Embed Size (px)
Citation preview

Mol Cell Toxicol (2011) 7:87-93DOI 10.1007/s13273-011-0012-2
Abstract Chronic obstructive pulmonary disease(COPD) is characterized by lung inflammation withneutrophil infiltration and increased levels of proin-flammatory cytokines. This study was conducted toevaluate the protective effect of Lonicera japonica (LJ)against lipopolysaccaride (LPS)-induced lung inflam-mation which resembles a COPD-like acute disease.Balb/c mice were treated once with LJ flower extractvia an oral injection, after which they were adminis-tered LPS (0.5 mg/kg body wt) to induce acute airwayinflammation. At 3 days after LPS stimulation, in vivostudy demonstrated that the influx of neutrophils andtotal cells were decreased significantly in LJ pretreatedgroup compared to LPS only treated group. In addi-tion, TNF-α and IL-6 levels in bronchoalveloar lavage(BAL) fluid were decreased in LJ pretreated group.The histological results demonstrated that LJ attenuat-ed the LPS induced lung inflammation. Furthermore,the expression of neutrophil elastase was decreased inLJ pretreated group. Taken together, these data sug-gest that LJ exerts protective effects against LPS-in-duced lung inflammation; therefore, this herbal medi-cine may represent a novel therapeutic agent for thetreatment of lung inflammation, particularly for thetreatment of COPD.
Keywords Chronic obstructive pulmonary disease,Herbal medicine, Lonicera japonica, TNF-α, IL-6
Chronic obstructive pulmonary disease (COPD) ischaracterized by airway obstruction and is associatedwith chronic bronchitis and emphysema1. In addition,COPD is associated with progressive and irreversiblefibrosis, tissue damage and inflammation of the smallairways. The pathogenesis of COPD involves severalpathogenetic processes including inflammation, alter-ations in cell growth, cellular apoptosis, abnormal cellrepair, destruction of the extracellular matrix, and oxi-dative stress2.
To prevent the progression of COPD, it was arguedthat inhaled corticosteroids might be beneficial. Theefficacy of corticosteroids in COPD is still uncertain,but this very uncertainty implied that they are of littlebenefit3. Most of patients with COPD respond poorlyto corticosteroid treatment, and even high doses of in-haled or oral corticosteroids fail to suppress inflam-mation4,5. Since the inflammatory process in COPD isessentially steroid resistant, new approaches for treat-ment of COPD have been done6. Several studies haverecently revealed that compounds originating fromplants have anti-inflammatory or immune-modulatingproperties7. In addition, there is attempt to use herbalmedicines for the treatment of COPD8.
The flower of Lonicera japonica (LJ) is a traditionaloriental medicine that has been used clinically for thetreatment of inflammation. In addition, experimentalstudy has demonstrated that extract from LJ exhibitinga strongly anti-inflammatory activity, can effectivelyinhibit the lipopolysaccharide (LPS)-induced tumornecrosis factor-α (TNF-α), interleukin-6 (IL-6) and in-ducible nitric oxide (NO) production in vitro9. Luteolin,a major flavonoid of LJ, also protects against LPS-in-duced lethal toxicity by inhibiting pro-inflammatorymolecule expression in murine macrophages10.
LPS is an endotoxin from gram-negative bacteria that
ORIGINAL PAPER
Lipopolysaccharide induced lung inflammation is inhibited byLonicera japonica
Hyojung Lee1, Dugjae Lee2, Youngeun Kim1, Gihyun Lee1, Soo-Jeong Kim1, Sungki Jung2, Heejae Jung2 & Hyunsu Bae1
Received: 16 August 2010 / Accepted: 24 January 2011�The Korean Society of Toxicogenomics and Toxicoporeteomics and Springer 2011
1Department of Physiology, College of Oriental Medicine, KyungHeeUniversity, #1 Hoeki-dong Dongdaemoon-gu, Seoul 130-701, Korea2Division of Allergy and Respiratory System, Department of OrientalInternal Medicine, College of Oriental Medicine, KyungHeeUniversity, #1 Hoeki-dong Dongdaemoon-gu, Seoul 130-701, KoreaCorrespondence and requests for materials should be addressed to H. Bae ( [email protected]), H. Jung ( [email protected])
induces influx of inflammatory cells such as macro-phages, neutrophils and lymphocytes, with increasingrelease of pro-inflammatory cytokines11. In addition,many studies have reported that repeated LPS expo-sure induces pathological changes similar to those ob-served in COPD patients such as goblet cell hyperpla-sia in the airways12 and chronic neutrophilia in thebronchi13.
Therefore, in the present study, we evaluated theanti-inflammatory effects of LJ on LPS-induced acutepulmonary inflammation in mouse and explained thepossible mechanism by which LJ suppress LPS-in-duced pulmonary injury. Our data suggest that LJ effec-tively attenuated LPS-induced pulmonary inflamma-tion through inhibition of the inflammatory cell infiltra-tion, decreases of the expression of neutrophil elastase(NE), and reduction of the proinflammatory cytokinesecretion in lung.
HPLC chromatograms
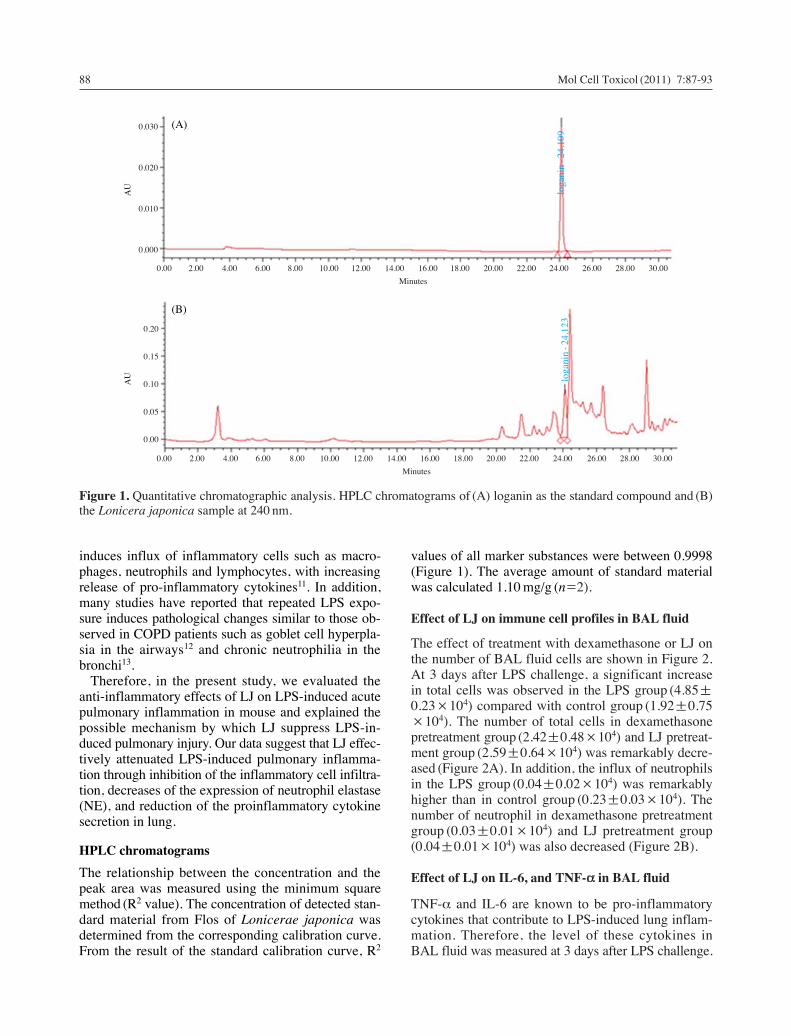
The relationship between the concentration and thepeak area was measured using the minimum squaremethod (R2 value). The concentration of detected stan-dard material from Flos of Lonicerae japonica wasdetermined from the corresponding calibration curve.From the result of the standard calibration curve, R2
values of all marker substances were between 0.9998(Figure 1). The average amount of standard materialwas calculated 1.10 mg/g (n=2).
Effect of LJ on immune cell profiles in BAL fluid
The effect of treatment with dexamethasone or LJ onthe number of BAL fluid cells are shown in Figure 2.At 3 days after LPS challenge, a significant increasein total cells was observed in the LPS group (4.85±0.23×104) compared with control group (1.92±0.75×104). The number of total cells in dexamethasonepretreatment group (2.42±0.48×104) and LJ pretreat-ment group (2.59±0.64×104) was remarkably decre-ased (Figure 2A). In addition, the influx of neutrophilsin the LPS group (0.04±0.02×104) was remarkablyhigher than in control group (0.23±0.03×104). Thenumber of neutrophil in dexamethasone pretreatmentgroup (0.03±0.01×104) and LJ pretreatment group(0.04±0.01×104) was also decreased (Figure 2B).
Effect of LJ on IL-6, and TNF-α in BAL fluid
TNF-α and IL-6 are known to be pro-inflammatorycytokines that contribute to LPS-induced lung inflam-mation. Therefore, the level of these cytokines inBAL fluid was measured at 3 days after LPS challenge.
88 Mol Cell Toxicol (2011) 7:87-93
Figure 1. Quantitative chromatographic analysis. HPLC chromatograms of (A) loganin as the standard compound and (B)the Lonicera japonica sample at 240 nm.
0.00 2.00 4.00 6.00 8.00 10.00 12.00 14.00 16.00 18.00 20.00 22.00 24.00 26.00 28.00 30.00
Minutes
0.00 2.00 4.00 6.00 8.00 10.00 12.00 14.00 16.00 18.00 20.00 22.00 24.00 26.00 28.00 30.00
Minutes
0.030
0.020
0.010
0.000
0.20
0.15
0.10
0.05
0.00
loga
nin
-24.
109
loga
nin
-24.
123
(A)
(B)
AU
AU

The levels of TNF-α were 1200.08±209.74 pg/mg inthe control group, 3458.30±431.83 pg/mg in the LPSgroup, 1969.93±251.62 pg/mg in the LJ treated group,1661.81±268.38 pg/mg in the dexamethasone treatedgroup (Figure 3A). The levels of IL-6 were 497.78±78.88 pg/mg in the control group, 878.57±106.44pg/mg in the LPS group, 517.75±44.55 pg/mg in theLJ treated group, 556.03±42.92 pg/mg in the dexame-thasone treated group (Figure 3B). These data indicat-ed that treatment with LJ 2 h prior to the administrationof LPS significantly reduced the levels of proimflam-matory cytokines as effectively as dexamethasonetreatment.
Effect of LJ on pulmonary damage
To determine if LJ exerted an effect on LPS-induced
lung damage, we stained lung sections with H&E. Aperibronchial cell count based on a five point scoringsystem was performed as previously described toestimate the severity of leukocyte infiltration. LPSchallenged mice showed a heavy infiltration of inflam-matory cells and exudative changes in the peribron-chial layers and intra-luminal areas of the large andsmall bronchi. These changes were less prominent inthe dexamethasone treated group and the LJ treatedgroup. Therefore treatment with LJ ameliorated thislung inflammation (Figure 4).
Immunohistochemical finding of LJ
To evaluate the effect of LJ on LPS-induced lung
Mol Cell Toxicol (2011) 7:87-93 89
Figure 2. Effect of LJ on immune cell profiles in BALfluid. The total number of cells (A) and of neutrophils (B)were determined in BAL fluid. Control: saline only treatedgroup, LPS: LPS only treated group, LPS++Dexa: Dexa-methasone and LPS treated group, LPS++LJ: Lonicerajaponica and LPS treated group. The value is presentedas the mean±S.E.M. (*P⁄0.05, **P⁄0.01 ***P⁄0.001versus LPS; n==6).
Figure 3. Effect of LJ on IL-6, and TNF-α in BAL fluid.Cytokine levels in BAL fluid were measured at 3 daysafter LPS challenge. Levels of TNF-α (A) and IL-6 (B) inBAL fluid were determined by ELISA. Control: salineonly treated group, LPS: LPS only treated group, LPS++Dexa: Dexamethasone and LPS treated group, LPS++LJ:Lonicera japonica and LPS treated group. The value ispresented as the mean±S.E.M. (*P⁄0.05, **P⁄0.01,***P⁄0.001 versus LPS; n==6).
8
6
4
2
0
0.4
0.3
0.2
0.1
0.0
Control LPS LPS++Dexa LPS++LJ
Control LPS LPS++Dexa LPS++LJ
**
***
***
***
*
*(A)
(B)
Tot
al c
ell(×
104 /
mL
)N
eutr
ophi
l(×
104 /
mL
)
5000
4000
3000
2000
1000
0
1200
1000
800
600
400
200
0
*****
*
*
***
TN
F-α
(pg/
mg
of p
rote
in)
IL-6
(pg/
mg
of p
rote
in)
(A)
(B)
Control LPS LPS++Dexa LPS++LJ
Control LPS LPS++Dexa LPS++LJ

damage, immunohistochemical staining for NE wasconducted. NE was strongly expressed in LPS group,while the levels of NE were notably reduced in the LJpre-treatment group (Figure 5).
Discussion
COPD is a very common public health concern world-wide, and the incidence of this disease is increasing
globally14. Current conventional treatments of COPDare geared toward relieving symptoms, preventingrecurrent exacerbations, preserving optimal lung func-tion and enhancing the quality of life15. Althoughmany drugs are used to treat COPD, adverse effectsare associated with several classes of drugs, includingsteroids; therefore, it is necessary to identify alterna-tive modes of treatment such as the use of herbal me-dicines16. Therefore we hypothesized that anti-inflam-matory effect of LJ may attenuate the progression oflung inflammation. Mouse model of LPS-induced lungneutrophilia was used to mimic a COPD-like acutedisease17.
In this study, infiltration of inflammatory cells inBAL fluid and in the lung parenchyma was observedfollowing exposure to LPS in mice. Concomitant withthe influx of neutrophils, elevated levels of the pro-in-flammatory cytokines, TNF-α and IL-6 were observedin the BAL fluid of LPS-exposed mice. In addition, theexpression of NE in the airway was found to increasefollowing LPS exposure. The pathological changesobserved in this study were similar to the clinicalfeatures of COPD patients18.
By contrast, at 3 days after LPS stimulation, theaccumulation of inflammatory cells in BAL fluid wasinhibited by pretreatment with either LJ or dexametha-sone. Furthermore, TNF-α and IL-6 were also decre-ased in the BAL fluid of LJ pretreated mice compar-ed to LPS only treated mice. In addition, the expres-sion of NE in the airway was significantly reduced ineither LJ or dexamethasone pretreated mice.
It is known that TNF-α plays a significant role inmany inflammatory in many inflammatory disease oflung such as chronic bronchitis, COPD, asthma, acutelung injury and acute respiratory distress syndrome.TNF-α is released from macrophage, T lymphocytes,mast cells, and epithelial cells19. It plays a significantrole in controlling cellular migration and permeabilityand stimulates the secretion of IL-6, and IL-820. TNF-α also activates nuclear factor-κB (NF-κB), whichincreases IL-8 gene transcription, thereby inducingthe release of IL-8 from the airway epithelium andneutrophils. IL-8, a CXC chemokine, is a neutrophilchemoattractant and activator18.
Luteolin, which is a major flavonoid found in LJ, isknown to inhibit an endotoxin-stimulated phosphory-lation cascade and pro-inflammatory cytokine produc-tion in macrophages10. It is reported that luteolin sup-presses inflammation-associated gene expression byblocking NF-κB and activator protein one activationpathway in mouse alveolar macrophages21. In addition,the aqueous extract of LJ has been shown to exertpotent inhibition of both NO production and TNF-αsecretion in a dose-dependent manner in an activated
90 Mol Cell Toxicol (2011) 7:87-93
Figure 4. Effect of LJ on lung inflammation. Lung sec-tions were obtained from control mice (A), LPS only treat-ed mice (B), dexamethasone+LPS treated mice (C) andLonicera japonica+LPS treated mice (D). After H&Estaining, histological examination was performed by lightmicroscopy (magnification ×400). The degree of inflam-mation was quantified (E) using a semiquantitative scale.Data are presented as means±SEM. (*P⁄0.05, **P⁄0.01 as compared with LPS; n=6).
3.5
3.0
2.5
2.0
1.5
1.0
0.5
*
**
**
Infl
amm
atio
n in
dex
(A)
(B)
Control LPS LPS+Dexa LPS+LJ

macrophage-like cell line9. Therefore our data indicatethat treatment with LJ may act on the influx of inflam-matory cells and the levels of mediators aggravatingthe inflammatory response.
Neutrophils are necessary in healthy lungs; they arean important component of innate immunity, protect-ing healthy individuals against infection22. However, inCOPD, they can be responsible for significant damagewhen they accumulate at sites of inflammation and areharmful to healthy tissue. NE from neutrophils playsa key role in the pathogenesis of both emphysema andlung fibrosis during the inflammatory process23. It isdocumented that neutrophil elastase-deficient micesignificantly protected from the development of em-physema after long-term cigarette smoke exposure24.In this study, influx of neutrophils and NE expressionlevels were remarkably reduced by treatment with LJ.Therefore our data demonstrates that LJ can preventthe neutrophilic inflammation in COPD.
In summary, the results of this study provide evi-dence that pre-treatment with LJ exerts preventiveeffects against LPS-induced lung inflammation invivo. The remarkable protective effect exerted by LJsuggests that it has the potential for use in the treat-ment of COPD patients. Therefore, further study toelucidate the mechanisms by which the effects of LJoccur should be conducted to aid in the discovery ofnew therapeutic agents for the prevention of COPD.
Materials & Methods
Reagents
The extract of the flower of Lonicera japonica (LJ)(Sun Ten Pharmaceutical, Taiwan) was dissolved in0.9% saline to give a final concentration of 10%(w/v).The herb suspension supernatant (HSS) was thenobtained by centrifugation at 27,000×g for 20 min at4�C. The HSS was then passed through a sterile 0.20μm pore size filter unit (Sartorius AG, Germany). LPS(Calbiocham, Germany) was dissolved in 0.9% salineat a concentration of 8 mg/mL.
Quantitative chromatographic analysis
The analysis was performed on a Waters system(Waters Co., USA) with a 717++ autosampler, 2996photodiode array detector (PDA) 2487 dual λ absor-bance detector, and 1525 binary HPLC pump, andWaters Millennium system (Waters Co., USA) wereused for data acquisition and integration. All solventsused for HPLC analysis were HPLC grade (J.T. BakerCo., Ltd., USA) and filtered and degassed before beingused. The standard compound used for quantitativeanalysis of loganin was purchased from Wako (Ja-pan)25. The standard compound (98%) weighing 1 mgwas dissolved with methanol in accordance with theanalysis conditions of standard compound. The dis-solved standard solution was diluted to 0.100, 0.050,
Mol Cell Toxicol (2011) 7:87-93 91
Figure 5. Effect of LJ onneutrophil elastase expres-sion. Lung sections wereobtained from control mice(A), LPS only treated mice(B), dexamethasone++LPStreated mice (C) and Loni-cera japonica++LPS treatedmice (D). The sections werestained using the immuno-histochemical method andthen incubated overnight at4�C with anti-Neutrophilelastease (NE) goat polyclo-nal antibody (1 : 50). Afterthe slides were incubatedwith avidin-biotin peroxi-dase complex, the color wasdeveloped with 3,3′-diami-nobenzidine tetrachloride.

0.025, 0.013 mg/mL respectively, and then the stan-dard HPLC chromatogram was obtained. The samplewas accurately weighed to about 2 g, dissolved in50 mL of methanol, ultrasonic for 15 min and centri-fuged at 15,000 rpm for 5 min. The supernatant of thesample was filtered through a 0.45μm syringe filter(PVDF, GELMAN, USA.). The chromatographicanalysis was carried out at room temperature on aXTerraTM RP18 column (250 mm×4.6 mm, 5 μm,Waters). A linear gradient elution of eluents A (water)and B (acetonitrile) was conducted as follows: a lineargradient of 3-5% B with the range of 0-10 min and alinear gradient of 5-40% B with the range of 10-30 min. The injection volume was 15μL, the peakswere detected at 240 nm and the solvent was kept at0.8 mL/min.
Animals
Balb/c male mice (6 wk of age, weighing 20-25 g)were purchased from Orient Bio Inc. (South Korea).Mice were kept under pathogen-free conditions andhad free access to food and water throughout the ex-periments.
Induction of COPD and Animals treatment
Mice (n=6 per group) were treated with 200μL of LJextract or saline via an oral injection. Mice in thepositive control group were treated with dexametasone(10 mg/kg body wt). Two hours later, mice were givenLPS (0.5 mg/kg body wt) or saline intranasally. At 3days after LPS stimulation, each group of mice wassacrificed for further studies.
Analysis of bronchoalveloar lavage (BAL) cells
Phosphate buffered saline was slowly infused into thelungs and then withdrawn via the canula that has beeninserted into the trachea. The number of cells in thelavage fluid was then determined using a hemacyto-meter. In addition, differential cell counts were per-formed on slides that were prepared by cytocentrifu-gation and Diff-Quick staining. Approximately 500cells were counted per slide. The BAL fluids were thencentrifuged, after which the supernatants were storedat -80�C until needed.
Measurements of IL-6 and TNF-α in BAL fluid
The levels of IL-6 and TNF-α in the BAL fluid weredetermined using a ELISA kit (BD PharMingen, SanDiego, USA). Briefly, flat-bottom 96-well plates werecoated with TNF-α or IL-6 monoclonal antibody(mAb) and incubated overnight at 4�C. The primary
mAbs were then discarded and the plates were blockedwith assay diluents (BD Pharmingen, San Diego, USA)for 1 h at room temperature. These plates were thenwashed 3 times with wash buffer (0.05% Tween 20 inphosphate buffered saline) and blotted on a papertowel. Next, diluted samples and standards were addedin triplicate and the plates were then incubated for 2 hat room temperature. The supernatant was then discard-ed, after which the wells were washed 5 times withwash buffer. Next, TNF-α or IL-6 mAb plus avidin-horseradish peroxidase was added to the samples,which were then incubated for 1 h at room temperature.The plates were then washed, after which tetramethyl-benzidine substrate solution (BD Bioscience, SanDiego, USA) was added. The color was allowed todevelop for 30 min in the dark before the reaction wasquenched with a stop solution (0.2 N H2SO4). Thedetection limits for the IL-6 and TNF-α ELISAs were7.8 pg/mL.
Preparation of lung tissues and histology andimmunohistochemistry
Lung tissues were fixed in 4% paraformaldehyde solu-tion and then embedded in paraffin. For histologicalexamination, 4μm sections of lung tissue were stainedsequentially with hematoxylin and eosin (H&E). Theseverity of peribronchial inflammation was gradedsemiquantitatively for the following features: 0, nor-mal; 1, few cells; 2, a ring of inflammatory cells 1 celllayer deep; 3, a ring of inflammatory cells 2-4 cellslayer deep; 4, a ring of inflammatory cells of ¤4 cellslayer deep26. For the immunohistochemistry of neutro-phil elastease (NE), 4μm sections of lung tissue weretreated with 0.3% H2O2-methanol for 30 min to blockthe endogenous peroxidase and then incubated at 4�Covernight with anti-NE goat polyclonal antibody (1 :50 dilution) (Santa Cruz Biotechnology, USA). Theslides were then incubated with avidin-biotin peroxi-dase complex (ABC kit, Vector Laboratories, USA),after which the color was developed with 3,3′-diamin-obenzidine tetrachloride (DAB, Vector Laboratories,USA). Following immunohistochemical staining, theslides were counterstained with Herris’s hematoxylinfor 2 min and then mounted with Canada balsam (Sho-wa Chemical Co. Ltd., Japan).
Statistical analysis
Data are presented as the means±S.E.M. Analysis ofdata was done using Graphpad Prism software (version4). Multiple comparisons between groups were evaluat-ed by One-way ANOVA and Tukey test. A P-valueof less than 0.05 was considered to indicate a signifi-cant difference.
92 Mol Cell Toxicol (2011) 7:87-93

Conflict of interests
Authors have no, real or perceived competing of inter-est that relate to this manuscript.
Acknowledgements This work was supported by agrant from Kyung Hee University in 2008 (20081254).
References
1. Barnes, P. J. Immunology of asthma and chronicobstructive pulmonary disease. Nat Rev Immunol8:183-192 (2008).
2. Yoshida, T. & Tuder, R. M. Pathobiology of cigarettesmoke-induced chronic obstructive pulmonary disease.Physiol Rev 87:1047-1082 (2007).
3. Keatings, V. M. et al. Effects of inhaled and oral glu-cocorticoids on inflammatory indices in asthma andCOPD. Am J Respir Crit Care Med 155:542-548(1997).
4. Barnes, P. J. Novel approaches and targets for treat-ment of chronic obstructive pulmonary disease. Am JRespir Crit Care Med 160:S72-79 (1999).
5. Loppow, D. et al. In patients with chronic bronchitis afour week trial with inhaled steroids does not attenuateairway inflammation. Respir Med 95:115-121 (2001).
6. Barnes, P. J. & Stockley, R. A. COPD: current thera-peutic interventions and future approaches. Eur RespirJ 25:1084-1106 (2005).
7. Calixto, J. B. et al. Anti-inflammatory compounds ofplant origin. Part II. modulation of pro-inflammatorycytokines, chemokines and adhesion molecules. PlantaMed 70:93-103 (2004).
8. Guo, R., Pittler, M. H. & Ernst, E. Herbal medicinesfor the treatment of COPD: a systematic review. EurRespir J 28:330-338 (2006).
9. Park, E. et al. Anti-inflammatory activity of herbalmedicines: inhibition of nitric oxide production andtumor necrosis factor-alpha secretion in an activatedmacrophage-like cell line. Am J Chin Med 33:415-424(2005).
10. Xagorari, A. et al. Luteolin inhibits an endotoxin-sti-mulated phosphorylation cascade and proinflammatorycytokine production in macrophages. J PharmacolExp Ther 296:181-187 (2001).
11. Hsueh, W. et al. The role of the complement systemin shock and tissue injury induced by tumour necrosisfactor and endotoxin. Immunology 70:309-314 (1990).
12. Rogers, D. F. Mucus pathophysiology in COPD: dif-
ferences to asthma, and pharmacotherapy. MonaldiArch Chest Dis 55:324-332 (2000).
13. Barnes, P. J. Mechanisms in COPD: differences fromasthma. Chest 117:10S-14S (2000).
14. Mannino, D. M. & Buist, A. S. Global burden ofCOPD: risk factors, prevalence, and future trends.Lancet 370:765-773 (2007).
15. Siafakas, N. M. et al. Optimal assessment and mana-gement of chronic obstructive pulmonary disease(COPD). The European Respiratory Society TaskForce. Eur Respir J 8:398-420 (1995).
16. George, J. et al. Use of complementary and alternativemedicines by patients with chronic obstructive pul-monary disease. Med J Aust 181:248-251 (2004).
17. Puljic, R. et al. Lipopolysaccharide-induced lung in-flammation is inhibited by neutralization of GM-CSF.Eur J Pharmacol 557:230-235 (2007).
18. Chung, K. F. Cytokines in chronic obstructive pul-monary disease. Eur Respir J Suppl 34:50s-59s (2001).
19. Mukhopadhyay, S., Hoidal, J. R. & Mukherjee, T. K.Role of TNFalpha in pulmonary pathophysiology.Respir Res 7:125 (2006).
20. Drost, E. M. & MacNee, W. Potential role of IL-8,platelet-activating factor and TNF-alpha in the seque-stration of neutrophils in the lung: effects on neutro-phil deformability, adhesion receptor expression, andchemotaxis. Eur J Immunol 32:393-403 (2002).
21. Chen, C. Y. et al. Luteolin suppresses inflammation-associated gene expression by blocking NF-kappaBand AP-1 activation pathway in mouse alveolar macro-phages. Life Sci 81:1602-1614 (2007).
22. Faurschou, M. & Borregaard, N. Neutrophil granulesand secretory vesicles in inflammation. Microbes Infect5:1317-1327 (2003).
23. Lungarella, G. et al. The dual role of neutrophil elastasein lung destruction and repair. Int J Biochem Cell Biol40:1287-1296 (2008).
24. Shapiro, S. D. et al. Neutrophil elastase contributes tocigarette smoke-induced emphysema in mice. Am JPathol 163:2329-2335 (2003).
25. Qian, Z. M. et al. Simultaneous qualitation and quanti-fication of thirteen bioactive compounds in Flos loni-cerae by high-performance liquid chromatographywith diode array detector and mass spectrometry.Chem Pharm Bull (Tokyo) 55:1073-1076 (2007).
26. Myou, S. et al. Blockade of inflammation and airwayhyperresponsiveness in immune-sensitized mice bydominant-negative phosphoinositide 3-kinase-TAT. JExp Med 198:1573-1582 (2003).
Mol Cell Toxicol (2011) 7:87-93 93








![Effect of two medicinal herbs ( Astragalus radix and Lonicera japonica ) on the growth performance and body composition of juvenile pikeperch [ Sander lucioperca (L.)]](https://img.pdfslide.net/doc/110x75/6324b12448d448ffa007433e/effect-of-two-medicinal-herbs-astragalus-radix-and-lonicera-japonica-on-the.jpg)




















