Embed Size (px)
Citation preview

http://tm.firebrandtech.com/WK/WK_FileRepository/WK_IMAGES/9781451191110.jpg[5/30/2014 12:55:29 PM]

Denise R. Ferrier, PhD Professor of Biochemistry Department of Biochemistry and Molecular Biology Drexel University College of Medicine Philadelphia, Pennsylvania
Lippincott Illustrated Reviews Flash CardsBIOCHEMISTRY
Bradford A. Jameson, PhD Professor of Biochemistry Department of Biochemistry and Molecular Biology Drexel University College of Medicine Philadelphia, Pennsylvania
Ferrier_FM.indd iFerrier_FM.indd i 5/3/14 4:48 AM5/3/14 4:48 AM

Acquisitions Editor: Tari Broderick Product Development Editor: Stephanie Roulias Production Project Manager: David Orzechowski Design Coordinator: Holly McLaughlin
Illustration Coordinator: Doug Smock Manufacturing Coordinator: Margie Orzech Prepress Vendor: Absolute Service, Inc.
Copyright © 2015 Wolters Kluwer Health
All rights reserved. This book is protected by copyright. No part of this book may be reproduced or transmitted in any form or by any means, including as photocopies or scanned-in or other electronic copies, or utilized by any information storage and retrieval system without written permission from the copyright owner, except for brief quotations embodied in critical articles and reviews. Materials appearing in this book prepared by individuals as part of their offi cial duties as U.S. government employees are not covered by the above-mentioned copyright. To request permission, please contact Wolters Kluwer Health at Two Commerce Square, 2001 Market Street, Philadelphia, PA 19103, via email at [email protected], or via our website at lww.com (products and services).
9 8 7 6 5 4 3 2 1
Printed in China
978-1-4511-9111-01-4511-9111-1 Library of Congress Cataloging-in-Publication Data is available upon request
Care has been taken to confi rm the accuracy of the information presented and to describe generally accepted practices. However, the author(s), editors, and publisher are not responsible for errors or omissions or for any consequences from application of the information in this book and make no warranty, expressed or implied, with respect to the currency, completeness, or accuracy of the contents of the publication. Application of this information in a particular situation remains the professional responsibility of the practitioner; the clinical treatments described and recommended may not be considered absolute and universal recommendations.
The author(s), editors, and publisher have exerted every effort to ensure that drug selection and dosage set forth in this text are in accordance with the current recommendations and practice at the time of publication. However, in view of ongoing research, changes in government regulations, and the constant fl ow of information relating to drug therapy and drug reactions, the reader is urged to check the package insert for each drug for any change in indications and dosage and for added warnings and precautions. This is particularly important when the recommended agent is a new or infrequently employed drug.
Some drugs and medical devices presented in this publication have Food and Drug Administration (FDA) clearance for limited use in restricted research settings. It is the responsibility of the health care provider to ascertain the FDA status of each drug or device planned for use in his or her clinical practice.
Ferrier_FM.indd iiFerrier_FM.indd ii 5/23/14 1:09 AM5/23/14 1:09 AM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Features: Three-Step Review
SPOT FLASHTest your grasp of key concepts or equations on a lecture-by-lecture basis!
COURSE REVIEWEnsure a thorough understanding of course material through in-depth questions. High-yield facts for course- and Board-exam review!
CLINICAL CORRELATIONSExplain how the basic science helps predict outcomes in a clinical setting!
Featuring the same visionary artwork found in Lippincott Illustrated Reviews: Biochemistry
With Lippincott Illustrated Reviews, Seeing is Understanding.
Ferrier_FM.indd iiiFerrier_FM.indd iii 5/3/14 4:48 AM5/3/14 4:48 AM

Ferrier_FM.indd ivFerrier_FM.indd iv 5/3/14 4:48 AM5/3/14 4:48 AM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Preface
Lippincott Illustrated Reviews Flash Cards: Biochemistry is a portable study tool designed for self-assessment and review of medical biochemistry. The fl ash cards were developed primarily for use by medical students studying biochemistry and preparing for United States licensing exams, but information is presented with a clarity and level of detail that makes them ideal supplements for any of the allied health sciences. The deck contains three card types: Question (Q) cards, Case cards, and Summary cards.
Q CARDS The majority of cards are Q cards that prompt the reader with questions (on the front) to assess level of understanding, depth of knowledge, and ability to apply biochemical concepts. The answers (on the back) are more inclusive than those found on typical fl ash cards.
Most Q cards contain three questions or sets of questions on a common topic: The fi rst tests for retention of basic facts, whereas the next two test understanding and/or application of related concepts and clinical correlations. Each question type is denoted by icons.
SPOT FLASH : Illustration-based questions test your grasp of key facts and are intended for use on a lecture-by-lecture assessment and review basis.
COURSE REVIEW: In-depth questions promote a thorough understanding of related concepts. The answers focus on high-yield facts to help consolidate and apply material during course- and licensing-exam review.
CLINICAL CORRELATIONS: Clinical questions highlight the basic science foundations of medicine. They help students apply biochemi-cal concepts to clinical problems and are particularly useful when studying for licensing exams.
Continued, over
Ferrier_FM.indd vFerrier_FM.indd v 5/3/14 4:48 AM5/3/14 4:48 AM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Preface
Q cards include several features to facilitate learning and retaining the material:
• Illustrations : Richly detailed illustrations from the popular companion text, Lippincott Illustrated Reviews: Biochemistry , appear on both sides of the cards. Many of the illustrations include narrative boxes that guide readers through complex concepts.
• Notes : Answers may be supplemented with information that goes beyond the need-to-know basics to provide context or to enrich and help anchor a concept.
• Emphasis: Key terms, disease names, and pathologic fi ndings are bolded for rapid review and assimilation.
CASE CARDS AND SUMMARY CARDS Case cards use common clinical presentations to highlight biochemical concepts. Summary cards (for the vitamins and the fed/fasted states) highlight key features of these information-rich areas of medical biochemistry.
The card deck is designed to be comprehensive, covering all signifi cant biochemical concepts.
Ferrier_FM.indd viFerrier_FM.indd vi 5/3/14 4:48 AM5/3/14 4:48 AM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Acknowledgments
The authors wish to thank John Swaney, PhD, our colleague at Drexel University College of Medicine, for his careful reading of the manuscript and constructive comments. Any errors are ours alone.
We thank the publishing team assembled by Wolters Kluwer. Stephanie Roulias, product development editor, and Kelly Horvath, freelance development editor, along with Doug Smock, Teresa Exley, and David Orzechowski, gave invaluable assistance in the development and production of the fi nished product. We also thank Robin R. Preston, PhD, for his design of the fl ash card format.
DedicationThe authors dedicate this work to the medical, biomedical graduate,
and professional studies students of Drexel University. You have challenged and inspired us, and have made us better teachers.
Ferrier_FM.indd viiFerrier_FM.indd vii 5/3/14 4:48 AM5/3/14 4:48 AM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Figure Credits
Card 3.6 Question and Answer: Modifi ed photo courtesy of Photodyne Incorporated, Hartland, WI.
Card 4.2 Answer: Kronauer and Buhler, Images in Clinical Medicine, The New England Journal of Medicine, June 15, 1995, Vol. 332, No. 24, p. 1611.
Card 4.5 Question and Answer: 1. Modifi ed photo from Web site Derma.de. 2. Modifi ed
from Jorde LB, Carey JC, Bamshad MJ, et al. Medical Genetics . 2nd ed. St. Louis, MO: Mosby; 2000. http://medgen.genetics.utah.edu/index.htm
Card 13.6 Answer: From the Crookston Collection, University of Toronto.
Card 21.2 Answer: Modifi ed from Rich MW. Porphyria cutanea tarda. Postgrad Med . 1999;105:208–214.
Card 21.4 Question and Answer: From Custom Medical School Stock Photo, Inc.
Card 22 Case Card Question: Modifi ed from WebMD Inc. http://www.samed.com/sam/forms/index.htm.
Card 23.6 Question and Answer: Modifi ed from Cryer PE, Fisher JN, Shamoon H. Hypoglycemia. Diabetes Care . 1994;17:734–753.
Ferrier_FM.indd viiiFerrier_FM.indd viii 5/3/14 4:48 AM5/3/14 4:48 AM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Contents
UNIT 1 Protein Structure and Function 1.1
UNIT 2 Bioenergetics and Carbohydrate Metabolism 6.1
UNIT 3 Lipid Metabolism 15.1
UNIT 4 Nitrogen Metabolism 19.1
UNIT 5 Metabolism Integration 23.1
UNIT 6 Genetic Information Storage and Expression 29.1
CHAPTER 34 Blood Clotting 34.1
APPENDIX Abbreviations A-1
Ferrier_FM.indd ixFerrier_FM.indd ix 5/3/14 4:48 AM5/3/14 4:48 AM

Ferrier_FM.indd xFerrier_FM.indd x 5/3/14 4:48 AM5/3/14 4:48 AM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
1.1 QuestionAmino Acid Structure
What effect will raising pH from an acidic value to the physiologic value of 7.4 have on the structural features shown in red at right?
At physiologic pH, what will be the charge on the side chain (R group) of free Asp? Of Lys?
Which amino acid(s) contains a side-chain hydroxyl group that can be glycosylated? A secondary amino group?
Is Val ionized when incorporated into a protein?
C+H3N
COOH
HC+H3N
COOH
H
These are common to all `-amino acids.
Free amino acid
RAminogroup
Carboxylgroup
`C H`
RRAminogroup
R
Side chain is distinctive for each amino acid.
`-Carbon islinked to the carboxyl, amino, and R groups.
Ferrier_Unit01.indd 1Ferrier_Unit01.indd 1 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
1.1 Answer Amino Acid Structure
Raising the pH from an acidic value to the physiologic value of 7.4 will result in deprotonation (ionization) of the �-carboxyl group (pK�2) to COO�. The �-amino group (pK�9) will remain protonated.
At physiologic pH, the charge on the side chain (R group) of free Asp is negative. Lys is positive.
Ser and Thr each contain a hydroxyl group that can be O-glycosylated. [Note: The hydroxyl group can also be phosphorylated.] Pro contains a secondary amino group. Its �-amino N and R group form a rigid ring.
Val is not ionized when incorporated into a protein because (1) the �-amino and �-carboxyl groups are involved in peptide bonds and, consequently, are unavailable for ionization, and (2) the side chain is nonpolar.
C+H3N
COO-
HC+H3N
CCOO-
H
These are common to all `-amino acids.
Free amino acid
RAminogroup
Carboxylgroup
`C H`
RRAminogroup
R
Side chain is distinctive for each amino acid.
`-Carbon islinked to the carboxyl, amino, and R groups.
COOH
H
Proline
C
CH2
+H2N
H2CCH2
Ferrier_Unit01.indd 2Ferrier_Unit01.indd 2 5/2/14 7:08 PM5/2/14 7:08 PM
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
1.2 QuestionAmino Acid Structure
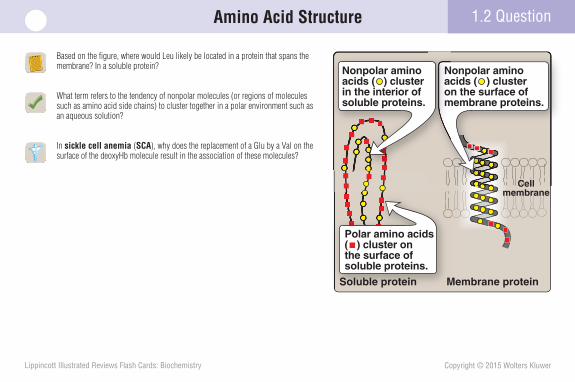
Based on the fi gure, where would Leu likely be located in a protein that spans the membrane? In a soluble protein?
What term refers to the tendency of nonpolar molecules (or regions of molecules such as amino acid side chains) to cluster together in a polar environment such as an aqueous solution?
In sickle cell anemia (SCA), why does the replacement of a Glu by a Val on the surface of the deoxyHb molecule result in the association of these molecules?
Cellmembrane
Polar amino acids( ) cluster onthe surface of soluble proteins.
CellCC ll
Nonpolar aminoacids ( ) cluster on the surface of membrane proteins.
Nonpolar amino acids ( ) cluster in the interior of soluble proteins.
Soluble protein Membrane protein
Ferrier_Unit01.indd 3Ferrier_Unit01.indd 3 5/2/14 7:08 PM5/2/14 7:08 PM
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Amino Acid Structure1.2 Answer
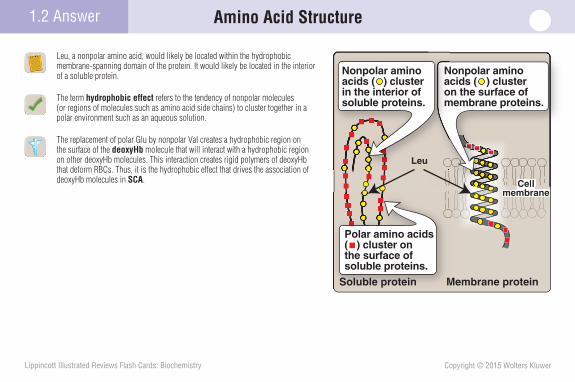
Leu, a nonpolar amino acid, would likely be located within the hydrophobic membrane-spanning domain of the protein. It would likely be located in the interior of a soluble protein.
The term hydrophobic effect refers to the tendency of nonpolar molecules (or regions of molecules such as amino acid side chains) to cluster together in a polar environment such as an aqueous solution.
The replacement of polar Glu by nonpolar Val creates a hydrophobic region on the surface of the deoxyHb molecule that will interact with a hydrophobic region on other deoxyHb molecules. This interaction creates rigid polymers of deoxyHb that deform RBCs. Thus, it is the hydrophobic effect that drives the association of deoxyHb molecules in SCA. Cell
membraneCell
Leu
Polar amino acids( ) cluster onthe surface of soluble proteins.
Nonpolar aminoacids ( ) cluster on the surface of membrane proteins.
Nonpolar amino acids ( ) cluster in the interior of soluble proteins.
Soluble protein Membrane protein
Ferrier_Unit01.indd 4Ferrier_Unit01.indd 4 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
1.3 QuestionAmino Acid Structure
Which structure shown (A or B) represents L-Ala?
Which amino acid does not possess a chiral (asymmetric) carbon?
Which peptide is less soluble in an aqueous (polar) environment, Ala-Gly-Asn-Ser-Tyr or Gly-Met-Phe-Leu-Ala?
H3C
HOOC
B
H C NH3+
CH3
COOH
A
HC+H3N
Ferrier_Unit01.indd 5Ferrier_Unit01.indd 5 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
1.3 Answer Amino Acid Structure
Structure A represents L-Ala. The L isomer of an amino acid has the �-amino group on the left. The D isomer has the �-amino group on the right. D and L isomers are mirror images of each other (enantiomers).
Gly, with its two H substituents, does not possess a chiral (asymmetric) carbon.
Because the Gly-Met-Phe-Leu-Ala peptide contains no charged or polar uncharged amino acids, it is less soluble than Ala-Gly-Asn-Ser-Tyr in an aqueous (polar) environment.
H3C
HOOC
D-Alanine
H C NH3+
CH3
COOH
L-Alanine
HC+H3N
Ferrier_Unit01.indd 6Ferrier_Unit01.indd 6 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
1.4 QuestionAcidic and Basic Properties of Amino Acids
What relationship is described by the Henderson–Hasselbalch equation shown?
Is an acid with a large pKa stronger or weaker than one with a small pKa?
The pKa of acetic acid (CH3COOH) is 4.8. What is the pH of a solution containing acetic acid and its conjugate base (CH3COO�) in a ratio of 10 to 1?
Physiologic buffers are important in resisting blood pH changes. Maximal buffering occurs when the pH is equal to the , while effective buffering can occur within .
pH pKa log[A–][HA]
+
Ferrier_Unit01.indd 7Ferrier_Unit01.indd 7 5/2/14 7:08 PM5/2/14 7:08 PM
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
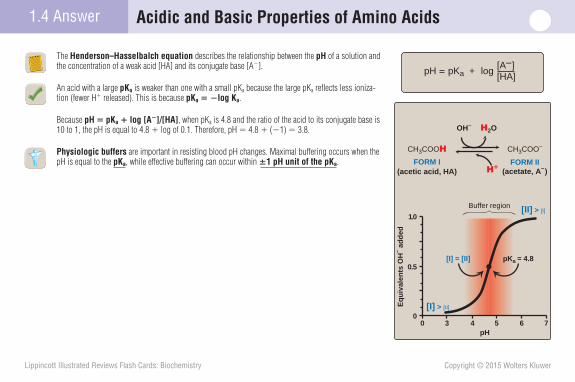
The Henderson–Hasselbalch equation describes the relationship between the pH of a solution and the concentration of a weak acid [HA] and its conjugate base [A�].
An acid with a large pKa is weaker than one with a small pKa because the large pKa refl ects less ioniza-tion (fewer H� released). This is because pKa � �log Ka.
Because pH � pKa � log [A�]/[HA], when pKa is 4.8 and the ratio of the acid to its conjugate base is 10 to 1, the pH is equal to 4.8 � log of 0.1. Therefore, pH � 4.8 � (�1) � 3.8.
Physiologic buffers are important in resisting blood pH changes. Maximal buffering occurs when the pH is equal to the pKa, while effective buffering can occur within �1 pH unit of the pKa.
1.4 Answer Acidic and Basic Properties of Amino Acids
0 3 4 5 6 70
0.5
1.0
pH
Eq
uiv
alen
ts O
H– a
dd
ed
Buffer region
CH3COOH CH3COO–
H2O
FORM I(acetic acid, HA)
FORM II(acetate, A–)
pKa = 4.8[I] = [II]
OH–
H+
[I] > [II]
[II] > [I]
pH pKa log[A–][HA]
+
Ferrier_Unit01.indd 8Ferrier_Unit01.indd 8 5/2/14 7:08 PM5/2/14 7:08 PM
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
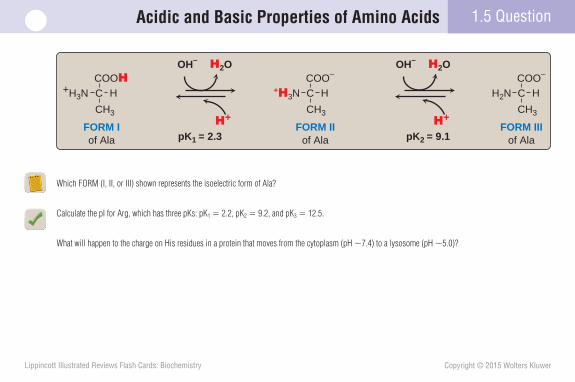
Which FORM (I, II, or III) shown represents the isoelectric form of Ala?
Calculate the pI for Arg, which has three pKs: pK1 � 2.2, pK2 � 9.2, and pK3 � 12.5.
What will happen to the charge on His residues in a protein that moves from the cytoplasm (pH �7.4) to a lysosome (pH �5.0)?
1.5 QuestionAcidic and Basic Properties of Amino Acids
COOH
FORM Iof Ala
FORM IIof Ala
FORM IIIof Ala
CH3
C+H3N HCOO–
CH3
C+H3N HCOO–
CH3
CH2N H
H2OOH–
H+
H2OOH–
H+
pK1 = 2.3 pK2 = 9.1
Ferrier_Unit01.indd 9Ferrier_Unit01.indd 9 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
1.5 Answer Acidic and Basic Properties of Amino Acids
COOH
FORM Iof Ala
FORM IIof Ala
FORM IIIof Ala
CH3
C+H3N HCOO–
CH3
C+H3N HCOO–
CH3
CH2N H
H2OOH–
H+
H2OOH–
H+
pK1 = 2.3 pK2 = 9.1
The isoelectric form has no net charge. It is the zwitterionic (“two ion”) form. Therefore, FORM II is the isoelectric form of Ala.
The pI corresponds to the pH at which an amino acid is electrically neutral, that is, the average of the pKs on either side of the isoelectric form. For Arg, a dibasic amino acid with pK1 (most acidic group) � 2.2, pK2 � 9.2, and pK3 (least acidic group) � 12.5, the pI is 10.8 (the average of 9.2 and 12.5).
In a protein, the imidazole R group of His can be charged or uncharged depending on the local environment. It will be uncharged (deprotonated) at pH 7.4 and charged (protonated) at pH 5.0. [Note: In free His the pK of the R group is 6.0.]
Ferrier_Unit01.indd 10Ferrier_Unit01.indd 10 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
1.6 QuestionAcidic and Basic Properties of Amino Acids
Based on the bicarbonate buffer system shown, what will happen to the availability of HCO 3 � when H � is lost, such as with emesis (vomiting)?
Use the Henderson–Hasselbalch equation to determine what will happen to pH when HCO 3 � is lost (e.g., with diarrhea) and when CO 2 is increased (e.g., with pulmonary obstruction).
Aspirin (pK a � 3.5) is largely protonated and uncharged in the stomach (pH 1.5). What percentage of the aspirin will be in this lipid-soluble form at pH 1.5?
H2CO3 HCO3-H+H2OCO2 + +
Ferrier_Unit01.indd 11Ferrier_Unit01.indd 11 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
1.6 Answer Acidic and Basic Properties of Amino Acids
With emesis ( vomiting ), the loss of H � (rise in pH) results in increased availability of HCO 3 � as the result of a compensatory rightward shift in the bicarbonate buffer system .
The Henderson–Hasselbalch equation is used to calculate how the pH of a system changes in response to changes in the concentration of an acid or its conjugate base. For the bicarbonate buffer system, pH � pK � log [HCO 3 � ]/[CO 2 ]. Therefore, both the loss of HCO 3 � (base) with diarrhea and the increase in CO 2 (acid) because of decreased elimination with pulmonary obstruction result in decreased pH.
pH � pK � log [Drug � ]/[Drug-H]. Therefore, for aspirin in the stomach, 1.5 � 3.5 � ( � 2). Because the antilog of � 2 is 0.01, the ratio of [Drug � ]/[Drug-H] is 1/100. This means that 1 out of 100 (1%) of the aspirin molecules will be the Drug � form and 99 out of 100 (99%) will be the uncharged, lipid-soluble, Drug-H form.
H2CO3 HCO3-H+H2OCO2 + +
DRUG ABSORPTION
At the pH of the stomach (1.5), a drug like aspirin (weak acid, pK = 3.5) will be largely protonated (COOH) and, thus, uncharged.
Uncharged drugs generally cross membranes more rapidly than do charged molecules.
pH = pK + log [Drug-H] [Drug– ]
A
HA
-
Lipidmembrane
LUMEN OF STOMACH
STOMACH
BLOOD
H+
H+
H+
A
HA
-H+
Remove B
Ferrier_Unit01.indd 12Ferrier_Unit01.indd 12 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.1 QuestionProtein Structure
Which level of protein structure depicted can be correctly described as the “three-dimensional shape of a folded polypeptide chain”?
Mutations that insert, delete, or replace amino acids change this level of protein structure.
How many different isoforms of the tetrameric enzyme PK can be made from M and/or L subunits?
How many different tetrapeptides could be generated from three different amino acids?
CN C
H
H
CN C
H
CH3O
H
NH
C
OC
O
CN
CNH
HCO
C
CNH O
CC
O
OH
N
C
C
NH
NH
R
CR
C R
C R
3
2
1H
4
Ferrier_Unit01.indd 13Ferrier_Unit01.indd 13 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.1 Answer Protein Structure
The “three-dimensional shape of a folded polypeptide chain” describes a protein’s tertiary structure (No. 3 shown).
At a minimum, the primary structure (amino acid sequence) will change with mutations that insert, delete, or replace amino acids. [ Note: Changes in the primary structure can also affect the higher levels of protein structure (No. 2 to 4 shown). Such changes frequently result in protein misfolding and can lead to loss of function, aggregation, or degradation.]
Five different forms of tetrameric PK can be made from M and/or L subunits: M 4 , M 3 L, M 2 L 2 , ML 3 , and L 4 . Because PK is composed of more than one subunit, it has a quaternary structure .
There are 3 4 or 81 (where 3 � the number of amino acids and 4 � the chain length) different tetrapeptides that could be generated from three different amino acids.
CN C
H
H
CN C
H
CH3O
H
NH
C
OC
O
CN
CNH
HCO
C
CNH O
CC
O
OH
N
C
C
NH
NH
R
CR
C R
C R
Quaternarystructure4
Tertiarystructure3
2 Secondarystructure
Primarystructure1
H
Ferrier_Unit01.indd 14Ferrier_Unit01.indd 14 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.2 QuestionPrimary Structure of Proteins
What is the name given to the bond outlined by the black box shown?
What are the characteristics of this bond?
With fever , why might proteins begin to unfold but not be hydrolyzed to peptides and free amino acids?
C COO–
H
Valine
Valylalanine
C+H3N COO–
H
CH3
Alanine
C C
H
CN COO–
H
CH3O
H
Free carboxyl end of peptide
CHH3C
CH3
H2O
Free amino end of peptide
+H3N
CHH3C
CH3
+H3N
Ferrier_Unit01.indd 15Ferrier_Unit01.indd 15 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.2 Answer Primary Structure of Proteins
A peptide bond , a type of amide bond, is outlined by the black box. Peptide bonds link the amino acid residues in a peptide or protein by joining the � -amino group of one amino acid to the � -carboxyl group of the next as water is released.
The peptide bond has partial double-bond character, is rigid and planar, uncharged but polar, and almost always in the trans confi guration that reduces steric interference by the R groups.
Peptide bonds are resistant to conditions (such as the heat from a fever ) that can denature proteins and cause them to unfold. However, they are susceptible to cleavage by enzymes known as proteases or peptidases . [ Note: Strong acids or bases at high temperatures can nonenzymatically cleave peptide bonds.]
C COO–
H
Valine
Valylalanine
C+H3N COO–
H
CH3
Alanine
C C
H
CN COO–
H
CH3O
H
Free carboxyl end of peptide
CHH3C
CH3
H2O
Free amino end of peptide
Peptide bond
+H3N
CHH3C
CH3
+H3NTrans peptidebond
C NH
O Cα
CαC N
HO
CαCα
Cis peptidebond R RR
R
Ferrier_Unit01.indd 16Ferrier_Unit01.indd 16 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.3 QuestionPrimary Structure of Proteins
Sequencing large polypeptides involves cleavage reactions, as shown. Which sites in a peptide are susceptible to cleavage by the endopeptidase trypsin ? By cyanogen bromide?
What is the Edman degradation method?
What is the amino acid sequence of a nonapeptide if trypsin digestion yields three products (Asn, Met-Gln-Lys, and Ala-Gly-Met-Leu-Arg) and cyanogen bromide cleavage yields three products (Leu-Arg-Met, Gln-Lys-Asn, and Ala-Gly-Met)?
1. Cleave with trypsin
Peptide of unknown sequence
2. Determine sequence of peptides using the Edman method
What is the correct order?
Peptide BPeptide A
Peptide X Peptide Y
Peptide C
1. Cleave with cyanogen bromide2. Determine sequence of peptides using the Edman method
1
2
Original sequence of peptide
A B C ?A C B ?B A C ?B C A ?C A B ?C B A ?
Peptide of unknown sequence
Ferrier_Unit01.indd 17Ferrier_Unit01.indd 17 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.3 Answer Primary Structure of Proteins
Trypsin , an endopeptidase , cleaves at the carboxyl side of Lys and Arg residues within a peptide. [ Note: Exopeptidases remove the terminal amino acid.] Cyanogen bromide cleaves at the carboxyl side of Met residues.
The Edman degradation method chemically determines the sequence of amino acids through the sequential removal and identifi cation of the N-terminal amino acids in the small peptides generated from a polypeptide by cleavage reactions.
Based on the overlapping amino acids in the products of the trypsin (Asn, Met-Gln-Lys, and Ala-Gly-Met-Leu-Arg) and the cyanogen bromide (Leu-Arg-Met, Gln-Lys-Asn, and Ala-Gly-Met) cleav-age reactions, the amino acid sequence of the nonapeptide is Ala-Gly-Met-Leu-Arg-Met-Gln-Lys-Asn. [ Note: The sequence of amino acids in a protein is always written from the N-terminal to the C-terminal amino acid.]
1. Cleave with trypsin at lysine and arginine
Peptide of unknown sequence
2. Determine sequence of peptides using the Edman method
What is the correct order?
Peptide BPeptide A
Peptide X Peptide Y
Peptide C
1. Cleave with cyanogen bromide at methionine2. Determine sequence of peptides using the Edman method
1
2
Original sequence of peptide
A B C ?A C B ?B A C ?B C A ?C A B ?C B A ?
Peptide of unknown sequence
Ferrier_Unit01.indd 18Ferrier_Unit01.indd 18 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.4 QuestionSecondary Structure of Proteins
Which type of secondary structure is illustrated at right?
How does the orientation of the hydrogen bonds differ between the � -helix and the � -sheet structures?
In proteins (e.g., the GPCRs for glucagon and the catecholamines) that contain several � -helical membrane-spanning domains, why would Pro not be one of the amino acids found in these domains?
Side chains ofamino acidsextend outward
NH
C
OC
O
CN
CNH
HCO
C
CNH O
CC
O
OH
N
C
C
NH
NH
R
C
C
C
R
R
R
Ferrier_Unit01.indd 19Ferrier_Unit01.indd 19 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.4 Answer Secondary Structure of Proteins
The fi gure illustrates an � -helix , a right-handed, helical, secondary structural element commonly encountered in both fi brous and globular proteins.
The hydrogen bonds in a coiled �-helix are intrachain bonds that are parallel to the polypeptide back-bone, whereas those in a � -sheet (an extended structure) can be intra- or interchain bonds (depending on whether they form between sections of one polypeptide or between two polypeptides) that are perpendicular to the backbone. [ Note: � -Helices and � -sheets may be components of supersecondary structures (motifs), such as a � -barrel.]
Pro contains a secondary amino group that is not compatible with the right-handed spiral of the � -helix because (1) it cannot participate in the hydrogen bonding and (2) it causes a kink in the protein. Consequently, Pro is not found in the membrane-spanning domains of proteins such as GPCRs . [ Note : Amino acids with bulky or charged R groups can also disrupt formation of an � -helix.]
Side chains ofamino acidsextend outwardIntrachain
hydrogenbond
NH
C
OC
O
CN
CNH
HCO
C
CNH O
CC
O
OH
N
C
C
NH
NH
R
C
C
C
R
R
R
COOH
H
Proline
C
CH2
+H2N
H2CCH2
Ferrier_Unit01.indd 20Ferrier_Unit01.indd 20 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.5 QuestionTertiary Structure of Proteins
What type of molecular interaction involved in stabilizing the tertiary structure of a protein is shown?
What type of interaction would likely occur between Asp and Lys?
The tertiary structures of proteins (such as albumin) that function in the extracellular environment are stabilized by the formation of covalent links between the oxidized side chains of which sulfur-containing amino acid(s)?
CH2
C CH3
CH3CH3
CH2
CHH3C CH3
HC C
H
N
OH
H
CNH
C
O
Polypeptidebackbone
Isoleucine
Leucine
Ferrier_Unit01.indd 21Ferrier_Unit01.indd 21 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.5 Answer Tertiary Structure of Proteins
Shown are hydrophobic interactions between Ile and Leu, two amino acids with nonpolar R groups.
Ionic interactions ( salt bridges ) would likely occur between Asp (acidic R group) and Lys (basic R group).
Two sulfur-containing Cys residues, brought into close proximity by the folding of the peptide(s), are covalently linked through oxidation of their thiol side chains. The disulfi de bonds formed stabilize the tertiary structure of the folded peptide, preventing it from becoming denatured in the oxidizing extracellular environment. [ Note: Cys-containing albumin transports hydrophobic molecules (e.g., fatty acids and bilirubin) in the blood. Its levels are used as an indicator of nutritional status.]
CH2
C CH3
CH3CH3
CH2
CHH3C CH3
HC C
H
N
OH
H
CNH
C
O
Polypeptidebackbone
Isoleucine
Leucine
CCCCCCCCCCC 333333333333333333333333HHHHHHHHCHCHCHCHCHCHCHCHCHCHCHCCCCCCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCH333333333333333333333333333333333333333333333333333333333333333333
CH2
CHHHH333CCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCC CHCCCCCCCCCCCCCCCCCC 3
H
CNH
C
O
peptidekbone
Leucine
Hydrophobicinteractions
Cystine residue
H
CN
CH2H
S
C C
H
C
O
CH2
N
O
H
Two cysteine residues
H
CN
CH2H
SH
SH
C C
H
C
O
CH2
N
O
H
S
Polypeptidebackbone
Cystine residue
H
CN
HHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCHCC 2HHHHHH
S
C
O
Disulfidebond
Oxidant(for example, O2)
Ferrier_Unit01.indd 22Ferrier_Unit01.indd 22 5/2/14 7:08 PM5/2/14 7:08 PM
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.6 QuestionProtein Misfolding
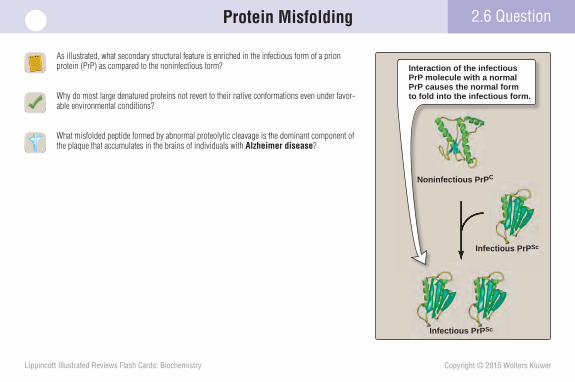
As illustrated, what secondary structural feature is enriched in the infectious form of a prion protein (PrP) as compared to the noninfectious form?
Why do most large denatured proteins not revert to their native conformations even under favor-able environmental conditions?
What misfolded peptide formed by abnormal proteolytic cleavage is the dominant component of the plaque that accumulates in the brains of individuals with Alzheimer disease ?
Infectious PrPSc
Infectious PrPSc
Infeectious PrP cSc
Interaction of the infectious PrP molecule with a normal PrP causes the normal form to fold into the infectious form.
Noninfectious PrPC
Ferrier_Unit01.indd 23Ferrier_Unit01.indd 23 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2.6 Answer Protein Misfolding
The � -sheet secondary structure is enriched in the infectious PrP Sc form of a PrP , which causes the transmissible spongiform encephalopathies , as compared to the noninfectious PrP C form that is � -helical rich.
The folding of most large proteins is a facilitated process that requires the assistance of proteins known as chaperones and ATP hydrolysis.
A � is the misfolded peptide produced by abnormal proteolytic cleavage of amyloid precursor protein by secretases . A � forms an extended � -sheet and spontaneously aggregates to form fi brils that are the dominant component of the amyloid plaque that accumulates in the brains of individuals with Alzheimer disease . [ Note: The � -sheets in A � have exposed hydrophobic amino acid residues. The hydrophobic effect drives the aggregation and precipitation of A � .]
Interaction of the infectious PrP molecule with a normal PrP causes the normal form to fold into the infectious form.
Infectious PrPSc
(contains a-sheets)
Infectious PrPSc
(contains a-sheets)
Noninfectious PrPC
(contains `-helix)
Aa
Cellmembrane
Amyloid
Spontaneousaggregation toform insolublefibrils of a-pleatedsheets
Ferrier_Unit01.indd 24Ferrier_Unit01.indd 24 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
3.1 QuestionMyoglobin Structure and Function
Which His residue (A or B), as shown, is the proximal His? What is its function? What is special about the location of this amino acid?
What type of secondary structure is most abundant in Mb? Does Mb have a quaternary structure?
Rhabdomyolysis (muscle destruction) caused by trauma, for example, is characterized by muscle pain, muscle weakness, and dark-colored urine. The dark color of the urine is the result of excretion of , a condition known as
.
Oxygenmolecule(O2)
Heme
F Helix E Helix
A
B
Fe
Ferrier_Unit01.indd 25Ferrier_Unit01.indd 25 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Choice A is the proximal His . It forms a coordination bond with the Fe 2 � in the heme prosthetic group . Polar His is located in the nonpolar crevice where heme binds.
Mb is rich in � -helices. Because it is a monomeric protein, Mb does not have a quaternary structure.
Rhabdomyolysis (muscle destruction) caused by trauma, for example, is characterized by muscle pain, muscle weakness, and dark-colored urine (shown). The dark color of the urine is the result of excretion of Mb , a condition known as myoglobinuria .
Oxygenmolecule(O2)
Heme
F Helix E Helix
Fe
Proximalhistidine(F8)
Distalhistidine(E7)
3.1 Answer Myoglobin Structure and Function
Ferrier_Unit01.indd 26Ferrier_Unit01.indd 26 5/2/14 7:08 PM5/2/14 7:08 PM
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
3.2 QuestionHemoglobin Structure and Function
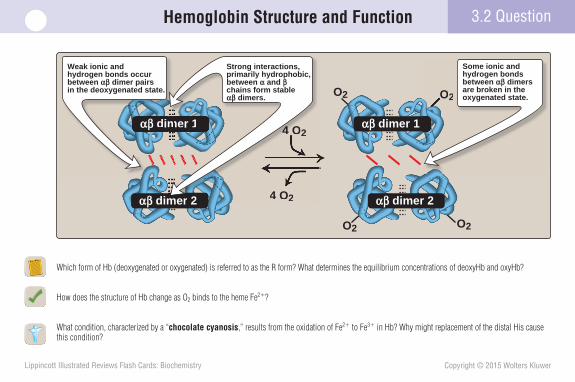
Which form of Hb (deoxygenated or oxygenated) is referred to as the R form? What determines the equilibrium concentrations of deoxyHb and oxyHb?
How does the structure of Hb change as O 2 binds to the heme Fe 2 � ?
What condition, characterized by a “ chocolate cyanosis ,” results from the oxidation of Fe 2 � to Fe 3 � in Hb? Why might replacement of the distal His cause this condition?
4 O2
O2 O2
O2O2
4 O2
αβ dimer 2
αβ dimer 1 αβ dimer 1
αβ dimer 2
αβ dim
O2
4 O2
4 O2
mememerr 2
mer 1m
Weak ionic and hydrogen bonds occurbetween αβ dimer pairs in the deoxygenated state.
Some ionic and hydrogen bonds between αβ dimers are broken in the oxygenated state.
Strong interactions,primarily hydrophobic, between α and β chains form stable αβ dimers.
Ferrier_Unit01.indd 27Ferrier_Unit01.indd 27 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
3.2 Answer Hemoglobin Structure and Function
The oxygenated, high-O 2 -affi nity form of Hb is referred to as the R form. The availability of O 2 determines the equilibrium concentrations.
The binding of O 2 to the heme Fe 2 � pulls the Fe 2 � into the plane of the heme. This causes salt bridges between the two �� dimers to rupture, thereby allowing movement that converts the T to the R form.
Methemoglobinemia , characterized by a “ chocolate cyanosis ” (dark-colored blood, bluish colored skin), results from the oxidation of Fe 2 � to Fe 3 � in Hb. Because the distal His stabilizes the binding of O 2 to the heme Fe 2 � , its replacement with another amino acid will favor oxidation of Fe 2 � to Fe 3 � and decreased binding of O 2 .
4 O2
O2 O2
O2O2
4 O2
"R," or relaxed, structure of oxyhemoglobin"T," or taut, structure of deoxyhemoglobin
αβ dimer 2
αβ dimer 1 αβ dimer 1
αβ dimer 2
αβ dim
O2
4 O2
4 O2
mememerr 2
mer 1m
Weak ionic and hydrogen bonds occurbetween αβ dimer pairs in the deoxygenated state.
Some ionic and hydrogen bonds between αβ dimers are broken in the oxygenated state.
Strong interactions,primarily hydrophobic, between α and β chains form stable αβ dimers.
Ferrier_Unit01.indd 28Ferrier_Unit01.indd 28 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
3.3 QuestionO2 Binding to Myoglobin and Hemoglobin
Use the fi gure to determine the approximate amount of O 2 that would be delivered by Mb and Hb when the pO 2 in the capillary bed is �26 mm Hg.
Why is the O 2 -dissociation curve for Hb sigmoidal and that for Mb hyperbolic?
How might RBC production be altered to compensate for changes to Hb that result in an abnormally high affi nity for O 2 ?
% S
atu
rati
on
wit
h O
2 (Y
)
00
40 80 120
100
Hemoglobin
Myoglobin
pO2 intissues
pO2 in lungs
50
Partial pressure of oxygen (pO2)(mm Hg)
Ferrier_Unit01.indd 29Ferrier_Unit01.indd 29 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
At a pO 2 of 26 mm Hg, Hb would have delivered 50% of its O 2 , while Mb would have delivered � 10%. Hb has a lower O 2 affi nity at all pO 2 values and a higher P 50 than does Mb, as shown. [ Note: P 50 is that pO 2 required to achieve 50% saturation of the O 2 -binding sites.]
Hb is a tetramer. The O 2 -dissociation curve for Hb is sigmoidal because the four subunits cooperate in binding O 2 . The fi rst O 2 binds to Hb with low affi nity. As subsequent subunits become occupied with O 2 , the affi nity increases such that the last O 2 binds with relative ease. Because Mb is a monomeric protein, it does not show cooperativity. Conse-quently, its O 2 -dissociation curve is hyperbolic , not sigmoidal.
RBC production typically is increased (a process known as erythrocytosis ) to compensate for changes to Hb that result in an abnormally high affi nity for O 2 : more RBCs � more Hb � more O 2 carried.
3.3 Answer O2 Binding to Myoglobin and Hemoglobin
% S
atu
rati
on
wit
h O
2 (Y
)
00
40 80 120
P50 = 1 P50 = 26
100
Hemoglobin
Myoglobin
pO2 intissues
pO2 in lungs
50
Partial pressure of oxygen (pO2)(mm Hg)
tio
n w
ith
O2
(Y)
100
Hemoglo nobin
Myoglobin
pO2 intissues
pO2 in lungs
50
The oxygen-dissociation curve for Hb is steepest at the oxygen concentrations that occur in the tissues. This permits oxygen delivery to respond to small changes in pO2.
Ferrier_Unit01.indd 30Ferrier_Unit01.indd 30 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
3.4 QuestionAllosteric Effects
Which curve (A or B), as shown, represents the lower pH?
List two other allosteric effectors that, when increased, result in a rightward shift of the Hb O 2 -dissociation curve. What does this shift refl ect? Do these allosteric effectors stabilize the R or the T form of Hb?
How does the binding of CO 2 to Hb stabilize Hb’s deoxygenated form?
What is the Bohr effect?
% S
atu
rati
on
wit
h O
2 (Y
)
Partial pressure of oxygen (pO2)(mm Hg)
00
40 80 120
100
B
A
50
Ferrier_Unit01.indd 31Ferrier_Unit01.indd 31 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Curve B represents the lower pH (higher H� concentration).
Increased amounts of CO 2 and 2,3-BPG also result in a rightward shift of the Hb O 2 -dissociation curve. The shift refl ects increased off-loading (delivery) of O 2 to the tissues. These allosteric effectors stabilize the T ( deoxygenated ) form of Hb, enabling O 2 delivery.
When CO 2 binds to the amino termini of the four Hb subunits, forming carbaminohemoglobin , the negative charge is used to form a salt bridge that helps to stabilize Hb’s deoxygenated (T) form.
Hb � NH 2 � CO 2 →← Hb � NH � COO � � H �
The Bohr effect refers to the increase in O 2 delivery when CO 2 or H � increases. In actively metabolizing tissue, Hb binds CO 2 and H � and releases O 2 . The process is reversed in the lungs.
3.4 Answer Allosteric Effects
Fe2+ Fe2+
Fe2+ Fe2+
O2
O2
O2
O2
Oxyhemoglobin
Fe2+ Fe2+
Fe2+ Fe2+
NHCOO–
NHCOO–
Carbaminohemoglobin
CO2 O2
O2CO2
O2CO2
C
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO2222222222222222222222222222OCCCCCCCCCCCOOOOOOOOOOOOOOOOOOCOOOOCOCCCCOCCCCCCCCCOCOOCOC 22222222222222222222
CO2 binds tohemoglobin.
O2 is released from hemoglobin.
O2 binds to hemoglobin.
CO2 is releasedfrom hemoglobin.
TISSUES
LUNGS
% S
atu
rati
on
wit
h O
2 (Y
)
Partial pressure of oxygen (pO2)(mm Hg)
00
40 80 120
100
pH = 7.2
pH = 7.6
50
O2
(
pH = 7.2
(Y) 100
pH = 7.6
Decrease in pH results in decreased oxygen affinity of hemoglobin and, therefore, a shift to the right in the oxygen-dissociation curve.
At lower pH, agreater pO2 isrequired to achieve any given oxygensaturation.
Ferrier_Unit01.indd 32Ferrier_Unit01.indd 32 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
3.5 QuestionMinor Hemoglobins
How does the subunit composition of HbF, as illustrated, infl uence the O 2 affi nity of HbF?
What form of Hb replaces HbF, and when does this occur?
What form of Hb is measured to assess glycemic control in individuals with diabetes ?
HbA α2β2
FormChain
composition
HbA1c α2β2-glucose
α2γ2HbF
HbA2 α2δ2
Ferrier_Unit01.indd 33Ferrier_Unit01.indd 33 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
HbF contains 2 � and 2 � subunits. Relative to the � subunits, the � subunits have a reduced affi nity for 2,3-BPG. This results in HbF having an increased affi nity for O 2 . [ Note: HbF is needed to obtain O 2 from maternal HbA, and its increased affi nity for O 2 enables this process.]
HbF is the major Hb found in the fetus and the newborn but represents � 2% of the Hb in most adults because it is replaced by HbA (2 � and 2 � subunits) by about 6 months after birth.
Nonenzymatically glycosylated ( glycated ) Hb, HbA 1c , is measured because its concentration in the blood is a refl ection of the average blood glucose concentration over the previous 3 months. [ Note: The goal value for HbA 1c in adults with diabetes is � 6.5%.]
3.5 Answer Minor Hemoglobins
Months before and after birth
Per
cen
tag
e o
f to
tal g
lob
in c
hai
ns
–9 –6 –3 3 6 90
25
50
0
25
50
`
a
c
d
f
y
`-Globin-like chains
a-Globin-like chains
Time of birth
0
HbA α2β2
FormChain
compositionFraction of
total hemoglobin
HbA1c α2β2-glucose
90%
3%–9%
α2γ2HbF <2%
HbA2 α2δ2 2%–5%
Ferrier_Unit01.indd 34Ferrier_Unit01.indd 34 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
3.6 QuestionHemoglobinopathies
How do the sickled RBCs illustrated cause infarction (cell/tissue death due to obstruction of blood fl ow)?
Which type of globin chain precipitates in � -thalassemia ?
Is HbC disease a sickling or nonsickling disease? Why?
Hydrophobic pocket
Fiber
?
Fibers
β-6-Valineβ Chain
...GTG...
...GAG...
Val.His.Leu.Thr.Pro.Glu.Glu.Lys
Val.His.Leu.Thr.Pro.Val.Glu.Lys
ibeFibeFibeibebebebebbFFibeibebebFF beibeFFFF beFFF rsrrsrsrsssssssssssrsssssrrrsrsrssssrsssrrsrTTTTTG
...G
Hi L Th P Gl G
G...
GAG...
β 6 V li
Glu
Glu.Lys
Glu.Lys
u Lys
L
3 Intracellular fibers of HbS distort the erythrocyte.
1 A point mutationin the DNA codes for structurally altered HbS.
2 In the deoxygenated state, HbS polymerizesinto long, rope-like fibers.
α1
α2
β1
β2
α1
α2
β1
β2
α1
α2
β1
β2
α1
α2
β1
β2
Ferrier_Unit01.indd 35Ferrier_Unit01.indd 35 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
3.6 Answer Hemoglobinopathies
Hydrophobic pocket
Fiber
Fibers
β-6-Valineβ Chain
...GTG...
...GAG...
Val.His.Leu.Thr.Pro.Glu.Glu.Lys
Val.His.Leu.Thr.Pro.Val.Glu.Lys
FiberFiberFFiberiberiberiberiberberbeberbbb rrFFiberb riberberF rF rerF ssssssssssssssssssssssssssssssGTTTTTG
...G
al.His.Leu.Thr.Pro.Glu
TG...
.GAG.....
β-6-Valine
l.Gl
u.Gl
u.Lys
u.Lys
3 Intracellular fibers of HbS distort the erythrocyte.
1 A point mutationin the DNA codes for structurally altered HbS.
2 In the deoxygenated state, HbS polymerizesinto long, rope-like fibers.
Rigid erythrocytes occlude blood flow in the capillaries.
4
α1
α2
β1
β2
α1
α2
β1
β2
α1
α2
β1
β2
α1
α2
β1
β2
Sickled RBCs cause infarction because the rigid polymer of HbS makes the sickled cells less deformable than the nonsickled cells and, therefore, less able to move through blood vessels. This can cause a blockage that obstructs the delivery of O 2 .
� -Thalassemia is a defect in the ability to make � globin. Consequently, it is the excess � -globin chains that precipitate.
HbC disease is a nonsickling disorder because Lys (a polar amino acid) is substituted for polar Glu. In contrast, in HbS disease ( SCA ), nonpolar Val is substituted for Glu.
Ferrier_Unit01.indd 36Ferrier_Unit01.indd 36 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
3Case Card
A woman, age 70 years, activates her medical alert system and is transported to the hospital by ambulance. The patient tells you she has a headache , feels weak , and is nauseated and drowsy . She vomited several times at home over the last few hours. She thinks she has the fl u. Upon talking with her, you discover that she has been without power for 2 days due to a recent snowstorm and has been using a kerosene space heater to keep warm. You suspect CO poisoning, send a blood sample to the clinical laboratory for analysis, and begin O2 therapy .
Why would CO poisoning cause an affected individual to feel weak and drowsy?
Ferrier_Unit01.indd 37Ferrier_Unit01.indd 37 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
CO is a colorless, odorless gas produced by incomplete combustion of hydrocarbons. CO binds reversibly to the Fe 2 � of Hb, forming HbCO (known as carboxyhemoglobin ). CO competes with O 2 and binds with a 200-fold higher affi nity. The bound CO stabilizes the R ( oxygenated ) form of Hb and shifts the O 2 -saturation curve to the left. Because CO does not easily dissociate from Hb, O 2 is not delivered. Treatment with O 2 is required to displace the CO. The patient’s blood test revealed that HbCO accounted for 16% of her Hb (reference value, � 2%; higher in smokers and urban dwellers). [ Note: At higher concen-trations of CO, use of hyperbaric O 2 therapy (100% O 2 under pressure) may be required to displace the CO.]
CO poisoning decreases O 2 delivery.
3 Case Card
Carbon monoxide (CO)
Carboxy-hemoglobin
High affinity for CO
“Left shift” of O2-saturation curve
Hyperbolic O2 saturation curve
characterized by
leads to
leads to
Stabilization ofthe relaxed state
leads to
binds
Effects ofcarbon monoxide
Increased affinity for bound O2
leads to
leads to
O2
Co
nte
nt
(ml/1
00 m
l blo
od
)
Partial pressure of oxygen (pO2)(mm Hg)
00
40 80 120
20
50% CO-Hb
0% CO-Hb
10A
Ferrier_Unit01.indd 38Ferrier_Unit01.indd 38 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
4.1 QuestionCollagen
In the collagen � chain shown, what amino acid (present at every third position) is represented by the black ball? What is special about this amino acid?
Which is/are descriptors of type 1 collagen? It is: A. a fi brous protein. B. an extracellular (secreted) protein. C. a fi bril-forming collagen. D. composed of three � -helical proteins. E. found only in bone.
What targets the prepro- � chains of collagen to the RER? Collagen α chain
Ferrier_Unit01.indd 39Ferrier_Unit01.indd 39 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
The black ball at every third position shown represents Gly. Gly is the smallest amino acid, having only an H for a side chain. Gly fi ts into the restricted space where the three � chains come together.
Type 1 collagen is: A. a fi brous protein. TRUE . B. an extracellular (secreted) protein. TRUE . C. a fi bril-forming collagen. TRUE . D. composed of three � -helical proteins. FALSE . Although the chains in
collagen are called � chains, the abundance of Pro in these chains prevents formation of the � helix.
E. found only in bone. FALSE . It also is found in skin, blood vessels, tendon, and the cornea of the eye, and is the most abundant protein in the body.
An amino acid sequence at the N terminus ( N-terminal signal sequence ) targets proteins such as the prepro- � chains of collagen to the RER .
4.1 Answer Collagen
Collagen α chain
Glycine
Ferrier_Unit01.indd 40Ferrier_Unit01.indd 40 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
4.2 QuestionCollagen Synthesis
What enzyme catalyzes the reaction shown? Where does the reaction occur?
What is the function of the reaction in the formation of collagen?
Which other amino acid undergoes the same posttranslational reaction during collagen synthesis?
A defi ciency in vitamin C ( ascorbate ), the coenzyme for the reaction shown, causes , a disease characterized by the production of collagen with decreased tensile strength.
CO
H
C
CH2
HN
CH2
H2C
CO
H
C
CH2
HN
CHH2C
OH
α-Ketoglutarate
Succinate + CO2
O2
H2O
Ascorbate, Fe2+
Prolyl residue
Pro-α chain
Hydroxyprolyl residue
Ferrier_Unit01.indd 41Ferrier_Unit01.indd 41 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
4.2 Answer
Prolyl hydroxylase , an enzyme of the RER, catalyzes the hydroxylation of Pro to Hyp.
Hydroxylation maximizes formation of the interchain H-bonds that stabilize the triple helical structure of collagen.
Lys also undergoes posttranslational hydroxylation to Hyl (which is formed by lysyl hydroxylase ) during collagen synthesis. [ Note: Hyl is a substrate for O-glycosylation.]
A defi ciency in vitamin C ( ascorbate ), the coenzyme for the reaction shown, causes scurvy . Vitamin C is the coenzyme for both prolyl hydroxylase and lysyl hydroxylase . Without the additional stability provided by Hyp and Hyl, collagen has decreased tensile strength. Patients with scurvy may have bruise-like ecchymoses (shown) as a result of blood vessel fragility.
Collagen Synthesis
CO
H
C
CH2
HN
CH2
H2C
CO
H
C
CH2
HN
CHH2C
OH
α-Ketoglutarate
Succinate + CO2
O2
H2O
Ascorbate, Fe2+
Prolyl residue
Pro-α chain
Hydroxyprolyl residue
Prolyl hydroxylase
Ferrier_Unit01.indd 42Ferrier_Unit01.indd 42 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Does the removal of the N- and C-terminal propeptides from procollagen (as shown) occur intracellularly or extracellularly? What is the fate of the triple-helical tropocollagen formed in the cleavage reaction?
Why are the disulfi de bonds in the C-terminal propeptide domain of procollagen important for the formation of functional collagen?
What name is given to the group of diseases that may result from defects in processing events during collagen synthesis?
4.3 Question Collagen Synthesis
N-terminalpropeptide
C-terminalpropeptide
S S
S S
SS
S S
SS
S S
S S
S S
S SS S
S S
Ferrier_Unit01.indd 43Ferrier_Unit01.indd 43 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Removal of the terminal N- and C-propeptides from procollagen occurs extracellularly and is catalyzed by N-terminal and C-terminal procollagen peptidases . The triple-helical tropocollagen molecules formed in the cleavage reaction spontaneously associate to form collagen fi brils that are organized into an overlapping parallel array. The array is then cross-linked to produce collagen fi bers . [ Note: The spontaneous association of tropocollagen is an example of the hydrophobic effect.]
The disulfi de bonds in the C-terminal propeptide domain bring the three � chains into correct alignment for triple helix formation. They are important for the formation of functional collagen.
Collagenopathies are diseases that may result from defects in collagen-processing events, such as removal of the terminal propeptides and hydroxylation of proline.
Collagen Synthesis4.3 Answer
N-terminalpropeptide
C-terminalpropeptide
S S
S S
SS
S S
SS
S S
S S
S S
S SS S
S S
Ferrier_Unit01.indd 44Ferrier_Unit01.indd 44 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
What enzyme catalyzes the oxidative deamination reaction shown?
Does the reaction occur within or outside of a cell? What is the function of the reaction?
Menkes syndrome is a disease of severe Cu 2 � defi ciency. Why is connective tissue fragility characteristic of this syndrome?
Collagen Synthesis 4.4 Question
HCH2 CH2 CC
NH
OH CH2CH2
C
HN
OC CH2
O
H
Lysineresidue
Allysineresidue
NH2 CH2C
Lysineresidue HCH2 CH2 C
C
NH
OCH2CH2NH2
O2
NH3 + H2O
HCC
NH
OH
C
HN
OC NH
CH2
Collagenchain
Collagenchain
CH2CH2 CH2 CH2 CH2CH2 CH2 CH2
Ferrier_Unit01.indd 45Ferrier_Unit01.indd 45 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
4.4 Answer Collagen Synthesis
Lysyl oxidase catalyzes the oxidative deamination of Lys to allysine.
The reaction occurs outside of a cell (extracellularly). It forms reactive aldehydes (such as allysine) that condense with Lys residues in neighboring collagen molecules to form the covalent cross-links characteristic of mature collagen. [ Note: Two allysine residues can form cross-links via aldol condensation.]
Connective tissue fragility is characteristic of Menkes syndrome because lysyl oxidase is a Cu 2 � -requiring enzyme. Decreased activity of this enzyme, as a consequence of decreased Cu 2 � , would impair the fi nal step in collagen synthesis. [ Note: X-linked Menkes syndrome ( kinky hair disease ) is the consequence of a defect in the transporter that moves dietary Cu 2 � out of intestinal cells. This decreases Cu 2 � availability for the rest of the body. In addition to lysyl oxidase , other Cu 2 � -requiring enzymes ( cytochrome c oxidase , dopamine hydroxylase , superoxide dismutase , and tyrosinase ) are affected.]
HCH2 CH2 CC
NH
OH CH2CH2
C
HN
OC CH2
O
H
Lysineresidue
Allysineresidue
NH2 CH2C
Lysineresidue
Lysyl oxidase
HCH2 CH2 CC
NH
OCH2CH2NH2
O2
NH3 + H2O
HCC
NH
OH
C
HN
OC NH
CH2
Collagenchain
Collagenchain
CH2CH2 CH2 CH2 CH2CH2 CH2 CH2
Cu2+
Ferrier_Unit01.indd 46Ferrier_Unit01.indd 46 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
4.5 Question Collagenopathies
Which heritable collagen-based disease is characterized by stretchy skin , as shown? Which type of collagen is affected in this disease? Which type of collagen is mutated in the vascular form of this disease that is associated with potentially lethal arterial rupture?
Which heritable collagen-based disease is characterized by bone fragility (as shown) and is the most severe form of the disease? Which type of collagen is affected in this disease?
Ferrier_Unit01.indd 47Ferrier_Unit01.indd 47 5/2/14 7:08 PM5/2/14 7:08 PM
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Collagenopathies4.5 Answer
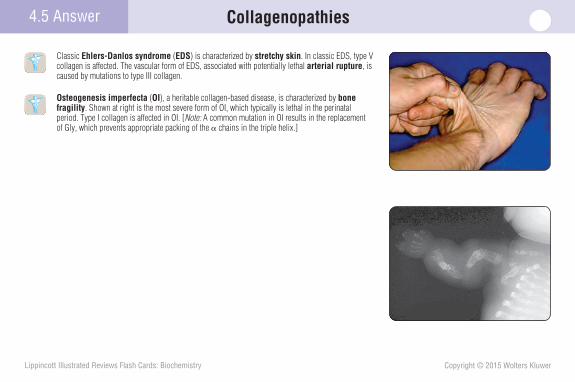
Classic Ehlers-Danlos syndrome ( EDS ) is characterized by stretchy skin . In classic EDS, type V collagen is affected. The vascular form of EDS, associated with potentially lethal arterial rupture, is caused by mutations to type III collagen.
Osteogenesis imperfecta ( OI ), a heritable collagen-based disease, is characterized by bone fragility . Shown at right is the most severe form of OI, which typically is lethal in the perinatal period. Type I collagen is affected in OI. [ Note: A common mutation in OI results in the replacement of Gly, which prevents appropriate packing of the � chains in the triple helix.]
Ferrier_Unit01.indd 48Ferrier_Unit01.indd 48 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
4.6 QuestionElastin
In elastin, a connective tissue protein that forms an extensively interconnected network with rubberlike properties, the interconnections are formed by cross-links, as shown. What name is given to these cross-links?
What is the role of fi brillin in the production of elastin?
Why does a defi ciency of the protease that normally destroys neutrophil elastase lead to lung pathology? Why might the liver also be affected?
CC C
C CN
CH2
CH2
CH2
CCHN
HO
CH2
CH2
CH2
CH2
CC NHHO
HCH2 CH2 CC
NH
OH CH2CH2
C
HN
OC
+
?cross-link
Ferrier_Unit01.indd 49Ferrier_Unit01.indd 49 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
4.6 Answer Elastin
Desmosine cross-links between three allysine side chains and one unaltered lysyl side chain provide the extensive interconnections that give elastin its mechanical ability to stretch.
Fibrillin is one of the glycoprotein microfi brils that functions as a scaffold onto which tropo-elastin is deposited. [ Note: Once deposited, tropoelastin undergoes the lysyl oxidase– mediated oxidative deamination required for cross-link formation.]
AAT is a protease inhibitor that normally destroys neutrophil elastase . The elastase , a protease , can destroy elastin in the walls of lung alveoli, thereby causing emphysema if unopposed by AAT. AAT defi ciency in the lungs is the result of mutations that cause polymerization and reten-tion of AAT in the liver, the primary site of its synthesis. Hepatic retention can damage the liver and result in cirrhosis .
CC C
C CN
CH2
CH2
CH2
CCHN
HO
CH2
CH2
CH2
CH2
CC NHHO
HCH2 CH2 CC
NH
OH CH2CH2
C
HN
OC
+
Desmosinecross-link
α1-Antitrypsin (AAT) deficiency
• In the alveoli, elastase released by activated and degenerating neutrophils is normally inhibited by AAT.
• Genetic defects in AAT can lead to emphysema (lung) and cirrhosis (liver). Smoking increases risk.
• The deficiency of elastase inhibitor can be reversed by weekly intravenous administration of AAT.
Ferrier_Unit01.indd 50Ferrier_Unit01.indd 50 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Enzyme Nomenclature and Properties 5.1 Question
Which one of the six major classes of enzymes is illustrated by the reaction shown?
Why is NAD said to function as a coenzyme– cosubstrate (not a coenzyme–prosthetic group) in enzymatic reactions such as the one shown?
McArdle disease type V GSD is caused by a defi ciency in muscle glycogen phosphorylase ( myophosphorylase ), an enzyme of glycogen degradation. How will a decrease in P i affect the activity of this enzyme?
C COO–HCH3
Lactate Pyruvate
NAD+ NADH+C COO–CH3
O2e-2H+
H++
OH
+
Ferrier_Unit01.indd 51Ferrier_Unit01.indd 51 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Enzyme Nomenclature and Properties5.1 Answer
Shown is an enzyme that belongs to the class known as oxidoreductases (that most commonly function as dehydrogenases ).
NAD functions as a coenzyme–cosubstrate in enzymatic reactions because it is only loosely bound to the enzyme and leaves the enzyme in a changed form. [ Note: FAD is an example of a coenzyme–prosthetic group. It is tightly bound to the enzyme and is returned to its original form on the enzyme.]
Based on its designation as a phosphorylase , myophosphorylase (defi cient in McArdle disease ) uses P i to cleave bonds in glycogen. Therefore, a decrease in P i will decrease enzymatic activity. [ Note: The enzyme cleaves the �(1→4) glycosidic bond in glycogen, thereby generating the phosphorylated product glucose 1-P.]
C COO–HCH3
Lactate Pyruvate
NAD+ NADH+C COO–CH3
O2e-2H+
Lactatedehydrogenase
H++
OH
+
Ferrier_Unit01.indd 52Ferrier_Unit01.indd 52 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Enzyme Properties 5.2 Question
Enzymes are protein that increase the of a chemical reaction. As shown, they contain an , which is a small on the surface of the enzyme to which a specifi c binds, forming an
complex leading to product formation. Binding may cause a conformational change in the enzyme, a process known as .
What is the difference between a holoenzyme and an apoenzyme?
Elevated blood ALP suggests a pathology. ALP is found primarily in the liver as ALP-1 and in bone as ALP-2 . Levels of the two forms can help differentiate between a liver and a bone pathology. What term is used to describe the tissue-specifi c forms of an enzyme?
?
?
Enzyme
Ferrier_Unit01.indd 53Ferrier_Unit01.indd 53 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Enzyme Properties5.2 Answer
Enzymes are protein catalysts that increase the rate ( velocity ) of a chemical reaction. As shown, they contain an active site , which is a small pocket ( or cleft) on the surface of the enzyme to which a specifi c substrate binds, forming an enzyme-substrate complex leading to product formation. Binding may cause a conformational change in the enzyme, a process known as induced fi t . [ Note: RNA catalysts are referred to as ribozymes.]
A holoenzyme is an enzyme with its nonprotein component, and an apoenzyme is missing the nonprotein component. The nonprotein component is required for enzymic activity.
Isozyme ( isoenzyme ) is the term used to describe the tissue-specifi c forms of an enzyme, such as ALP-1 and ALP-2 . Isozymes catalyze the same reaction but differ in their amino acid composition (primary structure).
Substrate
Active site
Enzyme
Ferrier_Unit01.indd 54Ferrier_Unit01.indd 54 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
5.3 QuestionHow Enzymes Work
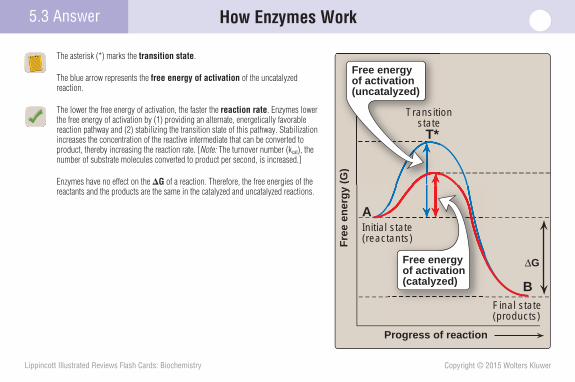
What name is given to that region of the curve shown at right marked by the asterisk (*)?
Which arrow (blue or red) represents the free energy of activation of the uncatalyzed reaction?
How do enzymes dramatically increase the reaction rate relative to the uncatalyzed reaction?
How do enzymes affect the G of a reaction?
Progress of reaction
Fre
e en
erg
y (G
)
Initial state(reactants)
*
Final state(products)
A
B
ΔG
Ferrier_Unit01.indd 55Ferrier_Unit01.indd 55 5/2/14 7:08 PM5/2/14 7:08 PM
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
How Enzymes Work5.3 Answer
The asterisk (*) marks the transition state .
The blue arrow represents the free energy of activation of the uncatalyzed reaction.
The lower the free energy of activation, the faster the reaction rate . Enzymes lower the free energy of activation by (1) providing an alternate, energetically favorable reaction pathway and (2) stabilizing the transition state of this pathway. Stabilization increases the concentration of the reactive intermediate that can be converted to product, thereby increasing the reaction rate. [ Note: The turnover number (k cat ), the number of substrate molecules converted to product per second, is increased.]
Enzymes have no effect on the � G of a reaction. Therefore, the free energies of the reactants and the products are the same in the catalyzed and uncatalyzed reactions.
Progress of reactionF
ree
ener
gy
(G)
Initial state(reactants)
Final state(products)
A
B
Transitionstate
T*
ΔG
(G)
Transitistate
T*
Free energyof activation(uncatalyzed)
statetants)
Free energyof activation(catalyzed)
Ferrier_Unit01.indd 56Ferrier_Unit01.indd 56 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
5.4 QuestionFactors Affecting Reaction Velocity
What processes are shown at right? What effect do they have on the velocity of an enzyme-catalyzed reaction?
What general name is given to the enzyme that catalyzes the forward reaction?
What other environmental factors infl uence the velocity of an enzyme-catalyzed reaction?
Tyrosinemia type 1 ( infantile tyrosinemia ) is caused by a defi ciency in fumarylacetoacetate hydrolase that catalyzes the last reaction in the degradation of Tyr. It is treated with a drug that inhibits an enzyme earlier in the pathway. What is the biochemi-cal rationale for this therapy?
Enzyme
OH
Enzyme
OP03
ATP ADP
HPO4 H2O2−
2−
Ferrier_Unit01.indd 57Ferrier_Unit01.indd 57 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Factors Affecting Reaction Velocity5.4 Answer
Phosphorylation and dephosphorylation , covalent modifi cations to proteins, are shown. Depending on the enzyme, these modifi cations may increase or decrease the velocity of an enzyme-catalyzed reaction. [ Note: The change in enzyme activity is the result of a conformational change in the enzyme caused by the covalent modifi cation.]
Kinases catalyze phosphorylation reactions using ATP as the phosphate source. They are opposed by phosphatases .
Changes in the concentration of the enzyme, coenzyme, and substrate; temperature; and pH are additional factors that infl uence the velocity of an enzyme-catalyzed reaction.
Nitisinone is prescribed for infantile tyrosinemia because it decreases production of the substrate for the hydrolase , thereby decreasing the velocity of the reaction. Addition-ally, by preventing substrate accumulation, this substrate reduction therapy prevents entry of the substrate into side reactions that produce harmful products.
Enzyme
OH
Enzyme
OP03
ATP ADP
HPO4 H2O
Proteinkinase
Phospho-protein
phosphatase2−
2−
Ferrier_Unit01.indd 58Ferrier_Unit01.indd 58 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
5.5 QuestionMichaelis–Menten Kinetics
Supply the missing terms in the Michaelis–Menten equation shown.
What is the steady state assumption?
True or false: When the [S] is much less than the K m , the V 0 is proportional to [S], and the reaction is said to be fi rst order.
If 1/V 0 and 1/[S] were plotted, what shape would result? What is the X intercept on this plot? The Y intercept?
If a mutation to the gene that codes for an enzyme results in a 12-fold increase in the K m of the enzyme for its physiologic substrate, what effect has the mutation had on the affi nity of the enzyme for the substrate?
vo = Vmax ?Km + ?
Ferrier_Unit01.indd 59Ferrier_Unit01.indd 59 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
[S] is the missing term in the Michaelis–Menten equation .
The steady state assumption is that the concentration of ES does not change with time. That is, the rate of formation of ES is equal to that of the breakdown of ES to E � S and E � P.
True: When [S] is much less than the K m , the V 0 is proportional to [S], and the reaction is said to be fi rst order , as shown.
A straight line would be seen if 1/V 0 and 1/[S] were plotted. The X intercept on this Lineweaver-Burk plot is � 1/K m , and the Y intercept is 1/V max .
Increasing the K m of the enzyme for its physiologic substrate decreases the affi nity of the enzyme for the substrate.
5.5 Answer Michaelis–Menten Kinetics
Vmax
Vmax
Rea
ctio
n v
elo
city
(v o
)
Km
[Substrate]00
Km
[Subst00
At low concentrations ofsubstrate ([S] << Km), the velocity of the reaction is first order . That is, it is proportional to substrateconcentration.
2
vo = Vmax [S]Km + [S]
Ferrier_Unit01.indd 60Ferrier_Unit01.indd 60 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
5.6 QuestionEnzyme Inhibition
What type of inhibition is shown?
Which line represents the uninhibited enzyme? Which line represents the highest concentration of inhibitor?
What type of inhibition results in a decrease in the apparent V max ? Is K m also affected by the inhibitor?
Orlistat, a weight-loss drug, covalently bonds to lipases that hydrolyze dietary fat (TAGs) and inhibits their enzymic activity. Is this an example of reversible or irreversible enzyme inhibition?
1vo
1[S]
Ferrier_Unit01.indd 61Ferrier_Unit01.indd 61 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Competitive inhibition is shown, in which the inhibitor and the S compete for the same binding site on the enzyme. As a result, the apparent K m increases because a higher [S] is required to achieve 1/2 V max .
The blue line represents the uninhibited enzyme. The black line represents the highest concentration of inhibitor.
Noncompetitive inhibition results in a decrease in apparent V max . K m is not affected. [ Note: In noncompetitive inhibition, the inhibitor does not compete with the S and can bind the E and the ES complex (as shown).]
Covalent bonding of an inhibitor to an enzyme (as seen with orlistat ) irreversibly inhibits the enzyme. [ Note: Covalent modifi cation of an enzyme, such as is seen with the acetylation of COX by aspirin, also causes irreversible enzyme inhibition.]
Enzyme Inhibition5.6 Answer
Enzyme (E)
Inhibitor (I)
Substrate (S)
ES complex
EI complex(inactive)
ESI complex(inactive)
1vo
1[S]
Competitiveinhibitor
Noinhibitor
(1 mM)
(3 mM)
1Vmax
1Km
Ferrier_Unit01.indd 62Ferrier_Unit01.indd 62 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Allosteric Enzyme Regulation 5.7 Question
Which curve shown represents an allosteric enzyme?
Will a positive allosteric effector that infl uences the K 0.5 shift the V 0 versus [S] plot to the left or to the right?
Sialuria (sialic acid in the urine) is a rare, AD condition caused by a mutation in the rate-limiting enzyme of sialic acid synthesis. The mutation decreases the en-zyme’s ability to bind CMP–sialic acid, the end product of the pathway. Why does this mutation result in increased production (and excretion) of sialic acid?
Vmax
Rea
ctio
n v
elo
city
(v o
)
[Substrate]00
Ferrier_Unit01.indd 63Ferrier_Unit01.indd 63 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
5.7 Answer Allosteric Enzyme Regulation
The green curve, with its sigmoidal shape , represents an allosteric enzyme .
A positive allosteric effector that infl uences K 0.5 will shift the V 0 versus [S] plot to the left (as shown), refl ecting a lower K 0.5 . [ Note: K 0.5 is that [S] required to achieve half maximal velocity.]
The CMP–sialic acid is a feedback inhibitor of the pathway. Loss of this allosteric inhibition (as the result of decreased binding to the regulated enzyme) results in overproduction of sialic acid and, consequently, sialuria .
Vmax
Rea
ctio
n v
elo
city
(v o
)
[Substrate]00
[Substrate]
ax
Enzymes following Michaelis-Menten kinetics show hyperbolic curve.
Allosteric enzymes show sigmoid curve.
Rea
ctio
n v
elo
city
(v o
)
[Substrate]K0.5 K0.5 K0.5
Vmax
+
Ferrier_Unit01.indd 64Ferrier_Unit01.indd 64 5/2/14 7:08 PM5/2/14 7:08 PM
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
5Case Card
A 66-year-old female is seen in the emergency department in the late evening. She was driven to the hospital by her husband. The woman reports she has had a “pressure” on her chest for the last few hours. She denies overt chest pain; jaw, neck, shoulder, arm, or epigastric pain; shortness of breath ( dyspnea ); and sweating ( diaphoresis ). The pressure does not seem to increase with exertion. The patient’s history is remarkable for hyperlipidemia that is being treated with diet and drugs. There is no family history of heart disease. The patient’s heart and respiratory rates are elevated. Blood is drawn and sent to the clinical laboratory for measurement of cardiac biomarkers. Sublingual nitroglycerin is given. An EKG is performed, and the results are consistent with a myocardial infarction ( MI ). Cardiac biomarker measurements reveal elevated levels of CK , the CK- MB (the isoform found predominately in cardiac muscle) to total CK ratio, and cTnI (a cardiac troponin).
What would be the characteristics of an ideal cardiac biomarker?
Ferrier_Unit01.indd 65Ferrier_Unit01.indd 65 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
5 Case Card
CK -MB is one of three isoforms of CK , an intracellular enzyme. CK -MB is the form found virtually exclusively in the heart, with CK -MM found in the brain, and CK -BB found in skeletal muscle. Troponins ( Tn ) are nonenzymatic, intracellular, regulatory proteins involved in contractility of skeletal and cardiac muscle. Both CK -MB and cTnI become elevated in the blood as a result of tissue necrosis in an MI, but their patterns are different. Although both cardiac biomarkers rise early in an MI, cTnI remains elevated for up to 10 days, whereas CK -MB remains elevated for up to 3 days.
An ideal cardiac biomarker would be (1) released by injury, (2) cardiac specifi c, (3) elevated shortly after the injury and remaining so for an extended period, and (4) easily measured.
Infarction
Upperreferencelimit
4N M
ult
iple
s o
f th
e u
pp
erre
fere
nce
lim
it
8
Days after onset of acute myocardial infarction
2
5
10
20
50
1
0
Cardiac troponin
CK-MB
A
Ferrier_Unit01.indd 66Ferrier_Unit01.indd 66 5/2/14 7:08 PM5/2/14 7:08 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
6.1 Question Free Energy Change
Will the reaction shown proceed spontaneously in the forward (B➔A) or the reverse (A➔B) direction?
Is the � G of this reaction positive or negative at equilibrium?
Compare and contrast � G and � G 0 .
Glutamine synthetase catalyzes the amidation of Glu to Gln. However, the reaction is endergonic. How is this problem solved in cells (e.g., skeletal myocytes) that synthesize Gln?
Initial state
Transitionstate
Progress of reaction
Fre
e en
erg
y (G
)
A
B A
B
Final state
Ferrier_Unit02.indd 67Ferrier_Unit02.indd 67 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Free Energy Change6.1 Answer
The reaction shown will proceed spontaneously in the reverse (A➔B) direction because the � G of the forward direction is positive. The forward reaction is endergonic , and it will not proceed unless energy is provided.
At equilibrium , the � G � 0 (neither positive nor negative). [ Note: Equilibrium is the point at which no net chemical change occurs. Therefore, for A➔B at equilib-rium, the ratio of [B] to [A] is constant regardless of their actual concentrations.]
G is a measure of the capacity of a system to do work as it proceeds to equilibrium . �G can be determined under standard conditions in which the concentration of the reactants and products is 1M ( � G 0 ), or it can be determined at any specifi ed con-centrations ( � G ). Thus, � G 0 is a constant (a reference value) and � G is a variable. Their relationship is shown in the equation at bottom right.
The problem of glutamine synthesis being endergonic is solved by the production of a common intermediate that couples the glutamine synthetase reaction to the exergonic hydrolysis of ATP, such that the net � G of the coupled reactions is negative.
Initial state
Transitionstate
Progress of reaction
Fre
e en
erg
y (G
)
A
B A
B
Final state
ΔG is positive
[B][A]
Ferrier_Unit02.indd 68Ferrier_Unit02.indd 68 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Electron Transport Chain
The ETC shown is an assembly of carriers that accept e � from the reduced coenzymes and generated in processes. As e � move through the ETC to , the terminal acceptor, they release that is used to pump across the mitochondrial membrane, thereby creating a
that drives the phosphorylation of to .
What is transferred from NADH to the FMN prosthetic group of NADH dehydrogenase in Complex I?
What are the two relatively mobile e � carriers of the ETC?
Primary CoQ defi ciency is an AR genetic condition that affects CoQ synthesis. What are the functional consequences of this defi ciency?
6.2 Question
Cristae
An electron transport assembly
NAD+
FMN CoQ b c a a3
Outer mitochondrial
membrane
Intermembrane space
Innermitochondrial
membrane
Ferrier_Unit02.indd 69Ferrier_Unit02.indd 69 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Electron Transport Chain
The ETC shown is an assembly of carriers that accept e � from the reduced coen-zymes NADH and FADH 2 generated in oxidative processes. As e � move through the ETC to O 2 , the terminal acceptor, they release energy that is used to pump H � across the inner mitochondrial membrane (into the intermembrane space), thereby creating a H � gradient that drives the phosphorylation of ADP to ATP .
NADH transfers a hydride ion and a proton (2 e � � 2 H � ) to the FMN prosthetic group of NADH dehydrogenase in Complex I of the ETC. The e� are subsequently transferred to CoQ via Fe-S proteins.
CoQ (a lipid-soluble component of the inner membrane) and cytochrome c (a protein in the intermembrane space) are relatively mobile e � carriers of the ETC. [ Note: CoQ accepts e � from several mitochondrial dehydrogenases .]
Primary CoQ defi ciency will impede e � transfer from both Complexes I and II, decreasing the production of ATP. This will typically manifest as muscle weak-ness and exercise intolerance .
6.2 Answer
Cristae
An electron transport assembly
NAD+
FMN CoQ b c a a3
ADP ATP
Outer mitochondrial
membrane
Intermembrane space
Innermitochondrial
membrane
Ferrier_Unit02.indd 70Ferrier_Unit02.indd 70 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Electron Transport Chain 6.3 Question
How do the cytochromes shown transfer e � ? Which one of the Complexes is also called cytochrome c oxidase ?
Trace the path through Complex II of the e � derived from the oxidation of succinate to fumarate.
Cyanide poisoning causes a cytotoxic hypoxia in which cells are unable to use O 2 , even if it is plentiful. Will cyanide poisoning affect the activity of NADH dehydrogenase ?
Intermembrane space
Complex I
Complex II
Inner mitochondrial membrane
Cytochrome c
NADH dehydrogenase
FMNFe-S
CoQ/CoQH2
Cytochrome b
Fe-S
Cytochrome c1
Complex III(Cytochrome bc1)
Complex IV(Cytochrome a + a3)
CuA
Cytochrome a
CuB-Cytochrome a3
H2O
O212
NADH + H+
NAD+
Succinate
Fumarate
?
Ferrier_Unit02.indd 71Ferrier_Unit02.indd 71 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Electron Transport Chain
The iron of the heme prosthetic group in cytochromes readily interconverts between the oxidized ferric form (Fe 3 � ) and the reduced ferrous form (Fe 2 � ), enabling cytochromes to transfer e � . Complex IV is called cytochrome c oxidase because the e � acceptor is O 2 and not the prosthetic group of a protein. Complex IV contains Fe (in the heme component) and Cu.
The e � from succinate are fi rst transferred to the FAD prosthetic group of SD , reducing it to FADH 2 , and then to the Fe 3 � of the Fe-S proteins, reducing it to Fe 2 � as the FADH 2 is reoxidized. The e � are picked up from the Fe 2 � by CoQ , reducing it to CoQH 2 as Fe 2 � is reoxidized. No H� are pumped at Complex II.
Cyanide binds and inactivates Complex IV. By preventing transfer of e � to O 2 , it causes the ETC to “back up,” resulting in accumulation of the reduced forms of its e � carriers. Therefore, NADH dehydrogenase will be inhibited, and the NADH/NAD � ratio in mitochondria will increase. [ Note: ETC inhibition results in inhibition of ATP synthesis in coupled mitochondria because ATP synthase requires the H � gradient.]
6.3 Answer
Intermembrane space
Complex I
Complex II
Succinate dehydrogenase
FADFe-S
Inner mitochondrial membrane
Cytochrome c
NADH dehydrogenase
FMNFe-S
CoQ/CoQH2
Cytochrome b
Fe-S
Cytochrome c1
Complex III(Cytochrome bc1)
Complex IV(Cytochrome a + a3)
CuA
Cytochrome a
CuB-Cytochrome a3
H2O
O212
NADH + H+
NAD+
Succinate
Fumarate
Ferrier_Unit02.indd 72Ferrier_Unit02.indd 72 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Electron Transport Chain
Does the fi gure show NADH being oxidized or reduced? FMN?
If the two reactions shown below were coupled, in which direction would the e � fl ow?
Ubiquinone � 2 H � � 2 e � ➔ ubiquinol Eo � � 0.045V
NAD � � 2 H � � 2 e � ➔ NADH � H � E o � � 0.320V
What is the consequence of the incomplete reduction of O 2 to 2 H 2 O by the ETC as seen in reperfusion injury ?
6.4 Question
NADH
NAD+ FMNH2
FMN
NADH + H+
NAD++ 2e– + 2H+ FMNH2
FMN + 2e– + 2H+
Redox pairEo = – 0.32 volt
Redox pairEo = – 0.22 volt
Component redox reactions
Overall oxidation-reduction reaction
+ H+
Ferrier_Unit02.indd 73Ferrier_Unit02.indd 73 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
The NADH is being oxidized to NAD � . The FMN is being reduced to FMNH 2 . Oxidation is the loss of e � and reduction the gain.
Ubiquinone � 2 H � � 2 e � ➔ ubiquinol E o � � 0.045V
NAD � � 2 H � � 2 e � ➔ NADH � H � E o � � 0.320V
Because e � fl ow is from the redox pair with the lowest E 0 to the pair with the highest, e � will fl ow from NADH to ubiquinone (CoQ). [ Note: Electrons subsequently will fl ow from ubiquinone to O 2 because the redox pairs involved in the transfer have increasingly positive E 0 values.]
Incomplete reduction of O 2 to 2 H 2 O by the ETC, as seen in reperfusion injury caused by the rapid return of O 2 (e.g., with thrombolytic therapy for an MI ), pro-duces ROS (e.g., O 2 � �, H 2 O 2 , and OH � ). ROS damage DNA and proteins and cause lipid peroxidation. [ Note: Enzymes such as superoxide dismutase , catalase , and glutathione peroxidase protect cells from ROS.]
Electron Transport Chain6.4 Answer
NADH
NAD+ FMNH2
FMN
NADH + H+
NAD++ 2e– + 2H+ FMNH2
FMN + 2e– + 2H+
Redox pairEo = – 0.32 volt
Redox pairEo = – 0.22 volt
Component redox reactions
Overall oxidation-reduction reaction
+ H+
Ferrier_Unit02.indd 74Ferrier_Unit02.indd 74 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Phosphorylation of ADP to ATP 6.5 Question
How is the fl ow of e � through the ETC coupled to ATP synthesis, as shown?
What will happen to e � fl ow through the ETC in the presence of oligomycin?
A myocardial infarction ( MI ) is usually caused by occlusion of a coronary artery by a thrombus. What would be the immediate effects on the mitochondrial ETC in the event of an MI?
ADP + Pi
ADP
ATP
ATP
NADH
H H H+ + +
INTERMEMBRANESPACE
MITOCHONDRIALMATRIX
+
cytc
H
ComplexIII
ComplexIV
ComplexI
Complex V(F0 domain)
Complex V(F1 domain)
NAD+ 1/2O2H2O
Electron flow
MITOCHONDRIONInner membrane
Intermembranespace
Outer membrane
Matrix
e–
e–e–
e–
ATP/ADP antiporter
Ferrier_Unit02.indd 75Ferrier_Unit02.indd 75 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Phosphorylation of ADP to ATP
Flow of e � through the ETC results in energy release used to pump H � from the mitochondrial matrix to the intermembrane space at Complexes I (4 H�), III (4 H�), and IV (2 H�), creating an electrochemical gradient . The energy of the gradient is used to drive the phosphorylation of ADP to ATP by Complex V ( ATP synthase , F 1 /F o ATPase ). Thus, the gradient is the common intermediate that couples the processes.
Oligomycin inhibits H � fl ux through the F o domain of ATP synthase , thereby inhibiting ATP production at the F 1 domain. In coupled mitochondria, inhibition of ATP synthesis inhibits the ETC because of the diffi culty of pumping additional H � against the steep gradient. Flow of e � will eventually stop.
Flow of e � through the ETC requires the reduction of O 2 to 2 H 2 O by Complex IV. As O 2 becomes limited during the MI , the ETC slows and stops. [ Note: Thrombolysis allows rapid reperfusion.]
6.5 Answer
ADP + Pi
ADP
ATP
ATP
NADH
H H H+ + +
INTERMEMBRANESPACE
MITOCHONDRIALMATRIX
+
cytc
H
ComplexIII
ComplexIV
ComplexI
Complex V(F0 domain)
Complex V(F1 domain)
NAD+ 1/2O2H2O
Electron flow
MITOCHONDRIONInner membrane
Intermembranespace
Outer membrane
Matrix
e–
e–e–
e–
ATP/ADP antiporter
Ferrier_Unit02.indd 76Ferrier_Unit02.indd 76 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Membrane Transport Systems
What is the function of the malate-aspartate shuttle shown?
The glycerophosphate shuttle delivers e � to the ETC via FADH 2 . Is this shuttle more or less effi cient than the malate-aspartate shuttle in generating ATP?
In mitochondrial myopathies , why are the mutations more likely to be in mtDNA rather than nuclear DNA?
6.6 Question
Oxaloacetate Glutamate
α-KetoglutarateAspartate
α-KetoglutarateAspartate
Malate
NADH+ H+
NAD+
Malate
GlutamateOxaloacetate
NADH+ H+
NAD+
Complex I of the electron transport chain
CYTOSOL
MITOCHONDRIAL MATRIX
Amino-transferase
Amino-transferase
Cytosolicmalatedehydrogenase
Mitochondrialmalatedehydrogenase
Ferrier_Unit02.indd 77Ferrier_Unit02.indd 77 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Membrane Transport Systems
The malate-aspartate shuttle moves reducing equivalents from the cytosol to the mitochondria because the inner mitochondrial membrane lacks a transporter for NADH. Cytosolic NADH is oxidized as OAA is reduced to malate, for which there is a membrane transporter. Mitochondrial malate is oxidized to OAA as NAD � is reduced to NADH � H � . [ Note: The OAA is transaminated to Asp.]
The NADH of the malate-aspartate shuttle is oxidized by Complex I, whereas the FADH 2 of the glycerophosphate shuttle is oxidized by CoQ. The P/O ratio for NADH is �3 and for FADH is �2. Therefore, more ATP will be generated using the malate-aspartate shuttle. [ Note: The lower P/O ratio for FADH 2 refl ects the smaller number of H � pumped (and, therefore, fewer ATP made) because FADH 2 is not oxidized by Complex I.]
Only a minority of the proteins required for OXPHOS is encoded by mtDNA , with most encoded by nuclear DNA. However, the mutational rate of mtDNA is about 10 times that for nuclear DNA.
6.6 Answer
Oxaloacetate Glutamate
α-KetoglutarateAspartate
α-KetoglutarateAspartate
Malate
NADH+ H+
NAD+
Malate
GlutamateOxaloacetate
NADH+ H+
NAD+
Complex I of the electron transport chain
CYTOSOL
MITOCHONDRIAL MATRIX
Amino-transferase
Amino-transferase
Cytosolicmalatedehydrogenase
Mitochondrialmalatedehydrogenase
Ferrier_Unit02.indd 78Ferrier_Unit02.indd 78 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
6
A 3-year-old girl is brought to the emergency department for suspected salicylate poisoning on the advice of the Poison Control Center her mother called after fi nding the child with an empty bottle of oil of wintergreen (used as a rub by the child’s grandfather to reduce his arthritic pain). At arrival, the child is hyperventilating and is shown to have a mixed acid–base disorder. Her breath has the odor of wintergreen . She is tachycardic and hyperactive . Her body temperature is elevated . The mother reports that the child vomited several times at home, was sweaty , and seemed to have trouble hearing . This constellation of signs and symptoms is suggestive of salicylate poisoning, and her blood level of salicylate was later determined to be 60 mg/dl (reference level is 0 mg/dl, with a therapeutic range � 30 mg/dl). Salicylate ingestion is a common cause of poisoning in children. [ Note: Oil of wintergreen is a non-aspirin source of salicylate and contains �7,000 mg of salicylate per teaspoon.]
Explain the fi nding of hyperthermia , given that salicylate can cause uncoupling of OXPHOS.
Case Card
Ferrier_Unit02.indd 79Ferrier_Unit02.indd 79 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
6
Salicylic acid (un-ionized) moves into the mitochondrial matrix where it ionizes to salicylate. [ Note: When the pH is above the pK, the acid deproton-ates. The pH is higher in the matrix because H � are pumped out by the ETC.] By bringing H � into the matrix, salicylic acid dissipates the H � gradient. Because the phosphorylation of ADP to ATP by ATP synthase depends on this gradient, ATP synthesis stops, thereby preventing energy capture from e � transport as ATP. Instead, the energy is lost as heat, causing hyperthermia . [ Note: The gradient allows H � fl ow through the F o domain of ATP synthase , causing rotation within the domain and resulting in conformational changes in the F 1 domain, which allow ADP phosphorylation.] Because the transport of e � is not inhibited, O 2 utilization will continue. Salicylic acid, therefore, uncouples the ETC from OXPHOS. The drug 2,4-DNP works in a similar manner. UCP1 is a physiologic uncoupler found in BAT . It works in a manner different than exogenous uncouplers, and forms channels in the inner mitochondrial membrane that allow H � to reenter the matrix, as shown. The resulting production of heat ( nonshivering thermogenesis ) maintains body temperature in neonates.
With uncouplers , the energy from e � transfer through the ETC is not captured as ATP but is lost as heat.
Case Card
ATP synthase
ATP
Uncouplingprotein
H+
H+
H+
H+
H+
O2
H2O
e–
H+
H+
MITOCHONDRIALMATRIX
Uncoupling proteins create a channel, allowing protons (H+1)to reenter the mitochondrial matrix without capturing any energy as ATP.
ADPA
Ferrier_Unit02.indd 80Ferrier_Unit02.indd 80 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
7.1 Question
What type of bond is displayed above the red question mark?
What enzyme joins monosaccharides to form a disaccharide?
Galactosemia is a rare metabolic disorder that inhibits an individual’s ability to metabolize the monosaccharide galactose. Why would those with galactosemia be advised to avoid dairy products?
Carbohydrate Structure
O
Lactose: galactosyl-β(1→4)-glucose
CH2OH
OH
OH
HOO
OCH2OH
OH
OH
HOH
OCH2OH
OH
HO
Carbon 1 ofgalactose
?
OCH2OH
OHOOOOOOOOOOOOOOOHOHO
Carbon 4 ofglucose
Ferrier_Unit02.indd 81Ferrier_Unit02.indd 81 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
7.1 Answer Carbohydrate Structure
It is a glycosidic bond between two hexoses. Specifi cally, it is a � (1➔4) glycosidic bond.
A glycosyltransferase joins monosaccharides to form a disaccharide. [ Note: Glycosyltransferases are also required for the formation of oligo- and polysaccharides.]
Dairy products contain lactose , which is a disaccharide of galactose and glucose. Because galactosemia is a defi ciency in the ability to metabolize galactose, individuals with the disorder are advised to avoid dairy products.
O
Lactose: galactosyl-β(1→4)-glucose
CH2OH
OH
OH
HOO
OCH2OH
OH
OH
HOH
OCH2OH
OH
HO
Carbon 1 ofgalactose
Glycosidic bond
OCH2OH
OHOOOOOOOOOOOOOOOHOHO
Carbon 4 ofglucose
Ferrier_Unit02.indd 82Ferrier_Unit02.indd 82 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Match the red letters shown with these three types of structural relationships: C-2 epimers, C-4 epimers, and isomers that are not epimers.
Defi ne the term enantiomer.
Formation of which type of glycoside is impaired in individuals who cannot attach carbohydrate to selected Asn residues in a protein?
Carbohydrate Structure 7.2 Question
CH2OH
HCOH
CHO
CH
HOCH
HCOH
Galactose
CH2OH
C
CHO
Glucose
CH2OH
HCOH
CHO
HOCHMannose
OHH
C OHH
C HHO
CH
HCOH
A
B
C
1
2
3
4
5
6
OH
HO
CHHO
CH2OH
C
CH2OH
OHH
C OHH
C HHO
C O
Fructose
Ferrier_Unit02.indd 83Ferrier_Unit02.indd 83 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
A � C-4 epimers and B � C-2 epimers. C � isomers that are not epimers because they differ in confi guration at more than one carbon. [ Note: Fructose has a keto group at the carbonyl C and is classifi ed as a ketose. The other sugars shown have an aldehyde group and are aldoses.]
An enantiomer is a special type of isomer in which the pair of structures is mirror images of one another, such as D- and L-glucose. [ Note: Most sugars exist as D isomers, whereas most amino acids exist as L isomers.]
N-glycoside formation is impaired in individuals who cannot attach carbohydrate to the amide N of selected Asn residues in a protein, a process known as N-glycosylation . Impairments in this process are classifi ed as congenital disorders of glycosylation ( CDGs ).
Carbohydrate Structure7.2 Answer
CH2OH
HCOH
CHO
CH
HOCH
HCOH
Galactose
CH2OH
C
CHO
Glucose
CH2OH
HCOH
CHO
HOCHMannose
OHH
C OHH
C HHO
CH
HCOH
C-2 epimers
C-4 epimers
1
2
3
4
5
6
OH
HO
CHHO
CH2OH
C
CH2OH
OHH
C OHH
C HHO
C O
Isomers
Fructose
Ferrier_Unit02.indd 84Ferrier_Unit02.indd 84 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Carbohydrate Structure 7.3 Question
Which red letter(s) shown identifi es an anomeric carbon?
What chemical feature identifi es a sugar as a reducing sugar?
Are reducing sugars normally detected in urine?
β-D-Gluco-pyranose
D-Glucose α-D-Gluco-pyranose
OHOCH2
OH
OH
H
H
H 5
11H
HOH
HOCH2
HC=OOH
OH
OH
OHH
H
HH
HOH
5
1
OHOCH2
OH
OH
OH
HH
HH
HOH
5
AB
C
Ferrier_Unit02.indd 85Ferrier_Unit02.indd 85 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Letters A and C identify anomeric carbons (carbonyl carbons now bound to two oxygens).
Reducing sugars contain a free hydroxyl group on the anomeric carbon of the cyclic form. In the acyclic form, the carbonyl carbon of the aldehyde group is oxidized (forming a carboxyl group) as a chromogenic agent (e.g., Benedict’s reagent ) is reduced. [ Note: Fructose is a reducing sugar because its ketone group can isomerize to an aldehyde.]
Reducing sugars are not normally detected in urine, and their presence is indicative of a pathology (e.g., galactosemia ). If urine gives a positive result with a reducing-sugar test (e.g., Benedict’s reagent), the identity of the sugar can be determined using more specifi c tests (such as the glucose oxidase test for glucose).
7.3 Answer Carbohydrate Structure
β-D-Gluco-pyranose
D-Glucose α-D-Gluco-pyranose
OHOCH2
OH
OH
H
H
H 5
11H
HOH
HOCH2
HC=OOH
OH
OH
OHH
H
HH
HOH
5
1
OHOCH2
OH
OH
OH
HH
HH
HOH
Carbonyl carbonAnomeric carbon
Anomeric carbon
5
Ferrier_Unit02.indd 86Ferrier_Unit02.indd 86 5/2/14 7:22 PM5/2/14 7:22 PM
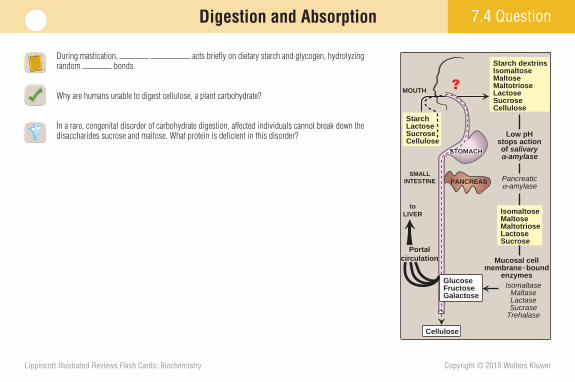
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
During mastication, acts briefl y on dietary starch and glycogen, hydrolyzing random bonds.
Why are humans unable to digest cellulose, a plant carbohydrate?
In a rare, congenital disorder of carbohydrate digestion, affected individuals cannot break down the disaccharides sucrose and maltose. What protein is defi cient in this disorder?
7.4 Question Digestion and Absorption
SMALLINTESTINE
toLIVER
MOUTH
StarchLactoseSucroseCellulose
Starch dextrinsIsomaltoseMaltoseMaltotrioseLactoseSucroseCellulose
Pancreaticα-amylase
Low pHstops actionof salivaryα-amylase
Mucosal cellmembrane–bound
enzymesIsomaltase
MaltaseLactaseSucrase
Trehalase
Cellulose
PANCREAS
?
STOMACHSTOMACHSTOMACH
GlucoseFructoseGalactose
Portalcirculation
IsomaltoseMaltoseMaltotrioseLactoseSucrose
Ferrier_Unit02.indd 87Ferrier_Unit02.indd 87 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
During mastication, salivary �-amylase acts briefl y on dietary starch and glycogen, hydrolyzing random � (1➔4) bonds .
Humans do not make the � (1➔4)-endoglucosidases that are necessary to digest cellulose .
The SI protein is defi cient in those who cannot break down sucrose and maltose. SI is synthesized and then cleaved into two functional subunits that form the sucrase–isomaltase (SI ) enzyme complex, which hydrolyzes dietary sucrose, maltose, and isomaltose in the small intestine.
7.4 Answer Digestion and Absorption
SMALLINTESTINE
toLIVER
MOUTH
StarchLactoseSucroseCellulose
Starch dextrinsIsomaltoseMaltoseMaltotrioseLactoseSucroseCellulose
Salivary α-amylase
Pancreaticα-amylase
Low pHstops actionof salivaryα-amylase
Mucosal cellmembrane–bound
enzymesIsomaltase
MaltaseLactaseSucrase
Trehalase
Cellulose
PANCREAS
STOMACHSTOMACHSTOMACH
GlucoseFructoseGalactose
Portalcirculation
IsomaltoseMaltoseMaltotrioseLactoseSucrose
Ferrier_Unit02.indd 88Ferrier_Unit02.indd 88 5/2/14 7:22 PM5/2/14 7:22 PM
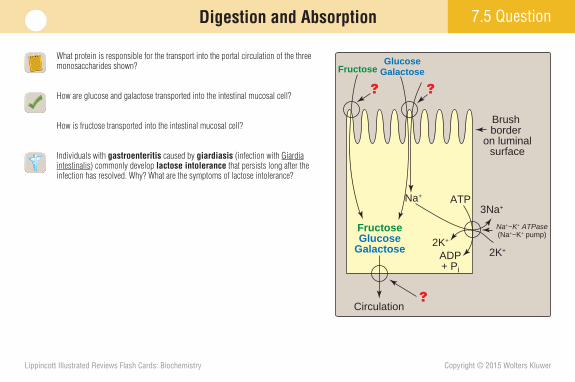
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
What protein is responsible for the transport into the portal circulation of the three monosaccharides shown?
How are glucose and galactose transported into the intestinal mucosal cell?
How is fructose transported into the intestinal mucosal cell?
Individuals with gastroenteritis caused by giardiasis (infection with Giardia intestinalis ) commonly develop lactose intolerance that persists long after the infection has resolved. Why? What are the symptoms of lactose intolerance?
7.5 QuestionDigestion and Absorption
Circulation?
??
FructoseGlucose
Galactose
Na+
FructoseGlucose
Galactose
ADP+ Pi
3Na+
2K+2K+
ATP
Brush border
on luminalsurface
Na+−K+ ATPase(Na+−K+ pump)
Ferrier_Unit02.indd 89Ferrier_Unit02.indd 89 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
The GLUT-2 transporter allows for the transport of glucose, galactose, and fructose into the portal circulation.
Glucose and galactose are transported into the intestinal mucosal cell by SGLT-1 .
Fructose enters the intestinal mucosal cell via GLUT-5 .
Brush border cells are damaged by the gastroenteritis caused by giardiasis , resulting in disaccharide accumulation in the large intestine due to defi ciency of the disaccharidases made by these cells. Lactase , the brush border disaccharidas e that hydrolyzes lactose, is the last to recover in giardiasis. The movement of lactose into the large intestine will draw in water, resulting in bloating and an osmotic diarrhea (shown). Treatment of lactose intolerance is lactose avoidance.
7.5 Answer Digestion and Absorption
Circulation GLUT-2
FructoseGlucose
Galactose
Na+
Na+
GLUT-5
FructoseGlucose
Galactose
ADP+ Pi
3Na+
2K+2K+
ATP
Brush border
on luminalsurface
SGLT-1
Na+−K+ ATPase(Na+−K+ pump)
BLOATINGDIARRHEA
DEHYDRATION
Lactose
CO2
H2Two-carbonmetabolites
(such asacetic acid)
Three-carbonmetabolites
(such aslactic acid)
BACTERIABACTERIABACTERIA
LARGE INTESTINE
H2O
H2 can bemeasuredin the breath.
Ferrier_Unit02.indd 90Ferrier_Unit02.indd 90 5/2/14 7:22 PM5/2/14 7:22 PM
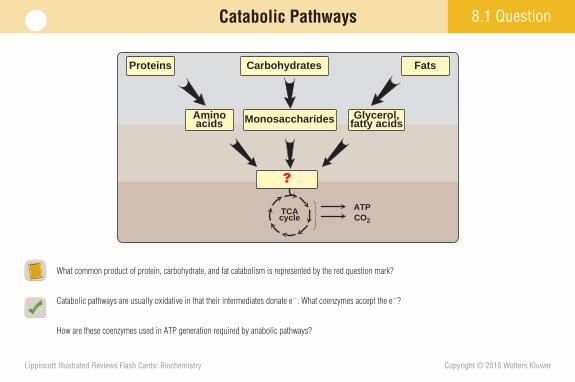
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
8.1 Question Catabolic Pathways
What common product of protein, carbohydrate, and fat catabolism is represented by the red question mark?
Catabolic pathways are usually oxidative in that their intermediates donate e � . What coenzymes accept the e � ?
How are these coenzymes used in ATP generation required by anabolic pathways?
Aminoacids Monosaccharides Glycerol,
fatty acids
TCAcycle
Proteins Carbohydrates Fats
ATPCO2
?
Ferrier_Unit02.indd 91Ferrier_Unit02.indd 91 5/2/14 7:22 PM5/2/14 7:22 PM
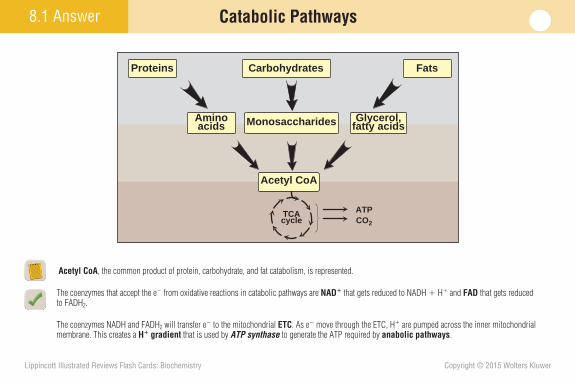
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
8.1 Answer Catabolic Pathways
Acetyl CoA , the common product of protein, carbohydrate, and fat catabolism, is represented.
The coenzymes that accept the e � from oxidative reactions in catabolic pathways are NAD � that gets reduced to NADH � H � and FAD that gets reduced to FADH 2 .
The coenzymes NADH and FADH 2 will transfer e � to the mitochondrial ETC . As e � move through the ETC, H � are pumped across the inner mitochondrial membrane. This creates a H � gradient that is used by ATP synthase to generate the ATP required by anabolic pathways .
Aminoacids Monosaccharides Glycerol,
fatty acids
TCAcycle
Proteins Carbohydrates Fats
ATPCO2
Acetyl CoA
Ferrier_Unit02.indd 92Ferrier_Unit02.indd 92 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
8.2 Question Metabolism Regulation
Upon ligand binding to (and activation of) the receptor, what happens to the trimeric G S protein shown?
What is a second messenger?
What second messenger is generated by activation of the receptor shown? How does it activate cellular pathways in the cell?
What is the effect of cholera toxin on G s proteins in intestinal epithelial cells?
Hormone or neuro-transmitter
Inactive adenylyl cyclaseCytosol
Extra-cellularspace
Unoccupied receptor does not interact with Gs protein.
GDP
α
Cell membrane
Receptor
Gs proteinwith bound GDP
γβ
1
Ferrier_Unit02.indd 93Ferrier_Unit02.indd 93 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Upon ligand binding, a conformational change in the activated receptor (a GPCR ) causes the GDP bound to the subunit of the trimeric G S protein to be replaced by GTP. The subunit then dissociates from the � and subunits and stimulates AC to produce cAMP . With time, the subunit hydrolyzes the bound GTP to GDP by its inherent GTPase activity and is inactivated.
A second messenger is an intracellularly generated molecule that links the original extracellular message (ligand binding) and the intracellular effects.
The second messenger generated by activation of the receptor shown is cAMP , which binds to the regulatory subunits of PKA , causing the release and activation of the catalytic subunits. PKA phosphorylates target proteins, either activating or inactivating them.
Cholera toxin causes ADP ribosylation of the subunit of G s proteins, thereby inhibiting the proteins’ inherent GTPase activity, which constitutively activates the proteins. [ Note: PKA phosphorylates and activates the CFTR protein, a Cl � channel. H 2 O, Cl � , Na � , K � , and HCO 3 � are secreted into the intestinal lumen, causing cholera’s characteristic watery diarrhea and dehydration.]
8.2 Answer Metabolism Regulation
GTP GDP
ATP
cAMP + PPi
Inactiveadenylylcyclase
Occupied receptor changes shape and interacts with α subunit of Gs protein. Gs protein releases GDP and binds GTP.
α Subunit of Gs protein dissociates from βγ and activates adenylyl cyclase.
When hormone is no longerpresent, the receptor revertsto resting state. GTP on the α subunit is hydrolyzed to GDP, α rejoins βγ, and adenylyl cyclase is deactivated.
Inactiveadenylylcyclase
Pi
γ
GDP
β
α
2
3
4
α
α
GTP
GTP
Activeadenylylcyclase
γβ
γβ
Ferrier_Unit02.indd 94Ferrier_Unit02.indd 94 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
8.3 Question Glucose Transport and Phosphorylation
This fi gure depicts glucose transport through the cell membrane by a GLUT that functions as a . The GLUT abundant in muscle and adipose tissue is the insulin-dependent .
How does the cell ensure that the glucose taken in by a GLUT remains inside rather than diffusing back out?
Why might inactivating mutations in glucokinase result in diabetes ?
Cytosol
Cytosol
Extracellularspace
Cell membrane
Glucosetransporter(state 1)
Glucose
Glucosetransporter(state 2)
Extracellularspace
GLUT
Ferrier_Unit02.indd 95Ferrier_Unit02.indd 95 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
8.3 Answer
This fi gure depicts facilitated glucose transport through the cell membrane by a GLUT that functions as a uniporter (in that it transports one specifi c molecule). The GLUT abundant in muscle and adipose tissue is the insulin-dependent GLUT-4 . [ Note: Glucose transport by GLUTs is down a concentration gradient. In contrast, SGLTs are energy-requiring transporters that move glucose against its concentration gradient in the intestine, kidney, and choroid plexus.]
Hexokinases irreversibly catalyze the phosphorylation of intracellular glucose to glucose 6-P , thereby trapping it inside the cell because no cell membrane transporter exists for phosphorylated sugars. [ Note: There are four isoforms of hexokinase . Hexokinases I–III are found in most tissues. Hexokinase IV ( glucokinase ) is found in the liver and pancreatic � cells.]
Glucokinase acts as a glucose sensor in pancreatic � cells and helps regulate insulin secretion. Inactivating mutations can impair insulin secretion, resulting in maturity-onset diabetes of the young ( MODY ). [ Note: In contrast to the other hexokinases , glucokinase has a high K m (it functions only when glucose concentration is high), a high V max (it functions effi ciently when glucose concentra-tion is high), and is not directly inhibited by glucose 6-P.]
Glucose Transport and Phosphorylation
Cytosol
Cytosol
Extracellularspace
Cell membrane
Glucosetransporter(state 1)
Glucose
Glucosetransporter(state 2)
Extracellularspace
GLUT
Ferrier_Unit02.indd 96Ferrier_Unit02.indd 96 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Fructose 6-Phosphate Phosphorylation
What are the positive and negative allosteric effectors of the enzyme PFK- 1 shown at the top of the fi gure?
How does insulin signaling affect the activity of PFK-1 ?
PFK-1 is a tetramer composed of different combinations of L and/or M subunits in different tissues. RBCs express both subunits. Patients with Tarui disease have a genetic defect in the M subunit and display muscle fatigue with exertion and myoglobinuria . What should be true about the ability of their RBCs to perform glycolysis?
8.4 Question
ATP
ADP
Fructose 1,6-bisphosphate
Fructose 6-phosphate
HCH OCH OHCH OH
CHO HCC
OCH OH
Phosphofructo-kinase-1
P
???
P
P
P
Dihydroxyacetone phosphate
Glyceraldehyde3-phosphate
HCHCC
OCH OH
HCH OCH OHC H
O Aldolase
Triosephosphate isomerase
OH
++
Ferrier_Unit02.indd 97Ferrier_Unit02.indd 97 5/2/14 7:22 PM5/2/14 7:22 PM
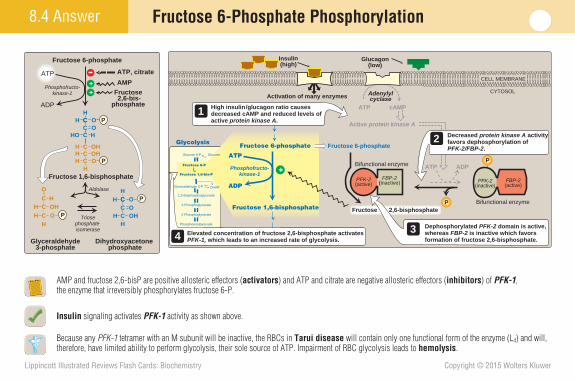
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
AMP and fructose 2,6-bisP are positive allosteric effectors ( activators ) and ATP and citrate are negative allosteric effectors ( inhibitors ) of PFK-1 , the enzyme that irreversibly phosphorylates fructose 6-P.
Insulin signaling activates PFK-1 activity as shown above.
Because any PFK-1 tetramer with an M subunit will be inactive, the RBCs in Tarui disease will contain only one functional form of the enzyme (L 4 ) and will, therefore, have limited ability to perform glycolysis, their sole source of ATP. Impairment of RBC glycolysis leads to hemolysis .
8.4 Answer Fructose 6-Phosphate Phosphorylation
ATP
ADP
Fructose 1,6-bisphosphate
Fructose 6-phosphate
HCH OCH OHCH OH
CHO HCC
OCH OH
Phosphofructo-kinase-1 Fructose
2,6-bis-phosphate
P
P
P
P
Dihydroxyacetone phosphate
Glyceraldehyde3-phosphate
HCHCC
OCH OH
HCH OCH OHC H
O Aldolase
Triosephosphate isomerase
ATP, citrate
AMP
OH
++
ATP
ADP
Fructose 6-phosphate Fructose 6-phosphate
Phosphofructo-kinase-1
Fructose 2,6-bisphosphate
Bifunctional enzyme
Bifunctional enzymeFructose 1,6-bisphosphate
PFK-2(active)
ATP ADP
Active protein kinase A
ATP cAMP
Adenylylcyclase
Receptor
Glucagon(low)
Receptor
Insulin(high)
Dephosphorylated PFK-2 domain is active, whereas FBP-2 is inactive which favors formation of fructose 2,6-bisphosphate.
FBP-2(inactive)
Activation of many enzymes
CELL MEMBRANE
CYTOSOL
Decreased protein kinase A activity favors dephosphorylation of PFK-2/FBP-2.
2
3
P
PGlucose 6-P Glucose
Fructose 6-P
Glycolysis
Fructose 1,6-bis-P
Glyceraldehyde 3-P
1,3-Bisphosphoglycerate
3-Phosphoglycerate
2-Phosphoglycerate
Phosphoenolpyruvate
Pyruvate
DHAP
Lactate
PFK-2(inactive)
FBP-2(active)
+
High insulin/glucagon ratio causes decreased cAMP and reduced levels of active protein kinase A.
1
Elevated concentration of fructose 2,6-bisphosphate activates PFK-1, which leads to an increased rate of glycolysis.4
Ferrier_Unit02.indd 98Ferrier_Unit02.indd 98 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Glyceraldehyde 3-Phosphate Oxidation
What is the signifi cance of the 2,3-BPG generation shown?
What is the fate of the NADH generated by glyceraldehyde 3-P oxidation?
How can arsenate (pentavalent arsenic) poisoning prevent net ATP production by glycolysis without inhibiting the pathway itself?
8.5 Question
1,3-Bisphosphoglycerate
3-Phosphoglycerate
HCH OCH OHCO
O~
HCH OCH OHCO
O-
ATP
ADPPhospho-glycerate
kinase
Glyceraldehyde3-phosphate
HCH OCH OHC HO
Glyceraldehyde3-phosphate
dehydrogenase
NAD+
NADH + H+
Pi
2,3-Bisphospho-glycerate
O-
HCH OCH OCO
P
Pi
P
H2O
Mutase
Phosphatase
P
P
P
P
Ferrier_Unit02.indd 99Ferrier_Unit02.indd 99 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
2,3-BPG is an important allosteric effector of Hb. It decreases the affi nity of Hb for O 2 , thereby increasing O 2 delivery to tissues. The mutase- catalyzed reaction that produces 2,3-BPG occurs to a signifi cant extent only in RBCs.
The NADH generated by glyceraldehyde 3-P oxidation is either oxidized by LDH as pyruvate is reduced to lactate, or its reducing equivalents are shuttled to the mitochondrial ETC . [ Note: In skeletal muscle, NADH production during intense exercise can exceed ETC oxidative capacity, resulting in an elevated NADH/NAD � ratio that favors lactate production.]
Arsenate can compete with P i as a substrate for glyceraldehyde 3-P dehydrogenase , forming a complex that spontaneously hydrolyzes to produce 3-phosphoglycerate. Consequently, the substrate-level phosphorylation reaction of glycolysis catalyzed by phosphoglycerate kinase is bypassed, decreasing the net yield of ATP from the pathway without inhibiting the pathway itself.
Glyceraldehyde 3-Phosphate Oxidation 8.5 Answer
1,3-Bisphosphoglycerate
3-Phosphoglycerate
HCH OCH OHCO
O~
HCH OCH OHCO
O-
ATP
ADPPhospho-glycerate
kinase
Glyceraldehyde3-phosphate
HCH OCH OHC HO
Glyceraldehyde3-phosphate
dehydrogenase
NAD+
NADH + H+
Pi
2,3-Bisphospho-glycerate
O-
HCH OCH OCO
P
Pi
P
H2O
Mutase
Phosphatase
P
P
P
P
Ferrier_Unit02.indd 100Ferrier_Unit02.indd 100 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
8.6 Question Pyruvate Kinase
What pancreatic hormone bound to its receptor causes the cascade of events shown?
How does fructose 1,6-bisP affect PK ?
PK defi ciency is the most common inherited metabolic disorder of glycolysis. How might a defi ciency of the RBC isozyme affect tissue oxygenation?
PEP
Pyruvate
ATP ADP
Active protein kinase A
ATP cAMP + PPi
Adenylylcyclase
?
ADP
ATP
Receptor
Pyruvatekinase(active)
Pyruvatekinase
(inactive)
P
Ferrier_Unit02.indd 101Ferrier_Unit02.indd 101 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
The pancreatic hormone is glucagon . Binding to its GPCR initiates the cascade that results in phosphorylation and inactivation of the hepatic isoform of PK . [ Note: A protein phosphatase can remove the phosphate group and reactivate PK .]
Fructose 1,6-bisP , the product of the earlier PFK-1 reaction, is a positive allosteric activator of PK and serves as a feedforward effector.
In RBCs, the reduced rate of conversion of PEP to pyruvate due to PK defi ciency will cause accumulation of the intermediates preceding this step. The increased pool of 2,3-BPG will lead to increased O 2 delivery to tissues (a rightward shift in the O 2 -saturation curve). [ Note: PK defi ciency decreases glycolysis and ATP production by this pathway, resulting in RBC hemolysis (insofar as RBCs depend completely on glycolysis for ATP production) in a manner similar to that seen with PFK-1 mutations.]
Pyruvate Kinase 8.6 Answer
PEP
Pyruvate
ATP ADP
Active protein kinase A
ATP cAMP + PPi
Adenylylcyclase
Glucagon
ADP
ATP
Receptor
Pyruvatekinase(active)
Pyruvatekinase
(inactive)
P
Ferrier_Unit02.indd 102Ferrier_Unit02.indd 102 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
9.1 Question Pyruvate Dehydrogenase Complex
List the fi ve coenzymes required by the nonregulatory enzymes of the PDHC . Do they function as prosthetic groups or as cosubstrates?
How do ATP, acetyl CoA, NADH, and pyruvate regulate the PDHC ? How does Ca 2 � regulate it?
Why does a defi ciency in PDHC activity cause lactic acidosis ?
PDHkinase
Ca2+
ATP
Pyruvate
Pyruvate
ADP
H2O
PiPyruvate
dehydrogenasecomplex(active)
P
ATPAcetyl CoA
NADH
Pyruvatedehydrogenase
complex(inactive)
P
PDHphosphatase
?
?
??
?
Acetyl CoANADH
CO2
Ferrier_Unit02.indd 103Ferrier_Unit02.indd 103 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Of the fi ve coenzymes required by the nonregulatory enzymes of the PDHC that cata-lyzes the oxidative decarboxylation of pyruvate, TPP of E1 ( pyruvate decarboxylase ), lipoic acid of E2 ( dihydrolipoyl transacetylase ), and FAD of E3 ( dihydrolipoyl dehydrogenase ) are tightly bound and function as coenzyme- prosthetic groups . CoA and NAD� (loosely associated with E2 and E3 , respectively) are coenzyme-cosubstrates. [ Note: Arsenite inhibits lipoic acid– requiring enzymes.]
ATP, acetyl CoA, and NADH ( PDHC products) are allosteric activators of PDH kinase . The kinase phosphorylates and inhibits E1 of the PDHC . Pyruvate ( PDHC substrate) is a potent inhibitor of the kinase . Ca 2 � , released during skeletal muscle contraction, is an allosteric activator of PDH phosphatase . The phosphatase dephosphorylates and activates the PDHC , increasing ATP availability to power contraction. NADH and acetyl CoA also affect PDHC nonregulatory enzymes by product inhibition .
A defi ciency of the PDHC results in a rise in pyruvate, thereby upregulating other reactions of pyruvate metabolism such as reduction to lactate by NADH-requiring LDH leading to lactic acidosis . [ Note: The most common form of PDHC defi ciency is caused by mutations to E1 .]
9.1 Answer Pyruvate Dehydrogenase Complex
PDHkinase
Pyruvate
Ca2+
ATP
ADP
H2O
PiPyruvate
dehydrogenasecomplex(active)
P
ATPAcetyl CoA
NADH
Pyruvatedehydrogenase
complex(inactive)
+
+
P
PDHphosphatase
Pyruvate Acetyl CoANADH
CO2
Ferrier_Unit02.indd 104Ferrier_Unit02.indd 104 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
9.2 Question Tricarboxylic Acid Cycle
What intermediate of the TCA (Krebs) cycle is combined with acetyl CoA to initiate the cycle (and is regenerated by the cycle), as shown?
Name the enzyme that catalyzes step 4 and compare it to the PDHC .
Which step generates GTP? How?
What is unique about the enzyme that catalyzes step 6?
Which TCA cycle enzyme will be directly affected with thiamine ( vitamin B 1 ) defi ciency ? What encephalopathy–psychosis syndrome can develop with this defi ciency?
Citrate
Isocitrate
α-Ketoglutarate
Succinyl CoASuccinate
?
28Malate
Fumarate
CO2
CO2
Acetyl CoA
4
37
6
1
5
Ferrier_Unit02.indd 105Ferrier_Unit02.indd 105 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
OAA is combined with acetyl CoA by CS to initiate the TCA cycle and is regenerated by the cycle.
The step 4 enzyme is the � -KGD complex , which catalyzes an oxidative decarboxylation reaction in a manner analogous to that of the PDHC . It is a protein aggregate of three nonregulatory enzymes that use the same coenzymes as the PDHC (their E3 components are identical). Like PDHC , its E2 is inhibited by arsenic. Unlike PDHC , it is not regulated covalently.
Substrate-level phosphorylation of GDP to GTP occurs during the conversion of succinyl CoA to succinate (step 5) by succinate thiokinase via cleavage of the high-energy thioester bond in succinyl CoA.
FAD-containing SD of step 6 is the only TCA cycle enzyme embedded in the inner mitochondrial membrane (the others are in the matrix). SD is a component of ETC Complex II .
The � -KGD complex of the TCA cycle will be directly inhibited by a thiamine ( vitamin B 1 ) defi ciency because of its requirement for TPP , a thiamine derivative. Wernicke-Korsakoff syndrome can develop with thiamine defi ciency (e.g., in alcohol abusers). [ Note: PDHC activity would also be inhibited with thiamine defi ciency.]
Tricarboxylic Acid Cycle 9.2 Answer
Citrate
Isocitrate
α-Ketoglutarate
Succinyl CoASuccinate
Oxaloacetate
Malate
Fumarate
CO2
CO2
Acetyl CoA
28
4
37
6
1
5
Ferrier_Unit02.indd 106Ferrier_Unit02.indd 106 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
How is the TCA cycle enzyme CS shown regulated?
What effect would elevated ATP and/or NADH levels have on ICD activity? Would Ca 2 � have the same effect?
Fluoroacetate is a plant toxin that is used as a pesticide. It inhibits aconitase of the TCA cycle. What effect will fl uoroacetate poisoning have on aerobic metabolism?
9.3 QuestionTricarboxylic Acid Cycle
Citratesynthase
Acetyl CoA
CoA
C
OCH3 + CoA CH2C-O
C C
O
O-O
Oxaloacetate
O
H2O
Citrate
CH2C-O
C C
O
O-
O
CH2 C O-O
HO
Isocitrate
α-Ketoglutarate
C-O
C
O
CH2 C O-O
H
C OHH
Aconitase
C-O C O
O
CH2 C O-O
CH2
NAD+
NADH + H+
OC O-
CO2
Isocitratedehydrogenase
ATP ?
?
NADH
ADPCa2+
Ferrier_Unit02.indd 107Ferrier_Unit02.indd 107 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
CS , which catalyzes the fi rst of three irreversible reactions of the TCA cycle, is nonallosterically inhibited by its product citrate (a tricarboxylic acid).
ATP and NADH (high-energy signals) are allosteric inhibitors of ICD , the second of three irreversible reactions of the cycle. In contrast, Ca 2 � (and ADP) allosterically activates the enzyme. Both Ca 2 � and ADP signal the need for energy.
Aerobic metabolism will be inhibited with fl uoroacetate poisoning . By inhibiting aconitase , fl uoroacetate will prevent NADH and FADH 2 production in the TCA cycle, thereby decreasing ATP production by OXPHOS (and of GTP by substrate-level phosphorylation). Anaerobic metabolism will increase, providing some ATP and causing a lactic acidosis .
9.3 Answer Tricarboxylic Acid Cycle
Citratesynthase
Acetyl CoA
CoA
C
OCH3 + CoA CH2C-O
C C
O
O-O
Oxaloacetate
O
H2O
Citrate
CH2C-O
C C
O
O-
O
CH2 C O-O
HO
Isocitrate
α-Ketoglutarate
C-O
C
O
CH2 C O-O
H
C OHH
Aconitase
C-O C O
O
CH2 C O-O
CH2
NAD+
NADH + H+
OC O-
CO2
Isocitratedehydrogenase
ATPNADH
ADPCa2+
Fluoroacetate
+
Ferrier_Unit02.indd 108Ferrier_Unit02.indd 108 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
What coenzyme is required for the MD reaction shown?
What role does this reaction play outside of the cycle (e.g., in glycolysis)?
The � G 0 for the conversion of malate to OAA is � 7.1 kcal/mol. What drives this reaction in the forward direction?
The addition of a small amount of malate or OAA to actively respiring muscle gives rise to a fi ve-fold increase in O 2 consumption. Why?
9.4 QuestionTricarboxylic Acid Cycle
L-Malate
CH2C-O
O
C C
O
O-HO
H
Malate dehydrogenase
?
?
Oxaloacetate
CH2C-O
C C
O
O-O
O
Ferrier_Unit02.indd 109Ferrier_Unit02.indd 109 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
The required coenzyme is NAD as NAD � in the forward reaction and NADH in the reverse.
The MD reaction carries reducing equivalents from glycolysis into the mitochondrial matrix as part of the malate-aspartate shuttle . [ Note: The NADH from glycolysis is oxidized as OAA is reduced to malate in the cytosol. Malate is transported from the cytosol into the mitochondrial matrix, where it is reoxidized to OAA as NAD � is reduced to NADH. No transporter exists to move NADH (or OAA) across the inner mitochondrial membrane.]
The endergonic conversion of malate to OAA ( � G 0 of � 7.1 kcal/mol) is driven in the forward direction because it is coupled to the highly exergonic CS reaction ( � G 0 of � 9.0 kcal/mol).
O 2 consumption is a measure of the activity of aerobic pathways such as the TCA cycle . The addition of malate or OAA stimulates the TCA cycle, thereby increasing production of reducing equivalents for the ETC , the major O 2 consumer.
9.4 Answer Tricarboxylic Acid Cycle
L-Malate
CH2C-O
O
C C
O
O-HO
H
Malate dehydrogenase
NAD+
NADH + H+
Oxaloacetate
CH2C-O
C C
O
O-O
O
Ferrier_Unit02.indd 110Ferrier_Unit02.indd 110 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
9.5 Question Tricarboxylic Acid Cycle Summary
How many ATPs will be produced from the four reducing equivalents generated in one round of the TCA cycle, as shown?
What are the major TCA cycle regulation sites, and what are the effectors?
What will be the effect on the P/O ratio in mitochondria exposed to an uncoupler (e.g., salicylate)?
Acetyl CoA
Citrate
Isocitrate
-Ketoglutarateα
Succinyl CoASuccinate
Oxaloacetate
Malate
Fumarate
3 NADH
CO2
NAD+
NAD+
NAD+
FADH2GTP GDP + Pi
(ATP)
CoA
CO2
FAD
Ferrier_Unit02.indd 111Ferrier_Unit02.indd 111 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Tricarboxylic Acid Cycle Summary 9.5 Answer
Three NADHs and one FADH 2 are generated in one round of the TCA cycle. Assuming a P/O ratio of 3 for NADH and 2 for FADH 2 , 11 ATPs will be generated by OXPHOS . Additionally, one GTP is produced by substrate-level phosphorylation . GTP and ATP are interconverted by nucleoside diphosphate kinase . Therefore, a total of 12 ATP are produced by one round of the TCA cycle.
The major sites of cycle regulation (and the regulators) are CS (inhibited by citrate, its product), ICD (allosterically inhibited by NADH and ATP and activated by ADP and Ca 2 � ), and the �-KGD complex (allosterically inhibited by NADH and succinyl CoA and activated by Ca 2 � ).
Uncouplers , whether endogenous (e.g., UCP1 ) or exogenous (e.g., 2,4-DNP and salicylate ), dissipate the H � gradient and prevent ATP generation by OXPHOS but not by substrate-level phosphorylation. The ETC is not inhibited, and O 2 use is not decreased. A decrease in ATP production without a decrease in O 2 utilization decreases the P/O ratio.
Acetyl CoA
Citrate
Isocitrate
-Ketoglutarateα
Succinyl CoASuccinate
Oxaloacetate
Malate
Fumarate
3 NADH
CO2
NAD+
NAD+
NAD+
FADH2GTP GDP + Pi
(ATP)
tyl CoA
Citrate
Isocitrate
-Ketoglutarateα
H
CCCCCCCO2
NAD++
Two molecules of CO2 are released.
SSuccinate
umarate
3 333
FADH2GTP
(ATP)
NADH
Four reduced coenzyme molecules produced per acetyl CoA oxidized to CO2.
GDP + Pi
ules etylCO2.
Ac
Oxaloacetate
cet
Substrate-level phosphorylation occurs.
CoA
Two carbon atoms enter the cycle.
CO2
FAD
Ferrier_Unit02.indd 112Ferrier_Unit02.indd 112 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Gluconeogenesis Overview
What is the function of gluconeogenesis, the pathway denoted by the blue arrows shown?
In what tissues does gluconeogenesis occur? What subcellular locales are involved? Which tissue is the primary gluconeogenesis site in a short-term fast?
What role does gluconeogenesis play in a long-term fast ( starvation )?
10.1 Question
2 GDP
2 GTP
2 Oxaloacetate
Glucose 6-P ?
Fructose 6-P
Fructose 1,6-bis-P
Glyceraldehyde 3-P
2 1,3-Bisphosphoglycerate
2 3-Phosphoglycerate
2 2-Phosphoglycerate
2 Phosphoenolpyruvate
2 Pyruvate
Dihydroxy-acetone-P
CO2
2
3
4
2 ADP + 2 Pi
2 ATP
2 ADP2 ATP
Pi2 NAD+
2 NADH + 2H+
1
Ferrier_Unit02.indd 113Ferrier_Unit02.indd 113 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Gluconeogenesis is the pathway that synthesizes glucose from noncarbohydrate precursor molecules, for example, pyruvate.
Gluconeogenesis occurs in the liver and the kidneys, with the majority of the reactions occurring in the cytosol. However, the enzyme that catalyzes reaction 1 ( PC ) is in the mitochondrial matrix, the enzyme that catalyzes reaction 2 ( PEPCK ) has cytosolic and mitochondrial isozymes, and the enzyme that catalyzes reaction 4 ( glucose 6-phosphatase ) is present in the ER membrane. Liver is the primary site in a short-term fast . [ Note: The kidneys become major glucose producers in a long-term fast.]
In a long-term fast ( starvation ), hepatic and renal gluconeogenesis provides sustained glucose synthesis that maintains blood glucose concentration, thereby ensuring glucose availability for those tissues such as the brain and RBCs that require a continuous supply.
Gluconeogenesis Overview 10.1 Answer
2 GDP
2 GTP
2 Oxaloacetate
Glucose 6-P Glucose
Fructose 6-P
Fructose 1,6-bis-P
Glyceraldehyde 3-P
2 1,3-Bisphosphoglycerate
2 3-Phosphoglycerate
2 2-Phosphoglycerate
2 Phosphoenolpyruvate
2 Pyruvate
Dihydroxy-acetone-P
CO2
2
3
4
2 ADP + 2 Pi
2 ATP
2 ADP2 ATP
Pi2 NAD+
2 NADH + 2H+
1
Ferrier_Unit02.indd 114Ferrier_Unit02.indd 114 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Gluconeogenesis Substrates 10.2 Question
What substrate for gluconeogenesis is denoted by the red question mark shown? What cycle is depicted?
What additional substrates can be used in gluconeogenesis?
Why cannot acetyl CoA be used as a substrate?
How does the lack of glycerol kinase expression in adipose tissue support gluconeogenesis in the liver and the kidneys in the fasted state?
?
?
Glucose
MUSCLE
BLOOD
??
Glucose
Glucose
LIVER
Ferrier_Unit02.indd 115Ferrier_Unit02.indd 115 5/2/14 7:22 PM5/2/14 7:22 PM
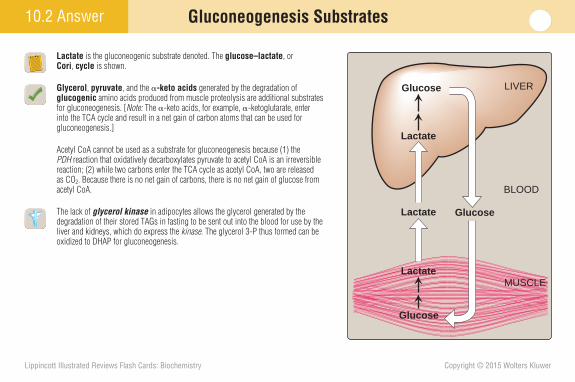
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Lactate is the gluconeogenic substrate denoted. The glucose–lactate , or Cori , cycle is shown.
Glycerol , pyruvate , and the -keto acids generated by the degradation of glucogenic amino acids produced from muscle proteolysis are additional substrates for gluconeogenesis. [ Note: The -keto acids, for example, -ketoglutarate, enter into the TCA cycle and result in a net gain of carbon atoms that can be used for gluconeogenesis.]
Acetyl CoA cannot be used as a substrate for gluconeogenesis because (1) the PDH reaction that oxidatively decarboxylates pyruvate to acetyl CoA is an irreversible reaction; (2) while two carbons enter the TCA cycle as acetyl CoA, two are released as CO 2 . Because there is no net gain of carbons, there is no net gain of glucose from acetyl CoA.
The lack of glycerol kinase in adipocytes allows the glycerol generated by the degradation of their stored TAGs in fasting to be sent out into the blood for use by the liver and kidneys, which do express the kinase . The glycerol 3-P thus formed can be oxidized to DHAP for gluconeogenesis.
10.2 Answer Gluconeogenesis Substrates
Lactate
Lactate
Glucose
MUSCLE
BLOOD
Lactate
Glucose
Glucose
LIVER
Ferrier_Unit02.indd 116Ferrier_Unit02.indd 116 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Gluconeogenesis Reactions
What enzyme, catalyzing the fi rst of four irreversible reactions of gluconeogenesis, is denoted by the red question mark?
What enzymes catalyze the other three irreversible reactions of the pathway?
What water-soluble vitamin is the coenzyme for the enzyme shown? What other enzymes require this coenzyme?
Why might decreased production of acetyl CoA result in hypoglycemia even though it cannot be used as a substrate for gluconeogenesis?
10.3 Question
Pyruvate
CH3
C C
O
O-O
CH2CO
-O
C C
O
O-O
Oxaloacetate (OAA)
?
Ferrier_Unit02.indd 117Ferrier_Unit02.indd 117 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Gluconeogenesis Reactions
The enzyme shown is PC , which catalyzes the fi rst of four irreversible gluconeogenesis reactions.
PEPCK , FBP-2 , and glucose 6-phosphatase catalyze the other irreversible gluconeogenesis reactions.
Biotin , a water-soluble vitamin, is the coenzyme for PC . Other carboxylases requiring biotin are acetyl CoA carboxylase , propionyl CoA carboxylase , and methylcrotonyl CoA c arboxylase . [ Note: Carboxylases also require ATP.]
Acetyl CoA is the allosteric activator of PC . Because it also inhibits PDH , acetyl CoA (primarily from FA oxidation) diverts pyruvate from oxidative degradation and to gluconeogenesis. Consequently, a decrease in acetyl CoA can result in hypoglycemia .
10.3 Answer
PDH complex
Pyruvate
Acetyl CoA Oxaloacetate
Glucose
+− Pyruvate carboxylase
Pyruvate
CH3
C C
O
O-O
CH2CO
-O
C C
O
O-O
Oxaloacetate (OAA)
Pyruvate carboxylase
Ferrier_Unit02.indd 118Ferrier_Unit02.indd 118 5/2/14 7:22 PM5/2/14 7:22 PM
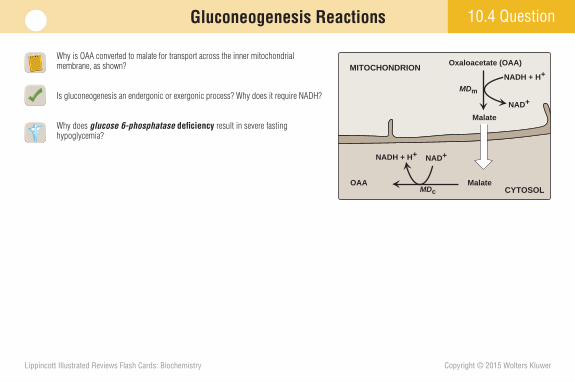
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Why is OAA converted to malate for transport across the inner mitochondrial membrane, as shown?
Is gluconeogenesis an endergonic or exergonic process? Why does it require NADH?
Why does glucose 6-phosphatase defi ciency result in severe fasting hypoglycemia?
10.4 QuestionGluconeogenesis Reactions
Oxaloacetate (OAA)
OAA
NADH + H+ NAD+
Malate
Malate
NAD+
NADH + H+MITOCHONDRION
CYTOSOL
MDm
MDc
Ferrier_Unit02.indd 119Ferrier_Unit02.indd 119 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
OAA has no mitochondrial transporter. Reduction to malate by MD m (as NADH is oxidized), transport across the inner mitochondrial membrane, and oxidation by MD c (as NAD � is reduced) makes the OAA and NADH needed for gluconeogenesis available in the cytosol. [ Note: With glycolysis, OAA ↔ malate is used to transfer reducing equivalents in the opposite direction.]
Gluconeogenesis is endergonic and uses energy from ATP and GTP hydrolysis. It requires NADH for the reduction of 1,3-bisphosphoglycerate to glyceraldehyde 3-P by glyceraldehyde 3-phosphate dehydrogenase , an enzyme common to gluconeogenesis and glycolysis.
Glucose 6-phosphatase , an ER membrane protein unique to liver and kidney, dephosphorylates intracellular glucose 6-P to free glucose, which can be transported into the blood by GLUT-2. Glucose 6-phosphatase defi ciency traps glucose 6-P within the cells of gluconeogenic tissues.
Gluconeogenesis Reactions10.4 Answer
Oxaloacetate (OAA)
OAA
NADH + H+ NAD+
Malate
Malate
NAD+
NADH + H+Oxaloacetate cannot cross the mitochondrial membrane so it is reduced to malate that can.
MDm
MDc
Glucose 6-phosphatase
D-Glucose
H
CH OH
CH OH
CH OH
CHO H
CH OH
C H
O
Glucose 6-phosphate
H
CH O
CH OH
CH OH
CHO H
CH OH
C H
O
H2O P
P
CYTOSOL
Ferrier_Unit02.indd 120Ferrier_Unit02.indd 120 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Gluconeogenesis Regulation
What effect does a decrease in the insulin to glucagon ratio have on the activity of FBP-1 shown? Why?
How are gluconeogenesis (glucose synthesis) and glycolysis (glucose oxidation) coordinately regulated?
Why might FBP-1 defi ciency cause hyperventilation ?
10.5 Question
H2O
Fructose 6-phosphate Fructose 6-phosphate
?FBP-1
Bifunctional enzymeFBP-1
PFK-2(active)
ATPADP
Active protein kinase A
ATP cAMP
Adenylylcyclase
Receptor
Glucagon(high)
Receptor
Insulin(low)
FBP-2(inactive)
CELL MEMBRANE
CYTOSOL
PP P
P
Glucose 6-P Glucose
Fructose 6-P
Gluconeogenesis
Fructose 1,6-bis-P
Glyceraldehyde 3-P
1,3-Bisphosphoglycerate
3-Phosphoglycerate
2-Phosphoglycerate
Phosphoenolpyruvate
Pyruvate
DHAP
Lactate
PFK-2(inactive)
FBP-2(active)
Ferrier_Unit02.indd 121Ferrier_Unit02.indd 121 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
A rise in glucagon results in decreased production of fructose 2,6-bisP , a FBP-1 inhibitor. Loss of the inhibitor increases FBP-1 activity and the rate of gluconeogenesis.
Fructose 2,6-bisP (a high glucose signal) and AMP (a low energy signal) coordinately downregulate gluconeogenesis (by inhibiting FBP-1 ) and upregulate glycolysis (by activating PFK-1 ).
FBP-1 defi ciency decreases gluconeogenesis. It does not affect glycolysis, which produces pyruvate or lactate that are substrates for gluconeogenesis. Accumulation of these acids causes a metabolic acidosis . The acidosis is compensated for by hyperventilation that decreases CO 2 , thereby reducing H � : H � � HCO 3 – ↔ H 2 CO 3 ↔ CO 2 � H 2 O.
Gluconeogenesis Regulation 10.5 Answer
H2O
Fructose 6-phosphate Fructose 6-phosphate
FBP-1
Fructose 2,6-bisphosphate Bifunctional enzyme
FBP-1
PFK-2(active)
ATPADP
Active protein kinase A
ATP cAMP
Adenylylcyclase
Receptor
Glucagon(high)
Receptor
Insulin(low)
FBP-2(inactive)
CELL MEMBRANE
CYTOSOL
PP P
P
Glucose 6-P Glucose
Fructose 6-P
Gluconeogenesis
Fructose 1,6-bis-P
Glyceraldehyde 3-P
1,3-Bisphosphoglycerate
3-Phosphoglycerate
2-Phosphoglycerate
Phosphoenolpyruvate
Pyruvate
DHAP
Lactate
PFK-2(inactive)
FBP-2(active)
High glucagon/insulin ratio causes elevated cAMP and increased levels of active protein kinase A.
Increased protein kinase A activity favors the phos-phorylated form of thebifunctional PFK-2/FBP-2.
Phosphorylation of the PFK-2 domain inactivates it, allowing the FBP-2 domain to be active.
Decreased levels of fructose 2,6-bisphosphate decrease the inhibition of FBP-1, whichleads to an increased rate of gluconeogenesis.
21
34
Ferrier_Unit02.indd 122Ferrier_Unit02.indd 122 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Gluconeogenesis Regulation
What effect does the phosphorylation of hepatic PK (shown) have on its activity?
In what pathway does this enzyme directly participate? How does its inhibition affect gluconeogenesis?
Is hypoglycemia an expected fi nding in an individual with hyperinsulinemia ? Why or why not?
10.6 Question
PEP
OAA
Glucose
Pyruvate
ATP ADP
Active protein kinase A
ATP cAMP + PPi
Adenylylcyclase
Glucagon
ADP
ATP
P
Receptor
Pyruvatekinase
Pyruvatekinase
Ferrier_Unit02.indd 123Ferrier_Unit02.indd 123 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Gluconeogenesis Regulation10.6 Answer
The hepatic isoform of PK is regulated by covalent phosphorylation (inactivated) and dephosphorylation (activated).
PK is an enzyme of glycolysis. PK inhibition by phosphorylation (or by allosteric effectors) decreases the conversion of PEP to pyruvate, thereby increasing PEP’s availability for gluconeogenesis.
Hypoglycemia is an expected fi nding in hyperinsulinemia , because gluconeogenesis is decreased as a result of (1) decreased transcription of the gene for PEPCK (as a consequence of decreased glucagon); (2) PFK-2 and PK dephosphorylation (activation), favoring glycolysis; and (3) decreased availability of gluconeogenic substrates, particularly amino acids from muscle protein degradation because insulin favors protein synthesis. [ Note: Insulin decreases FA degradation, thereby decreasing production of acetyl CoA, a PC activator.]
PEP
OAA
Glucose
Pyruvate
ATP ADP
Active protein kinase A
ATP cAMP + PPi
Adenylylcyclase
Glucagon
ADP
ATP
P
Receptor
Pyruvatekinase(active)
Pyruvatekinase
(inactive)
Ferrier_Unit02.indd 124Ferrier_Unit02.indd 124 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Glycogen Structure and Function
In what two tissues and in what subcellular locale is glycogen stored?
What is the function of stored glycogen?
In addition to glycogen, what are the other two sources of blood glucose?
What would be the expected signs and symptoms in someone with a defi ciency in the ability to store or utilize glycogen?
11.1 Question
UDP-Glucose
Glucose 1-P
Glucose 6-P
? ?
Glycogen
Ferrier_Unit02.indd 125Ferrier_Unit02.indd 125 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Glycogen, a branched homopolymer of glucose, is stored in the cytosol of liver and muscle cells primarily.
Glycogen serves as a rapidly mobilized glucose reserve. Glycogen stored in the liver is used to maintain blood glucose, whereas that stored in muscles is used to power contraction. [ Note: Liver glycogen can maintain blood glucose for 10–18 hours.]
In addition to glycogen stored in the liver, diet and gluconeogenesis (in the liver and kidneys) are sources of blood glucose.
Defi ciencies in the ability to store or use glycogen in the liver would result in fasting hypoglycemia . Defi ciencies in the storage or use of glycogen in muscles would result in muscle weakness (exercise intolerance) .
Glycogen Structure and Function11.1 Answer
Glucose
Glycogen
Glucose 6-P
Pi
Glucose 6-P
Glycogen
ENERGY
MUSCLE
LIVER
BLOODGLUCOSE
UDP-Glucose
Glycogen
MUSCLE LIVER
Glucose 1-P
Glucose 6-P
Ferrier_Unit02.indd 126Ferrier_Unit02.indd 126 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
11.2 Question Glycogenesis
As shown, glycogen is a branched homopolymer of glucose. What form of glucose is used as the substrate in glycogenesis?
What enzymes are required for glycogenesis?
What is glycogenin ?
How would branching enzyme defi ciency affect glycogen structure? What are the clinical consequences?
O
OH
OH
OH
OH
OH
OH
CH2OH CH2 CH2OH
O
OHOH
OH
CH2 OH
CH2 OH
OH
α(1→6) glycosidic bond
α(1→4) glycosidicbonds
O
O
O
O
O
O O
O O
Ferrier_Unit02.indd 127Ferrier_Unit02.indd 127 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
11.2 Answer Glycogenesis
The substrate for glycogenesis is UDP-glucose, which is made from glucose 1-P and UTP by UDP-glucose pyrophosphorylase .
GS and branching enzyme are required for glycogenesis from UDP-glucose.
Glycogenin is the enzyme that makes the primer for GS . It autoglucosylates (using UDP-glucose) at a specifi c Tyr and makes a short chain of glucose residues linked by (1➔4) glycosidic bonds. GS extends the chain. A primer is needed because GS cannot initiate synthesis from two molecules of UDP-glucose.
Branching enzyme ( 4:6 transfer-ase) moves up to 8 glucose residues from an end to an internal position, breaking an (1➔4) bond and forming an (1➔6) bond, thereby creating a branch. Defi ciency of 4:6 transferase activity ( Andersen disease , type IV GSD ) results in glycogen with few branches and long outer chains causing decreased solubility, which can result in cirrhosis .
GLYCOGEN
Further branching,making α(1→6) bonds.
Further elongation at the nonreducing ends by glycogen synthase, making α(1→4) bonds.
on
ml
k
j i hf e d c b aBranching
enzyme
Glycogensynthase
NONREDUCINGENDS
UDP
HO
Tyrosine
Glycogenin
Glucose 1-phosphate
UDP-glucosepyrophosphorylase
Pyrophosphatase
UDP-glucose(UDP - )
H2O
2 Pi
PPi
α(1→6) bond
α(1→4) bonds
o n m l k j i h g f e d c b a
Glucose 6-phosphate
Phosphoglucomutase
O
OO
UDP
UDP-glucose(UDP - )
UTP
4:6 transferase
Ferrier_Unit02.indd 128Ferrier_Unit02.indd 128 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
11.3 QuestionGlycogenolysis
What enzyme denoted by the red question mark catalyzes the reaction shown? Where in the cell is the enzyme found? What coenzyme does it require?
How would debranching enzyme defi ciency affect glycogen structure? What are the clinical consequences?
Glycogen chain
HO
OH
OH
HOO
O
OH
OH
O
Remaining glycogen
OH
OH
HOO
O
OH
OH
O
O
OH
OH
O
O
OH
OH
OHHO
HOO
OH
OH
O
O
OH
OH
OH
HO HO
HO HO HO
HO
Glucose 1-P
+
O
PO3
O
Pi
2–
?
Ferrier_Unit02.indd 129Ferrier_Unit02.indd 129 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
11.3 Answer Glycogenolysis
The enzyme is cytosolic glycogen phosphorylase , which uses P i to sequentially cleave (1➔4) bonds in glycogen to generate glucose 1-P. PLP (from vitamin B 6 ) is the coenzyme. The process stops when four glucose residues remain at the branch point, a structure known as a limit dextrin . [Note: Limited degradation of glycogen occurs in the lysosomes by �-glucosidase.]
Debranching enzyme is bifunctional. It moves the outer three glucose residues from a limit dextrin to an end ( 4:4 transferase activity). It then removes the terminal glucose residue as free (nonphosphorylated) glucose ( 1:6 glucosidase activity). Debranching enzyme defi ciency ( Cori disease , type III GSD ) results in glycogen with short branches. Hypoglycemia and muscle weakness can result from decreased ability to mobilize stored glycogen.
Glycogen chain
HO
OH
OH
PLP
HOO
O
OH
OH
O
Remaining glycogen
OH
OH
HOO
O
OH
OH
O
O
OH
OH
O
O
OH
OH
OHHO
HOO
OH
OH
O
O
OH
OH
OH
HO HO
HO HO HO
HO
Glucose 1-P
+
O
Glycogen phosphorylase
PO3
O
Pi
2–
Ferrier_Unit02.indd 130Ferrier_Unit02.indd 130 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
11.4 QuestionGlycogenolysis
What happens to the glucose 1-P produced by the glycogen phosphorylase reaction shown?
What is the role of glucose 6-phosphatase in glycogenolysis?
Would the hypoglycemia caused by glucose 6-phosphatase defi ciency be less or more severe than that caused by a defect in hepatic glycogen phosphorylase ? Glycogen chain
HO
OH
OH
PLP
HOO
O
OH
OH
O
OH
OH
HOO
HOO
OH
OH
O
O
OH
OH
OH
HO HO
HO
Glucose 1-P
O
Glycogen phosphorylase
PO3
O
Pi
2–
?
Ferrier_Unit02.indd 131Ferrier_Unit02.indd 131 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
11.4 Answer Glycogenolysis
The glucose 1-P produced by glycogen phosphorylase is converted to glucose 6-P by phosphogluco-mutase . Glucose 1,6-bisP is an intermediate in the reaction.
Glucose 6-phosphatase hydrolyzes glucose 6-P in the liver (and the kidneys), generating free glucose that can enter the blood. [ Note: Because glucose 6-phosphatase is not found in muscle, muscle glycogen degradation does not contribute to blood glucose maintenance.]
Glucose 6-P is produced by the penultimate reaction in both glycogenolysis and gluconeogenesis. Therefore, glucose 6-phosphatase defi ciency ( von Gierke disease , type Ia GSD ) would prevent blood glucose maintenance by both processes and result in a severe, fasting hypoglycemia . In contrast, hepatic glycogen phosphorylase defi ciency ( Hers disease , type VI GSD ) would affect only liver glycogenolysis.
Glycogen chain
HO
OH
OH
PLP
HOO
O
OH
OH
O
OH
OH
HOO
HOO
OH
OH
O
O
OH
OH
OH
HO HO
HO
Glucose 1-P Glucose 6-P
O
Glycogen phosphorylase
PO3
O
Pi
2–
Glucose 6-phosphatase
D-Glucose
H
CH OH
CH OH
CH OH
CHO H
CH OH
C H
O
Glucose 6-phosphate
H
CH O
CH OH
CH OH
CHO H
CH OH
C H
O
H2O P
P
Ferrier_Unit02.indd 132Ferrier_Unit02.indd 132 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
11.5 Question Glycogen Metabolism Regulation
Which enzyme(s) shown is inactivated by phosphorylation?
How do glucagon (in the liver) and epinephrine (in the liver and muscles) cause coordinated regulation of glycogen metabolism?
Why might endurance athletes greatly increase their carbohydrate consumption several days before an athletic event?
Glucagon(LIVER)
Phosphorylase
Phosphorylase kinase
Phosphorylates
Protein phosphatase-1inhibitor
Glycogensynthase
cAMP-mediated activation of PKA and phosphorylation of
Epinephrine(LIVER + MUSCLE)
Ferrier_Unit02.indd 133Ferrier_Unit02.indd 133 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
11.5 Answer Glycogen Metabolism Regulation
Phosphorylation inactivates GS , the regulated enzyme of glycogenesis. The phos-phorylated form of GS is the inactive, or “ b ,” form.
Glucagon and epinephrine, through cAMP-mediated activation of PKA , result in phosphorylation (inactivation) of GS of glycogenesis and phosphorylation of phosphorylase kinase and phosphorylase of glycogenolysis. The phosphory-lated form of phosphorylase kinase and phosphorylase is the active, or “ a ,” form.
Increased carbohydrate consumption is a strategy used by some athletes to replenish/increase their glycogen stores by increasing glucose, the glycogenesis substrate. The stored glycogen can be used to power muscle contraction, thereby improving performance (ideally).
Glucagon(LIVER)
Phosphorylase (active)
(Increased glycogenolysis)
Phosphorylase kinase (active)
Phosphorylates
Protein phosphatase-1inhibitor (active)
(Maintenance of phosphorylation)
Glycogensynthase(inactive)
(Decreased glycogenesis)
cAMP-mediated activation of PKA and phosphorylation of
Epinephrine(LIVER + MUSCLE)
Ferrier_Unit02.indd 134Ferrier_Unit02.indd 134 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
11.6 Question Glycogen Metabolism Regulation
What effect(s) do glucose 6-P and ATP have on the enzymes of glycogen metabolism (shown) in the liver? In muscle?
meet the needs of the body, and meet the needs of a particular tissue.
How does a rise in cytosolic Ca 2 � result in glycogen phosphorylase kinase activation?
What causes a rise in Ca 2 � in muscle? In liver?
MUSCLE
LIVER
Glucose 1-phosphate
Glycogen
Glycogensynthase
Glycogenphosphorylase
Glucose 1-phosphate
Glycogen
Glycogensynthase
Glycogenphosphorylase
A
B
Ferrier_Unit02.indd 135Ferrier_Unit02.indd 135 5/2/14 7:22 PM5/2/14 7:22 PM
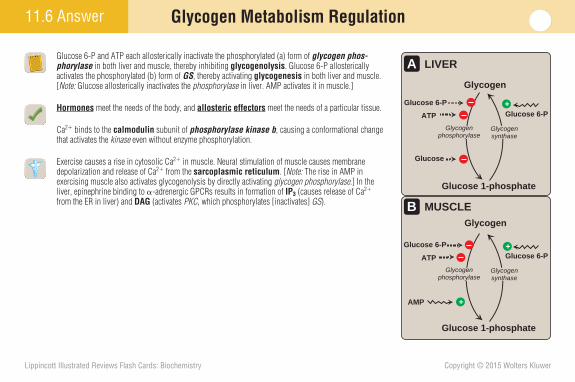
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Glycogen Metabolism Regulation11.6 Answer
Glucose 6-P and ATP each allosterically inactivate the phosphorylated (a) form of glycogen phos-phorylase in both liver and muscle, thereby inhibiting glycogenolysis . Glucose 6-P allosterically activates the phosphorylated (b) form of GS , thereby activating glycogenesis in both liver and muscle. [ Note: Glucose allosterically inactivates the phosphorylase in liver. AMP activates it in muscle.]
Hormones meet the needs of the body, and allosteric effectors meet the needs of a particular tissue.
Ca 2 � binds to the calmodulin subunit of phosphorylase kinase b , causing a conformational change that activates the kinase even without enzyme phosphorylation.
Exercise causes a rise in cytosolic Ca 2 � in muscle. Neural stimulation of muscle causes membrane depolarization and release of Ca 2 � from the sarcoplasmic reticulum . [ Note: The rise in AMP in exercising muscle also activates glycogenolysis by directly activating glycogen phosphorylase .] In the liver, epinephrine binding to -adrenergic GPCRs results in formation of IP 3 (causes release of Ca 2 � from the ER in liver) and DAG (activates PKC , which phosphorylates [inactivates] GS ). MUSCLE
LIVER
Glucose 1-phosphate
AMP
Glucose 6-P
Glycogen
Glycogensynthase
Glycogenphosphorylase
Glucose 1-phosphate
ATP
Glucose
Glucose 6-P
Glucose 6-P
Glycogen
Glycogensynthase
Glycogenphosphorylase
A
B
++
+
ATP
Glucose 6-P
Ferrier_Unit02.indd 136Ferrier_Unit02.indd 136 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
11
A 12-year-old boy is being evaluated for the cause of the muscle cramps and exertional fatigue that recently have caused him to sit on the sidelines during baseball drills. He reports that his urine was normal in color after the earlier episodes. A forearm lactate test is administered in which blood lactate , as well as CK , is measured before and after 30 hand contractions. Urinary myoglobin also is measured before and after the exercise. The results show that blood lactate failed to rise with the exercise, but urinary myoglobin levels did rise ( myoglobinuria ). CK was elevated before and after exercise. Based on the results, a diagnosis of muscle glycogen phosphorylase ( myophosphorylase ) defi ciency ( McArdle disease , GSD type V ) is made. No specifi c treatments are available for this AR disorder.
Why are most GSDs not lysosomal disorders?
Case Card
Ferrier_Unit02.indd 137Ferrier_Unit02.indd 137 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
11 Case Card
GSDs are rare genetic disorders that affect the various proteins of glycogen metabolism. They typically affect glycogen degradation (as with myophosphory-lase defi ciency , shown) or, more rarely, glycogen synthesis (as with branching enzyme defi ciency ). They result either in the formation of glycogen with an abnormal structure or excessive accumulation of normal glycogen. Severity ranges from mild to fatal in early childhood. Because liver and muscle are the primary sites of glycogen synthesis and use, the presenting symptoms are either hepatomegaly with hypoglycemia or muscle weakness . In the patient, blood lactate failed to rise with exercise because of decreased glucose availability for glycolysis as a result of a defi ciency in muscle glycogenolysis.
Glucose 1-P
Pi
Glycogenphosphorylase
`-1,6-bond
GLYCOGENIN
NONREDUCINGENDS
REMAINING GLYCOGEN
H2O
Lysosomala(1→4)-glucosidase
GLUCOSE
Lysosomal storage disease
Generalized (but primarily heart, liver, muscle)
Excessive glycogen concentrations found in abnormal vacuoles in the lysosomes
Normal blood sugar levels
Massive cardiomegaly
Enzyme replacement therapy available
Infantile form: early death typically from heart failure
Normal glycogen structure
TYPE II: POMPE DISEASE(LYSOSOMAL `(1→4)-GLUCOSIDASE DEFICIENCY)
Skeletal muscle affected; liver enzyme normal
Temporary weakness and cramping of skeletal muscle after exercise
No rise in blood lactate during strenuous exercise
Normal mental development
Myoglobinemia and myoglobinuria may be seen
Relatively benign, chronic condition
High level of glycogen with normal structure in muscle
Deficiency of the liver isozyme causes Type VI: Hers disease with mild fasting hypoglycemia.
TYPE V: McARDLE SYNDROME(SKELETAL MUSCLE GLYCOGEN PHOSPHORYLASE OR MYOPHOSPHORYLASE DEFICIENCY)
Glucose 1-P
Pi
Glycogenphosphorylase
`-1,6-bond
GLYCOGENIN
NONREDUCINGENDS
REMAINING GLYCOGEN
H2O
Lysosomala(1→4)-glucosidase
GLUCOSE
se
Lysosomala(1aa →4)-glucosidase
Lysosomal storage disease
Generalized (but primarily heart, liver, muscle)
Excessive glycogen concentrations found in abnormal vacuoles in the lysosomes
Normal blood sugar levels
Massive cardiomegaly
Enzyme replacement therapy available
Infantile form: early death typically from heart failure
Normal glycogen structure
TYPE II: POMPE DISEASE(LYSOSOMAL `(1→4)-GLUCOSIDASE DEFICIENCY)
Skeletal muscle affected; liver enzyme normal
Temporary weakness and cramping of skeletal muscle after exercise
No rise in blood lactate during strenuous exercise
Normal mental development
Myoglobinemia and myoglobinuria may be seen
Relatively benign, chronic condition
High level of glycogen with normal structure in muscle
Deficiency of the liver isozyme causes Type VI: Hers disease with mild fasting hypoglycemia.
TYPE V: McARDLE SYNDROME(SKELETAL MUSCLE GLYCOGEN PHOSPHORYLASE OR MYOPHOSPHORYLASE DEFICIENCY)
Because glycogen metabolism occurs primarily in the cytosol, most GSDs (in contrast to other storage diseases) are not lysosomal disorders. An exception is Pompe disease (shown). A
Ferrier_Unit02.indd 138Ferrier_Unit02.indd 138 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
12.1 Question Fructose Metabolism
Name the enzyme represented by the red question mark shown. In what tissue(s) is the enzyme found?
Is the rate of fructose metabolism faster or slower than that of glucose? Why?
How do the kinetics of fructokinase and glucokinase differ?
What is the primary dietary source of fructose?
Fructose
Fructose1-phosphate
CH OH
CH OH
CHO H
C O
Fructose1,6-bisphosphate
CH OH
CH OH
CHO H
C O
Fructose6-phosphate
ATP
ADP
ATP
ADP
Glyceraldehyde
CH OH
C H
O
Glyceraldehyde3-phosphate
CH OH
C H
O
? Aldolase A, B, C
CH2O CH2O
CH2OH
CH2OCH2OH
CH2O
P
P
P
P
Fructokinase Phosphofructokinase
FRUCTOSEMETABOLISM
GLYCOLYSIS
C O
H
CH OH
CH2O P
Dihydroxyacetonephosphate
Ferrier_Unit02.indd 139Ferrier_Unit02.indd 139 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
12.1 Answer Fructose Metabolism
The aldolase B isoform is shown. Aldolase B is found in the liver, kidneys, and small intestine. It can cleave both fructose 1-P and fructose 1,6-bisP into trioses, whereas the A isoform (found in many tissues) and the C isoform (found in the brain) cleave only the 1,6-bisP form.
Fructose metabolism is faster because it bypasses the key rate-limiting enzyme of glycolysis, PFK-1 .
Fructokinase has a high affi nity ( low K m ) for fructose and a high V max . Glucokinase , the hepatic hexokinase that phosphorylates glucose, has a low affi nity for fructose.
Dietary fructose is consumed primarily as the disaccharide sucrose (glucose � fructose), also called table sugar . Uptake of fructose is by insulin-independent GLUT-5 and does not promote insulin release.
Fructose
Fructose1-phosphate
CH OH
CH OH
CHO H
C O
Fructose1,6-bisphosphate
CH OH
CH OH
CHO H
C O
Fructose6-phosphate
ATP
ADP
ATP
ADP
Glyceraldehyde
CH OH
C H
O
Glyceraldehyde3-phosphate
CH OH
C H
O
Aldolase B Aldolase A, B, C
CH2O CH2O
CH2OH
CH2OCH2OH
CH2O
P
P
P
P
Fructokinase Phosphofructokinase
FRUCTOSEMETABOLISM
GLYCOLYSIS
Hexokinase
C O
H
CH OH
CH2O P
Dihydroxyacetonephosphate
Ferrier_Unit02.indd 140Ferrier_Unit02.indd 140 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
12.2 Question Fructose Metabolism Disorders
Which of the two enzymic defi ciencies (marked by red bars) results in a serious pathology?
What is the primary presenting sign of this defi ciency in an affected individual who consumes fructose?
Explain the basis of this sign.
FRUCTOSE
Glyceraldehyde
Fructose 1-P
ATP
ADP
Dihydroxyacetone P
Fructokinase
Aldolase B
Ferrier_Unit02.indd 141Ferrier_Unit02.indd 141 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Fructose Metabolism Disorders12.2 Answer
Aldolase B defi ciency results in a serious pathology. In contrast, fructokinase defi ciency (essential fructosuria) is a benign condition that results only in increased urinary excretion of fructose.
Aldolase B defi ciency (also known as hereditary fructose intolerance [ HFI ]) is characterized by severe hypoglycemia in affected individuals who consume fructose. Over time, patients develop an aversion to sweet foods.
With HFI , accumulation of fructose 1-P (the substrate of the defi cient aldolase B ) results in P i trapping . This causes a decrease in the ability to phosphorylate ADP to ATP, and the decrease in ATP decreases gluconeogenesis (an endergonic process). The drop in P i also inhibits glycogen phosphorylase . Therefore, neither gluconeogenesis nor glycogenolysis is able to maintain blood glucose. HFI becomes apparent when an affected baby is fi rst fed food containing fructose (typically when weaned). Treatment is the removal of fructose (and sucrose) from the diet. [ Note: As ATP levels fall, AMP levels rise. The AMP is degraded to uric acid, which competes with lactic acid for renal excretion, resulting in hyperuricemia and lactic acidemia. Thus, many of the signs of HFI are like those of GSD Ia .]
FRUCTOSE
Glyceraldehyde
Fructose 1-P
ATP
ADP
Dihydroxyacetone P
Fructokinase
Aldolase B
Ferrier_Unit02.indd 142Ferrier_Unit02.indd 142 5/2/14 7:22 PM5/2/14 7:22 PM
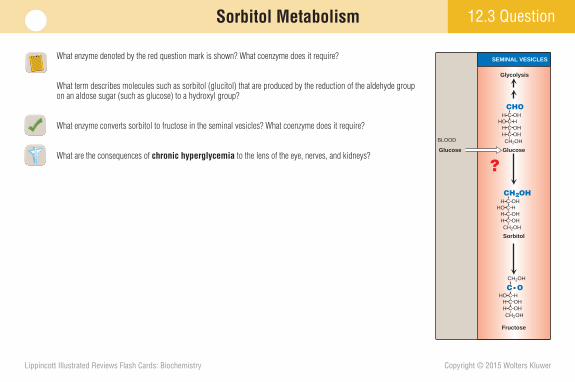
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
12.3 QuestionSorbitol Metabolism
What enzyme denoted by the red question mark is shown? What coenzyme does it require?
What term describes molecules such as sorbitol (glucitol) that are produced by the reduction of the aldehyde group on an aldose sugar (such as glucose) to a hydroxyl group?
What enzyme converts sorbitol to fructose in the seminal vesicles? What coenzyme does it require?
What are the consequences of chronic hyperglycemia to the lens of the eye, nerves, and kidneys?
Sorbitol
Fructose
Glycolysis
SEMINAL VESICLES
GlucoseGlucose
BLOOD
CH2OHCH OHCH OHCHO H
CH2OHCH OH
CH2OH
CH2OH
CH OHCH OHCHO H
CHOCH OH
CH2OHCH OHCH OHCHO HC O
?
Ferrier_Unit02.indd 143Ferrier_Unit02.indd 143 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Sorbitol Metabolism12.3 Answer
NADPH-requiring aldose reductase is shown.
Molecules such as sorbitol ( glucitol ) that are produced by the reduction of the aldehyde group on an aldose sugar (such as glucose) to a hydroxyl group are referred to as polyols or “ sugar alcohols .”
NAD � -requiring sorbitol dehydrogenase converts sorbitol to fructose in the seminal vesicles. [ Note: Fructose is the preferred energy source of sperm in the seminal vesicles.]
With chronic hyperglycemia , glucose uptake results in sorbitol accumulation because it either cannot be metabolized or is made faster than it can be metabolized. Sorbitol cannot effi ciently cross the cell membrane. It is osmotically active, drawing water into the cells, and causing an osmotic stress that has been related to cataract formation , peripheral neuropathy , and nephropathy in diabetes.
Sorbitol
Fructose
Sorbitoldehydrogenase
Aldosereductase
Glycolysis
SEMINAL VESICLES
GlucoseGlucose
BLOOD
CH2OHCH OHCH OHCHO H
CH2OHCH OH
CH2OH
CH2OH
CH OHCH OHCHO H
CHOCH OH
CH2OHCH OHCH OHCHO HC O
NADH + H+
NAD+
NADPH + H+
NADP+
Sorbitol
NADPH + H+
Aldosereductase
NADP+
Glucose
Glycolysis
H2O
H2O
H2O
LENSES NERVES KIDNEYS
In hyperglycemia
Ferrier_Unit02.indd 144Ferrier_Unit02.indd 144 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
12.4 QuestionGalactose Metabolism
What enzyme denoted by the red question mark catalyzes the exchange reaction involving galactose 1-P and UDP-glucose? What is the fate of the UDP-galactose product?
What is the primary dietary source of galactose?
What enzyme defi ciencies result in galactose metabolism disorders?
UDP-Glucose Galactose 1-P
Glycogen Galactose
UDP-GalactoseGlucose 1-P
Glucose 6-P Glucose
?
Ferrier_Unit02.indd 145Ferrier_Unit02.indd 145 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Galactose Metabolism12.4 Answer
The exchange reaction involving galactose 1-P and UDP-glucose is cata-lyzed by GALT . The UDP-galactose product serves as a galactose donor in biosynthetic reactions such as lactose synthesis. It can also be converted to its C-4 epimer (UDP-glucose) that is used in glycogenesis as shown.
Lactose ( milk sugar ), a disaccharide of galactose � glucose made in lactating mammary glands by lactose synthase , is the primary dietary source of galactose.
Galactokinase defi ciency causes a relatively benign disorder in which cataracts may be seen. GALT defi ciency ( � 5% of normal activity) causes classic galactosemia that results in liver damage, intellectual disability, and cataracts (likely the result of galactitol , a sugar alcohol derived from galactose). Dietary restriction of galactose is the treatment for both defi ciencies.
UDP-Glucose Galactose 1-P
Glycogen Galactose
UDP-GalactoseGlucose 1-P
Glucose 6-P Glucose
GALT
GALACTOSE
LACTOSE UDP-GALACTOSE
Galactose 1-P
ATP ADP
Glucose 1-P
GalactokinaseUDP-Glucose
UTP
PPi
UDP-Glucosepyrophosphorylase
Galactose 1-phosphateuridylyltransferase
Ferrier_Unit02.indd 146Ferrier_Unit02.indd 146 5/2/14 7:22 PM5/2/14 7:22 PM
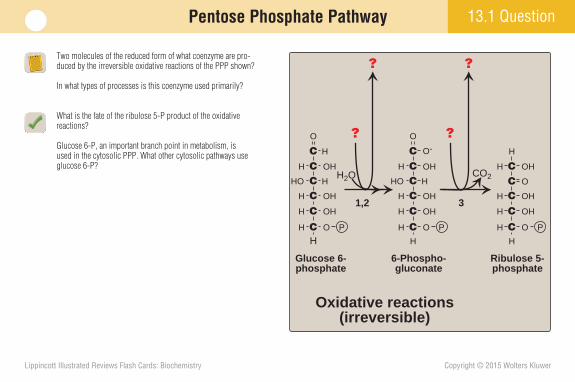
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
13.1 QuestionPentose Phosphate Pathway
Two molecules of the reduced form of what coenzyme are pro-duced by the irreversible oxidative reactions of the PPP shown?
In what types of processes is this coenzyme used primarily?
What is the fate of the ribulose 5-P product of the oxidative reactions?
Glucose 6-P, an important branch point in metabolism, is used in the cytosolic PPP. What other cytosolic pathways use glucose 6-P?
Glucose 6-phosphate
HCH O
CH OH
CH OH
CHO H
CH OH
C H
O
P
6-Phospho-gluconate
H
CH O
CH OH
CH OH
CHO H
CH OH
C O-O
P
Ribulose 5-phosphate
H
CH O
CH OH
CH OH
CH OH
H
P
C OH2O CO2
??
? ?
1,2 3
Oxidative reactions(irreversible)
Ferrier_Unit02.indd 147Ferrier_Unit02.indd 147 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Pentose Phosphate Pathway13.1 Answer
Two NADPH are produced by the oxidative reactions of the PPP. [ Note: NADPH is also produced by malic enzyme .]
NADPH is used as a coenzyme in reductive biosynthetic pathways, such as fatty acid, cholesterol, and steroid hormone synthesis. [ Note: NADP exists in the cell primarily as NADPH, a reductant (e � donor). This is in contrast to NAD, which exists primarily as NAD � , an oxidant (e � acceptor).]
The ribulose 5-P (produced by the oxidative decarboxylation of 6-phosphogluconate) can be reversibly isomerized to ribose 5-P and used in purine and pyrimidine nucleotide synthesis and xylulose 5-P that is used in sugar interconversions.
Glucose 6-phosphate
HCH O
CH OH
CH OH
CHO H
CH OH
C H
O
P
6-Phospho-gluconate
H
CH O
CH OH
CH OH
CHO H
CH OH
C O-O
P
Ribulose 5-phosphate
H
CH O
CH OH
CH OH
CH OH
H
P
C OH2O
NADP+ NADP+
CO2
NADPH,H+
NADPH,H+
1,2 3
Oxidative reactions(irreversible)
Ribulose 5-P
Ribose 5-P Xylulose 5-P
Glycolysis uses glucose 6-P directly. Glycogenesis uses UDP-glucose derived from glucose 6-P. [ Note: The pathways for the synthesis of the amino and acidic sugars of the GAGs also utilize nucleotide sugars derived from glucose 6-P.]
Ferrier_Unit02.indd 148Ferrier_Unit02.indd 148 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
13.2 QuestionPentose Phosphate Pathway
What enzyme catalyzes the two-carbon transfer shown? The three-carbon transfer?
What is the function of these sugar interconversions?
What B vitamin–derived coenzyme does the two-carbon transfer reaction require? What other enzymes require it?
Fructose 6-phosphate
H
CH O
CH OH
CH OH
H
P
Glyceraldehyde3-phosphate
H
CH O
CH OH
C H
O
P
Ribulose 5-phosphate
H
CH O
CH OH
CH OH
CH OH
H
P
C O
Xylulose 5-phosphate
H
CH O
CH OH
OH
P
O
CHO H
H
CH O
CH OH
CH OH
P
Sedoheptulose7-phosphate
H
CH O
CH OH
P
H
CH O
CH OH
P
CH OH
CH OH
C H
O
CH OH
CH OH C H
O
CH
H
C
CHO H
O
H
H OH
CC
CHO H
C O
CH OH
Ribose 5-phosphate
Δ2C
Erythrose 4-phosphate
Δ3C
Ferrier_Unit02.indd 149Ferrier_Unit02.indd 149 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
13.2 Answer Pentose Phosphate Pathway
Transketolase catalyzes the two-carbon transfer. Transaldolase catalyzes the three-carbon transfer.
The sugar interconversions allow the ribulose 5-P product of the PPP to be converted to the glycolytic intermediates glyceraldehyde 3-P and fructose 6-P. [ Note: In cells synthesizing nucleotides and nucleic acids, the ribulose 5-P product will be converted to PRPP. Under other conditions, the carbons enter glycolysis.]
Thiamine pyrophosphate ( TPP ) is the coenzyme for transketolase . The E1 components of � -keto acid dehydroge-nase complexes ( PDH , � -KGD of the TCA cycle, and BCKD of amino acid metabolism) also require TPP. [ Note: Defi ciency of thiamine (vitamin B 1 ), the precursor of TPP, may result in Wernicke-Korsakoff syndrome , a brain disorder. Activity of TPP-requiring enzymes will be impaired in this syndrome.]
Fructose 6-phosphate
H
CH O
CH OH
CH OH
H
P
Glyceraldehyde3-phosphate
H
CH O
CH OH
C H
O
P
Ribulose 5-phosphate
H
CH O
CH OH
CH OH
CH OH
H
P
C O
Xylulose 5-phosphate
H
CH O
CH OH
OH
P
O
CHO H
H
CH O
CH OH
CH OH
P
Sedoheptulose7-phosphate
H
CH O
CH OH
P
H
CH O
CH OH
P
CH OH
CH OH
C H
O
CH OH
CH OH C H
O
CH
H
C
CHO H
O
H
H OH
CC
CHO H
C O
CH OH
Ribose 5-phosphate
Δ2C
TransketolaseTPP
Transaldolase
Erythrose 4-phosphate
Δ3C
Ferrier_Unit02.indd 150Ferrier_Unit02.indd 150 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
13.3 QuestionNADPH
What molecule is shown?
What function does this molecule have in the prevention of damage by ROS (e.g., H 2 O 2 )?
Why is Se an essential micronutrient?
COO-HCNH3
+CH2 Glutamate
CH2
HNHS Cysteine
Glycine
C O
CH
C O
CH2
HN
CH2
COO-
Ferrier_Unit02.indd 151Ferrier_Unit02.indd 151 5/2/14 7:22 PM5/2/14 7:22 PM
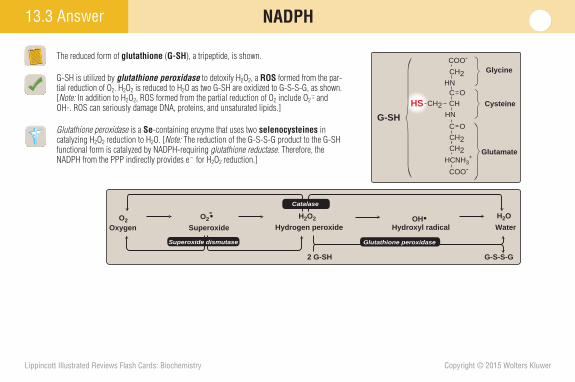
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
13.3 Answer NADPH
The reduced form of glutathione ( G-SH ), a tripeptide, is shown.
G-SH is utilized by glutathione peroxidase to detoxify H 2 O 2 , a ROS formed from the par-tial reduction of O 2 . H 2 O 2 is reduced to H 2 O as two G-SH are oxidized to G-S-S-G, as shown. [ Note: In addition to H 2 O 2 , ROS formed from the partial reduction of O 2 include O 2 � � and OH�. ROS can seriously damage DNA, proteins, and unsaturated lipids.]
Glutathione peroxidase is a Se -containing enzyme that uses two selenocysteines in catalyzing H 2 O 2 reduction to H 2 O. [ Note: The reduction of the G-S-S-G product to the G-SH functional form is catalyzed by NADPH-requiring glutathione reductase . Therefore, the NADPH from the PPP indirectly provides e � for H 2 O 2 reduction.]
COO-HCNH3
+CH2 Glutamate
CH2
HNHS Cysteine
Glycine
C O
CH
C O
CH2
HN
CH2
COO-
G-SH
O2 O2- H2O2 H2O
SuperoxideOxygen Hydrogen peroxide Hydroxyl radical
Superoxide dismutase
2 G-SH G-S-S-G
Water
Catalase
OH
Glutathione peroxidase
Ferrier_Unit02.indd 152Ferrier_Unit02.indd 152 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
NADPH 13.4 Question
The fi gure shows the CYP-mediated of the substrate A-H to the product as O 2 is reduced to using NADPH as the reductant.
What are monooxygenases (mixed-function oxidases)?
How might mutations in a CYP enzyme of the SER in liver infl uence the therapeutic dose of a drug? SubstrateA-H
A-H
A-H
P450-Fe3+
P450-Fe3+P450-Fe2+
A-HP450-Fe3+
e–
e–
e–
O2
O2
NADPH + H+ NADP+
P450-Fe3+
O=
Cytochrome P450reductase
e–
NADPH + H+NADP+
?
?
Cytochrome P450reductase
FAD, FMN
FAD, FMN
2H+
2
–
Product
Ferrier_Unit02.indd 153Ferrier_Unit02.indd 153 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
13.4 Answer NADPH
The fi gure shows the CYP -mediated oxidation of the substrate A-H to the product A-OH as O 2 is reduced to H 2 O using NADPH as the reductant.
Monooxygenases are enzymes that incorporate one O atom from O 2 into a substrate (creating a hydroxyl group). The other O atom gets reduced to H 2 O. In the heme-containing CYP monooxygenase system , the e � come from NADPH of the PPP.
The CYP enzymes of the SER in liver are important in the oxidation (detoxifi cation) of xenobiotics such as drugs. Mutations in a CYP enzyme could increase or decrease the ability of the liver to detoxify a particular drug, thereby infl uencing the therapeutic dose for patients with that mutation. For example, two variations from the wild type in CYP2C9 decrease warfarin (an anticoagulant) metabolism, allowing a lower therapeutic dose. [ Note: Mitochondrial CYP enzymes are involved in steroid hormone synthesis.]
Substrate
Product
A-H
A-H
A-H
P450-Fe3+
P450-Fe3+P450-Fe2+
A-HP450-Fe3+
e–
e–
e–
O2H2O
O2
A-OH
NADPH + H+ NADP+
P450-Fe3+
O=
Cytochrome P450reductase
e–
NADPH + H+NADP+
Cytochrome P450reductase
FAD, FMN
FAD, FMN
2H+
2
–
Ferrier_Unit02.indd 154Ferrier_Unit02.indd 154 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
13.5 Question NADPH
What is the amino acid substrate in the NADPH-requiring NOS reaction shown?
What function of NO is the rationale for using inhaled NO in acute respiratory distress syndrome (ARDS) treatment?
What NADPH-requiring enzyme initiates the cascade of events that result in the killing of bacteria within phagocytic cells such as leukocytes and macrophages?
?
C
NH2
O
NHCH2
CH2
CH2
HCNH3+
COO-
L-Citrulline
NO synthase (NOS)
NADP+NADPH + H+
NO
O2
Ferrier_Unit02.indd 155Ferrier_Unit02.indd 155 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
13.5 Answer NADPH
The amino acid substrate for NOS is L-arginine. [ Note: Three NOS isoforms are known: the constitutive, Ca 2 � -dependent endothelial ( eNOS ) and neuronal ( nNOS ) forms and the inducible, Ca 2 � -independent ( iNOS ) form in macrophages.]
NO, through cGMP -mediated activation of PKG , causes smooth muscle relaxation. Inhaled NO selectively causes pulmonary blood vessel vasodilation, thus improving systemic O 2 delivery in ARDS . Systemic vasodilation is avoided because Hb scavenges NO.
NADPH oxidase rapidly reduces O 2 to O 2 � � as NADPH is oxidized, as shown, initiating a cascade that results in the killing of bacteria within a phagocytic cell. [ Note: An NADPH oxidase defi ciency results in an immunodefi ciency known as chronic granulomatous disease .]
Spontaneously orby superoxidedismutase
O2–
H2O2
HOCl
Myelo-peroxidase
NADPH
NADP+
TER
IUM
BA
CTER
IUM
Cl– Fe2+
Fe3+
OH•
NADPHoxidase
RESPIRATORYBURST
O2
BA
CB
AC
C
NH2
NH2+
NHCH2
CH2
CH2
HCNH3+
COO-
L-Arginine
C
NH2
O
NHCH2
CH2
CH2
HCNH3+
COO-
L-Citrulline
NO synthase (NOS)
NADP+NADPH + H+
NO
O2
Ferrier_Unit02.indd 156Ferrier_Unit02.indd 156 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
13.6 QuestionNADPH
What X-linked enzyme is denoted by the red question mark shown?
In some individuals, the K m of this enzyme is increased for either the substrate or the coenzyme-cosubstrate. What effect will this have on the PPP?
Why might an individual with a defi ciency of the enzyme develop a hemolytic anemia under conditions of oxidative stress caused by infection, certain drugs, or certain foods?
6-Phospho-gluconolactone
NADP+
NADPH + H+
2 G-SH
G-S-S-G
H2O2
2 H2O
2 Lactate
2 ADP
2 ATP
Glucose
Glutathionereductase
Glutathioneperoxidase
Glucose 6-phosphate
ERYTHROCYTE
Glycolyticpathway
PPP
?
Ferrier_Unit02.indd 157Ferrier_Unit02.indd 157 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
13.6 Answer NADPH
The X-linked enzyme denoted is G6PD , which catalyzes the fi rst irreversible (and primary regulatory) step in the PPP. [ Note: A high NADPH/NADP � ratio inhibits G6PD .]
Increasing the K m decreases the binding affi nity of G6PD for glucose 6-P or NADP � , thereby decreasing enzyme activity. The PPP will be slowed because G6PD is rate limiting .
The PPP is the only means by which RBCs generate NADPH. G6PD defi ciency decreases NADPH and, consequently, the G-SH pool. In oxidative stress, this leads to an increase in ROS that can damage the cell membrane as well as a decrease in the ability to maintain thiol groups in proteins such as Hb. Damage to membranes causes the RBCs to be removed from circulation and destroyed (resulting in a hemolytic anemia ). Oxida-tion of thiol groups causes proteins to precipitate as Heinz bodies in RBCs.
6-Phospho-gluconolactone
NADP+
NADPH + H+
2 G-SH
G-S-S-G
H2O2
2 H2O
2 Lactate
2 ADP
2 ATP
Glucose
Glucose 6-phosphatedehydrogenase
Glutathionereductase
Glutathioneperoxidase
Certain drugsInfectionsFava beans
Oxidant stress
Glucose 6-phosphate
ERYTHROCYTE
NADP+ 2 G-SH
ucose
CIF
O
cose 6-phosphate
EEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEE Glucose 6-phosphate dehydrogenase deficiency impairs the ability of an erythrocyte to form NADPH, resulting in hemolysis.
Glycolyticpathway
PPP
Heinz bodies
Ferrier_Unit02.indd 158Ferrier_Unit02.indd 158 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
14.1 QuestionGAG Structure and Synthesis
What is an exception to the rule that GAGs are negatively charged heteropolysaccharide chains composed of a repeating disaccharide unit (acidic sugar–amino sugar), as shown?
What is produced when GAGs associate with small amounts of protein (core protein)?
Why might glucosamine or chondroitin sulfate supplementation benefi t patients with osteoarthritis ( OA )?
CH2OHO
COOH
OH
OH
O
HO
OO
NH
CH3
C O
Acidic sugarN-Acetylatedamino sugar
Acetylgroup n
Ferrier_Unit02.indd 159Ferrier_Unit02.indd 159 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
GAG Structure and Synthesis14.1 Answer
In negatively charged keratan sulfate , the acidic sugar has been replaced by galactose and is thus an exception to the rule that GAGs are composed of a repeating unit (acidic sugar–amino sugar). [ Note: In GAGs, the amino sugar (glucosamine or galactosamine) frequently is acetylated on the NH 2 group and sulfated (PAPS is the sulfate donor). The acidic (uronic) sugar (glucuronic acid or iduronic acid) is ionized at pH 7.4. The resulting net negative charge on GAGs results in a high degree of hydration that contributes to cartilage and synovial fl uid resilience.]
ECM and cell surface proteoglycans are produced when GAGs associate with a small amount of core protein. GAGs constitute �95% of a proteoglycan.
OA is a degenerative joint disease characterized by loss of cartilage. Supplementation with an amino sugar or a GAG of proteoglycans delays the loss of cartilage, decreasing the symptoms of OA in some patients.
CH2OHO
COOH
OH
OH
O
HO
OO
NH
CH3
C O
Acidic sugarN-Acetylatedamino sugar
Acetylgroup
n
H2O
H 2O
H2O
H2O
H2O
H2O
H2 O
H2O
H 2O
H2O
H2O
H2O
H2O
H2 O
H2 O
H2 O
Ferrier_Unit02.indd 160Ferrier_Unit02.indd 160 5/2/14 7:22 PM5/2/14 7:22 PM
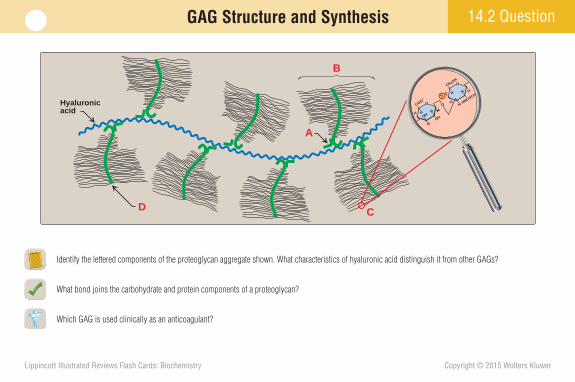
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
14.2 QuestionGAG Structure and Synthesis
Identify the lettered components of the proteoglycan aggregate shown. What characteristics of hyaluronic acid distinguish it from other GAGs?
What bond joins the carbohydrate and protein components of a proteoglycan?
Which GAG is used clinically as an anticoagulant?
Hyaluronicacid
D
B
A
C
CH 2OH
OCOO–
OHOH
O
HNCOCH 3
H
O
H
H
H
H
H
H
H
H
H
HO
S
Ferrier_Unit02.indd 161Ferrier_Unit02.indd 161 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
GAG Structure and Synthesis14.2 Answer
A � link protein , B � proteoglycan monomer ( bottlebrush ), C � GAG , and D � core protein . Hyaluronic acid is distinguished from other GAGs because it is neither sulfated nor covalently attached to protein and is not limited to animal tissue.
An O-glycosidic bond joins the OH of a Ser in the core protein to an OH of the xylose in the trisaccharide that connects the protein and the GAG (shown).
Heparin is a GAG used as an injectable anticoagulant . It binds to and activates ATIII, which then inactivates the serine proteases of coagulation.
Hyaluronicacid
Core protein
Proteoglycan monomer
Linkprotein
GAG
CH 2OH
OCOO–
OHOH
O
HNCOCH 3
H
O
H
H
H
H
H
H
H
H
H
HO
S
Amino sugar
Acidic sugar
Galactose
Galactose
Xylose
O
CH2
n
Core protein
Linkage region
Repeatingdisaccharide units
Serine side chain
Ferrier_Unit02.indd 162Ferrier_Unit02.indd 162 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
GAG Structure and Synthesis 14.3 Question
What nucleotide is used in the activation of amino sugars for GAG synthesis?
What is the structural relationship between the acidic sugars glucuronic and iduronic acids? What is the end product of glucuronic acid metabolism in humans? Which pathway uses it?
Why is glucuronic acid used in the transport, catabolism, and excretion of nonpolar endogenous substances (such as bilirubin and steroid hormones) and xenobiotics such as drugs?
Glutamine
Fructose6-phosphate
ATP
ADP
Glucose
Amidotransferase
Glucosamine6-phosphate
N-Acetylglucosamine 6-phosphate
N-Acetylmannosamine 6-phosphate ?-N-acetylglucosamine
?-N-acetylgalactosamine
PEP
CTPPPi
N-Acetylneuraminic acid (NANA)
Acetyl-CoACoA
Glucosamine1-phosphate
?
PPi
?-Glucosamine
Glycosaminoglycans
Glycosaminoglycans,glycoproteins
Glutamate
Glucose6-phosphate
Sialic acid,gangliosides,glycoproteins CMP-NANA
Ferrier_Unit02.indd 163Ferrier_Unit02.indd 163 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
GAG Structure and Synthesis14.3 Answer
UTP is used in the activation of amino sugars (to UDP-sugars) for GAG synthesis. [ Note: Acidic NANA is the only example of a sugar utilized as a nucleoside monophosphate (CMP-NANA).]
Glucuronic acid and iduronic acid are C-5 epimers . D-glucuronic acid is epimerized to L-iduronic acid after incorporation into GAGs. Xylulose is the end product of glucuronic acid metabolism in humans, and it is used in the PPP as xylulose 5-P.
Glucuronic acid is water soluble. It is transferred from UDP-glucuronic acid to nonpolar endogenous substances and xenobiotics ( glucuronidation ) to increase their solubility in aqueous solutions. Glucuronidation can occur after CYP -mediated hydroxylation as phase II of xenobiotic detoxifi cation.
Glutamine
Fructose6-phosphate
ATP
ADP
Glucose
Amidotransferase
Glucosamine6-phosphate
N-Acetylglucosamine 6-phosphate
N-Acetylmannosamine 6-phosphate UDP-N-acetylglucosamine
UDP-N-acetylgalactosamine
PEP
CTPPPi
N-Acetylneuraminic acid (NANA)
Acetyl-CoACoA
Glucosamine1-phosphate
UTP
PPi
UDP-Glucosamine
Glycosaminoglycans
Glycosaminoglycans,glycoproteins
Glutamate
Glucose6-phosphate
Sialic acid,gangliosides,glycoproteins CMP-NANA
Ferrier_Unit02.indd 164Ferrier_Unit02.indd 164 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
14.4 QuestionGAG Degradation
What specifi c GAG metabolism disorder is caused by iduronate sulfatase defi ciency? By �-L-iduronidase defi ciency?
To what class of disorders do these enzymic defi ciencies belong?
Which is a disorder of degradation, sulfur-related chondrodystrophy or multiple sulfatase defi ciency ?
IdUA GlcN GlcUA GlcNAc GlcUA
Iduronate sulfatase
IdUA GlcN GlcUA GlcNAc GlcUA
a-L-Iduronidase
IdUA
GlcN GlcUA GlcNAc GlcUA
S S
S
S S
S
S
S
Ferrier_Unit02.indd 165Ferrier_Unit02.indd 165 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
GAG Degradation14.4 Answer
Iduronate sulfatase defi ciency causes Hunter syndrome . � -L-Iduronidase defi ciency causes Hurler syndrome . Both syndromes result in neurologic problems, but only Hurler syndrome causes corneal clouding. Treatment for both includes enzyme replacement therapy.
Both Hunter and Hurler syndromes are classifi ed as mucopolysaccharidoses , lysosomal storage diseases caused by degradative lysosomal hydrolase defi ciency. [ Note: Hunter syndrome is the only X-linked mucopolysaccharidosis. The others are AR disorders.]
Multiple sulfatase defi ciency is a rare disorder of degradation in which all sulfatases (not just iduronate sulfatase ) are nonfunctional. Sulfur-related chondrodystrophies are defects in the ability to sulfate molecules such as GAGs during their synthesis. The defect may be in sulfate uptake or the synthesis of PAPS , the sulfate donor.
IdUA GlcN GlcUA GlcNAc GlcUA
Iduronate sulfatase
IdUA GlcN GlcUA GlcNAc GlcUA
a-L-Iduronidase
IdUA
GlcN GlcUA GlcNAc GlcUA
S S
S
S S
S
S
S
Ferrier_Unit02.indd 166Ferrier_Unit02.indd 166 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
14.5 QuestionGlycoproteins
Give an example in which glycoproteins play a role in cell-surface antigenicity, as shown.
Glycoproteins contain relatively short hetero-oligosaccharide chains that may be but neither contain units nor necessarily have a net charge. The chains are covalently attached to the protein at
selected or residues (and residues in collagen) through bonds and/or to selected Asn residues through bonds.
What processes use the UDP-glucose formed from glucose 1-P?
Glycoproteins
Cell-surface recognition
Cell-surface antigenicity
Mucins
Extracellular matrix
Ferrier_Unit02.indd 167Ferrier_Unit02.indd 167 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
14.5 Answer Glycoproteins
ABO blood group antigens are glycoproteins that play a role in cell-surface antigenicity.
Glycoproteins contain relatively short hetero-oligosaccharide chains that may be branched but neither contain repeating disaccharide units nor necessarily have a net negative charge. The chains are covalently attached to the protein at selected Ser or Thr residues (and Hyl residues in collagen) through O-glycosidic bonds and/or to selected Asn residues through N-glycosidic bonds .
Glucose 1-P (formed from glucose 6-P by phosphoglucomutase ) is converted to UDP-glucose by UDP-glucose pyrophosphorylase . The UDP-glucose can be used in glycogen synthesis, converted to UDP-galactose for lactose synthesis, and oxidized to UDP-glucuronate for GAG synthesis. [ Note: UDP-glucuronate is also used in detoxifi cation reactions (e.g., glucuronidation of bilirubin.)]
Glycoproteins
Cell-surface recognition
Cell-surface antigenicity
Mucins
Extracellular matrix
Ferrier_Unit02.indd 168Ferrier_Unit02.indd 168 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
14.6 QuestionGlycoproteins
To which organelle will the protein shown be targeted? What is the fate of such proteins if their targeting is defective?
What role do glycosyltransferases play in the synthesis of glycoconjugates such as proteoglycans and glycoproteins?
How can a defect in dolichol synthesis result in a congenital disorder of glycosylation ( CDG )?
AsnMan
CIS GOLGI
P
Phosphorylatedmannose
Ferrier_Unit02.indd 169Ferrier_Unit02.indd 169 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
14.6 Answer Glycoproteins
The mannose 6-P signal, generated in the cis Golgi, is a unique marker that targets acid hydrolases to the lysosomes . If targeting is defective, the proteins are secreted from the cell by default and appear in the blood and urine. Lack of the phosphotransferase needed to generate the signal causes I-cell disease , which is characterized by lysosomal inclusions of undegraded material.
Glycosyltransferases in the ER and Golgi catalyze monosaccharide transfer from their nucleotide sugar carrier to an acceptor (another sugar, a protein, or a lipid).
Dolichol (from the cholesterol synthesis pathway) is the RER membrane lipid onto which a branched oligosaccharide is built prior to transfer to an Asn in an acceptor protein, as shown. Defi ciency of dolichol (or any of the other components required for this N-glycosylation ) will result in a CDG .
Asn
Asn
Asn
NH2
NH2
NH2
PP
Dolichol +
Growing peptide
Ribosomes
mRNA
5'-End3'-End
2 A branched oligosaccharideis synthesized ondolichol pyrophosphate.
NH2
3 The oligosaccharide is transferred from dolichol to amide N of an asparagine residue of the growing polypeptide chain.
ROUGH ENDOPLASMIC RETICULUM
4 Trimming of the carbohydratechain begins as the proteinmoves through the RER.
A
1 Protein synthesis begins,and the polypeptide chain isextruded into the rough endo-plasmic reticulum (RER).
AsnMan
CIS GOLGI
P
Phosphorylatedmannose
Ferrier_Unit02.indd 170Ferrier_Unit02.indd 170 5/2/14 7:22 PM5/2/14 7:22 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
15.1 QuestionDietary Lipid Digestion
What general name is given to the enzymes that degrade dietary fat (TAGs) in the mouth, stomach, and small intestine, as shown?
Where in the body does the degradation of dietary TAGs containing LCFAs occur primarily? What are the two products? What enzyme catalyzes the process? What additional protein is needed?
What is the function of cholesterol esterase ? What are its products?
Pancreatic lipase concentration is low in neonates. How are they able to digest milk fat? PANCREASPANCREASPANCREAS
Dietary lipids
SMALLINTESTINE
TO BLOOD
MOUTH
CE, PL, TAG (unchanged)
PRIMARY PRODUCTS
?
Most of the CE, PL, TAG, and some short- andmedium-chain fatty acids
Remaining pieces of PL
CHYLOMICRONS(LYMPH)
Reesterified)
Bile salts emulsify,and pancreatic
enzymes degradedietary lipids
STOMACHSTOMACHSTOMACH
Ferrier_Unit03.indd 171Ferrier_Unit03.indd 171 5/2/14 7:30 PM5/2/14 7:30 PM
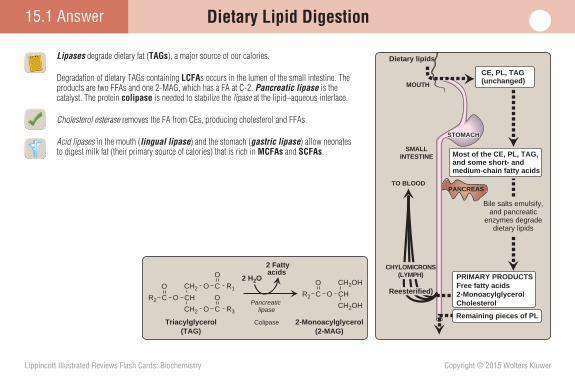
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
15.1 Answer Dietary Lipid Digestion
Lipases degrade dietary fat ( TAGs ), a major source of our calories.
Degradation of dietary TAGs containing LCFA s occurs in the lumen of the small intestine. The products are two FFAs and one 2-MAG, which has a FA at C-2. Pancreatic lipase is the catalyst. The protein colipase is needed to stabilize the lipase at the lipid–aqueous interface.
Cholesterol esterase removes the FA from CEs, producing cholesterol and FFAs.
Acid lipases in the mouth ( lingual lipase ) and the stomach ( gastric lipase ) allow neonates to digest milk fat (their primary source of calories) that is rich in MCFAs and SCFAs .
PANCREASPANCREASPANCREAS
Dietary lipids
SMALLINTESTINE
TO BLOOD
MOUTH
CE, PL, TAG (unchanged)
Most of the CE, PL, TAG, and some short- andmedium-chain fatty acids
Remaining pieces of PL
CHYLOMICRONS(LYMPH)
Reesterified)
Bile salts emulsify,and pancreatic
enzymes degradedietary lipids
STOMACHSTOMACHSTOMACH
CH2 O C R1
O
CHOC
O
R2
CH2 O C R3
O
Triacylglycerol(TAG)
CH2OH
CHOC
Colipase
O
R2
2-Monoacylglycerol(2-MAG)
CH2OHPancreatic lipase
2 Fatty acids
2 H2O PRIMARY PRODUCTSFree fatty acids2-MonoacylglycerolCholesterol
Ferrier_Unit03.indd 172Ferrier_Unit03.indd 172 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
15.2 QuestionDietary Lipid Digestion and Absorption
What are the functions of the hormones CCK and secretin in digestion?
What is the role of emulsifi cation in lipid digestion? How is it accomplished?
How and where are dietary lipids absorbed?
Why might individuals with cystic fi brosis ( CF ) be given supplemental pancreatic enzymes prior to eating?
STOMACHSTOMACHSTOMACH
Gastricmotility
Dietary lipids
Degradation of dietary lipids
CholecystokininCholecystokinin(in blood)(in blood)
Cholecystokinin(in blood)
GUTENDOCRINE
CELLS(enlarged)
Bicarbonate
Pancreaticenzymes
Bile
SecretinSecretin(in blood)(in blood)Secretin
(in blood)
GALL- BLADDER
Secretes
Secretes
Secretes
SMALLINTESTINE
++
PANCREASPANCREASPANCREAS
Ferrier_Unit03.indd 173Ferrier_Unit03.indd 173 5/2/14 7:30 PM5/2/14 7:30 PM
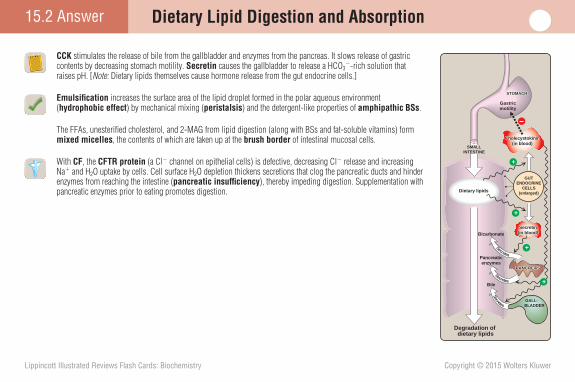
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
15.2 Answer Dietary Lipid Digestion and Absorption
CCK stimulates the release of bile from the gallbladder and enzymes from the pancreas. It slows release of gastric contents by decreasing stomach motility. Secretin causes the gallbladder to release a HCO 3 � -rich solution that raises pH. [ Note: Dietary lipids themselves cause hormone release from the gut endocrine cells.]
Emulsifi cation increases the surface area of the lipid droplet formed in the polar aqueous environment ( hydrophobic effect ) by mechanical mixing ( peristalsis ) and the detergent-like properties of amphipathic BSs .
The FFAs, unesterifi ed cholesterol, and 2-MAG from lipid digestion (along with BSs and fat-soluble vitamins) form mixed micelles , the contents of which are taken up at the brush border of intestinal mucosal cells.
With CF , the CFTR protein (a Cl � channel on epithelial cells) is defective, decreasing Cl � release and increasing Na � and H 2 O uptake by cells. Cell surface H 2 O depletion thickens secretions that clog the pancreatic ducts and hinder enzymes from reaching the intestine ( pancreatic insuffi ciency ), thereby impeding digestion. Supplementation with pancreatic enzymes prior to eating promotes digestion.
STOMACHSTOMACHSTOMACH
Gastricmotility
Dietary lipids
Degradation of dietary lipids
CholecystokininCholecystokinin(in blood)(in blood)
Cholecystokinin(in blood)
GUTENDOCRINE
CELLS(enlarged)
Bicarbonate
Pancreaticenzymes
Bile
SecretinSecretin(in blood)(in blood)Secretin
(in blood)
GALL- BLADDER
Secretes
Secretes
Secretes
SMALLINTESTINE
+
+
++
PANCREASPANCREASPANCREAS
Ferrier_Unit03.indd 174Ferrier_Unit03.indd 174 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
15.3 QuestionDietary Lipid Secretion and Use
What LP particle shown transports dietary lipids through blood?
What lipids are found in the core of the particle? What surface protein is characteristic of the particle?
Why might fecal fat be measured if lipid malabsorption is suspected?
AMP + PPiATP
2-Monoacylglycerol
Fat-soluble vitamins
Cholesterol
O-
Acyl CoA:monoacylglycerol acyltransferase
Acyl CoA:diacylglycerol acyltransferase
CoA CoA
Fatty acyl-CoA synthetase
CoALong-chain fatty acids
RCRC CoA
OO
Fatty acyl-CoA
Amino acidsINTESTINAL MUCOSAL CELL
Acyl CoA:cholesterol acyltransferase
CoA
?
?
?
?
Phospholipids
TO LYMPHATIC SYSTEM
Ferrier_Unit03.indd 175Ferrier_Unit03.indd 175 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
15.3 Answer Dietary Lipid Secretion and Use
CMs , formed in intestinal cells and secreted into the lymphatic system, are the LP particles that transport dietary lipids (and fat-soluble vitamins) through the blood.
Within the intestinal cells, FAs are activated and esterifi ed to the cholesterol and 2-MAG products of digestion, reforming the nonpolar TAGs and CEs that get packaged into CMs. Apolipoprotein ( apo ) B-48 is the characteristic surface protein of CMs. [ Note: PLs are also found on the surface.]
Fecal fat will be increased with defects in lipid digestion (such as in CF ) or absorption because dietary fat is primarily excreted rather than absorbed with such defects. Steatorrhea (loose, fatty, and foul-smelling feces) results.
Dietary lipids
STEATORRHEA(excess lipid in feces)
Pancreaticjuice Defective
cells
SMALLINTESTINE
LIVER
Bile
INTESTINALMUCOSAL
CELLS
GALL- BLADDER
PANCREASPANCREASPANCREAS
AMP + PPiATP
Triacylglycerol2-Monoacylglycerol
Fat-soluble vitamins
Cholesteryl esterCholesterol
O-
Acyl CoA:monoacylglycerol acyltransferase
Acyl CoA:diacylglycerol acyltransferase
CoA CoA
Fatty acyl-CoA synthetase
CoALong-chain fatty acids
RCRC CoA
OO
Fatty acyl-CoA
Amino acids Apolipoprotein B-48INTESTINAL MUCOSAL CELL
Acyl CoA:cholesterol acyltransferase
CoA
CHYLOMICRON
Phospholipids
TO LYMPHATIC SYSTEM
PANCREAS
Ferrier_Unit03.indd 176Ferrier_Unit03.indd 176 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
15.4 QuestionDietary Lipid Secretion and Use
What tissues (denoted by a red question mark) are the primary sites for the degradation of TAGs carried by CMs?
What enzyme (denoted by a green question mark) degrades the TAGs?
What is the fate of the products of TAG degradation in CMs?
Why might TAGs rich in MCFAs be used in the treatment of disorders of lipid digestion and/or absorption or of CM metabolism?
Chylomicrons
LYMPHATIC SYSTEM
BLOOD
secreted into
which transports them to
which transports TAG-rich chylomicrons to
?where ?
degrades TAG to
Fatty acids
taken up by
Glycerol
LIVER
metabolized by
MOST TISSUES
Ferrier_Unit03.indd 177Ferrier_Unit03.indd 177 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Dietary Lipid Secretion and Use15.4 Answer
Muscle and adipose tissues are the primary sites for degradation of TAGs carried by CMs.
LPL , located on the endothelial surface of capil-laries in muscle and adipose tissue, degrades the TAGs. LPL requires activation by apo CII located on CM surfaces.
The FA products are taken in by muscles (for energy) and adipocytes (for storage) and are transported on serum albumin, taken up, and used by the liver. The glycerol is picked up by liver and phosphorylated to glycerol 3-P, which can be used in hepatic TAG synthesis, for example.
TAGs rich in MCFAs might be used in the treatment of disorders of lipid digestion (e.g., pancreatitis ) because they are (1) rapidly degraded by lingual and gastric lipases , thereby eliminating the need for pancreatic lipase and (2) taken up by enterocytes without the aid of mixed micelles . Additionally, they are released from enterocytes directly into the blood and do not require incorporation into CMs. Coconut oil contains a high concentration of TAGs rich in MCFAs and is used in medical nutrition therapy for these disorders.
Chylomicrons
LYMPHATIC SYSTEM
BLOOD
secreted into
which transports them to
which transports TAG-rich chylomicrons to
MUSCLE, ADIPOSE
where lipoprotein lipasedegrades TAG to
Fatty acids
taken up by
Glycerol
LIVER
metabolized by
MOST TISSUES
Ferrier_Unit03.indd 178Ferrier_Unit03.indd 178 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
16.1 QuestionFatty Acid Structure
What term describes molecules such as FAs that have both hydrophobic and hydrophilic regions, as shown?
Which region predominates in FAs 14–20 carbons in length (LCFAs)? How does this affect their solubility?
What does it mean for a FA to be unsaturated? What is the structural meaning of the designation “ � -6” for an unsaturated FA?
Which FA(s) must be supplied by the diet?
CH3(CH2)n COO–
Hydrophobichydrocarbon chain
Hydrophiliccarboxyl group(ionized at pH 7)
Ferrier_Unit03.indd 179Ferrier_Unit03.indd 179 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Fatty Acid Structure16.1 Answer
The term amphipathic (or amphiphilic ) describes molecules such as FAs that have both hydrophobic and hydrophilic regions.
In a LCFA , the hydrophobic region predominates, making it water insoluble. Consequently, LCFAs must be transported through the blood in association with protein, either on albumin for “free” LCFAs or in LP particles for LCFA esters in TAG, CEs, and PLs. [ Note: SCFAs and MCFAs are more water soluble than LCFAs.]
An unsaturated FA has one (monounsaturated) or more (polyunsaturated) double bonds in the cis confi guration that causes a kink or bend in the molecule. If polyunsaturated, the double bonds are spaced at three-carbon intervals. An � -6 unsaturated FA has a double bond six carbons from the methyl ( � ) end, as shown for arachidonic acid [20:4(5,8,11,14)].
Linoleic acid [18:2(9,12), an � -6 FA] and � -linolenic acid [18:3(9,12,15), an � -3 FA] are not able to be synthesized by humans and are, therefore, required in the diet. They are essential FAs .
CH3(CH2)n COO–
Hydrophobichydrocarbon chain
Hydrophiliccarboxyl group(ionized at pH 7)
Double bonds relative to the ω end
HCCH2C
H HCH
CCH2
HCH
CH2HOOC(CH2)3C *H HC C(CH2)4CH3
Ferrier_Unit03.indd 180Ferrier_Unit03.indd 180 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
16.2 QuestionFatty Acid De Novo Synthesis
In what form are acetate units for FA synthesis transferred from the mitochondrial matrix to the cytosol, as shown? What enzymes are required in the process?
What is the rate-limiting, regulated step of FA synthesis? How is this step regulated in the short term?
How is the regulated step affected by the drug metformin used in type 2 diabetes ( T2D ) treatment?
CYTOSOL
MITOCHONDRIAL MATRIXOxaloacetate
(OAA)Acetyl CoA
ADP + Pi
ATP
CoA
?
?
OAA Acetyl CoA
CoA
INNER MITOCHONDRIAL MEMBRANE
H2O
H2O
Ferrier_Unit03.indd 181Ferrier_Unit03.indd 181 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
16.2 Answer Fatty Acid De Novo Synthesis
Citrate (made from OAA � acetyl CoA in the mitochondrial matrix by CS ) is transported across the inner mitochondrial membrane and cleaved to OAA � acetyl CoA in the cytosol by ATP–citrate lyase , thereby providing acetate units for FA synthesis. [ Note: No transporter for CoA (or its derivatives) exists in the membrane.]
Carboxylation of cytosolic acetyl CoA to malonyl CoA by ATP- and biotin -requiring ACC is the rate-limiting, regulated step of FA synthesis. In the short term, ACC is (1) allosterically activated by citrate and inhibited by LCFA CoAs that promote and prevent, respectively, the polymerization of ACC protomers and (2) covalently inhibited by AMPK- catalyzed phosphorylation as shown. [ Note: AMPK is allosterically activated by AMP. A decrease in the ATP/AMP ratio sig-nals a low-energy state. Acetyl CoA will be oxidized in the TCA cycle (or used for hepatic KB synthesis) rather than be used for FA synthesis under these conditions.]
Metformin (used in T2D treatment) lowers TAGs by activating AMPK , thereby inhibiting ACC and the syn-thesis of FAs needed for TAGs. [ Note: The main effect of metformin is reduction of blood glucose.]
Acetyl CoAcarboxylase-
(inactive)
Acetyl CoAcarboxylase
(active)
Protein phosphatasePi
AMP-activated proteinkinase (AMPK)ADP ATP
Insulin
P
+
+
+
GlucagonEpinephrine(covalent)
AMPK kinases(covalent)
AMP(allosteric)
CYTOSOL
MITOCHONDRIAL MATRIXOxaloacetate
(OAA)Acetyl CoA
ADP + Pi
ATP
CoA
OAA Acetyl CoA
CoA
INNER MITOCHONDRIAL MEMBRANE
H2O
H2O
Citrate
Citrate
ATP-citrate lyase
Citrate synthase
Ferrier_Unit03.indd 182Ferrier_Unit03.indd 182 5/2/14 7:30 PM5/2/14 7:30 PM
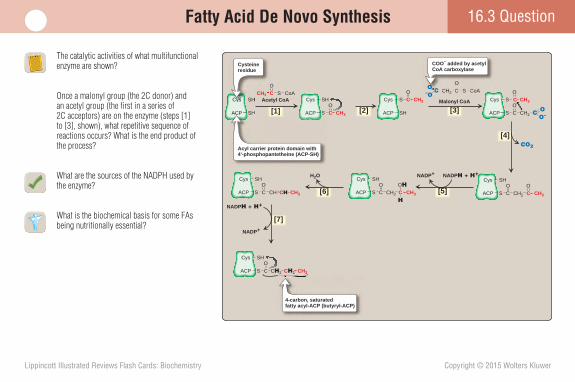
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
16.3 QuestionFatty Acid De Novo Synthesis
The catalytic activities of what multifunctional enzyme are shown?
Once a malonyl group (the 2C donor) and an acetyl group (the fi rst in a series of 2C acceptors) are on the enzyme (steps [1] to [3], shown), what repetitive sequence of reactions occurs? What is the end product of the process?
What are the sources of the NADPH used by the enzyme?
What is the biochemical basis for some FAs being nutritionally essential?
CH3CS
ACP
Cys
O
SH
CH3CS
ACP
Cys
O
CH2
CH2
CS
O
CH2C CH3SACP
SHCysO
CO
CHCHC CH3SACP
SHCysO
CCH3 S
O
CoAAcetyl CoA
C S
O
CoA
Malonyl CoA
–OCO
CH2
C OO–
[2] [3]
[4]CO2
NADP+ NADPH + H+H2O
NADP+
NADPH + H+
[5][6]
[7]
CH2CH2C CH3SACP
SHCysO
ACP CH3CS
OSHCys
ACP
SHCys
SH
CH3AceSHCys
Cysteineresidue
C S
O
CoACOOOOOOOOCH
COO– added by acetylCoA carboxylase
4-carbon, saturatedfatty acyl-ACP (butyryl-ACP)
C CH3SACP
SHCysO
C
H
OH
ACP SACP SH
Acyl carrier protein domain with4'-phosphopantetheine (ACP-SH)
[1]
Ferrier_Unit03.indd 183Ferrier_Unit03.indd 183 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
16.3 Answer Fatty Acid De Novo Synthesis
FAS is the multifunctional enzyme.
Once the malonyl 2C-donor and the acetyl 2C-acceptor are on the enzyme (steps [1] to [3]), the repetitive sequence catalyzed by FAS is condensation ( decarboxylation ) by 3-ketoacyl-ACP synthase [4], reduction by NADPH-requiring 3-ketoacyl-ACP reductase [5], dehydration by 3-hydroxyacyl-ACP dehydratase [6], and reduction by NADPH-requiring enoyl–ACP reductase [7]. [ Note: The ACP domain carries acyl units on its thiol group during FA synthesis.] Palmitic acid (16:0) , released by the t hioesterase activity of FAS , is the primary end product.
The NADPH is provided by the PPP and by malic enzyme , which catalyzes the oxidative decarboxylation of malate to pyruvate.
Humans are able to elongate and desaturate palmitate to longer chain–length saturated and unsaturated FAs using SER enzymes. However, we do not express desaturases able to introduce double bonds between C-10 and the � -C. Therefore, we cannot synthesize linoleic and linolenic acids, and they are dietary essentials.
CH3CS
ACP
Cys
O
SH
CH3CS
ACP
Cys
O
CH2
CH2
CS
O
CH2C CH3SACP
SHCysO
CO
CHCHC CH3SACP
SHCysO
CCH3 S
O
CoAAcetyl CoA
C S
O
CoA
Malonyl CoA
–OCO
CH2
C OO–
[2] [3]
[4]CO2
NADP+ NADPH + H+H2O
NADP+
NADPH + H+
[5][6]
[7]
CH2CH2C CH3SACP
SHCysO
ACP CH3CS
OSHCys
ACP
SHCys
SH
CH3AceSHCys
Cysteineresidue
C S
O
CoACOOOOOOOOCH
COO– added by acetylCoA carboxylase
4-carbon, saturatedfatty acyl-ACP (butyryl-ACP)
C CH3SACP
SHCysO
C
H
OH
ACP SACP SH
Acyl carrier protein domain with4'-phosphopantetheine (ACP-SH)
[1]
FATTY ACIDSYNTHASE
Ferrier_Unit03.indd 184Ferrier_Unit03.indd 184 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
16.4 QuestionTAG Storage and Mobilization
What molecule is the initial acceptor of FAs during TAG synthesis, as shown?
What are the sources of this molecule in liver, the primary site of TAG synthesis?
What is the fate of TAGs in liver? In WAT?
How does the body mobilize TAGs in WAT in times of need?
Acyltransferase
Acyltransferase
Acyltransferase
Phosphatase
CoA
CoA
CoA
CoA - FA2
CoA - FA1
CoA - FA3
H2O
Pi
Lysophosphatidic acid
?
Phosphatidic acid (DAG-P)
Diacylglycerol (DAG)
Triacylglycerol (TAG)
Ferrier_Unit03.indd 185Ferrier_Unit03.indd 185 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
16.4 Answer TAG Storage and Mobilization
Glycerol 3-P is the acceptor. The TAG product has three FAs esterifi ed to a glycerol backbone. [ Note: FAs must fi rst be activated to their CoA derivatives (CoA-FA) by ATP-dependent fatty acyl CoA synthetases .]
In the liver, the primary site of TAG synthesis, glycerol 3-P can be produced from the (1) reduction of DHAP from glycolysis by glycerol 3-phosphate dehy-drogenase and (2) phosphorylation of glycerol by glycerol kinase .
In the liver, TAGs are packaged into LP particles known as VLDLs and secreted into the blood. In WAT , TAGs are stored as anhydrous cytosolic droplets that represent the major energy reserve of the body.
Intracellular TAG lipolysis is catalyzed by lipases includ-ing HSL that is phosphorylated and activated by PKA in response to epinephrine. The products (3 FAs � glycerol) are sent into the blood. The FAs are carried on albumin to target tissues, taken up, and oxidized for energy. The glycerol is taken up by liver, phosphorylated to glycerol 3-P by glycerol kinase , and used in gluconeogenesis.
Hormone-sensitive lipase
(inactive)
ADP
Fatty acid
DIACYLGLYCEROL
MONOACYLGLYCEROL
ATP
Hormone-sensitive lipase
(active)
ATP cAMP + PPi
Adenylylcyclase
Epinephrine(high)
Insulin(low)
ReceptorReceptor
P
P
+
Phosphatase active Protein kinase A
Acyltransferase
Acyltransferase
Acyltransferase
Phosphatase
CoA
CoA
CoA
CoA - FA2
CoA - FA1
CoA - FA3
H2O
Pi
Lysophosphatidic acid
Phosphatidic acid (DAG-P)
Diacylglycerol (DAG)
Triacylglycerol (TAG)
Glycerol 3-phosphate
Ferrier_Unit03.indd 186Ferrier_Unit03.indd 186 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
16.5 QuestionFatty Acid Oxidation
In what form are LCFAs transported across the inner mitochondrial membrane to the mitochondrial matrix for degradation via � -oxidation, as shown? How is this transport process regulated?
What are the end products of the � -oxidation of palmitic acid (16:0)?
What aspect of FA degradation would be inhibited by biotin defi ciency ?
Fatty acid+
CoA
ATP
PPi + AMPAcyl CoAsynthetase
Translocase
Translocase? ?
? ?
Ferrier_Unit03.indd 187Ferrier_Unit03.indd 187 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Fatty Acid Oxidation16.5 Answer
LCFAs are linked to carnitine for transport across the inner mitochondrial membrane to the matrix for � -oxidation. [ Note: MCFAs and SCFAs are activated in the matrix and do not require carnitine. VLCFAs are oxidized in the peroxisome to MCFAs that travel to mitochondria for further oxidation.] Malonyl CoA (from ACC ) inhibits transfer of LCFAs from CoA to carnitine by CPT-1 , thereby preventing the simultaneous synthesis and degradation of FAs.
Eight acetyl CoA , 7 NADH , and 7 FADH 2 are the end products of mitochondrial � -oxidation of palmitate (16:0). [ Note: FA � -oxidation occurs by a repetitive four-step process of FAD-linked dehydrogenation, hydration, NAD+-linked dehydrogenation, and CoA-dependent cleavage.]
� -Oxidation of FAs with an odd number of carbons produces propionyl CoA (not acetyl CoA) in the fi nal thiolytic cleavage. The propionyl CoA is carboxylated to methylmalonyl CoA by biotin-dependent propionyl CoA carboxylase . Biotin defi ciency would prevent this process.
Fatty acid+
CoA
ATP
PPi + AMPAcyl CoAsynthetase
Translocase
Translocase
Ferrier_Unit03.indd 188Ferrier_Unit03.indd 188 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
16.6 QuestionKetone Body Metabolism
The acetyl CoA generated by FA � -oxidation is used for hepatic ketogenesis, as shown. What are the two functional KBs? What is the importance of the release of CoA during ketogenesis?
What pushes the acetyl CoA from FA � -oxidation to ketogenesis and away from the TCA cycle in the liver?
How do peripheral tissues use KBs? Why is the liver unable to use KBs?
What is the physiologic consequence of making KBs at a rate faster than they can be used?
Acetoacetyl CoA
CoA
O
C
O
CH2
HMG CoAsynthase
CoA
CoA
CoA
O
CH3C
HMG CoA
CoA
O
C
O
C CH2C
OH
CH3
CH2–O
HMG CoA lyaseCoA
O
CH3C
?
?
O
C CH3CH3
Acetone(metabolic dead end)
Spontaneous
CO2
3-Hydroxybutyratedehydrogenase
NAD+
NADH+ H+
CH3C
Acetyl CoA
Acetyl CoA
H2O
2 Acetyl CoA
Ferrier_Unit03.indd 189Ferrier_Unit03.indd 189 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
16.6 Answer Ketone Body Metabolism
Acetoacetate and � -hydroxybutyrate are the functional KBs . Volatile acetone is a metabolic dead end. The release of CoA in ketogenesis allows continued � -oxidation of activated FAs in the liver.
Acetyl CoA from FA �-oxidation is pushed to ketogenesis and away from the TCA cycle in liver because OAA is decreased as a consequence of (1) PDH inhibition and PC activation by acetyl CoA and (2) its reduction to malate by MD because of the increase in the NADH/NAD � ratio by FA � -oxidation.
Peripheral, but not hepatic, cells express thiophorase that transfers CoA from succinyl CoA to acetoacetate, generating acetoacetyl CoA that is thiolytically cleaved to two acetyl CoAs for oxidation in the TCA cycle. KBs are particularly important for the brain in long-term fasting.
Acetoacetate and � -hydroxybutyrate are 4C, water-soluble, nonvolatile, organic acids with a pK of �4. As they circulate in the blood, they ionize, thus lowering pH and causing ketoacidosis (a type of metabolic acidosis ). The acetone produced from acetoacetate may impart a fruity odor to the breath and provide a clue as to the cause of the acidosis (e.g., diabetic ketoacidosis [ DKA ]).
HMG CoA
CoA
O
C
O
C CH2C
OH
CH3
CH2–O
HMG CoA lyaseCoA
O
CH3C
Acetoacetate
O–
O
C
O
CH2CH3C
O–
O
CCH2C
H
OH
CH3
O
C CH3CH3
Acetone(metabolic dead end) 3-Hydroxybutyrate
Spontaneous
CO2
3-Hydroxybutyratedehydrogenase
NAD+
NADH+ H+
Acetyl CoA
Hepatic output of ketone bodies
Lipolysis
Free fatty acids in plasma
Ketoacidosis
Epinephrine/glucagon
Insulin
Acetoacetyl CoA
CoA
O
C
O
CH2
HMG CoAsynthase
CoA
CoA
O
CH3C
CH3C
Acetyl CoA
H2O
2 Acetyl CoA
CoA
Ferrier_Unit03.indd 190Ferrier_Unit03.indd 190 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
What is the cause of the baby’s fasting hypoketotic hypoglycemia ?
16Case Card
A 3-month-old boy was hospitalized following a seizure. History revealed that for about 2 days prior to admission, the baby had been fussy and had refused to nurse or take a bottle. (The baby subsequently was shown to have an ear infection.) At admission, his blood glucose was 24 mg/dl (age-referenced normal is 60–100). His urine was negative for KBs and positive for dicarboxylic acids 6–12 carbons in length, with 8-carbon acids (shown below) predominating. Blood carnitine and fatty acyl–carnitine levels were normal. A diagnosis of medium-chain fatty acyl CoA dehydrogenase ( MCAD ) defi ciency was made.
O
C C
H H H H H H
H H H H H H
C C C C C C−O O−
O
Ferrier_Unit03.indd 191Ferrier_Unit03.indd 191 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
16 Case Card
MCAD defi ciency , an AR disorder of FA � -oxidation, is the most common inborn error of FA metabolism (�1:14,000) and is seen primarily in Caucasians of Northern European descent. Symptoms typically appear before age 2 years. With MCAD defi ciency, metabolic stressors such as fasting and illness result in increased glucose utilization, decreased glucose synthesis, and reduced KB production. If undiagnosed, MCAD defi ciency has a mortality of up to 25%. Treatment involves avoiding fasting for more than 4 hours and use of IV glucose during acute episodes.
In the patient, the ability to oxidize LCFAs to a medium-chain length and the normal levels of carnitine and fatty acyl–carnitines suggest that carnitine synthe-sis and uptake are unaffected as are the enzymes that put a FA onto carnitine ( CPT-I ) and take it off ( CPT-II ). The dicarboxylic acids seen in the baby’s urine are caused by � -oxidation (oxidation at the � [methyl] end) of FAs. Normally a minor pathway in the ER, � -oxidation is upregulated in disorders such as MCAD defi ciency that limit FA � -oxidation.
The decreased ability to oxidize MCFAs results in their accumulation and in decreased production of acetyl CoA from � -oxidation and, therefore, of KBs. Decreased ketogenesis increases reliance on glucose. However, the decrease in MCFA � -oxidation decreases the availability of the ATP and NADH needed for gluconeogenesis. The result is a fasting hypoketotic hypoglycemia .
A
Ferrier_Unit03.indd 192Ferrier_Unit03.indd 192 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
17.1 QuestionPhospholipid Structure
To what carbon backbone are the FAs and polar head groups esterifi ed in the PLs shown? What name is given to this group of PLs? From what precursor are they derived?
What are ether PLs?
What are sphingophospholipids?
The Wassermann test for syphilis detects Abs against cardiolipin. Why would these Abs be formed? Phosphatidylserine
CH2CH
+NH3
COO–
MEMBRANE EXTRACELLULAR SPACE
Polar head
CH2
CHOC
O
OC
O
CH2
P
CH2
CHOC
O
OC
O
CH2
P
CH2
CHOC
O
OC
O
CH2
P
Hydrophobic tail
CH2CH2N+
CH2CH2
+NH3
CH3 CH3
CH3
Phosphatidylcholine
Phosphatidylethanolamine
?
Ferrier_Unit03.indd 193Ferrier_Unit03.indd 193 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
17.1 Answer Phospholipid Structure
The FAs and polar headgroups are esterifi ed to a glycerol backbone and are the glycerophospholipids . Glycerophospholipids are derived from PA (DAG-P). [ Note: PA is common to glycerophospholipid and TAG synthesis.]
Ether PLs (e.g., phosphatidalethanolamine, a plasmalogen ) have the FA attached to C-1 of the glycerol backbone by an ether link and not an ester link. [ Note: Platelet-activating factor is also an ether PL. It binds to membrane receptors and triggers potent thrombogenic and infl ammatory events.]
Sphingophospholipids (e.g., sphingomyelin of nerve myelin sheaths) are PLs that contain the amino alcohol sphingosine as the backbone and not glycerol.
Cardiolipin (a glycerophospholipid) is virtually exclu-sive to the inner mitochondrial membrane in eukaryotes, where it stabilizes the ETC complexes. With active syphilis , damage to infected cells exposes antigenic cardiolipin. Additionally, Abs are formed against car-diolipin found in the plasma membrane of the organism ( Treponema pallidum ) that causes syphilis.
Phosphatidylserine
CH2CH
+NH3
COO–
MEMBRANE EXTRACELLULAR SPACE
Polar head
CH2
CHOC
O
OC
O
CH2
P
CH2
CHOC
O
OC
O
CH2
P
CH2
CHOC
O
OC
O
CH2
P
Hydrophobic tail
CH2CH2N+
CH2CH2
+NH3
CH3 CH3
CH3
Phosphatidylcholine
Phosphatidylethanolamine
Glycerol backbone
Phosphatidalethanolamine
CH
C
O
O CH
C
CH2 O
CH2
O
O–PO OCH2CH2
+NH3
CH
Ether linkage
Glycerol backbone
Acyl group
Unsaturated
CholineOH
Ceramide
Fatty acids
Sphingosine
Sphingomyelin
P CH2CH2N+
CH3 CH3
CH3
CO
NH CH
CH
CH2
Ferrier_Unit03.indd 194Ferrier_Unit03.indd 194 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
17.2 QuestionPhospholipid Synthesis and Degradation
In the synthesis of glycerophospholipids from PA, as shown, either CDP-activated DAG or a CDP-activated alcohol is required. Which is used in the synthesis of PI? Of PC?
By what other process can PC be made in the liver?
What role does PLA 2 play in PL degradation?
What is the cause of Niemann-Pick disease (types A and B)?
Phospholipid
C
O
O C
H2C
H2C
H
C
O
O
Alcohol
C
O
O C
H2C
H2C
H
C
O
O
OH
CDP-diacylglycerol
Phosphatidic acid
Phosphatidic acidDiacylglycerol
C
O
O C
H2C
H2C
H
C
O
O
O CDP
CMP
CMP
PPi
Pi
CTP
ALCOHOL
CDP-ALCOHOL
POR
Ferrier_Unit03.indd 195Ferrier_Unit03.indd 195 5/2/14 7:30 PM5/2/14 7:30 PM
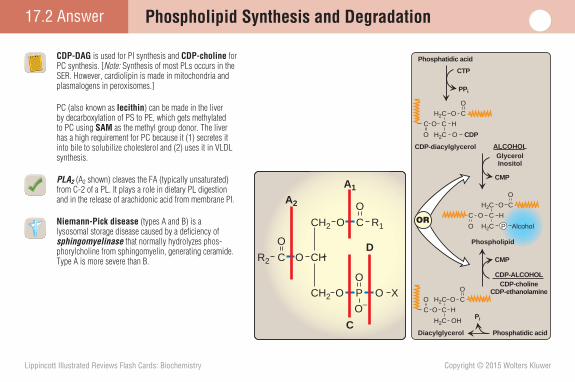
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Phospholipid Synthesis and Degradation17.2 Answer
CDP-DAG is used for PI synthesis and CDP-choline for PC synthesis. [ Note: Synthesis of most PLs occurs in the SER. However, cardiolipin is made in mitochondria and plasmalogens in peroxisomes.]
PC (also known as lecithin ) can be made in the liver by decarboxylation of PS to PE, which gets methylated to PC using SAM as the methyl group donor. The liver has a high requirement for PC because it (1) secretes it into bile to solubilize cholesterol and (2) uses it in VLDL synthesis.
PLA2 (A2 shown) cleaves the FA (typically unsaturated) from C-2 of a PL. It plays a role in dietary PL digestion and in the release of arachidonic acid from membrane PI.
Niemann-Pick disease (types A and B) is a lysosomal storage disease caused by a defi ciency of sphingomyelinase that normally hydrolyzes phos-phorylcholine from sphingomyelin, generating ceramide. Type A is more severe than B.
Phospholipid
C
O
O C
H2C
H2C
H
C
O
O
Alcohol
C
O
O C
H2C
H2C
H
C
O
O
OH
CDP-diacylglycerol
Phosphatidic acid
Phosphatidic acidDiacylglycerol
C
O
O C
H2C
H2C
H
C
O
O
O CDP
CMP
CMP
PPi
Pi
CTP
ALCOHOLGlycerolInositol
CDP-ALCOHOLCDP-choline
CDP-ethanolamine
PORR1
C
O
OR2
CH2
CH2
O
O–PO O
CH
C
O
O
X
A2
A1
C
D
Ferrier_Unit03.indd 196Ferrier_Unit03.indd 196 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
17.3 QuestionFunctions of Phospholipids
What second messengers are produced from PIP 2 , shown outlined by a red box in the cell membrane?
What structure tethers some proteins to membrane-bound PI on the extracellular surface of cells?
What is the clinical signifi cance of an L (lecithin) to S (sphingomyelin) ratio of � 2 in amniotic fl uid?
Hormone
Activatedreceptor
INTRACELLULAR EFFECTS
βγ
α
GTP
GTP
Ca2+
Ca2+
Ca2+
GDP
βγ
ααGTP
+
+
+
Proteinkinase C
ENDOPLASMICRETICULUM
Phosphorylated proteins
CELL MEMBRANE
Phospholipase C
?
?
Ferrier_Unit03.indd 197Ferrier_Unit03.indd 197 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
17.3 Answer Functions of Phospholipids
IP 3 and DAG are the second messengers produced from PIP 2 by PLC, activated when a hormone binds a Gq-type GPCR.
A GPI anchor , in which a protein is covalently attached through a carbohydrate bridge to membrane-bound PI, tethers some proteins (e.g., ALP ) to the extracellular surface.
Lung maturity results from the shift in synthesis from S to L, specifi cally dipalmitoylphosphatidylcholine ( DPPC ), in type II pneumocytes at �32 weeks of gestation. DPPC is the major lipid component of surfactant that decreases surface tension, thereby reducing the pressure needed to infl ate alveoli during inspiration. An L to S ratio � 2 elicits concern for respiratory distress.
Hormone
Activatedreceptor
Diacylglycerol(DAG)
INTRACELLULAR EFFECTS
Activatedreceptor
H
Occupied receptor interacts with Gq protein.
Gq protein releasesGDP and binds GTP.
βγ
α
GTP
GTP
Ca2+
Ca2+
Ca2+
GDP
βγ
αGTP
+
+
+
Proteinkinase C
1
23
6
7 Ca2+ and DAG activate protein kinase C.
Hormone binds to a specific G protein–coupled receptor.
IP3 binds to a specific receptor on the endoplasmic reticulum, causing release of sequestered Ca2+ from IP3-gated channels.
INTRACELLULAREFFECTS
2+
rmoneHor
`-Subunit of Gq protein dissociates and activatesphospholipase C.
ENDOPLASMICRETICULUM
Inositol 1,4,5-trisphosphate (IP3)
Protein kinase C catalyzes phosphorylation of cellular proteins that mediate cellular responseto the hormone.
Phosphorylated proteins
CELL MEMBRANE
8
4
Diacylglycerolcylglcylglcylglcylgcylgcylgcylgcylgcylgcylgcylgcylgylgylgylgylgylgylgylgylgylgylgylgylglgllllll(DAG)
CELL MEMB
Active phospholipase C cleaves phosphatidyl-inositol 4,5-bisphosphate (PIP2) to IP3 and DAG.
5
Phospholipase C
Ferrier_Unit03.indd 198Ferrier_Unit03.indd 198 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
17.4 QuestionGlycosphingolipids
What molecule is the immediate precursor of the glycosphingolipids and sphingomyelin (a sphingophospholipid), as shown?
How do glycosphingolipids and sphingophospholipids differ structurally?
What is the result of � -hexosaminidase A ( � subunit) defi ciency ?
Ganglioside
CMP
CMP-NANA
Globoside
Two or more UDP-sugars
Glucocerebroside
UDP
UDP-glucose
Sulfatide
PAPS
Galactocerebroside
UDP
UDP-galactose
Sphingomyelin(sphingophospholipid)
Phosphatidylcholine
Diacylglycerol
( Glycosphingolipids )
?
Ferrier_Unit03.indd 199Ferrier_Unit03.indd 199 5/2/14 7:30 PM5/2/14 7:30 PM
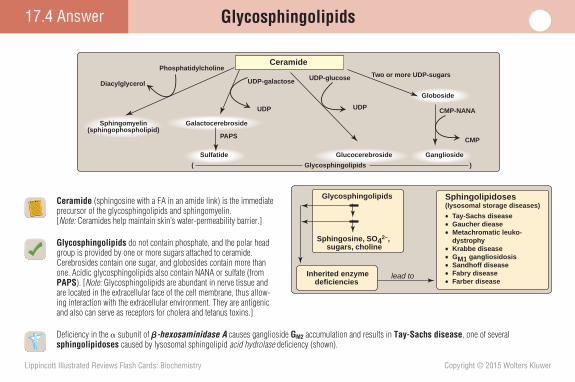
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
17.4 Answer Glycosphingolipids
Ceramide (sphingosine with a FA in an amide link) is the immediate precursor of the glycosphingolipids and sphingomyelin. [Note: Ceramides help maintain skin’s water- permeability barrier.]
Glycosphingolipids do not contain phosphate, and the polar head group is provided by one or more sugars attached to ceramide. Cerebrosides contain one sugar, and globosides contain more than one. Acidic glycosphingolipids also contain NANA or sulfate (from PAPS ). [Note: Glycosphingolipids are abundant in nerve tissue and are located in the extracellular face of the cell membrane, thus allow-ing interaction with the extracellular environment. They are antigenic and also can serve as receptors for cholera and tetanus toxins.]
Defi ciency in the � subunit of � -hexosaminidase A causes ganglioside G M2 accumulation and results in Tay-Sachs disease , one of several sphingolipidoses caused by lysosomal sphingolipid acid hydrolase defi ciency (shown).
Ganglioside
CMP
CMP-NANA
Globoside
Two or more UDP-sugars
Glucocerebroside
UDP
UDP-glucose
Sulfatide
PAPS
Galactocerebroside
UDP
UDP-galactose
Sphingomyelin(sphingophospholipid)
Phosphatidylcholine
Diacylglycerol
Ceramide
( Glycosphingolipids )
Glycosphingolipids
Sphingosine, SO42–, sugars, choline
lead to Inherited enzymedeficiencies
Sphingolipidoses(lysosomal storage diseases)
• Tay-Sachs disease• Gaucher diease• Metachromatic leuko- dystrophy• Krabbe disease• GM1 gangliosidosis• Sandhoff disease• Fabry disease• Farber disease
Ferrier_Unit03.indd 200Ferrier_Unit03.indd 200 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
17.5 QuestionEicosanoids
What 20-carbon, polyunsaturated, � -6 FA serves as the precursor for the synthesis of the predominate series of PGs, TXs, and LTs (collectively known as the eicosanoids), as shown?
Eicosanoids differ from endocrine hormones in that eicosanoids are produced in amounts in
tissues, are not , act , and have their biologic actions mediated by cell membrane and changes in the concentration of .
Why would a defi ciency of linoleic acid, an essential � -6 FA, decrease the synthesis of the eicosanoids?
is precursor to
Leukotrienes (LTs)Prostaglandins (PGs)Thromboxanes (TXs)
Membranephospholipids
cleaved by PLA2
cortisol?
Ferrier_Unit03.indd 201Ferrier_Unit03.indd 201 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
is precursor to
Arachidonic acid
Leukotrienes (LTs)Prostaglandins (PGs)Thromboxanes (TXs)
Membranephospholipids
cleaved by PLA2
cortisol
OH
O
COO–
PGH2
O
Peroxidase
OOH
O
COO–
PGG2
O
Cyclooxygenase2 O2
DesaturationElongation
Arachidonic acid20:4 (5,8,11,14)
(an ω-6 fatty acid)
Dietary linoleic acid18:2 (9,12)
(an ω-6 fatty acid)
COO–
COO–
2 G-SH
G-S-S-G
17.5 Answer Eicosanoids
The eicosatetraenoic FA, arachidonic acid [20:4(5,8,11,14)], is the precursor of the predominant series of eicosanoids .
Eicosanoids differ from endocrine hormones in that eicosanoids are produced in very small amounts in virtually all tissues, are not stored , act locally , and have their biologic actions mediated by cell membrane GPCRs and changes in the concentration of cAMP .
Because humans cannot insert double bonds after C-10 in a FA, we are unable to synthesize arachidonic acid de novo. However, we are able to elongate and desaturate dietary linoleic acid,18:2(9,12), to arachidonic acid. Therefore, linoleic acid defi ciency would decrease availability of the precursor for eicosanoid synthesis. [ Note: Arachidonic acid is incorporated into membrane PLs (primarily PI) at C-2 until it is released by PLA 2 . Cortisol inhibits PLA 2 activity.]
Ferrier_Unit03.indd 202Ferrier_Unit03.indd 202 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
17.6 QuestionEicosanoids
Which isozyme, COX-1 or COX-2 shown, is inducible (nonconstitutive)?
How do the NSAIDs (including aspirin) affect the activity of COX ? Of LOX ?
Why might inhibitors specifi c for COX-2 be associated with increased risk of an MI ?
is precursor to
PGE2
PGI2
PGF2
TXA2 PGH2
Arachidonic acid
PGG2
Cyclooxygenase 1(COX-1)
Cyclooxygenase 2(COX-2)
Peroxidase
Leukotrienes (LTs)Prostaglandins (PGs)Thromboxanes (TXs)
LTC4LTD4LTE4
LTA4 LTB4
5-Hydroperoxyeicosatetraenoic acid(5-HPETE)
5-Lipoxygenase(LOX )
Glutathione
Membranephospholipids
cleaved by PLA2
cortisol
Ferrier_Unit03.indd 203Ferrier_Unit03.indd 203 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
17.6 Answer Eicosanoids
COX-2 is inducible in a limited number of tissues. Induction results in the synthesis of PGs that mediate the pain, heat, redness and swelling of infl ammation, and the fever of infection. COX-1 , constitutively expressed in most tissues, maintains healthy gastric tissue and modulates renal function and platelet aggregation.
NSAIDs (including aspirin ) inhibit both COX isozymes. Aspirin, but not other NSAIDs, causes irreversible inhibition by covalent acetylation. Aspirin does not inhibit LOX and may even favor use of arachidonic acid by LOX for synthesis of the LTs , mediators of bronchoconstriction. [ Note: Cortisol indirectly inhibits both COX and LOX by directly inhibiting PLA 2 and the release of arachidonic acid, their substrate.]
COX-2 synthesizes PGI 2 ( prostacyclin ) that decreases platelet aggregation and vasoconstriction. Its specifi c inhibition would increase the risk of clotting (e.g., in a cardiac vessel in an MI ). [ Note: COX-1 synthesizes TXA 2 that increases platelet aggregation and vasoconstriction. COX-1 inhibition causes decreased clotting, the most common side effect of aspirin use.]
is precursor to
PGE2
PGI2
PGF2
TXA2 PGH2
Arachidonic acid
PGG2
AspirinIndomethacinPhenylbutazoneOther NSAIDs
Cytokines, endotoxin,growth factors, tumorpromoters
Selective COX-2 inhibitors (for example, celecoxib)
Cyclooxygenase 1(COX-1, constitutive)
Cyclooxygenase 2(COX-2, nonconstitutive)
Peroxidase
Leukotrienes (LTs)Prostaglandins (PGs)Thromboxanes (TXs)
+
Membranephospholipids
cleaved by PLA2
cortisol
LTC4LTD4LTE4
LTA4 LTB4
5-Hydroperoxyeicosatetraenoic acid(5-HPETE)
5-Lipoxygenase(LOX )
Glutathione
Ferrier_Unit03.indd 204Ferrier_Unit03.indd 204 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.1 QuestionCholesterol
In addition to de novo synthesis, what are the other two major sources of liver cholesterol, as shown?
Cholesterol is a structural component of , the precursor of in the liver, in the adrenal cortex, and in the skin.
In cholesterol synthesis, which enzymatic steps are identical to those required for KB synthesis? What is different?
Why might patients with hypercholesterolemia be prescribed ezetimibe ? Why should they include plant sterols (phytosterols) in their diet?
LiverCholesterol
Pool
De novo synthesis in the liver
Major sources of liver cholesterol
Major routes by which cholesterol leaves the liver
Free cholesterol secreted in the bile
Secretion of VLDL
Conversion to bile
acids/salts
? ?
Ferrier_Unit03.indd 205Ferrier_Unit03.indd 205 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.1 Answer Cholesterol
Liver receives cholesterol from the diet via CM remnants and from peripheral tissues via HDLs .
Cholesterol is a structural component of membranes , the precursor of bile acids in the liver, steroid hormones in the adrenal cortex, and vitamin D in the skin.
Two acetyl CoA → acetoacetyl CoA → HMG CoA are steps common to cholesterol and KB synthesis. The differ-ence is that the liver has two isozymes of HMG CoA synthase that convert acetoacetyl CoA to HMG CoA. The mitochondrial isoenzyme is used for KB synthesis, and the cytosolic one is used for cholesterol synthesis.
Ezetimibe and phytosterols decrease intestinal absorption of dietary cholesterol (via different mechanisms). Consequently, they have a hypocholesterolemic effect and are used to treat elevated blood cholesterol.
LiverCholesterol
Pool
Chylomicron remnants HDL
De novo synthesis in the liver
Dietary cholesterol
Cholesterol from
extrahepatic tissues
Major sources of liver cholesterol
Major routes by which cholesterol leaves the liver
Free cholesterol secreted in the bile
Secretion of VLDL
Conversion to bile
acids/salts
Ferrier_Unit03.indd 206Ferrier_Unit03.indd 206 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.2 QuestionCholesterol
What enzyme (denoted by the red question mark) is the rate-limiting, regulated enzyme in cholesterol biosynthesis?
How is the enzyme regulated at the transcriptional level when intracellular cholesterol is low? How else is it regulated?
How do statins affect cholesterol biosynthesis? HMG CoA
Mevalonate
CoA 2 NADP+
CH2CH2–O
OHCH3O
CC
2 NADPH + 2 H+
CH2OH
CH2CH2 CoA–O
OHCH3O OCCC
?
Ferrier_Unit03.indd 207Ferrier_Unit03.indd 207 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.2 Answer Cholesterol
The rate-limiting, regulated enzyme of cholesterol biosynthesis is HaMG CoA reductase .
When intracellular cholesterol is low , the SREBP–SCAP complex of the ER membrane moves to the Golgi, where SREBP is sequentially cleaved to a soluble fragment ( SREBP-2 ) that enters the nucleus, binds SRE regions on DNA, and functions as a TF that increases expression of HMG CoA reductase . A rise in cholesterol inhibits this process. [ Note: SREBP-1 upregulates FA and TAG synthesis.] Additional sterol-dependent regulation is the accelerated degradation of the reductase . Sterol-independent regulation includes phosphorylation of the reductase by AMPK . [ Note: When AMPK is active, acetyl CoA is oxidized in the TCA cycle and not used in FA and cholesterol synthesis.]
Statins are competitive inhibitors of HMG CoA reductase . Consequently, they increase the apparent K m of the enzyme (decrease the affi nity of enzyme for substrate) but do not affect the V max .
HMG CoA
Mevalonate
CoA 2 NADP+
HMG CoA reductase
CH2CH2–O
OHCH3O
CC
2 NADPH + 2 H+
CH2OH
Expression isinhibited bycholesterol
CH2CH2 CoA–O
OHCH3O OCCC
Translation
Transcription
HMG CoA reductase (active)
HMG CoA reductase (inactive)
HMG CoA
Mevalonate
Cholesterol
DNA
mRNA
mRNA
Endoplasmic reticulum
GolgiCYTOSOLNUCLEUS
ATP
AMP
ADP
H2O
AMPK
Phospho-protein
phosphatase
SREBP
SRE
P
P
+
Proteolyticcleavage
SREBP-SCAP
SREBP-SCAP
Ferrier_Unit03.indd 208Ferrier_Unit03.indd 208 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.3 QuestionBile Acids and Bile Salts
What enzyme (denoted by the red question mark) is the rate-limiting and regulated enzyme of BA synthesis? How is the enzyme regulated?
How does the amphipathic nature of BSs and TAG aid in dietary lipid emulsifi cation?
Why are agents such as cholestyramine that interfere with the enterohepatic circulation of BSs useful in hypercholesterolemia treatment?
7-α-Hydroxycholesterol
HO OH
CholesterolHOO2
NADPH + H+
NADP+
H2O
Cholic acid(a triol)
Chenodeoxycholic acid(a diol)
?
Ferrier_Unit03.indd 209Ferrier_Unit03.indd 209 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.3 Answer Bile Acids and Bile Salts
The rate-limiting and regulated enzyme of BA synthesis is cholesterol 7- � -hydroxylase , a CYP enzyme of the SER in hepatocytes. [ Note: The products, the primary BAs, undergo hepatic conjugation with taurine or Gly and form conjugated BAs that are stored in the gallbladder and released by CCK. At the pH of bile, the conjugated derivatives are negatively charged, contributing to their amphipathic nature, and are termed BSs. Intestinal bacteria can dehydroxylate them, generating secondary BSs.] Regulation is transcriptional: BAs (via a nuclear receptor) cause decreased transcription of the gene for the hydroxylase .
The amphipathic nature of BSs is largely the result of hydroxylation , which creates a water-soluble face (that interacts with the aqueous environment) and a water-insoluble face (that interacts with dietary lipids) that allow them to stabilize dietary lipid droplets (prevent their coalescence) as they become smaller ( emulsifi cation ).
Over 95% of BSs are reabsorbed in the proximal ileum, returned to the liver, and reused ( enterohepatic circulation ). Excretion of a small amount in stool is the primary mechanism by which cholesterol is removed from the body. [ Note: BS defi ciency can result in cholesterol stone formation (cholelithiasis).] Cholestyramine binds BSs, preventing their reabsorption and increasing the amount excreted. Consequently, more cholesterol is used for BA synthesis, thereby decreasing blood cholesterol levels.
7-α-Hydroxycholesterol
HO OH
CholesterolHO
Bile acids
Cholesterol 7-α-hydroxylase
O2
NADPH + H+
NADP+
H2O
Cholic acid(a triol)
Chenodeoxycholic acid(a diol)
Ferrier_Unit03.indd 210Ferrier_Unit03.indd 210 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.4 QuestionPlasma Lipoproteins
What molecules are contained in the core of a LP, as shown? What are the sources of these molecules? Which LP is the largest? Which is densest?
Compare and contrast CMs and VLDLs.
What is the total cholesterol (C) if LDL-C � 136 mg/dl, HDL-C � 45 mg/dl, and TAGs � 150 mg/dl?
Apolipo-protein
Phospholipids
Unesterifed cholesterol
Unesterifed cholesterol
Inner core of? and ?
Ferrier_Unit03.indd 211Ferrier_Unit03.indd 211 5/2/14 7:30 PM5/2/14 7:30 PM
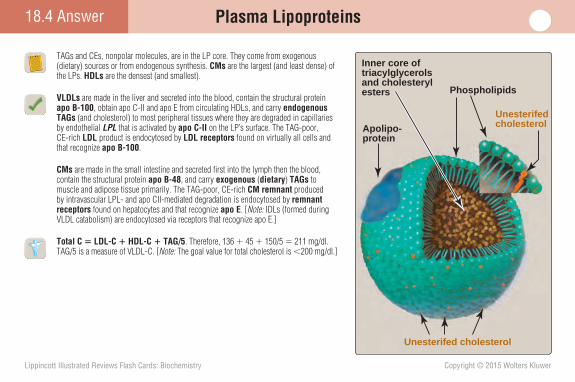
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.4 Answer Plasma Lipoproteins
TAGs and CEs, nonpolar molecules, are in the LP core. They come from exogenous (dietary) sources or from endogenous synthesis. CMs are the largest (and least dense) of the LPs. HDLs are the densest (and smallest).
VLDLs are made in the liver and secreted into the blood, contain the structural protein apo B-100 , obtain apo C-II and apo E from circulating HDLs, and carry endogenous TAGs (and cholesterol) to most peripheral tissues where they are degraded in capillaries by endothelial LPL that is activated by apo C-II on the LP’s surface. The TAG-poor, CE-rich LDL product is endocytosed by LDL receptors found on virtually all cells and that recognize apo B-100 .
CMs are made in the small intestine and secreted fi rst into the lymph then the blood, contain the structural protein apo B-48 , and carry exogenous ( dietary ) TAGs to muscle and adipose tissue primarily. The TAG-poor, CE-rich CM remnant produced by intravascular LPL- and apo CII-mediated degradation is endocytosed by remnant receptors found on hepatocytes and that recognize apo E . [ Note: IDLs (formed during VLDL catabolism) are endocytosed via receptors that recognize apo E.]
Total C � LDL-C � HDL-C � TAG/5 . Therefore, 136 � 45 � 150/5 � 211 mg/dl. TAG/5 is a measure of VLDL-C. [ Note: The goal value for total cholesterol is � 200 mg/dl.]
Apolipo-protein
Phospholipids
Unesterifed cholesterol
Unesterifed cholesterol
Inner core oftriacylglycerolsand cholesterylesters
Ferrier_Unit03.indd 212Ferrier_Unit03.indd 212 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.5 QuestionPlasma Lipoproteins
What mediates the decrease in LDL receptor synthesis when intracellular cholesterol is high, as shown?
What is reverse cholesterol transport (RCT)?
Match the hyperlipidemia to its cause: 1. Type I a. apo E-2 homozygosity 2. Type IIa b. LPL defi ciency 3. Type III c. LDL receptor defi ciency
Receptor protein
mRNA
ACAT
HMG CoA reductaseDNA
Ribosome
SYNTHESIS OFLDL RECEPTORS
SYNTHESIS OFCHOLESTEROL
OVERSUPPLYOF CHOLESTEROL
+
ER
Ferrier_Unit03.indd 213Ferrier_Unit03.indd 213 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.5 Answer Plasma Lipoproteins
Decreased LDL receptor synthe-sis when intracellular cholesterol is high is mediated by retention of the SREBP–SCAP complex in the ER membrane. This prevents formation (in the Golgi) of SREBP-2 , a TF that binds SREs on DNA and increases expression of the gene for the LDL receptor. The gene for HMG CoA reduc-tase , the rate-limiting enzyme of cholesterol synthesis, is regulated in the same way (see Card 18.2). [ Note: Cytosolic ACAT esterifi es the excess cholesterol to CE for storage in cytosolic droplets.]
RCT is an atheroprotective process by which cholesterol is sent out of peripheral cells (via ABCA1 ) for uptake onto nascent HDLs , esterifi ed by LCAT , and sequestered in the core. HDL (as HDL2) carries CEs to the liver, where they are selectively taken up by SR-B1 and used for BA synthesis or excreted into bile. [ Note: CETP exchanges HDL CEs for VLDL TAGs.]
Type I hyperlipidemia � b, LPL defi ciency; Type IIa � c, LDL receptor defi ciency; Type III � a, Apo E2 homozygosity.
LPL defi ciency results in a rise in CMs and hypertriglyceridemia . LDL receptor defi ciency results in a rise in LDLs and hypercholesterolemia . Apo E-2 homozygosity results in CM remnant and IDL accumulation (due to decreased uptake) and hypercholesterolemia .
Discoidal nascent HDL
PERIPHERALTISSUES
Apo A-I
LIVER
SMALLINTESTINE
C
C
+
+
HDL3
HDL2VLDL
VLDL
LCAT
CETP
CE
CE
C, CE
lyso-PC
PC
Apo A-1
Apo A-1
SR-B1
Free cholesterol
LCAT
ABCA1
Free
cholesterolHepatic lipase
LDL IDL
Apo E, C-II
Ferrier_Unit03.indd 214Ferrier_Unit03.indd 214 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.6 QuestionSteroid Hormones
What molecule (denoted by the red question mark) is the parent compound for all steroid hormones? What role does desmolase play in its synthesis?
What hormone stimulates cortisol synthesis and release? What are the effects of cortisol? How are these effects mediated?
Which congenital adrenal hyperplasia ( CAH ) is characterized by decreased aldosterone and cortisol production and increased androstenedione production?
Desmolase(CYP11A,P450scc )
3-β-Hydroxysteroiddehydrogenase
11-β-Hydroxylase(CYP11B1)
17-β-Hydroxysteroid dehydrogenase
Aromatase(CYP19 )
Corticosterone
21-α-Hydroxylase
17-α-Hydroxylase(CYP17)
NADPHO2
17, 20-Lyase(CYP17 )
Cholesterol (27C)
?
Progesterone (21C)
11-Deoxycorticosterone (21C) 11-Deoxycortisol (21C)
Testosterone (C19)
Androstenedione (19C)
17-α-Hydroxyprogesterone (21C)
Cortisol (21C) Estradiol (18C)Aldosterone (21C)
18-α-hydroxylase(aldosterone synthase)
(CYP11B2)
(11-β-hydroxylase) (CYP11B1)
Ferrier_Unit03.indd 215Ferrier_Unit03.indd 215 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
18.6 Answer Steroid Hormones
Pregnenolone , derived from cholesterol, is the parent of all steroid hormones. Desmolase, a CYP enzyme (CYP11A, or P450scc) of the inner mitochondrial membrane catalyzes cholesterol hydroxylation and side-chain cleavage (scc). This is the initial and rate-limiting step.
ACTH (or corticotropin ) from the pituitary gland stimulates cortisol synthesis and release. Cortisol binds to soluble receptors, and the receptor–hormone complex binds (as a dimer) to HREs on DNA, thereby altering gene expression. Changes in expression result in increased gluconeogenesis as well as weakened immune and infl ammatory responses.
Decreased aldosterone and cortisol production and increased androstenedione production are characteristic of 21- � -hydroxylase defi -ciency , the most common cause of CAH . In the classic form, salt wasting characterized by dehydration, hypotension, hyponatremia, and hyperka-lemia is seen because of aldosterone defi ciency. With 21- � -hydroxylase defi ciency, masculinization of female genitalia is seen because of androgen overproduction. In contrast, 17- � -hydroxylase defi ciency causes female-like genitalia in both sexes because of the absence of androgens.
Desmolase(CYP11A,P450scc )
3-β-Hydroxysteroiddehydrogenase
11-β-Hydroxylase(CYP11B1)
17-β-Hydroxysteroid dehydrogenase
Aromatase(CYP19 )
Corticosterone
21-α-Hydroxylase
17-α-Hydroxylase(CYP17)
NADPHO2
17, 20-Lyase(CYP17 )
Cholesterol (27C)
Pregnenolone (21C)
Progesterone (21C)
11-Deoxycorticosterone (21C) 11-Deoxycortisol (21C)
Testosterone (C19)
Androstenedione (19C)
17-α-Hydroxyprogesterone (21C)
Cortisol (21C) Estradiol (18C)Aldosterone (21C)
18-α-hydroxylase(aldosterone synthase)
(CYP11B2)
(11-β-hydroxylase) (CYP11B1)
Ferrier_Unit03.indd 216Ferrier_Unit03.indd 216 5/2/14 7:30 PM5/2/14 7:30 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Overall Nitrogen Metabolism 19.1 Question
What are the three inputs to the amino acid pool shown?
What is “protein turnover”?
Compare and contrast the proteasomal and lysosomal systems of protein degradation.
What does it mean for an individual to be in N balance? Positive N balance?
Amino acid pool
? ?
?
Ferrier_Unit04.indd 217Ferrier_Unit04.indd 217 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
19.1 Answer Overall Nitrogen Metabolism
Three inputs to the amino acid pool are the (1) degradation of body protein, (2) degradation of dietary protein, and (3) synthesis of nonessential amino acids.
“ Protein turnover ” is the ongoing synthesis and degradation of a protein. In a healthy adult, the rate of synthesis is just suffi cient to replace the amount of protein that was degraded, resulting in a steady state . Turnover rate varies among proteins.
Proteasomal protein degradation involves the three-step, ATP-dependent enzy-matic tagging of proteins with � 4 Ub followed by cleavage to small peptides in the cytosolic proteasome as Ub is recycled. The proteasomal system is selective and is infl uenced by structural aspects of the protein. In contrast, the relatively nonselective lysosomal system is ATP and Ub independent and uses acid hydrolases to cleave proteins.
N balance means that the amount of N going into the body equals the amount going out. In a state of positive N balance , however, more N is going in than is coming out, such as in periods of growth (including pregnancy) and in recovery from muscle atrophy (e.g., as occurs with prolonged immobilization or disease).
Varies
Bodyprotein
Amino acid pool
~400 g/day
Dietary protein can vary from none (for example, fasting) to over 600 g/day (high-protein diets), but 100 g/day is typical of the U.S. diet.
Synthesis ofnonessentialamino acids
Ferrier_Unit04.indd 218Ferrier_Unit04.indd 218 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
19.2 QuestionDietary Protein Digestion
What enzyme of protein digestion, denoted by the red question mark, is produced by the stomach?
What role does enteropeptidase play in digestion?
Why is celiac disease a pathology of malabsorption?
What amino acids are expected to be present in the urine of an individual with cystinuria ?
Amino- peptidasesDi- and tri- peptidases
Amino acids
TrypsinChymotrypsinElastaseCarboxy- peptidase
Oligopeptidesand amino acids
?Polypeptides
and amino acids
SMALLINTESTINE
Dietary protein
TO LIVER
STOMACH
PANCREAS
Ferrier_Unit04.indd 219Ferrier_Unit04.indd 219 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Dietary Protein Digestion19.2 Answer
Pepsin , an acid-stable endopeptidase , is secreted by gastric chief cells as the zymogen pepsinogen. [ Note: In the presence of HCL from gastric parietal cells, pepsinogen undergoes autocatalytic cleavage to pepsin.]
Enteropeptidase , a serine protease of the brush border membrane of intestinal mucosal cells, cleaves trypsinogen to trypsin , a serine protease that converts all other pancreatic zymogens to their active forms through cleavage at the carboxyl side of Arg and Lys residues in the proteins.
Celiac disease ( gluten enteropathy ) is a chronic disease of the gastrointestinal tract caused by an immune-mediated response to gluten (a protein in wheat, barley, and rye) that atrophies the brush border, resulting in malabsorption .
Cystinuria is an AR defect in the transporter that takes up cystine and the dibasic amino acids ornithine, Arg, and Lys (sometimes represented as COAL ) in the proximal tubules, causing them to appear in the urine. Cystine can precipitate at the acidic pH of urine and form stones in the urinary tract ( cystine urolithiasis ).
Amino- peptidasesDi- and tri- peptidases
Amino acids
TrypsinChymotrypsinElastaseCarboxy- peptidase
Oligopeptidesand amino acids
Pepsin
Polypeptidesand amino acids
SMALLINTESTINE
Dietary protein
TO LIVER
STOMACHSTOMACHSTOMACH
PANCREASPANCREASPANCREAS
Ferrier_Unit04.indd 220Ferrier_Unit04.indd 220 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
19.3 QuestionNitrogen Removal
What is the general name of the enzymes that catalyze the reversible transfer of amino groups from one carbon skeleton to another, as shown? What vitamin is the source of the coenzyme used in the reaction?
What is the primary fate of Glu during periods of amino acid catabolism?
Which set of clinical fi ndings in blood is more suggestive of liver disease ? A. ↑AST, ↑ALT, ↑bilirubin B. ↑AST, ↔ALT, ↔bilirubin
R
HC NH3+
COO–
α-Amino acid
CH2
α-KetoglutarateCOO–
O C
CH2
COO–
α-Keto acid
+
Glutamate
OH3N
CH2
COO–CH
CH2
COO–
R
CCOO–
Ferrier_Unit04.indd 221Ferrier_Unit04.indd 221 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
19.3 Answer Nitrogen Removal
Aminotransferases ( transaminases ) catalyze the reversible transfer of amino groups from most amino acids to �-KG, a process known as transamination . The products are an �-keto acid and Glu. [ Note: Lys and Thr are not substrates for aminotransferases .] The PLP coenzyme required by these enzymes is derived from vitamin B 6 ( pyridoxine ).
During amino acid catabolism, Glu is oxidatively deaminated to � -KG � NH 3 by the mitochondrial enzyme GDH that uses NAD � as a coenzyme as shown. ADP (a low-energy signal) is an allosteric activator. [ Note: The GDH reaction is reversible and the reductive biosynthesis of Glu uses NADPH.]
Choice A (↑ AST , ↑ ALT , ↑bilirubin) is more suggestive of liver disease . AST and ALT are intracel-lular enzymes that leak into the blood when liver cells are damaged. The rise in bilirubin indicates a problem with hepatic metabolism. ALT is found primarily in liver, whereas AST is also found in heart and skeletal muscle and RBCs. Therefore, a rise in AST with a normal value for ALT and bilirubin sug-gests damage to nonhepatic tissues.
R
HC NH3+
COO–
α-Amino acid
CH2
α-KetoglutarateCOO–
O C
CH2
COO–
α-Keto acid
+
Glutamate
PLP
OH3N
Aminotransferase
CH2
COO–CH
CH2
COO–
R
CCOO–
CH2
α-Ketoglutarate
COO–O C
CH2
COO–
+
Glutamate
NAD+ NADH
NADP+ NADPH
H3N
NH3
NH3
GlutamatedehydrogenaseCH2
COO–CH
CH2
COO–
Ferrier_Unit04.indd 222Ferrier_Unit04.indd 222 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
19.4 QuestionAmmonia and the Urea Cycle
What is the amino acid product of the reaction shown? Would you expect the enzyme that catalyzes the reaction to be a synthase or a synthetase ? What is the biologic signifi cance of the reaction?
What is the function of the UC, and where does it occur? What is the regulated enzyme? What is the fate of the urea product?
How do the liver and the kidneys metabolize Arg differently? How does this relate to Arg being nonessential?
?
CH2
GlutamateCOO–
CH2
COO–
HCNH3+
ADP + Pi
ATP + NH3
Ferrier_Unit04.indd 223Ferrier_Unit04.indd 223 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
19.4 Answer Ammonia and the Urea Cycle
Gln is the amino acid product. Because the catalyzing enzyme requires ATP, it is a synthetase ( glutamine synthetase ). The reaction utilizes toxic NH 3 (generated in amino acid catabolism) to form Gln, a nontoxic transporter of NH 3 through the blood. Gln, primarily generated by skeletal muscle, is taken up and metabolized by the liver, intestine, and kidneys.
The UC converts toxic NH 3 to nontoxic urea . This ATP-dependent process occurs in hepatocytes (the fi rst two reactions in the mitochondrial matrix, the remaining three in the cytosol). [ Note: Gluconeogenesis and heme synthesis also require enzymes of the matrix and the cytosol.] The regulated enzyme of the UC is CPS I , which requires N-AcGlu as an allosteric activator. Urea, the most important means of disposing of NH 3 , is transported through the blood to the kidneys for excretion. [ Note: The UC uses and regenerates ornithine.]
The liver expresses the full complement of UC enzymes, including arginase-1 that hydrolyzes Arg to urea and ornithine, whereas the kidney is able to make Arg from citrulline but does not contain arginase-1 . [ Note: Arg is used for renal NO synthesis.]
CH2
GlutamineCOO–
CH2
HCNH3+
Glutaminesynthetase
ATP + NH3
CH2
GlutamateCOO–
CH2
COO–
HCNH3+
ADP + Pi
CO NH2
Ferrier_Unit04.indd 224Ferrier_Unit04.indd 224 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
19.5 QuestionAmmonia and the Urea Cycle
What are the sources of the N that appears in urea?
What happens to the fumarate produced by argininosuccinate lyase ?
A 9-month-old boy was admitted to the hospital for evaluation of chronic vomiting and developmental delay. Lab studies revealed elevated levels of NH 3 , Gln, Ala, and ornithine. Citrulline was low. Which UC enzyme is defi cient in the patient?
Why might antibiotics be used to treat UC disorders ?
HCO3–
Glutamate
Glutamate
?
α-Ketoglutarate
α-Ketoglutarate
Oxaloacetate
NADH +
Argininosuccinate
Arginine
Ornithine
CarbamoylphosphateCitrulline
UREACYCLE
Urea
Fumarate
Oxidativedeamination
NAD+
Amino acids
α-Keto acids
Transamination
?
Ferrier_Unit04.indd 225Ferrier_Unit04.indd 225 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Ammonia and the Urea Cycle19.5 Answer
NH 3 , primarily from amino acid catabolism, provides one N of urea, and Asp provides the other. [ Note: Glu is the immediate precursor of the NH 3 (via GDH ) and of the Asp (via AST ).]
The fumarate produced by cytosolic argininosuccinate lyase is hydrated to malate, which can be transported into the mitochondrial matrix, enter the TCA cycle, and be oxidized to OAA . The OAA can be used in gluconeogenesis or transaminated to Asp and used in the UC.
Mitochondrial X-linked OTC is the defi cient enzyme. Its defi ciency is the most common UC disorder, resulting in elevated levels of NH3 and ornithine (substrates for the cycle and the OTC reaction, respectively). The rise in NH3 causes a rise in Gln. Ala, which transports N from amino acid catabolism, also increases. Citrulline (the product of OTC) decreases.
Because NH 3 is generated from urea by urease of intestinal bacteria, antibiotic use decreases this source of NH 3 in patients with impaired ability to detoxify it.
HCO3–
Glutamate
Glutamate
Aspartate
α-Ketoglutarate
α-Ketoglutarate
Oxaloacetate
NADH + NH3
Argininosuccinate
Arginine
Ornithine
CarbamoylphosphateCitrulline
UREACYCLE
Urea
Fumarate
Oxidativedeamination
NAD+
Amino acids
α-Keto acids
TransaminationNH2
C
Carbamoylphosphate
MITOCHONDRIALMATRIX
PO–
O
O–O
HCO3–
+2 ATP
NH3
+
NH3+
CH2
CH2
CH2
HCNH3+
COO–
L-Ornithine
CNH2
O
NHCH2
CH2
CH2
HCNH3+
COO–
L-Citrulline
Pi
3 H++
2 ADP+Pi
Carbamoylphosphate
synthetase I
Ornithine trans-carbamoylase O
Ferrier_Unit04.indd 226Ferrier_Unit04.indd 226 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
19.6 QuestionAmmonia Metabolism
How do the UC, glutaminase , and glutamine synthetase shown work together within hepatocytes to keep blood NH 3 levels low?
What is the signifi cance of NH 4 � production by the kidney?
What is blood BUN? UUN?
What role does phenylacetate play in UC disorder treatment?
Urea
Glutamate + ATP
Aminotransferases
NAD(P)+
NAD(P)H
BODY PROTEIN
α-Amino acids
α-Keto acids
NH3
NH4+
Glutamate
Urea cycle
H2O Glutamate
Glutaminase
Glutamine
Glutaminesynthetase
ADP + Pi
METABOLISM
URINE
Amide nitrogendonated in
biosyntheticreactions
DIET
α-Ketoglutarate
Glutamatedehydrogenase
H+
Carbamoyl phosphate synthetase I
Ferrier_Unit04.indd 227Ferrier_Unit04.indd 227 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
19.6 Answer Ammonia Metabolism
Periportal hepatocytes are rich in glutaminase , which produces toxic NH 3 (and Glu) from Gln (its nontoxic carrier), and in the enzymes of the UC that converts the NH 3 to nontoxic urea for transport to the kidneys. Any NH 3 missed by these reactions is “scavenged” by glutamine synthetase in the perivenous hepatocytes and used to convert Glu to Gln that is sent out into the blood. Together, these processes prevent hyperammonemia , a condition that has a neurotoxic effect.
NH 4 � production (NH 3 � H � → NH 4 � ) by the kidney helps to maintain acid–base balance through urinary excretion of H � , which is important when the rate of ketogenesis is faster than the rate of ketolysis, for example. [ Note: Loss of HCO 3 � in metabolic acidosis decreases the UC. Consequently, NH4
� production increases.]
BUN is a measure of the urea content in blood at a given point in time. UUN is a measure of the urea content in urine over 24 hours.
Phenylacetate (from the prodrug phenylbutyrate) conjugates with Gln (a nonessential amino acid) and is excreted in the urine, thereby decreasing the NH 3 load of the body. Such treatment has been shown to reduce the morbidity and mortality of UC disorders .
Urea
Glutamate + ATP
Aminotransferases
NAD(P)+
NAD(P)H
BODY PROTEIN
α-Amino acids
α-Keto acids
NH3
NH4+
Glutamate
Urea cycle
H2O Glutamate
Glutaminase
Glutamine
Glutaminesynthetase
ADP + Pi
METABOLISM
URINE
Amide nitrogendonated in
biosyntheticreactions
DIET
α-Ketoglutarate
Glutamatedehydrogenase
H+
Carbamoyl phosphate synthetase I
Ferrier_Unit04.indd 228Ferrier_Unit04.indd 228 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
20.1 QuestionCarbon Skeleton Catabolism
Which vertical column (A, B, or C) shown would most appropriately be labeled “(Solely) Ketogenic Amino Acids”?
Which horizontal row (1 or 2) would most appropriately be labeled “Essential Amino Acids”? What does it mean for an amino acid to be essential?
The pathways for catabolism of the C-skeletons of amino acids converge to form what seven intermediate products?
Asparaginase is used to treat childhood acute lymphoblastic leukemia ( ALL ). What is the biochemical basis of this treatment?
AlanineArginineAsparagineAspartateCysteineGlutamateGlutamineGlycineProline Serine
1 Tyrosine
HistidineMethionineThreonineValine
2 LeucineLysine
A CB
IsoleucinePhenyl- alanineTryptophan
Ferrier_Unit04.indd 229Ferrier_Unit04.indd 229 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
20.1 Answer Carbon Skeleton Catabolism
Column C contains the two solely ketogenic amino acids.
Row 2 contains the nine essential amino acids, which are the amino acids that cannot be synthesized (or synthesized in suffi cient quantities) by humans.
Catabolism of the C-skeletons of amino acids produces TCA intermediates ( � -KG, succinyl CoA, fumarate, and OAA) and pyruvate from the glucogenic amino acids, and acetoacetate (or its derivative acetyl CoA) from the ketogenic amino acids.
Asparaginase (from bacteria) is a treatment for ALL because it deamidates circulating Asn to Asp. Rapidly dividing leukemia cells require Asn for growth and have limited capacity to synthesize it.
AlanineArginineAsparagineAspartateCysteineGlutamateGlutamineGlycineProline Serine
Tyrosine
HistidineMethionineThreonineValine
LeucineLysine
No
nes
sen
tial
Ess
enti
al
Glucogenic KetogenicGlucogenic andKetogenic
IsoleucinePhenyl- alanineTryptophan
Ferrier_Unit04.indd 230Ferrier_Unit04.indd 230 5/2/14 7:36 PM5/2/14 7:36 PM
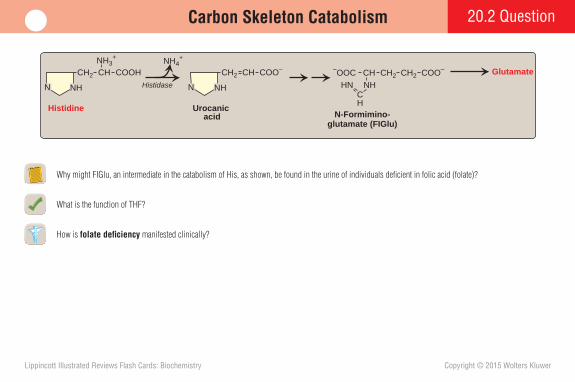
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Carbon Skeleton Catabolism 20.2 Question
Why might FIGlu, an intermediate in the catabolism of His, as shown, be found in the urine of individuals defi cient in folic acid (folate)?
What is the function of THF?
How is folate defi ciency manifested clinically?
N
CH2
Histidase
Histidine
NH
CH COOHNH3
+
Urocanic acid
Glutamate
N-Formimino-glutamate (FIGlu)
N
CH2
NH
CH COO– CH2CH COO–
NH
–OOC CH2
CH
HN
NH4+
Ferrier_Unit04.indd 231Ferrier_Unit04.indd 231 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
20.2 Answer Carbon Skeleton Catabolism
FIGlu reacts with THF to form N 5 -formimino-THF � Glu. If folate (and, consequently, THF) is defi cient, FIGlu accumulates and is excreted in the urine. [ Note: The FIGlu excretion test has been used in the diagnosis of folate defi ciency.]
THF is a carrier of one-C groups (attached to N 5 , N 10 , or both N 5 and N 10 of the molecule) in oxidation states that range from formyl to methyl. [ Note: N 10 -formyl-THF is used in synthesis of the purine ring; N 5 ,N 10 -methylene-THF is used in the synthesis of dTMP from dUMP; and N 5 -methyl-THF is used in the remethylation of Hcy to Met, a reaction that also requires vitamin B 12 . This remethylation reaction is the only time THF carries and donates a methyl group.] THF is made from folate in a two-step, NADPH-requiring reaction catalyzed by DHFR .
Folate defi ciency presents as a megaloblastic anemia (a type of macrocytic anemia ) in which cell growth occurs without cell division because of decreased availability of the purines and the dTMP needed for DNA synthesis. [ Note: Vitamin B 12 defi ciency presents in a similar manner.]
N
CH2
Histidase
Histidine
NH
CH COOHNH3
+
Urocanic acid
Glutamate
N5-Formimino- tetrahydrofolate
Tetrahydro-folateN-Formimino-
glutamate (FIGlu)
N
CH2
NH
CH COO– CH2CH COO–
NH
–OOC CH2
CH
HN
NH4+
Ferrier_Unit04.indd 232Ferrier_Unit04.indd 232 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
20.3 QuestionSulfur-Containing Amino Acids
What is the function of SAM, produced by the metabolism of Met, as shown?
Cys, produced from the sulfur of Met and the C-skeleton of Ser (shown), can be desulfurized to pyruvate. What is an important use of the sulfate released in this process?
Why is homocystinuria a concern? What role do vitamins B 6 , B 12 , and folate play in maintaining low Hcy levels?
L-Homocysteine
CH2
COO–HCNH3
+
CH2
SH
H2O
S-Adenosylhomocysteine (SAH)
S
CH2
COO–HCNH3
+
CH2
S-Adenosylmethionine (SAM)
S+
CH2
COO–HCNH3
+
CH2
Adenosine
Adenosine
CH3
Pi + PPi
2 Pi
ATP
H2O
L-Serine
Methionineadenosyl-
transferase
Mg2+
L-Methionine
Adenosine
SAHhydrolase
L-Cysteine
Ferrier_Unit04.indd 233Ferrier_Unit04.indd 233 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
20.3 Answer Sulfur-Containing Amino Acids
SAM (like THF) is a one-C carrier, but (unlike THF) SAM carries only methyl groups , which are transferred by methyltransferases to acceptors such as norepinephrine, PE, DNA, and RNA.
The sulfate released from the desulfurization of Cys can be used to synthesize PAPS , an activated sulfate donor with a variety of acceptors (e.g., the GAGs ).
Homocystinuria , caused by elevated Hcy levels, promotes endothelial dysfunction and is an independent risk factor for occlusive vascular disease . Hcy is kept low by (1) conversion to Cys, a two-step, B 6 -dependent process (shown) catalyzed by cystathionine synthase and cystathionase , and (2) remethylation to Met, a THF- and B 12 -requiring reaction catalyzed by methionine synthase . As the levels of vitamins B 6 , B 12 , and folate ↓, Hcy levels ↑. Mild elevations of Hcy are seen in a small percentage of individuals, but large elevations are rare and are primarily seen in cystathionine � -synthase defi ciency.
L-Cysteine
CH2
CystathionineCOO–
HCNH3+
γ-Cystathionase
α -Ketobutyrate + NH4+
CH2 S CH2
COO–HCNH3
+
H2O
H2O
L-SerineCystathionine
β-synthase
L-Homocysteine
CH2
COO–HCNH3
+
CH2
SH
H2O
S-Adenosylhomocysteine (SAH)
Methyl acceptors
Methylated products
Methyltransferases
S-Adenosylmethionine (SAM)
Pi + PPi
2 Pi
ATPMethionineadenosyl-
transferase
Mg2+
L-Methionine
Adenosine
B6
B6
SAHhydrolase
MethionineTetrahydrofolate
N5-Methyl-tetrahydrofolate
Homocysteine
Vitamin B12(methyl-
cobalamin)
Methionine synthase
Ferrier_Unit04.indd 234Ferrier_Unit04.indd 234 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
20.4 QuestionBranched-Chain Amino Acids
What coenzymes are required by BCKD , the enzyme that oxidatively decarboxylates the � -keto acid derivatives of the BCAAs, as shown? What other enzymes also require them?
In addition to Val and Ile, what other amino acids are metabolized to propionyl CoA and, ultimately, succinyl CoA?
Why are individuals with maple syrup urine disease ( MSUD ), a rare AR disorder caused by BCKD defi ciency, at particular risk during periods of physiologic stress?
ACETO-ACETATE
+ACETYL CoA
ACETYL CoA
Propionyl CoA
Isovaleryl CoA
Isobutyryl CoAα-Methyl-
butyryl CoA
α-Ketoiso-caproic acid
α-Ketoiso-valeric acid
α-Keto-β-methyl-valeric acid
Leucine Valine Isoleucine
TRANSAMINATION(Branched-chain amino acid aminotransferase)
OXIDATIVE DECARBOXYLATION(Branched-chain α-keto acid dehydrogenase
HMG CoA
β-Methyl-glutaconyl CoA
β-Methyl-crotonyl CoA
SUCCINYL CoA
Methylmalonyl CoA
Biotin
Biotin
5'-Deoxyadenosyl-cobalamin
(derivative of B12)
FAD-linked DEHYDROGENATION
Ferrier_Unit04.indd 235Ferrier_Unit04.indd 235 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
20.4 Answer Branched-Chain Amino Acids
BCKD , a mitochondrial enzyme, requires NAD � and CoA as cosubstrates and TPP, lipoic acid, and FAD as prosthetic groups. PDH and � -KGD are the other mitochondrial � -keto acid dehydrogenase complexes that require this group of coenzymes.
In addition to Val and Ile, Met and Thr are metabolized to propionyl CoA . Biotin-dependent propionyl CoA carboxylase converts propionyl CoA to methylmalonyl CoA, which is converted to succinyl CoA by a B 12 -dependent mutase . The other B 12 -requiring reaction in humans is the remethylation of Hcy to Met. [ Note: FAs with an odd number of C atoms produce propionyl CoA in the fi nal round of � -oxidation.]
Physiologic stress triggers skeletal muscle proteolysis to meet increased energy needs. Because Val and Ile provide glucose (from the metabolism of succinyl CoA to glucogenic Ala) and Leu and Ile provide acetyl CoA, these energy sources will be in decreased supply in individuals with MSUD , putting them at particular risk during periods of physiologic stress. Additionally, elevated Leu can cause neurologic dam-age. [ Note: BCKD defi ciency confers a maple syrup–like odor to body fl uids.]
ACETO-ACETATE
+ACETYL CoA
ACETYL CoA
Propionyl CoA
Isovaleryl CoA
Isobutyryl CoA`-Methyl-
butyryl CoA
`-Ketoiso-caproic acid
`-Ketoiso-valeric acid
`-Keto-a-methyl-valeric acid
Leucine Valine Isoleucine
TRANSAMINATION(Branched-chain amino acid aminotransferase)
HMG CoA
a-Methyl-glutaconyl CoA
a-Methyl-crotonyl CoA
SUCCINYL CoA
Methylmalonyl CoA
Biotin
Biotin
5'-Deoxyadenosyl- cobalamin
(derivative of B12)
FAD-linked DEHYDROGENATION
OXIDATIVE DECARBOXYLATION(Branched-chain a-keto acid dehydrogenase
Deficient in MSUDcoenzymes: NAD+, CoA, TPP, lipoic acid, FAD)
Ferrier_Unit04.indd 236Ferrier_Unit04.indd 236 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
20.5 QuestionAromatic Amino Acids
What coenzyme is required by the PAH reaction shown?
What other enzymes of amino acid metabolism require this coenzyme?
What is the cause of phenylketonuria ( PKU ), and how is it treated? Why are the CNS effects of PKU now rarely seen?
What is the clinical consequence of tyrosinase defi ciency ?
What are the causes and clinical consequences of alkaptonuria ? Phenylalaninehydroxylase
CH2
NH3+
L-Phenylalanine
C COO–H
CH2
NH3+
L-Tyrosine
HO
C COO–H
Ferrier_Unit04.indd 237Ferrier_Unit04.indd 237 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
20.5 Answer Aromatic Amino Acids
THB ( BH 4 ), made from GTP, is the coenzyme for the PAH reaction. Its defi ciency results in hyperphenylalaninemia and decreased Tyr production.
BH 4 is also used by tyrosine and tryptophan hydroxylases . Its defi ciency decreases synthesis of the catecholamines from Tyr and serotonin from Trp. Treatment includes replacement therapy. [ Note: Use of BH 4 by aromatic amino acid hydroxylases (and by NOS that synthesizes NO from Arg) is in contrast to the use of PLP in most other reactions involving amino acids.]
PAH defi ciencies cause PKU , which is characterized by a “mousey” odor. Treatment includes Phe restriction and supplementation with the now-essential Tyr. Newborn screening programs have allowed early diagnosis and treatment of PKU, preventing the microcephaly , intellectual disability , and seizures , characteristic of the untreated defi ciency. Because Phe is teratogenic , women with PKU can give birth to children with anatomic anomalies if Phe levels are not controlled ( maternal PKU syndrome ).
Lack of tyrosinase , which is required for the synthesis of melanin from Tyr, causes oculocutaneous albinism .
Defi ciency of homogentisic acid oxidase of Tyr catabolism causes alkap-tonuria . Symptoms include formation of a blue-black pigment-like polymer ( ochronosis ) in connective tissue (and urine) and early-onset arthritis.
Dihydro-biopterin + H2O
Tetrahydro-biopterin + O2
Phenylalaninehydroxylase
CH2
NH3+
L-Phenylalanine
C COO–H
CH2
NH3+
L-Tyrosine
HO
C COO–H
PKU
Ferrier_Unit04.indd 238Ferrier_Unit04.indd 238 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.1 QuestionHeme Structure and Synthesis
Based on the fi gure, to what series of the porphyrins (cyclic tetrapyrroles) does heme belong? What are some examples of heme-containing proteins?
What are the major sites of heme synthesis in the body? What subcellular sites are involved? What is the rate-limiting, committed reaction?
Why might use of statins , cholesterol-lowering drugs metabolized by the hepatic CYP system, cause an increase in heme synthesis in the liver?
Heme
Fe
CH2CH2–OOC
CH3
CH3
CH2
H2C CH
CH
CH3 CH3
CH2CH2 COO–
N N
N N
Ferrier_Unit04.indd 239Ferrier_Unit04.indd 239 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.1 Answer Heme Structure and Synthesis
In heme , the side chains are asymmetrically distributed on one of the pyrrole rings , placing heme in the III series of the porphyrins. [ Note: IX refl ects an older naming system and is equivalent to III.] Hb, Mb, CYP monooxygenases , NOS , and catalase , are examples of proteins that contain heme, a metalloporphyrin that functions as a prosthetic group .
The liver and RBC-producing cells of the marrow are the major sites of heme synthesis, with � 85% occurring in the marrow. Enzymes of the mitochondria and the cytosol are required. The rate-limiting, committed step is the mitochondrial synthesis of ALA from Gly and succinyl CoA by PLP-requiring isozymes, ALAS1 and ALAS2 .
ALAS1 (the ubiquitous isozyme) is regulated by heme (shown), which represses gene transcrip-tion, increases mRNA degradation, and decreases enzyme import into mitochondria. Use of heme in the synthesis of the hepatic CYP enzymes needed to metabolize the statins prevents heme from accumulating. This favors activation of ALAS1 and, consequently, heme synthesis in the liver. [ Note: ALAS2 (the isozyme specifi c to erythroid tissue) is regulated by iron: as iron ↑, synthesis of ALAS2 ↑.]
Heme (Fe2+ protoporphyrin IX)
Fe
CH2CH2–OOC
CH3
CH3
CH2
H2C CH
CH
CH3 CH3
CH2CH2 COO–
N N
N N
Glycine
CH2 COO–
NH3+
Succinyl CoA
CH2
COO–
O C CoA
CH2
CoA
ALAS1(mitochondrial
enzyme)
CO2
COO–
CH2
CH2
OC
CH2
NH3+
Heme
δ-Aminolevulinic acid (ALA)
PLP
Ferrier_Unit04.indd 240Ferrier_Unit04.indd 240 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.2 QuestionHeme Synthesis
What metal inhibits the reaction shown? Are any other reactions of heme synthesis similarly affected?
How is protoporphyrin IX synthesized from porphobilinogen?
What are the porphyrias , and how are they classifi ed? Which is most common?
N
C C
C CH
H
COO–
CH2
CH2
NH2
COO–
CH2
CH2
Porphobilinogen
δ-Aminolevulinicacid dehydratase
(cytosolic enzyme)
(Two moleculescondense)
δ-Aminolevulinic acid (ALA)
2 H2O
Ferrier_Unit04.indd 241Ferrier_Unit04.indd 241 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.2 Answer Heme Synthesis
Lead inhibits the ALA dehydratase - catalyzed condensation of two ALA to porphobilinogen , a pyrrole. Mitochondrial ferrochelatas e , which inserts Fe 2 � into protoporphyrin IX in the fi nal step of heme synthesis, is also inhibited. Consequently, lead poisoning causes microcytic anemia .
Four porphobilinogens are condensed in the cytosol to hydroxymethylbilane (a linear tetrapyrrole), which is enzymatically cyclized and isomerized to uroporphyrinogen III , which, in turn, undergoes UROD -catalyzed decarboxylation of all its acetate groups (to methyl) to produce coproporphyrinogen III . This product moves into the mitochondrion and undergoes decarboxylation and oxidation of two propionyl groups (to vinyl) to form protoporphyrinogen IX , which gets oxidized to protoporphyrin IX . Insertion of Fe 2 � yields heme. [Note: Defi ciency of uroporphyrinogen III synthase results in overproduction of the I series porphyrins.]
Porphyrias are rare, inherited (AD, primarily) or acquired (e.g., lead poisoning ) enzymatic defi -ciencies in heme synthesis in which porphyrins (or their precursors) accumulate and are excreted. They are classifi ed as hepatic or erythropoietic. Hepatic forms are further classifi ed as acute or chronic. PCT , a chronic porphyria caused by UROD defi ciency , is the most common. Patients are photosensitive due to the light-induced oxidation of porphyrinogens to porphyrins . Cutaneous symptoms (shown) and urine that turns reddish-brown are seen. [Note: In the hepatic porphyrias ↓ heme synthesis ↑ ALAS1 activity, thereby allowing synthesis of intermediates prior to the defective enzyme. Their accumulation causes the clinical manifestations of the porphyrias.]
N
C C
C CH
H
COO–
CH2
CH2
NH2
COO–
CH2
CH2
Porphobilinogen
Lead
δ-Aminolevulinicacid dehydratase
(cytosolic enzyme)
(Two moleculescondense)
δ-Aminolevulinic acid (ALA)
2 H2O
Ferrier_Unit04.indd 242Ferrier_Unit04.indd 242 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.3 QuestionHeme Degradation
What is the primary source of the heme that is degraded by macrophages of the RES, as shown? What enzyme catalyzes the initial step of degradation?
What is the function of bilirubin UGT ? What is the fate of its product?
What is the difference between Dubin-Johnson and Crigler-Najjar I syndromes ?
M V
NO C
M P
N CH
P M
N CHH
M V
N O
Heme
Fe2+
O2, NADPH + H+
NADP+
NADPH + H+
NADP+
M V
N CH
M P
N CH2
P M
N CH
M
HH
Bilirubin
Biliverdin
CO
Bilirubin–albumin complex
MACROPHAGE
BLOOD
Biliverdinreductase
H H
OO
V
NHH
Ferrier_Unit04.indd 243Ferrier_Unit04.indd 243 5/2/14 7:36 PM5/2/14 7:36 PM
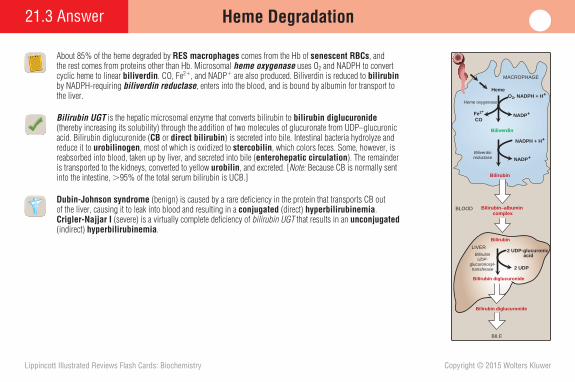
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.3 Answer Heme Degradation
About 85% of the heme degraded by RES macrophages comes from the Hb of senescent RBCs , and the rest comes from proteins other than Hb. Microsomal heme oxygenase uses O 2 and NADPH to convert cyclic heme to linear biliverdin . CO, Fe 2 � , and NADP � are also produced. Biliverdin is reduced to bilirubin by NADPH-requiring biliverdin reductase , enters into the blood, and is bound by albumin for transport to the liver.
Bilirubin UGT is the hepatic microsomal enzyme that converts bilirubin to bilirubin diglucuronide (thereby increasing its solubility) through the addition of two molecules of glucuronate from UDP–glucuronic acid. Bilirubin diglucuronide ( CB or direct bilirubin ) is secreted into bile. Intestinal bacteria hydrolyze and reduce it to urobilinogen , most of which is oxidized to stercobilin , which colors feces. Some, however, is reabsorbed into blood, taken up by liver, and secreted into bile ( enterohepatic circulation ). The remainder is transported to the kidneys, converted to yellow urobilin , and excreted. [ Note: Because CB is normally sent into the intestine, � 95% of the total serum bilirubin is UCB.]
Dubin-Johnson syndrome (benign) is caused by a rare defi ciency in the protein that transports CB out of the liver, causing it to leak into blood and resulting in a conjugated (direct) hyperbilirubinemia . Crigler-Najjar I (severe) is a virtually complete defi ciency of bilirubin UGT that results in an unconjugated (indirect) hyperbilirubinemia .
Heme
Fe2+
O2, NADPH + H+
NADP+
Bilirubin
CO
Bilirubin–albumin complex
Bilirubin
BILE
Bilirubin diglucuronide
2 UDP-glucuronic acid
2 UDP
MACROPHAGE
BLOOD
Bilirubin diglucuronide
LIVER
NADPH + H+
NADP+
Biliverdin
Biliverdinreductase
Heme oxygenase
BilirubinUDP-
glucuronosyl-transferase
Ferrier_Unit04.indd 244Ferrier_Unit04.indd 244 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.4 QuestionJaundice
Deposition of what molecule is responsible for the yellow color of the sclerae shown, a condition known as jaundice ?
What are the three major types of jaundice?
Which type of jaundice is best represented by the fi gure?
Heme
Biliverdin, CO, Fe2+
Hemoglobin,Cytochromes
Amino acids
Erythrocytes, heptocytes
Bilirubin glucuronide
Bilirubin
Urobilinogen
Bilirubin
StercobilinUrobilin
?
Ferrier_Unit04.indd 245Ferrier_Unit04.indd 245 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.4 Answer Jaundice
Jaundice ( icterus ) is caused by deposition of bilirubin secondary to hyperbilirubinemia.
The three major types of jaundice are (1) hemolytic ( prehepatic ) jaundice caused by production of bilirubin in excess of the liver’s capacity to conjugate it, resulting in an unconju-gated hyperbilirubinemia; (2) hepatocellular ( hepatic ) jaundice caused either by bilirubin UGT defi ciency, resulting in an unconjugated hyperbilirubinemia, or by impaired secretion of CB into bile, resulting in a conjugated hyperbilirubinemia; and (3) obstructive ( posthepatic ) jaundice caused by common bile duct blockage, resulting in a conjugated hyperbilirubinemia. [ Note: If less CB enters the intestine, stool is pale in color. The resulting increase in urinary bilirubin darkens the urine. Only CB is found in urine because it is water soluble. UCB is not.]
Hepatocellular jaundice , caused by decreased hepatic production or secretion of CB, is represented. [ Note: Physiologic jaundice of the newborn , a type of hepatocellular jaundice caused by a transient developmental delay in bilirubin UGT expression, is seen in the majority of neonates. If UCB levels exceed the binding capacity of albumin, UCB can cross the BBB and cause a toxic encephalopathy known as kernicterus . Treatment includes phototherapy to convert bilirubin to a more water-soluble isomer.]
Hepatocellar jaundice
Heme
Biliverdin, CO, Fe2+
Hemoglobin,Cytochromes
Amino acids
Erythrocytes, heptocytes
Bilirubin glucuronide
Bilirubin
Urobilinogen
Bilirubin
StercobilinUrobilin
Ferrier_Unit04.indd 246Ferrier_Unit04.indd 246 5/2/14 7:36 PM5/2/14 7:36 PM
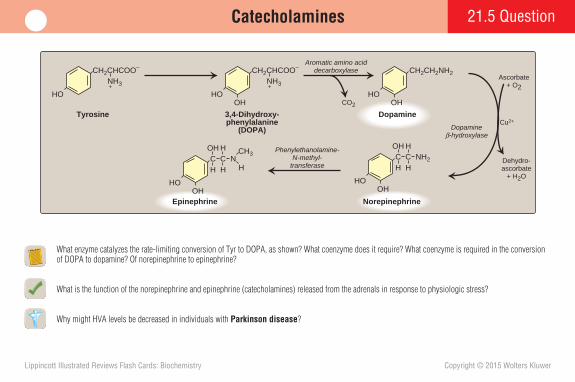
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.5 QuestionCatecholamines
What enzyme catalyzes the rate-limiting conversion of Tyr to DOPA, as shown? What coenzyme does it require? What coenzyme is required in the conversion of DOPA to dopamine? Of norepinephrine to epinephrine?
What is the function of the norepinephrine and epinephrine (catecholamines) released from the adrenals in response to physiologic stress?
Why might HVA levels be decreased in individuals with Parkinson disease ?
HO
CH2CHCOO–
NH3+
Tyrosine
HO
CH2CHCOO–
NH3+
3,4-Dihydroxy-phenylalanine
(DOPA)
OH CO2
Cu2+
Ascorbate+ O2
Dehydro-ascorbate
+ H2O
Dopamineβ-hydroxylase
Phenylethanolamine-N-methyl-
transferase
Epinephrine
HO
C N
OH
CH H
OH H
H
CH3
Norepinephrine
HO
C NH2
OH
CH H
OH H
Aromatic amino aciddecarboxylase
HO
CH2CH2NH2
OH
Dopamine
Ferrier_Unit04.indd 247Ferrier_Unit04.indd 247 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.5 Answer Catecholamines
Tyrosine hydroxylase converts Tyr to DOPA . As an aromatic amino acid hydroxylase , it requires THB as a coenzyme. The conversion of DOPA to dopamine is catalyzed by aromatic amino acid decarboxylase , which requires PLP . The methyltransferase that converts norepinephrine to epinephrine requires SAM . [ Note: Only the methylation of Hcy to Met uses THF.]
Catecholamines mediate the retrieval of energy-producing molecules from tissue stores in times of physiologic stress.
In Parkinson disease , the loss of dopamine-producing cells in the brain results in dopamine defi ciency. Dopamine is degraded to HVA by COMT and MAO , so a defi ciency results in decreased HVA generation. [ Note: COMT and MAO degrade epinephrine and norepinephrine to VMA.]
HO
CH2CHCOO–
NH3+
Tyrosine 3,4-Dihydroxy-phenylalanine
(DOPA)
Tyrosinehydroxylase
HO
CH2CHCOO–
NH3+
OH CO2
PLP
Cu2+Dopamine
β-hydroxylase
Phenylethanolamine-N-methyl-
transferase
Epinephrine
HO
C N
OH
CH H
OH H
H
CH3
Norepinephrine
HO
C NH2
OH
CH H
OH H
S-Adenosyl-methionine
S-Adenosyl-homocysteine
Tetrahydro-biopterin
+ O2
Dihydro-biopterin+ H2O
Dehydro-ascorbate
+ H2O
Ascorbate+ O2
Aromatic amino aciddecarboxylase
HO
CH2CH2NH2
OH
Dopamine
Homovanillic acid (HVA)
3-MethoxytyramineDihydroxyphenyl-acetic acid
Dopamine
MAO COMT
COMT MAO
Ferrier_Unit04.indd 248Ferrier_Unit04.indd 248 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.6 QuestionOther Nitrogen-Containing Compounds
What is the function of creatine phosphate, the synthesis of which from the amino acids Arg, Gly, and Met (as SAM) is shown?
Why are SSRIs used to treat depression and anxiety disorders?
Why do the antihistamines used to treat allergies have no effect on histamine-mediated gastric acid secretion?
Arginine
H20
Glycine
Amidino-transferaseOrnithine
Guanidinoacetate
Methyltransferase
S-Adenosylmethionine
S-Adenosylhomocysteine
Creatine
ATP
ADP + H+
ATP
ADP
Creatine phosphate
Creatinine
Creatinekinase
Pi
Ferrier_Unit04.indd 249Ferrier_Unit04.indd 249 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
21.6 Answer Other Nitrogen-Containing Compounds
Creatine phosphate provides a small, rapidly mobilized muscle reserve of high-energy phosphate groups that can be transferred to ADP to maintain ATP levels early in intense contraction. It sponta-neously cyclizes to creatinine , which is fi ltered by the kidney with little reabsorption. Elevated creatinine levels in the blood with low levels in the urine indicates impaired renal function.
Serotonin ( 5-HT ), made from Trp in presynaptic vesicles and then released into the synapse, causes a feeling of well-being. Its actions are terminated by reuptake. SSRIs target the 5-HT transporter and inhibit reuptake, thereby allowing a return of positive feelings.
Histamine , made from the PLP-requiring decarboxylation of His, binds to four GPCRs, H1–H4 . Allergy drugs block H1 receptors but have no effect on H2 receptors on acid-secreting parietal cells of the stomach. Specifi c H2 blockers are required to reduce acid secretion.
Arginine
H20
Glycine
Amidino-transferaseOrnithine
Guanidinoacetate
Methyltransferase
S-Adenosylmethionine
S-Adenosylhomocysteine
Creatine
ATP
ADP + H+
ATP
ADP
Creatine phosphate
Creatinine
Creatinekinase
Pi
NH
CH2CHCOO–
NH3+
Tryptophan
NH
CH2CHCOO–
NH3+
Aromatic amino acid decarboxylase
5-Hydroxy-tryptophan
CO2
HO
NH
CH2CH2NH2
Serotonin (5-HT)
HO
O2
Hydroxylase
Tetrahydro-biopterin
PLP
Dihydro-biopterin+ H2O
Ferrier_Unit04.indd 250Ferrier_Unit04.indd 250 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.1 QuestionNucleotide Structure and Function
Which nitrogenous base shown is used (as a component of a nucleotide) in DNA but not RNA synthesis? In addition to a purine or pyrimidine base, what are the other two components of a nucleotide?
Why are nucleotides and nucleosides referred to as N-glycosides?
What is the role of nucleotide sugars in the body? What group of disorders results from defects in nucleotide sugar-dependent protein N-glycosylation ?
NH2
Adenine (A)
O
Guanine (G)
H2N
Thymine (T)
OCH3
O
Cytosine (C)
NH2
O
Uracil (U)
O
O
N
N
NH
N
N
HN
NH
N
NH
HN
NH
N
NH
HN
Ferrier_Unit04.indd 251Ferrier_Unit04.indd 251 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.1 Answer Nucleotide Structure and Function
T (as dTTP ) is used in DNA synthesis, whereas U (as UTP ) is used in RNA synthesis. Structurally, T is methylated U. In addition to a purine or pyrimidine nitrogenous base, a nucleotide contains a pentose monosaccharide (ribose in RNA and 2-deoxyribose in DNA) plus one to three phosphate groups. [ Note: Compared to a nucleotide, a nucleoside lacks phosphate groups. The terms “nucleoside phosphate” and “nucleotide” are used interchangeably.]
Nucleotides and nucleosides are referred to as N-glycosides because a N in the base is linked to C-1' of the sugar. [ Note: The number of a C atom in the sugar includes a prime sign (') to distinguish it from the atoms in the base.]
Nucleotide sugars are activated monosaccharide donors in the synthesis of polysaccharides, glycoproteins, proteoglycans, and glycolipids. For example, UDP-glucose is used in glycogen synthesis, GDP-mannose in glycoprotein synthesis, and CMP-NANA in ganglioside (glycolipid) synthesis. Congenital disorders of glycosylation (CDG) result from defective production, transport, and processing of nucleotide sugars required for protein N-glycosylation.
NH2
Adenine (A)
O
Guanine (G)
H2N
Thymine (T)
OCH3
O
Cytosine (C)
NH2
O
Uracil (U)
O
O
DNA and RNA Purines
DNA Pyrimidines
N
N
NH
N
N
HN
NH
N
NH
HN
NH
N
NH
HN
RNA PyrimidinesO
Cytidine Deoxyadenosine
NH2
N
N
O
HO
123
4
65
1'4'
5'
NH2
N
N
321
6
45
N
N
9
78
3' 2 '
H
O
OH
1'4'
5'HO
3' 2 '
OH OH
Ferrier_Unit04.indd 252Ferrier_Unit04.indd 252 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.2 QuestionPurine Nucleotide De Novo Synthesis
The origins of the atoms in a purine base during nucleotide de novo synthesis are shown. What is the order of addition of these atoms?
What enzyme catalyzes the committed step of purine nucleotide de novo synthesis. How is it regulated? What is the fate of IMP, the fi rst purine nucleotide made?
Why does methotrexate cause a decrease in DNA synthesis? Why do sulfonamides decrease DNA synthesis in bacterial but not human cells?
N
N
NC
C
C
C
Glutamine
NC
CO2
Aspartate
N10-Formyl-tetrahydrofolate
Glycine
Ferrier_Unit04.indd 253Ferrier_Unit04.indd 253 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.2 Answer Purine Nucleotide De Novo Synthesis
The order of the addition of atoms in purine base synthesis is (1) the amide N from Gln, (2) the N � C atoms from Gly, (3) a C from N 10 -formyl-THF, (4) the amide N from another Gln, (5) the C from CO 2 , (6) the N of Asp, and (7) a C from another N 10 -formyl-THF.
The committed step of purine nucleotide de novo synthesis is catalyzed by glutamine:PRPP amidotransferase (shown). The enzyme is activated by PRPP and inhibited by AMP and GMP. IMP , the fi rst purine nucleotide made, is converted to AMP and GMP in separate two-step, energy-requiring processes.
Methotrexate inhibits DHFR , which catalyzes the reduction of DHF to the THF required (as N 10 -formyl-THF ) for purine synthesis. Sulfonamides inhibit folate (and consequently THF) synthesis in bacteria. With each drug, ↓ purines cause ↓ DNA synthesis. Humans, however, cannot synthesize folate and are unaffected by sulfonamides.
N
N
NC
C
C
C
Glutamine
NC
CO2
Aspartate
N10-Formyl-tetrahydrofolate
Glycine
1
23
4
56
7
2-O3POH2C O
OH
5-Phosphoribosylamine
OH
NH2Glutamine
+ H2O
Glutamine:phosphoribosyl-pyrophosphate amidotransferase
Glutamate+ PPi
2-O3POH2C O
OH
5-Phosphoribosyl-1-pyrophosphate
AMP, GMP
PRPP
OH
O PP O O-O O
O- O-
+
Ferrier_Unit04.indd 254Ferrier_Unit04.indd 254 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.3 QuestionPurine Nucleotide Degradation
What highly oxidized purine (indicated by a red question mark) is the end product of purine nucleotide degrada-tion? How is it excreted from the body? What enzyme catalyzes its production from xanthine? Where is this enzyme found primarily?
AMP can be deaminated to IMP by AMP deaminase and then converted to inosine by a 5 ' - nucleotidase . By what other path is AMP converted to inosine? What pathology results from an enzymatic defi ciency in this conversion?
Why might administration of recombinant uricase be a rational approach to gout treatment?
Nucleotide
Nucleoside
Free purine base
Xanthine
?
Ferrier_Unit04.indd 255Ferrier_Unit04.indd 255 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.3 Answer Purine Nucleotide Degradation
UA , a highly oxidized purine, is the end product of purine nucleotide degradation and is excreted (as urate ) primarily in urine and also in feces. XO catalyzes the oxidation of xanthine to UA. The enzyme is found in the intestine (for degradation of dietary purines) and the liver (for degradation of endogenously synthesized purines).
AMP can be converted by a 5'-nucleotidase to adenosine, which is deaminated to inosine by ADA . ADA defi ciency results in a type of SCIDS . [ Note: Less than 15% of SCIDS is caused by ADA defi ciency with the majority caused by an X-linked defi ciency in the common � chain of several cytokine receptors.] SCIDS results in a decrease in the number and/or function of T , B , and NK cells . A less severe immunodefi ciency that affects only T cells is caused by PNP defi ciency .
Humans do not express uricase , the enzyme that degrades UA (low solubility in aqueous solutions) to allantoin (high solubility). Because gout is initiated by hyperuricemia , conversion of urate to allantoin by administration of recombinant uricase reduces blood urate levels and, therefore, the risk for gout.
Inosine
H2O
Pi
5’ Nucleotidase
H2O
NH3
ADA
Adenosine
AMP
XO
Nucleotide
Nucleoside
Free purine base
Xanthine
Uric acid
Ferrier_Unit04.indd 256Ferrier_Unit04.indd 256 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.4 QuestionPurine Salvage and Hyperuricemia
Why do mutations that increase the activity of PRPP synthetase (shown) result in hyperuricemia ?
What is “purine salvage”? Why is it important? Why do defects in purine base salvage result in hyperuricemia ?
What disorder is caused by a nearly complete HGPRT defi ciency?
OH2CO
OH
Ribose 5-phosphate
OH
OH
O
OH
5-Phosphoribosyl-1-pyrophosphate (PRPP)
OATP AMP
Mg2+
PRPP synthetase
P
P
P
OH2CP
OH
ACTIVATOR INHIBITORSPurine
ribonucleotidesPi +Ferrier_Unit04.indd 257Ferrier_Unit04.indd 257 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.4 Answer Purine Salvage and Hyperuricemia
Increased PRPP synthetase activity increases production of PRPP , an activator of the regulated enzyme of purine nucleotide de novo synthesis glutamine:PRPP amidotransferase . Excess purine nucleotides are degraded to UA, resulting in hyperuricemia .
Purine salvage primarily refers to the HGPRT -catalyzed conversion of hypoxanthine and guanine (purine bases) to IMP and GMP (purine nucleotides) by the addition of ribose 5-P from PRPP, shown. Salvage allows recycling of the bases, the synthesis of which requires ATP. [ Note: Some salvage of adenine and adenosine to AMP does occur.] Salvage defects increase PRPP availability as a consequence of decreased use and increased production, the latter because there are fewer purine nucleotides from salvage to inhibit PRPP synthetase . ↑ PRPP results in ↑ UA.
Nearly complete defi ciency of X-linked HGPRT causes Lesch-Nyhan syndrome with accompanying hyperuricemia. [ Note: The most characteristic fi nding is behavioral disturbances that include self-mutilation. Motor dysfunction and cognitive defects also are seen. Less severe defi ciencies with less severe presenta-tions are known.]
OH2CO
OHRibose 5-phosphate
OH
OH
O
OH5-Phosphoribosyl-1-pyrophosphate (PRPP)
OATP AMP
Mg2+
PRPP synthetase
P
P
P
OH2CP
OH
ACTIVATOR INHIBITORSPurine
ribonucleotidesPi +
IMP
PRPP PPi
Hypoxanthine-guaninephosphoribosyltransferase
(HGPRT)
Hypoxanthine
GMP
PRPP PPi
Guanine
Hypoxanthine-guaninephosphoribosyltransferase
(HGPRT)
Ferrier_Unit04.indd 258Ferrier_Unit04.indd 258 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.5 QuestionPyrimidine Nucleotide Metabolism
What are the sources (A, B, and C shown) of the atoms in a pyrimidine base?
What is the regulated step in de novo pyrimidine synthesis? What is the fi rst pyrimidine base formed, and how is it converted to the fi rst pyrimidine nucleotide?
What is the cause of hereditary orotic aciduria ?
How is dTMP synthesis inhibited pharmacologically?
NC
C
C
CN
B
A
C
Ferrier_Unit04.indd 259Ferrier_Unit04.indd 259 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.5 Answer Pyrimidine Nucleotide Metabolism
The sources of the atoms in a pyrimidine base are the C of CO 2 , the amide N of Gln, and the N � 3C atoms of Asp. [ Note: Gln and Asp each provides a N in purine synthesis.]
The regulated step of pyrimidine synthesis is formation of CP from 2 ATP, CO 2 , and Gln by cytosolic CPS II , which is activated by PRPP and inhibited by UTP. Orotate is the fi rst pyrimidine base formed. [ Note: Defi ciency of OTC of the UC upregulates orotate synthesis by increasing CP availability.] A transferase uses PRPP to add ribose 5-P generating OMP , the fi rst nucleotide. A decarboxylase converts OMP to UMP, which is phosphorylated to UTP then aminated to CTP . [ Note: PRPP is used in purine and pyrimidine synthesis and salvage.]
Hereditary orotic aciduria is caused by a defect in bifunctional UMP synthase , which catalyzes the transferase and decarboxylase reactions of UMP synthesis. The treatment is administration of uridine, which gets salvaged to UMP.
dUMP is methylated to dTMP as shown . In this thymidylate synthase –catalyzed reaction, the methyl group is supplied by N 5 ,N 10 -methylene-THF (not SAM) as THF is oxidized to DHF. 5-FU (as 5-FdUMP) inhibits thymidylate synthase . Inhibition of DHFR by methotrexate inhibits the reduction of DHF to THF, thereby decreasing the availability of THF for purine and dTMP synthesis.
dTMP
Dihydrofolatereductase
NADPH + H+
NADP+
Tetrahydrofolate
Dihydrofolate
Metho-trexate
5-FdUMP
N5,N10-Methylene-tetrahydrofolate
5-Fluorouracil
Thymidylate synthase
dCMP
dCDP
Pi
dUMP
dUDP
Pi
NH4 +
NC
C
C
CN
Amide nitrogen(R-group) ofglutamine
CO2
Aspartate
Ferrier_Unit04.indd 260Ferrier_Unit04.indd 260 5/2/14 7:36 PM5/2/14 7:36 PM
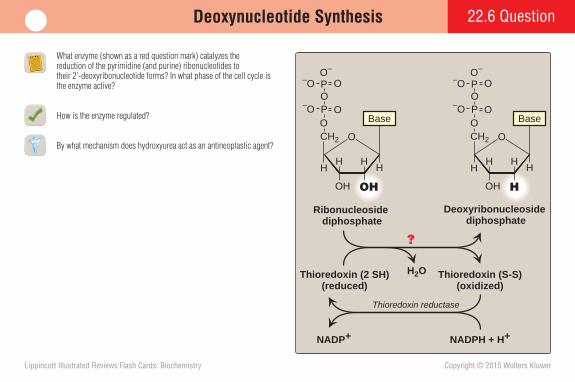
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.6 QuestionDeoxynucleotide Synthesis
What enzyme (shown as a red question mark) catalyzes the reduction of the pyrimidine (and purine) ribonucleotides to their 2'-deoxyribonucleotide forms? In what phase of the cell cycle is the enzyme active?
How is the enzyme regulated?
By what mechanism does hydroxyurea act as an antineoplastic agent? CH2
H
OH
H HH
Ribonucleoside diphosphate
Base
OH
CH2
O
H
H
H HH
Deoxyribonucleoside diphosphate
Base
OH
Thioredoxin (2 SH)(reduced)
Thioredoxin (S-S)(oxidized)
NADP+ NADPH + H+
Thioredoxin reductase
H2O
O O
PO
–O
–O
O–
O
O
P
OPO
–O
–O
O–
O
O
P
?
Ferrier_Unit04.indd 261Ferrier_Unit04.indd 261 5/2/14 7:36 PM5/2/14 7:36 PM
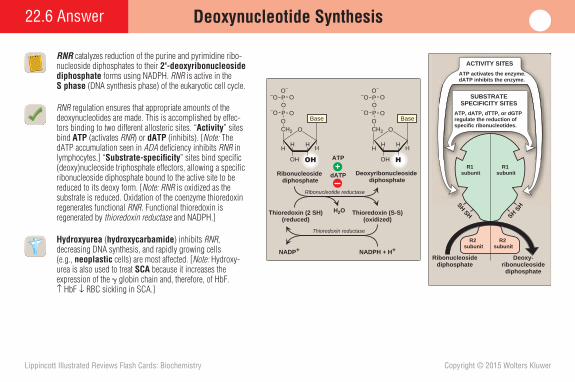
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22.6 Answer Deoxynucleotide Synthesis
RNR catalyzes reduction of the purine and pyrimidine ribo-nucleoside diphosphates to their 2'-deoxyribonucleoside diphosphate forms using NADPH. RNR is active in the S phase (DNA synthesis phase) of the eukaryotic cell cycle.
RNR regulation ensures that appropriate amounts of the deoxynucleotides are made. This is accomplished by effec-tors binding to two different allosteric sites. “ Activity ” sites bind ATP (activates RNR ) or dATP (inhibits). [ Note: The dATP accumulation seen in ADA defi ciency inhibits RNR in lymphocytes.] “ Substrate-specifi city ” sites bind specifi c (deoxy)nucleoside triphosphate effectors, allowing a specifi c ribonucleoside diphosphate bound to the active site to be reduced to its deoxy form. [ Note: RNR is oxidized as the substrate is reduced. Oxidation of the coenzyme thioredoxin regenerates functional RNR . Functional thioredoxin is regenerated by thioredoxin reductase and NADPH.]
Hydroxyurea ( hydroxycarbamide ) inhibits RNR , decreasing DNA synthesis, and rapidly growing cells (e.g., neoplastic cells) are most affected. [ Note: Hydroxy-urea is also used to treat SCA because it increases the expression of the � globin chain and, therefore, of HbF. ↑ HbF ↓ RBC sickling in SCA.]
CH2
H
OH
H HH
Ribonucleoside diphosphate
Base
OH
CH2
O
H
H
H HH
Deoxyribonucleoside diphosphate
Base
OH
Thioredoxin (2 SH)(reduced)
Thioredoxin (S-S)(oxidized)
NADP+ NADPH + H+
Ribonucleotide reductase
Thioredoxin reductase
H2O
O O
dATP
PO
–O
–O
O–
O
O
P
OPO
–O
–O
O–
O
O
P
ATP
+
Ribonucleosidediphosphate
Deoxy-ribonucleoside
diphosphate
SH
SH
SH
SH
ATP activates the enzyme.dATP inhibits the enzyme.
SUBSTRATESPECIFICITY SITES
ATP, dATP, dTTP, or dGTP regulate the reduction of specific ribonucleotides.
ACTIVITY SITES
R1 subunit
R1 subunit
R2 subunit
R2 subunit
Ferrier_Unit04.indd 262Ferrier_Unit04.indd 262 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Case Card 22
A 63-year-old woman was brought to the emergency department because of severe pain in her right big toe. The patient denied any trauma to the area. Gross examination revealed an overweight woman in distress. Examination of the toe revealed that it was swollen , red , and warm and tender to the touch. No other joints appeared to be affected. However, tophi were seen on the external part of her left ear. History revealed that this was the fi rst episode of joint pain. It also revealed that the patient had begun taking “water pills” for hypertension about 4 months ago. (Her daughter later identifi ed the medication as hydrochlorothia-zide.) The patient is a nondrinker. Fluid aspirated from the affected joint was negative for organisms but positive for needle-shaped crystals (shown). The patient was started on ibuprofen (an NSAID ) to reduce the infl ammation and associated pain and was given a prescription for allopurinol .
Why might individuals with certain disorders of carbohydrate metabolism develop tophi?
Ferrier_Unit04.indd 263Ferrier_Unit04.indd 263 5/2/14 7:36 PM5/2/14 7:36 PM

Case Card
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
22
The presence of needle-shaped MSU crystals is diagnostic for gout , an arthritic condition initiated by hyperuricemia caused either by decreased excretion of UA with impaired renal function or, more rarely, by increased production of UA (e.g., with ↑ PRPP synthetase and ↓ HGPRT activity). [ Note: Hyperuricemia is typically asymptomatic but may indicate comorbid conditions such as hypertension.] Treatment of acute gouty attacks includes anti-infl ammatory agents (e.g., NSAIDs , steroids , and colchicine ). However, they do not lower UA levels. Chronic therapies to lower UA levels include uricosuric agents (e.g., probenecid ) that increase renal excretion and XO inhibitors (e.g., allopurinol and febuxostat ) that decrease production. Patients are advised to lose weight; to decrease their consumption of ethanol, red meat, and shellfi sh; and to increase consumption of low-fat dairy products and vitamin C that increase UA excretion. Recent use of thiazide diuretics by the patient decreased her renal clearance of UA. She also had nodular masses of MSU crystals ( tophi ) in the soft tissue of the ear, an indication of long-standing hyperuricemia. Crystal deposition led to the observed infl ammatory response.
Disorders of carbohydrate metabolism that result in the “trapping” of P i (e.g., GSD Ia and HFI ) result in a decrease in the ATP/AMP ratio because of a decreased ability to phosphorylate ADP. Two ADP are converted to ATP � AMP by adenylate kinase . The AMP, a purine nucleotide, is degraded, a process that generates UA and can lead to the development of hyperuricemia and tophi.
Xanthine oxidase
O2 + H2O H2O2O
HN
NH
N
NH
O
Xanthine
O
HN
NH
NH
OO
Uric acid
HN
allopurinol−
A
Ferrier_Unit04.indd 264Ferrier_Unit04.indd 264 5/2/14 7:36 PM5/2/14 7:36 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
23.1 QuestionInsulin
How is the inactive precursor of insulin processed to produce the functional, mature product shown?
How does a rise in blood glucose lead to insulin secretion from pancreatic � cells?
Why does the same amount of glucose given orally induce a greater insulin response than if given IV?
Phe Val Asn Gln His Leu Cys Gly Ser His Leu Val Glu Ala Leu Tyr Leu Val Cys Gly Glu Arg Gly Phe Phe Tyr Thr Pro Lys Thr
Gly Ile Val Glu Gln Cys Cys Thr Ser Ile Cys Ser Leu Tyr Gln Leu Glu Asn Tyr Cys Asn
S
S S
S
S
S
A chain
B chain
Ferrier_Unit05.indd 265Ferrier_Unit05.indd 265 5/2/14 7:43 PM5/2/14 7:43 PM
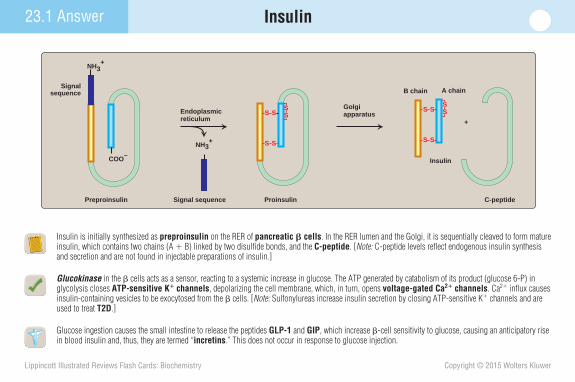
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
23.1 Answer Insulin
Insulin is initially synthesized as preproinsulin on the RER of pancreatic � cells . In the RER lumen and the Golgi, it is sequentially cleaved to form mature insulin, which contains two chains (A � B) linked by two disulfi de bonds, and the C-peptide . [ Note: C-peptide levels refl ect endogenous insulin synthesis and secretion and are not found in injectable preparations of insulin.]
Glucokinase in the � cells acts as a sensor, reacting to a systemic increase in glucose. The ATP generated by catabolism of its product (glucose 6-P) in glycolysis closes ATP-sensitive K � channels , depolarizing the cell membrane, which, in turn, opens voltage-gated Ca 2 � channels . Ca 2 � infl ux causes insulin-containing vesicles to be exocytosed from the � cells. [ Note: Sulfonylureas increase insulin secretion by closing ATP-sensitive K � channels and are used to treat T2D .]
Glucose ingestion causes the small intestine to release the peptides GLP-1 and GIP , which increase � -cell sensitivity to glucose, causing an anticipatory rise in blood insulin and, thus, they are termed “ incretins .” This does not occur in response to glucose injection.
Signalsequence
Endoplasmicreticulum
Golgiapparatus
ProinsulinPreproinsulin C-peptide
Insulin
NH3+
COO–
S S
S S
SS
B chain A chain
S S
S S
SS
Signal sequence
NH3+
+
Ferrier_Unit05.indd 266Ferrier_Unit05.indd 266 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
23.2 QuestionMetabolic Effects of Insulin
In which tissues are the effects of insulin denoted by arrows in the green boxes most prominent? What is the major stimulator of insulin secretion?
Contrast the effects of insulin on HSL and LPL .
Insulin promotes endergonic pathways of nutrient storage. How does the body mobilize these stores in the event of sudden physiologic stress ?
Glucose uptake
Glycogen synthesisProtein synthesis
Fat synthesis
Gluconeogenesis
Glycogenolysis
Lipolysis
Altered gene expression
Biologic effectsof insulin:
Ferrier_Unit05.indd 267Ferrier_Unit05.indd 267 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
23.2 Answer Metabolic Effects of Insulin
Insulin increases (1) glucose uptake in muscle and adipose via recruitment of GLUT-4 to the cell membrane; (2) glycogenesis in liver and muscle via activation of GS ; (3) amino acid uptake and protein synthesis in most tissues; and (4) fat synthesis in liver, lactating mammary glands and, to a lesser extent, adipose tissue via activation of ACC . [ Note: Insulin affects enzymatic activity by covalent (phosphorylation/dephosphorylation) and transcriptional regulation.] A rise in blood glucose is the major stimulator of insulin secretion as shown.
Insulin decreases the activity of intracellular HSL and increases the activity of membrane-associated extracellular LPL , enzymes that degrade TAGs stored in adipocytes and carried in circulating LP particles (CMs and VLDLs), respectively. Insulin activates a phosphatase that dephosphorylates (inactivates) HSL . In contrast, insulin increases expression of the gene for LPL in adipocytes. [ Note: Insulin decreases LPL expression in muscle.]
Physiologic stress (e.g., infection, hypoxia, and strenuous exercise) results in secretion of the catecholamines epinephrine and norepinephrine, which cause rapid mobilization of energy-yielding fuels (e.g., glucose from glycogenolysis and FAs from lipolysis). They also inhibit insulin secretion.
Glucose
Amino acidsFatty acids
Insulin
Prepro-insulin
Insulin
Insulin
BLOOD
β CELL
+Glucose uptake
Glycogen synthesisProtein synthesis
Fat synthesis
Gluconeogenesis
Glycogenolysis
Lipolysis
Altered gene expression
Biologic effectsof insulin:
Epinephrine toliver
Ferrier_Unit05.indd 268Ferrier_Unit05.indd 268 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
23.3 QuestionMechanism of Insulin Action
What happens to the inactive insulin receptor (shown) upon insulin binding? How are the receptors regulated?
What effect does insulin have on muscle and adipocyte cell membranes? Is the same effect seen on hepatocyte membranes?
What effect does blunting receptor responsiveness to insulin have on blood glucose levels in affected individuals?
S
SS
S
SSα α
β β
Tyrosine
Tyrosine
Insulin receptor(inactive)
Ferrier_Unit05.indd 269Ferrier_Unit05.indd 269 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
S
SS
IRS-Tyr—
Insulinreceptor (active)
IRS-Tyr
S
SS
S
SS
S
SS
Insulinα α
β
α α
β ββ
Tyrosine
Tyrosine —Tyrosine
—TyrosinePP
P
Insulin receptor(inactive)
SSS
TPPPP
Insulin binding activatesreceptor tyrosine kinaseactivity in the intracellular domain of the � subunit of the insulin receptor.
1
Tyrosine residues of the � subunit are auto-phosphorylated.
2
IRS-Tyr—
IRS-Tyry
— P
Receptor tyrosine kinase phosphorylates tyrosines in other proteins (for example, insulin receptor substrates [IRS]).
3
Activation of multiple signaling pathways
23.3 Answer Mechanism of Insulin Action
When insulin binds to its membrane receptor, the series of events shown occur. The process is regulated through internalization of the insulin–receptor complex, after which the insulin is degraded in the lysosomes, and the receptor is either recycled or degraded. Elevated insulin levels promote receptor degradation.
Insulin receptor binding initiates a signaling cascade that includes PKB ( Akt ) axactivation, which causes GLUT-4 recruitment from the intracellular vesicular pool to muscle and adipocyte cell membranes, thereby enabling facilitated uptake of glucose. In contrast, hepatocytes contain the insulin-insensitive GLUT-2 .
Blood glucose levels rise with decreased responsiveness of the insulin receptor as a result of decreased uptake by adipocytes and muscle cells because of a decrease in GLUT-4 on their surface.
Ferrier_Unit05.indd 270Ferrier_Unit05.indd 270 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
23.4 QuestionGlucagon
What are the major stimulators of glucagon secretion? What inhibits its secretion?
What is the major difference between preproglucagon and preproinsulin processing?
A popular approach for losing weight is a high-protein, low-carbohydrate diet. Why might such a diet be effective?
Glucagon
Precursors
Glucagon
Glucagon?
??
???
α CELLS
toliver
BLOOD
+
Ferrier_Unit05.indd 271Ferrier_Unit05.indd 271 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
23.4 Answer Glucagon
Epinephrine and norepinephrine, produced from Tyr in the adrenal medulla and sympathetic nervous system, stimulate glucagon secretion from pancreatic � cells . Amino acids (e.g., Arg) derived from a protein-containing meal also will induce glucagon release. [Note: Glucagon prevents the hypoglycemia that would otherwise result from postprandial insulin secretion.] Insulin and glucose are nega-tive regulators of the secretory pathway for glucagon.
Preproinsulin is made and processed (cleaved) to insulin only in pancreatic � cells. In contrast, preproglucagon is made in pancreatic � cells and in cells of the intestine and the brain. It undergoes tissue-specifi c processing that generates glucagon only in pancreatic � cells and GLP-1 in intestinal L cells and brain cells.
With a high-protein, low-carbohydrate diet, the free amino acids released from the protein component stimulate pancreatic glucagon secretion. The low level of carbohydrate minimizes the insulin response and reduces the rate of anabolic pathways. If sustained, these conditions lead to increased lipolysis, FA � -oxidation, and ketogenesis. The increased rate of TAG degradation results in weight loss.
EpinephrineAmino acids
Glucagon
Precursors
Glucagon
Glucagon
α CELLS
GlucoseInsulin to
liver
BLOOD
+
Ferrier_Unit05.indd 272Ferrier_Unit05.indd 272 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
23.5 QuestionMetabolic Effects of Glucagon
In which tissue are the effects of glucagon denoted by arrows in the green boxes most prominent?
How do glucagon and epinephrine work together to ensure short-term glucose homeostasis? Why are they termed “counterregulatory” hormones?
Why might inactivating mutations to the glucagon receptor (e.g., as seen in Mahvash disease ) cause hypoglycemia?
Biologic effects:Glycogenolysis
Gluconeogenesis
Ketogenesis
Uptake of aminoacids
Glycogenesis
Fatty acid oxidation
Ferrier_Unit05.indd 273Ferrier_Unit05.indd 273 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
23.5 Answer Metabolic Effects of Glucagon
Glucagon’s primary target is the liver, where it acts to maintain blood glucose levels. Like insulin, glucagon has covalent and transcriptional effects. [ Note: Skeletal muscles do not express the glucagon receptor.]
Glucagon bound to its membrane GPCR on hepatocytes promotes FA � -oxidation, ketogenesis, glycogenolysis, and gluconeogenesis, effects mediated through protein phosphorylation by PKA. [ Note: Hepatic FA oxidation supplies ATP and NADH for gluconeogenesis and acetyl CoA for keto-genesis.] Epinephrine inhibits insulin secretion and, when bound to its GPCR, is the primary signal in adipocytes for the PKA- mediated activation of HSL and subsequent lipolysis that provides FAs to the liver. It also promotes glycogenolysis. Glucagon and epinephrine (and norepinephrine, cortisol, and growth hormone) are termed “ counterregulatory ” hormones because they oppose the actions of insulin.
Impaired signaling by the glucagon GPCR, as in Mahvash disease , will decrease the body’s ability to maintain appropriate blood glucose levels through glycogenolysis and gluconeogenesis, thereby resulting in hypoglycemia. [ Note: In Mahvash disease, mutations in the receptor prevent its traffi cking to the plasma membrane thereby trapping it in the RER.]
ATP
Phospho-diesterase
cAMP-dependent protein kinase(inactive)
cAMP-dependent protein kinase
(active)
Enzyme(dephosphorylated)
Enzyme(phosphorylated)
ADP
H2O
5'-AMP
+
Activeadenylylcyclase
ATP
Glucagon receptor
cAMP ( )
CC
CC
R
R
CC
Glucagon
RR
Protein phosphatase
P
Pi
Ferrier_Unit05.indd 274Ferrier_Unit05.indd 274 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
23.6 QuestionHypoglycemia
Complete the chart to show the actions of cortisol, epinephrine, and glucagon in hypoglycemia.
What two categories of symptoms are seen with hypoglycemia?
What is the basis of ethanol-related hypoglycemia ?
Hypothalamic regulatorycenter
ACTH Autonomic nervous system
LOW BLOOD GLUCOSE(Blood glucose less than 40 mg/dl)
Cortisol EpinephrineNorepinephrine
Glucagon
Insulin
Glyco-genolysis
Gluconeo-genesis
Pituitary
PancreasAdrenal
Ferrier_Unit05.indd 275Ferrier_Unit05.indd 275 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
23.6 Answer Hypoglycemia
In hypoglycemia (a blood glucose level suffi ciently low to cause symptoms) cortisol activates gluconeogenesis, epinephrine activates glycogenolysis, and glucagon activates both. Glucagon and epinephrine work through cell membrane GPCRs , whereas cortisol (a steroid hormone) works through a nuclear receptor .
Adrenergic (neurogenic) and neuroglycopenic symptoms are seen in hypoglycemia. Adrenergic symptoms (e.g., palpitations, sweating, tremors, and anxiety) result when blood glucose falls abruptly and are mediated by epinephrine release. Neuroglycopenic symptoms result from glucose deprivation in the brain and begin with headache, slurred speech, and confusion but can lead to coma or death.
The basis of ethanol-related hypoglycemia is the rise in the NADH/NAD � ratio as a result of ethanol metabolism by ADH and ALDH , enzymes that oxidize ethanol and acetaldehyde, respectively, as their coenzyme NAD � is reduced. The NADH formed favors the reduction of pyruvate to lactate and OAA to malate, diverting these intermediates of gluconeogenesis into alternate pathways and decreasing glucose synthesis as shown.
Hypothalamic regulatorycenter
ACTH Autonomic nervous system
LOW BLOOD GLUCOSE(Blood glucose less than 40 mg/dl)
Cortisol EpinephrineNorepinephrine
Glucagon
Insulin
0 +++ ++
++ 0 ++
Glyco-genolysis
Gluconeo-genesis
Pituitary
PancreasAdrenal
Oxaloacetate
Phosphoenolpyruvate
Pyruvate Lactate
NADH NAD+
Malate
NADH
NAD+
NAD+
Acetaldehyde
Acetate
Alcoholdehydrogenase
Aldehydedehydrogenase
NADH
NAD+
NADH
Glucose 6-phosphate Glucose
NADH
EthanolEthanol consumed
Ferrier_Unit05.indd 276Ferrier_Unit05.indd 276 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
24.1 QuestionAbsorptive State
In the absorptive state, release of which pancreatic hormone is increased? Decreased?
Changes in enzymatic activity in the absorptive state primarily involve what three mechanisms? Which enzymes of intermediary metabolism are dephosphorylated and inactive in the absorptive state?
Why does short-bowel syndrome (seen when a large part of the small intestine has been removed) result in malabsorption? What are the expected symptoms? What would likely be included in the treatment?
leads to
Absorptive state Tissues involved
Glucose, amino acids in portal vein
leads to
leads to
Glucose, amino acids, and fatty acids in the intestine
Release of ? by α cells of pancreas
Pancreas
Intestine andportal vein
Release of ? by β cells of pancreas
Ferrier_Unit05.indd 277Ferrier_Unit05.indd 277 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
24.1 Answer
In the absorptive state (the 2- to 4-hour period after eating), insulin release from the pancreas is increased in response to the presence of digestive products in the portal vein. Glucagon release is decreased. [ Note: Insulin sup-presses glucagon release.]
Changes in enzymatic activity primarily involve (1) allosteric regulation; (2) covalent modifi cation; and (3) alterations in enzyme amount, primarily through transcriptional regula-tion but also through changes in degradation. Glycogen phosphorylase , phosphorylase kinase , and HSL are dephosphorylated and inactivated in the absorptive state.
Absorption of digestive products occurs in the small intestine: ↓intestine ↓absorption. Decreased absorption will cause weight loss, fatigue, diarrhea (from the increased osmotic load ), steatorrhea (from fat malabsorption), and fl atulence and abdominal distension (from gas production by microbial metabolism of unabsorbed digestive products). Anemia ( macrocytic with B 12 and folate defi ciency and microcytic with Fe defi ciency) and bleeding (with vitamin K defi ciency) may be seen. Treatment would include nutritional support ( including parenteral nutrition) to provide calories and amino acids; supplementation with minerals, pancreatic enzymes, and MCTs ; and restriction of fat and lactose, with gluten restriction as needed.
Absorptive State
leads to
Absorptive state Tissues involved
Glucose, amino acids in portal vein
leads to
leads to
Glucose, amino acids, and fatty acids in the intestine
Release of glucagon by α cells of pancreas
Pancreas
Intestine andportal vein
Release of insulin by β cells of pancreas
Ferrier_Unit05.indd 278Ferrier_Unit05.indd 278 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
24.2 QuestionLiver in the Absorptive State
What proteins are involved in blood glucose uptake and trapping by the liver in the absorptive state, as shown?
What pushes glucose to glycogenesis in the liver in the absorptive state? To glycolysis? To FA and TAG synthesis?
In an individual with G6PD defi ciency , which glucose utilization pathway is decreased?
LIVER
Glucose 6-P
Glycogen
Pyruvate
Glucose Glucose(from gut)
Amino acids Aminoacids
(from gut)
Fatty acid
TCA
VLDL (to adipose tissue)
Triacylglycerol (TAG)
Protein
PPP
Chylomicronremnants
VLDL
BLOOD
NH3
NH3Acetyl CoA
Ferrier_Unit05.indd 279Ferrier_Unit05.indd 279 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
24.2 Answer Liver in the Absorptive State
Hepatic uptake of blood glucose is through GLUT-2 . The glucose is phosphorylated to glucose 6-P by glucokinase , which has a high K m and V max for glucose, and trapped within the cell.
As shown, glucose is pushed to hepatic glycogenesis 2 by GS activation and to glycolysis 4 by PFK-1 and PK activation. [ Note: PFK-1 is allosterically activated by fructose 2,6-bisP made by PFK-2 . The kinase domain of PFK-2 is active when the bifunctional protein is dephosphorylated. The hepatic isoform of PK also is dephosphorylated and active.] FA synthesis 5 is favored by acetyl CoA availability ( PDH is active and the TCA cycle is inhibited) and ACC activation. TAG synthesis 6 is favored by the availability of the glycerol backbone from glycolysis and of FAs.
In G6PD defi ciency , the PPP 3 of glucose utilization is inhibited, decreasing the NADPH needed for hepatic FA (and cholesterol) synthesis.
Glucose uptake by insulin-independent GLUT-2 is driven by the rise in blood glucose.
Acetyl CoA carboxylase is activated covalently (dephosphorylated) and allosterically (by citrate).
The rise in glucose allows phosphorylation by glucokinase, which has a high Km for glucose.
LIVER
Glucose 6-P
Glycogen
Pyruvate
Glucose Glucose(from gut)
Amino acids Aminoacids
(from gut)
Fatty acid
TCA
VLDL (to adipose tissue)
Triacylglycerol (TAG)
Protein
PPP
Chylomicronremnants
2
4
4
3
1
5
VLDL 6
77 8
6BLOOD
6
NH3
NH37Acetyl CoA
The risphospwhich
Glucl os
Glyco
2
Glycogen synthase is activated covalently (dephosphorylated) and allosterically (by glucose 6-P).
3
Glucose 6-P availability stimulates the PPP, providing NADPH for fatty acid synthesis.
Pyruyy vPPPPP4
AcetAcetyll
PPPPActivation (dephosphorylation) of pyruvate dehydrogenase favors acetyl CoA production.
FFatttyy
ia
C55
AcetAce yl y p
TCA cycle inhibition at isocitrate dehydrogenase allows use of acetyl CoA in fatty acid synthesis.
VLDL (to adipo
TrriVLDLDL 6
Fattattyy
TTrriVVVLVLDVLDLDL 6
6hydrogenase allows use of tyl CoA in fatty acid synthesis.
Glycolysis provides the glycerol backbone for TAG synthesis.
Ferrier_Unit05.indd 280Ferrier_Unit05.indd 280 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
24.3 QuestionNonhepatic Tissues in the Absorptive State
Given that FA synthesis is not a major pathway in human adipocytes under most conditions, how do these cells obtain FAs?
What group of amino acids is metabolized primarily by muscle rather than by liver?
Why is the brain dependent on blood glucose?
What would be the expected effect on blood glucose levels with mutations that decrease the intracellular traffi cking of GLUT-4?
?
Acetyl CoATCAcycle
ADIPOCYTE
Glucose
Glucose Glucose 6-P
PyruvatePPP
Fatty acid
Triacylglycerol
?
2
3 2
6
4
5
5
1
Ferrier_Unit05.indd 281Ferrier_Unit05.indd 281 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
24.3 Answer Nonhepatic Tissues in the Absorptive State
Adipocytes obtain FAs primarily from the degradation of exogenous (dietary) TAGs in CMs exocytosed from the intestine and endogenous TAGs in VLDLs exocytosed from the liver. LPL attached to the endothelial lining of capillaries in adipose tissue (and activated by apo - CII on LP surfaces) degrades the TAGs to glycerol and FAs. [ Note: In adipose tissue, insulin upregulates LPL expression. It also causes HSL dephosphorylation and inactivation, thereby inhibiting intracellular lipolysis.]
BCAAs are catabolized primarily by muscles, the primary location of BCAA transaminase that initiates their degradation. [ Note : Metabolism of straight-chain amino acids occurs primarily in the liver, which has low levels of BCAA transaminase .]
The brain is dependent on blood glucose (requiring �140 g/day) because it has limited supplies of glycogen and TAGs. Additionally, FFAs do not effi ciently pass through the BBB , thus making little contribution to ATP production in brain.
GLUT-4, found in muscle and adipose tissue, is sequestered in intracellular vesicles. In response to insulin, the transporters move to the plasma membrane and allow blood glucose uptake. Mutations that decrease GLUT-4 traffi cking would prevent glucose uptake and cause hyperglycemia. [ Note: In T1D , the lack of insulin results in intracellular retention of GLUT-4 and, consequently, hyperglycemia.]
VLDL(from liver)
Acetyl CoATCAcycle
ADIPOCYTE
Glucose
Glucose Glucose 6-P
PyruvatePPP
Fatty acid
Triacylglycerol
Chylomicrons (from gut)
2
3 2
6
4
ADIPOCYTE
seAdipocytes contain the insulin-sensitive GLUT-4.
5
5
1
Ferrier_Unit05.indd 282Ferrier_Unit05.indd 282 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
24.4 QuestionFasting State
Which letter (A, B, or C) shown best represents the fat stores in a 70-kg individual at the start of a fast?
What are the two metabolic priorities in the fasting state?
Which enzymes of intermediary metabolism are phosphorylated and active in the fasting state?
What is the expected effect on blood glucose in an individual with Cushing disease , a pathology characterized by increased cortisol production?
C: 0.2 kg = 800 kcal
B: 6 kg = 24,000 kcal
A: 15 kg = 135,000 kcal
Ferrier_Unit05.indd 283Ferrier_Unit05.indd 283 5/2/14 7:43 PM5/2/14 7:43 PM
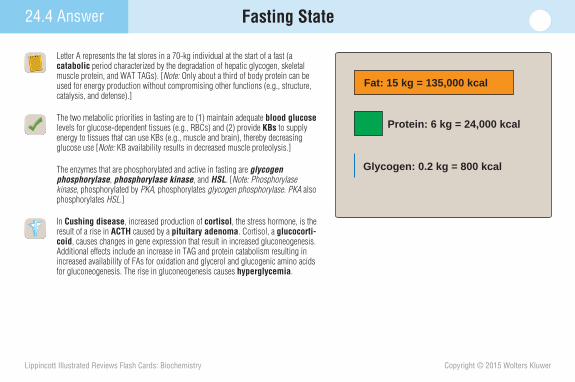
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
24.4 Answer Fasting State
Letter A represents the fat stores in a 70-kg individual at the start of a fast (a catabolic period characterized by the degradation of hepatic glycogen, skeletal muscle protein, and WAT TAGs). [ Note: Only about a third of body protein can be used for energy production without compromising other functions (e.g., structure, catalysis, and defense).]
The two metabolic priorities in fasting are to (1) maintain adequate blood glucose levels for glucose-dependent tissues (e.g., RBCs) and (2) provide KBs to supply energy to tissues that can use KBs (e.g., muscle and brain), thereby decreasing glucose use [Note: KB availability results in decreased muscle proteolysis.]
The enzymes that are phosphorylated and active in fasting are glycogen phosphorylase , phosphorylase kinase , and HSL . [ Note: Phosphorylase kinase , phosphorylated by PKA , phosphorylates glycogen phosphorylase . PKA also phosphorylates HSL .]
In Cushing disease , increased production of cortisol , the stress hormone, is the result of a rise in ACTH caused by a pituitary adenoma . Cortisol, a glucocorti-coid , causes changes in gene expression that result in increased gluconeogenesis. Additional effects include an increase in TAG and protein catabolism resulting in increased availability of FAs for oxidation and glycerol and glucogenic amino acids for gluconeogenesis. The rise in gluconeogenesis causes hyperglycemia .
Glycogen: 0.2 kg = 800 kcal
Protein: 6 kg = 24,000 kcal
Fat: 15 kg = 135,000 kcal
Ferrier_Unit05.indd 284Ferrier_Unit05.indd 284 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
24.5 QuestionLiver in the Fasting State
Contrast glycogenolysis and gluconeogenesis, processes that provide the blood glucose required by the body during fasting, as shown.
Describe the tissue interrelationships in the generation and use of KBs.
Why can KB production result in a metabolic acidosis?
In addition to long-term fasting, in what other conditions might KB concentration be increased and result in acidosis? In what conditions might KB production be impaired?
Glu
cose
use
d, g
/hr
0 8 16 24 10 200
40
Hours
20
Days40
Ingested glucose
Glycogen
Gluconeogenesis
Ferrier_Unit05.indd 285Ferrier_Unit05.indd 285 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Liver in the Fasting State24.5 Answer
Glycogenolysis is an immediate, short-lived response to fasting, whereas gluconeogenesis is slower, sustainable, and dependent on proteolysis and lipolysis. By 24 hours of fasting, gluconeogenesis provides all the blood glucose. [ Note: Glucose is generated from the glucose 6-P product of both processes by hepatic (and renal) glucose 6-phosphatase. ]
Catecholamine-mediated HSL activation causes degradation of WAT TAGs to FAs (and glycerol) that are sent into blood and taken up by the liver. The FAs are oxidized to acetyl CoA, which is used for ketogenesis (rather than being oxidized), because the rise in NADH from FA � -oxidation inhibits the TCA cycle. [ Note: Phosphorylation by AMPK inhibits ACC. The resulting drop in malonyl CoA relieves inhibition of CPT-1 , allowing FA oxidation.] The liver is unable to use KBs (it lacks thiophorase ), and they are sent out for use by nonhepatic tissues (e.g., brain and muscle).
Ketogenesis can result in metabolic acidosis if production outpaces use because the KBs acetoacetate and � -hydroxybutyrate are organic acids. Their dissocia-tion in aqueous solutions produces H � , thereby decreasing blood pH. [ Note: KBs spare glucose for glucose-dependent tissues (e.g., RBCs), reducing gluconeogen-esis and preserving muscle.]
KBs may be increased in T1D (causing DKA ) and in malnourished individuals who consume excessive amounts of ethanol (causing alcoholic ketoacidosis ). [Note: Hyperglycemia is seen with DKA whereas hypoglycemia is seen with alcoholic ketoacidosis.] KB production will be impaired in any condition that inhibits FA oxidation (e.g., MCAD or carnitine defi ciency ).
Glu
cose
use
d, g
/hr
0 8 16 24 10 200
40
Hours
20
Days40
Ingested glucose
Glycogen
Gluconeogenesis
Ferrier_Unit05.indd 286Ferrier_Unit05.indd 286 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
24.6 QuestionNonhepatic Tissues in the Fasting State
What is the brain’s primary fuel source in long-term fasting (starvation)?
Why is glucose metabolism decreased in both adipose and muscle tissue in the fasting state?
In addition to releasing FFAs into the blood, what else can adipocytes do with these products of intracellular lipolysis?
How might chronic kidney disease ( CKD ) decrease the body’s ability to compensate for ketoacidosis?
BLOOD
Glucose 6-P
PyruvateTCAcycle
Acetyl CoA
BRAIN
Glucose
Glucose
1
1
1
1
?
Ferrier_Unit05.indd 287Ferrier_Unit05.indd 287 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Nonhepatic Tissues in the Fasting State24.6 Answer
In long-term fasting ( starvation ), KBs are the brain’s primary fuel source. � -Hydroxybutyrate is oxidized to acetoacetate, which is converted by thiophorase to acetoacetyl CoA that is cleaved to two acetyl CoA for oxidation in the TCA cycle.
Glucose metabolism in adipose and muscle tissue is decreased in the fasting state because these tissues contain insulin-dependent GLUT-4. Consequently, they are not able to take up glucose from the blood when insulin is low.
In addition to releasing the FFAs from intracellular lipolysis into the blood, adipocytes can esterify them to the glycerol 3-P generated by glyceroneogenesis (an abbreviated version of gluconeogenesis) and store them as TAGs. This reduces FFAs, which have an infl ammatory effect.
Gln, released by the catabolism of BCAAs in skeletal muscle, is normally taken up by the kidneys. Renal glutaminase and GDH convert it to � -KG and NH 3 . The NH 3 picks up H � generated by KB dissociation and carries it into the urine as NH 4 � (shown). With CKD , this process may be compromised. [Note: The �-KG is a substrate for renal gluconeogenesis.]
BLOOD
Glucose 6-P
PyruvateTCAcycle
Acetyl CoA
BRAIN
Glucose
Glucose
1
1
1
1
Ketonebodies
2
Branched-chain amino acids (BCAAs)
Glutamate + NH3 → NH4+
α-Ketoglutarate + NH3 → NH4+
Glutaminase
Glutamatedehydrogenase
H+
H+
Glutamine
Ferrier_Unit05.indd 288Ferrier_Unit05.indd 288 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Absorptive State Summary
In the absorptive state : 1. Blood glucose levels and the
insulin/ glucagon ratio are increased.
2. Circulating TAG-rich LPs (CMs primarily but also VLDLs) are increased.
3. Amino acids from digestion are available in the blood.
4. KBs are virtually absent. 5. Synthesis of glycogen, TAGs,
and proteins is increased.
A useful “ rule of thumb ” for the absorptive state is that covalently regulated enzymes involved in nutrient storage processes (e.g., hepatic PK , the kinase domain of hepatic PFK-2 , GS , and ACC ) are active when they are dephosphorylated. PDH also is active when dephosphorylated, thereby allowing the conversion of glucose to acetyl CoA for FA (and cholesterol) biosynthesis. Enzyme induction (e.g., of ACC ) in response to hormonal signals also plays a role.
Acetyl CoATCAcycle
ADIPOCYTE
Glucose Glucose 6-P
PyruvatePPP
Acetyl CoA
Pyruvate
TCAcycle
Amino acids
Aminoacids
Protein
MUSCLE
Glucose 6-PGlycogen Glucose Glucose
Glucose 6-P
Pyruvate
TCAcycle
Acetyl CoA
BRAIN
Glucose
To alltissues
Chylomicronremnants
BLOOD
LIVER
Glucose 6-P
Glycogen
Pyruvate
Glucose
Amino acids
Fatty acid
VLDL
Triacylglycerol
Protein
PPP
NADPH
VLDL
NH3
NH3Acetyl CoA
VLDL(from liver)
Chylomicronremnants
Fatty acid
Triacylglycerol
Glucose
INTESTINE
Chylomicrons
Amino acids
Acetyl CoATCAcycle
ADIPOCYTE
Glucose Glucose 6-P
PyruvatePPP
FFFFFFFFFFFFFFFFFFFFFFFFFFFFFFatty acid
microns
DIETARY FAT CAN BE CONVERTED TO BODY FAT
When caloric intake exceeds energyexpenditure, dietary fat can be converted to triacylglycerol in the adipose tissue.
BLOOD
LIVER
P6 P6 P6 P6 P6 P6 P6 P6 Pucosososososososososososososososososososososesesesesesesesese 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-P
Glycogen
Pyyyyryrrrrrrrrrrrrrrrrrrrrrrrruvuvuvuvuvuvuvuvuvuvuvuvuvruvruvaruvaruvaruvaruvaruvauvauvauvatuvatuvatuvatuvateuvateuvateuvateuvateuvateuvateuvateuvateuvateuvateuvateuvateuvateuvateuvateuvatevatevatevatevatevatevatevatevatevatevate
GGlucoGlucoseGlucoseGlucoseGlucoseGlucoseGlucoseGlucoseGlucoseGlucoseGlucoseGlucose
A i idA i idA i idA i idA i idA i idA i idA i idA i idAmino acids
NH3
AAm
DIETARY CARBOHYDRATE AND DIETARY PROTEIN CAN BE CONVERTED TO BODY FAT
When caloric intake exceeds energyexpenditure, dietary carbohydrate and protein can be converted to triacylglycerol in the liver for ultimate deposition in the adipose tissue.
Glucagon
Pancreas
Insulinlin
Insulin is an anabolic signal that promotes synthesis of glycogen, protein, and triacylglycerol.
TCAcycle
Ferrier_Unit05.indd 289Ferrier_Unit05.indd 289 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Fasting State Summary
In the fasting state : 1. Blood glucose levels and the insulin/glucagon ratio
are decreased. However, glucose is maintained at an essential level by gluconeogenesis.
2. FAs bound to albumin are the predominating circulating lipids.
3. Ala and Gln are the predominating circulating amino acids.
4. KBs are present at concentrations that refl ect fast duration.
5. Degradation of glycogen, TAGs, and proteins is increased.
A useful “ rule of thumb ” for the fasting state is that covalently regulated enzymes involved in retrieval processes (e.g., glycogen phosphorylase , phosphorylase kinase , and HSL ) are active when phosphorylated. [ Note: PDH is inactive when phosphorylated, thereby decreasing glucose oxidation. Acetyl CoA from FA oxidation is used for ketogenesis because the TCA cycle in liver is inhibited by an increase in the NADH/NAD� ratio.] Enzyme induction (e.g., of PEPCK ) in response to hormonal signals also plays a role.
LIVER
Glycogen
Acetyl CoA TCAcycle
Glycerol
Glycerol
ADIPOCYTE
BLOOD
Fatty acids
Acetyl CoA
Ketone bodies
TCAcycle
Aminoacids
Protein
MUSCLE
BLOOD
Glucose 6-P
Pyruvate TCAcycle
BRAIN
GlucoseGlucose
Ketonebodies
Ketonebodies
Pancreas
Insulin
GlucagonCortisol Epinephrine
AdrenalPancreas
Fatty acids
Fatty acids
Triacylglycerol
Fatty acids
Acetyl CoA
Fatty acids
Ketone bodies Ketonebodies
Glucose 6-P Glucose
BLOOD
Pyruvate
TCAcycle
LIVER
enggggggggggggggggggggggggggggggggGlyyyyyyyccccccccccccccccccccccccccccogcogcogcogcogcooo
CCoCoCoCoACoACoACoACoA CoA CoA CoA CoA CoAAceAceAceAceAceAceAceAceAceAceAceAceAceAceAceAceAcececececececececececececececececececececececececececececececececececetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetcetycetycetycetycetycetycetycetyetyetyetyetyetyetyetyetyetyetyetyetyety AC AC AC Al C Al C Al C Al C Al C At l C At l C At l C Aetyl CoAetyl CoAetyl CoAetyl CoA
acidsaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaa a a ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y FatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatFatatatatatatatatatatatatatatatatatatatatatatatatattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattattatttttttttttttttttty tty tty tty
b db db db db dK b dK b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dK t b dKetone bod
Glucccccccoooooooooooooooooooooooooooooososososososososososososososososososeoseoseoseoseoseoseoseosesese 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-Pse 6-P G uG uGluGluGluGluGluGluGluGluGluGluGlu
ruvateruvaruvaruvruvruvruvruvyruvyruvyruvyruvyruvyruvyruvyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruvPyruPyruPyruPyruPyruPyruPyruPyru
TCAcycle
PRIORITY 1: FEED THE GLUCOSE-REQUIRING TISSUES
Blood glucose is maintained first by degradation ofliver glycogen, followed by hepatic gluconeogenesis.
Gluconeogenicprecursors
Amino acids
Acetyl CoA TTTTCTCTCTCTCCAcccccycycycyclee
Glycerol
ADIPOCYTE
idsidsidsidsidsidsidsidsidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidscidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidcidacidacidacidacidacidacidacidacidaciaciaciaciaciaciaciaciaciaciaciaciaciaciFattytytytytyyyyyyyyyyyyyyyyyyyyyyyyyyyyyyyyyyyyy y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y y ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay a aci aci aciaci
Triacylglycerolyceroyceroyceroycercerce lacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgacylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylgcylcylcylcylcylcylcylcylcylcylcylcylcylcyleeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeneeneeneeneeneeneeetonetonetKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetoneKetonetonKetonetononKetonetononKetonetononKetonetononKetonetononKetonetononKetonetononKetonetononKetonetononKetonetonoKetonetonoKetonetonoKetonetonoKetonetonoKetonetonoKetonetonoKetonetono
bodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesbodiesb dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib dib diii
BLOOD
PRIORITY 2: FEED THE NONGLUCOSE-REQUIRING TISSUES
Mobilization of triacylglycerols from adipose tissue providesfatty acids and precursors for ketone bodies.
Glucose
Acetyl CoA
Cortisol, epinephrine, and glucagon are catabolic signals that promote degradation of protein, triacylglycerol, and glycogen.
Ferrier_Unit05.indd 290Ferrier_Unit05.indd 290 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
25.1 QuestionType 1 Diabetes
What are the three symptoms of T1D that typically accompany the progressive onset of clinical disease, as shown?
How is the diagnosis of T1D confi rmed?
What is the oral glucose tolerance test (OGTT)? For what reason is the test most typically used?
Why is dehydration a common symptom of hyperglycemia ?
Type 1 diabetes
Autoimmune destruction of β cells in individuals with a
genetic predisposition
Loss of insulin secretory capacity
Immunologic trigger
Type 1 diabetes
leads to
leads to
?
often exhibits
leads to
associated with
Ferrier_Unit05.indd 291Ferrier_Unit05.indd 291 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
25.1 Answer Type 1 Diabetes
Patients with T1D typically present with three Ps: (1) polyuria (frequent urination), (2) polydipsia (excessive thirst), and (3) polyphagia (excessive hunger) accompanied by fatigue and weight loss. Progressive autoimmune pancreatic � -cell destruction results in absolute insulin defi ciency.
T1D diagnosis is confi rmed by a HbA 1c level � 6.5 mg/dl, a FBG � 126 mg/dl, or a non-FBG (random) � 200 mg/dl. T1D accounts for � 10% of the known cases of diabetes.
The OGTT reveals how quickly ingested glucose (75 g) is removed from the blood over a 2-hour period. The test is most typically used to screen those pregnant women at increased risk for gestational diabetes and is done between 24 and 28 weeks of pregnancy. About 4% of pregnancies are affected.
The renal tubules reclaim glucose via the SGLT-2 , which is saturated at �180 mg/dl of glucose. Above this concentration, glucose “spills” into the urine causing increased urine output ( osmotic diuresis ), which can result in severe dehydration . It also accounts for the character-istic polyuria and polydipsia of T1D.
Type 1 diabetes
Autoimmune destruction of β cells in individuals with a
genetic predisposition
Loss of insulin secretory capacity
Immunologic trigger
Type 1 diabetes
leads to
leads to
leads to
associated with
often exhibits
PolyuriaPolydipsiaPolyphagia
Ferrier_Unit05.indd 292Ferrier_Unit05.indd 292 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
25.2 QuestionMetabolic Changes in Type 1 Diabetes
What are the two causes of hyperglycemia in T1D?
Why is hypertriglyceridemia seen in T1D?
Why does ketoacidosis occur in T1D?
LIVER
Glycogen
Acetyl CoA TCAcycle
Glycerol
Glycerol
ADIPOCYTE
BLOODFatty acids
Fatty acids
Triacylglycerol
Fatty acids
Acetyl CoA
Fatty acids
Ketone bodies
Glucose 6-phosphate Glucose
BLOOD
Pyruvate
TCAcycle
Gluconeogenicprecursors
Amino acidsfrom muscle and other
peripheral tissues
Glucose
INTESTINE
Amino acids
VLDLs(accumulate)
Triacylglycerol
VLDLs
Chylomicrons(accumulate)
Pancreas
Insulin
Glucagon
Pancreas
Ketonebodies
Ferrier_Unit05.indd 293Ferrier_Unit05.indd 293 5/2/14 7:43 PM5/2/14 7:43 PM
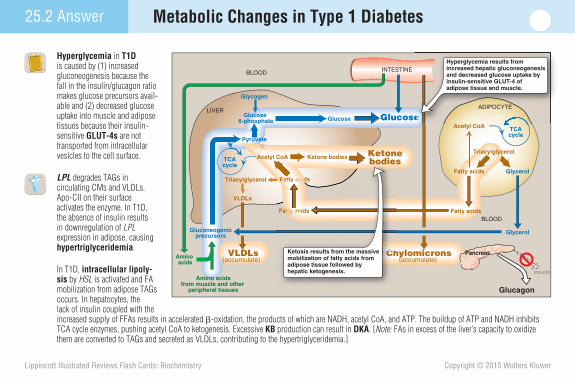
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
25.2 Answer Metabolic Changes in Type 1 Diabetes
Hyperglycemia in T1D is caused by (1) increased gluconeogenesis because the fall in the insulin/glucagon ratio makes glucose precursors avail-able and (2) decreased glucose uptake into muscle and adipose tissues because their insulin-sensitive GLUT-4s are not transported from intracellular vesicles to the cell surface.
LPL degrades TAGs in circulating CMs and VLDLs. Apo-CII on their surface activates the enzyme. In T1D, the absence of insulin results in downregulation of LPL expression in adipose, causing hypertriglyceridemia .
In T1D, intracellular lipoly-sis by HSL is activated and FA mobilization from adipose TAGs occurs. In hepatocytes, the lack of insulin coupled with the increased supply of FFAs results in accelerated � -oxidation, the products of which are NADH, acetyl CoA, and ATP. The buildup of ATP and NADH inhibits TCA cycle enzymes, pushing acetyl CoA to ketogenesis. Excessive KB production can result in DKA . [ Note: FAs in excess of the liver’s capacity to oxidize them are converted to TAGs and secreted as VLDLs, contributing to the hypertriglyceridemia.]
LIVER
Glycogen
Acetyl CoA TCAcycle
Glycerol
Glycerol
ADIPOCYTE
BLOODFatty acids
Fatty acids
Triacylglycerol
Fatty acids
Acetyl CoA
Fatty acids
Ketone bodies
Glucose 6-phosphate Glucose
BLOOD
Pyruvate
TCAcycle
Gluconeogenicprecursors
Amino acidsfrom muscle and other
peripheral tissues
Glucose
INTESTINE
Amino acids
VLDLs(accumulate)
Triacylglycerol
VLDLs
Chylomicrons(accumulate)
Pancreas
Insulin
Glucagon
PancreasCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCChCCCCh
Fattattattattattattattattattattttttttttttttttttttyttyttyttyttyttyttyttyttyttyttyttyttyttyttytytytytytytytytytytytytytytytyty ty ty tytytytyy y y y y y y ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay ay acy acy acy acy acy acy acy acy acy acy acacaciaciaciacidacidacidsacidsacidsacidsacidsacidsacids
Fatty acidsFatty acidFatty acidFatty idFatty idFatty idFatty idFatty idFatty idFatty acidFatty aciFatty aciFatty aciFatty aciFatty aciFatty aciFatty aciFatty aciFatty aciFatty aciFatty aciFatty ciFatty ciFatty ciFatty aciFatty aciFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty cFatty cFatty cFatty cFatty cFatty cFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty acFatty aFatty aFatty aFatty aFatty aFatty aFatty aFatty aFatty aFatty aFatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty aatty attyattyattytty
A t l C A
ADIPOCYTE
eeeeeeeeeeeeeeeeeeeeeeee
Ketosis results from the massive mobilization of fatty acids from adipose tissue followed by hepatic ketogenesis.
Hyperglycemia results from increased hepatic gluconeogenesis and decreased glucose uptake by insulin-sensitive GLUT-4 of adipose tissue and muscle.
Ketonebodies
Ferrier_Unit05.indd 294Ferrier_Unit05.indd 294 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
25.3 QuestionType 1 Diabetes Treatment
Which of the three colored arrows shown represents the typical mean blood glucose value obtained with standard insulin therapy for T1D?
Why does intensive insulin therapy result in a three-fold increase in the frequency of hypoglycemia? In spite of the risk, why might physicians choose intensive therapy in treating their patients with T1D?
What is “hypoglycemia unawareness”?
0 50 100 150 200 250 300 3500
2
4
6
8
10
Mean blood [glucose], mg/dl
Per
cen
t h
emo
blo
bin
A1C
12
Ferrier_Unit05.indd 295Ferrier_Unit05.indd 295 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
25.3 Answer Type 1 Diabetes Treatment
Standard insulin therapy (typically one or two injections of recombinant human insulin per day) for T1D is represented by the blue arrow. The glucose levels obtained with this treatment range from 225 to 275 mg/dl, with a HbA 1c level at �9% of the total Hb.
The goal of intensive insulin therapy (red arrow) is to maintain tight control of blood glucose levels, accomplished with more frequent glucose readings and three or more injections of insulin per day. However, it is diffi cult to accurately titrate the appropriate dosage of insulin and hypoglycemia is a common complication (shown). Nonetheless, the benefi ts of intensive therapy outweigh the risks in most populations. Patients on intensive therapy show a � 50% reduction in the long-term microvascular complications of diabetes (i.e., retinopathy , neuropathy , and nephropathy ) and lower HbA 1c values.
Patients with T1D develop glucagon secretion defi ciency early in the disease and rely on epinephrine to prevent severe hypoglycemia. However, as the disease progresses, epinephrine secretion is impaired, creating a symptom-free and dangerous condition ( hypoglycemia unawareness ) when blood glucose falls.
0 50 100 150 200 250 300 3500
2
4
6
8
10
Mean blood [glucose], mg/dl
Per
cen
t h
emo
blo
bin
A1C
Normal mean[glucose] innondiabeticindividuals
Intensiveinsulintherapy
Standardinsulintherapy
12
0
100
Hyp
og
lyce
mic
ep
iso
des
per
100
0 p
atie
nt
mo
nth
s
Conventionaltherapy
Intensivetherapy
INTENSIVE THERAPYIntensive therapy results in a threefold increase in the frequency of hypoglycemia.
Many clinicians believe the increased risk of hypo-glycemia that accompanies intensive therapy is justified by the substantial decrease in the incidence of long-term complications, such as diabeticretinopathy and nephropathy.
Ferrier_Unit05.indd 296Ferrier_Unit05.indd 296 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
25.4 QuestionType 2 Diabetes
Most obese individuals are insulin resistant (as shown). Do most develop T2D?
What is insulin resistance? How does obesity foster insulin resistance?
What is an acute complication of T2D?
ObeseNormal
Insu
lin (
μU/m
l)
160
120
80
40
0 8 12
noon4 8 12
midnight 4
Insulin level in blood
ulin
(μU
/ml)
160
120
80
Blood insulin rises from basal levels after each meal.Higher insulin
levels are required to control blood glucose in the insulin-resistant, obese individual.
Ferrier_Unit05.indd 297Ferrier_Unit05.indd 297 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
25.4 Answer Type 2 Diabetes
Most obese individuals with insulin resistance do not develop T2D , the most common form of diabetes, because still-functional pancreatic � cells produce suffi cient insulin to maintain normal blood glucose levels. [ Note: Patients who do develop T2D have a combination of insulin resistance and dysfunctional � cells but do not require insulin to sustain life.]
In insulin resistance, normal (or elevated) insulin levels fail to elicit the expected biologic response. Obesity fosters insulin resistance (shown) via changes in adipose secretions. The major secretory changes include increased infl ammatory cytokine (e.g., IL-6 ) and leptin production and decreased anti-infl ammatory adiponectin production. Infl ammation contributes to insulin resistance (and to CHD).
An acute complication of T2D is a hyperosmotic hyperglycemic state (most common in the elderly) that presents with very high blood glucose levels, severe dehydration, and altered mental status. Coma and death can result.
8
Glu
cose
(m
g/dl
)
12noon
4 8 12midnight
4
160
140
120
100
80
ObeseNormal
Glucose level in blood
Glu
cose
(m
g/dl
)
160
140
120
1000
Blood glucose is kept within the same narrow range thoughout the day in both normal-weight and obese individuals.
Changes in adipose secretions
Insulin resistance
Obesity
Adipose lipolysis
Fatty acidoxidation
Glucose uptakeby muscle andadipose tissue
Hepatic gluconeogenesis
Blood glucose
Freefattyacids
Ferrier_Unit05.indd 298Ferrier_Unit05.indd 298 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Type 2 Diabetes 25.5 Question
How is T2D development temporally related to the onset of insulin resistance and the decline of � -cell function shown?
Why is dyslipidemia one of the metabolic changes associated with T2D?
What is the treatment goal in T2D?
Insulin resistance
Hyperinsulinemia Decline of a-cell function
Type 2 diabetes
characterized by
leads to
in combination with
associated with
leads to
Obesity
Type 2 diabetes
Ferrier_Unit05.indd 299Ferrier_Unit05.indd 299 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
25.5 Answer Type 2 Diabetes
Obese individuals with insulin resistance may take � 10 years before they develop T2D. Initially, the � cells compensate by increasing insulin production. With time, however, they become increasingly dysfunctional and fail to produce enough insulin to correct the hyperglycemia.
Insulin resistance, coupled with decreased � -cell function, leads to decreased LPL expression in adipocytes and a decrease in TAG degradation in circulating VLDLs and CMs, causing hypertriglyceridemia (a dyslipidemia ).
The treatment goal in T2D is to maintain blood glucose within normal limits to avoid the long-term complications of hyperglycemia. Weight loss, exercise, and dietary modifi cations ( medical nutrition therapy ) can help correct hyperglycemia. Hypoglycemic drugs (e.g., metformin , which suppresses gluconeogenesis; sulfonylureas , which increase insulin secretion; and � -glucosidase inhibitors , which decrease carbohydrate absorption) are often prescribed. Insulin may be required.
–10
200
250
150
100
50
0
250
300
200
150
100
50
–5 0 5 10 15 20 25
–10 –5 5 10 15 20 25
Glu
cose
(mg
/dl)
Insu
lin s
ecre
tio
n(p
erce
nt
of
no
rmal
)
Years of diabetes
Insulin levels in untreated type 2 diabetes
Normal
Normal
Fasting glucose in untreated type 2 diabetes
Diagnosis of diabetes Years of diabetes–10 –5
Diagnosis of diabetes
20 25
Normal
etes
Normal
betes
5 10 15Years of diabetes
5
Patients diagnosed with type 2 diabetes initially show insulin resistance with compensatory hyperinsulinemia.
Subsequently, �-cell dysfunction occurs, marked by declining insulin secretion and worsening hyperglycemia.
Obese individuals develop insulin resistance, whichmay precede the develop-ment of diabetes by 10or more years.
1 2 3
0
Diagnosis of diabetes
Insulin resistance
Hyperinsulinemia Decline of β-cell function
Type 2 diabetes
characterized by
leads to
in combination with
associated with
leads to
Obesity
Type 2 diabetes
Ferrier_Unit05.indd 300Ferrier_Unit05.indd 300 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
25.6 QuestionType 2 Diabetes Effects
Why is T2D progression, as shown, not generally associated with DKA development?
What are “advanced glycation end products (AGEs)”?
How is T2D treatment different from that for T1D?
Insulin resistance
Hyper-insulinemia
GeneticsObesitySedentary lifestyleAging
GeneticsGlucose toxicityFree fatty acid toxicity
Impairedglucosetolerance
Decline of β-cellfunction
type 2 diabetes
+ +
MACROVASCULAR COMPLICATIONS (cardiovascular disease, stroke)
MICROVASCULAR COMPLICATIONS (retinopathy, neuropathy, nephropathy)
Ferrier_Unit05.indd 301Ferrier_Unit05.indd 301 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
25.6 Answer Type 2 Diabetes Effects
In T2D, the � cells have a diminished capacity to secrete insulin, but the amount is suffi cient to decrease glucagon secretion and prevent DKA .
Hyperglycemia promotes a reversible, nonenzymatic glycosylation of certain proteins, a process known as glycation . With time, these glycated proteins undergo irreversible reactions and become AGEs that are thought to play a causative role in the vascular complications and impaired wound healing seen with diabetes.
In diabetes, the treatment goal is glycemic control to reduce the development of long-term complications. Oral medications are used to reduce hyperglycemia in T2D, whereas insulin therapy is used in T1D. [ Note: The risk for developing T2D, a metabolic disorder, can be signifi cantly decreased by dietary modifi cations, exercise, and weight loss. In contrast, T1D results from autoimmune-mediated destruction of pancreatic � cells and no preventive treatment exists currently.]
Insulin resistance
Hyper-insulinemia
GeneticsObesitySedentary lifestyleAging
GeneticsGlucose toxicityFree fatty acid toxicity
Impairedglucosetolerance
Decline of β-cellfunction
type 2 diabetes
+ +
MACROVASCULAR COMPLICATIONS (cardiovascular disease, stroke)
MICROVASCULAR COMPLICATIONS (retinopathy, neuropathy, nephropathy)
24
Length of follow-up (years)
10%
9%
8%
7%Pre
vale
nce
of
reti
no
pat
hy (
%)
12
0 1 2 3 4 5 6 7 8 90
Mean HbA1c = 11%24
10%
9%Mean HbA1c = 11%
The benefits of an improvement in glycemic control occurred over the entire range of HbA1c values. Thus, any improvement in glycemic control is beneficial.
Ferrier_Unit05.indd 302Ferrier_Unit05.indd 302 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
26.1 QuestionFat Depots
How do differences in the anatomic distribution of body fat (stored TAGs), as shown, affect health risks in obesity?
What are the roles of the proteins adiponectin and leptin? How does their secretion from adipocytes in WAT change in obesity?
Why are the effects of adipocyte secretions different depending on the location of the stored fat?
A 28-year-old man presents for a physical. He is 5 � 11″ tall and weighs 240 pounds. What is his BMI? What additional measurement would help assess his risk for health problems? Thighs
Hips
Apple shaped =upper body
obesity
Pear shaped =lower body
obesity
WaistWaist
Body shape
Ferrier_Unit05.indd 303Ferrier_Unit05.indd 303 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
26.1 Answer Fat Depots
A waist/hip ratio � 0.8 for women and � 1.0 for men is defi ned as android , apple shaped , or upper body obesity. Lower body obesity (lower ratios) is defi ned as gynoid or pear shaped . Gynoid obesity (more common in women) presents a much lower risk of metabolic disease because the fat is mobilized more slowly than in android obesity, and the FFAs that contribute to insulin resistance are present at lower levels. [ Note: Of human fat, 80%–90% is stored as subcutaneous depots, with the rest stored as visceral (omental and mesenteric) fat.]
Adiponectin reduces FFA levels and is associated with an improved metabolic state. Leptin decreases appetite and increases energy use. As body weight increases, adiponectin levels fall and leptin levels rise.
FFAs and cytokines released from abdominal TAG stores enter the portal vein and have direct access to the liver. Those from lower body stores enter the general circulation and can be used by peripheral tissues, decreasing access by the liver.
BMI � [(weight in pounds) / (height in inches) 2 ] � 703 . With a height of 5 � 11 and weighing 240 pounds, the patient’s BMI is 33.4. A BMI � 30 is defi ned as obese and carries a risk of metabolic disease. Measuring his waist would be helpful because a waist size � 40 inches in men (�35 inches in women) is a risk factor for health problems.
ThighsHips
Apple shaped =upper body
obesity
Pear shaped =lower body
obesity
WaistWaist
Body shapeA
Location of abdominalsubcutaneous andvisceral fat
B
Subcutaneous fat
Visceral fat
Ferrier_Unit05.indd 304Ferrier_Unit05.indd 304 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
26.2 QuestionWeight Regulation
In a nonobese person, how does modest weight gain or loss affect adipocytes? How are adipocytes affected in obesity?
What are some of the environmental and behavioral contributions to the current obesity epidemic?
How can rare mutations in leptin lead to obesity?
Weight gain
Weight loss
Weight gain
Weight gain
Pre-adipocyte
Ferrier_Unit05.indd 305Ferrier_Unit05.indd 305 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
26.2 Answer Weight Regulation
In a nonobese person, modest weight change mainly affects the size but not the number of adipocytes. Weight gain results in an increase in fat cell size, and weight loss results in a decrease. In obesity , there is an increase in both size ( hypertrophy ) and number ( hyperplasia ) of adipocytes. When the adipocytes have reached their maximum size, further weight gain is accomplished by stimulating pre-adipocyte differentiation, thereby increasing the number of mature cells. [ Note: Once produced, adipocytes are diffi cult to lose.]
Although twin studies have demonstrated a genetic component to obesity, environmental and behavioral factors clearly play a role. The ready availability of palatable, energy dense foods; increasing portion size; sedentary lifestyles; and emotional responses to food are key factors. Obesity results when energy (caloric) intake exceeds energy expenditure. However, the susceptibility to obesity is multifactorial.
Individuals with rare mutations in the gene for the adipocyte hormone leptin that result in a defi ciency demonstrate hyperphagia (increased appetite for and consumption of food) and severe obesity.
Weight gain
Weight loss
Weight gain
Weight gain
Pre-adipocyte
Modest weight gain or loss in a non-obese person mainly affects the size, but not the number, of adipocytes.
When adipocytes reach their maximum size, further weightgain is achieved by recruitment and proliferation of new pre-adipocytes.
Weight loss occurs mainly by a decrease in adipocyte size.
Ferrier_Unit05.indd 306Ferrier_Unit05.indd 306 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
26.3 QuestionAppetite Control
As shown, what orexigenic (appetite-stimulating) hormone is secreted by the stomach?
As food is consumed, what anorexigenic (satiety-inducing) hormones are secreted by the intestine?
How does leptin affect appetite in the overnourished state?
HypothalamusUndernourished
STOMACH
ADIPOSE TISSUE
PANCREAS
Efferent signals: • Increased appetite• Decreased energy expenditure
Insulin
?
?
Leptin
Afferent satiety and adiposity signals
INTESTINE
Ferrier_Unit05.indd 307Ferrier_Unit05.indd 307 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
26.3 Answer Appetite Control
Ghrelin is the orexigenic hormone secreted by the stomach. Its rise in the blood triggers hunger, and its level falls after a meal.
After food has been consumed, the gastrointestinal tract secretes CCK and PYY , two anorexigenic peptide hormones that terminate eating via neural signals to the hypothalamus . [ Note: CCK also inhibits gastric motility and causes the gallbladder to release bile and the pancreas to release digestive enzymes.]
Leptin , an adipokine (a bioactive polypeptide made by adipocytes), is produced and secreted in direct proportion to the size of fat stores. Leptin binds to hypothalamic receptors and causes a decrease in appetite. Its anorexigenic effects are long term, in contrast to those of CCK and PYY. [ Note: Many obese individuals have elevated leptin levels but are resistant to its appetite-lowering effects. Other cues that stimulate appetite can apparently overcome leptin’s effects.]
HypothalamusUndernourished
STOMACH
ADIPOSE TISSUE
PANCREAS
Efferent signals: • Increased appetite• Decreased energy expenditure
Insulin
Ghrelin
CCK, PYY
Leptin
A
Afferent satiety and adiposity signals
INTESTINE
Overnourished
STOMACH
ADIPOSE TISSUE
PANCREAS
Efferent signals: • Decreased appetite• Increased energy expenditure
Insulin
Ghrelin
CCK, PYY
Leptin
BHypothalamus
INTESTINE
Afferent satiety and adiposity signals
Ferrier_Unit05.indd 308Ferrier_Unit05.indd 308 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
26.4 QuestionMetabolic Changes
What is the basis for the rise in TAGs with increasing BMI, as shown?
What can be done to decrease obesity complications, such as T2D and hypertension?
What two types of medical intervention are available for treating obesity?
mm
ol/l
Total cholesterol
Triacylglycerols
HDL cholesterol0.8
1.6
2.4
5.8
6.6
020 24 28 32
Body mass index (kg/m2)
Ferrier_Unit05.indd 309Ferrier_Unit05.indd 309 5/2/14 7:43 PM5/2/14 7:43 PM
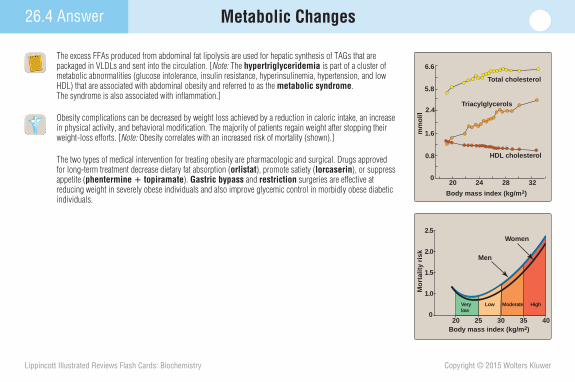
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
26.4 Answer Metabolic Changes
The excess FFAs produced from abdominal fat lipolysis are used for hepatic synthesis of TAGs that are packaged in VLDLs and sent into the circulation. [ Note: The hypertriglyceridemia is part of a cluster of metabolic abnormalities (glucose intolerance, insulin resistance, hyperinsulinemia, hypertension, and low HDL) that are associated with abdominal obesity and referred to as the metabolic syndrome . The syndrome is also associated with infl ammation.]
Obesity complications can be decreased by weight loss achieved by a reduction in caloric intake, an increase in physical activity, and behavioral modifi cation. The majority of patients regain weight after stopping their weight-loss efforts. [ Note: Obesity correlates with an increased risk of mortality (shown).]
The two types of medical intervention for treating obesity are pharmacologic and surgical. Drugs approved for long-term treatment decrease dietary fat absorption ( orlistat ), promote satiety ( lorcaserin ), or suppress appetite ( phentermine � topiramate ). Gastric bypass and restriction surgeries are effective at reducing weight in severely obese individuals and also improve glycemic control in morbidly obese diabetic individuals.
mm
ol/l
Total cholesterol
Triacylglycerols
HDL cholesterol0.8
1.6
2.4
5.8
6.6
020 24 28 32
Body mass index (kg/m2)
Men
Women
0
1.0
1.5
Mo
rtal
ity
risk
Body mass index (kg/m2)
HighLow ModerateVery low
30 35 4020 25
2.0
2.5
Ferrier_Unit05.indd 310Ferrier_Unit05.indd 310 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
27.1 QuestionDietary Reference Intakes
What is the DRI? What four DRI components are designated by the numbers shown?
Contrast EAR with RDA. What relationship does the AI have to the EAR and RDA?
What fi ve essential components must be supplied in the human diet? 1
2
4
3
DRI
Ferrier_Unit05.indd 311Ferrier_Unit05.indd 311 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
27.1 Answer Dietary Reference Intakes
The DRI is an estimate of the amount of nutrients required to prevent dietary defi ciencies and maintain optimal health. It does not include any special needs of the sick. DRI components are the (1) EAR , (2) RDA , (3) AI , and (4) UL (or TUL ). Values for these components can vary according to specifi c age-groups, physiologic status (e.g., pregnancy), and gender.
The EAR is the dietary intake at which there is a 50% risk of inadequacy. In contrast, the RDA (EAR � 2 SDs) is the intake at which the risk of inadequacy is 2%–3%. An AI is set when there is insuffi cient scientifi c information to establish an EAR or RDA (e.g., with biotin and vitamin K) and is based on the intake levels of apparently healthy individuals.
Essential dietary components are (1) energy sources (carbohydrates [4 kcal/g], fats [9 kcal/g], and proteins [4 kcal/g]), (2) the two essential fatty acids (linoleic and linolenic), (3) the nine essential amino acids (His, Ile, Leu, Lys, Met, Phe, Thr, Trp, and Val), (4) vitamins, and (5) minerals. Ethanol (7 kcal/g) is a source of calories in some diets. [Note: Restriction of one or more of these dietary components is required in certain conditions (e.g., Phe restriction in PAH defi ciency).]
Estimated Average Requirement
Recommended Dietary Allowance
Tolerable Upper Intake Level
Adequate Intake
DRI
DIET
Vitamins
Essential amino acids
Essential fatty acids
Energy sources
• Carbohydrates
• Fats
• Protein
• (Ethanol)
Minerals
Ferrier_Unit05.indd 312Ferrier_Unit05.indd 312 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
27.2 QuestionEnergy Requirements
What is the TEE? What three TEE components in healthy individuals are represented by the numbered pie slices shown?
What is the RMR? How is it measured? How does it differ from the BMR?
What is an AMDR?
Why might an injury factor be included in the TEE of hospitalized patients?
11,300 kcal = 60%
3210 kcal = 10%
2630 kcal = 30%
Ferrier_Unit05.indd 313Ferrier_Unit05.indd 313 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
27.2 Answer Energy Requirements
The TEE is the number of calories expended in a 24-hour period. TEE components in healthy individuals are (1) the REE , (2) physical activity (the most variable), and (3) the thermic effect of food.
The RMR is a measure of the energy expended in the resting, postabsorptive state. It is measured under less stringent conditions than the BMR and is �10% higher. [ Note: The BMR can be determined by indirect calorimetry (measuring O 2 consumed or CO 2 produced) or estimated by equations that include age, sex (BMR refl ects lean muscle mass, which is highest in the young and in males), height, and weight. A rough estimate commonly used is 1 kcal/kg/hour for men and 0.9 kcal/kg/hour for women.]
An AMDR is the range of intakes associated with reduced risk of chronic disease while providing adequate amounts for a given macronutrient. The AMDRs for adults are 45%–65% of total calories from carbohydrates, 20%–35% from fat, and 10%–35% from protein.
Because hospitalized patients are hypercatabolic , they have higher energy needs and an injury factor is included in their TEE.
Resting energy expenditure1,300 kcal = 60%
Thermic effectof food
210 kcal = 10% Physical activity630 kcal = 30%
Ferrier_Unit05.indd 314Ferrier_Unit05.indd 314 5/2/14 7:43 PM5/2/14 7:43 PM
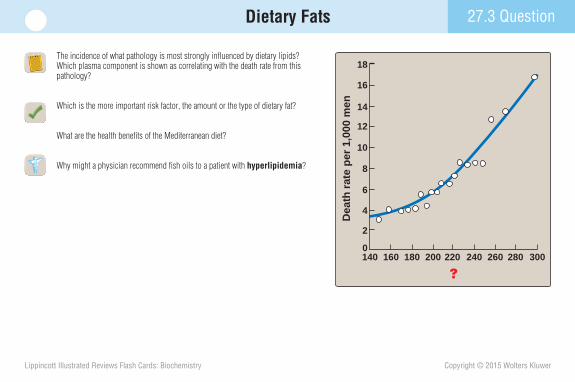
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
27.3 QuestionDietary Fats
The incidence of what pathology is most strongly infl uenced by dietary lipids? Which plasma component is shown as correlating with the death rate from this pathology?
Which is the more important risk factor, the amount or the type of dietary fat?
What are the health benefi ts of the Mediterranean diet?
Why might a physician recommend fi sh oils to a patient with hyperlipidemia ?
Dea
th r
ate
per
1,0
00 m
en
?
0
2
4
6
8
10
12
14
16
18
140 160 300180 200 220 240 260 280
Ferrier_Unit05.indd 315Ferrier_Unit05.indd 315 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Dietary Fats27.3 Answer
Dietary lipids most strongly infl uence the incidence of CHD . Total plasma cholesterol levels (from diet and de novo synthesis) correlate with the death rate from CHD. [ Note : An even stronger correlation is seen with LDL-C.]
The type of dietary fat is a more important risk factor than the amount. The presence, number, location, and confi guration of double bonds in the FAs of dietary fats infl uence cholesterol levels more than does dietary cholesterol. For example, MUFAs lower total and LDL-C but maintain or increase HDL-C when substituted for saturated FAs. Trans FAs , although unsaturated, behave like saturated FAs and are associated with a rise in LDL-C. Their consumption should be kept low. [Note: Most trans FAs are produced by food processing (hydrogenation).]
The Mediterranean diet is associated with decreased total cholesterol, LDL-C, and TAGs and with increased HDL-C compared to a typical Western diet. It is rich in MUFAs (from olive oil) and includes seasonally fresh food, an abundance of plant materials, and low amounts of red meat (and, therefore, saturated fats).
Fish oils contain the � -3 LCFAs EPA and DHA . These PUFAs reduce serum TAGs, suppress cardiac arrhyth-mias, decrease the risk of forming thrombi, lower blood pressure, and reduce the risk of cardiovascular mortality. [ Note: -3 FAs have little effect on blood cholesterol but are anti-infl ammatory.]
Fat = 38% Carbohydrate Protein
Carbohydrate ProteinFat = 38%
Typical Western diet
Typical Mediterranean diet
42%
42%
20%
20%
Polyunsaturated fatty acidMonounsaturated fatty acidSaturated fatty acidKey:
Fat = 20%
Low-fat diet
65% 15%Carbohydrate Protein
Dea
th r
ate
per
1,0
00 m
en
Plasma cholesterol, mg/dl
0
2
4
6
8
10
12
14
16
18
140 160 300180 200 220 240 260 280
Ferrier_Unit05.indd 316Ferrier_Unit05.indd 316 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
27.4 QuestionDietary Carbohydrates
What is the signifi cance of the GI shown? How is it related to the GR? The GL?
What are the most abundant disaccharides? What is the source of each?
Why is a diet rich in soluble fi ber advised for those with hypercholesterolemia ?
can be classified according to
Carbohydrates
leads to
formulated as
noteworthy because
also show
• Monosaccharides
• Disaccharides
• Polysaccharides
• Fiber Glycemic index
Foods richin fiber
Low glycemicindex
Structure anddigestibility
Effect on post-prandial blood
glucose concentration
Ferrier_Unit05.indd 317Ferrier_Unit05.indd 317 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
27.4 Answer Dietary Carbohydrates
The GI ranks carbohydrate-containing foods based on their GR relative to the same amount of carbohydrate (50 g) eaten as either glucose or white bread. Different foods can have very different GRs. The clinical importance of the GI is unresolved, but a low-GI diet appears to improve glycemic control in diabetes. [ Note: The GL is a measure of how much a typical serving size (not 50 g) of a particular food raises blood glucose. A food (e.g., carrots) can have a high GI and a low GL.]
The most abundant disaccharides are sucrose (glucose � fructose), lactose (galactose � glucose), and maltose (glucose � glucose). Sucrose (table sugar) is extracted from sugar cane and sugar beets, lactose (milk sugar) is made in lactating mammary glands, and maltose is the product of enzymatic digestion of polysaccharides and is also found in beer.
Soluble fi ber (e.g., oat bran) increases BA excretion and interferes with BA absorption. Because BAs are made from cholesterol, soluble fi ber lowers plasma cholesterol levels. It also delays gastric emptying, thereby reducing spikes in postprandial blood glucose. Consequently, a diet rich in fi ber is recommended for individuals with CHD and diabetes . [ Note: The AI for fi ber is 38 g/day for men and 25 g/day for women, but a typical American diet supplies only �15 g/day.]
can be classified according to
Carbohydrates
leads to
formulated as
noteworthy because
also show
• Monosaccharides
• Disaccharides
• Polysaccharides
• Fiber Glycemic index
Foods richin fiber
Low glycemicindex
Structure anddigestibility
Effect on post-prandial blood
glucose concentration
Ferrier_Unit05.indd 318Ferrier_Unit05.indd 318 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
27.5 QuestionDietary Proteins
What is meant by the PDCAAS value shown? What is its signifi cance?
Why might carbohydrates have a protein-sparing effect?
What is meant by negative N balance? What conditions might lead to it? In the formula used to determine N balance, what is “UUN”?
SourceAnimal proteins Egg Milk protein Beef/poultry/fish Gelatin
PDCAASvalue
1.001.00
0.82–0.920.08
Plant proteins Soybean protein Kidney beans Whole wheat bread
1.000.680.40
Ferrier_Unit05.indd 319Ferrier_Unit05.indd 319 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
27.5 Answer Dietary Proteins
The PDCAAS value is the standard by which the quality of a dietary protein is evaluated. It is based on the ability of the protein to provide the essential amino acids after correcting for its digestibility. The score provides a method to balance the intake of poorer quality proteins with ones of higher quality. [ Note: Proteins from plant sources have a lower quality (in general) than those from animal sources.]
When carbohydrate intake is too low to maintain normal blood glucose levels, amino acids (from skeletal muscle proteolysis) are degraded to provide gluconeo-genic substrates in response to the fall in insulin/counterregulatory hormone ratio. Increasing carbohydrate intake can spare proteins from degradation, preserving their structural, catalytic, and immunologic functions.
Negative N balance occurs when N loss exceeds intake. It arises with inadequate dietary protein intake, lack of essential amino acids, and physiologic stress (e.g., trauma, illness, and surgery). In the formula used to determine N balance ( N balance � protein N intake [in g/24 hours] � [UUN � 4 g] ), UUN rep-resents urinary urea N (in g/24 hours), which is quantitatively the most signifi cant N-containing molecule in human urine. [ Note: The 4 g account for urinary N loss in forms other than urea plus the loss in skin and feces.]
SourceAnimal proteins Egg Milk protein Beef/poultry/fish Gelatin
PDCAASvalue
1.001.00
0.82–0.920.08
Plant proteins Soybean protein Kidney beans Whole wheat bread
1.000.680.40
Ferrier_Unit05.indd 320Ferrier_Unit05.indd 320 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
27.6 QuestionProtein-Energy Malnutrition
Which column, A or B, best represents that form of extreme PEM known as kwashiorkor ?
Why is kwashiorkor nonadapted malnutrition?
In developed countries (e.g., the United States), in what populations is PEM most commonly seen?
Normal or decreased Markedly decreased
Present Absent
Irritable when picked up; apathetic when left alone Alert, irritable
Weight for height
Edema
Mood
Appetite Poor Good
Weight for age(% expected) 60–80 <60
ACHARACTERISTIC B
Ferrier_Unit05.indd 321Ferrier_Unit05.indd 321 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
27.6 Answer Protein-Energy Malnutrition
The two extreme forms of PEM are kwashiorkor (column A) and marasmus (column B).
Kwashiorkor occurs when protein deprivation is relatively greater than the reduction in total calories. Insulin levels are suffi cient to suppress lipolysis and proteolysis, reducing the availability of FFAs and amino acids and making kwashiorkor nonadapted malnutrition . [ Note: Edema results from inadequate blood proteins, especially albumin, decreasing oncotic pressure and allowing fl uid leakage from vessels.] In contrast, marasmus occurs when the caloric deprivation is relatively greater than the reduction in protein. Insulin levels are low and degradative pathways are activated, making essential amino acids avail-able for protein synthesis. Muscle wasting and emaciation are seen. Edema is not present.
In developed countries, PEM is most commonly seen in patients with decreased appetite, alterations in how nutrients are digested or absorbed, and major trauma and infections. It can also be seen in elderly individuals who are malnourished. Treatment may include IV ( parenteral ) or tube-based ( enteral ) nutrient administration.
Normal or decreased Markedly decreased
Present Absent
Irritable when picked up; apathetic when left alone Alert, irritable
Weight for height
Edema
Mood
Appetite Poor Good
Weight for age(% expected) 60–80 <60
CHARACTERISTIC KWASHIORKOR MARASMUS
Ferrier_Unit05.indd 322Ferrier_Unit05.indd 322 5/2/14 7:43 PM5/2/14 7:43 PM
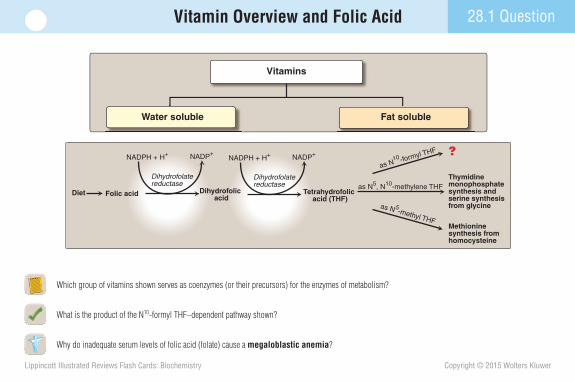
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.1 QuestionVitamin Overview and Folic Acid
Which group of vitamins shown serves as coenzymes (or their precursors) for the enzymes of metabolism?
What is the product of the N 10 -formyl THF–dependent pathway shown?
Why do inadequate serum levels of folic acid (folate) cause a megaloblastic anemia ?
Diet Folic acid
?
Methioninesynthesis from homocysteine
Thymidinemonophosphate synthesis and serine synthesis from glycine
Dihydrofolatereductase
NADPH + H+ NADP+
Dihydrofolatereductase
NADPH + H+ NADP+
Dihydrofolic acid
Tetrahydrofolic acid (THF)
as N10 -formyl THF
as N 5-methyl THF
as N5, N10-methylene THF
Vitamins
Water soluble Fat soluble
Ferrier_Unit05.indd 323Ferrier_Unit05.indd 323 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.1 Answer Vitamin Overview and Folic Acid
The water-soluble vitamins ( B complex � C ) are coenzymes (or their precursors). With the exception of vitamin B 12 , they are not stored.
Two molecules of N 10 -formyl THF are required as one-carbon donors in construction of the purine ring in purine nucleotide de novo synthesis.
Defi ciency of water-soluble folate can be caused by increased demand (in pregnancy); decreased absorption (in alcoholism); and treatment with the DHFR inhibitor methotrexate , which increases folate excretion by preventing conversion to THF (shown). Folate defi ciency results in megaloblastic anemia because decreased purine nucleotide and dTMP synthesis impairs cell division but allows cell growth. The result is production of fewer, larger than normal RBC precursors. [ Note: Women of childbearing age are advised to consume 0.4 mg/day of folate to reduce neural tube defect incidence.]
Diet Folic acid
Purinesynthesis
Methioninesynthesis from homocysteine
Thymidinemonophosphate synthesis and serine synthesis from glycine
Dihydrofolatereductase
NADPH + H+ NADP+
Methotrexate
-
Dihydrofolatereductase
NADPH + H+ NADP+
Methotrexate
-
Dihydrofolic acid
Tetrahydrofolic acid (THF)
as N10 -formyl THF
as N 5-methyl THF
as N5, N10-methylene THF
Dihydrofolate reductase is competitively inhibited by methotrexate, a folic acid analogue used to treat psoriasis, rheumatoid arthritis, and neoplastic diseases.
Vitamins
Water soluble Fat soluble
Ferrier_Unit05.indd 324Ferrier_Unit05.indd 324 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.2 QuestionVitamin B12 (Cobalamin)
What form of vitamin B 12 is required as the coenzyme for the mutase reaction shown?
What is the “folate trap,” and why does it lead to impaired DNA synthesis and cell division?
Follow-up blood tests on a patient with megaloblastic anemia reveal antiparietal cell Abs. What is the likely diagnosis?
Succinyl CoA
Methylmalonyl CoA
C
H2C
COO–
CoA
CH2
O
C
H3C
COO–
CoA
O
C H
Methylmalonyl CoAmutase
Odd-numbered fatty acidsSome amino acids
Ferrier_Unit05.indd 325Ferrier_Unit05.indd 325 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.2 Answer Vitamin B12 (Cobalamin)
Deoxyadenosylcobalamin is required to isomerize methylmalonyl CoA to succinyl CoA. Consequently, methylmalonic acid levels rise with B 12 defi ciency.
The “ folate trap ” links vitamin B 12 with folate. N 5 -methyl THF is the methyl group donor and B 12 is the initial acceptor (becoming methylcobalamin ) in the remethylation of Hcy to Met (shown). Because this is the only reaction in which THF carries and donates a methyl group, B 12 defi ciency will trap THF in a form that cannot be used in other reactions, preventing the N 10 -formyl THF formation required for purine synthesis and the N 5 ,N 10 -methylene THF required for dTMP synthesis. Consequently, DNA synthesis and cell division are impaired. Hcy levels rise with B 12 defi ciency.
Megaloblastic anemia with antiparietal cell Abs is diagnostic for pernicious anemia . B 12 absorption by mucosal cells of the ileum requires IF , a glycoprotein made by gastric parietal cells. Autoimmune destruction of these cells prevents IF synthesis and, consequently, B 12 absorption, thereby causing pernicious anemia. [ Note: Pernicious anemia also manifests with CNS effects if the disease is untreated. Because folate supplementation can mask B 12 defi ciency, thereby delaying diagnosis, the megaloblastic anemia is treated with both vitamins until the cause is determined.]
MethionineTetrahydrofolate
N5-Methyl-tetrahydrofolate
Homocysteine
Succinyl CoA
Methylmalonyl CoA
C
H2C
COO–
CoA
CH2
O
C
H3C
COO–
CoA
O
C H
Vitamin B12(deoxyadenosyl-
cobalamin)
Methylmalonyl CoAmutase
Vitamin B12(methyl-
cobalamin)
Odd-numbered fatty acidsSome amino acids
Methionine synthase
Ferrier_Unit05.indd 326Ferrier_Unit05.indd 326 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.3 QuestionVitamins B1, B6, and C
In what types of reactions does TPP (generated from thiamine, as shown) serve as a coenzyme?
How is thiamine (vitamin B1) defi ciency diagnosed?
What is the biologically active form of vitamin B 6 (pyridoxine)?
What syndrome is endemic in regions that rely on polished rice as a main staple in their diet?
Why might vitamin C (ascorbic acid) defi ciency result in defective connective tissue?
ATP
AMP
Thiamine
Thiamine pyrophosphate
CH3
NH2H
CH3
OP O–OOP O–OO–
CH3
NH2H
CH3
OH
Reactive carbon
N
N
S
N
N
S
N+
N+
Ferrier_Unit05.indd 327Ferrier_Unit05.indd 327 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.3 Answer Vitamins B1, B6, and C
TPP is the coenzyme in the transfer of a two-carbon unit (by transketolase [panel A]) and the oxidative decarboxylation of � -keto acids by PDH and � -KGD (panel B). [ Note: BCKD also requires TPP.]
Thiamine defi ciency can be diagnosed by an increase in RBC transketolase activity upon TPP addition.
The biologically active form of vitamin B 6 ( pyridoxine ) is PLP , a coenzyme in most reactions involving amino acids. [ Note: Aromatic amino acid hydroxylases require THB, not PLP.] Vitamin B 6 is the only water-soluble vitamin to show toxicity ( sensory neuropathy ) in excess.
Beriberi , endemic where polished rice is a dietary staple, is a severe thiamine-defi ciency syndrome characterized by neurologic and cardiac dysfunction. In the United States, thiamine ( vitamin B 1 ) defi ciency is seen primarily with chronic alcoholism and its associated decreased intake or absorption of the vitamin. Wernicke-Korsakoff syndrome , characterized by confusion, ataxia, nystagmus, memory loss, and hallucinations, may develop.
Vitamin C ( ascorbic acid ) defi ciency may result in scurvy , a connective tissue disease, because it is the coenzyme for prolyl and lysyl hydroxylase , enzymes that contribute to the tensile strength of collagen , a fi brous ECM protein.
Ribose 5-P
Pyruvate
Acetyl CoA
Glyceraldehyde 3-P
Citrate
Isocitrate
α-Ketoglutarate
CO
Succinyl CoASuccinate
Oxaloacetate
Malate
Fumarate
2
Xylulose 5-P
Sedoheptulose 7-P
CO2
CO2
Trans-ketolase
Pyruvatedehydrogenase
α-Ketoglutaratedehydrogenase
TPP
TPP
TPP
A
B
Ferrier_Unit05.indd 328Ferrier_Unit05.indd 328 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.4 QuestionVitamins B2, B3, and Biotin
What are the precursors for NAD � (shown), a coenzyme in many oxidation-reduction reactions?
What are the biologically active forms of vitamin B 2 (ribofl avin)? What general name is given to proteins that bind these active, coenzyme forms?
What nutritional defi ciency disease results from inadequate vitamin B3 (niacin) intake? Why might niacin be included in the treatment of familial combined (type IIb) hyperlipidemia in which both VLDL and LDL are elevated?
Why does a biotin cycle defect result in multiple carboxylase defi ciency ? O
HO
NAD+
O
HO OH
N+
H O
N
N N
N
NH2
O
PO O–
O
PO O–
O
OH
NH2
Ferrier_Unit05.indd 329Ferrier_Unit05.indd 329 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.4 Answer Vitamins B2, B3, and Biotin
The precursors of NAD � are vitamin B 3 ( niacin or nicotinic acid ), nicotinamide (which gets deaminated), and Trp (which gets metabolized to quinolinate ). However, Trp conversion to NAD� is ineffi cient. [ Note: NAD � can be phosphorylated to NADP � , and the oxidized forms reduced.]
The active, coenzyme forms of vitamin B 2 ( ribofl avin ) are FMN(H 2 ) and FAD(H 2 ) . They are prosthetic groups in fl avoprotein dehydrogenases such as NADH dehydrogenase (contains FMN) of the ETC and succinate dehydrogenase (FAD) of the ETC and the TCA cycle.
Inadequate niacin intake results in pellagra , a nutritional disorder characterized by the four Ds: diarrhea , derma-titis , dementia , and (if untreated) death . Niacin is use-ful in type IIb hyperlipidemia treatment because high doses (100 times the RDA) strongly inhibit adipose lipoly-sis, which reduces FFA availability for use in the hepatic synthesis of TAGs and, therefore, results in decreased VLDL synthesis (and, consequently, LDL production). [ Note: Niacin decreases Lp(a) and increases HDL.]
A biotin cycle defect results in multiple carboxylase defi ciency because of an inability to add biotin (by holocarboxylase synthetase ) during carboxylase synthesis or remove it (by biotinidase ) during degradation. Dermatologic and neurologic signs are characteristic. Biotin supplementation is the treatment.
O
HO
NAD+
O
HO OH
N+
H O
N
N N
N
NH2
O
PO O–
O
PO O–
O
OH
NH2
Tryptophan
Nicotinamide
Niacin(nicotinic acid)
+NH
+NH
O–C
O
NH2C
O
Quinolinate
Ferrier_Unit05.indd 330Ferrier_Unit05.indd 330 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.5 QuestionFat-Soluble Vitamin A
Which of the retinoids shown is required for vision? Which mediates the other actions of vitamin A?
How does retinoic acid (RA) lead to changes in gene expression?
How are the effects of vitamin A defi ciency related to keratin, a fi brous protein that helps to prevent moisture loss in epithelia?
OC
11-cis Retinal(formed by photoisomerization
of all-trans retinal)
OC
Retinol
Retinal
Retinoic acid(all trans)
OHCH2
OH
CH
O
H
Ferrier_Unit05.indd 331Ferrier_Unit05.indd 331 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.5 Answer Fat-Soluble Vitamin A
Retinal derived from retinol ( vitamin A ) oxidation is required for vision. The 11-cis form bound to the protein opsin forms rhodopsin , which, when bleached by light, triggers a nerve impulse from the optic nerve to the brain. Consequently, an early sign of defi ciency is night blindness . Prolonged defi ciency leads to an irreversible loss of visual cells. RA (from retinal oxidation) mediates other actions of the vitamin (e.g., epithelial tissue maintenance). [ Note: � -Carotene from plants can be cleaved to two molecules of vitamin A. The conversion is ineffi cient in humans, and most of our need is met by preformed vitamin A from animal sources.]
RA binds to a nuclear receptor (the RAR ) that functions as a STF. The RA–RAR complex binds to REs on DNA and alters expression of retinoid-responsive genes (e.g., the gene for keratin). The RAR is part of a family of nuclear receptors that includes those for steroid and thyroid hormones and calcitriol .
Expression of the gene for keratin is inhibited by vitamin A. Consequently, with vitamin A defi ciency, excess keratin is made, which can cause xerophthalmia (pathologic dryness of corneal epithelium) that can lead to blindness. [ Note: With excess vitamin A, a toxicity syndrome (hypervitaminosis A) can develop. In the chronic form, skin and hair are affected as a result of decreased keratin synthesis.]
OC
11-cis Retinal(formed by photoisomerization
of all-trans retinal)
OC
Retinol
Retinal
Retinoic acid(all trans)
OHCH2
OH
CH
O
H
Ferrier_Unit05.indd 332Ferrier_Unit05.indd 332 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.6 QuestionFat-Soluble Vitamin D
In addition to the preformed dietary precursors of active vitamin D shown, how else do humans obtain a precursor?
How and where is the active form of vitamin D generated? How is the process regulated?
What is the primary function of vitamin D?
What causes rickets and what are its effects?
Cholecalciferol (animals)
HO
H2C
C CH2 CH2 CH2 CHCH3
CH3
HCH3
Diet
Ergocalciferol (plants)HO
H2C
C CH CH CH CHCH3
CH3
HCH3
H3C
H3C
CH3
Ferrier_Unit05.indd 333Ferrier_Unit05.indd 333 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
28.6 Answer Fat-Soluble Vitamin D
Humans can synthesize the cholecalciferol ( vitamin D 3 ) precursor of active vitamin D from 7-dehydrocholesterol (an intermediate in cholesterol synthesis) in skin exposed to sunlight.
The active form of vitamin D ( calcitriol ) is produced from cholecalciferol by two sequential hydroxylation reactions: (1) hepatic 25-hydroxylase produces 25-OH-D 3 ( calcidiol ), the predominant form of vitamin D in the plasma and the major storage form; and (2) renal 25-hydroxycalciferol 1-hydroxylase produces 1,25-diOH-D 3 (calcitriol). 1-Hydroxylase activity is tightly regulated by plasma phosphate and Ca 2 � levels. Low phosphate stimulates the enzyme directly, and low Ca 2 � stimulates it indirectly through direct stimulation of PTH secretion. PTH upregulates 1-hydroxylase expression.
The primary function of 1,25-diOH-D 3 is to maintain adequate plasma levels of Ca 2 � . When blood Ca 2 � is low, it increases Ca 2 � uptake by the intestine, minimizes Ca 2 � loss by increasing renal reabsorption, and stimulates bone resorption (demineralization).
Vitamin D defi ciency impairs intestinal uptake of Ca 2 � causing net bone demineralization and resulting in nutritional rickets in children and osteomalacia in adults. Incomplete collagen mineralization results in soft, pliable bones. Insuffi cient exposure to sunlight is a risk factor for defi ciency. [ Note: Human milk is low in vitamin D.]
Synthesis in skin
7-Dehydrocholesterol
HO
H3C
H3CC CH2 CH2 CH2 CH
CH3
CH3
HCH3
Cholecalciferol
HO
H2C
C CH2 CH2 CH2 CHCH3
CH3
HCH3
Diet
ErgocalciferolHO
H2C
C CH CH CH CHCH3
CH3
HCH3
H3C
H3C
CH3
Ferrier_Unit05.indd 334Ferrier_Unit05.indd 334 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Vitamin Functions Summary Card
VITAMIN OTHER NAMES ACTIVE FORM FUNCTION
Folic acid
WATER SOLUBLE
FAT SOLUBLE
Vitamin B12
Vitamin C
Vitamin B6
Vitamin B1
Niacin
Vitamin B2
Biotin
Pantothenic acid
Vitamin A
Vitamin D
Vitamin K
Vitamin E
—
Cobalamin
Ascorbic acid
Pyridoxine, Pyridoxamine,PyridoxalThiamine
Riboflavin
Nicotinic acidNicotinamide
—
—
Retinol, RetinalRetinoic acida-Carotene
CholecalciferolErgocalciferol
Menadione, Menaquinone,Phylloquinone
`-Tocopherol
Transfer one-carbon units; synthesis of methionine, purines,and thymidine monophosphate
Coenzyme for reactions: Homocysteine → methionineMethylmalonyl CoA → succinyl CoA
AntioxidantCoenzyme for hydroxylation reactions, for example: In procollagen:Proline → hydroxyproline, Lysine → hydroxylysine
Coenzyme for enzymes, particularly in amino acid metabolism
Coenzyme of enzymes catalyzing:Pyruvate → acetyl CoA `-Ketoglutarate → Succinyl CoARibose 5-P + xylulose 5-P → Sedoheptulose 7-P + Glyceraldehyde 3-PBranched-chain `-keto acid oxidationElectron transfer
Electron transfer
Carboxylation reactions
Acyl carrier
Maintenance of reproduction, VisionPromotion of growth Differentiation and maintenanceof epithelial tissues, Gene expression
Calcium uptakeGene expression
f-Carboxylation of glutamate residues in clotting and other proteins
Antioxidant
Tetrahydrofolic acid
MethylcobalaminDeoxyadenosyl cobalamin
Ascorbic acid
Pyridoxal phosphate
Thiamine pyrophosphate
NAD+, NADP+
FMN, FAD
Enzyme-bound biotin
Coenzyme A
RetinolRetinalRetinoic acid
1,25-Dihydroxychole-calciferol
Menadione, Menaquinone,Phylloquinon
Any of severaltocopherol derivatives
Ferrier_Unit05.indd 335Ferrier_Unit05.indd 335 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Vitamin Defi ciencies and Toxicities Summary Card
DEFICIENCY SIGNS AND SYMPTOMS TOXICITY
InfertilityNight blindnessRetardation of growthXerophthalmia
Megaloblastic anemiaNeural tube defects
Pernicious anemia, Dementia,Spinal degeneration
Scurvy
Rare
BeriberiWernicke-Korsakoff syndrome (most commonin alcoholics)
Pellagra
Rare
Rare
Rare
Rare
Rickets (in children)Osteomalacia (in adults)
Newborn Rare in adults
AnemiaBirth defects
GlossitisNeuropathy
Megaloblastic anemiaNeuropsychiatric symptoms
Sore, spongy gums, Loose teeth, Poor wound healing
Tachycardia, vomiting, convulsionsApathy, loss of memory, dysregulated eye movements
Dermatitis, Diarrhea, Dementia
Dermatitis, Angular stomatitis
—
—
Increased visual threshold, Dryness of cornea
Soft, pliable bones
Bleeding
Red blood cell fragility leads to hemolytic anemia
None
None
None
Yes
None
None
None
None
None
Yes
Yes
Rare
None
VITAMIN
Folic acid
Vitamin B12
Vitamin C
Vitamin B6
Vitamin B1
Niacin
Vitamin B2
Biotin
Pantothenic acid
Vitamin A
Vitamin D
Vitamin K
Vitamin E
Ferrier_Unit05.indd 336Ferrier_Unit05.indd 336 5/2/14 7:43 PM5/2/14 7:43 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
29.1 QuestionDNA Structure
What type of bond links the dNMP monomers in each polymeric strand of the dsDNA molecule shown? What holds the strands together?
By convention, which strand of DNA is this: TTAGCCG? What dNMP is at the 5 � -end of the sequence?
What is the functional signifi cance of A- and T-rich DNA compared to G- and C-rich DNA?
A = T
C = G
C = G
T = A
G = C
A = T
T = A
C = G
A = T
G = C
T = A
C = G
Base pairs areperpendicular to the
helical axisMinor
groove
Majorgroove
Helical axis
5'-End
3'-End5'-End
Deoxyribose–phosphatebackbone
3'-End
Ferrier_Unit06.indd 337Ferrier_Unit06.indd 337 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
29.1 Answer DNA Structure
The dNMP monomers are linked by 3 � →5 � phosphodiester bonds that join the 3 � -OH group of the deoxyribose of one dNMP to the 5 � -OH group of the adjacent dNMP through a phosphoryl group. The comple-mentary and antiparallel strands are held by H-bonds between the AT and GC bps and by hydrophobic interactions between the stacked bases.
By convention, (1) if only one strand of dsDNA is shown, it is the coding strand, and (2) a nucleic acid sequence is written 5 � to 3 � , making T (dTMP) the 5 � -end of the TTAGCCG sequence.
AT bps are held together by two H-bonds , whereas GC bps are held by three. Consequently, AT pairs denature (“melt”) at a lower temperature than do GC pairs. [ Note: The site where DNA synthesis begins (the origin of replication) is rich in AT bps to allow the strands of the double helix to separate. Separation is maintained at the origin by SSB protein.]
A = T
C = G
C = G
T = A
G = C
A = T
T = A
C = G
A = T
G = C
T = A
C = G
Base pairs areperpendicular to the
helical axisMinor
groove
Majorgroove
Helical axis
5'-End
3'-End5'-End
Deoxyribose–phosphatebackbone
3'-End
Ferrier_Unit06.indd 338Ferrier_Unit06.indd 338 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
29.2 QuestionProkaryotic Replication
Use the fi gure to list the order in which the following enzymes of prokaryotic replication function: DNA pol I , DNA pol III , helicase , ligase , primase , and topoisomerase.
Describe the function of each of the listed enzymes.
What is the clinical signifi cance of DNA gyrase inhibitors?
DNA helicase
DNA polymerase
Primase
Single-stranded DNA-binding proteins (SSB)
Leading strand template
Newly synthesized strand
ParentalDNA helix
3'
5'
3'
3'
5'
5'
3'
Laggingstrandtemplate
RNAprimer
RNAprimer
RNAprimer
Newly synthesized DNA
Okazakifragment
3'RNAprimer
Newly synthesized DNA
Okazakifragment
DNA polymerase III recognizes the RNAprimer and begins to synthesize DNA.
Topoisomerase
Ferrier_Unit06.indd 339Ferrier_Unit06.indd 339 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
29.2 Answer Prokaryotic Replication
The order is: 1. helicase 2. topoisomerase 3. primase 4. DNA pol III 5. DNA pol I 6. ligase
Helicase unwinds dsDNA, and topoisomerases relieve the supercoiling created by unwinding via the cutting and rejoining of one strand (by topoisomerase I ) or both (by II ). Primase makes the RNA primer , then DNA pol III (a processive enzyme) elongates the primer with DNA ( 5 � →3 � polymerase activity) and removes errors ( proofreading 3 � →5 � exonuclease activity). DNA pol I removes the primer ( 5 � →3 � exonuclease activity), replaces it with DNA, and proofreads. Ligase joins the DNA made by pol I and pol III on the lagging strand, which is synthesized discontinuously (as Okazaki fragments ) in the 5 � →3 � direction (away from the replication fork). [ Note: Replication is semiconservative because one parental strand is retained in each new duplex.]
Fluoroquinolones are drugs that inhibit DNA gyrase (a bacterial topoisomerase II). They prevent the ATP-dependent neutralization of positive supercoils by gyrase , thereby inhibiting bacterial replication and causing bacterial death.
DNA helicase
DNA polymerase
Primase
Single-stranded DNA-binding proteins (SSB)
Leading strand template
Newly synthesized strand
ParentalDNA helix
3'
5'
3'
3'
5'
5'
3'
Laggingstrandtemplate
RNAprimer
RNAprimer
RNAprimer
Newly synthesized DNA
Okazakifragment
3'RNAprimer
Newly synthesized DNA
Okazakifragment
DNA polymerase III recognizes the RNAprimer and begins to synthesize DNA.
Topoisomerase
Ferrier_Unit06.indd 340Ferrier_Unit06.indd 340 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
29.3 QuestionEukaryotic Replication
Which one of the high-fi delity eukaryotic DNA pols shown initiates replication of eukaryotic nuclear DNA? Which one is recruited to elongate the leading strand? Which one replicates mtDNA?
In what phase of the eukaryotic cell cycle does scheduled replication occur?
Why is 2 � ,3 � -dideoxyinosine used in HIV infection treatment?
Pol α(alpha)
Pol β(beta)
Pol γ(gamma)
Pol δ(delta)
Pol ε(epsilon)
–
–
+
+
+
POLY-MERASE
PROOF-READING
Ferrier_Unit06.indd 341Ferrier_Unit06.indd 341 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
29.3 Answer Eukaryotic Replication
DNA pol � is a multisubunit, multifunctional enzyme that makes the RNA primer required for DNA synthesis and extends the primer with dNMPs. DNA pol � further extends the DNA on the leading strand. DNA pol � replicates mtDNA.
Scheduled DNA synthesis (in which the entire genome is replicated) occurs in the S phase (synthesis phase) of the eukaryotic cell cycle shown. [ Note: Unscheduled replication to fi ll in gaps occurs as part of DNA repair.]
2 � ,3 � -Dideoxyinosine ( ddI ), a purine nucleoside analog, is converted to ddATP in the cell. Because replication requires a 3 � -OH group for the formation of a 3 � →5 � phosphodiester bond with the incoming dNTP, absence of this group in a dideoxynucleotide terminates replication by HIV’s reverse transcriptase . [ Note: Dideoxynucleotides are also used in sequencing DNA.]
Pol α(alpha)
Pol β(beta)
Pol γ(gamma)
Pol δ(delta)
Pol ε(epsilon)
• Contains primase
• Initiates DNA synthesis
• Repair
• Replicates mitochondrial DNA
• Elongates Okazaki fragments of the lagging strand
• Elongates the leading strand
–
–
+
+
+
POLY-MERASE FUNCTION
PROOF-READING
Mitosis
Gap 1
Gap 2
DNAsynthesis
M
G2
G0
S
G1
Ferrier_Unit06.indd 342Ferrier_Unit06.indd 342 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Eukaryotic Replication 29.4 Question
What is the function of the 3�-UCCCAA-5� sequence shown as part of telomerase ? What are telomeres?
What is the basic structural unit of eukaryotic chromatin?
What is epigenetics?
New telomere repeat
Telomerase
?
5'3'5'
AGGGTT AGGGTT AGGGTT AGGGTT
TCCCAA
3'
UCCCAA
Ferrier_Unit06.indd 343Ferrier_Unit06.indd 343 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
29.4 Answer Eukaryotic Replication
The 3�-UCCCAA-5� sequence is the RNA template used to synthesize telomeric DNA , which consists of tandem repeats of the noncoding hexameric sequence AGGGTT. The RNA is a component of telomerase and is used by the enzymatic component (a reverse transcriptase ) to synthesize DNA in the 5 � →3 � direction. Telomeres are complexes of DNA and proteins that protect the ends of linear chromosomes. They normally shorten with each cell division, causing the cell to either senesce or apoptose, because most cells do not express telomerase. [Note: In some cells (e.g., cancer cells), telomerase expression allows unlimited division.]
The basic structural unit of eukaryotic chromatin is the nucleosome in which DNA is wound nearly twice around an octameric core of basic histone (H) proteins. Nucleosomes are joined by linker DNA bound by H1.
Epigenetics refers to heritable changes in gene expression without altering the nucleotide sequence of DNA. It includes covalent modifi cations to chromatin (e.g., the methylation of C in DNA, which decreases expression, and the acetylation of Lys in histones, which increases expression) and nucleosome repositioning. [ Note: Epigenetic changes have been linked to cancer (e.g., through silencing of tumor suppressor genes).]
New telomere repeat
Telomerase
RNA template
5'3'5'
AGGGTT AGGGTT AGGGTT AGGGTT
TCCCAA
3'
UCCCAA
Telomeraseextends the3'-end ofthe DNA.
Nucleosome core(H2A, H2B, H3, H4) 2
Linker DNA
H1
DNA
Ferrier_Unit06.indd 344Ferrier_Unit06.indd 344 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
29.5 QuestionDNA Repair
In BER of the deamination of C to U, what enzyme removes U?
In prokaryotic MMR, how is the “correct” strand identifi ed?
What two systems are used in the repair of ds breaks in DNA?
What unique DNA lesion is caused by UV radiation? What process repairs the lesion? Inability to perform this repair results in what rare genetic disease?
3'
5'
5'
3'
NH3
Spontaneousdeamination
3'
5'
5'
3'
U?
3'
5'
5'
3'
T G C A G T G
A C G T U A C
T G C A G T G
A C G T A C
T G C A G T G
A C G T C A C
Ferrier_Unit06.indd 345Ferrier_Unit06.indd 345 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
DNA Repair29.5 Answer
In BER , uracil N-glycosylase removes U by cleaving the glycosidic bond between the base and the phosphorylated sugar of the nucleotide. An endonuclease and a lyase remove the sugar, creating an AP site. DNA pol and ligase complete the repair process. [ Note: If not repaired, U will pair with A (rather than the correct CG pairing) in the next round of replication, causing a permanent change in DNA sequence (a mutation).]
In prokaryotic MMR , the degree of methylation identifi es the “correct” strand. The parental strand is more highly methyl-ated than the daughter strand immediately after replication and is assumed to be the correct strand. [ Note: Mutations to human MMR proteins result in hereditary nonpolyposis colorectal cancer ( HNPCC ).]
NHEJ and HR are two systems used in the repair of ds breaks in DNA. NHEJ is error prone because DNA lost in the process is not replaced.
UV radiation causes pyrimidine dimers , unique DNA lesions repaired by NER . [ Note: NER differs from BER in that an oligonucleotide, not just a single nucleotide, is removed.] Xeroderma pigmentosum ( XP ) is the disease caused by an inability to repair these dimers due to defects in any of several XP proteins required for NER. With XP, early and numerous skin cancers result (shown).
3'
5'
5'
3'
NH3
Spontaneousdeamination
3'
5'
5'
3'
UUracil-N-glycosylase
3'
5'
5'
3'
T G C A G T G
A C G T U A C
T G C A G T G
A C G T A C
T G C A G T G
A C G T C A C
Ferrier_Unit06.indd 346Ferrier_Unit06.indd 346 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
30.1 QuestionRNA
Which of the RNAs shown: 1. accounts for the largest percentage of cellular RNA? 2. carries amino acids to ribosomes? 3. is extensively modifi ed only in eukaryotes? 4. contains a high percentage of modifi ed bases? 5. is a ribozyme in translation? 6. contains extensive intrachain base-pairing?
Why is prokaryotic mRNA described as “polycistronic”?
How does RNA differ from DNA?
me-7Gppp pApApA?
Ribosome
?
DNA
?
28S5S
5.8S
18S
TRANSCRIPTION
Ferrier_Unit06.indd 347Ferrier_Unit06.indd 347 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
30.1 Answer RNA
1. rRNA accounts for the largest percentage of cellular RNA. 2. tRNA carries amino acids (bound to the 3 � -A) to ribosomes. 3. mRNA is extensively modifi ed only in eukaryotes. 4. tRNA contains a high percentage of unusual bases (e.g., dihydrouracil and pseudouracil ). 5. rRNA of the large ribosomal subunit is a ribozyme (RNA with catalytic activity) in translation and
forms the peptide bond between amino acids. 6. tRNA contains extensive intrachain base-pairing that leads to a characteristic secondary structure
( cloverleaf ).
Prokaryotic mRNA is polycistronic because it encodes more than one gene (or cistron ). [ Note: Eukaryotic mRNA is monocistronic.]
RNA differs from DNA in that it is smaller, contains ribose (not deoxyribose) and U (not T), and is single stranded. Its synthesis is selective (not “all or none”). [ Note: RNA is like DNA in that it is an unbranched polymer of NMPs linked by 3 � →5 � phosphodiester bonds, synthesized in the 5 � →3 � direction.]
me-7Gppp pApApAmRNA
Ribosome
tRNA
DNA
rRNA
28S5S
5.8S
18S
TRANSCRIPTION
Ferrier_Unit06.indd 348Ferrier_Unit06.indd 348 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
30.2 QuestionProkaryotic Transcription
How does prokaryotic RNA pol recognize and bind the appropriate region of DNA to initiate transcription, as shown? Is a primer required in transcription?
What is a “consensus sequence?”
What is the transcription product (conventionally shown) of the sequence TAGC (also conventionally shown)?
Individuals with tuberculosis are typically treated with a multidrug regimen that includes rifampin. How does rifampin work?
RNA polymerase
Template strand
RNA–DNA hybrid helix
Nontemplate strand
Negative supercoils
RNA
Positive supercoils
5'
3'
ase Po
3'
3'-End of RNA being elongated
Ferrier_Unit06.indd 349Ferrier_Unit06.indd 349 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
30.2 Answer Prokaryotic Transcription
Prokaryotic RNA pol initiates transcription through the binding of its � (sigma) subunit to consensus sequences within an untranscribed region of DNA known as the promoter . The Pribnow box (TATAAT), located upstream (toward the 5 � -end) of the transcription start site, is an example. RNA pol does not require a primer and does not appear to have 3 � →5 � exonuclease activity (proofreading).
A consensus sequence is one in which the nucleotide base shown is the one most frequently encountered at that position (e.g., TATAAT).
The product of the transcription of TAGC is UAGC. By convention, if only one strand of DNA is shown, it is the coding strand and is written 5 � to 3 � . The RNA product of transcription is identical to the coding strand, with U replacing T, and is written 5 � to 3 � .
Rifampin binds the � subunit of prokaryotic RNA pol , preventing chain extension beyond three nucleotides, thus having a bactericidal effect . [ Note: The core RNA pol contains 5 subunits: 2 � and 1 � (enzyme assembly), 1 � � (template binding), and 1 � (5 � →3 � polymerase activity). Addition of � forms the holoenzyme.]
RNA polymerase
Template strand
RNA–DNA hybrid helix
Nontemplate strand
Negative supercoils
RNA
Positive supercoils
5'
3'
ase Po
3'
3'-End of RNA being elongated
Ferrier_Unit06.indd 350Ferrier_Unit06.indd 350 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
30.3 QuestionProkaryotic Transcription
Which step in transcription is facilitated by formation of the hairpin structure shown? How else can this step be facilitated in prokaryotes?
What is the signifi cance of PP i formation in replication and transcription?
A 23-year-old man, recently diagnosed with testicular cancer , is started on a drug regimen that includes dactinomycin (actinomycin D). Why is this drug cytotoxic?
Hairpin
AGCCCGCNN
NNNGC
GGG
CU
UU U
Ferrier_Unit06.indd 351Ferrier_Unit06.indd 351 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Prokaryotic Transcription30.3 Answer
Transcription termination is facilitated by the hairpin structure (GC-rich stem � loop) formed when a sequence in the DNA template generates a self-complementary sequence in the nascent RNA. Just beyond the hairpin, a series of Us weakly base-pair to As in the template, facilitating separation of the DNA and RNA. This intrinsic termination is the norm. Termination can also be facilitated by bifunctional rho protein that binds to and moves along the RNA ( ATPase activity). When rho reaches RNA pol paused at the termination site, it separates the DNA–RNA hybrid helix ( helicase activity). [Note: Termination in eukaryotes is RNA pol-dependent. Pol II termination of mRNA transcription is linked to 3�-end polyadenylation.]
The PP i formed in replication and transcription is hydrolyzed to 2 P i by pyrophosphatase . The loss of product drives polymerization in the forward direction, making it essentially irreversible. This is a common theme in biochemistry.
Dactinomycin ( actinomycin D ) has antibiotic and anti-tumor activity. It intercalates between CG bps in DNA and interferes with the movement of RNA pol in both prokaryotes and eukaryotes. Because of its high cytotoxicity, dactinomycin is not used clinically as an antibiotic but is used to treat a variety of cancers.
Hairpin
AGCCCGCNNNNNGC
GGG
CU
UU U
CGCNNNNNGGGGGGGCGGGGG
Newly synthesized RNA folds to form a“hairpin” that is important in chain termination.
Ferrier_Unit06.indd 352Ferrier_Unit06.indd 352 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
30.4 QuestionEukaryotic Transcription
What role do the reactions shown play in eukaryotic transcription?
What is the function of RNA pol II ?
Based on the description below, does the cortisol receptor–cortisol complex function as a GTF or a STF?
The cortisol receptor is a trans-acting protein that functions as a transcriptional activator. It contains a hormone-binding domain, a DNA-binding domain that interacts with cis-acting consensus sequences in a promoter or an enhancer, and a transcription-activation domain that recruits other proteins (such as the GTFs and co-activators) to the DNA, forming a multiprotein complex that facilitates transcription initiation of cortisol-responsive genes (e.g., PEPCK of gluconeogenesis).
CN C
O
CH2
CH2 HAT
HDAC
CH2
CH2
NH 3+
CHH CN C
O
CH2
CH2
CH2
3
CH2
NH
C
C O
CH
HH
Ferrier_Unit06.indd 353Ferrier_Unit06.indd 353 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Eukaryotic Transcription30.4 Answer
The reactions shown covalently modify specifi c Lys residues in the histone components of eukaryotic chromatin. HAT acetylates Lys and eliminates its positive charge, thereby decreasing the strength of the interactions between histones and negatively charged DNA. This decondenses the chromatin, allowing access to DNA for transcription. HAT, then, is a co-activator. HDAC deacetylates Lys and favors chromatin condensation. [ Note: Decondensed, transcriptionally active chromatin is euchromatin, whereas the condensed, inactive form is heterochromatin.]
RNA pol II synthesizes nuclear pre-mRNA. It also synthesizes some small, noncoding RNAs such as snoRNA (for rRNA processing), snRNA (for mRNA splicing), and miRNA (for RNAi). [ Note: RNA pol I synthesizes rRNA, and RNA pol III synthesizes tRNA and 5S rRNA.]
Based on the description, the cortisol receptor in complex with cortisol, a steroid hormone, functions as a STF [Note: Cortisol mediates the stress response.].
CN C
O
CH2
CH2 HAT
HDAC
CH2
CH2
NH 3+
CHH CN C
O
CH2
CH2
CH2
3
CH2
NH
C
C O
CH
HH
Ferrier_Unit06.indd 354Ferrier_Unit06.indd 354 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
30.5 QuestionEukaryotic Transcription
What are GTFs? What is the function of the GTF TFIID shown?
What is an enhancer?
Why is � -amanitin (a cyclic peptide produced by some mushrooms) toxic to eukaryotic cells? Inr +1
DPE +25
Core promoter elements
TATAbox –25
TFIID(GTF)
Ferrier_Unit06.indd 355Ferrier_Unit06.indd 355 5/2/14 7:52 PM5/2/14 7:52 PM
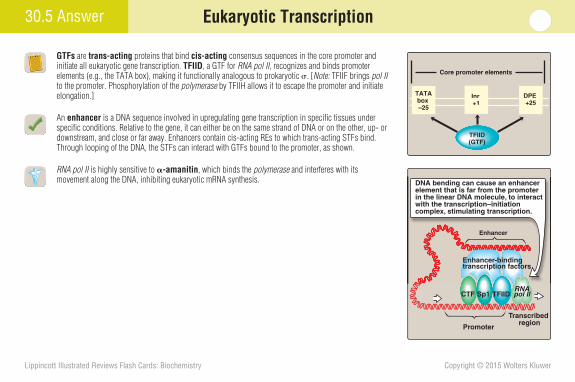
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
30.5 Answer Eukaryotic Transcription
GTFs are trans-acting proteins that bind cis-acting consensus sequences in the core promoter and initiate all eukaryotic gene transcription. TFIID , a GTF for RNA pol II , recognizes and binds promoter elements (e.g., the TATA box), making it functionally analogous to prokaryotic � . [ Note: TFIIF brings pol II to the promoter. Phosphorylation of the polymerase by TFIIH allows it to escape the promoter and initiate elongation.]
An enhancer is a DNA sequence involved in upregulating gene transcription in specifi c tissues under specifi c conditions. Relative to the gene, it can either be on the same strand of DNA or on the other, up- or downstream, and close or far away. Enhancers contain cis-acting REs to which trans-acting STFs bind. Through looping of the DNA, the STFs can interact with GTFs bound to the promoter, as shown.
RNA pol II is highly sensitive to � -amanitin , which binds the polymerase and interferes with its movement along the DNA, inhibiting eukaryotic mRNA synthesis.
Inr +1
DPE +25
Core promoter elements
TATAbox –25
TFIID(GTF)
Transcribed region
Promoter
EnhancerEnhancer
Enhancer-bindingtranscription factors
CTF Sp1 TFIIDRNApol II
DNA bending can cause an enhancer element that is far from the promoter in the linear DNA molecule, to interact with the transcription–initiation complex, stimulating transcription.
Ferrier_Unit06.indd 356Ferrier_Unit06.indd 356 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
30.6 QuestionPosttranscriptional Modifi cations
What four posttranscriptional processing events generate the functional tRNA molecule (whose secondary structure is shown) from the primary tRNA transcript?
What three posttranscriptional processing events convert eukaryotic pre-mRNA to its functional form?
Why do mutations to DNA that change or delete the conserved dinucleotide sequences at the 5 � or 3 � splice site end in the pre-mRNA for a Cu 2 � transporter result in the most severe phenotype of Menkes syndrome ?
OH 3'
C
C
CC
U
C
C
C
U
U
U
GG
G
A
C
G
AA
AAA
A
CC
G
GG G G
AA
AA
CC
G
GG
GA
A
A
5' P
CCCCC
UG
CUUG
C
UU
G
GG G G
A
A
CC
Gm
Gm
CmD
DD D
ψ
ψ
Am
ψD
Ferrier_Unit06.indd 357Ferrier_Unit06.indd 357 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
30.6 Answer Posttranscriptional Modifi cations
A functional tRNA molecule is generated from its primary transcript by (1) removal of nucleotides from the 5 � - and 3 � -ends, (2) addition of CCA (orange boxes) to the new 3 � -end, (3) removal of an intervening sequence from the anticodon loop by endo - and exonucleases , and (4) base modifi cations (yellow boxes).
Eukaryotic pre-mRNA is converted to functional mRNA by (1) addition of a methylated guanosine cap to the 5 � -end via an unusual 5 � →5 � triphosphate link, (2) addition of a polyA tail by polyadenylate polymerase to the 3 � -end created by cleavage just past an AAUAAA sequence, and (3) splicing (removal of noncoding introns and joining of coding [expressed] exons ) by two transesterifi cation reactions mediated by snRNPs of the spliceosome . The fi rst creates a lariat via an unusual 2 � →5 � phosphodiester linkage between the branch site A and the splice donor site G . The second cleaves the lariat and joins adjacent exons via a 3 � →5 � linkage.
Mutations that change or delete the conserved dinucleotide sequences at either the 5 � splice donor (GU) or 3 � splice acceptor (AG) site have severe consequences because they reduce functional mRNA generation and, therefore, its functional protein product such as the intestinal Cu 2 � transporter in Menkes syndrome .
OH 3'
C
C
CC
U
C
C
C
U
U
U
GG
G
A
C
G
AA
AAA
A
CC
G
GG G G
AA
AA
CC
G
GG
GA
A
A
5' P
CCCCC
UG
CUUG
C
UU
G
GG G G
A
A
CC
Gm
Gm
CmD
DD D
ψ
ψ
Am
ψD
pGU AGpA5' 3' EXON 1
INTRON
EXON 2
5' Splice donor site
3' Splice acceptor site
G
Ferrier_Unit06.indd 358Ferrier_Unit06.indd 358 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
31.1 QuestionGenetic Code
The genetic code is a triplet code of four nucleotide bases (U, C, A, and G, as shown). Why do only 61 of the 64 triplets code for amino acids in the translation of mRNA?
What are the three possible consequences of changing a single nucleotide base in the coding region of a mRNA?
Is cystic fi brosis ( CF ) a triplet expansion disease?
U
MIDDLE BASE3'-BASE
U C A GSerSer
TyrTyr
CysCys
5'-BASE
PhePhe
UC
Ferrier_Unit06.indd 359Ferrier_Unit06.indd 359 5/2/14 7:52 PM5/2/14 7:52 PM
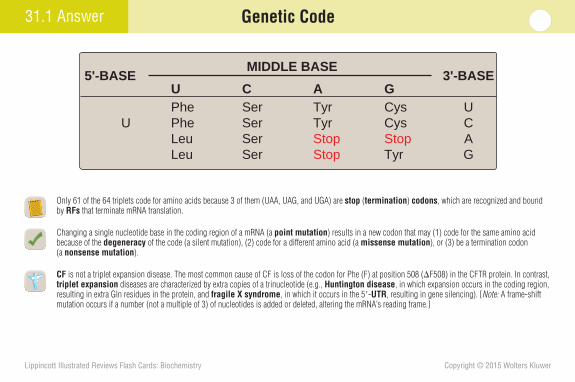
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
31.1 Answer Genetic Code
Only 61 of the 64 triplets code for amino acids because 3 of them (UAA, UAG, and UGA) are stop ( termination ) codons , which are recognized and bound by RFs that terminate mRNA translation.
Changing a single nucleotide base in the coding region of a mRNA (a point mutation ) results in a new codon that may (1) code for the same amino acid because of the degeneracy of the code (a silent mutation), (2) code for a different amino acid (a missense mutation ), or (3) be a termination codon (a nonsense mutation ).
CF is not a triplet expansion disease. The most common cause of CF is loss of the codon for Phe (F) at position 508 ( � F508) in the CFTR protein. In contrast, triplet expansion diseases are characterized by extra copies of a trinucleotide (e.g., Huntington disease , in which expansion occurs in the coding region, resulting in extra Gln residues in the protein, and fragile X syndrome , in which it occurs in the 5 � - UTR , resulting in gene silencing). [ Note: A frame-shift mutation occurs if a number (not a multiple of 3) of nucleotides is added or deleted, altering the mRNA’s reading frame.]
U
MIDDLE BASE3'-BASE
U C A GSerSerSerSer
UCAG
TyrTyrStopStop
CysCysStopTyr
5'-BASE
PhePheLeuLeu
Ferrier_Unit06.indd 360Ferrier_Unit06.indd 360 5/2/14 7:52 PM5/2/14 7:52 PM
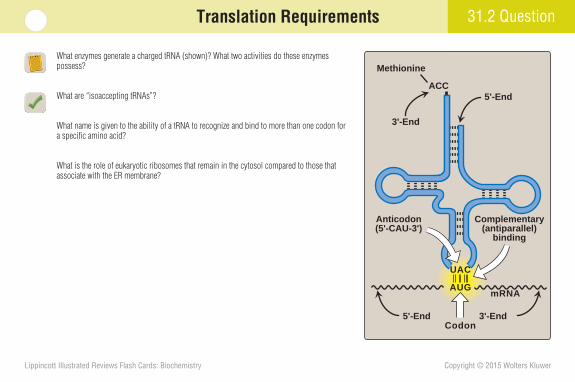
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
31.2 QuestionTranslation Requirements
What enzymes generate a charged tRNA (shown)? What two activities do these enzymes possess?
What are “isoaccepting tRNAs”?
What name is given to the ability of a tRNA to recognize and bind to more than one codon for a specifi c amino acid?
What is the role of eukaryotic ribosomes that remain in the cytosol compared to those that associate with the ER membrane?
5'-End 3'-End
5'-EndACC
3'-End
Methionine
Complementary(antiparallel)
binding
Anticodon(5'-CAU-3')
mRNA
UAC
AUG
Codon
Ferrier_Unit06.indd 361Ferrier_Unit06.indd 361 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
31.2 Answer Translation Requirements
Aminoacyl tRNA synthetases use ATP in the two-step process shown that generates a charged tRNA, one in which an amino acid is esterifi ed to the 3 � -A. The synthetases are also able to proofread and remove an incorrect amino acid from the enzyme or the tRNA.
Isoaccepting tRNAs are all the tRNAs that can be charged with the same amino acid. They have different anticodons .
A tRNA’s ability to recognize and bind more than one codon for a specifi c amino acid is known as wobble . It results from nontraditional pairing between the third (3 � ) base in the mRNA codon and the fi rst (5 � ) base in the tRNA anticodon. [ Note: Recall that two strands of nucleic acid orient in an antiparallel manner.]
Eukaryotic ribosomes that remain in the cytosol synthesize proteins required at that site or in the nucleus, mitochondria, or peroxisomes. In contrast, those on the ER membrane synthesize proteins that will be secreted; incorporated into the plasma membrane; reside in the ER, Golgi, or lysosomes or be incorporated into their membranes. [Note: ER with ribosomes attached is termed RER.]
E
Amino acid
ATP
PPi 2Pi
AMP
Aminoacyl-tRNA
CCA
CCA~Amino acid
E
E-AMP~Amino acid
Aminoacyl-tRNAsynthetase
(E )
Ferrier_Unit06.indd 362Ferrier_Unit06.indd 362 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
31.3 QuestionTranslation Process
Does the fi gure show the product of translation initiation in a prokaryote or eukaryote? Which ribosome is depicted, a 70S or an 80S? To which site on the ribosome is the charged tRNA i bound?
How is the start AUG distinguished from other AUGs in eukaryotic translation? Contrast with prokaryotes.
What NTP gets hydrolyzed in all three steps of translation?
Vanishing white matter disease ( VWM ) is a severe AR neurodegenerative disorder caused by mutations to eIF2B, a GEF of translation. What is the function of GEFs?
5' U U U A A G
U A C
A U G
fMet
Ferrier_Unit06.indd 363Ferrier_Unit06.indd 363 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
31.3 Answer Translation Process
fMet (made from N 10 -formyl-THF and Met after charging of the tRNA i ) is characteristic of prokaryotic initiation, so a 70S prokaryotic ribosome (30S � 50S subunits) is depicted. Eukaryotic ribosomes are 80S (40S � 60S). The charged tRNA i is bound to the P site of the ribosome and is the only tRNA that fi rst goes to this site. All others go to the A site .
In eukaryotes, the start AUG is distinguished by its proximity to the 5 � cap, which is bound by proteins of the eIF-4 family . The 40S subunit binds near the cap and scans the mRNA for the fi rst AUG, an ATP-requiring process. In prokaryotes, in contrast, the purine-rich SD sequence upstream of the start codon pairs with the 16S rRNA of the 30S subunit, positioning the subunit on the mRNA at the start codon without scanning.
GTP is hydrolyzed to GDP in translation initiation, elongation, and termination.
GEFs reactivate guanine nucleotide–binding factors by removing GDP and allowing GTP to bind. eIF-2-GTP recognizes the tRNA i and takes it to the P site of the 40S subunit. When the 60S subunit joins, the GTP is hydrolyzed to GDP. The GEF for eIF-2-GDP is eIF-2B mutated in VWM .
5' U U U A A G
U A C
A U G
fMet
Ferrier_Unit06.indd 364Ferrier_Unit06.indd 364 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
31.4 QuestionTranslation Process
How is the elongation intermediate shown achieved in prokaryotes?
What role does a ribozyme play in elongation?
Why are two GTP hydrolyzed for every amino acid added to a peptide during elongation?
Which aspects of prokaryotic translation are inhibited by chloramphenicol, erythromycin, streptomycin, and the tetracyclines?
5' A A GU U U
fMet Phe
U A C
A U G
A A A
Ferrier_Unit06.indd 365Ferrier_Unit06.indd 365 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
31.4 Answer Translation Process
The elongation intermediate is achieved in prokaryotes by EF-Tu-GTP , which brings all tRNAs (except tRNA i ) to the A site of the ribosome in response to codons on the mRNA, a process known as decoding . GTP is hydrolyzed to GDP, and the GEF EF-Ts facilitates its removal.
rRNA (23S in prokaryotes and 28S in eukaryotes) of the large subunit is the catalyst that forms a peptide bond by condensing the carboxyl end of the growing peptide at the P site with the amino group of the amino acid at the A site ( transpeptidation , shown). Therefore, the rRNA is a ribozyme . The catalytic activity is known as peptidyltransferase .
In addition to decoding and bond formation, elongation involves movement of the ribosome one codon in the 3 � direction. This puts the peptidyl-tRNA in the P site, leaving the A site available, as the uncharged tRNA exits the E site . EF-G-GTP mediates movement in prokaryotes. GTP is hydrolyzed to GDP.
Prokaryotic translation is inhibited at the peptidyltransferase reaction by chloramphenicol , translocation by erythromycin , initiation by streptomycin , and elongation by the tetracyclines . [ Note: Diptheria toxin covalently modifi es EF-2 and inhibits eukaryotic elongation.]
5' A A GU U U
fMet Phe
U A C
A U G
A A A
5' 3'
mRNA
OOCCHR'
HN
Peptide chain
OOCCHR''NH2
P A
Ferrier_Unit06.indd 366Ferrier_Unit06.indd 366 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
31.5 QuestionTranslation Process
Complete the chart by fi lling in the names of the factors that function in translation in a eukaryotic cell (denoted by the blue E).
What is the primary regulatory step of eukaryotic translation? How is it regulated?
What is a “polysome”?
Individuals with Swyer syndrome are genotypically 46,XY and phenotypically female. In some cases, the nuclear localization sequence (NLS) of the protein that functions as a STF to initiate maleness is mutated. How would this result in a 46,XY female?
E
E
Cell Factor Function
Initiation
PE
IF-2-GTP Bring charged initiat-ing tRNA to P site
P IF-3 Prevent association of subunits
Elongation
P EF-Tu-GTPBring all other
charged tRNAs to A site
P EF-Ts Guanine nucleotide exchange factor
P EF-G-GTPTranslocation
Termination
P RF-1, 2 Recognize "stop" codons
P RF-3-GTPRelease of other RFs
P
P
P
P
P
P
P
E
E
E
E
E
E
Ferrier_Unit06.indd 367Ferrier_Unit06.indd 367 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
31.5 Answer Translation Process
See the completed chart shown.
Initiation is the primary regulatory step of eukaryotic translation. It is inhibited by eIF-2 phosphorylation. Specifi c kinases phosphorylate the factor in response to the environ-mental stresses of unfolded proteins in the ER, amino acid deprivation, heme defi ciency in erythroid cells, and viral infection. Inhibiting translation at initiation conserves energy (primarily as GTP).
A polysome ( polyribosome ) is a complex of more than one ribosome simultaneously translating one mRNA.
STFs bind to response elements in nuclear DNA. Mutation to the NLS of the STF that initiates maleness would prevent its posttranslational targeting from the cytosol to the nucleus, preventing transcription of the genes required for maleness. Consequently, the fetus will develop as a 46,XY female.
E
E
Cell Factor Function
Initiation
PE
IF-2-GTP Bring charged initiat-ing tRNA to P site
P IF-3eIF-3
Prevent association of subunits
Elongation
P EF-Tu-GTPEF1α-GTP
Bring all other charged tRNAs to
A site
P EF-TsEF-1βY
Guanine nucleotide exchange factor
P EF-G-GTPEF-2-GTP
Translocation
Termination
P RF-1, 2eRF
Recognize "stop" codons
P RF-3-GTPeRF-3-GTP
Release of other RFs
P
P
P
P
P
P
P
E
E
E
E
E
E
eIF-2-GTP
Ferrier_Unit06.indd 368Ferrier_Unit06.indd 368 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
31.6 QuestionPosttranslational Modifi cations
What two effects does phosphorylation (shown) have on protein activity?
What proteins of coagulation undergo -carboxylation?
In I-cell disease , the inability to phosphorylate mannose to mannose 6-P prevents the cotranslational targeting of acid hydrolases . What is the effect on lysosomes? Where does the mannose originate?
Phosphorylation
Tyrosine
O–O–P–O
O
O–O–P–O
O
Serine
Phosphate
Protein
C O
CH
NH
CH2
C O
CH
NH
CH2
Ferrier_Unit06.indd 369Ferrier_Unit06.indd 369 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Posttranslational Modifi cations31.6 Answer
Phosphorylation , a covalent modifi cation, causes conformational changes in a protein that can lead to (1) activation (e.g., glycogen phosphorylase and the STF CREB) and (2) inactivation (e.g., glycogen synthase ).
The clotting proteins FII, FVII, FIX, and FX and the anticlotting proteins C and S undergo vitamin K– dependent � -carboxylation of specifi c Glu residues. [ Note: Biotin-dependent carboxylation of Lys residues is seen with carboxylases that use pyruvate, acetyl CoA, propionyl CoA, and methylcrotonyl CoA as substrates.]
In I-cell disease , lysosomes contain inclusion bodies of undegraded materials as a consequence of the mistargeting of acid hydrolases because of a defect in the phosphotransferase required to generate the mannose 6-P lysosomal targeting signal. The mannose is part of an oligosaccharide made on dolichol (an ER membrane lipid) and transferred en bloc to the amide N of an Asn residue in the hydrolase as it moves through the ER lumen. The glycosidic linkage between Asn and GlcNAc of the oligosaccharide (shown) is formed by N-glycosylation . [ Note: In O-glycosylation, sugars are sequentially added to the –OH group of selected Ser, Thr, or Hyl residues.]
N-Acetyl-glucosamine
O
O
OH
NH
H
HH
CH2OH
CH3
C O
C
O
NH
Asparagine
C O
CH
NH
CH2
Phosphorylation
Glycosylation
Tyrosine
O–O–P–O
O
O–O–P–O
O
Serine
Phosphate
Protein
C O
CH
NH
CH2
C O
CH
NH
CH2
Ferrier_Unit06.indd 370Ferrier_Unit06.indd 370 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
32.1 QuestionProkaryotic Gene Expression Regulation
How do proteins that function as trans-acting factors recognize and bind to cis-acting DNA elements, as shown?
Where are the genes that encode regulatory trans-acting factors located relative to the genes they regulate?
Give two examples of cis-acting elements and their trans-acting factors involved in regulation of the lac operon.
Why is the lac operon turned off in the presence of both glucose and lactose?
Directionof
transcription
Trans-actingfactor
Transcribed region
DNA
DNA
mRNA
Pol II
Cis-acting DNA regulatory sequences
Ferrier_Unit06.indd 371Ferrier_Unit06.indd 371 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
32.1 Answer Prokaryotic Gene Expression Regulation
Trans-acting proteins contain structural motifs (e.g., the helix-turn-helix and zinc fi nger) that recognize and bind specifi c cis-acting DNA elements.
Genes that encode trans-acting molecules can be upstream or downstream of the regulated gene. [ Note: They can be on a different chromosome in eukaryotes.]
The lac repressor / operator site and the CAP / CAP site are trans-acting factors and cis-acting ele-ments that regulate the lac operon . Prokaryotic operons contain the protein-coding genes (sequentially ordered) required for a pathway (e.g., the use of lactose and the synthesis of Trp) and the regulatory elements that control their transcription. Operons are not found in eukaryotes. [ Note: Transcription is the primary site for regulation of gene expression.]
In the presence of lactose, allolactose (its isomer) binds to the repressor protein and prevents it from binding the operator. However, if glucose is also present, cAMP is not available to form a complex with CAP protein and bind the CAP site, which prevents effi cient transcription initiation and turns off the operon.
Directionof
transcription
Trans-actingfactor
Transcribed region
DNA
DNA
mRNA
Transcribedregion
DNA
Pol II
Cis-acting elements are DNA sequences that are bound by trans-acting regulatory molecules.
Cis-acting DNA regulatory sequences
Directioof
transcript
Trans-actinfactor
DNA
mR
Trans-acting molecules, usually proteins, are synthesized from genes that are different from the genes targeted for regulation. Trans-acting molecules bind to cis-acting elements on DNA.
Ferrier_Unit06.indd 372Ferrier_Unit06.indd 372 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
32.2 QuestionProkaryotic Gene Expression Regulation
How does the trp operon detect the elevated levels of Trp that result in attenuation, as shown?
Why is the lac operon described as “inducible,” whereas the trp operon is “repressible”?
How do prokaryotes coordinate both transcriptional and translational responses to environmental stresses (e.g., amino acid starvation)?
Transcription terminator
“Terminated”RNA polymerase
+
Ribosome translating mRNA
Nascent peptide
mRNA
Hairpin structure
Transcription terminator
y
Self-complementary sequencesin certain regions of the mRNA cause a hairpin structure to form which attenuates (prematurely terminates) transcription.
Ribosome initiates translation of mRNA as it is being transcribed.
Ferrier_Unit06.indd 373Ferrier_Unit06.indd 373 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Prokaryotic Gene Expression Regulation32.2 Answer
The 5 � -end of the mRNA from the trp operon contains two consecutive codons for Trp. If charged tRNA Trp is plentiful, the ribosomes move past these codons as they translate the polycistronic mRNA, allowing a hairpin structure to form that attenuates transcription (stops it before completion). However, if charged tRNA Trp is in short supply, the ribosomes stall, an alternative structure forms, and transcription continues. [ Note: Attenuation is possible because prokaryotic translation begins during transcription.]
Lactose prevents the repressor binding to the operator, which relieves inhibition of the lac operon and allows it to be induced (turned on) when glucose is unavailable. In contrast, Trp (a corepressor ) facili-tates repressor binding, which maximizes trp operon inhibition and causes it to be repressed (turned off).
In amino acid starvation, an uncharged tRNA at the ribosomal A site activates stringent factor ( RelA ), which synthesizes ppGpp (an alarmone ) and results in inhibition of rRNA and tRNA synthesis. Conse-quently, ribosomes cannot be made, and excess ribosomal proteins bind their polycistronic mRNAs at the SD sequences, blocking translation. This keeps ribosomal protein and rRNA synthesis in balance.
Transcription terminator
“Terminated”RNA polymerase
+
Ribosome translating mRNA
Nascent peptide
mRNA
Hairpin structure
Transcriptionterminator
y
Self-complementary sequencesin certain regions of the mRNA cause a hairpin structure to form which attenuates (prematurely terminates) transcription.
Ribosome initiates translation of mRNA as it is being transcribed.
ppGpp (Guanosine 5’-diphosphate 3’-diphosphate)
AMP
Ribosomal RNA, transfer RNA (tRNA),
some messenger RNAs
Guanosine diphosphate ATP
Uncharged tRNA in the A site of the 70S ribosome activates stringent factor which synthesizes ppGpp.
Results in selective inhibition of transcription.
Ferrier_Unit06.indd 374Ferrier_Unit06.indd 374 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
32.3 QuestionEukaryotic Gene Expression Regulation
How does the binding of the hormone glucagon to its cell-membrane GPCR with production of the second messenger cAMP (as shown) alter the cell’s transcriptional profi le?
How do STFs mediate combinatorial control of transcription?
How does hydrocortisone, a glucocorticoid, decrease infl ammation ?
Glucagon
Cell membrane
Receptor
Adenylylcyclase
ATPcAMP
Ferrier_Unit06.indd 375Ferrier_Unit06.indd 375 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
32.3 Answer Eukaryotic Gene Expression Regulation
Glucagon binds to and activates its cell-membrane GPCR, upregulating production of cAMP by adenylyl cyclase and, consequently, activating PKA . The kinase phosphorylates and activates CREB , a trans-acting STF. CREB binds to cis-acting CREs throughout the genome, affecting the expression of glucagon-responsive genes (e.g., PEPCK ), thereby changing the cell’s transcription profi le.
STFs bound to DNA recruit proteins to their activation domain, forming a multiprotein complex that activates transcription. Regulation is achieved by the specifi c combinations of proteins in the complex, a process known as combinatorial control .
Hydrocortisone (cortisol) enters the cell and binds to its cytosolic receptor, which induces a conformational change in the receptor that allows the receptor–hormone complex to enter the nucleus. The complex, a STF, binds to GRE s throughout the genome, altering gene expression. Hydrocortisone induces expression of genes that code for proteins that have an anti-infl ammatory effect and represses pro-infl ammatory genes.
Glucagon
Cell membrane
Receptor
CRE
CREB Transcription factors
RNA polymerase II
Start of transcription
P
Adenylylcyclase
ATPcAMP
When CREB is phosphorylated,it can bind to CRE and activate the transcription machinery.
Ferrier_Unit06.indd 376Ferrier_Unit06.indd 376 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
32.4 QuestionEukaryotic Gene Expression Regulation
The eukaryotic gene shown contains fi ve exons. How can this one gene give rise to more than one protein product?
How do apo B-100 (made in the liver) and apo B-48 (made in the intestine) illustrate the use of one mature mRNA to produce different proteins in different tissues?
Why would inactivation of a gene encoding an IRP lead to decreased intracellular iron levels?
DNA
1
Exon
Gene
Exon Exon Exon Exon
2 3 4 5
Ferrier_Unit06.indd 377Ferrier_Unit06.indd 377 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
32.4 Answer Eukaryotic Gene Expression Regulation
A single gene can give rise to more than one protein by alternative splicing , in which the use of different splice sites gives rise to different mRNAs in different tissues, greatly increasing the number of proteins that can be made from the �21,000 protein-coding genes in the human genome.
In the liver, 100% of the mature mRNA is expressed, giving rise to apo B-100 for VLDL synthesis. In the intestine, the mRNA undergoes an additional (and uncommon) modifi cation, RNA editing , in which deamination of a C to a U converts a sense to a nonsense codon. Creation of this stop codon allows translation of only the fi rst 48% of the mRNA and production of apo B-48 for CM synthesis.
TfR mRNA has cis-acting IREs at the 3 � -end. When the iron levels in cells are low, trans-acting IRPs bind the IREs and stabilize the mRNA, resulting in increased TfR synthesis that allows cells to endocytose transferrin-bound iron from the blood. Inactivation of the gene for an IRP would result in less TfR being synthesized (due to increased mRNA degradation), in turn, causing decreased intracellular iron levels.
Protein A
Protein B
mRNA
mRNA
DNA
1
Exon
Gene
Exon Exon Exon Exon
2 3 4 5
1 2 4 5Translation
Translation
Alternativesplicing
3
1 2 4 5
CappingSplicingPolyadenylationEditing: C getsdeaminated to U
Translation
AUG UUACAA
(Gln)5’ 3’
AUG UUAUAA
(stop)5’ 3’
NH3+ COO–
pre-mRNA
mRNA
apo B-48protein
Ferrier_Unit06.indd 378Ferrier_Unit06.indd 378 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
32.5 QuestionEukaryotic Gene Expression Regulation
How does RNAi mediated by miRNA (as shown) regulate gene expression?
How can chemotherapy with methotrexate alter gene expression?
Why are methyltransferase inhibitors being explored as treatment for hemoglobinopathies that affect the � chain of Hb?
Guide strand of double-stranded miRNA associates with RISC and hybridizes with target mRNA
RISC
mRNA
Target
Guide strand
5'-cap
3'-tail
miRNA
DNA
RNA polymerase II
Drosha
Dicer
Pri-miRNA
Pre-miRNA
Nucleus
Cytoplasm
? ?
Ferrier_Unit06.indd 379Ferrier_Unit06.indd 379 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
32.5 Answer Eukaryotic Gene Expression Regulation
RNAi mediated by miRNA (a noncoding regulatory RNA) silences gene expression. Nuclear miRNA is processed as shown and sent to the cytosol as ds miRNA. One strand (the guide strand) associates with RISC and hybridizes to the target mRNA, causing either decreased mRNA translation or increased mRNA degradation by an endonuclease of RISC. [ Note: Synthetic siRNAs also can trigger RNAi and have clinical potential.]
Methotrexate inhibits DHFR , an enzyme required in the synthesis of dTMP and, consequently, DNA. In response to methotrexate, amplifi cation of the gene for DHFR occurs in some individuals, increasing DHFR production and leading to drug resistance.
Hypermethylation of C in CpG islands in the 5 � regulatory portion of many genes silences expression, whereas hypomethylation increases it. Hypermethylation of the gene for the chain of Hb is involved in the switch to � -chain expression shortly before birth. In hemoglobinopathies that affect the � chain, methyltransferase inhibitors could increase expression of the chains and improve the clinical picture.
Guide strand of double-stranded miRNA associates with RISC and hybridizes with target mRNA
Degradation oftarget mRNA by Argonaute/Ago/Slicer
Translationalrepression of target mRNA
RISC
mRNA
Target
Guide strand
5'-cap
3'-tail
miRNA
DNA
RNA polymerase II
Drosha
Dicer
Pri-miRNA
Pre-miRNA
Nucleus
Cytoplasm
Ferrier_Unit06.indd 380Ferrier_Unit06.indd 380 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
33.1 QuestionRestriction Endonucleases
How are the cohesive (“sticky”) ends shown created in dsDNA? Why are they useful in forming recombinant DNA?
What are the characteristics of a restriction endonuclease cleavage site?
Cloning of the gene for human insulin allowed for the production of the eukaryotic protein in a prokaryotic system. How can a DNA sequence be cloned?
Taq I : Cohesive ends
TGC
CG A
TTA G
CC
G AT
TA G
CC
G AT
“Sticky” ends
A+
Ferrier_Unit06.indd 381Ferrier_Unit06.indd 381 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
33.1 Answer Restriction Endonucleases
The sticky ends are created by specifi c restriction endonucleases that cleave DNA in a staggered manner, generating single-stranded ends. Two pieces of DNA (from different sources) cut with the same restriction enzyme will have complementary “sticky” ends that can anneal and be covalently joined by DNA ligase , creating recombinant DNA . Some restriction enzymes generate blunt ends (shown).
Restriction endonucleases recognize short (4–8 bps), specifi c stretches of dsDNA that are palindromes with two-fold rotational symmetry (i.e., the sequence is the same on both strands if read in the same direction).
To clone a DNA sequence, a vector (e.g., a plasmid) is used that (1) is capable of autonomous replication in the host, (2) contains a unique restriction site (also present in the DNA of interest), and (3) contains antibiotic resistance genes. The plasmid and the DNA are cleaved by the same restriction enzyme and ligated. The newly constructed plasmid is introduced into a bacterial host ( transformation ), which is grown in the presence of antibiotics to select for the recombinant form of the plasmid. After the DNA has been amplifi ed ( cloned ), it can be released from the vector and isolated [Note: Introduction of recombinant DNA into eukaryotic cells is termed “transfection”.]
Taq I : Cohesive ends
HaeIII: Blunt ends
CG
CG
GC
GC
CG
CG
GC
GC
TGC
CG A
TTA G
CC
G AT
TA G
CC
G AT
“Sticky” ends
“Blunt” ends
A+
+
Ferrier_Unit06.indd 382Ferrier_Unit06.indd 382 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
33.2 QuestionDNA Cloning
What specifi c type of plasmid vector is shown?
How is cDNA made?
Contrast a genomic library with a cDNA library. Which would be used to study mutations to promoter elements in the gene for � globin?
Fusion protein product
Bacterialpromoter
Bacterial gene
Cloned cDNA
Bacterial transcription and translation
—CN—
Ferrier_Unit06.indd 383Ferrier_Unit06.indd 383 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
33.2 Answer DNA Cloning
An expression vector that allows a eukaryotic protein to be made in a prokaryotic cell is shown. The plasmid contains a bacterial promoter (for transcrip-tion) and a SD sequence (for translation by bacterial ribosomes). Eukaryotic cDNA is inserted downstream of the promoter and within a gene expressed by the bacterium. The mRNA product contains some codons for the bacterial protein and all the codons for the eukaryotic protein, which enhances translation effi ciency and results in a fusion protein .
cDNA synthesis requires a mRNA template, an oligo-dT primer, reverse transcriptase , and the four dNTPs. The mRNA in the hybrid product is cleaved (e.g., by alkali or RNase H ) then removed and replaced by DNA pol . The resulting fragments are joined by DNA ligase , producing ds cDNA (shown).
A genomic library is a collection of fragments representing the entire genome of an organism, including introns and regulatory sequences, whereas a cDNA library is a collection of only the expressed sequences. As a dsDNA copy of mRNA, cDNA does not include introns and regulatory sequences. Because promoters and other regulatory elements are not expressed, a genomic library would be used to study them.
mRNA AAA . . A 3'
mRNA AAA . . A 3'T T T . . T 5'
mRNA
cDNA
Alkali cleaves mRNA
cDNA
DNA polymerases remove mRNA and replace it with DNA
DNA ligase
dATP, dCTP,dGTP, dTTP
AAA . . A 3'T T T . . T 5'
T T T . . T 5'
T T T . . T 5'
Reverse transcriptasedATP, dCTP,dGTP, dTTP
Add oligo-dT primer
A A A . . A 3'
5'
ds cDNAFusion protein product
Bacterialpromoter
Bacterial gene
Cloned cDNA
Bacterial transcription and translation
—CN—
Ferrier_Unit06.indd 384Ferrier_Unit06.indd 384 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
33.3 QuestionDNA Cloning
What is the value of developing a labeled probe, as shown?
What is the biochemical basis of the technique used to sequence cloned DNA?
How can a synthetic nucleotide probe be used to determine whether or not an individual carries the sickle cell mutation?
*CTCCTGTGGAGAAGT
Probe
...GAGGACACCTCTTCAGACG...
Ferrier_Unit06.indd 385Ferrier_Unit06.indd 385 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
33.3 Answer DNA Cloning
A probe (a short piece of labeled ssDNA or RNA) is a screening tool designed to hybridize with the DNA of interest. It is used to identify which band on a gel or clone in a library contains the target DNA.
Sequencing of cloned, ssDNA involves annealing a primer to the 3 � -end of the target DNA, adding DNA pol , all four dNTPs, and a limiting amount of the four ddNTPs linked to different fl uorescent dyes. DNA pol elongates the chain until a ddNMP is incorporated. The absence of a 3 � -OH group terminates elongation and produces strands of every length, with the shortest representing the 5 � -end. Separation of the products by size via gel electrophoresis followed by visualization of the fl uorescent labels will yield a pattern of bands from which the base sequence of the complementary strand can be read.
Under stringent hybridization conditions, a synthetic ASO probe will detect the sickle cell mutation in the gene for � globin because it will hybridize only to the � S sequence, as shown.
DNA from a patient with sickle cell disease
*CTCCTGTGGAGAAGT
Probe
...GAGGACACCTCTTCAGACG...
...CTCCTGTGGAGAAGTCTGC...
...GAGGACACCTCTTCAGACG...
....Pro Val Glu....5 6 7
DNA fragmentcoding for HbS
TCCTGTGGAGAAGT
obe
Portion of the gene for the �S-chain of hemoglobin S
Oligonucleotide probe hybridizes with a DNA fragment from the gene for the � chain of HbS.
DNA codes for valine (Val) instead of glutamate (Glu) in the sixth position of �-globin.
DNA
A
Probe
*CTCCTGTGGAGAAGT
...GAGGACTCCTCTTCAGACG...
Probe
*CTCCTGTGGAGAAGT
DNA fragmentcoding for HbA
Oligonucleotide probe fails to hybridize with the DNA fragment from the gene for the � chain of HbA.
DNA from a normal individual
B
Ferrier_Unit06.indd 386Ferrier_Unit06.indd 386 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
33.4 QuestionHybridization Techniques
What technique could be used to identify polymorphisms (variations in a particular DNA sequence) in two individuals, as shown?
What test would be performed to determine if a gene is being transcribed and the relative abundance of product?
How could a family with a child that has phenylketonuria (PKU) determine if their fetus will be born with the disease?
AG C TCAATCG
GC GC GC GC GC
GC GC GC
AG A TCAATCG
Individual 1
Individual 2
GC repeats
SNP
Individual 1
Individual 2
Polymorphisms can occur either in the sequence of bases at a given locus (called SNP if only one base is altered) or . . .
. . . where variable numbers of tandem repeats (VNTR) of DNA sequences occur. A specific number of tandem repeats defines a VNTR allele at a particular locus.
Ferrier_Unit06.indd 387Ferrier_Unit06.indd 387 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
33.4 Answer Hybridization Techniques
RFLP analysis is used to study polymorphisms . An RFLP is a genetic variant observable if the length of the restriction fragment is altered by creating or abolishing a restriction site or varying the number of short, tandem nucleotide repeats (shown). [ Note: In RFLP analysis, a restriction digest of the DNA from each individual is separated by gel electrophoresis, denatured, and transferred (by blotting) to a membrane. A labeled probe is used to detect the presence (or absence) of the target sequence. The technique of digesting, separating, blot-ting, and detecting DNA is known as Southern blotting.]
Northern blotting would be used to determine if a gene is being transcribed and the relative abundance of its RNA product. The technique is similar to Southern blotting except that it detects RNA, not DNA.
PAH is defi cient in PKU . Mutations in the gene for PAH usually do not affect restriction sites. To use RFLP analysis as a diagnostic screen for PKU, DNA from family members with and without PKU must be obtained to identify RFLPs closely linked to the gene ( indirect diagnosis ). [ Note: Direct diagnosis is rare because only a few diseases (e.g., sickle cell anemia ) are caused by the mutation that causes the RFLP.]
AG C TCAATCG
GC GC GC GC GC
GC GC GC
AG A TCAATCG
Individual 1
Individual 2
GC repeats
SNP
Individual 1
Individual 2
Polymorphisms can occur either in the sequence of bases at a given locus (called SNP if only one base is altered) or . . .
. . . where variable numbers of tandem repeats (VNTR) of DNA sequences occur. A specific number of tandem repeats defines a VNTR allele at a particular locus.
Ferrier_Unit06.indd 388Ferrier_Unit06.indd 388 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
33.5 QuestionMicroarrays, Transgenics, and PCR
How might the transcriptional profi le of a cancer cell (shown) be compared to that of a normal cell?
What are transgenic animals?
What is PCR?
How might PCR be used in genetic testing for cystic fi brosis (CF) caused by the � F508 mutation in the CFTR protein?
Normal cell
mRNA
Cancer cell
Ferrier_Unit06.indd 389Ferrier_Unit06.indd 389 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
33.5 Answer Microarrays, Transgenics, and PCR
The transcriptional (expression) profi le of a cancer cell and a normal cell can be compared by microarray analysis using gene chips , glass slides spotted (“arrayed”) with DNA fragments that represent specifi c coding regions. The mRNAs from each cell are converted to cDNAs, fl uo-rescently labeled, and exposed to a gene chip. The amount of fl uorescence bound to each spot is a measure of mRNA abundance in the sample.
Transgenic animals are those that have been genetically altered to carry a foreign gene ( transgene ) in their genome through use of recombinant DNA techniques.
PCR is a technique to amplify targeted sequences of DNA. It requires short primers designed to be complementary to the 5 � and 3 � sequences fl anking the target, a heat-stable DNA pol , and dNTPs. The mixture is heated to form ssDNA, then cooled to allow the primers to anneal and be extended. The process (a repetitive cycle of denature, anneal, and extend) leads to an exponential increase in target DNA amount.
The � F508 mutation in the gene for the CFTR protein causes a three-nucleotide deletion. Separation by size of the PCR product of the appropriate region of DNA can distinguish between homozygous normal , heterozygous ( carrier ), and homozygous mutant (CF-affected) individuals.
Normal cell
mRNA
cDNA
Cancer cell
Mix cDNAs and hybridizeto DNA microarray (gene chip)
Label with red fluorescent molecule
Label with greenfluorescent molecule
Yellow spot: Both cells produce the same amount of message.
Green spot: Normal cell produces more of its message.
Red spot: Cancer cell produces more of its message.
Dark (black) spot: Neither cell produces this message.
Ferrier_Unit06.indd 390Ferrier_Unit06.indd 390 5/2/14 7:52 PM5/2/14 7:52 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
34.1 QuestionFibrin Formation and Degradation
What traps RBCs within a blood clot, as shown? What term refers to the formation of a blood clot that occludes a vessel’s lumen?
What is � -carboxylation, and what role does it play in clotting?
How does warfarin affect clotting?
Endothelial layer
LUMEN OF VESSEL
?
laylayeerr
?
Trapped red blood cell?
Subendothelium
Ferrier_Ch34_Blood Clotting.indd 391Ferrier_Ch34_Blood Clotting.indd 391 5/2/14 7:54 PM5/2/14 7:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Fibrin Formation and Degradation34.1 Answer
Activated platelets form a soft plug ( primary hemostasis ) that is strengthened by a fi brin meshwork ( secondary hemostasis ), thereby trapping RBCs. Clotting is also facilitated by platelet-mediated vasoconstriction . “ Thrombosis ” refers to formation of a clot ( thrombus ) that occludes a vessel’s lumen.
� -Carboxylation (shown) is the posttranslational modifi cation by which specifi c Glu residues in FII, FVII, FIX, and FX get carboxylated at their � -carbon (shown in blue) by vitamin K–dependent � -glutamyl carboxylase and become Gla residues. The added negative charge allows coordination with Ca 2 � , facilitating the binding of Gla proteins to exposed negatively charged PLs in damaged membranes.
Vitamin K is oxidized in � -carboxylation, and the reduced form is regenerated by VKOR . Warfarin , a vitamin K antagonist , inhibits VKOR and is used to prevent inappropriate clotting. Knowledge of a patient’s genotype for VKOR can guide dosing with warfarin ( pharmacogenetics ), because some polymorphisms in the gene decrease enzyme production.
Endothelial layer
LUMEN OF VESSEL
Fibrin
Endothelilayer
LUMEN OF VESSELF VESSELLUMEN OFalLUMEN OF
Fibbrrin
Trapped red blood cellActivated platelet
Subendothelium
CH2
CH
COO– COO–
Vitamin K
Warfarin
g -Glutamyl carboxylase
O2, CO2Gla + 2H2O
CH2
CH2
COO–
Glu
Vitamin K epoxide reductase
Vitamin K(hydroquinone form) (epoxide form)(reduced) (oxidized)
R group
Polypeptide
Ferrier_Ch34_Blood Clotting.indd 392Ferrier_Ch34_Blood Clotting.indd 392 5/2/14 7:54 PM5/2/14 7:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
34.2 QuestionFibrin Formation and Activation
What is special about tissue factor (FIII) of the extrinsic pathway (shown) compared to other clotting proteins?
How is FX activated in the intrinsic pathway?
Why do individuals with hemophilia bleed even though their extrinsic pathway is not affected by the disease?
TF (FIII) FVII(Gla)
[FVIIa–TF(FIII)]
FX(Gla)
Fibrin clot
Ca2+
PL
Ca2+, PL
FXa
Ferrier_Ch34_Blood Clotting.indd 393Ferrier_Ch34_Blood Clotting.indd 393 5/2/14 7:54 PM5/2/14 7:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Fibrin Formation and Activation
Tissue factor (FIII) of the extrinsic pathway is not in the blood but is a transmembrane protein of the vascular subendothelium. Damage to a vessel exposes this extravascular factor. In the presence of Ca 2 � and PLs, FIII binds a circulating factor (FVII) and activates it to FVIIa via a conformational change. The complex then activates FX to FXa by proteolysis. Xa is required for fi brin formation.
In the intrinsic pathway , FVIIIa and FIXa , together with PLs and Ca 2 � , form a membrane-bound complex ( Xase ) with FX that proteolytically activates FX to FXa as shown. [ Note: The proteolytic factors are serine proteases . The active (a) product of one cleavage reaction initiates another, setting up a cascade.]
Individuals with hemophilia , a defect in either FVIII ( hemophilia A ) or FIX ( hemophilia B ) of the intrinsic pathway, bleed despite an intact extrinsic pathway because that path is rapidly inhibited by TFPI , resulting in reliance on the affected intrinsic pathway.
TF (FIII) FVII(Gla)
[FVIIa–TF(FIII)]
FX(Gla)
Fibrin clot
Ca2+
PL
Ca2+, PL
TFPI
FXa
FXIIa
FXIa
FIX(Gla)
FIXa Ca2+
FVIIIa [VWF–FVIII]
FX(Gla) Ca2+
Fibrin clot
PL
PL
VWF
FXI
FXa
34.2 Answer
Ferrier_Ch34_Blood Clotting.indd 394Ferrier_Ch34_Blood Clotting.indd 394 5/2/14 7:54 PM5/2/14 7:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Fibrin Formation and Degradation 34.3 Question
What factor combines with FXa to facilitate the generation of thrombin ( FIIa ) by the common pathway shown?
How is a initial (soft) fi brin clot strengthened?
What will be the clinical consequence of FIIa overexpression?
Prothrombin (FII)(Gla)
Ca2+
PLFXa
Intrinsic pathway
Extrinsic pathway Thrombin (FIIa) + Gla–containing peptide
?
Fibrin (FIa)Fibrinogen
?
Ferrier_Ch34_Blood Clotting.indd 395Ferrier_Ch34_Blood Clotting.indd 395 5/2/14 7:54 PM5/2/14 7:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
34.3 Answer
Nonproteolytic FVa combines with FXa and forms a com-plex ( prothrombinase ) that potentiates the proteolytic activity of FXa generated from both the extrinsic and intrinsic pathways. Prothrombinase activates FII to FIIa through cleavage that removes the Gla-containing region, releasing FIIa from the damaged membrane into the blood, where it activates FI to FIa.
The soft fi brin clot is strengthened by isopeptide cross-link formation between a Gln in one FIa molecule and a Lys in another by FXIIIa , a transglutaminase as shown. [ Note: Clotting factors include Gla-containing serine proteases (II, VII, IX, and X), non-Gla proteases (XI and XII), and accessory (nonproteolytic) proteins (III, V, and VIII), in addition to transglutaminase .]
Overexpression of FIIa (e.g., because of an activating mutation in the gene for prothrombin) causes thrombophilia , a condition characterized by increased tendency to clot.
Fibrin Formation and Degradation
Prothrombin (FII)(Gla)
Ca2+
PLFXa
Intrinsic pathway
Extrinsic pathway Thrombin (FIIa) + Gla–containing peptide
[FXa–FVa](prothrombinase)
Fibrin (FIa)Fibrinogen
FVa
FXa
CH2
CH2
CH2
CH2
NH2+NH2
R-group
R-group
Lysine
C=O
CH2
CH2
FXIIIa (transglutaminase)
CH2
CH2
CH2
CH2
NH
Glutamine
Lysine
C=O
CH2
CH2
+ NH3
Isopeptidebond
Glutamine
Ferrier_Ch34_Blood Clotting.indd 396Ferrier_Ch34_Blood Clotting.indd 396 5/2/14 7:54 PM5/2/14 7:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
34.4 QuestionFibrin Formation and Degradation
What is the function of the APC complex shown?
Why does FV Leiden lead to thrombophilia ?
What is the role of heparin in clotting? How is it used clinically?
How might TPA be used clinically?
Thrombin (FIIa)
Protein C
Fibrin (FIa)Fibrinogen
Activatedprotein C (APC) (Gla)
Protein S (Gla)
APC complex
?
Thrombomodulin
Ferrier_Ch34_Blood Clotting.indd 397Ferrier_Ch34_Blood Clotting.indd 397 5/2/14 7:54 PM5/2/14 7:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
34.4 Answer
The APC complex cleaves FVa and FVIIIa, accessory proteins in the production of FXa , thereby limiting clotting. Binding of FIIa to thrombomodulin (a membrane protein of endothelial cells) alters its function such that FIIa no longer activates fi brinogen, instead activating protein C . APC combines with protein S, forming the APC complex. As shown, proteins C and S contain Gla residues.
FV Leiden is a mutant form of FV that is resistant to cleavage by the APC complex. This results in inappropriate activation of FX and, therefore, of fi brinogen (and clotting). [ Note: FV Leiden is the most common cause of thrombophilia in the United States.]
Heparin (a GAG ) increases ATIII’s affi nity for the serine protease FIIa . ATIII binding causes FIIa to be taken to the liver, thereby decreasing its concentration in the blood. [ Note: ATIII is a serine protease inhibitor, or serpin.] Heparin is used clinically as an anticoagulant . It is fast-acting and short-lived, whereas warfarin is slow-acting and long-lived.
TPA activates plasminogen (bound to fi brin) to plasmin , a serine protease that cleaves fi brin to fi brin- degradation products as shown. Therapeutic fi brinolysis in patients with an MI or ischemic stroke can be achieved by treatment with recombinant TPA.
Fibrin Formation and Degradation
Thrombin (FIIa)
Protein C
Fibrin (FIa)Fibrinogen
Activatedprotein C (APC) (Gla)
Protein S (Gla)
APC complex
FVa, FVIIIaPeptide products
Thrombomodulin
Plasmini
FibrinPlasminogen
TPAi
α2-Antiplasmin
Fibrin–plasminogen
Fibrin–plasmin–TPAa
PAITPAi
+ Plasmin + TPAaFibrin degradation
products
Ferrier_Ch34_Blood Clotting.indd 398Ferrier_Ch34_Blood Clotting.indd 398 5/2/14 7:54 PM5/2/14 7:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
34.5 QuestionPlatelet Plug Formation
What molecule mediates the binding of platelets to sites of vessel injury, as shown?
Which protein of the clotting cascade plays a key role in platelet activation?
What is von Willebrand disease ( VWD )?
GPIb receptorExposed collagen of subendothelium
Endothelial layer
Platelets
Exposed collagen
ththth lielieli lalal
GPIb receptoren
PlateletsLUMEN
?
Ferrier_Ch34_Blood Clotting.indd 399Ferrier_Ch34_Blood Clotting.indd 399 5/2/14 7:54 PM5/2/14 7:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
34.5 Answer
VWF binds to exposed collagen in the subendothelium of damaged vessels. Platelets bind VWF via GP1b in a receptor complex (GP1b–V–IX) on their surface. Defects in the receptor cause Bernard-Soulier syndrome .
Thrombin ( FIIa ) is the most potent platelet activator. It binds a protease -activated GPCR and, via a Gq protein, activates PLC with production of DAG and IP 3 . DAG activates PKC , and IP 3 causes the release of Ca 2 � from platelet granules. PKC supports degranulation . Ca 2 � initiates platelet shape change (from discoidal to spherical with pseudopods). It also activates PLA 2 that cleaves membrane PLs, releasing the arachidonic acid substrate for TXA 2 synthesis by COX-1 . TXA 2 causes vasoconstriction, augments degranulation, activates additional platelets (by release of ADP), and supports fi brin formation (by release of stored FV and FXIII).
VWD is caused by defi ciency of VWF and results in decreased platelet binding to areas of injury. VWD is also characterized by a decrease in FVIII because VWF normally stabilizes circulating FVIII.
Platelet Plug Formation
GPIb receptorExposed collagen of subendothelium VWF
Endothelial layer
Platelets
Exposedof suben
EndoEndoEndothelthelthelialialial layelayeayerr
eceptorGPIb rd collagenndothelium VWF
PlateletsLUMEN
+DAGPIP2 IP3
Ca2+ release
Thrombin bound to protease-activated receptor
Phospholipase C
Protein kinase C
Phospholipase A2
TXA2
Degranulation
Serotonin
Vasoconstriction
Activation of additional platelets
ADPPDGF
VWF
FVa, FXIIIa
+
+
+
Ferrier_Ch34_Blood Clotting.indd 400Ferrier_Ch34_Blood Clotting.indd 400 5/2/14 7:54 PM5/2/14 7:54 PM
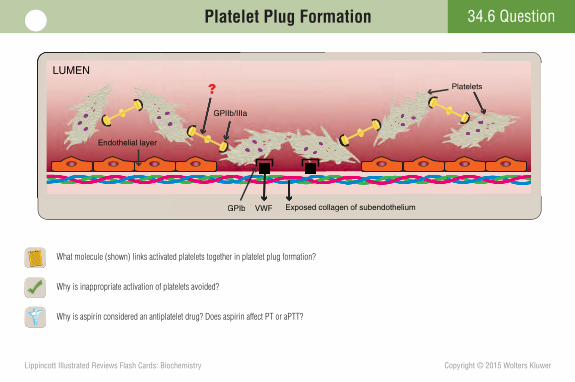
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
Platelet Plug Formation 34.6 Question
What molecule (shown) links activated platelets together in platelet plug formation?
Why is inappropriate activation of platelets avoided?
Why is aspirin considered an antiplatelet drug? Does aspirin affect PT or aPTT?
VWF
Endothelial layer
Platelets
GPIIb/IIIa
GPIb Exposed collagen of subendothelium
Platelets
n of subendotheliuG gVWF
Ia
PIb Exposed collagen
GPIIb//II
Endothelial layer
LUMEN
?
Ferrier_Ch34_Blood Clotting.indd 401Ferrier_Ch34_Blood Clotting.indd 401 5/2/14 7:54 PM5/2/14 7:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
34.6 Answer
Fibrinogen (FI) links activated platelets together, resulting in their aggregation. FI binds the exposed GPIIb/IIIa receptor on the surface of activated platelets, is activated by FIIa , and cross-linked by FXIIIa , strengthening the platelet plug. FI receptor defects cause Glanzmann thrombasthenia , whereas autoantibodies to it cause immune thrombocytopenia . [ Note: PL exposure on activated platelets causes Xase formation, FX activation, and subsequent FIIa generation.]
Inappropriate activation of platelets is avoided because (1) an intact vessel wall prevents platelet contact with collagen, (2) PGI 2 and NO made by endothelial cells cause vasodilation , and (3) ADPase on endothelial cells converts ADP (a platelet activator) to AMP.
Aspirin is considered an antiplatelet drug because it irreversibly inhibits COX and, subsequently, TXA 2 synthesis. [Note: Clopidogrel, another antiplatelet drug, is an ADP-receptor antagonist.] Because aspirin affects platelet function and not the clotting cascade, it has no effect on PT or aPTT .
Platelet Plug Formation
VWF
Endothelial layer
Platelets
GPIIb/IIIa
Fibrinogen
GPIb Exposed collagen of subendothelium
Platelets
n of subendotheliuG p gVWF
Ia
PIb Exposed collagen
GPIIb/
Fibrinogen
/II
n
Endothelial layer
LUMEN
Ferrier_Ch34_Blood Clotting.indd 402Ferrier_Ch34_Blood Clotting.indd 402 5/2/14 7:54 PM5/2/14 7:54 PM
Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
A-1Abbreviations
ABBREVIATION EXPANSION
[S] substrate concentration 2,3-BPG 2,3-bisphosphoglycerate 2,4-DNP 2,4-dinitrophenol 5-FdUMP 5-fl uorodeoxyuridine monophosphate 5-FU 5-fl uorouracil 5-HT 5-hydroxytryptamine (serotonin) 5 � -AMP 5 � -adenosine monophosphate a active A site aminoacyl site AAT � 1 -antitrypsin Ab antibody ABCA1 ATP-binding cassette protein A1 AC adenylyl cyclase ACAT acyl CoA:cholesterol acyltransferase ACC acetyl CoA carboxylase ACP acyl carrier protein ACTH adrenocorticotropic hormone AD autosomal dominant ADA adenosine deaminase ADH alcohol dehydrogenase ADP adenosine diphosphate AGE advanced glycation end product AI adequate intake ALA aminolevulinic acid ALAS1 , 2 aminolevulinic acid synthase1 , 2 ALDH aldehyde dehydrogenase ALL acute lymphoblastic leukemia ALP-1, 2 alkaline phosphatase-1, 2 ALT alanine transaminase
AMDR acceptable macronutrient distribution range AMP adenosine monophosphate AMPK adenosine monophosphate kinase AP site apurinic/apyrimidinic site APC activated protein C complex apo apolipoprotein aPTT activated partial thromboplastin time AR autosomal recessive ARDS acute respiratory distress syndrome ASO allele-specifi c oligonucleotide AST aspartate transaminase ATIII antithrombin III ATP adenosine triphosphate A � amyloid beta b inactive BA bile acid BAT brown adipose tissue BBB blood brain barrier BCAA branched-chain amino acid BCKD branched-chain � -keto acid dehydrogenase BER base excision repair BMI body mass index BMR basal metabolic rate bps base pairs BS bile salt BUN blood urea nitrogen CAH congenital adrenal hyperplasia cAMP cyclic adenosine monophosphate CAP catabolite activator protein
ABBREVIATION EXPANSION
Ferrier_Abbreviations.indd 1Ferrier_Abbreviations.indd 1 5/2/14 6:54 PM5/2/14 6:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
A-2 Abbreviations
CB conjugated (direct) bilirubin CCK cholecystokinin CDG congenital disorders of glycosylation cDNA complementary DNA CDP cytidine diphosphate CE cholesteryl ester CETP cholesteryl ester transfer protein CF cystic fi brosis CFTR cystic fi brosis transmembrane conductance regulator cGMP cyclic guanosine monophosphate CHD coronary heart disease CK creatine kinase CKD chronic kidney disease CM chylomicron CMP cytidine monophosphate CNS central nervous system CO carbon monoxide CO 2 carbon dioxide CoA coenzyme A COMT catechol-O-methyltransferase CoQ(H 2 ) coenzyme Q (or, ubiqunone) COX-1 , 2 cyclooxygenase-1 , 2 CP caramoyl phoshate C-peptide connecting peptide CPS I , II carbamoyl phosphate synthetase I , II CPT-I , II carnitine palmitoyltransferase-I , II CRE cAMP-response element CREB cAMP-response element binding (protein) CS citrate synthase
CTF CAAT box transcription factor cTnI cardiac troponin I CTP cytidine triphosphate CYP cytochrome P450 DAG diacylglycerol DAG-P diacylglycerol phosphate dATP deoxyadenosine triphosphate ddATP dideoxyadenosine triphosphate dCDP deoxycytidine diphosphate dCMP deoxycytidine monophosphate dCTP deoxycytidine triphosphate ddI 2 � ,3 � -dideoxyinosine ddNMP dideoxynucleoside monophosphate ddNTP dideoxynucleoside triphosphate dGTP deoxyguanosine triphosphate DHA docosahexaenoic acid DHAP dihydroxyacetone phosphate DHF dihydrofolate DHFR dihydrofolate reductase DKA diabetic ketoacidosis dNMP deoxynucleoside monophosphate dNTP deoxynucleoside triphosphate DNA deoxyribonucleic acid DOPA 3,4-dihydroxyphenylalanine DPE downstream promoter element DPPC dipalmitoylphosphatidylcholine DRI dietary reference intake ds double stranded dTMP deoxythymidine monophosphate
ABBREVIATION EXPANSIONABBREVIATION EXPANSION
Ferrier_Abbreviations.indd 2Ferrier_Abbreviations.indd 2 5/2/14 6:54 PM5/2/14 6:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
A-3Abbreviations
dTTP deoxythymidine triphosphate dUDP deoxyuridine diphosphate dUMP deoxyuridine monophosphate E 0 reduction potential EAR estimated average requirement ECM extracellular matrix EDS Ehlers-Danlos syndrome EF elongation factor eIF eukaryotic initiation factor EKG electrocardiogram eNOS endothelial nitric oxide synthase EPA eicosapentaenoic acid ER endoplasmic reticulum ES enzyme-substrate complex E-site exit site ETC electron transport chain F factor FA fatty acid FAD(H 2 ) fl avin adenine dinucleotide FAS fatty acid synthase FBG fasting blood glucose FBP-1 fructose1,6-bisphosphatase FBP-2 fructose 2,6-bisphosphatase FFA free fatty acid FI fi brinogen/fi brin FII prothrombin/thrombin FIII tissue factor FIGlu N-formiminoglutamate fMet formylated methionine
FMN(H 2 ) fl avin mononucleotide G-S-S-G glutathione (oxidized) G-SH glutathione (reduced) G6PD glucose 6-phosphate dehydrogenase GAG glycosaminoglycan GALT galactose 1-phosphate uridylyltransferase GDH glutamate dehydrogenase GDP guanosine diphosphate GEF guanine nucleotide exchange factor GI glycemic index GIP gastric-inhibitory polypeptide GL glycemic load Gla � -carboxyglutamate GlcN glucosamine GlcNAc N-acetylglucosamine GlcUA glucuronic acid GLP-1 glucagon-like protein-1 GLUT glucose transporter G M2 ganglioside M2 GMP guanosine monophosphate GPCR G protein–coupled receptor GPI glycosylphosphatidylinositol G protein guanine nucleotide-binding protein GR glycemic response GRE glucocorticoid response element G q phospholipase C -activating G protein G S adenylyl cyclase -activating G protein GS glycogen synthase GSD glycogen storage disease
ABBREVIATION EXPANSIONABBREVIATION EXPANSION
Ferrier_Abbreviations.indd 3Ferrier_Abbreviations.indd 3 5/2/14 6:54 PM5/2/14 6:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
A-4 Abbreviations
GTF general transcription factor GTP guanosine triphosphate H1–H4 histamine receptors H 2 O 2 hydrogen peroxide HAT histone acetyltransferase Hb hemoglobin HbA adult hemoglobin HbA 1c glycosylated hemoglobin HbCO carboxyhemoglobin HbF fetal hemoglobin HbS sickle hemoglobin HCl hydrochloric acid HCO 3 � bicarbonate ion Hcy homocysteine HDAC histone deacetylase HDL high-density lipoprotein HDL-C high-density lipoprotein cholesterol HFI hereditary fructose intolerance HGPRT hypoxanthine-guanine phosphoribosyltransferase HIV human immunodefi ciency virus HMG CoA 3-hydroxy-3-methylglutaryl coenzyme A HNPCC hereditary nonpolyposis colorectal cancer HOCl hypochlorous acid HR homologous recombination HRE hormone response element HSL hormone-sensitive lipase HVA homovanillic acid Hyl hydroxylysine Hyp hydroxyproline
ICD isocitrate dehydrogenase IDL intermediate-density lipoprotein IdUA iduronic acid IF intrinsic factor IL interleukin IMP inosine monophosphate iNOS inducible nitric oxide synthase Inr initiator IP 3 inositol trisphosphate IPP isopentenyl pyrophosphate IRE iron-responsive element IRP iron regulatory protein IV intravenous, -ly K 0.5 ligand concentration to attain half-maximal response KB ketone body k cat turnover number K m Michaelis constant L lecithin lac lactose LCAT lecithin:cholesterol acyltransferase LCFA long-chain fatty acid LDH lactate dehydrogenase LDL low-density lipoprotein LDL-C low-density lipoprotein cholesterol LOX lipoxygenase LP lipoprotein LPL lipoprotein lipase LT leukotriene MAG monoacylglycerol
ABBREVIATION EXPANSIONABBREVIATION EXPANSION
Ferrier_Abbreviations.indd 4Ferrier_Abbreviations.indd 4 5/2/14 6:54 PM5/2/14 6:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
A-5Abbreviations
MAO monoamine oxidase Mb myoglobin MCAD medium-chain fatty acyl CoA dehydrogenase MCFA medium-chain fatty acid MCT medium-chain triacylglycerol MD malate dehydrogenase MD c malate dehydrogenase ( cytosolic ) MD m malate dehydrogenase ( mitochondrial ) me- 7 Gppp 7-methylguanosine triphosphate MI myocardial infarction miRNA micro RNA MMR mismatch repair MODY maturity-onset diabetes of the young mRNA messenger RNA MSU monosodium urate MSUD maple syrup urine disease mtDNA mitochondrial DNA MUFA monounsaturated fatty acid N-AcGlu N-acetylglutamate NAD(H) nicotinamide adenine dinucleotide NADP(H) nicotinamide adenine dinucleotide phosphate NANA N-acetylneuraminic acid NER nucleotide excision repair NH 3 ammonia NH 4 � ammonium ion NHEJ nonhomologous end-joining NK natural killer NLS nuclear localization sequence NMP nucleoside monophosphate
nNOS neuronal nitric oxide synthase NO nitric oxide NOS nitric oxide synthase NSAID nonsteroidal anti-infl ammatory drug NTP nucleoside triphosphate O 2 � � superoxide OA osteoarthritis OAA oxaloacetate OGTT oral glucose tolerance test OH � hydroxyl radical OI osteogenesis imperfecta OMP orotate monophosphate OTC ornithine transcarbamoylase OXPHOS oxidative phosphorylation P phosphate P site peptidyl site P/O ATP made per O atom reduced to H 2 O P 50 partial pressure of O 2 at 50% saturation PA phosphatidic acid PAH phenylalanine hydroxylase PAI plasminogen activator inhibitor PAPS phosphoadenosine phosphosulfate PC pyruvate carboxylase PC phosphatidylcholine PCAT phosphatidylcholine:cholesterol acyltransferase PCR polymerase chain reaction PCT porphyria cutanea tarda PDCAAS protein digestibility-corrected amino acid score PDGF platelet-derived growth factor
ABBREVIATION EXPANSIONABBREVIATION EXPANSION
Ferrier_Abbreviations.indd 5Ferrier_Abbreviations.indd 5 5/2/14 6:54 PM5/2/14 6:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
A-6 Abbreviations
PDH(C) pyruvate dehydrogenase ( complex ) PE phosphatidylethanolamine PEM protein-energy malnutrition PEP phosphoenolpyruvate PEPCK phosphoenolpyruvate carboxykinase PFK-1 , 2 phosphofructokinase-1 , 2 PG prostaglandin PGI 2 prostacyclin pH negative logarithm of the H � concentration pI isoelectric point P i inorganic phosphate PI phosphatidylinositol PIP 2 phosphatidylinositol 4,5-bisphosphate PK pyruvate kinase pK a (pK) negative logarithm of the acid dissociation constant PKA protein kinase A PKB protein kinase B ( also known as Akt ) PKC protein kinase C PKG protein kinase G PKU phenylketonuria PL phospholipid PLA 2 phospholipase A 2 PLC phospholipase C PLP pyridoxal phosphate PNP purine nucleoside phosphorylase pO 2 partial pressure of oxygen pol polymerase ppGpp guanosine 5 � -diphosphate-3 � -diphosphate PP i pyrophosphate
PPP pentose phosphate pathway pri-miRNA primary micro RNA PrP prion particle PrP c prion particle cellular PrP sc prion particle scrapie PRPP 5-phosphoribosyl-1-pyrophosphate PS phosphatidylserine PT prothrombin time PTH parathyroid hormone PUFA polyunsaturated fatty acid PYY peptide YY R relaxed RA retinoic acid RAR retinoic acid receptor RBC red blood cell RBP retinol binding protein RCT reverse cholesterol transport RDA recommended dietary allowance RE response element REE resting energy expenditure RER rough endoplasmic reticulum RES reticuloendothelial system RF release factor RFLP restriction fragment length polymorphism RISC RNA-induced silencing complex RMR resting metabolic rate RNA ribonucleic acid RNAi RNA interference RNR ribonucleotide reductase
ABBREVIATION EXPANSIONABBREVIATION EXPANSION
Ferrier_Abbreviations.indd 6Ferrier_Abbreviations.indd 6 5/2/14 6:54 PM5/2/14 6:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
A-7Abbreviations
ROS reactive oxygen species rRNA ribosomal RNA S Svedberg unit SAM S-adenosylmethionine SCA sickle cell anemia SCAP SREBP cleavage-activating protein SCFA short-chain fatty acid SCIDS severe combined immunodefi ciency SD succinate dehydrogenase SD Shine-Dalgarno sequence SER smooth endoplasmic reticulum SGLT-1, 2 sodium-glucose cotransporter 1, 2 SH steroid hormone SI sucrase-isomaltase siRNA small interfering RNA snRNA small nuclear RNA snoRNA small nucleolar RNA snRNP small nuclear ribonucleoprotein particle SO 4 2� sulfate ion Sp1 specifi city factor 1 S phase synthesis phase SR-B1 scavenger receptor-B1 SRE sterol regulatory element SREBP sterol regulatory element-binding protein ss single stranded SSB single-stranded binding (protein) SSRI selective serotonin reuptake inhibitor STF specifi c transcription factor T tense
T1D type 1 diabetes T2D type 2 diabetes TAG triacylglycerol TCA tricarboxylic acid TEE total energy expenditure TF transcription factor TFPI tissue factor pathway inhibitor TfR transferrin receptor THB (BH 4 ) tetrahydrobiopterin THF tetrahydrofolate Tn troponin TPA tissue plasminogen activator TPP thiamine pyrophosphate tRNA transfer RNA tRNA i initiating transfer RNA TUL tolerable upper limit TX thromboxane UA uric acid Ub ubiquitin UC urea cycle UCB unconjugated (indirect) bilirubin UCP1 uncoupling protein 1 UDP uridine diphosphate UGT UDP-glucuronosyltransferase UL upper limit UMP uridine monophosphate UROD uroporphyrinogen III decarboxylase UTP uridine triphosphate UTR untranslated region
ABBREVIATION EXPANSIONABBREVIATION EXPANSION
Ferrier_Abbreviations.indd 7Ferrier_Abbreviations.indd 7 5/2/14 6:54 PM5/2/14 6:54 PM

Lippincott Illustrated Reviews Flash Cards: Biochemistry Copyright © 2015 Wolters Kluwer
A-8 Abbreviations
UUN urinary urea nitrogen UV ultraviolet V 0 initial velocity VKOR vitamin K epoxide reductase VLCFA very-long chain fatty acid VLDL very low-density lipoprotein VMA vanillylmandelic acid V max maximum velocity VWD von Willebrand disease
VWF von Willebrand factor VWM vanishing white matter disease WAT white adipose tissue XO xanthine oxidase XP xeroderma pigmentosum � -KG � -ketoglutarate � -KGD � -ketoglutarate dehydrogenase � G change in Gibbs free energy � G 0 standard change in Gibbs free energy
ABBREVIATION EXPANSIONABBREVIATION EXPANSION
Ferrier_Abbreviations.indd 8Ferrier_Abbreviations.indd 8 5/2/14 6:54 PM5/2/14 6:54 PM





























