Embed Size (px)
Citation preview

This article was downloaded by: [Wendy Magee]On: 21 October 2013, At: 15:18Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH,UK
NeuropsychologicalRehabilitation: An InternationalJournalPublication details, including instructions for authorsand subscription information:http://www.tandfonline.com/loi/pnrh20
Music Therapy Assessment Toolfor Awareness in Disordersof Consciousness (MATADOC):Standardisation of the principalsubscale to assess awarenessin patients with disorders ofconsciousnessWendy L. Mageea, Richard J. Siegertb, Barbara A.Davesonc, Gemma Lenton-Smithd & Steve M. Taylore
a Boyer College of Music and Dance, Temple University,Philadelphia, PA, USA and Royal Hospital for Neuro-disability, Londonb School of Rehabilitation and Occupational Studiesand School of Public Health and Psychosocial Studies,AUT University, Auckland, New Zealandc Cicely Saunders Institute, Department of PalliativeCare, Policy and Rehabilitation, King's College London,UKd Ealing Music Therapy, London, UKe School of Public Health and Psychosocial Studies,AUT University, Auckland, New ZealandPublished online: 18 Oct 2013.
To cite this article: Wendy L. Magee, Richard J. Siegert, Barbara A. Daveson, GemmaLenton-Smith & Steve M. Taylor , Neuropsychological Rehabilitation (2013): MusicTherapy Assessment Tool for Awareness in Disorders of Consciousness (MATADOC):Standardisation of the principal subscale to assess awareness in patients with disorders

of consciousness, Neuropsychological Rehabilitation: An International Journal, DOI:10.1080/09602011.2013.844174
To link to this article: http://dx.doi.org/10.1080/09602011.2013.844174
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all theinformation (the “Content”) contained in the publications on our platform.However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, orsuitability for any purpose of the Content. Any opinions and views expressedin this publication are the opinions and views of the authors, and are not theviews of or endorsed by Taylor & Francis. The accuracy of the Content shouldnot be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions,claims, proceedings, demands, costs, expenses, damages, and other liabilitieswhatsoever or howsoever caused arising directly or indirectly in connectionwith, in relation to or arising out of the use of the Content.
This article may be used for research, teaching, and private study purposes.Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expresslyforbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013

Music Therapy Assessment Tool for Awareness in
Disorders of Consciousness (MATADOC):
Standardisation of the principal subscale to assess
awareness in patients with disorders of consciousness
Wendy L. Magee1, Richard J. Siegert2, Barbara A. Daveson3,Gemma Lenton-Smith4, and Steve M. Taylor5
1Boyer College of Music and Dance, Temple University, Philadelphia, PA,
USA and Royal Hospital for Neuro-disability, London2School of Rehabilitation and Occupational Studies and School of Public
Health and Psychosocial Studies, AUT University, Auckland, New Zealand3Cicely Saunders Institute, Department of Palliative Care, Policy and
Rehabilitation, King’s College London, UK4Ealing Music Therapy, London, UK5School of Public Health and Psychosocial Studies, AUT University,
Auckland, New Zealand
(Received June 2012; accepted September 2013)
Establishing valid and reliable measures for use with patients with disorders ofconsciousness (DOC) following profound brain injury is challenging due to anumber of factors including the complex presentation of such patients andassessor variability. The auditory modality has been demonstrated to havegreater sensitivity for detecting awareness in DOC patients. However, thereare no measures developed to assess auditory responsiveness specifically.The objective of this study was to examine the psychometric properties ofthe principal subscale of a music therapy assessment tool (MATADOC) devel-oped for use with adult DOC patients. The subscale assesses behaviouraldomains essential for diagnosis of awareness. Twenty-one adult patientswere recruited from a specialist rehabilitation unit. In a prospective studywith repeated measures, internal consistency, inter-rater and test–retestreliability and dimensionality were examined. The five-item scale showed
Correspondence should be addressed to Dr Wendy L. Magee, Boyer College of Music and
Dance, Temple University, Presser Hall, 2001 North 13th Street, Philadelphia, PA 19122,
USA. E-mail: [email protected]
Neuropsychological Rehabilitation, 2013
http://dx.doi.org/10.1080/09602011.2013.844174
# 2013 Taylor & Francis
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013

satisfactory internal reliability (a ¼ .76) and a strong first principal component.Corrected item-total correlations were all . .45. Inter-rater intra-class corre-lations (ICCs) ranged from 0.65–1.00 and intra-rater ICCs from 0.77–0.90.Rasch analysis confirmed these impressions of a reliable, unidimensional andhomogenous scale. Diagnostic outcomes had 100% agreement with a validatedexternal reference standard. The results indicate that the MATADOC principalsubscale provides a new behavioural measure that can contribute to interdisci-plinary assessment of awareness with DOC patients.
Keywords: Music therapy; Disorders of consciousness; Assessment; Diagnosis;Awareness; Brain injuries; Vegetative state; Minimally conscious state.
INTRODUCTION
This paper presents the standardisation of an assessment tool developed tomeasure responsiveness to auditory stimuli which are finely manipulatedwithin a music therapy treatment protocol for patients with disorders of con-sciousness (DOC). The term DOC is used to encompass both the vegetativestate (VS) and minimally conscious state (MCS) following severe braininjury. VS is a syndrome where the individual displays spontaneous arousaland sleep–wake cycles, but in the absence of behaviours indicating awarenessof oneself or the environment, no interaction with others, and no sustained,purposeful or voluntary responses to sensory stimuli (Giacino & Kalmar,1997). Reflexive behaviours are typically observed. More recently, a newnomenclature of “unresponsive wakefulness syndrome” (UWS) has been pro-posed as an alternative to VS due to the pejorative image associated with theterm “vegetative” and the risk of permanent association of “unaware” with thepatient to whom such a diagnosis is ascribed (Gosseries et al., 2011; Laureyset al., 2010).
Individuals in MCS are in a condition of severely altered consciousnessalthough they are able to demonstrate goal-directed behaviours associatedwith conscious awareness, thus providing evidence of awareness of self andtheir environment (Giacino et al., 2002). Cognitively mediated behavioursare present and distinguishable from reflexive behaviours, although these pur-poseful behaviours remain typically inconsistent and only sometimes repro-ducible. Recently, more sensitive subcategories have been proposed for thisbroad grouping based on the level of complexity of observed non-heteroge-nous behavioural responses: high level behavioural responses can be cate-gorised as “MCS+” and low level responses as “MCS–” (Bruno,Vanhaudenhuyse, Thibaut, Moonen, & Laureys, 2011). Emergence fromMCS is indicated when the person is able to demonstrate functional interac-tive communication and/or functional use of two different objects (Giacino
2 MAGEE, SIEGERT, DAVESON, LENTON-SMITH, AND TAYLOR
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
et al., 2002). Disorders of consciousness can potentially be transient in nature(Giacino et al., 2002; Laureys et al., 2010) or chronic and irreversible (Bernat,2009). Discrimination between reflexive behaviours, which are non-contin-gent to stimuli, and purposeful behaviours distinguish VS from MCS.
Diagnosis in DOC and the issues of assessment measures
Although processes for diagnosis, rehabilitation and disability managementof persons with DOC are advancing, the diagnosis process in particularremains a complicated matter (Gill-Thwaites, 2006) albeit a primaryconcern and aim of clinical intervention (Hirschberg & Giacino, 2011).The rate of misdiagnosis remains high, estimated at between 30% and 40%(Hirschberg & Giacino, 2011) increasing the risk of poor decision-makingfor disability management, inadequate future care planning, insufficientfamily support and threatening the continuation of life-preserving interven-tions (Magee, 2007b). Several factors complicate diagnosis, including incon-sistent behaviours that are typical of both subcategories of the DOCpopulation, existing volitional behaviours which may be masked by the pro-found motor and sensory impairments typical of this population, fluctuatingarousal levels, and language impairments that cannot be accurately identifieddue to the complex motor, sensory and communication impairments (Gill-Thwaites, 2006).
It has been suggested that functional MRI scanning provides a more objec-tive measure of awareness (Coleman et al., 2009). However, at present, thereis still uncertainty about the accuracy of diagnoses resulting from such tests astechnical difficulties remain (Laureys & Schiff, 2011). Assessments using be-havioural methods are still considered essential, as multiple perspectives fromconvergent, independent sources are recommended in DOC diagnosis (Seelet al., 2010). The likelihood of receptive language impairment followingsevere brain injury questions whether language-based assessments are appro-priate tools (Laureys & Schiff, 2011). This has resulted in an array of assess-ment measures examining responsiveness to multi-modal stimuli rather thanprimarily verbal language (Seel et al., 2010). Increasing interest has beentaken in the auditory modality with this population, given its sensitivity indiagnosis (Gill-Thwaites, 1997; Gill-Thwaites & Munday, 1999; Owenet al., 2005), the prevalence of visual impairment following profound braininjury (Andrews, Murphy, Munday, & Littlewood, 1996), and the combi-nation of these factors contributing to the complexity of diagnosis. The sig-nificance of auditory stimuli (verbal and non-verbal) in the assessment ofDOC patients has been highlighted: there was international interest in acase of one “unresponsive” woman in VS who demonstrated brain activitycomparable to healthy individuals in response to verbal requests to“imagine playing tennis” and “imagine visiting all the rooms in your
MATADOC: PRINCIPAL SUBSCALE 3
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
home” (Owen et al., 2006). This case illustrates the potential significance ofthe auditory modality in the diagnosis of DOC and the progress that is yet tobe made regarding accurate diagnosis of those with DOC.
Saliency and the use of sensory stimuli
Using stimuli that hold personal meaning to the patient is a critical feature inDOC assessment. Visual tracking has been noted more to visual stimuli withemotional meaning, such as the reflection of one’s face, than to stimuli withless familiarity, such as a person moving in the patient’s environment (Van-haudenhuyse, Schnakers, Bredart, & Laureys, 2008). However, discrepancyexists between expert opinions on whether visual pursuit in VS patients is areflexive or conscious behaviour (Chatelle, Laureys, Majerus, & Schnakers,2010) as the research with VS patients suggests that visual fixation doesnot necessarily indicate conscious interaction between the patient and hisor her surroundings (Bruno et al., 2010). The use of auditory stimuli in assess-ment of consciousness is receiving increasing attention either with the use ofcalling names (Boly et al., 2004, 2005; Perrin et al., 2006; Schnakers et al.,2009), particularly the patient’s own name (Laureys, Perrin, & Bredart,2007), or using musical stimuli (Boyle & Greer, 1983; Formisano et al.,2001; Jones, Vaz Pato, Sprague, Stokes, & Haque, 2000; Puggina & Paesda Silva, 2009; Verville et al., 2012; Wilson, Cranny, & Andrews, 1992).This supports the use of auditory stimuli with emotional familiarity in theassessment of people with DOC. Non-language-based auditory stimuli holdparticular relevance given the complex communication and cognitive impair-ments typical of this population.
Music as a non-language-based medium for assessment
Music is well-placed to be considered as an assessment medium with thispopulation (Magee, 2007b) given its inherent emotion-inducing properties(Sloboda, 1991), particularly those linked with pleasure and reward (Blood& Zatorre, 2001). In addition to the possibility of structuring individually tai-lored treatment protocols using music of personal meaning, the use of livemusic enables the manipulation of specific parameters of auditory stimuli(e.g., volume, pitch, timbre) thus optimising the possibility for gaining amore accurate picture of the DOC patient’s auditory responsiveness(Magee, 2005). A number of empirical studies have examined the use ofmusic with this population (see Magee, 2005). However, measuring respon-siveness to musical stimuli in people with DOC faces the difficultiesalready outlined in the broader assessment issues with DOC to an evengreater degree: standardised music-based assessments are not sensitiveenough to detect the subtle and complex changes in DOC patients; and stan-dardised tools for use with DOC populations do not examine auditory
4 MAGEE, SIEGERT, DAVESON, LENTON-SMITH, AND TAYLOR
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
responsiveness to the degree of specificity which is possible in a musictherapy assessment protocol.
The Music Therapy Assessment Tool for Awareness in Disordersof Consciousness (MATADOC)
In response to the lack of sensitive tools to assess responses to finely manipu-lated auditory stimuli, the Music Therapy Assessment Tool for Awareness inDisorders of Consciousness (MATADOC, formerly the Music TherapyAssessment Tool for Low Awareness States or MATLAS) was developedfor use with patients with DOC (Magee, 2007a). The tool includes 14 itemsthat encompass five behavioural domains commonly assessed in DOC:motor responses, communication, arousal, and auditory and visual respon-siveness, that are described in more detail here (see Table 1) and also havebeen described in detail previously (Magee, 2007a). The MATADOC isdivided into three subscales with specific purposes. The Principal Subscale:Essential Categories (items 1–5) examines essential behaviours; themusical parameters subscale (items 6–7) informs clinical intervention; anda third subscale contains clinical items to inform goal setting and clinicalcare (items 8–14).
MATADOC rationale. Given the considerable attention to and critique ofthe existing assessment measures with this population (Seel et al., 2010) itmust be questioned as to why a music-specific assessment is warranted.The tool under examination in this study was developed to assist withimmediate local needs, i.e., structuring the behavioural observations madein music therapy sessions in order to contribute to interdisciplinary assess-ments. However, as time progressed it became apparent that a more refinedassessment of auditory responsiveness was warranted to assist the interdisci-plinary team in the assessment of complex cases; that is, cases where patientsseemed to show differentiated responses to auditory stimuli but not to stimuliin other sensory modalities (see Magee, 2005, 2007a, 2007b for illustrations).It should be stressed that, in line with recommendations for best practice(Giacino et al., 2002), the MATADOC does not stand alone as a measureof awareness, but can contribute to the range of diagnostic assessments thatare recommended for this complex population. Studies of DOC populationsrequire standardised behavioural assessment and outcome tools (Laureyset al., 2010).
There are a number of existing standardised tools and protocols for DOC,including the Sensory Modality Assessment and Rehabilitation Technique(SMART; Gill-Thwaites, 1997), the Wessex Head Injury Matrix (WHIM;Shiel et al., 2000) and the Coma-Recovery Scale–Revised (CRS-R;
MATADOC: PRINCIPAL SUBSCALE 5
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
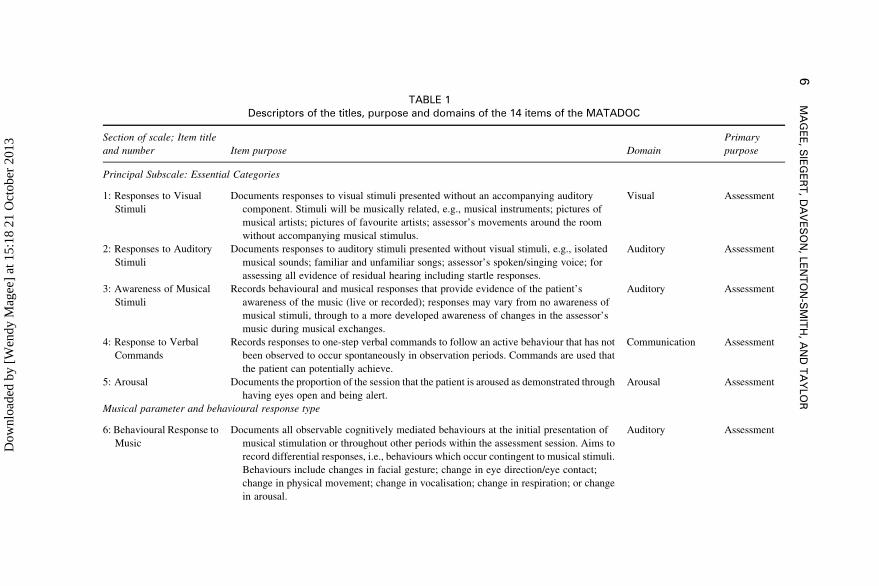
TABLE 1Descriptors of the titles, purpose and domains of the 14 items of the MATADOC
Section of scale; Item title
and number Item purpose Domain
Primary
purpose
Principal Subscale: Essential Categories
1: Responses to Visual
Stimuli
Documents responses to visual stimuli presented without an accompanying auditory
component. Stimuli will be musically related, e.g., musical instruments; pictures of
musical artists; pictures of favourite artists; assessor’s movements around the room
without accompanying musical stimulus.
Visual Assessment
2: Responses to Auditory
Stimuli
Documents responses to auditory stimuli presented without visual stimuli, e.g., isolated
musical sounds; familiar and unfamiliar songs; assessor’s spoken/singing voice; for
assessing all evidence of residual hearing including startle responses.
Auditory Assessment
3: Awareness of Musical
Stimuli
Records behavioural and musical responses that provide evidence of the patient’s
awareness of the music (live or recorded); responses may vary from no awareness of
musical stimuli, through to a more developed awareness of changes in the assessor’s
music during musical exchanges.
Auditory Assessment
4: Response to Verbal
Commands
Records responses to one-step verbal commands to follow an active behaviour that has not
been observed to occur spontaneously in observation periods. Commands are used that
the patient can potentially achieve.
Communication Assessment
5: Arousal Documents the proportion of the session that the patient is aroused as demonstrated through
having eyes open and being alert.
Arousal Assessment
Musical parameter and behavioural response type
6: Behavioural Response to
Music
Documents all observable cognitively mediated behaviours at the initial presentation of
musical stimulation or throughout other periods within the assessment session. Aims to
record differential responses, i.e., behaviours which occur contingent to musical stimuli.
Behaviours include changes in facial gesture; change in eye direction/eye contact;
change in physical movement; change in vocalisation; change in respiration; or change
in arousal.
Auditory Assessment
6M
AG
EE
,S
IEG
ER
T,
DA
VE
SO
N,
LE
NT
ON
-SM
ITH
,A
ND
TA
YLO
R
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
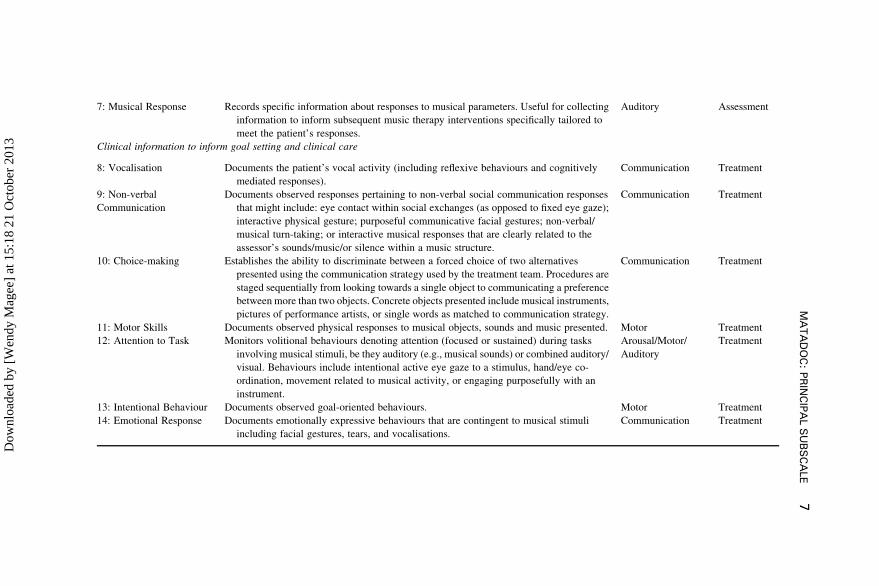
7: Musical Response Records specific information about responses to musical parameters. Useful for collecting
information to inform subsequent music therapy interventions specifically tailored to
meet the patient’s responses.
Auditory Assessment
Clinical information to inform goal setting and clinical care
8: Vocalisation Documents the patient’s vocal activity (including reflexive behaviours and cognitively
mediated responses).
Communication Treatment
9: Non-verbal
Communication
Documents observed responses pertaining to non-verbal social communication responses
that might include: eye contact within social exchanges (as opposed to fixed eye gaze);
interactive physical gesture; purposeful communicative facial gestures; non-verbal/
musical turn-taking; or interactive musical responses that are clearly related to the
assessor’s sounds/music/or silence within a music structure.
Communication Treatment
10: Choice-making Establishes the ability to discriminate between a forced choice of two alternatives
presented using the communication strategy used by the treatment team. Procedures are
staged sequentially from looking towards a single object to communicating a preference
between more than two objects. Concrete objects presented include musical instruments,
pictures of performance artists, or single words as matched to communication strategy.
Communication Treatment
11: Motor Skills Documents observed physical responses to musical objects, sounds and music presented. Motor Treatment
12: Attention to Task Monitors volitional behaviours denoting attention (focused or sustained) during tasks
involving musical stimuli, be they auditory (e.g., musical sounds) or combined auditory/
visual. Behaviours include intentional active eye gaze to a stimulus, hand/eye co-
ordination, movement related to musical activity, or engaging purposefully with an
instrument.
Arousal/Motor/
Auditory
Treatment
13: Intentional Behaviour Documents observed goal-oriented behaviours. Motor Treatment
14: Emotional Response Documents emotionally expressive behaviours that are contingent to musical stimuli
including facial gestures, tears, and vocalisations.
Communication Treatment
MA
TA
DO
C:
PR
INC
IPA
LS
UB
SC
ALE
7
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013

Giacino, Kalmar, & Whyte, 2004). The protocols of these tools are inadequatefor measuring sensitive manipulations of auditory stimuli, which can beachieved within a music-based assessment. Researching interventions withDOC where auditory stimuli are manipulated requires several particular fea-tures. First, measures need to be sensitive enough to discriminate betweenminimal responses typical of the DOC population and meet all other require-ments for evidence-based assessments as outlined by Seel et al. (2010).Second, measures need to measure specifically responses to auditorystimuli. Third, the procedures involved should be both well-defined andable to manipulate auditory components in a way to provide meaningful infor-mation. Current assessment protocols (e.g., CRS-R, SMART, WHIM) do notmanipulate components of auditory stimuli, but rather use loud sudden sounds(e.g., clapping hands) or generalised auditory stimuli such as calling thepatient’s name. Music is a useful tool for examining non-musical functionalbehaviours with this population (e.g., arousal, motor responses, visual respon-siveness) as well as musical behaviours which can be indicative of non-musical functional behaviours (e.g., non-verbal communication, vocalisation,see Magee, 2005). Thus, for reasons of validity, assessments of auditoryresponsiveness would benefit from using music-specific parameters. Onlytools that are sensitive and specific to the stimuli being used will reflect apatient’s optimal functioning.
The development of a standardised tool will enable further investigationsinto music as a diagnostic tool and treatment modality with this populationwhich has not previously been possible. Previous investigations havestruggled with the aspect of measurement, finding existing standardisedtools too insensitive to yield significant results necessitating the developmentof music-specific tools (Formisano et al., 2001) or relying on single casedesigns using individalised behavioural measures (Boyle & Greer, 1983; For-misano et al., 2001; Wilson et al., 1992). Valid tools with standardised proto-cols delivered by those with appropriate training and experience are importantwhen working with populations whose incidence is small enough to necessi-tate multisite (and often international) studies.
MATADOC protocol and scoring. A defined treatment protocol uses arange of musical stimuli, including single auditory stimuli, complexmusical sounds, and musical activities to measure a broad range of functionalnon-musical behaviours (Magee, Lenton-Smith, & Daveson, 2012). Deliver-ing the protocol requires advanced competency in the clinical application ofmusic and clinical experience with DOC populations. All tasks use music,which is predominantly presented live, although recorded music is occasion-ally used. The musical stimuli employ both music that is known to be person-ally meaningful to the patient and unfamiliar novel music which is based on
8 MAGEE, SIEGERT, DAVESON, LENTON-SMITH, AND TAYLOR
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
the patient’s physical presentation, e.g., aligning the musical tempo with thepatient’s breathing rate.
The protocol involves a minimum of four tasks to assess the items on theprincipal subscale. This subscale examines behaviours that are essential fordemonstrating awareness. However, depending on patient tolerance (e.g.,arousal) and responsiveness, the protocol can be extended to seven tasks.This means that during the process of MATADOC assessment all patientsare presented with the initial four tasks that examine preliminary responsive-ness across the auditory, visual, communication and arousal domains and canbe rated on the principal subscale. For patients who demonstrate little or noresponsiveness to the four tasks in the principal subscale and may not beable to tolerate a longer assessment (i.e., longer than approximately 12–15minutes), the assessment can be brief in duration. For patients who demon-strate tolerance for longer sessions, and particularly those who show respon-siveness in the first four tasks, additional tasks are presented that assessresponses more clearly aligned with MCS/MCS emergent states. In thisway, the MATADOC can assess the lowest level responses typical of VSpatients, but can be expanded to provide assessment tasks for patients whoare demonstrating responses typical of MCS and MCS emergent patients.Rating all 14 items for each patient on every clinical contact is essentialhowever, due to the inconsistent responses that are typical of this population.Thus, it is possible for a largely unresponsive patient to demonstrateoccasionally behaviours that are associated with higher levels of awareness(e.g., MCS) and these require careful documentation for interdisciplinary con-sideration to identify any patterns across interventions.
Although the data of behavioural ratings from the MATADOC are trans-formed into three scores, one for each subsection of the tool, only the Princi-pal Subscale score holds any diagnostic utility; the other subscales informtreatment planning and goal setting and thus hold primarily clinical utility.
Comparison of the MATADOC with existing DOC measures. Recommen-dations for diagnosis encourage the use of several different assessment toolsas the use of a single DOC assessment may prove less accurate than usingmultiple assessments (Seel et al., 2010). Best practice also recommendsthat assessments use a broad range of stimuli to elicit a range of differentresponses (Giacino et al., 2002). Within musical tasks, vocalisations can beassessed for evidence of behaviours that are volitional and related to theenvironment, thus bypassing the need for motor function which has beenfound to confound accurate scoring in other assessments. Stimuli that havepersonal meaning have been found to produce the greatest behaviouralchange in DOC populations (Boly et al., 2005; Shiel & Wilson, 2005), thusassessment using musical stimuli can optimise emotionally salient stimulithat are primarily non-verbal in nature, addressing the problems inherent in
MATADOC: PRINCIPAL SUBSCALE 9
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
language-based measures for DOC populations. Although musical stimulicould be used during the existing standardised assessments (e.g., CRS-R,SMART), protocols to ensure consistent testing are lacking. Furthermore,the tools are not structured to adequately capture subtle behaviours indicatingpatient responsiveness to musical stimuli, e.g., vocalising at pitch to environ-mental sounds.
In addition, the MATADOC places primary emphasis on the communi-cation domain (five items) and auditory domain (five items) which dis-tinguishes it from the available standardised DOC assessment tools such asthe SMART (Gill-Thwaites, 1997), the WHIM (Shiel et al., 2000) and theCRS-R (Giacino et al., 2004). However, the MATADOC also includesitems that assess the visual, motor and arousal domains as, in combinationwith auditory and communication function, these five domains are commonlyincluded in DOC assessment (Seel et al., 2010). Furthermore, neglecting tocapture data across these domains during multimodal stimulation risksmissing the inconsistent behaviours that typify the population in question(Seel et al., 2010). Thus the overlap between the MATADOC and the existingDOC measures is intentional in order to provide a comprehensive assessment,in addition to a providing a more sensitive assessment of the auditory domainand behaviours indicative of non-verbal communication.
The MATADOC administration is another point of difference, taking lesstime than the SMART for administration. On average, a MATADOC assess-ment takes 90 minutes per patient to complete (O’Kelly & Magee, 2013). Thisis completed in four contacts over one 10-day period. This is in comparison toapproximately 600 minutes over 10 occasions in 21 days for the SMART(Gill-Thwaites & Munday, 1999) with the required number of administrationsspecified as opposed to the CRS-R and WHIM that lack clear guidance(Godbolt, Stenson, Winberg, Frykberg, & Tengvar, 2011).
A pilot study comparing MATADOC outcomes with scores gained fromthe SMART (Gill-Thwaites, 1997) and the WHIM (Shiel et al., 2000)found strong concurrent validity with significant correlation (p , .01)ranging from .84 (WHIM) to .968 (SMART) (Daveson, Magee, Crewe, Beau-mont, & Kenealy, 2007). These findings warranted a more detailed compari-son specifically between items that assessed similar domains from theMATADOC and the SMART to examine sensitivities of each measure. Anaudit of 42 cases examining SMART and MATADOC outcomes from con-current assessments compared the scores of related items from each of themeasures to explore item sensitivity (O’Kelly & Magee, 2013). This auditdrew from a large sample of retrospective records including data that werecollected over a longer timeframe (i.e., MATADOC commencing days 10–20 of the commencement of SMART) and also drew from data collectedfor this current study where the assessments were administered within ashorter timeframe (i.e., MATADOC commencing between days 1–10 of
10 MAGEE, SIEGERT, DAVESON, LENTON-SMITH, AND TAYLOR
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013

the commencement of SMART). Items were compared that rated behavioursin the domains of visual, auditory and motor responsiveness, arousal andcommunication as well as overall diagnostic outcomes. A strong correlationwas found between MATADOC and SMART diagnostic outcome in thecohort (rs ¼ .80, p , .01, 2-tailed) that ranged across VS, MCS and border-line VS/MCS. As the SMART is a validated assessment tool for DOC popu-lations, this finding suggests that MATADOC has content validity for beingsensitive to behaviours representative of VS, MCS and MCS emerging beha-viours as outlined in the Aspen Workgroup criteria (Giacino et al., 2002).Although the SMART was found to have heightened sensitivity for themotor domain in relation to diagnosis when compared to the MATADOC,the MATADOC showed heightened sensitivity for the auditory and visualdomains. Scoring sensitivities may have contributed to these findings, asthe MATADOC offers smaller variations in the ratings for some items thanthe SMART. Overall the assessment tools were found to have contrasting sen-sitivities in different domains and also to record data on domains that aremutually exclusive (O’Kelly & Magee, 2013). The current study reportedhere tested the reliability, internal consistency and external validity of theMATADOC principal subscale specifically.
Testing the MATADOC principal subscale. In line with standardisedDOC assessment scales, the Principal Subscale: Essential Categories of theMATADOC can be compared with items on other DOC scales to examinevisual and auditory responsiveness, arousal, as well as responses to verbalcommands. This overlap with existing assessment tools was purposeful inorder to contribute to interdisciplinary assessments of awareness, followingrecommendations that patient responsiveness is examined in differentenvironments with contrasting stimuli and using a number of different toolsto measure responsiveness (Giacino et al., 2002). An additional item onthis subscale examines specific responses to musical stimuli (see Figure 1).These comparable features of the MATADOC principal subscale to otherDOC assessment tools and the promising concurrent validity found withSMART (Daveson et al., 2007) suggested that this particular section of theMATADOC was worth evaluating independently. This seemed importantgiven the different ratings systems used between the subscales (Guttmanand binary) and differences in the methods and relevance of scoringbetween subscales: the latter subscales have clinical rather than diagnosticutility.
Addressing evidence-based requirements in the MATADOC. This studyaimed to address several essential criteria that have been recommended forevidence-based behavioural assessment scales utilised in DOC populations(Seel et al., 2010). The MATADOC has a comprehensive manual and a
MATADOC: PRINCIPAL SUBSCALE 11
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
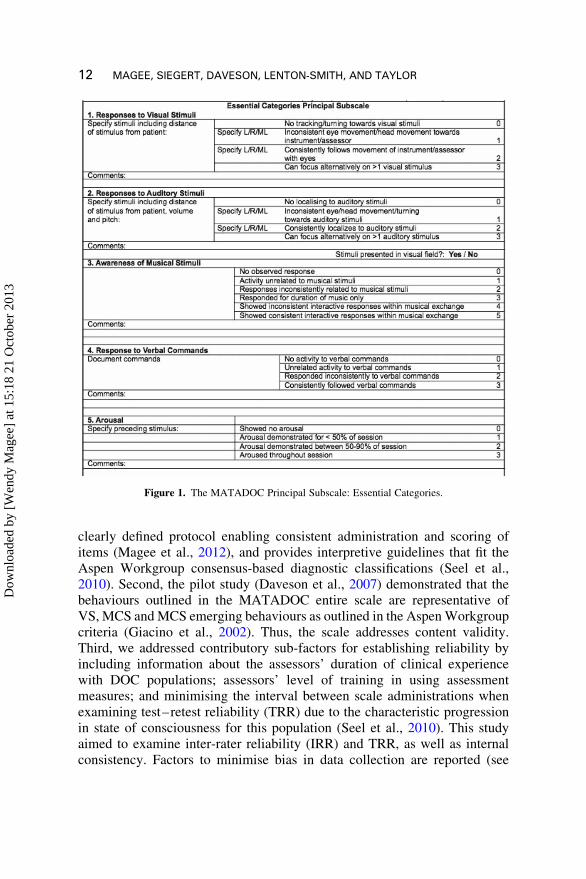
clearly defined protocol enabling consistent administration and scoring ofitems (Magee et al., 2012), and provides interpretive guidelines that fit theAspen Workgroup consensus-based diagnostic classifications (Seel et al.,2010). Second, the pilot study (Daveson et al., 2007) demonstrated that thebehaviours outlined in the MATADOC entire scale are representative ofVS, MCS and MCS emerging behaviours as outlined in the Aspen Workgroupcriteria (Giacino et al., 2002). Thus, the scale addresses content validity.Third, we addressed contributory sub-factors for establishing reliability byincluding information about the assessors’ duration of clinical experiencewith DOC populations; assessors’ level of training in using assessmentmeasures; and minimising the interval between scale administrations whenexamining test–retest reliability (TRR) due to the characteristic progressionin state of consciousness for this population (Seel et al., 2010). This studyaimed to examine inter-rater reliability (IRR) and TRR, as well as internalconsistency. Factors to minimise bias in data collection are reported (see
Figure 1. The MATADOC Principal Subscale: Essential Categories.
12 MAGEE, SIEGERT, DAVESON, LENTON-SMITH, AND TAYLOR
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013

Methods section). Fourth, evidence-based recommendations specify that con-struct validity is established using Rasch analysis where appropriate to thedata, which was implemented in the study reported here. Lastly, we aimedto examine criterion validity by comparing the MATADOC to an externalreference standard (the SMART).
Purpose of the current study
The purpose of this study was to examine the psychometric properties of theprincipal subscale of the MATADOC (reliability, repeatability, dimensional-ity and validity) in a prospective study across the domains of visual and audi-tory responsiveness, arousal, and responses to verbal commands and musicalstimuli. The research also aimed to examine the internal structure and internalconsistency of the principal subscale. In this regard we used both traditionalpsychometric methods and modern item-response methods (i.e., Rasch analy-sis; Nunnally & Bernstein, 1994). While Rasch analysis is increasingly usedin rehabilitation and strongly advocated by some authors (Hobart, Cano,Zajicek, & Thompson, 2007; Pallant & Tennant, 2007), it is still unfamiliarto many clinicians and researchers compared to classical test theorymethods (such as factor analysis). Moreover a robust measure should argu-ably stand up to scrutiny using either of these approaches (Siegert, Jackson,Tennant, & Turner-Stokes, 2010). Hence in the present study we used both.Lastly, the study aimed to conduct a validity analysis by comparing theitem scores and diagnostic outcomes of the MATADOC and SMART, withspecific comparison between items examining similar behavioural domainsfrom each measure, e.g., auditory responsiveness, visual responsiveness,and arousal, but within a narrower time frame in line with recommendationsfor validity research with DOC populations (Seel et al., 2010).
METHOD
Participants
Participants were recruited using convenience sampling from admissions to aspecialist unit for DOC over 36 months. Patients were admitted to this unitwith diagnoses of DOC but without any confirmed level of DOC, i.e., VS,MCS or MCS emerging. Admissions were for the purposes of diagnosis, dis-ability management and, where appropriate, rehabilitation. Patients were typi-cally admitted from acute general medical settings where there are nospecialist skills for assessing or treating people disabled to this level of pro-fundity. Thus, patients were typically admitted without specialist seatingsystems and without an assessment of cognitive capacity due to the level ofdisability.
MATADOC: PRINCIPAL SUBSCALE 13
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
The inclusion criteria were medically stable patients admitted to the unitfor diagnosis of awareness state, between the ages of 16 and 70 years ofage. A diagnosis of awareness (i.e., VS, MCS or emergent) had not been con-firmed for all patients recruited to the study. Participants excluded were thosewho had known pre-morbid hearing impairments, had a previous diagnosis ofmusicogenic epilepsy, had previously refused music therapy intervention,emerged from DOC during recruitment or assessment, or had a suspecteddiagnosis of locked-in syndrome. Mental capacity assessments were com-pleted before recruitment and standard procedures regarding the recruitmentof patients lacking capacity were followed. Ethical aproval was gained fromthe National Research Ethics Service (05/Q0406/185).
Assessors
Seven MATADOC assessors were involved in data collection, their experi-ence with DOC populations ranged from 0.25 to 19 years (mean ¼3.5 years). All assessors received training in both delivering the treatmentprotocol and completing the assessment rating prior to commencing involve-ment in the study. In each session, one assessor delivered the assessment pro-tocol and completed an assessment rating, and a second assessor observed andcompleted an assessment rating.
Protocol
Each participant received one complete MATADOC assessment, involvingfour individual sessions within a 10-day period. Sessions were scheduled inaccordance with the participant’s rehabilitation programme and thus tookplace at different times across a working day between 10.30 and 15.00hours. Three-minute observation periods were conducted at rest pre- andpost-treatment. The treatment protocol followed clearly defined procedures,involving the presentation of primarily live music and occasionally the useof recorded music (Magee et al., 2012). Musical stimuli involve both familiarmusic known to be salient (i.e., personally meaningful to the participant) aswell as unfamiliar music based on the participant’s behavioural presentation,e.g., breathing rate, vocal sounds, physical movements. Session duration wasbetween 12 and 25 minutes dependent on the participant’s arousal and behav-ioural responsiveness. Every MATADOC session assesses the five essentialbehavioural domains in addition to a further nine items which examinehigher level behaviours including musical behaviours elicited by the stimuli.
Each session was rated independently by two trained assessors (one whodelivered the protocol) using the MATADOC assessment schedule forinter-rater reliability analysis. In this study, the assessors were music thera-pists registered with the UK Health Professions Council. Assessors wereblind to each other’s ratings and one or both assessors were blind to the
14 MAGEE, SIEGERT, DAVESON, LENTON-SMITH, AND TAYLOR
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
participant’s clinical status and progress in interdisciplinary assessment.Additionally, sessions were video recorded enabling rating to take place bythe same two assessors independently at a later date (between 4 and24 weeks) for test–retest reliability. Thus, each single session was ratedduring live and video conditions by each assessor, producing four data setsfor a single clinical contact. In this way, 16 data sets were achieved for onecomplete MATADOC assessment for each of the 21 participants. Theviewing order of each participant’s video records was randomised to assistwith blinding for TRR.
All data were anonymised, entered into an EXCEL spreadsheet andimported into SPSS for statistical analysis (GLS). The Rasch analysis wascompleted using RUMM2020 software by an analyst who was blind to allaspects of data collection and data entry (RS). Apart from the IRR andTRR calculations, all the remaining psychometric analyses were completedusing the responses from the 168 live ratings of patients. This provided 168separate scores on each of the five items for analysis. We did not use theremaining 168 video ratings for these analyses since they could not be con-sidered completely independent.
Bias was minimised for IRR and TRR through addressing independence ofassessors, anonymisation of data, adequate time between test and retest con-ditions, randomisation of the viewing order of video records and blinding forall those involved in data management and analysis.
RESULTS
Sample
Twenty-one research participants (11 male, 10 female) were recruited, withages ranging from 19–67 years (mean ¼ 40.3 years, SD ¼ 15.65). Twenty-seven potential participants were identified, however, six were excluded as adiagnosis of DOC could not be confirmed or was contradicted. An uncon-firmed diagnosis of awareness was essential for inclusion in order to testthe validity of the MATADOC. Table 2 provides descriptive data for thecharacteristics of the people recruited to the study. The majority of thecases had sustained traumatic brain injury (n ¼ 9; 42.9%), then hypoxic-ischaemic brain damage (n ¼ 7; 33.3%), followed by haemorrhagicdamage (n ¼ 3; 14.3%) and viral infection (n ¼ 2; 9.5%). Individuals inthe recruited sample were assessed over four contacts using the WHIM(Shiel et al., 2000) to gauge behaviours indicative of severity of disabilityand emergence from DOC. The range of scores was from 0 (eyes openbriefly) to 14 (Mechanical vocalisation with yawn, sigh, etc.) with modeand median of 4 (n ¼ 14; Attention held momentarily by dominant
MATADOC: PRINCIPAL SUBSCALE 15
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
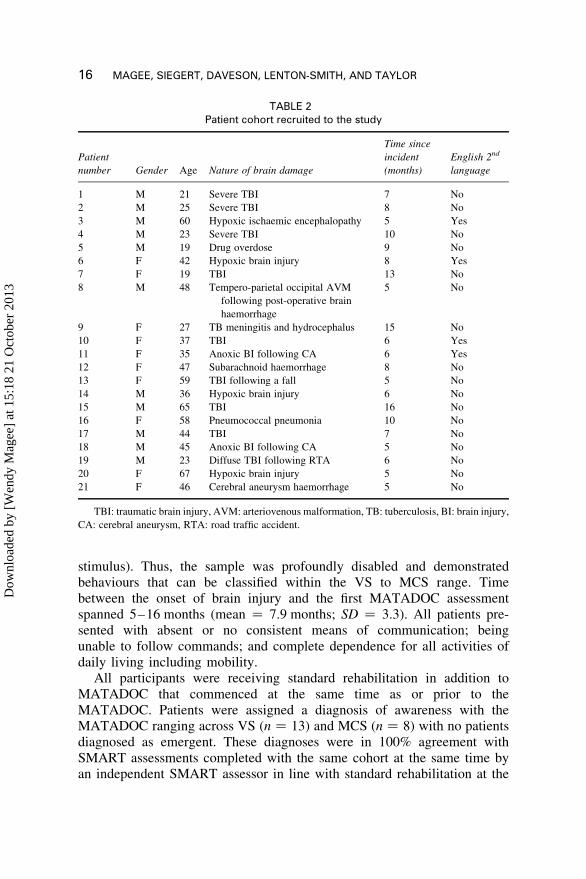
stimulus). Thus, the sample was profoundly disabled and demonstratedbehaviours that can be classified within the VS to MCS range. Timebetween the onset of brain injury and the first MATADOC assessmentspanned 5–16 months (mean ¼ 7.9 months; SD ¼ 3.3). All patients pre-sented with absent or no consistent means of communication; beingunable to follow commands; and complete dependence for all activities ofdaily living including mobility.
All participants were receiving standard rehabilitation in addition toMATADOC that commenced at the same time as or prior to theMATADOC. Patients were assigned a diagnosis of awareness with theMATADOC ranging across VS (n ¼ 13) and MCS (n ¼ 8) with no patientsdiagnosed as emergent. These diagnoses were in 100% agreement withSMART assessments completed with the same cohort at the same time byan independent SMART assessor in line with standard rehabilitation at the
TABLE 2Patient cohort recruited to the study
Patient
number Gender Age Nature of brain damage
Time since
incident
(months)
English 2nd
language
1 M 21 Severe TBI 7 No
2 M 25 Severe TBI 8 No
3 M 60 Hypoxic ischaemic encephalopathy 5 Yes
4 M 23 Severe TBI 10 No
5 M 19 Drug overdose 9 No
6 F 42 Hypoxic brain injury 8 Yes
7 F 19 TBI 13 No
8 M 48 Tempero-parietal occipital AVM
following post-operative brain
haemorrhage
5 No
9 F 27 TB meningitis and hydrocephalus 15 No
10 F 37 TBI 6 Yes
11 F 35 Anoxic BI following CA 6 Yes
12 F 47 Subarachnoid haemorrhage 8 No
13 F 59 TBI following a fall 5 No
14 M 36 Hypoxic brain injury 6 No
15 M 65 TBI 16 No
16 F 58 Pneumococcal pneumonia 10 No
17 M 44 TBI 7 No
18 M 45 Anoxic BI following CA 5 No
19 M 23 Diffuse TBI following RTA 6 No
20 F 67 Hypoxic brain injury 5 No
21 F 46 Cerebral aneurysm haemorrhage 5 No
TBI: traumatic brain injury, AVM: arteriovenous malformation, TB: tuberculosis, BI: brain injury,
CA: cerebral aneurysm, RTA: road traffic accident.
16 MAGEE, SIEGERT, DAVESON, LENTON-SMITH, AND TAYLOR
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
unit. The SMART and MATADOC assessors were blinded to the outcomes ofthe other’s assessment.
Reliability
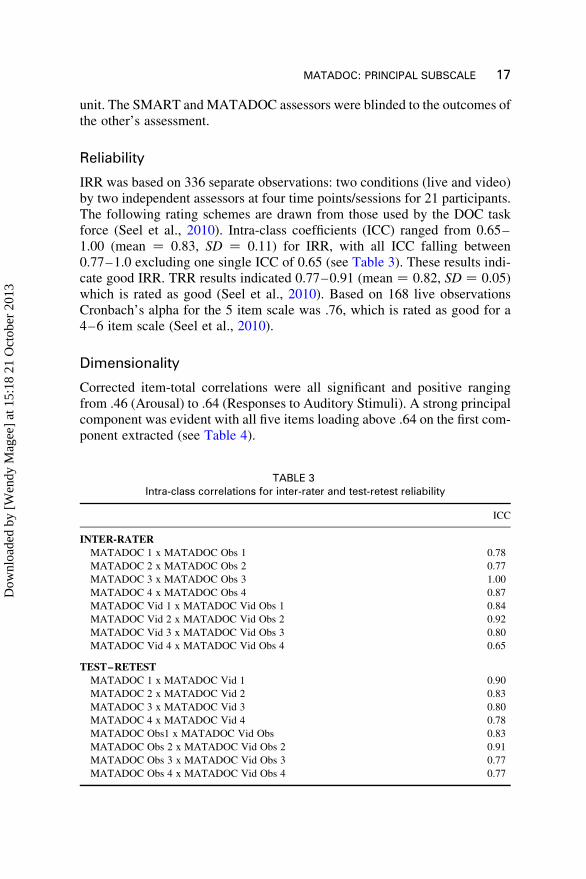
IRR was based on 336 separate observations: two conditions (live and video)by two independent assessors at four time points/sessions for 21 participants.The following rating schemes are drawn from those used by the DOC taskforce (Seel et al., 2010). Intra-class coefficients (ICC) ranged from 0.65–1.00 (mean ¼ 0.83, SD ¼ 0.11) for IRR, with all ICC falling between0.77–1.0 excluding one single ICC of 0.65 (see Table 3). These results indi-cate good IRR. TRR results indicated 0.77–0.91 (mean ¼ 0.82, SD ¼ 0.05)which is rated as good (Seel et al., 2010). Based on 168 live observationsCronbach’s alpha for the 5 item scale was .76, which is rated as good for a4–6 item scale (Seel et al., 2010).
Dimensionality
Corrected item-total correlations were all significant and positive rangingfrom .46 (Arousal) to .64 (Responses to Auditory Stimuli). A strong principalcomponent was evident with all five items loading above .64 on the first com-ponent extracted (see Table 4).
TABLE 3Intra-class correlations for inter-rater and test-retest reliability
ICC
INTER-RATER
MATADOC 1 x MATADOC Obs 1 0.78
MATADOC 2 x MATADOC Obs 2 0.77
MATADOC 3 x MATADOC Obs 3 1.00
MATADOC 4 x MATADOC Obs 4 0.87
MATADOC Vid 1 x MATADOC Vid Obs 1 0.84
MATADOC Vid 2 x MATADOC Vid Obs 2 0.92
MATADOC Vid 3 x MATADOC Vid Obs 3 0.80
MATADOC Vid 4 x MATADOC Vid Obs 4 0.65
TEST–RETEST
MATADOC 1 x MATADOC Vid 1 0.90
MATADOC 2 x MATADOC Vid 2 0.83
MATADOC 3 x MATADOC Vid 3 0.80
MATADOC 4 x MATADOC Vid 4 0.78
MATADOC Obs1 x MATADOC Vid Obs 0.83
MATADOC Obs 2 x MATADOC Vid Obs 2 0.91
MATADOC Obs 3 x MATADOC Vid Obs 3 0.77
MATADOC Obs 4 x MATADOC Vid Obs 4 0.77
MATADOC: PRINCIPAL SUBSCALE 17
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
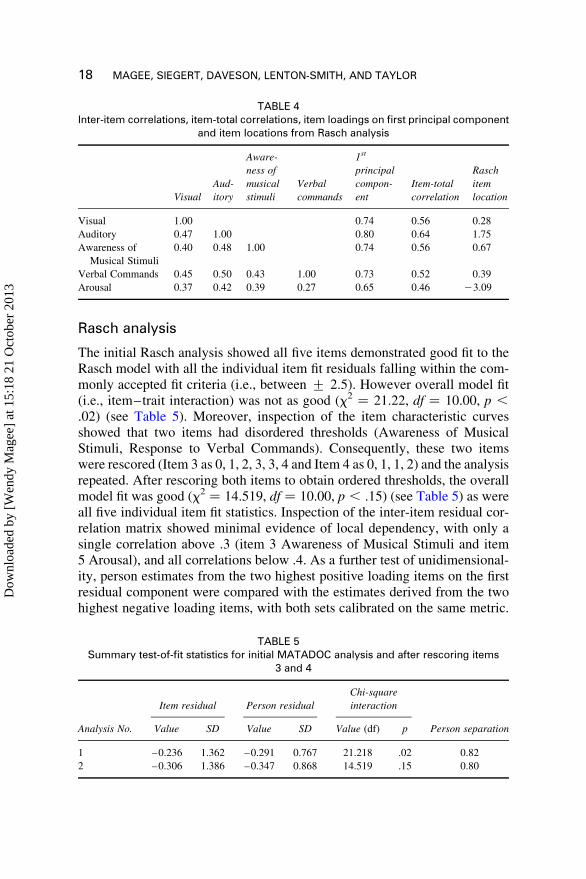
Rasch analysis
The initial Rasch analysis showed all five items demonstrated good fit to theRasch model with all the individual item fit residuals falling within the com-monly accepted fit criteria (i.e., between + 2.5). However overall model fit(i.e., item–trait interaction) was not as good (x2 ¼ 21.22, df ¼ 10.00, p ,
.02) (see Table 5). Moreover, inspection of the item characteristic curvesshowed that two items had disordered thresholds (Awareness of MusicalStimuli, Response to Verbal Commands). Consequently, these two itemswere rescored (Item 3 as 0, 1, 2, 3, 3, 4 and Item 4 as 0, 1, 1, 2) and the analysisrepeated. After rescoring both items to obtain ordered thresholds, the overallmodel fit was good (x2 ¼ 14.519, df ¼ 10.00, p , .15) (see Table 5) as wereall five individual item fit statistics. Inspection of the inter-item residual cor-relation matrix showed minimal evidence of local dependency, with only asingle correlation above .3 (item 3 Awareness of Musical Stimuli and item5 Arousal), and all correlations below .4. As a further test of unidimensional-ity, person estimates from the two highest positive loading items on the firstresidual component were compared with the estimates derived from the twohighest negative loading items, with both sets calibrated on the same metric.
TABLE 4Inter-item correlations, item-total correlations, item loadings on first principal component
and item locations from Rasch analysis
Visual
Aud-
itory
Aware-
ness of
musical
stimuli
Verbal
commands
1st
principal
compon-
ent
Item-total
correlation
Rasch
item
location
Visual 1.00 0.74 0.56 0.28
Auditory 0.47 1.00 0.80 0.64 1.75
Awareness of
Musical Stimuli
0.40 0.48 1.00 0.74 0.56 0.67
Verbal Commands 0.45 0.50 0.43 1.00 0.73 0.52 0.39
Arousal 0.37 0.42 0.39 0.27 0.65 0.46 23.09
TABLE 5Summary test-of-fit statistics for initial MATADOC analysis and after rescoring items
3 and 4
Item residual Person residual
Chi-square
interaction
Analysis No. Value SD Value SD Value (df) p Person separation
1 –0.236 1.362 –0.291 0.767 21.218 .02 0.82
2 –0.306 1.386 –0.347 0.868 14.519 .15 0.80
18 MAGEE, SIEGERT, DAVESON, LENTON-SMITH, AND TAYLOR
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013
Of the 155 t-test comparisons only three (1.94%) were significant. This is wellbelow the commonly accepted criterion for unidimensionality of 5% (Tennant& Pallant, 2006).
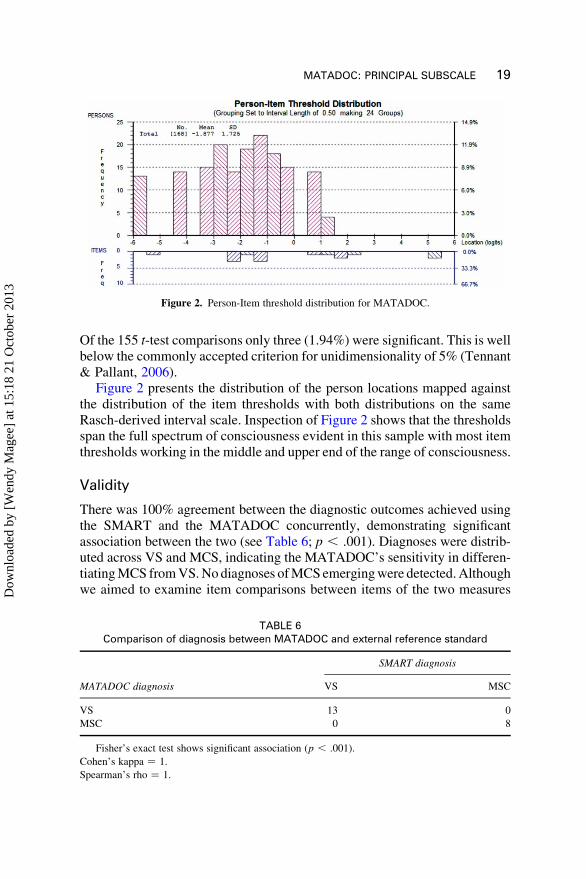
Figure 2 presents the distribution of the person locations mapped againstthe distribution of the item thresholds with both distributions on the sameRasch-derived interval scale. Inspection of Figure 2 shows that the thresholdsspan the full spectrum of consciousness evident in this sample with most itemthresholds working in the middle and upper end of the range of consciousness.
Validity
There was 100% agreement between the diagnostic outcomes achieved usingthe SMART and the MATADOC concurrently, demonstrating significantassociation between the two (see Table 6; p , .001). Diagnoses were distrib-uted across VS and MCS, indicating the MATADOC’s sensitivity in differen-tiating MCS from VS. No diagnoses of MCS emerging were detected. Althoughwe aimed to examine item comparisons between items of the two measures
Figure 2. Person-Item threshold distribution for MATADOC.
TABLE 6Comparison of diagnosis between MATADOC and external reference standard
SMART diagnosis
MATADOC diagnosis VS MSC
VS 13 0
MSC 0 8
Fisher’s exact test shows significant association (p , .001).
Cohen’s kappa ¼ 1.
Spearman’s rho ¼ 1.
MATADOC: PRINCIPAL SUBSCALE 19
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013

rating related behavioural domains, missing data for the SMART and the smallsample size (n ¼ 21) prevented meaningful analysis within this study.
DISCUSSION
This study examined the IRR and TRR of the principle subscale of a newmeasure that assesses responsiveness in DOC populations with greater sensi-tivity to measuring auditory responsiveness to a protocol that uses primarilymusical stimuli. The results suggest that the principal subscale of theMATADOC holds good IRR and good repeatability demonstrating TRR. Theresearch involved seven assessors who each functioned as observer-rater and/or the rater who administered the protocol. Reliability for DOC measures isdependent on protocols with adequate operational definitions as well as raterswho are trained in the protocol’s use. The reliability suggests that both the pro-tocol and the measure meet these standards. The measure can therefore be admi-nistered reliably across raters with varying years of experience with DOCpopulations who have been trained to a recognised level of competency in its use.
The internal consistency of the five items as a principal subscale is satis-factory. Both principal component and Rasch analyses confirmed theMATADOC principal subscale as a robust unidimensional and homogenoussubscale for assessing awareness in patients with DOC. Rasch analysis alsoclarified the hierarchy of item difficulty suggesting the most likely order inwhich the items will become achievable by patients emerging from disordersof consciousness. The person separation index from the Rasch analysis showsthat the five items of the principal subscale discriminate well among personsat different levels of consciousness. These findings indicate the measure’ssensitivity in differentiating between patients demonstrating responsestypical of VS and MCS, although sensitivity in further differentiation ofresponses indicative of MCS emergent have not been demonstrated.
The diagnostic outcomes of the MATADOC had 100% agreement with anexternal reference standard that is validated for assessing awareness.However, differences in the function of comparable items across the measurescould not be explored in this study due to the sample size and the prevalenceof missing data for the external reference standard. Given the complexity ofthis population, the level of agreement between the two measures supports theuse of the MATADOC in the clinical care of people with DOC, and a tool forspecifically researching the role of auditory stimuli in the diagnosis of DOC.
Testing the strength of the MATADOC principal subscale initially wasimportant as these five items examine behavioural domains that are importantindicators of awareness in other validated assessment measures for DOC(Daveson et al., 2007; Seel et al., 2010). Specifically, the items examinevisual responsiveness, arousal, and auditory responsiveness, including
20 MAGEE, SIEGERT, DAVESON, LENTON-SMITH, AND TAYLOR
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013

responses to verbal and non-verbal musical stimuli. Given the strength of thissubscale, the analysis of IRR and TRR for all 14 items of the MATADOC iswarranted. However, psychometric testing of the remaining two subscales isnot a priority given the differences in scoring and their emphasis on clinicalrather than diagnostic utility.
This investigation focused on the potential of the MATADOC as a diag-nostic tool, which is the priority issue in the care of people with DOC.However, the MATADOC functions as a tool for measuring patient progressover time as well as an assessment for use in an interdisciplinary programme.In line with evidence-based recommendations for DOC assessment scales forhaving items that cover behaviours representative of VS, MCS and MCSemergent and the ability to distinguish between these categories, the otheritems on the MATADOC (i.e., items 6–14) assess “higher” level responsessuch as communication, social behaviours, cognition, and attention, whichhave been included in some other DOC scales (Shiel et al., 2000). Thus,although it was not demonstrated in this study, the tool may hold potentialto evaluate responsiveness indicative of emergence from DOC in additionto having sensitivity to measure changes within the VS/MCS categories.The items yet to be assessed specifically contribute to goal setting (items8–14) and responses to musical stimuli in order to formulate individually tai-lored treatment (items 6–7). So, the measure records which musical par-ameters elicit responses. In this way, treatment can be tailored within aninterdisciplinary programme to the patient’s emergent strengths if they pro-gress through the DOC categories and emerge from MCS.
The MATADOC can be considered an objective tool as operational defi-nitions have been provided for the protocol and the ratings. Furthermore,the behavioural nature of the scale enhances the information that may begained from observing patients in musical conditions. Auditory responsive-ness in DOC populations has received particular attention historically(Boyle & Greer, 1983) as well as recently (Verville et al., 2012) and it is rel-evant that music has remained a stimulus of interest for 30 years. Music’svalue as an assessment medium with this complex population has been pro-posed (Magee, 2007b) and explored to some degree (Boyle & Greer, 1983;Formisano et al., 2001; Jones et al., 2000; Puggina et al., 2009; Vervilleet al., 2012; Wilson et al., 1992). However, without objective measurementtools that are sensitive to the population’s needs and can optimise the capacityfor manipulating auditory components, this has remained as conjecture. Thedevelopment of a standardised tool will address this.
Conclusion
The standardisation of this new subscale is clinically relevant as MATADOCholds particular sensitivity for the auditory modality and this modality has
MATADOC: PRINCIPAL SUBSCALE 21
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013

been found to be more sensitive for detecting awareness in DOC populations(Gill-Thwaites, 1997). Therefore, MATADOC should be used within inter-disciplinary assessment of awareness in patients with DOC and rehabilitationof this population to complement existing DOC measures that may be lesssensitive to assessing the auditory modality. Furthermore, as the first standar-dised measure for assessing responses to musical and auditory-specific stimuliwith this population, this tool will enable research on the outcomes of music-based interventions with DOC populations.
REFERENCES
Andrews, K., Murphy, L., Munday, R., & Littlewood, C. (1996). Misdiagnosis of the vegetative
state: Retrospective study in a rehabilitation unit. British Medical Journal (Clinical
Research Edn.), 313(7048), 13–16.
Bernat, J. L. (2009). Chronic consciousness disorders. Annual Review of Medicine, 60(1), 381–
392. doi:10.1146/annurev.med.60.060107.091250
Blood, A. J., & Zatorre, R. J. (2001). Intensely pleasurable responses to music correlate with
activity in brain regions implicated in reward and emotion. Proceedings of the National
Academy of Sciences of the United States of America, 98(20), 11818–11823.
Boly, M., Faymonville, M., Peigneux, P., Lambermont, B., Damas, P., Del Fiore, G., . . .
Laureys, S. (2004). Auditory processing in severely brain injured patients: Differences
between the minimally conscious state and the persistent vegetative state. Archives of Neu-
rology, 61(2), 233–238. doi:10.1001/archneur.61.2.233
Boly, M., Faymonville, M., Peigneux, P., Lambermont, B., Damas, F., Luxen, A., . . . Laureys,
S. (2005). Cerebral processing of auditory and noxious stimuli in severely brain injured
patients: Differences between VS and MCS. Neuropsychological Rehabilitation, 15(3),
283–289. doi:10.1080/09602010443000371
Boyle, M. E., & Greer, R. D. (1983). Operant procedures and the comatose patient. Journal of
Applied Behavioral Analysis, 16(1), 3–12.
Bruno, M., Vanhaudenhuyse, A., Schnakers, C., Boly, M., Gosseries, O., Demertzi, A., . . .
Laureys, S. (2010). Visual fixation in the vegetative state: An observational case series
PET study. BioMedCentral Neurology, 10, 35–40. doi:10.1186/1471-2377-10-35
Bruno, M., Vanhaudenhuyse, A., Thibaut, A., Moonen, G., & Laureys, S. (2011). From unre-
sponsive wakefulness to minimally conscious PLUS and functional locked-in syndromes:
Recent advances in our understanding of disorders of consciousness. Journal of Neurology,
258(7), 1373–1384. doi:10.1007/s00415-011-6114-x
Chatelle, C., Laureys, S., Majerus, S., & Schnakers, C. (2010). Eye gaze and conscious processing
in severely brain-injured patients [commentary]. Behavioral Brain Sciences, 33, 442–443.
Coleman, M. R., Davis, M. H., Rodd, J. M., Robson, T., Ali, A., Owen, A. M., Pickard, J. D.
(2009). Towards the routine use of brain imaging to aid the clinical diagnosis of disorders
of consciousness. Brain: A Journal of Neurology, 132, 2541–2552.
Daveson, B. A., Magee, W. L., Crewe, L., Beaumont, G., & Kenealy, P. (2007). The music
therapy assessment tool for low awareness states. International Journal of Therapy & Reha-
bilitation, 14(12), 545–549.
Formisano, R., Vinicola, V., Penta, F., Matteis, M., Brunelli, S., & Weckel, J. W. (2001). Active
music therapy in the rehabilitation of severe brain injured patients during coma recovery.
Annali dellIstituto Superiore di Sanita, 37(4), 627–630.
22 MAGEE, SIEGERT, DAVESON, LENTON-SMITH, AND TAYLOR
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013

Giacino, J. T., Ashwal, S., Childs, N., Cranford, R., Jennet, B., Katz, D. I., . . .Zasler, N. D. (2002).
The minimally conscious state: Definition and diagnostic criteria. Neurology, 58, 349–353.
Giacino, J. T., & Kalmar, K. (1997). The vegetative and minimally conscious states: A comparison
of clinical features and functional outcome. Journal of Head Trauma Rehabilitation, 12, 36–51.
Giacino, J., Kalmar, K., & Whyte, J. (2004). The JFK Coma Recovery Scale – Revised:
Measurement characteristics and diagnostic utility. Archives of Physical Medicine and
Rehabilitation, 85(12), 2020–2029.
Gill-Thwaites, H. (1997). The sensory modality assessment rehabilitation Technique – A tool
for assessment and treatment of patients with severe brain injury in a vegetative state. Brain
Injury, 11(10), 723–734. doi:10.1080/026990597123098
Gill-Thwaites, H. (2006). Lotteries, loopholes and luck: Misdiagnosis in the vegetative state
patient. Brain Injury, 20(13–14), 1321–1328. doi:10.1080/02699050601081802
Gill-Thwaites, H., & Munday, R. (1999). The sensory modality assessment and rehabilitation
technique (SMART): A comprehensive integrated assessment and treatment protocol for
the vegetative state and minimally responsive patient. Neuropsychological Rehabilitation,
9(3–4), 305–320. doi:10.1080/096020199389392
Godbolt, A. K., Stenson, S., Winberg, M., Frykberg, G. E., & Tengvar, C. (2011). Disorders of
consciousness: Recommendations are welcome but further guidance is needed. Archives of
Physical Medicine and Rehabilitation, 92(7), 1181. doi:10.1016/j.apmr.2011.03.034
Gosseries, O., Vanhaudenhuyse, A., Bruno, M., Demertzi, A., Schnakers, C., Boly, M., . . .
Laureys, S. (2011). Disorders of consciousness: Coma, vegetative and minimally conscious
states. In D. Cvetkovic, I. Cosic, D. Cvetkovic, & I. Cosic (Eds.), States of consciousness:
Experimental insights into meditation, waking, sleep and dreams (pp. 29–55). New York,
NY: Springer-Verlag Publishing.
Hirschberg, R., & Giacino, J. T. (2011). The vegetative and minimally conscious states: Diag-
nosis, prognosis and treatment. Neurologic Clinics, 29(4), 773–786. doi:10.1016/
j.ncl.2011.07.009
Hobart, J. C., Cano, S. J., Zajicek, J. P., & Thompson, A. J. (2007). Rating scales as outcome
measures for clinical trials in neurology: Problems, solutions, and recommendations. Lancet
Neurology, 6, 1094–1105.
Jones, S. J., Vaz Pato, M., Sprague, L., Stokes, M., & Haque, N. (2000). Auditory evoked poten-
tials to spectro-temporal modulation of complex tones in normal subjects and patients with
severe brain injury. Brain, 123(5), 1007–1016.
Laureys, S., Celesia, G. G., Cohadon, F., Lavrijsen, J., Leon-Carrion, J., Sannita, W. G., . . . The
European Task Force on Disorders of Consciousness. (2010). Unresponsive wakefulness
syndrome: A new name for the vegetative state or apallic syndrome. BioMedCentral Medi-
cine, 8, 68–71. doi:10.1186/1741-7015-8-68
Laureys, S., Perrin, F., & Bredart, S. (2007). Self-consciousness in non-communicative patients.
Consciousness & Cognition, 16(3), 722–741. doi:10.1016/j.concog.2007.04.004
Laureys, S., & Schiff, N. D. (2011). Coma and consciousness: Paradigms (re)framed by neuroi-
maging. NeuroImage, 61(2), 478–491. doi:10.1016/j.neuroimage.2011.12.041
Magee, W. L. (2005). Music therapy with patients in low awareness states: Approaches to
assessment and treatment in multidisciplinary care. Neuropsychological Rehabilitation,
15(3–4), 522–536. doi:10.1080/09602010443000461
Magee, W. L. (2007a). Development of a music therapy assessment tool for patients in low
awareness states. NeuroRehabilitation, 22(4), 319–324.
Magee, W. L. (2007b). Music as a diagnostic tool in low awareness states: Considering limbic
responses. Brain Injury, 21(6), 593–599. doi:10.1080/02699050701426907
Magee, W. L., Lenton-Smith, G., & Daveson, B. A. (2012). The Music Therapy Assessment
Tool for Awareness in Disorders of Consciousness: Manual and protocol. London: Royal
Hospital for Neuro-disability.
MATADOC: PRINCIPAL SUBSCALE 23
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013

Nunnally, J. C., & Bernstein, I. H. (1994). Psychometric theory. New York, NY: McGraw-Hill.
O’Kelly, J., & Magee, W. L. (2013). The complementary role of music therapy in the detection
of awareness in disorders of consciousness: An audit of concurrent SMART and
MATADOC assessments. Neuropsychological Rehabilitation, 23(2), 287–298.
Owen, A. M., Coleman, M. R., Boly, M., Davis, M. H., Laureys, S., & Pickard, J. D. (2006).
Detecting awareness in the vegetative state. Science (New York), 313(5792), 1402–1402.
Owen, A. M., Coleman, M. R., Menon, D. K., Berry, E. L., Johnsrude, I. S., Rodd, J. M., . . .
Pickard, J. D. (2005). Using a hierarchical approach to investigate residual auditory cogni-
tion in persistent vegetative state. Progress in Brain Research, 150, 457–471.
Pallant, J. F., & Tennant, A. (2007). An introduction to the Rasch measurement model: An
example using the Hospital Anxiety and Depression Scale (HADS). British Journal of Clini-
cal Psychology, 46, 1–18.
Perrin, F., Schnakers, C., Schabus, M., Degeuldre, C., Goldman, S., Bredart, S., . . . Laureys, S.
(2006). Brain response to one’s own name in vegetative state, minimally conscious state and
locked-in syndrome. Archives of Neurology, 63, 562–569.
Puggina, A. C. G., & Paes da Silva, M. J. (2009). Sinais vitais e expressao facial de pacientes em
estado de coma. Revista Brasileira de Enfermagem, 62(3), 435–441.
Schnakers, C., Chatelle, C., Vanhaudenhuyse, A., Majerus, S., Ledoux, D., Boly, M., . . .
Laureys, S. (2010). The Nociception Coma Scale: A new tool to assess nociception in dis-
orders of consciousness. Pain, 148(2), 215–219. doi:10.1016/j.pain.2009.09.028
Schnakers, C., Perrin, F., Schabus, M., Hustinx, R., Majerus, S., Moonen, G., . . . Laureys, S.
(2009). Detecting consciousness in a total locked-in syndrome: An active event related para-
digm. Neurocase, 25, 1–7.
Seel, R. T., Sherer, M., Whyte, J., Katz, D. I., Giacino, J. T., Rosenbaum, A. M., . . . Zasler, N.
(2010). Assessment scales for disorders of consciousness: Evidence-based recommen-
dations for clinical practice and research. Archives of Physical Medicine and Rehabilitation,
91(12), 1795–1813. doi:10.1016/j.apmr.2010.07.218
Shiel, A., Horn, S. A., Wilson, B. A., Watson, M. J., Campbell, M. J., & McLellan, D. L. (2000).
The Wessex Head Injury Matrix (WHIM) main scale: A preliminary report on a scale to
assess and monitor patient recovery after severe head injury. Clinical Rehabilitation,
14(4), 408–416.
Shiel, A., & Wilson, B. A. (2005). Can behaviours observed in the early stages of recovery after
traumatic brain injury predict poor outcome? Neuropsychological Rehabilitation, 15(3–4),
494–502.
Siegert, R. J., Jackson, D. J., Tennant, A., & Turner-Stokes, L. (2010). Factor analysis and
Rasch analysis of the Zarit Burden Interview for acquired brain injury carer research.
Journal of Rehabilitation Medicine, 42, 302–309.
Sloboda, J. (1991). Empirical studies of emotional response to music. In M. R. Jones & S. Hol-
leran (Eds.), Cognitive bases of musical communication (pp. 33–46). Washington, DC:
American Psychological Association.
Tennant, A., & Pallant, J. (2006). Unidimensionality matters! (A tale of two Smiths?). Rasch
Measurement Transactions, 20(1), 1048–1051.
Vanhaudenhuyse, A., Schnakers, C., Bredart, S., & Lauroys, S. (2008). Assessment of visual
pursuit in post-comatose states: Use a mirror. Journal of Neurology, Neurosurgery & Psy-
chiatry, 79(2), 223–223. doi:10.1136/jnnp.2007.121524
Verville, V. C., Sela, L., Plotkin, A., Chatelle, C., Sobel, N., & Laureys, S. (2012). Detecting
signs of consciousness in severely brain injured patients with voluntary control of sniffing:
A cohort study (Accepted Abstracts from the International Brain Injury Association’s Ninth
World Congress on Brain Injury). Brain Injury, 26(4–5), 721.
Wilson, S. L., Cranny, S. M., & Andrews, K. (1992). The efficacy of music for stimulation in
prolonged coma – Four single case experiments. Clinical Rehabilitation, 6, 181–187.
24 MAGEE, SIEGERT, DAVESON, LENTON-SMITH, AND TAYLOR
Dow
nloa
ded
by [
Wen
dy M
agee
] at
15:
18 2
1 O
ctob
er 2
013





























