Embed Size (px)
Citation preview

www.elsevier.com/locate/braindev
Brain & Development 32 (2010) 855–862
Original article
Migraine in junior high-school students: A prospective3-academic-year cohort study
Anannit Visudtibhan *, Lunliya Thampratankul, Chaiyos Khongkhatithum,Chusak Okascharoen, Vorasith Siripornpanich, Surang Chiemchanya,
Pongsakdi Visudhiphan
Department of Pediatrics, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand
Received 20 July 2009; received in revised form 12 December 2009; accepted 15 December 2009
Abstract
Migraine is a common childhood illness with expected favorable outcome. A study of the long-term clinical course of childhoodmigraine will provide information of evolution of migraine. A cohort study for 3-academic-year was conducted in Thai junior high-school children from July 2005 to February 2008 to determine the clinical course of migraine. Two hundred and forty-eight studentsin four junior high schools diagnosed with migraine according to ICHD-II in July 2005 were recruited. Each student was seriallyevaluated twice yearly from 7th grade during each semester of the academic year until the second semester of 9th grade. Determi-nation of the characteristics, severity, frequency, and treatment of headache were obtained by questionnaire and direct interview. Atthe final evaluation, clinical course of headache was categorized into seven patterns. Among enrolled students, 209 (84.3%) com-pleted the study. Twenty-eight (13.5%) students had no recurrent headache while that of 153 (73.5%) improved. No improvementof migraine and worsened migraine were observed in four students (1.8%) and 24 students (11.2%), respectively. Spontaneous remis-sion and avoidance of precipitating causes contributed to relief of migraine in the majority of the students. Stress-related dailyschool activities and inadequate rest were reported as common precipitating factors among students with non-improving or wors-ening outcome. Chronic daily headache and tension-type headache was observed in 6 and 30 students, respectively. This study con-firms that clinical course of migraine in schoolchildren is benign. Frequency and intensity of headache can be reduced withreassurance and appropriate guidance. Early recognition and appropriate prevention of migraine attack will decrease the risk ofchronic migraine and disease burden.� 2009 Elsevier B.V. All rights reserved.
Keywords: Migraine; Cohort study; Thailand; Schoolchildren
1. Introduction
Childhood migraine has been extensively studied inWestern countries since it was brought to attention byBille in 1962 [1]. There has been various studies in chil-dren at various ages. Prevalence of migraine is variableaccording to different ages and various countries [2–6].Follow-up evaluation ranging from 1 to 20 years con-
0387-7604/$ - see front matter � 2009 Elsevier B.V. All rights reserved.
doi:10.1016/j.braindev.2009.12.004
* Corresponding author. Tel.: +66 2 201 1488; fax: +66 2 201 1850.E-mail address: [email protected] (A. Visudtibhan).
firmed the likely benign course in children [2,7,8].Short-term studies ranging from 1 to 3 years were con-ducted in Taiwanese, Norwegians, and Finnish childrenwith headache and migraine [9–11]. Recently, a German1-year cohort study in 8800 households with the childrenage of 7–14 years revealed improved and worsenedheadache status in 22.3% and 20.7%, respectively [12].Persistent rate of migraine of 41–63% was determinedby three studies in children [2,9,11]. However, there werevariable children’s ages from 7 to 15 years and variableduration of follow-up ranging from 1 to 7 years in these
856 A. Visudtibhan et al. / Brain & Development 32 (2010) 855–862
studies [2,9,11]. The longest follow-up duration was a40-year study by Bille, who demonstrated migraineremission of 23% in this cohort study [13].
In Asian children, recent studies point to the risingmigraine prevalence [14,15]. The racial and socioeco-nomic differences among different countries werehypothesized as the explanation [14]. In Thailand, therehave not been many studies in childhood headache andmigraine [15–18]. Most of these studies were hospital-based studies. One such study determined the short-termoutcome of tension-type and migraine from 2 weeks to2 months in children younger than 16 years revealed aminimal response to medical treatment. Reassuranceand avoidance of precipitating causes contributed tofavorable outcome [18]. However, there have been nostudies focusing on the clinical course of migraine ingeneral population. Therefore, the authors haveembarked upon the evolution of childhood migraineby conducting a 3-year cohort study specifically injunior high-school students. The data obtained from thisstudy will enhance the knowledge of migraine for fur-ther appropriate management of migraine in this age-specific group.
2. Subjects and methods
This study was a continuation of the previous studyin July 2004. A cross-sectional study in the 7th gradestudents in four junior high schools in Bangkok, Thai-land to determine the prevalence of migraine in school-children was conducted then. The enrolled schools werethe schools in the Adolescent Health-Promotion Pro-gram, which was a pilot program under the supervisionof the Department of Pediatrics, Ramathibodi Hospital.The detail of migraine diagnosed in these students waspublished [15]. After identification of 248 schoolchildrenin first semester of 7th grade, a 3-year prospective cohortstudy was then carried out. All 248 students were seriallyfollowed for a total of five sessions with one visit foreach semester until they were in the 9th grade. Afterenrolled visit, these students received a brief verbalcounselling for migraine, which included a self-careinstruction and precipitating causes of migraine avoid-ance. In addition, each student received a one-pagepamphlet describing general information of migraine.The contents also included the list of the precipitatingcauses, a general advice for self-care during migraineattack and the red-flag symptoms of dangerous causeof headache. In each follow-up visit, the studentsreceived person-to-person interview for the severityand frequency of migraine attack, school absencedirectly caused by headache, treatment for headache,menstruation history, overall subjective health condi-tion, and school performance. Physical examinationincluding measurement of blood pressure was also inte-grated in each visit. Interview checklist included the
frequency of migraine, duration, possible precipitatingcauses of migraine, school performance, and subjectiveself-determination of overall headache in comparisonto previous visit. The subjective self-determinations wereclassified as (1) no recurrent migraine, (2) improvingsymptoms or less frequent attack, (3) no change insymptoms, (4) worsened headache. The methods ofself-management of migraine were (1) doing nothing,(2) symptomatic medication, (3) precaution/avoidingof precipitating causes, (4) combination of symptomaticmedication and precaution/avoiding of precipitatingcause.
Primary headache was classified into migraine andtension-type headache, according to ICHD-II [19]. Ifany student had daily headache more than 14 days ina month, which was not compatible with the classifica-tion of tension-type headache and the duration of head-ache was longer than 4 h without specific associatesymptoms; the diagnosis of a possible chronic dailyheadache would be assigned to that student.
In each interview, the verification and the classifica-tion of headache was finalized by the principal investiga-tor (AV), who is a pediatric neurologist. Precipitatingcauses of headache were reported by each student inthe checklist, which was conducted in the same mannerin previous study [15]. For the final evaluation day in thesecond semester of 9th grade, evolutions of migrainewere categorized into seven groups. Group 1 (no recur-rence) there was no recurrent migraine headache. Group2 (improving headache) students experienced less head-ache severity or frequency in comparison to previousevaluation. Group 3 (occasional migraine headache);there were occasional migraine attacks with a periodof headache-free between the fourth and the last evalu-ation. Group 4 (initial deterioration with final improv-ing); there were some degree of headache deteriorationwith a period of headache-free between the fourth andthe last evaluation. Group 5 (no change); there wereno improving or worsening of the headache severityand frequency during the 3-year periods. Group 6 (min-imal deterioration); there were some degrees of deterio-ration such as increase in frequency or severity ofheadache, which were occasional discontinuation ofdaily activities and/or occasional bed-rests, and therewere no improving symptoms in comparison to previousevaluation. Group 7 (worsened headache); there wereprogressive increase in frequency and intensity ofmigraine, which were discontinuation of daily activitiesand bed-rest was in need every recurrent migraine.
Descriptive analysis was the main statistical analy-sis. Whenever appropriate, analyzed using Chi squaretest or Fisher’s exact test was used instead. P-valueless than 0.05 is considered statistically significant.STATA V-10 (College Station, Texas, USA) was thestatistic packed program applied for all statisticalanalysis.

A. Visudtibhan et al. / Brain & Development 32 (2010) 855–862 857
3. Results
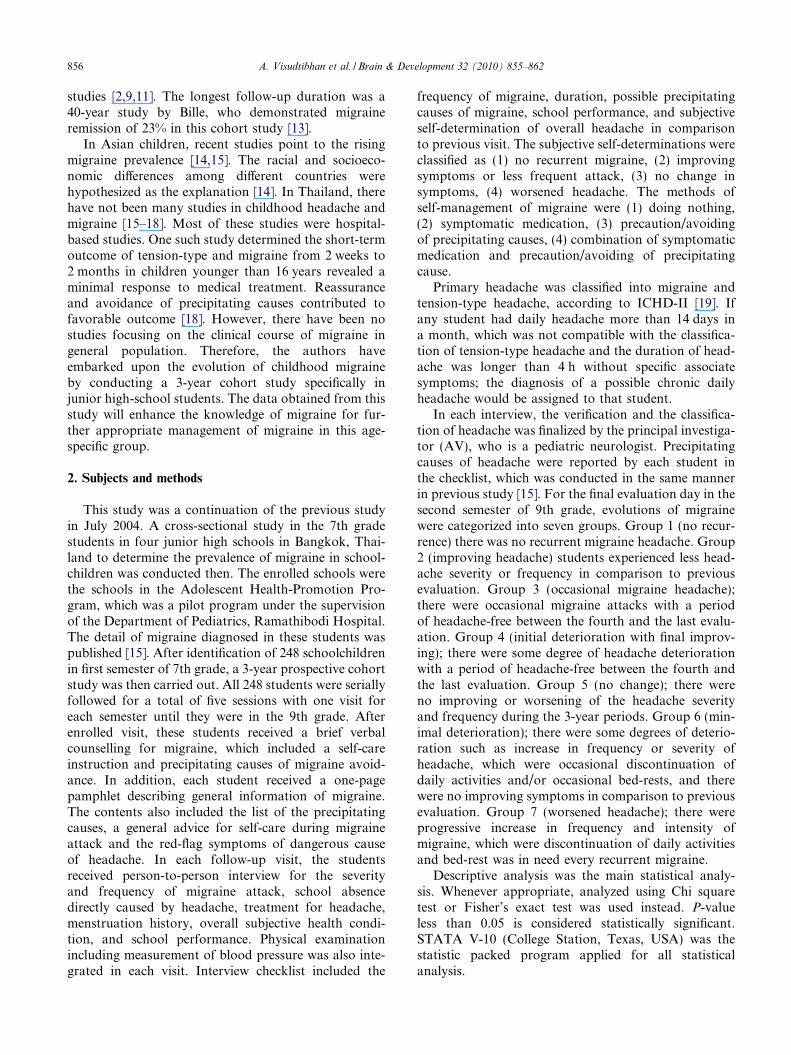
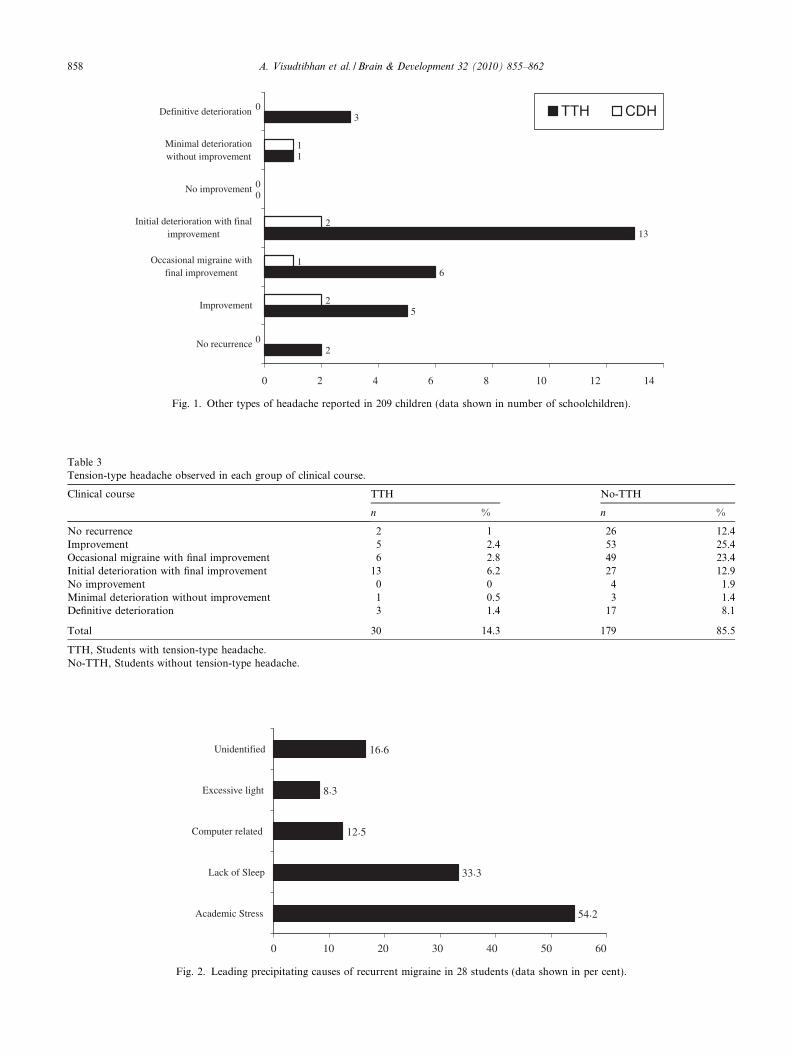
Among 248 students, there were 27 students whoeither quitted or transferred to other schools duringthe 3-year period. Twelve students were excluded fromthe study because they failed to participate the five ses-sions of interview and examination. At the final visit,there were 209 students included for analysis. Therewere 87 boys (41.6%) and 122 girls (58.4%). There wasno significant statistical difference between boys andgirls in each clinical course. The detail of the clinicalcourse finalized on the last evaluation is shown in Table1. Among those who dropped out from this study, theresult according to the last evaluation is shown in Table2. There were 181 students who experienced migraineheadache during the 3-year period. Among these stu-dents, there were 14 students who experienced migrainewith aura. Eleven of these 14 students were initiallydiagnosed as migraine with aura when they were firstseen in the first semester of 7th grade. In contrast,among students who were initially classified intomigraine without aura then, only three students experi-enced migraine with aura during this 3-year period.There were 30 and six children who had tension-typeheadache and chronic daily headache, respectively.Fig. 1 demonstrates other types of headache accordingto clinical course in 209 students. Number of childrenwith and without tension-type headache in each clinicalcourse are shown in Table 3. Tension-type headache was
Table 1Clinical course of migraine in 209 students from 7th to 8th grade according
Category according to the overall clinical course Boys
N
No recurrence 16Improvement 25Occasional migraine with final improvement 21Initial deterioration with final improvement 16No improvement 2Minimal deterioration without improvement 1Definitive deterioration 6Total 87
Table 2Result of the latest evaluation among the dropout students.
Quit or tr
No recurrence 2Improvement 15Occasional migraine with final improvement 2Initial deterioration with final improvement 2No improvement 4Minimal deterioration without improvement 0Definitive deterioration 2
Total 27
highly reported in students who initially experienceddeterioration of migraine with final improvement (13/40). However, there was no statistical difference betweenstudents with and without tension-type headache amongvarious clinical courses.
There were 28 students whose headache was notimproving during the 3-year period. Among these stu-dents, the most common precipitating cause of headachewas the stress caused by daily school activities. Fig. 2reveals the leading precipitating causes of recurrentmigraine in 28 students. Two students reported com-puter-related activity and lack of sleep as the top twoprecipitating causes of their headache.
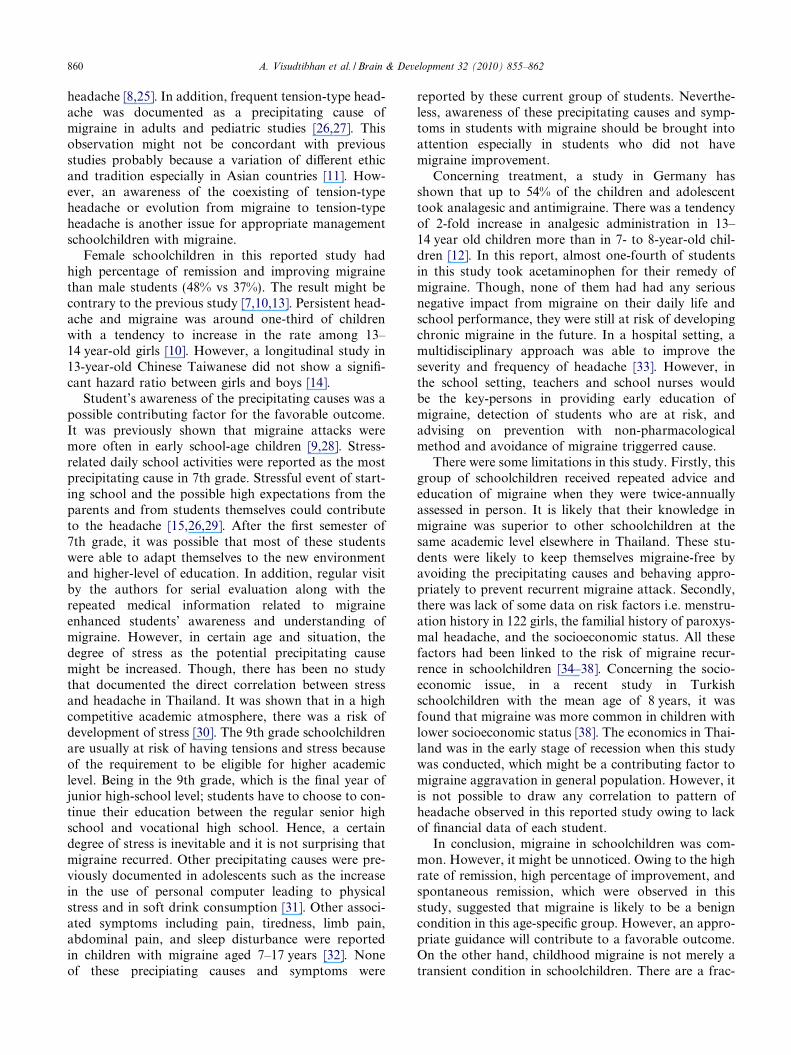
Among 181 students who still had recurrent migraineduring 3-year period, most of these students did notreceive any specific prevention or medication. Avoid-ance of precipitating cause of migraine according tothe migraine information guidance was reported in31% of 209 students. There were 17.1% of the studentswho received acute abortive medication. Acetamino-phen was the main analgesic drug taken by these stu-dents (Table 4).
There were 20 students who were classified into thegroup with definitive deterioration; there was only onestudent who took ibuprofen for his headache. Thisboy had migraine without aura and occasionally visitedgeneral practitioners for symptomatic treatment of hismigraine. The other 16 students took either acetamino-phen or combination of acetaminophen and sought
to gender.
Girls P
% N %
7.7 12 5.7 0.0712 33 15.8 0.810 34 16.3 0.57.6 24 11.5 0.80.95 2 0.95 0.90.5 3 1.4 0.62.9 14 6.7 0.341.65 122 58.35 N/A
ansfer Incomplete visit Total
0 24 192 42 44 80 02 4
12 39
2
5
6
13
0
1
3
0
2
1
2
0
1
0
0 2 4 6 8 10 12 14
No recurrence
Improvement
Occasional migraine withfinal improvement
Initial deterioration with finalimprovement
No improvement
Minimal deteriorationwithout improvement
Definitive deterioration TTH CDH
Fig. 1. Other types of headache reported in 209 children (data shown in number of schoolchildren).
Table 3Tension-type headache observed in each group of clinical course.
Clinical course TTH No-TTH
n % n %
No recurrence 2 1 26 12.4Improvement 5 2.4 53 25.4Occasional migraine with final improvement 6 2.8 49 23.4Initial deterioration with final improvement 13 6.2 27 12.9No improvement 0 0 4 1.9Minimal deterioration without improvement 1 0.5 3 1.4Definitive deterioration 3 1.4 17 8.1
Total 30 14.3 179 85.5
TTH, Students with tension-type headache.No-TTH, Students without tension-type headache.
54.2
33.3
12.5
8.3
16.6
0 10 20 30 40 50 60
Academic Stress
Lack of Sleep
Computer related
Excessive light
Unidentified
Fig. 2. Leading precipitating causes of recurrent migraine in 28 students (data shown in per cent).
858 A. Visudtibhan et al. / Brain & Development 32 (2010) 855–862
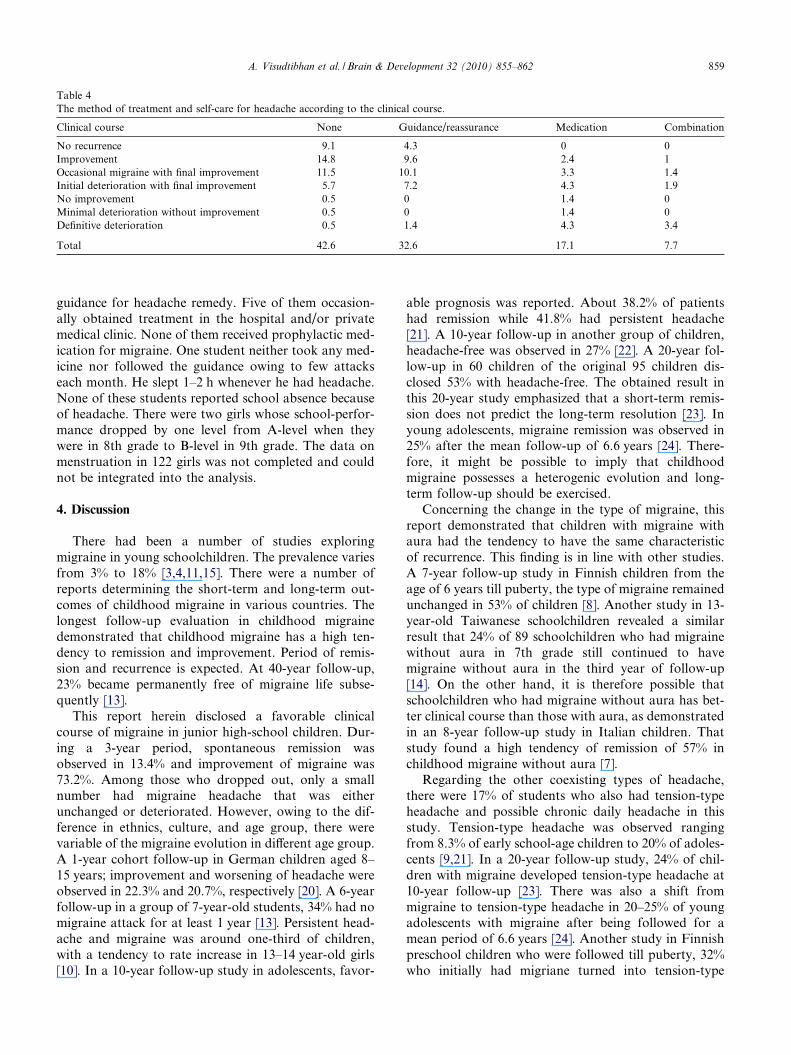
Table 4The method of treatment and self-care for headache according to the clinical course.
Clinical course None Guidance/reassurance Medication Combination
No recurrence 9.1 4.3 0 0Improvement 14.8 9.6 2.4 1Occasional migraine with final improvement 11.5 10.1 3.3 1.4Initial deterioration with final improvement 5.7 7.2 4.3 1.9No improvement 0.5 0 1.4 0Minimal deterioration without improvement 0.5 0 1.4 0Definitive deterioration 0.5 1.4 4.3 3.4
Total 42.6 32.6 17.1 7.7
A. Visudtibhan et al. / Brain & Development 32 (2010) 855–862 859
guidance for headache remedy. Five of them occasion-ally obtained treatment in the hospital and/or privatemedical clinic. None of them received prophylactic med-ication for migraine. One student neither took any med-icine nor followed the guidance owing to few attackseach month. He slept 1–2 h whenever he had headache.None of these students reported school absence becauseof headache. There were two girls whose school-perfor-mance dropped by one level from A-level when theywere in 8th grade to B-level in 9th grade. The data onmenstruation in 122 girls was not completed and couldnot be integrated into the analysis.
4. Discussion
There had been a number of studies exploringmigraine in young schoolchildren. The prevalence variesfrom 3% to 18% [3,4,11,15]. There were a number ofreports determining the short-term and long-term out-comes of childhood migraine in various countries. Thelongest follow-up evaluation in childhood migrainedemonstrated that childhood migraine has a high ten-dency to remission and improvement. Period of remis-sion and recurrence is expected. At 40-year follow-up,23% became permanently free of migraine life subse-quently [13].
This report herein disclosed a favorable clinicalcourse of migraine in junior high-school children. Dur-ing a 3-year period, spontaneous remission wasobserved in 13.4% and improvement of migraine was73.2%. Among those who dropped out, only a smallnumber had migraine headache that was eitherunchanged or deteriorated. However, owing to the dif-ference in ethnics, culture, and age group, there werevariable of the migraine evolution in different age group.A 1-year cohort follow-up in German children aged 8–15 years; improvement and worsening of headache wereobserved in 22.3% and 20.7%, respectively [20]. A 6-yearfollow-up in a group of 7-year-old students, 34% had nomigraine attack for at least 1 year [13]. Persistent head-ache and migraine was around one-third of children,with a tendency to rate increase in 13–14 year-old girls[10]. In a 10-year follow-up study in adolescents, favor-
able prognosis was reported. About 38.2% of patientshad remission while 41.8% had persistent headache[21]. A 10-year follow-up in another group of children,headache-free was observed in 27% [22]. A 20-year fol-low-up in 60 children of the original 95 children dis-closed 53% with headache-free. The obtained result inthis 20-year study emphasized that a short-term remis-sion does not predict the long-term resolution [23]. Inyoung adolescents, migraine remission was observed in25% after the mean follow-up of 6.6 years [24]. There-fore, it might be possible to imply that childhoodmigraine possesses a heterogenic evolution and long-term follow-up should be exercised.
Concerning the change in the type of migraine, thisreport demonstrated that children with migraine withaura had the tendency to have the same characteristicof recurrence. This finding is in line with other studies.A 7-year follow-up study in Finnish children from theage of 6 years till puberty, the type of migraine remainedunchanged in 53% of children [8]. Another study in 13-year-old Taiwanese schoolchildren revealed a similarresult that 24% of 89 schoolchildren who had migrainewithout aura in 7th grade still continued to havemigraine without aura in the third year of follow-up[14]. On the other hand, it is therefore possible thatschoolchildren who had migraine without aura has bet-ter clinical course than those with aura, as demonstratedin an 8-year follow-up study in Italian children. Thatstudy found a high tendency of remission of 57% inchildhood migraine without aura [7].
Regarding the other coexisting types of headache,there were 17% of students who also had tension-typeheadache and possible chronic daily headache in thisstudy. Tension-type headache was observed rangingfrom 8.3% of early school-age children to 20% of adoles-cents [9,21]. In a 20-year follow-up study, 24% of chil-dren with migraine developed tension-type headache at10-year follow-up [23]. There was also a shift frommigraine to tension-type headache in 20–25% of youngadolescents with migraine after being followed for amean period of 6.6 years [24]. Another study in Finnishpreschool children who were followed till puberty, 32%who initially had migriane turned into tension-type
860 A. Visudtibhan et al. / Brain & Development 32 (2010) 855–862
headache [8,25]. In addition, frequent tension-type head-ache was documented as a precipitating cause ofmigraine in adults and pediatric studies [26,27]. Thisobservation might not be concordant with previousstudies probably because a variation of different ethicand tradition especially in Asian countries [11]. How-ever, an awareness of the coexisting of tension-typeheadache or evolution from migraine to tension-typeheadache is another issue for appropriate managementschoolchildren with migraine.
Female schoolchildren in this reported study hadhigh percentage of remission and improving migrainethan male students (48% vs 37%). The result might becontrary to the previous study [7,10,13]. Persistent head-ache and migraine was around one-third of childrenwith a tendency to increase in the rate among 13–14 year-old girls [10]. However, a longitudinal study in13-year-old Chinese Taiwanese did not show a signifi-cant hazard ratio between girls and boys [14].
Student’s awareness of the precipitating causes was apossible contributing factor for the favorable outcome.It was previously shown that migraine attacks weremore often in early school-age children [9,28]. Stress-related daily school activities were reported as the mostprecipitating cause in 7th grade. Stressful event of start-ing school and the possible high expectations from theparents and from students themselves could contributeto the headache [15,26,29]. After the first semester of7th grade, it was possible that most of these studentswere able to adapt themselves to the new environmentand higher-level of education. In addition, regular visitby the authors for serial evaluation along with therepeated medical information related to migraineenhanced students’ awareness and understanding ofmigraine. However, in certain age and situation, thedegree of stress as the potential precipitating causemight be increased. Though, there has been no studythat documented the direct correlation between stressand headache in Thailand. It was shown that in a highcompetitive academic atmosphere, there was a risk ofdevelopment of stress [30]. The 9th grade schoolchildrenare usually at risk of having tensions and stress becauseof the requirement to be eligible for higher academiclevel. Being in the 9th grade, which is the final year ofjunior high-school level; students have to choose to con-tinue their education between the regular senior highschool and vocational high school. Hence, a certaindegree of stress is inevitable and it is not surprising thatmigraine recurred. Other precipitating causes were pre-viously documented in adolescents such as the increasein the use of personal computer leading to physicalstress and in soft drink consumption [31]. Other associ-ated symptoms including pain, tiredness, limb pain,abdominal pain, and sleep disturbance were reportedin children with migraine aged 7–17 years [32]. Noneof these precipiating causes and symptoms were
reported by these current group of students. Neverthe-less, awareness of these precipitating causes and symp-toms in students with migraine should be brought intoattention especially in students who did not havemigraine improvement.
Concerning treatment, a study in Germany hasshown that up to 54% of the children and adolescenttook analagesic and antimigraine. There was a tendencyof 2-fold increase in analgesic administration in 13–14 year old children more than in 7- to 8-year-old chil-dren [12]. In this report, almost one-fourth of studentsin this study took acetaminophen for their remedy ofmigraine. Though, none of them had had any seriousnegative impact from migraine on their daily life andschool performance, they were still at risk of developingchronic migraine in the future. In a hospital setting, amultidisciplinary approach was able to improve theseverity and frequency of headache [33]. However, inthe school setting, teachers and school nurses wouldbe the key-persons in providing early education ofmigraine, detection of students who are at risk, andadvising on prevention with non-pharmacologicalmethod and avoidance of migraine triggerred cause.
There were some limitations in this study. Firstly, thisgroup of schoolchildren received repeated advice andeducation of migraine when they were twice-annuallyassessed in person. It is likely that their knowledge inmigraine was superior to other schoolchildren at thesame academic level elsewhere in Thailand. These stu-dents were likely to keep themselves migraine-free byavoiding the precipitating causes and behaving appro-priately to prevent recurrent migraine attack. Secondly,there was lack of some data on risk factors i.e. menstru-ation history in 122 girls, the familial history of paroxys-mal headache, and the socioeconomic status. All thesefactors had been linked to the risk of migraine recur-rence in schoolchildren [34–38]. Concerning the socio-economic issue, in a recent study in Turkishschoolchildren with the mean age of 8 years, it wasfound that migraine was more common in children withlower socioeconomic status [38]. The economics in Thai-land was in the early stage of recession when this studywas conducted, which might be a contributing factor tomigraine aggravation in general population. However, itis not possible to draw any correlation to pattern ofheadache observed in this reported study owing to lackof financial data of each student.
In conclusion, migraine in schoolchildren was com-mon. However, it might be unnoticed. Owing to the highrate of remission, high percentage of improvement, andspontaneous remission, which were observed in thisstudy, suggested that migraine is likely to be a benigncondition in this age-specific group. However, an appro-priate guidance will contribute to a favorable outcome.On the other hand, childhood migraine is not merely atransient condition in schoolchildren. There are a frac-
A. Visudtibhan et al. / Brain & Development 32 (2010) 855–862 861
tion of schoolchildren in junior high school who still hadmigraine throughout the 3-year follow-up and carry therisk of severe recurrent migraine. This concern was alsoemphasized in the study in Taiwanese children of thesame age [14]. Early identification of these studentsand appropriate management of their migraine wouldbe able to decrease the risk of developing chronicmigraine in their adulthood.
Acknowledgements
The authors would like to express their gratitude tothe teachers and students of the 7th grade in the four ju-nior high schools (Nawamintharachutis BadindechaSchool, Kunnatheerutharam School, Sri AyudhayaSchool, and Wat Benjamabapitr School) for their excel-lent cooperation and to Dr. Mahippathorn Chinnaphafor his kind English editing of the manuscript.
References
[1] Bille BS. Migraine in school children: a study of the incidence andshort-term prognosis, and a clinical, psychological and electroen-cephalographic comparison between children with migraine andmatched controls.. Acta Paediatr Suppl 1962;136:1–151.
[2] Sillanpaa M. Prevalence of headache in prepuberty. Headache1983;23:10–4.
[3] Abu-Arefeh I, Russell G. Prevalence of headache and migraine inschoolchildren. Brit Med J 1994;309:765–9.
[4] Al Jumah M, Awada A, Al Azzam S. Headache syndromesamongst schoolchildren in Riyadh, Saudi Arabia. Headache2002;42:281–6.
[5] Ando N, Fujimoto S, Ishikawa T, Teramoto J, Kobayashi S,Hattori A, et al. Prevalence and features of migraine in Japanesejunior high-school students aged 12–15 years. Brain Dev2007;29:482–5.
[6] Karli N, Akis� N, Zarifoglu M, Akgoz S, Irgil E, Ayvacioglu U,et al. Headache prevalence in adolescents age 12–17: a student-based epidemiological study in Bursa. Headache 2006;46:649–55.
[7] Guidetti V, Galli F. Evolution of headache in childhood andadolescence. An 8-year follow-up. Cephalalgia 1998;18:449–54.
[8] Virtanen R, Aromaa M, Rautava P, Metsahonkala L, Anttila P,Helenius H, et al. Changing headache from preschool age topuberty: a controlled study. Cephalalgia 2007;27:294–303.
[9] Metsahonkala L, Sillanpaa M, Tuominen J. Outcome of earlyschool-age migraine. Cephalalgia 1997;17:662–5.
[10] Larsson B, Sund AM. One-year incidence, course, and outcomepredictors of frequent headaches among early adolescents. Head-ache 2005;45:684–91.
[11] Wang SJ, Fuh JL, Juang KD, Lu SR. Rising prevalence ofmigraine in Taiwanese adolescents aged 13–15 years. Cephalalgia2005;25:433–4338.
[12] Kroner-Herwig B, Heinrich M, Morris L. Headache in Germanchildren and adolescents: a population-based epidemiologicalstudy. Cephalalgia 2007;27:519–27.
[13] Bille B. A 40-year follow-up of school children with migraine.Cephalalgia 1997;17:488–91.
[14] Wang SJ, Fuh JL, Juang KD, Lu SR, Hsu LC, Chen WT, et al.Evolution of migraine diagnoses in adolescents: a 3-year annualsurvey. Cephalalgia 2005;25:333–8.
[15] Visudtibhan A, Siripornpanich V, Khongkhatithum C, Chiem-chanya S, Sirijunpen S, Ruangkanchanasetr S, et al. Migraine inThai children: prevalence in junior high-school students. J ChildNeurol 2007;22:1117–20.
[16] Visudtibhan A, Lusawat A, Chiemchanya S, Visudhiphan P.Flunarizine for prophylactic treatment of childhood migraine. JMed Assoc Thai 2004;87:1466–70.
[17] Ruangsuwan S, Sriudomkajorn S. 375 childhood primaryheadache: clinical features, the agreement between clinicaldiagnosis and diagnoses using the international classificationof headache disorders in Thai children. J Med Assoc Thai2007;90:1309–16.
[18] Sri-udomkajorn S, Ruangsuwan S. Short-term outcomes oftension type and migraine headache in children. J Med AssocThai 2008;91(Suppl. 3):S104–8.
[19] Headache Classification Subcommittee of the InternationalHeadache Society. The international classification of headachedisorders: 2nd edition. Cephalalgia 2004;24 Suppl. 1:9-160.
[20] Gassmann J, Morris L, Heinrich M, Kroner-Herwig B. One-yearcourse of paediatric headache in children and adolescents aged 8–15 years. Cephalalgia 2008;28:1154–62.
[21] Monastero R, Camarda C, Pipia C, Camarda R. Prognosis ofmigraine headaches in adolescents: a 10-year follow-up study.Neurology 2006;67:1353–6.
[22] Dooley J, Bagnell A. The prognosis and treatment of headaches inchildren-a 10-year follow-up. Can J Neurol Sci 1995;22:47–9.
[23] Brna P, Dooley J, Gordon K, Dewan T. The prognosis ofchildhood headache: a 20-year follow-up. Arch Pediatr AdolescMed 2005;159:1157–60.
[24] Kienbacher C, Wober C, Zesch HE, Hafferl-Gattermayer A,Poach M, Karwautz A, et al. Clinical features, classification andprognosis of migraine and tension-type headache in children andadolescents: a long-term follow-up study. Cephalalgia2006;26:820–30.
[25] Aromaa M, Sillanpaa ML, Rautava P, Helenius H. Childhoodheadache at school entry: a controlled clinical study. Neurology1998;50:1729–36.
[26] Laurell K, Larsson B, Mattsson P, Eeg-Olofsson O. A 3-yearfollow-up of headache diagnoses and symptoms in Swedishschoolchildren. Cephalalgia 2006;26:809–15.
[27] Lyngberg AC, Rasmussen BK, Jørgensen T, Jensen R. Incidenceof primary headache: a Danish epidemiologic follow-up study.Am J Epidemiol 2005;161:1066–73.
[28] Metsahonkala L, Sillanpaa M, Tuominen J. Social environmentand headache in 8- to 9-year-old children: a follow-up study.Headache 1998;38:222–8.
[29] Anttila P, Metsahonkala L, Sillanpaa M. School start andoccurrence of headache. Pediatrics 1999;103:e80.
[30] Saipanish R. Stress among medical students in a Thai medicalschool. Med Teach 2003;25:502–6.
[31] Anttila P, Metsahonkala L, Sillanpaa M. Long-term trends in theincidence of headache in Finnish schoolchildren. Pediatrics2006;117:e1197–201.
[32] Laurell K, Larsson B, Eeg-Olofsson O. Headache in schoolchil-dren: association with other pain, family history and psychosocialfactors. Pain 2005;119:150–8.
[33] Kabbouche MA, Powers SW, Vockell AL, LeCates SL, EllinorPL, Segers A, et al. Outcome of a multidisciplinary approach topediatric migraine at 1, 2, and 5 years. Headache 2005;45:1298–303.
[34] Mavromichalis I, Anagnostopoulos D, Metaxas N, Papanastas-siou E. Prevalence of migraine in schoolchildren and some clinicalcomparisons between migraine with and without aura. Headache1999;39:728–36.
[35] Anttila P, Metsahonkala L, Helenius H, Sillanpaa M. Predispos-ing and provoking factors in childhood headache. Headache2000;40:351–6.

862 A. Visudtibhan et al. / Brain & Development 32 (2010) 855–862
[36] Bugdayci R, Ozge A, Sasmaz T, Kurt AO, Kaleagasi H,Karakelle A, et al. Prevalence and factors affecting headache inTurkish schoolchildren. Pediatr Int 2005;47:316–22.
[37] Scharfman HE, MacLusky NJ. Estrogen-growth factor interac-tions and their contributions to neurological disorders. Headache2008;48(Suppl. 2):S77–89.
[38] Is�ik U, Topuzoglu A, Ay P, Ersu RH, Arman AR, Onsuz MF,et al. The prevalence of headache and its association withsocioeconomic status among schoolchildren in Istanbul, Turkey.Headache 2009;49:697–703.





























