Embed Size (px)
Citation preview

Distal Radius Fractures: Strategic Alternativesto Volar Plate Fixation
Christopher J. Dy, MD MSPHScott W. Wolfe, MD
Jesse B. Jupiter, MDPhilip E. Blazar, MDDavid S. Ruch, MD
Douglas P. Hanel, MD
Fractures of the distal radius arecommon, and the incidence of theseinjuries continues to increase.1 Abroad range of individuals are affected,from young patients with high-energyinjuries to elderly patients with osteo-porotic fragility fractures. Treatmentstrategies have evolved along with anunderstanding of these injuries, withrecent epidemiologic studies indicat-ing the growing use of internal fixa-tion.2,3 Volar locking plates haveprovided surgeons with enhanced ca-pability to reliably repair both simpleand complex fractures while avoidingthe hardware-related complications as-sociated with dorsal plating.4 How-ever, there is a growing body of litera-ture reporting the frequency and typesof complications and failures associ-ated with distal radius fracture fixationwith volar locking plates.5 An assess-ment of fracture characteristics willallow the surgeon to select an individ-ualized treatment strategy that maxi-mizes the chances of success.
Dr. Dy or an immediate family member serves as a board member, owner, officer, or committee member of theAccreditation Council for Graduate Medical Education. Dr. Wolfe or an immediate family member has receivedroyalties from Extremity Medical; is a member of a speakers’ bureau or has made paid presentations on behalf ofTriMed; serves as a paid consultant to or is an employee of Extremity Medical; has received research or institu-tional support from Integra AxoGen; and serves as a board member, owner, officer, or committee member of theNew York Society for Surgery of the Hand. Dr. Jupiter or an immediate family member serves as a paid consul-tant to or is an employee of OHK; serves as an unpaid consultant to Synthes TriMed; has received research or in-stitutional support from the AO Foundation; has stock or stock options held in OHK; and is a member of aspeakers’ bureau or has made paid presentations on behalf of the AAHS Board Curriculum Committee. Dr. Bla-zar or an immediate family member serves as a paid consultant to or is an employee of Auxillium Pharmaceuti-cals and has received research or institutional support from Auxillium Pharmaceuticals. Dr. Ruch or an imme-diate family member has received research or institutional support from Synthes and serves as a board member,owner, officer, or committee member of the American Society for Surgery of the Hand. Dr. Hanel or an imme-diate family member serves as a paid consultant to or is an employee of Aptis Medical.
AbstractVolar locking plates have provided surgeons with enhanced capability to reliablyrepair both simple and complex fractures and avoid the hardware-related compli-cations associated with dorsal plating. However, there have been an increasingnumber of published reports on the frequency and types of complications and fail-ures associated with volar locked plating of distal radius fractures. An informed,critical assessment of distal radius fracture characteristics will allow surgeons to se-lect an individualized treatment strategy that maximizes the likelihood of a suc-cessful outcome. Knowledge of the anatomy, patterns, and characteristics of the di-verse types of distal radius fractures and the complications and failures associatedwith volar locked plating will be helpful to orthopaedic surgeons who treat patientswith these injuries.
Instr Course Lect 2014;63:27-37.
3
© 2014 AAOS Instructional Course Lectures, Volume 63 27
Anatomic and BiomechanicalConsiderationsCurrent approaches to the managementof distal radius fractures are based on theprinciple that restoration of normalanatomy will facilitate an expeditious re-turn to function.6,7 Careful consider-ation of the anatomy and biomechan-ics of the injury will help the surgeonchoose a treatment strategy to restorethe normal stability and load-bearingcharacteristics of the wrist.
The three-column theory of the dis-tal radius and ulna is particularly help-ful in understanding the biomechani-cal rationale for treating distal radiusfractures.8,9 The lateral (radial) col-umn, composed of the radial styloidand the scaphoid fossa, provides radio-carpal stability through the styloid’s os-seous buttress and the origin of thepalmar radiocarpal ligaments. Restor-ing the intermediate column, com-posed of the lunate fossa and sigmoidnotch, reestablishes the primary load-
bearing surface of the radiocarpaljoint.9 Reducing the articular surfaceof the sigmoid notch provides congru-ity to the distal radioulnar joint(DRUJ) and tensions its soft-tissue at-tachments.10,11 Restoring the volar lu-nate facet provides radiocarpal stabilityvia a bony buttress (the teardrop orcritical corner) and the ligamentoussupport of the short radiolunate liga-ment.12 Restoring the integrity of themedial (or ulnar) column, composedof the distal ulna and triangular fibro-cartilage complex (TFCC), allows it toserve as a fulcrum for rotating the ra-dius and share in load transmissionfrom the carpus.9
The optimal management of a dis-tal radius fracture will ensure restora-tion of each column. The radial andintermediate columns are anatomicallyreduced and rigidly fixed, and the me-dial column is stabilized as necessarythrough bony fixation, TFCC repair,and/or immobilization.8 During pre-
operative planning, careful attentionshould be paid to fractures that areparticularly prone to radiocarpal insta-bility (such as articular shearing frac-tures),13 loss of fixation (such as lunatefacet fractures), and fractures that mayrequire direct articular visualizationand reconstruction (such as extensivelyimpacted articular fractures). Each ofthese fracture characteristics shouldalert the surgeon that adequate frac-ture fixation may not be possible usingonly volar plating; however, the frac-ture can be successfully managed ifthese characteristics are recognizedpreoperatively or intraoperatively.14,15
Complications AssociatedWith Volar Locking PlatesSince their introduction, volar lockingplates have been reliably used to treatdisplaced distal radius fractures.16,17
The fixed-angle construct minimizesthe load transmitted to the often-comminuted metaphysis while de-creasing the risks of screw looseningand loss of reduction.18 Successful re-ports of fixation with volar platingwere contemporaneous with the in-creasing frequency of hardware-relatedcomplications from dorsal plating,leading to the rapid adoption of volarplating to fix dorsally angulated frac-tures.4,19
Although volar plates are increas-ingly used to manage many injury pat-terns, complications are associatedwith these implants. These complica-tions can be divided into two main cat-egories: tendon-related and loss of fixa-tion (Table 1). Other complications,including complex regional pain syn-drome and neurologic injury, occurless frequently and are less directly re-lated to the hardware.5,20,21
Tendon-Related ComplicationsExtensor TendonsAlthough avoidance of extensor ten-don irritation was seen as a key advan-
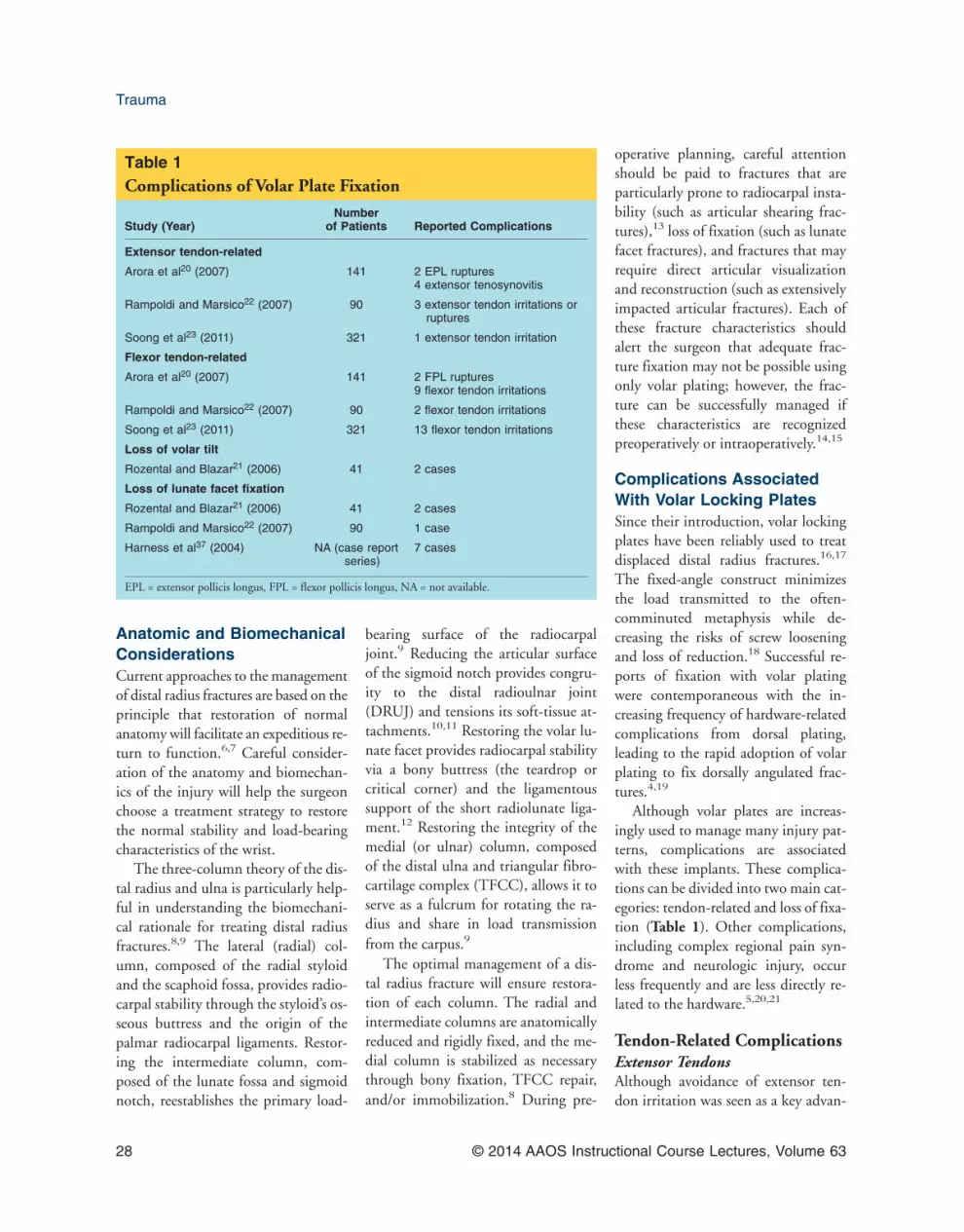
Table 1Complications of Volar Plate Fixation
Study (Year)Number
of Patients Reported Complications
Extensor tendon-related
Arora et al20 (2007) 141 2 EPL ruptures4 extensor tenosynovitis
Rampoldi and Marsico22 (2007) 90 3 extensor tendon irritations orruptures
Soong et al23 (2011) 321 1 extensor tendon irritation
Flexor tendon-related
Arora et al20 (2007) 141 2 FPL ruptures9 flexor tendon irritations
Rampoldi and Marsico22 (2007) 90 2 flexor tendon irritations
Soong et al23 (2011) 321 13 flexor tendon irritations
Loss of volar tilt
Rozental and Blazar21 (2006) 41 2 cases
Loss of lunate facet fixation
Rozental and Blazar21 (2006) 41 2 cases
Rampoldi and Marsico22 (2007) 90 1 case
Harness et al37 (2004) NA (case reportseries)
7 cases
EPL = extensor pollicis longus, FPL = flexor pollicis longus, NA = not available.
Trauma
28 © 2014 AAOS Instructional Course Lectures, Volume 63
tage of volar locking plate fixation fordorsally displaced fractures, damage tothe extensor tendons still occurs fromdrill tips, prominent screws, and dis-placed bony fragments (Figure 1).Arora et al20 reported 2 ruptures of theextensor pollicis longus and 4 patientswith extensor tenosynovitis in a seriesof 141 consecutive patients with dor-sally displaced distal radius fracturestreated with a volar locking plate. In astudy of 90 patients with distal radiusfractures treated with volar plate fixa-tion, Rampoldi and Marisco22 re-ported 3 extensor tendon irritations orruptures.22 In the largest series of pa-tients followed for complications aftervolar plating, Soong et al23 reportedthat 1 of 321 patients had plate-relatedextensor tendon irritation.
Despite its relative rarity, this chap-ter’s authors attempt to prevent intra-operative extensor tendon damage andpostoperative extensor tendon irrita-tion by drilling only the volar cortexand inserting unicortical locked screwsthat are slightly shorter than the mea-
sured amount, particularly in the set-ting of dorsal comminution. Alterna-tively, if the fracture necessitatesbicortical fixation, full-length smoothpegs are preferred. This practice is sub-stantiated by a biomechanical study byWall et al24 that reported no differencein axial or sagittal stiffness force amongfull-length bicortical screws, unicorti-cal screws (full length, 75% length,and 50% length), and unicortical pegsin an osteoporotic distal radius model.
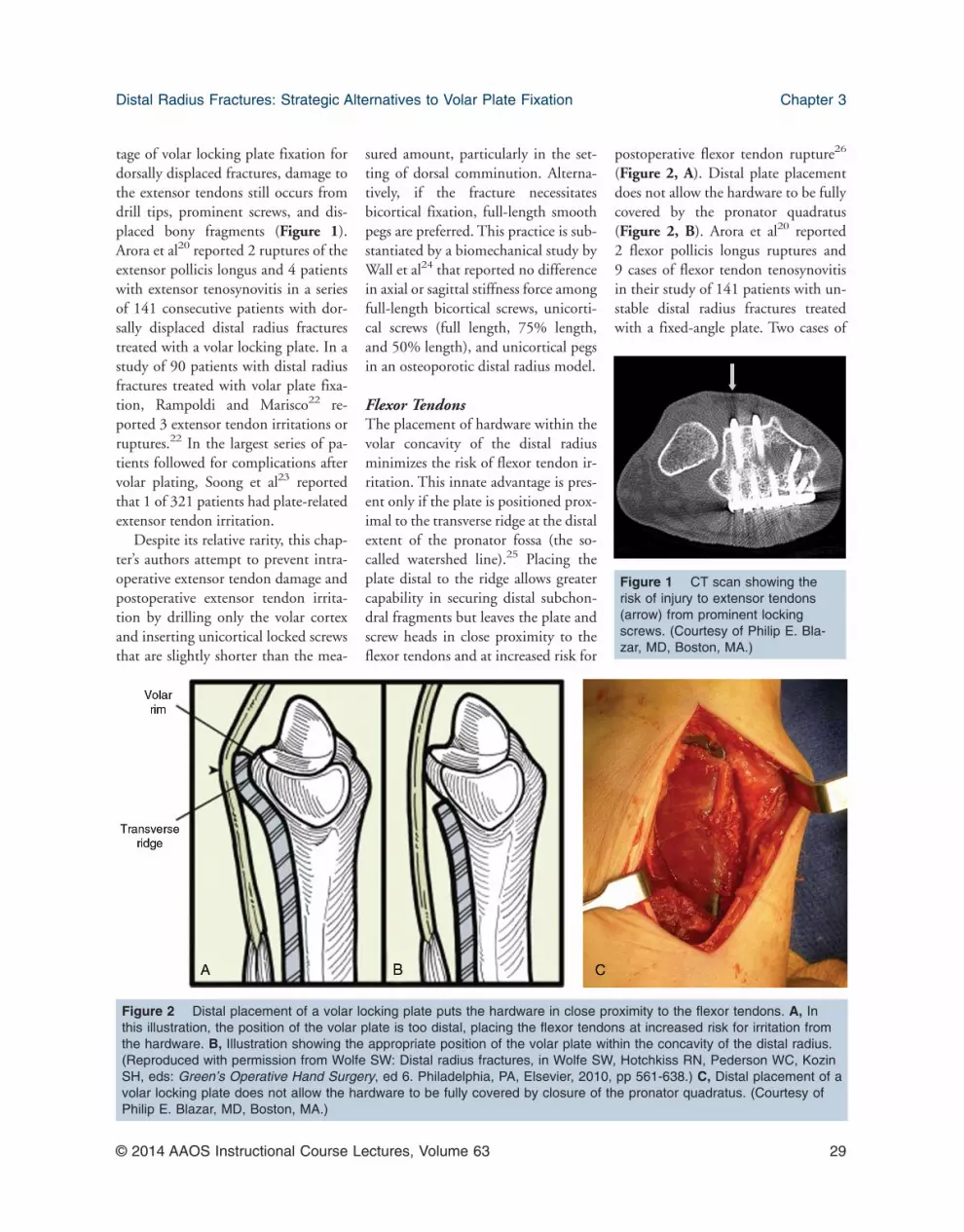
Flexor TendonsThe placement of hardware within thevolar concavity of the distal radiusminimizes the risk of flexor tendon ir-ritation. This innate advantage is pres-ent only if the plate is positioned prox-imal to the transverse ridge at the distalextent of the pronator fossa (the so-called watershed line).25 Placing theplate distal to the ridge allows greatercapability in securing distal subchon-dral fragments but leaves the plate andscrew heads in close proximity to theflexor tendons and at increased risk for
postoperative flexor tendon rupture26
(Figure 2, A). Distal plate placementdoes not allow the hardware to be fullycovered by the pronator quadratus(Figure 2, B). Arora et al20 reported2 flexor pollicis longus ruptures and9 cases of flexor tendon tenosynovitisin their study of 141 patients with un-stable distal radius fractures treatedwith a fixed-angle plate. Two cases of
Figure 1 CT scan showing therisk of injury to extensor tendons(arrow) from prominent lockingscrews. (Courtesy of Philip E. Bla-zar, MD, Boston, MA.)
Figure 2 Distal placement of a volar locking plate puts the hardware in close proximity to the flexor tendons. A, Inthis illustration, the position of the volar plate is too distal, placing the flexor tendons at increased risk for irritation fromthe hardware. B, Illustration showing the appropriate position of the volar plate within the concavity of the distal radius.(Reproduced with permission from Wolfe SW: Distal radius fractures, in Wolfe SW, Hotchkiss RN, Pederson WC, KozinSH, eds: Green’s Operative Hand Surgery, ed 6. Philadelphia, PA, Elsevier, 2010, pp 561-638.) C, Distal placement of avolar locking plate does not allow the hardware to be fully covered by closure of the pronator quadratus. (Courtesy ofPhilip E. Blazar, MD, Boston, MA.)
Distal Radius Fractures: Strategic Alternatives to Volar Plate Fixation Chapter 3
© 2014 AAOS Instructional Course Lectures, Volume 63 29

flexor tendon irritation in 90 patientswere reported by Rampoldi and Mar-sico,22 and 13 cases of plate-relatedflexor tendon irritation were reportedin 321 patients by Soong et al.23 Giventhat delayed flexor tendon rupture hasbeen reported up to 5 years after volarplating,27 there should be a low thresh-old of consideration for hardware re-moval if there is concern about flexortendon irritation. Ultrasound or MRIcan be useful in identifying synovitisor attritional changes in at-risk flexortendons. Retained drilling guides fromscrew insertion and loosening of im-properly engaged locking screws havebeen reported as mechanisms for flexortendon irritation after volar plat-ing.20,28
Loss of Fixation AfterVolar PlatingLoss of Volar TiltThe restoration of radiocarpal align-ment in the sagittal plane substantiallyinfluences functional outcomes andgrip strength after distal radius fracturetreatment.29 After achieving intraoper-ative reduction of anatomic sagittaltilt, the volar fixed-angle construct canbe used to secure reduction withoutapplying an implant to the dorsal sur-face. However, long-term clinical suc-cess has been correlated with mainte-nance of sagittal collinearity of theradius and the carpus.29 The biome-chanical stability of the construct iscontingent on the distance of the distalscrews from subchondral bone, withthe highest resistance to metaphysealsettling seen with screws inserted asclose to subchondral bone as possi-ble.30 Because fractures with extensivedorsal comminution are believed to beat greatest risk for loss of volar tilt,multiple fluoroscopic views should beused to maximize subchondral screwpurchase distal to the zone of commi-nution.21,31
Loss of Fixationin the Lunate FacetThe importance of the volar lunatefacet as the cornerstone of stability forthe radiocarpal joint and the DRUJwas reported by Melone.10 The effectsof this fragment on radiocarpal insta-bility have been emphasized, andawareness of its importance for DRUJstability is increasing.32-35 The volaraspect of the lunate facet contains a ra-diographic prominence (teardrop) thatprovides stability against volar sublux-ation by serving as a bony buttress atthe origin of the short radiolunate liga-ment.12,36 Loss of fixation of the volarlunate facet has been widely recog-nized as a mechanism of failure aftervolar plating.21,22,37 Because the tear-drop is less than 5 mm wide and has arelatively steep volar slope, it is diffi-cult for the ulnar limb of volar lockingplates to provide adequate stabiliza-tion.37,38 This chapter’s authors be-lieve that at least two points of fixationare needed within this critical corner ofthe intermediate column. The newestvolar locking plates feature two distalrows of multiaxial locking screws, pro-viding the potential to achieve addi-tional screw purchase within the volarlunate facet.39 However, it is unlikelythat the additional proximal row ofscrews provides sufficient distal cap-ture for this small fragment, and distalplacement of the entire plate comes atthe expense of potential flexor tendonirritation. Given this risk, alternatemethods of fixation are often preferredto secure the volar lunate facet frag-ment. Plating of the intermediate col-umn can be accomplished through avolar-ulnar incision using a buttresspin, a mini plate-and-screw construct,or a tension banding tech-nique.14,34,40,41 These fixation tech-niques can be used as part of a multi-column internal fixation approach oran approach augmented by externalfixation.8,34
What Cannot Be FixedWith a Volar Plate?Dorsal Ulnar FragmentThe displaced dorsal ulnar fragment isparticularly challenging to controlwith a volar implant. Although not alldorsal ulnar fragments require stabili-zation, it is important to recognize thatthis fragment comprises a portion ofboth the radiolunate and radioulnararticular surfaces, and displacement oflarger fragments can lead to instabilityof either joint. The inability to securethe dorsal ulnar fragment, dependingon its size, can prevent the mainte-nance of adequate sagittal radiocarpalalignment and predispose the fractureto dorsal collapse. Although dorsalcomminution and articular impactioncan be addressed using an extendedflexor carpi radialis approach,42 thistechnique relies on indirect articularreduction and gaining adequate indi-rect purchase of the dorsal fragmentswith volarly to dorsally placed screws.A dorsal approach provides the sur-geon with the advantage of visualizingand directly reducing the articular sur-face, often through a limited and tar-geted approach. The application of adorsally based implant also provides abuttress against dorsal fragment dis-placement, which decreases the risk ofsecondary collapse.
As previously mentioned, the fre-quency of hardware-related irritationof the extensor tendons was a majorlimitation of conventional dorsally ap-plied implants. This prompted the de-velopment of low-profile dorsal plates;however, these plates had inherentlyless material strength. In recognizingthe need to strategically apply thesesmaller plates, Rikli and Regazzoni8
introduced the concept of multicol-umn fixation. They achieved stable fix-ation and promising clinical results us-ing 2.0-mm plates positioned on thelateral and intermediate columns at50° to 70° from each other.8,43 Biome-
Trauma
30 © 2014 AAOS Instructional Course Lectures, Volume 63

chanical studies supported the multi-column strategy, with superior stiffnesscompared with both augmented exter-nal fixation and conventional dorsalplates.44,45 Because of persistent im-plant irritation, a system of even lower-profile pin-plates and wireforms wasdeveloped.40,43,46 This fragment-specific implant system allows the sur-geon greater versatility in selecting im-plants for challenging fracturepatterns, such as those that include adorsal ulnar fragment. Using a pin-plate to secure the dorsal ulnar cornerallows buttressing of the deformitywhile minimizing the risk of soft-tissueirritation. Multicolumn fixation withfragment-specific implants has beenused with good to excellent results andno reported extensor tendon rup-tures.40,47,48
The specific utility of multicolumnfixation for stabilizing the dorsal ulnarfragment is substantiated by biome-chanical testing. During loads ex-pected in the rehabilitation phase, thedorsal ulnar pin-plate provided a but-tress effect against dorsal closure of theosteotomy that was not provided bythe volar locking plate.49 A biome-chanical evaluation by Taylor et al50
demonstrated that a multicolumn ap-proach using a dorsal ulnar pin-plateprovided greater stiffness for the ulnar-sided fracture fragment than a volarlocking plate. When viewed in con-junction, these studies indicate thatmulticolumn plating provides an ad-vantage over volar locking plates in se-curing the intermediate column andopposing dorsal fracture collapse.
Volar Ulnar FragmentAs previously mentioned, the volar ul-nar fragment is regarded as the corner-stone of the radiocarpal joint and theDRUJ because it plays critical roles inmaintaining sagittal alignment, trans-mitting the load from the carpus, andproviding sigmoid notch congru-
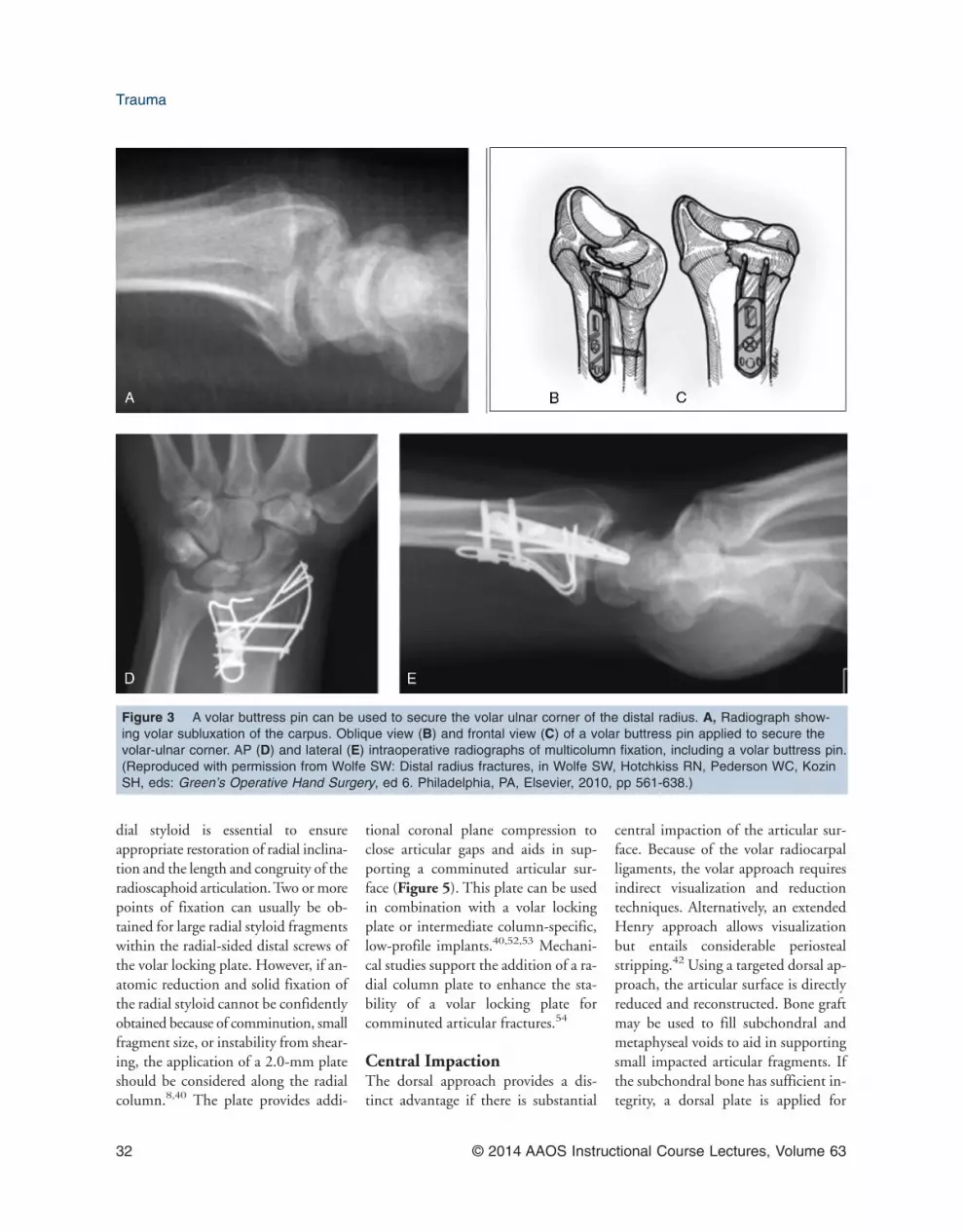
ity.9,10,37 The challenges of securingthe volar ulnar fragment with a volarlocking plate mainly arise from thesmall size and sloping morphology ofthe fragment.38 Given the contour ofcurrently available volar locking plates,it is difficult to achieve multiple pointsof fixation within the volar ulnar frag-ment. Moving the plate more distallyputs the flexor tendons at increasedrisk for irritation, whereas using a mul-tiaxial guide to obtain more distal andulnar screw trajectories increases therisk of screw placement within the ra-diocarpal joint or the DRUJ. Theshortcomings of using volar lockingplate fixation in this situation havebeen recognized along with the needfor smaller implants that can be placedmore distally.21,37 It has been reportedthat Kirschner wires, tension-bandwiring, and miniplates provide ade-quate fixation of the volar ulnar cor-ner.34,41 The volar buttress pin hasbeen reported to provide rapid and se-cure fixation of small critical cornerfragments.14,15,40 Provisional fixationof the fragment is performed with aKirschner wire, and sagittal radiocar-pal alignment and stability are care-fully assessed. The buttress pin has twoprongs that provide fixed-angle sup-port within the subchondral bone(Figure 3). The proximal aspect of thevolar buttress pin implant is secured tothe intact diaphysis with 2.0-mmscrews and washers. Although the im-plant can be applied through the stan-dard volar approach, a limited ap-proach between the flexor tendons andthe ulnar neurovascular bundle is help-ful when performing multicolumn fix-ation with multiple incisions.14,15
Care must be taken to avoid tractionon the median nerve and the palmarcutaneous branch if applying an ulnar-sided implant through a standardHenry approach.
Marginal ArticularShear FracturesMarginal shearing fractures (Fernan-dez type II) are difficult to treat withvolar locking plates for many of thesame reasons described for dorsal andvolar ulnar fragments13 (Figure 4).Dorsal shearing fractures (reverse Bar-ton fractures) are associated with ra-diocarpal subluxation or dislocation.These fractures are relatively uncom-mon; are usually caused by high-energy mechanisms; and often have aspectrum of associated volar injuries,including carpal ligament tears, articu-lar impaction, and volar marginalshearing.51 Because of the direction ofthe associated radiocarpal instability,these injuries are often best ap-proached from the dorsal side. Articu-lar impaction can be directly assessedfrom this approach, and bone graftingis often helpful to provide subchondralsupport. The fracture is then but-tressed with a dorsally based implantto minimize the risk of recurrent insta-bility.51 Low-profile implants of vari-ous sizes, ranging from 2.0-mm to3.5-mm dorsal plates to fragment-specific pin-plates or wireforms can beused (Figure 4). The surgeon choosesthe implant based on the fracture char-acteristics and the soft-tissue coveragecapability. Volar shearing fractures(and the treatment of volar injuries as-sociated with dorsal marginal shearingfractures) require an analogous ap-proach. Larger fragments can be stabi-lized with volar locking plates; how-ever, marginal shear fragmentstypically require the use of low-profile,distally positioned implants to buttressthe articular surface.
Unstable Radial StyloidThe radial styloid plays a critical rolein radiocarpal stability, providing bothan osseous buttress and the ligamen-tous origin of the stout palmar radio-carpal ligaments.9 Reduction of the ra-
Distal Radius Fractures: Strategic Alternatives to Volar Plate Fixation Chapter 3
© 2014 AAOS Instructional Course Lectures, Volume 63 31
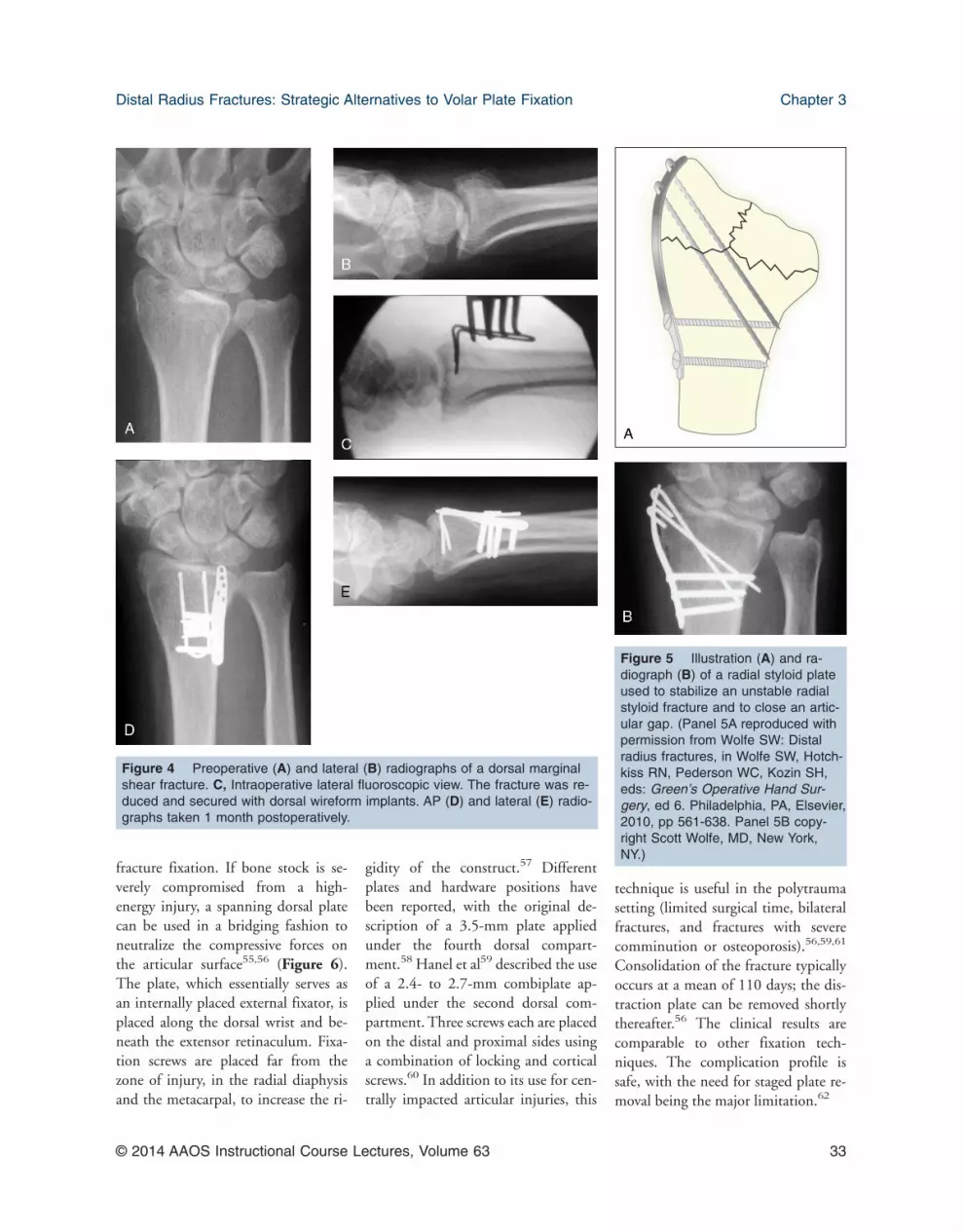
dial styloid is essential to ensureappropriate restoration of radial inclina-tion and the length and congruity of theradioscaphoid articulation. Two or morepoints of fixation can usually be ob-tained for large radial styloid fragmentswithin the radial-sided distal screws ofthe volar locking plate. However, if an-atomic reduction and solid fixation ofthe radial styloid cannot be confidentlyobtained because of comminution, smallfragment size, or instability from shear-ing, the application of a 2.0-mm plateshould be considered along the radialcolumn.8,40 The plate provides addi-
tional coronal plane compression toclose articular gaps and aids in sup-porting a comminuted articular sur-face (Figure 5). This plate can be usedin combination with a volar lockingplate or intermediate column-specific,low-profile implants.40,52,53 Mechani-cal studies support the addition of a ra-dial column plate to enhance the sta-bility of a volar locking plate forcomminuted articular fractures.54
Central ImpactionThe dorsal approach provides a dis-tinct advantage if there is substantial
central impaction of the articular sur-face. Because of the volar radiocarpalligaments, the volar approach requiresindirect visualization and reductiontechniques. Alternatively, an extendedHenry approach allows visualizationbut entails considerable periostealstripping.42 Using a targeted dorsal ap-proach, the articular surface is directlyreduced and reconstructed. Bone graftmay be used to fill subchondral andmetaphyseal voids to aid in supportingsmall impacted articular fragments. Ifthe subchondral bone has sufficient in-tegrity, a dorsal plate is applied for
Figure 3 A volar buttress pin can be used to secure the volar ulnar corner of the distal radius. A, Radiograph show-ing volar subluxation of the carpus. Oblique view (B) and frontal view (C) of a volar buttress pin applied to secure thevolar-ulnar corner. AP (D) and lateral (E) intraoperative radiographs of multicolumn fixation, including a volar buttress pin.(Reproduced with permission from Wolfe SW: Distal radius fractures, in Wolfe SW, Hotchkiss RN, Pederson WC, KozinSH, eds: Green’s Operative Hand Surgery, ed 6. Philadelphia, PA, Elsevier, 2010, pp 561-638.)
Trauma
32 © 2014 AAOS Instructional Course Lectures, Volume 63
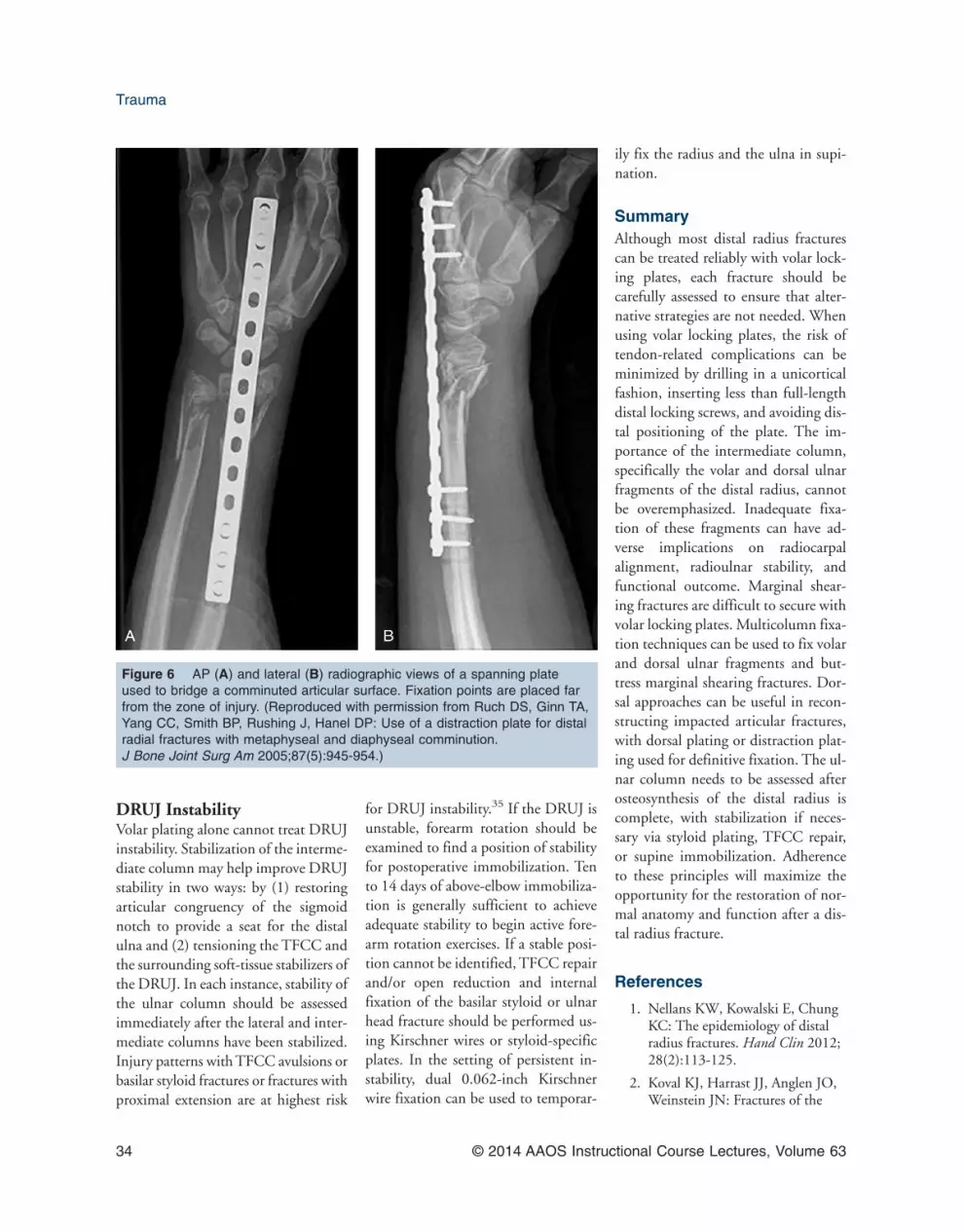
fracture fixation. If bone stock is se-verely compromised from a high-energy injury, a spanning dorsal platecan be used in a bridging fashion toneutralize the compressive forces onthe articular surface55,56 (Figure 6).The plate, which essentially serves asan internally placed external fixator, isplaced along the dorsal wrist and be-neath the extensor retinaculum. Fixa-tion screws are placed far from thezone of injury, in the radial diaphysisand the metacarpal, to increase the ri-
gidity of the construct.57 Differentplates and hardware positions havebeen reported, with the original de-scription of a 3.5-mm plate appliedunder the fourth dorsal compart-ment.58 Hanel et al59 described the useof a 2.4- to 2.7-mm combiplate ap-plied under the second dorsal com-partment. Three screws each are placedon the distal and proximal sides usinga combination of locking and corticalscrews.60 In addition to its use for cen-trally impacted articular injuries, this
technique is useful in the polytraumasetting (limited surgical time, bilateralfractures, and fractures with severecomminution or osteoporosis).56,59,61
Consolidation of the fracture typicallyoccurs at a mean of 110 days; the dis-traction plate can be removed shortlythereafter.56 The clinical results arecomparable to other fixation tech-niques. The complication profile issafe, with the need for staged plate re-moval being the major limitation.62
Figure 4 Preoperative (A) and lateral (B) radiographs of a dorsal marginalshear fracture. C, Intraoperative lateral fluoroscopic view. The fracture was re-duced and secured with dorsal wireform implants. AP (D) and lateral (E) radio-graphs taken 1 month postoperatively.
Figure 5 Illustration (A) and ra-diograph (B) of a radial styloid plateused to stabilize an unstable radialstyloid fracture and to close an artic-ular gap. (Panel 5A reproduced withpermission from Wolfe SW: Distalradius fractures, in Wolfe SW, Hotch-kiss RN, Pederson WC, Kozin SH,eds: Green’s Operative Hand Sur-gery, ed 6. Philadelphia, PA, Elsevier,2010, pp 561-638. Panel 5B copy-right Scott Wolfe, MD, New York,NY.)
Distal Radius Fractures: Strategic Alternatives to Volar Plate Fixation Chapter 3
© 2014 AAOS Instructional Course Lectures, Volume 63 33
DRUJ InstabilityVolar plating alone cannot treat DRUJinstability. Stabilization of the interme-diate column may help improve DRUJstability in two ways: by (1) restoringarticular congruency of the sigmoidnotch to provide a seat for the distalulna and (2) tensioning the TFCC andthe surrounding soft-tissue stabilizers ofthe DRUJ. In each instance, stability ofthe ulnar column should be assessedimmediately after the lateral and inter-mediate columns have been stabilized.Injury patterns with TFCC avulsions orbasilar styloid fractures or fractures withproximal extension are at highest risk
for DRUJ instability.35 If the DRUJ isunstable, forearm rotation should beexamined to find a position of stabilityfor postoperative immobilization. Tento 14 days of above-elbow immobiliza-tion is generally sufficient to achieveadequate stability to begin active fore-arm rotation exercises. If a stable posi-tion cannot be identified, TFCC repairand/or open reduction and internalfixation of the basilar styloid or ulnarhead fracture should be performed us-ing Kirschner wires or styloid-specificplates. In the setting of persistent in-stability, dual 0.062-inch Kirschnerwire fixation can be used to temporar-
ily fix the radius and the ulna in supi-nation.
SummaryAlthough most distal radius fracturescan be treated reliably with volar lock-ing plates, each fracture should becarefully assessed to ensure that alter-native strategies are not needed. Whenusing volar locking plates, the risk oftendon-related complications can beminimized by drilling in a unicorticalfashion, inserting less than full-lengthdistal locking screws, and avoiding dis-tal positioning of the plate. The im-portance of the intermediate column,specifically the volar and dorsal ulnarfragments of the distal radius, cannotbe overemphasized. Inadequate fixa-tion of these fragments can have ad-verse implications on radiocarpalalignment, radioulnar stability, andfunctional outcome. Marginal shear-ing fractures are difficult to secure withvolar locking plates. Multicolumn fixa-tion techniques can be used to fix volarand dorsal ulnar fragments and but-tress marginal shearing fractures. Dor-sal approaches can be useful in recon-structing impacted articular fractures,with dorsal plating or distraction plat-ing used for definitive fixation. The ul-nar column needs to be assessed afterosteosynthesis of the distal radius iscomplete, with stabilization if neces-sary via styloid plating, TFCC repair,or supine immobilization. Adherenceto these principles will maximize theopportunity for the restoration of nor-mal anatomy and function after a dis-tal radius fracture.
References
1. Nellans KW, Kowalski E, ChungKC: The epidemiology of distalradius fractures. Hand Clin 2012;28(2):113-125.
2. Koval KJ, Harrast JJ, Anglen JO,Weinstein JN: Fractures of the
Figure 6 AP (A) and lateral (B) radiographic views of a spanning plateused to bridge a comminuted articular surface. Fixation points are placed farfrom the zone of injury. (Reproduced with permission from Ruch DS, Ginn TA,Yang CC, Smith BP, Rushing J, Hanel DP: Use of a distraction plate for distalradial fractures with metaphyseal and diaphyseal comminution.J Bone Joint Surg Am 2005;87(5):945-954.)
Trauma
34 © 2014 AAOS Instructional Course Lectures, Volume 63

distal part of the radius: The evo-lution of practice over time.Where’s the evidence? J Bone JointSurg Am 2008;90(9):1855-1861.
3. Chung KC, Shauver MJ, Birk-meyer JD: Trends in the UnitedStates in the treatment of distalradial fractures in the elderly.J Bone Joint Surg Am 2009;91(8):1868-1873.
4. Orbay JL, Fernandez DL: Volarfixation for dorsally displaced frac-tures of the distal radius: A pre-liminary report. J Hand Surg Am2002;27(2):205-215.
5. Berglund LM, Messer TM: Com-plications of volar plate fixationfor managing distal radius frac-tures. J Am Acad Orthop Surg2009;17(6):369-377.
6. Gartland JJ Jr, Werley CW: Eval-uation of healed Colles’ fractures.J Bone Joint Surg Am 1951;33(4):895-907.
7. McQueen M, Caspers J: Collesfracture: Does the anatomicalresult affect the final function?J Bone Joint Surg Br 1988;70(4):649-651.
8. Rikli DA, Regazzoni P: Fracturesof the distal end of the radiustreated by internal fixation andearly function: A preliminary re-port of 20 cases. J Bone Joint SurgBr 1996;78(4):588-592.
9. Rikli DA, Honigmann P, BabstR, Cristalli A, Morlock MM, Mit-tlmeier T: Intra-articular pressuremeasurement in the radioulnocar-pal joint using a novel sensor: Invitro and in vivo results. J HandSurg Am 2007;32(1):67-75.
10. Melone CP Jr: Articular fracturesof the distal radius. Orthop ClinNorth Am 1984;15(2):217-236.
11. Moritomo H: The distal in-terosseous membrane: Currentconcepts in wrist anatomy andbiomechanics. J Hand Surg Am2012;37(7):1501-1507.
12. Medoff RJ: Essential radiographicevaluation for distal radius frac-tures. Hand Clin 2005;21(3):279-288.
13. Fernández DL: Fractures of thedistal radius: Operative treatment.Instr Course Lect 1993;42:73-88.
14. Wolfe SW: Green’s OperativeHand Surgery, ed 6. Philadelphia,PA, Elsevier, 2010.
15. Lam JW, Wolfe SW: Distal radiusfractures: What cannot be fixedwith a volar plate? The role offragment-specific fixation in mod-ern fracture treatment. Oper TechSports Med 2010;18(3):181-188.
16. Gesensway D, Putnam MD,Mente PL, Lewis JL: Design andbiomechanics of a plate for thedistal radius. J Hand Surg Am1995;20(6):1021-1027.
17. Orbay JL: The treatment of unsta-ble distal radius fractures withvolar fixation. Hand Surg 2000;5(2):103-112.
18. Orbay JL, Touhami A: Currentconcepts in volar fixed-angle fixa-tion of unstable distal radius frac-tures. Clin Orthop Relat Res 2006;445:58-67.
19. Drobetz H, Kutscha-Lissberg E:Osteosynthesis of distal radialfractures with a volar lockingscrew plate system. Int Orthop2003;27(1):1-6.
20. Arora R, Lutz M, Hennerbi-chler A, Krappinger D, Espen D,Gabl M: Complications followinginternal fixation of unstable distalradius fracture with a palmarlocking-plate. J Orthop Trauma2007;21(5):316-322.
21. Rozental TD, Blazar PE: Func-tional outcome and complicationsafter volar plating for dorsallydisplaced, unstable fractures of thedistal radius. J Hand Surg Am2006;31(3):359-365.
22. Rampoldi M, Marsico S: Compli-cations of volar plating of distalradius fractures. Acta Orthop Belg2007;73(6):714-719.
23. Soong M, van Leerdam R, Guit-ton TG, Got C, Katarincic J,Ring D: Fracture of the distalradius: Risk factors for complica-
tions after locked volar plate fixa-tion. J Hand Surg Am 2011;36(1):3-9.
24. Wall LB, Brodt MD, Silva MJ,Boyer MI, Calfee RP: The effectsof screw length on stability ofsimulated osteoporotic distal ra-dius fractures fixed with volarlocking plates. J Hand Surg Am2012;37(3):446-453.
25. Orbay J: Volar plate fixation ofdistal radius fractures. Hand Clin2005;21(3):347-354.
26. Soong M, Earp BE, Bishop G,Leung A, Blazar P: Volar lockingplate implant prominence andflexor tendon rupture. J Bone JointSurg Am 2011;93(4):328-335.
27. Koo SC, Ho ST: Delayed ruptureof flexor pollicis longus tendonafter volar plating of the distalradius. Hand Surg 2006;11(1-2):67-70.
28. Bhattacharyya T, WadgaonkarAD: Inadvertent retention of an-gled drill guides after volar lockingplate fixation of distal radial frac-tures: A report of three cases.J Bone Joint Surg Am 2008;90(2):401-403.
29. McQueen MM, Hajducka C,Court-Brown CM: Redisplacedunstable fractures of the distalradius: A prospective randomisedcomparison of four methods oftreatment. J Bone Joint Surg Br1996;78(3):404-409.
30. Drobetz H, Bryant AL, PokornyT, Spitaler R, Leixnering M, Jupi-ter JB: Volar fixed-angle plating ofdistal radius extension fractures:Influence of plate position onsecondary loss of reduction. Abiomechanic study in a cadavericmodel. J Hand Surg Am 2006;31(4):615-622.
31. Soong M, Got C, Katarincic J,Akelman E: Fluoroscopic evalua-tion of intra-articular screw place-ment during locked volar platingof the distal radius: A cadavericstudy. J Hand Surg Am 2008;33(10):1720-1723.
Distal Radius Fractures: Strategic Alternatives to Volar Plate Fixation Chapter 3
© 2014 AAOS Instructional Course Lectures, Volume 63 35

32. Apergis E, Darmanis S, Theodo-ratos G, Maris J: Beware of theulno-palmar distal radial frag-ment. J Hand Surg Br 2002;27(2):139-145.
33. Smith RS, Crick JC, Alonso J,Horowitz M: Open reduction andinternal fixation of volar lip frac-tures of the distal radius. J OrthopTrauma 1988;2(3):181-187.
34. Ruch DS, Yang C, Smith BP:Results of palmar plating of thelunate facet combined with exter-nal fixation for the treatment ofhigh-energy compression fracturesof the distal radius. J OrthopTrauma 2004;18(1):28-33.
35. Cole DW, Elsaidi GA, KuzmaKR, Kuzma GR, Smith BP, RuchDS: Distal radioulnar joint insta-bility in distal radius fractures:The role of sigmoid notch andtriangular fibrocartilage complexrevisited. Injury 2006;37(3):252-258.
36. Berger RA, Landsmeer JM: Thepalmar radiocarpal ligaments: Astudy of adult and fetal humanwrist joints. J Hand Surg Am1990;15(6):847-854.
37. Harness NG, Jupiter JB, OrbayJL, Raskin KB, Fernandez DL:Loss of fixation of the volar lunatefacet fragment in fractures of thedistal part of the radius. J BoneJoint Surg Am 2004;86(9):1900-1908.
38. Andermahr J, Lozano-Calderon S,Trafton T, Crisco JJ, Ring D: Thevolar extension of the lunate facetof the distal radius: A quantitativeanatomic study. J Hand Surg Am2006;31(6):892-895.
39. Buzzell JE, Weikert DR, WatsonJT, Lee DH: Precontoured fixed-angle volar distal radius plates: Acomparison of anatomic fit.J Hand Surg Am 2008;33(7):1144-1152.
40. Konrath GA, Bahler S: Open re-duction and internal fixation ofunstable distal radius fractures:Results using the trimed fixation
system. J Orthop Trauma 2002;16(8):578-585.
41. Chin KR, Jupiter JB: Wire-loopfixation of volar displaced osteo-chondral fractures of the distalradius. J Hand Surg Am 1999;24(3):525-533.
42. Orbay JL, Badia A, Indriago IR,et al: A new perspective for thedistal radius fracture. Tech HandUp Extrem Surg 2001;5(4):204-211.
43. Jakob M, Rikli DA, Regazzoni P:Fractures of the distal radiustreated by internal fixation andearly function: A prospectivestudy of 73 consecutive patients.J Bone Joint Surg Br 2000;82(3):340-344.
44. Dodds SD, Cornelissen S, Jos-san S, Wolfe SW: A biomechani-cal comparison of fragment-specific fixation and augmentedexternal fixation for intra-articulardistal radius fractures. J HandSurg Am 2002;27(6):953-964.
45. Peine R, Rikli DA, Hoffmann R,Duda G, Regazzoni P: Compari-son of three different plating tech-niques for the dorsum of the distalradius: A biomechanical study.J Hand Surg Am 2000;25(1):29-33.
46. Leslie BM, Medoff RJ: Fracturespecific fixation of distal radiusfractures. Tech Orthop 2000;15(4):336-352.
47. Benson LS, Minihane KP, SternLD, Eller E, Seshadri R: The out-come of intra-articular distal ra-dius fractures treated withfragment-specific fixation. J HandSurg Am 2006;31(8):1333-1339.
48. Gerostathopoulos N, Kalliakma-nis A, Fandridis E, Georgoulis S:Trimed fixation system for dis-placed fractures of the distal ra-dius. J Trauma 2007;62(4):913-918.
49. Cooper EO, Segalman KA, ParksBG, Sharma KM, Nguyen A: Bio-mechanical stability of a volarlocking-screw plate versus
fragment-specific fixation in adistal radius fracture model. Am JOrthop (Belle Mead NJ) 2007;36(4):E46-E49.
50. Taylor KF, Parks BG, SegalmanKA: Biomechanical stability of afixed-angle volar plate versusfragment-specific fixation system:Cyclic testing in a C2-type distalradius cadaver fracture model.J Hand Surg Am 2006;31(3):373-381.
51. Lozano-Calderón SA, DoornbergJ, Ring D: Fractures of the dorsalarticular margin of the distal partof the radius with dorsal radiocar-pal subluxation. J Bone Joint SurgAm 2006;88(7):1486-1493.
52. Tang P, Ding A, Uzumcugil A:Radial column and volar plating(RCVP) for distal radius fractureswith a radial styloid component orsevere comminution. Tech HandUp Extrem Surg 2010;14(3):143-149.
53. Bae DS, Koris MJ: Fragment-specific internal fixation of distalradius fractures. Hand Clin 2005;21(3):355-362.
54. Grindel SI, Wang M, Gerlach M,McGrady LM, Brown S: Biome-chanical comparison of fixed-angle volar plate versus fixed-anglevolar plate plus fragment-specificfixation in a cadaveric distal radiusfracture model. J Hand Surg Am2007;32(2):194-199.
55. Ginn TA, Ruch DS, Yang CC,Hanel DP: Use of a distractionplate for distal radial fractureswith metaphyseal and diaphysealcomminution: Surgical technique.J Bone Joint Surg Am 2006;88(suppl pt 1):29-36.
56. Ruch DS, Ginn TA, Yang CC,Smith BP, Rushing J, Hanel DP:Use of a distraction plate for distalradial fractures with metaphysealand diaphyseal comminution.J Bone Joint Surg Am 2005;87(5):945-954.
57. Behrens F, Johnson W: Unilateralexternal fixation: Methods to in-
Trauma
36 © 2014 AAOS Instructional Course Lectures, Volume 63

crease and reduce frame stiffness.Clin Orthop Relat Res 1989;241:48-56.
58. Burke EF, Singer RM: Treatmentof comminuted distal radius withthe use of an internal distractionplate. Tech Hand Up Extrem Surg1998;2(4):248-252.
59. Hanel DP, Lu TS, Weil WM:Bridge plating of distal radiusfractures: The Harborviewmethod. Clin Orthop Relat Res2006;445:91-99.
60. Wolf JC, Weil WM, Hanel DP,Trumble TE: A biomechanic com-parison of an internal radiocarpal-spanning 2.4-mm locking plateand external fixation in a model ofdistal radius fractures. J HandSurg Am 2006;31(10):1578-1586.
61. Richard MJ, Katolik LI, HanelDP, Wartinbee DA, Ruch DS:Distraction plating for the treat-ment of highly comminuted distalradius fractures in elderly patients.
J Hand Surg Am 2012;37(5):948-956.
62. Hanel DP, Ruhlman SD, KatolikLI, Allan CH: Complicationsassociated with distraction platefixation of wrist fractures. HandClin 2010;26(2):237-243.
Distal Radius Fractures: Strategic Alternatives to Volar Plate Fixation Chapter 3
© 2014 AAOS Instructional Course Lectures, Volume 63 37






























