Embed Size (px)
Citation preview

Liver Disease in Rabbits Anna Meredith, MA, VetMB, CertLAS, CertZooMed, MRCVS, * and Louise Rayment, BVetMed, CertZooMed, MRCVSI
In clinical practice, a specific diagnosis of liver disease is rarely made in rabbits. Presenting signs are often vague and nonspecific, and a full range of diagnostic tests are needed to reach a conclusion. However, many condi- tions can affect the liver, and a variety of clinical signs may indicate liver impairment, as either a primary or secondary condition. Historically, pet rabbits have been perceived as a low-value animal, and financial con- straints are often placed on the application of a full diagnostic workup in the sick animal. This is perhaps why there are few references to pet rabbit liver disease in the literature. This article is intended to provide a practical overview for veterinarians, showing a system- atic approach to the diagnostic process and applying techniques that are well described in other species. The major hepatic diseases have been summarized in the text. Liver disease is relatively common in other compan- ion species, so it is more likely that the lack of published information is from underdiagnosis than a species rar- ity. A more thorough diagnostic approach may provide more information in the future. Copyright �9 2000 by W. B. Saunders Company,
Key words: Rabbit, liver, hepatic.
125 mL/kg/day) ,~ and the primary bile pigment is biliverdin rather than bilirubin. The bile and pancreatic ducts open separately into the duode- num in the rabbit.
Diagnosis of Liver Disease A number of diagnostic tests are available to
evaluate symptoms that may be indicative of liver disease) -5 It is important, particularly when faced with nonspecific signs of ill health, to take a detailed history and per form a thorough clinical examination, followed by a broad base of diagnos- tic tests. Once liver involvement has been estab- lished, more specific tests can be done to catego- rize this (Tables 1 and 2).
Laboratory Tests for Liver Disease
e rabbit liver is divided by a deep cleft into ht and left lobes, which are each divided
into anterior and posterior lobules. The right lobe has a fur ther division into the (iuadrate lobe, which lies caudal to the gallbladder. There is also a small circular caudate lobe adjacent to the right kidney, which has a narrow attach- ment. 1 This makes the lobe susceptible to detach- ment or torsion. 2 The gallbladder is found deep within the right anterior lobule. The common bile duct joins the cystic bile duct and opens into the duodenum just distal to the pylorus. Rabbits secrete a large amount of bile ~ (approximately
Alanine Aminotrans ferase
Alanine aminotransferase (ALT) is of limited use for evaluating hepatic damage in the rabbit, because it has little tissue specificity. For ex- ample, ALT in rabbit hear t muscle and liver is similar, and rabbit liver has only half the ALT level of that in the dog. The half-life of ALT is only 5 hours in the rabbit, compared with 45 to 60 hours in the dog. However, significant eleva- tions in ALT can be found in conditions of hepatic damage and necrosis, such as hepatic coccidiosis and hepatic lipidosis.
From the *Royal (Dick) School of Veterinary Studies, University of Edinburgh, Hospital for Small Animals, Roslin, UK; and i'Westover Veterinary Centre, North Walsham, Norfolk, UK.
Address correspondence to Anna Meredith, MA, VetMB, Cert- LAS, CertZooMed, MRCVS, Head of Exotic Animal Service, Royal (Dick) School of Veterinary Studies, University of Edinburgh, Hospital for Small Animals, Roslin, UK EH25 9RG.
Copyright �9 2000 by W. B. Saunders Company. 1055-937X/00/0903-0005510. 00/0 doi: l O. 1053/ax. 2000. 7135
A lka l ine Phospha tase
Alkaline phosphatase (ALP) originates f rom many tissues, including bone, intestine, kidney, and placenta, as well as liver, with highest levels in intestine and kidney. The highest levels of ALP activity in the liver are found in the mem- branes border ing the bile canaliculi, and levels increase in conditions of biliary stasis. Rabbits have 2 liver ALP isoenzymes.
146 Seminars in Avian and Exotic Pet Medicine, Vol 9, No 3 (July), 2000: pp 146-152

Liver Disease in Rabbits 14 7
Table 1. Clinical Signs and Diagnostic Tests for Liver Disease in-Rabbits
Clinical Signs of Tests for Liver Disease Liver Disease
Anorexia Ill thrift Lethargy, depression, list-
lessness Weight loss Diarrhea Polydipsia and polyuria Jaundice, icterus
Liver enzymes (ALT, ALP, AST, GGT)
Liver function tests (biliru- bin, bile acids)
Fecal analysis---parasites, bacteriology
Peritoneal tap and analysis of fluid
Ascites, abdominal disten- Radiography--hepatic size sion and shape
Dyspnea Ultrasonography--echo- Coagulopathies, bleeding genicity, masses Neurological symptoms Endoscopy Seizures , Laparotomy Collapse, lateral recum- Liver biopsy
bency Impression smear Death Histopathology
Culture and sensitivity Cytology
Abbreviations: ALT, alanine aminotransferase; ALP, alkaline phosphatase; AST, aspartate aminotransferase; GGT, gamma glutamyltransferase.
Aspartate Aminotransferase
Aspartate aminotransferase (AST) is found in the rabbit liver, cardiac and skeletal muscle, kidney, and pancreas, with highest levels in the liver and skeletal muscle. Elevation of AST is seen with conditions causing hepatocellular ne- crosis.
Gamma Glutamyltransferase
Gamma glutamyltransferase (GGT) is found in the liver and kidney, but that of renal origin is not found in the circulation. Thus, serum GGT is all of hepatic origin, and levels are raised with hepatocellular damage and biliary stasis.
Bilirubin and Bile Acids
The main product of heme breakdown is biliverdin in the rabbit, al though some is con- verted to bilirubin, which is present at measur- able levels. 6 Biliverdin assays are not commer- cially available. Serum bilirubin levels reflect hepatocellular and biliary tree function. Visible icterus is a rare presenting sign in the rabbit. Significant hyperbilirubinemia is usually associ- ated with biliary obstruction and cholestasis,
such as neoplasia of the biliary tree and hepatic coccidiosis:
Bile acids (cholic acid and chenodeoxycholic acid) are synthesized in the liver from choles- terol and are essential for fat digestion and absorption. There is normally a highly efficient enterohepatic circulation of bile acids, and blood levels will only rise if liver function is impaired. There is little information on the use of bile acids as an indicator of liver function in the rabbit, but it is presumed that it will be a sensitive indicator, as in other species. Because the rabbit is a herbivore and always has ingesta in its gastrointestinal tract, the taking of fasting and postprandial levels is not practical.
Table 2. Hematologic and Biochemical Values for the Domestic Rabbit
Range Units
RBC 5-8 • PCV 34-50 % Hemoglobin 10-17.5 g/dL WBC 5-12 X109/L Neutrophils 34-60 % Lymphocytes 43-62 % Eosinophils 0-2 % Monocytes 0-4 % Basophils 0-1 % Platelets 240-600 • 109/L Total protein 49-71 g/L Albumin 27-36 g/L Globulin 24-33 g/L Glucose 6-8.9 mmol/L Urea 9.1-22.7 mmol/L Creatinine 53-124 mmol/L Bilirubin--total 4.3-12.8 mmol/L Cholesterol 0.62-1.68 mmol/L Calcium 2.17-4.59 mmol/L Phosphorous 1.0-2.2 mmol/L Sodium 134-150 mmol/L Potassium 3.3-5.7 mmol/L Chloride 92-120 mmol/L ALP 12-96 IU/L AST 33-99 1U/L Amylase 400-3,600 IU/L CK 140-372 IU/L LDH 132-252 IU/L ALT 55-260 IU/L GGT 0-5 IU/L Bile acids 3-20 mmol/L
Abbreviations: RBC, red blood cell count; PCV, packed cell volume; WBC, white blood cell count; ALP, alkaline phospha- tase; AST, aspartate aminotransferase; CK, creatinine kinase; LDH, lactic dehydrogenase; ALT, alanine aminotransferase; GGT, gamma glutamyltransferase. Printed with permission from Cooke SW at Greendale Laboratories.

148 Meredith and Rayment
Other Liver Function Tests
Cholephilic dyes such as sulphobromophtha- lein and indocyanine green are not generally used in clinical practice to assess liver function. These dyes are administered intravenously, and the rate of removal from the plasma by the liver is measured from subsequent blood samples. Data are available for rabbits, but it should be remembered that dehydration, drug competi- tion, and shock can give faise elevations in levels, and the tests are not valid if biliary obstruction is present.
Serum protein
Total protein levels vary in rabbits with breed and age. The albumin fraction is approximately 60%, higher than for most o ther mammals. Hypoproteinemia will occur in rabbits with signifi- cant liver disease, because of decreased produc- tion.
Table 2 gives normal ranges of hematologic and biochemical values for rabbits.
Diagnostic Imaging
Radiography
This is the most basic and accessible form of diagnostic imaging available to the general prac- titioner. Two views, most commonly lateral and ventrodorsal, of the liver should be used to provide information on size, shape, density, and position. Radiographs can show the position of other viscera and also the presence of peritoneal fluid, which will obscure visceral detail.
Ultrasonography
The ultrasonographic scanner is becoming a more f requent item of equipment in general practice. This provides another noninvasive imag- ing technique to visualize the liver, its size, echogenicity, and position. Masses both external to and within the liver parenchyma can be measured and evaluated. Ascitic fluid provides an echolucent standoff for visualizing the liver. This technique can be used to pe r fo rm guided biopsies of masses and abnormalities. Doppler ultrasound can be used to visualize blood flow within the liver and show shunting, for example.
Ultrasound can be used without the need for sedation or anesthesia and thus is ideal in the compromised patient. However, it is often neces-
sary, and usually essential when performing biop- sies, to use sedation or general anesthesia. If severe liver compromise is suspected, assessment of blood clotting parameters should be under- taken before liver biopsy.
Endoscopy
Rigid endoscopy is a minimally invasive proce- dure, pe r fo rmed under general anaesthesia, which allows direct visualization of the liver in situ (Fig 1). It can be used as an alternative to laparotomy, but the presence of ascitic fluid and intraabdominal fat can make this technique of limited use in t h e rabbit. A ventral midline approach is generally employed. Endoscopy al- lows biopsy directly f rom any liver lesion to provide an temor tem histopathological diagno- sis. If severe liver compromise is suspected, assessment of blood clotting parameters should be under taken before liver biopsy.
Other
Abdominocentesis
Ascites can be detected by the presence of abdominal distension, a fluid "thrill ," and b y radiography and ultrasonography. To obtain a sample of fluid, the abdomen is aseptically pre- pared and a needle and syringe int roduced through the midline at a shallow angle. Great care must be taken not to puncture the intes- tines. This is done with the animal in a normal upright position if possible, al though sedation is usually required. Fluid then can be analyzed for protein content and the presence of inflamma- tory or neoplastic cells and submitted for culture and sensitivity.
Fecal Analysis
Fecal analysis is a useful screening tool, particu- larly in group situations, because it is noninva- sive. Both culture and sensitivity and parasitic oocyst counts are pe r fo rmed routinely, but it is important to bear in mind that in acute out- breaks fecal shedding of either oocysts or bacte- ria may not have started, so false negatives may occur.
Laparotomy
Less invasive tests may have drawn a blank or given indication for a laparotomy. A cranial

Liver Disease in Rabbits 149
Figure 1. Endoscopic examination and biopsy of the liver of a rabbit. (A) Endoscopic view of the liver. (B) Advancing the biopsy forceps toward the liver. (C) Biopsy. (D) Posthiopsy view of the liver. Minor hemorrhage is common after biopsy. Images courtesy of S. Divers.
abdominal ventral midline approach is used to visualize the liver, take excisional wedge biopsies, or pe r fo rm surgery. It is impor tan t to remember , as with any biopsy or surgery considered where there is hepatic disease, that the blood 's ability to clot may be impaired. Any indication of pro- longed bleeding times would make this tech- nique extremely risky and perhaps contraindi- cated. As a last resort, it may be necessary, but with a less favorable prognosis. Circulatory sup- port, such as colloidal fluids or whole blood transfusions, should be considered.
Hepatic Diseases and Treatment
Trea tment for liver disease depends on the initiating cause, but is largely supportive. 7 Main- tenance of hydration status is vital. Fluid and electrolyte imbalances should be evaluated and corrected before nutrit ional suppor t is insti- tuted. Fluids can be administered orally (by syringe, orogastric, or nasogastric intubation) or parenterally (intraperitoneal, subcutaneous, in- travenous or intraosseous) (Fig 2). Maintenance requirements are a m i n i m u m of 100 mL/kg /day .

150 Meredith and Rayment
Figure 2. Nasogastric intubation for fluid and nutri- tional support on a anorexic rabbit.
The type and level of dehydration determine choice of fluids. Crystalloids are generally used, but colloids should be considered ifhypovolemia is severe and there is hypoproteinemia.
Many animals with liver disease are anorexic, and because of the rabbit's complex gastrointes- tinal physiology, there should be a constant throughput of food of a high fiber content. Anorexia is of serious concern if it lasts more than 2 to 3 days, and nutritional support should be instituted at the earliest opportuni ty to pre- vent mucosal atrophy, gastrointestinal stasis, and hepatic lipidosis (see below). Rabbits can be force-fed easily with a syringe or nasogastric tube. Suitable foods are proprietary rabbit pellets or alfalfa meal liquidized into a slurry. Fiber con- tent should be at least 12%. Commercial baby foods are often fed but are very low in fiber, and the addition of alfalfa meal will improve fiber content. Cisapride (0.5 m g / k g 3 times daily) and metoclopramide (0.5 mg /kg 3 times daily) should be given to stimulate and maintain gastrointesti- nal motility. Fresh timothy hay, greens such as dandelions, and the rabbit's normal diet should be offered at all times to stimulate appetite.
Minimization of stress is also of importance. Hospitalized rabbits should be kept away from carnivores, in a quiet environment. Other sup- portive measures include the use of short-acting corticosteroids, anabolic steroids, and vitamins, especially vitamins B and K if the rabbit is anorexic.
Parasitic Diseases
Hepatic Coccidiosis
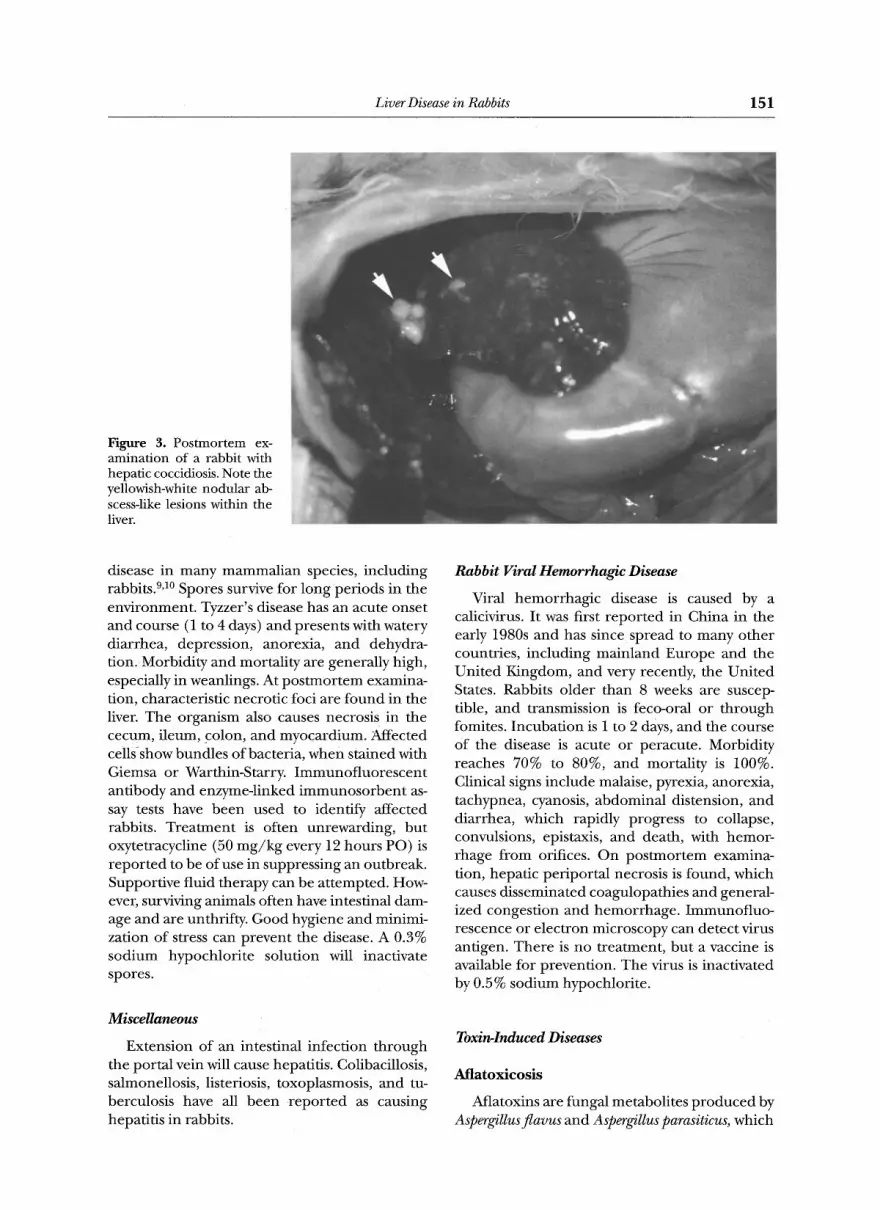
Eimeria stiedae is ubiquitous in open rabbitries, where feed has not been treated with coccidio- stats. Symptoms range from ill thrift and reduced weight gain to anorexia, diarrhea, abdominal distension, icterus, and death, s,9 Radiography can show hepatic enlargement and ascites, and serum ALP, ALT, and total bilirubin levels may be elevated. Diagnosis is reached by detection of oocysts in feces or at postmortem examination, where the liver will be enlarged and contain yellowish-white nodular abscess-like lesions (Fig 3). The gallbladder is often grossly enlarged, and oocysts can be seen in the bile or on histological examination of liver tissue. Sulfa preparations such as sulfamethoxine (15 mg /kg by mouth every [PO] every 12 hours for 10 days) and trimethoprim-sulfa combinations (30 m g / k g ev- ery 12 hours PO for 10 days) can be effective in preventing and treating hepatic coccidiosis. The main role of drug t reatment is to control the organism until immunity develops. Prevention depends on good hygiene and avoidance of fecal contamination of feed and water bowls.
Liver Fluke
Fasciola hepatica causing cachexia, lethargy, and death, can affect rabbits that graze in wet pasture affected by carrier snails. Diagnosis is made by the detection of oocysts on fecal exami- nation or at postmortem examination, finding the flukes in the bile ducts. Treatment of af- fected individuals is with a single dose of praziqu- antel (5 to 10 mg/kg) . Infestation can be con- trolled by avoidance of contaminated grazing.
Microbiological Diseases
Abscessation
Hepatic abscessation caused by bacteremia or septicemia with organisms such as Pasteurella multocida can occur in the rabbit. Antibiotic therapy is usually unrewarding because of the thick inspissated nature of rabbit pus and the formation of a thick capsule.
Tyzzer' s Disease ( Clostridium piliformis )
Clostridium piliformis is a gram-negative, spore- forming obligate intracellular organism, which is transmitted by the feco-oral route. It causes
Liver Disease in Rabbits 151
Figure 3. Postmortem ex- amination of a rabbit with hepatic coccidiosis. Note the yellowish-white nodular ab- scess-like lesions within the liver.
disease in many mammalian species, including rabbits. 9a~ Spores survive for long periods in the environment. Tyzzer's disease has an acute onset and course (1 to 4 days) and presents with watery diarrhea, depression, anorexia, and dehydra- tion. Morbidity and mortality are generally high, especially in weanlings. At postmortem examina- tion, characteristic necrotic foci are found in the liver. The organism also causes necrosis in the cecum, ileum, colon, and myocardium. Affected cells~show bundles of bacteria, when stained with Giemsa or Warthin-Starry. Immunofluorescent antibody and enzyme-linked immunosorbent as- say tests have been used to identify affected rabbits. Treatment is often unrewarding, but oxytetracycline (50 mg /kg every 12 hours PO) is repor ted to be of use in suppressing an outbreak. Supportive fluid therapy can be attempted. How- ever, surviving animals often have intestinal dam- age and are unthrifty. Good hygiene and minimi- zation of stress can prevent the disease. A 0.3% sodium hypochlori te solution will inactivate spores.
Miscellaneous
Extension of an intestinal infection through the portal vein will cause hepatitis. Colibacillosis, salmonellosis, listeriosis, toxoplasmosis, and tu- berculosis have all been repor ted as causing hepatitis in rabbits.
Rabbit Viral Hemorrhagic Disease
Viral hemorrhagic disease is caused by a calicivirus. It was first repor ted in China in the early 1980s and has since spread to many other countries, including mainland Europe and the United Kingdom, and very recently, the United States. Rabbits older than 8 weeks are suscep- tible, and transmission is feco-oral or through fomites. Incubation is 1 to 2 days, and the course of the disease is acute or peracute. Morbidity reaches 70% to 80%, and mortality is 100%. Clinical signs include malaise, pyrexia, anorexia, tachypnea, cyanosis, abdominal distension, and diarrhea, which rapidly progress to collapse, convulsions, epistaxis, and death, with hemor- rhage from orifices. On postmortem examina- tion, hepatic periportal necrosis is found, which causes disseminated coagulopathies and general- ized congestion and hemorrhage. Immunofluo- rescence or electron microscopy can detect virus antigen. There is no treatment, but a vaccine is available for prevention. The virus is inactivated by 0.5% sodium hypochlorite.
Toxin-Induced Diseases
Atlatoxicos is
Aflatoxins are fungal metabolites p roduced by Aspergillus flavus and Aspergillus parasiticus, which

152 Meredith and Rayment
can be present in moldy f o o d . 11'12 Rabbits are very sensitive to the hepatotoxic effects of aflatox- ins, and levels of aflatoxin B1 greater than 100 ppm have been shown to cause morbidity and mortality.
Lead Toxicity
Although not a specific liver disease, lead toxicity affects the liver as in other species. ~3,14 Clinical signs include anorexia, weight loss, de- pression, and neurological signs. Diagnosis is made on radiographic detection of a metallic foreign body, elevated blood lead levels, anemia, and the presence of nucleated red blood cells or basophil ic stippling. Trea tment is by chelation with calcium ethylenediaminetetra-acetic acid at 27.5 mg /kg subcutaneously 4 times daily for 5 days, with an additional course of t reatment 1 week later if required.
Hepatic Lipidosis
Any cause of anorexia can rapidly lead to hepatic lipidosis in the rabbit. Anorexia leads to a mobilization of fat stores, elevation of serum lipid levels, and ketoacidosis. Hepatocytes can become overwhelmed with lipid and become necrotic. Common causes of anorexia in the rabbit are dental disease and gastrointestinal stasis attributable to a low-fiber diet. Obese animals are especially susceptible, and lipidosis is also seen in pregnant does as part of the preg- nancy toxemia syndrome. These animals show signs including depression, anorexia, abortion, convulsion, and death. Radiography will show an enlarged liver, and there will be elevated serum bile acids. Ketone will be present in blood and urine. At pos tmor tem examination, the liver is pale and friable, and histological examination shows that the hepatocytes are distended with lipid. Trea tment is supportive: parenteral or oral fluid therapy with lactated Ringer's solution and 5% dextrose, and force-feeding, but the progno- sis for recovery is poor. Nutritional support should be instituted at an early stage as possible for any anorexic rabbit to prevent the occur- rence of hepatic lipidosis.
Neoplasia
Lymphoma, bile duct adenoma, and carci- noma are primary tumors that affect the liver. Metastatic disease, usually uterine adenocarci- noma, commonly affects the liver, s All hepatic neoplasia carries a grave prognosis, and surgical resection is generally not attempted. Chemother- apy protocols used in canine and feline patients may help to increase the lifespan of rabbits affected with lymphoma.
References 1. Manning PJ, Ingler DH, Newcomer CE: The Biology of
the Laboratory Rabbit (ed 2). San Diego, CA, Academic, 1994
2. Evering W, Edwards JF: Hepatic lobe deformity in a rabbit. Lab Anim 21:14-16, 1992
3. Jenkins JR: Rabbit and ferret liver and gastrointestinal testing, in Fudge AM (ed): Laboratory Medicine, Avian and Exotic Pets. Philadelphia, PA, Saunders, 1999, pp 291-304
4. Clampitt RB, Hart RJ: The tissue activities of some diagnostic enzymes in ten mammalian species. J Comp Pathol 88:607-621, 1978
5. Benson KG, Paul-Murphy J: Clinical pathology of the domestic rabbit. Vet Clin North Am (Exotic Anim Pract) 2:3, 539-551, 1999
6. Munoz ME, Gonzales J, Esteller A: Bile pigment forma- tion and excretion in the rabbit. Comp Biochem Physiol 85A:67-71, 1986
7. Paul-Murphy J, Ramer J: Urgent care of the pet rabbit. Vet Clin North Am (Exotic An Pract) 1:127-152, 1998
8. Jenkins JR: Gastrointestinal diseases, in Hillyer EV, Que- senbery KE (eds): Ferrets, Rabbits and Rodents: Clinical Medicine and Surgery. Philadelphia, PA, Saunders, 1997, pp 176-188
9. Harkness JE, Wagner JE: The Biology and Medicine of Laboratory Rabbits and Rodents (ed 3). Philadelphia, PA, Lea & Fabiger, 1989
10. Besch-Williford C: Tyzzer's disease in rabbits, in House Rabbit Society Veterinary Conference National Sympo- sium Program and Abstracts, 1997, pp 113-116
11. Clard JD, Jain AV, Hatch RC: Experimentally induced chronic aflatoxicosis in rabbits. Am J Vet Res 41:1841- 1845, 1980
12. Makkar HPS, Singh B: Aflatoxicosis in rabbits. J Appl Rabbit Res 14:218-222, 1991
13. Morgan RV, Moore FM, Pearce LK, et al: Clinical and laboratory findings in small companion animals with lead poisoning: 347 cases (1977-1986). J Am Vet Med Assoc 199:93-97, 1991
14. Swartout MS, Gerken DF: Lead-induced toxicosis in two domestic rabbits. J Am Vet Med Assoc 197:717-719, 1987





























