Embed Size (px)
Citation preview
PSYCHIATRY
RESEARCH
ELSEVIER Psychiatry Research 64 (1996) 35-45
Neurocognitive function in alcoholic, schizophrenic, and dually diagnosed patients
Sara Jo Nixon*, H. Gene Hallford, Rick D. Tivis
Cognitive Studies Laboratory, Oklahoma Center for Alcohol and Drug-Related Studies, Depatiment of Psychiatry and Behavioral Sciences, University of Oklahoma Health Sciences Center, 800 NE 15th Street, Suite 410, Oklahoma Civ,
OK 73104, USA
Received 8 September 1995; revised 1 April 1996; accepted 30 May 1996
Abstract
Neurocognitive functions were compared in alcoholic, schizophrenic, and dually diagnosed (schizophrenic and alcoholic) patients and community control volunteers. Participants (N = 52, n = 13 in each group) completed a brief battery including two measures of neuropsychological function and two affective measures. The neuropsychological tests included the Trail-Making Test Forms A and B and a face-recognition test. The affective measures included assessment of anxiety and depression. The major objective was to compare the patterns of neurocognitive perfor- mance among the four groups. The groups did not differ in mean age (35.37) or years of education (12.46). Compared with the community control and alcoholic groups, the schizophrenic groups reported higher mean depression (12.92 vs. 5.54) and mean state anxiety scores (60.73 vs. 46.04). Control subjects were generally, although not always significantly, superior to the other groups. Contrary to expectations, alcoholic patients were not consistently better than the schizophrenic groups, and dually diagnosed participants were not more impaired than schizophrenic patients without substance abuse histories. Thus, the interaction of schizophrenia and substance abuse did not have an additive effect on neurocognitive performance assessed in this study. More research using this complete four-group design and a larger neurocognitive batteq is needed.
Keywords: Neuropsychology; Substance abuse; Depression; Anxiety
*Corresponding author. Tel.: + 1 405 2712474; fax: + 1 405 2716236.
0169-2607/96/$15.00 0 1996 Elsevier Science Ireland Ltd. All rights reserved. PII SO169-2607(96) 0291 l-3
36 S.J. N&on et al. / PJychiatty Research 64 (1996) 35-45
1. Introduction
Interest in schizophrenia and alcohol use dis- orders is longstanding in the psychiatric litera- ture. Of immediate relevance are studies that have examined neuropsychological functions. These studies have revealed a wide array of im- pairment in both groups, including problems in attentional processes, memory, and abstracting (Gold and Harvey, 1993; Parsons, 1993; Kremen et al., 1994). Patients with schizophrenia, how- ever, exhibit more significant impairment. For example, schizophrenic subjects frequently score in the clinically impaired range, i.e., from - 1.5 to 3 SD below the standard mean performance (Harvey et al., 1986; Gold and Harvey, 1993). Subjects with alcohol use disorders, on the other hand, typically exhibit mild, generalized dysfunc- tion (Tivis et al., 1995). Their level of function is often statistically inferior to that in community controls, but the deficit is not of sufficient magni- tude to place them in the clinically impaired range (Nixon, 1995; Parsons et al., 1987). Interest- ingly, current research suggests that the underly- ing cognitive processes compromised in the two groups may also be different (Sullivan et al., 1992, 1993).
Considering the two psychiatric diagnoses sepa- rately, however, may not provide the most mean- ingful information. Clinicians have long recog- nized that the coexistence or comorbidity of mul- tiple disorders is common (e.g., Drake et al., 1993; Ries, 1993; Greenfield et al., 1995). Epidemiologi- cal research also supports this conclusion. Recent studies indicate that multiple diagnoses may char- acterize a significant percentage of individuals with psychiatric disorders (Regier et al., 1990; Kessler et al., 1994). Specifically, Kessler et al. (1994) conclude that approximately 56% of the respondents who meet criteria for one psychiatric disorder also meet criteria for two or more psy- chiatric disorders.
Particularly appropriate for the current work are those studies that consider the overlap between schizophrenia and substance abuse diag- noses. Although the data are highly variable, they suggest that a substantial percentage, perhaps 47%, of those persons with a diagnosis of
schizophrenia also meet criteria for a lifetime diagnosis of substance abuse (Barbee et al., 1989; Regier et al., 1990; Drake et al., 1990; Cuffel, 1992) with alcohol apparently being the most frequently used/abused drug (see Cuffel, 1992; Selzer and Lieberman, 1993). The reciprocal rela- tion is also evidenced: alcohol-abusing/depen- dent persons (alcoholics) are three to four times more likely to meet criteria for schizophrenia than are nonalcoholic persons (Regier et al., 1990).
Despite the wealth of data regarding neurocog- nitive functioning in alcoholics and schizophrenic patients, few empirical data regarding persons dually diagnosed with these disorders are avail- able. Given the obvious clinical and research im- plications of this dual diagnosis (Dixon et al., 1991; Selzer and Lieberman, 19931, such research appears to be overdue. The current study was an initial step in clarifying the neurocognitive func- tioning in dually diagnosed schizophrenic patients and their control groups: schizophrenic patients without other diagnoses, alcoholics without other diagnoses, and community controls.
A large number of neurocognitive tests might have been applied in this study (for review, see Nixon, 1995), but the resource restraints of this pilot work dictated a restricted battery. The bat- tery included the administration of several psy- chosocial measures and two neurocognitive tests. In the selection of neurocognitive tests, two pri- mary criteria were applied: (1) Tests should assess performance in areas known to be compromised in these clinical populations and enhance our understanding of the underlying processes. (2) Tasks should be brief, easily administered, and easily comprehended by the patient groups. Given these criteria, the Trail-Making Test, Forms A and B (Rennick et al., 1972) and a face-recogni- tion test (Yin, 1969) were selected.
The Trail-Making Test is a standard measure of perceptual-motor and set-shifting skills. It is sensitive to brain injury and insult resulting from a variety of disorders including alcoholism and schizophrenia (Parsons, 1987; Sweeney et al., 1991). Trails B appears to be more sensitive than Trails A to alcohol-related dysfunction (see Nixon, 1995).
S.J. Nixon et al. /Psychiatry Research 64 (I 996) 35-45 37
Previous work has suggested both alcohol-re- lated (Schaeffer and Parsons, 1987) and schizophrenia-related deficits (Feinberg et al., 1986) in learning/memory tasks using facial sti- muli. Schaeffer and Parsons (1987) found that alcoholics were inferior to control subjects in learning faces and names in multi-trial learning tests. Feinberg et al. (1986) showed that schizophrenic patients showed a deficit, when compared with community controls, in the recog- nition of faces presented in the usual (upright) orientation. Schizophrenic patients were not, however, impaired in their ability to recognize faces when presented in the inverted (upside down) orientation. That is, schizophrenic patients failed to demonstrate the normally obtained dif- ferential benefit associated with the upright as opposed to inverted positioning of faces. If, and how, this finding may be linked to the differential involvement of the cerebral hemispheres in schizophrenia is not yet clear.
Within this pilot study, three hypotheses and one empirical question were posited. The hy- potheses were: (1) Community controls will per- form better than the clinical groups. (2) Al- coholics will perform better than the other clini- cal groups. (3) If the negative effects of alcohol and schizophrenia are additive, dually diagnosed patients should perform worse than all other groups. The empirical question was whether the three clinical groups would exhibit differential impairment, depending on the cognitive task.
2. Methods
2.1. Subjects
Subjects (N= 52) were 13 schizophrenic (9 males, 4 females), 13 alcoholic (9 males, 4 fe- males), 13 dually diagnosed (10 males, 3 females), and 13 community control (7 males, 6 females) subjects. All participants had at least an eighth grade education and were between 21 and 55 years of age. Although a minimum level of educa- tion was required, subject groups were not inten- tionally matched for educational level. As shown below, however, the groups did not differ on this variable.
Clinical groups were recruited from inpatient facilities across Oklahoma, including both private and state-maintained units. Clinical groups met E&f-III-R (American Psychiatric Association, 1987) criteria as determined by clinical review and independent measurement using alcoholism and schizophrenia diagnostic checklists. Only those psychiatric patients (schizophrenic and dual) with a consistent clinical diagnosis for at least 5 years were asked to participate.
For alcoholics, the length of sobriety ranged from 21 to 45 days at the time of test administra- tion. All clinical patients (alcoholic, schizophrenic, and dual) had incurred fewer than 45 days of inpatient care for the current hospitalization. These criteria were used to minimize the poten- tial negative consequences of longer term hospi- talization (e.g., increased social deprivation) which might, separate from the disease state, influence cognitive performance.
Community controls were recruited from the Oklahoma City catchment area by newspaper ad- vertisements, fliers, and word-of-mouth.
Subjects were excluded on the basis of medical, neurological or concomitant psychiatric condi- tions not related to group selection criteria. Po- tential control subjects who indicated a current or past psychiatric or substance abuse/dependence diagnosis were not included. Also, alcohol abuse/dependent and community control sub- jects were excluded if currently taking medica- tions that might affect cognitive function. Medi- cated schizophrenic and dually diagnosed patients, however, were tested. Participation was voluntary; all subjects read and signed informed consent forms before testing and were paid for their par- ticipation.
2.2. Procedure
2.2.1. Group screening packet A screening packet, adapted from the instru-
ment developed at the Oklahoma Center for Al- cohol and Drug-Related Studies, was used to gather basic demographic and health-related in- formation. Self-report measures of the quantity and frequency of alcohol use and the conse- quences resulting from alcohol abuse and/or de-
38 S.J. Nixon et al. /Pychiatry Research 64 (1996) 35-45
pendence were also obtained with this instru- ment. Despite the limitations of self-report, this mechanism has been shown to be valid and reli- able with both alcoholic and schizophrenic sam- ples (Hesselbrock et al., 1983; Loethen and Khavari, 1990; Smith and Pristach, 1990; Bryant et al., 1992).
After reviewing the screening materials, ex- aminers recruited subjects appropriate for further study to participate in the cognitive assessment. As noted previously, subjects provided written informed consent.
2.2.2. Affective measures Because levels of depression and anxiety may
affect task performance independent of psychi- atric diagnosis, standardized tests were given to assess affect. The instruments included the Beck Depression Inventory (BDI; Beck et al., 1988) and the Spielberger State Anxiety Inventory (STAI; Spielberger, 1983). Standard administra- tion procedures were followed. The affective measures were obtained before neurocognitive testing.
2.2.3. Trail-Making forms A and B (Trails A and B) The task was administered following the design
and implementation described by Rennick et al. (1972). Trails A requires the sequential connec- tion of a series of numbered dots. Subjects are provided with instructions and a practice trial with correction before the test is administered. Performance on the test is evaluated for both errors and time to completion.
Trails B, an extension of Trails A, requires completing the same basic motor skill (connecting the dots) but adds the requirement of alternating between numbers and letters (connecting ‘1’ to ‘A’ then to ‘2’ then to ‘By>. Again, subjects are given detailed instruction with corrected practice before the test phase begins.
2.2.4. Face-recognition test The face-recognition task, developed after Yin
(1969, 19701, was constructed from a pool of 40 high-contrast black-and-white photographs devoid of obvious cues such as unusual clothing and jewelry. Men and women were equally repre-
sented in the set of pictures. The photographs were divided into two sets, the first to be pre- sented in the normal upright orientation and the second set to be presented inverted. Pairs were assigned to maximize similarity and, thus, to in- crease task difficulty, particularly in light of the 50% chance of correct recognition. Because Yin (1969) found no order effect, the presentation of upright faces followed by inverted faces was maintained for all subjects, without counter- balance.
Before they viewed the individual faces, sub- jects were given instructions for a standard recog- nition test. They were told that they would be shown 10 individual faces, one at a time and that each face would be visible for only 2 s. To ensure that the presentation rate would be constant, subjects were not allowed to touch the test mate- rials while the individual faces were being pre- sented. They were instructed to examine each face carefully because pairs of faces would be shown later and they would be asked to identify the one seen previously.
After the upright presentation/test of the faces, subjects were told that they would be shown an- other set of faces and that their task was, again, to study each picture individually and then, when the pairs of faces were presented, to select the one from each pair that they had seen before. They were told that these faces would be pre- sented upside down. Accuracy and reaction-time measures were recorded for all responses.
3. Results
3.1. Demographic data and affective measures (Table 1)
Groups did not differ in age (F = 0.74, df = 3,49, P = 0.53) or years of completed education (F = 1.59, df = 3,49, P = 0.20). Significant group effects were found for depression (F = 3.19, df = 3,49, P = 0.03) and anxiety (F = 11.36, df = 3,49, P= 0.0001). Neither of the affective measures was in the clinically significant range.
3.1.1. Statistical corrections Reaction times are often skewed, although the
significance of this fact is controversial when ade-
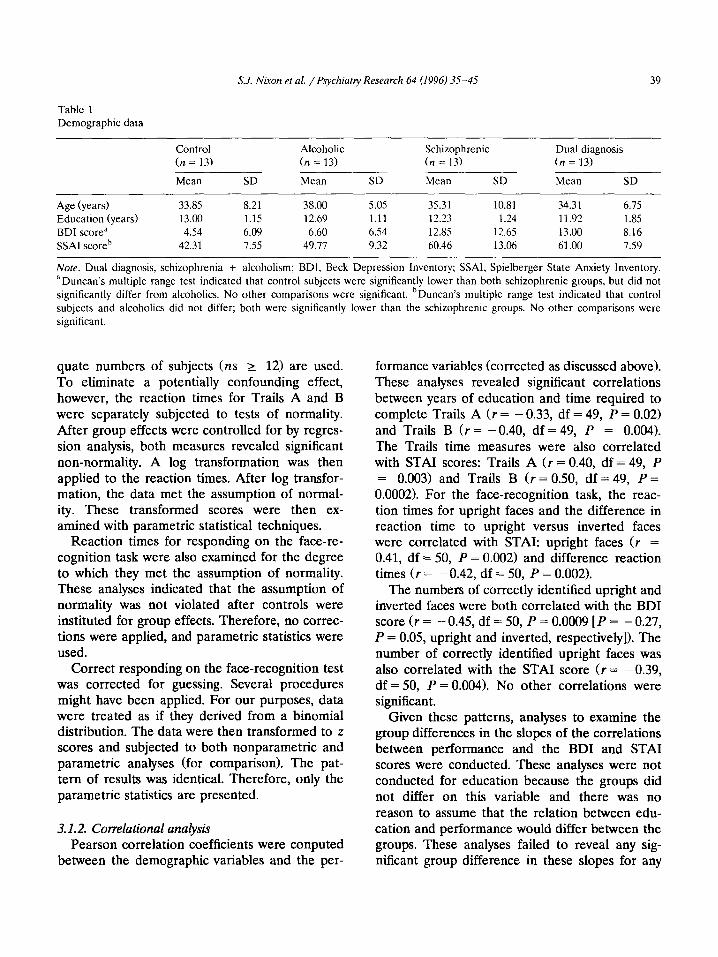
Table 1
Demographic data
S.J. Nixon et al. / Psychiaty Research 64 (1996) 35-45 39
Control
(n = 13)
Mean SD
Alcoholic
(n = 13)
Mean SD
Schizophrenic Dual diagnosis
(n = 13) (n = 13)
Mean SD Mean SD
Age (years) 33.85 8.21 38.00 5.05 35.31 10.81 34.31 6.75
Education (years) 13.00 1.15 12.69 1.11 12.23 1.24 11.92 1.85
BDI scorea 4.54 6.09 6.60 6.54 12.85 12.65 13.00 8.16
SSAl scorch 42.31 7.55 49.77 9.32 60.46 13.06 61 .OO 7.59
Note. Dual diagnosis, schizophrenia + alcoholism; BDI, Beck Depression Inventory; SSAI, Spielberger State Anxiety Inventory.
aDuncan’s multiple range test indicated that control subjects were significantly lower than both schizophrenic groups, but did not
significantly differ from alcoholics. No other comparisons were significant. hDuncan’s multiple range test indicated that control
subjects and alcoholics did not differ; both were significantly lower than the schizophrenic groups. No other comparisons were
significant.
quate numbers of subjects (ns 2 12) are used. To eliminate a potentially confounding effect, however, the reaction times for Trails A and B were separately subjected to tests of normality. After group effects were controlled for by regres- sion analysis, both measures revealed significant non-normality. A log transformation was then applied to the reaction times. After log transfor- mation, the data met the assumption of normal- ity. These transformed scores were then ex- amined with parametric statistical techniques.
Reaction times for responding on the face-re- cognition task were also examined for the degree to which they met the assumption of normality. These analyses indicated that the assumption of normality was not violated after controls were instituted for group effects. Therefore, no correc- tions were applied, and parametric statistics were used.
Correct responding on the face-recognition test was corrected for guessing. Several procedures might have been applied. For our purposes, data were treated as if they derived from a binomial distribution. The data were then transformed to z scores and subjected to both nonparametric and parametric analyses (for comparison). The pat- tern of results was identical. Therefore, only the parametric statistics are presented.
3.1.2. Correlational analysis Pearson correlation coefficients were conputed
between the demographic variables and the per-
formance variables (corrected as discussed above). These analyses revealed significant correlations between years of education and time required to complete Trails A (r = - 0.33, df = 49, P = 0.02) and Trails B (r = - 0.40, df = 49, P = 0.004). The Trails time measures were also correlated with STAI scores: Trails A (r = 0.40, df = 49, P = 0.003) and Trails B (r = 0.50, df = 49, P = 0.0002). For the face-recognition task, the reac- tion times for upright faces and the difference in reaction time to upright versus inverted faces were correlated with STAI: upright faces (r = 0.41, df = 50, P = 0.002) and difference reaction times (r = -0.42, df = 50, P = 0.002).
The numbers of correctly identified upright and inverted faces were both correlated with the BDI score (r = - 0.45, df = 50, P = 0.0009 [P = - 0.27, P = 0.05, upright and inverted, respectively]). The number of correctly identified upright faces was also correlated with the STAI score (r = - 0.39, df = 50, P = 0.004). No other correlations were significant.
Given these patterns, analyses to examine the group differences in the slopes of the correlations between performance and the BDI and STAI scores were conducted. These analyses were not conducted for education because the groups did not differ on this variable and there was no reason to assume that the relation between edu- cation and performance would differ between the groups. These analyses failed to reveal any sig- nificant group difference in these slopes for any
40 Xl. Nixon et al. / Psychiaty Research 64 (1996) 35-45
of the significant correlations (I;s I 1.75, Ps L 0.17). On the basis of this finding, the individual performance measures were regressed (linear re- gression) on the basis of the significant covariate identified in the correlational analysis.
3.2. Neurocognitive measures
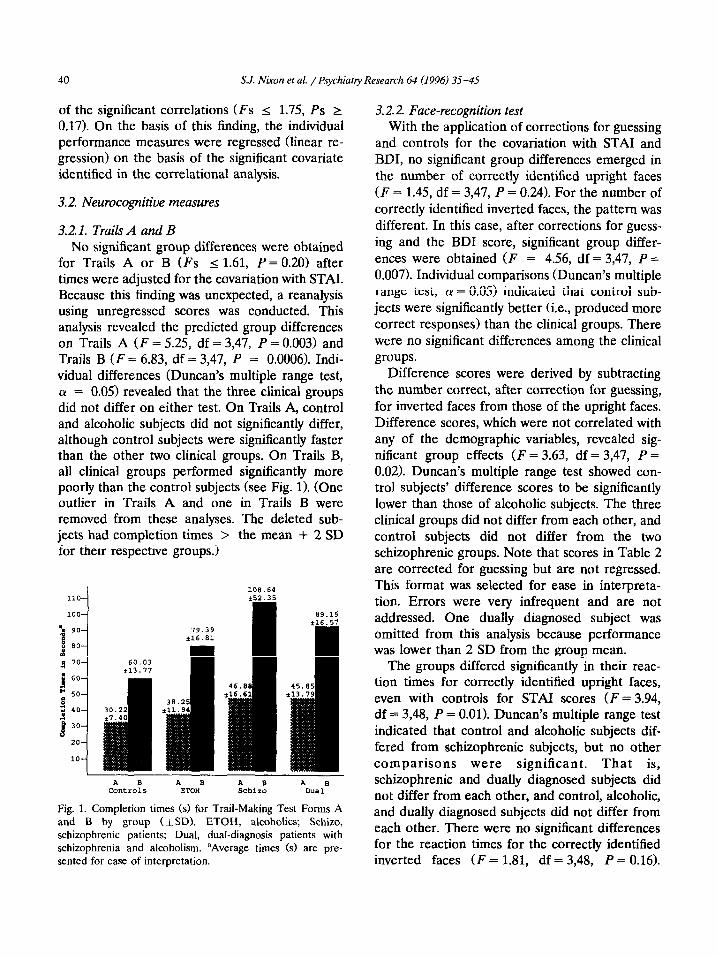
3.2.1. Trails A and B No significant group differences were obtained
for Trails A or B (Fs < 1.61, P = 0.20) after times were adjusted for the covariation with STAI. Because this finding was unexpected, a reanalysis using unregressed scores was conducted. This analysis revealed the predicted group differences on Trails A (F = 5.25, df = 3,47, P = 0.003) and Trails B (F = 6.83, df = 3,47, P = 0.0006). Indi- vidual differences (Duncan’s multiple range test, (Y = 0.05) revealed that the three clinical groups did not differ on either test. On Trails A, control and alcoholic subjects did not significantly differ, although control subjects were significantly faster than the other two clinical groups. On Trails B, all clinical groups performed significantly more poorly than the control subjects (see Fig. 1). (One outlier in Trails A and one in Trails B were removed from these analyses. The deleted sub- jects had completion times > the mean + 2 SD for their respective groups.)
110
100
% 90
1 ” 80 x a ‘O - J 60
* so g z 40
-j 30
20
10
A B A s A B A S Controls ETOH Schiro Dual
Fig. 1. Completion times (s) for Trail-Making Test Forms A and B by group (*SD). ETOH, alcoholics; Schizo, schizophrenic patients; Dual, dual-diagnosis patients with schizophrenia and alcoholism. aAverage times (s) are pre- sented for east of interpretation.
3.2.2. Face-recognition test With the application of corrections for guessing
and controls for the covariation with STAI and BDI, no significant group differences emerged in the number of correctly identified upright faces (F = 1.45, df = 3,47, P = 0.24). For the number of correctly identified inverted faces, the pattern was different. In this case, after corrections for guess- ing and the BDI score, significant group differ- ences were obtained (F = 4.56, df = 3,47, P = 0.007). Individual comparisons (Duncan’s multiple range test, (Y = 0.05) indicated that control sub- jects were significantly better (i.e., produced more correct responses) than the clinical groups. There were no significant differences among the clinical groups.
Difference scores were derived by subtracting the number correct, after correction for guessing, for inverted faces from those of the upright faces. Difference scores, which were not correlated with any of the demographic variables, revealed sig- nificant group effects (F = 3.63, df = 3,47, P = 0.02). Duncan’s multiple range test showed con- trol subjects’ difference scores to be significantly lower than those of alcoholic subjects. The three clinical groups did not differ from each other, and control subjects did not differ from the two schizophrenic groups. Note that scores in Table 2 are corrected for guessing but are not regressed. This format was selected for ease in interpreta- tion. Errors were very infrequent and are not addressed. One dually diagnosed subject was omitted from this analysis because performance was lower than 2 SD from the group mean.
The groups differed significantly in their reac- tion times for correctly identified upright faces, even with controls for STAI scores (I; = 3.94, df = 3,48, P = 0.01). Duncan’s multiple range test indicated that control and alcoholic subjects dif- fered from schizophrenic subjects, but no other comparisons were significant. That is, schizophrenic and dually diagnosed subjects did not differ from each other, and control, alcoholic, and dually diagnosed subjects did not differ from each other. There were no significant differences for the reaction times for the correctly identified inverted faces (F = 1.81, df = 3,48, P = 0.16).
S.J. Nixon et al. /Psychiatry Research 64 (1996) 35-45 41
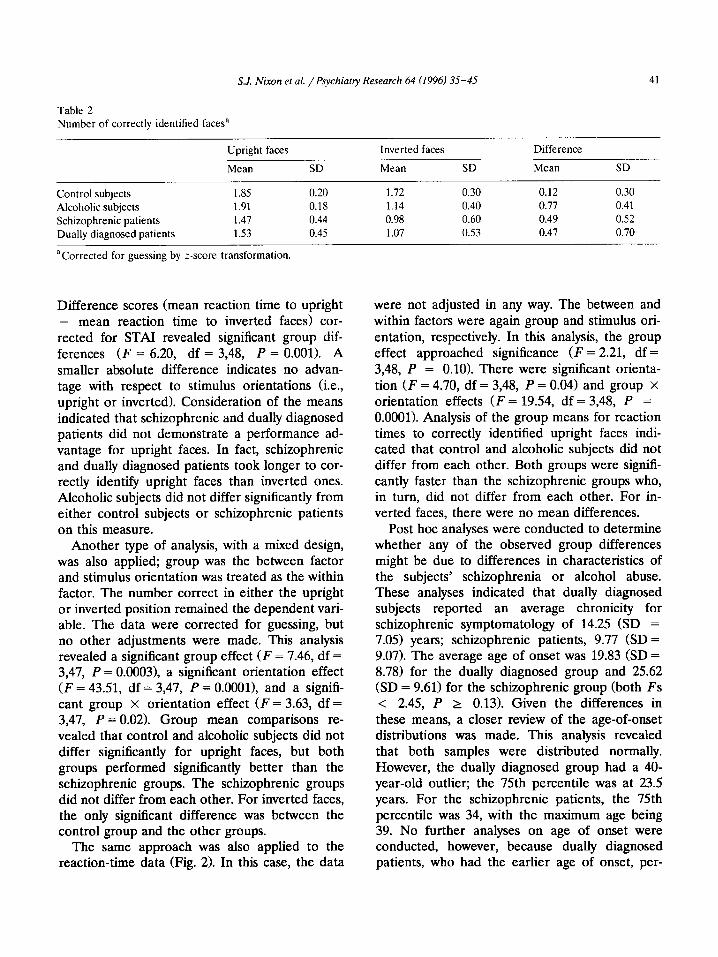
Table 2 Number of correctly identified faces”
Upright faces
Mean SD
Inverted faces Difference
Mean SD Mean SD
Control subjects 1.85 0.20 Alcoholic subjects 1.91 0.18 Schizophrenic patients 1.47 0.44 Dually diagnosed patients 1.53 0.45
aCorrected for guessing by z-score transformation.
Difference scores (mean reaction time to upright - mean reaction time to inverted faces) cor- rected for STAI revealed significant group dif- ferences (F = 6.20, df = 3,48, P = 0.001). A smaller absolute difference indicates no advan- tage with respect to stimulus orientations (i.e., upright or inverted). Consideration of the means indicated that schizophrenic and dually diagnosed patients did not demonstrate a performance ad- vantage for upright faces. In fact, schizophrenic and dually diagnosed patients took longer to cor- rectly identify upright faces than inverted ones. Alcoholic subjects did not differ significantly from either control subjects or schizophrenic patients on this measure.
Another type of analysis, with a mixed design, was also applied; group was the between factor and stimulus orientation was treated as the within factor. The number correct in either the upright or inverted position remained the dependent vari- able. The data were corrected for guessing, but no other adjustments were made. This analysis revealed a significant group effect (F = 7.46, df = 3,47, P = 0.0003>, a significant orientation effect (F = 43.51, df = 3,47, P = O.OOOl>, and a signifi- cant group x orientation effect (F = 3.63, df = 3,47, P = 0.02). Group mean comparisons re- vealed that control and alcoholic subjects did not differ significantly for upright faces, but both groups performed significantly better than the schizophrenic groups. The schizophrenic groups did not differ from each other. For inverted faces, the only significant difference was between the control group and the other groups.
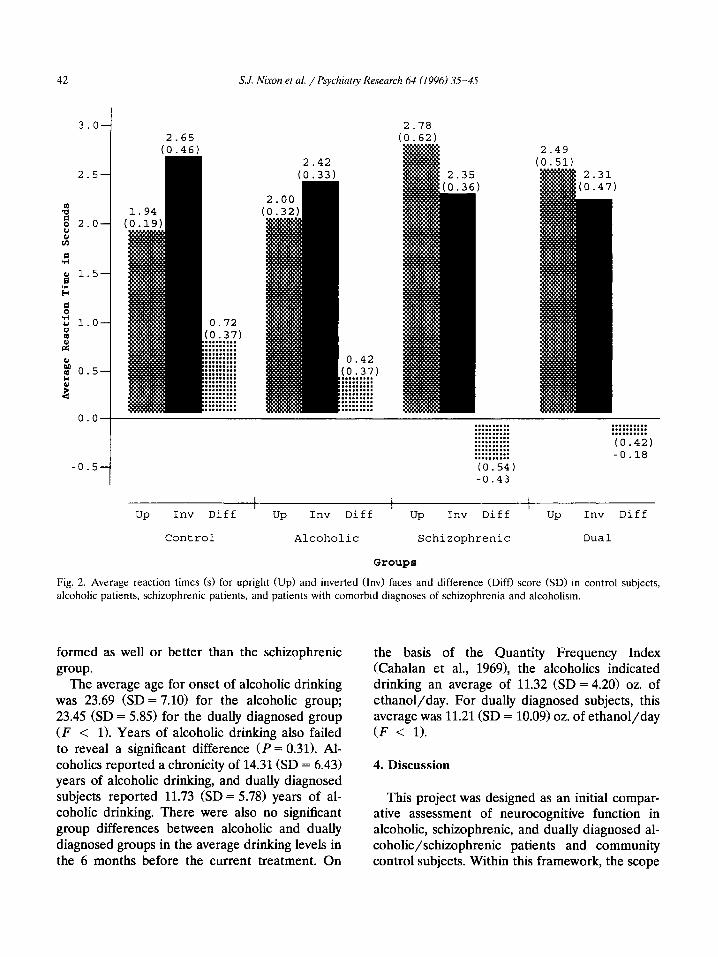
The same approach was also applied to the reaction-time data (Fig. 2). In this case, the data
1.72 0.30 0.12 0.30 1.14 0.40 0.71 0.41 0.98 0.60 0.49 0.52 1.07 0.53 0.41 0.70
were not adjusted in any way. The between and within factors were again group and stimulus ori- entation, respectively. In this analysis, the group effect approached significance (F = 2.21, df = 3,48, P = 0.10). There were significant orienta- tion (F = 4.70, df = 3,48, P = 0.04) and group X
orientation effects (F = 19.54, df = 3,48, P = 0.0001). Analysis of the group means for reaction times to correctly identified upright faces indi- cated that control and alcoholic subjects did not differ from each other. Both groups were signifi- cantly faster than the schizophrenic groups who, in turn, did not differ from each other. For in- verted faces, there were no mean differences.
Post hoc analyses were conducted to determine whether any of the observed group differences might be due to differences in characteristics of the subjects’ schizophrenia or alcohol abuse. These analyses indicated that dually diagnosed subjects reported an average chronicity for schizophrenic symptomatology of 14.25 (SD = 7.05) years; schizophrenic patients, 9.77 (SD = 9.07). The average age of onset was 19.83 (SD = 8.78) for the dually diagnosed group and 25.62 (SD = 9.61) for the schizophrenic group (both Fs < 2.45, P 2 0.13). Given the differences in these means, a closer review of the age-of-onset distributions was made. This analysis revealed that both samples were distributed normally. However, the dually diagnosed group had a 40- year-old outlier; the 75th percentile was at 23.5 years. For the schizophrenic patients, the 75th percentile was 34, with the maximum age being 39. No further analyses on age of onset were conducted, however, because dually diagnosed patients, who had the earlier age of onset, per-
42
3.0-
2.5-
4 ; 2.0-
:
a
g 1.5-
3 u l.O- s !J
0 nl 0.5- : %
o.o-
-0.5-
1
S.J. Nixon et al. /Psychiatry Research 64 (1996) 35-45
2.65 (0.46)
2.42 (0.33)
.......... .......... .......... .......... .......... ..........
..........
..........
..........
(0.54) -0.43
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (0.42) -0.18
UP Inv Diff ’ Up Inv Diff ’ Up Inv Diff ’ Up Inv Diff
Control Alcoholic Schizophrenic Dual
Groups
Fig. 2. Average reaction times (s) for upright (Up) and inverted (IIN) faces and difference (Diff) score (SD) in control subjects,
alcoholic patients, schizophrenic patients, and patients with comorbid diagnoses of schizophrenia and alcoholism.
formed as well or group.
The average age
better than the schizophrenic
for onset of alcoholic drinking was 23.69 (SD = 7.10) for the alcoholic group; 23.45 (SD = 5.85) for the dually diagnosed group (F < 1). Years of alcoholic drinking also failed to reveal a significant difference 0’ = 0.31). Al- coholics reported a chronicity of 14.31 (SD = 6.43) years of alcoholic drinking, and dually diagnosed subjects reported 11.73 (SD = 5.78) years of al- coholic drinking. There were also no significant group differences between alcoholic and dually diagnosed groups in the average drinking levels in the 6 months before the current treatment. On
the basis of the Quantity Frequency Index (Cahalan et al., 19691, the alcoholics indicated drinking an average of 11.32 (SD = 4.20) oz. of ethanol/day. For dually diagnosed subjects, this average was 11.21 (SD = 10.09) oz. of ethanol/day (F < 1).
4. Discussion
This project was designed as an initial compar- ative assessment of neurocognitive function in alcoholic, schizophrenic, and dually diagnosed al- coholic/schizophrenic patients and community control subjects. Within this framework, the scope
S.J. Nixon et al. /Psychiatry Research 64 (1996) 35-45 43
of the work was intentionally restricted: only two neuropsychological and two affective measures were used.
The study revealed several interesting results. First, consistent with our first hypothesis, control subjects were superior to other groups on the neurocognitive tests. Control subjects correctly identified more inverted faces and were signifi- cantly faster on the Trails A and B. However, the latter finding was observed only if the STAI score was not used as a covariate. This outcome may reflect the fact that affective characteristics (e.g., increased anxiety) constitute an inherent at- tribute of certain psychiatric disorders and at- tempts to control for this variance reduce the observed group effect. This conclusion is sup- ported by the mixed design analyses applied to the face-recognition task. When the data were not corrected for scores on the affective mea- sures, significant group effects were obtained for both recognition and reaction time variables.
Also, it should be noted that control subjects were not significantly better on all measures. For example, there were no significant group differ- ences in the reaction time to correctly identified inverted faces. The reason for the failure to ob- tain significant differences on the reaction time for inverted faces is not obvious, particularly given the significant effects on reaction time for upright faces.
The fact that schizophrenic subjects appeared less affected by the orientation of the faces de- serves further study. A number of studies have attempted to localize the schizophrenic cognitive deficiency. These studies have not produced con- sistent results, with right, left and frontal func- tions being separately and jointly implicated (Ditchfield and Hemsley, 1990; Gruzelier et al., 1990; Fishman et al., 1991; Schwartz et al., 1992; Braff et al., 1991). The current data speak to this issue only indirectly. If one assumes that right- hemisphere functions are differentially spared in schizophrenia, and that inverted faces are more complex visual spatial stimuli than are upright faces and therefore demand greater right-hemi- sphere involvement, the relative sparing of per- formance of inverted face performance would be predicted. Obviously, additional studies incor-
porating a variety of tasks and neuropsychological domains are needed to examine this possibility.
Our second hypothesis was not supported. Con- trary to our predictions, alcoholics were not supe- rior to the other clinical groups on most mea- sures. It is not clear if the fact that the groups did not differ in education influenced this outcome. As noted by some researchers, matching psychi- atric patients, particularly schizophrenic patients and control subjects, on educational level may dilute group differences through the so-called matching fallacy (e.g., Kremen et al., 1996). It should be reiterated, however, that subjects were not intentionally matched on education in the current study. It was coincidental that the groups were equated on this variable. Future studies, however, should include other measures of pre- morbid intellectual function such as reading and spelling scores (Kremen et al., 1996).
Our third hypothesis also was not supported. Dually diagnosed subjects were not significantly more impaired than those schizophrenic subjects without other diagnoses. Thus, the data do not suggest that the effects of alcohol abuse and schizophrenia are additive. In fact, these data are similar to work conducted by Dixon et al. (1991) who found that dually diagnosed patients were less affected than others.
Finally, the data do not reveal an interaction between clinical group and cognitive task. In large part, the three clinical groups performed quite similarly, across both tasks. However, schizophrenic subgroups were not examined. Given the literature that suggests differential neurocognitive patterns in behaviorally defined (e.g., paranoid vs. nonparanoid, negative vs. posi- tive symptoms) subgroups (Ditchfield and Hems- ley, 1990; Braff et al., 1990, such subtyping might be an important factor in future studies. In sum- mary, this preliminary project generally failed to support the proposed hypotheses. However, it provides pertinent data for directing future re- search in the area of dual diagnosis.
Acknowledgements
This project was support by a grant from the Warren Foundation (Tulsa, OK) and grants K21-
44 S.J. Nixon et al. /Psychiatry Research 64 (1996) 35-45
AA-00134 and ROl-AA-09163 from the National Institute of Alcohol Abuse and Alcoholism to Sara Jo Nixon (principal investigator). This pro- ject would not have been possible without the cooperative efforts of psychiatric facilities at Griffin Memorial Hospital (Dr. Head, Medical Director), the Laureate Psychiatric Facility (Dr. R. Tompkins, Medical Director), University Hos- pital (Dr. L. Dabiri, Medical Director), the Veter- ans Administration Medical Center (Dr. Warren, Medical Director), and Western State Hospital (S. Norwood, Superintendent).
References
American Psychiatric Association. (1987) DSM-III-R: Diagnos- tic and Statistical Manual of Mental Disorders. 3rd rev. edn.
American Psychiatric Press, Washington, DC.
Barbee, J.G., Clark, P.D., Crapanzano, M.S., Heintz, G.C. and
Kehoe, C.E. (1989) Alcohol and substance abuse among
schizophrenic patients presenting to an emergency psychi-
atric service. J Nerv Ment Dis 177, 400-407. Beck, A.T., Steer, R.A. and Garbin, M.G. (1988) Psychometric
properties of the Beck Depression Inventory: Twenty-five
years of evaluation. Clin Psycho1 Rev 8, 77-100. Braff, D.L., Heaton, R., Kuck, J., Cullum, M., Moranville, J.,
Grant, I. and Zisook, S. (1991) The generalized pattern of
neuropsychological deficits in outpatients with chronic
schizophrenia with heterogeneous Wisconsin Card Sorting
Test results. Arch Gen Psychiatry 48, 891-898. Bryant, K.J., Rounsaville, B., Spitzer, R.L. and Williams, J.B.W.
(1992) Reliability of dual diagnosis substance dependence
and psychiatric disorders. J Nerv Ment Dis 180, 251-257.
Cahalan, D., Cissin, I.H. and Crossley, H.M. (1969) American Drinking Practices: A National Study of Drinking Behavior andAttitudes. Monograph No. 6. Rutgers Center of Alcohol
Studies, New Brunswick, NJ.
Cuffel, B.J. (1992) Prevalence estimates of substance abuse in
schizophrenia and their correlates. J Nerv Ment Dis 180, 589-592.
Ditchfield, H. and Hemsley, D.R. (1990) Interhemispheric
transfer of information and schizophrenia. EurArch Psychi- atry Neural Sci 239,309-313.
Dixon, L., Haas, G., Weiden, P.J., Sweeney, J. and Frances,
A.J. (1991) Drug abuse in schizophrenic patients: Clinical
correlates and reasons for use. Am J Psychiatry 148, 224-230.
Drake, R.E., Aherman, A.I. and Rosenberg, S.R. (1993) De-
tection of substance use disorders in severely mentally ill
patients. Communily Ment Health J 29, 175-192. Drake, R.E., Osher, F.C., Noordsy, D.L., Hulbut, S.C., Teague,
G.B. and Beaudett, M.S. (1990) Diagnosis of alcohol use
disorders in schizophrenia. Schizophr Bull 16, 57-67.
Feinberg, T.E., Rifkin, A., Schaffer, C. and Walker, E. (1986)
Facial discrimination and emotional recognition in
schizophrenia and affective disorders. Arch Gen Psychiatry 43, 276-279.
Fishman, J., Schwartz, F., Bertuch, E., Lesser, B., Rescigno, D.
and Viegener, B. (1991) Laterality in schizophrenia: A
reaction time study. Eur Arch Psychiatry Clin Neurosci 241, 126-130.
Gold, J.M. and Harvey, P.D. (1993) Cognitive deficits in
schizophrenia. Schizophrenia 16, 295-311.
Greenfield, S.F., Weiss, R.D. and Tohen, M. (1995) Substance
abuse and the chronically mentally ill: A description of
dual diagnosis treatment services in a psychiatric hospital.
Community Ment Health J 31, 265-277.
Gruzelier, J., Liddiard, D., Davis, L. and Wilson, L. (1990)
Topographical EEG differences between schizophrenic
patients and controls during neuropsychological functional
activation. Int J Psychophysiology 8, 275-282.
Harvey, P.D., Walker, E. and Wielgus, M.S. (1986) Psychologi-
cal markers of vulnerability to schizophrenia. In: Maher,
B.A. (Ed.), Progress in Experimental Personality Research. Vol. 14. Academic Press, New York, p. 231.
Hesselbrock, M., Babor, T.F., Hesselbrock, V., Meyer, R.E.
and Workman, K. (1983) Never believe an alcoholic? On
the validity of self-report measures of alcohol dependence
and related constructs. Int J Addict 18, 593-609.
Kessler, R.C., McGonagle, K.A., Zhao, S., Nelson, C.B.,
Hughes, M., Eshleman, S., Wittchen, H.-U. and Kendler,
K.S. (1994) Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: Results from the
National Comorbidity Survey. Arch Gen Psychiatry 51.8-19.
Kremen, W.S., Seidman, L.J., Faraone, S.V., Pepple, J.R.,
Lyons, M.J. and Tsuang, M.T. (1996) The 3 Rs and neu-
ropsychological function in schizophrenia: An empirical
test of the matching fallacy. Nemopsychology 10, 22-31.
Kremen, W.S., Seidman, L.J., Pepple, J.R., Lyons, M.J.,
Tsuang, M.T. and Faraone, S.V. (1994) Neuropsychological
risk indicators for schizophrenia: A review of family stud-
ies. Schizophr Bull 20, 103-l 19.
Loethen, G.J. and Khavari, K.A. (1990) Comparison of the
Self-Administered Alcoholism Screening Test (SAAST) and
the Khavari Alcohol Test (KAT): Results from an alcoholic
population and their collaterals. Alcohol Clin _!?q Res 14, 756-760.
Nixon, S.J. (1995) Assessing cognitive impairment. Alcohol Health and Research World 19, 97-103.
Parsons, O.A. (1987) Neuropsychological consequences of al-
cohol abuse: Many questions - Some answers. In: Par-
sons, O.A., Butters, N. and Nathan, P.E. (Eds.), Neumpsy- chology of Alcoholism Implications for Diagnosis and Treat- ment. Guilford Press, New York, pp. 153-175.
Parsons, O.A. (1993) Impaired neuropsychological cognitive
functioning in sober alcoholics. In: Hunt, W.A. and Nixon,
S.J. (Eds.), Alcohol-Induced Bruin Damage. National Insti-
tute on Alcohol Abuse and Alcoholism, Washington, DC,
pp. 173-194.

S.J. Nixon et al. /Psychiatry Research 64 (1996) 35-45 45
Parsons, O.A., Butters, N. and Nathan, P.E. (Eds.) (1987) Neuropsychology of Alcoholism: Implications for Diagnosis and Treatment. Guilford Press, New York.
Regier, D.A., Farmer, M.E., Rae, D.S., Locke, B.Z., Kietk, S.J., Judd, L.L. and Goodwin, F.K. (1990) Comorbidity of mental disorders with alcohol and other drug abuse: Re- sults from the Epidemiologic Catchment Area (ECA) study. JAMA 264, 2.511-2518.
Rennick, P.M., Russell, M., Kempler, H. and Schwartz, M. (1972) The effect of d-amphetamine on cognitive and per- ceptual-motor functions of hyperkinetic children. Pre- sented at the Midwestern Psychological Association Con- vention, Chicago, IL.
Ries, R. (1993) Clinical treatment matching models for dually diagnosed patients. Recent Adu Addict Disord 16, 167-175.
Schaeffer, K.W. and Parsons, O.A. (1987) Learning impair- ment in alcoholics using an ecologically relevant test. J Neru Ment Dis 175, 213-218.
Schwartz, B.L., Rosse, R.B. and Deutsch, S.I. (1992) Toward a neuropsychology of memory in schizophrenia. Psychophar- macol Bull 28, 341-35 1.
Seizer, J.A. and Lieberman, J.A. (1993) Schizophrenia and substance abuse. Schizophrenia 16.401-412.
Smith, C.M. and Pristach, CA. (1990) Utility of the Self-Ad- ministered Alcoholism Screening Test (SAAST) in
schizophrenic patients. Alcohol Clin Exp Res 14, 690-694.
Spielberger, C.D. (1983) Manual for the State-Trait Anxiety Inuentory. Consulting Psychologists Press, Palo Alto, CA.
Sullivan, E.V., Mathalon, D.H., Ha, C.N., Zipursky, R.B. and Pfefferbaum, A. (1992) The contribution of constructional accuracy and organizational strategy to nonverbal recall in schizophrenia and chronic alcoholism. Biol Psychiatry 32, 312-333.
Sullivan, E.V., Mathalon, D.H., Zipursky, R.B., Kersteen- Tucker, Z., Knight, R.T. and Pfefferbaum, A. (1993) Fac- tors of the Wisconsin Card Sorting Test as measures of frontal-lobe function in schizophrenia and in chronic al- coholism. Psychiatry Res 46, 175-199.
Sweeney, J.A., Haas, G.L., Kelib, J.G. and Long, M. (1991) Evaluation of the stability of neuropsychological function- ing after acute episodes of schizophrenia: One-year fol- lowup study. Psychiatry Res 38, 63-76.
Tivis, R.D., Beatty, W.W., Nixon, S.J. and Parsons, O.A. (1995) Patterns of cognitive impairment among alcoholics: Are there subtypes? Alcohol Clin Eup Res 19,496-500.
Yin, R.K. (1969) Looking at upside down faces. J Exp Psycho/ 81, 141-145.
Yin, R.K. (1970) Face recognition by brain-injured patients: A dissociable reality? Neuropsychologia 8, 395-402.



























![[Neurocognitive insight in schizophrenia: a meta-analysis]](https://img.pdfslide.net/doc/110x75/635df1f0095e4caf2205fb8a/neurocognitive-insight-in-schizophrenia-a-meta-analysis.jpg)

