Embed Size (px)
Citation preview
Reduction techniques in distal radius fractures
W. De ea,*, W. Kleinb, H. Riegerc
aDepartment of Trauma and Hand Surgery, BruÈderkrankenhaus St. Josef, Paderborn, D-33098 Paderborn, GermanybClinic of Trauma Surgery, StaÈdtisches Krankenhaus Wolfsburg, Sauerbruchstraûe 7, D-38440 Wolfsburg, Germany
cClinic for Trauma and Hand Surgery, Clemens Krankenhaus MuÈnster, D-48149 MuÈnster, Germany
Abstract
External skeletal ®xation is an important minimal invasive procedure in the management of fractures at the distal end of theradius. Attention to detail is important not only in the recognition of indications and function of the external ®xator but also in
its speci®c application. To improve anatomical restoration (e.g. palmar tilt) multi-planar ligamentotaxis is recommended. Thedemonstrated dynamic ®xator is easy to apply and the double ball joint facilitates reduction after mounting by multi-planarligamentotaxis. This transarticular unilateral external ®xation system permits restoration of anatomy with the wrist in neutral orextension, thereby allowing full ¯exion of the metacarpophalangeal joints, with ®ngers and wrist extensor tendons relatively
relaxed. Multi-planar ligamentotaxis, combined with a limited approach for supplementary procedures (®xation of articularfragments and/or bone grafting) and with early wrist motion, o�ers an encouraging treatment option in the management ofunstable distal radial fractures by providing better anatomical restoration, especially of the palmar tilt and reduces the risk of
wrist and ®nger sti�ness. # 2000 Published by Elsevier Science Ltd. All rights reserved.
Keywords: Unstable distal radius fractures; External ®xation; Reduction; Multi-planar ligamentotaxis
1. Introduction
In unstable dislocated distal radius fractures treat-ment aims at anatomical reduction as the incidence ofsequelae of fractures healed in anatomical position islower than in malunited fractures. Functional resultsare directly correlated to the residual deformity [1,2].The list of complications in malunited distal radiusfractures is extensive and includes limitation of wristmobility due to joint incongruencies, loss of radiallength leading to impingement or subluxation of thedistal radial joint, all causing a painful wrist, reducedgrip strength, problems with the median nerve and inthe later stage carpal instability and secondary arthriticchanges [1±4].
Closed reduction of Colles' fractures even when un-stable normally is straight-forward, retention of thefragments being the challenge. The classic reduction
according to Charnley follows three steps: under con-tinuous longitudinal traction the fracture is disim-pacted and dorsal angulation is increased, followed bythe Robert±Jones manoeuver: the ``reducing'' handforces the distal fragment to the volar side under con-tinuous traction while the ``stabilizing'' hand holds theproximal radius. In the last step of the manoeuver theresult of the reposition is maintained by pronating thedistal fragment and traction can be stopped [5]. Stablefractures of the distal radius, accounting for 80% offractures can be reduced with this approach and mana-ged conservatively. As Charnley already stated in 1961``some continuous traction must be applied in order tomaintain the styloid process of the radius in itsreduced position'', probably referring to fractures plussubluxation of the distal radio-ulnar joint and frac-tures with metaphysal bone loss. When a dorsal angu-lar displacement greater than 208, loss of radial lengthof more than 5 mm, ulnar separation and/or extendeddorsal comminution (all criteria of an unstable frac-ture) are present, operative treatment is mandatory [6].
Injury, Int. J. Care Injured 31 (2000) 48±55
0020-1383/00/$ - see front matter # 2000 Published by Elsevier Science Ltd. All rights reserved.
PII: S0020-1383(99 )00263 -6
www.elsevier.com/locate/injury
* Corresponding author.
Using either trans-styloid or intrafocal k-wires accord-
ing to Kapandji gradual loss of anatomical reduction
and loss of radial length are described [7]. Open re-
duction of the fracture and internal ®xation is not fea-
sable in severely comminuted fractures with badly
contused soft tissues. External ®xation is a minimally-
invasive method to retain reduction with adequate
stability [8] and maintains the longitudinal traction rec-
ommended by Charnley [5]. Intact soft tissue can
reduce the fragments by longitudinal traction (referred
to as ligamentotaxis by Vidal [9]). External ®xation is
reliable in securing the radial length even in grossly
unstable distal radius fractures [10].
Our retrospective analysis of 103 unstable distal
radius fractures showed maintenance of the radial
length and radial angle even after removal of the uni-
lateral wrist ®xator [11,12] (Tables 1 and 2), but the
palmar tilt could not be reconstituted su�ciently by
our original method (Table 3). This was also described
by Szabo and Weber [13] and Agee [14,15]. Bartosh et
al. [16] showed experimentally that longitudinal trac-
tion, like uni-planar ligamentotaxis alone, could not
restore and preserve anatomical palmar tilt.
We changed our reduction manoeuvre according to
the results of Gupta [17] and Agee et al. [15] in order
to gain anatomical reduction by multi-planar ligamen-
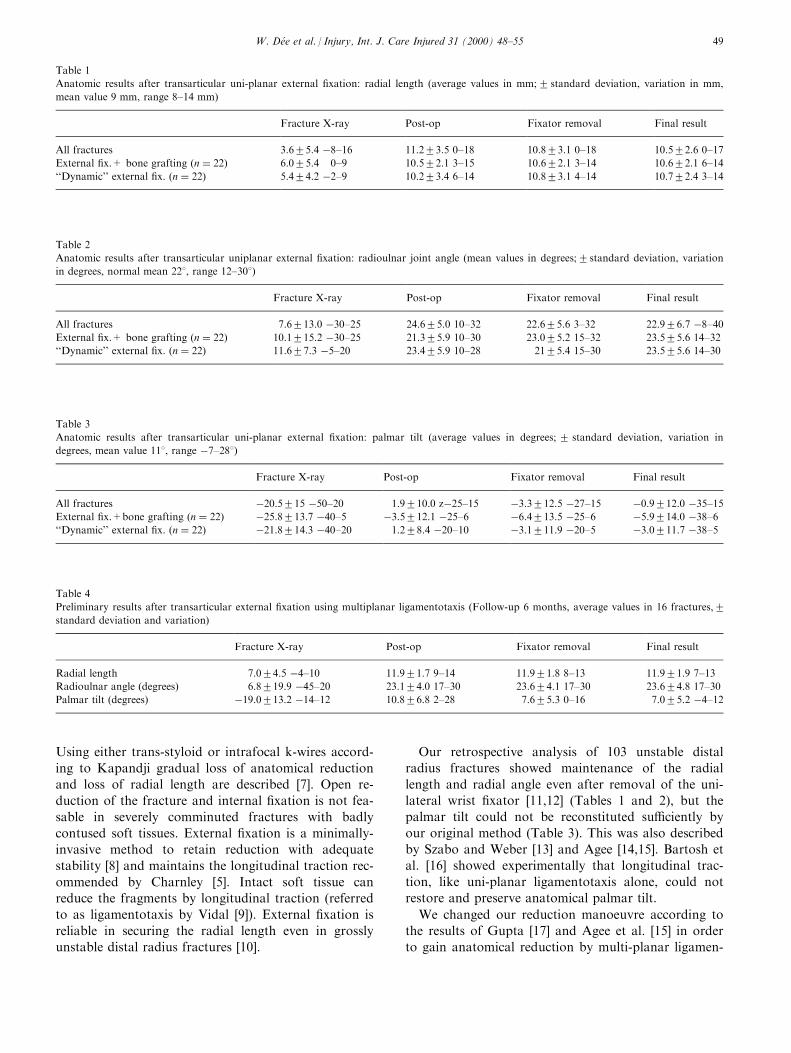
Table 1
Anatomic results after transarticular uni-planar external ®xation: radial length (average values in mm;2 standard deviation, variation in mm,
mean value 9 mm, range 8±14 mm)
Fracture X-ray Post-op Fixator removal Final result
All fractures 3.625.4 ÿ8±16 11.223.5 0±18 10.823.1 0±18 10.522.6 0±17
External ®x.+ bone grafting �n � 22) 6.025.4 0±9 10.522.1 3±15 10.622.1 3±14 10.622.1 6±14
``Dynamic'' external ®x. �n � 22) 5.424.2 ÿ2±9 10.223.4 6±14 10.823.1 4±14 10.722.4 3±14
Table 2
Anatomic results after transarticular uniplanar external ®xation: radioulnar joint angle (mean values in degrees;2standard deviation, variation
in degrees, normal mean 228, range 12±308)
Fracture X-ray Post-op Fixator removal Final result
All fractures 7.6213.0 ÿ30±25 24.625.0 10±32 22.625.6 3±32 22.926.7 ÿ8±40External ®x.+ bone grafting �n � 22) 10.1215.2 ÿ30±25 21.325.9 10±30 23.025.2 15±32 23.525.6 14±32
``Dynamic'' external ®x. �n � 22) 11.627.3 ÿ5±20 23.425.9 10±28 2125.4 15±30 23.525.6 14±30
Table 3
Anatomic results after transarticular uni-planar external ®xation: palmar tilt (average values in degrees; 2 standard deviation, variation in
degrees, mean value 118, range ÿ7±288)
Fracture X-ray Post-op Fixator removal Final result
All fractures ÿ20.5215 ÿ50±20 1.9210.0 zÿ25±15 ÿ3.3212.5 ÿ27±15 ÿ0.9212.0 ÿ35±15External ®x.+bone grafting �n � 22) ÿ25.8213.7 ÿ40±5 ÿ3.5212.1 ÿ25±6 ÿ6.4213.5 ÿ25±6 ÿ5.9214.0 ÿ38±6``Dynamic'' external ®x. �n � 22) ÿ21.8214.3 ÿ40±20 1.228.4 ÿ20±10 ÿ3.1211.9 ÿ20±5 ÿ3.0211.7 ÿ38±5
Table 4
Preliminary results after transarticular external ®xation using multiplanar ligamentotaxis (Follow-up 6 months, average values in 16 fractures,2standard deviation and variation)
Fracture X-ray Post-op Fixator removal Final result
Radial length 7.024.5 ÿ4±10 11.921.7 9±14 11.921.8 8±13 11.921.9 7±13
Radioulnar angle (degrees) 6.8219.9 ÿ45±20 23.124.0 17±30 23.624.1 17±30 23.624.8 17±30
Palmar tilt (degrees) ÿ19.0213.2 ÿ14±12 10.826.8 2±28 7.625.3 0±16 7.025.2 ÿ4±12
W. DeÂe et al. / Injury, Int. J. Care Injured 31 (2000) 48±55 49
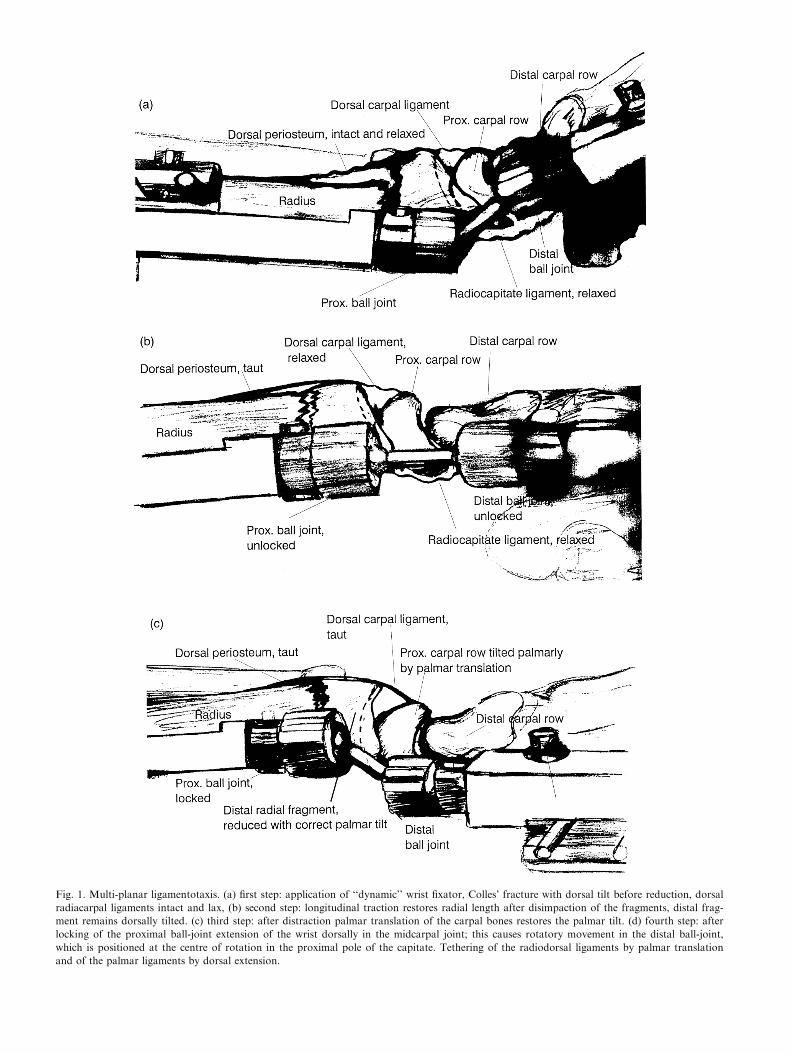
Fig. 1. Multi-planar ligamentotaxis. (a) ®rst step: application of ``dynamic'' wrist ®xator, Colles' fracture with dorsal tilt before reduction, dorsal
radiacarpal ligaments intact and lax, (b) second step: longitudinal traction restores radial length after disimpaction of the fragments, distal frag-
ment remains dorsally tilted. (c) third step: after distraction palmar translation of the carpal bones restores the palmar tilt. (d) fourth step: after
locking of the proximal ball-joint extension of the wrist dorsally in the midcarpal joint; this causes rotatory movement in the distal ball-joint,
which is positioned at the centre of rotation in the proximal pole of the capitate. Tethering of the radiodorsal ligaments by palmar translation
and of the palmar ligaments by dorsal extension.
totaxis. The external ®xator with integrated doubleball joint is an ideal device for three dimensional liga-mentotaxis at the level of the fracture and the carpalrows (Fig. 1). The ®xator comprises a double balljointlinking two bars combined with two sliding clamps(Pennig wrist ®xator, Ortho®x Srl, Italy) [18,19]. The®xator is mounted on two predrilled pins in the distalradial diaphysis and near the base into the secondmetacarpal from the radial side via limited approaches[8], leaving su�cient mobility in all planes for re-duction by the un®xed ball joints and sliding bars.
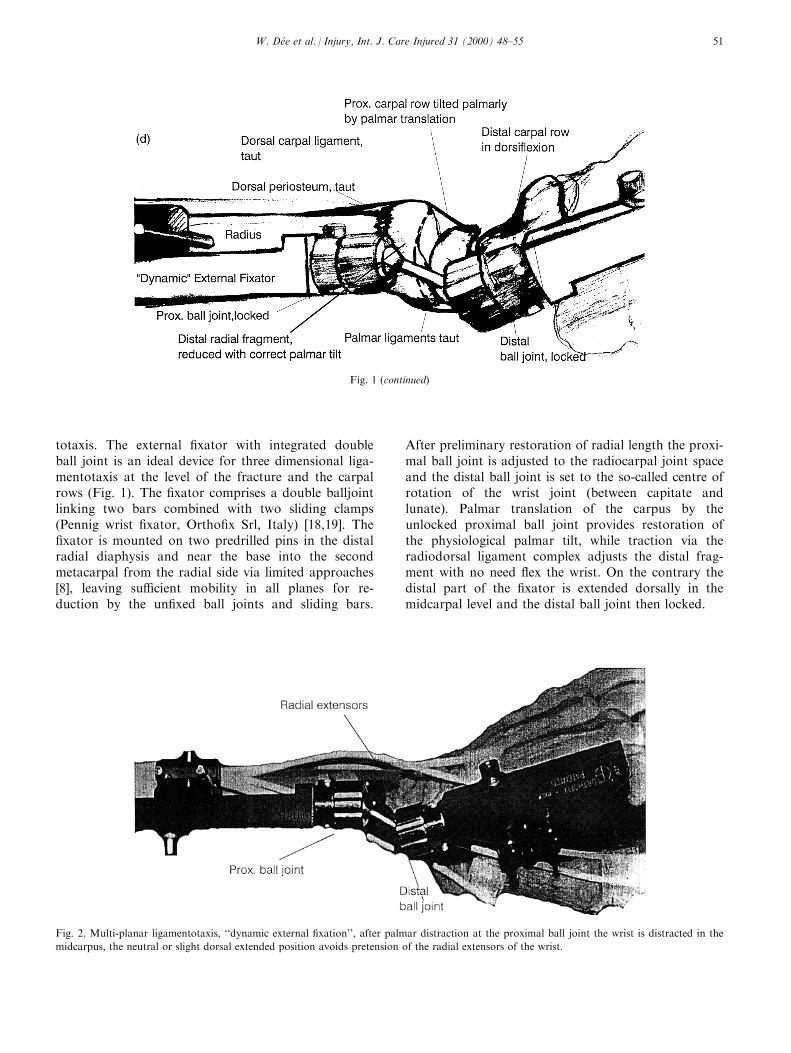
After preliminary restoration of radial length the proxi-mal ball joint is adjusted to the radiocarpal joint spaceand the distal ball joint is set to the so-called centre ofrotation of the wrist joint (between capitate andlunate). Palmar translation of the carpus by theunlocked proximal ball joint provides restoration ofthe physiological palmar tilt, while traction via theradiodorsal ligament complex adjusts the distal frag-ment with no need ¯ex the wrist. On the contrary thedistal part of the ®xator is extended dorsally in themidcarpal level and the distal ball joint then locked.
Fig. 1 (continued)
Fig. 2. Multi-planar ligamentotaxis, ``dynamic external ®xation'', after palmar distraction at the proximal ball joint the wrist is distracted in the
midcarpus, the neutral or slight dorsal extended position avoids pretension of the radial extensors of the wrist.
W. DeÂe et al. / Injury, Int. J. Care Injured 31 (2000) 48±55 51
This was described by Gupta who stated that ¯exionin the midcarpus does not control the dorsally tilteddistal fragment because of the mainly proximal inser-tion of the dorsal wrist ligaments on the proximal car-pal row [17], but translation and dorsi¯exion tethersthe stronger palmar ligaments [16] thus stabilising thereduction result while the added longitudinal tractionprotects against redisplacement [15,16]. Overdistractionmay lead to loss of reduction and dorsal tilt of thefragment, raises pressure in the carpal tunnel [20] andcan cause re¯ex dystrophy in animal experiments [21].Direct tissue pressure recordings in the carpal tunnelduring reduction showed 26 mm Hg after preliminaryreduction and 19 mm Hg after Gupta's manoeuvre,which later was normal at 11 mm Hg [11]. This re-duction technique allows anatomical positioning of thedistal radius in neutral or even dorsi¯exion and avoidsoverdistraction and the so-called ``extrinsic-extensor-
plus'' position (Cotton±Loder or Schede-position)which may lead to ®nger sti�ness and increased carpaltunnel pressure [20]. The metacarpophalangeal jointsshould move freely and be able to fully ¯ex after re-duction. This is of major importance while maintainingreduction. Furthermore the strong extensor musclesare weakened using transarticular external ®xation inmild dorsi¯exion which helps to prevent redisplace-ment [17] (Fig. 2). Control over the distal fragment ofthe radius is achieved by palmar translation thus load-ing the radiodorsal capsule with the proximal ball jointbeing locked. Ligamentotaxis can only be transmittedto the fragment with intact capsular attachments [22].As a common ®nding even in unstable radius fractureswith metaphyseal comminution the dorsal capsule isnot completely disrupted. After bone grafting of themetaphyseal defect using a limited dorsal approachthrough the fourth extensor tendon compartment the
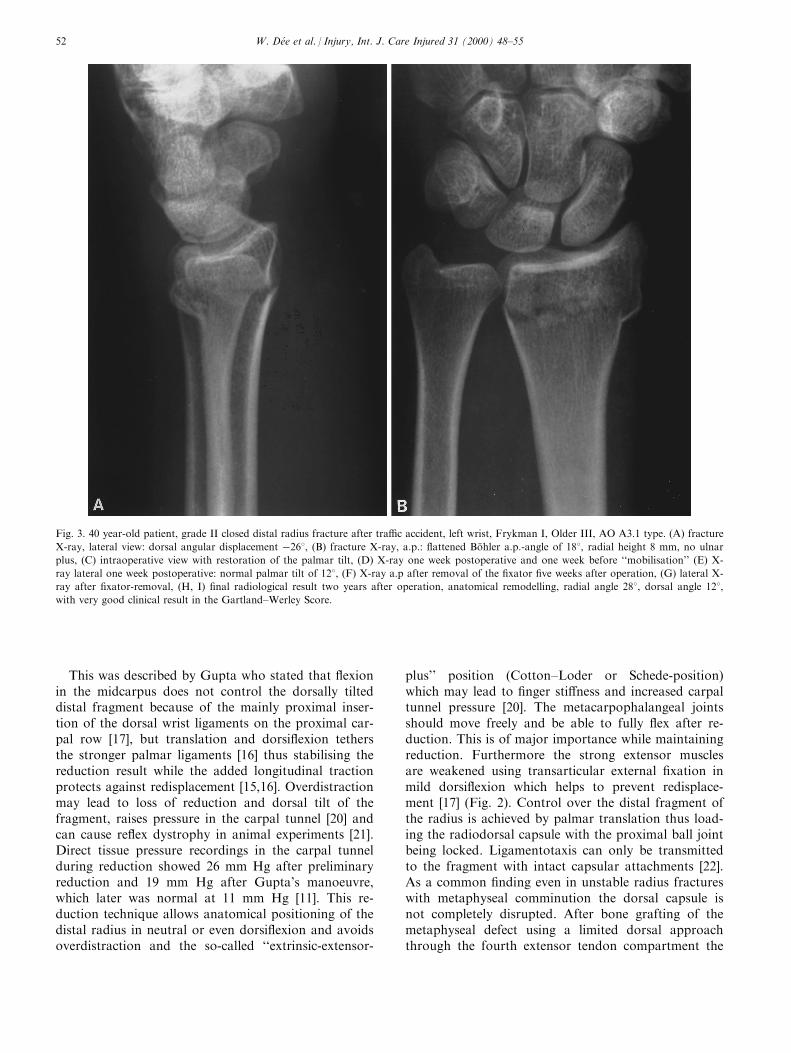
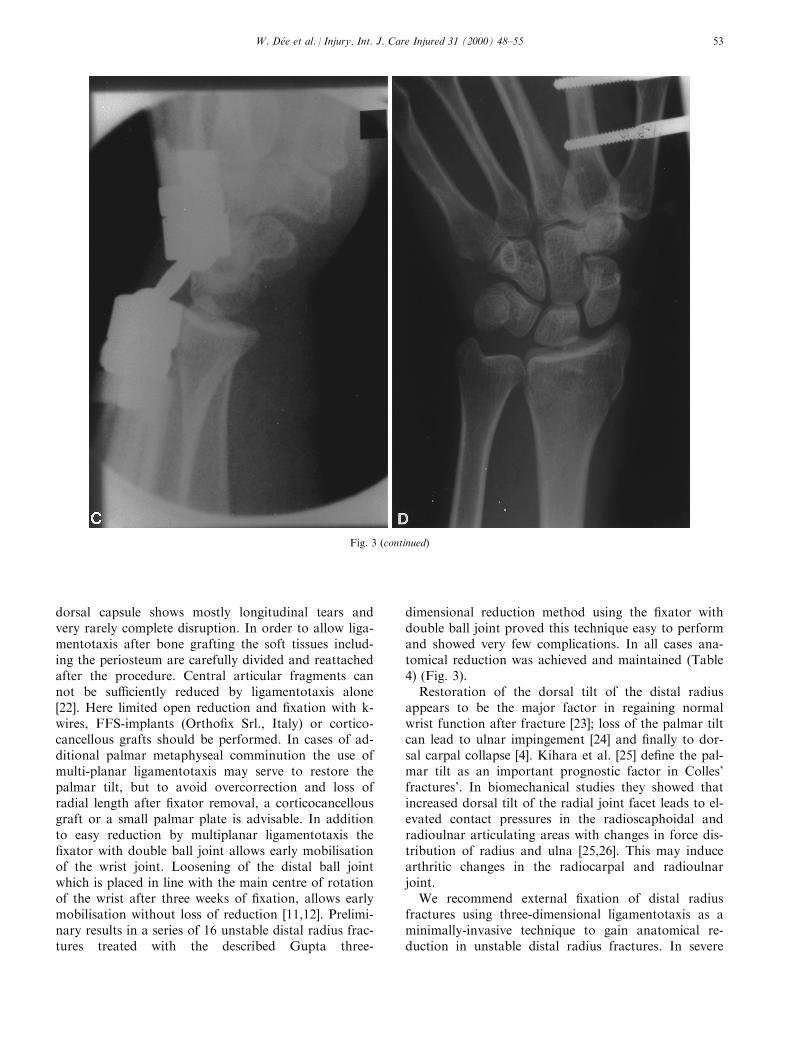
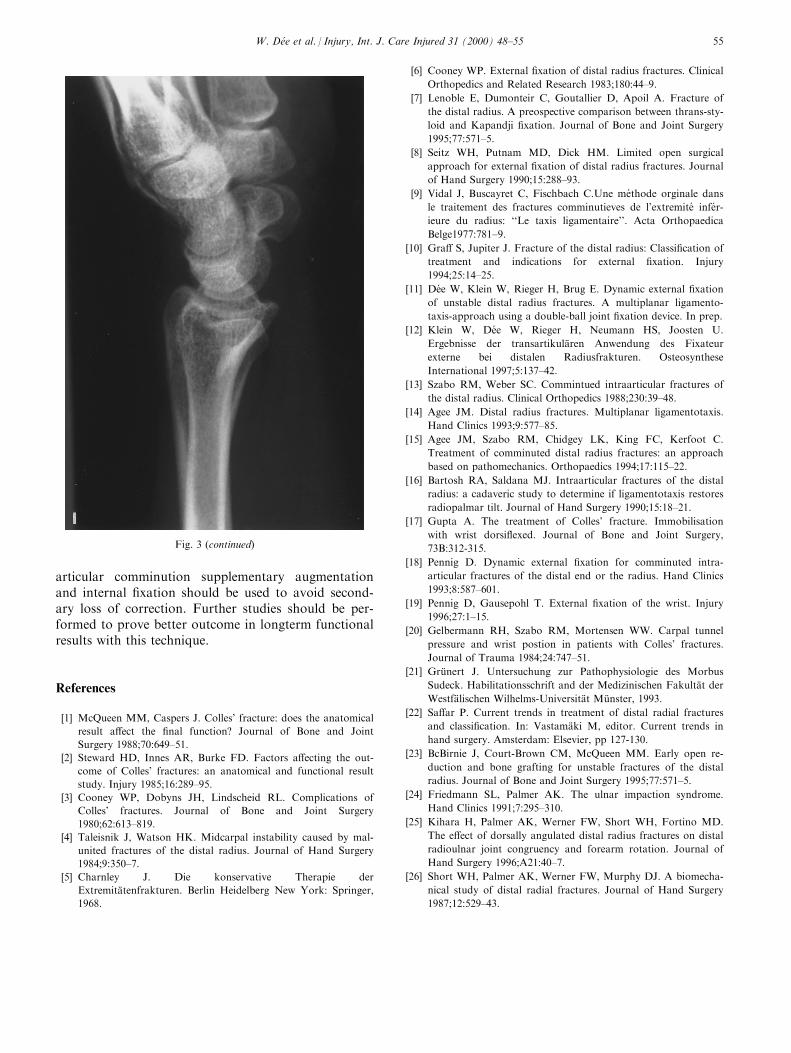
Fig. 3. 40 year-old patient, grade II closed distal radius fracture after tra�c accident, left wrist, Frykman I, Older III, AO A3.1 type. (A) fracture
X-ray, lateral view: dorsal angular displacement ÿ268, (B) fracture X-ray, a.p.: ¯attened BoÈ hler a.p.-angle of 188, radial height 8 mm, no ulnar
plus, (C) intraoperative view with restoration of the palmar tilt, (D) X-ray one week postoperative and one week before ``mobilisation'' (E) X-
ray lateral one week postoperative: normal palmar tilt of 128, (F) X-ray a.p after removal of the ®xator ®ve weeks after operation, (G) lateral X-
ray after ®xator-removal, (H, I) ®nal radiological result two years after operation, anatomical remodelling, radial angle 288, dorsal angle 128,with very good clinical result in the Gartland±Werley Score.
W. DeÂe et al. / Injury, Int. J. Care Injured 31 (2000) 48±5552
dorsal capsule shows mostly longitudinal tears andvery rarely complete disruption. In order to allow liga-mentotaxis after bone grafting the soft tissues includ-ing the periosteum are carefully divided and reattachedafter the procedure. Central articular fragments cannot be su�ciently reduced by ligamentotaxis alone[22]. Here limited open reduction and ®xation with k-wires, FFS-implants (Ortho®x Srl., Italy) or cortico-cancellous grafts should be performed. In cases of ad-ditional palmar metaphyseal comminution the use ofmulti-planar ligamentotaxis may serve to restore thepalmar tilt, but to avoid overcorrection and loss ofradial length after ®xator removal, a corticocancellousgraft or a small palmar plate is advisable. In additionto easy reduction by multiplanar ligamentotaxis the®xator with double ball joint allows early mobilisationof the wrist joint. Loosening of the distal ball jointwhich is placed in line with the main centre of rotationof the wrist after three weeks of ®xation, allows earlymobilisation without loss of reduction [11,12]. Prelimi-nary results in a series of 16 unstable distal radius frac-tures treated with the described Gupta three-
dimensional reduction method using the ®xator withdouble ball joint proved this technique easy to performand showed very few complications. In all cases ana-tomical reduction was achieved and maintained (Table4) (Fig. 3).
Restoration of the dorsal tilt of the distal radiusappears to be the major factor in regaining normalwrist function after fracture [23]; loss of the palmar tiltcan lead to ulnar impingement [24] and ®nally to dor-sal carpal collapse [4]. Kihara et al. [25] de®ne the pal-mar tilt as an important prognostic factor in Colles'fractures'. In biomechanical studies they showed thatincreased dorsal tilt of the radial joint facet leads to el-evated contact pressures in the radioscaphoidal andradioulnar articulating areas with changes in force dis-tribution of radius and ulna [25,26]. This may inducearthritic changes in the radiocarpal and radioulnarjoint.
We recommend external ®xation of distal radiusfractures using three-dimensional ligamentotaxis as aminimally-invasive technique to gain anatomical re-duction in unstable distal radius fractures. In severe
Fig. 3 (continued)
W. DeÂe et al. / Injury, Int. J. Care Injured 31 (2000) 48±55 53
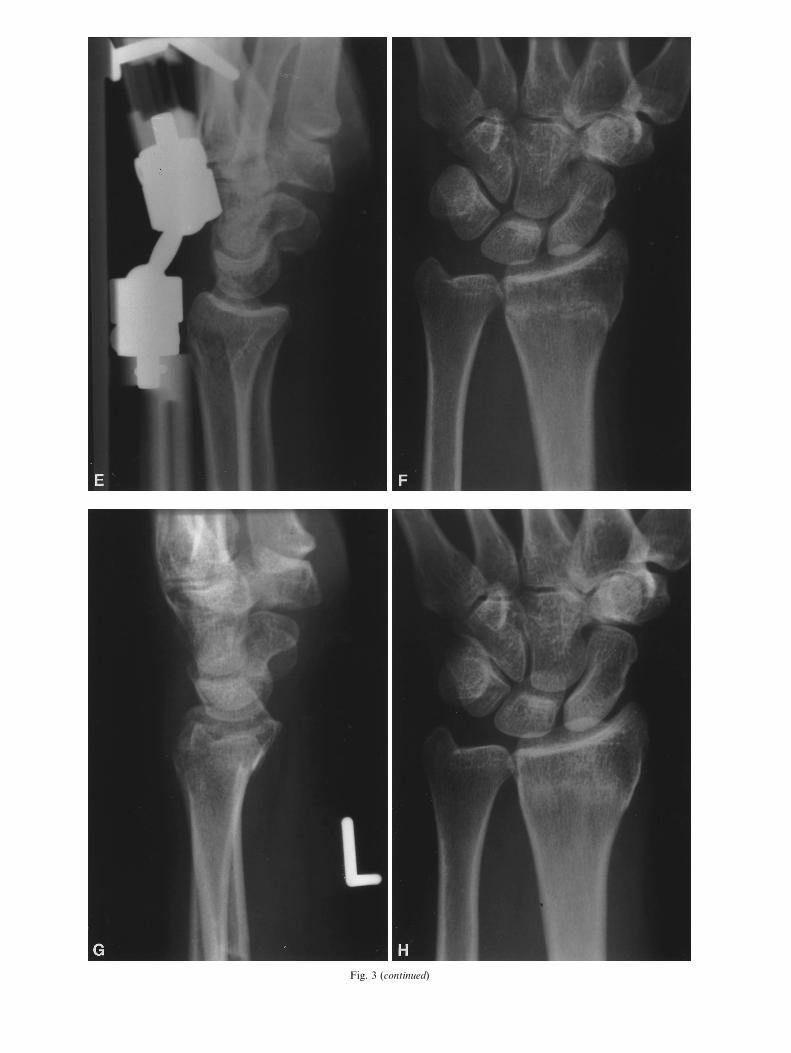
Fig. 3 (continued)
articular comminution supplementary augmentationand internal ®xation should be used to avoid second-ary loss of correction. Further studies should be per-formed to prove better outcome in longterm functionalresults with this technique.
References
[1] McQueen MM, Caspers J. Colles' fracture: does the anatomical
result a�ect the ®nal function? Journal of Bone and Joint
Surgery 1988;70:649±51.
[2] Steward HD, Innes AR, Burke FD. Factors a�ecting the out-
come of Colles' fractures: an anatomical and functional result
study. Injury 1985;16:289±95.
[3] Cooney WP, Dobyns JH, Lindscheid RL. Complications of
Colles' fractures. Journal of Bone and Joint Surgery
1980;62:613±819.
[4] Taleisnik J, Watson HK. Midcarpal instability caused by mal-
united fractures of the distal radius. Journal of Hand Surgery
1984;9:350±7.
[5] Charnley J. Die konservative Therapie der
ExtremitaÈ tenfrakturen. Berlin Heidelberg New York: Springer,
1968.
[6] Cooney WP. External ®xation of distal radius fractures. Clinical
Orthopedics and Related Research 1983;180:44±9.
[7] Lenoble E, Dumonteir C, Goutallier D, Apoil A. Fracture of
the distal radius. A preospective comparison between thrans-sty-
loid and Kapandji ®xation. Journal of Bone and Joint Surgery
1995;77:571±5.
[8] Seitz WH, Putnam MD, Dick HM. Limited open surgical
approach for external ®xation of distal radius fractures. Journal
of Hand Surgery 1990;15:288±93.
[9] Vidal J, Buscayret C, Fischbach C.Une me thode orginale dans
le traitement des fractures comminutieves de l'extremite infe r-
ieure du radius: ``Le taxis ligamentaire''. Acta Orthopaedica
Belge1977:781±9.
[10] Gra� S, Jupiter J. Fracture of the distal radius: Classi®cation of
treatment and indications for external ®xation. Injury
1994;25:14±25.
[11] De e W, Klein W, Rieger H, Brug E. Dynamic external ®xation
of unstable distal radius fractures. A multiplanar ligamento-
taxis-approach using a double-ball joint ®xation device. In prep.
[12] Klein W, De e W, Rieger H, Neumann HS, Joosten U.
Ergebnisse der transartikulaÈ ren Anwendung des Fixateur
externe bei distalen Radiusfrakturen. Osteosynthese
International 1997;5:137±42.
[13] Szabo RM, Weber SC. Commintued intraarticular fractures of
the distal radius. Clinical Orthopedics 1988;230:39±48.
[14] Agee JM. Distal radius fractures. Multiplanar ligamentotaxis.
Hand Clinics 1993;9:577±85.
[15] Agee JM, Szabo RM, Chidgey LK, King FC, Kerfoot C.
Treatment of comminuted distal radius fractures: an approach
based on pathomechanics. Orthopaedics 1994;17:115±22.
[16] Bartosh RA, Saldana MJ. Intraarticular fractures of the distal
radius: a cadaveric study to determine if ligamentotaxis restores
radiopalmar tilt. Journal of Hand Surgery 1990;15:18±21.
[17] Gupta A. The treatment of Colles' fracture. Immobilisation
with wrist dorsi¯exed. Journal of Bone and Joint Surgery,
73B:312-315.
[18] Pennig D. Dynamic external ®xation for comminuted intra-
articular fractures of the distal end or the radius. Hand Clinics
1993;8:587±601.
[19] Pennig D, Gausepohl T. External ®xation of the wrist. Injury
1996;27:1±15.
[20] Gelbermann RH, Szabo RM, Mortensen WW. Carpal tunnel
pressure and wrist postion in patients with Colles' fractures.
Journal of Trauma 1984;24:747±51.
[21] GruÈ nert J. Untersuchung zur Pathophysiologie des Morbus
Sudeck. Habilitationsschrift and der Medizinischen FakultaÈ t der
WestfaÈ lischen Wilhelms-UniversitaÈ t MuÈ nster, 1993.
[22] Sa�ar P. Current trends in treatment of distal radial fractures
and classi®cation. In: VastamaÈ ki M, editor. Current trends in
hand surgery. Amsterdam: Elsevier, pp 127-130.
[23] BcBirnie J, Court-Brown CM, McQueen MM. Early open re-
duction and bone grafting for unstable fractures of the distal
radius. Journal of Bone and Joint Surgery 1995;77:571±5.
[24] Friedmann SL, Palmer AK. The ulnar impaction syndrome.
Hand Clinics 1991;7:295±310.
[25] Kihara H, Palmer AK, Werner FW, Short WH, Fortino MD.
The e�ect of dorsally angulated distal radius fractures on distal
radioulnar joint congruency and forearm rotation. Journal of
Hand Surgery 1996;A21:40±7.
[26] Short WH, Palmer AK, Werner FW, Murphy DJ. A biomecha-
nical study of distal radial fractures. Journal of Hand Surgery
1987;12:529±43.
Fig. 3 (continued)
W. DeÂe et al. / Injury, Int. J. Care Injured 31 (2000) 48±55 55



























![[Fixation of distal radial fractures with the Targon DR nail]](https://img.pdfslide.net/doc/110x75/634b651f9fa0ab3f6b087795/fixation-of-distal-radial-fractures-with-the-targon-dr-nail.jpg)

