Embed Size (px)
Citation preview

C(J)SYMPOSIUM ON GERIATRICS-Part VI
Rehabilitation of Geriatric Patients
DAVID C. WEBER, M.D., KEVIN C. FLEMING, M.D., AND JONATHAN M. EVANS, M.D.
• Objective: To describe the role of geriatric rehabilitation, the methods of practice, and the mechanisms underlying integrated care in rehabilitationmedicine.
• Design: We reviewed the rehabilitation-relatedmedical literature and outlined an approach to theevaluation of impairment in older patients and subsequent rehabilitation planning.
• Results: For optimal rehabilitation of geriatricpatients, knowledge of general principles of rehabilitation and key areas affecting the elderly population isimportant. A rehabilitation program will be mostsuccessful if a team approach-including a physician,rehabilitation nurse, physical therapist, occupational
Rehabilitation has been defined as "the development of aperson to the fullest physical, psychological, social, vocational, avocational, and educational potential consistent withhis or her physiological or anatomic impairment and environmental Iimitations."! More simply, rehabilitation involves maximizing functional independence within the constraints imposed by disease, illness, and injury. Because thequality of life for elderly persons is closely linked to preservation offunctional independence, the principles of rehabilitation are particularly applicable to the geriatric population.Indeed, the American Geriatrics Society affirms the importance of rehabilitation in serving the needs of the elderlypopulation' (Table 1). In this article, we review the conceptsof impairment, disability, and handicap. In addition, wediscuss general principles of rehabilitation, special considerations for rehabilitation of elderly patients, patient assessment and rehabilitation planning, sites for providing rehabilitation, the rehabilitation team, and barriers to geriatricrehabilitation.
From the Department of Physical Medicine and Rehabilitation (D.C.W.)and Section of Geriatrics (K.C.F., J.M.E.), Mayo Clinic Rochester, Rochester, Minnesota.
Individual reprints of this article are not available. The entire Symposiumon Geriatrics will be available for purchase as a bound booklet from theProceedings Circulation Office at a later date.
therapist, psychologist, medical social worker, andrecreational therapist-is used. Attention should bepaid to special considerations in older patients (suchas the presence of comorbid conditions) and potentialbarriers to care in order to maximize benefit.
• Conclusion: Rehabilitation of elderly patients canassist in preserving functional independence and improving the quality of life. Assessment and management in an individual patient ate best performed by ateam approach.
(Mayo Clin Proc 1995; 70:1198-1204)
ADLs =activities of daily living; OT =occupational therapist;PT =physical therapist
DEFINITIONSThe World Health Organization approach to rehabilitationissues is well defined and easily applied'< (Table 2). Theyhave defined a "disease" as a process that causes a change inthe structure or function of the body. "Impairment" refers tothe loss or abnormality of structure or function, as a result ofdisease, illness, or injury. A "disability" is a functionallimitation as a result of disease or impairments. A "handicap" is a societally determined disadvantage that resultsfrom impairment or disability. In essence, an impairment occurs at the organ level, a disability occurs at the levelof individual Junction, and a handicap is at the level ofsociety:'
As an example, a person who sustains a cerebral infarction might have right hemiparesis as one impairment.The ensuing disability might include the inability to drive orinability to ambulate without assistance, and a subsequenthandicap might be social isolation because of limited mobility. Of importance, the degree of impairment may not correlate directly with the degree of disability or handicap; theextent of a disability or handicap from a given impairment isspecific to an individual. For example, if two persons hadtheir nondominant fifth finger traumatically amputated(identical impairment), their ensuing disability and handicapwould differ dramatically if one were a farmer and the otherwere a concert violinist.
Mayo Clin Proc 1995; 70:1198-1204 1198 © 1995 Mayo Foundation/or Medical Education and Research
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

MayoClin Proc, December1995,Vol70
Table I.-American Geriatrics SocietyPublic Policy Committee Position Statements:
Geriatric Rehabilitation
1. Rehabilitation services should be available in all settings inwhich older persons receive health care
2. An interdisciplinary approach should be used in the delivery ofcomprehensive geriatric rehabilitative services
3. Primary-care providers should be trained to assess the need forrehabilitative services and should be actively involved in theprovision of these services
4. Funding for rehabilitative services of various durations andintensities should be provided for older persons
5. Research is needed in order to determine the optimalapplication of rehabilitative services for the older person
From the AGS Public Policy Committee." By permission.
The World Health Organization outlines four major goalsof intervention for disabilities: prevention, enhancement,supplementation, and substitution." We discuss preventionin a subsequent section of this article (see Approach toGeriatric Rehabilitation). Enhancement or supplementationbecomes necessary when prevention fails and independentperformance of functional activities becomes difficult. Forexample, impaired vision may be enhanced or supplementedwith reading glasses, improved illumination, and largeprint." When the severity of an impairment precludes performance of a particular activity (even with enhancement orsupplementation), substitution becomes necessary. With themodel of impaired vision, examples of substitution includeuse of radio, recorded books, or braille (for material thatformerly was read visually)." In this model, interventionmay occur at any level-that is, disease, impairment, disability, or handicap. Medical or surgical intervention generallyoccurs at the level of disease or impairment. In contrast,rehabilitation intervention may occur at the level of impairment, disability, or handicap. Usually, social service intervention occurs at the handicap level.
Another useful concept is "active life expectancy," whichrefers to the portion of a person's remaining life span inwhich functional independence is maintained' As medicaldevelopments increase life expectancy to the biologic limitsof the natural life span, functional assessment and rehabilitation intervention will become increasingly important to ensure that active life expectancy increases as well."
GENERAL PRINCIPLES OF REHABILITATIONSeveral key principles are involved in the rehabilitation approach to care. First, rehabilitation consists of a functionoriented approach-a paradigm shift from the usual diseaseor illness-oriented model." Specific diagnosis and treatmentof disease, illness, or injury are still primary objectives. In
REHABILITAnON OF GERIATRIC PATIENTS I 199
rehabilitation, however, assessment of the functional effectof the pathologic change is emphasized, inasmuch as thequality of life may be dramatically altered. Another keyconcept is the interdisciplinary team approach of the rehabilitation model. Interdisciplinary should be distinguishedfrom multidisciplinary. Multidisciplinary denotes merelythat multiple disciplines are involved with a patient's care,whereas interdisciplinary implies active communication andcooperation among the various disciplines." Such team cooperation is crucial in ensuring that patient and family goalsare appropriately addressed. In a purely multidisciplinaryapproach, suboptimal communication among multiple consulting physicians may result in inadequate or inappropriatepatient care.
SPECIAL CONSIDERATIONS INREHABILITATION OF ELDERLY PATIENTSSeveral characteristics distinguish geriatric rehabilitationfrom rehabilitation in younger patients. In general, the agedpopulation has more comorbid conditions, each of whichmust be considered when rehabilitation is planned. Forexample, an ankle sprain may have only a minor and shortlived effect on a young person. In an elderly patient, however, comorbid conditions such as proximal weakness fromgeneral deconditioning or severe arthritis may preclude theuse of a walker or crutches. Thus, return to completelyindependent living may not be possible until full weightbearing activity can be tolerated. Another example is cognitive impairment. Although a person may be physicallycapable of self-care, cognitive limitations may preclude living in an unsupervised setting. In addition, comorbid conditions such as cardiac or pulmonary disease may limit exercise tolerance and restrict the patient's ability to participatein rehabilitation. Elderly patients also tend to have lower
Table 2.-Definitions of Rehabilitation-Related TermsEstablished by the World Health Organization
DiseaseIntrinsic pathology or disorder that gives rise to changes in the
structure or function of the body"
ImpairmentAny loss or abnormality of psychologic, physiologic, or
anatomic structure or function"
DisabilityAny restriction or lack (resulting from an impairment) of
ability to perform an activity in the manner or within therange considered normal for a human being"
HandicapA disadvantage for a given individual, resulting from an
impairment or disability, that limits or prevents thefulfillment of a role that is normal (depending on age, sex,and social and cultural factors) for that individual"
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

1200 REHABILITATION OF GERIATRIC PATIENTS
functional reserves and more difficulty maintaining homeostasis than do younger populations. For these reasons, geriatric patients are more vulnerable to functional decline, evenwhen the acute illness or impairment is relatively mild.Functional decline in hospitalized elderly patients is common but often unrecognized; hence, the result may be longerhospital stays and an increased need for assistance.F'
Although vocational issues are less prominent than inyoung patients (because many of these patients are retired),avocational interests may be a focal point of the patient'slifestyle. Thus, returning to these pursuits will be an important goal in rehabilitation planning. Avocational activitiesmay be a major source of life satisfaction for older adults andshould not be overlooked or considered unimportant.
APPROACH TO GERIATRIC REHABILITATIONThe initial step in geriatric rehabilitation involves prevention(Table 3), which can encompass preventing deterioration offunction and anticipating or avoiding complications of aging, disease, illness, or injury. 10 Adjustments in lifestyle (forexample, cessation of smoking, regular exercise, and dietarymodifications), preventive health maintenance measures,and timely medical intervention may need emphasis. Ofutmost importance is prevention of deconditioning, definedas "the multiple changes in organ system physiology that areinduced by inactivity and reversed by activity."!' It can besubdivided into acute deconditioning from bed rest andchronic deconditioning from a sedentary lifestyle. II Acutedeconditioning may be prevented by bedside range-of-motion exercises, gentle strengthening exercises, and encouragement of activity (such as bathroom privileges,ambulation with assistance, and seated in chair for meals) assoon as it is medically appropriate.
After initiation of appropriate preventive care, the nextstep is to identify impairments, disabilities, and handicaps.Detailed methods of functional assessment have been published elsewhere.F-" Distinguishing between a patient'sreport of physical capabilities and actual performance isimportant. Fear of nursing home placement may cause apatient to exaggerate functional abilities. Alternatively,anxiety, apprehension, or poor motivation may cause performance at a lower level than expected. For example, a patientmay be capable of ambulating safely and independently witha walker yet prefer physical assistance because of fear offalling. Direct observation is still the best means of ensuringaccuracy of the assessment; many rehabilitation departmentshave simulated home environments to observe function inthe kitchen, bath, and other areas directly.
Once impairments, disabilities, and handicaps have beenidentified, realistic goals must be established. Ideally, goalsetting involves discussion with both the patient and thefamily. Goals should be precisely defined and measurable
Mayo Clin Proc, December 1995, Vol 70
Table 3.-Approach to Rehabilitation of Geriatric Patients
I. Recommend preventive measures (forexample, avoiddeconditioning, maintain propernutrition, stop smoking,schedule periodic medical examinations)
2. Identifyimpairments, disabilities, and handicaps
3. Set realistic goalsafterdiscussion withpatientand family;considerthe following factors:
Potential site of dispositionDegree of physical independenceUse of adaptive equipmentHomeaccessibility or modifications neededAssistance available (spouse, relatives, friends)
4. Determine realistic timeframefor goals
5. Determine site for provisionof rehabilitationAcute-care hospitalDesignated rehabilitation unit withinacute-care hospitalFreestanding rehabilitation facilitySkillednursingfacilityOutpatient centerHome
6. Review andreevaluate progress periodically
when possible (for example, "Will independently ambulate100 feet with rolling walker") rather than vague and nonspecific (for instance, "Will improve level of functional independence"). Several factors should be considered whensetting goals (Table 3). The patient's living situation isimportant in determining the required level of independence;however, disposition, in itself, should not determine rehabilitation plans. For example, patients entering a long-termcare facility may still be appropriate candidates for inpatientrehabilitation if this arrangement decreases caregiver needsor improves mobility or safety.
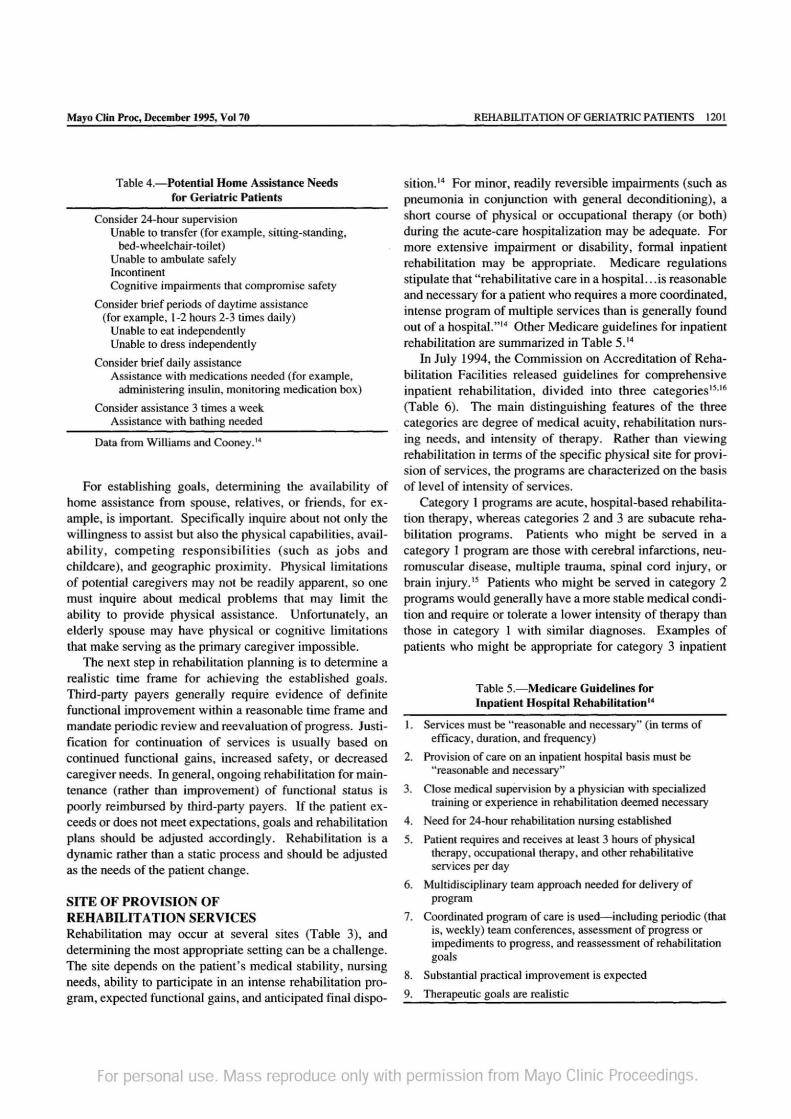
The degree of physical dependence will determine thelevel of intensity of home care, as outlined in Table 4. Theserecommendations are intended only as guidelines and shouldbe individualized. Use of adaptive equipment may decreasethe need for care and potentially enable a patient to remain athome rather than being placed in a nursing home. Unless aperson is independent (even with the use of adaptive equipment), however, some type of home assistance will obviously be necessary.
Determining accessibility of the home setting is important in planning disposition. Narrow hallways, small bathrooms, and multilevel homes are a few of the architecturalbarriers encountered. Many barriers can be easily overcomewith simple modifications such as bath benches, grab bars,handheld showerheads, removal of doors to increase wheelchair accessibility, and substitution of a ramp for a multistepentry. A home visit by a physical or occupational therapistmay be useful for assessing the home accessibility and appropriate home modifications.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
Mayo elin Proc, December 1995, Vol 70
Table 4.-Potential Home Assistance Needsfor Geriatric Patients
Consider24-hoursupervisionUnableto transfer(for example,sitting-standing,
bed-wheelchair-toilet)Unableto ambulate safelyIncontinentCognitiveimpairments that compromise safety
Considerbrief periodsof daytimeassistance(for example, 1-2hours 2-3 timesdaily)
Unableto eat independentlyUnable to dress independently
Considerbriefdaily assistanceAssistance withmedications needed (for example,
administering insulin, monitoring medication box)
Considerassistance 3 timesa weekAssistance with bathingneeded
Data from Williamsand Cooney.14
For establishing goals, determining the availability ofhome assistance from spouse, relatives, or friends, for example, is important. Specifically inquire about not only thewillingness to assist but also the physical capabilities, availability, competing responsibilities (such as jobs andchildcare), and geographic proximity. Physical limitationsof potential caregivers may not be readily apparent, so onemust inquire about medical problems that may limit theability to provide physical assistance. Unfortunately, anelderly spouse may have physical or cognitive limitationsthat make serving as the primary caregiver impossible.
The next step in rehabilitation planning is to determine arealistic time frame for achieving the established goals.Third-party payers generally require evidence of definitefunctional improvement within a reasonable time frame andmandate periodic review and reevaluation of progress. Justification for continuation of services is usually based oncontinued functional gains, increased safety, or decreasedcaregiver needs . In general, ongoing rehabilitation for maintenance (rather than improvement) of functional status ispoorly reimbursed by third-party payers. If the patient exceeds or does not meet expectations, goals and rehabilitationplans should be adjusted accordingly. Rehabilitation is adynamic rather than a static process and should be adjustedas the needs of the patient change.
SITE OF PROVISION OFREHABILITATION SERVICESRehabilitation may occur at several sites (Table 3), anddetermining the most appropriate setting can be a challenge.The site depends on the patient's medical stability, nursingneeds, ability to participate in an intense rehabilitation program, expected functional gains, and anticipated final dispo-
REHABILITATION OF GERIATRIC PATIENTS 1201
sition." For minor, readily reversible impairments (such aspneumonia in conjunction with general deconditioning), ashort course of physical or occupational therapy (or both)during the acute-care hospitalization may be adequate. Formore extensive impairment or disability, formal inpatientrehabilitation may be appropriate. Medicare regulationsstipulate that "rehabilitative care in a hospital. . .is reasonableand necessary for a patient who requires a more coordinated,intense program of multiple services than is generally foundout of a hospital. "14 Other Medicare guidelines for inpatientrehabilitation are summarized in Table 5. 14
In July 1994, the Commission on Accreditation of Rehabilitation Facilities released guidelines for comprehensiveinpatient rehabilitation, divided into three categories15.16
(Table 6). The main distinguishing features of the threecategories are degree of medical acuity, rehabilitation nursing needs, and intensity of therapy. Rather than viewingrehabilitation in terms of the specific physical site for provision of services, the programs are characterized on the basisof level of intensity of services.
Category I programs are acute, hospital-based rehabilitation therapy, whereas categories 2 and 3 are subacute rehabilitation programs. Patients who might be served in acategory 1 program are those with cerebral infarctions, neuromuscular disease, multiple trauma, spinal cord injury, orbrain injury ." Patients who might be served in category 2programs would generally have a more stable medical condition and require or tolerate a lower intensity of therapy thanthose in category 1 with similar diagnoses. Examples ofpatients who might be appropriate for category 3 inpatient
Table 5.-Medicare Guidelines forInpatient Hospital Rehahilitation"
1. Servicesmust be "reasonableand necessary"(in termsofefficacy, duration, and frequency)
2. Provisionof care on an inpatienthospitalbasis must be"reasonable and necessary"
3. Close medicalsupervision by a physicianwith specializedtrainingor experiencein rehabilitation deemednecessary
4. Need for 24-hour rehabilitation nursingestablished
5. Patientrequires and receivesat least 3 hours of physicaltherapy, occupational therapy, and other rehabilitativeservices per day
6. Multidisciplinary team approachneededfor deliveryofprogram
7. Coordinated programof care is used-including periodic (thatis, weekly)team conferences, assessmentof progressorimpediments to progress, and reassessment of rehabilitationgoals
8. Substantial practical improvement is expected
9. Therapeutic goals are realistic
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

1202 REHABILITATION OF GERIATRIC PATIENTS Mayo Clin Proc, December 1995, Vol 70
Table 6.-Stratification of Comprehensive Inpatient Medical Rehabilitation Programs Based onGuidelines From the Commission on Accreditation of Rehabilitation Facilities's
FactorCategory I
(acute)Category 2(subacute)
Category 3(subacute)
Site of rehabilitation*
Risk of medical instabilityRehabilitation nursing needs
Hospital
HighMultiple, complex, or
both
Hospital, hospital-basedSNF,SNF
VariableMultiple, complex, or
both
Hospital-based SNF,SNF
LowRoutine
Low riskReturn to community
with appropriatesupport
YesProgress to another level
of rehabilitation or returnto community withappropriate support
Minimum-I-3 h/day, Minimum-I-3 h/day,5 days/wk 5 days/wk
All require regular direct contact by rehabilitation physicianAll require education and training opportunities for patient and family members
on an ongoing basis
YesProgress to another level
of rehabilitation or returnto community withappropriate support
Minimum-3 h/day,5 days/wk
Potential need for high medicalacuity skilled nursing
Expected outcome
Therapy by interdisciplinaryteamt
Physician contactPatient and family education
*SNF = skilled nursing facility.tlnterdisciplinary team includes an occupational therapist, a physical therapist, a psychologist, a-social worker, a speech
language pathologist, and a therapeutic recreation specialist.
rehabilitation are those with orthopedic conditions (such asuncomplicated total hip or knee arthroplasty), amputations,and multiple trauma without complications. IS
When a rehabilitation facility is evaluated for the care of aparticular patient, the quality and quantity of the staff areimportant factors. The number of staff members, their levelof training, and any subspecialty experience (geriatrics,stroke, amputations) should be considered. In general, advanced training and experience better equip the rehabilitation team to address more complex needs. For simplestrengthening activities and mobility or gait training, a highlevel of expertise is unnecessary, whereas complex neuromuscular reeducation of a patient with hemiparesis requiresa high degree of knowledge and experience. The trainingand experience of the staff should be concordant with thecomplexity of the rehabilitation needed.
THE REHABILITATION TEAMAlthough many different disciplines may participate in rehabilitation of geriatric patients, the core team usually consistsof a physician, a rehabilitation nurse, a physical therapist(PT), an occupational therapist (OT), a psychologist, a medical social worker, and a recreational therapist. Practicepatterns and specific roles of team members may vary between institutions, but the team approach is an essentialcomponent in a successful rehabilitation program. The corerehabilitation team is well suited to both inpatient and outpatient rehabilitation, including programs at long-term andsubacute care facilities. Typical roles of the various rehabili-
tation team members have been described elsewhere.l-'? Thefollowing descriptions are of potential general roles of thevarious disciplines.
The physician member of a geriatric rehabilitation teammay be a rehabilitation specialist (physiatrist) with geriatricexperience, a geriatrician with rehabilitation experience, oranother primary-care physician with rehabilitation and geriatric experience. More important than credentials are anunderstanding of the process of rehabilitation and an abilityto lead an interdisciplinary team effectively. Good communication and leadership skills are crucial to being an effectiveteam leader.'? Typically, team meetings involve brief reviews of a patient's status by each team member and discussion of goals and plans for ongoing care. The team conceptensures consistency of purpose, fosters group evaluation ofproblems, and allows efficient planning of therapies anddisposition.
Rehabilitation nurses are important members of any rehabilitation team. They integrate all the knowledge and skillsobtained by the patient in various therapies and apply themto achieve practical self-care goals. The acute-care hospitalenvironment may unintentionally foster dependence." Patients are often assisted (in the interest of time) with tasksthat they are capable of performing independently, albeitmore slowly. Rehabilitation nurses encourage independence, provide physical assistance or verbal cues, and have arole in the following activities: monitoring of skin integrity,educating patients about skin care, evaluating bowel andbladder management programs, discussing information
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc, December 1995, Vol 70
about medications , providing general patient and familyeducation, and training patients and family members fordismissal.
PTs can assist a patient in improving level of function inseveral ways. They can design an exercise program toincrease range of motion, strength, coordination, balance,and endurance. They address bed mobility (for example,turning side-to-side or adjusting from supine to sitting), sitting balance, transfers (for example, from sitting to standing,from bed to wheelchair, or getting in and out of a car), andstanding balance. PTs evaluate ambulation and train thepatient in ambulation skills (either wheelchair or bipedal),including traversing barriers such as curbs, stairs, and ramps.In addition, they may assess various splints and braces,evaluate various gait aids and train patients in their properuse, apply various modalities (heat, cold, hydrotherapy, electrical stimulation, traction, and massage) for control of pain,review a stretching program for management of spasticity,access wheelchair needs and assist with wheelchair prescription, perform home evaluations for accessibility and safety,and fabricate orthoses (splints).
A major emphasis of OTs is self-care skills or activities ofdaily living (ADLs), including basic ADLs (such as bathing,grooming, dressing, toileting, personal hygiene, and eating)needed to live without constant supervision. They also focuson instrumental ADLs, which are community skills necessary to live completely independently-for example, cooking, light housekeeping, telephone use, shopping, and moneymanagement (such as paying bills and balancing a checkbook). An OTcan assess a patient's ability to perform ADLsindependently and safely. If the evaluation reveals problemswith performance of ADLs, an OT can assist with education,training, compensatory skills, and adaptive equipment tofacilitate independence. OTs (in addition to PTs) also suggest ways to increase range of motion, strength, coordination, balance, and endurance . Although practice patternsvary considerably, OTs often focus more on upper extremityactivities, whereas PTs focus more on lower extremity activities. Other responsibilities of an OT may include instruction in principles of joint protection in patients with arthritis,instruction in energy conservation principles (for example,in those with rheumatoid arthritis, cardiac disease, or pulmonary disease), fabrication of orthoses (splints), training inupper extremity fine motor activities, performing homeevaluations of accessibility and safety, performingpredriving evaluations, training in use of upper extremityprostheses, application of modalities for control of pain,evaluating and treating dysphagia (for example, after stroke,aspiration pneumonia, dementia, or parkinsonism), cognitive retraining and compensatory skills (such as after strokeor brain injury), and remediation and compensation forvisuospatial difficulties.
REHABILITATION OF GERIATRIC PATIENTS 1203
Speech-language pathologists evaluate and treat disorders of speech (dysarthrias), disorders of language and communication (aphasias), and disorders of coordination ofspeech (apraxia). They train patients in compensatory skillsto improve their communication abilities, and they also educate families about appropriate compensations to facilitatecommunication. Furthermore, they may assist with augmentative communication (for example, after stroke orlaryngectomy), evaluation and treatment of dysphagia, cognitive retraining and compensatory skills, and remediationand compensation for visuospatial difficulties.
Certified therapeutic recreation specialists (or recreational therapists) use "recreational activities for purposiveintervention ... to promote the growth and development of thepatient."! Avocational interests and activities, includinghobbies, games, sports, and other recreational activities, areassessed for appropriateness and the ability of the patient toparticipate. Patients are then educated about adapted recreation or sports, new leisure skills, and social interests. Often,geriatric patients with disabilities 'are apprehensive aboutreentering the community. Recreational therapists can assist with community reentry by coordinating trips into thecommunity (for example, for theater, restaurant, or shopping excursions) in a supportive, nonthreatening setting.They are also an invaluable resource for assessing adaptations and modifications to enable a patient to continue toenjoy recreational interests. Recreational therapists oftenarrange group social activities (such as movies, games, visiting lecturers, and musical performances) in the rehabilitationunit.
Rehabilitation psychologists can help to identify and define cognitive, visuoperceptual, and psychiatric issues. Theyconduct clinical interviews as well as perform and interpretspecific tests of intelligence, memory, learning, and personality. Through interviewing and testing, they can assist therehabilitation team in better characterizing the patient andoffering the appropriate strategies for unique needs andgoals. They may also counsel patients to assist with theiradjustment to impairments, disabilities, or handicaps ; in addition, they can evaluate and address other mental healthneeds. A rehabilitation psychologist can also assist the teamin understanding and managing behavioral issues, a component of which might include development of a behavioralmanagement program for appropriate patients.
The medical social worker has a crucial role in numerousaspects of rehabilitation care. The social worker often servesas the primary communicator between the rehabilitationteam and the family and is an invaluable resource for coordinating disposition planning, including home care needs,transportation needs, and continued outpatient therapies .Counseling and financial concerns of the patient and familymay also be addressed by the social worker.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

1204 REHABILITATION OF GERIATRIC PATIENTS
BARRIERS TO GERIATRIC REHABILITAnONPotential barriers to geriatric rehabilitation include ageism,right of dependence, and apathy of fatigue." Ageism is anegatively biased perception of aging and the elderly population. It is often as pervasive among elderly persons themselves as in the general population." Geriatric patients mayaccept a decline in functional status as an inevitable part ofaging, even when faced with a potentially reversible situation that is amenable to rehabilitation. Such nihilism on thepart of the patient may be inappropriately interpreted as"poor motivation" for rehabilitation, when in reality it represents inadequate education of the patient about the potentialbenefits of rehabilitation. 18 Exposure to the rehabilitationenvironment (that is, seeing other patients in physical, occupational, speech, and recreational therapy) can be helpful inimproving attitudes because other patients in a similar agerange and with similar impairments are noted as activelyparticipating in and benefiting from rehabilitation.
A related concept is the right of dependence, which is theexpectation by elderly persons that, because they have takencare of other relatives, they now have a right to be cared forby others even though they may be capable of independentself-care. A plan should be formulated to allow the patient toretain a role as the respected elder without assuming thedependent-sick role."
Another barrier to geriatric rehabilitation is the apathy offatigue. Physical or emotional fatigue may leave the patientpoorly motivated for rehabilitation. Potential nutritional,metabolic, or other causes of fatigue must be identified andcorrected." The patient should be educated about potentialsequelae of continued immobility and deconditioning." Acommitment should be obtained from the patient to participate in a mutually agreeable amount of therapy each day."With the cost-containment emphasis by third-party payers,poor progress can result in termination of reimbursement forrehabilitation services. Because many of these patients willnot be allowed another opportunity for rehabilitation, "thereshould be a sense of urgency in identifying and interveningin any process that interferes with needed rehabilitation.''"Attention paid to the potential benefits of rehabilitation forolder patients can result in appreciable functional improvements and enhanced quality of life.
REFERENCES1. DeLisa JA, Martin GM, Currie DM. Rehabilitation medi
cine: past, present, and future. In: DeLisa JA, Gans BM,editors. Rehabilitation Medicine: Principles and Practice.2nd ed. Philadelphia: Lippincott, 1993: 3-27
Mayo Clio Proc, December 1995, Vol 70
2. AGS Public Policy Committee. Geriatric rehabilitation. JAm Geriatr Soc 1990; 38:1049-1050
3. Hoening H, Mayer-Oakes SA, Siebens H, Fink A, BrummelSmith K, Rubenstein LV. Geriatric rehabilitation: what dophysicians know about it and how should they use it? J AmGeriatr Soc 1994; 42:341-347
4. World Health Organization. International Classification ofImpairments, Disabilities, and Handicaps: A Manual of Classification Relating to the Consequence of Disease. Geneva:World Health Organization, 1980
5. Katz S, Branch LG, Branson MH, Papsidero JA, Beck JC,Greer DS. Active life expectancy. N Engl J Med 1983;309:1218-1224
6. Williams ME, Hadler NM. The illness as the focus of geriatric medicine. N Engl J Med 1983; 308:1357-1360
7. Melvin JL. Interdisciplinary and multidisciplinary activitiesand the ACRM. Arch Phys Med Rehabil 1980; 61:379-380
8. Creditor MC. Hazards of hospitalization of the elderly. AnnIntern Med 1993; 118:219-223
9. Hirsch CH, Sommers L, Olsen A, Mullen L, WinogradCH. The natural history of functional morbidity in hospitalized older patients. J Am Geriatr Soc 1990; 38:12961303
10. Clark GS, Bray GP. Development of a rehabilitation plan.In: Williams TF, editor. Rehabilitation in the Aging. NewYork: Raven Press, 1984: 125-143
11. Siebens H. Deconditioning. In: Kemp B, Brummel-SmithK, Ramsdell JW, editors. Geriatric Rehabilitation. Boston:Little, Brown, 1990: 177-191
12. Fleming KC, Evans JM, Weber DC, Chutka DS. Practicalfunctional assessment of elderly persons: a primary-careapproach. Mayo Clin Proc 1995; 70:890-910
13. Applegate WB, Blass JP, Williams TF. Instruments for thefunctional assessment of older patients. N Engl J Med 1990;322:1207-1214
14. Williams TF, Cooney LM Jr. Principles of rehabilitation inolder persons. In: Hazzard WR, Bierman EL, Blass JP,Ettinger WH Jr, Halter JB, Andres R, editors. Principles ofGeriatric Medicine and Gerontology. 3rd ed. New York:McGraw-Hill, 1994: 343-348
15. Commission on Accreditation of Rehabilitation Facilities.Section 2.n.A: Medical rehabilitation programs; comprehensive inpatient, categories one through three. In: Supplementto the 1994 Standards Manual and Interpretive Guidelines forOrganizations Serving People With Disabilities. Tucson(AZ): CARF, 1994: 1-14
16. Standards released for subacute care. Physiatrist 1994 Sep;10:8-9
17. Clark GS. Rehabilitation team: process and roles. In:Fe1senthalG, Garrison SJ, Steinberg FU, editors. Rehabilitation of the Aging and Elderly Patient. Baltimore: Williams &Wilkins, 1994: 439-448
18. Hesse KA, Campion EW, Karamouz N. Attitudinal stumbling blocks to geriatric rehabilitation. J Am Geriatr Soc1984; 32:747-750
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.





























