Embed Size (px)
Citation preview
Restenosis in clinical practice
Modern risk factors and treatment options in patients at increased risk for coronary restenosis after balloon
angioplasty and stenting
B.M. Rahel

Cover St. Tropez – Simone van Doornum Lay-out B.M. Rahel Printed by Grafische Producties Budde – Elinkwijk, Nieuwegein ISBN 90-367-2233-0 © Copyright 2005 B.M. Rahel All rights are reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, mechanically, by photocopying, recording or otherwise, without the written permission of the author.

Rijksuniversiteit Groningen
Restenosis in clinical practice
Modern risk factors and treatment options in patients at increased risk for coronary restenosis
after balloon angioplasty and stenting
Proefschrift
ter verkrijging van het doctoraat in de Medische Wetenschappen
aan de Rijksuniversiteit Groningen op gezag van de
Rector Magnificus, dr. F. Zwarts, in het openbaar te verdedigen op
woensdag 18 mei 2005 des namiddags om 1.15 uur
door
Braim Mohamed Rahel
Geboren op 23 mei 1972 te Kerkrade

Promotor: Prof. dr. F. Zijlstra
Co-promotores: Dr. H.W.M. Plokker Dr. M.J. Suttorp Beoordelingscommissie: Prof. dr. P.W. Boonstra Dr. J.M.P.G. Ernst
Prof. dr. J.J. Piek Prof. dr. N.H.J. Pijls
ISBN 90-367-2233-0

Aan mijn ouders aan Paulien en Nouri

Financial support by the Netherlands Heart Foundation and the Jacques H. de Jong Stichting for the publication of this thesis is gratefully acknowledged. Financial support by the J.E. Jurriaanse Stichting, AstraZeneca BV, Biotronik Nederland BV, Boston Scientific BV, Cordis BV, Guidant BV, Medtronic BV, Menarini Farma Nederland, Merck Sharp & Dohme BV, Novartis Pharma BV, Pfizer BV, sanofi-aventis, Servier BV and
St. Jude Medical BV for the publication of this thesis is gratefully acknowledged.

Contents
CHAPTER 1 CHAPTER 2 CHAPTER 3 CHAPTER 4 CHAPTER 5 CHAPTER 6 CHAPTER 7 CHAPTER 8 CHAPTER 9 CHAPTER 10 CHAPTER 11
Introduction: Coronary Restenosis. Preprocedural serum levels of acute-phase reactants and prognosis after percutaneous coronary intervention. Published in Cardiovascular Research 2003;60:136-140 Pre-procedural ACE-activity does not predict in-stent restenosis. Accepted by the International Journal of Cardiology Cytomegalovirus and Chlamydia pneumoniae as predictors for major adverse clinical events and angina pectoris after percutaneous coronary intervention. Published in the American Heart Journal 2004;148:670-675 Is Direct Stent Implantation Without Predilatation Safe? Acute and Long-Term Outcome. Published in the Journal of Interventional Cardiology 2002;15:263-268 Stenting for Restenotic Lesions with the BARD XT Stent. Published in the Journal of Interventional Cardiology 2003;16:227-230 Cutting Balloon for in-stent restenosis: acute and long-term results. Published in the Journal of Interventional Cardiology 2004;17:197-201 Primary Stenting of Occluded Native Coronary Arteries: Final Results of the PRISON Study. Published in the American Heart Journal 2004;147:e22 Primary Stenting of Occluded Native Coronary Arteries II: Rationale and design of the PRISON II study. Accepted by the American Heart Journal Summary/Samenvatting Dankwoord Curriculum vitae
9 21 33 45 57 69 77 87 99 105 117 121


9
Chapter 1
Introduction: Coronary Restenosis

CHAPTER 1
10
Introduction: Coronary Restenosis History The concept of transluminal angioplasty - enlargement of the lumen of a stenotic vessel by a catheter technique - was first proposed by Dotter and Judkins in 1964 using rigid dilators.1 This technique was modified by Gruentzig, who replaced the rigid dilator with an inflatable balloon resulting in the first percutaneous balloon angioplasty of a stenotic human coronary artery on September 16, 1977. However, the long-term success of this revascularization technique has been limited by restenosis.2,3. To overcome this problem, stents were introduced in the mid 1980’s.4 Two landmark studies, the BENESTENT and STRESS studies5,6, showed that coronary stenting significantly decreases restenosis. Although stenting has improved the results of percutaneous coronary revascularization, it also introduced in-stent restenosis (ISR). The introduction of drug-eluting stents7 meant a further improvement of percutaneous coronary intervention (PCI), possibly preventing restenosis in various subsets of patients.8,9 Pathophysiology: The response to injury Restenosis is the arterial healing response after injury incurred during transluminal coronary revascularization.10 The most widely used definition of restenosis is a diameter stenosis of more than 50%. Clinically significant restenosis generally occurs between one and three months after angioplasty and occurs in 20-50% of patients after balloon angioplasty and in 10-30% of patients receiving a stent. The pathophysiology of restenosis is very complex and has as yet not been fully clarified. Restenosis after ‘plain old balloon angioplasty’ (POBA) is distinct from ISR.11 Restenosis after POBA is thought to involve vessel elastic recoil, negative remodeling and neointima formation.12,13
Remodeling Remodeling can be defined by changes in vessel size. In positive remodeling, the artery expands to accommodate neointima formation. This accommodation totally compensates on a volume-for-volume basis, thus preventing luminal narrowing. When the artery fails to expand or even shrinks, remodeling leads to luminal narrowing.14 Negative remodeling is the result of adventitial thickening and fibrosis after arterial injury, resulting in vessel shrinkage (fig. 1).

CORONARY RESTENOSIS
11
Positive remodeling
Fig. 1 Arterial remodeling after injury.
Negative remodeling
Stenting virtually eliminates vessel elastic recoil and negative remodeling and ISR is mainly the result of neointima formation alone.15,16 Neointima formation Neointima formation has been examined in animal and human coronary arteries. All forms of PCI cause neointima formation (fig.2), which is proportional to the severity of injury and can be divided in 3 stages12,14,17-20: Stage I: Thrombotic phase: days 0-3 The initial response to arterial injury is activation, adhesion, and aggregation of platelets. Within 24 hours, fibrin-rich thrombus accumulates around the platelet site. Stage II: Recruitment phase: days 3-8 The thrombus at arterial injury sites develops an endothelial cell layer. Shortly after the endothelial cells appear, cellular infiltration of mainly monocytes occurs. The monocytes become macrophages as they leave the bloodstream and migrate into the subendothelial mural thrombus. Stage III: Proliferative phase: day 8 to final healing. Smooth muscle cells migrate and proliferate into the degenerated thrombus, increasing neointimal volume. The smooth muscle cells migrate from sites distant to the injury location, and the resorbing thrombus becomes a matrix for neointimal cells.

CHAPTER 1
12
Fig. 2a Fig. 2b Figure 2a/b: Coronary angiography 8 months after stenting of the right coronary artery showing 50% ISR (arrows). Figure 2c: Intravascular ultrasound at the lesion side showing the intimal hyperplasia inside the stent struts (arrows). (Catheterization laboratory, St. Antonius hospital, Nieuwegein, The Netherlands) Fig. 2c Risk factors for restenosis Traditional patient factors
Of the traditional atherosclerotic risk factors, diabetes mellitus is among the most consistent to predict restenosis. In addition to restenosis diabetics, especially insulin-requiring diabetics, have higher rates of myocardial infarction, target vessel revascularization, and death rates after PCI.21-23 Intravascular ultrasound observations have demonstrated that the increased restenosis rate in diabetics is explained by an exaggerated intimal hyperplasia in both stented and nonstented lesions.24 Moreno et al. showed that restenotic tissue in patients with diabetes mellitus has less intimal hypercellular tissue and an increased collagen-rich sclerotic content, suggesting that restenosis in diabetics is an accelerated fibrotic rather than a proliferative response.25 Several biological and metabolic abnormalities confer vulnerability to diabetic individuals, like hyperinsulinemia, increased thrombotic and inflammatory state.26 Coronary stents, especially sirolimus-eluting stents, have improved clinical outcomes of diabetic patients compared with balloon angioplasty.27,28

CORONARY RESTENOSIS
13
Studies on the effect of serum cholesterol levels on the risk of restenosis have been controversial, mainly suggesting that hypercholesterolaemia should not be regarded as an established risk factor for restenosis.29-31 Lowering cholesterol levels with statins did not result in lower rates of restenosis after PCI.32,33 The possible exception is the serum lipoprotein(a) level, which might be regarded as a risk factor for restenosis.34,35
Like plasma glucose and cholesterol levels, the plasma homocysteine level is a predictor of cardiovascular risk and correlates with the severity of coronary artery disease.36-38 Data regarding homocysteine levels and the risk of restenosis after PCI have been conflicting.39-42 Also the effect of vitamin therapy to lower homocysteine levels (folate therapy) is not unambiguous.43,44 Neither smoking nor gender seem to be unequivocal related to restenosis.45-49 In some studies, smoking even was a negative predictor. Several studies indicate that hypertension is a risk factor for restenosis, but again results are contradictory.50-54 Severe or unstable angina however clearly predicts restenosis after PCI.50-
54 ‘Modern’ patient factors The renin-angiotensin system is probably involved in the progress of restenosis as angiotensin II, the effector molecule, is able to induce proliferation of vascular smooth muscle cells via its angiotensin II type 1 receptor.55-57 Although initial studies on the insertion/deletion polymorphism in the gene for angiotensin-converting enzyme (ACE) suggested a relation between the ACE D/D genotype and restenosis58-60, this was not confirmed in larger study populations.61,62 Results of studies which tested the effect of ACE inhibitors on restenosis failed to show a consistent protective effect.63-66 Inflammatory markers, in particular C-reactive protein have shown consistent associations with cardiovascular events in healthy people67,68 and in patients with established coronary heart disease69-71. C-reactive protein might also predict restenosis after PCI.72,73 Micro-organisms are suggested to be related to the development of atherosclerosis. Especially cytomegalovirus (CMV) and Chlamydia pneumoniae (CP) are two potential candidates. Whether restenosis is linked to infection by CMV or CP is under debate.74-80 Angiographic risk factors Studies are clearer about angiographic predictors of restenosis. The most important predictors are48-54,81-89: - Post-procedural mean luminal diameter - Small vessels - Long lesions - Multiple stents - Chronic total occlusions - Bifurcation lesions - Restenotic lesions - Left anterior descending artery - Saphenous vein grafts - Ostial lesions

CHAPTER 1
14
Objectives of this thesis 1. To assess the value of several ‘modern’ risk factors to predict coronary restenosis:
In chapter 2, a study describing the relation between pre-procedural acute-phase reactants and clinical signs of restenosis is presented. Chapter 3 discusses the possible role of angiotensin converting enzyme in the process of in-stent restenosis. In chapter 4 the impact of prior cytomegalovirus and Chlamydia pneumoniae infection on prognosis after PCI is described.
2. To assess the value of various treatment modalities to prevent coronary restenosis:
To test whether less injury will lead to less response (restenosis) the effect of stenting without predilatation is studied. The results are described in chapter 5. In chapter 6 the effect of stenting in restenotic lesions is described. In chapter 7 the results of the ‘cutting balloon’ to treat ISR are presented. In chapter 8 the results of stenting versus POBA in a group of patients with chronic total occlusions (CTO) are described. To compare bare metal stents with sirolimus-eluting stents in CTO a randomized study is started. The trial design of this study is described in chapter 9.

CORONARY RESTENOSIS
15
References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17.
Dotter CT, Judkins MP. Transluminal treatment of arteriosclerotic obstruction. Circulation 1964;30:654-670. Gruentzig A. Transluminal dilatation of coronary artery stenosis (letter). Lancet 1978;1:263. Serruys PW, Luijten HE, Beatt KJ, Geuskens R, de Feyter PJ, van den Brand M, Reiber JHC, ten Katen HJ, van Es GA, Hugenholtz PG. Incidence of restenosis after successful coronary angioplasty: a time related phenomenon: a quantitative angiographic study in 342 consecutive patients at 1, 2, 3, and 4 months. Circulation 1988;77:361-71. Sigwart U, Puel J, Mirkovitch V, Joffre F, Kappenberger L. Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty. N Engl J Med 1987;316:701-706. Serruys PW, De Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G, Emanuelson H, Marco J, Legrand V, Materne P, Belardi J, Sigwart U, Colombo A, Goy JJ, van den Heuvel P, Delcan J, Morel M-A, for the Benestent Study group. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331:489-95. Fischman DL, Leon MB, Baim DS, Schatz RA, Savage MP, Penn I, Detre K, Veltri L, Ricci D, Nobuyoshi M, Cleman M, Heuser R, Almond D, Teirstein PS, Fish RD, Colombo A, Brinker J, Moses J, Shaknovich A, Hirshfeld J, Bailey S, Ellis S, Rake R, Goldberg S. For the Stent Restenosis Study Investigators. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331:496-501. Sousa JE, Costa MA, Abizaid A, Abizaid AS, Feres F, Pinto IMF, Seixas AC, Staico R, Mattos LA, Sousa AGMR, Falotico R, Jaeger J, Popma JJ, Serruys PW. Lack of neointimal proliferation after implantation of sirolimus-coated stents in human coronary arteries. A quantitative coronary angiography and three-dimensional intravascular ultrasound study. Circulation 2001;103:192-195. Morice M-C, Serruys PW, Sousa JE, Fajadet J, Hayashi EB, Perin M, Colombo A, Schuler G, Barragan P, Guagliumi G, Molnàr F, Falotico R. for the RAVEL study group. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med 2002;346:1773-1780. Grube E, Silber S, Hauptman KE, Mueller R, Beullesfeld, Gerckens U, Russel ME. TAXUS I, Six- and twelve-month results from a randomised, double-blind trial on a slow-release paclitaxel-eluting stent for de novo coronary lesions. Circulation 2003;107:38-42. Topol, Textbook of interventional cardiology, 4th edition 2003. Moreno PR, Palacios IF, Leon MN, Rhodes J, Fuster V, Fallon JT. Histopathologic comparison of human coronary in-stent and post-angioplasty restenotic tissue. Am J Cardiol 1999;84:462-66. Schwartz RS, Henry TD. Pathophysiology of coronary artery restenosis. Rev Cardiovasc Med. 2002;3(suppl5):S4-S9. Mintz GS, Kent KM, Pichard AD, Satler LF, Popma, JJ, Leon MB. Contribution of inadequate arterial remodeling to the development of focal coronary artery stenoses. An intravascular ultrasound study. Circulation 1997;95:1791-98. Schwartz RS. Pathophysiology of restenosis: interaction of thrombosis, hyperplasia, and/or remodeling. Am J Cardiol 1998;81(7A):14E-17E. Lowe HC, Oesterle SN, Khachigian. Coronary in-stent restenosis: current status and future strategies. J Am Coll Cardiol 2002;39:183-93. Haude M, Erbel R, Issa H, Meyer J. Quantitative analysis of elastic recoil after balloon angioplasty and after intracoronary implantation of balloon-expandable Palmaz-Schatz stents. J Am Coll Cardiol 1993;21:26-34. Grewe PH, Deneke T, Machraoui A, Barmeyer J, Muller K-M. Acute and chronic tissue response to coronary stent implantation: pathologic findings in human specimen. J Am Coll Cardiol 1999;35:157-63.
CHAPTER 1
16
18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34.
Farb A, Sangiorgi G, Carter AJ, Walley VM, Edwards WD, Schwartz RS, Virmani R. Pathology of acute and chronic coronary stenting in humans. Circulation 1999;99:44-52. Schwartz RS, Murphy JG, Edwards WD, Camrud AR, Vlietstra RE, Holmes. Restenosis after balloon angioplasty. A practical proliferative model in porcine coronary arteries. Circulation 1990;82:2190-2200. Schwartz RS, Huber KC, Murphy JG, Edwards WD, Camrud AR, Vlietstra RE, Holmes DR. Restenosis and the proportional neointimal response to coronary artery injury: results in a porcine model. J Am Coll Cardiol 1992;19:267-274. Stein B, Weintraub WS, Gebhart SSP, Cohen-Bernstein CL, Grosswald R, Liberman HA, Douglas JS, Morris DC, King III SB. Influence of diabetes mellitus on early and late outcome after percutaneous transluminal coronary angioplasty. Circulation. 1995;91: 979-989. Abizaid A, Kornowski R, Mintz GS, Hong MK, Abizaid AS, Mehran R, Pichard AD, Kent KM, Satler LF, Hongsheng WU, Popma JJ, Leon MB. The influence of diabetes mellitus on acute and late clinical outcomes following coronary stent implantation. J Am Coll Cardiol 1998;32:584-589. Verghese M, Gersh BJ, Williams BA, Laskey WK, Willerson JT, Tilbury RT, Davis BR, Holmes DR. Outcomes in patients with diabetes mellitus undergoing percutaneous coronary intervention in the current era. A report from the prevention of restenosis with tranilast and its outcomes (PRESTO) trial. Circulation 2004;109:476-480. Kornowski R, Mintz GS, Kent KM, Pichard AD, Satler LF, Bucher TA, Hong MK, Popma JJ, Leon MB. Increased restenosis in diabetes mellitus after coronary interventions is due to exaggerated intimal hyperplasia: a serial intravascular ultrasound study. Circulation. 1997;95:1366-1369. Moreno PR, Fallon JT, Murcia AM, Leon MN, Simosa H, Fuster V, Palacios IF. Tissue characteristics of restenosis after percutaneous transluminal coronary angioplasty in diabetic patients. J Am Coll Cardiol 1999;34:1045-9. Roffi M, Topol EJ. Percutaneous coronary intervention in diabetic patients with non-ST-segment elevation acute coronary syndromes. Eur Heart J 2004;25:190-198. Savage MP, Fischman DL, Schatz RA, et al. Coronary intervention in the diabetic patient: improved outcome following stent implantation compared with balloon angioplasty. Clin Cardiol. 2002;25:213-217. Moussa I, Leon MB, Baim DS, O’Neill WW, Popma JJ, Buchbinder MB, Widwall J, Simonton CA, Keim E, Wang P, Kuntz RE, Moses JW. Impact of sirolimus-eluting stents on outcome in diabetic patients. A Sirius substudy. Circulation. 2004;109:2273-2278. Reis GJ, Kuntz RE, Silverman DI, Pasternak RC. Effects of serum lipid levels on restenosis after coronary angioplasty. Am J Cardiol 1991;68:1431-1435 Violaris AG, Melkert R, Serruys PW. Influence of serum cholesterol and cholesterol subfractions on restenosis after successful coronary angioplasty. A quantitative angiographic analysis of 3336 lesions. Circulation 1994;90:2267-2279. Roth A, Eshchar Y, Keren G, Sheps D, Kerbel S, Laniado S, Miller HI, Rubinstein A, and the Ichilov Magnesium Study group. Serum lipids and restenosis after successful percutaneous transluminal coronary angioplasty. Am J Cardiol 1994;73:1154-1158. Bertrand ME, McFadden EP, Fruchart J-C, Van Belle E, Commeau P, Grollier G, Bassand J-P, Machecourt J, Cassagnes J, Mossard J-M, Vacheron A, Castaigne A, Danchin N, Lablanche J-M, for the PREDICT trial Investigators. Effect of pravastatin on angiographic restenosis after coronary balloon angioplasty. J Am Coll Cardiol 1997;30:863-869. Serruys PW, Foley DP, Jackson G, Bonnier H, Macaya C, Vrolix M, Branzi A, Shepherd J, Suryapranata H, de Feyter PJ, Melkert R, van Es G-A, Pfister PJ on behalf of the FLARE study group. A randomized placebo-controlled trial of fluvastatin for prevention of restenosis after successful coronary balloon angioplasty. Eur Heart J 1999;20:58-69. Desmarais RL, Sarembock IJ, Ayers CR, Vernon SM, Powers ER, Gimple LW. Elevated serum levels of lipoprotein(a) is a risk factor for clinical recurrence after coronary balloon angioplasty. Circulation 1995;91:1403-1409.

CORONARY RESTENOSIS
17
35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51.
Yamamoto H, Imazu M, Yamabe T, Ueda H, Hattori Y, Yamakido M. Risk factors for restenosis after percutaneous transluminal coronary angioplasty: role of lipoprotein(a). Am Heart J 1995;130:1168-73. Boushey CJ, Beresford SAA, Omenn GS, Motulsky AG. A quantitative assessment of plasma homocysteine as a risk for vascular disease: probable benefits of increasing folic acid intakes. JAMA 1995;274:1049-57. Chao CL, Tsai HH, Lee CM, Hsu SM, Kao JT, Chien KL, Sung FC, Lee YT. The grade effect of hyperhomocysteinemia on the severity and extent of coronary atherosclerosis. Atherosclerosis 1999;147:379-86. Schnyder G, Pin R, Roffi M, Flammer Y, Hess OM. Association of plasma homocysteine with the number of major coronary arteries severely narrowed. Am J Cardiol 2001;88:1027-30. Schnyder G, Roffi M, Flammer Y, Pin R, Hess OM. Association of plasma homocysteine with restenosis after percutaneous coronary angioplasty. Eur Heart J 2002;23:726-733. Kosokabe T, Okumura K, Sone T, Kondo J, Tsuboi H, Mukawa H, Tomida T, Suzuki T, Kamiya H, Matsui H, Hayakawa T. Relation of a common methylenetetrahydrofolate reductase mutation and plasma homocysteine with intimal hyperplasia after coronary stenting. Circulation 2001;103:2048-54. Genser D, Prachar H, Hauer R, Halbmayer WM, Mlczoch J, Elmadfa I. Relation of homocysteine, vitamin B(12), and folate to coronary in-stent restenosis. Am J Cardiol 2002;89:495-499. Miner SE, Hegele RA, Sparkes J, Teitel JM, Bowman KA, Connelly PW, Banijamali H, Lau HK, Chisholm RJ, Babaei S, Strauss BH. Homocysteine, lipoprotein(a), and restenosis after percutaneous transluminal coronary angioplasty: a prospective study. Am Heart J 2000;140:272-278. Schnyder G, Roffi M, Pin R, Flammer Y, Lange H, Eberli FR, Meier B, Turi ZG, Hess AM. Decrease rate of coronary restenosis after lowering of plasma homocysteine levels. N Engl J Med 2001;345:1593-600. Lange H, Suryapranata H, De Luca G, Börner C, Dille J, Kallmayer K, Noor Pasalary M, Scherer E, Dambrink J-H. Folate therapy and in-stent restenosis after coronary stenting. N Engl J Med 2004;350:2673-81. Cohen DJ, Doucet M, Cutlip DE, Ho KKL, Popma JJ, Kuntz RE. Impact of smoking on clinical and angiographic restenosis after percutaneous coronary intervention. Another smoker’s paradox? Circulation 2001;104:773-778. Violaris AG, Thury A, Regar E, Melkert R, Serruys PW. Influence of a history of smoking on short term (six month) clinical and angiographic outcome after successful coronary angioplasty. Heart 2000;84:299-306. Mehilli J, Kastrati A, Bollwein H, Dibra A, Schühlen H, Dirschinger J, Schömig A. Gender and restenosis after coronary artery stenting. Eur Heart J 2003;24:1523-1530. Kishi K, Hiasa Y, Suzuki N, Takahashi T, Hosokawa S, Tanimoto M, Otani R. Predicors of recurrent restenosis after coronary stenting: an analysis of 197 patients. J Invasive Cardiol 2002;14:187-91. Lemos PA, Hoye A, Goedhart D, Arampatzis CA, Saia F, van der Giessen WJ, McFadden E, Sianos G, Smits PC, Hofma SH, de Feyter PJ, van Domburg RT, Serruys PW. Clinical, angiographic, and procedural predictors of angiographic restenosis after sirolimus-eluting stent implanation in complex patients. An evaluation from the rapamycin-eluting evaluated at Rotterdam cardiology hospital (RESEARCH) study. Circulation 2004;109:1366-1370. Singh M, Gersh BJ, McClelland RL, Ho KKL, Willerson JT, Penny WF, Holmes DR. Clinical and angiographic predictors of restenosis after percutaneous coronary intervention. Insights from the prevention of restenosis with tranilast and its outcomes (PRESTO) trial. Circulation 2004;109:2727-2731. Rupprecht HJ, Brennecke R, Bernhard G, Erbel R, Pop T, Meyer J. Analysis of risk facors for restenosis after PTCA. Cathet Cardiovasc Diagn 1990;19:151-159.

CHAPTER 1
18
52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. 64. 65. 66.
Bourassa MG, Lespérance J, Eastwood C, Schwartz L, Côté G, Kazim F, Hudon G. Clinical, physiologic, anatomic, and procedural factors predictive of restenosis after percutaneous transluminal coronary angioplasty. J Am Coll Cardiol 1991;18:368-376. Weintraub WS, Kosinski AS, Brown III CL, King III SB. Can restenosis after coronary angioplasty be predicted from clinical variables? J Am Coll Cardiol 1993;21:6-14. Cutlip DE, Chauhan MS, Baim DS, Ho KKL, Popma JJ, Carrozza JP, Cohen DJ, Kuntz RE. Clinical restenosis after coronary stenting: perspectives from multicenter clinical trials. J Am Coll Cardiol 2002;40:2082-2089. Daemen MJ, Lombardi DM, Bosman FT, Schwartz SM. Angiotensin II induces smooth muscle cell proliferation in the normal and injured rat arterial wall. Circ Res 1991;68:450-456. Pratt RE, Dzau VJ. Pharmacological strategies to prevent restenosis. Lessons learned from blockade of the rennin-angiotensin system. Circulation 1996;93:848-852. Wagenaar LJ, van Boven AJ, van der Wal AC, Amoroso G, Tio RA, van der Loos CM, Becker AE, van Gilst WH. Differential localisation of the rennin-angiotensin system in de-novo lesions and in-stent restenotic lesions in in-vivo human coronary arteries. Cardiovasc Res 2003;59:980-987. Van Bockxmeer FM, Mamotte CDS, Gibbons FA, Burke V, Taylor RR. Angiotensin-converting enzyme and apolipoprotein E genotypes and restenosis after coronary angioplasty. Circulation 1995;92:2066-2071. Ribichini F, Steffenino G, Dellavalle A, Matullo G, Colajanni E, Camilla T, Vado A, Benetton G, Uslenghi E, Piazza A. Plasma activity and insertion/deletion polymorphism of angiotensin I-converting enzyme. A major risk factor and a marker of risk for coronary stent restenosis. Circulation 1998;97:147-154. Amant C, Bauters C, Bodart J-C, Lablanche J-M, Grollier G, Danchin N, Hamon M, Richard F, Helbecque N, McFadden EP, Amouyel P, Bertrand ME. Circulation 1997;96:56-60. Koch W, Kastrati A, Mehilli J, Böttiger C, von Beckerath N, Schömig A. Insertion/deletion polymorphism of the angiotensin I-converting enzyme gene is not associated with restenosis after coronary stent placement. Circulation 2000;102:197-202. Jørgensen E, Kelbæk H, Helqvist S, Jensen GVH, Saunamäki K, Kastrup J, Havndrup O, Bundgaard H, Madsen JK, Christiansen M, Andersen PS, Reiber JHC. Predictors of coronary in-stent restenosis: importance of angiotensin-converting enzyme gene polymorphism and treatment with angiotensin-converting enzyme inhibitors. J Am Coll Cardiol 2001;38:1434-1439. Hermans WR, Rensing BJ, Foley DP, Tijssen JG, Rutsch W, Emanuelsson H, Danchin N, Wijns W, chappuis F, Serruys PW. Patient, lesion, and procedural variables as risk factors for luminal re-narrowing after successful coronary angioplasty: a quantitative analysis in 653 patients with 778 lesions. Multicenter European Research Trial with cilazapril after angioplasty to prevent transluminal coronary obstruction and restenosis (MERCATOR) study group. J Cardiovasc Pharmacol 993;22:S45-57. Kondo J, Sone T, Tsuboi H, Mukawa H, Kosokabe T, Tsuzuki M, Tomida T, Suzuki T, Kamiya H, Hayashi K, Matsui H, Okumura K. Effect of quinapril on intimal hyperplasia after coronary stenting as assessed by intravascular ultrasound. Am J Cardiol;87:443-445. Ellis SG, Lincoff AM, Whitlow PL, Raymond RE, Franco I, Schneider JP, Topol EJ. Evidence that angiotensin-converting enzyme inhibitor use diminishes the need for coronary revascularization after stenting. Am J Cardiol 2002;89:937-940. Meurice T, Bauters C, Hermant X, Codron V, VanBelle E, Mc Fadden EP, Lablanche J-M, Bertand ME, Amouyel P. Effect of ACE inhibitors on angiographic restenosis after coronary stenting (PARIS): a randomised, double-blind, placebo-controlled trial. Lancet 2001;357:1321-1324.

CORONARY RESTENOSIS
19
67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84.
Kuller L, Tracy R, Shaten J, Meilahn E. Relation of C-reactive protein and coronary heart disease in MRFIT nested case-control study. Multiple Risk Factor Intervention Trial Am J Epidemiol 1996;144:537-547. Ridker P, Cushman M, Stampfer M, Tracy R, Hennekens C. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med 1997;336:973-979. Haverkate F, Thompson S, Pyke S, Gallimore J, Pepys M. Production of C-reactive protein and risk of coronary events in stable and unstable angina. Lancet 1997;349:462- 466. Ridker P, Rifai N, Pfeffer M, Sacks F, Moye L Goldman S, Flaker G, Braunwald E. Inflammation, pravastatin, and the risk of coronary events after myocardial infarction in patients with average cholesterol levels. Circulation 1998;98:839-844. Zebrack J, Muhlestein J, Horne B, Anderson J. C-reactive protein and angiographic coronary artery disease: independent and additive predictors of risk in subjects with angina. J Am Coll Cardiol 2002;39:632-637. Buffon A, Liuzzo G, Biasucci L, Pasqualetti P, Ramazzotti V, Rebuzzi A, Crea F, Maseri A. Preprocedural serum levels of C-reactive protein predict early complications and late restenosis after coronary angioplasty. J Am coll Cardiol 1999;34:1512-1521. Walter D, Fichtlscherer S, Sellwig M, Auch-Schwelk W, Schächinger V, Zeiher A. Preprocedural C-reactive protein levels and cardiovascular events after coronary stent implantation J Am Coll Cardiol 2001;37:839-846. Adam E, Melnick JL, Probtsfield JL, Petrie BL, Burek J, Bailey KR, McCollum CH, DeBakey ME. High level of cytomegalovirus antibody in patients requiring vascular surgery for atherosclerosis. Lancet 1987;2:291-93. Epstein SE, Speir E, Zhou YF, Guetta E, Leon M, Finkel T. The role of infection in restenosis and atherosclerosis: focus on cytomegalovirus. Lancet 1996; 348:13-17. Blum A, Giladi M, Weinberg W, Kaplan G, Pasternack H, Laniado S, Miller H. High anti-cytomegalovirus (CMV) IgG antibody titer is associated with coronary artery disease and may predict post-coronary balloon angioplasty restenosis. Am J Cardiol 1998;81:866-68. Rassu M, Cazzavillan S, Scagnelli M, Peron A, Bevilacqua PA, Facco M, Bertoloni G. Lauro FM, Zambello R. Demonstration of Chlamydia pneumoniae in atherosclerotic arteries from various vascular regions. Atherosclerosis 2001;158:73-79. Tutuncu NB, Guvener N, Tutuncu T, Yilmaz M, Guvener M, Boke E, Pasaoglu I, Erbas T. Chlamydia pneumonia seropositivity correlates with serum fibrinogen and lipoprotein a levels: any role in atherosclerosis? Endocr J 2001;48:269-74. Rutherford JD. Chlamydia pneumoniae and atherosclerosis. Curr Atheroscler Rep 2000;2:218-25. Carlsson J, Miketic S, Mueller K-H, Brom J, Ross R, von Essen R, Tebbe U. Previous cytomegalovirus or Chlamydia pneumoniae infection and risk of restenosis after percutaneous transluminal coronary angioplasty. Lancet 1997; 350:1225. Hirshfeld JW, Schwartz JS, Jugo R, Macdonald RG, Goldberg S, Savage MP, Bass TA, Vetrovec G, Cowley M, Taussig AS, Whitworth HB, Margolis JR, Hill JA, Pepine CJ, and the M-HEART investigators. Restenosis after coronary angioplasty: a multivariate statistical model to relate lesion and procedure variables to restenosis. J Am Coll Cardiol 1991;18:647-656. Elezi S, Kastrati A, Neumann F-J, Hadamitzky M, Dirschinger J, Schömig A. Vessel size and long-term outcome after coronary stent implantation. Circulation 1998;98:1875-1880. Quigley PJ, Hlatky MA, Hinohara T, Rendall DS, Perez JA, Phillips HR, Califf RM, Stack RS. Repeat percutaneous transluminal coronary angioplasty and predictors of recurrent restenosis. Am J Cardiol 1989;63:409-413. Serruys PW, Foley DP, Kirkeeide RL, King SB 3rd. Restenosis revisited: insights provided by quantitative coronary angiography. Am Heart J 1993;126:1263-1267.

CHAPTER 1
20
85. 86. 87. 88. 89.
Serruys PW, Umans V, Heyndrickx GR, van den Brand M, de Feyter PJ, Wijns W, Jaski B, Hugenholtz PG Elective PTCA of totally occluded coronary arteries not associated with myocardial infarction; short-term and long-term results. Eur Heart J 1985;6:2-12. Kereiakes DJ, Selmon MR, McAuley BJ, McAuley DB, Sheehan DJ, Simpson JB. Angioplasty in total coronary occlusion: Experience in 76 consecutive patients. J Am Coll Cardiol 1985;6:526-33. Meier B. Total coronary occlusion: a different animal? J Am Coll Cardiol 1991;17:50B-57B. Ellis SG, Shaw RE, Gershony G, Thormas R, Roubin GS, Douglas JS Jr, Topol EJ, Startzer SH, Myler RK, King SB 3rd. Risk factors, time course and treatment effect for restenosis after succesful percutaneous transluminal coronary angioplasty of chronic total occlusion. Am J Cardiol 1989;63:897-901. Arjomand H, Turi ZG, McCormick D, Goldberg S. Percutaneous coronary intervention: Historical perspectives, current status, and future directions. Am Heart J 2003;146:787-796.

21
Chapter 2
Preprocedural serum levels of acute-phase reactants and prognosis after percutaneous coronary intervention
Braim M. Rahel 1Frank L.J. Visseren Maarten-Jan Suttorp
Thijs H.W. Plokker Johannes C. Kelder
2Bartelt M. de Jongh 3 K. Paul Bouter
4Rob J.A. Diepersloot
St. Antonius Hospital Nieuwegein, Dept of Cardiology, 1University Medical Centre Utrecht, Dept of Internal and Vascular Medicine,
2St. Antonius Hospital Nieuwegein, Dept of Microbiology, 3Jeroen Bosch Hospital, Den Bosch, Dept of Internal Medicine,
4Diakonessen Hospital Utrecht, Dept of Microbiology, the Netherlands
Published in Cardiovascular Research 2003;60:136-140

CHAPTER 2
22
ABSTRACT Objective: In this study we evaluate the value of baseline concentrations of acute-phase reactants on prognosis after percutaneous coronary intervention (PCI). Methods: Blood samples were drawn immediately before PCI to measure baseline concentrations of C-reactive protein (CRP), interleukin-6 (IL-6), lipoprotein(a) (Lp(a)), and fibrinogen. Follow-up data were collected at 8 months. Repeat PCI, CABG, myocardial infarction, and death were recorded as major adverse clinical events (MACE). Furthermore the recurrence of angina pectoris was noted. Results: The study included 600 consecutive patients after a successful PCI. Sixty-four percent of the patients were stented. The mean age was 61.6 years and 68.9% were male. CRP levels were significantly higher in patients who were to have repeat angina as compared with those who were not (p=0.0322). IL-6 levels were not correlated with angina or MACE. Lp(a) and fibrinogen concentrations were both significantly related to MACE (p=0.0337 and p=0.0253 respectively). Conclusion: Our study clearly supports the role of inflammation in restenosis after PCI as measured in statistically higher levels of Lp(a) and fibrinogen in patients with MACE and CRP in patients with repeat angina.

ACUTE-PHASE REACTANTS AND PROGNOSIS AFTER PCI
23
INTRODUCTION Case-control studies have established consistent associations between circulating inflammatory markers, in particular C-reactive protein (CRP), and the subsequent risk of cardiovascular events in healthy people1,2 and in patients with established coronary heart disease.3-5 Percutaneous coronary intervention (PCI) has been shown to elicit an inflammatory response by itself.6,7 In addition, preprocedural CRP levels appear to predict outcome in patients undergoing balloon angioplasty and stent implantation.8,9 Also other acute-phase reactants like interleukin-6 (IL-6), lipoprotein(a) (Lp(a)) and fibrinogen possibly play a role in the biologic response after PCI.10,11,12 So far, there are only limited data on the prognostic value of these acute-phase reactants measured preprocedural. METHODS Patients All consecutive patients scheduled for elective PCI in the St. Antonius Hospital in Nieuwegein, the Netherlands were eligible in the period between July 1998 and December 1999. Patients were included if there was a successful procedure of a de novo lesion with signs of ischemia related to this vessel (signs of ischemia found during an abnormal excercise test, defined as ST depression of at least 1.0 mm that is horizontal or down-sloping or upsloping ST depression of at least 2.0 mm or signs of ischemia found during nuclear imaging with excercise, dobutamine or adenosine). The minimum age for inclusion was 18 years. Exclusion criteria were acute coronary syndromes, prior PCI or CABG of the target lesion, current treatment for a malignancy or infection, or use of immunosuppressive drugs. The study was conducted according to the principles of the Declaration of Helsinki, and all patients gave written informed consent to use routinely drawn preprocedural blood samples for further analysis. The institutional ethics committee approved the study. Hypertension was defined as a systolic tension higher than 140 mmHg and/or a diastolic tension higher than 90 mmHg or use of anti-hypertensive drugs. Diabetes mellitus was defined as fasting venous glucose concentrations ≥ 7.8 mmol/L or use of glucose lowering drugs. Hypercholesterolaemia was defined as a fasting plasma cholesterol level higher than 5.0 mmol/L or use of cholesterol lowering drugs. A positive family history was defined as the presence of coronary heart disease in a first degree family member before the age of 55 in male and 60 in female. Blood Samples and Laboratory Analysis Blood samples were routinely drawn prior to each procedure, separated and serum and plasma samples kept frozen at -80º C until analysis of C-reactive protein (CRP-EIA (HS), ELISA set, Kordia BV, Leiden, the Netherlands), fibrinogen (FG-EIA fibrinogeen, ELISA set, Kordia), Lipoprotein(a) (Tint ELIZE Lp(a), Kordia), and IL-6 (M1916, Pelikine IL-6, Compact ELISA CLB, Amsterdam, the Netherlands). The laboratory personnel were blinded for the clinical outcome. The clinical outcome investigators committee was blinded to the laboratory results.

CHAPTER 2
24
Angioplasty Procedure Aspirin was started before the procedure and continued during the follow-up period. At the start of the procedure, patients received a bolus of 10,000 U of heparin intravenously. Percutaneous coronary intervention was performed from the femoral artery approach with standard techniques. Stents were used to the discretion of the operator. Procedural success was defined as a residual stenosis less than 20% at the angioplasty site. Before and after angioplasty, 100-500 µg intracoronary nitroglycerine was given and repeated if necessary. Directly following stent implantation patients received 300 mg clopidogrel and were instructed to take 75 mg clopidogrel once daily during 1 month. Long-Term Follow-Up Clinical follow-up was performed at 8 months by mailing a questionnaire to the patient or relatives of the patient. In case of non-response patients were contacted by telephone. Repeat PCI, CABG, myocardial infarction (defined as the presence of new significant Q waves or an elevation of creatine kinase or its MB isoenzyme to at least two times the upper limit), or death (of all causes) were recorded as major adverse clinical events (MACE). Repeat angina was defined as chest pain recognised from cardiac origin by the patient. Statistical Analysis Statistical analysis was done using the Statcalc module of Epi Info® and SAS version 8.2. The t-test was used to test differences in quantitative values. Variables are expressed as means (± standard deviation) unless otherwise stated. Variables are called independent after multivariate logistic regression analysis. The crude and adjusted odds ratios, as estimates for the relative risk, were calculated using unconditional logistic regression. Adjustment was made for the following potentially confounding factors: age and smoking. RESULTS The study included 600 consecutive patients scheduled for PCI. In 64% of the patients one or more stents were implanted. The baseline characteristics are shown in Table 1. Mean age was 61.6 years, 68.9% were male. Two patients were lost to follow-up (1 patient emigrated to Brazil, 1 patient moved to the United Kingdom and could not be traced). Only 54 patients (9%) had a major adverse clinical event during follow-up (repeat PCI: 57%, CABG: 13%, myocardial infarction: 23%, death: 7%, all deaths are cardiac or presumed cardiac). We found statistically significant higher fibrinogen levels in patients developing MACE as compared with patients without MACE (p=0.0253). Also Lp(a) levels were found higher in patients with MACE as compared to patients without MACE (p=0.0337). C-reactive protein showed a trend towards higher levels in patients with MACE (Table 2). During 8 months follow-up 196 patients (32.7%) reported recurrence of anginal complaints. As shown in Table 3, CRP showed higher levels in the group with complaints as compared with patients without repeat angina (p=0.0322). Subanalysis of only stented patients yielded similar results. Comparison of stented patients versus patients with only balloon angioplasty showed no significant differences with respect to MACE or angina pectoris (p=0.7629 and p=0.1711 respectively). Also comparison of patients on statins versus patients without statins and diabetics versus non-diabetics yielded no significant differences in MACE or angina pectoris.

ACUTE-PHASE REACTANTS AND PROGNOSIS AFTER PCI
25
Table 1. Baseline characteristics of 600 PCI patients.
Age (y) (mean±sd) Women (%) Active smoker (%) Hypercholesterolaemia (%) Hypertension (%) Diabetes mellitus (%) Positive family history (%) Medication (%) aspirin calcium antagonists beta blockers nitrates statins
61.6±10.5 31.1 36.6 75.0 30.0 11.2 52.3 88.6 50.5 77.3 64.4 50.0
PCI, Percutaneous Coronary Intervention.
Multivariate subanalysis of the permutations of two or more acute-phase reactants yielded no additional risk factor for MACE or repeat angina. Fibrinogen was found the strongest independent predictor for MACE. Even after adjustment of the acute-phase reactants (CRP, IL-6, Lp(a)), both single and in combinations (CRP and IL-6, CRP and Lp(a), IL-6 and Lp(a), CRP and IL-6 and Lp(a)) or after adjustment for stenting, age, statin treatment, or diabetes, we found no important change in the odds ratio’s for fibrinogen (ranging between 1.6 - 2.4). Adjustment for the confounding factors age and smoking showed a significant increase in the odds ratio of fibrinogen (table 4).

CHAPTER 2
26
Table 2. MACE during 8 months follow-up
MACE n=54 (9%)
No MACE n=546 (91%)
p-value
IL-6 (pg/mL) fibrinogen (g/L) Lp(a) (mg/L) CRP (mg/L)
1.93±2.36 3.50±0.84 280±331 5.83±9.37
2.97±8.30 3.09±0.88 192±274 4.33±5.16
0.3560 0.0253 0.0337 0.0759
MACE, Major Adverse Clinical Events, (combined endpoint of repeat PCI/CABG, myocardial infarction and death). IL-6, Interleukin-6. Lp(a), Lipoprotein(a). CRP, C-reactive protein.
Table 3. Repeat angina pectoris at 8 months follow-up
Repeat AP n=196 (32.7%)
No repeat AP n=404 (67.3%)
p-value
IL-6 (pg/mL) fibrinogen (g/L) Lp(a) (mg/L) CRP (mg/L)
2.72±5.34 3.16±0.83 221±299 5.17±6.98
2.97±9.02 3.08±0.89 184±256 4.06±4.78
0.7197 0.4647 0.1451 0.0322
AP, angina pectoris. IL-6, Interleukin-6. Lp(a), Lipoprotein(a). CRP, C-reactive protein

ACUTE-PHASE REACTANTS AND PROGNOSIS AFTER PCI
27
Table 4. Odds ratios after adjustment for age and smoking Adjustment IL-6 fibrinogen Lp(a) CRP MACE No Age Age and Smoking
1st tertile 2nd tertile 3rd tertile 1st tertile 2nd tertile 3rd tertile 1st tertile 2nd tertile 3rd tertile
1 0.71 (0.35-1.42) 0.91 (0.47-1.74) 1 0.71 (0.36-1.42) 0.86 (0.43-1.65) 1 0.84 (0.39-1.77) 0.75 (0.35-1.62)
1 0.82 (0.24-2.76) 2.53 (0.94-6.86) 1 1.01 (0.28-3.64) 3.17 (1.06-9.51)* 1 0.85 (0.18-3.99) 3.74 (1.08-12.95)*
1 0.78 (0.36-1.72) 1.61 (0.81-3.19) 1 0.79 (0.36-1.73) 1.55 (0.78-3.10) 1 1.03 (0.42-2.50) 1.66 (0.73-3.76)
1 0.99 (0.46-2.15) 1.56 (0.77-3.18) 1 1.0 (0.46-2.15) 1.55 (0.76-3.17) 1 0.95 (0.40-2.22) 1.39 (0.62-3.10)
Repeat angina pectoris No Age Age and Smoking
1st tertile 2nd tertile 3rd tertile 1st tertile 2nd tertile 3rd tertile 1st tertile 2nd tertile 3rd tertile
1 0.72 (0.47-1.10) 0.97 (0.64-1.45) 1 0.73 (0.48-1.11) 0.94 (0.62-1.42) 1 0.71 (0.44-1.14) 0.87 (0.55-1.38)
1 1.15 (0.63-2.08) 1.81 (1.02-3.21)* 1 1.08 (0.59-1.98) 1.73 (0.95-3.15) 1 1.42 (0.69-2.90) 2.27 (1.12-4.59)*
1 1.0 (0.64-1.56) 1.17 (0.75-1.82) 1 0.99 (0.63-1.54) 1.17 (0.75-1.83) 1 0.85 (0.51-1.41) 1.12 (0.68-1.83)
1 0.99 (0.63-1.55) 1.41 (0.91-2.19) 1 1.01 (0.64-1.59) 1.42 (0.91-2.22) 1 1.09 (0.66-1.79) 1.22 (0.74-2.01)
* p<0.05 MACE, Major Adverse Clinical Adverse Events (combined endpoint of repeat PCI/CABG, myocardial infarction and death). CRP, C-reactive protein. IL-6, Interleukin-6. Lp(a), Lipoprotein(a).

CHAPTER 2
28
DISCUSSION To our knowledge, this prospective study is the first investigating the independent and combined prognostic value of several acute-phase reactants in a large consecutive group of patients undergoing PCI. Of the acute-phase reactants C-reactive protein has been studied most extensively. An early study investigating this subject could not detect an association between preprocedural CRP levels and restenosis in a relatively small patient group.13 However, more recently published data suggested that preprocedural CRP levels consistently were associated with adverse events after percutaneous coronary intervention.8,14,15 Also in a cohort solely consisting of stented patients, preprocedural CRP appears to predict cardiovascular events, supporting the role of inflammation in neointimal hyperplasia.9 Also in our population, CRP levels were higher in patients with MACE as compared with patients without MACE, but this difference reached no statistically significance. Looking at patients experiencing repeat anginal complaints however, we found significantly higher levels of CRP as compared to patients free of complaints. The precise mechanisms by which elevated CRP levels lead to events remain to be elucidated. CRP is synthesised and secreted by hepatocytes in response to cytokines, especially IL-6. CRP levels reflect the degree of underlying inflammation, which in turn is known to be related to restenosis.16,17 CRP has been shown to bind to damaged tissues and to act synergistically with lipopolysaccharide in the activation of endothelial cells and to induce tissue factor production by monocytes.18,19,20 Considering that IL-6 is the principal regulator of CRP release by the liver and IL-6 can be produced by various cells, including endothelial cells, hepatocytes, monocytes, and smooth muscle cells, we hypothesised that raised IL-6 levels are the link between circulating CRP concentrations and coronary events. In this study we found no correlation between IL-6 levels and development of MACE after PCI. In two small studies a positive correlation between increased IL-6 levels and restenosis was shown.10,21 This could partly be explained by the fact that we measured preprocedural IL-6 concentrations, whereas these two studies reported postprocedural IL-6 levels. In our study Lp(a) levels were found significantly higher in patients with MACE as compared with patients without MACE. Previous data about Lp(a) and adverse events after percutaneous coronary intervention are inconsistent. In the FLARE study, in which 823 patients were followed after angioplasty, baseline Lp(a) failed to predict restenosis or major adverse cardiac events.22 In the same year Chiarugi et al. showed significantly higher baseline levels of Lp(a) in patients developing restenosis. Earlier restenosis was observed with Lp(a) values >450 mg/L and >300 mg/L if associated with anticardiolipin antibodies.23
Sirikci et al. found higher Lp(a) levels in patients with restenosis, but this difference was only statistically significant in a small subgroup of women.24 The exact mechanism by which Lp(a) acts in smooth muscle cell hyperplasia is not fully understood. Lp(a) consists of two parts. One part is LDL cholesterol which could explain the development of atherosclerosis. The other part is apolipoprotein(a) which resembles plasminogen resulting in competition for fibrin and thus increasing basal clotting levels. In the present study baseline fibrinogen levels also appeared to be significantly higher in patients with MACE as compared to patients without MACE. Montalescot et al.25 also found a relation between elevated fibrinogen levels during follow-up after angioplasty and restenosis. Patients with a fibrinogen concentration exceeding 3.5 g/L at follow-up evaluation had higher restenosis rates than patients with a fibrinogen concentration below 3.5 g/L. This cut-off point fits well in the concentrations found in our study-groups. The rationale for
ACUTE-PHASE REACTANTS AND PROGNOSIS AFTER PCI
29
fibrinogen as a risk factor for restenosis is supported by the results of Naito et al. who concluded that fibrin degradation products stimulate smooth muscle cell outgrowth leading to restenosis.26 This could be in agreement with our own study on the effect of coumadin on restenosis.27 Although Schumacher et al. also demonstrated higher fibrinogen levels in patients with restenosis versus patients without restenosis, the difference was not significant. 28 The combination of two or more of the discussed acute-phase reactants yielded no additional risk factor for MACE or repeat angina. CONCLUSIONS Our study clearly supports the role of inflammation in restenosis after PCI as measured in statistically higher levels of Lp(a) and fibrinogen in patients with MACE and CRP in patients with repeat angina.

CHAPTER 2
30
References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16.
Kuller L, Tracy R, Shaten J, Meilahn E. Relation of C-reactive protein and coronary heart disease in MRFIT nested case-control study. Multiple Risk Factor Intervention Trial Am J Epidemiol 1996;144:537-547. Ridker P, Cushman M, Stampfer M, Tracy R, Hennekens C. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med 1997;336:973-979. Haverkate F, Thompson S, Pyke S, Gallimore J, Pepys M. Production of C-reactive protein and risk of coronary events in stable and unstable angina. Lancet 1997;349:462- 466. Ridker P, Rifai N, Pfeffer M, Sacks F, Moye L Goldman S, Flaker G, Braunwald E. Inflammation, pravastatin, and the risk of coronary events after myocardial infarction in patients with average cholesterol levels. Circulation 1998;98:839-844. Zebrack J, Muhlestein J, Horne B, Anderson J. C-reactive protein and angiographic coronary artery disease: independent and additive predictors of risk in subjects with angina. J Am Coll Cardiol 2002;39:632-637. Liuzzo G, Buffon A, Biasucci L, Gallimore J, Caligiuri G, Vitelli A, Altamura S, Ciliberto G, Rebuzzi A, Crea F, Pepys M, Maseri A. Enhanced inflammatory response to coronary angioplasty in patients with severe unstable angina. Circulation 1998;98:2370- 2376. Gaspardone A, Crea F, Versaci F, Tomai F, Pellegrino A, Chiariello L, Gioffre P. Predictive value of C-reactive protein after successful coronary artery stenting in patients with stable angina. Am J Cardiol 1998:82:515-518. Buffon A, Liuzzo G, Biasucci L, Pasqualetti P, Ramazzotti V, Rebuzzi A, Crea F, Maseri A. Preprocedural serum levels of C-reactive protein predict early complications and late restenosis after coronary angioplasty. J Am Coll Cardiol 1999;34:1512-1521. Walter D, Fichtlscherer S, Sellwig M, Auch-Schwelk W, Schächinger V, Zeiher A. Preprocedural C-reactive protein levels and cardiovascular events after coronary stent implantation J Am Coll Cardiol 2001;37:839-846. Hojo Y, Ikeda U, Katsuki T, Mizuno O, Fukazawa H, Kurosaki K, Fujikawa H, Shimada K. Interleukin 6 expression in coronary circulation after coronary angioplasty as a risk factor for restenosis. Heart 2000;84:83-87. Cooke T, Sheahan R, Foley D, Reilly M, D’Arcy G, Jauch W, Gibney M, Gearty G, Crean P, Walsh M. Lipoprotein(a) in restenosis after percutaneous transluminal coronary angioplasty and coronary artery disease. Circulation 1994;89:1593-1598. Montalescot G, Ankri A, Vicaut E, Drobinski G, Grosgogeat Y, Thomas D. Fibrinogen after coronary angioplasty as a risk factor for restenosis. Circulation 1995;92:31-38. Zhou Y, Csako G, Grayston J, Wing S, Yu Z, Shou M, Leon M, Epstein S. Lack of association of restenosis following coronary angioplasty with elevated C-reactive protein levels or seropositivity to Chlamydia pneumoniae. Am J Cardiol 1999;84:595-598. Chew D, Bhatt D, Robbins M, Penn M, Schneider J, Lauer M, Topol E, Ellis S. Incremental prognostic value of elevated baseline C-reactive protein among established markers of risk in percutaneous coronary intervention. Circulation 2001;104:992-997. De Winter R, Heyde G, Koch K, Fischer J, van Straalen J, Bax M, Schotborgh C, Mulder K, Sanders G, Piek J, Tijssen J. The prognostic value of pre-procedural plasma C-reactive protein in patients undergoing elective coronary angioplasty. Eur Heart J 2002;23:960-966. Serrano C, Ramires J, Venturinelli M, Arie S, D’Amico E, Zweier J, Pileggi F, da Luz P. Coronary angioplasty results in leukocyte and platelet activation with adhesion molecule expression. Evidence of inflammatory responses in coronary angioplasty. J Am Coll Cardiol 1997;29:1276-1283.

31
17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28.
Biasucci L, Liuzzo G, Buffon A, Maseri A. The variable role of inflammation in acute coronary syndromes and in restenosis. Semin Interv Cardiol 1999;4:105-110. Yeh E, Anderson H, Pasceri V, Willerson J. C-reactive protein. Linking inflammation to cardiovascular complications. Circulation 2001;104:974-975. Du Clos T. Function of C-reactive protein. Ann Med. 2000;32:274-278. Nakagomi A, Freedman S, Geczy C. Interferon-gamma and lipopolysaccharide potentiate monocyte tissue factor induction by C-reactive protein: relationship with age, sex, and hormone replacement treatment. Circulation. 2000;101:1785-1791. Suzuki T, Ishiwata S, Hasegawa K, Yamamoto K, Yamazaki T. Raised interleukin 6 concentrations as a predictor of postangioplasty restenosis. Heart 2000;83:578. Lloyd G, Jackson G, Foley D, Boersma E, Shepherd J, Serruys P. The influence of plasma lipoprotein(a) on angiographic restenosis and coronary events in patients undergoing planned coronary balloon angioplasty. Ancillary analysis of the Fluvastatin Angioplasty Restenosis (FLARE) trial. Atherosclerosis 2001;158:445-454. Chiarugi L, Prisco D, Antonucci E, Capanni M, Fedi S, Liotta A, Margheri M, Simonetti I, Gensini G, Abbate R. Lipoprotein(a) and anticardiolipin antibodies are risk factors for clinically relevant restenosis after elective balloon percutaneous transluminal coronary angioplasty. Atherosclerosis 2001;154:129-135. Sirikci O, Aytekin V, Demiroglu I, Demiroglu C, Marcovina S. Association of lipoprotein(a) concentration and apo(a) isoform size with restenosis after percutaneous transluminal coronary angioplasty. Int J Clin Lab Res; 2000;30:93-99. Montalescot G, Ankri A, Vicaut E, Drobinski G, Grosgogeat Y, Thomas D. Fibrinogen after coronary angioplasty as a risk factor for restenosis. Circulation 1995;92:31-38. Naito M, Stirk C, Smith E, Thompson W. Smooth muscle cell outgrowth stimulated by fibrin degradation products. The potential role of fibrin E in restenosis and atherogenesis. Thromb Res 2000;98:165-174. ten Berg J, Hutten B, Kelder J, Verheugt F, Plokker H. Oral anticoagulant therapy during and after coronary angioplasty the intensity and duration of anticoagulation are essential to reduce thrombotic complications. Circulation 2001;103:2042-2047. Schumacher M, Eber B, Tiran A, Toplak H, Luka O, Gasser R, Klein W. Fibrinogen values in patients with and without restenosis following percutaneous transluminal coronary angioplasty. Cardiology 1992;80:345-348.

CHAPTER 2
32

33
Chapter 3
Pre-procedural ACE-activity does not predict in-stent restenosis
L.J. Wagenaar B.M. Rahel
1A.J. van Boven 1A.A. Voors
2A.C. van der Wal H.W.M. Plokker
1,3W.H. van Gilst
St. Antonius Hospital Nieuwegein, Dept of Cardiology, 1University Hospital Groningen, Dept of Cardiology,
2Academic Medical Center, Amsterdam, Dept of Cardiovascular Pathology, 3University of Groningen, Dept of Clinical Pharmacology,
the Netherlands
Accepted by the International Journal of Cardiology

34
ABSTRACT
Background: Several studies indicate that ACE-activity is related to atherosclerosis. We investigated the correlation between ACE-activity, in plasma as well as in the atherosclerotic plaque, and in-stent restenosis.
Methods and results: ACE-activity was measured in blood samples from 178 patients who underwent a percutaneous coronary intervention with stent placement. During 8 months follow-up, 51 of these patients had an adverse clinical event. ACE-activity did not differ between patients with or without adverse events (21.5 vs. 23.1 nM/ml/min; P=0.36)
Tissue samples were obtained with an atherectomy catheter before elective stent placement in another group of 13 patients with de novo stenosis. In this tissue, we determined the ACE-content immunohistologically. These patients were scheduled for follow-up quantitative coronary angiography after 12 months. In this group, the quantity of ACE was not correlated to the late luminal loss (0.31 vs. 0.38 mm; P=0.76).
Conclusion: In this study, pre-procedural ACE-activity, in plasma as well as in the atherosclerotic plaque, does not predict the occurrence of in-stent restenosis.

ACE-ACTIVITY AND IN-STENT RESTENOSIS
35
INTRODUCTION The introduction of the stent reduced the incidence of restenosis after percutaneous coronary interventions (PCI) remarkably.1,2 But still 10-21% of the patients develops in-stent restenosis 3 Several prognostic factors have been determined, such as length of the stent4, strut thickness 5, the type of the stent6, diabetes7 and the post-procedural minimal lumen diameter.8 Also the plaque burden outside the stent appears to correlate with the amount of neointimal proliferation inside the stent in rabbits9, as well as in humans.10 In-stent restenosis is mainly caused by growth of vascular smooth muscle cells within the stent11, which can be induced by angiotensin II via its type 1 (AT1) receptor.12 In a previous study, we demonstrated that vascular smooth muscle cells in human in-stent restenotic lesions carry the AT1 receptor.13 Therefore, it is likely that angiotensin II plays an important role in the genesis of in-stent restenosis. We hypothesized that ACE-activity, either local or in plasma, is related to the occurrence in-stent restenosis. The aim of this study was to evaluate the correlation between plasma ACE-activity and the occurrence of in-stent restenosis. Therefore, we determined the amount of ACE in the original atherosclerotic plaque as well as the ACE-activity in plasma in a different group of patients.
MATERIALS AND METHODS Plasma ACE All consecutive patients scheduled for elective PCI in the St. Antonius Hospital in Nieuwegein, the Netherlands were eligible in the period between July 1998 and December 1999. Patients were included if there was a successful procedure of a de novo lesion with signs of ischemia related to this vessel (signs of ischemia found during an abnormal excercise test, defined as ST depression of at least 1.0 mm that is horizontal or down-sloping or upsloping ST depression of at least 2.0 mm or signs of ischemia found during nuclear imaging with excercise, dobutamine or adenosine). The minimum age for inclusion was 18 years. Exclusion criteria were acute coronary syndromes, prior PCI or CABG of the target lesion, current treatment for a malignancy or infection, the use of immunosuppressive drug and the use of an ACE-inhibitor and/or an angiotensin II type 1 receptor blocker. The study was conducted according to the principles of the Declaration of Helsinki, and all patients gave written informed consent to use routinely drawn pre-procedural blood samples for further analysis. The institutional ethics committee approved the study.
Hypertension was defined as a systolic tension higher than 140 mmHg and/or a diastolic tension higher than 90 mmHg or use of anti-hypertensive drugs. Diabetes mellitus was defined as fasting venous glucose concentrations 7.8 mmol/L or use of glucose lowering drugs. Hypercholesterolaemia was defined as a fasting plasma cholesterol level higher than 5.0 mmol/L or use of cholesterol lowering drugs. A positive family history was defined as the presence of coronary heart disease in a first degree family member before the age of 55 in male and 60 in female.
Blood samples were drawn immediately before coronary angioplasty. Plasma samples were kept frozen at –80 ºC until analysis. ACE-activity in plasma (35 times diluted) was measured according to the method of Cushman and Cheung [14], using 10 minutes of incubation with 7

CHAPTER 3
36
mmol/L of hippuryl-L-histidyl-L-leucine (HHL) at 37ºC. The clinical investigators were blinded to the laboratory results. Clinical follow-up was performed at 8 months by mailing a questionnaire to the patient or his relatives. Occurrence of angina pectoris, (target) PCI or CABG, myocardial infarction, and death were all recorded as adverse clinical events. Repeat angina pectoris was defined as chest pain recognized from cardiac origin by the patient.
Tissue ACE
Tissue was collected from patients with significant, stable de-novo coronary lesions in the proximal left anterior descending artery or the circumflex artery. These patients did not use an ACE-inhibitor or an angiotensin II type 1 receptor blocker. Percutaneous coronary atherectomy was performed using a pullback atherectomy catheter (Arrow int., Reading, PA, USA). In all patients, a biopsy was taken out of the culprit lesion. Coronary angiography before and after the atherectomy confirmed that the sample was taken from the lesion. The samples were immediately frozen in liquid nitrogen and stored in a –80 °C freezer. Following the atherectomy procedure, a stent was placed, and the minimal luminal diameter (MLD) was measured using quantitative coronary angiography (QCA)(CAAS-system, PIE-medical, Maastricht, the Netherlands). Of each specimen, 5 µm sections were mounted on glass slides. One slide was stained with haematoxylin & eosin (H&E) and another was used for immunohistochemistry with an anti-ACE antibody (mouse antibody; clone 9B9; Chemicon, Temecula, CA, USA). Sections of alveolar lung tissue and infarcted myocardium served as positive controls for anti-ACE staining. The amount of ACE staining was applied by two independent investigators in order to evaluate the number of ACE-positive cells in each biopsy. The number of ACE-positive cells was expressed as a percentage of the total number of cells present in the biopsy as visualized in the adjacent H&E stained sections. The investigators were blinded to the patient characteristics. The patients were divided into two groups. Group 1: absent ACE staining, a few scattered cells or clusters <5 cells with positive ACE-staining; group 2: more than 5% of cells ACE-positive. After 12 months, the patients underwent repeat angiography, during which QCA was performed and the MLD was measured. Luminal loss was defined as the difference between the MLD at baseline and after 12 months. Both studies comply with the Declaration of Helsinki. The protocols were approved by the local ethics committees and informed consent of all patients was obtained. Statistical analysis Two-tailed T-test and Chi-square tests were performed to compare continuous and categorical variables, respectively. Differences were considered statistically significant at a level of P<0.05.
RESULTS ACE-activity was measured in 178 patients who underwent a percutaneous coronary intervention with stent placement. The characteristics of these patients are summarized in table 1. In this group, 51 patients suffered from an adverse clinical event. As shown in figure 1, the ACE-activity in the plasma did not correlate with the occurrence of these adverse events (23.1 vs. 21.5 nM/ml/min; P=0.36).

ACE-ACTIVITY AND IN-STENT RESTENOSIS
37
Thirteen patients underwent an atherectomy. The biopsy tissue existed mainly of myxoid tissue with stellate shaped cells (‘neointimal tissue’) as has been described previously for in-stent restenotic lesions [15]. Anti-ACE staining revealed scattered positive cells in all but one lesion, but the total amount of positive staining was very low. Six patients had no (n=5) or only a few ACE-positive cells (n=1) in the biopsy of their original plaque. Of the other 7, the biopsy of six patients contained 5-50% ACE-positive cells, and in one case, more than 50% of the cells were ACE-positive. There were no differences in the characteristics between the two groups (see table 2). At repeat angiography with QCA, no relation between the amount of ACE in the original plaque and late luminal loss could be found (0.31 vs. 0.38 mm; P=0.76)(see figure 2). Also the degree of in-stent restenosis did not differ (34.2 VS. 30.3%; P=0.59).
Table 1. Patient characteristics patient group A
No adverse events (n=127)
Adverse events (n=51)
P
Age (years) 59.4 61.6 0.24
Male (%) 72.9 63.5 0.21
Smoking (%) 43.5 34.7 0.30
Hypertension (%) 20.6 23.1 0.72
Positive Family History (%) 49.1 46.7 0.78
Diabetes (%) 9.4 9.6 0.97
Total cholesterol (mmol/l) 5.86 6.22 0.14
Beta Blockers (%) 76.0 71.2 0.50
Calcium antagonists (%) 51.2 46.2 0.54
Nitrates (%) 59.7 61.5 0.82
Cholesterol lowering drugs (%) 41.9 42.3 0.96
Heparin (%) 14.0 9.6 0.43
Coumarin (%) 36.4 36.5 0.99

CHAPTER 3
38
Table 2. Patient characteristics patient group B
No or few ACE-positive cells (n=6)
>5% ACE-positive cells (n=7)
P
Age (years) 52.7 53.3 0.88
Male (%) 100 85.7 1.00
Smoking (%) 50.0 28.6 0.59
Hypertension (%) 50.0 57.1 1.00
Positive Family History (%) 66.7 28.6 0.20
Diabetes (%) 0.0 0.0 1.00
Total cholesterol (mmol/l) 4.84 5.76 0.07
Beta Blockers (%) 83.3 71.4 1.00
Calcium antagonists (%) 50.0 71.4 0.59
Nitrates (%) 16.7 71.4 0.10
Cholesterol lowering drugs (%) 50.0 42.9 1.00
Heparin (%) 33.3 0.0 0.19
Coumarin (%) 0.0 0.0 1.00

ACE-ACTIVITY AND IN-STENT RESTENOSIS
39
P = NS
Figure 1. Plasma ACE-activity (nM/ml/min) in patients with (grey bars) or without (black bars) adverse clinical events in the 8 months following a percutaneous coronary intervention with stent placement.
P=NS
Figure 2. Luminal loss (determined with quantitative coronary angiography) 12 months after stent placement in patients with no or few ACE in their atherosclerotic plaque (black bars) or with >5% of ACE-positive cells in their plaque (grey bars).
0
5
10
15
20
25
30
AE- AE+
AC
E-a
ctiv
itity
(nM
/ml/m
in)
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
Few or no ACE >5% of cells ACE-positive
Late
lum
inal
loss
(m
m)

CHAPTER 3
40
DISCUSSION In-stent restenosis is a process that is mainly due to proliferation of vascular smooth muscle cells forming a variable amount of neointima within the stent.11,16 In the first four weeks after stent placement, other processes like platelet deposition and inflammation at the strut sites play a role too, but after approximately one month, neither thrombi nor acute inflammatory cells are found in the neointima.15,17 At that time, the plaque consists for 96% of vascular smooth muscle cells and proteoglycan matrix.11 Chronic inflammation cells are only found at the strut sites.16
In a previous study, we demonstrated that VSMCs in the neointima of human in-stent restenotic lesions were mostly AT1 receptor-positive.13 The renin-angiotensin system is probably involved in the progress of in-stent restenosis as angiotensin II, the effector molecule of the renin-angiotensin system, is able to induce proliferation of VSMCs via its AT1 receptor.12,18,19 Indeed, the AT1 receptor blocker valsartan was able to prevent in-stent restenosis in the Val-PREST study.20
Whether inhibition of ACE is effective in preventing in-stent restenosis is still unclear. Several studies reported that the ACE-inhibitor quinapril reduces in-stent intimal hyperplasia, late luminal loss and restenosis rate.21-23 A recent retrospective study in 1598 patients suggested that ACE-inhibitors decrease late revascularisation after stent placement.24 In the PARIS study, on the other hand, the ACE-inhibitor quinapril did not prevent in-stent restenosis in patients with the DD genotype of ACE.25
In this study, we demonstrated that plasma ACE-activity is not correlated with the incidence of adverse clinical events after stent placement. Moreover, in a small group of patients, we found that the content of ACE in the plaque during percutaneous coronary intervention did not predict the amount of in-stent restenosis after 12 months.
The absence of a correlation between ACE-activity and in-stent restenosis might have several causes. A limitation of our study is that we measured ACE-activity (both in the plasma as well as in the plaque) before stent placement. It is possible that the ACE-expression significantly changes as a reaction to the injury made by the balloon and/or the stent during PCI, as it does in animal models.26 Another limitation of our study is that, in the group in which we measured serum-ACE, we only counted adverse events as reported by the patients in the questionnaire. Therefore, we cannot be sure whether these patients suffer from in-stent restenosis. Another possibility is that ACE is not the rate-limiting step in the cascade of the renin-angiotensin system. This implicates that even in case of low ACE-activity, enough ACE is present to convert angiotensin I to angiotensin II. It remains controversial whether patients with the DD-allele of the ACE-polymorphism are especially at risk for in-stent restenosis, due to their higher ACE-activity. The D-allele has been identified as a prognostic factor for in-stent restenosis in some studies27,28, but other larger studies did not confirm this.29-31 A third explanation for the absent correlation between ACE-activity and in-stent restenosis is that angiotensin I is not only converted to angiotensin II by ACE, but also by other enzymes. This hypothesis is supported by a study by Hojo et al., who showed that ACE-inhibitors had no inhibiting effect on the increased angiotensin production during PCI in humans.32 Several studies have proven that in human vessels non-ACE converting enzymes, such as chymase and cathepsin G, could be involved in the production of angiotensin II .33,34

ACE-ACTIVITY AND IN-STENT RESTENOSIS
41
In human coronary arteries, chymase is mainly found in mast cells in the adventitia35 , and can therefore not be found in our biopsies. The number of chymase-positive cells is increased in atherosclerotic plaques in human aortas as well as in coronary arteries.35,36 In a canine model, chymase is upregulated after balloon injury.26 Notably, in the normal human heart chymase already appears to be the predominant enzyme for the angiotensin I conversion.37 Since we only measured ACE-activity in our study, we cannot prove the importance of other enzymes in the genesis of in-stent restenosis.
In conclusion, we studied the relationship between the angiotensin converting enzyme (ACE) and the incidence of in-stent restenosis. We found that the ACE-activity in plasma at the time of the initial percutaneous coronary intervention was not correlated with the extent of in-stent restenosis. Furthermore, the presence of ACE in the initial plaque was also not associated with in-stent restenosis. Therefore, our study does not confirm that pre-procedural plasma and tissue ACE-activity are related to in-stent restenosis, although a relation between the renin-angiotensin system and in-stent restenosis remains undisputed.
Acknowledgments
We want to thank D.I.K. Versteeg for his valuable assistance in performing the quantitative coronary angiographies.

CHAPTER 3
42
References
1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15.
Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G, Emanuelsson H, Marco J, Legrand V, Materne P, . A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. Benestent Study Group. N Engl J Med 1994;331,489-495. Fischman DL, Leon MB, Baim DS, Schatz RA, Savage MP, Penn I, Detre K, Veltri L, Ricci D, Nobuyoshi M, . A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. Stent Restenosis Study Investigators. N Engl J Med 1994;331,496-501. Serruys PW, Kay IP, Disco C, Deshpande NV, de Feyter PJ. Periprocedural quantitative coronary angiography after Palmaz-Schatz stent implantation predicts the restenosis rate at six months: results of a meta-analysis of the BElgian NEtherlands Stent study (BENESTENT) I, BENESTENT II Pilot, BENESTENT II and MUSIC trials. Multicenter Ultrasound Stent In Coronaries. J Am Coll Cardiol 1999;34,1067-1074. Kobayashi Y, Gregorio Jd, Kobayashi N, Akiyama T, Reimers B, Finci L, Mario Cd, Colombo A. Stented segment length as an independent predictor of restenosis. J Am Coll Cardiol 1999;34,651-659. Kastrati A, Mehilli J, Dirschinger J, Dotzer F, Schuhlen H, Neumann FJ, Fleckenstein M, Pfafferott C, Seyfarth M, Schomig A. Intracoronary stenting and angiographic results: strut thickness effect on restenosis outcome (ISAR-STEREO) trial. Circulation 2001;103,2816-2821. Kastrati A, Mehilli J, Dirschinger J, Pache J, Ulm K, Schuhlen H, Seyfarth M, Schmitt C, Blasini R, Neumann FJ, Schomig A. Restenosis after coronary placement of various stent types. Am J Cardiol 2001;87,34-39 Abizaid A, Kornowski R, Mintz GS, Hong MK, Abizaid AS, Mehran R, Pichard AD, Kent KM, Satler LF, Wu H, Popma JJ, Leon MB. The influence of diabetes mellitus on acute and late clinical outcomes following coronary stent implantation. J Am Coll Cardiol 1998;32,584-589. Fitzgerald PJ, Oshima A, Hayase M, Metz JA, Bailey SR, Baim DS, Cleman MW, Deutsch E, Diver DJ, Leon MB, Moses JW, Oesterle SN, Overlie PA, Pepine CJ, Safian RD, Shani J, Simonton CA, Smalling RW, Teirstein PS, Zidar JP, Yeung AC, Kuntz RE, Yock PG. Final results of the Can Routine Ultrasound Influence Stent Expansion (CRUISE) study. Circulation 2000;102,523-530. Carter AJ, Farb A, Gould KE, Taylor AJ, Virmani R. The degree of neointimal formation after stent placement in atherosclerotic rabbit iliac arteries is dependent on the underlying plaque. Cardiovasc Pathol 1999;8,73-80. Prati F, di Mario C, Moussa I, Reimers B, Mallus MT, Parma A, Lioy E, Colombo A. In-stent neointimal proliferation correlates with the amount of residual plaque burden outside the stent: an intravascular ultrasound study. Circulation 1999;99,1011-1014. Moreno PR, Palacios IF, Leon MN, Rhodes J, Fuster V, Fallon JT. Histopathologic comparison of human coronary in-stent and post-balloon angioplasty restenotic tissue. Am J Cardiol 1999;84,462-466. Daemen MJ, Lombardi DM, Bosman FT, Schwartz SM. Angiotensin II induces smooth muscle cell proliferation in the normal and injured rat arterial wall. Circ Res 1991;68,450-456. Wagenaar LJ, van Boven AJ, van der Wal AC, Amoroso G, Tio RA, van der Loos CM, Becker AE, van Gilst WH. Differential localisation of the renin-angiotensin system in de-novo lesions and in-stent restenotic lesions in in-vivo human coronary arteries. Cardiovasc Res 2003;59,980-987. Cushman DW, Cheung HS. Spectrophotometric assay and properties of the angiotensin-converting enzyme of rabbit lung. Biochem Pharmacol 1971;20,1637-1648 Farb A, Sangiorgi G, Carter AJ, Walley VM, Edwards WD, Schwartz RS, Virmani R. Pathology of acute and chronic coronary stenting in humans. Circulation 1999;99,44-52

ACE-ACTIVITY AND IN-STENT RESTENOSIS
43
16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32.
Komatsu R, Ueda M, Naruko T, Kojima A, Becker AE. Neointimal tissue response at sites of coronary stenting in humans: macroscopic, histological, and immunohistochemical analyses. Circulation 1998;98,224-233. Virmani R, Farb A. Pathology of in-stent restenosis. Curr Opin Lipidol 1999;10,499-506. Pratt RE, Dzau VJ. Pharmacological strategies to prevent restenosis: lessons learned from blockade of the renin-angiotensin system. Circulation 1996;93,848-852. Hafizi S, Chester AH, Allen SP, Morgan K, Yacoub MH. Growth response of human coronary smooth muscle cells to angiotensin II and influence of angiotensin AT1 receptor blockade. Coron Artery Dis 1998;9,167-175. Peters S, Gotting B, Trummel M, Rust H, Brattstrom A. Valsartan for Prevention of Restenosis after Stenting of Type B2/C Lesions: The Val-PREST Trial. J Invasive Cardiol 2001;13,93-97. Okimoto T, Imazu M, Hayashi Y, Gomyo Y, Sekiguchi Y, Yanagihara K, Shimohara Y, Sumii K, Yamamoto H, Tadehara F, Toyofuku M, Kohno N. Quinapril with high affinity to tissue angiotensin-converting enzyme reduces restenosis after percutaneous transcatheter coronary intervention. Cardiovasc Drugs Ther 2001;15,323-329. Kondo J, Sone T, Tsuboi H, Mukawa H, Kosokabe T, Tsuzuki M, Tomida T, Suzuki T, Kamiya H, Hayashi K, Matsui H, Okumura K. Effect of quinapril on intimal hyperplasia after coronary stenting as assessed by intravascular ultrasound. Am J Cardiol 2001;87,443-5, A6. Okumura K, Sone T, Kondo J, Tsuboi H, Mukawa H, Tsuzuki M, Imai H, Kamiya H, Mabuchi Y, Matsui H, Hayakawa T. Quinapril prevents restenosis after coronary stenting in patients with angiotensin-converting enzyme D allele. Circ J 2002;66,311-316. Ellis SG, Lincoff AM, Whitlow PL, Raymond RE, Franco I, Schneider JP, Topol EJ. Evidence that angiotensin-converting enzyme inhibitor use diminishes the need for coronary revascularization after stenting. Am J Cardiol 2002;89,937-940 Meurice T, Bauters C, Hermant X, Codron V, VanBelle E, Mc Fadden EP, Lablanche J, Bertrand ME, Amouyel P. Effect of ACE inhibitors on angiographic restenosis after coronary stenting (PARIS): a randomised, double-blind, placebo-controlled trial. Lancet 2001;357,1321-1324. Shiota N, Okunishi H, Fukamizu A, Sakonjo H, Kikumori M, Nishimura T, Nakagawa T, Murakami K, Miyazaki M. Activation of two angiotensin-generating systems in the balloon-injured artery. FEBS Lett 1993;323,239-242. Amant C, Bauters C, Bodart JC, Lablanche JM, Grollier G, Danchin N, Hamon M, Richard F, Helbecque N, McFadden EP, Amouyel P, Bertrand ME. D allele of the angiotensin I-converting enzyme is a major risk factor for restenosis after coronary stenting. Circulation 1997;96,56-60. Ribichini F, Steffenino G, Dellavalle A, Matullo G, Colajanni E, Camilla T, Vado A, Benetton G, Uslenghi E, Piazza A. Plasma activity and insertion/deletion polymorphism of angiotensin I-converting enzyme: a major risk factor and a marker of risk for coronary stent restenosis. Circulation 1998;97,147-154. Koch W, Kastrati A, Mehilli J, Bottiger C, von Beckerath N, Schomig A. Insertion/Deletion polymorphism of the angiotensin I-converting enzyme gene is not associated with restenosis after coronary stent placement. Circulation 2000;102,197-202. Agema WR, Jukema JW, Pimstone SN, Kastelein JJ. Genetic aspects of restenosis after percutaneous coronary interventions;towards more tailored therapy. Eur Heart J 2001;22,2058-2074. Jorgensen E, Kelbaek H, Helqvist S, Jensen GV, Saunamaki K, Kastrup J, Havndrup O, Bundgaard H, Kyst MJ, Christiansen M, Andersen PS, Reiber JH. Predictors of coronary in-stent restenosis: importance of angiotensin- converting enzyme gene polymorphism and treatment with angiotensin- converting enzyme inhibitors. J Am Coll Cardiol 2001;38,1434-1439. Hojo Y, Ikeda U, Katsuki T, Mizuno O, Fujikawa H, Shimada K. Inhibition of angiotensin converting enzyme cannot prevent increases in angiotensin II production in coronary circulation. Heart 2000;83,574-576.

CHAPTER 3
44
33. 34. 35. 36. 37.
Voors AA, Pinto YM, Buikema H, Urata H, Oosterga M, Rooks G, Grandjean JG, Ganten D, van Gilst WH. Dual pathway for angiotensin II formation in human internal mammary arteries. Br J Pharmacol 1998;125,1028-1032. Okunishi H, Miyazaki M, Okamura T, Toda N. Different distribution of two types of angiotensin II-generating enzymes in the aortic wall. Biochem Biophys Res Commun 1987;149,1186-1192. Ohishi M, Ueda M, Rakugi H, Naruko T, Kojima A, Okamura A, Higaki J, Ogihara T. Relative localization of angiotensin-converting enzyme, chymase and angiotensin II in human coronary atherosclerotic lesions. J Hypertens 1999;17,547-553. Ihara M, Urata H, Kinoshita A, Suzumiya J, Sasaguri M, Kikuchi M, Ideishi M, Arakawa K. Increased chymase-dependent angiotensin II formation in human atherosclerotic aorta. Hypertension 1999;33,1399-1405. Katugampola SD, Davenport AP. Radioligand binding reveals chymase as the predominant enzyme for mediating tissue conversion of angiotensin I in the normal human heart. Clin Sci (Lond) 2002;102,15-21.

45
Chapter 4
Cytomegalovirus and Chlamydia pneumoniae as predictors for adverse events and angina pectoris after percutaneous coronary
intervention
Braim M. Rahel 1Frank L.J. Visseren Maarten-Jan Suttorp
Thijs H.W. Plokker Johannes C. Kelder
2 Bartelt M. de Jongh 3Rob J.A. Diepersloot
4Roel P.A.J. Verkooyen 5K. Paul Bouter
St. Antonius Hospital Nieuwegein, Dept of Cardiology, 1University Medical Centre Utrecht, Dept of Internal and Vascular Medicine,
2St. Antonius Hospital Nieuwegein, Dept of Microbiology, 3Diakonessen Hospital Utrecht, Dept of Microbiology,
4Erasmus University Hospital Rotterdam, Dept of Microbiology, 5Jeroen Bosch Hospital, Den Bosch, Dept of Internal Medicine,
the Netherlands
Published in the American Heart Journal 2004;148:670-675

CHAPTER 4
46
ABSTRACT Background: The aim of our study was to investigate the influence of prior cytomegalovirus (CMV) or Chlamydia pneumoniae (CP) infection on prognosis after percutaneous coronary intervention (PCI). Methods: Using the enzyme-linked immunosorbent assay technique preprocedural anti-CMV immunoglobulin G and anti-CP immunoglobulin A (CP IgA), immunoglobulin M and immunoglobulin G antibodies were measured. Repeat anginal complaints and major adverse clinical events (MACE), including PCI, coronary artery bypass grafting, myocardial infarction, and death, were recorded at 8-month follow-up. Results: Six hundred consecutive patients were included after successful PCI. Sixty-four percent of the patients were stented. The mean age was 61.6 years and 68.9% were male. The rate of seropositivity for CP IgA in patients with MACE as compared with patients without MACE was 50.9% versus 35.4% (p=0.0276). In patients with repeat anginal complaints CP IgA seropositivity was 41.6% versus 34.6% in patients without repeat angina (p=0.1057). The negative effect of CP on prognosis was confirmed after calculating the odds ratios for MACE (1.9, 95% CI 1.1-3.3). The rates of seropositivity for anti-CMV immunoglobulin G were not significantly different between both groups, although we found an association between infectious burden and repeat angina pectoris (odds ratio 1.8, 95% CI 1.1-3.0). Conclusions: We conclude that preprocedural seropositivity of CP IgA is a risk factor for MACE and angina pectoris after PCI. Although no such relation was found for CMV alone, the cumulative infectious burden was also related to these clinical manifestations of restenosis.

CMV AND CHLAMYDIA PNEUMONIAE AND PROGNOSIS AFTER PCI
47
INTRODUCTION The development of atherosclerosis is determined by many factors. Micro-organisms are suggested to be one of them with cytomegalovirus (CMV) and Chlamydia pneumoniae (CP) as 2 potential candidates.1-5 Multiple routes of action by which CP infection could lead to atherosclerosis and/or vascular smooth muscle cell proliferation have been described, influencing inflammatory mediators like fibrinogen, lipoprotein(a), tissue factor, and plasminogen activator inhibitor 1.5-8 CMV may also act by its immediate-early gene products, which inhibit the tumour suppressor protein p53 and thereby decrease smooth muscle cell apoptosis, leading to restenosis and development of atherosclerotic lesions.9,10 Restenosis after percutaneous coronary intervention (PCI) is mainly due to smooth muscle cell proliferation. Whether this process is linked to infection by CMV or CP is under debate.3,11-14 So far, there are no large studies evaluating the influence of CMV and/or CP infection on the long-term prognosis after PCI with plain old balloon angioplasty and provisional stenting. We conducted this study to evaluate the possible impact of prior CMV or CP infection on prognosis after PCI in a consecutive group of patients with and without stent implantation. METHODS Patients All consecutive patients scheduled for elective PCI in the St. Antonius Hospital in Nieuwegein, the Netherlands, were eligible in the period between July 1998 and December 1999. Patients were included if they underwent a successful procedure of a de novo lesion with signs of ischemia related to this vessel (signs of ischemia found during an abnormal exercise test, defined as ST depression of at least 1.0 mm that is horizontal or down-sloping, or upsloping ST depression of at least 2.0 mm, or signs of ischemia found during nuclear imaging with exercise, dobutamine, or adenosine). The minimum age for inclusion was 18 years. Exclusion criteria were acute coronary syndromes, prior PCI or coronary artery bypass graft (CABG) of the target lesion, current treatment for a malignancy or infection, or use of immunosuppressive drugs. The study was conducted according to the principles of the Declaration of Helsinki, and all patients gave written informed consent to use routinely drawn preprocedural blood samples for further analysis. The institutional ethics committee approved the study. Hypertension was defined as a systolic tension higher than 140 mmHg and/or a diastolic tension higher than 90 mmHg or use of anti-hypertensive drugs. Diabetes mellitus was defined as fasting venous glucose concentrations ≥ 140.5 mg/dL or use of glucose lowering drugs. Hypercholesterolaemia was defined as a fasting plasma cholesterol level higher than 193 mg/dL or use of cholesterol lowering drugs. A positive family history was defined as the presence of coronary heart disease in a first degree family member at age < 55 years in men and <60 years in women.

CHAPTER 4
48
Blood Samples and Laboratory Analysis Blood samples were drawn immediately before coronary angioplasty and separated. Serum and plasma samples were kept frozen at -80º C until analysis. Using the enzyme-linked immunosorbent assay (ELISA) technique anti-CMV immunoglobulin G (IgG) antibodies (AxSYM, Abbott, Abbott Park, Ill), and anti-CP immunoglobulin A (IgA), immunoglobulin M (IgM), and IgG antibodies (Medac, Hamburg, Germany) were measured. The agreement between the Medac ELISA and the micro-immunofluorescence as expressed by the к has been demonstrated previously to be 0.234.15 The cutoff for seropositivity for anti-CMV IgG was 50 AU/mL, cut-offs for anti-CP IgA, IgM and IgG titers all were 100 AU/mL. To evaluate the influence of inflammation on clinical outcome, the plasma levels of C-reactive protein (CRP) (CRP-EIA (HS), ELISA set, Kordia BV, Leiden, the Netherlands), Interleukin-6 (IL-6) (M1916, Pelikine IL-6, Compact ELISA CLB, Amsterdam, the Netherlands) and Lp(a) (Tint ELIZE Lp(a), Kordia) were measured. The laboratory personnel were blinded for the clinical outcome. The clinical outcome investigators’ committee were blinded to the laboratory results. Angioplasty procedure Aspirin was started before the procedure and continued during the follow-up period. At the start of the procedure, patients received a bolus of 10,000 U of heparin intravenously. PCI was performed from the femoral artery approach with standard techniques. Stents were used at the discretion of the operator. Procedural success was defined as a residual stenosis less than 20% at the angioplasty site. Before and after angioplasty, intracoronary nitroglycerin 100 to 500 µg was given and repeated if necessary. Directly following stent implantation, patients received clopidogrel 300 mg and were instructed to take clopidogrel 75 mg once daily during 1 month. Long-term follow-up Clinical follow-up was performed at 8 months by mailing a questionnaire to the patient or relatives of the patient. In case of nonresponse patients were contacted by telephone. Repeat PCI, CABG, myocardial infarction (defined as the presence of new significant Q waves or an elevation of creatine kinase or its MB isoenzyme to at least 2 times the upper limit), or death (from all causes) were recorded as major adverse clinical events (MACE). Repeat angina was defined as chest pain that the patient recognized as being of cardiac origin. Power calculation and statistical analysis To determine a difference of 10% in restenosis rate between seropositive and seronegative patients, with an α of 0.05 at least 600 patients had to be included. Statistical analysis was done using the Statcalc module of Epi Info (CDC, Atlanta, Ga). We used the Wilcoxon signed ranks test for non-normally distributed variables and the Spearman correlation coefficient and t-test for normally distributed variables. The crude and adjusted odds ratios as estimates for the relative risk of MACE and repeat angina pectoris were calculated using logistic regression. The impact of seropositivity was assessed with a Kaplan-Meier survival analysis and difference calculated with a log-rank test. Adjustment was made for the potentially confounding factors of stent, age, and smoking. The number of infections was determined for each participant. The adjusted odds ratios were calculated in patients with 1 and 2 infections. Plasma levels of CRP, IL-6, and Lp(a) were dichotomized with the median value as cutoff point.

CMV AND CHLAMYDIA PNEUMONIAE AND PROGNOSIS AFTER PCI
49
RESULTS The study included 600 consecutive patients scheduled for PCI. One or more stents were implanted in 64%. The baseline characteristics are shown in Table I. The mean age was 61.6 years and 68.9% were male. Two patients were lost to follow-up (1 patient emigrated to Brazil, 1 patient moved to the United Kingdom and could not be traced). Table I. Baseline characteristics
Age (y) Women (%) Active smoker (%) Hypercholesterolaemia (%) Hypertension (%) Diabetes mellitus (%) Positive family history (%) Medication (%) aspirin calcium antagonists beta blockers nitrates statins
61.6±10.5 31.1 36.6 77.2 30.0 11.2 52.3 88.6 50.5 77.3 64.4 50.0
Only 54 patients (9%) had MACE during follow-up (repeat PCI, 57%; CABG, 13%; myocardial infarction, 23%; death, 7%; all deaths are cardiac or presumed cardiac). We found a statistically significant difference in the rate of seropositivity for CP IgA between patients with MACE as compared with patients without MACE: 50.9% versus 35.4% respectively (p=0.0276), graphically depicted as a Kaplan-Meier curve in Figure 1. The rates of seropositivity for CP IgG and IgM were not significantly different between both groups. In the group with a MACE, 68.6% were seropositive for CMV IgG versus 65.6% in the group without MACE (p=0.7600) (Table II). During 8 months follow-up, 196 patients (32.7%) reported recurrence of anginal complaints. We found a trend towards higher levels of CP IgA seropositivity in this group as compared with the group free of anginal complaints, but the difference was not statistically significant (41.6% vs. 34.6%, p=0.1057). The rates of seropositivity for CP IgG and IgM were not significantly different between both groups. In the group with repeat angina the rate of CMV IgG seropositivity was 68.0%, compared with 64.9% in the group without complaints (p=0.5000) (Table III). We found no statistically significant difference between the lowest versus the highest quartile of CMV-IgG titers. In all cases CMV is no predictor of adverse events after PCI. CP IgA, IgG, IgM titers were higher than 100 AU/mL (cut-off point) in only 22%, 13%, and 5% respectively, so additional subdivision in quartiles was not feasible.

CHAPTER 4
50
We found similar results in baseline characteristics and seropositivity for CP and CMV between patients with or without a stent, nor was stenting a predictor for better outcome. The odds ratios and the 95% CI for MACE and repeat angina pectoris are shown in Table IV. The crude odds ratio for MACE was 1.9 (95% CI 1.1-3.3) for CP and 1.1 (0.6-2.0) for CMV. The crude odds ratio for repeat angina pectoris was 1.3 (0.9-1.9) for CP and 1.2 (0.8-1.7) for CMV. After adjustment for potential confounders no relevant changes were found. The adjusted odds ratios for MACE or repeat angina pectoris showed a consistent trend to increase with the cumulative number of infections. This trend did not change after correction for CRP, IL-6, or Lp(a) (Table V).
Table II. Major Adverse Clinical Events during 8 months follow-up
MACE n=54 (9%)
No MACE n=546 (91%)
p-value
Chlamydia IgG positive (%) Chlamydia IgA positive (%) Chlamydia IgM positive (%) CMVIgG positive (%)
38.2 50.9 10.8 68.6
44.0 35.4 8.0 65.6
0.4766 0.0276 0.5294 0.7600
Major Adverse Clinical Events, MACE, combined endpoint of repeat PCI/CABG, myocardial infarction and death
Table III. Repeat angina pectoris at 8 months follow-up
Repeat AP n=196 (32.7%)
No repeat AP n=404 (67.3%)
p-value
Chlamydia IgG positive (%) Chlamydia IgA positive (%) Chlamydia IgM positive (%) CMVIgG positive (%)
44.7 41.6 9.7 68.0
42.8 34.6 7.0 64.9
0.6625 0.1057 0.3348 0.5000

CMV AND CHLAMYDIA PNEUMONIAE AND PROGNOSIS AFTER PCI
51
Table IV. Crude and adjusted odds ratios (95%CI) for CP or CMV and MACE or repeat angina pectoris Adjustment MACE Repeat AP CMV
No Stent Stent, age Stent, age, smoking
1.116 (0.621-2.004) 1.261 (0.682-2.333) 1.234 (0.664-2.295) 1.234 (0.664-2.296)
1.198 (0.829-1.732) 1.319 (0.904-1.924) 1.280 (0.873-1.875) 1.276 (0.870-1.870)
CP*
No Stent Stent, age Stent, age, smoking
1.891 (1.084-3.298) 1.612 (0.905-2.871) 1.588 (0.887-2.840) 1.588 (0.887-2.841)
1.341 (0.946-1.900) 1.279 (0.897-1.825) 1.245 (0.869-1.784) 1.244 (0.868-1.782)
*CPIgA positive Table V. Adjusted odds ratios (95% CI) for number of infections and MACE or repeat angina pectoris Adjustment Number of
infections *
MACE Stent, age 0 1 2
1 1.344 (0.617-2.930) 1.936 (0.826-4.537)
Repeat AP
CRP, stent, age IL-6, stent, age Lp(a), stent, age Stent, age CRP IL-6, stent, age Lp(a), stent, age
0 1 2 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2
1 2.930 (0.606-3.096) 4.537 (0.631-3.992) 1 1.364(0.625-2.977) 1.942 (0.828-4.553) 1 1.347(0.595-3.049) 1.608(0.637-4.057) 1 1.262 (0.799-1.993) 1.797 (1.060-3.045) 1 1.084 (0.666-1.765) 1.711 (0.974-3.004) 1 1.264 (0.800-1.998) 1.797 (1.060-3.047) 1 1.058 (0.649-1.725) 1.733 (0.984-3.053)
*Infection with CP or CMV or both; 1 versus 0 and 2 versus 0.

CHAPTER 4
52
0 50 100 150 200 250
80
90
100
Days after PCI
Eve
nt-f
ree
surv
iva
lfro
mm
ajor
adv
ers
e cl
inic
al e
vent
s(
%)
p=0.0485
CP IgA negativeCP IgA positive
Figure 1: Kaplan-Meier curve of event-free survival after percutaneous coronary intervention (PCI) for Chlamydia pneumoniae (CP) IgA negative and positive patients DISCUSSION Whether or not cytomegalovirus and Chlamydia pneumoniae are involved in the restenosis process after PCI is still under debate, with recent studies showing contradictory results. Therefore we investigated the possible role of CMV and CP in a large consecutive patient group who underwent PCI with provisional stenting. The results of our study do not suggest that previous CMV infection affects restenosis after PCI. The prevalence of seropositivity for CMV IgG was not significantly higher in patients with MACE or repeat angina versus patients without clinical signs of restenosis. The theoretical basis for CMV involvement in coronary artery disease includes that CMV is present in a latent state in vascular endothelial and smooth muscle cells and is reactivated by angioplasty-induced injury. CMV is thought to interact with the tumour suppressor gene p53 present in these cells. The gene product of p53 inhibits cell cycle progression and therefore cell proliferation, and can lead to programmed cell death (apoptosis). One of the virus’s immediate early proteins (IE84) binds to p53 and inhibits its transcriptional activity thereby leading to enhanced smooth muscle cell proliferation and restenosis.2,9,10,16 Another effect of CMV is its ability to induce procoagulant activity in infected endothelial cells.17 Indeed, Zhou et al. demonstrated an association between prior CMV infection and the risk of restenosis after coronary atherectomy.18 Blum et al. found a similar result after
CMV AND CHLAMYDIA PNEUMONIAE AND PROGNOSIS AFTER PCI
53
balloon angioplasty.3 In contrast, Manegold et al. found no association between previous CMV infection and restenosis after balloon angioplasty.12 We found similar results for patients who received stents and those who did not, indicating that previous CMV infection does not influence prognosis after stent implantation. These results are supported by a study by Neumann et al. in which no increased risk of CMV infection on restenosis after stent implantation could be detected.11 Other studies also could not confirm the previous described association between cytomegalovirus and restenosis.13,14 The positive result found by Zhou et al. might be explained by the ‘deeper’ injury caused by atherectomy compared with balloon angioplasty with or without stent implantation. This could lead to a stronger stimulus for CMV reactivation. Nevertheless, conclusions are contradictory with a majority showing no relation between CMV infection and restenosis. In this study we found significantly higher rates of CP IgA, but not IgG, seropositivity in patients with MACE compared with the group without MACE. The negative effect of CP IgA on prognosis was confirmed after calculating the odds ratios. The lacking difference in CP IgM seropositivity between the 2 groups suggests that only chronic CP infection can contribute to the restenosis process after PCI. CP IgA seropositivity showed a trend towards higher levels in patients with repeat anginal complaints versus patients without angina, but this difference was not statistically significant. The role of CP in atherosclerosis is attributed to its ability to promote inflammatory responses in the vessel wall.19 A possible mechanism could be due to their influence on the serum fibrinogen and Lp(a) levels, which are higher in CP-seropositive patients versus CP-seronegative patients.5 In an in vitro study Fryer et al. demonstrated that CP can infect endothelial cells and stimulate the expression of tissue factor and platelet adhesion.20 Also plasminogen activator inhibitor-1 and IL-6 expression is increased in vascular smooth muscle and endothelial cells by CP.21 Despite a theoretical basis for the involvement of CP infection, several clinical studies could not demonstrate an association with restenosis.13,14,22 The reason that some studies support the role of CP in restenosis and other studies did not is unclear. The most likely explanation is the complex and multifactorial mechanism of restenosis. In the recently published Intracoronary Stenting and Antibiotic Regimen (ISAR-3) study, roxithromycin was used in CP-seropositive patients to prevent restenosis after coronary stenting. The restenosis rate in this study could only be reduced in the subgroup with high antibody titres.23 In this subgroup CP infection apparently becomes a more distinct risk for restenosis, suggesting that in patients with lower titres the effect of CP infection is concealed by other factors. On the contrary, in patients with coronary artery disease seropositive for CP, azithromycin failed to reduce ischemic events.24 In a recent study, Espinola-Klein et al. measured antibodies against herpes simplex, CMV, Ebstein-Barr virus, Haemophilus influenzae, CP, Mycoplasma pneumoniae, and Helicobacter pylori in 572 patients with coronary, carotid, and peripheral atherosclerosis. Their conclusion was that there is an association between infectious burden and the risk for an adverse long-term outcome in patients with atherosclerosis.25 However, this effect seems mainly driven by the bacterial infections and not the viral burden. Horne et al. measured antibodies to CP, CMV, and Helicobacter pylori in patients undergoing elective PCI, showing that pathogen burden is related to the risk of clinical restenosis.26 The study by Schiele et al. who also measured CMV, CP, and Helicobacter pylori IgG, failed to show an association between infectious burden and restenosis after stent implantation.14 In the present study we also found an association between infectious burden and MACE or residual anginal complaints.

CHAPTER 4
54
CONCLUSIONS In our study population preprocedural seropositivity of CP IgA is a risk factor for MACE and angina pectoris after PCI. Although no such relation was found for CMV alone, the cumulative infectious burden was also related to these clinical manifestations of restenosis.
CMV AND CHLAMYDIA PNEUMONIAE AND PROGNOSIS AFTER PCI
55
References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18.
Adam E, Melnick JL, Probtsfield JL, et al. High level of cytomegalovirus antibody in patients requiring vascular surgery for atherosclerosis. Lancet 1987;2:291-93. Epstein SE, Speir E, Zhou YF, et al. The role of infection in restenosis and atherosclerosis: focus on cytomegalovirus. Lancet 1996; 348:13-17. Blum A, Giladi M, Weinberg W, et al. High anti-cytomegalovirus (CMV) IgG antibody titer is associated with coronary artery disease and may predict post-coronary balloon angioplasty restenosis. Am J Cardiol 1998;81:866-68. Rassu M, Cazzavillan S, Scagnelli M, et al. Demonstration of Chlamydia pneumoniae in atherosclerotic arteries from various vascular regions. Atherosclerosis 2001;158:73-79. Tutuncu NB, Guvener N, Tutuncu T, et al. Chlamydia pneumonia seropositivity correlates with serum fibrinogen and lipoprotein a levels: any role in atherosclerosis? Endocr J 2001;48:269-74. Rutherford JD. Chlamydia pneumoniae and atherosclerosis. Curr Atheroscler Rep 2000;2:218-25. Krüll M, Klucken AD, Wuppermann FN, et al. Signal transduction pathways activated in endothelial cells following infection with Chlamydia pneumoniae. J. Immunol. 1999;162:4834-41. Dechend R, Maass M, Gieffers J, et al. Chlamydia pneumoniae infection of vascular smooth muscle and endothelial cells activates NF-κB and induces tissue factor and PAI-1 expression. A potential link to accelerated arteriosclerosis. Circulation 1999;100:1369-73. Speir E, Modali R, Huang ES, et al. Potential role of human cytomegalovirus and p53 interaction in coronary restenosis. Science 1994;165:391-94. Tanaka K, Zou JP, Takeda K, et al. Effects of human cytomegalovirus immediate-early proteins on p53-mediated apoptosis in coronary artery smooth muscle cells. Circulation 1999;99:1656-59. Neumann FJ, Kastrati A, Miethke T, et al. Previous Cytomegalovirus infection and restenosis after coronary stent placement. Circulation 2001; 104:1135-39. Manegold C, Alwazzeh M, Jablonowski H, et al. Prior cytomegalovirus infection and the risk of restenosis after percutaneous transluminal coronary balloon angioplasty. Circulation 1999;99:1290-94. Carlsson J, Miketic S, Mueller KH, et al. Previous cytomegalovirus or Chlamydia pneumoniae infection and risk of restenosis after percutaneous transluminal coronary angioplasty. Lancet 1997; 350:1225. Schiele F, Batur MK, Seronde MF, et al. Cytomegalovirus, Chlamydia pneumoniae, and Helicobacter pylori IgG antibodies and restenosis after stent implantation: an angiographic and intravascular ultrasound study. Heart 2001;85:304-11. Hoymans, VY, Bosmans JM, Van Renterghem L, et al. Importance of methodology in determination of Chlamydia pneumoniae seropositivity in healthy subjects and in patients with coronary atherosclerosis. J Clin Microbiol. 2003;41: 4049-53. Bertrand ME, Bauters C. Cytomegalovirus infection and coronary restenosis. Circulation 1999;99:1278-79. Visseren FLJ, Bouwman JJM, Bouter KP, et al. Procoagulant activity of endothelial cells after infection with respiratory viruses. Thromb Haemost 2000;84:319-24. Zhou YF, Leon MB, Waclawiw MA, et al. Association between prior cytomegalovirus infection and the risk of restenosis after coronary atherectomy. N Engl J Med 1996;335:624-30.

CHAPTER 4
56
19. 20. 21. 22. 23. 24. 25. 26.
Ross R. Atherosclerosis-an inflammatory disease. N Engl J Med 1999;340:115-26. Fryer RH, Schwobe EP, Woods ML, et al. Chlamydia species infect human vascular endothelial cells and induce procoagulant activity. J Investig Med 1997;45:168-74. Dechend R, Maass M, Gieffers J, et al. Chlamydia pneumoniae infection of vascular smooth muscle and endothelial cells activates NF-kappaB and induces tissue factor and PAI-1 expression: a potential link to accelerated arteriosclerosis. Circulation 1999;100:1369-73. Zhou YF, Csako G, Grayston JT, et al. Lack of association of restenosis following coronary angioplasty with elevated C-reactive protein levels or seropositivity to Chlamydia pneumoniae. Am J Cardiol 1999;84:595-98. Neumann FJ, Kastrati A, Miethke T, et al. Treatment of Chlamydia pneumoniae infection with roxithromycin and effect on neointima proliferation after coronary stent placement (ISAR-3): a randomised, double- blind, placebo-controlled trial. Lancet 2001;357:2085-89. Muhlestein JB, Anderson JL, Carlquist JF, et al. Randomized secondary prevention trial of azithromycin in patients with coronary artery disease. Primary clinical results of the ACADEMIC study. Circulation 2000;102:1755-60. Espinola-Klein C, Rupprecht HJ, Blankenberg S, et al. for the AtheroGene Investigators. Impact of infectious burden on extent and long-term prognosis of atherosclerosis. Circulation 2002;105:15-21. Horne BD, Muhlestein JB, Strobel GG, et al. Greater pathogen burden but not elevated C-reactive protein increases the risk of clinical restenosis after percutaneous coronary intervention. Am Heart J 2002;144:491-500.

57
Chapter 5
Is Direct Stent Implantation Without Predilatation Safe? Acute and
Long-Term Outcome.
Braim M. Rahel
Maarten Jan Suttorp Jurriën M. ten Berg,
Egbert T. Bal Sjef M.P.G. Ernst
Gijs Mast Johannes C. Kelder H.W. Thijs Plokker
St. Antonius Hospital Nieuwegein, Dept of Cardiology, the Netherlands
Published in the Journal of Interventional Cardiology 2002;15:263-268

CHAPTER 5
58
ABSTRACT Introduction: Direct stenting could potentially lead to a reduction in dissections, time, and restenosis at 6 month follow-up. Methods: Using the premounted Palmaz-Schatz Crown stent elective stenting was performed without predilatation in 61 consecutive patients who were compared with a control group of provisional stenting. All patients underwent clinical and angiographic follow-up at 6 months. Results: Direct stenting was successful in 81% of patients. In 16% of the patients predilatation was needed. In 3% the stent could not be implanted despite predilatation. Stent dislodgment occurred in 2% of patients, without embolization. Six-month angiographic follow-up was performed in 51 (84%) of 61 patients. In the direct stenting group the mean preprocedural minimal luminal diameter (MLD) increased from 0.96±0.47 mm to 3.09±0.54 mm directly after the procedure. At 6 month follow-up the MLD measured 2.32±0.79 mm. In the provisional stenting group the mean MLD increased from 0.92±0.51 to 2.44±0.58 mm and was 1.84±0.70 mm at 6 month follow-up. Restenosis, defined as a diameter stenosis > 50%, occurred in 8% of the direct stenting group compared with 28% in the provisional stenting group (p<0.001). Conclusion: Direct coronary stent implantation can be attempted safely and efficaciously. The risk of stent loss is low. The initial and long-term angiographic results are significantly better as compared with provisional stenting. The risk of restenosis is significantly lower.

STENTING WITHOUT PREDILATATION
59
INTRODUCTION Today coronary stents are used in up to 70% or even 80% of all percutaneous transluminal coronary angioplasty (PTCA) procedures. Although initially intended for use in case of suboptimal angioplasty results and threat of occlusion1,2, stents were proven to reduce restenosis rates after PTCA in various groups of patients.3-5 Stenting has been proven to be feasible and safe and stent dislodgment has become a rare event with new premounted stents. A new development is direct stenting without predilatation (SWOP). This technique is an inexpensive alternative that is expected to yield better long-term results. Based on preclinical research, this technique causes less damage to the vessel wall and results in a “lower response to injury”. Therefore, application of SWOP is likely to result in a lower rate of restenosis.6,7 In addition, a procedure without predilatation may result in shorter procedural and ischemic time period, fewer dissection, and to the use of less disposables. Recent clinical series on SWOP have reported encouraging initial procedural results.8-12 However, there are no available data describing the long-term angiographic follow-up as compared with a control group. This study investigated the acute and long-term results of SWOP using the premounted Palmaz-Schatz Crown stent (Johnson&Johnson Interventional systems, Warren, NJ, USA) and compared them with a control group of provisional stenting (PRS). PATIENTS AND METHODS Patient Population SWOP was applied in a consecutive group of patients in a single center prospective study. Patients were included if they had a de novo lesion in a native coronary artery with signs of ischemia related to this vessel. Exclusion criteria were a lesion location at a large side branch, a totally occluded coronary artery, severe calcification, an aorto-ostial lesion, prior PTCA or coronary bypass surgery of the study artery, myocardial infarction within 1 week before inclusion, contraindications to the use of ticlopidine or aspirin, or unable or unwilling to provide informed consent. Control Group For the control group, a subset of the Balloon Angioplasty and Anticoagulation Study (BAAS) study was used.13 The BAAS study, which was performed in the same center, included 1,056 consecutive patients from March 1996 until November 1997 and randomized patients to aspirin alone or aspirin plus coumadin pre-PTCA; a sub-randomization allocated 50% of patients to 6-month follow-up angiography. The angiography subset of patients was used, and patients were excluded according to the exclusion criteria for the present study. From the BAAS study, 317 patients were eligible for the control group. Angiographic Definitions Single vessel coronary artery disease was defined as > 50% diameter stenosis in one coronary artery or one of its major side branches. Multivessel (two or three vessel) coronary artery disease was defined as a >70% diameter stenosis in one major coronary artery or its major side branches in addition to a >50% diameter stenosis in one or more other major coronary arteries. Acute gain was defined as the increase in the MLD of the treated artery from before to immediately after angioplasty.

CHAPTER 5
60
Late loss was defined as the subsequent decrease in MLD of the treated artery at the follow-up angiography. Net gain was defined as the difference between the acute gain and the late loss. Angioplasty Procedure Patients were pretreated with 100 mg of aspirin once daily and calcium antagonists. At the start of the procedure, patients received a bolus dose of 10,000 U heparin. PTCA was performed by means of the femoral artery approach with standard balloon and stent implantation techniques using a High-Torque Floppy wire (Guidant, Inc., St. Paul, MN, USA). In all SWOP patients the new premounted Palmaz-Schatz Crown stent was implanted, which has a non-expanded profile (uncrimped) of 1.4 mm and may be delivered by 6Fr and 7Fr guiding catheters. The rate of stenting in the PRS group was 34.9%. Before and after angioplasty, 100-500 µg intracoronary nitroglycerin was given and repeated if necessary. After successful stent implantation, both groups were instructed to take aspirin permanently and ticlopidine 250 mg bid for 4 weeks. Long-Term Follow-Up Clinical and angiographic follow-up was performed at 6 months or earlier, if symptoms occurred. Death, myocardial infarction, defined as the presence of new significant Q waves or an elevation of creatine kinase or its MB isoenzyme to at least two times the upper limit, occurrence of angina pectoris (Canadian cardiovascular society class III or IV), or target lesion revascularization were all recorded as major clinical events. Quantitative Measurements Prestent, poststent implantation, and 6-month follow-up angiographic measurements were performed under standard conditions with an on-line automatic computer-based edge-detection system (DCI, Philips Medical Systems, Eindhoven, The Netherlands) in the angiographic projection with the lowest MLD. The guiding catheter was used as the calibration standard. Restenosis Angiographic restenosis at follow-up was defined as >50% residual diameter stenosis at the previous angioplasty site. Statistical Analysis Continuous variables were expressed as mean ± SD and were compared by the paired or unpaired Student’s t-test where appropriate. The 95% confidence intervals (CI) for rates were computed by means of the exact method. RESULTS Patient Characteristics In 1997 the authors attempted SWOP in 61 consecutive patients. In the SWOP group 69% of the patients had angina class III or IV; this figure was 70% in the PRS group. The baseline clinical characteristics showed no significant differences between both study groups (Table 1). There was a significantly higher prevalence of calcified lesions in the PRS group (p<0.001). The angiographic characteristics are listed in Table 2.

STENTING WITHOUT PREDILATATION
61
Table 1. Baseline clinical characteristics Variable PRS (N=317) SWOP (N=61) Age (yr) Male gender (%) Angina pectoris CCS class (%) I II III IV Risk factors (%) Smoking Hypertension Diabetes Mellitus Previous stroke Mean Cholesterol (mmol/L) > 5.5 mmol/L (%) Previous MI (%)
59.4±10.4 81 1 29 49 21 34 22 9 1 6.1±1.2 63 37
59.7±11.3 74 2 29 30 39 25 21 11 0 6.2±1.2 77 31
MI, myocardial infarction; CCS, Canadian cardiovascular society Table 2. Angiographic characteristics Variable PRS (N=317) SWOP (N=61) Target vessel (%) Right coronary Left anterior descending Left circumflex Ejection fraction (%) >50% 20-50% <20% Eccentricity concentric eccentric Calcification (%) Angulation (%) <45° >45° ACC/AHA lesion type (%) A B C
30 45 25 82 18 0 33 67 23 81 19 52 38 10
50 45 5 92 8 0 28 72 4 90 10 28 66 6
ACC/AHA, American College of Cardiology/American Heart Association

CHAPTER 5
62
Procedural Success Direct stenting was succesful in 81% of patients. Predilatation was necessary in ten patients (16%). In two lesions (3%) the Crown stent could not be placed even after predilatation. In one patient a stent was dislodged from the balloon, but could be retrieved. Because of proximal and distal dissection during the procedure, four additional stents were implanted in three patients. In one patient a distal dissection was seen 2 hours after the procedure necessitating re-PTCA. The mean procedure time was 22±13 minutes (time from arterial sheath insertion until acceptance of stent implantation result). Angiographic Results Follow-up coronary angiography after 6 months was performed in 84% (51/61) of the patients. Reasons for nonperformance of follow-up angiography were refusal in six patients and lost to follow-up due to emigration in one case. The three patients in whom the Crown stent could not be placed did not undergo angiographic follow-up. The quantitative coronary angiographic results are shown in Table 3. The SWOP resulted in a larger postprocedural MLD than did PRS, and this difference was maintained at follow-up. Accordingly, the restenosis rate was 8% in the SWOP group versus 28% in the PRS group (p<0.001). Late loss was not significantly different in the two groups, but the net gain was higher in the SWOP group (p=0.000). Long-Term Clinical Follow-Up Patients were monitored for a mean of 7.6 ± 1.9 months (range 2.3-12.0 months) from the time of the initial angioplasty procedure. Recurrence of angina pectoris was more frequent in the PRS group than in the SWOP group (18% and 11%, respectively), but this difference was not significant (p=0.177). In the SWOP group, none of the patients died, no patients had a myocardial infarction, no patients underwent repeat angioplasty at the stent site, and no patients had elective coronary artery bypass graft surgery. Two patients underwent PTCA for a new stenosis showing a patent study-stent. Although there was a higher prevalence of adverse clinical events in the PRS group, this difference was not significant (Fig. 1).
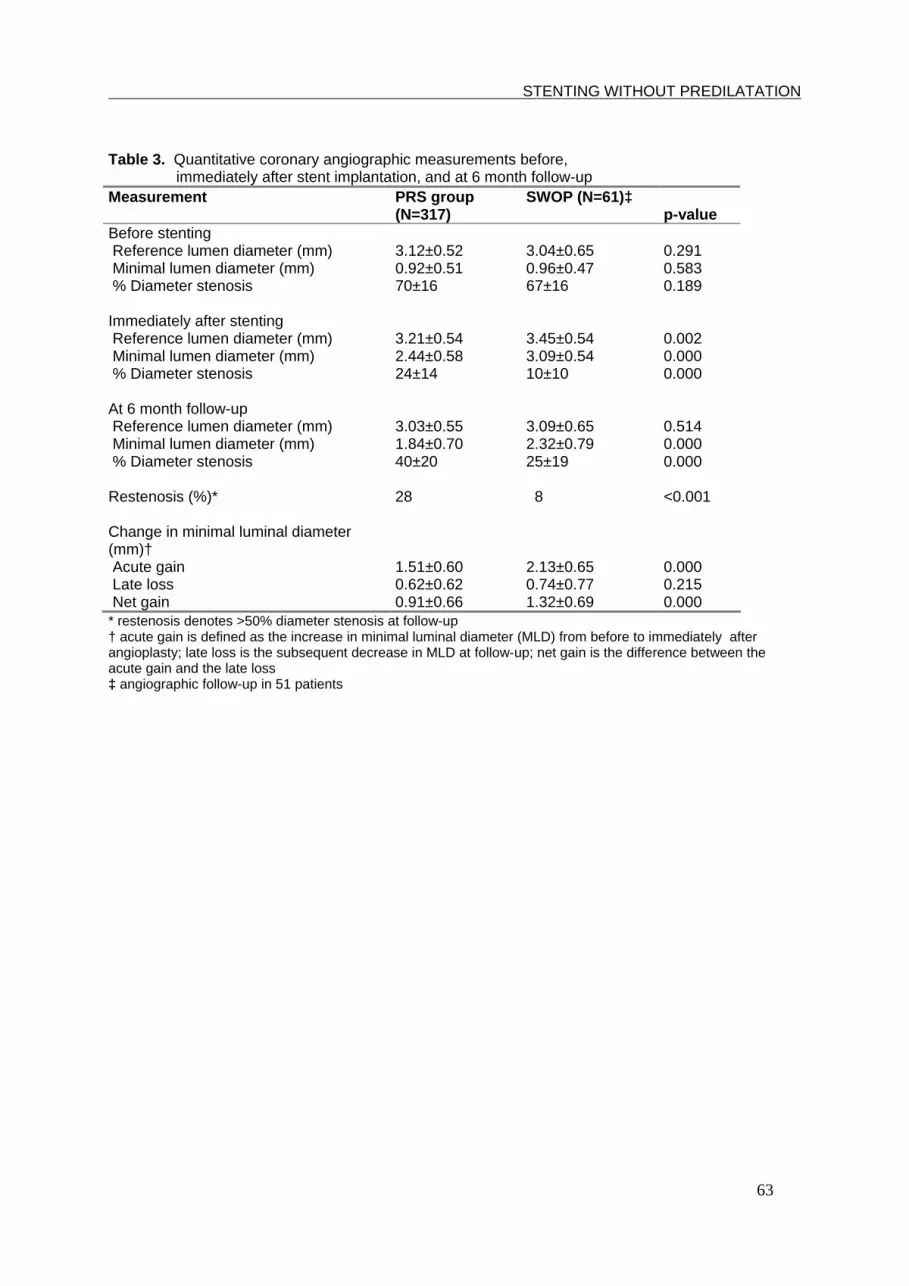
STENTING WITHOUT PREDILATATION
63
Table 3. Quantitative coronary angiographic measurements before, immediately after stent implantation, and at 6 month follow-up Measurement PRS group
(N=317) SWOP (N=61)‡
p-value Before stenting Reference lumen diameter (mm) Minimal lumen diameter (mm) % Diameter stenosis Immediately after stenting Reference lumen diameter (mm) Minimal lumen diameter (mm) % Diameter stenosis At 6 month follow-up Reference lumen diameter (mm) Minimal lumen diameter (mm) % Diameter stenosis Restenosis (%)* Change in minimal luminal diameter (mm)† Acute gain Late loss Net gain
3.12±0.52 0.92±0.51 70±16 3.21±0.54 2.44±0.58 24±14 3.03±0.55 1.84±0.70 40±20 28 1.51±0.60 0.62±0.62 0.91±0.66
3.04±0.65 0.96±0.47 67±16 3.45±0.54 3.09±0.54 10±10 3.09±0.65 2.32±0.79 25±19 8 2.13±0.65 0.74±0.77 1.32±0.69
0.291 0.583 0.189 0.002 0.000 0.000 0.514 0.000 0.000 <0.001 0.000 0.215 0.000
* restenosis denotes >50% diameter stenosis at follow-up † acute gain is defined as the increase in minimal luminal diameter (MLD) from before to immediately after angioplasty; late loss is the subsequent decrease in MLD at follow-up; net gain is the difference between the acute gain and the late loss ‡ angiographic follow-up in 51 patients

CHAPTER 5
64
Fig.1 MI, myocardial infarction; TLR, target lesion revascularization
0 1 2 3 4 5 6 7
100
90
80
70
tim e since index PCI (m onths)
Freedom from death, MI, or TVR (%)
SW OP
PRS
p=0.064
//

STENTING WITHOUT PREDILATATION
65
DISCUSSION Increasing the Efficacy of Stenting Today, coronary stents are used in up to 70-80% of the cases in interventional centers in the Netherlands. Since the indications for stent implantation are evolving, it is likely that numbers will increase further. For example, stent placement for restenotic lesions14, small vessels15, saphenous vein grafts16, long lesions17, and chronic total occlusions18,19 is under investigation. In addition, the availability of ticlopidine20 and abciximab21 and modern techniques like high pressure stent implantation22 has dramatically reduced the rate of subacute stent thrombosis. The continued focus on research efforts will increase the therapeutic benefit and improve the ease of the procedures. Krishna et al.23 showed that using one balloon for both lesion predilatation and poststent deployment significantly reduced resource utilization and costs. Another approach is direct stent implantation without predilatation, which may be of further advantage. First, the immediate results of stenting may be improved by means of reducing the procedural time. Second, SWOP could also result in a decrease in radiation and ischemic time and a reduction of complications. Third, considering that less trauma to the vessel wall results in less response to injury6,7, SWOP may lead to a lower frequency of in-stent restenosis. However, direct stenting seems to be less attractive in heavily calcified11, tortuous, and small vessels, and in chronic total occlusions, due to stent delivery problems. In the setting of primary PTCA for acute myocardial infarction, direct stenting is less feasible due to difficulties in properly assessing the lesion length. Several studies8-12 have demonstrated that SWOP is safe, leads to shorter radiation exposure times, and uses a smaller amount of contrast media and balloons. Direct stenting bears the potential advantage of fewer ischemic complications as compared with stent procedures with predilatation. In these studies, SWOP was successful demonstrating rates from 80%11 to 98.1%10 and 81% in the present study. Direct Stenting Without Predilatation This study focused on the angiographic results of direct stenting using the premounted Palmaz-Schatz Crown stent. This stent has a non-expanded profile of 1.4 mm (although the mean MLD before implantation was 0.96 mm). Also vulnerable lesions, like type C lesions, which occurred in 8% of the cases appeared to be well suited for direct stenting. Direct stenting is not restricted to straight vessel segments. In 55% of cases, the right coronary artery or left circumflex arteries were directly stented, which are by nature more tortuous vessels than the left anterior descending artery. At six month angiographic follow-up, only 8% of the SWOP group presented with a significant in-stent restenosis. This is a favorable result when compared with 28% restenosis in the PRS group. These data fit in the assumption that less injury results in less reaction of the vessel wall. Furthermore, this study also compares the results of routine stenting with PRS. The higher rate of stenting in the SWOP group will contribute to the better results in this group. Limitations of Stenting Without Predilatation Potential disadvantages of SWOP could be stent dislodgment, unpredictable stent expansion, and invisible lesion borders during stent placement. Direct stent implantation failed in 3% of the patients due to dislodgment. This figure is similar to the 4% in the initial series with the Palmaz-Schatz stent24,25 and the 2% presented by Laarman et al.12. The risk of stent dislodgment is clearly related to vessel and lesion characteristics, to the fixation of the stent on the balloon, and to the efforts of the operator.

CHAPTER 5
66
It could be argued that in difficult lesions the risk of incomplete stent deployment is unpredictable when no predilatation has been performed. Visibility of the lesion border during direct stent placement was no problem in the patient group. However, in case of application of SWOP for acute myocardial infarction this might be a draw back as in this setting the lesion length can often not be visualized. CONCLUSION Direct coronary stent implantation can be safe and efficacious. The risk of stent loss is low. The initial and long-term angiographic results are significantly better as compared with PRS. The risk of restenosis is significantly lower.

STENTING WITHOUT PREDILATATION
67
References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19.
Roubin GS, Cannon AD, Agrawal SK, et al. Intracoronary stenting for acute and threatened closure complicating percutaneous transluminal coronary angioplasty. Circulation 1992;85:916-927. George BS, Voorhees III WD, Roubin GS, et al. Multicenter investigation of coronary stenting to treat acute or threatened closure after percutaneous transluminal coronary angioplasty: Clinical and angiographic outcomes. J Am Coll Cardiol 1993;22:135-143. Sigwart U, Puel J, Mirkowitch V, et al. Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty. N Engl J Med 1987;316:701-706. Serruys PW, De Jaegere P, Kiemeneij F, et al. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331:489-495. Fischman DL, Leon MB, Baim DS, et al. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331:496-501. Edelman ER, Rogers C. Hoop Dreams, Stents without restenosis. Circulation 1996;94:1199-1202. Rogers C, Parikh S, Seifert P, et al. Endogenous cell seeding. remnant endothelium after stenting enhances vascular repair. Circulation 1996;94(11):2909-2914 Herz I, Assali A, Solodky A, et al. Coronary stenting without predilatation (SWOP): Applicable technique in everyday practice. Cathet Cardiovasc Intervent 2000; 49:384-388. Oemrawsingh PV, Schalij MJ, Srimahachota S, et al. Clinical and angiographic outcome of stent implantation without predilatation using the jostent flex stent. J Invasive Cardiol 2000;12:187-193. Chan AW, Carere RG, Solankhi N, et al. Coronary stenting without predilatation in a broad spectrum of clinical and angiographic situations. J Invasive Cardiol 2000;12:75-79. Figulla HR, Mudra H, Reifart N, et al. Direct Coronary Stenting Without Predilatation: A new therapeutic approach with a special balloon catheter design. Cathet Cardiovasc Diagn 1998;43:245-252. Laarman GJ, Muthusamy TS, Swart H, et al. Direct coronary stent implantation: safety, feasibility, and predictors of success of the strategy of direct coronary stent implantation. Cathet Cardiovasc Intervent 2001;52: 443-448. ten Berg JM, Kelder JC, Suttorp MJ, et al. Effect of coumarins started before coronary angioplasty on acute complications and long-term follow-up. A randomized trial. Circulation 2000;102:386-391. Erbel R, Haude M, Höpp HW, et al. Coronary -artery stenting compared with balloon angioplasty for restenosis after initial balloon angioplasty. N Engl J Med 1998;339:1672-1678. Savage MP, Fischman DL, Rake R, et al. Efficacy of coronary stenting versus balloon angioplasty in small coronary arteries. Stent restenosis Study (STRESS) Investigators. J Am Coll Cardiol 1998;31:307-311. Savage MP, Douglas JS, Fischman DL, et al. Stent placement compared with balloon angioplasty for obstructed coronary bypass grafts. Saphenous Vein De Novo Trial Investigators. N Engl J Med 1997;337:740-747. Antoniucci D, Valenti R, Santoro GM, et al. Preliminary experience with stent-supported coronary angioplasty in long narrowings using the long Freedom Force stent: Acute and six-month clinical and angiographic results in a series of 27 consecutive patients. Cathet Cardiovasc Diagn 1998;43:163-167. Sirnes PA, Golf S, Myreng Y, et al. Stenting in chronic coronary occlusions (SICCO): A randomized, controlled trial of adding stent implantation after successful angioplasty. J Am Coll Cardiol 1996;28:1444-1451. Buller CE, Dzavik V, Carere RG, et al. Primary stenting versus balloon angioplasty in occluded coronary arteries: The Total Occlusion Study of Canada (TOSCA). Circulation 1999;100:236-242.

CHAPTER 5
68
20. 21. 22. 23. 24. 25.
Goods CM, al-Shaibi KF, Liu MW, et al. Comparison of aspirin alone versus aspirin plus ticlopidine after coronary artery stenting. J Am Coll Cardiol 1996;78:1042-1044. The EPISTENT Investigators: Randomised placebo-controlled and balloon angioplasty-controlled trial to assess safety of coronary stenting with use of platelet glycoprotein IIb/IIIa blockade. Lancet 1998;352:87-92. Colombo A, Hall P, Nakamura S, et al. Intracoronary stenting without anticoagulation accomplished with intravascular ultrasound guidance. Circulation 1995;91:1676-1688. Krishna JRS, Trask RV, Lucore CL, et al. One Balloon, One Stent: An Effective Cost-Containment Strategy for Elective Stent Deployment. Cathet Cardiovasc Diagn 1997;40:17-20. Schatz RA, Baim DS, Leon M, et al. Clinical experience with the Palmaz-Schatz coronary stent. Initial results of a multicenter study. Circulation 1991;83:148-161. Shaknovich A: Complications of coronary stenting. Coronary Artery Dis 1994;5:583-589.

69
Chapter 6
Stenting for Restenotic Lesions with the BARD XT Stent
Braim M. Rahel Maarten J. Suttorp
1Hans A.M. te Riele Egbert T. Bal
Sjef M.P.G. Ernst E. Gijs Mast
Jurriën M. ten Berg Johannes C. Kelder H.W. Thijs Plokker
St. Antonius Hospital Nieuwegein, Dept of Cardiology,
1Thoraxcenter Ignatius Breda, Dept of Cardiology, the Netherlands
Published in the Journal of Interventional Cardiology 2003;16:227-230
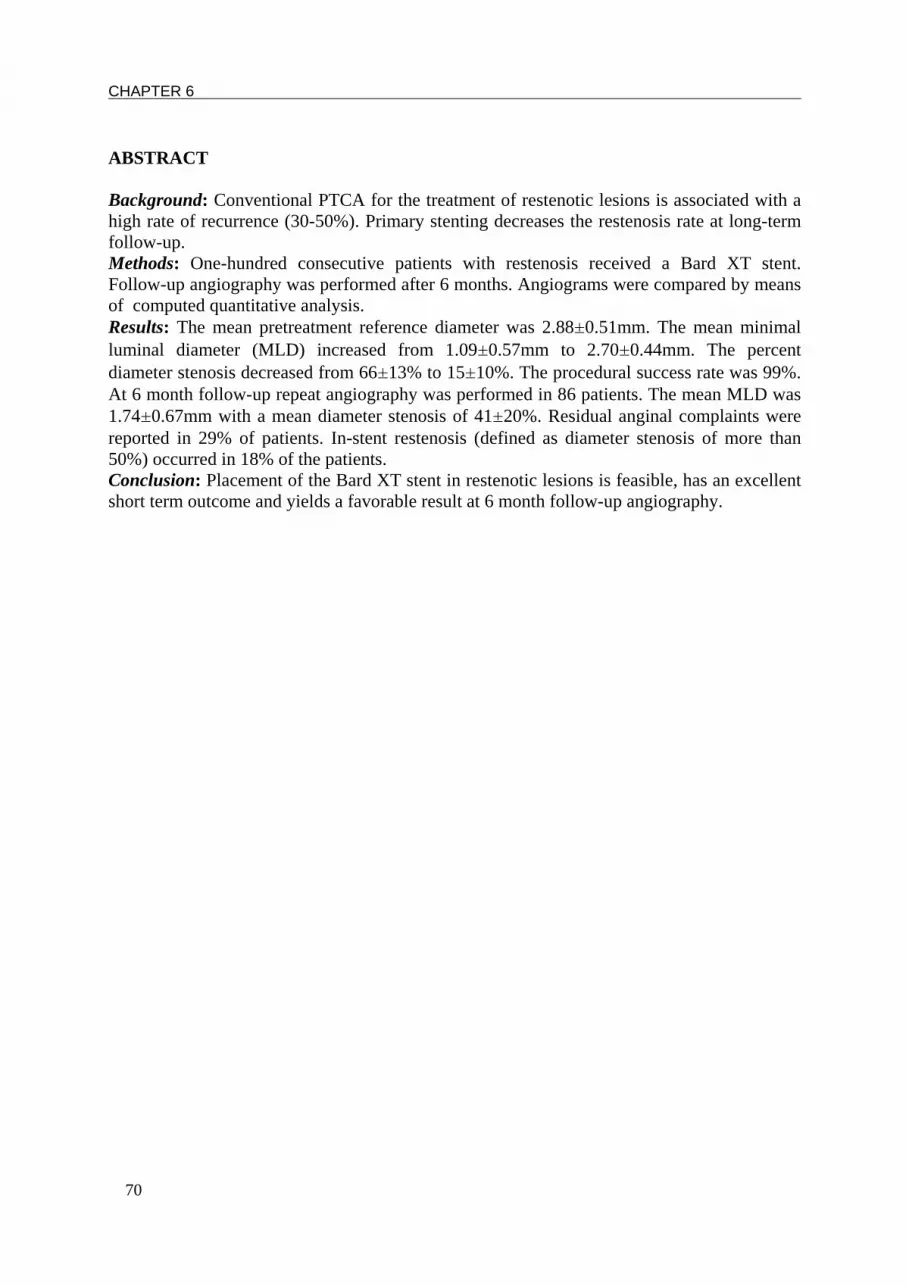
CHAPTER 6
70
ABSTRACT Background: Conventional PTCA for the treatment of restenotic lesions is associated with a high rate of recurrence (30-50%). Primary stenting decreases the restenosis rate at long-term follow-up. Methods: One-hundred consecutive patients with restenosis received a Bard XT stent. Follow-up angiography was performed after 6 months. Angiograms were compared by means of computed quantitative analysis. Results: The mean pretreatment reference diameter was 2.88±0.51mm. The mean minimal luminal diameter (MLD) increased from 1.09±0.57mm to 2.70±0.44mm. The percent diameter stenosis decreased from 66±13% to 15±10%. The procedural success rate was 99%. At 6 month follow-up repeat angiography was performed in 86 patients. The mean MLD was 1.74±0.67mm with a mean diameter stenosis of 41±20%. Residual anginal complaints were reported in 29% of patients. In-stent restenosis (defined as diameter stenosis of more than 50%) occurred in 18% of the patients. Conclusion: Placement of the Bard XT stent in restenotic lesions is feasible, has an excellent short term outcome and yields a favorable result at 6 month follow-up angiography.

STENTING FOR RESTENOSIS
71
INTRODUCTION Angiographic restenosis after percutaneous transluminal coronary angioplasty (PTCA) has been reported to occur in up to 50% of patients.1,2 Although a restenotic lesion can be treated successfully by means of repeat balloon angioplasty, a second restenosis after re-dilatation is reported to occur once again in 30-50% of patients.1,3 In de novo lesions, a significant reduction of restenosis was demonstrated in the Benestent and STRESS trials by using the Palmaz-Schatz stent.4,5 In a randomized study, Erbel et al. reported a beneficial effect of coronary stent implantation as compared with balloon dilatation in restenotic lesions.6 However, the lesion length in this group was too short. Although many studies investigated different treatment modalities for restenosis after conventional balloon angioplasty, data concerning ‘simple’ stent implantation are scarce. The purpose of this study is to test the immediate and 6-month angiographic results of stent implantation in restenotic lesions of any length using the Bard XT stent. METHODS Patients The study group consists of 100 consecutive patients. The study was conducted at two centers. Patients were included if they had a restenotic lesion in a native coronary artery with signs of ischemia related to this vessel. There were no limitations to lesion length. Exclusion criteria were in-stent restenosis, bifurcation lesions, pregnant or nursing women, contraindications for aspirin or ticlopidine, or use of anticoagulants that could not be discontinued before the procedure. The study was carried out according to the principles of the Declaration of Helsinki. Written informed consent was obtained from all patients. Angiographic Definitions Single-vessel coronary artery disease was defined as > 70% diameter stenosis in one coronary artery or one of its major side branches. Multivessel (two- or three-vessel) coronary artery disease was defined as a >70% diameter stenosis in one major coronary artery or its major side branches in addition to a >50% diameter stenosis in one or more other major coronary arteries. The early gain was defined as the difference between the minimal luminal diameter (MLD) after intervention and the diameter before intervention. Late loss was defined as the subsequent decrease in MLD of the treated artery at the 6-month follow-up angiography. Net gain was defined as the difference between the early gain and the late loss. The loss index was defined as the late loss divided by the early gain. Restenosis at follow-up was defined as >50% residual diameter stenosis at the previous angioplasty site, or death. Angioplasty Procedure Patients were pretreated with 100 mg aspirin once daily as well as calcium-channel antagonists. At the start of the procedure, patients received a bolus dose of 10,000 U heparin. No glycoprotein IIb/IIIa receptor blockers were used. PTCA was performed by means of either the femoral artery approach or the radial artery approach. Standard balloon and stent implantation techniques were applied. In all patients the bare Bard XT stent (Bard, Ireland) was used. This stent has a high radial strength and a maximum unexpanded (uncrimped) diameter of 1.45 mm (0.057 inch) and can be delivered by means of both 6 and 7 French guiding catheters. We used variable lengths of 11, 15, 19 and 24 mm.

CHAPTER 6
72
All stents had a similar nominal diameter which covered 3.0-4.0 mm and were adjusted to the individual vessel diameter. Final dilatation was performed at high balloon inflation pressures (>10 atm). Investigators attempted to achieve an optimal result with stent implantation, which was defined as a residual stenosis of less than 20% of the luminal diameter, according to a visual estimate. Before control angiography was performed, 500 µg intracoronary nitroglycerin was given and repeated if necessary. After successful stent implantation, all patients were prescribed long-term daily aspirin, ticlopidine 250 mg bid for 4 weeks, and calcium-channel antagonists for 3 months. Study End Points Patients were required to have clinical follow-up at 1 and 6 months. Coronary angiography was performed at 6 months or earlier, in case when symptoms occurred. The primary end point was angiographic evidence of restenosis, defined as a stenosis of more than 50% of the luminal diameter. Secondary end points included death, myocardial infarction, defined as the presence of new significant Q waves or an elevation of creatine kinase or its MB isoenzyme to at least two times the upper limit, and target lesion revascularization. Revascularization of the target lesion was defined as angioplasty or coronary artery bypass surgery because of recurrent angina pectoris or signs of ischemia. Other events recorded included bleeding in the groin (defined as major if requiring transfusion or surgery), and stroke. Angiographic Analysis Prestent, poststent implantation, and 6-month follow-up angiographic measurements were made under standard conditions with an on-line automatic computer-based edge-detection system (DCI, Philips Medical Systems, Eindhoven, The Netherlands) in the angiographic projection with the lowest MLD. The guiding catheter was used as the calibration standard. Statistical Analysis The main statistical analysis is descriptive. Continuous parameters are expressed as mean ± standard deviation; categorical parameters are expressed as percentage. Univariate and multivariate regression were used for baseline and angiographic characteristics. RESULTS Patient Characteristics Between September 1997 and March 1999, 100 patients at two centers were enrolled in the study. The baseline characteristics of the study group are shown in Table 1. Most of the patients had angina pectoris Canadian Cardiovascular Society (CCS) class III or IV. We could not demonstrate a significant relationship between the baseline characteristics and restenosis after univariate as well as multivariate analysis. The median duration of stent implantation after the previous PTCA was 5 months (Inter Quartile Range 3.5 - 7.6 months). The median duration after the previous PTCA and re-occurrence of anginal complaints was 1.7 months (IQR 0.9 - 3.4 months). After univariate and multivariate analysis both time-intervals were not found to predict restenosis after stent implantation. The angiographic characteristics are listed in table 2. Total stent length was univariately significant related to restenosis. The total stent length in the patient group with restenosis was 18.5±6.8 cm vs. 15.2±2.6 cm in the group without restenosis (p=0.044). Multivariate analysis revealed no other angiographic risk factor than stent length.
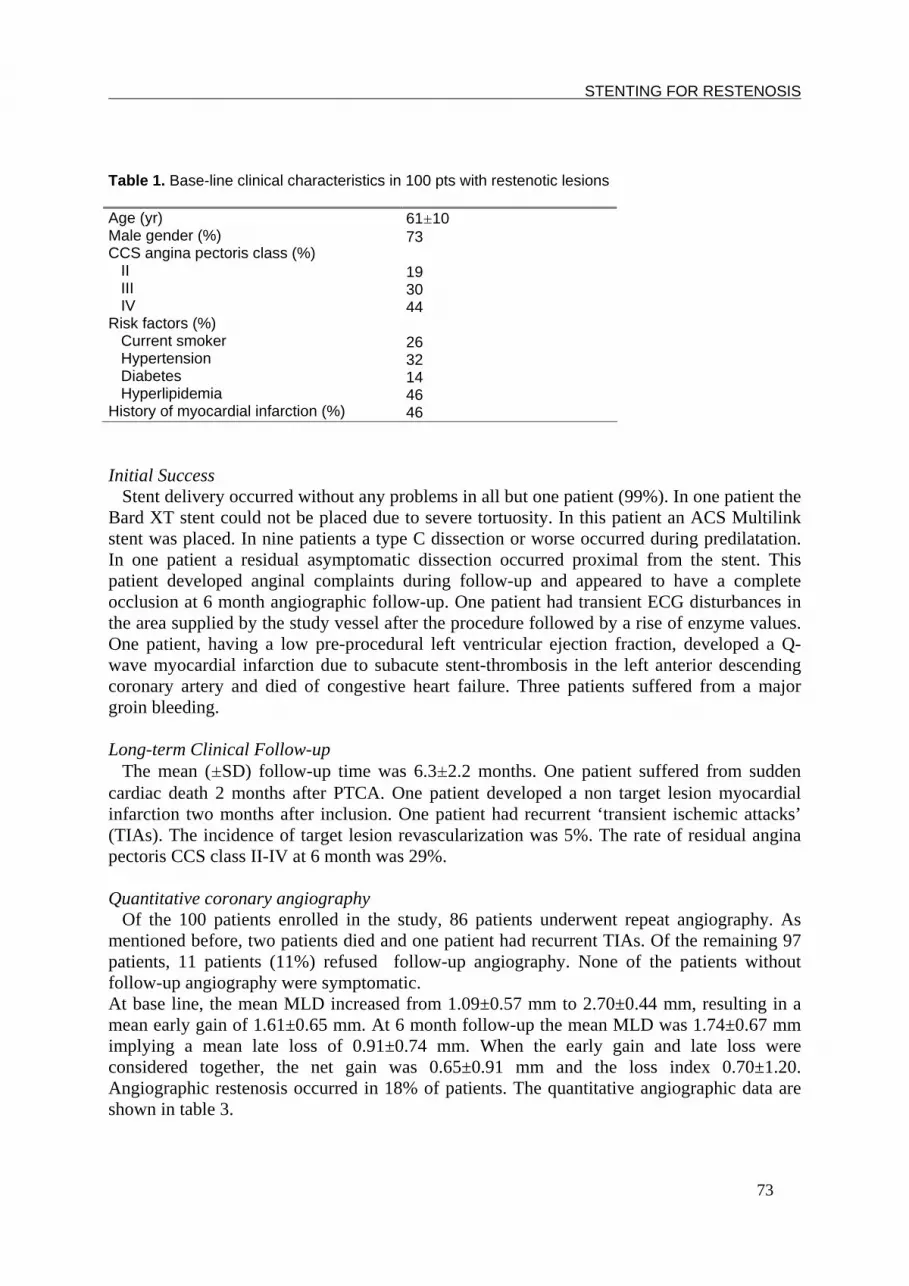
STENTING FOR RESTENOSIS
73
Table 1. Base-line clinical characteristics in 100 pts with restenotic lesions
Age (yr) Male gender (%) CCS angina pectoris class (%) II III IV Risk factors (%) Current smoker Hypertension Diabetes Hyperlipidemia History of myocardial infarction (%)
61±10 73 19 30 44 26 32 14 46 46
Initial Success Stent delivery occurred without any problems in all but one patient (99%). In one patient the Bard XT stent could not be placed due to severe tortuosity. In this patient an ACS Multilink stent was placed. In nine patients a type C dissection or worse occurred during predilatation. In one patient a residual asymptomatic dissection occurred proximal from the stent. This patient developed anginal complaints during follow-up and appeared to have a complete occlusion at 6 month angiographic follow-up. One patient had transient ECG disturbances in the area supplied by the study vessel after the procedure followed by a rise of enzyme values. One patient, having a low pre-procedural left ventricular ejection fraction, developed a Q-wave myocardial infarction due to subacute stent-thrombosis in the left anterior descending coronary artery and died of congestive heart failure. Three patients suffered from a major groin bleeding. Long-term Clinical Follow-up The mean (±SD) follow-up time was 6.3±2.2 months. One patient suffered from sudden cardiac death 2 months after PTCA. One patient developed a non target lesion myocardial infarction two months after inclusion. One patient had recurrent ‘transient ischemic attacks’ (TIAs). The incidence of target lesion revascularization was 5%. The rate of residual angina pectoris CCS class II-IV at 6 month was 29%. Quantitative coronary angiography Of the 100 patients enrolled in the study, 86 patients underwent repeat angiography. As mentioned before, two patients died and one patient had recurrent TIAs. Of the remaining 97 patients, 11 patients (11%) refused follow-up angiography. None of the patients without follow-up angiography were symptomatic. At base line, the mean MLD increased from 1.09±0.57 mm to 2.70±0.44 mm, resulting in a mean early gain of 1.61±0.65 mm. At 6 month follow-up the mean MLD was 1.74±0.67 mm implying a mean late loss of 0.91±0.74 mm. When the early gain and late loss were considered together, the net gain was 0.65±0.91 mm and the loss index 0.70±1.20. Angiographic restenosis occurred in 18% of patients. The quantitative angiographic data are shown in table 3.

CHAPTER 6
74
Table 2. Angiographic characteristics in 100 pts with restenotic lesions No. of diseased vessels pre-procedural (%) 1 2 3 Ejection fraction (%) >50% 20-50% <20% Target vessel (%) Left anterior descending Left circumflex Right coronary artery Lesion length (mm) Lesion type (%) A B C Stent length (mm) (number) 11 15 19 24 Stent diameter after dilatation (mm±SD)*
62 27 11 90 9 1 59 19 22 12.1±4.6 (range 3.0-30.0 mm) 24 66 10 12 68 21 7 3.50±0.35
* according to balloon diameter/inflation pressure Table 3. Quantitative coronary angiographic measurements pre-procedural post-procedural 6 month follow-up Ref. lum. diam.(mm)* 2.88±0.51 3.13±0.41 2.88±0.57 MLD (mm) % diameter stenosis
1.09±0.57 66.31±13.06
2.70±0.44 15.34±9.57
1.74±0.67 40.53±20.45
* Reference lumen diameter

STENTING FOR RESTENOSIS
75
DISCUSSION Restenosis remains the most important limitation with regard to the long-term benefit of percutaneous balloon angioplasty. The technique of balloon angioplasty in its widest sense has shown a dramatic improvement ever since this technique was started by Grüntzig in 1977.7 However, this is still not the ultimate solution for restenosis8 since a second restenosis after re-dilatation is reported to occur once again in 30-50% of the patients.1,3 Until now, there are only few data describing the effect of coronary stent implantation for restenosis after conventional balloon angioplasty. In this study, the major finding is that coronary stent implantation for the treatment of restenosis after balloon angioplasty is associated with an angiographic second restenosis rate of 18%. This figure is a favorable outcome as compared with conventional balloon angioplasty for restenosis.1,3 This is not surprising since the main advantage of placement of a stent over balloon angioplasty is the larger luminal diameter achieved. A higher residual diameter stenosis is a risk factor for restenosis.9,10 Erbel et al.6 reported an in-stent restenosis rate of 18% after stent implantation which is similar to our results. However, contrary to our study, only patients with short lesions were included in that study. Another difference is that we did not use the Palmaz-Schatz stent but the Bard XT stent .11,12 The main advantages of the latter are that it has a lower profile and is available at different lengths. Despite the inclusion of relatively long lesions in our study we experienced few difficulties in stent delivery. In addition, a low rate of stent thrombosis was noted. This study was not designed as a randomized trial. Comparing the Bard XT stent with other stents in the treatment of restenosis after conventional balloon angioplasty would be of interest. Especially drug-eluting stents, such as the rapamycin stent, seem very promising.13 CONCLUSION The Bard XT stent can be placed in restenotic lesions of any length with excellent acute angiographic results. The incidence of in-hospital adverse effects is low. In addition, a favorable outcome is noted at 6 month angiographic follow-up.

CHAPTER 6
76
References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13.
Serruys PW, Foley DP, Kirkeeide RL, et al. Restenosis revisited: insights provided by quantitative coronary angiography. Am Heart J 1993;126:1263-1267. Rupprecht HJ, Brennecke R, Bernhard G, et al. Analysis of risk factors for restenosis after PTCA. Cath Cardiovasc Diagn 1990;19:151-159. Quigley PJ, Hlatky MA, Hinohara T, et al. Repeat percutaneous transluminal coronary ngioplasty and predictors of recurrent restenosis. Am J Cardiol 1989;63:409-413. Serruys PW, De Jaegere P, Kiemeneij F, et al. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331:489-495. Fischman DL, Leon MB, Baim DS, et al. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331:496-501. Erbel R, Haude M, Höpp HW, et al. for the Restenosis Stent Study Group. Coronary-artery stenting compared with balloon angioplasty for restenosis after initial balloon angioplasty. N Engl J Med 1998;339:1672-1678. Grüntzig AR, Sennig A, Siegenthaler WE: Non-operative dilatation of coronary-artery stenosis: Percutaneous transluminal coronary angioplasty. N Engl J Med 1979;301:61-68. Sugrue DD, Vlietstra RE, Hammes LN, et al.: Repeat balloon coronary angioplasty for symptomatic restenosis: a note of caution. Eur Heart J 1987;8:697-701. Bourassa MG, Lespérance J, Eastwood C, et al. Clinical, physiologic, anatomic and procedural factors predictive of restenosis after percutaneous transluminal coronary angioplasty.J Am Coll Cardiol 1991;18:368-376. Rupprecht HJ, Brennecke R, Bernhard G, et al. J. Analysis of risk factors for restenosis after PTCA. Cath Cardiovasc Diagn 1990;19:151-159. Ravat H, Cannon A. Early experience with the Bard XT stent. Cathet Cardiovasc Diagn 1998;45:462-470. Bueno RR, Guerios EE, Tarastchuk JC, et al. Angiographic results and late clinical follow-up after Bard-XT intracoronary stent implantation. J Invasive Cardiol 1999;11:661-666 Chan AW, Chew DP, Lincoff AM. Update on pharmacology for restenosis. Curr Interv Cardiol Rep 2001;3:149-155.

77
Chapter 7
Cutting Balloon for in-stent restenosis: acute and longterm results
Braim M. Rahel
Maarten Jan Suttorp Jurriën M. ten Berg
Egbert T. Bal Sjef M.P.G. Ernst Benno J. Rensing
Johannes C. Kelder H.W. Thijs Plokker
St. Antonius Hospital Nieuwegein, Dept of Cardiology, the Netherlands
Published in the Journal of Interventional Cardiology 2004;17:197-201

CHAPTER 7
78
ABSTRACT Introduction: Conventional percutaneous coronary intervention for the treatment of in-stent restenosis (ISR) has shown a high rate of ISR (30-55%). Considering the need for both extrusion of hyperplastic intima and additional stent expansion, a cutting balloon might be more effective for the treatment of ISR. Methods: We prospectively assessed the immediate and 8-month outcome of balloon angioplasty using the BARATH Cutting Balloon in 100 consecutive patients (mean age 60.5±10.8 yrs, 71% male). Results: In 73 lesions (73%) a good result was reached with the cutting balloon only. In 21 lesions (21%) postdilatation and in 6 lesions (6%) predilatation with a conventional balloon was necessary. The mean inflation pressure was 8.7±2.0 (range 6.0-18.0) atm. Before the procedure the mean minimal luminal diameter (MLD) was 0.95±0.45mm. Quantitative coronary analysis showed a mean diameter stenosis of 65±16%. Immediately after the procedure the mean MLD was 2.42±0.54mm with a mean diameter stenosis of 19±13%. Two patients died during the follow-up period (1 stroke, 1 nonvascular). At 8 month follow-up 26 patients (26%) reported to have anginal complaints CCS class 2 to 4 of whom 16 (16%) needed target lesion revascularization. Conclusion: Treatment of ISR using the Barath Cutting Balloon can be performed safely with good immediate results and a relatively low need for repeated target lesion revascularization at 8 month follow-up.

CUTTING BALLOON FOR IN-STENT RESTENOSIS
79
INTRODUCTION Coronary stent implantation has been shown superior to plain old balloon angioplasty (POBA) in the prevention of restenosis after percutaneous coronary intervention (PCI).1,2 In the past decade, stenting has replaced POBA for the treatment of obstructive coronary artery disease. The long-term success of stenting, however, remains limited by the occurrence of in-stent restenosis (ISR), which may occur in 20-30% of cases. Balloon angioplasty for ISR has been performed with excellent immediate results but the angiographic restenosis rate is high. 3,4 The mechanism of PCI for ISR is a combination of additional stent expansion and tissue extrusion out of the stent.5 It is thought that the incisions made by the cutting balloon facilitate maximum dilatation with less dilating force, making cutting balloon a preferable treatment modality for ISR compared with POBA . The aim of this study was to evaluate the immediate and long-term efficacy of cutting balloon angioplasty (CBA) in the treatment of ISR. METHODS Patients The study group consisted of 100 consecutive patients admitted to our hospital in a prospective, nonrandomized study. Patients were included if they had an ISR in a native coronary artery with signs of ischemia related to this vessel. There were no limitations to lesion-length. Exclusion criteria were contraindications for aspirin, and factors making long-term follow-up difficult or unlikely. Angiographic Definitions Single vessel disease was defined as >70% diameter stenosis in one coronary artery or one of its major side branches. Multivessel (two or three vessel) coronary artery disease was defined as >70% diameter stenosis in one major coronary artery or its major side branches in addition to a >50% diameter stenosis in one or more other major coronary arteries. Acute gain was defined as the increase in the minimal luminal diameter of the treated artery from before to immediately after angioplasty. Patterns of ISR were defined as follows: diffuse type: ISR extending greater than half the length of the stent; focal: less than half the length of the stent; edge: ISR limited to one of the edges of the stent; total: (functional) occlusion, with Thrombolysis in Myocardial Infarction (TIMI) grade 0 or 1 flow. Angioplasty Procedure Patients were pretreated with 100 mg aspirin. At the beginning of the procedure patients received a bolus dose of 10,000 U heparin. In all patients the cutting balloon was used, which was originally developed by Barath6, and manufactured by Boston Scientific (Natick, MA). The cutting balloon consists of a noncompliant dilatation balloon with 3 or 4 atherotomes (microsurgical blades) mounted longitudinally on its outer surface. The balloon is engineered to protect the edges of the microblades when the balloon is collapsed, thus preventing injury to the artery as the catheter is passed. When the balloon is inflated, the blades incise the plaque, relieving its hoop stress. It is expected that these incisions facilitate maximum dilatation of the lesion with the least amount of dilating force.

CHAPTER 7
80
Long-Term Follow-Up
Clinical follow-up was performed at 8 months. Repeat angina pectoris, a positive exercise test, or abnormal nuclear imaging were considered as clinical signs of restenosis. Death, MI (defined as the presence of new significant Q waves or an elevation of creatine kinase or its MB isoenzyme to at least two times the upper limit), or target lesion revascularization (TLR, defined as percutaneous or surgical revascularization of the target lesion after the initial procedure) were all recorded as major adverse clinical events (MACE). At 8 months follow-up patients were asked to return for exercise testing. An exercise test was defined as positive if there was ST depression of at least 1.0 mm, that is horizontal or down-sloping or upsloping ST depression of at least 2.0 mm. The test was defined as nonconclusive if the patient did not meet the criteria for a positive test and stopped before 80% of the predicted maximal heart rate was achieved. Repeat angiography was planned if there were clinical signs of restenosis and eventual followed by target lesion revascularization. RESULTS Patient Characteristics Between March 1998 and May 2002 we treated 100 patients for ISR with a cutting balloon. The mean duration of the recurrence of anginal complaints after stent implantation was 8.6 months. No patient presented with acute MI as a sign of ISR. The baseline characteristics are shown in Table 1. Most of the patients had angina pectoris Canadian Cardiovascular Society (CCS) class III or IV. The angiographic data are listed in Tables 2 and 3. Table 1. Baseline characteristics in 100 patients with in-stent restenosis. Age (yr) Male gender (%) CCS angina pectoris class (%) II III IV Smoking (%) Hypertension (%) Hyperlipidemia* (%) History of MI †(%) History of stroke (%)
60.5±10.8 71 18 44 36 12 36 36 46 4
*defined as total cholesterol > 5.0 mmol/L † MI: Myocardial infarction
Initial Success Predilatation with a conventional balloon was necessary in 6 patients (6%). In 21 patients (21%) postdilatation with other (high pressure) balloons was necessary for an optimal result. Two patients needed urgent stent implantation within 1 hour after the procedure (one dissection distal to the stent, one stent occlusion). One patient developed transient anginal complaints, showing a type B dissection at urgent re-angiography, and was treated conservatively. This patient did well during follow-up. No patient had a subacute stent thrombosis.

CUTTING BALLOON FOR IN-STENT RESTENOSIS
81
Long-Term Clinical Follow-Up Clinical follow-up was completed in 100% of the patients. One patient had a stroke one day after the procedure and subsequently died. One patient died due to a traffic accident. During follow-up 26 patients (26%) developed recurrent angina pectoris CCS class II to IV. Fifty-nine patients returned for an exercise test which was positive in 20%, non-conclusive in 19% and negative in 61%. At 8 month follow-up 16 patients (16%) needed target lesion revascularization (9 patients re-PCI, 7 patients CABG). No patient had a myocardial infarction. Subanalysis of the baseline characteristics yielded no predictor for TLR (Table 4). Table 2. Angiographic characteristics. No. of diseased vessels pre-procedural (%) 1 2 3 Left ventricular ejection fraction (%) >50% 20-50% <20% Target vessel (%) Right coronary artery Left main stem Left anterior descending Left circumflex In-stent lesion type (%) focal edge diffuse total Stent length (%) <10 mm 10-20 mm > 20 mm Mean inflation pressure (atm)(±SD)
76 20 4 93 7 0 29 2 44 25 34 7 51 8 10 64 26 8.5±2.2 (range:6.0-18.0)
Table 3. Quantitative coronary angiographic measurements. Measurements before the procedure Reference lumen diameter (mm) Minimal lumen diameter (mm) %Diameter stensosis Measurements after the procedure Reference lumen diameter (mm) Minimal lumen diameter (mm) %Diameter stensosis Acute gain (mm)
2.79±0.62 0.95±0.45 65±16 2.96±0.66 2.42±0.54 19±13 1.45±0.68

CHAPTER 7
82
Table 4. Comparison baseline characteristics between patients with and without TLR. TLR+
(n=16) TLR- (n=84)
p-value
Age (yr) Male gender (%) CCS angina pectoris class (%) II III IV Smoking (%) Hypertension (%) Hyperlipidemia(%) History of MI (%) History of stroke (%) Lesion type (%) focal edge diffuse total Lesion length, mm (±sd) Max. pressure, atm (±sd) Acute gain, mm (±sd)
60.5±11.0 50.0 31.3 25.0 37.5 18.8 31.3 43.6 25.0 0.0 31.3 0.0 62.5 6.3 17.0±7.2 8.4±1.5 1.52±0.67
59.8±12.6 75.9 14.9 46.0 36.8 10.7 37.2 34.1 49.4 4.7 34.1 8.2 49.4 8.2 13.8±7.7 8.6±2.3 1.44±0.69
0.837 0.065 0.183 0.402 0.781 0.571 0.101 0.999 0.823 0.513 0.337 0.814 0.108 0.737 0.690
TLR, Target lesion revascularization
DISCUSSION Treatment of ISR has become an increasing challenge due to the increased use of coronary stents in the past decade. The mechanism of ISR parallels wound healing responses, with thrombus deposition and acute inflammation processes in the early phase followed by smooth muscle cell proliferation.7,8 In a recent histopathologic study Moreno et al. showed that in-stent restenotic tissue as compared with restenotic tissue after POBA is composed of larger areas of smooth muscle cells (96% of total plaque area vs. 46%) at the expense of macrophages and collagen.9 Increased damage to the vessel wall has been proposed as a responsible mechanism for this enhanced neointimal growth.7,8 It is believed that the incisions made by the atherotomes of the cutting balloon facilitate maximum dilatation with less dilating force, thus minimizing trauma to the vessel wall. The cutting balloon enlarges the coronary lumen mainly by in-stent tissue reduction associated with a moderate degree of additional stent expansion.10 The purpose of this study was to evaluate the immediate and long-term clinical outcome of CBA in the treatment of ISR. The present series demonstrate that, when ISR occurs, the stent usually can be recrossed and the lesion effectively dilated using the cutting balloon.

CUTTING BALLOON FOR IN-STENT RESTENOSIS
83
Predilatation was only necessary in 6% of the patients, but in all lesions the cutting balloon eventually passed. The mean inflation pressure needed for successful redilatation was 8.5±2.2 atm.. This relatively low pressure is comparable with the mean dilating pressure of 10.7±2.8 atm. used in the study performed by Adamian et al.11, 8.7±1.2 atm. used by Miyamoto et al.12, and 9±1.2 atm. used by Chevalier et al..13 During long-term follow-up 26 patients (26%) developed recurrent anginal complaints CCS class II to IV. TLR was necessary in 16 patients (16%), which is similar to the 15.8% shown by Adamian et al.11, and 12% shown by Chevalier et al.13 but lower than the 32% shown by Miyamoto et al..12 One study reported an extremely low TLR percentage of 3.8%.14 There are multiple alternative percutaneous revascularization techniques for ISR. The most simple treatment for ISR is POBA, which is associated with good immediate results but has a high need for repeat TLR varying from 20% to 35%. Balloon angioplasty for diffuse in-stent restenosis shows the highest incidence of repeat ISR.3,4,15,16 Stenting for ISR also has good immediate results but has a similar high TLR rate of 20%- 35%.11,17,18 Pretreatment with atheroablative techniques prior to balloon dilatation yields, as compared with historical data, no better results. The TLR percentage after rotational atherectomy is 26%-32%11,19,20 and 23%- 26% after excimer laser angioplasty.21,22 Intra-coronary radiation therapy might be the best alternative. Rates of TLR after beta-radiation vary from 17% in the START trial to as low as 3% in the BRITE I trial.23-25 Use of gamma-radiation resulted in TLR rates of 12-28% in the SCRIPPS and GAMMA-1 trials.26,27 Drug-eluting stents, which show no clinically significant ISR, might be a very promising treatment option to prevent repeat ISR28,29 However, further data have to be awaited. Study limitations The present study is not randomized, compelling any comparison to historical data. There was no angiographic follow-up which makes it difficult to relate residual anginal complaints to target lesion restenosis. CONCLUSION Angioplasty for ISR using a cutting balloon has excellent immediate results and a low rate of long-term clinical events and a low need for repeated target lesion revascularization. Until now there are no superior treatment modalities for ISR, which makes the cutting balloon a good alternative with relatively low expenses and no need for further operator training.

CHAPTER 7
84
References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21.
Serruys PW, de Jaegere P, Kiemeneij F, et al., for the Benestent Study Group. A comparison of balloon-expandable stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331:489-495. Fischman DL, Leon MB, Baim DS, et al. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331:496-501. Eltchaninoff H, Koning R, Tron C, et al. Balloon angioplasty for the treatment of coronary in-stent restenosis: Immediate results and 6-month angiographic recurrent restenosis rate. J Am Coll Cardiol 1998;32:980-984. Bauters C, Banos JL, Van Belle E, et al. Six-month angiographic outcome after successful repeat percutaneous intervention for in-stent restenosis. Circulation 1998;97:318-321. Mehran R, Mintz GS, Popma JJ, et al. Mechanisms and results of balloon agnioplasty for the treatment of in-stent restenosis. Am J Cardiol 1996;78:618-622. Barath P, Fischbein MC, Vari S, et al. Cutting Balloon: a novel approach to percutaneous angioplasty. Am J Cardiol 1991;68:1249-1252. Farb A, Sangiorgi G, Carter AJ, et al.Pathology of acute and chronic coronary stenting in humans. Circulation 1999;99:44-52. Virmani R, Farb A. Pathology of in-stent restenosis. Curr Opin Lipidol 1999;10(6):499-506. Moreno PR, Palacios IF, Leon MN, et al. Histopathologic comparison of human in-stent and post-balloon angioplasty restenotic tissue. Am J Cardiol 1999;84:462-466. Montorsi P, Galli S, Fabbiocchi F, et al. Mechanism of cutting balloon angioplasty for in-stent restenosis: an intravascular ultrasound study. Catheter Cardiovasc Interv 2002; 56:166-173. Adamian M, Colombo A, Briguori C, et al. Cutting balloon angioplasty for the treatment of in-stent restenosis: a matched comparison with rotational atherectomy, additional stent implantation and balloon angioplasty. J Am Coll Cardiol 2001;38:672-679. Miyamoto T, Araki T, Hiroe M, et al. Standalone cutting balloon angioplasty for the treatment of stent-related restenosis: acute results and 3- to 6- month angiographic recurrent restenosis rates. Catheter Cardiovasc Interv 2001;54:301-308. Chevalier B, Royer T, Guyon P, et al. Treatment of in-stent restenosis: short and midterm results of a pilot randomized study between balloon and cutting balloon. J Am Coll Cardiol 1999;33:62A (Abstract). Mizobe M, Oohata K, Osada T. The efficacy of cutting balloon for in-stent re-restenosis: compared with conventional balloon angioplasty. Circulation 1999;100:I-308 (Abstract). Macander PJ, Roubin GS, Agrawal SK, et al. Balloon angioplasty for treatment of in-stent restenosis: feasibility, safety, and efficacy. Cathet Cardiovasc Diagn 1994;32:125-131. Bossi I, Klersy C, Black AJ, et al. In-stent restenosis: long-term outcome and predictors of subsequent target lesion revascularization after repeat balloon angioplasty. J Am Coll Cardiol 2000;35:1569-1576. Al-Sergani HS, Ho PC, Nesto RW, et al. Stenting for in-stent restenosis: A long term clinical follow-up. Catheter Cardiovasc Interv 1999;48:143-148. Antoniucci D, Valenti R, Moschi G, et al. Stenting for in-stent restenosis. Catheter Cardiovasc Interv 2000;49:376-381. Sharma SK, Duvvuri S, Dangas G, et al. Rotational atherectomy for in-stent restenosis: acute and long-term results of the first 100 cases. J Am Coll Cardiol 1998;32:1358-1365. Dauerman HL, Baim DS, Cutlip DE, et al. Mechanical debulkin versus balloon angioplasty for the treatment of diffuse in-stent restenosis. Am J Cardiol 1998;82:277-284. Mehran R, Dangas G, Mintz GS, et al. Treatment of in-stent restenosis with excimer laser coronary angioplasty versus rotational atherectomy: comparative mechanisms and results. Circulation 2000;101:2484-2489.

85
22. 23. 24. 25. 26. 27. 28. 29.
Dahm JB, Kuon E. High-energy eccentric excimer laser angioplasty for debulking diffuse in-stent restenosis leads to better acute- and 6-month follow-up results. J Invasive Cardiol 2000;12:335-342. Popma JJ, Suntharalingam M, Lansky AJ, et al. Stents And Radiation Therapy (START) Investigators. Randomized trial of 90Sr/90Y beta-radiation versus placebo control for treatment of in-stent restenosis. Circulation 2002;106:1090-1096. Moustapha A, Salloum J, Saika S, et al. Combined cutting balloon angioplasty and intracoronary beta radiation for treatment of in-stent restenosis: clinical outcomes and effect of pullback radiation for long lesions. Catheter Cardiovasc Interv 2002;57:325-329. Waksman R, Buchbinder M, Reisman M, et al. Balloon-based radiation therapy for treatment of in-stent restenosis in human coronary arteries, results from the BRITE I study. Catheter Cardiovasc Interv 2002;57:295-296. Teirstein PS, Massullo V, Jani S, et al. Catheter-based radiotherapy to inhibit restenosis after coronary stenting. N Engl J Med 1997;336:1697-1703. Leon MB, Teirstein PS, Moses JW, et al. Localized intracoronary gamma-radiation therapy to inhibit the recurrence of restenosis after stenting. N Engl J Med 2001;344:250-256. Morice MC, Serruys PW, Sousa JE, et al. RAVEL Study Group. Randomized study with the sirolimus-coated Bx Velocity balloon-expandable stent in the treatment of patients with de novo native coronary artery lesions. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med 2002;346:1773-1780. Sousa JE, Costa MA, Abizaid A, et al. Sirolimus-eluting stent for the treatment of in-stent restenosis: a quantitative coronary angiography and three-dimensional intravascular ultrasound study. Circulation 2003;107:24-27.

CHAPTER 7
86

87
Chapter 8
Primary Stenting of Occluded Native Coronary Arteries: Final Results of the Primary Stenting of Occluded Native
Coronary Arteries (PRISON) Study.
Braim M. Rahel Maarten J. Suttorp
1Gert J. Laarman 1Ferdinand Kiemeneij
Egbert T. Bal Benno J. Rensing Sjef M.P.G. Ernst
Jurriën M. ten Berg Johannes C. Kelder H.W. Thijs Plokker
St Antonius Hospital Nieuwegein, Dept of Cardiology, 1Onze Lieve Vrouwe Gasthuis Amsterdam, Dept of Cardiology,
The Netherlands
Published in the American Heart Journal 2004;147:e22

CHAPTER 8
88
ABSTRACT Background: Primary intracoronary stent placement after successfully crossing chronic total coronary occlusions may decrease the high restenosis rate at long-term follow-up compared with conventional balloon angioplasty. Methods: In a prospective, randomized trial, balloon angioplasty was compared with stent implantation for the treatment of chronic total occlusions. Patients were followed for 12 months with angiographic follow-up at 6 months. Quantitative coronary analysis was performed by an independent core lab. Results: A total of 200 patients were enrolled. Baseline characteristics were evenly distributed. After the procedure the mean minimal luminal diameter in the conventional group was 2.34±0.46mm versus 2.90±0.41mm in the stented group (p<0.0001). The 6-month angiographic follow-up showed a mean minimal luminal diameter of 1.57±0.74mm in the conventional group versus 1.93±0.85mm in the stented group (p=0.009) and a mean diameter stenosis of 44.7±25.0% versus 35.5±26.5% (p=0.036). Binary angiographic restenosis (>50% diameter stenosis) was seen in 33% in the conventional group versus 22% in the stented group (p=0.137). The reocclusion rates were 7.3% and 8.2% respectively (p=1.00). At 12 month follow-up, the rate of target lesion revascularization was significantly higher in the conventional group (29% versus 13%, p<0.0001). Conclusion: These data demonstrate that stenting of chronic total occlusions is superior to balloon angioplasty alone with a statistically significant reduction in the need for target lesion revascularization and a lower, but not significant, restenosis rate.

STENTING OF CHRONIC TOTAL OCCLUSIONS
89
INTRODUCTION Since the introduction of percutaneous coronary intervention (PCI) by Gruentzig in 1977 1, this revascularization technique has been applied for an increasing number of indications. Chronic total occlusions were considered to be a relative contraindication for PCI because of a low success rate (between 51% and 73%) and a high restenosis rate (up to 68%).2-6 Therefore many of these patients have been referred for coronary artery bypass graft surgery instead of balloon angioplasty. Recent studies showed an improved outcome after coronary stent implantation for chronic total occlusions, with restenosis rates between 32% and 55%. In most of these trials first generation stents were used in relatively small numbers of patients lacking long-term follow-up.7-12 We performed a prospective randomized study in 200 patients with chronic total occlusions. The aim of our trial was to compare the immediate, 6-month, and 12-month results of balloon angioplasty with primary intracoronary stent placement using the NIR stent (Boston Scientific, Maple Grove, Minn). METHODS Patients The PRImary Stenting of Occluded Native coronary arteries (PRISON) study was a randomized, 2-center trial of 200 patients recruited between January 1998 and November 1999. We investigated the effect of coronary NIR stent implantation versus balloon angioplasty in chronic coronary occlusions. Patients were included if the estimated duration of the chronic total occlusion was at least 2 weeks with evidence of ischemia related to the occluded coronary artery. Patients were excluded if the lesion could not be crossed or if the target lesion length was >30mm. The study was conducted according to the principles of the Declaration of Helsinki, and all patients gave written informed consent before they underwent the procedure. Angiographic definitions Chronic total coronary artery occlusion was defined by the absence of antegrade flow of contrast distal to the occlusion (flow grade 0 according to the Thrombolysis and Myocardial Infarction [TIMI] score) or only minimal flow of contrast distal to the occluded vessel (TIMI flow I).13 The duration of the total occlusion was estimated by clinical information, sequential angiographic information, or both. The estimated length of the occlusion was measured from the point of the chronic occlusion to the most proximal point of the distal vessel, which was visualized by collateral filling with contrast. Angioplasty procedure Percutaneous coronary intervention was performed from either the femoral artery or radial artery approach with standard recanalization and stent implantation techniques. The major goal was to achieve a residual luminal diameter stenosis <30% on visual assessment. Randomization was performed after crossing the lesion, but before initial dilatation. Patients were randomized by a telephone allocation service, which was provided with the randomization list before recruitment of the first patient. Patients were equally assigned to either the balloon group or stent group. In all stented lesions the NIR stent (Boston Scientific) was used. Final dilatation was performed with high inflation pressures in all patients. At the beginning of the procedure patients received a single dose of heparin 10,000 U.

CHAPTER 8
90
All patients received aspirin before the procedure. Ticlopidine or clopidogrel was added for 1 month for the patients who received stents. Quantitative coronary analysis The angiograms were analyzed by an independent core angiography laboratory (Heart Core B.V., Leiden, The Netherlands). The observers were not provided with the clinical information of the patients. Before angiography 500 µg nitroglycerin was given intracoronary. The guiding catheter was used as the calibration standard. All lesions were assessed in ≥ 2 orthogonal views and the projection showing the smallest diameter was used for quantitative coronary angiography analysis, and views with the least foreshortening were used for measuring the length of the occlusion. In disease-free proximal segments the reference diameter was measured. Cineangiograms were obtained before, immediately after and at 6 months, using the same views. Any coronary angiography performed within 3 months after the initial procedure was considered unscheduled. When an unscheduled angiography was followed by target lesion revascularization (TLR), no further angiograms were needed. If no TLR took place, repeat angiography at 6 months was still required. If the angiography took place after 3 months, 6 months angiographic assessment was not mandatory. The early gain was defined as the difference between the minimal luminal diameter (MLD) after intervention and the diameter before intervention. Late loss was defined as the subsequent decrease in MLD of the treated artery at the 6-month follow-up angiography. The loss index was defined as the late loss divided by the early gain. Long-term follow-up Clinical follow-up was performed at 6 and 12 months. Repeat angina pectoris, a positive exercise test, or abnormal nuclear imaging were considered as clinical signs of restenosis. Follow-up angiography was performed earlier if there were clinical signs of restenosis and eventual followed by TLR. Death, myocardial infarction (MI) (defined as the presence of new significant Q waves or an elevation of creatine kinase or its MB isoenzyme to ≥ 2 times the upper limit), occurrence of angina pectoris (Canadian Cardiovascular Society class III or IV), or TLR (defined as percutaneous or surgical revascularization of the target lesion after the initial procedure) were all recorded as major adverse clinical events. Restenosis and reocclusion Angiographic restenosis at follow-up was defined as > 50% residual diameter stenosis at the previous angioplasty site. Reocclusion was defined as a recurrent total occlusion at the previous angioplasty site. End-points The primary end point was the binary angiographic restenosis/reocclusion rate at 6-month follow-up as assessed by an independent core lab. Prespecified secondary endpoints were: MLD and diameter stenosis at 6-month follow-up as assessed by an independent core laboratory and rates of TLR, MI, stroke, and death until the 12-month clinical follow-up. Statistical analysis Continuous variables were expressed as mean ± SD and were compared by the paired and unpaired Student’s t test where appropriate; for correlations, the Pearson correlation coefficient (r) was computed; for categorical data, Fischer’s exact test; for ordinal data, the p for trend was computed. A sample size of 200 patients was calculated.

STENTING OF CHRONIC TOTAL OCCLUSIONS
91
The formal statistical power calculation for 2 groups of 100 patients yields a power of at least 80% for detecting a statistically significant rate difference of 19.7% for angiographic restenosis (that is for the rates 60.0% in the conventional balloon angioplasty group versus 40.3% in the stent group). Taking into account 10% loss to follow-up, the power of 2 groups of 90 patients is at least 80% for detecting a difference of 20.7% (ie, for rates 60.0% vs 39.3%). Logistic regression was used for multivariate statistical analysis. RESULTS Baseline and procedural data Between January 1998 and November 1999 a total of 252 patients were screened for the study. Of these, 21 were excluded because the lesion could not be crossed, 14 because of spontaneous reperfusion to TIMI flow ≥ II in the time between the diagnostic angiogram and the actual procedure, and 17 for other reasons (according to the exclusion criteria). The baseline clinical characteristics are shown in Table 1. Most of the patients were severely symptomatic. After crossing the lesion, procedural success was achieved in all patients of the stent group. In the balloon group, 16 patients needed additional stent implantation due to flow impairing dissection or suboptimal lesion expansion. The angiographic characteristics are shown in Table 2. Both mean maximal balloon size and pressure were higher in the stent group (p<0.0001, p<0.05 respectively). There was no death, MI, or emergency revascularization in either group during hospitalization. Minor bleeding occurred in 2 patients in the stent group and 1 patient in the balloon group.
Table 1. Baseline Clinical Characteristics of 200 patients with chronic total occlusions Balloon group
(n = 100) Stent group (n=100)
Age (yr) Women (%) CCS angina class (%) II III IV Risk factors (%) Smoking Diabetes mellitus Hyperlipidemia* Hypertension Previous MI (%) Previous intervention (%) PCI CABG Previous stroke
57.4±9.2 22 24 44 28 41 11 42 27 49 9 2 6
58.8±10.1 22 18 37 38 35 13 43 18 68 14 4 1
*total cholesterol > 5.5 mmol/L

CHAPTER 8
92
Angiographic results Angiographic follow-up was obtained in 180 patients (90%), 16 refused (8 balloon, 8 stent), and angiography was not possible in 4 patients (2 deaths, 2 strokes). The quantitative coronary angiographic results are shown in Table 3. Stent implantation resulted in a larger immediate postprocedural MLD than did balloon angioplasty (2.90±0.41mm vs 2.34±0.46 mm, p<0.0001). Follow-up angiograms obtained at 6 months demonstrated that patients assigned to stent implantation continued to have a larger MLD than those assigned to angioplasty alone (1.93±0.85 mm vs 1.57±0.74 mm, p=0.009), with less residual stenosis (35.5±26.5 % vs. 44.7±25.0 %, p=0.036). As a result of these differences, the rate of restenosis (including reocclusions) in the stent group was lower than that in the balloon group (21.9 % vs. 33.3 %, p=0.137). The rate of reocclusion was similar in both groups (8.2% vs. 7.3% respectively, p=1.000). Subanalysis In the stent group the rate of TIMI 0 flow before the procedure was 61% versus 43% in the conventional balloon angioplasty group (p=0.02). Although the stent group showed a higher rate of TIMI flow grade 0, this was without causing any statistically significant imbalance. For patients with TIMI flow grade 0, the rate of restenosis in the stented group was 27.3% versus 40.0% in the balloon group (p=0.296). For patients with TIMI flow grade 1, the rate of restenosis was 13.8% versus 31% respectively (p=0.156). Occlusion duration >3 months as compared with <3 months did not predict restenosis in either the stent group or the balloon group (p=0.067 and p=0.194, respectively). Stratification for occlusion length (<10 mm, 10-20mm, >20mm) in the stent and the balloon group did not show any lesion length with a higher risk for restenosis (p for trend = 0.673 and 0.686, respectively). Long-term follow-up Patients were followed for a mean of 13.1±2.4 months from the time of the initial procedure. TLR, which was only performed if patients reported anginal complaints and/or had a positive exercise test, was more frequently performed in the balloon group than in the stent group (29 % vs. 13 %, p<0.0001). The clinical events during follow-up are shown in Table 4.

STENTING OF CHRONIC TOTAL OCCLUSIONS
93
Table 2. Angiographic characteristics of 200 patients with chronic occlusions Balloon group
(n = 100) Stent group (n = 100)
p-value
Duration of occlusion > 3 mo (%) Coronary artery disease (%) 1-vessel 2-vessel 3-vessel LVEF (%) >50 20-50 <20 Occluded vessel (%) LAD LCX RCA Maximal balloon size (mm) Maximal balloon pressure (atm)
45 57 37 6 85 13 2 38 25 37 3.33±0.35 12.2±3.1
38 58 32 10 75 21 4 28 29 43 3.55±0.37 13.2±2.6
p<0.0001 p=0.0320
LVEF = left ventricular ejection fraction; LAD = left anterior descending coronary artery; LCX = left circumflex coronary artery; RCA = right coronary artery Table 3. Quantitative coronary angiographic data Balloon group
Stent group
p-value
Before procedure RD (mm) After procedure RD (mm) MLD (mm) DS (%) At follow-up RD (mm) MLD (mm) DS (%) Restenosis rate (% of pts) * Reocclusion rate (% of pts) Late loss (mm) Loss index
2.97±0.67 2.98±0.45 2.34±0.46 21.56±10.62 2.93±0.53 1.57±0.74 44.70±25.00 33.3 7.3 0.76±0.79 0.32±0.32
3.11±0.61 3.19±0.44 2.90±0.41 8.71±7.22 2.96±0.47 1.93±0.85 35.54±26.51 21.9 8.2 0.97±0.77 0.34±0.27
0.0020 <0.0001 <0.0001 0.6702 0.0088 0.0359 0.1374 1.000 0.1026 0.6183
*including reocclusions

CHAPTER 8
94
Table 4. Clinical events during follow-up Balloon group
(n = 100) Stent group (n = 100)
p-value
6 month follow-up Recurrent angina CCS class (%) II III IV Death Myocardial infarction Targel lesion revascularization Coronary bypass surgery Repeated angioplasty Stroke 6 - 12 month follow-up Recurrent angina CCS class (%) II III IV Death Myocardial infarction Target lesion revascularization Coronary bypass surgery Repeated angioplasty Stroke
9 16 7 1 1 1 19 0 7 7 1 0 0 3 6 0
6 12 3 1 1 0 5 2 7 5 4 0 2 4 4 0
0.3335 0.0022 0.4975 0.5752 0.4974 0.8007
DISCUSSION Since data from 2 landmark studies, the Belgian Netherlands Stent Study (BENESTENT) and the Stent Restenosis Study (STRESS)14,15, showed that coronary stenting significantly decreases restenosis as compared with conventional balloon angioplasty, this treatment modality has been suggested to be superior in an increasing number of clinical and angiographic indications. The generally accepted indication for recanalization of a chronic total occlusion is ischemia related to the occluded vessel. According to the “open artery” concept, recanalization of an occluded coronary artery could have long-term benefits with respect to morbidity and mortality following MI.16,17 Opening of an “old” chronic total occlusion is also beneficial by restoring blood flow to a hibernating myocardium and thus improving left ventricular function. 18,19

STENTING OF CHRONIC TOTAL OCCLUSIONS
95
In a pilot study, we already showed that stenting in chronic total occlusions is safe and efficacious.7 Several randomized studies have been published, suggesting the superiority of coronary stent implantation over conventional balloon angioplasty in chronic total occlusions.8,9,10 In all of these studies the Palmaz-Schatz stent was used. In the Stents in Total Occlusion for Restenosis Prevention (STOP) and Stent versus PTCA After recanalization of Chronic Total Occlusion (SPACTO) trials similar results were found with the AVE Microstent (Medtronic, Minneapolis, Minn) and the Wiktor stent (Medtronic, San Diego, Calif), respectively.11,12 However, the total number of patients in these 2 trials was limited and randomization took place after achieving an optimal angioplasty result. We studied 200 patients using the Boston Scientific NIR stent. Randomization was performed after crossing the occlusion with the guidewire, but before initial dilatation, committing operators to a treatment assignment without knowing all lesion characteristics in advance. Furthermore, patients were followed during a longer time period, with a mean follow-up of 13.1±2.4 months. The restenosis percentage (defined as diameter stenosis > 50%) in the present study was 33% in the balloon group versus 22% in the stent group. The restenosis rate in both our balloon group as in the stent group is lower as compared with the Stenting in Chronic Coronary Occlusion (SICCO; 74 vs 32%), Gruppo Italiano di Studio sullo Stent nelle Occlusioni Coronariche (GISSOC; 68 vs 32%), Total Occlusion Study of Canada (TOSCA; 70 vs 55%), SPACTO (64 vs 32%), and STOP (71 vs 42%) trials. We can think of 2 possible explanations for the low restenosis rate in the balloon group. First, high inflation pressures were applied in both treatment arms. This technique, which is known to reduce the complications of stent implantation20,21, might also be more effective in balloon angioplasty without the intention of stent implantation. The pressures in the balloon group were almost as high as in the stent group (12.2±3.1 atm vs 13.2±2.6 atm, respectively). The balloon angioplasty groups in most of the mentioned trials received lower balloon inflation pressures than in the stent groups: GISSOC (7.7±2.9 atm vs 11.3±3.5 atm), TOSCA (10.0±3.3 atm vs 15.4±3.3 atm), STOP (8.8±2.1 atm vs 13.2±2.5 atm), and SICCO (9.7±2.3 atm vs 9.5±3.0 atm). A second explanation could be the higher rate of diabetes in most of the other studies: in this study the rate was 11% in the balloon group and 13% in the stented group. In the other trials the rates of diabetes were as follows: GISSOC, 9.2% vs 11%; TOSCA, 18% vs 15%; STOP, 25% vs 25%; and SPACTO, 32.6% vs. 35.7%. The complete absence of subacute stent thrombosis was another notable result. The SICCO and GISSOC trials presented relatively high percentages of stent thrombosis (6.9% and 5.4%, respectively). Besides lower pressures, warfarin was used in stead of ticlopidine or clopidogrel in both studies. Today these antiplatelet agents are mandatory after coronary stent implantation.22-24 At 6-month follow-up 32% of the patients in the balloon group reported recurrent anginal complaints versus 21% in the stent group, which is in line with other studies. Limitations of the study
As in most device studies, treatment assignment could not be blinded. A bias influencing subsequent patient management and interpretation of anginal status could have existed. Stent placement could result in a more conservative management during follow-up with regard to TLR. An independent core laboratory, however, analyzed the angiograms. The results of our study cannot be extrapolated to other stent types. Other trials on chronic total occlusions, using different stents, draw the same conclusion.

CHAPTER 8
96
CONCLUSION These data demonstrate that stenting of CTO is superior to balloon angioplasty alone with a statistically significant reduction in the need for TLR and a lower, but not significant, restenosis rate.

STENTING OF CHRONIC TOTAL OCCLUSIONS
97
References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20.
Gruentzig A. Transluminal dilatation of coronary artery stenosis (letter). Lancet 1978;1:263. Holmes DR, Vlietstra RE, Reeder GS. Angioplasty in total artery occlusion. J Am Coll Cardiol 1984;3:845-9. Serruys PW, Umans V, Heyndrickx GR. Elective PTCA of totally occluded coronary arteries not associated with myocardial infarction; short-term and long-term results. Eur Heart J 1985;6:2-12. Kereiakes DJ, Selmon MR, McAuley BJ. Angioplasty in total coronary occlusion: Experience in 76 consecutive patients. J Am Coll Cardiol 1985;6:526-33. Meier B. Total coronary occlusion: a different animal? J Am Coll Cardiol 1991;17:50B- 57B. Ellis SG, Shaw RE, Gershony G. Risk factors, time course and treatment effect for restenosis after succesful percutaneous transluminal coronary angioplasty of chronic total occlusion. Am J Cardiol 1989;63:897-901. Suttorp MJ, Mast EG, Plokker HWM. Primary coronary stenting after successful balloon angioplasty of chronic total occlusions: A single-center experience. Am Heart J 1998;135:318-22. Sirnes PA, Golf S, Myreng Y. Stenting in chronic coronary occlusion (SICCO): A randomized, controlled trial of adding stent implantation after succesful angioplasty. J Am Coll Cardiol 1996;28:1444-51. Rubartelli P, Niccoli L, Verna E. Stent implantation versus balloon angioplasty in chronic coronary occlusions: results from the GISSOC trial. J Am Coll Cardiol 1998;32:90-6. Buller CE, Dzavik V, Carere RG. Primary stenting versus balloon angioplasty in occluded coronary arteries. The total occlusion study of Canada (TOSCA). Circulation 1999;100:236-42. Lotan C, Rozenman Y, Hendler A. Stents in total occlusion for restenosis prevention. The multicenter randomized STOP study. Eur Heart J 2000;21:1960-6. Höher M, Wöhrle J, Grebe OC. A randomized trial of elective stenting after balloon recanalization of chronic total occlusions. J Am Coll Cardiol 1999;34:722-9. TIMI study group. The thrombolysis and myocardial infarction (TIMI) trial: phase I findings. N Engl J Med 1988;318:265-70. Serruys PW, De Jaegere P, Kiemeneij F. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331:489-95. Fischman DL, Leon MB, Baim DS. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331:496-501. Ellis CJ, French JK, White HD. Coronary artery patency and survival in clinical trials. J Thromb Thrombolysis 1997;4:239-50. Califf RM. The GUSTO trial and the open artery theory. Eur Heart J 1997;18 suppl F:F2- 10. Sirnes PA, Myreng Y, Mølstad P. Improvement in left ventricular ejection fraction and wall motion after successful recanalization of chronic coronary occlusions. Eur Heart J 1998;19:273-81. Rambaldi R, Hamburger JN, Geleijnse ML. Early recovery of wall motion abnormalities after recanalization of chronic totally occluded coronary arteries: a dobutamine echocardiographic, prospective, single-center experience. Am Heart J 1998;136:831-36. Colombo A, Hall P, Nakamura S. Intracoronary stenting without anticoagulation accomplished with intravascular ultrasound guidance. Circulation 1995;91:1676-88.

98
21. 22. 23. 24.
Lawrence ME, Burtt DM, Shaftel PA. Intracoronary stent placement without coumadin or intravascular ultrasound. J Invasive Cardiol 1996;8:428-32. Goods CM, al-Shaibi KF, Liu MW. Comparison of aspirin alone versus aspirin plus ticlopidine after coronary artery stenting. J Am Coll Cardiol 1996;78:1042-44. Moussa I, Oetgen M, Roubin G. Effectiveness of clopidogrel and aspirin versus ticlopidine and aspirin in preventing stent thrombosis after coronary stent implantation. Circulation 1999;99:2364-66. Bertrand ME, Rupprecht HJ, Urban P. Double-blind study of the safety of clopidogrel with and without a loading dose in combination with aspirin compared with ticlopidine in combination with aspirin after coronary stenting: the clopidogrel aspirin international cooperative study (CLASSICS). Circulation 2000;102:624-29.

99
Chapter 9
Primary Stenting of Occluded Native Coronary Arteries II:
Rationale and design of the PRISON II study
A randomized comparison of bare metal stent implantation with sirolimus-eluting
stent implantation for the treatment of chronic total coronary occlusions
Braim M. Rahel 1Gert J. Laarman
Maarten J. Suttorp on behalf of the PRISON II study investigators.
St. Antonius Hospital Nieuwegein, Dept of Cardiology, 1Onze Lieve Vrouwe Gasthuis Amsterdam, Dept of Cardiology,
The Netherlands
Accepted by the American Heart Journal

100
ABSTRACT Primary intracoronary stent placement after successfully crossing chronic total occlusions (CTO) decreases the high restenosis rate at long-term follow-up compared with conventional balloon angioplasty. Several studies have shown the efficacy of sirolimus-eluting stents in selected groups of patients. Whether sirolimus-eluting stents are superior to bare metal stents in CTO is unknown. In this prospective, randomized trial, bare metal stent implantation will be compared with sirolimus-eluting stent implantation for the treatment of CTO. A total of 200 patients will be followed for 12 months with angiographic follow-up at 6 months. Quantitative coronary analysis will be performed by an independent core lab. The primary end-point is the binary angiographic restenosis and re-occlusion rate.

SIROLIMUS STENT FOR CHRONIC TOTAL OCCLUSIONS
101
INTRODUCTION Since data from the two landmark studies, the BENESTENT and STRESS studies1,2, showed that coronary stenting significantly decreases restenosis as compared with conventional balloon angioplasty, this treatment modality has shown to be superior in an increasing number of indications.1,2 Percutaneous coronary intervention (PCI) of chronic total occlusions (CTO) however is still limited by high restenosis rates. Although coronary stenting using bare metal stents significantly decreases restenosis in CTO, restenosis rates still reach 32-55%.3-8 In 200 patients with CTO randomized in the PRISON I study we demonstrated a restenosis rate of 22% after bare metal stent implantation as compared with 33% after conventional balloon angioplasty.9 During the past few years, sirolimus (rapamycin), a cytostatic macrocyclic lactone with anti-inflammatory and antiproliferative properties10-12, delivered from a polymer-encapsulated stent was shown to almost eliminate the risk of restenosis in selected groups of patients.13-16 In this study we will investigate the results of sirolimus-eluting stent implantation as compared with bare metal stent implantation in CTO. METHODS Patients The PRImary Stenting of Occluded Native coronary arteries II (PRISON II) study is a randomized, two-center trial in which 200 patients will be recruited. We will investigate the effect of a bare metal stent (Bx VELOCITY™)(Cordis corporation, Johnson&Johnson) versus a sirolimus-eluting stent (Cypher™) in chronic coronary occlusions. The bare metal stent and the sirolimus-eluting stent have the same design. Patients are included if the estimated duration of the chronic total occlusion is at least 2 weeks with evidence of ischemia related to the occluded coronary artery (signs of ischemia found during an abnormal exercise test, defined as ST depression of at least 1.0 mm that is horizontal or down-sloping or upsloping ST depression of at least 2.0 mm or signs of ischemia found during nuclear imaging with exercise, dobutamine or adenosine). Patients are excluded if the lesion can not be crossed or if the use of aspirin and clopidogrel is prohibited. The study is conducted according to the principles of the Declaration of Helsinki, and all patients have to give written informed consent before they undergo the procedure. Hypertension is defined as a systolic tension higher than 140 mmHg and/or a diastolic tension higher than 90 mmHg or use of anti-hypertensive drugs. Diabetes mellitus is defined as fasting venous glucose concentrations ≥ 7.8 mmol/L (140.5 mg/dL) or use of glucose lowering drugs. Hypercholesterolemia is defined as a fasting plasma cholesterol level higher than 5.0 mmol/L (193 mg/dL) or use of cholesterol lowering drugs. Angiographic definitions Chronic total coronary artery occlusion is defined by the absence of antegrade flow of contrast distal to the occlusion (flow grade 0 according to the Thrombolysis and Myocardial Infarction [TIMI] score) or only minimal flow of contrast distal to the occluded vessel (TIMI flow I).17 The duration of the chronic occlusion has to be at least 2 weeks and is estimated by clinical information, sequential angiographic information, or both.

CHAPTER 9
102
The estimated length of the occlusion is measured from the point of the chronic occlusion to the most proximal point of the distal vessel, which is visualized by collateral filling with contrast. The total coronary analysis segment is defined as the stented segment including the margins 5 mm distal and proximal to the stents. Angioplasty procedure Percutaneous coronary intervention is performed from either the femoral artery or radial artery approach with standard recanalization and stent implantation techniques. The major goal is to achieve a residual luminal diameter stenosis <30% on visual assessment. Randomization is performed after crossing the lesion, but before initial dilatation. Patients are randomized by a telephone allocation service, which was provided with the randomization list before recruitment of the first patient. Patients are equally assigned to either the conventional bare metal stent group or the sirolimus-eluting stent group. Both patient and treating physician are blinded for allocation. Poststent dilatation is performed with high inflation pressures in all patients. At the beginning of the procedure patients receive a single dose of 10,000 U heparin. All patients receive aspirin and clopidogrel before the procedure. Clopidogrel will be continued for 1 year and aspirin is given lifelong. Quantitative coronary analysis The angiograms will be analyzed by an independent core angiography laboratory (Research&Development department, cardiology department, St. Antonius Hospital, Nieuwegein, The Netherlands). The observers are not provided with the clinical information of the patients. Before angiography 500 µg nitroglycerine is given intracoronary. The guiding catheter is used as the calibration standard. All lesions are assessed in at least two orthogonal views and the projection showing the smallest diameter is used for quantitative coronary angiography analysis, and views with the least foreshortening are used for measuring the length of the occlusion. In disease-free proximal segments the reference diameter is measured. Cineangiograms will be obtained before, immediately after and at 6 months, using the same views. Any coronary angiography performed within 3 months after the initial procedure will be considered unscheduled. When an unscheduled angiography is followed by target lesion revascularization no further angiograms are needed. If no target lesion revascularization takes place, repeat angiography at 6 months still will be required. If the angiography takes place after 3 months, 6 months angiographic assessment is not mandatory. The early gain is defined as the difference between the minimal luminal diameter (MLD) after intervention and the diameter before intervention. Late loss is defined as the subsequent decrease in MLD of the treated artery at the 6-month follow-up angiography. The loss index is defined as the late loss divided by the early gain. Long-term follow-up Clinical follow-up will be performed at 6 months, 1 year, and 5 years. Recurrent angina, a positive exercise test, or abnormal nuclear imaging are considered as clinical signs of restenosis. Follow-up angiography will be performed earlier if there are clinical signs of restenosis and if indicated, followed by target lesion revascularization. Death, myocardial infarction (MI, defined as the presence of new significant Q waves or an elevation of creatine kinase or its MB isoenzyme to at least two times the upper limit), occurrence of angina (Canadian Cardiovascular Society [CCS] class III or IV), or target lesion revascularization (TLR, defined as percutaneous or surgical revascularization of the target lesion after the initial procedure) will be recorded as major adverse clinical events (MACE).

SIROLIMUS STENT FOR CHRONIC TOTAL OCCLUSIONS
103
Restenosis and reocclusion Angiographic in-stent restenosis at follow-up is defined as > 50% residual diameter stenosis in the stent. Edge restenosis at follow-up is defined as >50% residual diameter stenosis located at the proximal or distal edge. Reocclusion is defined as a recurrent total occlusion at the previous angioplasty site. End-points The primary end-point is the binary angiographic restenosis/re-occlusion rate at 6-month follow-up as assessed by an independent core lab. Pre-specified secondary endpoints are: in-stent/in-segment MLD and diameter stenosis at 6 months follow-up as assessed by an independent core laboratory and rates of TLR, MI, stroke and death until the 12 months clinical follow-up. Statistical analysis Assuming the restenosis rate in the conventional PCI group to be 22% and projecting the restenosis rate in the sirolimus-eluting stent group to be between 5% and 7%, furthermore setting the alpha level at 5% (two-sided) and the power to be at least 80%, this study needs to evaluate 93 patients in both study groups. Allowing for a low dropout rate, comparable to the PRISON I study9, 100 patients in each group is the target sample size. The primary endpoint is the angiographic restenosis/reocclusion rate at 6 months follow-up. The comparison between the two groups will be assessed by means of Fisher’s exact test for a 2x2 table. The in-segment and in-stent percent diameter stenosis, MLD, and late loss will be compared by means of the Student’s t-test. Additional multivariate analyses will only be performed as hypothesis generating method. CONCLUSIONS Despite bare metal coronary stents, chronic total occlusions continue to pose a problem both to the interventionalist and the patient due to the high rate of restenosis. The PRISON II study will allow determination of the value of sirolimus-eluting stents in patients with chronic total occlusions.

CHAPTER 9
104
References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17.
Serruys PW, De Jaegere P, Kiemeneij F, et al. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331:489-95.
Fischman DL, Leon MB, Baim DS, et al. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331:496-501. Sirnes PA, Golf S, Myreng Y, et al. Stenting in chronic coronary occlusion (SICCO): A randomized, controlled trial of adding stent implantation after succesful angioplasty. J Am Coll Cardiol 1996;28:1444-51. Rubartelli P, Niccoli L, Verna E, et al. Stent implantation versus balloon angioplasty in chronic coronary occlusions: results from the GISSOC trial. J Am Coll Cardiol 1998;32:90-6. Buller CE, Dzavik V, Carere RG, et al. Primary stenting versus balloon angioplasty in occluded coronary arteries. The total occlusion study of Canada (TOSCA). Circulation 1999;100:236-42. Lotan C, Rozenman Y, Hendler A, et al. Stents in total occlusion for restenosis prevention. The multicenter randomized STOP study. Eur Heart J 2000;21:1960-66. Höher M, Wöhrle J, Grebe OC, et al. A randomized trial of elective stenting after balloon recanalization of chronic total occlusions. J Am Coll Cardiol 1999;34:722-29. Suttorp MJ, Mast EG, Plokker HWM, et al. Primary coronary stenting after successful balloon angioplasty of chronic total occlusions: A single-center experience. Am Heart J 1998;135:318-22. Rahel BM, Suttorp MJ, Laarman GJ, et al. Primary Stenting of Occluded Native Coronary Arteries: Final Results of the PRISON Study. Am Heart J 2004;147:e22. Gallo R, Padurean A, Jayaraman T, et al. Inhibition of intimal thickening after balloon angioplasty in porcine coronary arteries by targeting regulators of the cell cycle. Circulation 1999;99:2164-70. Marx SO, Marks AR, Bench to bedside: the development of rapamycin and its application to stent restenosis. Circulation 2001;104:852-55. Suzuki T, Kopia G, Hayashi S, et al. Stent-based delivery of sirolimus reduces neointimal formation in a porcine coronary model. Circulation 2001;104:1188-93. Rensing BJ, Vos J, Smits PC, et al. Coronary restenosis elimination with a sirolimus eluting stent: first European human experience with 6-month angiographic and intravascular ultrasonic follow-up. Eur Heart J 2001;22:2125-30. Sousa JE, Costa MA, Abizaid AC, et al. Sustained suppression of neointimal proliferation by sirolimus-eluting stents: one-year angiographic and intravascular ultrasound follow-up. Circulation 2001;104:2007-11. Morice MC, Serruys PW, Sousa JE, et al, for the RAVEL Study Group. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med 2002;346:1773-80. Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003;349:1315-23. TIMI study group. The thrombolysis and myocardial infarction (TIMI) trial: phase I findings. N Engl J Med 1988;318:265-70.
105
Chapter 10
Summary

CHAPTER 10
106
Despite considerable progress, restenosis remains a major limitation of percutaneous coronary intervention (PCI). Restenosis is determined by many factors in which the ‘response to injury’ plays a central role. There are two possible approaches in the prevention of restenosis. Unraveling the complex pathophysiology of this vascular response has lead to a better understanding of its mechanisms and to the identification of numerous risk factors. This has lead to the development of new pharmacological and nonpharmacological treatment options, with more or less success. Another approach is to prevent restenosis mechanically, irrespective of its cause. Today, coronary stents are the corner stone of mechanical vessel support, thereby also decreasing the restenosis rate in various subsets of patients at increased risk. In chapters 2, 3, and 4 of this thesis, the prognostic value of several “modern” risk factors is described, further unraveling the pathophysiology of restenosis. In chapters 5, 6, 7, and 8 of this thesis, several “mechanical” treatment modalities are tested to prevent restenosis. Chapter 1: Introduction Chapter 1 gives a short overview of the pathophysiology of restenosis, which can be divided in elastic recoil, remodeling, and neointima proliferation. Stenting virtually eliminates elastic recoil and remodeling, and in-stent restenosis is mainly caused by neointima proliferation. Furthermore, patient related risk factors and lesion specific angiographic risk factors are described. Chapter 2: Preprocedural serum levels of acute-phase reactants and prognosis after percutaneous coronary intervention Circulating inflammatory markers, in particular C-reactive protein (CRP), belong to the most prominent “modern” risk factors of coronary heart disease. In chapter 2 the influence of these acute-phase reactants on prognosis after PCI is described. In a group of 600 patients preprocedural levels of CRP, interleukin-6 (IL-6), lipoprotein(a) (Lp(a)), and fibrinogen were measured. At 8 months follow-up, the occurrence of repeat PCI, coronary artery bypass grafting, myocardial infarction, and death were noted as major adverse clinical events (MACE). Furthermore, the recurrence of angina was noted. CRP levels were significantly higher in patients with repeat angina as compared with patients without recurrent angina (p<0.05). Lp(a) and fibrinogen were both higher in patients with MACE as compared with patients without MACE (p<0.05 and p<0.05, respectively). IL-6 levels were not correlated with MACE or repeat angina. Conclusion: This study clearly supports the role of inflammation in restenosis after PCI. Chapter 3: Preprocedural ACE-activity does not predict in-stent restenosis Chapter 3 describes the correlation between angiotensin converting enzyme (ACE) activity, in plasma as well as in the atherosclerotic plaque, and the occurrence of in-stent restenosis. The ACE activity in peripheral blood was measured in 178 patients before they underwent PCI with stent placement. After 8 months adverse cardiovascular events were counted as a measure of clinical recurrence due to in-stent restenosis, and related to the ACE-activity. In a second group of patients, tissue samples were obtained with an atherectomy catheter before elective stent placement in 13 patients with de novo stenosis. In these samples, the ACE content was determined immunohistologically.

SUMMARY
107
Recatheterisation was performed after 12 months to determine the degree of in-stent restenosis in relation to the amount of ACE in the original plaque. Conclusion: In both substudies, no relation between the amount of preprocedural ACE or ACE-activity and in-stent restenosis could be established. Chapter 4: Cytomegalovirus and Chlamydia pneumoniae as predictors for major adverse clinical events and angina pectoris after percutaneous coronary intervention The development of restenosis is enhanced by several patient related risk factors. Studies investigating the role of microorganisms on restenosis are contradictory. Therefore we investigated the role of two potential candidates: cytomegalovirus (CMV) and Chlamydia pneumoniae (CP). We measured preprocedural anti-CMV immunoglobulin G and anti-CP immunoglobulin A (IgA), immunoglobulin M, and immunoglobulin G antibodies in 600 patients. At 8 months follow-up, the occurrence of MACE and angina was noted. We found a higher rate of seropositivity for CP IgA in patients with MACE as compared with patients without MACE (50.9% vs 35.4%, p<0.05). Seropositivity for CMV was not related to adverse events. Conclusion: Preprocedural seropositivity of CP IgA is a risk factor for MACE after PCI. Chapter 5: Is Direct Stent Implantation Without Predilatation Safe? Acute and Long-Term Outcome The lower the injury, the lower the response. Therefore, stenting without predilatation (SWOP) is likely to result in a lower rate of restenosis. Using the Palmaz-Schatz Crown stent SWOP was attempted in 61 patients who were compared with a control group of provisional stenting. The results of this study are described in chapter 5. In the SWOP group the mean preprocedural minimal luminal diameter (MLD) increased from 0.96±0.47 mm to 3.09±0.54 mm directly after the procedure. At 6 month follow-up the MLD measured 2.32±0.79 mm. In the provisional stenting group the mean MLD increased from 0.92±0.51 to 2.44±0.58 mm and was 1.84±0.70 mm at 6 month follow-up. Restenosis occurred in 8% of the SWOP group compared with 28% in the group of provisional stenting (p<0.001) . Conclusion: The acute and long-term results of SWOP are better as compared with provisional stenting. Chapter 6: Stenting for Restenotic Lesions with the BARD XT Stent A history of restenosis after balloon angioplasty is among the most important and relatively frequent occurring risk factors for recurrent restenosis. Many treatment modalities have been investigated for the treatment of restenotic lesions. In chapter 6 the immediate and 6-month clinical and angiographic results of stenting for restenosis are described. One-hundred patients with restenosis after conventional balloon angioplasty were stented using the BARD XT stent. The mean MLD increased from 1.09±0.57mm to 2.70±0.44mm. The procedural success rate was 99%. The mean MLD at follow-up was 1.74±0.67mm with a mean diameter stenosis of 41±20%. Residual anginal complaints were reported in 29% of patients. In-stent restenosis occurred in 18% of the patients. Conclusion: Coronary stenting for restenotic lesions results in a good immediate result and yields a favorable long-term outcome.

CHAPTER 10
108
Chapter 7: Cutting Balloon for in-stent restenosis: acute and long-term results The long-term success of stenting is limited by the occurrence of in-stent restenosis. Repeat balloon angioplasty shows good immediate results, but the rate of recurrent in-stent restenosis is high. In-stent restenotic tissue, which is mainly composed of smooth muscle cells, is not as compressible as compared with an atherosclerotic plaque. Chapter 7 describes the results of the cutting balloon for in-stent restenosis. The incisions made by the blades of the cutting balloon decrease the radial force of the restenotic tissue and facilitate dilatation. In this study 100 consecutive patients with in-stent restenosis were treated with the Barath cutting balloon. The mean inflation pressure was 8.7±2.0 (range 6.0-18.0) atm. Before the procedure the mean MLD was 0.95±0.45mm. Immediately after the procedure the mean MLD was 2.42±0.54 mm. At 8 month follow-up 26 patients (26%) reported to have anginal complaints CCS class 2 to 4 of whom 16 (16%) needed target lesion revascularization. Conclusion: angioplasty for in-stent restenosis using a cutting balloon has good immediate results and a low need for repeated target lesion revascularization. Chapter 8: Primary Stenting of Occluded Native Coronary Arteries: Final Results of the PRISON Study Chronic total coronary occlusions have long been considered to be an indication for coronary artery bypass graft surgery because of the low success rate of balloon angioplasty. Coronary stent implantation is expected to improve the outcome of PCI for chronic total occlusions. Chapter 8 describes the results of the Primary Stenting of Occluded Native Coronary Arteries (PRISON) study. In this randomized study, the results of stent implantation are compared with balloon angioplasty in 200 patients. After the procedure the mean MLD in the balloon group was 2.34±0.46 mm versus 2.90±0.41 mm in the stented group (p<0.0001). The 6-month angiographic follow-up showed a mean MLD of 1.57±0.74 mm in the conventional group versus 1.93±0.85mm in the stented group (p<0.01). Angiographic restenosis was seen in 33% in the conventional group versus 22% in the stented group (p=0.14). The reocclusion rates were 7.3% and 8.2% respectively (p=1.0). At 12 month follow-up, the rate of target lesion revascularization was significantly higher in the balloon group (29% versus 13%, p<0.0001). Conclusion: Stenting of chronic total occlusions is superior to balloon angioplasty alone. Chapter 9: Primary Stenting of Occluded Native Coronary Arteries II: Rationale and design of the PRISON II study A randomized comparison of bare metal stent implantation with sirolimus-eluting stent implantation for the treatment of chronic total coronary occlusions. Although chapter 8 showed that coronary stenting using bare metal stents is superior to balloon angioplasty in chronic total occlusions, restenosis continues to pose a problem to the interventionalist and the patient. During the past few years, studies evaluating stents coated with sirolimus (rapamycin) have shown promise at reducing restenosis rates in selected groups of patients. Chapter 9 describes the rationale and design of the Primary Stenting of Occluded Native Coronary Arteries II (PRISON II) study. This randomized study will investigate the results of sirolimus-eluting stent implantation as compared with bare metal stent implantation in chronic total occlusions. A total of 200 patients will be followed for 5 years, with angiographic follow-up at 6 months.

SUMMARY
109

110
111
Samenvatting

CHAPTER 10
112
Ondanks verbeteringen in de techniek van percutane coronaire interventie (PCI), blijft restenose een belangrijk probleem. De reactie van de vaatwand op beschadiging speelt een centrale rol in de vele factoren die leiden tot restenose. De preventie van restenose is op twee manieren te benaderen. Ten eerste heeft het ontrafelen van de complexe pathofysiologie geleid tot een beter begrip van het mechanisme van restenose en tot het identificeren van verscheidene risicofactoren. Mechanische preventie van restenose is een tweede benadering. Hierbij maakt het niet precies uit wat de oorzaak is. Tegenwoordig vormen coronaire stents de hoeksteen van mechanische vaatwandondersteuning. Het blijkt tevens dat stents de kans op restenose verminderen in patiënten met een verhoogd risico op restenose. In de hoofdstukken 2, 3 en 4 van dit proefschrift wordt de prognostische waarde van verscheidene ‘moderne’ risicofactoren beschreven. De studies uit deze hoofdstukken bieden een beter inzicht in de pathofysiologie van restenose. In de hoofdstukken 5, 6, 7 en 8 worden verscheidene ‘mechanische’ behandelingsmethoden beschreven. Hoofdstuk 1: Introductie Hoofdstuk 1 geeft een kort overzicht in de pathofysiologie van restenose. Restenose kan worden onderverdeeld in elastisch ‘terugveren’, remodelleren en neointima proliferatie van de vaatwand. Door het plaatsen van een stent in de kransslagader worden terugveren en remodelleren praktisch voorkomen en in-stent restenose wordt dan ook met name veroorzaakt door neointima proliferatie. Verder worden in dit hoofdstuk patiënt-gerelateerde en angiografische risicofactoren beschreven. Hoofdstuk 2: Preprocedurele serum waarden van acute-fase reagentia en de prognose na percutane coronaire interventie Circulerende ontstekingsmarkers, en met name het C-reactive protein (CRP), behoren tot de meest prominente ‘moderne’ risicofactoren voor kransslagaderlijden. In hoofdstuk 2 wordt de invloed van deze acute-fase reagentia op de prognose na een PCI beschreven. In 600 patiënten werd voor de procedure de concentratie van CRP, interleukine-6 (IL-6), lipoproteine(a) (Lp(a)) en fibrinogeen gemeten. Na 8 maanden follow-up werd het voorkomen van re-PCI, coronaire bypass chirurgie, myocardinfarct en overlijden genoteerd als major adverse clinical events (MACE). Verder werd het hernieuwd optreden van angina pectoris bijgehouden. CRP concentraties bleken significant hoger in patiënten met recidief angina pectoris ten opzichte van patiënten zonder recidief klachten (p<0,05). De concentraties van Lp(a) en fibrinogeen waren beiden hoger in patiënten met MACE ten opzichte van patiënten zonder MACE (p<0,05 en p<0,05 respectievelijk). De concentratie van IL-6 bleek geen voorspellende waarde te hebben voor deze klinische uitingen van restenose. Conclusie: Deze studie ondersteunt de rol van inflammatie in restenose na PCI. Hoofdstuk 3: Preprocedurele ACE-activiteit voorspelt in-stent restenose niet Hoofdstuk 3 beschrijft de correlatie tussen enerzijds angiotensin converting enzyme (ACE) activiteit in plasma alsook in de atherosclerotische plaque en anderzijds het voorkomen van in-stent restenose. Voor het ondergaan van een PCI met stentimplantatie werd de ACE-activiteit in plasma van 178 patiënten gemeten. Acht maanden later werd gekeken hoeveel van deze patiënten een MACE hadden meegemaakt (als maat voor in-stent restenose). In een tweede groep bestaande uit 13 patiënten werd voor het plaatsen van een stent weefsel uit een de novo stenose verkregen met behulp van een atherectomie-catheter. In dit weefsel werd het

SAMENVATTING
113
ACE gehalte immunohistologisch bepaald. Na 12 maanden vond controle coronairangiografisch onderzoek plaats om de ernst van in-stent restenose te relateren aan de hoeveelheid ACE in de oorspronkelijke plaque. Conclusie: In beide substudies werd geen relatie gevonden tussen de hoeveelheid preprocedureel ACE of ACE-activiteit en in-stent restenose. Hoofdstuk 4: Cytomegalovirus en Chlamydia pneumoniae als voorspellers van ‘major adverse clinical events’ en angina pectoris na percutane coronaire interventie De ontwikkeling van restenose wordt bevorderd door verscheidene patiënt-gerelateerde risicofactoren. De literatuur is tegenstrijdig omtrent de rol van micro-organismen in restenose. Daarom onderzochten we de rol van 2 potentiële kandidaten: cytomegalovirus (CMV) en Chlamydia pneumoniae (CP). In 600 patiënten werd preprocedureel de concentratie van anti-CMV immunoglobuline G en anti-CP immunoglobuline A (IgA), immunoglobuline M en immunoglobuline G gemeten. Gedurende 8 maanden follow-up werd het voorkomen van MACE en angina pectoris bijgehouden. Seropositiviteit voor CP IgA bleek vaker voor te komen bij patiënten met MACE ten opzichte van patiënten zonder MACE (50,9% versus 35,4%, p<0,05). Seropositiviteit voor CMV bleek niet gecorreleerd aan MACE. Conclusie: Preprocedurele seropositiviteit voor CP IgA is een risicofactor voor MACE na een PCI. Hoofdstuk 5: Is het direkt plaatsen van een stent zonder predilatatie veilig? Korte en lange-termijn resultaten Hoe minder de beschadiging, des te minder is de reactie van de vaatwand. Stentimplantatie zonder predilatatie zou derhalve tot minder restenose kunnen leiden. Stenten zonder predilatatie werd gepoogd in 61 patiënten, die vergeleken werden met een controle groep waarin alleen op indicatie een stent geplaatst werd. De resultaten van deze studie worden beschreven in hoofdstuk 5. In de studie groep werd de Palmaz-Schatz Crown stent gebruikt. De gemiddelde preprocedurele minimale lumen diameter (MLD) groeide van 0,96±0,47 mm naar 3,09±0,54 mm direct na de procedure. Na 6 maanden follow-up bedroeg de MLD 2,32±0,79 mm. In de controle groep groeide de gemiddelde MLD van 0,92±0,51 mm naar 2,44±0,58 mm en was 1,84±0,70 mm na 6 maanden follow-up. Restenose kwam in 8% van de studie-populatie voor in vergelijking met 28% in de controle groep (p<0,001). Conclusie: De korte en lange termijn resultaten van stenten zonder predilatatie zijn beter dan stenten op indicatie. Hoofdstuk 6: Stenten in restenotische laesies met behulp van de BARD XT stent Restenose na een eerdere ballondilatatie vormt een van de belangrijkste en meest voorkomende risicofactoren voor het opnieuw optreden van restenose. De behandeling van restenose is reeds op vele manieren onderzocht. In hoofdstuk 6 worden de korte en lange termijn resultaten van stentimplantatie voor restenose beschreven. Honderd patiënten met restenose na een eerdere ballondilatatie kregen een of meerdere BARD XT stents. De gemiddelde MLD groeide van 1,09±0,57 mm naar 2,70±0,44 mm. Stentimplantatie was succesvol in 99%. De gemiddelde MLD tijdens follow-up angiografie bedroeg 1,74±0,67 mm met een gemiddelde diameter stenose van 41±20%. Negenentwintig procent van de patiënten meldden recidief angina pectoris. In 18% van de patiënten bleek sprake van in-stent restenose.

CHAPTER 10
114
Conclusie: Stentimplantatie in restenotische laesies resulteert in goede korte en lange termijn resultaten. Hoofdstuk 7: De ‘Cutting Balloon’ voor in-stent restenose: korte en lange termijn resultaten In-stent restenose is een belangrijke beperkende factor van coronaire stentimplantatie. Ballondilatatie voor in-stent restenose heeft welliswaar goede korte termijn resultaten, maar op de lange termijn recidiveert de in-stent restenose in veel gevallen. Het weefsel in de stent bestaat voornamelijk uit glad spierweefsel en is derhalve minder comprimeerbaar ten opzichte van een atherosclerotische plaque. In hoofdstuk 7 worden de resultaten van het gebruik van een zogenaamde ‘cutting balloon’ voor in-stent restenose beschreven. De cutting balloon bevat 3 tot 4 mesjes in longitudinale richting op het oppervlak. De incisies ten gevolge van deze mesjes verlagen de radiale kracht van het restenotisch weefsel in de stent en vereenvoudigen zodoende de dilatatie. In deze studie werden 100 patiënten met in-stent restenose behandeld met de Barath cutting balloon. De gemiddelde inflatie-druk bedroeg 8,7±2,0 (range 6,0-18,0) atm. Voor de procedure was de gemiddelde MLD 0,95±0,45 mm. Direct na procedure bedroeg de gemiddelde MLD 2,42±0,54 mm. Na 8 maanden follow-up meldden 26 patiënten (26%) recidief angina pectoris Canadian Cardiovascular Society klasse 2 tot 4. In 16 van deze patiënten (16%) was een revascularisatie nodig van het studieletsel. Conclusie: PCI voor in-stent restenose met behulp van een cutting balloon heeft goede directe resultaten. Na deze behandeling behoeven weinig patiënten een herhaalde revascularisatie van het studieletsel. Hoofdstuk 8: Primair stenten van geoccludeerde natieve coronairen: Eindresultaten van de PRISON studie Vanwege het lage succespercentage van ballondilatatie werden chronische totale occlusies beschouwd als een indicatie voor coronaire bypass chirurgie. Door het gebruik van stents is het te verwachten dat het resultaat van PCI voor chronische totale occlusies verbetert. Hoofdstuk 8 beschrijft de resultaten van de ‘Primair Stenten van Geoccludeerde Natieve Coronairen’ (PRISON) studie. In deze gerandomiseerde studie worden de resultaten van stentimplantatie vergeleken met ballondilatatie in 200 patiënten. Na de procedure was de gemiddelde MLD in the ballon groep 2,34±0,46 mm versus 2,90±0,41 mm in de groep die één of meerdere stents ontving (p<0,0001). Tijdens de angiografische controle na 6 maanden bedroeg de gemiddelde MLD in de ballon groep 1,57±0,74 mm versus 1,93±0,85 mm in de gestente groep (p<0,01). Restenose werd in 33% van de patiënten uit de ballon groep gezien versus 22% patiënten uit de stent groep (p=0,14). Het percentage reocclusies bedroeg respectievelijk 7,3% en 8,2% (p=1,0). Na 12 maanden follow-up was het aantal revascularisaties van het studieletsel significant hoger in de ballon groep (29% versus 13%, p<0,0001). Conclusie: PCI met stentimplantatie van chronisch totale occlusies is superieur aan PCI met enkel ballondilatatie.

SAMENVATTING
115
Hoofdstuk 9: Primair stenten van geoccludeerde natieve coronairen II: Achtergrond en doel van de PRISON II studie Een gerandomiseerde vergelijking tussen het gebruik van ongecoate en sirolimus-gecoate stents in de behandeling van chronische totale occlusies. In hoofdstuk 8 werd reeds aangetoond dat het gebruik van ongecoate stents in chronische totale occlusies superieur is aan enkel ballondilatatie. Ondanks het gebruik van stents blijft restenose echter een probleem voor de interventie-cardioloog en de patiënt. Stents bedekt met sirolimus (rapamycine) hebben de afgelopen jaren (zeer) goede resultaten laten zien in een geselecteerde groep patiënten. In hoofdstuk 9 worden de achtergrond en het doel van de ‘Primair stenten van geoccludeerde natieve coronairen II (PRISON II)’ studie beschreven. In deze studie zal onderzocht worden wat de resultaten zijn van implantatie van sirolimus-gecoate stents versus ongecoate stents in chronische totale occlusies. In totaal zullen 200 patiënten gedurende 5 jaar vervolgd worden met een angiografische controle na 6 maanden.

CHAPTER 10
116

117
Chapter 11
Dankwoord
CHAPTER 11
118
Het voltooien van een proefschrift is niet het werk van slechts één persoon. Ook ik heb de bereidwillige inbreng van anderen ervaren waarvoor ik, nu mijn proefschrift is voltooid, zeer dankbaar ben. Zonder iemand tekort te willen doen, zal ik proberen een aantal van hen mijn dank te betuigen. Allereerst mijn co-promotores dr. H.W.M. Plokker en dr. M.J. Suttorp. Beste Thijs, jij was vanaf het begin betrokken bij het ontstaan van dit proefschrift. Het schijnt dat ik bij m’n aanstelling heb gezegd dat ik én in opleiding wilde komen én wilde promoveren. Dat jij hierbij enige scepsis had, kan ik nu pas echt goed begrijpen. Het is echter mede dankzij jou dat het uiteindelijk gelukt is. Hiervoor mijn hartelijke dank. Beste Maarten-Jan, zonder jouw aanvoer van ideeën zou dit proefschrift nooit tot stand zijn gekomen. Toen ik in 1997 naar ‘het Antonius’ kwam, kreeg ik al gauw enkele studies onder m’n hoede met de mededeling dat ik dan mogelijk zou kunnen promoveren. Aangezien het doen van onderzoek niet altijd even gemakkelijk is (met name niet na berichten als: "Unfortunately, we cannot ...."), kwam jouw niet aflatende vertrouwen op een goede afloop goed van pas. Mijn promotor prof. dr. F. Zijlstra. Geachte prof. Zijlstra, alhoewel u pas in een later stadium bij het onderzoek van dit proefschrift betrokken raakte, wist u feilloos op een rijdende trein te springen en deze de goede richting te geven. Ik dank u hartelijk voor het in mij gestelde vertrouwen. De leden van de beoordelingscommissie, Prof. dr. P.W. Boonstra, Dr. J.M.P.G. Ernst, Prof. dr. J.J. Piek en Prof. dr. N.H.J. Pijls, dank ik voor de tijd en aandacht die zij hebben besteed aan de beoordeling van deze thesis. De overige (oud-)leden van de maatschap cardiologie van het St. Antonius Ziekenhuis te Nieuwegein: dr. C.A.P.L. Ascoop, dr. J.M. ten Berg, dr. L.V.A. Boersma, drs. E.T. Bal, drs. F.D. Eefting, dr. J.M.P.G. Ernst, drs. E.G. Mast, dr. W. Jaarsma, Prof. dr. N.M. van Hemel, dr. B.J.W.M. Rensing en dr. E.F.D. Wever ben ik niet alleen zeer erkentelijk voor de opleiding die ik tot nu toe bij hen heb genoten, maar ook voor de geboden faciliteiten om onderzoek te kunnen doen. Dr. R.J.A. Diepersloot en Dr. F.L.J. Visseren. Beste Rob en Frank, als ‘denk-tank’ zijn jullie onmisbaar geweest voor dit proefschrift. Naast jullie kennis op het gebied van ‘infectie en ontsteking’ heb ik ook van jullie statistische kennis mogen profiteren. Met veel plezier denk ik terug aan de avondjes bij jullie thuis. Dr. B.M. de Jongh. Beste Bartelt, dankzij jou had ik ‘carte blanche’ als ik voor de zoveelste keer buisjes bloed naar het microbiologisch lab kwam brengen. Drs. J.C. Kelder. Beste Hans, jouw geduld met ‘statistisch minder bedeelden’ is ongeëvenaard. Over hopelijk niet al te lange tijd is het voor jou ook zover. Succes! Afdeling Research en Development. Alle medewerkers van de RenD ben ik erkentelijk voor de hulp bij het in goede banen leiden van de diverse studies.
119
Medewerkers van het catheterisatie laboratorium. Het gehele team van het 'cathlab' wil ik bedanken voor het bewaren van de cathetertips, het noteren van de standen en de overige hulp als ik niet op tijd aanwezig kon zijn. Nitrobordje? Mw. O.A. Klompstra, secretariaat cardiologie Groningen. Beste Olga, nog nooit heb ik zoveel hulp van iemand gekregen zonder de persoon in kwestie ontmoet te hebben. Ik dank je hiervoor hartelijk. Drs. R.M. van Tooren. Beste Rob, samen begonnen wij in het Antonius, in de run voor die ene opleidingsplaats. In de loop der jaren hebben we nogal wat meegemaakt. Ik voel me vereerd dat jij met mij de arena wilt betreden. Mijn schoonouders dank ik voor alle keren dat jullie bij kwamen springen ('ga jij maar achter de computer zitten'). Jullie geven Nouri waarlijk een tweede thuis. Mijn ouders wil ik bedanken voor de hulp die ik telkens weer krijg. Lieve pa en ma, het moet een hele taak geweest zijn om twee kinderen goed op de rails te zetten. Het is niet voor niets dat dit proefschrift ook aan jullie is opgedragen. Lieve Paulien, inmiddels calculeer jij automatisch in dat effe een kwartiertje achter de computer al gauw anderhalf uur betekent. Ook voor jou betekent promoveren minder tijd voor elkaar. Dat we ook nog gezinsuitbreiding tegemoet gaan lijkt jouw kalmte niet te deren. Dé datum behelst voor ons een andere dag en heeft een andere betekenis: echt meer tijd voor elkaar.

120

121
Curriculum vitae
Born
Nationality
State Children
1984-1990
1990-1996
1996-1997
1997-1999
1999-2001
2001- Nov. 2005
Kerkrade, the Netherlands, May 23, 1972 Dutch Married to Paulien Elberse One son: Nouri, and ? Secondary school, Katholiek Gymnasium Rolduc, Kerkrade Medical school, State University Limburg, Maastricht Research-assistant cardiology, Academic Hospital Maastricht, dr. A.P.M. Gorgels House officer at the Department of Cardiology, Atrium Medical Centre, Heerlen House officer at the Department of Cardiology, St. Antonius Hospital Nieuwegein Resident at the Department of Internal Medicine, Diakonessenhuis Utrecht, Prof. dr. J.B.L. Hoekstra Resident at the Department of Cardiology, St. Antonius Hospital Nieuwegein, Dr. W. Jaarsma





























