Embed Size (px)
Citation preview

Schizophrenia Research 152 (2014) 255–260
Contents lists available at ScienceDirect
Schizophrenia Research
j ourna l homepage: www.e lsev ie r .com/ locate /schres
Olanzapine and clozapine differently affect sleep in patients withschizophrenia: Results from a double-blind, polysomnographic studyand review of the literature
Michael Kluge a,b,⁎, Alexander Schacht c, Hubertus Himmerich a, Christine Rummel-Kluge a,Peter M. Wehmeier d, Mira Dalal b, Dunja Hinze-Selch e, Thomas Kraus f, Ralf W. Dittmann d,Thomas Pollmächer b,g, Andreas Schuld g
a Department of Psychiatry, University of Leipzig, Leipzig, Germanyb Max Planck Institute of Psychiatry, Munich, Germanyc Lilly Deutschland GmbH, Medical Department, Bad Homburg, Germanyd Department of Child and Adolescent Psychiatry, Central Institute of Mental Health Mannheim, University of Heidelberg, Germanye Fachklinik St. Marienstift, Center for Psychiatric and Psychotherapeutic Treatment for Traumatized Males, Neuenkirchen, Germanyf Frankenalb-Klinik, District Hospital of Psychiatry, Psychotherapy, Psychosomatics and Addiction Rehabilitation, Engelthal, Germanyg Klinikum Ingolstadt, Center of Mental Health, Ingolstadt, Germany
⁎ Corresponding author at: University of Leipzig, DPsychotherapy, Semmelweisstrasse 10, 04103 Leipzig, Gerfax: +49 341/97 24539.
E-mail address: [email protected]
0920-9964/$ – see front matter © 2013 Elsevier B.V. All rihttp://dx.doi.org/10.1016/j.schres.2013.11.009
a b s t r a c t
a r t i c l e i n f oArticle history:Received 29 July 2013Received in revised form 4 November 2013Accepted 11 November 2013Available online 5 December 2013
Keywords:SleepREMSlow-wave-sleepOlanzapineClozapineRestless legs syndromeRLS
Schizophrenia is associated with impaired sleep continuity. The second generation antipsychotics clozapine andolanzapinehavebeen reported to improve sleep continuity but also to rarely induce restless legs syndrome (RLS).The aimsof this randomized double-blind studywere to compare the effects of clozapine and olanzapine on sleepand the occurrence of RLS. Therefore, polysomnographies were recorded and RLS symptomswere assessed in 30patients with schizophrenia before and after 2, 4 and 6 weeks of treatment with either clozapine or olanzapine.Treatment with both antipsychotics increased total sleep time, sleep period time and sleep efficiency and de-creased sleep onset latency. These changes were similar in both groups, occurred during the first 2 treatmentweeks and were sustained. For example, sleep efficiency increased from 83% (olanzapine) and 82% (clozapine)at baseline to 95% at week 2 and 97% at week 6 in both treatment groups. Sleep architecture was differently af-fected: clozapine caused a significantly stronger increase of stage 2 sleep (44%) than olanzapine (11%) butolanzapine a significantly stronger increase of REM-sleep. Olanzapine caused an 80% increase of slow wavesleep whereas clozapine caused a 6% decrease. No patient reported any of 4 RLS defining symptoms at baseline.During treatment, 1 patient of each group reported at one visit all 4 symptoms, i.e. met the diagnosis of an RLS. Inconclusion, sleep continuity similarly improved and sleep architecture changed more physiologically witholanzapine. Neither of the antipsychotics induced RLS symptoms that were clinically relevant.
© 2013 Elsevier B.V. All rights reserved.
1. Introduction
Sleep in patients with schizophrenia is impaired comparing tohealthy subjects. Delayed sleep onset, decreased total sleep time andreduced sleep efficiency are the most consistent findings from studiesin drug naïve patients. In addition, several studies demonstrated ashorter REM latency and less slow wave or non-REM stage 4 sleepin drug naïve patients than healthy controls (Cohrs, 2008; Montiet al., 2013). Sleep disturbances affect up to 80% of patients with schizo-phrenia (Cohrs, 2008) and are associated with impaired cognitive
epartment of Psychiatry andmany. Tel.: +49 341/97 24673;
(M. Kluge).
ghts reserved.
functioning (Bromundt et al., 2011), decreased quality of life(Hofstetter et al., 2005) and severity of illness (Sarkar et al., 2010).Therefore, improvement of sleep disturbance is an important goal inthe treatment of patients with schizophrenia.
The second generation antipsychotics (SGAs) clozapine andolanzapine share similar receptor binding patterns (Bymaster et al.,1996), good efficacy (Leucht et al., 2013), unfavourable metabolic sideeffects (Rummel-Kluge et al., 2010) but a favourable extrapyramidalside effect profile (Rummel-Kluge et al., 2012). In addition, severalsleep-EEG studies, mostly open, suggested a sleep-improving effect ofolanzapine and clozapine (Rüther et al., 1976; Touyz et al., 1977,1978; Wetter et al., 1996; Hinze-Selch et al., 1997; Salin-Pascual et al.,1999; Sharpley et al., 2000; Lee et al., 2001; Lindberg et al., 2002;Armitage et al., 2004; Müller et al., 2004; Salin-Pascual et al., 2004;Sharpley et al., 2005; Gimenez et al., 2007; Moreno et al., 2007; Göder
256 M. Kluge et al. / Schizophrenia Research 152 (2014) 255–260
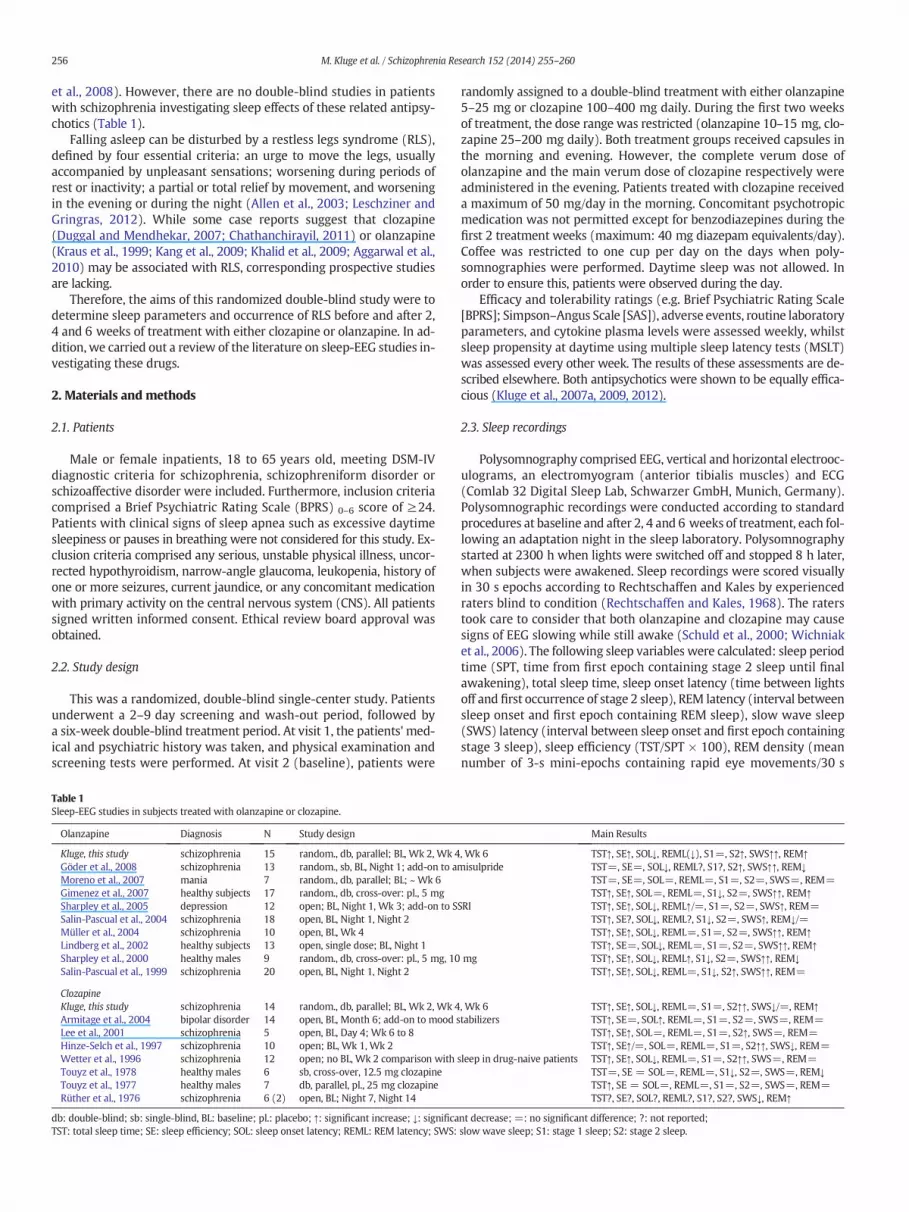
et al., 2008). However, there are no double-blind studies in patientswith schizophrenia investigating sleep effects of these related antipsy-chotics (Table 1).
Falling asleep can be disturbed by a restless legs syndrome (RLS),defined by four essential criteria: an urge to move the legs, usuallyaccompanied by unpleasant sensations; worsening during periods ofrest or inactivity; a partial or total relief by movement, and worseningin the evening or during the night (Allen et al., 2003; Leschziner andGringras, 2012). While some case reports suggest that clozapine(Duggal and Mendhekar, 2007; Chathanchirayil, 2011) or olanzapine(Kraus et al., 1999; Kang et al., 2009; Khalid et al., 2009; Aggarwal et al.,2010) may be associated with RLS, corresponding prospective studiesare lacking.
Therefore, the aims of this randomized double-blind study were todetermine sleep parameters and occurrence of RLS before and after 2,4 and 6 weeks of treatment with either clozapine or olanzapine. In ad-dition, we carried out a review of the literature on sleep-EEG studies in-vestigating these drugs.
2. Materials and methods
2.1. Patients
Male or female inpatients, 18 to 65 years old, meeting DSM-IVdiagnostic criteria for schizophrenia, schizophreniform disorder orschizoaffective disorder were included. Furthermore, inclusion criteriacomprised a Brief Psychiatric Rating Scale (BPRS) 0–6 score of ≥24.Patients with clinical signs of sleep apnea such as excessive daytimesleepiness or pauses in breathing were not considered for this study. Ex-clusion criteria comprised any serious, unstable physical illness, uncor-rected hypothyroidism, narrow-angle glaucoma, leukopenia, history ofone or more seizures, current jaundice, or any concomitant medicationwith primary activity on the central nervous system (CNS). All patientssigned written informed consent. Ethical review board approval wasobtained.
2.2. Study design
This was a randomized, double-blind single-center study. Patientsunderwent a 2–9 day screening and wash-out period, followed bya six-week double-blind treatment period. At visit 1, the patients' med-ical and psychiatric history was taken, and physical examination andscreening tests were performed. At visit 2 (baseline), patients were
Table 1Sleep-EEG studies in subjects treated with olanzapine or clozapine.
Olanzapine Diagnosis N Study design
Kluge, this study schizophrenia 15 random., db, parallel; BL, Wk 2, Wk 4Göder et al., 2008 schizophrenia 13 random., sb, BL, Night 1; add-on to aMoreno et al., 2007 mania 7 random., db, parallel; BL; ~ Wk 6Gimenez et al., 2007 healthy subjects 17 random., db, cross-over: pl., 5 mgSharpley et al., 2005 depression 12 open; BL, Night 1, Wk 3; add-on to SSalin-Pascual et al., 2004 schizophrenia 18 open, BL, Night 1, Night 2Müller et al., 2004 schizophrenia 10 open, BL, Wk 4Lindberg et al., 2002 healthy subjects 13 open, single dose; BL, Night 1Sharpley et al., 2000 healthy males 9 random., db, cross-over: pl., 5 mg, 10Salin-Pascual et al., 1999 schizophrenia 20 open, BL, Night 1, Night 2
ClozapineKluge, this study schizophrenia 14 random., db, parallel; BL, Wk 2, Wk 4Armitage et al., 2004 bipolar disorder 14 open, BL, Month 6; add-on to mood sLee et al., 2001 schizophrenia 5 open, BL, Day 4; Wk 6 to 8Hinze-Selch et al., 1997 schizophrenia 10 open; BL, Wk 1, Wk 2Wetter et al., 1996 schizophrenia 12 open; no BL, Wk 2 comparison withTouyz et al., 1978 healthy males 6 sb, cross-over, 12.5 mg clozapineTouyz et al., 1977 healthy males 7 db, parallel, pl., 25 mg clozapineRüther et al., 1976 schizophrenia 6 (2) open, BL; Night 7, Night 14
db: double-blind; sb: single-blind, BL: baseline; pl.: placebo; ↑: significant increase; ↓: significaTST: total sleep time; SE: sleep efficiency; SOL: sleep onset latency; REML: REM latency; SWS:
randomly assigned to a double-blind treatment with either olanzapine5–25 mg or clozapine 100–400 mg daily. During the first two weeksof treatment, the dose range was restricted (olanzapine 10–15 mg, clo-zapine 25–200 mg daily). Both treatment groups received capsules inthe morning and evening. However, the complete verum dose ofolanzapine and the main verum dose of clozapine respectively wereadministered in the evening. Patients treated with clozapine receiveda maximum of 50 mg/day in the morning. Concomitant psychotropicmedication was not permitted except for benzodiazepines during thefirst 2 treatment weeks (maximum: 40 mg diazepam equivalents/day).Coffee was restricted to one cup per day on the days when poly-somnographies were performed. Daytime sleep was not allowed. Inorder to ensure this, patients were observed during the day.
Efficacy and tolerability ratings (e.g. Brief Psychiatric Rating Scale[BPRS]; Simpson–Angus Scale [SAS]), adverse events, routine laboratoryparameters, and cytokine plasma levels were assessed weekly, whilstsleep propensity at daytime using multiple sleep latency tests (MSLT)was assessed every other week. The results of these assessments are de-scribed elsewhere. Both antipsychotics were shown to be equally effica-cious (Kluge et al., 2007a, 2009, 2012).
2.3. Sleep recordings
Polysomnography comprised EEG, vertical and horizontal electrooc-ulograms, an electromyogram (anterior tibialis muscles) and ECG(Comlab 32 Digital Sleep Lab, Schwarzer GmbH, Munich, Germany).Polysomnographic recordings were conducted according to standardprocedures at baseline and after 2, 4 and 6 weeks of treatment, each fol-lowing an adaptation night in the sleep laboratory. Polysomnographystarted at 2300 h when lights were switched off and stopped 8 h later,when subjects were awakened. Sleep recordings were scored visuallyin 30 s epochs according to Rechtschaffen and Kales by experiencedraters blind to condition (Rechtschaffen and Kales, 1968). The raterstook care to consider that both olanzapine and clozapine may causesigns of EEG slowing while still awake (Schuld et al., 2000; Wichniaket al., 2006). The following sleep variables were calculated: sleep periodtime (SPT, time from first epoch containing stage 2 sleep until finalawakening), total sleep time, sleep onset latency (time between lightsoff and first occurrence of stage 2 sleep), REM latency (interval betweensleep onset and first epoch containing REM sleep), slow wave sleep(SWS) latency (interval between sleep onset and first epoch containingstage 3 sleep), sleep efficiency (TST/SPT × 100), REM density (meannumber of 3-s mini-epochs containing rapid eye movements/30 s
Main Results
, Wk 6 TST↑, SE↑, SOL↓, REML(↓), S1=, S2↑, SWS↑↑, REM↑misulpride TST=, SE=, SOL↓, REML?, S1?, S2↑, SWS↑↑, REM↓
TST=, SE=, SOL=, REML=, S1=, S2=, SWS=, REM=TST↑, SE↑, SOL=, REML=, S1↓, S2=, SWS↑↑, REM↑
SRI TST↑, SE↑, SOL↓, REML↑/=, S1=, S2=, SWS↑, REM=TST↑, SE?, SOL↓, REML?, S1↓, S2=, SWS↑, REM↓/=TST↑, SE↑, SOL↓, REML=, S1=, S2=, SWS↑↑, REM↑TST↑, SE=, SOL↓, REML=, S1=, S2=, SWS↑↑, REM↑
mg TST↑, SE↑, SOL↓, REML↑, S1↓, S2=, SWS↑↑, REM↓TST↑, SE↑, SOL↓, REML=, S1↓, S2↑, SWS↑↑, REM=
, Wk 6 TST↑, SE↑, SOL↓, REML=, S1=, S2↑↑, SWS↓/=, REM↑tabilizers TST↑, SE=, SOL↑, REML=, S1=, S2=, SWS=, REM=
TST↑, SE↑, SOL=, REML=, S1=, S2↑, SWS=, REM=TST↑, SE↑/=, SOL=, REML=, S1=, S2↑↑, SWS↓, REM=
sleep in drug-naive patients TST↑, SE↑, SOL↓, REML=, S1=, S2↑↑, SWS=, REM=TST=, SE = SOL=, REML=, S1↓, S2=, SWS=, REM↓TST↑, SE = SOL=, REML=, S1=, S2=, SWS=, REM=TST?, SE?, SOL?, REML?, S1?, S2?, SWS↓, REM↑
nt decrease; =: no significant difference; ?: not reported;slow wave sleep; S1: stage 1 sleep; S2: stage 2 sleep.

257M. Kluge et al. / Schizophrenia Research 152 (2014) 255–260
epoch of REM sleep) and the absolute time spent at each sleep stage. Aquantitative analysis of sleep was not performed.
2.4. Restless legs syndrome (RLS)
RLS was assessed weekly using a binary scale, capturing the pres-ence or absence of the 4 symptoms defining RLS (Allen et al., 2003) dur-ing the preceding week in the judgment of the rating physicianfollowing an unstructured interview (i.e. urge to move the legs, usuallyaccompanied by unpleasant sensations; worsening during periods ofrest or inactivity; a partial or total relief by movement, and worseningin the evening or during the night).
2.5. Statistical methods
All analyses were carried out on the intent-to-treat-population, i.e.,all randomized patients. All patients were treated according to the ran-domization scheme. The baseline characteristics were analyzed usingdescriptive statistics. Changes from baseline in the various sleep param-eters were analyzed using mixed models repeated measurement(MMRM) with unstructured covariance and fixed effects for baseline,sex, visit, and visit–treatment interaction. In case of non-convergenceof the mixed models, an autoregressive type of covariance was used.Based on earlier studies (Hinze-Selch et al., 1997), changes in non-REM stage 2 were chosen as a primary endpoint of this study and ana-lyzed using Analysis of Co-variance (ANCOVA). Differences to baselinewere assessed based on the MMRM results. All results are presentedas mean (± standard deviation).
3. Results
3.1. Patient demographics
Thirty-seven patients were screened for this study. A total of 30patients (12 male, 18 female) were randomized. Four patientsdiscontinued the study early, three patients in the clozapine groupdue to adverse event, lack of efficacy, or physician's decision, and onepatient in the olanzapine group discontinued due to patient's decision.The olanzapine group consisted of 8 women and 7 men, the clozapinegroup of 10 women and 5 men. In the clozapine group, 12 patientshad schizophrenia, 2 patients a schizoaffective and 1 patient aschizophreniform disorder. In the olanzapine group, 14 patients hadschizophrenia and 1 patient had a schizoaffective disorder. Except forone patient in the olanzapine group, all patients had been treated withan antipsychotic medication before the wash-out period, predominant-ly with risperidone and haloperidol. At baseline, treatment groups didnot significantly differ regarding age (clozapine 36.7 ± 13.0 years,olanzapine 32.8 ± 8.3 years), age at first episode (clozapine group:30 ± 8 years, olanzapine group: 28 ± 11 years), number of previousepisodes (clozapine group: 1 ± 2, olanzapine group: 1 ± 1), and sever-ity of baseline psychopathology (BPRS0–6: clozapine 36.6 ± 8.8;olanzapine 36.7 ± 9.9). During the study period, BPRS0–6 total scoresignificantly improved from baseline to endpoint in both groups.There were no significant differences between groups at the endof treatment (clozapine group: 18.9 ± 13.7, olanzapine group:19.1 ± 13.8).
3.2. Dosage
During the first twoweeks of double-blind treatment, all 15 patientstreated with olanzapine had a modal dose of 15 mg. 14 of 15 patientstreated with clozapine had a modal dose of 200 mg, one patientreceived just 150 mg clozapine. The mean modal dose administeredin the last four weeks of the double blind treatment phase were266.7 ± 77.9 mg of clozapine or 21.2 ± 2.5 mg of olanzapine,respectively.
3.3. Sleep parameters
Treatment with both olanzapine and clozapine increased total sleeptime, sleep period time and sleep efficiency and decreased sleep onsetlatency. These changes were similar in both treatment groups and oc-curred for the very most part already during the first 2 weeks of treat-ment (Table 2). For example, sleep efficiency (SEI) increased from 83%(olanzapine) and 82% (clozapine) at baseline to 95% at week 2 and to97% at week 6 in both treatment groups. Also, total sleep time (TST)increased from 350.9 ± 75.4 min to 444.2 ± 14.8 min (olanzapine)and from 354.4 ± 90.7 to 446.5 ± 25.3 min within the first 2 weeks.During the remaining study period, both compounds caused furthermean increases of only 15.6 (olanzapine) min or 10.7 min (clozapine),respectively.
While effects on these global sleep parameters were similar,olanzapine and clozapine had different effects on sleep architecture(Table 2). Clozapine was associated with a significantly stronger meanincrease of stage 2 sleep of about 44% (baseline: 205.1 ± 45.2; end ofthe study: 296.6 ± 49.3 min) as compared to olanzapine (11%; base-line: 183.4 ± 60.7 min, week 6: 206.1 ± 40.7 min). Contrary effectswere observed on slow wave sleep. Olanzapine caused an 80% increaseof slow wave sleep from baseline (53.2 ± 39.7 min) to end of study(95.8 ± 47.6 min), whereas clozapine caused a 6% decrease (baseline:41.0 ± 39.3; end of study: 38.4 ± 37.0). Interestingly, suppression ofslow wave sleep after only two weeks of treatment was much strongerand gradually approached baseline level (Table 2). These effects werealso significant when both subtypes of slowwave sleep, nonREM stages3 and 4, were analyzed separately.
Amount of REM-sleep significantly increased with both antipsy-chotics, but increase was significantly greater in patients treated witholanzapine (Table 2). Sleep onset REM periods (SOREMPs) as definedas the occurrence of REM sleep within 10 min after sleep onset (Klugeet al., 2007b) did not occur at any point in time.
3.4. Restless legs syndrome (RLS)
At baseline, none of the patients had any of the 4 symptoms definingRLS. Few patients transiently developed at least one symptom of RLSduring the treatment period. One patient of each treatment groupreported all 4 definition criteria for RLS but only at 1 visit (Table 3).
4. Discussion
Sleep continuity improved during treatment as indicated by a signif-icant increase of total sleep time, sleep period time, sleep efficiency anda decrease of sleep onset latency. These changes were similar in bothtreatment groups, occurred early in treatment, were sustained andwere clinically relevant. For example, sleep onset latency decreased bymore than half in both drug treatment groups. In contrast to theseglobal sleep parameters, sleep architecture differently changed withboth drugs. Here, olanzapine resulted in more physiological changes(Ohayon et al., 2004), specifically an increase of slow wave sleep and astronger increase of REM sleep, while clozapine resulted in amuch stron-ger increase of light stage 2 sleep. Taken together, these findings indicatethat both olanzapine and clozapine improve sleep inpatientswith schizo-phrenia, but olanzapine does so to a greater extent.
While our findings are generally in line with previous, mostly open-label, sleep studies (Table 1), we feel that we can now provide a clearerpicture on the effects on sleep over time due to the double-blindcomparator-controlled design with 4 repeated polysomnographies. Interms of olanzapine, we have confirmed an early increase of totalsleep time, sleep efficiency, slow wave sleep and decrease of sleep onsetlatency observed in most groups. In addition, we found an early increaseof stage 2 sleep andREMsleep, previously rarely reported (Table 2). Inter-estingly, all of these findings in our studywere observedwith remarkableconsistency at three time-points during treatment. With respect to

Table 2Sleep parameters (mean (SD) in patients treated with olanzapine (n = 15) or clozapine (n = 14).
Baseline Week 2 Week 4 Week 6
Ola Clz Ola Clz Ola Clz Ola Clz
Total sleep time (min)a 350.9 (75.4) 354.4 (90.7) 444.2 (14.8) 446.5 (25.3) 451.3 (23.5) 460.4 (13.9) 459.6 (24.8) 457.2 (24.0)Sleep period time (min)a 415.9 (44.8) 425.4 (75.2) 460.0 (13.8) 466.6 (16.6) 460.4 (8.8) 468.9 (11.4) 460.7 (20.9) 468.1 (20.8)Sleep efficiencya 0.83 (0.14) 0.82 (0.13) 0.95 (0.03) 0.95 (0.04) 0.97 (0.01) 0.98 (0.03) 0.97 (0.01) 0.97 (0.03)Sleep onset latency (min)a 42.2 (30.2) 29.9 (26.6) 20.7 (14.6) 14.9 (13.4) 18.7 (22.3) 11.1 (11.6) 19.4 (20.4) 14.0 (18.0)REM latency (min) 116.4 (57.6) 94.0 (40.5) 79.8 (37.8) 103.3 (48.9) 87.9 (57.5) 89.1 (16.7) 88.0 (55.9) 105.0 (48.0)REM density 2.62 (1.53) 3.11 (0.84) 3.43 (1.16) 2.98 (0.93) 2.94 (0.92) 3.53 (1.36) 3.25 (1.05) 3.07 (1.45)Stage 1 sleep (min) 35.2 (20.9) 29.6 (15.1) 38.1 (19.1) 21.4 (16.3) 28.5 (11.2) 23.1 (20.2) 31.5 (19.1) 20.1 (12.4)Stage 2 sleep (min)ab 183.4 (60.7) 205.1 (45.2) 201.5 (52.5) 309.4 (41.7) 200.3 (56.1) 297.0 (39.2) 206.7 (40.7) 296.6 (49.3)Stage 3 sleep (min)b 21.9 (15.5) 24.3 (22.6) 43.6 (28.4) 17.5 (16.2) 45.3 (28.2) 19.4 (17.9) 47.0 (22.7) 22.6 (10.4)Stage 4 sleep (min)b 32.3 (30.5) 16.6 (23.1) 42.4 (33.4) 6.7 (12.0) 56.5 (38.4) 12.3 (16.6) 50.1 (34.6) 15.8 (18.5)Slow wave sleep (min)b 54.2 (39.7) 41.0 (39.3) 86.1 (54.0) 24.2 (27.4) 101.7 (58.7) 31.7 (31.8) 95.8 (47.6) 38.4 (37.0)REM sleep (min)ab 77.7 (24.2) 77.9 (34.7) 115.9 (26.0) 89.8 (22.5) 118.2 (26.1) 106.5 (37.4) 115.2 (25.5) 99.9 (44.5)
a Significant time effect b significant time-by-treatment effect.
258 M. Kluge et al. / Schizophrenia Research 152 (2014) 255–260
clozapine, we showed an increase of total sleep time and sleep efficiencyand stage 2 sleep and a decrease of slow wave sleep, corroborating find-ings from several other studies. A new finding is that slow wave sleepstep-wise normalized during the 6 weeks of treatment. A further newfinding is that clozapine increased REM sleep. There is only one studythat compared sleep parameters of six patients during treatment withthose of two patients before treatment, that also showed an increase ofREM sleep (Rüther et al., 1976). Reasons for the inconsistent results in-clude different study designs, treatment duration, co-medication andthe relatively small sample size of less than 10 subjects.
While receptor profiles of clozapine and olanzapine are related(Kroeze et al., 2003) there are some differences which may partly ex-plain the different effects on sleep: There is evidence that antagonisticaction at serotonergic 5HT2a and 5HT2c receptors increases amountof SWS (Landolt and Wehrle, 2009). In line with these findings andour own findings, olanzapine has a higher affinity to both of these re-ceptors (Kroeze et al., 2003). In addition, the relatively higher dose ofolanzapine as compared to clozapine in our study may have contributedto the increase of SWS observed with olanzapine, but not with clozapine.REM sleep occurs when monoaminergic REM-off neurons are inhibitedand cholinergic REM-on neurons are active (Espana and Scammell,2011). Thus, the stronger anticholinergic potency of clozapine may par-tially explain the different effects on REM sleep of both drugs. Clearly,other receptors are involved in sleep regulation also and are differently af-fected by clozapine and olanzapine, such as adrenergic and histaminergicreceptors (Broese et al., 2012; Unno et al., 2012).
There are inconsistent findings as to how clozapine-induced fever af-fects sleep. While an early study reported a very strong increase of REMsleep to 85–100% of total sleep time in 5 patients (Blum and Girke,1973), a single case report described a strong suppression of REM sleepto about 20% of initial REM sleepduring fever followed by a normalizationafter fever had ceased (Hinze-Selch et al., 1995). The finding that cloza-pine-induced fever is associated with high levels of interleukin-6
Table 3Number (proportion) of patients reporting RLS symptoms in patients treated with olanzapine
Urge to move the legs/unpleasant sensations
Worsening duringinactivity
Ola Clz Ola Clz
N (%) N (%) N (%) N (%
Baseline 0 (0) 0 (0) 0 (0) 0 (0Week 1 1 (7) 0 (0) 0 (0) 0 (0Week 2 3 (20) 1 (7) 1 (7) 0 (0Week 3 1 (7) 1 (7) 1 (7) 1 (7Week 4 2 (13) 1 (7) 1 (7) 1 (7Week 5 1 (7) 1 (7) 1 (7) 2 (1Week 6 0 (0) 1 (7) 0 (0) 1 (7
There were no significant group differences.
(Kluge et al., 2009) and that interleukin-6 suppresses REM sleep(Späth-Schwalbe et al., 1998) is more in line with the latter report. Inour study, there were no sleep recordings during fever.
In the untreated patients with schizophrenia (baseline), sleepefficiency and total sleep time were reduced and sleep latencyprolonged as compared to healthy subjects (Ohayon et al., 2004), afinding which is in agreement with previous reports. In contrast, REMlatency tended to be prolonged rather than shortened as found in onereport (Monti et al., 2013). SOREMPs did occur neither before nor dur-ing treatment. Interestingly, in the MSLT, a method to determine sleeppropensity where subjects get 5 sleep opportunities, SOREMPs occurredmore often than normally during the treatment period (Kluge et al.,2012).
To our knowledge, this is the first study prospectively investigatingsymptoms of RLS during treatment with antipsychotics. Overall, RLSsymptoms tended to occur occasionally. Furthermore, only one patientof each treatment group transiently met all RLS criteria. Thus, ourstudy confirmed findings that both drugs may induce RLS or abortiveforms (Aggarwal et al., 2010; Chathanchirayil, 2011). We do not thinkthat the abortive forms of RLS represent extrapyramidal side effects(e.g. akathisia), since scores of the SAS decreased during the course ofthe study (Kluge et al., 2007a). Considering the short sleep onset latencyduring treatment in both groups, RLS symptoms did not compromisesleep to a relevant degree. Overall, antipsychotic-related RLS seems tooccur rarely or may be recognized rarely (Jagota et al., 2012; Perez-Lloret et al., 2012). The risk for developing RLSmay differ between anti-psychotics and could be greaterwith stronger antagonistic action on do-pamine D2 receptors (Wetter et al., 2002). Apart from the finding thatantipsychotics (dopamine antagonists) may trigger RLS, the findingthat dopamine agonists are effective in treating RLS indicates that thedopaminergic system is involved in RLS. There is now increasing evi-dence that this altered dopaminergic activity is secondary to centraliron dysfunction (Dauvilliers and Winkelmann, 2013).
(n = 15) or clozapine (n = 15).
Relief by movement Worsening in the evening
Ola Clz Ola Clz
) N (%) N (%) N (%) N (%)
) 0 (0) 0 (0) 0 (0) 0 (0)) 0 (0) 0 (0) 0 (0) 0 (0)) 0 (0) 0 (0) 0 (0) 0 (0)) 0 (0) 0 (0) 0 (0) 0 (0)) 1 (7) 0 (0) 0 (0) 0 (0)3) 1 (7) 0 (0) 1 (7) 0 (0)) 0 (0) 1 (7) 0 (0) 1 (7)

259M. Kluge et al. / Schizophrenia Research 152 (2014) 255–260
In our opinion, this is the soundest study so far investigating sleepduring treatment with olanzapine or clozapine. Nevertheless, thereare two limitations that need to be acknowledged. First, the samplesize was too small for a meaningful calculation of results regarding theimpact of baseline characteristics on the treatment difference. Largerstudies would be needed to better understand whether the one treat-ment or the other is better in particular subgroups of patients with re-spect to sleep outcomes. In spite of this limitation, the sample size inthis studywas larger than inmost other studies. Secondly,wedidnot pro-vide a quantitative analysis of sleep data.
In conclusion, olanzapine and clozapine similarly improved sleep con-tinuity. However, their effects on sleep architecture differed. Olanzapinecaused a strong increase of slow wave sleep that was not observed withclozapine, a stronger increase of REM sleep and a much weaker increaseof stage 2 sleep than clozapine. Neither of the antipsychotics inducedRLS symptoms that were clinically relevant.
Role of the funding sourceThe study was funded by the Lilly Deutschland GmbH, Bad Homburg, Germany. Lilly
was not involved in the interpretation of data, writing the manuscript, or in the decisionto submit the paper for publication.
ContributorsM. Kluge: Data control, data interpretation, writing the manuscriptA. Schuld: Protocol development, study conduction, data control, data interpretation,
review of the manuscriptA. Schacht: statistical analysis, review of the manuscriptH. Himmerich,M.A. Dalal, D. Hinze-Selch, T. Kraus: Study conduction, data control, re-
view of the manuscriptC. Rummel-Kluge, P. M. Wehmeier: Data interpretation, review of the manuscriptR. W. Dittmann: Protocol development, review of the manuscriptT. Pollmächer: Protocol development, data interpretation, review of the manuscriptAll authors contributed to and have approved the final manuscript.
Conflict of interestM. Kluge received a travel grant from Lilly Deutschland. A. Schacht is a full-time em-
ployee of Lilly Deutschland. P. M.Wehmeierwas a full-time employee of Lilly Deutschlandand has received travel grants and speaker honoraria from Eli Lilly since then. H.Himmerich received speaker honoraria from AstraZeneca, Servier and Lilly, consultingfees from Servier and Bristol-Myers Squibb, and chemical substances for study supportfrom AstraZeneca, Novartis and Wyeth. R. W. Dittmann, a former full-time employee ofLilly Deutschland, received research funding and travel grants from Eli Lilly & Co. and isalso a stockholder of Eli Lilly & Co. shares. All other authors declare that there are noconflicts of interest in relation to the subject of this study.
AcknowledgmentWe would like to thank Martin Lehmann who did the study monitoring.
References
Aggarwal, S., Dodd, S., Berk, M., 2010. Restless leg syndrome associatedwith olanzapine: acase series. Curr. Drug Saf. 5, 129–131.
Allen, R.P., Picchietti, D., Hening, W.A., Trenkwalder, C., Walters, A.S., Montplaisi, J., 2003.Restless legs syndrome: diagnostic criteria, special considerations, and epidemiology.A report from the restless legs syndrome diagnosis and epidemiology workshop at theNational Institutes of Health. Sleep Med. 4, 101–119.
Armitage, R., Cole, D., Suppes, T., Ozcan, M.E., 2004. Effects of clozapine on sleep in bipolarand schizoaffective disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 28,1065–1070.
Blum, A., Girke,W., 1973. Marked increase in REM sleep produced by a new antipsychoticcompound. Clin. Electroencephalogr. 4, 80–84.
Broese, M., Riemann, D., Hein, L., Nissen, C., 2012. alpha-Adrenergic receptor function, arous-al and sleep: mechanisms and therapeutic implications. Pharmacopsychiatry 45,209–216.
Bromundt, V., Koster, M., Georgiev-Kill, A., Opwis, K.,Wirz-Justice, A., Stoppe, G., Cajochen, C.,2011. Sleep-wake cycles and cognitive functioning in schizophrenia. Br. J. Psychiatry198, 269–276.
Bymaster, F.P., Calligaro, D.O., Falcone, J.F., Marsh, R.D., Moore, N.A., Tye, N.C., Seeman, P.,Wong, D.T., 1996. Radioreceptor binding profile of the atypical antipsychoticolanzapine. Neuropsychopharmacology 14, 87–96.
Chathanchirayil, S.J., 2011. Restless legs syndrome probably due to clozapine. Aust. N. Z.J. Psychiatry 45, 1005–1006.
Cohrs, S., 2008. Sleep disturbances in patients with schizophrenia: impact and effect ofantipsychotics. CNS Drugs 22, 939–962.
Dauvilliers, Y., Winkelmann, J., 2013. Restless legs syndrome: update on pathogenesis.Curr. Opin. Pulm. Med. 19, 594–600.
Duggal, H.S., Mendhekar, D.N., 2007. Clozapine-associated restless legs syndrome. J. Clin.Psychopharmacol. 27, 89–90.
Espana, R.A., Scammell, T.E., 2011. Sleep neurobiology from a clinical perspective. Sleep 34,845–858.
Gimenez, S., Clos, S., Romero, S., Grasa, E., Morte, A., Barbanoj, M.J., 2007. Effects ofolanzapine, risperidone and haloperidol on sleep after a single oral morning dose inhealthy volunteers. Psychopharmacology (Berl) 190, 507–516.
Göder, R., Fritzer, G., Gottwald, B., Lippmann, B., Seeck-Hirschner, M., Serafin, I., Aldenhoff,J.B., 2008. Effects of olanzapine on slow wave sleep, sleep spindles and sleep-relatedmemory consolidation in schizophrenia. Pharmacopsychiatry 41, 92–99.
Hinze-Selch, D., Mullington, J., Pollmächer, T., 1995. Sleep during clozapine-induced feverin a schizophrenic patient. Biol. Psychiatry 38, 690–693.
Hinze-Selch, D., Mullington, J., Orth, A., Lauer, C.J., Pollmächer, T., 1997. Effects of clozapineon sleep: a longitudinal study. Biol. Psychiatry 42, 260–266.
Hofstetter, J.R., Lysaker, P.H., Mayeda, A.R., 2005. Quality of sleep in patients with schizo-phrenia is associated with quality of life and coping. BMC Psychiatry 5, 13.
Jagota, P., Asawavichienjinda, T., Bhidayasiri, R., 2012. Prevalence of neuroleptic-induced restless legs syndrome in patients taking neuroleptic drugs. J. Neurol. Sci.314, 158–160.
Kang, S.G., Lee, H.J., Kim, L., 2009. Restless legs syndrome and periodic limb movementsduring sleep probably associated with olanzapine. J. Psychopharmacol. 23, 597–601.
Khalid, I., Rana, L., Khalid, T.J., Roehrs, T., 2009. Refractory restless legs syndrome likelycaused by olanzapine. J. Clin. Sleep Med. 5, 68–69.
Kluge, M., Schuld, A., Himmerich, H., Dalal, M., Schacht, A., Wehmeier, P.M., Hinze-Selch,D., Kraus, T., Dittmann, R.W., Pollmächer, T., 2007a. Clozapine and olanzapine are as-sociated with food craving and binge eating: results from a randomized double-blindstudy. J. Clin. Psychopharmacol. 27, 662–666.
Kluge, M., Schüssler, P., Dresler, M., Yassouridis, A., Steiger, A., 2007b. Sleep onset REM pe-riods in obsessive compulsive disorder. Psychiatry Res. 152, 29–35.
Kluge, M., Schuld, A., Schacht, A., Himmerich, H., Dalal, M.A., Wehmeier, P.M., Hinze-Selch,D., Kraus, T., Dittmann, R.W., Pollmächer, T., 2009. Effects of clozapine and olanzapineon cytokine systems are closely linked to weight gain and drug-induced fever.Psychoneuroendocrinology 34, 118–128.
Kluge, M., Himmerich, H., Wehmeier, P.M., Rummel-Kluge, C., Dalal, M., Hinze-Selch, D.,Kraus, T., Dittmann, R.W., Pollmächer, T., Schuld, A., 2012. Sleep propensity atdaytime as assessed by Multiple Sleep Latency Tests (MSLT) in patients with schizo-phrenia increases with clozapine and olanzapine. Schizophr. Res. 135, 123–127.
Kraus, T., Schuld, A., Pollmacher, T., 1999. Periodic leg movements in sleep and restlesslegs syndrome probably caused by olanzapine. J. Clin. Psychopharmacol. 19, 478–479.
Kroeze, W.K., Hufeisen, S.J., Popadak, B.A., Renock, S.M., Steinberg, S., Ernsberger, P.,Jayathilake, K., Meltzer, H.Y., Roth, B.L., 2003. H1-histamine receptor affinitypredicts short-term weight gain for typical and atypical antipsychotic drugs.Neuropsychopharmacology 28, 519–526.
Landolt, H.P., Wehrle, R., 2009. Antagonism of serotonergic 5-HT2A/2C receptors: mutualimprovement of sleep, cognition and mood? Eur. J. Neurosci. 29, 1795–1809.
Lee, J.H., Woo, J.I., Meltzer, H.Y., 2001. Effects of clozapine on sleep measures and sleep-associated changes in growth hormone and cortisol in patients with schizophrenia.Psychiatry Res. 103, 157–166.
Leschziner, G., Gringras, P., 2012. Restless legs syndrome. BMJ 344, e3056.Leucht, S., Cipriani, A., Spineli, L., Mavridis, D., Orey, D., Richter, F., Samara, M., Barbui, C.,
Engel, R.R., Geddes, J.R., Kissling, W., Stapf, M.P., Lassig, B., Salanti, G., Davis, J.M.,2013. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophre-nia: a multiple-treatments meta-analysis. Lancet 382, 951–962.
Lindberg, N., Virkkunen, M., Tani, P., Appelberg, B., Virkkala, J., Rimon, R., Porkka-Heiskanen, T., 2002. Effect of a single-dose of olanzapine on sleep in healthy femalesand males. Int. Clin. Psychopharmacol. 17, 177–184.
Monti, J.M., BaHammam, A.S., Pandi-Perumal, S.R., Bromundt, V., Spence, D.W., Cardinali,D.P., Brown, G.M., 2013. Sleep and circadian rhythm dysregulation in schizophrenia.Prog. Neuropsychopharmacol. Biol. Psychiatry 43, 209–216.
Moreno, R.A., Hanna, M.M., Tavares, S.M., Wang, Y.P., 2007. A double-blind comparison ofthe effect of the antipsychotics haloperidol and olanzapine on sleep in mania. Braz.J. Med. Biol. Res. 40, 357–366.
Müller, M.J., Rossbach, W., Mann, K., Röschke, J., Muller-Siecheneder, F., Blumler, M.,Wetzel, H., Russ, H., Dittmann, R.W., Benkert, O., 2004. Subchronic effects of olanzapineon sleep EEG in schizophrenic patients with predominantly negative symptoms.Pharmacopsychiatry 37, 157–162.
Ohayon, M.M., Carskadon, M.A., Guilleminault, C., Vitiello, M.V., 2004. Meta-analysisof quantitative sleep parameters from childhood to old age in healthy individuals:developing normative sleep values across the human lifespan. Sleep 27, 1255–1273.
Perez-Lloret, S., Rey, M.V., Bondon-Guitton, E., Rascol, O., Montastruc, A.J., 2012. Drugs as-sociated with restless legs syndrome: a case/noncase study in the Frenchpharmacovigilance database. J. Clin. Psychopharmacol. 32, 824–827.
Rechtschaffen, A., Kales, A., 1968. A Manual of Standardized Terminology, Techniques andScoring System for Sleep Stages of Hunman Subjects Brain Information Service BrainResearch Institute. University of California, Los Angeles.
Rummel-Kluge, C., Komossa, K., Schwarz, S., Hunger, H., Schmid, F., Lobos, C.A., Kissling,W., Davis, J.M., Leucht, S., 2010. Head-to-head comparisons of metabolic side effectsof second generation antipsychotics in the treatment of schizophrenia: a systematicreview and meta-analysis. Schizophr. Res. 123, 225–233.
Rummel-Kluge, C., Komossa, K., Schwarz, S., Hunger, H., Schmid, F., Kissling, W., Davis, J.M.,Leucht, S., 2012. Second-generation antipsychotic drugs and extrapyramidal side ef-fects: a systematic review and meta-analysis of head-to-head comparisons. Schizophr.Bull. 38, 167–177.
Rüther, E., Davis, L., Papousek, M., Reichinger, M., Reiter, H., Rudolph, M., 1976.Pharmakologische Beeinflussung zentraler serotonergerMechanismen amMenschenund Auswirkungen auf den Schlaf. Arzneimittelforschung 26, 1071–1073.

260 M. Kluge et al. / Schizophrenia Research 152 (2014) 255–260
Salin-Pascual, R.J., Herrera-Estrella, M., Galicia-Polo, L., Laurrabaquio, M.R., 1999.Olanzapine acute administration in schizophrenic patients increases delta sleep andsleep efficiency. Biol. Psychiatry 46, 141–143.
Salin-Pascual, R.J., Herrera-Estrella, M., Galicia-Polo, L., Rosas, M., Brunner, E., 2004. Lowdelta sleep predicted a good clinical response to olanzapine administration in schizo-phrenic patients. Rev. Investig. Clin. 56, 345–350.
Sarkar, S., Katshu, M.Z., Nizamie, S.H., Praharaj, S.K., 2010. Slow wave sleep deficits as atrait marker in patients with schizophrenia. Schizophr. Res. 124, 127–133.
Schuld, A., Kuhn, M., Haack, M., Kraus, T., Hinze-Selch, D., Lechner, C., Pollmächer, T., 2000.A comparison of the effects of clozapine and olanzapine on the EEG in patients withschizophrenia. Pharmacopsychiatry 33, 109–111.
Sharpley, A.L., Vassallo, C.M., Cowen, P.J., 2000. Olanzapine increases slow-wave sleep:evidence for blockade of central 5-HT(2C) receptors in vivo. Biol. Psychiatry 47,468–470.
Sharpley, A.L., Attenburrow, M.E., Hafizi, S., Cowen, P.J., 2005. Olanzapine increasesslow wave sleep and sleep continuity in SSRI-resistant depressed patients. J. Clin.Psychiatry 66, 450–454.
Späth-Schwalbe, E., Hansen, K., Schmidt, F., Schrezenmeier, H., Marshall, L., Burger, K., Fehm,H.L., Born, J., 1998. Acute effects of recombinant human interleukin-6 on endocrine and
central nervous sleep functions in healthy men. J. Clin. Endocrinol. Metab. 83,1573–1579.
Touyz, S.W., Beumont, P.J., Saayman, G.S., Zabow, T., 1977. A psychophysiological investi-gation of the short-term effects of clozapine upon sleep parameters of normal youngadults. Biol. Psychiatry 12, 801–822.
Touyz, S.W., Saayman, G.S., Zabow, T., 1978. A psychophysiological investigation of thelong-term effects of clozapine upon sleep patterns of normal young adults. Psycho-pharmacology (Berl) 56, 69–73.
Unno, K., Ozaki, T., Mohammad, S., Tsuno, S., Ikeda-Sagara, M., Honda, K., Ikeda, M., 2012.First and second generation H(1) histamine receptor antagonists produce differentsleep-inducing profiles in rats. Eur. J. Pharmacol. 683, 179–185.
Wetter, T.C., Lauer, C.J., Gillich, G., Pollmächer, T., 1996. The electroencephalographic sleeppattern in schizophrenic patients treated with clozapine or classical antipsychoticdrugs. J. Psychiatr. Res. 30, 411–419.
Wetter, T.C., Brunner, J., Bronisch, T., 2002. Restless legs syndrome probably induced byrisperidone treatment. Pharmacopsychiatry 35, 109–111.
Wichniak, A., Szafranski, T., Wierzbicka, A., Waliniowska, E., Jernajczyk, W., 2006. Electroen-cephalogram slowing, sleepiness and treatment response in patients with schizophre-nia during olanzapine treatment. J. Psychopharmacol. 20, 80–85.





























