Embed Size (px)
Citation preview

haematologica 2004; 89(2):February 2004 207
[haematologica]2004;89:207-214
A B S T R A C TLIVIO PAGANO
MASSIMO OFFIDANI
LUANA FIANCHI
ANNAMARIA NOSARI
ANNA CANDONI
MARCO PICCARDI
LAURA CORVATTA
DOMENICO D’ANTONIO
CORRADO GIRMENIA
PIETRO MARTINO
ALBANO DEL FAVERO
FOR THE GIMEMA(GRUPPO ITALIANO
MALATTIE EMATOLOGICHE
DELL'ADULTO) INFECTION PROGRAM
From the Istituto di Ematologia,Università Cattolica S. Cuore,Roma (LP, LF); Clinica diEmatologia, Università di Ancona(MO, LC); Divisione Talamona,Ospedale Niguarda Cà Granda,Milan (AN); Cattedra di Ematolo-gia, Università di Udine (AC);Cattedra di Ematologia, Univer-sità Umberto I, Napoli (MP);Unità di Microbiologia, Divisionedi Ematologia, Ospedale CivileSpirito Santo, Pescara (DD);Dipartimento di BiotecnologieCellulari ed Ematologia, Univer-sità «La Sapienza», Roma (CG,PM); Istituto di Clinica Medica 1,Università di Perugia (ADF), Italy
Correspondence: Dr. LivioPagano, Istituto di EmatologiaUniversità Cattolica del S.Cuorelargo A. Gemelli 8, 00168 Rome,Italy.E-mail: [email protected]
©2004, Ferrata Storti Foundation
Mucormycosis in hematologic patients
Background and Objectives. To evaluate the clinical characteristics of patients affectedby hematologic malignancies who developed mucormycosis and to ascertain the factorswhich influenced the outcome following mycotic infection.
Design and Methods. This was a retrospective study conducted over a 15-year period(1987-2001). The study included 59 patients with hematologic malignancies with a provenor probable mucormycosis admitted in 18 Hematology Divisions in tertiary care or univer-sity hospitals.
Results. The most frequent sites of infection were lung (64%) and orbito-sinus-facial(24%); cerebral involvement observed in 19% of cases was always associated with othersites of infection. Antifungal treatment was empirically administered in 49 patients (83%);7 patients underwent radical surgical debridement (12%). Therapy was successful for only18 patients (37%). Forty-seven patients died within 3 months of the diagnosis of fungalinfection: the cause of death was mucormycosis in 41 patients (87%) and progression ofhematologic disease in 6 patients (13%). At univariate analysis, the factors that correlat-ed with a positive outcome from infection were the following: male sex, amphotericin Btreatment, neutrophil recovery from post-chemotherapy aplasia. At multivariate analysis,the only factor that significantly correlated with recovery from infection was the liposo-mal amphotericin B treatment.
Interpretation and Conclusions. Mucormycosis is a rare filamentous fungal infectionthat occurs most frequently in neutropenic patients with acute leukemia. It does not seemto have increased in recent years. Although a reduction of mortality has been observedrecently, the mortality rate still remains high. Extensive and aggressive diagnostic and ther-apeutic procedures are essential in order to improve the prognosis in these patients.
Key words: mucormycosis, leukemia, lymphoma.
Mucormycosis is an invasive fungalinfection caused by various mem-bers of the class Phycomycetes,
especially Mucoraceae, subdivided into thegenera Absidia, Rhizopus and Mucor. Afteraspergillosis, mucormycosis is the secondmost common mycosis caused by filamen-tous fungi. Overall, genera of the orderMucorales represent the third leading causeof invasive fungal infections followingAspergillus and Candida species.1-5 Amongpatients with hematologic disorders, mucor-mycosis most commonly occurs in those withacute leukemia or lymphoma who havedeveloped neutropenia due to malignancy orto chemotherapy, and in transplantedpatients receiving immunosuppressive treat-ment.2,6-8 Rhino-cerebral, maxillo-facial andpulmonary infections are the most frequentclinical forms, but neutropenic patients areat a high risk of developing a disseminated
mucormycosis. In fact dissemination occursin up to 40% of mucormycosis in patientswith hematologic malignancies2,9,10-12 and allof these manifestations are characterized bya high rate of mortality.2,13
We have already analyzed the epidemio-logical characteristics of mucormycosis inpatients with hematologic disorders.2 Thisnew analysis is an update of the previousstudy and a re-evaluation of some of itsaspects; in fact the recent availability of moreeffective diagnostic tools and new antifungaldrugs, together with a larger series ofpatients, could provide interesting new con-siderations. We reviewed the clinical featuresof 59 patients with a hematologic malignan-cy who developed mucormycosis in order toevaluate the clinical spectrum of the disease,its diagnosis and its treatment. Factors thatmay have influenced the outcome of thisinfectious complication were also considered.
A B S T R A C T

Design and Methods
Eighteen Hematology Departments took part in thisstudy. The clinical records of patients affected by ahematologic malignancy with a diagnosis of mucormy-cosis in the period between January 1987 and Decem-ber 2001 were reviewed.
The diagnosis of mucormycosis was made in vivo andat autopsy by demonstrating the organism in the tissueof a biopsy specimen, according to previously reportedcriteria.2
The following information was extracted from theclinical records of these patients: demographic charac-teristics; type and stage of hematologic malignancy;clinical symptoms and signs of infection; radiologicalfindings; site of infection; laboratory findings (e.g. neu-trophil count, microbiological isolates); treatmentsreceived; cause of death; autopsy findings.
Statistical methodsDefinitions and end-points of the study were agreed
upon prior to data retrieval from the clinical records.Success was defined as the disappearance of all signsand symptoms of the treated fungal infection or con-tinuous improvement and clinical evolution compatiblewith responding disease Failure was defined as deathattributed to the fungal infection as a primary or con-tributing cause, or progressive infection while on ther-apy or within 1 month of last therapy.
Data were analyzed by descriptive statistical methodsand differences between groups were calculated usingthe χ2 test or Fisher's exact test when appropriate.
Factors affecting infection outcome (death vs nodeath) were investigated using a stepwise backwardmethod and were also excluded from the model whenthe probability was higher than 0.1. Results are pre-sented as odds ratios (with the 95% confidence inter-val). The best cut-off of continuous variables was ascer-tained empirically using correlation coefficients.
Statistical significance was established at p <0.05(two sides). Data were analyzed using an SPSS statisti-cal package (SPSS, Chicago, IL, USA).
Results
Clinical and laboratory features of the patientsDuring the study period (1987-2001) 59 episodes of
mucormycosis were documented in patients withhematologic malignancies. These patients’ characteris-tics are summarized in Table 1. The great majority (78%)of patients had acute leukemia: acute myeloid leukemia(AML) in 30 patients (51%) and acute lymphoblasticleukemia (ALL) in 16 patients (27%). Non-Hodgkin'slymphoma (NHL) was the underlying malignancy in 6
patients (10%), myelodysplastic syndrome and hairy cellleukemia in 2 patients each (3%) and multiple myelo-ma (MM), Hodgkin’s disease, and chronic myeloidleukemia in 1 patient each.
All but two patients had been previously treated withaggressive chemotherapy regimens. In particular 5patients (9%) developed the infection during trans-plantation procedures (4 autologous and 1 allogeneicbone marrow transplantation). Twenty-nine patientsreceived 6-methyl-prednisolone (median total dose of500 mg [range 8-5000] over a median time of 22 days,[range 2-180]). In all these cases glucocorticoids wereadministered for the treatment of the hematologic dis-ease. Only 10 of the patients (17%) had concomitantdiabetes mellitus. None of the patients had a history ofprevious mycotic infection. Five patients (8.5%) devel-oped mucormycosis despite protective isolation in alaminar airflow room.
When the clinical diagnosis of fungal infection wasmade, 47 patients were neutropenic and, in particular,43 of them had a neutrophil count below 0.5×109/L; themedian duration of neutropenia prior to the diagnosisof mucormycosis was 12 days (range 1-60). Thirty-threeof these 47 patients (70%) recovered from neutropenia(neutrophil count >1×109/L) in a median time of 7 daysafter the clinical diagnosis of infection (range 4-30)and 18 of them received granulocyte colony-stimulat-ing factor (rhG-CSF).
haematologica 2004; 89(2):February 2004208
L. Pagano et al.
Table 1. Demographic and clinical characteristics ofpatients with mucormycosis.
Patients, n. 59Age in years: mean (range) 48 (13-80)Sex: M/F 30/29Underlying disease: n. (%)• Acute myeloid leukemia 30 (51%)• Acute lymphoblastic leukemia 16 (27%)• Non Hodgkin’s lymphoma 6 (10%)• Hairy cell leukemia 2 (3%)• Myelodyspalstic syndromes 2 (3%)• Multiple myeloma 1 (2%)• Chronic myeloid leukemia 1 (2%)• Hodgkin’s disease 1 (3%)
Primary site of infection:• Lung 38 (64%)
Alone 28Plus other sites [involving CNS] 10 [7]
• Sinus 12 (20%)• Systemic 5 (8%)• Eye 3 (5%)• Other* 3 (5%)
CNS: central enrvous system. *Heart: 1 case, Oral cavity: 1 case; Bowel: 1 case.
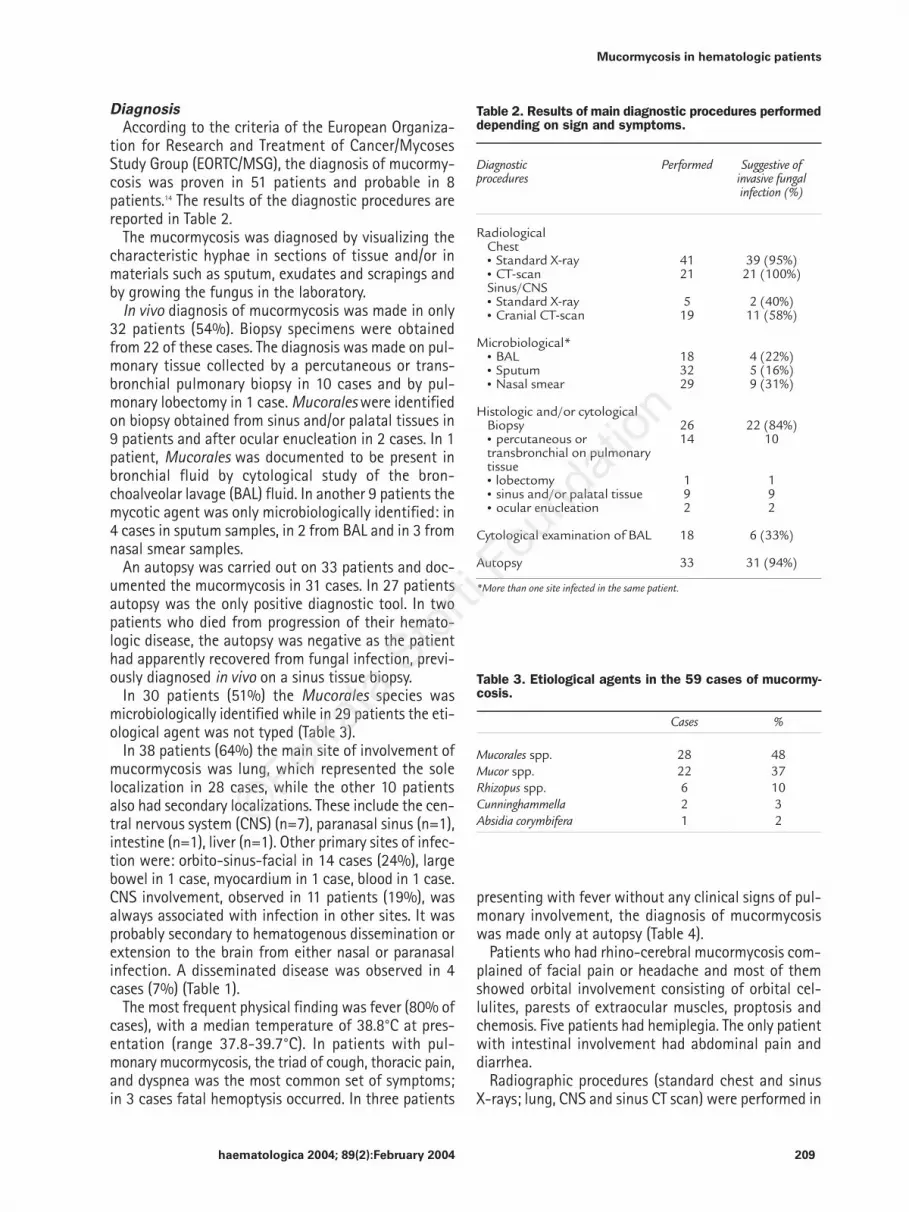
DiagnosisAccording to the criteria of the European Organiza-
tion for Research and Treatment of Cancer/MycosesStudy Group (EORTC/MSG), the diagnosis of mucormy-cosis was proven in 51 patients and probable in 8patients.14 The results of the diagnostic procedures arereported in Table 2.
The mucormycosis was diagnosed by visualizing thecharacteristic hyphae in sections of tissue and/or inmaterials such as sputum, exudates and scrapings andby growing the fungus in the laboratory.
In vivo diagnosis of mucormycosis was made in only32 patients (54%). Biopsy specimens were obtainedfrom 22 of these cases. The diagnosis was made on pul-monary tissue collected by a percutaneous or trans-bronchial pulmonary biopsy in 10 cases and by pul-monary lobectomy in 1 case. Mucorales were identifiedon biopsy obtained from sinus and/or palatal tissues in9 patients and after ocular enucleation in 2 cases. In 1patient, Mucorales was documented to be present inbronchial fluid by cytological study of the bron-choalveolar lavage (BAL) fluid. In another 9 patients themycotic agent was only microbiologically identified: in4 cases in sputum samples, in 2 from BAL and in 3 fromnasal smear samples.
An autopsy was carried out on 33 patients and doc-umented the mucormycosis in 31 cases. In 27 patientsautopsy was the only positive diagnostic tool. In twopatients who died from progression of their hemato-logic disease, the autopsy was negative as the patienthad apparently recovered from fungal infection, previ-ously diagnosed in vivo on a sinus tissue biopsy.
In 30 patients (51%) the Mucorales species wasmicrobiologically identified while in 29 patients the eti-ological agent was not typed (Table 3).
In 38 patients (64%) the main site of involvement ofmucormycosis was lung, which represented the solelocalization in 28 cases, while the other 10 patientsalso had secondary localizations. These include the cen-tral nervous system (CNS) (n=7), paranasal sinus (n=1),intestine (n=1), liver (n=1). Other primary sites of infec-tion were: orbito-sinus-facial in 14 cases (24%), largebowel in 1 case, myocardium in 1 case, blood in 1 case.CNS involvement, observed in 11 patients (19%), wasalways associated with infection in other sites. It wasprobably secondary to hematogenous dissemination orextension to the brain from either nasal or paranasalinfection. A disseminated disease was observed in 4cases (7%) (Table 1).
The most frequent physical finding was fever (80% ofcases), with a median temperature of 38.8°C at pres-entation (range 37.8-39.7°C). In patients with pul-monary mucormycosis, the triad of cough, thoracic pain,and dyspnea was the most common set of symptoms;in 3 cases fatal hemoptysis occurred. In three patients
presenting with fever without any clinical signs of pul-monary involvement, the diagnosis of mucormycosiswas made only at autopsy (Table 4).
Patients who had rhino-cerebral mucormycosis com-plained of facial pain or headache and most of themshowed orbital involvement consisting of orbital cel-lulites, parests of extraocular muscles, proptosis andchemosis. Five patients had hemiplegia. The only patientwith intestinal involvement had abdominal pain anddiarrhea.
Radiographic procedures (standard chest and sinusX-rays; lung, CNS and sinus CT scan) were performed in
haematologica 2004; 89(2):February 2004 209
Mucormycosis in hematologic patients
Table 2. Results of main diagnostic procedures performeddepending on sign and symptoms.
Diagnostic Performed Suggestive of procedures invasive fungal
infection (%)
RadiologicalChest• Standard X-ray 41 39 (95%)• CT-scan 21 21 (100%)Sinus/CNS• Standard X-ray 5 2 (40%)• Cranial CT-scan 19 11 (58%)
Microbiological*• BAL 18 4 (22%)• Sputum 32 5 (16%)• Nasal smear 29 9 (31%)
Histologic and/or cytologicalBiopsy 26 22 (84%)• percutaneous or 14 10transbronchial on pulmonary tissue• lobectomy 1 1• sinus and/or palatal tissue 9 9• ocular enucleation 2 2
Cytological examination of BAL 18 6 (33%)
Autopsy 33 31 (94%)
*More than one site infected in the same patient.
Table 3. Etiological agents in the 59 cases of mucormy-cosis.
Cases %
Mucorales spp. 28 48Mucor spp. 22 37Rhizopus spp. 6 10Cunninghammella 2 3Absidia corymbifera 1 2

52 patients (88%) and the result was suggestive of fun-gal infection in 41 of them (80%). Chest X-rays wereabnormal in 39 of 41 patients examined; chest CT scanshowed a pattern compatible with fungal infection in20 of these patients. In 1 case chest CT scan diagnoseda lung infiltrate not identified by standard X-ray (Table2). Radiography revealed various patterns such as focalconsolidation and widespread infiltrates or nodules.Cavitation was observed in 25% of cases.
Cranial CT scan was performed in 19 patients andrevealed evidence of sinus involvement associated withopacification in 11 cases; in 8 cases the presence ofbrain abscesses was revealed.
TreatmentDuring neutropenia, 47 patients (80%) had received
oral antifungal prophylaxis (18 with fluconazole, 15
with itraconazole, 8 with nystatin, 4 with oral ampho-tericin B and 2 with ketoconazole) for a median time of18 days (range 5-90). These 47 neutropenic patientsbecame febrile and received empirical treatment withbroad-spectrum antibiotics (β lactam plus aminogly-coside with or without a glycopeptide), which wasadministered for a median of 10 days (1-35).
Antifungal treatment was empirically administeredin 49 patients (83%) after a median time of 90 hoursof fever unresponsive to broad-spectrum antibiotics.
Thirty-nine patients were treated with intravenousdeoxycholate amphotericin B (AmB) (in 12 patients oralazoles were associated) at a median daily dose of 1mg/kg (total median dose 1000 mg, range 500-1200);6 patients received fluconazole (3 cases) or itraconazole(3 cases) only.
Liposomal amphotericin B (L-AmB) was administeredin 12 patients at a median daily dose of 3 mg/kg (totalmedian dose 5000 mg, range 2100-19000). In 4 casesthis drug was the first line treatment while in theremaining 8 cases it was administered after prior treat-ment with Amb. They switched from AmB to L-AmBbecause of renal impairment, intolerance to AmB orbecause the physicians considered the treatment withAmB a failure.
Seven patients underwent radical surgical clearance:eye enucleation in 2 cases, sinus debridements in 4 cas-es, and lung lobectomy in 1 case.
OutcomeTherapy was successful in 18 patients (37%). Nine of
the 39 patients who received only AmB (23%) and 7 ofthe 12 patients who received L-AmB (58%) respondedto therapy. In 2 of the 6 patients treated with azoles(33%), there was an improvement in clinical status.
Forty-seven patients died within 3 months of thediagnosis of fungal infection. Mucormycosis was thecause of death in 41 of them (87%) while 6 patientswho responded to antifungal therapy died from pro-gression of their hematologic disease without signs orsymptoms of a new relapsed infection.
Statistical resultsThe factors considered in the univariate analysis are
summarized in Table 5; those statistically significantlyassociated with recovery from infection are shown inbold. The factors which correlated with a positive out-come from infection were male sex (p = 0.033), AmBtreatment (p = 0.012), neutrophil recovery from post-chemotherapy aplasia (p = 0.01). However, at multi-variate analysis the only factor that was significantlycorrelated with recovery from infection was L-AmBtreatment [RR=0.5 (CI 0.3-0.8; p = 0.0001)].
In order to examine the effect of the introduction ofL-AmB into the clinical use, we divided the overall pop-
haematologica 2004; 89(2):February 2004210
L. Pagano et al.
Table 4. Signs and symptoms of the patients at diagno-sis by site of infection.*
Sign/symptom N° %
Pulmonary localization 38 64Fever 38 100Cough 36 92Dyspnea 28 72Chest pain 15 38Hemoptysis 3 8
Orbito-sinus-facial localization 15 25Facial edema 15 100Nasal obstruction 12 80Facial pain 10 67Rhinorrhea 8 53Fever 7 46Proptosis 4 27Chemosis 3 20Palate destruction 3 20
Central nervous system involvement 11 19Fever 8 53Headache 7 63Hemiplegia 7 19Ptosis, diplopia 4 11Epilepsy 1 5
Gastro-intestinal tract 1 2Fever 1Abdominal pain 1Diarrhea 1Rectorrhagia 1
Myocardium 1 2Fever 1Dyspnea 1Thoracic pain 1
Blood 1 2Fever 1
*More than one site infected in the same patient

haematologica 2004; 89(2):February 2004 211
Mucormycosis in hematologic patients
ulation of patients into two different groups: those inwhom the diagnosis of mucormycosis was madebetween 1987 and 1994 and those diagnosed between1995 and 2001. We then compared the features of thetwo groups (Table 6). The most relevant difference thatwe found was a higher number of patients treated withL-AmB. However, in spite of an apparent improvement
of diagnostic procedures and the use of more effectiveantifungal drugs (i.e. L-AmB), only a slight, not signifi-cant reduction of mortality was observed (72% versus60%).
Discussion
Mucormycosis is a rare filamentous fungal infectionwhich most frequently arises in patients with hemato-logic malignancies.5,8,9,11,12,15-18 The main cause of thisinfections is probably the prolonged and profound neu-tropenia secondary to the myeloablative treatmentsused for the underlying hematologic malignancy. Infact, mucormycosis occurs more commonly in patientswith acute leukemia (in our series 78%) than in patientswith other types of hematologic malignancies, and theinfection is characterized by a high rate of mortality(~70%).
In the past, various factors negatively influenced mor-tality, including the diagnostic difficulties and theincorrect belief that antifungal prophylaxis could beefficacious against these filamentous fungi.
The diagnosis of mucormycosis is not simple and thedemonstration of fungal elements from cytologicpreparations (i.e. sputum samples, inflammatory fluidaspirates from sinusitis infection, and broncho-alveo-lar lavage) is complicated by the difficulty in extract-ing fungal elements from invaded tissues. Fungal ele-ments may be rare in cytological specimens and whenpresent are often fragmented. Additionally, hyphae maybe very focal and may appear in only part of a speci-men. A delayed diagnosis means that appropriate dos-es of antifungal treatment are started late, which canhave the consequence of increasing the number of fail-ures.
The present survey represents an update of our pre-vious study. The larger number of cases collected, theavailability of better laboratory and radiological diag-nostic tools and the introduction of new antifungaldrugs in the routine treatment of fungal infections (i.e.lipid formulation of AmB) led us to make a new re-appraisal of the characteristics and outcome of mucor-mycosis in patients with a hematologic malignancy. Asalready demonstrated, oral antimycotic prophylaxisseems unable to prevent mucormycosis.2 In fact flu-conazole and, in some cases, itraconazole should not beused either for prophylaxis or for treating mucormyco-sis given the lack of both in vitro and in vivo suscepti-bility.19-23
The main preventive measure against filamentousfungal infections remains the reduction of environ-mental exposure;24 in fact in our series only 5 patientsamong those who developed mucormycosis wereadmitted in hepa-filtered rooms.
Table 5. Univariate analysis of factors that influencedrecovery from infection.
Prognostic factor Patient Patient pTotal patients cured died value(n=59) (n = 13)(%) (n= 46)(%)
Age≤ 50 years 8 (25) 24 (75) ns>50 years 5 (18) 22 (82)
SexMale 10 (33) 20 (67) 0.033Female 3 (10) 26 (90)
Phase of underlying hematologic treatmentInduction 8 (20) 31 (80) nsOther 5 (25) 15 (75)
Use of steroidsYes 7(24) 22(76) nsNo 6(20) 24(80)
Neutropenia< 0.5×109/L 8 (18) 35 (82) 0.311≥ 0.5×109/L 5(31) 11(69)
Duration of neutropenia≤14 days 9 (14) 28 (76) 0.742> 14 days 4 (18) 18 (82)
Neutrophils recoveryYes 6 (33) 16 (57) 0.01No 7 (17) 26 (89)
ProphylaxisNo 2 (17) 10 (83) 0.755Itraconazole 4 (29) 10 (71)Other 7 (21) 26 (79)
FeverYes 11 (23) 36 (77) 1No 2 (17) 10 (83)
Sites of primary infectionLung 9 (24) 29 (76) 0.754Other 4 (19) 17 (81)
TherapyAmB + L-AmB 13 (30) 30 (70) 0.01Other 0 16 (100)
AmB dosage≤18 g 2 (10) 17 (90) 0.189> 18 g 11 (27) 29 (73)
TherapyL-AmB 7 (64) 4 (36) 0.001Other 6 (12) 42 (88)

The treatment of mucormycosis in patients withhematologic malignancies may require several simulta-neous approaches including surgery, antifungal thera-py, and medical management of the neutropenia.
In general, surgical resection of isolated pulmonarydisease greatly improves survival compared to patientswho receive antifungal therapy alone.13,25 There are evennotable cases of mucormycosis being cured by surgeryalone.25-28 However, the clinical conditions of neu-tropenic patients (low platelet count, low performance
status), and the presence of multiple mycotic abscess-es frequently do not allow a surgical resection. In ourexperience surgical resection significantly improves therecovery from infection; however, in the present seriesonly 7 patients underwent surgery. It is remarkable that6 of them recovered from infection and that 4 of these6 patients received L-Amb as antifungal treatment. Itis possible that more widespread use of combined med-ical-surgical therapy could further reduce mortality, asalready stressed by other authors.6,11
When surgical intervention is not possible or difficultto perform because of the site of the infection, anti-fungal therapy alone can be used, but a successful out-come is rare.18,29-31
Deoxycholate AmB is the first-line drug of choice formucormycosis. In our series AmB treatment statistical-ly improved the patients’ outcome, even though it maynot be effective in all cases, particularly in patients pre-senting late in the course of their disease and with dis-seminated disease. The therapeutic activity of AmB islimited by its potentially severe side effects. Impairedrenal function often leads to cessation of therapy.9,19,20
Furthermore it must be taken in account that AmB doesnot penetrate the blood-brain barrier readily, so it canbe ineffective in CNS mucormycosis. The majority ofzygomycetes demonstrate resistance to fluconazole,itraconazole and 5-fluorocytosine.9,19-23 In vitro activity ofinvestigational triazoles such as posaconazole, andravuconazole has been tested. These studies showedthat posaconazole was effective in vitro against zygo-mycetes; however its efficacy in vivo remains to bedetermined.23,32,33
In vitro studies have demonstrated that pneumo-cadin34 and the echinocandins35 do not inhibit fungalgrowth. Furthermore recent clinical trials have statedthat both echinocandins36 and voriconazole,21 two new-er antifungal drugs, are ineffective in the treatment ofmucormycosis. In this discouraging situation, L-AmBrepresents the only possible alternative to convention-al AmB, without a significantly increased toxicity evenif applied at higher dosage (3-5 mg/kg).
In fact, the liposomal formulations enable the drug todeposit in the reticulo-endothelial system includinglocal sites of infection. The drug is released within thesesites through the action of lipases from surroundinginflammatory cells. Furthermore L-AmB penetrates thebrain parenchyma and results in high drug concentra-tions in the brain;37 a similar effect has also beendemonstrated for AmB lipid complex.38
The characteristics of our study, retrospective and notrandomized, do not allow a demonstration of the supe-rior efficacy of L-AmB, with respect to other treatmentsbut the rarity of mucormycosis excludes the possibilityof conducting prospective randomized trials with a sig-nificant number of patients, particularly those with
haematologica 2004; 89(2):February 2004212
L. Pagano et al.
Table 6. Demographic and clinical characteristics ofpatients with mucormycosis and univariate analysis divid-ed into two study periods.
Parameters 1987-1994 1995-2001 Total (39) (20) (59)
Age
Median (range) 47(19-75) 51 (13-80)≤ 50 years (%) 22 (56) 10 (50) 0.841>50 years (%) 17 (44) 10 (50) 0.423
SexMale 18 (46) 12 (60) 0.232Female 21 (54) 8 (40)
DiagnosisAML 22 (56) 8 (40)ALL 11 (28) 5 (25)NHL 2 (5) 4 (20)HD 0 1 (5) 0.161CML 1 (3) 0MM 0 1 (5)MDS 1 (3) 1 (5)HCL 2 (5) 0 BMTNo 39 (100) 15 (75) 0.005Autologous 0 4 (20)Allogeneic 0 1 (5)
SteroidsYes 16 (41) 13 (65)Median dosage [mg] 1200 510(range) (200-5000) (20-4800)Median duration 24 (4-66) 15 (2-180) 0.103(days)No 23 (59) 7 (35)
Previous neutropeniaMedian duration [day] 12 10.5 0.160(range) (3-60) (0-30)
Neutrophils at diagnosis< 0.1×109/L 26 (67) 8 (40) 0.1690.1-0.49×109/L 4 (10) 5 (25)0.5-0.99×109/L 3 (8) 1 (5)≥ 1×109/L 6 (15) 6 (30)
Neutrophil recoveryYes 21 (54) 11 (34) 0.933No 18 (46) 9 (45)

213haematologica 2004; 89(2):February 2004
Mucormycosis in hematologic patients
hematologic malignancies. However, our collection ofdata on a large group of patients does allow some inter-esting considerations. In our series, we observed a sig-nificant reduction in mortality from mucormycosis inthose patients who received L-AmB, which resulted tobe the most relevant factor influencing the mortalityassociated with recovery from neutropenia. In fact, inmultivariate analysis, L-AmB was the only parametercorrelated with survival from the infection. In our seriesa median daily L-AmB dosage of 3 mg/kg resulted effi-cacious.
The importance of neutropenia as a factor contribut-ing to the development of infection in patients withhematologic malignancies has already been demon-strated,39 and the recovery of neutrophils plays a mainrole in the cure of mucormycosis. In our experience therecovery from aplasia is strictly correlated with a low-er mortality rate. Various studies of improved recoveryfrom infection by correcting neutropenia either withgranulocyte transfusions40,41 or by enhancing endoge-nous neutrophil production using growth factors42-44
have been published. The use of growth factors recon-stituting altered host defenses and reducing the dura-tion of neutropenia might increase the recovery frommucormycosis, even though in our statistical evalua-tion, this therapeutic approach did not result signifi-cant, perhaps because of the low number of cases treat-ed with growth factors.
When we stratified patients according to two differ-ent time periods (1987-1994 and 1995-2001), some
relevant differences were observed. In vivo diagnosisseems to be achieved more easily in recent years andthe fungal agent is now frequently specified, but themost important difference we found was the slightreduction in the mortality rate, even if not statisticallysignificant.
In conclusion, mucormycosis is a rare filamentousfungal infection, which does not seem to have increasedin the last years. Although a slight reduction in mor-tality has been observed, the mortality rate still remainshigh. Among the drugs effective against Mucorales, L-AmB seems to be more effective than AmB, probablybecause high daily doses can be used for longer periodswith fewer side effects. Recent pharmacokinetic stud-ies demonstrated the safety and tolerance of high dos-es of L-AmB (since 15 mg/kg/day);45 this kind of treat-ment could be the appropriate approach to mucormy-cosis, in consideration that literature reviews show thatthe new antifungal drugs (i.e. voriconazole, caspofun-gin) do not seem to add new ammunition against thesedangerous fungal infections, and we are awaiting datafrom treatment studies using posaconazole to assessthe efficacy of this azole agent in zygomycosis.
Contributions. LP co-ordinated the study; LP and LF wrote thepaper; MO and LF were responsible for the data analysis; all the oth-er co-authors collected the clinical data; PM and ADF criticallyreviewed and approved the final version. This work was supported bya grant from the Ministry of University and Scientific and Techno-logical Research (MURST) of Italy. The authors indicated no potentialconflicts of interest.
Received on August 27, 2003, accepted December 1, 2003.
References
1. Eucker J, Sezer O, Graf B, Possinger K.Mucormycoses. Mycoses 2001;44:253-60.
2. Pagano L, Ricci P, Tonso A, et al. Mucormy-cosis in patients with haematologicalmalignancies: a retrospective clinicalstudy of 37 cases. Br J Haematol 1997;99:331-6.
3. Bodey GP, Vartivarian S. Aspergillosis. EurJ Clin Microbiol Infect Dis 1989;8:413-37.
4. Pfaffenbach B, Donhuijsen K, Pahnke J,Bug R, Adamek RJ, Wegener M, et al. Sys-temic fungal infections in hematologicneoplasms. An autopsy study of 1,053patients. Med Klin 1994;89:299-304.
5. Pagano L, Ricci P, Nosari A, Tonso A, Buel-li M, Montillo Met al. Fatal haemoptysis inpulmonary filamentous mycosis: anunderevaluated cause of death in patientswith acute leukaemia in haematologicalcomplete remission. A retrospective studyand review of the literature. GimemaInfection Program (Gruppo Italiano Ma-lattie Ematologiche dell'Adulto). Br JHaematol 1995;89:500-5.
6. Sugar AM. Mucormycosis. Clin Infect Dis1992; 14 Suppl 1:S126-9.
7. Lehrer RI, Howard DH, Sypherd PS,Edwards JE, Segal GP, Winston DJ. Mucor-
mycosis. Ann Intern Med 1980; 93:93-108.
8. Morrison VA, McGlave PB. Mucormycosisin the BMT population. Bone MarrowTransplant 1993;11:383-8.
9. St-Germain G, Robert A, Ishak M, Trem-blay C, Claveau S Infection due to Rhi-zomucor pusillus: report of four cases inpatients with leukemia and review. ClinInfect Dis 1993;16:640-5.
10. Nosari A, Oreste P, Montillo M, Carrafiel-lo G, Draisci M, Muti G, et al. Mucormy-cosis in hematologic malignancies: anemerging fungal infection. Haematologi-ca 2000;85:1068-71.
11. Tedder M, Spratt JA, Anstadt MP, HedgeSS, Tedder SD, Lowe JE. Pulmonary mucor-mycosis: results of medical and surgicaltherapy. Ann Thorac Surg 1994; 57:1044-50.
12. Kontoyiannis DP, Wessel VC, Bodey GP,Rolston KV. Zygomycosis in the 1990s ina tertiary-care cancer center. Clin InfectDis 2000;30:851-6.
13. Marr KA, Carter RA, Crippa F, Wald A,Corey L. Epidemiology and outcome ofmould infections in hematopoietic stemcell transplant recipients. Clin Infect Dis2002;34:909-17.
14. Ascioglu S, Rex JH, de Pauw B, Bennett JE,Bille J, Crokaert F, et al. Defining oppor-tunistic invasive fungal infections inimmunocompromised patients with can-
cer and hematopoietic stem cell trans-plants: an international consensus. Inva-sive Fungal Infections Cooperative Groupof the European Organization for Researchand Treatment of Cancer; Mycoses StudyGroup of the National Institute of Allergyand Infectious Diseases. Clin Infect Dis2002;34:7-14.
15. Parfrey NA. Improved diagnosis and prog-nosis of mucormycois. A clinicopatholog-ic study of 33 cases. Medicine 1986;65:113-23.
16. Dykhuizen RS, Kerr KN, Soutar RL. Aircrescent sign and fatal haemoptysis inpulmonary mucormycosis. Scand J InfectDis 1994;26:498-501.
17. Tonso A, Ricci P, Cenacchi A, Bonini A,Ficara F, Pagano L, et al. Invasive infec-tions by fylamentous mycetes in adultpatients with hematological neoplasticdiseases (polycentric and retrospectivestudy of 162 cases). Haematologica 1993;78 Suppl 4:24.
18. Fingeroth JD, Roth RS, Talcott JA, RinaldiMG. Zygomycosis due to Mucor circinel-loides in a neutropenic patient receivingchemotherapy for acute myelogenousleukemia. Clin Infect Dis 1994; 19:135-7.
19. Eng RHK, Person A, Mangura C, Chmel H,Corrado M. Susceptibility of zygomycetesto amphotericin B, miconazole, and keto-conazole. Antimicrob Agents Chemother1981;20:688-90.

haematologica 2004; 89(2):February 2004214
L. Pagano et al.
20. Otcenasek M, Buchta V. In vitro suscep-tibility to 9 antifungal agents of 14strains of Zygomycetes isolated from clin-ical specimens. Mycopathologia 1994;128:135-7.
21. Johonson LB, Kauffman CA. Voriconazole:a new triazole antifungal agent. ClinInfect Dis 2003;36:630-7.
22. Gomez-Lopez A, Cuenca-Estrella M,Monzon A, Rodriguez-Tudela JL. In vitrosusceptibility of clinical isolates ofZygomycota to amphotericin B, flucyto-sine, itraconazole and voriconazole. JAntimicrob Chemother 2001;48:919-21.
23. Pfaller MA, Messer SA, Hollis RJ, Jones RN.Antifungal activities of posaconazole,ravuconazole, and voriconazole comparedto those of itraconazole and amphotericinB against 239 clinical isolates of Asper-gillus spp. and other filamentous fungi:report from SENTRY Antimicrobial Surveil-lance Program, 2000. The SENTRY Partici-pants Group. Antimicrob Agents Chemo-ther 2002;46:1032-7.
24 Walsh TJ, Dixon DM. Nosocomial asper-gillosis: environmental microbiology, hos-pital epidemiology, diagnosis and treat-ment. Eur J Epidemiol 1989;5:131-42.
25. DeSousa R, MacKinnon S, Spagnolo SV,Fossieck BE. Treatment of localized pul-monary phycomycosis. South Med J 1979;72:609-12.
26. Chakrabarti A, Kumar P, Padhye AA,Chatha L, Singh SK, Das AJ, et al. Prima-ry cutaneous zygomycosis due to Sakse-naea vasiformis and Apophysomyces ele-gans. Clin Infect Dis 1997;24:580-3.
27. Pritchard RC, Muir DB, Archer KH, BeithJM. Subcutaneous zygomycosis due toSaksenaea vasiformis in an infant. Med JAust 1986;145:630-1.
28. Tomford JW, Whittlessey D, Ellner JJ,Tomashefski JF. Invasive primary cuta-neous phycomycosis in diabetic leg ulcers.Arch Surg 1980;115:770-1.
29. Lye GR, Wood G, Nimmo G. Subcutaneouszygomycosis due to Saksenaea vasiformis:rapid isolate identification using a modi-fied sporulation technique. Pathology1996;28:364-5.
30. Meyers BR, Wormser G, Hirschman SZ,Blitzer A. Rhinocerebral mucormycosis:pre-mortem diagnosis and therapy. ArchIntern Med 1979;139:557-60.
31. Ng TTC, Campbell CK, Rothera M,Houghton JB, Hughes D, Denning DW.Successful treatment of sinusitis causedby Cunninghamella bertholletiae. ClinInfect Dis 1994;19:313-6.
32. Dannaoui E, Meletiadis J, Mouton JW,Meis JF, Verweij PE. In vitro susceptibili-ties of zygomycetes to conventional andnew antifungals. J Antimicrob Chemoth-er 2003;51:45-52.
33. Sun QN, Najvar LK, Bocanegra R, Loeben-berg D, Graybill JR. In vivo activity ofposaconazole against Mucor spp. in animmunosuppressed-mouse model. Antimi-crob Agents Chemother 2002;46:2310-2.
34. Del Poeta M, Schell WA, Perfect JR. In vit-ro antifungal activity of Pneumocadin L-743,872 against a variety of clinically sig-nificant molds. Antimicrob Agents Che-mother 1997;41:1835-6.
35. Pfaller MA, Marco F, Messer SA, Jones RN.In vitro activities of two echinocadinderivatives, LY303366 and MK-0991 (L-743,792), against clinical isolates ofAspergillus, Fusarium, Rhizopus, and oth-er filamentous fungi. Diagn MicrobiolInfect Dis 1998;30:251-5.
36. Cornely OA, Schmitz K, Aisenbrey S. Thefirst echinocandin: caspofungin. Mycoses2002;45:56-60.
37. Adler-Moore J, Proffitt RT. Effect of tissuepenetration on AmBisome efficacy. CurrOpin Invest Drugs 2003;4:179-85.
38. Mondy KE, Haughey B, Custer PL, Wip-pold FJ 2nd, Ritchie DJ, Mundy LM.Rhinocerebral mucormycosis in the era of
lipid-based amphotericin B: casereport and literature review. Pharmaco-therapy 2002;22:519-26.
39. Pizzo PA. Management of fever inpatients with cancer and treatment-induced neutropenia. N Engl J Med 1993;328:1323-32.
40. Bodey GP, Anaissie E, Gutterman J, Vad-han-Raj S. Role of granulocyte-macro-phage colony-stimulating factor as adju-vant therapy for fungal infection inpatients with cancer. Clin Infect Dis 1993;17:705-7.
41. Ryan ME, Ochs J. Primary cutaneousmucormycosis: superficial and gangre-nous infections. Pediatr Infect Dis J 1982;1:110-4.
42. Goodman NL, Rinaldi MG. Agents ofzygomycosis. I: A. Balows, W. J. Hausler,KL Herrmann, H. D. Isenberg, and H. J.Shadoomy, eds. Manual of clinical micro-biology, 5th ed. ASM Press; Washington,D.C. 1991. p. 674-92.
43. Leong KW, Crowley B, White B, CrottyGM, O'Brian DS, Keane C, et al. Cutaneousmucormycosis due to Absidia corymbiferaoccurring after bone marrow transplan-tation. Bone Marrow Transplant 1997;19:513-5.
44. Liles WC, Huang JE, Van Burik JH, BowdenRA, Dale DC. Granulocyte colony-stimu-lating factor administered in vivo aug-ments neutrophil-mediated activityagainst opportunistic fungal pathogens.J Infect Dis 1997;175:1012-5.
45. Walsh TH, Goodman JL, Pappas P, Beker-sky I, Buell DN, Roden M, et al. Safety, tol-erance, and pharmacokinetics of high-dose liposomal amphotericin B (AmBi-some) in patients infected with asper-gillus species and other filamentous fun-gi: maximum tolerated dose study. AgentsChemother 2001;15:3487-96.





























