCHORDAL TUMOURSndash Chordoma
bull VASCULAR TUMOURSndash Haemangioma ndash Angiosarcoma
bull SMOOTH MUSCLE TUMOURSndash Leiomyoma ndash Leiomyosarcoma
bull LIPOGENIC TUMOURSndash Lipoma ndash Liposarcoma
Continuedbull NEURAL TUMOURS
ndash Neurilemmoma bull MISCELLANEOUS TUMOURS
ndash Adamantinoma ndash Metastatic malignancy
bull MISCELLANEOUS LESIONSndash Aneurysmal bone cystndash Simple cystndash Fibrous dysplasiandash Osteofibrous dysplasiandash Langerhans cell histiocytosis ndash Erdheim-Chester diseasendash Chest wall hamartoma
bull JOINT LESIONSndash Synovial chondromatosis
Osteochondroma Hard smooth nodularswelling of the distal femur skin and soft tissues are
easily movable and the knee joint is freely mobile
Osteosarcoma causing swelling in the distalfemur Soft tissues poorly movable consistency
ranging from tough to hard hyperthermia of the skinand marked veins
Ewing sarcoma of the proximal humeruspresenting as tightly elastic tense ulcerated
lesion with shining skin on a grey-white backgroundNote the marked veins and skin striation
The choice of the imaging technique
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Continuedbull FIBROGENIC TUMOURS
ndash Desmoplastic fibroma ndash Fibrosarcoma
bull FIBROHISTIOCYTIC TUMOURSndash Benign fibrous histiocytoma ndash Malignant fibrous histiocytoma
bull EWING SARCOMAPRIMITIVE NEUROECTODERMAL TUMOURndash Ewing sarcoma
bull HAEMATOPOIETIC TUMOURSndash Plasma cell myeloma ndash Malignant lymphoma
Continuedbull GIANT CELL TUMOUR
ndash Giant cell tumour ndash Malignancy in giant cell tumour
bull NOTOCHORDAL TUMOURSndash Chordoma
bull VASCULAR TUMOURSndash Haemangioma ndash Angiosarcoma
bull SMOOTH MUSCLE TUMOURSndash Leiomyoma ndash Leiomyosarcoma
bull LIPOGENIC TUMOURSndash Lipoma ndash Liposarcoma
Continuedbull NEURAL TUMOURS
ndash Neurilemmoma bull MISCELLANEOUS TUMOURS
ndash Adamantinoma ndash Metastatic malignancy
bull MISCELLANEOUS LESIONSndash Aneurysmal bone cystndash Simple cystndash Fibrous dysplasiandash Osteofibrous dysplasiandash Langerhans cell histiocytosis ndash Erdheim-Chester diseasendash Chest wall hamartoma
bull JOINT LESIONSndash Synovial chondromatosis
Osteochondroma Hard smooth nodularswelling of the distal femur skin and soft tissues are
easily movable and the knee joint is freely mobile
Osteosarcoma causing swelling in the distalfemur Soft tissues poorly movable consistency
ranging from tough to hard hyperthermia of the skinand marked veins
Ewing sarcoma of the proximal humeruspresenting as tightly elastic tense ulcerated
lesion with shining skin on a grey-white backgroundNote the marked veins and skin striation
The choice of the imaging technique
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Continuedbull GIANT CELL TUMOUR
ndash Giant cell tumour ndash Malignancy in giant cell tumour
bull NOTOCHORDAL TUMOURSndash Chordoma
bull VASCULAR TUMOURSndash Haemangioma ndash Angiosarcoma
bull SMOOTH MUSCLE TUMOURSndash Leiomyoma ndash Leiomyosarcoma
bull LIPOGENIC TUMOURSndash Lipoma ndash Liposarcoma
Continuedbull NEURAL TUMOURS
ndash Neurilemmoma bull MISCELLANEOUS TUMOURS
ndash Adamantinoma ndash Metastatic malignancy
bull MISCELLANEOUS LESIONSndash Aneurysmal bone cystndash Simple cystndash Fibrous dysplasiandash Osteofibrous dysplasiandash Langerhans cell histiocytosis ndash Erdheim-Chester diseasendash Chest wall hamartoma
bull JOINT LESIONSndash Synovial chondromatosis
Osteochondroma Hard smooth nodularswelling of the distal femur skin and soft tissues are
easily movable and the knee joint is freely mobile
Osteosarcoma causing swelling in the distalfemur Soft tissues poorly movable consistency
ranging from tough to hard hyperthermia of the skinand marked veins
Ewing sarcoma of the proximal humeruspresenting as tightly elastic tense ulcerated
lesion with shining skin on a grey-white backgroundNote the marked veins and skin striation
The choice of the imaging technique
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Continuedbull NEURAL TUMOURS
ndash Neurilemmoma bull MISCELLANEOUS TUMOURS
ndash Adamantinoma ndash Metastatic malignancy
bull MISCELLANEOUS LESIONSndash Aneurysmal bone cystndash Simple cystndash Fibrous dysplasiandash Osteofibrous dysplasiandash Langerhans cell histiocytosis ndash Erdheim-Chester diseasendash Chest wall hamartoma
bull JOINT LESIONSndash Synovial chondromatosis
Osteochondroma Hard smooth nodularswelling of the distal femur skin and soft tissues are
easily movable and the knee joint is freely mobile
Osteosarcoma causing swelling in the distalfemur Soft tissues poorly movable consistency
ranging from tough to hard hyperthermia of the skinand marked veins
Ewing sarcoma of the proximal humeruspresenting as tightly elastic tense ulcerated
lesion with shining skin on a grey-white backgroundNote the marked veins and skin striation
The choice of the imaging technique
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Osteochondroma Hard smooth nodularswelling of the distal femur skin and soft tissues are
easily movable and the knee joint is freely mobile
Osteosarcoma causing swelling in the distalfemur Soft tissues poorly movable consistency
ranging from tough to hard hyperthermia of the skinand marked veins
Ewing sarcoma of the proximal humeruspresenting as tightly elastic tense ulcerated
lesion with shining skin on a grey-white backgroundNote the marked veins and skin striation
The choice of the imaging technique
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
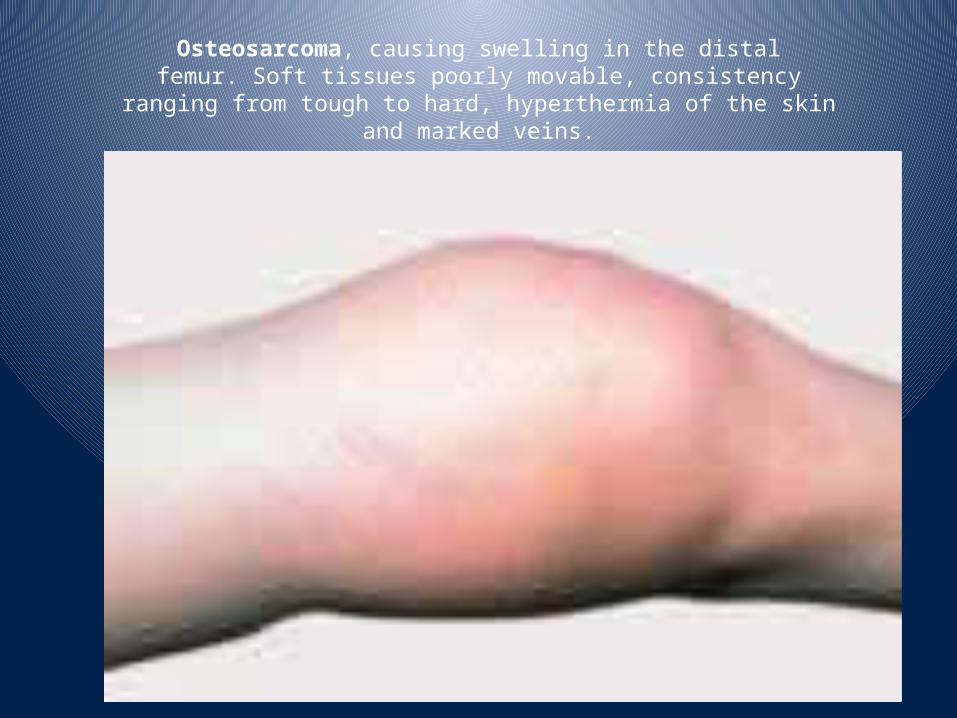
Osteosarcoma causing swelling in the distalfemur Soft tissues poorly movable consistency
ranging from tough to hard hyperthermia of the skinand marked veins
Ewing sarcoma of the proximal humeruspresenting as tightly elastic tense ulcerated
lesion with shining skin on a grey-white backgroundNote the marked veins and skin striation
The choice of the imaging technique
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
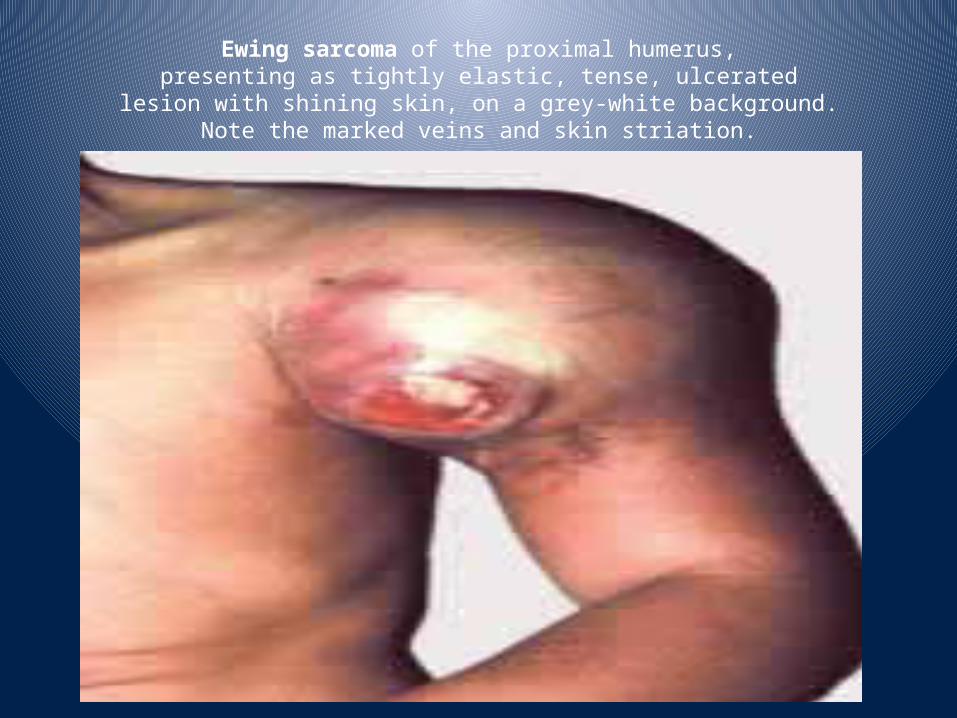
Ewing sarcoma of the proximal humeruspresenting as tightly elastic tense ulcerated
lesion with shining skin on a grey-white backgroundNote the marked veins and skin striation
The choice of the imaging technique
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
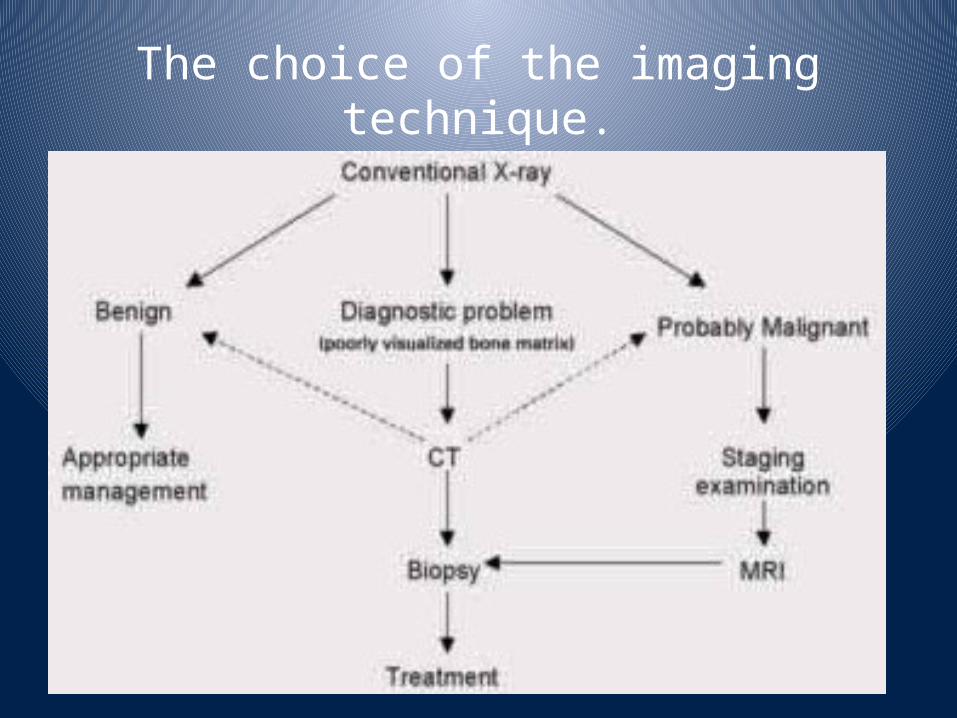
The choice of the imaging technique
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
TNM Classification of bone tumours
bull Primary tumour (T) ndash TX primary tumour cannot be assessedndash T0 no evidence of primary tumourndash T1 tumour 1048617 8 cm in greatest dimensionndash T2 tumour gt 8 cm in greatest dimensionndash T3 discontinuous tumours in the primary bone site
bull Regional lymph nodes (N) ndash NX regional lymph nodes cannot be assessedndash N0 no regional lymph node metastasisndash N1 regional lymph node metastasis
bull Note Regional node involvement is rare and cases in which nodal status is not assessed either
bull clinically or pathologically could be considered N0 instead of NX or pNX
bull Distant metastasis (M) ndash MX distant metastasis cannot be assessedndash M0 no distant metastasisndash M1 distant metastasisndash M1a lungndash M1b other distant sites
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Histopathological Grading
bull Stage IA T1 N0NX M0 Low gradebull Stage IB T2 N0NX M0 Low gradebull Stage IIA T1 N0NX M0 High gradebull Stage IIB T2 N0NX M0 High gradebull Stage III T3 N0NX M0 Any gradebull Stage IVA Any T N0NX M1a Any grade
bull Stage IVB Any T N1 Any M Any gradebull Any T Any N M1b Any grade
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Musculoskeletal Tumour Society staging of malignant
bone lesionsbull Stage Definitionbull III Any grade metastatic
bull IIB High grade extracompartmental
bull IIA High grade intracompartmental
bull IB Low grade extracompartmental
bull IA Low grade intracompartmental
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Musculoskeletal Tumour Society staging Surgical margins
Type Plane of Dissectionbull Intralesional Within lesionbull Marginal Within reactive zone-extracapsular
bull Wide Beyond reactive zone through normal tissue within compartment
bull Radical Normal tissue extracompartmental
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Malignant bone tumorsbull Rarebull 6 of all childhood malignanciesbull Annual US Incidence in children lt 20 yrsbull 87 per million~ 650 to 700 childrenyear
bull For perspective Annual US Incidencebull Overall 4697 per millionbull Lung 610 per millionbull Breast 633 per million
bull Most often occur in young patients lt 25 yrsbull Most common bone tumorsbull Osteosarcoma 56bull Ewing sarcoma34
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Osteosarcoma (OS)bull Primary malignant tumor of bonebull Derived from primitive bone forming mesenchyme
bull Malignant spindle cells produce immature neoplastic bone matrix ndash osteoid
bull Can look heterogeneous under the microscope
bull Cell of origin
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
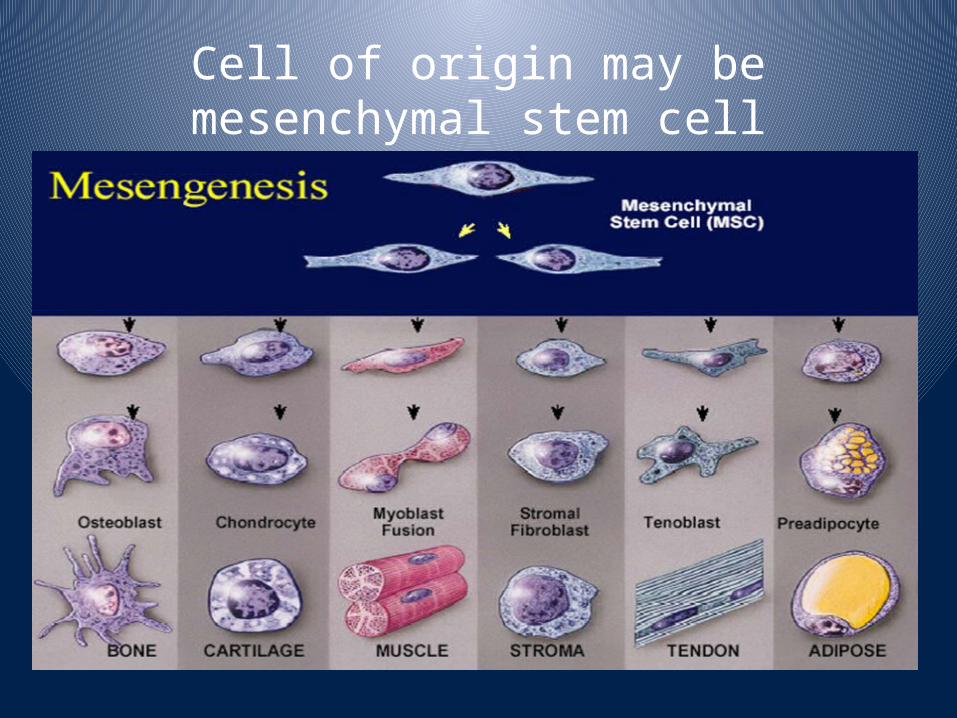
Cell of origin may be mesenchymal stem cell
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Epidemiologybull Most common during 2nd decadebull 75 between 10 and 20 yrsbull Peak during adolescent growth spurt
bull Taller than averagebull Occurs earlier in girlsbull MF 151bull African-AmericanCaucasian 141
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Associations or Risk Factors
bull Ionizing radiationbull Hereditary retinoblastoma (Rb mutations)
bull Li-Fraumeni syndrome (p53 mutations)bull Rothmund-Thomson syndrome
bull No environmental risk factors
bull No consistent cytogenetic abnormality
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Clinical presentationbull Pain dull aching constant worse at night often attributed to trauma
bull Average duration of symptoms prior to diagnosis is three months
bull May or may not have a massbull Diagnosis of pelvic lesions often delayed
bull 20 have detectable metastases at diagnosis ndash most often (gt90) pulmonary
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Age of Tumorsbull 20gthellipOsteogenic Sarcoma Ewings
bull 40helliphellipGCT Chondrosarcoma MFH Lymphoma Mets
bull 60helliphellipMets Myeloma Chondrosarcoma late Osteogenic MFH Fibrosarcoma
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Locationbull Most common in long bonesbull May have altered gait or functionbull 90 are metaphysealbull May cross growth platebull Locationbull 1 distal femurbull 2 proximal tibiabull 3 proximal humerus
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Sites of Tumorsbull Diaphyseal Ewings Osteoid Osteoma Mets Adamantinoma Fibrous Dysplasia
bull Epiphyseal Chondroblastoma Clear Cell Chondrosarcoma GCT Ganglion of Bone
bull Metaphyseal Everything
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Diagnostic Workupbull History and physical examination
bull Laboratory testsndash Blood tests include LDH Alkaline phosphataseAlso CBC liverkidney function tests
bull Pathologyndash Biopsy (open preferred)
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Diagnostic Workupbull Radiologic tests
ndash Plain films of involved bone ndash MRI of entire involved bonendash Whole body Bone Scanndash CXR and CT of Chestndash PET scan
bull Pre-therapy evaluation also includes Audiogram echocardiogram GFRcreatinine clearance
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Radiographic Features of the Various Tumors
bull Benign well circumscribed narrow transition no reaction sclerotic border lsquodoes one thingrsquo
bull Benign Aggressive neocorticalization expansion thinning of cortex usually lytic +-reaction +- narrow zone of transition
bull Malignant ++++reaction large permeative moth eaten lsquodoes more than one thingrsquo
bull ConditionsMets more than one bone symmetry
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
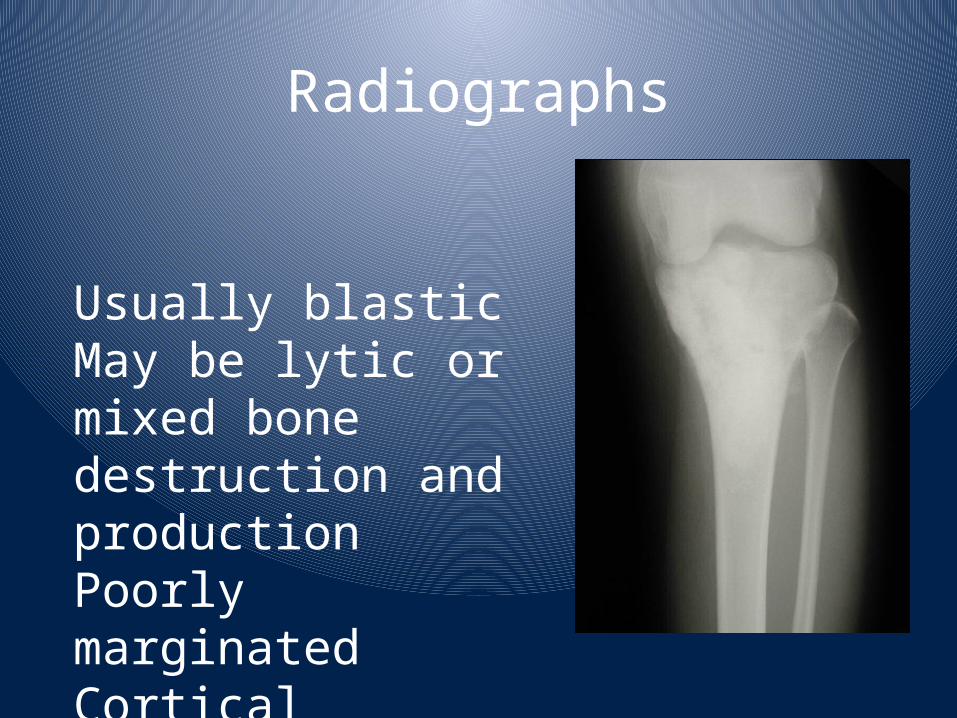
Radiographs
Usually blasticMay be lytic or mixed bone destruction and productionPoorly marginatedCortical destructionSoft tissue ossification
Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases

Osteosarcoma
Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases

Prognostic Factorsbull Tumor Grade amp Histologybull Parosteal favorable telangiectatic unfavorablebull Disease Extentbull metastatic disease unfavorablebull Tumor Size Sitebull axial skeletal primaries unfavorablebull Agebull lt 10 yrs unfavorablebull Response of the primary tumor to pre-operative chemotherapy very powerful predictor
bull gt 80-90 necrosis favorable
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
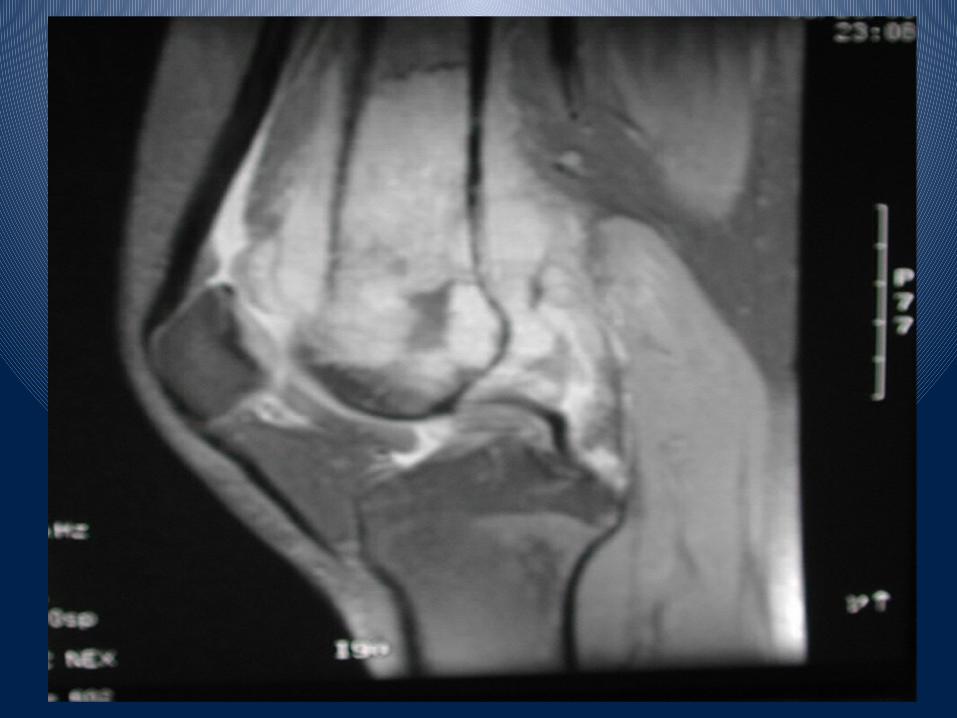
Treatment Multimodalbull Surgery
ndash control of bulk disease
bull Chemotherapyndash control of micrometastases
bull Radiation ndash Tumors not very radiosensitive so this usually reserved for palliation
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
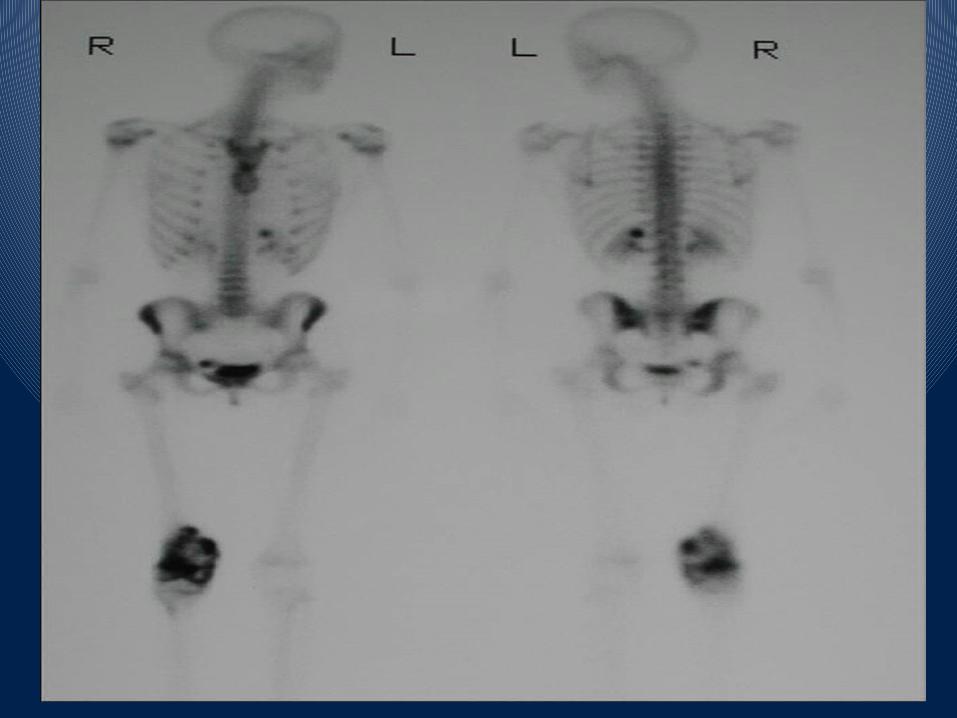
Treatment Surgerybull Removal of all gross tumor with wide (gt5cm) margins en bloc and biopsy site through normal tissue planes is required
bull Type of surgical procedure depends on tumor location size extramedullary extent presence of distant metastatic disease age skeletal development and life-style preference
bull limb-sparingbull amputationbull Metastatic sites must also be resectedbull Ifwhen relapse occurs retrieval therapy must include resection
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Operative Findings
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Resection of Tumour
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Gross Specimen
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
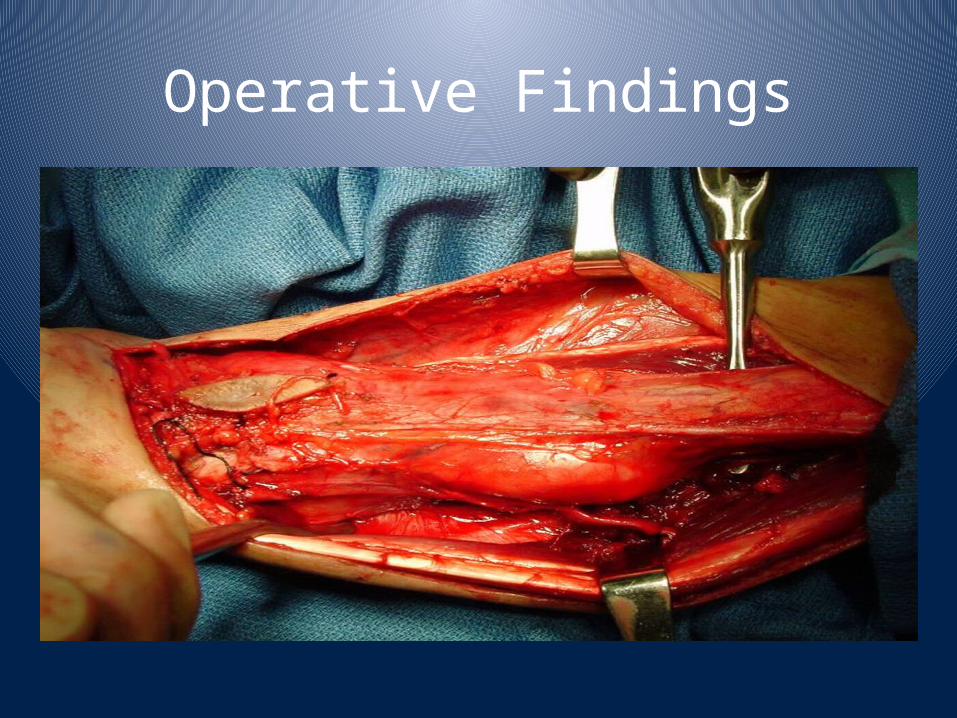
Prosthesis
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
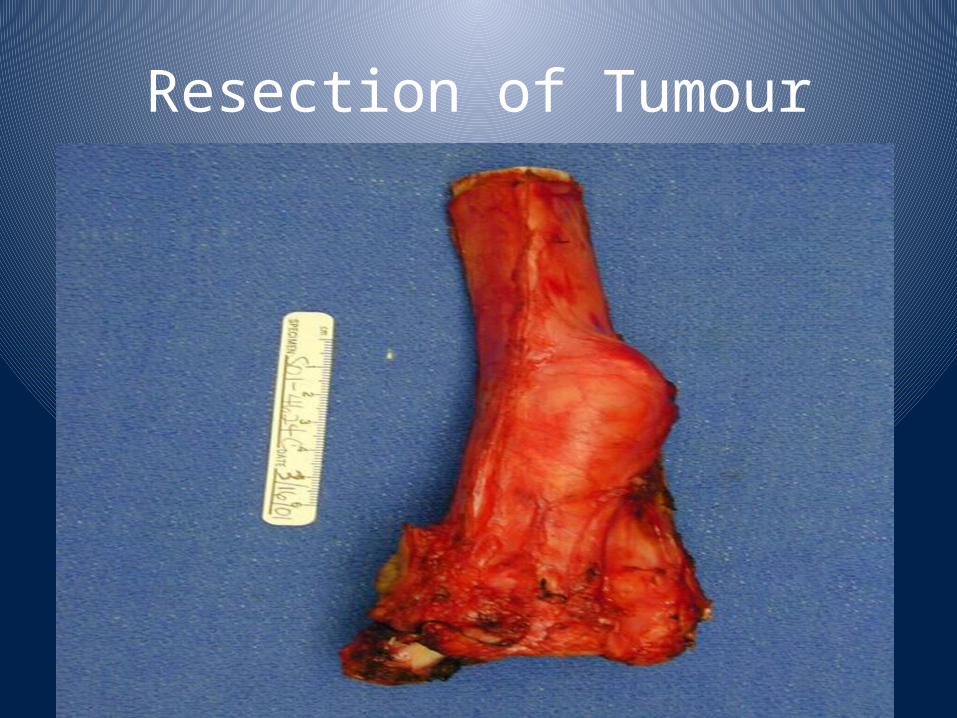
Upper Limb Prosthesis
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
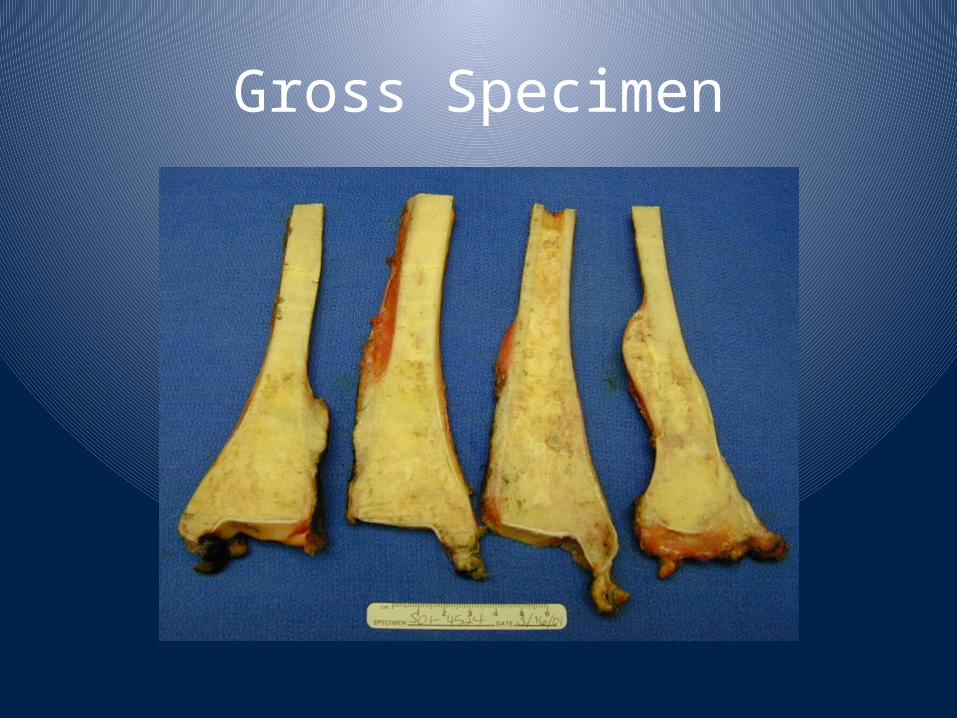
Outcomesbull Surgery alone1048617 15-25 5 year survivalbull Recurrence with local and (50) metastatic disease within 6 months of resection
bull With multiagent chemotherapy 1048617 55-68bull No difference between adjuvant or neoadjuvant chemotherapy
bull Those with gt90 tumor necrosis and complete resection 1048617 80-85
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Treatment Chemotherapybull Bulky disease is considered somewhat chemotherapy resistant
bull Subclinical metastases are sensitive to chemotherapy
bull Most active agents include bull adriamycin cisplatinum high-dose methotrexate ifosfamide etoposide
bull Best and schedule of chemotherapy unclearbull Role of intensification after local control unclear
bull Immune modulators under studybull Role of adjuvant chemotherapy after thoracotomy for recurrent disease unclear
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
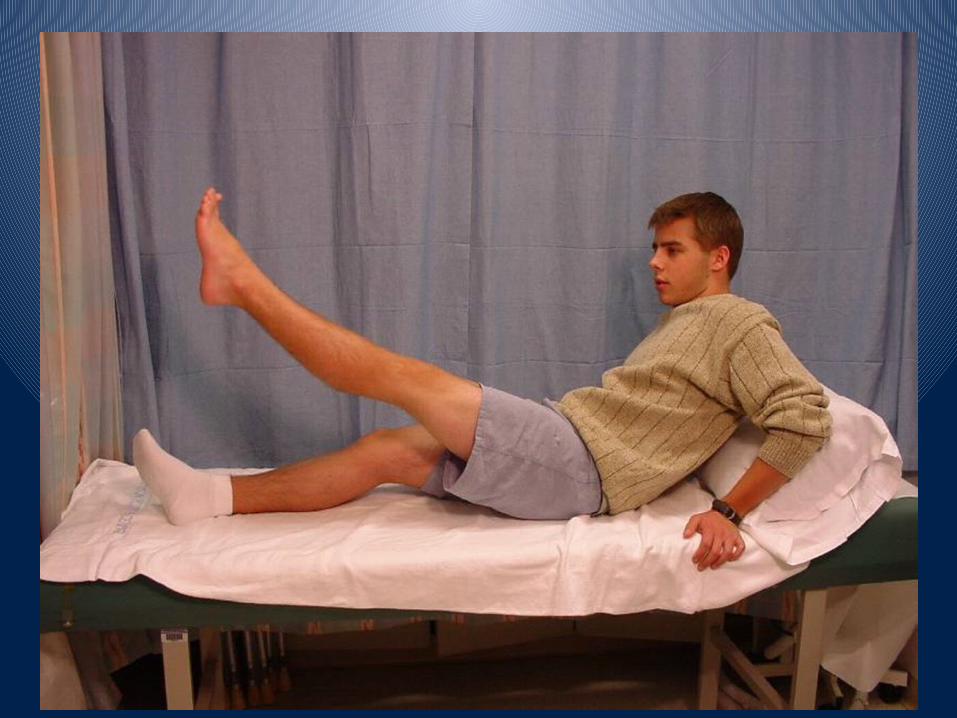
Outcomesbull 60-68 of patients with nonmetastatic osteosarcoma of the extremity will survive without recurrence and be cured
bull 20 of patients with metastatic disease will be cured
bull Therapy with curative intent is possible following relapse 10-20 of these patients may achieve long term survival
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
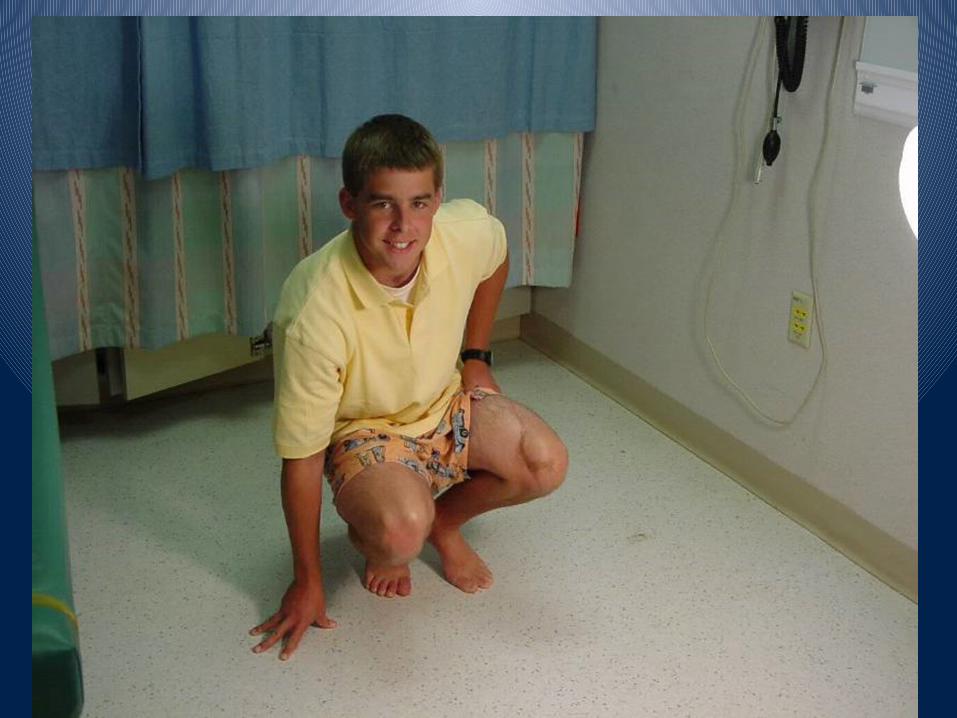
Complications Late effects of Therapy
bull Surgicalndash Functional outcomes of limb salvage vs amputation under study
bull Chemotherapyndash Anthracycline induced cardiomyopathyndash may arise 15+ years after therapyndash Cis-platinum induced ototoxicity and renal toxicity
ndash Ifosfamide induced renal tubular dysfunction
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Ewing Sarcoma (EWS)bull Represents a family of tumors includingndash Ewing sarcoma of bonendash extraosseous Ewing sarcoma and ndash peripheral neuroectodermal tumor (PNET) of bone or soft tissue
bull 2nd most common bone tumor in children
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Ewing Sarcoma
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Chondrosarcomabull Definition
ndash Malignant tumor of chondroblasts
bull Etiologyndash The tumor may arise de novo (primary) or secondary to preexisting enchondroma exostosis (osteochondromas) or Pagetrsquos disease
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Chondrosarcomabull Clinicallybull Malegt femalesbull Age 30-60 yearsbull Enlarged mass with pain and swelling
bull Typically involves the pelvic bones spine and shoulder girdle
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Chondrosarcoma
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Giant cell tumor (Osteoclastoma)
bull Uncommon malignant neoplasm containing mult-inucleated giant cells admixed with stromal cells
bull It is a locally malignant bone tumor with a high rate of recurrence
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
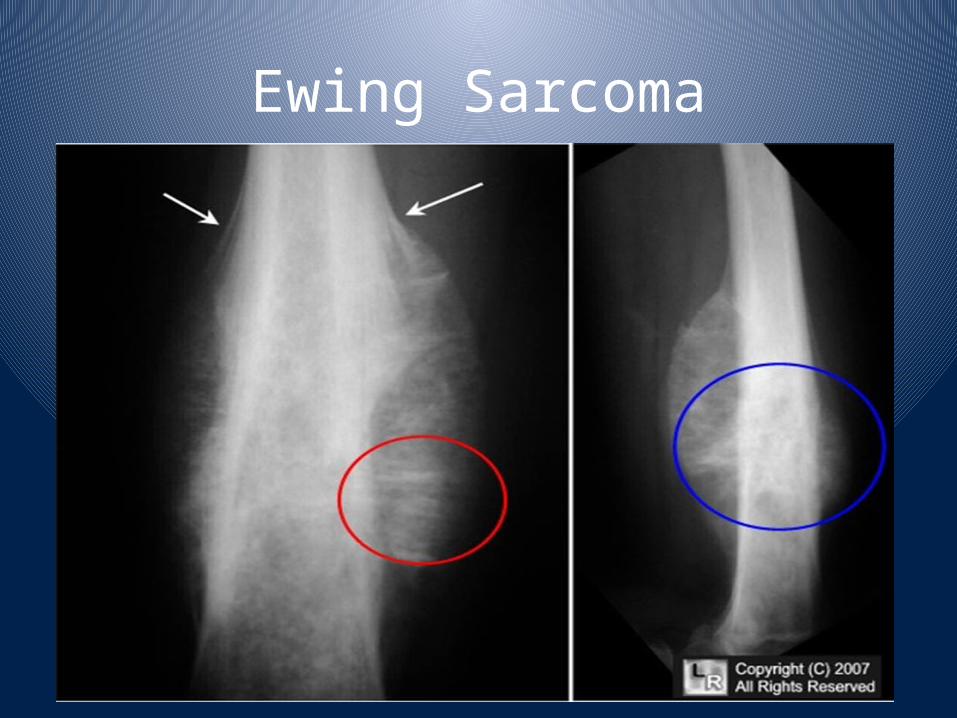
Osteoclastomabull Clinically
ndash Femalesgtmalesndash Age 20-50 yearsndash Bulky mass with pain and fractures
bull X-rayndash Expanding lytic lesion surrounded by a thin rim of bone
ndash It may have a soap-bubble appearance
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Osteoclastoma
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases
Metastatic tumors bull Metastatic tumors are the most common malignant tumor of bone
bull Pathways of spread Blood Lymphatic Direct
bull Origin Thyroid Breast Lungs Kidneys Prostate
bull The radiologic appearance of metastases