Embed Size (px)
Citation preview

ELSEVIER
Int. J. Radiation Oncology Biol. Phys., Vol. 37, No. 4, pp. X97-905, 1997 Copyright 0 1997 Elsevier Science Inc.
Printed in the USA. All rights reserved 0360-3016/97 $17.00 + .@I
PI1 SO360-3016(96)00539-l
l Biology Contribution
PROLIFERATION AND HYPOXIA IN HUMAN SQUAMOUS CELL CARCINOMA OF THE CERVIX: FIRST REPORT OF COMBINED
IMMUNOHISTOCHEMICAL ASSAYS
ANDREW S. KENNEDY, M.D.,* JAMES A. RALEIGH, PH.D.,* GERARDO M. PEREZ, M.D.,’ DENNISE P. CALKINS, B.S.,* DONALD E. THRALL, D.V.M., PH.D.,$ DEBRA B. NOVOTNY, M.D.§
AND MAHESH A. VARIA, M.B., CH.B, F.A.C.R.*
Departments of *Radiation Oncology, ‘Gynecologic Oncology, and §Pathology, University of North Carolina School of Medicine, Chapel Hill, NC and $College of Veterinary Medicine, NC State University, Raleigh, NC
Purpose: To characterize the distribution of hypoxia and proliferation in human squamous cell carcinoma of the cervix via an immunohistochemical approach prior to initiation of therapy. Methods and Materials: Patients with primary squamous cell carcinoma of the cervix uteri received a single infusion of the 2-nitrobnldazole, pimonidazole (0.5 g/m’ i.v.), and 24 h later punch biopsies of the primary tumor were taken. Tissue was formalin fixed, paraffin embedded, and sectioned for immunohistochemistry. Hypoxia was detected by monoclonal antibody binding to adducts of reductively activated pimonidazole in malignant cells. Staining for endogenous MIB-1 and PCNA was detected in tumor cells via commercially available monoclonal antibodies. Point counting was used to quantitate the fraction of tumor cells immunostained for MIB-1, PCNA, and hypoxia marker binding. Results: Immunostaining for pimonidazole binding was distant from blood vessels. There was no staining in necrotic regions, and only minimal nonspecific staining, mostly in keratin. In general, cells immunostaining for MIB-1 and PCNA did not immunostaln for pimonldazole binding. Cells lmmunostalning for MIB-1 and PCNA showed no obvious geographic predilection such as proximity to vasculature. Quantitative comparison showed an inverse relationship between hypoxia marker binding and proliferation. Conclusions: Immunohistochemical staining for pimonidazole binding is consistent with the presence of hypoxic cells in human tumors and may be useful for estimating tumor hypoxia prior to radiation therapy. Immunostain- ing for pimonidazole binding is an ideal complement to immunohistochemical assays for endogenous proliferation markers allowing for comparisons of tumor hypoxia with other physiological parameters. These parameters might be used to select patients for radiation protocols specifically designed to offset the negative impact of hypoxia and/or proliferation on therapy. The inverse relationship between pimonidazole binding and proliferation mark- ers is a preliminary result requiring verification. 0 1997 Elsevier Science Inc.
Hypoxia, Proliferation, Hypoxia marker, Pimonidazole, MIB-1, PCNA, Cervix carcinoma.
INTRODUCTION
Hypoxia, proliferation, and intrinsic radiosensitivity are potential prognostic indicators for radiation therapy outcome, and each has been the subject of independent investigation in recent years. Tumor hypoxia measured by either oxygen electrodes or noninvasive hypoxia markers has an inverse relationship with the radiation response of neck node metastases and malignancies of the uterine cervix (17, 22, 30). Tumor cell proliferation correlates with radiation therapy outcome, but the par-
ticulars depend on the treatment plan. Proliferation in- dices measured prior to treatment were not correlated with overall outcome for patients with rectal or cervix cancers (11, 42) receiving preoperative radiation and surgery but were directly correlated with actuarial 5- year survival for rectal carcinoma patients (42). The picture is different when tumors are treated with radi- ation alone. In this case, proliferation was inversely cor- related with outcome (29, 37). Similarly, patients with head and neck tumors with potential doubling times (T,,,) of less than 4 days were reported to do signifi-
Reprint requests to: Andrew Kennedy, M.D., UNC School of Council at UNC Chapel Hill; and the State of North Carolina. Medicine, Dept. of Radiation Oncology, Campus Box #7512, The authors thank Dr. E. M. Zeman, Dr. J. E. Tepper, Dr. J. M. Chapel Hill, NC 27599-7512. Cline, and Mr. G. E. Arteel for helpful discussions; Ms. E. Ken- Acknowledgements-Financial support was provided by DHHS nedy for help with manuscript preparation; and Dr. Y. W. Lee NC1 CA.50995, CA68826, and MO1 RR00046; the Lineberger for the preparation of pimonidazole hydrochloride. Comprehensive Cancer Center and the University Research Accepted for publication 1 November 1996.
897

898 I. J. Radiation Oncology 0 Biology 0 Physics
cantly worse than patients with slower growing tumors, although the significance of these early results for long- term outcome now appears to be in question (2).
In addition to hypoxia and proliferation, intrinsic radio- sensitivity of cells isolated from solid tumors has been shown to be correlated with radiation therapy outcome. Patients with radioresistant tumors, defined as having a median surviving fraction at 2 Gy for cells isolated from the tumors of >0.40, had a significantly lower 3-year sur- vival level than those with sensitive tumours for a series of patients receiving radical radiation therapy for carci- noma of the uterine cervix (39, 40). Other studies have shown a similar trend (3), but there are cases where a relationship between SF2 and outcome could not be dem- onstrated (36).
The possibility that hypoxia, proliferation, and intrin- sic radiosensitivity are linked phenomena in tumors has received little attention. Hypoxia is believed to compro- mise radiation response by decreasing the interaction of oxygen with free radicals in target molecules and by arresting cells in a radiation resistant phase of the cell cycle. However, it is also possible that hypoxia (or hyp- oxia/reperfusion) affects radiation response by chang- ing the intrinsic radiosensitivity of tumor cells by in- ducing antioxidant peptides such as metallothionein; DNA damage inducible genes (e.g., GADD45); cyto- kines (e.g., NF-KB), and differentiation, and possibly by inducing clonal selection in favor of cells that have lost an apoptotic pathway to lysis (18, 19, 35, 43). Under- standing the relationships among hypoxia, proliferation, and intrinsic radiation sensitivity could be crucial in treatment planning. This consideration led us to develop a method for comparing hypoxia marker binding and proliferation in human tumors to complement intrinsic radiosensitivity assays developed elsewhere.
The immunohistochemical hypoxia marker assay for tu- mor hypoxia (32) is an ideal complement to immuno- chemical assays for tumor proliferation based on endog- enous MIB-1 or PCNA. Both types of assays are routine, robust, relatively inexpensive, and can be performed on the same, formalin-fixed tissue. Furthemlore, the relation- ship between hypoxia and proliferation is revealed at the cellular and microregional levels. Oxygen microelec- trodes cannot do this and, in fact, give a very different picture of microregional hypoxia when compared to im- munohistochemical hypoxia marker assays (30). Other immunochemical assays based on hypoxia markers such as ELISA (3 1, 38) or flow cytometry (14,23) and various noninvasive hypoxia marker techniques [review (30)] suf- fer from the same loss of microregional information.
The usefulness of the immunohistochemical hypoxia marker approach has been demonstrated in extensive studies of spontaneous canine tumors in which antibod-
Volume 37, Number 4, 1997
ies to the hypoxia marker CCI-103F were used (7, 8, 27, 32). More limited studies of the relationship of hyp- oxia marker binding and proliferation have also been performed (33, 45). In order to extend the study to hu- man tumors, hypoxia markers have been developed from the pool of 2-nitroimidazole radiosensitizers. Hu- man pharmacokinetic and toxicity data are available for these compounds so that costly preclinical studies can be avoided. One particularly attractive compound was pimonidazole hydrochloride from European radiosen- sitizer trials (13). Pimonidazole hydrochloride has a high, 0.4 M water solubility, which makes it convenient to handle and administer. On average, it concentrates in human tumors 3.411 relative to plasma levels (34) so that the effective tumor dose of the drug is increased. Pimonidazole binds to hypoxic cells with an oxygen de- pendence similar to that for other 2-nitroimidazoles (1) and shows binding characteristics in spheroids, rodent tumors, and canine tumors indistinguishable from CCI- 103F (30). The maximum tolerated dose (MTD) for a single infusion of pimonidazole hydrochloride is 2 g/ m2, while the maximum multiple dose during a frac- tionated course of radiation therapy is 1 g/m” given every second day or 0.75 g/m2 given every day for 20 days. The plasma half-life for pimonidazole for a single dose of 1 g/m* is 5.2 h in the elimination phase. No toxicity or symptoms were recorded at, or below 0.5 g/ mz (34), and this dose of pimonidazole was chosen for the hypoxia marker studies.
For the purposes of the present investigation, com- mercially available antibodies to MIB-I and prolifer- ating cell nuclear antigen (PCNA) were chosen as mark- ers for proliferation to complement pimonidazole as the marker of hypoxia. MIB-1 recognizes native Ki-67 an- tigen and recombinant fragments of the molecule in par- affin-embedded specimens (24). The advantage of MIB- 1 and PCNA over Ki-67 is that both can be detected in formalin-fixed tissue, whereas Ki-67 requires snap-fro- zen specimens. Investigations of the merits of various endogenous markers of proliferation are ongoing [e.g., (21)] and it seemed prudent to investigate more than one marker of proliferation in the present study. We report the first comparison of immunohistochemical assays for hypoxia marker binding with endogenous proliferation markers in human tumors.
METHODS AND MATERIALS
Pimonidazole Pimonidazole hydrochloride, I-[(Zhydroxy-3-piperi-
dinyI)propyl]-2-nitroimidazole hydrochloride, was pre- pared and characterized for us. ’ Standard chromato- graphic, spectroscopic, and elemental analyses, including
‘Natural Pharmacia International, Inc., Research Triangle Park, NC.

Proliferation and hypoxia in human squamous cell carcinoma l A. S. KENNEDY et al. 899
analysis for heavy metal contamination were carried out. The preparation was shown to be pathogen free and py- rogen free prior to use. United States Food and Drug Ad- ministration clearance has been obtained for the use of pimonidazole hydrochloride as an Investigational New Drug (IND#36,783). A dose of 0.5 g/m2 pimonidazole hydrochloride was dissolved in 110 ml of normal saline under sterile conditions and infused intravenously into pa- tients over 20 min. This dose is one-quarter of the maxi- mum tolerated dose (MTD) for single infusions and two- thirds of the MTD for repeated, daily infusions (34).
Patients Patients were eligible to enter the study if they (a) had
a biopsy-proven cervix carcinoma; (b) had an accessible lesion for punch biopsy; (c) were age > 18 years; and (d) did not have concurrent infections, leukopenia, hemoglo- bin level < 10 g/dl, elevated liver enzymes, or neuropa- thies. All patients provided a signed, informed consent on a form approved by the Institutional Review Board at the University of North Carolina Hospital. Patients were ad- mitted for 3 days to complete the study. This entailed in- fusion of pimonidazole on day 1, biopsy of the tumor on day 2, and discharge on day 3. Toxicities of the infusion and biopsy procedures were graded by Gynecological On- cology Group Adverse Effects Criteria (Gynecological Oncology Group, October, 1988). To date, five patients have been entered in the study. Patient distribution by FIG0 stage was IB (one patient), IIB (two patients), IIIB (one patient), and IVA (one patient).
Biopsy and tissue section preparation Twenty-four hours after pimonidazole hydrochloride
infusion, multiple punch biopsies of primary cervical tu- mors were performed. Fresh tissue was immediately placed in 10% neutral buffered formalin, and then pro- cessed into paraffin blocks. All quadrants of the tumor were biopsied, and regions of obvious necrosis were avoided. Prior to immunostaining, multiple 4 pm sections from each block were placed on capillary-action clear glass slides, with one slide per block stained on standard slides with hematoxylin and eosin for pathologic review to confirm the presence of tumor. Comparison of MIB-I, PCNA, and hypoxia marker immmunostaining was car- ried out on three contiguous slides taken from three to four biopsies from each tumor.
Immunohistochemistry Immunostaining for pimonidazole binding was accom-
plished by means of the capillary-action Microprobe
Staining System including Probe-on Plus slides’ and a mouse monoclonal antibody (MAb) produced for us3 and characterized as described previously (1). Isotyping showed the MAb to be IgG, with no detectable contami- nation with other immunoglobulins. Hybridoma superna- tants containing the antipimonidazole MAb were used without further purification. Tissue sections were heated at 40°C for 2 h, then deparaffinized by treatment with xy- lene, a graded series of alcohol and water mixtures and finally with water. Hydrogen peroxide (3%) was used with 40°C heat for 20 min to quench endogenous peroxidase in the tissue. Protease” (0.01%) was used with heat for 30 min to enhance entry of the MAb into cells. Phosphate- buffered saline (PBS, 10 n&I) plus BRIJ-35 (0.2%)” were used to wash slides between steps. Nonspecific binding to endogenous biotin or biotin-binding proteins, lectins, or other nonspecific binding substances was blocked prior to application of the primary MAb. 6 Antipimonidazole MAb was added (1: 100 dilution of hybridoma supematant) to the slides, which were then warmed for 2 h at 40°C. The secondary antibody was composed of rat-absorbed, horse antimouse antibody conjugated to peroxidase, and was incubated with the fixed tissue sections for 30 min at 40°C. A biotin-streptavidin-peroxidase indirect staining method7 was used to visualize the MAb-pimonidazole complex. The chromogen, 3-amino-9-ethyl-carbazole (AEC), imparted a red color to the cell cytoplasm and/or nucleus of pimonidazole labeled cells. Tissue sections were exposed to AEC at room temperature for 20 min, rinsed with water, counterstained with Mayer’s” hematox- ylin, and mounted with aqueous Crystal/Mount.9
Sections contiguous to those stained for pimonidazole binding were stained for MIB- 1 or PCNA. For MIB-1, the mouse antihuman anti-MIB- 1 antigen MAb (MIB- 1) lo was used. Staining for MIB-1 began with the heating of slides at 60°C for 15 min. Removal of paraffin was ac- complished in the manner described above for pimoni- dazole staining. Hydrogen peroxide (3%) was used for 5 min with heat (40°C) but protease treatment was not used on the tissue sections. Microwave heating was used in the presence of 10 mM citrate buffer, pH 6.0 for 10 min prior to the application of MIB-1 (1:lOO dilution). As with staining for pimonidazole, nonspecific binding was blocked prior to the application of MIB-1. Heat (40°C) was used in conjunction with MIB-1, and subsequently with secondary antibody which was composed of horse antimouse biotinylated IgG. The biotin-streptavidin-per- oxidase indirect staining method was used as described above for pimonidazole staining. Visualization of the an- tibody complex was achieved with 3,3’-diaminobenzidine
*Fisher Scientific Company, Pittsburgh, PA. 3Hybridoma Facility, North Carolina State University, Ra-
leigh, NC. 4Pronase, Biomeda, Foster City, CA. ‘Biomeda, Foster City, CA. 6Vector Blocking Kit, Vector Laboratories, Burlingame, CA.
‘Vectastainm ABC Elite Kit, Vector Laboratories, Burlin- game, CA.
‘Biomeda, Foster City, CA. 9Crystalb40unt, Biomeda, Foster City, CA. ‘“Immunotech, Inc., Westbrook, ME.

900 I. J. Radiation Oncology 0 Biology 0 Physics
(DAB) I1 chromogen, which gave a brown color after 10 min of exposure at room temperature. Completion of the counterstaining and mounting was accomplished as de- scribed for pimonidazole staining. Immunostaining for PCNA using a commercially available mouse monoclonal antibody12 was carried out in a way similar to that de- scribed previously for canine tumors (33,45).
Immunostained sections were viewed under low mag- nification (10 X 1 and 10 X 4) and high magnification (10 X 10 and 10 X 40) in a Zeiss Axioskop 50 microscope13 connected to a high-resolution color video camera. Images were displayed on a high-resolution RGB color monitor and could be captured and stored via a software program l4 on a workstation (486/33 microprocessor) personal com- puter running MS DOS 5.0. For quantitative analysis, im- ages were not stored but were analyzed directly for hyp- oxia and proliferation markers.
Quantitating proliferation and hypoxia marker binding Sets of four contiguous tissue sections were chosen
from regions within each tumor biopsy. In each set, one slide was stained with hematoxylin and eosin in order to confirm that the region was replete with tumor cells; one slide was immunstained for pimonidazole binding, one immunostained for MIB-1 antigens, and one immuno- stained for PCNA antigens. In this way a comparison was made among the markers that were in close proximity within the tumors. Four sets of contiguous slides were available from four biopsies for four out of the five tumors while three sets of contiguous slides were available from three biopsies from the fifth tumor. Quantitative analyses for pimonidazole binding, MIB- 1, and PCNA were carried out on images of highly magnified, microscopic fields (200 km x 200 pm) captured from immunostained tissue sections. For pimonidazole, typically, 100 images were analyzed from each tissue section. The images were dis- played on the video screen and a 10 X 12 grid superim- posed on each image. The number of “hits” lying at the intersections of the grid lines was recorded. Immuno- stained and unstained tumor cells comprised the “hits.” No other features were scored. For pimonidazole binding, the whole area of each immunostained tissue section was analyzed. Typically, for each tissue section a total of 3000-5000 tumor cells were scored as stained or un- stained for pimonidazole binding. For MIB- 1 and PCNA, where a more uniform distribution of immunostaining oc- curred, fewer fields (typically 30) were analyzed and a total of 1000 tumor cells per slide were scored as stained or unstained. The data for pimonidazole binding, MIB-1 and PCNA were expressed as the ratio of immunostained tumor cells to total number of tumor cells counted.
Volume 37, Number 4, 1997
RESULTS
Patients Five patients entered the study, and all five received the
full dose (0.5 g/m’) of pimonidazole hydrochloride with- out difficulty. One patient with a long history of chronic headaches and migraine attacks reported a mild unilateral (ipsilateral with infusion site) headache coinciding with the infusion of pimonidazole (GOG Grade 1) that lasted a few minutes and then resolved spontaneously. There were no other adverse effects to either the infusion of pi- monidazole or the biopsy procedure.
Staining patterns Pimonidazole. Immunostaining patterns for pimonida-
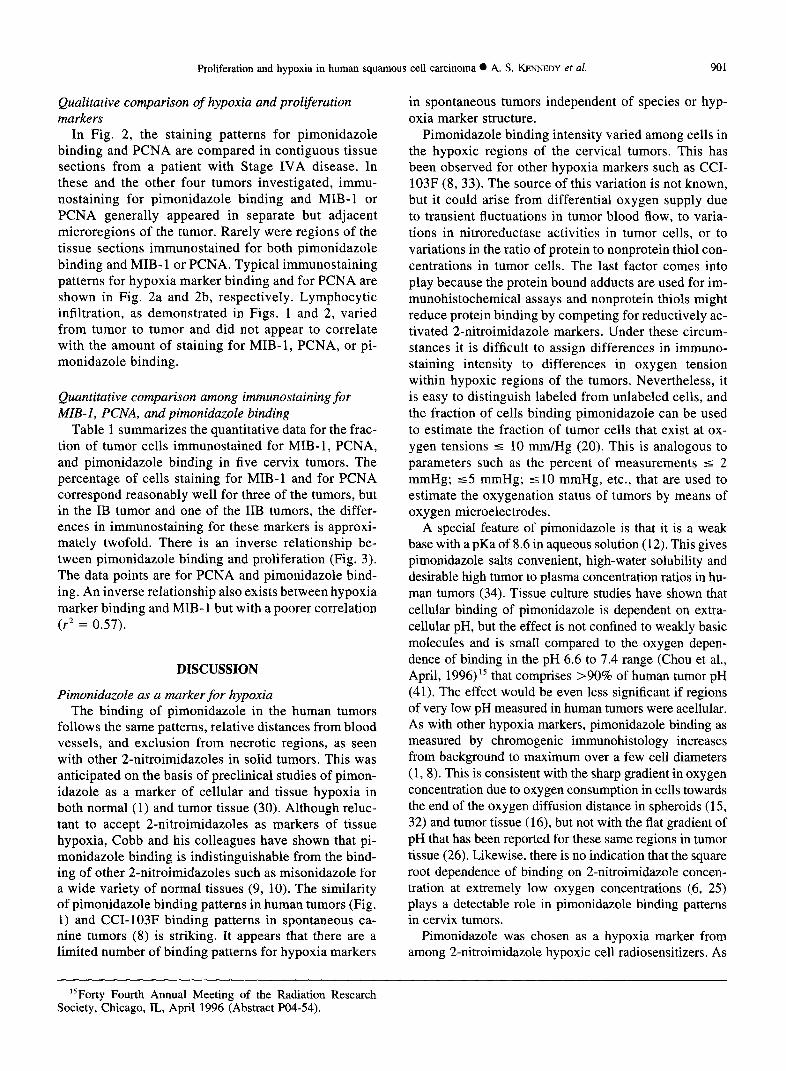
zole binding shown in Fig. 1 were indistinguishable from those observed previously for CCI-103F binding in spon- taneous canine tumors (8). Focal and zonal patterns oc- curred on nearly every slide. Occasionally, reticular bind- ing was observed. Reticular binding is defined as that which follows along tumor cores when viewed at low magnification. At high magnification, reticular binding could appear as zonal binding. Pimonidazole staining var- ied in intensity between slides, and within the same slide. The range of intensities, however, was quite similar throughout the entire collection of tissue sections exam- ined. In general, the most intense staining was in focal or zonal patterns, and the least intense staining was seen at the periphery of zonal-pattern staining. Pimonidazole binding was always at a distance from vascular structures and was consistent with diffusion limited oxygen supply; that is, with chronic hypoxia. Pimonidazole staining was usually observed close to regions of necrosis (Fig. 1B) but staining also occurred in the absence of frank necrosis (Fig. 1C). None of the necrotic foci immunostained for pimonidazole binding, but nonspecific immunostaining did occur in densely keratinized regions of tissue. Pimon- idazole binding was seen to increase from background lev- els to maximum binding over a few cell diameters (Figs. 1 and 2.
MB-1 and PCNA. Cells positively immunostained for the proliferation markers were dispersed throughout most regions of the cervix tumors, which is consistent with ob- servations by other investigators. Considerable variation in staining intensity was observed in the same slide, even in tumor foci in close proximity, and between biopsies. No significant staining of normal tissues was observed, with most staining confined to the aggregates of tumor cells. Cells immunostaining for proliferation markers were dispersed throughout the tumor bundles despite the pres- ence or absence of observable vessels or lymphatics. Ne- crotic regions did not stain positive, and very little staining was seen in the area surrounding necrosis.
“Vector Laboratories, Burlingame, CA. %one PClO; Dako Corporation, Carpenteria, CA.
“Carl Zeiss, Inc., Microscope Division, Thornwood, NY. “Zmage I, Universal Imaging Corporation, West Chester. PA
Proliferation and hypoxia in human squamous cell carcinoma l A. S. KENNEDY et al. 901
Qualitative comparison of hypoxia and prolferation markers
In Fig. 2, the staining patterns for pimonidazole binding and PCNA are compared in contiguous tissue sections from a patient with Stage IVA disease. In these and the other four tumors investigated, immu- nostaining for pimonidazole binding and MIB-1 or PCNA generally appeared in separate but adjacent microregions of the tumor. Rarely were regions of the tissue sections immunostained for both pimonidazole binding and MIB-1 or PCNA. Typical immunostaining patterns for hypoxia marker binding and for PCNA are shown in Fig. 2a and 2b, respectively. Lymphocytic infiltration, as demonstrated in Figs. 1 and 2, varied from tumor to tumor and did not appear to correlate with the amount of staining for MIB-1, PCNA, or pi- monidazole binding.
Quantitative comparison among immunostaining for MB-I, PCNA, and pimonidazole binding
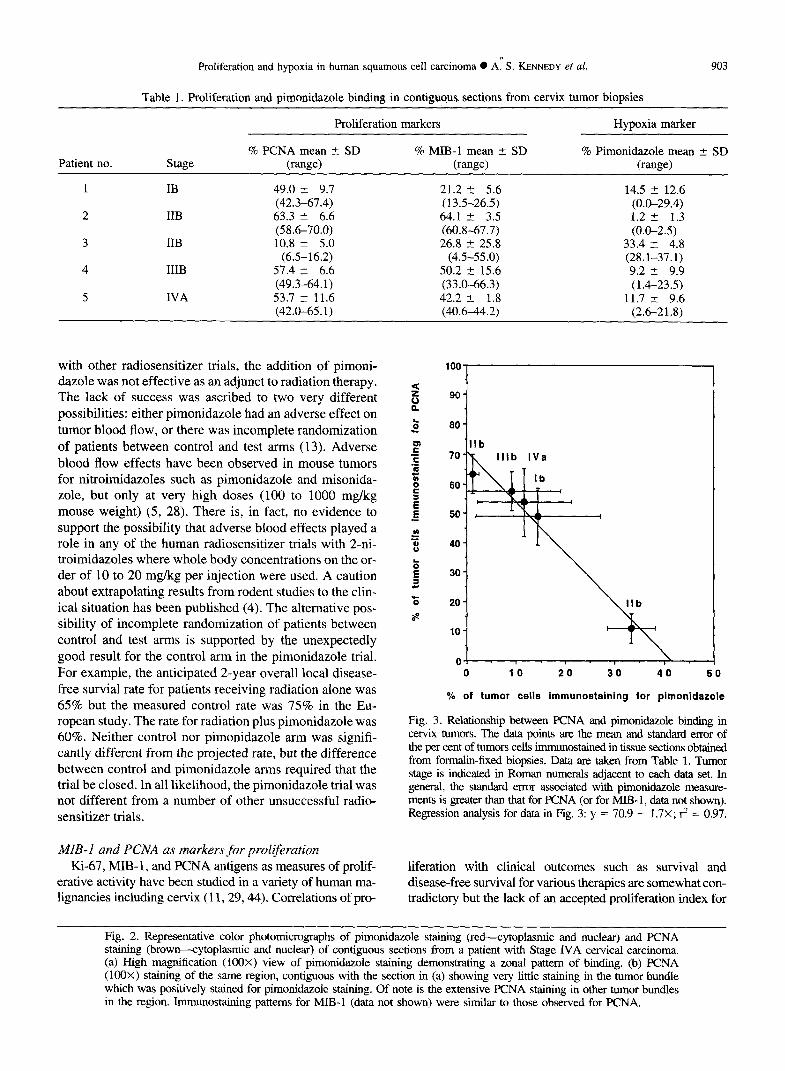
Table 1 summarizes the quantitative data for the frac- tion of tumor cells immunostained for MIB-1, PCNA, and pimonidazole binding in five cervix tumors. The percentage of cells staining for MIB-1 and for PCNA correspond reasonably well for three of the tumors, but in the IB tumor and one of the IIB tumors, the differ- ences in immunostaining for these markers is approxi- mately twofold. There is an inverse relationship be- tween pimonidazole binding and proliferation (Fig. 3). The data points are for PCNA and pimonidazole bind- ing. An inverse relationship also exists between hypoxia marker binding and MIB-1 but with a poorer correlation (r2 = 0.57).
DISCUSSION
Pimonidazole as a marker for hypoxia The binding of pimonidazole in the human tumors
follows the same patterns, relative distances from blood vessels, and exclusion from necrotic regions, as seen with other 2-nitroimidazoles in solid tumors. This was anticipated on the basis of preclinical studies of pimon- idazole as a marker of cellular and tissue hypoxia in both normal (1) and tumor tissue (30). Although reluc- tant to accept 2-nitroimidazoles as markers of tissue hypoxia, Cobb and his colleagues have shown that pi- monidazole binding is indistinguishable from the bind- ing of other 2-nitroimidazoles such as misonidazole for a wide variety of normal tissues (9, 10). The similarity of pimonidazole binding patterns in human tumors (Fig. 1) and CCI-103F binding patterns in spontaneous ca- nine tumors (8) is striking. It appears that there are a limited number of binding patterns for hypoxia markers
in spontaneous tumors independent of species or hyp- oxia marker structure.
Pimonidazole binding intensity varied among cells in the hypoxic regions of the cervical tumors. This has been observed for other hypoxia markers such as CCI- 103F (8, 33). The source of this variation is not known, but it could arise from differential oxygen supply due to transient fluctuations in tumor blood flow, to varia- tions in nitroreductase activities in tumor cells, or to variations in the ratio of protein to nonprotein thiol con- centrations in tumor cells. The last factor comes into play because the protein bound adducts are used for im- munohistochemical assays and nonprotein thiols might reduce protein binding by competing for reductively ac- tivated 2-nitroimidazole markers. Under these circum- stances it is difficult to assign differences in immuno- staining intensity to differences in oxygen tension within hypoxic regions of the tumors. Nevertheless, it is easy to distinguish labeled from unlabeled cells, and the fraction of cells binding pimonidazole can be used to estimate the fraction of tumor cells that exist at ox- ygen tensions I 10 mm/Hg (20). This is analogous to parameters such as the percent of measurements 5 2 mmHg; ~5 mmHg; ~10 mmHg, etc., that are used to estimate the oxygenation status of tumors by means of oxygen microelectrodes.
A special feature of pimonidazole is that it is a weak base with a pKa of 8.6 in aqueous solution (12). This gives pimonidazole salts convenient, high-water solubility and desirable high tumor to plasma concentration ratios in hu- man tumors (34). Tissue culture studies have shown that cellular binding of pimonidazole is dependent on extra- cellular pH, but the effect is not confined to weakly basic molecules and is small compared to the oxygen depen- dence of binding in the pH 6.6 to 7.4 range (Chou et al., April, 1996) l5 that comprises >90% of human tumor pH (41). The effect would be even less significant if regions of very low pH measured in human tumors were acellular. As with other hypoxia markers, pimonidazole binding as measured by chromogenic immunohistology increases from background to maximum over a few cell diameters (1,8). This is consistent with the sharp gradient in oxygen concentration due to oxygen consumption in cells towards the end of the oxygen diffusion distance in spheroids (15, 32) and tumor tissue (16), but not with the flat gradient of pH that has been reported for these same regions in tumor tissue (26). Likewise, there is no indication that the square root dependence of binding on 2-nitroimidazole concen- tration at extremely low oxygen concentrations (6, 25) plays a detectable role in pimonidazole binding patterns in cervix tumors.
Pimonidazole was chosen as a hypoxia marker from among 2-nitroimidazole hypoxic cell radiosensitizers. As
IsForty Fourth Annual Meeting of the Radiation Research Society, Chicago, IL, April 1996 (Abstract PO4-54).
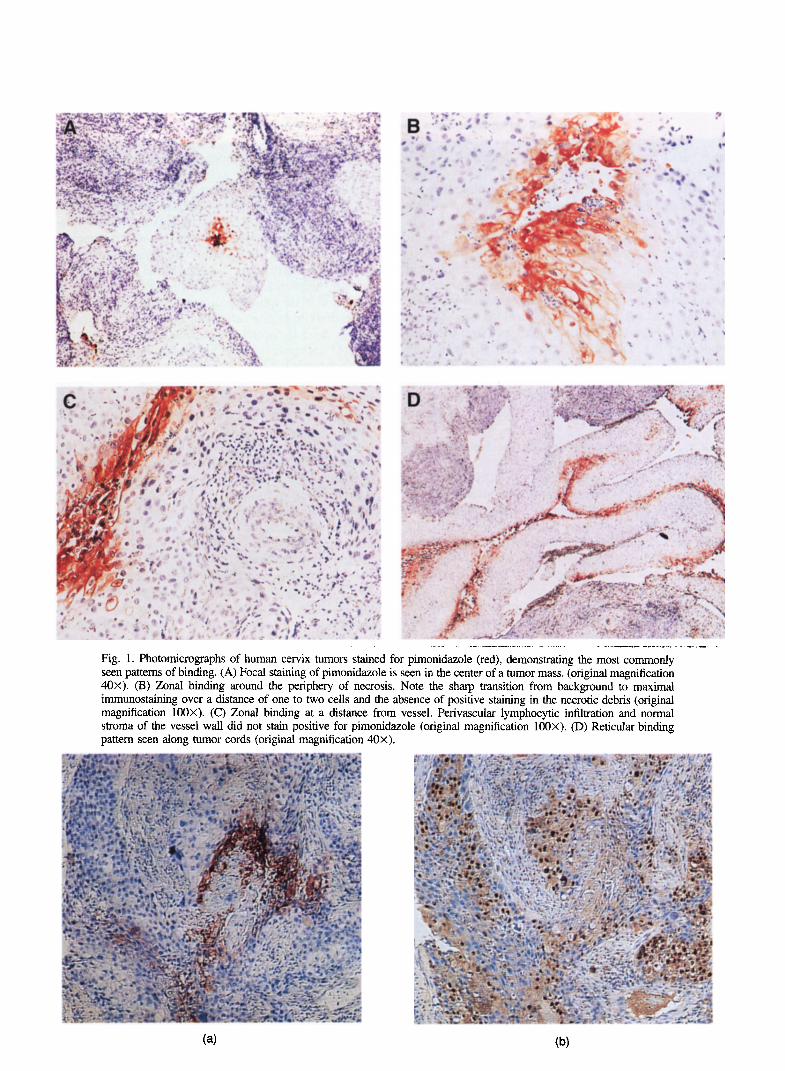
Fig. 1. Photomicrographs of human cervix tumors stained for pimonidazole (red), demonstrating the most commonly seen patterns of binding. (A) Focal staining of pimonidazole is seen in the center of a tumor mass. (original magnification 40x). (B) Zonal binding around the periphery of necrosis. Note the sharp transition from background to maximal immunostaining over a distance of one to two cells and the absence of positive staining in the necrotic debris (original magnification 100X). (C) Zonal binding at a distance from vessel. Perivascular lymphocytic infiltration and normal strorna of the vessel wall did not stain positive for pimonidazole (original magnification 100X). (D) Reticular binding pattern seen along tumor cords (original magnification 40x).
Proliferation and hypoxia in human squamous cell carcinoma 0 A:’ S. KENNEDY ef al. 903
Table 1. Proliferation and pimonidazole binding in contiguous sections from cervix tumor biopsies
Patient no. Stage
1 IB
2 IIB
3 IIB
4 IIIB
5 IVA
Proliferation markers
% PCNA mean t- SD % MIB-1 mean + SD (range) (rws)
49.0 5 9.7 21.2 2 5.6 (42.3-67.4) (13.5-26.5) 63.3 + 6.6 64.1 I 3.5 (X6-70.0) (60.8-67.7) 10.8 + 5.0 26.8 i 25.8
(6.5-16.2) (4.5-55.0) 57.4 2 6.6 50.2 + 15.6 (49.3-64.1) (33.0-66.3) 53.7 ? 11.6 42.2 -+ 1.8 (42.0-65.1) (40.6-44.2)
Hypoxia marker
% Pimonidazole mean ? SD (range)
14.5 +- 12.6 (0.0-29.4) 1.2 2 1.3 (0.0-2.5)
33.4 + 4.8 (28.1-37.1) 9.2 + 9.9 (1.4-23.5)
11.7 r 9.6 (2.6-21.8)
with other radiosensitizer trials, the addition of pimoni- dazoie was not effective as an adjunct to radiation therapy. The lack of success was ascribed to two very different possibilities: either pimonidazole had an adverse effect on tumor blood flow, or there was incomplete randomization of patients between control and test arms (13). Adverse blood flow effects have been observed in mouse tumors for nitroimidazoles such as pimonidazole and misonida- zole, but only at very high doses (100 to 1000 mg/kg mouse weight) (5, 28). There is, in fact, no evidence to support the possibility that adverse blood effects played a role in any of the human radiosensitizer trials with 2-ni- troimidazoles where whole body concentrations on the or- der of 10 to 20 mg/kg per injection were used. A caution about extrapolating results from rodent studies to the clin- ical situation has been published (4). The alternative pos- sibility of incomplete randomization of patients between control and test arms is supported by the unexpectedly good result for the control arm in the pimonidazole trial. For example, the anticipated 2-year overall local disease- free survial rate for patients receiving radiation alone was 65% but the measured control rate was 75% in the Eu- ropean study. The rate for radiation plus pimonidazole was 60%. Neither control nor pimonidazole arm was signifi- cantly different from the projected rate, but the difference between control and pimonidazole arms required that the trial be closed. In all likelihood, the pimonidazole trial was not different from a number of other unsuccessful radio- sensitizer trials.
h&B-f and PCNA as markers for proliferation Ki-67, MIB- 1, and PCNA antigens as measures of prolif-
erative activity have been studied in a variety of human ma- lignancies including cervix ( 11,29,44). Correlations of pro-
‘Ilb
01 0 10 20 30 40 50
% of tumor cells immunostaining for pimonidazole
Fig. 3. Relationship between PCNA and pimonidazole binding in cervix tumors. The data points are the mean and standard error of the per cent of tumors cells immunostained in tissue sections obtained from formalin-fixed biopsies. Data are taken from Table 1. Tumor stage is indicated in Roman numerals adjacent to each data set. In general, the standard error associated with pimonidazole measure- ments is greater than that for PCNA (or for MIB- 1, data not shown). Regression analysis for data in Fig. 3: y = 70.9 - 1.7X; rz = 0.97.
liferation with clinical outcomes such as survival and disease-free survival for various therapies are somewhat con- tradictory but the lack of an accepted proliferation index for
Fig. 2. Representative color photomicrographs of pimonidazole staining (red-cytoplasmic and nuclear) and PCNA staining (brown-cytoplasmic and nuclear) of contiguous sections from a patient with Stage IVA cervical carcinoma. (a) High magnification (100X) view of pimonidazole staining demonstrating a zonal pattern of binding. (b) PCNA (100X) staining of the same region, contiguous with the section in (a) showing very little staining in the tumor bundle which was positively stained for pimonidazole staining. Of note is the extensive PCNA staining in other tumor bundles in the region. Immunostaining patterns for MEL1 (data not shown) were similar to those observed for PCNA.

904 I. J. Radiation Oncology l Biology 0 Physics
categorizing tumors and unwarranted cross comparisons among tumor types and therapies, has, perhaps, contributed to this. Ki-67, PCNA, mitotic index, or Tpot results in the radiation studies described above are self-consistent if the intent of the radiation treatment is taken into account. If a distinction is made between short-term responsiveness for preoperative downstaging (42) and long-term responsiveness for disease-free survival (2,29, 37), then the significance of correlations between proliferation and outcome perhaps be- come clearer. It remains to be seen if endogenous indices of proliferation (MIH-1, PCNA, etc.) will give the same cor- relations with outcome as those based on the administration of exogenous probes of tumor proliferation (T,,, iododeoxy- midine labeling index, etc.).
Comparison of hypoxia and proliferation Quantitative comparison of immunostaining for hyp-
oxia and proliferation indicates an inverse relationship exists between proliferation (MIB-1 and PCNA) and hypoxia in the limited number of tumors studied to date
Volume 37, Number 4, 1997
(Table 1, Fig. 3). The correlation is particularly strong when PCNA is the marker of proliferation. However, the number of tumors investigated is small, and further investigation is required to confirm the inverse relation- ship. It does appear that a high percentage of prolifer- ating cells in a tumor is not necessarily associated with increased tumor hypoxia.
SUMMARY
Preliminary data establishes pimonidazole as a useful probe for human tumor hypoxia. Although different in chemical structure and properties, pimonidazole is indis- tinguishable from other markers in its binding to hypoxic cells in human tumors. Pimonidazole hydrochloride is convenient to administer and is well tolerated when given as single intravenous infusion of 0.5 g/m’. Comparison of immunostaining for pimonidazole binding and for PCNA or MIB-1 shows an inverse relationship between prolif- eration and hypoxia.
REFERENCES
1. Arteel, G. E.; Thurman, R. G.; Yates, J. M.; Raleigh, J. A. Evidence that hypoxia markers detect oxygen gradients in liver: Pimonidazole and retrograde perfusion of rat liver. Br. J. Cancer 72:889-895; 1995.
2. Begg, A. C. The clinical status of Tpot as a predictor? Or why no tempest in the Tpot! Int. J. Radiat. Oncol. Biol. Phys. 32:1539-1540; 1995.
3. Brock, W. A.; Baker, F. L.; Wike, J. L.; Sivon, S. L.; Peters, L. J. Cellular radiosensitivity of primary head and neck squa- mous cell carcinomas and local tumor control. Int. J. Radiat. Oncol. Biol. Phys. 18:1283-1286; 1990.
4. Chaplin, D. J. The effect of therapy on tumour vascular func- tion. Int. J. Radiat. Biol. 60:31 l-325; 1991.
5. Chaplin, D. J.; Horsman, M. R. Tumor blood flow changes induced by chemical modifiers of radiation response. Int. J. Radiat. Oncol. Biol. Phys. 22:459-462; 1992.
6. Chapman, J. D.; Baer, K.; Lee, J. Characteristics of the me- tabolism-induced binding of misonidazole to hypoxic mam- malian cells. Cancer Res. 43:1523-1528; 1983.
7. Cline, J. M.; Thrall, D. E.; Page, R. L.; Franko, A. J.; Ra- leigh, J. A. Immunohistochemical detection of a hypoxia marker in spontaneous canine turnours. Br. J. Cancer 62:925-931; 1990.
8. Cline, J. M.; Thrall, D. E.; Rosner, G. L.; Raleigh, J. A. Distribution of the hypoxia marker Ccl-103F in canine tumors. Int. J. Radiat. Oncol. Biol. Phys. 28:921-933; 1994.
9. Cobb, L. M.; Nolan, J.; Butler, S. A. Distribution of pimon- idazole and RSU 1069 in tumour and normal tissues. Br. J. Cancer 62:915-915; 1990.
10. Cobb, L. M.; Nolan, J.; Hacker, T. Retention of misonidazole in normal and malignant tissues: Interplay of hypoxia and reductases. Int. J. Radiat. Oncol. Biol. Phys. 22:655-659; 1992.
11. Cole, D. J.; Brown, D. C.; Crossley, E.; Alcock, C. J.; Gatter, K. C. Carcinoma of the cervix uteri: An assessment of the relationship of tumour proliferation to prognosis. Br. J. Can- cer 65:783-785; 1992.
12. Dermis, M. F.; Stratford, M. R.; Wardman, P.; Watts, M. E. Cellular uptake of misonidazole and analogues with
acidic or basic functions. Int. J. Radiat. Biol. 47:629-643; 1985.
13. Dische, S.; Machin, D.; Chassange, D. A trial of Ro 03-8799 (pimonidazole) in carcinoma of the uterine cervix: An in- terim report from the Medical Research Council Working Party on advanced carcinoma of the cervix. Radiother. On- col. 26:93-103; 1993.
14. Evans, S. M.; Joiner, B.; Jenkins, W. T.; Laughlin, K. M.; Lord, E. M.; Koch, C. J. Identification of hypoxia in cells and tissues of epigastric 9L rat glioma using EF5 [2-(2-nitro- lH-imidazol-l-yl)-N-(2,2,3,3,3-pentafluoropropyl) aceta- mide]. Br. J. Cancer 72:875-882; 1995.
15. Franko, A. J. Hypoxic fraction and binding of misonidazole in EMT6/Ed multicellular tumor spheroids. Radiat. Res. 103:89-97; 1985.
16. Franko, A. J.; Koch, C. J.; Garrecht, B. M.; Sharplin, J.; Hughes, D. Oxygen dependence of binding of misonidazole to rodent and human tumors in vitro. Cancer Res. 47:5367- 5376; 1987.
17. Gatenby, R.; Kessler, H.; Rosenblum, J.; Cola, L.; Moldov- sky, P.; Hartz, W.; Broder, G. Oxygen distribution in squa- mous cell carcinoma metastases and its relationship to out- come of radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 14:831-838; 1988.
18. Giaccia, A. J. Hypoxic stress proteins: Survival of the fittest. Semin. Radiat. Oncol. 6:46-58; 1996.
19. Graeber, T. G.; Peterson, J. F.; Tsai, M.; Monica, K.; For- nace, A. J. J.; Giaccia, A. J. Hypoxia induces accumulation of p53 protein, but activation of a Gl-phase checkpoint by low-oxygen conditions is independent of p53 status. Mol. Cell. Biol. 14:6264-6277; 1994.
20. Gross, M. W.; Karbach, U.; Groebe, K.; Franko, A. J.; Mueller-Klieser, W. Calibration of misonidazole labeling by simultaneous measurement of oxygen tension and labeling density in multicellular spheroids. Int. J. Cancer 61:567-573; 1995.
21. Hepburn, P. J.; Glynne-Jones, E.; Goddard, L.; Gee, J. M.; Harper, M. E. Cell proliferation in prostatic carcinoma: Comparative analysis of Ki-67, MIB-1 and PCNA. Histo- them. J. 27:196-203; 1995.
Proliferation and hypoxia in human squamous cell carcinoma l A. S. KENIUXDY et af. 905
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
Hockel, M.; Schlenger, K.; Mitze, M.; Schaffer, U.; Vaupel, of Ro 03-8799-Pharmacokinetics, toxicology, tissue and P. Hypoxia and radiation response in human tumors. Semin. tumor concentrations. Int. J. Radiat. Oncol. Biol. Phys. Radiat. Oncol. 6:3-9; 1996. 10:1759-1763; 1984. Hodgkiss, R. J.; Wardman, P. The measurement of hypoxia in tumours. Br. J. Radiol. Suppl. 24:105-l 10; 1992. Key, G.; Becker, M. H.; Duchrow, M.; Schliiter, C.; Flad, H. D.; Gerdes, J. New Ki-67 equivalent murine monoclonal antibodies (MIBl-3) generated against bacterially expressed parts of the Ki-67 cDNA containing three 62 base pair re- petitive elements encoding for the Ki-67 epitope. Lab. In- vest. 68:629-636; 1993. Koch, C. J.; Stobbe, C. C.; Baer, K. A. Metabolism induced binding of “C-misonidazole to hypoxic cells: Kinetic de- pendence on oxygen concentration and misonidazole con- centration. Int. J. Radiat. Oncol. Biol. Phys. 10:1327-1331; 1984.
35.
36.
37.
38. Martin, G. R.; Jain, R. K. Noninvasive measurement of in- terstitial pH profiles in normal and neoplastic tissue using fluorescence ratio imaging microscopy. Cancer Res. 545670-5674; 1994. Miller, G.; Best, M.; Franko, A.; Koch, C.; Raleigh, J. Quantitation of hypoxia in multicellular spheroids by video image analysis. Int. J. Radiat. Oncol. Biol. Phys. 16:949-952; 1989. Murray, J. C.; Randhawa, V.; Denekamp, J. The effects of melphalan and misonidazole on the vasculature of a murine sarcoma. Br. J. Cancer 55:233-238; 1987. Nakano, T.; Oka, K. Differential values of Ki-67 index and mitotic index of proliferation cell population. Cancer 72:2401-2408; 1993. Raleigh, J. A.; Dewhirst, M. W.; Thrall, D. E. Measuring tumor hypoxia. Semin. Radiat. Oncol. 6:37-45; 1996. Raleigh, J. A.; La Dine, J. K.; Cline, J. M.; Thrall, D. E. An enzyme-linked immunosorbent assay for hypoxia marker binding in tumours. Br. J. Cancer 69:6671; 1994. Raleigh, .I. A.; Miller, G. G.; Franko, A. J.; Koch, C. J.; Fuciarelli, A. F.; Kelly, D. A. Fluorescence immunohisto- chemical detection of hypoxic cells in spheroids and tu- mours. Br. J. Cancer 56:395-400; 1987. Raleigh, J. A.; Zeman, E. M.; Calkins, D. P.; McEntee, M. C.; Thrall, D. E. Distribution of hypoxia and proliferation associated markers in spontaneous canine tumors. Acta On- col. 34:345-349; 1995. Saunders, M. I.; Anderson, P. J.; Bennett, M. H.; Dische, S.; Minchinton, A. I.; Stratford, M. R. L. The clinical testing
39.
40.
41.
42.
43.
44.
45.
Sutherland, R. M.; Ausserer, W. A.; Murphy, B. J.; Laderoute, K. R. Tumor hypoxia and heterogeneity: Challenges and op- portunities for the future. Semin. Radiat. Oncol. 6:59-70; 1996. Taghian, A.; Ramsay, J.; Allalunis-Turner, J.; Budach, W.; Gioioso, D.; Pardo, F.; Okunieff, P.; Bleehen, N.; Urtasun, R.; Suit, H. Intrinsic radiation sensitivity may not be the major de- terminant of the poor clinical outcome of glioblastoma multi- forme. Int. J. Radiat. Oncol. Biol. Phys. 25:243-249; 1993. Theon, A. P.; Madewell, B. R.; Shearn, V. J.; Moulton, J. E. Prognostic factors associated with radiotherapy of squa- mous cell carcinoma of the nasal plane in cats. J. Am. Vet. Med. Assoc. 206:991-996; 1995. Thrall, D. E.; McEntee, M. C.; Cline, J. M.; Raleigh, J. A. ELISA quantification of CCI- 103F binding in canine tumors prior to and during irradiation. hit. J. Radiat. Oncol. Biol. Phys. 28:649-659; 1994. West, C. M.; Davidson, S. E.; Burt, P. A.; Hunter, R. D. The intrinsic radiosensitivity of cervical carcinoma: Correlations with clinical data. Int. J. Radiat. Oncol. Biol. Phys. 31:841- 846; 1995. West, C. M.; Davidson, S. E.; Roberts, S. A.; Hunter, R. D. Intrinsic radiosensitivity and prediction of patient re- sponse to radiotherapy for carcinoma of the cervix. Br. J. Cancer 68:819-823; 1993. Wike-Hooley, J. L.; Haveman, J.; Reinhold, H. S. The rel- evance of tumour pH to the treatment of malignant disease. Radiother. Oncol. 2:343-366; 1984. Willett, C. G.; Warland, G.; Hagan, M. P.; Daly, W. J.; Coen, J.; Shellito, P. C.; Compton, C. C. Tumor proliferation in rectal cancer following preoperative irradiation. J. Clin. On- col. 13:1417-1424; 1995. Wilson, R. E.; Sutherland, R. M. Enhanced synthesis of spe- cific proteins, RNA, and DNA caused by hypoxia and reox- ygenation. Int. J. Radiat. Oncol. Biol. Phys. 16:957-961; 1989. Yu, C.; Filipe, M. I. Update on proliferation-associated an- tibodies applicable to formalin-fixed paraffin-embedded tis- sue and their clinical applications. Histochem. J. 25:843- 853; 1993. Zeman, E. M.; Calkins, D. P.; Cline, J. M.; Thrall, D. E.; Raleigh, J. A. The relationship between proliferative and ox- ygenation status in spontaneous canine tumors. Int. J. Radiat. Oncol. Biol. Phys. 27:891-898; 1993.





























