Embed Size (px)
Citation preview

ODHHYDT
apmoada
1wawc
6
TuaasameMcriapwnaeaaar
A
ASM
©P
CA
RD
IOV
AS
CU
LA
R
ptimal Method of Coronary Endarterectomy foriffusely Diseased Coronary Arteries
iroyuki Nishi, MD, Satoru Miyamoto, MD, Shuichiro Takanashi, MD,irokazu Minamimura, MD, Takumi Ishikawa, MD, Yasuyuki Kato, MD, andoshihiro Shimizu, MDepartment of Cardiovascular Surgery, Osaka City General Hospital, Osaka, and Department of Cardiovascular Surgery, Shin-
okyo Hospital, Chiba, JapanpiA7pp8
wwtsta
Background. Although several techniques for coronaryrtery bypass grafting have been introduced that incor-orate coronary endarterectomy (CE), there is little infor-ation about late patency among the various CE meth-
ds. To clarify the quality of CE, we assessed clinical andngiographic results of our experience with this proce-ure on 127 patients who had diffusely diseased coronaryrteries.Methods. Between January 1994 and December 2002,
27 patients underwent coronary artery bypass graftingith CE. Sixty-eight patients undergoing CE with long
rteriotomies and on-lay patch bypass grafting (group O)ere compared with 59 patients undergoing CE with the
onventional pull-out method (group P).Results. Thirty-day mortality was 2.9% in group O and
.8% in group P. The early angiographic results of 115
tc[osd1pceir
cicowc
P
STcvO
urgery, Osaka City General Hospital, 2–13–22, Miyakojimahondori,iyakojima-ku, Osaka, 534–0021, Japan; e-mail: [email protected].
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
atients revealed a patency rate of 92.1% (grade A: 79.4%)n group O and 88.6% (grade A: 68.6%) in group P.ctuarial survival at 5 years was 90.7% in group O and
4.0% in group P (p � 0.1). Angiograms performed on 78atients after a mean period of 21 � 16 months showed aatency rate of 89.1% (grade A:76.1%) in group O and1.0% (grade A: 38.1%) in group P (grade A: p < 0.001).
Conclusions. The midterm angiographic results of CEith long arteriotomies and on-lay patch bypass graftingere better than the results obtained with the conven-
ional pull-out method. This procedure was found to beafe and effective for complete revascularization in pa-ients with a severely and diffusely diseased coronaryrtery.
(Ann Thorac Surg 2005;79:846–53)
© 2005 by The Society of Thoracic Surgeonshe progressive application of noninvasive methods toachieve myocardial revascularization has contrib-
ted to the selection of patients with distinctly lessttractive anatomic substrates for surgery. With recentdvances in percutaneous catheter intervention such astents, the results of percutaneous catheter interventionre now improving, and some reports show the sameortality for multivessel disease with percutaneous cath-
ter intervention and coronary artery bypass grafting [1].oreover, the lesions of coronary arteries treated surgi-
ally have become more severe [2], and the populationeferred for revascularization is increasingly character-zed by advanced age and coexisting diabetes mellitusnd lipid disorders [3]. Several studies indicate thatatients with a diffusely diseased coronary artery inhom standard coronary artery bypass grafting tech-iques cannot be performed constitute 0.8% to 25.1% ofll patients with coronary artery disease [4–7]. Coronaryndarterectomy (CE) was first described by Baily andssociates, in 1957 [8], as a method of treating coronaryrtery disease without using cardiopulmonary bypassnd coronary artery bypass grafting. This procedure waseported to have high postoperative morbidity and mor-
ccepted for publication June 16, 2004.
ddress reprint requests to Dr Nishi, Department of Cardiovascular
ality during the 1960s and 1970s [9, 10]; as a result, CEame under scrutiny and its feasibility was controversial6]. However, with the recent trend of treating more casesf diffuse coronary artery disease, increasingly indicatedurgical therapy for severe and diffuse coronary arteryisease has resulted in a revival of interest in CE [3,1–19]. In an effort to expand surgical options for theseatients, several techniques have been introduced, in-luding CE and different methods for reconstructingndarterectomized vessels [11, 13, 15, 18]. However, theres little information available about the angiographicesults of endarterectomized vessels [14, 15, 18].
In 1994, we introduced this method as an adjunct tooronary artery bypass grafting and have been develop-ng and evaluating it angiographically for 10 years. Tolarify the optimal method of CE, we reviewed the resultsf recatheterization in our experience with 127 patientsho had diffusely diseased coronary artery necessitating
oronary artery bypass grafting with CE.
atients and Methods
tudy Populationhis study includes 127 patients with diffusely diseasedoronary artery requiring operation for myocardial re-ascularization between January 1994 and April 2003 at
saka City General Hospital. The mean age of the0003-4975/05/$30.00doi:10.1016/j.athoracsur.2004.06.070

pwaamCb(5ma
itprt
AAcopaFegwoampt
SCcMacpldmbVmtrwat
satbram
mw
nanflafetfiasom
Ltrit
DLtaf�vBawmlsa
R
PBdrfibcgcdpmgp
OTd
847Ann Thorac Surg NISHI ET AL2005;79:846–53 OPTIMAL METHOD OF CORONARY ENDARTERECTOMY
CA
RD
IOV
AS
CU
LA
R
atients was 63.8 � 8.8 years, and 34 patients (27%) wereomen. Two patients (2%) had single-vessel coronary
rtery disease, 20 patients (16%) had two-vessel disease,nd 105 patients (83%) had three-vessel disease. Theean number of distal anastomoses was 4.2 � 1.2.oronary endarterectomy was performed in 148ranches, including 71 left anterior descending arteries
LAD), 7 diagonal arteries, 17 left circumflex arteries, and3 right coronary arteries. The institutional ethics com-ittee approved this technique, and the patients signed
n informed consent before surgery.The 127 patients were divided into two groups accord-
ng to the operative method for coronary endarterec-omy. Group P, who underwent CE by the conventionalull-out method, included 59 patients. Group O, whichequired long arteriotomy and on-lay patch grafting ofhe endarterectomized vessels, numbered 69 patients.
ngiographic Protocolll surviving patients were requested for postoperative
atheterization at 1 month, 1 year, and 5 years after theperation. Postangiographic control was obtained if theatients agreed to the procedure. The quality of thenastomosis was graded according to the classification ofitzgibbon and colleagues [20]. Briefly, grade A stands forxcellent graft patency, grade B for graft stenosis ofreater than 50%, and grade O for occlusion. String sign,hich was defined as a severe and extensive narrowingf the whole body of the graft, was classified as grade Bnastomosis. The criterion for diagnosing perioperativeyocardial infarction is defined as the maximum level of
ostoperative creatine kinase myocardial band greaterhan 100 IU/L.
urgical Technique for Coronary Endarterectomyoronary artery bypass grafting was performed during
ardiopulmonary bypass with normothermia (35°C).yocardial protection was achieved by induction of
ntegrade and retrograde intermittent cold crystalloidardioplegic solution. Coronary endarterectomy was ap-lied in patients having a primary proximal significant
esion of the major coronary artery but with a diffuselyiseased or calcified coronary artery, often with involve-ent of the distal portion, which was considered not to
e amenable to other more conventional bypass grafting.essels undergoing CE were arteries supplying viableyocardium and had many segmental narrowings, so
hat anastomosing one segment would not adequatelyevascularize the territory of that vessel. Most of the CEas scheduled before operation, but the final decision of
pplying which technique was made during the opera-ion according to the surgeon’s preference.
The pull-out method (group P) was simple, as de-cribed previously [21]. A short arteriotomy was made,nd the closed traction method was applied in a mannerhat included the proximal and distal branches. Then,ypass grafting was performed to the arteriotomy. Foremoving as much plaque as possible, two or threerteriotomies were sometimes made distally to pull out
ore atheromatous core. Bypass grafting was anasto- gosed to the most proximal arteriotomy, and the othersere closed with a patch.In group O, the long arteriotomy was extended until
ondiseased arterial lumen was reached. The coronaryrtery at the level of the first major proximal lesion waseither opened nor reconstructed to avoid competitiveow between the bypass graft and the native coronaryrtery. Coronary endarterectomy was routinely per-ormed through an extended arteriotomy, permittingxtraction of material from the origins of septal perfora-ors and diagonal branches under direct vision. Afterxing the distal coronary artery intima, on-lay patchnastomosis using the internal thoracic artery (ITA) oraphenous vein graft was constructed over the arteriot-my, with a running suture so that the graft wall made upost of the reconstructed vessel.Patients received anticoagulation postoperatively.
ow-molecular-weight heparin was initiated 6 hours af-er arrival in the intensive care unit. After 2 days, this waseplaced by warfarin sodium and aspirin and continuedndefinitely, maintaining an international normalized ra-io of 2.0.
ata Analysis and Follow-Upate follow-up information was obtained by postal ques-
ionnaire or telephone interview between April 1, 2003,nd June 1, 2003. Three patients were lost to follow-up,or a follow-up rate of 97.6%; mean follow-up time was 52
31 months (range, 5 to 109 months). All continuousariables are presented as mean � standard deviation.asic methods of univariate analysis included the �2 testnd Student’s t test. Actuarial estimates of morbid eventsere calculated by the Kaplan-Meier survival analysisethod and compared with log-rank tests. Values of p
ess than 0.05 were considered significant. StatView ver-ion 5.0 (SAS Institute, Cary, NC) was used for statisticalnalysis.
esults
atient Demographicsetween group O and group P there were no significantifferences in terms of patient characteristics, coronaryisk factors, preoperative comorbidities, or cardiac pro-les (Table 1). In group P, CE was performed in 76ranches, including 24 LAD, 5 diagonal arteries, 10 leftircumflex arteries, and 37 right coronary arteries. Inroup O, the sites of the CEs were LAD in 47, leftircumflex arteries in 7, right coronary arteries in 16, andiagonal arteries in 2 cases. The mean length of on-layatch bypass grafting was 4.9 � 2.1 cm. The pull-outethod tended to be most frequently performed for
rafting to the right coronary arteries. To the LAD, on-layatch grafting was the more frequent method of CE.
perative Resultshere were no intraoperative deaths. The mean number ofistal anastomoses in group O was smaller than that in
roup P (Table 2). The ITA was most often used to recon-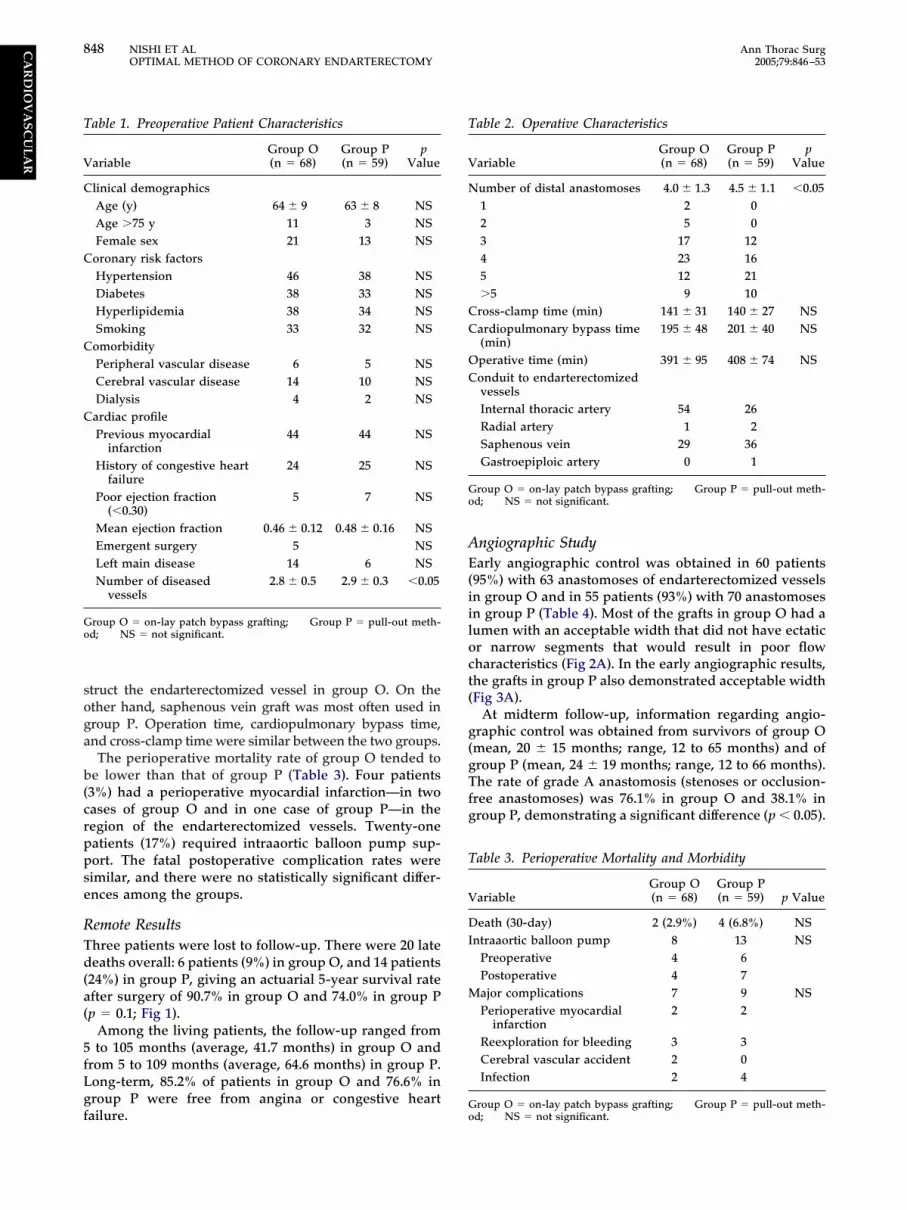
soga
b(crppse
RTd(a(
5fLgf
AE(iiloct(
g(gTfg
T
V
N
CC
OC
Go
T
V
DI
M
T
V
C
C
C
C
Go
848 NISHI ET AL Ann Thorac SurgOPTIMAL METHOD OF CORONARY ENDARTERECTOMY 2005;79:846–53
CA
RD
IOV
AS
CU
LA
R
truct the endarterectomized vessel in group O. On thether hand, saphenous vein graft was most often used inroup P. Operation time, cardiopulmonary bypass time,nd cross-clamp time were similar between the two groups.
The perioperative mortality rate of group O tended toe lower than that of group P (Table 3). Four patients
3%) had a perioperative myocardial infarction—in twoases of group O and in one case of group P—in theegion of the endarterectomized vessels. Twenty-oneatients (17%) required intraaortic balloon pump sup-ort. The fatal postoperative complication rates wereimilar, and there were no statistically significant differ-nces among the groups.
emote Resultshree patients were lost to follow-up. There were 20 lateeaths overall: 6 patients (9%) in group O, and 14 patients
24%) in group P, giving an actuarial 5-year survival ratefter surgery of 90.7% in group O and 74.0% in group Pp � 0.1; Fig 1).
Among the living patients, the follow-up ranged fromto 105 months (average, 41.7 months) in group O and
rom 5 to 109 months (average, 64.6 months) in group P.ong-term, 85.2% of patients in group O and 76.6% inroup P were free from angina or congestive heart
able 1. Preoperative Patient Characteristics
ariableGroup O(n � 68)
Group P(n � 59)
pValue
linical demographicsAge (y) 64 � 9 63 � 8 NSAge �75 y 11 3 NSFemale sex 21 13 NS
oronary risk factorsHypertension 46 38 NSDiabetes 38 33 NSHyperlipidemia 38 34 NSSmoking 33 32 NS
omorbidityPeripheral vascular disease 6 5 NSCerebral vascular disease 14 10 NSDialysis 4 2 NS
ardiac profilePrevious myocardial
infarction44 44 NS
History of congestive heartfailure
24 25 NS
Poor ejection fraction(�0.30)
5 7 NS
Mean ejection fraction 0.46 � 0.12 0.48 � 0.16 NSEmergent surgery 5 NSLeft main disease 14 6 NSNumber of diseased
vessels2.8 � 0.5 2.9 � 0.3 �0.05
roup O � on-lay patch bypass grafting; Group P � pull-out meth-d; NS � not significant.
ailure.Go
ngiographic Studyarly angiographic control was obtained in 60 patients
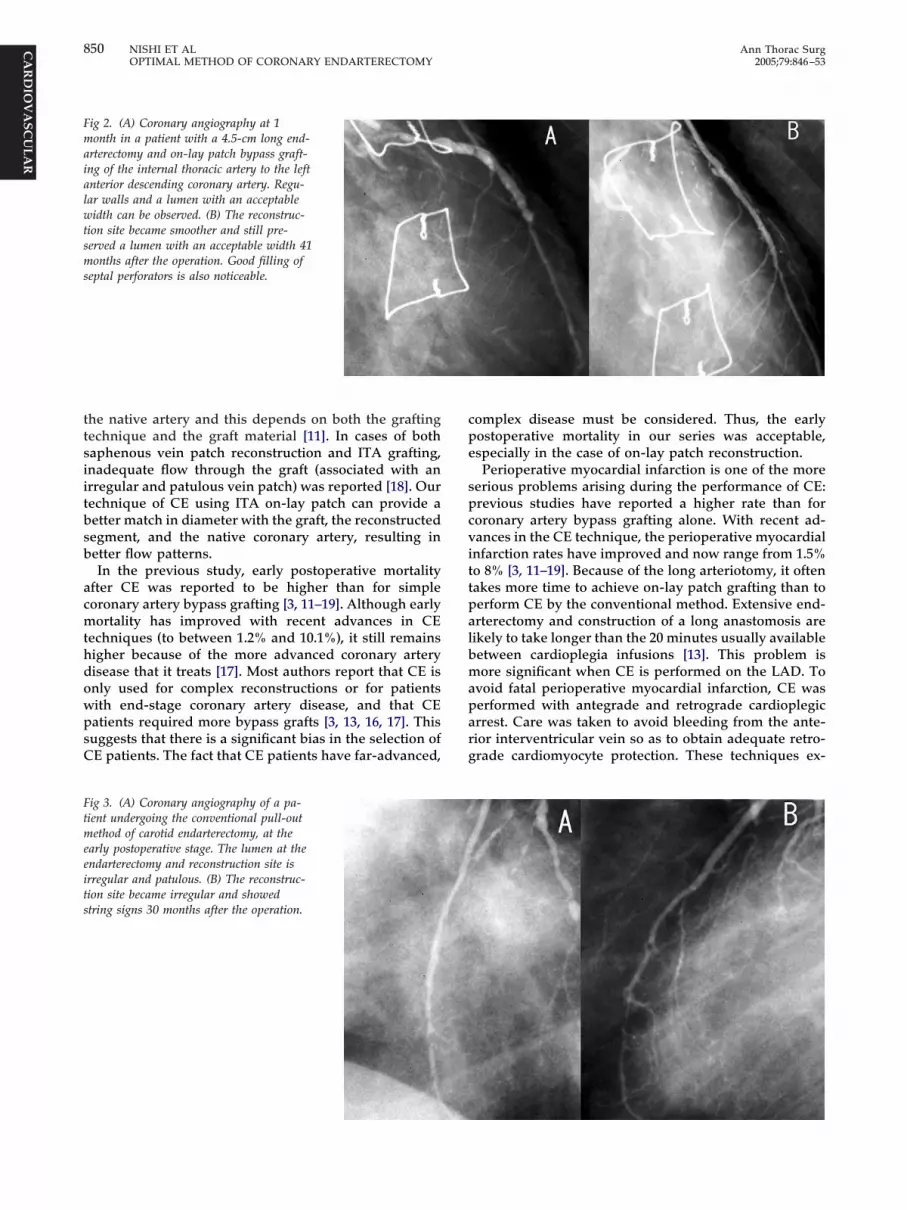
95%) with 63 anastomoses of endarterectomized vesselsn group O and in 55 patients (93%) with 70 anastomosesn group P (Table 4). Most of the grafts in group O had aumen with an acceptable width that did not have ectaticr narrow segments that would result in poor flowharacteristics (Fig 2A). In the early angiographic results,he grafts in group P also demonstrated acceptable widthFig 3A).
At midterm follow-up, information regarding angio-raphic control was obtained from survivors of group Omean, 20 � 15 months; range, 12 to 65 months) and ofroup P (mean, 24 � 19 months; range, 12 to 66 months).he rate of grade A anastomosis (stenoses or occlusion-
ree anastomoses) was 76.1% in group O and 38.1% inroup P, demonstrating a significant difference (p � 0.05).
able 2. Operative Characteristics
ariableGroup O(n � 68)
Group P(n � 59)
pValue
umber of distal anastomoses 4.0 � 1.3 4.5 � 1.1 �0.051 2 02 5 03 17 124 23 165 12 21�5 9 10
ross-clamp time (min) 141 � 31 140 � 27 NSardiopulmonary bypass time(min)
195 � 48 201 � 40 NS
perative time (min) 391 � 95 408 � 74 NSonduit to endarterectomizedvesselsInternal thoracic artery 54 26Radial artery 1 2Saphenous vein 29 36Gastroepiploic artery 0 1
roup O � on-lay patch bypass grafting; Group P � pull-out meth-d; NS � not significant.
able 3. Perioperative Mortality and Morbidity
ariableGroup O(n � 68)
Group P(n � 59) p Value
eath (30-day) 2 (2.9%) 4 (6.8%) NSntraaortic balloon pump 8 13 NS
Preoperative 4 6Postoperative 4 7ajor complications 7 9 NSPerioperative myocardial
infarction2 2
Reexploration for bleeding 3 3Cerebral vascular accident 2 0Infection 2 4
roup O � on-lay patch bypass grafting; Group P � pull-out meth-d; NS � not significant.

Wgestwa2vy
bat8tP
C
Tolurpecbait8snbatpttimsteTatbawttos
Fwg
T
V
E
I
S
M
I
S
G
849Ann Thorac Surg NISHI ET AL2005;79:846–53 OPTIMAL METHOD OF CORONARY ENDARTERECTOMY
CA
RD
IOV
AS
CU
LA
R
hereas the midterm rate of grade A anastomosis inroup O was not different from that of the early postop-rative stage, the rate of grade A anastomosis in group Pignificantly dropped from the early period to the mid-erm. Most patients in group P had patent CE segmentsith a thin or absent lumen of the distal coronary artery,
nd the grafts were still patent despite poor runoff (FigB). On the other hand, most of the endarterectomizedessels in group O had excellent patency even severalears after the operation (Fig 3B).In 21 patients of the conventional group (group P),
ypass grafting was anastomosed to the most proximalrteriotomy, and the rest were closed with a patch. Earlyerm and midterm graft patency rate in that group were6.3% and 69.2%, respectively. On the other hand, earlyerm and midterm graft patency rate in the rest of group
were 92.3% and 83.3%, respectively.
ig 1. Actuarial estimates of survival after coronary endarterectomyith two different techniques. Group O � on-lay patch bypass
rafting; Group P � pull-out method. (Pts. � patients.)
able 4. Postoperative Angiographic Results
ariableGroup O(n � 68)
arly patency rate 92.1% (58/63)Grade A 50 (79.4%)Grade B 8
nternal thoracic artery 90.1% (38/42)Grade B 6
aphenous vein 95.0% (19/20)Grade B 2idterm patency rate 89.1% (41/46)Grade A 35 (89.1%)Grade B 6
nternal thoracic artery 93.5% (29/31)Grade B 4
aphenous vein 76.9% (10/13)Grade B 1
roup O � on-lay patch bypass grafting; Group P � pull-out method;
omment
he results of this study indicate that CE can be carriedut with an acceptable operative risk, especially when
ong arteriotomies and on-lay patch bypass grafting issed as a CE method. There are several reasons for betteresults with the on-lay patch method. First, CE can beerformed under direct vision with a long arteriotomy,xposing the whole arterial lumen and side branchesontaining atherosclerotic occlusive material, so that itecomes possible to avoid residual material in the lumens well as in the dissections. Second, on-lay patch graft-ng of the ITA consists of new coronary lumen. We madehe on-lay patch technique so that the ITA wall makes up0% of the reconstructed vessel, and the newly recon-tructed coronary artery retains 20% of the native coro-ary artery. Coronary artery reconstruction is performedy covering the arteriotomy with an ITA in such a fashions to exclude atheromatous plaques from the lumen ofhe coronary arteries. As previously reported, once CE iserformed, the resulting lack of endothelium exposes to
he flowing blood all the subendothelial material that canrigger the coagulation cascade [11, 13, 22]. Although anncomplete endothelial covering of the endarterecto-
ized arterial wall enhances myocyte proliferation, it istopped when the endothelial covering is complete. Ourechnique of on-lay patch grafting reduced the endarter-ctomized area and presented new coronary artery wall.his might achieve rapid complete endothelial coveringnd should decrease the risk of intimal proliferation. Thehird reason is the function of the ITA. This providesetter vasomotor function, particularly the capacity todjust the flow rate in proportion to the distal runoff, aidely known paracrine function of living endothelium
hat produces and releases prostacyclin and other endo-helium-dependent relaxation factors [23]. The diameterf the coronary artery is also important. The recon-tructed segment in endarterectomy is often wider than
Group P(n � 59) p Value
88.6% (62/70) NS48 (68.6%) NS
1477.0% (23/26) NS
887.5% (35/40) NS
381.0% (34/42) NS16 (38.1%) �0.05
1873.7% (14/19) NS
1085.0% (17/20) NS
6
NS � not significant.
ttsiitbsb
acmthdowpsC
cpe
spcvittpalbmaparg
Fmaialwtsms
Ftmeeits
850 NISHI ET AL Ann Thorac SurgOPTIMAL METHOD OF CORONARY ENDARTERECTOMY 2005;79:846–53
CA
RD
IOV
AS
CU
LA
R
he native artery and this depends on both the graftingechnique and the graft material [11]. In cases of bothaphenous vein patch reconstruction and ITA grafting,nadequate flow through the graft (associated with anrregular and patulous vein patch) was reported [18]. Ourechnique of CE using ITA on-lay patch can provide aetter match in diameter with the graft, the reconstructedegment, and the native coronary artery, resulting inetter flow patterns.In the previous study, early postoperative mortality
fter CE was reported to be higher than for simpleoronary artery bypass grafting [3, 11–19]. Although earlyortality has improved with recent advances in CE
echniques (to between 1.2% and 10.1%), it still remainsigher because of the more advanced coronary arteryisease that it treats [17]. Most authors report that CE isnly used for complex reconstructions or for patientsith end-stage coronary artery disease, and that CEatients required more bypass grafts [3, 13, 16, 17]. Thisuggests that there is a significant bias in the selection ofE patients. The fact that CE patients have far-advanced,
ig 2. (A) Coronary angiography at 1onth in a patient with a 4.5-cm long end-
rterectomy and on-lay patch bypass graft-ng of the internal thoracic artery to the leftnterior descending coronary artery. Regu-ar walls and a lumen with an acceptableidth can be observed. (B) The reconstruc-
ion site became smoother and still pre-erved a lumen with an acceptable width 41onths after the operation. Good filling of
eptal perforators is also noticeable.
ig 3. (A) Coronary angiography of a pa-ient undergoing the conventional pull-outethod of carotid endarterectomy, at the
arly postoperative stage. The lumen at thendarterectomy and reconstruction site isrregular and patulous. (B) The reconstruc-ion site became irregular and showedtring signs 30 months after the operation.
omplex disease must be considered. Thus, the earlyostoperative mortality in our series was acceptable,specially in the case of on-lay patch reconstruction.Perioperative myocardial infarction is one of the more
erious problems arising during the performance of CE:revious studies have reported a higher rate than fororonary artery bypass grafting alone. With recent ad-ances in the CE technique, the perioperative myocardialnfarction rates have improved and now range from 1.5%o 8% [3, 11–19]. Because of the long arteriotomy, it oftenakes more time to achieve on-lay patch grafting than toerform CE by the conventional method. Extensive end-rterectomy and construction of a long anastomosis areikely to take longer than the 20 minutes usually availableetween cardioplegia infusions [13]. This problem isore significant when CE is performed on the LAD. To
void fatal perioperative myocardial infarction, CE waserformed with antegrade and retrograde cardioplegicrrest. Care was taken to avoid bleeding from the ante-ior interventricular vein so as to obtain adequate retro-rade cardiomyocyte protection. These techniques ex-

tcAig
wfnccs
lBiotbst9wrwSoe
icl[gaclpd
omcAfasoasstsihpitc4bgtabtaeg
tawlcwwmCptroe
R
FspwaOert
851Ann Thorac Surg NISHI ET AL2005;79:846–53 OPTIMAL METHOD OF CORONARY ENDARTERECTOMY
CA
RD
IOV
AS
CU
LA
R
ended the limits of safe arrest and the optimalonditions for endarterectomy and multivessel grafting.s a result, a favorable rate of perioperative myocardial
nfarction could be achieved in the case of on-lay patchrafting.Our late results (5-year actuarial survival) for patientsith on-lay patch reconstruction was better than those
or patients who underwent the conventional CE tech-ique. This feature was probably a reflection of theomplete removal of all atherosclerotic material and theomplete revascularization of the endarterectomized ves-els in group O patients.
The size of our angiographic study in CE patients wasarger than in previous studies [11, 12, 15, 17, 18, 24, 25].ecause most of the patency quoted in the literature
nvolved selective restudy of certain subgroups of theriginal cohort, the only way to obtain a true picture ofhe natural history of endarterectomized grafts was to useoth early and late coronary angiography to study, pro-pectively, a consecutive group of patients. In the litera-ure, the patency rate of CE at 1 year is between 56% and8% [4–6, 26]. This is dependent on CE technique and onhether or not threadlike arteries are considered to
epresent graft failure. About 10% of our patent casesere ranked as grade B in the early postoperative stage.ome of these included stenosis of the graft with patencyf the native coronary artery in which the proximally
ig 4. Evaluation of the status of the intima by intravascular ultra-ound sonography at the early and late postoperative stages. In theull-out method, although the diameters of endarterectomized vesselsere wide in the early postoperative stage (A), they became narrows a result of intimal hyperplasia in the late postoperative stage (B).n the other hand, intimal hyperplasia rarely occurred in group P,
ven in the late postoperative stage. The intima of the internal tho-acic artery became circumferential, and intima was reconstructed inhe endarterectomized vessels: (C) early, (D) late.
xtended CE had removed all the stenoses. Of course,
ncomplete removal of atheromatous plaque might alsoause this phenomenon. There is little information onate graft patency, with rates ranging from 40% to 81.5%11, 17, 19, 24]. Our late patency rate in the on-lay patchroup was better than those previously reported and wascceptable when compared with the patency rate oflassic ITA bypass grafts on nondiffuse coronary arteryesions [27]. Coronary endarterectomy with the on-layatch method does not increase the rate of graft failureespite the presence of diffuse coronary lesions.In our angiographic study, long arteriotomy and ITA
n-lay patch grafting is considered to be the preferredethod after CE is performed for diffusely diseased
oronary artery. Although the number of midterm gradeanastomoses in the on-lay patch group did not differ
rom the early postoperative stage, the rate of grade Anastomoses in the conventional CE method droppedignificantly. These changes may be owing to the devel-pment of myofibrointimal proliferation and localizedtheroma in the conventional CE method group. In thetudy on the status of the intima by intravascular ultra-ound sonography, although the diameter of endarterec-omized vessels was wide in the early postoperativetage, it became narrow as a result of intimal hyperplasian the late postoperative stage (Figs 4A, 4B). On the otherand, intimal hyperplasia rarely occurred in the on-layatch group, even in the late postoperative stage. In the
ntravascular ultrasound sonography study, the intima ofhe ITA became circumferential, and new intima wasonstructed in the endarterectomized vessels (Figs 4C,D). This coronary reconstruction may be the reasonehind the good results in this group. The conventionalroup included fewer patients receiving endarterectomyo the LAD. However, we do not consider that thisccounts for the inferior results in the conventional groupecause there were no obvious differences of graft pa-
ency of ITA or saphenous vein graft between group Ond group P. Moreover, there were no obvious differ-nces of graft patency between ITA and saphenous veinraft in the two groups.The indication of CE is also important. We consider
hat elective CE should be reserved only for arteries thatre truly inoperable by other means and for instances inhich the involved vessel supplies a coronary bed of at
east moderate size, so that failure to graft the vessel at allould be expected to result in residual angina. Vesselsith extensive noncalcific atheroma and a small lumen,ith a severely diseased distal right coronary artery withultiple small branches, might also be indications forE. A prospective randomized trial will be needed torove the superiority of the on-lay patch method; this is
he limitation of the present study. Because we nowoutinely perform CE with the on-lay patch techniquewing to the superiority of this method, the fate ofndarterectomized grafts should be followed carefully.
eferences
1. Williams DO, Holubkov R, Yeh W, et al. Percutaneouscoronary intervention in the current era compared with

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
I
SntaenwNcpatr
oomt
852 NISHI ET AL Ann Thorac SurgOPTIMAL METHOD OF CORONARY ENDARTERECTOMY 2005;79:846–53
©P
CA
RD
IOV
AS
CU
LA
R
1985–1986: the National Heart, Lung, and Blood InstituteRegistries. Circulation 2000;102:2945–51.
2. Rodriguez A, Rodriguez Alemparte M, Baldi J, et al. Coronarystenting versus coronary bypass surgery in patients with mul-tiple vessel disease and significant proximal LAD stenosis:results from the ERACI II study. Heart 2003;89:184–8.
3. Sundt TM III, Camillo CJ, Mendeloff EN, Barmer HB, GayWA Jr. Reappraisal of coronary endarterectomy for thetreatment of diffuse coronary artery disease. Ann ThoracSurg 1999;68:1272–7.
4. Brenowitz JB, Kayser KL, Johnson WD. Results of coronaryartery endarterectomy and reconstruction. J Thorac Cardio-vasc Surg 1988;95:1–10.
5. Shapira N, Lumia FJ, Gottdiener JS, Germon P, Lemole GM.Adjunct endarterectomy of the left anterior descendingcoronary artery. Ann Thorac Surg 1988;46:289–96.
6. Ladowski JS, Schatzlein MH, Underhill DJ, Peterson AC.Endarterectomy, vein patch, and mammary bypass of theanterior descending artery. Ann Thorac Surg 1991;52:1187–9.
7. CASS Principal Investigators and Their Associates. Coro-nary Artery Surgery Study (CASS): a randomized trial ofcoronary artery bypass surgery. Survival data. Circulation1983;68:939–50.
8. Baily CP, May A, Lemmon WM. Survival after coronaryendarterectomy in man. JAMA 1957;164:641–6.
9. Parsonet V, Gilbert L, Gielchinsky I, et al. Endarterectomy ofthe left anterior descending and maintain coronary arteries:a technique for reconstruction of inoperable arteries. Sur-gery 1976;80:662–73.
0. Effler DB, Groves LK, Sone FM Jr, Shirey EK. Endarterec-tomy in the treatment of coronary artery disease. J ThoracCardiovasc Surg 1964;47:98–108.
1. Tasdemir O, Kiziltepe U, Karagoz HY, Yamak B, Korkmaz S,Bayazit K. Long-term results of reconstructions of the leftanterior descending coronary artery in diffuse atheroscle-rotic lesions. J Thorac Cardiovasc Surg 1996;112:745–54.
2. Gill IS, Beanlands DS, Boyd WD, Finlay S, Keon WJ. Leftanterior descending endarterectomy and internal thoracicartery bypass for diffuse coronary disease. Ann Thorac Surg1998;65:659–62.
3. Abrahamov D, Tamaris M, Guru V, et al. Clinical results ofendarterectomy of the right and left anterior descendingcoronary arteries. J Card Surg 1999;14:16–25.
4. Asimakopoulos G, Taylor KM, Ratnatunga CP. Outcome ofcoronary endarterectomy: a case-control study. Ann Thorac
Surg 1999;67:989–93.hat found early. In contrast, the rate of grade A anasto-
msro
tdetplmt
poha
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
5. Barra JA, Bezon E, Mondine P, Resk A, Gilard M, Boshat J.Coronary artery reconstruction for extensive coronary dis-ease: 108 patients and two year follow-up. Ann Thorac Surg2000;70:1541–5.
6. Shapira OM, Akopian G, Hussain A, et al. Improved clinicaloutcomes in patients undergoing coronary artery bypassgrafting with coronary endarterectomy. Ann Thorac Surg1999;68:2273–8.
7. Ferraris VA, Harrah JD, Moritz DM, Stritz M, Stritz D,Ferraris SP. Long-term angiographic results of coronaryendarterectomy. Ann Thorac Surg 2000;69:1737–43.
8. Santini F, Casali G, Lusini M, et al. Mid-term results afterextensive vein patch reconstruction and internal mammarygrafting of the diffusely diseased left anterior descendingcoronary artery. Eur J Cardiothorac Surg 2002;21:1020–5.
9. Marinelli G, Chiappini B, Eusanio MD, et al. Bypass graftingwith coronary endarterectomy: immediate and long-termresults. J Thorac Cardiovasc Surg 2002;124:553–60.
0. Fitzgibbon GM, Kafka HP, Leach AJ, Keon WJ, Hooper D,Burton JR. Coronary bypass graft fate and patient outcome:angiographic follow-up of 5,065 grafts related to survival andre-operation in 1,388 patients during 25 years. J Am CollCardiol 1996;28:616–26.
1. Mills NL. Coronary endarterectomy: surgical techniques forpatients with extensive distal atherosclerotic coronary dis-ease. Adv Card Surg 1998;10:197–227.
2. Walley VM, Byard RW, Keon WJ. A study of the sequentialmorphologic changes after manual coronary endarterec-tomy. J Thorac Cardiovasc Surg 1991;102:890–4.
3. Lüscher TF, Diederich D, Siebenmann R, et al. Differencebetween endothelium dependent relaxations in arterial andvenous coronary bypass grafts. N Engl J Med 1988;319:462–7.
4. Djalilian AR, Shumway SJ. Adjunctive coronary endarter-ectomy: improved safety in modern cardiac surgery. AnnThorac Surg 1995;60:1749 –54.
5. Goldstein J, Cooper E, Saltups A, Boxall J. Angiographicassessment of graft patency after coronary endarterectomy.J Thorac Cardiovasc Surg 1991;102:539–45.
6. Beretta L, Lemma M, Vanelli D, et al. Coronary “open”endarterectomy and reconstruction: short- and long-termresults of revascularization with saphenous vein versusIMA-graft. Eur J Cardiothorac Surg 1992;6:382–7.
7. Zeff RH, Kongtahworn C, Iannone LA, et al. Internal mam-mary artery versus saphenous vein graft to the left anteriordescending coronary artery: prospective randomized study
with 10-year follow-up. Ann Thorac Surg 1988;45:533–6.NVITED COMMENTARY
everal studies indicate that patients with diffuse coro-ary artery disease in whom standard coronary bypass
echniques cannot be performed constitute up to 25% ofll patients with coronary artery disease. In the modernra of invasive interventional cardiology, the referralumber of patients with diffuse coronary artery diseaseill continue to increase. Therefore, the present study byishi and colleagues offers some major contributions to
oronary surgery, by providing valuable early and lateostoperative angiograms of patients with coronary end-rterectomy. The authors should be congratulated forheir high rate of postoperative angiographies whicheached more than 80%.
The most important finding of this study is that withpen endarterectomy and on-lay patch grafting, the ratef grade A anastomosis (free of stenosis or occlusion) atid-term angiographic studies was not different from
osis in conventional pull out endarterectomy groupignificantly dropped from early to mid-term. This is aemarkable finding and should be kept in mind whileperating with diffusely diseased coronary arteries.While describing the conventional pull out method,
he authors mention application of closed traction foristal and proximal branches. According to our experi-nce, proximal dissection plane should end at the end ofhe arteriotomy and plaque should be transected at thisoint. Blind proximal endarterectomy, particularly on the
eft anterior descending artery, may disrupt flow intoajor proximal branches, including the circumflex ar-
ery, a ramus artery or septal arteries.One other technical issue, although not advocated but
erformed by the authors needs some discussion. Somef the conventional endarterectomy patients in this studyad more than one arteriotomy. Bypass grafts were
nastomosed to the most proximal arteriotomy and the0003-4975/05/$30.00doi:10.1016/j.athoracsur.2004.07.056





























