Embed Size (px)
Citation preview
PerinatologyISSN: 0972-2408
J o u r n a l o f P e r i n a t a l a n d N e o n a t a l C a r e
Vol. 13 • No. 2Jul–Sep 2012
Indexed in EMBASE and CINAHL

Indexed in EMBASE and CINAHL
Dr Kamini A Rao, Bangalore
Dr Prathima Radhakrishnan, Bangalore
Dr Meenakshi Bhat, Bangalore
Dr DK Guha, Delhi
Dr Uma Ram, Chennai
Dr Hisham Mirghani, UAE
Dr RS Prasad, UK
Dr Ravi GP Krishnan, USA
Dr David Ellwood, Australia
Dr Arvind Shenoi, Bangalore
Dr Sulochana Gunasheela, Bangalore
Dr MKC Nair, Trivandrum
Dr Purnima Satoskar, Mumbai
Dr Rajam S Ramamurthy, USA
Dr Koravangattu Sankaran, Canada
Dr Bhavani Sriram, Singapore
Editor in chief
Dr Ranjan Kumar PejaverBangalore
Editorial Board
National Advisory Committee
International Advisory Committee
Managing Editor
Dr Jayashree B KeshavBangalore
Vol. 13 • No. 2Jul–Sep 2012
Indexed in EMBASE and CINAHL
PerinatologyJ o u r n a l o f P e r i n a t a l a n d N e o n a t a l C a r e
General Information
The Journal
Perinatology (ISSN 0972-2408), one of the few journals dedicated to the emerging multidisciplinary field of perinatal medicine, is published and distributed quarterly (in the months of January, April, July, and October every year) at The Himalaya Drug Company. The journal publishes original research articles, review articles, brief reports on clinical and laboratory observations, case reports, and clinical studies. The journal is indexed in EMBASE, the Excerpta Medica database, CINAHL® database, and Cumulative Index to Nursing and Allied Health Literature® print index.
Information for Authors
There are no page charges for Perinatology submissions. Please see the last section of the journal for guidelines to be followed while preparing and submitting a manuscript.
Subscription Information
Perinatology allows its readers to recommend this journal to two of their friends/colleagues using the invitation/free subscription form provided in every issue. The readers can send the invitation/free subscription form attached in the journal to the editor with complete postal addresses of two of their friends/colleagues.
Subsequent issues of the journal will be sent to the invitees on a regular basis, without any subscription charges.
Copies of the journal are sent directly from the publisher’s address. It is illegal to acquire copies from any other source. If a copy is received for personal use, one cannot resale or give away the copy for commercial or library use. The copies of the journal are sent by ordinary post/courier. If a copy returns due to incomplete, incorrect, or changed
address of a subscriber on two consecutive occasions, names of such members will be deleted from the mailing list of the journal. Providing complete, correct, and up-to-date address is the responsibility of the subscriber. Information regarding change of address should be communicated to the publisher at [email protected].
Copyright
The entire contents of Perinatology are protected under Indian and international copyrights. The journal, however, grants its subscribers the right of access and a license to copy, use, distribute, perform, and display the information/article publicly and to make and distribute derivative works in any digital medium for any reasonable noncommercial purpose. For commercial use, one has to obtain permission from the publisher. In either case, the authorship and ownership of the information/article should be attributed properly. For permission to reproduce articles/information published in this journal, please write to [email protected].
Address for Correspondence
The Managing Editor – Perinatology Scientific Publications Division The Himalaya Drug Company Makali, Bangalore – 562 123
Email: [email protected]
Published at
The Himalaya Drug Company Makali, Bangalore – 562 123
Printed at
M/s Sri Sudhindra Offset Process #97, DT Street, 8th Cross, Malleswaram, Bangalore – 560 003
Vol. 13 • No. 2 • Jul–Sep 2012PerinatologyJ o u r n a l o f P e r i n a t a l a n d N e o n a t a l C a r e
ContentsVol. 13 • No. 2 • Jul–Sep 2012Perinatology
J o u r n a l o f P e r i n a t a l a n d N e o n a t a l C a r e
Research Articles
Glutathione as an Indicator of Oxidative Stress in Neonates Bilakhia K, D’ Souza J, Kudalkar K, Dasgupta D, Mohite M, Jalan A 41
Low-cost Hand Hygiene Regimen Nair IS, Shenoi A 46
Review Articles
Counseling in Perinatal Practice Nayak S 54
Perinatal Congenital Cytomegalovirus Infection Nair IS 57
Picture Quiz 66
Self-assessment Quiz 67
Abstracts from Literature 70
Short Communications 74
Significance of Prenatal Cytogenetic and Molecular Diagnosis of Triploidy and the Need for Genetic Counseling–A Report of 2 Cases Dhanya V, Smitha C, Pradeep S, Chitra P, Pooja SK, Kadandale JS, Sundareshan TS
Special Features
A Neonate Narrates 50
Human Resources for Facility-based Newborn Care in India 52
World Breastfeeding Week 64
EMBLEM
New look!
Vol. 13 • No. 2 • Jul–Sep 2012PerinatologyJ o u r n a l o f P e r i n a t a l a n d N e o n a t a l C a r e
Editorial
Dear friends,
I am glad to present to you the second issue of Volume 13 of Perinatology. This issue features articles on encouraging breastfeeding and improving the health of babies.
We all know that breast milk is the optimal source of nutrients for infants; therefore, the World Breastfeeding Week is celebrated from August, 1 to 7, to enable mothers to establish and sustain exclusive breastfeeding in infants up to the age of 6 months. The prime duty of all of us involved in the care of the mother and child is to bring to the notice of women, all over the world, the importance of breastfeeding.
The World Population Day is observed on July 11 every year. The world population, especially of our country, is exploding. It is well-known that the resources of the country are limited, yet they are not being protected and utilized promptly. Rapid urbanization and migration of people to towns and cities are leading to imbalance, creation of slums, pollution, and suboptimal living conditions. We have to act quickly and efficiently to save the world for our future generations.
I sincerely thank the publisher for maintaining the standard of the journal through their persistent support, cooperation, and help. The regular features have also been improved in quality. In addition, I earnestly appreciate the readers for their precious feedback as it plays a very essential role in our growth; and request the readers to send in their contributions in the form of research papers, case reports, brief articles, and review articles.
I hope that you will find this issue to be enlightening and interesting.
Dr Ranjan Kumar PejaverEditor in chief
Email: [email protected]
ThemeVol. 13 • No. 2 • Jul–Sep 2012Perinatology
J o u r n a l o f P e r i n a t a l a n d N e o n a t a l C a r e
20th World Breastfeeding Week (2012)
Understanding the Past - Planning the FutureCelebrating 10 years of WHO/UNICEF’s Global Strategy for Infant and Young Child Feeding
World Breastfeeding Week is celebrated every year from August 1 to 7, in more than 170 countries with the aim to encourage breastfeeding and improve the health of babies around the world. The objectives of the 20th World Breastfeeding Week (2012) are as follows:
1. To recall what had happened in the past 20 years as regards infant and young child feeding.
2. To celebrate successes and achievements nationally, regionally, and globally as well as showcase the national work at a global level.
3. To assess the status of implementation of the Global Strategy (GS) for Infant and Young Child Feeding.
4. To bridge the remaining gaps existing in policy and programs on breastfeeding and infant and young child feeding.
5. To draw public attention on the state of policy and programs on breastfeeding and infant and young child feeding.
…read more on page 64
RESEARCH ARTICLES PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
41
*Correspondence
Dr Anil B Jalan Senior Scientific Officer Navi Mumbai Institute of Research in Mental and Neurological Handicap C116-Om Rachana Society, Sector-17, Vashi Navi Mumbai, Mumbai 400705 Maharashtra, India
Phone: +91-9821124578 Email: [email protected]
Research Articles
Glutathione as an Indicator of Oxidative Stress in NeonatesBilakhia K, D’ Souza J, Kudalkar K, Dasgupta D, Mohite M, Jalan A*
AbstractBackground: When the production of free radicals exceeds the cells’ capacity to eliminate them, the outcome is oxidative stress. Neonates are highly susceptible to oxidative stress especially, preterm and low-birth weight infants.
Glutathione (GSH), a potent antioxidant, is synthesized from amino acids in the human body. It plays a critical role in pro-tecting the cells from oxidative damage by removing reactive species and maintaining homeostasis. Levels of GSH in RBCs serve as an indicator of the redox state of cells.
Methods: GSH levels were analyzed in 68 neonates. They were-categorized into 4 groups according to their gestational age and birth weight as follows: full term and appropriate for gesta-tional age (FT- AGA), full term and small for gestational age (FT-SGA), preterm and appropriate for gestational age (PT-AGA), and preterm and small for gestational age (PT-SGA). GSH levels in the RBCs were assayed using the standard method described by Ernest Beutler et al; its levels were correlated with the clinical data and the gas chromatographic/mass spectrometric (GC/MS) results.
Results: The levels of GSH were found to decrease among the 4 study groups: FT-AGA, PT-AGA, FT-SGA, and PT-SGA. Although a decreasing trend was seen, GSH levels in FT-SGA and PT-AGA neonates were not significantly different from GSH levels in FT-AGA neonates. However, the GSH levels in PT-SGA neonates were significantly different from the GSH levels in PT-AGA as well as FT-AGA (P < .05).
Conclusions: GSH levels in PT-SGA neonates were lower as com-pared to that in PT-AGA and FT-AGA. PT-SGA neonates are at a high risk of stress and oxidative-damage related complications.
Key words: Glutathione, neonates, oxidative stress
RESEARCH ARTICLES
42 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
Bilakhia K, et al. Glutathione, an oxidative stress indicator in neonates.
Research Articles
IntroductionOxidative stress causes cellular damage and has been implicated in several diseases such as cardiovascular disorders, neurodegenerative disorders, asthma, and cancer. The process of child birth is accompanied by an increase in oxidative stress.1 The antioxidant enzymes mature during late gestation leading to an increased transfer of antioxidants across the placenta, particularly during the last few days of gestation.2–4 Therefore, it is likely for the antioxidant system to be highly stressed in premature or immature infants.
Glutathione (GSH) plays a critical role in maintaining oxidative homeostasis and protecting the cells from oxidative damage by removal of many reactive species.5 It plays a crucial role in overcoming the early oxidative stress at the time of birth.4 Low GSH levels are inad-equate to overcome the oxidative stress at the time of birth and may affect the prognosis in the early post-natal life of a neonate. With these considerations in mind, we analyzed blood samples of neonates, specu-lating that increased oxidative stress in preterm and premature neonates would result in low GSH levels. Low levels of GSH were indeed seen in PT-SGA neonates. This correlation between levels of GSH and maturity in neonates offers a new motive to measure oxidative stress. These measures may provide a means of addressing oxidative stress in early neonatal life and aid in the development of therapies and precautionary measures.
Materials and MethodsThe study population consisted of 68 neonates admitted to the neonatal intensive care unit (NICU) of Sai Child Care Clinic (New Panvel, Mumbai). Neonates below 60 days of age were included in the study. Some of these neonates had sepsis, birth asphyxia, convulsions, fetal distress, etc. Neonates above 60 days of age were excluded from the study due to variations in their blood antioxidant status varies according to age. None of the neonates were on any antioxidant supplements at the time of analysis.
Estimation of GSH in the peripheral blood samples from these neonates was made an integral part of basic
investigations. The erythrocytes were separated and hemolyzed immediately, and the protein fraction was precipitated with trichloroacetic acid. The superna-tants were stored at 4°C until analysis. Biochemical colorimetric analysis for quantification of GSH was performed using the method described by Beutler E, et al. This method uses Ellman’s reagent (ie, 5,5’-dithio-bis-2-[nitrobenzoic acid], [DTNB]), which reacts with the sulfhydryl group of GSH to produce a yellow colored 5-thio-2-nitrobenzoic acid (TNB) derivative that can be estimated by measuring its absorbance at 405 nm.6 Values of GSH were calculated as nanomole per gram of Hb of the hemolysate for each sample.
The levels of GSH in the neonates of all study groups were compared and statistical analysis was carried out using Student’s t-test.
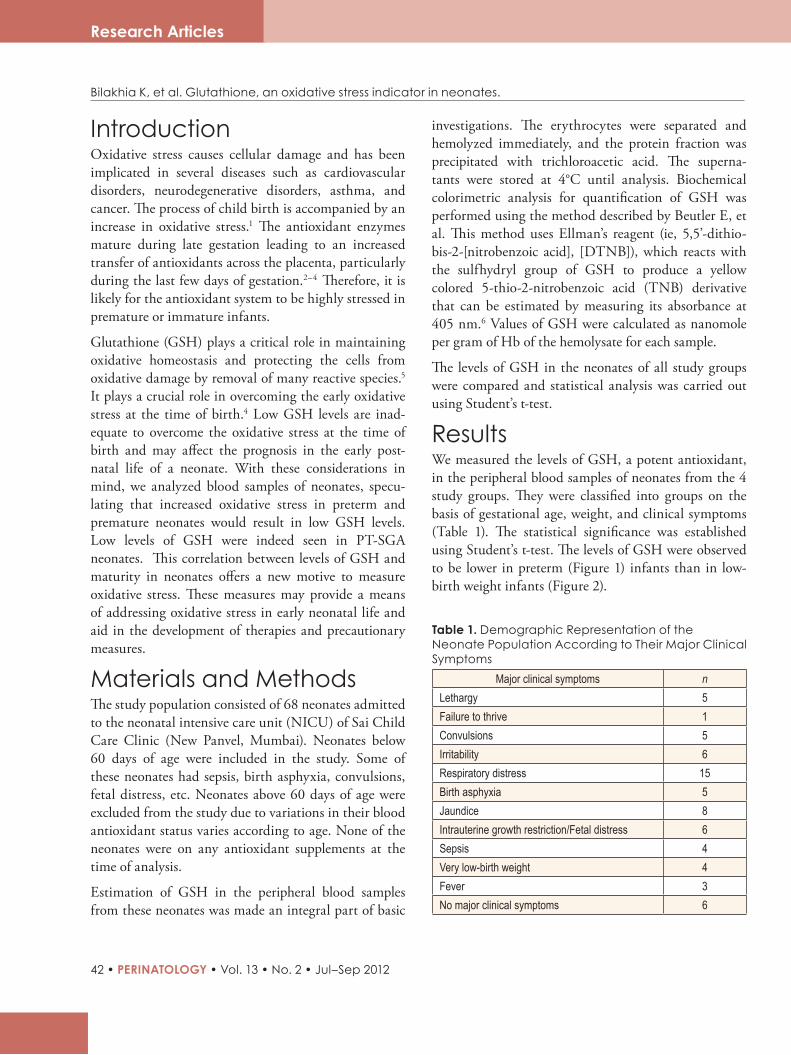
ResultsWe measured the levels of GSH, a potent antioxidant, in the peripheral blood samples of neonates from the 4 study groups. They were classified into groups on the basis of gestational age, weight, and clinical symptoms (Table 1). The statistical significance was established using Student’s t-test. The levels of GSH were observed to be lower in preterm (Figure 1) infants than in low-birth weight infants (Figure 2).
Table 1. Demographic Representation of the Neonate Population According to Their Major Clinical Symptoms
Major clinical symptoms nLethargy 5Failure to thrive 1Convulsions 5Irritability 6Respiratory distress 15Birth asphyxia 5Jaundice 8Intrauterine growth restriction/Fetal distress 6Sepsis 4Very low-birth weight 4Fever 3No major clinical symptoms 6
RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 43
Bilakhia K, et al. Glutathione, an oxidative stress indicator in neonates.
Research Articles
Figure 1. Demographic representation of GSH levels based on gestational age
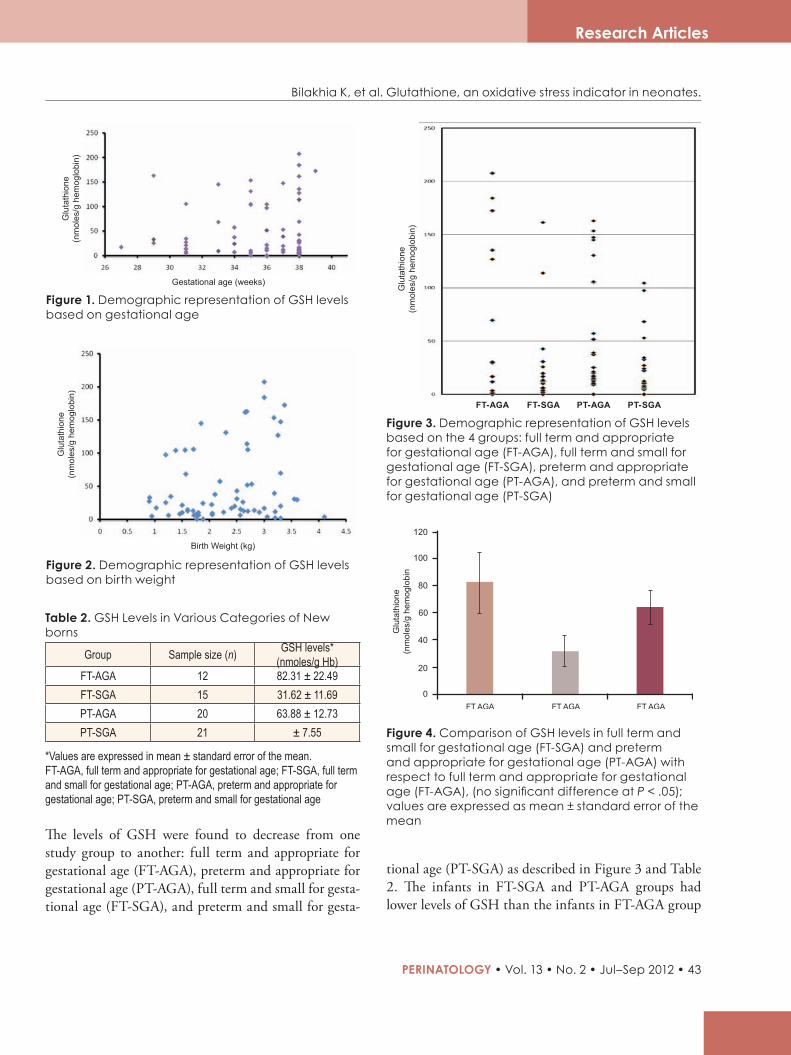
Figure 2. Demographic representation of GSH levels based on birth weight
Table 2. GSH Levels in Various Categories of New borns
Group Sample size (n) GSH levels* (nmoles/g Hb)
FT-AGA 12 82.31 ± 22.49FT-SGA 15 31.62 ± 11.69PT-AGA 20 63.88 ± 12.73PT-SGA 21 ± 7.55
*Values are expressed in mean ± standard error of the mean. FT-AGA, full term and appropriate for gestational age; FT-SGA, full term and small for gestational age; PT-AGA, preterm and appropriate for gestational age; PT-SGA, preterm and small for gestational age
tional age (PT-SGA) as described in Figure 3 and Table 2. The infants in FT-SGA and PT-AGA groups had lower levels of GSH than the infants in FT-AGA group
The levels of GSH were found to decrease from one study group to another: full term and appropriate for gestational age (FT-AGA), preterm and appropriate for gestational age (PT-AGA), full term and small for gesta-tional age (FT-SGA), and preterm and small for gesta-
Figure 3. Demographic representation of GSH levels based on the 4 groups: full term and appropriate for gestational age (FT-AGA), full term and small for gestational age (FT-SGA), preterm and appropriate for gestational age (PT-AGA), and preterm and small for gestational age (PT-SGA)
PT-AGAFT-SGA PT-SGAFT-AGA
Figure 4. Comparison of GSH levels in full term and small for gestational age (FT-SGA) and preterm and appropriate for gestational age (PT-AGA) with respect to full term and appropriate for gestational age (FT-AGA), (no significant difference at P < .05); values are expressed as mean ± standard error of the mean
Glu
tath
ione
(n
mol
es/g
hem
oglo
bin)
Glu
tath
ione
(n
mol
es/g
hem
oglo
bin)
Glu
tath
ione
(n
mol
es/g
hem
oglo
bin)
Gestational age (weeks)
Birth Weight (kg)
RESEARCH ARTICLES
44 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
Research Articles
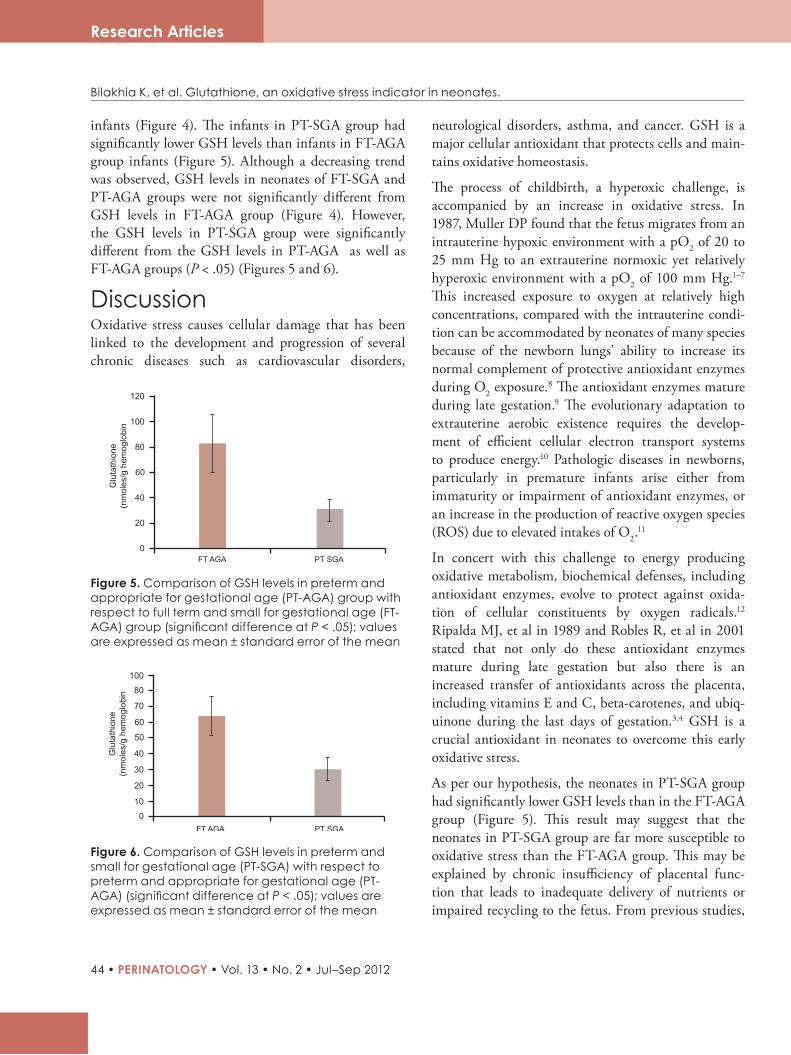
Figure 5. Comparison of GSH levels in preterm and appropriate for gestational age (PT-AGA) group with respect to full term and small for gestational age (FT-AGA) group (significant difference at P < .05); values are expressed as mean ± standard error of the mean
Figure 6. Comparison of GSH levels in preterm and small for gestational age (PT-SGA) with respect to preterm and appropriate for gestational age (PT-AGA) (significant difference at P < .05); values are expressed as mean ± standard error of the mean
infants (Figure 4). The infants in PT-SGA group had significantly lower GSH levels than infants in FT-AGA group infants (Figure 5). Although a decreasing trend was observed, GSH levels in neonates of FT-SGA and PT-AGA groups were not significantly different from GSH levels in FT-AGA group (Figure 4). However, the GSH levels in PT-SGA group were significantly different from the GSH levels in PT-AGA as well as FT-AGA groups (P < .05) (Figures 5 and 6).
DiscussionOxidative stress causes cellular damage that has been linked to the development and progression of several chronic diseases such as cardiovascular disorders,
neurological disorders, asthma, and cancer. GSH is a major cellular antioxidant that protects cells and main-tains oxidative homeostasis.
The process of childbirth, a hyperoxic challenge, is accompanied by an increase in oxidative stress. In 1987, Muller DP found that the fetus migrates from an intrauterine hypoxic environment with a pO2 of 20 to 25 mm Hg to an extrauterine normoxic yet relatively hyperoxic environment with a pO2 of 100 mm Hg.1–7
This increased exposure to oxygen at relatively high concentrations, compared with the intrauterine condi-tion can be accommodated by neonates of many species because of the newborn lungs’ ability to increase its normal complement of protective antioxidant enzymes during O2 exposure.8 The antioxidant enzymes mature during late gestation.9 The evolutionary adaptation to extrauterine aerobic existence requires the develop-ment of efficient cellular electron transport systems to produce energy.10 Pathologic diseases in newborns, particularly in premature infants arise either from immaturity or impairment of antioxidant enzymes, or an increase in the production of reactive oxygen species (ROS) due to elevated intakes of O2.
11
In concert with this challenge to energy producing oxidative metabolism, biochemical defenses, including antioxidant enzymes, evolve to protect against oxida-tion of cellular constituents by oxygen radicals.12 Ripalda MJ, et al in 1989 and Robles R, et al in 2001 stated that not only do these antioxidant enzymes mature during late gestation but also there is an increased transfer of antioxidants across the placenta, including vitamins E and C, beta-carotenes, and ubiq-uinone during the last days of gestation.3,4 GSH is a crucial antioxidant in neonates to overcome this early oxidative stress.
As per our hypothesis, the neonates in PT-SGA group had significantly lower GSH levels than in the FT-AGA group (Figure 5). This result may suggest that the neonates in PT-SGA group are far more susceptible to oxidative stress than the FT-AGA group. This may be explained by chronic insufficiency of placental func-tion that leads to inadequate delivery of nutrients or impaired recycling to the fetus. From previous studies,
Bilakhia K, et al. Glutathione, an oxidative stress indicator in neonates.

RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 45
Research Articles
it is known that preterm neonates have higher levels of glutathione peroxidase compared with full term neonates,13 thereby supporting our results. The rise in glutathione peroxidase may be a predominant cause of GSH depletion. A study of antioxidant defense poten-tial of erythrocytes during late fetal development revealed that erythrocyte catalase, glutathione peroxi-dase, and vitamin E levels correlated positively with increasing fetal weight. A low-birth weight infant is more frequently exposed to the conditions associated with increased generation of free oxygen radicals such as reperfusion and hypoxia,14 thereby supporting our results of significantly lower GSH levels in PT-SGA group compared with PT-AGA group. The GSH levels in FT-SGA group were not quite significantly different from those in FT-AGA group. This result may suggest that the full-term neonates are capable of adapting to the defense mechanism against high levels of free oxygen radicals.
Human neonates have a relative deficiency of brain superoxide dismutase and glutathione peroxidase. Also, the neuronal membranes are rich in polyunsatu-rated fatty acids.15 Hence, the brain may be at a high risk of free-radical damage. Conditions such as birth asphyxia may further increase oxidative stress and result in oxidative brain damage.16 In our cohort, we observed low levels of GSH in 3 out of 5 neonates with a clinical history of birth asphyxia. Two out of 4 neonates with birth asphyxia in the group PT-AGA group had lower levels of GSH (39 and 37.32 nmol/g Hb) compared with the mean GSH levels in PT-AGA group (63.88 ± 12.73, n = 20). Only 1 neonate in the FT-SGA group had a history of birth asphyxia. The GSH levels in this neonate (9.85 nmol/g Hb) were significantly lower compared with the group (31.62 ± 11.69, n =15).
Thus, our results indicate that neonates, particularly preterm, premature, and with a history of birth asphyxia are at a high risk of oxidative stress and are susceptible to oxidative damage. This increased oxidative stress accompanied by reduced endogenous defenses may play a role in the pathogenesis of a number of diseases. Furthermore, the evaluation of oxidative stress in these neonates may be helpful in targeting therapeutic
options to avoid oxidative-stress related complications.
AcknowledgmentThe authors whole heartedly thank all the pediatricians and neonatologists who supported them throughout this study.
References1. RobertsonNJ.Airor100%oxygenforasphyxiatedbabies?
Timetodecide. Crit Care.2005;9(2):128–130.2. GerdenE,etal.Thedevelopmentofantioxidantenzymatic
defense in the perinatal rat lung: activities of superoxidedismutase,glutathioneperoxidaseandcatalase. Pediatr Res.1985;19:687–691.
3. RoblesR,etal.Oxidativestressintheneonate. Early Hum Dev.2001;65:S75–S81.
4. RipaldaMJ, et al.Developmental patterns of antioxidantdefensemechanisms in human erythrocytes. Pediatr Res.1989;26:366–369.
5. FormanHJ, et al.Glutathione: overviewof its protectiveroles,measurement and biosynthesis. Mol Aspects Med.2009;30(1-2):1–12.
6. BeutlerE,etal.Improvedmethodfordeterminationofbloodglutathione. J Lab Clin Med.1963;61:88.
7. MullerDP.Freeradicalproblemsofthenewborn. Proc Nutr Soc.1987;46:69–75.
8. FrankL. Effects of oxygen on the newborn. Fed Proc.1985;44:2328–2334.
9. GerdinE,etal.Thedevelopmentofantioxidantenzymaticdefense in the perinatal rat lung: activities of superoxidedismutase,glutathioneperoxidase,andcatalase. Pediatr Res.1985;19:687–691.
10. FrankL, et al. Prenatal development of lung antioxidantenzymesinfourspecies. J Pediatr.1987;110:106–110.
11. Friel JK, et al. Evidence of oxidative stress in full-termhealthyinfants. Pediatr Res.2004;56(6):878–882.
12. VlessisAA, et al. Perinatal development of heart, kidneyand livermitochondrial antioxidant defense. Pediatr Res.1989;26:220–226.
13. SarkarPD,etal.Oxidativestressandantioxidantsinpretermlabor. Biomed Res.2006;17(1):41–43.
14. FrankL, et al. Failure of premature rabbits to increaseantioxidantenzymesduringhypertoxicexposure:increasedsusceptibilitytopulmonaryoxygentoxicitycomparedwithtermrabbits. Pediatr Res.1991;29:292–296.
15. BuonocoreG,etal.Freeradicalsandbraindamageinthenewborns. Biol Neonate.2001;79:180–186.
16. GittoE, et al.Causes of oxidative stress in the pre- andperinatalperiod. Biol Neonate.2002;81:146–157.
Bilakhia K, et al. Glutathione, an oxidative stress indicator in neonates.
RESEARCH ARTICLES
46 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
Research Articles
*Correspondence
Dr Indu S Nair Consultant Neonatologist 98, Manipal Hospital, Old Airport Road Bangalore - 560017 Karnataka, India
Email: [email protected]
Dr Arvind ShenoiConsultant Neonatologist and Medical Director 115, Cloudnine Hospital, Old Airport Road Bangalore - 560017 Karnataka, India
Email: [email protected]
Low-cost Hand Hygiene RegimenIndu S Nair,* Arvind Shenoi*
AbstractIntensive health care in India is very expensive and neonatal intensive care can be an economic burden on young parents. Hence, it is imperative that we search for newer strategies to reduce health-care costs without compromising quality. Most studies done on cost analysis of intensive care have discussed the strategies for cost reduction with respect to equipment used, clinical, and nonclinical support services, consumables, and manpower costs.
Implementing certain evidence based practices in neonatal intensive care units (NICUs) throughout India can be the key to reducing associated costs. This article particularly provides insight into cost-effective hand hygiene practices.
The World Health Organization (WHO) has set out the goal of “Clean care is safer care” in its World Alliance for Patient Safety Guidelines to ensure that clean care is acknowledged univer-sally as an essential basis for patient safety. In this regard, hand hygiene is the simplest and most effective measure for pre-venting health care-associated infections (HAIs).
There are two basic methods of maintaining hand hygiene—water-based and waterless methods. Water-based methods require clean water, clean soap, and clean methods of drying the hand whereas waterless methods are mainly alcohol-based; also referred to as alcohol-based hand rubs (ABHR).
It is essential to change hand hygiene practices from traditional hand washing techniques to the use of ABHR. Existing evidence suggests that ABHR is as efficacious as water-based methods, less expensive than traditional hand washing, and also finds greater compliance among health-care personnel. However, the role of traditional hand washing when there is visible soiling of hands remains unchallenged by many clinical guidelines.6-9

RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 47
Research Articles
Nair IS, et al. Low-cost hand hygiene regimen
IntroductionHealth care has become very costly and often unafford-able. Intensive care, in particular, is very expensive as it is resource-intensive. Perhaps, neonatal intensive care is relatively less expensive. However, the economic burden on young parents can be quite immense. Hence, it is imperative that we search for newer strategies to reduce health care costs without compromising on quality. There are few studies,1,2 some from India,3,4 regarding cost of neonatal intensive care unit (NICU), and 1 exhaustive review article5 that describes a methodology for cost analysis. This is a series of review articles that aims to discuss implementation of certain evidence -based practices in NICUs throughout India, which would result in reducing the cost of neonatal intensive care. This article particularly deals with cost effective hand hygiene practices.
Hand hygiene is one of the key initiatives set out by the WHO- world alliance for patient safety guidelines with the goal of ”Clean Care is Safer Care.”6 Health care-associated infection (HAI) occurs worldwide and affects both developed and developing countries. In high risk settings such as intensive care units, more than one-third of patients can be affected. Adherence to hand hygiene recommendations is the single most important practice to prevent transmission of patho-gens in health care settings and is the responsibility of all individuals involved in health care.
Effective hand hygiene is the simplest and most effec-tive measure for preventing HAIs. An ineffective hand-washing technique is as significant as the lack of hygiene itself. Adherence to recommended hand hygiene practice is unacceptably low in healthcare workers, presenting a risk to patients.7 Studies on hand hygiene compliance among health-care workers suggest that the mean baseline rate ranges from 5% to 81%, with an overall average of 40% compliance.7
Hand Washing TechniquesThere are 2 basic methods of maintaining hand hygiene—water-based hand washing and waterless methods. Waterless methods are also known as alcohol-based hand rubs (ABHR). Hand washing consists of
clean water, clean soap, and clean methods of drying the hand.
Water-based hand washingUnfortunately, clean water is a difficult commodity to get and no Indian city can boast of it.8 The cost of acquiring, storing, and providing clean water is beyond the purview of this review. However, one needs to know that hand washing with soap and water is essen-tial when the hands are visibly soiled and either ABHR or soap and water can be used if hands are visibly clean.6,7,9,10
Clean soap is generally available but dispensers can get colonized with Pseudomonas aeruginosa.11 Further, the cost of using liquid soaps that require a dispenser versus a bar of soap that needs a soap dish has never been compared. Needless to say, theoretically both, the soap dish as well as dispenser are prone to contamination.
An array of products such as, paper towels, cloth towels, and air driers are used to dry washed hands,12
but there is conflicting evidence pertaining to the effi-cacy of each method in removing bacteria from washed hands.10,13,14 Ideally, hands should be dried using either individual paper towels or hand dryers, which can dry hands effectively and quickly as with paper towels, but both add on to the cost.15
Alcohol-based hand rubsThere are many studies16–19 that state ABHRs are better than traditional hand washing among patients in an intensive care setting. Pittet, et al showed that there was a significant reduction of HAI from 16.9% to 9.9%; and several other studies have demonstrated low infec-tion rates.17–19 One study has shown that alcohol hand rub was even equivalent to traditional surgical scrub protocols (2.44% and 2.48%, respectively).20 A study carried out by Larson et al in neonatal intensive care has shown that alcohol is at least equivalent to tradi-tional antiseptic hand washing in terms of impact on infection rates.21 ABHRs require less time to use (mean:12.7 seconds with hand rub and 21.1 s with hand wash, respectively; P=.0001); acts faster; does not need a sink, water, and drying agents as in traditional
RESEARCH ARTICLES
48 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
Research Articles
Nair IS, et al. Low-cost hand hygiene regimen
hand washing; therefore, it is less cumbersome and perhaps more cost-effective.22
Increased hand hygiene compliance with an alcohol-based rub has been attributed to product placement in the environment, convenience of use, and less skin irri-tation.17,23,24 Observations after introduction of the new, increasingly accessible, alcohol-based, waterless hand antiseptic revealed significantly higher hand washing rates (P < .05), and hand washing compliance improved as accessibility was enhanced—before 19% and after 41% with 1 dispenser per 4 beds; and before 23% and after 48% with 1 dispenser for each bed.25
Cost of Water-Based Hand Washing Versus ABHRVery few studies have examined the direct cost of hand asepsis, out of which, the studies by Stone, et al and Cimiotti, et al have carried out exhaustive cost analyses of various hand hygiene products. 22, 26–28 A recent study in a dental setting has reported that use of ABHR to be more cost-effective than antimicrobial soap.20 A study by Larson, et al has documented a 50% reduction in material costs with ABHR and suggested that changes in hand hygiene practices in acute care settings from the traditional antiseptic wash to the use of an alcohol-based product should be considered.22
The study by Stone et al, has shown that paper towels were on an average the most expensive hand hygiene product, with annual costs of almost $10,000 per 100 beds; soap on an average costs almost $4,000 per 100 beds; while the average cost of alcohol-based products was approximately $2,000 per 100 beds.27 This study again highlights that handrubs are cheaper than the other hand hygiene products.
A study conducted at a 450-bed community teaching hospital has revealed that $22,000 was spent annually on hand hygiene products at a cost of $0.72 per patient per day.26 It was reported that 2% of chlorhexidine gluconate was 1.7 times as expensive as the plain soap and the alcohol-based gel, twice as expensive. Similar results were found by Cimiotti et al.28
Despite the high costs of hand hygiene products, use of alcohol-based products has proven to be less costly
compared to traditional hand washing. Traditional hand washing requires longer time and comes with the added costs of paper towels and water. Cimiotti, et al have documented that though product cost was more for ABHR, the total cost per 1,000 hand hygiene episodes was less, as the amount of product used and the time consumed was less (P = .79 and P = .006, respectively). The study concludes that the chlorhexi-dine hand hygiene regimen costs significantly more than the ABHR ($184, SD±194 and $147, SD± 67, respectively; P = .007). Although the ABHR cost was nearly $750 per 1,000 patient-days more, it was found to be less costly due to its shorter application time than traditional hand washing. Traditional hand washing requires approximately 5 s more per episode than the ABHR.28 These results could be more dramatic if cost of water- and paper towel-usage were included.
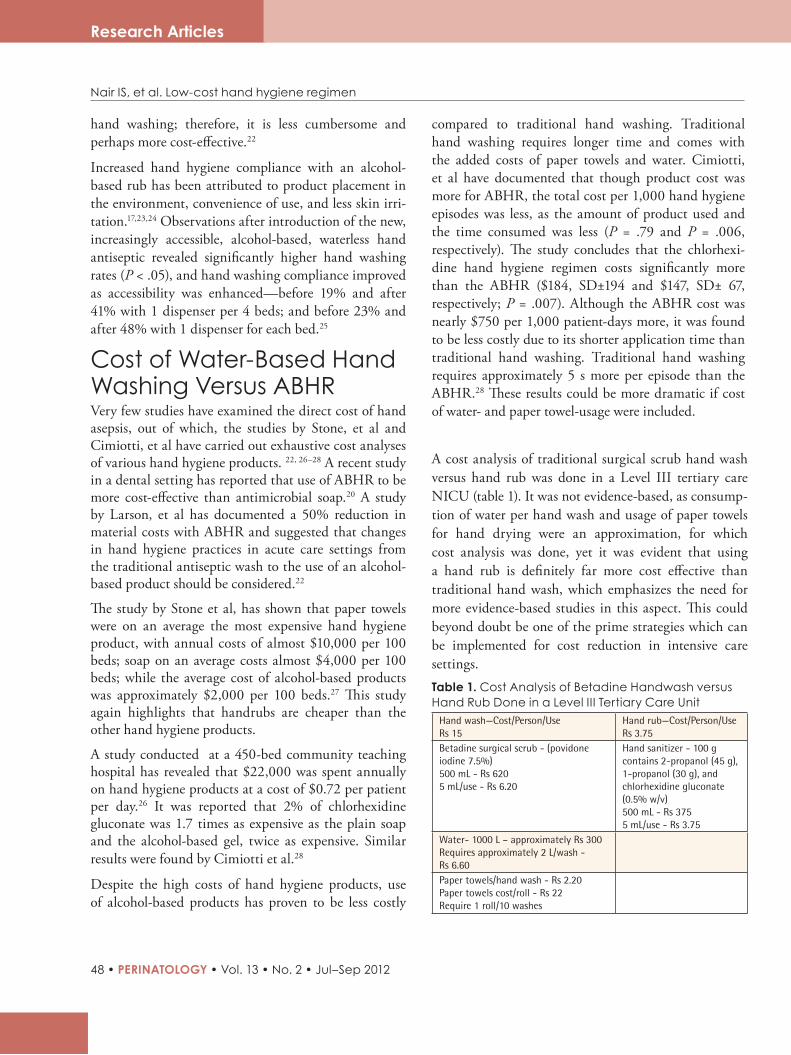
A cost analysis of traditional surgical scrub hand wash versus hand rub was done in a Level III tertiary care NICU (table 1). It was not evidence-based, as consump-tion of water per hand wash and usage of paper towels for hand drying were an approximation, for which cost analysis was done, yet it was evident that using a hand rub is definitely far more cost effective than traditional hand wash, which emphasizes the need for more evidence-based studies in this aspect. This could beyond doubt be one of the prime strategies which can be implemented for cost reduction in intensive care settings.Table 1. Cost Analysis of Betadine Handwash versus Hand Rub Done in a Level III Tertiary Care Unit
Hand wash—Cost/Person/Use Rs 15
Hand rub—Cost/Person/Use Rs 3.75
Betadine surgical scrub - (povidone iodine 7.5%)500 mL - Rs 6205 mL/use - Rs 6.20
Hand sanitizer - 100 g contains 2-propanol (45 g), 1-propanol (30 g), and chlorhexidine gluconate (0.5% w/v)500 mL - Rs 3755 mL/use - Rs 3.75
Water- 1000 L – approximately Rs 300Requires approximately 2 L/wash - Rs 6.60Paper towels/hand wash - Rs 2.20Paper towels cost/roll - Rs 22 Require 1 roll/10 washes

RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 49
Research Articles
ConclusionMost studies done on cost analysis of intensive care4,5
have discussed the strategies for cost reduction with respect to equipment, clinical, and nonclinical support services, consumables, and manpower costs. The infor-mation available challenges the concept that tradi-tional hand washing is cheaper than ABHR. However, it needs to be investigated and would go a long way in reducing the cost in neonatal intensive care. Existing evidence suggests that a change in hand hygiene prac-tices from the traditional hand washing to use of ABHR needs to be implemented as it has been proven to be as efficacious and less expensive than traditional hand washing, with greater compliance among health care personnel. However, the role of handwashing when there is visible soiling of hands remains unchallenged by many clinical guidelines.6–9
References1. RichardsonDK, et al.A critical reviewof cost reduction
in neonatal intensive care. II. Strategies for reduction. J Perinatol.2001;2(2):121–127.
2. RichardsonDK,etal.Acriticalreviewofcostreductioninneonatalintensivecare. I.Thestructureofcosts.J Perinatol.2001;21(2):107–115.
3. ShanmugasundaramR,etal.Costofneonatalintensivecare. Indian J Pediatr.1998;65:249–255.
4. NarangA,etal.Costofneonatalintensivecareinatertiarycarecenter. Indian Pediatr.2005;42:989–997.
5. JayaramR,etal.CostofintensivecareinIndia. Indian J Crit Care Med.2008;12(2):55–61.
6. WorldAllianceforPatientSafety.WHOGuidelinesonHandHygieneinHealthCare(AdvancedDraft). 2006.
7. BoyceJM,etal.Guidelineforhandhygieneinhealth-caresettings. RecommendationsofthehealthcareinfectioncontrolpracticeadvisoryandtheHICPAC/SHEA/APIC/IDSAhandhygienetaskforce.Infect Control Hosp Epidemiol.23(12):S3–S39.
8. http://en.wikipedia.org/wiki/Water_supply_and_sanitation_in_India.AccessedApril31,2012.
9. WorldHealthOrganization.WHOguidelinesonhandhygieneinhealthcare. In:WorldAlliance forPatientSafety.First Global Patient Safety. Challenge “Clean Care is Safer Care.”Geneva:WorldHealthOrganizationPress;2009.
10. GraysonLM,etal.Handhygienemanual. Australia.2010.11. LaniniS,etal.MolecularepidemiologyofaPseudomonas
aeruginosa hospital outbreak driven by a contaminateddisinfectant-soapdispenser. PLoS One.2011;6(2):e17064.
12. AnsariSA,etal.Comparisonofcloth,paper,andwarmairdryingineliminatingvirusesandbacteriafromwashedhands. Am J Infect Control.1991;19(5):243–249.
13. YamamotoY,etal.Efficiencyofhanddryingforremovingbacteria fromwashed hands:Comparison of paper toweldryingwithwarmairdrying. Infect Control Hosp Epidemiol.2005;26(3):316–320.
14. NgeowYF,etal.Dispersalofbacteriabyanelectricairhanddryer. Malays J Pathol.1989;11:53–56.
15. SnellingAM,etal.Comparativeevaluationofthehygienicefficacyofanultra-rapidhanddryervsconventionalwarmairhanddryers. J Appl Microbiol.2011;110(1):19–26.
16. GirouE,etal.Efficacyofhandrubbingwithalcoholbasedsolutionversusstandardhandwashingwithantisepticsoap:randomisedclinicaltrial. BMJ.2002;325:362.
17. PittetD,etal.Effectivenessofahospital-wideprogrammeto improve compliance with hand hygiene. Lancet.2000;356:1307–1312.
18. HilburnJ,etal.Useofalcoholhandsanitizerasaninfectioncontrolstrategyinanacutecarefacility. Am J Infect Control.2003;31:109–116.
19. BrownSM, et al.Use of an alcohol-based hand rub andqualityimprovementinterventionstoimprovehandhygieneinaRussianneonatalintensivecareunit. Infect Control Hosp Epidemiol.2003;24:172–179.
20. HuberMA, et al. Cost analysis of hand hygiene usingantimicrobialsoapandwaterversusanalcohol-basedhandrub. J Contemp Dent Pract.2006;7(2):37–45.
21. Larson EL, et al. Effect of antiseptic handwashing vsalcohol sanitizer on health care–associated infections inneonatal intensive care units. Arch Pediatr Adolesc Med.2005;159:377–383.
22. Larson EL, et al.Assessment of two hand hygieneregimensforintensivecareunitpersonnel. Crit Care Med.2001;29(5):944–951.
23. BoyceJM,etal.Skinirritationanddrynessassociatedwithtwohand-hygieneregimens:Soap-and-waterhandwashingversus hand antisepsiswith an alcoholic hand gel. Infect Control Hosp Epidemiol.2000;21:442–448.
24. WinnefeldM,etal.Skintoleranceandeffectivenessoftwohanddecontaminationproceduresineverydayhospitaluse. Br J Dermatol.2000;143:546–550.
25. BischoffWE, et al. The impact of introducing anaccessible,alcohol-basedhandantiseptic. Arch Intern Med.2000;160:1017–1021.
26. BoyceJM.Antiseptictechnology:Access,affordability,andacceptance. Emerg Infect Dis.2001;7(2):231–233.
27. StonePW,etal.Effectofguidelineimplementationoncostsofhandhygiene. Nurs Econ.2007;25(5):279–284.
28. Cimiotti JP, et al.A cost comparison of hand hygieneregimens. Nurs Econ.2004;22(4):196–199.
Nair IS, et al. Low-cost hand hygiene regimen
RESEARCH ARTICLESPERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
50
A Neonate Narrates
Hooray! I have finally made it from a wet, watery, restricted chamber (womb) to this big, bright world. Mind you, it was not easy. In fact I was not prepared for this. I was taken by surprise. It was that fateful moment when I suddenly noticed a gaping hole in the roof of my chamber and the water around me draining out. Have you ever been in a bathtub full of water and foam, and all of a sudden without your knowl-edge, all the water has run out? It was a horrible experience! Later 2 green heads with face half-covered, peered down the hole. Do they want to hide their identity, lest I may take revenge? Before I could blink, two rubberized hands grabbed me, pulled me out, and severed my lifeline. In addition, one of them held me upside down and raised his hand, as if he was about to spank me. Just then, out of sheer fright, I gave out a loud shriek and funnily, this made all people around me heave a sigh of relief! Anyway, I was spared the bash and passed onto another person in green who placed me on a green towel at the corner of the room. Strangely, though it was a shock to me, I believe that people around me had planned and arranged this calculated mission of dislodging me from my private chamber.
As I was celebrating my escape from spanking, all of a sudden a tube was shoved into my nostril. I spluttered, sneezed, and cried in protest, which in turn stopped them from continuing this assault. Next was the act of rubbing me with a green dry cloth. I enjoyed it as it was exhilarating, and thought that life was going to be fun. Just then I heard somebody saying, “He is 3 weeks early, we have to keep a close eye on him.” I felt like a convict who had escaped from prison. In a moments time, I started feeling this heat from above. Goodness gracious! It was a heater coil above me. Instead of a baby boy, I felt like a beef burger on the barbecue!
I was then shifted to a room and placed in a glass case akin to an empty aquarium. This was mean; but worse was yet to come. The people around me, most of them in green or blue gown, did all sort of nasty things like shoving tubes up and down my various orifices. I was tired and wanted to be left alone to take a nap. This I thought they did, when nothing happened for few moments. Later, a young lady entered with a needle in hand. She may be pretty at other times, but at that moment she looked scared and nervous, even more than me! She poked me 3 times before drawing some blood and shoving a cannula into me. I was wondering whether she was one of Dracu-la’s assistants and how often was she going to do this to me?
It was time for some food. They brought a bottle of milk, the smell of which was very appetizing. Believe me, as I was priming my taste buds, they again shoved a tube down
Special Feature
RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 51
Pejaver RK. A neonate narrates
my nostril and let the milk downward without any of it touching my lips and tongue. This was the height of cruelty. The amount given was few spoonfuls, stingy stinkers! When I looked around the room, I could see a few babies in other glass cabinets. Around 1 or 2 babies were chubby and resembled sumo wrestlers while some seemed to be quite shriveled. I was wondering as to why they did not fight this imprisonment? The veteran across was appearing to say “You fella, if you think that being a neonate is all about breast milk and honey, then wait till you see everything. The fun has just begun.”
During the last 3 days there were some interesting moments, and some not so interesting ones. Every morning a group of doctors and nurses, all trying to
look smart and intelligent but make a fool of them-selves when they start talking, visit the room. Wait, until I get my hands on these people who bang things on my cabinet. Least are they aware that it is like living through an explosion or earthquake. Hey, we are not wearing ear muffs, you know. I am determined to teach them a lesson when they come to change my nappies. Wish me success. I have been listening to mumblings and statements that I may have to stay here for atleast 3 weeks before I am released. I just cannot live in this hell with daily prodding and poking and food being poured in a minute ration down a tube. Do I have a choice?
– Dr Ranjan Kumar Pejaver, DCH, DEXPI, DEXPXH(UK)
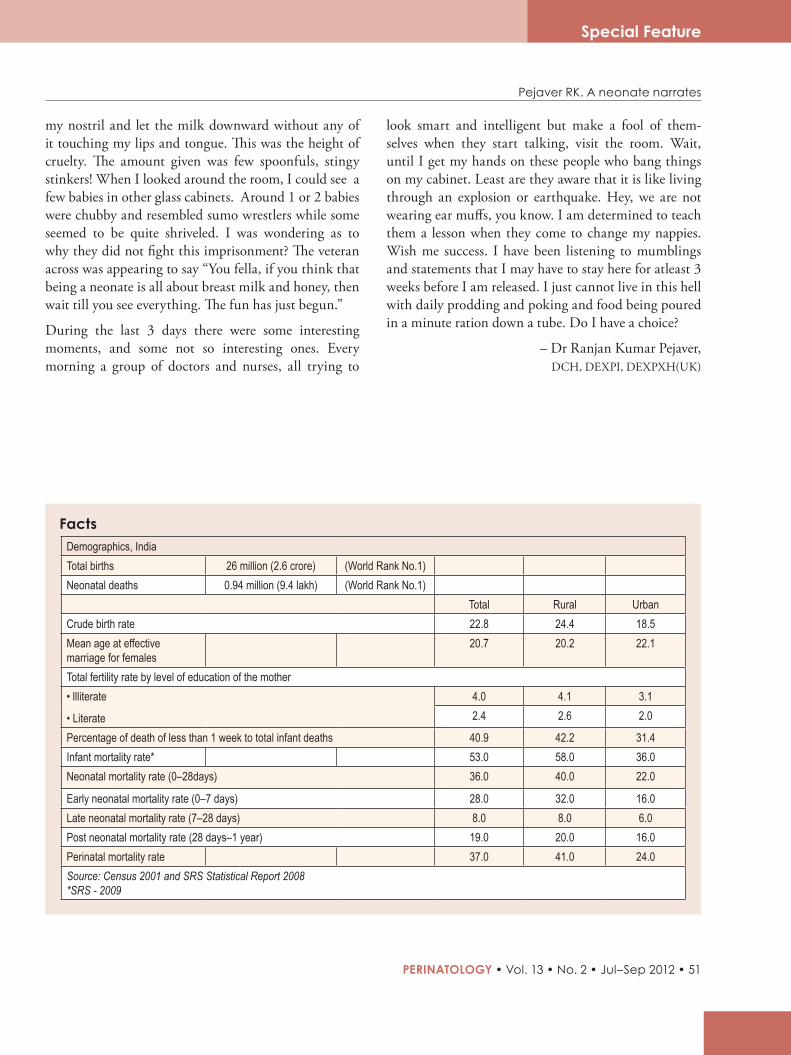
Demographics, IndiaTotal births 26 million (2.6 crore) (World Rank No.1)Neonatal deaths 0.94 million (9.4 lakh) (World Rank No.1)
Total Rural UrbanCrude birth rate 22.8 24.4 18.5Mean age at effective marriage for females
20.7 20.2 22.1
Total fertility rate by level of education of the mother• llliterate
• Literate
4.0 4.1 3.12.4 2.6 2.0
Percentage of death of less than 1 week to total infant deaths 40.9 42.2 31.4Infant mortality rate* 53.0 58.0 36.0Neonatal mortality rate (0–28days) 36.0 40.0 22.0
Early neonatal mortality rate (0–7 days) 28.0 32.0 16.0Late neonatal mortality rate (7–28 days) 8.0 8.0 6.0Post neonatal mortality rate (28 days–1 year) 19.0 20.0 16.0Perinatal mortality rate 37.0 41.0 24.0Source: Census 2001 and SRS Statistical Report 2008 *SRS - 2009
Facts
Special Feature
RESEARCH ARTICLESPERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
52
Human Resources for Facility-based Newborn Care in India
Issues and Options
Facility-based newborn care has a significant poten-tial for improving newborn survival in India. It has been estimated that health facility-based interventions can reduce neonatal mortality by as much as 23% to 50% in different settings. In this course, large numbers of special care newborn units (SCNUs) are being set-up in some of the remotest districts of the country. Initial evidence suggests that the mortality rate among newborns admitted in these units has been low over the last few years. However, there are several challenges in managing and scaling-up these units; first and fore-most being the requirement of a large number of skilled human resources.
While availability of skilled human resources is essential in providing quality care for all in-patients, in general, it is critical for providing special care for newborns. Among all categories of human resources, availability of an adequate number of nurses is the most crucial factor. It has been estimated that the odds of mortality of newborns admitted in SCNUs increase significantly when one nurse cares for more than 1.7 newborns. Shortage of nursing staff is frequently experienced in remote areas and during the night; even encountered in developed countries, often with adverse consequences.
Infection outbreak is one of the major consequences of inadequacy of nursing staff, affecting the survival rates of infants. When nurses are insufficient in number, they are less likely to follow hand hygiene and other infec-tion prevention practices that can be time-intensive. While the availability of nurses is critical, availability of doctors is important, especially in those units providing
higher levels of sophisticated care such as ventilation, and in the care of very low birth weight babies.
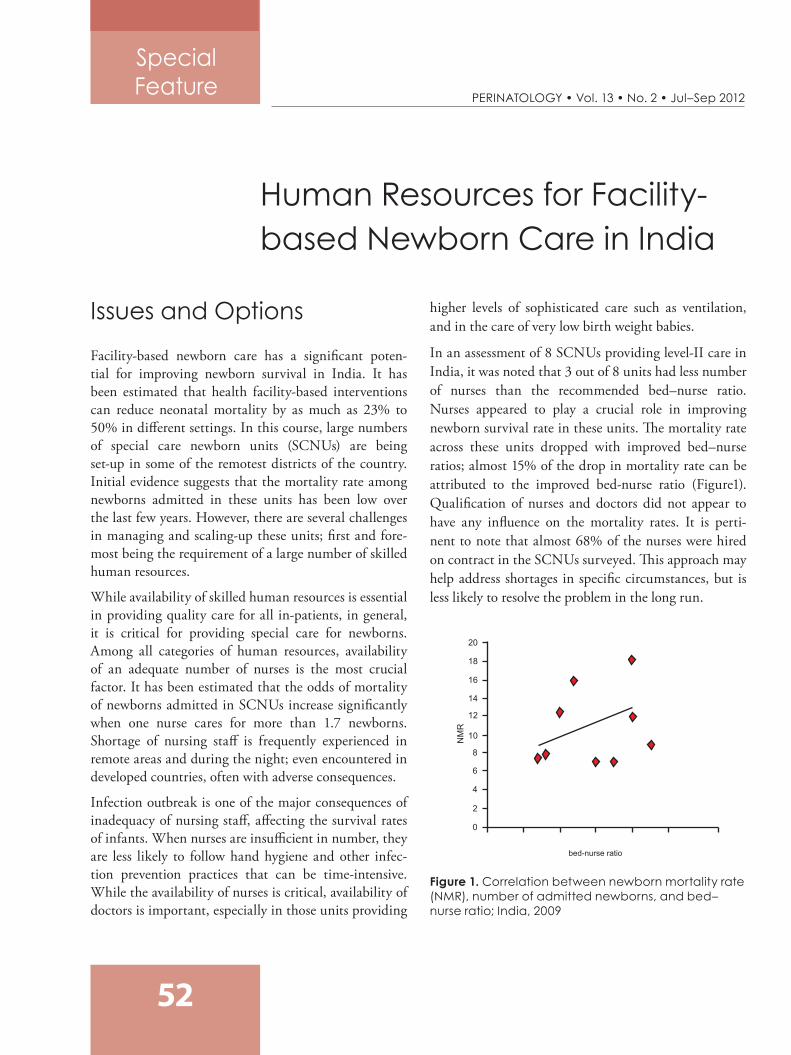
In an assessment of 8 SCNUs providing level-II care in India, it was noted that 3 out of 8 units had less number of nurses than the recommended bed–nurse ratio. Nurses appeared to play a crucial role in improving newborn survival rate in these units. The mortality rate across these units dropped with improved bed–nurse ratios; almost 15% of the drop in mortality rate can be attributed to the improved bed-nurse ratio (Figure1). Qualification of nurses and doctors did not appear to have any influence on the mortality rates. It is perti-nent to note that almost 68% of the nurses were hired on contract in the SCNUs surveyed. This approach may help address shortages in specific circumstances, but is less likely to resolve the problem in the long run.
Figure 1. Correlation between newborn mortality rate (NMR), number of admitted newborns, and bed–nurse ratio; India, 2009
Special Feature
RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 53
Ensuring Adequate Human Resources for Facility-based Newborn Care in IndiaThe following section provides some solutions to address the shortage of skilled and motivated human resources for facility-based newborn care.
Task-shifting: Lowering the Bar From pediatricians to graduate doctorsIn tackling the shortage of skilled doctors for the special care of newborns, the Gujarat, government has launched a training program on “Emergency Newborn Care” (EmNC) for medical officers. The duration of the training is 120 days, of which 30 days are spent in a First Referral Unit (FRU) or a district hospital managing newborns. The state government also assures to place the medical officers in any of the pre-identi-fied FRUs or community health centers on successful completion of the training. .
The Government of Bihar in association UNICEF is contemplating on hosting a short-term certificate course in facility-based newborn care (FBNC) for doctors holding a basic Diploma in Pediatrics. Addi-tionally, doctors certified for FBNC would get pref-erential posting in the upcoming SCNUs on a higher remuneration.
From nurses to nursing aidesFunctions performed by the nurses are of two types: (i) those that are specialized, (ii) those that can be conducted by less skilled persons. In Purulia district, West Bengal, India, newborn aides are engaged in order to partly overcome the problem of severe shortage of trained nurses for SCNUs. Local young women with 10 to 12 years of school education are provided hands-on training for 6 months, followed by an internship for 6 months at a SCNU. They perform simple tasks related to housekeeping and care of newborns under the supervision of trained nurses. Assessment of the aides by external experts suggested that these women had acquired a reasonable level of skills essential for newborn-care. Their involvement in simple tasks freed the nurses (limited number of them) for more special-ized functions.
Proximity of newborns with mothersMaternal involvement in the care of their sick newborns is well recognized to be beneficial for a variety of reasons—increased bonding, early and improved breastfeeding, and better health outcome. Maternal involvement can also be extremely important for reducing the workload of nurses and ensuring adequate bed–nurse ratio. Mothers can play an effective role in the care of newborns that require more-than-usual attention, but may not require admission to an SCNU.
Attract, retain, and motivate human resourcesProviding special care to newborns requires higher level of skills and often involves more strenuous work conditions than in many other medical care disci-plines. The government of Madhya Pradesh in associa-tion with UNICEF has been able to attract and retain paediatricians and nurses for SCNUs by providing them improved work conditions, higher remunera-tion, and public recognition for their work. In many cases, these initiatives have also led to a reversal of brain drain; many doctors have left private practice, while a few others have even sacrificed their career overseas to join these specialized units. Besides improving the remuneration and working conditions for staff SCNUs, the government of Madhya Pradesh has also identi-fied some pediatricians working at the primary health centers (PHC) where their skills are under-utilized and moved them to functional SCNUs.
SummaryAdequacy of skilled human resources is critical for facility-based newborn care. Inadequate human resources, especially nurses, increase the chances of infection outbreaks and thus, increase newborn mortality in SCNUs. Ample number of skilled nurses is an absolute prerequisite for setting up a SCNU. Improving remuneration and working conditions for doctors and nurses can attract and retain specialized human resources at SCNUs in the public sector.
Sources: UNICEF
Indian Institute of Public Health, Delhi National Neonatology Forum
Special Feature
RESEARCH ARTICLESPERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
54
Counseling is a term that denotes a wide variety of procedures aimed to help individuals achieve cultural adjustment and bring about a voluntary change in their lifestyle. By definition, counseling is a special kind of helping relationship, a set of activities and methods, or a defined area in which services are provided.1 When viewed as a helping relationship, it extends an empa-thetic understanding of the client’s problems and provides a genuine solution for the client to exert his potentials to accept and face the reality situations. When viewed as a set of activities or methods, the coun-selor uses his skills, including psychoanalytic or behav-ioral, to assist the client to accept the reality.
When viewed as an area in which services are provided, counseling is a definite method to help the disturbed clients achieve their potentials and enable them to over-come their obstacles, to lead a more meaningful and fuller life. Thus understood, counseling is an interaction between 2 persons, the counselor and the counselee, which takes place in a professional setting, with an aim of bringing about a voluntary change in the behavior of the counselee by making a suitable choice.
Counseling is a learning-oriented process carried out in a simple one-to-one social environment. The counselor, who is professionally competent in relevant psycholog-
ical skills and knowledge, seeks to assist the client by methods appropriate to the latter’s need and within the total personal program such that the client becomes a content and more productive member of the society.
Role of CounselorsCounselors need to be aware of the influence they exert on the client, and hence should be authentic, honest, and sincere in their dealings with the client. They should be deeply involved in their work and have a sincere interest in the welfare of their clients. They must convey empathy and genuineness while speaking, and should be able to convince the client about their earnestness in feeling the client’s pain and suffering. They must develop a supportive alliance that is condu-cive to openness, trust, and respect with the client. They should also develop understanding skills that will assist them in accepting all the client’s reactions and feelings.
The Counseling SessionsIt is preferable to conduct the counseling sessions in a professional manner, with the clients seated comfort-ably while facing the counselor. In medical counseling, normally, the child’s parents are primarily involved, and the decision to include any other responsible family member for the counseling sessions must be
*Correspondence
Dr Sumitha Nayak44, NTI Colony 2nd Main Road RMV Extension 2nd Stage, Bangalore - 560025, Karnataka India
Counseling in Perinatal PracticeSumitha Nayak*
Review Articles

RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 55
Review Articles
Nayak S. Counseling in Perinatal Practice
made by the parents alone. The senior most member of the treating team/counseling team is the person who conducts the sessions. Presence of other team members involved in the active part of the treatment during counseling is an added benefit.2 Normally, the nursing team members are the ones who handle the child most often, hence it is desirous to have them present during the counseling process, as they can provide supportive details of the child’s behavior and responses to the ongoing treatment.
Counseling must be carried out in a vacant room, providing privacy and warmth, with comfortable and adequate seating arrangements for all present, so that there is no feeling of intimidation or coercion for the parents. The doctor/counselor must provide a brief summary of the child’s condition, including diagnosis, investigations done, and treatment that has been initi-ated. This must be followed by a report of the child’s response to the treatment and the possible outcome and prognosis. The parents must be allowed to ask questions and clarify any lingering doubts. The doctor/counselor must at all times provide a patient hearing and certain means for the parents to accept their child’s suffering.
The child’s condition must be explained through simple and understandable terms, especially using the language that the parents are familiar with. Use of too many technical terms should be avoided, unless the parents are well educated to understand what is being said. If possible, a written material relating to the baby’s condition could be provided, as it will have a better rele-vance and impact in understanding the medical condi-tion. The local culture and traditions must be respected at all times. At the end of the session, the discussions could be summarized and signatures of the parents and a witness could be taken at the end of the document, to preserve it along with the baby’s case file.
Situations Requiring CounselingPrenatal counseling This could be a preconception counseling or antenatal counseling.
Preconception counselingPreconception counseling is done before concep-tion. It is usually done in cases where there is a likeli-hood of a genetic disorder in the offspring, in cases of consanguineous marriages, or in cases where a previous offspring has suffered from some genetic conditions in the immediate family. The counseling done here provides an insight into the cause and probability of having a baby with a genetic mutation.
Antenatal counselingAntenatal counseling is done after conception, where a diagnosis of genetic disorder is likely from the ultra-sound reports in case of previous infant mortality, or in case where a previous sibling suffered from congen-ital disorder. Apart from this, in case of oligo- or poly-hydramnios in pregnancy, the likelihood of having an offspring with a genetic abnormality is high.3 There-fore, the parents need to be counseled on the possible outcomes of the pregnancy. This could give them the necessary options to make an informed decision with regard to the pregnancy and to explore other possibili-ties available.4
Perinatal counseling In cases where there is a possibility of any interventions required or any adverse neonatal outcomes, the parents need to be counseled, so that they are made aware of the situation that could arise upon the delivery of the child. It is essential to provide statistical evidence, so that the parents’ have an opportunity to make informed choices and decisions.
Neonatal counselingThe newborn babies’ need utmost care and attention as during this stage they are prone to many complications such as resuscitation, metabolic disorders, and congen-ital anomalies. Under these conditions, the parents need to be counseled with regard to the condition, treatment modalities, and possible outcome and prognosis of the condition. In cases where the newborns need surgery to correct any deformity or genetic anomaly, the parents should be briefly informed about the surgical proce-

RESEARCH ARTICLES
56 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
Nayak S. Counseling in Perinatal Practice
Review Articles
dure, postoperative needs and care, and subsequent follow-up that may be required. Also they need to know about the continuance of care, after discharge care, etc. All this information should be provided during the course of the counseling sessions.
Predischarge counselingThis is essential for all neonatal intensive care unit (NICU) graduates, at the time of discharge. The parents are told about their baby’s condition, follow-up requirements, methods to care for the baby at home, immunization requirements and schedules, feeding medication instructions, etc. Additionally, the possible danger signs that need to be watched for are explained in detail.
Bereavement counselingIn cases where the neonatal outcome is adverse, that is, the baby is either stillborn or has expired despite all resuscitative efforts, the parents are usually shattered. This situation should be handled extremely delicately. The treating doctor must break the news with utmost empathy toward the bereaved family. Neonatal loss is always hard to cope with, especially for the mother.
Hence, the counseling must be guided toward accept-ance of the loss. This is probably the most challenging task any counselor has to face during his career. Support groups and social workers go a long way in continuing the counseling process and providing the much needed support to the bereaved family.
Key MessagesCounseling is a helping relationship, a set of activities, and a definite area in which help is provided for a client.
Counseling needs to be conducted in a professional manner with utmost empathy toward the client.
Perinatal and neonatal counseling needs to be done routinely to keep the parents aware and up-to-date about their child’s progress and development.
References1. Principles ofGuidance andCounselingCoursebook II,
AnnamalaiUniversity:Pg4-7,2012.2. PejaverR.Parentcounselingonperinatalcare:Textbookof
Perinatology. 3. PejaverR.Parentcounseling:TextbookofPerinatology. 4. Nelson’s textbook of Pediatrics: 18th edition:Genetic
counseling,chapter83.1.
RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 57
Review Articles
*Correspondence
Indu S NairConsultant Neonatologist Manipal Hospital, Airport Road Bangalore - 560017 Karnataka, India
Email: [email protected]
Perinatal Congenital Cytomegalovirus InfectionIndu S Nair*
SummaryCytomegalovirus (CMV) has a high prevalence rate of 65% to 90% in the west and 80% to 90% in India with a risk of 2% to 2.5% seroconversion in pregnancy. Maternal infection during pregnancy can be primary infection, reactivation, or recurrent infection. Diagnosis of primary maternal CMV infection in preg-nancy is through the detection of specific IgM antibodies asso-ciated with low IgG avidity. The prenatal diagnosis of fetal CMV infection is based on amniocentesis.
Hearing impairment is seen in 10% to 15% of congenital CMV infections and in 30% to 65% of symptomatic neonates. CMV infection is also the single most important cause of sensorineural hearing loss in children.
Recommended antiviral drugs for the treatment of CMV infection are ganciclovir (intravenous) and valaganciclovir (oral). Real time polymerase chain reaction (RT-PCR) assays of liquid or dried saliva samples could be adopted for large scale screening of newborns. Until a new vaccine is available, hygienic measures are important as prophylaxis.
RESEARCH ARTICLES
58 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
IntroductionHuman CMV (HCMV) is a double stranded DNA virus of the Herpesviridae family. Margaret G Smith recovered the first isolate of the virus in 1956 from the submaxillary gland tissue of a dead infant.1
Although CMV has a worldwide distribution with a prevalence of 65% to 90% in USA, it is more prevalent in developing countries and among women in lower socioeconomic groups of developed countries.2,3 Sero-logical surveys from India have shown in a prevalence rate of 80% to 90% CMV IgG antibodies in women of childbearing age.4 Risk of seroconversion during preg-nancy averages 2.0% to 2.5%.
Transmission and Patho-genesis of Congenital Cytomegalovirus Infection There are 3 modes of transmissions through which CMV can infect newborns. They are: (i) intrauterine, (ii) intrapartum, and (iii) postnatal (breast milk acquisi-tion or through blood transfusions given postnatally).
Maternal infections during pregnancy includes primary infection, reactivation of latent infection, or recurrence of infection with a new strain.
Primary CMV infections are reported in 1% to 4% of seronegative women during pregnancy with a 30% to 40% risk of viral transmission to the fetus, of which 5% to 15% cause symptomatic infection in the neonate.5,6 Reactivation of CMV infection during pregnancy is reported in 10% to 30% of seropositive women and the risk of transmission is about 1% to 3%.6 Recur-rent infections are caused either by reinfection with new CMV strain or reactivation of a latent infection. The congenital infection rate in infants born to mothers with preconception immunity is between 0.2% and 2%, and they are rarely symptomatic.7
Among pregnant women, 40% to 60% are susceptible to CMV at conception. Of these, 1% to 4% will acquire CMV during pregnancy. On an average, about 40% to 50% of these infected women transmit the virus to the
fetus resulting in about one-third of the infants devel-oping severe neurological impairment and sequelae.8
The transmission rate is 35% if infection is acquired in the first trimester and increases to 75% in the last trimester, but infections early in gestation probably result in more severe congenital disease. Infant hearing-loss was observed in those infants born of women who had recurring infections, but it was not found to be as profound as that observed in children born to mothers without preconception immunity.9
Diagnosis and Management of Cytomegalovirus Infec- tion During PregnancyDiagnosisSerologic diagnosis of primary CMV infection during pregnancy is documented by seroconversion (appear-ance of CMV-specific IgG antibodies in a previously seronegative woman).11,12 In the absence of universal serial serologic screening of pregnant women, diagnosis through seroconversion is seldom achieved as an initial seronegative serum is rarely available.
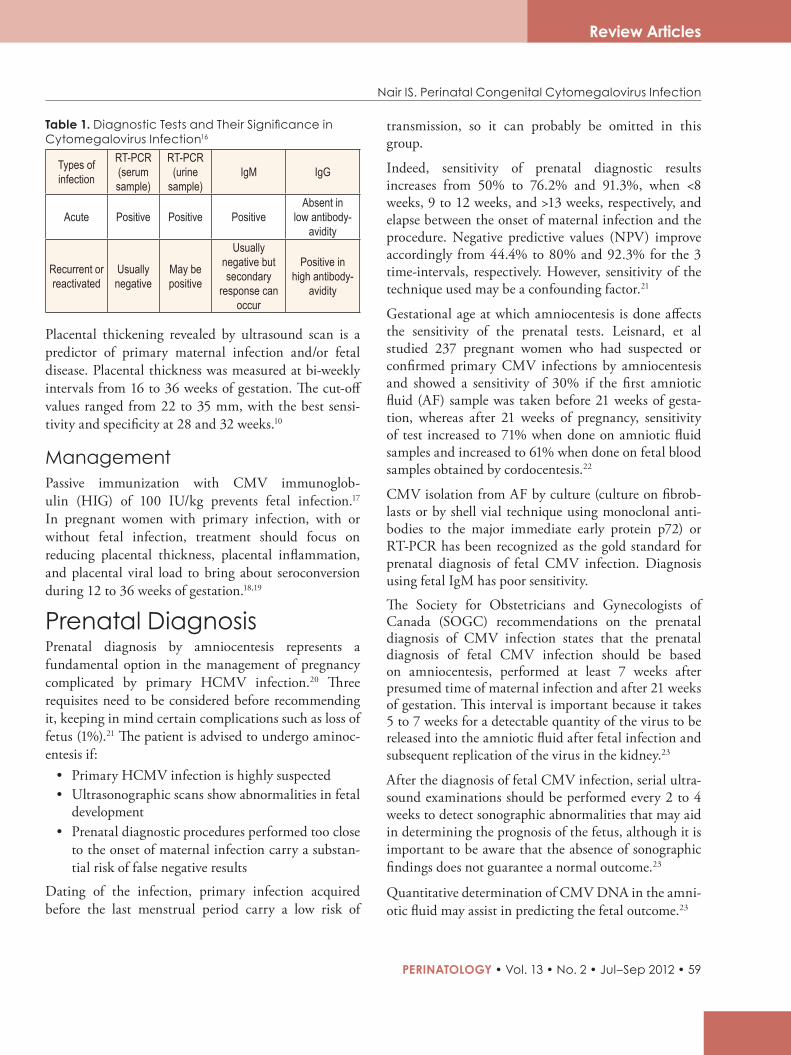
When the immune status before pregnancy is unknown, determination of primary CMV infection should be based on the detection of specific IgM anti-bodies. But, serum can even test positive for IgM for about 9 to 12 months after an acute infection or due to anamnestic responses of the immune system trig-gered by recurrent or reactivated infection.13 In such instances, IgG avidity assay can be extremely helpful in differentiating the primary infection from past or recurrent infection. Antibody avidity is an indirect measure of the tightness of antibody binding to its target antigen. Avidity levels are reported as avidity index expressing the percentage of IgG bound to the antigen after treatment with denaturing agents. An avidity index >60% is highly suggestive of past or secondary infection, while an avidity index <30% is highly suggestive of a recent primary infection (dura-tion <3 months).14,15 Table 1 lists the key tests for the diagnosis of CMV during pregnancy.16
Review Articles
Nair IS. Perinatal Congenital Cytomegalovirus Infection
RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 59
Table 1. Diagnostic Tests and Their Significance in Cytomegalovirus Infection16
Types of infection
RT-PCR (serum sample)
RT-PCR (urine
sample)IgM IgG
Acute Positive Positive PositiveAbsent in
low antibody-avidity
Recurrent or reactivated
Usually negative
May be positive
Usually negative but secondary
response can occur
Positive in high antibody-
avidity
Placental thickening revealed by ultrasound scan is a predictor of primary maternal infection and/or fetal disease. Placental thickness was measured at bi-weekly intervals from 16 to 36 weeks of gestation. The cut-off values ranged from 22 to 35 mm, with the best sensi-tivity and specificity at 28 and 32 weeks.10
ManagementPassive immunization with CMV immunoglob-ulin (HIG) of 100 IU/kg prevents fetal infection.17 In pregnant women with primary infection, with or without fetal infection, treatment should focus on reducing placental thickness, placental inflammation, and placental viral load to bring about seroconversion during 12 to 36 weeks of gestation.18,19
Prenatal DiagnosisPrenatal diagnosis by amniocentesis represents a fundamental option in the management of pregnancy complicated by primary HCMV infection.20 Three requisites need to be considered before recommending it, keeping in mind certain complications such as loss of fetus (1%).21 The patient is advised to undergo aminoc-entesis if:
• Primary HCMV infection is highly suspected • Ultrasonographic scans show abnormalities in fetal
development• Prenatal diagnostic procedures performed too close
to the onset of maternal infection carry a substan-tial risk of false negative results
Dating of the infection, primary infection acquired before the last menstrual period carry a low risk of
transmission, so it can probably be omitted in this group.
Indeed, sensitivity of prenatal diagnostic results increases from 50% to 76.2% and 91.3%, when <8 weeks, 9 to 12 weeks, and >13 weeks, respectively, and elapse between the onset of maternal infection and the procedure. Negative predictive values (NPV) improve accordingly from 44.4% to 80% and 92.3% for the 3 time-intervals, respectively. However, sensitivity of the technique used may be a confounding factor.21
Gestational age at which amniocentesis is done affects the sensitivity of the prenatal tests. Leisnard, et al studied 237 pregnant women who had suspected or confirmed primary CMV infections by amniocentesis and showed a sensitivity of 30% if the first amniotic fluid (AF) sample was taken before 21 weeks of gesta-tion, whereas after 21 weeks of pregnancy, sensitivity of test increased to 71% when done on amniotic fluid samples and increased to 61% when done on fetal blood samples obtained by cordocentesis.22
CMV isolation from AF by culture (culture on fibrob-lasts or by shell vial technique using monoclonal anti-bodies to the major immediate early protein p72) or RT-PCR has been recognized as the gold standard for prenatal diagnosis of fetal CMV infection. Diagnosis using fetal IgM has poor sensitivity.
The Society for Obstetricians and Gynecologists of Canada (SOGC) recommendations on the prenatal diagnosis of CMV infection states that the prenatal diagnosis of fetal CMV infection should be based on amniocentesis, performed at least 7 weeks after presumed time of maternal infection and after 21 weeks of gestation. This interval is important because it takes 5 to 7 weeks for a detectable quantity of the virus to be released into the amniotic fluid after fetal infection and subsequent replication of the virus in the kidney.23
After the diagnosis of fetal CMV infection, serial ultra-sound examinations should be performed every 2 to 4 weeks to detect sonographic abnormalities that may aid in determining the prognosis of the fetus, although it is important to be aware that the absence of sonographic findings does not guarantee a normal outcome.23
Quantitative determination of CMV DNA in the amni-otic fluid may assist in predicting the fetal outcome.23
Review Articles
Nair IS. Perinatal Congenital Cytomegalovirus Infection
RESEARCH ARTICLES
60 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
Presence of the virus in fetal blood can be ascertained by means of rapid assays of (i) viremia, infectious HCMV in leukocytes; (ii) antigenemia, presence of pp65-positive leukocytes; (iii) DNAemia, detection of viral DNA; and more recently, (iv) IEmRNAemia—detection of IE-messenger RNA in whole blood.
Determination of IEmRNA and pp67 mRNA by the nucleic acid sequence-based amplification (NASBA) assay in fetal blood provides sensitivities comparable to PCR (84.6%) and antigenemia (63.6%), respectively, with 100% specificities.20
Congenital CytomegalovirusOnly 10% of those infected are symptomatic, with multiorgan involvement, especially the reticuloen-dothelial system and central nervous system (CNS). The patients have retarded growth and with jaundice as well as petechiae; hepatosplenomegaly; neurological disabilities like microcephaly, seizures, learning disabil-ities, mental retardation, and autism; hearing impair-ment; and visual deficits.
Central nervous system damageAbout 10% to 20% neonates showed neurological damage on follow-up. One-third of symptomatic neonates had a normal outcome, conversely not all asymptomatic neonates will have a normal outcome. Mortality was around 30%. Predictors of poor cogni-tive outcome were ventriculomegaly, brain atrophy, involvement of deep parietal white matter, and intracra-nial calcifications.
Hearing impairmentHearing impairment was seen in 10% to 15% of congenital CMV and in 30% to 65% of symptomatic neonates, and was the single most important cause of sensorineural hearing loss in children. A neonatal screening program can detect less than half of all the sensorineural deafness caused by CMV infection.24 Visual-incidence of chorioretinitis in symptomatic newborns was 15% to 30%.
Diagnosis and Treatment of Congenital Cytomegalovirus InfectionDiagnosis is through demonstration of the virus by (i) isolation from urine samples; (ii) detection of CMV-DNA in urine, blood/dried blood spots (DBS), saliva, or cerebrospinal fluid samples (before 3 weeks of age) by PCR; and (iii) detection of antigen or CMV–IgM in blood. The shell vial assay (72 h) and detec-tion of viral DNA in urine by PCR have become the standard tests carried out in most laboratories.25
Currently, there are 4 licensed drugs for the systemic treatment of CMV infection—ganciclovir, valgan-ciclovir (oral prodrug of ganciclovir), cidofovir, and foscarnet. In addition, fomivirisen is licensed for intrav-itreal administration to treat CMV retinitis in patients with AIDS.26 Only ganciclovir and valganciclovir are used in the treatment of congenital CMV. National Institute of Allergy and Infectious Diseases’ Collaborative Antiviral Study Group (NIAID CASG) conducted a pharmacokinetic/pharmacodynamic study that established a safe dose of intravenous (IV) ganci-clovir for administration to infected infants.27 A phase III study of ganciclovir therapy at 6 mg/kg per dose intravenously every 12 h for 6 weeks showed improved hearing in the treatment group as compared to the control group; after 6 months follow-up when assessed by brainstem-evoked response (BSER) audiometry.28 The use of ganciclovir should be limited (causes severe neutropenia) to pregnant women and those children with symptomatic disease, as the medication is muta-genic, teratogenic, and carcinogenic. The drug has been approved for treatment in neonates.29 A study by Kimberlin, et al showed that administration of 6 mg/kg of ganciclovir (IV) and 16 mg/kg of oral valganciclovir for 6 weeks had similar results.30,31
Currently, the NIAID CASG is conducting a controlled clinical trial of 6 weeks versus 6 months of valganci-clovir therapy to determine whether longer duration of treatment is associated with improved hearing and developmental benefits. A recent study reported better auditory outcome at 12 months when symptomatic congenital CMV infection was treated with IV ganci-
Review Articles
Nair IS. Perinatal Congenital Cytomegalovirus Infection
RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 61
clovir for 6 weeks followed by oral valganciclovir for 12 months.32
Maribavir, a benzimidazole L-riboside, whose mecha-nism of activity has been mapped to the viral protein products of UL97 and UL27, may provide a new option for the treatment of congenital CMV disease.25 as maribavir does not need to be phosphorylated by UL97 kinase, as does ganciclovir, it has the potential to be useful in the treatment of ganciclovir resistant strains of CMV.
Screening for Congenital Cytomegalovirus InfectionCongenital CMV infection occurs in 0.2% to 2% of births in developed countries and is a leading cause of nongenetic sensorineural hearing loss. Screening of newborns for CMV infection will permit early iden-tification of at-risk infants so that timely interven-tion during critical stages of speech and language development can prevent further damage. Tradition-ally, screening of congenital CMV infection has been performed by culturing CMV from urine or saliva samples collected within 3 weeks of child birth. Few studies have examined the use of DBSs for congen-ital CMV diagnosis though DBS-based assays are of limited sensitivity, has low virus loads in blood (in asymptomatic cases), and needs efficient DNA extrac-tion and sensitive PCR assays.33-36
Recently, a large multicentic study on 21,000 neonates in Japan conducted using urine samples on filter cards and quantitative PCR, identified congenital CMV infection in 0.13% of neonates (65% CI: 0.24%–0.39%), of whom 30% were symptomatic with a posi-tive predictive value of 94%.37
A large prospective study of CMV screening in newborns showed that the RT-PCR assay of dried-saliva samples has excellent sensitivity (97.4%) and specificity (99.9%). The sensitivity and specificity of the liquid-saliva PCR assay were 100% and 99.9%, respec-tively.38 This indicates that RT-PCR assays of liquid or dried saliva samples should be adopted for large-scale screening of newborns, and will help identify most infants who have congenital CMV infection.38
PreventionThe ultimate goal in prevention of congenital CMV infection is to develop a vaccine that would be adminis-tered to seronegative women of childbearing age. These experimental vaccines include a live attenuated strain of CMV (Towne), and a recombinant protein vaccine that uses major glycoprotein B of CMV and an adju-vant (MF59).39,40
Until then it is recommended that pregnant women be counseled regarding hygienic interventions as many studies have proved their efficacy in reducing their risk of CMV infection.41
References1. ChakravartiA,etal.Cytomegalovirusinfection:anIndian
perspective. Ind J Med Microbiol.2009;27:3–11.2. ChakravartyA, et al.The seroepidemiological study on
cytomegalovirusinwomenofchildbearingagewithspecialreferencetopregnancyandmaternal-fetaltransmission. Ind J Pathol Microbiol.2005;48:518–521.
3. Staras SAS, et al. Seroprevalence of cytomegalovirusinfectionintheUnitedStates,1988–1994. Clin Infect Dis.2006;43:1143–1151.
4. GandhokeI,etal.CongenitalCMVinfectioninsymptomaticinfants inDelhi and surrounding areas. Ind J Pediatr.2006;73:1095–1097.
5. Ahlfors K, et al. Primary and secondary maternalcytomegalovirusinfectionsandtheirrelationtocongenitalinfection. Analysis ofmaternal sera.Acta Pediatr Scand.1982;71:109–113.
6. Stagno S, et al. Congenital cytomegalovirus infection,the relative importanceofprimaryandrecurrentmaternalinfections. N Engl J Med.1982;306:945–949.
7. Stuart P, et al. Recent advances in the prevention andtreatmentofcongenitalcytomegalovirusinfections. Semin Perinatol.2007;31:10–18.
8. NigroG,etal.Passiveimmunizationduringpregnancyforcongenital cytomegalovirus infection. N Engl J of Med.2005;353(13):1350–1362.
9. RossSA, et al.Hearing loss in childrenwith congenitalcytomegalovirusinfectionborntomotherswithpreexistingimmunity. J Pediatr.2006;148(3):332–336.
10. Fowler KB, et al.Maternal immunity and preventionof congenital cytomegalovirus infection. JAMA.2003;289(8):1008–1011.
11. Lagrou K, et al. Evaluation of the new architectcytomegalovirus immunoglobulinM(IgM),IgG,andIgGavidityassays. J Clin Microbiol.2009;47(6):1695–1699.
Review Articles
Nair IS. Perinatal Congenital Cytomegalovirus Infection
RESEARCH ARTICLES
62 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
12. CarlierP,etal.LaboratoryevaluationofthenewAccess®cytomegalovirusimmunoglobulinIgMandIgGassays. J Clin Virol.2010;49(3):192–197.
13. RevelloMG,GernaG.Diagnosisandmanagementofhumancytomegalovirusinfectioninthemother,fetus,andnewborninfant. Clin Microbiol Rev.2002;15(4):680–715.
14. Lazzarotto T, et al.Anticytomegalovirus (anti-CMV)immunoglobulinGavidityindentificationofpregnantwomenatriskoftransmittingcongenitalCMVinfection. Clin Diagn Lab Immunol.1999;6(1):127–129.
15. Grangeot-KerosL,etal.Valueofcytomegalovirus(CMV)IgGavidityindexforthediagnosisofprimaryCMVinfectioninpregnantwomen. J Infect Dis.1997;175:944–946.
16. PatrickDuff.DiagnosisandmanagementofCMVinfectioninpregnancy. Perinatology.2010;1:1.
17. NigroG, et al. Passive immunization during pregnancyfor congenital cytomegalovirus infection. N Engl J Med.2005:353(13):1350–1362.
18. LaTorreR, et al. Placental enlargement inwomenwithprimarymaternal cytomegalovirus infection is associatedwithfetalandneonataldisease. Clin Infect Dis.2006;43(8):994–1000.
19. MaidjiE,etal.Antibodytreatmentpromotescompensationfor human cytomegalovirus-induced pathogenesis and ahypoxia-likeconditioninplacentaswithcongenitalinfection. Am J Pathol.2010;177(3):1298–1310.
20. RevelloMG,GernaG.Diagnosisandmanagementofhumancytomegalovirusinfectioninthemother,fetusandnewborninfants. Clin Microbiol Rev.2002;15:680–715.
21. RevelloMG,GernaG.Pathogenesisandprenataldiagnosisofhumancytomegalovirusinfection. J Clin Virol.2004;29:71-83.
22. Liesnard C, et al. Prenatal diagnosis of congenitalcytomegalovirus infection: prospective study of 237pregnanciesatrisk. Obstet Gynecol.2000;95:881–888.
23. YoavYinonY,etal.Cytomegalovirusinfectioninpregnancy. SOGCclinicalpracticeguideline.J Obstet Gynaecol Can.2010;32(4):348–354.
24. FowlerKB,etal.Newbornhearingscreening:willchildrenwith hearing loss caused by congenital cytomegalovirusinfectionbemissed?J Pediatr. 1999;35:60–64.
25. MocarskiES,etal.Cytomegalovirus. In:FieldsBN,KnipeDM,HowleyPM,etal.eds.Virology.5thed.Philadelphia:LippincottWilliamsandWilkins;2007:2701–2772.
26. NassettaL,etal.Treatmentofcongenitalcytomegalovirusinfection: implications for future therapeutic strategies. J Antimicrob Chemother.2009;63:862–867.
27. WhitleyRJ, et al.Ganciclovir treatment of symptomaticcongenitalcytomegalovirusinfection:resultsofaphaseIIstudy. J Infect Dis.1997;53:1080–1086.
28. KimberlinDW,etal.Effectofganciclovirtherapyonhearinginsymptomaticcongenitalcytomegalovirusdiseaseinvolvingthecentralnervoussystem:arandomized,controlledtrial. J Pediatr.2003;143:16–25.
29. AmericanAcademy of Pediatrics. Cytomegalovirusinfection. In:PickeringLK,ed.2006 Red Book: Report of the Committee on Infectious Disease. 27th ed.ElkGroveVillage,IL:AmericanAcademyofPediatrics;2006:273–277.
30. KimberlinDW,etal.Pharmacokineticandpharmacodynamicassessment of oral valganciclovir in the treatment ofsymptomatic congenital cytomegalovirus disease. J Infect Dis.2008;197(6):836–845.
31. AcostaEP,etal.Ganciclovirpopulationpharmacokineticsinneonatesfollowingintravenousadministrationofganciclovirandoraladministrationofaliquidvalganciclovirformulation. Clin Pharmacol Ther.2007;81(6):867–872.
32. Amir J, et al. Treatment of symptomatic congenitalcytomegalovirus infectionwith intravenous ganciclovirfollowedby long-termoral valganciclovir. Eur J Pediatr.2010;169(9):1061–1067.
33. BarbiM, et al.Multicity Italian study of congenitalcytomegalovirus infection. Pediatr Infect Dis J. 2006;25:156–159.
34. Scanga L, et al. Diagnosis of human congenitalcytomegalovirus infection by amplification of viralDNAfromdried blood spots on perinatal cards. J Mol Diagn.2006;8:240–245.
35. Boppana SB, et al. National Institute onDeafness andOther Communication Disorders CMV and HearingMulticenter Screening (CHIMES) Study. Dried bloodspot real-timepolymerase chain reaction assays to screennewbornsforcongenitalcytomegalovirusinfection.JAMA.2010;303:1375–1382.
Review Articles
Nair IS. Perinatal Congenital Cytomegalovirus Infection
RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 63
36. InoueN,Koyano S. Evaluation of screening tests forcongenitalcytomegalovirusinfection. Pediatr Infect Dis J.2008;27:182–184.
37. ShinKoyano,etal.Screeningforcongenitalcytomegalovirusinfectionusingnewbornurine samples collectedonfilterpaper: feasibility andoutcomes fromamulticentre study. BMJ.2011;1(1).doi:1:e000118doi:10.113.
38. BoppanaSB,etal.Salivapolymerase-chain-reactionassayforcytomegalovirusscreeninginnewborns. N Engl J Med.2011;364(22):2111–2118.
39. AdlerSP,et al.Safetyand immunogenicityof theTownestrain cytomegalovirus vaccine. Pediatr Infect Dis J.1998;17:200–206.
40. PassRF,etal.AsubunitcytomegalovirusvaccinebasedonrecombinantenvelopeglycoproteinBandanewadjuvant. J Infect Dis.1999;180:970–975.
41. Adler SP, et al. Recent advances in the prevention andtreatmentofcongenitalcytomegalovirusinfections. Semin Perinatol.2007;31:10–18.
Review Articles
Prevalence of Risk Factors for Sensorineural Hearing Loss in NICU Newborns
Speleman K, et al.
B-ENT. 2012;8(1):1–6.
The aim of this study was to determine the prevalence and significance of traditional risk factors associated with sensorineural hearing loss (SNHL). The study included a population of 615 neonates who attended the neonatal intensive care unit (NICU) of the University Hospital in Leuven, Belgium between January 2005 and December 2007.
Auditory brainstem response (ABR) audiometry using 40 dB stimuli was performed in all 615 neonates. A ret-rospective medical database analysis was carried out to evaluate the influence of 14 predetermined risk factors. The evaluated risk factors included ototoxic medication, hyperbilirubinemia, in-utero infections (together with CMV, rubella, syphilis, herpes, and toxoplasmosis), craniofacial anomalies, syndromes asso-ciated with SNHL, low-birth weight (< 1500 g), low Apgar score, mechanical ventilation lasting for 5 days or longer, bacterial meningitis, family history of hereditary childhood SNHL, endocranial hemorrhage, hypoxic ischemic encephalopathy, convulsions, and sepsis.
Uni- or bilateral hearing impairment was diagnosed in 25 of 615 neonates (4.1%). The significant risk factors observed in correlation with SNHL were in-utero infections (especially CMV), craniofacial anomalies, and syn-dromes known to include SNHL, whereas for the remaining risk factors, no significant correlation with SNHL was found.
In this study, only in-utero infections (especially CMV), craniofacial anomalies, and syndromes known to include SNHL were significant risk factors associated with SNHL. Adequate management of hyperbiliru-binemia and ototoxic drug administration may eliminate some of the major historical risk factors associated with SNHL in NICU neonates.
Nair IS. Perinatal Congenital Cytomegalovirus Infection
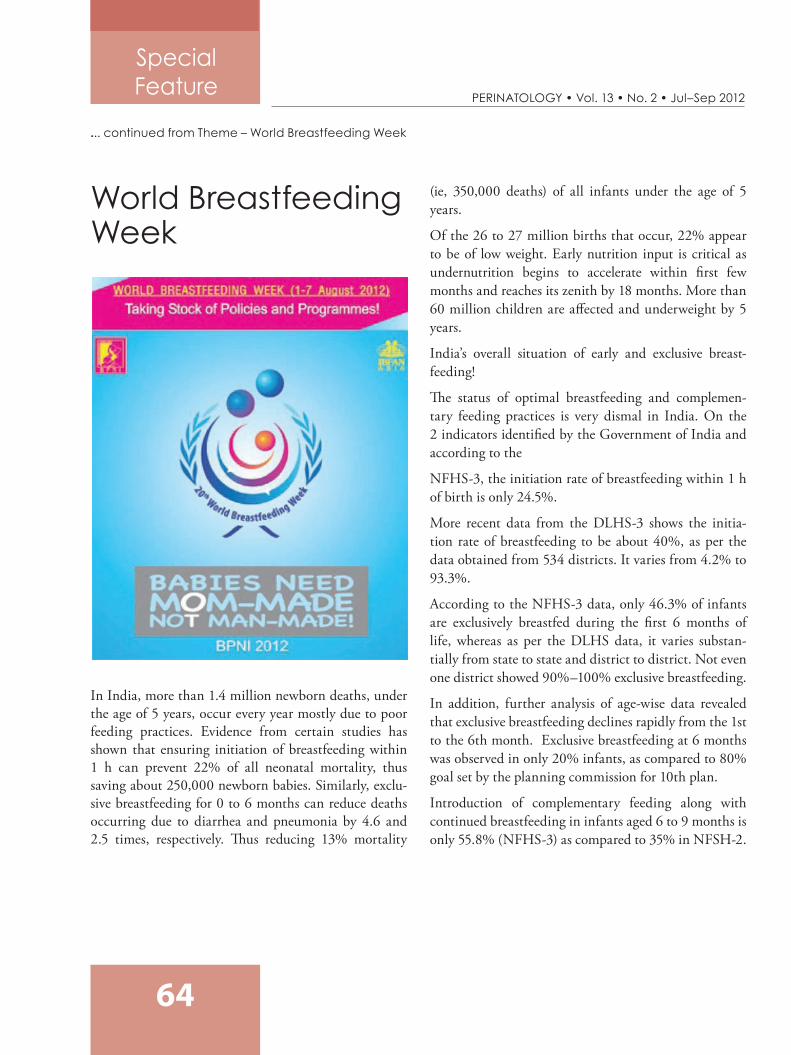
RESEARCH ARTICLESPERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
64
World Breastfeeding Week
In India, more than 1.4 million newborn deaths, under the age of 5 years, occur every year mostly due to poor feeding practices. Evidence from certain studies has shown that ensuring initiation of breastfeeding within 1 h can prevent 22% of all neonatal mortality, thus saving about 250,000 newborn babies. Similarly, exclu-sive breastfeeding for 0 to 6 months can reduce deaths occurring due to diarrhea and pneumonia by 4.6 and 2.5 times, respectively. Thus reducing 13% mortality
(ie, 350,000 deaths) of all infants under the age of 5 years.
Of the 26 to 27 million births that occur, 22% appear to be of low weight. Early nutrition input is critical as undernutrition begins to accelerate within first few months and reaches its zenith by 18 months. More than 60 million children are affected and underweight by 5 years.
India’s overall situation of early and exclusive breast-feeding!
The status of optimal breastfeeding and complemen-tary feeding practices is very dismal in India. On the 2 indicators identified by the Government of India and according to the
NFHS-3, the initiation rate of breastfeeding within 1 h of birth is only 24.5%.
More recent data from the DLHS-3 shows the initia-tion rate of breastfeeding to be about 40%, as per the data obtained from 534 districts. It varies from 4.2% to 93.3%.
According to the NFHS-3 data, only 46.3% of infants are exclusively breastfed during the first 6 months of life, whereas as per the DLHS data, it varies substan-tially from state to state and district to district. Not even one district showed 90%–100% exclusive breastfeeding.
In addition, further analysis of age-wise data revealed that exclusive breastfeeding declines rapidly from the 1st to the 6th month. Exclusive breastfeeding at 6 months was observed in only 20% infants, as compared to 80% goal set by the planning commission for 10th plan.
Introduction of complementary feeding along with continued breastfeeding in infants aged 6 to 9 months is only 55.8% (NFHS-3) as compared to 35% in NFSH-2.
... continued from Theme – World Breastfeeding Week
Special Feature
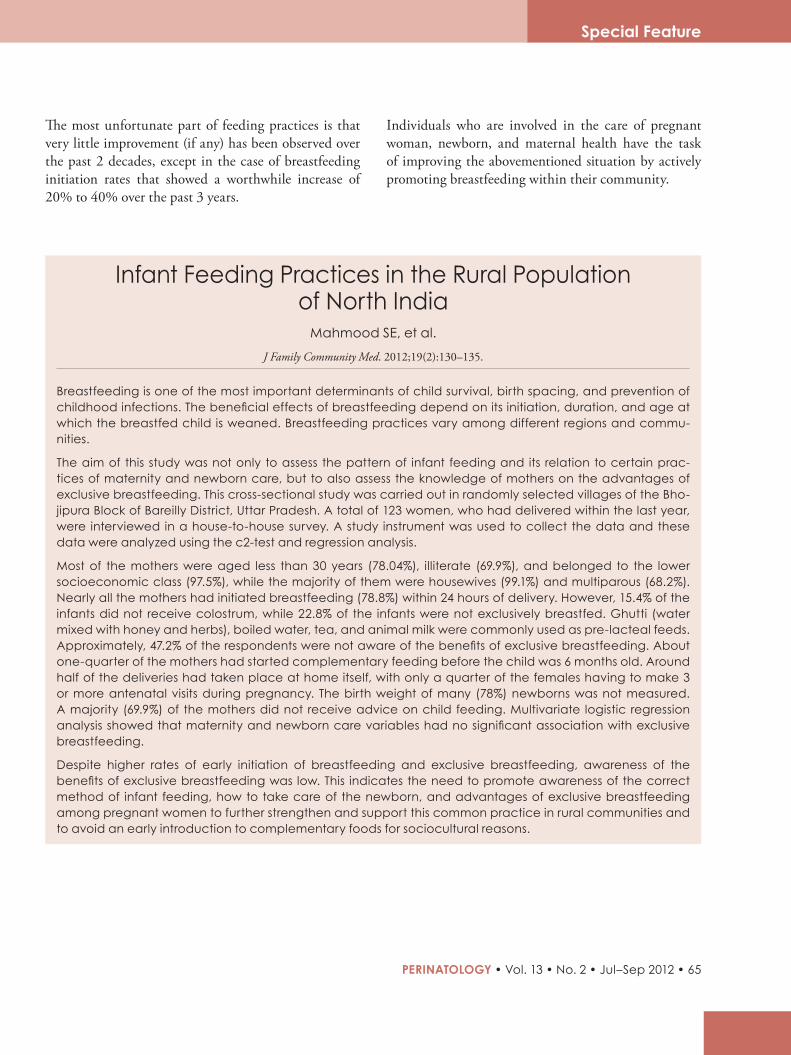
RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 65
The most unfortunate part of feeding practices is that very little improvement (if any) has been observed over the past 2 decades, except in the case of breastfeeding initiation rates that showed a worthwhile increase of 20% to 40% over the past 3 years.
Individuals who are involved in the care of pregnant woman, newborn, and maternal health have the task of improving the abovementioned situation by actively promoting breastfeeding within their community.
Infant Feeding Practices in the Rural Population of North India
Mahmood SE, et al.
J Family Community Med. 2012;19(2):130–135.
Breastfeeding is one of the most important determinants of child survival, birth spacing, and prevention of childhood infections. The beneficial effects of breastfeeding depend on its initiation, duration, and age at which the breastfed child is weaned. Breastfeeding practices vary among different regions and commu-nities.
The aim of this study was not only to assess the pattern of infant feeding and its relation to certain prac-tices of maternity and newborn care, but to also assess the knowledge of mothers on the advantages of exclusive breastfeeding. This cross-sectional study was carried out in randomly selected villages of the Bho-jipura Block of Bareilly District, Uttar Pradesh. A total of 123 women, who had delivered within the last year, were interviewed in a house-to-house survey. A study instrument was used to collect the data and these data were analyzed using the c2-test and regression analysis.
Most of the mothers were aged less than 30 years (78.04%), illiterate (69.9%), and belonged to the lower socioeconomic class (97.5%), while the majority of them were housewives (99.1%) and multiparous (68.2%). Nearly all the mothers had initiated breastfeeding (78.8%) within 24 hours of delivery. However, 15.4% of the infants did not receive colostrum, while 22.8% of the infants were not exclusively breastfed. Ghutti (water mixed with honey and herbs), boiled water, tea, and animal milk were commonly used as pre-lacteal feeds. Approximately, 47.2% of the respondents were not aware of the benefits of exclusive breastfeeding. About one-quarter of the mothers had started complementary feeding before the child was 6 months old. Around half of the deliveries had taken place at home itself, with only a quarter of the females having to make 3 or more antenatal visits during pregnancy. The birth weight of many (78%) newborns was not measured. A majority (69.9%) of the mothers did not receive advice on child feeding. Multivariate logistic regression analysis showed that maternity and newborn care variables had no significant association with exclusive breastfeeding.
Despite higher rates of early initiation of breastfeeding and exclusive breastfeeding, awareness of the benefits of exclusive breastfeeding was low. This indicates the need to promote awareness of the correct method of infant feeding, how to take care of the newborn, and advantages of exclusive breastfeeding among pregnant women to further strengthen and support this common practice in rural communities and to avoid an early introduction to complementary foods for sociocultural reasons.
Special Feature
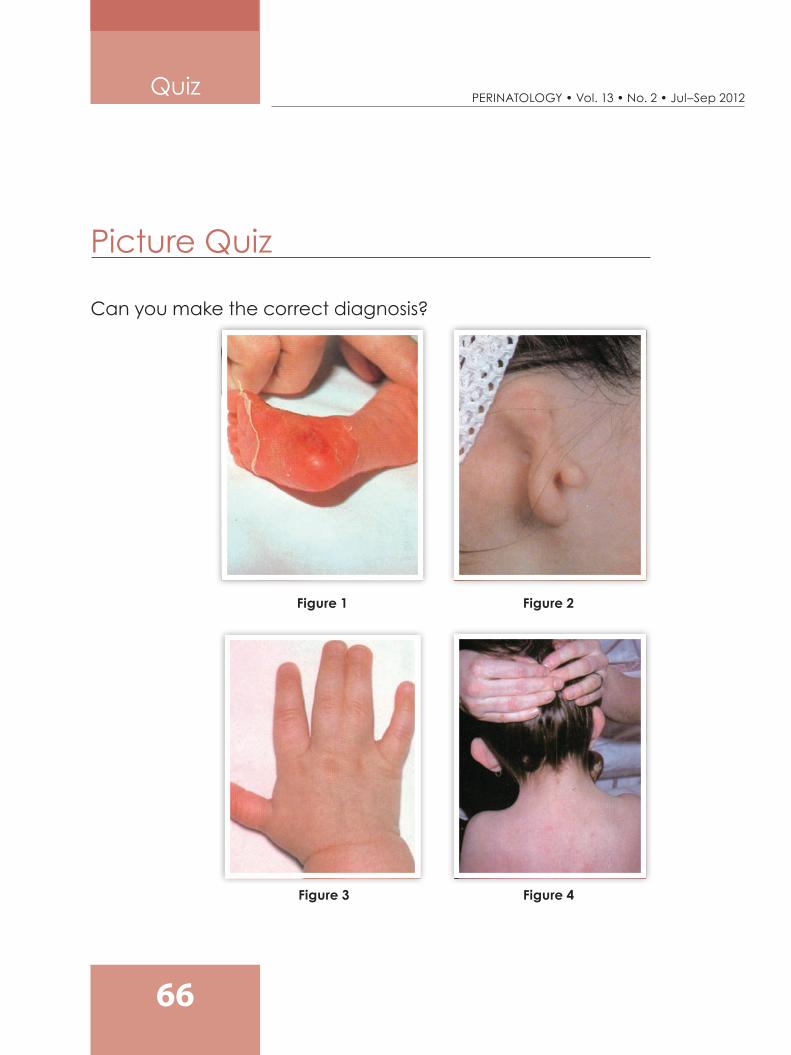
RESEARCH ARTICLESPERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
66
Quiz
Can you make the correct diagnosis?
Figure 1
Figure 3
Figure 2
Figure 4
Picture Quiz
RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 67
Quiz
Self-assessment Quiz
Self-assessment Quiz
1. Prostaglandins
a. are small peptidesb. are synthesized by vascular endotheliumc. are stored in granulesd. are metabolized in plateletse. have plasma half-live of one hour
2. Progesterone
a. relaxes the myometriumb. stimulates respirationc. is given orally for therapeutic purposesd. causes a fall in basal body temperaturee. is a glycoprotein
3.Neisseriagonorrhoeae
a. is a diplococcusb. is usually found extracellularlyc. is a commensal in the nasopharynxd. may be detected by fluorescent staininge. is a commensal in the rectum
4.Candidaalbicans
a. is an anaerobeb. is a commensal in the bowelc. has flagellaed. is Gram-positivee. colonies appear as sulphur granules
5. A patient who is 32 weeks pregnant and who has an antepartum hemorrhage
a. requires admission to hospitalb. requires placental localizationc. should be delivered forthwithd. should not be examined vaginally under any
circumstancese. usually requires a blood transfusion
6. External cephalic version is contraindi-cated in patients with
a. an antepartum hemorrhageb. placenta previac. multiple pregnanciesd. hypertensione. a scarred uterus
7. Serum fructosamine concentration
a. is dependent on hemoglobin concentrationb. is dependent on plasma protein concentrationc. falls during pregnancyd. is a useful guide for current blood glucose con-
centratione. is a useful guide for blood glucose concentra-
tions in the recent past
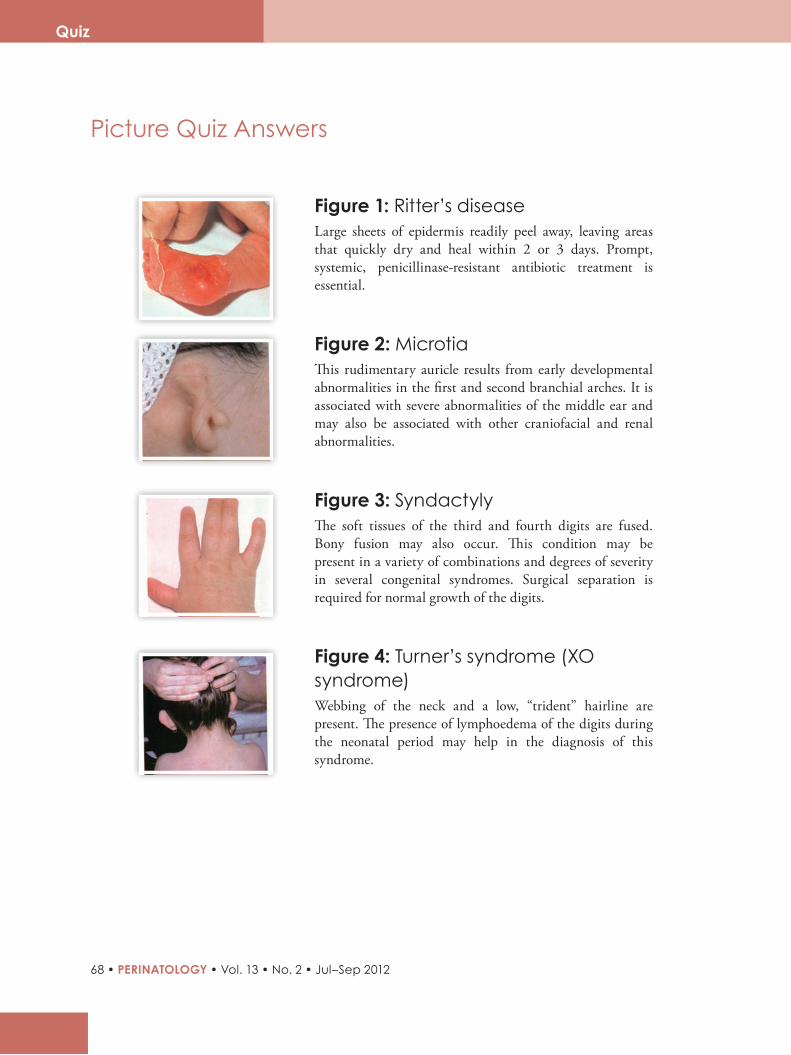
RESEARCH ARTICLES
68 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
Quiz
Picture Quiz Answers
Figure 1: Ritter’s diseaseLarge sheets of epidermis readily peel away, leaving areas that quickly dry and heal within 2 or 3 days. Prompt, systemic, penicillinase-resistant antibiotic treatment is essential.
Figure 2: MicrotiaThis rudimentary auricle results from early developmental abnormalities in the first and second branchial arches. It is associated with severe abnormalities of the middle ear and may also be associated with other craniofacial and renal abnormalities.
Figure 3: SyndactylyThe soft tissues of the third and fourth digits are fused. Bony fusion may also occur. This condition may be present in a variety of combinations and degrees of severity in several congenital syndromes. Surgical separation is required for normal growth of the digits.
Figure 4: Turner’s syndrome (XO syndrome)Webbing of the neck and a low, “trident” hairline are present. The presence of lymphoedema of the digits during the neonatal period may help in the diagnosis of this syndrome.
RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 69
Self-assessment Quiz Answers
Quiz
1. Question 1: b, d
Prostaglandins are derivatives of prostanoic acid (20-carbon saturated fatty acid). They are synthe-sized in vascular endothelium and are not stored but produced as needed. It is rapidly metabolized in the lungs and platelets.
2. Question 2: a, b
Progesterone is a steroid hormone that is produced mainly by the corpus luteum and placenta. It is not active when given orally. In the second half of the ovulatory menstrual cycle, it causes a rise in basal body temperature, whereas it relaxes smooth muscle, including the myometrium, and stimulates respiration during pregnancy.
3. Question 3: a, d
Neisseria gonorrhea is an intracellular diplococcus that is not a commensal anywhere. It can be detected using fluorescent staining.
4. Question 4: b, d
Candida albicans, responsible for thrush, is a Gram-positive aerobic organism that is not flagellate. It is a common commensal in the bowel. It consists of charac-teristic sulphur granules.
5. Question 5: a, b
The majority of hemorrhages at 32 weeks of preg-nancy is fairly minor and does not warrant transfusion or delivery. There may be a sign of placenta previa in which case an ultrasound would be required to localize the placental site. Until then, vaginal examination should be avoided, unless the bleeding is so severe that an immediate delivery after examination needs to be performed.
6. Question 6: All are true
Leaving aside the advisability of performing an ECV, in these cases either the mother is at risk, of placental sepa-ration or uterine rupture, or it is pointless as cesarean section would be undertaken in any case.
7. Question 7: b, c, e
Serum fructosamine does not depend on hemoglobin concentration; therefore, it is a more stable and useful substance to measure in diabetic pregnancies than glyc-osylated hemoglobin. It is dependent on plasma protein concentration, and falls during pregnancy. This is a reasonably stable event for a given pregnancy, as glyc-osylated hemoglobin reflects long term rather than current blood-glucose concentration.
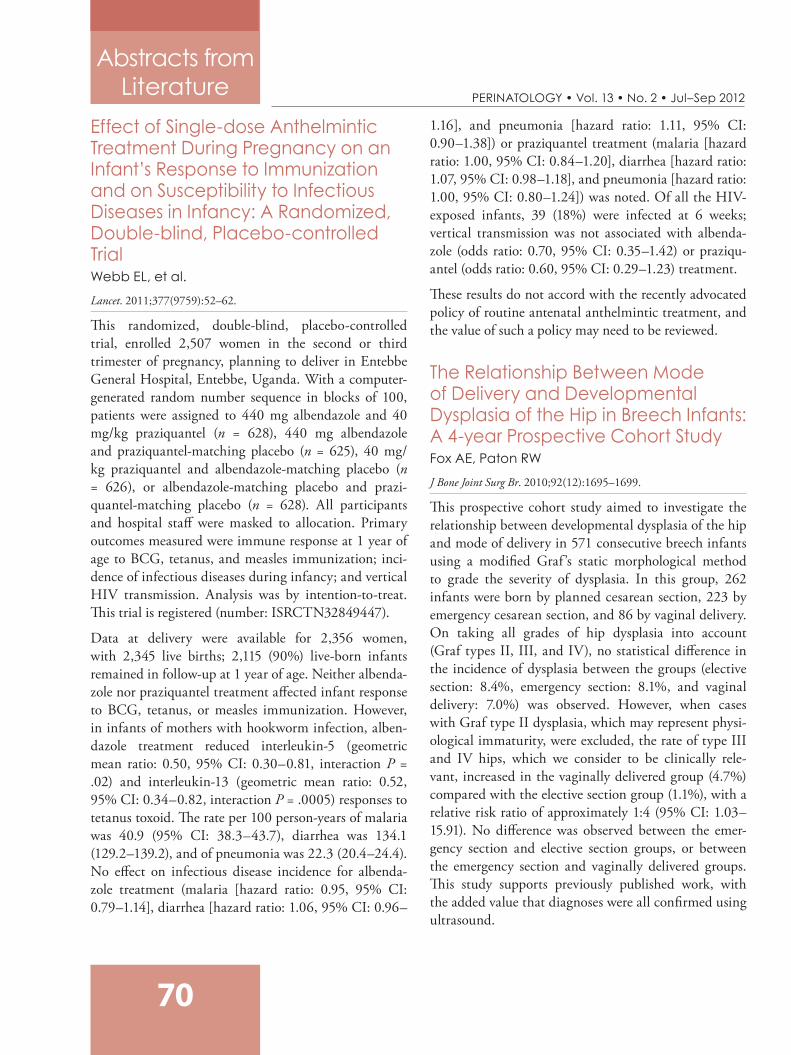
RESEARCH ARTICLESPERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
70
Abstracts from Literature
Effect of Single-dose Anthelmintic Treatment During Pregnancy on an Infant’s Response to Immunization and on Susceptibility to Infectious Diseases in Infancy: A Randomized, Double-blind, Placebo-controlled TrialWebb EL, et al.
Lancet. 2011;377(9759):52–62.
This randomized, double-blind, placebo-controlled trial, enrolled 2,507 women in the second or third trimester of pregnancy, planning to deliver in Entebbe General Hospital, Entebbe, Uganda. With a computer-generated random number sequence in blocks of 100, patients were assigned to 440 mg albendazole and 40 mg/kg praziquantel (n = 628), 440 mg albendazole and praziquantel-matching placebo (n = 625), 40 mg/kg praziquantel and albendazole-matching placebo (n = 626), or albendazole-matching placebo and prazi-quantel-matching placebo (n = 628). All participants and hospital staff were masked to allocation. Primary outcomes measured were immune response at 1 year of age to BCG, tetanus, and measles immunization; inci-dence of infectious diseases during infancy; and vertical HIV transmission. Analysis was by intention-to-treat. This trial is registered (number: ISRCTN32849447).
Data at delivery were available for 2,356 women, with 2,345 live births; 2,115 (90%) live-born infants remained in follow-up at 1 year of age. Neither albenda-zole nor praziquantel treatment affected infant response to BCG, tetanus, or measles immunization. However, in infants of mothers with hookworm infection, alben-dazole treatment reduced interleukin-5 (geometric mean ratio: 0.50, 95% CI: 0.30–0.81, interaction P = .02) and interleukin-13 (geometric mean ratio: 0.52, 95% CI: 0.34–0.82, interaction P = .0005) responses to tetanus toxoid. The rate per 100 person-years of malaria was 40.9 (95% CI: 38.3–43.7), diarrhea was 134.1 (129.2–139.2), and of pneumonia was 22.3 (20.4–24.4). No effect on infectious disease incidence for albenda-zole treatment (malaria [hazard ratio: 0.95, 95% CI: 0.79–1.14], diarrhea [hazard ratio: 1.06, 95% CI: 0.96–
1.16], and pneumonia [hazard ratio: 1.11, 95% CI: 0.90–1.38]) or praziquantel treatment (malaria [hazard ratio: 1.00, 95% CI: 0.84–1.20], diarrhea [hazard ratio: 1.07, 95% CI: 0.98–1.18], and pneumonia [hazard ratio: 1.00, 95% CI: 0.80–1.24]) was noted. Of all the HIV-exposed infants, 39 (18%) were infected at 6 weeks; vertical transmission was not associated with albenda-zole (odds ratio: 0.70, 95% CI: 0.35–1.42) or praziqu-antel (odds ratio: 0.60, 95% CI: 0.29–1.23) treatment.
These results do not accord with the recently advocated policy of routine antenatal anthelmintic treatment, and the value of such a policy may need to be reviewed.
The Relationship Between Mode of Delivery and Developmental Dysplasia of the Hip in Breech Infants: A 4-year Prospective Cohort StudyFox AE, Paton RW
J Bone Joint Surg Br. 2010;92(12):1695–1699.
This prospective cohort study aimed to investigate the relationship between developmental dysplasia of the hip and mode of delivery in 571 consecutive breech infants using a modified Graf ’s static morphological method to grade the severity of dysplasia. In this group, 262 infants were born by planned cesarean section, 223 by emergency cesarean section, and 86 by vaginal delivery. On taking all grades of hip dysplasia into account (Graf types II, III, and IV), no statistical difference in the incidence of dysplasia between the groups (elective section: 8.4%, emergency section: 8.1%, and vaginal delivery: 7.0%) was observed. However, when cases with Graf type II dysplasia, which may represent physi-ological immaturity, were excluded, the rate of type III and IV hips, which we consider to be clinically rele-vant, increased in the vaginally delivered group (4.7%) compared with the elective section group (1.1%), with a relative risk ratio of approximately 1:4 (95% CI: 1.03–15.91). No difference was observed between the emer-gency section and elective section groups, or between the emergency section and vaginally delivered groups. This study supports previously published work, with the added value that diagnoses were all confirmed using ultrasound.

RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 71
Abstracts from Literature
Treatment of Neonatal Sepsis with Intravenous Immune GlobulinINIS Collaborative Group, et al.
N Engl J Med. 2011;365(13):1201–1211.
In this experimental study, the authors enrolled 3,493 infants receiving antibiotics for suspected or proven serious infection at 113 hospitals in 9 countries, and randomly assigned them to receive 2 infusions of either polyvalent IgG immune globulin (at a dose of 500 mg per kilogram of body weight) or matching placebo at a time interval of 48 h. The primary outcome was death or major disability at the age of 2 years. No significant between-group difference in the rates of the primary outcome, which occurred in 686 of 1,759 infants (39.0%) who received intravenous immune globulin and in 677 of 1,734 infants (39.0%) who received placebo (RR: 1.00; 95% CI: 0.92–1.08) was observed. Similarly, there were no significant differences in the rates of secondary outcomes, including the incidence of subsequent sepsis episodes. In follow-up of 2-year-old infants, there were no significant differences in the rates of major or nonmajor disability or of adverse events. Analysis of these data suggests that therapy with intra-venous immune globulin had no effect on the outcomes of suspected or proven neonatal sepsis.
Long-term Neuroprotective Effects of Allopurinol After Moderate Perinatal Asphyxia: Follow-up of 2 Randomized Controlled TrialsKaandorp JJ, et al.
Arch Dis Child Fetal Neonatal Ed. 2012;97(3):F162–F166.
In this study, the long-term outcome of neonatal allop-urinol treatment after birth asphyxia was examined through the follow-up of 4 to 8 years of 2 randomized controlled trials performed earlier at the Leiden Univer-sity Medical Center, University Medical Center Gron-ingen, and University Medical Center Utrecht, the Netherlands. Fifty-four term infants suffering from moderate-to-severe birth asphyxia in 2 previously performed trials were included in this study. Infants
either received 40 mg/kg allopurinol (with an interval of 12 h) starting within 4 h after birth or served as controls. Children, who survived, were assessed with the Wechsler Preschool and Primary Scales of Intelli-gence test or Wechsler Intelligence Scale for Children, and underwent a neurological examination. The effect of allopurinol on severe adverse outcome (defined as mortality or severe disability at the age of 4-8 years) was examined in the total group of asphyxiated infants and in a predefined subgroup of moderately asphyxiated infants (based on the amplitude integrated electroen-cephalogram).
The mean age during follow-up (n = 23) was 5 years and 5 months (SD: 1 year and 2 months). There were no differences observed in long-term outcome between the allopurinol-treated infants and controls. However, subgroup analysis of the moderately asphyxiated group showed significantly less severe adverse outcome in the allopurinol-treated infants compared with controls (25% vs. 65%; RR: 0.40, 95% CI: 0.17–0.94). The reported data may suggest a (neuro) protective effect of neonatal allopurinol treatment on moderately asphyxi-ated infants.
Predictors of Early Nasal CPAP Failure and Effects of Various Intubation Criteria on the Rate of Mechanical Ventilation in Preterm Infants of <29 Weeks Gestational AgeFuchs H, et al.
Arch Dis Child Fetal Neonatal Ed. 2011;96(5):F343–F347.
The objective of this study was to identify factors asso-ciated with early nCPAP failure and effects of various intubation criteria on rate and time of intubation. A retrospective analysis of the first 48 h in infants of 23–28 weeks gestational age (GA) treated with sustained inflations followed by early nCPAP was carried out. Of the 225 infants (GA: 26.2±1.6 weeks), 140 (62%) could be stabilized with nCPAP in the delivery room, of whom 68 (49%; GA 26.9±1.5 weeks) succeeded on nCPAP with favorable outcome and 72 infants (51%; GA 26.3±1.4 weeks) failed on nCPAP

RESEARCH ARTICLES
72 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
within 48 h at a median (IQR) age of 5.6 (3.3–19.3) h. Intubation at fraction of inspired oxygen (FiO[2]) ≥ 0.35 versus 0.4 versus 0.45 instead of ≥ 0.6 would have resulted in unnecessary intubations of 16% versus 9% versus 6% of infants with nCPAP success, but decreased the age at intubation of infants with nCPAP failure to 3.1 (2.2–5.2) versus 3.8 (2.5–8.7) versus 4.4 (2.7–10.9) h. Data suggested that medical history or initial blood gas values are poor predictors of subsequent nCPAP failure. A threshold FiO[2] of ≥ 0.35–0.45 compared to ≥ 0.6 for intubation would shorten the time to surfactant delivery without a relevant increase in intu-bation rate. An individualized approach with a trial of early nCPAP and prompt intubation and surfactant treatment at low thresholds may be the best approach in infants with very low birthweight.
China’s Facility-based Birth Strategy and Neonatal Mortality: A Population-based Epidemiological StudyFeng XL, et al.
Lancet. 2011;378(9801):1493–1500.
In this study, authors aimed to establish the effect of a large-scale facility-based strategy on neonatal mortality by assessing how the institutional strategy of intrapartum care has affected neonatal mortality and its regional inequalities. They carried out a popu-lation-based epidemiological study of China’s National Maternal and Child Mortality Surveillance System between 1996 and 2008. Data from 116 surveillance sites in China (37 urban districts and 79 rural coun-ties) were used to examine neonatal mortality by cause, socioeconomic region, and place of birth, with Poisson regression to calculate relative risks. Rural counties were categorized into types 1 to 4, with type 4 being the least developed. Attributable risks and preventable fractions for hospital births versus home births were also reported. It was observed that neonatal mortality decreased by 62% between 1996 and 2008. The rate of neonatal mortality was much lower for hospital births than for home births in all regions, with relative risks
ranging from 0.30 (95% CI: 0.22–0.40) in type 2 rural counties, to 0.52 (0.33–0.83) in type 4 counties (P < .0001). The proportion of neonatal deaths prevented by hospital birth ranged from 70% (95% CI: 59.7–77.8) to 48% (16.9–67.3). Babies born in urban hospitals had a low rate of neonatal mortality (5.7 per 1,000 live births); but those born in type 4 rural county hospitals were almost 4 times more likely to die than the chil-dren born in urban hospitals (relative risk: 3.80, 2.53–5.72). Data suggested that other countries can learn from China’s substantial progress in reducing neonatal mortality. The major effect of China’s facility-based strategy on neonatal mortality is much greater than that reported for community-based interventions. Data of this study will provide a great impetus for countries to increase demand for and quality of facility-based intrapartum care.
Avoidance of Mechanical Ventilation by Surfactant Treatment of Spontaneously Breathing Preterm Infants: An Open-label, Randomized, Controlled TrialGöpel W, et al.
Lancet. 2011;378(9803):1627–1634.
This study aimed to test a new method of surfactant application on spontaneously breathing preterm infants to avoid mechanical ventilation (AMV). In a parallel-group, randomized controlled trial, 220 preterm infants with a gestational age between 26 and 28 weeks and a birthweight less than 1.5 kg were enrolled in 12 German neonatal intensive care units. Infants were independently randomized in a 1:1 ratio with variable block sizes, to standard treatment or intervention, and randomization was stratified according to center and multiple birth status. Masking was not possible. Infants were stabilized with continuous positive airway pres-sure and received rescue intubation, if necessary. In the intervention group, infants received surfactant treat-ment during spontaneous breathing through a thin catheter inserted into the trachea by laryngoscopy, if they needed a fraction of inspired oxygen more than
Abstracts from Literature

RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 73
0.30. The primary endpoint was need for any mechan-ical ventilation, or not being ventilated but having a partial pressure of carbon dioxide more than 65 mm Hg (8.6 kPa) or a fraction of inspired oxygen more than 0.60, or both, for more than 2 h, between 25 h and 72 h of age. Analysis was by intention-to-treat. This study is registered, number ISRCTN05025922. About 108 infants were assigned to the intervention group and 112 infants to the standard treatment group. All infants were analyzed. On day 2 or 3 after birth, 30 (28%) infants in the intervention group were mechanically ventilated versus 51 (46%) in the standard treatment group (number needed to treat 6, 95% CI: 3–20, abso-lute risk reduction 0.18, 95% CI: 0.30–0.05, P = .008). Thirty-six (33%) infants in the intervention group were mechanically ventilated during their stay in the hospital compared with 82 (73%) in the standard treat-ment group (number needed to treat: 3, 95% CI: 2–4, P < .0001). The intervention group had significantly fewer median days on mechanical ventilation, (0 days; IQR: 0–3 vs. 2 days, 0–5) and a lower need for oxygen therapy at 28 days (30 infants [30%] vs. 49 infants [45%], P = .032) compared with the standard treatment group. We recorded no differences between groups for mortality (7 deaths in the intervention group vs. 5 in the standard treatment group) and serious adverse events (21 vs. 28). The data suggested that the applica-tion of surfactant through a thin catheter to spontane-ously breathing preterm infants receiving continuous positive airway pressure reduces the need for mechan-ical ventilation.
Rotavirus Vaccine and Health-care Utilization for Diarrhea in US ChildrenCortes JE, et al.
N Engl J Med. 2011;365(12):1108–1117.
Using MarketScan databases, the authors assessed the pentavalent rotavirus vaccine (RV5) coverage and diarrhea-associated health care use from July 2007 through June 2009 versus July 2001 through June 2006 in children aged below 5 years, and compared the rates of diarrhea-associated health care use in unvac-
cinated children during January through June (when rotavirus was most prevalent) in 2008 and 2009 with the prevaccine rates to estimate indirect benefits. They also estimated national reductions in the number of hospitalizations for diarrhea, and associated costs, by extrapolation. By December 31, 2008, at least one dose of RV5 had been administered in 73% of children aged below 1 year, 64% of children aged 1 year, and 8% of children aged 2 to 4 years. Among children aged below 5 years, rates of hospitalization for diarrhea in 2001–2006, 2007–2008, and 2008–2009 were 52, 35, and 39 cases per 10,000 person-years, respectively, for rela-tive reductions from 2001 to 2006 by 33% (95% CI: 31–35) in 2007–2008 and by 25% (95% CI: 23–27) in 2008–2009; rates of hospitalization specifically coded for rotavirus infection were 14, 4, and 6 cases per 10,000 person-years, respectively, for relative reduc-tions in the rate from 2001 to 2006 by 75% (95% CI: 72–77) in 2007–2008 and by 60% (95% CI: 58–63) in 2008–2009. During January–June 2008 and 2009, the respective relative rate reductions among vaccinated children as compared with unvaccinated children were as follows: hospitalization for diarrhea, 44% (95% CI: 33–53) and 58% (95% CI: 52–64); rotavirus-coded hospitalization, 89% (95% CI: 79–94) and 89% (95% CI: 84–93); emergency department visits for diarrhea, 37% (95% CI: 31–43) and 48% (95% CI: 44–51); and outpatient visits for diarrhea, 9% (95% CI: 6–11) and 12% (95% CI: 10–15). Indirect benefits (in unvacci-nated children) were seen during 2007-2008 but not in 2008-2009. Nationally, during 2007-2009, there was an estimated reduction of 64,855 hospitalizations, saving approximately $278 million in treatment costs. The data inferred that since the introduction of rota-virus vaccine, diarrhea-associated health care utiliza-tion and medical expenditures for children in US have decreased substantially.
Abstracts from Literature
RESEARCH ARTICLESPERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
74
*Correspondence
Dr Sundareshan TSDepartment of Cytogenetics, Anand Diagnostic Laboratory, Blue Cross Chambers, Infantry Road Cross Bangalore -560001, Karnataka, India.
Email: [email protected]
Significance of Prenatal Cytogenetic and Molecular Diagnosis of Triploidy and the Need for Genetic Counseling—A Report of 2 CasesDhanya V, Smitha C, Pradeep S, Chitra P, Pooja SK, Kadandale JS, Sundareshan TS*
AbstractTriploidy is a numerical chromosomal abnormality in human con-ceptions, which most frequently results in spontaneous abortion within 20 weeks of gestation. It has an incidence of 1 in 10,000 live births. Here, we describe 2 case reports of triploidy with 69, XXX karyotype from amniotic fluid samples with an indication of intrauterine growth retardation (IUGR) and less amniotic fluid in case 1 and multiple fetal malformations in case 2. Cytogenetic analysis and fluorescence in-situ hybridization (FISH) confirmed the triploid nature of the fetus in both the cases. The present report indicates the significance of a cytogenetic study in deter-mining the genetic make-up of the fetus, and highlights the importance of karyotyping and FISH in prenatal samples over other methods. Although maternal serum screening tests and other investigations provide a risk ratio, confirmation can be obtained only after genetic analysis. Parents should be informed about detailed ultrasonography (USG) scans and the need for prenatal cytogenetic diagnosis and genetic counseling for future pregnancies.
Key words: Amniotic fluid, FISH, karyotyping, prenatal diagnosis, triploidy
Short Communications

RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 75
IntroductionTriploidy is the most common chromosomal abnor-mality in human conceptions resulting in a total of 69 chromosomes that originates from three haploid gametes or 1 diploid and 1 haploid gamete. Placental changes, fetal malformations, and IUGR occur in trip-loid pregnancies.1,2 Facial or body asymmetry, syndac-tyly of the third and fourth fingers, characteristic dysmorphic features, and mental retardation are the main symptoms.3 Triploidy is estimated to occur in about 2% of the conceptuses.4 The present case report describes 2 cases of triploidy with 69, XXX karyotype that were detected by prenatal cytogenetics and molec-ular analysis of amniotic fluid cultures.
Case 1A 27-year-old woman at 17 weeks of gestation with an indication of IUGR and reduced amount of amniotic fluid was referred to our laboratory for both cytoge-netic analysis and FISH. There was no family history of genetic abnormalities and the couple were non-consan-guineous. Biochemical screening tests done during the first trimester showed high risk of trisomy 18 and trisomy 21. Ultrasonography showed a single live active fetus withbreech presentation. The amount of amniotic fluid liquor was less (AFI 5.7). Placenta was in the ante-rior right lateral location; nasal bone length was 3 mm; transcerebellar diameter was 1.4 cm; skull was normal without ventriculomegaly. Stomach was not seen on the left side and echogenic bowel was not visualized. Head, abdomen, and limbs showed a lag of 2 to 3 weeks.
Case 2A 34-year-old woman at 21 weeks of gestation was referred due to multiple fetal malformations and suspected trisomy. The first trimester biochemical screening tests showed an increased risk for trisomy 13 and 18. Ultrasonography at 21 weeks of gestation showed a single live fetus with breech presentation and oligohydraminos (AFI 9.5 mm). There were multiple fetal defects such as unilateral cerebral ventriculom-egaly on the left side measuring about 17.7 mm, mild micrognathia, echogenic intracardiac focus in the left
Short Communications
Dhanya V et al. Prenatal Cytogenetic and Molecular Diagnosis of Triploidy
Figure1. Autopsy findings
Figure 2. Autopsy findings
ventricle, and fixed flexion deformity of both the wrists and reduced asymmetrical growth restriction. Fetal cardiac scan, uterine artery doppler, and cervical length showed normal values. There was no family history of genetic abnormalities and the couple were non-consan-guineous.
Autopsy findings of case 2A gross examination of the fetus revealed low set ears and mild micrognathia. Cerebellum was found to be small for the age. On coronal slicing, mild asym-metry was observed. The cortical mantle was thicker on the left side. Posterior part of the lateral ventricle, the trigone, and the occipital horns were dilated. The aqueduct appeared slightly narrowed. No aqueductal infection or glial nodules were found in the lumen. The cervical, thoracic, and lumbar cord showed normal maturation of neurons (Figures 1 and 2). The basal ganglia (head of caudate nucleus), the paraventricular zone at trigone, irregular nodular mantle of immature fetal neuroblastic cells were also observed. In the right, a mushroom-like projection was seen in the trigone (paraventricular stem cells).
a b
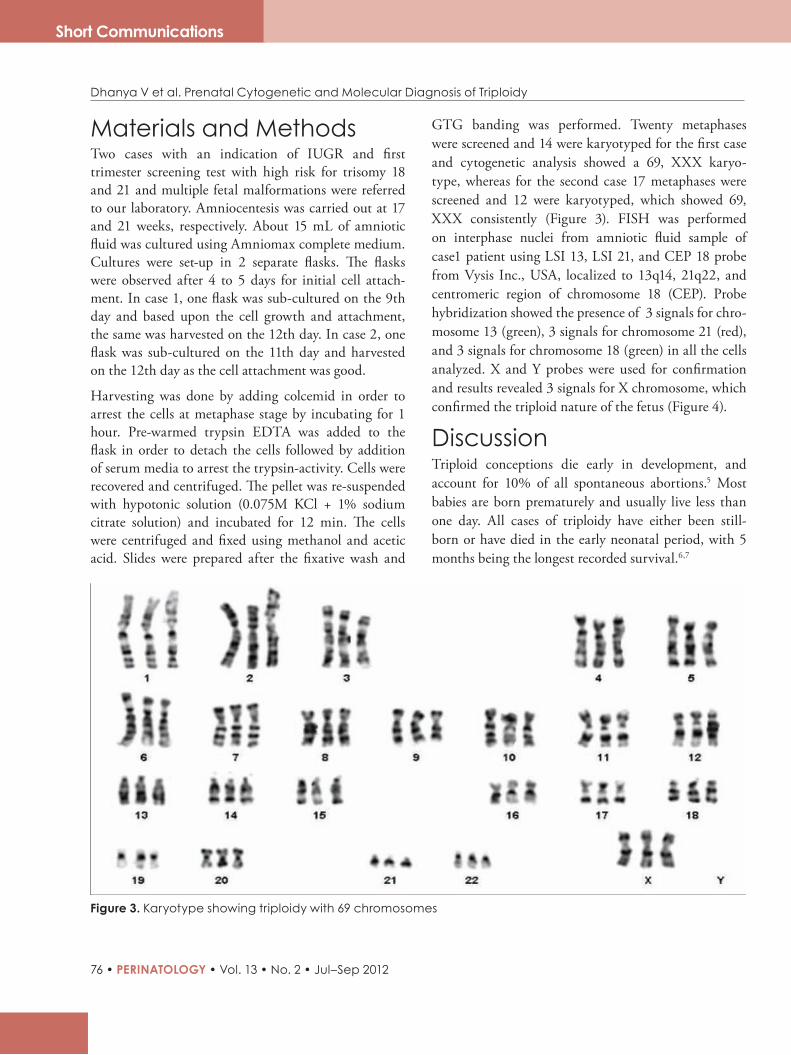
RESEARCH ARTICLES
76 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
Short Communications
Materials and MethodsTwo cases with an indication of IUGR and first trimester screening test with high risk for trisomy 18 and 21 and multiple fetal malformations were referred to our laboratory. Amniocentesis was carried out at 17 and 21 weeks, respectively. About 15 mL of amniotic fluid was cultured using Amniomax complete medium. Cultures were set-up in 2 separate flasks. The flasks were observed after 4 to 5 days for initial cell attach-ment. In case 1, one flask was sub-cultured on the 9th day and based upon the cell growth and attachment, the same was harvested on the 12th day. In case 2, one flask was sub-cultured on the 11th day and harvested on the 12th day as the cell attachment was good.
Harvesting was done by adding colcemid in order to arrest the cells at metaphase stage by incubating for 1 hour. Pre-warmed trypsin EDTA was added to the flask in order to detach the cells followed by addition of serum media to arrest the trypsin-activity. Cells were recovered and centrifuged. The pellet was re-suspended with hypotonic solution (0.075M KCl + 1% sodium citrate solution) and incubated for 12 min. The cells were centrifuged and fixed using methanol and acetic acid. Slides were prepared after the fixative wash and
GTG banding was performed. Twenty metaphases were screened and 14 were karyotyped for the first case and cytogenetic analysis showed a 69, XXX karyo-type, whereas for the second case 17 metaphases were screened and 12 were karyotyped, which showed 69, XXX consistently (Figure 3). FISH was performed on interphase nuclei from amniotic fluid sample of case1 patient using LSI 13, LSI 21, and CEP 18 probe from Vysis Inc., USA, localized to 13q14, 21q22, and centromeric region of chromosome 18 (CEP). Probe hybridization showed the presence of 3 signals for chro-mosome 13 (green), 3 signals for chromosome 21 (red), and 3 signals for chromosome 18 (green) in all the cells analyzed. X and Y probes were used for confirmation and results revealed 3 signals for X chromosome, which confirmed the triploid nature of the fetus (Figure 4).
DiscussionTriploid conceptions die early in development, and account for 10% of all spontaneous abortions.5 Most babies are born prematurely and usually live less than one day. All cases of triploidy have either been still-born or have died in the early neonatal period, with 5 months being the longest recorded survival.6,7
Figure 3. Karyotype showing triploidy with 69 chromosomes
Dhanya V et al. Prenatal Cytogenetic and Molecular Diagnosis of Triploidy

RESEARCH ARTICLES
PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012 • 77
Short Communications
Dhanya V et al. Prenatal Cytogenetic and Molecular Diagnosis of Triploidy
Figure 4. Fluorescence in-situ hybridization using chromosome X/Y,13/21, and 18 probes
X/Y 13/21 18
Triploidy may result from either digynic or diandric fertilizations. Digynic triploid most often arises from fertilization of a primary oocyte or a diploid ovum by a normal haploid sperm. The diploid ovum results from an error during meiosis I and meiosis II or from reten-tion of the second polar body. Alternatively, a diandric triploid usually originates from fertilization of a normal haploid ovum by two separate sperms, or by a diploid sperm. The parental origin of the extra haploid chro-mosome set has been delineated into 2 distinct diploid phenotypes. Type I (diandric triploid) is characterized by a relatively well grown fetus with or without micro-cephaly and a large cystic placenta showing partial molar changes. Type II (digynic triploid) presents a fetus with severe IUGR, relative macrocephaly and a small non-cystic placenta.8,9 In addition to IUGR and relative macrocephaly, triploid fetuses have been reported to be associated with various abnormal pheno-types, including facial dysmorphism, limb defects, major cardiovascular and urogenital anomalies and abnormalities involving central nervous system (CNS), endocrine, and respiratory systems.10 The present cases correlate to digynic triploidy having IUGR and fetal malformations as indicated in ultrasound scanning. The most common clinical features of triploidy include IUGR, total syndactyly of third and fourth fingers, and CNS heart and renal defects. Hydatidiform mole, one of the characteristic features of pure triploidy, is found in more than 90% of cases.11-15
The identification of fetal abnormalities during ultra-sound examination initiated a request for rapid deter-mination of ploidy status through prenatal FISH analysis of uncultured amniocytes which indicated the triploid nature. It was still recommended that the result
needed confirmation by conventional cytogenetics along with karyotyping. FISH is used as an investiga-tional technique and no irreversible therapeutic action should be taken on the basis of FISH results in the absence of other confirmatory diagnostic information such as ultrasound findings and karyotype results.16 In both the cases discussed, ultrasound findings showed IUGR and oligohydraminos and were referred for karyotyping. Both the cases were confirmed as trip-loidy after cytogenetic and molecular analyses that led the couples to terminate the pregnancies. Autopsy was done for one of the cases. These cases highlight the importance of karyotyping and molecular analysis (FISH) in prenatal samples over any other methods to establish the genetic makeup of the fetus. Although maternal serum screening tests and other investigations provide a risk ratio, confirmation is obtained only after cytogenetic and molecular analyses. Parents should be informed in detail about ultrasonographic scans, all the investigation reports, and the value of prenatal diag-nosis not only for the present fetus but also for planning the future pregnancies.
Acknowledgments Authors thank Dr R Narayanan, Consultant, obgyn; Dr Prathima Radhakrishnan, Consultant, fetal medi-cine, Bangalore Fetal Medicine Centre and Dr Shankar SK, Human Brain Tissue Repository, Department of Neuropathology, NIMHANS for their expert opinions.
References1. ClaseinvanderHouwen,etal.Transientearlypreeclampsia
intwinpregnancywithatriploidfetus:acasereport. J Med Case Rep.2009;3:7311.
2. YilmazZ,etal.TriploidiesinfirstandsecondtrimestersofpregnanciesinTurkey. BJMG.2007;10(2):71-76.
3. GrahamJM,etal.Diploidtriploidmixoploidy:clinicalandcytogeneticaspect. Pediatrics.1981;68:23–28.
4. Jones KL. Triploidy syndrome and diploid/triploidmixoploidysyndrome. In: Smith’s Recognizable Patterns of Human Malformation, 4th ed.Philadelphia;1988:32–33.
5. JonesKL.Chromosomalabnormalitysyndromes. In: JonesKL,SmithDW,eds.Smith’sRecognizablePatternsofHumanMalformation.6thed.Philadelphia:ElsevierSaunders;2006:28–31.
6. GarzenaE,etal.Triploidysyndrome:acasereport. Minerva Pediatr.1995;47:307–311.
RESEARCH ARTICLES
78 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
Short Communications
7. ArvidssonCG.Aboywithcompletetriploidyandunusuallylongsurvival. Acta Paediatr Scand.1986;75:507–510.
8. McFaddenDE,etal.Twodifferentphenotypesoffetuseswithchromosomaltriploidy:correlationwithparentaloriginofthehaploidset. Am J Med Genet.1991;38:535–538.
9. McFaddenE, et al. Prenatal origin of triploidy in humanfetuses:evidenceforgenomicimprinting. Hum Genet.1993;92:465–469.
10. MittalTK,etal.Triploidy:antenatalsonographicfeatureswithpost-mortemcorrelation. Prenat Diagn.1998;18:1253–1262.
11. GalánF,etal.69,XXXkaryotypeinamalformedlivebornfemale. Maternal origin of triploidy.Ann Genet. 1991;34:37–39.
12. GrahamJM,etal.Diploid-triploidmixoploidy:clinicalandcytogeneticaspects. Pediatrics.1981;68:23–28.
13. HasegawaT,etal.Digynictriploidinfantsurvivingfor46days. Am J Med Genet.1999;87:306–310.
14. McFaddenDE,etal.Placentalpathologyoftriploidy. Hum Pathol.1996;27:1018–1020.
15. ObersztynE,etal.Clinicalexpressionoftriploidy.Med Wieku Rozwoj.2002;6:329–336.
16. GersenSL, et al.Rapidprenataldiagnosisof14casesoftriploidy using FISHwithmultiple probes In:Prenatal diagnosis. Massachusetts,USA:JohnWileyandSons;1995:1–5.
Length of Postnatal Hospital Stay in Healthy Newborns and Re-hospitalization After Early Discharge
Farhat R, Rajab M.
N Am J Med Sci. 2011;3(3):146–151.
The length of postnatal hospital stay for healthy newborns remains controversial. Proponents of early hospital
discharge claim that it is safe as it decreases the risk of iatrogenic infection, promotes family bonding and
attachment, and reduces hospitalization care and patient costs. Disadvantages include delayed breast-
feeding, manifestation of new conditions affecting newborns after early discharge, and improper discharge
planning.
The main aim of this study was to compare early discharge versus late discharge with the risk of re-admission.
The length of hospital stay was recorded for all healthy newborns and infants followed by investigation of any
medical problem arising after discharge. Factors associated with re-admission to the hospital were analyzed
by c2- test and Mantel–Haenszel common odds ratio estimate (OR) with confidence limits (CL).
This study enrolled a total of 478 babies of whom 307 were discharged ≤ 48 h. The overall length of stay was 39
h (1.6 days). Thirty-eight (7.9%) newborns were re-hospitalized, with the most common cause being neonatal
jaundice. Factors associated with re-admission for jaundice were breastfeeding (OR: 10.3; CL: 3.10–32.20)
and length of stay ≤ 48 h (OR: 13.8; CL: 4.04–47.05).
Hospital discharge at any time ≤ 48 h significantly increases the risk for re-admission due to hyperbilirubinemia
as well as re-admissions due to certain other factors. Planning and implementing a structured program for
follow-up of infants who are discharged at ≤ 48 h are vital in order to decrease the risk for re-admission, mor-
bidity, and neonatal mortality.
Dhanya V et al. Prenatal Cytogenetic and Molecular Diagnosis of Triploidy
RESEARCH ARTICLES
79
Perinatology, one of the few journals dedicated to the emerging multidisciplinary field of perinatal medicine, is published quarterly. The journal publishes original articles, brief reports on clinical and laboratory observations, case reports of substantiate value, invited editorials, invited papers on recent advances, clinical diagnosis, announcements of meetings, and summary reports of conferences.
The journal is multidisciplinary and welcomes articles in English from metabolic specialists, clinical biochemists, obstetricians, neonatolo-gists, pathologists, geneticists, endocrinologists, neurologists, devel-opmental pediatricians, and any other person whose work is related to metabolic disorders and genetics.
The articles should not exceed 2500 words, with not more than six figures, tables, and photographs. Brief reports and case reports should not exceed 1200 words, with not more than two tables and figures or photographs and six references. Brief accounts of new observations can also be presented as letters not exceeding 400 words.
Guidelines to be followed while preparing and submitting a manu-script are given below.
MANUSCRIPT CHECKLIST
Typescript and other inputs• Send original (unpublished and not submitted elsewhere)
manuscript along with two photocopies to the address* given below
• Send a softcopy (CD) of the manuscript in MS Word format• Send two sets of illustrations, photographs, and drawings
– Line art/graphs/illustrations should be provided in “.eps” or “.ai” format or in a camera-ready form with redundant areas trimmed
– Line drawings can be submitted as photographic prints or high-quality photocopies. All other illustrations should be black-and-white photographic prints
– Resolution of photographs or their scanned copies should be 300 or more dpi
– If the subjects of the photographs are identifiable, either their eyes should be masked or their written permission to use the photograph should be submitted along with the typescripts
– Color illustrations can be used if essential to the article• Provide complete details of the corresponding author,
including address for communication, telephone and fax numbers, and email address
• Keep a copy of the manuscript for your reference
Statements/permissions• Include statements signed by each author on:
– Authorship criteria and responsibility – Financial disclosure – Copyright transfer
• Include statement signed by corresponding author that written permission has been obtained from all persons named in the Acknowledgment
• Include research or project support/funding in an acknowl-edgment
Instructions to Authors
Instructions to Authors• Include written permission from each individual identified as a
source for personal communication• Include informed consent forms for identifiable patient descrip-
tions, photographs, and pedigrees• Include written permission from publishers and authors to
reproduce or adapt previously published illustrations and tables
Postsubmission• An acknowledgement will be sent against the receipt of the
manuscript• Manuscripts not accepted for publication will not be returned• Editor has the right to make necessary changes in the manu-
script and also to reduce the length of the manuscript, if required
• Two copies of the journal will be provided to the author free of cost after the issue has been published. No reprints will be sent
MANUSCRIPT FORMAT
Titles and subtitlesTitles should be short, concise, specific, and informative.
AbstractAbstract of a research paper summarizes the main points of an article: (1) the study objective and background, (2) the study design and methods, (3) results, and (4) conclusion.
Key wordsKey words are descriptors representing the key topics presented in the article.
IntroductionThe introduction should provide the objective of the study and state the hypothesis or research question, how and why the hypothesis was developed, and why it is important.
MethodsThis section includes a description of:
• Study design or type of analysis and period of study• Condition, factors, or disease studied• Details of sample (eg, study subjects and the setting from which
they were drawn)• Intervention(s)• Outcome measures• Statistical analysis
ResultsThe results given in the manuscript should be specific and relevant to the research hypothesis.
DiscussionThis section should be a formal consideration and critical exami-nation of the study. The results should be considered in this section in the context of other studies.
ConclusionThis section summarizes the consensus statement. It may include benefits and harms of the study. The type of future studies, if appro-priate, should be mentioned here.
AcknowledgmentsAcknowledgments are considered to be a continuation of the text and precede the references. Only those who have made substantial contributions to the study and/or preparation of the paper should be acknowledged. The source(s) of grant support, equipment, and drugs should be included.
Vol. 13 • No. 2 • Jul–Sep 2012PerinatologyJ o u r n a l o f P e r i n a t a l a n d N e o n a t a l C a r e
* The Managing Editor – Perinatology Scientific Publications Division The Himalaya Drug Company Makali, Bangalore, Karnataka, India – 562123
RESEARCH ARTICLES
80 • PERINATOLOGY • Vol. 13 • No. 2 • Jul–Sep 2012
ReferencesAuthors cite a reference:
• To support their arguments or lay the foundation for their theses• As a source of information or to credit other authors
General Style Points (US Spelling and Style)• Use American English, “ize” spelling• Numbers under 10 are spelled out, except for measurements
with a unit (8 mmol/L) or age (6-week old), or when in a list with other numbers (14 dogs, 12 cats, and 9 gerbils)
• Use list comma. For example: The bishops of Durham, Can-terbury, Bath and Wells, and York were invited. OR I used to help my mother with the cooking, cleaning, washing and ironing, and yard work
• Use double quotes: Generally, quotes are outside punctuation. For example: poliomyelitis is commonly referred to as “polio.”
• For range use “to” in text, for example 40 to 50 mg, and “–” (en dash) in parenthesis (35–47 cm)
• Use P value as: P = .05, P<.005, P>.05 (no “0” before period and “P” is capital and italics; no space between the symbols (<,>) and “P”; rule of exception: insert space before and after the symbol “=”)
• Closed-up em dash “—” should be used for parenthetical phrases
• Parenthesis style: First priority is parenthesis followed by square bracket, that is, ([]), (World Health Organization [WHO])
• Date: December 5, 2008 (US style)• Foreign words listed in “Merriam-Webster’s” online dictionary
should not be italicized and hyphenated (in vitro, in vivo, etc.)
Tables• All tables should be cited in the text and it should be in
sequential order• Table should be cited as Table 1/Tables 1 and 2/Tables 1 to 3 (or
Tables 1–3, inside parenthesis)• Table caption should be provided and its first part should be in
bold form as given below
For example:
Table 1. Table Caption in Title Case (no full point at the end)
Figures• All figures should be cited in the text and it should be in
sequential order• Figure should be cited as Figure 1/Figures 1 and 2/Figures 1 to 3
(or Figures 1–3, inside parenthesis)• Figure caption should be provided and its first part should be in
bold form as given below
For example:
Figure 1. Figure caption in sentence case. (Note the full point at the end.)
AbbreviationsMost abbreviations should be spelled out at first mention (in text); some very common abbreviations need not be expanded. Abbre-viations should not be introduced in titles.
Some notes on the use of abbreviations are given below. • In general, use uppercase letters without period for acronyms
and initialisms such as CHF, GFR, and WBC and also for routes of administration and dosage schedules such as PO, IV, BID, and TID. Some abbreviations—such as PhD and pH—do contain lowercase letters
• Use abbreviations consistently. In general, write out the term or phrase at first mention, followed by the abbreviation in paren-theses; use only the abbreviation thereafter
• Write lowercase abbreviations without period; “et al” and “vs” are examples. Rule of exception: Use lowercase abbreviations, preceded by a comma and followed by a full point at the end of “etc.” For example: sun, moon, etc.
– Write “for example” or “that is,” preceded and followed by a comma, if it is not the beginning of the sentence, in a running text. Write “eg” or “ie” followed by a comma when used in parenthesis (ie, or eg,)
Genus and speciesItalicize when used in singular: Species, variety or subspecies, genus (eg, first occurrence in text—Escherichia coli; following occurrences—E coli—without any period)
Use lowercase (unless it is not a beginning of the sentence) and nonitalic style for plural form of organisms
Bacillus bacilli
Staphylococcus staphylococci
Streptococcus streptococci
UnitsUse standard abbreviations for units of measure.
ReferencesAll references should be cited in the text, tables, or figures in con-secutive numerical order (as presented in the text) by means of superscript Arabic numerals, outside punctuation.
Article in journalsTypical entry for journal with more than two authors (if more than two authors, list first author, then et al).
For example:
Hunter DJ, et al. Plasma organochlorine levels and the risk of breast cancer. N Engl J Med. 1997;337(suppl 1):1253-1258.
Morris LA. The risk revolution: an experimentation of the regulatory environment [editorial]. J Am Pharm Assoc. 2001;41:S5-S10.
BooksAuthor name: Same as journal.
Aronoff GR, et al. Drug Prescribing in Renal Failure. Vol. 1. 4th edn. Philadelphia, PA: American College of Physicians; 1999:39.
Dukes MNG, Aronson JK, eds. Meyler’s Side Effects of Drugs. 14th edn. Amsterdam, Netherlands: Elsevier; 2000:xvi-xvii.
OTHER PUBLISHED MATERIAL
Electronic mediaPerneger TV, et al. Randomized trial of heroin maintenance pro-gramme for adults who fail in conventional drug treatments. TBMJT [serial online]. 1998;317:20-24. Available at: http://www.bmj.com/cgi/content/full/317/7150/13. Accessed March 4, 2003.
Rennie D, Guyatt G, eds. Users’ Guides to the Medical Literature: A Manual for Evidence-Based Clinical Practice [book online]. Chicago, IL: AMA Press; 2002. Available at: http://www.usersguides.org/textbooks.asp. Accessed February 26, 2004.
Unpublished materialDo not include material that has been submitted for publication but has not yet been accepted. This material, with its date, should be noted in the text as “unpublished data,” as follows:
For example:
These findings have recently been corroborated (Mariman, unpub-lished data, January 1996).
Instructions to Authors


MAG (3) NPP/43/2011/12
Printed and published by Dr Pralhad S Patki on behalf of The Himalaya Drug Company, Makali, Bangalore - 562123.Published at The Himalaya Drug Company, Makali, Bangalore - 562123.
Printed at Sri Sudhindra Offset Process, No. 27/28, DT Street, 8th Cross, Malleshwaram, Bangalore - 560003.Edited by Dr Ranjan K Pejaver.
RNI Regd No. KARENG/1999/35





























