Embed Size (px)
Citation preview
Abstract Our experience of providing an NF1 gene
diagnostic mutation detection service as part of the UK
Genetic Testing Network (UKGTN) is presented. A
total of 169 unrelated individuals suspected of having
neurofibromatosis type I (NF1) were referred for NF1
diagnostic testing over a 2 year period. Mutation
analysis of the entire NF1 coding region and the
flanking splice sites was carried out, and included the
use of a combination of FISH, dHPLC and MLPA.
Possible disease causing mutations were identified in
109 (64%) cases. These comprised 88 different se-
quence alterations, of which 57 were novel. Out of the
169 cases referred, there were 102 patients with reliable
clinical data, of whom 78 satisfied the NIH diagnostic
criteria for NF1. Within this better defined cohort of
NF1 patients, NF1 mutations were identified in 61
individuals (78%), showing the importance of clinical
selection on overall test sensitivity, and highlighting
the problem of full clinical data collection in the audit
of routine services. As mutation detection technologies
advance, facilitating direct sequencing of all coding and
flanking non-coding regions of the NF1 gene, the
development of an even more cost-effective, quick and
sensitive diagnostic test for future testing of NF1 is
discussed.
Keywords Denaturing High Performance Liquid
Chromatography (dHPLC) Æ Fluorescence In-Situ
Hybridisation (FISH) Æ Multiplex Ligation-Dependent
Probe Amplification (MLPA) Æ Mutation ÆNeurofibromatosis Type 1 (NF1) Æ Polymerase chain
reaction (PCR) Æ Polymorphism Æ Sequencing ÆUK Genetic Testing Network (UKGTN)
Introduction
Neurofibromatosis type 1 (NF1) is a common familial
syndrome that afflicts all ethnic groups, equally affects
males and females, and all age groups. The disease is
transmitted in an autosomal dominant fashion, with a
prevalence of approximately one in 3,500 individuals
worldwide.
The NF1 gene is one of the largest human genes and
spans ~350 kb of 17q11.2, contains 60 exons, of which 3
are alternatively spliced and encodes a 12 kb mRNA
transcript. Intron 27 b of the NF1 gene contains three
embedded genes (OMGP, EVI2B and EVI2A), which
are all transcribed in the opposite orientation to the
NF1 gene. Neurofibromin, the NF1 gene protein
product, is ubiquitously expressed and exhibits struc-
tural and sequence similarity to an evolutionarily
conserved family of proteins, the mammalian GTPase-
activating proteins (GAP). The most highly conserved
region of neurofibromin is the GAP-related domain
(GRD) encoded by exons 21–27a [1, 2].
The germline mutation rate for the NF1 gene is
some 10-fold higher than that observed in most other
comparable inherited disease genes, and de novo
mutations are present in almost half of all index NF1
cases [3]. Approximately 800 different NF1 mutations
are reported to-date (http://www.hgmd.org), but there
is no evidence of localised clustering. Examination of
these germline mutations demonstrates that some 80%
S. Griffiths Æ P. Thompson Æ I. Frayling ÆM. Upadhyaya (&)Institute of Medical Genetics, University Hospital of Wales,Cardiff CF14 4XN, UKe-mail: [email protected]
Familial Cancer (2007) 6:21–34
DOI 10.1007/s10689-006-9001-3
123
ORIGINAL PAPER
Molecular diagnosis of neurofibromatosis type 1: 2 yearsexperience
Sian Griffiths Æ Peter Thompson Æ Ian Frayling ÆMeena Upadhyaya
Received: 23 January 2006 / Accepted: 11 July 2006 / Published online: 31 August 2006� Springer Science+Business Media B.V. 2006

are predicted to be truncating mutations, with about
30% of these expected to result in RNA splicing
abnormalities [4]. Efforts to identify and characterise
all NF1 gene mutations continue to present a consid-
erable research and diagnostic challenge due to a
combination of the large gene size, the absence of any
localised mutation clustering, little evidence of repeat
mutation and the wide diversity of mutation types
observed. Furthermore, the presence of a number of
highly homologous partial NF1 pseudogene-like se-
quences located throughout the human genome has
increased the complexity of PCR-based mutation
analysis [5–7]. Indeed, most diagnostic laboratories
were until recently only able to offer molecular testing
in families using linked markers, a strategy that is
obviously not possible in de novo cases which con-
tribute almost half of all new cases [8, 9].
NF1 is characterised by the presence of multiple
cafe-au-lait spots (CAL), benign neurofibromas, and
Lisch nodules in the eye [3]. The often extreme vari-
ability in the presentation of extent and severity of NF1
clinical signs and symptoms, even within the same
family, affected by the same mutation has meant that
establishing definitive clinical diagnostic criteria has
often been problematic. Recognition of this issue led
the National Institute of Health (NIH) in 1988 to issue
a ‘‘Consensus Statement’’ which defined the standard
diagnostic criteria for NF1 to help clinicians to be able
to distinguish it from other related disorders [10].
A number of clinical complications may also occur
in patients and these include abnormalities of the car-
diovascular, gastrointestinal, renal and endocrine sys-
tems; the presence of major orthopedic problems;
facial and body disfigurement; the presence of cogni-
tive deficit and the development of malignancy. There
is an increased risk of development of malignant tu-
mours of the peripheral nerve sheath and the central
nervous systems (CNS). About a quarter of NF1 pa-
tients may eventually develop one or more of these
various clinical complications, underlining the signifi-
cant morbidity and increased mortality associated with
this disorder. It is noteworthy that while the majority of
NF1 patients exhibit only mild symptoms, the lifetime
risk of developing a MPNST in NF1 patients is about
8–13% [11].
While the initial diagnosis is almost always made on
a clinical basis, additional specialist examination is
often needed for those NF1 children who present with
no major disease complications, and who often repre-
sent the first case in the family. It is such families who
may be especially aided by the identification of a
specific NF1 gene mutation. Early diagnosis of the
disease is considered essential so that such patients and
their families can be offered appropriate counselling,
and the affected children can be regularly monitored
for complications, such as learning difficulties, optic
glioma and hypertension.
Genetic counselling in NF1 is greatly complicated by
the marked intra- and inter-familial variation in NF1
disease expression [12]. The combination of this clini-
cal variability and the extensive mutational heteroge-
neity in NF1, necessitating labour-intensive mutation
screening, has meant that attempts to produce geno-
type–phenotype correlations for this disorder are still
very much in their infancy [13, 14].
Another consequence of the variability of clinical
expression in NF1 is that disease progression and
severity cannot be readily predicted. As a result, there
has been little demand to date for prenatal diagnosis,
possibly because most couples would want to know the
clinical severity of the disease in their baby, which
currently cannot be predicted [8]. Despite this lack of
demand, there is still an urgent need for a cost-effective,
rapid and accurate DNA-based test for NF1, and
development of a suitable preimplantation test for NF1
has been reported [15, 16].
Here we describe our experiences from 2 years of
offering an NF1 molecular diagnostic service. To date,
we have analysed the entire NF1 coding region and
the flanking splice site in 169 unrelated individuals,
suspected of having NF1. Possible disease-causing
mutations have been identified in 109 of them.
Materials and methods
Patient samples
Over a 2 year period from April 2003 to June 2005, 169
unrelated patients were referred for NF1 mutation
analysis from medical genetics centres throughout the
UK. Patients were referred for three main reasons: (1)
confirmation of a clinical diagnosis of NF1, in partic-
ular for those individuals who do not fully meet the
diagnostic criteria for NF1, or for children in whom a
precise clinical diagnosis is often difficult (115 indi-
viduals), (2) For NF1 families requesting or consider-
ing prenatal diagnosis in the near future (19
individuals), and (3) A cohort of 32 patients who all
display a severe clinical phenotype, suggesting the
presence of a large NF1 gene deletion. For the
remaining three patients, the reason for referral was
not mentioned. Full clinical details were available on
102 of these patients.
123
22 Familial Cancer (2007) 6:21–34

DNA samples
Genomic DNA was isolated from peripheral blood
cells by our previously published method [17], an
aliquot of each DNA sample being taken and stored
for later confirmation of any identified mutation.
Fluorescent in-situ hybridisation (FISH)
FISH analysis was performed using probes P1-9 and
P1-12 as previously described [17, 18].
Point mutation detection
PCR reactions
PCR reactions were set up using a Biomek FX
automated robotic platform (Beckman Coulter) in a
final volume of 25 ll, using the buffer provided with
the enzyme and containing 25 ng of genomic DNA,
10 pmol of each primer, 10 mM dNTPs, and 1U Taq
DNA polymerase or Hotstar Taq DNA polymerase
(Qiagen). The amplification cycles for reactions using
Taq DNA polymerase consisted of an initial dena-
turation at 94�C for 5 minutes, followed by 35–40
cycles of 94�C for 30 s, Ta �C for 30 s and 72�C for
30 s. Each reaction was terminated with a final
extension step at 72�C for 10 min. For those PCR
reactions using the Hotstar Taq DNA polymerase the
initial denaturation at 94�C was for 15 min followed
by 35 cycles at 94�C for 1 min, Ta �C for 1 min and
72�C for 1 min completed with a final extension of
72�C for 10 min.
Oligonucleotide PCR primers
PCR amplification of the 57 coding exons of the NF1
gene was carried out. The three alternatively spliced
exons (9b, 23a and 48a) were not analysed as no
mutations have yet been identified in these exons
despite NF1 mutational screen of over 1000 unrelated
patients [1, 19–21]. The oligonucleotide primers are
based on those previously described [22], with twenty
nine pairs being re-designed using Primer3-primer de-
sign software [http://frodo.wi.mit.edu/cgi-bin/primer3/
primer3_www.cgi] either to optimise PCR amplifica-
tion, or to extend the sequence analysed around indi-
vidual splice sites (primer sequences available on
request). For exon 19b, nested PCR primers were
designed in order to sequence the fragment. All
oligonucleotides were synthesised by MWG Biotech,
Milton Keynes UK.
Denaturing HPLC analysis
Denaturing high performance liquid chromatography
(dHPLC) was performed on a WAVE DNA fragment
analysis system (Transgenomic, Crewe, UK) using a
DNAsep column. Full diagnostic details are available
from the authors, but in brief, heteroduplex formation
was enhanced by subjecting the untreated PCR
product to denaturation at 95�C for 5 min and then
allowing the reaction mix to gradually reanneal over
30 min by decreasing the temperature to 50�C. PCR
products were analysed for heteroduplexes by sub-
jecting 5 ll of PCR product to a 2% linear acetoni-
trile gradient at a rate of 0.9 ml/min. The starting
concentrations of buffer B were selected by the
WaveMaker software version 4.1. The temperatures
for optimal heteroduplex separation were determined
from the melting profiles produced for each fragment
using the WAVEmaker software. Depending on the
melting domains predicted by the software, the use of
one, two or three different melting temperatures (Tm)
may be required to allow individual PCR fragments
to be successfully analysed.
Sequencing
PCR products were purified using the Montage PCR96
Plates (Millipore), according to the manufacturer’s
protocol, with 5 ll of each purified PCR product being
sequenced in both orientations using ABI Prism
BigDye terminator cycle sequencing kit version 3.1
(Applied Biosystems). Sequencing reactions were also
purified using the Montage SEQ96 Plates (Millipore),
with the addition of 10 ll of Hi-DI formamide and
analysis on an ABI Prism 3100 genetic analyzer.
Sequence analysis was performed to characterise each
identified aberrant fragment, with each of the muta-
tions identified confirmed independently by two expe-
rienced molecular genetic scientists.
Analysis for either complete gene or multi-exon
deletions
DNA samples from all patients in whom neither a
sequence variation or a mutation could be identified
were genotyped using a panel of five highly polymor-
phic extragenic and intragenic markers (from 5¢ to 3¢:pHHH202/RsaI [23], intron 12b (unpublished),
IVS27CA 28.4 [23], IVS38GT53 [23] and 3¢NF1-1 [24]).
The polymorphic markers were analysed either by
restriction fragment length polymorphism (RFLP)
analysis or microsatellite analysis using the ABI Prism
123
Familial Cancer (2007) 6:21–34 23

3100 Genetic Analyzer with ROX 500 (Applied Bio-
systems) as an internal size standard.
Multiplex Ligation Probe Amplification (MLPA)
With the availability of the NF1 MLPA commercial
probe sets, samples in which dHPLC failed to identify
a point mutation were analysed for the presence of
complete or partial NF1 gene deletions. Approxi-
mately 250 ng of DNA was used for MLPA analysis
using the SALSA P081 and P082 NF1 MLPA kits from
MRC-Holland (Amsterdam, NL), these together con-
tain probes for 51 of the 57 NF1 coding exons, as well
as a probe for a sequence located 17 kb downstream of
the NF1 gene and two probes specific for the OMG
gene located in intron 27. Information regarding the
probe sequences and ligation sites may be obtained at
www.mlpa.com. Hybridization, ligation, and amplifi-
cation of the MLPA probes was carried out as
described [25].
Results
Of the 169 patient samples referred to us for NF1
diagnostic analysis over a two year period, mutations
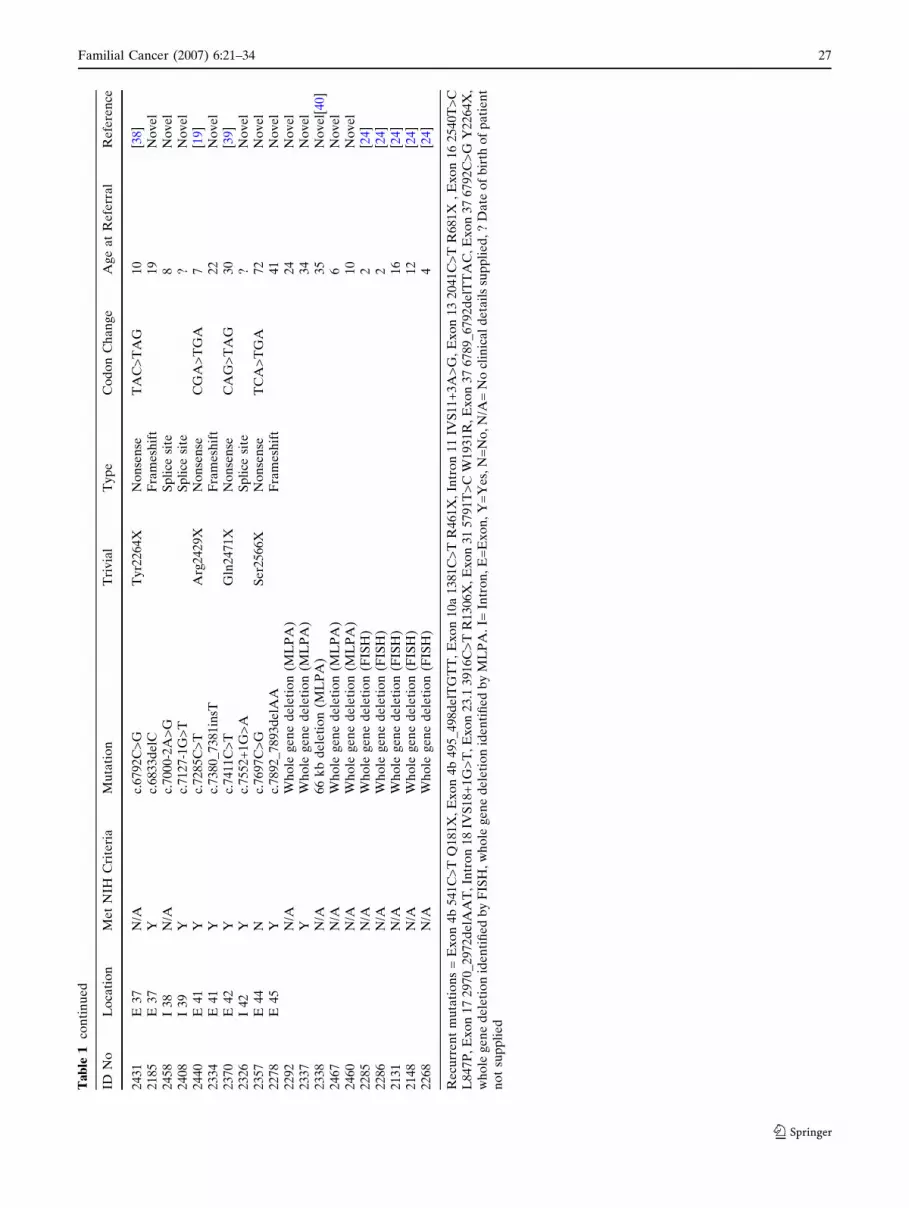
were identified in 109 (64%) cases (Table 1). Of the
46 sporadic NF1 patients, clinical details were avail-
able from 41, of which, 35 individuals met the diag-
nostic criteria of NF1. Mutations which could be
confidently assessed as pathogenic (large exonic
deletions, nonsenses, frameshifts and splice-site
mutations) were identified in 26/35 (74%) of these. In
the remaining six sporadic cases with clinical infor-
mation, but who did not fulfil the diagnostic criteria
for NF1, only one disease causing mutation was
identified (Table 1 2340: Ex17 c.2970_2972delATT).
Thirty three cases are known to be familial and clin-
ical details were available from 26 of these, of which,
21 individuals met the diagnostic criteria for NF1.
Disease-causing mutations were identified in 17/21
(81%). In the remaining 5 cases who did not fulfil the
diagnostic criteria, only one possible disease causing
mutation was identified (Table 1 2404: Ex21 3560
T>C L1187P).
Mutation spectrum
We have identified NF1 mutations in 109 individuals,
comprising 88 different mutations. 57 mutations are
novel (Table 1).
Twelve of the 99 mutations identified by dHPLC were
present in more than one individual:c.1383C>T (R461X)
found in three unrelated patients, whilst another eleven
mutations (c. 541C>T Q181X, c.495_498delTGTT,
c.1721+3A>G, c.2041C>T R681X, c.2540T>C L847P,
c. 5791T>C W1931R, c.2970_2972delAAT (delMet990),
c.6792C>G (Y2264X), c.3113+1G>T, c.3916C>T
(R1306X) and c.6789_6792delTTAC) being identified in
at least two unrelated patients. These may represent
recurrent de novo mutations at ‘hot spots’, or common
alleles due to some founder effect, or a combination of
both factors. We have not carried out haplotype analysis
to help establish this.
Thirty of the 109 (27.5%) possibly pathogenic se-
quence changes identified are predicted to cause
frameshift mutations, including 22 deletions, 7 inser-
tions and 1 insertion/deletion (indel). Two of these
were found in more than two unrelated individuals. Of
these, five mutations have been previously published.
The largest deletion identified by dHPLC was a 22 bp
deletion in exon 16, although the majority of the
frameshift mutations were due to single base pair
deletions or insertions. The single indel was identified
in exon 34. Two unrelated patients had an identical
in-frame deletion in exon 17 (c.2970_2972delAAT).
Nonsense mutations were identified in 30/109
(27.5%) patients and of these 20 have previously been
reported. Thus, 81 (74%) of the 109 mutations identi-
fied were predicted to result in the formation of a
premature termination codon and can be considered
highly likely to be pathogenic.
Mutations predicted to cause missense changes in the
NF1 protein accounted for 16 (15%) of the sequence
variants observed, of which ten have not been previously
described: c.667T>C (W223R), c.1658A>C (H553P),
c.1658A>G (H553R), c.2339C>G (T780R), c.2352G>T
(W784C), c.3447G>A (M1149I), c.3560T>C (L1187P),
c.3604 G>T (A1202S) c.5426G>T (R1809L) and
c.5435T>C (L1812P). Each of these sequence variants
observed is at a highly conserved amino-acid residue and
has not been observed in more than 200 normal chro-
mosomes studied. Whenever possible, parental DNA
was also obtained in order to help determine the po-
tential pathogenicity of such mutations. Two patients
could be identified as having definite de novo mutations,
these include the missense c.5793G>A (W1931R) and
c.3447G>A (M1149I) alterations. In neither case was the
sequence change identifiable in DNA from the parent,
thus implying probable pathogenicity. In another
patient with a family history of NF1, the missense
mutation c.1658A>G (H553P) identified in exon 11
segregated with 2 affected members of the family
123
24 Familial Cancer (2007) 6:21–34

Ta
ble
1S
um
ma
ryo
fN
F1
Mu
tati
on
sid
en
tifi
ed
in1
09
ind
ivid
ua
lsb
yF
ISH
,d
HP
LC
or
ML
PA
IDN
oL
oca
tio
nM
et
NIH
Cri
teri
aM
uta
tio
nT
riv
ial
Ty
pe
Co
do
nC
ha
ng
eA
ge
at
Re
ferr
al
Re
fere
nce
23
73
I1
N/A
c.6
0+
1G
>C
Sp
lice
site
5.5
No
ve
l2
51
6E
3N
/Ac.
24
5C
>T
Se
r8
2P
he
Mis
sen
seT
CT
>T
TT
28
[26]
21
62
E3
Yc.
28
8G
>T
Gly
96
Gly
Sp
lice
site
GG
G>
GG
T2
4N
ov
el
23
60
E3
N/A
c.2
46
_2
47
de
lTC
Fra
me
shif
t2
2N
ov
el
24
09
I4
aN
/Ac.
48
0-1
G>
TS
pli
cesi
te7
No
ve
l2
27
1E
4a
Yc.
31
1T
>G
Le
u1
04
XN
on
sen
seT
TA
>T
GA
38
[27]
23
80
E4
aN
/Ac.
42
1_
42
2in
sGF
ram
esh
ift
45
No
ve
l2
16
1E
4b
Yc.
54
0_
54
1in
sAF
ram
esh
ift
23
[28]
23
64
E4
bN
/Ac.
54
1C
>T
Gln
18
1X
No
nse
nse
CA
G>
TA
G2
8N
ov
el
24
48
E4
bN
/Ac.
54
1C
>T
Gln
18
1X
No
nse
nse
CA
G>
TA
G6
1N
ov
el
24
34
E4
bN
/Ac.
49
5_
49
8d
elT
GT
TF
ram
esh
ift
2N
ov
el
24
35
E4
bY
c.4
95
_4
98
de
lTG
TT
Fra
me
shif
t2
2N
ov
el
24
35
I4
cN
/Ac.
65
5-1
G>
CS
pli
cesi
te3
9N
ov
el
24
32
E5
Yc.
66
7T
>C
Trp
22
3A
rgM
isse
nse
TG
G>
CG
G2
5N
ov
el
23
18
E6
Yc.
77
5d
elA
Fra
me
shif
t5
4N
ov
el
23
01
E7
Yc.
97
8d
elA
Fra
me
shif
t3
3N
ov
el
24
57
I7
Yc.
10
63
-4T
>G
Sp
lici
ng
?4
3N
ov
el
22
94
E1
0a
Yc.
12
78
G>
AT
rp4
26
XN
on
sen
seT
GG
>T
GA
42
No
ve
l2
27
3E
10
aY
c.1
31
8C
>T
Arg
44
0X
No
nse
nse
CG
A>
TG
A4
1[2
9]
20
70
E1
0a
Yc.
13
81
C>
TA
rg4
61
XN
on
sen
seC
GA
>T
GA
31
[19]
23
91
E1
0a
N/A
c.1
38
1C
>T
Arg
46
1X
No
nse
nse
CG
A>
TG
A3
3[1
9]
23
92
E1
0a
N/A
c.1
38
1C
>T
Arg
46
1X
No
nse
nse
CG
A>
TG
Ad
ied
6m
on
ths
[19]
24
39
E1
0b
Yc.
14
22
de
lCF
ram
esh
ift
38
No
ve
l2
40
6I
10
cY
c.1
64
1+
3A
>G
Sp
lici
ng
?2
1N
ov
el
21
50
E1
1N
/Ac.
16
58
A>
CH
is5
53
Pro
Mis
sen
seC
AT
>C
CT
25
No
ve
l2
29
0E
11
N/A
c.1
65
8A
>G
His
55
3A
rgM
isse
nse
CA
T>
CG
T2
7N
ov
el
22
97
I1
1N
/Ac.
17
21
+3
A>
GS
pli
cin
g?
[5]
24
46
I1
1Y
c.1
72
1+
3A
>G
Sp
lici
ng
1[5
]2
36
8E
12
aN
/Ac.
17
48
A>
GL
ys5
83
Arg
Mis
sen
seA
AG
>A
GG
41
[19]
23
28
E1
2a
Yc.
17
56
_1
75
9d
elA
CT
AF
ram
esh
ift
5[3
0]
24
02
E1
2a
Yc.
18
31
_1
83
8d
elC
TT
CT
TA
AF
ram
esh
ift
35
No
ve
l2
10
4I
12
bY
c.2
00
2-1
G>
AS
pli
cesi
te3
No
ve
l2
39
4E
12
bN
/Ac.
18
85
G>
AG
ly6
29
Arg
Mis
sen
seG
GG
>A
GG
21
[31]
23
44
E1
3N
/Ac.
20
41
C>
TA
rg6
81
XN
on
sen
seC
GA
>T
GA
43
[4]
24
41
E1
3N
/Ac.
20
41
C>
TA
rg6
81
XN
on
sen
seC
GA
>T
GA
25
[4]
23
72
E1
3N
/Ac.
20
50
de
lCF
ram
esh
ift
8?
No
ve
l2
19
7E
13
N/A
c.2
24
6C
>G
Se
r74
9X
No
nse
nse
TC
A>
TG
A3
0N
ov
el
23
96
E1
3N
/Ac.
22
51
G>
AG
ly7
51
Arg
Sp
lice
site
GG
A>
AG
A2
1N
ov
el
24
33
E1
5N
/Ac.
23
39
C>
GT
hr7
80
Arg
Mis
sen
seA
CA
>A
GA
20
No
ve
l2
40
3E
15
N/A
c.2
35
2G
>T
Trp
78
4C
ys
Mis
sen
seT
GG
>T
GT
65
No
ve
l2
34
6E
16
Yc.
24
36
_2
45
7d
el2
2(d
elT
GT
TA
AG
AG
GC
GA
AT
GT
CC
CA
T)
Fra
me
shif
t3
1N
ov
el
24
59
E1
6N
/Ac.
25
40
T>
CL
eu
84
7P
roM
isse
nse
CT
T>
CC
T2
[19]
24
38
E1
6Y
c.2
54
0T
>C
Le
u8
47
Pro
Mis
sen
seC
TT
>C
CT
47
[19]
22
03
E1
6N
/Ac.
25
10
G>
AT
rp8
37
XN
on
sen
seT
GG
>T
AG
4N
ov
el
123
Familial Cancer (2007) 6:21–34 25

Ta
ble
1co
nti
nu
ed
IDN
oL
oca
tio
nM
et
NIH
Cri
teri
aM
uta
tio
nT
riv
ial
Ty
pe
Co
do
nC
ha
ng
eA
ge
at
Re
ferr
al
Re
fere
nce
24
33
I1
6N
/Ac.
28
50
+1
G>
AS
pli
cesi
te2
7[1
8]
23
40
E1
7N
c.2
97
0_
29
72
de
lAA
TIn
fra
me
de
leti
on
11
[19
]2
39
7E
17
Yc.
29
70
_2
97
2d
elA
AT
Infr
am
ed
ele
tio
n8
[19
]1
11
2I
18
Yc.
31
13
+1
G>
TS
pli
cesi
te9
[21
]2
36
2I
18
N/A
c.3
11
3+
1G
>T
Sp
lice
site
37
[21
]2
36
7E
19
bY
c.3
20
3_
32
04
insT
Fra
me
shif
t2
7N
ov
el
24
63
E1
9b
Yc.
32
10
de
lGF
ram
esh
ift
?N
ov
el
23
56
E1
9b
Yc.
32
41
_3
24
9d
elC
TG
GT
CT
CF
ram
esh
ift
2N
ov
el
23
12
E1
9b
N/A
c.3
24
6_
32
47
insT
Fra
me
shif
t3
2N
ov
el
24
47
E2
0Y
c.3
36
7G
>T
Glu
11
23
XN
on
sen
seG
AA
>T
AA
3[2
0]
21
98
E2
0N
/Ac.
34
47
G>
AM
et1
14
9Il
eM
isse
nse
AT
G>
AT
A2
6N
ov
el
23
99
I2
1Y
c.3
70
9-1
G>
CS
pli
cesi
te3
0N
ov
el
24
04
E2
1N
c.3
56
0T
>C
Le
u1
18
7P
roM
isse
nse
CT
T>
CC
T1
2N
ov
el
22
77
E2
2Y
c.3
72
1_
37
22
insA
Fra
me
shif
t2
No
ve
l2
35
9E
22
N/A
c.3
82
2_
38
23
de
lCT
Fra
me
shif
t1
7[1
9]
22
29
E2
2Y
c.3
82
6C
>T
Arg
12
76
XN
on
sen
seC
GA
>T
GA
20
[29
]2
35
5I
23
.1Y
c.3
97
5-2
A>
GS
pli
cesi
te1
7[1
9]
23
90
E2
3.1
N/A
c.3
91
6C
>T
Arg
13
06
XN
on
sen
seC
GA
>T
GA
2[3
0]
15
63
E2
3.1
Yc.
39
16
C>
TA
rg1
30
6X
No
nse
nse
CG
A>
TG
A3
5[3
0]
23
29
E2
5Y
c.4
30
8d
elA
Fra
me
shif
t2
6N
ov
el
21
33
E2
7a
N/A
c.4
54
9A
>T
Ly
s15
17
XN
on
sen
seA
AG
>T
AG
52
No
ve
l2
44
3E
27
bY
c.4
70
6T
>G
Le
u1
56
9X
No
nse
nse
TT
A>
TG
A3
1[3
2]
23
36
E2
7b
N/A
c.4
76
1T
>A
Ty
r15
87
XN
on
sen
seT
AT
>T
AA
4N
ov
el
20
13
E2
8N
/Ac.
48
20
T>
AL
eu
16
07
XN
on
sen
seT
TA
>T
AA
30
No
ve
l2
23
5E
28
Yc.
50
50
de
lAF
ram
esh
ift
29
No
ve
l2
40
5E
29
Yc.
52
42
C>
TA
rg1
74
8X
No
nse
nse
CG
A>
TG
A3
0[3
3]
21
84
E2
9N
c.5
42
6G
>T
Arg
18
09
Ieu
Mis
sen
seC
GC
>C
TC
10
No
ve
l2
44
4E
29
Yc.
54
35
T>
CL
eu
18
12
Pro
Mis
sen
seC
TG
>C
CG
20
No
ve
l2
32
7I
29
N/A
c.5
54
6+
5G
>A
Sp
lici
ng
?1
0N
ov
el
22
36
E3
0Y
c.5
71
9G
>T
Glu
19
07
XN
on
sen
seG
AA
>T
AA
28
[34
]2
38
9I
31
N/A
c.5
94
4-2
A>
GS
pli
cesi
te2
3[1
9]
21
32
E3
1Y
c.5
79
1T
>C
Trp
19
31
Arg
Mis
sen
seT
GG
>C
GG
5[3
5]
23
93
E3
1N
/Ac.
57
91
T>
CT
rp1
93
1A
rgM
isse
nse
TG
G>
CG
G1
4[3
5]
23
51
E3
1Y
c.5
79
3G
>A
Trp
19
31
Arg
No
nse
nse
TG
G>
TG
A1
0N
ov
el
22
75
E3
1Y
c.5
83
9C
>T
Arg
19
47
XN
on
sen
seC
GA
>T
GA
23
[36
]2
20
0E
31
Yc.
59
17
de
lGF
ram
esh
ift
24
No
ve
l2
34
8E
34
N/A
c.6
52
2_
65
23
de
lGA
Fra
me
shif
t2
2N
ov
el
24
00
E3
4Y
c.6
54
7_
65
49
de
lAC
Ain
sCC
ind
el
20
No
ve
l2
39
8E
35
Yc.
65
82
de
lAF
ram
esh
ift
22
No
ve
l2
40
7I
36
N/A
c.6
75
6+
3A
>G
an
dIV
S3
6+
4C
>T
Sp
lici
ng
?5
1N
ov
el
24
42
E3
7N
/Ac.
67
89
_6
79
2d
elT
TA
CF
ram
esh
ift
6[3
7]
24
36
E3
7Y
c.6
78
9_
67
92
de
lTT
AC
Fra
me
shif
t2
[37
]2
27
6E
37
Yc.
67
92
_6
79
3in
sAF
ram
esh
ift
18
[19
]2
34
3E
37
Yc.
67
92
C>
AT
yr2
26
4X
No
nse
nse
TA
C>
TA
A1
9[3
7]
23
71
E3
7N
/Ac.
67
92
C>
AT
yr2
26
4X
No
nse
nse
TA
C>
TA
A5
?[3
7]
123
26 Familial Cancer (2007) 6:21–34
Ta
ble
1co
nti
nu
ed
IDN
oL
oca
tio
nM
et
NIH
Cri
teri
aM
uta
tio
nT
riv
ial
Ty
pe
Co
do
nC
ha
ng
eA
ge
at
Re
ferr
al
Re
fere
nce
24
31
E3
7N
/Ac.
67
92
C>
GT
yr2
26
4X
No
nse
nse
TA
C>
TA
G1
0[3
8]
21
85
E3
7Y
c.6
83
3d
elC
Fra
me
shif
t1
9N
ov
el
24
58
I3
8N
/Ac.
70
00
-2A
>G
Sp
lice
site
8N
ov
el
24
08
I3
9Y
c.7
12
7-1
G>
TS
pli
cesi
te?
No
ve
l2
44
0E
41
Yc.
72
85
C>
TA
rg2
42
9X
No
nse
nse
CG
A>
TG
A7
[19]
23
34
E4
1Y
c.7
38
0_
73
81
insT
Fra
me
shif
t2
2N
ov
el
23
70
E4
2Y
c.7
41
1C
>T
Gln
24
71
XN
on
sen
seC
AG
>T
AG
30
[39]
23
26
I4
2Y
c.7
55
2+
1G
>A
Sp
lice
site
?N
ov
el
23
57
E4
4N
c.7
69
7C
>G
Se
r25
66
XN
on
sen
seT
CA
>T
GA
72
No
ve
l2
27
8E
45
Yc.
78
92
_7
89
3d
elA
AF
ram
esh
ift
41
No
ve
l2
29
2N
/AW
ho
leg
en
ed
ele
tio
n(M
LP
A)
24
No
ve
l2
33
7Y
Wh
ole
ge
ne
de
leti
on
(ML
PA
)3
4N
ov
el
23
38
N/A
66
kb
de
leti
on
(ML
PA
)3
5N
ov
el[
40
]2
46
7N
/AW
ho
leg
en
ed
ele
tio
n(M
LP
A)
6N
ov
el
24
60
N/A
Wh
ole
ge
ne
de
leti
on
(ML
PA
)1
0N
ov
el
22
85
N/A
Wh
ole
ge
ne
de
leti
on
(FIS
H)
2[2
4]
22
86
N/A
Wh
ole
ge
ne
de
leti
on
(FIS
H)
2[2
4]
21
31
N/A
Wh
ole
ge
ne
de
leti
on
(FIS
H)
16
[24]
21
48
N/A
Wh
ole
ge
ne
de
leti
on
(FIS
H)
12
[24]
22
68
N/A
Wh
ole
ge
ne
de
leti
on
(FIS
H)
4[2
4]
Re
curr
en
tm
uta
tio
ns
=E
xo
n4
b5
41
C>
TQ
18
1X
,E
xo
n4
b4
95
_4
98
de
lTG
TT
,E
xo
n1
0a
13
81
C>
TR
46
1X
,In
tro
n1
1IV
S1
1+
3A
>G
,E
xo
n1
32
04
1C
>T
R6
81
X,
Ex
on
16
25
40
T>
CL
84
7P
,E
xo
n1
72
97
0_
29
72
de
lAA
T,
Intr
on
18
IVS
18
+1
G>
T,
Ex
on
23
.13
91
6C
>T
R1
30
6X
,E
xo
n3
15
79
1T
>C
W1
93
1R
,E
xo
n3
76
78
9_
67
92
de
lTT
AC
,E
xo
n3
76
79
2C
>G
Y22
64
X,
wh
ole
ge
ne
de
leti
on
ide
nti
fie
db
yF
ISH
,w
ho
leg
en
ed
ele
tio
nid
en
tifi
ed
by
ML
PA
.I=
Intr
on
,E
=E
xo
n,
Y=
Ye
s,N
=N
o,
N/A
=N
ocl
inic
al
de
tail
ssu
pp
lie
d,
?D
ate
of
bir
tho
fp
ati
en
tn
ot
sup
pli
ed
123
Familial Cancer (2007) 6:21–34 27

provided for analysis, again providing good evidence for
its probable pathogenicity.
Fifteen sequence variants occurred at splice donor
or acceptor sites, and a further 6 sequence changes
were detected in the adjacent intronic sequences,
within five base pairs of the intron/exon boundary. Five
of these previously reported variants include, 4
involving the donor or acceptor splice sites
(c.2850+1G>A [21], c.3113+1G>T [21], c.3975-2A>
G[19], c.5944-2A>G [19]) and one in the adjacent in-
tronic sequence of exon 11 (c.1721+3A>G [5]). Two
variants c.6756+3A>G and c.6756+4C>T (both within
the accepted consensus region of the donor splice site)
occurred simultaneously in one individual. On further
investigation it was determined that both variants
segregated with two affected family members provid-
ing evidence that they probably are pathogenic.
The spectrum of different mutation types identified
in this study is illustrated in Fig. 1. Of all the point
mutations identified, 74% are predicted to result in
truncated mRNA transcript.
Table 2 displays the 23 sequence variants detected
in this study. Variants were classed as polymorphisms if
they were either found in association with a pathogenic
mutation, or if they have been detected in unaffected
individuals, or have been established as such in previ-
ous publications [19, 22, 27].
Table 3 shows the seven sequence variants for which
pathogenicity has yet to be definitively established.
However, none of these sequence changes were found
in 200 normal chromosome 17.
Distribution of NF1 mutations
The distribution of mutations across the NF1 gene is
illustrated in Fig. 2. Most mutations detected were
located in exons 4b,10a, 13, 16, 31 and 37 and no
27%
15%
27%
19%
2%
1%
9%
Nonsense
Missense
Frameshift
Splicing
In frame deletion
Indel
Large deletion
Fig. 1 NF1 mutational spectrum derived from 109 NF1 patients.Indel = Insertion and deletion
Table 2 Summary of non pathogenic sequence variants identified
Location Mutation Trivial Pathogenic mutation foundin association
Reference
5¢ UTR c.1-22G>C Mattocks et al. [27] Found with definite mutation and in unaffected [27]Intron 3 c.288+41G>A Exon 28, c.5050delA This ReportExon 4b c.528T>A D176E Exon 23.1, c.3916C>T R1306X This Report and [21]Intron 4c c.655-83T>C Exon 10a, c.1318C>T R440X This ReportExon 5 c.702G>A L234L Exon 28, c.5050delA This Report and [41]Exon 6 c.846G>A Q282Q Exon 17, c.2970_2973delAAT This ReportIntron 10b c.1528-35delT Exon 30, c.5719G>T E1907X This ReportExon 12a c.1810T>C L604L Exon 16, c.2433_2456del22 This ReportExon 13 c.2034G>A P678P Exon 31, c.5917_delG This ReportIntron 16 c.2851-16T>C Exon 28, c.4820T>A L1607X This ReportIntron 17 c.2991-96T>C Exon 30, c.5719G>T E1907X This ReportExon 21 c.3564A>G Q1188Q Exon 21, c.3560T>C L1187P This ReportExon 22 c.3867C>T F1289F Mattocks et al. [27] Found with definite mutation [27]Exon 23.2 c.4020T>C L1340L IVS23.1-2G>A This ReportIntron 23.2 c.4111-7delTTG Exon 7, 1017_1019delA This ReportIntron 25 c.4368-46 Exon 13, 2050delC fs687X This ReportIntron 28 c.5205+23T>C Exon 19b, 3241_3249delCTGGTCTC This ReportIntron 29 c.5546+19T>A Exon 44, 7697C>G S2566X This ReportIntron 32 c.6084+8C>G Mattocks et al. [27] Found with definite mutation[27]Intron 39 c.7126+37G>C Exon 28, c.4820T>A L1607X This ReportIntron 40 c.7258+19delCAAA Exon 19b, 3241_3249delCTGGTCTC This ReportIntron 41 c.7395-17C>T Exon 30, c.5719G>T E1907X This ReportExon 46 c.7978A>G I2660V Exon 23.1, c.3916C>T R1306X This Report
Twenty three non pathogenic sequence variants were identified, 19 of these were detected with a definite mutation in this study andanother with a possible missense mutation, the remaining 3 have been established as non pathogenic in previous studies
123
28 Familial Cancer (2007) 6:21–34

mutations were found in exons 2, 8, 9, 14, 19a, 23.2, 24,
26, 32, 33, 40, 43 and 46–49. The most common muta-
tion, occurring three times (3%) in our series, was the
nonsense mutation, c.1381 (R461X) in exon 10a. A
direct comparison of the number of mutations detected
in each exon compared to the physical size of that exon
is shown in Fig. 3 and illustrates that for its size, exon
37 has the most mutations.
Complete or partial NF1 gene deletions
On the basis of severe clinical presentation of NF1
disease, 32 samples were tested by FISH for large
deletions encompassing NF1, in 5 cases a whole NF1
gene deletion was identified. The remaining 27 samples
were screened by DHPLC and mutations were identi-
fied in 23 of them. Therefore, in total 164 samples were
screened by dHPLC, 25 of which failed to display ei-
ther a polymorphism or a definitive mutation, indicat-
ing the possibility of either a whole or partial NF1 gene
deletion. These samples were genotyped with a panel
of 5 highly polymorphic markers. Patients 2292, 2337
and 2363 were apparently homozygous for all of these
markers, suggesting a whole gene deletion, sample
2338 was apparently homozygous for two markers,
IVS27AC and IVS38. With the introduction of MLPA
kits P081 and P082 for NF1, confirmation of a whole
gene deletion in two of the samples (2292, 2337) and a
multi exon deletion extending exons 2–10a in the other
(2338) was possible. Furthermore, MLPA analysis was
carried out on samples without point mutations pro-
vided that the DNA quantity was sufficient and of
adequate quality. To date, 33 cases out of 63 have been
analysed and deletions identified in five (2292, 2337,
2338, 2467, 2460) (Table 1). High resolution CGH
micro-array analysis has also confirmed that samples
2292 and 2337 harbour complete gene deletions, and
that sample 2338 has a 66 kb genomic deletion [40].
Discussion
Definition of the complete sequence of the human NF1
gene has provided the means to offer both presymp-
tomatic and prenatal diagnosis, either via linkage or by
direct mutation analysis of the NF1 gene. In practice,
however, it has been observed that despite this very
few families express a wish to pursue either of these
options. This may be because they either do not per-
ceive NF1 as a serious debilitating illness, or it may be
more related to the issue that even successful mutation
Table 3 Summary ofsequence variants ofunknown pathogenicityidentified
In eight NF1 patients,sequence variants wereidentified but thepathogenicity of thesechanges is not defined
ID No. Location Sequence Change Reference
2147 Intron 10c c.1641+39C>T Novel2354 Intron 12a c.1845+45G>A Novel2295 Intron 22 c.3871-39G>A Novel2192 Intron 26 c.4514+11C>G Novel2134 Intron 26 c.4514+12C>T Novel2134 Intron 34 c.6579+45T>A [19]2333 Intron 43 c.7675+46G>A Novel
0
1
2
3
4
5
6
7
8
1 4B 5 10B 11 12B 14 16 18 19B 21 24 26 27B 29 31 33 35 37 39 41 43 45 47 49
Exon
Nu
mb
er o
f m
uta
tio
ns
3 7 9 23.1
Fig. 2 Histogram representing the distribution of NF1 mutations identified in 99 patients by dHPLC. The exons or their consensussplice sites in which the mutations were identified are represented on the X axis and the number of mutations identified on the Y axis
123
Familial Cancer (2007) 6:21–34 29

analysis is often of little help in accurately predicting
the disease severity expected in any future offspring.
Insensitivity at detecting mutations may also have been
a factor in the past, but this has become less of an issue
with the recent introduction of more efficient mutation
detection techniques. Whether the patient without an
identifiable NF1 mutation may have a mutation in
some other gene(s) is also a slight possibility.
Gross DNA re-arrangements and multi-exon dele-
tions account for between 5% and 10% [1, 19, 42, 43]
to 15 [44] of all NF1 mutations. In this series we
identified complete gene deletions in 9/169 (5 %)
individuals, while a multi-exon deletion was identified
in only 1 patient (0.6%).
The absence of any obvious clustering of mutations
within the NF1 gene clearly necessitates screening of
the entire gene for mutations. Furthermore, no single
mutation detection test system is currently able to
identify the entire spectrum of NF1 mutations, which
includes everything from point mutations through sin-
gle and multiple exon lesions up to 1.5 Mb genomic
deletions [19–21, 44, 45]. In addition, some 30% of
mutations in the NF1 gene are predicted to cause
aberrant splicing [4]. While the majority of mutations
affect consensus acceptor and donor splice site se-
quences, a number of missense, nonsense and silent
mutations may also result in splicing abnormalities,
either by creating a novel donor or acceptor site, or by
their direct effect on exonic splicing enhancer (ESE) or
exonic splicing silencer (ESS) regulatory sequences
[34, 42, 45].
No mutations were identified in exon 19b in a pre-
vious study which analysed 500 unrelated NF1 patients
[19]. In this study, nested primers were designed to
sequence exon 19b to overcome the difficulty in
sequencing this exon caused by the tract of 26 T’s in
intron 19a before the beginning of exon 19b. Using
nested PCR primers, however, we identified three
disease-causing mutations in this study. Fahsold and
colleagues found, multiple NF1 mutations in exon 4b,
in this study we identified three different mutations in
exon 4b, two of the mutations were recurrent, occur-
ring in two unrelated individuals. ‘Warm’ hot spots for
mutations in the NF1 gene have been reported in exons
31 and 37 [1], this is also confirmed in this series:
mutations in exon or intron 31 were identified in six
individuals (one of which is a previously described
recurrent nonsense mutation, c.5839C>T R1947X,
whilst another c.5791 T>C Trp1931Arg occurred in two
unrelated individuals in this study), and seven indi-
viduals harboured a mutation in exon 37 (one of which
is novel c.6833delC, another two were recurrent
c.6792C>A Y2264X and c.6789_6792delTTAC) even
though this exon represents just over 1.2% of the
coding region.
It is often difficult to judge the diagnostic signifi-
cance of missense mutations without some level of
functional analysis [45]. However, all mutations iden-
tified in this series predict changes in evolutionarily
conserved aminoacid residues in mouse v. human, and
none of the sequence alterations has been seen in at
least 200 normal chromosomes 17. Without suitable
family histories, and thus the possibility of segregation
studies to assist in deciding pathogenicity, either RNA-
based analysis or the use of a minigene splicing assay
might be usefully applied in such situations [20, 42, 45,
46]. However, the problems involved in collecting and
analysing mRNA on a routine diagnostic basis are not
to be underestimated, as are the potential issues with
the testing of illegitimate transcripts derived from
lymphocytes [47].
Ideally, diagnostic mutation screening tests should
have high sensitivity, preferably approaching 100%,
although any such estimates are inherently dependent
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
1 4B 5 9 10B 11 12B 18 2123.1 24 26 27B 31 33 37
Exon
Rel
ativ
e m
uta
tio
n f
req
uen
cy (
wei
gh
ted
)
3 7 14 16 19B 29 35 39 41 43 45 47 49
Fig. 3 Weighted distributionof mutations over the NF1gene, calculated for each exonby dividing the number ofpossible pathogenic mutationsidentified in that exon, by thenumber of base-pairscomprising the exon, plus tenbase pairs added to allow forsplice-site mutations. Thevalues are ratios between theexon-specific mutationdensities and the averagemutation density for thewhole gene (99/9054bp)
123
30 Familial Cancer (2007) 6:21–34

on the accuracy of relevant clinical diagnosis. It is
therefore encouraging that NF1 mutation detection
rates of 89–95% have been reported [20, 27]. Auto-
mated comparative sequence analysis identifies muta-
tions in 89% of NF1 patients and confirms a mutation
cluster in exons 11–17 distinct from the GAP related
domain [27]. Messiaen and colleagues [20] used a
combination of techniques to maximise sensitivity:
inherently, the more techniques that are applied, then
the greater will be the yield of mutations. However,
especially in a publicly-funded healthcare system such
as the UK National Health Service, resources are fi-
nite, and we feel that our approach is more cost-
effective for a routine diagnostic service. Any reduc-
tion in sensitivity, however, has potentially important
implications for NF families. Given the high pene-
trance of NF1 mutations, coupled with less than 100%
sensitivity of the test, then any negative mutation result
will always be difficult to interpret in individual cases,
and in series such as this audit of activity. The
mutation detection rate of 78% achieved in this audit
is lower than that obtained in other centres as our
service involves only DNA analysis, and no RNA
work. Therefore, the techniques we use will obviously
not identify ‘deep’ intronic and some splicing changes
which are located outside the region of sequence
analysed. It is also possible that methylation of the
NF1 gene promoter region may be involved in the
inactivation of NF1 gene in some patients, although
this feature has not been reported to be a common
mechanism of NF1 gene inactivation [48–51]. An
additional factor reducing the apparent sensitivity of
our analytical technique is likely to be clinical ascer-
tainment bias, in that clinicians often ask for NF1
molecular testing in circumstances where the pheno-
type is less obvious, i.e. in cases where the prior
probability of a mutation is lower, and they are
seeking the laboratory’s help in making a firm diag-
nosis. Inevitably, this will lower the overall percentage
yield of mutations, and it should be noted that this is
a report of an audit of activity, not a research study
designed to demonstrate the maximum possible
mutation detection rate in clinically definite cases,
useful though it is to know what that figure is.
Publication of the complete human genome
sequence has led to the identification of a number of
additional NF1-like genomic sequences located on
several other chromosomes [6]. Their potential inter-
ference in any diagnostic NF1 test is significant and
thus secure PCR strategies are warranted. As a result
we have re-designed new primers for twenty nine exons
in order to make this test more robust. We have also
developed an RNA-based diagnostic test which
permits the analysis of the entire NF1 transcript in a
series of 24 overlapping amplimers [17].
No obvious genotype–phenotype relationships have
yet been found in NF1 [12, 13]. Different mutations in
the NF1 gene are associated with Neurofibromatosis-
Noonan syndrome (NFNS) [52, 53]. The general lack
of a genotype–phenotype relationship in NF1 is
somewhat intriguing. It may be due to modifier loci
[12], or a subtle effect in terms of the nature of the
germline mutation determining the nature of the so-
matic mutations in NF1 tumours, as has been seen in
Familial Adenomatous Polyposis [54]. The pathogenic
and non-pathogenic variants identified in this study will
add to the body of data able to contribute to any such
understanding of genotype phenotype relationship in
NF1.
There are, nonetheless, some interesting observa-
tions that can be made from this data set. Firstly, two
unrelated patients, both with the same in-frame dele-
tion in exon 17 (c.2970_2972delAAT), have only CAL
spots without any obvious dermal neurofibromas. This
preliminary finding has been supported by similar
clinical findings in 18 unrelated NF1 patients with this
mutation (Upadhyaya et al. submitted). Secondly,
while a relationship between the presence of large NF1
gene deletions and dysmorphic features, learning dis-
ability and developmental delay has previously been
described [55], we were unable to confirm that all such
patients with NF1 deletions have this specific pheno-
type [56]. It is difficult to comment on a genotype-
phenotype correlation with certainty in this report in
view of the often limited clinical data given to us by
referring clinicians. These findings may indicate that
unlinked modifying genes and the normal NF1 allele
may well be involved in the development of particu-
lar clinical features in NF1, and that their relative
contributions may vary for different features.
The lack of definitive clinical information on some
67 patients included in this study, almost 40% of all
referrals, made it difficult to assess accurately the
mutation detection rate in this cohort of patients.
Recalculation of our results based only on those pa-
tients with a definitive clinical diagnosis, demonstrates
that of the 102 patients with reliable clinical data, 78
patients satisfied the NIH diagnostic criteria for NF1.
Within this defined cohort of NF1 patients, mutations
were characterised in 61 cases (78%), an increase over
the 64% in unselected cases.
The 57 novel NF1 mutations identified in this study
will expand the germline mutational spectrum of the
NF1 gene. In contrast to earlier findings [21], however,
our series would indicate that there are only a small
number of recurrent mutations in NF1 (Fig. 2). There is
123
Familial Cancer (2007) 6:21–34 31
no clustering of mutations in either the Cys-Ser rich
domain encoded by exons 11–17 [19, 27], or within the
GAP-related domain encoded by exons 21–27a. We
have found that exons 4b, 10a, 13, 16, 31 and 37 do appear
to harbour more mutations than do any other exons.
A sensitive genetic test for NF1 is warranted in or-
der to define better the clinical status of those patients
who fail to satisfy the diagnostic criteria for NF1, which
is often the case with young patients and atypical cases.
Given that almost half of all NF1 patients represent
new NF1 gene mutations, the possible presence of
germline mosaicism often makes it difficult to predict
the risk to offspring of inheriting NF1 mutations. Some
de novo patients will undoubtedly be somatic mosaics,
but we have not observed any cases of even possible
mosaicism in this series. While it is possible to detect
mosaicism by careful sequencing, the detection of
somatic mosaicism will always be challenging.
Over the two years that we have offered a complete
NF1 mutational screening service as part of the UK
Genetic Testing Network (UKGTN: http://www.ukgt-
n.org/index.html ), we have continued to modify and
improve our mutation detection technique. Our
reporting time for a complete NF1 gene mutational
screen ranges from 3 weeks up to 3 months for the
more complex mutations, however, our average
reporting time is currently about 6 weeks. The test
performance data we present here is of relevance in the
audit and development of genetic tests, as exemplified
by the requirements of the UKGTN in its gene dossier
system (http://www.ukgtn.org/dossier.html), which in-
volves assessment of genetic tests against set criteria.
The sensitivity of genetic testing is increasingly also
becoming a factor in establishing guidelines for clinical
genetic care, e.g. familial breast cancer (NICE Guide-
line CG014, May 2004, England and Wales: http://
www.nice.org.uk ) which states ‘‘A search/screen for a
mutation in a gene should aim for as close to 100%
sensitivity as possible for detecting coding alterations
and the whole gene should be searched.’’ In addition,
there is pressure on laboratory and clinical genetics
services to reduce the time spent in the diagnostic
process, as well as the public health considerations of
equity of testing. Thus, while we acknowledge that our
current system for NF1 testing could be improved, it
does go a considerable way to addressing such issues.
With the application of robotisation to increase labo-
ratory throughput, as we have started to use, it is
envisaged that turnaround times will be further
reduced. With the advancement of mutation detection
technologies including direct sequencing of all coding
and flanking non-coding regions of the NF1 gene, it
should be possible to develop a quicker and even more
sensitive diagnostic test for NF1, however, any such
testing will always be a compromise based on cost-
effectiveness.
Acknowledgments We thank all the clinicians for their help inproviding the clinical information. We are grateful to the WalesGene Park for their financial support, and the staff of theMolecular Genetics Laboratory of the All-Wales Genetics Lab-oratory Service. We thank Dr Nick Thomas for his help with thesplice prediction program.We wish to thank Dr Susan Huson forher support in initially setting up a diagnostic service, LindaSelwood for her administrative support and Andrew Wallace fordeveloping MLPA data analysis spreadsheets.
References
1. Upadhyaya M, Cooper DN (1998) Neurofibromatosis Type 1from genotype to phenotype. In: Upadhyaya M, Cooped DN(eds) BIOS Scientific, Oxford
2. Cichowski K, Jacks T (2001) NF1 tumor suppressor genefunction: 1narrowing the GAP. Cell 104(4):593–604
3. Huson SM, Hughes RAC (1994) The neurofibromatoses: apathogenetic and clinical overview. Chapman and HallMedical, London
4. Ars E, Serra E, Garcia J, Kruyer H, Gaona A, Lazaro C,Estivill X (2000) Mutations affecting mRNA splicing are themost common molecular defects in patients with neurofi-bromatosis type 1. Hum Mol Genet 9(2):237–247
5. Purandare SM, Huntsman Breidenbach H, Li Y, Zhu XL,Sawada S, Neil SM, Brothman A, White R, Cawthon R,Viskochil D (1995) Identification of neurofibromatosis 1(NF1) homologous loci by direct sequencing, fluorescence insitu hybridization, and PCR amplification of somatic cellhybrids. Genomics 30(3):476–485
6. Luijten M, Wang Y, Smith BT, Westerveld A, Smink LJ,Dunham I, Roe BA, Hulsebos TJ (2000) Mechanism ofspreading of the highly related neurofibromatosis type 1(NF1) pseudogenes on chromosomes 2, 14 and 22. Eur JHum Genet 8(3):209–214
7. Yu H, Zhao X, Su B, Li D, Xu Y, Luo S, Xiao C, Wang W(2005) Expression of NF1 pseudogenes. Hum Mutat26(5):487–488
8. Upadhyaya M, Fryer A, MacMillan J, Broadhead W, HusonSM, Harper PS (1992) Prenatal diagnosis and presymptom-atic detection of neurofibromatosis type 1. J Med Genet29(3):180–183
9. Lazaro C, Ravella A, Casals T, Volpini V, Estivill X (1992)Prenatal diagnosis of sporadic neurofibromatosis 1. Lancet339(8785):119–20
10. NIH (1988) NIH Consensus development conference state-ment. Neurofibromatosis. Arch Neurol 45:575–8
11. Evans DG, Baser ME, McGaughran J, Sharif S, Howard E,Moran A (2002) Malignant peripheral nerve sheath tumoursin neurofibromatosis 1. J Med Genet 39(5):311–314
12. Easton DF, Ponder MA, Huson SM, Ponder BA (1993) Ananalysis of variation in expression of neurofibromatosis (NF)type 1 (NF1): evidence for modifying genes. Am J HumGenet 53(2):305–313
13. Castle B, Baser ME, Huson SM, Cooper DN, Upadhyaya M(2003) Evaluation of genotype-phenotype correlations inneurofibromatosis type 1. J Med Genet 40(10):e109
14. Viskochil DH (1998) Gene structure and expression. In:Upadhyaya M, Cooper DN (eds) Neurofibromatosis Type 1from genotype to phenotype. BIOS Scientific, Oxford
123
32 Familial Cancer (2007) 6:21–34

15. Verlinsky Y, Rechitsky S, Verlinsky O, Chistokhina A,Sharapova T, Masciangelo C, Levy M, Kaplan B, Lederer K,Kuliev A (2002) Preimplantation diagnosis for neurofibro-matosis. Reprod Biomed Online 4(3):218–222
16. Spits C, De Rycke M, Van Ranst N, Joris H, Verpoest W,Lissens W, Devroey P, Van Steirteghem A, Liebaers ISer-mon K (2005) Preimplantation genetic diagnosis for neuro-fibromatosis type 1. Mol Hum Reprod 11(5):381–387
17. Upadhyaya M, Han S, Consoli C, Majounie E, Horan M,Thomas NS, Potts C, Griffiths S, Ruggieri M, von DeimlingA, Cooper DN (2004) Characterization of the somaticmutational spectrum of the neurofibromatosis type 1 (NF1)gene in neurofibromatosis patients with benign and malig-nant tumors. Hum Mutat 23(2):134–146
18. Wu R, Lopez-Correa C, Rutkowski JL, Baumbach LL,Glover TW, Legius E (1999) Germline mutations in NF1patients with malignancies. Genes Chromosomes Cancer26(4):376–380
19. Fahsold R, Hoffmeyer S, Mischung C, Gille C, Ehlers C,Kucukceylan N, Abdel-Nour M, Gewies A, Peters H, Ka-ufmann D, Buske A, Tinschert S, Nurnberg P (2000) Minorlesion mutational spectrum of the entire NF1 gene does notexplain its high mutability but points to a functional domainupstream of the GAP-related domain. Am J Hum Genet66(3):790–818
20. Messiaen LM, Callens T, Mortier G, Beysen D, Van-denbroucke I, Van Roy N, Speleman F, Paepe AD (2000)Exhaustive mutation analysis of the NF1 gene allows iden-tification of 95% of mutations and reveals a high frequencyof unusual splicing defects. Hum Mutat 15(6):541–555
21. Ars E, Kruyer H, Morell M, Pros E, Serra E, Ravella A,Estivill X, Lazaro C (2003) Recurrent mutations in the NF1gene are common among neurofibromatosis type 1 patients. JMed Genet 40(6):e82
22. Han SS, Cooper DN, Upadhyaya MN (2001) Evaluation ofdenaturing high performance liquid chromatography(DHPLC) for the mutational analysis of the neurofibroma-tosis type 1 (NF1) gene. Hum Genet 109(5):487–497
23. Oguzkan S, Cinbis M, Ayter S, Anlar B, Aysun S (2003)Molecular analysis of neurofibromatosis type 1 in Turkishfamilies using polymorphic markers. Turk J Pediatr 45(3):192–7
24. Lopez Correa C, Brems H, Lazaro C, Estivill X, Clementi M,Mason S, Rutkowski JL, Marynen P, Legius E (1999)Molecular studies in 20 submicroscopic neurofibromatosistype 1 gene deletions. Hum Mutat 14(5):387–393
25. Schouten JP, McElgunn CJ, Waaijer R, Zwijnenburg D,Diepvens F, Pals G (2002) Relative quantification of 40 nu-cleic acid sequences by multiplex ligation-dependent probeamplification. Nucleic Acids Res 30(12):e57
26. Kluwe L, Friedrich RE, Korf B, Fahsold R, Mautner VF(2002 Mar) NF1 mutations in neurofibromatosis 1 patientswith plexiform neurofibromas. Hum Muta 19(3):309
27. Mattocks C, Baralle D, Tarpey P, ffrench-Constant C,Bobrow M, Whittaker J (2004) Automated comparative se-quence analysis identifies mutations in 89% of NF1 patientsand confirms a mutation cluster in exons 11–17 distinct fromthe GAP related domain. J Med Genet 41(4):e48
28. Toliat MR, Erdogan F,Gewies A, Fahsold, Buske A, Tinsc-hert S, Nurnberg P (2000) Analysis of the NF1 gene bytemperature gradient gel electrophoresis reveals a highincidence of mutations in exon 4b. Electrophoresis21(3):541–544
29. Heim RA, Kam-Morgan L, N.Binnie CG, Corns DD, Cay-ouette MC, Farber RA, Aylsworth AS, Silverman LM, LuceMC (1995) Distribution of 13 truncating mutations in theneurofibromatosis 1 gene. Hum Mol Genet 4(6):975–981
30. Park VM, Pivnick EK (1998) Neurofibromatosis type 1(NF1): a protein truncation assay yielding identification ofmutations in 73% of patients. J Med Genet 35(10):813–820
31. Gasparini P, D’Agruma L, Pio de Cillis G, Balestrazzi P,Mingarelli R, Zelante L (1996) Scanning the first part of theneurofibromatosis type 1 gene by RNA-SSCP: identificationof three novel mutations and of two new polymorphisms.Hum Genet 97(4):492–495
32. Upadhyaya M, Maynard J, Osborn M, Harper PS (1997) Sixnovel mutations in the neurofibromatosis type 1 (NF1) gene.Hum Mutat 10(3):248–250
33. Valero MC, Velasco E, Moreno F, Hernandez-Chico C(1994) Characterization of four mutations in the neurofi-bromatosis type 1 gene by denaturing gradient gel electro-phoresis (DGGE). Hum Mol Genet 3(4):639–641
34. Zatkova A, Messiaen L, Vandenbroucke I, Wieser R,Fonatsch C, Krainer AR, Wimmer K (2004) Disruption ofexonic splicing enhancer elements is the principal cause ofexon skipping associated with seven nonsense or missensealleles of NF1. Hum Mutat 24(6):491–501
35. Hudson J, Wu CL, Tassabehji M, Summers EM, Simon S,Super M, Donnai D, Thakker N (1997) Novel and recurrentmutations in the neurofibromatosis type 1 (NF1) gene. HumMutat 9(4):366–367
36. Cawthon RM, Weiss R, Xu GF, Viskochil D, Culver M,Stevens J, Robertson M, Dunn D, Gesteland R, O’Connell P(1990) A major segment of the neurofibromatosis type 1gene: cDNA sequence genomic structure and pointmutations. Cell 62(1):193–201
37. Robinson PN, Boddrich A, Peters H, Tinschert S, Buske A,Kaufmann D, Nurnberg P (1995) Two recurrent nonsensemutations and a 4 bp deletion in a quasi-symmetric elementin exon 37 of the NF1 gene. Hum Genet 96(1):95–98
38. Messiaen L, Callens T, De Paepe A, Craen M, Mortier G(1997) Characterisation of two different nonsense mutationsC6792A and C6792G causing skipping of exon 37 in the NF1gene. Hum Genet 101(1):75–80
39. Origone P, Bellini C, Sambarino D, Banelli B, Morcaldi G,La Rosa C, Stanzial F, Castellan C, Coviello DA, Garre C,Bonioli E (2003) Neurofibromatosis type 1 (NF1): Identifi-cation of eight unreported mutations in NF1 gene in Italianpatients [corrected]. Hum Mutat 22(2):179–180
40. Mantripragada KK, Thuresson AC, Piotrowski A, Diaz deStahl T, Menzel U, Grigelionis G, Ferner RE, Griffiths S,Bolund L, Mautner V, Nordling M, Legius E, Vetrie D, DahlN, Messiaen L, Upadhyaya M, Bruder CE, Dumanski JP(2006 Jan) Identification of novel deletion breakpoints bor-dered by segmental duplications in the NF1 locus usinghigh-resolution array-CGH. J Med Genet 43(1):28–38
41. Hoffmeyer S, Assum G, Griesser J, Kaufmann D, NurnbergP, Krone W (1995) On unequal allelic expression of theneurofibromin gene in neurofibromatosis type 1. Hum MolGenet 4:1267–1272
42. Upadhyaya M, Osborn M, Cooper DN (2003) Detection ofNF1 mutations utilizing the protein truncation test (PTT).Methods Mol Biol 217:315–27
43. Kluwe L, Siebest R, Gesk S, Fridrich RE, Tinschert S,Kehrer-Sawatzki H, MautnerVF (2004) Screening 500unselected neurofibromatosis 1 patients for deletions of theNF1 gene. Hum Mut 23(2):111–116
44. Korf BR (1998) The NF1 genetic analysis consortium. In:Upadhyaya M, Cooper DN (eds) Neurofibromatosis Type 1from genotype to phenotype. BIOS Scientific, Oxford
45. Messiaen LM, Wimmer K (2005) Pitfalls of automatedcomparative sequence analysis as a single platform forroutine clinical testing for NF1. J Med Genet 42(5):e25
123
Familial Cancer (2007) 6:21–34 33

46. Baralle M, Baralle D, De Conti L, Mattocks C, Whittaker J,Krezevich A, ffrench-constant C, Baralle E (2003) Identifi-cation of a mutation that perturbs NF1 gene splicing usinggenomic DNA samples and a minigene assay. J Med genet40:220–222
47. Wimmer K, Eckart M, Rehder H, Fonatsch C (2000) Ille-gitimate splicing of the NF1 gene in healthy individualsmimics mutation induced splicing alterations in NF1 patients.Hum Genet 106(3):311–313
48. Horan MP, Cooper DN, Upadhyaya M (2000) Hyperme-thylation of the neurofibromatosis type 1 (NF1) gene pro-moter is not a common event in the inactivation of the NF1gene in NF1-specific tumours. Hum Genet 107(1):33–39
49. Harder A, Rosche M, Reuss DE, Holtkamp N, Uhlmann K,Friedrich R, Mautner VF, von Deimling A (2004) Methyla-tion analysis of the neurofibromatosis type 1 (NF1) promoterin peripheral nerve sheath tumours. Eur J Cancer40(18):2820–2828
50. Fishbein L, Eady B, Sanek N, Muir D, Wallace MR (2005)Analysis of somatic NF1 promoter methylation in plexiformneurofibromas and Schwann cells. Cancer Genet Cytogenet157(2):181–186
51. Ebinger M, Senf L, Wachowski O, Scheurlen W (2005) Noaberrant methylation of neurofibromatosis 1 gene (NF1)promoter in pilocytic astrocytoma in childhood. PediatrHematol Oncol 22(1):83–87
52. Baralle D, Mattocks C, Kalidas K, Elmslie F, Whittaker J,Lees M, Ragge N, Patton MA, Winter RM, ffrench-ConstantC (2003) Different mutations in the NF1 gene are associatedwith Neurofibromatosis-Noonan syndrome (NFNS). Am JMed Genet 119(1):1–8
53. DeLuca A, Bottillo I, Sarkozy A, Carta C, Neri C, BellacchioE, Schirinzi A, Conti E, Zampino G, Battaglia A, Majore S,Rinaldi MM, Cavella M, Marion B, Pizzuti A, Digilio MC,Tartaglia M, Dallapiccola B (2005 Dec NF1 gene mutationsrepresent the major molecular event underlying Neurofi-bromatosis Noonan syndrome. Am J Hum Genet77(6):1092–1101
54. Lamlum H, Ilyas M, Rowan A, Clark S, Johnson V, Bell J,Frayling I, Efstathiou J, Pack K, Payne S, Roylance R,Gorman P, Sheer D, Neale K, Phillips R, Talbot I, BodmerW, Tomlinson I (1999) The type of somatic mutation at APCin familial adenomatous polyposis is determined by the siteof the germline mutation: a new facet to Knudson’s ‘two-hit’hypothesis. Nat Med 5(9):1071–1075
55. Kayes LM, Burke W, Riccardi VM, Bennett R, Ehrlich P,Rubenstein A, Stephens K (1994) Deletions spanning theneurofibromatosis 1 gene: identification and phenotype offive patients. Am J Hum Genet 54(3):424–436
56. Upadhyaya M, Ruggieri M, Maynard J, Osborn M, HartogC, Mudd S, Penttinen M, Cordeiro I, Ponder M, Ponder BA,Krawczak M, Cooper DN (1998) Gross deletions of theneurofibromatosis type 1 (NF1) gene are predominantly ofmaternal origin and commonly associated with a learningdisability, dysmorphic features and developmental delay.Hum Genet 102(5):591–597
123
34 Familial Cancer (2007) 6:21–34





























