Embed Size (px)
Citation preview

Lung Cancer 28 (2000) 187–202
Lung cancer and positron emission tomography withfluorodeoxyglucose
Edith M. Marom *, Jeremy J. Erasmus, Edward F. Patz JrDepartment of Radiology, Duke Uni6ersity Medical Center, P.O. Box 3808, Durham, NC 27710, USA
Received 27 September 1999; received in revised form 20 December 1999; accepted 22 December 1999
Abstract
Over the past years, positron emission tomography (PET) with fluoro-2-deoxy-D-glucose (FDG) has emerged as animportant imaging modality. In the thorax, FDG-PET has been shown to differentiate benign from malignantpulmonary lesions and stage lung cancer. Preliminary studies have shown its usefulness in assessing tumor recurrence,and assisting in radiotherapy planning. FDG-PET is often more accurate than conventional imaging studies, and hasbeen proven to be cost-effective in evaluating lung cancer patients. This review will discuss the current applicationsof FDG-PET as compared with conventional imaging in diagnosing, staging, and following patients with lung cancer.© 2000 Elsevier Science Ireland Ltd. All rights reserved.
Keywords: Lung cancer; Positron emission tomography; Diagnosis; Staging; Treatment; Prognosis
www.elsevier.nl/locate/lungcan
1. Introduction
Lung cancer is a significant world-wide healthproblem with approximately 3 000 000 new casesin 1998. In the United States alone, there were181 000 cases diagnosed in 1998, and lung cancernow accounts for more cancer-related deaths inmen and women annually than colon, breast andprostate cancer combined [1]. Conventional imag-ing modalities with chest radiography, computedtomography (CT) and, occasionally, magnetic res-onance imaging (MRI) play an essential role indiagnosing, staging, and assessing response to
treatment in patients with lung cancer. Theseimaging modalities provide exquisite anatomicand morphologic detail, but do not alwaysprovide the requisite information for a definitivediagnosis, and tissue sampling is often required.
More recently, positron emission tomography(PET) with F-18–2-fluoro-2-deoxy-D-glucose(FDG), a D-glucose analog labeled with positron-emitting fluorine-18, has been shown to be anaccurate imaging modality that complements con-ventional studies in evaluating these patients.FDG-PET takes advantage of one characteristicfeature of malignant cells, increased glucose con-sumption [2–7]. Because tumors are metabolicallyhyperactive, FDG is taken up by the cancer cellsin greater amounts than in normal tissue, and
* Corresponding author. Tel.: +1-919-6847367; fax: +1-919-6847123.
E-mail address: [email protected] (E.M. Marom)
0169-5002/00/$ - see front matter © 2000 Elsevier Science Ireland Ltd. All rights reserved.
PII: S 0169 -5002 (00 )00096 -9

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202188
then enters the glycolytic pathway. It becomesphosphorylated, however, due to an abnormalhexose�phosphate bond, FDG-6 phosphate can-not be further metabolized, and thus it becomestrapped within the cell. This increased uptake,trapping, and subsequent accumulation permitsdifferentiation between benign and malignant le-sions [8–11]. These principals form the fundamen-tal basis for tumor imaging with FDG-PET.
This review will describe the current applica-tions of FDG-PET imaging in diagnosing, stag-ing, and following patients with lung cancer.
2. Diagnosis
The radiological manifestations of lung cancerare variable. The primary mass typically presentsas a focal pulmonary opacity or solitary pul-monary nodule. Not all pulmonary lesions, how-ever, are malignant, and differentiating a benignfrom malignant abnormality can be difficult.Standard evaluation usually includes comparisonwith prior radiographs or CT to determinegrowth. Absence of growth over a 2-year period,although not diagnostic, is highly suggestive of abenign lesion [12–15]. Further imaging, includingcontrast-enhanced CT, can also be useful in dif-ferentiating benign from malignant nodules [16].If the lesion remains indeterminate after conven-tional radiological evaluation then, according tothe likelihood of malignancy, the lesion can eitherbe observed, biopsied or resected.
More recently, FDG-PET has become an addi-tional option that can be used to evaluate patientswith indeterminate lung lesions. FDG-PET is ac-curate in differentiating benign from malignantlesions as small as 10 mm with an overall sensitiv-ity, specificity and accuracy of 96, 88 and 94%,respectively, shown in prospective [17–20] andretrospective trials [21–23]. These studies havesuggested several important features of FDG-PETimaging in the evaluation of an indeterminatepulmonary abnormality.1. The negative predictive value of a FDG-PET
study is clinically useful [20,24]. Patients with afocal lung lesion without significant FDG up-take can be followed, as this is highly sugges-
tive of a benign abnormality. False negativestudies of the primary lesion (a negative FDG-PET that proves to be a tumor) are unusual,but may be seen with small (B10 mm) lungcancers. This is thought to be due to limita-tions in spatial resolution and the paucity oftumor cells within the abnormality. Other falsenegative studies have been reported with car-cinoid tumors and bronchioloalveolar car-cinomas [25–28]. Because malignancies rarelyhave low FDG uptake, patients with negativeFDG-PET studies should be followed radio-logically for 2 years. The radiological follow-up will eliminate unnecessary surgery forbenign nodules, but will detect those uncom-mon, small, slowly progressing lung cancerssuch as carcnoid and bronchioalveolar car-cinoma that may have been falsely negative byFDG-PET. If a lesion grows during this pe-riod of time, it should be considered malignantand removed. This short delay in these malig-nancies is not considered as a significant risk,and is often the standard of care in the ab-sence of an available PET study.
2. The positive predictive value is also usefulbecause the probability of malignancy with apositive FDG-PET, in most places, is high(90% if the patient is older than 60 years).False positive studies of the primary lesion (apositive FDG-PET that proves to be benign)have been reported with infectious and inflam-matory processes such as tuberculosis, histo-plasmosis and rheumatoid nodules [18,29–32].Lesions with increased FDG uptake, however,should be considered malignant until provenotherwise and managed accordingly.
FDG-PET is currently used to further evaluateabnormalities detected on conventional radiologi-cal imaging studies (Fig. 1). The combination ofCT and FDG-PET imaging is clinically useful andcost-effective in evaluating patients with focal pul-monary lesions [33]. FDG-PET has been shown toreduce the number of patients with indeterminatenodules undergoing unnecessary resection of be-nign lesions by 15% [33]. It has been estimatedthat the combination of FDG-PET and CT toevaluate indeterminate focal pulmonary lesionscan save $1192 per patient ($62.7 million annu-

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202 189
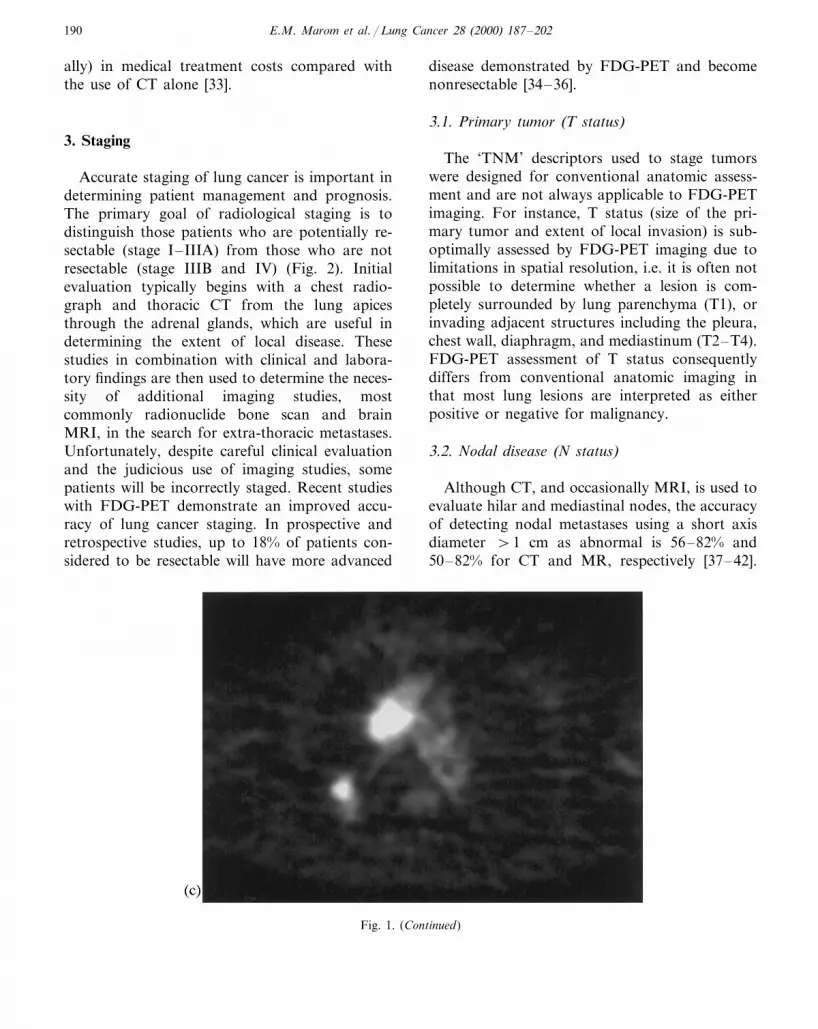
Fig. 1. Sixty-five-year-old male with a new right upper lobe pulmonary nodule on routine chest radiograph. (a) Axial thoracic CTat the level of the aortic arch confirms the indeterminate 1 cm nodule in the posterior segment of the right upper lobe (arrow). (b)Soft tissue windows at the same level demonstrate an enlarged right paratracheal lymph node (arrow). (c) Axial FDG-PETdemonstrates increased FDG uptake in the pulmonary nodule and the right paratracheal node. This proved to be stage IIIA (T1N2)nonsmall-cell lung cancer.
E.M. Marom et al. / Lung Cancer 28 (2000) 187–202190
ally) in medical treatment costs compared withthe use of CT alone [33].
3. Staging
Accurate staging of lung cancer is important indetermining patient management and prognosis.The primary goal of radiological staging is todistinguish those patients who are potentially re-sectable (stage I–IIIA) from those who are notresectable (stage IIIB and IV) (Fig. 2). Initialevaluation typically begins with a chest radio-graph and thoracic CT from the lung apicesthrough the adrenal glands, which are useful indetermining the extent of local disease. Thesestudies in combination with clinical and labora-tory findings are then used to determine the neces-sity of additional imaging studies, mostcommonly radionuclide bone scan and brainMRI, in the search for extra-thoracic metastases.Unfortunately, despite careful clinical evaluationand the judicious use of imaging studies, somepatients will be incorrectly staged. Recent studieswith FDG-PET demonstrate an improved accu-racy of lung cancer staging. In prospective andretrospective studies, up to 18% of patients con-sidered to be resectable will have more advanced
disease demonstrated by FDG-PET and becomenonresectable [34–36].
3.1. Primary tumor (T status)
The ‘TNM’ descriptors used to stage tumorswere designed for conventional anatomic assess-ment and are not always applicable to FDG-PETimaging. For instance, T status (size of the pri-mary tumor and extent of local invasion) is sub-optimally assessed by FDG-PET imaging due tolimitations in spatial resolution, i.e. it is often notpossible to determine whether a lesion is com-pletely surrounded by lung parenchyma (T1), orinvading adjacent structures including the pleura,chest wall, diaphragm, and mediastinum (T2–T4).FDG-PET assessment of T status consequentlydiffers from conventional anatomic imaging inthat most lung lesions are interpreted as eitherpositive or negative for malignancy.
3.2. Nodal disease (N status)
Although CT, and occasionally MRI, is used toevaluate hilar and mediastinal nodes, the accuracyof detecting nodal metastases using a short axisdiameter \1 cm as abnormal is 56–82% and50–82% for CT and MR, respectively [37–42].
Fig. 1. (Continued)

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202 191
Fig. 2. Sixty-year-old male complained of increasing shortness of breath. (a) Axial CT image demonstrates a 4 cm cavitary mass inthe posterior segment of the left upper lobe, scattered atelectasis, and small bilateral effusions. (b) Axial FDG-PET at the same levelshows increased FDG uptake within the periphery of the left upper lobe mass (arrow) and both pleura (curved arrows). The rightpleural effusion was found to contain malignant cells consistent with nonsmall-cell lung cancer.

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202192
Normal sized lymph nodes may harbor tumor,and enlarged nodes may be reactive [43,44]. FDG-PET, however, relying on the metabolic propertiesof tumor cells is more sensitive and specific thanCT, with accuracy reported to be 81–100% in aretrospective [45] and prospective trials [18,19,46–50]. In a prospective study, FDG-PET correctlyincreased or decreased nodal staging as deter-mined by CT in 24% of pre-surgical patients [51].A retrospective study found mediastinoscopy un-necessary in patients with CT evidence for stage Idisease and a negative FDG-PET of the regionalnodes [52]. Additionally, increased FDG uptakein hilar and mediastinal lymph nodes was used todirect surgical nodal sampling.
A decision analysis model showed that the useof both CT and FDG-PET to stage intra-thoracicnodal metastases is not only clinically useful, butalso cost-effective [53]. FDG-PET reduces theprobability that a patient with unresectable me-diastinal nodal metastases will undergo an at-tempt at curative resection, and has been shownto save $1154 per patient with a small increase inlife expectancy [53]. Although additional cost sav-ings may be obtained by eliminating the chest CTin staging nodal disease [54], it is unlikely to gainclinical acceptance. As stated previously, theTNM staging system was designed for conven-tional anatomic assessment and is important insurgical planning. FDG-PET does not offer thesame anatomic detail, but compliments conven-tional studies with the metabolic information.
3.3. Distant metastases (M status)
Lung cancer most commonly metastasizes tothe regional lymph nodes, adrenal glands, bones,brain, and liver [37,55]. Up to 44% of patients willhave distant disease at presentation [1,56]; how-ever, routine radiological evaluation for metas-tases in the absence of clinical or laboratoryfindings remains controversial and not clearlydefined [37,57–59].
FDG-PET imaging appears to improve thenon-invasive detection of extra-thoracic disease.Whole-body FDG-PET has the capability to stageboth intra- and extra-thoracic disease in a singleexamination and has an overall greater accuracy
than conventional imaging [34–36,51,60–63].Whole-body FDG-PET alters management in upto 40% of cases [34,35,51].
The adrenal glands are the most commonmetastatic site in nonsmall-cell lung cancer [64–66]. Adrenal metastases are found by autopsy in38% of patients, 1 month following curativesurgery [65]. Adrenal masses are found in up to20% of patients at initial presentation [67–71].They are occasionally difficult to distinguish frombenign abnormalities as up to two-thirds ofadrenal lesions detected by CT in patients withlung cancer are benign [67,61–73]. Consequently,FDG-PET has been advocated to evaluateadrenal masses as the sensitivity and specificity ofFDG-PET for detecting adrenal metastases inlung cancer patients are 100 and 80–100%, re-spectively [36,63,74].
The bones are another common site ofmetastatic disease, and metastases are found in12–19% of patients at presentation [62,75,76]. Atleast 20% are asymptomatic [77,78], and bonescintigraphy using 99m-Tc-MDP has a low spe-cificity (61%) with a modest sensitivity (90%).FDG-PET imaging, however, detects lesions notfound on conventional studies. The accuracy, sen-sitivity, specificity, positive and negative predic-tive values of FDG-PET for bone metastases havebeen reported to be 96, 90, 98, 90 and 98%,respectively [76]. Additional prospective studiesconfirm FDG-PET superiority in detecting lungcancer bone metastases [35,36,61,62,51].
Lung cancer also metastasizes to the brain, andup to 6% of patients with brain metastases areasymptomatic at presentation [79,80]. CT is typi-cally performed, although MRI is slightly moresensitive, particularly for leptomeningeal disease.Since the normal brain has significant glucoseuptake, metastases may be difficult to detect onFDG-PET [81]. Because of this, FDG-PET imag-ing has a low sensitivity (68%) in detecting brainmetastases [82] and should not be used to replaceCT or MRI.
Although lung cancer commonly metastasizesto the liver, it is a very unusual isolated site ofdisease, particularly in the absence of metastaticdisease to regional lymph nodes. Thus, in mostcases, liver metastases do not significantly alter

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202 193
Fig. 3. Seventy-six-year-old male with nonsmall-cell lung cancer returned for follow-up 18 months after partial left upper loberesection. (a) Posterior-anterior (PA) chest radiograph demonstrates a new lobular lingular mass adjacent to the left heart border(arrow head). (b) Axial CT image at the level of the carina confirms the lingular mass (arrow head) without evidence for hilar ormediastinal lymphadenopathy. (c) Axial FDG-PET shows increased FDG uptake in the primary mass as well as in a subcarinal andright hilar lymph node. Biopsy confirmed recurrent nonsmall-cell lung cancer.

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202194
Fig. 3. (Continued)
patient management [83]. Whole-body FDG-PETmay be useful in the evaluation of hepatic lesionsthat are indeterminate by conventional imaging.Preliminary data from studies that evaluated liverlesions discovered, while staging nonsmall celllung cancer, suggested that FDG-PET was morespecific than CT in detecting liver metastases[35,36,61]. Data from a study that evaluated livermetastases from several different primaries hasshown FG-PET’s accuracy, sensitivity, and spe-cificity to be 92, 97 and 88%, respectively, incomparison with 85, 93 and 75% by CT [84], withsimilar findings supported by other workers [85–88]. False positive FDG-PET readings can rarelyoccur with other lesions such as liver abscesses orother malignant primary liver lesions (cholangio-carcinoma and hepatocellular carcinoma [85]).
In summary, the use of FDG-PET for routinestaging of nonsmall-cell lung cancer appears tomarkedly improve lesion detection, with reducedcost and morbidity associated with unnecessarysurgical intervention. If FDG-PET is consideredas an addition to conventional staging, the ratioof saving to cost should be greater than 2:1 [54].With the use of FDG-PET, preliminary data sug-gests bone scintigraphy may be eliminated, al-though brain imaging is still required, if clinicallyindicated.
4. Evaluation of recurrent disease
Once patients have been treated for lung can-cer, anatomic and morphological changes includ-ing airway distortion, focal ground glass opacitiesand soft tissue opacities occur within the thoraxand, occasionally, the chest wall. Depending onthe therapeutic intervention (surgical or irradia-tion), benign abnormalities including post-treat-ment scarring and fibrosis may be impossible todistinguish from tumor on conventional imagingstudies (Figs. 3 and 4).
Unfortunately, once patients have had first-linetherapy, additional therapeutic options are notvery effective and, in many cases, detecting earlyrecurrence does not clearly improve survival [89].If it becomes important to distinguish benignpost-treatment changes from recurrent tumor,FDG-PET has an accuracy of 78–98%, sensitivityof 97–100% and specificity of 62–100% [22,90–94]. False positive studies, however, may occurimmediately following surgery or irradiation (Fig.5). It is therefore recommended that FDG-PETstudies in this situation be obtained approxi-mately 4–5 months after completion of the ther-apy, to allow the inflammatory changes to subsideand to provide a more accurate assessment oftumor viability [90].

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202 195
Fig. 4. Sixty-seven-year-old male with squamous cell carcinoma presented 1 year following left pneumonectomy with general malaiseand hypercalcemia. (a) Axial CT demonstrates thickening and nodularity of the left pleural space extending into the soft tissues ofthe chest wall (arrows). (b) Coronal whole-body FDG-PET demonstrates increased FDG uptake in the left pleural rind and in theperiphery of the chest wall soft tissue mass. Fine needle biopsy confirmed recurrent nonsmall-cell lung cancer.

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202196
Fig. 5. Sixty-eight-year-old male with nonsmall-cell lung cancer returned for follow-up 3 months after completing radiotherapy. (a)Axial CT image at the level of the carina demonstrates bilateral paramediastinal opacities with straight lateral margins suggestiveof radiation changes. (b) Axial FDG-PET scan at the same level demonstrates bilateral paramediastinal uptake with a linearappearance correlating to the radiation port. One-year follow-up showed stable opacities by CT with no evidence of recurrence.
5. Radiotherapy planning
Radiation treatment planning traditionally usesconventional imaging including chest radiographs,CT or MRI for an anatomic description of thetumor. As already stated, this relies on morpho-
logic features, which do not always provide aclear distinction between benign and malignanttissue. FDG-PET is more accurate than theseother imaging studies in making this distinction.
Radiation ports are typically planned to treatthe primary lesion with prophylactic doses to the

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202 197
mediastinum in order to treat microscopic tumorfoci not identified by conventional imaging studies[95]. It is common to use small margins on CTdefined targets when planning three-dimensionaltreatment, to minimize radiation damage to adja-cent normal tissues. The use of FDG-PET inconjunction with CT when planning radiationports has been shown to influence treatment in26.7–34% [95,96], with the result of enlargingportions of the irradiated margins up to 15 cm.The use of morphologic imaging alone in thesecases would have meant inadequate coverage anda higher chance of local recurrence. In addition,in poorly demarcated tumors, FDG-PET canidentify the neoplastic focus to be smaller thansuspected by conventional imaging [97,98], poten-tially allowing irradiation of smaller portals withless morbidity. Thus, for radiation planning, inte-grating FDG-PET with CT appears to be moreaccurate in defining tumor extent, and futurestudies will show if this indeed is associated withincreased survival and reduced morbidity.
6. Therapeutic response and prognostic potential
Preliminary studies have suggested FDG-PETmay be usefully used as a prognostic marker inpredicting survival and response to therapy[90,92,93,99–101]. Once patients have beentreated for lung cancer, a positive FDG-PET inthe thorax is associated with statistically worsesurvival than those patients with a negative FDG-PET [102]. Two retrospective studies showed thatthe amount of FDG uptake in the primary lesionat the time of diagnosis, independent of stage,correlated with survival [103,104]. Other prospec-tive studies suggest that complete reduction inmetabolic activity of tumor site to backgroundactivity (complete response) is indicative of truelocal remission of the disease with a specificity of100% [94,97,99].
When assessing patient’s operability followinginduction chemotherapy (stage IIIa-N2), a prelim-inary study [101] showed promise for FDG-PETas a non-invasive method for selecting those pa-tients who should proceed with surgical resection.Re-mediastinoscopy in these irradiated patients is
difficult due to fibrosis, and neither the disappear-ance of lymphadenopathy, nor a greater than 50%decrease of the primary tumor diameter on CT,was significantly associated with survival. FDG-PET, on the other hand, showed that patientswith a greater than 50% reduction in FDG uptakein the primary tumor following inductionchemotherapy had a more favorable outcome.
7. Cost and future development
Recent meta-analysis studies have suggestedconventional imaging and FDG-PET to be morecost-effective than conventional modalities alone[53,54] as unnecessary invasive procedures wereeliminated and management changed in a signifi-cant number of cases. Because of these extensiveclinical data, PET studies for the evaluation of thesolitary pulmonary nodule and staging of lungcancer has been approved for reimbursement inthe United States [105,106].
Few studies have addressed changes in treat-ment decisions based on PET findings, and noprospective studies documented changes in out-comes of care or costs of care associated withFDG-PET incorporation into the diagnostic strat-egy in lung cancer. Future large-scale studies willhopefully address the efficacy of PET for otherindications as well, while taking into account pa-tient outcome and reimbursement issues.
The price of a whole-body FDG-PET scanthese days costs approximately $1500–2000 [105].It is assumed that with increasing demand, itsprice will drop. This high cost and the rapidtechnological advances in nuclear medicine, elec-tronics and computer science has lead to thedevelopment of FDG imaging on a variety ofPET scanners and modified gamma cameras. Thealternatives are less expensive but are not equiva-lent to a dedicated PET scanner in terms ofperformance. Comparitive studies assessing FDGimaging on a dedicated PET scanner to amodified gamma camera have shown that gammacamera imaging had lower image contrast thatdeteriorated with decrease in lesion size. Gammacamera was useful in detecting lesions greaterthan 2 cm in diameter [107–109]. In a preliminary
E.M. Marom et al. / Lung Cancer 28 (2000) 187–202198
study, the gamma camera depicted only 55% ofthe neoplastic lesions that a dedicated PET scan-ner depicted [110]. If a gamma camera were usedfor staging lung cancer, a wrong therapeutic deci-sion would have been made in 29% of patients[111]. Therefore, modified gamma-camera FDGimaging cannot yet replace dedicated FDG-PETscanning in oncology patients. However, furtherperfection of this imaging modality and computerdevelopments may also lead to its future use withFDG imaging in oncology.
8. Conclusion
Over the past years, a tremendous amount ofinformation concerning FDG-PET imaging andlung cancer has been generated. It has becomeclear that this non-invasive imaging modalitycompliments conventional studies in evaluatingpatients with lung cancer. The current clinicalindications include differentiating a benign frommalignant focal pulmonary abnormality and stag-ing lung cancer. Preliminary studies show promisefor the use of FDG-PET in evaluating for recur-rent disease and radiotherapy planning. FDG-PET has provided a new model for tumorimaging and, with an increased understanding oftumor biology, improvements in detection, char-acterization and staging will hopefully lead to anincrease in survival.
References
[1] Parker SL, Tong T, Bolden S, Wingo PA. Cancer Stat1997;47:5–27.
[2] Warburg O, Posener K, Negelein E. The metabolism ofthe carcinoma cell. In: Warburg O, editor. TheMetabolism of Tumors. New York: Richard R. Smith,1931:129–69.
[3] Weber G. Enzymology of cancer cells (first of twoparts). N Eng J Med 1977;296:486–92.
[4] Golshani S. Insulin, growth factors, and cancer cellenergy metabolism: an hypothesis on oncogene action.Biochem Med Metab Biol 1992;47:108–15.
[5] Merrall NW, Plevin R, Gould GW. Growth factors,mitogens, oncogenes and the regulation of glucose trans-port. Cell Signal 1993;5:667–75.
[6] Yamamoto T, Seino Y, Fukumoto H, Koh G, Yano H,Inagaki N, Yamada Y, Inoue K, Manabe T, Imura H.Over-expression of facilitative glucose transporter genesin human cancer. Biochem Biophys Res Commun1990;170:223–30.
[7] Brown RS, Wahl RL. Overexpression of Glut-1 glucosetransporter in human breast cancer. An immunohisto-chemical study. Cancer 1993;72:2979–85.
[8] Nolop KB, Rhodes CG, Brudin LH. Glucose utilizationin vivo by human pulmonary neoplasm. Cancer1987;60:2682–9.
[9] Wahl RL, Hutchins CD, Buchsbaum DJ, Liebert M,Grossman HB, Fisher S. 18F-2-deoxy-2-fluoro-D-glucoseuptake into human tumor xenografts: feasibility studiesfor cancer imaging with positron emission tomography.Cancer 1991;67:1544–50.
[10] Hatanaka M. Transport of sugars in tumor cell mem-branes. Biochim Biophys Acta 1974;355:77–104.
[11] Patz EF Jr, Goodman PC. Positron emission tomogra-phy imaging of the thorax. Radiol Clin North Am1994;32:811–23.
[12] Good CA. Management of patient with solitary mass inlung. Chin Med Soc Bull 1953;55:893–6.
[13] Good CA, Wilson TW. The solitary circumscribed pul-monary nodule. J Am Med Assoc 1958;166:210–5.
[14] Lillington GA, Caskey CI. Evaluation and managementof solitary multiple pulmonary nodules. Clin Chest Med1993;14:111–9.
[15] Yankelevitz DF, Henschke CI. Does 2-year stabilityimply that pulmonary nodules are benign? Am J Radiol1997;168:325–8.
[16] Swensen SJ, Brown LR, Colby TV, Weaver AL,Midthun DE. Lung nodule enhancement at CT:prospective findings. Radiology 1996;201:447–55.
[17] Gupta N, Gill H, Graeber G, Bishop H, Hurst J,Stephens T. Dynamic positron emission tomographywith F-18 fluorodeoxyglucose imaging in differentiatingof benign from malignant lung/mediastinal lesions.Chest 1998;114:1105–11.
[18] Patz EF, Lowe VJ, Hoffman JM, Paine SS, Burrowes P,Coleman RE, Goodman PC. Focal pulmonary abnor-malities: evaluation with F-18 fluorodeoxyglucose PETscanning. Radiology 1993;188:487–90.
[19] Gupta NC, Frank AR, Dewan NA, Redepenning LS,Rothberg ML, Mailliard JA, Phalen JJ, Sunderland JJ,Frick MP. Solitary pulmonary nodules: detection ofmalignancy with PET with 2-[F-18]-fluoro-2-deoxy-D-glucose. Radiology 1992;184:441–4.
[20] Gupta NC, Maloof J, Gunel E. Probability of malig-nancy in solitary pulmonary nodules using fluorine-18-FDG and PET. J Nucl Med 1996;37:943–8.
[21] Hubner KF, Buonocore E, Gould HR, Thie J, SmithGT, Stephens S, Dickey J. Differentiating benign frommalignant lung lesions using ‘quantitative’ parameters ofFDG PET images. Clin Nucl Med 1996;21:941–9.
[22] Conti PS, Lilien DL, Hawley K, Keppler J, Grafton ST,Bading JR. PET and [18F]-FDG in oncology: a clinicalupdate. Nucl Med Biol 1996;23:717–35.

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202 199
[23] Scott WJ, Schwabe JL, Gupta NC, Dewan NA, ReebSD, Sugimoto JT. Positron emission tomography of lungtumors and mediastinal lymph nodes using[18F]fluorodeoxyglucose. Ann Thorac Surg 1994;58:698–703.
[24] Dewan NA, Shehan CJ, Reeb SD, Gobar LS, Scott WJ,Ryschon K. Likelihood of malignancy in a solitarypulmonary nodule. Chest 1997;112:416–22.
[25] Lowe VJ, Fletcher JW, Gobar L, Lawson M, KirchnerP, Valk P, Karis J, Hubner K, Delbeke D, Heiberg EV,Patz EF, Coleman RE. Prospective investigation of PETin lung nodules (PIOPILN). J Clin Oncol 1998;16:1075–84.
[26] Erasmus JJ, McAdams HP, Patz EF Jr, Coleman RE,Ahuja V, Goodman PC. Evaluation of primary pul-monary carcinoid tumors using FDG PET. Am J Radiol1998;170:1369–73.
[27] Higashi K, Ueda Y, Seki H, Yuasa K, Oguchi M,Noguchi T, Taniguchi M, Tonami H, Okimura T, Ya-manato I. Fluorine-18-FDG PET imaging is negative inbronchioloalveolar lung carcinoma. J Nucl Med1998;39:1016–20.
[28] Kim BT, Kim Y, Lee KS, Yoon SB, Cheon EM, KwonOJ, Rhee CH, Han J, Shin MH. Localized form ofbronchioloalveolar carcinoma: FDG PET findings. Am JRadiol 1998;170:935–9.
[29] Strauss LG, Conti PS. The applications of PET inclinical oncology. J Nucl Med 1991;32:623–48.
[30] Kubota K, Matsuzawa T, Fujiwara T, et al. Differentialdiagnosis of lung tumor with positron emission tomogra-phy: a prospective study. J Nucl Med 1990;31:1927–33.
[31] Quint LE, Francis IR, Wahl RL, Gross BH, GlazerGM. Preoperative staging of non-small cell carcinoma ofthe lung: imaging methods. Am J Roentgenol1995;164:1349–59.
[32] Dewan NA, Gupta NC, Redepenning LS, Phalen JJ,Frick MP. Diagnostic efficacy of PET-FDG imaging insolitary pulmonary nodules. Chest 1993;104:997–1002.
[33] Gambhir SS, Shepherd JE, Shah BD, Hart E, Hoh CK,Valk PE, Emi T, Phelps ME. Analytical decision modelfor the cost-effective management of solitary pulmonarynodules. J Clin Oncol 1998;16:2113–25.
[34] Lewis P, Griffin S, Marsden P, Gee T, Nunan T, MalseyM, Dussek J. Whole-body 18F-fluorodeoxyglucosepositron emission tomography in preoperative evalua-tion of lung cancer. Lancet 1994;344:1265–6.
[35] Weder W, Schmidt RA, Bruchhaus H, Hillinger S, vonSchulthess GK, Steinert HC. Detection of extrathoracicmetastases by positron emission tomography in lungcancer. Ann Thorac Surg 1998;66:886–93.
[36] Marom EM, McAdmas HP, Erasmus JJ, Goodman PC,Culhane DK, Coleman RE, Herndon JE, Patz EF Jr.Staging non-small cell lung cancer with whole bodyPET. Radiology 1999;212:803–9.
[37] Klein JS, Webb WR. The radiologic staging of lungcancer. J Thorac Imaging 1991;7:29–47.
[38] Martini N, Heelan R, Westcott J, Bains MS, McCor-mack P, Caravelli J, Watson R, Zaman M. Comparitivemerits of conventional, computed tomographic, andmagnetic resonance imaging in assessing mediastinal in-volvement in surgically confirmed lung carcinoma. JThorac Cardiovasc Surg 1985;90:639–48.
[39] Musset D, Grenier P, Carette MF, Frija G, Hauuy MP,Desbleds MT, Girard P, Bigot JM, Lallemand D. Pri-mary lung cancer staging: prospective comparative studyof MR imaging with CT. Radiology 1986;160:607–11.
[40] Webb WR, Gatsonis C, Zerhouni EA, Heelan RT,Glazer GM, Francis IR, McNeil BJ. CT and MR imag-ing in staging non-small cell bronchogenic carcinoma:report of the radiologic diagnostic Oncology Group.Radiology 1991;178:705–13.
[41] Webb WR. MR imaging in the evaluation and staging oflung cancer. Semin Ultrasound CT MRI 1988;9:53–66.
[42] Staples CA, Muller NL, Miller RR, Evans KG, NelemsB. Mediastinal nodes in bronchogenic carcinoma: com-parison between CT and mediastinoscopy. Radiology1988;167:367–72.
[43] Gdeedo A, Van Schill P, Corthouts B, Van Mieghem F,Van Meerbeek J, Van Mark E. Prospective evaluation ofcomputed tomography and medistinoscopy in medistinallymph node staging. Eur Respir J 1997;10:1547–51.
[44] McLoud TC, Bourgouin PM, Greenberg RW, KosijukJP, Templeton PA, Shepard JA, Moore EH, Wain JC,Mathisen DJ, Grillo HC. Bronchogenic carcinoma: anal-ysis of staging in the mediastinum with CT by correla-tive lymph node mapping and sampling. Radiology1992;182:319–23.
[45] Guhlmann A, Storck M, Kotzerke J, Moog F, Sunder-Plassmann L, Reske SN. Lymph node staging in non-small cell lung cancer: evaluation by [18F]FDG positronemission tomography (PET). Thorax 1997;52:438–41.
[46] Steinert H, et al. Non-small cell lung cancer: nodalstaging with FDG PET versus CT with correlativelymph node mapping and sampling. Radiology1997;202:441–6.
[47] Wahl RL, Quint LE, Greenough RL, Meyer CR, WhiteRI, Orringer MB. Staging of mediastinal non-small celllung cancer with FDG PET, CT, and fusion images:preliminary prospective evaluation. Radiology1994;191:371–7.
[48] Sazon DA, Santiago SM, Soo Hoo GW, Khonsary A,Brown C, Mandelkern M, Blahd W, Williams AJ. Fluo-rodeoxyglucose-positron emission tomography in the de-tection and staging of lung cancer. Am J Respir CritCare Med 1996;153:417–21.
[49] Patz EF Jr, Lowe VJ, Goodman PC, Herndon J. Tho-racic nodal staging with positron emission tomography(PET) and 18-F-2 fluoro-2-deoxy-D-glucose in patientswith bronchogenic carcinoma. Chest 1995;108:1617–21.
[50] Vansteenkiste JF, Stroobants SG, De Leyn PR, DupontPJ, Bogaert J, Maes A, Deneffe GJ, Nackaerts KL,Verschakelen JA, Lerut TE, Mortelmans LA, DemedtsMG. Lymph node staging in non-small-cell lung cancer

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202200
with FDG-PET scan: a prospective study on 690 lymphnode stations from 68 patients. J Clin Oncol1998;16:2142–9.
[51] Valk PE, Pounds TR, Hopkins DM, Haseman MK,Hofer GA, Greiss HB, Myers RW, Lutrin CL. Stagingnon-small cell lung cancer by whole-body positron emis-sion tomographic imaging. Ann Thorac Surg1995;60:1573–82.
[52] Farrell MA, McAdams HP, Patz Jr EF. Accuracy ofFDG-PET imaging in determining nodal status for earlystage lung cancer. In: Proceedings of the AmericanRoentgen Ray Society 99th Annual Meeting, 9–14 May.New Orleans, LA. Am J Radiol 1999;172:54 [abstract].
[53] Gambir SS, Hoh CK, Phelps ME, Madar I, MadddahiJ. Decision tree sensitivity analysis for cost-effectivenessof FDG-PET in the staging and management of non-small-cell lung carcinoma. J Nucl Med 1996;37:1428–36.
[54] Valk PE, Pounds TR, Tesa RD, Hopkins DM, HasemanMK. Cost-effectiveness of PET imaging in clinical oncol-ogy. Nucl Med Biol 1996;23:737–43.
[55] Quint LE, Tummala S, Brisson LJ, Francis IR, Krup-nick AS, Kazerooni EA, Iannettoni MD, Whyte RI,Orringer MB. Distribution of distant metastases fromnewly diagnosed non-small cell lung cancer. Ann ThoracSurg 1996;62:246–50.
[56] Boring CC, Squires TS, Tong T. Cancer Stat1992;42:19–43.
[57] Little AG, Stitik FP. Clinical staging of patients withnon-small cell lung cancer. Chest 1990;97:1431–8.
[58] Templeton PA, Caskey CI, Zerhouni EA. Current usesof CT and MR imaging in the staging of lung cancer.Radiol Clin North Am 1990;28:631–46.
[59] Stitik FP. Staging of lung cancer. Radiol Clin North Am1990;28:619–30.
[60] Rege SD, Hoh CK, Glaspy JA. Imaging of pulmonarymass lesions with whole-body positron emission tomog-raphy and fluoro-deoxyglucose. Cancer 1993;72:82–90.
[61] Bury T, Dowalti A, Paulus P, Hustinx R, RadermeckerM, Rigo P. Staging of non-small-cell lung cancer bywhole-body fluorine-18 deoxyglucose positron emissiontomography. Eur J Nucl Med 1996;23:204–6.
[62] Bury T, Dowalti A, Paulus P, Corhay JL, Hustinx R,Ghaye B, Radermecker M. Whole-body 18FDG positronemission tomography in the staging of non-small celllung cancer. Eur Respir J 1997;10:2529–34.
[63] Erasmus JJ, Patz EF, McAdams HP, Murray JG, Hern-don JE, Coleman RE, Goodman PC. Evaluation ofadrenal masses in patients with bronchogenic carcinomaby using 18F-fluorodeoxyglucose positron emission to-mography. AJR 1997;168:1357–60.
[64] Winstanley DP, Smith RA. Selection of patients for thesurgical treatment of bronchial carcinoma. Thorax1968;23:327 [abstract].
[65] Mathews MJ, Kanhouwa S, Pickren J, Robinette D.Frequency of residual and metastatic tumor in patientsundergoing curative surgical resection for lung cancer.Cancer Treat Rep (part 3) 1973;4:63–7.
[66] Englemen RM, McNamara WL. Bronchogenic car-cinoma: a statistical review of two hundred twenty fourautopsies. J Thorac Surg 1954;27:227–37.
[67] Oliver TW Jr, Bernardino ME, Miller JI, Mansour K,Greene D, Davis WA. Isolated adrenal masses in nons-mall-cell bronchogenic carcinoma. Radiology1984;153:217–8.
[68] Sparup J, Merete F, Brenoe J, Vejilsted H, Villumsen B,Olesen KP, Borgeskov S, Bertelsen S. Computed tomog-raphy and the TNM claasification of lung cancer. ScandJ Thorac Cardiovasc Surg 1990;24:207–11.
[69] Nielsen ME Jr, Heaston DK, Dunnick NR, KorobkinM. Preoperative CT evaluation of adrenal glands innon-small cell bronchogenic carcinoma. Am JRoentgenol 1982;139:317–20.
[70] Pagani JJ. Normal adrenal glands in small cell lungcarcinoma: CT-guided biopsy. Am J Radiol1983;140:949–51.
[71] Pagani JJ. Non-small cell lung carcinoma adrenal metas-tases. Cancer 1984;53:1058–60.
[72] Pagani JJ, Bernardino ME. Incidence and significance ofserendipitous CT findings in the oncologic patient. JComput Assisted Tomogr 1982;6:268–75.
[73] Ettinghausen SE, Burt ME. Prospective evaluation ofunilateral adrenal masses in patients with operable non-small-cell lung cancer. J Clin Oncol 1991;9:1462–6.
[74] Boland GW, Goldberg MA, Lee MJ, Mayo-Smith WW,Dixon J, McNicholas MM, Mueller PR. Indeterminateadrenal mass in patients with cancer: evaluation at PETwith 2-[F-18]-fluoro-2-deoxy-D-glucose. Radiology1995;194:131–4.
[75] Salvatierra A, Baamonde C, Llamas JM, Cruz F, Lopez-Pujol J. Extrathoracic staging of bronchogenic car-cinoma. Chest 1990;97:1052–8.
[76] Bury T, Barreto A, Daenen F, Barthelemy N, Ghaye B,Rigo P. Fluorine-18 deoxyglucose positron emission to-mography for the detection of bone metastases in pa-tients with non-small cell lung cancer. Eur J Nucl Med1998;25:1244–7.
[77] Hillers TK, Sauve MD, Guyatt GH. Analysis of pub-lished studies on the detection of extrathoracic metas-tases in patients presumed to have operable non-smallcell lung cancer. Thorax 1994;49:14–9.
[78] Tornyos K, Garcia O, Karr B, LeBeaud R. A correla-tion study of bone scanning with clinical and laboratoryfindings in the staging of nonsmall-cell lung cancer. ClinNucl Med 1991;16:107–9.
[79] Tarver RD, Richmond BD, Klatte EC. Cerebral metas-tases from lung carcinoma: neurological and CT correla-tion. Radiology 1984;153:689–92.
[80] Yokoi K, Miyazawa N, Arai T. Brain metastasis inresected lung cancer: value of intensive follow-up withcomputed tomography. Ann Thorac Surg 1996;61:546–51.
[81] Larcos G, Maisey MN. FDG-PET screening for cerebralmetastases in patients with suspected malignancy. NuclMed Commun 1996;17:197–8.

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202 201
[82] Griffeth LK, Rich KM, Dehadashti F, Simpson JR,Fusselman MJ, Mcguire AH, Siegel BA. Brain metas-tases from non-central nervous system tumors: evalua-tion by PET. Radiology 1993;186:37–44.
[83] Patz EF Jr, Erasmus JJ, McAdams HP, Connoly JE,Marom EM, Goodman PC, Leder RA, Keogan MT,Herndon JE. Lung cancer staging and management:comparison of contrast-enhanced and nonenhanced heli-cal CT of the thorax. Radiology 1999;212:56–60.
[84] Hustinx R, Paulus P, Jacquet N, Jerusalem G, Bury T,Rigo P. Clinical evaluation of whole-body 18F-fluorodeoxyglucose positron emission tomography in thedetection of liver metastases. Ann Oncol 1998;9:397–401.
[85] Delbeke D, Martin WH, Sandler MP, Chapman WC,Wright JK Jr, Pinson CW. Evaluation of benign vs,malignant hepatic lesions with positron emission tomog-raphy. Arch Surg 1998;133:510–5.
[86] Nakamato Y, Higashi T, Sakahara H, Tamaki N, Ko-gire M, Imamura M, Konishi J. Contribution of PET inthe detection of liver metastases from pancreatic tu-mours. Clin Radiol 1999;54:248–52.
[87] Rankin SC, Taylor H, Cook GJ, Mason R. Computedtomography and positron emission tomography in thepre-operative staging of oesophageal carcinoma. ClinRadiol 1998;53:659–65.
[88] Abdel-Nabi H, Doer RJ, Lamonica DM, Cronin VR,Galantowicz PJ, Carbone GM, Spaulding MB. Stagingof primary colorectal carcinomas with fluorine-18fluorodeoxyglucose whole-body PET: correlation withhistopathologic and CT findings. Radiology1998;206:755–60.
[89] Younes RN, Gross JL, Deheinzelin D. Follow-up inlung cancer. How often and for what purpose? Chest1999;115:1494–9.
[90] Frank A, Lefkowitz D, Jaeger S, Gobar L, SunderlandJ, et al. Decision logic for retreatment of asymptomaticlung cancer recurrence based on positron emission to-mography findings. Int J Radiat Oncol Biol Phys1995;32:1495–512.
[91] Hubner KF, Buonocore E, Singh SK, Gould HR, Cot-ton DW. Characterization of chest masses by FDGpositron emission tomography. Clin Nucl Med1995;20:293–8.
[92] Inoue T, Kim EE, Komaki R, Wong FC, Bassa P,Wong WH, Yang DJ, Endo K, Podoloff DA. Detectingrecurrent or residual lung cancer with FDG-PET. J NuclMed 1995;36:788–93.
[93] Kubota K, Yamada S, Ishiwata K, Ito M, Ido T.Positron emission tomography for treatment evaluationand recurrence detection compared with CT in long-termfollow-up cases of lung cancer. Clin Nucl Med1992;17:877–81.
[94] Patz EF, Lowe VJ, Hoffman JM, Paine SS, Harris KK,Goodman PC. Persistent or recurrent bronchogenic car-cinoma: detection with PET and 2-[F-18] fluoro-2-deoxy-D-glucose. Radiology 1994;191:379–82.
[95] Munley MT, Marks LB, Scarfone C, Sibley GS, Patz EFJr, Turkington T, Jaszczak RJ, Gilland DR, AnscherMS, Coleman RE. Multimodality nuclear medicineimaging in three-dimensional radiation treatment plan-ning for lung cancer: challenges and prospects. LungCancer 1999;23:105–14.
[96] Kiffer JD, Berlangieri SU, Scott AM, Quong G, FeigenM, Schumer W, Clarke CP, Knight SR, Daniel FJ. Thecontribution of 18F-fluoro-2-deoxy-glucose positronemission tomographic imaging to radiotherapy in lungcancer. Lung Cancer 1998;19:167–77.
[97] Hebert ME, Lowe VJ, Hoffman JM, Patz EF, AnscherMS. Positron emission tomography in the pretreatmentevaluation and follow-up of non-small cell lung cancerpatients treated with radiotherapy: preliminary findings.Am J Clin Oncol 1996;19:416–21.
[98] Nestle U, Walter K, Schmidt S, Licht N, Nieder C,Motaref B, Hellwig D, et al. 18F-Deoxyglucose positronemission tomography (FDG-PET) for the planning ofradiotherapy in lung cancer: high impact in patients withatelectasis. Int J Radiat Oncol Biol Phys 1999;44:593–7.
[99] Duhaylongsod FG, Lowe VJ, Patz EF Jr. Detection ofprimary and recurrent lung cancer by means of F-18fluorodeoxyglucose positron emission tomography(FDG PET). J Thorac Cardiovasc Surg 1995;110:130–9.
[100] Abe Y, Matzuzawa T, Fujiwara T. Clinical assessmentof therapeutic effects on lung cancer using FDG andPET: preliminary study of lung cancer. Int J RadiatOncol Biol Phys 1990;19:1005–10.
[101] Leuven Lung Cancer Group, Vansteenkiste JF,Stroobants SG, De Leyn PR, Dupont PJ, Verbeken EK.Potential use of FDG-PET scan after inductionchemotherapy in surgically staged IIIa-N2 non-small-celllung cancer: a prospective pilot study. Ann Oncol1998;9:1193–8.
[102] Patz EF, Jr, Connolly JE, Herndon JE. Prognostic valueof FDG-PET imaging following treatment for non-smallcell lung cancer. Am J Radiol (in press).
[103] Ahuja V, Coleman RE, Herndon J, Patz EF Jr. Theprognostic significance of fluorodeoxyglucose positronemission tomography imaging for patients with nonsmallcell lung carcinoma. Cancer 1998;83:918–24.
[104] Leuven Lung Cancer Group, Vansteenkiste JF,Stroobants SG, Dupont PJ, De Leyn PR, Verbeken EK,Deneffe GJ, Mortelmans LA, Demedts MG. Prognosticimportance of standardized uptake value on 18F-fluoro-2-deoxy-glucose-positron emission tomography scan innon-small-cell lung cancer: an analysis of 125 cases. JClin Oncol 1999;17:3201–6.
[105] McCann J. PET scans approved for detecting metastaticnon-small-cell lung cancer. J Natl Cancer Inst1998;90:94–6.
[106] Coleman RE, Tesar RD. Clinical PET: are we ready? JNucl Med 1997;38:8N–9N.
[107] Zimny M, Kaiser HJ, Cremerius U, Sabri O, Schrecken-berger M, Reinartz P, Bull U. F-18-FDG positron imag-ing in oncological patients: gamma camera coincidence

E.M. Marom et al. / Lung Cancer 28 (2000) 187–202202
detection versus dedicated PET. Nuklearmedizin1999;38:108–14.
[108] Tatsumi M, Yutani K, Watanabe Y, Miyoshi S,Tomiyama N, Johkoh T, Kusuoka H, Nakamura H,Nishimura T. Feasibility of gluorodeoxyglucose dual-head gamma camera coincidence imaging in evaluationof lung cancer: comparison with FDG-PET. J NuclMed 1999;40:566–73.
[109] Weber WA, Neverve J, Sklarek J, Ziegler SI, Barten-stein P, King B, Treumann T, Enterrottacher A, KrapfM, Haussinger KE, Lichte H, Prauer HW, Thetter O,Schwaiger M. Imaging of lung cancer with fluorine-18fluorodeoxyglucose: comparison of a dual-head gammacamera in coincidence mode with a full-ring positron
emission tomography system. Eur J Nucl Med1999;26:388–95.
[110] Shreve PD, Stevenson RS, Deters EC, Kison PV,Gross MD, Wahl RL. Oncologic diagnosis with 2-[fluorine-18]fluoro-2-deoxy-D-glucose imaging: dual-head coincidence gamma camera versus positronemission tomographic scanner. Radiology 1998;207:431–7.
[111] Lonneux M, Dleval D, Bausart R, Moens R, Will-cockx R, Van Mael P, Declerck P, Jamar F, Zreik H,Pauwels S. Can dual-headed 18F-FDG SPET imagingreliably supersede PET in clinical oncology? A com-parative study in lung and gastrointestinal tract cancer.Nucl Med Commun 1998;19:1047–54.
.
![The metabolic anatomy of Parkinson's disease: Complementary [18F]fluorodeoxyglucose and [18F]fluorodopa positron emission tomographic studies](https://img.pdfslide.net/doc/110x75/634c1d4b526bce8bbe0c08da/the-metabolic-anatomy-of-parkinsons-disease-complementary-18ffluorodeoxyglucose-1700043549.jpg)













![Time dependence of residual tissue viability after myocardial infarction assessed by [18F]fluorodeoxyglucose and positron emission tomography](https://img.pdfslide.net/doc/110x75/6351d1825c21d80fde0aac15/time-dependence-of-residual-tissue-viability-after-myocardial-infarction-assessed.jpg)














