Embed Size (px)
Citation preview

Exp Brain Res (2007) 182:249–260
DOI 10.1007/s00221-007-1037-6RESEARCH NOTE
Proprioceptive deWcits of the lower limb following anterior cruciate ligament deWciency aVect whole body steering control
Rebecca J. Reed-Jones · Lori Ann Vallis
Received: 14 May 2007 / Accepted: 15 June 2007 / Published online: 18 August 2007© Springer-Verlag 2007
Abstract The role of lower limb proprioception in thesteering control of locomotion is still unclear. The purposeof the current study was to determine whether steering con-trol is altered in individuals with reduced lower limb pro-prioception. Anterior cruciate ligament deWciency (ACLD)results in a decrease in proprioceptive information from theinjured knee joint (Barrack et al. 1989). Therefore thewhole body kinematics were recorded for eight unilateralACLD individuals and eight CONTROL individuals duringthe descent of a 20° incline ramp followed by either a redi-rection using a side or cross cutting maneuver or a continu-ation straight ahead. Onset of head and trunk yaw,mediolateral displacement of a weighted center of mass(COMHT) and mediolateral displacement of the swing footwere analyzed to evaluate diVerences in the steering con-trol. Timing analyses revealed that ACLD individualsdelayed the reorientation of body segments compared toCONTROL individuals. In addition, ACLD did not use atypical steering synergy where the head leads whole bodyreorientation; rather ACLD individuals reoriented the head,trunk and COMHT in the new direction at the same time.These results suggest that when lower limb proprioceptiveinformation is reduced, the central nervous system (CNS)may delay whole body reorientation to the new travel direc-tion, perhaps in order to integrate existing sensory informa-tion (vision, vestibular and proprioception) with thereduced information from the injured knee joint. Thiscontrol strategy is maintained when visual information is
present or reduced in a low light environment. Addition-ally, the CNS may move the head and trunk segments as,eVectively, one segment to decrease the number of degreesof freedom that must be controlled and increase whole bodystability during the turning task.
Keywords Steering control · Locomotion · Segment reorientation · Spatial reference frame · Anticipatory control · Coordination · Reduced ambient lighting · Head and trunk control · Anterior Cruciate Ligament
Introduction
Multimodal sensory information must be integrated inorder to produce an internal spatial reference frame for theexecution of appropriate anticipatory locomotor adjust-ments (for reviews see: Berthoz and Viaud-Delmon 1999;Mergner and Rosemeier 1998; Patla 1997). Vision has beenshown to contribute a majority of the advance informationrequired for online modiWcations of locomotor patterns(Hollands et al. 2002; Patla 1997). For example, vision canprovide information of inanimate features, such as objectsin the path or potential surface irregularities. Advancedknowledge of these features can then be used to plan amethod of avoidance, for example, altering the coordina-tion of segments by adjusting foot placement or using trunkroll to navigate around an obstacle (Patla 1997; Patla et al.1999).
Experimental paradigms involving a change in traveldirection have provided interesting insight into adaptivelocomotor control strategies. A distinctive sequence ofbody segment reorientation in a new travel direction isobserved when performing quick changes in travel direction.
R. J. Reed-Jones · L. A. Vallis (&)Department of Human Health and Nutritional Sciences, College of Biological Science, University of Guelph, Animal Science/Nutrition Building, Guelph, ON, Canada N1G 2W1e-mail: [email protected]
123

250 Exp Brain Res (2007) 182:249–260
The sequence of segmental reorientation has been referredto as a ‘steering synergy’ in the literature. In this synergy,the head leads the reorientation in the new travel directionfollowed by the trunk, center of mass (COM) and feet(Grasso et al. 1996, 1998a, b; Patla et al. 1999). The pur-pose of the head leading the body reorientation is that thehead itself contains the visual and vestibular sensoryorgans. Therefore, a head-leading reorientation allows foradvanced integration of visual information of the newtravel direction prior to whole body commitment and pro-vides a stable reference for segment coordination (Hollandset al. 2001; Vallis and Patla 2004). The steering synergyhas been examined during the absence of visual informa-tion, and a similar orienting behavior is observed betweenvisual and impeded visual conditions, though diVerences intiming and magnitudes of movement are present (Grassoet al. 1998a). Typically, impeding vision involves using aneyes-closed or a blindfold-like protocol (Grasso et al. 1996,1998a, b). However, another method of manipulating visualinformation is by reducing ambient room lighting.
The same order of body segmental reorientation has alsobeen observed in diVerent locomotor contexts. Vallis andPatla (2004) reported the presence of the steering strategyfollowing unexpected externally applied head yaw move-ments and, though modiWed to ensure whole body safety,the synergy was even present during voluntary head yawmovements. While collectively these results suggest thatthe steering synergy is a fundamental component of thehuman locomotor repertoire (Vallis and Patla 2004), it isclear that the synergy can be modiWed to the context of thewalking task. It is not immutable and is hierarchically con-trolled by the central nervous system (CNS) under volun-tary or proactive situations, such as when making avoluntary head turn (Vallis and Patla 2004). Similarly, itcan be adapted to both external (environmental) and inter-nal (body conWguration) constraints (Grasso et al. 1998a;Hollands et al. 2001). Interestingly, this steering synergyhas not been observed in situations involving transientdeviations of the travel trajectory, such as when circum-venting an obstacle (Vallis and McFadyen 2003). Duringthis circumvention task, initially the trunk and head arecoupled; there is a simultaneous onset of trunk and headmovement prior to clearance of the obstacle. Observationsof greater maximum trunk yaw movement post-obstacleclearance indicated that these segments were later decou-pled. It was proposed that this initial coupling might serveas a strategy to ensure a stable platform for redirectingwhole body movement. First, visual information could becollected about body position with respect to the transienttravel path, distance to obstacle and travel path end point.Additionally, as a large percentage of body mass is locatedin the trunk segment, moving the two segments togethercould also ensure a stable platform for the head and reduce
the number of degrees of freedom that must be initiallycontrolled by the CNS. Finally, initiating movement of thehead and trunk together may facilitate a more controlled,transient change in travel path and reduce the risk of veer-ing behavior that has been observed during previous steer-ing tasks (e.g. Patla et al. 1999). By reducing the body’snumber of degrees of freedom requiring control, the overallbody coordination required to perform the task is simpliWed(Hicheur and Berthoz 2005).
In addition to vision and vestibular information, proprio-ception also plays an important role during adaptive loco-motor tasks. For example, the loss or disruption of localknee joint proprioception in the lower limb results in modi-Wcations to interjoint coordination and COM control duringlocomotion in both animals and humans (Abelew et al.2000; Ivanenko et al. 2000; Sorenson et al. 2002). Whilethe contributions of the visual and vestibular systems to thesteering control of locomotion have been detailed in the lit-erature (Karnath et al. 1994; Kennedy et al. 2003, 2005;Bent et al. 2000; Deshpande and Patla 2005), contributionsfrom proprioception, speciWcally of the lower limb, havebeen limited and inconclusive. Courtine et al. (2007) sys-tematically examined contributions of whole body musclespindle aVerents on the locomotor trajectory of a straight,level-walking task. This particular paradigm has been con-sistently used to demonstrate sensory contributions to loco-motor steering control (Karnath et al. 1994; Kennedy et al.2003, 2005; Bent et al. 2000; Deshpande and Patla 2005).These authors observed that neck and trunk muscle vibra-tion resulted in signiWcant deviations in locomotor trajec-tory, while lower limb muscle vibration did not aVectsteering control. These results suggest that proprioceptionfrom the lower limb does not make signiWcant contributionsto the steering control of locomotion. However, as theauthors state themselves; this may not be the case when thelocomotor task requires speciWc control of lower limb tra-jectory (Courtine et al. 2007). For example, podokineticparadigms have demonstrated that lower limb sensoryinformation is integrated for whole body spatial orientation.These paradigms involve stepping in place on a platformthat rotates about the vertical axis and therefore presents atask that requires very speciWc control of lower limb move-ments. In order to maintain a straight-ahead orientation, arecalibration of foot position with respect to upper bodyorientation must continuously occur. As a result, an aftereVect of trunk rotation is observed when participants returnto a stable surface and step in place blindfolded (Weberet al. 1998). Although podokinetic paradigms have success-fully demonstrated that lower limb sensory information isused in whole body spatial orientation during a locomotortask, they do not provide evidence for the role of lowerlimb proprioception in the anticipatory control of discreteredirection tasks.
123

Exp Brain Res (2007) 182:249–260 251
Cutting tasks require complex control of the lower limbsegment to initiate an abrupt redirection of the COM trajec-tory in the new travel direction (Besier et al. 2001; Houck2003; Lloyd et al. 2005). These maneuvers cause large rota-tional and valgus/varus moments to occur in the knee jointand thus lower limb trajectory must be tightly controlled(Besier et al. 2001; Lloyd et al. 2005). As a result, sensoryinformation from the lower limb during these movementsmay be critical for task execution.
Rupture of the anterior cruciate ligament (ACL) of theknee is well established to cause proprioceptive deWcits inthe knee joint. Barrack et al. (1989), published one of themost cited studies on the eVects of ACL deWciency (ACLD)on knee proprioception. By measuring the threshold todetection of a slow passive knee joint movement, theseauthors demonstrated that ACL-deWcient individuals have asigniWcantly greater threshold for detecting a knee jointposition change on their injured limb in comparison to theiruninjured limb. These results provide direct evidence ofreduced knee proprioception as a result of ACLD. A num-ber of studies have replicated the methods of this work andproduced similar results; of particular note is the contribu-tion by Corrigan et al. (1992). Moreover, neurophysiologi-cal studies have demonstrated reduced cortical activationvia direct somatosensory evoked potentials of the ACL lig-ament and common peroneal nerve in individuals who havesuVered an ACLD (Pitman et al. 1992; Valeriani et al.1996). In fact, Valeriani et al. (1996) observed that corticalactivity evoked from the stimulation of the common pero-neal nerve in ACL-deWcient individuals was signiWcantlyreduced in magnitude suggesting that the knee joint, andparticularly ACL aVerents, contribute to a majority of thesensory aVerents located within that speciWc nerve.Recently, Kapreli and Athanasopoulos (2006) published anoverview of scientiWc literature investigating propriocep-tive deWcits that result following ACLD. Based on thisreview, the authors proposed that ACLD is not simply amusculoskeletal injury, but may in fact result in a neuro-physiological disorder following the de-aVerentation thatoccurs following injury to the ACL.
The purpose of the current study was to determine if thesequence of upper body segmental reorientation observed inhealthy individuals during changes in travel direction werealso produced by individuals with reduced lower limb pro-prioceptive information. Prior evidence indicates that theCNS uses multimodal sensory information in the creation ofa body reference frame used to coordinate segments duringsteering tasks. Thus, it was hypothesized that the loss of theACL, which contributes considerably to proprioceptiveinformation about knee joint position, would result in thesame segmental control sequence, but would cause a delayin the timing of segmental reorientation during a steeringtask. This may be due to a more cautious control strategy
used by ACL-deWcient individuals, who may delay commit-ting movement of their COM in the new direction of traveluntil the CNS has enough time to integrate available sen-sory information and create a safe and stable movement ref-erence frame relevant to the task at hand. Given thatprevious studies have stressed the importance of visualinformation during steering tasks, a secondary purpose ofthe current study was designed to investigate if reducedvisual information about self-motion, via reduced ambientlighting, aVected the order or timing of segmental reorienta-tion for a healthy and ACL-deWcient population. It washypothesized that if visual cues were indeed critical in steer-ing tasks, we would observe a signiWcantly earlier onset ofhead reorientation under reduced lighting compared to nor-mal lighting conditions, in order to acquire as much visualinformation in advance of the new travel direction as possi-ble. In an ACL-deWcient population, with reduced visualinput and altered lower limb proprioceptive information, weexpected that head reorientation to occur even earlier than inthe healthy individuals during reduced lighting conditions.The results presented in the current work represent datafrom a larger study. Preliminary results of lower limb elec-tromyography and kinematic analyses were previously pub-lished in abstract form (Reed and Vallis 2005).
Methodology
Participants
Eight persons with a unilateral ACLD (four males, fourfemales, age 31.2 § 8.9 years, height 170 § 8.0 cm, weight78 § 20.9 kg) and eight healthy matched control individu-als (CONTROL; four males, four females, age 29.5 § 8.9years, height 171 § 10.0 cm, weight 75.5 § 14.8 kg) vol-unteered to participate in the study. Ethics approval wasobtained from the University of Guelph Research EthicsBoard prior to the start of subject recruitment and clinical/experimental testing.
Inclusion criterion for the ACLD group was an arthro-scopic or magnetic resonance imaging diagnosis of unilat-eral ACL rupture. All ACLD participants had receivedrehabilitation following diagnosis that ranged from 5 to 168months post injury. Prior to experimental testing ACLDparticipants underwent assessment with a certiWed physio-therapist using excerpts from the 2000 International KneeDocumentation Committee (IKDC) forms. SpeciWcally,this included the Subjective Knee Evaluation Form consist-ing of self-reports of knee function and the ExaminationForm involving range of motion and joint laxity assess-ments as well as a Functional One-Leg Hop Test (Noyeset al. 1991). ACLD participants were excluded from thestudy if the IKDC evaluation indicated excessive mechanical
123

252 Exp Brain Res (2007) 182:249–260
deWcits and/or knee joint instability, knee joint eVusion,pain, decreased range of motion, as well as multiple liga-ment and/or extensive meniscal damage.
All study participants (ACLD and CONTROL) wereexcluded from the study if a history of neurological disor-ders, signiWcant medical conditions (e.g. diabetes), or mus-culoskeletal injuries or diseases were self-reported in awritten questionnaire. In addition, all ACLD were requiredto perform a hop test and were excluded if hop performanceon the injured limb was less than 90% of their uninjuredlimb performance. The hop test is a standard measure ofknee function in ACLD; an uninjured to injured hop sym-metry of 90% indicates a stable knee joint (Noyes et al.1991; Rudolph et al. 2000). Although self reporting of neu-rological or medical deWcits was not ideal, further strengthtests of maximal peak extensor and Xexor muscle contrac-tions (velocity = 60°/s) using the System 3 Isokinetic Dyna-mometer (Biodex Medical Systems, New York) for allparticipants (CONTROL and ACLD) would have revealeddiVerences if severe underlying neurological or musculo-skeletal injuries were present. Torque values were normal-ized to percentage of body weight to facilitate inter-subjectcomparisons. ACLD group mean extensor muscle: injured55.7 § 17.1%, uninjured 67.8 § 17.1%; mean Xexor mus-cle torque: injured 35.9 § 11.7%, uninjured 36.1 § 11.8%.The CONTROL group mean extensor muscle torque:matched limb 67.5 § 7.1%, other limb 70.3 § 13.8%;mean Xexor muscle torque: matched limb 40.9 § 5.7%,other limb 46 § 14.1%. Results of these tests revealed thatalthough the mean injured limb extensor torque was lowerin the ACLD group, this diVerence was not statistically sig-niWcant (P = 0.308). Further, no signiWcant diVerence wasobserved between ACLD and CONTROL for magnitude ofpeak Xexion torque (P = 0.990), or between the uninjuredand injured limbs (P = 0.518 and P = 0.709, respectively).
Experimental protocol
Three-dimensional kinematic data were recorded at 60 Hzusing the Optotrak Motion Analysis system (Model 3020;NDI, Waterloo, Canada). An optoelectric active markerconWguration was used with three infrared-emitting diodemarkers mounted non-collinearly on a triangular rigid sur-face. These rigid bodies were aYxed to the head, trunk, pel-vis, thighs, tibias and feet. In addition, anatomical points(e.g. heels) were digitized creating an anatomical standingcalibration prior to commencing experimental trials.
Descent of a ramp creates peak anterior shear forces atthe knee joint of up to two times greater than those of levelwalking during early stance (Kuster et al. 1994). This loco-motor task presents a signiWcant challenge to the CNS assensory information, speciWcally proprioceptive informa-tion from the knee joint, is required to control and coordi-
nate knee joint loading while maintaining knee jointstability (Kuster et al. 1994, 1995a, b; Redfern and Dip-asquale 1997). Given the nature of our research questions,a locomotor task that required descent of an inclined sur-face and then performance of a cutting maneuver was cho-sen to further enhance potential diVerences between ahealthy and ACL deWcient population. As such, all partici-pants were asked to descend a 20° ramp, 3.7 m in lengthwith a start height of 90 cm. At the end of the ramp theywere required to ‘plant’ their injured (ACL) or matched(CONTROL) leg on level ground and either continuestraight ahead (control trials) or deviate their travel trajec-tory by 40° using either a cross step (plant with injuredlimb and uninjured limb was swung across and in front) orside step (plant with injured limb and step to side). Thirtyrandomly presented trials (ten per direction) were collectedin the LIGHT and in the LOW LIGHT ambient lightingconditions (total of 60 trials). Presentation of ambient light-ing conditions was counterbalanced among participants.The LIGHT condition involved a fully lit room (lux 200;simulating normal oYce lighting) achieved with overheadlighting in the laboratory. The LOW LIGHT condition wasachieved using rope lighting attached to the undersurfaceof the ramp platform which illuminated the ramp itself, butseverely limited the amount of visual information availableabout the remainder of the environment. This produced areduced lighting environment similar to that experienced ina darkened cinema theater (measured lighting levels were10 lux). Previously published studies have also used thismethod to create a reduced ambient lighting condition (e.g.Reed et al. 2006). Participants were given a 10-min breakbetween lighting conditions to allow for visual adaptation.Directional cues were given prior to the start of each trialso that participants could plan their descent. Participantswere given two to three practice descents prior to the startof data collection.
Data analysis
For analysis of kinematic variables, three-dimensional rawkinematic data were low-pass Wltered (6 Hz: dual pass sec-ond order Butterworth) and windowed for each heel con-tact. Heel contacts were identiWed using 0 crossings ofvirtual heel marker velocity proWles for each foot (Hollandset al. 2001) for the three steps prior to the plant step (P ¡ 3,P ¡ 2, P ¡ 1), the plant step (P) and one step followingplant (P + 1). The gait parameter step width and gait speedwere determined for these Wve steps for each of the controland cutting direction trials. Displacement of the heels wasused to determine step widths (lateral distance between heelcontacts) during each locomotor task. Gait speed was calcu-lated as the mean velocity of the left iliac crest virtualmarker over the windowed P ¡ 3 to P ¡ 1 period. This
123

Exp Brain Res (2007) 182:249–260 253
period corresponded to the stride preceding the landing stepwhen onset of steering behaviour was observed.
Virtual anatomical reference points (e.g. ears, glenohu-meral joint, iliac crest) were used to estimate the COMlocation of the head and trunk segment. A weighted headand trunk segment anthropometric model was then used toestimate the center of mass of the head and trunk unit(COMHT) displacement during walking trials. Anthropo-metric data tables used to estimate COM of these segmentswere from Winter (2005). A weighted COMHT model hasbeen used in previously published research in this area toanalyse body displacement in the anterior–posterior andmedial–lateral (M–L) directions (Vallis and McFadyen2003; Lowrey et al. 2007).
The magnitude of head and trunk yaw (rotation) andtrunk roll was examined using the range values determinedfrom calculation of maximum and minimum peak anglesduring the windowed three steps (P ¡ 3 to P + 1). The tim-ing of segment reorientation was calculated for the head,trunk, COMHT and uninjured (swing) foot. Trunk roll pro-Wles did not deviate from the ensemble-averaged trajecto-ries of the straight trials in the same manner as head andtrunk yaw angle proWles. During all directional trials, trunkroll deviations did not exceed §6° and were always similarto the proWles observed during control trials. Therefore, ananalysis of trunk roll deviations from control during thecutting maneuvers could not be performed.
Displacement proWles of head and trunk yaw (rotationabout the longitudinal axis), M–L displacement proWles ofCOMHT and the M–L displacement proWles of the virtualtoe marker of the uninjured (swing) foot were ensembleaveraged for the ten control (straight ahead) trials. Onset ofreorientation was then calculated for each directional trialand measured as the point in time when the instantaneousposition data deviated from the mean trajectory for the con-trol trials, providing the deviation continued beyond onestandard deviation. This onset was reported with respect toplant during cutting step performance (Hollands et al. 2001;Vallis and McFadyen 2003).
Statistical measures
Gait speed and step width were evaluated using two sepa-rate mixed model repeated measures ANOVAs. A 95%conWdence interval (critical � = 0.05) was used to deter-mine the eVects of the two within participant-independentvariables: lighting (LIGHT and LOW LIGHT) and direc-tion (Straight, Cross, Side), and one between participant-independent variable, injury (ACLD and CONTROL).Degrees of freedom were adjusted using the Huynh–Feldtcorrection for any sphericity assumption violations. Posthoc pair-wise comparison of signiWcant eVects was con-ducted using Bonferroni corrected t-tests.
Magnitude of head and trunk yaw and trunk roll angulardisplacement were also analysed using the same statisticalmodel and independent factors as those used for analysis ofgait events.
Similar analyses were performed for the timing of seg-mental reorientation measures, head and trunk yaw, M–LCOMHT and M–L foot. A single mixed model repeated mea-sures ANOVA was used to evaluate the eVects of the threewithin participant-independent variables: lighting (LIGHTand LOW LIGHT), direction (cross, side) and segment(head yaw, trunk yaw, M–L COM, M–L foot), and onebetween participant-independent variable: injury (ACLDand CONTROL) on the above-mentioned timing measures.
Results
Gait parameters
Gait speed
No signiWcant alterations to gait speed were found to occur asa result of lighting condition or direction. In addition, no sig-niWcant eVect of injury was observed. The mean gait speed foreach group collapsed across lighting and direction was ACLD= 0.98 § 0.12 m/s and CONTROL = 1.04 § 0.11 m/s.
Step width
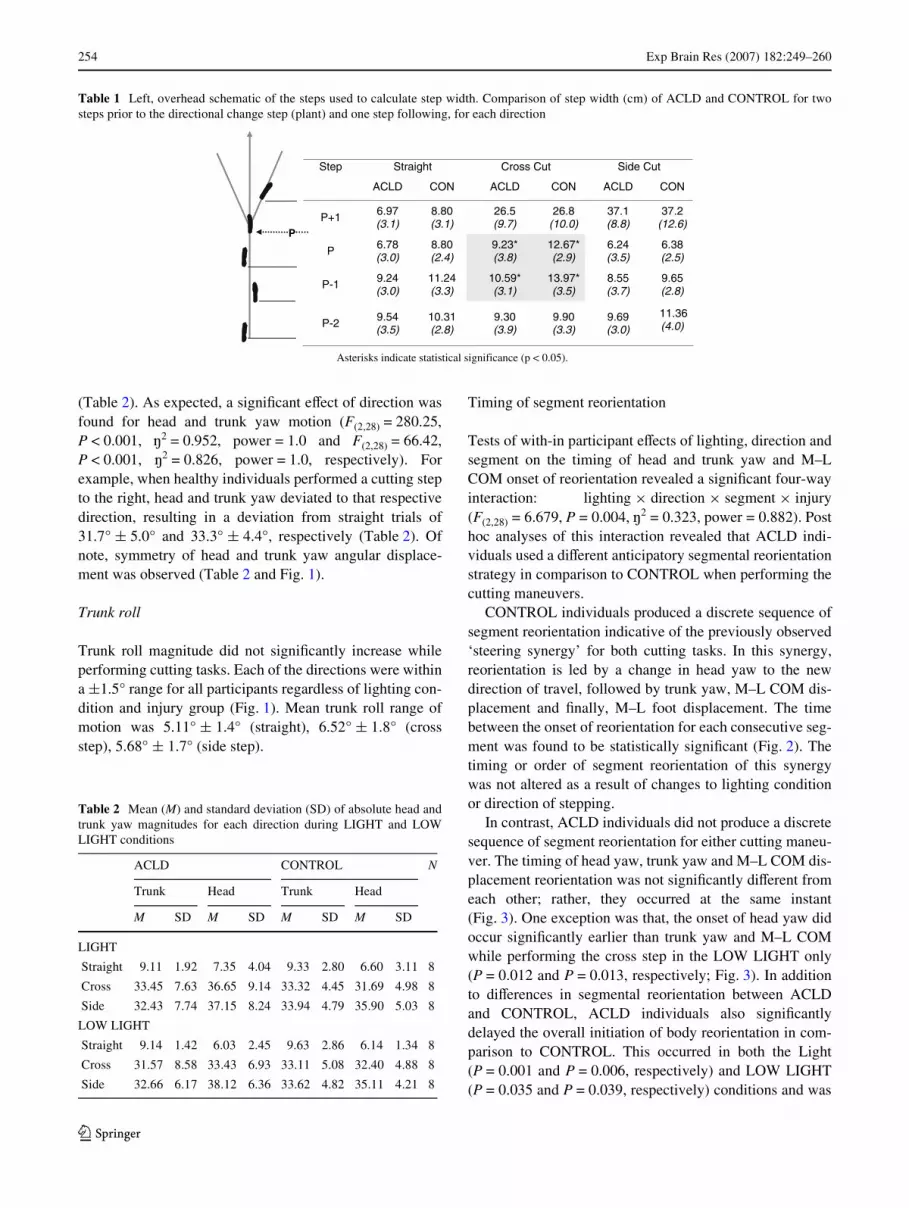
A comparison of step width was conducted for each of therespective steps (P ¡ 3, P ¡ 2, P ¡ 1, P and P + 1). A sig-niWcant interaction (direction £ injury) was determined forthe P ¡ 1 (F(2,48) = 4.030, P = 0.024, ¢2 = 0.144 (eVectsize), power = 0.692), and Plant (F(2,48) = 4.557, P = 0.015,¢2 = 0.160, power = 0.748) steps only. Post hoc analysisrevealed that ACL-deWcient individuals adopted a signiW-cantly smaller step width at both P ¡ 1 (10.59 § 3.1 cm,P = 0.017) and Plant (9.23 § 3.8 cm, P = 0.016) in compar-ison to CONTROL (13.97 § 3.5 cm and 12.67 § 2.9 cm,respectively) when performing the crosscut maneuver(Table 1). In addition, a main eVect of cutting direction wasobserved for P + 1 (F(2,48) = 119.22, P < 0.001, ¢2 = 0.832,power = 1.0). Post hoc testing revealed that cross and sidecutting resulted in a greater step width than continuingstraight ahead. No signiWcant eVect of lighting conditionwas found for step width measures.
Magnitude of head and trunk angles
Head and trunk yaw
No signiWcant eVects of either lighting condition or injurywere found for the magnitude of head and trunk yaw
123
254 Exp Brain Res (2007) 182:249–260
(Table 2). As expected, a signiWcant eVect of direction wasfound for head and trunk yaw motion (F(2,28) = 280.25,P < 0.001, ¢2 = 0.952, power = 1.0 and F(2,28) = 66.42,P < 0.001, ¢2 = 0.826, power = 1.0, respectively). Forexample, when healthy individuals performed a cutting stepto the right, head and trunk yaw deviated to that respectivedirection, resulting in a deviation from straight trials of31.7° § 5.0° and 33.3° § 4.4°, respectively (Table 2). Ofnote, symmetry of head and trunk yaw angular displace-ment was observed (Table 2 and Fig. 1).
Trunk roll
Trunk roll magnitude did not signiWcantly increase whileperforming cutting tasks. Each of the directions were withina §1.5° range for all participants regardless of lighting con-dition and injury group (Fig. 1). Mean trunk roll range ofmotion was 5.11° § 1.4° (straight), 6.52° § 1.8° (crossstep), 5.68° § 1.7° (side step).
Timing of segment reorientation
Tests of with-in participant eVects of lighting, direction andsegment on the timing of head and trunk yaw and M–LCOM onset of reorientation revealed a signiWcant four-wayinteraction: lighting £ direction £ segment £ injury(F(2,28) = 6.679, P = 0.004, ¢2 = 0.323, power = 0.882). Posthoc analyses of this interaction revealed that ACLD indi-viduals used a diVerent anticipatory segmental reorientationstrategy in comparison to CONTROL when performing thecutting maneuvers.
CONTROL individuals produced a discrete sequence ofsegment reorientation indicative of the previously observed‘steering synergy’ for both cutting tasks. In this synergy,reorientation is led by a change in head yaw to the newdirection of travel, followed by trunk yaw, M–L COM dis-placement and Wnally, M–L foot displacement. The timebetween the onset of reorientation for each consecutive seg-ment was found to be statistically signiWcant (Fig. 2). Thetiming or order of segment reorientation of this synergywas not altered as a result of changes to lighting conditionor direction of stepping.
In contrast, ACLD individuals did not produce a discretesequence of segment reorientation for either cutting maneu-ver. The timing of head yaw, trunk yaw and M–L COM dis-placement reorientation was not signiWcantly diVerent fromeach other; rather, they occurred at the same instant(Fig. 3). One exception was that, the onset of head yaw didoccur signiWcantly earlier than trunk yaw and M–L COMwhile performing the cross step in the LOW LIGHT only(P = 0.012 and P = 0.013, respectively; Fig. 3). In additionto diVerences in segmental reorientation between ACLDand CONTROL, ACLD individuals also signiWcantlydelayed the overall initiation of body reorientation in com-parison to CONTROL. This occurred in both the Light(P = 0.001 and P = 0.006, respectively) and LOW LIGHT(P = 0.035 and P = 0.039, respectively) conditions and was
Table 1 Left, overhead schematic of the steps used to calculate step width. Comparison of step width (cm) of ACLD and CONTROL for twosteps prior to the directional change step (plant) and one step following, for each direction
Step Straight Cross Cut Side Cut
ACLD CON ACLD CON ACLD CON
P+1 6.97(3.1)
8.80(3.1)
26.5(9.7)
26.8(10.0)
37.1(8.8)
37.2(12.6)
P 6.78(3.0)
8.80(2.4)
9.23*(3.8)
12.67*(2.9)
6.24(3.5)
6.38(2.5)
P-1 9.24(3.0)
11.24(3.3)
10.59*(3.1)
13.97*(3.5)
8.55(3.7)
9.65(2.8)
P-2 9.54(3.5)
10.31(2.8)
9.30(3.9)
9.90(3.3)
9.69(3.0)
11.36(4.0)
P
Asterisks indicate statistical significance (p < 0.05).
Table 2 Mean (M) and standard deviation (SD) of absolute head andtrunk yaw magnitudes for each direction during LIGHT and LOWLIGHT conditions
ACLD CONTROL N
Trunk Head Trunk Head
M SD M SD M SD M SD
LIGHT
Straight 9.11 1.92 7.35 4.04 9.33 2.80 6.60 3.11 8
Cross 33.45 7.63 36.65 9.14 33.32 4.45 31.69 4.98 8
Side 32.43 7.74 37.15 8.24 33.94 4.79 35.90 5.03 8
LOW LIGHT
Straight 9.14 1.42 6.03 2.45 9.63 2.86 6.14 1.34 8
Cross 31.57 8.58 33.43 6.93 33.11 5.08 32.40 4.88 8
Side 32.66 6.17 38.12 6.36 33.62 4.82 35.11 4.21 8
123

Exp Brain Res (2007) 182:249–260 255
most pronounced during the cross cutting step (Figs. 1, 2).Thus unlike CONTROL, individuals without an ACL didalter segment reorientation when presented with diVerentstepping directions and lighting conditions.
Although obvious upper body segment coordinationdiVerences were observed between the ACLD and CON-TROL groups, the onset of foot reorientation was not foundto be statistically diVerent between the groups (Figs. 2, 3).
Fig. 1 Ensemble-averaged pro-Wles (over ten trials in each direction) of the medial–lateral center of mass displacement, trunk roll, trunk yaw and head yaw for one representation sub-ject from each experimental group (ACLD and CONTROL). ProWles for the LIGHT (unshad-ed) and the LOW LIGHT (shad-ed) are presented. The reference coordinate system is shown: positive values equal rightward movements. Note, in the trunk roll proWle, the arrow indicates that trunk roll movement oc-curred in the same direction as the change in travel direction
ssaM fo ertneC L-M)m( tnemecalpsiD
)°( waY daeH
)°( waY knurT
)°( lloR knurT
4.04.0-
2121-
0404-
0404-
4.04.0-
2121-
0404-
0404-
4.04.0-
2121-
0404-
0404-
4.04.0-
2121-
0404-
0404-
petS-ediS
petS-X
thgiartS
P
P
P
P
ZthgiR+
XnoissergorP
YlacitreV
DLCALORTNOC LORTNOC ACLD
Fig. 2 Control participants: initiation of head yaw (Hy), trunk yaw(Ty), mediolateral center of mass displacement (COMHT) and medial–lateral foot displacement (F). Onset timing of these anticipatory eventsis with respect to the plant step (P). Therefore, negative values equaltime prior to P and positive values equal time after P. The average val-
ues plus one standard error across the control (CON) group are shownfor cross cut (top) and side cut (bottom) during LIGHT (unshaded) andLOW LIGHT (shaded) conditions. Timing of onset of reorientation be-tween Hy, Ty and COMHT was statistically signiWcant (P < 0.05); crosscut in the LIGHT (P < 0.001) for control participants
tuC ssorC
tuC ediS
Dire
ctio
n of
Pro
gres
sion
4.1-
2.0-
8.0-
2.0
P
4.1-
2.0-
8.0-
2.0
P
MOCyTyH TH F
yH yT MOC TH F yH yT MOC TH F
THGIL THGIL WOL
MOCyTyH TH F
lortnoC
P
P
trw emiT )ces( tnalP
trw emiT )ces( tnalP
* 100. < p
123

256 Exp Brain Res (2007) 182:249–260
Nor was foot reorientation aVected by lighting condition orstepping direction in the ACLD group.
Discussion
The steering synergy has been proposed as a feed-forwardprocess that facilitates optimal gathering of sensory infor-mation for the dynamic updating of spatial orientation rep-resentations (Grasso et al. 1996, 1998a; Patla et al. 1999;Hollands et al. 2001). It has been demonstrated to be acontext-dependent component of the human locomotorrepertoire, as forms of the synergy are released duringperformance of a number of very diVerent locomotor tasks(i.e. circular walking, Grasso et al. 1996; walking around acorner, Grasso et al. 1998a; and voluntary head move-ments, Vallis and Patla 2004).
The current study presented a novel locomotor task thatnot only required the descent of an inclined surface (20°),but also a complex whole body redirection maneuver. Cut-ting tasks arguably require much more complex wholebody coordination than stepping tasks performed on levelground (Besier et al. 2001; Houck 2003; Lloyd et al. 2005).To date, research on steering control has focused on redi-rection tasks which require a step out (on level ground) at aself-selected walking speed (Hollands et al. 2001; Patlaet al. 1999; Vallis et al. 2001) and, the investigation ofsegmental control strategies when performing a step where
the swing limb must actually move across and in front ofthe stance limb, has not been reported in the literature.
Despite the novelty and complexity of the locomotortask presented in the current study, a slightly modiWedsteering synergy was used by control individuals with accu-rate lower limb proprioception (i.e. an intact ACL). Thesteering synergy is characteristically deWned by the onset ofhead yaw followed by trunk yaw, trunk roll, mediolateraldisplacement of the COM and Wnally, mediolateral foot dis-placement (Hollands et al. 2001; Patla et al. 1999). Thistypical sequence was observed clearly in the control indi-viduals during performance of both cross and side-cuttingsteps (Figs. 2, 3) with the exception of trunk roll which willbe discussed later (Discussion: Mechanism for body trans-lation). Head yaw led reorientation (1.0–0.9 s) is followedby trunk yaw (0.2–0.4 s); this reorientation timing is similarto values reported in previous studies (Grasso et al. 1998a;Hollands et al. 2001; Patla et al. 1999).
In the absence of visual information (blindfolded or eyesclosed) the head has been observed to delay the onset ofyaw reorientation to the new travel direction as well asundergo smaller ranges of motion (Grasso et al. 1996,1998a). ModiWcation to the steering synergy in the absenceof visual input is thought to occur due to increased relianceon vestibular and neck proprioceptive information. In thissituation, it is important for the head to be stabilized andaligned with the direction of travel so that appropriate spa-tial reference frames can be created and used to coordinate
Fig. 3 ACLD participants: initiation of head yaw (Hy), trunk yaw(Ty), mediolateral center of mass displacement (COMHT) and medial–lateral foot displacement (F). Timing of these anticipatory events iswith respect to the landing step (P). Therefore, negative values equaltime prior to P and positive values equal time after P. The averagevalues plus one standard error across the anterior cruciate ligament
deWcient (ACLD) group are shown for cross cut (top) and side cut (bot-tom) during LIGHT (unshaded) and LOW LIGHT (shaded) condi-tions. Timing of onset of reorientation between Hy, Ty and COMHTwas not statistically signiWcant with the exception of Hy during thecross cut in LOW LIGHT for ACLD participants
DLCA
trw emiT )ces( tnalP
4.1-
2.0-
8.0-
2.0
P
4.1-
2.0-
8.0-
2.0P
yH yT MOC TH FyH yT MOC TH F
yH yT MOC TH FyH yT MOC TH F
THGIL THGIL WOL
tuC ssorC
P
tuC ediS
P
trw emiT )ces( tnalP
Dire
ctio
n of
Pro
gres
sion
* 210.=p
123

Exp Brain Res (2007) 182:249–260 257
body movements (Grasso et al. 1996, 1998a; Pozzo et al.1991). In contrast, the current study used reduced ambientlighting to impede visual information, but not to completelyobliterate it. In our LOW LIGHT condition, vision couldpotentially still be used as a source of information for spa-tial orientation; however, it would likely require more timeto gain the same information as that obtained in LIGHTambient conditions. By using ambient lighting to reducevision as opposed to completely removing visual input, wecould investigate whether visual information about the newtravel direction was critical during the steering task. Wehypothesized that, if visual information was primarily usedfor successful performance of the ramp and cutting taskthen a signiWcantly earlier onset of head reorientationwould be observed in the LOW LIGHT in comparison tothe LIGHT condition. Earlier head reorientation wouldfacilitate the acquisition of as much visual information aspossible in this low light environment prior to committingthe body to move in the new direction of travel. While priorexperience of executing the ramp task may have alsoaVected the timing of reorientation of the head segment,eVorts were made to minimize a potential learning eVect;lighting conditions were counterbalanced between partici-pants and cutting directions were randomized for each par-ticipant.
In fact, we observed that the timing of segment reorien-tation by CONTROL individuals in the LOW LIGHT wassimilar to that observed in the LIGHT condition (Fig. 2).The head did not initiate a signiWcantly earlier reorienta-tion. This is in contrast to previous observations that with-out vision, the head delays reorientation (Grasso et al.1996); it appears that when vision is available albeitreduced in low lighted conditions, there is still a drive toreorient the head in the new travel direction. Visual gazedata were not available for the current study and withoutthis data it is not possible to deWnitively state whethervision was used in the same way during the LOW LIGHTcondition as in the LIGHT condition. What can be con-cluded however, is that by using a protocol where vision isstill an available source of sensory information, the steeringsynergy remained similar as when under optimal visualinformation conditions.
EVect of deWcient lower limb proprioception on steering control
Participants of the study were matched so that each ACLDparticipant had a gender, height, weight and age-matchedCONTROL ‘twin’. In addition, a rigorous clinical evalua-tion of knee function was performed on all participants toensure that the two groups had similar knee joint mechani-cal function. Thus, the diVerence between the two experi-mental groups was that one group had a unilateral ACLD
and therefore reduced lower limb proprioceptive input(Barrack et al. 1989). Recent studies investigating the roleof proprioception in steering control have used a vibrationtechnique applied to healthy individuals in order to disruptproprioceptive information from the lower limb (Courtineet al. 2007; Ivanenko et al. 2000; Sorenson et al. 2002). Thecurrent work examined the relationship between reducedlower limb proprioception in an ACLD population to deter-mine how altered proprioceptive information from the kneejoint might aVect the coordination of body segments duringa steering task. As hypothesized, the timing of segmentreorientation was delayed in the ACLD group (Figs. 1, 3).ACLD individuals signiWcantly delayed the onset of reori-entation of the head and trunk segments during perfor-mance of both the cross and side-cutting step. The mostsigniWcant delay was observed during the cross step whereonset of head yaw occurred at 0.5 s and onset of trunk yawoccurred at 0.3 s prior to plant (Fig. 3). Thus, unlike CON-TROL who initiated head yaw and trunk yaw reorientationin the step prior to plant, ACLD individuals delayed thereorientation onset to occur within the plant step. Delayedonset of the steering synergy was expected to occur in theACLD individuals, as altered proprioceptive informationfrom the injured lower limb would result in a compromisedability to use this mode of sensory information for the crea-tion of the whole body frame of reference or body schema(Berthoz and Viaud-Delmon 1999). An unexpected resultwas that instead of a discrete sequence of reorientation withthe head leading followed by the trunk and M–L COMHT,reorientation of the head, trunk and M–L COMHT occurredalmost simultaneously (Figs. 2, 3). This is in contrast to thesequence of reorientation that was observed by the CON-TROL individuals of this study and those typicallyobserved during steering tasks (Grasso et al. 1996, 1998a,b; Hollands et al. 2001; Patla et al. 1999).
In the LOW LIGHT, the ACLD individuals maintainedthe modiWed and delayed steering strategy they produced inthe LIGHT condition. The timing of segment reorientationwas not signiWcantly diVerent between the lighting condi-tions, except for the cross step in the LOW LIGHT.Figure 3 illustrates that for this particular directional task,head yaw did in fact initiate reorientation signiWcantly ear-lier than the trunk yaw and M–L COMHT. As well, theonset of this head movement occurred approximately 0.8 sprior to plant; this timing is consistent with the timing ofhead reorientation observed in CONTROL and those typi-cally observed in the steering literature (Grasso et al. 1996,1998a; Hollands et al. 2001; Patla et al. 1999). Thus, itseems that when the ACLD group was presented with themost diYcult task (cross step in the LOW LIGHT), thehead was reoriented earlier than any other segment. Whywould this particular environmental situation result in adiVerent control strategy in ACLD individuals?
123

258 Exp Brain Res (2007) 182:249–260
In the LOW LIGHT, visual acuity may be reduced; how-ever, reorientation of the head segment may still provide addi-tional sensory information, e.g. from the vestibular and neckproprioception systems that could be used for spatial reorien-tation. Although, head reorientation in ACLD preceded reori-entation of the other segments in the LOW LIGHT, the timingof this movement was not signiWcantly earlier than the onsetof head movement in the LIGHT. This suggests that ACLDindividuals were not relying on the increased visual informa-tion in the LOW LIGHT condition; however, they mayrequire additional sensory input from the head segment (ves-tibular and neck proprioception) to establish a safe referenceframe for locomotion during this novel task.
These striking results raise a number of questions. Whywould the steering synergy be modiWed in an ACL-deW-cient population? Does this altered control strategy serveany particular advantages to those with a lower limb propri-oception deWciency? We propose that there are two possi-ble scenarios that could explain these observations.
First, a delayed simultaneous reorientation of the wholebody could reXect a cautious control strategy in the ACLDpopulation. The descent of the ramp followed by an abruptcutting maneuver was a novel task and therefore, the use ofa previous learnt synergy for this speciWc task would beminimal. As a result, these individuals likely used a strat-egy, which would ensure that stability of the knee joint; infact dynamic stability of the whole body, was maintainedthroughout the current task. Vallis and McFadyen (2003)observed a similar simultaneous head–trunk coupling ofyaw motion during circumvention of an obstacle in thetravel path. These authors proposed that this couplingmight serve as a strategy to ensure a stable platform forredirecting the whole body movement. By reducing thenumber of degrees of freedom requiring control, the overallbody coordination required to perform the task is simpliWed(Hicheur and Berthoz 2005). Stabilization of the head to thetrunk has also been reported as a premature steering strat-egy in children developing locomotor skills (Grasso et al.1998b). In the situation where proprioceptive informationof limb position may be deWcient (as is the case of the kneein ACLD; Barrack et al. 1989) this strategy may serve as anadvantage. Reducing the number of body segments thatrequire individual control, may possibly allow for anincreased focus on segments that may require greater stabil-ization control (ACLD knee). Furthermore, simultaneoushead–trunk movement may reduce potential destabilizingeVects on the whole body resulting from the reactive trunktorque that is produced by a head yaw movement (Vallisand Patla 2004). Thus, using a coordinated head–trunkreorientation or an ‘en bloc’ strategy (Hicheur and Berthoz2005) may be advantageous during more complex reorien-tation situations for ensuring whole body stabilization inACLD individuals.
Alternatively, compromised proprioceptive information(either altered or delayed) from the lower limb via the lossof the ACL may aVect the eYciency of creating the body’sinternal spatial reference frame or body schema. Recently,the contribution of proprioceptive information to spatialorientation during level gait was examined (Courtine et al.2007). It was found that lower limb aVerents did not signiW-cantly contribute to steering control. However, in the inter-pretation of their results, these authors stated that thisWnding might be very diVerent under circumstances wherelower limb proprioception is of more importance. Ourstudy provides evidence that this may in fact be the case.Ramp descent requires complex control of lower limb mus-culature in particular to stabilize the knee joint, whichundergoes extreme loading (Kuster et al. 1994, 1995a; Red-fern and Dipasquale 1997). A signiWcant amount of lowerlimb sensory information, particularly from the knee joint,would be required in addition to already available visual,vestibular and upper body proprioceptive input. WhenaVerent information from the lower limb is reduced, e.g.following an ACL injury, a delay in segment reorientationoccurs whether vision is present or absent. This modiWca-tion to the steering synergy may provide additional time forthe CNS to integrate all available, online sensory informa-tion in order to ensure the planning and execution of anappropriate locomotor plan, which, in turn, ensures wholebody stability during this complex locomotor task.
Mechanism for body translation
A change in travel direction requires a redirection of thebody’s COM. Modulation of the COM in the frontal planecan be done through either medial lateral foot placement orthrough the use of a hip strategy (MacKinnon and Winter1993; Patla et al. 1999; Hollands et al. 2001). A foot place-ment strategy is typically used when cues are given earlierto the commencement of the directional change, with thehip strategy possibly being used as a secondary strategy toWne-tune M–L COM displacement during turning (Patlaet al. 1999; Hollands et al. 2001). The hip strategy isachieved through muscle action at the hip and trunk, wherethe body behaves like a double pendulum (upper and lowerbody moving in opposing directions) and is reXected in themeasure of trunk roll (Patla et al. 1999). As such, measuressuch as step width and trunk roll are important in examin-ing overall whole body control during these movements.
Despite the signiWcant diVerences in timing of head andtrunk coordination between the ACLD and control individ-uals, the actual timing of M–L COMHT and foot displace-ment was similar between the populations (Fig. 1). Asparticipants of the current study were given directional cuesprior to ramp descent and execution of the subsequentdirectional change, it was expected that a foot placement
123

Exp Brain Res (2007) 182:249–260 259
strategy would be used in order to redirect the COM in thenew travel direction. Indeed, the use of a foot placementstrategy was evident during the performance of the crosscutting step. Step width adopted at P ¡ 1 was greater thanduring the previous step (P ¡ 2) for all participants; how-ever, ACLD individuals did not increase step width asmuch as CONTROL. In contrast, no indication of a step-ping strategy was observed during the side-cutting step foreither participant group (Table 1). It is possible that due tothe nature of the side cut step, a diVerent control strategyover the lateral COM displacement was used. This will befurther discussed in relation to observed trunk roll in thecurrent study.
Previous works on steering behaviour have observedincreased trunk roll when changing direction (7.90°, Patlaet al. 1999; 5.0°, Hollands et al. 2001). However, theabsence of signiWcant trunk roll deviations from straight tri-als during transient changes in direction have also beenreported when perhaps the Wne tuning of COM displace-ment via trunk roll is not necessary (Vallis and McFadyen2003). Although changes in travel direction were completeredirections (similar to those used by Patla et al. 1999 andHollands et al. 2001), we did not observe signiWcant devia-tions of trunk roll from straight-ahead trials. The exact rela-tionship between trunk roll and the control of M–L COMdisplacement is not known and therefore deriving conclu-sions as to the relation between these two variables shouldbe made with caution (Hollands et al. 2001). For the currentparadigm, perhaps trunk roll measures cannot adequatelycharacterize the use of a hip strategy to redirect M–L COMin the new direction of travel. Certainly, trunk roll behav-iour observed during side cutting steps certainly suggeststhat this may be the case. Characteristically, during anabrupt redirection movement, the direction of trunk roll isopposite to the new trajectory (Hollands et al. 2001). Forexample, during a turn to the left, a rightward trunk roll isobserved. This is due to the double pendulum action of thehip strategy where movement of the upper and lower bodyis opposed. This opposite movement of the upper and lowerbody eVectively redirects the COM towards the direction ofthe feet, the intended new trajectory (Patla et al. 1999). Thetrunk roll proWle of the crosscutting task follows this con-vention; however, during side cutting, trunk roll movementactually occurred towards the same direction as the new tra-jectory (as indicated by the arrow in Fig. 1). This matcheddirection of COM displacement and trunk roll contradictsthe biomechanical mechanism of the hip strategy. We sug-gest that this result could reXect what is not yet knownabout how trunk roll contributes to the control of M–LCOM displacement during changes in direction; speciW-cally, the unique control-mechanism used by the CNS tocontrol landing from a ramp descent and perform a side cutstep.
Magnitude of head and trunk angles
The diVerences observed between ACLD and CONTROLin the timing of reorienting behaviour in itself revealsimportant implications that a lower limb proprioceptivedeWciency has on feed-forward mechanisms of whole bodylocomotor control. However, what is further interesting isthat despite such large modiWcations in the timing andsequence of orienting behaviour, the magnitude of segmen-tal movements and COMHT displacement was similarbetween the two participant groups. Magnitudes of headand trunk yaw observed in the current work (Table 2) wereconsistent with values published previously (Grasso et al.1996; Hollands et al. 2001; Patla et al. 1999; Vallis andMcFadyen 2003), and were equally observed in bothACLD and CONTROL individuals. The consistency ofthese magnitudes across studies indicates the range ofangular motion that is maintained for these segments forredirection during diVerent walking tasks.
Conclusion
This is the Wrst study to examine strategies used by anACL-deWcit population to control the head and trunk seg-ments during an abrupt change in travel direction. Resultspresent preliminary evidence that adaptive changes follow-ing ACLD are not limited to lower limb control, as hasbeen the focus of published research to date; ACLDappears to inXuence motor coordination on a global level,including head and trunk movement strategies. Recently,ACLD has been proposed to be a neurophysiological disor-der, and that observed compensations following injury tothe anterior cruciate ligament provide a valid model of neu-rological plasticity (Kapreli and Athanasopoulos 2006).Results from the present study oVers evidence to supportthis hypothesis and provide some insight into the complexnature of motor control adaptations following peripheraljoint injury. Clearly, further research is required to eluci-date the role of lower limb proprioceptive information, andspeciWcally input from the ACL, in the central control oflocomotor movement strategies in complex environments.
Acknowledgements Financial support for this project was providedby OGS (RRJ). We would like to thank the staV, particularly JackieSinkledam, Tony Downes, Val Brouwer, and Teresa Piotrowski of theHealth and Performance Centre and the participants at the Universityof Guelph for all their work and support on this project.
References
Abelew TA, Miller MD, Cope TC, Nichols TR (2000) Local loss ofproprioception results in disruption of interjoint coordinationduring locomotion in the cat. J Neurophysiol 84:2709–2714
123

260 Exp Brain Res (2007) 182:249–260
Barrack RL, Skinner HB, Buckley SL (1989) Proprioception in theanterior cruciate deWcient knee. Am J Sports Med 17(1):1–6
Bent LR, McFadyen BJ, Merkley VF, Kennedy PM, Inglis JT (2000)Magnitude eVects of galvanic vestibular stimulation on the trajec-tory of human gait. Neurosci Lett 279:157–160
Berthoz A, Viaud-Delmon I (1999) Multisensory integration in spatialorientation. Curr Opin Neurobiol 9:708–712
Besier TF, Lloyd DG, Cochrane JL, Ackland TR (2001) External load-ing of the knee joint during running and cutting manoeuvre. MedSci Sports Exerc 33:1168–1175
Corrigan JP, Cashman WF, Brady MP (1992) Proprioception in thecruciate deWcient knee. J Bone Joint Surg Br 14:247–250
Courtine G, De Nunzio AM, Schmid M, Beretta MV, Schieppati M(2007) Stance- and locomotion-dependent processing of vibra-tion-induced proprioceptive inXow from multiple muscles inhumans. J Neurophysiol 97(1):772–779
Deshpande N, Patla AE (2005) Dynamic visual–vestibular integrationduring goal directed human locomotion. Exp Brain Res 166:237–247
Grasso R, Glasauer S, Takei Y, Berthoz A (1996) The predictive brain:anticipatory control of head direction for the steering of locomo-tion. Neuroreport 7:1170–1174
Grasso R, Prevost P, Ivanenko Y, Berthoz A (1998a) Eye-head coordi-nation for the steering of locomotion in humans: an anticipatorysynergy. Neurosci Lett 253:115–118
Grasso R, Assaiante C, Prevost P, Berthoz A (1998b) Development ofanticipatory orienting strategies during locomotor tasks in chil-dren. Neurosci Biobehav Rev 22(4):533–539
Hicheur H, Berthoz A (2005) How do humans turn? Head and bodymovements for the steering of locomotion. In: IEEE proceedingsof the international conference on humanoid robots, Tsukuba,Japan, pp 265–270
Hollands MA, Sorenson KL, Patla AE (2001) EVects of head immobi-lization on the coordination and control of head and body reorien-tation and translation during steering. Exp Brain Res 120:223–233
Hollands MA, Patla AE, Vickers JN (2002) “Look where you’re go-ing!”: gaze behaviour associated with maintaining and changingthe direction of locomotion. Exp Brain Res 143:221–230
Houck JR (2003) Muscle activation patterns of selected lower extrem-ity muscles during stepping and cutting tasks. J Electromyogr Ki-nesiol 13(6):545–554
Ivanenko YP, Grasso R, Laquaniti F (2000) InXuence of leg musclevibration on human walking. J Neurophysiol 84:1737–1747
Kapreli E, Athanasopoulos S (2006) The anterior cruciate ligamentdeWciency as a model of brain plasticity. Med Hypotheses67:645–650
Karnath HO, Sievering D, Fetter M (1994) The interactive contributionof neck muscle proprioception and vestibular stimulation to sub-jective “straight ahead” orientation in man. Exp Brain Res101:140–146
Kennedy PM, Carlsen AN, Inglis JT, Chow R, Franks IM, Chua R(2003) Relative contributions of visual and vestibular informationon the trajectory of human gait. Exp Brain Res 153:113–117
Kennedy PM, Cressman EK, Carlsen AN, Chua R (2005) Assessingvestibular contributions during changes in gait trajectory. Neuro-report 16:1097–1100
Kuster M, Wood GA, Sakurai S, Blatter G (1994) Winner of the 1994Nicola Cerulli Young Researchers Award. Downhill walking: astressful task for the anterior cruciate ligament? Knee Surg SportsTraumatol Arthrosc 2:2–7
Kuster M, Sakurai S, Wood GA (1995a) Kinematic and kinetic com-parison of downhill and level walking. Clin Biomech 10(2):79–84
Kuster M, Sakurai S, Wood GA (1995b) The anterior cruciate liga-ment-deWcient knee: compensatory mechanisms during downhillwalking. Knee 2(2):105–111
Lloyd DG, Buchanan TS, Besier TF (2005) Neuromuscular biome-chanical modeling to understand knee ligament loading. Med SciSports Exerc 37(11):1939–1947
Lowrey CR, Reed RJ, Vallis LA (2007) Control strategies used by old-er adults during multiple obstacle avoidance. Gait Posture25(4):502–508
MacKinnon CD, Winter DA (1993) Control of whole body balance inthe frontal plane during human walking. J Biomech 26:633–644
Mergner T, Rosemeier T (1998) Interaction of vestibular, somatosen-sory and visual signals for postural control and motion perceptionunder terrestrial and microgravity conditions-a conceptual model.Brain Res Rev 28:118–135
Noyes FR, Barber SD, Mangine RE (1991) Abnormal lower limbsymmetry determined by function hop tests after anterior cruciateligament rupture. Am J Sports Med 19:513–518
Patla AE (1997) Understanding the roles of vision in the control ofhuman locomotion. Gait Posture 5:54–69
Patla AE, Adkin A, Ballard T (1999) Online steering: coordination andcontrol of body center of mass, head and body reorientation. ExpBrain Res 129:629–634
Pitman MI, Nainzadeh N, Menche D, Gasalberti R, Song EK (1992)The intraoperative evaluation of the neurosensory function of theanterior cruciate ligament in humans using somatosensory evokedpotentials. Arthroscopy 8(2):442–447
Pozzo T, Berthoz A, Lefort L, Vitte E (1991) Head stabilization duringvarious locomotor tasks in humans II. Patients with bilateral ves-tibular deWcits. Exp Brain Res 85:208–217
Redfern MS, Dipasquale J (1997) Biomechanics of descending ramps.Gait Posture 6:119–125
Reed RJ, Vallis LA (2005) Ramped descent and directional changes: anew paradigm for investigating the anterior cruciate ligament dur-ing locomotor control. International Society for Posture and GaitResearch Abstract. Gait Posture 21:S81
Reed RJ, Lowrey CR, Vallis LA (2006) Middle–old and old–old retire-ment dwelling adults respond diVerently to locomotor challengesin cluttered environments. Gait Posture 23(4):486–491
Rudolph KS, Axe MJ, Snyder-Mackler L (2000) Dynamic stabilityafter ACL injury: who can hop? Knee Surg Sports Traumatol,Athrosc 8:262–269
Sorenson KA, Hollands MA, Patla AE (2002) The eVects of humanankle muscle vibration on posture and balance during adaptivelocomotion. Exp Brain Res 143(1):24–34
Valeriani M, Restuccia D, Di Lazzaro V, Franceschi F, Fabbriciani C,Tonali P (1996) Central nervous system modiWcations in patientswith lesion of the anterior cruciate ligament of the knee. Brain119:1751–1762
Vallis LA, McFadyen BJ (2003) Locomotor adjustments for circumven-tion of an obstacle in the travel path. Exp Brain Res 152:409–414
Vallis LA, Patla AE (2004) Expected and unexpected head yaw move-ments result in diVerent modiWcations of gait and whole bodycoordination strategies. Exp Brain Res 157:94–110
Vallis LA, Patla AE, Adkin AL (2001) Control of steering in the pres-ence of unexpected head yaw movements. InXuence on sequenc-ing of subtasks. Exp Brain Res 138(1):128–134
Weber KD, Fletcher WA, Gordon CR, Jones GM, Block EW (1998)Motor learning in the “podokinetic” system and its role in spatialorientation during locomotion. Exp Brain Res 120:377–385
Winter DA (2005) Biomechanics and motor control of human move-ment, 3rd edn. Wiley, Hoboken
123




























