Embed Size (px)
Citation preview
J Head Trauma RehabilCopyright c© 2015 Wolters Kluwer Health, Inc. All rights reserved.
Polysomnographic Sleep Patterns inChildren and Adolescents inUnresponsive Wakefulness Syndrome
Paolo Avantaggiato, MD; Erika Molteni, PhD; Francesca Formica, MD;Gian Luigi Gigli, MD; Mariarosaria Valente, MD; Simone Lorenzut, MD;Stefano de Biase, MD; Salvatore Arcieri, MD; Federica Locatelli, MD; Sandra Strazzer, MD
Objectives: We aimed (i) to search for qualitative sleep patterns for pediatric unresponsive wakefulness syndrome(SPPUWS) in prolonged polysomnographic (PSG) recordings in children and adolescents with subacute severedisorders of consciousness due to an acquired brain damage; (ii) to investigate the clinical relevance of SPPUWS andof possible neurophysiological markers (rapid eye movement sleep and sleep spindles) in PSG recordings of pediatricpatients with unresponsive wakefulness syndrome (UWS). Methods: We performed a PSG study in 27 children withUWS due to acquired brain damage in the subacute phase. Patients received a full neurological examination anda clinical assessment with standardized scales. In addition, outcome was assessed after 36 months. Results: Weidentified 6 PSG patterns (SPPUWS) corresponding to increasing neuroelectrical complexity. The presence of anorganized sleep pattern, as well as rapid eye movement sleep and sleep spindles, in the subacute stage appearedhighly predictive of a more favorable outcome. Correlation was found between SPPUWS and recovery, as assessed byseveral clinical and rehabilitation scales. Conclusions: Polysomnography can be used as a prognostic tool, as it canhelp determine the capability to recover from a pediatric UWS and predict outcome well before the confirmationprovided by suitable clinical scales. Key words: brain injury prognosis, electroencephalography, encephalopathy, pediatricbrain injury, pediatric brain tumor, persistent vegetative state, polysomnography, unresponsive wakefulness syndrome
EMERGING FROM COMA, a state of completeunconsciousness, reflects a transition to the unre-
sponsive wakefulness syndrome (UWS). Unresponsivewakefulness syndrome was first introduced by Laureyset al1 in 2010 to overcome the in-use definitions of veg-etative state (VS) and apallic state and to specify thosecomatose patients who begin to show sleep-wake cycles
Author Affiliations: Acquired Brain Injury Unit,Scientific Institute“Eugenio Medea,” Bosisio Parini, Lecco, Italy (Drs Avantaggiato,Molteni, Formica, Arcieri, Locatelli, and Strazzer); Department ofExperimental and Clinical Medicine, University of Udine Medical School,Udine, Italy (Drs Gigli and Valente); and Neurology Unit and Center ofSleep Medicine, "Santa Maria della Misericordia" University Hospital,Udine, Italy (Drs Lorenzut and de Biase).
This study was supported by the Italian Department of Health (Ricerca Corrente2008–2009, Bando Ricerca Finalizzata 2008). The authors acknowledgeDrs Katia Colombo, Valentina Pastore, and Federica Villa for their flawlessassistance in the clinical scale administration.
Supplemental digital content is available for this article. Direct URL citationsappear in the printed text and are provided in the HTML and PDF versionsof this article on the journal’s Web site (www.headtraumarehab.com).
The authors declare no conflicts of interest.
Corresponding Author: Erika Molteni, PhD, Scientific Institute E. Medea,Acquired Brain Injury Unit, Via Don Luigi Monza 20, Bosisio Parini, Lecco23842, Italy ([email protected]).
DOI: 10.1097/HTR.0000000000000122
(ie, eye closing/opening and muscles inactivity/activity)while (still) presenting a number of clinical signs of unre-sponsiveness. Be it transient or persistent, UWS is char-acterized by the absence of self-awareness behaviors ofthe environment.2–4
Diagnosis of UWS nowadays relies on 2 mainstaysperformed behaviorally: clinical examination and neu-ropsychological assessments. Both tools have seriouslimitations,5,6 as they result in approximately 35% ofmisdiagnoses7 and more often in insufficient prognos-tic indications for predicting or excluding the progresstoward some responsiveness. On the contrary, neuro-physiological studies have shown that, in time, pa-tients with UWS develop some electrophysiologicaldifferentiation.8–10 This fact has fostered an increasinginterest in the sleep patterns of patients with disorders ofconsciousness (DOC) and has steered research towardthe use of polysomnography (PSG).
One of the major difficulties encountered in sleepstudies of UWS is the absence of specific staging cri-teria. Indeed, the official electrophysiological scoringsystem of sleep11 is currently based on the electroen-cephalographic (EEG) features of healthy individuals,hardly applicable for sleep staging in patients with se-vere brain damage.10 Alternative criteria, tailored andadapted to adult and pediatric cohorts of patients, have
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
1

2 JOURNAL OF HEAD TRAUMA REHABILITATION
to be applied for pediatric cases.12 Among them, manystudies have attempted to use additional data, such aselectromyographic (EMG) measurement, heart rate, orblood pressure, for the interpretation of sleep and todetect differentiated stages of DOC.13–16 Furthermore,studies investigating the hormonal effects on sleep inbrain-injured patients with DOC and testing the effectof substances acting on the sleep-wake cycle, such asmelatonin, are still lacking.
Prolonged PSG recordings have been plumbed forpossible correlations between neuroelectrical activityand functional levels of impairment. Studies suggest thatthe presence of specific EEG patterns, ascribed to differ-ent DOC,13,17,18 could be proposed as specific prognos-tic indicators for recovery.18–20 Similar to what has beenobserved in adults,21 a previous study on comatose chil-dren supports the finding that the reappearance of sleep-related waveforms (eg, spindles, K-complexes) during re-covery from brain injury is a sign of a good prognosis.13
Other works compared the PSG prognostic value of PSGwaveforms with the Level of Cognitive Functional As-sessment Scale,19 as well as Glasgow Coma Scale ratingsin patients who had sustained an acute brain injury.20
Furthermore, a number of PSG studies specificallyfocusing on VS9,21–26 were written before the definitionof minimally conscious state (MCS) in 2002,27 makingit possible that many patients reported as being in a VSmight, in fact, have been in a MCS. As a consequence,the present work can be compared stricto sensu with thefew works written only in the last decade.17,28–31 Earlierand recent literature, however, agrees in reporting thatthe presence of spindles and sleep-stage differentiationin EEG tracks is a potential marker of good outcome23,28
and that the presence of rapid eye movement (REM)sleep is predictive of better cognitive recovery (see alsothe work by Ron et al32).
A decade after the pioneering effort of Cheliout-Heraut et al,13 we conducted a retrospective clinical andPSG analysis of 27 children and adolescents with suba-cute or chronic UWS due to an acquired brain damage.We searched for possible neurophysiological markersof sleep-wake EEG organization that could predict thechildren’s outcome. Our analysis isolated 6 qualitativesleep characteristics that we termed sleep patterns for pe-diatric unresponsive wakefulness syndrome (SPPUWS)and which were tested for correlations with the clinicaloutcome at 36 months after PSG recordings.
METHODS
Participants
Thirty-five brain-injured pediatric patients with UWSparticipated in the study. The group was made up ofin-patients, admitted to our hospital for intensive neu-rorehabilitation treatment (physical therapy, dysphagiatherapy, and sensory stimulation therapy) throughout a
period of 4 years. Inclusion criteria were as follows: (a)severe acquired brain lesion; (b) age 18 years or less; and(c) time since injury 1 year or less at the study enroll-ment. Exclusion criteria were as follows: (a) congenitalneurological pathology; (b) need of mechanical venti-lation (due to the interfering effect of ventilation onsleep33,34); and (c) administration of drugs in compo-sition and dosages capable of significantly altering theEEG frequency content (however, a complete list ofsedative drugs and dosages is provided for each patientin Table 1).
At enrollment in the study, a multidisciplinary team(neurologist, neuropsychiatrist, neuropsychologist, anddysphagia therapist) evaluated all patients and con-cluded that they fulfilled the criteria for UWS diagnosis,according to the diagnostic criteria of the Royal Collegeof Physicians2 and of Giacino et al.27 Seven patients wereexcluded from the study because of recurrent epilepticseizures/activity that would have dominated the EEGactivity and would have impeded the correct sleep stag-ing, and one patient was excluded because of recurrentmovement artifacts that would have overwhelmed theneurophysiological evidences. A final group of 27 pa-tients (mean age = 8.44 years, SD = 5.33 years; 21 malepatients) was selected. Among the final cohort, none ofthe patients exhibited epileptic activity with duration ofmore than 15% of the whole PSG track. Epileptic dis-charges consisted of all cases in short isolated sequencesof epileptiform anomalies, deemed not to interfere withsleep architecture. Table 1 reports the demographic andclinical characteristics of the patients.
Ethics statement
This study was carried out in compliance with theDeclaration of Helsinki and was approved by the“I.R.C.C.S. E. Medea—Ass. La Nostra Famiglia” EthicsCommittee, located in Bosisio Parini (Lecco, Italy). Pa-tients’ relatives and/or legal guardians provided writteninformed consent for the participation in the study.
Clinical evaluation and measures
On admission, the patients’ medical history was col-lected, including their Glasgow Coma Scale (GCS) scoreat insult (see Table 1).35,36 At the time of study (T0),the Disability Rating Scale (DRS),37,38 which focuseson the functional abilities, and the Level of Cogni-tive Functioning Assessment Scale (LOCFAS),39 whichis specifically used for the punctual evaluation of thecognitive functions, were administered. Patients alsounderwent clinical magnetic resonance imaging exam-ination (see Supplemental Digital Content Table ST2,available at http://links.lww.com/JHTR/A134). A clini-cal follow-up (T1) was performed after 36 months fromthe first evaluation (T0); the follow-up included patients’evaluation with the standardized Glasgow Outcome
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.

Polysomnographic Sleep Patterns in Unresponsive Wakefulness Syndrome 3
TA
BLE
1D
emog
raph
ican
dcl
inic
alda
ta
Ca
se
Ag
e,
y/s
ex
Pri
ma
ryd
ise
ase
GC
Ssco
re(a
tin
su
lt)
GO
Ssco
re( T
1)
LO
CF
AS
sco
re( T
0/T
1)
DR
Ssco
re( T
0/T
1)
C/N
CS
sco
re( T
1)
Sta
teo
fco
nscio
usn
ess
a
(T0/T
1)
SP
PU
WS
bE
pil
ep
sy
Dru
gs
c
111
/MH
ead
trau
ma
44
2/8
24/7
1U
WS
/exi
t-M
CS
6N
oE
=0.
62
14/M
Hea
dtr
aum
a7
22/
224
/22
3U
WS
/UW
S2
No
Non
e3
16/M
Hea
dtr
aum
a4
42/
623
/91
UW
S/e
xit-
MC
S5
No
E=
0.7
45/
MH
ypox
icda
mag
e3
42/
524
/91
UW
S/e
xit-
MC
S5
No
C=
0.4
4∗ ;
F=
15
2/M
Bra
intu
mor
31
2/2
24/3
04
UW
S/U
WS
4Y
esA
=5
614
/MH
ead
trau
ma
31
2/2
28/2
42
UW
S/U
WS
3N
oE
=1.
8;H
=2
713
/MH
ead
trau
ma
63
2/2
24/2
32
UW
S/M
CS
3N
oE
=2.
3;F
=0.
8;H
=12
84/
ME
ncep
halit
is4
32/
224
/20
2U
WS
/MC
S3
No
E=
2.8
∗
95/
MH
ead
trau
ma
63
2/3
23/2
01
UW
S/M
CS
6N
oN
one
1014
/MB
rain
tum
or6
22/
224
/22
2U
WS
/UW
S2
No
Non
e11
5/M
Enc
epha
litis
63
2/3
24/1
91
UW
S/M
CS
5Y
esA
=5
1212
/FH
ead
trau
ma
54
2/7
22/8
2U
WS
/exi
t-M
CS
6N
oA
=6;
D=
0.0
5∗ ;
E=
0.8
1313
/FH
ead
trau
ma
34
2/5
23/9
1U
WS
/exi
t-M
CS
6N
oN
one
1413
/MH
ead
trau
ma
33
2/3
24/1
91
UW
S/M
CS
4N
oC
=0.
1;D
=0.
04;E
=2.
515
15/F
Hea
dtr
aum
a5
32/
623
/71
UW
S/e
xit-
MC
S5
No
E=
2.2;
F=
0.3
165/
FE
ncep
halit
is4
32/
324
/21
2U
WS
/MC
S6
No
E=
0.2;
F=
0.9
174/
MH
ead
trau
ma
44
2/6
22/8
1U
WS
/exi
t-M
CS
5N
oN
one
184/
MH
ead
trau
ma
63
2/3
27/1
71
UW
S/M
CS
5Y
esC
=0.
04;E
=1.
719
9/M
Hea
dtr
aum
a4
32/
325
/18
4U
WS
/MC
S5
No
A=
5;D
=0.
04;E
=0.
1;F
=1
203/
MH
ypox
icda
mag
e3
32/
325
/20
1U
WS
/MC
S5
No
C=
0.8
∗ ;E
=2.
3;F
=1
.4∗
2118
/MH
ead
trau
ma
43
3/3
25/2
02
UW
S/M
CS
3N
oE
=1.
4;G
=0.
522
6/F
Bra
intu
mor
33
1/5
26/6
1U
WS
/exi
t-M
CS
5N
oN
one
2314
/MH
ead
trau
ma
33
3/5
26/7
2U
WS
/exi
t-M
CS
6N
oN
one
244/
FH
ypox
icda
mag
e3
22/
224
/22
2U
WS
/UW
S3
Yes
E=
1.8;
F=
0.2
252/
MH
ypox
icda
mag
e3
22/
223
/22
2U
WS
/UW
S4
Yes
F=
426
2/M
Hyp
oxic
dam
age
33
2/3
23/2
01
UW
S/M
CS
5Y
esB
=0.
015;
E=
2.3
271/
MH
ypox
icda
mag
e5
22/
226
/24
3U
WS
/UW
S1
Yes
E=
0.8;
F=
0.8
Abb
revi
atio
ns:C
/NC
S,C
oma/
Nea
rC
oma
Sca
leat
follo
w-u
p;D
RS
,Dis
abili
tyR
atin
gS
cale
attim
eof
EE
Gan
dat
follo
w-u
p;E
EG
,ele
ctro
ence
phal
ogra
m;G
CS
,Gla
sgow
Com
aS
cale
scor
eat
insu
lt;G
OS
,G
lasg
owO
utco
me
Sca
lesc
ore
atfo
llow
-up;
LOC
FAS
,Le
velo
fC
ogni
tive
Func
tioni
ngA
sses
smen
tS
cale
attim
eof
EE
Gan
dat
follo
w-u
p;S
PP
UW
S,
slee
ppa
tter
nsfo
rpe
diat
ricun
resp
onsi
vew
akef
ulne
sssy
ndro
me;
T 0,t
ime
atst
udy;
T 1,t
ime
atfo
llow
-up.
a Sta
teof
cons
ciou
snes
sat
time
ofE
EG
and
atfo
llow
-up
(UW
Sis
unre
spon
sive
wak
eful
ness
synd
rom
ean
dve
geta
tive
stat
e;M
CS
ism
inim
ally
cons
ciou
sst
ate;
exit-
MC
Sis
the
reco
very
ofco
nsci
ousn
ess)
.bS
leep
grou
pac
cord
ing
toS
PP
UW
S.
c Dos
age
ofdr
ugs
with
seda
tive
effe
cts:
A=
phen
obar
bita
l(m
g/kg
/d);
B=
clon
azep
am(m
g/kg
/d);
C=
diaz
epam
(mg/
kg/d
);D
=lo
raze
pam
(mg/
kg/d
);E
=ba
clof
en(m
g/kg
/d);
F=
niap
razi
ne(m
g/kg
/d);
G=
hydr
oxyz
ine
dich
lorh
ydra
te(m
g/kg
/d);
H=
tizia
nidi
nech
lorh
ydra
te(m
g/d)
.The
valu
esw
ith“∗
”in
dica
tedo
sage
sex
ceed
ing
the
reco
mm
ende
dra
nges
.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com

4 JOURNAL OF HEAD TRAUMA REHABILITATION
Scale (GOS),40,41 which provides the general degree ofrecovery, the DRS, the LOCFAS, and the Coma/NearComa Scale (C/NCS),42 which estimates the level ofresponsiveness damage, depending on responses tothe stimulation of the different sensory channels. TheC/NCS was applied in compliance with the AmericanCongress of Rehabilitation Medicine Disorders of Con-sciousness Task Force guidelines.43 High scores on theGCS, LOCFAS, and GOS reflected a less impaired clin-ical picture. In contrast, the higher the DRS and C/NCSscores, the more marked the difficulties. The staff (DrsValentina Pastore, Federica Villa, and Katia Colombo)who administered the clinical scales were blinded to theresearch study rationale.
PSG recordings
After admission to our rehabilitation center, PSGrecordings of all the 27 patients were obtained overnight,uninterruptedly from the afternoon to the morning ofthe following day. We agreed to record the longestrecording possible, with respect to the daily rehabilita-tion schedules and the patients’ compliance and needs.Mean time since injury was 106 days (SD = 58 days).Mean duration of recordings was 828 minutes (SD =197 minutes). Patients received no specific sedation forthe execution of EEG examination. EEG tracks wereacquired with an Embla RemLogic digital system, with500-Hz sampling rate. In compliance with the mini-mal requirements provided in the American Academyof Sleep Medicine (AASM) recommendations for mon-tage, 8 Ag/AgCl electrodes were placed on the patients’head, corresponding to the standard 10/20 system44
in F3, F4, C3, C4, T3, T4, O1, and O2 positions.EEG recording was performed with reference to 2 ad-ditional electrodes, placed in A1 and A2 positions, atthe mastoids. A set of polygraphic channels was alsoadded: 2 electrodes for electro-oculogram (EOG) incross-montage, at least 1 bipolar EMG channel for del-toid activity, and 1 bipolar electrocardiographic (ECG)derivation. Digital bandpass filtering was applied to theEEG and EOG channels in the 0.3- to 35-Hz range, tothe EMG in the 10- to 200-Hz range, and to the ECG inthe 0.3- to 70-Hz range. EEG impedances were kept un-der 5 k�. During the recording, patients’ caregivers wereinstructed to accurately report any event in a standardform, also called “sleep diary.”
Because of the partial absence of the skull, in patient18, we could not place electrodes over F3 and F4; in-stead, we were able to place Fpz electrode. Similarly, pa-tients 19, 21, and 23 completely lacked EEG recordingfrom the frontal area, as the placement of frontopolarand frontal electrodes was impossible.
For each patient, PSG tracks were visualized and an-alyzed by Somnologica software (Reykjavik, Iceland).
Sleep was partitioned into 30-second epochs for furtherstaging. After visual selection and exclusion of the arti-factual periods, including intervals affected by muscularelectrical activity, 2 trained and certified neuropsychia-trists (P.A., F.F.) and 2 experienced neurologists (S.L., S.de B.), belonging to 2 different hospitals, scored thetracks independently. They performed a preliminaryscoring of the PSG tracks, using the age-appropriatecriteria of the AASM.1 In doing so, they isolated thespecific PSG periods for which the criteria were clearlynot applicable. Unscored periods were discussed by theteam in 2 independent scoring sessions, and scoringconflicts were partially resolved. Then, alternative cri-teria were developed on the basis of previous works(see Supplemental Digital Content Table ST1, avail-able at http://links.lww.com/JHTR/A134).13,28,45 Suchcriteria helped in the attribution of sleep-wake statusand in the identification of possible sleep stages inunscored epochs, during a second double-blind scor-ing process. However, segments with debatable score(<20% of the total duration in all cases) were not in-cluded in the following analyses. Then, we attemptedsystematization into different stages, further graded ac-cording to the global neuroelectrical complexity of eachpatient’s PSG recording. Such systematization gave riseto the sleep patterns for pediatric unresponsive wake-fulness syndrome (SPPUWS), detailed into the “Re-sults” section. Finally, the duration of REM periodsand the number of spindles were quantified for eachpatient located in SPPUWS 5 and SPPUWS 6 (seeSupplemental Digital Content Table ST2, available athttp://links.lww.com/JHTR/A134).
Statistics
Demographic and clinical characteristics were re-ported by descriptive statistics. The Student t test wasused for pairwise comparison of the age at injury in thetraumatic and nontraumatic groups of patients. Becauseall data, with the only exception of the age at injury,proved to be nonnormally distributed after the Shapiro-Wilks and Kolmogorov-Smirnov tests, and because ofthe small size of the data set, we applied nonparametrictests for inferential statistics. The Mann-Whitney U testwas used for testing differences between traumatic andnontraumatic patients at the time of the study (T0) andfor testing differences in clinical scores between patientsshowing PSG tracks with and without spindles andREM. Multiple comparisons were adjusted for the age atinjury and were investigated by the Quade test. We setsignificance at P values below .05; to adjust for multiplecomparisons, we used a Bonferroni correction (α =.025). Spearman rank correlation coefficients, adjustedfor the age at injury, were obtained to determine therelationship between quantitative variables. Qualitative
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.

Polysomnographic Sleep Patterns in Unresponsive Wakefulness Syndrome 5
variable comparisons were done using the χ2 test. Allstatistical analyses were carried out using the NCSSstatistical package (Kaysville, Utah).
RESULTS
Demographic data and clinical scales
In this section, we report the clinical characteristics of27 children and adolescents with UWS (see also Table 1).Mean age at injury was 8.44 years (SD = 5.33 years) forthe group. With respect to the etiology, 15 children(56%) presented with an acquired brain lesion due toa brain trauma whereas 12 patients (44%) had a non-traumatic etiology (6 cases of anoxia due to drowning,suffocation, or cardiac arrest; 3 cases of brain lesionssecondary to brain tumor treatments; and 3 cases of in-fectious or immune-mediated lesions). Median value forthe GCS score at insult was 4 (range, 3-7). At the time ofthe study (T0), median value for the LOCFAS score was2, with the majority of patients (n = 24; 89%) at LOC-FAS level = 2 (range, 1-3); moreover, median value forthe DRS score was 24, with the majority of patients atDRS level = 24 (n = 11; 41%) and level = 23 (n = 6;22%) (range, 22-28).
At the follow-up (T1), median value for the GOS scorewas 3 (range, 1-4); median value for the LOCFAS scorewas 3, with the patients equally distributed at LOCFASlevel = 2 and level = 3 (n = 9; 33% each) (range, 2-8);moreover, median value for the DRS score was 20, withscores widely spread in the range from 6 to 30. Medianvalue for the C/NCS score was 2 (range, 1-4), with 13 pa-tients (48%) at level = 1, 10 patients (38%) at level = 2,2 patients (7%) at level = 3, and 2 patients (7%) at level= 4. In the group, 7 patients (26%) exhibited epilepsy.Finally, at the time of the study, 4 patients (15%) were re-ceiving pharmacological treatment including drugs withpotential sedative effects in dosages exceeding the rec-ommended ranges. At follow-up (T1), 9 patients (33% ofthe total sample) recovered consciousness (exited MCS),11 patients (41%) were in an MCS, and 7 patients (26%)had UWS.
According to the etiology of their lesions (traumaticand nontraumatic), 2 patient groups were formed. A sta-tistical comparison was made between the 2 groups onthe main clinical variables to verify their homogeneity.No significant differences were found, with the excep-tion of the “age at insult” variable (t = 4.75; P < .001).Indeed, patients with a traumatic brain injury were sig-nificantly older at the time of insult than patients withbrain lesions due to other etiologies (mean age = 11.67± 4.32 years vs 4.42 ± 3.40 years); nonetheless, the2 groups were comparable on the other clinical fea-tures. Consequently, further comparisons and correla-tions were adjusted for the “age at insult.”
Sleep patterns for pediatric unresponsive wakefulnesssyndrome
On the basis of previous works,13,18,28 we attempteda search for comparable sleep characteristics among ourgroup of pediatric patients with UWS. The 4 sleep ex-perts (P.A., F.F., S.L., and S. de B.) agreed on the identi-fication of 6 different EEG patterns, which were termedSPPUWS. The isolated SPPUWS show increasing orga-nizational complexity of sleep. Figure 1 describes theobserved SPPUWS.
The 6 patterns are identified as follows:1. Monophasic pattern: No distinction between wake
and sleep cycles can be deduced on the basis of anelectroencephalogram. The neuroelectrical patternconsists of continuous low-voltage monomorphicactivity (<75 μV) at a specific frequency (no powerpeak at any specific frequency can be observed) (seeFigure 2).
2. Biphasic pattern: Presence of 2 distinguishablephases:(1). A stage attributed to wakefulness (stage W)
and conforming to the general criteria re-ported in Figure 1. The stage is character-ized by dominant, diffuse, low-voltage thetaactivity (4-7 Hz; 50%-70% of the epoch), in-termingled with waves in the delta band (1-4 Hz; 50%-30%), and with rapid low-voltageactivity in the 14- to 18-Hz band (<30 μV)of clear neuronal origin (as also described inthe AASM manual). Rapid activity due tomovements and muscle tone can be addition-ally present and is considered an additionalevidence.
(2). A stage attributed to sleep (stage S). Thestage manifests with high-voltage delta activ-ity (>75% of the epoch; amplitude >75 μV).
3. Aspecific triphasic pattern: Presence of 3 distinguish-able phases:(1) A stage attributed to wakefulness (stage W).
The stage is characterized by dominant, dif-fuse, low-voltage theta activity (≥80% of theepoch), intermingled with rare and sporadicwaves in the delta band (<20%). Superim-posed, rapid, low-voltage beta activity of clearneuronal origin is observed. Globally, this stageis characterized by more rapid activity, with re-spect to stage W of the biphasic pattern (see Sup-plemental Digital Content Figure SF1a, avail-able at: http://links.lww.com/JHTR/A135).
(2) A first phase attributed to sleep. In this stage,theta activity alternates with delta band activ-ity (<20% of epoch) (see Supplemental Digi-tal Content Figure SF1b, available at: http://links.lww.com/JHTR/A135).
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com

6 JOURNAL OF HEAD TRAUMA REHABILITATION
Figure 1. Criteria for the identification of the sleep patterns, according to SPPUWS. REM indicates rapid eye movement;SWA, short-wave activity; EEG, electroencephalogram; EMG, electromyogram; RAT, rhythmic theta anterior activity; NREM,nonrapid eye movement; SPPUWS, sleep patterns for pediatric unresponsive wakefulness syndrome.
(3) A second phase attributed to sleep, charac-terized by periods longer than 3 consecutiveepochs showing prevalent delta activity (≥20%of epoch) (see Supplemental Digital Con-tent Figure SF1c, available at: http://links.lww.com/JHTR/A135).
Globally, sleep (phases 2 and 3) shows slowdownof the neuroelectrical activity. In addition, thetheta/delta alternated activity observed in phases
2 and 3 is clearly not classifiable as nonrapid eyemovement (NREM) sleep because no K-complexesor spindles can be found.
4. REM triphasic pattern: Presence of 3 distinguishablephases:(1) Wakefulness (stage W), as observed in the aspe-
cific triphasic pattern (see Supplemental DigitalContent Figure SF2a, available at: http://links.lww.com/JHTR/A136).
Figure 2. Example of EEG spectrum at the frontopolar (Fp1), temporal (T3) and occipital (O1) locations. FFT indicates FastFourier Transform.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.

Polysomnographic Sleep Patterns in Unresponsive Wakefulness Syndrome 7
(2) A first phase attributed to sleep, characterizedby slow-wave activity with duration of 20%or more of the epoch (see SupplementalDigital Content Figure SF2b, available at:http://links.lww.com/JHTR/A136). Slow-wave activity structures as a slow rhythm,comprising delta and theta frequency bands,and not corresponding to REM sleep stage.
(3) A second phase attributed to sleep (R). Desyn-chronization of electrical activity is found inthe absence of criteria related to wakefulness.This stage is characterized by low-amplitude,mixed-frequency, rudimentary REM sleep ele-ments such as (i) variable presence of REMs,(ii) trains of monomorphic, triangular delta-subdelta waves (50-75 μV), located in the fron-tocentral head region, and suggesting a saw-tooth wave morphology, (iii) rhythmic thetaanterior activity (RAT), and (vi) low-chin EMGtone (see Supplemental Digital Content FigureSF2c, available at: http://links.lww.com/JHTR/A136). NREM sleep elements such asspindles and K-complexes are absent.
5. Atypical NREM-REM sleep: Standard REM sleep,alternated with atypical NREM sleep. AtypicalNREM sleep is characterized by sleep elementsatypical in morphology and frequency, such asfrontocentral slow spindles, as in the work of Colo-gan et al.28 A clear distinction between stages N1and N2 is not identifiable in this stage. As a conse-quence, a “light sleep” stage, grouping N1- and N2-like activities, is used, as in the work of Cheliout-Heraut et al.13
6. Fully structured sleep: Presence of standard NREMand REM sleep elements. This pattern complieswith the standard AASM11 criteria.
Each SPPUWS group (groups 1-6) shows increasingneurophysiological complexity. The numbers given toeach group were then considered a quantitative variableand entered into statistics as such.
The monophasic pattern (SPPUWS 1) was observedonly in 1 patient (4% of the total sample), the bipha-sic pattern (SPPUWS 2) in 2 patients (7%), the aspe-cific triphasic pattern (SPPUWS 3) in 5 patients (19%),and the REM triphasic pattern (SPPUWS 4) in 3 pa-tients (11%). The atypical NREM-REM sleep pattern(SPPUWS 5) was the most common sleep pattern for ourpatients (n = 10; 37%), followed by the fully structuredsleep pattern (SPPUWS 6; n = 6; 22%) (see Table 1).
Correlations between PSG patterns and the clinicalscales
Statistical analysis of the correlations between thePSG patterns (SPPUWS) and the clinical scales could
not show any significant result for the measures reg-istered in T0. On the contrary, statistically signifi-cant results were obtained for all the measures in T1
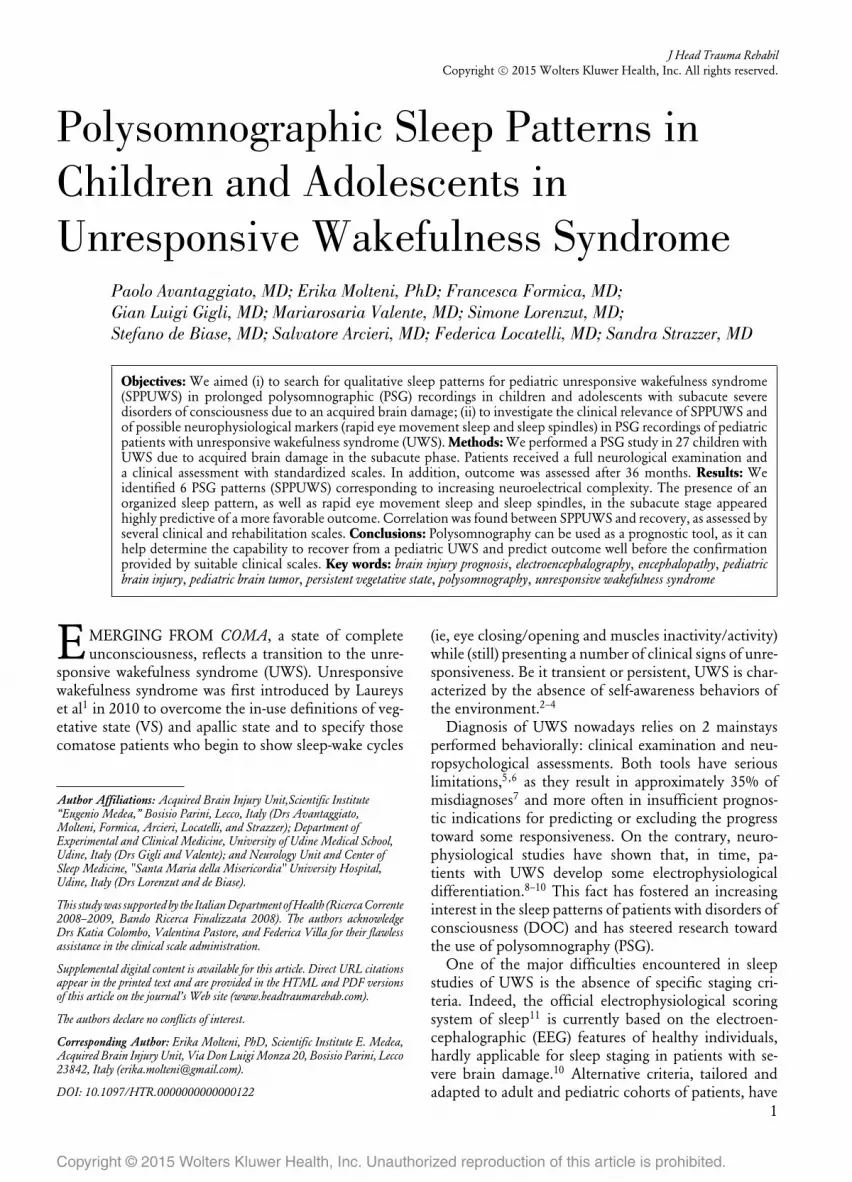
(see Table 2). Specifically, SPPUWS were positively re-lated to the GOS and LOCFAS scores at follow-upwhereas a significant negative correlation was foundwith the DRS and C/NCS scores. Moreover, SPPUWSshowed strong positive correlation with the state of con-sciousness in T1 (ρ = 0.775; P < .001).
As can be seen in Figure 3, increasing complexity ofthe PSG pattern is associated with improved state ofconsciousness.
Neurophysiological markers of prognostic relevance
The outcome (state of consciousness at T1) was sig-nificantly different in the group of children whose PSGtracks showed the presence of spindles and REM sleep,with respect to the patients providing PSG recordingsin which spindles and REM sleep had not been iso-lated (U = 2.031, P = .021, and U = 2.673, P = .008,respectively).
TABLE 2 Age-corrected correlationsbetween the 6 SPPUWS and the clinicalscales
SPPUWS
GCSρ 0.250P .218
LOCFAS (T0)ρ 0.017P .935
DRS (T0)ρ − 0.290P .151
GOSρ 0.659P <.001a
LOCFAS (T1)ρ 0.709P <.001a
DRS (T1)ρ − 0.669P <.001a
C/NCSρ − 0.466P .017b
Abbreviations: C/NCS, Coma/Near Coma Scale; DRS, DisabilityRating Scale; GCS, Glasgow Coma Scale; GOS, Glasgow Out-come Scale; LOCFAS, Level of Cognitive Functioning Assess-ment Scale; SPPUWS, sleep patterns for pediatric unresponsivewakefulness syndrome; T0, time of enrollment; T1, follow-up(36 months later).aP ≤ .001.bP ≤ .05.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com
8 JOURNAL OF HEAD TRAUMA REHABILITATION
Figure 3. SPPUWS distribution, with respect to the levels ofconsciousness. More complex sleep patterns (ie, higher SP-PUWS) correlate with higher levels of consciousness. SPPUWSindicates sleep patterns for pediatric unresponsive wakefulnesssyndrome; VS, vegetative state; MCS, minimally consciousstate; NC, normal consciousness.
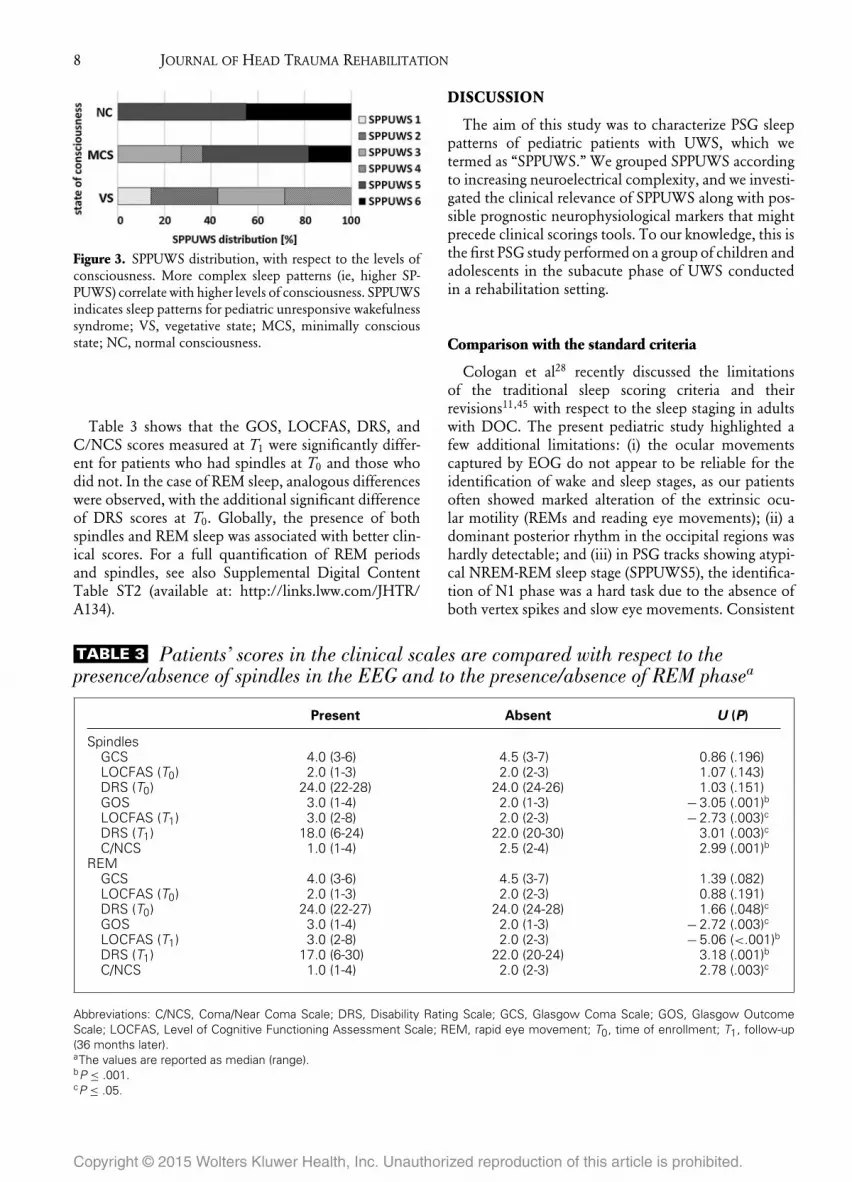
Table 3 shows that the GOS, LOCFAS, DRS, andC/NCS scores measured at T1 were significantly differ-ent for patients who had spindles at T0 and those whodid not. In the case of REM sleep, analogous differenceswere observed, with the additional significant differenceof DRS scores at T0. Globally, the presence of bothspindles and REM sleep was associated with better clin-ical scores. For a full quantification of REM periodsand spindles, see also Supplemental Digital ContentTable ST2 (available at: http://links.lww.com/JHTR/A134).
DISCUSSION
The aim of this study was to characterize PSG sleeppatterns of pediatric patients with UWS, which wetermed as “SPPUWS.” We grouped SPPUWS accordingto increasing neuroelectrical complexity, and we investi-gated the clinical relevance of SPPUWS along with pos-sible prognostic neurophysiological markers that mightprecede clinical scorings tools. To our knowledge, this isthe first PSG study performed on a group of children andadolescents in the subacute phase of UWS conductedin a rehabilitation setting.
Comparison with the standard criteria
Cologan et al28 recently discussed the limitationsof the traditional sleep scoring criteria and theirrevisions11,45 with respect to the sleep staging in adultswith DOC. The present pediatric study highlighted afew additional limitations: (i) the ocular movementscaptured by EOG do not appear to be reliable for theidentification of wake and sleep stages, as our patientsoften showed marked alteration of the extrinsic ocu-lar motility (REMs and reading eye movements); (ii) adominant posterior rhythm in the occipital regions washardly detectable; and (iii) in PSG tracks showing atypi-cal NREM-REM sleep stage (SPPUWS5), the identifica-tion of N1 phase was a hard task due to the absence ofboth vertex spikes and slow eye movements. Consistent
TABLE 3 Patients’ scores in the clinical scales are compared with respect to thepresence/absence of spindles in the EEG and to the presence/absence of REM phasea
Present Absent U (P)
SpindlesGCS 4.0 (3-6) 4.5 (3-7) 0.86 (.196)LOCFAS (T0) 2.0 (1-3) 2.0 (2-3) 1.07 (.143)DRS (T0) 24.0 (22-28) 24.0 (24-26) 1.03 (.151)GOS 3.0 (1-4) 2.0 (1-3) − 3.05 (.001)bLOCFAS (T1) 3.0 (2-8) 2.0 (2-3) − 2.73 (.003)cDRS (T1) 18.0 (6-24) 22.0 (20-30) 3.01 (.003)cC/NCS 1.0 (1-4) 2.5 (2-4) 2.99 (.001)b
REMGCS 4.0 (3-6) 4.5 (3-7) 1.39 (.082)LOCFAS (T0) 2.0 (1-3) 2.0 (2-3) 0.88 (.191)DRS (T0) 24.0 (22-27) 24.0 (24-28) 1.66 (.048)cGOS 3.0 (1-4) 2.0 (1-3) − 2.72 (.003)cLOCFAS (T1) 3.0 (2-8) 2.0 (2-3) − 5.06 (<.001)bDRS (T1) 17.0 (6-30) 22.0 (20-24) 3.18 (.001)bC/NCS 1.0 (1-4) 2.0 (2-3) 2.78 (.003)c
Abbreviations: C/NCS, Coma/Near Coma Scale; DRS, Disability Rating Scale; GCS, Glasgow Coma Scale; GOS, Glasgow OutcomeScale; LOCFAS, Level of Cognitive Functioning Assessment Scale; REM, rapid eye movement; T0, time of enrollment; T1, follow-up(36 months later).aThe values are reported as median (range).bP ≤ .001.cP ≤ .05.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.

Polysomnographic Sleep Patterns in Unresponsive Wakefulness Syndrome 9
with Cheliout-Heraut et al,13 we identified a light sleepphase comprising both N1 and N2 phases.
On the contrary, the eye blinking activity, the muscletone evaluation, and the artifact detection movementwere crucial at least for the identification of the wakestage. Conversely, we deemed it improper to use thecardiac frequency as a criterion due to the insufficientmodulation of the cardiac circadian rhythm oftenobserved in patients in a subacute phase of UWS.Cologan et al28 plotted the EEG, EMG, EOG, andEKG along the 24 hours of recording into a spectralmap. This appeared to be especially useful to locatethe periods of rest that were characterized by a globalreduction of all activities. However, the decrease of theheart rate was not systematically observed during the vi-sual scoring of sleep stages. This is also the case in someof our recordings. Furthermore, we observed transientpathological overactivations of the body temperature,respiratory rate, heart rate, and muscular tone duringthe wake and sleep stages in some of our patients. Theinvestigation of the neurovegetative system activityduring the different vigilance states of brain-injured
patients could therefore be the matter of futurework.
However, following the observations listed earlier, wepropose the criteria described in Figure 1, including (i)the use of a “sleep diary,” filled in by the caregiver, orvideo-recording; (ii) monitoring of the massive muscularactivity by EMG, as suggested also by Kohyama et al14
and Landsness et al17; and (iii) evaluation of the eyeblinks, as suggested also by Cologan et al.28
Previous studies (see Table 4), which observed disso-ciation between neuroelectrical and clinical evidences,due to the fact that the presence of alternating periodsof eyes opening/closing did not agree with the expectedEEG wakefulness/sleep architectures. This observationis confirmed in the present study, despite the average du-ration of the recordings being remarkably shorter than24 hours and the sleep-wake cycle only being able to beinvestigated partially.
Discussion of SPPUWS
In our database, we found only 1 case of “monopha-sic” pattern (SPPUWS 1): in this patient, distinguishing
TABLE 4 Previous studies discussing signs of favorable outcome in altered sleep due tosevere brain injury
Signs of favorable outcome
StudyAdults/children Etiology
Sleep-stagedifferentiation
Presence of stablesleep-wake cycles
Sleepspindles
de Biase et al (2014)31 A Head/brain trauma + + +Hypoxic damageHemorrhagic stroke
Cologan et al (2013)28 A Head/brain trauma + + +Hypoxic damageCerebral vascular
accidentUrakami (2012)46 A Head/brain trauma +Landsness et al (2011)17 A Head/brain trauma +
Hypoxic damageBagnato et al (2010)19 A Head/brain trauma +
Hypoxic damage in comaValente et al (2002)18 A Head/brain trauma +Cheliout-Heraut et al (2001)13 C Head/brain trauma +
Hypoxic damage + +Evans and Bartlett (1995)20 A, C Head/brain traumaGiubilei et al (1995)24 A Head/brain trauma + +D’Aleo et al (1994)23 A Head/brain trauma +
Hypoxic damageHulihan and Syna (1994)47 A Hypoxic damage +Synek (1988)48 A Head/brain trauma +
Hypoxic damageKohyama et al (1986)14 C Hypoxic damage +
EncephalitisRumpl et al (1983)49 A Head/brain trauma +Ron et al (1980)32 A, C Head/brain trauma +
Abbreviations: A, adults; C, children.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com

10 JOURNAL OF HEAD TRAUMA REHABILITATION
between 2 EEG states was not feasible and electroclin-ical dissociation was highly evident, despite the subjectfully meeting the criteria for UWS. In some patients,the global slowing of the neuroelectrical activityduring sleep appeared in the concurrent absence ofphysiological elements of sleep, primarily spindles. Thisevidence did not find confirmation in the AASM11
criteria and led to the definition and characterization ofspecific SSPUWS: a subgroup of patients manifestinghigh-voltage delta activity during sleep was identifiedand included in SPPUWS 2, whereas children present-ing high-voltage delta activity interleaved with periodsof prevalently theta activity were grouped in a specificpattern numbered SPPUWS 3.
Figure 1 shows that the appearance of REM sleep isthe main feature of SPPUWS 4 and that it manifestswith the presence of low, mixed-frequency, and saw-tooth activity. These features seem to be the most reli-able criteria for REM sleep staging in these patients. Inline with Cheliout-Heraut et al,13 in 4 of our patients,REM sleep did not show atony. Remarkably, we neverfound NREM elements (spindles and K-complexes) inthe absence of REM sleep. As a consequence, we hypoth-esize that REM activity restructures before NREM ele-ments. However, a longitudinal study on patients withSPPUWS 4 is needed for confirmation.
The progressive restructuring of sleep in patients withUWS seems to retrace ontogenetic milestones: it initiallymanifests with paradoxical sleep, which is a precursor ofREM sleep. Indeed, REM sleep plays a major role dur-ing the first weeks of life of a child.50,51 In contrast,spindles—which are among the early elements of NREMsleep—appear from the second month of life. Our resultssuggest parallelism between the neonatal electrophysiol-ogy and the recovery from pediatric coma.
Clinical discussion
With regard to prognosis, the clinical validity of theSPPUWS is confirmed by significant correlations withthe scores at T1 on all the clinical scales. Specifically,the LOCFAS, measured at T1, showed the highest cor-relation with SPPUWS. Interestingly, among the clini-cal scales used in this study, the LOCFAS is the onespecifically used for the punctual evaluation of the cog-nitive functions; moreover, it was recently proved thatthe LOCFAS alone is capable of providing reliable in-formation about the state of consciousness of pediatricpatients exiting from coma, if administered by trainedpersonnel.52
In addition, the correlation between SPPUWS and theclinical scales fosters the hypothesis that slow-wave ac-tivity stabilizes across the progression of the conscious-ness after the injury, in parallel with the appearance ofthe spindles and their thickening, as also affirmed in thework of Cologan et al.28
Wakefulness is associated with instant awareness,which is a function of the thalamocortical network.The transition from wakefulness to sleep is effectedby an arousal inhibitory mechanism based on a par-tial blockade of the thalamus and the upper brain stem.Such mechanism is generally associated with both tha-lamic sleep spindles and cortical slow-wave activity inthe EEG.53 Considering that patients in subacute andchronic UWS often show postconcussive/atrophic tha-lamic anomalies,54 Cologan et al10 examined the antag-onistic role of thalamic disruption in the restructuringof sleep, finding that the presence of spindles correlatesboth quantitatively and qualitatively with the severity ofthe thalamocortical injury in adults in a VS/UWS andMCS. According to the literature, REM sleep is absent17
or occasionally present9,10,18,31 in the UWS. However,standard REM sleep is associated with dreams that areby definition a form of consciousness in healthy sub-jects. The persistence of REM sleep is therefore a signof a less severe diagnostic because of less damages inthe dedicated brain networks and could even reflect anMCS undetected by behavioral scales (such as in thework of Cruse et al6). This would support why patientswith UWS having REM sleep have a better outcomeduring neurorehabilitation.
Nearly a half of the children enrolled in our studyshowed thalamic atrophy and/or multifocal lesions onmagnetic resonance imaging (see Supplemental DigitalContent Table ST3, available at: http://links.lww.com/JHTR/A134), in line with previous literature on adults;nevertheless, we could not draw any inference from thecorrelation with the presence of spindles, probably dueto the small sample size. Rather, the presence of spin-dles and REM sleep in PSG tracings was related to betteroutcome, as suggested by all the clinical scales applied atT1. These results confirm the aforementioned previousfindings in adults, showing that the observation of spin-dles and REM in PSG is a positive marker of recovery(see also Table 4).10,28,49
General issues and limitations
Despite this work attempted to face and overcomesome of the limitations arisen in previous studies, still anumber of issues remain unsolved:
1. Methodological limitations: The Coma RecoveryScale–Revised55 is the standard clinical tool for as-sessing responsiveness. Nevertheless, a validationin pediatric populations is not available to date.For this reason, a number of alternative scales havebeen chosen on the basis of previous pediatricliterature.56,57
Polysomnographic montage was obtainedaccording to the AASM guidelines.11 Neverthe-less, the AASM criteria have been formulatedfor patients with undamaged brains and we
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.

Polysomnographic Sleep Patterns in Unresponsive Wakefulness Syndrome 11
cannot rule out the fact that the recordingfrom parietal channels would have providedadditional relevant information to the study. Infuture studies, the use of comprehensive PSGmontages (eg, by using PSG caps) should beconsidered.
Moreover, PSG tracks were acquired in a rehabil-itation center rather than in an intensive care unit.This fact provided a more ecological setting withrespect to previous studies, as it helped minimizeassistive interferences. On the contrary, the record-ing duration was limited to less than 24 hours (ie,the duration of a circadian cycle) due to the sched-uled rehabilitative treatments; as a consequence,some sleep stages may have been missed by therecordings.
2. Clinical limitations: As documented in Table 1,at the time of PSG recording, some of the chil-dren were undergoing light sedative therapy, whichcould not be interrupted because of ethical rea-sons. Sedative drugs can consistently alter the EEGactivity.58 However, the number of patients whoreceived the highest dosages of sedative drugs doesnot coincide with the number of patients whoshowed the worst clinical scores in T0, nor withthe number of those who manifested the worsestate of consciousness at follow-up. Consequently,no link can be established between the sedativetherapy and prognosis. However, administration ofbenzodiazepines could be a potential confoundingvariable of the study, as they can increase spindledensity.
In addition, some patients had pharmaco-logically treated epilepsy at the time of PSGrecording. Epilepsy can sensibly distort the sleepmacrostructure and the EEG frequency contentand can relevantly mask the sleep microstructure.59
To minimize the disturbance of epilepsy, PSGsegments affected by manifest epileptic activitywere not used for SPPUWS attribution. Moreover,the reader should note that patients with severe
epileptic encephalopathy were not enrolled in thestudy.Polysomnography is an inexpensive, ambulatorytechnique that has high time resolution and goodsensitivity in recording the electrical activity of sev-eral body compartments. It can help assess thefunctional integrity of major brain networks, mean-while recording a virtually unlimited number ofsubsidiary measures (such as respiration, heart rate,etc). Importantly, it easily adapts to the clinical rou-tine of brain-injured patients and can be applied atthe bedside. Thanks to its ecological virtue, PSG isconsidered as the elective tool for pediatric applica-tions and rehabilitation settings. On the contrary,long recording times, limited spatial resolution,and time-consuming signal evaluation/processingconstitute relevant drawbacks and, in some cases,limiting its use. All these aspects considered, wereckon that PSG remains an essential tool in theassessment of pediatric UWS.
CONCLUSIONS
Accordingly with previous works on adults and chil-dren, our pediatric study gives relevance to the reemer-gence of sleep spindles and REM sleep as prognosticmarkers for a possible recovery from UWS to the MCSand exit-MCS. Moreover, we put forward the anticipa-tory role of REM with respect to NREM activity. In ad-dition, our data confirm the statement that “the higheris the level of complexity in the PSG signal, the bet-ter is the functional outcome generally gained”30 previ-ously formulated for adult patients. Since studies in thefield were conducted on patients’ cohorts comparable insize with ours, or even smaller, further prospective, pos-sibly multicentric, studies are needed to double-checkSPPUWS on a larger scale. However, our study confirmsthe capability of PSG to provide some prediction ofthe outcome for children and adolescents in a subacutephase of UWS, well before the confirmation providedby suitable clinical scales.
REFERENCES
1. Laureys S, Celesia GG, Cohadon F, et al. Unresponsive wake-fulness syndrome: a new name for the vegetative state or apallicsyndrome. BMC Med. 2010;8:68.
2. Royal College of Physicians. The Permanent Vegetative State: Guid-ance on Diagnosis and Management. Report of a Working Party. Lon-don, England: Royal College of Physicians; 2003
3. Laureys S, Boly M. What is it like to be vegetative or minimallyconscious? Curr Opin Neurol. 2007;20:609–613.
4. Laureys S, Boly M. The changing spectrum of coma. Nat Clin PractNeurol. 2008;4:544–546.
5. Owen AM, Coleman MR, Boly M, Davis MH, Laureys S,Pickard JD. Detecting awareness in the vegetative state. Science.2006;313:1402.
6. Cruse D, Chennu S, Chatelle C, et al. Bedside detection of aware-ness in the vegetative state: a cohort study. Lancet. 2011;378:2088–2094.
7. Majerus S, Gill-Thwaites H, Andrews K, Laureys S. Behavioralevaluation of consciousness in severe brain damage. Prog BrainRes. 2005;150:397–413.
8. Vanhaudenhuyse A, Noirhomme Q, Tshibanda LJ, et al. Defaultnetwork connectivity reflects the level of consciousness in non-communicative brain-damaged patients. Brain. 2010;133:161–171.
9. Oksenberg A, Gordon C, Arons E, Sazbon L. Phasic activitiesof rapid eye movement sleep in vegetative state patients. Sleep.2001;24:703–706.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com

12 JOURNAL OF HEAD TRAUMA REHABILITATION
10. Cologan V, Schabus M, Ledoux D, Moonen G, Maquet P, LaureysS. Sleep in disorders of consciousness. Sleep Med Rev. 2010;14:97–105.
11. American Academy of Sleep Medicine. The AASM Manual for theScoring of Sleep and Associated Events. Rules, Terminology and Tech-nical Specifications. Westchester, IL: American Academy of SleepMedicine; 2007.
12. Himanen SL, Hasan J. Limitations of Rechtschaffen and Kales.Sleep Med Rev. 2000;4:149–167.
13. Cheliout-Heraut F, Rubinsztajn R, Ioos C, Estournet B. Prognosticvalue of evoked potentials and sleep recordings in the prolongedcomatose state of children. Preliminary data. Neurophysiol Clin.2001;31:283–292.
14. Kohyama J, Shishikura J, Nakano I, Iwakawa Y, Mori K. Sleepstudy on patients with severe brain damage—polysomnographicalexamination. Brain Dev. 1986;8:583–589.
15. Pattoneri P, Tirabassi G, Pela G, Astorri E, Mazzucchi A, BorghettiA. Circadian blood pressure and heart rate changes in patients ina persistent vegetative state after traumatic brain injury. J ClinHypertens (Greenwich). 2005;7:734–739.
16. Fukudome Y, Abe I, Saku Y, et al. Circadian blood pres-sure in patients in a persistent vegetative state. Am J Physiol.1996;270:R1109–R1114.
17. Landsness E, Bruno MA, Noirhomme Q, et al. Electrophysiolog-ical correlates of behavioural changes in vigilance in vegetativestate and minimally conscious state. Brain. 2011;134:2222–2232.
18. Valente M, Placidi F, Oliveira AJ, et al. Sleep organization patternas a prognostic marker at the subacute stage of posttraumatic coma.Clin Neurophysiol. 2002;113:1798–1805.
19. Bagnato S, Boccagni C, Prestandrea C, Sant’Angelo A, CastiglioneA, Galardi G. Prognostic value of standard EEG in traumaticand nontraumatic disorders of consciousness following coma. ClinNeurophysiol. 2010;121:274–280.
20. Evans BM, Bartlett JR. Prediction of outcome in severe head injurybased on recognition of sleep related activity in the polygraphicelectroencephalogram. J Neurol Neurosurg Psychiatry. 1995;59:17–25.
21. D’Aleo G, Bramanti P, Silvestri R, Saltuari L, Gerstenbrand F, DiPerri R. Sleep spindles in the initial stages of the vegetative state.Ital J Neurol Sci. 1994;15:347–351.
22. Gordon CR, Oksenberg A. Spontaneous nystagmus across thesleep-wake cycle in vegetative state patients. Electroencephalogr ClinNeurophysiol. 1993;86:132–137.
23. D’Aleo G, Saltuari L, Gerstenbrand F, Bramanti P. Sleep in thelast remission stages of vegetative state of traumatic nature. FunctNeurol. 1994;9:189–192.
24. Giubilei F, Formisano R, Fiorini M, et al. Sleep abnormali-ties in traumatic apallic syndrome. J Neurol Neurosurg Psychiatry.1995;58:484–486.
25. Oksenberg A, Arons E, Sazbon L, Mizrahi A, Radwan H. Sleep-related erections in vegetative state patients. Sleep. 2000;23:953–957.
26. Isono M, Wakabayashi Y, Fujiki MM, Kamida T, Kobayashi H.Sleep cycle in patients in a state of permanent unconsciousness.Brain Inj. 2002;16:705–712.
27. Giacino JT, Ashwal S, Childs N, et al. The minimally consciousstate: definition and diagnostic criteria. Neurology. 2002;58:349–353.
28. Cologan V, Drouot X, Parapatics S, et al. Sleep in the unrespon-sive wakefulness syndrome and minimally conscious state. J Neu-rotrauma. 2013;30:339–346.
29. Fingelkurts AA, Fingelkurts AA, Bagnato S, Boccagni C, GalardiG. Life or death: prognostic value of a resting EEG with regards tosurvival in patients in vegetative and minimally conscious states.PLoS One. 2011;6:e25967.
30. Fingelkurts AA, Fingelkurts AA, Bagnato S, Boccagni C, GalardiG. Prognostic value of resting-state electroencephalographystructure in disentangling vegetative and minimally consciousstates: a preliminary study. Neurorehabil Neural Repair. 2013;27:345–354.
31. de Biase S, Gigli GL, Lorenzut S, et al. The importance ofpolysomnography in the evaluation of prolonged disorders ofconsciousness: sleep recordings more adequately correlate thanstimulus-related evoked potentials with patients’ clinical status.Sleep Med. 2014;15(4):393–400.
32. Ron S, Algom D, Hary D, Cohen M. Time-related changes inthe distribution of sleep stages in brain injured patients. Electroen-cephalogr Clin Neurophysiol. 1980;48:432–441.
33. Watson PL, Pandharipande P, Gehlbach BK, et al. Atypical sleepin ventilated patients: empirical electroencephalography findingsand the path toward revised ICU sleep scoring criteria. Crit CareMed. 2013;41(8):1958–1967.
34. Cabello B, Parthasarathy S, Mancebo J. Mechanical ventila-tion: let us minimize sleep disturbances. Curr Opin Crit Care.2007;13(1):20–26.
35. Jennett B, Teasdale G. Prognosis after severe head injury. In: Jen-nett B, Graham D, eds. Management of Head Injuries. Philadelphia,PA: FA Davis; 1981:317–332.
36. Jennett B, Teasdale G, Braakman R, Minderhoud J, Knill-Jones R.Predicting outcome in individual patients after severe head injury.Lancet. 1976;1:1031–1034.
37. Rappaport M, Herrero-Backe C, Rappaport ML, Winterfield KM.Head injury outcome up to ten years later. Arch Phys Med Rehabil.1989;70:885–892.
38. Hall K, Cope DN, Rappaport M. Glasgow Outcome Scale andDisability Rating Scale: comparative usefulness in following re-covery in traumatic head injury. Arch Phys Med Rehabil. 1985;66:35–37.
39. Flannery J, Korcheck S. Use of the Levels of Cognitive FunctioningAssessment Scale (LOCFAS) by acute care nurses. Appl Nurs Res.1993;6:167–169.
40. Wilson JT, Pettigrew LE, Teasdale GM. Structured interviews forthe Glasgow Outcome Scale and the extended Glasgow OutcomeScale: guidelines for their use. J Neurotrauma. 1998;15:573–585.
41. Teasdale GM, Pettigrew LE, Wilson JT, Murray G, Jennett B.Analyzing outcome of treatment of severe head injury: a reviewand update on advancing the use of the Glasgow Outcome Scale.J Neurotrauma. 1998;15:587–597.
42. Rappaport M, Dougherty AM, Kelting DL. Evaluation of comaand vegetative states. Arch Phys Med Rehabil. 1992;73:628–634.
43. American Congress of Rehabilitation Medicine, Brain Injury-Interdisciplinary Special Interest Group, Disorders of Conscious-ness Task Force; Seel RT, Sherer M, Whyte J, et al. Assessmentscales for disorders of consciousness: evidence-based recommen-dations for clinical practice and research. Arch Phys Med Rehabil.2010;91:1795–1813.
44. Jasper HH. The ten-twenty electrode system of the internationalfederation. Electroencephalogr Clin Neurophys. 1958;10:371–375.
45. Rechtschaffen A, Kales A. A Manual of Standardized Terminology,Techniques and Scoring System for Sleep Stages of Human Subjects.Bethesda, MD: US Department of Health, Education, and WelfarePublic Health Service—NIH/NIND; 1968.
46. Urakami Y. Relationship between, sleep spindles and clinical re-covery in patients with traumatic brain injury: a simultaneous EEGand MEG study. Clin EEG Neurosci. 2012;43(1):39–47.
47. Hulihan JF Jr, Syna DR. Electroencephalographic sleep patternsin postanoxic stupor and coma. Neurology. 1994;44(4):758–760.
48. Synek VM. Prognostically important EEG coma patterns in dif-fuse anoxic and traumatic encephalopathies in adults. J ClinNeurophysiol. 1988;5(2):161–174.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.

Polysomnographic Sleep Patterns in Unresponsive Wakefulness Syndrome 13
49. Rumpl E, Prugger M, Bauer G, Gerstenbrand F, Hackl JM, PalluaA. Incidence and prognostic value of spindles in posttraumaticcoma. Electroencephalogr Clin Neurophysiol. 1983;56:420–429.
50. Scher MS, Johnson MW, Holditch-Davis D. Cyclicity of neonatalsleep behaviors at 25 to 30 weeks’ postconceptional age. PediatrRes. 2005;57:879–882.
51. Coons S, Guilleminault C. Development of consolidated sleepand wakeful periods in relation to the day/night cycle in infancy.Dev Med Child Neurol. 1984;26:169–176.
52. Villa F, Colombo K, Pastore V, et al. LOCFAS-assessed evolu-tion of cognitive and behavioral functioning in a sample of pe-diatric patients with severe acquired brain injury in the postacutephase [published online ahead of print November 4, 2014]. J ChildNeurol. doi:10.1177/0883073814553798.
53. Evans BM. Sleep, consciousness and the spontaneous and evokedelectrical activity of the brain. Is there a cortical integrating mech-anism? Neurophysiol Clin. 2003;33(1):1–10.
54. Leunissen I, Coxon JP, Caeyenberghs K, Michiels K, Sunaert S,Swinnen SP. Subcortical volume analysis in traumatic brain in-
jury: the importance of the fronto-striato-thalamic circuit in taskswitching. Cortex. 2014;51:67–81.
55. Giacino JT, Kalmar K, Whyte J. The JFK Coma Recovery Scale–Revised: measurement characteristics and diagnostic utility. ArchPhys Med Rehabil. 2004;85:2020–2029.
56. Liscio M, Adduci A, Galbiati S, et al. Cognitive-behaviouralstimulation protocol for severely brain damaged patients in thepostacute stage in developmental age. Disabil Rehabil. 2008;30:275–285.
57. Eilander HJ, Timmerman RB, Scheirs JG, Van Heugten CM, DeKort PL, Prevo AJ. Children and young adults in a prolongedunconscious state after severe brain injury: long-term functionaloutcome as measured by the DRS and the GOSE after early in-tensive neurorehabilitation. Brain Inj. 2007;21:53–61.
58. Constant I, Sabourdin N. The EEG signal: a window onthe cortical brain activity. Paediatr Anaesth. 2012;22:539–552.
59. Aneja S, Gupta M. Sleep and childhood epilepsy. Indian J Pediatr.2005;72:687–690.
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
www.headtraumarehab.com





























