Embed Size (px)
Citation preview

Infect Dis Clin N Am
21 (2007) 103–132
Management of AntiretroviralTreatment–Related Complications
Risa M. Hoffman, MD, MPHa,*,Judith S. Currier, MDb
aUCLA Division of Infectious Diseases, Department of Medicine,
David Geffen School of Medicine at the University of California,
10833 Le Conte Avenue, 37-121 CHS, Los Angeles, CA 90095, USAbCenter for Clinical AIDS Research and Education, Division of Infectious Diseases,
Department of Medicine, David Geffen School of Medicine at the University of California,
9911 West Pico Boulevard, Suite 980, Los Angeles, CA 90035, USA
The year 2006 marks the 25th anniversary of the discovery of the firstreported case of acquired immunodeficiency syndrome (AIDS). With thislandmark comes celebration of tremendous advances in the understandingof pathogenesis and treatment of infection; however, the anniversary alsobrought the opportunity to analyze future challenges in HIV treatment.Although developing countries are now gaining access to basic antiretrovi-ral regimens (ARVs), only approximately 20% of 6 million individuals indeveloping countries needing treatment have access to ARVs [1]. Withthe success of these medications in restoring immune function and control-ling viral replication, HIV has been transformed into a chronic condition,requiring long-term therapy. Health care providers are increasingly con-fronted with complications of therapy, and expanded worldwide accessand ongoing treatment advances in developed countries have highlightedthe need for increased knowledge of adverse consequences and theirmanagement.
This article reviews six common complications of antiretroviral therapy(ART), including hyperlactatemia/lactic acidosis, hypersensitivity reactions,abnormal glucose metabolism, dyslipidemia, body composition changes,
Dr. Currier is supported by NIH Grants U01 A127660 and K24 AI56933.
* Corresponding author.
E-mail address: [email protected] (R.M. Hoffman).
0891-5520/07/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.idc.2007.01.007 id.theclinics.com

104 HOFFMAN & CURRIER
and cardiovascular disease. Each section provides a brief discussion of riskfactors and clinical features, with primary emphasis on clinical managementand monitoring.
Hyperlactatemia/lactic acidosis
Risk factors and clinical features
Among patients undergoing nucleoside reverse transcriptase (NRTI)therapy, the incidence of lactic academia ranges from 8% to 21%. Stavudine(d4T, Zerit) is the most frequently implicated NRTI [2]. The proposedmechanism for lactic acid accumulation is inhibition of mitochondrial poly-merase-g. Poisoning of mitochondria pressures the cell to meet energy re-quirements through anaerobic metabolism, with generation of lactate.Affinity for polymerase-g is strongest for stavudine, but didanosine (ddI,Videx) and zidovudine (ZDV, AZT, Retrovir) follow in predilection forbinding the enzyme. Abacavir (ABC, Ziagen), tenofovir (TDF, Viread),and lamivudine (3TC, Epivir) are least implicated in symptomatic lactic ac-ademia, although case reports link both drugs to life-threatening episodes oflactate elevation [3,4]. A twofold increase in risk for symptomatic lactate el-evation has been noted for each NRTI added to a regimen, and the combi-nation of stavudine and didanosine is now discouraged by the United StatesPublic Health service because of a high risk for fatal lactic acidosis experi-enced with this combination, particularly in pregnant women [5].
NRTI-associated lactic academia can occur after months or years ontherapy. However, the overall incidence of this complication remains lowat less than 2% [6]. Demographic and genetic risk factors for the develop-ment of lactic academia are ill-defined. Possible predisposing conditionsinclude treatment for chronic hepatitis B or C coinfection, chronic muscledisorders, kidney disease, and combination therapy with metformin andNRTIs [7–11]. In the Swiss HIV Cohort Study, independent predictors forlactic academia included older age, severe immunodeficiency, liver dysfunc-tion, and stavudine-containing regimens. Increased waist-to-hip ratio wasalso found to be associated with development of severe hyperlactatemia[12]. Recent research from South Africa has described higher rates of symp-tomatic lactic academia than previously reported in developed countries,with highest risk in overweight women, and an overall mortality rate of29% [13]. All cases occurred in patients on South Africa’s first-line regimenof stavudine, lamivudine, and a non–nucleoside reverse transcriptase inhib-itor (NNRTI).
The clinical presentation of NRTI-associated lactic academia is variableand ranges from generalized weakness, myalgias, and paresthesias to non-specific abdominal symptoms. Physical findings can include weight loss,hepatomegaly, and fat redistribution. Laboratory evaluation reveals an ele-vated lactate with increased anion gap and acidemia on arterial blood gas

105ANTIRETROVIRAL TREATMENT COMPLICATIONS
testing. Other laboratory abnormalities may include elevated creatininekinase, lactate dehydrogenase, C-reactive protein, lipase, and amylase [14].Ultrasonography or CT may reveal an enlarged, fatty liver.
Diagnosis is achieved when lactate is elevated in the context of a compat-ible clinical syndrome. Lactate measurements should be drawn as venoussamples, without a tourniquet in place. Samples require storage on iceand processing within 4 hours. Recent exercise, dehydration, and blooddraw technique can falsely elevate lactate levels. Hyperlactatemia is definedas a lactate level from 2.5 to 5 mmol/L without acidosis. When lactate levelsexceed 5 mmol/L and are associated with bicarbonate less than 20 mmol/L,arterial pH less than 7.34, and anion gap more than 12, patients have lacticacidosis and are typically symptomatic. Mortality in excess of 60% has beendescribed for patients with a lactate level exceeding 15 mmol/L [15].
Management
The cornerstone of management is withdrawal of offending NRTIs andsupportive care. As a single intervention, drug cessation often leads toimprovement in clinical status and reversal of laboratory abnormalities.Supportive management of acidosis may include intravenous fluids, intuba-tion, and dialysis. Evidence for bicarbonate infusion is lacking, and data aremixed on the use of dichloroacetate, which acts on pyruvate dehydrogenaseto reduce the production of lactate [16]. Some authors recommend ‘‘mito-chondrial supportive care,’’ including the use of coenzyme Q10, L-carnitine,vitamin C, and riboflavin. Supplementation has been effective for patientswho have inherited mitochondrial disorders, but for NRTI-associated lacticacademia, data are limited to the case report or case series level [17–20].
Small studies have shown safety of switching to non–stavudine-contain-ing regimens in patients with mild lactate elevations [21,22]. For patientswho have a history of severe lactic acidosis, rechallenge with NRTI shouldbe performed with careful monitoring and attention to choice of drug, per-haps using tenofovir or abacavir given their lesser affinity for polymerase-g.Options also include use of an NRTI-sparing regimen, such as combinationprotease inhibitor and NNRTI. Risk for recurrent lactic acidosis must bebalanced against regimen potency.
Monitoring
Monitoring for lactate elevation is not generally recommended. Of onequarter of patients taking NRTIs who will have an elevated lactate duringtheir treatment course, 85% will be asymptomatic and have no clinical se-quelae [23]. Additionally, asymptomatic elevations do not predict episodesof severe lactic acidemia [24]. In the Swiss HIV Cohort Study, $11,268 wasspent to detect 42 episodes of severe hyperlactatemia. In this study, abnormalliver function tests were an independent predictor of severe

106 HOFFMAN & CURRIER
hyperlactatemia, and the authors propose that liver function monitoringmay be a more cost-effective approach [12]. Other reasonable strategies in-clude selective monitoring of serum lactate in presumed high-risk popula-tions, such as older individuals, those who have abnormal liver function,hepatitis B or C coinfection, and those being treated with stavudine- or di-danosine-containing regimens. The latter criterion would not be feasible indeveloping countries where stavudine is used in the first-line regimen, andhighlights the tremendous challenge of creating a safe and cost-effectiveapproach to hyperlactatemia in this setting.
Drug hypersensitivity
Risk factors and clinical features
Non–nucleoside reverse transcriptase inhibitorsDrug reactions in association with antiretroviral therapy are common,
with manifestations of rash or transaminitis representing most syndromes.Risk factors for the development of a specific type of drug reaction are be-coming more elucidated. Drug class is one of the most important determi-nants, with NNRTIs posing the highest risk. Approximately 10% to 17%of patients taking NNRTIs will develop rash [25]. Maculopapular rash onthe trunk, face, and extremities occurs in 16% of patients on nevirapine(NVP, Viramune) during the first 6 weeks of therapy. Severe rash hasbeen seen in approximately 6.5% of patients on nevirapine and 4% on efa-virenz [26–28]. Female sex, CD4 cell counts less than 100 cells/mL, and ageolder than 40 years are independent risk factors for the development of cu-taneous reactions to NNRTIs [25]. Hepatotoxicity frequently accompaniesrash as part of a hypersensitivity reaction or can occur as a singularfinding.
Women have emerged as being at high risk for NNRTI hypersensitivity,with 3- to 12-fold risk for cutaneous reactions and increased likelihood ofnevirapine-associated severe skin rash and hepatotoxicity [29]. Other identi-fied risk factors include coexistent hepatitis B or C, obesity, pregnancy, andless-advanced stage of immunosuppression (CD4 cell count, O250 cells/mLin women and O400 cells/mL in men) [30,31]. In the United States, nevira-pine now carries a boxed warning regarding risks for severe hepatotoxicreactions in women and individuals with increased CD4 cell counts.
In the case of suspected drug reaction, the timing of symptoms in rela-tion to initiation of a drug, specific clinical features of the patient, andcomplete evaluation of medication history are important to note. Clinicallydistinguishing features for typical NNRTI reactions are (1) occurrencewithin the first 6 weeks of therapy (although manifestations remain com-mon through the first 12 to 18 weeks of therapy); (2) rash, ranging frommorbilliform to Stevens-Johnson syndrome, with severe involvement ofskin and mucous membranes; and (3) hypotoxicity, occurring along the
107ANTIRETROVIRAL TREATMENT COMPLICATIONS
same timeline, and often asymptomatic and developing in association withrash. Of concern, individuals can develop fulminant liver failure withoutpreceding systemic hypersensitivity symptoms or other warning signs.
Abacavir
Abacavir hypersensitivity typically occurs within 6 weeks of drug initia-tion, with a mean of 12 to 14 days; however, reactions have been describedup to 12 months on therapy. In contrast to NNRTI hypersensitivity, rashwith abacavir is often mild and may be absent in up to 30% of cases [32].Abnormal laboratory studies can accompany systemic symptoms and in-clude leukopenia, anemia, thrombocytopenia, elevated blood urea nitrogen,creatinine, and lactate dehydrogenase. Eosinophilia is uncommon. The pres-ence of systemic symptoms such as fever, malaise, respiratory symptoms,and abdominal complaints, especially if they worsen with continued dosing,are highly suggestive of this diagnosis. Nonetheless, identification of thissyndrome is challenging because symptoms substantially overlap with othercommon processes, such as immune reconstitution, viral infections, andother drug reactions, and no single test can confirm or exonerate abacaviras causative.
The overall incidence of abacavir hypersensitivity ranges from 3% to 5%but is as high as 8% in Caucasians [33]. Two independent research groupshave shown a strong association with HLA-B*5701 and abacavir hypersen-sitivity [34,35], and in Australia, prospective screening for HLA-B*5701reduced the incidence of abacavir reactions from 8% to 2% [36]. The useful-ness and generalizability of this approach is now being tested in larger stud-ies. Because HLA-B*5701 is rare in certain African and Asian populations,ultimate cost-effectiveness of this approach varies according to geographicarea. The advent of abacavir patch testing may diminish cost and has shownstrong correlation with HLA-B*5701 positivity [37,38]. Testing for presenceof HLA type cannot be used to supersede clinical judgment, and presence orabsence of the allele should not be used as criteria for rechallenge with aba-cavir, but rather to guide therapy for treatment-naı̈ve subjects [33].
Management
Non–nucleoside reverse transcriptase inhibitorsIf patients develop mild to moderate rash during the first 2 weeks of
once-daily therapy, nevirapine can be continued but typical escalation totwice-daily regimen should be deferred until the rash has resolved. Useof prednisone and antihistamines (cetirizine) during the first few weeksof nevirapine has failed to show effectiveness in preventing hypersensitivityreactions [39,40]. Any patient presenting with rash should have testing ofliver function, a complete blood cell count with differential, and measure-ment of renal function. Treatment should be discontinued immediately for
108 HOFFMAN & CURRIER
severe skin reactions or when rash occurs with any of the following sys-temic symptoms: fever, urticaria, wheezing, clinical hepatitis, muscle orjoint aches, exfoliation, mucosal involvement or conjunctivitis, elevated al-anine aminotransferase or aspartate aminotransferase five times or morethe upper limit of normal (ULN), eosinophilia, granulocytopenia, or sig-nificant renal dysfunction. Patients who show evidence of these systemicsymptoms should undergo close observation and appropriate supportivecare. Limited data exist regarding the use of efavirenz in patients whohave a history of severe hypersensitivity reaction to nevirapine. Proteaseinhibitor (PI)–based therapy should be considered the safest alternativein these patients.
Abacavir
Treatment for suspected abacavir hypersensitivity is supportive andshould include immediate withdrawal of antiretroviral drugs. Symptomaticmanagement includes intravenous hydration, antiemetics, and analgesics.Corticosteroids are of no proven benefit. If abacavir is etiologic, improve-ment should occur within 1 to 2 days of drug cessation. Patients whohave a history of abacavir reactions should never be rechallenged withthis medication. Extremely high rates of anaphylactic reactions with cardio-vascular collapse and death have occurred in patients re-exposed to abacavirafter an initial reaction [32].
Monitoring
Non–nucleoside reverse transcriptase inhibitorsOptimal monitoring for NNRTIs has not been defined, but because of
high rates of severe skin reactions and hypotoxicity during the initial 3months of nevirapine, vigilance for skin changes and hepatotoxicity is war-ranted. Nevirapine (Boehringer Ingelheim, Germany) carries a manufac-turer’s recommendation for a dose escalation protocol to preventdevelopment of cutaneous reactions. This protocol includes initiation ofthe drug at a dose of 200 mg once daily for 2 weeks, followed by an increaseto twice-daily dosing if the patient is tolerating therapy. Before therapy, pa-tients should be screened for hepatitis B and C infection. Baseline liver func-tion should be obtained, with repeat testing 2 weeks after initiation and thenmonthly for the first 3 months. Coinfection with hepatitis B or C or under-lying liver disease is not a contraindication to NNRTI therapy, but morefrequent monitoring of liver function may be required. Transaminitis upto five times ULN is considered tolerable as long as close observation is con-tinued and associated systemic hypersensitivity is not present. Monitoringliver function does not always predict or prevent fulminant liver failure. Aproposed approach to nevirapine hypersensitivity is included in Fig. 1.

109ANTIRETROVIRAL TREATMENT COMPLICATIONS
Abacavir
No monitoring laboratory tests are predictive of abacavir hypersensitiv-ity. Patient education at drug initiation is crucial and appropriate documen-tation after initial reaction is essential to prevent rechallenge in a patientwith prior abacavir reaction.
Abnormal glucose metabolism
Risk factors and clinical features
An association between ART and abnormal glucose metabolism wasestablished in 1987 when the U.S. Food and Drug Administration (FDA)issued a public health advisory reporting 83 cases of new-onset hyperglyce-mia in patients taking PIs [41]. Since then, impaired glucose tolerance, insu-lin resistance, and diabetes mellitus have emerged as important clinicalsequelae of HIV therapy. Precise mechanisms are unknown, but HIV infec-tion seems to confer some increased risk for diabetes in the absence of ART.Retrospective data suggest that individuals infected with HIV have in-creased incidence and age-specific risk for diabetes [42] compared with thosewho are not. Other risk factors are similar to the general population and in-clude obesity, family history, nonwhite race, and older age. HIV-specific
*Baseline LFTs, *Hepatitis B and C Screen, CD4 <250 (women)
Or <400 (men):Initiate nevirapine 200 mg once daily
No adverse reaction and 2 week LFT
< 5 times ULN, proceed with dose
escalation to 200 mg twice daily
Rash within first 2 weeks. Check LFTS, CBC with
differential, and renal function, and evaluate for
mucositis and other systemic symptoms.
LFT > 5 times ULN, severe rash,
or rash with any of the following
systemic features: fever, clinical
hepatitis, muscle or joint aches,
urticaria, mucosal or
conjunctival involvement,
eosinophilia, granulocytopenia,
or significant renal dysfunction.
DISCONTINUE NEVIRAPINE
AND MONITOR
No features of Stevens-Johnson
(conjunctivital involvement, mucositis)
and LFTs < 5 times ULN: Continue
nevirapine at dose of 200 mg once daily
until symptoms resolve
Rash completely resolved and LFTs normal or stable, increase
dose to 200 mg twice daily and monitor with monthly LFTs.
If normal after 3 months, decrease frequency of monitoring
Routine Monitoring with
LFTs monthly through
first 3 months. If normal,
decrease frequency of
monitoring
When symptoms resolve, consider
initiation of PI-based regimen
*Baseline LFT abnormalities
and hepatitis co-infection is
not a contradiction to therapy but may warrant closer monitoring
CBC: Complete blood countLFT: Liver function tests ULN: Upper limit of normal
2 weeks
Fig. 1. Approach to nevirapine hypersensitivity.

110 HOFFMAN & CURRIER
factors include lipodystrophy, stavudine exposure, and hepatitis C coinfec-tion [43–45]. Gender-specific risk has been less well characterized, but a re-cent study showed increased rates of abnormal glucose metabolism amongmiddle-aged women on ART, although PI-use was not independently asso-ciated with insulin resistance [46]. Despite this finding, use of PIs remains thestrongest risk factor for abnormal glucose metabolism in HIV patients onART, with studies suggesting a prevalence of 8% to 46% for the spectrumof abnormalities, most commonly described as insulin resistance with im-paired glucose tolerance and normal fasting glucose [47,48]. The proportionof individuals with insulin resistance and impaired glucose tolerance thatwill progress to frank diabetes mellitus is unknown.
Diagnostic criteria for impaired glucose tolerance and diabetes in patientswho have HIV undergoing ART is based on fasting, random, or oral glu-cose tolerance testing (OGTT) (Box 1). Insulin measurements are problem-atic given variability among assays and lack of formalized normative values.
Management
Treatment options for diabetes reflect recommendations for the generalpopulation, with diet, exercise, and weight reduction of critical importance[49]. Additionally, medications (eg, corticosteroids, growth hormone, di-uretics, niacin) should be reviewed for contributions to abnormal glucosemetabolism. Pharmacologic management of hyperglycemia is largely extrap-olated from experience with type 2 diabetes in adults not infected with HIV,with careful attention to drug interactions and overlapping toxicities in pa-tients on ART. Metformin (Glucophage) is a biguanide that increases theaction of insulin, decreases hepatic glucose generation, and increases glucoseuptake by peripheral tissues. In populations infected with HIV, metforminhas been shown in small studies to improve insulin resistance and decrease
Box 1. Diagnosis of abnormal glucose metabolism
Impaired fasting glucose: 100–125 mg/dLImpaired glucose tolerance: 2-hour post-glucose 140–199 mg/dLDiabetes mellitus: fasting glucose >126 mg/dL or 2-hour
post-glucose >200 mg/dL. For a diagnosis of diabetes,patients must have symptoms (polyuria, polydipsia, weightloss) and a casual glucose >200 mg/dL OR fasting glucose>126 mg/dL OR a 2-hour post-glucose by OGTT >200 mg/dL
From the American Diabetes Association, Expert Committee on the Diagnosisand Classification of Diabetes Mellitus. Follow-up report on the diagnosis of dia-betes mellitus. Diabetes Care 2003;26:3160.

111ANTIRETROVIRAL TREATMENT COMPLICATIONS
body weight after 3 months of therapy, particularly for patients who haveassociated lipodystrophy [21,50,51]. Metformin is a less attractive optionfor patients who have renal insufficiency or are taking NRTIs because ofthe risk for lactate elevations.
Thiazolidinediones bind to peroxisome proliferator-activated receptor-gamma (PPARs) and increase insulin sensitivity and glucose use, and de-crease glucose production. Because the two available drugs, rosiglitazone(Avandia) and pioglitazone (Actos), have slight differences in affinity forPPARs (gamma versus alpha), they therefore have theoretical and practicaldifferences in efficacy and toxicity. They have been shown to improve insulinsensitivity in patients who have HIV, but are associated with weight gainand fluid retention. Rosiglitazone has been associated with increases inlow-density lipoprotein (LDL), but a recent large study showed that piogli-tazone is less offensive in regard to lipid profile, and may even have a favor-able effect on triglyceride levels [52–54]. The entire class of medications hasbeen associated with hepatic dysfunction and should be used cautiously inpatients with preexisting liver disease. All patients taking thiazolidinedionesshould undergo close monitoring of transaminases, particularly in the firstyear of therapy. Sulfonylureas can stimulate insulin secretion and improveplasma glucose, but do not improve insulin resistance and may induce seri-ous hypoglycemia. Combination therapy for diabetes mellitus may be re-quired and has been shown to be effective in patients not infected withHIV [55]. When oral regimens fail to normalize glucose, insulin therapyshould be used to achieve adequate control of blood sugar.
Proper management of glucose abnormalities without frank diabetes isunclear. Preventive therapies are promising, with recent data showingthat rosiglitazone can reduce incident diabetes in adults not infected withHIV who have impaired fasting glucose or impaired glucose tolerance[56]. In the same study, ramipril (Altace) for individuals who have impairedfasting glucose levels or impaired glucose tolerance did not influence the in-cidence of diabetes but significantly increased regression to normoglycemia[57]. Whether longer duration of therapy with ramipril will decrease the in-cidence of diabetes is unclear, and although both drugs show promise, theyhave not been explored as preventive approaches to diabetes in patients in-fected with HIV who have impaired fasting glucose or impaired glucosetolerance.
For further management of abnormal glucose metabolism or frank dia-betes, consideration of substitution of PI for NNRTI is warranted in cer-tain cases, particularly when other metabolic abnormalities are present.Studies with amprenavir and atazanavir (ATV, Reyataz) have not beenlinked to the development of insulin resistance and may be feasible alterna-tives to class-switching [58–60]. Substituting PI for abacavir or NNRTI hasbeen shown to improve insulin resistance, but changes that offset toxicitymay compromise regimen potency and cause loss of viral suppression[61–63].

112 HOFFMAN & CURRIER
Monitoring
Before ART is initiated, patients should undergo risk assessment, includ-ing review of family history, body mass index, and medication list. A base-line evaluation for abnormal glucose metabolism should be considered withfasting glucose or, if high-risk, OGTT with 75 g of glucose. Once on ART,follow-up testing should be performed at 6 to 12 weeks and then once every3 months during the first year of therapy. If values are reassuring, monitor-ing can be performed once yearly for patients at low risk. Ongoing counsel-ing regarding diet, exercise, and other risk factor reduction is recommendedfor all patients, regardless of risk.
Lipid disorders
Risk factors and clinical features
The characteristic lipid profile associated with chronic HIV infection in-cludes elevated triglycerides and decreased high-density lipoprotein (HDL)and LDL, associated with subtypes of LDL that are particularly proathero-genic. PI therapy has been closely linked with the development of hypertri-glyceridemia and increased LDL, with lipid changes occurring in 25% ofpatients at 1 year [64]. Ritonavir has induced similar lipid abnormalitiesin healthy volunteers after only 2 weeks of therapy, suggesting a strongrole for PIs as opposed to viral effect [65]. All PIs with the exception of ata-zanavir share this property. NNRTIs have also been linked to unfavorablelipid changes. Nevirapine increases LDL cholesterol, whereas efavirenz in-creases total cholesterol and has been associated with hypertriglyceridemiawith longer duration of exposure [66,67].
Genetic patterns may increase risk for lipid alterations in the setting ofART. Higher triglyceride levels have been linked to heterozygous or homo-zygous expression of the apolipoprotein E-2 genotype [68,69]. This findingunderlies the importance of obtaining family history and baseline fastinglipid panel before choosing an HIV regimen.
Management
Recommendations from the Infectious Disease Society of America(IDSA) and AIDS Clinical Trials Group (ACTG) have provided a frame-work for approaching dyslipidemia in individuals infected with HIV(Fig. 2) [70]. These guidelines call for management based on the NationalCholesterol Education Program (NCEP) Expert Panel on Detection, Evalu-ation, and Treatment of High Blood Cholesterol in Adults (Adult Treat-ment Panel III). Assessment of risk factors (Box 2) is used to guide choiceof therapy and treatment goals.When appropriate, Framingham calculationsare used to determine 10-year coronary heart disease risk. Non-HDL choles-terol can be used as a target in patients who are hypertriglyceridemic in

113ANTIRETROVIRAL TREATMENT COMPLICATIONS
whomLDL is difficult to determine. Table 1 provides a suggested guideline fortiming of initiation and goals of treatment for dyslipidemia based on the afore-mentioned factors. This table considers data published after NCEP ATP III(Heart Protection Study, PROVE-IT), which supports choosing an LDL cho-lesterol goal of less than 70 mg/dL (non-HDL !100 mg/dL) in highest-risk
Baseline fasting lipid profile
Modifiable risk factor modification: diet,exercise, smoking cessation
LDL above threshold for risk category (or non-HDL above
threshold): STATIN
CHD Risk Assessment. If ≥ 2 risk factors,perform 10 year risk calculation.
Assess lipid goal based on risk factors andresults of lifestyle interventions (Table 1)
Serum triglycerides >500mg/dL: FIBRATE
Fig. 2. General approach to dyslipidemia and cardiovascular risk in patients infected with HIV
taking ART. (Adapted from Dube MP, Stein JH, Aberg JA, et al. Guidelines for the evaluation
and management of dyslipidemia in human immunodeficiency virus (HIV)-infected adults re-
ceiving antiretroviral therapy: recommendations of the HIV Medical Association of the Infec-
tious Disease Society of America and the Adult AIDS Clinical Trials Group. Clin Infect Dis
2003;37(5):613–27; with permission.)
Box 2. Major risk factors that modify low-density lipoproteingoals
Cigarette smokingHypertensionHDL cholesterol <40 mg/dLFamily history of premature coronary heart disease
(men <55 years; women <65 years)Age (men ‚45 years; women ‚55 years)Diabetes is a coronary heart disease risk equivalent.HDL level >60 mg/dL is protective and allows subtraction of one
of the above risk factors.
Adapted from the NCEP Expert Panel on Detection, Evaluation, and Treatmentof High Blood Cholesterol in Adults (Adult Treatment Panel III). Circulation2002;106:3143–21; with permission.

114 HOFFMAN & CURRIER
patients, such as those who have baseline LDL levels less than 100 mg/dL, re-cent acute coronary syndrome, andmultiple poorly controlled risk factors (ie,diabetes, smoking, metabolic syndrome) [71–73]. These data must be extrap-olated to theHIV-infectedpopulation carefully, because high-dose statin ther-apy or statin-fibrate combinationsmay be required to reach a goal of LDL lessthan 70 mg/dL. Patients undergoing ART may experience unacceptabletoxicity from this approach.
The NCEP ATP III gives special consideration to the metabolic syn-drome defined by three or more of the following: (1) triglyceride levels of150 mg/dL or more, (2) low HDL (women !50 mg/dL, men !40 mg/dL),(3) abdominal obesity, (4) hypertension, and (5) fasting glucose more than110 mg/dL. Whether the metabolic manifestations of HIV and ART repre-sent the same entity with equivalent risk has yet to be determined, but pend-ing further data, metabolic changes should be considered as a secondarytarget of therapy when addressing dyslipidemia.
Diet and exercise should be encouraged for all individuals (Box 3). Forelevated total cholesterol and LDL, HMG-CoA reductase inhibitors
Table 1
Low-density lipoprotein goals for risk categories
Risk category
(see Box 2
for risk factors) LDL goal
Initiate
therapeutic
lifestyle changes
Consider drug
therapy
High risk: CHD or
CHD risk
equivalenta
(10-year risk
O20%)
!100 mg/dL
Optional goal:
! 70 mg/dL
(if high
triglycerides,
non-HDL goal
!100 mg/dL)
R100 mg/dL R100 mg/dL (!100
mg/dL consider
pharmacotherapy
to reach goal
!70 mg/dL)
Moderately high
risk: 2þ risk
factors (10-year
risk 10%–20%)
!130 mg/dL
(non-HDL
!160 mg/dL)
R130 mg/dL R130 mg/dL
(100–129 mg/dL
consider drug
options)
Moderate risk:
2þ risk factors
(10-year risk
!10%)
!130 mg/dL
(non-HDL
!160 mg/dL)
R130 mg/dL R160 mg/dL
Lower risk: 0–1 risk
factors
!160 mg/dL
(non-HDL
!190 mg/dL)
R160 mg/dL R190 mg/dL
(160–189 mg/dL:
consider
pharmacotherapy)
a Diabetes, noncoronary atherosclerotic disease, or 2þ risk factors with 10-year risk O20%.
Adapted from the NCEP Expert Panel on Detection, Evaluation, and Treatment of High
Blood Cholesterol in Adults (Adult Treatment Panel III). Circulation 2002;106:3143–21 and
Grundy SM, et al. Implications of recent clinical trials for the National Cholesterol Education
Program Adult Treatment Panel III Guidelines. J Am Coll Cardiol 2004;44(5):1011–7.

115ANTIRETROVIRAL TREATMENT COMPLICATIONS
(statins) have shown success among patients infected with HIV. The para-mount principle is avoiding statins that have substantial interaction with cy-tochrome p450 3A4. For patients taking PIs, simvastatin (Zocor) andlovastatin (Mevacor) should be avoided, but atorvastatin (Lipitor), fluvasta-tin (Lescol), and combination pravastatin (Pravachol) (with or without fe-nofibrate) have been used safely [74]. Pravastatin and fluvastatin are leastlikely to have drug interactions and are therefore considered safest in thestatin class.
Rosuvastatin (Crestor) is emerging as a new option for patients infectedwith HIV undergoing PI or NNRTI therapy. In one study, 16 patients un-dergoing PI-based regimens who were treated with rosuvastatin for 24 weeksexperienced significant decreases in total cholesterol, LDL, and triglyceridesand significant increase in HDL [75]. Rosuvastatin has outstanding potencyand is not dependent on cytochrome P450 for metabolism. Larger studiesare needed before this drug can be recommended broadly.
All statins should be initiated at low dose and titrated with careful mon-itoring of liver function, both before starting therapy and after 4 to 6 weekson therapy. Routine monitoring of muscle enzymes is not recommended,but patients should be educated about symptoms of myopathy so that clin-ically significant myositis or rhabdomyolysis can be identified early.
Ezetimibe (Zetia) is a new cholesterol absorption inhibitor that can besafely used with statins to decrease LDL, but studies have not been reportedin large numbers of patients infected with HIV. Bile acid sequestrants arenot recommended because of possible chelation of concurrent medicationsand tendency to cause hypertriglyceridemia. For PI-associated hypertrigly-ceridemia, particularly when levels exceed 500 mg/dL, fibric acid derivatives(gemfibrozil or fenofibrate) are effective. Alternatives for treatment includefish oil (3–6 g/d) and extended-release niacin. Fish oil can increase LDLlevels and niacin can worsen insulin resistance, so these risks must be
Box 3. Dietary interventions for dyslipidemia
Total fat: 25% to 35% of total caloric intakeSaturated fat: <7% of total caloriesPolyunsaturated fat: up to 10% of total caloriesMonounsaturated fat: up to 20% of total caloriesCholesterol: <200 mg/dayFiber: 20–30 grams/dayPlant sterols: 2 grams/day
Adapted from the NCEP Expert Panel on Detection, Evaluation, and Treatmentof High Blood Cholesterol in Adults (Adult Treatment Panel III). Circulation2002;106:3143–21; with permission.

116 HOFFMAN & CURRIER
balanced against benefits of treatment. In accordance with IDSA/ACTGguidelines, risk factor reduction is paramount. When pharmacotherapy isrequired, it should be prescribed with utmost attention to potential druginteractions and close observation for complications.
Although switching from any PI to atazanavir or class-switching to anNNRTI may be a reasonable option depending on a patient’s resistance pro-file, it has not been shown to be as effective as pharmacotherapy for man-aging dyslipidemia [76]. In recent studies, lipid abnormalities have beenprevented in naı̈ve patients initiated on atazanavir-based regimens. This ef-fect is somewhat attenuated by ritonavir boosting of atazanavir, but this ap-proach still offers lipid advantages over other PI-based regimens [77,78].Switching to nevirapine has been associated with rapid reversal of hypertri-glyceridemia without significant changes in total cholesterol [79,80]. Resultsfrom PI-to-efavirenz switches have yielded conflicting results [81–83].
Monitoring
Before starting ART, a fasting lipid panel should be obtained andfollowed at 3 to 6 monthly intervals during the first year. For patientswho have triglyceride levels greater than 400 mg/dL, calculated LDL isunreliable, and direct measurement should be obtained for further riskassessment and management decisions. Alternatively, non-HDL cholesterol(total cholesterol minus HDL cholesterol) can be monitored when directLDL measurement is not feasible. Lipids should be reassessed beforetherapy changes and once yearly for individuals undergoing stable HIVtreatment regimens. Ongoing lifestyle counseling and surveillance forsecondary causes of dyslipidemia should be integrated into routine visits(monitoring for thyroid disease, liver disease, renal disease, diabetes, anduse of exacerbating medications such as hormones and corticosteroids).
Body composition changes
Body fat abnormalities have been described in large numbers of patientsinfected with HIV, both on and off therapy. The term lipodystrophy has beenused to describe all forms of body fat redistribution and metabolic changes,and is not precise. Fat abnormalities fall into distinct categories of lipoatro-phy and lipohypertrophy, each syndrome with different risk factors, clinicalfeatures, and treatments.
Lipoatrophy: risk factors and clinical features
Lipoatrophy is defined as fat wasting of the face, extremities, and but-tocks. In fact, most patients with peripheral lipoatrophy have fat loss inthe subcutaneous tissue both centrally and peripherally [84]. Risk factorsfor the development of lipoatrophy include therapy with certain NRTIs
117ANTIRETROVIRAL TREATMENT COMPLICATIONS
(eg, stavudine, didanosine, and zidovudine), older age, higher triglyceridesat the start of therapy, nadir CD4 count less than 200 cells/mL, and immunereconstitution/response to therapy. Additionally, lipoatrophy with or with-out other metabolic complications of ART seems to be a risk factor for car-diovascular disease [85,86]. HIV infection in the absence of therapy is a riskfactor for lipoatrophy, as shown in at least one study comparing limb fat inindividuals infected with HIV versus those who were uninfected [84]. Theprecise mechanism by which lipoatrophy occurs is unknown and is the sub-ject of ongoing studies. Mitochondrial toxicity, increased oxidative stress,and abnormal cytokine expression have been implicated in pathogenesis[87]. Fat biopsies in patients on stavudine and other thymidine analogshave shown severe mitochondrial depletion, and healthy volunteers havebeen noted to develop mitochondrial enzyme depletion after 2 weeks ofNRTI therapy with thymidine-containing drugs [3]. Diagnosing lipoatrophyis challenging, because formal criteria have not been developed. Objectivemeasurement of limb fat using dual energy x-ray absorptiometry (DEXA)scans is not generally recommended outside of the research setting. Carefulphysical examination and patient self-report may be adequate to monitorperipheral fat loss in clinical settings.
Lipoatrophy: management and monitoring
The decision to treat fat redistribution is frequently determined in thecontext of associated findings such as insulin resistance and hyperlipidemia.No consensus exists regarding whether treatment of body fat changes shouldbe undertaken in the absence of an associated metabolic syndrome. Thiazo-lidinediones have received significant attention as an investigational treat-ment of lipoatrophy because they stimulate PPAR-g and increaseadipogenesis in vitro. Most studies have shown minimal benefit, and showthat glitazone therapy for patients who remain on stavudine (a potent inhib-itor of PPAR-g) will have no impact on fat redistribution [53,88,89]. Twosmall studies have shown that uridine supplementation after 3 months oftherapy increases limb fat to a greater degree than seen in ARV switch stud-ies. In patients taking uridine, mitochondrial DNA levels did not changeand the mechanism of fat gain remains unclear [90,91]. In a single random-ized, placebo-controlled study of 33 men infected with HIV, 4 weeks of pra-vastatin significantly improved limb fat as assessed in baseline and follow-upDEXA measurement [92]. Larger studies are needed to confirm this unex-pected finding. Various plastic surgery techniques have emerged as treat-ment options for lipoatrophy, although only polylactic acid (Sculptra) hasbeen adequately tested in individuals infected with HIV and is FDA-approved for use [93]. Insurance coverage of polylactic acid is poor, becausethe procedure is usually designated as cosmetic. Autologous fat transfer andpolymethylmethacrylate have had mixed results and require larger studiesbefore widespread use can be recommended [94].

118 HOFFMAN & CURRIER
Changing ART may be appropriate for patients who have lipoatrophy,particularly among those currently receiving stavudine or zidovudinewhen tenofovir or abacavir are available therapeutic options. A recent studyshowed that after 48 weeks of therapy with either zidovudine or tenofovir,individuals taking zidovudine had clear limb fat losses, whereas those takingtenofovir had increased limb fat. Interpretation of the study is limited by thelack of baseline DEXA testing. Another study showed that switching froma thymidine-containing regimen (d4T or AZT) to either tenofovir or abaca-vir resulted in small but statistically significant gains in limb fat, with mostmarked improvement seen in patients switching from stavudine-containingregimens [95]. Fat losses from stavudine improved, but only approximately10% of fat recovery was seen at 1-year follow-up, and whether longer inter-vals would lead to substantial gains or whether these individuals would everreturn to pretreatment baseline is unclear [95–97].
Lipohypertrophy: risk factors and clinical features
Lipohypertrophy is defined by fat accumulation in the abdomen,breasts, and posterior neck (buffalo hump). Risk factors include PI use,older age, white race, more advanced degree of immunosuppression, andfemale gender [44,98,99]. The prevalence of PI-associated fat redistributionhas been reported to range from 2% to 84% [100–102]. The wide intervalreflects lack of consensus definition and diagnostic criteria. Patient andphysician report are most commonly used for diagnosis, but cross-sec-tional imaging techniques such as CT and MRI are the gold standardfor measuring body fat in the research setting. Routine use of these tech-niques is limited by expense and availability, and diagnosis can be madewith specific waist-to-hip ratio (O0.95 in men and O0.85 in women) orenlarged abdominal circumference (R102 cm in men and R88 cm inwomen) [103].
Management and monitoring
Lifestyle changes can be helpful in the management of lipohypertrophy,including dietary limitations of saturated fat, simple carbohydrates, andalcohol, and avoidance of rapid weight loss which can worsen lean tissueloss. Aerobic and resistance exercise can improve fat accumulation in indi-viduals infected with HIV, but excessive exercise has been shown to worsenlipoatrophy [104–106].
Recombinant human growth hormone (rhGH) has been found todecrease visceral fat, but also exacerbates insulin resistance and worsenslipoatrophy in clinical trials [48,107]. Benefits gained from rhGH seemto be reversed on cessation of the drug [108]. Growth hormone releasingfactor has been shown to decrease visceral fat and improve lipid profile,but until final results of phase 3 trials are available, cannot be

119ANTIRETROVIRAL TREATMENT COMPLICATIONS
recommended. Testosterone may have some benefit in hypogonadal menby reducing visceral fat and improving insulin sensitivity, but also leadsto decreased limb fat and is not recommended for chronic treatment ofisolated lipohypertrophy [109,110]. Metformin has been shown to improveglucose tolerance, reduce weight and visceral fat, and decrease triglyceridelevels in randomized trials of individuals infected with HIV who have cen-tral fat accumulation and insulin resistance [50,51]. Benefits in reductionof visceral fat may be offset by worsening of preexisting lipoatrophy;therefore, metformin is not a recommended approach to lipohypertrophyin the absence of associated metabolic changes. Buffalo hump liposuctionhas been associated with surgical complications and high recurrence rate,and may not be covered by insurance. Unlike switch therapy for lipoatro-phy, switching off PI-based regimens has not been shown to improvelipohypertrophy [63,111].
Is cardiovascular risk increased?
Most observational and retrospective data support the association be-tween increased cardiovascular risk and ART, but studies not defined theextent of this risk. Although an early study from the Veterans Affairs system
Box 4. Monitoring for cardiovascular risk
ModifiableHypertensionObesityDietExerciseDyslipidemiaAbnormal glucoseMedications, including PIs*Cigarette smokingElevated homocysteineElevated lipoprotein(a)
NonmodifiableAdvancing ageFamily historyGenderChronic kidney diseaseMetabolism
* May be nonmodifiable if resistant virus.

Table 2
Summary of the major co
Monitoring
Hyperlactatemia/
lactic acidosis
s: If on
log,
nitor. If
lly or
regimen.
continue
resolved,
nalog,
e with
No established role for monitoring
asymptomatic individuals. Role for
selective monitoring of high-risk
patients unclear.
Nevirapine
hypersensitivity
less than
without
rapine
14 days,
oms
evens-
han five
tinue
gimen.
Baseline LFTs prior to starting
therapy, after 2 weeks of therapy,
and then monthly through the first 3
months. If patient develops skin rash
or gastrointestinal symptoms at any
point on therapy, check LFTs, CBC
with differential, and renal function.
120
HOFFMAN
&CURRIE
R
mplications of antiretroviral therapy
Risk factors Management
Definite or probable: stavudine,
didanosine, zidovudine, female
gender, higher body weight
Possible: chronic hepatitis or other liver
disease, NRTI plus metformin, older
age, advanced immunodeficiency.
Mild hyperlactatemia with symptom
stavudine or other thymidine ana
switch to non-thymidine and mo
on non-thymidine, observe carefu
consider switch to NRTI-sparing
Moderate-severe lactic acidosis: dis
all ARVs. Supportive care. When
if prior regimen was thymidine a
consider non-thymidine backbon
careful monitoring.
Definite or probable: female gender,
CD4 O 250 cells/mL for women and
O400 cells/mL for men (particularly
for hepatotoxicity), age O40 years,
hepatitis B or C coinfection, obesity,
pregnancy
Mild-moderate rash or transaminitis
five times upper limit of normal,
fever or mucositis: Continue nevi
and monitor. If develops in first
defer dose escalation until sympt
resolve.
Severe rash, systemic symptoms, St
Johnson, or transaminitis more t
times upper limit normal: Discon
nevirapine. Consider PI-based re

Abacavir
h
HLA-B*5701 Mild rash without systemic symptoms:
with careful monitoring.
with or without rash,
sening with additional
abacavir, document
future exposure to
No established monitoring or screening
currently recommended. HLA typing
for B*5701 is under study as possible
screening tool.
Ins
(
g
(
d
(
s: Diet and Exercise
rove IR and decrease
y if lipohypertrophy.
f potential for increased
improve IR, but
ight gain. Risk of
ect on IR, can cause
ed if oral therapy fails to
Before ART: Risk stratify with review
of family history, medication list, and
body mass index. Check fasting
glucose. Consider oral glucose
tolerance test for high-risk patients.
During ART: fasting glucose 6–12
weeks after starting therapy,
particularly for PI based regimens or
high-risk patients, then every 3
months during the first year of
therapy. Intensity of further
monitoring is based on individual
risk. PLUS Ongoing counseling
regarding diet and exercise,
regardless of risk.
(continued on next page)
121
ANTIR
ETROVIR
ALTREATMENTCOMPLIC
ATIO
NS
ypersensitivity continue abacavir
Systemic symptoms
particularly if wor
doses: Discontinue
allergy and avoid
abacavir.
ulin resistance
IR), impaired
lucose tolerance
IGT), and
iabetes mellitus
DM)
Definite or probable: HIV infection,
PIs, fat redistribution, stavudine,
hepatitis C coinfection, obesity,
family history, older age.
Possible: female gender
Lifestyle intervention
Metformin: may imp
weight, particularl
Caution because o
lactate.
Thiazolidinediones:
associated with we
hepatotoxicity.
Sulfonylureas: no eff
hypoglycemia
Insulin: should be us
control DM.
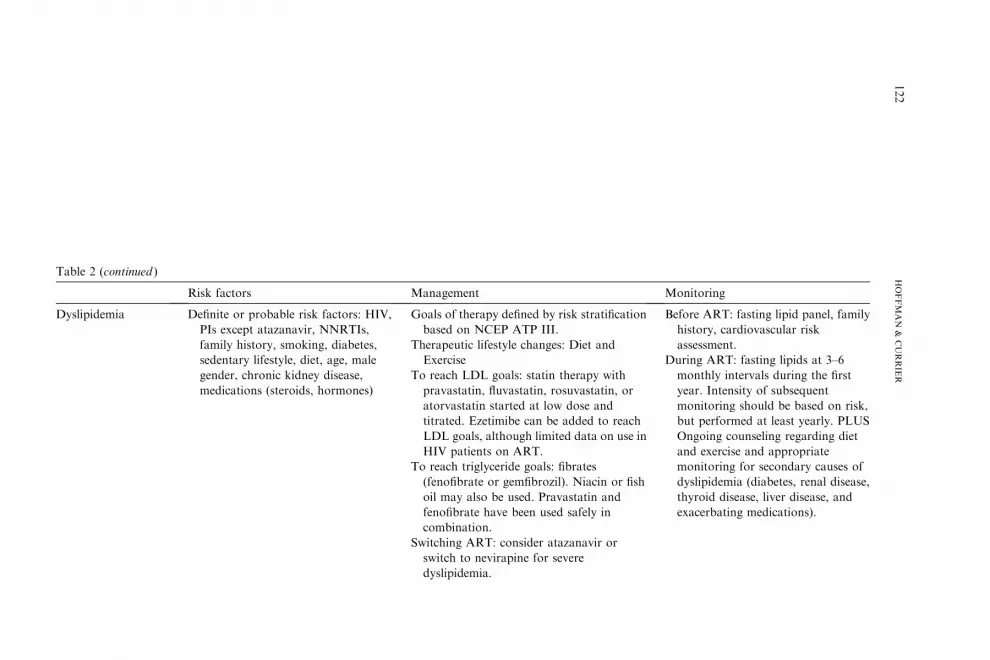
Table 2 (continued )
Risk fact Monitoring
Dyslipidemia Definite o
PIs exc
family
sedenta
gender,
medica
atification
and
with
atin, or
and
to reach
on use in
in or fish
and
in
ir or
Before ART: fasting lipid panel, family
history, cardiovascular risk
assessment.
During ART: fasting lipids at 3–6
monthly intervals during the first
year. Intensity of subsequent
monitoring should be based on risk,
but performed at least yearly. PLUS
Ongoing counseling regarding diet
and exercise and appropriate
monitoring for secondary causes of
dyslipidemia (diabetes, renal disease,
thyroid disease, liver disease, and
exacerbating medications).
122
HOFFMAN
&CURRIE
R
ors Management
r probable risk factors: HIV,
ept atazanavir, NNRTIs,
history, smoking, diabetes,
ry lifestyle, diet, age, male
chronic kidney disease,
tions (steroids, hormones)
Goals of therapy defined by risk str
based on NCEP ATP III.
Therapeutic lifestyle changes: Diet
Exercise
To reach LDL goals: statin therapy
pravastatin, fluvastatin, rosuvast
atorvastatin started at low dose
titrated. Ezetimibe can be added
LDL goals, although limited data
HIV patients on ART.
To reach triglyceride goals: fibrates
(fenofibrate or gemfibrozil). Niac
oil may also be used. Pravastatin
fenofibrate have been used safely
combination.
Switching ART: consider atazanav
switch to nevirapine for severe
dyslipidemia.

Lipoatrophy Definite or probable risk factors:
NRTIs (especially stavudine,
Presence of IR and dyslipidemia favors
decision to treat:
inimal
if
show
e
ns.
ing off
h
with
No monitoring beyond routine physical
examination and vigilance for
development of body fat
redistribution. Patients who
experience fat redistribution should
have screening for abnormal glucose
metabolism and dyslipidemia.
L rs
nd
visceral
s, but
benefit
:
y
R and
with
ching
No monitoring beyond routine physical
examination and vigilance for
development of body fat
redistribution. Patients with fat
redistribution should have screening
for abnormal glucose metabolism
and dyslipidemia.
(continued on next page)
123
ANTIR
ETROVIR
ALTREATMENTCOMPLIC
ATIO
NS
didanosine, and zidovudine) older
age, higher triglycerides at initiation
of therapy, nadir CD4 count !200
cells/mL, immune reconstitution.
Thiazolidinediones: investigational. M
benefit for lipoatrophy particularly
patient remains on stavudine.
Uridine: investigational. Small studies
limb fat increases greater than thos
achieved by switching ART regime
Plastic surgery: polylactic acid.
Switching ART: fat losses after switch
stavudine improve. Substitution wit
tenofovir or abacavir is associated
increase in limb fat.
ipohypertrophy Definite or probable risk factors: higher
body mass index before antiretroviral
therapy, PIs, older age, white race,
advanced immunosuppression,
female gender.
Presence of IR and dyslipidemia favo
decision to treat:
Lifestyle changes: limit saturated fat a
carbohydrates in diet; aerobic and
resistance exercise.
Metformin: investigational. Improves
fat and has other metabolic benefit
can worsen lipoatrophy.
Testosterone: investigational. Possible
in hypogonadal men, but worsens
lipoatrophy.
Recombinant human growth hormone
investigational. Results in temporar
decrease in visceral fat but worsens I
lipoatrophy.
Plastic surgery: liposuction associated
high recurrence rate.
Switching ART: No benefit from swit
off PI therapy.
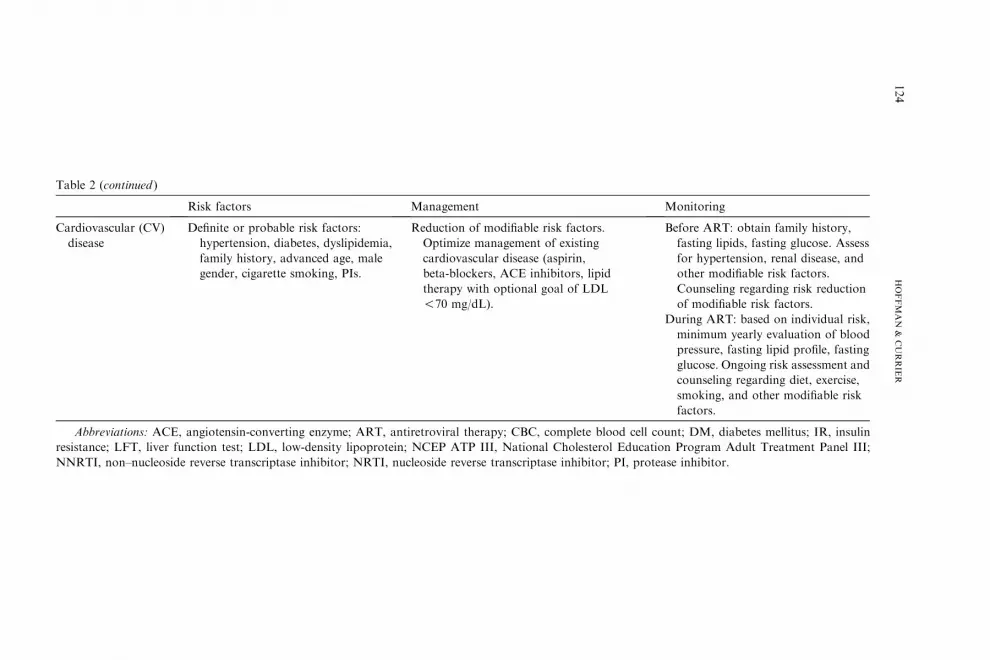
Table 2 (continued )
Monitoring
Cardiovascular (CV)
disease
factors.
existing
irin,
tors, lipid
l of LDL
Before ART: obtain family history,
fasting lipids, fasting glucose. Assess
for hypertension, renal disease, and
other modifiable risk factors.
Counseling regarding risk reduction
of modifiable risk factors.
During ART: based on individual risk,
minimum yearly evaluation of blood
pressure, fasting lipid profile, fasting
glucose. Ongoing risk assessment and
counseling regarding diet, exercise,
smoking, and other modifiable risk
factors.
Abbreviations: A plete blood cell count; DM, diabetes mellitus; IR, insulin
resistance; LFT, live holesterol Education Program Adult Treatment Panel III;
NNRTI, non–nucleo inhibitor; PI, protease inhibitor.
124
HOFFMAN
&CURRIE
R
Risk factors Management
Definite or probable risk factors:
hypertension, diabetes, dyslipidemia,
family history, advanced age, male
gender, cigarette smoking, PIs.
Reduction of modifiable risk
Optimize management of
cardiovascular disease (asp
beta-blockers, ACE inhibi
therapy with optional goa
!70 mg/dL).
CE, angiotensin-converting enzyme; ART, antiretroviral therapy; CBC, com
r function test; LDL, low-density lipoprotein; NCEP ATP III, National C
side reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase

125ANTIRETROVIRAL TREATMENT COMPLICATIONS
in patients infected with HIV who had limited PI exposure found a slightdecrease in cerebrovascular and cardiovascular events, other large studieshave shown small but significantly increased risk [112]. A French cohortstudy of patients undergoing PI-based therapy showed the incidence of myo-cardial infarction was increased threefold when therapy lasted longer than30 months [113]. The HIV Outpatient Study (HOPS) followed more than5500 patients and also found greater risk for myocardial infarction in pa-tients who used PIs, but an overall low event rate [114]. The French andHOPS data are supported by the findings of the Data Collection on AdverseEvents of Anti-HIV Drugs (D:A:D) study group. This study, the largest todate, prospectively followed more than 20,000 patients on ART representingmore than 35,000 person-years of follow-up, and showed a 26% relative in-crease in the rate of myocardial infarction per year of exposure during thefirst 4 to 6 years of use [115]. Predictors of myocardial infarction includeda history of cardiovascular disease, current or former smoking, anyARVs, age, and male gender. As of February 2005 the D:A:D study grouphad 94,469 person-years of follow-up and found that time on PI was asso-ciated with increased risk for myocardial infarction (16% per year of expo-sure), partially explained by dyslipidemia [116]. The absolute risk was low at0.4% per year of follow-up, and the absolute risk of events has been consis-tently low in subsequent studies. Any risk must be weighed against clearbenefits of HIV therapy.
Because the absolute cardiovascular event rate in HIV infection has re-mained low, use of validated surrogates has been increasingly used to studycardiovascular risk from HIV and ART. Impaired endothelium-dependentvasodilation is an indicator of atherosclerotic disease and has led to interestin surrogate markers such as carotid intima-media thickness (IMT), brachialartery flow-mediated dilation (FMD), and aortic pulse-wave velocity(PWV). Many of these studies have shown subclinical atherosclerosis in pa-tients undergoing ART, but the strongest predictors have been traditionalcardiovascular risk factors as opposed to specific antiretroviral regimensor features of HIV infection [117,118]. Additional risk factors describedinclude advanced degree of immunodeficiency [119], any ARVs [120], andPI-based therapy [121]. Pathogenesis of endothelial dysfunction in HIV isbeing actively explored, and validated surrogate markers may eventuallybe available to stratify and monitor high-risk patients [122–124].
Management of cardiovascular risk
Experience from research on cardiovascular disease highlights that tra-ditional cardiac risk factors may be more contributory than HIV-specificfactors. Thus, emphasis on changing these modifiable risks is of utmostimportance (Box 4). Before ART is initiated, patients should undergocardiovascular risk assessment with evaluation for hypertension, dyslipide-mia, and glucose abnormalities, and receive counseling on risk reduction

126 HOFFMAN & CURRIER
(eg, diet, exercise, smoking cessation). Patients undergoing on chronic ARTshould be intermittently monitored for diabetes and dyslipidemia, most in-tensively in the first year (approximately every 3 months) and then at leastyearly if no abnormalities are identified. Smoking is a critical modifiablerisk factor that should be addressed in the setting of HIV infection.
Summary
Successful treatment of HIV results in immune restoration, viral suppres-sion, prevention of opportunistic infections, and probable extension of aninfected individual’s lifespan to near-normal. These remarkable benefitsare accompanied by an array of treatment complications, with an impactthat has yet to be fully understood. A comprehensive approach to manage-ment of complications includes knowledge in three areas: (1) risk factors foradverse reactions, (2) clinical syndromes suggestive of an evolving complica-tion, and (3) informed treatment approaches to preventing and managingthese complications. Systematic evaluation has led to emerging informationabout risk factors for drug complications, such as gender, immune status,HLA subtypes, coinfections, and comorbidities. Knowledge of these riskscan inform choice of drug regimen and intensity of monitoring. An under-standing of clinical presentation of complications empowers the clinician forearly recognition of an adverse drug reaction, rapid response, and avoidanceof further morbidity. Fluency in options for preventing and treating compli-cations can provide maximal opportunity to balance treatment effects withquality of life (Table 2).
References
[1] Organization WH. Global access to HIV therapy tripled in past two years, but significant
challenges remain. JointNewsReleaseWHO/UNAIDS.Available at: http://www.who.int/
hiv/mediacentre/news57/en/index.html. March 28, 2006.
[2] Vrouenraets SM, TreskesM, Regez RM, et al. Hyperlactataemia in HIV-infected patients:
the role of NRTI-treatment. Antivir Ther 2002;7(4):239–44.
[3] Birkus G, Hitchcock MJ, Cihlar T. Assessment of mitochondrial toxicity in human cells
treated with tenofovir: comparison with other nucleoside reverse transcriptase inhibitors.
Antimicrob Agents Chemother 2002;46(3):716–23.
[4] GiolaM, Basilico C, Grossi P. Fatal lactic acidosis associated with tenofovir and abacavir.
Int J Infect Dis 2005;9(4):228–9.
[5] James JS. d4T plus ddI: warning for pregnant women. AIDS Treat News. January 12,
2001:358:8.
[6] Gerard Y, Maulin L, Yazdanpanah Y, et al. Symptomatic hyperlactataemia: an emerging
complication of antiretroviral therapy. AIDS 2000;14(17):2723–30.
[7] Bonnet F, Bonarek M, Abrij A, et al. Metabolic acidosis in HIV-infected patients. Clin
Infect Dis 2002;34(9):1289–90.

127ANTIRETROVIRAL TREATMENT COMPLICATIONS
[8] Moyle GJ, Datta D, Mandalia S, et al. Hyperlactataemia and lactic acidosis during antire-
troviral therapy: relevance, reproducibility and possible risk factors. AIDS 2002;16(10):
1341–9.
[9] Laguno M, Milinkovic A, de Lazzari E, et al. Incidence and risk factors for mito-
chondrial toxicity in treated HIV/HCV-coinfected patients. Antivir Ther 2005;10(3):
423–9.
[10] Moreno A, Quereda C, Moreno L, et al. High rate of didanosine-related mitochon-
drial toxicity in HIV/HCV-coinfected patients receiving ribavirin. Antivir Ther 2004;
9(1):133–8.
[11] Wyles DL, Gerber JG. Antiretroviral drug pharmacokinetics in hepatitis with hepatic
dysfunction. Clin Infect Dis 2005;40(1):174–81.
[12] Imhof A, Ledergerber B, Gunthard HF, et al. Risk factors for and outcome of hyperlacta-
temia in HIV-infected persons: is there a need for routine lactate monitoring? Clin Infect
Dis 2005;41(5):721–8.
[13] Geddes R, Knight S,MoosaMY, et al. A high incidence of nucleoside reverse transcriptase
inhibitor (NRTI)-induced lactic acidosis in HIV-infected patients in a South African con-
text. S Afr Med J 2006;96(8):722–4.
[14] Smith KY. Selected metabolic and morphologic complications associated with highly
active antiretroviral therapy. J Infect Dis 2002;185(Suppl 2):S123–7.
[15] Falco V, CrespoM,Ribera E. Lactic acidosis related to nucleoside therapy in HIV-infected
patients. Expert Opin Pharmacother 2003;4(8):1321–9.
[16] Stacpoole PW,Wright EC, Baumgartner TG, et al. A controlled clinical trial of dichloroa-
cetate for treatment of lactic acidosis in adults. The Dichloroacetate-Lactic Acidosis Study
Group. N Engl J Med 1992;327(22):1564–9.
[17] Patel V,Hedayati SS. Lactic acidosis in anHIV-infected patient receiving highly active anti-
retroviral therapy. Nat Clin Pract Nephrol 2006;2(2):109–14 [quiz: 115].
[18] Carter RW, Singh J, Archambault C, et al. Severe lactic acidosis in association with reverse
transcriptase inhibitors with potential response to L-carnitine in a pediatric HIV-positive
patient. AIDS Patient Care STDS 2004;18(3):131–4.
[19] Claessens YE, Cariou A, Chiche JD, et al. L-Carnitine as a treatment of life-threatening
lactic acidosis induced by nucleoside analogues. AIDS 10 2000;14(4):472–73.
[20] Brinkman K, Vrouenraets S, Kauffmann R, et al. Treatment of nucleoside reverse tran-
scriptase inhibitor-induced lactic acidosis. AIDS 2000;14(17):2801–2.
[21] Saint-Marc T, Touraine JL. The effects of discontinuing stavudine therapy on clinical and
metabolic abnormalities in patients suffering from lipodystrophy. AIDS 1999;13(15):
2188–9.
[22] Lonergan JT, Barber RE,MathewsWC. Safety and efficacy of switching to alternative nu-
cleoside analogues following symptomatic hyperlactatemia and lactic acidosis. AIDS 2003;
17(17):2495–9.
[23] Ogedegbe AE, Thomas DL, Diehl AM. Hyperlactataemia syndromes associated with HIV
therapy. Lancet Infect Dis 2003;3(6):329–37.
[24] BrinkmanK, Smeitink JA, Romijn JA, et al.Mitochondrial toxicity induced by nucleoside-
analogue reverse-transcriptase inhibitors is a key factor in the pathogenesis of antiretrovi-
ral-therapy-related lipodystrophy. Lancet 1999;354(9184):1112–5.
[25] Carr A, Cooper DA. Adverse effects of antiretroviral therapy. Lancet 2000;356(9239):
1423–30.
[26] Montessori V, Press N, Harris M, et al. Adverse effects of antiretroviral therapy for HIV
infection. CMAJ 2004;170(2):229–38.
[27] Fagot JP, MockenhauptM, Bouwes-Bavinck JN, et al. Nevirapine and the risk of Stevens-
Johnson syndrome or toxic epidermal necrolysis. AIDS 2001;15(14):1843–8.
[28] van Leth F, Phanuphak P, Ruxrungtham K, et al. Comparison of first-line antiretroviral
therapy with regimens including nevirapine, efavirenz, or both drugs, plus stavudine and

128 HOFFMAN & CURRIER
lamivudine: a randomised open-label trial, the 2NN Study. Lancet 2004;363(9417):
1253–63.
[29] Ofotokun I, Pomeroy C. Sex differences in adverse reactions to antiretroviral drugs. Top
HIV Med 2003;11(2):55–9.
[30] Stern JO,RobinsonPA,Love J, et al. A comprehensive hepatic safety analysis of nevirapine
in different populations of HIV infected patients. J Acquir Immune Defic Syndr 2003;
34(Suppl 1):S21–33.
[31] Lyons F, Hopkins S, Kelleher B, et al. Maternal hepatotoxicity with nevirapine as part of
combination antiretroviral therapy in pregnancy. HIV Med 2006;7(4):255–60.
[32] Clay PG. The abacavir hypersensitivity reaction: a review. Clin Ther 2002;24(10):1502–14.
[33] Phillips EJ. Genetic screening to prevent abacavir hypersensitivity reaction: are we there
yet? Clin Infect Dis 2006;43(1):103–5.
[34] Mallal S, Nolan D, Witt C, et al. Association between presence of HLA-B*5701, HLA-
DR7, and HLA-DQ3 and hypersensitivity to HIV-1 reverse-transcriptase inhibitor abaca-
vir. Lancet 2002;359(9308):727–32.
[35] Hetherington S, Hughes AR, Mosteller M, et al. Genetic variations in HLA-B region and
hypersensitivity reactions to abacavir. Lancet 2002;359(9312):1121–2.
[36] RauchA,NolanD,MartinA, et al. Prospective genetic screening decreases the incidence of
abacavir hypersensitivity reactions in theWesternAustralianHIV cohort study. Clin Infect
Dis 2006;43(1):99–102.
[37] Phillips EJ, Sullivan JR, Knowles SR, et al. Utility of patch testing in patients with hyper-
sensitivity syndromes associated with abacavir. AIDS 2002;16(16):2223–5.
[38] Martin AM, Nolan D, Gaudieri S, et al. Pharmacogenetics of antiretroviral therapy:
genetic variation of response and toxicity. Pharmacogenomics 2004;5(6):643–55.
[39] Launay O, Roudiere L, Boukli N, et al. Assessment of cetirizine, an antihistamine, to pre-
vent cutaneous reactions to nevirapine therapy: results of the Viramune-Zyrtec double-
blind, placebo-controlled trial. Clin Infect Dis 2004;38(8):e66–72.
[40] Knobel H, Miro JM, Domingo P, et al. Failure of a short-term prednisone regimen to pre-
vent nevirapine-associated rash: a double-blind placebo-controlled trial: the GESIDA 09/
99 study. J Acquir Immune Defic Syndr 2001;28(1):14–8.
[41] Gelato MC. Insulin and carbohydrate dysregulation. Clin Infect Dis 2003;36(Suppl 2):
S91–5.
[42] Currier JS, Taylor A, Boyd F, et al. Coronary heart disease in HIV-infected individuals.
J Acquir Immune Defic Syndr 2003;33(4):506–12.
[43] Brown TT, Cole SR, Li X, et al. Antiretroviral therapy and the prevalence and incidence of
diabetes mellitus in the multicenter AIDS cohort study. Arch Intern Med 2005;165(10):
1179–84.
[44] Justman JE, Benning L,DanoffA, et al. Protease inhibitor use and the incidence of diabetes
mellitus in a large cohort of HIV-infected women. J Acquir Immune Defic Syndr 2003;
32(3):298–302.
[45] Jones CY, Wilson IB, Greenberg AS, et al. Insulin resistance in HIV-infected men and
women in the nutrition for healthy living cohort. J Acquir Immune Defic Syndr 2005;
40(2):202–11.
[46] Howard AA, Floris-Moore M, Arnsten JH, et al. Disorders of glucose metabolism among
HIV-infected women. Clin Infect Dis 2005;40(10):1492–9.
[47] Behrens G, Dejam A, Schmidt H, et al. Impaired glucose tolerance, beta cell function and
lipid metabolism in HIV patients under treatment with protease inhibitors. AIDS 1999;
13(10):F63–70.
[48] Mauss S, Wolf E, Jaeger H. Impaired glucose tolerance in HIV-positive patients receiving
and those not receiving protease inhibitors. Ann Intern Med 1999;130(2):162–3.
[49] Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of
type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002;
346(6):393–403.

129ANTIRETROVIRAL TREATMENT COMPLICATIONS
[50] HadiganC, CorcoranC, BasgozN, et al.Metformin in the treatment of HIV lipodystrophy
syndrome: a randomized controlled trial. JAMA 2000;284(4):472–7.
[51] vanWijk JP, deKoningEJ, CabezasMC, et al. Comparison of rosiglitazone andmetformin
for treating HIV lipodystrophy: a randomized trial. Ann Intern Med 2005;143(5):337–46.
[52] Hadigan C, Yawetz S, Thomas A, et al. Metabolic effects of rosiglitazone in HIV lipodys-
trophy: a randomized, controlled trial. Ann Intern Med 2004;140(10):786–94.
[53] Sutinen J, Hakkinen AM,Westerbacka J, et al. Rosiglitazone in the treatment of HAART-
associated lipodystrophyda randomized double-blind placebo-controlled study. Antivir
Ther 2003;8(3):199–207.
[54] Goldberg RB, Kendall DM, DeegMA, et al. A comparison of lipid and glycemic effects of
pioglitazone and rosiglitazone in patients with type 2 diabetes and dyslipidemia. Diabetes
Care 2005;28(7):1547–54.
[55] Fonseca V, Rosenstock J, Patwardhan R, et al. Effect of metformin and rosiglitazone com-
bination therapy in patients with type 2 diabetes mellitus: a randomized controlled trial.
JAMA 2000;283(13):1695–702.
[56] Gerstein HC, Yusuf S, Bosch J, et al. Effect of rosiglitazone on the frequency of diabetes in
patients with impaired glucose tolerance or impaired fasting glucose: a randomised con-
trolled trial. Lancet 2006;368(9541):1096–105.
[57] Bosch J, Yusuf S, Gerstein HC, et al. Effect of ramipril on the incidence of diabetes. N Engl
J Med 2006;355(15):1551–62.
[58] Noor MA, Parker RA, O’Mara E, et al. The effects of HIV protease inhibitors atazanavir
and lopinavir/ritonavir on insulin sensitivity in HIV-seronegative healthy adults. AIDS
2004;18(16):2137–44.
[59] Dube MP, Qian D, Edmondson-Melancon H, et al. Prospective, intensive study of meta-
bolic changes associated with 48 weeks of amprenavir-based antiretroviral therapy. Clin
Infect Dis 2002;35(4):475–81.
[60] Yan Q, Hruz PW. Direct comparison of the acute in vivo effects of HIV protease inhibitors
on peripheral glucose disposal. J Acquir Immune Defic Syndr 2005;40(4):398–403.
[61] Carr A, Workman C, Smith DE, et al. Abacavir substitution for nucleoside analogs in
patients with HIV lipoatrophy: a randomized trial. JAMA 2002;288(2):207–15.
[62] Smith DE, Carr A, LawM, et al. Thymidine analogue withdrawal for lipoatrophic patients
on protease-sparing therapy improves lipoatrophy but compromises antiviral control: the
PIILR extension study. AIDS 2002;16(18):2489–91.
[63] Martinez E, Garcia-ViejoMA, Blanco JL, et al. Impact of switching from human immuno-
deficiency virus type 1 protease inhibitors to efavirenz in successfully treated adults with
lipodystrophy. Clin Infect Dis 2000;31(5):1266–73.
[64] Thiebaut R, Dequae-Merchadou L, Ekouevi DK, et al. Incidence and risk factors of severe
hypertriglyceridaemia in the era of highly active antiretroviral therapy: the Aquitaine
Cohort, France, 1996-1999. HIV Med 2001;2(2):84–8.
[65] Purnell JQ, Zambon A, Knopp RH, et al. Effect of ritonavir on lipids and post-heparin
lipase activities in normal subjects. AIDS 2000;14(1):51–7.
[66] van der ValkM,Kastelein JJ,MurphyRL, et al. Nevirapine-containing antiretroviral ther-
apy in HIV-1 infected patients results in an anti-atherogenic lipid profile. AIDS 2001;
15(18):2407–14.
[67] Young J, Weber R, Rickenbach M, et al. Lipid profiles for antiretroviral-naive patients
starting PI- and NNRTI-based therapy in the Swiss HIV cohort study. Antivir Ther
2005;10(5):585–91.
[68] Schmidt HH, Behrens G, Genschel J, et al. Lipid evaluation in HIV-1-positive patients
treated with protease inhibitors. Antivir Ther 1999;4(3):163–70.
[69] Behrens G, Schmidt HH, Stoll M, et al. ApoE genotype and protease-inhibitor-associated
hyperlipidaemia. Lancet 1999;354(9172):76.
[70] DubeMP, Stein JH, Aberg JA, et al. Guidelines for the evaluation andmanagement of dys-
lipidemia in human immunodeficiency virus (HIV)-infected adults receiving antiretroviral

130 HOFFMAN & CURRIER
therapy: recommendations of the HIVMedical Association of the Infectious Disease Soci-
ety of America and the Adult AIDS Clinical Trials Group. Clin Infect Dis 2003;37(5):
613–27.
[71] Heart Protection Study Collaborative Group MB. MRC/BHF heart protection study
of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised
placebo-controlled trial. Lancet 2002;360:7–22.
[72] Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid lowering
with statins after acute coronary syndromes. N Engl J Med 2004;350(15):1495–504.
[73] Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the
National cholesterol education program adult treatment panel III guidelines. J Am Coll
Cardiol 2004;44(3):720–32.
[74] HenryK,Melroe H,Huebesch J, et al. Atorvastatin and gemfibrozil for protease-inhibitor-
related lipid abnormalities. Lancet 1998;352(9133):1031–2.
[75] Calza L, Colangeli V,Manfredi R, et al. Rosuvastatin for the treatment of hyperlipidaemia
in HIV-infected patients receiving protease inhibitors: a pilot study. AIDS 2005;19(10):
1103–5.
[76] Calza L,ManfrediR, Colangeli V, et al. Substitution of nevirapine or efavirenz for protease
inhibitor versus lipid-lowering therapy for the management of dyslipidaemia. AIDS 2005;
19(10):1051–8.
[77] Mobius U, Lubach-RuitmanM, Castro-Frenzel B, et al. Switching to atazanavir improves
metabolic disorders in antiretroviral-experienced patients with severe hyperlipidemia.
J Acquir Immune Defic Syndr 2005;39(2):174–80.
[78] Cahn PE, Gatell JM, Squires K, et al. Atazanavir–a once-daily HIV protease inhibitor that
does not cause dyslipidemia in newly treated patients: results from two randomized clinical
trials. J Int Assoc Physicians AIDS Care (Chic Ill) 2004;3(3):92–8.
[79] Barreiro P, SorianoV, Blanco F, et al. Risks and benefits of replacing protease inhibitors by
nevirapine in HIV-infected subjects under long-term successful triple combination therapy.
AIDS 2000;14(7):807–12.
[80] De Luca A, Baldini F, Cingolani A, et al. Benefits and risks of switching from protease in-
hibitors to nevirapine with stable background therapy in patients with low or undetectable
viral load: a multicentre study. AIDS 2000;14(11):1655–6.
[81] DrechslerH, PowderlyWG. Switching effective antiretroviral therapy: a review. Clin Infect
Dis 2002;35(10):1219–30.
[82] Viciana P, Alarcon A, Martin D, et al. Partial improvement in lipodystrophy after switch-
ing from HIV-1 protease inhibitors to efavirenz. Paper Presented at the 7th Conference on
Retroviruses and Opportunistic Infections. San Francisco (CA), January 30–February 2,
2000.
[83] Bonnet E, Lepec R, Bluteau M, et al. Evaluation of lipodystrophy syndrome and lipid
profile in HIV patients after switching from protease inhibitors to efavirenz. Presented
at the 7th Conference on Retroviruses and Opportunistic Infections. San Francisco
(CA), January 30–February 2, 2000.
[84] Bacchetti P, Gripshover B, Grunfeld C, et al. Fat distribution in men with HIV infection.
J Acquir Immune Defic Syndr 2005;40(2):121–31.
[85] Carr A. HIV lipodystrophy: risk factors, pathogenesis, diagnosis and management. AIDS
2003;17(Suppl 1):S141–8.
[86] Hadigan C, Meigs JB, Wilson PW, et al. Prediction of coronary heart disease risk in HIV-
infected patients with fat redistribution. Clin Infect Dis 2003;36(7):909–16.
[87] McComsey GA, Walker UA. Role of mitochondria in HIV lipoatrophy: insight into path-
ogenesis and potential therapies. Mitochondrion 2004;4(2–3):111–8.
[88] Carr A, Workman C, Carey D, et al. No effect of rosiglitazone for treatment of HIV-1 lip-
oatrophy: randomised, double-blind, placebo-controlled trial. Lancet 2004;363(9407):
429–38.
131ANTIRETROVIRAL TREATMENT COMPLICATIONS
[89] Slama L, Lanoy E, Valentin M, et al. Effect of pioglitazone on HIV-1 related lipoatrophy:
a randomized double-blind placebo controlled trial (ANRS 113) with 130 patients.
Presented at the 13th Conference on Retrovirus and Opportunistic Infections. Denver,
February 5–8, 2006.
[90] Sutinen J, Walker U, Sevastianova K, et al. Uridine supplementation increases subcutane-
ous fat in patients with HAART-associated lipodystrophy: a randomized, placebo-con-
trolled trial. Presented at the 7th International Workshop on Adverse Drug Reactions
and Lipodystrophy in HIV. Dublin (Ireland), November 13–17, 2005.
[91] McComsey G, Riordan M, Setzer B, et al. Effect of Nucleomaxx on fat and blood mito-
chondrial DNA in D4T-treated subjects with clinical lipoatrophy. Presented at the 7th
International Workshop on Adverse Drug Reactions and Lipodystrophy in HIV. Dublin
(Ireland), November 13–17, 2005.
[92] Mallon PW, Miller J, Kovacic JC, et al. Effect of pravastatin on body composition and
markers of cardiovascular disease inHIV-infectedmenda randomized, placebo-controlled
study. AIDS 2006;20(7):1003–10.
[93] ValantinMA, Aubron-Olivier C, Ghosn J, et al. Polylactic acid implants (New-Fill) to cor-
rect facial lipoatrophy in HIV-infected patients: results of the open-label study VEGA.
AIDS 2003;17(17):2471–7.
[94] Guaraldi G, Orlando G, De Fazio D, et al. Comparison of three different interventions for
the correction ofHIV-associated facial lipoatrophy: a prospective study. Antivir Ther 2005;
10(6):753–9.
[95] MoyleGJ, Sabin CA, Cartledge J, et al. A randomized comparative trial of tenofovir DF or
abacavir as replacement for a thymidine analogue in persons with lipoatrophy. AIDS 2006;
20(16):):2043–50.
[96] Martin A, Smith DE, Carr A, et al. Reversibility of lipoatrophy in HIV-infected patients 2
years after switching from a thymidine analogue to abacavir: theMITOXExtension Study.
AIDS 2004;18(7):1029–36.
[97] McComsey GA,Ward DJ, Hessenthaler SM, et al. Improvement in lipoatrophy associated
with highly active antiretroviral therapy in human immunodeficiency virus-infected pa-
tients switched from stavudine to abacavir or zidovudine: the results of the TARHEEL
study. Clin Infect Dis 2004;38(2):263–70.
[98] Lichtenstein KA, Delaney KM, Armon C, et al. Incidence of and risk factors for lipoatro-
phy (abnormal fat loss) in ambulatory HIV-1-infected patients. J Acquir Immune Defic
Syndr 2003;32(1):48–56.
[99] Gervasoni C, Ridolfo AL, Trifiro G, et al. Redistribution of body fat in HIV-infected
women undergoing combined antiretroviral therapy. AIDS 1999;13(4):465–71.
[100] Miller J, Carr A, Emery S, et al. HIV lipodystrophy: prevalence, severity and correlates of
risk in Australia. HIV Med 2003;4(3):293–301.
[101] Saves M, Raffi F, Capeau J, et al. Factors related to lipodystrophy and metabolic alter-
ations in patients with human immunodeficiency virus infection receiving highly active
antiretroviral therapy. Clin Infect Dis 2002;34(10):1396–405.
[102] Carter VM, Hoy JF, Bailey M, et al. The prevalence of lipodystrophy in an ambu-
lant HIV-infected population: it all depends on the definition. HIV Med 2001;2(3):
174–80.
[103] LeanME,Han TS,Morrison CE.Waist circumference as a measure for indicating need for
weight management. BMJ 1995;311(6998):158–61.
[104] Smith BA, Neidig JL, Nickel JT, et al. Aerobic exercise: effects on parameters related to fa-
tigue, dyspnea, weight and body composition in HIV-infected adults. AIDS 2001;15(6):
693–701.
[105] Roubenoff R, McDermott A, Weiss L, et al. Short-term progressive resistance training in-
creases strength and lean bodymass in adults infected with human immunodeficiency virus.
AIDS 1999;13(2):231–9.

132 HOFFMAN & CURRIER
[106] Roubenoff R, Weiss L, McDermott A, et al. A pilot study of exercise training to re-
duce trunk fat in adults with HIV-associated fat redistribution. AIDS 1999;13(11):
1373–5.
[107] Wanke C, Gerrior J, Kantaros J, et al. Recombinant human growth hormone improves the
fat redistribution syndrome (lipodystrophy) in patients with HIV. AIDS 1999;13(15):
2099–103.
[108] Engelson ES, Glesby MJ, Mendez D, et al. Effect of recombinant human growth hormone
in the treatment of visceral fat accumulation in HIV infection. J Acquir Immune Defic
Syndr 2002;30(4):379–91.
[109] Rebuffe-ScriveM,Marin P, BjorntorpP. Effect of testosterone on abdominal adipose tissue
in men. Int J Obes 1991;15(11):791–5.
[110] Marin P, Holmang S, Jonsson L, et al. The effects of testosterone treatment on body
composition and metabolism in middle-aged obese men. Int J Obes Relat Metab Disord
1992;16(12):991–7.
[111] MartinezE, Conget I, LozanoL, et al. Reversion ofmetabolic abnormalities after switching
from HIV-1 protease inhibitors to nevirapine. AIDS 1999;13(7):805–10.
[112] Bozzette SA, Ake CF, Tam HK, et al. Cardiovascular and cerebrovascular events in
patients treated for human immunodeficiency virus infection. N Engl J Med 2003;348(8):
702–10.
[113] Mary-Krause M, Cotte L, Simon A, et al. Increased risk of myocardial infarction with
duration of protease inhibitor therapy in HIV-infected men. AIDS 2003;17(17):2479–86.
[114] Holmberg SD,MoormanAC,Williamson JM, et al. Protease inhibitors and cardiovascular
outcomes in patients with HIV-1. Lancet 2002;360(9347):1747–8.
[115] Friis-Moller N, Weber R, Reiss P, et al. Cardiovascular disease risk factors in HIV
patients–association with antiretroviral therapy. Results from the DAD study. AIDS
2003;17(8):1179–93.
[116] Friis-Moller N, Reiss P, El-Sadr W, et al. Exposure to PI and NNRTI and risk of myocar-
dial infarction: results from the D:A:D study. Presented at the 13th Conference on Retro-
viruses and Opportunistic Infections. Denver (CO), February 5–8, 2006.
[117] Currier JS, Kendall MA, Zackin R, et al. Carotid artery intima-media thickness and HIV
infection: traditional risk factors overshadow impact of protease inhibitor exposure. AIDS
2005;19(9):927–33.
[118] Depairon M, Chessex S, Sudre P, et al. Premature atherosclerosis in HIV-infected individ-
ualsdfocus on protease inhibitor therapy. AIDS 2001;15(3):329–34.
[119] Hsue PY, Lo JC, Franklin A, et al. Progression of atherosclerosis as assessed by carotid in-
tima-media thickness in patients with HIV infection. Circulation 2004;109(13):1603–8.
[120] Blanco JJ, Garcia IS, Cerezo JG, et al. Endothelial function in HIV-infected patients with
low or mild cardiovascular risk. J Antimicrob Chemother 2006;58(1):133–9.
[121] Maggi P, Serio G, Epifani G, et al. Premature lesions of the carotid vessels in HIV-1-
infected patients treated with protease inhibitors. AIDS 2000;14(16):F123–8.
[122] Twu C, Liu NQ, PopikW, et al. Cardiomyocytes undergo apoptosis in human immunode-
ficiency virus cardiomyopathy through mitochondrion- and death receptor-controlled
pathways. Proc Natl Acad Sci U S A 2002;99(22):14386–91.
[123] van Wijk JP, de Koning EJ, Cabezas MC, et al. Functional and structural markers of
atherosclerosis in human immunodeficiency virus-infected patients. J Am Coll Cardiol
2006;47(6):1117–23.
[124] Stein JH. Cardiovascular risk in patients with human immunodeficiency virus infection:
incomplete data. J Am Coll Cardiol 2006;47(6):1124–5.





























