Embed Size (px)
Citation preview

lable at ScienceDirect
Journal of Cranio-Maxillo-Facial Surgery xxx (2010) 1e6
Contents lists avai
Journal of Cranio-Maxillo-Facial Surgery
journal homepage: www.jcmfs.com
Neurofibromatosis type 1 associated with bilateral central giant cellgranuloma of the mandible
Bruno Ramos Chrcanovic*, Ricardo Santiago Gomez, Belini Freire-MaiaDepartment of Oral and Maxillofacial Surgery, School of Dentistry, (Head: Belini Freire-Maia), Pontifícia Universidade Católica de Minas Gerais,Av. Dom José Gaspar, 500 Prédio 45, Coração Eucarístico-30535-610, Belo Horizonte, MG, Brazil
a r t i c l e i n f o
Article history:Paper received 17 October 2009Accepted 4 October 2010
Keywords:Neurofibromatosis type 1Central giant cell granulomaMandibleTreatment
* Corresponding author. Av. Raja Gabaglia 1000/120Minas Gerais, CEP 30441-070, Brazil. Tel.: þ55 31(home)/91625090 (mobile); fax: þ55 31 25151579.
E-mail address: [email protected] (B
1010-5182/$ e see front matter � 2010 European Assdoi:10.1016/j.jcms.2010.10.014
Please cite this article in press as: Chrcanovmandible, Journal of Cranio-Maxillo-Facial S
a b s t r a c t
Neurofibromatosis type 1, or von Recklinghausen disease, is one of the most common hereditary neu-rocutaneous disorders in humans. Clinically, Neurofibromatosis type 1 is characterized by café-au-laitspots, freckling, skin neurofibroma, plexiform neurofibroma, bony defects, Lisch nodules and tumors ofthe central nervous system. Central giant cell granuloma is a benign central lesion of bone, primarilyinvolving the jaws, of variably aggressive nature characterized by aggregates of multinucleated giant cellsin a background of cellular vascular fibrous connective tissue and spindle-shaped mononuclear stromalcells. The association between neurofibromatosis and central giant cell granuloma has been reported inthe literature. A case of mandibular bilateral central giant cell granuloma in a patient with Neurofibro-matosis type 1 was conservatively but successfully treated by adequate surgical curettage of mandibularbone lesions.
� 2010 European Association for Cranio-Maxillo-Facial Surgery.
1. Introduction
Neurofibromatosis type 1 (NF1) is an autosomal dominant,multisystem disorder affecting approximately 1 in 3500 people(Boyd et al., 2009), caused by a spectrum of mutations affecting theneurofibromatosis 1 (Nf1) gene. The central giant cell granuloma(CGCG)of the jaws isusuallyanon-neoplastic bone lesionaccountingfor fewer than7%ofall benign tumorsof the jaws (Regezi, 2002),withan incidence rate of 1.1/million population annually (de Lange et al.,2004). The classification of the World Health Organization (Barneset al., 2005) defined this entity as localized benign but sometimesaggressive osteolytic proliferation. Reports of CGCG in patients withNF1 have been described in the literature (Kerl and Schroll,1971; Davis and Tideman, 1977; Van Damme and Mooren, 1994;Ardekian et al., 1999; Ruggieri et al., 1999; Krammer et al., 2003;de Lange and Van den Akker, 2005; Edwards et al., 2006).
In the present report, a case of mandibular bilateral CGCG ina patient with NF1 was conservatively but successfully treated byadequate surgical curettage of mandibular bone lesions. It is alsodiscussed in the differential diagnosis and treatment options.
9, Gutierrez, Belo Horizonte,32920997 (office)/33356892
.R. Chrcanovic).
ociation for Cranio-Maxillo-Facial
ic BR, et al., Neurofibromatosurgery (2010), doi:10.1016/j.j
2. Case report
An 18-year-old female presented at his dentist in order to makea orthodontic treatment. A panoramic radiograph was requested aspart of the complementary exams. The radiograph revealed a smallradiolucent lesion between the right second mandibular molar andthe impacted third molar, and a larger radiolucent lesion at the leftside, covering the impacted thirdmolar and reaching the ascendingmandibular ramus, and the distal root of the second molar wastotally involved (Fig. 1a). However, the orthodontist decided only tofollow the case.
The orthodontic device was mounted and 2 months later thepatient was referred to another dentist, in order to perform theremoval of the impacted third molars. This second professional sawthe lesions and decided to request a more recent radiograph, toverify the evolution of the lesions. The second panoramic radio-graph showed that the right radiolucent lesionwas larger (Fig.1b). Aright enlargedmandibular foramen, an inferiorly bilateral displacedcoronoid notch, and a bilateral pseudoelongation of condylarprocess were seen in these radiographs (Fig. 1a and 1b). There wereno signs of a possible diffusely invasive plexiform neurofibromaextending to themandibular angle. The patient was then referred tothe Department of Oral and Maxillofacial Surgery of the PontifíciaUniversidade Católica de Minas Gerais, Belo Horizonte, Brazil.
The patient’s examination showed prominent and posteriorlyangulated ears but no swelling of bilateral cheeks, peripheralcutaneous neurofibromas mainly in the back and belly, café-au-lait
Surgery.
is type 1 associated with bilateral central giant cell granuloma of thecms.2010.10.014

Fig. 1. (a) Panoramic radiograph showing bilateral radiolucences in the mandible;(b) Radiograph 2 months after the first one, showing growing of the right lesions.
B.R. Chrcanovic et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2010) 1e62
spots, Lisch nodules of the iris, and scoliosis. There were no axillaryfreckling, optic gliomas, fibrocystic lesions of the long bones, andcardiac anomalies. The patient presented learning disabilities andattention deficit hyperactivity disorder. There was no history offamiliar occurrence. The patient fulfilled the diagnostic criteria forNF1 according to Gutmann et al. (1997).
A computed tomography (CT) scan without contrast materialwas carried out to show the true extent of the lesion. The coronalsections showed the radiolucency involving tooth 48 and reachingthe basilar (Fig. 2a), radiolucency at the lingual aspect of the tooth47 with lingual cortical resorbed (Fig. 2b), radiolucency involvingtooth 38 (Fig. 2c), and radiolucency at the buccal aspect of the tooth37 (Fig. 2d). The CT did not show signs of lesion extending to themandibular angle.
Under local anesthesia, the third molars were removed togetherwith the complete lesions. As the secondmolars were also involved,these were also removed. The osseous region affected by the lesionin the resorbed lingual cortical (Fig. 2b) detached easily from thenormal adjacent periosteum, which showed no clinical signs ofperforation and soft tissue involvement. Histopathologic exami-nation revealed the presence of a lesion containing multiple benignmultinucleated giant cells and cellular spindle cell stroma withoutmitotic activity, trabecules of reactive bone and extravasation of redblood cells (Figs. 3 and 4). Therefore, a diagnosis of bilateral centralgiant cell granuloma was made, based on the radiological findings,along with compatible histopathologic features.
An immediate postoperative radiograph was made (Fig. 5a), andanother at 7months of follow-up (Fig. 5b), which showed advancedbone regeneration.
3. Discussion
NF1 is an inherited disorder characterized by the presence ofcafé-au-lait macules, peripheral neurofibromas, Lisch nodules,axillary freckling, skeletal dysplasia, and optic gliomas and a first-degree relative with NF1. Also, bone abnormalities may occur inNF1 that reflect the basic mesodermal dysplasia, such as bowing,pathological fractures, and pseudoarthrosis of the long bones (VanDamme and Mooren, 1994).
Please cite this article in press as: Chrcanovic BR, et al., Neurofibromatosmandible, Journal of Cranio-Maxillo-Facial Surgery (2010), doi:10.1016/j.j
A right enlarged mandibular foramen, an inferiorly bilateraldisplaced coronoid notch, and a bilateral pseudoelongation ofcondylar process were also seen in the patient, which are three ofseveral pathognomonic changes in the mandible in neurofibro-matosis (Sailer et al., 1988). This is important because of thepossible association of a unilateral diffusely invasive plexiformneurofibroma extending to the mandibular angle (Friedrich et al.,2003). The vascularization is dense and vascular malformationsare commonly seen in NF1 (Hamilton and Friedman, 2000), andsevere bleeding is usually associated with plexiform neurofibromasurgery (McMaster, 1972). This putative association would beinteresting to surgeons when planning surgery in this region withrespect to increased risk of bleeding. The deepening of the sigmoidnotch combined with a large mandibular foramen can be explainedby the increase in size and diameter of the plexiform neurofibromaof the inferior alveolar nerve proximal to the mandibular foramen(Friedrich et al., 2003), although the present patient did not presentlesion extending to the mandibular angle.
The clinical features of CGCGs range from painless, slow-growing, asymptomatic non-aggressive masses to aggressivepainful lesions with root resorptions, cortical bone perforation, andtendency to recur after curettage (Chuong et al., 1986; de Langeet al., 2007b).
The appearance of CGCG in combination with other benignlesions or cysts of the jaws also has been reported in the literature(Jaffe, 1953; Ficarra et al., 1993) and the association betweenneurofibromatosis and CGCG has been reported in cases with(Davis and Tideman, 1977; Krammer et al., 2003) and withouthyperparathyroid disease (Van Damme and Mooren, 1994;Ardekian et al., 1999; Ruggieri et al., 1999; de Lange and Van denAkker, 2005; Edwards et al., 2006). Cherubism has also beenreported in association with NF1 (Martínez-Tello et al., 2005;Friedrich et al., 2007; van Capelle et al., 2007) and Noonan-like/multiple giant cell lesion syndrome, and also with multiple osteo-lytic polyostotic bone lesions (Cohen and Gorlin, 1991; Addante andBreen, 1996). However, the clinical presentation, radiographicfindings, and histologic appearance of the central mandibular in thepresent lesions were consistent with CGCG.
CGCG lesions associated with Noonan-like syndrome could arisefrom additional somatic PTPN11 gene mutations (Sarkozy et al.,2004). Multiple CGCG have been reported in association withNF1, and a novel splice mutation (A4268 G) was found in one familyaffected by NF1 with CGCGs (Krammer et al., 2003). Friedrich et al.(2007) revealed loss of heterozygosity of the NF1 gene in geneticanalysis of CGCG and blood of a 7-year-old female NF1 patient usingseven microsatellite markers. However, further genetic studies arenecessary to determine the genetic background of alterationsassociated with CGCG development (Carvalho et al., 2009).
CGCG is characterized by aggregates of multinucleated giantcells in a background of cellular vascular fibrous connective tissueand spindle-shaped mononuclear stromal cells, often with extrav-asation of red blood cells (Jaffe, 1953). Currently there are no reli-able criteria for correlating clinical aggressiveness with histologicalpresentation (Chuong et al., 1986). An attempt to improvemorphological diagnosis by measuring the mitotic activity oftumors using proliferation markers has been made. The growthfraction, i.e. the proportion of the cells committed to the cycle, maybe easily assessed by Ki67 or MIB-1 antibodies, which identify anantigen expressed in G1, S and G2 phases of cycling cells (Cattorettiet al., 1992). Proliferation markers such as the Ki67 have been usedas prognostic value, for example, in oral squamous cell carcinomas(Motta et al., 2009), odontogenic keratocyst (Mitrou et al., 2009),oral epithelial dysplasias (Torres-Rendon et al., 2009), in the effectsof smoking on the proliferation of the epithelium in periodontallydiseased marginal gingiva (Gültekin et al., 2008), and in Burkitt
is type 1 associated with bilateral central giant cell granuloma of thecms.2010.10.014

Fig. 2. CT coronal sections. (a) Radiolucency involving tooth 48 and reaching the basilar; (b) Radiolucency at the lingual aspect of the tooth 47 with lingual cortical resorbed;(c) Radiolucency involving tooth 38; (d) Radiolucency at the buccal aspect of the tooth 37.
B.R. Chrcanovic et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2010) 1e6 3
lymphoma of the oral cavity (Balasubramaniam et al., 2009). To ourknowledge, there is no research using proliferation markers in theprognostic value of oral CGCG.
Radiographically, radiolucency is one of the most consistentfeatures of jaw CGCGs. According to the literature, CGCGs areunilocular in 39e85% (de Lange et al., 2007a) and havewell-definedmargins in 19e69% (Kruse-Losler et al., 2006; de Lange et al., 2007a).In the present case, the left side showed a multilocular with ill-defined margins pattern and the right side unilocular with well-defined margins. Tooth displacement may be found in between 18%and 80% of CGCGs (Gungormus and Akgul, 2003; de Lange et al.,2007a). Root resorption occurs in 0e43% of CGCGs and is consid-ered tobe an important indicator of aggressiveness (Gungormus andAkgul, 2003; de Lange et al., 2007a). Varying degrees of expansionand cortical destruction may be seen, suggesting a possibleinvolvement of the surrounding soft tissues (Sun et al., 2009).
Please cite this article in press as: Chrcanovic BR, et al., Neurofibromatosmandible, Journal of Cranio-Maxillo-Facial Surgery (2010), doi:10.1016/j.j
Despite the radiographic features described above, CGCG has nopathognomonic radiographic finding. Although the lesion in theright side of the mandible has shown some growth in 2months andcortical destruction was observed in the lingual aspect of tooth 47,root resorption and involvement of the soft tissues were not noted.
CGCG may mimic a variety of other jaw lesions, such as cysts,odontogenic tumors, fibro-osseous lesions, vascular malforma-tions, and even malignancies (Kruse-Losler et al., 2006). Radio-logically, CGCGs should be differentially diagnosed with otherentities containing giant cells such as giant cell tumor (Hochet al., 2007), cherubism (Martínez-Tello et al., 2005), browntumor of hyperparathyroidism (Scholl et al., 1999; Regezi, 2002),and aneurismal bone cyst (Scholl et al., 1999; Murphey et al.,2001). In the present case, the right enlarged mandibularforamen could also be differentially diagnosed with an intra-osseous neurofibroma (Polak et al., 1989; Apostolidis et al., 2001).
is type 1 associated with bilateral central giant cell granuloma of thecms.2010.10.014
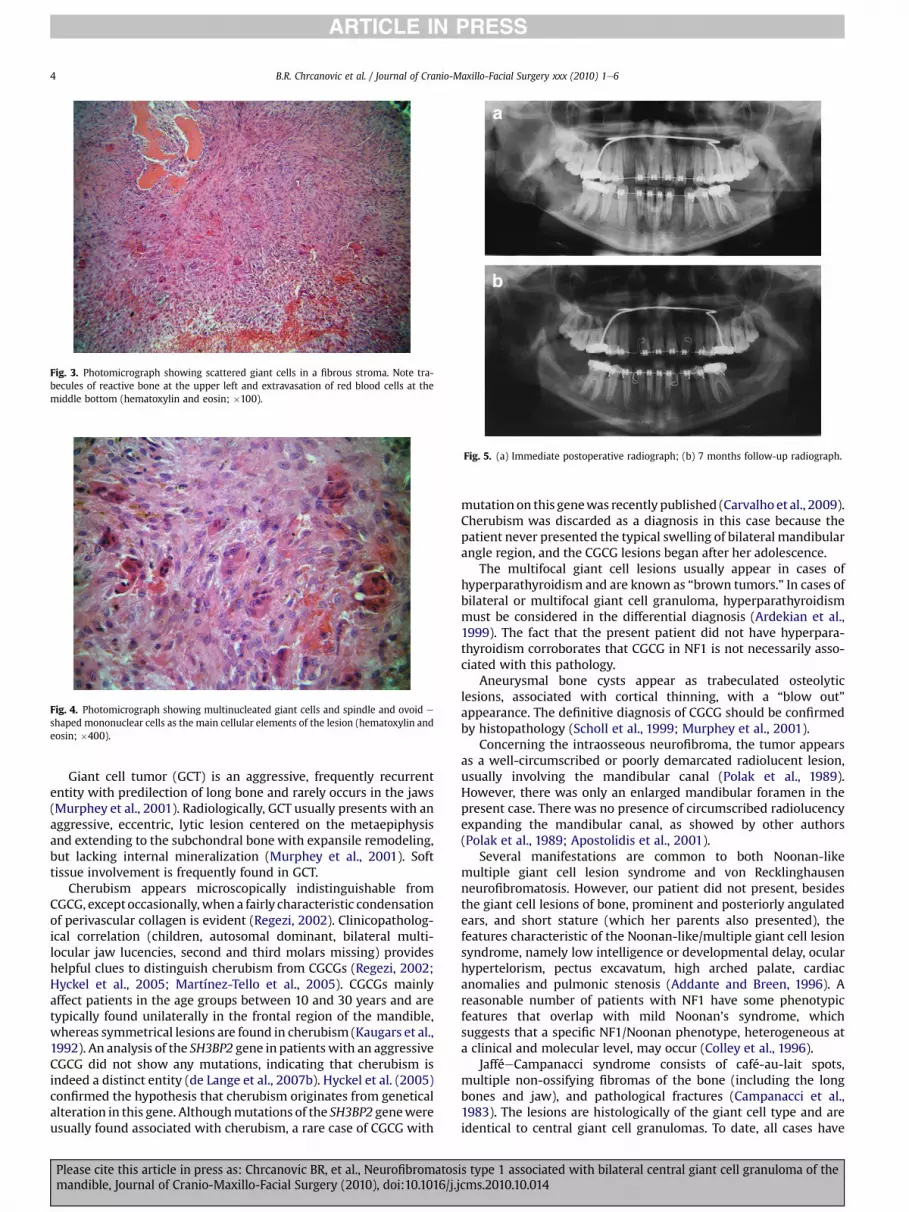
Fig. 3. Photomicrograph showing scattered giant cells in a fibrous stroma. Note tra-becules of reactive bone at the upper left and extravasation of red blood cells at themiddle bottom (hematoxylin and eosin; �100).
Fig. 4. Photomicrograph showing multinucleated giant cells and spindle and ovoid e
shaped mononuclear cells as the main cellular elements of the lesion (hematoxylin andeosin; �400).
Fig. 5. (a) Immediate postoperative radiograph; (b) 7 months follow-up radiograph.
B.R. Chrcanovic et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2010) 1e64
Giant cell tumor (GCT) is an aggressive, frequently recurrententity with predilection of long bone and rarely occurs in the jaws(Murphey et al., 2001). Radiologically, GCT usually presents with anaggressive, eccentric, lytic lesion centered on the metaepiphysisand extending to the subchondral bone with expansile remodeling,but lacking internal mineralization (Murphey et al., 2001). Softtissue involvement is frequently found in GCT.
Cherubism appears microscopically indistinguishable fromCGCG, except occasionally,when a fairly characteristic condensationof perivascular collagen is evident (Regezi, 2002). Clinicopatholog-ical correlation (children, autosomal dominant, bilateral multi-locular jaw lucencies, second and third molars missing) provideshelpful clues to distinguish cherubism from CGCGs (Regezi, 2002;Hyckel et al., 2005; Martínez-Tello et al., 2005). CGCGs mainlyaffect patients in the age groups between 10 and 30 years and aretypically found unilaterally in the frontal region of the mandible,whereas symmetrical lesions are found in cherubism (Kaugars et al.,1992). An analysis of the SH3BP2 gene in patients with an aggressiveCGCG did not show any mutations, indicating that cherubism isindeed a distinct entity (de Lange et al., 2007b). Hyckel et al. (2005)confirmed the hypothesis that cherubism originates from geneticalalteration in this gene. Althoughmutations of the SH3BP2 genewereusually found associated with cherubism, a rare case of CGCG with
Please cite this article in press as: Chrcanovic BR, et al., Neurofibromatosmandible, Journal of Cranio-Maxillo-Facial Surgery (2010), doi:10.1016/j.j
mutation on this genewas recently published (Carvalho et al., 2009).Cherubism was discarded as a diagnosis in this case because thepatient never presented the typical swelling of bilateral mandibularangle region, and the CGCG lesions began after her adolescence.
The multifocal giant cell lesions usually appear in cases ofhyperparathyroidism and are known as “brown tumors.” In cases ofbilateral or multifocal giant cell granuloma, hyperparathyroidismmust be considered in the differential diagnosis (Ardekian et al.,1999). The fact that the present patient did not have hyperpara-thyroidism corroborates that CGCG in NF1 is not necessarily asso-ciated with this pathology.
Aneurysmal bone cysts appear as trabeculated osteolyticlesions, associated with cortical thinning, with a “blow out”appearance. The definitive diagnosis of CGCG should be confirmedby histopathology (Scholl et al., 1999; Murphey et al., 2001).
Concerning the intraosseous neurofibroma, the tumor appearsas a well-circumscribed or poorly demarcated radiolucent lesion,usually involving the mandibular canal (Polak et al., 1989).However, there was only an enlarged mandibular foramen in thepresent case. There was no presence of circumscribed radiolucencyexpanding the mandibular canal, as showed by other authors(Polak et al., 1989; Apostolidis et al., 2001).
Several manifestations are common to both Noonan-likemultiple giant cell lesion syndrome and von Recklinghausenneurofibromatosis. However, our patient did not present, besidesthe giant cell lesions of bone, prominent and posteriorly angulatedears, and short stature (which her parents also presented), thefeatures characteristic of the Noonan-like/multiple giant cell lesionsyndrome, namely low intelligence or developmental delay, ocularhypertelorism, pectus excavatum, high arched palate, cardiacanomalies and pulmonic stenosis (Addante and Breen, 1996). Areasonable number of patients with NF1 have some phenotypicfeatures that overlap with mild Noonan’s syndrome, whichsuggests that a specific NF1/Noonan phenotype, heterogeneous ata clinical and molecular level, may occur (Colley et al., 1996).
JafféeCampanacci syndrome consists of café-au-lait spots,multiple non-ossifying fibromas of the bone (including the longbones and jaw), and pathological fractures (Campanacci et al.,1983). The lesions are histologically of the giant cell type and areidentical to central giant cell granulomas. To date, all cases have
is type 1 associated with bilateral central giant cell granuloma of thecms.2010.10.014

B.R. Chrcanovic et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2010) 1e6 5
been sporadic and no patient has had skin nodules or documentedneurofibromas (Cohen and Gorlin, 1991).
Surgery is still the most frequently applied treatment in CGCGs(Kruse-Losler et al., 2006; de Lange et al., 2007a). The extent ofsurgery depends on the size and localization of the lesion and rangesfrom simple curettage to extensive resection. Several studies evalu-ated the results of surgery, reporting recurrence rates ranging from11.0%to49.0% (Kruse-Losleret al., 2006;deLangeetal., 2007a). Thesedata indicate that surgical curettage is suitable for the treatment ofjaw CGCGs without aggressive signs (Kruse-Losler et al., 2006), asseen in the present case. Simple curettage of clinico-radiographicaggressive lesions proved not to be adequate (Kruse-Losler et al.,2006) and resection has been suggested to be the surgical treat-ment method of choice for removal of aggressive CGCGs and recur-rent lesions (Kruse-Losler et al., 2006; de Lange et al., 2007a; Boydet al., 2009). Recurrence in patients showing aggressive signs ismore frequent (Kruse-Losler et al., 2006; de Lange et al., 2007a).
Recently, non-aggressive treatment methods such as systemicdaily application of calcitonin (de Lange et al., 2007a), intralesionalinjections of corticosteroids (Carlos and Sedano, 2002), and subcu-taneous injections of alpha-interferon (Goldman et al., 2005) havebeen applied. Latest treatment strategies such as Imatinib� (Glivec,Novartis Pharma, Basel, Switzerland) targeting the activity of oste-oclasts directly have also been reported (de Lange et al., 2009).
Calcitonin causes an increased influx of calcium into the bonesand thus functions antagonistically to parathyroid hormone. It hasbeen demonstrated that giant cells express calcitonin receptors(Nickolson et al., 1987). It is assumed that giant cells are directlyinhibited in their function by calcitonin (de Lange et al., 2007a).
The mode of action of corticosteroids on CGCG is not fullyunderstood. In vitro it was shown that dexamethasone on the onehand stimulates the proliferation and differentiation of osteoclastprecursors, but on the other hand inhibits lacunar resorption bymature osteoclasts isolated from giant cells tumors of the bone(Hirayama et al., 2002). It is hypothesized that the extracellularproduction of bone resorption mediating lysosomal proteases bythe giant cells is inhibited and steroids induce apoptosis of osteo-clast like cells (Abdo et al., 2005). As a result, the administration ofcorticosteroids inhibits bone resorption. However, the fact thatcorticosteroids are also known to enhance bone resorption andcause osteoporosis is contradictory (de Lange et al., 2007a).
Interferon is an antiviral and anti-angiogenic agent, which isused in various conditions, including life-threatening haemangio-mas and several types of malignant tumor (de Lange et al., 2009). Itis unlikely that central giant cell granuloma is a true proliferativevascular lesion (Vered et al., 2006), but the immunoreactivity of thelesionalmononuclear and giant cells for angiogenic factors probablyhas an important role in the osteoclastogenic process and therebycontributes to the growth of the lesion. Interferon alpha given alonefor aggressive central giant cell granuloma is capable of terminatingthe rapid growth of the lesion and reducing its size (de Lange et al.,2006), but to date a total remission after treatment with interferonalpha has been reported in only one patient (Collins, 2000).
Imatinib is a protein tyrosine kinase inhibitor that is used totreat chronic myeloid leukaemia and gastrointestinal stromaltumors by inhibiting bcreabl and stem cell factor receptor (c-kit)tyrosine kinases, respectively (Druker et al., 1996). Imatinib is welltolerated and has mild to moderate side-effects. Imatinib promotesosteoblast differentiation (Fitter et al., 2008). This finding stronglysuggests that Imatinib may be an effective anti-osteolytic agent andcould therefore be useful in the treatment of skeletal diseasesinvolving excessive osteoclast activity, such as central giant cellgranuloma (de Lange et al., 2009). de Lange et al. (2009) proposedthat the combination of imatinib and alpha-interferon couldtheoretically be effective on separate levels in osteoclastogenesis
Please cite this article in press as: Chrcanovic BR, et al., Neurofibromatosmandible, Journal of Cranio-Maxillo-Facial Surgery (2010), doi:10.1016/j.j
and, therefore, be more potent than a single drug. In line with theseefforts to improve medical treatment is the current experimentalresult that imatinib not only is useful in the treatment of CGCG butalso reduces plexiform neurofibromas (PNF) Schwann cell viabilityand reduces size of transplanted human PNFs to the nude mouse(Demestre et al., 2010).
Related to the results of the long-term follow-up, CGCG mayrecur within 2 years after the surgical treatment, emphasizinga close follow-up to be of utmost importance. Extensive surgicaltreatment proved to be effective in aggressive lesions; however, itresulted in inevitable loss of bone, teeth, tooth germs and func-tional disorders of the inferior alveolar nerve (Boyd et al., 2009).
4. Conclusions
In cases of bilateral mandibular CGCG, Neurofibromatosis type 1,hyperparathyroidism and cherubism must be considered in thedifferential diagnosis (Ardekian et al., 1999, Regezi, 2002; Hyckelet al., 2005; Martínez-Tello et al., 2005).
Differentiation between aggressive and non-aggressive CGCGsshould be considered to improve individual treatment planning(Boyd et al., 2009). Surgical curettage is suitable for the treatmentof jaw CGCGs without aggressive signs.
References
Abdo EN, Alves LC, Rodrigues AS, Mesquita RA, Gomez RS: Treatment of a centralgiant cell granuloma with intralesional corticosteroid. Br J Oral Maxillofac Surg43: 74e76, 2005
Addante RR, Breen GH: Cherubism in a patient with Noonan’s syndrome. J OralMaxillofac Surg 54: 210e213, 1996
Apostolidis C, Anterriotis D, Rapidis AD, Angelopoulos AP: Solitary intraosseousneurofibroma of the inferior alveolar nerve: report of a case. J Oral MaxillofacSurg 59: 232e235, 2001
Ardekian L, Manor R, Peled M, Laufer D: Bilateral central giant cell granulomas ina patient with neurofibromatosis: report of a case and review of the literature.J Oral Maxillofac Surg 57: 869e872, 1999
Balasubramaniam R, Goradia A, Turner LN, Stoopler ET, Alawi F, Frank DM, et al:Burkitt lymphoma of the oral cavity: an atypical presentation. Oral Surg OralMed Oral Pathol Oral Radiol Endod 107: 240e245, 2009
Barnes L, Eveson JW, Reichart P, Sidransky D: World Health Organization classifi-cation of tumors: pathology and genetics of head and neck tumors, Lyon: IARC,2005
Boyd KP, Korf BR, Theos A: Neurofibromatosis type 1. J Am Acad Dermatol 61: 1e14,2009
Campanacci M, Laus M, Boriani S: Multiple non-ossifying fibromata with extra-skeletal abnormalities: a new syndrome? J Bone Joint Surg 65B: 627e632, 1983
Carlos R, Sedano HO: Intralesional corticosteroids as an alternative treatment forcentral giant cell granuloma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod93: 161e166, 2002
Carvalho VM, Perdigão PF, Amaral FR, de Souza PE, De Marco L, Gomez RS: Novelmutations in the SH3BP2 gene associated with sporadic central giant cell lesionsand cherubism. Oral Dis 15: 106e110, 2009
Cattoretti G, Becker MHG, Key G, Duchrow M, Schlüter C, Galle J, et al: Monoclonalantibodies against recombinant parts of the Ki-67 antigen (MIB-1 and MIB-3)detect proliferating cells in microwave-processed formalin-fixed paraffinsections. J Pathol 168: 357e363, 1992
Chuong R, Kaban LB, Kozakewich H, Perez-Atayde A: Central giant cell lesions of thejaws: a clinicopathologic study. J Oral Maxillofac Surg 44: 708e713, 1986
Cohen MM, Gorlin RJ: Noonan-like/multiple giant cell lesion syndrome. Am J MedGenet 40: 159e166, 1991
Colley A, Donnai D, Evans DGR: Neurofibromatosis/Noonan phenotype: a variablefeature of type 1 neurofibromatosis. Clin Genet 49: 59e64, 1996
Collins A: Experience with anti-angiogenic therapy of giant cell granuloma of thefacial bones. Ann R Australas Coll Dent Surg 15: 170e175, 2000
Davis GB, Tideman H: Multiple recurrent central giant cell granulomas of the jaws:case report. J Oral Maxillofac Surg 5: 127e129, 1977
de Lange J, van den Akker HP, Klip H: Incidence and disease-free survival aftersurgical therapy of central giant cell granulomas of the jaw in The Netherlands:1990e1995. Head Neck 26: 792e795, 2004
de Lange J, van den Akker HP, van den Berg H, Richel DJ, Gortzak RA: Limitedregression of central giant cell granuloma by interferon alpha afterfailed calcitonin therapy: a report of two cases. Int J Oral Maxillofac Surg35: 865e869, 2006
de Lange J, van den Akker HP, van den Berg H: Central giant cell granuloma of thejaw: a review of the literature with emphasis on therapy options. Oral Surg OralMed Oral Pathol Oral Radiol Endod 104: 603e615, 2007a
is type 1 associated with bilateral central giant cell granuloma of thecms.2010.10.014

B.R. Chrcanovic et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2010) 1e66
de Lange J, Van den Akker HP: Clinical and radiological features of central giant-celllesions of the jaw. Oral Surg Oral Med Oral Pathol Oral Radiol Endod99: 464e470, 2005
de Lange J, van Maarle MC, van den Akker HP, Redeker EJ: DNA analysis of theSH3BP2 gene in patients with aggressive central giant cell granuloma. Br J OralMaxillofac Surg 45: 499e500, 2007b
de Lange J, van Rijn RR, van den Berg H, van den Akker HP: Regression of centralgiant cell granuloma by a combination of imatinib and interferon: a case report.Br J Oral Maxillofac Surg 47: 59e61, 2009
Demestre M, Herzberg J, Holtkamp N, Hagel C, Reuss D, Friedrich RE, et al: Imatinibmesylate (Glivec) inhibits Schwann cell viability and reduces the size of humanplexiform neurofibroma in a xenograft model. J Neurooncol 98: 11e19, 2010
Druker BJ, Tamura S, Buchdunger E, Ohno S, Segal GM, Fanning S, et al: Effects ofa selective inhibitor of the Abl tyrosine kinase on the growth of BcreAblpositive cells. Nat Med 2: 561e566, 1996
Edwards PC, Fantasia JE, Saini T, Rosenberg TJ, Sachs SA, Ruggiero S: Clinicallyaggressive central giant cell granulomas in two patients with neurofibromatosis1. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 102: 765e772, 2006
Ficarra G, Sapp P, Eversole LR: Multiple peripheral odontogenic fibroma, WorldHealth Organization type, and central giant cell granuloma: a case report of anunusual association. J Oral Maxillofac Surg 51: 325e328, 1993
Fitter S, Dewar AL, Kostakis P, To LB, Hughes TP, Roberts MM, et al: Long-termimatinib therapy promotes bone formation in CML patients. Blood111: 2538e2547, 2008
Friedrich RE, Giese M, Schmelzle R, Mautner VF, Scheuer HA: Jaw malformationsplus displacement and numerical aberrations of teeth in neurofibromatosistype 1: a descriptive analysis of 48 patients based on panoramic radiographsand oral findings. J Craniomaxillofac Surg 31: 1e9, 2003
Friedrich RE, Mautner VF, Scheuer HA: Loss of heterozygosity in tumor cells ofa recurrent mandibular giant cell granuloma in neurofibromatosis type 1.Anticancer Res 27: 2079e2083, 2007
Goldman KE, Marshall MK, Alessandrini E, Bernstein ML: Complications of alpha-interferon therapy for aggressive central giant cell lesion of the maxilla. OralSurg Oral Med Oral Pathol Oral Radiol Endod 100: 285e291, 2005
Gültekin SE, Sengüven B, Karaduman B: The effect of smoking on epithelialproliferation in healthy and periodontally diseased marginal gingival epithe-lium. J Periodontol 79: 1444e1450, 2008
Gungormus M, Akgul HM: Central giant cell granuloma of the jaws: a clinical andradiologic study. J Contemp Dent Pract 4: 87e97, 2003
Gutmann DH, Aylsworth A, Carey JC, Korf B, Marks J, Pyeritz RE, et al: The diagnosticevaluation and multidisciplinary management of neurofibromatosis 1 andneurofibromatosis 2. JAMA 278: 51e57, 1997
Hamilton SJ, Friedman JM: Insights into the pathogenesis of neurofibromatosis 1vasculopathy. Clin Genet 58: 341e344, 2000
Hirayama T, Sabokbar A, Athanasou NA: Effect of corticosteroids on human osteo-clast formation and activity. J Endocrinol 175: 155e163, 2002
Hoch B, Hermann G, Klein MJ, Abdelwahab IF, Springfield D: Giant cell tumorcomplicating Paget disease of long bone. Skeletal Radiol 36: 973e978, 2007
Hyckel P, Berndt A, Schleier P, Clement JH, Beensen V, Peters H, et al: Cherubism e
new hypotheses on pathogenesis and therapeutic consequences. J Craniomax-illofac Surg 33: 61e68, 2005
JaffeHL:Giant-cell reparativegranuloma, traumaticbonecyst, andfibrous (fibro-osseous)dysplasia of the jawbones. Oral Surg Oral Med Oral Pathol 6: 159e175, 1953
Kaugars GE, Niamtu I, Svirsky JA: Cherubism: diagnosis, treatment, and comparisonwith central giant cell granulomas and giant cell tumors. Oral Surg Oral MedOral Pathol Oral Radiol Endod 73: 369e374, 1992
Kerl H, Schroll K: [Multiple giant cell granulomas of the jaws associated with Reck-linghausen’s neurofibromatosis]. Wien Klin Wochenschr 83: 938e941, 1971
Please cite this article in press as: Chrcanovic BR, et al., Neurofibromatosmandible, Journal of Cranio-Maxillo-Facial Surgery (2010), doi:10.1016/j.j
Krammer U, Wimmer K, Wiesbauer P, Rasse M, Lang S, Müllner-Eidenböck A, et al:Neurofibromatosis 1: a novel NF1 mutation in an 11-year-old girl with a giantcell granuloma. J Child Neurol 18: 371e373, 2003
Kruse-Losler B, Diallo R, Gaertner C, Mischke KL, Joos U, Kleinheinz J: Central giantcell granuloma of the jaws: a clinical, radiologic, and histopathologic study of26 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101: 346e354, 2006
Martínez-Tello FJ, Manjón-Luengo P, Martin-Pérez M, Montes-Moreno S: Cherubismassociated with neurofibromatosis type 1, and multiple osteolytic lesions ofboth femurs: a previously undescribed association of findings. Skeletal Radiol34: 793e798, 2005
McMaster P: Massive hemorrhage in elephantiasis neurofibroma. Br J Surg 59:984e985, 1972
Mitrou GK, Tosios KI, Kyroudi A, Sklavounou A: Odontogenic keratocyst expressesvascular endothelial growth factor: an immunohistochemical study. J OralPathol Med 38: 470e475, 2009
Motta Rda R, Zettler CG, Cambruzzi E, Jotz GP, Berni RB: Ki-67 and p53 correlationprognostic value in squamous cell carcinomas of the oral cavity and tongue.Braz J Otorhinolaryngol 75: 544e549, 2009
Murphey MD, Nomikos GC, Flemming DJ, Gannon FH, Temple HT, Kransdorf MJ:From the archives of AFIP. Imaging of giant cell tumor and giant cell reparativegranuloma of bone: radiologic-pathologic correlation. Radiographics 21:1283e1309, 2001
Nickolson GC, Horton MA, Sexton PM, D’Santos CS, Mosely JM, Kemp BE, et al: Calci-tonin receptors of human osteoclastoma. HormMetab Res 19: 585e589, 1987
PolakM, PolakG, Brocheriou C, Vigneul J: Solitary neurofibromaof themandible: casereport and review of the literature. J Oral Maxillofacial Surg 47: 65e68, 1989
Regezi JA: Odontogenic cysts, odontogenic tumors, fibro-osseous, and giant celllesions of the jaws. Mod Pathol 15: 331e341, 2002
Ruggieri M, Pavone V, Polizzi A, Albanese S, Magro G, Merino M, et al: Unusual formof recurrent giant cell granuloma of the mandible and lower extremities ina patient with neurofibromatosis type 1. Oral Surg Oral Med Oral Pathol OralRadiol Endod 87: 67e72, 1999
Sailer HF, Kunzler A, Makek MS: Neurofibrohämangiomatöse Weichteilverander-ungen mit pathognomonischer Unterkieferdeformität. Fortschr Kief GesichtsChirurgie 33: 84e86, 1988
Sarkozy A, Obregon MG, Conti E, Esposito G, Mingarelli R, Pizzuti A, et al: A novelPTPN11 gene mutation bridges Noonan syndrome, multiple lentigines/LEOPARDsyndrome and Noonan-like/multiple giant cell lesion syndrome. Eur J HumGenet 12: 1069e1072, 2004
Scholl RJ, Kellett HM, Neumann DP, Lurie AG: Cysts and cystic lesions ofthe mandible: clinical and radiologic-histopathologic review. Radiographics19: 1107e1124, 1999
Sun ZJ, Cai Y, Zwahlen RA, Zheng YF, Wang SP, Zhao YF: Central giant cell granulomaof the jaws: clinical and radiological evaluation of 22 cases. Skeletal Radiol38: 903e909, 2009
Torres-Rendon A, Roy S, Craig GT, Speight PM: Expression of Mcm2, geminin andKi67 in normal oral mucosa, oral epithelial dysplasias and their correspondingsquamous-cell carcinomas. Br J Cancer 100: 1128e1134, 2009
van Capelle CI, Hogeman PH, van der Sijs-Bos CJ, Heggelman BG, Idowu B,Slootweg PJ, et al: Neurofibromatosis presenting with a cherubism phenotype.Eur J Pediatr 166: 905e909, 2007
Van Damme PhA, Mooren REC: Differentiation of multiple giant cell lesions,Noonan-like syndrome, and (occult) hyperparathyroidism. Case report andreview of the literature. Int J Maxillofac Surg 23: 32e36, 1994
Vered M, Buchner A, Dayan D: Giant cell granuloma of the jawbones- a prolifera-tive vascular lesion? Immunohistochemical study with vascular endothelialgrowth factor and basic fibroblast growth factor. J Oral Pathol Med 35:613e619, 2006
is type 1 associated with bilateral central giant cell granuloma of thecms.2010.10.014





























