Embed Size (px)
Citation preview
MATERNITY NURSING(CA MAMAY)
ANNISAULFALAH (011007 D3KI)
SITI FATIMAH (0110 D3KI)
INTERNATIONAL CLASS OF NURSING DIPLOMA PROGRAM
BANJARMASIN MUHAMMADIYAH HEALTY COLLEGE
ACADEMIC YEAR 2012/2013
ANATOMY AND PHYSIOLOGY MAMMAY
A. BREAST ANATOMY AND PHYSIOLOGY
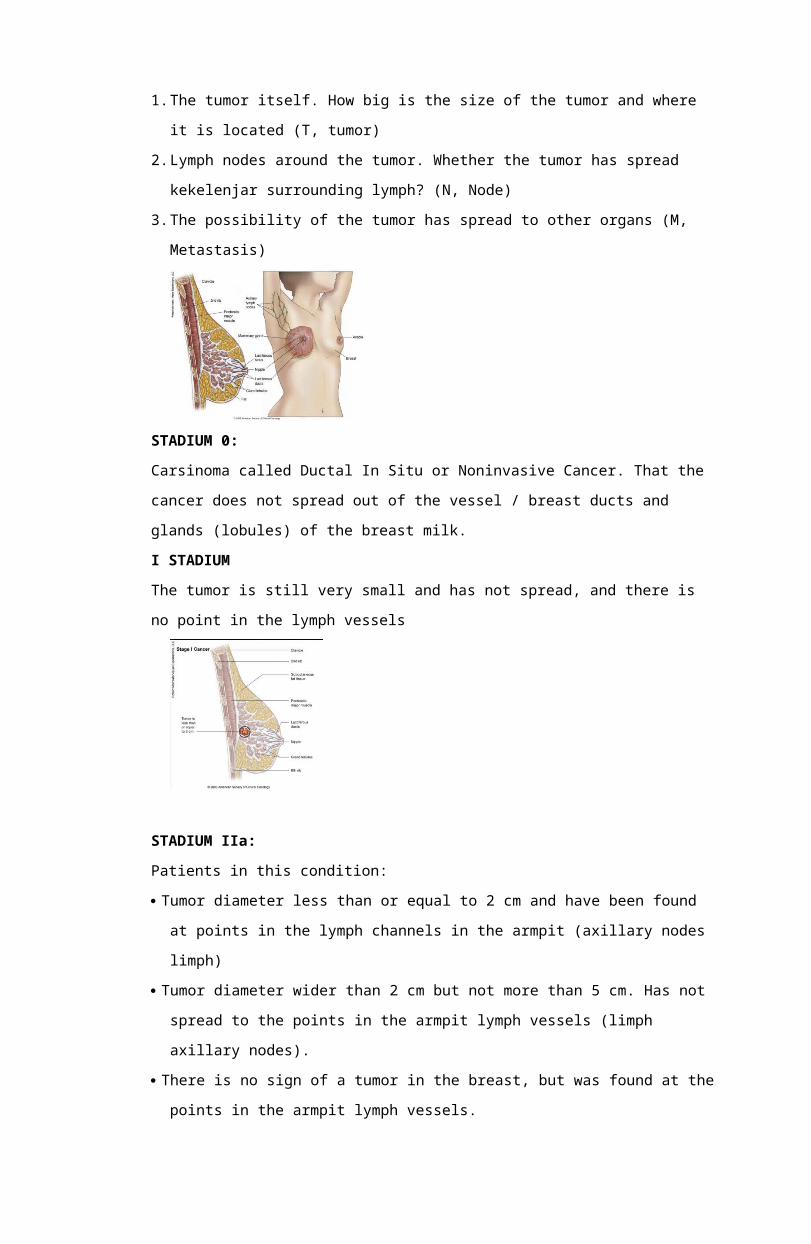
1.Breast Anatomy
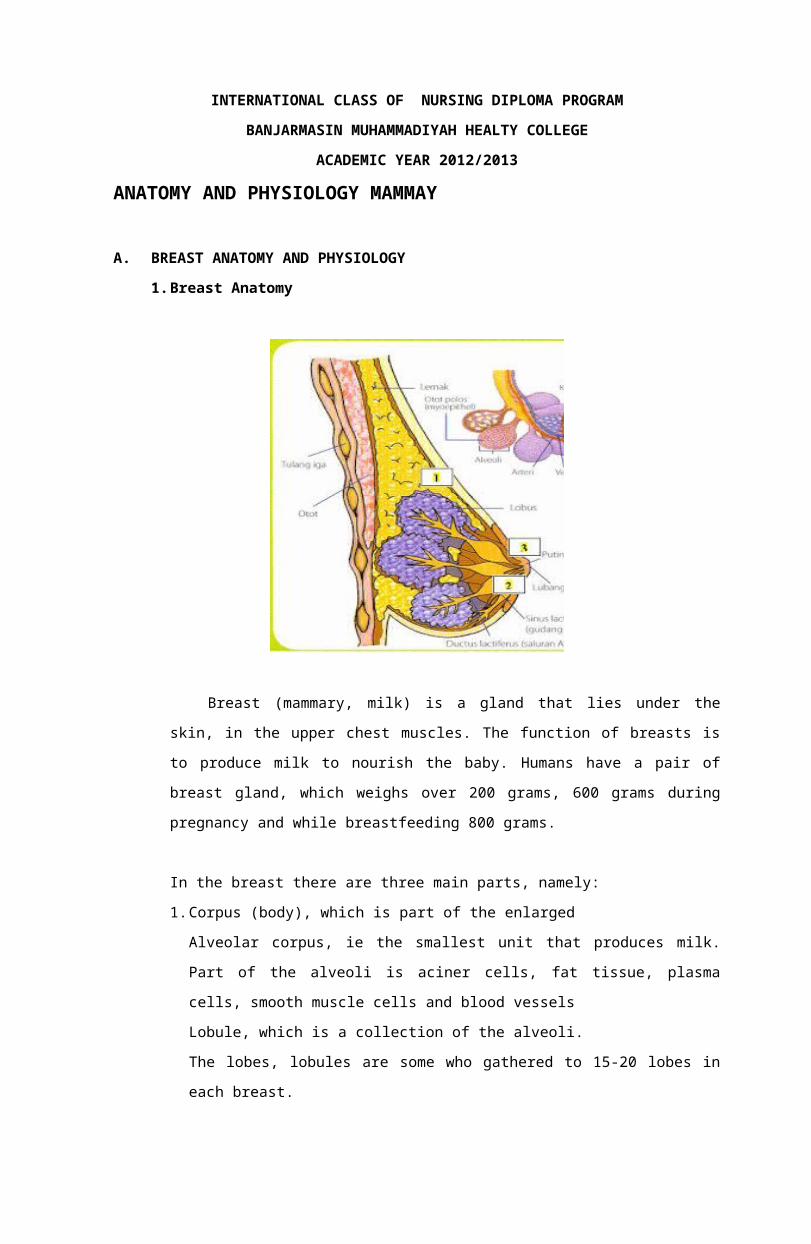
Breast (mammary, milk) is a gland that lies under the
skin, in the upper chest muscles. The function of breasts is
to produce milk to nourish the baby. Humans have a pair of
breast gland, which weighs over 200 grams, 600 grams during
pregnancy and while breastfeeding 800 grams.
In the breast there are three main parts, namely:
1.Corpus (body), which is part of the enlarged
Alveolar corpus, ie the smallest unit that produces milk.
Part of the alveoli is aciner cells, fat tissue, plasma
cells, smooth muscle cells and blood vessels
Lobule, which is a collection of the alveoli.
The lobes, lobules are some who gathered to 15-20 lobes in
each breast.
Breast milk is transferred from the alveoli into the small
channel (duktulus), then some duktulus combine to form a
larger channel (lactiferous duct)
2.Areola, the dark part in the middle
Lactiferous sinuses, which channels beneath the areola
widens, eventually converging to the nipple and empties out.
Inside the walls of the alveoli and ducts are muscle
contraction can be plain when pumping out.
3.Papilla or nipple, that protrusions at the top of the breast
Menojol parts are inserted into the baby's mouth for a
stream of milk
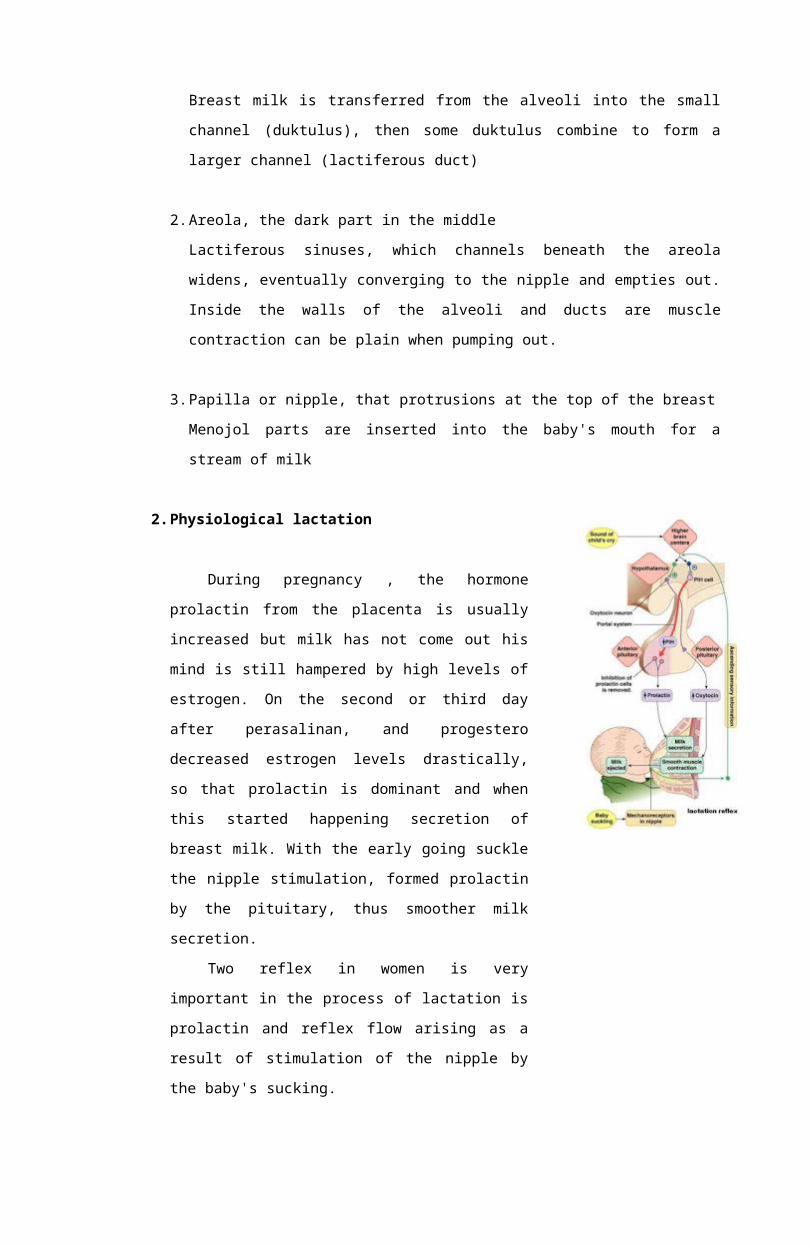
2.Physiological lactation
During pregnancy , the hormone
prolactin from the placenta is usually
increased but milk has not come out his
mind is still hampered by high levels of
estrogen. On the second or third day
after perasalinan, and progestero
decreased estrogen levels drastically,
so that prolactin is dominant and when
this started happening secretion of
breast milk. With the early going suckle
the nipple stimulation, formed prolactin
by the pituitary, thus smoother milk
secretion.
Two reflex in women is very
important in the process of lactation is
prolactin and reflex flow arising as a
result of stimulation of the nipple by
the baby's sucking.
1)reflexes prolactin
At the end of the pregnancy hormone prolactin plays a
role to make colostrum, is limited due to the activity of
prolactin is inhibited by estrogen and progesterone is still
high. Post oersalinan, the release of the placenta and
reduced function of the corpus luteum estrogen and
progesterone also reduced. Will stimulate the baby sucking
the nipple and breast prop because sensory nerve endings
that serve as mechanical receptors. Stimulation was
continued through the spinal cord to the hypothalamus
hypothalamus and inhibiting factors will depress spending
and otherwise stimulate prolactin secretion spending hyper
factor prolactin secretion. Factors hyper prolactin
secretion that stimulates the anterior pituitary prolactin
exit. This hormone stimulates the cells of the alveoli which
is used to make milk.
Prolactin levels in breastfeeding mothers will be a
normal 3 months after giving birth to weaning children and
at that time there will be no increase in prolactin despite
the baby's sucking, but the milk remains ongoing expenses.
In women postpartum who are not breastfeeding, prolactin
levels will be normal at week 2-3. While in nursing Ibi
prolactin will increase in a state such as stress or
psychological effects, anesthesia, surgery and nipple
stimulation.
2)let down reflex
Along with the formation of prolactin by the anterior
pituitary, stimulation from the baby's sucking continued to
posterior pituitary (neurohipofise) were then removed
oxytocin. Through this hormone into the bloodstream, causing
uterine contractions. Contraction of the cells to squeeze
out the milk that has been made out of the alveoli and enter
through the duct into the mouth lactiferus Created,
CA MAMMAY
A. DEFINITION
Ca breast is a group of abnormal cells that continue to grow
in the jaringanmammae (Tapan, 2005).
Ca breast is a cancer that attacks the breast tissue and
breast tissue causes cells to change shape to become abnormal
and multiply in an uncontrolled manner (Mardiana, 2004).
A condition in which cells lose their ability to control the
speed of division and growth. Normally, dead cells equals the
number of cells that grow. If the cell is already experiencing
malignancy / malignant or cancerous cells that divide
continuously without regard to need, thus forming a tumor or
developing "new growth" but not all that new growth is a
carcinogen. (Daniele gale 1996).
Breast cancer is a group of abnormal cells in the breast
that continues to grow in the form of a double. Eventually these
cells to form in the breast bejolan. If it is not a cancerous
lump removed or controlled, cancer cells can spread (metastasis)
to other body parts. Metastases can occur in lymph nodes (lymph
nodes) in the armpit or shoulder blades. Besides cancer cells
could be lodged in the bones, lungs, liver, skin, and
subcutaneous. (Erik T, 2005, p: 39-40)
B. ETIOLOGY
Currently, the data are certainly not found the main causes
mammary penyakitca. Until now, the occurrence of breast ca
allegedly caused by a complex interaction of many factors such
as genetic, environmental, and hormonal levels of the hormone
estrogen in the body excessively (Harianto, 2005).
C. RISK FACTORS
The etiology of breast cancer is not known with certainty.
However, some risk factors in patients were related to the
incidence of breast cancer. There are several risk factors that
may increase the occurrence of breast ca namely:
1.Family history
Women who have a family history of breast ca no one
suffers like the mother, sister, or brother / sister has
breast ca risk 2 to 3 times higher.
2.Hormone
The first menstruation (menarche) before age 10 years,
menopause (menopause) after the age of 55 years old, not
married or never have children, have children after the age of
35 years and never feed a child.
3.Age
Women aged> 30 years have a greater chance of breast
cancer and possibly got the increase after menopause.
4.Women who have had an infection, trauma / impact, breast
surgery due to benign tumors atatu contralateral malignant
tumor.
5.Women who received prior radiation to the breast or chest
wall.
6.Significant weight gain in adulthood.
7.Women who have had ovarian tumor surgery risk is 3 to 4 times
higher (Dalimartha, 2004).
8.Older oral contraceptives
9.Pattern of consumption of fatty foods
10. Lack of physical activity (Indarti, 2005).
D. PATHOPHYSIOLOGY
Ca mammary, like other malignancies cause of this malignancy
is multifaktoral both environmental and hereditary factors, such
as lesions in the DNA causing genetic mutations, mutations in
this gene can cause breast ca, immune system failure, abnormal
growth of the growth factor causes abnormal stimulation between
stromal cells with epithelial cells, a defect in DNA repair
genes such as BRCA1, BRCA2, which, in principle, increase the
activity and cell proliferation disorders that reduce or
eliminate the regulation of cell death (Heffner, 2005).
Ca mammary occur due to loss of control or breast cell
proliferation and apoptosis that breast cells proliferating
continuously. Loss of function of the inability to detect
apoptosis causes cell damage caused by DNA damage. When the p53
gene mutation as a function of the detection of DNA damage will
be lost, so that abnormal cells are continuously proliferating.
The increase in the number of abnormal cells form a lump is
generally called a tumor or cancer. Benign tumors usually a fat
blob encased in a container that resembles a pouch. Through the
bloodstream or lymph system, tumor cells and the toxins produced
out of the herd and spread to other parts of the body.
The cells are spread would then grow in a new place, which
eventually form a swarm of malignant tumor cells or a new
cancer. Malignancy of breast cancer cells to invade surrounding
nomal, especially the weak cells. Cancer cells will grow leaps
and bounds, so the patient will be larger breasts than usual.
Ca from the mammary gland epithelium and breast duct. Growth
begins in the ducts or glands called lobules noninvasive
carcinoma. Then the tumor broke through the outside wall of the
duct or lobule area kelenjarr and invasion into the stroma,
which is known as invasive carcinoma. The spread of tumor occurs
through the lymphatic vessels, and grow deposits in the lymph
nodes, so that the axillary lymph nodes or enlarged
supraklavikuler. Ca mammary gland was first spread to the
axillary region. What most distant metastases are bone, liver,
lung, pleura, and brain (Heffner, 2005).
E. TYPES
Type Ca mammae by histopathologic picture:
1.Ductal carcinoma menginflitrasi
Is the most common histopathological type, constitute 75% of
all breast cancers. Cancer is very clear because it is hard on
palpation. This type of cancer often metastasizes to the
axillary nodes, bone, lung, liver and brain
2.Infiltrating lobular carcinoma
This type is generally multisentris, some areas of
thickening can occur in one or both mammary. Lobular
carcinomas usually metastasize to the meningeal surface.
3.Carcinoma of the modular
At 6% modular carcinoma grows in a capsule, it can be
great but spread slowly, so the prognosis is often better.
4.Mucinous carcinoma
At 3% mucinous carcinoma is mucus, also grow slowly.
5.Ductal carcinoma-tubular
Only 2% and rarely occurs, because axillary metastases
histologically unusual the prognosis is very good.
6.Carcinoma inflamantori
It is a rare type of breast carcinoma (1-2%) and cause
symptoms that are different from other breast carcinomas.
These tumors tenderness and intense pain, abnormal mammary
hard and enlarged. Red skin over the tumor and a little black.
It often happens mammary papilla edema and retraction
(Prawirohardjo, 2005).
F. STAGE BREAST CANCER
stadium in cancer, is to describe the condition of the
cancer, the location, to which the distribution, the extent of
its influence on other organs. Doctors use tests to determine
the stage of cancer. So the stage could not be determined if the
tests do not complete / finished. By knowing the stage, this is
one way which helps your doctor to determine what is the
appropriate treatment for patients.
One way that doctors use to describe the stage of the cancer is the TNM system.
This system uses three criteria to determine the stage of cancer. Namely:
1.The tumor itself. How big is the size of the tumor and where
it is located (T, tumor)
2.Lymph nodes around the tumor. Whether the tumor has spread
kekelenjar surrounding lymph? (N, Node)
3.The possibility of the tumor has spread to other organs (M,
Metastasis)
STADIUM 0:
Carsinoma called Ductal In Situ or Noninvasive Cancer. That the
cancer does not spread out of the vessel / breast ducts and
glands (lobules) of the breast milk.
I STADIUM
The tumor is still very small and has not spread, and there is
no point in the lymph vessels
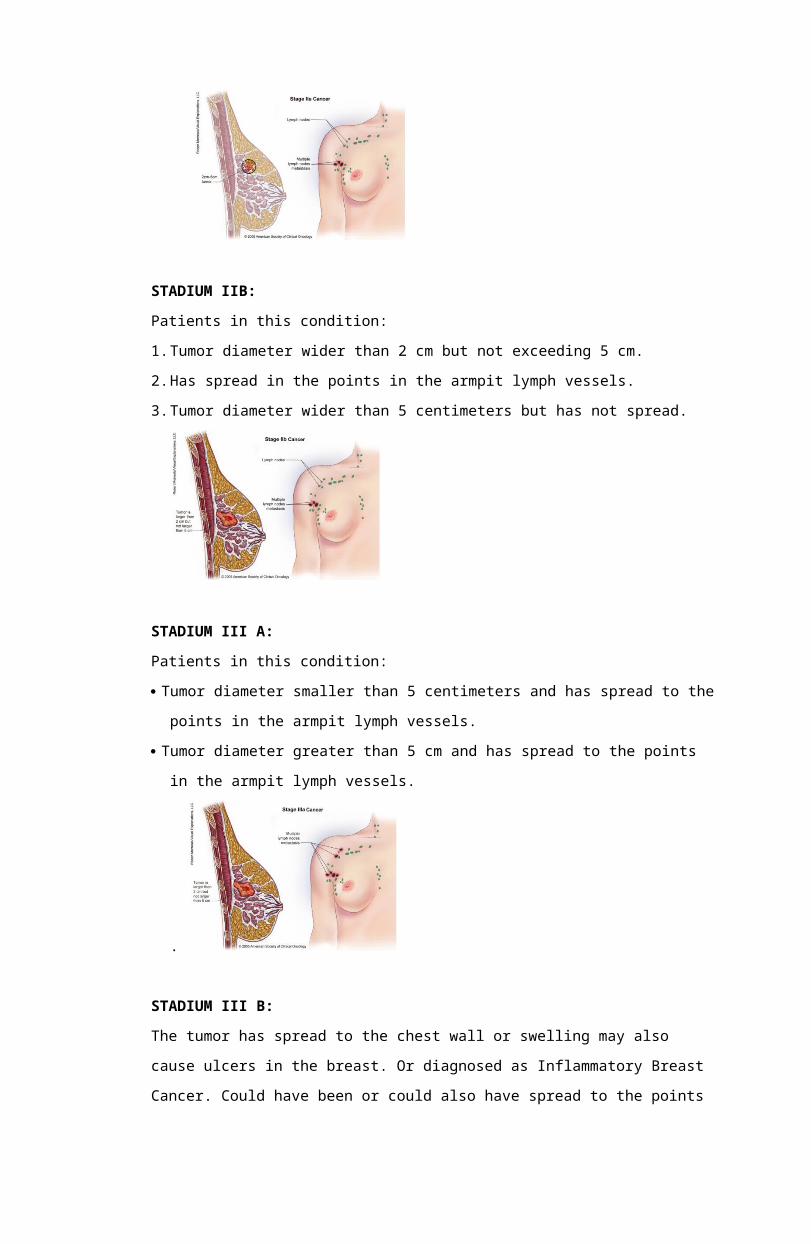
STADIUM IIa:
Patients in this condition:
Tumor diameter less than or equal to 2 cm and have been found
at points in the lymph channels in the armpit (axillary nodes
limph)
Tumor diameter wider than 2 cm but not more than 5 cm. Has not
spread to the points in the armpit lymph vessels (limph
axillary nodes).
There is no sign of a tumor in the breast, but was found at the
points in the armpit lymph vessels.
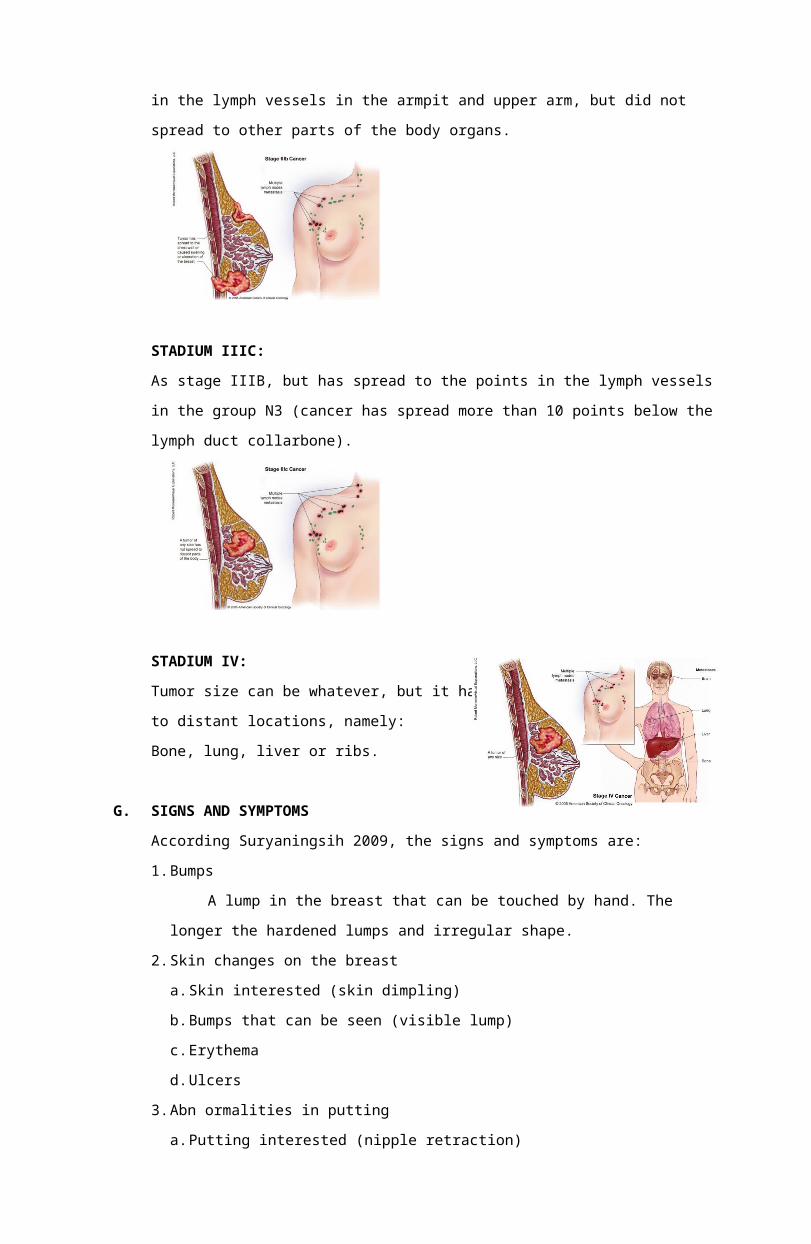
STADIUM IIB:
Patients in this condition:
1.Tumor diameter wider than 2 cm but not exceeding 5 cm.
2.Has spread in the points in the armpit lymph vessels.
3.Tumor diameter wider than 5 centimeters but has not spread.
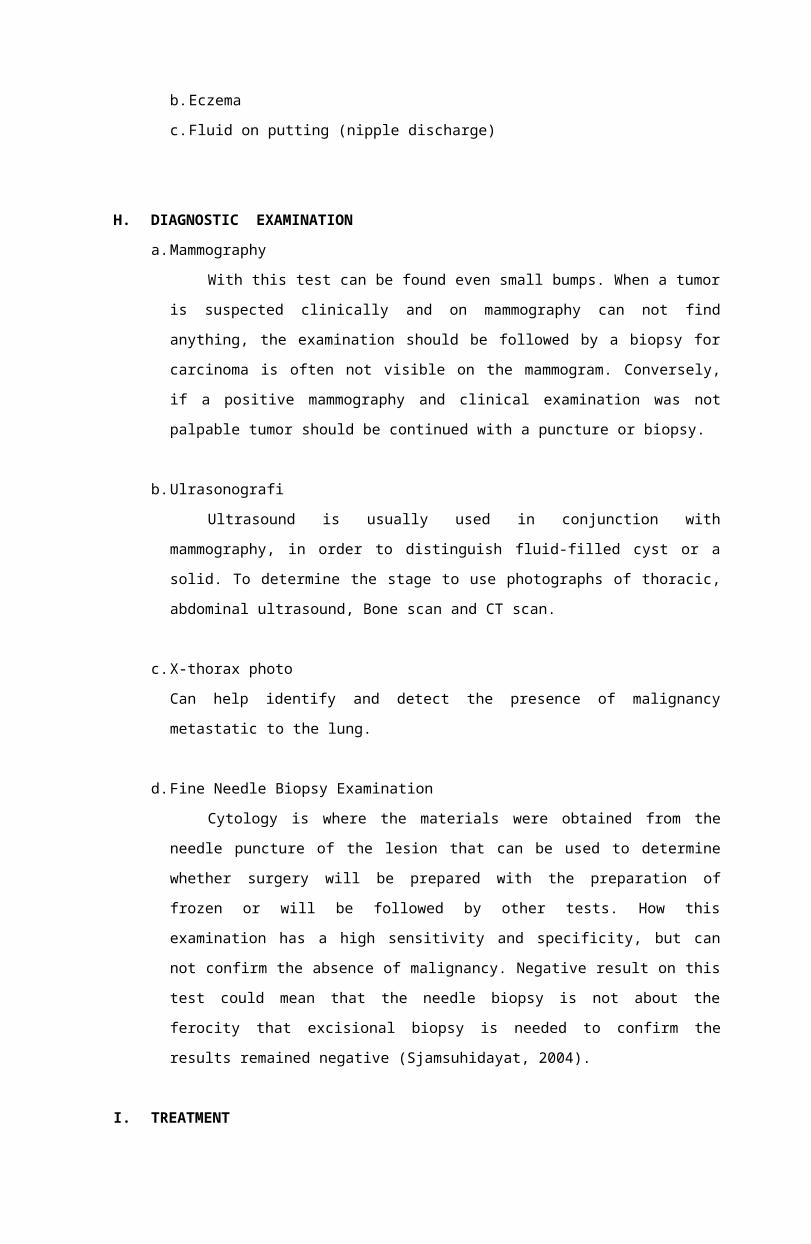
STADIUM III A:
Patients in this condition:
Tumor diameter smaller than 5 centimeters and has spread to the
points in the armpit lymph vessels.
Tumor diameter greater than 5 cm and has spread to the points
in the armpit lymph vessels.
.
STADIUM III B:
The tumor has spread to the chest wall or swelling may also
cause ulcers in the breast. Or diagnosed as Inflammatory Breast
Cancer. Could have been or could also have spread to the points
in the lymph vessels in the armpit and upper arm, but did not
spread to other parts of the body organs.
STADIUM IIIC:
As stage IIIB, but has spread to the points in the lymph vessels
in the group N3 (cancer has spread more than 10 points below the
lymph duct collarbone).
STADIUM IV:
Tumor size can be whatever, but it has spread
to distant locations, namely:
Bone, lung, liver or ribs.
G. SIGNS AND SYMPTOMS
According Suryaningsih 2009, the signs and symptoms are:
1.Bumps
A lump in the breast that can be touched by hand. The
longer the hardened lumps and irregular shape.
2.Skin changes on the breast
a.Skin interested (skin dimpling)
b.Bumps that can be seen (visible lump)
c.Erythema
d.Ulcers
3.Abn ormalities in putting
a.Putting interested (nipple retraction)
b.Eczema
c.Fluid on putting (nipple discharge)
H. DIAGNOSTIC EXAMINATION
a.Mammography
With this test can be found even small bumps. When a tumor
is suspected clinically and on mammography can not find
anything, the examination should be followed by a biopsy for
carcinoma is often not visible on the mammogram. Conversely,
if a positive mammography and clinical examination was not
palpable tumor should be continued with a puncture or biopsy.
b.Ulrasonografi
Ultrasound is usually used in conjunction with
mammography, in order to distinguish fluid-filled cyst or a
solid. To determine the stage to use photographs of thoracic,
abdominal ultrasound, Bone scan and CT scan.
c.X-thorax photo
Can help identify and detect the presence of malignancy
metastatic to the lung.
d.Fine Needle Biopsy Examination
Cytology is where the materials were obtained from the
needle puncture of the lesion that can be used to determine
whether surgery will be prepared with the preparation of
frozen or will be followed by other tests. How this
examination has a high sensitivity and specificity, but can
not confirm the absence of malignancy. Negative result on this
test could mean that the needle biopsy is not about the
ferocity that excisional biopsy is needed to confirm the
results remained negative (Sjamsuhidayat, 2004).
I. TREATMENT
Treatment begins after a thorough assessment of the
condition of the patient, which is about 1 week or more after
the biopsy. Treatment consists of surgery, radiation therapy,
chemotherapy and hormone inhibitors.
1.Surgery
a.Mastectomy
Mastectomy is the surgical removal of the breast. There
are three types of mastectomy are:
1)Radycal Modified Mastectomy, the surgical removal of the
entire breast, breast tissue in the sternum, collarbone
and ribs, and lump around the armpit.
2)Total (Simple) Mastectomy, the surgical removal of the
entire breast, without glands in the armpit.
3)Radical Mastectomy, the surgical removal of part of the
breast. Lumpectomy is usually called, is merely the
removal of tissue containing cancer cells, instead of the
whole breast. Usually lumpectomydirekomendasikan in
patients with large tumor less than 2 cm and located on
the edge of the breast.
b.Lymph node (KGB) Armpit.
Appointment Armpit KGB carried out on patients with
breast ca spread but large tumor more than 2.5 cm (Tapan,
2005).
2.Non Surgery
a.Radiation Therapy
Radiation is the process of radiation to the affected
area ca using X-rays and gamma rays are aimed at killing any
remaining cancer cells after surgery dimammae. The effect of
this treatment is the body becomes weak, poor appetite, skin
color around the breast to black and hemoglobin and
leukocytes tended to decline as a result of radiation.
b.Chemotherapy
Chemotherapy is the administration of anti-cancer drugs
in pill or capsule or liquid through the infusion aimed at
killing cancer cells. These drugs not only kill cancer cells
in the breast, but also all the cells in the body. The
effects of chemotherapy are patients experienced nausea and
vomiting and hair loss. Systematic after mastectomy,
palliative in advanced disease.
c.Hormone therapy and endocrine
Hormone made if the disease has systemic form distant
metastases. Hormonal therapy is usually given prior
palliative chemotherapy.
Inhibiting hormone medications (drugs that affect the
hormones that support the growth of cancer cells) is used to
suppress the growth of cancer cells throughout the body.
Given to cancer that has spread, taking estrogen, androgen,
antiestrogen, coferektomi hipofisektomi adrenalectomy
(Tapan, 2005).
FETAL CONDITION DUE TO BREAST CANCER MOM
No deleterious effects on the fetus from the mother's breast
cancer has been proven, and there are no reported cases of breast
cancer cell transfer of fetal-maternal.
CONSEQUENCES OF PREGNANCY IN PATIENTS WITH A HISTORY OF BREAST CANCER
Based on retrospective data, pregnancy does not seem to
jeopardize the survival of women with a history of breast cancer, and
no deleterious effects have been demonstrated in the fetus. Some
doctors recommend that patients wait 2 years after diagnosis before
trying to conceive.
Effective treatment, including surgery and chemotherapy can be
administered at certain phases of pregnancy. Treatment is based on
the stage of fetal development and the stage of cancer development.
The use of radiation therapy during the first and second trimester of
pregnancy is not recommended because of the inability to protect
babies from cancer radiation. In early pregnancy, the treatment given
is usually composed of a mastectomy followed by chemotherapy in the
second trimester. Chemotherapy given after the first trimester so do
not put the fetus at greater risk, although low birth weight.
Women in advanced stages of cancer have more difficult choices,
whether they should postpone treatment until after birth, or using a
less aggressive treatment of chemotherapy that may not be effective
against their cancer. It is important for women to face transform and
discuss the implications of these options with doctors and
specialists, as well as to get support from their friends, family,
and partners.
Some women can get pregnant after breast cancer, but because not
enough research has been done, then women should consult a doctor if
considering pregnancy. It is important to realize that certain cancer
treatments can affect a person's ability to bear children will
require careful consideration and planning to preserve fertility
before and during treatment.
There are several clinical issues that need to be considered
when thinking about pregnancy after breast cancer:
Estrogen - receptor status of the cancer cells.
If the cancer cells have estrogen receptor positive, it may be more
at risk of getting pregnant. With the hormonal surges of estrogen and
progesterone associated with pregnancy, it can allow for the cancer
cells to become active inactive.
The impact of chemotherapy on the ovaries. (Impact of
chemotherapy on the ovaries)
At birth, every woman is born with a complete egg in the ovaries for
a lifetime, spending a month each in accordance with the menstrual
cycle. However, chemotherapy can damage ovrium in a variety of ways.
Even if the women who had experienced menopause cancer, chemotherapy
may actually kill more eggs, or it may have damaged the remaining
egg, so they may not be able to conceive or can cause genetic
defects. To some extent, the content specialist can determine the
quality of the eggs, and if she is successful pregnancy. Treatment
did not cause immediate menopause but accelerate the menopause.
Year of survival Although there is little debate, some
oncologists recommend to wait until the past five years since the
success of therapy to consider pregnancy because it may impact on
your body. Others recommend just waiting for two years.
Limited fertility options: Patients with a history of cancer may not
be able to get pregnant the natural way, for various reasons, some of
which may have nothing to do with your cancer history. But as a
victim of cancer, fertility treatment options may be more limited, as
many fertility programs including significant hormonal stimulation.
Extended Treatment: Some women require additional hormonal
therapy after treatment, such as 5 years of tamoxifen, which could
further delay pregnancy.
J. NURSING CARE REPORT
1.Assessment
a.Data biography / bio
Includes client identity: name, age, gender, religion,
education, occupation, and address.
b.History of complaints
1)Complaints in the breast or armpit and a history of the
disease:
Bumps, speed of growth, pain, nipple discharge, nipple
retraction, and since when, crusting on the areola, skin
disorders: dimpling, peau d'orange, ulceration, venektasi,
skin discoloration, lump armpit, arm edema.
2)Complaints elsewhere related to metastasis:
Painful bone (vertebra, femur), a feeling of fullness
in the pit of the stomach, coughing, tightness, severe
headache.
c.Risk Factors
Patient age, age of first child, have a child or
unlicensed, history of breastfeeding, history of
menstruation: first menstrual age, regularity of menstrual
cycle, menopause age, history of hormonal drug use, family
history of breast cancer or with respect to other cancers, a
history of surgery ever breast tumors, a history of chest
wall radiation.
d.The physical examination includes:
1.Status generalist
2.Status location:
Right and left breast should be checked
Period tumors: location, size, consistency, surface, shape
and boundaries of the tumor, number of tumors, fixed or
not to the surrounding breast tissue, skin, m. pectoral
and chest wall.
Skin changes: redness, dimpling, edema, nodules, peau
d'orange, ulceration.
Nipple: interested, erosion, crusting, discharge.
Lymph node status:
Axillary Lymph node: the number, size, consistency
Lymph node infra clavicle
Supraclavicular Lymph node
Examination of the area of suspected metastasis: What
organs (lung, bone, liver, brain).
3.Body weight and height
4.Head to toe assessment
e.Laboratory tests include:
1.Blood tests are usually decreased hemoglobin, increased
leukocytes, platelets increase if there is spread of urea
and creatinine.
2.Examination of the urine, examined whether increased urea
and creatinine.
3.Diagnostic tests commonly performed on patients with
breast ca is the X-ray, ultrasound, xerora diagrafi,
diaphanografi and examination hormone receptors.
f.Assessment of patterns of everyday life include:
1.Nutrition
Eating habits, frequency of eating, appetite, food
taboos, food preferences, the number of drinking. Studied
history before and after admission.
2.Elimination
CHAPTER habit / bladder, frequency, color, consistency,
before and after admission.
3.Rest and sleep
Sleeping habits, the amount of sleep the day before and
after illness.
4.Personal hygiene
The frequency of bathing and brushing your teeth
daily, the frequency of washing hair in a week, assessed
before and at the hospital.
5.Identification of psychological problems, social, and
spiritual.
Psychological Status: Emotions are usually irritable,
angry, anxious, patients expect a speedy recovery, feel
foreigners stay in the hospital, feeling inferior,
negative coping mechanisms.
Social Status: Feeling isolated due to lack of clients
interact with other people.
Spiritual Status: Client in worship.
NURSING DIAGNOSIS
a.Acute Pain / Chronic related to the suppression of tumor mass
b.Integrity of the skin or tissue damage associated with changes in
circulation, edema, tissue destruction
c.Imbalance nutrition less than body requirements related to
inadequate intake and hipermetabolisme.
d.The risk of infection associated with wound infection
e.Anxiety associated with changes in body image
f.Body image disturbance associated with loss or alteration of
mammary and mammary picture.
g.Lack of knowledge about the condition, prognosis, and treatment of
illnesses related to lack of information.
INTERVENTION
a.Acute Pain / Chronic related to the suppression of tumor mass.
Goal: Pain is reduced or the client can be resolved
Expected outcomes:
1)Clients say the pain is reduced, pain scale 2-3 or lost.
2)Tender no.
3)Facial expressions quiet, rest, sleep.
4)Identifying the causes and uses measures to prevent pain.
Intervention (NIC) Rational a.komphrehensif Assess the
location, characteristics,
duration, frequency, scale,
and intensity of pain.
b.Provide information on pain
a. To determine the extent to
which the development of
the pain felt by the
client so that it can be
used as a reference for
further intervention.
clients include causing pain
and pain intensity.
c.Position the patient to
provide comfort.
d.Teach the use of non-
pharmacological techniques
(relaxation, guided
emergency, music therapy,
distraction, hot and cold
applications, massage, TENS,
hypnosis, play therapy,
activity therapy
acupressure).
e.Increase sleep / rest.
f.Monitor TTV before and after
the first analgesic.
g.Determine the analgesic of
choice, route of
administration and optimal
dosage
b. Clients can control the
pain.
c. May affect the client's
ability to relax / rest
effectively and can reduce
pain.
d. Relaxation techniques can
make the client feel
comfortable and a little
distraction to divert the
attention of clients to
pain so that it can help
reduce the pain.
e. The need for sleep / rest
being met and how to
reduce the pain.
f. Changes in vital signs,
especially temperature and
pulse rate is one
indication of increased
pain experienced by the
client.
g. Analgesic drugs block the
pain receptors so that the
pain can be perceived
tidat.
b.Integrity of the skin or tissue damage associated with changes in
circulation, edema, tissue destruction.
Goal: Damage to skin integrity can be resolved.
Criteria results:
a.Good skin integrity can be maintained (sensation, elasticity,
temperature, hydration, pigmentation)
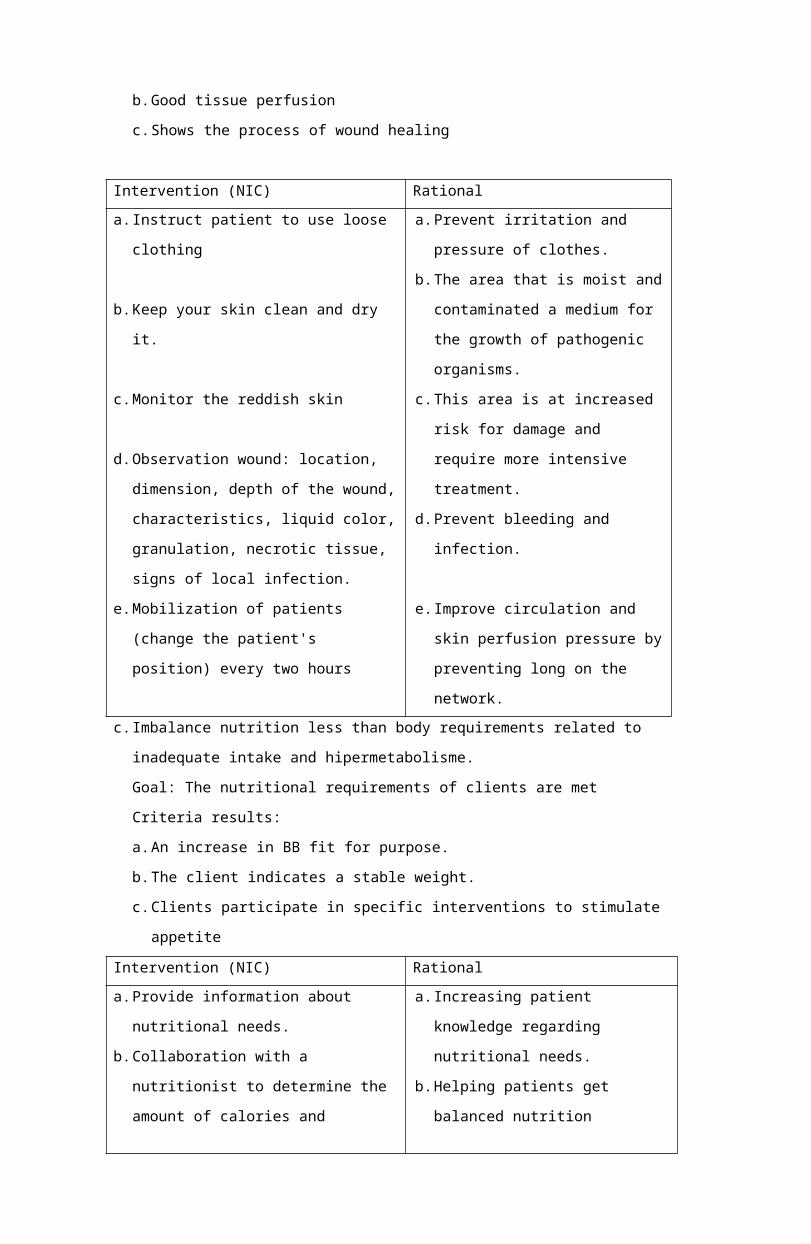
b.Good tissue perfusion
c.Shows the process of wound healing
Intervention (NIC) Rational a.Instruct patient to use loose
clothing
b.Keep your skin clean and dry
it.
c.Monitor the reddish skin
d.Observation wound: location,
dimension, depth of the wound,
characteristics, liquid color,
granulation, necrotic tissue,
signs of local infection.
e.Mobilization of patients
(change the patient's
position) every two hours
a.Prevent irritation and
pressure of clothes.
b.The area that is moist and
contaminated a medium for
the growth of pathogenic
organisms.
c.This area is at increased
risk for damage and
require more intensive
treatment.
d.Prevent bleeding and
infection.
e.Improve circulation and
skin perfusion pressure by
preventing long on the
network. c.Imbalance nutrition less than body requirements related to
inadequate intake and hipermetabolisme.
Goal: The nutritional requirements of clients are met
Criteria results:
a.An increase in BB fit for purpose.
b.The client indicates a stable weight.
c.Clients participate in specific interventions to stimulate
appetite
Intervention (NIC) Rational a.Provide information about
nutritional needs.
b.Collaboration with a
nutritionist to determine the
amount of calories and
a.Increasing patient
knowledge regarding
nutritional needs.
b.Helping patients get
balanced nutrition
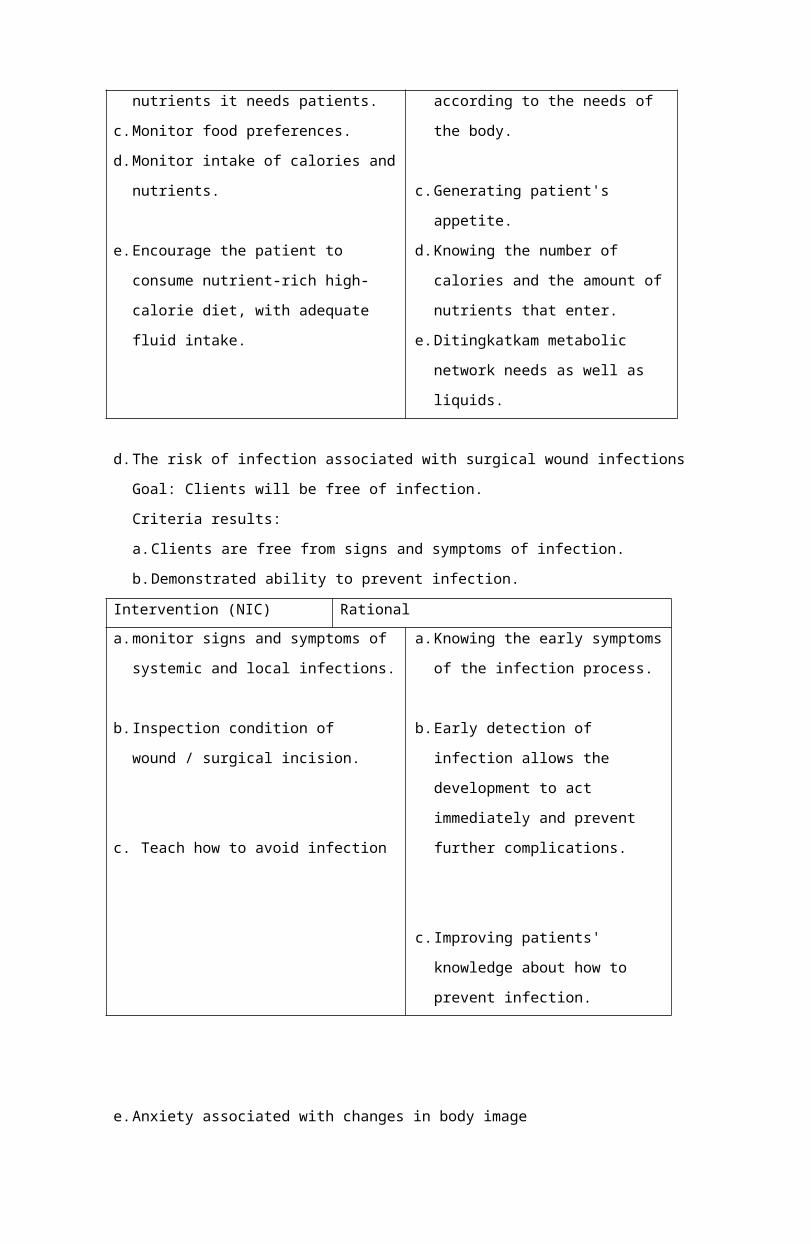
nutrients it needs patients.
c.Monitor food preferences.
d.Monitor intake of calories and
nutrients.
e.Encourage the patient to
consume nutrient-rich high-
calorie diet, with adequate
fluid intake.
according to the needs of
the body.
c.Generating patient's
appetite.
d.Knowing the number of
calories and the amount of
nutrients that enter.
e.Ditingkatkam metabolic
network needs as well as
liquids.
d.The risk of infection associated with surgical wound infections
Goal: Clients will be free of infection.
Criteria results:
a.Clients are free from signs and symptoms of infection.
b.Demonstrated ability to prevent infection.
Intervention (NIC) Rational a.monitor signs and symptoms of
systemic and local infections.
b.Inspection condition of
wound / surgical incision.
c. Teach how to avoid infection
a.Knowing the early symptoms
of the infection process.
b.Early detection of
infection allows the
development to act
immediately and prevent
further complications.
c.Improving patients'
knowledge about how to
prevent infection.
e.Anxiety associated with changes in body image
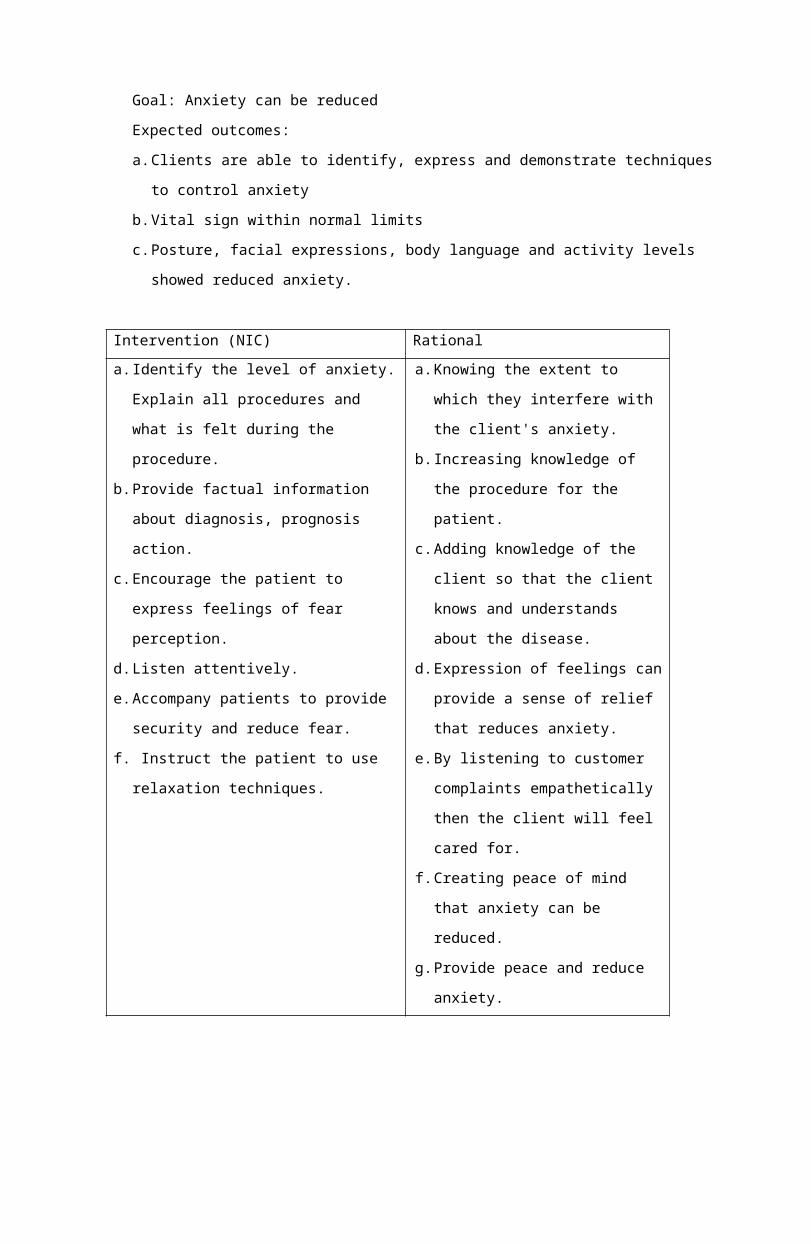
Goal: Anxiety can be reduced
Expected outcomes:
a.Clients are able to identify, express and demonstrate techniques
to control anxiety
b.Vital sign within normal limits
c.Posture, facial expressions, body language and activity levels
showed reduced anxiety.
Intervention (NIC) Rational a.Identify the level of anxiety.
Explain all procedures and
what is felt during the
procedure.
b.Provide factual information
about diagnosis, prognosis
action.
c.Encourage the patient to
express feelings of fear
perception.
d.Listen attentively.
e.Accompany patients to provide
security and reduce fear.
f. Instruct the patient to use
relaxation techniques.
a.Knowing the extent to
which they interfere with
the client's anxiety.
b.Increasing knowledge of
the procedure for the
patient.
c.Adding knowledge of the
client so that the client
knows and understands
about the disease.
d.Expression of feelings can
provide a sense of relief
that reduces anxiety.
e.By listening to customer
complaints empathetically
then the client will feel
cared for.
f.Creating peace of mind
that anxiety can be
reduced.
g.Provide peace and reduce
anxiety.
REFERENCE
Azamris. 2006. Analisis Faktor Risiko pada Pasien Kanker
Payudara di Rumah Sakit Dr. M. Djamil Padang. Jurnal Cermin
Dunia Kedokteran No. 152.
Dalimartha, Setiawan. 2004. Deteksi Dini Kanker dan Simplisia
Anti Kanker. Jakarta : Penebar Swadaya.
Harianto, Rina M dan Hery S. 2005. Risiko Penggunaan Pil
Kontrasepsi Kombinasi Terhadap Kejadian Kanker Payudara pada
Reseptor KB di RS Dr. Cipto Mangunkusumo, Jakarta:Majalah Ilmu
Kefarmasian, Vol. 2, No.1, hh. 84-99.
Heffner, Linda J dan Danny J Schust. 2005. At Glance Sistem
Reproduksi Edisi Kedua.Jakarta : Erlangga.
Ibrahim, Syarif dan Syarifuddin Wahid. 2010. Immunotherapy on
Breast Cancer. The Indonesia Journal of Medical Science Volume 2
No 1 Juli 2010 p.54-60.
Indarti, Rini dan Henry Setiawan. 2005. Faktor-Faktor Risiko
yang Berpengaruh Terhadap Kejadian Kanker Payudara. Magister
Programme of Epidemiology, University ofDiponegoro, Semarang,
Indonesia No 5248.
Mardiana, Lina. 2004. Kanker pada Wanita, Pencegahan dan
Pengobatan dengan Tanaman. Jakarta : Penebar Swadaya.
Prawirohardjo, Sarwono. 2005. Ilmu Kandungan. Jakarta : Yayasan
Bina Pustaka.
Sjamsuhidayat, R. 2004. Buku Ajar Ilmu Bedah Edisi 2. Jakarta :
EGC.
Tapan, Erik. 2005. Kanker, Antioksidan, dan Terapi Komplementer.
Jakarta : Elex Media Komputindo.
Tim Penanggulangan dan Pelayanan Kanker Payudara Terpadu
Paripurna RS Kanker Dharmais. 2002. Penatalaksanaan Kanker
Payudara Terkini Edisi 1 Cetakan 1. Jakarta : Pustaka Populer
Obor.
Tjindarbumi, D. 2002. Deteksi Dini Kanker Payudara dan
Penanggulangannya dalam Deteksi Dini Kanker. Jakarta : FK UI.
http://ainicahayamata.wordpress.com/2011/03/30/askep-ca-mammae-
pada-ibu-hamil-dan-menyusui/





























