Embed Size (px)
Citation preview
page 1 of 3 Shropshire Community Health NHS Trust Board Agenda
William Farr House
Mytton Oak Road Shrewsbury Shropshire
SY3 8XL
Dear Colleague
I enclose the agenda for the meeting of the Shropshire Community Health NHS Trust Board to be held by MS Teams due to the Covid-19 pandemic. Questions or comments from members of the public are invited by email in advance of the virtual meeting and a recording of the meeting will be available on-line after the meeting. If you would prefer to put your question(s) in writing, please write to Ms Nuala O’Kane, Chair, Shropshire Community Health NHS Trust, William Farr House, Mytton Oak Road, Shrewsbury, SY3 8XL
Yours sincerely
Nuala O’Kane Chair
A G E N D A
ITEM Purpose Lead Format Time
1.
Welcome and Chair’s Award
N O’Kane
10:00
2. Apologies and quorum
N O’Kane
3. Declarations of Interest - www.shropscommunityhealth.nhs.uk/foi-lists-and-registers
Assurance N O’Kane
4. Patient/Staff story
Information 10:05
5. Minutes of the meeting held on: 7 October 2021
Approval N O’Kane Enc. 1 10:30
6. Matters arising and review of action log
Assurance N O’Kane Enc. 2 10:35
7. Chair’s Communications including:
• Brief report of any private board meetings held
Information N O’Kane Enc. 3 10:40
8. Non-Executive Directors’ Communications Information
Non-Executive Directors
10:50
9. Chief Executive’s Report
Information P Davies
Enc. 4 10:55
QUALITY, SAFETY AND PEOPLE Purpose Lead Format Time
10. Update from the Quality & Safety Committee Chair including the following appendices:-
Assurance T Long
Verbal 11:10
Appendix 1 Integrated Quality & Safety Performance Report
Assurance C Hobbs
Enc. 5
MEETING OF THE BOARD OF DIRECTORS (held in public) Thursday 2 December 2021 Virtual Via MS Teams 10:00am – 12:30pm
1 - Welcome and Chair's Award
1 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
page 2 of 3 Shropshire Community Health NHS Trust Board Agenda
Appendix 2 Quarterly Guardian for Junior Doctor Safe Working Report
Assurance J Povey
Enc 6
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
Assurance J Povey Enc. 7
Appendix 4 Learning from Deaths Report Assurance J Povey Enc 8
REFRESHMENT BREAK 11:30
RESOURCE & PERFORMANCE
Purpose Lead Format Time
12. Update from the Resource & Performance Committee Chair including the following appendices:-
Assurance
P Featherstone
Verbal 11.40
Appendix 1 Performance Report
Assurance S Lloyd
Enc. 9
Appendix 2 Finance Report Assurance S Lloyd Enc. 10
13 2020/21 Charitable Funds Accounts Approval S Lloyd Enc. 11 11.50
GOVERNANCE AND AUDIT
Purpose Lead Format Time
14. Governance Report, update from the Audit Committee including the following appendices:-
Assurance H Darbhanga Enc. 12 11:55
Appendix 1 Board Assurance Framework Assurance S Ramtuhul
Appendix 2 Corporate Risk Register Assurance S Ramtuhul
Appendix 3 Risk Appetite Statement Assurance S Ramtuhul
15. Trust Constitutional Documents and Committee Terms of Reference
Approval S Ramtuhul Enc. 13 12.00
16. Questions or Comments from Members of the Public
12:10
17.
Any Other Business
• With prior agreement of the Chair N O’Kane 12:15
18.
MEETING EVALUATION
18.1 Reflections on the meeting: effectiveness and any new risks and assurances
Consider for Action
N O’Kane Verbal 12:20
19.
DATE OF FUTURE MEETING
Thursday 3 February 2022
TO RESOLVE ‘that representatives of the press and other members of the public be excluded from the remainder of the meeting, having regard to the confidential nature of the business to be transacted, publicity of which would be prejudicial to the public interest’ (in accordance with Section 1(2) Public Bodies (Admission to Meetings) Act 1960
Patricia Davies
Chief Executive Nuala O’Kane Chair
1 - Welcome and Chair's Award
2 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 1 of 11 Shropshire Community Health NHS Trust Board Meeting – 7 October 2021
MINUTES OF THE BOARD MEETING
HELD VIRTUALLY VIA MICROSOFT TEAMS
AT 10.00AM ON THURSDAY 7 OCTOBER 2021
PRESENT
Chair and Non-Executive Members (Voting) Ms. Nuala O’Kane Ms. Tina Long Mr. Harmesh Darbhanga Mr. Peter Featherstone Ms. Cathy Purt Non-Executive Members (Non-Voting) Mr. Mike McDonald Executive Members (Voting) Ms. Patricia Davies, Dr. Jane Povey Ms. Sarah Lloyd Executive Members (Non-Voting) Mr Greg Moores In attendance Mr. Michael Wuestefeld-Gray, Mrs. Louise Tompson Malcolm Thomson Samantha Young Claudette Elliot Fiona Macpherson
(Chair) (Non-Executive Director and Vice Chair) (Non-Executive Director) (Non-Executive Director) (Non-Executive Director) (Associate Non-Executive Director) (Chief Executive) (Medical Director) (Director of Finance) (Director of People) (Interim Director of Governance) Executive Personal Assistant (to take the minutes of the meeting) Interim COO Interim Director of Nursing Local Care Group Director HR Manager
Ms O’Kane welcomed everyone to the meeting, reminding those present that the meeting would be recorded and uploaded on to our website. Ms O’Kane introduced Malcolm and Samantha Chair’s Award Ms O’Kane presented Chair’s Awards to the following people or teams: Linda Hamilton, Senior Management Accountant nominated by Gemma McIver, Deputy Director of Operations Linda is part of an amazing team and since I joined the Trust 12 months ago the support from finance has been incredible, they are by far the most aligned and supportive finance team to operations that I have ever worked with providing daily respectful challenge but also integral to driving joined up delivery. Linda is one of the Trust’s true stars from within the finance team– in one of our operational senior meetings last week the appreciation for her and all that she does was raised in abundance with everyone supporting her name to be put forward to you so that her hard work and ‘can do’ approach can be formally recognised hopefully through an award. Linda really stretches our operational thinking in terms of cost improvement but also always maintains integrity advocating for the patient and balancing our financial pressures with quality discussions making her a key partner to our teams. Linda is always approachable, responsive, articulate, and very solution focused. Her approach always reflects our Trust values, and she is certainly someone SCHT should be very proud to have as part of our workforce Ms O’Kane said finance is an important function but quite often this work goes on behind the scenes, but it was very nice to read and receive this nomination. We are very proud to acknowledge
5 - Minutes of the Meeting Held 7 October 2021
3 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 2 of 11 Shropshire Community Health NHS Trust Board Meeting – 7 October 2021
the great work that Linda does and on behalf of the Trust Ms O’Kane thanked her for her contribution.
DAART RSH Team: Laura Stewart Team Leader Saffie Roberts Sister Dawn Meredith Staff nurse Josephine Murillo Staff nurse Marny Ricafort Staff nurse Susan Van Straaten Admin Julia Bishop Admin Chrissy Davies HCA Dr Emily Peer GPwSI Dr Emma Watts GPwSI
Regular bank team members: Amy Hayes Staff nurse Philippa Saunders Staff nurse Vivian Pahal Staff nurse Lynne Bebb Staff nurse Eileen Swan Staff Nurse Dr Elizabeth Anderson Dr Prasanth Kandepalli Dr Jane Eden
Oswestry DAART team: Maria Jones Sister Denise Stone Emma Smith Janet Good Karen Price Helen Fischer
I have been managing a team of staff for the past two years and would like to nominate them all for the Chairman's Award please. Times have been difficult over the past eighteen months for everyone, but the team have pulled out all the stops and risen over and above their call of duty. MIU staff have moved willingly to cover shifts at short notice and our fellow county MIU's have helped us too. Theresa, our receptionist has created this superhero's board in a bid to help children relate and feel at ease to staff wearing masks. Last year MIU were nominated for the Nursing Times Student Nurse awards, and we have just been awarded 100% for our educational audit.
The small team in DAART have continued to function brilliantly, again moving shifts patterns to accommodate and support each other and provide care for their patients. I am so very proud of them all and would very much like them recognised for this please.
Cheryl Kinson - Specialist Nursery Nurse, Paulson Arancheril – Deputy Ward Manager, Liz Dambrauskas – School Staff Nurse, nominated by Fiona MacPherson, Human Resources Manager Liz, Cheryl and Paulson have been part of the BAME network since it started back in 2019. It is recognised that BAME staff don’t always have the same experience as white staff so the network is instrumental in trying to change experiences and listen. Liz, Cheryl and Paulson have always been committed to the network and prepared to share their stories through various channels which has included videos and speaking up at events – as a result an excellent system event for Cultural Diversity Day took place on 21 May 2021. Paulson also volunteered to be a member of the Workforce Race Equality Standard (WRES) Frontline Forum which involved travel to London as a representative for Shropcom. I would like to take this opportunity to thank them for their commitment and support to the network and I look forward to continuing to work with them on changing people’s experiences within Shropcom and the system. Liz thanked the Trust and Fiona for giving her the opportunity to do this and Paulson and Cheryl for working with her and hoped that as a Trust we can continue with the work we have been doing. Cheryl and Paulson a greed and thanked Mark Donovan and Fiona, and the Trust for giving them the opportunity. Mr Darbhanga congratulated the team, adding that they great ambassadors for the Trust. Ms Davies agreed adding that they are having an amazing contribution on top of a very busy day job. The work that is being done is great, the Cultural Diversity day was phenomenal and very exciting.
5 - Minutes of the Meeting Held 7 October 2021
4 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 3 of 11 Shropshire Community Health NHS Trust Board Meeting – 7 October 2021
Elinor Phillips Memory and Wellbeing worker, Ludlow and Bishop’s Castle nominated by Anthony Archambault Nurse Specialist – Safeguarding Adults I would like to put forward Elinor Phillips, memory and wellbeing worker who works across Ludlow and Bishops Castle, for a chairs award. Elinor has always demonstrated a ‘can do’ attitude. She works above and beyond her role and is always willing to help support staff. Elinor has recently been involved in identifying safeguarding concerns in her work area. She has demonstrated a in depth working knowledge of the key principles of safeguarding and ‘making safeguarding personal’ and professional curiosity, by working with a patient and asking them there wishes and views and identifying initial concerns that required follow up. As a result of Elinor’s positive work, a safeguarding plan was put in place and full multi-agency involvement. This meant that the patient was kept safe and was able to be fully involved and state their wishes. Elinor went above and beyond her role in this instance, and this was a shining example of someone ‘going the extra mile’. She continued to work with the patient and gave them the time and space to discuss their concerns, and for them to be given the correct information to make an informed choice. Without Elinor’s pro-active approach, these concerns may not have been picked up. Elinor encourages others around her, and she demonstrates excellent knowledge base. She has been instrumental in helping to develop recent resources around Mental Capacity and Deprivation of Liberty Safeguards and has been keen to get involved and has provided invaluable feedback to the process. Elinor remains dedicated, and it is clear to see she is a well-respected and invaluable member of her team. Ms O’Kane commented that Elinor acts with great empathy care and compassion and see’s situations from the patient perspective. It is a great pleasure to acknowledge her work with the Chair’s award, she is a great asset to the Trust. Ms O’Kane said that it is always such a pleasure to present the Chair’s awards for their over and above contribution to the work of the Trust. Patient and Staff Story Stacey Harrison, previous Shropcom Admiral Nurse attended the meeting today to share Audrey’s story along with Audrey’s daughter Lisa and her father Michael. Lisa had taken part in a video to share Audrey and her families experience, and this video was shared to the Board. In the video Lisa explained that Audrey did not contract Covid, but she went on to say that everything that was put in place to stop her getting Covid stopped Audrey from seeing her family and ultimately, she felt that not getting Covid killed her. Audrey had been diagnosed with dementia 5 years previously and had support from lots of services and lived with her husband, daughter, and family. Lisa explained that in August 2020 Audrey needed to move to a care home due to the family home suffering a flood. Lisa explained that when Audrey was in the care home the family was not included in decision-making, despite them having power of attorney. The care home changed Audrey’s GP and Pharmacist without consulting the family. A ReSPECT document was completed without the input of her family. Covid restrictions meant family and other services who had been working with Audrey were not allowed to visit the home and Audrey’s health began to rapidly deteriorate. Lisa explained that the family felt powerless and it was hard when they could hear Audrey becoming so frail and confused. Audrey did not see her grandchildren again, and by the time her husband could see her she was unaware that he was there. When in hospital Audrey experienced further negative experiences which impacted her dementia. She was moved wards in the middle of the night and was later moved again and spent four days in
5 - Minutes of the Meeting Held 7 October 2021
5 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 4 of 11 Shropshire Community Health NHS Trust Board Meeting – 7 October 2021
the discharge ward waiting to be taken to a new care home. When she moved to the new care home Audrey was assessed as being at end of life and Lisa and her family could visit. Lisa felt there could have been a much more person-centred approach to Audrey’s care, and everything could be risk managed. Ms O’Kane thanked Lisa and Michael and offered her condolences to them and the whole family on the loss of their wife and mother. Ms O’Kane thanked Stacey for helping to tell the story. She asked was there more the Trust could have done to make the situation better at the time. Stacey said the blanket ban on visitors to the care home was difficult but if someone could have gone into the care home that knew her from when she was at home, they could have seen that she was deteriorating. Ms O’Kane commented that the Trust works very closely with care homes, but they are independent organisations who make their own rules, and this can sometimes be difficult for the Trust to work with. Lisa said that there was a lot of community care involved for Audrey but the care home shut the door on that and that felt horrendous. Lisa went on to say that the family really needed the extra support and she wanted to try and prevent this happening again to another family. Ms O’Kane asked if the family have had communication with the care home since Audrey had passed away. Lisa said that she had been in touch with the CQC and Healthwatch had assisted in writing a letter of complaint, but this had not yet been finalised. Claudette Elliot, Local Care Director said that our local care programme will give us the opportunity to pick up some of the learning from some of the issues Lisa had identified. Tracey Lee, Admiral Nurse Team Lead said that during Covid-19 there has been trauma caused to families from not being able to see each other and the lack of stimulation. Ms O’Kane thanked Lisa and Michael for sharing their story adding that seeing their photos of happier times was very powerful and showed what a lovely mum she was, she wished the family all the very best. Minute No 2021.5.1 - Apologies None received Minute No. 2021.5.2 - Minutes of the Meeting held on 5 August 2021 Agreed as an accurate record Minute No. 2021.5.3 Review of action log No outstanding actions Minute No. 2021.5.4 - Declarations of Interest No new declarations Minute No. 2021.5.5 - Chair’s Communications Ms O’Kane reported that it has been a very busy time, especially in relation to system work. She visited the League of Friends at Ludlow and has also attended the AGM at Bridgnorth League of Friends. She spoke about the great work of the League of Friends at Bridgnorth, in particular the weekly memory café. Ms O’Kane paid tribute to the work of the League of Friends and the volunteer workforce and the fantastic work they do which adds value to the Trust’s.
The Board accepted the assurance provided by the Chair’s report
5 - Minutes of the Meeting Held 7 October 2021
6 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 5 of 11 Shropshire Community Health NHS Trust Board Meeting – 7 October 2021
Minute No. 2021.5.6 – Non – Executive’s Report Ms O’Kane welcomed any updates from the Non-Executive Directors. Ms Long said that the since the last meeting she had attended two meetings of the Local Care Programme. Significant progress is being made and the detail is becoming much clearer. Moving forward it will be important to engage with the public effectively. Mr Featherstone has continued to provide support across the system, and he has been involved with some light touch engagement with local authorities around how co working can be developed. Mr Darbhanga has attended the Equality and Diversity Steering Group where lots of good work is taking place. The group considered the health inequalities plan and difficulties faced accessing secondary care. The group is also mindful of digital isolation affecting some of our older population. He also attended the ICS Sustainability Committee and Benefit Realisation Group meetings. Ms Purt attended the Regional Health and Wellbeing meeting looking at the role of the Guardian and how we can support staff in Shropcom, she also attends the Estates and Capital Planning meetings. Ms O’Kane recognised the enormous contribution of Non-Executives, their skills and experience is valuable Minute No. 2021.5.7 - Chief Executive’s Report Ms Davies presented national and local issues relevant to the Board and not covered elsewhere on the agenda. She reported that the Trust has successfully appointed to Executive posts based on the revised structure that the Board signed off in May. Sarah Lloyd has been appointed as Finance Director after many years with the Trust and most recently as Acting Director of Finance. Ms Davies confirmed that Angie Wallace has been appointed as Chief Operating Officer and Clair Hobbs as Director of Nursing. Both currently work in the Shropshire, Telford, and Wrekin System, with the local acute trust and they will join the executive team in November. Ms Davies remarked that system partners have given great feedback on the appointments. Ms Davies went on to thank Ms Young and Mr Thomson for being Interim Directors over the next month. Ms Davies formally thanked Mr Gregory who retired from Shropcom last week as Director of Operations and Nursing, having provided 37 years of service for the NHS. Mr Gregory was also awarded a Gold Award by the Chief Nurse for NHS England, Ruth May, and she wished Steve well for the Future. The Trust is the first Community Trust to be part of the levelling up coalition which is focussing on the levelling up agenda which is a group looking at the social impact of institutions and how inequalities can be reduced. Ms Davies said that she was very proud that the Trust is part of this, and she will report back to the Board on the progress of the group. In relation to Covid-19, in Shropshire there are higher rates of transmission than other areas of the region. Originally it was thought this was due to tourism factors but now it is thought this could be being driven by students returning to universities and schools. There are now 40 patients in SaTH with Covid-19 but none of the patients are in critical care. There have been two Covid-19 outbreaks in the Trust’s Community Hospitals, one of these was stood down last week. Ms Davies emphasised that no staff have had Covid-19 in these areas and the outbreak has been well managed by the Infection Control Team. Ms Davies went on to explain that the system continues to see long waits for ambulances and a level 4 escalation has been put in place. The system has been working well together but there is more that can be done. The system is working with pharmacists and 111 appropriately to redirect patients to the right professional, Ms Davies expressed concerns with this as it is not yet winter. The Trust’s winter plan has been submitted to the region, a big part of this is around the Covid-19 vaccine boosters as well as flu vaccinations. Flu vaccinations have started with staff and the Trust’s performance on this will be brought back to the Board at regular times.
5 - Minutes of the Meeting Held 7 October 2021
7 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 6 of 11 Shropshire Community Health NHS Trust Board Meeting – 7 October 2021
Mr Featherstone asked what is driving elective pressures and the impact on Shropcom and its capacity to support patients. Ms Davies said causes are multifactorial but it is due to Covdi-19, and also the need to address the back log. The Trust is now trying to make an impact on the waiting list as well as deal with new referrals. Ms Purt asked how community diagnostic hubs will help relieve the pressure in the system. Ms Davies commented that the diagnostic hubs will help in the future and will have an impact on supporting elective flow. Mr Darbhanga asked a question relating to emergency planning processes as a system and what impact did the recent national fuel situation have on waiting lists or elective management. The Board noted that regular internal emergency planning meetings are held which link to ICS meetings. Ms O’Kane thanked Ms Davies for the update and recognised that there are significant challenges in the system now. She expressed support to GP colleagues who are impacted and under the same pressures as the Trust but who are suffering criticisms currently. The Board acknowledged that the Local Care Programme will be working very closely with GP services so that care can be co-ordinated. Dr Povey welcomed the ambition to work closely with primary care, adding that an initial meeting with GPs who work with the Trust in Community Hospitals and DAART had been positive. Wider communication would be needed moving forward and further education for the community that there is more than one way to access healthcare.
The Board accepted the assurance provided by the report.
QUALITY, SAFETY AND PEOPLE
Minute No 2021.5.8 – Update from Quality and Safety Committee Chair Mr Featherstone presented the report which provided a summary of discussions at the last meeting. He reported that Tina Long will now be Chair as Mr Featherstone will move to Chair the Resource and Performance Committee. At the last meeting of the Quality Committee a good report was received on patient experience, including key learning for the Trust to consider relating to compliments and complaints. Some services have tested the use of QR codes, and a higher response rate was seen. Ms O’Kane thanked Mr Featherstone for his effective chairing of the Committee.
The Board accepted the assurance provided by the report.
Appendix 1 Integrated Quality & Safety Performance Report Ms Young highlighted key points from the most recent Quality and Safety (Q&S) Committee meeting which were set out in the summary report. The decrease in the number of inpatient falls is testament to the work of the falls group who are looking at assisted technology and the grading of falls. She reported an increase in the number of pressure ulcers which is reflective of pressures in IDT Teams, there are plans in place to address this. There has been an increase in the number of new birth visits taking place, 50% of visits not able to take place in the first 2 weeks were due to parent choice and the other 50% had taken place in day 15 or 16 after birth. Ms Young went on to update the Board on two outbreaks of Covid-19 at Community Hospitals. The outbreak at Ludlow is coming to an end and work is ongoing around an outbreak at Whitchurch.
5 - Minutes of the Meeting Held 7 October 2021
8 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 7 of 11 Shropshire Community Health NHS Trust Board Meeting – 7 October 2021
The Trust Infection, Prevention and Control team is working closely with NHSEI to ensure guidance and policies are followed. Ms O’Kane expressed concerns around pressure ulcers and requested further assurance around this.
The Board accepted the assurance provided by the report.
Appendix 2 Quarterly Guardian for Junior Doctor Safe Working Report Dr Povey presented the report which provided assurance to the Board that trainee doctors at Shropshire Community Health NHS Trust have safe working hours and conditions to maintain doctor and patient safety. This assurance is collated from Shrewsbury and Telford Hospitals NHS Trust’s (SATH) Guardian of Safe Working Hours (GOSW), our trainees being employed by SATH. During the reporting period 1 May – 31 July 2021 there were four doctors in training working in SCHT) They raised no concerns during this period.
The Board accepted the assurance provided by the report.
Appendix 3 Equality, Diversity, and Inclusion Update Ms MacPherson attended the meeting and provided an overview of the report. She said that a lot of work has been implemented since she last reported in March including, implementing cultural ambassadors, reverse mentoring, and the Cultural Diversity Day. She asked the Board to approve the publication of our Workforce Disability Equality Standard (WDES) and Workforce Race Equality Standard (WRES) metrics and associated action plans to ensure compliance with our legal obligations. Ms MacPherson recognised that there are some areas of focus and she is working with networks to address these. She also noted that there are some significant areas of improvement and the Trust has come a long way in last 18 months- 2 years in relation to Equality, Diversity, and Inclusion. Ms Lloyd asked if there were actions focussed on areas of shortlisting through to appointment Ms Macpherson said that the recruitment process and paperwork have been worked through with the networks and changes have taken place. Network members are also being trained so they can be on panels and the Trust is also implementing the cultural ambassadors programme to support having people on recruitment panels etc. Mr Darbhanga asked what impact Covid-19 has had on percentages for example bullying and harassment and whether some of these results had reduced because of circumstances, for example working from home. Ms Macpherson said that it was difficult to tell what is attributed to the results, however networks are reporting that their experiences of bullying and harassment have not changed because of Covid-19. Ms O’Kane thanked Ms MacPherson, acknowledging that this is very important work, and that the Trust takes it very seriously.
The Board approved the publication of the WRES and WDES matrix on the website.
5 - Minutes of the Meeting Held 7 October 2021
9 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 8 of 11 Shropshire Community Health NHS Trust Board Meeting – 7 October 2021
RISK AND FINANCIAL STABILITY
Minute No 2021.5.9 – Update from Resources and Performance Committee Mr Darbhanga was pleased to report that the Resource and Performance Committee held a positive meeting but will be reporting an adverse position. He noted that the ICS Sustainability Committee approved the work to develop the Community Diagnostic Hub, although ongoing funding relating to this is uncertain, work is ongoing to mitigate this risk; this is a system-wide programme of work. Mr Darbhanga said that he is no longer Chair of Resource and Performance Committee and is now Chair of Audit Committee. Peter Featherstone will now Chair the Committee and Tina Long will now Chair Quality and Safety Committee. Ms O’Kane thanked Mr Darbhanga for all his work as Chair of the Resource and Performance Committee,
The Board accepted the assurance provided by the report.
Appendix 1 Performance Report Ms Lloyd reported that much of the issues in the report have been discussed earlier on the agenda. The Board noted that there is limited assurance almost entirely due to waiting times of services, this was discussed earlier on the agenda, however the Trust is not on outlier compared to other organisations. The Board noted that Ms Young had provided assurance relating to clinical triage while patients wait. Shropcom are ensuring that measures are taken to ensure patients are kept safe whilst they are waiting for appointments. The Board acknowledged that it is going to take some time to recover the waiting lists from the last 18 months. Ms O’Kane recognised the limited assurance and noted that Board will be looking for further assurance on this in the future.
The Board accepted the limited assurance provided by the report.
Appendix 2 Finance Report Ms Lloyd presented the report which highlighted the following key areas. The Trust is reporting a year-to-date deficit of £1,223k against a planned deficit £1,426k, showing a favourable variance of £204k against the Stabilisation Plan. The Trust’s H1 plan includes non-recurrent items, and the Trust is reporting a year-to-date surplus of £234k against a planned surplus £150k, showing a favourable variance of £84k. The key risk to achievement of the financial plan remains identifying and delivering a recurrent CIP. To date £1,627k recurrent schemes have been identified against planned delivery of £2,641k. £320k of the identified schemes are high risk. To close the gap the focus continues on developing additional recurrent schemes and actions include: • Further Executive CIP Confirm and Challenge sessions have been arranged with corporate and SDG leads to identify potential schemes and completed QEIAs as required • All schemes still requiring PIDs and QEIAs now have leads identified and a date to complete the documentation
5 - Minutes of the Meeting Held 7 October 2021
10 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 9 of 11 Shropshire Community Health NHS Trust Board Meeting – 7 October 2021
The Board • Considered the adjusted financial position against our H1 plan at month 5, which is a surplus of £234k compared to plan of £150k, a favourable variance of £84k • Recognised that performance against the Stabilisation Plan at month 5 is a deficit of £1,223k compared to the planned deficit of £1,426k which is a favourable variance of £204k • Considered that recurrent CIP development remains a challenge and is the Trust’s most material financial risk; work continues to identify additional schemes • Recognised the transfer of the Covid Vaccination service to SCHT where the costs of delivery are fully reimbursed by NHSEI
Minute No 2021.5.10 – H2 2021/22 Planning Update Ms Lloyd presented the report, highlighting 2 key areas:
1. Local care and huge amount of good work going on in this area. 2. H2 plans - system level financial allocations have been made and the system is considering
what this means. There is a lot of work to do around restoring activity and how to tackle the waiting list and work is ongoing to address this. Ms Lloyd reported that there are difficulties restoring activity in a couple of areas which are in the report but there are actions in place to address this.
3. Summary of development of integrated care system. Ms Long asked what the level of confidence is that the recovery of services will be successful. Ms Lloyd emphasised that services have done an amazing job on this to date. Mr Thomson commented that in relation to pulmonary rehab the Trust is well on the way to addressing this delay, improvement plans are in place and there is excellent leadership in the team. Addressing TEMs and the Wheelchair Service Mr Thomson said there are national issues impacting on this. TEMs have external relationship and capacity issues that need to be worked through with the system. Mr Thomson said that meetings are taking place weekly to monitor progress. Responding to a question from Mr Featherstone relating to falls, Ms Young said that the team is considering different ways in which patients can be assessed, including the use of digital. Ms Purt asked what the impact of the need is to revamp the community equipment store; this has been a concern of the Resource and Performance Committee for some time. Mr Thomson said there is a lot of work going on around the store, reviewing where and how we purchase. There is a lot of equipment on back order, noting international issues. Mr Thomson said the team have excellent leadership and there is a strong workforce. He commented that there are ongoing amnesties to get equipment back into the service.
The Board accepted the limited assurance provided by the report and noted the areas of concern.
REPORTS CONSIDERED BY AUDIT COMMITTEE
Minute No 2021.4.11 – Governance Report Mr Wuestefeld-Gray thanked the team for the report and work to date on the BAF and Corporate Register. He confirmed that the updated internal audit report will go to the next Audit Committee meeting. Ms O’Kane noted the progress being made and thanked Mr Wuestefeld-Gray for the report.
5 - Minutes of the Meeting Held 7 October 2021
11 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 10 of 11 Shropshire Community Health NHS Trust Board Meeting – 7 October 2021
Appendix 1 Board Assurance Framework Appendix 2 Corporate Risk Register Appendix 3 NHS Resolution Report
The Board approved the report and appendices.
QUESTIONS OR COMMENTS FROM MEMBERS OF THE PUBLIC
Minute No. 2021.5.12 Questions or Comments from Members of the Public
Question from Geeta Patel sent via email
1. Page 46 of 167: Under Well-led and sickness- Good to see that a humanistic review of staff with long term sickness has taken place. What do the Board see as an outcome of the review?
The Director of Nursing and Ops completed this review alongside the Interim Director of People to review all ongoing long term sickness cases over 6 months in duration. The findings of the review have been fed into the People Delivery Plan which will be presented at the Q&S Committee in November. Specifically, the delivery plan will feature a continued focus on proactive health and wellbeing programmes and strengthening measures around reasonable adjustments.
2. On the WRES/DES papers- What are the Trust's plans to examine intersectionality- Staff who may be disabled and BAME.
The Trust plans to do further engagement with its staff on what they would like to see from the networks and intersectionality will form part of those discussions. The Trust is also in the planning stage of how it will refresh of its EDI strategy which will include discussions around intersectionality. Mr Moores emphasised that the Trust’s staff networks have huge value to add.
ANY OTHER BUSINESS – with prior agreement of the Chair
Minute No. 2021.5.13 – Any Other Business There was none
MEETING EVALUATION
Minute No. 2021.5.14 – Reflections on the meeting: effectiveness and any new risks and assurances The Board acknowledged that no new risks were identified at the meeting. The Board had the opportunity to ask detailed questions. Ms O’Kane thanked the contribution of the NEDs and the support they are giving to the Trust and executive colleagues. Mr Darbhanga commented that the staff receiving awards are great ambassadors for the organisation.
5 - Minutes of the Meeting Held 7 October 2021
12 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 11 of 11 Shropshire Community Health NHS Trust Board Meeting – 7 October 2021
Board members suggested that they would welcome a shortened more concise agenda, both length and number of papers that come to Board meetings, so that the burden on executive colleagues can be reduced.
DATE OF FUTURE MEETING
Minute No. 2021.5.15– Date of Future Meeting 10am – 12.30pm, Thursday 2 December 2021 Ms O’Kane thanked everyone for attending the meeting.
IT WAS RESOLVED that representatives of the press, and other members of the public, be excluded from the remainder of the meeting, having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest (in accordance with Section 1(2) Public Bodies (Admission to Meetings) Act 1960).
5 - Minutes of the Meeting Held 7 October 2021
13 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Meeting Date: December 2021
Part 1 – Trust Board Meeting Action Log
Action Completed
Action is not yet complete but on track
Action has slipped
Meeting Date
Minute Ref and Agenda
Issue Action Update Lead Target Date
October 2021
Integrated Quality & Safety Performance Report
Pressure Ulcers
Ms O’Kane expressed concerns around pressure ulcers and requested further assurance around this.
Themes identified with associated ongoing work to improve pressure ulcer management include: • Patient Compliance/Non-concordance and its management • Interservice communication and MDT working • Completion of a full assessment on admission to the case load A weekly Pressure ulcer panel where all PU are reviewed by TVN A weekly PU scrutiny group and review of all new Inservice pressure ulcer reported in the last 7 days From 1st December Accountability meetings chaired by the Director of Nursing will be held to further review ongoing themes, closure of actions and a focus on learning and prevention Coo and operational support are reviewing current workloads for the District Nursing Service and how this may be impacting
C Hobbs December
21
6 - Review
of the Action Log
14 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
1 Accountable Director: Nuala O’Kane Meeting Date: 3 December 2020
REPORT COVER SHEET Report Title: Chair’s Update
Meeting: Trust Board of Directors
Author: Nuala O’Kane Accountable Director:
Nuala O’Kane
Other meetings or Committee presented to or previously agreed at:
Meeting or Committee Date Reviewed
N/A N/A
Strategic goals this report relates to: (tick as appropriate)
To deliver high quality care
To deliver integrated care
To support people to live the lives they want
to lead
To deliver sustainable community services
Relevance to Board Assurance Framework : (tick as appropriate)
Clinical Quality &
Safety
Long term financial
sustainability of the Trust
Healthcare Systems
Organisational culture
Optimising use of technology
Covid19
Relevance to Well-led domains (CQC & NHSE/I): (tick as appropriate)
leadership capacity and capability
clear vision and credible strategy
culture clear roles and responsibilities
clear and effective risk management
appropriate and accurate information
learning, continuous improvement and innovation
Stakeholders engaged and involved
Relevance to CQC domains: (tick as appropriate)
Safe Caring Responsive Effective Well led
Impacts and Implications? YES or NO
If yes, what impact or implication
Patient safety & experience
Equality & Inclusion
Financial (revenue & capital)
IG Governance Toolkit
OD/Workforce
Legal
Relevance to Corporate Risk
Meeting Date: 2 December 2021
Agenda Item: 7
Enclosure Number: 3
7 - Chair's Communications
15 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2 Accountable Director: Nuala O’Kane Meeting Date: 3 December 2020
Register (Risk No/Name)
Aim of the report (a concise statement of the purpose of this report)
To update the Board on developments and activities in the last two months, October and November 2021
Assessment and summary of key points in report (include analysis and consideration of issues, options,
risks and mitigations. Also include good practice, required improvements, and timescales. If appropriate, include a judgement on the level of assurance the report provides: Substantial: Moderate: Limited: None)
Private Meeting of the Board – 4 November 2021 Items discussed included a high level update on the vaccination programme, Health and Safety policy and standard operating procedures updates, financial reports and 2022/23 Planning and Priorities. Meetings and Visits Together with Patricia Davies I met with Friends Group members and Patient Represetative groups in Ludlow and Bishops Castle, to explain the issues around the temporary closure of BC hospital and how we are planning to support patients in the interim. Over the last two months I have interviewed for Non Executive Directors, we were fortunate in having a high level of interest in these roles and I am pleased that we have appointed one Non Executive Director and one Associate NED, who will both join the Board on 1 January 2022. I have also been assisting with the recruitment of a number of NEDs for a neighbouring Trust, which has been a useful and interesting experience. Thanks and appreciation are extended to Mike McDonald as he reaches the end of his term of office. Mike has brought valuable insights to our meetings and he will be missed, but we wish him all the best in his future ventures. I have attended a number of meetings of the ICS Board and Sub Committee, and Regional Briefings. I was also asked to lead discussion organized by the Good Governance Institute on the role of Community Health Services and how we can help to transform health care by initiatives such as Community Diagnostic Hubs and Virtual Wards. Trust Board We held the Trust Annual General Meeting in November, when we reflected on the challenges and successes of the past year, which we acknowledged had been the most extraordinary in the history of the NHS.. We also had a presentation by Mark Brandreth, the Executive Lead for Shropshire, Telford and Wrekin Integrated Care System. He outlined the progress that has been made in partnership working across the ICS area and the strengths we have all realised through working together.
Purpose of the Report (tick as appropriate)
Consider for Action
Give Approval Accept Assurance
Provide Information
Key Recommendations
The Board is asked to note and accept the Chair’s Report.
7 - Chair's Communications
16 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21

3 Accountable Director: Nuala O’Kane Meeting Date: 3 December 2020
7 - Chair's Communications
17 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1 Accountable Director: Patricia Davies, Chief Executive Meeting Date: Trust Board – 2nd December 2021
REPORT COVER SHEET Report Title: Chief Executive’s report
Meeting: Board of Directors
Author: Patricia Davies, Chief Executive
Accountable Director:
N/A
Other meetings or Committee presented to or previously agreed at:
Meeting or Committee Date Reviewed
N/A
Strategic goals this report relates to: (tick as appropriate)
To deliver high quality care
To deliver integrated care
To support people to live the lives they want
to lead
To deliver sustainable community
services
√ √ √ √
Relevance to Board Assurance Framework : (tick as appropriate)
Clinical Quality &
Safety
Long term financial
sustainability of the Trust
Healthcare Systems
Organisational culture
Optimising use of technology
Covid19
√ √ √ √
Relevance to Well-led domains (CQC & NHSE/I): (tick as appropriate)
leadership capacity and capability
√clear vision and credible strategy
√ culture √clear roles and responsibilities
√
clear and effective risk management
appropriate and accurate information
learning, continuous improvement and innovation
Stakeholders engaged and involved
Relevance to CQC domains: (tick as appropriate)
Safe Caring Responsive Effective Well led √
Impacts and Implications? YES or NO
If yes, what impact or implication
Patient safety & experience Yes
Consequence of coronavirus will be evaluated as the pandemic develops.
Equality & Inclusion
Financial (revenue & capital)
Yes
The Trust will monitor the financial impact of our response to the pandemic. There is a national commitment that these costs will be funded.
IG Governance Toolkit No
OD/Workforce Yes
Our response to coronavirus will have a direct and indirect impact on staff.
Meeting Date: 2 December 2021
Agenda Item: 9
Enclosure Number: 4
9 - Chief Executive's Report
18 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2 Accountable Director: Patricia Davies, Chief Executive Meeting Date: Trust Board – 2nd December 2021
Legal N/A
Relevance to Corporate Risk
Register (Risk No/Name)
Aim of the report (a concise statement of the purpose of this report)
To update the Board on key policies, issues and events and to stimulate debate regarding potential impact on strategy and levels of assurance.
Assessment and summary of key points in report (include analysis and consideration of issues, options,
risks and mitigations. Also include good practice, required improvements, and timescales. If appropriate, include a judgement on the level of assurance the report provides: Substantial: Moderate: Limited: None)
This report sets out the national and local issues of strategic importance to the organisation, highlighting relevant policy, guidance and information that may have an impact on our strategic objectives or organisational risks, as set out in the Board Assurance Framework (BAF).
Purpose of the Report (tick as appropriate)
Consider for Action
Give Approval √Accept Assurance
√Provide Information
√
Key Recommendations
The Board of Directors is asked to consider the potential impact of the national issues and local issues on strategy and levels of assurance for the Trust
9 - Chief Executive's Report
19 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1 | P a g e
CHIEF EXECUTIVE’S REPORT – 2nd December 2021
1. Introduction
This report sets out the national and local issues of strategic importance to the organisation (for information) not picked up through other Board reports. The Board is asked to consider the impact of these issues on the Trust.
2. Key Issues
2.1 Temporary Closure of Bishops Castle: Board members will be aware that
Bishop’s Castle hospital was temporarily closed from the 1st November on safety
grounds. Prior to this decision, the Trust’s Quality and Safety Committee had
considered several staffing related issues over a period of months which, when
considered in the round, presented a significant ongoing safety risk to patients which
the Trust was unable to mitigate in the short term.
The Board will be aware that the Trust had undertaken numerous recruitment
campaigns with little success. Given the increasing staffing pressures generally
because of the pandemic and the need for staff to self-isolate, the situation was
considered by the Board and felt to no longer be sustainable without a real risk that
patients could come to harm. A full quality impact assessment has been undertaken
and this confirmed that the safest option for our patients was to temporarily close the
service and ensure that their ongoing care needs could be met elsewhere. The Trust
is exploring how it can build and restore services in a safe way, that meets the needs
of the community locally and across South Shropshire in the most clinically sustainable
way. To this end a full options appraisal is being undertaken, considering the known
challenges and any potential mitigations. The speed with which the decision was
taken to protect patients did not provide time for a full and thorough options appraisal
or for consultation by commissioners with the public. We seek to rectify this by fully
engaging with the community and key partners as part of our system Local Care
Transformation Programme, overseen by commissioners, and through this
programme engage on models of care that also have a focus on prevention and
promoting good health and wellbeing. The first phase of this will commence during the
winter months with the view to publishing the options appraisal following on from this
period of engagement in the spring with our commissioners in line with any required
formal consultation.
9 - Chief Executive's Report
20 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2 | P a g e
During this time and since the 1st November, some of the staff from Bishop’s Castle
Hospital are working alongside local GPs to put in place a model of care that will allow
us to care for more people in the comfort and familiarity of their own home. We have
also relocated the community physiotherapy clinic that has run from the hospital within
the local area so that this service is not disrupted.
2.2 Covid-19 infection rates: Covid-19 infection rates: the latest seven-day
infection rates per 100,000 residents as of 17 November. Figures (those in brackets
are those from the previous briefing) are:
Shropshire: 497.8 (375.8)
Telford & Wrekin 510.7 (466.6)
West Midlands 362.5 (347.8)
England 376.4 (356.1)
Outbreaks: Transmissions for both Telford and Wrekin and Shropshire remain higher
than for the rest of the West Midlands, although take up of the vaccine remains within
the upper quartile for the region.
The previously reported outbreaks of Covid at two of our community hospitals are now
closed. Whilst cohorting remains in place for known transfers of patients with COVID
19 from other providers, I am pleased to report that we have had no further IPC
breakouts relating to COVID 19 within our community hospitals.
The acute Trust has recently seen higher numbers of admissions relating to COVID.
On 5th November there were 60 COVID patients (2 wards) occupying beds. This
reduced to 40 on 8th November. The higher levels of COVID inpatients are putting
further pressure on services across the system.
Regional Non-Elective Pressures: The pressures relating to non-elective
attendances and admissions continue, with high levels of ambulance calls and calls to
111 and local GPs. We continue to support the system through the work we are doing
with all partners to prevent unnecessary admission to hospital by maintaining and
supporting people with long term conditions in their home. Over 85% of what we do
as a community Trust is within people’s homes. Likewise, the system is re-focusing
efforts on discharge planning from the point of admission, so once acute treatment
has been completed, a person can be discharged quickly and safely back to their home
to receive rehabilitation, care and reablement if this is needed. The evidence is clear
that ‘home first’ has the greatest impact on optimising a person’s independence and
wellbeing for the long term.
I would urge the public to use local pharmacies and access their GP appropriately for
advice, guidance, and treatment as a first port of call. Primary Care can be accessed
via several routes, including the phone. As a recent resident in Shropshire, having
come back home and used the service, I have to say that the response from my local
GP practice was exceptional. Not everything requires face to face contact and many
consultations can be done using the phone or via video call, which is quick, effective
and was less hassle for me as the patient in terms of taking time out of work to travel
9 - Chief Executive's Report
21 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
3 | P a g e
to an appointment. And the consultation can be done with other clinicians such as
paramedics, therapists, nurses, and pharmacists that are attached to or associated
with the practice. Your GP practice will decide what type of consultation is required
and yes, in high pressure times the phone may take a few minutes, but that is the case
in all sectors including trying to get through to your bank, insurance, phone provider,
etc. Primary care is open, it is under immense pressure and we can help ourselves
and primary care to help us by using technology as much as possible and our local
chemist and pharmacist likewise is a wealth of support, information, and advice in
terms of managing conditions and our health. The one thing we can all do, of course,
to support our health and wellbeing this winter is to get the flu vaccine and COVID
vaccine (if you haven’t had your two jabs yet) and Booster. Likewise, following and
continuing with the COVID guidelines of wearing a mask in public places, washing
hands regularly, using hand sanitisers in public places and keeping a distance really
does make a difference in terms of not only keeping COVID at bay, but other winter
bugs including flu at bay too.
I say this in every report, but I want to reiterate and thank all our fantastic staff
personally on behalf of this Board for what you do, under what is exceptional pressure
and I extend that thanks to all staff across the system. MPFT, RJAH, WMAS, our GPs
and our fantastic council staff and voluntary sector who pull it out of the bag every day.
Thank you! Particularly so as this report is the last before Christmas and New Year
and want to wish all staff a very warm Seasons Greetings and to remind us all that
many of our staff will be working over this period and away from their loved ones.
2.3 Covid-19 Vaccination Programme- The vaccination programme across Shropshire, Telford and Wrekin continues to go at pace and remains strong in terms of delivery. In terms of 12–15-year-olds, we are the second highest performers in the region in terms of numbers vaccinated and highest performers in terms of the 16–17-year-old vaccines. Likewise, in terms of vaccinating pregnant woman this is now over 75% and within the top performers regionally and nationally. 2.4 Flu – Delivery of the flu vaccine has commenced for all over 50s across the country
and it is important that we encourage the wider population to take up the offer for flu;
this is a second plank in our armour over the winter. In terms of vaccinating our staff
against the flu, our occupational health team have been running clinics across the
Trust. Take up has been good. As of the 15th November 64% of staff received the
vaccine, compared to 62% this time last year.
2.5 Covid vaccination – The Board is asked to note the change in regulations
regarding covid vaccination for staff working in care homes has now come into effect.
As you can imagine many Shropcom staff are required to visit care homes as part of
their roles. The People function have been leading preparations for this change,
working very closely with colleagues from Operations and Nursing, and in partnership
with staff side, communications have been issued and no major concerns raised to
date. The Secretary of State has announced that the same requirement will apply to
NHS staff with effect from April 2022; further detail and guidance is expected, and I
9 - Chief Executive's Report
22 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
4 | P a g e
will ensure the Board is updated in due course. Latest data shows 93% of Shropcom
workers (including employed, bank, and regular agency workers) have received both
primary doses of the Covid vaccine.
3. ICS and Placed Based working
3.1 The ICS - The STW ICS has been operating in Shadow form since April 2021. In line with the Interim Guidance on the Function and Governance of the Integrated Care Board (ICB), the ICS will be formally established as an ICB in April 2022. This ICB will be a new organisation that bind partner organisations together with a common purpose. The Shropshire, Telford & Wrekin ICB will lead integration within the NHS, bringing together all those involved in planning and providing NHS services, to take a collaborative approach to agreeing and delivering ambitions for the health of their population. Our Shropshire, Telford & Wrekin ICB will be a unitary board, responsible for ensuring the ICB plays its role in achieving the four purposes of the ICS and will therefore be constituted in a way that ensures a focus on improving outcomes in population health and healthcare; tackling inequalities in outcomes, experience, and access; enhancing productivity and value for money; and contributing to broader social and economic development. Our Board of the ICB will also be responsible for:
Developing and delivering the ICB’s strategy
Ensuring the ICB operates effectively, fairly and openly
Seeking assurance that systems of control are robust and reliable
Shaping a healthy culture for the ICB and wider Integrated Partnerships and Placed Based boards
Our ICB will oversee the delivery off specific functions that will enable us as a system to achieve the four core purposes/ quadruple aim of an ICS. The statutory functions currently exercised by the CCG will also be conferred to the ICB from April 2022. This includes duties regarding health inequalities, quality, safeguarding, children in care and children and young people with special educational needs and/or disability. A clearly defined due diligence process led by the CCG is currently underway to ensure the safe passage of duties, assets and liabilities to the ICS. This is being overseen by the ICS Transformation Group and assured via both the CCG and ICS Audit Committees. The ICS are in the process of formally recruiting key roles within the ICB including a CEO, Executive and Partner members. A Designate ICB Chair, Sir Neil McKay has already been appointed and the ICS is in the process of recruiting two Independent Non-Executive Directors.
9 - Chief Executive's Report
23 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
5 | P a g e
Chief Executives across health and Local Authorities within the STW system meet regularly and have strong, high-trust relationships. This has been accelerated by the recent challenges (and successes) associated with rolling out the vaccination programme to our population. Our ICS CEO Group membership is enhanced by the presence of clinical leadership to ensure that the clinical voice is given appropriate prominence. Multi-professional (i.e., clinical, care, public health) leadership and engagement to drive our ICS and this is being strengthened through several channels. This includes our inclusive Multi-Professional Leadership Network and Professional Executive Leads Team feeding in and out of the ICS CEO Group. 3.2 Placed-Based Working – As described in the NHSE guidance Thriving Places: Guidance on the Development of Place-based Partnerships, all ICS’s must confirm their proposed Place-Based Partnerships for 2022/23 including their boundaries, leadership and membership.
As an ICS, we build from a position of strength with markedly strong pre-existing Health and Wellbeing Boards in both Telford & Wrekin and Shropshire respectively. These boards have a statutory responsibility for developing the health and wellbeing strategies for each local authority area and meet in public.
Within our system we have also already established 2 Integrated Place Partnerships, reporting to our CEO Group both with representation from the local authority, local NHS trusts, Primary Care Networks (PCNs) and the voluntary, charity and social enterprise sector:
Shropshire Integrated Place Partnership (ShIPP)
Telford & Wrekin Integrated Place Partnership (TWIPP)
Our Integrated Place Partnerships clearly correspond to the pre-existing footprints of both our Places of Shropshire, and Telford & Wrekin. Integrated Place Partnerships have emerged locally as collaborative arrangements formed by the organisations responsible for arranging and delivering health and care services in a locality or community. Our Integrated Place Partnerships will remain as the foundations of Shropshire, Telford & Wrekin Integrated Care System. In an important change, it is proposed that they will operate as a committee of the ICB as the ICB becomes the statutory. The placed based boards are chaired by the LA and this gives a level of strength and focus, given only 20% of health and wellbeing is driven by clinical care. The rest depends on health behaviours, the environment in which people live and wider determinants of health. Place with its local connections and great understanding of the neighbourhoods it serves, is best placed to tackle the whole agenda. Both Ship and Twip have a clear plan for delivery that meets the Health and Wellbeing Boards of each council and reflects the key priorities of the ICS. Furthermore, there is a clear roadmap to formalise the boards going forward. The most recent key areas of focus
9 - Chief Executive's Report
24 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21

6 | P a g e
that shrop comm have been leading on relates to local care. The focus of the local care programme, achievements to date and milestones for the coming year are as follows: 3.3 Local Care - The Local Care Transformation Programme is making good progress
in the implementation of 2021/22 priorities. Board members will recall that the system
was successful in receiving investment committee approval to access Ageing Well
funds to focus on 3 key areas: Advanced Care planning in Care Homes; Intermediate
Respiratory Care Service and expansion to the integrated Rapid Response team. The
aim and objectives to promote selfcare and supported management of patients at
home and prevent unnecessary admission to acute care. I am pleased to report that
for advanced care planning and the respiratory services, we are ahead of trajectory in
terms of recruiting clinical staff across these integrated teams, that allow for the wider
expansion and skill set, linking to wider community and primary care teams. In terms
of Rapid response, Recruitment is underway for both health and social care additional
posts, which to date this has been mainly successful. We have had some challenges
in recruitment to social care posts, however our local authority colleagues have put
steps in place to mitigate risks associated with on-going recruitment, that will be
monitored through the Local Care Transformation Programme Delivery Group. Where
it is practically possible, we will be accelerating/bringing forward subsequent phase to
the programme to support the current demands for urgent and emergency care during
the winter period.
Finally, I wanted to update the board on the work related to children’s services, which
is in its early stages and again reflects the ambition of both our organisation and the
ICS in terms of collaboration, joint working and integration to deliver the best
population health outcomes.
4 Children’s Services
On the 11th November I joined a facilitated workshop, alongside colleagues from
Shropshire Council and MPFT, exploring the potential to improve outcomes for
children in the County through strengthened integration and partnership working. It
was a very positive session, hearing from other areas that have taken this journey as
well as exploring our local context. We produced tangible outcomes which will now
be shaped into a programme to be delivered through an integrated Board. I will be
delighted to share more detail about this exciting programme as it shapes up.
The above are the main updates to the Board not included elsewhere within officer
reports. I would like to take the opportunity to wish the Board, staff and members of
the public a very Happy Christmas and peaceful New Year.
9 - Chief Executive's Report
25 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
REPORT COVER SHEET Report Title: November 2021 Quality Report Meeting: Trust Board
Author: Liz Hagon Adult AHP Professional Lead Claire Horsfield - Deputy Director of AHPs & Quality
Accountable Director:
Clair Hobbs - Executive Director of Nursing /Director of Infection Prevention and Control
Other meetings or Committee presented to or previously agreed at:
Meeting or Committee Date Reviewed
Quality and Safety Committee Nov 2021
Strategic goals this report relates to: (tick as appropriate)
To deliver high quality care
To deliver integrated care
To support people to live the lives they want
to lead
To deliver sustainable community
services
Relevance to Board Assurance Framework : (tick as appropriate)
Clinical Quality &
Safety
Long term financial
sustainability of the Trust
Healthcare Systems
Organisational culture
Optimising use of technology
Covid19
Relevance to Well-led domains (CQC & NHSE/I): (tick as appropriate)
leadership capacity and capability
clear vision and credible strategy
culture clear roles and responsibilities
clear and effective risk management
appropriate and accurate information
learning, continuous improvement and innovation
Stakeholders engaged and involved
Relevance to CQC domains: (tick as appropriate)
Safe Caring Responsive Effective Well led
Impacts and Implications? YES or NO
If yes, what impact or implication
Patient safety & experience YES CQC quality performance domains and Trust performance.
Equality & Inclusion
Financial (revenue & capital)
IG Governance Toolkit
OD/Workforce
Meeting Date: 2 December 2021
Agenda Item: 10
Enclosure Number: 5
Appendix 1 Integrated Quality and Safety Performance Report
26 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Legal YES CQC regulatory requirements
Relevance to Corporate Risk
Register (Risk No/Name)
Aim of the report
1. To provide assurance to Trust Board to support the organisation in the provision of evidence against key lines of enquiry and to contribute to the Trust strategic goals and priorities. The report aims to do this by:- a. Providing Board with an executive summary focussing on areas for and areas of improvement. b. Access to the suite of detailed quantifiable information from the Trust’s single data performance repository for reliability and accuracy. c. Analysis to provide evidence through external benchmarking, Trust historical performance and triangulation of softer intelligence to strengthen both reliability and confidence in content. 2. To report improvement headlines from the Service Delivery Groups
Assessment and summary of key points in report
Inpatient falls have increased to 14 this month despite a reduced bed occupancy rate. The Inpatient Falls Steering Group is continuing with a programme of work to influence this trend.
The volume of pressure ulcers increased to 45 in October, the highest reported volume this year. District Nursing Teams reported 35% Level 3, 65% Level 2 for October. This led to higher cancelled and rescheduled visits than the previous month.
New Birth Visit compliance continued to improve with the Trust achieving the overall target of 95% at 95.14%.
Purpose of the Report (tick as appropriate)
Consider for Action
Give Approval Accept Assurance
Provide Information
Key Recommendations
The Board/ Committee is asked to:
Note and accept the report as assurance
Appendix 1 Integrated Quality and Safety Performance Report
27 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
3 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
1.0 Quality Metrics
The first part of this Quality and Performance Report provides the Quality and Safety Committee
with key exceptions across a range of quality and performance measures for the service delivery
groups, to ensure the Quality and Safety Committee are informed on the following key areas:
1. Services that have improved, are consistently performing well and meeting both CQC descriptors for ‘Good’ and Trust quality KPI’s
2. Services falling below CQC descriptors for ‘Good’ and Trust quality KPI’s that are on an improvement plan
3. Services where quality and performance is considered to meet or exceed CQC descriptors for ‘Outstanding’ and Trust performance
4. Learning from when things go well and not so well
5. New or increased risks identified by the service delivery groups
6. Trust overview of key mandatory safety training, information governance and appraisal performance.
Commissioners receive Trust Quality Performance Reports as part of our monthly Clinical Quality Review meetings and these reports also contribute to the suite of information required as part of Care Quality Commission (CQC) informal engagement visits with the Director of Nursing and Operations and Deputy Director of Nursing and Quality.
As well as our Trust quality performance KPI’s, the CQC as our regulatory body for quality set fundamental standard below which care must never fail. It is therefore essential quality performance relates to CQC as well as referencing other relevant national quality standards accordingly.
Appendix 1 Integrated Quality and Safety Performance Report
28 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
4 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Safe
Falls – Number of Falls Standard outcome
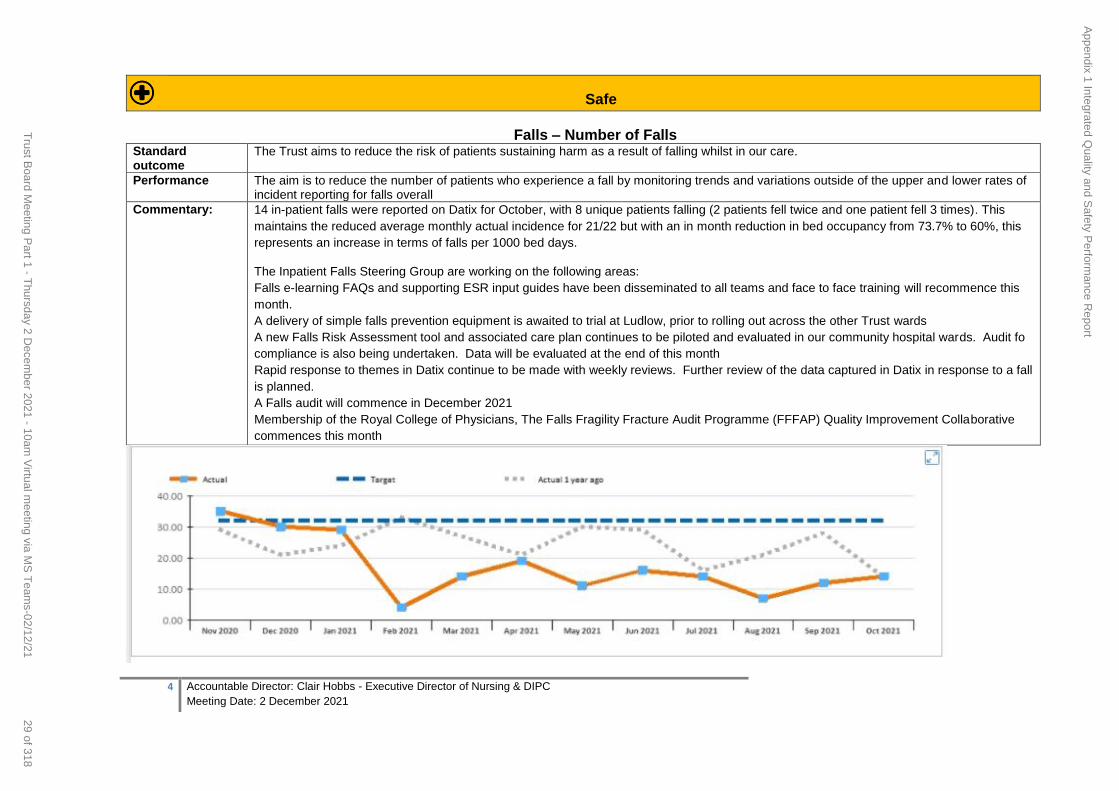
The Trust aims to reduce the risk of patients sustaining harm as a result of falling whilst in our care.
Performance The aim is to reduce the number of patients who experience a fall by monitoring trends and variations outside of the upper and lower rates of incident reporting for falls overall
Commentary: 14 in-patient falls were reported on Datix for October, with 8 unique patients falling (2 patients fell twice and one patient fell 3 times). This
maintains the reduced average monthly actual incidence for 21/22 but with an in month reduction in bed occupancy from 73.7% to 60%, this
represents an increase in terms of falls per 1000 bed days.
The Inpatient Falls Steering Group are working on the following areas:
Falls e-learning FAQs and supporting ESR input guides have been disseminated to all teams and face to face training will recommence this
month.
A delivery of simple falls prevention equipment is awaited to trial at Ludlow, prior to rolling out across the other Trust wards
A new Falls Risk Assessment tool and associated care plan continues to be piloted and evaluated in our community hospital wards. Audit fo
compliance is also being undertaken. Data will be evaluated at the end of this month
Rapid response to themes in Datix continue to be made with weekly reviews. Further review of the data captured in Datix in response to a fall
is planned.
A Falls audit will commence in December 2021
Membership of the Royal College of Physicians, The Falls Fragility Fracture Audit Programme (FFFAP) Quality Improvement Collaborative
commences this month
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
29 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
5 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
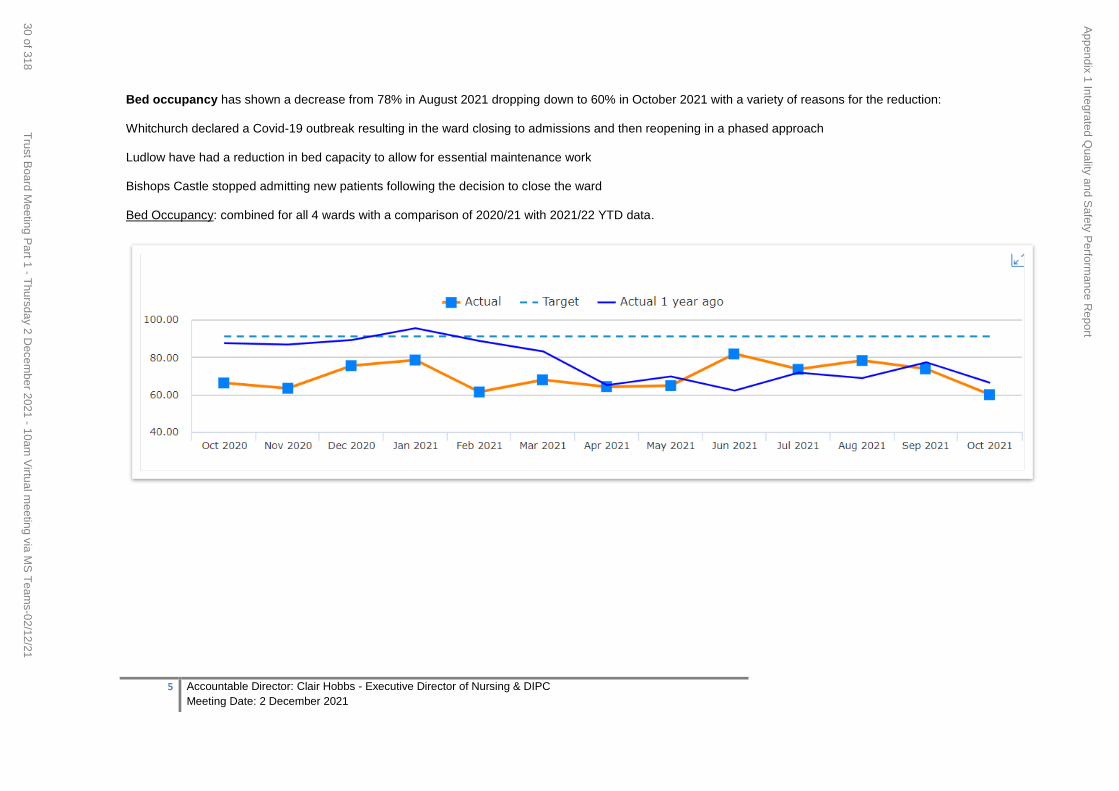
Bed occupancy has shown a decrease from 78% in August 2021 dropping down to 60% in October 2021 with a variety of reasons for the reduction:
Whitchurch declared a Covid-19 outbreak resulting in the ward closing to admissions and then reopening in a phased approach
Ludlow have had a reduction in bed capacity to allow for essential maintenance work
Bishops Castle stopped admitting new patients following the decision to close the ward
Bed Occupancy: combined for all 4 wards with a comparison of 2020/21 with 2021/22 YTD data.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
30 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
6 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Safe
VTE (Venous Thromboembolism Risk Assessment)
Standard and outcomes:
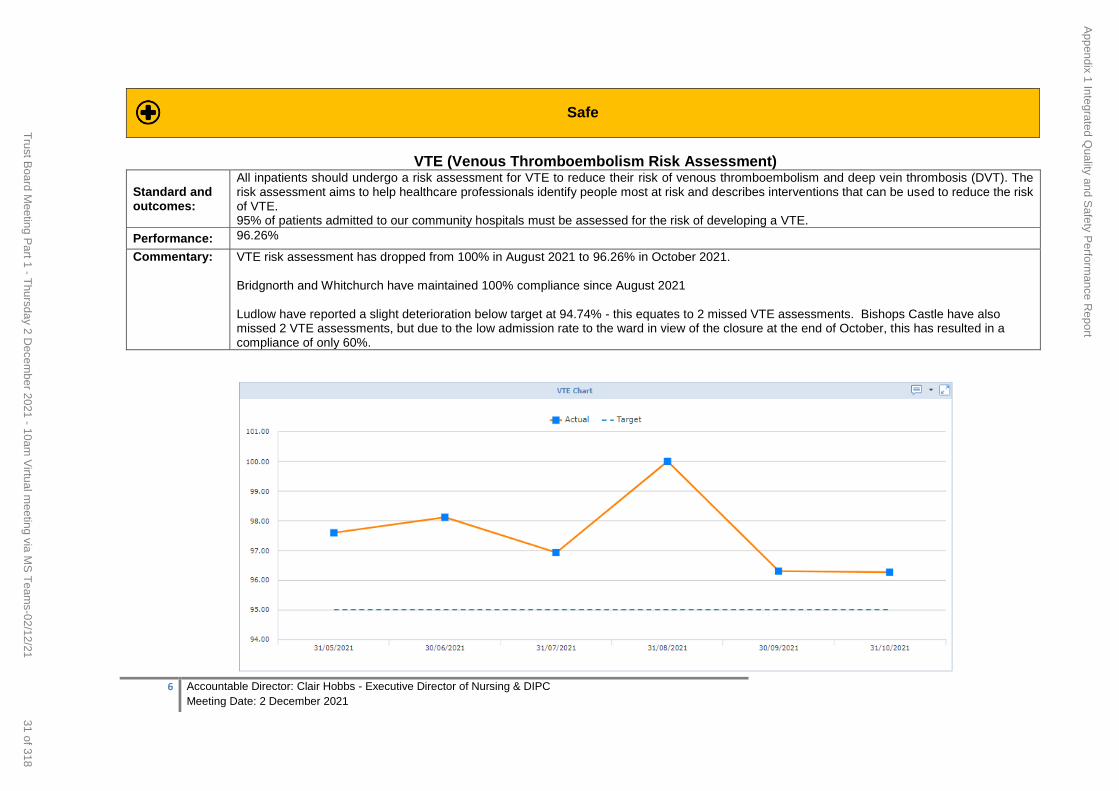
All inpatients should undergo a risk assessment for VTE to reduce their risk of venous thromboembolism and deep vein thrombosis (DVT). The risk assessment aims to help healthcare professionals identify people most at risk and describes interventions that can be used to reduce the risk of VTE. 95% of patients admitted to our community hospitals must be assessed for the risk of developing a VTE.
Performance: 96.26%
Commentary: VTE risk assessment has dropped from 100% in August 2021 to 96.26% in October 2021. Bridgnorth and Whitchurch have maintained 100% compliance since August 2021 Ludlow have reported a slight deterioration below target at 94.74% - this equates to 2 missed VTE assessments. Bishops Castle have also missed 2 VTE assessments, but due to the low admission rate to the ward in view of the closure at the end of October, this has resulted in a compliance of only 60%.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
31 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
7 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Safe
Serious Incidents (all)
Standard and outcomes:
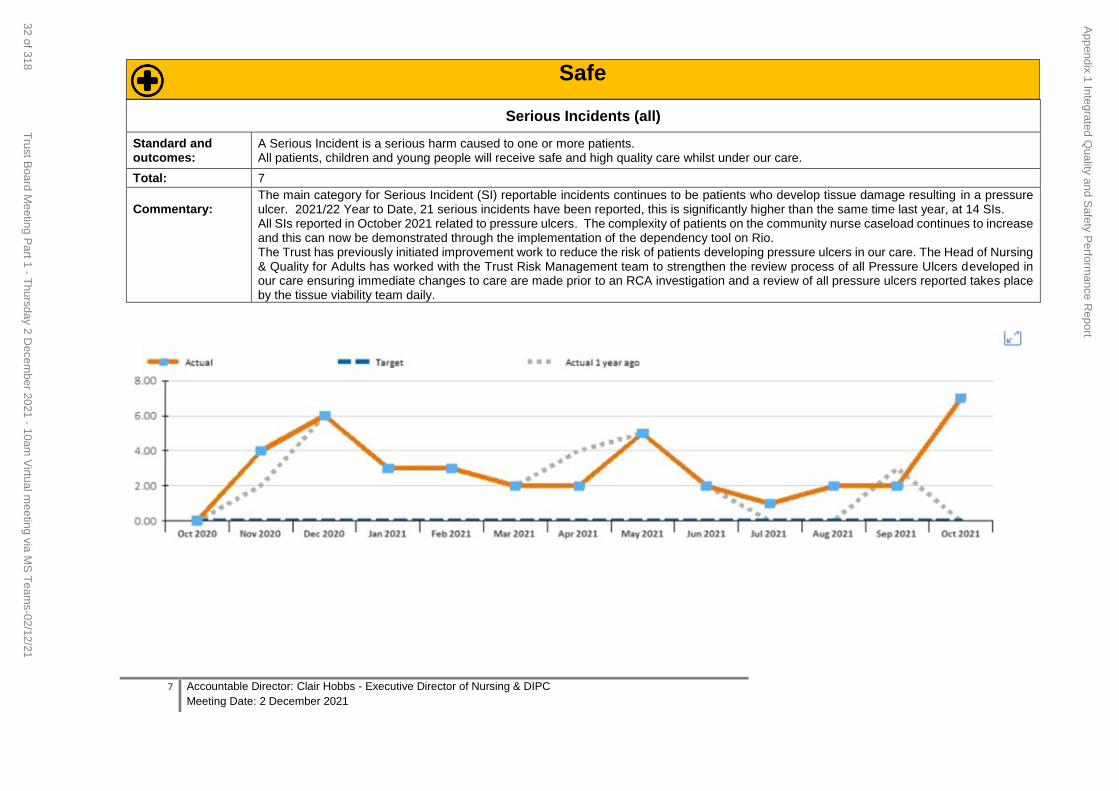
A Serious Incident is a serious harm caused to one or more patients. All patients, children and young people will receive safe and high quality care whilst under our care.
Total: 7
Commentary:
The main category for Serious Incident (SI) reportable incidents continues to be patients who develop tissue damage resulting in a pressure ulcer. 2021/22 Year to Date, 21 serious incidents have been reported, this is significantly higher than the same time last year, at 14 SIs. All SIs reported in October 2021 related to pressure ulcers. The complexity of patients on the community nurse caseload continues to increase and this can now be demonstrated through the implementation of the dependency tool on Rio. The Trust has previously initiated improvement work to reduce the risk of patients developing pressure ulcers in our care. The Head of Nursing & Quality for Adults has worked with the Trust Risk Management team to strengthen the review process of all Pressure Ulcers developed in our care ensuring immediate changes to care are made prior to an RCA investigation and a review of all pressure ulcers reported takes place by the tissue viability team daily.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
32 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
8 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Safe
Pressure Ulcers
Standard and outcomes:
Pressure ulcers form part of the ‘harm free’ care reporting suite which are reflective of ‘hospital acquired harm’. Pressure ulcers remain a concerning and mainly avoidable harm associated with healthcare delivery. We aim to reduce the number of patients in our care from developing a pressure ulcer
Position : 45
Commentary: There is a further increase in pressure ulcers reported in service this month with 45 reported in October compared to 41 in August, with 73% of pressure ulcers reported as Category 2.
Pressure ulcer numbers remain high – benchmarking completed with MPFT who report a similar picture. There is a joint quality project underway with MPFT to look at themes from RCAs and action plans to address
Nursing home incidents – Safeguarding submitted for St Georges Park due to 2 patients with unstageable pressure damage and equipment issues
Residential homes –safeguarding issues raised by SCHT due to 4 patients with pressure damage. These are currently being investigated
Barrier products have been found to not be used as a preventative measure, so this could be a significant factor contributing to the increase in category 2 damage
Actions:
Pressure Ulcer policy with Clinical Policy Group for approval
New skin care range (Medi derma Range) has been evaluated and approved at wound steering group, for final approval at Area Prescribing Committee, with a soft launch of the product range and pathways on Stop the Pressure Day (18th November) prior to a full launch with an educational programme in January 2022
Procurement exercise looking at pressure relieving cushions, followed by a review of mattresses to standardise and reduce variation in the products clinicians can order through CES
Development of Accountability meetings with staff to ensure rapid assessment of risks, mitigations and immediate actions for PU prevention
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
33 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
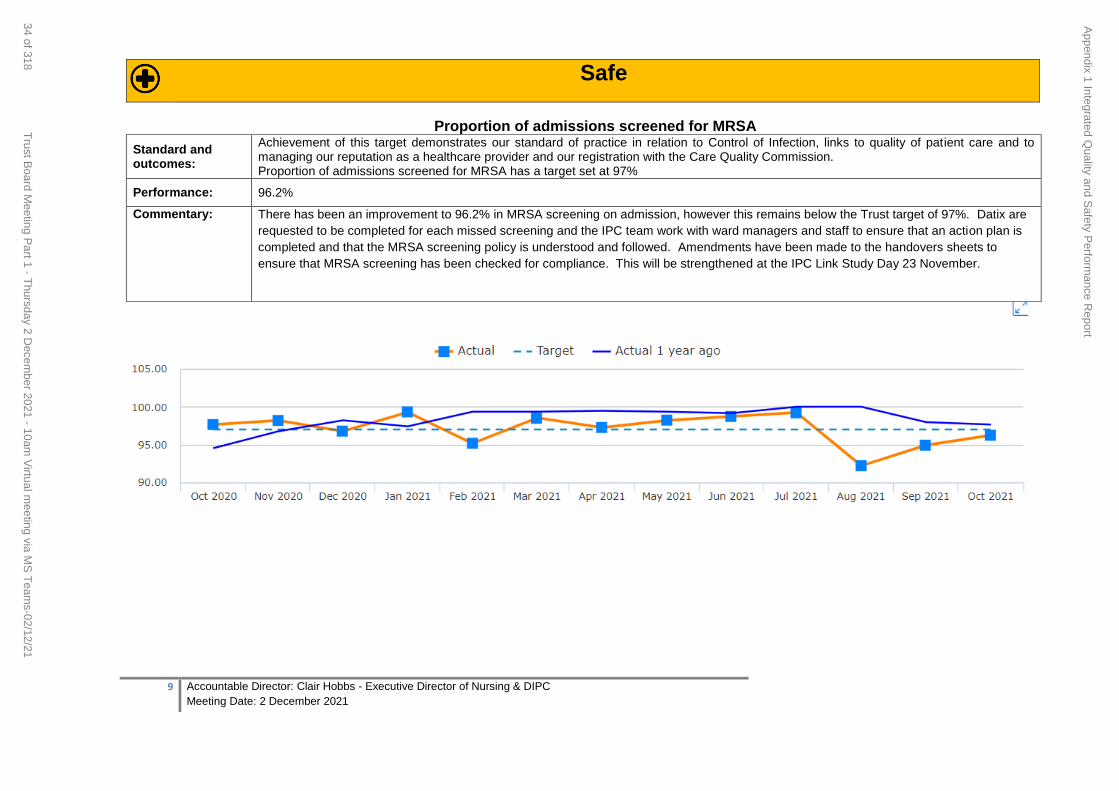
9 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Safe
Proportion of admissions screened for MRSA
Standard and outcomes:
Achievement of this target demonstrates our standard of practice in relation to Control of Infection, links to quality of patient care and to managing our reputation as a healthcare provider and our registration with the Care Quality Commission. Proportion of admissions screened for MRSA has a target set at 97%
Performance: 96.2%
Commentary: There has been an improvement to 96.2% in MRSA screening on admission, however this remains below the Trust target of 97%. Datix are
requested to be completed for each missed screening and the IPC team work with ward managers and staff to ensure that an action plan is
completed and that the MRSA screening policy is understood and followed. Amendments have been made to the handovers sheets to
ensure that MRSA screening has been checked for compliance. This will be strengthened at the IPC Link Study Day 23 November.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
34 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
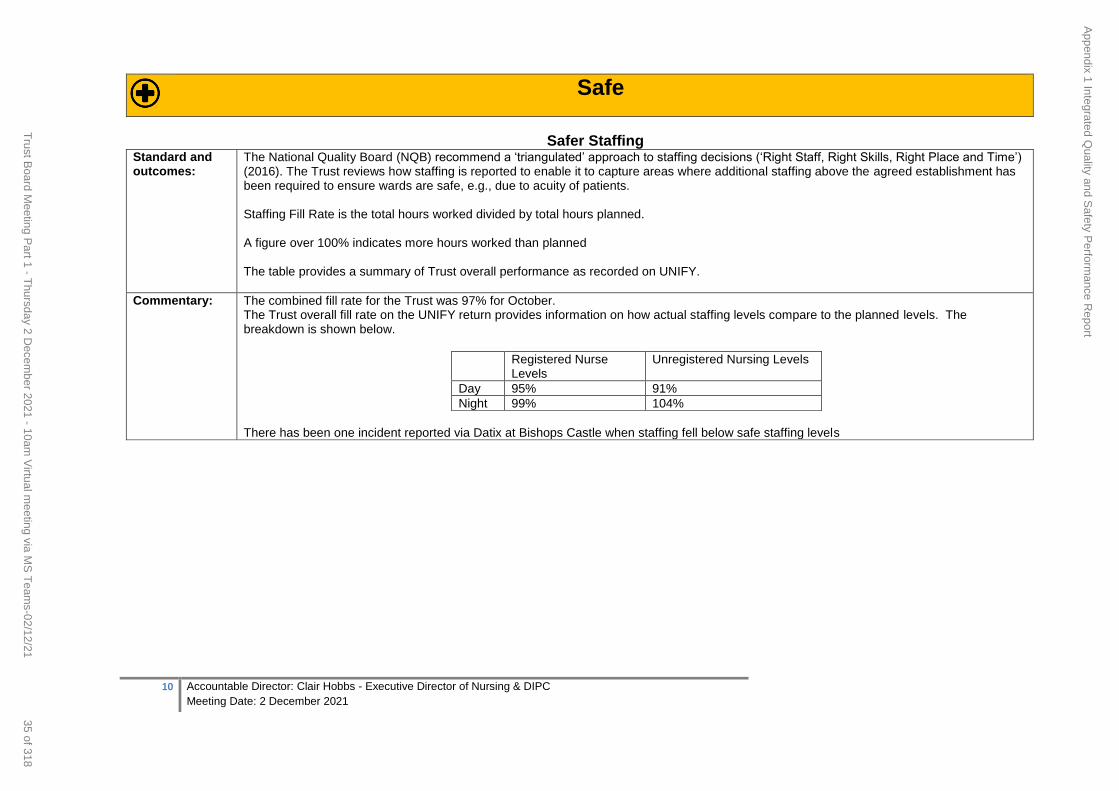
10 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Safer Staffing Standard and outcomes:
The National Quality Board (NQB) recommend a ‘triangulated’ approach to staffing decisions (‘Right Staff, Right Skills, Right Place and Time’) (2016). The Trust reviews how staffing is reported to enable it to capture areas where additional staffing above the agreed establishment has been required to ensure wards are safe, e.g., due to acuity of patients. Staffing Fill Rate is the total hours worked divided by total hours planned. A figure over 100% indicates more hours worked than planned The table provides a summary of Trust overall performance as recorded on UNIFY.
Commentary: The combined fill rate for the Trust was 97% for October. The Trust overall fill rate on the UNIFY return provides information on how actual staffing levels compare to the planned levels. The breakdown is shown below.
Registered Nurse Levels
Unregistered Nursing Levels
Day 95% 91%
Night 99% 104%
There has been one incident reported via Datix at Bishops Castle when staffing fell below safe staffing levels
Safe
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
35 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
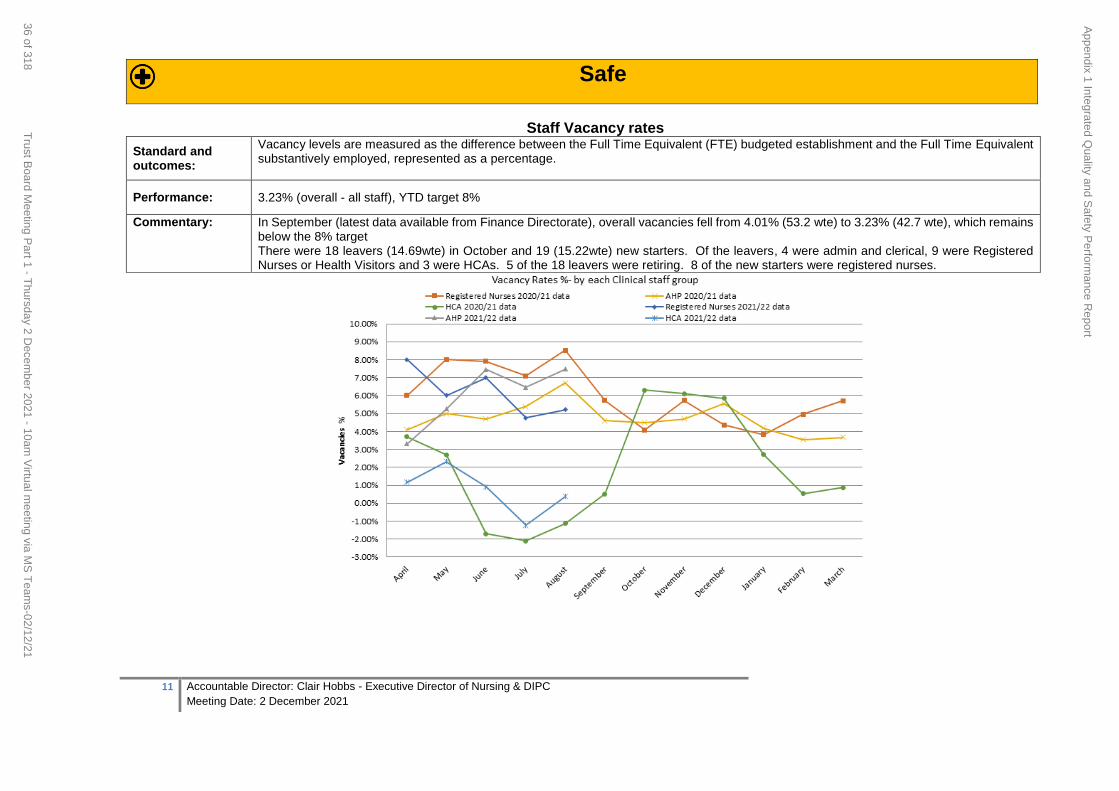
11 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Safe
Staff Vacancy rates
Standard and outcomes:
Vacancy levels are measured as the difference between the Full Time Equivalent (FTE) budgeted establishment and the Full Time Equivalent substantively employed, represented as a percentage.
Performance: 3.23% (overall - all staff), YTD target 8%
Commentary: In September (latest data available from Finance Directorate), overall vacancies fell from 4.01% (53.2 wte) to 3.23% (42.7 wte), which remains below the 8% target There were 18 leavers (14.69wte) in October and 19 (15.22wte) new starters. Of the leavers, 4 were admin and clerical, 9 were Registered Nurses or Health Visitors and 3 were HCAs. 5 of the 18 leavers were retiring. 8 of the new starters were registered nurses.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
36 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
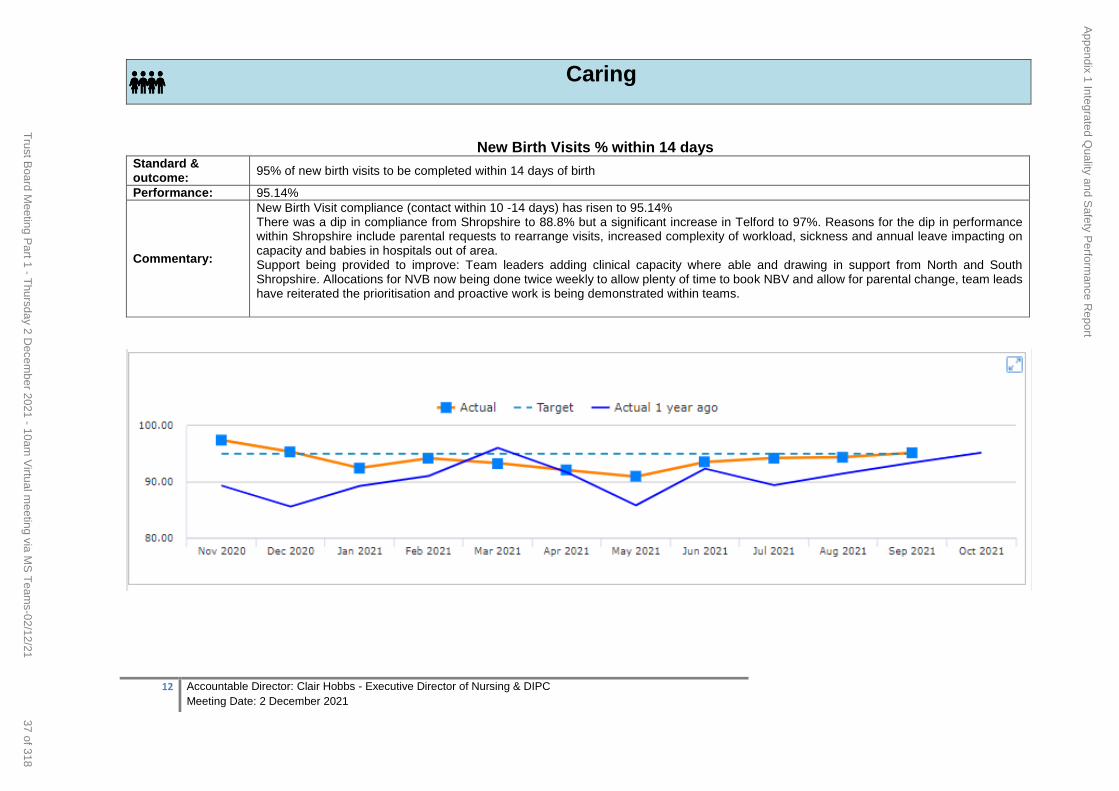
12 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Caring
New Birth Visits % within 14 days Standard & outcome:
95% of new birth visits to be completed within 14 days of birth
Performance: 95.14%
Commentary:
New Birth Visit compliance (contact within 10 -14 days) has risen to 95.14% There was a dip in compliance from Shropshire to 88.8% but a significant increase in Telford to 97%. Reasons for the dip in performance within Shropshire include parental requests to rearrange visits, increased complexity of workload, sickness and annual leave impacting on capacity and babies in hospitals out of area. Support being provided to improve: Team leaders adding clinical capacity where able and drawing in support from North and South Shropshire. Allocations for NVB now being done twice weekly to allow plenty of time to book NBV and allow for parental change, team leads have reiterated the prioritisation and proactive work is being demonstrated within teams.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
37 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
13 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Caring
Friends and Family Test The monthly Community FFT data submission commenced on 1st February and is now being submitted on a monthly basis.
278 responses were received in October 2021, with 99.3% providing positive feedback across the whole range of clinical services delivered by the Trust. Paper
responses continue to make up 30% of feedback mechanism. Updates have been made to appointment letters generated through Trust electronic paper records,
with a QR Code to access FFT to provide options to our service users to facilitate increased opportunities for feedback.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
38 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
14 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Responsive
Complaints
Standard and outcomes:
The number of written complaints. Complaints provide valuable feedback to improve care & outcomes
Performance: 6
Commentary:
6 complaints have been received in October 2021. Quality of Care accounted for the majority of the complaints received. A total of 19 complaints were closed during quarter 2 of which 11 were found to be upheld or partly upheld. Training opportunities are being sourced for frontline staff, both admin and clinical, to further develop and enhance communication skills. In response to quality of care elements, refresher and enhanced training is being implemented. There is an ongoing process in place to share learning from complaints across Service Delivery Groups. 33 Compliments were received in October 2021
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
39 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
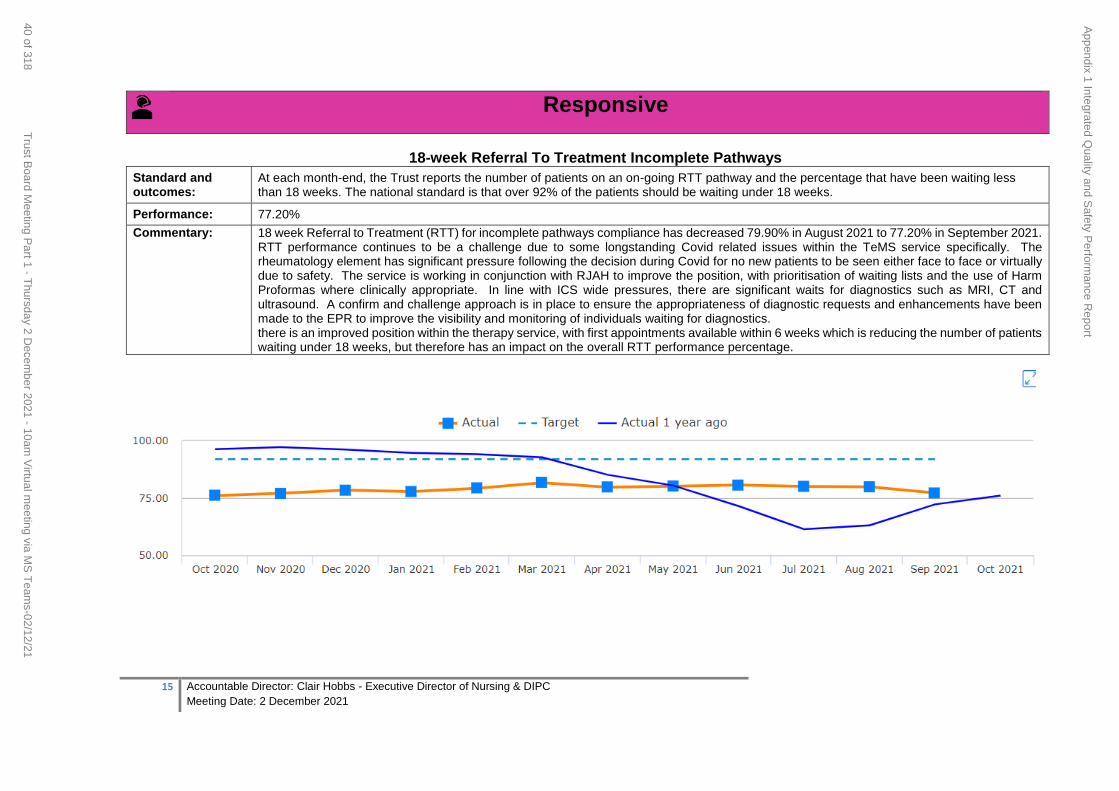
15 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Responsive
18-week Referral To Treatment Incomplete Pathways
Standard and outcomes:
At each month-end, the Trust reports the number of patients on an on-going RTT pathway and the percentage that have been waiting less than 18 weeks. The national standard is that over 92% of the patients should be waiting under 18 weeks.
Performance: 77.20%
Commentary: 18 week Referral to Treatment (RTT) for incomplete pathways compliance has decreased 79.90% in August 2021 to 77.20% in September 2021. RTT performance continues to be a challenge due to some longstanding Covid related issues within the TeMS service specifically. The rheumatology element has significant pressure following the decision during Covid for no new patients to be seen either face to face or virtually due to safety. The service is working in conjunction with RJAH to improve the position, with prioritisation of waiting lists and the use of Harm Proformas where clinically appropriate. In line with ICS wide pressures, there are significant waits for diagnostics such as MRI, CT and ultrasound. A confirm and challenge approach is in place to ensure the appropriateness of diagnostic requests and enhancements have been made to the EPR to improve the visibility and monitoring of individuals waiting for diagnostics. there is an improved position within the therapy service, with first appointments available within 6 weeks which is reducing the number of patients waiting under 18 weeks, but therefore has an impact on the overall RTT performance percentage.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
40 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
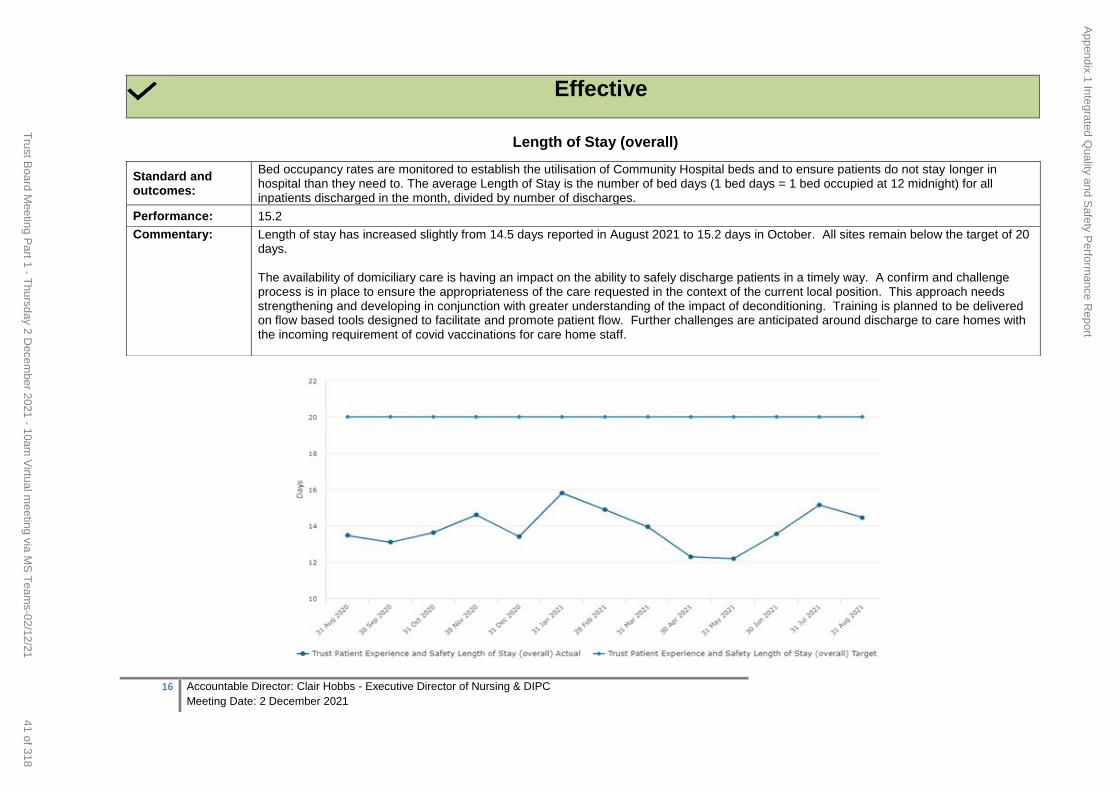
16 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Effective
Length of Stay (overall)
Standard and outcomes:
Bed occupancy rates are monitored to establish the utilisation of Community Hospital beds and to ensure patients do not stay longer in hospital than they need to. The average Length of Stay is the number of bed days (1 bed days = 1 bed occupied at 12 midnight) for all inpatients discharged in the month, divided by number of discharges.
Performance: 15.2
Commentary: Length of stay has increased slightly from 14.5 days reported in August 2021 to 15.2 days in October. All sites remain below the target of 20 days. The availability of domiciliary care is having an impact on the ability to safely discharge patients in a timely way. A confirm and challenge process is in place to ensure the appropriateness of the care requested in the context of the current local position. This approach needs strengthening and developing in conjunction with greater understanding of the impact of deconditioning. Training is planned to be delivered on flow based tools designed to facilitate and promote patient flow. Further challenges are anticipated around discharge to care homes with the incoming requirement of covid vaccinations for care home staff.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
41 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
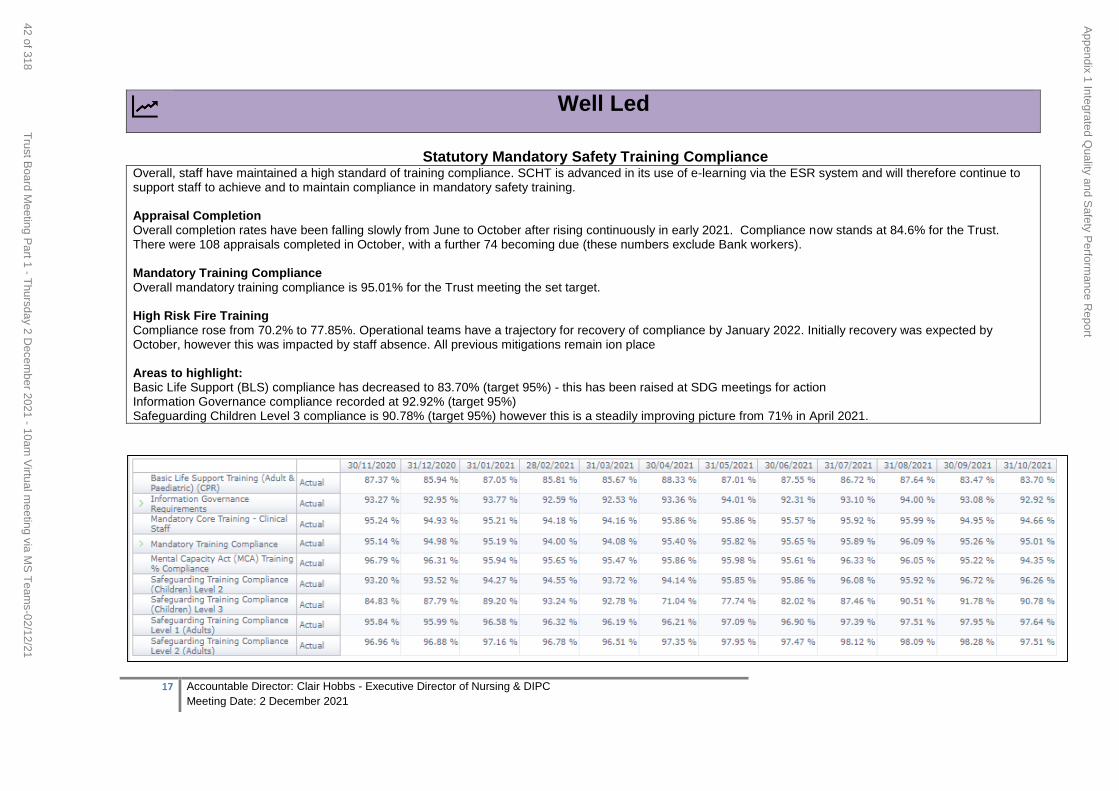
17 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Well Led
Statutory Mandatory Safety Training Compliance
Overall, staff have maintained a high standard of training compliance. SCHT is advanced in its use of e-learning via the ESR system and will therefore continue to support staff to achieve and to maintain compliance in mandatory safety training. Appraisal Completion Overall completion rates have been falling slowly from June to October after rising continuously in early 2021. Compliance now stands at 84.6% for the Trust. There were 108 appraisals completed in October, with a further 74 becoming due (these numbers exclude Bank workers). Mandatory Training Compliance Overall mandatory training compliance is 95.01% for the Trust meeting the set target. High Risk Fire Training Compliance rose from 70.2% to 77.85%. Operational teams have a trajectory for recovery of compliance by January 2022. Initially recovery was expected by October, however this was impacted by staff absence. All previous mitigations remain ion place Areas to highlight: Basic Life Support (BLS) compliance has decreased to 83.70% (target 95%) - this has been raised at SDG meetings for action Information Governance compliance recorded at 92.92% (target 95%) Safeguarding Children Level 3 compliance is 90.78% (target 95%) however this is a steadily improving picture from 71% in April 2021.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
42 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
18 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Well Led
Sickness Rates - Trust Standard and outcomes:
Supporting staff attendance at work - aiming for less than 4.5% of our staff to be absent from work at any one time
Performance: 5.24%
Commentary:
Recorded sickness absence in October at 5.24% was higher than average for recent years. Mental health remains the most common reason for sickness absence, with infectious disease as the second most prevalent cause. Coronavirus accounted for 14% of all sickness absence, equating to just over 9wte people absent on any given day (unchanged from September). Of these, 9 people (6.1wte) were long term cases and 29 people (6.4wte over the month) were short term. By staff group, estates and ancillary and additional clinical services are showing the highest sickness rates in October 2021. The 3 operational areas showing the highest rates of sickness during the month are Single Point of Referral, Whitchurch Ward and Bishops Castle Ward.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
43 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21

19 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
44 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
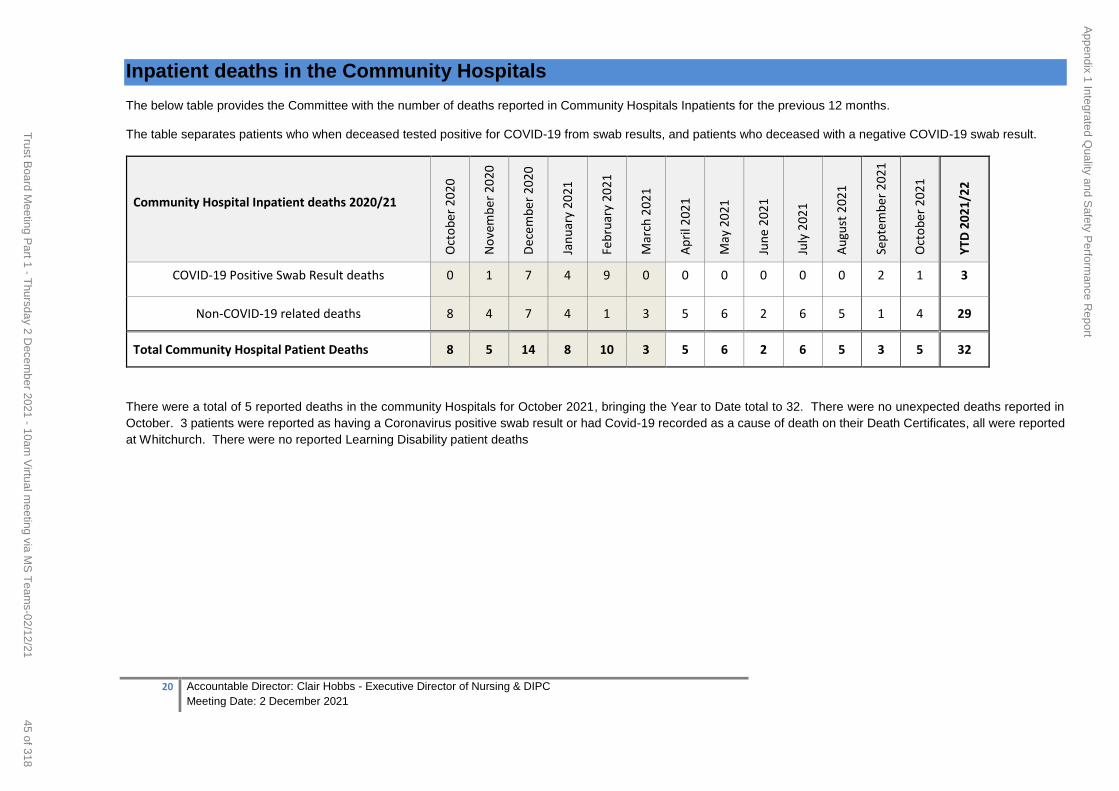
20 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Inpatient deaths in the Community Hospitals
The below table provides the Committee with the number of deaths reported in Community Hospitals Inpatients for the previous 12 months.
The table separates patients who when deceased tested positive for COVID-19 from swab results, and patients who deceased with a negative COVID-19 swab result.
Community Hospital Inpatient deaths 2020/21
Oct
ob
er 2
020
No
vem
ber
20
20
Dec
emb
er 2
020
Jan
uar
y 20
21
Feb
ruar
y 20
21
Mar
ch 2
021
Ap
ril 2
021
May
20
21
Jun
e 2
021
July
202
1
Au
gust
202
1
Sep
tem
ber
20
21
Oct
ob
er 2
021
YT
D 2
021
/22
COVID-19 Positive Swab Result deaths 0 1 7 4 9 0 0 0 0 0 0 2 1 3
Non-COVID-19 related deaths 8 4 7 4 1 3 5 6 2 6 5 1 4 29
Total Community Hospital Patient Deaths 8 5 14 8 10 3 5 6 2 6 5 3 5 32
There were a total of 5 reported deaths in the community Hospitals for October 2021, bringing the Year to Date total to 32. There were no unexpected deaths reported in
October. 3 patients were reported as having a Coronavirus positive swab result or had Covid-19 recorded as a cause of death on their Death Certificates, all were reported
at Whitchurch. There were no reported Learning Disability patient deaths
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
45 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
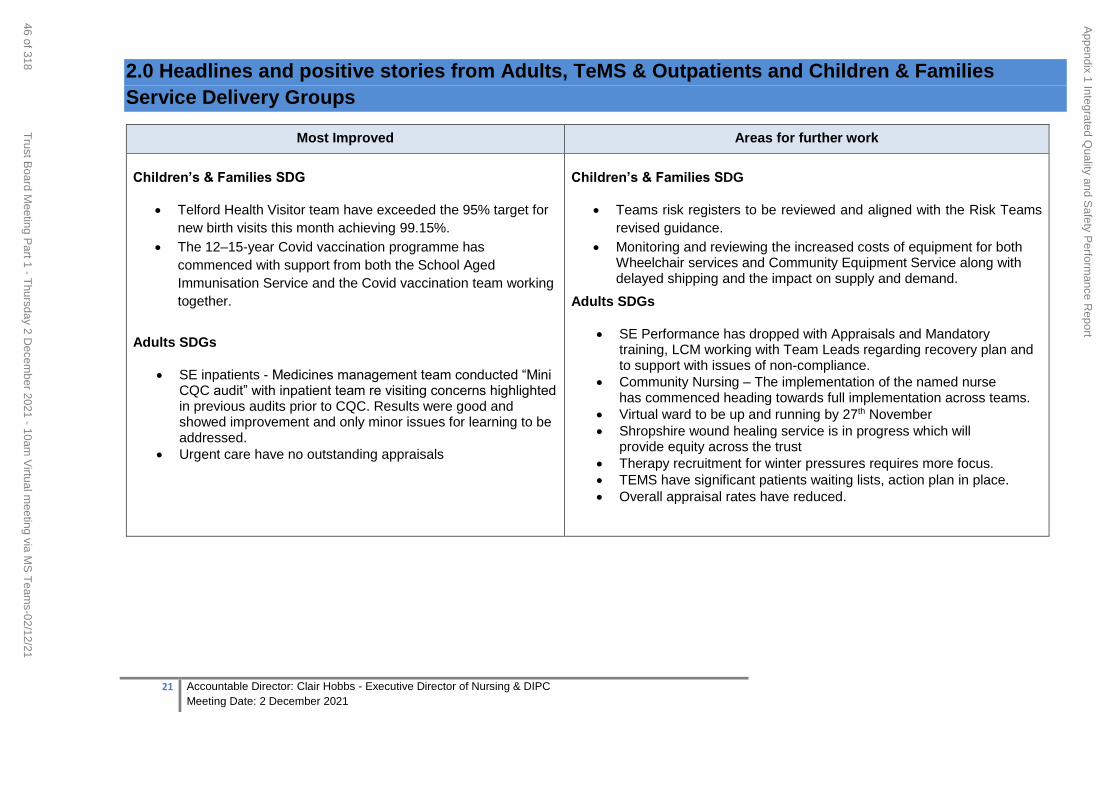
21 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
2.0 Headlines and positive stories from Adults, TeMS & Outpatients and Children & Families
Service Delivery Groups
Most Improved Areas for further work
Children’s & Families SDG
Telford Health Visitor team have exceeded the 95% target for
new birth visits this month achieving 99.15%.
The 12–15-year Covid vaccination programme has
commenced with support from both the School Aged
Immunisation Service and the Covid vaccination team working
together.
Adults SDGs
SE inpatients - Medicines management team conducted “Mini CQC audit” with inpatient team re visiting concerns highlighted in previous audits prior to CQC. Results were good and showed improvement and only minor issues for learning to be addressed.
Urgent care have no outstanding appraisals
Children’s & Families SDG
Teams risk registers to be reviewed and aligned with the Risk Teams
revised guidance.
Monitoring and reviewing the increased costs of equipment for both Wheelchair services and Community Equipment Service along with delayed shipping and the impact on supply and demand.
Adults SDGs
SE Performance has dropped with Appraisals and Mandatory training, LCM working with Team Leads regarding recovery plan and to support with issues of non-compliance.
Community Nursing – The implementation of the named nurse has commenced heading towards full implementation across teams.
Virtual ward to be up and running by 27th November
Shropshire wound healing service is in progress which will provide equity across the trust
Therapy recruitment for winter pressures requires more focus.
TEMS have significant patients waiting lists, action plan in place.
Overall appraisal rates have reduced.
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
46 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
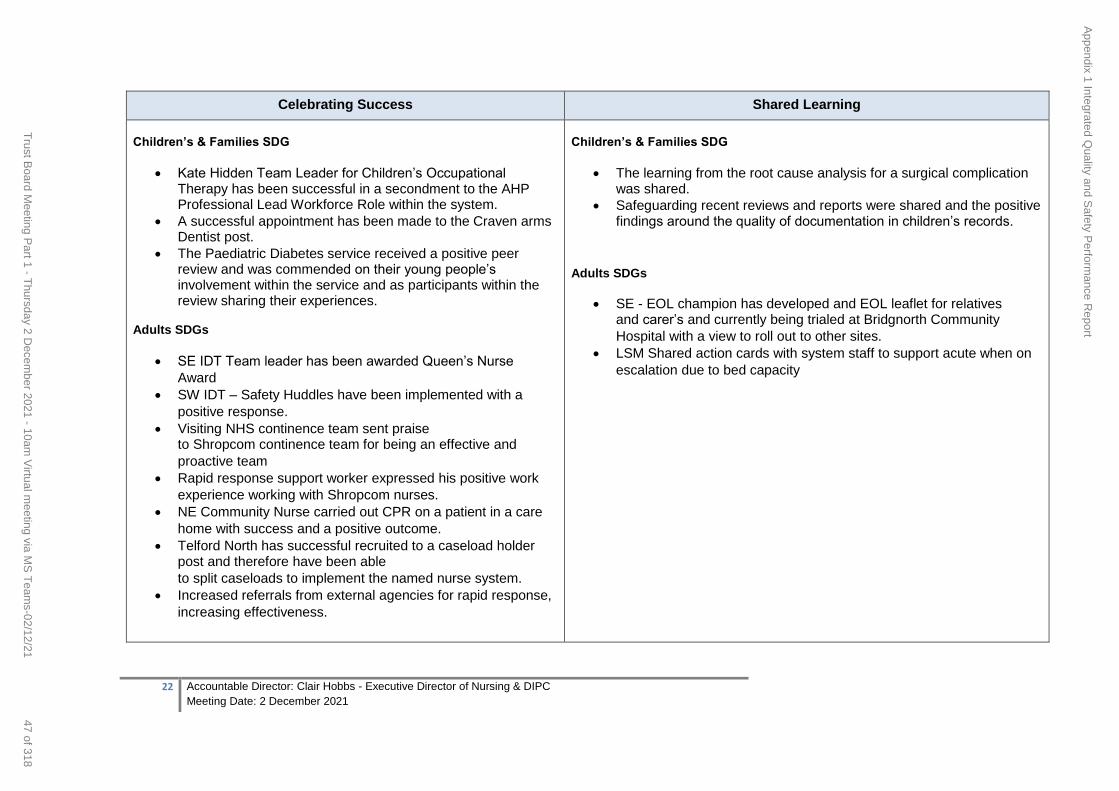
22 Accountable Director: Clair Hobbs - Executive Director of Nursing & DIPC
Meeting Date: 2 December 2021
Celebrating Success Shared Learning
Children’s & Families SDG
Kate Hidden Team Leader for Children’s Occupational Therapy has been successful in a secondment to the AHP Professional Lead Workforce Role within the system.
A successful appointment has been made to the Craven arms Dentist post.
The Paediatric Diabetes service received a positive peer review and was commended on their young people’s involvement within the service and as participants within the review sharing their experiences.
Adults SDGs
SE IDT Team leader has been awarded Queen’s Nurse
Award SW IDT – Safety Huddles have been implemented with a
positive response. Visiting NHS continence team sent praise
to Shropcom continence team for being an effective and
proactive team Rapid response support worker expressed his positive work
experience working with Shropcom nurses. NE Community Nurse carried out CPR on a patient in a care
home with success and a positive outcome. Telford North has successful recruited to a caseload holder
post and therefore have been able
to split caseloads to implement the named nurse system. Increased referrals from external agencies for rapid response,
increasing effectiveness.
Children’s & Families SDG
The learning from the root cause analysis for a surgical complication was shared.
Safeguarding recent reviews and reports were shared and the positive findings around the quality of documentation in children’s records.
Adults SDGs
SE - EOL champion has developed and EOL leaflet for relatives and carer’s and currently being trialed at Bridgnorth Community
Hospital with a view to roll out to other sites. LSM Shared action cards with system staff to support acute when on
escalation due to bed capacity
Appendix 1 Integrated Q
uality and Safety P
erformance R
eport
47 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
REPORT COVER SHEET Report Title: Quarterly Guardian for Junior Doctor Safe Working Report Meeting: Quality and Safety Committee Author: Dr Jane Povey Accountable
Director: Dr Jane Povey
Other meetings or Committee presented to or previously agreed at:
Meeting or Committee Date Reviewed
Strategic goals this report relates to: (tick as appropriate) To deliver high
quality care To deliver integrated
care To support people to
live the lives they want to lead
To deliver sustainable community
services
√ √ √ √
Relevance to Board Assurance Framework : (tick as appropriate) Clinical
Quality & Safety
Long term financial
sustainability of the Trust
Healthcare Systems
Organisational culture
Optimising use of technology
Covid19
√
Relevance to Well-led domains (CQC & NHSE/I): (tick as appropriate) leadership capacity and capability
√
clear vision and credible strategy
culture clear roles and responsibilities
clear and effective risk management
appropriate and accurate information
learning, continuous improvement and innovation
Stakeholders engaged and involved
Relevance to CQC domains: (tick as appropriate)
Safe √ Caring √ Responsive √ Effective √ Well led √
Impacts and Implications? YES or NO
If yes, what impact or implication
Patient safety & experience YES
Yes, quality assurance to the process from a safety perspective
Equality & Inclusion
Financial (revenue & capital) YES
Yes, compensation if worked more than their Contractual hours
IG Governance Toolkit
101 of 560Quality & Safety Committee meeting 18.11.2021 - 9.30 a.m. - 12.30 p.m.. via MS Teams-18/11/21
Meeting Date: 2 Dec 2021 Agenda Item: 10
Enclosure Number: 6
1 Accountable Director: Dr Jane Povey Meeting Date: 2 December 2021
Appendix 2 - Quarterly Guardian for Junior Doctor Safe Working Report
48 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
OD/Workforce YES Yes, challenges to rota compliance
Legal
Relevance to Corporate Risk Register (Risk No/Name)
Aim of the report (a concise statement of the purpose of this report)
This report provides assurance to the Board that trainee doctors at Shropshire Community Health NHS Trust have safe working hours and conditions in order to maintain doctor and patient safety. This assurance is collated from and Shrewsbury and Telford Hospitals NHS Trust’s (SATH) Guardian of Safe Working Hours (GOSW), our trainees being employed by SATH. To respond to the committee’s request to receive feedback from our junior doctors on their experience working in SCHT. Assessment and summary of key points in report (include analysis and consideration of issues, options,
risks and mitigations. Also include good practice, required improvements, and timescales. If appropriate, include a judgement on the level of assurance the report provides: Substantial: Moderate: Limited: None)
The GoSW for Shrewsbury and Telford Hospital NHS Trust and for the Shropshire Community Health NHS Trust continues in the role since July 2016 to champion safe working hours and ensure compliance with an Exception Reporting system as mandated in the TCS Junior Doctor Contact 2016. Junior trainees can use this process to report hours worked over, missed rest breaks, and differences in service commitments and variations in educational opportunities. The GoSW maintains an oversight of all reports and ensures that all reports are addressed in a timely manner.
During the reporting period 1 Aug – 31 Oct 2021 there were 3 doctors in training working in SCHT) They raised no concerns during this period.
During October the GoSW held two informal ‘Drop in Sessions’ that were kindly sponsored by the British Medical Association (BMA) and held at each site to ensure trainees have an opportunity to share and raise concerns.
Purpose of the Report (tick as appropriate)
Consider for Action
Give Approval Accept Assurance
√Provide Information
Key Recommendations
The Board are asked to agree the level of assurance provided by this report.
2 Accountable Director: Dr Jane Povey Meeting Date: 2 December 2021
Appendix 2 - Quarterly Guardian for Junior Doctor Safe Working Report
49 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
REPORT COVER SHEET
Report Title: Clinical Effectiveness Report Apr-21 to Sep-21
Meeting: Board
Author: M Bramble F Davies
Accountable Director:
Dr J Povey
Other meetings or Committee presented to or previously agreed at:
Meeting or Committee Date Reviewed
Quality and Safety Committee 18 November 2021
Quality and Safety Delivery Group
10 November 2021
Strategic goals this report relates to: (tick as appropriate)
To deliver high quality care
To deliver integrated care
To support people to live the lives they
want to lead
To deliver sustainable community
services
Relevance to Board Assurance Framework : (tick as appropriate)
Clinical Quality &
Safety
Long term financial
sustainability of the Trust
Healthcare Systems
Organisational culture
Optimising use of
technology
Covid19
Relevance to Well-led domains (CQC & NHSE/I): (tick as appropriate)
leadership capacity and capability
clear vision and credible strategy
culture clear roles and responsibilities
clear and effective risk management
appropriate and accurate information
learning, continuous improvement and innovation
Stakeholders engaged and involved
Relevance to CQC domains: (tick as appropriate)
Safe Caring Responsive Effective Well led
Impacts and Implications? YES or NO
If yes, what impact or implication
Patient safety & experience YES
Compliance with audit standards and adherence to NICE recommendations will result in improved outcomes for patients
Meeting Date: 2 December 2021
Agenda Item: 10
Enclosure Number: 7
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
50 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
Equality & Inclusion
Financial (revenue & capital)
IG Governance Toolkit
OD/Workforce
Legal
Relevance to Corporate Risk
Register (Risk No/Name)
Aim of the report
To provide assurance to Quality and Safety Committee around the delivery of Clinical Audit and NICE Guidance for the period of April 2021 – September 2021. To provide an update on our evolving Research & Innovation programme and ambition.
Assessment and summary of key points in report
Clinical Audit & NICE Guidance
Implementation of the clinical audit plan has progressed well over the period of this report
Only three audits were delayed as at 30/9/21, with evidence of actions to get back on track in all
Eight audits were completed, four demonstrated full compliance with audit standards and four partial compliance. Action plans have been developed and approved in relation to the latter; two had been implemented and two were still in progress at period end
The Trust submitted data to four of the five National Clinical Audits in which it was eligible to take part. Data is no longer being directly submitted to the National Early Inflammatory Arthritis audit as The Robert Jones and Agnes Hunt Orthopaedic Hospital (RJAH) has taken over management of the Early Arthritis clinic and is now responsible for all aspects of the audit submission
The Trust is again signed up to participate in the NHSE/I learning disability improvement standards project
The 2021/22 CQUIN programme remains suspended although the scheme for 2022/23 is currently in development
The Trust was fully compliant in one of the two NICE baseline assessments completed during the period. An action plan has been developed to address in areas of non-compliance in the other
Research & Innovation
The amount of research undertaken in SCHT continues to grow
The R&I team have been successful in attracting the first commercially funded research to the Trust
The Team was a finalist in the West Midlands Clinical Research Network Annual Awards for the third year in succession
The collaboration agreement with MPFT has now been extended to five years The report was reviewed at Quality and Safety Delivery Group on 10/11/21 – feedback from the Group was that the report was helpful. The report was reviewed at Quality and Safety Committee on 18/11/21. Following an update at the meeting on the issue of pressure ulcers in community teams, Committee was assured by the fact that an audit of use of the ADDER and self-neglect framework had been undertaken and that an audit on assessment and documentation of pressure ulcers would be included in the 2022/23 clinical audit plan.
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
51 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
3 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
Purpose of the Report (tick as appropriate)
Consider for Action
Give Approval Accept Assurance
Provide Information
Key Recommendations
The Board is asked to:
Receive the report and accept as assurance against clinical audit and NICE guidance adherence
Accept the Research & Innovation update
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
52 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
4 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
CLINICAL EFFECTIVESS REPORT APRIL 2021 – SEPTEMBER 2021
The purpose of this report is to provide assurance to Quality and Safety Committee around the delivery of the Clinical Audit, NICE Guidance and Research and Development Programmes. The report will form the basis of discussion on how to evolve these programmes going forward, with the focus being on their impact of the quality and safety of care provided to patients.
2.0 Context
In terms of the national context:
National Asthma and Chronic Obstructive Pulmonary Disease Audit Programme (NACAP). Pulmonary Rehabilitation Service. Data is submitted to the clinical audit element of this project on a continuous basis, with the last reporting period being 1/10/20-31/3/21. The Trust submitted data to the case ascertainment and workforce planning survey of PR services in October 2021 and is about to start submission to the organisational element, completion of which is due by 26/11/21. The most recent report published for cases assessed between 1/6/19 and 30/11/19 has been reviewed by the Trust and an action plan produced to address areas of non-compliance; the outcomes from this audit are detailed in Section 3.0 of this report.
National Audit of Care at the End of Life (NACEL). The Trust has submitted data to all elements of the third round of NACEL which includes: an organisational level audit, a case note review, a quality survey of bereaved relatives and carers and a staff reported measure to garner staff review and experiences on delivery end of life care in hospital. As the maximum number of staff survey submissions allowed was 20, the survey has also been implemented locally to enable all staff – clinical and non-clinical – providing care, treatment and support to patients at the end of their lives to take part.
National Audit of Inpatient Falls. A report has been published for the organisational element of this audit undertaken in 2020 and is under review by the Trust Falls Steering Group. The Trust is still not submitting data to the clinical audit element of this project because no cases have been identified for inclusion via the National Hip Fracture Database (NHFD). Notification to the NHFD of a fracture sustained as a result of an inpatient fall is the responsibility of the local acute trust but identification of the location of the fall as SCHT should generate an alert to SCHT that a case for audit has been identified. Discussions are taking place with SaTH to resolve this issue.
National Diabetes Foot Audit. Data continues to be submitted by the Trust to this audit which
is run on a continuous data collection basis.
1.0 Introduction
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
53 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
5 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
National Early Inflammatory Arthritis Audit. The Trust is no longer submitting data directly
to this audit. The Robert Jones and Agnes Hunt Orthopaedic Hospital (RJAH) will be taking
over management of the Early Arthritis clinic in relation to the TeMS Rheumatology service and
it has been agreed that RJAH will be responsible for the submission going forward.
NHSE/I Learning Disability Improvement Standards. The Trust has once again signed up to
participate in this project which includes an organisational level data collection, a staff survey
and a patient survey. The project opens in November 2021 and closes in February 2022.
CQUIN. The operation of CQUIN will remain suspended for the remainder of this financial year due to the impact of the C19 pandemic, although the 2022/23 scheme is currently in development. One CQUIN being considered for Community Services is a malnutrition assessment CQUIN for people in community hospitals (underpinned by NICE quality standard 24). It was in the 2020/21 CQUIN scheme and NHSE/I is seeking views on this CQUIN to check that it remains appropriate. MUST scores (Malnutrition Universal Screening Tool) are already being recorded on Rio.
NICE guidance. The well-established process for reviewing and implementing NICE guidance within the Trust has continued throughout the period of this report. Major pieces of work have commenced in relation to the following guidance and will be reported on in the next Clinical Effectiveness report to Committee:
o NG197 Shared decision making o NG204 Babies, children and young people’s experience of healthcare o QS13 end of life care for adults
At a local health economy level:
The Trust is exploring the possibility of setting up a Quality Improvement Patient and Volunteer Group in conjunction with RJAH, with the aim of improving and increasing patient and volunteer involvement in QI activity locally. Both clinical audit and NICE guidance will be included as part of the remit of this group.
Discussions are being held about the possibility of procuring software from InPhase to assist with managing the programmes of clinical audit across the ICS. This software has already been procured by SaTH for this purpose.
Within the Trust, the progamme of clinical audit has progressed well over the period of this report.
Of the 28 projects listed on the programme, 8 were completed, 14 were in progress, three were delayed and four were not due to start within the period of this report1.
1 The breakdown of projects adds up to 29 not 28 because one national project is a continuous audit, for which a report
has also been published in respect of 2019 data collection and reviewed by the Trust
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
54 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
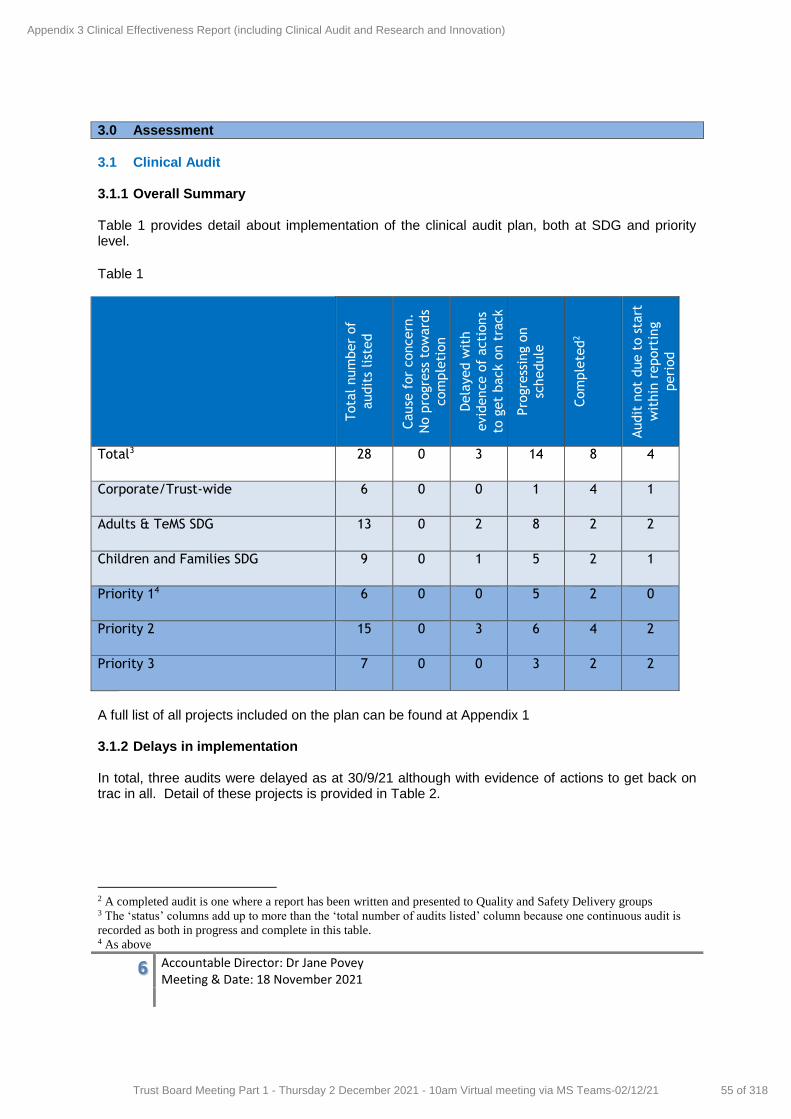
6 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
3.0 Assessment
3.1 Clinical Audit 3.1.1 Overall Summary Table 1 provides detail about implementation of the clinical audit plan, both at SDG and priority level.
Table 1
Tota
l num
ber
of
audit
s list
ed
Cause
for
concern
.
No p
rogre
ss t
ow
ard
s
com
ple
tion
Dela
yed w
ith
evid
ence o
f acti
ons
to g
et
back o
n t
rack
Pro
gre
ssin
g o
n
schedule
Com
ple
ted
2
Audit
not
due t
o s
tart
wit
hin
report
ing
peri
od
Total3 28 0 3 14 8 4
Corporate/Trust-wide 6 0 0 1 4 1
Adults & TeMS SDG 13 0 2 8 2 2
Children and Families SDG 9 0 1 5 2 1
Priority 14 6 0 0 5 2 0
Priority 2 15
0 3 6 4 2
Priority 3 7 0 0 3 2 2
A full list of all projects included on the plan can be found at Appendix 1 3.1.2 Delays in implementation In total, three audits were delayed as at 30/9/21 although with evidence of actions to get back on trac in all. Detail of these projects is provided in Table 2.
2 A completed audit is one where a report has been written and presented to Quality and Safety Delivery groups 3 The ‘status’ columns add up to more than the ‘total number of audits listed’ column because one continuous audit is
recorded as both in progress and complete in this table. 4 As above
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
55 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
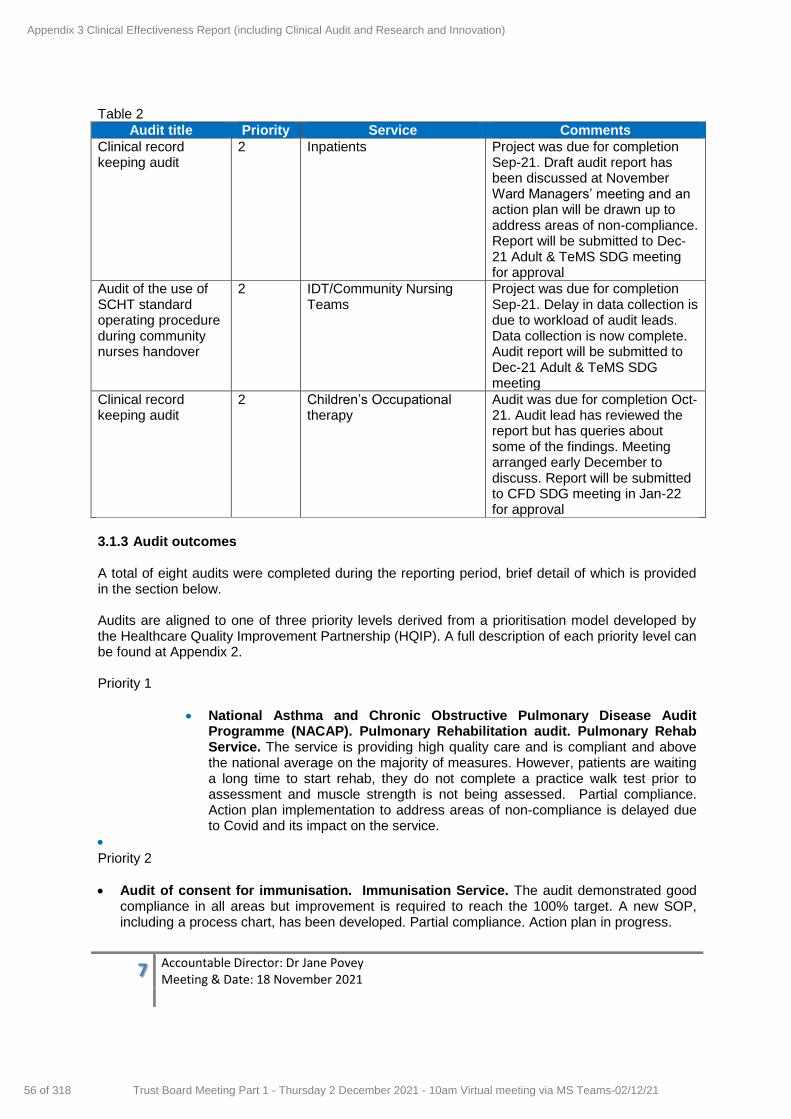
7 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
Table 2
Audit title Priority Service Comments
Clinical record keeping audit
2 Inpatients Project was due for completion Sep-21. Draft audit report has been discussed at November Ward Managers’ meeting and an action plan will be drawn up to address areas of non-compliance. Report will be submitted to Dec-21 Adult & TeMS SDG meeting for approval
Audit of the use of SCHT standard operating procedure during community nurses handover
2 IDT/Community Nursing Teams
Project was due for completion Sep-21. Delay in data collection is due to workload of audit leads. Data collection is now complete. Audit report will be submitted to Dec-21 Adult & TeMS SDG meeting
Clinical record keeping audit
2 Children’s Occupational therapy
Audit was due for completion Oct-21. Audit lead has reviewed the report but has queries about some of the findings. Meeting arranged early December to discuss. Report will be submitted to CFD SDG meeting in Jan-22 for approval
3.1.3 Audit outcomes
A total of eight audits were completed during the reporting period, brief detail of which is provided in the section below. Audits are aligned to one of three priority levels derived from a prioritisation model developed by the Healthcare Quality Improvement Partnership (HQIP). A full description of each priority level can be found at Appendix 2. Priority 1
National Asthma and Chronic Obstructive Pulmonary Disease Audit Programme (NACAP). Pulmonary Rehabilitation audit. Pulmonary Rehab Service. The service is providing high quality care and is compliant and above the national average on the majority of measures. However, patients are waiting a long time to start rehab, they do not complete a practice walk test prior to assessment and muscle strength is not being assessed. Partial compliance. Action plan implementation to address areas of non-compliance is delayed due to Covid and its impact on the service.
Priority 2
Audit of consent for immunisation. Immunisation Service. The audit demonstrated good compliance in all areas but improvement is required to reach the 100% target. A new SOP, including a process chart, has been developed. Partial compliance. Action plan in progress.
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
56 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
8 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
Rio alerts for Looked After Children (LAC). LAC Service. Full compliance was achieved in relation to adding alerts and removing alerts. No alerts were added by anyone outside of the LAC service. The proportion of alerts being reviewed increased from 61% to 73%. The review of alerts has been embedded into the Administrator process and is completed at the time of the health assessment. The SOP has been updated. Partial compliance. Action plan fully implemented.
Quality assurance audit of the LAC initial health assessment (Qs 1 & 2). LAC Service. This is a quarterly audit. The results remain good across all sections for both local authorities, with the overall quality of reports identified as outstanding. The detail and the actions plans continue to improve along with all medicals reinstated. Full compliance.
Quality assurance audit of the LAC review health assessment (Qs 1 & 2). LAC Service. Overall improvements were maintained and high-quality assessments recorded. Full compliance.
Quality assessment of leaving care health summaries (Qs 1 & 2). LAC Service. All of the 21 summaries reviewed were rated as Good overall. Four young people did not contribute to the summary but this was because they declined to do so. In three cases, the young person’s Social Worker was not informed about or given the opportunity to contribute to the summary but this was at the request of the young person. Full compliance.
Audit of completion of the WHO Checklist. Bridgnorth Day Surgery Unit. This audit is carried out annually. The checklist was present in the notes, completed and signed in 100% of the cases audited. Full compliance.
Priority 3
Audit of NICE guidance CG128 Autism spectrum disorder in under 19s: recognition, referral and diagnosis. Community Paediatrics. The audit findings highlighted that the final CDC assessment process meets all quality statements. However, Wood’s light is not being used for skin assessments, history, examination and discussion about possible ASD is not always documented, there is a long wait between Community Paediatric decision to refer to the CDC and triage of referral and a six-week following up is not being routinely offered. Psychology input is also missing. Wood’s light is to be made available at all assessment areas, team are to be reminded of the need to complete documentation fully, process mapping, technology review and backlog initiative to be undertaken to address long waits following referral, as well as an alternative pathway for very young children. Partial compliance. Action plan in progress.
3.2 NICE guidance An update of newly-published NICE guidance is produced each month and reviewed for relevance by the Quality Facilitator, the Chief Pharmacist and the Clinical Leads for Quality prior to submission to SDGs.
Between 1/4/21 and 30/9/21 126 separate pieces of guidance or advice were published by NICE, 11 of which were relevant to the Trust for information only. Baseline assessments of compliance are only undertaken in relation to NICE guidelines and NICE quality standards and seven were requested during the period as is shown in table 3 below.
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
57 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
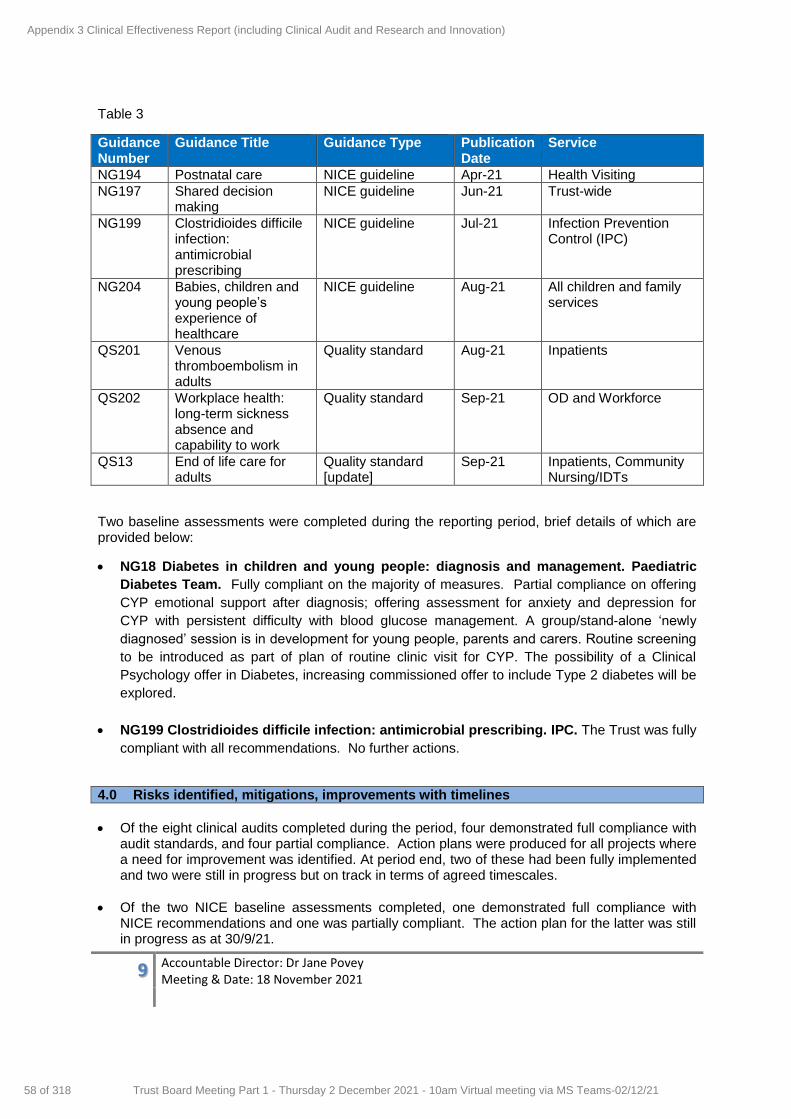
9 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
Table 3
Guidance Number
Guidance Title Guidance Type Publication Date
Service
NG194 Postnatal care NICE guideline Apr-21 Health Visiting
NG197 Shared decision making
NICE guideline Jun-21 Trust-wide
NG199 Clostridioides difficile infection: antimicrobial prescribing
NICE guideline Jul-21 Infection Prevention Control (IPC)
NG204 Babies, children and young people’s experience of healthcare
NICE guideline Aug-21 All children and family services
QS201 Venous thromboembolism in adults
Quality standard Aug-21 Inpatients
QS202 Workplace health: long-term sickness absence and capability to work
Quality standard Sep-21 OD and Workforce
QS13 End of life care for adults
Quality standard [update]
Sep-21 Inpatients, Community Nursing/IDTs
Two baseline assessments were completed during the reporting period, brief details of which are provided below:
NG18 Diabetes in children and young people: diagnosis and management. Paediatric
Diabetes Team. Fully compliant on the majority of measures. Partial compliance on offering
CYP emotional support after diagnosis; offering assessment for anxiety and depression for
CYP with persistent difficulty with blood glucose management. A group/stand-alone ‘newly
diagnosed’ session is in development for young people, parents and carers. Routine screening
to be introduced as part of plan of routine clinic visit for CYP. The possibility of a Clinical
Psychology offer in Diabetes, increasing commissioned offer to include Type 2 diabetes will be
explored.
NG199 Clostridioides difficile infection: antimicrobial prescribing. IPC. The Trust was fully
compliant with all recommendations. No further actions.
4.0 Risks identified, mitigations, improvements with timelines
Of the eight clinical audits completed during the period, four demonstrated full compliance with audit standards, and four partial compliance. Action plans were produced for all projects where a need for improvement was identified. At period end, two of these had been fully implemented and two were still in progress but on track in terms of agreed timescales.
Of the two NICE baseline assessments completed, one demonstrated full compliance with NICE recommendations and one was partially compliant. The action plan for the latter was still in progress as at 30/9/21.
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
58 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21

10 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
Research and Innovation update
The R&I team have continued to grow the amount of research being undertaken in SCHT services and are currently 8th regionally for the number of participants recruited. The team have also been successful in attracting the first commercially funded research to the Trust, with trials being set up in Rheumatology and Dentistry; and a new research nurse being recruited to the Team to help to deliver this work. This success is reflected in the Team’s being finalists in the West Midlands Clinical Research Network Annual Awards for the third year in succession – this year for Team of the Year – and in receiving a Chair’s Award from the SCHT Board. The new Research PPIE Champions have continued to work alongside the team and receive support from the CRN and the team at MPFT and engagement with the CRN Participant in Research Experience Survey (PRES) continues; there is also a new suite of training materials on the R&I SharePoint site. The collaboration agreement with MPFT has now been extended to a five-year agreement to cement this activity and success, with the ambition to have the research delivery team employed directly with SCHT by the end of the year.
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
59 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
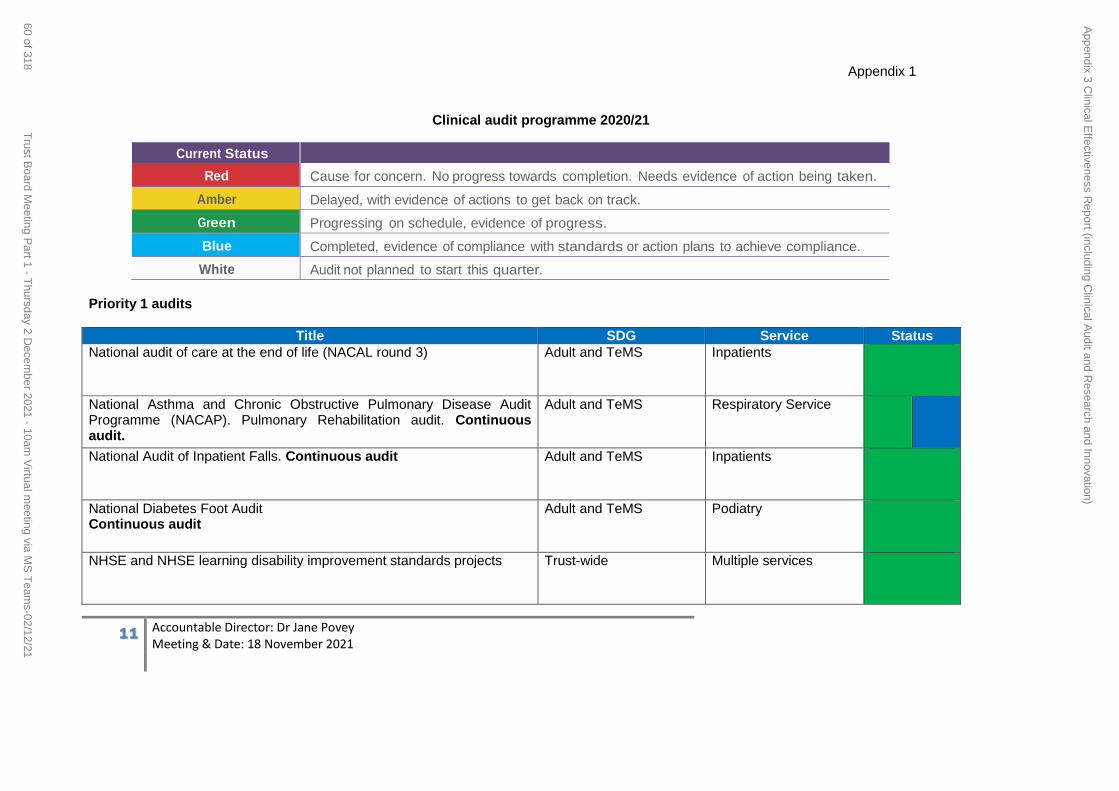
11 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
Clinical audit programme 2020/21
Current Status
Red Cause for concern. No progress towards completion. Needs evidence of action being taken.
Amber Delayed, with evidence of actions to get back on track.
Green Progressing on schedule, evidence of progress.
Blue Completed, evidence of compliance with standards or action plans to achieve compliance.
White Audit not planned to start this quarter.
Priority 1 audits
Title SDG Service Status
National audit of care at the end of life (NACAL round 3) Adult and TeMS Inpatients
National Asthma and Chronic Obstructive Pulmonary Disease Audit Programme (NACAP). Pulmonary Rehabilitation audit. Continuous audit.
Adult and TeMS Respiratory Service
National Audit of Inpatient Falls. Continuous audit Adult and TeMS Inpatients
National Diabetes Foot Audit Continuous audit
Adult and TeMS Podiatry
NHSE and NHSE learning disability improvement standards projects Trust-wide Multiple services
Appendix 1
Appendix 3 C
linical Effectiveness R
eport (including Clinical A
udit and Research and Innovation)
60 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
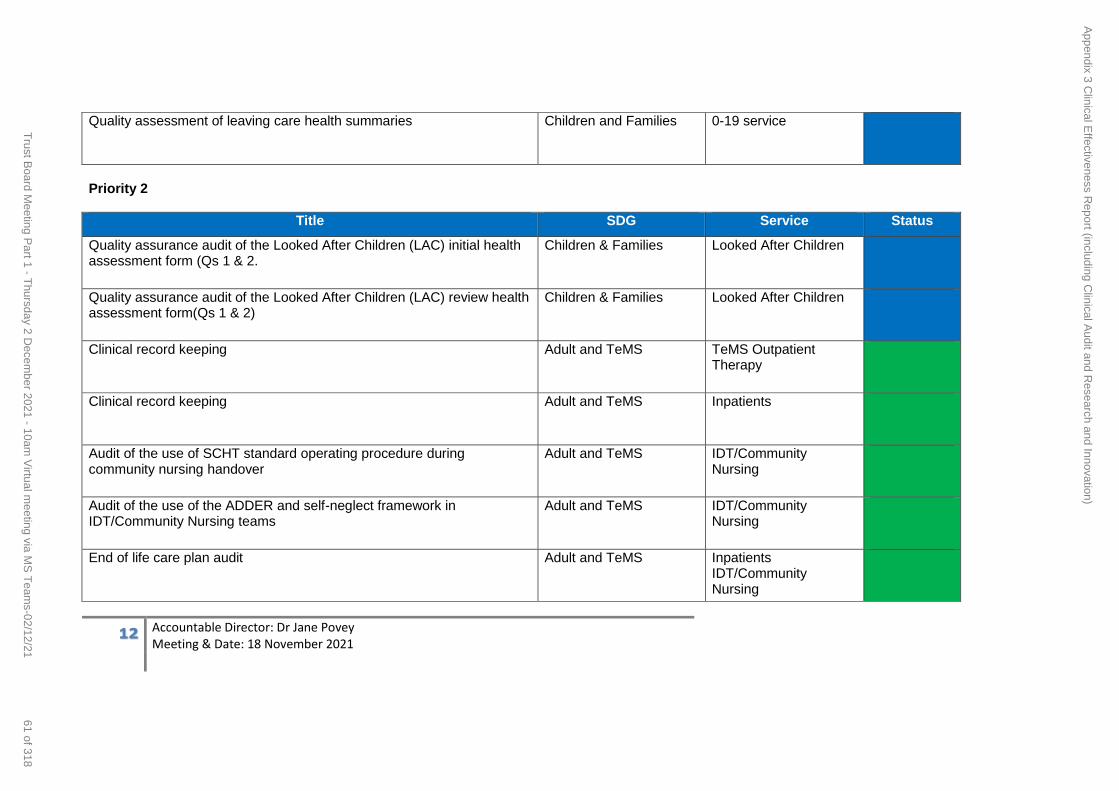
12 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
Quality assessment of leaving care health summaries Children and Families 0-19 service
Priority 2
Title SDG Service Status
Quality assurance audit of the Looked After Children (LAC) initial health assessment form (Qs 1 & 2.
Children & Families Looked After Children
Quality assurance audit of the Looked After Children (LAC) review health assessment form(Qs 1 & 2)
Children & Families Looked After Children
Clinical record keeping Adult and TeMS TeMS Outpatient Therapy
Clinical record keeping Adult and TeMS Inpatients
Audit of the use of SCHT standard operating procedure during community nursing handover
Adult and TeMS IDT/Community Nursing
Audit of the use of the ADDER and self-neglect framework in IDT/Community Nursing teams
Adult and TeMS IDT/Community Nursing
End of life care plan audit Adult and TeMS Inpatients IDT/Community Nursing
Appendix 3 C
linical Effectiveness R
eport (including Clinical A
udit and Research and Innovation)
61 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
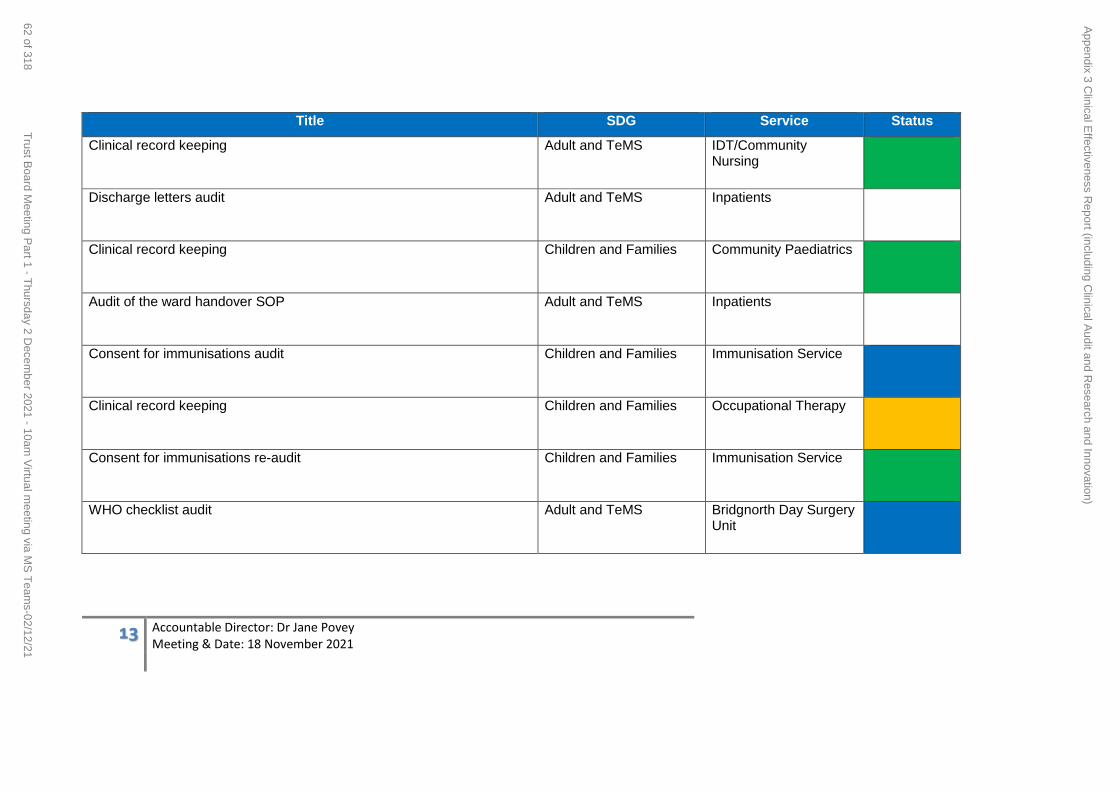
13 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
Title SDG Service Status
Clinical record keeping Adult and TeMS IDT/Community Nursing
Discharge letters audit Adult and TeMS Inpatients
Clinical record keeping Children and Families Community Paediatrics
Audit of the ward handover SOP Adult and TeMS Inpatients
Consent for immunisations audit Children and Families Immunisation Service
Clinical record keeping Children and Families Occupational Therapy
Consent for immunisations re-audit Children and Families Immunisation Service
WHO checklist audit Adult and TeMS Bridgnorth Day Surgery Unit
Appendix 3 C
linical Effectiveness R
eport (including Clinical A
udit and Research and Innovation)
62 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
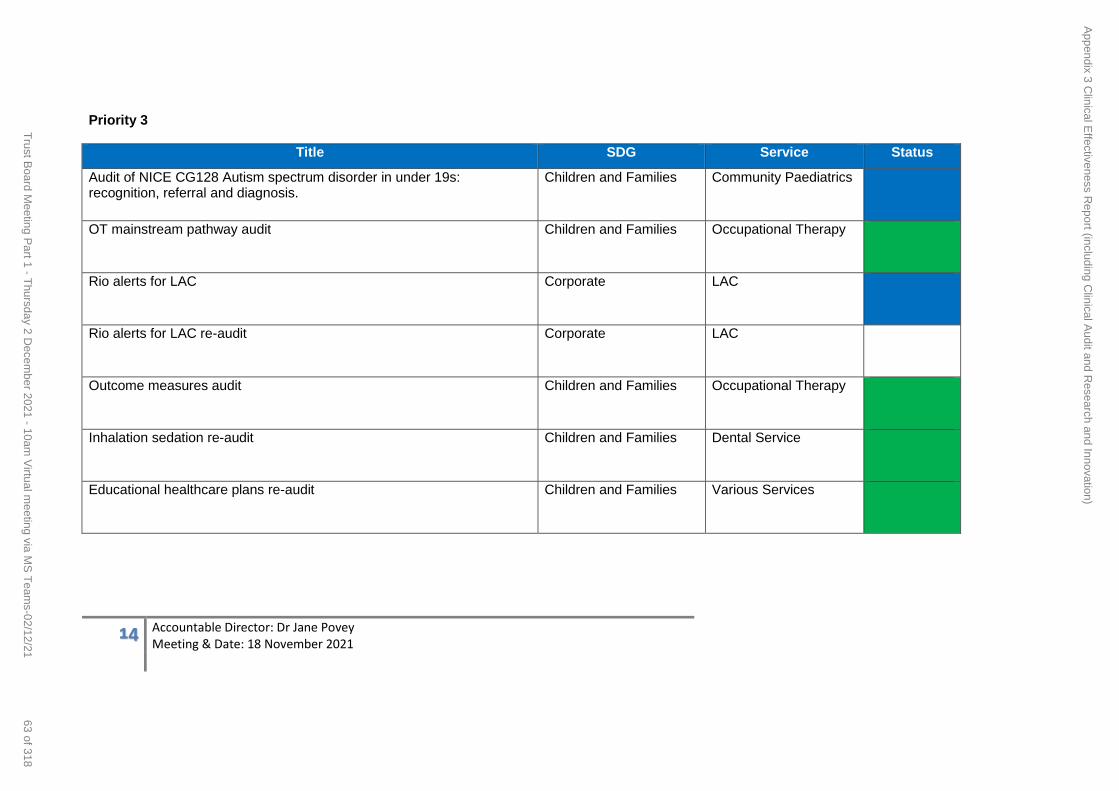
14 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
Priority 3
Title SDG Service Status
Audit of NICE CG128 Autism spectrum disorder in under 19s: recognition, referral and diagnosis.
Children and Families Community Paediatrics
OT mainstream pathway audit Children and Families Occupational Therapy
Rio alerts for LAC Corporate LAC
Rio alerts for LAC re-audit Corporate LAC
Outcome measures audit Children and Families Occupational Therapy
Inhalation sedation re-audit Children and Families Dental Service
Educational healthcare plans re-audit Children and Families Various Services
Appendix 3 C
linical Effectiveness R
eport (including Clinical A
udit and Research and Innovation)
63 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
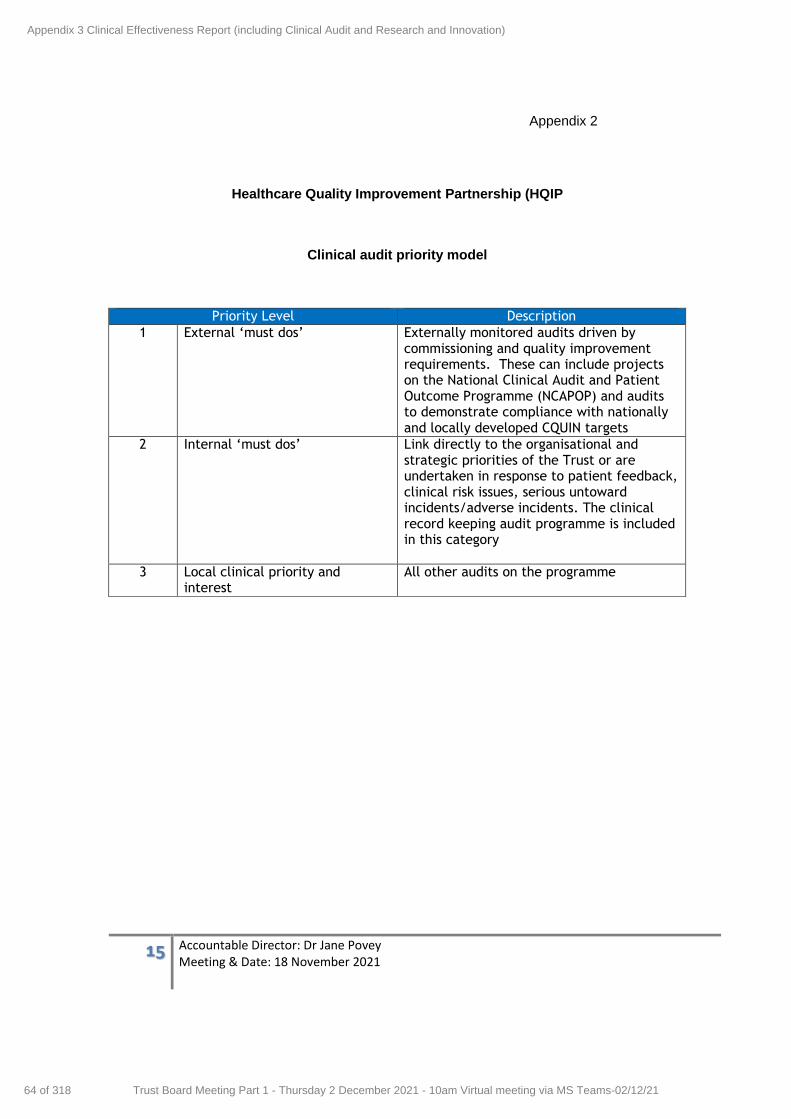
15 Accountable Director: Dr Jane Povey Meeting & Date: 18 November 2021
Healthcare Quality Improvement Partnership (HQIP
Clinical audit priority model
Priority Level Description
1 External ‘must dos’
Externally monitored audits driven by commissioning and quality improvement requirements. These can include projects on the National Clinical Audit and Patient Outcome Programme (NCAPOP) and audits to demonstrate compliance with nationally and locally developed CQUIN targets
2 Internal ‘must dos’ Link directly to the organisational and strategic priorities of the Trust or are undertaken in response to patient feedback, clinical risk issues, serious untoward incidents/adverse incidents. The clinical record keeping audit programme is included in this category
3 Local clinical priority and interest
All other audits on the programme
Appendix 2
Appendix 3 Clinical Effectiveness Report (including Clinical Audit and Research and Innovation)
64 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1 Accountable Director: Jane Povey Meeting Date: 02 Dec 2021
REPORT COVER SHEET Report Title: Learning from Deaths Report
Meeting: Trust Board Meeting
Author(s): Jane Povey, Sam Young, Alan Ferguson
Accountable Director:
Jane Povey Medical Director
Other meetings or Committee presented to or previously agreed at:
Meeting or Committee Date Reviewed
Quality and Safety Delivery Group
10 November 2021
Quality and Safety Committee
18 November 2021
Strategic goals this report relates to: (tick as appropriate)
To deliver high quality care
To deliver integrated care
To support people to live the lives they want
to lead
To deliver sustainable community
services
Relevance to Board Assurance Framework: (tick as appropriate)
Clinical Quality &
Safety
Long term financial
sustainability of the Trust
Healthcare Systems
Organisational culture
Optimising use of technology
Covid19
Relevance to Well-led domains (CQC & NHSE/I): (tick as appropriate)
leadership capacity and capability
clear vision and credible strategy
culture clear roles and responsibilities
clear and effective risk management
appropriate and accurate information
learning, continuous improvement and innovation
Stakeholders engaged and involved
Relevance to CQC domains: (tick as appropriate)
Safe Caring Responsive Effective Well led
Impacts and Implications? YES or NO
If yes, what impact or implication
Patient safety & experience Yes
Improving patient safety and experience
Equality & Inclusion Yes Personalising end of life care
Financial (revenue & capital)
IG Governance Toolkit
Meeting Date: 02 Dec 2021
Agenda Item: 10
Enclosure Number: 8
Appendix 4 Learning from Deaths Report
65 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2 Accountable Director: Jane Povey Meeting Date: 02 Dec 2021
OD/Workforce
Legal
Relevance to Corporate Risk
Register (Risk No/Name)
The Care Quality Commission
Regulations - this report
provides assurance as
follows:
Outcome 4 (Regulation 9) Care and welfare of people who use services
Outcome 14 (Regulation 23) Supporting staff
Outcome 16 (Regulation 10) Assessing and monitoring the quality of service provision
Duty of Candour (Regulation 20)
Aim of the report (a concise statement of the purpose of this report)
To provide the Trust Board with assurance that Shropshire Community Health NHS Trust (SCHT) has a robust internal Learning from Deaths review process to ensure that we learn from any patient deaths and ensure patient safety, clinical effectiveness and user experience form the core practice and principles of services.
To meet the National Learning from Deaths Framework requirement to collect and publish data to monitor trends in patients’ deaths within the Trust and report quarterly to the Trust Public Board meeting. To provide an update on work to learn from deaths beyond that required statutorily and the emergent system (ICS) approach to Learning from Deaths.
The key points of the report are:
For this Quarter 2 and Oct 2021 there have been 19 deaths reported within the Community Hospitals. Three deaths were reported with COVID-19 as their primary cause of death. There have been no unexpected deaths.
There has been one death of a patient with a Learning Disability
In addition to exploring and responding locally to learning from each community hospital death, the following themes have been recognised and are being addressed and impact demonstrated through our Learning from Deaths Lessons Learnt Improvement Plan.
Improving End of Life care
Improving monitoring of patient nutrition and hydration status and oral care
Improving clinical record keeping
Improving the timeliness of Learning from Death reporting
Use of self-neglect framework (safeguarding)
Staff wellbeing
Following the Learning from Deaths Reporting Audit, processes for reviewing and learning from deaths are being reviewed and strengthened. A new initial Learning from Deaths report form has been agreed is being piloted within the community hospitals and the community teams to enable us to learn from deaths in the community as well as in community hospitals.
A STW ICS Learning from Deaths Group has been established (reporting to System Quality Group). This group will:
enable us to approach learning from deaths opportunities as a system in addition to within organisations, including responding to the recommendations of the Niche review,
Appendix 4 Learning from Deaths Report
66 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
3 Accountable Director: Jane Povey Meeting Date: 02 Dec 2021
oversee the expansion of Medical Examiner function into community and primary care services.
Representatives are attending the new Regional Learning from Deaths Group.
No new risks have been identified
Assessment and summary of key points in report (include analysis and consideration of issues, options,
risks and mitigations. Also include good practice, required improvements, and timescales. If appropriate, include a judgement on the level of assurance the report provides: Substantial: Moderate: Limited: None)
Purpose of the Report (tick as appropriate)
Consider for Action
Give Approval Accept Assurance
Provide Information
Key Recommendations
The Trust Board are asked to:
Note the mortality data and themes detailed
Discuss and question the issues and work highlighted in the report
To agree the level of assurance provided by this report as recommended by the Quality and Safety Committee which proposed Substantive Assurance
Appendix 4 Learning from Deaths Report
67 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
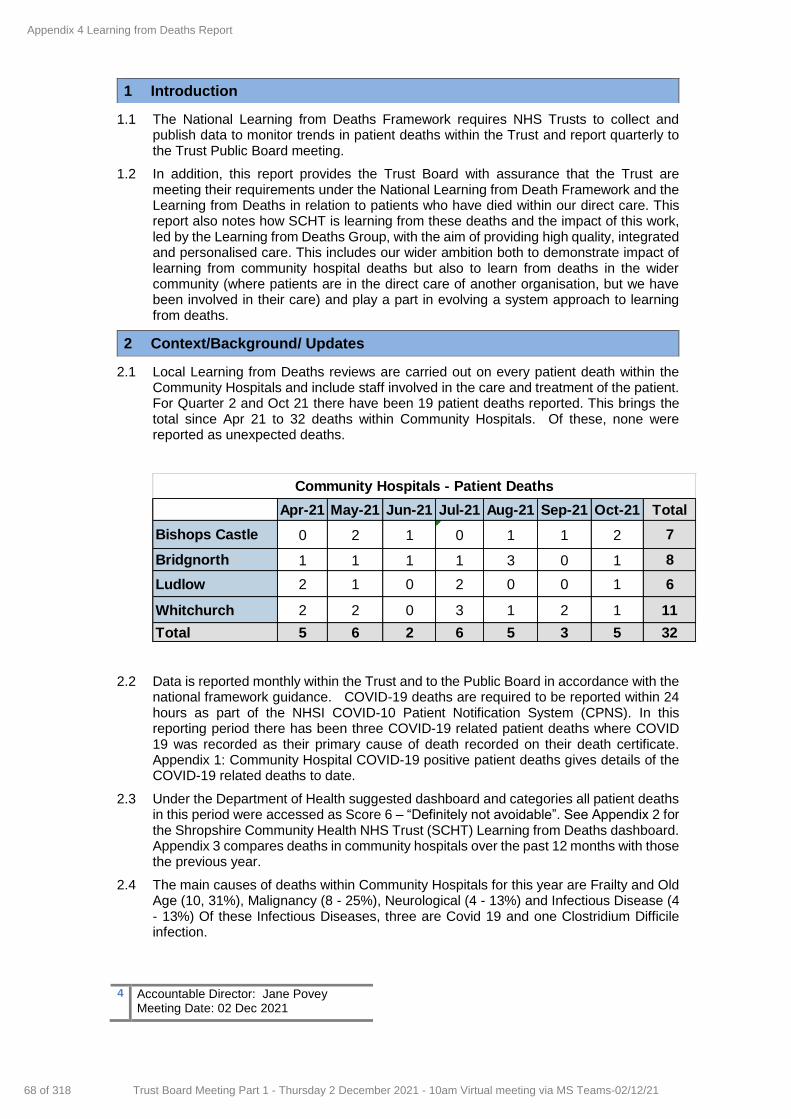
4 Accountable Director: Jane Povey Meeting Date: 02 Dec 2021
1.1 The National Learning from Deaths Framework requires NHS Trusts to collect and publish data to monitor trends in patient deaths within the Trust and report quarterly to the Trust Public Board meeting.
1.2 In addition, this report provides the Trust Board with assurance that the Trust are meeting their requirements under the National Learning from Death Framework and the Learning from Deaths in relation to patients who have died within our direct care. This report also notes how SCHT is learning from these deaths and the impact of this work, led by the Learning from Deaths Group, with the aim of providing high quality, integrated and personalised care. This includes our wider ambition both to demonstrate impact of learning from community hospital deaths but also to learn from deaths in the wider community (where patients are in the direct care of another organisation, but we have been involved in their care) and play a part in evolving a system approach to learning from deaths.
2 Context/Background/ Updates
2.1 Local Learning from Deaths reviews are carried out on every patient death within the Community Hospitals and include staff involved in the care and treatment of the patient. For Quarter 2 and Oct 21 there have been 19 patient deaths reported. This brings the total since Apr 21 to 32 deaths within Community Hospitals. Of these, none were reported as unexpected deaths.
2.2 Data is reported monthly within the Trust and to the Public Board in accordance with the national framework guidance. COVID-19 deaths are required to be reported within 24 hours as part of the NHSI COVID-10 Patient Notification System (CPNS). In this reporting period there has been three COVID-19 related patient deaths where COVID 19 was recorded as their primary cause of death recorded on their death certificate. Appendix 1: Community Hospital COVID-19 positive patient deaths gives details of the COVID-19 related deaths to date.
2.3 Under the Department of Health suggested dashboard and categories all patient deaths in this period were accessed as Score 6 – “Definitely not avoidable”. See Appendix 2 for the Shropshire Community Health NHS Trust (SCHT) Learning from Deaths dashboard. Appendix 3 compares deaths in community hospitals over the past 12 months with those the previous year.
2.4 The main causes of deaths within Community Hospitals for this year are Frailty and Old Age (10, 31%), Malignancy (8 - 25%), Neurological (4 - 13%) and Infectious Disease (4 - 13%) Of these Infectious Diseases, three are Covid 19 and one Clostridium Difficile infection.
Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Total
Bishops Castle 0 2 1 0 1 1 2 7
Bridgnorth 1 1 1 1 3 0 1 8
Ludlow 2 1 0 2 0 0 1 6
Whitchurch 2 2 0 3 1 2 1 11
Total 5 6 2 6 5 3 5 32
Community Hospitals - Patient Deaths
1 Introduction
Appendix 4 Learning from Deaths Report
68 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
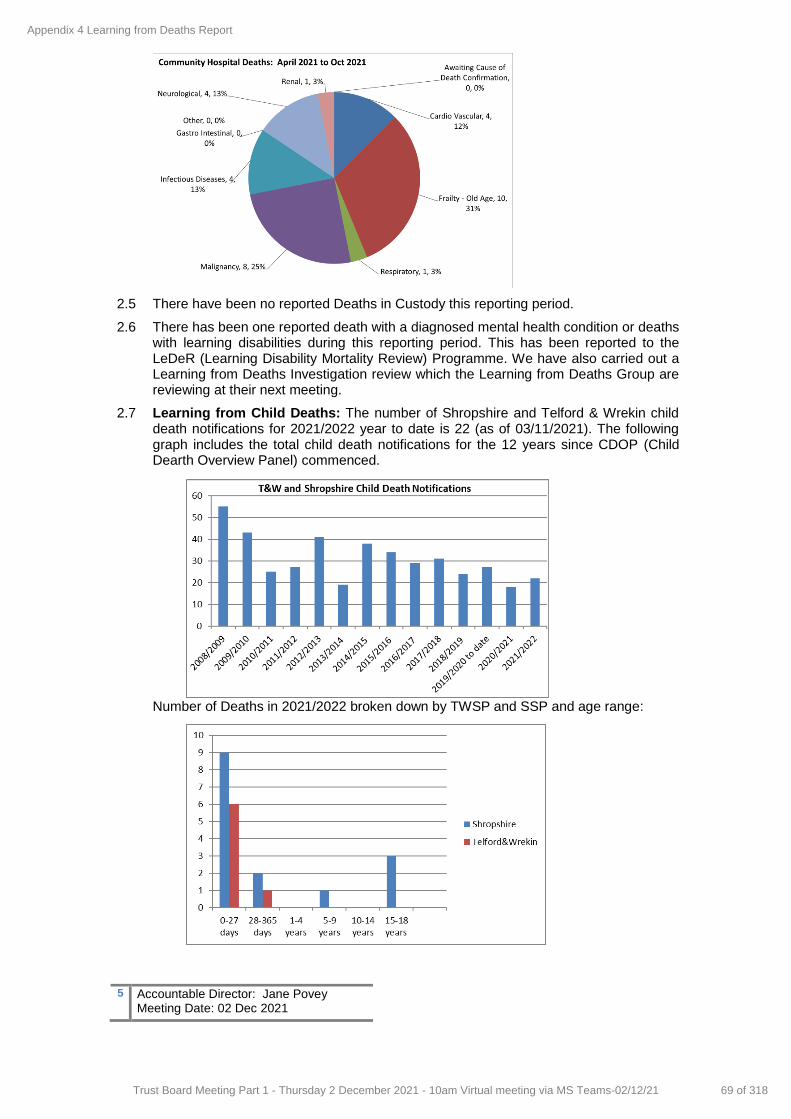
5 Accountable Director: Jane Povey Meeting Date: 02 Dec 2021
2.5 There have been no reported Deaths in Custody this reporting period.
2.6 There has been one reported death with a diagnosed mental health condition or deaths with learning disabilities during this reporting period. This has been reported to the LeDeR (Learning Disability Mortality Review) Programme. We have also carried out a Learning from Deaths Investigation review which the Learning from Deaths Group are reviewing at their next meeting.
2.7 Learning from Child Deaths: The number of Shropshire and Telford & Wrekin child death notifications for 2021/2022 year to date is 22 (as of 03/11/2021). The following graph includes the total child death notifications for the 12 years since CDOP (Child Dearth Overview Panel) commenced.
Number of Deaths in 2021/2022 broken down by TWSP and SSP and age range:
Appendix 4 Learning from Deaths Report
69 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
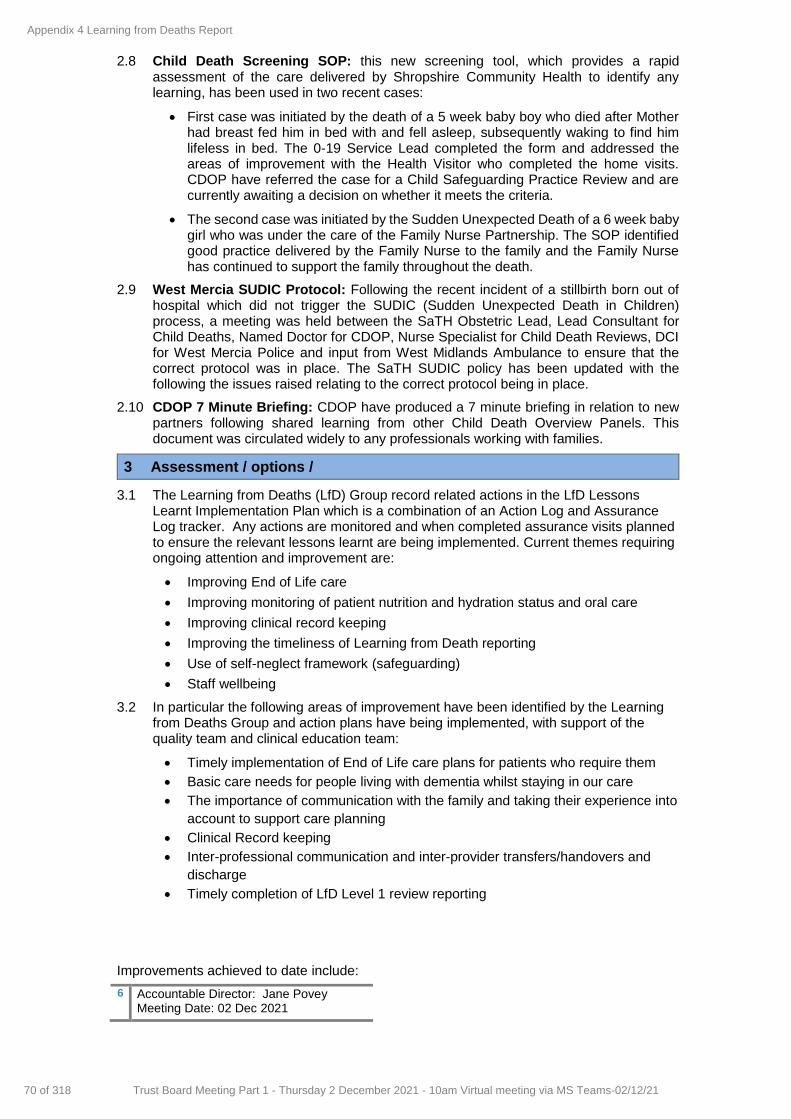
6 Accountable Director: Jane Povey Meeting Date: 02 Dec 2021
2.8 Child Death Screening SOP: this new screening tool, which provides a rapid assessment of the care delivered by Shropshire Community Health to identify any learning, has been used in two recent cases:
First case was initiated by the death of a 5 week baby boy who died after Mother had breast fed him in bed with and fell asleep, subsequently waking to find him lifeless in bed. The 0-19 Service Lead completed the form and addressed the areas of improvement with the Health Visitor who completed the home visits. CDOP have referred the case for a Child Safeguarding Practice Review and are currently awaiting a decision on whether it meets the criteria.
The second case was initiated by the Sudden Unexpected Death of a 6 week baby girl who was under the care of the Family Nurse Partnership. The SOP identified good practice delivered by the Family Nurse to the family and the Family Nurse has continued to support the family throughout the death.
2.9 West Mercia SUDIC Protocol: Following the recent incident of a stillbirth born out of hospital which did not trigger the SUDIC (Sudden Unexpected Death in Children) process, a meeting was held between the SaTH Obstetric Lead, Lead Consultant for Child Deaths, Named Doctor for CDOP, Nurse Specialist for Child Death Reviews, DCI for West Mercia Police and input from West Midlands Ambulance to ensure that the correct protocol was in place. The SaTH SUDIC policy has been updated with the following the issues raised relating to the correct protocol being in place.
2.10 CDOP 7 Minute Briefing: CDOP have produced a 7 minute briefing in relation to new partners following shared learning from other Child Death Overview Panels. This document was circulated widely to any professionals working with families.
3 Assessment / options /
3.1 The Learning from Deaths (LfD) Group record related actions in the LfD Lessons Learnt Implementation Plan which is a combination of an Action Log and Assurance Log tracker. Any actions are monitored and when completed assurance visits planned to ensure the relevant lessons learnt are being implemented. Current themes requiring ongoing attention and improvement are:
Improving End of Life care
Improving monitoring of patient nutrition and hydration status and oral care
Improving clinical record keeping
Improving the timeliness of Learning from Death reporting
Use of self-neglect framework (safeguarding)
Staff wellbeing
3.2 In particular the following areas of improvement have been identified by the Learning from Deaths Group and action plans have being implemented, with support of the quality team and clinical education team:
Timely implementation of End of Life care plans for patients who require them
Basic care needs for people living with dementia whilst staying in our care
The importance of communication with the family and taking their experience into
account to support care planning
Clinical Record keeping
Inter-professional communication and inter-provider transfers/handovers and
discharge
Timely completion of LfD Level 1 review reporting
Improvements achieved to date include:
Appendix 4 Learning from Deaths Report
70 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
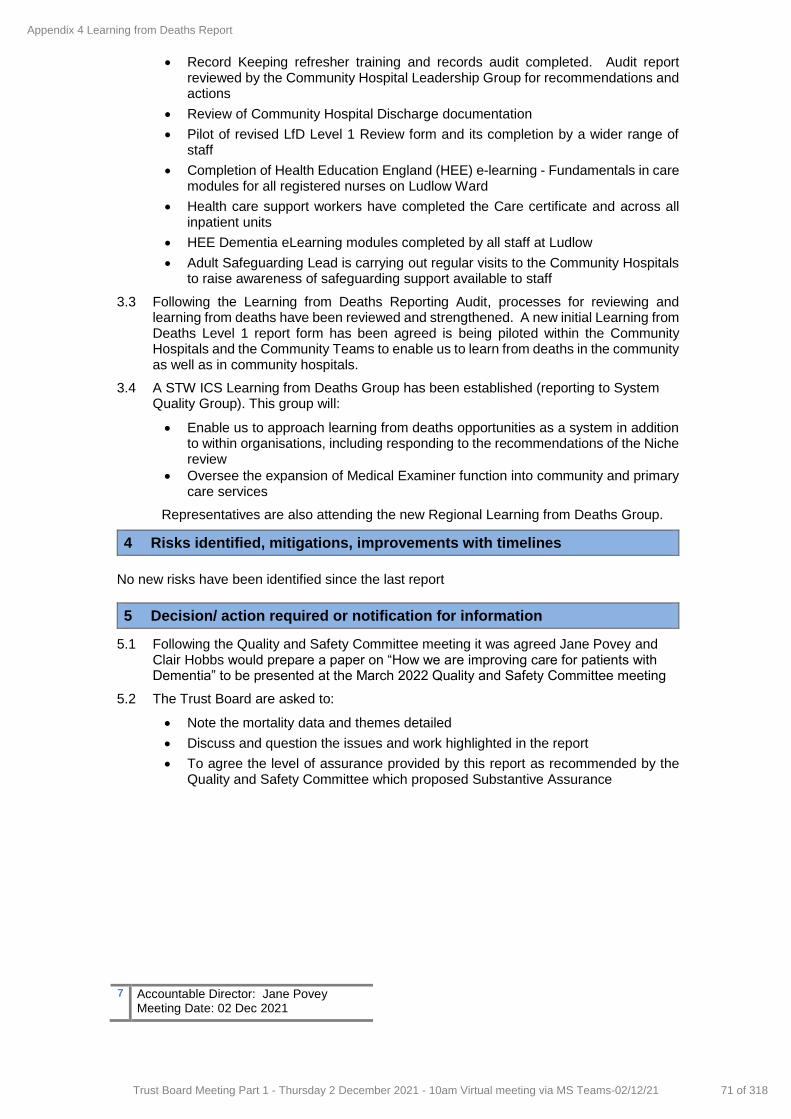
7 Accountable Director: Jane Povey Meeting Date: 02 Dec 2021
Record Keeping refresher training and records audit completed. Audit report reviewed by the Community Hospital Leadership Group for recommendations and actions
Review of Community Hospital Discharge documentation
Pilot of revised LfD Level 1 Review form and its completion by a wider range of staff
Completion of Health Education England (HEE) e-learning - Fundamentals in care modules for all registered nurses on Ludlow Ward
Health care support workers have completed the Care certificate and across all inpatient units
HEE Dementia eLearning modules completed by all staff at Ludlow
Adult Safeguarding Lead is carrying out regular visits to the Community Hospitals to raise awareness of safeguarding support available to staff
3.3 Following the Learning from Deaths Reporting Audit, processes for reviewing and learning from deaths have been reviewed and strengthened. A new initial Learning from Deaths Level 1 report form has been agreed is being piloted within the Community Hospitals and the Community Teams to enable us to learn from deaths in the community as well as in community hospitals.
3.4 A STW ICS Learning from Deaths Group has been established (reporting to System Quality Group). This group will:
Enable us to approach learning from deaths opportunities as a system in addition to within organisations, including responding to the recommendations of the Niche review
Oversee the expansion of Medical Examiner function into community and primary care services
Representatives are also attending the new Regional Learning from Deaths Group.
4 Risks identified, mitigations, improvements with timelines
No new risks have been identified since the last report
5 Decision/ action required or notification for information
5.1 Following the Quality and Safety Committee meeting it was agreed Jane Povey and Clair Hobbs would prepare a paper on “How we are improving care for patients with Dementia” to be presented at the March 2022 Quality and Safety Committee meeting
5.2 The Trust Board are asked to:
Note the mortality data and themes detailed
Discuss and question the issues and work highlighted in the report
To agree the level of assurance provided by this report as recommended by the Quality and Safety Committee which proposed Substantive Assurance
Appendix 4 Learning from Deaths Report
71 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
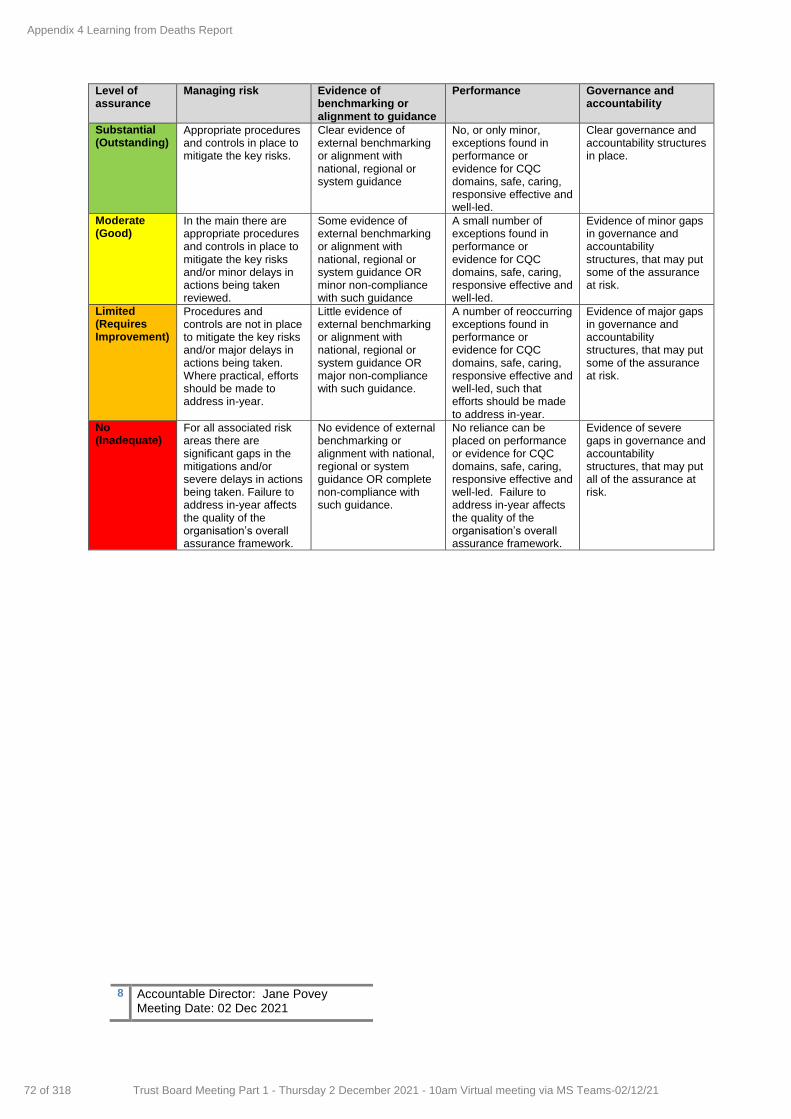
8 Accountable Director: Jane Povey Meeting Date: 02 Dec 2021
Level of assurance
Managing risk Evidence of benchmarking or alignment to guidance
Performance Governance and accountability
Substantial (Outstanding)
Appropriate procedures and controls in place to mitigate the key risks.
Clear evidence of external benchmarking or alignment with national, regional or system guidance
No, or only minor, exceptions found in performance or evidence for CQC domains, safe, caring, responsive effective and well-led.
Clear governance and accountability structures in place.
Moderate (Good)
In the main there are appropriate procedures and controls in place to mitigate the key risks and/or minor delays in actions being taken reviewed.
Some evidence of external benchmarking or alignment with national, regional or system guidance OR minor non-compliance with such guidance
A small number of exceptions found in performance or evidence for CQC domains, safe, caring, responsive effective and well-led.
Evidence of minor gaps in governance and accountability structures, that may put some of the assurance at risk.
Limited (Requires Improvement)
Procedures and controls are not in place to mitigate the key risks and/or major delays in actions being taken. Where practical, efforts should be made to address in-year.
Little evidence of external benchmarking or alignment with national, regional or system guidance OR major non-compliance with such guidance.
A number of reoccurring exceptions found in performance or evidence for CQC domains, safe, caring, responsive effective and well-led, such that efforts should be made to address in-year.
Evidence of major gaps in governance and accountability structures, that may put some of the assurance at risk.
No (Inadequate)
For all associated risk areas there are significant gaps in the mitigations and/or severe delays in actions being taken. Failure to address in-year affects the quality of the organisation’s overall assurance framework.
No evidence of external benchmarking or alignment with national, regional or system guidance OR complete non-compliance with such guidance.
No reliance can be placed on performance or evidence for CQC domains, safe, caring, responsive effective and well-led. Failure to address in-year affects the quality of the organisation’s overall assurance framework.
Evidence of severe gaps in governance and accountability structures, that may put all of the assurance at risk.
Appendix 4 Learning from Deaths Report
72 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
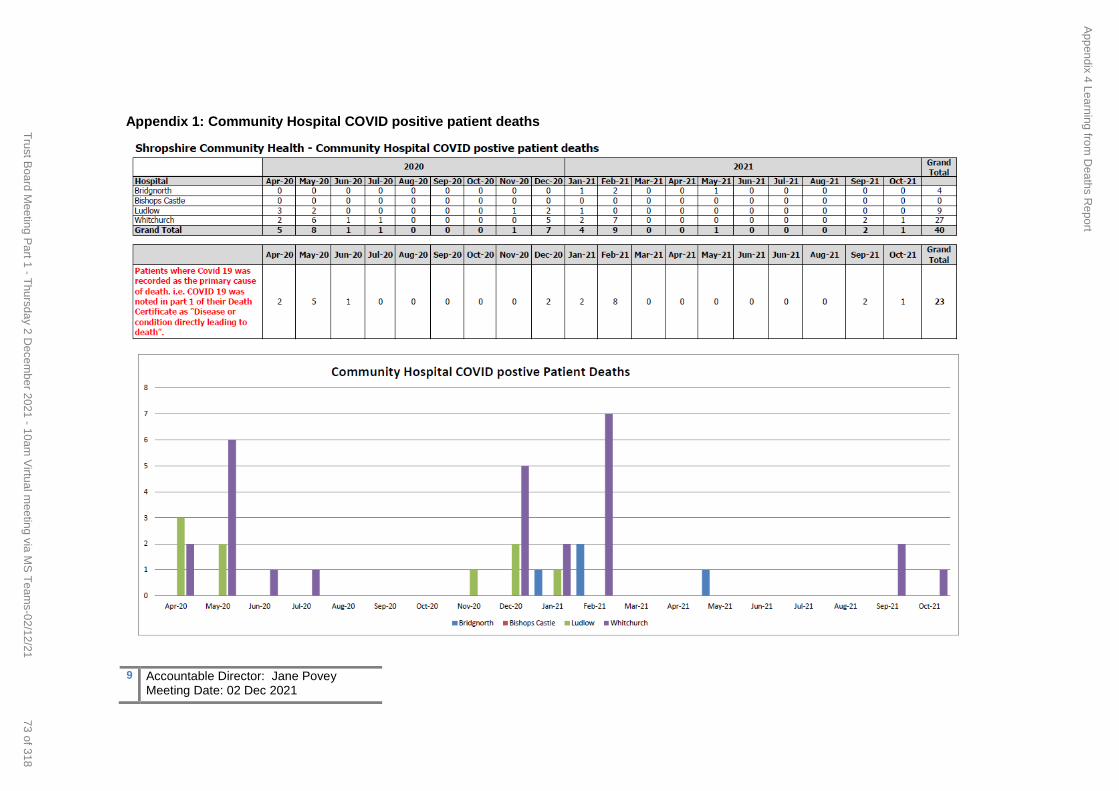
9 Accountable Director: Jane Povey Meeting Date: 02 Dec 2021
Appendix 1: Community Hospital COVID positive patient deaths
Appendix 4 Learning from
Deaths R
eport
73 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
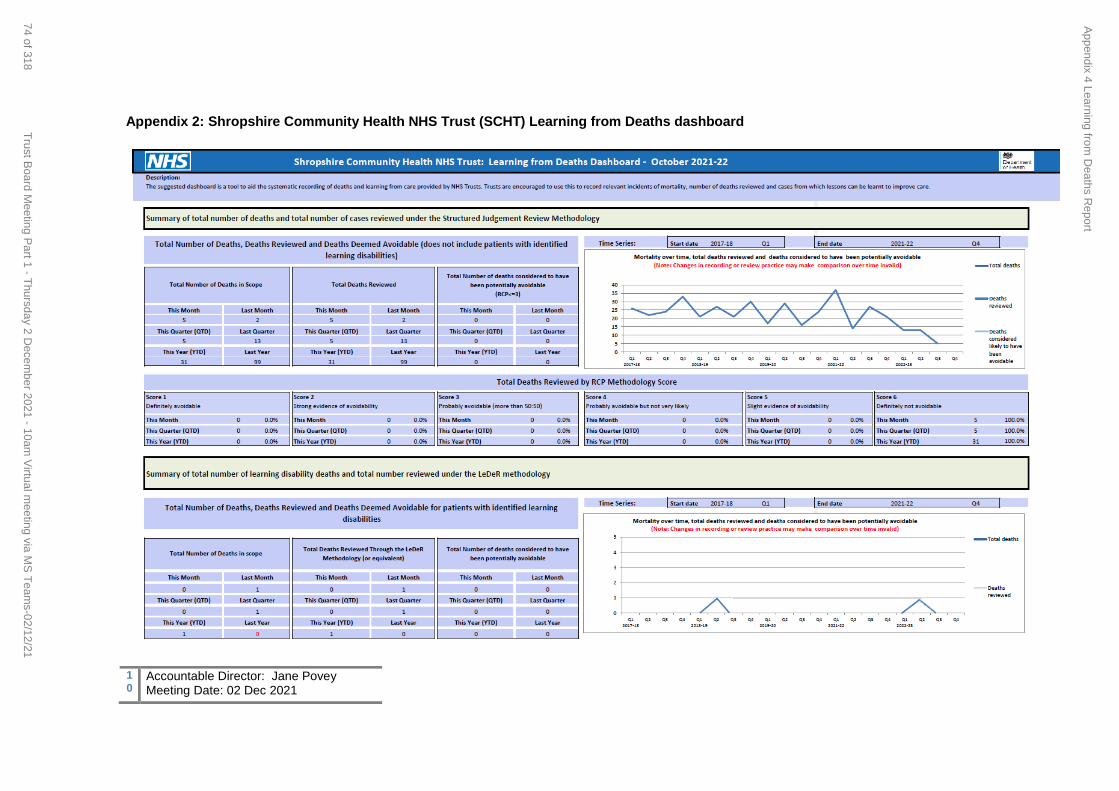
10
Accountable Director: Jane Povey Meeting Date: 02 Dec 2021
Appendix 2: Shropshire Community Health NHS Trust (SCHT) Learning from Deaths dashboard
Appendix 4 Learning from
Deaths R
eport
74 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
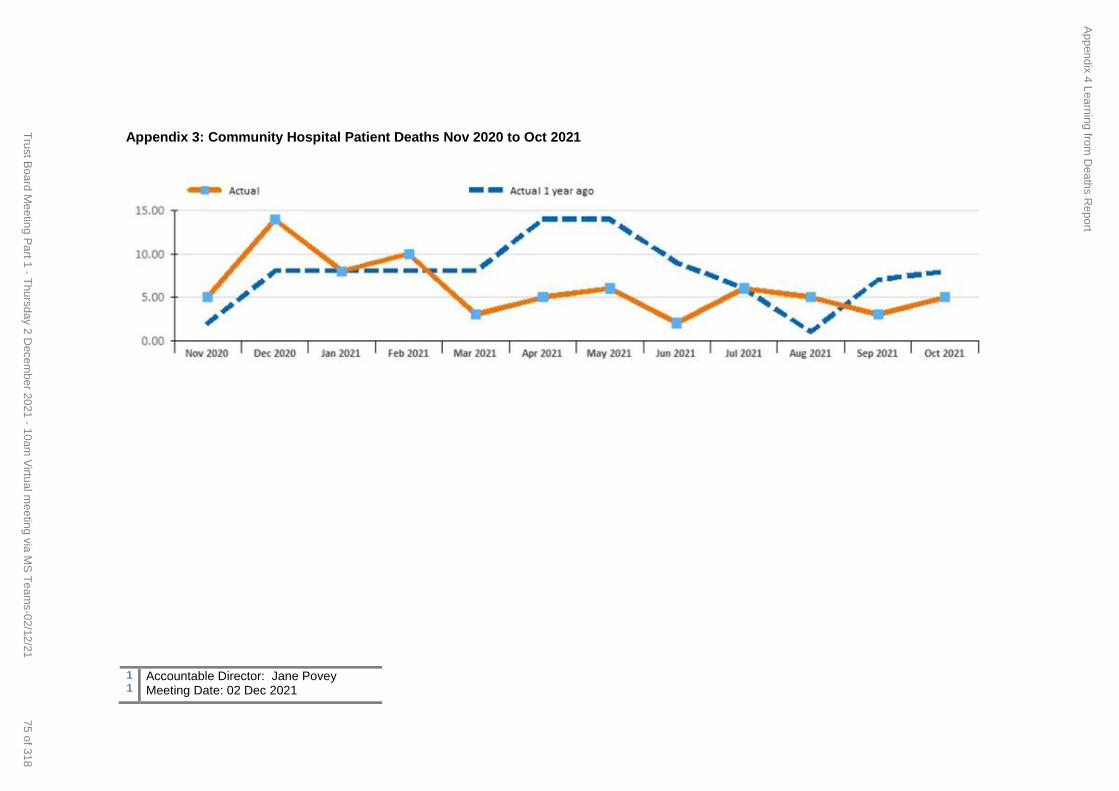
11
Accountable Director: Jane Povey Meeting Date: 02 Dec 2021
Appendix 3: Community Hospital Patient Deaths Nov 2020 to Oct 2021
Appendix 4 Learning from
Deaths R
eport
75 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
1 Accountable Director: Sarah Lloyd, Director of Finance Meeting Date: 2 December 2021
REPORT COVER SHEET Report Title: Performance Update
Meeting: Trust Board
Author: Steve Price, Information Programme Manager
Accountable Director:
Sarah Lloyd, Director of Finance
Other meetings or Committee presented to or previously agreed at:
Meeting or Committee Date Reviewed
Key Points/ Recommendation
Resource and Performance Committee
22 November 2021
As noted within this report
Strategic goals this report relates to: (tick as appropriate)
Good and Beyond Continuous Improvement to
Deliver Outstanding Care
Transforming Services Implement our Clinical and
Quality Strategy
Making Best Use of Resources People, Technology, Finances,
Estates and Networks
Relevance to Board Assurance Framework : (tick as appropriate)
Clinical Quality & Safety
Long term financial
sustainability of the Trust
Healthcare Systems
Organisational culture
Optimising use of
technology
Covid19
Relevance to Well-led domains (CQC & NHSE/I): (tick as appropriate)
leadership capacity and capability
clear vision and credible strategy culture
clear roles and responsibilities
clear and effective risk management
appropriate and accurate information
learning, continuous improvement and innovation
Stakeholders engaged and involved
Relevance to CQC domains: (tick as appropriate)
Safe Caring Responsive Effective Well led
Impacts and Implications? YES or NO
If yes, what impact or implication
Patient safety & experience Yes
The report, actions taken and recovery plans will provide a basis for assurance on safety and experience
Equality & Inclusion Yes
Access to services including specific measures
Financial (revenue & capital) Yes
Number of financial indicators including temporary staffing
IG Governance Toolkit Yes
Reporting of elements such as IG Training and Data Quality
Meeting Date: 2 December 2021
Agenda Item: 12
Enclosure Number: 9
Tab 3.1 Appendix 1 Performance Report
76 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2 Accountable Director: Sarah Lloyd, Director of Finance Meeting Date: 2 December 2021
OD/Workforce Yes
Any actions through services/teams regarding performance and any improvements
Legal Yes Potential impact from claims
Relevance to Corporate Risk
Register (Risk No/Name) Yes
Measures included in the report may link to certain risks
Summary of key points in report
The purpose of this report is to provide a focussed assessment of our performance. The Resource and Performance Committee reviewed the trust’s non-clinical performance in detail at its meeting on 22 November. The key areas of discussion related to waiting times and recovery of activity across some of our services. In addition, a number of Well Led metrics, which are currently showing as Amber, but with a deteriorating trend, were also discussed. For this reason, only limited assurance is given in relation to performance in these areas. Our performance is now summarised through a number of dashboards, as follows: Appendix 1 – Summary Covid Employee and Patient Focused Dashboard Appendix 2 – Summary Covid Restoration and Recovery Dashboard Appendix 3 – Recovery Plan Performance Dashboard – this summarises all metrics where a recovery plan is in place or where performance is outside the agreed performance tolerance Appendix 4 - the Integrated Performance Dashboard – this summaries performance across all KPIs monitored across the Trust up to 31 October 2021. Performance is relatively stable between months and 19 performance indicators are designated ‘red’ at the end of October compared to 21 ‘red’ performance measures within the pervious report. The changes are as follows:
o Measures moving to red (1); Basic Life Support Training (Adult & Paediatric) (CPR)
o Measure moving from red (3); Data Quality Maturity Index, Number of patients
not treated within 28 days of last minute cancellation and Clostridium Difficile incidence rate
The major difference in performance to business as usual at this time is the impact the pandemic has had on waiting times/access standards. In September, we have reported 87 breaches of the RTT 52 Week standard and 18 week Referral To Treatment (RTT) incomplete pathways has been deteriorating for the last few months. In terms of RTT services there are 2 patients that have exceeded 104 weeks wait as at 21st November, both are within TeMS. The Operational leads are regularly reviewing these patients, working with system partners to ensure the patients receive appropriate interventions and plans are in place to list the patients. The weekly RTT/Waiting List meeting, chaired by Head of Development and Transformation / Deputy Director of Operations, focuses on RTT/Waiting List performance and recovery plans. The Board is guided to pay attention to the areas of restore and recovery in this regard to ensure any potential impacts on patients and staff are minimised.
Purpose of the Report (tick as appropriate)
Tab 3.1 Appendix 1 Performance Report
77 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21

3 Accountable Director: Sarah Lloyd, Director of Finance Meeting Date: 2 December 2021
Consider for Action
Give Approval Accept Assurance
Provide Information
Key Recommendations
The Board is asked to:
Consider the current performance indicators and discuss actions being taken to minimise any risks
Discuss whether current performance monitoring enables oversight of the risk and actions required
Tab 3.1 Appendix 1 Performance Report
78 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
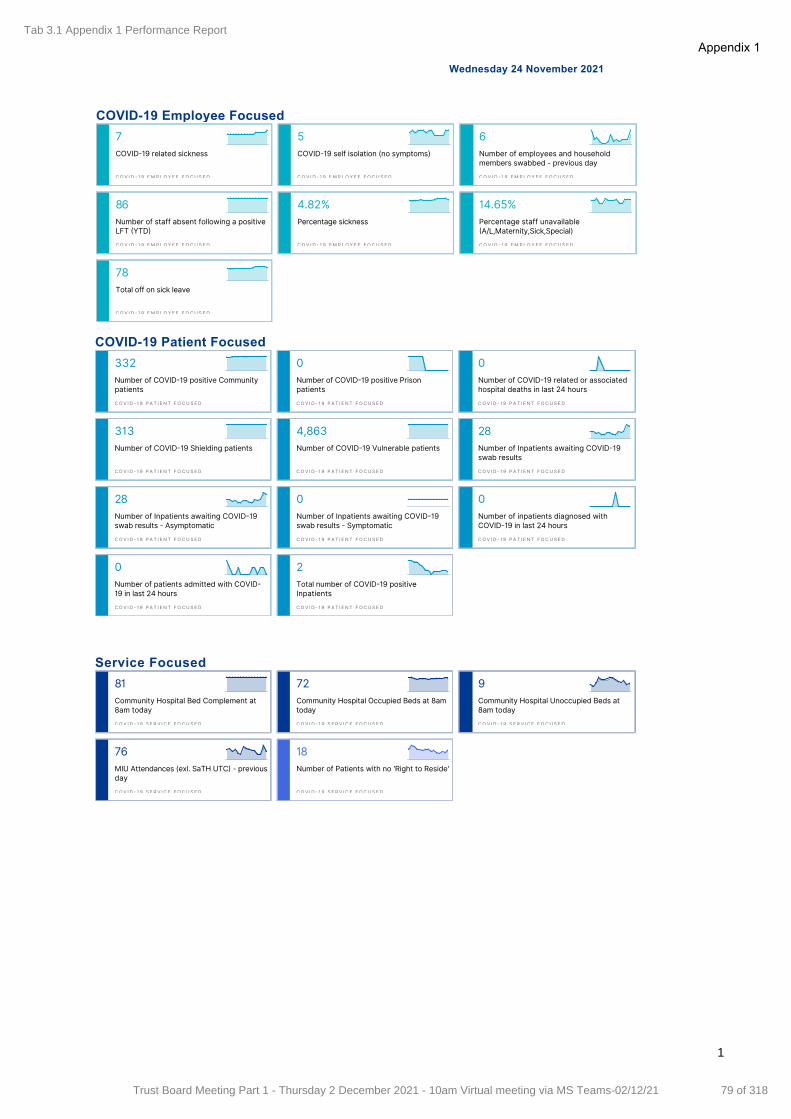
Wednesday 24 November 2021
COVID19 Employee Focused
7COVID 19 related sickness
COV I D 1 9 EM P LO Y E E F OCU S E D
5COVID 19 self isolation (no symptoms)
COV I D 1 9 EM P LO Y E E F OCU S E D
6Number of employees and householdmembers swabbed - previous day
COV I D 1 9 EM P LO Y E E F OCU S E D
86Number of staff absent following a positiveLFT YTD
COV I D 1 9 EM P LO Y E E F OCU S E D
4.82%Percentage sickness
COV I D 1 9 EM P LO Y E E F OCU S E D
14.65%Percentage staff unavailable A/L,Maternity,Sick,Special)
COV I D 1 9 EM P LO Y E E F OCU S E D
78Total off on sick leave
COV I D 1 9 EM P LO Y E E F OCU S E D
COVID19 Patient Focused
332Number of COVID 19 positive Communitypatients
COV I D 1 9 P A T I E NT FOCUS ED
0Number of COVID 19 positive Prisonpatients
COV I D 1 9 P A T I E NT FOCUS ED
0Number of COVID 19 related or associatedhospital deaths in last 24 hours
COV I D 1 9 P A T I E NT FOCUS ED
313Number of COVID 19 Shielding patients
COV I D 1 9 P A T I E NT FOCUS ED
4,863Number of COVID 19 Vulnerable patients
COV I D 1 9 P A T I E NT FOCUS ED
28Number of Inpatients awaiting COVID 19swab results
COV I D 1 9 P A T I E NT FOCUS ED
28Number of Inpatients awaiting COVID 19swab results - Asymptomatic
COV I D 1 9 P A T I E NT FOCUS ED
0Number of Inpatients awaiting COVID 19swab results - Symptomatic
COV I D 1 9 P A T I E NT FOCUS ED
0Number of inpatients diagnosed withCOVID 19 in last 24 hours
COV I D 1 9 P A T I E NT FOCUS ED
0Number of patients admitted with COVID 19 in last 24 hours
COV I D 1 9 P A T I E NT FOCUS ED
2Total number of COVID 19 positiveInpatients
COV I D 1 9 P A T I E NT FOCUS ED
Service Focused
81Community Hospital Bed Complement at8am today
COV I D 1 9 S E R V I C E F OCUS ED
72Community Hospital Occupied Beds at 8amtoday
COV I D 1 9 S E R V I C E F OCUS ED
9Community Hospital Unoccupied Beds at8am today
COV I D 1 9 S E R V I C E F OCUS ED
76MIU Attendances (exl. SaTH UTC - previousday
COV I D 1 9 S E R V I C E F OCUS ED
18Number of Patients with no 'Right to Reside'
COV I D 1 9 S E R V I C E F OCUS ED
1
Appendix 1Tab 3.1 Appendix 1 Performance Report
79 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
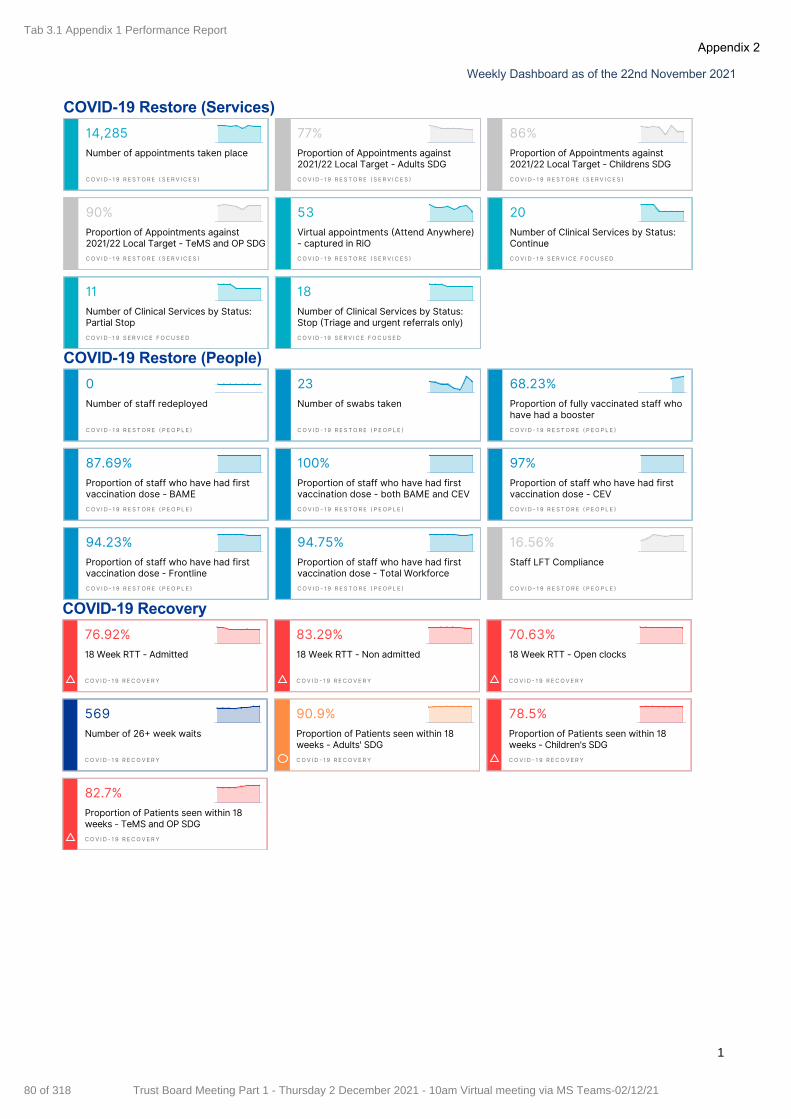
Weekly Dashboard as of the 22nd November 2021
COVID19 Restore (Services)
14,285Number of appointments taken place
COV I D 1 9 R E S TOR E S E R V I C E S
77%Proportion of Appointments against2021/22 Local Target - Adults SDG
COV I D 1 9 R E S TOR E S E R V I C E S
86%Proportion of Appointments against2021/22 Local Target - Childrens SDG
COV I D 1 9 R E S TOR E S E R V I C E S
90%Proportion of Appointments against2021/22 Local Target - TeMS and OP SDG
COV I D 1 9 R E S TOR E S E R V I C E S
53Virtual appointments Attend Anywhere)- captured in RiO
COV I D 1 9 R E S TOR E S E R V I C E S
20Number of Clinical Services by Status:Continue
COV I D 1 9 S E RV I C E FOCUSED
11Number of Clinical Services by Status:Partial Stop
COV I D 1 9 S E RV I C E FOCUSED
18Number of Clinical Services by Status:Stop Triage and urgent referrals only)
COV I D 1 9 S E RV I C E FOCUSED
COVID19 Restore (People)
0Number of staff redeployed
COV I D 1 9 R E S TO R E P E O P L E
23Number of swabs taken
COV I D 1 9 R E S TO R E P E O P L E
68.23%Proportion of fully vaccinated staff whohave had a booster
COV I D 1 9 R E S TO R E P E O P L E
87.69%Proportion of staff who have had firstvaccination dose - BAME
COV I D 1 9 R E S TO R E P E O P L E
100%Proportion of staff who have had firstvaccination dose - both BAME and CEV
COV I D 1 9 R E S TO R E P E O P L E
97%Proportion of staff who have had firstvaccination dose - CEV
COV I D 1 9 R E S TO R E P E O P L E
94.23%Proportion of staff who have had firstvaccination dose - Frontline
COV I D 1 9 R E S TO R E P E O P L E
94.75%Proportion of staff who have had firstvaccination dose - Total Workforce
COV I D 1 9 R E S TO R E P E O P L E
16.56%Staff LFT Compliance
COV I D 1 9 R E S TO R E P E O P L E
COVID19 Recovery
76.92%18 Week RTT - Admitted
COV I D 1 9 R E COV E RY
83.29%18 Week RTT - Non admitted
COV I D 1 9 R E COV E RY
70.63%18 Week RTT - Open clocks
COV I D 1 9 R E COV E RY
569Number of 26 week waits
COV I D 1 9 R E COV E RY
90.9%Proportion of Patients seen within 18weeks - Adults' SDG
COV I D 1 9 R E COV E RY
78.5%Proportion of Patients seen within 18weeks - Children's SDG
COV I D 1 9 R E COV E RY
82.7%Proportion of Patients seen within 18weeks - TeMS and OP SDG
COV I D 1 9 R E COV E RY
1
Appendix 2Tab 3.1 Appendix 1 Performance Report
80 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21

Ethnic coding data quality 68.13 67.61 67.26 67.14 68.52 68.37 67.50 70.72 76.47 75.30 74.26 73.87 74.45 90.00 73.28 95.00
Proportion of temporary staff 4.40% 4.90% 5.40% 6.00% 4.40% 5.00% 4.70% 4.50% 5.20% 5.40% 4.70% 4.70% 4.60% 4.20% 4.83% 3.40%
Data Quality Maturity Index 86.2% 86.8% 84.1% 84.1% 83.9% 84.7% 88.0% 84.6% 90.5% 90.6% ? ? ? 95.0% 90.6% 95.0%
Safeguarding Training Compliance (Children) Level 3 85.5… 84.8… 87.7… 89.2… 93.2… 92.7… 71.0… 77.7… 82.0… 87.4… 90.5… 91.7… 90.7… 95.00% 90.7… 95.0…
Community Equipment Store Response within 7 days 90.39 88.66 91.43 91.14 95.55 95.68 93.94 92.24 89.24 91.00 91.43 93.52 ? 95.00 91.90 95.00
Referral to Treatment Incomplete 52+ Week Waiters 9 18 23 32 52 71 49 31 47 70 83 87 ? 90 87 0
18 week Referral To Treatment (RTT) incomplete pathways 76.03 77.05 78.41 77.80 79.27 81.70 79.76 80.13 80.67 80.09 79.90 77.20 ? 68.70 77.20 92.00
Total shifts exceeding NHSI capped rate 408 458 472 455 452 539 473 514 587 581 484 491 416 ? 507 0
Complaints upheld or partly upheld 2 8 4 5 3 2 1 1 3 1 3 5 3 ? 17 0
Total shifts on a nonframework agreement 9 12 54 42 25 9 8 13 2 7 8 8 1 ? 47 0
Category 2 Pressure Ulcers 19 14 23 24 23 30 22 20 19 22 25 14 24 ? 24 0
Serious Incidents (reported) 0 4 6 3 3 2 2 5 2 1 2 2 7 ? 21 0
Proportion of Delayed Transfers of Care (Days) 2.50% 1.05% 4.25% 21.6… 12.8… 15.2… 9.26% 9.41% ? ? ? ? ? ? 9.41% 3.50%
Diagnostics for Audio/Ultrasound 54.8… 55.5… 45.9… 39.9… 57.7… 96.3… 90.0… 98.5… 99.5… 100.… 100.… 100.… ? ? 97.6… 99.0…
Unstageable Pressure Ulcers 1 7 2 4 6 7 2 2 5 2 10 0 7 ? 7 0
Sickness Absence Nursing Workforce 5.68% 7.92% 6.09% 7.05% 6.71% 5.88% 5.51% 6.64% 5.73% 5.70% 4.63% 4.41% 4.50% ? 5.30% 4.50%
Agency expenditure 214 240 269 302 220 290 232 218 253 260 226 220 ? ? 1,409 1,137
Actual efficiency recurring compared to plan Actual (YTD) 0 0 0 75 100 124 39 95 228 325 412 492 ? ? 492 660
Proportion of patients within 18 weeks 73.65 75.34 77.12 76.07 78.77 79.20 77.50 77.36 77.22 79.00 78.89 75.97 81.12 ? 81.12 92.00
Leavers All (FTE) 0.76% 0.88% 0.72% 0.96% 0.57% 3.24% 1.30% 1.32% 0.79% 1.08% 1.01% 1.47% 1.15% ? 1.16% 0.80%
Basic Life Support Training (Adult & Paediatric) (CPR) 87.7… 87.3… 85.9… 87.0… 85.8… 85.6… 88.3… 87.0… 87.5… 86.7… 87.6… 83.4… 83.7… ? 83.7… 95.0…
Indicator Oct20Nov20
Dec20
Jan21 Feb21 Mar21 Apr21May21
Jun21 Jul21 Aug21 Sep21 Oct21Recov…Traject…
RecoveryStatus
ActualYTD
YTDTarget
YTDStatus
1
Appendix 3T
ab 3.1 Appendix 1 P
erformance R
eport
81 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
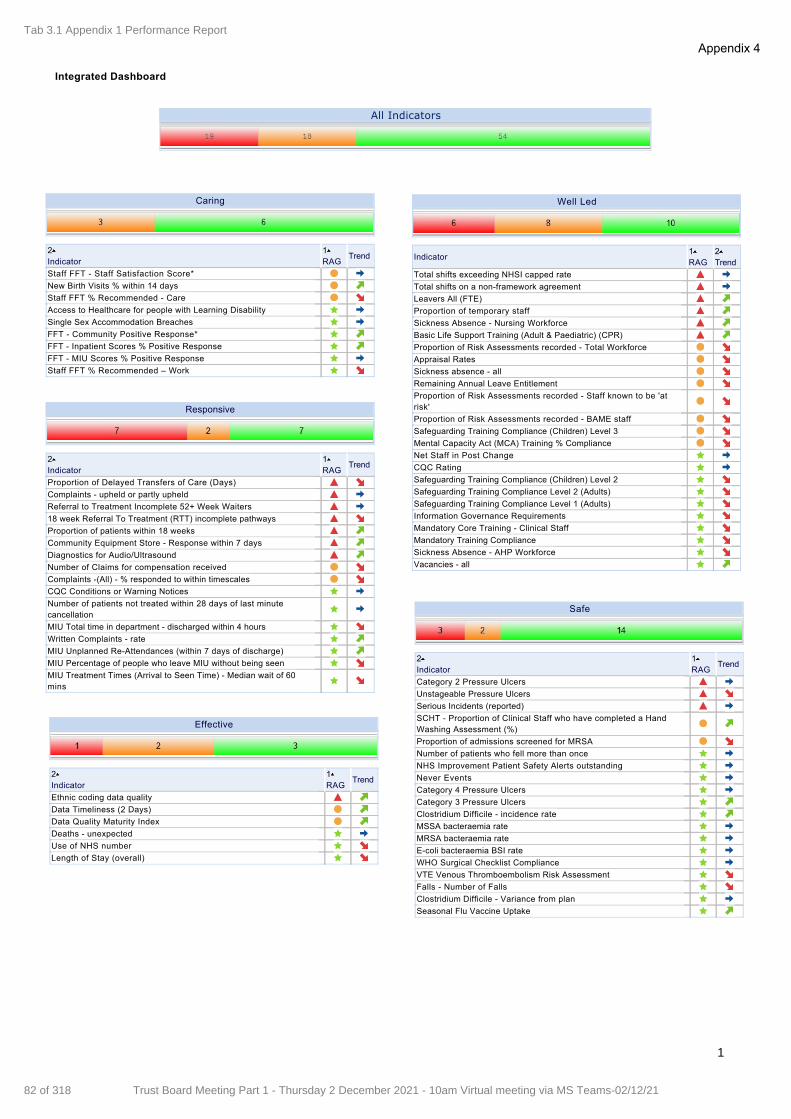
Integrated Dashboard
All Indicators
Staff FFT Staff Satisfaction Score*
New Birth Visits % within 14 days
Staff FFT % Recommended Care
Access to Healthcare for people with Learning Disability
Single Sex Accommodation Breaches
FFT Community Positive Response*
FFT Inpatient Scores % Positive Response
FFT MIU Scores % Positive Response
Staff FFT % Recommended – Work
Caring
2Indicator
1RAG
Trend
Total shifts exceeding NHSI capped rate
Total shifts on a nonframework agreement
Leavers All (FTE)
Proportion of temporary staff
Sickness Absence Nursing Workforce
Basic Life Support Training (Adult & Paediatric) (CPR)
Proportion of Risk Assessments recorded Total Workforce
Appraisal Rates
Sickness absence all
Remaining Annual Leave Entitlement
Proportion of Risk Assessments recorded Staff known to be 'atrisk'
Proportion of Risk Assessments recorded BAME staff
Safeguarding Training Compliance (Children) Level 3
Mental Capacity Act (MCA) Training % Compliance
Net Staff in Post Change
CQC Rating
Safeguarding Training Compliance (Children) Level 2
Safeguarding Training Compliance Level 2 (Adults)
Safeguarding Training Compliance Level 1 (Adults)
Information Governance Requirements
Mandatory Core Training Clinical Staff
Mandatory Training Compliance
Sickness Absence AHP Workforce
Vacancies all
Well Led
Indicator1RAG
2Trend
Proportion of Delayed Transfers of Care (Days)
Complaints upheld or partly upheld
Referral to Treatment Incomplete 52+ Week Waiters
18 week Referral To Treatment (RTT) incomplete pathways
Proportion of patients within 18 weeks
Community Equipment Store Response within 7 days
Diagnostics for Audio/Ultrasound
Number of Claims for compensation received
Complaints (All) % responded to within timescales
CQC Conditions or Warning Notices
Number of patients not treated within 28 days of last minutecancellation
MIU Total time in department discharged within 4 hours
Written Complaints rate
MIU Unplanned ReAttendances (within 7 days of discharge)
MIU Percentage of people who leave MIU without being seen
MIU Treatment Times (Arrival to Seen Time) Median wait of 60mins
Responsive
2Indicator
1RAG
Trend
Category 2 Pressure Ulcers
Unstageable Pressure Ulcers
Serious Incidents (reported)
SCHT Proportion of Clinical Staff who have completed a HandWashing Assessment (%)
Proportion of admissions screened for MRSA
Number of patients who fell more than once
NHS Improvement Patient Safety Alerts outstanding
Never Events
Category 4 Pressure Ulcers
Category 3 Pressure Ulcers
Clostridium Difficile incidence rate
MSSA bacteraemia rate
MRSA bacteraemia rate
Ecoli bacteraemia BSI rate
WHO Surgical Checklist Compliance
VTE Venous Thromboembolism Risk Assessment
Falls Number of Falls
Clostridium Difficile Variance from plan
Seasonal Flu Vaccine Uptake
Safe
2Indicator
1RAG
Trend
Ethnic coding data quality
Data Timeliness (2 Days)
Data Quality Maturity Index
Deaths unexpected
Use of NHS number
Length of Stay (overall)
Effective
2Indicator
1RAG
Trend
Early Supported Discharge
Admission Avoidance
Designed around the Patient
2Indicator
1RAG
Trend
Delivery of maintenance programmes
Development of estates strategy
Peat Rating
Delivered in Suitable Environments
2Indicator
1RAG
Trend
Actual efficiency recurring compared toplan Actual (YTD)
Agency expenditure
Bottom line I&E position full yearforecast
Forecast year end charge to capitalresource limit
Is the trust forecasting a fundingrequirement for liquidity purposes?
Use of Resources Risk Rating
Forecast underlying surplus/(deficit)
Actual efficiency recurring/nonrecurringcompared to plan Actual (YTD)
Bottom line I&E position Actual (YTD)
Actual efficiency nonrecurring comparedto plan Actual (YTD)
Financially Sustainable
IndicatorRAG
Trend
EPR implementation
HSCN Implementation
Making best use of Technology
2Indicator
1RAG
Trend
1
Appendix 4Tab 3.1 Appendix 1 Performance Report
82 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
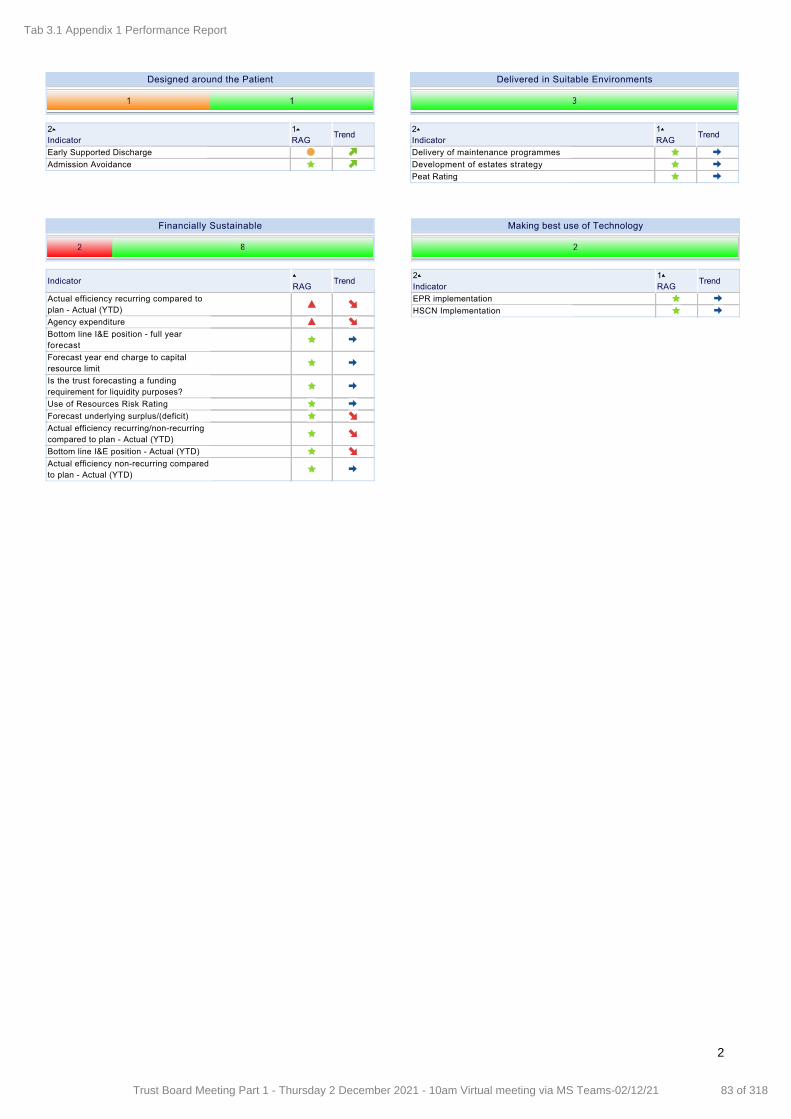
Integrated Dashboard
All Indicators
Staff FFT Staff Satisfaction Score*
New Birth Visits % within 14 days
Staff FFT % Recommended Care
Access to Healthcare for people with Learning Disability
Single Sex Accommodation Breaches
FFT Community Positive Response*
FFT Inpatient Scores % Positive Response
FFT MIU Scores % Positive Response
Staff FFT % Recommended – Work
Caring
2Indicator
1RAG
Trend
Total shifts exceeding NHSI capped rate
Total shifts on a nonframework agreement
Leavers All (FTE)
Proportion of temporary staff
Sickness Absence Nursing Workforce
Basic Life Support Training (Adult & Paediatric) (CPR)
Proportion of Risk Assessments recorded Total Workforce
Appraisal Rates
Sickness absence all
Remaining Annual Leave Entitlement
Proportion of Risk Assessments recorded Staff known to be 'atrisk'
Proportion of Risk Assessments recorded BAME staff
Safeguarding Training Compliance (Children) Level 3
Mental Capacity Act (MCA) Training % Compliance
Net Staff in Post Change
CQC Rating
Safeguarding Training Compliance (Children) Level 2
Safeguarding Training Compliance Level 2 (Adults)
Safeguarding Training Compliance Level 1 (Adults)
Information Governance Requirements
Mandatory Core Training Clinical Staff
Mandatory Training Compliance
Sickness Absence AHP Workforce
Vacancies all
Well Led
Indicator1RAG
2Trend
Proportion of Delayed Transfers of Care (Days)
Complaints upheld or partly upheld
Referral to Treatment Incomplete 52+ Week Waiters
18 week Referral To Treatment (RTT) incomplete pathways
Proportion of patients within 18 weeks
Community Equipment Store Response within 7 days
Diagnostics for Audio/Ultrasound
Number of Claims for compensation received
Complaints (All) % responded to within timescales
CQC Conditions or Warning Notices
Number of patients not treated within 28 days of last minutecancellation
MIU Total time in department discharged within 4 hours
Written Complaints rate
MIU Unplanned ReAttendances (within 7 days of discharge)
MIU Percentage of people who leave MIU without being seen
MIU Treatment Times (Arrival to Seen Time) Median wait of 60mins
Responsive
2Indicator
1RAG
Trend
Category 2 Pressure Ulcers
Unstageable Pressure Ulcers
Serious Incidents (reported)
SCHT Proportion of Clinical Staff who have completed a HandWashing Assessment (%)
Proportion of admissions screened for MRSA
Number of patients who fell more than once
NHS Improvement Patient Safety Alerts outstanding
Never Events
Category 4 Pressure Ulcers
Category 3 Pressure Ulcers
Clostridium Difficile incidence rate
MSSA bacteraemia rate
MRSA bacteraemia rate
Ecoli bacteraemia BSI rate
WHO Surgical Checklist Compliance
VTE Venous Thromboembolism Risk Assessment
Falls Number of Falls
Clostridium Difficile Variance from plan
Seasonal Flu Vaccine Uptake
Safe
2Indicator
1RAG
Trend
Ethnic coding data quality
Data Timeliness (2 Days)
Data Quality Maturity Index
Deaths unexpected
Use of NHS number
Length of Stay (overall)
Effective
2Indicator
1RAG
Trend
Early Supported Discharge
Admission Avoidance
Designed around the Patient
2Indicator
1RAG
Trend
Delivery of maintenance programmes
Development of estates strategy
Peat Rating
Delivered in Suitable Environments
2Indicator
1RAG
Trend
Actual efficiency recurring compared toplan Actual (YTD)
Agency expenditure
Bottom line I&E position full yearforecast
Forecast year end charge to capitalresource limit
Is the trust forecasting a fundingrequirement for liquidity purposes?
Use of Resources Risk Rating
Forecast underlying surplus/(deficit)
Actual efficiency recurring/nonrecurringcompared to plan Actual (YTD)
Bottom line I&E position Actual (YTD)
Actual efficiency nonrecurring comparedto plan Actual (YTD)
Financially Sustainable
IndicatorRAG
Trend
EPR implementation
HSCN Implementation
Making best use of Technology
2Indicator
1RAG
Trend
2
Tab 3.1 Appendix 1 Performance Report
83 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1 Accountable Director: Sarah Lloyd, Associate Director of Finance
Board Meeting: 5 August 2021
APPENDIX 2
Meeting Date: 2 December 2021
Agenda Item: 12
Enclosure Number: 10
Meeting: Board of Directors
Title: Finance Report – Month 7 (2021/22)
Author: Sarah Lloyd, Director of Finance
Reviewing Committee: Resource & Performance Committee
Assurance level Moderate
Requirement: This report is required to meet the obligation of the NHS constitution, to be open and transparent with respect the use of resources.
Tab 3.2 Appendix 2 Finance Report
84 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1 Accountable Director: Sarah Lloyd, Director of Finance Board Meeting: 2 December 2021
1. Introduction
1.1 Financial arrangements were amended during the response to the Covid-19 pandemic. These
arrangements were confirmed to continue for the first six months of 2021/22 and the Shropshire and Telford & Wrekin (STW) Integrated Care System (ICS) submitted a financial plan for this period, referred to as the H1 plan.
1.2 These arrangements are now continuing into the second six months of this financial year, after adjusting for inflation, Covid-19 funding, and efficiency requirements, and both the ICS and our Trust have submitted financial plans for this period, referred to as the H2 plan.
1.3 A summary of the draft ICS financial plan, and the headlines of Shropcom’s plan, were
presented at the Extraordinary Resource and Performance Committee (RPC) meeting on 12 November and our trust plan was approved.
1.4 Following a number of adjustments across the ICS, final headline numbers were presented to
RPC on 22 November and the Trust’s financial plan for H2 was approved. The trust is now planning to deliver a surplus of £1,193k in H2.
1.5 Since presenting the financial plan to RPC, it has been confirmed that the full year plan will be
the H1 plan (not the H1 actual performance) plus the H2 plan. Shropcom’s H1 plan was £158k surplus and, as shown above the H2 plan is £1,193k, giving a full year plan of £1,351k surplus.
1.6 At the time of writing the RPC paper, the full year plan calculation had not been confirmed and month 7 reporting within this report therefore focusses on the in-month performance against plan only.
1.7 In addition, the ICS committed to a stabilisation plan that covers the full financial year and
measures recurrent (on-going) expenditure only. The ICS made a commitment that its recurrent expenditure will not increase during 2021/22. This plan is being reviewed to reflect H2 planning guidance however is the ICS is assessed to be on track at this time.
1.8 CIP delivery remains our most significant risk to the 2021/22 financial plan, especially in
relation to recurrent CIP target. Our in-year CIP target for 2021/22 is a lower risk because we are able include non-recurrent CIP to achieve it.
1.9 The Trust is measured on its financial performance in a number of ways, but the principal measure is total Income & Expenditure at Adjusted Financial Performance level. This excludes a number of technical accounting adjustments and is the level at which performance is reported to and managed by NHSE&I.
2. Financial Performance against the H2 Plan – Month 7
The dashboard below summarises the key areas of performance in relation to our financial
position. Our current in-month financial performance is a favourable variance of £9k compared to our month 7 plan.
It is of note that, although CIP delivery shows a favourable position compared to the in-year
plan for the year to date this is due to non-recurrent CIP delivery. The recurrent CIP position is a £186k adverse variance to plan for the year to date and further detail is included within section 4 of this report.
Title: Finance Performance for the Period Ended 31 October 2021 (Month 7 2020/21)
Tab 3.2 Appendix 2 Finance Report
85 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
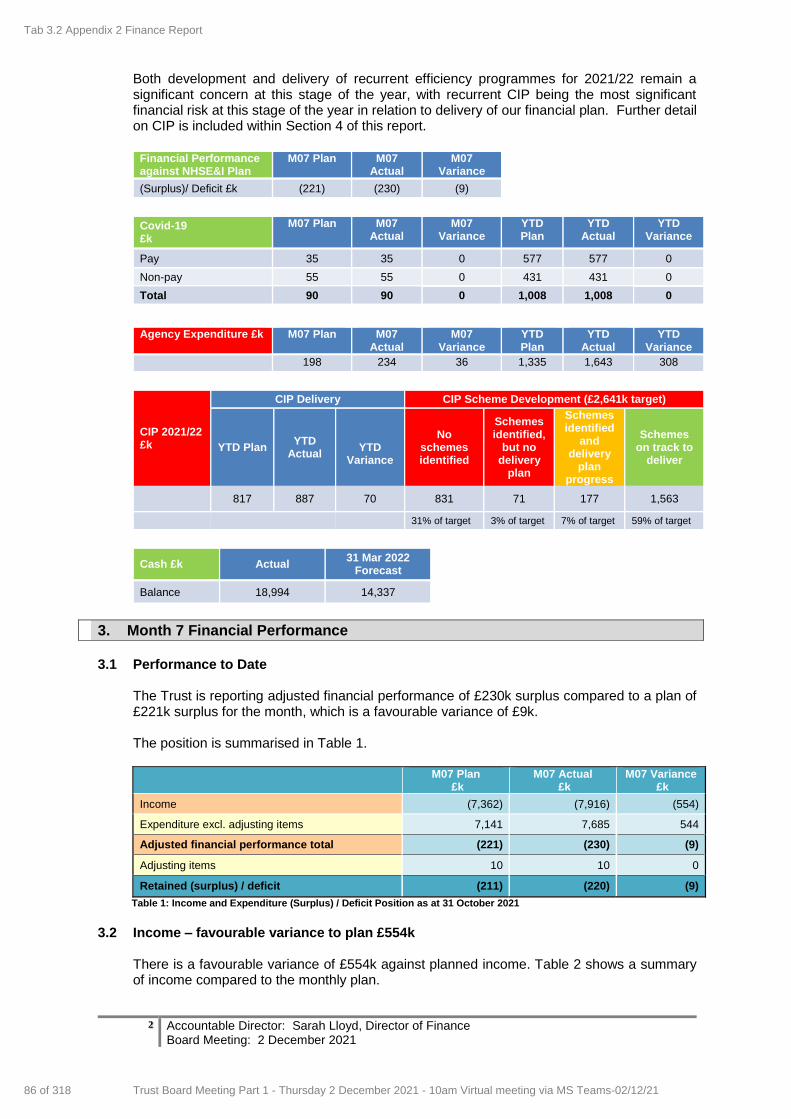
2 Accountable Director: Sarah Lloyd, Director of Finance Board Meeting: 2 December 2021
Both development and delivery of recurrent efficiency programmes for 2021/22 remain a significant concern at this stage of the year, with recurrent CIP being the most significant financial risk at this stage of the year in relation to delivery of our financial plan. Further detail on CIP is included within Section 4 of this report.
Financial Performance against NHSE&I Plan
M07 Plan M07 Actual
M07 Variance
(Surplus)/ Deficit £k (221) (230) (9)
Covid-19 £k
M07 Plan M07 Actual
M07 Variance
YTD Plan
YTD Actual
YTD Variance
Pay 35 35 0 577 577 0
Non-pay 55 55 0 431 431 0
Total 90 90 0 1,008 1,008 0
Agency Expenditure £k M07 Plan M07
Actual M07
Variance YTD Plan
YTD Actual
YTD Variance
198 234 36 1,335 1,643 308
CIP 2021/22 £k
CIP Delivery CIP Scheme Development (£2,641k target)
YTD Plan YTD
Actual
YTD
Variance
No schemes identified
Schemes identified,
but no delivery
plan
Schemes identified
and delivery
plan progress
Schemes on track to
deliver
817 887 70 831 71 177 1,563
31% of target 3% of target 7% of target 59% of target
Cash £k Actual 31 Mar 2022
Forecast
Balance 18,994 14,337
3. Month 7 Financial Performance
3.1 Performance to Date
The Trust is reporting adjusted financial performance of £230k surplus compared to a plan of £221k surplus for the month, which is a favourable variance of £9k. The position is summarised in Table 1.
M07 Plan
£k M07 Actual
£k M07 Variance
£k
Income (7,362) (7,916) (554)
Expenditure excl. adjusting items 7,141 7,685 544
Adjusted financial performance total (221) (230) (9)
Adjusting items 10 10 0
Retained (surplus) / deficit (211) (220) (9)
Table 1: Income and Expenditure (Surplus) / Deficit Position as at 31 October 2021
3.2 Income – favourable variance to plan £554k
There is a favourable variance of £554k against planned income. Table 2 shows a summary of income compared to the monthly plan.
Tab 3.2 Appendix 2 Finance Report
86 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
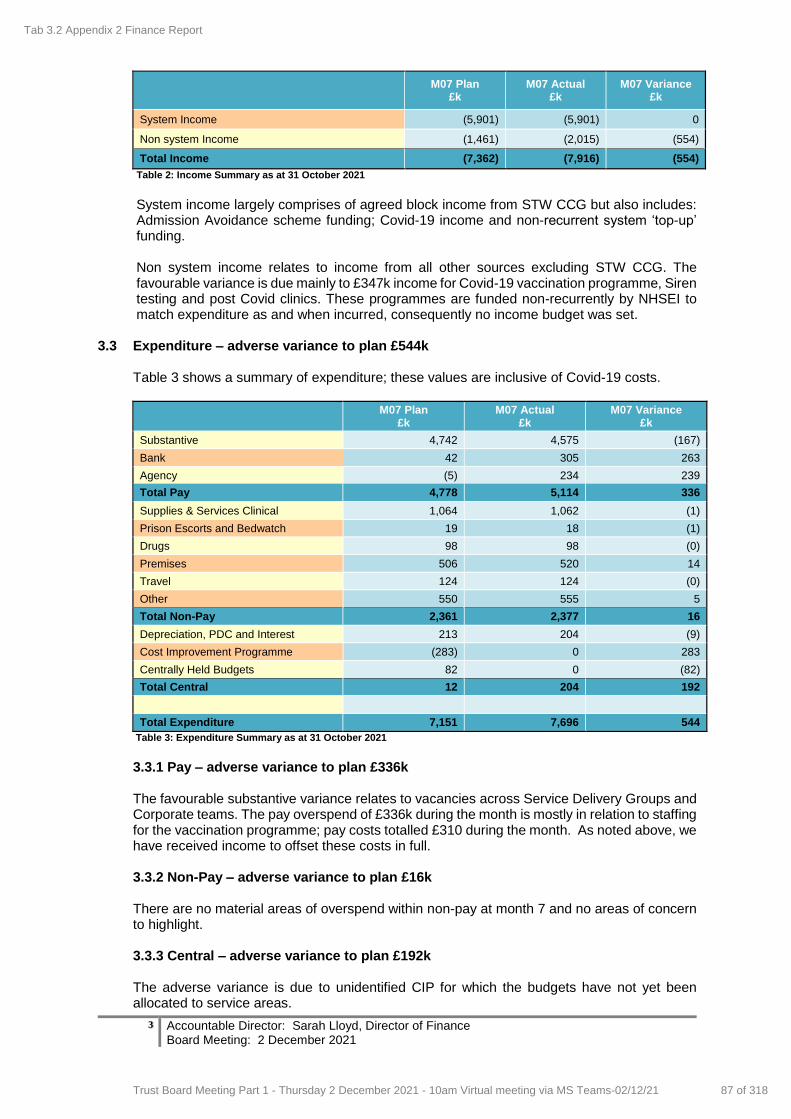
3 Accountable Director: Sarah Lloyd, Director of Finance Board Meeting: 2 December 2021
M07 Plan
£k M07 Actual
£k M07 Variance
£k
System Income (5,901) (5,901) 0
Non system Income (1,461) (2,015) (554)
Total Income (7,362) (7,916) (554)
Table 2: Income Summary as at 31 October 2021
System income largely comprises of agreed block income from STW CCG but also includes: Admission Avoidance scheme funding; Covid-19 income and non-recurrent system ‘top-up’ funding.
Non system income relates to income from all other sources excluding STW CCG. The favourable variance is due mainly to £347k income for Covid-19 vaccination programme, Siren testing and post Covid clinics. These programmes are funded non-recurrently by NHSEI to match expenditure as and when incurred, consequently no income budget was set.
3.3 Expenditure – adverse variance to plan £544k
Table 3 shows a summary of expenditure; these values are inclusive of Covid-19 costs.
M07 Plan
£k M07 Actual
£k M07 Variance
£k
Substantive 4,742 4,575 (167)
Bank 42 305 263
Agency (5) 234 239
Total Pay 4,778 5,114 336
Supplies & Services Clinical 1,064 1,062 (1)
Prison Escorts and Bedwatch 19 18 (1)
Drugs 98 98 (0)
Premises 506 520 14
Travel 124 124 (0)
Other 550 555 5
Total Non-Pay 2,361 2,377 16
Depreciation, PDC and Interest 213 204 (9)
Cost Improvement Programme (283) 0 283
Centrally Held Budgets 82 0 (82)
Total Central 12 204 192
Total Expenditure 7,151 7,696 544
Table 3: Expenditure Summary as at 31 October 2021 3.3.1 Pay – adverse variance to plan £336k The favourable substantive variance relates to vacancies across Service Delivery Groups and Corporate teams. The pay overspend of £336k during the month is mostly in relation to staffing for the vaccination programme; pay costs totalled £310 during the month. As noted above, we have received income to offset these costs in full. 3.3.2 Non-Pay – adverse variance to plan £16k There are no material areas of overspend within non-pay at month 7 and no areas of concern to highlight. 3.3.3 Central – adverse variance to plan £192k The adverse variance is due to unidentified CIP for which the budgets have not yet been allocated to service areas.
Tab 3.2 Appendix 2 Finance Report
87 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
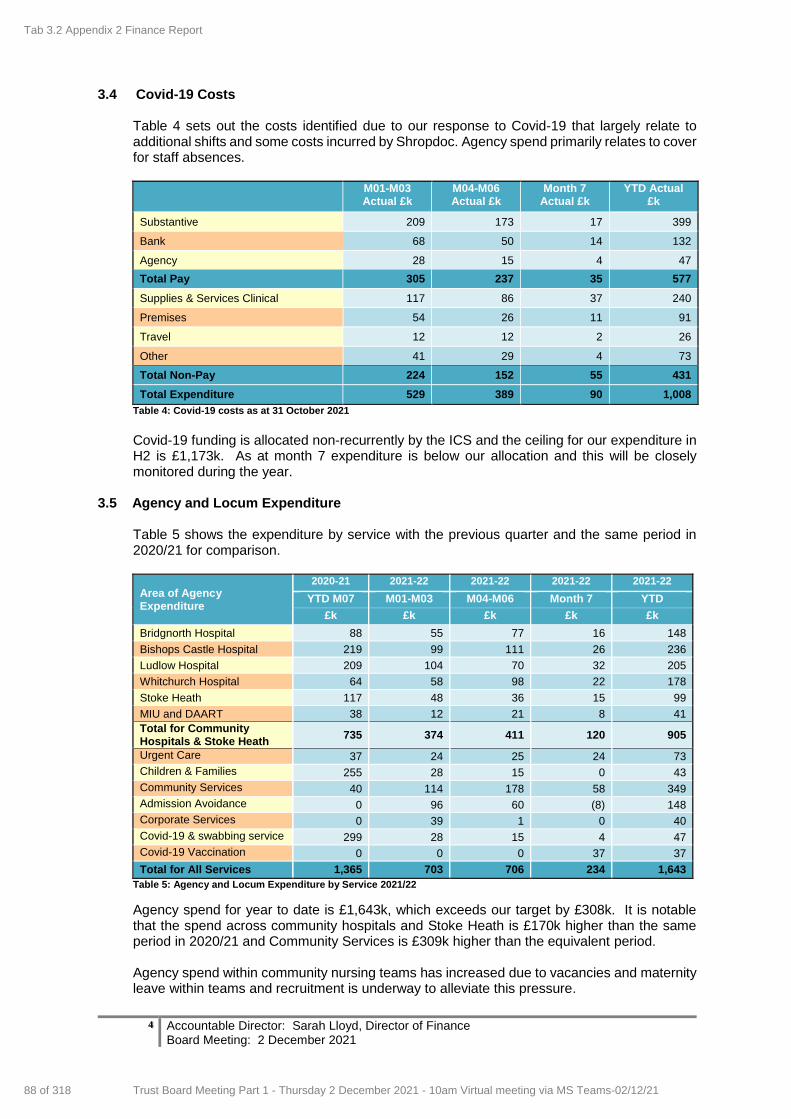
4 Accountable Director: Sarah Lloyd, Director of Finance Board Meeting: 2 December 2021
3.4 Covid-19 Costs
Table 4 sets out the costs identified due to our response to Covid-19 that largely relate to additional shifts and some costs incurred by Shropdoc. Agency spend primarily relates to cover for staff absences.
M01-M03 Actual £k
M04-M06 Actual £k
Month 7 Actual £k
YTD Actual £k
Substantive 209 173 17 399
Bank 68 50 14 132
Agency 28 15 4 47
Total Pay 305 237 35 577
Supplies & Services Clinical 117 86 37 240
Premises 54 26 11 91
Travel 12 12 2 26
Other 41 29 4 73
Total Non-Pay 224 152 55 431
Total Expenditure 529 389 90 1,008
Table 4: Covid-19 costs as at 31 October 2021
Covid-19 funding is allocated non-recurrently by the ICS and the ceiling for our expenditure in H2 is £1,173k. As at month 7 expenditure is below our allocation and this will be closely monitored during the year.
3.5 Agency and Locum Expenditure Table 5 shows the expenditure by service with the previous quarter and the same period in 2020/21 for comparison.
Area of Agency Expenditure
2020-21 2021-22 2021-22 2021-22 2021-22
YTD M07 M01-M03 M04-M06 Month 7 YTD
£k £k £k £k £k
Bridgnorth Hospital 88 55 77 16 148
Bishops Castle Hospital 219 99 111 26 236
Ludlow Hospital 209 104 70 32 205
Whitchurch Hospital 64 58 98 22 178
Stoke Heath 117 48 36 15 99
MIU and DAART 38 12 21 8 41
Total for Community Hospitals & Stoke Heath
735 374 411 120 905
Urgent Care 37 24 25 24 73
Children & Families 255 28 15 0 43
Community Services 40 114 178 58 349
Admission Avoidance 0 96 60 (8) 148
Corporate Services 0 39 1 0 40
Covid-19 & swabbing service 299 28 15 4 47
Covid-19 Vaccination 0 0 0 37 37
Total for All Services 1,365 703 706 234 1,643
Table 5: Agency and Locum Expenditure by Service 2021/22
Agency spend for year to date is £1,643k, which exceeds our target by £308k. It is notable that the spend across community hospitals and Stoke Heath is £170k higher than the same period in 2020/21 and Community Services is £309k higher than the equivalent period. Agency spend within community nursing teams has increased due to vacancies and maternity leave within teams and recruitment is underway to alleviate this pressure.
Tab 3.2 Appendix 2 Finance Report
88 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
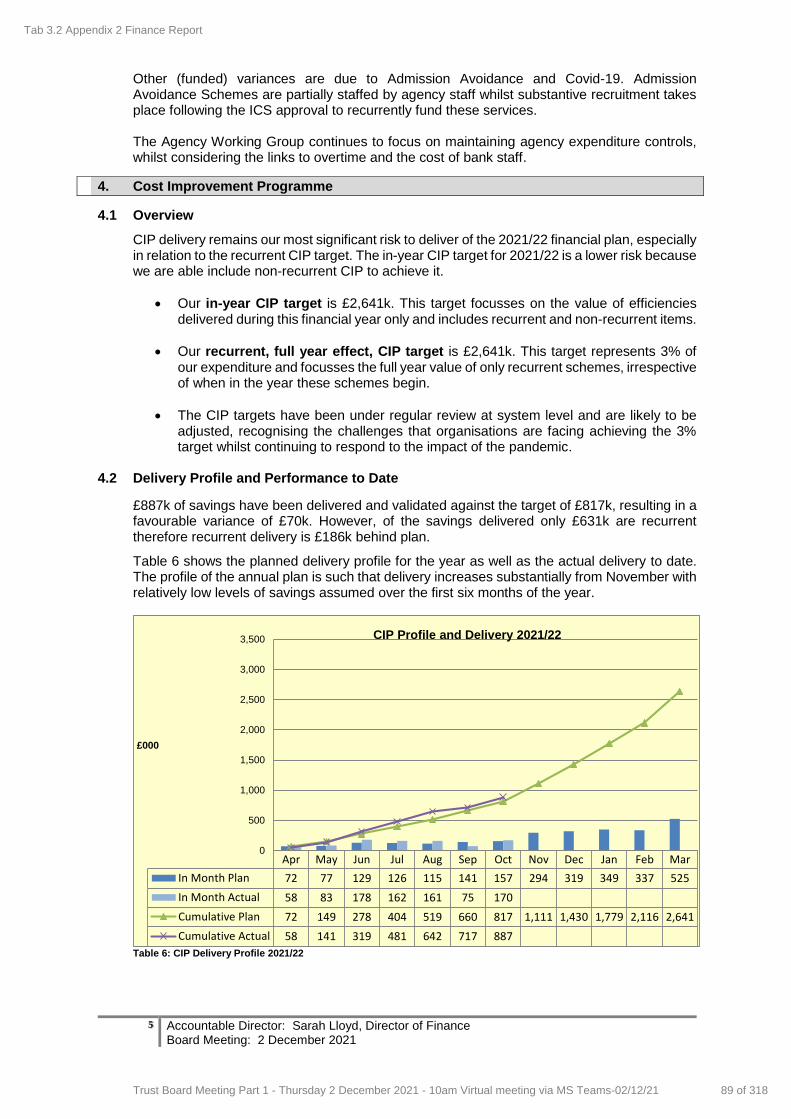
5 Accountable Director: Sarah Lloyd, Director of Finance Board Meeting: 2 December 2021
Other (funded) variances are due to Admission Avoidance and Covid-19. Admission Avoidance Schemes are partially staffed by agency staff whilst substantive recruitment takes place following the ICS approval to recurrently fund these services. The Agency Working Group continues to focus on maintaining agency expenditure controls, whilst considering the links to overtime and the cost of bank staff.
4. Cost Improvement Programme
4.1 Overview
CIP delivery remains our most significant risk to deliver of the 2021/22 financial plan, especially in relation to the recurrent CIP target. The in-year CIP target for 2021/22 is a lower risk because we are able include non-recurrent CIP to achieve it.
Our in-year CIP target is £2,641k. This target focusses on the value of efficiencies delivered during this financial year only and includes recurrent and non-recurrent items.
Our recurrent, full year effect, CIP target is £2,641k. This target represents 3% of our expenditure and focusses the full year value of only recurrent schemes, irrespective of when in the year these schemes begin.
The CIP targets have been under regular review at system level and are likely to be adjusted, recognising the challenges that organisations are facing achieving the 3% target whilst continuing to respond to the impact of the pandemic.
4.2 Delivery Profile and Performance to Date
£887k of savings have been delivered and validated against the target of £817k, resulting in a favourable variance of £70k. However, of the savings delivered only £631k are recurrent therefore recurrent delivery is £186k behind plan.
Table 6 shows the planned delivery profile for the year as well as the actual delivery to date. The profile of the annual plan is such that delivery increases substantially from November with relatively low levels of savings assumed over the first six months of the year.
Table 6: CIP Delivery Profile 2021/22
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
In Month Plan 72 77 129 126 115 141 157 294 319 349 337 525
In Month Actual 58 83 178 162 161 75 170
Cumulative Plan 72 149 278 404 519 660 817 1,111 1,430 1,779 2,116 2,641
Cumulative Actual 58 141 319 481 642 717 887
0
500
1,000
1,500
2,000
2,500
3,000
3,500
£000
CIP Profile and Delivery 2021/22
Tab 3.2 Appendix 2 Finance Report
89 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
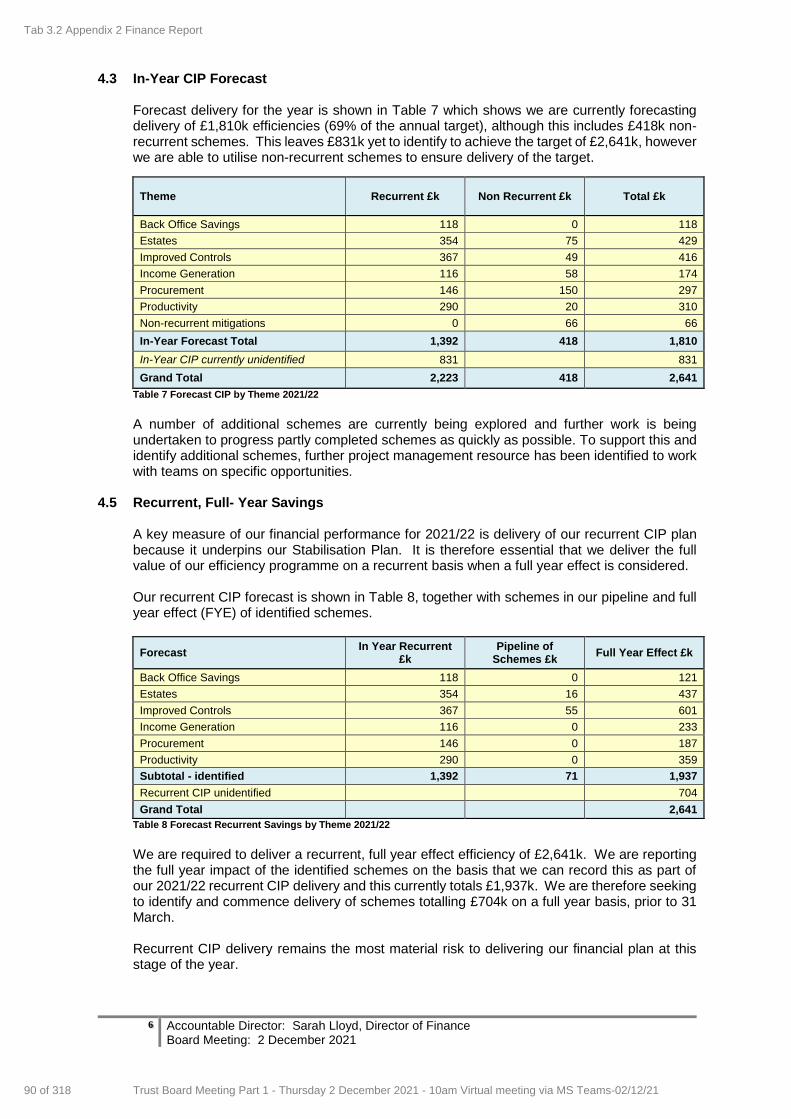
6 Accountable Director: Sarah Lloyd, Director of Finance Board Meeting: 2 December 2021
4.3 In-Year CIP Forecast Forecast delivery for the year is shown in Table 7 which shows we are currently forecasting delivery of £1,810k efficiencies (69% of the annual target), although this includes £418k non-recurrent schemes. This leaves £831k yet to identify to achieve the target of £2,641k, however we are able to utilise non-recurrent schemes to ensure delivery of the target.
Theme Recurrent £k Non Recurrent £k Total £k
Back Office Savings 118 0 118
Estates 354 75 429
Improved Controls 367 49 416
Income Generation 116 58 174
Procurement 146 150 297
Productivity 290 20 310
Non-recurrent mitigations 0 66 66
In-Year Forecast Total 1,392 418 1,810
In-Year CIP currently unidentified 831 831
Grand Total 2,223 418 2,641
Table 7 Forecast CIP by Theme 2021/22
A number of additional schemes are currently being explored and further work is being undertaken to progress partly completed schemes as quickly as possible. To support this and identify additional schemes, further project management resource has been identified to work with teams on specific opportunities.
4.5 Recurrent, Full- Year Savings A key measure of our financial performance for 2021/22 is delivery of our recurrent CIP plan because it underpins our Stabilisation Plan. It is therefore essential that we deliver the full value of our efficiency programme on a recurrent basis when a full year effect is considered. Our recurrent CIP forecast is shown in Table 8, together with schemes in our pipeline and full year effect (FYE) of identified schemes.
Forecast In Year Recurrent
£k Pipeline of
Schemes £k Full Year Effect £k
Back Office Savings 118 0 121
Estates 354 16 437
Improved Controls 367 55 601
Income Generation 116 0 233
Procurement 146 0 187
Productivity 290 0 359
Subtotal - identified 1,392 71 1,937
Recurrent CIP unidentified 704
Grand Total 2,641
Table 8 Forecast Recurrent Savings by Theme 2021/22
We are required to deliver a recurrent, full year effect efficiency of £2,641k. We are reporting the full year impact of the identified schemes on the basis that we can record this as part of our 2021/22 recurrent CIP delivery and this currently totals £1,937k. We are therefore seeking to identify and commence delivery of schemes totalling £704k on a full year basis, prior to 31 March. Recurrent CIP delivery remains the most material risk to delivering our financial plan at this stage of the year.
Tab 3.2 Appendix 2 Finance Report
90 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
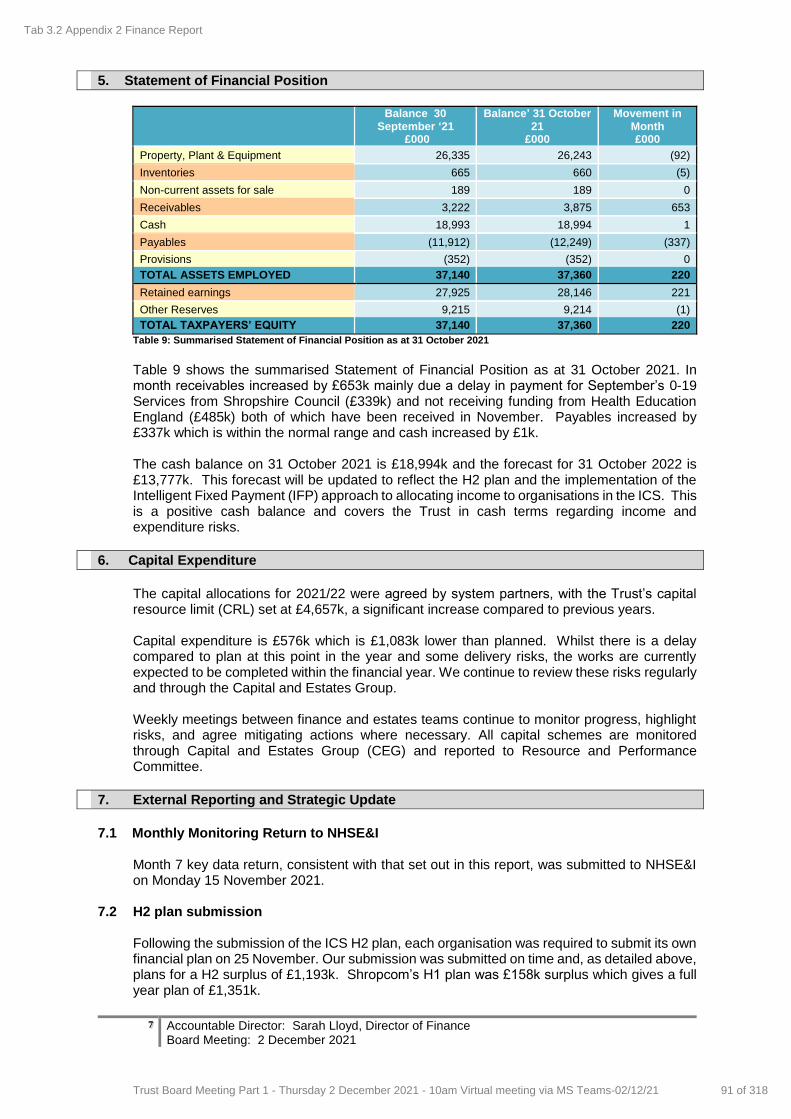
7 Accountable Director: Sarah Lloyd, Director of Finance Board Meeting: 2 December 2021
5. Statement of Financial Position
Balance 30
September ‘21 £000
Balance’ 31 October 21
£000
Movement in Month £000
Property, Plant & Equipment 26,335 26,243 (92)
Inventories 665 660 (5)
Non-current assets for sale 189 189 0
Receivables 3,222 3,875 653
Cash 18,993 18,994 1
Payables (11,912) (12,249) (337)
Provisions (352) (352) 0
TOTAL ASSETS EMPLOYED 37,140 37,360 220
Retained earnings 27,925 28,146 221
Other Reserves 9,215 9,214 (1)
TOTAL TAXPAYERS’ EQUITY 37,140 37,360 220
Table 9: Summarised Statement of Financial Position as at 31 October 2021 Table 9 shows the summarised Statement of Financial Position as at 31 October 2021. In month receivables increased by £653k mainly due a delay in payment for September’s 0-19 Services from Shropshire Council (£339k) and not receiving funding from Health Education England (£485k) both of which have been received in November. Payables increased by £337k which is within the normal range and cash increased by £1k. The cash balance on 31 October 2021 is £18,994k and the forecast for 31 October 2022 is £13,777k. This forecast will be updated to reflect the H2 plan and the implementation of the Intelligent Fixed Payment (IFP) approach to allocating income to organisations in the ICS. This is a positive cash balance and covers the Trust in cash terms regarding income and expenditure risks.
6. Capital Expenditure
The capital allocations for 2021/22 were agreed by system partners, with the Trust’s capital resource limit (CRL) set at £4,657k, a significant increase compared to previous years. Capital expenditure is £576k which is £1,083k lower than planned. Whilst there is a delay compared to plan at this point in the year and some delivery risks, the works are currently expected to be completed within the financial year. We continue to review these risks regularly and through the Capital and Estates Group. Weekly meetings between finance and estates teams continue to monitor progress, highlight risks, and agree mitigating actions where necessary. All capital schemes are monitored through Capital and Estates Group (CEG) and reported to Resource and Performance Committee.
7. External Reporting and Strategic Update
7.1 Monthly Monitoring Return to NHSE&I
Month 7 key data return, consistent with that set out in this report, was submitted to NHSE&I on Monday 15 November 2021.
7.2 H2 plan submission Following the submission of the ICS H2 plan, each organisation was required to submit its own
financial plan on 25 November. Our submission was submitted on time and, as detailed above, plans for a H2 surplus of £1,193k. Shropcom’s H1 plan was £158k surplus which gives a full year plan of £1,351k.
Tab 3.2 Appendix 2 Finance Report
91 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
8 Accountable Director: Sarah Lloyd, Director of Finance Board Meeting: 2 December 2021
7.3 Transfer of Covid-19 Vaccination Service to Shropcom
We became the lead provider and employer for this service from October. The cost of the service is fully reimbursed, and payments are made based on the quarterly cost returns which we submit.
7.4 Lease renewal for Hortonwood
The main site for the Community Equipment Service is at Hortonwood in Telford. We are proposing to renew the lease for 5 years, which includes a break clause at 3 years. The lease cost is £96k per year and the RPC recommended this lease renewal to the Board for approval.
8. Recommendations
The Board is asked to:
Consider the adjusted financial position for month 7, which is a surplus of £230k compared to a plan of £221k which is a favourable variance of £9k
Consider that recurrent CIP development remains a challenge and is our most material financial risk; work continues to identify additional schemes
Recognise that Shropcom submitted its detailed H2 financial plan on 25 November 2021 which includes a planned surplus of £1,193k
Approve the lease renewal for the Community Equipment Services property at Hortonwood
Tab 3.2 Appendix 2 Finance Report
92 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1 Accountable Director: Sarah Lloyd, Director of Finance Meeting Date: 2 December 2021
REPORT COVER SHEET Report Title: Charitable Funds Annual Report & Accounts 2020/21
Meeting: Trust Board
Author: David Court, Head of Financial Accounting
Accountable Director:
Sarah Lloyd, Director of Finance
Other meetings or Committee presented to or previously agreed at:
Meeting or Committee Date Reviewed
Charitable Funds Committee
25 November 2021
Strategic goals this report relates to: (tick as appropriate)
To deliver high quality care
To deliver integrated care
To support people to live the lives they want
to lead
To deliver sustainable community
services
Relevance to Board Assurance Framework : (tick as appropriate)
Clinical Quality &
Safety
Long term financial
sustainability of the Trust
Healthcare Systems
Organisational culture
Optimising use of technology
Covid19
Relevance to Well-led domains (CQC & NHSE/I): (tick as appropriate)
leadership capacity and capability
clear vision and credible strategy
culture clear roles and responsibilities
clear and effective risk management
appropriate and accurate information
learning, continuous improvement and innovation
Stakeholders engaged and involved
Relevance to CQC domains: (tick as appropriate)
Safe Caring Responsive Effective Well led
Impacts and Implications? YES or NO
If yes, what impact or implication
Patient safety & experience No
Equality & Inclusion No
Financial (revenue & capital) Yes
The Board has overall responsibility for approving the charitable funds annual report & accounts
IG Governance Toolkit No
Meeting Date: 2 December 2021
Agenda Item: 13
Enclosure Number: 11
Tab 4 13. 2020/21 Charitable Funds Accounts
93 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2 Accountable Director: Sarah Lloyd, Director of Finance Meeting Date: 2 December 2021
OD/Workforce No
Legal No
Relevance to Corporate Risk
Register (Risk No/Name) No
Aim of the report (a concise statement of the purpose of this report)
To request the Board, as the Corporate Trustee, to formally approve the Charitable Funds Annual Report and Accounts for 2020/21, as recommended by the Charitable Funds Committee on 25 November 2021
Assessment and summary of key points in report (include analysis and consideration of issues, options,
risks and mitigations. Also include good practice, required improvements, and timescales. If appropriate, include a judgement on the level of assurance the report provides: Substantial: Moderate: Limited: None)
The Charitable Funds Committee have considered and endorsed the Charitable Funds Annual Report & Accounts 2020/21 on behalf of the Board in line with their delegated responsibility and recommended these for formal approval by the Board. The accounts show an overall decrease in fund balances during the year of £77k from £241k to £164k, consisting of income of £298k and expenditure of £375k. Income of £298k included Grants from NHS Charities together of £98k, Donations of £153k and a Legacy of £47k. Generous donations were received from: The League of Friends of Bridgnorth Hospital £131,000 and The League of Friends of Whitchurch Hospital £7,000, a total of £138,000. These donations were mainly in respect of medical equipment. Expenditure of £375k included £336k on patient welfare and amenities comprising of: - a new X Ray machine at Whitchurch Hospital £159k, at Bridgnorth Hospital a new AER (Automated Endoscope Reprocessor) machine £105k, four High low beds £19k and a new bladder scanner £5k all from League of Friends donations. £23k, was spent on patient welfare in relation to the NHS Charities together Stage 1 COVID Grant, this included a variety of items to enhance the well-being of patients impacted by the pandemic. Expenditure on staff welfare and amenities totalled £39k, this included £37k in relation to the NHS Charities together Stage 1 COVID Grant. A variety of items were purchased to enhance the well-being of staff impacted by the pandemic. Given the value of the funds, they are not subject to a full external audit, however the Trust’s External Auditors carried out an independent examination, resulting in no change in the reported position. The annual report and accounts, and the draft audit findings report are attached. The Annual Report and Accounts will be submitted to the Charity Commission as part of the annual return prior to 31st January 2022.
Purpose of the Report (tick as appropriate)
Consider for Action
Give Approval Accept Assurance
Provide Information
Tab 4 13. 2020/21 Charitable Funds Accounts
94 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21

3 Accountable Director: Sarah Lloyd, Director of Finance Meeting Date: 2 December 2021
Key Recommendations
The Board is asked to: formally adopt the Charitable Funds Annual Report & Accounts for 2020/21, as approved by the Charitable Funds Committee on 25 November 2021 and in accordance with their delegated authority.
Tab 4 13. 2020/21 Charitable Funds Accounts
95 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Charitable Funds
Annual Report & Accounts 2020/21
Charity Registration Number 1056698
Cover
Tab 4 13. 2020/21 Charitable Funds Accounts
96 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Select suitable accounting policies and then apply them consistently
Make judgments and estimates that are reasonable and prudent
Signed on behalf of the trustees:
Chair : ……………………………………………. Date : …………………………
Trustee : ………………….……………………… Date : …………………………
Statement of Trustees' Responsibilities in respect of the Trustees' Annual Report and
Accounts
The trustees are required to act in accordance with the trust deed and the rules of the charity, within the
framework of trust law. The trustees are responsible for keeping proper accounting records, sufficient to
disclose at any time, with reasonable accuracy, the financial position of the charity at that time, and to
enable the trustees to ensure that, where any statements of accounts are prepared by the trustees under
section 132(1) of the Charities Act 2011, those statements of accounts comply with the requirements of
regulations under that provision. The trustees have general responsibility for taking such steps as are
reasonably open to the trustees to safeguard the assets of the charity and to prevent and detect fraud and
other irregularities.
The trustees confirm that they have met the responsibilities set out above and complied with the
requirements for preparing the accounts. The financial statements set out on pages 4 to 11 have been
compiled from and are in accordance with the financial records maintained by the trustees.
Under charity law, the trustees are responsible for preparing the trustees’ annual report and
accounts for each financial year which show a true and fair view of the state of affairs of the
charity and of the excess of expenditure over income for that period.
In preparing these financial statements, generally accepted accounting practice requires that the trustees:
State whether the recommendations of the SORP have been followed, subject to any material
departures disclosed and explained in the financial statements
State whether the financial statements comply with the trust deed, subject to any material departures
disclosed and explained in the financial statements
Prepare the financial statements on the going concern basis unless it is inappropriate to presume that
the charity will continue its activities.
Tab 4 13. 2020/21 Charitable Funds Accounts
97 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Commercial in confidence
Independent examiner's report to the corporate trustee of NHS Shropshire
Community Health NHS Trust Charitable Funds
I report on the accounts of Shropshire Community Health NHS Trust Charitable Funds (the "charity") for the year ended 31
March 2021, which are set out on pages 3 to 13.
Independent examiner's statement
In connection with my examination, no matter has come to my attention:
which gives me reasonable cause to believe that in any material respect, the requirements:
to keep accounting records in accordance with section 130 of the Charities Act 2011; and
to prepare accounts which accord with the accounting records; and
to comply with the applicable requirements concerning the form and content of accounts set out in the Charities
(Accounts and Reports) Regulations 2008
have not been met, or
to which, in my opinion, attention should be drawn in order to enable a proper understanding of the accounts to be
reached.
Basis of independent examiner's statement
My examination was carried out in accordance with the general Directions given by the Charity Commission. An examination
includes a comparison of the accounts with the accounting records kept by the charity. It also includes consideration of any
unusual items or disclosures in the accounts and seeking explanations from you as corporate trustee concerning any such
matters. The procedures undertaken do not provide all the evidence that would be required in an audit, and consequently no
opinion is given as to whether the accounts present a 'true and fair' view and the report is limited to those matters set out in
the statement above.
Respective responsibilities of corporate trustee and examiner
The charity’s corporate trustee is responsible for the preparation of the accounts. The charity’s trustee considers that an audit
is not required for this year under section 149(2) of the Charities Act 2011 and that an independent examination is needed.
It is my responsibility to:
examine the accounts under section 149 of the Charities Act 2011;
to follow the procedures laid down in the general Directions given by the Charity Commission under section 149(5) of the
Charities Act 2011; and
to state whether particular matters have come to my attention.
Your attention is drawn to the fact that the charity's trustee has prepared the charity's accounts in accordance with the
Statement of Recommended Practice 'Accounting and Reporting by Charities: Statement of Recommended Practice
applicable to charities preparing their accounts in accordance with the Financial Reporting Standard applicable in the UK and
Republic of Ireland (FRS 102) issued in October 2019 in preference to the Statement of Recommended Practice 'Accounting
and Reporting by Charities: Statement of Recommended Practice (revised 2005)' issued in April 2005 which is referred to in
the Charities (Accounts and Reports) Regulations 2008 but has been withdrawn. I understand that the charity's trustee has
done this in order for the charity's accounts to give a true and fair view in accordance with United Kingdom Generally
Accepted Accounting Practice effective for reporting periods beginning on or after 1 January 2019.
Use of this report
This report is in respect of an examination carried out under section 149(3) of the Charities Act 2011. This report is made
solely to the charity's corporate trustee, as a body, in accordance with the regulations made under section 154 of the
Charities Act 2011. My work has been undertaken so that I might state to the charity's trustees those matters I am required to
state to them in an independent examiner's report and for no other purpose. To the fullest extent permitted by law, I do not
accept or assume responsibility to anyone other than the charity and the charity's trustee, as a body, for my work, for this
report or for the opinions I have formed.
XXX
Grant Thornton UK LLP
Chartered Accountants
Birmingham
XX November 2021
Tab 4 13. 2020/21 Charitable Funds Accounts
98 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Reference & Administrative Details
Name of charity:
Registered charity number: 1056698
Address of charity: Trust Headquarters, William Farr House,
Mytton Oak Road, Shrewsbury, SY3 8XL
Trustee Arrangements
During 2020/21 they were as follows:
David Stout
Ros Preen
Jane Povey
Steve Gregory
Sarah Lloyd
Jaki Lowe (1st April 2020 to 23rd August 2020)
Victoria Rankin
Louise Brereton (20th July 2020 to 7th January 2021)
Michael Wuesterfeld-Gray (7th January to 31st March 2021))
Nuala O'Kane
Peter Phillips
Harmesh Darbhanga
Peter Featherstone
Tina Long
Cathy Purt
Mike McDonald
Governance & Management
The committee has responsibility for ensuring that:
Spending is in line with agreed objects and priorities.
All legal duties and regulations in relation to charitable funds are complied with.
Devolved decision making and delegation is in accordance with the policies and procedures set out
by the Board.
Annual Report
In its role as corporate trustee, the Trust Board takes into account the Charity Commission guidance
on independence. A Charitable Funds Committee has therefore been set up with delegated
responsibility for managing the charity, ensuring that the use of charitable funds is focussed on the
needs of patients. This committee operates within the Terms of Reference and delegated powers as
set by the Board.
In accordance with the Charities Act 2011, the charity is included in the Charity Commission's
Register of Charities with the following details:
There are 16 separate sub-funds registered within the group registration. There are further sub-
divisions for the purpose of local management of funds.
The original governing document was a deed dated June 1996, as amended by supplementary deeds
due to NHS re-organisations over the years.
The Trust is the sole corporate trustee of the charity. Since the Trust must act through individuals in
order to express its will, trusteeship is assumed by the members of the Trust Board.
Shropshire Community Health NHS Trust General Charitable
Fund
3
Tab 4 13. 2020/21 Charitable Funds Accounts
99 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Objectives & Activities
Patients Expenditure
Improving patient facilities and amenities to improve the environment.
Staff Expenditure
Motivation of staff, by improving staff facilities and providing services that improve staff wellbeing.
Education of staff by providing training over and above what would normally be provided.
Relationships with Related Parties/External Bodies
Review of Finances, Activities, Achievements & Performance
The charity is accounted for and administered on a day to day basis by the Finance Department of
Shropshire Community Health NHS Trust.
The strategy of the charity is to provide support by providing funds to benefit patients of Shropshire
Community Health NHS Trust. It does this by purchasing supplementary and complementary equipment or
services for which the Trust is unable to provide funding through exchequer sources.
The charity does not currently actively fundraise and relies upon the generosity of patients and their relatives
and other donors who are familiar with, or have experienced the care of the Trust services and hospitals, or
who are sympathetic and generous in their support to their local NHS services.
The objective of the charity is that the Trustees shall apply the income and, at their discretion, so far as may
be permissible, the capital, for any charitable purposes relating to the NHS wholly or mainly for the services
provided within Shropshire Community Health NHS Trust.
The charity is funded by donations and legacies received from patients, their relatives, the general public
and other organisations. The overall strategy of the charity is to provide support to the above Trust by the
following means:
Purchase of medical equipment and provision of services not normally provided by or in addition to that
normally provided by the NHS.
Close links are also maintained with individual hospital League of Friends organisations. The charity is
pleased to work with these organisations in the provision of charitable support to the related hospitals and
health services.
Grants to the related NHS organisation, Shropshire Community Health NHS Trust, are made in accordance
with donors' wishes and in line with Charity Commission guidance on the public benefit.
The charity works closely with the Trust. Staff within the organisation identify and advise the charity on local
priorities and assist the corporate trustee in monitoring the use of the charitable funds.
The strong relationship with members of staff is particularly valued and enables the charitable funds to be
directed to ensure an effective contribution is made in support of local services.
4
Tab 4 13. 2020/21 Charitable Funds Accounts
100 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Finances
Patient welfare and amenities
Staff welfare and amenities
Future Plans
Reserves policy
In the 2020/21 financial year the charity received Grants of £98,000 from NHS Charities Together,
Donations of £153,000 and a Legacy of £47,000. Total incoming resources for the year were therefore
£298,000.
The overall financial performance recorded a net decrease in funds of £77,000.
Patients’ welfare expenditure totalled £336,000. The majority of this expenditure related to medical
equipment and the most significant items were:
£132,000 from the Bridgnorth Hospital Patient Welfare Fund and relates to donations from the
League of Friends for an AER (Automated Endoscope Reprocessor) Machine £105,000, 4 Hi low beds
£19,000, a new bladder scanner £5,000 and a Lockable Suture trolley £1,500. With a further £1,500
spent on smaller items from a number of donations.
In particular the League of Friends of Bridgnorth Hospital donated £131,000 and the League of Friends
of Whitchurch Hospital donated £7,000, a total of £138,000 between them. These donations were
mainly for medical equipment.
£169,000 from the Whitchurch Hospital Patient Welfare Fund and relates to donations from the
League of Friends for a new X Ray machine £159,000 relating to the donation given in 2019/20, £5,000
for a new bladder scanner and £2,500 for a patient transfer scale. With a further £2,500 spent on
smaller items from a number of donations.
The charity's intention is that funds are spent within a reasonable period of receipt, and therefore
reserves should not be built up. Managers are encouraged to spend the funds to continue to reduce the
level of funds held.
Expenditure from the Staff welfare funds totalled £39,000. £37,000 from the General Fund in relation to
the NHS Charities Together Stage 1 COVID Grant for a variety of items to enhance the well-being of
NHS Staff and volunteers impacted by COVID-19.
The trustees do not expect any significant changes in the objectives of the charity in the forthcoming
years, and intends to continue to reduce fund balances where suitable projects and schemes can be
identified.
£23,000 from the General Fund in relation to the NHS Charities together Stage 1 COVID Grant on a
variety of items to enhance the well-being patients impacted by COVID-19.
The charity can only continue to support the work of Shropshire Community Health NHS Trust as long
as donations and legacies continue to be received. The charity is therefore indebted to the generosity of
patients, their families and carers, well-wishers and friends, who have donated so generously to the
work of the charity. This includes people who have left legacies in their will, and we are aware that we
receive these monies at a sensitive time for the remaining family.
5
Tab 4 13. 2020/21 Charitable Funds Accounts
101 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
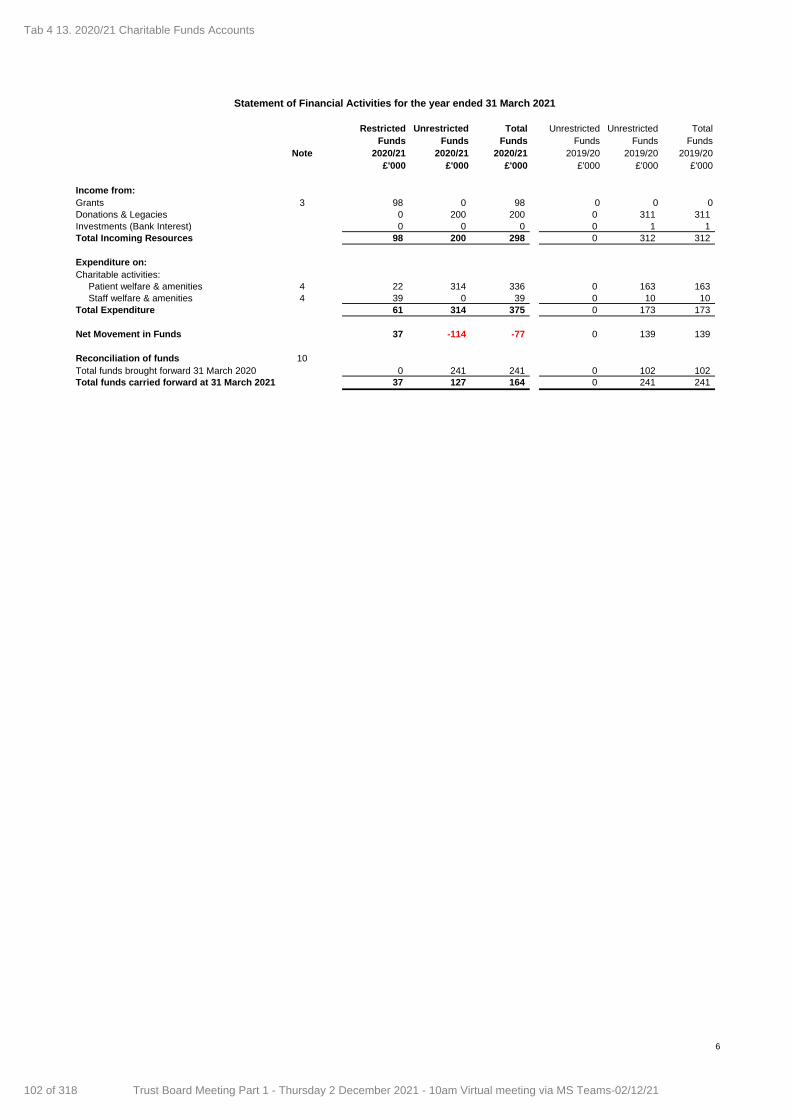
Restricted Unrestricted Total Unrestricted Unrestricted Total
Funds Funds Funds Funds Funds Funds
Note 2020/21 2020/21 2020/21 2019/20 2019/20 2019/20
£'000 £'000 £'000 £'000 £'000 £'000
Income from:
Grants 3 98 0 98 0 0 0
Donations & Legacies 0 200 200 0 311 311
Investments (Bank Interest) 0 0 0 0 1 1
Total Incoming Resources 98 200 298 0 312 312
Expenditure on:
Charitable activities:
Patient welfare & amenities 4 22 314 336 0 163 163
Staff welfare & amenities 4 39 0 39 0 10 10
Total Expenditure 61 314 375 0 173 173
Net Movement in Funds 37 -114 -77 0 139 139
Reconciliation of funds 10
Total funds brought forward 31 March 2020 0 241 241 0 102 102
Total funds carried forward at 31 March 2021 37 127 164 0 241 241
Statement of Financial Activities for the year ended 31 March 2021
6
Tab 4 13. 2020/21 Charitable Funds Accounts
102 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
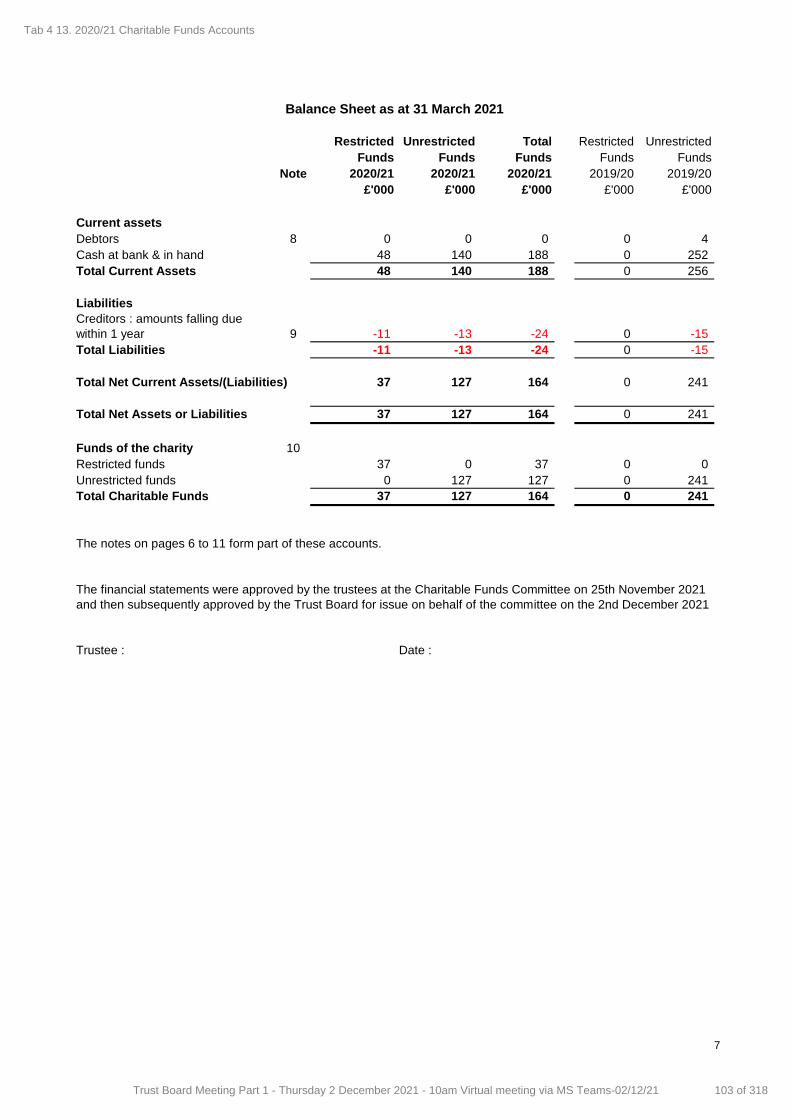
Restricted Unrestricted Total Restricted Unrestricted
Funds Funds Funds Funds Funds
Note 2020/21 2020/21 2020/21 2019/20 2019/20
£'000 £'000 £'000 £'000 £'000
Current assets
Debtors 8 0 0 0 0 4
Cash at bank & in hand 48 140 188 0 252
Total Current Assets 48 140 188 0 256
Liabilities
9 -11 -13 -24 0 -15
Total Liabilities -11 -13 -24 0 -15
Total Net Current Assets/(Liabilities) 37 127 164 0 241
Total Net Assets or Liabilities 37 127 164 0 241
Funds of the charity 10
Restricted funds 37 0 37 0 0
Unrestricted funds 0 127 127 0 241
Total Charitable Funds 37 127 164 0 241
The notes on pages 6 to 11 form part of these accounts.
Trustee : Date :
Balance Sheet as at 31 March 2021
Creditors : amounts falling due
within 1 year
The financial statements were approved by the trustees at the Charitable Funds Committee on 25th November 2021
and then subsequently approved by the Trust Board for issue on behalf of the committee on the 2nd December 2021
7
Tab 4 13. 2020/21 Charitable Funds Accounts
103 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
a) Basis of preparation
The financial statements have been prepared under the historic cost convention.
b) Funds structure
c) Incoming resources
There are 16 separate sub-funds registered within the group registration with the Charity Commission,
with further sub-divisions for the purpose of local management of funds.
All incoming resources are recognised once the charity has entitlement to the resources, it is probable
(more likely than not) that the resources will be received, and the monetary value of the incoming
resources can be measured with sufficient reliability.
Where there are terms or conditions attached to incoming resources, particularly grants, then these
terms or conditions must be met before the income is recognised as the entitlement condition will not
be satisfied until that point. Where terms or conditions have not been met or uncertainty exists as to
whether they can be met, then the relevant income is not recognised in the year but deferred and
shown on the balance sheet as deferred income.
NOTES TO THE ACCOUNTS
Note 1 : Accounting Policies
The accounts (financial statements) have been prepared to give a "true and fair view" and have
departed from the Charities (Accounts and Reports) Regulations 2008 only to the extent required to
provide a "true and fair view". This departure has involved following Accounting and Reporting by
Charities preparing their accounts in accordance with the Financial Reporting Standard applicable in the
UK and Republic of Ireland (FRS 102) issued on 16 July 2014 rather than Accounting and Reporting by
Charities : Statement of Recommended Practice effective from 1 April 2005 which has since been
withdrawn.
The accounts (financial statements) have been prepared in accordance with the Statement of
Recommended Practice : Accounting and Reporting by Charities preparing their accounts in
accordance with the Financial Reporting Standard applicable in the UK and Republic of Ireland (FRS
102) issued on 16 July 2014 and the Charities Act 2011 and UK Generally Accepted Accounting
Practice as it applies from 1 January 2015.
The trustees consider that there are no material uncertainties about the charity's ability to continue as a
going concern. There are no material uncertainties affecting the current year's accounts.
An endowment fund - where the donor has expressly provided that the gift is to be invested and only
the income of the fund may be spent.
A restricted income fund - where the donor has provided for the donation to be spent in furtherance of
a specified charitable purpose.
Where there is a legal restriction on the purpose to which a fund may be put, the fund is classified
either as:
Update Bulletin 1 of the Charities SORP (FRS 102) was implemented in 2015/16.
The charity currently has no endowment funds but does have restricted income funds in the form of
Grants received from NHS Charities Together in relation to COVID.
Update Bulletin 2 of the Charities SORP (FRS 102) was implemented in 2019/20.
8
Tab 4 13. 2020/21 Charitable Funds Accounts
104 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
d) Incoming resources from legacies
Receipt is probable when all the following conditions are met:
All conditions attached to the legacy have been fulfilled or are within the charity's control.
e) Resources expended and irrecoverable VAT
There is a present legal or constructive obligation resulting from a past event.
The amount of the obligation can be measured or estimated reliably.
Irrecoverable VAT is charged against the category of resources expended for which it was incurred.
f) Recognition of expenditure and associated liabilities as a result of grant
g) Allocation of support costs
h) Charitable activities
NOTES TO THE ACCOUNTS
Grants payable are payments made to linked, related party or third party NHS bodies and non NHS bodies, in
furtherance of the charitable objectives of the funds held on trust, primarily relief of those who are sick.
Legacies are accounted for as incoming resources either upon receipt or where the receipt of the legacy is
probable.
Confirmation has been received from the estate representatives that probate has been granted
The executors have established that there are sufficient assets in the estate to pay the legacy
If there is uncertainty as to the amount of the legacy and it cannot be reliably estimated, then the legacy is
shown as a contingent asset until all of the conditions for income recognition are met.
All expenditure is accounted for on an accruals basis and has been classified under headings that aggregate
all costs related to each category of expense shown in the Statement of Financial Activities. Expenditure is
recognised when the following criteria are met:
It is more likely than not that a transfer of benefits (usually a cash payment) will be required in settlement.
Grant payments are recognised as expenditure when the conditions for their payment have been met or
where there is a constructive obligation to make a payment:
Approval and authorisation have been granted in accordance with the Scheme of Delegation operated by
the Trustee.
Receipt of goods or services have been confirmed as appropriate and payment authorised in accordance
with the Trustee's Standing Financial Instructions.
Support costs are those costs which do not relate directly to a single activity. These include costs of
administration, internal and external audit costs and bank charges. Support costs have been apportioned
across the categories of charitable expenditure on an appropriate basis. The analysis of support costs and
the basis of apportionment applied are shown in note 5.
Costs of charitable activities comprise all costs incurred in the pursuit of the charitable objects of the charity.
These costs, where not wholly attributable, are apportioned between the categories of charitable expenditure
in addition to the direct costs. The total costs of each category of charitable expenditure include an
apportionment of support costs as shown in note 4.
9
Tab 4 13. 2020/21 Charitable Funds Accounts
105 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
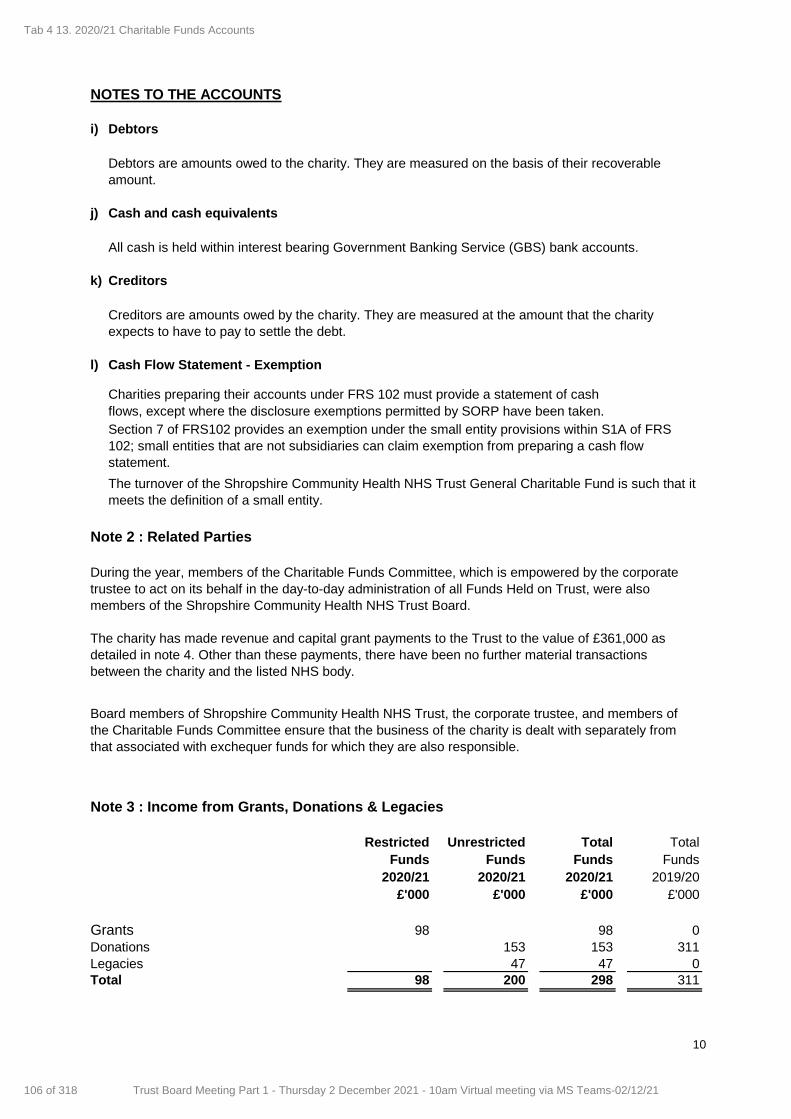
i) Debtors
j) Cash and cash equivalents
All cash is held within interest bearing Government Banking Service (GBS) bank accounts.
k) Creditors
l) Cash Flow Statement - Exemption
flows, except where the disclosure exemptions permitted by SORP have been taken.
Restricted Unrestricted Total Total
Funds Funds Funds Funds
2020/21 2020/21 2020/21 2019/20
£'000 £'000 £'000 £'000
Grants 98 98 0
Donations 153 153 311
Legacies 47 47 0
Total 98 200 298 311
Note 3 : Income from Grants, Donations & Legacies
Board members of Shropshire Community Health NHS Trust, the corporate trustee, and members of
the Charitable Funds Committee ensure that the business of the charity is dealt with separately from
that associated with exchequer funds for which they are also responsible.
NOTES TO THE ACCOUNTS
Debtors are amounts owed to the charity. They are measured on the basis of their recoverable
amount.
Creditors are amounts owed by the charity. They are measured at the amount that the charity
expects to have to pay to settle the debt.
Note 2 : Related Parties
During the year, members of the Charitable Funds Committee, which is empowered by the corporate
trustee to act on its behalf in the day-to-day administration of all Funds Held on Trust, were also
members of the Shropshire Community Health NHS Trust Board.
The charity has made revenue and capital grant payments to the Trust to the value of £361,000 as
detailed in note 4. Other than these payments, there have been no further material transactions
between the charity and the listed NHS body.
Charities preparing their accounts under FRS 102 must provide a statement of cash
Section 7 of FRS102 provides an exemption under the small entity provisions within S1A of FRS
102; small entities that are not subsidiaries can claim exemption from preparing a cash flow
statement.
The turnover of the Shropshire Community Health NHS Trust General Charitable Fund is such that it
meets the definition of a small entity.
10
Tab 4 13. 2020/21 Charitable Funds Accounts
106 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
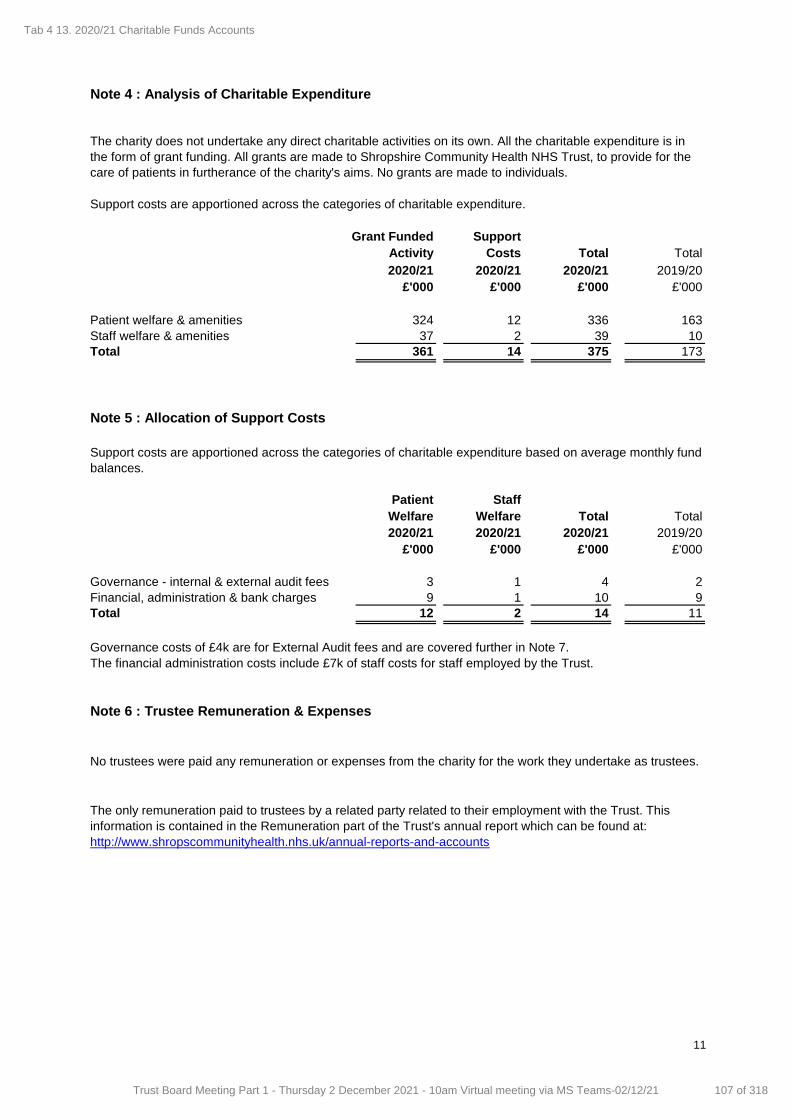
Grant Funded Support
Activity Costs Total Total
2020/21 2020/21 2020/21 2019/20
£'000 £'000 £'000 £'000
Patient welfare & amenities 324 12 336 163
Staff welfare & amenities 37 2 39 10
Total 361 14 375 173
Patient Staff
Welfare Welfare Total Total
2020/21 2020/21 2020/21 2019/20
£'000 £'000 £'000 £'000
Governance - internal & external audit fees 3 1 4 2
Financial, administration & bank charges 9 1 10 9
Total 12 2 14 11
Governance costs of £4k are for External Audit fees and are covered further in Note 7.
The financial administration costs include £7k of staff costs for staff employed by the Trust.
No trustees were paid any remuneration or expenses from the charity for the work they undertake as trustees.
The only remuneration paid to trustees by a related party related to their employment with the Trust. This
information is contained in the Remuneration part of the Trust's annual report which can be found at:
http://www.shropscommunityhealth.nhs.uk/annual-reports-and-accounts
Support costs are apportioned across the categories of charitable expenditure based on average monthly fund
balances.
Note 4 : Analysis of Charitable Expenditure
Support costs are apportioned across the categories of charitable expenditure.
The charity does not undertake any direct charitable activities on its own. All the charitable expenditure is in
the form of grant funding. All grants are made to Shropshire Community Health NHS Trust, to provide for the
care of patients in furtherance of the charity's aims. No grants are made to individuals.
Note 5 : Allocation of Support Costs
Note 6 : Trustee Remuneration & Expenses
11
Tab 4 13. 2020/21 Charitable Funds Accounts
107 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
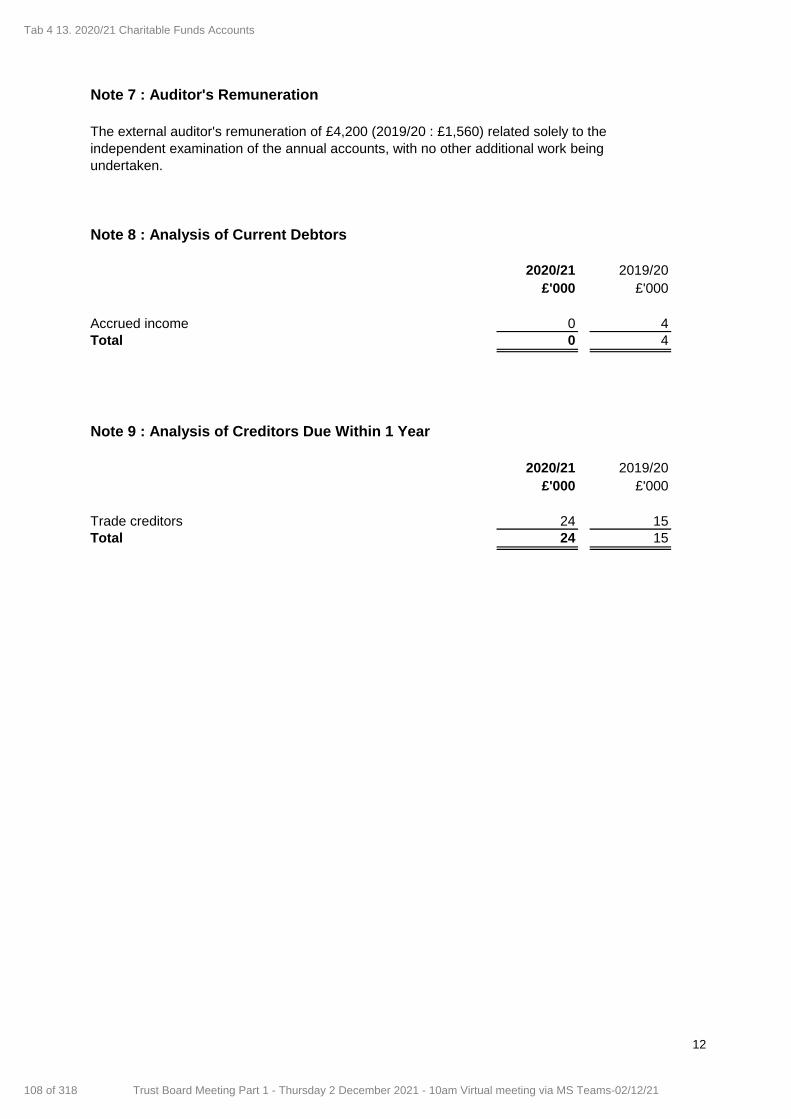
2020/21 2019/20
£'000 £'000
Accrued income 0 4
Total 0 4
2020/21 2019/20
£'000 £'000
Trade creditors 24 15
Total 24 15
Note 7 : Auditor's Remuneration
The external auditor's remuneration of £4,200 (2019/20 : £1,560) related solely to the
independent examination of the annual accounts, with no other additional work being
undertaken.
Note 8 : Analysis of Current Debtors
Note 9 : Analysis of Creditors Due Within 1 Year
12
Tab 4 13. 2020/21 Charitable Funds Accounts
108 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
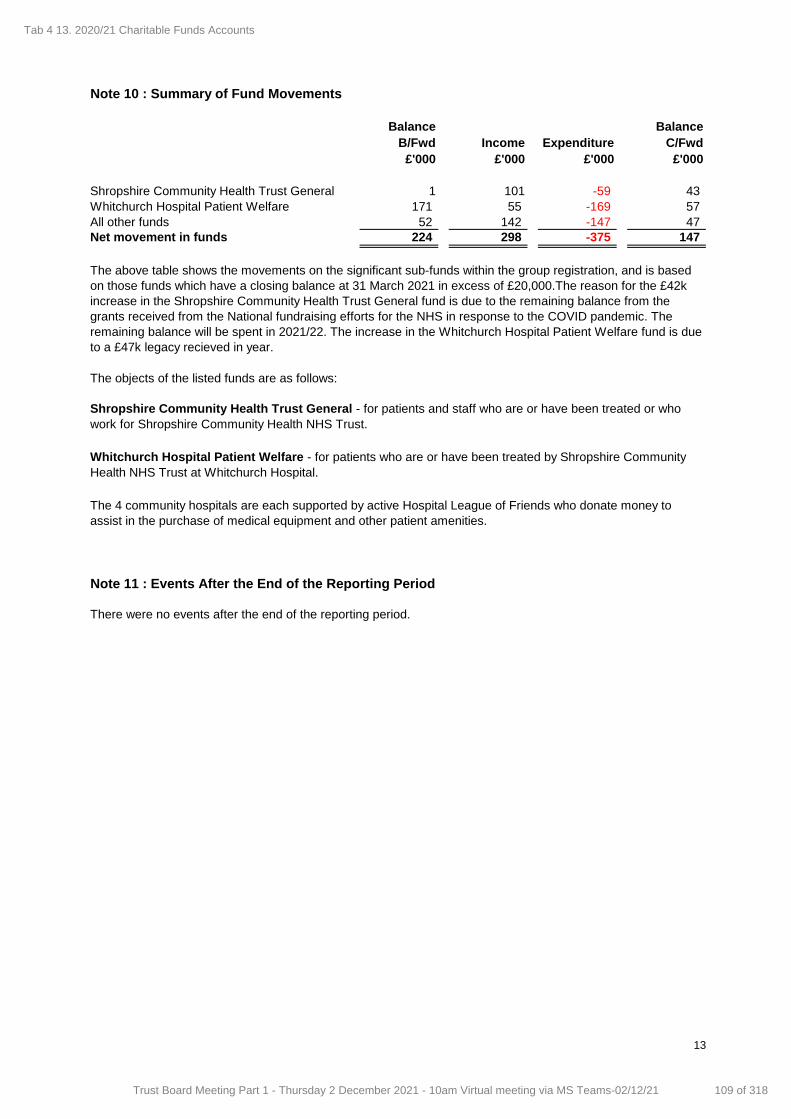
Balance Balance
B/Fwd Income Expenditure C/Fwd
£'000 £'000 £'000 £'000
Shropshire Community Health Trust General 1 101 -59 43
Whitchurch Hospital Patient Welfare 171 55 -169 57
All other funds 52 142 -147 47
Net movement in funds 224 298 -375 147
The objects of the listed funds are as follows:
There were no events after the end of the reporting period.
Note 11 : Events After the End of the Reporting Period
The 4 community hospitals are each supported by active Hospital League of Friends who donate money to
assist in the purchase of medical equipment and other patient amenities.
Note 10 : Summary of Fund Movements
The above table shows the movements on the significant sub-funds within the group registration, and is based
on those funds which have a closing balance at 31 March 2021 in excess of £20,000.The reason for the £42k
increase in the Shropshire Community Health Trust General fund is due to the remaining balance from the
grants received from the National fundraising efforts for the NHS in response to the COVID pandemic. The
remaining balance will be spent in 2021/22. The increase in the Whitchurch Hospital Patient Welfare fund is due
to a £47k legacy recieved in year.
Whitchurch Hospital Patient Welfare - for patients who are or have been treated by Shropshire Community
Health NHS Trust at Whitchurch Hospital.
Shropshire Community Health Trust General - for patients and staff who are or have been treated or who
work for Shropshire Community Health NHS Trust.
13
Tab 4 13. 2020/21 Charitable Funds Accounts
109 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1 Accountable Director: Shelley Ramtuhul, Director of Governance Meeting Date: 2 December 2021
REPORT COVER SHEET Report Title: Governance Report
Meeting: Board Meeting
Author: Stanley Mukwenya, Head Governance and Risk
Accountable Director:
Shelley Ramtuhul, Director of Governance, Harmesh Darbhanga, Non-Executive Director and Chairman of the Audit Committee
Other meetings or Committee presented to or previously agreed at:
Meeting or Committee Date Reviewed
Key Points/ Recommendation
Strategic goals this report relates to: (tick as appropriate)
Good and Beyond Continuous Improvement to Deliver
Outstanding Care
Transforming Services Implement our Clinical and Quality Strategy
Making Best Use of Resources People, Technology, Finances, Estates and
Networks
Relevance to Board Assurance Framework : (tick as appropriate)
Clinical Quality & Safety Long term financial
sustainability of the Trust
Healthcare Systems
Organisational culture
Optimising use of
technology
Covid19
Relevance to Well-led domains (CQC & NHSE/I): (tick as appropriate)
leadership capacity and capability
clear vision and credible strategy
culture clear roles and responsibilities
clear and effective risk management
appropriate and accurate information
learning, continuous improvement and innovation
Stakeholders engaged and involved
Relevance to CQC domains: (tick as appropriate)
Safe Caring Responsive Effective Well led
Impacts and Implications? YES or NO
If yes, what impact or implication
Patient safety & experience
Good risk management will have a positive impact on patient safety and experience
Equality & Inclusion
Identification of diversity and inclusion risks will have positive staff experience outcomes across the Trust.
Meeting Date: 2 December 2021
Agenda Item: 14
Enclosure Number: 12
14 - Governance and Audit
110 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2 Accountable Director: Shelley Ramtuhul, Director of Governance Meeting Date: 2 December 2021
Financial (revenue & capital)
Identification of risks will have a positive impact on the Trusts financial management
IG Governance Toolkit
Identification and monitoring of IG risks will promote compliance with IG requirements
OD/Workforce
Identification of risks will have a positive impact on the Trust’s workforce and OD development
Legal
Management of risk in these areas helps avoid legal challenge
Relevance to Corporate Risk Register
(Risk No/Name) All risks on Corporate Risk Register
Summary of key points in report
Board Assurance Framework The Board Assurance Framework (BAF) is one of the key mechanisms which the Board uses to hold itself to account. It provides a structure to focus on risks that may impact the Trust in achieving its strategic objectives. The BAF also confirms adequacy of controls in place whether they provide effective sufficient assurance to the board members. Since the Board last reviewed the BAF, there has not been any major changes. Controls and actions were refreshed and revised on the Organisational culture does not support the values of the Trust, Optimising the Use of Technology, Clinical Quality and Safety and Covid-19 BAF entries. Due to the Trust executive structure reconfiguration and appointments Healthcare Systems and Covid-19 BAF risks ownership has been allocated to the Chief Operating Officer, Clinical Quality and Safety risk to the Director of Nursing and the Health and Safety Compliance with Legislation risk to the Director of People respectively. The Long- Term Financial Sustainability entry remain the highest scored risk on the BAF at C 5 X L 5. The Trust remain waiting for national RCS Financial Strategy Framework review outcome. A deep dive on Health and Safety Compliance with legislation BAF risk was presented and discussed as part of the BAF risks assurance processes at the last Audit Committee meeting. As part of the BAF assurance process the Board Sub-Committees continue to assess strength of controls, adequacy on assurance and identifying gaps that may exist on current controls and assurance on risks related to their Committees. As such the Quality and Safety Committee recommended that a new Workforce (Staffing) risk be escalated to the BAF. The new BAF entry will be linked with other workforce related risks e.g., staffing pressures, staff absenteeism and well-being. The new risk will be presented in the next Board meeting. Corporate Risk Register Discussions were held with all individual risk owners and changes were agreed as reflected on the current CRR attached below. Section 2 Audit Committee The committee met on the 27th October 2021. The report highlights significant issues received, discussed and agreed at the meeting.
14 - Governance and Audit
111 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
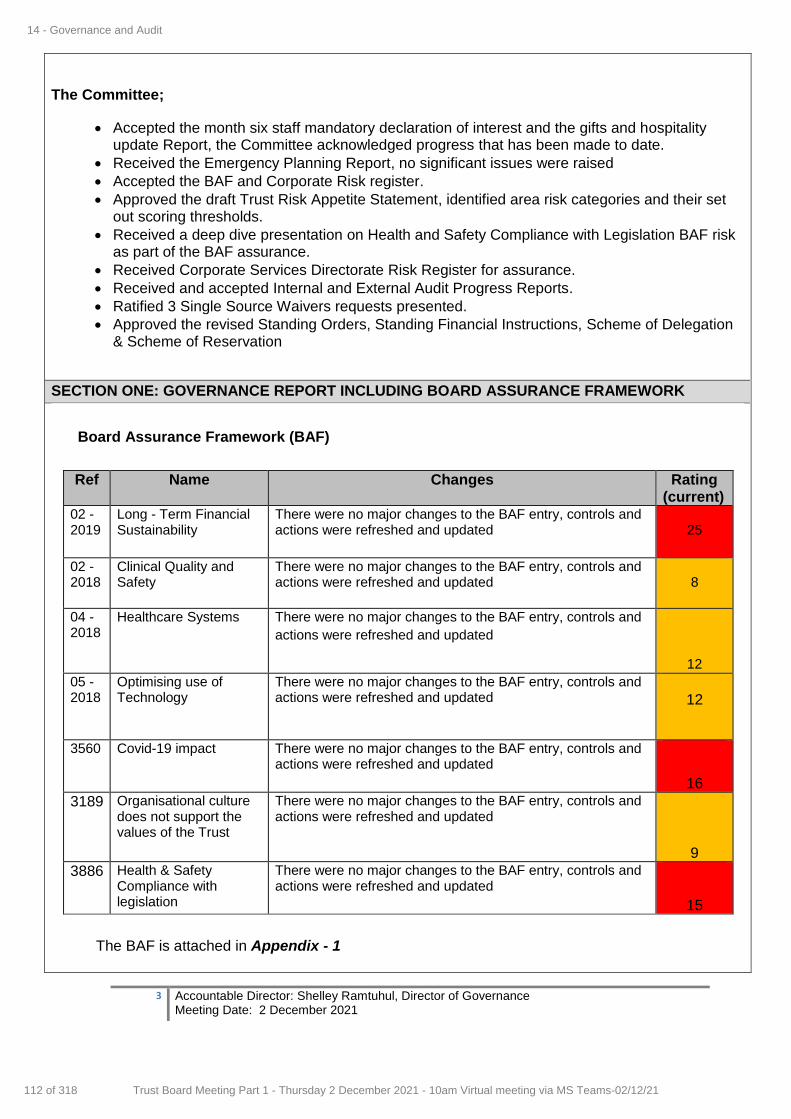
3 Accountable Director: Shelley Ramtuhul, Director of Governance Meeting Date: 2 December 2021
The Committee;
Accepted the month six staff mandatory declaration of interest and the gifts and hospitality update Report, the Committee acknowledged progress that has been made to date.
Received the Emergency Planning Report, no significant issues were raised
Accepted the BAF and Corporate Risk register.
Approved the draft Trust Risk Appetite Statement, identified area risk categories and their set out scoring thresholds.
Received a deep dive presentation on Health and Safety Compliance with Legislation BAF risk as part of the BAF assurance.
Received Corporate Services Directorate Risk Register for assurance.
Received and accepted Internal and External Audit Progress Reports.
Ratified 3 Single Source Waivers requests presented.
Approved the revised Standing Orders, Standing Financial Instructions, Scheme of Delegation & Scheme of Reservation
SECTION ONE: GOVERNANCE REPORT INCLUDING BOARD ASSURANCE FRAMEWORK
Board Assurance Framework (BAF)
Ref Name Changes Rating (current)
02 -2019
Long - Term Financial Sustainability
There were no major changes to the BAF entry, controls and actions were refreshed and updated
25
02 -2018
Clinical Quality and Safety
There were no major changes to the BAF entry, controls and actions were refreshed and updated
8
04 -2018
Healthcare Systems There were no major changes to the BAF entry, controls and
actions were refreshed and updated
12
05 -2018
Optimising use of Technology
There were no major changes to the BAF entry, controls and actions were refreshed and updated
12
3560 Covid-19 impact There were no major changes to the BAF entry, controls and actions were refreshed and updated
16
3189 Organisational culture does not support the values of the Trust
There were no major changes to the BAF entry, controls and actions were refreshed and updated
9
3886 Health & Safety Compliance with legislation
There were no major changes to the BAF entry, controls and actions were refreshed and updated
15
The BAF is attached in Appendix - 1
14 - Governance and Audit
112 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
4 Accountable Director: Shelley Ramtuhul, Director of Governance Meeting Date: 2 December 2021
Corporate Risk Register (CRR)
As part of the Internal Audit recommendation on risk and BAF maturity, the Corporate Risk Register template was reformatted to capture individual risk categories. All the categories are linked to the Trust risk appetite. Risks on the Corporate Risk Register are linked to the BAF risks. The CRR also effectively captures operational risks not assessed as high enough to be on the Board Assurance Framework (BAF). The Corporate Risk Register (CRR) currently holds 21 risks. Discussions have been held with all individual risk owners to review current risk descriptions, controls/actions and scoring. Major changes from the reviews were on the following,
New risks escalated to the CRR since the last update
ID 4235. Workforce Assurance Information and Workforce Planning Expertise.
Only one new risk has been added to the CRR since the last update, the risk have been given a
current scoring of C 4 X L 4.
Due to the earlier than planned resignation of the Head of Workforce Planning, Systems &
Information, there is a risk that the Trust may be unable to meet requests for routine, ad hoc or
bespoke workforce analytics to support operational business decisions, NHSEI reporting, CQC
compliance reporting etc. There is also a risk that the Trust will be unable to continue to deliver
workforce plans for operational use within ShropCom and the System. Both issues will impact on
the whole Trust's ability to make business decisions related to workforce information, on the whole
Trust's ability to create specialist workforce plans in support of operational delivery and the whole
Trust's reputation. Lack of workforce information may also impact on the Trust's ability to bid for
funds to support service development (e.g., international recruitment)
Changes to the CRR since the last update
ID 1571 Waiting times.
The Waiting times risk description has been revised to reflect all services impacted. The scoring
has been increased from C 4 X L 4 to C 4 X L 5.
There is a risk of harm to patients due to long waiting times accessing services and treatment, as
well as a risk to the Trust in failing to meet its local and national targets which may impact patient
health, clinical outcomes and Trust's reputation.
ID 2495 Vacancies and the effect on service delivery
Due to continuous staffing pressures the Trust is currently experiencing the Vacancies and the
effect on service delivery risk scoring has been increased from C 3 X L 4 to C 4 X L 5.
There is a risk that if the Trust fails to have an appropriately resourced, focused, resilient
workforce in place that meet service requirements, as a result of an inability to recruit, retain
and/or appropriately deploy a workforce with the necessary skills and experience, may result in
unplanned disruption to services leading to poor clinical outcomes.
14 - Governance and Audit
113 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
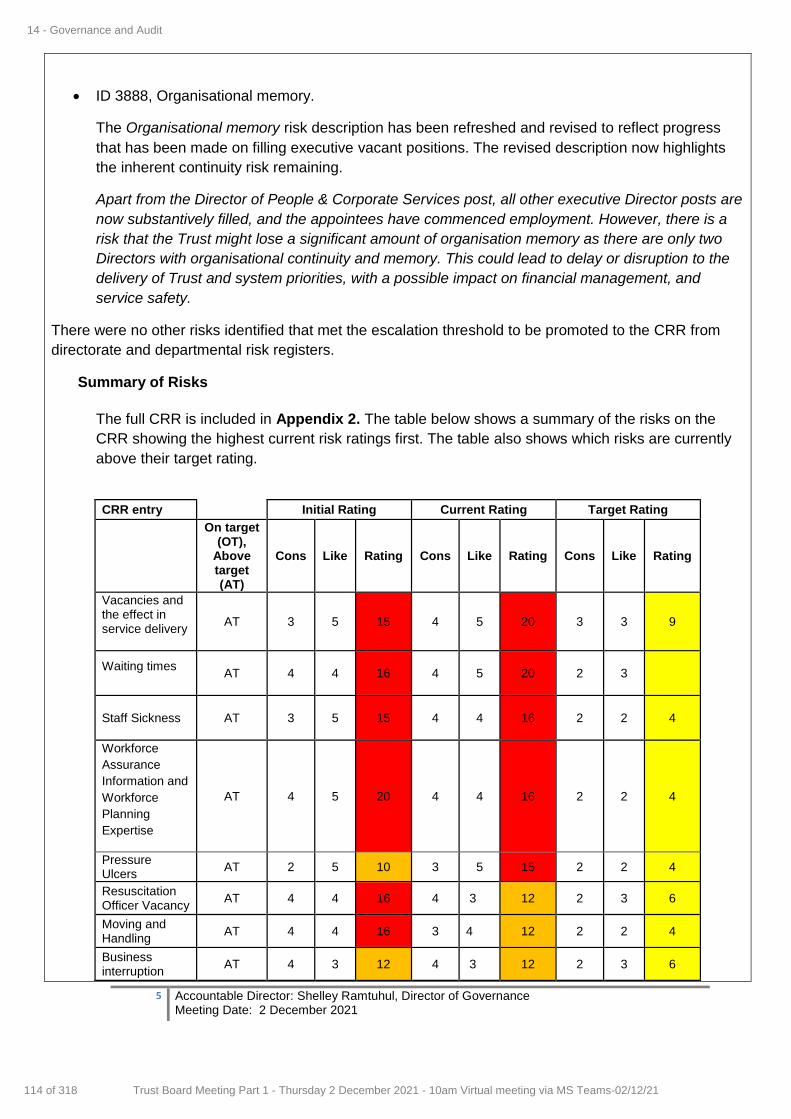
5 Accountable Director: Shelley Ramtuhul, Director of Governance Meeting Date: 2 December 2021
ID 3888, Organisational memory.
The Organisational memory risk description has been refreshed and revised to reflect progress
that has been made on filling executive vacant positions. The revised description now highlights
the inherent continuity risk remaining.
Apart from the Director of People & Corporate Services post, all other executive Director posts are
now substantively filled, and the appointees have commenced employment. However, there is a
risk that the Trust might lose a significant amount of organisation memory as there are only two
Directors with organisational continuity and memory. This could lead to delay or disruption to the
delivery of Trust and system priorities, with a possible impact on financial management, and
service safety.
There were no other risks identified that met the escalation threshold to be promoted to the CRR from
directorate and departmental risk registers.
Summary of Risks
The full CRR is included in Appendix 2. The table below shows a summary of the risks on the
CRR showing the highest current risk ratings first. The table also shows which risks are currently
above their target rating.
CRR entry Initial Rating Current Rating Target Rating
On target (OT),
Above target (AT)
Cons Like Rating Cons Like Rating Cons Like Rating
Vacancies and the effect in service delivery
AT 3 5 15 4 5 20 3 3 9
Waiting times
AT 4 4 16 4 5 20 2 3
Staff Sickness AT 3 5 15 4 4 16 2 2 4
Workforce
Assurance
Information and
Workforce
Planning
Expertise
AT 4 5 20 4 4 16 2 2 4
Pressure Ulcers
AT 2 5 10 3 5 15 2 2 4
Resuscitation Officer Vacancy
AT 4 4 16 4 3 12 2 3 6
Moving and Handling
AT 4 4 16 3 4 12 2 2 4
Business interruption
AT 4 3 12 4 3 12 2 3 6
14 - Governance and Audit
114 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
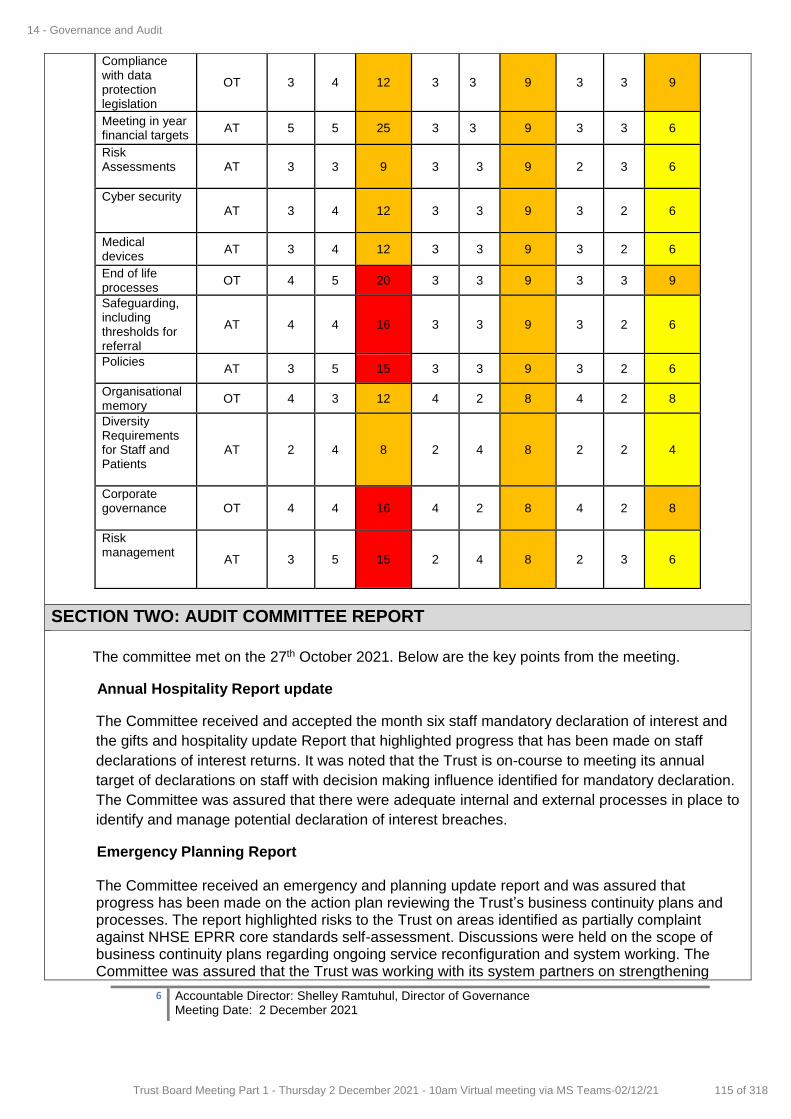
6 Accountable Director: Shelley Ramtuhul, Director of Governance Meeting Date: 2 December 2021
SECTION TWO: AUDIT COMMITTEE REPORT
The committee met on the 27th October 2021. Below are the key points from the meeting.
Annual Hospitality Report update
The Committee received and accepted the month six staff mandatory declaration of interest and
the gifts and hospitality update Report that highlighted progress that has been made on staff
declarations of interest returns. It was noted that the Trust is on-course to meeting its annual
target of declarations on staff with decision making influence identified for mandatory declaration.
The Committee was assured that there were adequate internal and external processes in place to
identify and manage potential declaration of interest breaches.
Emergency Planning Report
The Committee received an emergency and planning update report and was assured that progress has been made on the action plan reviewing the Trust’s business continuity plans and processes. The report highlighted risks to the Trust on areas identified as partially complaint against NHSE EPRR core standards self-assessment. Discussions were held on the scope of business continuity plans regarding ongoing service reconfiguration and system working. The Committee was assured that the Trust was working with its system partners on strengthening
Compliance with data protection legislation
OT 3 4 12 3 3 9 3 3 9
Meeting in year financial targets
AT 5 5 25 3 3 9 3 3 6
Risk Assessments
AT 3 3 9 3 3 9 2 3 6
Cyber security
AT 3 4 12 3 3 9 3 2 6
Medical devices
AT 3 4 12 3 3 9 3 2 6
End of life processes
OT 4 5 20 3 3 9 3 3 9
Safeguarding, including thresholds for referral
AT 4 4 16 3 3 9 3 2 6
Policies
AT 3 5 15 3 3 9 3 2 6
Organisational memory
OT 4 3 12 4 2 8 4 2 8
Diversity Requirements for Staff and Patients
AT 2 4 8 2 4 8 2 2 4
Corporate governance
OT 4 4 16 4 2 8 4 2 8
Risk management
AT 3 5 15 2 4 8 2 3 6
14 - Governance and Audit
115 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
7 Accountable Director: Shelley Ramtuhul, Director of Governance Meeting Date: 2 December 2021
plans and identifying business continuity gaps in the system organisations. The Committee agreed that good progress had been made towards achieving adequate plans. Draft Risk Appetite Statement The Committee received and approved the draft Trust Risk Appetite Statement, seven risk areas categories identified and their set tolerance scoring thresholds. The Committee was assured that a successful consultation and engagement exercise had been undertaken with the Executive Team and Service Heads on the report as requested on its initial presentation to the Committee. Discussions were held on areas of further improvement and need for the Trust BAF to be alignment to the system BAF. Further discussions were held on the adequacy of the current BAF risks, the Committee was assured that a BAF Board Workshop session was being planned for early 2022 which will review the current risks and discuss emerging risks. The Committee also received the draft Risk Management Guidance document which has been developed to complement the Trust Risk Policy by providing staff with step-by-step guidance on identifying risks, entering risks in Datix system registers, how risks are escalated and how to write appropriate qaulity risk descriptions. Appendix 3 – Copy of the Trust Risk Appetite Statement Report that was approved at the Audit Committee.
BAF Assurance Presentation (Health and Safety Compliance with Legislation)
The Committee received a deep dive presentation on the Health and safety Compliance with Legislation BAF entry as part of BAF risk assurance. The Committee noted that progress had been made in mitigating and providing assurance to the BAF entry. The Committee agreed that the current risk scoring was appropriate for the risk based on the current mitigations. Discussions and recommendations were provided on gaps and areas of future focus in mitigating the risk.
Single Source Arrangements for Goods and Services
The Committee ratified 3 Single Source Waivers on, replacement of leaking flat roof covering at Newport
Cottage, additional works required to complete the new boiler house installation at Bridgnorth and provision of new control panel in old boiler house at Bridgnorth as unsupported. Annual Review of Standing Orders, Standing Financial Instructions, Scheme of Delegation & Scheme of Reservation
The Committee received and ratified revised changes made to the Standing Orders, Standing Financial Instructions, Scheme of Delegation & Scheme of Reservation Trust Constitutional documents. Consideration was given on areas that had been amended, comments and recommendations were made on areas of improvement.
Internal Audit
Consideration was given to the Internal Audit Progress Report. Concerns were raised on outstanding delayed audits on Care Plans, Community Equipment, Waiting Times as well as outstanding historical past audits recommendations. The Committee was also informed that positive progress had been made on the Risk and BAF Maturity Audit recommendations. Discussions were held on challenges that had been faced by Internal Auditors accessing data and information for the waiting times audit, the Committee agreed that the issue must be escalated to
14 - Governance and Audit
116 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
8 Accountable Director: Shelley Ramtuhul, Director of Governance Meeting Date: 2 December 2021
the Board and executive team. The Committee strongly recommended that action was required to clear outstanding historical audit recommendations.
External Audit
The Committee was informed that planning process for 2021-22 external audit had started. Also, the Committee was informed that external auditors were not anticipating any significant changes to the audit plan. Focus areas of external auditors’ report for the January 2022 Audit meeting were provided. It was also indicated that there were no changes to the risk profile. Further discussions were also held on value for money ICS impact, and potential changes to NHS accounts submission deadlines. Use of Trust Seal
The Trust Seal has not been used since the last Board meeting update.
Purpose of the Report (tick as appropriate)
Consider for Action Give Approval Accept Assurance Provide Information
Key Recommendations
The Board is asked to:
Section 1: Governance Report
Accept assurances provided by the Audit Committee
Confirm They are satisfied the BAF entries accurately reflect the risks to the Trust strategic priorities.
Request additional assurance where there are concerns
Approve changes to the Corporate Risk Register risks
Approve draft Trust Risk Appetite Statement, approved by the Audit Committee on 27
October.
14 - Governance and Audit
117 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
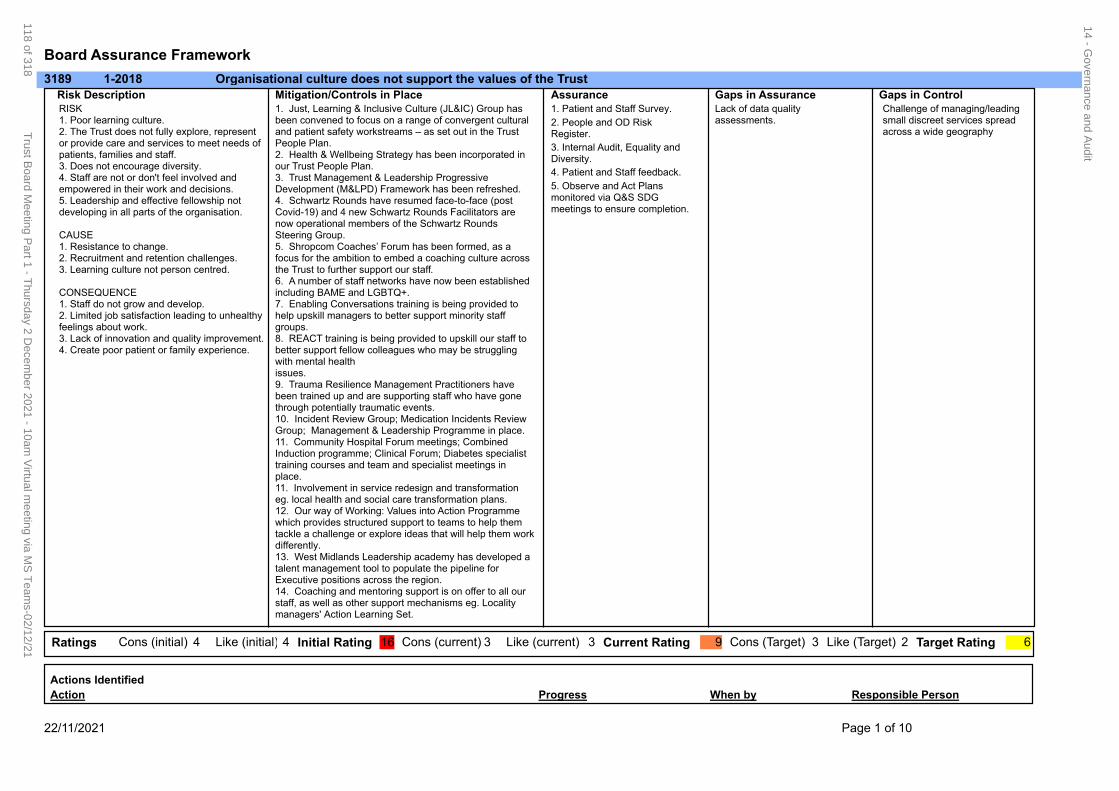
Board Assurance Framework
3189 Organisational culture does not support the values of the Trust1-2018
RISK1. Poor learning culture. 2. The Trust does not fully explore, represent or provide care and services to meet needs of patients, families and staff.3. Does not encourage diversity.4. Staff are not or don't feel involved and empowered in their work and decisions.5. Leadership and effective fellowship not developing in all parts of the organisation.
CAUSE1. Resistance to change.2. Recruitment and retention challenges.3. Learning culture not person centred.
CONSEQUENCE1. Staff do not grow and develop.2. Limited job satisfaction leading to unhealthy feelings about work.3. Lack of innovation and quality improvement.4. Create poor patient or family experience.
1. Just, Learning & Inclusive Culture (JL&IC) Group has been convened to focus on a range of convergent cultural and patient safety workstreams – as set out in the Trust People Plan.2. Health & Wellbeing Strategy has been incorporated in our Trust People Plan.3. Trust Management & Leadership Progressive Development (M&LPD) Framework has been refreshed.4. Schwartz Rounds have resumed face-to-face (post Covid-19) and 4 new Schwartz Rounds Facilitators are now operational members of the Schwartz Rounds Steering Group.5. Shropcom Coaches’ Forum has been formed, as a focus for the ambition to embed a coaching culture across the Trust to further support our staff.6. A number of staff networks have now been established including BAME and LGBTQ+.7. Enabling Conversations training is being provided to help upskill managers to better support minority staff groups.8. REACT training is being provided to upskill our staff to better support fellow colleagues who may be struggling with mental health issues.9. Trauma Resilience Management Practitioners have been trained up and are supporting staff who have gone through potentially traumatic events.10. Incident Review Group; Medication Incidents Review Group; Management & Leadership Programme in place.11. Community Hospital Forum meetings; Combined Induction programme; Clinical Forum; Diabetes specialist training courses and team and specialist meetings in place.11. Involvement in service redesign and transformation eg. local health and social care transformation plans.12. Our way of Working: Values into Action Programme which provides structured support to teams to help them tackle a challenge or explore ideas that will help them work differently.13. West Midlands Leadership academy has developed a talent management tool to populate the pipeline for Executive positions across the region.14. Coaching and mentoring support is on offer to all our staff, as well as other support mechanisms eg. Locality managers' Action Learning Set.
Risk Description Mitigation/Controls in Place1. Patient and Staff Survey.
2. People and OD Risk Register.
3. Internal Audit, Equality and Diversity.
4. Patient and Staff feedback.
5. Observe and Act Plans monitored via Q&S SDG meetings to ensure completion.
Lack of data quality assessments.
Challenge of managing/leading small discreet services spread across a wide geography
Assurance Gaps in ControlGaps in Assurance
3Ratings 4Cons (initial) 16Initial Rating Cons (current) Like (current) Current Rating Target RatingCons (Target) Like (Target) 9 3 2 64 Like (initial) 3
Responsible PersonWhen byProgressAction
Actions Identified
22/11/2021 Page 1 of 10
14 - Governance and A
udit
118 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
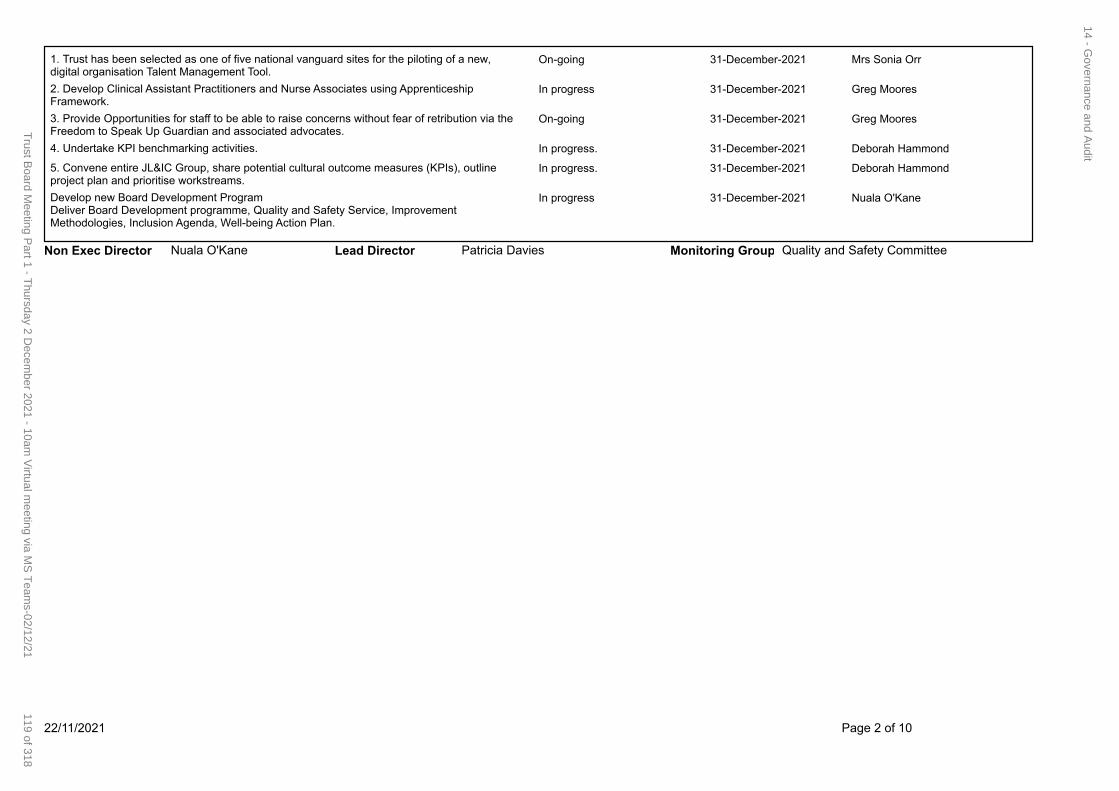
On-going 31-December-2021 Mrs Sonia Orr1. Trust has been selected as one of five national vanguard sites for the piloting of a new, digital organisation Talent Management Tool.
In progress 31-December-2021 Greg Moores2. Develop Clinical Assistant Practitioners and Nurse Associates using Apprenticeship Framework.
On-going 31-December-2021 Greg Moores3. Provide Opportunities for staff to be able to raise concerns without fear of retribution via the Freedom to Speak Up Guardian and associated advocates.
In progress. 31-December-2021 Deborah Hammond4. Undertake KPI benchmarking activities.
In progress. 31-December-2021 Deborah Hammond5. Convene entire JL&IC Group, share potential cultural outcome measures (KPIs), outline project plan and prioritise workstreams.
In progress 31-December-2021 Nuala O'KaneDevelop new Board Development ProgramDeliver Board Development programme, Quality and Safety Service, Improvement Methodologies, Inclusion Agenda, Well-being Action Plan.
Quality and Safety CommitteePatricia DaviesLead Director Monitoring GroupNon Exec Director Nuala O'Kane
22/11/2021 Page 2 of 10
14 - Governance and A
udit
119 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
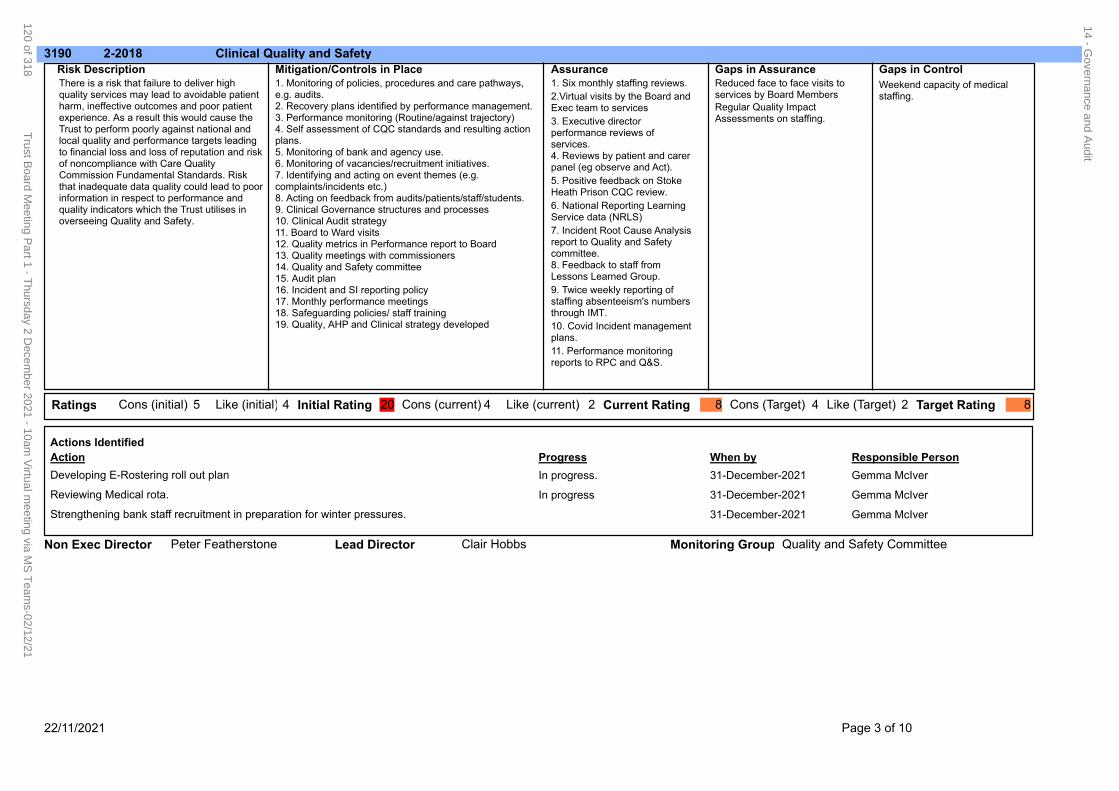
3190 Clinical Quality and Safety2-2018
There is a risk that failure to deliver high quality services may lead to avoidable patient harm, ineffective outcomes and poor patient experience. As a result this would cause the Trust to perform poorly against national and local quality and performance targets leading to financial loss and loss of reputation and risk of noncompliance with Care Quality Commission Fundamental Standards. Risk that inadequate data quality could lead to poor information in respect to performance and quality indicators which the Trust utilises in overseeing Quality and Safety.
1. Monitoring of policies, procedures and care pathways, e.g. audits.2. Recovery plans identified by performance management. 3. Performance monitoring (Routine/against trajectory)4. Self assessment of CQC standards and resulting action plans.5. Monitoring of bank and agency use.6. Monitoring of vacancies/recruitment initiatives.7. Identifying and acting on event themes (e.g. complaints/incidents etc.)8. Acting on feedback from audits/patients/staff/students.9. Clinical Governance structures and processes10. Clinical Audit strategy11. Board to Ward visits12. Quality metrics in Performance report to Board13. Quality meetings with commissioners14. Quality and Safety committee15. Audit plan16. Incident and SI reporting policy17. Monthly performance meetings18. Safeguarding policies/ staff training 19. Quality, AHP and Clinical strategy developed
Risk Description Mitigation/Controls in Place1. Six monthly staffing reviews.
10. Covid Incident management plans.
11. Performance monitoring reports to RPC and Q&S.
2.Virtual visits by the Board and Exec team to services
3. Executive director performance reviews of services.4. Reviews by patient and carer panel (eg observe and Act).
5. Positive feedback on Stoke Heath Prison CQC review.
6. National Reporting Learning Service data (NRLS)
7. Incident Root Cause Analysis report to Quality and Safety committee.8. Feedback to staff from Lessons Learned Group.
9. Twice weekly reporting of staffing absenteeism's numbers through IMT.
Reduced face to face visits to services by Board Members
Regular Quality Impact Assessments on staffing.
Weekend capacity of medical staffing.
Assurance Gaps in ControlGaps in Assurance
4Ratings 4Cons (initial) 20Initial Rating Cons (current) Like (current) Current Rating Target RatingCons (Target) Like (Target) 8 4 2 85 Like (initial) 2
Responsible PersonWhen byProgressAction
Actions Identified
In progress. 31-December-2021 Gemma McIverDeveloping E-Rostering roll out plan
In progress 31-December-2021 Gemma McIverReviewing Medical rota.
31-December-2021 Gemma McIverStrengthening bank staff recruitment in preparation for winter pressures.
Quality and Safety CommitteeClair HobbsLead Director Monitoring GroupNon Exec Director Peter Featherstone
22/11/2021 Page 3 of 10
14 - Governance and A
udit
120 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
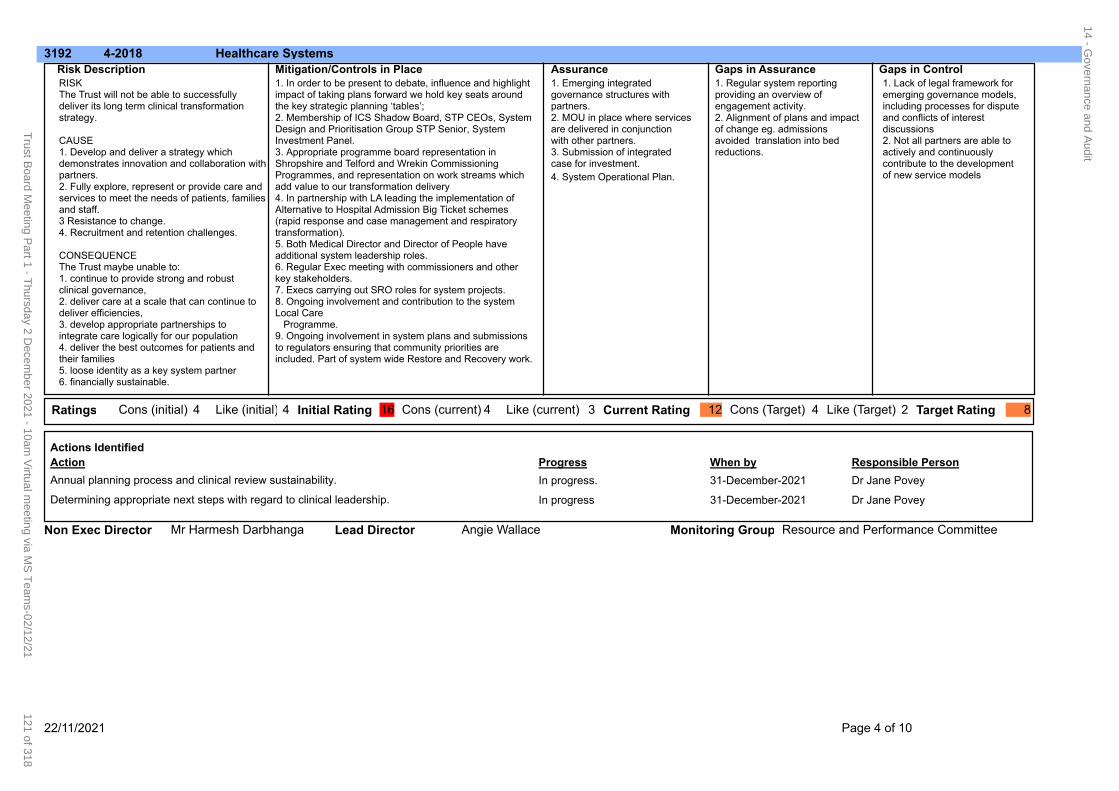
3192 Healthcare Systems4-2018
RISKThe Trust will not be able to successfully deliver its long term clinical transformation strategy.
CAUSE1. Develop and deliver a strategy which demonstrates innovation and collaboration with partners.2. Fully explore, represent or provide care and services to meet the needs of patients, families and staff.3 Resistance to change.4. Recruitment and retention challenges.
CONSEQUENCEThe Trust maybe unable to:1. continue to provide strong and robust clinical governance,2. deliver care at a scale that can continue to deliver efficiencies, 3. develop appropriate partnerships to integrate care logically for our population4. deliver the best outcomes for patients and their families5. loose identity as a key system partner6. financially sustainable.
1. In order to be present to debate, influence and highlight impact of taking plans forward we hold key seats around the key strategic planning ‘tables’; 2. Membership of ICS Shadow Board, STP CEOs, System Design and Prioritisation Group STP Senior, System Investment Panel.3. Appropriate programme board representation in Shropshire and Telford and Wrekin Commissioning Programmes, and representation on work streams which add value to our transformation delivery4. In partnership with LA leading the implementation of Alternative to Hospital Admission Big Ticket schemes (rapid response and case management and respiratory transformation).5. Both Medical Director and Director of People have additional system leadership roles.6. Regular Exec meeting with commissioners and other key stakeholders.7. Execs carrying out SRO roles for system projects.8. Ongoing involvement and contribution to the system Local Care Programme.9. Ongoing involvement in system plans and submissions to regulators ensuring that community priorities are included. Part of system wide Restore and Recovery work.
Risk Description Mitigation/Controls in Place1. Emerging integrated governance structures with partners.2. MOU in place where services are delivered in conjunction with other partners.3. Submission of integrated case for investment.
4. System Operational Plan.
1. Regular system reporting providing an overview of engagement activity.2. Alignment of plans and impact of change eg. admissions avoided translation into bed reductions.
1. Lack of legal framework for emerging governance models, including processes for dispute and conflicts of interest discussions2. Not all partners are able to actively and continuously contribute to the development of new service models
Assurance Gaps in ControlGaps in Assurance
4Ratings 4Cons (initial) 16Initial Rating Cons (current) Like (current) Current Rating Target RatingCons (Target) Like (Target) 12 4 2 84 Like (initial) 3
Responsible PersonWhen byProgressAction
Actions Identified
In progress. 31-December-2021 Dr Jane PoveyAnnual planning process and clinical review sustainability.
In progress 31-December-2021 Dr Jane PoveyDetermining appropriate next steps with regard to clinical leadership.
Resource and Performance CommitteeAngie WallaceLead Director Monitoring GroupNon Exec Director Mr Harmesh Darbhanga
22/11/2021 Page 4 of 10
14 - Governance and A
udit
121 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
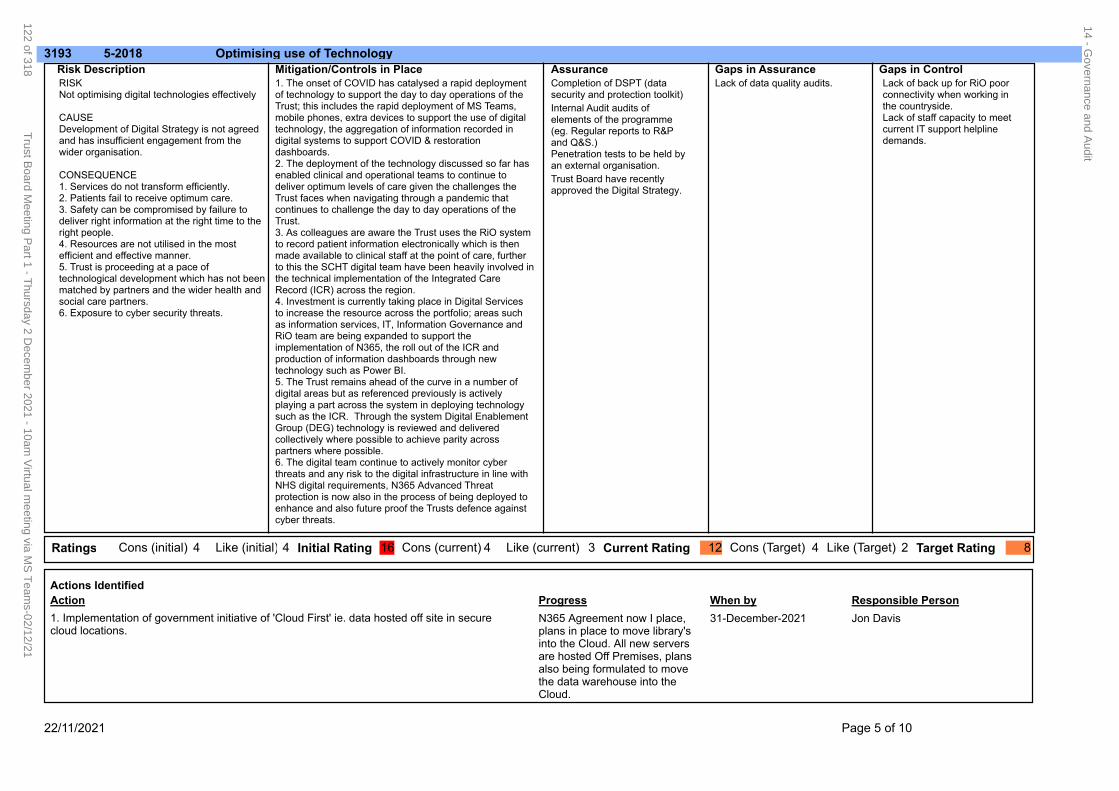
3193 Optimising use of Technology5-2018
RISKNot optimising digital technologies effectively
CAUSEDevelopment of Digital Strategy is not agreed and has insufficient engagement from the wider organisation.
CONSEQUENCE1. Services do not transform efficiently.2. Patients fail to receive optimum care.3. Safety can be compromised by failure to deliver right information at the right time to the right people.4. Resources are not utilised in the most efficient and effective manner.5. Trust is proceeding at a pace of technological development which has not been matched by partners and the wider health and social care partners.6. Exposure to cyber security threats.
1. The onset of COVID has catalysed a rapid deployment of technology to support the day to day operations of the Trust; this includes the rapid deployment of MS Teams, mobile phones, extra devices to support the use of digital technology, the aggregation of information recorded in digital systems to support COVID & restoration dashboards.2. The deployment of the technology discussed so far has enabled clinical and operational teams to continue to deliver optimum levels of care given the challenges the Trust faces when navigating through a pandemic that continues to challenge the day to day operations of the Trust.3. As colleagues are aware the Trust uses the RiO system to record patient information electronically which is then made available to clinical staff at the point of care, further to this the SCHT digital team have been heavily involved in the technical implementation of the Integrated Care Record (ICR) across the region.4. Investment is currently taking place in Digital Services to increase the resource across the portfolio; areas such as information services, IT, Information Governance and RiO team are being expanded to support the implementation of N365, the roll out of the ICR and production of information dashboards through new technology such as Power BI.5. The Trust remains ahead of the curve in a number of digital areas but as referenced previously is actively playing a part across the system in deploying technology such as the ICR. Through the system Digital Enablement Group (DEG) technology is reviewed and delivered collectively where possible to achieve parity across partners where possible.6. The digital team continue to actively monitor cyber threats and any risk to the digital infrastructure in line with NHS digital requirements, N365 Advanced Threat protection is now also in the process of being deployed to enhance and also future proof the Trusts defence against cyber threats.
Risk Description Mitigation/Controls in PlaceCompletion of DSPT (data security and protection toolkit)
Internal Audit audits of elements of the programme (eg. Regular reports to R&P and Q&S.)Penetration tests to be held by an external organisation.
Trust Board have recently approved the Digital Strategy.
Lack of data quality audits. Lack of back up for RiO poor connectivity when working in the countryside.Lack of staff capacity to meet current IT support helpline demands.
Assurance Gaps in ControlGaps in Assurance
4Ratings 4Cons (initial) 16Initial Rating Cons (current) Like (current) Current Rating Target RatingCons (Target) Like (Target) 12 4 2 84 Like (initial) 3
Responsible PersonWhen byProgressAction
Actions Identified
N365 Agreement now I place, plans in place to move library's into the Cloud. All new servers are hosted Off Premises, plans also being formulated to move the data warehouse into the Cloud.
31-December-2021 Jon Davis1. Implementation of government initiative of 'Cloud First' ie. data hosted off site in secure cloud locations.
22/11/2021 Page 5 of 10
14 - Governance and A
udit
122 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
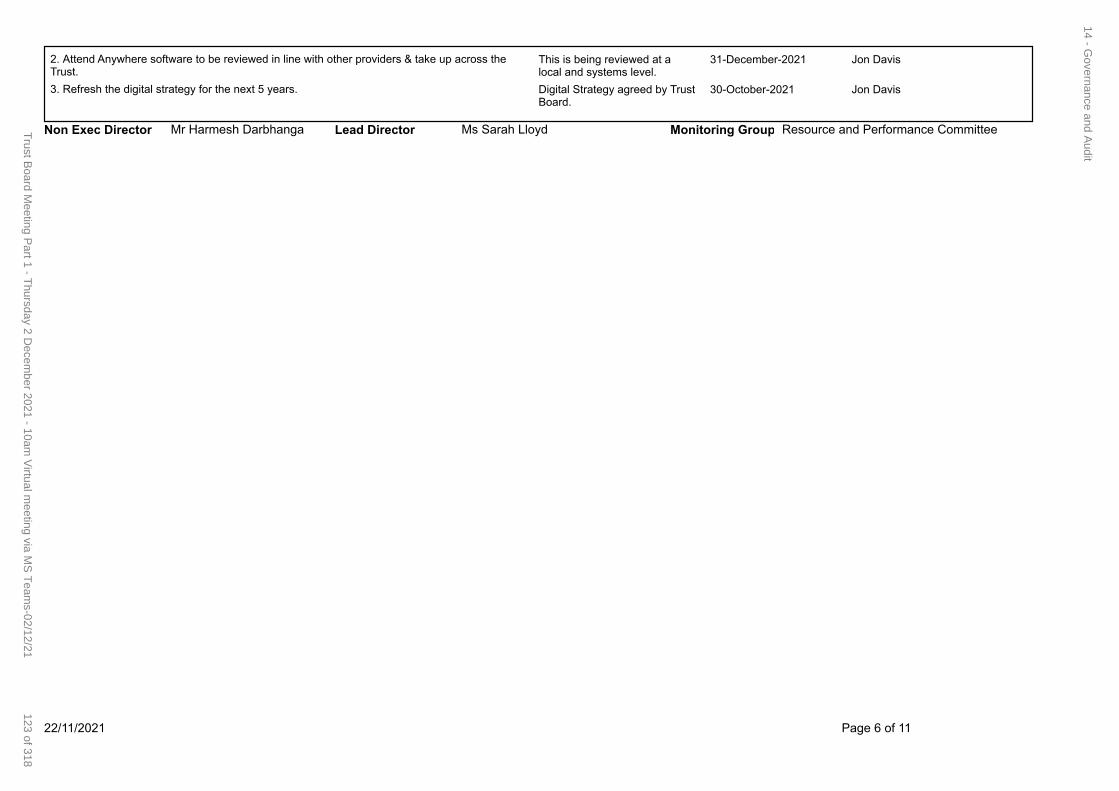
This is being reviewed at a local and systems level.
31-December-2021 Jon Davis2. Attend Anywhere software to be reviewed in line with other providers & take up across the Trust.
Digital Strategy agreed by Trust Board.
30-October-2021 Jon Davis3. Refresh the digital strategy for the next 5 years.
Resource and Performance CommitteeMs Sarah LloydLead Director Monitoring GroupNon Exec Director Mr Harmesh Darbhanga
22/11/2021 Page 6 of 11
14 - Governance and A
udit
123 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
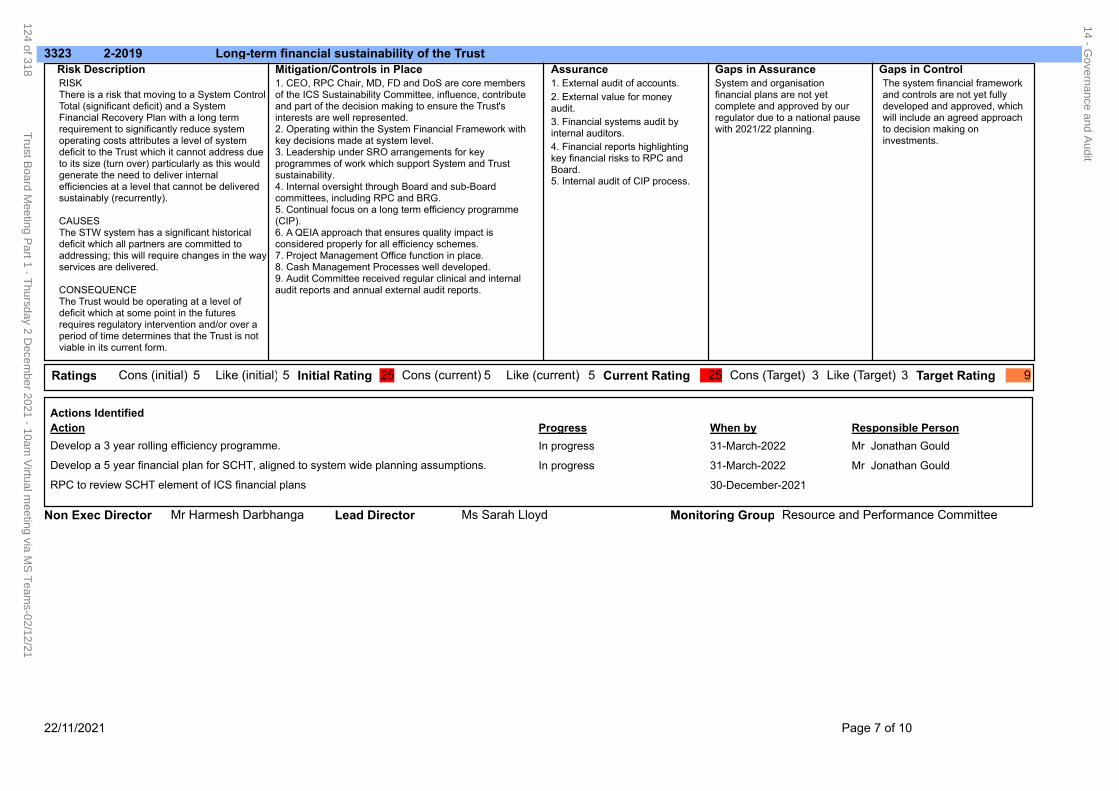
3323 Long-term financial sustainability of the Trust2-2019
RISK There is a risk that moving to a System Control Total (significant deficit) and a System Financial Recovery Plan with a long term requirement to significantly reduce system operating costs attributes a level of system deficit to the Trust which it cannot address due to its size (turn over) particularly as this would generate the need to deliver internal efficiencies at a level that cannot be delivered sustainably (recurrently).
CAUSESThe STW system has a significant historical deficit which all partners are committed to addressing; this will require changes in the way services are delivered.
CONSEQUENCEThe Trust would be operating at a level of deficit which at some point in the futures requires regulatory intervention and/or over a period of time determines that the Trust is not viable in its current form.
1. CEO, RPC Chair, MD, FD and DoS are core members of the ICS Sustainability Committee, influence, contribute and part of the decision making to ensure the Trust's interests are well represented.2. Operating within the System Financial Framework with key decisions made at system level.3. Leadership under SRO arrangements for key programmes of work which support System and Trust sustainability.4. Internal oversight through Board and sub-Board committees, including RPC and BRG.5. Continual focus on a long term efficiency programme (CIP).6. A QEIA approach that ensures quality impact is considered properly for all efficiency schemes.7. Project Management Office function in place.8. Cash Management Processes well developed.9. Audit Committee received regular clinical and internal audit reports and annual external audit reports.
Risk Description Mitigation/Controls in Place1. External audit of accounts.
2. External value for money audit.
3. Financial systems audit by internal auditors.
4. Financial reports highlighting key financial risks to RPC and Board.5. Internal audit of CIP process.
System and organisation financial plans are not yet complete and approved by our regulator due to a national pause with 2021/22 planning.
The system financial framework and controls are not yet fully developed and approved, which will include an agreed approach to decision making on investments.
Assurance Gaps in ControlGaps in Assurance
5Ratings 5Cons (initial) 25Initial Rating Cons (current) Like (current) Current Rating Target RatingCons (Target) Like (Target) 25 3 3 95 Like (initial) 5
Responsible PersonWhen byProgressAction
Actions Identified
In progress 31-March-2022 Mr Jonathan GouldDevelop a 3 year rolling efficiency programme.
In progress 31-March-2022 Mr Jonathan GouldDevelop a 5 year financial plan for SCHT, aligned to system wide planning assumptions.
30-December-2021RPC to review SCHT element of ICS financial plans
Resource and Performance CommitteeMs Sarah LloydLead Director Monitoring GroupNon Exec Director Mr Harmesh Darbhanga
22/11/2021 Page 7 of 10
14 - Governance and A
udit
124 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
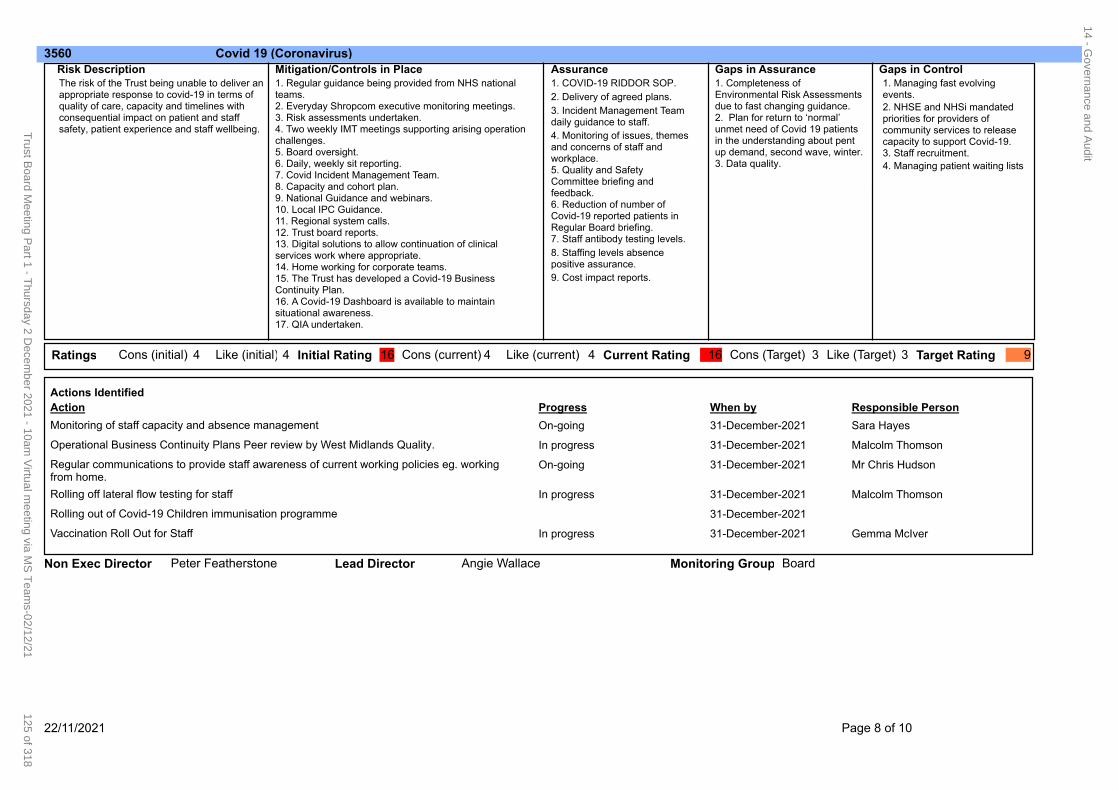
3560 Covid 19 (Coronavirus)
The risk of the Trust being unable to deliver an appropriate response to covid-19 in terms of quality of care, capacity and timelines with consequential impact on patient and staff safety, patient experience and staff wellbeing.
1. Regular guidance being provided from NHS national teams.2. Everyday Shropcom executive monitoring meetings.3. Risk assessments undertaken.4. Two weekly IMT meetings supporting arising operation challenges.5. Board oversight.6. Daily, weekly sit reporting.7. Covid Incident Management Team.8. Capacity and cohort plan.9. National Guidance and webinars.10. Local IPC Guidance.11. Regional system calls.12. Trust board reports.13. Digital solutions to allow continuation of clinical services work where appropriate.14. Home working for corporate teams. 15. The Trust has developed a Covid-19 Business Continuity Plan.16. A Covid-19 Dashboard is available to maintain situational awareness.17. QIA undertaken.
Risk Description Mitigation/Controls in Place1. COVID-19 RIDDOR SOP.
2. Delivery of agreed plans.
3. Incident Management Team daily guidance to staff.
4. Monitoring of issues, themes and concerns of staff and workplace.5. Quality and Safety Committee briefing and feedback.6. Reduction of number of Covid-19 reported patients in Regular Board briefing.7. Staff antibody testing levels.
8. Staffing levels absence positive assurance.
9. Cost impact reports.
1. Completeness of Environmental Risk Assessments due to fast changing guidance.2. Plan for return to ‘normal’ unmet need of Covid 19 patients in the understanding about pent up demand, second wave, winter.3. Data quality.
1. Managing fast evolving events.
2. NHSE and NHSi mandated priorities for providers of community services to release capacity to support Covid-19.3. Staff recruitment.
4. Managing patient waiting lists
Assurance Gaps in ControlGaps in Assurance
4Ratings 4Cons (initial) 16Initial Rating Cons (current) Like (current) Current Rating Target RatingCons (Target) Like (Target) 16 3 3 94 Like (initial) 4
Responsible PersonWhen byProgressAction
Actions Identified
On-going 31-December-2021 Sara HayesMonitoring of staff capacity and absence management
In progress 31-December-2021 Malcolm ThomsonOperational Business Continuity Plans Peer review by West Midlands Quality.
On-going 31-December-2021 Mr Chris HudsonRegular communications to provide staff awareness of current working policies eg. working from home.
In progress 31-December-2021 Malcolm ThomsonRolling off lateral flow testing for staff
31-December-2021Rolling out of Covid-19 Children immunisation programme
In progress 31-December-2021 Gemma McIverVaccination Roll Out for Staff
BoardAngie WallaceLead Director Monitoring GroupNon Exec Director Peter Featherstone
22/11/2021 Page 8 of 10
14 - Governance and A
udit
125 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
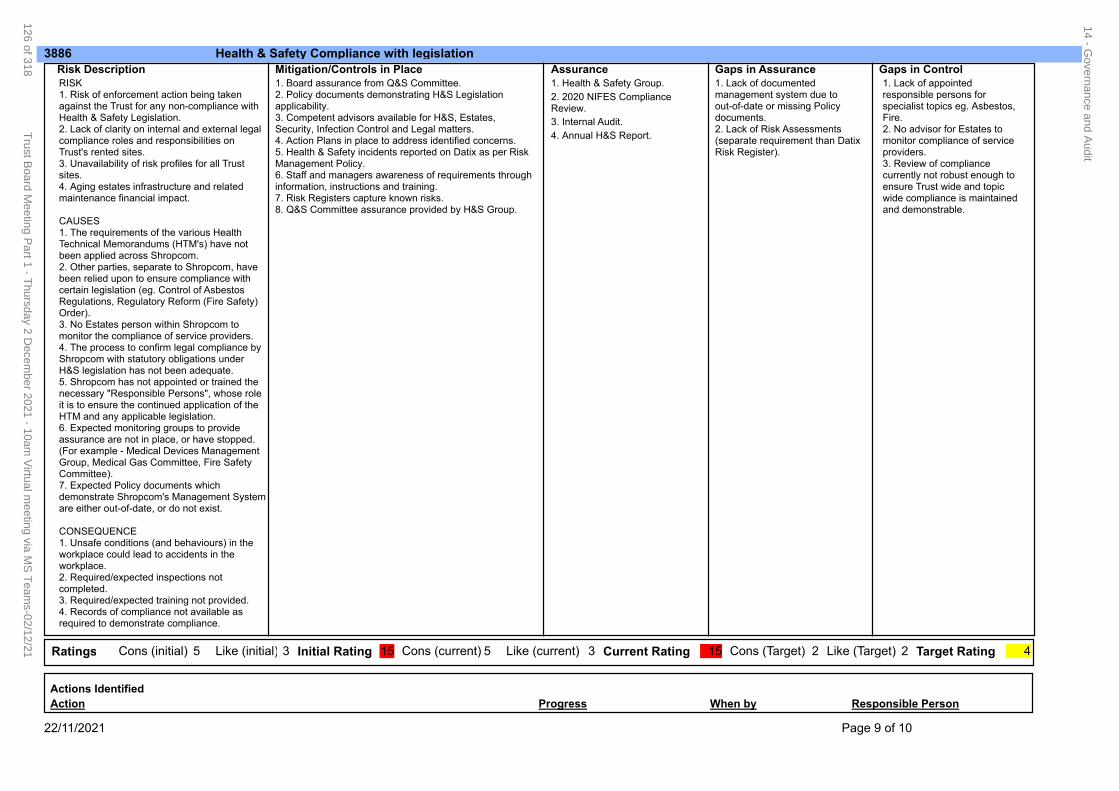
3886 Health & Safety Compliance with legislation
RISK1. Risk of enforcement action being taken against the Trust for any non-compliance with Health & Safety Legislation.2. Lack of clarity on internal and external legal compliance roles and responsibilities on Trust's rented sites.3. Unavailability of risk profiles for all Trust sites.4. Aging estates infrastructure and related maintenance financial impact.
CAUSES1. The requirements of the various Health Technical Memorandums (HTM's) have not been applied across Shropcom.2. Other parties, separate to Shropcom, have been relied upon to ensure compliance with certain legislation (eg. Control of Asbestos Regulations, Regulatory Reform (Fire Safety) Order).3. No Estates person within Shropcom to monitor the compliance of service providers.4. The process to confirm legal compliance by Shropcom with statutory obligations under H&S legislation has not been adequate.5. Shropcom has not appointed or trained the necessary "Responsible Persons", whose role it is to ensure the continued application of the HTM and any applicable legislation.6. Expected monitoring groups to provide assurance are not in place, or have stopped. (For example - Medical Devices Management Group, Medical Gas Committee, Fire Safety Committee).7. Expected Policy documents which demonstrate Shropcom's Management System are either out-of-date, or do not exist.
CONSEQUENCE1. Unsafe conditions (and behaviours) in the workplace could lead to accidents in the workplace.2. Required/expected inspections not completed.3. Required/expected training not provided.4. Records of compliance not available as required to demonstrate compliance.
1. Board assurance from Q&S Committee.2. Policy documents demonstrating H&S Legislation applicability.3. Competent advisors available for H&S, Estates, Security, Infection Control and Legal matters.4. Action Plans in place to address identified concerns.5. Health & Safety incidents reported on Datix as per Risk Management Policy.6. Staff and managers awareness of requirements through information, instructions and training.7. Risk Registers capture known risks.8. Q&S Committee assurance provided by H&S Group.
Risk Description Mitigation/Controls in Place1. Health & Safety Group.
2. 2020 NIFES Compliance Review.
3. Internal Audit.
4. Annual H&S Report.
1. Lack of documented management system due to out-of-date or missing Policy documents.2. Lack of Risk Assessments (separate requirement than Datix Risk Register).
1. Lack of appointed responsible persons for specialist topics eg. Asbestos, Fire.2. No advisor for Estates to monitor compliance of service providers.3. Review of compliance currently not robust enough to ensure Trust wide and topic wide compliance is maintained and demonstrable.
Assurance Gaps in ControlGaps in Assurance
5Ratings 3Cons (initial) 15Initial Rating Cons (current) Like (current) Current Rating Target RatingCons (Target) Like (Target) 15 2 2 45 Like (initial) 3
Responsible PersonWhen byProgressAction
Actions Identified
22/11/2021 Page 9 of 10
14 - Governance and A
udit
126 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
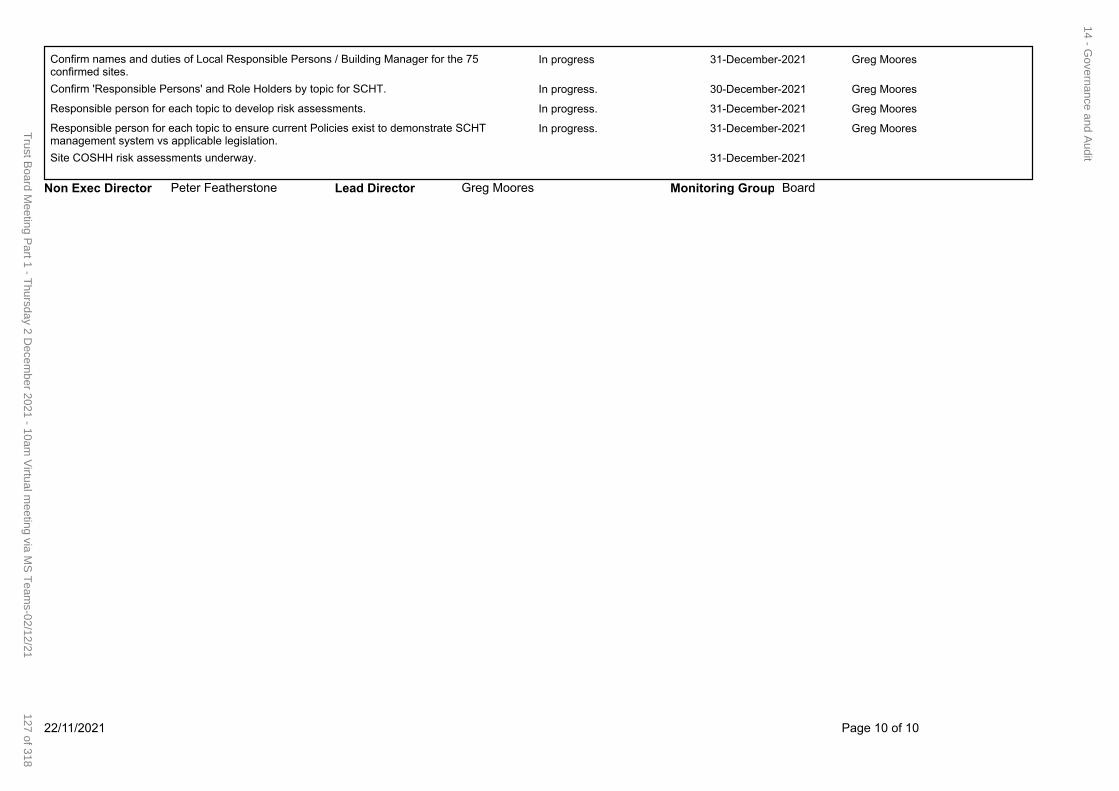
In progress 31-December-2021 Greg MooresConfirm names and duties of Local Responsible Persons / Building Manager for the 75 confirmed sites.
In progress. 30-December-2021 Greg MooresConfirm 'Responsible Persons' and Role Holders by topic for SCHT.
In progress. 31-December-2021 Greg MooresResponsible person for each topic to develop risk assessments.
In progress. 31-December-2021 Greg MooresResponsible person for each topic to ensure current Policies exist to demonstrate SCHT management system vs applicable legislation.
31-December-2021Site COSHH risk assessments underway.
BoardGreg MooresLead Director Monitoring GroupNon Exec Director Peter Featherstone
22/11/2021 Page 10 of 10
14 - Governance and A
udit
127 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
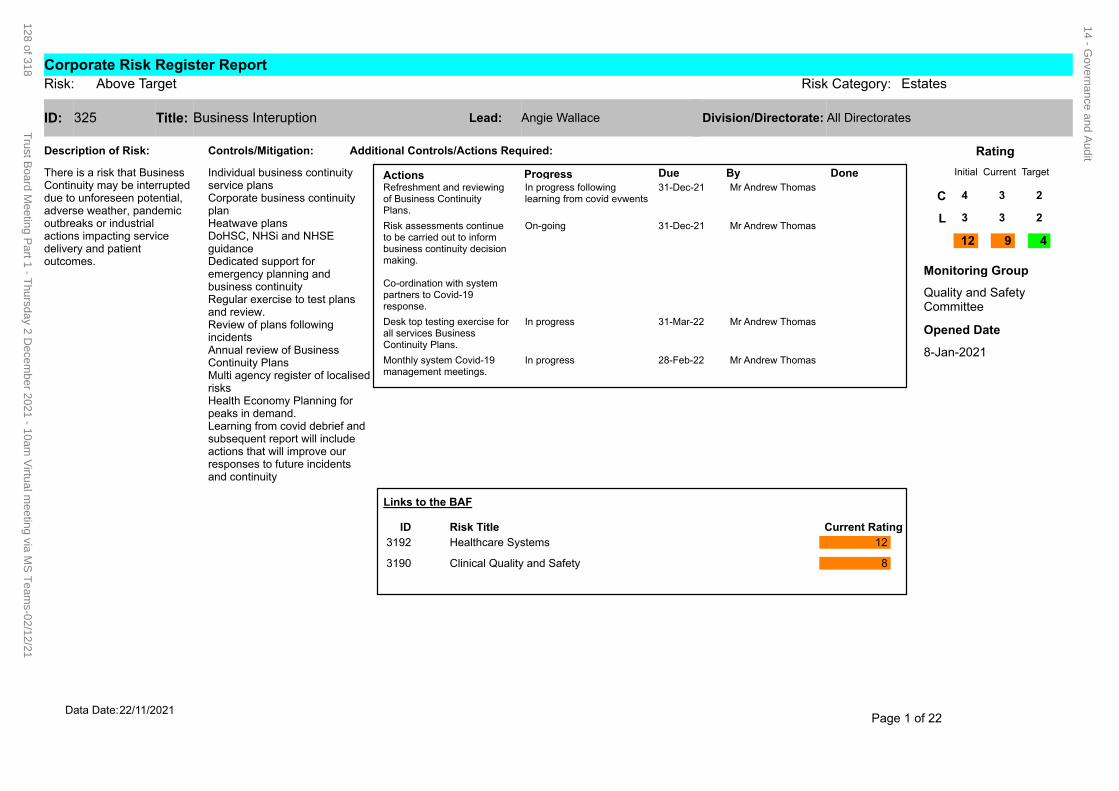
325 Business InteruptionID: Title:
Description of Risk:
Actions Progress Due By Done31-Dec-21 Mr Andrew ThomasRefreshment and reviewing
of Business Continuity Plans.
In progress following learning from covid evwents
31-Dec-21 Mr Andrew ThomasRisk assessments continue to be carried out to inform business continuity decision making.
Co-ordination with system partners to Covid-19 response.
On-going
31-Mar-22 Mr Andrew ThomasDesk top testing exercise for all services Business Continuity Plans.
In progress
28-Feb-22 Mr Andrew ThomasMonthly system Covid-19 management meetings.
In progress
Additional Controls/Actions Required:Controls/Mitigation:
Individual business continuity service plansCorporate business continuity planHeatwave plansDoHSC, NHSi and NHSE guidanceDedicated support for emergency planning and business continuityRegular exercise to test plans and review.Review of plans following incidentsAnnual review of Business Continuity PlansMulti agency register of localised risksHealth Economy Planning for peaks in demand.Learning from covid debrief and subsequent report will include actions that will improve our responses to future incidents and continuity
Initial Current Target
Rating
Quality and Safety Committee
Monitoring Group
Angie Wallace All DirectoratesLead: Division/Directorate:
C
L
12 9 4
8-Jan-2021
Opened Date
4 3 2
3 3 2
There is a risk that Business Continuity may be interrupted due to unforeseen potential, adverse weather, pandemic outbreaks or industrial actions impacting service delivery and patient outcomes.
Links to the BAF
Current RatingRisk TitleID
3192 Healthcare Systems 12
3190 Clinical Quality and Safety 8
Page 1 of 2222/11/2021Data Date:
Corporate Risk Register ReportAbove TargetRisk: Risk Category: Estates
14 - Governance and A
udit
128 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
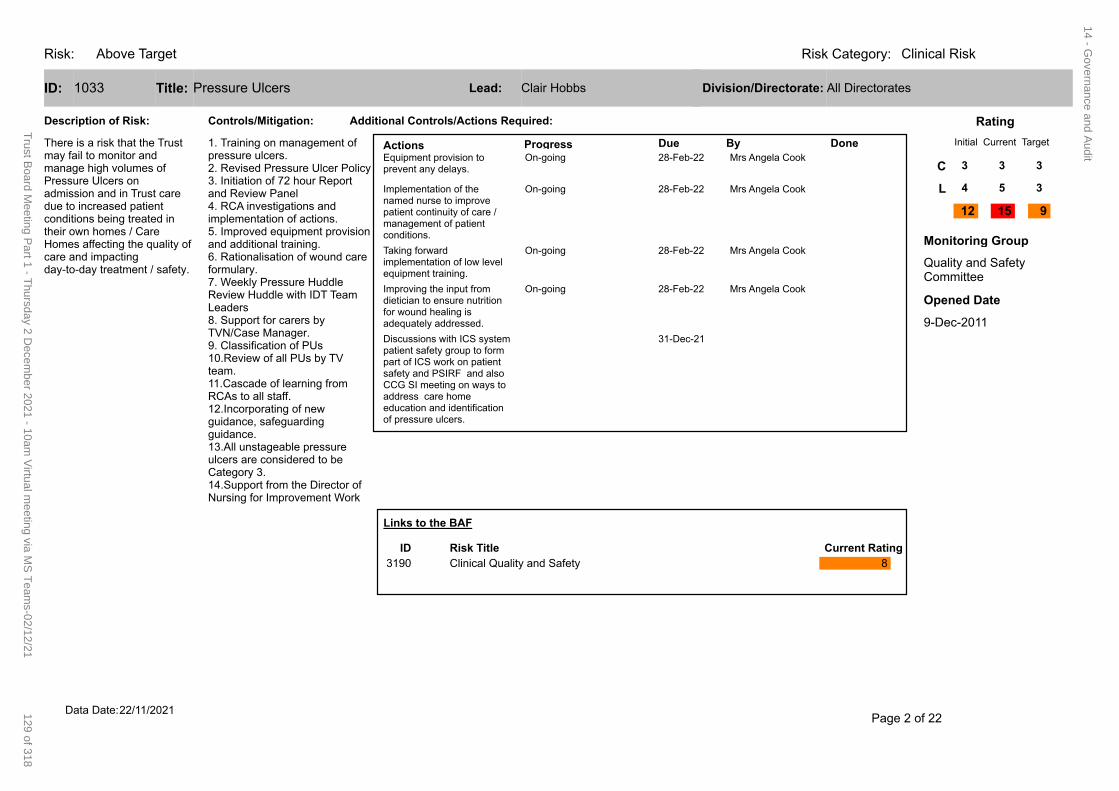
Risk: Clinical RiskRisk Category:Above Target
1033 Pressure UlcersID: Title:
Description of Risk:
Actions Progress Due By Done28-Feb-22 Mrs Angela CookEquipment provision to
prevent any delays.On-going
28-Feb-22 Mrs Angela CookImplementation of the named nurse to improve patient continuity of care / management of patient conditions.
On-going
28-Feb-22 Mrs Angela CookTaking forward implementation of low level equipment training.
On-going
28-Feb-22 Mrs Angela CookImproving the input from dietician to ensure nutrition for wound healing is adequately addressed.
On-going
31-Dec-21Discussions with ICS system patient safety group to form part of ICS work on patient safety and PSIRF and also CCG SI meeting on ways to address care home education and identification of pressure ulcers.
Additional Controls/Actions Required:Controls/Mitigation:
1. Training on management of pressure ulcers.2. Revised Pressure Ulcer Policy3. Initiation of 72 hour Report and Review Panel4. RCA investigations and implementation of actions. 5. Improved equipment provision and additional training.6. Rationalisation of wound care formulary.7. Weekly Pressure Huddle Review Huddle with IDT Team Leaders8. Support for carers by TVN/Case Manager.9. Classification of PUs 10.Review of all PUs by TV team.11.Cascade of learning from RCAs to all staff.12.Incorporating of new guidance, safeguarding guidance. 13.All unstageable pressure ulcers are considered to be Category 3.14.Support from the Director of Nursing for Improvement Work
Initial Current Target
Rating
Quality and Safety Committee
Monitoring Group
Clair Hobbs All DirectoratesLead: Division/Directorate:
C
L
12 15 9
9-Dec-2011
Opened Date
3 3 3
4 5 3
There is a risk that the Trust may fail to monitor and manage high volumes of Pressure Ulcers on admission and in Trust care due to increased patient conditions being treated in their own homes / Care Homes affecting the quality of care and impacting day-to-day treatment / safety.
Links to the BAF
Current RatingRisk TitleID
3190 Clinical Quality and Safety 8
Page 2 of 2222/11/2021Data Date:
14 - Governance and A
udit
129 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
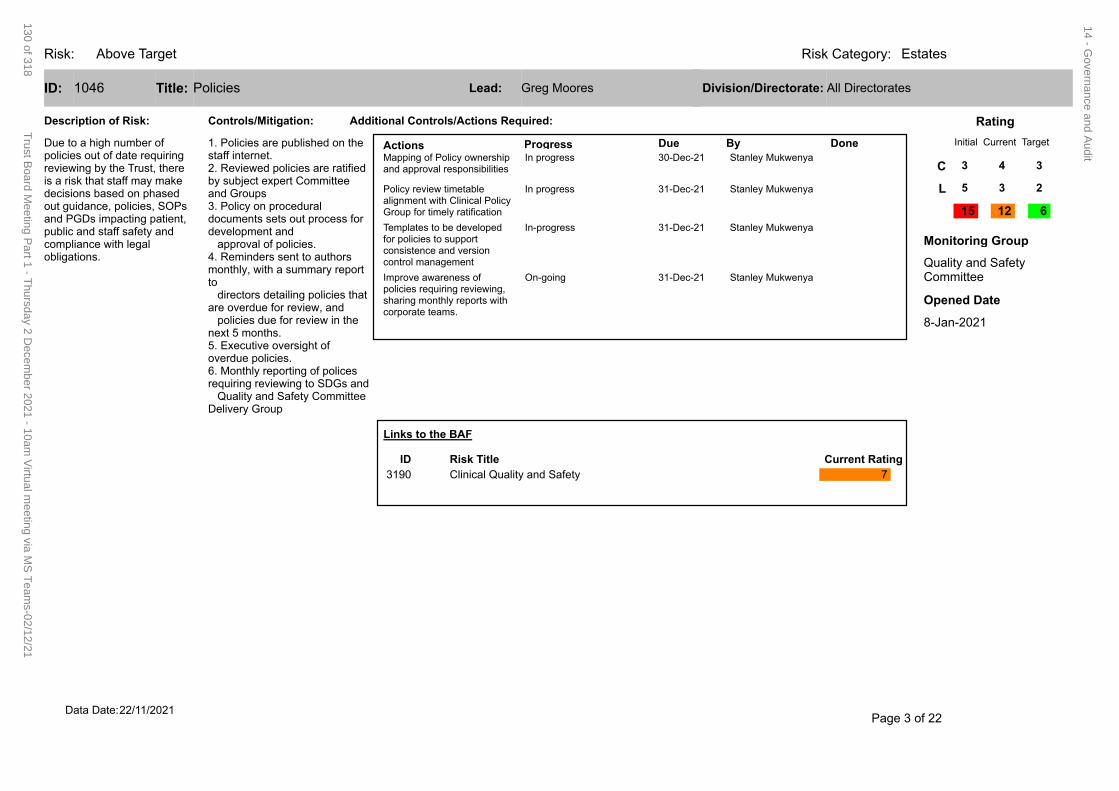
Risk: EstatesRisk Category:Above Target
1046 PoliciesID: Title:
Description of Risk:
Actions Progress Due By Done30-Dec-21 Stanley MukwenyaMapping of Policy ownership
and approval responsibilitiesIn progress
31-Dec-21 Stanley MukwenyaPolicy review timetable alignment with Clinical Policy Group for timely ratification
In progress
31-Dec-21 Stanley MukwenyaTemplates to be developed for policies to support consistence and version control management
In-progress
31-Dec-21 Stanley MukwenyaImprove awareness of policies requiring reviewing, sharing monthly reports with corporate teams.
On-going
Additional Controls/Actions Required:Controls/Mitigation:
1. Policies are published on the staff internet.2. Reviewed policies are ratified by subject expert Committee and Groups3. Policy on procedural documents sets out process for development and approval of policies.4. Reminders sent to authors monthly, with a summary report to directors detailing policies that are overdue for review, and policies due for review in the next 5 months.5. Executive oversight of overdue policies.6. Monthly reporting of polices requiring reviewing to SDGs and Quality and Safety Committee Delivery Group
Initial Current Target
Rating
Quality and Safety Committee
Monitoring Group
Greg Moores All DirectoratesLead: Division/Directorate:
C
L
15 12 6
8-Jan-2021
Opened Date
3 4 3
5 3 2
Due to a high number of policies out of date requiring reviewing by the Trust, there is a risk that staff may make decisions based on phased out guidance, policies, SOPs and PGDs impacting patient, public and staff safety and compliance with legal obligations.
Links to the BAF
Current RatingRisk TitleID
3190 Clinical Quality and Safety 7
Page 3 of 2222/11/2021Data Date:
14 - Governance and A
udit
130 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
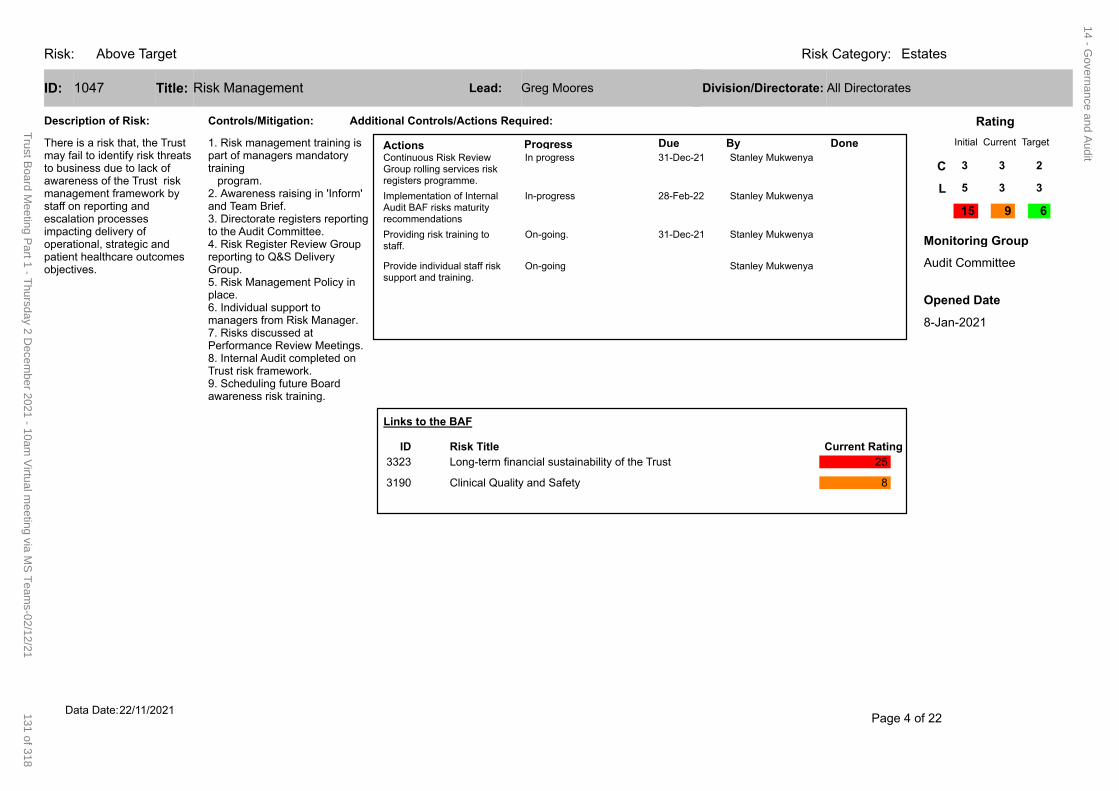
Risk: EstatesRisk Category:Above Target
1047 Risk ManagementID: Title:
Description of Risk:
Actions Progress Due By Done31-Dec-21 Stanley MukwenyaContinuous Risk Review
Group rolling services risk registers programme.
In progress
28-Feb-22 Stanley MukwenyaImplementation of Internal Audit BAF risks maturity recommendations
In-progress
31-Dec-21 Stanley MukwenyaProviding risk training to staff.
On-going.
Stanley MukwenyaProvide individual staff risk support and training.
On-going
Additional Controls/Actions Required:Controls/Mitigation:
1. Risk management training is part of managers mandatory training program.2. Awareness raising in 'Inform' and Team Brief.3. Directorate registers reporting to the Audit Committee. 4. Risk Register Review Group reporting to Q&S Delivery Group.5. Risk Management Policy in place.6. Individual support to managers from Risk Manager.7. Risks discussed at Performance Review Meetings.8. Internal Audit completed on Trust risk framework.9. Scheduling future Board awareness risk training.
Initial Current Target
Rating
Audit Committee
Monitoring Group
Greg Moores All DirectoratesLead: Division/Directorate:
C
L
15 9 6
8-Jan-2021
Opened Date
3 3 2
5 3 3
There is a risk that, the Trust may fail to identify risk threats to business due to lack of awareness of the Trust risk management framework by staff on reporting and escalation processes impacting delivery of operational, strategic and patient healthcare outcomes objectives.
Links to the BAF
Current RatingRisk TitleID
3323 Long-term financial sustainability of the Trust 25
3190 Clinical Quality and Safety 8
Page 4 of 2222/11/2021Data Date:
14 - Governance and A
udit
131 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
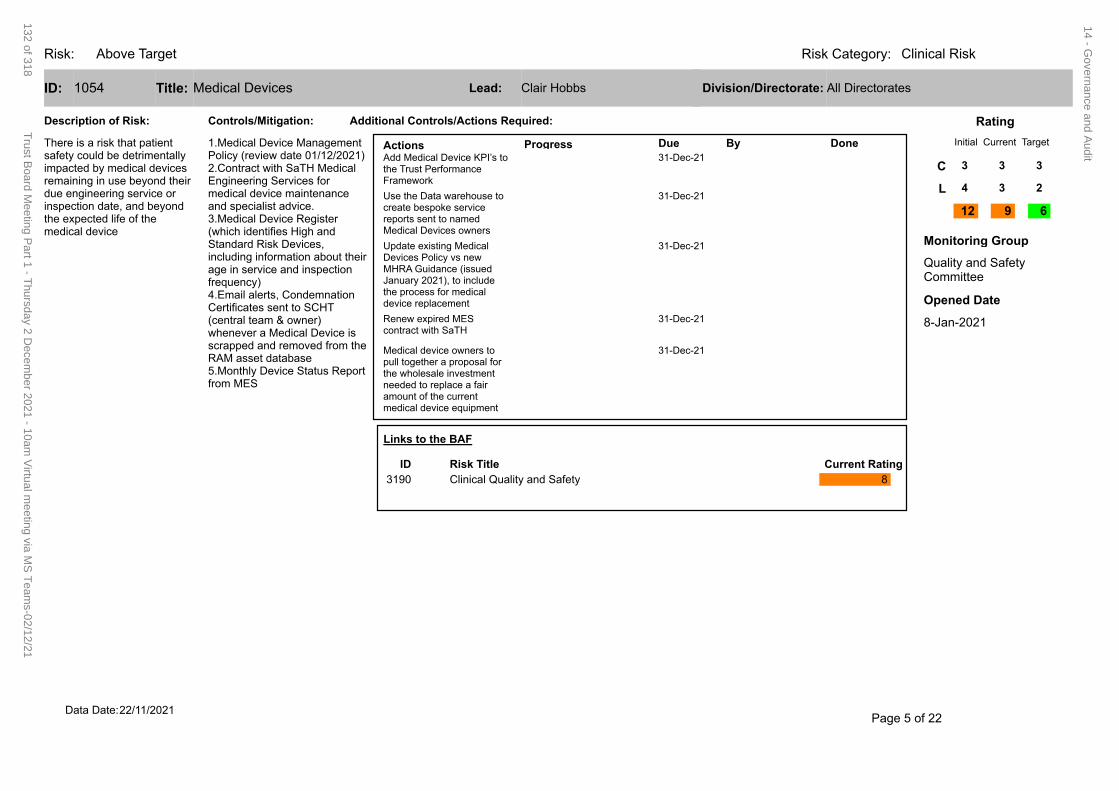
Risk: Clinical RiskRisk Category:Above Target
1054 Medical DevicesID: Title:
Description of Risk:
Actions Progress Due By Done31-Dec-21Add Medical Device KPI’s to
the Trust Performance Framework
31-Dec-21Use the Data warehouse to create bespoke service reports sent to named Medical Devices owners
31-Dec-21Update existing Medical Devices Policy vs new MHRA Guidance (issued January 2021), to include the process for medical device replacement
31-Dec-21Renew expired MES contract with SaTH
31-Dec-21Medical device owners to pull together a proposal for the wholesale investment needed to replace a fair amount of the current medical device equipment
Additional Controls/Actions Required:Controls/Mitigation:
1.Medical Device Management Policy (review date 01/12/2021)2.Contract with SaTH Medical Engineering Services for medical device maintenance and specialist advice. 3.Medical Device Register (which identifies High and Standard Risk Devices, including information about their age in service and inspection frequency)4.Email alerts, Condemnation Certificates sent to SCHT (central team & owner) whenever a Medical Device is scrapped and removed from the RAM asset database5.Monthly Device Status Report from MES
Initial Current Target
Rating
Quality and Safety Committee
Monitoring Group
Clair Hobbs All DirectoratesLead: Division/Directorate:
C
L
12 9 6
8-Jan-2021
Opened Date
3 3 3
4 3 2
There is a risk that patient safety could be detrimentally impacted by medical devices remaining in use beyond their due engineering service or inspection date, and beyond the expected life of the medical device
Links to the BAF
Current RatingRisk TitleID
3190 Clinical Quality and Safety 8
Page 5 of 2222/11/2021Data Date:
14 - Governance and A
udit
132 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
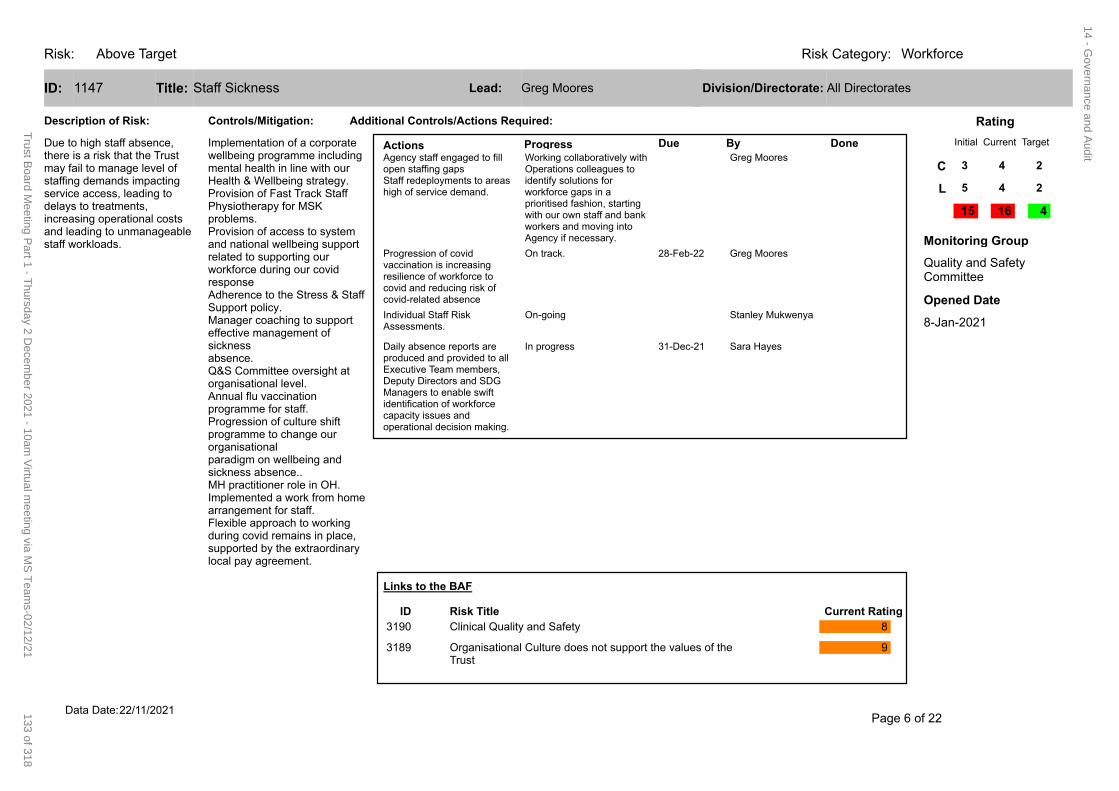
Risk: WorkforceRisk Category:Above Target
1147 Staff SicknessID: Title:
Description of Risk:
Actions Progress Due By DoneGreg MooresAgency staff engaged to fill
open staffing gapsStaff redeployments to areas high of service demand.
Working collaboratively with Operations colleagues to identify solutions for workforce gaps in a prioritised fashion, starting with our own staff and bank workers and moving into Agency if necessary.
28-Feb-22 Greg MooresProgression of covid vaccination is increasing resilience of workforce to covid and reducing risk of covid-related absence
On track.
Stanley MukwenyaIndividual Staff Risk Assessments.
On-going
31-Dec-21 Sara HayesDaily absence reports are produced and provided to all Executive Team members, Deputy Directors and SDG Managers to enable swift identification of workforce capacity issues and operational decision making.
In progress
Additional Controls/Actions Required:Controls/Mitigation:
Implementation of a corporate wellbeing programme including mental health in line with our Health & Wellbeing strategy.Provision of Fast Track Staff Physiotherapy for MSK problems.Provision of access to system and national wellbeing support related to supporting our workforce during our covid responseAdherence to the Stress & Staff Support policy.Manager coaching to support effective management of sickness absence.Q&S Committee oversight at organisational level.Annual flu vaccination programme for staff.Progression of culture shift programme to change our organisational paradigm on wellbeing and sickness absence..MH practitioner role in OH.Implemented a work from home arrangement for staff.Flexible approach to working during covid remains in place, supported by the extraordinary local pay agreement.
Initial Current Target
Rating
Quality and Safety Committee
Monitoring Group
Greg Moores All DirectoratesLead: Division/Directorate:
C
L
15 16 4
8-Jan-2021
Opened Date
3 4 2
5 4 2
Due to high staff absence, there is a risk that the Trust may fail to manage level of staffing demands impacting service access, leading to delays to treatments, increasing operational costs and leading to unmanageable staff workloads.
Links to the BAF
Current RatingRisk TitleID
3190 Clinical Quality and Safety 8
3189 Organisational Culture does not support the values of the Trust
9
Page 6 of 2222/11/2021Data Date:
14 - Governance and A
udit
133 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
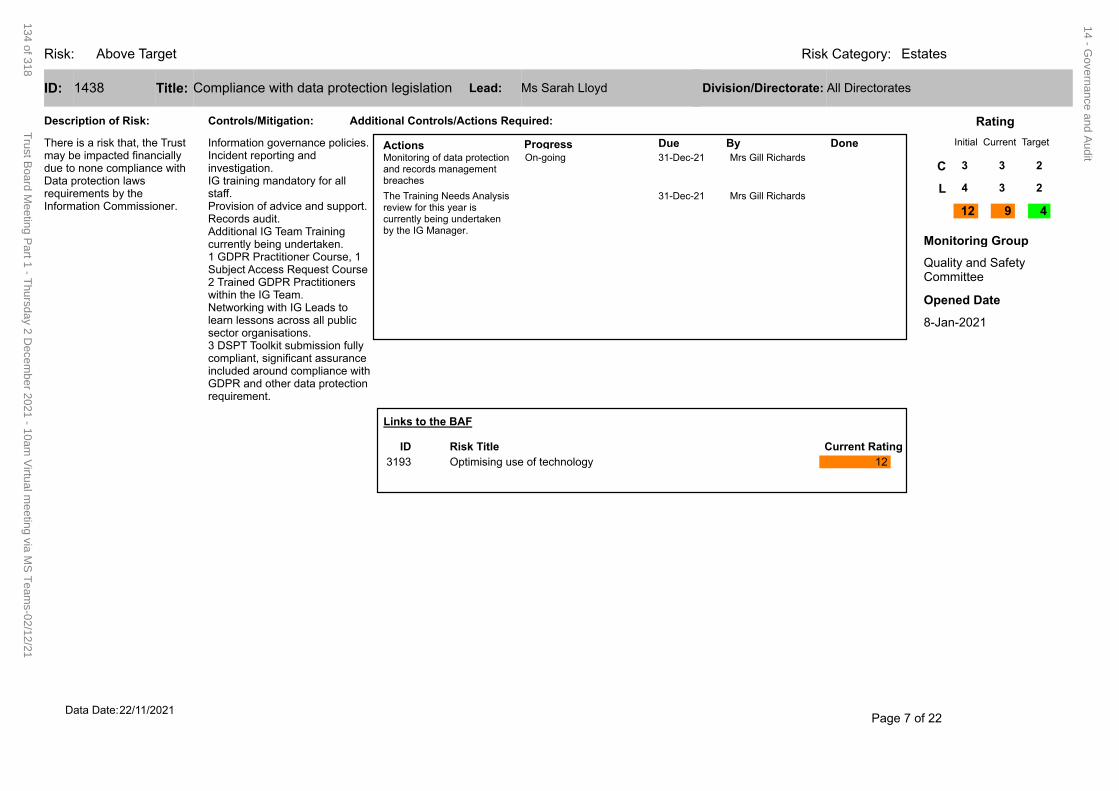
Risk: EstatesRisk Category:Above Target
1438 Compliance with data protection legislationID: Title:
Description of Risk:
Actions Progress Due By DoneOn-going
Additional Controls/Actions Required:Controls/Mitigation:
Information governance policies.Incident reporting and investigation.IG training mandatory for all staff.Provision of advice and support.Records audit.Additional IG Team Training currently being undertaken.1 GDPR Practitioner Course, 1 Subject Access Request Course2 Trained GDPR Practitioners within the IG Team.Networking with IG Leads to learn lessons across all public sector organisations.3 DSPT Toolkit submission fully compliant, significant assurance included around compliance with GDPR and other data protection requirement.
Initial Current Target
Rating
Quality and Safety Committee
Monitoring Group
Ms Sarah Lloyd All DirectoratesLead: Division/Directorate:
C
L
12 9 4
8-Jan-2021
Opened Date
3 3 2
4 3 2
There is a risk that, the Trust may be impacted financially due to none compliance with Data protection laws requirements by the Information Commissioner.
Links to the BAF
Current RatingRisk TitleID
3193 Optimising use of technology 12
Page 7 of 2222/11/2021Data Date:
Monitoring of data protection 31-Dec-21 Mrs Gill Richardsand records management breaches
The Training Needs Analysis 31-Dec-21 Mrs Gill Richardsreview for this year is currently being undertaken by the IG Manager.
14 - Governance and A
udit
134 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
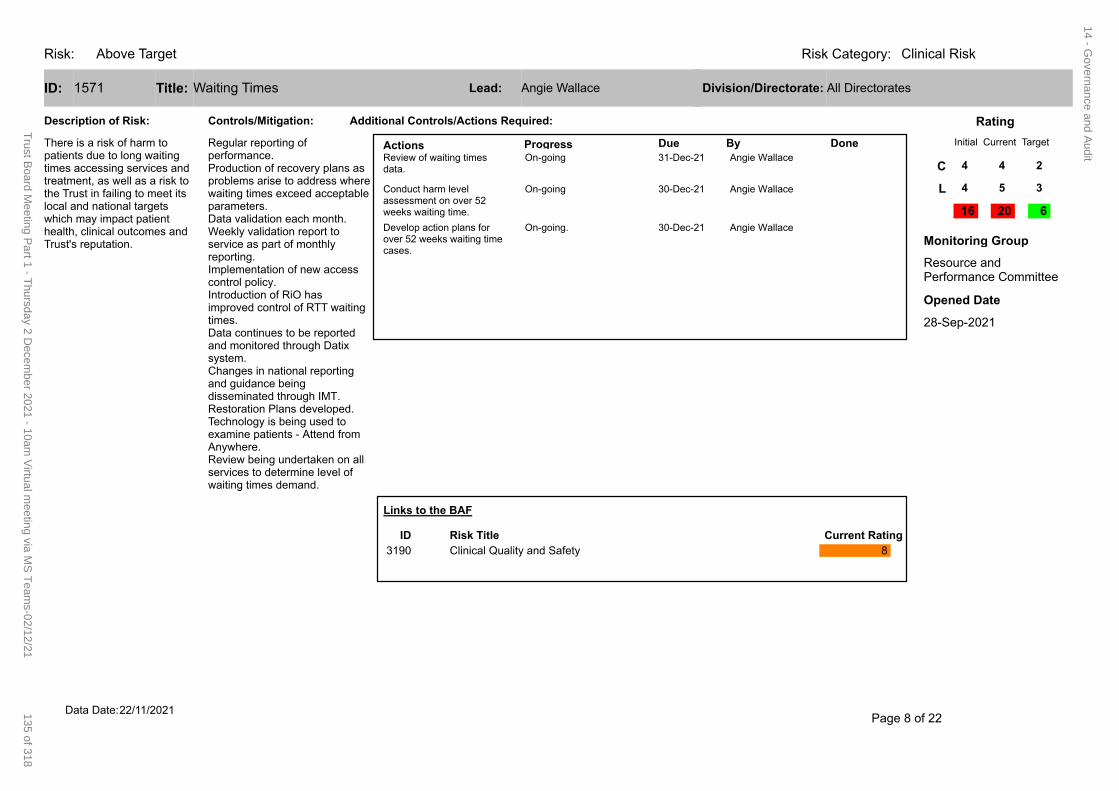
1571 Waiting TimesID: Title:
Description of Risk:
Actions Progress Due By DoneOn-going
On-going
On-going.
Additional Controls/Actions Required:Controls/Mitigation:
Regular reporting of performance.Production of recovery plans as problems arise to address where waiting times exceed acceptable parameters.Data validation each month.Weekly validation report to service as part of monthly reporting.Implementation of new access control policy.Introduction of RiO has improved control of RTT waiting times.Data continues to be reported and monitored through Datix system.Changes in national reporting and guidance being disseminated through IMT.Restoration Plans developed.Technology is being used to examine patients - Attend from Anywhere.Review being undertaken on all services to determine level of waiting times demand.
Initial Current Target
Rating
Resource and Performance Committee
Monitoring Group
Angie Wallace All DirectoratesLead: Division/Directorate:
C
L
16 20 6
28-Sep-2021
Opened Date
4 4 2
4 5 3
There is a risk of harm to patients due to long waiting times accessing services and treatment, as well as a risk to the Trust in failing to meet its local and national targets which may impact patient health, clinical outcomes and Trust's reputation.
Links to the BAF
Current RatingRisk TitleID
3190 Clinical Quality and Safety 8
Page 8 of 2222/11/2021Data Date:
Review of waiting times 31-Dec-21 Angie Wallace data.
Conduct harm level 30-Dec-21 Angie Wallace assessment on over 52 weeks waiting time.
Develop action plans for 30-Dec-21 Angie Wallace over 52 weeks waiting time cases.
Risk: Above Target Risk Category: Clinical Risk
14 - Governance and A
udit
135 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
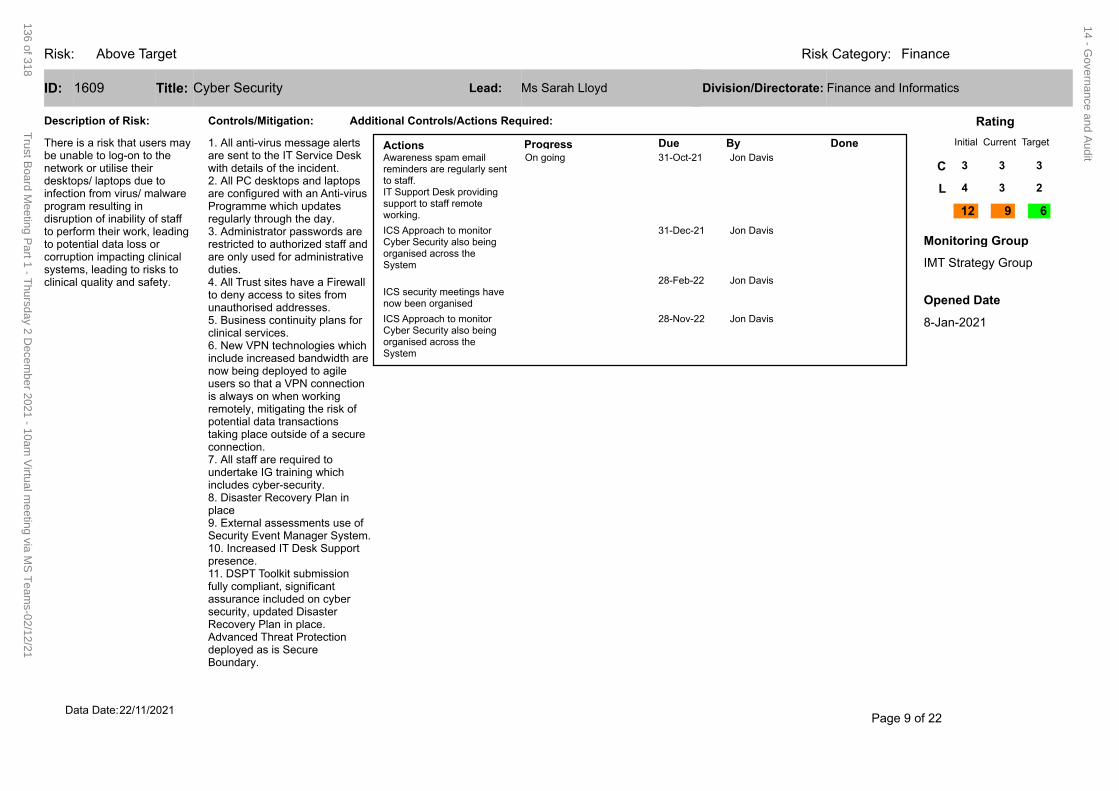
Risk: FinanceRisk Category:Above Target
1609 Cyber SecurityID: Title:
Description of Risk:
Actions Progress Due By Done31-Oct-21 Jon DavisAwareness spam email
reminders are regularly sent to staff. IT Support Desk providing support to staff remote working.
On going
31-Dec-21 Jon DavisICS Approach to monitor Cyber Security also being organised across the System
28-Feb-22 Jon DavisICS security meetings have now been organised
28-Nov-22 Jon DavisICS Approach to monitor Cyber Security also being organised across the System
Additional Controls/Actions Required:Controls/Mitigation:
1. All anti-virus message alerts are sent to the IT Service Desk with details of the incident. 2. All PC desktops and laptops are configured with an Anti-virus Programme which updates regularly through the day.3. Administrator passwords are restricted to authorized staff and are only used for administrative duties. 4. All Trust sites have a Firewall to deny access to sites from unauthorised addresses.5. Business continuity plans for clinical services.6. New VPN technologies which include increased bandwidth are now being deployed to agile users so that a VPN connection is always on when working remotely, mitigating the risk of potential data transactions taking place outside of a secure connection.7. All staff are required to undertake IG training which includes cyber-security.8. Disaster Recovery Plan in place9. External assessments use of Security Event Manager System.10. Increased IT Desk Support presence. 11. DSPT Toolkit submission fully compliant, significant assurance included on cyber security, updated Disaster Recovery Plan in place. Advanced Threat Protection deployed as is Secure Boundary.
Initial Current Target
Rating
IMT Strategy Group
Monitoring Group
Ms Sarah Lloyd Finance and InformaticsLead: Division/Directorate:
C
L
12 9 6
8-Jan-2021
Opened Date
3 3 3
4 3 2
There is a risk that users may be unable to log-on to the network or utilise their desktops/ laptops due to infection from virus/ malware program resulting in disruption of inability of staff to perform their work, leading to potential data loss or corruption impacting clinical systems, leading to risks to clinical quality and safety.
Page 9 of 2222/11/2021Data Date:
14 - Governance and A
udit
136 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
Risk: FinanceRisk Category:Above Target
Links to the BAF
Current RatingRisk TitleID
3193 Optimising use of technology 12
Page 10 of 2222/11/2021Data Date:
14 - Governance and A
udit
137 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
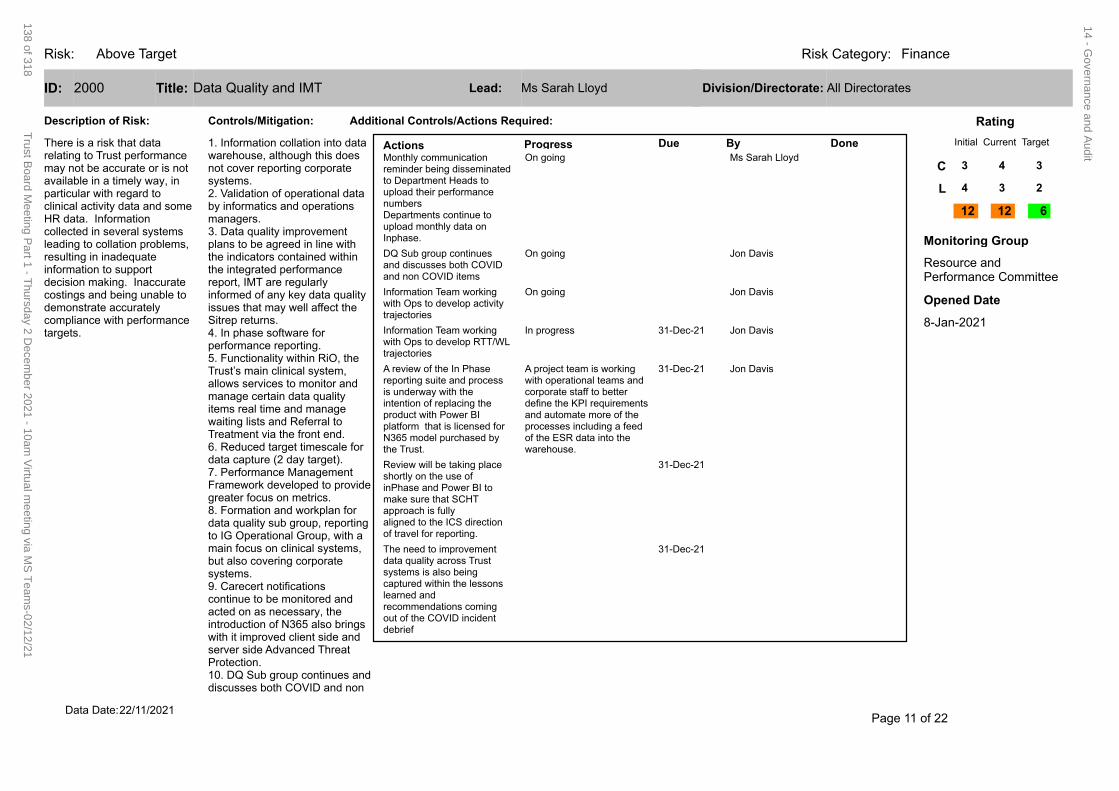
Risk: FinanceRisk Category:Above Target
2000 Data Quality and IMTID: Title:
Description of Risk:
Actions Progress Due By DoneMs Sarah LloydMonthly communication
reminder being disseminated to Department Heads to upload their performance numbersDepartments continue to upload monthly data on Inphase.
On going
Jon DavisDQ Sub group continues and discusses both COVID and non COVID items
On going
Jon DavisInformation Team working with Ops to develop activity trajectories
On going
In progress
31-Dec-21 Jon DavisA review of the In Phase reporting suite and process is underway with the intention of replacing the product with Power BI platform that is licensed for N365 model purchased by the Trust.
A project team is working with operational teams and corporate staff to better define the KPI requirements and automate more of the processes including a feed of the ESR data into the warehouse.
31-Dec-21Review will be taking place shortly on the use of inPhase and Power BI to make sure that SCHT approach is fullyaligned to the ICS direction of travel for reporting.
31-Dec-21The need to improvement data quality across Trust systems is also being captured within the lessons learned and recommendations coming out of the COVID incident debrief
Additional Controls/Actions Required:Controls/Mitigation:
1. Information collation into data warehouse, although this does not cover reporting corporate systems.2. Validation of operational data by informatics and operations managers.3. Data quality improvement plans to be agreed in line with the indicators contained within the integrated performance report, IMT are regularly informed of any key data quality issues that may well affect the Sitrep returns.4. In phase software for performance reporting.5. Functionality within RiO, the Trust’s main clinical system, allows services to monitor and manage certain data quality items real time and manage waiting lists and Referral to Treatment via the front end.6. Reduced target timescale for data capture (2 day target).7. Performance Management Framework developed to provide greater focus on metrics.8. Formation and workplan for data quality sub group, reporting to IG Operational Group, with a main focus on clinical systems, but also covering corporate systems.9. Carecert notifications continue to be monitored and acted on as necessary, the introduction of N365 also brings with it improved client side and server side Advanced Threat Protection.10. DQ Sub group continues and discusses both COVID and non
Initial Current Target
Rating
Resource and Performance Committee
Monitoring Group
Ms Sarah Lloyd All DirectoratesLead: Division/Directorate:
C
L
12 12 6
8-Jan-2021
Opened Date
3 4 3
4 3 2
There is a risk that data relating to Trust performance may not be accurate or is not available in a timely way, in particular with regard to clinical activity data and some HR data. Information collected in several systems leading to collation problems, resulting in inadequate information to support decision making. Inaccurate costings and being unable to demonstrate accurately compliance with performance targets.
Page 11 of 2222/11/2021Data Date:
Information Team working 31-Dec-21 Jon Daviswith Ops to develop RTT/WL trajectories
14 - Governance and A
udit
138 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
Risk: FinanceRisk Category:Above Target
COVID items.11. Information Team working with Ops to develop activity trajectories12. Information Team working with Ops to develop RTT/WL trajectories13. COVID related dashboard regularly reviewed at IMT and distributed to RPC/Board.13. Data quality is being managed in conjunction with the DSPT workplan and submission
Links to the BAF
Current RatingRisk TitleID
3193 Optimising use of technology 12
3192 Healthcare Systems 12
3190 Clinical Quality and Safety 8
Page 12 of 2222/11/2021Data Date:
14 - Governance and A
udit
139 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
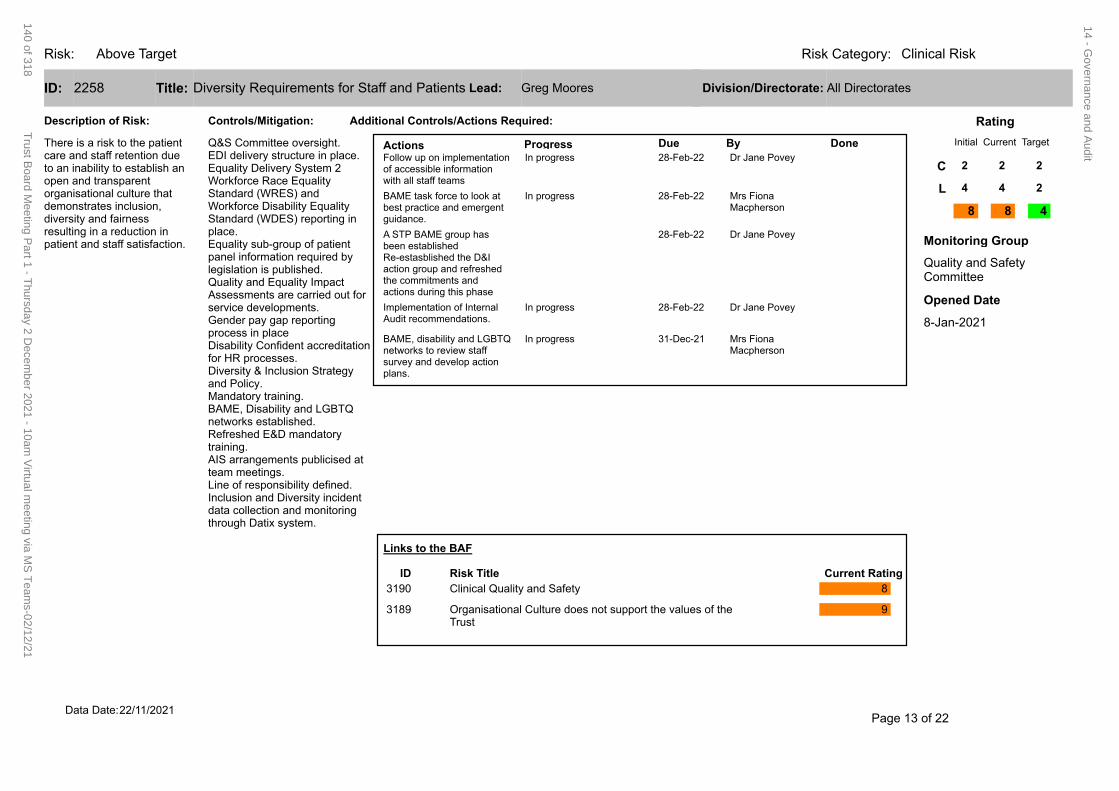
Risk: Clinical RiskRisk Category:Above Target
2258 Diversity Requirements for Staff and PatientsID: Title:
Description of Risk:
Actions Progress Due By Done28-Feb-22 Dr Jane PoveyFollow up on implementation
of accessible information with all staff teams
In progress
28-Feb-22 Mrs Fiona Macpherson
BAME task force to look at best practice and emergent guidance.
In progress
28-Feb-22 Dr Jane PoveyA STP BAME group has been establishedRe-estasblished the D&I action group and refreshed the commitments and actions during this phase
28-Feb-22 Dr Jane PoveyImplementation of Internal Audit recommendations.
In progress
31-Dec-21 Mrs Fiona Macpherson
BAME, disability and LGBTQ networks to review staff survey and develop action plans.
In progress
Additional Controls/Actions Required:Controls/Mitigation:
Q&S Committee oversight.EDI delivery structure in place.Equality Delivery System 2 Workforce Race Equality Standard (WRES) and Workforce Disability Equality Standard (WDES) reporting in place.Equality sub-group of patient panel information required by legislation is published.Quality and Equality Impact Assessments are carried out for service developments.Gender pay gap reporting process in placeDisability Confident accreditation for HR processes.Diversity & Inclusion Strategy and Policy.Mandatory training.BAME, Disability and LGBTQ networks established.Refreshed E&D mandatory training.AIS arrangements publicised at team meetings.Line of responsibility defined.Inclusion and Diversity incident data collection and monitoring through Datix system.
Initial Current Target
Rating
Quality and Safety Committee
Monitoring Group
Greg Moores All DirectoratesLead: Division/Directorate:
C
L
8 8 4
8-Jan-2021
Opened Date
2 2 2
4 4 2
There is a risk to the patient care and staff retention due to an inability to establish an open and transparent organisational culture that demonstrates inclusion, diversity and fairness resulting in a reduction in patient and staff satisfaction.
Links to the BAF
Current RatingRisk TitleID
3190 Clinical Quality and Safety 8
3189 Organisational Culture does not support the values of the Trust
9
Page 13 of 2222/11/2021Data Date:
14 - Governance and A
udit
140 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
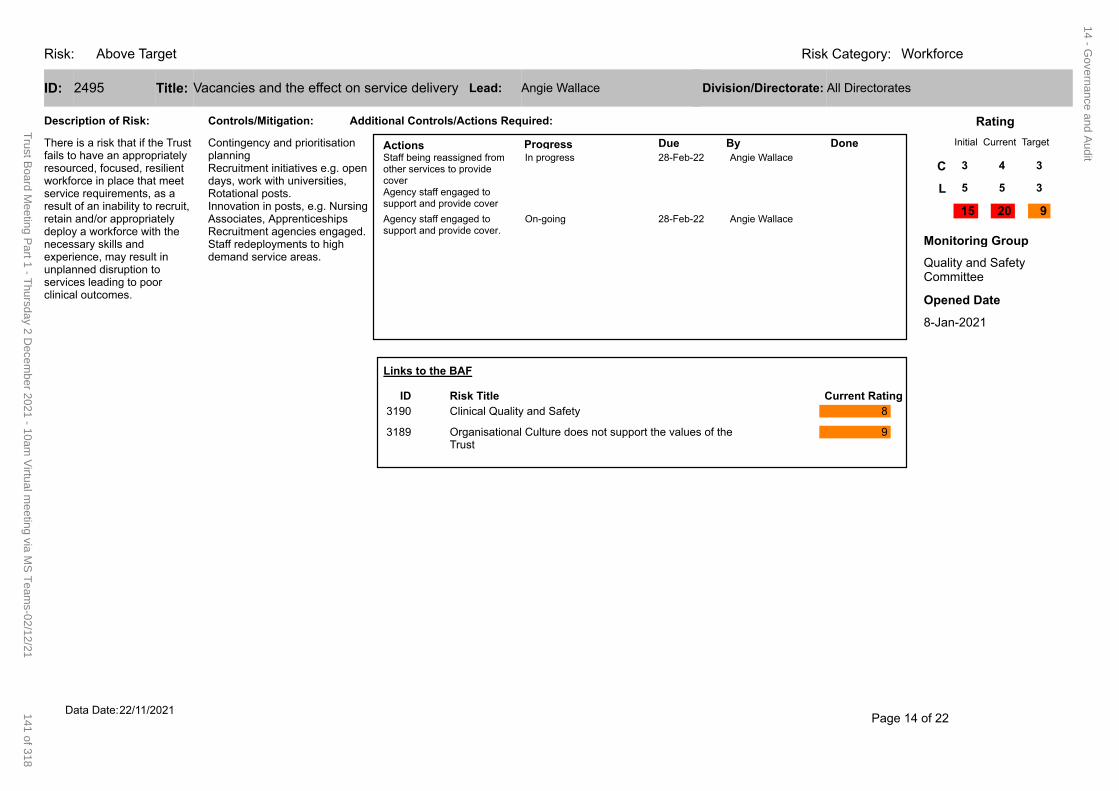
Risk: WorkforceRisk Category:Above Target
2495 Vacancies and the effect on service deliveryID: Title:
Description of Risk:
Actions Progress Due By Done28-Feb-22 Angie WallaceStaff being reassigned from
other services to provide coverAgency staff engaged to support and provide cover
In progress
28-Feb-22 Angie WallaceAgency staff engaged to support and provide cover.
On-going
Additional Controls/Actions Required:Controls/Mitigation:
Contingency and prioritisation planningRecruitment initiatives e.g. open days, work with universities, Rotational posts.Innovation in posts, e.g. Nursing Associates, ApprenticeshipsRecruitment agencies engaged.Staff redeployments to high demand service areas.
Initial Current Target
Rating
Quality and Safety Committee
Monitoring Group
Angie Wallace All DirectoratesLead: Division/Directorate:
C
L
15 20 9
8-Jan-2021
Opened Date
3 4 3
5 5 3
There is a risk that if the Trust fails to have an appropriately resourced, focused, resilient workforce in place that meet service requirements, as a result of an inability to recruit, retain and/or appropriately deploy a workforce with the necessary skills and experience, may result in unplanned disruption to services leading to poor clinical outcomes.
Links to the BAF
Current RatingRisk TitleID
3190 Clinical Quality and Safety 8
3189 Organisational Culture does not support the values of the Trust
9
Page 14 of 2222/11/2021Data Date:
14 - Governance and A
udit
141 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
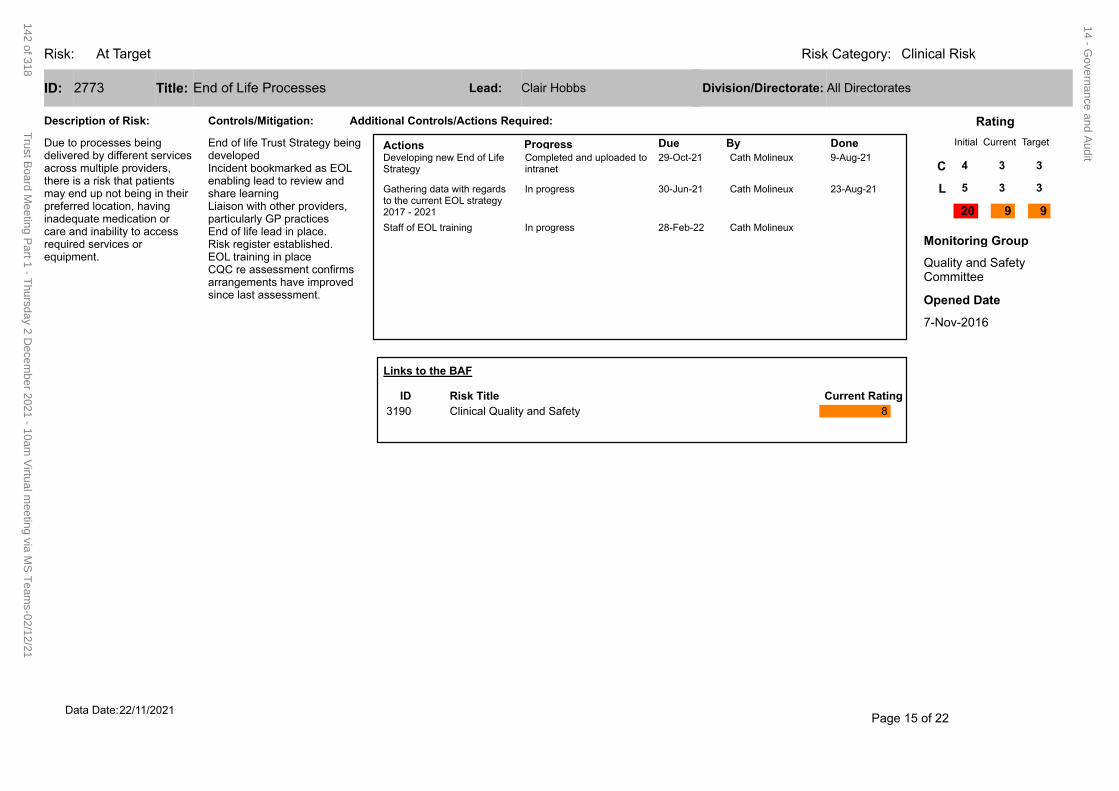
Risk: Clinical RiskRisk Category:At Target
2773 End of Life ProcessesID: Title:
Description of Risk:
Actions Progress Due By Done29-Oct-21 Cath Molineux 9-Aug-21Developing new End of Life
StrategyCompleted and uploaded to intranet
30-Jun-21 Cath Molineux 23-Aug-21Gathering data with regards to the current EOL strategy 2017 - 2021
In progress
28-Feb-22 Cath MolineuxStaff of EOL training In progress
Additional Controls/Actions Required:Controls/Mitigation:
End of life Trust Strategy being developedIncident bookmarked as EOL enabling lead to review and share learningLiaison with other providers, particularly GP practicesEnd of life lead in place.Risk register established.EOL training in placeCQC re assessment confirms arrangements have improved since last assessment.
Initial Current Target
Rating
Quality and Safety Committee
Monitoring Group
Clair Hobbs All DirectoratesLead: Division/Directorate:
C
L
20 9 9
7-Nov-2016
Opened Date
4 3 3
5 3 3
Due to processes being delivered by different services across multiple providers, there is a risk that patients may end up not being in their preferred location, having inadequate medication or care and inability to access required services or equipment.
Links to the BAF
Current RatingRisk TitleID
3190 Clinical Quality and Safety 8
Page 15 of 2222/11/2021Data Date:
14 - Governance and A
udit
142 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
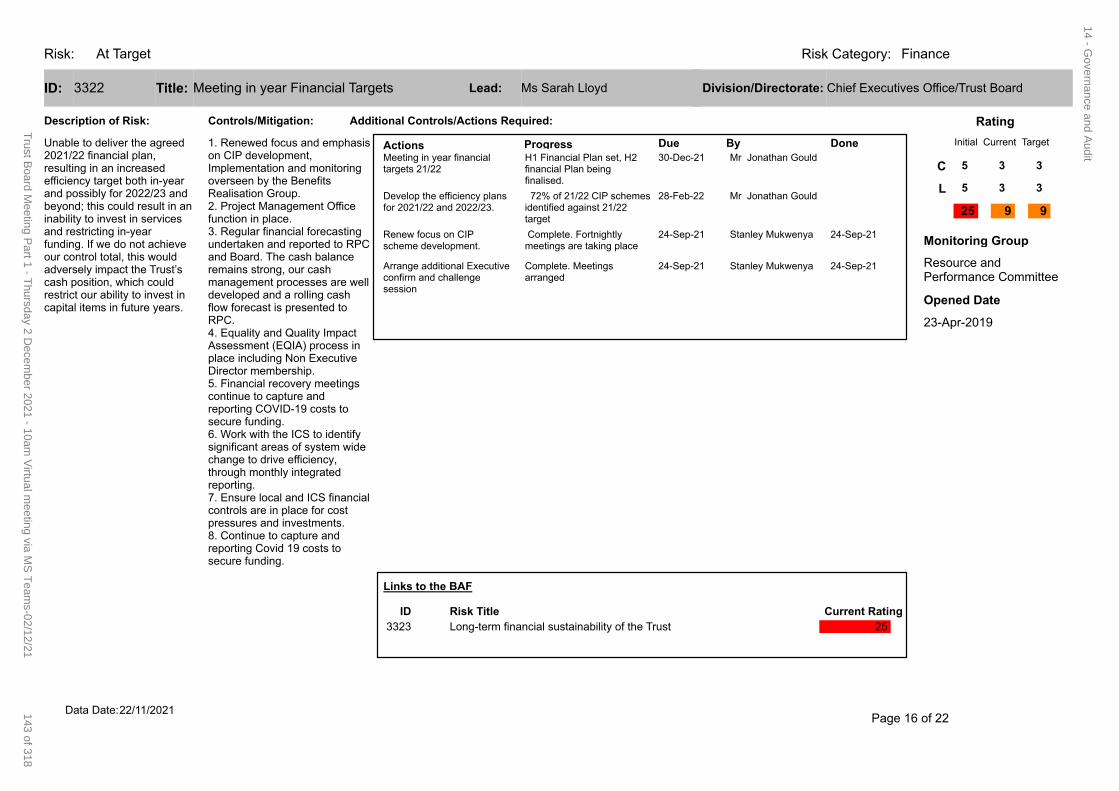
Risk: FinanceRisk Category:At Target
3322 Meeting in year Financial TargetsID: Title:
Description of Risk:
Actions Progress Due By Done30-Dec-21 Mr Jonathan GouldMeeting in year financial
targets 21/22H1 Financial Plan set, H2 financial Plan being finalised.
28-Feb-22 Mr Jonathan GouldDevelop the efficiency plans for 2021/22 and 2022/23.
72% of 21/22 CIP schemes identified against 21/22 target
24-Sep-21 Stanley Mukwenya 24-Sep-21Renew focus on CIP scheme development.
Complete. Fortnightly meetings are taking place
24-Sep-21 Stanley Mukwenya 24-Sep-21Arrange additional Executive confirm and challenge session
Complete. Meetings arranged
Additional Controls/Actions Required:Controls/Mitigation:
1. Renewed focus and emphasis on CIP development, Implementation and monitoring overseen by the Benefits Realisation Group. 2. Project Management Office function in place. 3. Regular financial forecasting undertaken and reported to RPC and Board. The cash balance remains strong, our cash management processes are well developed and a rolling cash flow forecast is presented to RPC. 4. Equality and Quality Impact Assessment (EQIA) process in place including Non Executive Director membership. 5. Financial recovery meetings continue to capture and reporting COVID-19 costs to secure funding. 6. Work with the ICS to identify significant areas of system wide change to drive efficiency, through monthly integrated reporting.7. Ensure local and ICS financial controls are in place for cost pressures and investments. 8. Continue to capture and reporting Covid 19 costs to secure funding.
Initial Current Target
Rating
Resource and Performance Committee
Monitoring Group
Ms Sarah Lloyd Chief Executives Office/Trust BoardLead: Division/Directorate:
C
L
25 9 9
23-Apr-2019
Opened Date
5 3 3
5 3 3
Unable to deliver the agreed 2021/22 financial plan, resulting in an increased efficiency target both in-year and possibly for 2022/23 and beyond; this could result in an inability to invest in services and restricting in-year funding. If we do not achieve our control total, this would adversely impact the Trust’s cash position, which could restrict our ability to invest in capital items in future years.
Links to the BAF
Current RatingRisk TitleID
3323 Long-term financial sustainability of the Trust 25
Page 16 of 2222/11/2021Data Date:
14 - Governance and A
udit
143 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
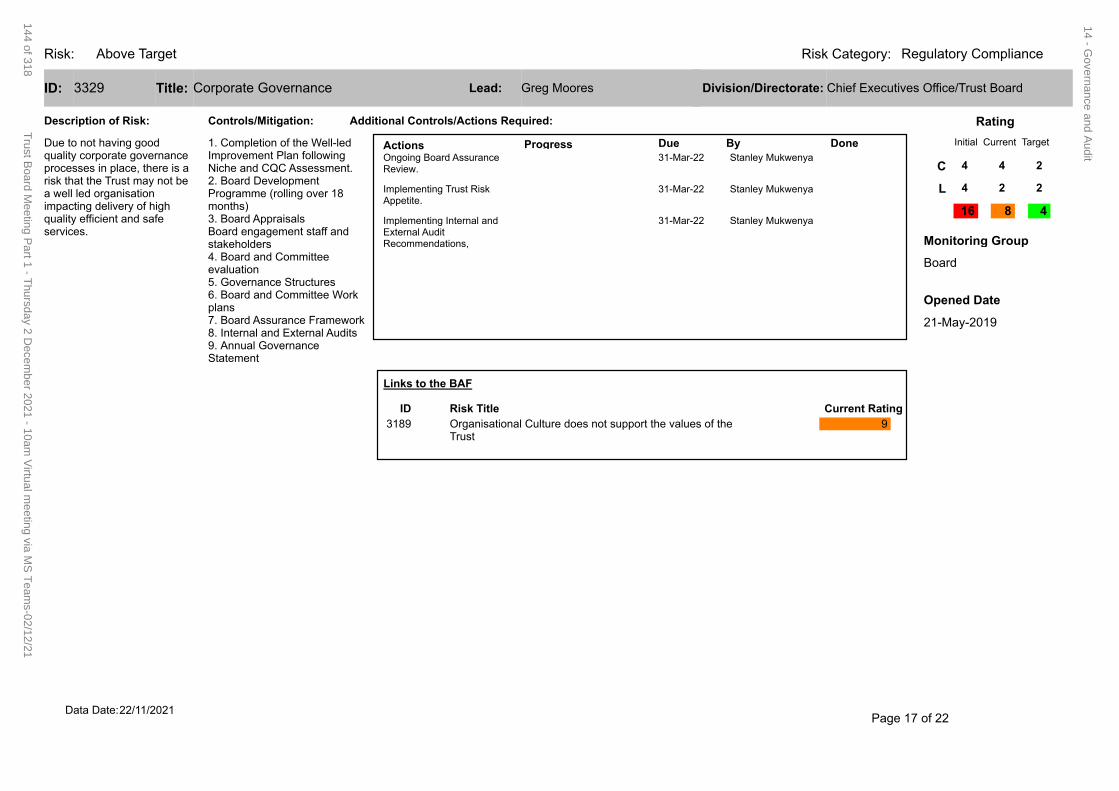
Risk: Regulatory ComplianceRisk Category:Above Target
3329 Corporate GovernanceID: Title:
Description of Risk:
Actions Progress Due By Done31-Mar-22 Stanley MukwenyaOngoing Board Assurance
Review.
31-Mar-22 Stanley MukwenyaImplementing Trust Risk Appetite.
31-Mar-22 Stanley MukwenyaImplementing Internal and External Audit Recommendations,
Additional Controls/Actions Required:Controls/Mitigation:
1. Completion of the Well-led Improvement Plan following Niche and CQC Assessment.2. Board Development Programme (rolling over 18 months)3. Board AppraisalsBoard engagement staff and stakeholders4. Board and Committee evaluation5. Governance Structures6. Board and Committee Work plans7. Board Assurance Framework8. Internal and External Audits9. Annual Governance Statement
Initial Current Target
Rating
Board
Monitoring Group
Greg Moores Chief Executives Office/Trust BoardLead: Division/Directorate:
C
L
16 8 4
21-May-2019
Opened Date
4 4 2
4 2 2
Due to not having good quality corporate governance processes in place, there is a risk that the Trust may not be a well led organisation impacting delivery of high quality efficient and safe services.
Links to the BAF
Current RatingRisk TitleID
3189 Organisational Culture does not support the values of the Trust
9
Page 17 of 2222/11/2021Data Date:
14 - Governance and A
udit
144 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
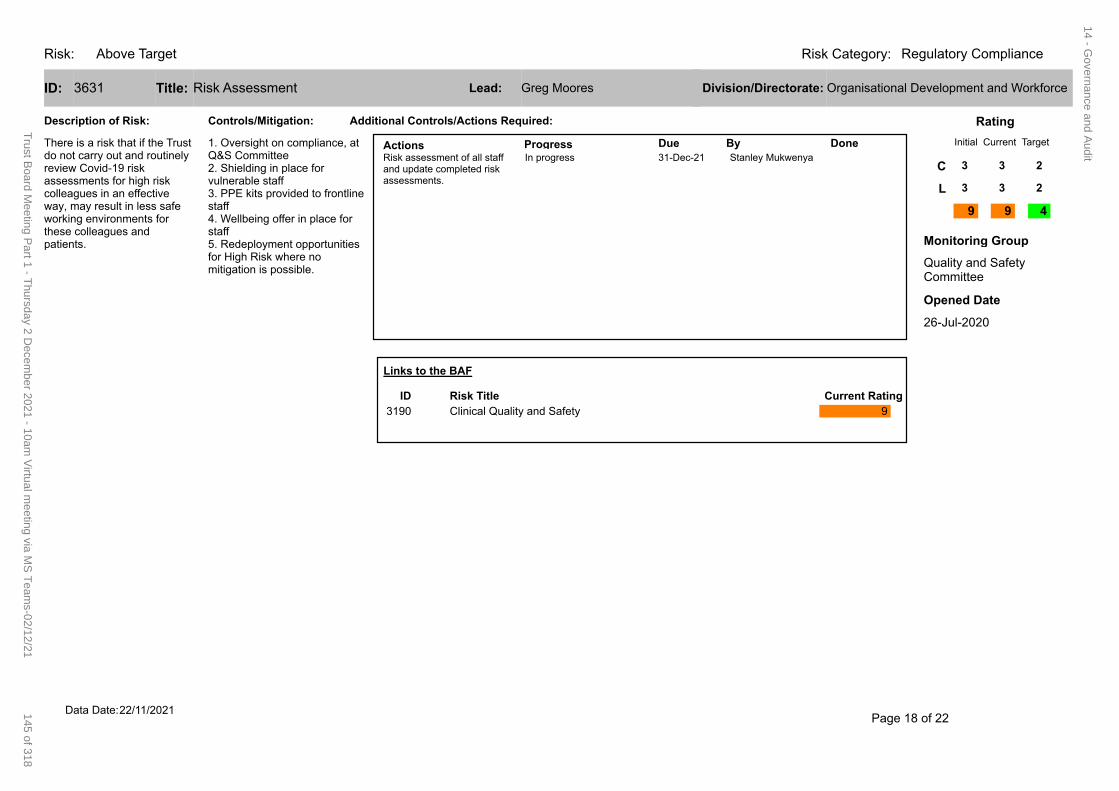
Risk: Regulatory ComplianceRisk Category:Above Target
3631 Risk AssessmentID: Title:
Description of Risk:
Actions Progress Due By Done31-Dec-21 Stanley MukwenyaRisk assessment of all staff
and update completed risk assessments.
In progress
Additional Controls/Actions Required:Controls/Mitigation:
1. Oversight on compliance, at Q&S Committee2. Shielding in place for vulnerable staff3. PPE kits provided to frontline staff4. Wellbeing offer in place for staff5. Redeployment opportunities for High Risk where no mitigation is possible.
Initial Current Target
Rating
Quality and Safety Committee
Monitoring Group
Greg Moores Organisational Development and WorkforceLead: Division/Directorate:
C
L
9 9 4
26-Jul-2020
Opened Date
3 3 2
3 3 2
There is a risk that if the Trust do not carry out and routinely review Covid-19 risk assessments for high risk colleagues in an effective way, may result in less safe working environments for these colleagues and patients.
Links to the BAF
Current RatingRisk TitleID
3190 Clinical Quality and Safety 9
Page 18 of 2222/11/2021Data Date:
14 - Governance and A
udit
145 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
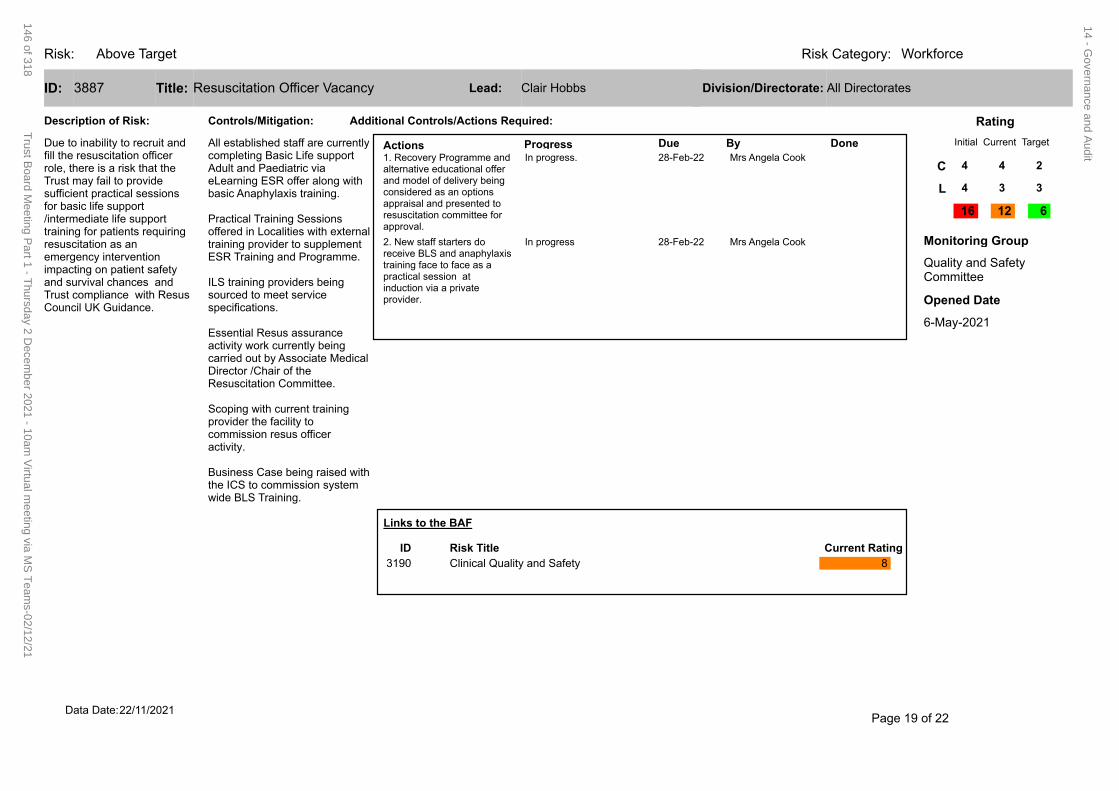
Risk: WorkforceRisk Category:Above Target
3887 Resuscitation Officer VacancyID: Title:
Description of Risk:
Actions Progress Due By Done28-Feb-22 Mrs Angela Cook1. Recovery Programme and
alternative educational offer and model of delivery being considered as an options appraisal and presented to resuscitation committee for approval.
In progress.
28-Feb-22 Mrs Angela Cook2. New staff starters do receive BLS and anaphylaxis training face to face as a practical session at induction via a private provider.
In progress
Additional Controls/Actions Required:Controls/Mitigation:
All established staff are currently completing Basic Life support Adult and Paediatric via eLearning ESR offer along with basic Anaphylaxis training.
Practical Training Sessions offered in Localities with external training provider to supplement ESR Training and Programme.
ILS training providers being sourced to meet service specifications.
Essential Resus assurance activity work currently being carried out by Associate Medical Director /Chair of the Resuscitation Committee.
Scoping with current training provider the facility to commission resus officer activity.
Business Case being raised with the ICS to commission system wide BLS Training.
Initial Current Target
Rating
Quality and Safety Committee
Monitoring Group
Clair Hobbs All DirectoratesLead: Division/Directorate:
C
L
16 12 6
6-May-2021
Opened Date
4 4 2
4 3 3
Due to inability to recruit and fill the resuscitation officer role, there is a risk that the Trust may fail to provide sufficient practical sessions for basic life support /intermediate life support training for patients requiring resuscitation as an emergency intervention impacting on patient safety and survival chances and Trust compliance with Resus Council UK Guidance.
Links to the BAF
Current RatingRisk TitleID
3190 Clinical Quality and Safety 8
Page 19 of 2222/11/2021Data Date:
14 - Governance and A
udit
146 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
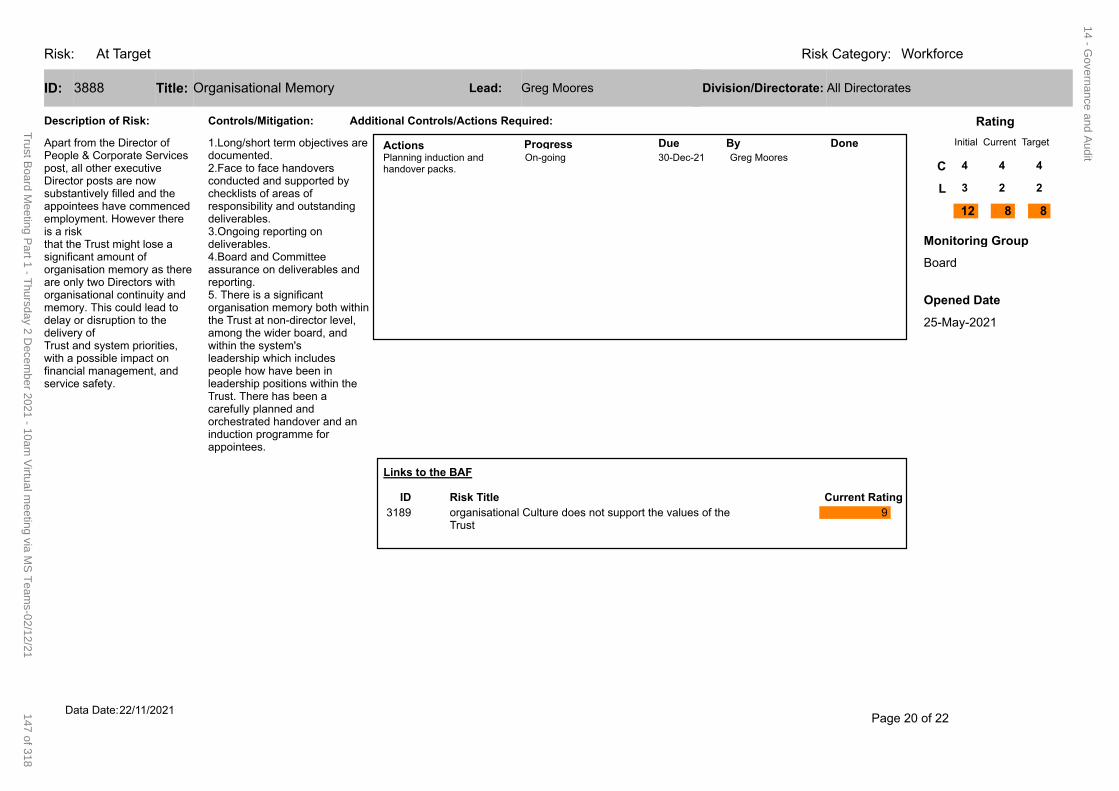
Risk: WorkforceRisk Category:At Target
3888 Organisational MemoryID: Title:
Description of Risk:
Actions Progress Due By Done30-Dec-21 Greg MooresPlanning induction and
handover packs.On-going
Additional Controls/Actions Required:Controls/Mitigation:
1.Long/short term objectives are documented.2.Face to face handovers conducted and supported by checklists of areas of responsibility and outstanding deliverables.3.Ongoing reporting on deliverables.4.Board and Committee assurance on deliverables and reporting.5. There is a significant organisation memory both within the Trust at non-director level, among the wider board, and within the system'sleadership which includes people how have been in leadership positions within the Trust. There has been a carefully planned and orchestrated handover and an induction programme for appointees.
Initial Current Target
Rating
Board
Monitoring Group
Greg Moores All DirectoratesLead: Division/Directorate:
C
L
12 8 8
25-May-2021
Opened Date
4 4 4
3 2 2
Apart from the Director of People & Corporate Services post, all other executive Director posts are now substantively filled and the appointees have commenced employment. However there is a riskthat the Trust might lose a significant amount of organisation memory as there are only two Directors with organisational continuity and memory. This could lead to delay or disruption to the delivery ofTrust and system priorities, with a possible impact on financial management, and service safety.
Links to the BAF
Current RatingRisk TitleID
3189 organisational Culture does not support the values of the Trust
9
Page 20 of 2222/11/2021Data Date:
14 - Governance and A
udit
147 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
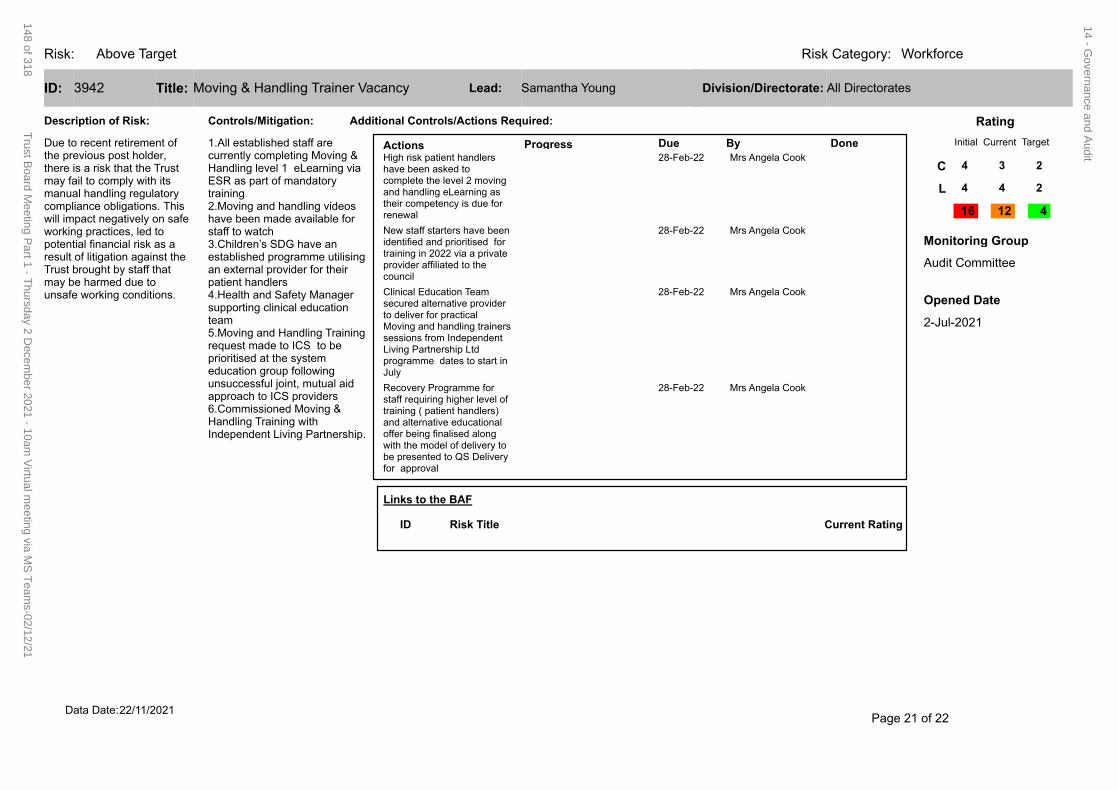
Risk: WorkforceRisk Category:Above Target
3942 Moving & Handling Trainer VacancyID: Title:
Description of Risk:
Actions Progress Due By Done28-Feb-22 Mrs Angela CookHigh risk patient handlers
have been asked to complete the level 2 moving and handling eLearning as their competency is due for renewal
28-Feb-22 Mrs Angela CookNew staff starters have been identified and prioritised for training in 2022 via a private provider affiliated to the council
28-Feb-22 Mrs Angela CookClinical Education Team secured alternative provider to deliver for practical Moving and handling trainers sessions from Independent Living Partnership Ltd programme dates to start in July
28-Feb-22 Mrs Angela CookRecovery Programme for staff requiring higher level of training ( patient handlers) and alternative educational offer being finalised along with the model of delivery to be presented to QS Delivery for approval
Additional Controls/Actions Required:Controls/Mitigation:
1.All established staff are currently completing Moving & Handling level 1 eLearning via ESR as part of mandatory training 2.Moving and handling videos have been made available for staff to watch 3.Children’s SDG have an established programme utilising an external provider for their patient handlers 4.Health and Safety Manager supporting clinical education team 5.Moving and Handling Training request made to ICS to be prioritised at the system education group following unsuccessful joint, mutual aid approach to ICS providers 6.Commissioned Moving & Handling Training with Independent Living Partnership.
Initial Current Target
Rating
Audit Committee
Monitoring Group
Samantha Young All DirectoratesLead: Division/Directorate:
C
L
16 12 4
2-Jul-2021
Opened Date
4 3 2
4 4 2
Due to recent retirement of the previous post holder, there is a risk that the Trust may fail to comply with its manual handling regulatory compliance obligations. This will impact negatively on safe working practices, led to potential financial risk as a result of litigation against the Trust brought by staff that may be harmed due to unsafe working conditions.
Links to the BAF
Current RatingRisk TitleID
Page 21 of 2222/11/2021Data Date:
14 - Governance and A
udit
148 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
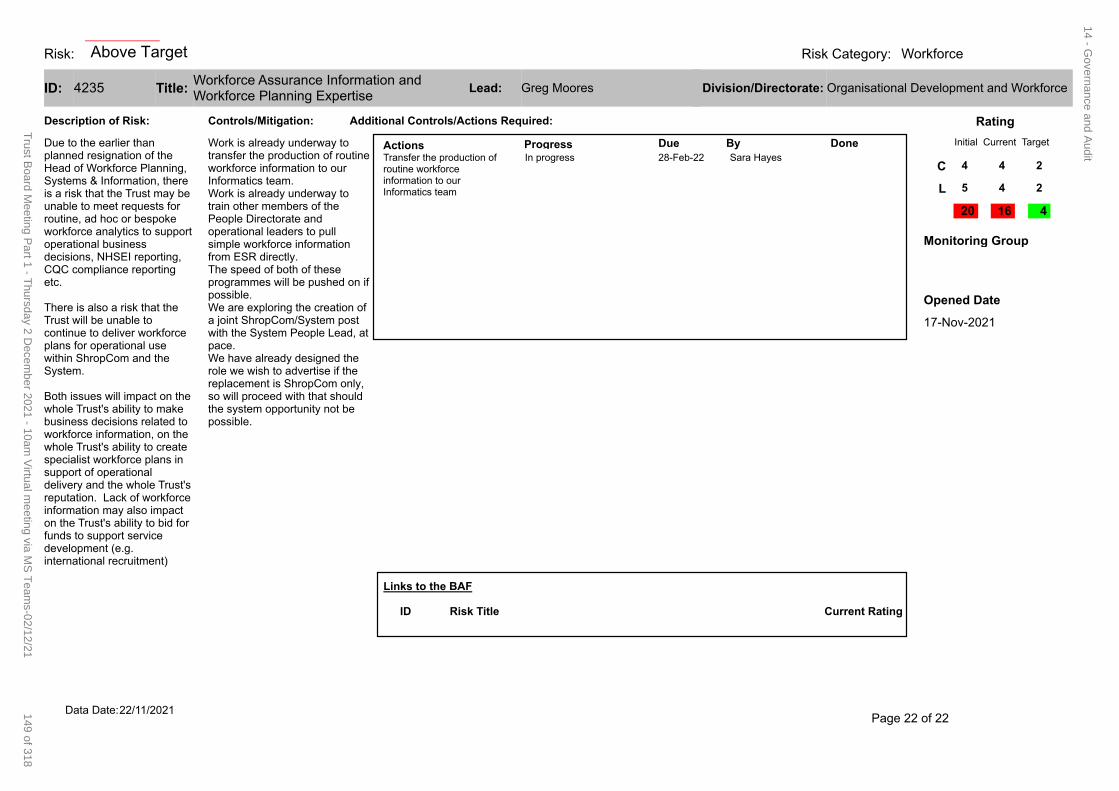
Risk: WorkforceRisk Category:
4235Workforce Assurance Information and Workforce Planning Expertise
ID: Title:
Description of Risk:
Actions Progress Due By Done28-Feb-22 Sara HayesTransfer the production of
routine workforce information to our Informatics team
In progress
Additional Controls/Actions Required:Controls/Mitigation:
Work is already underway to transfer the production of routine workforce information to our Informatics team.Work is already underway to train other members of the People Directorate and operational leaders to pull simple workforce information from ESR directly.The speed of both of these programmes will be pushed on if possible.We are exploring the creation of a joint ShropCom/System post with the System People Lead, at pace.We have already designed the role we wish to advertise if the replacement is ShropCom only, so will proceed with that should the system opportunity not be possible.
Initial Current Target
Rating
Monitoring Group
Greg Moores Organisational Development and WorkforceLead: Division/Directorate:
C
L
20 16 4
17-Nov-2021
Opened Date
4 4 2
5 4 2
Due to the earlier than planned resignation of the Head of Workforce Planning, Systems & Information, there is a risk that the Trust may be unable to meet requests for routine, ad hoc or bespoke workforce analytics to support operational business decisions, NHSEI reporting, CQC compliance reporting etc.
There is also a risk that the Trust will be unable to continue to deliver workforce plans for operational use within ShropCom and the System.
Both issues will impact on the whole Trust's ability to make business decisions related to workforce information, on the whole Trust's ability to create specialist workforce plans in support of operational delivery and the whole Trust's reputation. Lack of workforce information may also impact on the Trust's ability to bid for funds to support service development (e.g. international recruitment)
Links to the BAF
Current RatingRisk TitleID
Page 22 of 2222/11/2021Data Date:
Above Target 14 - G
overnance and Audit
149 of 318T
rust Board M
eeting Part 1 - T
hursday 2 Decem
ber 2021 - 10am V
irtual meeting via M
S T
eams-02/12/21
1 Accountable Director: Governance Support Consultant Meeting Date: 20 July 2021
REPORT COVER SHEET Report Title: Risk Appetite Statement Report
Meeting: Audit Committee
Author: Stanley Mukwenya Head of Governance & Risk
Accountable Director:
Michael Wuestefeld-Gray Governance Support Consultant
Other meetings or Committee presented to or previously agreed at:
Meeting or Committee Date Reviewed
Key Points/ Recommendation
Strategic goals this report relates to: (tick as appropriate)
Good and Beyond Continuous Improvement to Deliver
Outstanding Care
Transforming Services Implement our Clinical and
Quality Strategy
Making Best Use of Resources People, Technology, Finances, Estates and
Networks
Relevance to Board Assurance Framework: (tick as appropriate)
Clinical Quality & Safety Long term financial
sustainability of the Trust
Healthcare Systems
Organisational culture
Optimising use of
technology
Covid-19
Relevance to Well-led domains (CQC & NHSE/I): (tick as appropriate)
leadership capacity and capability
clear vision and credible strategy culture
clear roles and responsibilities
clear and effective risk management
appropriate and accurate information
learning, continuous improvement and innovation
Stakeholders engaged and involved
Relevance to CQC domains: (tick as appropriate)
Safe Caring Responsive Effective Well led
Impacts and Implications? YES or NO
If yes, what impact or implication
Patient safety & experience Yes
Effective risk management will have a positive impact on safety and staff experience
Equality & Inclusion No
Financial (revenue & capital)
Yes
Identification and effective management of financial risks will have a positive impact on the Trust’s long-term sustainability and quality care
Meeting Date: 27 October 2021
Agenda Item:
Enclosure Number:
14 - Governance and Audit
150 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2 Accountable Director: Governance Support Consultant Meeting Date: 20 July 2021
IG Governance Toolkit Yes
Identification and monitoring of risks will promote compliance with IG requirements
OD/Workforce Yes
Identification of risks will have a positive impact on the Trust’s workforce and OD development
Legal Yes
Management of risk in these areas helps avoid legal challenge
Relevance to Corporate Risk Register
(Risk No/Name) Yes BAF & CRR entries
Summary of key points in report
Purpose Firstly, to ask the Audit Committee to discuss, approve and adopt the draft Risk Appetite Statement. Secondly, the Committee is asked to agree on proposed areas of risk categories identified, and level of scoring thresholds presented. Finally, the Committee is asked to accept the insertion of the Risk Appetite Statement into the Trust Risk Management Policy
Background
The Board recognises that risk is inherent in the provision of healthcare, therefore, a defined approach is
required and necessary to identify context ensuring that the Trust understands and is aware of risks it is
prepared to accept in pursuing delivery of its objectives. It is important to provide clarity on acceptable
levels of risk the Trust is willing and unwilling to take through defining its risk appetite. The Risk Appetite
Statement will set out Board’s strategic approach to risk by defining its boundaries, tolerance levels and
delivery of the Trust’s Risk Management Strategy and Policy.
A defined level of appetite will be a facilitating tool for decision making where there is uncertainty on outcomes in pursuit of value, not for stifling development and innovation. The Trust may still take considered risks were for example, long term benefits outweigh any short-term losses. The risk Appetite Statement will support safe service planning, provide assurance to regulators and maximise opportunities through a balanced risk taking versus reward. The NHSE/I 2017 Well Led guidance references regular review of the Board’s risk appetite and tolerance as part of evidence that the Trust has clear and effective processes for managing risks, issues and performance (KLOE 5).
Role of
risk
appetite
Support risk
management
decisions
Support risk
governance
and internal
control
activities
Support
strategic
decision
making
14 - Governance and Audit
151 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
3 Accountable Director: Governance Support Consultant Meeting Date: 20 July 2021
Proposed Risk Appetite Statement ‘Shropshire Community Health NHS Trust will seek to prevent, mitigate, cope with, share, accept and/or avoid risks which have the potential to;
Adversely impact the reputation of the Trust
Expose patients, staff, visitors and stakeholders to harm
Limit ability to deliver strategic and operational priorities
Cause significant financial consequences which would jeopardise ability to deliver and carry out mandated priorities
Cause non-compliance with the law and regulation
Result in barriers to active engagement with system partners, research and innovation being embedded into the Trust’s culture’
Seven risk categories linked with scoring thresholds have been identified for use when determining level
of appetite and risk using guidance from the ‘Good Governance Institute Risk Appetite for NHS
Organisations Matrix’ provided in appendix 1. Each risk category has its own appetite statement which
will help provide direction and guidance to risk owners on extent to which different types of risk can be
accepted, mitigated, or avoided.
Definitions of risk terminology;
• Risk, ‘the potential of an event occurring with the combined likelihood and consequence of harm, injury, damage or loss occurring or impacting the achievement of the Trust’s objectives or strategic goals’.
• Risk tolerance, ‘the threshold levels of risk exposure that, with appropriate approvals can be exceeded, but which when exceeded, will trigger some form of response’.
• Risk capacity, ‘the maximum amount of risk that an organisation, or subset of it can bear, linked to factors such as its reputation, capital, assets and ability to raise additional funds’.
• Inherent risk, ‘the exposure arising from a specific risk before any action has been taken to manage it’.
• Residual risk, ‘the risk remaining after the risk response has been successfully applied’. • Risk appetite; ‘The amount of risk an entity is willing to accept in pursuit of value (it also
refers to the degree of risk, on a broad-based level, that a company or other entity is willing to accept in pursuit of its goals’, COSO. ‘The amount of risk that is judged to be tolerable and justifiable’, HM Treasury’s Orange Book.
14 - Governance and Audit
152 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
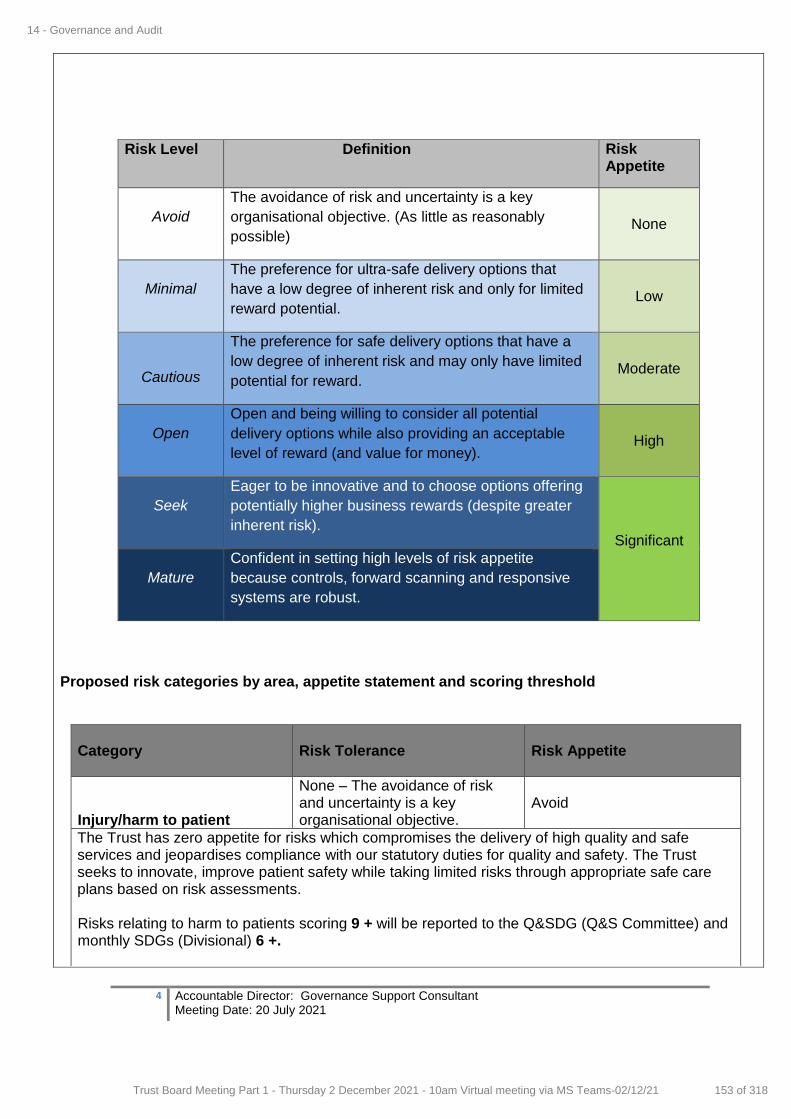
4 Accountable Director: Governance Support Consultant Meeting Date: 20 July 2021
Risk Level Definition Risk Appetite
Avoid
The avoidance of risk and uncertainty is a key
organisational objective. (As little as reasonably
possible) None
Minimal
The preference for ultra-safe delivery options that
have a low degree of inherent risk and only for limited
reward potential. Low
Cautious
The preference for safe delivery options that have a
low degree of inherent risk and may only have limited
potential for reward. Moderate
Open
Open and being willing to consider all potential
delivery options while also providing an acceptable
level of reward (and value for money). High
Seek
Eager to be innovative and to choose options offering
potentially higher business rewards (despite greater
inherent risk). Significant
Mature
Confident in setting high levels of risk appetite
because controls, forward scanning and responsive
systems are robust.
Proposed risk categories by area, appetite statement and scoring threshold
Category
Risk Tolerance
Risk Appetite
Injury/harm to patient
None – The avoidance of risk and uncertainty is a key organisational objective.
Avoid
The Trust has zero appetite for risks which compromises the delivery of high quality and safe services and jeopardises compliance with our statutory duties for quality and safety. The Trust seeks to innovate, improve patient safety while taking limited risks through appropriate safe care plans based on risk assessments. Risks relating to harm to patients scoring 9 + will be reported to the Q&SDG (Q&S Committee) and monthly SDGs (Divisional) 6 +.
14 - Governance and Audit
153 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
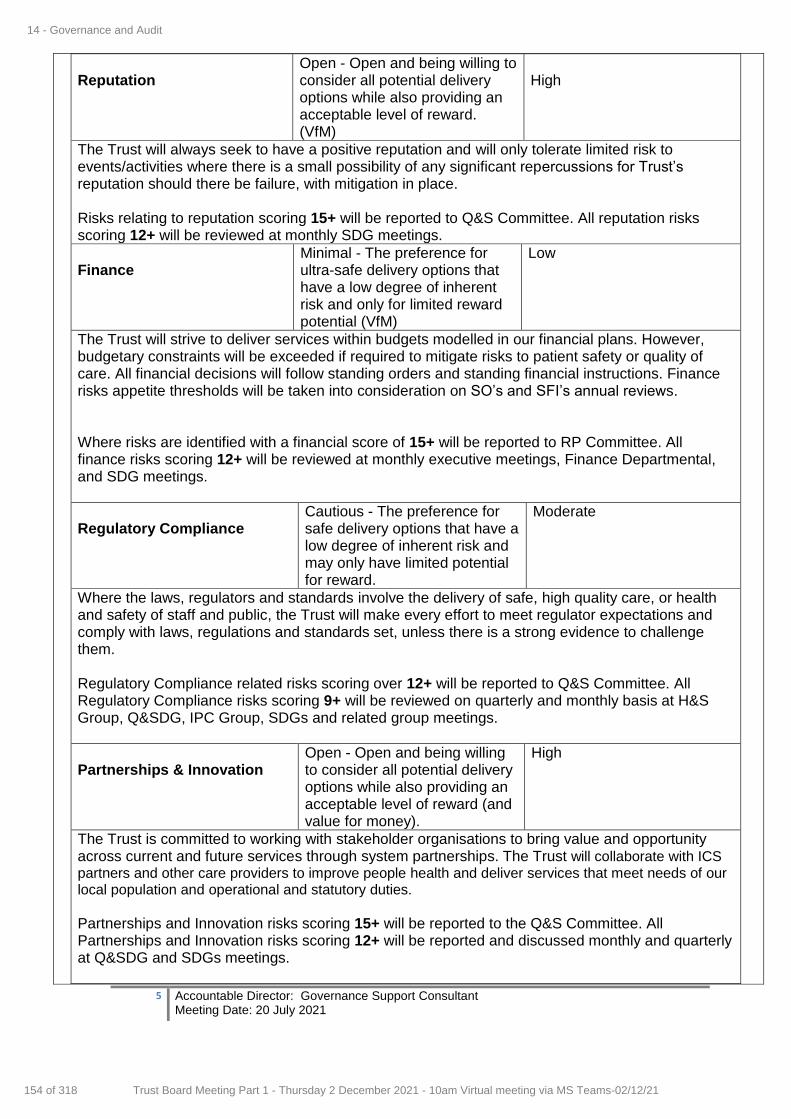
5 Accountable Director: Governance Support Consultant Meeting Date: 20 July 2021
Reputation
Open - Open and being willing to consider all potential delivery options while also providing an acceptable level of reward. (VfM)
High
The Trust will always seek to have a positive reputation and will only tolerate limited risk to events/activities where there is a small possibility of any significant repercussions for Trust’s reputation should there be failure, with mitigation in place. Risks relating to reputation scoring 15+ will be reported to Q&S Committee. All reputation risks scoring 12+ will be reviewed at monthly SDG meetings.
Finance
Minimal - The preference for ultra-safe delivery options that have a low degree of inherent risk and only for limited reward potential (VfM)
Low
The Trust will strive to deliver services within budgets modelled in our financial plans. However, budgetary constraints will be exceeded if required to mitigate risks to patient safety or quality of care. All financial decisions will follow standing orders and standing financial instructions. Finance risks appetite thresholds will be taken into consideration on SO’s and SFI’s annual reviews. Where risks are identified with a financial score of 15+ will be reported to RP Committee. All finance risks scoring 12+ will be reviewed at monthly executive meetings, Finance Departmental, and SDG meetings.
Regulatory Compliance
Cautious - The preference for safe delivery options that have a low degree of inherent risk and may only have limited potential for reward.
Moderate
Where the laws, regulators and standards involve the delivery of safe, high quality care, or health and safety of staff and public, the Trust will make every effort to meet regulator expectations and comply with laws, regulations and standards set, unless there is a strong evidence to challenge them. Regulatory Compliance related risks scoring over 12+ will be reported to Q&S Committee. All Regulatory Compliance risks scoring 9+ will be reviewed on quarterly and monthly basis at H&S Group, Q&SDG, IPC Group, SDGs and related group meetings.
Partnerships & Innovation
Open - Open and being willing to consider all potential delivery options while also providing an acceptable level of reward (and value for money).
High
The Trust is committed to working with stakeholder organisations to bring value and opportunity across current and future services through system partnerships. The Trust will collaborate with ICS partners and other care providers to improve people health and deliver services that meet needs of our local population and operational and statutory duties. Partnerships and Innovation risks scoring 15+ will be reported to the Q&S Committee. All Partnerships and Innovation risks scoring 12+ will be reported and discussed monthly and quarterly at Q&SDG and SDGs meetings.
14 - Governance and Audit
154 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
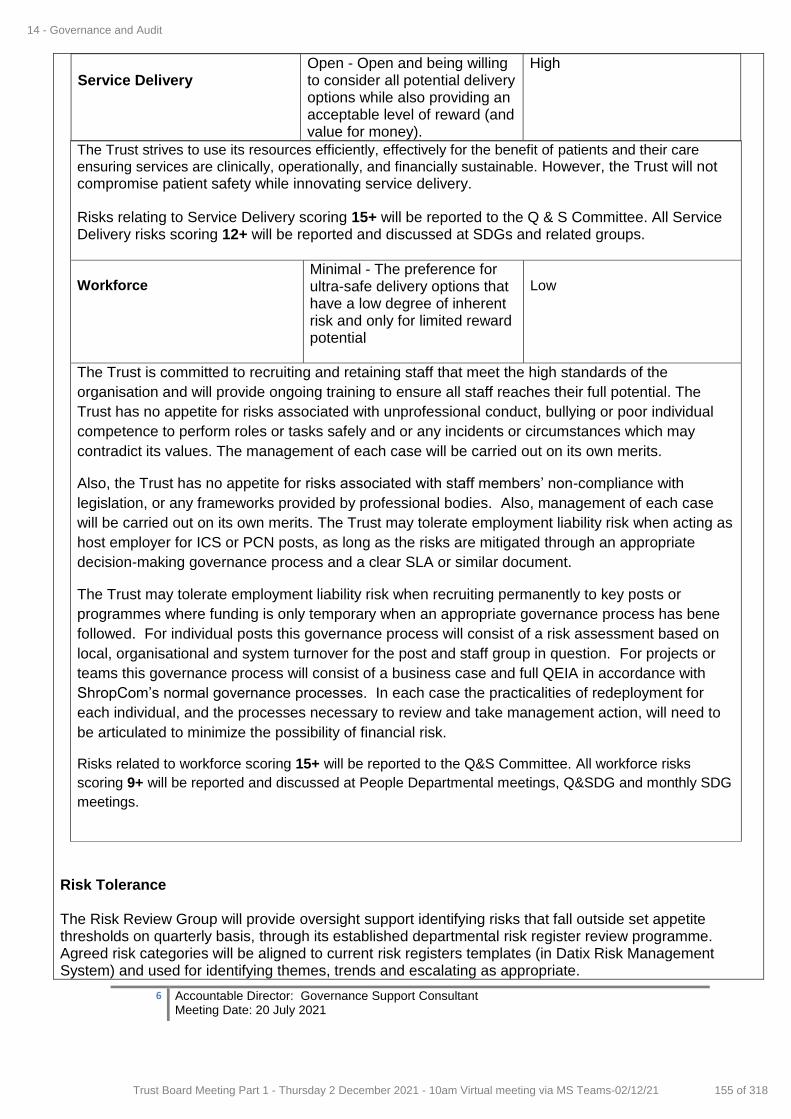
6 Accountable Director: Governance Support Consultant Meeting Date: 20 July 2021
Service Delivery
Open - Open and being willing to consider all potential delivery options while also providing an acceptable level of reward (and value for money).
High
The Trust strives to use its resources efficiently, effectively for the benefit of patients and their care
ensuring services are clinically, operationally, and financially sustainable. However, the Trust will not compromise patient safety while innovating service delivery.
Risks relating to Service Delivery scoring 15+ will be reported to the Q & S Committee. All Service Delivery risks scoring 12+ will be reported and discussed at SDGs and related groups. Workforce
Minimal - The preference for ultra-safe delivery options that have a low degree of inherent risk and only for limited reward potential
Low
The Trust is committed to recruiting and retaining staff that meet the high standards of the
organisation and will provide ongoing training to ensure all staff reaches their full potential. The
Trust has no appetite for risks associated with unprofessional conduct, bullying or poor individual
competence to perform roles or tasks safely and or any incidents or circumstances which may
contradict its values. The management of each case will be carried out on its own merits.
Also, the Trust has no appetite for risks associated with staff members’ non-compliance with
legislation, or any frameworks provided by professional bodies. Also, management of each case
will be carried out on its own merits. The Trust may tolerate employment liability risk when acting as
host employer for ICS or PCN posts, as long as the risks are mitigated through an appropriate
decision-making governance process and a clear SLA or similar document.
The Trust may tolerate employment liability risk when recruiting permanently to key posts or
programmes where funding is only temporary when an appropriate governance process has bene
followed. For individual posts this governance process will consist of a risk assessment based on
local, organisational and system turnover for the post and staff group in question. For projects or
teams this governance process will consist of a business case and full QEIA in accordance with
ShropCom’s normal governance processes. In each case the practicalities of redeployment for
each individual, and the processes necessary to review and take management action, will need to
be articulated to minimize the possibility of financial risk.
Risks related to workforce scoring 15+ will be reported to the Q&S Committee. All workforce risks
scoring 9+ will be reported and discussed at People Departmental meetings, Q&SDG and monthly SDG
meetings.
Risk Tolerance The Risk Review Group will provide oversight support identifying risks that fall outside set appetite thresholds on quarterly basis, through its established departmental risk register review programme. Agreed risk categories will be aligned to current risk registers templates (in Datix Risk Management System) and used for identifying themes, trends and escalating as appropriate.
14 - Governance and Audit
155 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
7 Accountable Director: Governance Support Consultant Meeting Date: 20 July 2021
Executive Directors have oversight of the groups and committees informing the Trust Board, and its sub-committees. The Executive Directors will provide direction and challenge on risks, ensuring any deviation from the Trust’s appetite for risk is appropriate and/or highlighted where applicable. Appendix 1 - Good Governance Institute Risk Appetite Matrix Appendix 2 – Risk Management Policy (Risk Appetite Statement inserted on Pages 6 – 8)
Purpose of the Report (tick as appropriate)
Consider for Action Give Approval Accept Assurance Provide Information
Key Recommendations
The committee is asked to:
Agree and accept proposed draft Trust Risk Appetite Statement
Agree and accept areas of proposed categories
Accept proposed categories
Accept insertion of Risk Appetite Statement into the Trust Risk Management Policy
Agree on proposed individual categories scoring thresholds
Agree on continuous future annual reviewing of the Trust Risk Appetite Statement.
14 - Governance and Audit
156 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1 Accountable Director: Shelley Ramtuhul Meeting Date: 02.12.2021
REPORT COVER SHEET
Report Title: Trust Constitutional Documents and Committee Terms of Reference
Meeting: Trust Board
Author: Michael Wuestefeld-Gray
Accountable Director:
Shelley Ramtuhul
Other meetings or Committee presented to or previously agreed at:
Meeting or Committee Date Reviewed
Key Points/ Recommendation
Executive Team and Trust Committees
Various
Committee’s comments have been included in the revised documents.
Strategic goals this report relates to: (tick as appropriate)
Good and Beyond Continuous Improvement to
Deliver Outstanding Care
Transforming Services Implement our Clinical and
Quality Strategy
Making Best Use of Resources People, Technology, Finances,
Estates and Networks
Relevance to Board Assurance Framework : (tick as appropriate)
Clinical Quality & Safety
Long term financial
sustainability of the Trust
Healthcare Systems
Organisational culture
Optimising use of
technology
Covid19
Relevance to Well-led domains (CQC & NHSE/I): (tick as appropriate)
leadership capacity and capability
clear vision and credible strategy
culture clear roles and responsibilities
clear and effective risk management
appropriate and accurate information
learning, continuous improvement and innovation
Stakeholders engaged and involved
Relevance to CQC domains: (tick as appropriate)
Safe Caring Responsive Effective Well led
Impacts and Implications? YES or NO
If yes, what impact or implication
Patient safety & experience Yes Safe environment
Equality & Inclusion No
Financial (revenue & capital) Yes
IG Governance Toolkit No
OD/Workforce Yes
Meeting Date: 2 December 2021
Agenda Item: 15
Enclosure Number: 13
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
157 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2 Accountable Director: Shelley Ramtuhul Meeting Date: 02.12.2021
Legal Yes
Relevance to Corporate Risk
Register (Risk No/Name) Yes
Summary of key points in report
Review of Trust Constitutional Documents
The Trust is supported by four key documents that underpin its structures and processes. They
allocate responsibilities to both individuals and groups, and set the limits that they can work
within.
There are four key documents:
Standing Orders;
Standing Financial Instructions;
Scheme of Reservation;
Scheme of Delegation.
The documents, appended to this paper, have been reviewed as part of an annual cycle of
reviews. Changes are highlighted in “track changes” and substantive changes to the Standing
Orders have explanatory comments attached. There are no significant changes in terms of the
Trust’s structures, or the allocation of responsibilities. Changes are mainly:
grammatical or “tidying up”;
to remove references that are no longer need such as to “EU directives” or “Director of
Governance”;
to reflect other recent changes to executive portfolios and responsibilities;
to make the documents more consistent with each other e.g. in terms of committee names
and definitions of terms.
The reviews were conducted by the Head of Financial Account, Local Counter Fraud Specialist
and Trust leads for security and for governance. In addition reviews and updates have been
provided by the Director of Finance and Head of Governance and Risk
In addition the terms of reference of Committee have also been reviewed and updated, with
changes presented to committees for discussion and approval. These have been amended as set
out above – to improve consistency, to clarify membership in the light of changes to the Executive
Team, and to generally improve structures and content.
These documents are presented for approval but it is not the intention that the Board should go
through them all in detail. Instead they are shared so the changes can be seen, and for assurance
that they have had the appropriate level of in-depth review and oversight.
Next Steps
The Board is asked to approve the:
Standing Orders;
Standing Financial Instructions;
Scheme of Reservation;
Scheme of Delegation.
Committee terms of reference.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
158 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
3 Accountable Director: Shelley Ramtuhul Meeting Date: 02.12.2021
These documents will be kept under review, particularly in the light of the establishment of the
ICS as a statutory body from 1 April 2022.
Purpose of the Report (tick as appropriate)
Consider for Action
Give Approval Accept Assurance
Provide Information
Key Recommendations
The Board is asked to approve the:
Standing Orders;
Standing Financial Instructions;
Scheme of Reservation;
Scheme of Delegation.
Committee terms of reference.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
159 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
Policies, Procedures, Guidelines and Protocols
Document Details
Title Standing Orders
Trust Ref No
Local Ref (optional)
Main points the document covers
These orders set out the Governance arrangements for the Trust. Appended to these are the Standards of Business Conduct
Who is the document aimed at?
All staff
Author Head of Financial Accounting
Approval process
Approved by (Committee/Director)
Trust Board
Approval Date December 2021
Initial Equality Impact Screening
Yes
Full Equality Impact Assessment
No
Lead Director Sarah Lloyd, Director of Finance
Category Finance
Sub CategorySubcategory Standing Orders
Review date September 2022
Distribution
Who the policy will be distributed to
Distributed to senior staff as defined by Directors
Method Electronically to senior staff & available to all staff via the Trust website
Document Links Required by CQC
Required by NHSR
Other
Amendments History No Date Amendment
2 May 2014 Minor amendments to terminology & updates in line with current practice
3 May 2015 Amend para 2.3 & 7.1 re Fit & Proper Persons Amend para 4.8 re Board sub-committees Minor amendments to terminology
4 November 2016 Para 4.8.1 : add reference to the Audit Committee acting as the Auditor Panel
5 November 2017 Para 2.1.2 & 2.7.6 change references to NHS Trust Development Authority and replace with NHS Improvement. Para 7.1.3 change reference to Company Secretary and replace with Director of Corporate Affairs. Para 7.1.3 change reference to Financial Reporting Standard 8 and change to International Accounting Standard 24 (Related Party Disclosure).
6 November 2019 Changed Chairman to Chair throughout. Replaced NHS Act 1977 with NHS Act 2006 Replaced Local Involvement Networks (LiNks) with Healthwatch England. Removed Appendix 1 as guidance replaced by Managing Conflicts of Interest in the NHS. This is now incorporated in the Trusts Code of Business Conduct, including Managing Conflicts of Interest Policy. Added 1.4.31 & 1.4.32 for definitions of a “Motion” and NHS Improvement/England. Removed para’s 5.12 & 5.1.3 as not relevant Removed NHS Trust Development Authority as incorporated into NHSI/E Referenced the Health and Social Care Act 2012 throughout Added para 2.2.2 Appointment of Associate Non-Executive Directors Added para 2.11 for Acting up Arrangements Added para 3.8 for Written Resolutions Added para 3.20 for Meetings held by electronic means
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
160 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 2
7 September 2020 Change NHS Improvement (NHSI) to NHS Improvement/England (NHSI/E).
Removed para 4.8.6 Information Governance Committee as Trust doesn’t have one.
Added further specific guidance to Para. 6.4
Para 7.1.3 changed reference to Director of Corporate Affairs and replaced with Director of Governance/Corporate Secretary
Minor amendments to terminology
8 September 2021 Change to structure and titles of executive director team.
Addition of information to give clarity on: appointment of directors and non-
executive directors; and statutory restrictions on functions and duties
Minor grammatical amendments
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
161 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 3
CONTENTS
Page 1. INTRODUCTION 4
Statutory Framework NHS Framework Delegation of Powers
Interpretation & Definitions 2. THE TRUST BOARD: COMPOSITION OF MEMBERSHIP, TENURE & ROLE OF MEMBERS 8 Composition of the Membership of the Trust Board
Appointment of the Chair & Members of the Trust Terms of Office of the Chair & Members Appointment & Powers of Vice-Chair Joint Members Healthwatch England Role of Members Corporate Role of the Board Scheme of Reservation & Scheme of Delegation Lead Roles for Board Members Acting up Arrangements
3. MEETINGS OF THE TRUST 12
Calling Meetings Notice of Meetings & the Business to be Transacted Agenda & Supporting Papers Petitions Notice of Motion Emergency Motions Motions: Procedure at & During a Meeting Written Resolutions Motion to Rescind a Resolution Chair of Meeting Chair’s Ruling Quorum Voting Suspension of Standing Orders Variation & Amendment of Standing Orders Record of Attendance Minutes Admission of the Public & the Press Observers at Trust Meetings Meetings held by electronic means
4. APPOINTMENT OF COMMITTEES & SUB-COMMITTEES 20
Appointment of Committees Joint Committees Applicability of SO’s & SFIs to Committees Terms of Reference
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
162 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 4
Delegation of Powers by Committees to Sub-Committees Approval of Appointments to Committees Appointments for Statutory Functions Committees Established by the Trust Board
5. ARRANGEMENTS FOR THE EXERCISE OF TRUST FUNCTIONS BY DELEGATION 23 Delegation of Functions to Committees, Officers or Other Bodies Emergency Powers & Urgent Decisions Delegation to Committees Delegation to Officers
Scheme of Reservation & Scheme of Delegation Duty to Report Non-Compliance with SOs & SFIs 6. OVERLAP WITH OTHER TRUST POLICY STATEMENTS/PROCEDURES,
REGULATIONS & SFIs 25 Policy Statements: General Principles Specific Policy Statements Standing Financial Instructions Specific Guidance 7. DUTIES & OBLIGATIONS OF BOARD MEMBERS/DIRECTORS & SENIOR
MANAGERS UNDER THESE SOs 26 Declaration of Interests Register of Interests Exclusion of Chair & Members in Proceedings on Account of Pecuniary Interest Standards of Business Conduct
8. CUSTODY OF SEAL, SEALING OF DOCUMENTS & SIGNATURE OF DOCUMENTS 32
Custody of Seal Sealing of Documents Register of Sealing Use of Seal – General Guidance Signature of Documents
9. MISCELLANEOUS 33
Standing Orders to be given to Members & Officers Review of Standing Orders Joint Finance Arrangements
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
163 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 5
1. INTRODUCTION
1.1 Statutory Framework
1.1.1 The Shropshire Community Health NHS Trust (the Trust) is a statutory body which came into existence on 1 July 2011 under The Shropshire Community Health NHS Trust (Establishment) Order 2011 No. 1519 (the Establishment Order).
1.1.2 The principal place of business of the Trust is the county of
Shropshire.
1.1.3 NHS Trusts are governed by aActs of Parliament, mainly the National Health Service Act 2006 (Chapter 3 and Schedule 4) (NHS Act 2006) and the Health and Social Care Act 2012.
1.1.4 The functions of the Trust are conferred by this legislation.
1.1.5 As a statutory body, the Trust has specified powers to contract in its
own name and to act as a corporate trustee. In the latter role it is accountable to the Charity Commission for those funds deemed to be charitable as well as to the Secretary of State for Health. The Trust also has a common law duty as a Bailee for property held by the Trust on behalf of patients.
1.1.6 The Trust also has statutory powers under Section 75 of the NHS Act
2006, to fund projects jointly planned with local authorities. 1.1.7 The Code of Accountability requires the Trust to adopt Standing
Orders for the regulation of its proceedings and business. The Trust must also adopt Standing Financial Instructions (SFIs) as an integral part of Standing Orders setting out the responsibilities of individuals.
1.1.8 The Trust will also be bound by such other statutes and legal
provisions which govern the conduct of its affairs. 1.2 NHS Framework
1.2.1 In addition to the statutory requirements the Secretary of State
through the Department of Health issues further directions and guidance. These are normally issued under cover of a circular or letter.
1.2.2 The Code of Accountability requires that, inter alia, Boards draw up a
Schedule of Decisions Reserved to the Board and ensure that management arrangements are in place to enable responsibility to be clearly delegated to senior executives (a Scheme of Delegation). The code also requires the establishment of audit and remuneration committees with formally agreed terms of reference. The Code of
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
164 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 6
Conduct makes various requirements concerning possible conflicts of interest of Board members.
1.2.3 The Code of Practice on Openness in the NHS, as revised by the Freedom of Information Act 2000 and the Environmental Information Regulations 2004 sets out the requirements for public access to information on the NHS.
1.3 Delegation of Powers
1.3.1 The Trust has powers to delegate and make arrangements for
delegation. The Standing Orders set out the detail of these arrangements. Under Standing Order No. 5 relating to the “Arrangements for the Exercise of Trust Functions by Delegation”, the Trust is given powers to “make arrangements for the exercise, on behalf of the Trust of any of their functions by a committee, sub-committee or joint committee appointed by virtue of Standing Order No. 4 “Appointment of Committees and Sub-Committees” or by an officer of the Trust, in each case subject to such restrictions and conditions as the Trust thinks fit or as the Secretary of State may direct”.
1.3.2 Delegated Powers are covered in separate documents (Scheme of
Reservation and Scheme of Delegation). These documents have effect as if incorporated into the Standing Orders and Standing Financial Instructions.
1.4 Interpretation & Definitions
1.4. 1 The Chair of the Trust is the final authority on the interpretation of Standing Orders (on which they should be advised by the Chief Executive or Secretary to the Board).
1.4.2 Any expression to which a meaning is given in the National Health
Service Act 2006, Health and Social Care Act 2012, National Health Service and Community Care Act 1990 and other Acts relating to the National Health Service or in the Financial Regulations made under the Acts shall have the same meaning in these Standing Orders and in addition, those definitions given below.
1.4.3 "Accountable Officer" means the NHS Officer responsible and
accountable for funds entrusted to the Trust. The officer shall be responsible for ensuring the proper stewardship of public funds and assets. For this Trust it shall be the Chief Executive.
1.4.4 "Trust" means the Shropshire Community Health NHS Trust.
1.4.5 "Board" means the Chair, executive and non-executive dDirectors of
the Trust who are members of the Board collectively as a body.
1.4.6 "Budget" means a plan, expressed in financial terms, proposed by the Board for the purpose of carrying out, for a specific period, any, or all of the functions of the Trust.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
165 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 7
1.4.7 “Director” means the executive officer with delegated authority to
manage finances (income and expenditure) for a specific area of the organisation.
1.4.8 “Budget Manager” means second level delegation by a Director to
another Senior Manager. They can either be an employee of the Trust or of another organisation and be authorised by the Director.
1.4.9 “Resource Manager” means third level delegation by a Budget
Manager to another Senior Manager. They can either be an employee of the Trust or of another organisation and be authorised by the Director.
1.4.10 “Service Lead” means an officer who has delegated responsibility
from a Resource Manager for the day-to-day management of a defined budget. They can either be an employee of the Trust or of another organisation and be authorised by the Director.
1.4.11 "Chair of the Board (or Trust)" is the person appointed by the
Secretary of State for Health to lead the Board and to ensure that it successfully discharges its overall responsibility for the Trust as a whole. The expression “the Chair of the Trust” shall be deemed to include the Vice-Chairanyone acting as the Chair of the Trust if the Chair is absent from the meeting or is otherwise unavailable.
1.4.12 "Chief Executive" means the chief officer of the Trust. 1.4.13 "Director of Finance and Strategy" and “Associate Director of
Finance” means the chief financial officer of the Trust. 1.4.14 "Clinical Governance Committee" means thea committee whose
functions are concerned with the arrangements for the purpose of monitoring and improving the quality of health care for which the Trust has responsibility.
1.4.15 "Commissioning" means the process for determining the need for
and for obtaining the supply of healthcare and related services by the Trust within available resources.
1.4.16 "Committee" means a committee or sub-committee created and
appointed by the Trust.
1.4.17 "Committee members" means persons formally appointed by the Board to sit onbe members of or to chair specific committees.
1.4.18 "Contracting and procuring" means the systems for obtaining the
supply of goods, materials, manufactured items, services, building and engineering services, works of construction and maintenance and for disposal of surplus and obsolete assets.
1.4.19 “Funds Held on Trust” means those funds which the Trust holds on
date of incorporation, receives on distribution by statutory instrument or chooses subsequently to accept under powers derived under Part
Commented [CD(CHNT1]: Checking we have one,
Commented [MWG2R1]: Yes it is QSC – have amended to allow for differences in names
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
166 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 8
11(Eleven) of the NHS Act 2006. Such funds may or may not be charitable.
1.4.20 "Member" means executive or non-executive Director of the Board
as the context permits. Member in relation to the Board does not include its Chair.
1.4.21 “Associate Director” means a person appointed to perform specific
statutory and non-statutory duties which have been delegated by the Trust Board for them to perform and these duties have been recorded in an appropriate Trust Board minutes or other suitable record.
1.4.22 "Membership, Procedure and Administration Arrangements
Regulations" means NHS Membership and Procedure Regulations (SI 1990/2024) and subsequent amendments.
1.4.23 "Nominated officer" means an officer charged with the responsibility
for discharging specific tasks within Standing Orders and Standing Financial Instructions.
1.4.24 "Non-executive Director" means a member of the Trust who is not
an officer of the Trust and is not to be treated as an officer by virtue of regulation 1(3) of the Membership, Procedure and Administration Arrangements Regulations.
1.4.25 "Officer" means employee of the Trust or any other person holding a
paid appointment or office with the Trust. 1.4.26 "Executive Director " means a member of the Trust who is either an
officer of the Trust or is to be treated as an officer by virtue of regulation 1(3) (i.e., the Chair of the Trust or any person nominated by such a Committee for appointment as a Trust member).
1.4.27 "Secretary" means a person appointed to act independently of the
Board to provide advice on corporate governance issues to the Board and the Chair and monitor the Trust's compliance with the law, Standing Orders, and Department of Health guidance.
1.4.28 "SFIs" means Standing Financial Instructions.
1.4.29 "SOs" means Standing Orders.
1.4.30 "Vice-Chair" means the non-executive Director appointed by the
Board to take on the Chair’s duties if the Chair is absent for any reason.
1.4.31 “Motion” is a formal proposition to be discussed and voted on during
the course of a Trust Board or cCommittee meeting. 1.4.32 “NHS Improvement/England (NHSI/E)” is responsible for the
oversight of NHS trusts and has delegated authority from the Secretary of State for Health for the appointment of the Non-Executive Directors, including the Chair of the Trust.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
167 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 9
2. THE TRUST BOARD: COMPOSITION OF MEMBERSHIP, TENURE AND ROLE
OF MEMBERS
2.1 Composition of the Membership of the Trust Board
2.1.1 In accordance with the Membership, Procedure and Administration Arrangements Regulations the composition of the Board shall be as follows:
2.1.2 The Chair of the Trust (appointed by NHS Improvement/England).
2.1.3 Up to 5 non-executive Directors (appointed by NHS
Improvement/England). 2.1.4 Up to 5 executive Directors (but not exceeding the number of non-
executive Directors) including: -
the Chief Executive
the Director of Finance and Strategy or Associate Director of Finance
the Director of Nursing
the Medical Director
the Chief Operating Officer
2.1.5 The Trust shall have not more than 11 and not less than 8 members (unless otherwise determined by the Secretary of State for Health and set out in the Trust’s Establishment Order or such other communication from the Secretary of State).
2.1.6 The Trust may appoint additional executive directors who may be
attendees at, but not members of, the Board. These additional executive directors may be members of committees of the Board.
2.2 Appointment of the Chair and Members of the Trust
2.2.1 Appointment of the Chair and Members of the Trust - Schedule 4 to the 2006 Act, , provides that the Chair is appointed by the Secretary of State, but otherwise the appointment and tenure of office of the Chair and members are set out in the Membership, Procedure and Administration Arrangements Regulations.
2.2.2 Appointment of Associate Non-Executive Directors - The Board may
appoint Associate Non-Executive Directors on terms and conditions to be specified by the Board to provide additional advice and expertise to the Board and/or its committees.are appointed by the Secretary of State with the involvement of the Chair in the recruitment process, as administered by NHS I/E.
2.2.3 The Board may appoint Associate Non-Executive Directors who will
not be members of the Board and as such will be non-voting appointees without executive or delegated executive functions but. They will be accountable to the Board for the responsibilities detailed
Commented [MWG3]: This section has been updated to reflect statutory requirements.
Commented [MWG4]: To reflect planned make up of executive director portfolios
Commented [MWG5]: Common in NHS SOs
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
168 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 10
in their terms and conditions of appointment, which shall never exceed 3 years but may be renewed by the Board.
2.2.4 Appointment of the Chief Executive – The Chief Executive is
appointed by the Chair and Non-Executive Directors following a process as approved by the Trust’s Remuneration Committee
2.2.5 Appointment of Executive Directors – executive directors are
appointed jointly by the Chair and Chief Executive following a process as approved by the Trust’s Remuneration Committee
2.3 Terms of Office of the Chair and Members
2.3.1 The regulations setting out the period of tenure of office of the Chair and members and for the termination or suspension of office of the Chair and members are contained in Sections 2 to 4 of the Membership, Procedure and Administration Arrangements Regulations.
2.3.2 The Trust will seek assurance that any individuals under
consideration for appointment as Chair or member of the Board satisfy the Fit & Proper Person requirements.
2.4 Appointment and Powers of Vice-Chair
2.4.1 Subject to Standing Order 2.4.2 below, the Chair and members of the Trust may appoint one of their numbers, who is not also an executive Director, to be Vice-Chair, for such period, not exceeding the remainder of his/her term as a member of the Trust, as they may specify on appointing him/her.
2.4.2 Any member so appointed may at any time resign from the office of
Vice-Chair by giving notice in writing to the Chair. The Chair and members may thereupon appoint another member as Vice-Chair in accordance with the provisions of Standing Order 2.4.1.
2.4.3 The Vice Chair shall not be the Chair of the Audit Committee or act
as the Trust’s Senior Independent Director.
2.4.43 Where the Chair of the Trust has died or has ceased to hold office, or where they have been unable to perform their duties as Chair owing to illness or any other cause, the Vice-Chair shall act as Chair until a new Chair is appointed or the existing Chair resumes their duties, as the case may be; and references to the Chair in these Standing Orders shall, so long as there is no Chair able to perform those duties, be taken to include references to the Vice-Chair.
2.5 Joint Members
2.5.1 Where more than one person is appointed jointly to a post mentioned in regulation 2(4)(a) of the Membership, Procedure and Administration Arrangements Regulations those persons shall count for the purpose of Standing Order 2.1 as one person.
Commented [MWG6]: Added for completeness of appointment
of members given scope of members as set out above
Commented [MWG7]: Reflects statutory requirements
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
169 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 11
2.5.2 Where the office of a member of the Board is shared jointly by more than one person: a) Either or both of those persons may attend or take part in
meetings of the Board, b) If both are present at a meeting, they should cast one vote if
they agree, c) In the case of disagreements, no vote should be cast, d) The presence of either or both of those persons should count
as the presence of one person for the purposes of Standing Order 3.12 “Quorum”.
2.6 Healthwatch England
2.6.1 Healthwatch England was established under the Health and Social Care Act 2012 to understand the needs, experiences and concerns of people who use health and social care services and to speak out on their behalf. It is a statutory committee of the Care Quality Commission (CQC). Their main statutory functions are to: i) Provide leadership, guidance, support, and advice to local Healthwatch organisations. ii) Escalate concerns about health and social care services which have been raised by local Healthwatch to CQC. CQC are required to respond to advice from the Healthwatch England Committee. iii) Provide advice to the Secretary of State for Health and Social Care, NHS England, and English local authorities, when in their view the quality of service provided is not adequate. Bodies to whom advice is given are required to respond in writing. The Secretary of State for Health and Social Care is also required to consult Healthwatch England on the NHS mandate, which sets the objectives for the NHS.
2.7 Role of Members
2.7.1 The Board will function as a corporate decision-making body the Executive Directors set out above and the Non-Executive Directors will be full and equal members. Their role as members of the Board of Directors will be to consider the key strategic and managerial issues facing the Trust in carrying out its statutory and other functions.
2.7.2 Executive Directors
Executive Directors shall exercise their authority within the terms of these Standing Orders and Standing Financial Instructions and the Scheme of Delegation.
2.7.3 Chief Executive
The Chief Executive shall be responsible for the overall performance of the executive functions of the Trust. He/she is the Accountable Officer for the Trust and shall be responsible for ensuring the discharge of obligations under Financial Directions and in line with the requirements of the Accountable Officer Memorandum for Trust Chief Executives.
2.7.4 Director of Finance and Strategy and Associate Director of Finance
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
170 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 12
The Director of Finance and Strategy and Associate Director of Finance shall be responsible for the provision of financial advice to the Trust and to its members and for the supervision of financial control and accounting systems. He/she shall be responsible along with the Chief Executive for ensuring the discharge of obligations under relevant Financial Directions.
2.7.5 Non-Executive Directors
The Non-Executive Directors shall not be granted, nor shall they seek to exercise any individual executive powers on behalf of the Trust. They may however, exercise collective authority when acting as members of or when chairing a committee of the Trust which has delegated powers.
2.7.6 Chair
The Chair shall be responsible for the operation of the Board and chair all Board Meetings when present. The Chair has certain delegated executive powers. The Chair must comply with the terms of appointment and with these Standing Orders.
The Chair shall liaise with the NHS Improvement/England over the
appointment of Non-Executive Directors and once appointed shall take responsibility either directly or indirectly for their induction, their portfolios of interests and assignments, and their performance.
The Chair shall work in close harmony with the Chief Executive and shall ensure that key and appropriate issues are discussed by the Board in a timely manner with all the necessary information and advice being made available to the Board to inform the debate and ultimate resolutions.
2.8 Corporate Role of the Board
2.8.1 All business shall be conducted in the name of the Trust (Shropshire Community Health NHS Trust).
2.8.2 All funds received in trust shall be held in the name of the Trust as
corporate trustee.
2.8.3 The powers of the Trust established under statute shall be exercised by the Board meeting in public session except as otherwise provided for in Standing Order No. 3 “Meetings of the Trust”.
2.8.4 The Board shall define and regularly review the functions it exercises
on behalf of the Secretary of State and Charity Commission 2.9 Scheme of Reservation and Scheme of Delegation
2.9.1 The Board has resolved that certain powers and decisions may only be exercised by the Board in formal session. These powers and decisions are set out in the Scheme of Reservation and have effect as if incorporated into the Standing Orders. Those powers which it has delegated to officers and other bodies are contained in the Scheme of Delegation.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
171 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 13
2.10 Lead Roles for Board Members
2.10.1 The Chair will ensure that the designation of lead roles or
appointments of Board members as required by the Department of Health or as set out in any statutory or other guidance, will be made in accordance with that guidance or statutory requirement (e.g., appointing a Lead Board Member with responsibilities for Infection Control or Child Protection Services, etc.).
2.11 Acting up Arrangements
2.11.1 An officer who has been appointed formally by the Board of Directors
to act up for an Executive Director during a period of incapacity or temporarily to fill an Executive Director vacancy, shall be entitled to exercise the voting rights of the Executive Director. An officer attending the Board of Directors to represent an Executive Director during a period of incapacity or temporary absence without formal acting up status may not exercise the voting rights of the Executive Director. An officer’s status when attending a meeting shall be recorded in the minutes.
3. MEETINGS OF THE TRUST 3.1 Calling Meetings
3.1.1 Ordinary meetings of the Board shall be held at regular intervals at such times and places as the Board may determine.
3.1.2 The Chair of the Trust may call a meeting of the Board at any time. 3.1.3 One-third or more members of the Board may requisition request a
meeting in writing. If the Chair refuses, or fails, to call a meeting within seven days of a requisition request being presented, the members signing the requisitionmaking the request may forthwith then call a meeting.
3.1.4 For such meetings the normal quoracy requirements for meetings of
the Board shall apply.
3.2 Notice of Meetings and the Business to be Transacted
3.2.1 Before each meeting of the Board a written notice specifying the business proposed to be transacted shall be delivered to every member or sent by post to the usual place of residence of each member, so as to being available to members at least three 6 clear days before the meeting. The notice shall be signed by the Chair or by an officer authorised by the Chair to sign on their behalf. Want of service of such a notice on any member shall not affect the validity of a meeting.
3.2.2 In the case of a meeting called by members in default of the Chair
calling the meeting, the notice shall be signed by those members.
Commented [MWG8]: To be consistent with the following sections
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
172 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 14
3.2.3 No business shall be transacted at the meeting other than that specified on the agenda, or emergency motions allowed under Standing Order 3.6 “Emergency Motions”.
3.2.4 A member desiring a matter to be included on an agenda shall make
his/her request in writing to the Chair at least 10 5 clear days before the meeting. The request should state whether the item of business is proposed to be transacted in the presence of the public and should include appropriate supporting information. Requests made less than 10 days before a meeting may be included on the agenda at the discretion of the Chair.
3.2.5 Before each meeting of the Board a public notice of the time and
place of the meeting, and the public part of the agenda, shall be displayed at the Trust's principal offices at least three clear days before the meeting, (required by the Public Bodies (Admission to Meetings) Act 1960 S.I.(4)(a)).
3.3 Agenda and Supporting Papers
3.3.1 The Agenda will be sent to members 6 5 days before the meeting and
supporting papers, whenever possible, shall accompany the agenda, but will certainly be despatched no later than three clear days before the meeting, save in emergency.
3.3.2 The Board may determine that certain matters shall appear on every
agenda for a meeting and shall be addressed prior to any other business being conducted. (Such matters may be identified within these Standing Orders or following subsequent resolution shall be listed in an Appendix to the Standing Orders.)
3.4 Petitions
3.4.1 Where a petition has been received by the Trust the Chair shall include the petition as an item for the agenda of the next meeting.
3.5 Notice of Motion
3.5.1 Subject to the provision of Standing Orders 3.7 “Motions: Procedure at and During a Meeting” and 3.9 “Motion to Rescind a Resolution”, a member of the Board wishing to move a motion shall send a written notice to the Chief Executive who will ensure that it is brought to the immediate attention of the Chair.
3.5.2 The notice shall be delivered at least 10 5 clear days before the
meeting. The Chief ExecutiveChair shall include in the agenda for the meeting all notices so received that are in order and permissible under governing regulations. This Standing Order shall not prevent any motion being withdrawn or moved without notice on any business mentioned on the agenda for the meeting.
3.6 Emergency Motions
Commented [MWG9]: Can’t be 10 days if the member has only three (or six) days’ notice of the meeting
Commented [MWG10]: As the Trust Chair chair’s the Board not clear why notices should go to the Chief Executive?
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
173 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 15
3.6.1 Subject to the agreement of the Chair, and subject also to the provision of Standing Order 3.7 “Motions: Procedure at and During a Meeting”, a member of the Board may give written notice of an emergency motion after the issue of the notice of meeting and agenda, up to one hour before the time fixed for the meeting. The notice shall state the grounds of urgency. If in order, it shall be declared to the Trust Board at the commencement of the business of the meeting as an additional item included in the agenda. The Chair's decision to include the item shall be final.
3.7 Motions: Procedure at and During a Meeting 3.7.1 Who may propose?
A motion may be proposed by the Chair of the meeting or any member present. It must also be seconded by another member.
3.7.2 Contents of motions
The Chair may exclude from the debate at their discretion any such motion of which notice was not given on the notice summoning the meeting other than a motion relating to : -
the reception of a report
consideration of any item of business before the Trust Board
the accuracy of minutes
that the Board proceed to next business
that the Board adjourn
that the question be now put.
3.7.3 Amendments to motions A motion for amendment shall not be discussed unless it has been
proposed and seconded. Amendments to motions shall be moved relevant to the motion and
shall not have the effect of negating the motion before the Board. If there are a number of amendments, they shall be considered one
at a time. When a motion has been amended, the amended motion shall become the substantive motion before the meeting, upon which any further amendment may be moved.
3.7.4 Rights of reply to motions
The mover of an amendment may reply to the debate on their amendment immediately prior to the mover of the original motion, who shall have the right of reply at the close of debate on the amendment but may not otherwise speak on it.
The member who proposed the substantive motion shall have a right of reply at the close of any debate on the motion.
3.7.5 Withdrawing a motion
A motion, or an amendment to a motion, may be withdrawn.
3.7.6 Motions once under debate When a motion is under debate, no motion may be moved other than:
-
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
174 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 16
an amendment to the motion
the adjournment of the discussion, or the meeting
that the meeting proceeds to the next business
that the question should now be put
the appointment of an ad hoc committee to deal with a specific item of business
that a member/Director be not further heard
a motion under Section 1(2) or Section 1(8) of the Public Bodies (Admission to Meetings) Act 1960 resolving to exclude the public, including the press (see Standing Order 3.18 “Admission of the Public and Press”).
In those cases where the motion is either that the meeting proceeds to the “next business” or “that the question be now put” in the interests of objectivity these should only be put forward by a member of the Board who has not taken part in the debate and who is eligible to vote.
If a motion to proceed to the next business or that the question be now put, is carried, the Chair should give the mover of the substantive motion under debate a right of reply, if not already exercised. The matter should then be put to the vote.
3.8 Written Resolutions
3.8.1 Where a decision needs to be taken by the Committee outside
the normal cycle of meetings, and where the matter is not
deemed by the Chair to require an additional meeting to be
called, the decision may be made via e-mail. The preference is
for decisions to be taken at committee meetings. The decisions
via e-mail process will be used on an exceptionsby exception
basis. The process for decision via e-mail will be as follows.
a) An e-mail setting out the matter for decision will be sent to all
committee members on the same working dayat the same time. This shall include a statement setting out how the Board or
committee should signify what their view on the matter is and the deadline for doing so.
b) Board or committee members will be given no less than three working days in which to respond.
c) For a decision to be passed, all of the members of the committee or Board must express the same view on the matter. This view can be expressed by action or inaction.
d) Where Board or committee members have comments on the
proposed decision or recommendation/s these will be circulated to other committee members by the Corporate Secretary within one
working day of receipt.
e) If any individual Board or committee member wishes to debate an item proposed for decision via e-mail at a Board or committee
meeting instead they may ask the Chair to arrange an additional meeting or defer the item for decision until the next Board or
committee meeting. If the Chair agrees a full meeting of the Board or committee will be arranged.
f) Decisions made via e-mail will be reported to the next scheduled
Commented [MWG11]: Amended to be in line with committee terms of reference
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
175 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 17
meeting and the wording of the decision minuted. Any decision
made in this manner will be effective from the date of agreement of all of the Board or committee members and confirmed by email
by the Chair or Board or Committee Secretariat
3.9 Motion to Rescind a Resolution
3.9.1 Notice of motion to rescind any resolution (or the general substance of any resolution) which has been passed within the preceding 6 calendar months shall bear the signature of the member who gives it and also the signature of 3 other members, and before considering any such motion of which notice shall have been given, the Trust Board may refer the matter to any appropriate Committee or the Chief Executive for recommendation.
3.9.2 When any such motion has been dealt with by the Trust Board, it
shall not be competent for any Director/member other than the Chair to propose a motion to the same effect within 6 months. This Standing Order shall not apply to motions moved in pursuance of a report or recommendations of a Committee or the Chief Executive.
3.10 Chair of Meeting
3.10.1 At any meeting of the Trust Board, the Chair, if present, shall preside. If the Chair is absent from the meeting, the Vice-Chair (if the Board has appointed one), if present, shall preside.
3.10.2 If the Chair and Vice-Chair are absent, such member (who is not also
an Executive Director of the Trust) as the members present shall choose who shall preside.
3.11 Chair’s Ruling
3.11.1 The decision of the Chair of the meeting on questions of order, relevancy, and regularity (including procedures on handling motions) and their interpretation of Standing Orders and Standing Financial Instructions, at the meeting, shall be final.
3.12 Quorum
3.12.1 No business shall be transacted at a meeting unless at least one-third of the whole number of the Chair and members (including at least one member who is also an Executive Director of the Trust and one member who is not) is present.
3.12.2 An officer in attendance for an Executive Director but without formal
acting up status may not count towards the quorum. 3.12.3 If the Chair or member has been disqualified from participating in the
discussion on any matter and/or from voting on any resolution by reason of a declaration of a conflict of interest (see Standing Orders No.7.1 “Declaration of Interests” and 7.2 “Register of Interests”) that person shall no longer count towards the quorum. If a quorum is then not available for the discussion and/or the passing of a resolution on
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
176 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 18
any matter, that matter may not be discussed further or voted upon at that meeting. Such a position shall be recorded in the minutes of the meeting. The meeting must then proceed to the next business.
3.13 Voting
3.13.1 Save as provided in Standing Orders 3.14 “Suspension of Standing Orders” and 3.15 “Variation and Amendment of Standing Orders” every question put to a vote at a meeting shall be determined by a majority of the votes of members present and voting on the question. In the case of an equal vote, the person presiding (i.e., the Chair of the meeting) shall have a second and casting vote.
3.13.2 At the discretion of the Chair all questions put to the vote shall be determined by oral expression or by a show of hands, unless the Chair directs otherwise, or it is proposed, seconded, and carried that a vote be taken by paper ballot.
3.13.3 If at least one-third of the members present so request, the voting on any question may be recorded so as to show how each member present voted or did not vote (except when conducted by paper ballot).
3.13.4 If a member so requests, their vote shall be recorded by name.
3.13.5 In no circumstances may an absent member vote by proxy. Absence is defined as being absent at the time of the vote.
3.13.6 A manager,person who has been formally appointed to act up for an Executive Director during a period of incapacity or temporarily to fill an Executive Director vacancy, shall be entitled to exercise the voting rights of the Executive Director.
3.13.7 A manager person attending the Trust Board meeting to represent an Executive Director during a period of incapacity or temporary absence without formal acting up status may not exercise the voting rights of the Executive Director. An officer’s status when attending a meeting shall be recorded in the minutes.
3.13.8 For the voting rules relating to joint members see Standing Order 2.5 “Joint Members”.
3.14 Suspension of Standing Orders
3.14.1 Except where this would contravene any statutory provision or any direction made by the Secretary of State or the rules relating to the Quorum (Standing Order 3.12), any one or more of the Standing Orders may be suspended at any meeting, provided that at least two-thirds of the whole number of the members of the Board are present (including at least one member who is an Executive Director and one member who is not) and that at least two-thirds of those members present signify their agreement to such suspension. The reason for the suspension shall be recorded in the Trust Board’s minutes.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
177 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 19
3.14.2 A separate record of matters discussed during the suspension of Standing Orders shall be made and shall be available to the Chair and members of the Trust.
3.14.3 No formal business may be transacted while Standing Orders are
suspended. 3.14.4 The Audit Committee shall review every decision to suspend
Standing Orders.
3.15 Variation and Amendment of Standing Orders
3.15.1 These Standing Orders shall not be varied except in the following circumstances:
upon a notice of motion under Standing Order 3.5 “Notice of Motion”,;
upon a recommendation of the Chair or Chief Executive included on the agenda for the meeting,
that two-thirds of the Board members are present at the meeting where the variation or amendment is being discussed, and that at least half of the Trust’s Non-Executive Directors vote in favour of the amendment,
providing that any variation or amendment does not contravene a statutory provision or direction made by the Secretary of State.
3.16 Record of Attendance
3.16.1 The names of the Chair and Directors/members present at the meeting shall be recorded in the minutes.
3.16.2 If a Director is not present for the entirety of the meeting, the minutes
shall record the items that were considered whilst they were present. 3.17 Minutes
3.17.1 The minutes of the proceedings of a meeting shall be drawn up and submitted for agreement at the next ensuing meeting. where they will be signed by the person presiding at it.
3.17.2 No discussion shall take place upon the minutes except upon their
accuracy or where the Chair considers discussion appropriate.
3.18 Admission of the Public and the Press
3.18.1 Admission and exclusion on grounds of confidentiality of business to be transacted The public and representatives of the press may attend all meetings of the Trust, but shall be required to withdraw upon the Trust Board as follows: "That representatives of the press, and other members of the public, be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity on
Commented [MWG12]: In line with current practice where meetings are accepted at meetings and such acceptance is recorded
in the next set of minutes
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
178 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 20
which would be prejudicial to the public interest" (Section 1(2) Public Bodies (Admission to Meetings) Act 1960). Guidance should be sought from the Trust’s Freedom of Information Lead to ensure correct procedure is followed on matters to be included in the exclusion.
3.18.2 General disturbances
The Chair (or Vice-Chair if one has been appointed and the Chair is absent) or the person presiding over the meeting shall give such directions as he/she thinks fit with regard to the arrangements for meetings and accommodation of the public and representatives of the press such as to ensure that the Trust 's business shall be conducted without interruption and disruption and, without prejudice to the power to exclude on grounds of the confidential nature of the business to be transacted, the public will be required to withdraw upon the Trust Board resolving as follows: “That in the interests of public order the meeting adjourn for (the period to be specified) to enable the Trust Board to complete its business without the presence of the public" (Section 1(8) Public Bodies (Admission to Meetings) Act 1960).
3.18.3 Business proposed to be transacted when the press and public have been excluded from a meeting
Matters to be dealt with by the Trust Board following the exclusion of representatives of the press, and other members of the public, as provided in 3.18.1 and 3.18.2 above shall be confidential to the members of the Board.
Members and Officers or any employee of the Trust in attendance shall not reveal or disclose the contents of papers marked “In Confidence” or minutes headed “Items Taken in Private” outside of the Trust, without the express permission of the Trust. This prohibition shall apply equally to the content of any discussion during the Board meeting which may take place on such reports or papers.
3.18.4 Use of mechanical or electrical equipment for recording or
transmission of meetings Nothing in these Standing Orders shall be construed as permitting the introduction by the public, or press representatives, of recording, transmitting, video or similar apparatus into meetings of the Trust or Committee thereof. Such permission shall be granted only upon resolution of the Trust.
3.19 Observers at Trust Meetings
3.19.1 The Trust will decide what arrangements and terms and conditions it
feels are appropriate to offer in extending an invitation to observers to attend and address any of the Trust Board's meetings and may change, alter, or vary these terms and conditions as it deems fit.
3.20 Meetings held by electronic means
3.20.1 Any Bboard/committee member may participate in a meeting by way of telephone, computer, or any other electronic means of
Commented [MWG13]: Removed as what may or may not be
disclosed under FOI cannot be pre-determined (instead a decision must be made at the time a request is made); and private board
papers and minutes are still disclosable.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
179 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 21
communication provided that each person is able to hear and speak. A person participating in this way is deemed to be present in person although their actual location shall be noted in the minutes and is counted in a quorum and entitled to vote. The meeting is deemed to take place where the largest group of those participating is assembled, or if there is no such group, where the Chair of the meeting is located.
4. APPOINTMENT OF COMMITTEES AND SUB-COMMITTEES
4.1 Appointment of Committees
4.1.1 Subject to such directions as may be given by the Secretary of State for Health, the Trust Board may appoint committees of the Trust.
4.1.2 The Trust shall determine the membership and terms of reference of
committees and sub-committees and shall if it requires to, receive, and consider reports of such committees.
4.2 Joint Committees
4.2.1 Joint committees may be appointed by the Trust by joining together with one or more other health service bodies consisting of, wholly or partly of the Chair and members of the Trust or other health service bodies or wholly of persons who are not members of the Trust or other health service bodies in question.
4.2.2 Any committee or joint committee appointed under this Standing
Order may, subject to such directions as may be given by the Secretary of State or the Trust or other health bodies in question, appoint sub-committees consisting wholly or partly of members of the committee or joint committee (whether or not they are members of the Trust or health bodies in question) or wholly of persons who are not members of the Trust or health bodies in question or the committee of the Trust or health bodies in question.
4.3 Applicability of Standing Orders and Standing Financial Instructions to
Committees
4.3.1 The Standing Orders and Standing Financial Instructions of the Trust, as far as they are applicable, shall as appropriately apply to meetings and any committees established by the Trust. In which case the term “Chair” is to be read as a reference to the Chair of other committees as the context permits, and the term “member” is to be read as a reference to a member of other committees also as the context permits. (There is no requirement to hold meetings of committees established by the Trust in public.)
4.4 Terms of Reference
4.4.1 Each such committee shall have such terms of reference and powers
and be subject to such conditions (as to reporting back to the Board), as the Board shall decide and shall be in accordance with any
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
180 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 22
legislation and regulation or direction issued by the Secretary of State. Such terms of reference shall have effect as if incorporated into the Standing Orders.
4.5 Delegation of Powers by Committees to Sub-Committees
4.5.1 Where committees are authorised to establish sub-committees, they
may not delegate executive powers to the sub-committee unless expressly authorised by the Trust Board.
4.6 Approval of Appointments to Committees
4.6.1 The Board shall approve the appointments to each of the committees
which it has formally constituted. Where the Board determines, and regulations permit, that persons, who are neither members nor officers, shall be appointed to a committee the terms of such appointment shall be within the powers of the Board as defined by the Secretary of State. The Board shall define the powers of such appointees and shall agree allowances, including reimbursement for loss of earnings, and/or expenses in accordance where appropriate with national guidance.
4.7 Appointments for Statutory Functions
4.7.1 Where the Board is required to appoint persons to a committee
and/or to undertake statutory functions as required by the Secretary of State, and where such appointments are to operate independently of the Board such appointment shall be made in accordance with the regulations and directions made by the Secretary of State.
4.8 Committees Established by the Trust Board
The committees, sub-committees, and joint committees established by the Board are: 4.8.1 Audit Committee
In line with the requirements of the NHS Audit Committee Handbook, NHS Codes of Conduct and Accountability, and the Finance Reporting Council Guidance on Board Effectiveness, an Audit Committee will be established and constituted to provide the Trust Board with an independent and objective review on its financial systems, financial information and compliance with laws, guidance, and regulations governing the NHS. The Terms of Reference will be approved by the Trust Board and reviewed on a periodic basis.
In addition, the Audit Committee acts as the Trust’s Auditor Panel, the main function being to advise on the appointment of external auditors.
A minimum of three Non-Executive Directors should be appointed, unless the Board decides otherwise, of which one must have significant, recent, and relevant financial experience.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
181 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 23
4.8.2 Appointments, Nomination & Remuneration Committee
In line with the requirements of the NHS Codes of Conduct and Accountability, and the Finance Reporting Council Guidance on Board Effectiveness, an Appointments, Nomination and Remuneration Committee will be established and constituted.
The Committee should be comprised exclusively of Non-Executive Directors, a minimum of three, who are independent of management.
The purpose of the Committee will be to advise the Trust Board about appropriate remuneration and terms of service for the Chief Executive and other Executive Directors including: - (i) all aspects of salary (including any performance-related
elements/bonuses),; (ii) provisions for other benefits, including pensions and cars, (iii) arrangements for termination of employment and other
contractual terms. 4.8.3 Resource & Performance Committee
The Resource and Performance Committee has delegated authority from the Board to oversee, co-ordinate, review and assess the financial and performance management arrangements within the Trust.
4.8.4 Charitable Funds Committee In line with its role as a corporate trustee for any funds held on trust, either as charitable or non-charitable funds, the Trust Board delegate authority to the Charitable Funds Committee to administer those funds in accordance with any statutory or other legal requirements, or best practice required by the Charity Commission.
4.8.5 Quality and Safety Committee
The purpose of the Quality and Safety Committee is to assure the Board of the quality of clinical services across the Trust.
4.8.6 Information Governance Committee
The Information Governance Committee oversees the development of the Trust’s Information Governance strategy and provides assurance to the Board that arrangements for handling and using information, including personal information, are safe and secure, and compliant with all legal requirements and national standards.
4.8.7 Other Committees The Board may also establish such other committees as required to
discharge the Trust’s responsibilities.
Commented [MWG14]: No such committee currently exists
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
182 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 24
5. ARRANGEMENTS FOR THE EXERCISE OF TRUST FUNCTIONS BY
DELEGATION
5.1 Delegation of Functions to Committees, Officers or Other Bodies
5.1.1 Subject to such directions as may be given by the Secretary of State, the Board may make arrangements for the exercise, on behalf of the Board, of any of its functions by a committee, sub-committee appointed by virtue of Standing Order 4 “Appointment of Committees and Sub-Committees”, or by an officer of the Trust. In each case these arrangements shall be subject to such restrictions and conditions as the Trust thinks fit.
5.2 Emergency Powers and Urgent Decisions
5.2.1 The powers which the Board has reserved to itself within these Standing Orders (see Standing Order 2.8 “Corporate Role of the Board”) may in emergency or for an urgent decision be exercised by the Chief Executive and the Chair after having consulted at least two non-executive dDirectors. The exercise of such powers by the Chief Executive and Chair shall be reported to the next formal meeting of the Trust Board in public session for formal ratification.
5.3 Delegation to Committees
5.3.1 The Board shall agree from time to time to the delegation of executive powers to be exercised by other committees, or sub-committees, or joint committees, which it has formally constituted in accordance with directions issued by the Secretary of State. The constitution and terms of reference of these committees, or sub-committees, or joint committees, and their specific executive powers shall be approved by the Board.
5.3.2 When the Board is not meeting as the Trust in public session it shall
operate as a committee and may only exercise such powers as may have been delegated to it by the Trust in public session.
5.4 Delegation to Officers
5.4.1 Those functions of the Trust which have not been retained as reserved by the Board or delegated to other committee or sub-committee or joint committee shall be exercised on behalf of the Trust by the Chief Executive. The Chief Executive shall determine which functions he/she will perform personally and shall nominate officers to undertake the remaining functions for which he/she will still retain accountability to the Trust.
5.4.2 The Chief Executive shall prepare a Scheme of Delegation identifying
his/her proposals which shall be considered and approved by the Board. The Chief Executive may periodically propose amendment to the Scheme of Delegation, which shall be considered and approved by the Board.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
183 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 25
5.4.3 Nothing in the Scheme of Delegation shall impair the discharge of the direct accountability to the Board of the Director of Finance and Strategy and Associate Director of Finance to provide information and advise the Board in accordance with statutory or Department of Health requirements. Outside these statutory requirements the roles of the Director of Finance and Strategy and Associate Director of Finance shall be accountable to the Chief Executive for operational matters.
5.5 Scheme of Reservation and Scheme of Delegation
5.5.1 The arrangements made by the Board as set out in the Scheme of Reservation and Scheme of Delegation shall have effect as if incorporated in these Standing Orders.
5.6 Duty to Report Non-Compliance with Standing Orders and Standing
Financial Instructions
5.6.1 If for any reason these Standing Orders are not complied with, full details of the non-compliance and any justification for non-compliance and the circumstances around the non-compliance, shall be reported to the next formal meeting of the Board for action or ratification. All members of the Trust Board and staff have a duty to disclose any non-compliance with these Standing Orders to the Chief Executive as soon as possible.
6. OVERLAP WITH OTHER TRUST POLICY STATEMENTS/PROCEDURES,
REGULATIONS AND STANDING FINANCIAL INSTRUCTIONS 6.1 Policy Statements: General Principles
6.1.1 The Trust Board will from time to time agree and approve Policy statements/procedures which will apply to all or specific groups of staff employed by the Trust. The decisions to approve such policies and procedures will be recorded in an appropriate Trust Board minute and will be deemed where appropriate to be an integral part of the Trust's Standing Orders and Standing Financial Instructions.
6.2 Specific Policy Statements
6.2.1 Notwithstanding the application of Standing Order 6.1 above, these
Standing Orders and Standing Financial Instructions must be read in conjunction with the following Policy statements:
Code of Business Conduct, including Managing Conflicts of Interest Policy,
Staff Disciplinary and Appeals Procedures adopted by the Trust both of which shall have effect as if incorporated in these Standing Orders.
6.3 Standing Financial Instructions 6.3.1 Standing Financial Instructions adopted by the Trust Board in
accordance with the Financial Regulations shall have effect as if incorporated in these Standing Orders.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
184 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 26
6.4 Specific Guidance
6.4.1 Notwithstanding the application of Standing Order 6.1 above, these
Standing Orders and Standing Financial Instructions must be read in conjunction with the following guidance and any other issued by the Secretary of State for Health:
Caldicott Guardian 1997,
Human Rights Act 1998,
Freedom of Information Act 2000,
Companies Act 2006,
Bribery Act 2010,
Equality Act 2010,
Health and Social Care Act 2012,
Social Care Act 2012,
Care Act 2014. 7. DUTIES & OBLIGATIONS OF BOARD MEMBERS/DIRECTORS & SENIOR
MANAGERS UNDER THESE STANDING ORDERS
7.1 Declaration of Interests
7.1.1 Requirements for declaring interests and applicability to Board members
The NHS Code of Accountability requires Trust Board members to declare interests which are relevant and material to the NHS Board of which they are a member. All existing Board members should declare such interests. Any Board members appointed subsequently should do so on appointment.
7.1.2 Interests which are relevant and material
Interests which should be regarded as "relevant and material" are those with any potential impediment to the fitness to act in the role of a Director or non-officer member. Examples are: (i) Directorships, including non-executive Directorships held in
private companies or PLCs (with the exception ofexcept for those of dormant companies),
(ii) Ownership or part-ownership of private companies, businesses, or consultancies likely or possibly seeking to do business with the NHS,
(iii) Majority or controlling shareholdings in organisations likely or possibly seeking to do business with the NHS,
(iv) A position of authority in a charity or voluntary organisation in the field of health and social care,
(v) Any connection with a voluntary or other organisation contracting for NHS services,
(vi) Research funding/grants that may be received by an individual or their department,
(vii) Interests in pooled funds that are under separate management.
Any member of the Trust Board who comes to know that the Trust has entered into or proposes to enter into a contract in which he/she or any person connected with him/her (as defined in Standing Order 7.3 below and elsewhere) has any pecuniary interest, direct or
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
185 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 27
indirect, the Board member shall declare his/her interest by giving notice in writing of such fact to the Trust as soon as practicable.
7.1.3 Advice on interests
If Board members have any doubt about the relevance of an interest, this should be discussed with the Chair of the Trust or with the Trust’s Director of Governance/Corporate Secretary.
The relevant standard is IAS 24, Related Party Disclosures, interpreted as set out in Chapter 4 Annex 1: Standards and applicability to the DH group (issued by the International Accounting Standards Board), specifies that influence and control rather than the immediacy of the relationship is more important in assessing the relevance of an interest. The interests of partners in professional partnerships including general practitioners should also be considered.
7.1.4 Recording of interests in Trust Board minutes
At the time Board members' interests are declared, they should be recorded in the Trust Board minutes. Any changes in interests should be declared at the next Trust Board meeting following the change occurring and recorded in the minutes of that meeting.
7.1.5 Publication of declared interests in the Annual Report
Board members' Directorships of companies likely or possibly seeking to do business with the NHS should be published in the Trust's annual report. The information should be kept up to date for inclusion in succeeding annual reports.
7.1.6 Conflicts of interest which arise during the course of a meeting
During the course of a Trust Board or committee meeting, if a conflict of interest is established, the Board or committee member concerned should withdraw from the meeting and play no part in the relevant discussion or decision (see overlap with Standing Order 7.3).
7.2 Register of Interests
7.2.1 The Chief Executive will ensure that a Register of Interests is
established to record formally declarations of interests of Board members. In particular tThe Register will include details of all Directorships and other relevant and material interests (as defined in Standing Order 7.1.2) which have been declared by both executive and non-executive Trust Board members.
7.2.2 These details will be kept up to date by means of an annual review of
the Register in which any changes to interests declared during the preceding twelve months will be incorporated.
7.2.3 The Register will be available to the public and the Chief Executive
will take reasonable steps to bring the existence of the Register to the attention of local residents and to publicise arrangements for viewing it.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
186 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 28
7.3 Exclusion of Chair and Members in Proceedings on Account of Pecuniary Interest
7.3.1 Interpretation of “pecuniary interest”
For the sake of clarity, the following definition of terms is to be used in interpreting this Standing Order: (i) “spouse” shall include any person who lives with another
person in the same household (and any pecuniary interest of one spouse shall, if known to the other spouse, be deemed to be an interest of that other spouse),
(ii) “contract” shall include any proposed contract or other course of dealing,
(iii) subject to the exceptions set out in this Standing Order, a person shall be treated as having an indirect pecuniary interest in a contract if: -
he/she or a nominee of his/her, is a member of a company or other body (not being a public body), with which the contract is made, or to be made or which has a direct pecuniary interest in the same, or
he/she is a partner, associate, or employee of any person with whom the contract is made or to be made or who has a direct pecuniary interest in the same.
(iv) a person shall not be regarded as having a pecuniary interest in any contract if: -
neither he/she or any person connected with him/her has any beneficial interest in the securities of a company of which he/she or such person appears as a member, or
any interest that he/she or any person connected with him/her may have in the contract is so remote or insignificant that it cannot reasonably be regarded as likely to influence him/her in relation to considering or voting on that contract, or
those securities of any company in which he/she (or any person connected with him/her) has a beneficial interest do not exceed £10,000 in nominal value or one per cent of the total issued share capital of the company or of the relevant class of such capital, whichever is the less.
However, where bullet point 3 above applies the person shall nevertheless be obliged to disclose/declare their interest in accordance with Standing Order 7.1.2.
7.3.2 Exclusion in proceedings of the Trust Board
(i) Subject to the following provisions of this Standing Order, if the Chair or a member of the Trust Board has any pecuniary interest, direct or indirect, in any contract, proposed contract or other matter and is present at a meeting of the Trust Board at which the contract or other matter is the subject of consideration, they shall at the meeting and as soon as practicable after its commencement disclose the fact and shall not take part in the consideration or discussion of the contract or other matter or vote on any question with respect to it.
(ii) The Secretary of State may, subject to such conditions as he/she may think fit to impose, remove any disability imposed by this Standing Order in any case in which it appears to
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
187 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 29
him/her in the interests of the National Health Service that the disability should be removed. (see Standing Order 7.3.3 on the “waiver” which has been approved by the Secretary of State for Health).
(iii) The Trust Board may exclude the Chair or a member of the Board from a meeting of the Board while any contract, proposed contract, or other matter in which he has a pecuniary interest, is under consideration.
(iv) Any remuneration, compensation, or allowances payable to the Chair or a member by virtue of paragraph 233, Part 11 of the NHS Act 2006 shall not be treated as a pecuniary interest for the purpose of this Standing Order.
(v) This Standing Order applies to a committee or sub-committee and to a joint committee or sub-committee as it applies to the Trust and applies to a member of any such committee or sub-committee (whether or not he/she is also a member of the Trust) as it applies to a member of the Trust.
7.3.3 Waiver of Standing Orders made by the Secretary of State for Health
(i) Power of the Secretary of State to make waivers
Under regulation 11(2) of the NHS (Membership and Procedure Regulations SI 1999/2024 (“the Regulations”), there is a power for the Secretary of State to issue waivers if it appears to the Secretary of State in the interests of the health service that the disability in regulation 11 (which prevents a Chair or a member from taking part in the consideration or discussion of, or voting on any question with respect to, a matter in which he has a pecuniary interest) is removed. A waiver has been agreed in line with sub-sections (ii) to (iv) below.
(ii) Definition of “Chair” for the purpose of interpreting this waiver
For the purposes of paragraph 7.3.3. (iii) (below), the “relevant Chair” is: –
at a meeting of the Trust, the Chair of that Trust,
at a meeting of a Committee: in a case where the member in question is the Chair of that Committee, the Chair of the Trust; or in the case of any other member, the Chair of that Committee.
(iii) Application of waiver
A waiver will apply in relation to the disability to participate in the proceedings of the Trust on account of a pecuniary interest.
It will apply to: -
a member of the Trust, who is a healthcare professional, and who is providing or performing, or assisting in the provision or performance, of: – a) services under the National Health Service Act 2006; or b) services in connection with the Health and Social Care Act 2012; for the benefit of persons for whom the Trust is responsible.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
188 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 30
where the pecuniary interest of the member in the matter which is the subject of consideration at a meeting at which he/she is present: - a) arises by reason only of the member’s role as such a
professional providing or performing, or assisting in the provision or performance of, those services to those persons,
b) has been declared by the relevant Chair as an interest which cannot reasonably be regarded as an interest more substantial than that of the majority of other persons who are members of the same profession as the member in question or who are providing or performing, or assisting in the provision or performance of, such of those services as he provides or performs, or assists in the provision or performance of, for the benefit of persons for whom the Trust is responsible.
(iv) Conditions which apply to the waiver and the removal of
having a pecuniary interest The removal is subject to the following conditions:
the member must disclose his/her interest as soon as practicable after the commencement of the meeting and this must be recorded in the minutes,
the relevant Chair must consult the Chief Executive before making a declaration in relation to the member in question pursuant to paragraph 7.3.3(ii) above, except where that member is the Chief Executive,
in the case of a meeting of the Trust the member may take part in the consideration or discussion of the matter which must be subjected to a vote and the outcome recorded but may not vote on any question with respect to it.
in the case of a meeting of a Committee the member may take part in the consideration or discussion of the matter which must be subjected to a vote and the outcome recorded and may vote on any question with respect to it, but the resolution which is subject to the vote must comprise a recommendation to, and be referred for approval by, the Trust Board.
7.4 Standards of Business Conduct
7.4.1 Trust Policy and National Guidance
All Trust staff and members of the Board must comply with the Trust’s Code of Business Conduct, including Managing Conflicts of Interest and the national guidance contained in “Managing Conflicts of Interest in the NHS” which has been incorporated into the above policy.
7.4.2 Interest of Officers in Contracts Any officer or employee of the Trust who comes to know that the Trust has entered into or proposes to enter into a contract in which he/she or any person connected with him/her (as defined in Standing Order 7.3) has any pecuniary interest, direct or indirect, the Officer
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
189 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 31
shall declare their interest by giving notice in writing of such fact to the Chief Executive or Trust’s Company Secretary as soon as practicable.
An officer should also declare to the Chief Executive any other employment or business or other relationship of his/her, or of a cohabiting spouse, that conflicts, or might reasonably be predicted could conflict with the interests of the Trust. The Trust will require interests, employment or relationships so declared to be entered in a register of interests of staff.
7.4.3 Canvassing of and Recommendations by Members in Relation to Appointments Canvassing of members of the Trust or of any Committee of the Trust directly or indirectly for any appointment under the Trust shall disqualify the candidate for such appointment. The contents of this paragraph of the Standing Orders shall be included in application forms or otherwise brought to the attention of candidates. Members of the Trust shall not solicit for any person any appointment under the Trust or recommend any person for such appointment: but this paragraph of this Standing Order shall not preclude a member from giving written testimonial of a candidate's ability, experience, or character for submission to the Trust.
7.4.4 Relatives of Members or Officers
Candidates for any staff appointment under the Trust shall, when making an application, disclose in writing to the Trust whether they are related to any member or the holder of any office under the Trust. Failure to disclose such a relationship shall disqualify a candidate and, if appointed, render him/her liable to instant dismissal. The Chair and every member and officer of the Trust shall disclose to the Trust Board any relationship between himself and a candidate of whose candidature that member or officer is aware. It shall be the duty of the Chief Executive to report to the Trust Board any such disclosure made. On appointment, members (and prior to acceptance of an appointment in the case of Executive Directors) should disclose to the Trust whether they are related to any other member or holder of any office in the Trust. Where the relationship to a member of the Trust is disclosed, the Standing Order headed “Exclusion of Chair and Members in Proceedings on Account of Pecuniary Interest” (Standing Order 7.3) shall apply.
8. CUSTODY OF SEAL, SEALING OF DOCUMENTS AND SIGNATURE OF
DOCUMENTS
8.1 Custody of Seal
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
190 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 32
8.1.1 The Common Seal of the Trust shall be kept by the Chief Executive or a nominated manager by them in a secure place.
8.2 Sealing of Documents
8.2.1 Where it is necessary that a document shall be sealed, the seal shall be affixed in the presence of two senior managers duly authorised by the Chief Executive, and not also from the originating department, and shall be attested by them.
8.2.2 When it is not possible to affix the seal to a document the authorisation of the application of the seal by two senior managers duly authorised by the Chief Executive shall be sufficient to treat the document as if it has been sealed.
8.3 Register of Sealing
8.3.1 An entry of every sealing shall be made and numbered consecutively in a book provided for that purpose and shall be signed by the persons who shall have approved and authorised the document and those who attested the seal.
8.4 Use of Seal – General Guide
8.4.1 The seal should be used for:
all contracts for the purchase/lease of land and/or buildings
all contracts for capital works exceeding £100,000
all lease agreements where the annual lease charge exceeds £10,000 per annum and the period of the lease exceeds beyond five years
any other lease agreement where the total payable under the lease exceeds £100,000
any contracts or agreements with organisations other than NHS or other government bodies including local authorities where the annual costs exceed or are expected to exceed £100,000.
8.5 Signature of Documents
8.5.1 Where any document will be a necessary step in legal proceedings
on behalf of the Trust, it shall, unless any enactment otherwise requires or authorises, be signed by the Chief Executive or any Executive Director.
8.5.2 In land transactions, the signing of certain supporting documents will
be delegated to Managers and set out clearly in the Scheme of Delegation but will not include the main or principal documents effecting the transfer (e.g., sale/purchase agreement, lease, contracts for construction works and main warranty agreements or any document which is required to be executed as a deed).
Commented [MWG15]: Reflects a need that came about during the pandemic
Commented [MWG16]: It is not normal for the circumstances when the seal should be used to be listed in the SOs. This should be
considered for deletion; and if not deleted the figures should be reviewed as they are not consistent with approval thresholds in the
Standing Financial Instruction
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
191 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021
Page 33
9. MISCELLANEOUS
9.1 Standing Orders to be Given to Members and Officers
9.1.1 It is the duty of the Chief Executive to ensure that existing members and officers and all new appointees are notified of and understand their responsibilities within Standing Orders and Standing Financial Instructions.
9.2 Review of Standing Orders
9.2.1 Standing Orders shall be reviewed annually by the Board. The requirement for review extends to all documents having the effect as if incorporated in Standing Orders.
9.3 Joint Finance Arrangements
See overlap with Standing Financial Instruction 10.3 “Joint Finance Arrangements with Local Authorities”.
9.3.1 The Board may confirm contracts to purchase from a local authority
using its powers under Section 75 of the NHS Act 2006. The Board may confirm contracts to transfer money from the NHS to the health-related functions of local authorities where such a transfer is to fund services to improve the health of the local population more effectively than equivalent expenditure on NHS services.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
192 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Policies, Procedures, Guidelines and Protocols
Document Details
Title Scheme of Reservation
Trust Ref No
Local Ref (optional)
Main points the document covers
This document details decisions reserved for the Board
Who is the document aimed at?
All staff
Author Head of Financial Accounting
Approval process
Approved by (Committee/Director)
Trust Board
Approval Date December 2021
Initial Equality Impact Screening
Yes
Full Equality Impact Assessment
No
Lead Director Sarah Lloyd, Director of Finance
Category Finance
Sub CategorySubcategory Standing Orders
Review date September 2022
Distribution
Who the policy will be distributed to
Distributed to senior staff as defined by directors
Method Electronically to senior staff & available to all staff via the Trust web-site
Document Links
Required by CQC
Required by NHSR
Other
Amendments History
No Date Amendment
1 September 2018 D.15 changed reference to ‘NHS Litigation Authority’ and replaced with ‘NHS Resolution’
2 September 2019 Minor amendments to terminology
3 September 2020 No amendments required
4 September 2021 Added Director of Finance Removed Director of Finance and Strategy and Associate Director of Finance Minor grammatical amendments
5
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
193 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 2 of 4 September 20210
SHROPSHIRE COMMUNITY HEALTH NHS TRUST SCHEME OF RESERVATION
DECISIONS RESERVED TO THE BOARD
A. General Enabling Provision
1. The Board may determine any matter, for which it has delegated or statutory authority, it wishes in full session within its statutory powers.
B. Regulations and Control
1. Approval, variation, and amendment of Standing Orders (SOs), a Scheme of Reservation and Standing Financial Instructions (SFIs) for the regulation of its proceedings and business.
2. Suspension of Standing Orders.
3. Ratifying any urgent decisions taken by the Chair or Chief Executive in public session in accordance with SO 5.2.
4. Approval of a Scheme of Delegation of powers from the Board to committees.
5. Requiring and receiving the declaration of Board members’ interests which may conflict with those of the Trust and determining the extent to which that member may remain involved with the matter under consideration.
6. Requiring and receiving the declaration of officers’ interests which may conflict with those of the Trust.
7. Approval of arrangements for dealing with complaints.
8. Adoption of the organisation structures, processes, and procedures to facilitate the discharge of business by the Trust and to agree modifications thereto.
9. Receipt of reports from committees including those which the Trust is required by the Secretary of State or other regulation to establish and to take appropriate action on.
10. Confirmation of the recommendations of the Trust’s committees where the committees do not have executive powers.
11. Approval of arrangements relating to the discharge of the Trust’s responsibilities as a corporate trustee for charitable funds.
12. Establishing terms of reference and reporting arrangements of all committees and sub-committees that are established by the Board.
13. Approval of arrangements relating to the discharge of the Trust’s responsibilities as a bailer for patients’ property.
14. Authorising the use of the seal.
15. Disciplining of members of the Board or employees who are in breach of statutory requirements or SOs.
16. Ratifying or otherwise instances of failure to comply with Standing Orders brought to the Chief Executive’s attention in accordance with SO 5.6.
C. Appointments/ Dismissal
1. Appointment of the Vice Chair of the Board.
2. Appointment and dismissal of committees (and individual members) that are directly accountable to the Board.
3. Appointment, appraisal, disciplining and dismissal of Executive Directors subject to SO 2.2.
4. Confirmation of appointment of members of any committee of the Trust as representatives
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
194 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 3 of 4 September 20210
DECISIONS RESERVED TO THE BOARD
on outside bodies.
5. Appointment appraisal, disciplining and dismissal of the Secretary (if the appointment of a Secretary is required under SOs).
6. Approving the proposals of the Appointments, Nomination & Remuneration Committee regarding directors and senior employees and those of the Chief Executive for staff not covered by the Appointments, Nomination & Remuneration Committee.
D. Strategy, Plans and Budgets
1. Definition of the strategic aims and objectives of the Trust.
2. Identification of the key strategic risks, evaluation of them and ensuring that adequate responses are in place and are monitored.
3. Approval of proposals for ensuring quality and developing clinical governance in services provided by the Trust, having regard to any guidance issued by the Secretary of State.
4. Approval of the Trust’s policies and procedures for the management of risk.
5. Approval of Outline and Final Business Cases for Capital Investment.
6. Approval of budgets.
7. Approval annually of the Trust’s proposed organisational development proposals.
8. Ratification of proposals for acquisition, disposal or change of use of land and/or buildings
9. Approval of PFI proposals.
10. Approval of the opening of bank accounts.
11. Approval of proposals on individual contracts (other than NHS contracts) of a capital or revenue nature amounting to, or likely to amount to over £100,000 over a 3- year period or the period of the contract if longer.
12. Approval of proposals in individual cases for the write off, of losses or making of special payments above the limits of delegation to the Chief Executive and Director of Finance and Strategy or Associate Director of Finance and other officers (for losses and special payments) previously approved by the Board.
13. Approval of individual compensation payments.
14. Approval of proposals for action on litigation against or on behalf of the Trust.
15. Review of the use of the NHS Resolution risk pooling schemes (LPST/CNST/RPST).
E. Policy Determination
1. Approval of management policies including personnel policies incorporating the arrangements for the appointment, removal, and remuneration of staff.
F. Audit
1. Receiving the annual management letter received from the External Auditor and agreement of proposed action, taking account of the advice, where appropriate, of the Audit Committee.
2. Receiving the annual report from the Internal Auditor and agreement of proposed action, taking account of the advice, where appropriate, of the Audit Committee.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
195 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page 4 of 4 September 20210
DECISIONS RESERVED TO THE BOARD
G. Annual Report and Accounts
1. Receipt and approval of the Trust’s Annual Report and Annual Accounts.
2. Receipt and approval of the Annual Report and Annual Accounts for Charitable Funds.
H. Monitoring
1. Receipt of such reports as the Board sees fit from committees in respect of its exercise of powers delegated.
2. Continuous appraisal of the affairs of the Trust by means of the provision to the Board as the Board may require from directors, committees, and officers of the Trust as set out in management policy statements. All monitoring returns required by the Department of Health shall be reported, at least in summary, to the Board.
3. Receipt of reports from the Director of Finance and Strategy or Associate Director of Finance on actual and forecast income from SLAs.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
196 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Policies, Procedures, Guidelines and Protocols
Document Details
Title Scheme of Delegation
Trust Ref No
Local Ref (optional)
Main points the document covers
This scheme details the levels of delegation the Board gives to individuals & committees
Who is the document aimed at?
All staff
Author Head of Financial Accounting
Approval process
Approved by (Committee/Director)
Trust Board
Approval Date December 2021
Initial Equality Impact Screening
Yes
Full Equality Impact Assessment
No
Lead Director Sarah Lloyd, Director of Finance
Category Finance
Sub CategorySubcategory
Standing Orders
Review date September 2022
Distribution
Who the policy will be distributed to
Distributed to senior staff as defined by Directors
Method Electronically to senior staff & available to all staff via the Trust website
Document Links
Required by CQC
Required by NHSR
Other
Amendments History No Date Amendment
1 April 2014 Amendments to section 5(quotations/tendering) & section 10 (disposals) plus other amendments to terminology
2 May 2015
Significant amendments to section 2 (capital scheme approval), section 6 (charitable fund expenditure), section 9 (redundancy & early retirements) & section 34 (new & core business developments) Other minor amendments
3 January 2016
Amendment to section 8 (engagement of staff not on the establishment) relating to consultancy
4 November 2016 Amend Audit Committee responsibilities to reflect role as Auditor Panel
5 November 2017 Changed references to ‘Estates Advisor’ and replaced with ‘Director of Finance’
6 September 2018 New section 35; requirement for PDC or loan draw down utilisation request authorised signatories. Added ‘Associate Director of Finance’ alongside Director of Finance and Director.
7 September 2019 Reference to SFIs as SFIs renumbered Removed reference to Appendix 1 in SO’s as no longer relevant and replaced with reference to the Trusts Code of Business Conduct, including Managing Conflicts of Interest Policy. Changed Transformational & CIP Programme Board to Benefits Realisation Group
8 September 2020 Change NSHI to NHSI/E Changed reference to Director of Corporate Affairs and replaced with Director of Governance/Corporate Secretary
9 September 2021 Added Director of Finance Removed Director of Finance and Strategy and Associate Director of Finance
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
197 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
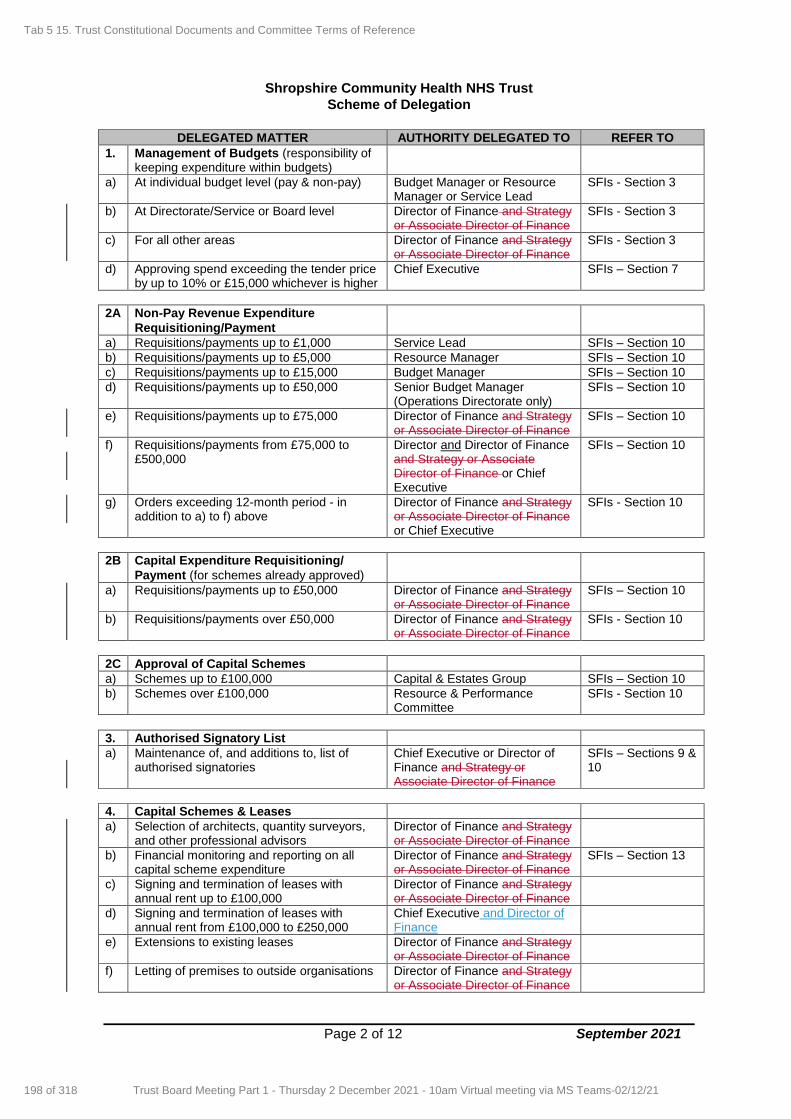
Shropshire Community Health NHS Trust
Scheme of Delegation
Page 2 of 12 September 2021
DELEGATED MATTER AUTHORITY DELEGATED TO REFER TO
1. Management of Budgets (responsibility of keeping expenditure within budgets)
a) At individual budget level (pay & non-pay) Budget Manager or Resource Manager or Service Lead
SFIs - Section 3
b) At Directorate/Service or Board level Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 3
c) For all other areas Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 3
d) Approving spend exceeding the tender price by up to 10% or £15,000 whichever is higher
Chief Executive SFIs – Section 7
2A Non-Pay Revenue Expenditure
Requisitioning/Payment
a) Requisitions/payments up to £1,000 Service Lead SFIs – Section 10
b) Requisitions/payments up to £5,000 Resource Manager SFIs – Section 10
c) Requisitions/payments up to £15,000 Budget Manager SFIs – Section 10
d) Requisitions/payments up to £50,000 Senior Budget Manager (Operations Directorate only)
SFIs – Section 10
e) Requisitions/payments up to £75,000 Director of Finance and Strategy or Associate Director of Finance
SFIs – Section 10
f) Requisitions/payments from £75,000 to £500,000
Director and Director of Finance and Strategy or Associate Director of Finance or Chief Executive
SFIs – Section 10
g) Orders exceeding 12-month period - in addition to a) to f) above
Director of Finance and Strategy or Associate Director of Finance or Chief Executive
SFIs - Section 10
2B Capital Expenditure Requisitioning/
Payment (for schemes already approved)
a) Requisitions/payments up to £50,000 Director of Finance and Strategy or Associate Director of Finance
SFIs – Section 10
b) Requisitions/payments over £50,000 Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 10
2C Approval of Capital Schemes
a) Schemes up to £100,000 Capital & Estates Group SFIs – Section 10
b) Schemes over £100,000 Resource & Performance Committee
SFIs - Section 10
3. Authorised Signatory List
a) Maintenance of, and additions to, list of authorised signatories
Chief Executive or Director of Finance and Strategy or Associate Director of Finance
SFIs – Sections 9 & 10
4. Capital Schemes & Leases
a) Selection of architects, quantity surveyors, and other professional advisors
Director of Finance and Strategy or Associate Director of Finance
b) Financial monitoring and reporting on all capital scheme expenditure
Director of Finance and Strategy or Associate Director of Finance
SFIs – Section 13
c) Signing and termination of leases with annual rent up to £100,000
Director of Finance and Strategy or Associate Director of Finance
d) Signing and termination of leases with annual rent from £100,000 to £250,000
Chief Executive and Director of Finance
e) Extensions to existing leases Director of Finance and Strategy or Associate Director of Finance
f) Letting of premises to outside organisations Director of Finance and Strategy or Associate Director of Finance
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
198 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
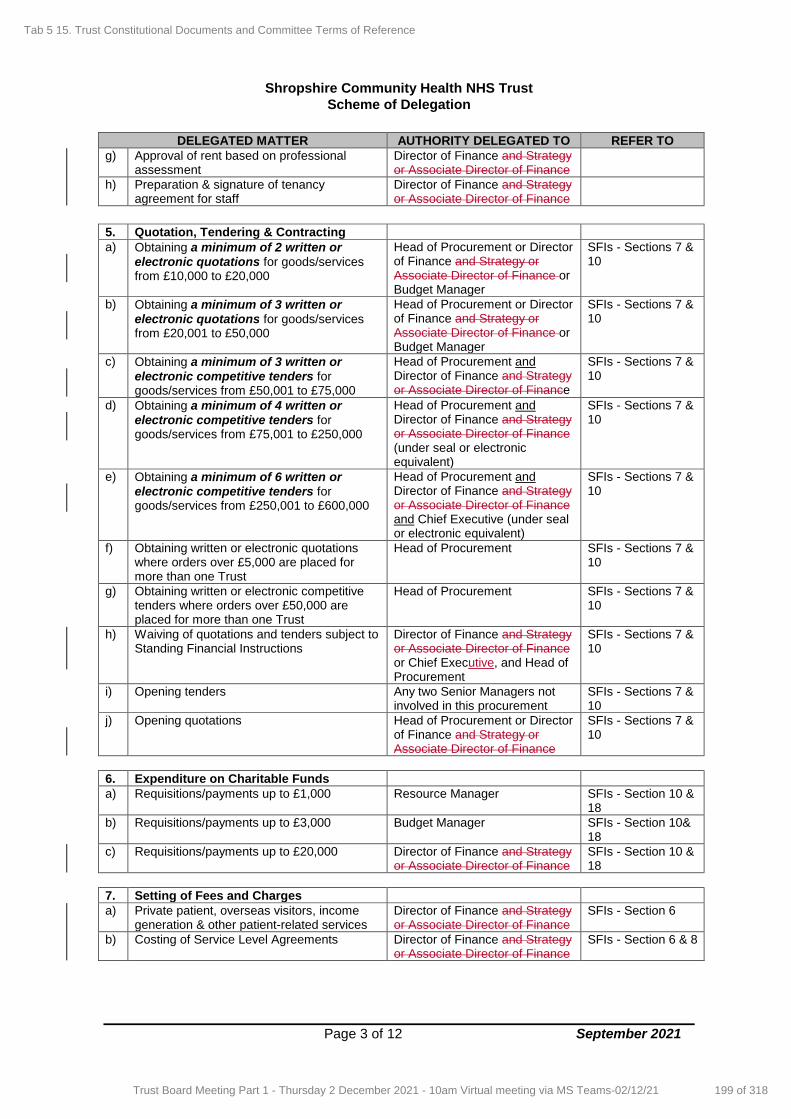
Shropshire Community Health NHS Trust
Scheme of Delegation
Page 3 of 12 September 2021
DELEGATED MATTER AUTHORITY DELEGATED TO REFER TO
g) Approval of rent based on professional assessment
Director of Finance and Strategy or Associate Director of Finance
h) Preparation & signature of tenancy agreement for staff
Director of Finance and Strategy or Associate Director of Finance
5. Quotation, Tendering & Contracting
a) Obtaining a minimum of 2 written or electronic quotations for goods/services from £10,000 to £20,000
Head of Procurement or Director of Finance and Strategy or Associate Director of Finance or Budget Manager
SFIs - Sections 7 & 10
b) Obtaining a minimum of 3 written or electronic quotations for goods/services from £20,001 to £50,000
Head of Procurement or Director of Finance and Strategy or Associate Director of Finance or Budget Manager
SFIs - Sections 7 & 10
c) Obtaining a minimum of 3 written or electronic competitive tenders for goods/services from £50,001 to £75,000
Head of Procurement and Director of Finance and Strategy or Associate Director of Finance
SFIs - Sections 7 & 10
d) Obtaining a minimum of 4 written or electronic competitive tenders for goods/services from £75,001 to £250,000
Head of Procurement and Director of Finance and Strategy or Associate Director of Finance (under seal or electronic equivalent)
SFIs - Sections 7 & 10
e) Obtaining a minimum of 6 written or electronic competitive tenders for goods/services from £250,001 to £600,000
Head of Procurement and Director of Finance and Strategy or Associate Director of Finance and Chief Executive (under seal or electronic equivalent)
SFIs - Sections 7 & 10
f) Obtaining written or electronic quotations where orders over £5,000 are placed for more than one Trust
Head of Procurement SFIs - Sections 7 & 10
g) Obtaining written or electronic competitive tenders where orders over £50,000 are placed for more than one Trust
Head of Procurement SFIs - Sections 7 & 10
h) Waiving of quotations and tenders subject to Standing Financial Instructions
Director of Finance and Strategy or Associate Director of Finance or Chief Executive, and Head of Procurement
SFIs - Sections 7 & 10
i) Opening tenders Any two Senior Managers not involved in this procurement
SFIs - Sections 7 & 10
j) Opening quotations Head of Procurement or Director of Finance and Strategy or Associate Director of Finance
SFIs - Sections 7 & 10
6. Expenditure on Charitable Funds
a) Requisitions/payments up to £1,000 Resource Manager SFIs - Section 10 & 18
b) Requisitions/payments up to £3,000 Budget Manager SFIs - Section 10& 18
c) Requisitions/payments up to £20,000 Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 10 & 18
7. Setting of Fees and Charges
a) Private patient, overseas visitors, income generation & other patient-related services
Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 6
b) Costing of Service Level Agreements Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 6 & 8
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
199 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
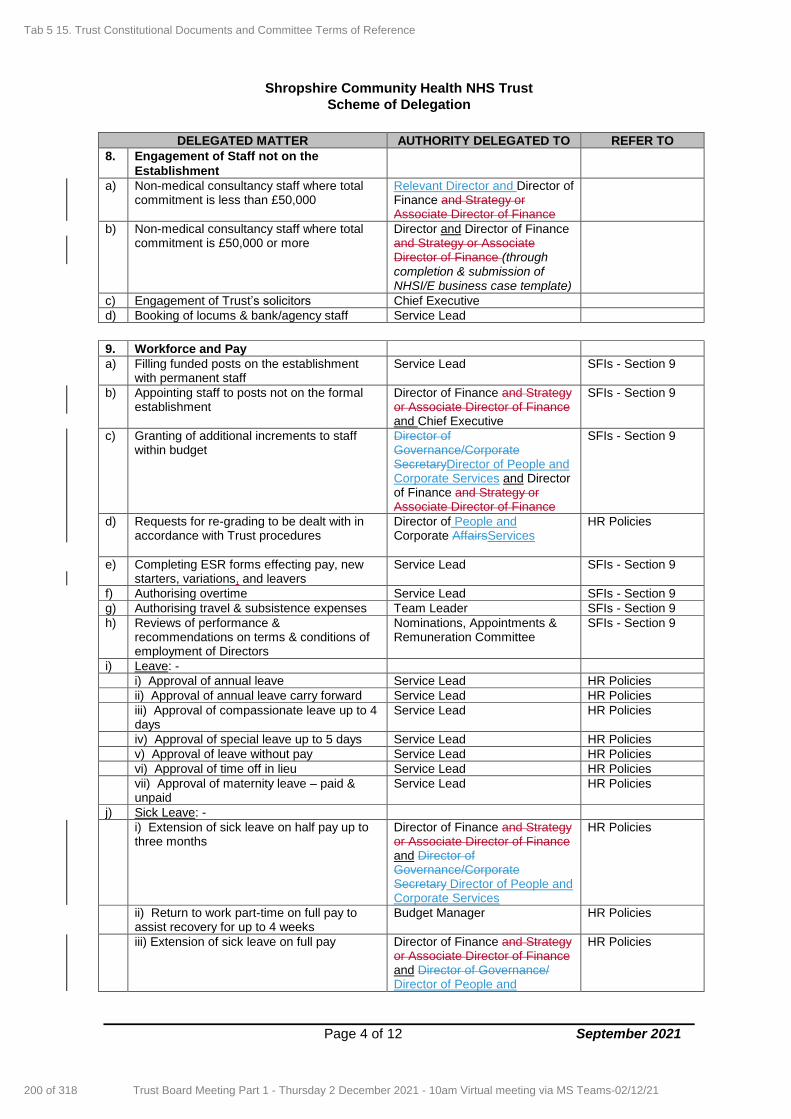
Shropshire Community Health NHS Trust
Scheme of Delegation
Page 4 of 12 September 2021
DELEGATED MATTER AUTHORITY DELEGATED TO REFER TO
8. Engagement of Staff not on the
Establishment
a) Non-medical consultancy staff where total commitment is less than £50,000
Relevant Director and Director of Finance and Strategy or Associate Director of Finance
b) Non-medical consultancy staff where total commitment is £50,000 or more
Director and Director of Finance and Strategy or Associate Director of Finance (through completion & submission of NHSI/E business case template)
c) Engagement of Trust’s solicitors Chief Executive
d) Booking of locums & bank/agency staff Service Lead
9. Workforce and Pay
a) Filling funded posts on the establishment with permanent staff
Service Lead SFIs - Section 9
b) Appointing staff to posts not on the formal establishment
Director of Finance and Strategy or Associate Director of Finance and Chief Executive
SFIs - Section 9
c) Granting of additional increments to staff within budget
Director of Governance/Corporate SecretaryDirector of People and Corporate Services and Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 9
d) Requests for re-grading to be dealt with in accordance with Trust procedures
Director of People and Corporate AffairsServices
HR Policies
e) Completing ESR forms effecting pay, new starters, variations, and leavers
Service Lead SFIs - Section 9
f) Authorising overtime Service Lead SFIs - Section 9
g) Authorising travel & subsistence expenses Team Leader SFIs - Section 9
h) Reviews of performance & recommendations on terms & conditions of employment of Directors
Nominations, Appointments & Remuneration Committee
SFIs - Section 9
i) Leave: -
i) Approval of annual leave Service Lead HR Policies
ii) Approval of annual leave carry forward Service Lead HR Policies
iii) Approval of compassionate leave up to 4 days
Service Lead HR Policies
iv) Approval of special leave up to 5 days Service Lead HR Policies
v) Approval of leave without pay Service Lead HR Policies
vi) Approval of time off in lieu Service Lead HR Policies
vii) Approval of maternity leave – paid & unpaid
Service Lead HR Policies
j) Sick Leave: -
i) Extension of sick leave on half pay up to three months
Director of Finance and Strategy or Associate Director of Finance and Director of Governance/Corporate Secretary Director of People and Corporate Services
HR Policies
ii) Return to work part-time on full pay to assist recovery for up to 4 weeks
Budget Manager HR Policies
iii) Extension of sick leave on full pay Director of Finance and Strategy or Associate Director of Finance and Director of Governance/ Director of People and
HR Policies
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
200 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
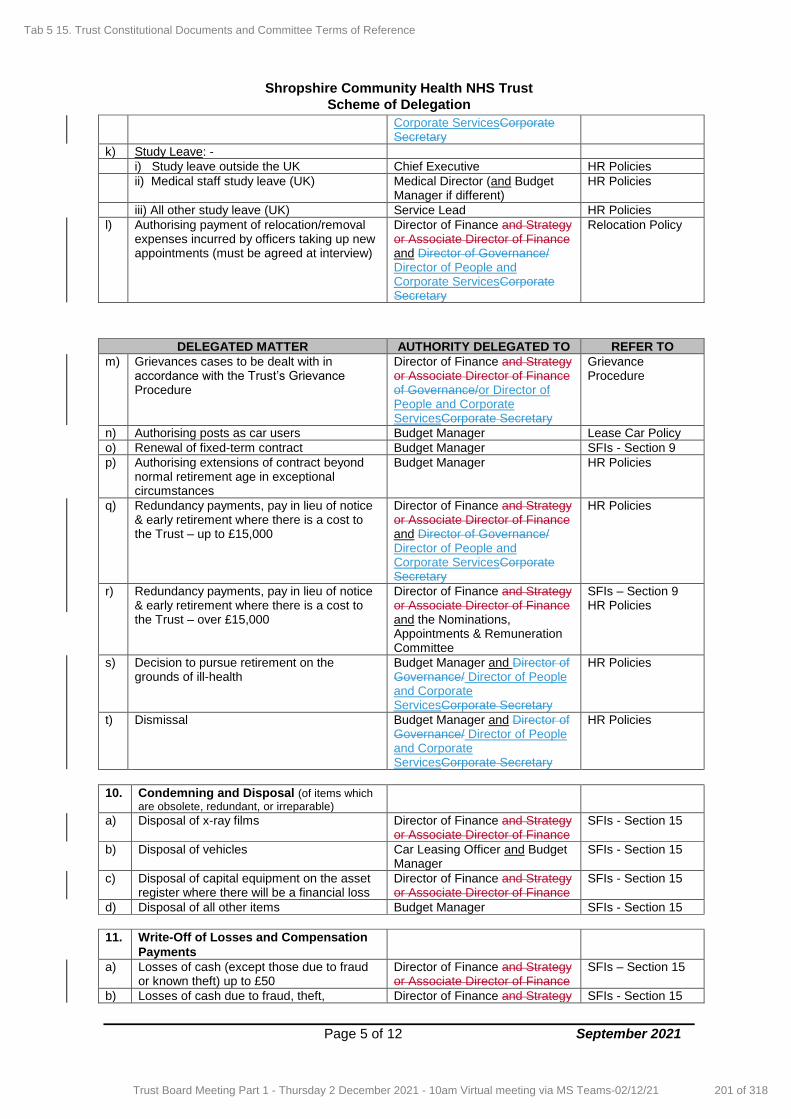
Shropshire Community Health NHS Trust
Scheme of Delegation
Page 5 of 12 September 2021
Corporate ServicesCorporate Secretary
k) Study Leave: -
i) Study leave outside the UK Chief Executive HR Policies
ii) Medical staff study leave (UK) Medical Director (and Budget Manager if different)
HR Policies
iii) All other study leave (UK) Service Lead HR Policies
l) Authorising payment of relocation/removal expenses incurred by officers taking up new appointments (must be agreed at interview)
Director of Finance and Strategy or Associate Director of Finance and Director of Governance/ Director of People and Corporate ServicesCorporate Secretary
Relocation Policy
DELEGATED MATTER AUTHORITY DELEGATED TO REFER TO
m) Grievances cases to be dealt with in accordance with the Trust’s Grievance Procedure
Director of Finance and Strategy or Associate Director of Finance of Governance/or Director of People and Corporate ServicesCorporate Secretary
Grievance Procedure
n) Authorising posts as car users Budget Manager Lease Car Policy
o) Renewal of fixed-term contract Budget Manager SFIs - Section 9
p) Authorising extensions of contract beyond normal retirement age in exceptional circumstances
Budget Manager HR Policies
q) Redundancy payments, pay in lieu of notice & early retirement where there is a cost to the Trust – up to £15,000
Director of Finance and Strategy or Associate Director of Finance and Director of Governance/ Director of People and Corporate ServicesCorporate Secretary
HR Policies
r) Redundancy payments, pay in lieu of notice & early retirement where there is a cost to the Trust – over £15,000
Director of Finance and Strategy or Associate Director of Finance and the Nominations, Appointments & Remuneration Committee
SFIs – Section 9 HR Policies
s) Decision to pursue retirement on the grounds of ill-health
Budget Manager and Director of Governance/ Director of People and Corporate ServicesCorporate Secretary
HR Policies
t) Dismissal Budget Manager and Director of Governance/ Director of People and Corporate ServicesCorporate Secretary
HR Policies
10. Condemning and Disposal (of items which
are obsolete, redundant, or irreparable)
a) Disposal of x-ray films Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 15
b) Disposal of vehicles Car Leasing Officer and Budget Manager
SFIs - Section 15
c) Disposal of capital equipment on the asset register where there will be a financial loss
Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 15
d) Disposal of all other items Budget Manager SFIs - Section 15
11. Write-Off of Losses and Compensation
Payments
a) Losses of cash (except those due to fraud or known theft) up to £50
Director of Finance and Strategy or Associate Director of Finance
SFIs – Section 15
b) Losses of cash due to fraud, theft, Director of Finance and Strategy SFIs - Section 15
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
201 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
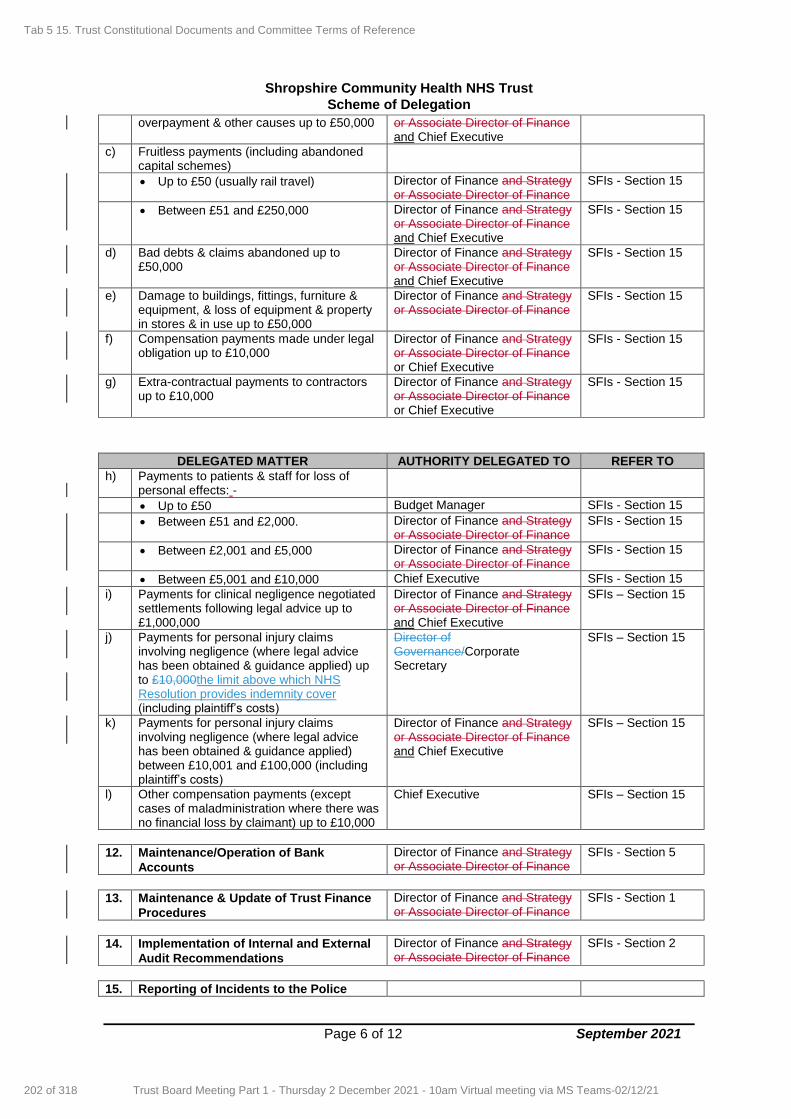
Shropshire Community Health NHS Trust
Scheme of Delegation
Page 6 of 12 September 2021
overpayment & other causes up to £50,000 or Associate Director of Finance and Chief Executive
c) Fruitless payments (including abandoned capital schemes)
Up to £50 (usually rail travel) Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 15
Between £51 and £250,000 Director of Finance and Strategy or Associate Director of Finance and Chief Executive
SFIs - Section 15
d) Bad debts & claims abandoned up to £50,000
Director of Finance and Strategy or Associate Director of Finance and Chief Executive
SFIs - Section 15
e) Damage to buildings, fittings, furniture & equipment, & loss of equipment & property in stores & in use up to £50,000
Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 15
f) Compensation payments made under legal obligation up to £10,000
Director of Finance and Strategy or Associate Director of Finance or Chief Executive
SFIs - Section 15
g) Extra-contractual payments to contractors up to £10,000
Director of Finance and Strategy or Associate Director of Finance or Chief Executive
SFIs - Section 15
DELEGATED MATTER AUTHORITY DELEGATED TO REFER TO
h) Payments to patients & staff for loss of personal effects: -
Up to £50 Budget Manager SFIs - Section 15
Between £51 and £2,000. Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 15
Between £2,001 and £5,000 Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 15
Between £5,001 and £10,000 Chief Executive SFIs - Section 15
i) Payments for clinical negligence negotiated settlements following legal advice up to £1,000,000
Director of Finance and Strategy or Associate Director of Finance and Chief Executive
SFIs – Section 15
j) Payments for personal injury claims involving negligence (where legal advice has been obtained & guidance applied) up to £10,000the limit above which NHS Resolution provides indemnity cover (including plaintiff’s costs)
Director of Governance/Corporate Secretary
SFIs – Section 15
k) Payments for personal injury claims involving negligence (where legal advice has been obtained & guidance applied) between £10,001 and £100,000 (including plaintiff’s costs)
Director of Finance and Strategy or Associate Director of Finance and Chief Executive
SFIs – Section 15
l) Other compensation payments (except cases of maladministration where there was no financial loss by claimant) up to £10,000
Chief Executive SFIs – Section 15
12. Maintenance/Operation of Bank
Accounts
Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 5
13. Maintenance & Update of Trust Finance
Procedures
Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 1
14. Implementation of Internal and External
Audit Recommendations
Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 2
15. Reporting of Incidents to the Police
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
202 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
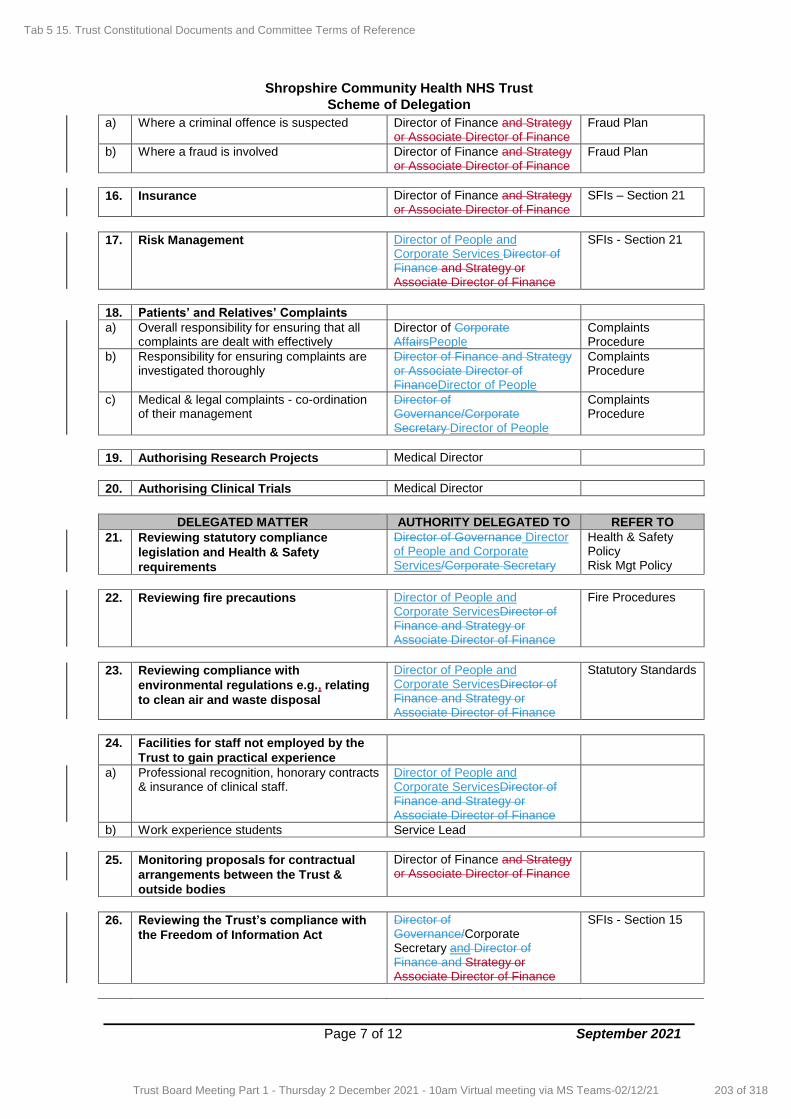
Shropshire Community Health NHS Trust
Scheme of Delegation
Page 7 of 12 September 2021
a) Where a criminal offence is suspected Director of Finance and Strategy or Associate Director of Finance
Fraud Plan
b) Where a fraud is involved Director of Finance and Strategy or Associate Director of Finance
Fraud Plan
16. Insurance Director of Finance and Strategy or Associate Director of Finance
SFIs – Section 21
17. Risk Management Director of People and Corporate Services Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 21
18. Patients’ and Relatives’ Complaints
a) Overall responsibility for ensuring that all complaints are dealt with effectively
Director of Corporate AffairsPeople
Complaints Procedure
b) Responsibility for ensuring complaints are investigated thoroughly
Director of Finance and Strategy or Associate Director of FinanceDirector of People
Complaints Procedure
c) Medical & legal complaints - co-ordination of their management
Director of Governance/Corporate Secretary Director of People
Complaints Procedure
19. Authorising Research Projects Medical Director
20. Authorising Clinical Trials Medical Director
DELEGATED MATTER AUTHORITY DELEGATED TO REFER TO
21. Reviewing statutory compliance
legislation and Health & Safety
requirements
Director of Governance Director of People and Corporate Services/Corporate Secretary
Health & Safety Policy Risk Mgt Policy
22. Reviewing fire precautions Director of People and Corporate ServicesDirector of Finance and Strategy or Associate Director of Finance
Fire Procedures
23. Reviewing compliance with
environmental regulations e.g., relating
to clean air and waste disposal
Director of People and Corporate ServicesDirector of Finance and Strategy or Associate Director of Finance
Statutory Standards
24. Facilities for staff not employed by the
Trust to gain practical experience
a) Professional recognition, honorary contracts & insurance of clinical staff.
Director of People and Corporate ServicesDirector of Finance and Strategy or Associate Director of Finance
b) Work experience students Service Lead
25. Monitoring proposals for contractual
arrangements between the Trust &
outside bodies
Director of Finance and Strategy or Associate Director of Finance
26. Reviewing the Trust’s compliance with
the Freedom of Information Act
Director of Governance/Corporate Secretary and Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 15
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
203 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
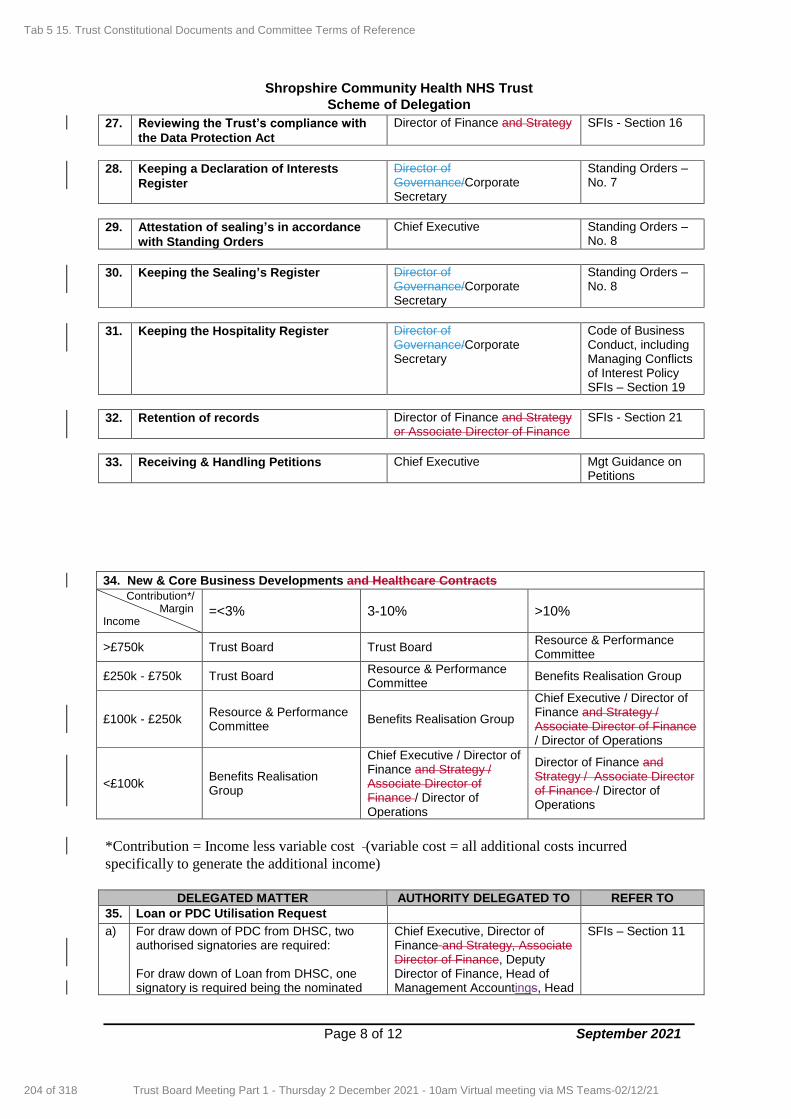
Shropshire Community Health NHS Trust
Scheme of Delegation
Page 8 of 12 September 2021
27. Reviewing the Trust’s compliance with
the Data Protection Act
Director of Finance and Strategy SFIs - Section 16
28. Keeping a Declaration of Interests
Register
Director of Governance/Corporate Secretary
Standing Orders – No. 7
29. Attestation of sealing’s in accordance
with Standing Orders
Chief Executive Standing Orders – No. 8
30. Keeping the Sealing’s Register Director of Governance/Corporate Secretary
Standing Orders – No. 8
31. Keeping the Hospitality Register Director of Governance/Corporate Secretary
Code of Business Conduct, including Managing Conflicts of Interest Policy SFIs – Section 19
32. Retention of records Director of Finance and Strategy or Associate Director of Finance
SFIs - Section 21
33. Receiving & Handling Petitions Chief Executive Mgt Guidance on Petitions
34. New & Core Business Developments and Healthcare Contracts
Contribution*/ Margin Income
=<3% 3-10% >10%
>£750k Trust Board Trust Board Resource & Performance Committee
£250k - £750k Trust Board Resource & Performance Committee
Benefits Realisation Group
£100k - £250k Resource & Performance Committee
Benefits Realisation Group
Chief Executive / Director of Finance and Strategy / Associate Director of Finance / Director of Operations
<£100k Benefits Realisation Group
Chief Executive / Director of Finance and Strategy / Associate Director of Finance / Director of Operations
Director of Finance and Strategy / Associate Director of Finance / Director of Operations
*Contribution = Income less variable cost (variable cost = all additional costs incurred
specifically to generate the additional income)
DELEGATED MATTER AUTHORITY DELEGATED TO REFER TO
35. Loan or PDC Utilisation Request
a)
For draw down of PDC from DHSC, two authorised signatories are required: For draw down of Loan from DHSC, one signatory is required being the nominated
Chief Executive, Director of Finance and Strategy, Associate Director of Finance, Deputy Director of Finance, Head of Management Accountings, Head
SFIs – Section 11
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
204 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21

Shropshire Community Health NHS Trust
Scheme of Delegation
Page 9 of 12 September 2021
representative as stated in the board minute. of Financial Accountings, Head of Costing & Contracting.
Note In all cases where amounts are higher than those listed in the Scheme of Delegation, approval must be by the Board.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
205 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
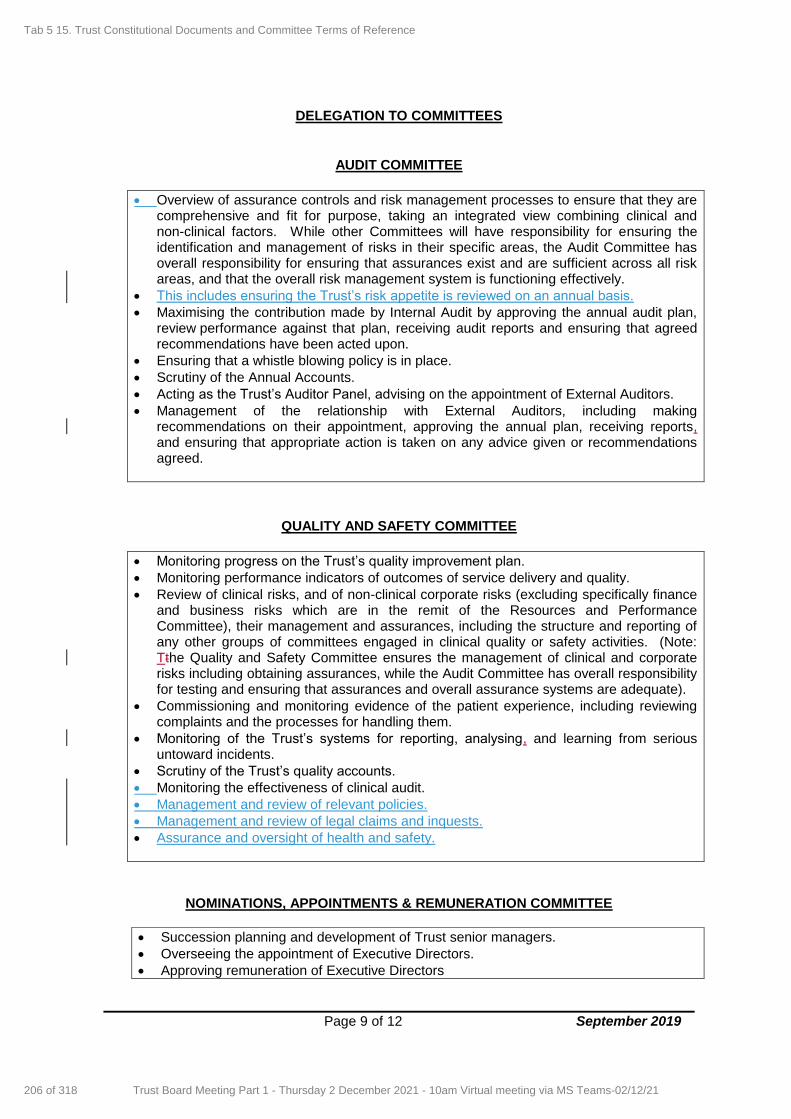
Page 9 of 12 September 2019
DELEGATION TO COMMITTEES
AUDIT COMMITTEE
Overview of assurance controls and risk management processes to ensure that they are comprehensive and fit for purpose, taking an integrated view combining clinical and non-clinical factors. While other Committees will have responsibility for ensuring the identification and management of risks in their specific areas, the Audit Committee has overall responsibility for ensuring that assurances exist and are sufficient across all risk areas, and that the overall risk management system is functioning effectively.
This includes ensuring the Trust’s risk appetite is reviewed on an annual basis.
Maximising the contribution made by Internal Audit by approving the annual audit plan, review performance against that plan, receiving audit reports and ensuring that agreed recommendations have been acted upon.
Ensuring that a whistle blowing policy is in place.
Scrutiny of the Annual Accounts.
Acting as the Trust’s Auditor Panel, advising on the appointment of External Auditors.
Management of the relationship with External Auditors, including making recommendations on their appointment, approving the annual plan, receiving reports, and ensuring that appropriate action is taken on any advice given or recommendations agreed.
QUALITY AND SAFETY COMMITTEE
Monitoring progress on the Trust’s quality improvement plan.
Monitoring performance indicators of outcomes of service delivery and quality.
Review of clinical risks, and of non-clinical corporate risks (excluding specifically finance and business risks which are in the remit of the Resources and Performance Committee), their management and assurances, including the structure and reporting of any other groups of committees engaged in clinical quality or safety activities. (Note: Tthe Quality and Safety Committee ensures the management of clinical and corporate risks including obtaining assurances, while the Audit Committee has overall responsibility for testing and ensuring that assurances and overall assurance systems are adequate).
Commissioning and monitoring evidence of the patient experience, including reviewing complaints and the processes for handling them.
Monitoring of the Trust’s systems for reporting, analysing, and learning from serious untoward incidents.
Scrutiny of the Trust’s quality accounts.
Monitoring the effectiveness of clinical audit.
Management and review of relevant policies.
Management and review of legal claims and inquests.
Assurance and oversight of health and safety.
NOMINATIONS, APPOINTMENTS & REMUNERATION COMMITTEE
Succession planning and development of Trust senior managers.
Overseeing the appointment of Executive Directors.
Approving remuneration of Executive Directors
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
206 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21

Shropshire Community Health NHS Trust
Scheme of Delegation
Page 2 of 12 September 2021
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
207 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
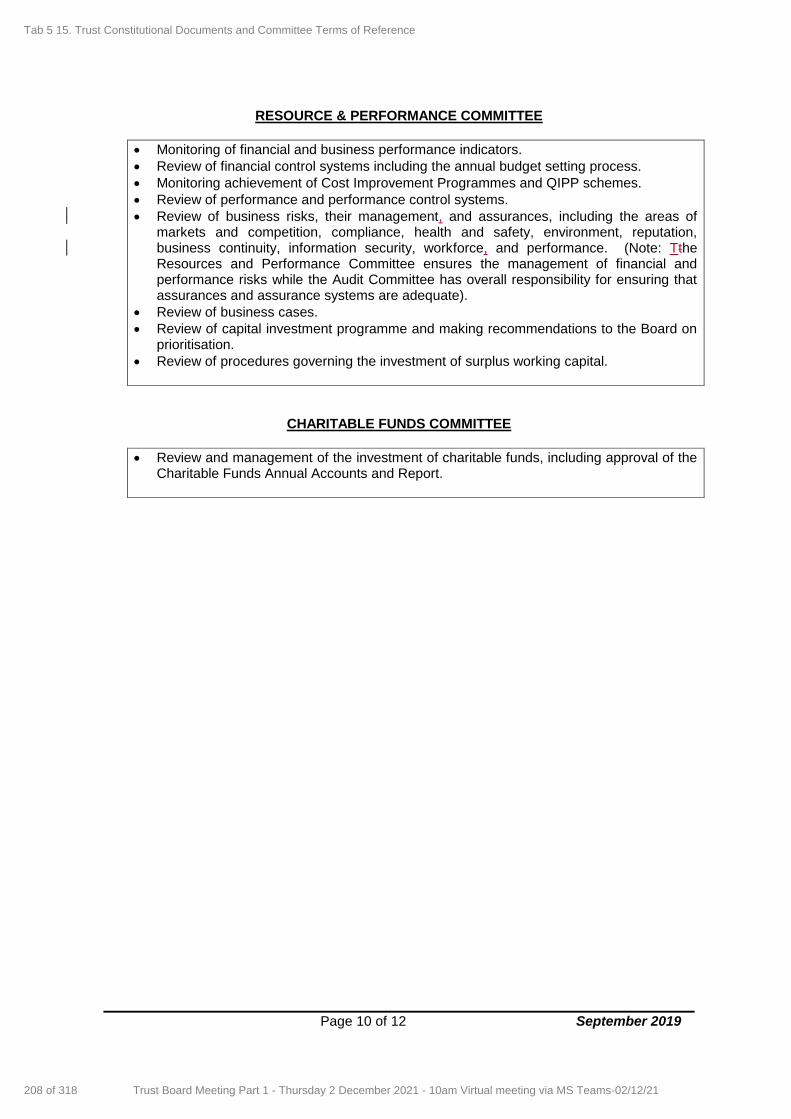
Page 10 of 12 September 2019
RESOURCE & PERFORMANCE COMMITTEE
Monitoring of financial and business performance indicators.
Review of financial control systems including the annual budget setting process.
Monitoring achievement of Cost Improvement Programmes and QIPP schemes.
Review of performance and performance control systems.
Review of business risks, their management, and assurances, including the areas of markets and competition, compliance, health and safety, environment, reputation, business continuity, information security, workforce, and performance. (Note: Tthe Resources and Performance Committee ensures the management of financial and performance risks while the Audit Committee has overall responsibility for ensuring that assurances and assurance systems are adequate).
Review of business cases.
Review of capital investment programme and making recommendations to the Board on prioritisation.
Review of procedures governing the investment of surplus working capital.
CHARITABLE FUNDS COMMITTEE
Review and management of the investment of charitable funds, including approval of the Charitable Funds Annual Accounts and Report.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
208 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
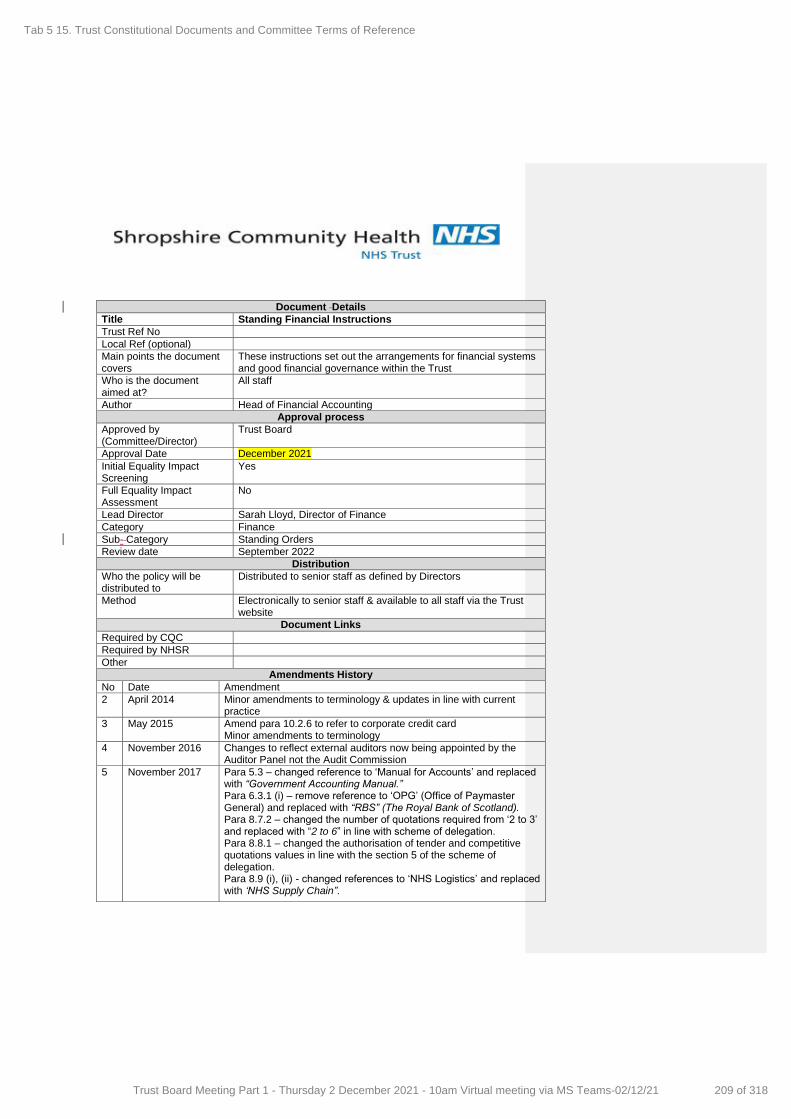
Document Details
Title Standing Financial Instructions
Trust Ref No
Local Ref (optional)
Main points the document covers
These instructions set out the arrangements for financial systems and good financial governance within the Trust
Who is the document aimed at?
All staff
Author Head of Financial Accounting
Approval process
Approved by (Committee/Director)
Trust Board
Approval Date December 2021
Initial Equality Impact Screening
Yes
Full Equality Impact Assessment
No
Lead Director Sarah Lloyd, Director of Finance
Category Finance
Sub- Category Standing Orders
Review date September 2022
Distribution
Who the policy will be distributed to
Distributed to senior staff as defined by Directors
Method Electronically to senior staff & available to all staff via the Trust website
Document Links
Required by CQC
Required by NHSR
Other
Amendments History
No Date Amendment
2 April 2014 Minor amendments to terminology & updates in line with current practice
3 May 2015 Amend para 10.2.6 to refer to corporate credit card Minor amendments to terminology
4 November 2016 Changes to reflect external auditors now being appointed by the Auditor Panel not the Audit Commission
5 November 2017 Para 5.3 – changed reference to ‘Manual for Accounts’ and replaced with “Government Accounting Manual.” Para 6.3.1 (i) – remove reference to ‘OPG’ (Office of Paymaster General) and replaced with “RBS” (The Royal Bank of Scotland). Para 8.7.2 – changed the number of quotations required from ‘2 to 3’ and replaced with “2 to 6” in line with scheme of delegation. Para 8.8.1 – changed the authorisation of tender and competitive quotations values in line with the section 5 of the scheme of delegation. Para 8.9 (i), (ii) - changed references to ‘NHS Logistics’ and replaced with ‘NHS Supply Chain”.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
209 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 1
Policies, Procedures, Guidelines and Protocols
6 September 2018 Para 13.1.5 - add requirement that loan utilisation request requires one signature and stated in the board minute. Para 13.1.7 – new NHSI PDC draw down signatory requirement. Changed references to ‘NHS Litigation Authority’ to ‘NHS Resolution’ instead. Removed para 22 payments to independent contractors as it is not applicable. Added ‘Associate Director of Finance’ alongside Director of Finance, Para 1.2.11 explains the authority level of the Associate Director of Finance.
7 September 2019 Removed Section 3 and 10 as not relevant. Minor amendments to terminology Replaced NHS Act 1977 with NHS Act 2006 throughout. Removed NHS Protect and replaced with the NHS Counter Fraud Authority Removed PASA and replaced with NHS Supply Chain Removed reference to Healthcare Commission and Standards of Better Healthcare as now CQC. Replaced reference to Standards of Business conduct as guidance replaced by Managing Conflicts of Interest in the NHS. Replaced a number ofa few Acts in 7.6.9 (ii) as now within Equality Act 2010. Replaced Deputy Director of Finance with Head of Finance. Changed Data Protection Act 1998 to Data Protection Act 2018 Added para 6.1.3 on due diligence checks for new customers per Internal Audit recommendation. Added to para 10.2.6 (vi) to exempt off-framework emergency agency staff from an official order as agreed by the Agency Working Group and changed per recommendation from Internal Audit.
8 September 2020 Change NHS Improvement (NHSI) to NHS Improvement/England (NHSI/E). Para 10.2.6(vi) added exemption for using an official order for goods, services or works that causes a reduction in financial control and/or an increase in processing time. Minor changes to terminology.
9 September 2021 Replaced Director of Finance and Strategy with Director of Finance Removed Associate Director Finance Updated section 2.5 on Arrangements for Anti-Fraud, Bribery and Corruption per Lead Local Counter Fraud Specialist
Updated section 2.6 on Security Management per Local Security
Management Specialist review Minor grammatical amendments
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
210 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 2
CONTENTS
Section Page 1. INTRODUCTION 3 2. AUDIT 8 3 ALLOCATIONS, PLANNING, BUDGETS, BUDGETARY CONTROL & MONITORING 14 4 ANNUAL ACCOUNTS & REPORTS 17 5. BANK & GBS ACCOUNTS 18 6. INCOME, FEES & CHARGES & SECURITY OF CASH, CHEQUES & OTHER NEGOTIABLE INSTRUMENT 20 7. TENDERING & CONTRACT PROCEDURE 22 8. NHS SERVICE AGREEMENTS FOR PROVISION OF SERVICES 35
9. TERMS OF SERVICE, ALLOWANCES & PAYMENT OF MEMBERS OF THE TRUST BOARD & EMPLOYEES 36 10. NON-PAY EXPENDITURE 40 11. EXTERNAL BORROWING & INVESTMENTS 45 12. FINANCIAL FRAMEWORK 47 13. CAPITAL INVESTMENT, PRIVATE FINANCING, FIXED ASSET REGISTERS & SECURITY OF ASSETS 48 14. STORES & RECEIPT OF GOODS 52 15. DISPOSALS & CONDEMNATIONS, LOSSES & SPECIAL PAYMENTS 54 16. INFORMATION TECHNOLOGY 56 17. PATIENTS' PROPERTY 59 18. FUNDS HELD ON TRUST 60 19. ACCEPTANCE OF GIFTS BY STAFF & LINK TO STANDARDS OF BUSINESS CONDUCT 61 20. RETENTION OF RECORDS 62 21. RISK MANAGEMENT & INSURANCE 63
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
211 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 3
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
212 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 4
1. INTRODUCTION 1.1. General
1.1.1. These Standing Financial Instructions (SFIs) are issued in accordance with the Trust (Functions) Directions 2000 issued by the Secretary of State which require that each Trust shall agree SFIs for the regulation of the conduct of its members and officers in relation to all financial matters with which they are concerned. They shall have effect as if incorporated in the Standing Orders.
1.1.2 These SFIs detail the financial responsibilities, policies and
procedures adopted by the Trust. They are designed to ensure that the Trust's financial transactions are carried out in accordance with the law and Government policy in order to achieve probity, accuracy, economy, efficiency, and effectiveness. They should be used in conjunction with the Scheme of Reservation and the Scheme of Delegation adopted by the Trust.
1.1.3 These SFIs identify the financial responsibilities, which apply to
everyone working for the Trust and its constituent organisations including trading units. They do not provide detailed procedural advice and should be read in conjunction with the detailed departmental and financial procedure notes. All financial procedures must be approved by the Director of Finance and Strategy or Associate Director of Finance.
1.1.4. Should any difficulties arise regarding the interpretation or application
of any of the SFIs then the advice of the Director of Finance and Strategy or Associate Director of Finance must be sought before acting. The user of these SFIs should also be familiar with and comply with the provisions of the Trust’s Standing Orders.
1.1.5. Failure to comply with SFIs and Standing Orders can in certain
circumstances be regarded as a disciplinary matter that could result in dismissal.
1.1.6. Overriding SFIs – if for any reason these SFIs are not complied with,
full details of the non-compliance and any justification for non-compliance and the circumstances around the non-compliance shall be reported to the next formal meeting of the Audit Committee for referring action or ratification. All members of the Board and staff have a duty to disclose any non-compliance with these SFIs to the Director of Finance and Strategy or Associate Director of Finance as soon as possible.
1.2. Interpretation and Definitions
1.2.1 "Accountable Officer" means the NHS Officer responsible and
accountable for funds entrusted to the Trust. The officer shall be responsible for ensuring the proper stewardship of public funds and assets. For this Trust it shall be the Chief Executive.
Formatted: Highlight
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
213 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 5
1.2.2 "Trust" means the Shropshire Community Health NHS Trust.
1.2.3 "Board" means the Chair, executive Directors, and non-executive
Directors of the Trust collectively as a body.
1.2.4 "Budget" means a resource, expressed in financial terms, proposed by the Board for the purpose of carrying out, for a specific period, any, or all of the functions of the Trust.
1.2.5 “Director” means the Director with delegated authority to manage
finances (income and expenditure) for a specific area of the organisation.
1.2.6 “Budget Manager” means second level delegation by a Director to
another Senior Manager. They can either be an employee of the Trust or of another organisation and be authorised by the Director.
1.2.7 “Resource Manager” means third level delegation by a Budget
Manager to another Senior Manager. They can either be an employee of the Trust or of another organisation and be authorised by the Director.
1.2.8 “Service Lead” means an officer who has delegated responsibility
from a Resource Manager for the day-to-day management of a defined budget. They can either be an employee of the Trust or of another organisation and be authorised by the Director.
1.2.9 "Chair of the Board (or Trust)" is the person appointed by the
Secretary of State for Health to lead the Board and to ensure that it successfully discharges its overall responsibility for the Trust as a whole. The expression “the Chair of the Trust” shall be deemed to include the Vice-Chair of the Trust if the Chair is absent from the meeting or is otherwise unavailable.
1.2.10 "Chief Executive" means the chief officer of the Trust. 1.2.11 "Director of Finance and Strategy" or “Associate Director of
Finance” meansFinance” means the chief financial officer of the Trust.
1.2.12 "Quality & Safety Committee"”Clinical Governance Committee” means a the committee whose functions are concerned with the arrangements for the purpose of monitoring and improving the quality of health care for which the Trust has responsibility.
1.2.13 "Commissioning" means the process for determining the need for
and for obtaining the supply of healthcare and related services by the Trust within available resources.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
214 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 6
1.2.14 "Committee" means a committee or sub-committee created and appointed by the Trust.
1.2.15 "Committee members" means persons formally appointed by the
Board to sit onbe members of or to chair specific committees.
1.2.16 "Contracting and procuring" means the systems for obtaining the supply of goods, materials, manufactured items, services, building and engineering services, works of construction and maintenance and for disposal of surplus and obsolete assets.
1.2.17 “Funds Held on Trust” means those funds which the Trust holds on
date of incorporation, receives on distribution by statutory instrument or chooses subsequently to accept under powers derived under Part 11 (eleven) of the NHS Act 2006. Such funds may or may not be charitable.
1.2.18 "Member" means Executive or Non-Executive Director of the Board
as the context permits. Member in relation to the Board does not include its Chair.
1.2.19 “Associate Member” means a person appointed to perform specific
statutory and non-statutory duties which have been delegated by the Trust Board for them to perform and these duties have been recorded in an appropriate Trust Board minute or other suitable record.
1.2.20 "Membership, Procedure and Administration Arrangements
Regulations" means NHS Membership and Procedure Regulations (SI 1990/2024) and subsequent amendments.
1.2.21 "Nominated officer" means an officer charged with the responsibility
for discharging specific tasks within Standing Orders and Standing Financial Instructions.
1.2.22 "Non-executive member" means a member of the Trust who is not
a Director of the Trust and is not to be treated as an officer by virtue of regulation 1(3) of the Membership, Procedure and Administration Arrangements Regulations.
1.2.23 "Officer" means employee of the Trust or any other person holding a
paid appointment or office with the Trust. 1.2.24 "Officer member" means a member of the Trust who is either an
officer of the Trust or is to be treated as an officer by virtue of regulation 1(3) (i.e., the Chair of the Trust or any person nominated by such a Committee for appointment as a Trust member).
1.2.25 "Secretary" means a person appointed to act independently of the
Board to provide advice on corporate governance issues to the Board and the Chair and monitor the Trust's compliance with the law, Standing Orders, and Department of Health guidance.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
215 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 7
1.2.26 "SFIs" means Standing Financial Instructions.
1.2.27 "SOs" mean Standing Orders.
1.2.28 “Vice-Chair" means the Non-Executive Director appointed by the Board to take on the Chair’s duties if the Chair is absent for any reason.
1.2.29 Wherever the title Chief Executive, Director of Finance and Strategy
or Associate Director of Finance, or other nominated officer is used in these instructions, it shall be deemed to include such other Director or employees who have been duly authorised to represent them. This will include officers from another NHS organisation where shared service arrangements are in place.
1.2.30 Wherever the term "employee" is used and where the context permits
it shall be deemed to include employees of third parties contracted to the Trust when acting on behalf of the Trust.
1.3. Responsibilities and Delegation
1.3.1. The Trust Board The Board exercises financial supervision and control by: (i) formulating the financial strategy; (ii) requiring the submission and approval of budgets within an
approved control total, (iii) defining and approving essential features in respect of
important procedures and financial systems (including the need to obtain value for money),
(iv) defining specific responsibilities placed on members of the Board and employees as indicated in the Scheme of Delegation document.
1.3.2. The Board has resolved that certain powers and decisions may only
be exercised by the Board in formal session. These are set out in the “Scheme of Reservation” document. All other powers have been delegated to such other Committees as the Trust has established.
1.3.3. The Chief Executive and, Director of Finance and Strategy and
Associate Director of Finance The Chief Executive and, Director of Finance and Strategy and
Associate Director of Finance will, as far as possible, delegate their detailed responsibilities, but they remain accountable for financial control. Within the SFIs, it is acknowledged that the Chief Executive is ultimately accountable to the Board and, as Accountable Officer, to the Secretary of State, for ensuring that the Board meets its obligation to perform its functions within the available financial resources. The Chief Executive has overall executive responsibility for the Trust’s activities, is responsible to the Chair and the Board for ensuring that its financial obligations and targets are met and has overall responsibility for the Trust’s system of internal control.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
216 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 8
1.3.4. It is a duty of the Chief Executive to ensure that members of the Board and employees and all new appointees are notified of, and put in a position to understand, their responsibilities within these Instructions.
1.3.5. The Director of Finance and Strategy and the Associate Director of Finance The Director of Finance and Strategy and the Associate Director of Finance are is responsible for: (i) implementing the Trust’s financial policies and for co-
ordinating any corrective action necessary to further these policies,
(ii) maintaining an effective system of internal financial control including ensuring that detailed financial procedures and systems incorporating the principles of separation of duties and internal checks are prepared, documented and maintained to supplement these instructions,
(iii) ensuring that sufficient records are maintained to show and explain the Trust’s transactions, in order to disclose, with reasonable accuracy, the financial position of the Trust at any time.
In addition, without prejudice to any other functions of the Trust, and
employees of the Trust, the duties of the Director of Finance and Strategy and Associate Director of Finance include: (iv) the provision of financial advice to other members of the
Board and employees, (v) the design, implementation, and supervision of systems of
internal financial control, (vi) the preparation and maintenance of such accounts,
certificates, estimates, records, and reports as the Trust may require for the purpose of carrying out its statutory duties.
1.3.6. Board Members and Employees
All members of the Board and employees, severally and collectively, are responsible for:
(i) the security of the property of the Trust, (ii) avoiding loss, (iii) exercising economy and efficiency in the use of resources, (iv) conforming with the requirements of Standing Orders, SFIs,
Financial Procedures and the Scheme of Delegation.
1.3.7. Contractors and their Employees Any contractor or employee of a contractor who is empowered by the Trust to commit the Trust to expenditure or who is authorised to obtain income shall be covered by these instructions. It is the responsibility of the Chief Executive to ensure that such persons are made aware of this.
1.3.8. For all members of the Board and any employees who carry out a
financial function, the form in which financial records are kept, and
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
217 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 9
the way manner in which members of the Board and employees discharge their duties, must be to the satisfaction of the Director of Finance and Strategy or Associate Director of Finance.
2. AUDIT 2.1. Audit Committee
2.1.1 An independent Audit Committee is a central means by which a Board ensures effective internal control arrangements are in place. In accordance with Standing Orders the Board shall formally establish an Audit Committee, with clearly defined terms of reference and following guidance from the NHS Audit Committee Handbook (2018) to perform the following tasks: -
(i) Ensuring there is an effective Internal Audit function
established by management, that meets mandatory NHS Internal Audit Standards and provides appropriate independent assurance to the Audit Committee, Chief Executive and Board,
(ii) Acting as the Trust’s Auditor Panel (the main function being to
advise on the appointment of external auditors), reviewing the work and findings of the external auditors and considering the implications of and management’s responses to their work,
(iii) Reviewing the findings of other significant assurance
functions, both internal and external to the organisation, and considering the implications for the governance of the organisation,
(iv) Ensuring that the systems for financial reporting to the Board,
including those of budgetary control, are subject to review as to completeness and accuracy of the information provided to the Board,
(v) Reviewing financial and information systems and monitoring
the integrity of the financial statements and reviewing significant financial reporting judgments,
(vi) Reviewing the establishment and maintenance of an effective
system of integrated governance, risk management and internal control, across the whole of the organisation’s activities (both clinical and non-clinical), that supports the achievement of the organisation’s objectives,
(vii) Monitoring compliance with Standing Orders and SFI, (viii) Reviewing schedules of losses and compensations and
making recommendations to the Board, (ix) Reviewing the Annual Report and annual financial statements
and recommending their approval to the Board,
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
218 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 10
(x) Reviewing the External Auditors report on the financial
statements and the annual management letter, (xi) Reviewing any incident of fraud or corruption or possible
breach of ethical standards or legal or statutory requirements that could have a significant impact on the Trust’s published financial accounts or reputation,
(xii) Reviewing major findings from Internal and External Audit
reports and ensure appropriate action is taken, (xiii) Reviewing “value for money” audits reporting on the
effectiveness and efficiency of the selected departments or activities,
(xiv) Reviewing the mechanisms and levels of authority (e.g.,
Standing Orders, SFIs, Delegated Limits) and make recommendations to the Trust Board,
(xv) Reviewing the scope of both Internal and External Audit
including the agreement on the number of audits per year for approval by the Trust Board,
(xvi) Reviewing waivers to Standing Orders, (xvii) Reviewing hospitality and sponsorship registers, (xviii) Reviewing the information prepared to support the controls
assurance statements prepared on behalf of the Board and advising the Board accordingly.
(xix) Reviewing all appropriate security management related
issues.
2.1.2 The minutes of the Audit Committee meetings shall be formally recorded by the Trust Secretary and submitted to the Board. The Chair of the Committee shall draw to the attention of the Board any issues that require disclosure to the full Board or require executive action. The Committee will report to the Board annually on its work in support of the Statement of Internal Control, specifically commenting on the fitness for purpose of the Assurance Framework, the completeness and embeddedness of risk management in the organisation, the integration of governance arrangements and the appropriateness of the self-assessment against the Key Lines of Enquiry (KLOEs) inspected by CQC.
2.1.3 Where the Audit Committee considers there is evidence of ultra vires
transactions, evidence of improper acts, or if there are other important matters that the Committee wishes to raise, the Chair of the Audit Committee should raise the matter at a full meeting of the Board.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
219 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 11
Exceptionally, the matter may need to be referred to the Department of Health.
2.2 Director of Finance and Strategy and Associate Director of Finance
2.2.1 The Director of Finance and Strategy and the Associate Director of Finance are is responsible for:
(i) ensuring there are arrangements to review, evaluate and report on the effectiveness of internal financial control including the establishment of an effective Internal Audit function,
(ii) ensuring that the Internal Audit function meets the NHS mandatory audit standards and provides sufficient independent and objective assurance to the Audit Committee and the Accountable Officer,
(iii) deciding at what stage to involve the police in cases of misappropriation and other irregularities not involving fraud or corruption,
(iv) ensuring that an annual Internal Audit report is prepared for the consideration of the Audit Committee and the Board. The report must cover:
a clear opinion on the effectiveness of internal control in accordance with current assurance framework guidance issued by the Department of Health including for example compliance with control criteria and standards,
major internal financial control weaknesses discovered,
progress on the implementation of Internal Audit recommendations,
progress against plan over the previous year,
strategic audit plan covering the coming three years,
a detailed plan for the coming year.
2.2.2 The Director of Finance and Strategy or Associate Director of Finance or designated Internal or External Auditors are entitled without necessarily giving prior notice to require and receive:
(i) access to all records, documents and correspondence relating
to any financial or other relevant transactions, including documents of a confidential nature,
(ii) access at all reasonable times to any land, premises or
members of the Board or employee of the Trust,
(iii) the production of any cash, stores, or other property of the Trust under a member of the Board and or an employee’s control,
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
220 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 12
(iv) explanations concerning any matter under investigation.
2.3. Role of Internal Audit 2.3.1 Internal Audit is an independent and objective appraisal service within
an organisation which provides: (i) an independent and objective opinion to the Accountable
Officer, the Board, and the Audit Committee on the degree to which risk management, control, and governance, support the achievement of the organisation’s agreed objectives,
(ii) an independent and objective consultancy service specifically
to help line management improve the organisation’s risk management, control, and governance arrangements.
2.3.2 Internal Audit will review, appraise, and report upon policies,
procedures, and operations in place to: (i) establish and monitor the achievement of the organisation’s
objectives,
(ii) identify, assess, and manage the risks to achieving the organisation’s objectives,
(iii) ensure the economical, effective, and efficient use of
resources, (iv) ensure compliance with established policies (including
behavioural and ethical expectations), procedures, laws, and regulations,
(v) safeguard the organisation’s assets and interests from losses
of all kinds, including those arising from fraud, irregularity, or corruption,
(vi) ensure the integrity and reliability of information, accounts,
and data, including internal and external reporting and accountability processes.
2.3.3 The Head of Internal Audit will provide to the Audit Committee:
(i) a risk-based plan of Internal Audit work, agreed with
management and approved by the Audit Committee, based upon the management’s Assurance Framework that will enable the auditors to collect sufficient evidence to give an opinion on the adequacy and effective operation of the organisation,
(ii) regular updates on the progress against plan,
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
221 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 13
(iii) reports of management’s progress on the implementation of
action agreed as a result of Internal Audit findings, (iv) an annual opinion based upon and limited to the work
performed, on the overall adequacy and effectiveness of the organisation’s risk management, control, and governance processes (i.e., the organisation’s system of internal control). This opinion is used by the Board to inform the Statement of Internal Control,
(v) additional reports as requested by the Audit Committee.
2.3.4 Whenever any matter arises which involves, or is thought to involve,
irregularities concerning cash, stores, or other property or any suspected irregularity in the exercise of any function of a pecuniary nature, the Director of Finance and Strategy or Associate Director of Finance must be notified immediately.
2.3.5 The Head of Internal Audit will normally attend Audit Committee
meetings and has a right of access to all Audit Committee members, the Chair and Chief Executive of the Trust.
2.3.6 The Head of Internal Audit reports to the Audit Committee and is
managed by the Director of Finance and Strategy and the Associate Director of Finance. The reporting system for Internal Audit shall be agreed between the Director of Finance and Strategy or Associate Director of Finance, the Audit Committee and the Head of Internal Audit. The agreement shall be in writing and shall comply with the guidance on reporting contained in the NHS Internal Audit Standards. The reporting system shall be reviewed at least every three years.
2.3.7 The appointment and termination of the Head of Internal Audit and/or
the Internal Audit Service must be approved by the Audit Committee. 2.4 External Audit
2.4.1 The External Auditor is appointed by the Audit Committee acting as the Auditor Panel. The Audit Committee must ensure a cost effective and efficient service. If there are any problems relating to the service provided by the External Auditor, then this should be raised with them.
2.5 Arrangements for Anti-Fraud, Bribery and Corruption 2.5.1 Finance Under the NHS Standard Contract, the Trust are required to
put in place and maintain appropriate arrangements to address counter fraud issues having regard to the NHS Counter Fraud Authority Standards for NHS Providers. The clauses relating to counter-fraud are set out in Service Condition 24 of the contract. As a consequenceConsequently, and in line with their responsibilities, the Trust Chief Executive and, Director of Finance and Strategy and
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
222 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 14
Associate Director of Finance shall monitor and ensure compliance with the NHS Standard Contract and the NHS Counter Fraud Authority Standards for NHS Providers.
2.5.2 The Trust shall nominate a suitable person (who is accredited) to
carry out the duties of the Lead Local Counter Fraud Specialist (LCFS) as specified by the NHS Counter Fraud Authority NHS Counter Fraud Manual, Standards for NHS Providers, and other guidance published. The Lead LCFS has access to the audit committee and audit chair as may be required.
The Trust shall nominate a suitable person as the Trust Anti- Fraud
Champion to provide support at a Strategic level to the Lead LCFS. The Trust may appoint more than one anti-fraud champion but will appoint at least one person to the role.
2.5.3 The Lead LCFS shall report to and is managed by the Trusts Director of Finance and Strategy and Associate Director of Finance and shall work with staff in the NHS Counter Fraud Authority in accordance with the NHS Counter Fraud Authority NHS Counter Fraud Manual, NHS CFA Standards for NHS Providers under the Functional Standard GovS 013: Counter Fraud (Functional Standards), and other guidance published.
2.5.4 The NHS Counter Fraud Authority requires the Trust to provide an
annual statement of assurance against the fraud, bribery, and corruption under the NHS CFA Standards for NHS Providers under the Functional Standard GovS 013: Counter Fraud (Functional Standards). This statement of assurance is provided through the completion and submission of an online self-assessment against the Functional Standards. The online form is completed for the Trust by the Lead LCFS and it is required to be signed off by both the Director of Finance and the Chair of the Audit Committee before a submission can be made to NHS CFA. Standards for NHS Providers. This statement of assurance is provided through the completion of a Self-Review Tool.
2.5.5 The Lead LCFS Local Counter Fraud Specialist will provide a written
progress report, at least annually, on counter fraud work within the Trust.
2.6 Security Management 2.6.1 The Trust are required under Service Condition 24 of the NHS
Standard Contract to have put in place and maintain appropriate arrangements to address all security management related issues, having regard to previously published NHS security management standards (Standards for Providers), and other all appropriate guidance issued.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
223 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 15
2.6.2 In line with previously published Standards for Providers and other guidance, Tthe Chief Executive has overall responsibility for controlling and coordinating security. However, these tasks are delegated to the Trust Director of Finance and Strategy and Associate Director of Finance in the role of Security Management Director, who shall monitor and ensure compliance with the previously published Standards for Providers, and other guidance issued.
2.6.3 The Trust shall nominate a suitable accredited person to carry out the
duties of the Local Security Management Specialist (LSMS), taking into account previously published guidance on NHS Security Management.
2.6.4 The Local Security Management Specialist shall report to the Trust
Director of Finance on all security related matters and Strategy and Associate Director of Finance in accordance with the previously published Standards for Providers, and other guidance issued
2.6.5 The Local Security Management Specialist LSMS will provide a
written report, at least annually, on security management work within the Trust.
3. ALLOCATIONS, PLANNING, BUDGETS, BUDGETARY CONTROL AND
MONITORING
3.1. Preparation and Approval of Plans and Budgets
3.1.1. The Chief Executive will compile and submit to the Board a Local Delivery Plan (LDP) which takes into accountconsiders financial targets and forecast limits of available resources. The plan will contain:
(i) a statement of the significant assumptions on which the plan
is based, (ii) details of major changes in workload, delivery of services or
resources required to achieve the plan.
3.1.2. Prior to the start of the financial year the Director of Finance and Strategy or Associate Director of Finance will, on behalf of the Chief Executive, prepare and submit budgets for approval by the Board. Such budgets will:
(i) be in accordance with the aims and objectives set out in the
LDP,
(ii) accord with workload and manpower plans;
(iii) be produced following discussion with appropriate budget managers;
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
224 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 16
(iv) be prepared within the limits of available funds; (v) identify potential risks.
3.1.3. The Director of Finance and Strategy or Associate Director of Finance shall monitor financial performance against budget and plan, periodically review them, and report to the Board.
3.1.4. All budget managers must provide information as required by the
Director of Finance and Strategy and Associate Director of Finance to enable budgets to be compiled.
3.1.5 All budget managers will sign up to their allocated budgets at the
commencement of each financial year.
3.1.6. The Director of Finance and Strategy and Associate Director of Finance hasve a responsibility to ensure that adequate training is delivered on an on-going basis to budget managers to help them manage effectively.
3.2. Budgetary Delegation
3.2.1. The Chief Executive may delegate the management of a budget to
permit the performance of a defined range of activities. This delegation must be in writing and be accompanied by a clear definition of:
(i) the amount of the budget, (ii) the purpose(s) of each budget heading, (iii) individual and group responsibilities, (iv) authority to exercise virement,
(v) achievement of planned levels of service, (vi) the provision of regular reports.
3.2.2. The Chief Executive and delegated budget managers must not
exceed the budgetary total or virement limits set by the Board.
3.2.3. Any budgeted funds not required for their designated purpose(s) revert to the immediate control of the Chief Executive, subject to any authorised use of virement.
3.2.4. Non-recurring budgets should not be used to finance recurring
expenditure without the authority in writing of the Chief Executive, as advised by the Director of Finance and Strategy or Associate Director of Finance.
3.3. Budgetary Control and Reporting
3.3.1. The Director of Finance and Strategy or Associate Director of Finance
will devise and maintain systems of budgetary control. These will include: -
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
225 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 17
(i) monthly financial reports to the Board in a form approved by
the Board, containing:
income and expenditure to date showing trends and forecast year-end position,
Statement of Financial Position,
movements in cash and capital,
capital projects spend and projected outturn against plan,
explanations of any material variances from plan,
details of any corrective action where necessary, and the Chief Executive’s and/or Director of Finance’s and Strategy or Associate Director of Finance’s view of whether such actions are sufficient to correct the situation.
(ii) the issue of timely, accurate and comprehensible advice and
financial reports to each budget manager, covering the areas for which they are responsible,
(iii) investigation and reporting of variances from financial,
workload and manpower budgets, (iv) monitoring of management action to correct variances; and
(v) arrangements for the authorisation of budget transfers.
3.3.2 Each Budget Manager is responsible for ensuring that: (i) any likely overspending or reduction of income which cannot
be met by virement is not incurred without the prior consent of the Board,
(ii) the amount provided in the approved budget is not used in
whole or in part for any purpose other than that specifically authorised, subject to the rules of virement,
(iii) no permanent employees are appointed without the approval
of the Chief Executive other than those provided for within the available resources and manpower establishment as approved by the Board.
3.3.3. The Chief Executive is responsible for identifying and implementing
cost improvements and income generation initiatives in accordance with the requirements of the Local Delivery Plan and a balanced budget.
3.4 Capital Expenditure
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
226 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 18
3.4.1 The general rules applying to delegation and reporting shall also apply to capital expenditure. (The particular applicationsapplications relating to capital are in SFI No.13).
3.5. Monitoring Returns
3.5.1 The Chief Executive is responsible for ensuring that the appropriate monitoring forms are submitted to the requisite monitoring organisation.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
227 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 19
4. ANNUAL ACCOUNTS AND REPORTS
4.1. The Director of Finance and Strategy or Associate Director of Finance, on behalf of the Trust, will:
(i) prepare financial returns in accordance with the accounting policies
and guidance given by the Department of Health and the Treasury, the Trust’s accounting policies, and generally accepted accounting practice,
(ii) prepare and submit annual financial reports to the Department of
Health certified in accordance with current guidelines,
(iii) submit financial returns to the Department of Health for each financial year in accordance with the timetable prescribed by the Department of Health.
4.2 The Trust’s annual accounts must be audited by an auditor appointed by the
Auditor PanelAudit Committee. The Trust’s audited annual accounts must be presented to a public meeting and made available to the public.
4.3 The Trust will publish an Annual Report, in accordance with guidelines on
local accountability, and present it at a public meeting. The document will comply with the Department of Health’s Group Accounting Manual.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
228 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 20
5. BANK AND GBS ACCOUNTS
5.1. General
5.1.1. The Director of Finance and Strategy and Associate Director of Finance are is responsible for managing the Trust’s banking arrangements and for advising the Trust Board on the provision of banking services and operation of accounts. This advice will take into accountconsider guidance/directions issued from time to time by the Department of Health. In line with “Cash Management in the NHS” Trusts should minimise the use of commercial bank accounts and consider using Government Banking Services (GBS) accounts for all banking services.
5.1.2. The Board shall approve the banking arrangements.
5.2. Bank and GBS Accounts
5.2.1. The Director of Finance and Strategy and Associate Director of
Finance is responsible for:
(i) bank accounts and Government Banking Service (GBS) accounts,
(ii) establishing separate bank accounts for the Trust’s non-
exchequer funds,
(iii) ensuring payments made from bank or GBS accounts do not exceed the amount credited to the account except where arrangements have been made,
(iv) reporting to the Board all arrangements made with the Trust’s
bankers for accounts to be overdrawn,
5.3. Banking Procedures
5.3.1. The Director of Finance and Strategy or Associate Director of Finance
will prepare detailed instructions on the operation of bank and GBS accounts, which must include:
(i) the conditions under which each bank and GBS account is to
be operated; (ii) those authorised to sign cheques or other orders drawn on the
Trust’s accounts,
5.3.2. The Director of Finance and Strategy or Associate Director of Finance
must advise the Trust’s bankers in writing of the conditions under which each account will be operated.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
229 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 21
5.4. Tendering and Review
5.4.1 The Director of Finance and Strategy or Associate Director of Finance will review the commercial banking arrangements of the Trust at regular intervals to ensure they reflect best practice and represent best value for money, by periodically seeking competitive tenders for the Trust’s commercial banking business.
5.4.2 Competitive tenders should be sought at least every 5 years. The
results of the tendering exercise should be reported to the Board. This review is not necessary for GBS accounts.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
230 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 22
6. INCOME, FEES AND CHARGES AND SECURITY OF CASH, CHEQUES AND OTHER NEGOTIABLE INSTRUMENTS
6.1. Income Systems
6.1.1. The Director of Finance and Strategy and Associate Director of
Finance are is responsible for designing, maintaining, and ensuring compliance with systems for the proper recording, invoicing, collecting, and coding of all monies due.
6.1.2. The Director of Finance and Strategy and Associate Director of
Finance are is also responsible for the prompt banking of all monies received.
6.1.3 When creating significant new customers due diligence and
background checks will be carried out.
6.2. Fees and Charges
6.2.1. The Trust shall follow NHS Improvement/England’s advice in the Approved Costing Guidance in informing and setting prices for NHS service agreements.
6.2.2. The Director of Finance and Strategy and Associate Director of
Finance are is responsible for approving and regularly reviewing the level of all fees and charges other than those determined by the Department of Health or by Statute. Independent professional advice on matters of valuation shall be taken as necessary. Where sponsorship income (including items in kind such as subsidised goods or loans of equipment) is considered the guidance in NHS Improvement/England’s Managing Conflicts of Interest in the NHS shall be followed.
6.2.3. All employees must inform the Director of Finance and Strategy or
Associate Director of Finance promptly of money due arising from transactions which they initiate/deal with, including all contracts, leases, tenancy agreements, private patient undertakings and other transactions.
6.3. Debt Recovery
6.3.1. The Director of Finance and Strategy and the Associate Director of
Finance are is responsible for the appropriate recovery action on all outstanding debts.
6.3.2 Income not received should be dealt with in accordance with losses
procedures. 6.3.3 Overpayments should be detected (or preferably prevented) and
recovery initiated.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
231 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 23
6.4 Security of Cash, Cheques and Other Negotiable Instruments
6.4.1. The Director of Finance and Strategy and the Associate Director of Finance are is responsible for:
(i) approving the form of all receipt books, agreement forms, or
other means of officially acknowledging or recording monies received or receivable,
(ii) ordering and securely controlling any such stationery, (iii) the provision of adequate facilities and systems for employees
whose duties include collecting and holding cash, including the provision of safes or lockable cash boxes, the procedures for keys, and for coin operated machines,
(iv) prescribing systems and procedures for handling cash and
negotiable securities on behalf of the Trust.
6.4.2. Official money shall not under any circumstances be used for the encashment of private cheques or IOUs.
6.4.3. All cheques, postal orders, cash etc., shall be banked intact.
Disbursements shall not be made from cash received, except under arrangements approved by the Director of Finance and Strategy or Associate Director of Finance.
6.4.4. The holders of safe keys shall not accept unofficial funds for depositing
in their safes unless such deposits are in special sealed envelopes or locked containers. It shall be made clear to the depositors that the Trust is not to be held liable for any loss, and written indemnities must be obtained from the organisation or individuals absolving the Trust from responsibility for any loss.
6.4.5. To comply with money laundering legislation, under no circumstances
will the Trust accept cash payments in excess of £10,000 in respect of any single transaction. Any attempts by an individual to effect payment above this amount should be notified immediately to the Director of Finance and Strategy or Associate Director of Finance.
6.5 Income Generation
6.5.1 The Director of Finance and Strategy and the Associate Director of Finance are is responsible for carrying out a full financial appraisal of all proposed schemes, and producing documented procedures advising scheme proposers of the correct format for submission, and the factors which will be considered when deciding whether or not to approve an income generation scheme.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
232 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 24
6.5.2 The appropriate Director is responsible for preparing a Memorandum Trading Account in respect of each income generation scheme with a turnover in excess of £50,000.
Formatted: Highlight
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
233 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 25
7. TENDERING AND CONTRACT PROCEDURE
7.1 Duty to comply with Standing Orders and Standing Financial Instructions
7.1.1 The procedure for making all contracts by or on behalf of the Trust
shall comply with these Standing Orders and Standing Financial Instructions (except where Standing Order 3.14 “Suspension of Standing Orders” is applied).
7.2 EU Directives Governing Public Procurement
7.2.1 Directives by the Council of the European Union promulgated by the Department of Health (DH) prescribing procedures for awarding all forms of contracts shall have effect as if incorporated in these Standing Orders and Standing Financial Instructions.
7.3 Reverse E-Auctions
7.3.1 The Trust should have policies and procedures in place for the control of all tendering activity carried out through Reverse E-Auctions. For further guidance on Reverse E-Auctions refer to https://www.gov.uk/guidance/eauctions
7.4 Capital regime, investment and property business case approval guidance and Other NHS Improvement/England Guidance
7.4.1 The Trust shall comply as far as is practicable with the requirements
of NHS Improvement/England’s "Capital regime, investment and property business case approval guidance for NHS providers and the Department of Health guidance on the efficient management of healthcare estates and facilities (HBN 00-08) “. In the case of management consultancy contracts the Trust shall comply as far as is practicable with NHS Improvement/England’s guidance Consultancy spending approval criteria for providers.
7.5 Formal Competitive Tendering
7.5.1 General Applicability The Trust shall ensure that competitive tenders are invited for: -
the supply of goods, materials, and manufactured articles,
the rendering of services including all forms of management consultancy services (other than specialised services sought from or provided by the DH),
the design, construction and maintenance of building and engineering works (including construction and maintenance of grounds and gardens),
for disposals.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
234 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 26
7.5.2 Healthcare Services Where the Trust elects to invite tenders for the supply of healthcare services these Standing Orders and Standing Financial Instructions shall apply as far as they are applicable to the tendering procedure and need to be read in conjunction with Standing Financial Instruction No.8 “NHS Service Agreements for Provision of Services”.
7.5.3 Exceptions and instances where formal tendering need not be applied Formal tendering procedures need not be applied where: - (i) the estimated expenditure or income does not, or is not
reasonably expected to, exceed £50,000, (ii) where the supply is proposed under special arrangements
negotiated by the DOH in which event the said special arrangements must be complied with,
(iii) regarding disposals as set out in Standing Financial Instruction No.15 “Disposals and Condemnations, Losses and Special Payments”.
Formal tendering procedures may be waived in the following circumstances: - (iv) in very exceptional circumstances where the Chief Executive
decides that formal tendering procedures would not be practicable or the estimated expenditure or income would not warrant formal tendering procedures, and the circumstances are detailed in an appropriate Trust record,
(v) where the requirement is covered by an existing contract, (vi) where NHS Supply Chain agreements are in place and have
been approved by the Board, (vii) where a consortium arrangement is in place and a lead
organisation has been appointed to carry out tendering activity on behalf of the consortium members,
(viii) where the timescale genuinely precludes competitive tendering but failure to plan the work properly would not be regarded as a justification for a single tender,
(ix) where specialist expertise is required and is available from only one source,
(x) when the task is essential to complete the project, and arises as a consequence ofbecause of a recently completed assignment and engaging different consultants for the new task would be inappropriate,
(xi) where there is a clear benefit to be gained from maintaining continuity with an earlier project. However, in such cases the benefits of such continuity must outweigh any potential financial advantage to be gained by competitive tendering,
(xii) for the provision of legal advice and services providing that any legal firm or partnership commissioned by the Trust is regulated by the Law Society for England and Wales for the conduct of their business (or by the Bar Council for England and Wales in relation to the obtaining of Counsel’s opinion) and are generally recognised as having sufficient expertise in the area of work for which they are commissioned. The Director of
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
235 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 27
Finance and Strategy or Associate Director of Finance will ensure that any fees paid are reasonable and within commonly accepted rates for the costing of such work.
(xiii) Where allowed and provided for in the Capital regime, investment, and property business case approval guidance for NHS providers
(xiv) Where the League of Friends is paying for an item and has specified the supplier.
The waiving of competitive tendering procedures should not be used to avoid competition or for administrative convenience or to award further work to a consultant originally appointed through a competitive procedure. Where it is decided that competitive tendering is not applicable and should be waived, the fact of the waiver and the reasons should be documented and recorded in an appropriate Trust record and authorised by the Director of Finance and Strategy or Associate Director of Finance or Chief Executive.
7.5.4 Fair and Adequate Competition
Where the exceptions set out in 7.5.3 above apply, the Trust shall ensure that invitations to tender are sent to a sufficient number ofenough firms/individuals to provide fair and adequate competition as appropriate, and in no case less than two firms/individuals, having regard to their capacity to supply the goods or materials or to undertake the services or works required.
7.5.5 List of Approved Firms
The Trust shall ensure that the firms/individuals invited to tender (and where appropriate, quote) are among those on approved lists. Where in the opinion of the Director of Finance and Strategy or Associate Director of Finance it is desirable to seek tenders from firms not on the approved lists, the reason shall be recorded in writing to the Chief Executive (see Standing Financial Instruction 7.6.9 “List of Approved Firms”).
7.5.6 Building and Engineering Construction Works
Competitive Tendering cannot be waived for building and engineering construction works and maintenance (other than in accordance with Concode) without Departmental of Health approval.
7.5.7 Items which subsequently breach thresholds after original approval
Items estimated to be below the limits set in this Standing Financial Instruction for which formal tendering procedures are not used which subsequently prove to have a value above such limits shall be reported to the Chief Executive and be recorded in an appropriate Trust record.
Commented [CD(CHNT1]: Do we need to change this?
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
236 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 28
7.6 Contracting/Tendering Procedure
7.6.1 Paper based or electronic tenders The tendering process may be entirely paper based, using an electronic tendering system, or part using a system (e.g., sending out invitations to tender electronically, but receiving tenders back on paper). The following paragraphs indicate where the tendering process is different between paper and electronic.
7.6.2 Invitation to tender
(i) All invitations to tender shall state the date and time as being the latest time for the receipt of tenders.
(ii) For paper tenders, all invitations to tender shall state that no
tender will be accepted unless: -
submitted in a plain, sealed package or envelope bearing a pre-printed label supplied by the Trust (or the word “Tender” followed by the subject to which it relates) and the latest date and time for the receipt of such tender addressed to the Chief Executive or nominated manager,
that tender envelopes/packages shall not bear any names or marks indicating the sender. The use of courier/postal services must not identify the sender on the envelope or on any receipt so required by the deliverer.
(iii) For electronic tenders, the invitation shall state that only
tenders submitted electronically will be considered.
(iv) Every tender for goods, materials, services, or disposals shall embody such of the NHS Standard Contract Conditions as are applicable.
(v) Every tender for building and engineering works (except for
maintenance work, when Estmancode guidance shall be followed) shall embody or be in the terms of the current edition of one of the Joint Contracts Tribunal Standard Forms of Building Contract or Department of the Environment (GC/Wks) Standard Forms of Contract amended to comply with Concode, or when the content of the work is primarily engineering, the General Conditions of Contract recommended by the Institution of Mechanical and Electrical Engineers and the Association of Consulting Engineers (Form A) or (in the case of civil engineering work) the General Conditions of Contract recommended by the Institute of Civil Engineers, the Association of Consulting Engineers and the Federation of Civil Engineering Contractors. These documents shall be modified and/or amplified to accord with Department of Health/ NHS Improvement/England’s guidance and, in minor respects, to cover special features of individual projects.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
237 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 29
(vi) Every tenderer must have given, or give, a written undertaking not to engage in collusive tendering or other restrictive practice.
7.6.3 Receipt and safe custody of tenders (i) For paper tenders, the Chief Executive or his/her nominated
representative will be responsible for the receipt, endorsement and safe custody of tenders received until the time appointed for their opening.
The date and time of receipt of each tender shall be endorsed on the tender envelope/package.
(ii) For electronic tenders, the tenders are locked automatically
until the published date and time of opening. The date and time of receipt of each tender is stored electronically.
7.6.4 Opening tenders and register of tenders
(i) As soon as practicable after the date and time stated as being
the latest time for the receipt of tenders, they shall be opened by two senior officers/managers designated by the Chief Executive and not from the originating department. The “originating department” will be taken to mean the department responsible for sponsoring or commissioning the tender.
(ii) The involvement of Finance Directorate staff in the
preparation of a tender proposal will not preclude the Director of Finance and Strategy or Associate Director of Finance or any approved Senior Manager from the Finance Directorate from serving as one of the two senior managers to open tenders.
(iii) All Executive Directors/members will be authorised to open
tenders regardless of whether they are from the originating department provided that the other authorised person opening the tenders with them is not from the originating department. The Trust’s Company Secretary will count as a Director for the purposes of opening tenders.
(iv) For paper tenders, every tender received shall be marked with
the date of opening and initialled by those present at the opening. This will be automatic for electronic tenders.
(v) A register shall be maintained by the Chief Executive, or a
person authorised by him/her, to show for each set of competitive tender invitations despatched: -
the names of all firms/individuals invited,
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
238 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 30
the names of firms/individuals from which tenders have been received,
the date the tenders were received and opened,
the persons present at the opening,
the price shown on each tender,
a note where price alterations have been made on the tender and suitably initialled,
a note if any one tender price has had so many alterations that it cannot be readily read or understood.
Each entry on this register shall be signed by those present.
(vi) Incomplete tenders, i.e., those from which information necessary for the adjudication of the tender is missing, and amended tenders i.e., those amended by the tenderer upon his/her own initiative either orally or in writing after the due time for receipt, but prior to the opening of other tenders, should be dealt with in the same way as late tenders (see 7.6.6 below).
7.6.5 Admissibility
(i) If for any reason the designated officers are of the opinion that
the tenders received are not strictly competitive (for example, because their numbers are insufficient or any are amended, incomplete or qualified) no contract shall be awarded without the approval of the Chief Executive.
(ii) Where only one tender is sought and/or received, the Chief
Executive and, Director of Finance and Strategy or Associate Director of Finance shall, as far practicable, ensure that the price to be paid is fair and reasonable and will ensure value for money for the Trust.
7.6.6 Late tenders
(i) Tenders received after the due time and date, but prior to the
opening of the other tenders, may be considered only if the Chief Executive or his/her nominated officer decides that there are exceptional circumstances i.e., despatched in good time but delayed through no fault of the tenderer.
(ii) Only in the most exceptional circumstances will a tender be
considered which is received after the opening of the other tenders and only then if the tenders that have been duly opened have not left the custody of the Chief Executive or his/her nominated officer or if the process of evaluation and adjudication has not started.
(iii) While decisions as to the admissibility of late, incomplete, or amended tenders are under consideration, the tender
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
239 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 31
documents shall be kept strictly confidential, recorded, and kept in safe custody by the Chief Executive or his/her nominated officer.
(iv) Accepted late tenders will be reported to the Board.
7.6.7 Acceptance of formal tenders
(i) Any discussions with a tenderer which are deemed necessary
to clarify technical aspects of his/her tender before the award of a contract will not disqualify the tender.
(ii) The lowest tender, if payment is to be made by the Trust, or
the highest, if payment is to be received by the Trust, shall be accepted unless there are good and sufficient reasons to the contrary. Such reasons shall be set out in either the contract file, or other appropriate record.
It is accepted that for professional services such as management consultancy, the lowest price does not always represent the best value for money. Other factors affecting the success of a project include: -
experience and qualifications of team members,
understanding of client’s needs,
feasibility and credibility of proposed approach,
ability to complete the project on time. Where other factors are taken into accountconsidered in selecting a tenderer, these must be clearly recorded and documented in the contract file, and the reason(s) for not accepting the lowest tender clearly stated.
(iii) No tender shall be accepted which will commit expenditure in
excess of that which has been allocated by the Trust and which is not in accordance with these iInstructions except with the authorisation of the Chief Executive.
(iv) The use of these procedures must demonstrate that the award
of the contract was not in excess of the going market rate/price current at the time the contract was awarded, and that best value for money was achieved.
(v) All tenders should be treated as confidential and should be
retained for inspection.
7.6.8 Tender reports to the Trust Board Reports to the Trust Board will be made on an exceptional circumstance basis only.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
240 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 32
7.6.9 List of approved firms
(i) Responsibility for maintaining list A manager nominated by the Chief Executive shall on behalf of the Trust maintain lists of approved firms from whom tenders, and quotations may be invited. These shall be kept under frequent review. The lists shall include all firms who have applied for permission to tender and as to whose technical and financial competence the Trust is satisfied. All suppliers must be made aware of the Trust’s terms and conditions of contract.
(ii) Building and engineering construction works
Invitations to tender shall be made only to firms included on the approved list of tenderers compiled in accordance with this iInstruction or on the separate maintenance lists compiled in accordance with Estmancode guidance (Health Notice HN(78)147).
Firms included on the approved list of tenderers shall ensure
that when engaging, training, promoting, or dismissing employees or in any conditions of employment, shall not discriminate against any person because of colour, race, ethnic or national origins, religion, or sex, and will comply with the provisions of the Equality Act 2010 and any amending and/or related legislation.
Firms shall conform at least with the requirements of the
Health and Safety at Work Act and any amending and/or other related legislation concerned with the health, safety and welfare of workers and other persons, and to any relevant British Standard Code of Practice issued by the British Standard Institution. Firms must provide to the appropriate manager a copy of its safety policy and evidence of the safety of plant and equipment, when requested.
(iii) Financial standing and technical competence of contractors
The Director of Finance and Strategy and the Associate Director of Finance may make or institute any enquiries he/she deems appropriate concerning the financial standing and financial suitability of approved contractors. The Director with lead responsibility for clinical governance will similarly make such enquiries as is felt appropriate to be satisfied as to their technical/medical competence.
7.6.10 Exceptions to using approved contractors If in the opinion of the Chief Executive and the Director of Finance and Strategy or Associate Director of Finance or the Director with lead responsibility for clinical governance it is impractical to use a potential contractor from the list of approved firms/individuals (for example where specialist services or skills are required and there are insufficient suitable potential contractors on the list), or where a list for
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
241 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 33
whatever reason has not been prepared, the Chief Executive should ensure that appropriate checks are carried out as to the technical and financial capability of those firms that are invited to tender or quote. An appropriate record in the contract file should be made of the reasons for inviting a tender or quote other than from an approved list.
7.7 Quotations: Competitive and Non-Competitive
7.7.1 General position on quotations
Quotations are required where formal tendering procedures are not adopted and where the intended expenditure or income exceeds or is reasonably expected to exceed £10,000 but not exceed £50,000.
7.7.2 Competitive quotations
(i) Quotations should be obtained from 2 to 6 firms/individuals (in
line with the Scheme of Delegation) based on specifications or terms of reference prepared by, or on behalf of, the Trust.
(ii) Quotations should be in writing unless the Chief Executive or
his nominated officer determines that it is impractical to do so, in which case quotations may be obtained by telephone. Confirmation of telephone quotations should be obtained as soon as possible and the reasons why the telephone quotation was obtained should be set out in a permanent record.
(iii) All quotations should be treated as confidential and should be
retained for inspection.
(iv) The Chief Executive or his nominated officer should evaluate the quotations and select the one which gives the best value for money. If this is not the lowest quotation if payment is to be made by the Trust, or the highest if payment is to be received by the Trust, then the choice made, and the reasons why should be recorded in a permanent record.
7.7.3 Non-competitive quotations
Non-competitive quotations in writing may be obtained in the following circumstances: - (i) the supply of proprietary or other goods of a special character
and the rendering of services of a special character, for which it is not, in the opinion of the responsible officer, possible or desirable to obtain competitive quotations,
(ii) the supply of goods or manufactured articles of any kind which are required quickly and are not obtainable under existing contracts,
(iii) miscellaneous services, supplies, and disposals, (iv) where the goods or services are for building and engineering
maintenance the responsible works manager must certify that the first two conditions of this SFI apply.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
242 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 34
7.7.4 Quotations to be within financial limits
No quotation shall be accepted which will commit expenditure in excess of that which has been allocated by the Trust and which is not in accordance with Standing Financial Instructions except with the authorisation of either the Chief Executive or Director of Finance and Strategy or Associate Director of Finance.
7.8 Authorisation of Tenders & Competitive Quotations
7.8.1 Providing all the conditions and circumstances set out in these SFIs have been fully complied with, formal authorisation of a contract may be decided by the following staff to the value of the contract as follows: - (i) Designated Budget Manager Up to £50,000 (ii) Directors & Head of Procurement Up to £75,000 (iii) Directors & Head of Procurement (under seal) Up to £250,000 (iv) Chief Executive & Director of Finance and Strategy or Associate Director of Finance & Head of Procurement (under seal) Up to £600,000.
(v) Trust Board Over £600,000
7.8.2 These levels of authorisation may be varied or changed and need to be read in conjunction with the Trust Board’s Scheme of Delegation.
7.8.3 Formal authorisation must be put in writing. In the case of authorisation
by the Trust Board this shall be recorded in their minutes. 7.9 Instances Where Formal Competitive Tendering or Competitive
Quotation is Not Required
7.9.1 Where competitive tendering or a competitive quotation is not required, the Trust should adopt one of the following alternatives: - (i) the Trust shall use NHS Supply Chain for procurement of all
goods and services unless the Chief Executive or nominated officers deem it inappropriate. The decision to use alternative sources must be documented.
(ii) if the Trust does not use NHS Supply Chain - where tenders or quotations are not required, because expenditure is below £10,000, the Trust shall procure goods and services in accordance with procurement procedures approved by the Director of Finance and Strategy or Associate Director of Finance.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
243 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 35
7.10 Private Finance for Capital Procurement
(See overlap with Standing Financial Instruction No.13).
7.10.1 The Trust should normally market-test for PFI (Private Finance Initiative funding) when considering a capital procurement. When the Board proposes, or is required, to use finance provided by the private sector the following should apply: (i) The Chief Executive shall demonstrate that the use of private
finance represents value for money and genuinely transfers risk to the private sector.
(ii) Where the sum exceeds delegated limits, a business case must be referred to the NHS Improvement/England for approval or treated as per current guidelines.
(iii) The proposal must be specifically agreed by the Trust Board. (iv) The selection of a contractor/finance company must be on the
basis ofbased on competitive tendering or quotations.
7.11 Compliance Requirements for all Contracts
7.11.1 The Board may only enter into contracts on behalf of the Trust within the statutory powers delegated to it by the Secretary of State and shall comply with the following:
(i) The Trust’s Standing Orders and SFIs, (ii) EU Directives and other statutory provisions, (iii) Any relevant directions/guidance, (iv) Such of the NHS Standard Contract Conditions as are
applicable, (v) Contracts with Foundation Trusts must be in a form compliant
with appropriate NHS guidance, (vi) Where appropriate, contracts shall be in or embody the same
terms and conditions of contract as was the basis on which tenders or quotations were invited,
(vii) In all contracts made by the Trust, the Board shall endeavour to obtain best value for money by use of all systems in place. The Chief Executive shall nominate an officer who shall oversee and manage each contract on behalf of the Trust.
7.12 Personnel and Agency or Temporary Staff Contracts
7.12.1 The Chief Executive shall nominate officers with delegated authority to enter into contracts of employment, regarding staff, agency staff or temporary staff service contracts.
7.13 Healthcare Services Agreements
(See overlap with Standing Financial Instruction No.8).
7.13.1 Service agreements with NHS providers for the supply of healthcare
services shall be drawn up in accordance with the NHS and Community Care Act 1990 and administered by the Trust. Service agreements are not contracts, in law and are not enforceable by the
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
244 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 36
courts. However, a contract with a Foundation Trust, being a PBC, is a legal document and is enforceable in law.
7.14 Disposals
(See overlap with Standing Financial Instruction No.15).
7.14.1 Competitive Tendering or Quotation procedures shall not apply to the disposal of:
(i) any matter in respect of which a fair price can be obtained
only by negotiation or sale by auction as determined (or pre-determined in a reserve) by the Chief Executive or their nominated officer,
(ii) obsolete or condemned articles and stores, which may be
disposed of in accordance with the supplies policy of the Trust,
(iii) items to be disposed of with an estimated sale value of less
than £100 this figure to be reviewed on a periodic basis,
(iv) items arising from works of construction, demolition, or site clearance, which should be dealt with in accordance with the relevant contract,
(v) land or buildings concerning which Department of Health
guidance has been issued but subject to compliance with such guidance.
7.15 In-House Services
7.15.1 The Chief Executive shall be responsible for ensuring that best value for money can be demonstrated for all services provided on an in-house basis. The Trust may also determine from time to time that in-house services should be market tested by competitive tendering.
7.15.2 In all cases where the Board determines that in-house services
should be subject to competitive tendering, the following groups should be set up: (i) Specification group, comprising the Chief Executive or
nominated officer/s and specialist. (ii) In-house tender group, comprising a nominee of the Chief
Executive and technical support. (iii) Evaluation team, comprising normally a specialist officer, a
supplies officer, and a Director of Finance and Strategy or Associate Director of Finance representative.
7.15.3 All groups should work independently of each other and individual
officers may be a member of more than one group, but no member of the in-house tender group may participate in the evaluation of the tenders.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
245 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 37
7.15.4 The evaluation team shall make recommendations to the Board.
7.15.5 The Chief Executive shall nominate an officer to oversee and manage
the contract on behalf of the Trust.
7.16 Applicability of SFIs on Tendering and Contracting to Funds Held on Trust
(See overlap with Standing Financial Instruction No.18).
7.16.1 These instructions shall not only apply to expenditure from Exchequer
funds but also to works, services and goods purchased from the Trust’s trust funds and private resources.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
246 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 38
8. NHS SERVICE AGREEMENTS FOR PROVISION OF SERVICES (See overlap with Standing Financial Instruction No.7.13)
8.1 Service Level Agreements (SLAs)
8.1.1 The Chief Executive, as the Accountable Officer, is responsible for ensuring the Trust enters into suitable SLAs with service commissioners for the provision of NHS Services.
8.1.2 All SLAs should aim to implement the agreed priorities contained
within the Local Delivery Plan (LDP) and wherever possible, be based upon integrated care pathways to reflect expected patient experience. In discharging this responsibility, the Chief Executive should take into accountconsider: -
the standards of service quality expected,
the relevant national service framework (if any),
the provision of reliable information on cost and volume of services,
the NHS Outcomes Framework,
that SLAs build where appropriate on existing Joint Investment Plans,
that SLAs are based on integrated care pathways,
that SLAs are based upon cost-effective services.
8.2 Involving Partners and Jointly Managing Risk
8.2.1 A good SLA will result from a dialogue of clinicians, users, carers, public health professionals and managers. It will reflect knowledge of local needs and inequalities. This will require the Chief Executive to ensure that the Trust works with all partner agencies involved in both the delivery and the commissioning of the service required. The SLA will apportion responsibility for handling a particular risk to the party or parties in the best position to influence the event and financial arrangements should reflect this. In this way the Trust can jointly manage risk with all interested parties.
8.3 Reports to the Board on SLAs 8.3.1 The Chief Executive, as the Accountable Officer, will need to ensure
that regular reports are provided to the Board detailing actual and forecast income from the SLA. This will include information on costing arrangements, which increasingly should be based upon Healthcare Resource Groups (HRGs). Where HRGs are unavailable for specific services, all parties should agree a common currency for across the range of SLAs.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
247 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 39
9. TERMS OF SERVICE, ALLOWANCES AND PAYMENT OF MEMBERS OF THE TRUST BOARD AND EMPLOYEES
9.1 Remuneration and Terms of Service
(See overlap with Standing Order No.4).
9.1.1. In accordance with Standing Orders the Board shall establish a Nominations, Appointments and Remuneration Committee, with clearly defined terms of reference, specifying which posts fall within its area of responsibility, its composition, and the arrangements for reporting (see NHS guidance contained in the Higgs report).
9.1.2. The Committee will:
(i) advise the Board about appropriate remuneration and terms of
service for the Chief Executive, other Executive Directors employed by the Trust and other senior employees including: -
all aspects of salary (including any performance-related elements/ bonuses),
provisions for other benefits, including pensions and cars,
arrangements for termination of employment and other contractual terms,
(ii) make such recommendations to the Board on the
remuneration and terms of service of Executive Directors of the Board (and other senior employees) to ensure they are fairly rewarded for their individual contribution to the Trust - having proper regard to the Trust’s circumstances and performance and to the provisions of any national arrangements for such staff where appropriate,
(iii) monitor and evaluate the performance of individual Executive
Directors (and other senior employees),
(iv) advise on and oversee appropriate contractual arrangements for such staff including the proper calculation and scrutiny of termination payments, taking account of such national guidance as is appropriate,
(v) Approve any redundancy payments over £15,000.
9.1.3. The Committee shall report in writing to the Board the basis for its
recommendations. The Board shall use the report as the basis for their decisions but remain accountable for taking decisions on the remuneration and terms of service of Executive Directors. Minutes of the Board’s meetings should record such decisions.
9.1.4. The Board will consider and need to approve proposals presented by
the Chief Executive for the setting of remuneration and conditions of
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
248 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 40
service for those employees and officers not covered by the Committee.
9.1.5. The Trust will pay allowances to the Chair, and Non-Executive
Directors of the Board in accordance with instructions issued by the Secretary of State for Health.
9.2. Funded Establishment
9.2.1. The manpower plans incorporated within the annual budget will form
the funded establishment.
9.2.2. The funded establishment of any department may not be varied without the approval of the Chief Executive or the delegated officer.
9.3. Staff Appointments
9.3.1. No officer or member of the Trust Board or employee may engage,
re-engage, or re-grade employees, either on a permanent or temporary basis, or hire agency staff, or agree to changes in any aspect of remuneration: (i) unless authorised to do so by the Chief Executive, or the
officer(s) so delegated; and (ii) within the limit of their approved budget and funded
establishment.
9.3.2. The Board will approve procedures presented by the Chief Executive for the determination of commencing pay rates, conditions of service etc. for employees.
9.4 Processing of Payroll
9.4.1 “Payroll” includes payments for all hours worked at agreed rates,
Statutory Sick and Maternity Pay, Annual Leave, Travel and Subsistence Expenses, Relocation Expenses and any other employment related payments authorised by the Trust Board.
9.4.2. The Director of Finance and Strategy and the Associate Director of
Finance are is responsible for:
(i) specifying timetables for submission of properly authorised time records and other notifications,
(ii) the final determination of pay and allowances,
(iii) making payment on agreed dates; and
(iv) agreeing method of payment.
9.4.3. The Director of Finance and Strategy or Associate Director of Finance
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
249 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 41
(i) verification and documentation of data,
(ii) the timetable for receipt and preparation of payroll data and
the payment of employees and allowances,
(iii) maintenance of subsidiary records for superannuation, income tax, social security, and other authorised deductions from pay,
(iv) security and confidentiality of payroll information,
(v) checks to be applied to completed payroll before and after
payment,
(vi) authority to release payroll data under the provisions of the Data Protection Act,
(vii) methods of payment available to various categories of
employees and officers,
(viii) procedures for payment by cheque, bank credit or cash to employees and officers,
(ix) procedures for the recall of cheques and bank credits,
(x) pay advances and their recovery,
(xi) maintenance of regular and independent reconciliation of pay
control accounts;
(xii) separation of duties of preparing records and handling cash,
(xiii) a system to ensure the recovery from those leaving the employment of the Trust of sums of money and property due by them to the Trust.
9.4.4. Appropriately nominated managers have delegated responsibility for:
(i) submitting time records and other notifications in accordance
with agreed timetables,
(ii) completing time records and other notifications in accordance with the Director of Finances and Strategy’s or the Associate Director of Finances instructions, and in the form prescribed by the Director of Finance and Strategy or Associate Director of Finance,
(iii) submitting termination forms in the prescribed form
immediately upon knowing the effective date of an employee’s or officer’s resignation, termination, or retirement. Where an employee fails to report for duty or to fulfil obligations in circumstances that suggest they have left without notice, the
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
250 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 42
Director of Finance and Strategy or Associate Director of
9.4.5. Regardless of the arrangements for providing the payroll service, the Director of Finance and Strategy or Associate Director of Finance shall ensure that the chosen method is supported by appropriate (contracted) terms and conditions, adequate internal controls and audit review procedures, and that suitable arrangements are made for the collection of payroll deductions and payment of these to appropriate bodies.
9.5. Contracts of Employment
9.5.1. The Board shall delegate responsibility to an officer for:
(i) ensuring that all employees are issued with a Contract of
Employment in a form approved by the Board, and which complies with employment legislation; and
(ii) dealing with variations to, or termination of, contracts of
employment.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
251 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 43
10. NON-PAY EXPENDITURE
10.1. Delegation of Authority
10.1.1. The Board will approve the level of non-pay expenditure on an annual basis, and the Chief Executive will determine the level of delegation to budget managers (see the Scheme of Delegation for details).
10.1.2. The Chief Executive will set out:
(i) the list of managers who are authorised to place requisitions
for the supply of goods and services,
(ii) the maximum level of each requisition, and the system for authorisation above that level.
10.1.3. The Chief Executive shall set out procedures on the seeking of
professional advice regarding the supply of goods and services.
10.2. Choice, Requisitioning, Ordering, Receipt and Payment for Goods and Services
(See overlap with Standing Financial Instruction No.7).
10.2.1. Requisitioning The requisitioner, in choosing the item to be supplied (or the service to be performed) shall always obtain the best value for money for the Trust. In so doing, the advice of the Trust’s advisor on supply shall be sought. Where this advice is not acceptable to the requisitioner, the Director of Finance and Strategy or Associate Director of Finance (and/or the Chief Executive) shall be consulted.
10.2.2. System of Payment and Payment Verification
The Director of Finance and Strategy and the Associate Director of Finance shall be responsible for the prompt payment of accounts and claims. Payment of contract invoices shall be in accordance with contract terms, or otherwise, in accordance with national guidance.
10.2.3. The Director of Finance and Strategy and the Associate Director of
Finance will:
(i) advise the Board regarding the setting of thresholds above which quotations (competitive or otherwise) or formal tenders must be obtained; and, once approved, the thresholds should be incorporated in Standing Financial Instructions and regularly reviewed,
(ii) prepare procedural instructions (where not already provided in
the Scheme of Delegation or procedure notes for budget managers) on the obtaining of goods, works and services, incorporating the thresholds,
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
252 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 44
(iii) be responsible for the prompt payment of all properly authorised accounts and claims,
(iv) be responsible for designing and maintaining a system of
verification, recording and payment of all amounts payable. The system shall provide for:
(a) a list of Board members and employees (including
specimens of their signatures) authorised to certify invoices,
(b) certification that:
goods have been duly received, examined and are in accordance with specification, and the prices are correct,
work done or services rendered have been satisfactorily carried out in accordance with the order and, where applicable, the materials used are of the requisite standard, and the charges are correct,
in the case of contracts based on the measurement of time, materials or expenses, the time charged is in accordance with the time sheets, the rates of labour are in accordance with the appropriate rates, the materials have been checked as regards quantity, quality and price, and the charges for the use of vehicles, plant and machinery have been examined,
where appropriate, the expenditure is in accordance with regulations, and all necessary authorisations have been obtained,
the account is arithmetically correct,
the account is in order for payment.
(c) a timetable and system for submission to the Director of Finance and Strategy or Associate Director of Finance of accounts for payment; provision shall be made for the early submission of accounts subject to cash discounts or otherwise requiring early payment,
(d) instructions to employees regarding the handling and
payment of accounts within the Finance Department.
(v) be responsible for ensuring that payment for goods and services is only made once the goods and services are received. The only exceptions are set out in SFI 10.2.4 below.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
253 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 45
10.2.4 Prepayments Prepayments are only permitted where exceptional circumstances apply. In such instances: (i) Prepayments are only permitted where the financial
advantages outweigh the disadvantages (i.e., cash flows must be discounted to NPV using the National Loans Fund (NLF) rate plus 2%).
(ii) The appropriate officer must provide, in the form of a written
report, a case setting out all relevant circumstances of the purchase. The report must set out the effects on the Trust if the supplier is, at some time during the course of the prepayment agreement, unable to meet his commitments.
(iii) The Director of Finance and Strategy or Associate Director of
Finance will need to be satisfied with the proposed arrangements before contractual arrangements proceed (taking into account the EU public procurement rules where the contract is above the stipulated financial threshold).
(iv) The budget manager is responsible for ensuring that all items
due under a prepayment contract are received and they must immediately inform the appropriate Director or Chief Executive if problems are encountered
10.2.5 Official orders
Official orders must:
be consecutively numbered,
be in a form approved by the Director of Finance and Strategy or Associate Director of Finance,
state the Trust’s terms and conditions of trade; and
only be issued to, and used by, those duly authorised by the Chief Executive.
10.2.6 Duties of managers and officers
Managers and officers must ensure that they comply fully with the guidance and limits specified by the Director of Finance and Strategy or Associate Director of Finance, and that:
(i) all contracts (except as otherwise provided for in the Scheme
of Delegation), leases, tenancy agreements and other commitments which may result in a liability are notified to the Director of Finance and Strategy or Associate Director of Finance in advance of any commitment being made,
(ii) contracts above specified thresholds are advertised and
awarded in accordance with EU rules on public procurement,
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
254 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 46
(iii) where consultancy advice is being obtained, the procurement of such advice must be in accordance with guidance issued by the Department of Health,
(iv) no order shall be issued for any item or items to any firm,
which has made an offer of gifts, reward or benefit to Directors or employees, other than: a. isolated gifts of a trivial character, or inexpensive seasonal
gifts, such as calendars, b. conventional hospitality, such as lunches in the course of
working visits. This provision needs to be read in conjunction with the principles outlined in national guidance contained in the Trusts Policy Code of Business Conduct, including Managing Conflicts of interest.
(v) no requisition/order is placed for any item or items for which
there is no budget provision, unless authorised by the Director of Finance and Strategy or Associate Director of Finance on behalf of the Chief Executive,
(vi) all goods, services or works are ordered on an official order,
except works and services executed in accordance with a contract, or for off–framework emergency agency staff, purchases from petty cash and if financial control and processing time are not enhanced.
(vii) verbal orders must only be issued very exceptionally - by an
employee designated by the Chief Executive and only in cases of emergency or urgent necessity. These must be confirmed by an official order and clearly marked “Confirmation Order”,
(viii) orders are not split or otherwise placed in a manner devised
so as toto avoid the financial thresholds, (ix) goods are not taken on trial or loan in circumstances that
could commit the Trust to a future uncompetitive purchase, (x) changes to the list employees and officers authorised to certify
invoices are notified to the Director of Finance and Strategy or Associate Director of Finance,
(xi) purchases from petty cash and the corporate credit card are
restricted in value and by type of purchase in accordance with instructions issued by the Director of Finance and Strategy or Associate Director of Finance,
(xii) petty cash records are maintained in a form as determined by
the Director of Finance and Strategy or Associate Director of Finance.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
255 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 47
10.2.7 The Chief Executive and, Director of Finance and Strategy and
Associate Director of Finance shall ensure that the arrangements for financial control and financial audit of building and engineering contracts and property transactions comply with the guidance contained within Concode and Estatecode. The technical audit of these Contracts shall be the responsibility of the relevant Director.
10.3 Joint Finance Arrangements with Local Authorities
(See overlap with Standing Order 9.3 “Joint Finance Arrangements”). 10.3.1 Payments to local authorities made under the powers of section 75 of
the NHS Act 2006 shall comply with procedures laid down by the Director of Finance and Strategy or Associate Director of Finance
which shall be in accordance with that Act.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
256 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 48
11. EXTERNAL BORROWING AND INVESTMENTS 11.1 External Borrowing
11.1.1 The Director of Finance and Strategy or Associate Director of Finance will advise the Board concerning the Trust’s ability to pay dividend on, and repay Public Dividend Capital and any proposed new borrowing, within the limits set by the Department of Health. The Director of Finance and Strategy and Associate Director of Finance are is also responsible for reporting periodically to the Board concerning the PDC debt and all loans and overdrafts.
11.1.2 The Board will agree the list of employees (including specimens of
their signatures) who are authorised to make short term borrowings on behalf of the Trust. This must contain the Chief Executive and the Director of Finance and Strategy or Associate Director of Finance.
11.1.3 The Director of Finance and Strategy or Associate Director of Finance
must prepare detailed procedural instructions concerning applications for loans and overdrafts.
11.1.4 All short-term borrowings should be kept to the minimum period of
time possible, consistent with the overall cash-flow position, represent good value for money, and comply with the latest guidance from the Department of Health.
11.1.5 Any short-term borrowing must be with the authority of two members
of an authorised panel, one of which must be the Chief Executive or the Director of Finance and Strategy or Associate Director of Finance. The Board must be made aware of all short-term borrowings at the next Board meeting. For loan draws NHSI/E require a utilisation request with one signature, the nominated representative as stated in the board minute.
11.1.6 All long-term borrowing must be consistent with the plans outlined in
the current LDP and be approved by the Trust Board. 11.1.7 For PDC draws two signatures are required on the utilisation request;
the signatories are individuals who are authorised by the Board under the Trust’s Standing Financial Instructions, and Scheme of Delegation to make the request for funding. The following authorised individuals are able tocan sign PDC utilisation requests:
Chief Executive, Director of Finance and Strategy, Associate Director of Finance, Head of Finance, Head of Management Accounting, Head of Financial Accounting, Head of Costing & Contracting
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
257 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 49
NHSI/E also require a Capital Cash Flow Forecast template to be completed with the signed utilisation request.
11.2 Investments 11.2.1 Temporary cash surpluses must be held only in such public or private
sector investments as notified by the Secretary of State and authorised by the Board.
11.2.2 The Director of Finance and Strategy and the Associate Director of
Finance are is responsible for advising the Board on investments and shall report periodically to the Board concerning the performance of investments held.
11.2.3 The Director of Finance and Strategy or Associate Director of Finance
will prepare detailed procedural instructions on the operation of investment accounts and on the records to be maintained.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
258 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 50
12. FINANCIAL FRAMEWORK
12.1. The Director of Finance and Strategy and the Associate Director of Finance should ensure that members of the Board are aware of the Operating Framework. This document contains directions, which the Trust must follow. The Director of Finance and Strategy and the Associate Director of Finance
should also ensure that the direction and guidance in the framework is followed by the Trust.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
259 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 51
13. CAPITAL INVESTMENT, PRIVATE FINANCING, FIXED ASSET REGISTERS AND SECURITY OF ASSETS
13.1 Capital Investment
13.1.1. The Chief Executive: -
(i) shall ensure that there is an adequate appraisal and approval
process in place for determining capital expenditure priorities, and the effect of each proposal upon business plans,
(ii) is responsible for the management of all stages of capital
schemes, and for ensuring that schemes are delivered on time and to cost,
(iii) shall ensure that the capital investment is not undertaken
without confirmation of purchaser(s) support and the availability of resources to finance all revenue consequences, including capital charges.
13.1.2. For every capital expenditure proposal, the Chief Executive shall
ensure: -
(i) that a business case (in line with the guidance contained within the Capital Investment Manual) is produced, setting out:
an option appraisal of potential benefits compared with known costs, to determine the option with the highest ratio of benefits to costs,
the involvement of appropriate Trust personnel and external agencies,
appropriate project management and control arrangements,
(ii) that the Director of Finance and Strategy or Associate Director
of Finance has certified professionally to the costs and revenue consequences detailed in the business case.
13.1.3 For capital schemes where the contracts stipulate stage payments,
the Chief Executive will issue procedures for their management, incorporating the recommendations of Estatecode.
13.1.4 The Director of Finance and Strategy or Associate Director of Finance
shall assess on an annual basis the requirement for the operation of the Construction Industry tax deduction scheme in accordance with Inland Revenue guidance.
13.1.5 The Director of Finance and Strategy or Associate Director of Finance
shall issue procedures for the regular reporting of expenditure and commitment against authorised expenditure.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
260 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 52
13.1.6 The approval of a capital programme shall not constitute approval for expenditure on any scheme. The Chief Executive shall issue to the manager responsible for any scheme: -
specific authority to commit expenditure,
authority to proceed to tender,
approval to accept a successful tender. The Chief Executive will issue a Scheme of Delegation for capital investment management in accordance with Estatecode guidance and the Trust’s Standing Orders.
13.1.7 The Director of Finance and Strategy or Associate Director of Finance
shall issue procedures governing the financial management, including variations to contract, of capital investment projects, and valuation for accounting purposes. These procedures shall fully take into accountconsider the delegated limits for capital schemes included in NHS Improvements Capital regime, investment and property business case approval guidance for NHS Trusts and Foundation Trusts.
13.2. Private Finance (See overlap with Standing Financial Instruction 7.10 “Private Finance for
Capital Procurement”).
13.2.1. The Trust should normally test for PFI when considering capital procurement. When the Trust proposes to use finance, which is to be provided other than through its own or NHS resources, the following procedures shall apply: -
(i) The Director of Finance and Strategy or Associate Director of
Finance shall demonstrate that the use of private finance represents value for money and genuinely transfers significant risk to the private sector.
(ii) Where the sum involved exceeds delegated limits, the
business case must be referred to NHS Improvement/England or in line with any current guidelines.
(iii) The proposal must be specifically agreed by the Board.
13.3. Asset Registers
13.3.1. The Chief Executive is responsible for the maintenance of registers of
assets, taking account of the advice of the Director of Finance and Strategy or Associate Director of Finance concerning the form of any register and the method of updating, and arranging for a physical check of assets against the asset register to be conducted at least once a year.
13.3.2. Each Trust shall maintain an asset register recording capital assets.
The minimum data set to be held within these registers shall be as
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
261 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 53
specified in the Capital Accounting Manual as issued by the Department of Health. This shall be expanded wherever possible.
13.3.3. Additions to the capital asset register must be clearly identified to an
appropriate budget manager and be validated by reference to: (i) properly authorised and approved agreements, architect’s
certificates, supplier’s invoices, and other documentary evidence in respect of purchases from third parties,
(ii) stores, requisitions and wages records for own materials and
labour, including appropriate overheads,
(iii) lease agreements in respect of assets held under a finance lease and capitalised.
13.3.4. Where capital assets are sold, scrapped, lost, or otherwise disposed
of, their value must be removed from the accounting records, and each disposal must be validated by reference to authorisation documents and invoices (where appropriate).
13.3.5. The Director of Finance and Strategy or Associate Director of Finance
shall approve procedures for reconciling balances on capital assets accounts in ledgers against balances on capital asset registers.
13.3.6. The value of each asset shall be indexed to current values in
accordance with methods specified in the Capital Accounting Manual issued by the Department of Health.
13.3.7. The value of each asset shall be depreciated using methods and
rates as specified in the Capital Accounting Manual issued by the Department of Health.
13.3.8 The Director of Finance and Strategy or Associate Director of Finance
of the Trust shall calculate and pay capital charges as specified in the Capital Accounting Manual issued by the Department of Health.
13.4. Security of Assets
13.4.1. The overall control of capital assets is the responsibility of the Chief
Executive.
13.4.2. Asset control procedures (including capital assets, cash, cheques, and negotiable instruments, and also including donated assets) must be approved by the Director of Finance and Strategy or Associate Director of Finance. The procedures shall make provision for: (i) recording managerial responsibility for each asset, (ii) identification of additions and disposals, (iii) identification of all repairs and maintenance expenses, (iv) physical security of assets, (v) periodic verification of the existence, condition of, and title to
assets recorded,;
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
262 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 54
(vi) identification and reporting of all costs associated with the retention of an asset,
(vii) reporting, recording and safekeeping of cash, cheques, and negotiable instruments.
13.4.3. All discrepancies revealed by verification of physical assets to the
capital asset register shall be notified to the Director of Finance and Strategy or Associate Director of Finance.
13.4.4. Whilst each employee and officer have a responsibility for the security
of property of the Trust, it is the responsibility of Board members and senior employees in all disciplines to apply such appropriate routine security practices in relation to NHS property as may be determined by the Board. Any breach of agreed security practices must be reported in accordance with agreed procedures.
13.4.5. Any damage to the Trust’s premises, vehicles and equipment, or any
loss of equipment, stores or supplies must be reported by Board members and employees in accordance with the procedure for reporting losses.
13.4.6. Where practical, assets should be marked as Trust property.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
263 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 55
14. STORES AND RECEIPT OF GOODS
14.1 General Position
14.1.1. Stores, defined in terms of controlled stores and departmental stores (for immediate use) should be:
kept to a minimum,
subjected to annual stock take,
valued at the lower of cost and net realisable value.
14.2 Control of Stores, Stocktaking, Condemnations and Disposals
14.2.1. Subject to the responsibility of the Director of Finance and Strategy and Associate Director of Finance for the systems of control, overall responsibility for the control of stores shall be delegated to an employee by the Chief Executive. The day-to-day responsibility may be delegated by him/her to departmental employees and stores managers/keepers, subject to such delegation being entered in a record available to the Director of Finance and Strategy and the Associate Director of Finance. The control of Pharmaceutical stocks shall be the responsibility of a designated Pharmaceutical Officer, the control of any fuel oil and coal of a designated Estates Manager.
14.2.2. The responsibility for security arrangements and the custody of keys
for all stores and locations shall be clearly defined in writing by the designated manager/Pharmaceutical Officer. Wherever practicable, stocks should be marked as health service property.
14.2.3. The Director of Finance and Strategy or Associate Director of Finance
shall set out procedures and systems to regulate the stores, including records for receipt of goods, issues and returns to stores, and losses.
14.2.4. Stocktaking arrangements shall be agreed with the Director of
Finance and Strategy or Associate Director of Finance and there shall be a physical check covering all items in store at least once a year.
14.2.5. Where a complete system of stores control is not justified, alternative
arrangements shall require the approval of the Director of Finance and Strategy or Associate Director of Finance.
14.2.6. The designated manager/pharmaceutical officer shall be responsible
for a system approved by the Director of Finance and Strategy or Associate Director of Finance for a review of slow moving and obsolete items, and for condemnation, disposal, and replacement of all unserviceable articles. The designated officer shall report to the Director of Finance and Strategy or Associate Director of Finance any evidence of significant overstocking, and of any negligence or malpractice (see also overlap with SFI No.15 “Disposals and Condemnations, Losses and Special Payments). Procedures for the disposal of obsolete stock shall follow the procedures set out for disposal of all surplus and obsolete goods.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
264 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 56
14.3. Departmental Stores
14.3.1. Senior Managers are responsible for all goods stored in their
departments and required for immediate use, and for systems for control of those stores.
14.4 Bankruptcies, Liquidations and Receiverships
14.4.1. The Director of Finance and Strategy and the Associate Director of Finance should make every effort to appraise him/herself, at the earliest point possible, of the bankruptcy, liquidation, or receivership of any supplier.
14.4.2. When a bankruptcy, liquidation or receivership is discovered, all
payments should be ceased pending confirmation of the bankruptcy etc. As a matter of urgency, a statement must be prepared listing the amounts due to and from the Trust.
14.4.3 The Director of Finance and Strategy or Associate Director of Finance
must ensure that any payments due by the Trust are made to the correct person.
14.4.4 The Director of Finance and Strategy or Associate Director of Finance
must ensure that any claim by the Trust is properly lodged with the correct party, and without delay.
14.4.5 If the Trust has a contract with a person or body which is bankrupt
etc., it normally has the right to summarily terminate the contract. However, there are ramifications arising from this and, in any case, it will probably be prudent to take legal advice.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
265 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 57
15. DISPOSALS AND CONDEMNATIONS, LOSSES AND SPECIAL PAYMENTS 15.1 Disposals and Condemnations
15.1.1 The Director of Finance and Strategy or Associate Director of Finance must prepare detailed procedures for the disposal of assets including condemnations and ensure that these are notified to managers.
15.1.2. When it is decided to dispose of a Trust asset, the head of
department or authorised deputy will determine and advise the Director of Finance and Strategy or Associate Director of Finance, or officer so delegated by him/her, of the estimated market value of the item, taking account of professional advice where appropriate.
15.1.3. All unserviceable articles shall be:
(i) condemned or otherwise disposed of by an employee
authorised for that purpose by the Director of Finance and Strategy or Associate Director of Finance. The advice of the Supplies Department shall be sought regarding the manner of disposal, to ensure that such articles are disposed of safely and in accordance with any prevailing disposal regulations,
(ii) recorded by the condemning officer in a form approved by the
Director of Finance and Strategy or Associate Director of Finance, which will indicate whether the articles are to be converted, destroyed, or otherwise disposed of. All entries shall be confirmed by the countersignature of a second employee authorised for the purpose by the Director of Finance and Strategy or Associate Director of Finance.
15.1.4. The condemning officer shall satisfy himself as to whether or not
there is evidence of negligence in use and shall report any such evidence to the Director of Finance and Strategy or Associate Director of Finance who will take the appropriate action.
15.2 Losses and Special Payments
15.2.1 The Director of Finance and Strategy or Associate Director of Finance
must prepare procedural instructions on the recording of and accounting for condemnations, losses, and special payments.
15.2.2 Any employee or officer discovering or suspecting a loss of any kind
must either immediately inform their head of department, who must immediately inform the Chief Executive and the Director of Finance and Strategy or Associate Director of Finance or inform an officer charged with responsibility for responding to concerns involving loss. This officer will then appropriately inform the Director of Finance and Strategy and /or Associate Director of Finance and/or Chief Executive. Where a criminal offence is suspected, the Director of Finance and Strategy or Associate Director of Finance must immediately inform the police if theft or arson is involved. In cases of
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
266 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 58
fraud and corruption or of anomalies which may indicate fraud or corruption, the Director of Finance and Strategy or Associate Director of Finance must inform the relevant Local Counter Fraud Specialist (LCFS) and the NHS Counter Fraud Authority, and in line with the Trust Anti-Fraud, Bribery and Corruption Response Policy.
15.2.3 The Director of Finance and Strategy or Associate Director of Finance
must notify the NHS Counter Fraud Authority and the External Auditor of all frauds.
15.2.4 For losses apparently caused by theft, arson, neglect of duty or gross
carelessness, except if trivial, the Director of Finance and Strategy or Associate Director of Finance must immediately notify the Board and the External Auditor.
15.2.5 Within limits delegated to it by the Department of Health, the Board
shall approve the writing off, of losses. 15.2.6 The Director of Finance and Strategy and the Associate Director of
Finance shall be authorised to take any necessary steps to safeguard the Trust’s interests in bankruptcies and company liquidations.
15.2.7 For any loss, the Director of Finance and Strategy or Associate
Director of Finance should consider whether any insurance claim can be made.
15.2.8 The Director of Finance and Strategy or Associate Director of Finance
shall maintain a Losses and Special Payments Register, in which write-off action is recorded, and will produce an annual summary for consideration by the Audit Committee.
15.2.9 No special payments exceeding delegated limits shall be made
without the prior approval of the Department of Health.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
267 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 59
16. INFORMATION TECHNOLOGY
16.1 Responsibilities and Duties of the Director of Finance and Strategy and Associate Director of Finance
16.1.1 The Director of Finance and Strategy and Associate Director of
Finance, who is are responsible for the accuracy and security of the computerised financial data of the Trust, shall:
(i) devise and implement any necessary procedures to ensure
adequate (reasonable) protection of the Trust's data, programs, and computer hardware for which the Director is responsible from accidental or intentional disclosure to unauthorised persons, deletion or modification, theft, or damage, having due regard for the Data Protection Act 2018,
(ii) ensure that adequate (reasonable) controls exist over data
entry, processing, storage, transmission, and output to ensure security, privacy, accuracy, completeness, and timeliness of the data, as well as the efficient and effective operation of the system,
(iii) ensure that adequate controls exist such that the computer
operation is separated from development, maintenance, and amendment,
(iv) ensure that an adequate management (audit) trail exists
through the computerised system and that such computer audit reviews as the Director may consider necessary are being carried out.
16.1.2 The Director of Finance and Strategy or Associate Director of Finance
shall need to ensure that new financial systems and amendments to current financial systems are developed in a controlled manner and thoroughly tested prior to implementation. Where this is undertaken by another organisation, assurances of adequacy must be obtained from them prior to implementation.
16.1.3 The Head of Informatics shall publish and maintain a Freedom of
Information (FOI) Publication Scheme or adopt a model Publication Scheme approved by the Information Commissioner. A Publication Scheme is a complete guide to the information routinely published by a public authority. It describes the classes or types of information about our Trust that we make publicly available.
16.2 Responsibilities and Duties of Other Directors and Officers in Relation
to Computer Systems of a General Application
16.2.1 In the case of computer systems which are proposed General Applications (i.e., normally those applications which the majority of Trusts in the Region wish to sponsor jointly) all responsible Directors and employees will send to the Director of Finance and Strategy or
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
268 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 60
(i) details of the outline design of the system, (ii) in the case of packages acquired either from a commercial
organisation, from the NHS, or from another public sector organisation, the operational requirement.
16.3 Contracts for Computer Services with Other Health Bodies or Outside
Agencies
16.3.1 The Director of Finance and Strategy or Associate Director of Finance shall ensure that contracts for computer services for financial applications with another health organisation or any other agency shall clearly define the responsibility of all parties for the security, privacy, accuracy, completeness, and timeliness of data during processing, transmission, and storage. The contract should also ensure rights of access for audit purposes.
16.3.2 Where another health organisation or any other agency provides a
computer service for financial applications, the Director of Finance and Strategy or Associate Director of Finance shall periodically seek assurances that adequate controls are in operation via an appropriate mechanism such as a service level agreement.
16.4 Risk Assessment
16.4.1 The Director of Finance and Strategy or Associate Director of Finance shall ensure that risks to the Trust rising from the use of I/T are effectively identified and considered and appropriate action taken to mitigate or control risk. This shall include the preparation and testing of appropriate disaster recovery plans.
16.5 Requirements for Computer Systems Which Have an Impact on
Corporate Financial Systems
16.5.1 Where computer systems have an impact on corporate financial systems the Director of Finance and Strategy or Associate Director of Finance shall need to be satisfied that:
(i) systems acquisition, development and maintenance are in line
with corporate policies such as an Information Technology Strategy,
(ii) data produced for use with financial systems is adequate,
accurate, complete, and timely, and that a management (audit) trail exists,
(iii) Director of Finance and Strategy and the Associate Director of
Finance ensures staff have access to such data,
(iv) such computer audit reviews as are considered necessary are being carried out.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
269 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 61
17. PATIENTS' PROPERTY
17.1 The Trust has a responsibility to provide safe custody for money and other personal property (hereafter referred to as "property") handed in by patients, in the possession of unconscious or confused patients, or found in the possession of patients dying in hospital or dead-on arrival.
17.2 The Chief Executive is responsible for ensuring that patients or their
guardians, as appropriate, are informed before or at admission by: -
notices and information booklets (subject to sensitivity guidance),
hospital admission documentation and property records,
the oral advice of administrative and nursing staff responsible for admissions,
that the Trust will not accept responsibility or liability for patients' property brought into Health Service premises, unless it is handed in for safe custody and a copy of an official patients' property record is obtained as a receipt.
17.3 The Director of Finance and Strategy or Associate Director of Finance must
provide detailed written instructions on the collection, custody, investment, recording, safekeeping, and disposal of patients' property (including instructions on the disposal of the property of deceased patients and of patients transferred to other premises) for all staff whose duty is to administer, in any way, the property of patients. Due care should be exercised in the management of a patient's money in order to maximise the benefits to the patient.
17.4 Where Department of Health instructions require the opening of separate
accounts for patients' moneys, these shall be opened and operated under arrangements agreed by the Director of Finance and Strategy or Associate Director of Finance.
17.5 In all cases where property of a deceased patient is of a total value in excess
of £5,000 (or such other amount as may be prescribed by any amendment to the Administration of Estates, Small Payments, Act 1965), the production of Probate or Letters of Administration shall be required before any of the property is released. Where the total value of property is £5,000 or less, forms of indemnity shall be obtained.
17.6 Staff should be informed, on appointment, by the appropriate departmental
or senior manager of their responsibilities and duties for the administration of the property of patients.
17.7 Where patients' property or income is received for specific purposes and held
for safekeeping the property or income shall be used only for that purpose , unless any variation is approved by the donor or patient in writing.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
270 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 62
18. FUNDS HELD ON TRUST 18.1 Corporate Trustee
18.1.1 Standing Order 2.8 “Corporate Role of the Board” outlines the Trust’s
responsibilities as a corporate trustee for the management of funds it holds on trust. There is also a requirement for compliance with the Charities Commission latest guidance and best practice.
18.1.2 The discharge of the Trust’s corporate trustee responsibilities isare
distinct from its responsibilities for exchequer funds and may not necessarily be discharged in the same manner, but there must still be adherence to the overriding general principles of financial regularity, prudence, and propriety. Trustee responsibilities cover both charitable and non-charitable purposes.
18.1.3 The Director of Finance and Strategy or Associate Director of Finance
shall ensure that each trust fund which the Trust is responsible for managing is managed appropriately with regard toregarding its purpose and to its requirements.
18.2 Accountability to the Charity Commission and Secretary of State for
Health
18.2.1 The trustee responsibilities must be discharged separately, and full recognition given to the Trust’s dual accountabilities to the Charity Commission for charitable funds held on trust and to the Secretary of State for Health for all funds held on trust.
18.2.2 The Scheme of Reservation and the Scheme of Delegation make
clear where decisions regarding the exercise of discretion regarding the disposal and use of funds are to be taken and by whom. All Trust Board members and Trust officers must take account of that guidance before taking action.
18.3 Applicability of SFIs to Funds Held on Trust
18.3.1 In so far as it is possible to do so, most of the sections of these SFIs will apply to the management of funds held on trust. (See overlap with Standing Financial Instruction No.7.16).
18.3.2 The over-riding principle is that the integrity of each Trust must be
maintained, and statutory and Trust obligations met. Materiality must be assessed separately from Exchequer activities and funds.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
271 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 63
19. ACCEPTANCE OF GIFTS BY STAFF AND LINK TO STANDARDS OF BUSINESS CONDUCT
19.1 The Director of Finance and Strategy and the Associate Director of Finance
shall ensure that all staff are made aware of the Trust policy on acceptance of gifts and other benefits in kind by staff. This policy follows the guidance contained in the Trusts Code of Business Conduct, including Managing Conflicts of Interest, and is also deemed to be an integral part of these Standing Orders and SFIs (see overlap with Standing Order No.7).
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
272 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 64
20. RETENTION OF RECORDS
20.1 The Chief Executive shall be responsible for maintaining archives for all records required to be retained in accordance with Department of Health guidelines.
20.2 The records held in archives shall be capable of retrieval by authorised
persons.
20.3 Records held in accordance with latest Department of Health guidance shall only be destroyed at the express instigation of the Chief Executive. Detail shall be maintained of records so destroyed.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
273 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 65
21. RISK MANAGEMENT AND INSURANCE 21.1 Programme of Risk Management
21.1.1 The Chief Executive shall ensure that the Trust has a programme of
risk management, in accordance with current Department of Health assurance framework requirements, which must be approved and monitored by the Board.
21.1.2 The programme of risk management shall include:
(i) a process for identifying and quantifying risks and potential liabilities,
(ii) engendering among all levels of staff a positive attitude
towards the control of risk, (iii) management processes to ensure all significant risks and
potential liabilities are addressed including effective systems of internal control, cost effective insurance cover, and decisions on the acceptable level of retained risk,
(iv) contingency plans to offset the impact of adverse events, (v) audit arrangements including internal audit, clinical audit,
health and safety review, (vi) a clear indication of which risks shall be insured, (viii) arrangements to review the risk management programme.
21.1.3 The existence, integration and evaluation of the above elements will
assist in providing a basis to make a statement on the effectiveness of Internal Control (SIC) within the Annual Report and Accounts as required by current Department of Health guidance.
21.2 Insurance: Risk Pooling Schemes Administered by the NHR
21.2.1 The Board shall decide if the Trust will insure through the risk pooling schemes administered by NHS Resolution or self-insure for some or all of the risks covered by the risk pooling schemes. If the Board decides not to use the risk pooling schemes for any of the risk areas (clinical, property and employers/third party liability) covered by the scheme this decision shall be reviewed annually.
21.3 Insurance Arrangements with Commercial Insurers
21.3.1 There is a general prohibition on entering into insurance arrangements with commercial insurers. There are however three exceptions when Trusts may enter into insurance arrangements with commercial insurers. The exceptions are: -
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
274 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Shropshire Community Health NHS Trust
September 2021 Page 66
(i) for insuring motor vehicles owned by the Trust including insuring third party liability arising from their use,
(ii) where the Trust is involved with a consortium in a Private
Finance Initiative contract and the other consortium members require that commercial insurance arrangements are entered into,
(iii) where income generation activities take place. Income
generation activities should normally be insured against all risks using commercial insurance. If the income generation activity is also an activity normally carried out by the Trust for aan NHS purpose the activity may be covered in the risk pool. Confirmation of coverage in the risk pool must be obtained from NHS Resolution. In any case of doubt concerning a Trust’s powers to enter into commercial insurance arrangements the Director of Finance and Strategy or the Associate Director of Finance should consult the Department of Health.
21.4 Arrangements to be followed by the Board in Agreeing Insurance Cover
21.4.1 Where the Board decides to use the risk pooling schemes
administered by NHS Resolution the Director of People and Corporate
Services Director of Finance and Strategy or Associate Director of Finance shall ensure that the arrangements entered into are appropriate and complementary to the risk management programme. Director of People and Corporate Services The Director of Finance and Strategy or Associate Director of Finance shall ensure that documented procedures cover these arrangements.
21.4.2 Where the Board decides not to use the risk pooling schemes
administered by NHS Resolution for one or other of the risks covered by the schemes, the Director of People and Corporate Services Director of Finance and Strategy or Associate Director of Finance shall ensure that the Board is informed of the nature and extent of the risks that are self-insured as a result ofbecause of this decision. The Director of
People and Corporate ServicesDirector of Finance and Strategy or Associate Director of Finance will draw up formal documented procedures for the management of any claims arising from third parties and payments in respect of losses, which will not be reimbursed.
21.4.3 All the risk-pooling schemes require scheme members to make some
contribution to the settlement of claims (the “deductible”). The Director
of People and Corporate Services Director of Finance and Strategy or Associate Director of Finance should ensure documented procedures also cover the management of claims and payments below the deductible in each case.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
275 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page | 1
Version: 4.1 Approved by: Trust Board
Date approved
Date issued: July 2011
Review date: July 2013, updated January 2014, October 2014, January 2016, January 2017, January 2018, January 2019, October 2021
Shropshire Community Health NHS Trust AUDIT COMMITTEE Terms of Reference
Document History:
Version: 5.1
Ratified by: Shropshire Community Health NHS Trust Board
Date ratified:
Name of author(s): Michael Wuestefeld-Gray, Interim Governance Lead
Sarah Lloyd, Deputy Director of Finance
Committee Chair Harmesh Darbhanga Non-Executive Director
This Committee/Group reports to: Shropshire Community Health NHS Trust Board Target audience: Shropshire Community Health NHS Trust Board and staff
Audit Committee Terms of Reference
Enclosure 17
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
276 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page | 2
Contents
Section Page 1. Introduction 4 2. Constitution 4 3. Membership 4 4. Meetings and Quorum 5 5. Authority 6 6. Role and Duties 6 7. Auditor Panel 7 8. Monitoring Effectiveness 8 9. Administrative Arrangements 8 10. Relationships and Reporting 9 11. Review of Terms of Reference 9 12. Committee Structure 9 1. Introduction
These Terms of Reference build on original work based around the UK Corporate Governance Code and uses the model from the HFMA NHS Audit Committee Handbook 2018. They reflect the particular nature of Audit Committees in the NHS and the growing role of the Committee in developing integrated governance arrangements and providing assurance that NHS bodies are well managed across the whole range of their activities.
2. Constitution The Board hereby resolves to establish a Committee of the Board of Shropshire Community Health NHS Trust (the Trust) to be known as the Audit Committee (the Committee). The Committee is a Non-Executive committee of the Board and has no executive powers, other than those specifically delegated in these Terms of Reference.
3. Membership The membership of the Committee will comprise at least three independent Non-executive Directors who will be appointed as members of the Committee by the Board, at least one of which will have significant, recent and relevant financial experience. One of the members will be appointed Chair of the Committee by the Board. The Chair of the Committee shall be seen as independent and therefore should not chair any other governance committees. The Chair of the Trust shall not be a member of the Committee. The Non-Executive Chair of the Quality and Safety Committee will be one of the Non-Executive Director Members.
Other directors or their deputies may be asked to attend meetings or part meetings for discussions on matters relating to their portfolio, if required. The provisions of the Trust’s Standing Orders relating to acting up arrangements and joint members will apply to this Committee. Other attendees may be invited for specific items as follows:
Director of Finance
Head of Governance/Corporate Secretary
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
277 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page | 3
A representative from Internal Audit
A representative from External Audit
The Risk Manager
Local Counter Fraud Specialist (LCFS)
Local Security Management Specialist (LSMS) All Non- Executive Directors will be informed of the dates of the Committee meetings and can attend meetings if they wish to. The Chief Executive shall be invited to attend, at least annually, to discuss with the Committee the process for assurance that supports the Annual Governance Statement and the annual report and accounts. The Chief Executive, other Executive Directors and Senior Managers shall be invited to attend for discussions when the Committee is discussing areas of risk or operation that are the responsibility of that Director/Manager. The Corporate Secretary will provide support to the Chair and Committee members and ensure that the Committee receives the appropriate administrative and secretarial support. A secretary/minute taker will also be in attendance at all committee meetings. The Risk Manager should also be invited to attend the meetings to advise as a standing item on issues around the Assurance Framework and other matters related to the Trust’s Internal Control and risk management systems. The Local Counter Fraud Specialist (LCFS) has the right of access to the Committee. The LCFS will be invited to at least two meetings a year to update the Committee on the LCFS’s work, including presenting an annual report and Annual Work plan. The Local Security Management Specialist (LSMS) has the right of access to the Committee. The LSMS will be invited to at least one meeting a year to update the Committee on the LSMS’s work, including presenting an annual report. Representatives from other organisations e.g. NHS Protect may be invited to attend on occasions. At least once a year the Committee will meet privately with the External and Internal Auditors (and LCFS), without any Executive Director present. These discussions should not be minuted unless both the Committee and the auditors agree that a record is required. The Head of Internal Audit and representative of External Audit have the right of direct access to the Committee Chair. Membership will be reviewed annually.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
278 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page | 4
4. Meetings and Quorum
The Chair will preside at all meetings. In extraordinary circumstances where the Chair cannot attend, the Chair will nominate one of the other NEDs to act as vice-chair. Quorum A quorum shall be two members of the Committee. If the Committee is not quorate the meeting may be postponed at the discretion of the Chair. If the meeting does take place and is not quorate, no decision shall be made at that meeting and such matters must be deferred until the next quorate meeting. Frequency Meetings shall be held not less than four times a year. The current work plan for the Trust is four regular meetings together with an additional meeting to focus on the annual accounts. The Board, Chief Executive or External Auditor or Head of Internal Audit may request additional meetings, through the Chair of the Committee, if they consider that one is necessary. Where a decision needs to be taken by the Committee outside the normal cycle of meetings, and where the matter is not deemed by the Chair to require an additional meeting to be called, the decision may be made via e-mail. The preference is for decisions to be taken at committee meetings. The decisions via e-mail process will be used on an exceptions basis. The process for decision via e-mail will be as follows. a) An e-mail setting out the matter for decision will be sent to all committee members on the same
working day. This shall include a statement setting out how the committee members should signify what their view on the matter is and the deadline for doing so.
b) Committee members will be given no less than three working days in which to respond.
c) For a decision to be passed, all of the committee members must express the same view on the matter. Views can be expressed by action or inaction
d) Where committee members have comments on the proposed decision or recommendation/s these will be circulated to other committee members by the Corporate Secretary within one working day of receipt.
e) If any individual committee member wishes to debate an item proposed for decision via e-mail at a committee meeting instead they may ask the Chair to arrange an additional meeting or defer the item for decision until the next committee meeting.
f) Decisions via e-mail will be reported to the next committee meeting and the wording of the decision minuted. Any decision made in this manner will be effective from the date of agreement of all of the committee members and confirmed by email by the Corporate Secretary.
Attendance Committee members are expected to attend all meetings. Apologies must be received by the Corporate Secretary in advance of the meetings. All members will be required to attend a minimum of two thirds of all meetings held annually. Members should not be absent for more than two consecutive meetings without the agreement of the Chair. Any committee member may participate in a meeting by way of telephone, computer or any other electronic means of communication provided that each person is able to hear and speak. A person participating in this way is deemed to be present in person although their actual location shall be noted in the minutes and is counted in a quorum and entitled to vote. The meeting is deemed to take place where the largest group of those participating is assembled, or if there is no such group, where the Chair of the meeting is located. Where a specific matter is deemed to be of a confidential or commercially sensitive nature the Chair has the authority to restrict attendance at the Committee meeting to members only and to ask all attendees to leave the meeting. If any Committee member or attendee has an interest, pecuniary or otherwise, in any matter and is present at the meeting at which the matter is under discussion, he / she will declare that interest as early as possible
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
279 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page | 5
and shall not participate in the discussions. The Chair will have the power to request that member or invitee to withdraw until the Committee’s consideration has been completed. Notice of meetings Meetings of the committee shall be called by the secretary to the committee at the request of the Chair or any of its members. Unless otherwise agreed, notice of each meeting and agenda of items to be discussed, shall be forwarded to each Committee member, any other person required to attend no later than four working days before the date of the meeting. Supporting papers shall be sent to committee members and to other attendees as appropriate, at the same time. Notices, agendas and supporting papers can be sent in electronic form where the recipient has agreed to receive documents in such a way. The Committee will agree a meeting calendar on an annual basis, setting out the main work items to be carried out by the Committee at each meeting to ensure that adequate time is given to the main duties of the Committee.
5. Authority The Committee is authorised by the Board to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised by the Board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. The budget for such advice should be within agreed financial constraints. In addition to the above the Board has nominated the Committee to act as its Auditor Panel.
6. Role and Duties of the Committee The Committee will provide an overarching governance role and review the work of other governance committees within the Trust, whose work can provide relevant assurance to the Committee’s own scope of work. This will particularly include the Quality and Safety Committee and Resources and Performance Committee. Minutes of the meetings of such committees and associated action plans will be presented to the Committee for review. The Committee will uphold the values of the Trust in the work it does. In particular it will look for assurances that these values are being delivered in the Trust, as part of its overall governance role on behalf of the Board. Our values are: Improving Lives
We make things happen to improve peoples’ lives in Shropshire. Everyone Counts
We make sure no-one feels excluded or left behind - patients, carers, staff and the whole community.
Commitment to Quality We all strive for excellence and getting it right for patients, carers and staff every time.
Working Together for Patients Patients come first. We work and communicate closely with other teams, services and organisations to make that a reality.
Compassionate Care We put compassionate care at the heart of everything we do.
Respect and Dignity We see the person every time - respecting their values, aspirations and commitments in life – for patients, carers and staff
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
280 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page | 6
The Committee’s duties can be categorised as follows: Integrated governance, risk management and internal control Reviewing the establishment and maintenance of an effective system of integrated governance, risk management and internal control, across the whole of the organisation’s activities (both clinical and non-clinical), that supports the achievement of the organisation’s objectives. In particular the Committee will review the adequacy and effectiveness of:
All risk and control- related disclosure statements, in particular the annual governance statement, auditor opinions and any other appropriate independent assurance prior to submission to the Board
The assurance processes that indicates the degree of achievement of the organisational objectives and the effectiveness of the management of principal risks.
The policies for ensuring compliance with relevant regulatory legal and code of conduct requirements and any related reporting and self certifications
The policies and procedures for all work related to counter fraud and security as required by NHS Counter Fraud Authority, or other nominated NHS bodies.
In carrying out this work the committee will primarily use the work of internal and external audit. It will also use any other appropriate assurance source, including reports from directors and managers. This work will be focussed through the principal risks, and the assurance framework. As part of its integrated approach the Committee will have effective relationships with other key Committees e.g. Quality and Safety Committee and Resources and Performance Committee so that it understands processes and linkages. These other committees must not usurp the Committee’s role. Internal audit Ensuring there is an effective internal audit function established by management, that meets the Public Sector Internal Audit Standards 2017 and provides appropriate independent assurance to the Committee, Chief Executive and Board. This will be achieved by:
Considering the provision of the internal audit and the costs involved Reviewing and approving the internal audit plan and programme of work, and ensuring that it is
consistent with the needs of the organisation Considering the major findings of audit, the managements responses and the implementation of
risk controls where the need is identified. Ensuring co-ordination of internal and external auditors to optimise the use of audit resources Ensuring that the internal audit function is adequately resourced and has appropriate standing
within the organisation Monitoring the effectiveness of internal audit and carrying out an annual review.
External audit Reviewing and monitoring the independence, objectivity, work and findings of the external auditor appointed and considering the implications of and management’s responses to their work. This will be achieved by:
Considering the appointment and performance of external audit, as far as the rules governing the appointment permit.
Discussing and agreeing with the external auditors the nature and scope of the annual audit plan. Discussing with auditors the evaluation of audit risks and assessment of the organisation and the
impact on the audit fee. Reviewing all external audit reports, including management responses, and the implementation of
additional controls where the need is identified Reviewing any engagement of External Auditors to supply non audit services.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
281 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page | 7
Other assurance functions The Committee shall review the findings of other assurance functions, both internal and external to the organisation, and consider the implications for the governance of the organisation. These will include, but will not be limited to, any reviews by Department of Health and Social Care arm’s length bodies or regulators/inspectors (for example CQC. NHS Resolution etc.) and professional bodies with responsibility for the performance of staff or functions. The Committee will review the work of other committees within the organisation, whose work can provide relevant assurance to the Committee’s own areas of responsibility. In particular this will include the Quality and Safety Committee and Resource and Performance Committee. In reviewing the work related to clinical quality the Committee will satisfy itself that assurance can be gained from the clinical audit function. The committee will review the governance arrangements for procurement Counter Fraud The Committee shall satisfy itself that the organisation has adequate arrangements in place for counter fraud and security that meets NHS Counter Fraud Authority, or other nominated NHS bodies, standards and will review the work from these areas. Management The Committee shall request and review reports, evidence and assurances from directors and managers on the overall arrangements for governance, risk management and internal control. The Committee may also request specific reports from individual functions within the Trust, e.g. clinical audit. Financial reporting The Committee shall monitor the integrity of the financial statements of the organisation and any formal announcements relating to its financial performance. The Committee will ensure that the systems for financial reporting to the board, including those of budgetary control, are subject to review as to the completeness and accuracy of the information provided. The Committee shall review the annual report and financial statements before submission to the Board, focusing particularly on:
The wording in the annual governance statement and other disclosures relevant to the terms of reference of the committee
Changes in, and compliance with, accounting policies, practices and estimation techniques Unadjusted mis-statements in the financial statements Significant judgements in preparation of the financial statements Significant adjustments resulting from the audit Letters of representation Explanations of significant variances
Whistleblowing The Committee shall review the adequacy and security of the arrangements in place for allowing staff and contractors to raise (in confidence) concerns about possible improprieties in financial, clinical or safety matters and ensure that any such concerns are investigated proportionately and independently.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
282 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page | 8
7. Auditor Panel 7.1 Auditor panel arrangements The Board resolved at its meeting in January 2015 to nominate the Audit Committee to act as its Auditor Panel in line with the requirements of the Local Audit (Health Service Bodies Auditor Panel and Independence) Regulations 2015 The panel shall comprise the entire membership of the Audit Committee, i.e. will consist of at least three Non-executive Directors. In line with the regulations each member’s independence will be reviewed against the criteria laid down in the regulations. The Chair of the Audit Committee will act as the Chair of the Auditor Panel. The quorum for the panel will be the same as the Audit Committee, i.e. two non-executive directors. The Auditor Panel Chair will invite executive directors and others to attend depending on the requirements of the meeting agenda. These invitees are not members of the Auditor Panel. Auditors will not attend the Auditor Panel meeting. The Auditor Panel will meet on the same day as the Committee. The frequency and timing of the panel meetings will be dependent on the need to discharge its business, i.e. to advise the Board on the selection of external auditors. Auditor Panel business will be identified clearly separately on the agenda and minutes and Audit Committee members shall deal with these matters as Auditor Panel members not as the Audit Committee. The Chair will formally state at the start of each meeting that the Auditor Panel is meeting in that capacity and not as the Audit Committee Conflicts and interests must be declared in accordance with the Trust’s code of conduct. In respect of the Auditor Panel the Board is authorised to carry out the functions listed in 7.2. The panel is authorised to seek any information it requires from employees and relevant third parties 7.2 Auditor Panel Functions The Auditor Panel’s functions are to:
• advise the Board on the selection and appointment of the External Auditor. This includes: o agreeing and overseeing a robust process for selecting the External Auditors in line with the
organisation’s normal procurement rules o making a recommendation to the board body as to who should be appointed o ensuring that any conflicts of interest are dealt with effectively
• Advise the Board on the maintenance of an independent relationship with the appointed External Auditor
• Advise (if asked) the Board on whether or not any proposal from the External Auditor to enter into a liability limitation agreement as part of the procurement process is fair and reasonable
• Advise on (and approve) the contents of the Trust’s policy on the purchase of non-audit services from the appointed External Auditor
• Advise the Board on any decision about the removal or resignation of the External Auditor.
7.3 Reporting The Chair of the Auditor Panel must report to the Board on how the Auditor Panel discharges its responsibilities. The minutes of the panel’s meetings must be formally recorded and submitted to the Board by the panel’s Chair. The Chair of the Auditor Panel must draw to the attention of the B oard any issues that require disclosure to the full board or require executive action.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
283 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Page | 9
7.4 Remuneration Payments to Auditor Panel members shall be in line with the Trust’s existing approach to remuneration and allowances 7.5 Administration. The administration arrangements will be the same as for the Audit Committee
8. Monitoring Effectiveness
The Committee shall at least once a year, review its own performance, constitution and terms of reference to ensure it is operating at maximum effectiveness and recommend any changes it considers necessary to the Board for approval. The Committee also assesses itself against the HFMA NHS Audit Committee Handbook checklist and draws up an action plan where further work is required. This will be submitted to the Board. The Committee shall be provided with appropriate and timely training, both in the form of an induction programme for new members and on an ongoing basis for all members. The Committee shall arrange for periodic reviews of its own performance and, at least annually, review its constitution and terms of reference to ensure it is operating at maximum effectiveness and recommend any changes it considers necessary to the Board. A record of the frequency of attendance by members, quoracy and the frequency of meetings will be maintained. Any areas of concern will be highlighted to the Chair of the Committee.
9. Administrative Arrangements The Committee will be supported by a nominated secretary who will:
produce a schedule of meetings and maintain the annual work plan for the Committee
prepare the agenda and papers with the Chair and circulate 4 working days prior to the meeting;
maintain accurate records of attendance, key discussion points and decisions taken and issue necessary action logs within five full working days of the meeting;
draft minutes recording where the Committee has gained assurance through relevant reports and subsequent discussion, debate and challenge, and where further assurance is required for circulation to members within five full working days of the meeting;
maintain a database of any documents discussed and/or approved and recall them to the Committee when due;
organise future meetings; and
file and maintain records of the work of the Committee.
10. Relationships and Reporting The Committee will report to the Board on how it discharges its responsibilities. The minutes of Committee meetings will be formally recorded and submitted to the Board. The Chair of the Committee will draw to the attention of the Board any issues that require disclosure to the full Board, or require executive action. The Committee will report to the Board annually on its work in support of the Annual Governance Statement, specifically commenting on the fitness for purpose of the Assurance Framework, the completeness and embeddedness of risk management in the organisation, the integration of governance arrangements and the appropriateness of the self-assessment against regulatory arrangements including the CQC essential standards and any subsequent regulatory regime, and the robustness of the processes behind the quality accounts. As part of its Annual Report to the Board, the Committee will prepare an ‘impact assessment’ to identify specific areas where the Committee has made important positive differences to the governance of the Trust.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
284 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
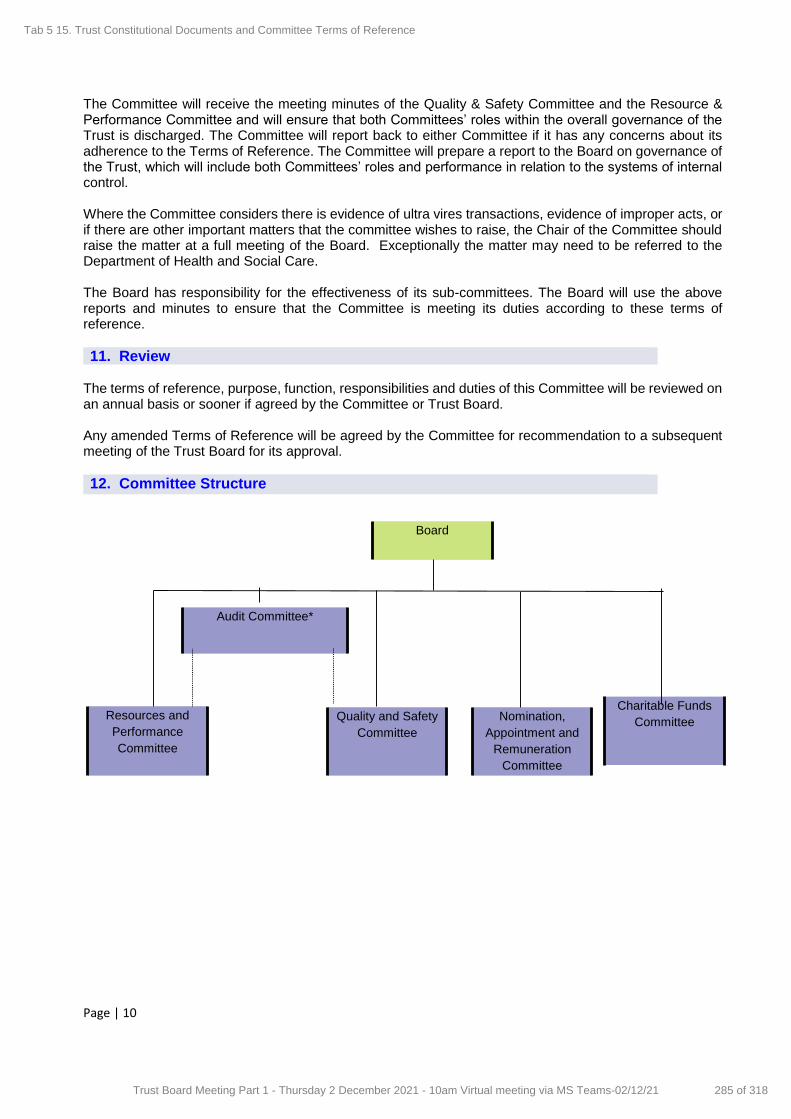
Page | 10
The Committee will receive the meeting minutes of the Quality & Safety Committee and the Resource & Performance Committee and will ensure that both Committees’ roles within the overall governance of the Trust is discharged. The Committee will report back to either Committee if it has any concerns about its adherence to the Terms of Reference. The Committee will prepare a report to the Board on governance of the Trust, which will include both Committees’ roles and performance in relation to the systems of internal control. Where the Committee considers there is evidence of ultra vires transactions, evidence of improper acts, or if there are other important matters that the committee wishes to raise, the Chair of the Committee should raise the matter at a full meeting of the Board. Exceptionally the matter may need to be referred to the Department of Health and Social Care. The Board has responsibility for the effectiveness of its sub-committees. The Board will use the above reports and minutes to ensure that the Committee is meeting its duties according to these terms of reference.
11. Review The terms of reference, purpose, function, responsibilities and duties of this Committee will be reviewed on an annual basis or sooner if agreed by the Committee or Trust Board. Any amended Terms of Reference will be agreed by the Committee for recommendation to a subsequent meeting of the Trust Board for its approval.
12. Committee Structure
Board
Quality and Safety
Committee
Nomination,
Appointment and
Remuneration
Committee
Resources and
Performance
Committee
Audit Committee*
Charitable Funds
Committee
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
285 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1
Draft Nomination, Appointments and Remuneration Committee Terms of Reference
Version: 54
Approved by: Trust Board (in due course)
Date approved Date issued: September 2011
Review date: September 2012, updated June 2015, updated December 2019; Updated September 2021
Shropshire Community Health NHS Trust NOMINATION, APPOINTMENTS AND REMUNERATION COMMITTEE Terms of Reference
Document History:
Version: 45.0 Ratified by: Shropshire Community Health NHS Trust Board
Date ratified:
Name of author(s): Michael Wuestefeld-Gry Interim Governance Lead
Committee Chair Nuala O’Kane - Non-Executive Director
This Committee/Group reports to: Shropshire Community Health NHS Trust Board
Target audience: Shropshire Community Health NHS Trust Board and staff
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
286 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2
1. Introduction and Establishment
All NHS Trust’s are required in law to establish a remuneration committee that sets the terms of service of certain senior managers. The terms of service of non-executive directors, including trust chairs are set by the Secretary of State. The Board hereby resolves to establish a Committee of the Board to be known as the Nominations, Appointments and Remuneration Committee (the Committee). The Committee is a has no executive powers, other than those specifically delegated in these terms of reference. All members of the Committee must be non-executive directors (NEDs).
The Committee has an overall responsibility in respect of the structure, size and composition of the bBoard and matters of pay and employment conditions of service for the Chief Executive, eExecutive dDirectors and sSenior mManagers (including the Corporate Board Secretary) . In order that the Trust shall deliver sound stewardship of public funds the Committee must ensure that the Trust conducts its business in accordance with:
• legal requirements, • the principles of probity, • good people management practice, and • proper corporate governance.
It must also work in a co-operative manner with the NHS England and Improvement Authority (NHSINHSE/I) whose main functions in this regard are to:
appoint, re-appoint and, where necessary, to terminate the appointment of chairs and non- executive directors of NHS trusts
ensure chairs and non-executive directors receive relevant and appropriate training
ensure through annual performance review that chairs and non-executive directors are supported and developed in their role and feel valued
ensure chairs and non-executive directors receive all necessary support through mentoring programmes
ensure that overall NHS boards add value to the NHS locally and more widely.
2. Constitution
The Board hereby resolves to establish a Committee of the Board to be known as the Nominations, Appointments and Remuneration Committee (the Committee). The Committee is a Non-Executive committee of the Board and has no executive powers, other than those specifically delegated in these Terms of Reference.
32. Membership
In line with the Higgs Report recommendations, all members of the Committee must be non-
executive directors (NEDs)
The Committee shall be appointed by the Board and shall consist of all of the non-executive
directors of Shropshire Community Health NHS Trust including the Chair of the Trust, who shall be
appointed as Chair of the Committee by the Board. Any associate non-executive directors will be
attendees at the Committee.
The Chief Executive will attend the Committee in an advisory capacity, except where his/her own
salary, performance or position is being discussed; on such occasions they must not be present
during the meeting.
The Director of Governance/Corporate Secretary should attend and provide support to the Chair
and Committee members, except where his/her own salary, performance or position is being
discussed; on such occasions they must not be present during the meeting. The Corporate
Secretary will ensure that the Committee receives the appropriate administrative and secretarial
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
287 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
3
support, including the co-ordination of papers and the taking of minutes. A secretary/minute taker
may also be in attendance at all committee meetings if appropriate.
Other Executive Directors (EDs) and Senior Managers shall be invited to attend for discussions
when the Committee is discussing areas of risk or operation that are the responsibility of that
Director/Manager. The provisions of the Trust’s Standing Orders relating to acting up
arrangements and joint members will apply to this Committee.
Membership will be reviewed annually.
3. Meetings, and Quorum, and Decision Making
The Chair will preside at all meetings. In extraordinary circumstances where the Chair cannot
attend, the Chair will nominate the Trust’s Deputy Chair or Senior Independent Director to act as
vice-chairChair.
A quorum shall be the Chair and two members of the Committee. If the Committee is not quorate the meeting may be postponed at the discretion of the Chair. If the meeting does take place and is not quorate, no decision shall be made at that meeting and such matters must be deferred until the
next quorate meeting.
Frequency
Meetings shall be held not less than twice per year. Additional meetings shall be held as
necessary, and may be requested by:The current work plan for the Committee is two regular meetings together with any additional meetings as required. The Board or the Chief Executive or
the External Auditor or Head of Internal Audit may request additional meetings,
the Chair; or in consultation with the Chair by
the Chief Executive;
any non-executive director
any executive director
the Trust’s internal and external auditors
the Trust’s corporate secretary
Meetings may be held in-person or remotely.
Reaching Decisions
Like all Trust Committees decisions should be reached by consensus. Where this is not possible the Chair may
resolve to hold a vote, and a decision shall be reached by a simple majority of members voting for or against the
proposal. If there is deadlock the Chair shall have a second, casting vote.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
288 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
4
through the Chair of the Committee, if they consider that one is necessary.
Where a decision needs to be taken by the Committee outside the normal cycle of meetings, and
where the matter is not deemed by the Chair to require an additional meeting to be called, the
decision may be made via e-mail. The preference is for decisions to be taken at committee meetings. The decisions via e-mail process will be used on an exceptionsby exception basis. The
process for decision via e-mail will be as follows.
a) An e-mail setting out the matter for decision will be sent to all committee members on the
same working dayat the same time. This shall include a statement setting out how the committee members should signify what their view on the matter is and the deadline for
doing so. b) Committee members will be given no less than five three working days in which to respond.
c) For a decision to be passed, all of the committee members must express the same view on the matter. This view can be expressed by action or inaction.
d) Where committee members have comments on the proposed decision or
recommendation/s these will be circulated to other committee members by the Corporate
Secretary within one working day of receipt.
e) If any individual committee member wishes to debate an item proposed for decision via e- mail at a committee meeting instead they may ask the Chair to arrange an additional
meeting or defer the item for decision until the next committee meeting (such agreement
by the Chair not to be unreasonably withheld). If the Chair agrees a full meeting of the
Committee will be arranged.
f) Decisions made via e-mail will be reported to the next committee meeting and the wording of the decision minuted. Any decision made in this manner will be effective from the date of
agreement of all of the committee members and confirmed by email by the Corporate
Secretary.Chair or Committee Secretariat
Attendance
Members are expected to attend all meetings.; however, as a minimum should attend at least two
thirds of all meetings. Apologies must be received by the Corporate SecretaryChair or Committee
Secretary in advance of the meetings.any meeting. Members should not be absent for more than
two consecutive meetings, without the permission of the Chair.
Any committee member may participate in a meeting by way of telephone, computer or any other electronic means of communication provided that each person is able to hear and speak. A person participating in this way is deemed to be present in person although their actual location shall be noted in the minutes and is counted in a quorum and entitled to vote. The meeting is deemed to take place where the largest group of those participating is assembled, or if there is no such group, where the Chair of the meeting is located.
Where a specific matter is deemed to be of a confidential or commercially sensitive nature the Chair has the authority to restrict attendance at the Committee meeting to members only and to ask all invitees to leave the meeting.
If any member has an interest, pecuniary or otherwise, in any matter and is present at the meeting at which the matter is under discussion, he / she will declare that interest as early as possible and shall not participate in the discussions. The Chair will have the power to request that member to withdraw until the Committee’s consideration has been completed.
Notice of meetings Meetings of the committee shall be called by the secretary to the committeeconvened by the Committee Secretariat at the request of the Chair .or any of its members.
Unless otherwise agreed, notice of each meeting and agenda of items to be discussed, shall be forwarded to each Committee member, any other person required to attend no later than four working
Formatted: Font color: Text 1
Formatted: No underline, Underline color: Auto, Font
color: Text 1
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
289 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
5
5. Role and Duties of the Committee
days before the date of the meeting. Supporting papers shall be sent to committee members and to other attendees as appropriate, at the same time.
Notices, agendas and supporting papers willcan be sent in electronic form where the recipient has agreed to receive documents in such a way. The Committee will agree a meeting calendar on an annual basis, setting out the main work items to be carried out by the Committee at each meeting to ensure that adequate time is given to the main duties of the Committee.
4. Authority
The Committee is authorised by the Board to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co- operate with any request made by the Committee.
The Committee is authorised by the Board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. The budget for such advice should be within agreed financial constraints.
The Committee is authoriszed to:
approve the performance criteria of the Chief Executive and, in consultation with the Chief Executive, the Executive Directors/Directors of the Trust Board and the Trust’s senior management, as designated.
consider and approve annual pay and remuneration packages, following satisfactory assessment of performance of the Chief Executive, and eExecutive dDirectors, and/ Directors/sSenior mManagers (as designated), having proper regard to the organisation's circumstances and performance and to the provisions of any national arrangements for such staff, where appropriate.
approve the appointment and remuneration packages for new Executive Director/Director appointments to the Trust Board and other members of the Trust’s senior management as designated, including the approval or interim or acting-up arrangements..
to establish an Appointment Panel of the Committee for the appointment of the Executive
Directors/Directors of the Trust Board
to maintain oversight and seek assurance of the management of any interests declared by executive directors and senior managers (as designated).
to maintain oversight and seek assurance of the continued compliance of executive directors and senior managers (as designated) with fit and proper person requirements.
to maintain oversight and seek assurance of the management and mitigation of those risks relating to organisational memory, succession planning, the skills experience and make-up of the Board etc.
contribute as needed to the development of and appointment to leadership positions within the local Integrated Care System or of system partners.
The Committee will uphold the values of the Trust in the work it does. In particular it will look
for assurances that these values are being delivered upheld in the Trust, as part of its overall
governance role on behalf of the Board. Our values are:
Improving Lives: we make things happen to improve peoples’ lives in our communities
Everyone Counts: we make sure no-one feels excluded or left behind - patients, carers, staff and the whole community.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
290 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
6
Commitment to Quality: we all strive for excellence and getting it right for patients, carers and staff every time.
Working Together for Patients: patients come first. We work and communicate closely with other teams, services and organisations to make that a reality.
Compassionate Care: we put compassionate care at the heart of everything we do.
Respect and Dignity: we see the person every time - respecting their values, aspirations and commitments in life – for patients, carers and staff.
The Committee’s duties can be categorised as follows:
Nomination – the identification of key skills, capacity and capability to ensure the
composition of a well-led and healthy NHS board
regularly review the structure, size and composition (including the skills, knowledge and experience) required of the board compared to its current position, and make recommendations to the board with regard to any changes (and to the NHSI in respect of any changes to NED appointments);
give full consideration to succession planning for all board members in the course of its
work, taking into account the challenges and opportunities facing the trust, and what skills
and expertise are therefore needed on the board of directors in the future;
before any appointment is made by to the board of directors, evaluate the balance of
skills, knowledge and experience on the board, and, in the light of this evaluation
prepare a description of the role and capabilities required for a particular appointment.
keep under review the leadership needs of the organisation, with a view to ensuring the
continued ability of the organisation to deliver services effectively;
keep up to date and fully informed about strategic issues and commercial changes
affecting the trust and the environment in which it operates; and
Appointments – overseeing an open and transparent process for the appointment, appraisal and removal of Chief Executive, the Executive Directors/Directors of the Trust Board and the Trust’s senior management, as designated.
In identifying suitable candidates for a NED appointment the committee shall work in
conjunction with the NHSI’s appointment processes
In identifying suitable candidates for executive director ED appointments the c Committee shall – use open advertising or the services of external advisers to facilitate the search – consider candidates from a wide range of backgrounds – consider candidates on merit and against objective criteria, taking care that
appointees have enough time available to devote to the position; – consider any matter relating to the appointment of an individual in relation to the
‘Fit and Proper Test for Directors’.
to consider any matter relating to the continuation in office at any time of any Board member, (for example in relation to the ‘Fit and Proper Person Test For Directors’) including suspension or termination of service. For NED appointments this will be in conjunction with the NHSI.
to receive reports on any matter relating to the continuation in office at any time including the suspension or termination of service of any senior manager as an employee/officer of the Trust.
review the job descriptions of the executive director and senior manager roles as required;
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
291 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
7
review annually the performance evaluation process for executive directors and senior managers EDs ensuring it is fit for purpose
Remuneration – determining the remuneration policy and packages for Executive
Director/Director appointments to the Trust Board and other members of the Trust’s senior
management as designated
To determine salary levels for any of those the appointments specified above not on
Agenda for Change or other national terms and conditions, ensuring that basic salaries are maintained at a level which allows the organisation to retain and compete in the market place.
Consider the pension consequences and associated costs to the Trust of any salary
increases.
To make external comparisons with other similar sized trusts to ensure
competitiveness using nationally available benchmarking information.
To ensure that annual pay increases are awarded both in relation to performance and to
an assessment of market movement based on independent data and in accordance with
overall NHS Executive Director guidance.
To ensure that any supplementary/performance payments relate to the satisfactory
performance of the organisation.
To ensure that contractual obligations are honoured and that contracts are reviewed from
time to time to ensure that they remain up to date and defensible.
To agree any associated benefits that will form part of the overall remuneration package,
including car allowances and removal expenses.
Severance Payments
To receive from the Chairman, details of appraisal of the Chief Executive.
To monitor and evaluate the performance of individual eExecutive Ddirectors/ Directors
and other members of the Trust’s senior management (as designated) annually and or
more frequently if the Chief Executive considers it appropriaterequested by the Chief
Executive.
To agree and ratify all non-statutory severance payments to be made on behalf of the Trust ensuring including seeking assurance that necessarythat all necessary reporting processes are followed to HM Treasury and the NHSI. This will include redundancy payments in accordance with delegated limits – below £50,000, the chief executive will authorise payments and report these to the remuneration committee at its next meeting. For payments of a value of £50,000 and above, a business case will be presented to the remuneration committee for approvalset out in the Trust’s constitutional documents
To agree any disputes settlements for any staff groups above £10,000.
To monitor and make recommendations on all discretionary policies in lieu of a supplement to pay benefit or expenses entitlements of employees.
6. Monitoring Effectiveness
The Committee shall at least once a year, review its own performance, constitution and terms of reference to ensure it is operating at maximum effectiveness and recommend any changes it considers necessary to the Audit Committee and then the Board for approval.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
292 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
8
Members of The Committee shall be provided with appropriate and timely training, both in the form of an induction programme for new members and on an ongoing basis for all members.
The Committee shall arrange for periodic reviews of its own performance and, at least annually, review its constitution and terms of reference to ensure it is operating at maximum effectiveness and recommend any changes it considers necessary to the Board.
A record of the frequency of attendance by members, quoracy and the frequency of meetings will
be maintained. Any areas of concern will be highlighted to the Chair of the Committee.
7. Administrative Arrangements
The Director of Governance/Corporate Affairs/Board SsecretaryCorporate Secretary will ensure that the Committee receives appropriate administrative support. Duties will include:
produce a schedule of meetings and maintain the annual work plan for the Committee
prepare the agenda and papers with the Chair and circulate 4 working days prior to the meeting;
maintain accurate records of attendance, key discussion points and decisions taken and issue necessary action logs within five full working days of the meeting;
draft minutes recording where the Committee has gained assurance through relevant reports and subsequent discussion, debate and challenge, and where further assurance is required for circulation to members within five full working days of the meeting;
maintain a database of any documents discussed and/or approved and recall them to the Committee when due;
organise future meetings; and file and maintain records of the work of the Committee.
8. Relationships and Reporting
The Minutes of the Committee shall be formally recorded and a summary of decisions taken
submitted to the Trust Board by the Chair of the Committee. The Chair of the Committee shall draw to the attention of the Trust Board any issues that require disclosure to the full Trust Board, or require executive action.
The Committee shall make a Remuneration Report in the Trust’s annual report about its activities
and the process used to make appointments.
9. Review of Terms of Reference
The terms of reference, purpose, function, responsibilities and duties of this Committee will be reviewed on an annual basis or sooner if agreed by the Committee or Trust Board.
Any amended Terms of Reference will be agreed by the Committee for recommendation to a subsequent meeting of the Trust Board for its approval.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
293 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Quality and Safety Committee Terms of Reference for review July 2022 Page 1 of 9
Version: 11 Approved by:
Date approved
Date issued: 24 May 2012
Review date: 15 July 2021
Shropshire Community Health NHS Trust QUALITY AND SAFETY COMMITTEE Terms of Reference
Document History:
Version: 11
Ratified by: Shropshire Community Health NHS Trust Board
Date ratified: TBC – Aim is for Board Meeting September 2021
Name of author(s): Steve Gregory Director of Nursing and Operations Claire Lea, Corporate Governance Director
Committee Chair Peter Featherstone, Non-Executive Director
This Committee/Group reports to: Shropshire Community Health NHS Trust Board Target audience: Shropshire Community Health NHS Trust Board and Staff
Quality and Safety Committee Terms of Reference
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
294 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Quality and Safety Committee Terms of Reference for review July 2022 Page 2 of 9
Contents
Section Page 1. Introduction 1 2. Constitution 1 3. Membership 3 4. Meetings and Quorum 3 5. Authority 6. Role and duties of the Committee 4 7. Monitoring effectiveness 6 8. Administrative Arrangements 6 9. Relationships and Reporting 6 10. Review 6 11. Committee Structure 7
1. Introduction The Quality and Safety Committee is a sub-committee of the Board of Shropshire Community Health NHS Trust (the Trust) and has delegated authority from the Board to oversee, co-ordinate, review and assess the quality and clinical safety arrangements within the Trust. The Quality & Safety Committee will provide scrutiny and challenge with regard to all aspects of quality and clinical safety, including strategy, delivery, clinical governance, research and clinical audit, in order to obtain assurance and make appropriate reports or recommendations to the Board. 2. Constitution The Board hereby resolves to establish a committee of the Board to be known as the Quality and Safety Committee (the Committee). The Committee has no executive powers other than those specifically delegated in these Terms of Reference. 3. Membership The membership of the Committee will comprise:
• Three Two Non-Executive Directors (including Committee Chair & Deputy Chair) as appointed by the Board
• Director of Nursing & Operations • Medical Director • Director of People • Director of Governance/Corporate Secretary • Chief Operating Officer
Other directors or their deputies may be asked to attend meetings or part meetings for discussions on matters relating to their portfolio, if required. The provisions of the Trust’s Standing Orders relating to acting up arrangements and joint members will apply to this Committee. Other attendees may be invited for specific items as follows:
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
295 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Quality and Safety Committee Terms of Reference for review July 2022 Page 3 of 9
• Deputy Director of Allied Health ProfessionalsOperations • Deputy Director of Nursing & Quality • Chief Pharmacist • Heads of Nursing and Quality • Head of Safeguarding • Head of IPC • Head of HR and WorkforceDeputy Director of People
All Board members will be informed of the dates of the Committee meetings and can attend meetings if they wish to. The Corporate SecretaryHead of Governance will provide support to the Chair and Committee members of the Committee and ensure that the Committee receives the appropriate administrative and secretarial support. A secretary/minute taker will also be in attendance at all committee meetings. Membership will be reviewed annually. 4. Meetings and Quorum The Chair will preside at all meetings. In circumstances where the Chair cannot attend, the Deputy Chair will chair the meeting.another non-executive director shall act as chair Quorum A quorum will be three members and must include two Non-Executive Directors and 1 one Executive Director including the Chair or Deputy Chair and the Director of Nursing and Operations or Medical Director. If the Committee is not quorate the meeting may be postponed at the discretion of the Chair. If the meeting does take place and is not quorate, no decision shall be made at that meeting and such matters must be deferred until the next quorate meeting. Frequency The Committee will meet every monthno less than six times a year. Additional meetings of the Committee can be arranged for specific purposes as necessary, with agreement by the Chair or Deputy Chair. Where a decision needs to be taken by the Committee outside the normal cycle of meetings, and where the matter is not deemed by the Chair to require an additional meeting to be called, the decision may be made via e-mail. The preference is for decisions to be taken at committee meetings. The dDecisions via e-mail process will be used on an by done by exceptions basis. The process for decision via e-mail will be as follows.
a) The Chair shall agree that a matter can be decided by email. b) An e-mail setting out the matter for decision will be sent to all committee members
on the same working day. This shall include a statement setting out how the committee members should signify what their view on the matter is and the deadline for doing so.
b) Committee members will be given no less than five working days in which to
respond.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
296 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Quality and Safety Committee Terms of Reference for review July 2022 Page 4 of 9
c) For a decision to be passed, all of the committee members must express the same view on the matter.made all members of the Committee must indicate their agreement, and this can be done by action or in-action (i.e. a non-response may be taken as agreement).
d) Where committee members have comments on the proposed decision or
recommendation/s these will be circulated to other committee members by the Corporate SecretaryCommittee Secretariat or person making the prosposal. within one working day of receipt.
e) If any individual member of the Ccommittee member wishes to debate discuss
thean item proposed for decision via e-mail at a Ccommittee meeting instead they may ask the Chair to arrangefor an additional meeting or defer the item for decision until the next committee meeting (such agreement by the Chair not to be unreasonably withheld).
f) Decisions via e-mail will be reported to the next committee meeting and the wording
of the decision will be minuted. Any decision made in this manner will be effective from the date of agreement of all of the committee members and confirmed by email by the Corporate Secretaryor the date proposed by the person seeking the decision.
Attendance Committee members are expected to attend all meetings. Apologies must be received by the Corporate SecretaryChair or Committee Secretariat in advance of the meetings. All members will be required to attend a minimum of two thirds of all meetings held annually. Members should not be absent for more than two consecutive meetings without the agreement of the Committee Chair. Any Ccommittee member may participate in a meeting by way of telephone, computer or any other electronic means of communication provided that each person is able to hear and speak. A person participating in this way is deemed to be present in person although their actual location shall be noted in the minutes and is counted in a quorum and entitled to vote. The meeting is deemed to take place where the largest group of those participating is assembled, or if there is no such group, where the Chair of the meeting is located. Where a specific matter is deemed to be of a confidential or commercially sensitive nature the Chair has the authority to restrict attendance at the Committee meeting to members only and to ask some or all attendees and invitees to leave the meeting. If any Committee member, attendee or invitee has an interest, pecuniary or otherwise, in any matter and is present at the meeting at which the matter is under discussion, he / she will declare that interest as early as possible and shall not participate in the discussions. The Chair will have the power to request that member, attendee or invitee to withdraw until the Committee’s consideration has been completed. Notice of meetings Meetings of the committee shall be called by the secretary to the cCommittee at the request of the Chair or any of its members. Unless otherwise agreed, notice of each meeting and agenda of items to be discussed, shall be forwarded to each Committee member, any other person required to attend no later than four working days before the date of the meeting. Supporting papers shall be sent to committee Committee members and to other attendees as appropriate, at the same time.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
297 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Quality and Safety Committee Terms of Reference for review July 2022 Page 5 of 9
Notices, agendas and supporting papers can shall be sent provided in electronic form where the recipient has agreed to receive documents in such a way.. The Committee will agree a meeting calendar on an annual basis, setting out the main work items to be carried out by the Committee at each meeting to ensure that adequate time is given to the main duties of the Committee. 5. Authority The Committee is authorised by the Board to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised by the Board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. The budget for such advice should be within agreed financial constraints. 6. Roles and duties of the Committee The Committee will uphold the values of the Trust in the work it does. In particular it will look for assurances that these values are being delivered in the Trust, as part of its overall governance role on behalf of the Board. Our values are: Improving Lives
We make things happen to improve peoples’ lives in our communities.
Everyone Counts We make sure no-one feels excluded or left behind - patients, carers, staff and the
whole community.
Commitment to Quality We all strive for excellence and getting it right for patients, carers and staff every
time. Working Together for Patients
Patients come first. We work and communicate closely with other teams, services and organisations to make that a reality.
Compassionate Care We put compassionate care at the heart of everything we do.
Respect and Dignity We see the person every time - respecting their values, aspirations and commitments
in life – for patients, carers and staff The Committee’s duties can be categorised as follows:
To ensure the Trust’s compliance against the statutory requirements laid down by the Care Quality Commission
To drive and monitor the any improvement plan following the a CQC inspection
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
298 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Quality and Safety Committee Terms of Reference for review July 2022 Page 6 of 9
To provide assurance to the Board that the actions identified in thate iImprovement pPlan following the CQC inspection are being completed within timescales are and monitored on a regular basis through the Quality and Safety Governance processes.
To ensure treat patients, carers and members of the public are treated as equal partners in the review and redesign of services ensuring that engagement results in comprehensive and involved patients, carers and service users in Trust day to day activity.
To provide assurance to the Board that there are adequate systems and processes in place to ensure and continuously improve patient safety and management of risk across all Trust services.
To provide assurance to the Board that there are effective structures to measure and continuously improve the effectiveness of care.
To maintain oversight of and provide assurance to the Board that the Trust is complying with its statutory duties in terms of health and safety.
To provide assurance to the Board that the Trust is listening to patients about their experiences of care and taking action to improve the experience of those using its services.
To provide assurance to the Board that the Trust is also listening to staff about their experience of working within the Trust and taking action where required to improve those experiences.
To provide assurance to the Board that the Trust is working with partners and priority groups in relation to the equality agenda.
To review, approve and monitor implementation of the Quality and Clinical Strategy and the Quality Accounts.
To receive regular reports in order to monitor capability and organisational cultural issues as they impact on quality and patient safety and will agree strategies for improvement
To oversee the groups that report to the Committee in relation to quality, effectiveness and patient and staff experience in order to assure members and the Board that clinical services are giving appropriate priority to continuous improvement in quality and patient safety and experience.
To receive the monthly quality dashboard report for the Trust around an agreed set of Key Performance Indicators that will provide assurance in relation to the indicators required by NHS Improvement.
Where performance in respect of quality, effectiveness, patient or staff safety has fallen short of agreed standards, to request evidence of assurance that the concerns have been investigated, corrective action has been taken and lessons have been learnt
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
299 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21

Quality and Safety Committee Terms of Reference for review July 2022 Page 7 of 9
To review service changes and the Quality Equality Impact Assessment (QEIA) of Cost Improvement Programmes/Quality Innovation Prevention & Productivity initiatives within the Trust.
To escalate key issues to Directors and the Board and provide regular feedback to the Board on the activity of the Committee in the form of a bi monthly report.
To receive reports on significant concerns or adverse findings highlighted by external bodies in relation to clinical quality and safety and the actions being taken by management to address these
To annually review the quality aspects of the Board Assurance Framework 7. Monitoring Effectiveness The Committee shall at least once a year, review its own performance, constitution membership and terms of reference to ensure it is operating at maximum effectiveness and recommend any changes it considers necessary to the Board for approval. The Committee shall be provided with appropriate and timely training, both in the form of an induction programme for new members and on an ongoing basis for all members. The Committee shall arrange for periodic reviews of its own performance and, at least annually, review its constitution work plan and terms of reference to ensure it is operating at maximum effectiveness and recommend any changes it considers necessary to the Board. A record of the frequency of attendance by members, quoracy and the frequency of meetings will be maintained. Any areas of concern will be highlighted to the Chair of the Committee. 8. Administrative Arrangements The Committee will be supported by a nominated secretary who will:
produce a schedule of meetings and maintain the annual work plan for the Committee
prepare the agenda and papers with the Chair and circulate four working days prior to the meeting;
maintain accurate records of attendance, key discussion points and decisions taken and issue necessary action logs within five full working days of the meeting;
draft minutes recording where the Committee has gained assurance through relevant reports and subsequent discussion, debate and challenge, and where further assurance is required for circulation to members within five full working days of the meeting;
maintain a database of any documents discussed and/or approved and recall them to the Committee when due;
organise future meetings; and
file and maintain records of the work of the Committee. 9. Relationships and Reporting The Committee will obtain assurance from the working groups shown in the structure chart below
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
300 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
Quality and Safety Committee Terms of Reference for review July 2022 Page 8 of 9
The Committee will report to the Board on how it discharges its responsibilities. The Audit Committee will receive the meeting minutes of the Committee and will ensure that the Committee’s role within the overall governance of the Trust is discharged. The Audit Committee will report back to the Committee if it has any concerns about its adherence to the Terms of Reference. The Audit Committee will prepare a report to the Board on governance of the Trust, which will include the Committee’s role and performance in relation to the systems of internal control. The minutes of the Committee shall be formally recorded and a summary of decisions taken submitted reported to the Trust Board by the Chair of the Committee. The minutes will also be submitted to the Board. The Chair of the Committee shall draw to the attention of the Trust Board any issues that require disclosure to the full Trust Board, or require executive action. The Committee will receive standing monthly reports and additional reports as part of the scheduled programme of annual reports. The Trust’s integrated quality and safety report will be provided quarterly with an exception report provide monthly updates. In addition, the Committee will receive thematic ‘deep dive’ reports or reviews accordingly to provide more quality-orientated discussions about specific issues and to facilitate in depth discussions between the Committee members and staff providing services. The Quality and Safety Delivery Group will meet monthly and will receive a schedule of reports prior to Committee. Internal Auditors will carry out an audit of the governance systems within the Trust, including the role of the Committee, and will use this audit to prepare the annual Head of Internal Audit Opinion. The Board has responsibility is responsible for the effectiveness of sub-its committees. The Board will use the above reports to ensure that the Committee is meeting its duties according to these Terms of Reference. 10. Review The terms of reference, purpose, function, responsibilities and duties of this Committee will be reviewed on an annual basis or sooner if agreed by the Committee or Trust Board. Any amended Terms of Reference will be agreed by the Committee for recommendation to a subsequent meeting of the Trust Board for its approval. 10. Committee Structure The Committee structure to the Board is shown in the chart below. The committee structure is reflected in the chart below, however reporting groups may
change to reflect operational requirements.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
301 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
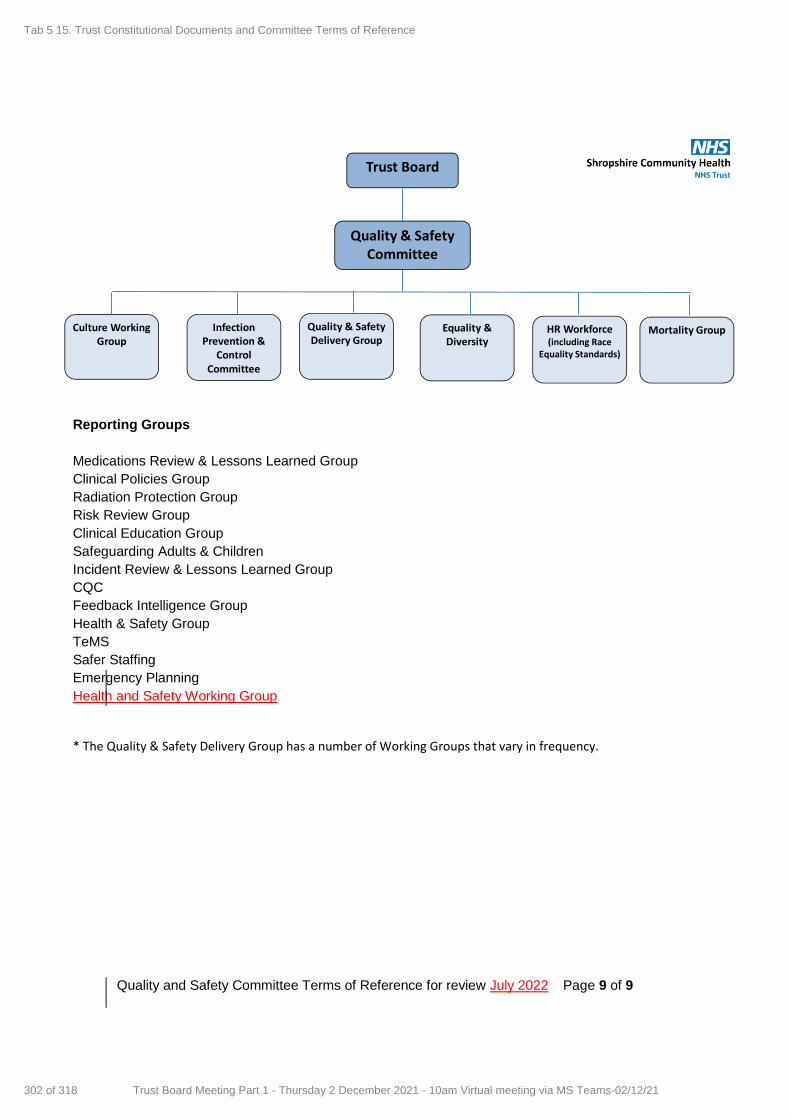
Quality and Safety Committee Terms of Reference for review July 2022 Page 9 of 9
Quality & Safety Delivery Group
Trust Board
Quality & SafetyCommittee
Culture Working Group
Infection Prevention &
Control Committee
Equality & Diversity
HR Workforce (including Race
Equality Standards)
Mortality Group
Reporting Groups
Medications Review & Lessons Learned Group
Clinical Policies Group
Radiation Protection Group
Risk Review Group
Clinical Education Group
Safeguarding Adults & Children
Incident Review & Lessons Learned Group
CQC
Feedback Intelligence Group
Health & Safety Group
TeMS
Safer Staffing
Emergency Planning
Health and Safety Working Group
* The Quality & Safety Delivery Group has a number of Working Groups that vary in frequency.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
302 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1
Resource and Performance Committee Terms of Reference
Version 10.4 Approved by Trust Board
Date approved Date issued: September 2021
Review date: July 2022
Shropshire Community Health NHS Trust RESOURCE AND PERFORMANCE COMMITTEE Terms of Reference
Document History: Version: 10.4
Ratified by: TBC Aim is Trust Board September 2021
Date ratified: Update:
20 March 2014 26 August 2014 25 January 2016 23 January 2017 March 2018 November 2019 October 2020
Name of author(s): Ros Preen, Director of Finance and Strategy Claire Lea, Corporate Governance Consultant
Name of responsible committee/individual: Shropshire Community Health NHS Trust Board Target audience: Shropshire Community Health NHS Trust Board and staff
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
303 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2
Contents
Section Page
1. Introduction 2 2. Constitution 2 3. Membership 2 4. Meeting and Quorum 3 5. Authority 6. Roles and Duties of the Committee 3 7. Monitoring Effectiveness 4 8. Administrative Arrangements 4 9. Relationships & reporting 4 10. Review 4 11. Committee Structure 5
1. Introduction
The Resource and Performance Committee is a sub-committeeCommittee of the Board of Shropshire Community Health NHS Trust (the Trust) and has delegated authority from the Board to oversee, co-ordinate, review and assess the financial and performance management arrangements within the Trust.
The Resource and Performance Committee will assist in ensuring that Board members have a sufficiently robust understanding of key performance and financial issues to enable sound decision-making.
2. Constitution
The Board hereby resolves to establish a committee of the Board to be known as the Resource and Performance Committee (the Committee). The Committee has no executive powers other than those specifically delegated in these Terms of Reference.
3. Membership
The membership of the Committee will comprise:
Three Non-Executive Directors (including Committee Chair & Deputy Chair) as appointed by the Board
Associate Director of Finance
Director of Nursing & Operations
Director of Governance/Corporate SecretaryChief Operating Officer
Representative from the Patient & Carer Panel
Other directors or their deputies may be asked to attend meetings or part meetings for discussions on matters relating to their portfolio, if required. The provisions of the Trust’s Standing Orders relating to acting up arrangements and joint members will apply to this Committee.
Other attendees may be invited for specific items as follows:
Medical Director
Head of Finance
Head of Informatics
Head of HR & WorkforceDeputy Director of People
Deputy Director of Operations
Deputy Director of Nursing
Head of Development and Transformation
Information Programme Manager
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
304 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
3
All Board members will be informed of the dates of the Committee meetings and can attend meetings if they wish to.
The Corporate Secretary will provide support to the Chair and Committee members and ensure that the Committee receives the appropriate administrative and secretarial support. A secretary/minute taker will also be in attendance at all committee meetings.
Membership will be reviewed annually.
4. Meetings and Quorum
The Chair will preside at all meetings. In extraordinary circumstances where the Chair cannot attend, the Deputy Chair will chair the meeting.anoher non-executive director shall act as chair.
Quorum A quorum will be three members and must include two Non-Executive Directors and 1 one Executive Director including the Chair or Vice Chair . If the Committee is not quorate the meeting may be postponed at the discretion of the Chair. If the meeting does take place and is not quorate no decisions shall be made at that meeting and such matters must be deferred until the next quorate meeting.
Frequency The Committee will meet every month no less than six times a year. Additional meetings of the Committee can be arranged for specific purposes as necessary, with agreement by the Chair or Deputy Chair.
Where a decision needs to be taken by the Committee outside the normal cycle of meetings, and where the matter is not deemed by the Chair to require an additional meeting to be called, the decision may be made via e-mail. The preference is for decisions to be taken at committee meetings. The dDecisions via e-mail process will be used on an exceptions basisdone by exception. The process for decision via e-mail will be as follows.
a) The Chair shall agree that a matter can be decided by email. b) An e-mail setting out the matter for decision will be sent to all committee members on
the same working day. This shall include a statement setting out how the committee members should signify what their view on the matter is and the deadline for doing so.
b) Committee members will be given no less than five working days in which to respond. c) For a decision to be passed, all of the committee members must express the same view
on the matter. made all members of the Committee must indicate their agreement, and this can be done by action or in-action (i.e. a non-response may be taken as agreement).
d) Where committee members have comments on the proposed decision or
recommendation/s these will be circulated to other committee members by the Committee Secretariat or person making the prosposalCorporate Secretary within one working day of receipt.
e) If any individual member of the cCommittee member wishes to debate anto discuss the
item proposed for decision via e-mail at a committee meeting instead they may ask the Chair to arrangefor an additional meeting or defer the item for decision until the next committee meeting (such agreement by the Chair not to be unreasonably withheld).
f) Decisions via e-mail will be reported to the next committee meeting and the wording of
the decision will be minuted. Any decision made in this manner will be effective from the date of agreement of all of the committee members and confirmed by email by the Corporate Secretary.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
305 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
4
Attendance Committee members are expected to attend all meetings. Apologies must be received by the Corporate SecretaryChair or Committee Secretariat in advance of the meetings. All members will be required to attend a minimum of two thirds of all meetings held annually. Members should not be absent for more than two consecutive meetings without the agreement of the Committee Chair.
Any Ccommittee member may participate in a meeting by way of telephone, computer or any other electronic means of communication provided that each person is able to hear and speak. A person participating in this way is deemed to be present in person although their actual location shall be noted in the minutes and is counted in a quorum and entitled to vote. The meeting is deemed to take place where the largest group of those participating is assembled, or if there is no such group, where the Chair of the meeting is located.
Where a specific matter is deemed to be of a confidential or commercially sensitive nature the Chair has the authority to restrict attendance at the Committee meeting to members only and to ask some or all attendees and invitees to leave the meeting.
If any Committee member, attendee or invitee has an interest, pecuniary or otherwise, in any matter and is present at the meeting at which the matter is under discussion, he / she will declare that interest as early as possible and shall not participate in the discussions. The Chair will have the power to request that member, attendee or invitee to withdraw until the Committee’s consideration has been completed.
Notice of meetings Meetings of the committee shall be called by the secretary to the Ccommittee at the request of the Chair or any of its members.
Unless otherwise agreed, notice of each meeting and agenda of items to be discussed, shall be forwarded to each Committee member, any other person required to attend no later than four working days before the date of the meeting. Supporting papers shall be sent to Ccommittee members and to other attendees as appropriate, at the same time.
Notices, agendas and supporting papers can shall be sent provided in electronic form where the recipient has agreed to receive documents in such a way.
The Committee will agree a meeting calendar on an annual basis, setting out the main work items to be carried out by the Committee at each meeting to ensure that adequate time is given to the main duties of the Committee.
5. Authority
The Committee is authorised by the Board to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee.
The Committee is authorised by the Board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. The budget for such advice should be within agreed financial constraints.
6. Role and Duties of the Committee
The Committee will uphold the values of the Trust in the work it does. In particular it will look for assurances that these values are being delivered in the Trust, as part of its overall governance role on behalf of the Board. Our values are:
Improving Lives We make things happen to improve peoples’ lives in Shropshire.
Everyone Counts We make sure no-one feels excluded or left behind - patients, careers, staff and the whole community.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
306 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
5
Commitment to Quality We all strive for excellence and getting it right for patients, carers and staff every time.
Working Together for Patients Patients come first. We work and communicate closely with other teams, services and organisations to make that a reality.
Compassionate Care We put compassionate care at the heart of everything we do.
Respect and Dignity We see the person every time - respecting their values, aspirations and commitments in life – for patients, carers and staff
The Committee’s duties can be categorised as follows:
Oversee and monitor the financial and performance management systems of the organisation responding the requirements of the Board.
Continue to develop and improve effective financial and performance management systems, highlighting risks and areas for consideration and providing reports to the Board.
Receive assurance from the Benefits Realisation Group and monitor performance against the Cost Improvement Programme (CIP) / Quality, Innovation, Productivity and Prevention (QIPP) programme and the organisation’s contribution to system transformation in Shropshire.
Receive and consider business development proposals, progress updates and post implementation evaluations.
Consider all financial and performance risks and whether these should be added to the Board Assurance Framework or Directorate risk register.
Review progress and issues relating to the delivery of the targets resulting from the organisation’s strategy and business plan. In particular review and monitor:
contractual targets;
efficiency indicators; and
financial performance of the organisation against budgets
Approve and monitor action plans where remedial steps are required to improve financial and system management performance.
Approve the Trust’s capital programme and receive regular information on its implementation through the finance report and from the Transformation Programme Board.
Receive minutes from the Digital Programme Group chaired by the Director of Finance and Strategy.
Receive reports on and consider the outcome of periodic performance reviews to assess Directorate performance against key objectives and targets.
Receive reports from working groups as appropriate:
7. Monitoring Effectiveness
The Committee shall at least once a year, review its own performance, constitution and terms of reference to ensure it is operating at maximum effectiveness and recommend any changes it considers necessary to the Board for approval.
The Committee shall be provided with appropriate and timely training, both in the form of an induction programme for new members and on an ongoing basis for all members.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
307 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
6
The Committee shall arrange for periodic reviews of its own performance and, at least annually, review its constitution and terms of reference to ensure it is operating at maximum effectiveness and recommend any changes it considers necessary to the Board.
A record of the frequency of attendance by members, quoracy and the frequency of meetings will be maintained. Any areas of concern will be highlighted to the Chair of the Committee.
8. Administrative Arrangements
The Committee will be supported by a nominated secretary who will:
produce a schedule of meetings and maintain the annual work plan for the Committee
prepare the agenda and papers with the Chair and circulate 4 working days prior to the meeting;
maintain accurate records of attendance, key discussion points and decisions taken and issue necessary action logs within five full working days of the meeting;
draft minutes recording where the Committee has gained assurance through relevant reports and subsequent discussion, debate and challenge, and where further assurance is required for circulation to members within five full working days of the meeting;
maintain a database of any documents discussed and/or approved and recall them to the Committee when due;
organise future meetings; and
file and maintain records of the work of the Committee. 9. Relationships and reporting
The Committee will obtain assurance from the working groups shown in the structure chart below
The Committee will report to the Board on how it discharges its responsibilities.
The Audit Committee will receive the meeting minutes of the Committee and will ensure that the Committee’s role within the overall governance of the Trust is discharged. The Audit Committee will report back to the Committee if it has any concerns about its adherence to the Terms of Reference. The Audit Committee will prepare a report to the Board on governance of the Trust, which will include the Committee’s role and performance in relation to the systems of internal control.
The minutes of Committee meetings will be formally recorded and a summary of decisions taken submitted to the Trust Board by the Chair of the Committee. The minutes will also be submitted to the Board. The Chair of the Committee will draw to the attention of the Board any issues that require disclosure to the full Board, or require executive action.
The Committee will receive standing monthly reports and additional reports as part of the scheduled programme of annual reports.
The Trust’s integrated performance report will be provided monthly with exception reporting..
In addition, the Committee will receive thematic ‘deep dive’ reports or reviews accordingly to provide more resource or performance orientated discussions about specific issues and to facilitate in depth discussions between the Committee members and staff providing services.
Internal Auditors will carry out an audit of the governance systems within the Trust, including the role of the Committee, and will use this audit to prepare the annual Head of Internal Audit Opinion.
The Board has responsibility for the effectiveness of its sub-committees. The Board will use the above reports and minutes to ensure that the Committee is meeting its duties according to these terms of reference.
10. Review
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
308 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21

7
The terms of reference, purpose, function, responsibilities and duties of this Committee will be reviewed on an annual basis or sooner if agreed by the Committee or Trust Board.
Any amended Terms of Reference will be agreed by the Committee and the Audit Committee for recommendation to a subsequent meeting of the Trust Board for its approval.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
309 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
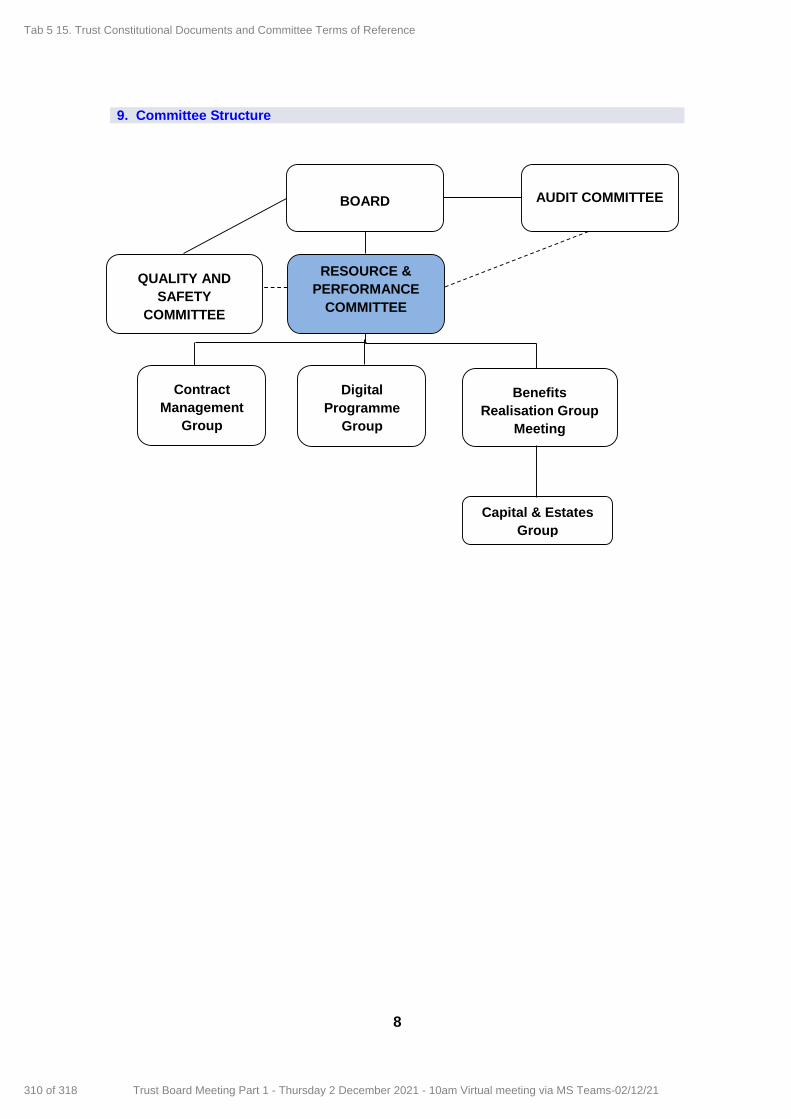
8
9. Committee Structure
BOARD AUDIT COMMITTEE
RESOURCE &
PERFORMANCE
COMMITTEE
Digital
Programme
Group
Benefits
Realisation Group
Meeting
Capital & Estates
Group
Contract
Management
Group
QUALITY AND
SAFETY
COMMITTEE
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
310 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
1
Charitable Funds Committee Terms of Reference Version: 3.1 Approved by: Shropshire Community Health NHS Trust Board
Date approved
Date issued:
Review date: November 202219
Shropshire Community Health NHS Trust CHARITABLE FUNDS COMMITTEE Terms of Reference
Document History:
Version: 3.1
Ratified by: Shropshire Community Health NHS Trust Board
Date ratified: 24th November 2017TBC
Name of author(s): Sarah Lloyd, Associate Director of Finance
Claire Lea, Corporate Governance Consultant
J Flexman, Interim Head of Financial AccountingMichael Wuestefeld-Gray, Interim Governance Lead
Name of responsible committee/individual: Shropshire Community Health NHS Trust Board Target audience: Shropshire Community Health NHS Trust Board and staff
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
311 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
2
Contents
Section Page
1. Introduction 2 2. Constitution 2 3. Membership and Attendance 2 4. Meetings and Quorum 3 5. Authority 6. Roles and Duties of the Charitable Funds Committee 3 7. Monitoring Effectiveness 4 8. Administrative Arrangements 4 9. Reporting and relationships 10. Review 4 11. Committee structure
1. Introduction
The Charitable Funds Committee is a sub-Ccommittee of the Board of Shropshire Community NHS Trust (the Trust) and has delegated authority to oversee, review and assess charitable funds arrangements within the Trust. All activities must be in line with the Charity’s objects as registered with the Charity Commission, which state that activities are for any charitable purpose relating to the services provided by Trust. In order to comply with Charity Commission regulations the Charity Committee can only act in an advisory capacity and cannot be an approving body, as the Board of Directors being the Corporate Trustee retains overall responsibility. 2. Constitution
The Trust is the Charity’s Corporate Trustee. The Charities Act 2011 defines “charity trustees” as “the persons having the general control and management of the administration of the charity”. The Directors are not tTrustees themselves, however, they act on behalf of the Corporate Trustee. The Charity is separate from the Trust and independent of it, but the tTrustees always aim to work closely with the Trust. The Corporate Trustee can delegate certain powers to agents and/or employees but will always retain the ultimate responsibility for the management of the Charity. The Board hereby resolves to establish a committee to be known as the Charitable Funds Committee (the Committee). The Committee has no executive powers other than those specifically delegated in these Terms of Reference. 3. Membership and Attendance
The membership of the Committee will comprise:
One Two 1 Non-Executive Directors, (as committee Chair and appointed by the Board)one of which will act as Chair
Associate the Director of Finance (who will act as Deputy Chair and appointed by the Board);
the Director of Nursing & OperationsPeople. Standing attendees shall include:
Director of Corporate Governance/Corporate Secretarythe Chief Operating Officer
the Director of Nursing
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
312 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
3
Other directors or their deputies may be asked to attend meetings or part meetings for discussions on matters relating to their portfolio, if required. The provisions of the Trust’s Standing Orders relating to acting up arrangements and joint members will apply to this Committee. Other attendees may be invited for specific items as follows:
The Head of Financial Accounting
League of Friends representatives All Board members will be informed of the dates of the Committee meetings and can attend meetings if they wish to. A Committee secretariatThe Corporate Secretary will provide support to the Chair and Committee members and ensure that the Committee receives the appropriate administrative and secretarial support. A secretary/minute taker will also be in attendance at all committee meetings., including the taking of minutes. Membership will be reviewed annually. 4. Meetings and Quorum
The Chair will preside at all meetings. In extraordinary circumstances where the Chair cannot attend, the Deputy Chair will chair the meeting. Quorum A quorum will be 2 members and must include 1 Non-Executive Directors and 1 Executive Director including the Chair or Vice Chair. If the Committee is not quorate the meeting may be postponed at the discretion of the Chair. If the meeting does take place and is not quorate no decisions shall be made at that meeting and such matters must be deferred until the next quorate meeting. Frequency The Committee will meet every quarter. Additional meetings of the Committee can be arranged for specific purposes as necessary, with agreement by the Chair or Deputy Chair. Where a decision needs to be taken by the Committee outside the normal cycle of meetings, and where the matter is not deemed by the Chair to require an additional meeting to be called, the decision may be made via e-mail. The preference is for decisions to be taken at committee meetings. The decisions via e-mail process will be used on an exceptions basis. The process for decision via e-mail will be as follows. a) An e-mail setting out the matter for decision will be sent to all committee members on the
same working dayat the same time. This shall include a statement setting out how the committee members should signify what their view on the matter is and the deadline for doing so.
b) Committee members will be given no less than five three working days in which to respond.
c) For a decision to be passed, all of the committee members must express the same view on the matter which can be done by action or inaction..
d) Where committee members have comments on the proposed decision or recommendation/s these will be circulated to other committee members by the Corporate SecretaryCommittee secretariat within one working day of receipt.
e) If any individual committee member wishes to debate an item proposed for decision via e-mail at a committee meeting instead they may ask the Chair to arrange an additional meeting or defer the item for decision until the next committee meeting. (such agreement by the Chair not to be unreasonably withheld).
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
313 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
4
f) Decisions via e-mail will be reported to the next committee meeting and the wording of the decision minuted. Any decision made in this manner will be effective from the date of agreement of all of the committee members and confirmed by email by the Corporate Secretary.Chair or Committee Secretariat.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
314 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
5
Attendance Committee members are expected to attend all meetings. Apologies must be received by the Corporate Secretary in advance of the meetings. All members will be required to attend a minimum of two thirds of all meetings held annually. Members should not be absent for more than two consecutive meetings without the agreement of the Chair. Any committee member may participate in a meeting by way of telephone, computer or any other electronic means of communication provided that each person is able to hear and speak. A person participating in this way is deemed to be present in person although their actual location shall be noted in the minutes and is counted in a quorum and entitled to vote. The meeting is deemed to take place where the largest group of those participating is assembled, or if there is no such group, where the Chair of the meeting is located. Where a specific matter is deemed to be of a confidential or commercially sensitive nature the Chair has the authority to restrict attendance at the Committee meeting to members only and to ask all inviteesother people attending to leave the meeting. If any Committee member or inviteeattendee has an interest, pecuniary or otherwise, in any matter and is present at the meeting at which the matter is under discussion, he / she will declare that interest as early as possible and shall not participate in the discussions. The Chair will have the power to request that member or attendeeinvitee to withdraw until the Committee’s consideration has been completed. Notice of meetings Meetings of the committee shall be called by the secretary to the committee at the request of the Chair or any of its members. Unless otherwise agreed, notice of each meeting and agenda of items to be discussed, shall be forwarded to each Committee member, any other person required to attend no later than four working days before the date of the meeting. Supporting papers shall be sent to committee members and to other attendees as appropriate, at the same time. Notices, agendas and supporting papers can be sent in electronic form where the recipient has agreed to receive documents in such a way. The Committee will agree a meeting calendar on an annual basis, setting out the main work items to be carried out by the Committee at each meeting to ensure that adequate time is given to the main duties of the Committee. 5. Authority
The Committee is authorised by the Board to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised by the Board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. The budget for such advice should be within agreed financial constraints. The Committee is authorised by the Board to make decisions that are not of a significant matter to the Board. Reference should be made, as appropriate to the Standing Orders and Standing Financial Instructions of the Trust. The following matters that must be referred to the Board:
Where there is significant revenue, capital or cash implications as determined by the Trust’s Standing Financial Instructions;
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
315 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
6
Conflict with statutory obligations, or have significant governance implications;
Change the strategic direction of the Charitable Fund;
Likely to arouse significant public or media interest. The Committee will meet quarterly, and is accountable to the Trust Board. 6. Role and Duties of the Committee
The Committee will uphold the values of the Trust in the work it does. In particular it will look for assurances that these values are being delivered in the Trust, as part of its overall governance role on behalf of the Board. Our values are: Improving Lives We make things happen to improve peoples’ lives in our communities.
Everyone Counts We make sure no-one feels excluded or left behind - patients, carers, staff and the whole community.
Commitment to Quality We all strive for excellence and getting it right for patients, carers and staff every time. Working Together for Patients Patients come first. We work and communicate closely with other teams, services and organisations to make that a reality. Compassionate Care
We put compassionate care at the heart of everything we do.
Respect and Dignity We see the person every time - respecting their values, aspirations and commitments in life – for patients, carers and staff The Committee’s duties can be categorised as follows: The Committee will apply scrutiny and constructive challenge to the Charity’s financial information and systems of control, including the Annual Accounts, to provide assurance to the Board of Directors that the administration of charitable funds is distinct from its exchequer funds and compliant with legislation and the Charity’s objectives. The purpose of the Committee is to maintain a detailed overview of the Charity’s assets and resources in relation to the achievement of the agreed Charity strategy. The Committee shall develop the objectives and strategy for the Charity for consideration by the Board of Directors, ensuring that they are consistent with the strategic direction of the Trust and ensuring statutory compliance with Charity Commission Regulations The Committee shall monitor achievement of the strategy and objectives and consider annually whether any updating is to be recommended. The Committee will provide assurance that the activities of the Charity do not cause conflict with those undertaken by others supporting the Trust e.g. League of Friends.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
316 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
7
Overseeing the Charity’s Expenditure: The Committee will:
Review policies and procedures and implementation for the identification of projects for charitable funding, ensuring they are consistent with the Charities Act and Charity Commission guidance.
Receive quarterly updates on Charitable Funds income and expenditure, and monitor the effectiveness of spending.
Monitor the level of funds held and take action where necessary to reduce balances.
Approve individual items of expenditure over £20,000, or a group of related items totalling more than £20,000ensuring that spending is appropriate with the objectives of the Charity.
Approve the Charitable Funds Annual Accounts and report prior to ratification by the Trust Board.
Review approval thresholds for Charitable Fund expenditure prior to the Trust’s annual review of the Scheme of Delegation.
Oversee the rationalisation of existing funds; new individual funds can only be established with the express approval of the Committee.
Monitor the performance of all aspects of the charity’s activities and ensure it adheres to the principles of good governance.
Oversee the Charity’s Income:
The Charity does not itself actively engage in fundraising activities, although it is prepared to encourage individuals and groups, provided that such activities are appropriate with the objectives of the Charity.
In line with our values, the Trust will support the League of Friends and others with their fundraising as appropriate on behalf of our patients, through communications and engagement.
Review and approve investment policies and decisions. 7. Monitoring Effectiveness
The Committee shall at least once a year, review its own performance, constitution and terms of reference to ensure it is operating at maximum effectiveness and recommend any changes it considers necessary to the Board for approval. The Committee shall be provided with appropriate and timely training, both in the form of an induction programme for new members and on an ongoing basis for all members. The Committee shall arrange for periodic reviews of its own performance and, at least annually, review its constitution and terms of reference to ensure it is operating at maximum effectiveness and recommend any changes it considers necessary to the Board. A record of the frequency of attendance by members, quoracy and the frequency of meetings will be maintained. Any areas of concern will be highlighted to the Chair of the Committee. 8. Administrative Arrangements
The Committee will be supported by a nominated secretary who will:
produce a schedule of meetings and maintain the annual work plan for the Committee
prepare the agenda and papers with the Chair and circulate 4 working days prior to the meeting;
maintain accurate records of attendance, key discussion points and decisions taken and issue necessary action logs within five full working days of the meeting;
draft minutes recording where the Committee has gained assurance through relevant reports and subsequent discussion, debate and challenge, and where further assurance is required for circulation to members within five full working days of the meeting;
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
317 of 318Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21
8
maintain a database of any documents discussed and/or approved and recall them to the Committee when due;
organise future meetings; and
file and maintain records of the work of the Committee. 9. Review
The Committee will report to the Board on how it discharges its responsibilities. The Audit Committee will receive the meeting minutes of the Committee and will ensure that the Committee’s role within the overall governance of the Charity is discharged. The Audit Committee will report back to the Committee if it has any concerns about its adherence to the Terms of Reference. The Audit Committee will prepare a report to the Board on governance of the Charity, which will include the Committee’s role and performance in relation to the Charity’s systems of internal control. The minutes of Committee meetings will be formally recorded and a summary of decisions taken submitted to the Trust Board by the Chair of the Committee. The minutes will also be submitted to the Board. The Chair of the Committee will draw to the attention of the Board any issues that require disclosure to the full Board, or require executive action. The Committee will receive standing monthly reports and additional reports as part of the scheduled programme of annual reports. In addition, the Committee will receive thematic ‘deep dive’ reports or reviews accordingly to enable greater discussion about specific issues and to facilitate in depth discussions between the Committee members and staff providing services. The Board has responsibility for the effectiveness of its sub-committees. The Board will use the above reports and minutes to ensure that the Committee is meeting its duties according to these terms of reference.
Tab 5 15. Trust Constitutional Documents and Committee Terms of Reference
318 of 318 Trust Board Meeting Part 1 - Thursday 2 December 2021 - 10am Virtual meeting via MS Teams-02/12/21





























