Embed Size (px)
Citation preview

Mantle cell lymphoma with aberrant expression of CD10
U Zanetto, H Dong,1 Y Huang,2 K Zhang,3 M Narbaitz,4 S Sapia,5 I Kostopoulos,6 H Liu,2
M-Q Du2 & C M Bacon2
Department of Pathology, City Hospital, Birmingham, UK, 1Genzyme Genetics, New York, NY, USA, 2Department of
Pathology, University of Cambridge, Cambridge, UK, 3Geisinger Medical Center, Danville, PA, USA, 4Pathology Service,
Instituto de Investigaciones Hematologicas, Academia Nacional de Medicina, 5Department of Haematopathology, Fundaleu,
Buenos Aires, Argentina, and 6Department of Pathology, Aristotle University of Thessaloniki, Thessaloniki, Greece
Date of submission 13 December 2007Accepted for publication 25 January 2008
Zanetto U, Dong H, Huang Y, Zhang K, Narbaitz M, Sapia S, Kostopoulos I, Liu H, Du M-Q & Bacon CM
(2008) Histopathology 53, 20–29
Mantle cell lymphoma with aberrant expression of CD10
Aims: Morphological, immunophenotypic and geneticheterogeneity amongst mantle cell lymphomas (MCLs)can lead to difficulties in diagnosis and management.The aim was to describe the clinical and patho-logical features of MCLs with aberrant expression ofCD10.Methods and results: Of 17 specimens from 13 patients,14 expressed CD10 and three (presenting before orafter a CD10+ specimen) did not. All expressed cyclinD1 and carried the t(11;14)(q13;q32) ⁄ CCND1-IGHtranslocation. Similar to non-selected MCL patients,most patients had disseminated disease and an adverseclinical course. Five specimens showed pleomorphicblastoid morphology and blastoid transformation was
associated with a change in phenotype, including gainor loss of CD10. Additional phenotypic variations likelyto cause diagnostic difficulty were present in eightspecimens: five were CD5) and five (all CD10+)expressed Bcl-6. One Bcl-6+ case carried a BCL-6translocation and three others had extra copies of theBCL-6 gene. Sequence analysis of the immunoglobulinheavy chain variable region in five cases showed onlyone to have low-level somatic mutation, indicating thatthey did not arise from germinal centre B cells.Conclusions: Expression of CD10 by MCL is oftenassociated with other variant morphological, immuno-phenotypic or genetic features, but does not reflectderivation from germinal centre B cells.
Keywords: Bcl-6, CD10, genetics, immunohistochemistry, mantle cell lymphoma
Abbreviations: FISH, fluorescence in situ hybridization; IGVH, immunoglobulin heavy chain variable; MCL, mantlecell lymphoma
Introduction
Mantle cell lymphoma (MCL)1–4 is a relatively well-defined type of non-Hodgkin’s lymphoma that typicallypresents with disseminated disease and pursues anaggressive clinical course. Most MCLs are neoplasms ofsmall centrocyte-like B cells with a characteristicCD20+ CD5+ CD43+ CD10) Bcl-6) CD23) immuno-phenotype. The majority lack significant somatichypermutation of immunoglobulin genes and are
thought to derive from naive, pre-germinal centre,mantle zone B lymphocytes.5–8 MCLs share a commonmolecular pathogenesis, associated in virtually all caseswith overexpression of the cell cycle regulatory proteincyclin D1 as a result of the t(11;14)(q13;q32) ⁄ CCND1-IGH translocation.1,9,10 Amongst the small B-cell lym-phomas, the detection of cyclin D1 expression is highlyspecific for, and the presence of the t(11;14)(q13;q32) isvirtually pathognomonic of, MCL.8,11–13
Despite these rather uniform typical features, it isnow recognized that MCLs display both clinical andbiological heterogeneity, which can cause difficulty inboth management and diagnosis. Several morphologi-cal variants are recognized, including lymphoblast-like
Address for correspondence: Ulises Zanetto, Department of Pathology,
City Hospital, Dudley Road, Birmingham B18 7QH, UK.
e-mail: [email protected]
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Limited.
Histopathology 2008, 53, 20–29. DOI: 10.1111/j.1365-2559.2008.03060.x

and pleomorphic blastoid variants, which may beassociated with additional genetic changes and anadverse prognosis.1,3,14–16 Recently, several studieshave demonstrated that approximately 15–30% ofMCLs show somatic mutation of immunoglobulinheavy chain variable (IGVH) genes, raising the possi-bility that these may derive from germinal centreor post-germinal centre B cells rather than naive Bcells.5–8 Variation from the typical immunophenotypeis also recognized. Up to 10% of cases lack expressionof CD5 detectable by immunohistochemistry and ⁄ orflow cytometry.17,18 A recent study has reported fivecases expressing the germinal centre protein Bcl-6 inassociation with genetic abnormalities of the BCL-6gene.19 In addition, rare cases of MCL have beenshown to express the germinal centre proteinCD10.20–22 The significance and clinicopathologicalassociations of such infrequent variant immunopheno-types are largely unknown.
In the present study 13 cases of MCL with aberrantexpression of CD10 were investigated. The clinical,morphological, immunophenotypic and genetic fea-tures of these cases are described, highlighting featuresof importance to diagnostic histopathologists. Weexamine the possibility that expression of CD10 mightreflect a germinal centre origin for these cases byanalysis of IGVH gene mutation.
Materials and methods
case material, immunophenotyping and
fluorescence in s itu hybridization
Seventeen specimens from 13 patients were identifiedfrom the archives of the authors’ institutions. Four ofthe cases were included (but not extensively described)in a previous series of CD5+ CD10+ B-cell lympho-mas.21 In each case, the diagnosis of MCL was made onclinical, histological, immunophenotypic and geneticfeatures according to the World Health OrganizationClassification of Tumours of Haematopoietic and Lymph-oid Tissues.2 Immunohistochemistry, flow cytometricimmunophenotyping and fluorescence in situ hybridiza-tion (FISH) were performed during routine diagnosticwork-up of the cases. In all cases, immunohisto-chemistry was performed on paraffin sections followingheat-mediated antigen retrieval using the streptavidin–immunoperoxidase method with diaminobenzidinechromogen, according to standard procedures. In sixcases multicolour flow cytometric immunophenotypingwas also performed using standard techniques. FISHusing dual-colour dual-fusion CCND1-IGH, IGH-BCL-2probes and BCL-6 dual-colour break-apart probes was
performed in 10, five and seven cases, respectively,according to standard procedures.
igvh
mutational analys is
DNA was extracted from paraffin sections using theQIAmp DNA Mini kit (Qiagen, Crawley, UK) and itsquality assessed using the BIOMED-2 control geneprimer set.23 Five of the eight cases tested yielded DNAof sufficient quality for assessment of IGH generearrangement. Rearranged IGH genes were amplifiedusing the BIOMED-2 IGVH FR1-JH primer set23 and theproducts visualized by electrophoresis through a 7%polyacrylamide gel. A single clonal product was seen ineach case. This was excised and DNA was purifiedusing the Qiaquick Gel Extraction kit (Qiagen). PurifiedDNA was directly sequenced using the consensus JH
primer and the ABI dRhodamine Terminator CycleSequencing kit (Applied Biosystems, Warrington, UK)on an ABI 377 Automated DNA Sequencer (AppliedBiosystems). IGVH gene usage and mutation statuswere determined by comparison with germ-linesequences using VBASE 2 and IMGT online databases.Cases with less than the standard threshold of 98%germ-line homology were considered to show IGVH
somatic mutation.
Results
clinical features
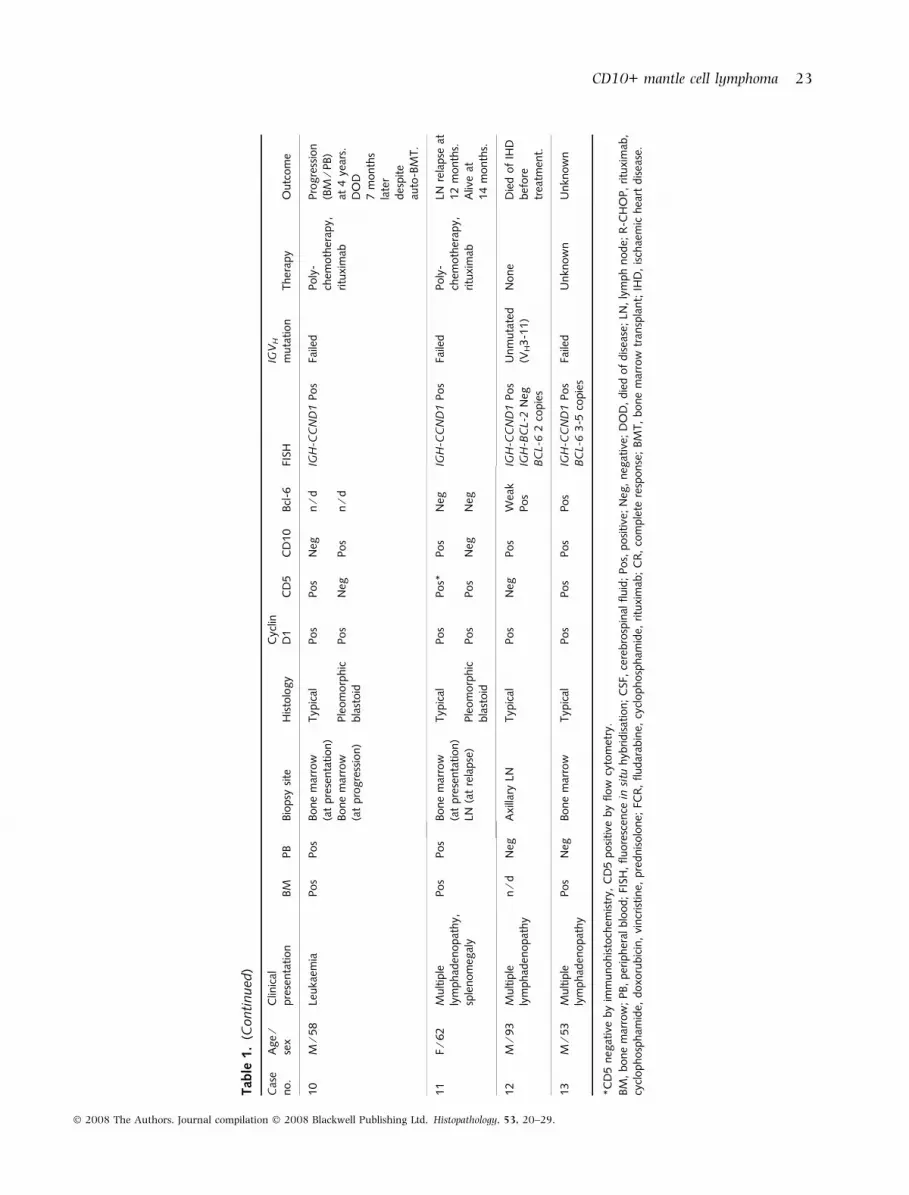
The clinical details of the patients studied are summa-rized in Table 1. There were eight men and five women,with a median age of 67 years (range 53–93 years).Most patients presented with multiple lymphadenopa-thy with or without splenomegaly and the bone marrowwas involved in each of the five cases in which the resultof bone marrow investigation is known. One patienthad a primarily leukaemic presentation and, in all, fiveof the 13 patients had peripheral blood involvement.Details of treatment and outcome were available for sixpatients. Five patients received multi-agent chemother-apy, four with Rituximab and one was not treated dueto comorbidity. One patient had progressive primaryrefractory disease and three progressed or relapsedfollowing initial responses to therapy (1–4 years fromdiagnosis). At last follow-up, four of the six patients haddied (0 months to 4 years from diagnosis).
morphology
Table 1 also shows the morphological features of thecases studied. Biopsy material from the time of first
CD10+ mantle cell lymphoma 21
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 20–29.

Tab
le1.
Clin
ical
,m
orp
holo
gic
al,
imm
unophen
oty
pic
and
gen
etic
feat
ure
sof
CD
10-p
osi
tive
man
tle
cell
lym
phom
a
Cas
eno.
Age
⁄se
xC
linic
alpre
senta
tion
BM
PB
Bio
psy
site
His
tolo
gy
Cyc
linD
1C
D5
CD
10
Bcl
-6FI
SHIG
VH
muta
tion
Ther
apy
Outc
om
e
1M
⁄75
Multip
lely
mphad
enopat
hy,
sple
nom
egal
y,bone,
CSF
Pos
Pos
Tes
tis,
skin
Typ
ical
Pos
Pos
Pos
Neg
IGH
-CC
ND
1Pos
IGH
-BC
L-2
Neg
Unm
uta
ted
(VH5-5
1)
Poly
-ch
emoth
erap
yPro
gre
ssiv
edis
ease
.D
OD
at6
month
s.C
onju
nct
iva
(2m
onth
sla
ter)
Ple
om
orp
hic
bla
stoid
Pos
Neg
Pos
Neg
BC
L-6
2co
pie
s
2F
⁄73
Multip
lely
mphad
enopat
hy
?N
egC
ervi
calLN
(at
pre
senta
tion)
Typ
ical
Pos
Pos
Neg
Neg
IGH
-CC
ND
1Pos
IGH
-BC
L-2
Neg
Unm
uta
ted
(VH5-5
1)
R-C
HO
PR
elap
seat
2ye
ars.
Furt
her
R-C
HO
P.
Die
dof
sepsi
s.
Soft
tiss
ue,
arm
(at
rela
pse
)Ple
om
orp
hic
bla
stoid
Pos
Neg
Pos
Neg
BC
L-6
3co
pie
s
3F
⁄72
Multip
lely
mphad
enopat
hy
?N
egA
xilla
ryLN
Ple
om
orp
hic
bla
stoid
Pos
Pos
Pos
Pos
IGH
-CC
ND
1Pos
x3IG
H-B
CL-2
Neg
BC
L-6
3-5
copie
s
Unm
uta
ted
(VH3-1
5)
Unkn
ow
nU
nkn
ow
n
4M
⁄68
Multip
lely
mphad
enopat
hy
?N
egR
etro
per
itonea
lLN
Typ
ical
Pos
Pos
Pos
Pos
IGH
-CC
ND
1Pos
BC
L-6
tran
sloca
tion
n⁄d
Unkn
ow
nU
nkn
ow
n
5F
⁄76
Ches
tw
allm
ass
?N
egC
hes
tw
all
mas
sTyp
ical
Pos
Pos
Pos
Neg
n⁄d
n⁄d
Unkn
ow
nU
nkn
ow
n
6M
⁄67
Cer
vica
lly
mphad
enopat
hy
?N
egC
ervi
calLN
Typ
ical
Pos
Pos
Pos
Neg
n⁄d
n⁄d
Unkn
ow
nU
nkn
ow
n
7M
⁄54
Multip
lely
mphad
enopat
hy
?Pos
Cer
vica
lLN
Typ
ical
Pos
Pos
Pos
Neg
IGH
-CC
ND
1Pos
n⁄d
Unkn
ow
nU
nkn
ow
n
8F
⁄63
Phar
yngea
lm
ass
?N
egPhar
yngea
lm
ass
Typ
ical
Pos
Pos
Pos
Neg
n⁄d
n⁄d
Unkn
ow
nU
nkn
ow
n
9M
⁄65
Multip
lely
mphad
enopat
hy,
sple
nom
egal
y
Pos
Pos
Axi
llary
LNTyp
ical
Pos
Neg
Pos
Wea
kPos
IGH
-CC
ND
1Pos
IGH
-BC
L-2
Neg
BC
L-6
5-8
copie
s
Low
leve
lm
uta
tion
(VH3-3
0)
FCR
CR
(1ye
ar)
22 U Zanetto et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 20–29.
Tab
le1.
(Conti
nued)
Cas
eno.
Age
⁄se
xC
linic
alpre
senta
tion
BM
PB
Bio
psy
site
His
tolo
gy
Cyc
linD
1C
D5
CD
10
Bcl
-6FI
SHIG
VH
muta
tion
Ther
apy
Outc
om
e
10
M⁄5
8Le
uka
emia
Pos
Pos
Bone
mar
row
(at
pre
senta
tion)
Typ
ical
Pos
Pos
Neg
n⁄d
IGH
-CC
ND
1Pos
Faile
dPoly
-ch
emoth
erap
y,ritu
xim
ab
Pro
gre
ssio
n(B
M⁄P
B)
at4
year
s.D
OD
7m
onth
sla
ter
des
pite
auto
-BM
T.
Bone
mar
row
(at
pro
gre
ssio
n)
Ple
om
orp
hic
bla
stoid
Pos
Neg
Pos
n⁄d
11
F⁄6
2M
ultip
lely
mphad
enopat
hy,
sple
nom
egal
y
Pos
Pos
Bone
mar
row
(at
pre
senta
tion)
Typ
ical
Pos
Pos*
Pos
Neg
IGH
-CC
ND
1Pos
Faile
dPoly
-ch
emoth
erap
y,ritu
xim
ab
LNre
lapse
at12
month
s.A
live
at14
month
s.LN
(at
rela
pse
)Ple
om
orp
hic
bla
stoid
Pos
Pos
Neg
Neg
12
M⁄9
3M
ultip
lely
mphad
enopat
hy
n⁄d
Neg
Axi
llary
LNTyp
ical
Pos
Neg
Pos
Wea
kPos
IGH
-CC
ND
1Pos
IGH
-BC
L-2
Neg
BC
L-6
2co
pie
s
Unm
uta
ted
(VH3-1
1)
None
Die
dof
IHD
bef
ore
trea
tmen
t.
13
M⁄5
3M
ultip
lely
mphad
enopat
hy
Pos
Neg
Bone
mar
row
Typ
ical
Pos
Pos
Pos
Pos
IGH
-CC
ND
1Pos
BC
L-6
3-5
copie
sFa
iled
Unkn
ow
nU
nkn
ow
n
*C
D5
neg
ativ
eby
imm
unohis
toch
emis
try,
CD
5posi
tive
by
flow
cyto
met
ry.
BM
,bone
mar
row
;PB,
per
ipher
alblo
od;
FISH
,fluore
scen
cein
situ
hyb
ridis
atio
n;
CSF
,ce
rebro
spin
alfluid
;Pos,
posi
tive
;N
eg,
neg
ativ
e;D
OD
,die
dof
dis
ease
;LN
,ly
mph
node;
R-C
HO
P,
ritu
xim
ab,
cycl
ophosp
ham
ide,
doxo
rubic
in,
vincr
istine,
pre
dnis
olo
ne;
FCR
,fludar
abin
e,cy
clophosp
ham
ide,
ritu
xim
ab;
CR
,co
mple
tere
sponse
;BM
T,
bone
mar
row
tran
spla
nt;
IHD
,is
chae
mic
hea
rtdis
ease
.
CD10+ mantle cell lymphoma 23
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 20–29.

diagnosis was available in all cases. In 12 suchspecimens, the neoplastic infiltrate showed the typicalcytomorphology of MCL: small to medium-sized cen-trocyte-like cells with irregular nuclear outlines,slightly clumped chromatin and inconspicuous nucleoli(e.g. Figure 1). In lymph node and extranodal biopsyspecimens the lymphomas had a nodular and ⁄ ordiffuse growth pattern; in bone marrow trephinespecimens neoplastic cells formed predominantly non-paratrabecular lymphoid aggregates. In one initialdiagnostic specimen the lymphoma comprised a diffuseinfiltrate of cells with pleomorphic blastoid morphol-ogy: a heterogeneous population of medium-sizedand ⁄ or large cells with moderately condensed chro-matin, one or more small but readily visible nucleoli,and scanty cytoplasm (Figure 2).
In four cases a second biopsy specimen was takenduring the course of disease progression or at relapse.In each of these cases, although the original diagnostic
specimen had shown typical MCL morphology, thesubsequent specimen showed pleomorphic blastoidmorphology as described above (e.g. Figure 3). Thus,overall, pleomorphic blastoid morphology was shown byfive of 17 (29%) specimens from five of 13 (38%) patients.
immunophenotype
Immunohistochemistry (see Table 1) showed all spec-imens to express cyclin D1 with a nuclear pattern ofimmunoreactivity, in keeping with the diagnoses ofMCL. All MCLs except one expressed CD20. Thisspecimen was taken following rituximab therapy,known to induce CD20 negativity in mature B-celllymphomas.24 At first diagnosis, nine cases had aCD5+ CD10+ immunophenotype (e.g. Figure 2), twowere CD5) CD10+ (e.g. Figure 1), and two expressedCD5 but were CD10) at this stage of their evolution(e.g. Figure 3). CD43 was expressed by 10 of 12 cases
H&E Cyclin D1
CD5 CD10
Figure 1. Case 12. H&E-stained sections show the typical centrocyte-like morphology of mantle cell lymphoma. Immunohistochemistry shows
the neoplastic cells to express cyclin D1 and CD10, but not CD5. Scattered CD5+ T cells are present.
24 U Zanetto et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 20–29.

studied, and Bcl-2 by nine of 11 cases. One case (case10) showed partial and dim expression of CD23 by flowcytometry but not by immunohistochemistry; CD23was not expressed by any other case. Three of 12 casesexamined showed strong nuclear positivity for Bcl-6 inthe majority of neoplastic cells (e.g. Figure 2); in twofurther cases there was weak expression of Bcl-6 byapproximately 50% of cells. These specimens were allCD10+, but included specimens with both pleomorphicblastoid and typical morphology and specimens bothpositive and negative for CD5. The five cases examinedfor expression of IgD were all positive. Where flow
cytometry was performed, this was concordant withthe immunohistochemistry, except in one specimen inwhich staining for CD5 was negative by immuno-histochemistry and positive by flow cytometry (case 11,considered CD5+ in this study).
Immunophenotyping was also performed on the fourfollow-up specimens available. In each, the changefrom typical to pleomorphic blastoid morphology wasaccompanied by an alteration in phenotype. In oneCD5+ CD10+ case (case 1) there was loss of CD5 inthe second specimen, and in another (case 11) therewas loss of CD10 in the second specimen. In two
H&E Cyclin D1
CD10
CD5
Bcl-6 BCL-6 FISH
Figure 2. Case 3. H&E-stained sections show the lymphoma cells to have pleomorphic blastoid morphology. Immunohistochemistry shows the
neoplastic cells to express cyclin D1, CD5, CD10 and Bcl-6. Fluorescence in situ hybridization using a dual-colour BCL-6 break-apart probe shows
three to five copies of BCL-6 without evidence of a BCL-6 translocation.
CD10+ mantle cell lymphoma 25
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 20–29.

CD5+ CD10) cases (cases 2 and 10), the secondspecimen showed a CD5) CD10+ immunophenotype(e.g. Figure 3). In case 10, flow cytometric immuno-phenotyping showed progressive accumulation ofCD10+ CD5) B cells in the peripheral blood in theperiod between the two bone marrow trephine biopsyspecimens. In total, CD5 negativity was shown by fiveof 17 (29%) specimens, three of which showed pleo-morphic blastoid morphology, from five of 13 (38%)patients. Expression of the other antigens tested,including cyclin D1 and Bcl-6, remained unchangedbetween specimens taken at presentation and atrelapse.
molecular genetics
The results of the molecular studies undertaken arealso presented in Table 1. FISH for the t(11;14)(q13;q32) ⁄ CCND1-IGH translocation was performed
in the diagnostic specimens of 10 of the 13 cases. Inkeeping with the diagnoses of MCL, each showed signalpatterns consistent with the presence of a CCND1-IGHtranslocation. The translocation was also detected inthe three follow-up specimens tested. Because theaberrant expression of Bcl-6 seen in five of the casescould be due to abnormalities of the BCL-6 gene, theseand two Bcl-6) cases (cases 1 and 2) were assessed byFISH using a BCL-6 break-apart probe. Of the caseswith Bcl-6 protein expression, one (case 4) showed atranslocation involving BCL-6 (and also evidence of anIGH translocation in addition to CCND1-IGH, suggest-ing the presence of a BCL-6)IGH translocation), three(cases 3, 9 and 13) showed multiple (three to eight)signals consistent with extra copies or amplification ofBCL-6 (e.g. Figure 2), and one (case 12) showednormal signals. One of the two Bcl-6) cases (case 2)also showed three copies of BCL-6. FISH for IGH-BCL-2was negative in all five cases examined.
H&E
2nd Biopsy
1st Biopsy
H&E
Cyclin D1
Cyclin D1 CD5
CD10
CD10
CD5
Figure 3. Case 2. H&E-stained sections from the first diagnostic biopsy (‘‘1st biopsy’’) show the typical morphology of mantle cell lymphoma.
Immunohistochemistry of this specimen shows the neoplastic cells to express cyclin D1 and CD5, but not CD10. A germinal centre shown is
negative for cyclin D1 and CD5, but positive for CD10. H&E-stained sections from a biopsy at relapse (‘‘2nd biopsy’’) show transformation to
pleomorphic blastoid morphology. Immunohistochemistry of this biopsy specimen shows that the neoplastic cells now express cyclin D1 and
CD10, but not CD5.
26 U Zanetto et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 20–29.

To determine whether expression of CD10 by theseMCLs might reflect their derivation from germinalcentre B cells with somatic hypermutation of immuno-globulin genes, the sequences of the variable regions ofthe clonal rearranged IGH genes from five cases wereanalysed. Two cases utilized VH5-51 and one eachutilized VH3-11, VH3-15 and VH3-30. Four cases hadunmutated IGVH genes (using the accepted cut-offvalue of 98% germ-line homology) with 98.7–100%germ-line homology; the fifth showed low-level muta-tion of IGVH (97.4% germ-line homology). Attempts toanalyse three additional specimens (bone marrowtrephine biopsies) were unsuccessful. These resultssuggest that CD10+ MCLs are no different from othermantle cell lymphomas with regard to their IGVH
mutation status and do not suggest a germinal centrederivation for these tumours.
Discussion
Although MCLs are a relatively discrete group oflymphoid neoplasms with well-defined characteristicfeatures,1–4 it is clear that within this group there ismorphological, immunophenotypic and genetic varia-tion, the biological, diagnostic and clinical significanceof which is unclear. In this study we have described 13cases of MCL with aberrant expression of CD10. Despitethis unusual feature, all cases could be definitivelyidentified as MCLs by a combination of morphology, theexpression of cyclin D1, the remaining immunopheno-type and, most importantly, the detection of at(11;14)(q13;q32) translocation by FISH. The clinicalfeatures of these patients were similar to those of largerseries of unselected MCL patients:1–4 most presentedwith disseminated disease with or without peripheralblood involvement and, despite multi-agent therapy,outcome was generally poor.
Other studies have also documented aberrant expres-sion of CD10 by rare MCLs. Dong et al. have reported aseries of CD5+ CD10+ B-cell lymphomas, whichrepresented 0.4% of all B-cell lymphomas seen at onelarge diagnostic laboratory.21 Of these, one-quarterwere MCLs. In a flow cytometric study of 100 CD10+small B-cell lymphomas, Xu et al. identified a singleCD10+ MCL,22 and Camacho et al. included a CD10+MCL in their series, discussed in more detail below.19
Five of our specimens, including three pleomorphicblastoid tumours, showed a CD5) CD10+ phenotyperarely recognized before. Morice et al. have reported aleukaemic MCL with a CD5) CD10+ blastoid compo-nent,20 Yin et al. have reported a CD5) CD10+immunophenotype in a blastoid MCL and Kostopouloset al. have described a lymphoma with follicular
architecture, a CCND1 translocation detected by FISHand a CD5) CD10+ cyclin D1+ immunophenotype,consistent with an MCL.25 Such variant immunopheno-types can lead to considerable diagnostic difficulty andpossibly misdiagnosis of MCLs as follicular lymphoma,atypical CD10+ chronic lymphocytic leukaemia ⁄ smalllymphocytic lymphoma or even, in the case of blastoidtumours, diffuse large B-cell lymphoma or lymphoblas-tic lymphoma.21 Difficulties may be greatest whenassessing small needle core biopsy specimens or ‘‘fluid’’specimens by flow cytometry, when histological fea-tures helpful in diagnosis may be absent. Accuratediagnosis of cases such as these requires carefulintegration of morphological findings, a discriminatoryimmunophenotyping panel (including cyclin D1) and,increasingly, genetic findings.
Amongst our CD10+ MCLs, pleomorphic blastoidmorphology was seen in 29% of specimens. However,as the incidence of blastoid morphology varies fromapproximately 6% to approximately 26% in larger,unselected series of MCLs,3,26–28 analysis of additionalCD10+ MCLs will be required to ascertain if these twovariant features are linked. Interestingly, in all fourcases in which blastoid transformation of a previouslytypical MCL occurred, this transformation was accom-panied by an alteration in immunophenotype. In threecases there was loss of CD5 and in two of these therewas, in addition, gain of CD10 by a previously CD10)tumour. In one other case, CD10 expression was lostupon transformation. Similar immunophenotypicchanges were seen in two of the five cases of blastoidtransformation reported by Yin et al.29 The recognitionthat blastoid transformation of MCL may be accompa-nied by such phenotypic shifts has important impli-cations for the use of these markers in follow-upspecimens from MCL patients.
A further interesting finding of our study is that five(29%) of our specimens showed aberrant expression ofBcl-6, a transcription factor largely restricted duringB-cell differentiation to germinal centre B cells and thuscharacteristically found in B-cell lymphomas of germi-nal centre derivation. Bcl-6 protein expression was seenin both CD5+ and CD5) MCLs and in specimens withboth typical and blastoid morphology. Camacho et al.have recently reported a series of five Bcl-6+ MCLs, oneof which also expressed CD10.19 As these casesrepresented only 1.6% of all MCLs diagnosed in theirdepartment, our data suggests that Bcl-6 expressionmay be more frequent in CD10+ MCLs than amongstunselected cases. In diagnostic practice, cyclin D1immunohistochemistry and FISH for CCND1-IGH andIGH-BCL2 translocations may be necessary to distin-guish these cases from CD5+ follicular lymphomas.
CD10+ mantle cell lymphoma 27
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 20–29.

In the series of Camacho et al., four of the five casescarried translocations of BCL-6 with undisclosed part-ner genes and the remaining case had three copies ofthe BCL-6 gene.19 Similarly, in our study one Bcl-6+case contained a translocation of BCL-6 (probably withIGH), and three others showed extra copies or ampli-fication of BCL-6. It is possible therefore that Bcl-6expression in some of our cases is the result ofchromosomal alterations involving the BCL-6 gene,rather than a programmed expression of Bcl-6 resultingfrom a germinal centre origin of the lymphomas.However, the effect of BCL-6 translocations or copynumber increases on Bcl-6 expression is unclear. In therecent study of MCLs by Salaverria et al., gain ofchromosomal material at 3q27-28 detected by array-based comparative genomic hybridization was notassociated with increased expression of BCL-6 mRNAdetected by Lymphochip cDNA microarray.30 Similarly,although copy number gains and translocations ofBCL-6 are well recognized in other non-germinalcentre-derived lymphomas, such as activated B-cell-like diffuse large B-cell lymphomas, these often do notcorrelate with increased Bcl-6 protein or mRNAexpression.31 These genetic aberrations may insteadlead to functional dysregulation of BCL-6 expressionand potentially to altered expression of Bcl-6 targetgenes, without being associated with a detectableincrease in protein level. Furthermore, Bcl-6 expressionmay be regulated by additional mechanisms, such astranscriptional regulation and mutation of the BCL-6promoter,32 not studied in the present work.
The above discussion notwithstanding, as CD10positivity is a feature of both normal and malignantgerminal centre cells, the expression of CD10 didraise the possibility that this small subset of MCLsmight be derived from germinal centre cells. Likeother germinal centre-derived lymphomas, such MCLswould be expected to show evidence of somaticmutation of immunoglobulin genes. Indeed, someauthors have interpreted the detection of low-levelsomatic mutation of IGVH genes in up to 30% ofMCLs as evidence of a germinal centre orpost-germinal centre origin in these cases.6,33 How-ever, we found that only one of the five cases wesuccessfully examined showed significant somaticmutation, and this was at a lower level thantypically seen in germinal centre neoplasms.34 Thereis thus no evidence that CD10 expression by an MCLreflects a germinal centre derivation. Moreover,although the presence of IGVH mutation in someMCLs suggests the influence of antigen stimulationduring the development of these lymphomas, the lowlevel of mutation, the infrequent identification of
intraclonal variation and evidence of antigen selec-tion and the lack of immunoglobulin class switchingin these cases5–8,33,35,36 raise questions as to theprecise role of the germinal centre in this process.
Also known as membrane metallo-endopeptidase,CD10 is a cell surface neutral endopeptidase with anunknown role in lymphocyte biology. It is charac-teristically expressed by lymphoid populations with ahigh rate of apoptosis,37 suggesting a role in regu-lation of cell survival. However, the molecularpathogenesis of mantle cell lymphoma appears to bedominated by dysregulated cell proliferation ratherthan abnormal survival10 and both the mechanismof CD10 expression and its function on this smallsubset of MCLs remain unascertained. Nevertheless,an understanding of the expression of CD10 by MCLis important for diagnostic histopathologists. In thisstudy, we have shown in particular that CD10expression often occurs with other phenotypic vari-ations, may be induced or lost upon blastoid trans-formation and may be associated with geneticabnormalities of BCL-6 and Bcl-6 protein expression.There is no evidence from analysis of IGVH muta-tions that CD10+ MCLs derive from germinal centreB cells.
Acknowledgements
The authors are grateful to laboratory staff andhaemato-oncologists at their institutions for theircontribution to the diagnostic work-up of the casesand for provision of clinical data. We thank Dr HongtaoYe for help with additional FISH. C.M.B. is supported bya Senior Clinician Scientist Fellowship from The HealthFoundation, The Royal College of Pathologists andThe Pathological Society of Great Britain and Ireland.The Du lab is supported by The Leukaemia ResearchFund, UK.
References
1. Swerdlow SH, Williams ME. From centrocytic to mantle cell
lymphoma: a clinicopathologic and molecular review of 3
decades. Hum. Pathol. 2002; 33; 7–20.
2. Swerdlow SH, Berger F, Isaacson PG et al. Mantle cell lymphoma.
In Jaffe ES, Harris NL, Stein H, Vardiman JW eds. World Health
Organisation classification of tumour. Pathology and genetics of
tumours of haematopoietic and lymphoid tissues. Lyon: IARC Press,
2001; 168–170.
3. Argatoff LH, Connors JM, Klasa RJ, Horsman DE, Gascoyne RD.
Mantle cell lymphoma: a clinicopathologic study of 80 cases.
Blood 1997; 89; 2067–2078.
4. Zucca E, Stein H, Coiffier B. European lymphoma task force
(ELTF): report of the workshop on mantle cell lymphoma (MCL).
Ann. Oncol. 1994; 5; 507–511.
28 U Zanetto et al.
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 20–29.

5. Camacho FI, Algara P, Rodriguez A et al. Molecular heterogene-
ity in MCL defined by the use of specific VH genes and the
frequency of somatic mutations. Blood 2003; 101; 4042–4046.
6. Walsh SH, Thorselius M, Johnson A et al. Mutated VH genes and
preferential VH3-21 use define new subsets of mantle cell
lymphoma. Blood 2003; 101; 4047–4054.
7. Kienle D, Krober A, Katzenberger T et al. VH mutation status and
VDJ rearrangement structure in mantle cell lymphoma: correla-
tion with genomic aberrations, clinical characteristics, and
outcome. Blood 2003; 102; 3003–3009.
8. Orchard J, Garand R, Davis Z et al. A subset of t(11;14)
lymphoma with mantle cell features displays mutated IgVH
genes and includes patients with good prognosis, nonnodal
disease. Blood 2003; 101; 4975–4981.
9. Rosenberg CL, Wong E, Petty EM et al. PRAD1, a candidate BCL1
oncogene: mapping and expression in centrocytic lymphoma.
Proc. Natl. Acad. Sci. U.S.A. 1991; 88; 9638–9642.
10. Rosenwald A, Wright G, Wiestner A et al. The proliferation gene
expression signature is a quantitative integrator of oncogenic
events that predicts survival in mantle cell lymphoma. Cancer Cell
2003; 3; 185–197.
11. Zukerberg LR, Yang WI, Arnold A, Harris NL. Cyclin D1
expression in non-Hodgkin’s lymphomas. Detection by immuno-
histochemistry. Am. J. Clin. Pathol. 1995; 103; 756–760.
12. Swerdlow SH, Zukerberg LR, Yang WI, Harris NL, Williams ME.
The morphologic spectrum of non-Hodgkin’s lymphomas with
BCL1 ⁄ cyclin D1 gene rearrangements. Am. J. Surg. Pathol. 1996;
20; 627–640.
13. Bosch F, Jares P, Campo E et al. PRAD-1 ⁄ cyclin D1 gene
overexpression in chronic lymphoproliferative disorders: a highly
specific marker of mantle cell lymphoma. Blood 1994; 84; 2726–
2732.
14. Bea S, Ribas M, Hernandez JM et al. Increased number of
chromosomal imbalances and high-level DNA amplifications in
mantle cell lymphoma are associated with blastoid variants.
Blood 1999; 93; 4365–4374.
15. Ott G, Kalla J, Hanke A et al. The cytomorphological spectrum of
mantle cell lymphoma is reflected by distinct biological features.
Leuk. Lymphoma 1998; 32; 55–63.
16. Zoldan MC, Inghirami G, Masuda Y et al. Large-cell variants of
mantle cell lymphoma: cytologic characteristics and p53 anom-
alies may predict poor outcome. Br. J. Haematol. 1996; 93; 475–
486.
17. Liu Z, Dong HY, Gorczyca W et al. CD5- mantle cell lymphoma.
Am. J. Clin. Pathol. 2002; 118; 216–224.
18. Kaptain S, Zukerberg LR, Ferry JA, Harris NL. BCL-1 cyclin D1+
CD5- mantle cell lymphoma. Mod. Pathol. 1998; 11; 133A.
19. Camacho FI, Garcia JF, Cigudosa JC et al. Aberrant Bcl6 protein
expression in mantle cell lymphoma. Am. J. Surg. Pathol. 2004;
28; 1051–1056.
20. Morice WG, Hodnefield JM, Kurtin PJ, Hanson CA. An unusual
case of leukemic mantle cell lymphoma with a blastoid compo-
nent showing loss of CD5 and aberrant expression of CD10. Am.
J. Clin. Pathol. 2004; 122; 122–127.
21. Dong HY, Gorczyca W, Liu Z et al. B-cell lymphomas with
coexpression of CD5 and CD10. Am. J. Clin. Pathol. 2003; 119;
218–230.
22. Xu Y, McKenna RW, Kroft SH. Assessment of CD10 in the
diagnosis of small B-cell lymphomas: a multiparameter flow
cytometric study. Am. J. Clin. Pathol. 2002; 117; 291–300.
23. van Dongen JJ, Langerak AW, Bruggemann M et al. Design and
standardization of PCR primers and protocols for detection of
clonal immunoglobulin and T-cell receptor gene recombinations
in suspect lymphoproliferations: report of the BIOMED-2 Con-
certed Action BMH4-CT98-3936. Leukemia 2003; 17; 2257–
2317.
24. Foran JM, Norton AJ, Micallef IN et al. Loss of CD20 expression
following treatment with rituximab (chimaeric monoclonal anti-
CD20): a retrospective cohort analysis. Br. J. Haematol. 2001;
114; 881–883.
25. Kostopoulos I, Cocco M, Ginanneschi C et al. Overlapping
morphologic and immunophenotypic profiles in small B-cell
lymphoma. A report of two cases. Virchows Arch. 2006; 449;
320–327.
26. Weisenburger DD, Vose JM, Greiner TC et al. Mantle cell
lymphoma. A clinicopathologic study of 68 cases from the
Nebraska Lymphoma Study Group. Am. J. Hematol. 2000; 64;
190–196.
27. Bernard M, Gressin R, Lefrere F et al. Blastic variant of mantle
cell lymphoma: a rare but highly aggressive subtype. Leukemia
2001; 15; 1785–1791.
28. Tiemann M, Schrader C, Klapper W et al. Histopathology, cell
proliferation indices and clinical outcome in 304 patients with
mantle cell lymphoma (MCL): a clinicopathological study from
the European MCL Network. Br. J. Haematol. 2005; 131; 29–38.
29. Yin CC, Medeiros LJ, Cromwell CC et al. Sequence analysis proves
clonal identity in five patients with typical and blastoid mantle
cell lymphoma. Mod. Pathol. 2007; 20; 1–7.
30. Salaverria I, Zettl A, Bea S et al. Specific secondary genetic
alterations in mantle cell lymphoma provide prognostic infor-
mation independent of the gene expression-based proliferation
signature. J. Clin. Oncol. 2007; 25; 1216–1222.
31. Iqbal J, Greiner TC, Patel K et al. Distinctive patterns of BCL6
molecular alterations and their functional consequences in
different subgroups of diffuse large B-cell lymphoma. Leukemia
2007; 21; 2332–2343.
32. Saito M, Gao J, Basso K et al. A signaling pathway mediating
downregulation of BCL6 in germinal center B cells is blocked by
BCL6 gene alterations in B cell lymphoma. Cancer Cell 2007; 12;
280–292.
33. Lai R, Lefresne SV, Franko B et al. Immunoglobulin VH somatic
hypermutation in mantle cell lymphoma: mutated genotype
correlates with better clinical outcome. Mod. Pathol. 2006; 19;
1498–1505.
34. Muller-Hermelink HK, Greiner A. Molecular analysis of human
immunoglobulin heavy chain variable genes (IgVH) in
normal and malignant B cells. Am. J. Pathol. 1998; 153;
1341–1346.
35. Pittaluga S, Tierens A, Pinyol M et al. Blastic variant of mantle
cell lymphoma shows a heterogenous pattern of somatic muta-
tions of the rearranged immunoglobulin heavy chain variable
genes. Br. J. Haematol. 1998; 102; 1301–1306.
36. Cogliatti SB, Bertoni F, Zimmermann DR et al. IgV H mutations
in blastoid mantle cell lymphoma characterize a subgroup with a
tendency to more favourable clinical outcome. J. Pathol. 2005;
206; 320–327.
37. Chu PG, Chang KL, Weiss LM, Arber DA. Immunohistochemical
detection of CD10 in paraffin sections of hematopoietic neo-
plasms: a comparison with flow cytometry detection in 56 cases.
Appl. Immunohistochem. Mol. Morphol. 2000; 8; 257–262.
CD10+ mantle cell lymphoma 29
� 2008 The Authors. Journal compilation � 2008 Blackwell Publishing Ltd, Histopathology, 53, 20–29.





























