Embed Size (px)
Citation preview

European Journal of Cancer (2014) 50, 679–689
A v a i l a b l e a t w w w . s c i e n c e d i r e c t . c o m
ScienceDirect
journa l homepag e : www.e j cancer . com
Review
International expert opinion on patient-tailoredmanagement of soft tissue sarcomas
0959-8049/$ - see front matter � 2013 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.ejca.2013.11.011
⇑ Corresponding author: Address: Universite Claude Bernard, Centre Leon Berard, 28, rue Laennec, 69008 Lyon, France. Tel.: +33 4787E-mail address: [email protected] (J.-Y. Blay).
Jean-Yves Blay a,⇑, Stefan Sleijfer b, Patrick Schoffski c, Akira Kawai d,Thomas Brodowicz e, George D. Demetri f, Robert G. Maki g
a Universite Claude Bernard, Lyon, Franceb Erasmus MC Cancer Institute, Rotterdam, The Netherlandsc University Hospitals Leuven, KU Leuven, Belgiumd National Cancer Center Hospital, Tokyo, Japane Clinical Division of Oncology, Comprehensive Cancer Center – MusculoSkeletal Tumors, Medical University Vienna – General Hospital, Austriaf Center for Sarcoma and Bone Oncology, Dana-Farber Cancer Institute, Boston, MA, USAg Mount Sinai Medical Center, NY, USA
Available online 29 November 2013
KEYWORDS
Soft tissue sarcomaManagementTreatment
Abstract Background: Soft tissue sarcomas (STS) are a heterogeneous group of cancerscomprising over 50 histological subtypes. Current treatment strategies for sarcomas areincreasingly adapted to histological and molecular subtype, and several patient- andtumour-related factors influence treatment decision.Methods: Seven oncologists specialising in the management of STS, from Europe, the UnitedStates of America and Japan, met to develop a practical model to identify parameters guidingtreatment decision-making in advanced STS. Literature searches were carried out to identifykey published evidence, in particular phase II and III randomised trials, to validate the model,and extensive clinical experience was used as expert evidence. A document was developed toprovide a logical approach to advanced STS management and was analysed critically by a sec-ond group of STS specialists.Results: Broad consensus was reached during this exercise and the following parameters wereidentified as key factors influencing treatment decision: chemosensitivity of histological sub-type, natural history of the diagnosis, tumour burden, tumour site, locally advanced primaryand/or metastases, patient’s general condition, relevant comorbidities, previous chemother-apy, treatment goal and patient acceptance. These parameters, judged useful for treatmentselection, were based on published literature, the selection process within clinical trials andexpert opinion (some factors have not been formerly defined in published literature).
82 757.

680 J.-Y. Blay et al. / European Journal of Cancer 50 (2014) 679–689
Conclusion: A model describing factors affecting treatment decisions in sarcoma was estab-lished. The model requires validation and several of its parameters require standardisation.
� 2013 Elsevier Ltd. All rights reserved.
1. Introduction
Soft tissue sarcomas (STS) are a heterogeneous groupof uncommon cancers of mesenchymal origin compris-ing over 50 different major histological subtypes [1–3].Annual incidence in Europe averages five cases per100,000 people [3]. Historically, all STS subtypes havebeen treated similarly, given the lack of defined outcomedifferences for conventional chemotherapy agents suchas doxorubicin, ifosfamide and dacarbazine.
The first evidence of kinase-specific therapy activeagainst specific STS subtypes was provided by studiesof imatinib in gastrointestinal stromal tumours and der-matofibrosarcoma protuberans [4,5]. Other agents havedemonstrated activity subsequently in various STS sub-types [6–13]. Consequently, current treatment strategiesfor sarcomas are increasingly adapted to histologicalsubtype and incorporate both cytotoxic chemotherapyand newer agents.
In addition to histological subtype, many othertumour- and patient-related characteristics affect prog-nosis and should be taken into consideration when tai-loring STS treatment [14–18]. The increasing numberof systemic treatment options available for advanceddisease, the fact that histological classifications andnames continue to change over time and the rarity ofSTS, increase the difficulty of managing patients withadvanced STS.
Recognising the need for greater practical guidance inthe management of advanced STS patients, an expertpanel was convened to develop an evidence- and experi-ence-based, patient-focused model to aid clinicians man-aging the care of patients with advanced STS. We seekto identify the main factors that influence treatmentchoice in advanced STS; an approach that is distinctfrom current STS management guidelines.
This paper represents an initial attempt at developinga model for clinical practice and at gaining agreementon the factors that clinicians must consider when choos-ing a treatment plan for advanced, inoperable STS.
2. Materials and methods
2.1. Expert panel and development of the patient-focused
model
Seven oncologists, specialising and focusing on STSmanagement, planned and attended a meeting todevelop a patient-focused treatment model in advancedSTS. Advanced disease was defined as metastatic and/orinoperable disease, not amenable to curative surgery
and/or radiotherapy. Key factors agreed upon by theexperts are often not validated in existing publisheddata; some represent exclusion criteria in clinical trials(e.g. poor performance status [PS], poor patient accep-tance and relevant comorbidities), whilst other factorsare not standardised (e.g. tumour burden, diseaseaggressiveness).
2.2. Literature review and analysis
Literature searches identified published evidence toinform the model. Given the scarcity of high-quality,randomised, prospective clinical trials, which are usuallythe basis for evidence-based practice guidelines, themodel focuses on extensive clinical experience, whilstdrawing on published evidence where possible.
Electronic searches of Medline and the CochraneLibrary (performed between December 2012 and May2013) identified relevant published evidence involvingfactors influencing prognosis in STS and current STSmanagement guidelines.
2.3. Development, review and validation of consensus
A second meeting was held to create a workable for-mat for the model and to evaluate evidence supportingthe inclusion of selected factors. All members of thepanel contributed to the development of the patient-focused treatment model, review of the literature anddevelopment of the subsequent manuscript. Three fur-ther experts in STS, who did not directly participate inthese planning and discussion meetings, reviewed themanuscript. The final patient-focused treatment modeland accompanying text represent content that all panelmembers agree on.
3. Results
3.1. A patient-focused treatment model
The model is divided into sections representingparameters to consider when deciding on the clinicalapproach and treatment for patients with advancedSTS (Fig. 1). Data obtained from prospective random-ised clinical trials were included as key evidence, wher-ever possible. Given the relative lack of randomiseddata, most evidence was derived from phase II trialsor retrospective analyses. Published evidence for certainparameters included in the model does not exist. Theinclusion of such factors was based on clinical
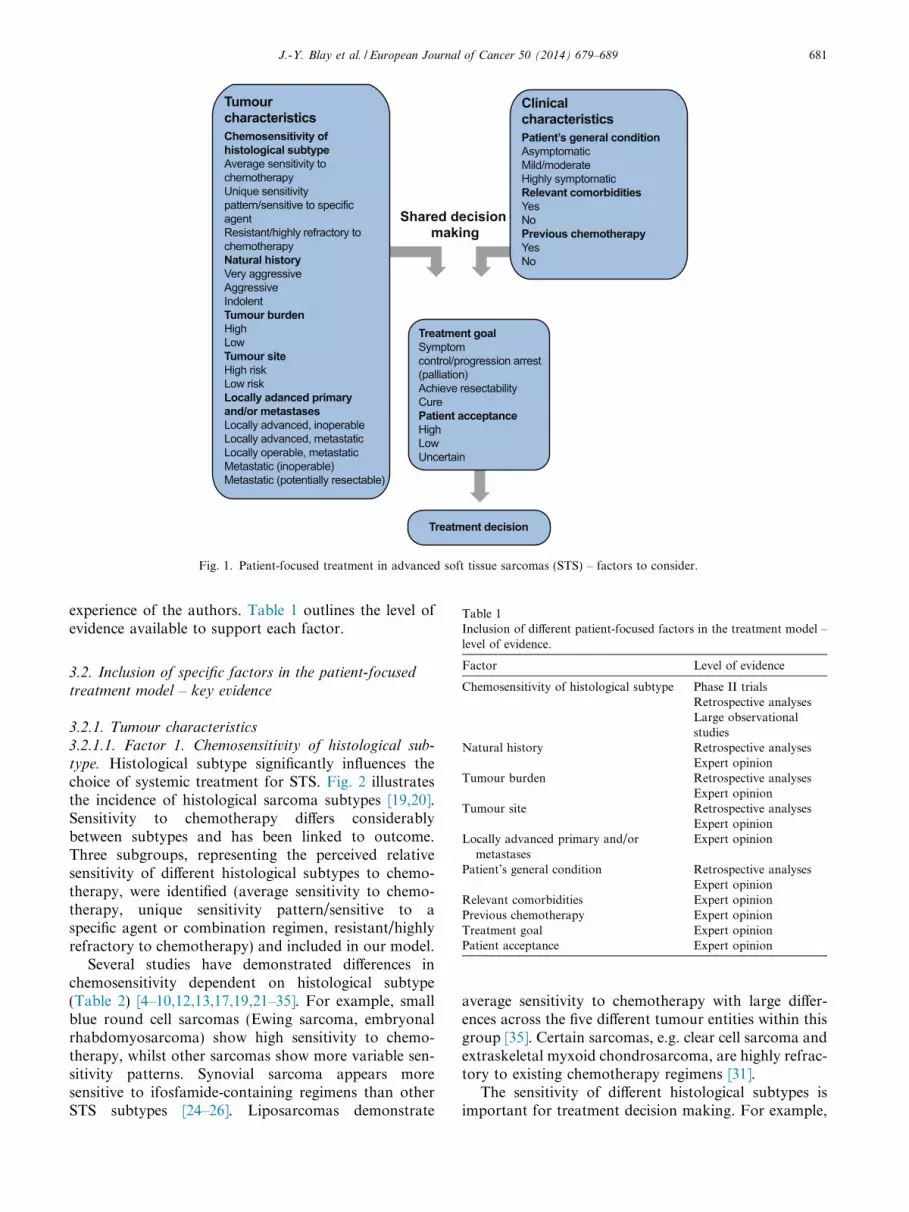
Tumour characteristics
Clinicalcharacteristics
Shared decision making
Treatment goalSymptom control/progression arrest (palliation)Achieve resectabilityCure Patient acceptanceHighLowUncertain
Patient’s general conditionAsymptomaticMild/moderateHighly symptomaticRelevant comorbiditiesYesNoPrevious chemotherapyYesNo
Chemosensitivity of histological subtypeAverage sensitivity to chemotherapyUnique sensitivity pattern/sensitive to specific agentResistant/highly refractory tochemotherapyNatural historyVery aggressiveAggressiveIndolentTumour burdenHighLowTumour siteHigh riskLow riskLocally adanced primaryand/or metastasesLocally advanced, inoperableLocally advanced, metastaticLocally operable, metastaticMetastatic (inoperable)Metastatic (potentially resectable)
Treatment decision
Fig. 1. Patient-focused treatment in advanced soft tissue sarcomas (STS) – factors to consider.
Table 1Inclusion of different patient-focused factors in the treatment model –
J.-Y. Blay et al. / European Journal of Cancer 50 (2014) 679–689 681
experience of the authors. Table 1 outlines the level ofevidence available to support each factor.
level of evidence.
Factor Level of evidence
Chemosensitivity of histological subtype Phase II trialsRetrospective analysesLarge observationalstudies
Natural history Retrospective analysesExpert opinion
Tumour burden Retrospective analysesExpert opinion
Tumour site Retrospective analysesExpert opinion
Locally advanced primary and/ormetastases
Expert opinion
Patient’s general condition Retrospective analysesExpert opinion
Relevant comorbidities Expert opinionPrevious chemotherapy Expert opinionTreatment goal Expert opinionPatient acceptance Expert opinion
3.2. Inclusion of specific factors in the patient-focused
treatment model – key evidence
3.2.1. Tumour characteristics
3.2.1.1. Factor 1. Chemosensitivity of histological sub-
type. Histological subtype significantly influences thechoice of systemic treatment for STS. Fig. 2 illustratesthe incidence of histological sarcoma subtypes [19,20].Sensitivity to chemotherapy differs considerablybetween subtypes and has been linked to outcome.Three subgroups, representing the perceived relativesensitivity of different histological subtypes to chemo-therapy, were identified (average sensitivity to chemo-therapy, unique sensitivity pattern/sensitive to aspecific agent or combination regimen, resistant/highlyrefractory to chemotherapy) and included in our model.
Several studies have demonstrated differences inchemosensitivity dependent on histological subtype(Table 2) [4–10,12,13,17,19,21–35]. For example, smallblue round cell sarcomas (Ewing sarcoma, embryonalrhabdomyosarcoma) show high sensitivity to chemo-therapy, whilst other sarcomas show more variable sen-sitivity patterns. Synovial sarcoma appears moresensitive to ifosfamide-containing regimens than otherSTS subtypes [24–26]. Liposarcomas demonstrate
average sensitivity to chemotherapy with large differ-ences across the five different tumour entities within thisgroup [35]. Certain sarcomas, e.g. clear cell sarcoma andextraskeletal myxoid chondrosarcoma, are highly refrac-tory to existing chemotherapy regimens [31].
The sensitivity of different histological subtypes isimportant for treatment decision making. For example,

18
16
1511
5
4
4
4
33
32
22
1 6
GIST
Unclassified
Liposarcoma
Leiomyosarcoma
DermatofibrosarcomaprotuberansOsteosarcoma
Chondrosarcoma
Ewing sarcoma/PNET
Rhabdomyosarcoma
Kaposi sarcoma
Angiosarcoma
Myxofibrosarcoma
Synovial sarcoma
Endometrial stromal sarcoma
Malignant solitary fibrous tumour
Other
Fig. 2. Crude incidence of histological subtypes of all sarcomas (per 100,000 [%]) [20]. GIST, gastrointestinal stromal tumour; PNET, primitiveneuroectodermal tumour.
682 J.-Y. Blay et al. / European Journal of Cancer 50 (2014) 679–689
cytotoxic chemotherapy may be a reasonable option forpatients with poor PS and pain due to metastases from achemosensitive tumour, whilst for patients with thesame clinical features but a chemoresistant tumour type,pure palliative care measures may be more appropriate.
3.2.1.2. Factor 2. Natural history. Natural history refersto disease aggressiveness (i.e. the expected clinical courseof metastatic STS in a given patient). Natural history isdescribed in our patient-focused model as very aggres-sive, aggressive or indolent. Currently, no reported def-initions for these terms exist. However, we propose thatprogression within 1 month as defined by ResponseEvaluation Criteria in Solid Tumours (RECIST) guide-lines [36] would represent ‘very aggressive’ disease.Aggressive disease could be described as disease thathas progressed or is expected to progress within a shorttime frame (e.g. 3–6 months). Finally, we propose dis-ease that is not expected to meet the criteria for objectiveprogression within 6 months is described as indolent.We recognise that more than one assessment may beneeded to determine the natural history of disease inany individual and that the growth dynamics of tumoursin general, and STS in particular, can change over time.
Many STS subtypes are characterised by an unpre-dictable clinical behaviour and it is well recognised thatthere is a great heterogeneity in tumour aggressiveness,even between tumours belonging to the same histologi-cal subgroup and grade.
Unsurprisingly, rapidly progressive disease is linkedto poor survival in STS [37–39]. For patients with
aggressive tumours, a more intensive treatmentapproach can be considered. In contrast, watchful wait-ing may be an option for patients with indolent tumours.
3.2.1.3. Factor 3. Tumour burden. We describe tumourburden as the total mass of tumour in the body, includ-ing the primary tumour, local relapse and metastaticspread. We have described tumour burden as ‘high’ or‘low’ in our model. There is currently no valid definitionof high or low tumour burden. However, we suggest thathigh tumour burden be defined as cumulative tumourdiameter >10 cm (‘bulky disease’) and/or >10 metasta-ses in various organs.
Greater tumour burden (large tumour size or highnumber of metastatic sites) is linked to poorer prognosisin STS [15,18]. In a retrospective study of 1024 patientswith metastatic STS, the number of affected sites (P2)was an adverse prognostic factor for overall survival(OS) [15]. Furthermore, a trend towards improvedsurvival in patients with locally advanced diseasecompared with metastatic disease in a single organ ormultiple sites was observed in a study of 488 patientswith advanced STS (median survival: 15, 13 and9 months, respectively) [37].
Tools that evaluate tumour burden in a comparative,reproducible manner do not exist currently. Therefore,defining tumour burden remains at the discretion ofthe treating clinician. For patients with a low tumourburden, less intensive intervention may be considered,whilst a more intensive approach might be consideredfor patients with a high tumour burden.

Table 2Soft tissue sarcoma tumour subtype by chemosensitivity.
Average sensitivity to chemotherapya Unique sensitivity pattern/sensitive to specific agent orcombination regimenb
Resistant/highly refractory tochemotherapyc
Leiomyosarcoma [19,32,35] Gastrointestinal stromal tumour (imatinib, sunitinib,regorafenib) [5,12,22]
Clear cell sarcoma [31]Undifferentiated pleomorphic sarcomad [17] Extraskeletal myxoid
chondrosarcoma [31]Myxofibrosarcoma [31] Angiosarcoma (taxane) [6,7] Well-differentiated liposarcoma [31]De-differentiated liposarcoma [19] Myxoid round cell liposarcoma (trabectedin) [8,9,23]Pleomorphic liposarcoma [19] Synovial sarcoma (ifosfamide) [24–26]Malignant peripheral nerve sheath tumour [19] Endometrial stromal sarcoma (aromatase inhibitor
[hormone receptor positive tumours]) [10]Pleomorphic rhabdomyosarcoma [21] Dermatofibrosarcoma protuberans (imatinib) [4]Desmoid tumour/deep fibromatosis [31] Tenosynovial giant cell tumour (imatinib) [27]Intermediate and high-grade fibrosarcoma [19] Solitary fibrous tumour/hemangiopericytoma
(bevacizumab in combination with temozolomide [33];sunitinib [12,34])
Epithelioid sarcoma [19]Unclassified sarcoma not otherwise specifiede
Osteosarcoma of soft tissuee Alveolar soft part sarcoma (sunitinib, cediranib)[13,28]Extraskeletal Ewing sarcoma [29]Alveolar rhabdomyosarcoma [19]Embryonal rhabdomyosarcoma [19]Inflammatory myofibroblastic tumour (crizotinib) [30]Small round blue cell Ewing-like sarcomae
a >20% to <70% non-progression rate at 3 months.b P70% Non-progression rate at 3 months.c620% Non-progression rate at 3 months.
d Formerly malignant fibrous histiocytoma.e No specific published evidence for subtype sensitivity to chemotherapy, expert opinion.
J.-Y. Blay et al. / European Journal of Cancer 50 (2014) 679–689 683
3.2.1.4. Factor 4. Tumour site. Tumour site includes theprimary tumour site and sites of metastases and isdescribed in our model as ‘high risk’ or ‘low risk’.High-risk tumours are those involving certain sites thatcan be anticipated to endanger a patient in the shortterm or are associated with poorer prognosis, e.g. adja-cent to or involving major blood vessels, nerves, medias-tinum, base of the skull, the liver or bone. Lower-risktumours are those located at sites unlikely to be danger-ous to a patient within a short time frame.
Studies have shown that tumour site (specifically siteof metastases) is associated with outcome, independentfrom other prognostic factors. For example, a patientwith liver or bone metastases may have poorer progno-sis, compared with other sites (e.g. lung). In a retrospec-tive study of 2187 patients with advanced STS,significantly fewer patients with liver metastases were5-year survivors compared with other patients (6%versus 21%) [40]. In a large cohort study of patients withadvanced STS, liver metastasis was a significant risk fac-tor for decreased survival [14]. Bone and liver metastasesadversely affected progression-free survival (PFS) in astudy of 1997 patients with advanced STS [16].
Such findings can be applied to populations ofpatients, but are not reliably prognostic on or predictiveon an individual patient basis. Other important factors(including histopathology) may prove more potent thanlocation of disease in impacting the likely clinical out-comes of a patient. Nevertheless, the location of diseaseis a factor to be considered for treatment decisions. For
a patient with an unfavourable location such as liver orbone, symptomatic treatment rather than chemotherapycan be an option. For patients with only lung metasta-ses, but an otherwise similar clinical status, the oppositemay apply. Systemic or local therapy should be initiatedquickly for patients with disease in high-risk sites, whilstfor patients with tumours in lower-risk sites, a moreconservative approach can be chosen.
3.2.1.5. Factor 5. Locally advanced primary and/or
metastases. We categorised clinical status as follows:(1) locally advanced and inoperable; (2) locallyadvanced and metastatic; (3) locally operable and meta-static; (4) metastatic (inoperable) and (5) metastatic(potentially resectable). Palliative surgery for the pri-mary tumour site may be appropriate in patients withlocally operable disease and metastases, especially ifthe primary tumour is symptomatic or located in closeproximity to vital anatomical structures [31]. Surgeryor radiotherapy of metastases may be options dependingon patient symptoms, the sites of disease and number ofmetastases, especially in patients with a good generalcondition and indolent course [3,41]. Long-term survivalrates have been reported in a subset of such patients [42].
3.2.2. Clinical characteristics
3.2.2.1. Factor 6. Patient’s general condition. The generalcondition of a patient significantly influences treatmentchoice. In our model we have divided general conditioninto three categories: highly symptomatic (PS P 2); mild

684 J.-Y. Blay et al. / European Journal of Cancer 50 (2014) 679–689
to moderate (PS 1); and asymptomatic (PS 0). Apatient’s general condition is linked to PS and is influ-enced significantly by comorbidities. However, pub-lished data to validate this factor are limited as manyclinical studies have excluded patients with PS > 1.
In a retrospective study of 2187 patients withadvanced STS, the proportion of patients who werealive at 5 years with an initial PS of 0 was greater com-pared with patients who died within 5 years (63% versus41%) [40]. In a large retrospective cohort study of 3297patients with advanced STS, poorer PS was a significantrisk factor for early death [14]. Good PS was a favour-able prognostic factor and associated with longer PFS
Table 3Contraindications and comorbidities effecting treatment choice in advance
Treatment Contraindication
Licensed treatments
Doxorubicin [44] Overt heart failureSevere hyperbilirubinemia (>�5 mg/dL)
Ifosfamide [46] Severe renal impairment
Dacarbazine [32] Severe renal impairment
Trabectedinb [45] Significant hepatic impairmentCombination with Yellow Fever vaccineConcomitant use with alcoholHepatic impairmentRenal impairment
Pazopanib [43]
Unlicensed treatments
Gemcitabine [47] Thrombocytopenia
Paclitaxelc [48] Insufficient or low platelet count/white bloodcountSerious, uncontrolled infectionSevere hepatic impairment
Docetaxel [49] Insufficient or low white blood cell countSevere hepatic impairment
Aromatase inhibitorsd
[50,51]
a Treatments described here are those most commonly used in advancedb Trabectedin is not licensed in the United States of America but is licenc Paclitaxel is licensed for Acquired Immunodeficiency Syndrome (AIDS
other types of sarcoma [48].d Contraindication dependant on agent used.
in a retrospective analysis of 1997 adults with advancedSTS [16]. The general condition of a patient informshow aggressively STS is treated, e.g. patients with a poorgeneral condition may not tolerate aggressive treatment.
3.2.2.2. Factor 7. Relevant comorbidities. Patient comor-bidities impact treatment choice in STS. Many treat-ments are contraindicated or used with caution incertain comorbidities (e.g. cardiac disease, neurologicaldeficits, poor liver or kidney function). We haveincluded ‘relevant comorbidities – yes or no’ in ourmodel to reflect the influence of comorbidities on treat-ment choice. Table 3 outlines relevant comorbidities
d soft tissue sarcoma.a
Precautionary comorbidity
Decreased cardiac functionPoor bone marrow reserveIncreased bleeding tendencyInfectionElevated serum creatinine/renal impairmentInability to tolerate fluid challengesAge (elderly)Known urothelial injuryDiabetes mellitusInfectionPoor bone marrow reserveNeurological disordersHepatic impairmentPoor bone marrow reservePoor bone marrow reserveAlcohol use (due to hepatotoxicity of product)InfectionCombination with live, attenuated vaccines
Severe hepatic impairmentSevere renal impairmentUncontrolled hypertensionCardiac dysfunctionHistory of bleeding diathesisPre-existing risk of bowel perforationRisk or history of pneumothorax
Impaired hepatic or renal functionYellow Fever vaccine administration (or other live attenuatedvaccines)
cell
Pre-menopauseHistory of fractures or osteoporosisSevere hepatic or renal impairmentPrevious thrombolic event
soft tissue sarcomas (STS).sed in Europe and Asia.)-related Kaposi’s sarcoma only and used off-label in the treatment of

J.-Y. Blay et al. / European Journal of Cancer 50 (2014) 679–689 685
when considering certain agents for the treatment ofadvanced STS [32,43–51]. Again, some of these comor-bidities are exclusion criteria in clinical trials and areincompletely captured in published evidence.
3.2.2.3. Factor 8. Previous chemotherapy. We include‘previous chemotherapy’ in our model, which refers towhether a patient has received prior systemic treatmentfor cancer or are treatment naıve. This factor is impor-tant when considering treatment choice. For example,if a patient has received the maximum cumulative life-time doses of anthracyclines in the adjuvant setting,
Tumour characteristics
Clinicalcharacteristics
Shared decision making
Treatment goalAchieve resectabilityPatient acceptanceHigh
Patient’s general conditionMild/moderateRelevant comorbiditiesNoPrevious chemotherapyNo
Chemosensitivity of histological subtypeAverage sensitivity to chemotherapy (pleiomorphic liposarcoma)Natural historyAggressiveTumour burdenLowTumour siteLow riskLocally advanced primary and/or metastasesPotentially resectable metastases
Treatment decisionAnthracycline and ifosfamide
Tumour characteristics
Clinicalcharacteristics
Shared decision making
Treatment goalSymptom control/ progression arrestPatient acceptanceHigh
Treatment decisionAromatase inhibitor
Patient’s general conditionMild/moderateRelevant comorbiditiesNoPrevious chemotherapyNo
Chemosensitivity of histological subtypeUnique sensitivity pattern/sensitive to specific agent (endometrial stromal sarcoma†)Natural historyIndolentTumour burdenLowTumour siteLow riskLocally advanced primary and/or metastasesMetastatic
a b
c d
Fig. 3. Using the patient-focused model in clinical practice – case study exalicensed in the treatment of advanced soft tissue sarcomas (STS), howevereceptor positive.
treatment with doxorubicin is usually not a viable optionfor metastatic disease. The interval between chemother-apy regimens is also important, as a shorter interval(e.g. <3 months) may be associated with poorer outcome.
3.2.3. Shared decision making
Once the characteristics of the tumour and thepatient’s clinical condition have been determined, thenext step in the decision-making process is to assessthe treatment goal. Shared decision making is extremelyimportant and is highlighted in guidelines on the man-agement of STS [3,41].
Tumour characteristics
Clinicalcharacteristics
Shared decision making
Treatment goalSymptom control / progression arrestPatient acceptanceHigh
Patient’s general conditionMild/moderateRelevant comorbiditiesNoPrevious chemotherapyNo
Chemosensitivity of histological subtypeAverage sensitivity to chemotherapy (pleiomorphic liposarcoma)Natural historyAggressiveTumour burdenLowTumour siteLow riskLocally advanced primaryand/or metastasesLocally advanced, metastatic
Treatment decisionDoxorubicin or doxorubicin/dacarbazine
Tumour characteristics
Clinicalcharacteristics
Shared decision making
Treatment goalSymptom control/ progression arrestPatient acceptanceHigh
Treatment decisionTrabectedin
Patient’s general conditionMild/moderateRelevant comorbiditiesNoPrevious chemotherapyYes – previous anthracycline and ifosfamide
Chemosensitivity of histological subtypeUnique sensitivity pattern/sensitive to specific agent/combination (myxoid round-cell liposarcoma)Natural history AggressiveTumour burdenLowTumour siteLow riskLocally advanced primary and/or metastasesMetastatic
mples*. *Some of the suggestions cite combinations/agents that are notr, these agents are used in clinical practice. �Oestrogen/progesterone

Tumour characteristics
Clinicalcharacteristics
Shared decision making
Treatment goalSymptom control/ progression arrestPatient acceptanceHigh
Treatment decision
Patient’s general conditionHighly symptomaticRelevant comorbiditiesNoPrevious chemotherapyNo
Chemosensitivity of histological subtypeAverage sensitivity to chemotherapy (pleiomorphicliposarcoma)Natural history AggressiveTumour burdenLowTumour siteLow riskLocally advanced primary and/or metastasesMetastatic
Doxorubicin or doxorubicin/dacarbazine
Tumour characteristics
Clinicalcharacteristics
Shared decision making
Treatment goalSymptom control/ progression arrestPatient acceptanceHigh
Treatment decision
Patient’s general conditionMild/moderateRelevant comorbiditiesNoPrevious chemotherapyYes – previous anthracycline and ifosfamide
Chemosensitivity of histological subtypeAverage sensitivity to chemotherapy (synovial sarcoma)Natural history AggressiveTumour burdenLowTumour siteLow riskLocally advanced primary and/or metastasesMetastatic
Pazopanib
e f
Fig 3. (continued)
686 J.-Y. Blay et al. / European Journal of Cancer 50 (2014) 679–689
3.2.3.1. Factor 9. Treatment goal. Appropriate informa-tion on treatment goal is essential for adequate shareddecision making. A study reporting the expectations ofpatients with advanced cancer showed that 69% and81% of patients (with metastatic lung and colorectalcancer, respectively) being treated with palliativechemotherapy did not understand that their treatmentwas not curative [52]. It is likely that numbers will besimilar for patients with advanced STS. In general,palliative care (symptom control or progression arrest[prolongation of disease control]) is the primary intentof treatment for advanced STS. Even minor tumourshrinking can achieve symptom control and the onsetof symptoms can likely be delayed by prolonging diseasestabilisation [31].
We have included: (1) symptom control/progressionarrest (palliative aims); (2) achievement of resectability;and (3) cure, as the three main treatment goals forpatients with advanced STS. Cure is included in themodel as it is essentially the ultimate aim of treatment.However, cure is currently not possible for the greatmajority of patients with advanced STS; in a retrospec-tive analysis of outcomes in patients with advanced STS(n = 2187) median OS was 11.7 months and OS at5 years only 8% [40].
3.2.3.2. Factor 10. Patient acceptance. Some patientsaccept greater levels of toxicities and more aggressivetreatment than others to reach their treatment goal. Thiscan be described as ‘patient acceptance’. Patient accep-tance also includes ‘tolerability’ of patients to disruptionin their lifestyle, which also impacts on the choice oftreatment.
Patient acceptance of risk is described as ‘high’, ‘low’or ‘uncertain’ in our model. The treating clinicianshould carefully address the level of risk and patientpreferences before deciding on any treatment.
3.2.4. Using the patient-focused model in clinical practice
– case study examples
Our patient-focused model can be used to help tailortreatment to individual patients. Fig. 3 demonstrateshow the model can be used in clinical practice to aiddecision making. We present six scenarios, demonstrat-ing how changing different parameters (patient ortumour characteristic) can change treatment decision.
4. Discussion
This is a first attempt to develop a model that identi-fies critical factors affecting treatment choice inadvanced STS, and is aimed at specialists in trainingand non-specialists with an interest in STS. Our objec-tive was to identify and organise key relevant factorsto be considered whilst determining the optimal man-agement of patients with advanced STS. This model isintended to provide a framework to assess patients withSTS and develop an optimal management plan.
The model focuses on the factors that influence treat-ment decisions by physicians routinely treatingadvanced sarcomas. Given the complexity of STS andthe differences in patient presentation, development ofa treatment algorithm detailing all treatment optionsfor all patients would be extremely challenging and iswell beyond the scope of this paper. We suggest that fur-

J.-Y. Blay et al. / European Journal of Cancer 50 (2014) 679–689 687
ther studies could use our model to investigate the extentto which it proves useful.
Where possible, the model is based on publishedevidence. However, robust evidence was often unavail-able and several parameters included in the modelwere based on expert opinion. Several of these param-eters have not been captured in clinical trials becausethey represent exclusion criteria. Other factors, e.g.natural history or tumour burden, are consideredessential for inclusion by this group of experts butlack standardisation. Classification of STS has beensubject to repeated modifications and STS are still fre-quently misclassified or classed as ‘STS not otherwisespecified’. This limits the value of histological subtypeas a prognostic factor. The involvement of an expertpathologist with extensive experience in the field ofSTS is essential to clearly define the specific diagnosisof STS. Further studies are needed relating the mod-ern classification of STS and the factors that influencetreatment decision in this group of tumours, ensuringthat clinicians have robust evidence with which tobase their decisions.
This model differs from current evidence-based orconsensus-based practice guidelines and may not coverall practical situations, as many factors beyond clinicalparameters impact decision-making. Individualisedmedicine is increasingly important in cancer manage-ment, especially in rare cancers such as STS where fewrandomised data are available to guide treatment deci-sions. In these cases clinician and patient rapportbecomes even more critical compared with situationswith well-defined treatment pathways.
This model has the goal to describe factors determin-ing treatment selection by a sarcoma specialist. It isintended to evolve over time and may contribute toguide future clinical research. In the process of creatingthis model, several important scientific questions wereidentified on the factors selected. Further validation ofthe model is needed and the authors welcome furtherresearch on the multiple factors affecting treatmentchoice in advanced STS.
Sources of support
GlaxoSmithKline funded editorial assistance of themanuscript which included collation of comments, edit-ing the manuscript and submission and independentmedical facilitation of the expert meetings.
Role of funding source
GlaxoSmithKline funded editorial assistance of themanuscript which included collation of comments, edit-ing the manuscript and submission and also fundedmedical facilitation of the expert meetings. The aca-demic authors maintained complete control over all con-tent and phrasing in the final manuscript and accept full
responsibility for the content. Neither GlaxoSmithKlinenor any other corporate entity had any editorial inputinto the preparation of the manuscript and at no timedid any employee of GlaxoSmithKline or any other cor-porate entity review the manuscript or provide editorialcomments.
Conflict of interest statement
Jean-Yves Blay: Research support and honorariafrom GlaxoSmithKline, Novartis, Roche, Merck andPharmaMar.
Stefan Sleijfer: Research funding from Glaxo-SmithKline, Roche, Bayer, Pfizer, Novartis andPharmaMar.
Patrick Schoffski: Research funding and honorariafor scientific advisory and educational functions fromGlaxoSmithKline, Roche, Bayer, Pfizer, Novartis andPharmaMar.
Akira Kawai: Research funding from GlaxoSmithK-line, MSD, Eisai and TAIHO.
Thomas Brodowicz: Lecture fees: Amgen, GSK,Novartis and PharmaMar.
George Demetri: Research funding from Bayer,Novartis, Pfizer, GSK, Janssen, PharmaMar and Merck.Consulting stipends for Bayer, Novartis, Pfizer, Sanofi,Janssen, GSK, Merck, Ariad, EMD Serono, FoundationMedicine, ZioPharm, Champions Oncology, Kolltan,Blueprint Medicines. Equity: Kolltan and BlueprintMedicines.
Robert G. Maki: Research funding: Eisai, Ziopharm,Roche and Imclone/Lilly. Consulting fees: Glaxo-SmithKline, Morphotek/Eisai, Imclone/Lilly, Merckand Pfizer. Salary support: Sarcoma Alliance forResearch through Collaboration (SARC). Honoraria:Novartis, Ziopharm.
Acknowledgements
The authors thank the following advisors who re-viewed the manuscript and provided editorial input: PeterReichardt, Alexander Fedenko and Carlos Barrios.
Writing and editing assistance was provided byJoanne Parker of FWG Scientific Communications,with financial support from GlaxoSmithKline. Dr. PaulGandhi of Bridge Medical Consulting, with financialsupport from GlaxoSmithKline, facilitated the expertmeetings.
References
[1] Fletcher CDM, Unni K, Mertens F. World Health Organizationclassification of tumours. Pathology and genetics of tumours ofsoft tissue and bone. Lyon: IARC Press; 2002.
[2] Riedel RF. Systemic therapy for advanced soft tissue sarcomas:highlighting novel therapies and treatment approaches. Cancer2012;118:1474–85.

688 J.-Y. Blay et al. / European Journal of Cancer 50 (2014) 679–689
[3] ESMO/European Sarcoma Network Working Group. Soft tissueand visceral sarcomas: ESMO Clinical Practice Guidelines fordiagnosis, treatment and follow-up. Ann Oncol 2012;23(Suppl.7):vii92–9.
[4] Rutkowski P, Van Glabbeke M, Rankin CJ, et al. Imatinib mesylatein advanced dermatofibrosarcoma protuberans: pooled analysis oftwo phase II clinical trials. J Clin Oncol 2010;28:1772–9.
[5] Demetri GD, von Mehren M, Antonescu CR, et al. NCCN TaskForce report: update on the management of patients withgastrointestinal stromal tumors. J Natl Comp Canc Netw2010;8(Suppl. 2):S1–S41, quiz S42–4.
[6] Penel N, Bui BN, Bay JO, et al. Phase II trial of weekly paclitaxelfor unresectable angiosarcoma: the ANGIOTAX study. J ClinOncol 2008;26:5269–74.
[7] Schlemmer M, Reichardt P, Verweij J, et al. Paclitaxel in patientswith advanced angiosarcomas of soft tissue: a retrospective studyof the EORTC soft tissue and bone sarcoma group. Eur J Cancer2008;44:2433–6.
[8] Garcia-Carbonero R, Supko JG, Maki RG, et al. Ecteinascidin-743 (ET-743) for chemotherapy-naive patients with advanced softtissue sarcomas: multicenter phase II and pharmacokinetic study.J Clinc Oncol 2005;23:5484–92.
[9] Gronchi A, Bui BN, Bonvalot S, et al. Phase II clinical trial ofneoadjuvant trabectedin in patients with advanced localizedmyxoid liposarcoma. Ann Oncol 2012;23:771–6.
[10] Pink D, Lindner T, Mrozek A, Kretzschmar A, Thuss-PatiencePC, Dorken B, et al. Harm or benefit of hormonal treatment inmetastatic low-grade endometrial stromal sarcoma: single centerexperience with 10 cases and review of the literature. GynecolOncol 2006;101:464–9.
[11] Casali PG. Histology- and non-histology-driven therapy fortreatment of soft tissue sarcomas. Ann Oncol 2012;23(Suppl10):x167–9.
[12] George S, Blay JY, Casali PG, Le Cesne A, Stephenson P, DeprimoSE, et al. Clinical evaluation of continuous daily dosing of sunitinibmalate in patients with advanced gastrointestinal stromal tumourafter imatinib failure. Eur J Cancer 2009;45:1959–68.
[13] Stacchiotti S, Tamborini E, Marrari A, et al. Response tosunitinib malate in advanced alveolar soft part sarcoma. ClinCancer Res 2009;15:1096–104.
[14] Penel N, Glabbeke MV, Mathoulin-Pelissier S, et al. Performancestatus is the most powerful risk factor for early death amongpatients with advanced soft tissue sarcoma: the EuropeanOrganisation for Research and Treatment of Cancer-Soft Tissueand Bone Sarcoma Group (STBSG) and French Sarcoma Group(FSG) study. Br J Cancer 2011;104:1544–50.
[15] Italiano A, Mathoulin-Pelissier S, Cesne AL, et al. Trends insurvival for patients with metastatic soft-tissue sarcoma. Cancer2011;117:1049–54.
[16] Sleijfer S, Ouali M, van Glabbeke M, et al. Prognostic andpredictive factors for outcome to first-line ifosfamide-containingchemotherapy for adult patients with advanced soft tissuesarcomas: an exploratory, retrospective analysis on large seriesfrom the European Organization for Research and Treatment ofCancer-Soft Tissue and Bone Sarcoma Group (EORTC-STBSG).Eur J Cancer 2010;46:72–83.
[17] Van Glabbeke M, van Oosterom AT, Oosterhuis JW, et al.Prognostic factors for the outcome of chemotherapy in advancedsoft tissue sarcoma: an analysis of 2,185 patients treated withanthracycline-containing first-line regimens – a European Orga-nization for Research and Treatment of Cancer Soft Tissue andBone Sarcoma Group Study. J Clin Oncol 1999;17:150–7.
[18] Kasper B, Ouali M, van Glabbeke M, et al. Prognostic factors inadolescents and young adults (AYA) with high risk soft tissuesarcoma (STS) treated by adjuvant chemotherapy: A study basedon pooled European Organisation for Research and Treatment ofCancer (EORTC) clinical trials 62771 and 62931. Eur J Cancer2013;49:449–56.
[19] Eriksson M. Histology-driven chemotherapy of soft-tissue sar-coma. Ann Oncol 2010;21(Suppl 7):vii270–6.
[20] Ducimetiere F, Lurkin A, Ranchere-Vince D, et al. Incidence ofsarcoma histotypes and molecular subtypes in a prospectiveepidemiological study with central pathology review and molec-ular testing. PLoS One 2011;6:e20294.
[21] Ferrari A, Dileo P, Casanova M, et al. Rhabdomyosarcoma inadults. A retrospective analysis of 171 patients treated at a singleinstitution. Cancer 2003;98:571–80.
[22] Demetri GD, Reichardt P, Kang YK, et al. Efficacy and safety ofregorafenib for advanced gastrointestinal stromal tumours afterfailure of imatinib and sunitinib (GRID): an international,multicentre, randomised, placebo-controlled, phase 3 trial. Lancet2013;381:295–302.
[23] Garcia-Carbonero R, Supko JG, Manola J, et al. Phase II andpharmacokinetic study of ecteinascidin 743 in patients withprogressive sarcomas of soft tissues refractory to chemotherapy. JClin Oncol 2004;22:1480–90.
[24] Lee SH, Chang MH, Baek KK, et al. High-dose ifosfamide assecond- or third-line chemotherapy in refractory bone and softtissue sarcoma patients. Oncology 2011;80:257–61.
[25] Edmonson JH, Ryan LM, Blum RH, et al. Randomizedcomparison of doxorubicin alone versus ifosfamide plus doxoru-bicin or mitomycin, doxorubicin, and cisplatin against advancedsoft tissue sarcomas. J Clin Oncol 1993;11:1269–75.
[26] Edmonson JH, Ryan LM, Falkson CI, Hicks DG, Blum RH.Phase II study of ifosfamide+doxorubicin in patients withadvanced synovial sarcomas (e1793): a trial of the EasternCooperative Oncology group. Sarcoma 2003;7:9–11.
[27] Cassier PA, Gelderblom H, Stacchiotti S, et al. Efficacy ofimatinib mesylate for the treatment of locally advanced and/ormetastatic tenosynovial giant cell tumor/pigmented villonodularsynovitis. Cancer 2012;118:1649–55.
[28] Kummar S, Allen D, Monks A, et al. Cediranib for metastaticalveolar soft part sarcoma. J Clin Oncol 2013;31:2296–302.
[29] Tural D, Molinas Mandel N, Dervisoglu S. Extraskeletal Ewing’ssarcoma family of tumors in adults: prognostic factors andclinical outcome. Jpn J Clin Oncol 2012;42:420–6.
[30] Butrynski JE, D’Adamo DR, Hornick JL, et al. Crizotinib inALK-rearranged inflammatory myofibroblastic tumor. N Engl JMed 2010;363:1727–33.
[31] Grimer R, Judson I, Peake D, Seddon B. Guidelines for themanagement of soft tissue sarcomas. Sarcoma 2010;2010:506182.
[32] Dacarbazine Summary of Product Characteristics. 2011. Avail-able from: http://www.medicines.org.uk/EMC/medicine/1088/SPC/Dacarbazine+100mg%2c+200mg%2c+500mg%2c+1000mg/.Accessed January 2013.
[33] Park MS, Patel SR, Ludwig JA, et al. Activity of temozolomideand bevacizumab in the treatment of locally advanced, recurrent,and metastatic hemangiopericytoma and malignant solitaryfibrous tumor. Cancer 2011;117:4939–47.
[34] Casali PG, Stacchiotti S, Palassini E, et al. Evaluation of theantitumor activity of sunitinib malate (SM) in solitary fibroustumor (SFT). J Clin Oncol 2009;27:10571.
[35] Italiano A, Toulmonde M, Cioffi A, Penel N, Isambert N,Bompas E, et al. Advanced well-differentiated/dedifferentiatedliposarcomas: role of chemotherapy and survival. Ann Oncol2012;23:1601–7.
[36] Eisenhauer EA, Therasse P, Bogaerts J, et al. New responseevaluation criteria in solid tumours: revised RECIST guideline(version 1.1). Eur J Cancer 2009;45:228–47.
[37] Karavasilis V, Seddon BM, Ashley S, Al-Muderis O, Fisher C,Judson I. Significant clinical benefit of first-line palliative chemo-therapy in advanced soft-tissue sarcoma: retrospective analysisand identification of prognostic factors in 488 patients. Cancer2008;112:1585–91.
[38] Fayette J, Martin E, Piperno-Neumann S, et al. Angiosarcomas, aheterogeneous group of sarcomas with specific behavior depend-

J.-Y. Blay et al. / European Journal of Cancer 50 (2014) 679–689 689
ing on primary site: a retrospective study of 161 cases. Ann Oncol2007;18:2030–6.
[39] Wiklund T, Saeter G, Strander H, Alvegard T, Blomqvist C. Theoutcome of advanced soft tissue sarcoma patients with completetumour regression after either chemotherapy alone or chemo-therapy plus surgery. The Scandinavian Sarcoma Group experi-ence. Eur J Cancer 1997;33:357–61.
[40] Blay JY, van Glabbeke M, Verweij J, et al. Advanced soft-tissuesarcoma: a disease that is potentially curable for a subset ofpatients treated with chemotherapy. Eur J Cancer 2003;39:64–9.
[41] Demetri GD, Antonia S, Benjamin RS, et al. Soft tissue sarcoma.J Natl Comp Cancer Network 2010;8:630–74.
[42] Putnam Jr JB, Roth JA. Surgical treatment for pulmonarymetastases from sarcoma. Hematol Oncol Clin North Am 1995;9:869–87.
[43] Votrient 200 mg and 400 mg film coated tablets. Summary ofproduct characteristics. Available from: http://www.medicines.org.uk/EMC/medicine/23148/SPC/Votrient+200+mg+and+400+mg+film+coated+tablets/. Accessed December 2012.
[44] Doxorubicin 2 mg/ml concentrate for solution for infusion. Sum-mary of product characteristics. Available from: http://www.medicines.org.uk/EMC/medicine/25946/SPC/Doxorubicin+2+mg+ml+Concentrate+for+Solution+for+Infusion/. AccessedDecember 2012.
[45] Yondelis 0.25 mg powder for concentrate for solution forinfusion/Yondelis 1 mg powder for solution for infusion. Avail-able from: http://www.medicines.org.uk/EMC/medicine/20457/SPC/Yondelis+0.25+mg+powder+for+concentrate+for+solution+
for+infusion+Yondelis+1+mg+powder+for+concentrate+for+solution+for+infusion/. Acessed January 2013.
[46] Ifosfamide injection 2 g. Summary of product characteristics.Available from: http://www.ecomm.baxter.com/ecatalog/loadRe-source.do?bid=53536. Accessed December 2012.
[47] EMC. Gemcitabine 100 mg/ml concentrate for solution forinfusion 2012. Available from: http://www.medicines.org.uk/EMC/medicine/27136/SPC/Gemcitabine+100+mg+ml+Concen-trate+for+Solution+for+Infusion/. Accessed December 2012.
[48] EMC. Paclitaxel 6 mg/ml concentrate for solution for infusion2012. Available from: http://www.medicines.org.uk/EMC/medicine/15842/SPC/Paclitaxel+6+mg+ml+concentrate+for+solution+for+infusion/. Accessed December 2012.
[49] EMC. Docetaxel Accord 160 mg/8 ml concentrate for solution forinfusion 2012. Available from: http://www.medicines.org.uk/EMC/medicine/26771/SPC/Docetaxel+Accord+160+mg+8+ml+concentrate+for+solution+for+infusion/. Accessed December2012.
[50] Letrozole 2.5 mg film-coated tablets summary of productcharacteristics. Available from: http://www.medicines.org.uk/emc/medicine/24764/SPC/Letrozole+2.5+mg+film-coated+tablets/.Accessed December 2012.
[51] Anastrozole 1 mg film-coated tablets Available from: http://www.medicines.org.uk/emc/medicine/27391/SPC/Anastrozole+1+mg+film-coated+tablets/. Accessed December 2012.
[52] Weeks JC, Catalano PJ, Cronin A, et al. Patients’ expectationsabout effects of chemotherapy for advanced cancer. N Engl J Med2012;367:1616–25.





























