Embed Size (px)
Citation preview

at SciVerse ScienceDirect
Clinical Radiology 66 (2011) 1181e1192
Contents lists available
Clinical Radiology
journal homepage: www.elsevierheal th.com/journals /crad
Low-dose contrast-enhanced time-resolved MRangiography at 3 T: Diagnostic accuracy for treatmentplanning and follow-up of vascular malformationsM. Anzidei a,*, B. Cavallo Marincola a, A. Napoli a, L. Saba b, F. Zaccagna a, P. Lucatelli a,F. Fanelli a, E. Bassetti a, F.M. Salvatori a, C. Catalano a, R. Passariello a
aDepartment of Radiological Sciences, University of Rome “La Sapienza”, Rome, ItalybUniversity of Cagliari, Polo Ospedaliero Monserrato, Italy
article information
Article history:Received 27 February 2011Received in revised form24 July 2011Accepted 1 August 2011
* Guarantor and correspondent: M. Anzidei,Sapienza”, Department of Radiological Sciences00161 Rome- Italy. Tel.: þ0039 06 44 55 602; fa
E-mail address: [email protected] (M
0009-9260/$ e see front matter � 2011 The Royal Codoi:10.1016/j.crad.2011.08.003
AIM: To assess the accuracy of low-dose contrast-enhanced time-resolved 3 T magneticresonance angiography (MRA) for the morphological and functional assessment of vascularmalformations (VM), and to evaluate its diagnostic potential for the depiction oftreatment-induced changes.MATERIALS AND METHODS: Twenty-fivepatientswithknownVMunderwentMRAto evaluate
the locationandextentof lesions and theirhaemodynamic characteristics. Three-dimensional (3D)T1-weighted time-resolved sequences were acquired following the administration of 0.05 mmol/kg of gadobenate dimeglumine. VM were classified according to their morphology and haemo-dynamic characteristics. All patients thereafter underwent conventional angiography to confirmthe diagnosis and to treat the lesions (embolization or sclerotherapy). Follow-up MRA was per-formed 30 days after treatment to assessmorphological and functional changes. Avisual analoguescale (VAS) was used to clinically assess the severity of symptoms before and after therapy.RESULTS: Based on haemodynamic characteristics, VM were classified as predominantly
arterial [4 (16%)], artero-venous [19 (76%)] or venous [2 (8%)]. Twenty-three (92%) lesions wereclassified as high-flow VM and two (8%) as low-flow VM. Intralesional thrombosis was presentin 17 (68%) lesions before therapy and in 10 lesions (40%) after therapy. The median VAS scoreswere 5� 1 before treatment and 4� 2 after treatment. Very good correlation (Spearman’scorrelation coefficient: rho¼ 0.87; p¼ 0.000) was noted between the reduction of lesion sizeon follow-up MRA and pain relief as assessed by VAS.CONCLUSION: Low-dose contrast-enhanced time-resolved 3 T MRA can be used to define
morphological and functional aspects of VM accurately during treatment planning and follow-up, and can identify post-therapy changes that positively correlate with treatment outcome.
� 2011 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.
University of Rome “La, Viale Regina Elena 324,x: þ0039 06 49 02 43.. Anzidei).
llege of Radiologists. Published by
Introduction
Vascular malformations (VM) are relatively commonespecially in younger patients.1 VM vary in terms of structuraland topographic appearance andmay be congenital in nature,occurringdue tounknowngenetic or environmental effects ontheprimitivevascular systeminearlyembryonic life, orarise in
Elsevier Ltd. All rights reserved.

Table 2Baseline demographic characteristics of the patient population and classifi-cation of vascular malformations (VMs) based on morphological andfunctional criteria. [F/N] Age (years) and size (cm) are expressed asmean� standard deviation with minimum and maximum values inparentheses. Other values are expressed as numbers of patients withpercentage in parentheses.
Agea 24� 7 yrs [12e52]Male/Femaleb 11/14 (44/66)Size (cm) 7.1� 4 cm [2.3e17.9]Location (anatomic region):Extremities 15 (60)Torso 2 (8)Head-neck 7 (28)Visceral 1 (4)
Haemodynamic characteristics:Predominantly arterial 4 (16)Artero-venous 19 (76)Predominantly venous 2 (8)
Flow:High 23 (92)Low 2 (8)
a mean� SD [min-max].b n (%).
Table 3Baseline and follow-up size of vascular malformations (VMs; in cm) and VASscore [F/N]. Differences between baseline and follow-up values are expressedfor size and visual analogue scores (VAS).
Patients Size VAS
Baseline Follow-up D Baseline Follow-up D
1 7,3 4,3 �41 5 3 �22 6,4 4,9 �22 7 4 �33 9,7 4,6 �53 7 4 �34 14 11,9 �15 5 5 05 2,3 2 �12 4 4 06 17,9 10,9 �39 6 3 �37 4,5 6,2 37 6 7 1
M. Anzidei et al. / Clinical Radiology 66 (2011) 1181e11921182
response to trauma. In certain cases VM may becomecomplicated and become symptomatic (pain, swelling,bleeding, and functio laesa) resulting in the need fortreatment.1e8
In order to define the appropriate interventional proce-dure, it is essential to differentiate accurately high-flowlesions (e.g., arterial malformations), which typically requireembolization or palliative therapy, from low-flow lesions (e.g.,haemangiomas and VMs), which can be treated with scle-rotherapy or laser therapy.9e14 Moreover, it is essential toensure that treatment is completed successfully as incom-plete treatment may render the residual malformation moreaggressive and symptomatic. Thus, detailed anatomicalmapping is required to increase the rate of therapy success.One approach to obtaining specific morphological andfunctional information prior to treatment is to use digitalsubtraction angiography (DSA). However, DSA is aninvasive, costly, and time-consuming procedure that carriesa significant risk to the patient. An alternative procedure isdynamic contrast-enhanced magnetic resonance angiog-raphy (MRA), which can provide the same time-relevantinformation on the extent of the VM, location, and physio-pathology as DSA with the advantage of being non-invasiveand comparatively rapid and inexpensive. Several studieshave shown that the implementation of dedicated 3D time-resolved acquisitions allow real-time evaluation of thespecific haemodynamic features of lesions, while eliminatingthe need for breath-holding and bolus timing (15e19). Forsimilar reasons dynamic MRA is an appropriate technique toevaluate treatment response, even if it’s diagnostic perfor-mance was never explored in this clinical setting.
Hence the aim of the present study was to assess theaccuracy of 3 T MRA using a reduced dose of contrast agentfor the morphological and functional assessment of VM andto evaluate its diagnostic potential for the depiction oftreatment-induced changes.
Methods and materials
Patient population and study timeline
Between February 2009 and May 2010, 30 consecutivepatients with untreated, symptomatic VM previously
Table 1Magnetic resonance sequences parameters.
TR(msec)
TE(msec)
FlipAngle (�)
SliceThickness(mm)
AcquisitionTime (sec)
3D T1-weightedspin-echo (withand withoutfat saturation)
4 2 12 6 58
T2-weighted fastspin-echo(with and withoutfat saturation)
1240 79 90 5 42
3D T1-weighted timeresolved
4 1 25� 1.7 157
3D T1-weightedhigh-resolution
7 3 10 0.7 186
diagnosed at computed tomography (CT), MR and/orultrasound were prospectively enrolled. In accordance withthe institution’s review board guidelines, each patient orparental guardian provided written informed consent forinclusion in the study group after being thoroughlyinformed of the potential benefits and contraindications ofMRA, DSA, and subsequent treatment. The study protocolwas as follows1: pre-interventional MRA to confirm theinitial diagnosis and to assess the anatomy and
8 7 9,3 33 5 8 39 9 5,8 �35 5 2 �310 10,1 5,5 �45 5 2 �311 11,3 6,4 �43 4 2 �212 15,3 9,6 �37 7 4 �313 6 8,6 43 4 7 314 6,2 8 30 6 7 115 5,6 3,5 �38 7 4 �316 4,3 6 40 6 8 217 3,7 2,7 �27 5 3 �218 5,7 8,2 43 5 6 119 2,8 3,8 35 6 6 020 3,5 2,7 �23 5 2 �321 7,5 4,9 �34 6 4 �222 3,9 3,6 �8 5 5 023 3 2,2 �28 7 7 024 5 2,7 �45 5 3 �225 4,9 3,8 �21 5 2 �3

M. Anzidei et al. / Clinical Radiology 66 (2011) 1181e1192 1183
physiopathology of the VM; patients were also assessedusing a visual analogue scale (VAS) to establish the severityof clinical symptoms2; percutaneous treatment underDSA guidance in eligible patients3; post-interventionalfollow-up MRA performed 1 month after treatment toassess morphological and functional changes to treated VM.Patients were again assessed (VAS) to clinically assess therelief of symptoms after treatment.
MRA
MRA examinations were performed on a 3 T MRI system(Discovery MR750, GE Healthcare, Milwaukee-WIS, USA)using a dedicated surface coil. Unenhanced T1-weighted andT2-weighted sequences (Table 1) were initially acquired withandwithout fat suppression in order to identify theVMand toevaluate its topographic anatomy. Time-resolved three-di-mensional (3D) T1-weighted MRA sequences (Table 1) werethen acquired following the administration of 0.05 mmol/kggadobenatedimeglumine (MultiHance�; Bracco Imaging SpA,
Figure 1 A 32-year-old woman with swelling of the left arm. Time-resolinvolving soft tissues of the shoulder and the whole left upper limb (arrartery and by forearm arteries. High-resolution T1 weighted sequences (defilling for several minutes after the injection of gadobenate dimeglumine
Milan, Italy). Contrast agent administrationwas performed ata rateof2 ml/s througha22G intravenous catheterpositionedin an antecubital vein and was followed by 10 ml of salineflush at a rate of 1 ml/s. Image acquisition was startedimmediately after contrast agent administration in order toobserve in real-time the passage of the contrast agent bolusthrough the vascular bed of the lesion. Background subtrac-tion andmaximum intensity projection (MIP) reconstructionswere used to generate fluoroscopic-like MRA datasets forfunctional imageevaluation,with a temporal resolutionof 3 s/acquisition. Finally, a modified 3D T1-weightedhigh-resolution sequence (Table 1) was acquired during theequilibrium phase of contrast circulation at 3 min aftercontrast agent administration in order to obtain a detailedvascular map and to depict intralesional thrombosis.
DSA and treatment
Eligible patients underwent conventional catheter-basedDSA during the treatment of diagnosed VM. DSA-guided
ved MRA (aec) shows the presence of a wide vascular malformationows). Arterial feeding is predominantly supported by the subclavianf) demonstrate the extension of the vascular malformation that keeps(asterisks).

Figure 2 Same patient as Fig 1. DSA confirms the MRA findings (aed); the lesions were treated with a combined approach: embolization wasused for the vessels originating from the subclavian and forearm arteries (arrows), while sclerotheraphy was preferred in the extremities, wherevenous vessels were more superficial.
M. Anzidei et al. / Clinical Radiology 66 (2011) 1181e11921184

M. Anzidei et al. / Clinical Radiology 66 (2011) 1181e1192 1185
procedures were performed on a standard angiography unit(Integris 500, Philips Medical Systems, Best, The Netherlands)with acquisition speed of 2 frames/s. All procedures wereperformedwith a common femoral artery access. To reach thedifferent anatomical site of the vascular malformations themost suitable 4 F catheter [such as Simmons, Vertebral, Ber-stein, Multipurpose (Johnson & Johnson Cordis, Miami, Fl,USA)] was employed. The catheter tip was then positionedproximal to the vascular malformation to verify the arterialblood supply. If arterial feeders were observed, they weresuperselective catheterized with coaxial technique by usinga microcatheter (Progreat, Terumo, Tokyo, Japan). Vascularmalformation’s feeders were embolized using an embolicagent [Contour (Boston Natick, MA, USA) or Onyx�-34(MicroTherapeutics, Irvine, CA, USA)]. If the lesion hada predominantly venous outflow, percutaneous sclerotizationwas performed by injecting 95% ethanol (S.A.L.F. SpA, Ber-gamo, Italy) through a 22 G spinal needle (Becton DickinsonSA, Madrid, Spain) using a 21 G infusion set (Artsana, Como,
Figure 3 Same patient as Fig 1, 1 month follow-up. MRA (aec) reveals(arrows). Also the extension of the lesion is reduced as seen on T2-weightein the shoulder and the forearm. Treatment-induced thrombosis is also evVM into the humeral shaft (arrowhead).
Italy). All treated patients underwent MRA follow-up at 1month after the procedure.
Image analysis
Two radiologists (MA and AN with 6 and 8 yearsexperience in vascular imaging, respectively) evaluated allpre-treatment and 1-month follow-up MRA image sets inconsensus. A third radiologist with 10 years experience ininterventional procedures evaluated all DSA images. VMwere evaluated morphologically in terms of location(anatomic region), size (cm), and extent in thesurrounding soft tissue (subcutaneous, muscular and bonetissues) and haemodynamically in terms of whether theVM had a predominantly arterial or venous componentbased on the circulation time and the presence of thrombi.All VM were classified according to Van Rijswijk et al.15 aseither high-flow malformations [early lesion enhance-ment (�6 s after the start of arterial filling) in association
delayed filling of the VM, which is more evident in the late phasesd (d) and high-resolution T1-weighted sequences (e, f), predominatelyident (large arrow). High-resolution sequences reveal extension of the

Figure 4 A 21-year-old man with a VM of the soft tissues involving the right maxillary and mandibular region (e, arrowhead). Time-resolvedsequences (aed) demonstrate arterial feeding supported by internal maxillary and facial arteries and their collateral branches (arrows). Inthe late acquisition (f, g), the high-resolution sequence reveals late filling of the venous reservoirs (asterisks).
M. Anzidei et al. / Clinical Radiology 66 (2011) 1181e11921186
with internal flow voids and absence of dilated venousspaces] or low-flow malformations [late enhancement(>6 s after arterial filling) in association with dilatedvenous spaces and no flow voids]. To calculate the lesion
Figure 5 Same patient as Fig 4. Selective DSA of the right external carotimaxilla (a, b; arrows). Due to the predominant venous nature of the VM
enhancement time after the start of arterial filling bothMRA and DSA images were reviewed in cine mode onoff-line workstations. The diagnostic performance of MRAwas compared with DSA as the reference standard.
d artery confirms the presence of a low-flow VM involving the right, percutaneous alcohol ablation was performed (arrowhead).
M. Anzidei et al. / Clinical Radiology 66 (2011) 1181e1192 1187
Statistical analysis
Statistical comparison of MRA and DSA datasets wasperformed using dedicated software (SPSS 13.0 for Macin-tosh; SPSS, Chicago, IL, USA). In the present study therewere no patients without VM (i.e., no negative patients).Therefore comparison of findings on MRA with those onDSA as reference standard was performed using the Wil-coxon rank-sum test. Baseline and follow-up VAS valueswere similarly compared using theWilcoxon rank-sum test.The response to treatment in terms of dimension modifi-cation (decrease, increase or no change) on MRA wascorrelated with VAS criteria before and after treatmentusing Spearman’s correlation coefficient (rho; p< 0.05).
Results
Of the 30 patients initially enrolled, five were excludedfrom the definitive study population. In two cases exclusionwas due to extensive visceral VM requiring surgical treat-ment, in two cases due to concurrent renal failure, and inone case due to patient dropout at follow-up. The definitivestudy population, therefore, comprised 25 patients
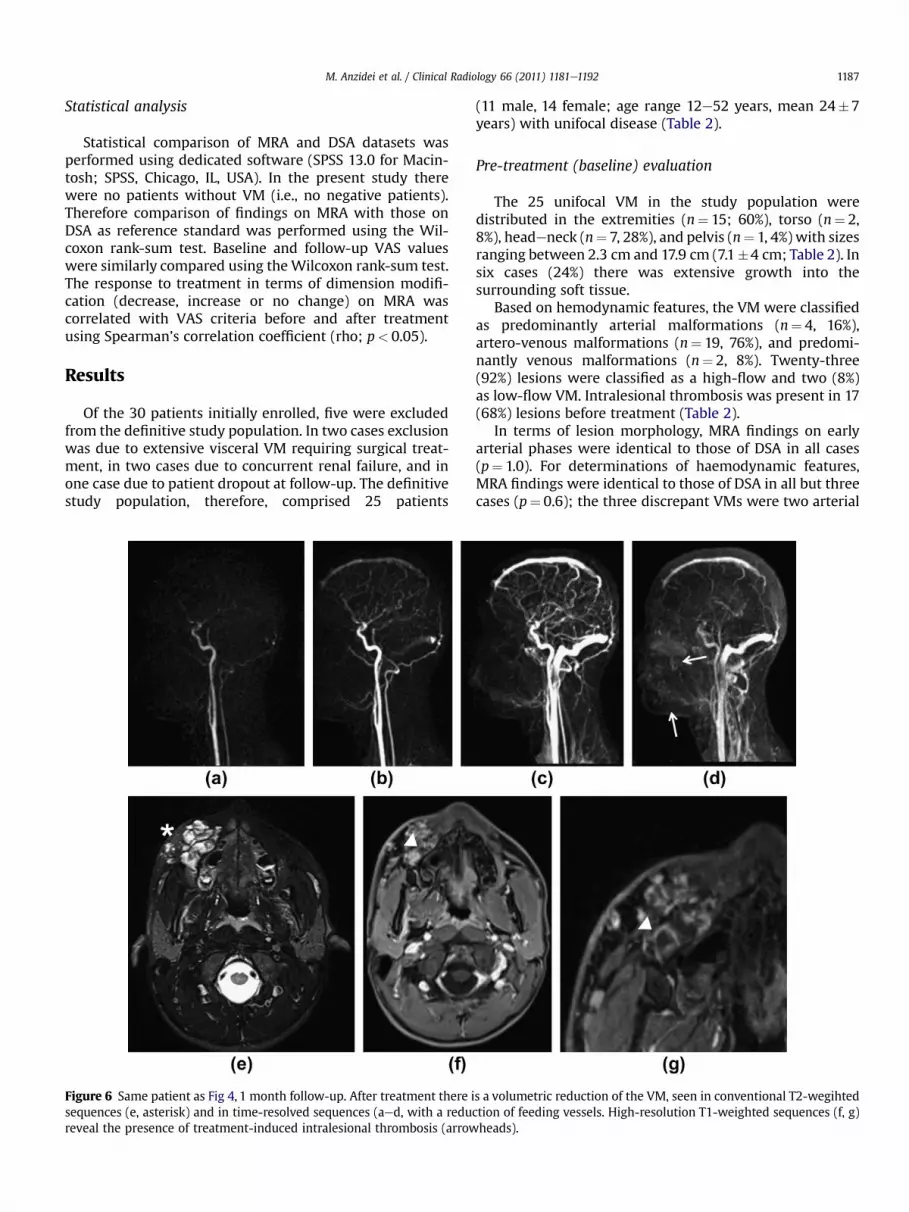
Figure 6 Same patient as Fig 4, 1 month follow-up. After treatment there isequences (e, asterisk) and in time-resolved sequences (aed, with a reducreveal the presence of treatment-induced intralesional thrombosis (arrow
(11 male, 14 female; age range 12e52 years, mean 24�7years) with unifocal disease (Table 2).
Pre-treatment (baseline) evaluation
The 25 unifocal VM in the study population weredistributed in the extremities (n¼ 15; 60%), torso (n¼ 2,8%), headeneck (n¼ 7, 28%), and pelvis (n¼ 1, 4%) with sizesranging between 2.3 cm and 17.9 cm (7.1�4 cm; Table 2). Insix cases (24%) there was extensive growth into thesurrounding soft tissue.
Based on hemodynamic features, the VM were classifiedas predominantly arterial malformations (n¼ 4, 16%),artero-venous malformations (n¼ 19, 76%), and predomi-nantly venous malformations (n¼ 2, 8%). Twenty-three(92%) lesions were classified as a high-flow and two (8%)as low-flow VM. Intralesional thrombosis was present in 17(68%) lesions before treatment (Table 2).
In terms of lesion morphology, MRA findings on earlyarterial phases were identical to those of DSA in all cases(p¼ 1.0). For determinations of haemodynamic features,MRA findings were identical to those of DSA in all but threecases (p¼ 0.6); the three discrepant VMs were two arterial
s a volumetric reduction of the VM, seen in conventional T2-wegihtedtion of feeding vessels. High-resolution T1-weighted sequences (f, g)heads).

M. Anzidei et al. / Clinical Radiology 66 (2011) 1181e11921188
lesions that were artero-venous at DSA and one singleartero-venous malformation that was completely venous atDSA. Finally, in terms of flow velocity, MRA was identical toDSA in all but one case (p¼ 0.3). The solitary VM in whichdiscrepancy between MRA and DSA was reported wasa high-flow lesion that showed low-flow at DSA.Pre-treatment (baseline) individual VAS scores are reportedin Table 3. The median pre-treatment VAS score was 5�1.
Follow-up evaluation
At follow-up MRA the post-treatment size of treated VMranged between 2 and 12 cm (mean 5.7� 2.8 cm; Table 3). Aclinically-relevant reduction in VM size (�30% across themaximum diameter) was noted in 10 (40%) cases (twopredominantly arterial VM, two predominantly venous VM,and six arterovenous VM; Figs 1e6). In eight further cases(32%, all arterovenous VM), there was a smaller or absentreduction in size (<30% across the maximum diameter;Figs 7e9), and in sevencases (28%, twopredominantlyarterialVM and five artero-venous VM) there was an increase in size(�30% across the maximum diameter). Post-procedural
Figure 7 An 18-year-old woman in which a high-flow VM in the left forethe lesion was clearly depicted if compared with the blood flow withincollateral vessels originating from radial, ulnar, and interosseous arterieslast two fingers (d, e; arrowheads). Involvement of the radius was also n
intralesional thrombosis, intended as newly developedthrombus not present at baseline MRA, was observed in 10(40%) lesions after therapy, mostly in larger VM.
Post-treatment individual VAS scores are reported inTable 3. Themedian post-treatment VAS scorewas 4� 2. Theoverall mean difference between pre- and post-treatmentVAS scores was statistically significant (p¼ 0.017) and therewas also a very good correlation between the reduction oflesion size on follow-up MRA and pain relief as assessed byVAS (Spearman’s correlation coefficient rho¼ 0.87;p< 0.001). The VAS score was found to be lower (medianscore 3� 0.8) in all patients with a clinically-relevant reduc-tion inVMsize (�30%) and in four patientswith a smaller sizereduction (<30%). Conversely, no change was noted (medianscore 5�1.1) in four patients with smaller size reduction andin one patient with a larger VM at follow-up. An increase inVAS score (median score 7� 0.7) was noted in the remainingsix patients with larger VMs at follow-up.
None of the patients presented with treatment-relatedcomplications (skin necrosis, neuropathy, muscle atrophy orcontracture, deep vein thrombosis, pulmonary embolus,disseminated intravascular coagulation, or cardiopulmonary
arm was depicted using time-resolved MRA (a, b, c). The high flow ofthe contralateral arm (arrows). Arterial feeding was supported by
. The wide malformation also determined hypovascularization of theoted on high resolution T1 sequences (e; big arrow).

Figure 8 Same patient as Fig 7. DSA confirmed the presence of thehigh-flow vascular malformation in the left forearm and wrist. Thenidus is fed mainly by the interosseous artery that appears hyper-trophic (a, c). DSA after embolization of the interosseous artery (b, d)with 3 ml of Onyx�-34, shows complete exclusion of the main feederof the nidus (arrowheads).
M. Anzidei et al. / Clinical Radiology 66 (2011) 1181e1192 1189
collapse). All patients with incomplete or poor symptomregressionwere scheduled for further DSA-guided treatmentand MRA follow-up; these additional procedures were notconsidered part of the present study.
Discussion
The updated classification of VM based on flow charac-teristics and clinical behaviour in addition to morphology,
allows high-flow lesions to be distinguished from low-flowlesions,1,4 thereby permitting more appropriate treatmentapproaches for the different VM types (i.e., endovascularembolization for high-flow lesions with a well-definedarterial component; percutaneous sclerotherapy forlow-flow lesions with a predominantly venous component).Historically, diagnosis, treatment planning, and follow-upof VM was based on Doppler ultrasonography (DUS) asa first-line examination20,21 and DSA for confirmation andinterventional guidance. However, with the advent ofhigh-end gradient technology and the introduction ofadvanced k-space sampling techniques, contrast-enhancedMRA has recently emerged as a technique of choice forthe routine acquisition of real-time fluoroscopic-like MRAimages. As yet, however, most studies gave focused on VMevaluation in the central nervous system22e24; only a fewstudies have addressed the potential of MRA for the diag-nosis of body VMs and almost none have looked at thepossible added value of the latest 3 T systems.
The present study shows that the use of a 3 T systemfeaturing both parallel imaging and dedicated k-spacesampling techniques enables the acquisition of dynamicMRA series with high spatial and temporal resolution thatpermits real-time visualization of both high-flow andlow-flow VMs with a quality similar to that of conventionalDSA. This can be ascribed to the fact that the higher fieldstrength leads to increase in signal-to-noise ratio (SNR)which, in conjunction with parallel imaging, enables theacquisition of images of high diagnostic quality withina short acquisition time. This in turn permits sequenceparameters (matrix and section thickness) to be modified inorder to increase spatial resolution without compromisingfunctional information.22e25 Furthermore, the use of a highrelaxivity contrast agent (gadobenate dimeglumine) inconjunctionwith the inherently increased SNR at 3 T allowsthe contrast agent dose to be halved to just 0.05 mmol/kgbodyweight compared to the dose approved for MRA at1.5 T.26e28 The results of the present stud show that this doseis sufficient to acquire good-quality dynamic images notonly during the first pass of contrast agent through the VMvascular bed, but also during recirculation of the contrastagent during the equilibrium phase after contrast agentinjection. Importantly, the equilibrium phase acquisitioncan be performed with increased spatial resolution usingmodified 3D sequences for precise anatomical mapping andidentification of intralesional thrombosis, which is oftendifficult to identify on time-resolved images alone.29,30 Thiscombined approach allowed a diagnostic performance to beobtained that is similar or superior to that described inpreviously published papers with the use of 1.5 T systemsand standard or high-doses of contrast agents.15e19
Regarding clinical utility, it should be borne in mind thattheultimate goal of imagingwhenmanagingpatients affectedby symptomatic VM is to identify the central nidus andfeeding vessels in order to allow their destruction and theregressionof symptoms. To this end, vascularmapping shouldbe accurate in terms of both the topographyand physiology ofthe lesions in order to better direct the treatment choicetowards either sclerotherapy or embolotherapy or both. The

Figure 9 Same patient as Fig 7, 1 month follow-up. The lesion is substantially unchanged. At time-resolved MRA (aec) there is no reduction inthe number or volume of the arterial and venous feeders (arrows). Also the involvement of the radial shaft is identical at high-resolution MRA(arrowheads; d, e). No signs of internal thrombosis are depicted (e, f; large arrow).
M. Anzidei et al. / Clinical Radiology 66 (2011) 1181e11921190
present study suggests that MRA is a highly accurate tool forthe evaluation of VM prior to therapy decision-making, withmorphological and functional findings superimposable onthose of DSA in almost all cases. Moreover, the excellentcorrelation demonstrated between VAS scores and MRAfindings before and after treatment represents further vali-dation for MRA, not only as an advanced confirmatory test inpatients with suspected VM on first-line examinations, butprincipally for its use as the non-invasive imaging techniqueof choice during follow-up (morphology, dimension, flow,numbers of feeders, thrombosis).
With regard to the few discrepancies between DSA andMRA findings at baseline (two arterial lesions that resultedartero-venous at DSA, one single artero-venous malforma-tion that was completely venous at DSA and a high-flowlesion at MRA that was low-flow at DSA), it may be
postulated that some minor difficulties still persist for MRAin the evaluation of complex flow dynamics and in theidentification of smaller vessels, such as perilesional veins:these data reflect the higher spatial and temporal resolutionof DSA. However, this observation does not diminish therole of MRA as a treatment-planning tool, as some diag-nostic alternatives (DUS) are not accurate enough forpanoramic imaging and others (CT angiography and DSAitself) expose patients to unnecessary radiation.
Regarding the interventional aspect of the present study,the success rate for endovascular and percutaneous treatmentwas essentially in line with data presented elsewhere.9,15
Although it can be argued that incomplete or clinically inef-fective treatment is frequent, it must be borne in mind thatmany VMs are comprised of complex, interconnectednetworksofnumerousmicroandmacroartero-venousshunts.

M. Anzidei et al. / Clinical Radiology 66 (2011) 1181e1192 1191
As a result, the probability of an incomplete response ortreatment failure is high, particularly in cases of extensivehigh-flow lesions, which often require multipletreatments.31e33 Furthermore, while the presence of intrale-sional thrombosis is often considered a complication, it isimportant tonote that sclerotheraphyperformedwith ethanolresults in protein damage and denaturation of the endothelialcell layer of the VM, with vessel wall denudation, andprogressive obliteration of the lumen due to thrombusformation: in these conditions the subsequent vessel fibrosisand stenosis represent the natural cascade response totherapy, culminating in alteration of blood-flow patterns thatdefine a positive response to treatment.14,34,35 In light of theseconsiderations, the appearance of intralesional thrombosismay represent a normal post-treatment response rather thana complication and should be specifically reported in follow-up examinations.
Although thepresent studyhighlights the valueofMRA forthe pre-treatment assessment and post-treatment follow-upof VMs, it is perhaps limited by the relatively short follow-upperiod (1 month, only one post-treatment examination).Moreover, only 25 VMs in 25 patientswere evaluated (mainlydue to the comparative rarity of the diagnosed VM) andcertain types of low-flow VMs (e.g., lymphatic malforma-tions) were not present in the lesion population.
Last, validation data of the above described techniquewas not included; this for two main reasons: first, MRA hasalready been validated as a diagnostic tool in patients withartero-VMs and, with respect to previously publishedpapers, the results obtained from the present study witha 3 T system and a low dose of contrast agent are notdifferent from those reported in literature. Second, it wasassumed that the described technique is inter-individuallyreproducible, as pre- and post-treatment examinationshave been adequately evaluated and compared for theanalysis of morphological and functional findings.
Nevertheless, despite these limitations, the presentstudy demonstrates that 3 T time-resolved MRA with a lowdose of a high-relaxivity contrast agent can accuratelydefine both morphological and functional aspects of VM inboth the treatment planning and follow-up phases.Furthermore, MRA can identify post-therapy changes thatpositively correlate with treatment outcomes.
Conflict of interest
For all authors there is no potential conflict of interestthat could be perceived to bias our work. Authors had fullcontrol of all the data and information presented in thismanuscript. Written informed consent was obtained by allthe patients involved in the study and the whole studyprotocol was approved by the local ethics committee.
References
1. Mulliken JB, Glowacki J. Hemangiomas and vascular malformations ininfants and children: a classification based on endothelial characteris-tics. Plast Reconstr Surg 1982;69:412e22.
2. Mulliken JB, Zetter BR, Folkman J. In vitro characteristics of endotheliumfromhemangiomas and vascularmalformations. Surgery 1982;92:348e53.
3. Fishman SJ, Mulliken JB. Hemangiomas and vascular malformations ofinfancy and childhood. Pediatr Clin North Am 1993;40:1177e200.
4. Enjolras O. Classification and management of the various superficialvascular anomalies: hemangiomas and vascular malformations. J Der-matol 1997;24:701e10.
5. Cohen JM, Weinreb JC, Redman HC. Arteriovenous malformations of theextremities: MR imaging. Radiology 1986;158:475e9.
6. Jackson IT, Carreno R, Potparic Z, et al. Hemangiomas, vascular malfor-mations, and lymphovenous malformations: classification and methodsof treatment. Plast Reconstr Surg 1993;91:1216e30.
7. Finn MC, Glowacki J, Mulliken JB. Congenital vascular lesions: clinicalapplication of a new classification. J Pediatr Surg 1983;18:894e900.
8. Meyer JS, Hoffer FA, Barnes PD, et al. Biological classification of soft-tissue vascular anomalies: MR correlation. AJR Am J Roentgenol1991;157:559e64.
9. Ohgiya Y. Dynamic MRI for distinguishing high-flow from low-flowperipheral vascularmalformations.AJR Am J Roentgenol2005;185:1131e7.
10. Yakes WF, Rossi P, Odink H. How I do it: arteriovenous malformationmanagement. Cardiovasc Intervent Radiol 1996;19:65e71.
11. Yakes WF, Haas DK, Parker SH, et al. Symptomatic vascular malforma-tions: ethanol embolotherapy. Radiology 1989;170:1059e66.
12. Burrows PE, Mulliken JB, Fellows KE, et al. Childhood hemangiomas andvascular malformations: angiographic differentiation. AJR Am J Roent-genol 1983;141:483e8.
13. Rak KM, Yakes WF, Ray RL, et al. MR imaging of symptomatic peripheralvascular malformations. AJR Am J Roentgenol 1992;159:107e12.
14. Boll DT, Merkle EM, Lewin JS. Low-flow vascular malformations: MR-guided percutaneous sclerotherapy in qualitative and quantitativeassessment of therapy and outcome. Radiology 2004;233:376e84.
15. Van Rijswijk CS, van der Linden E, van der Woude HJ, et al. Value ofdynamic contrast-enhanced MR imaging in diagnosing and classifyingperipheral vascular malformations. AJR Am J Roentgenol 2002;178:1181e7.
16. Herborn CU, Goyen M, Lauenstein TC, et al. Comprehensive time-resolved MRI of peripheral vascular malformations. AJR Am J Roent-genol 2003;181:729e35.
17. Swan JS, Carroll TJ, Kennell TW, et al. Time-resolved three-dimensionalcontrast-enhanced MR angiography of the peripheral vessels. Radi-ology 2002;225:43e52.
18. Carroll TJ, Korosec FR, Petermann GM, et al. Carotid bifurcation: evalu-ation of time-resolved three-dimensional contrast-enhanced MR angi-ography. Radiology 2001;220:525e32.
19. Kramer U, Ernemann U, Fenchel M, et al. Pretreatment evaluation ofperipheral vascular malformations using low-dose contrast-enhancedtime-resolved 3D MR angiography: initial results in 22 patients. AJR Am JRoentgenol 2011;196:702e11.
20. Trop I, Dubois J, Guibaud L, et al. Soft-tissue venous malformations inpediatric and young adult patients: diagnosis with Doppler US. Radi-ology 1999;212:841e5.
21. Paltiel HJ, Burrows PE, Kozakewich HPW, et al. Soft-tissue vascularanomalies: utility of US for diagnosis. Radiology 2000;214:747e54.
22. Farb RI, Agid R, Willinsky RA, et al. Cranial dural arteriovenous fistula:diagnosis and classification with time-resolved MR angiography at 3T.AJNR Am J Neuroradiol 2009;30:1546e51. Epub 2009 May 27.
23. Oleaga L, Dalal SS,Weigele JB, et al. The role of time-resolved 3D contrast-enhanced MR angiography in the assessment and grading of cerebralarteriovenous malformations. Eur J Radiol 2010;74:e117e212009. Epub20 May 2009.
24. Petkova M, Gauvrit JY, Trystram D, et al. Three-dimensional dynamictime-resolved contrast-enhanced MRA using parallel imaging anda variable rate k-space sampling strategy in intracranial arteriovenousmalformations. J Magn Reson Imaging 2009;29:7e12.
25. Cornfeld D, Mojibian H. Clinical uses of time-resolved imaging in thebody and peripheral vascular system. AJR Am J Roentgenol 2009;193:W546e57.
26. Nael K, Krishnam M, Nael A, et al. Peripheral contrast-enhanced MRangiography at 3.0 T, improved spatial resolution and low dose contrast:initial clinical experience. Eur Radiol 2008;18:2893e900. Epub 11 Jul 2008.
27. Kramer U, Fenchel M, Laub G, et al. Low-dose, time-resolved,contrast-enhanced 3D MR angiography in the assessment of the

M. Anzidei et al. / Clinical Radiology 66 (2011) 1181e11921192
abdominal aorta and its major branches at 3 Tesla. Acad Radiol2010;17:564e76. Epub 20 Feb 2010.
28. Lohan DG, Tomasian A, Saleh RS, et al. Ultra-low-dose, time-resolvedcontrast-enhanced magnetic resonance angiography of the carotidarteries at 3.0 tesla. Invest Radiol 2009;44:207e17.
29. Anzidei M, Napoli A, Marincola BC, et al. Gadofosveset-enhanced MRangiography of carotid arteries: does steady-state imaging improveaccuracy of first-pass imaging? Comparison with selective digitalsubtraction angiography. Radiology 2009;251:457e66.
30. Anzidei M, Napoli A, Marincola BC, et al. High-resolution steady statemagnetic resonance angiography of the carotid arteries: are intravas-cular agents necessary? Feasibility and preliminary experience withgadobenate dimeglumine. Invest Radiol 2009;44:784e92.
31. Dickey K, Pollak J,Meier GH.Management of large high-flowarteriovenousmalformations of the shoulder and upper extremity with transcatheterembolotherapy. J Vasc Interv Radiol 1995;6:765e73.
32. Do YS, Park KB, Park HS, et al. Extremity arteriovenous malformationsinvolving the bone: therapeutic outcomes of ethanol embolotherapy.J Vasc Interv Radiol 2010;21:807e16.
33. Tan KT, Simons ME, Rajan DK. Peripheral high-flow arteriovenousvascular malformations: a single-center experience. J Vasc Interv Radiol2004;15:1071e80.
34. Connor WE, Hoak JC, Warner ED. Massive thrombosis produced by fattyacid infusion. J Clin Invest 1963;42:860e6.
35. Do Y-S, Wayne F, Yakes WF, et al. Ethanol embolization of arteriovenousmalformations: interim results. Radiology 2005;235:674e82.





























