Embed Size (px)
Citation preview

Aliment Pharmacol Ther 1997; 11: 147–156.
Lansoprazole heals erosive reflux oesophagitis in patients with
Barrett’s oesophagus
S. J. SONTAG, T. G. SCHNELL, G. CHEJFEC, C. KURUCAR, J. KARPF & G. LEVINE
Departments of Medicine and Pathology, Veterans Affairs Hospital, Hines, Illinois, Loyola University of Chicago Stritch
School of Medicine, Maywood, Illinois, USA
Accepted for publication 3 September 1996
SUMMARY
Background : Barrett’s oesophagus is thought to be a
complication of severe gastro-oesophageal reflux.
Aim : To determine whether the proton pump inhibitor,
lansoprazole, is effective in healing erosive reflux
oesophagitis in patients with Barrett’s oesophagus.
Methods : An 8-week, randomized, double-blind study
was conducted using patients with both erosive reflux
oesophagitis and Barrett’s oesophagus. Erosive reflux
oesophagitis was defined as grades 2–4 oesophagitis ;
Barrett’s oesophagus, as specialized columnar
epithelium obtained by biopsy from the tubular
oesophagus ; and healing, as a return to grade 0 or 1
oesophageal mucosa (complete re-epithelialization).
One-hundred and five (105) patients from one centre
were randomized to receive either lansoprazole 30 mg
daily or ranitidine 150 mg twice daily. Unhealed or
symptomatic lansoprazole patients at week 4 were
INTRODUCTION
Barrett’s oesophagus is generally believed to be a com-
plication of long standing, severe gastro-oesophageal
reflux." Patients with co-existing Barrett’s oesophagus
and erosive reflux oesophagitis are therefore considered
to have severe gastro-oesophageal reflux requiring potent
anti-reflux therapy to achieve healing. Two lansoprazole
studies have been performed on refractory erosive reflux
oesophagitis patients, some of whom have had Barrett’s
oesophagus.#,$ One study of 13 patients with Barrett’s
Correspondence to : Dr S. J. Sontag, Veterans Affairs Hospital, PO Box 5000
(11C3) Hines, IL 60141–5000, USA.
randomized to receive the same 30 mg dose daily or an
increased dose of 60 mg daily. Endoscopy was
performed at baseline and at weeks 2, 4, 6 and 8.
Results : The treatment groups were similar in regards
to baseline characteristics, erosive reflux oesophagitis
grades and length of Barrett’s oesophagus. At each 2-
week interval, lansoprazole patients had significantly
greater healing rates and less day and night heartburn
and regurgitation than ranitidine patients. There were
no significant differences between treatment groups in
antacid use, quality of life parameters, or rate of
reported adverse events. Median values for fasting
serum gastrin levels remained within the normal range
for both groups.
Conclusion : In patients with both Barrett’s oesophagus
and erosive reflux oesophagitis, lansoprazole is
significantly more effective than ranitidine in relieving
reflux symptoms and healing erosive reflux
oesophagitis.
oesophagus demonstrated that high dose lansoprazole
healed the erosive oesophagitis for up to 3 years.%
Another refractory oesophagitis study showed that a
subset of patients with Barrett’s oesophagus healed in 16
weeks with 40 mg omeprazole daily.& No lansoprazole
study to our knowledge has made the presence of
Barrett’s oesophagus the major inclusion criterion.
Since no comparative or placebo-controlled studies have
been conducted with proton pump inhibitors exclusively
in patients with Barrett’s oesophagus, it is not known
whether anti-reflux therapy with the proton pump
inhibitor, lansoprazole, is more effective than therapy
with the H#
receptor antagonist, ranitidine, in healing
# 1997 Blackwell Science Ltd 147

148 S. J. SONTAG et al.
the erosive reflux oesophagitis in the presence of Barrett’s
oesophagus.
To determine whether anti-reflux therapy is effective in
healing the erosive reflux oesophagitis in patients with
co-existing Barrett’s oesophagus, we conducted a study
using the new proton pump inhibitor, lansoprazole, and
the histamine#-receptor antagonist, ranitidine.
MATERIALS AND METHODS
Study design
The study was conducted as a double-blind, randomized,
active-controlled, single-centre clinical trial in which
patients with erosive reflux oesophagitis co-existing with
Barrett’s oesophagus were randomized to receive (in a
1:2 allocation) ranitidine 150 mg twice daily or lanso-
prazole 30 mg once daily. Lansoprazole patients who
were still unhealed or symptomatic at week 4 received
either the same dose of lansoprazole 30 mg or an
increased dose of lansoprazole 60 mg daily before break-
fast for the final four weeks ; ranitidine patients continued
to receive ranitidine 150 mg twice daily. To achieve the
described dosing in a blinded fashion, all patients who at
week 4 were not healed or had reflux symptoms received
an additional bottle that contained lansoprazole 30 mg
or placebo. The ‘double-dummy’ technique was used to
maintain the double-blind status. Gelusil tablets,
9.7 mmol}per tablet (Parke-Davis, Morris Plains, NJ), to
be taken for heartburn, were dispensed at each visit
along with the study medication. Randomization was
performed within 7 days of the baseline endoscopic
demonstration of erosive reflux oesophagitis and Barrett’s
oesophagus.
Patient Selection
One-hundred and five (105) patients, 18 years of age or
older, from one Veterans Affairs Hospital (Hines, IL) were
enrolled in the study. Patients were eligible for enrolment
if they had endoscopic evidence of at least grade 2
(erosive) oesophagitis (Table 1) and histological evidence
of Barrett’s oesophagus, which included specialized
columnar epithelium obtained from biopsy specimens of
the tubular oesophagus. Table 1 shows the oesophagitis
grading scale, which was modified to include patients
with Barrett’s oesophagus. Patients were not eligible for
the study if they had any of the following: oesophageal
stricture requiring dilation; oesophagitis associated with
Table 1. Oesophagitis grading scale
Grade Description
0 Normal-appearing mucosa
1 Mucosal oedema, hyperaemia, and}or friability
2 One or more erosions involving less than 10% of the
distal 5 cm of the oesophagus proximal to the
squamocolumnar junction*
3 Erosions involving 10% to 50% of the distal 5 cm of the
oesophagus proximal to the squamocolumnar
junction,* or a single ulcer measuring 3–5 mm in
diameter
4 Multiple erosions involving more than 50% of the distal
5 cm of the oesophagus proximal to the
squamocolumnar junction,* or a single large ulcer
greater than 5 mm in diameter
* To adjust for the Barrett’s columnar epithelium, the distal 5 cm
of the oesophageal mucosa was considered as the 5 cm segment
above the endoscopically determined squamocolumnar junction.
scleroderma; active ulcer in the stomach, pyloric chan-
nel, or duodenum; current malignancy; clinically signifi-
cant abnormal laboratory values or disease ; or con-
current need for anticoagulants, motility drugs, cortico-
steroids or non-steroidal anti-inflammatory drugs.
Endoscopic assessment
Endoscopy was performed at baseline and at weeks 2, 4,
6 (if not healed at week 4) and 8. At each endoscopy, the
severity of the oesophagitis was scored from grade 0 to
grade 4 (Table 1). Oesophageal mucosal healing was
defined as complete re-epithelization of all ulcers and
erosions (grade 0 or grade 1). Directed mucosal biopsies
of the oesophagus were obtained at baseline to document
the presence of specialized columnar epithelium in the
tubular oesophagus. Patients were eligible for the study
only if there was histological evidence of Barrett’s
oesophagus.
Histological assessment
Four directed mucosal biopsies of the greater curvature of
the gastric body were taken at the initial and final
endoscopies. Two of the biopsy specimens were placed in
Bouin’s solution for later analysis of the following: (i)
inflammation and neoplasia using haematoxylin & eosin
staining and (ii) gastric endocrine cell growth using
Grimelius silver stain.',( The two remaining biopsy
specimens were placed in 2.5% glutaraldehyde in 0.1
molar phosphate buffer at pH 7.4 for future analysis by
# 1997 Blackwell Science Ltd, Aliment Pharmacol Ther 11, 147–156

149LANSOPRAZOLE IN BARRETT’S OESOPHAGUS
electron microscopy. Biopsy specimens were analysed at
the Medical College of Pennsylvania, Philadelphia, PA.
Symptom assessment
Symptoms were assessed using three methods : (i) no-
tation of symptoms at each study visit by study
coordinator, (ii) patient diary, and (iii) quality-of-life
questionnaire.
Notation of symptoms. Patients were asked about an
overall symptom assessment and were questioned about
the presence of specific symptoms, including upper
abdominal burning, day and night heartburn, painful
swallowing, dysphagia, belching, regurgitation,
fullness}bloating}early satiety, abdominal distension,
anorexia, nausea, vomiting, day abdominal pain, night
abdominal pain, flatulence and}or abdominal rumbling,
diarrhoea, constipation, haematemesis, and melena.
Symptoms were recorded as none, mild (symptom of
short duration that was easily tolerated), moderate
(symptom that caused discomfort and that interrupted
usual activities), or severe (symptom that was potentially
incapacitating and that greatly interfered with usual
activities).
Patient diary. Patients were seen at baseline and at the
end of weeks 2, 4, 6 and 8 of treatment. At each visit,
patients were given diary cards to record daily antacid
use, missed doses of study medications, and the frequency
and severity of day and night heartburn. The severity of
symptoms was similarly recorded as none, mild, mod-
erate or severe.
Quality-of-life questionnaire. The patients completed a
‘quality-of-life ’ questionnaire that was designed to
evaluate the effect of oesophagitis on physical, psycho-
logical, and social functioning. The questionnaire was
completed at each study visit prior to all other procedures.
Clinical laboratory determinations
The clinical laboratory tests were analysed at SciCor Inc.,
Indianapolis, IN. Patients fasted for at least 8 h before
blood samples were drawn. Laboratory tests consisted of
a complete blood count and blood chemistries, which
included liver enzymes, lipid determinations, electrolytes,
glucose, albumin and total protein. Fasting serum gastrin
levels were drawn prior to or 24 h after the endoscopy
procedure. Except for baseline screening results,
investigators were blinded to the results of the serum
gastrin levels for the duration of the study.
Statistical analysis
The database remained blinded until all the data were
screened to identify protocol violators. As specified in the
protocol, analyses combined the two lansoprazole groups
(lansoprazole 30 mg for all 8 weeks and lansoprazole
30 mg for 4 weeks followed by lansoprazole 60 mg for 4
weeks) so that all patients receiving lansoprazole are
referred to as the lansoprazole group.
Data were analysed using two approaches : The ‘per
protocol ’ approach, which includes only data considered
acceptable for efficacy evaluation; the ‘all-patients-
treated’ approach (also known as the ‘ intention-to-treat ’
approach), which includes all patients who entered the
study regardless of whether their outcomes were known
or the protocol was followed. In the ‘per protocol ’
analysis, a patient with no endoscopy in a given time
interval was considered healed if healing was docu-
mented previously ; otherwise the patient is not included
in the analysis of that time interval. The ‘all-patients-
treated’ analysis considers all patients to be treatment
failures unless proven to be healed by endoscopy.
Baseline analyses. Baseline demographic data and clinical
characteristics were compared between the two treat-
ment groups (ranitidine group and lansoprazole group)
using a χ# test or a one-way analysis of variance ().
The severity of oesophageal symptoms (including day
and night heartburn, upper abdominal burning, painful
swallowing, belching and regurgitation) was compared
between the two treatment groups using Cochran–
Mantel–Haenszel methodology for ordered response
variables.
Efficacy analyses. The proportions of patients healed
(cumulatively) at each time point were compared be-
tween treatment groups using the Mantel–Haenszel
method. The effect on healing adjusting for various
concomitant factors was assessed using Cochran–
Mantel–Haenszel methodology. Treatment-by-factor in-
teraction was determined using the Breslow–Day Test.
Symptom changes were compared between treatment
groups using the Cochran–Mantel–Haenszel method for
ordered response variables with baseline value as a
stratification factor.
# 1997 Blackwell Science Ltd, Aliment Pharmacol Ther 11, 147–156

150 S. J. SONTAG et al.
Differences between treatment groups were determined
using Wilcoxon two-sample test for average daily heart-
burn scores, percentage of days with heartburn, per-
centage of days antacid was used, and number of antacid
tablets taken.
Eleven measures were derived and validated from the
‘quality-of-life ’ questionnaire. Changes from baseline to
week 8 were compared within and between treatment
groups using analysis of variance.
Safety analysis. Clinical adverse experiences were
analysed using Fisher’s Exact Test. The analysis of the
distribution of patients by predefined limits of change for
clinical laboratory measurements was performed using
the Cochran–Mantel–Haenszel method for ordered re-
sponse categories and mean change analysed using one-
way . The percentage change from baseline of the
serum gastrin levels was calculated for each patient ;
between-group comparisons were made using the
Wilcoxon Two-Sample Test. Changes in gastric biopsies
were compared between both treatment groups using a
one-way analysis of covariance with baseline density as
a covariate.
The study was approved by the Hines Veterans Affairs
Hospital Internal Review Board.
RESULTS
One-hundred and five (105) patients (104 males and 1
female) were randomized to the two treatment groups :
lansoprazole, 69 patients ; ranitidine, 36 patients. Figure
1 shows the demographic and clinical characteristics of
Figure 1. Demographic and clinical characteristics of evaluable
patients. There were no significant differences between
lansoprazole and ranitidine patients at baseline. Both groups
were comparable in regards to age, sex, race, baseline
oesophagitis grade, and use of tobacco, alcohol and caffeine.
the 95 evaluable patients that were included in the ‘per
protocol ’ efficacy evaluations. The two treatment groups
were comparable at baseline with respect to age, sex,
race, baseline grade of oesophagitis, smoking and alcohol
habits, caffeine use, and the presence of hiatal hernia.
Healing rates
Per-protocol analysis. Ten patients (9 in the lansoprazole
group and 1 in the ranitidine group) were excluded from
the per-protocol analysis for reasons shown in Table 2.
Large and significant differences in healing rates were
noted between lansoprazole treatment and ranitidine
treatment. At week 4, the percentage of patients with
complete oesophageal mucosal healing was 85.7% for
the lansoprazole group and 48.4% for the ranitidine
group (P!0.001). After 8 weeks of treatment the
healing rates were 91.4% and 58.1% for the two groups,
respectively, (P!0.001). The healing rates for the 95
evaluable patients are shown in Figure 2.
All-patients-treated analysis. The results of the all-patients-
treated analysis were similar to those of the per-protocol
analysis. At week 4 the percentage of patients with
complete mucosal healing was 76.8% for the lanso-
prazole group and 41.7% for the ranitidine group (P!0.001). After 8 weeks of treatment, the healing rates
were 84.1% and 50.0% for the two groups, respectively,
(P!0.001).
Concomitant factor analysis. Concomitant factors, includ-
ing age, tobacco, alcohol and caffeine consumption,
baseline oesophagitis grade, length of Barrett’s oesoph-
agus, and hiatal hernia were analysed to determine
whether they influenced the healing of oesophagitis or
explained the treatment group differences. Figure 3
shows the percentage of patients with complete healing
stratified by concomitant factors. The differences between
the lansoprazole group and the ranitidine group prevailed
regardless of the concomitant factors considered.
Effect of higher dose lansoprazole. Doubling the dose of
lansoprazole for the final 4 weeks of study did not appear
to influence healing. Of the 7 patients unhealed at 4
weeks, 2 of 3 patients who continued on 30 mg lanso-
prazole healed compared with 3 of 4 who had the dose
increased to 60 mg lansoprazole.
# 1997 Blackwell Science Ltd, Aliment Pharmacol Ther 11, 147–156

151LANSOPRAZOLE IN BARRETT’S OESOPHAGUS
Group Lansoprazole Ranitidine
Number of patients entered 69 36
Number of patients excluded 9 1
Reason excluded
E endoscopic grade not appropriate for entry 1 0
E no histological evidence of Barrett’s oesophagus 3 0
E no data after start of treatment 1 0
E received less than 14 days of therapy 3 1
E malignancy (adenocarcinoma of oesophagus) 1 0
Number of patients evaluable 60 35
Table 2. Reasons for exclusion from per
protocol analysis of efficacy
Figure 2. Percentage of patients with complete endoscopic
healing. At 2, 4, and 8 weeks of treatment, lansoprazole had
statistically significantly greater healing rates in evaluable
patients when compared to ranitidine at all time points (P!0.01).
Symptom Improvement
Notation of symptoms. Of the six primary symptoms of
reflux oesophagitis (including day and night heartburn,
upper abdominal burning, painful swallowing, belching
and regurgitation) lansoprazole was superior to
ranitidine in producing symptom relief in two: day
heartburn and night heartburn.
Lansoprazole patients had statistically significantly
greater relief of day and night heartburn than ranitidine
patients at week 8 (P!0.05). There were no significant
differences between lansoprazole and ranitidine at week
8 in other primary symptoms. The effect on symptom
relief of higher doses of lansoprazole for the final 4 weeks
of study could not be determined because of an
insufficient number of symptomatic patients.
Quality-of-life assessment. Quality-of-life questionnaires
were used to assess the impact of lansoprazole as
compared to ranitidine on certain measures of both
functional status and quality-of-life. Both treatment
groups showed significant improvement from baseline in
the following quality-of-life measures : limitations in
social activities, current health perceptions, health dis-
tress and health index, transitional rating of symptoms,
problem index, sleep index and the overall assessment
index. The lansoprazole group also had significant
improvement in the limitation in daily activity measure
while the ranitidine group improved on the energy}fatigue measure. There were no differences between the
lansoprazole 30 mg group and the lansoprazole 60 mg
group for any of quality-of-life measure.
Diary assessment. Figure 4 shows the mean severity of
daily and nightly heartburn in evaluable patients ac-
cording to the results of the diary. Compared to ranitidine
patients, lansoprazole patients reported significantly
fewer days and nights with heartburn, and less severe
day and night heartburn, (P!0.01). Although the
lansoprazole group used numerically less Gelusil than
the ranitidine group, the difference was not statistically
significant.
Safety
Adverse events. The incidence of adverse events was
similar in both lansoprazole and ranitidine patients.
Table 3 shows the most frequently reported ‘possibly ’ or
‘probably ’ treatment-related adverse events. The table
includes the adverse events that occurred in either group
with an incidence of at least 3% and were judged by the
investigator to be possibly or probably related to the
study drug. The most commonly reported adverse
reactions with lansoprazole were headache, diarrhoea
and asthenia.
# 1997 Blackwell Science Ltd, Aliment Pharmacol Ther 11, 147–156

152 S. J. SONTAG et al.
Figure 3. Effect of concomitant factors on
healing of oesophagitis at week 8 for
evaluable patients. Concomitant factors,
including age, habits, baseline oesophagitis
grade, length of Barrett’s oesophagitis, and
hiatal hernia did not influence healing of
oesophagitis or explain the treatment
group healing differences. The difference in
healing rates between groups prevailed
regardless of the concomitant factors
considered.
Figure 4. Heartburn severity. From the
symptom severity score, as recorded in the
daily diary, lansoprazole patients had
significantly less severe day and night
heartburn as compared with ranitidine
patients (P!0.01).
Table 4 lists the adverse events contributing to with-
drawal from the study. Eight patients (six in the lanso-
prazole group and two in the ranitidine group) withdrew
from the study at least in part due to adverse reactions.
There were no clinically significant treatment-related
changes in either the lansoprazole or the ranitidine group
in physical examinations, electrocardiograms, blood
chemistries or haematology or urinalysis parameters.
Serum gastrins. The lansoprazole group had statistically
significantly larger increases from baseline in fasting
serum gastrin values at weeks 4 and 8 than the ranitidine
groups (P!0.05). Figure 5 shows the median per-
centage increases from baseline for both groups. After
week 4 there was no further increase in median gastrin
levels in the lansoprazole-treated patients. No significant
differences were noted among patients receiving lanso-
prazole 60 mg for the final weeks (although the number
of patients was small) compared to those continuing on
lansoprazole 30 mg. The median percentage increases in
serum gastrin levels from baseline to weeks 4 and 8 were
74% and 76% for the lansoprazole group, compared
with 36% and 25% for the ranitidine group, respectively,
(P!0.05 between groups for week 4 and week 8).
Figure 6 shows the final gastrin levels in patients with
normal baseline gastrins. The percentage of patients that
remained in the normal range at week 8 (% 100 pg}mL)
was 63% in the lansoprazole group and 79% in the
ranitidine group.
# 1997 Blackwell Science Ltd, Aliment Pharmacol Ther 11, 147–156

153LANSOPRAZOLE IN BARRETT’S OESOPHAGUS
Table 3. Percentage of patients with possible or probable
treatment-related adverse events occurring with a prevalence of
at least 3% (n[%])
Adverse Lansoprazole Ranitidine
event (n¯69) (n¯36)
Headache 12 (17.4) 2 (5.6)
Diarrhoea 4 (5.8) 0 (0.0)
Asthenia 3 (4.3) 1 (2.8)
Table 4. Adverse events contributing to withdrawal of eight
patients from study
Treatment Reason for Relation to
Patient Group withdrawal study drug
1 Lansoprazole Nausea Possible
2 Lansoprazole Headache Possible
3 Lansoprazole Aesthenia Possible
4 Lansoprazole Dizziness, Aesthenia Possible
5 Lansoprazole Diarrhoea Possible
6 Lansoprazole Asthenia, Dizziness, Possible
Abnormal Thinking,
Headache
7 Ranitidine Migraine Possible
8 Ranitidine Acute diverticulitis None
Figure 5. Fasting serum gastrin levels. The median percentage
increases in serum gastrin levels from baseline to the final visit
(weeks 4 and 8) were 74% and 76% for the lansoprazole group
compared with 36% and 25% for the ranitidine group,
respectively (P!0.05 between groups for weeks 4 and 8).
Gastric histology. Histological specimens were obtained
from the greater curvature of the gastric body at baseline
and the final visit in all patients. Figure 7 shows the effect
Figure 6. Final gastrin levels in patients with normal baseline
gastrins. The percentage of patients that remained in the normal
range (% 100 pg}mL) was 63% in the lansoprazole group and
79% in the ranitidine group. Gastrin levels greater than
200 pg}mL were found in 8% of the lansoprazole group and 8%
of the ranitidine group.
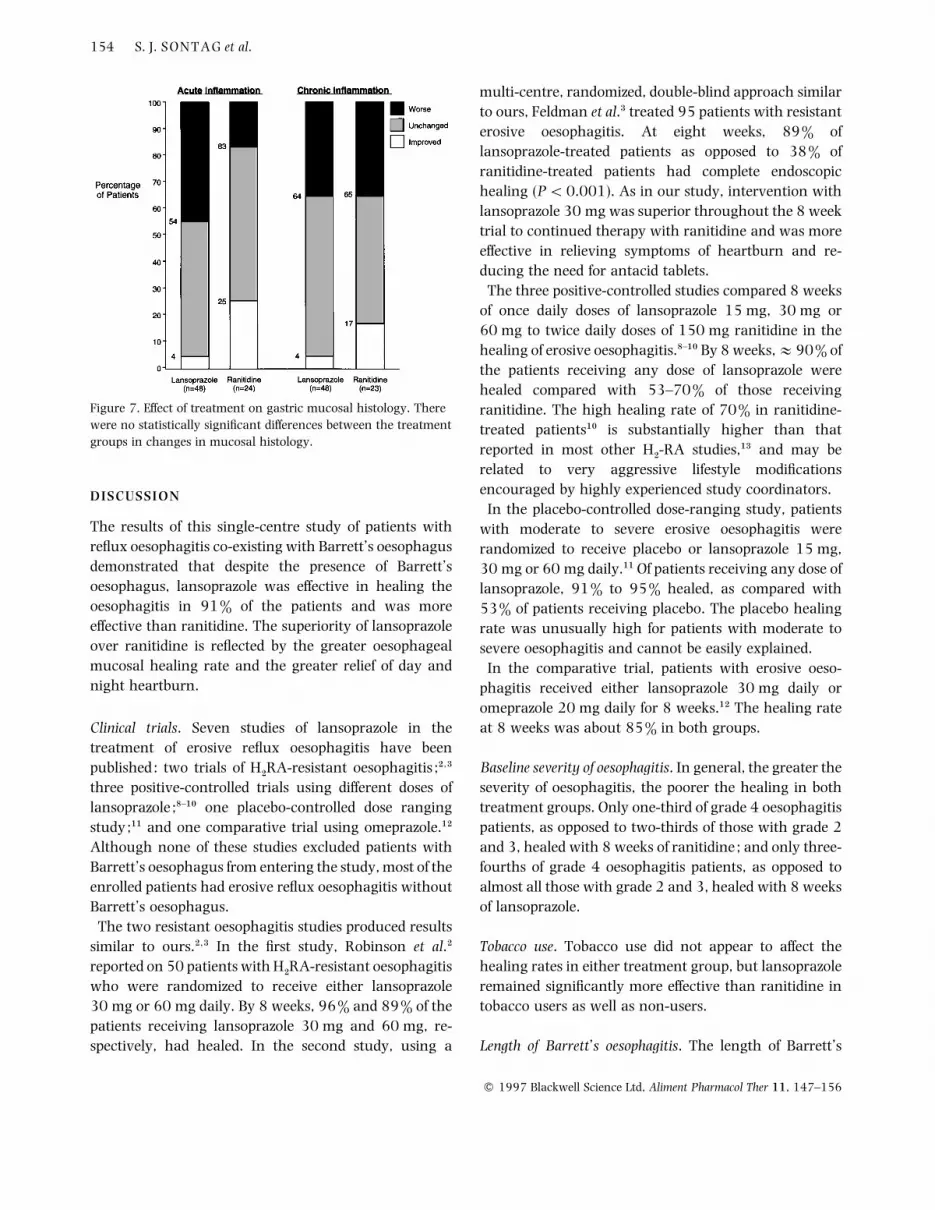
of treatment on gastric mucosal histology. Assessment of
acute inflammation in the lansoprazole group showed
that 50% of patients remained unchanged, 4.2% showed
improvement, and 45.8% showed worsening. In the
ranitidine group, 58.3% of patients remained unchanged
from baseline, 25% showed improvement, and 16.7%
showed worsening.
Assessment of chronic inflammation in the lansoprazole
group showed that 60.4% of patients remained un-
changed from baseline, 4.2% showed improvement, and
35.4% showed worsening. In the ranitidine group,
47.8% of patients remained unchanged from baseline,
17.4% showed improvement and 34.8% showed
worsening.
There were no statistical differences between the lanso-
prazole and ranitidine treatment groups in mean change
from baseline in Grimelius-positive cell densities, Solcia
classification of gastric endocrine growth,',( or level of
inflammation. Furthermore, no cells in either group were
classified as greater than simple (diffuse) hyperplasia.
Light microscopic examination of biopsy specimens
revealed no evidence of carcinoid tumours or of any
visible neuro-endocrine proliferation in any patient.
# 1997 Blackwell Science Ltd, Aliment Pharmacol Ther 11, 147–156
154 S. J. SONTAG et al.
Figure 7. Effect of treatment on gastric mucosal histology. There
were no statistically significant differences between the treatment
groups in changes in mucosal histology.
DISCUSSION
The results of this single-centre study of patients with
reflux oesophagitis co-existing with Barrett’s oesophagus
demonstrated that despite the presence of Barrett’s
oesophagus, lansoprazole was effective in healing the
oesophagitis in 91% of the patients and was more
effective than ranitidine. The superiority of lansoprazole
over ranitidine is reflected by the greater oesophageal
mucosal healing rate and the greater relief of day and
night heartburn.
Clinical trials. Seven studies of lansoprazole in the
treatment of erosive reflux oesophagitis have been
published: two trials of H#RA-resistant oesophagitis ;#,$
three positive-controlled trials using different doses of
lansoprazole ;)–"! one placebo-controlled dose ranging
study;"" and one comparative trial using omeprazole."#
Although none of these studies excluded patients with
Barrett’s oesophagus from entering the study, most of the
enrolled patients had erosive reflux oesophagitis without
Barrett’s oesophagus.
The two resistant oesophagitis studies produced results
similar to ours.#,$ In the first study, Robinson et al.#
reported on 50 patients with H#RA-resistant oesophagitis
who were randomized to receive either lansoprazole
30 mg or 60 mg daily. By 8 weeks, 96% and 89% of the
patients receiving lansoprazole 30 mg and 60 mg, re-
spectively, had healed. In the second study, using a
multi-centre, randomized, double-blind approach similar
to ours, Feldman et al.$ treated 95 patients with resistant
erosive oesophagitis. At eight weeks, 89% of
lansoprazole-treated patients as opposed to 38% of
ranitidine-treated patients had complete endoscopic
healing (P!0.001). As in our study, intervention with
lansoprazole 30 mg was superior throughout the 8 week
trial to continued therapy with ranitidine and was more
effective in relieving symptoms of heartburn and re-
ducing the need for antacid tablets.
The three positive-controlled studies compared 8 weeks
of once daily doses of lansoprazole 15 mg, 30 mg or
60 mg to twice daily doses of 150 mg ranitidine in the
healing of erosive oesophagitis.)–"! By 8 weeks,E90% of
the patients receiving any dose of lansoprazole were
healed compared with 53–70% of those receiving
ranitidine. The high healing rate of 70% in ranitidine-
treated patients"! is substantially higher than that
reported in most other H#-RA studies,"$ and may be
related to very aggressive lifestyle modifications
encouraged by highly experienced study coordinators.
In the placebo-controlled dose-ranging study, patients
with moderate to severe erosive oesophagitis were
randomized to receive placebo or lansoprazole 15 mg,
30 mg or 60 mg daily."" Of patients receiving any dose of
lansoprazole, 91% to 95% healed, as compared with
53% of patients receiving placebo. The placebo healing
rate was unusually high for patients with moderate to
severe oesophagitis and cannot be easily explained.
In the comparative trial, patients with erosive oeso-
phagitis received either lansoprazole 30 mg daily or
omeprazole 20 mg daily for 8 weeks."# The healing rate
at 8 weeks was about 85% in both groups.
Baseline severity of oesophagitis. In general, the greater the
severity of oesophagitis, the poorer the healing in both
treatment groups. Only one-third of grade 4 oesophagitis
patients, as opposed to two-thirds of those with grade 2
and 3, healed with 8 weeks of ranitidine ; and only three-
fourths of grade 4 oesophagitis patients, as opposed to
almost all those with grade 2 and 3, healed with 8 weeks
of lansoprazole.
Tobacco use. Tobacco use did not appear to affect the
healing rates in either treatment group, but lansoprazole
remained significantly more effective than ranitidine in
tobacco users as well as non-users.
Length of Barrett’s oesophagitis. The length of Barrett’s
# 1997 Blackwell Science Ltd, Aliment Pharmacol Ther 11, 147–156

155LANSOPRAZOLE IN BARRETT’S OESOPHAGUS
oesophagus did not affect the healing rates in either
group. Lansoprazole healed 85% of patients with greater
than 3 cm of Barrett’s oesophagus and 97% of those with
less than 2 cm. Lansoprazole was significantly more
effective than ranitidine in healing the oesophagitis
regardless of the length of Barrett’s oesophagus.
Quality-of-life. The quality-of-life questionnaire, designed
to detect a change in the feeling of relative well being,
revealed an improvement in well-being for both
lansoprazole- and ranitidine-treated patients.
Safety. Lansoprazole and ranitidine were well-tolerated.
There were no clinically significant changes in physical
examination, ECGs or standard clinical laboratory tests.
Adverse reactions occurred in both treatment groups
with similar frequency.
As expected, the increase in serum gastrin levels was
greater in patients treated with lansoprazole than in
those treated with ranitidine. Median fasting serum
gastrin levels increased by 74% after 4 weeks of
lansoprazole therapy and by 76% after 8 weeks of
lansoprazole therapy. Corresponding increases in serum
gastrin with ranitidine at 4 and 8 weeks were 36% and
25%.
In the 24 ranitidine-treated patients with normal
gastrin levels at baseline, 19 (79%) remained within
normal limits at week 8, and 3 (13%) had 8-week levels
between 100 and 200 pg}mL. Two (8%) ranitidine-
treated patients had gastrin levels greater than
200 pg}mL. The differences in gastrin levels were un-
doubtedly due to the more potent acid inhibitory property
of lansoprazole as compared with ranitidine.
Of the 49 lansoprazole patients with normal baseline
fasting serum gastrin levels, 31 (63%) at week 8
remained within normal limits, 14 (29%) at week 8 had
levels between 100 and 200 pg}mL, and 4 (8%) at week
8 had levels above 200 pg}mL. Of the 8 patients with
levels greater than 200 pg}mL at week 8, one had a level
of 795 pg}mL at 8 weeks and one had a level of
390 pg}mL at 8 weeks. In general, serum gastrin levels
increased from baseline to week 4 of lansoprazole
therapy, and appeared to taper off with no additional
increase after week 4.
Biopsies of the gastric mucosa taken from the greater
curvature of the stomach in this study failed to reveal any
increase in enterochromaffin-like cell density or neuro-
endocrine cell proliferation.
CONCLUSION
From previous studies it is apparent that in patients with
reflux oesophagitis and H#-RA-resistant reflux oeso-
phagitis, lansoprazole in doses of 30 and 60 mg daily is
superior to ranitidine in the complete healing of moderate
and severe reflux oesophagitis and in the complete relief
of primary and secondary symptoms associated with
gastro-oesophageal reflux. From our present study we
conclude that lansoprazole is equally effective for healing
of reflux oesophagitis in patients with coexisting Barrett’s
oesophagus.
ACKNOWLEDGEMENTS
This study was supported by a grant from TAP Holdings.
This material is based upon work supported by the Office
of Research and Development (R&D) at the Department
of Veteran Affairs (VA), Hines, IL. We gratefully ac-
knowledge the support of Jean Seidel for her expertise
in preparing this manuscript, Larry Brand for the high
quality figures and Kathy Franke, Sue O’Connell and
Rose Todd for clinical assistance. We also thank the
Hines VA pharmacy staff for their assistance in dis-
tributing the medications. Additionally, we thank Dr
Marion Haber (TAP Holdings) for reading all the biopsy
material.
REFERENCES
1 Spechler SJ. Epidemiology and natural history of gastro-
oesophageal reflux disease. Digestion 1992; 51(Suppl. 1) :
24–9.
2 Robinson MG, Campbell DR, Sontag S, et al. Lansoprazole heals
H#
RA-resistant erosive reflux esophagitis. Gastroenterology
1990; 98: A113(Abstract).
3 Feldman M, Harford WV, Fisher RS, et al. Lansoprazole heals
erosive reflux esophagitis resistant to histamine H#-receptor
antagonist therapy. Am J Gastroenterol 1993; 88: 1212–7.
4 Sampliner RE. Effect of up to 3 years high dose lansoprazole in
Barrett’s esophagus. Am J Gastroenterol 1994; 89: 1844–8.
5 Klingenberg-Knol EC, Festen HPM, Jansen JBMJ, et al. Long-
term treatment with omeprazole for refractory reflux
esophagitis : safety and efficacy. Ann Int Med 1994; 121:
161–7.
6 Solcia E, Capella C, Vassallo G, et al. Endocrine cells of the
gastric mucosa. Int Rev Cytol 1975; 42: 223–86.
7 Solcia E, Bordi C, Creutzfeldt W, et al. Histopathological
classification of nonantral gastric endocrine growths in man.
Digestion 1988; 41: 185–200.
8 Benhaim MC, Evreux M, Salducci J, Petite JP, Lemaire M.
# 1997 Blackwell Science Ltd, Aliment Pharmacol Ther 11, 147–156

156 S. J. SONTAG et al.
Lansoprazole and ranitidine in treatment of reflux oesophagitis :
double blind comparative trial. Gastroenterology 1990; 98(2) :
A20(Abstract).
9 Bardhan KD, Long R, Hawkey CJ, et al. Lansoprazole, a new
proton-pump inhibitor, vs. ranitidine in the treatment of reflux
erosive esophagitis. Gastroenterology 1991; 100(2) :
A30(Abstract).
10 Robinson M, Kogut D, Jennings D, et al. Lansoprazole heals
erosive reflux esophagitis better than ranitidine. Gastro-
enterology 1992; 102(2) : A153(Abstract).
11 Dorsch E, Jones J, Padgett C, et al. Lansoprazole heals moderate
to severe reflux esophagitis. Am J Gastroenterol 1991; 86:
A1294(Abstract).
12 Hatlebakk JG, Berstad A, Carling L, et al. Lansoprazole vs.
omeprazole in short-term treatment of reflux oesophagitis—
Results of a Scandinavian Multicentre Trial. Scand J Gastro-
enterol 1993; 28: 224–8.
13 Sontag SJ. Rolling review: gastro-oesophageal reflux disease.
Aliment Pharmacol Ther 1993; 7: 293–12.
14 Sontag S, Hendrix T, Hirschowitz B, et al. Omeprazole for
esophagitis and ulcers refractory to H#-blockers. Gastro-
enterology 1988; 94(2) : A436(Abstract).
# 1997 Blackwell Science Ltd, Aliment Pharmacol Ther 11, 147–156





























