Embed Size (px)
Citation preview

Journal of Immunological Methods 326 (2007) 63–75www.elsevier.com/locate/jim
Research paper
Large scale expansion of γ9δ2 T lymphocytes: Innacell γδ™ celltherapy product
Samuel Salot a,⁎, Catherine Laplace a, Soraya Saïagh b, Sylvain Bercegeay b,Isabelle Tenaud b, Alain Cassidanius b, François Romagne a,
Brigitte Dreno b, Jérôme Tiollier a
a Innate Pharma, 119-121 Ancien chemin de Cassis, 13009 Marseille, Franceb Unité de Thérapie Cellulaire et Génique (UTCG), Institut de Biologie, 9 quai Moncousu, 44093 Nantes cedex 01, France
Received 4 December 2006; received in revised form 6 June 2007; accepted 9 July 2007Available online 7 August 2007
Abstract
γ9δ2 T lymphocytes are non-conventional lymphocytes presenting a direct cytotoxic effect against a broad range of tumourtargets. These cells also secrete inflammatory cytokines that can boost the other components of the immune system. In contrast toconventional CD8+ T cells, the cytotoxic effect of γ9δ2 T lymphocytes does not depend on the expression of majorhistocompatibility complex molecules by target tumour cells. INNACELL γδ™ is a cell therapy product obtained by ex vivoamplification of mononuclear cells. The stimulation is achieved by a specific synthetic agonist of γ9δ2 T lymphocytes,bromohydrin pyrophosphate (BrHPP). After a single stimulation with BrHPP, γ9δ2 T lymphocytes are expanded for 2 weeks in aclosed system in culture medium with interleukin-2 (IL-2). On day 15, cells are washed and harvested in 4% human serumalbumin. In this manufacturing process, the total cell population is expanded by approximately 10-fold and γ9δ2 T lymphocytesundergo a specific 1000-fold expansion, corresponding to a γ9δ2 T lymphocyte enrichment of more than 70% at the end of theculture. This manufacturing process is much simpler than most current cellular therapy approaches using conventional CD8+ T-celllines or clones: there is no final or initial separation, no purification step and no use of feeder cells; the specific T-cell receptor-mediated signal provided by BrHPP is sufficient to trigger the IL-2-dependent expansion of the γ9δ2 subset, which then becomespredominant in the cell culture in large amounts.© 2007 Elsevier B.V. All rights reserved.
Keywords: γ9δ2 T lymphocytes; Cell therapy product; Phosphoantigen; BrHPP
Abbreviations: BrHPP; bromohydrin pyrophosphate; CTP; celltherapy product; DC; dendritic cells; FCS; foetal calf serum; 4%; HA;4%; human serum albumin; mRCC; metastatic renal cell carcinoma;MNC; mononuclear cell; MM; multiple myeloma; NHL; non-Hodgkin's lymphoma; TNFα; tumour necrosis factor α.⁎ Corresponding author. Tel.: +33 4 96 19 05 50; fax: +33 4 96 19 06
55.E-mail address: [email protected] (S. Salot).
0022-1759/$ - see front matter © 2007 Elsevier B.V. All rights reserved.doi:10.1016/j.jim.2007.07.010
1. Introduction
Most current immuno-therapeutic approaches aim toinduce anti-tumour response via stimulation of theadaptive immune system, which depends on majorhistocompatibility complex (MHC) restricted αβT lymphocytes. Despite major advances in our under-standing of adaptive immunity against tumours and the

64 S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
introduction of vaccine-based strategies, durable re-sponses are rare and yet active immuno-therapy is notan established treatment modality. Adaptive immuno-therapeutic approaches have several disadvantages: αβT lymphocytes need specific tumour-associated antigensand appropriate co-stimulating molecules for activation.Failure or loss of tumour-associated antigens, MHCmolecules and/or co-stimulatingmolecules render tumourcells resistant to αβ T-cell-mediated cytotoxicity orinduce anergy of specific T cells (Schultze and Nadler,1999).
On the other hand, the ability of γδ T lymphocytes torespond to non-processed and non-peptidic phosphoan-tigens in an MHC-unrestricted manner is an importantfeature distinguishing them from αβ T lymphocytes(Brenner et al., 1987; Constant et al., 1994; Bukowskiet al., 1995; Tanaka et al., 1995). In addition, γδT lymphocytes are thought to be involved in thecoordination of the interplay between innate andadaptive immunity and, in particular, to guide theestablishment of acquired immunity contributing to thedefinition of αβ T lymphocyte responses towards Th1 orTh2 phenotype (Fearon and Locksley, 1996; Mak andFerrick, 1998). γδ T lymphocytes regulate the initiation,progression and resolution of the immune response toinfectious pathogens and γδ T-cell-mediated immuneresponses have been demonstrated in many microbialinfections, suggesting that anti-viral immuno-surveil-lance may be one of the primary γδ T-cell functions(Poupot and Fournie, 2004).
In contrast to γδ T lymphocytes expressing the TCRvariable region Vδ1, which are prevalent in late foetal,postnatal thymus and the red pulp of spleen, more than70% of the circulating human γδ T cells express theVγ9Vδ2 TCR chains (Parker et al., 1990). γ9δ2T lymphocytes, which represent 0.5–5.0% of wholeperipheral blood T cells, are referred to as innate-likeT cells owing to: (i) their ability to recognize conservedantigens expressed by a broad range of infected, stressedand/or transformed cells, (ii) their pre-activated statusresulting from an early (postnatal) acquisition ofmemory markers and (iii) their high frequency inparticular tissue locations (Hayday, 2000; Bonnevilleand Fournie, 2005; Bendelac et al., 2001). Two kinds ofAg selectively stimulating γ9δ2 T cells have beenidentified: (i) small phosphorylated compounds referredto as phosphoantigens (Constant et al., 1994; Espinosaet al., 2001a) which are produced through the isoprenoidbiosynthetic pathway of mammalian cells, such asisopentenyl pyrophosphate (IPP) (Tanaka et al., 1995)and non-mammalian cells such as 4-hydroxy-3-dimethylallyl pyrophosphate (Hintz et al., 2001) and
(ii) complexes comprising ATP synthase subunits,which are found on the surface of some tumour cells(Scotet et al., 2005). Besides their anti-infectiousactivity, γ9δ2 T lymphocytes participate together withdendritic cells (DC) (Kroca et al., 2001), NK cells, andNK-T cells in the innate immunity response to cancerprocesses (Walzer et al., 2005). It was shown incytotoxicity assays that γ9δ2 T lymphocytes are ableto kill a wide variety of tumour cell lines from verydiverse origins: lymphoma and leukaemia from B cell,T cell or myeloid lineages (Sturm et al., 1990; Fischet al., 1997), multiple myeloma (B. Klein, personalcommunication), breast carcinoma (Bank et al., 1993),glioblastoma (Fujimiya et al., 1997), renal cell carcino-ma (Mitropoulos et al., 1994), nasopharyngeal carcino-ma (Zheng et al., 2001), neuroblastoma (Otto et al.,2005), colon carcinoma (Corvaisier et al., 2005), lungadenocarcinoma (Ferrarini et al., 1996) and hepatocar-cinoma (F. Bouet, personal communication). This directin vitro anti-tumour activity was also demonstrated inautologous contexts and with fresh tumour cells orshort-term cancer cell lines (Fujimiya et al., 1997;Yamaguchi et al., 1997; Viey et al., 2005a).
The first clinical evidence for in vivo manipulation ofhuman γ9δ2 T lymphocytes induced by γ9δ2 T-cellagonists came unexpectedly from the finding of circulat-ing γ9δ2 T lymphocyte increases in some adults withmultiple myeloma (MM) following intravenous injectionof the aminobisphosphonate, pamidronate. Pamidronateis an indirect inducer of γ9δ2 T-cell responses via theinhibition of an enzyme of the mevalonate pathway,which leads to accumulation of IPP metabolite, a weakagonist of γ9δ2 T cells. A clinical trial evaluated theeffects of pamidronate and interleukin-2 (IL-2) co-treatment in 19 patients: 11 patients with non-Hodgkin'slymphoma (NHL) and 8 patients with MM (Wilhelmet al., 2003). This study showed that pamidronate and IL-2 co-treatment induce specific γ9δ2 T lymphocyteamplification in the periphery, and clinical response(disease stabilization or partial remission) related to invivo γ9δ2 T lymphocyte expansion. Pamidronate, andmore generally bisphosphonates, however, are not idealdrugs to induce in vivo activation of γ9δ2 T lymphocytes:first, their in vitro activity is in the μM range (Jomaa et al.,1999) compared to the nM range for (E)-4-hydroxy-3-methyl-but-2-enyl pyrophosphate (HMB-PP) (Hintzet al., 2001). Second, unlike phosphoantigens, aminobi-sphosphonates activateγ9δ2 T lymphocytes in an indirectfashion, through the blockade of the mevalonate pathway,which can have undesirable effects if only immuno-manipulation is sought (Gober et al., 2003). Third,bisphosphonates rapidly bind to bone tissue with a very

65S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
long half-life, which may be detrimental to immuno-stimulation (Lin, 1996; Lin et al., 1999).
In contrast to conventional cytotoxic and cytostaticagents which directly target tumour cells, the syntheticphosphoantigen BrHPP, a specific agonist of γ9δ2T lymphocytes activates the subpopulation of γ9δ2T lymphocytes that in turn has been shown to exert anti-tumour activity (Belmant et al., 2000). It is therefore likelythat increasing the state of activation and the number ofthese effector cells will enhance anti-tumour activity(Sicard et al., 2001). Moreover, BrHPP alone, like otherphosphoantigens, is sufficient to trigger the production ofcytokines and expression of activation markers such asCD25 by γ9δ2 T lymphocytes; in vitro proliferation ofγ9δ2 T lymphocytes still requires exogenous IL-2(Espinosa et al., 2001b;Wesch et al., 1997). Furthermore,a recent in vivo study on cynomologus monkeys treatedwith BrHPP combined with a low dose of IL-2 showed asystematic expansion of CD45RA−CD27−/effector-memory phenotype γ9δ2 T-cell subsets, associated witha Th1 response (Sicard et al., 2005).
It has been previously reported that γ9δ2 T lympho-cytes could be expanded in vitro from cultured humanPBMCs and then enriched by immuno-magnetic separa-tion (Lopez et al., 2000), and this protocol could be usedin a clinical trial (Guo et al., 2005; Liu et al., 2005).However, such a process requires cell separation, use offeeder cells, purification steps, and it would thus bedifficult to adapt it to an extensive therapeutic scale in theindustrial setting. In comparison, our process has severaladvantages, the most important being that it does notinvolve either a final or an initial separation or purificationstep and does not use feeder cells. A single stimulation ofMNCs cells with BrHPP is required to obtain a celltherapeutic product (CTP) highly enriched in γ9δ2T lymphocytes after 2 weeks of culture with IL-2. Thepresent study aims to describe the main parameters thatinfluence the proliferation and specific expansion of γ9δ2T lymphocytes ex vivo, and to propose a new protocol forγ9δ2 T lymphocyte amplification applicable in theindustrial setting. This new adoptive immuno-therapyapproach could offer a complementary treatment toconventional cancer therapies.
2. Materials and methods
Written informed consent was obtained from eachpatient before enrolment and completion of any studyprocedure. The clinical trial registered under thereference Innacell GD® D001-101, and entitled “Aphase I/II dose ranging tolerance study of Innacell GD®in combination with a fixed dose of IL-2 in patients with
metastatic renal cell carcinoma” was approved by theIndependent Ethics Committee of Nantes, France, andby the French National Committee of Cell Therapy. Thetrial was conducted in compliance with the principleslaid down by the Declaration of Helsinki, subsequentamendments and Good Clinical Practice.
The following products were used throughout thestudy: lymphocyte separationmedium (LSM), LSM1077,PAA Laboratories, Pasching, Austria; RPMI-1640, Cam-brex Biosciences, Verviers, Belgium; non-decomplemen-ted irradiated foetal calf serum (FCS), Foetal Clone-I,HyClone, Erembodegem, Belgium; DMSO, Braun Med-ical, Boulogne, France; BrHPP, IPH1101-Phosphostim200™, Innate Pharma, Marseille, France; human recom-binant interleukin-2 (IL-2), Proleukin®, Chiron Thera-peutics, Emeryville CA, USA; RPMI–FCS (RPMI-1640supplemented with 9% FCS).
Isolation of MNCs and the large scale amplificationprocess were performed under good manufacturingpractice (GMP) conditions.
2.1. Small scale in vitro amplification assay
Knowing that the γ9δ2 T-cell response to BrHPPstimulation is dependent on the individual, evaluation ofthe amplification potential of each volunteer wasconducted in a small scale in vitro assay prior to thelarge scale amplification process. Blood samples werediluted 1/2 in RPMI. After loading 2 vol of diluted bloodsample on 1 vol of LSM, PBMCs were separated bycentrifugation. The white blood cell ring fraction waswashed in 1 vol of RPMI by centrifugation and plateletswere removed by centrifugation at 200 ×g. PBMCs werefrozen in CryoTube vials (size 1.8ml, Nalgen® Labware,Neerijse, Belgium) at 10×106 viable cells/ml FCS with7.5% DMSO and stored at −80 °C for 2 days prior totransfer to liquid nitrogen. PBMCs were briefly thawed ina water bath at 37 °C, washed and re-suspended in RPMI–FCS. Triplicate aliquots of 1.5million viable PBMCswerestimulated with 3 μM BrHPP in RPMI–FCS and IL-2 at20 ng/ml under 1.5ml in a 24-well plate (day 0 of culture).From day 4 to day 14, cells were maintained at 1×106
viable cells/ml in RPMI–FCS with IL-2 at 60 ng/ml.Cell counts were determined using a Malassez cham-
ber in which cells were diluted in 0.15% eosin in order toevaluate cell viability; the cell amplification factor wascalculated as (viable cell number at day 14/viable cellnumber at day 0). The selection criteria evaluated at day14 of culture, and which were required to perform a largescale amplification, were the following: mean total viablecell amplification rate≥10; mean CD3+Vδ2+≥70%;mean cell viability≥70%.

66 S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
2.2. Isolation of mononuclear cells
Patients showing anaemia, poor venous access, poorcirculation in the legs, Hbb10 g/dl, polymorphonuclearleukocyte (PMN)b2.0×109/l or plateletsb150×109/lwere not eligible for leukapheresis. Mononuclear cells(MNCs) were collected using a continuous-flow bloodcell separator, COBE Spectra® Apheresis System(Gambro BCT, Lakewood, USA). The blood flow ratewas 75−100 ml/min and cell density was followed upwith the help of spectra colourgrams (1.05bdb1.055).Approximately 6–9 l of blood were processed over 3–4 hin order to collect a final volume of approximately 150 ml(containing 1 to 16 billion MNCs). Acid citrate dextrose(Braun Medical, Boulogne, France) was used as anti-coagulant. One leukapheresis provides enough MNCs toinoculate at least one cell culture bag with 600 millionviable cells, which represents the minimum amount re-quired to initiate the production process.
On the day of leukapheresis, the collected cells werefirst washed in RPMI-1640 and platelets were thenremoved by centrifugation at 200 ×g. MNCs werefrozen in FCS supplemented with 7.5% DMSO at a celldensity of 60 million viable cells/ml in freezing vials(5.0 ml CryoTube, Nalgene®, Neerijse, Belgium)containing 4.5 ml of cells and then stored at −80 °Cfor 2 days prior to transfer to liquid nitrogen.
2.3. Large scale amplification process
Freezing vials were thawed in a water bath at 37 °C andtransferred in RPMI–FCS. After 1 h incubation in tubes at37 °C, 5% CO2, in RPMI–FCS, white blood celldifferential counts were carried out to quantify the ratiosof cell types. Six hundred million viable cells wereinoculated in a 3-l cell culture bag (Lifecell 3L, Baxter,Deerfield IL, USA) under 500 ml of RPMI–FCS, with3 μMBrHPP and 20 ng/ml of IL-2. From day 4 to day 14,cell culture maintenance medium was prepared extempo-raneously (RPMI–FCS and IL-2 60 ng/ml) and prior toaddition of the medium, the cell suspensions were dividedinto two when the final volume was upper than 2.2 l. Onday 4, medium was added depending on the cell concen-tration (C): if Cb0.7×106 viable cells/ml, 250 ml of me-dium were added per bag; if 0.7×106 cells/ml≤C≤1.3×106 cells/ml, 500 ml of medium were added per bag;ifCN1.3×106 cells/ml, 1 l of medium was added per bag.At day 7, the cell concentration was adjusted to0.5×106 cells/ml. At day 11, the cell concentration wasadjusted to 1.0×106 cells/ml and to 1.5×106 cells/ml atday 14. Cell counts were determined using a Malassezchamber in which cells were diluted with 0.15% eosin in
order to evaluate the cell viability; the cell amplifica-tion factor was calculated as (viable cell number at day14/viable cell number at day 0). At day 15, the end ofthe expansion phase, the cell culture volume wasreduced and the cells were washed with buffered 0.9%NaCl solution, pH 7 (formule TS 590, Braun Medical,Boulogne, France). This harvesting step was performedeither manually with several centrifugations or auto-mated (CytoMate™, Baxter, Deerfield, IL, USA). Inthe manual approach, after transferring the cell culturein a transfer bag (DGR2089, Baxter, Deerfield IL,USA), three centrifugation steps were required. WithCytoMate™, the procedure was totally automated andno manual centrifuge steps were necessary. In a finalstep for both harvesting methods, the cells were harvestedin transfer bags at 10–100 million total cells/ml in 4%HA (4% Vialebex, LFB Laboratory, Courtabœuf, France)and stored at +5±3 °C.
2.4. Flow cytometry
Immuno-phenotypic analyses were performed ondays 0, 4, 7, 11, 14 and 15 of culture. The followingmouse anti-human antibodies from Beckman Coulterwere used: CD3-FITC (A07746), CD8-FITC (A07756),Vδ2-FITC (IM1464), CD14-FITC (IM0645F), CD3-PE(A07744), pan αβ-PE (IM1467), CD56-PE (IM2073),CD19-PE (A07769), HLA-DR-PE (IM1639),CD45RA-PE (IM1834), CD27-PC5 (6607107), CD3-PC5 (A07749), CD4-PC5 (IM2636), CD69-PC5(IM2656), IgG1-FITC (A07795), IgG1-PE (A07796)and IgG1-PC5 (A07798); CD25-PE clone 2A3(341011) was obtained from Becton-Dickinson. Twohundred thousand live cells were stained in a finalvolume of 50 μl of 0.1% PBS–BSA (Sigma, St Louis,USA); antibodies were diluted 1/5 (FITC- and PE-labelled) or 1/10 (PC5-labelled). Sample acquisition wasperformed on a four-colour flow cytometer (FACScali-bur, BD Biosciences, Franklin Lakes, USA) andanalysed using Cell Quest software (BD Biosciences,Franklin Lakes, USA); after gating out low forwardscatter elements (red blood cells and debris), samplecollection was run with at least 200 CD3+Vδ2+ eventsand a minimum of 10,000 total events collected.
2.5. Cytokine titration by enzyme-linked immuno-sorbent assay (ELISA)
IL-2 concentration was determined using a commer-cial immuno-assay kit according to the manufacturer'sinstructions (IM3583, Beckman Coulter, Fullerton,USA).

67S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
TNFα release assay and dosage was performed asfollows: the cell concentration of a sample of γδ CTPsuspension was adjusted at 125,000 cells/ml in RPMI–FCS. Triplicates of 22,500 cells/well were distributed in aU-bottom 96-well plate in a final volume of 180 μl/well.Cell stimulation was triggered by adding 20 μl of RPMI–FCS containing 30 μM BrHPP (final BrHPP concentra-tion 3 μM). The same volume of RPMI–FCS withoutBrHPP was added to control cultures. The plate wasincubated for 20±2 h in 5% CO2 at 37 °C. TNFα releasewas determined on the culture supernatant following themanufacturer's instructions for the immuno-assay kit(IM1121, Beckman Coulter, Fullerton, USA).
2.6. 51Cr-release cytotoxicity test
The primary study in a small scale assay showed thatexpanded cells at day 14 were able to lyse many RCC celllines from ATCC, such as 786-0, 769-P, Caki-1, G-401,
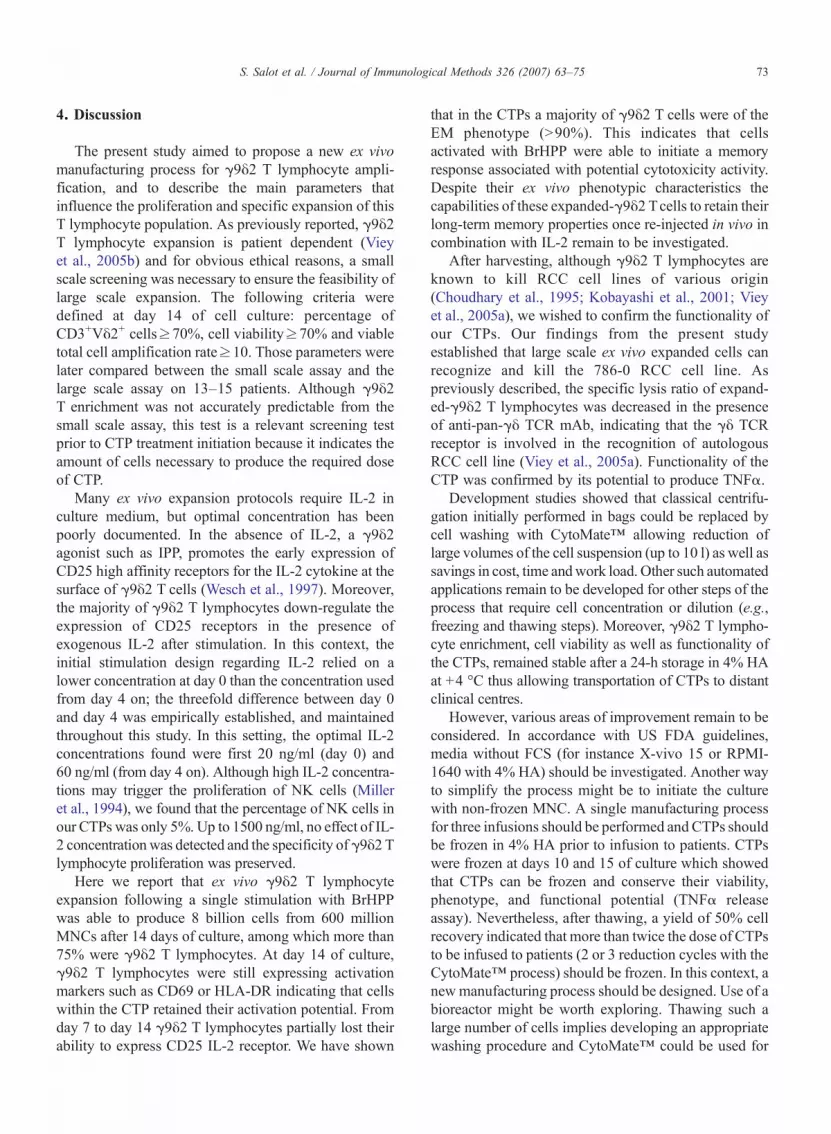
Fig. 1. Cell characteristics of the large scale amplification process. From the M3 CTPs per patient); each CTP was generated from 600 million MNCs stimulamaintained for 15 days in RPMI–FCS–IL2 (60 ng/ml). Cell numbers (A), cellday 14 (C), calculated as (viable Vδ2+CD3+ cell number at day 14/viable Vδ2manual cell counting: T cells (CD3+), NK cells (CD3−/CD56+), T-cell subpo
G-402, SK-NEP-1 (data not shown); since the highestspecific lysis ratios were observed against the 786-0 cellline, it was retained as the reference sensitive targetthroughout the study. Expanded cells were tested forcytotoxicity against a negative control B-EBV+ targetobtained as previously described (Ibisch et al., 2000) and apositive (RCC) cell line (786-0, CRL-1932, ATCC). Onemillion target cells were labelled with 50 μl (50 μCi) of51Cr (Amersham Pharmacia Biotech, Piscataway, USA)for 1 h at 37 °C in 5% CO2. The cells were then washedfour times and re-suspended in RPMI–FCS and 50 μlwere plated (3000 cells/well) in 96-well V-bottommicrotitre trays. Fifty microlitres of negative effectorcontrol αβ T-cell clone “A 4.5” (Vely et al., 2001),positive effector control γ9δ2 T-cell clone “G 12”(Davodeau et al., 1993) or CTP effector cells wereadded to the target cells in order to get the followingeffector/target ratios 0.3/1; 3/1; 30/1. In maximum andspontaneous release control wells, 50 μl/well of 0.1%
NCs collected from 10 mRCC patients, 27 CTPs were produced (up toted once (day 0) with 3 μMBrHPP in RPMI–FCS–IL2 (20 ng/ml) andpopulation ratios (B) and the specific Vδ2+CD3+ amplification factor at+CD3+ cell number at day 0), were determined by flow cytometry andpulations (CD3+Vδ2+ and CD3+αβ+).

68 S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
Triton X-100 or RPMI–FCS were added in place ofeffector cells. After 4 h incubation at 37 °C and 5% CO2,25 μl of supernatant was collected to determine 51Crrelease. The percentage of specific target-cell lysis wascalculated as the mean of triplicate determinations:[(experimental release−spontaneous release) / (maximumrelease−spontaneous release)]×100.
3. Results
The clinical trial required three distinct infusions ofCTPs to patients which were produced 3 weeks apart(Bompas et al., 2006); hence the following resultsshow up to three distinct productions of CTPs for eachpatient.
3.1. Large scale amplification process
After thawing, lymphocyte cell recovery yield was57±16% (range 41–82; n=23 CTPs) and polynuclearneutrophils (PNN), which represented up to 65% of theMNCs, were lysed after 1 h incubation. No correlationcould be made between the number of monocytes orpolynuclear neutrophils in the initial leukapheresismaterial and the amplification of γ9δ2 T cells duringthe culture (data not shown).
Out of 10 distinct mRCC patients, 27 CTPs wereproduced and characterized as shown in Fig. 1; from600 million viable MNCs, 7.8±3.9 billion of total cells(range 1.7–22.0 billion) and 6.3±3.7 ofγ9δ2 Tcells wereproduced within 14 days of culture (Fig. 1A), i.e. a totalcell amplification of 10.8±4.9 (range 2.0–26.7); the cellcomposition of CTPs was highly enriched in T lympho-
Table 1Functionality and CD3+Vδ2+ enrichment at day 14 of 27 CTPs produced fro
Patient/CTP ID
PODA/I1 PODA/I2 PODA/I3 VICL/I1 D
Cell viability (%) 67 80 78 90CD3+Vδ2+ (%) 68 46 79 81TNFα release (pg/ml) 246 336 460 1260 5
BOMA/I1 BOMA/I2 BOMA/I3 SADA/I1 S
Cell viability (%) 87 91 80 89CD3+Vδ2+ (%) 95 96 96 65TNFα release (pg/ml) 826 708 579 632 3
MARE/I2 SOAL/I1 SOAL/I2 SOAL/I3 D
Cell viability (%) 82 88 74 74CD3+Vδ2+ (%) 46 92 92 91TNFα release (pg/ml) 130 435 645 346 1
TNFα titration of CTP cells was performed by ELISA on the supernatantCD3+Vδ2+ cells were determined by manual cell counting and flow cytome
cytes, with 95±5% of CD3+ cells, of which 18±18% ofαβ T lymphocytes were left; the T-cell population wasdrastically enriched inCD3+Vδ2+ cells rising from2±3%(range 0.3–8.0%) to 77±17% (range 39–96%). TheCD3+Vδ2+ lymphocyte population reached a plateau atday 7 and remained stable until day 14. The NK cell ratiodecreased down to 5% during the culture (Fig. 1B). Theenrichment was illustrated by the powerful capacity of theγ9δ2 T lymphocytes to amplify upon single BrHPP stim-ulation (Fig. 1C) showing a CD3+Vδ2+ cell amplificationfactor of 1585±1493 (range 150–4700). Cell viabilityrecorded in theCTPswas greater than 80% (mean 82±7%;range 67–91%) and only 9CTPs out of 27 (from4 separatepatients) showed a percentage of CD3+Vδ2+ cells lowerthan 70% at the end of culture (Table 1).
3.2. Analytical characterization of the cell therapyproduct
3.2.1. Memory phenotype of γ9δ2 T cellsOut of 27CTPs produced, five issued from two separate
patients were analysed at day 14 for CD3+Vδ2+ subsetdistribution (as defined by Dieli et al., 2003): effector-memory (EM: CD27−CD45RA−) cells represented 91±5% (range 87–98%); central memory (CM: CD27+/CD45RA−) cells represented 8±5% (range 1–12%);T effector-memory RA+ (TEMRA: CD27−/CD45RA+)cells represented 1±1% (range 0–2%), and no naïve (N)cells were detected (Fig. 2).
3.2.2. Expression of activation markersAll activation markers analysed from 25 CTPs were
found to be up-regulated during γ9δ2 T lymphocyte
m 10 mRCC patients
EGI/I1 DEGI/I2 DEGI/I3 GUGU/I1 GUGU/I2 GUGU/I3
74 88 84 84 83 8396 95 94 84 65 7332 1113 728 486 111 400
ADA/I2 SADA/I3 DODA/I1 DODA/I2 DODA/I3 MARE/I1
68 75 83 77 91 8548 39 87 76 87 6365 63 447 388 457 218
ONI/I1 DONI/I2 DONI/I3 MEAN SD
87 90 87 82 769 88 78 77 1718 627 776 497 288
from overnight BrHPP stimulation. Percentages of cell viability andtry.

Fig. 2. CD45RA and CD27 expression on CD3+Vδ2+ cells at day 14.Representative example of CTP cell subsets analysed by flowcytometry gating on the CD3+Vδ2+ population to identify effector/memory phenotype: naïve (N), central memory (CM), effectormemory (EM) and T effector-memory RA+ (TEMRA).
69S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
expansion between day 0 and day 7 and were stillexpressed at day 14, as shown in Fig. 3. However, theexpression of CD25 by CD3+Vδ2+ lymphocytes wastransient, with 51% (mean 51±8%; range 9–86%) ofCD25+ cells at day 7 versus 23% (mean 23±21%; range5–99%) at day 14. In contrast, the expression by γ9δ2T lymphocytes of other early activation markers such asHLA-DR (mean 85±6%; range 59–97%) and CD69(mean 78±12%; range 23–100%) reached about 80% atday 7 and then remained stable at day 14 (≥60%).
3.2.3. Cytotoxicity and TNFα productionThe lytic potential of CTPs generated from 3 mRCC
patients was assessed in a classical cytotoxic assayagainst the RCC (786-0) and the B-EBV+ cell lines used
Fig. 3. Surface expression of CD69, CD25 and HLA-DR activation markCD3+Vδ2+ cell enrichment is depicted on the black curve and histograms repras analysed by flow cytometry at days 0, 7 and 14 of culture.
as sensitive and resistant cell targets, respectively. TheCTP exhibited a specific lysis at a 30/1 effector-to-target-cell ratio of 44±19% (range 23–59%) against theRCC cell line (Fig. 4A) versus 10±12% (range 2–24%)specific lysis against the control B-EBV+ target(Fig. 4B).
Analysis of TNFα production provided additionaldata supporting the functional activity of the expandedcells. The CTP was considered functional if, afterstimulation with BrHPP, TNFα concentration in theculture medium was greater than 100 pg/ml (maximumTNFα release observed in unstimulated controls).Twenty-six out of 27 CTPs showed a positive response(Table 1). The low percentage of CD3+Vδ2+ cells (39%)in CTPs from patent SADA I3 may explain the negativeresponse in the TNFα production test.
3.3. Development of the manufacturing process
3.3.1. Influence of IL-2 concentration on γδ T-cellproliferation
Considering the role of IL-2 on T lymphocyteexpansion, evaluation of the influence of IL-2 concen-tration on proliferation and specifically expanded γ9δ2T lymphocytes was a key parameter to investigateduring process development. IL-2 concentrations rang-ing from 0.015 to 1500 ng/ml were tested on PBMCsfrom three healthy volunteers in a small scale amplifi-cation assay. A dose–response relationship was ob-served between IL-2 concentration and T lymphocyteexpansion (Fig. 5); maximal response observed at day14 of culture in terms of total cell amplification (Fig. 5A)and enrichment in CD3+Vδ2+ population (Fig. 5B) wasobtained when using an IL-2 concentration of 60 ng/ml
ers on CD3+Vδ2+ cells along the large scale amplification process.esent the percentage of CD3+Vδ2+ cells expressing activation markers,

Fig. 4. Cytotoxic activity of CTPs from three distinct mRCC patients against the RCC target 786-0. After large scale expansion of MNCs, the lyticpotential of the three CTPs was analysed by the classical 4-h chromium release assay performed at day 14 of culture. A αβ T-cell clone (A4.5) and aγ9δ2 T-cell clone (G12) were used as negative and positive effector controls, respectively. γ9δ2 T-cell effectors recognize the RCC cell line (786-0)as a sensitive target-cell line (A) but not the B-EBV+ resistant target (B). Data are presented as the mean percentage of specific target lysis at differenteffector/target ratios (0.3/1, 3/1 and 30/1).
70 S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
from day 4 on (i.e. 20 ng/ml at day 0). When cultureswere maintained with high concentration of IL-2(1500 ng/ml) from day 4 on (i.e. 500 ng/ml at day 0)
Fig. 5. Influence of IL-2 concentration on total cell amplification and CD3+Vstimulated in RPMI–FCS, 3 μM BrHPP and variable concentrations of IL-2 (the onset of culture. Three healthy donors were tested in triplicate for IL-2results obtained at day 14 of culture are shown as the mean of triplicate detCD3+Vδ2+ cell enrichment (B).
no effect on proliferation and specifically expandedγ9δ2 T lymphocytes was observed. There were inter-individual variations in response to IL-2 among cells
δ2+ cell enrichment on day 14 of the small scale assay. PBMCs were3 times lower at day 0 than IL-2 concentration added from day 4 on) atconcentrations ranging from 0.015 to 1500 ng/ml from day 4 on. Theerminations of the total cell amplification factor A) and percentage of

Table 3Comparison of two harvesting methods
Mean SD Range n
CytoMate™Cell recovery yield (%) 87 8 70–100 17TNFα release (pg/ml) 456 233 63–826 17Cell viability (%) 83 7 74–91 17
CentrifugeCell recovery yield (%) 70 12 52–89 10TNFα release (pg/ml) 567 367 111–1260 10Cell viability (%) 81 7 67–90 10
After 14 days of culture, CTPs from mRCC patients were conditionedin 4% HA either by classical, successive, centrifugations or by anautomated method (CytoMate™). For each harvesting method, cellrecovery yield, calculated as (total cell number after harvesting/totalcell number before harvesting×100) and cell viability were deter-mined by manual cell counting. TNFα titration of conditioned CTPcells was performed by ELISA on supernatant from overnight BrHPPstimulation.
71S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
from different donors (Fig. 5); in cells from donor 3, IL-2concentration did not show any influence on CD3+Vδ2+
population enrichment which remained elevated what-ever concentration was tested. In contrast, IL-2 showed adose-related effect in cells from donor 1 on CD3+Vδ2+
population enrichment (Fig. 5B). Moreover, for the threehealthy donors, cell viability was always higher than87%when culturing with IL-2 at 60 ng/ml from day 4 on(i.e. 20 ng/ml at day 0).
These results were confirmed on PBMCs from9 mRCC patients in the same small scale assay(Table 2), where two different IL-2 concentrationswere used from day 4 of culture on (and three times lessIL-2 at day 0): 20 ng/ml versus 60 ng/ml. The followingresults were obtained: a total cell amplification factor of9 versus 14, percentage of CD3+Vδ2+ of 47% versus62% and cell viability of 67% versus 77% at 20 ng/mland 60 ng/ml respectively.
3.3.2. Cell washing and harvestingInitially, cell washing and harvesting were carried out
via classical centrifugation in buffered 0.9% NaClsolution (pH 7) and the cells were collected in 4% HA.During process development, an improvement in the cellharvesting procedure was implemented bymaking use ofautomated cell collection (Cytomate™). For all produc-tion runs, the cell recovery yields were 70±12% (range52–89; n=10) when harvesting by classical centrifuga-tion and 87±8% (range 70–100; n=17) with automatedharvesting (Table 3); CTPs were always viable (Cyto-mate™: mean 83±7%; range 74–91; n=17 versuscentrifugation: mean 81±7%; range 67–90; n=10) andfunctional (Cytomate™: mean 456±233 pg/ml; range63–826; n=17 versus centrifugation: mean 567±
Table 2Influence of IL-2 concentration on CD3+Vδ2+ cells expanded at day14 in the small scale assay
IL2 concentration from day 4 on(ng/ml)
20 60
Total cell amplification factor atday 14 (range)
9±7 (2–26) 14±9 (2–32)
Percentage of CD3+Vδ2+ at day14 (range)
47±28 (2–89) 62±27 (2–90)
Cell viability at day 14 (range) 67±14 (48–92) 77±11 (60–95)
PBMCs were stimulated with 3 μM BrHPP in RPMI–FCS andvariable IL-2 concentration (3 times lower at day 0 than the IL-2concentration added from day 4 on) at the onset of culture. Ninepatients were tested in triplicate with 20 ng/ml or 60 ng/ml of IL-2from day 4 on. Total cell amplification factor, calculated as (viableVδ2+CD3+ cell number at day 14/viable Vδ2+CD3+ cell number at day0), the percentage of CD3+Vδ2+ cell enrichment and cell viability weredetermined by flow cytometry and manual cell counting.
367 pg/ml; range 111–1260; n=10) with both methodsused. In addition, automated cell reduction is timesaving: 1 h less for 4 to 5 billion cells (about 3 l),compared to the classical centrifugation procedure (datanot shown).
3.3.3. CTP stabilityGelofusine (4%; AMM no. 563 091.2, Braun
Médical, Boulogne, France), Ringer's lactate (AMMno. 560 228-7, Braun Médical, Boulogne, France),Ringer's Aguettant (AMM no. 560 212.3, AguettantLaboratory, Lyon, France), buffered 0.9% NaCl at pH 7(formule TS 590, Braun Medical, Boulogne, France),FCS and pure human serum (EFS, Lyon), andautologous sera had previously been tested as storagemedia at +4 °C compared to reference 4% HA. Only 4%Gelofusine showed results comparable with those of the4% HA in terms of cell survival, CD3+Vδ2+ratio,CD3+Vδ2+ activation ratio (CD69+) and functionalpotential as evaluated by TNFα release assay (data notshown); high inter-patient variability using autologousserum hampered its used as storage medium.
Results obtained from 6 CTPs generated out of MNCof 5 mRCC patients and stored either in 4% HA or in 4%Gelofusine are depicted in Table 4; after 24 h storage at+4 °C in 4% HA, residual cell viability of the CTPs was93±14% (range 74–109%), similar to that when storedin 4% Gelofusine (mean 91±10%, range 71–100%);total cell survival was greater when cells were stored in4% HA (mean 90±24%, range 66–125%) than whenstored in 4% Gelofusine (74±16%, range 66–95%);CD3+Vδ2+ and CD3+Vδ2+CD69+ cells survived and

Table 4Stability comparison of 6 CTPs from 5 mRCC patients conditioned either in 4% HA or in 4% Gelofusine
Ratio aftera 24-hstorage
Recovery yield (%)
Cell viability Total cell CD3+Vd2+ CD3+Vd2+CD69+
HA Gelofusine HA Gelofusine HA Gelofusine HA Gelofusine
BOMA/I2 83 71 125 78 99 99 104 109MECL/I0 98 92 66 66 101 101 99 100DEGI/R&D 109 99 76 48 99 98 100 99DEGI/I0 88 91 113 76 101 101 92 116MAJE/I0 74 91 84 81 99 101 109 110DODA/I3 107 100 73 95 ND ND ND NDMean 93 91 90 74 100 100 101 107SD 14 10 24 16 1 1 6 7
Cell viability, total cell number, CD3+Vδ2+ and CD3+Vδ2+CD69+ percentages were determined by manual cell counting and flow cytometry beforeand after a 24-h conditioning in each media at 5±3 °C. Recovery yields were calculated for each parameter as %=(parameter at T 24 h /parameter atT 0 h)×100.
72 S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
even grew when stored in either conditions (n=5 CTPs,4 patients); CTPswere still functional after a 24-h storageat +4 °C as shown by themean of the TNFα release assay(n=3 CTPs, 3 patients; data not shown). The maximumduration of CTP storage in 4% HA prior to infusion topatients was therefore extended to 24 h at +4 °C.
3.4. Eligibility for large scale expansion as assessed bysmall scale assay
Considering the inter-individual variability of γ9δ2T lymphocyte response to stimulation by BrHPP,correlation parameters between results from the small
Fig. 6. Correlation at day 14 of the expansion between the small and large scacalculated from expansions of 15 mRCC patients (A) and the correlation coefof 13 mRCC patients as (viable cell number at day 14/viable cell number at
scale assay and those of the large scale assay wereexamined. Correlation analysis between both amplifi-cation assays was performed on mRCC patients and isdepicted in Fig. 6. The CD3+Vδ2+ T-cell correlationcoefficient was low (0.65) and 10 out of 15 patientstested offered a lower purity in CD3+Vδ2+ at day 14 inthe small scale assay than in the large scale manufac-turing assay (Fig. 6A). In contrast to CD3+Vδ2+ cellenrichment, the total cell amplification factor highlycorrelated between both assays (correlation coefficientof 0.96). This suggests that the cell amplification factordetermined in the small scale assay can be used as apredictive factor for large scale cell expansion feasibility.
le assays. The correlation coefficient of Vδ2+CD3+ cell enrichment wasficient of total cell amplification factor was calculated from expansionsday 0) (B).
73S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
4. Discussion
The present study aimed to propose a new ex vivomanufacturing process for γ9δ2 T lymphocyte ampli-fication, and to describe the main parameters thatinfluence the proliferation and specific expansion of thisT lymphocyte population. As previously reported, γ9δ2T lymphocyte expansion is patient dependent (Vieyet al., 2005b) and for obvious ethical reasons, a smallscale screening was necessary to ensure the feasibility oflarge scale expansion. The following criteria weredefined at day 14 of cell culture: percentage ofCD3+Vδ2+ cells≥70%, cell viability≥70% and viabletotal cell amplification rate≥10. Those parameters werelater compared between the small scale assay and thelarge scale assay on 13–15 patients. Although γ9δ2T enrichment was not accurately predictable from thesmall scale assay, this test is a relevant screening testprior to CTP treatment initiation because it indicates theamount of cells necessary to produce the required doseof CTP.
Many ex vivo expansion protocols require IL-2 inculture medium, but optimal concentration has beenpoorly documented. In the absence of IL-2, a γ9δ2agonist such as IPP, promotes the early expression ofCD25 high affinity receptors for the IL-2 cytokine at thesurface of γ9δ2 T cells (Wesch et al., 1997). Moreover,the majority of γ9δ2 T lymphocytes down-regulate theexpression of CD25 receptors in the presence ofexogenous IL-2 after stimulation. In this context, theinitial stimulation design regarding IL-2 relied on alower concentration at day 0 than the concentration usedfrom day 4 on; the threefold difference between day 0and day 4 was empirically established, and maintainedthroughout this study. In this setting, the optimal IL-2concentrations found were first 20 ng/ml (day 0) and60 ng/ml (from day 4 on). Although high IL-2 concentra-tions may trigger the proliferation of NK cells (Milleret al., 1994), we found that the percentage of NK cells inour CTPs was only 5%. Up to 1500 ng/ml, no effect of IL-2 concentrationwas detected and the specificity ofγ9δ2 Tlymphocyte proliferation was preserved.
Here we report that ex vivo γ9δ2 T lymphocyteexpansion following a single stimulation with BrHPPwas able to produce 8 billion cells from 600 millionMNCs after 14 days of culture, among which more than75% were γ9δ2 T lymphocytes. At day 14 of culture,γ9δ2 T lymphocytes were still expressing activationmarkers such as CD69 or HLA-DR indicating that cellswithin the CTP retained their activation potential. Fromday 7 to day 14 γ9δ2 T lymphocytes partially lost theirability to express CD25 IL-2 receptor. We have shown
that in the CTPs a majority of γ9δ2 T cells were of theEM phenotype (N90%). This indicates that cellsactivated with BrHPP were able to initiate a memoryresponse associated with potential cytotoxicity activity.Despite their ex vivo phenotypic characteristics thecapabilities of these expanded-γ9δ2 Tcells to retain theirlong-term memory properties once re-injected in vivo incombination with IL-2 remain to be investigated.
After harvesting, although γ9δ2 T lymphocytes areknown to kill RCC cell lines of various origin(Choudhary et al., 1995; Kobayashi et al., 2001; Vieyet al., 2005a), we wished to confirm the functionality ofour CTPs. Our findings from the present studyestablished that large scale ex vivo expanded cells canrecognize and kill the 786-0 RCC cell line. Aspreviously described, the specific lysis ratio of expand-ed-γ9δ2 T lymphocytes was decreased in the presenceof anti-pan-γδ TCR mAb, indicating that the γδ TCRreceptor is involved in the recognition of autologousRCC cell line (Viey et al., 2005a). Functionality of theCTP was confirmed by its potential to produce TNFα.
Development studies showed that classical centrifu-gation initially performed in bags could be replaced bycell washing with CytoMate™ allowing reduction oflarge volumes of the cell suspension (up to 10 l) as well assavings in cost, time andwork load. Other such automatedapplications remain to be developed for other steps of theprocess that require cell concentration or dilution (e.g.,freezing and thawing steps). Moreover, γ9δ2 T lympho-cyte enrichment, cell viability as well as functionality ofthe CTPs, remained stable after a 24-h storage in 4% HAat +4 °C thus allowing transportation of CTPs to distantclinical centres.
However, various areas of improvement remain to beconsidered. In accordance with US FDA guidelines,media without FCS (for instance X-vivo 15 or RPMI-1640 with 4% HA) should be investigated. Another wayto simplify the process might be to initiate the culturewith non-frozen MNC. A single manufacturing processfor three infusions should be performed and CTPs shouldbe frozen in 4% HA prior to infusion to patients. CTPswere frozen at days 10 and 15 of culture which showedthat CTPs can be frozen and conserve their viability,phenotype, and functional potential (TNFα releaseassay). Nevertheless, after thawing, a yield of 50% cellrecovery indicated that more than twice the dose of CTPsto be infused to patients (2 or 3 reduction cycles with theCytoMate™ process) should be frozen. In this context, anewmanufacturing process should be designed. Use of abioreactor might be worth exploring. Thawing such alarge number of cells implies developing an appropriatewashing procedure and CytoMate™ could be used for

74 S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
this application. In the next few years, a cell therapyprocess using allogenic cells could also be considered. Itcould also be interesting to focus on the effects of IL-7and IL-15 on γ9δ2 T lymphocyte proliferation andrelated lymphocyte effector/memory profiles (Baccalaet al., 2005).
In conclusion, this study has defined culture conditionsfor simple ex vivo expansion of γ9δ2 T lymphocytes.Mononuclear cells grown with IL-2 and BrHPP yielded a10-fold increase in total cell number within 2 weeks, withγ9δ2 T-cell enrichment; a direct correlation between thesmall scale assay and large scale expansion process wasfound. Cell therapeutic products generated from mRCCpatients demonstrated functional capabilities in terms ofactivation marker, cytotoxicity and TNFα production.The 24-h stability of CTPs allows multicentric clinicaltrials avoiding freezing CTP prior to infusion to patients.Considering the current literature, Innacell γδ™ offers apromising approach for the treatment of a large spectrumof cancers.
Acknowledgements
The authors would like to thank Dr Jaafar Bennounaand Mireille Drouet from the Department of MedicalOncology, Centre René Gauducheau, Nantes, France,for the expert clinical investigation; Dr Marc Bonnevillefrom Inserm U601, Nantes, France, for the helpfuldiscussion; Dr Michel Perrocheau from the FrenchBlood Center (EFS), Nantes, France; Dr Marie Audrain,from the Immunology Laboratory, University Hospital,Nantes, France; Dr Irène Philip and Gilles Clapissonfrom Centre Léon-Bérard, Lyon, France; Ariane Thie-lens and Céline Galéa from Innate Pharma, Marseille,for the excellent collaboration and all the patients andhealthy volunteers for donating blood.
References
Baccala, R., Witherden, D., Gonzalez-Quintial, R., Dummer, W., Surh,C.D., Havran, W.L., Theofilopoulos, A.N., 2005. Gamma deltaT cell homeostasis is controlled by IL-7 and IL-15 together withsubset-specific factors. J. Immunol. 174, 4606.
Bank, I., Book, M., Huszar, M., Baram, Y., Schnirer, I., Brenner, H.,1993. V delta 2+gamma delta T lymphocytes are cytotoxic to theMCF 7 breast carcinoma cell line and can be detected among theT cells that infiltrate breast tumors. Clin. Immunol. Immunopathol.67, 17.
Belmant, C., Espinosa, E., Halary, F., Tang, Y., Peyrat, M.A., Sicard,H., Kozikowski, A., Buelow, R., Poupot, R., Bonneville, M.,Fournie, J.J., 2000. A chemical basis for selective recognition ofnonpeptide antigens by human γδ T cells. FASEB J. 14, 1669.
Bendelac, A., Bonneville, M., Kearney, J.F., 2001. Autoreactivity bydesign: innate B and T lymphocytes. Nat. Rev. Immunol. 1, 177.
Bompas, E., Neidhardt, E.M., Rolland, F., Philip, I., Galéa, C., Salot, S.,Tiollier, J., Saiagh, S., Negrier, S., Bennouna, J., 2006.An autologousVγ9Vδ2 T lymphocytes cell therapy product generated by BrHPP(INNACELL Gamma Delta [GD]) in metastatic renal cell carcinomapatients: phase I clinical trial results. J. Clin. Oncol. 24, 2550MeetingAbstracts.
Bonneville, M., Fournie, J.J., 2005. Sensing cell stress andtransformation through Vγ9Vδ2 T cell-mediated recognition ofthe isoprenoid pathway metabolites. Microbes Infect. 7, 503.
Brenner, M.B., McLean, J., Scheft, H., Riberdy, J., Ang, S.L.,Seidman, J.G., Devlin, P., Krangel, M.S., 1987. Two forms of theT-cell receptor gamma protein found on peripheral blood cytotoxicT lymphocytes. Nature 325, 689.
Bukowski, J.F., Morita, C.T., Tanaka, Y., Bloom, B.R., Brenner, M.B.,Band, H., 1995. V gamma 2 V delta 2 TCR-dependent recognitionof non-peptide antigens and Daudi cells analyzed by TCR genetransfer. J. Immunol. 154, 998.
Choudhary, A., Davodeau, F., Moreau, A., Peyrat, M.A., Bonneville,M., Jotereau, F., 1995. Selective lysis of autologous tumor cells byrecurrent gamma delta tumor-infiltrating lymphocytes from renalcarcinoma. J. Immunol. 154, 3932.
Constant, P., Davodeau, F., Peyrat, M.A., Poquet, Y., Puzo, G.,Bonneville, M., Fournie, J.J., 1994. Stimulation of human gammadelta T cells by nonpeptidic mycobacterial ligands. Science 264,267.
Corvaisier, M., Moreau-Aubry, A., Diez, E., Bennouna, J., Mosnier, J.F.,Scotet, E., Bonneville, M., Jotereau, F., 2005. V gamma 9V delta 2T cell response to colon carcinoma cells. J. Immunol. 175, 5481.
Davodeau, F., Peyrat, M.A., Hallet, M.M., Gaschet, J., Houde, I.,Vivien, R., Vie, H., Bonneville, M., 1993. Close correlationbetween Daudi and mycobacterial antigen recognition by humangamma delta T cells and expression of V9JPC1 gamma/V2DJCdelta-encoded T cell receptors. J. Immunol. 151, 1214.
Dieli, F., Poccia, F., Lipp, M., Sireci, G., Caccamo, N., Di Sano, C.,Salerno, A., 2003. Differentiation of effector/memory Vdelta2T cells and migratory routes in lymph nodes or inflammatory sites.J. Exp. Med. 198, 391.
Espinosa, E., Belmant, C., Pont, F., Luciani, B., Poupot, R., Romagne, F.,Brailly, H., Bonneville, M., Fournie, J.J., 2001a. Chemical synthesisand biological activity of bromohydrin pyrophosphate, a potentstimulator of human γδ T cells. J. Biol. Chem. 276, 18337.
Espinosa, E., Belmant, C., Sicard, H., Poupot, R., Bonneville, M.,Fournié, J.J., 2001b. Y2K_1 state-of-the-art on non-peptidephosphoantigens, a novel category of immunostimulatory mole-cules. Microbes Infect. 3, 645.
Fearon, D.T., Locksley, R.M., 1996. The instructive role of innateimmunity in the acquired immune response. Science 272, 50.
Ferrarini, M., Heltai, S., Pupa, S.M., Mernard, S., Zocchi, R., 1996.Killing of laminin receptor-positive human lung cancers by tumorinfiltrating lymphocytes bearing gammadelta(+) T-cell receptors.J. Natl. Cancer Inst. 88, 436.
Fisch, P., Meuer, E., Pende, D., Rothenfusser, S., Viale, O., Kock, S.,Ferrone, S., Fradelizi, D., Klein, G.,Moretta, L., Rammensee, H.G.,Boon, T., Coulie, P., van der Bruggen, P., 1997. Control of B celllymphoma recognition via natural killer inhibitory receptorsimplies a role for human Vgamma9/Vdelta2 T cells in tumorimmunity. Eur. J. Immunol. 27, 3368.
Fujimiya, Y., Suzuki, Y., Katakura, R., Miyagi, T., Yamaguchi, T.,Yoshimoto, T., Ebina, T., 1997. In vitro interleukin 12 activationof peripheral blood CD3(+)CD56(+) and CD3(+)CD56(−)gammadelta T cells from glioblastoma patients. Clin. CancerRes. 3, 633.

75S. Salot et al. / Journal of Immunological Methods 326 (2007) 63–75
Gober,H.J., Kistowska,M., Angman, L., Jeno, P.,Mori, L., DeLibero,G.,2003. Human Tcell receptor gammadelta cells recognize endogenousmevalonate metabolites in tumor cells. J. Exp. Med. 197, 163.
Guo, B.L., Liu, Z., Aldrich, W.A., Lopez, R.D., 2005. Innate anti-breast cancer immunity of apoptosis-resistant human gammadelta-T cells. Breast Cancer Res. Treat. 93, 169.
Hayday, A.C., 2000. γδ cells: a right time and a right place for aconserved third way of protection. Annu. Rev. Immunol. 18, 975.
Hintz, M., Reichenberg, A., Altincicek, B., Bahr, U., Gschwind, R.M.,Kollas, A.K., Beck, E., Wiesner, J., Eberl, M., Jomaa, H., 2001.Identification of (E)-4-hydroxy-3-methyl-but-2-enyl pyrophos-phate as a major activator for human T cells in Escherichia coli.FEBS Lett. 509, 317.
Ibisch, C., Saulquin, X., Gallot, G., Vivien, R., Ferrand, C.,Tiberghien, P., Houssaint, E., Vie, H., 2000. The T cell repertoireselected in vitro against EBV: diversity, specificity, and improvedpurification through early IL-2 receptor alpha-chain (CD25)-positive selection. J. Immunol. 164, 4924.
Jomaa, H., Feurle, J., Luhs, K., Kunzmann, V., Tony, H.P., Herderich,M., Wilhelm, M., 1999. Vγ9Vδ2 T cell activation induced bybacterial low molecular mass compounds depends on the 1-deoxy-d-xylulose 5-phosphate pathway of isoprenoid biosynthesis.FEMS Immunol. Med. Microbiol. 25, 371.
Kobayashi, H., Tanaka, Y., Yagi, J., Toma, H., Uchiyama, T., 2001.Gamma/delta T cells provide innate immunity against renal cellcarcinoma. Cancer Immunol. Immunother. 50, 115.
Kroca, M., Johansson, A., Sjostedt, A., Tarnvik, A., 2001. V gamma9V delta 2 T cells in human legionellosis. Clin. Diagn. Lab.Immunol. 8, 949.
Lin, J.H., 1996. Bisphosphonates: a review of their pharmacokineticproperties. Bone 18, 75.
Lin, J.H., Russell, G., Gertz, B., 1999. Pharmacokinetics ofalendronate: an overview. Int. J. Clin. Pract., Suppl. 101, 18.
Liu, Z., Guo, B.L., Gehrs, B.C., Nan, L., Lopez, R.D., 2005. Ex vivoexpanded human Vgamma9Vdelta2+ gammadelta-T cells mediateinnate antitumor activity against human prostate cancer cells invitro. J. Urol. 173, 1552.
Lopez, R.D., Xu, S., Guo, B., Negrin, R.S., Waller, E.K., 2000. CD2-mediated IL-12-dependent signals render human gamma delta-Tcells resistant to mitogen-induced apoptosis, permitting the large-scale ex vivo expansion of functionally distinct lymphocytes:implications for the development of adoptive immunotherapystrategies. Blood 96, 3827.
Mak, T.W., Ferrick, D.A., 1998. The gammadelta T-cell bridge: linkinginnate and acquired immunity. Nat. Med. 4, 764.
Miller, J.S., Klingsporn, S., Lund, J., Perry, E.H., Verfaillie, C.,McGlave, P., 1994. Large scale ex vivo expansion and activation ofhuman natural killer cells for autologous therapy. Bone MarrowTransplant. 14, 555.
Mitropoulos, D., Kooi, S., Rodriguez-Villanueva, J., Platsoucas, C.D.,1994. Characterization of fresh (uncultured) tumour-infiltratinglymphocytes (TIL) and TIL-derived T cell lines from patients withrenal cell carcinoma. Clin. Exp. Immunol. 97, 321.
Otto, M., Barfield, R.C., Martin, W.J., Iyengar, R., Leung, W., Leimig,T., Chaleff, S., Gillies, S.D., Handgretinger, R., 2005. Combinationimmunotherapy with clinical-scale enriched human gammadeltaT cells, hu14.18 antibody, and the immunocytokine Fc-IL7 indisseminated neuroblastoma. Clin. Cancer Res. 11, 8486.
Parker, C.M., Groh, V., Band, H., Porcelli, S.A., Morita, C., Fabbi, M.,Glass, D., Strominger, J.L., Brenner, M.B., 1990. Evidence forextrathymic changes in the T cell receptor gamma/delta repertoire.J. Exp. Med. 171, 1597.
Poupot, M., Fournie, J.J., 2004. Non-peptide antigens activatinghuman Vgamma9/Vdelta2 T lymphocytes. Immunol. Lett. 95, 129.
Schultze, J.L., Nadler, L.M., 1999. T cell mediated immunotherapy forB cell lymphoma. J. Mol. Med. 77, 322–331.
Scotet, E., Martinez, L.O., Grant, E., Barbaras, R., Jeno, P., Guiraud,M., Monsarrat, B., Saulquin, X., Maillet, S., Estève, J.P., 2005.Tumor recognition following Vγ9Vδ2 T cell receptor interactionswith a surface F1-ATPase-related structure and apolipoprotein A-I.Immunity 22, 71.
Sicard, H., Al Saati, T., Delsol, G., Fournie, J.J., 2001. Syntheticphosphoantigens enhance human Vg9Vd2 T lymphocytes killingof non-Hodgkin's B lymphoma. Mol. Med. 7, 711.
Sicard,H., Ingoure, S., Luciani, B., Serraz,C., Fournie, J.J., Bonneville,M.,Tiollier, J., Romagne, F., 2005. In vivo immunomanipulation ofV gamma 9V delta 2 T cells with a synthetic phosphoantigen in apreclinical nonhuman primate model. J. Immunol. 175, 5471.
Sturm, E., Braakman, E., Fisch, P., Vreugdenhil, R.J., Sondel, P.,Bolhuis, R.L., 1990. Human V gamma 9-V delta 2 T cell receptor-gamma delta lymphocytes show specificity to Daudi Burkitt'slymphoma cells. J. Immunol. 145, 3202.
Tanaka, Y., Morita, C.T., Tanaka, Y., Nieves, E., Brenner, M.B.,Bloom, B.R., 1995. Natural and synthetic non-peptide antigensrecognized by human gamma delta T cells. Nature 375, 155.
Vely, F., Peyrat, M., Couedel, C., Morcet, J., Halary, F., Davodeau,F., Romagne, F., Scotet, E., Saulquin, X., Houssaint, E.,Schleinitz, N., Moretta, A., Vivier, E., Bonneville, M., 2001.Regulation of inhibitory and activating killer-cell Ig-like receptorexpression occurs in T cells after termination of TCR rearrange-ments. J. Immunol. 166, 2487.
Viey, E., Fromont, G., Escudier, B., Morel, Y., Da Rocha, S., Chouaib,S., Caignard, A., 2005a. Phosphostim-activated gamma deltaT cells kill autologous metastatic renal cell carcinoma. J. Immunol.174, 1338.
Viey, E., Laplace, C., Escudier, B., 2005b. Peripheral gammadelta T-lymphocytes as an innovative tool in immunotherapy for metastaticrenal cell carcinoma. Expert Rev. Anticancer Ther. 5, 973.
Walzer, T., Dalod, M., Vivier, E., Zitvogel, L., 2005. Natural killer cell-dendritic cell crosstalk in the initiation of immune responses.Expert Opin. Biol. Ther. Suppl. 1, S49.
Wesch, D., Marx, S., Kabelitz, D., 1997. Comparative analysis ofalpha beta and gamma delta T cell activation by Mycobacteriumtuberculosis and isopentenyl pyrophosphate. Eur. J. Immunol. 27,952.
Wilhelm, M., Kunzmann, V., Eckstein, S., Reimer, P., Weissinger, F.,Ruediger, T., Tony, H.P., 2003. Gammadelta T cells for immunetherapy of patients with lymphoid malignancies. Blood 102, 200.
Yamaguchi, T., Fujimiya, Y., Suzuki, Y., Katakura, R., Ebina, T., 1997.A simple method for the propagation and purification of gammadelta T cells from the peripheral blood of glioblastoma patientsusing solid-phase anti-CD3 antibody and soluble IL-2. J. Immunol.Methods 205, 19.
Zheng, B.J., Chan, K.W., Im, S., Chua, D., Sham, J.S., Tin, P.C., He, Z.M.,Ng, M.H., 2001. Anti-tumor effects of human peripheral gammadeltaT cells in a mouse tumor model. Int. J. Cancer 92, 421.





























