Embed Size (px)
Citation preview
This article was downloaded by: [Ms Patricia Fobair]On: 24 August 2012, At: 12:43Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Psychosocial OncologyPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/wjpo20
The Relationship of Purpose in Lifeand Hope in Shaping Happiness AmongPatients with Cancer in PolandMarcin Wnuk PhD a , Jerzy T. Marcinkowski MD a & Patricia FobairMSW, MPH ba Poznan University of Medical Sciences, Poznan, Polandb Stanford University Hospital, Cancer Center, Supportive CareProgram, Stanford, CA, USA
Accepted author version posted online: 01 May 2012. Version ofrecord first published: 02 Jul 2012
To cite this article: Marcin Wnuk PhD, Jerzy T. Marcinkowski MD & Patricia Fobair MSW, MPH (2012):The Relationship of Purpose in Life and Hope in Shaping Happiness Among Patients with Cancer inPoland, Journal of Psychosocial Oncology, 30:4, 461-483
To link to this article: http://dx.doi.org/10.1080/07347332.2012.684988
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representationthat the contents will be complete or accurate or up to date. The accuracy of anyinstructions, formulae, and drug doses should be independently verified with primarysources. The publisher shall not be liable for any loss, actions, claims, proceedings,demand, or costs or damages whatsoever or howsoever caused arising directly orindirectly in connection with or arising out of the use of this material.
Journal of Psychosocial Oncology, 30:461–483, 2012Copyright © Taylor & Francis Group, LLCISSN: 0734-7332 print / 1540-7586 onlineDOI: 10.1080/07347332.2012.684988
The Relationship of Purpose in Life and Hopein Shaping Happiness Among Patients
with Cancer in Poland
MARCIN WNUK, PhD and JERZY T. MARCINKOWSKI, MDPoznan University of Medical Sciences, Poznan, Poland
PATRICIA FOBAIR, MSW, MPHStanford University Hospital, Cancer Center, Supportive Care Program, Stanford, CA, USA
The authors investigated the relationship of purpose of life, andhope in the happiness and life satisfaction of patients with cancerduring or following cancer treatment. Fifty cancer patients wereinterviewed during recovery in two Warsaw medical centers. Theprimary measures used were Purpose in Life Test, Herth Hope In-dex, Happiness and Social Well-Being tools by Czapinski, and theCantril Ladder of Satisfaction with Life, as well as medical and de-mographic measures. Purpose in life was correlated with measuresof happiness, and satisfaction with life. Hope was correlated withcurrent happiness, and four measures of satisfaction with life. Pa-tients who had cancer longer, that is, duration of disease, showedlower scores for purpose in life, and number of friends. The longerthe time of cancer treatment, the lower were patients’ scores for de-sire for life. Purpose in life and hope were positively correlated witheleven measures of happiness and satisfaction in life. The cancervariables negatively correlated with loss of friends and six vari-ables of happiness, and satisfaction in life, suggesting the impactthat having cancer treatment had on patients’ lives. Psychologicalsupport in the cancer center was helpful to patients in and out oftreatment.
KEYWORDS purpose in life, hope, happiness, satisfaction inlife, cancer patients, cancer treatment, duration of disease, socialsupport
Address correspondence to Patricia Fobair, MSW, MPH, 1943 Mount Vernon Court, #203,Mountain View, CA 94040. E-mail: [email protected]
461
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

462 M. Wnuk et al.
INTRODUCTION
Study Setting in Poland
Poland has a lower rate of cancer incidence than many countries, rankingninth among countries with the lowest cancer incidence in a study by Ferlayet al. (2010b). But, in terms of relative survival for all cancers, Poland’s 1-and 5-year survival rate was lowest among the countries in the Eurocarestudy (Coleman, Alexe, Albreht, & McKee, 2008). For lung cancer patients,Poland’s mortality rate is second only to Hungary, as highest among Euro-pean countries (Organisation for Economic Cooperation and Development[OECD], 2010).
The population of Europe is aging, and the rate of new cases of can-cer is expected to increase (OECD, 2010). Concerns about the increas-ing cancer incidence are accompanied by concerns for the quality of lifeamong surviving patients. Czapinski and Panek (2007, 2009) describedthe general conditions of life in Poland, including psychological, physi-cal, and material well-being and life stresses, but there was little exami-nation of psychosocial issues among specific diagnostic subgroups, that is,cancer.
Research on quality of life following a cancer trajectory is an areaof growing interest in Poland (Janiszewska et al., 2008; Osmanska, Bor-lowska, & Makarewicz, 2010; Rzewnicki & Jackiewicz, 2009; Wierzbicka,Kusnierkiewicz, Wojtowica, Maune, & Szyfter, 2001; Wronska, 2003). As psy-chosocial issues among r patients who survive cancer becomes an area ofgreater interest, we believe it important to this study results to describe theimpact of having cancer and cancer treatment had on purpose of life andhope, among a sample of patients treated in Warsaw, Poland.
Background: Specific Interest, “Purpose in Life,” “Hope”
The role that purpose in life and hope play in the happiness and life sat-isfaction of the individual has been a subject of interest since the days ofPlato and Aristotle (Annas, 1995; Broadie, 2007). Viktor Frankl brought theseconcepts to life in the 20th century as part of the wisdom he gleaned fromhis experiences caring for patients hospitalized for attempted suicide, andliving with men in concentration camps during World War II. He found thatthe human desire for meaning and purpose in life was a fundamental drivingforce that helped motivate men to stay alive. The prisoner who lost hope inthe future often became subject to mental and physical decay (Frankl, 1959;Ryff, 1989).
Although Frankl’s signature work, Man’s Search for Meaning was firstpublished and distributed in Poland in 2009 (Frankl, 2009), the first author,Wnuk, used Crumbaugh and Maholick’s (1964) purpose in life measurement,
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

Purpose in Life and Hope Among Patients with Cancer in Poland 463
inspired by Frankl’s work, in previous research (Crumbaugh & Maholick,1964; Wnuk, 2006, 2008). Wnuk and his colleagues working clinically aspsychologists with patients with cancer in Poznan and Warsaw decided toexamine how purpose in life and hope might relate to the lives of cancerpatients in Warsaw.
Questions about one’s purpose of life and hope are important to patientswith cancer, especially in difficult or crisis-like situations. The rapid personalchanges that occur following a cancer diagnosis require one’s reassessmentof personal aims and goals, as adjustments to the new circumstances (Frankl,1959, 2009; Moadel et al., 1998). Current research regarding, hope points toan important role that hope plays in the well-being of people who have suf-fered from chronic diseases (Abayomi-Akinsola, 2001; Craig, Weinert, Wal-ton, & Derwinski-Robinson, 2006; Gelling, Iddon, McVicar, & Pickard, 2004;Shapiro, McCue, Heyman, Dey, & Haller, 2010; Weaver & Flannelly, 2004),or with patients undergoing palliative care and their families (Benzein, 2005;Penson, 2000).
When people cope with a cancer diagnosis, the situation prompts manyto search for the meaning of the diagnosis in their life (Breitbart, 2002).There is evidence that cancer patients’ who find purpose or meaning in theirsituation are happier than others who have problems making sense of theirdisease (Meraviglia, 2004, 2006; Weebers, 2006). In a recent study, 90 patientswith advanced solid tumor cancers were assigned to either meaning-centeredgroup psychotherapy or supportive group psychotherapy. The patients in themeaning-centered group showed significantly greater improvements in spiri-tual well-being and a sense of meaning. At the second follow-up assessmentimprovements were even more substantial. Anxiety and desire for deathwere significantly lower (Breitbart et al., 2010)
Purpose in life is a cognitive process that defines life goals and providespersonal meaning (McKnight & Kashdan, 2009). Frankl (1979/1995) con-cluded that finding meaning in life is a self-discovery within each person’slife (Auhagen, 2000).
Hope, is an emotional factor related to the patient’s level of happi-ness. Hope relies on the belief of a successful outcome of events and circ-umstances in one’s life, for example, optimism about achieving goals, orhope for a good outcome from cancer treatment (Snyder et al., 1991). Pur-pose in life and hope have overlapping but slightly different meanings. Theyare conceptual, linked to goals, and require active, problem-focused copingstyles. Although finding one’s purpose in life may be thought of as a cerebralprocess, whose objective could include “obtaining a better life, realizing one’spotential, surviving as long as possible, seeking wisdom, contributing to thewell-being of others, or attaining spiritual enlightenment” (Cameron, 2001,p. 52), hope is seen as an emotional state, a feeling that events will turn outfor the “best” (The American Heritage Dictionary of the English Language,2006; Snyder, 2000). Hope often comes into play when circumstances are dire
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

464 M. Wnuk et al.
(The American Heritage Dictionary of the English Language, 2006; Fredrick-son, 2009; Snyder, 2000).
Hope may also play a role as a defense mechanism moderating thepatient’s worry about his or her diagnosis (Kwon, 2000) According to Kozi-elecki (2006) hope consists of cognitive, emotional, agency, temporal, andcausative factors. The cognitive dimension of hope is directed toward one’soptimism about completing goals or realization of values. The agency sub-scale of hope concerns the belief that one is able to perform the actionsnecessary to reach a desired goal. As stated by Stephenson (1991), the tem-poral aspect of hope concentrates on the future, based on experiences fromone’s past and present. The causative dimension of hope has a motivationalrole in maintaining activity and behaviors directed toward reaching a de-sired goal. With hope, the personally valuable and significant goal becomesachievable (Dufault & Martocchio, 1985; Stephenson, 1991).
‘Purpose in life and hope are components of existential well-being thatincludes realizing values, having goals, controlling one’s destiny, and findingself-acceptance (Baumeister, Vohs, & Snyder, 2002). In a study by Cohen,Mount, Tomas, and Mount (1996) the existential subscale was as important asany other subscale (physical, support, etc.) in predicting the overall quality oflife of patients with cancer (Cohen et al.). The subscale was more importantin determining the quality of life among patients with local or metastaticdisease, than in patients with no evidence of disease.
Other studies have found that purpose in life and hope are importantconcepts for patients treated for cancer. Among 258 patients with cancerlocated in urban areas, 40% were concerned about finding purpose in life,42% wished to find hope, and 51% desired help in overcoming fear (Moadelet al., 1998). Women with ovarian cancer found that concerns with purposein life and hope had influence on their feelings of well-being or sense of de-spair (Bowes, Tamlyn, & Butler, 2002). In other research, purpose in life andhope were found to have influence on the quality of life of patients with can-cer (Benzein, 2005; Majkowicz, de Walden-Galuszko, & Trojanowski, 1997;Weebers, 2006). Among 490 patients suffering from prostate cancer, hopeproved to be a significant factor in positive affect and sense of happinessand was negatively correlated with depression and negative affect (Blank &Bellizzi, 2005). Social support was a significant contributor to hope among73 women with breast cancer who were questioned twice during a 12-monthsurvey (Ebright & Lyon, 2002).
Additional study results support the view that patients with cancer expe-rience fewer problems with emotional distress when purpose in life and hopeis high. In a study among women with breast cancer (Stages 1–3, 5 years afterdiagnosis), it was found that having a problem finding purpose in life wasnegatively correlated with positive affect, feelings of happiness, and mentalhealth (Tomich & Helgeson, 2002). When the same sample group had a goalin life, their physical and mental health showed higher positive affect scores
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

Purpose in Life and Hope Among Patients with Cancer in Poland 465
(Tomich & Helgeson, 2002). In studies by Meraviglia (2004, 2006), patientswith breast cancer and patients with lung cancer with higher meaning inlife scores also enjoyed better psychological well-being and lower symptomdistress scores. A study carried out among people age 65 years and older,with various cancer diagnoses, found that low levels of hope were associ-ated with low levels of quality of life (Esbenzen, Osterlind, Roer, & Hallberg,2004).
The concepts of happiness, life satisfaction, and well-being are interre-lated ideas that describe one aspect of quality of life (Phillips, 2006). Aris-totle’s defined, happiness as “flourishing or living well,” the highest goodand the end which our activities ultimately aimed. Aristotle believed thathappiness included the state of personal well-being, living well, and doingwell in the world (Broadie, 2007). Life satisfaction is an overall assessmentof feelings and attitudes about one’s life at a particular point in time, rangingfrom negative to positive. It is an indicator of well-being (Diener, Emmons,Larsen, & Griffin, 1985). In this study, happiness was defined as a state ofwell-being, contentment, and joy. Satisfaction in life was defined as an over-all assessment of feelings about one’s life. Happiness and satisfaction in lifeare important in an individual’s sense of well-being. Given the overlappingnature of the terms, happiness was defined as a cognitive balance betweenthe patient’s desire for life, passion for life, evaluation of life up to now,and evaluation of life from the perspective of recent days. Satisfaction in lifewas considered from three different life time perspectives: past, present, andfuture.
According to Czapinski’s (1992) theory, happiness is a multilayer struc-ture in which the most stable and constant element, and the one moststrongly immune to outside influence, is desire for life, and passion forlife. Czapinski found that desire for life and the passion for life were relatedto stable dispositions connected with the process of achieving important lifegoals. An intermediate layer of happiness is satisfaction with one’s life asa whole. The layer closest to the surface is the evaluation connected withfeelings about different time periods of life, that is, current, past, and an-ticipated future. The individual who identifies goals for oneself is workingtoward his or her purpose in life. One’s satisfaction with life as a whole maybe more dependent on external factors in relation to desire for life. There is amiddle layer of satisfaction with life that estimates goals undertaken in othertime periods of life, (past, current, future). Evaluating the middle layer maybe determined by the objective conditions of life, that is, illness, education,income, employment, and marital status (Czapinski, 1992). In the presentresearch model, the level of happiness was examined by referring to two ofthe more stable layers of happiness, that is, desire for life and passion forlife.
The interaction between psychosocial, medical, and demographic vari-ables is important to understand, as each may contribute to research
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

466 M. Wnuk et al.
outcomes (Fobair et al., 2006; Spiegel, Bloom, Kraemer, & Gottheil, 1989).The duration of patients’ disease and length of treatment time are two suchvariables. Fobair et al. (1986) found that patients more recently treated dif-fered from those with longer time since diagnosis and that their researchoutcomes differed by how intense their treatment was, how long it lasted.Younger age and greater education are variables are important considera-tions in reviewing research outcome (Fobair et al., 2006). Does younger orolder age make a difference in purpose, hope, happiness, or life satisfactionof patients with cancer? Do patients with greater education have a morepositive outlook on purpose of life, hope, happiness, and/or life satisfaction?This study looked at these questions.
Social support is defined as help from other people in a difficult lifesituation (Dalgard, 2011) and as the individual belief that one is cared forand loved, esteemed and valued, and belongs to a network of communi-cation and mutual obligations (Cobb, 1976). There is evidence that socialsupport has a protective affect against the health consequences of variouslife stresses (Cobb, 1976), and that it plays an important role in the pro-cess of recovery among patients with cancer (Neuling & Winefield, 1988).Previous research found that the number of friends added to the quality oflife in the patient with cancer (Bloom, Stewart, Johnston, Banks, & Fobair,2001). It has been suggested that an individual’s social support system maymediate or buffer the effects of undesirable life events, and that those withlittle social support may be more vulnerable to life changes (Thoits, 1982).Close friends can support patients in finding meaning in their cancer expe-rience and help them develop hope for their recovery, facilitating a senseof well-being. Social support is one of the factors correlating with happi-ness (Nanthamongkolchai, Munsawaengsub, & Charupoonphol, 2009) andlife satisfaction (Young, 2006). Providing counselling to patients with can-cer during and after treatment has been found to be effective in improvingpatient mood (Breitbart et al., 2010; Fobair, 2007).
Study Design
This preliminary cross-sectional study examines the relationship betweenpurpose in life and happiness and life satisfaction, as well as hope, and hap-piness and life satisfaction among a sample of oncology patients in Poland.We want to examine whether purpose in life and hope will positively cor-relate with happiness and satisfaction in life among patients with cancer.We hope to learn what role medical (duration of disease and cancer treat-ment), demographic (patient’s age and education), and social support vari-ables (friends, feeling loved, or lonely, and past and present psychologicalsupport) play in affecting patients’ purpose in life and hope.
We count the frequency of correlations found between variables in thematrix correlation as an indicator of each variables’ significance.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012
Purpose in Life and Hope Among Patients with Cancer in Poland 467
METHOD
Data Sources: Sample and Recruitment
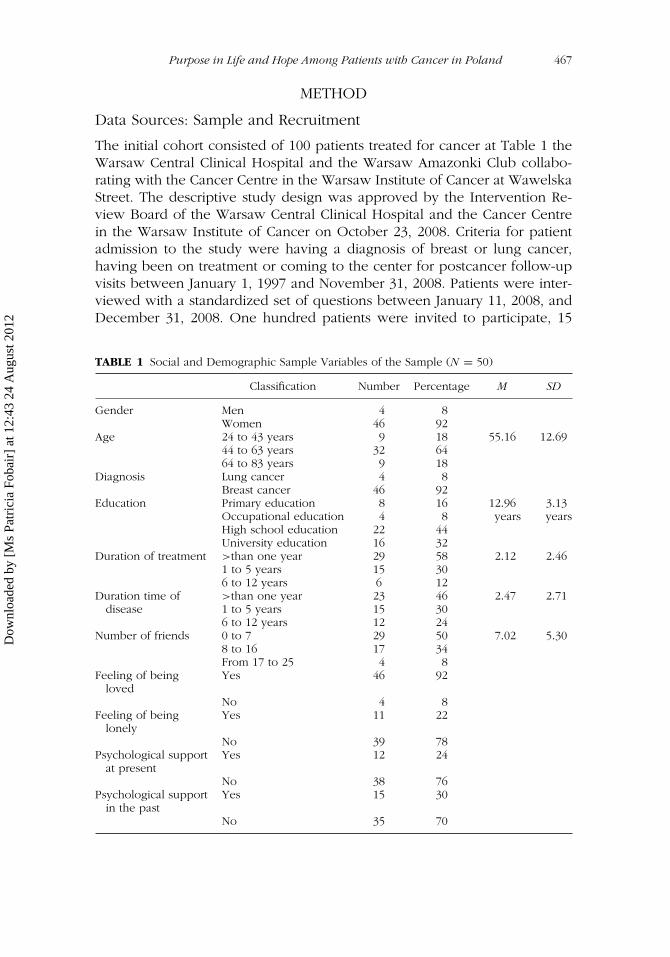
The initial cohort consisted of 100 patients treated for cancer at Table 1 theWarsaw Central Clinical Hospital and the Warsaw Amazonki Club collabo-rating with the Cancer Centre in the Warsaw Institute of Cancer at WawelskaStreet. The descriptive study design was approved by the Intervention Re-view Board of the Warsaw Central Clinical Hospital and the Cancer Centrein the Warsaw Institute of Cancer on October 23, 2008. Criteria for patientadmission to the study were having a diagnosis of breast or lung cancer,having been on treatment or coming to the center for postcancer follow-upvisits between January 1, 1997 and November 31, 2008. Patients were inter-viewed with a standardized set of questions between January 11, 2008, andDecember 31, 2008. One hundred patients were invited to participate, 15
TABLE 1 Social and Demographic Sample Variables of the Sample (N = 50)
Classification Number Percentage M SD
Gender Men 4 8Women 46 92
Age 24 to 43 years 9 18 55.16 12.6944 to 63 years 32 6464 to 83 years 9 18
Diagnosis Lung cancer 4 8Breast cancer 46 92
Education Primary education 8 16 12.96 3.13Occupational education 4 8 years yearsHigh school education 22 44University education 16 32
Duration of treatment >than one year 29 58 2.12 2.461 to 5 years 15 306 to 12 years 6 12
Duration time of >than one year 23 46 2.47 2.71disease 1 to 5 years 15 30
6 to 12 years 12 24Number of friends 0 to 7 29 50 7.02 5.30
8 to 16 17 34From 17 to 25 4 8
Feeling of beingloved
Yes 46 92
No 4 8Feeling of being
lonelyYes 11 22
No 39 78Psychological support
at presentYes 12 24
No 38 76Psychological support
in the pastYes 15 30
No 35 70
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012
468 M. Wnuk et al.
were too sick to participate, 26 declined to participate, and 9 patients didnot completely fill Table 2 the questionnaires. Data analysis was completedfor the 50 remaining patients. Sample demographics are illustrated in . Theresearch staff consisted of two psycho-oncologists, one at the Warsaw Cen-tral Clinical Hospital at Banach Street and the other at the Warsaw AmazonkiClub, collaborating with the Cancer Centre in the Warsaw Institute of Cancerat Wawelska Street.
Measures
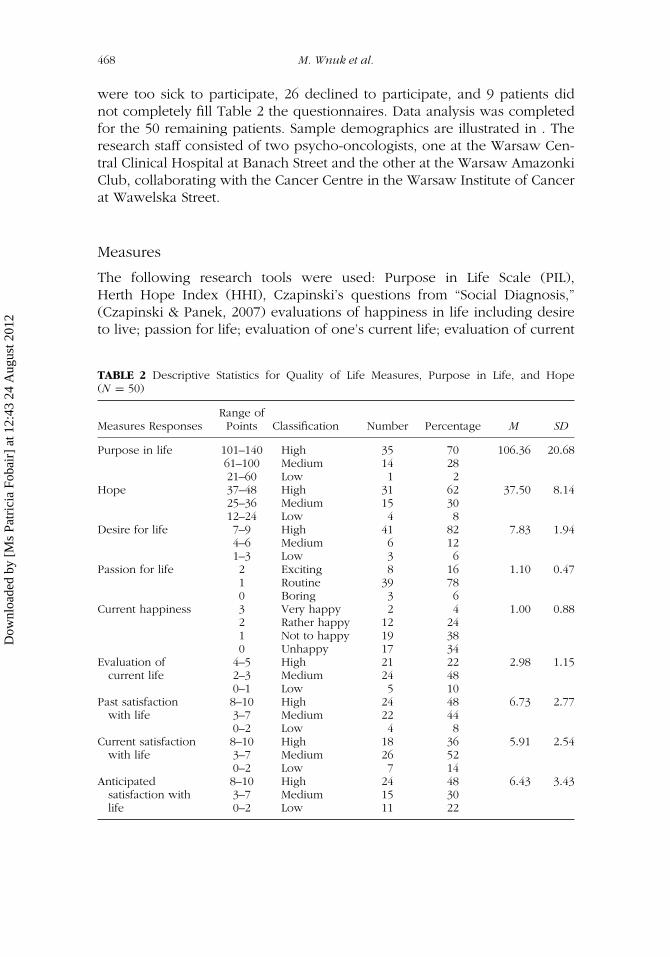
The following research tools were used: Purpose in Life Scale (PIL),Herth Hope Index (HHI), Czapinski’s questions from “Social Diagnosis,”(Czapinski & Panek, 2007) evaluations of happiness in life including desireto live; passion for life; evaluation of one’s current life; evaluation of current
TABLE 2 Descriptive Statistics for Quality of Life Measures, Purpose in Life, and Hope(N = 50)
Range ofMeasures Responses Points Classification Number Percentage M SD
Purpose in life 101–140 High 35 70 106.36 20.6861–100 Medium 14 2821–60 Low 1 2
Hope 37–48 High 31 62 37.50 8.1425–36 Medium 15 3012–24 Low 4 8
Desire for life 7–9 High 41 82 7.83 1.944–6 Medium 6 121–3 Low 3 6
Passion for life 2 Exciting 8 16 1.10 0.471 Routine 39 780 Boring 3 6
Current happiness 3 Very happy 2 4 1.00 0.882 Rather happy 12 241 Not to happy 19 380 Unhappy 17 34
Evaluation ofcurrent life
4–5 High 21 22 2.98 1.152–3 Medium 24 480–1 Low 5 10
Past satisfactionwith life
8–10 High 24 48 6.73 2.773–7 Medium 22 440–2 Low 4 8
Current satisfactionwith life
8–10 High 18 36 5.91 2.543–7 Medium 26 520–2 Low 7 14
Anticipatedsatisfaction withlife
8–10 High 24 48 6.43 3.433–7 Medium 15 300–2 Low 11 22
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012
Purpose in Life and Hope Among Patients with Cancer in Poland 469
happiness in life; life satisfaction past, current, and anticipated future; aswell as social support questions including the number of friends, feelingsof being loved, feeling lonely, and psychological support, past, and present.The Cantril Ladder of Life Satisfaction was an additional measure includedin the study. provides the descriptive statistics for quality of life measures aswell as purpose in life and hope (N = 50).
The Purpose in Life Test (PIL) (Crumbaugh & Maholick, 1964) was de-signed to measure the ideas of Victor Frankl, to determine an individual’sexperience of meaning and purpose in life (Adler, 1997). It consists of 20statements concerning the need for meaning of life. Each question is an-swered by marking the fields placed on the continuum between 1 and 7,with 7 indicating maximum intensity related to the meaning of life, and 1indicating a minimum intensity. The overall result is obtained by adding thescore from all answers (Cekiera, 1985). The highest score is 140, the lowestis 20. The higher score indicates stronger purpose in life; the lower the resultthe greater the existential frustration. The reliability of this tool measured bythe coefficient of correlation (r-Pearson) was 0.82 with the Spearman-Browncorrection = 0.90 (Crumbaugh & Maholick, 1964). In a Polish version of thescale, when a test–retest method was used during a 6-month interval, thereliability ranged from 0.64 to 0.70 depending on the population studied(Siek, 1993).
Hope Herth Index (HHI) (Dufault & Martocchio, 1985; Herth, 1992) isa scale used for the measurement of hope based on a definition of hope,that states that hope is a multidimensional, dynamic life force, rather thantrait oriented and one dimensional. Hope, considered always possible, canbe characterized as the certainty of achieving a good result in a goal thatis personally significant (Dufault & Martocchio, 1985). Participants answered12 questions expressed on the 4-step Likert-type scale. For Items 3 and 5,total agreement with the items equalled a score of 1, total disagreementequalled 4. Total agreement with the rest of the items in the questionnaireequalled 4, and total disagreement equalled 1 (Herth, 1992). The reliability ofthis scale has satisfactory psychometrical features—in reference to patientsscores α = 0.97 (Herth, 1992) were evaluated with the test–retest methodscores = .91 (Herth, 1992), and in the previous research scores –Cronbach’sα = .91.
To measure happiness and life satisfaction, we used Cantril’s Ladder(Cantril, 1965, 1981) and tests formulated by Czapinski for his onion theoryof happiness (Czapinski, 1992; Czapinski & Panek, 2009).
The Cantril Ladder (Cantril, 1965, 1981) is a popular measure of life satis-faction that is used in psychosocial research (Arnold, et al., 2005; Hagedoornet al., 2000; Johnson, Thomas, & Matre, 1990; Kivett & Palmore, 1977; Luttik,Jaarsma, Jeeger, & van Veldhuisen, 2005; Schaar, 2003; Spanier & Lachman,1980). It is a simple and understandable tool for all groups of respondentsregardless of education. The Cantril Ladder consists of one question in which
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

470 M. Wnuk et al.
the respondent evaluates his or her overall satisfaction with life on a scalefrom 0 (minimum) to 10 (maximum), life satisfaction. This measure wasused from three different life perspectives (past, present, and future). In ad-dition to past and present, the questionnaire asked about anticipating one’sevaluation of life, 5 years in the future. Variations of the reliability coeffi-cient between studies have been noted. Czapinski used this scale during a2-month interval, obtaining a reliability score of 0.76 (Czapinski, 1992). Inanother project the coefficient of reliability at a 2-year interval measured 0.65(Kivett & Palmore, 1977).
Czapinski’s test of his onion theory of happiness includes the Desirefor Life Scale (Czapinski, 1992) that consists of one statement in which therespondent chooses an estimates placed on a 0 to 9 continuum. 0 in thisscale means total lack of desire to live (the answer: “I don’t want to live”)and 9 means the strongest possible desire to live (answer: “I want to live verymuch”). Desire for life results were M = 6.55, SD = 2.32. Passion for life(Czapinski, 1992) is a one statement measure. The respondent chooses oneanswer among three alternatives (Is life boring 0, bland 1, or 2 exciting).Passion for life results were M = 1.20, SD = .68. Using the current happinessscale, the respondent estimates his or her level of happiness by marking oneof the four alternative answers: not happy (0), happy (1), quite happy (2), andvery happy (3). Current happiness (in recent days) results were M = 1.11,SD = .97. In the current life evaluation (Czapinski, 1992) the respondent hasseven statements to choose from: unhappy (0), not too successful (1), neithergood nor bad (2), quite good (3), successful (4), wonderful (5). Answering thisquestion, the research participant evaluates his or her current life and choosesa statement that is closest to his or her opinion. Current life evaluation resultswere M = 3.00, SD = 1.34.
Medical and demographic questions included three medical questions:“What was the diagnosis that led to treatment for cancer?” “What is thenumber of months or years since your diagnosis?” “What was the lengthof time of your treatment for cancer?” Demographic information includedquestions about gender, age, and number of years of education.
Social support was measured using questions from Czapinski andPanek’s “Social Diagnosis” (2007, 2009). Patients were asked to provide thenumber of people they felt close to, to rate the lack of having feelings ofbeing lonely, and their sense of being loved and trusted (Czapinski & Panek,2009). In the factor analysis of life quality dimensions with varimax rotation,social well-being accounted for 0.618 and explained 11.8% of the variance(Czapinski & Panek, 2009).
An additional social support resource was noted. Psychological supporthad been offered to patients during medical treatment and in follow-upvisits. Patients were asked on a yes/no basis whether they had participatedin psychological counselling in the past or present time.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

Purpose in Life and Hope Among Patients with Cancer in Poland 471
Data Analysis
To examine whether purpose in life and hope positively correlated withmeasures of the happiness and satisfaction in life of patients with cancer, theSPSS version 12 Statistical Paquet was used. Means and standard deviations(SDs) were calculated to describe the distribution of patients’ psychologicaland quality of life factors measured on a continuous scale. Percentageswere computed to describe the distributions of the medical, demographic,and social support variables that were assessed using categorical measures.Pearson’s correlation coefficient was computed between all variables ex-amined in this study to create the correlation matrix. Chi-square evaluationswere carried out between variables where patients’ answers to purpose inlife and hope appeared to contrasted with current happiness, evaluationwith life up to now and current satisfaction with life. The correlation matrixwas the central means used to determine relationships between variables.Due to the small patient sample size other forms of analysis were lessappropriate. The number of times a variable correlated with other variableswas noted, as a proxy of the variables strength in relation to purpose of lifeand hope.
RESULTS
Table 1 presents the demographic, medical, and social support variables.Ninety-two percent of the patients were women with breast cancer. Themean age, 55.16 years, (SD = 12.69), and 64% of patients fell between age44 and 63 years. Forty-four percent completed high school, and 32% receiveduniversity education. Most of the patients were interviewed during the first12 months following diagnosis. Fifty-four percent had cancer for more thana year, whereas 58% had been in treatment for less than one year. Fiftypercent of the patients cited 0 to 7 friends, and 50% mentioned 8 to 25friends. Ninety-two percent of the patients felt ‘loved. Psychological serviceswere utilized by 30% of the patients during treatment, and 24% of the patientsduring follow-up visits, at the time of the data collection.
Table 2 provides the descriptive statistics for the measures used for pur-pose in life and hope, and the measures for happiness and satisfaction withlife (N = 50). Purpose in life was marked “high” by 70% of the patients. Hope’was marked “high” for 62% of the patients. Desire for life, a measure of hap-piness (Czapinski, 1992), ranked highest of all the measures used with 82%of the patients rating desire for life, as “high.” In contrast, passion for life wasconsidered “routine” or “boring” by 84%, with only 16% rating it “high.” Only28% patients rated their current happiness as “high,” whereas 72% rated cur-rent happiness as “not to happy” or “unhappy.” Evaluation of current life was“high” for 42% of the patients, but “medium” or “low” for 58%. Satisfaction
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

472 M. Wnuk et al.
with current life was “high” for 34% of the patients, but “medium” or “low”for 66%.
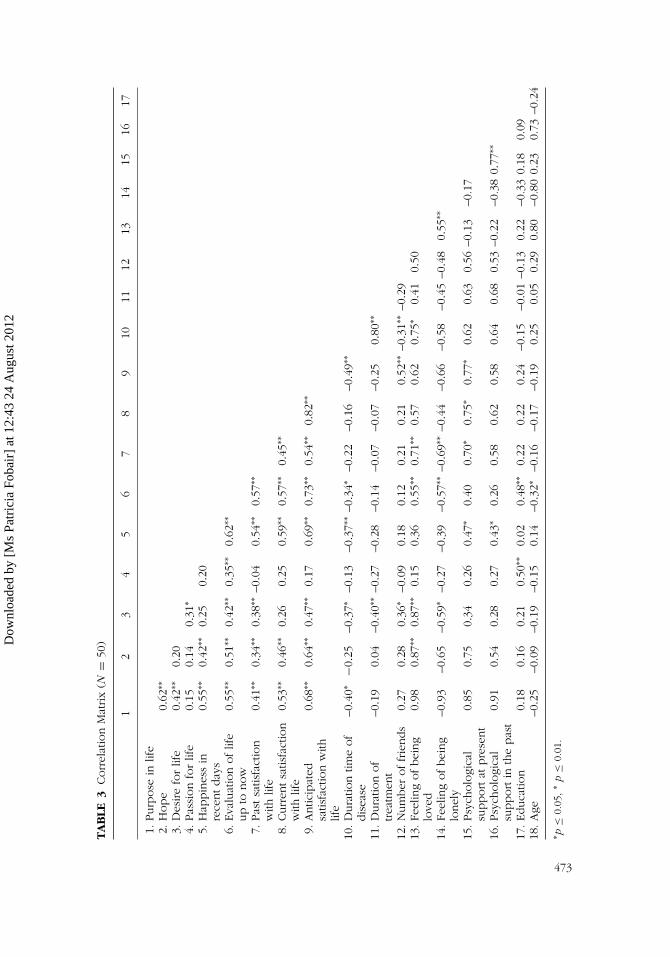
Table 3 presents the results of the correlation matrix of all measuresexamined. Purpose in life correlated positively with six out of seven measuresof happiness and satisfaction: all measures except passion for life (see Table3). There was a negative correlation between purpose in life and durationof disease. Purpose in life was not correlated with duration of treatment,number of friends, feeling loved, being lonely, or psychological support pastor present’, age’ or education. It should be noted that a correction factor,was not applied.
Hope was positively correlated with purpose in life, and five measuresof happiness and life satisfaction, all measures except for desire for life, andpassion for life. Hope was correlated with feelings of being loved. Hope’ wasnot correlated with duration of disease, or treatment, psychological supportpast or present, number of friends, feeling lonely, or age, and education.
Among the happiness and satisfaction in life variables, desire for life waspositively correlated with six variables: purpose in life, passion for life, eval-uation of one’s current life, past satisfaction with life, anticipated satisfactionwith life, number of friends, and feelings of being loved. Desire for life wasnegatively correlated with duration time of disease, duration of treatment,and feelings of being lonely.
Passion for life was positively correlated with only three variables: desirefor life, current evaluation of one’s life, and greater educational achievement.
Current happiness was positively correlated with eight variables: pur-pose in life’ and hope, evaluation of one’s current life, past satisfaction withlife, current satisfaction with life, and anticipated satisfaction with life, psy-chological support in the past and present. Current happiness was negativelycorrelated with longer duration of disease.
Evaluation of one’s current life was the most frequently correlated withother measures in the study. It was positively correlated with 10 variables:positive correlations were found for purpose in life, hope, desire for life, pas-sion for life, current happiness, past satisfaction with life, current and futuresatisfaction with life, feelings of being loved, and having greater education.Evaluation of one’s current life negatively correlated with longer duration ofdisease, greater feelings of being lonely, and younger age.
Past satisfaction with life was positively correlated with nine variables:purpose in life, hope, desire for life, current happiness, evaluation of one’scurrent life, current and future satisfaction with life, feelings of being loved,and psychological support at present. Past satisfaction with life was nega-tively correlated with greater feelings of being lonely.
Current satisfaction with life was positively correlated with seven vari-ables: purpose in life, hope, current happiness, one’s evaluation of currentlife, past satisfaction with life, anticipated satisfaction with life, and psycho-logical support at present.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012
TA
BLE
3Corr
elat
ion
Mat
rix
(N=
50)
12
34
56
78
910
1112
1314
1516
17
1.Purp
ose
inlif
e2.
Hope
0.62
∗∗
3.D
esire
for
life
0.42
∗∗0.
204.
Pas
sion
for
life
0.15
0.14
0.31
∗
5.H
appin
ess
inre
centday
s0.
55∗∗
0.42
∗∗0.
250.
20
6.Eva
luat
ion
oflif
eup
tonow
0.55
∗∗0.
51∗∗
0.42
∗∗0.
35∗∗
0.62
∗∗
7.Pas
tsa
tisfa
ctio
nw
ithlif
e0.
41∗∗
0.34
∗∗0.
38∗∗
–0.0
40.
54∗∗
0.57
∗∗
8.Curr
entsa
tisfa
ctio
nw
ithlif
e0.
53∗∗
0.46
∗∗0.
260.
250.
59∗∗
0.57
∗∗0.
45∗∗
9.A
ntic
ipat
edsa
tisfa
ctio
nw
ithlif
e
0.68
∗∗0.
64∗∗
0.47
∗∗0.
170.
69∗∗
0.73
∗∗0.
54∗∗
0.82
∗∗
10.D
ura
tion
time
of
dis
ease
–0.4
0∗−0
.25
–0.3
7∗–0
.13
–0.3
7∗∗–0
.34∗
–0.2
2–0
.16
–0.4
9∗∗
11.D
ura
tion
of
trea
tmen
t–0
.19
0.04
–0.4
0∗∗–0
.27
–0.2
8–0
.14
–0.0
7–0
.07
–0.2
50.
80∗∗
12.N
um
ber
offr
iends
0.27
0.28
0.36
∗–0
.09
0.18
0.12
0.21
0.21
0.52
∗∗–0
.31∗∗
–0.2
913
.Fe
elin
gofbei
ng
love
d0.
980.
87∗∗
0.87
∗∗0.
150.
360.
55∗∗
0.71
∗∗0.
570.
620.
75∗
0.41
0.50
14.Fe
elin
gofbei
ng
lonel
y–0
.93
–0.6
5–0
.59∗
–0.2
7–0
.39
–0.5
7∗∗–0
.69∗∗
–0.4
4–0
.66
–0.5
8–0
.45
–0.4
80.
55∗∗
15.Psy
cholo
gica
lsu
pport
atpre
sent
0.85
0.75
0.34
0.26
0.47
∗0.
400.
70∗
0.75
∗0.
77∗
0.62
0.63
0.56
–0.1
3–0
.17
16.Psy
cholo
gica
lsu
pport
inth
epas
t0.
910.
540.
280.
270.
43∗
0.26
0.58
0.62
0.58
0.64
0.68
0.53
–0.2
2–0
.38
0.77
∗∗
17.Educa
tion
0.18
0.16
0.21
0.50
∗∗0.
020.
48∗∗
0.22
0.22
0.24
–0.1
5–0
.01
–0.1
30.
22–0
.33
0.18
0.09
18.A
ge–0
.25
–0.0
9–0
.19
–0.1
50.
14–0
.32∗
–0.1
6–0
.17
–0.1
90.
250.
050.
290.
80–0
.80
0.23
0.73
–0.2
4
∗ p≤
0.05
,∗
p≤
0.01
.
473
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

474 M. Wnuk et al.
Anticipated (future) satisfaction with one’s life was positively correlatedwith nine variables: purpose in life, hope, desire for life, current happiness,evaluation of one’s current life, past and current satisfaction with life, numberof friends, and psychological support at present. Anticipating future satisfac-tion with one’s life was negatively correlated with length of illness, that is,duration of disease.
Of the two medical variables, the length of time since diagnosis, durationtime of disease, correlated negatively with six variables with (less) purposein life,’(less)’desire for life, (less) current happiness, (lower) evaluation ofone’s current life, (lower) anticipation of future satisfaction with life, and(fewer) friends. Duration of treatment correlated negatively with desire forlife, and duration of disease.
Purpose in life was not correlated with any of the social support vari-ables. Feeling loved was the only social support variable correlated withhope. Feeling loved also correlated with five other variables: desire for life,current evaluation of life, past satisfaction with life, duration of disease, andfeelings of being lonely. Psychological support at present correlated with fivevariables: current happiness, past, current and future satisfaction with life,and psychological support in the past. Feelings of being lonely negativelycorrelated with three variables, desire for life, evaluation of one’s currentlife, and past satisfaction with life, but correlated positively with feelings ofbeing loved. Having a greater number of friends correlated positively withpatients’ desire for life, and anticipated future satisfaction with life but neg-atively correlated with longer duration of disease. Psychological support atfollow- up correlated with current happiness, current satisfaction with life,and anticipated satisfaction with life. Psychological support during treatmentcorrelated with current happiness, and psychological support at present.
Younger or older age, in this study, was not correlated significantlywith purpose in life or hope. Younger age was found to have a negativecorrelation with one’s current evaluation of life. Having greater educationwas positively correlated with passion for life and current evaluation of life,but not with “purpose in life’ or hope.
To learn if the differences in Table 2 between the patients’ high scoresfor purpose in life and hope, and their lower scores on measures of happi-ness and life satisfaction were due to chance alone, or significantly different,we carried out a chi-square probability evaluations between purpose of life,hope, and four variables (see Tables 4 and 5). The results were significantdifferences were found in six of the eight equations. The chi-square eval-uation of passion for life and purpose in life was nonsignificant. But, theevaluation for purpose of life and current happiness, was significant, χ2 =4.64, df (1), p = .03, as it was for patients evaluation of current life, χ2 =8.74, df (1), p = .01, and for current satisfaction with life as χ2 = 5.29, df(1), p = .03. Three of the chi-square evaluations indicated that the differencebetween responses were unlikely to have occurred by chance alone.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

Purpose in Life and Hope Among Patients with Cancer in Poland 475
TABLE 4 Purpose in Life and Other Indicators of Happiness Among Oncology Patients(N = 50): Test Results χ 2
χ 2 df p
Passion for life 5.02 2 0.08Current happiness 4.64 1 0.03∗
Evaluation of current life 8.74 1 0.01∗
Current satisfaction with life 5.29 1 0.03∗
∗p ≤ 0.05.
It also appeared to be more than chance that hope was rated “high” bypatients, but passion for life was rated “routine” or “boring, χ2 = 7.58, df(2), p = .02, or their current happiness as “not happy,” χ2 = 4.13, df (1),p = .04, or their current evaluation of life as “medium” or “low” χ2 = 12.83,df (1), p = .01. There appear to be factors not evaluated in this study thataccount for the lower scores on passion for life, current happiness, currentlife evaluation, and satisfaction with current life. Yet the high proportion ofpeople scoring “high,” in rating purpose in life and hope and desire for life,implies that this is the dominant view in the patient group.
DISCUSSION
This research suggests that purpose in life and hope contributed to the levelof happiness and life satisfaction experienced by the 50 cancer patients inthis study. As Frankl found, the purpose in life of patients with cancer wasassociated with desire for life, and recent happiness (Frankl, 1977). Purposein life’ was positively associated with the patients’ evaluation of current life;past, current, and future satisfaction with life; and their sense of hope andnegatively affected by greater length of time since diagnosis, longer durationof disease. Hope correlated with current happiness, evaluation of life, lifesatisfaction, and feelings of being loved.
The results of this research are similar to those found in other researchwith patients with cancer. As with Meraviglia’s (2004, 2006) work, we found
TABLE 5 Hope and Other Indicators of Happiness Among Oncology Patients (N = 50): TestResults χ 2
χ 2 df p
Passion for life 7.58 2 0.02∗
Current happiness 4.13 1 0.04∗
Evaluation of current life 12.83 1 0.01∗
Current satisfaction with life 0.58 1 0.33
∗p ≤ 0.05.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

476 M. Wnuk et al.
that, purpose of life was negatively correlated to duration of the disease butwas positively correlated with desire for life, evaluation of happiness, evalu-ation of current life, as well as the past, current, and anticipated satisfactionwith life. Duration of treatment had a negative impact on the patients’ desirefor life (Meraviglia, 2004, 2006).
Like Shapiro et al. (2010), we found that high ratings of hope were asso-ciated with high levels of happiness. The correlation of hope, with feelings ofbeing loved was a result similar to Ebright and Lyon (2002) who found thatsocial support was a significant contributor to hope, in a study with patientswith breast cancer. It also recalls the work of Kozielecki (2006), who wroteof the “emotional, agency, and temporal factors-” of hope. Kozielecki (2006)and Stephenson (1991) noticed that there was a temporal aspect of hope thatconcentrated on the future. Our results showed a strong correlation betweenpatients’ hope and their anticipation of future satisfaction in life.
Although Czapinski (1992) found that desire for life, and passion forlife were the most stable of the happiness variables, we found that patients’current evaluation of life showed greater strength, correlating more oftenwith the other variables (Czapinski, 1992; Czapinski & Panek, 2009). One’scurrent evaluation of life correlated with purpose of life, hope, and 10 othervariables, whereas desire for life correlated with 10 variables, past satisfactionwith life (10), anticipated satisfaction with life (10), current happiness (9),and current satisfaction (7), or passion for life (3).
Partially consistent with recent studies, patients with a larger numberof friends were more likely to indicate a desire for life and anticipate lifesatisfaction in the future (Cobb, 1976). However, when duration of diseasewas longer, patients’ friendships diminished, as did patients’ purpose inlife, current happiness, evaluation of current life, and satisfaction with life.This result supports research (Bloom et al., 2001; Bloom, Stewart, Oakley-Girvan, Banks, & Shema, 2011; Fobair et al., 1986) showing that survivorsof cancer frequently report more psychosocial and physical problems assurvival time from diagnosis continues. Fobair et al. (1986) found that thepatients’ treated for Hodgkin’s disease with longer times from diagnosis weremore likely to express symptoms of depression, suffer fatigue, and report lessenergy than those patients treated more recently. Bloom and her colleaguesreinterviewed women 10 years after breast cancer diagnosis who reportedincreased problems with their general health and physical well-being, lesssexual activity, and more chronic conditions than they had reported in earlieryears (Bloom et al., 2011).
Among the demographic variables having greater education correlatedwith the patients’ passion for life and their evaluation of current life. Youngerpatients (age) had a negative correlation with their evaluation of current life.Neither number of friends, age, education, or having psychological supportwere correlated with the patients’ purpose in life’ or hope.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

Purpose in Life and Hope Among Patients with Cancer in Poland 477
We have shown that purpose in life and hope’ are important variablesaffecting the happiness and life satisfaction’ among the patients with cancerin this study. Contrary to Czapinski’s theory (1992) that the most stable andconstant element of happiness is desire and passion for life, we found thatpatients in this study indicated through frequency of their correlation scoresthat evaluation of one’s current life was most important. We found that dura-tion of disease and duration of treatment had negative effects on the patients’desire for life. Although the patients’ passion for life was positively correlatedwith greater education, it was not correlated with purpose of life, hope, themedical variables, nor other happiness’ measures except evaluation of one’scurrent life. This suggests that passion of life may be a more autonomousindicator of happiness.
We also found an interesting anomaly to be examined in future research.Although the patients gave high scores to purpose in life’ and hope, theyranked their current happiness, current evaluation of life, and current lifesatisfaction in the middle and lower ranges. Chi-square evaluation suggeststhat factors other than chance account for this difference. Future researchmay examine additional aspects of the population to answer question ofwhy these patients were less positive about their current happiness andsatisfaction with life. The first author suggests that the public consciousnessin Poland experiences a “cancer diagnosis” as a “death warrant.” Cancerstatistics in Poland are less optimistic for patients than in other parts ofEurope. Wnuk’s thoughtful concerns are supported by recent health statistics(Coleman et al., 2008; Ferlay et al., 2010a; OECD, 2010), referred to in theBackground section. This lower cancer survival rate creates an unfortunatesituation for patients, and a challenge for health care services in Poland toprovide additional cancer prevention and effective medical treatment servicesin greater abundance.
Interpreting the results of this article is limited by several factors:(1) this was a preliminary study to examine the hypothesis that purposein life and hope would make difference in the happiness and life satisfactionin a population of Polish cancer patients. (2) The questionnaire was limited;it was not exhaustive of important content. (3) The small size of the sam-ple does not represent the breadth of patients treated at this institution, orthe population as a whole. (4) The small size of the sample made analysislimited to a descriptive, corelational design. (5) As the research design wascorelational, our comments are limited to the associations found betweenvariables.
We hope to collect a larger sample of patients with cancer in futuremonths and compare results of Polish cancer patients with a group of healthyadults having similar demographic variables. In further research amongoncology patients we want to use additional measures of happiness andquality of life, in relation to the patient’s purpose of life and hope.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

478 M. Wnuk et al.
IMPLICATIONS FOR CLINICAL PRACTICE
Even tentative results, like those described here, suggest possibilities forinterventions in patient care. Interventions are needed for supportive carewith a patients’ focus, encouraging patients to examine their purpose oflife and hope, and reimagine goals that will add to their happiness and lifesatisfaction. Nurses, doctors, and social workers are encouraged to look forways to help patients build hope and purpose in their life, as these variablesare important to the patient’s quality of life.
IMPLICATIONS FOR FUTURE RESEARCH
There is a growing interest in Poland in examining the quality of life ofsurvivors of cancer. Our group has a particular interest in the existential andspiritual aspects of personal life that may play a positive role in recovery fromtreatment and survival issues. We look forward to continuing the researchreported here, expanding our patient population, and adding control groupsfor comparison. We hope to collect a larger sample of patients with cancerin future months and compare results of Polish patients with cancer with agroup of healthy adults having similar demographic variables.
IN SUMMARY
We have shown that though the purpose of life and hope in this group ofpatients ranked “high,” and there was an active positive relationship betweenthe happiness and life satisfaction variables with purpose of life and hope,some aspects of the patients’ happiness and life satisfaction were “medium”or “low.” In future research we want to learn more about the relationshipfound between high patient scores for purpose in life’ and hope and lowerscores on measures of happiness and life satisfaction. We will further exploreand confirm the role of medical variables in effecting patients’ purpose inlife, hope, and we will use additional measures to explore other aspects ofpatients’ lives related to happiness and satisfaction with life, as they affectpatients’ purpose of life and hope.
REFERENCES
Abayomi-Akinsola, H. (2001). Fostering hope in people living with AIDS in Africa:The role of primary health-care workers. Australian Journal of Rural Health,9(4), 158–165.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012
Purpose in Life and Hope Among Patients with Cancer in Poland 479
Adler, N. S. J. (1997). The MacArthur Scale of Subjective Social Status PsychosocialNotebook. MacArthur Research Network on SES and Health. Retrieved January 4,2011 from http://www.macses.ucsf.edu/research/psychosocial/subjective.php
The American Heritage Dictionary of the English Language (4th ed.). (2006). Boston,MA: Houghton Mifflin.
Annas, J. (1995). Making sense of my life as a whole. In J. Annas (Ed.), The moralityof happiness (Chapter 1, pp. 36–37). Oxford: Oxford University Press.
Arnold, R., Ranchor, A. V., DeJongste, M. J., Koeter, G. H., Ten Hacken, N. H.,Aalbers, R., & Sanderman, R. (2005). The relationship between self-efficacy andself-reported physical functioning in chronic obstructive pulmonary disease andchronic heart failure. Behavioral Medicine, 31(3), 107–115.
Auhagen, E. A. (2000). On the psychology of meaning of life. Swiss Journal ofPsychology, 59(1), 34–48.
Baumeister, R. F., Vohs, K., & Snyder, C. R. (Eds.). (2002). The pursuit of meaning-fulness in life. New York: Oxford University Press.
Benzein, E. G. (2005). The level of and relation between hope, hopelessness andfatigue in patients and family members in palliative care. Palliative Medicine,19(3), 234–240.
Blank, T. O., & Bellizzi, K. M. (2005). After prostate cancer: Predictors of well-being among long-term prostate cancer survivors. Cancer, 106(10), 2128–2135.
Bloom, J. R., Stewart, S. L., Johnston, M., Banks, P., & Fobair, P. (2001). Sources ofsupport and the physical and mental well-being of young women with breastcancer. Social Science & Medicine, 53(11), 1513–1524.
Bloom, J. R., Stewart, S. L., Oakley-Girvan, I., Banks, P. J., & Shema, S. (2011).Quality of life of younger breast cancer survivors: Persistence of problems andsense of well-being. Psycho-Oncology, doi:10.1002/pon.1965.
Bowes, D. E., Tamlyn, D., & Butler, L. J. (2002). Women living with ovarian can-cer: Dealing with an early death. Health Care for Women International, 23(2),135–148.
Breitbart, W. (2002). Spirituality and meaning in supportive care: Spirituality andmeaning centered group psychotherapy interventions in advanced cancer. Sup-port Care Cancer, 10(1), 272–280.
Breitbart, W., Rosenfeld, B., Gibson, C., Pessin, H., Poppito, S., Nelson, C., . . .
Olden, M. (2010). Meaning centered group psychotherapy for patients forpatients with advanced cancer: A pilot randomized controlled trial. Psycho-Oncology, 19(1), 21–28.
Broadie, S. (2007). What should we mean by ‘the highest good’? In Aristotle andbeyond: Essays in metaphysics and ethics (pp. 153–165). Cambridge, UK: Cam-bridge University Press.
Cameron, D. (2001). The purpose of life. London, UK: Woodhull Publishing.Cantril, H. (1965). The patterns of human concern. New Brunswick, NJ: Rutgers
University Press.Cantril, H. (1981). Life satisfaction and chronic disease: Exploration of a theoretical
model. Medical Care, 29, 1136–1146.Cekiera, C. (1985). Toxic obsession, drug addiction, medicine addiction, alcoholism,
nicotine addiction. Warsaw, Poland: State Scientific Publishing.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012

480 M. Wnuk et al.
Cobb, S. (1976). Social support as a moderator of life stress. Psychosomatic Medicine,38, 300–314.
Cohen, S. R., Mount, B. M., Tomas, J. J. N., & Mount, L. F. (1996). Existential well-being is an important determinant of quality of life. Cancer, 77(3), 576–586.
Coleman, M. P., Alexe, D. M., Albreht, T., & McKee, M. (2008). Responding to thechallenge of cancer in Europe. Ljubljana, Slovenia: Institute of Public Health ofthe Republic of Slovenia.
Craig, C., Weinert, C., Walton, J., & Derwinski-Robinson, B. (2006). Spirituality,chronic illness and rural life. Journal of Holistic Nursing, 24(1), 27–35.
Crumbaugh, J., & Maholick, L. (1964). An experimental study of existentialism: Thepsychometric approach to Frankl’s concept of noogenic neurosis. Journal ofClinical Psychology, 20, 200–207.
Czapinski, J. (1992). Psychology of happiness: Research review and outline of theonion theory. Warszawa-Poznan, Poland: Akademos.
Czapinski, J., & Panek, T. (2007). Social diagnosis 2007. In J. Czapinski & T. Panek(Eds.), Social diagnosis 2007 (pp. 1–237). Warsaw, Poland: Council for SocialMonitoring.
Czapinski, J., & Panek, T. (2009). Social diagnosis 2009. In J. Czapinski & T. Panek(Ed.), Social diagnosis (pp. 214–225). Warsaw, Poland: University of Warsaw,Council for Social Monitoring.
Dalgard, O. S. (2011). Social support: Definition and scope. EUphact, 1–2. Retrievedfrom http://www.euphix.org/object_document/05479n27411.html
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The Satisfaction WithLife Scale. Journal of Personality Assessment, 49, 71–75.
Dufault, K., & Martocchio, B. C. (1985). Symposium on compassionate care andthe dying experience. Hope its sphere and dimensions. Nursing Clinical NorthAmerican, 20(2), 379–391.
Ebright, P. R., & Lyon, B. (2002). Understanding hope and factors that enhance hopein women with breast cancer. Oncology Nursing Forum, 29(3), 561–568.
Esbenzen, B. A., Osterlind, K., Roer, O., & Hallberg, I. R. (2004). Quality of lifeof elderly persons with newly diagnosed cancer. European Journal of CancerCare, 13(5), 443–453.
Ferlay, J., Shin, H. R., Bray, F., Forman, D., Mathers, C., & Parkin, D. M.(2010a). Cancer incidence and mortality worldwide ( IARC CancerBase No. 10).Lyon, France: International Agency for Research on Cancer. GLOBOCAN 2008v1.2.
Ferlay, J., Shin, H. R., Bray, F., Forman, D., Mathers, C., & Parkin, D. M. (2010b). Esti-mates of worldwide burden of cancer in 2008: GLOBOCAN 2008. InternationalJournal of Cancer, 127(12), 2893–2917.
Fobair, P. (2007). Oncology social work for survivorship. In P. Ganz (Ed.), Cancersurvivorship: Today and tomorrow (pp. 14–27). New York, NY: Springer.
Fobair, P., Hoppe, R. T., Bloom, J., Cox, R., Varghese, A., & Spiegel, D. (1986). Psy-chosocial problems among survivors of Hodgkin’s disease. Journal of ClinicalOncology, 4(5), 805–814.
Fobair, P., Stewart, S. L., Chang, S., D’Onofrio, C. D., Banks, P. J., & Bloom, J. R.(2006). Body image and sexual problems in young women with breast cancer.Psycho-Oncology, 15, 579–594.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012
Purpose in Life and Hope Among Patients with Cancer in Poland 481
Frankl, V. (1959). Man’s search for meaning. Boston, MA: Beacon Press.Frankl, V. E. (1977). Paradoxes of happiness. Life and Thought, 1, 33–45.Frankl, V. E. (1979/1995). Der Mensch vor der Frage nach Sinn. Munchen: Piper.Frankl, V. E. (2009). Man’s search for meaning. Warsaw, Poland: Black Sheep Press.Fredrickson, B. L. (2009). Why choose hope? Retrieved from http://www.
psychologytoday.com/blog/positivity/200903/why-choose-hopeGelling, L., Iddon, J., McVicar, A., & Pickard, J. D. (2004). CSF circulation disorders:
Measuring progress through quality of life and hope. Journal of Clinical Nursing,13, 589–600.
Hagedoorn, M., Buunk, B. P., Kuijer, R. G., Bram, P., Wobbes, T., & Sanderman,P. (2000). Couples dealing with cancer: Role and gender differences regard-ing psychological distress and quality of life. Psycho-Oncology, 9(3), 232–242.
Herth, K. A. (1992). Abbreviated instrument to measure hope: Development andpsychometric evaluation. Journal of Advanced Nursing, 17, 1251–1259.
Janiszewska, J., Buss, T., de Walden-Galuszko, K., Majkowicz, M., Lichodziejewska-Niemierko, M., & Modlinska, A. (2008). The religiousness as a way of copingwith anxiety in women with breast cancer at different disease stages. SupportiveCare in Cancer, 16(12), 1361–1366.
Johnson, G. D., Thomas, J. S., & Matre, M. (1990). Race, social ties, social support,and subjective wellbeing: Evidence from a community study. Sociological Focus,23(4), 341–354.
Kivett, E., & Palmore, E. (1977). Change in life satisfaction: A longitudinal study ofpersons aged 46–70. Journal of Gerontology, 32, 311–316.
Kozielecki, J. (2006). Psychology of hope. Warsaw, Poland: Zak Academic Publishing.Kwon, P. (2000). Hope and dysphoria: The moderating role of defense mechanisms.
Journal of Personality, Sociology, Psychology, 68(2), 199–223.Luttik, M. L., Jaarsma, T., Jeeger, N., & van Veldhuisen, D. J. (2005). For better and
for worse: Quality of life impaired in HF patients as well as in their partners.European Journal of Cardiovascular Nursing, 4(1), 11–14.
Majkowicz, M., de Walden-Galuszko, K., & Trojanowski, L. (1997). The role ofassessment of social functioning, mental and spiritual experience in the globalassessment of quality of life. Psycho-Cancer, 1, 78–85.
McKnight, P. E., & Kashdan, T. B. (2009). Purpose in life as a system that createsand sustains health and well-being: An integrative, testable theory. Review ofGeneral Psychology, 13(3), 242–251.
Meraviglia, M. G. (2004). The effects of spirituality on well-being of people withlung cancer. Oncology Nursing Forum, 31(1), 89–94.
Meraviglia, M. G. (2006). Effects of spirituality in breast cancer survivors. OncologyNursing Forum, 33(1), E1–E7.
Moadel, A., Morgan, K., Fatone, A., Grennan, J., Carter, J., Laruffa, G., Skummy,A., & Dutcher, J. (1999). Seeking meaning and hope: Self-reported spiritualand existential needs among an ethnically-diverse cancer patient population.Psycho-Oncology, 8, 378–385. doi: 10.1002/(SICI)1099-1611
Nanthamongkolchai, S. T., Munsawaengsub, D., & Charupoonphol, P. (2009). Factorsinfluencing life happiness among elderly female in Rayong Province, Thailand.Journal Medical Association Thailand, 92(Suppl 7), S8–S12.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012
482 M. Wnuk et al.
Neuling, J., & Winefield, H. R. (1988). Social support and recovery after surgery forbreast cancer: Frequency and correlates of supportive behaviours by family,friends and surgeon. Social Science and Medicine, 27(4), 385–392.
Organisation for Economic Cooperation and Development. (2010). Health at aglance: Europe 2010. Retrieved from http://dx.doi.org/10.1787/health_glance-2010-en
Osmanska, M., Borlowska, A., & Makarewicz, R. (2010). Evaluation of quality of life,anxiety and depression in testicular cancer patients during chemotherapy andafter anticancer treatment. Psychiatry Polish, 44(4), 543–556.
Penson, J. (2000). A hope is not a promise: Fostering hope within palliative care.International Journal of Palliative Nursing, 6(2), 94–98.
Phillips, D. (2006). Quality of life: Concept, policy and practice. New York, NY:Routledge, Taylor & Francis Group.
Ryff, C. D. (1989). Happiness is everything, or is it? Explorations on the meaningof psychological well-being. Journal of Personality, Sociology, Psychology, 57,1069–1081.
Rzewnicki, I., & Jackiewicz, M. (2009). The quality of life after the surgery of laryngealor hypopharynx. Polish Merkur Lekarski, 26(151), 40–42.
Schaar, I., & Ojehagen, A. (2003). Predictors of improvement in quality of life ofseverely mentally ill substance abusers during 18 months of co-operation be-tween psychiatric and social services. Social Psychiatry and Psychiatric Epi-demiology, 38(2), 83–87.
Shapiro, J. P., McCue, K., Heyman, E. N., Dey, T., & Haller, H. S. (2010). Coping-related variables associated with individual differences in adjustment to cancer.Journal of Psychosocial Oncology, 28, 1–22.
Snyder, C. R. (2000). Hypothesis: There is hope. In C. R. Snyder (Ed.), Handbook ofhope (pp. 3–21). San Diego, CA: Academic Press.
Snyder, C. R., Harris, C., Anderson, J. R., Holleran, S. A., Irving, L. M., Sigmon, S.T., . . . Harney, P. (1991). The will and the ways: Development and validationof an individual-differences measure of hope. Journal of Personality and SocialPsychology, 60, 570–585.
Spanier, G. B., & Lachman, M. E. (1980). Factors associated with adjustment tomarital separation. Sociological Focus, 13(4), 369–381.
Spiegel, D., Bloom, J. R., Kraemer, H. C., & Gottheil, E. (1989). Effect of psychosocialtreatment on survival of patients with metastatic breast cancer. Lancet, 2(8668),888–891.
Stephenson, C. (1991). The concept of hope revisited for nursing. Journal of Ad-vanced Nursing, 16, 1456–1461.
Thoits, P. A. (1982, June). Conceptual, methodological, and theoretical problems instudying social support as a buffer against life stress. Journal of Health andSocial Behavior, 23, 145–159.
Tomich, P. L., & Helgeson, V. S. (2002). Five years later: A cross-sectional compari-son of breast cancer survivors with health women. Psycho-Oncology, 11, 154–169.
Weaver, A. J., & Flannelly, K. J. (2004). The role of religion/spirituality for can-cer patients and their caregivers. Southern Medical Association, 97, 1210–1214.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012
Purpose in Life and Hope Among Patients with Cancer in Poland 483
Weebers, J. E. (2006). The role of meaning in the prediction of psychosocial well-being of testicular cancer survivors. Quality of Life Research, 15(4), 705–717.
Wierzbicka, M., Kusnierkiewicz, M., Wojtowica, J. G., Maune, S., & Szyfter, W. (2001).The quality of life in head and neck cancer patients: Description of randomizedexamination formula based on standardized questionnaires EORTC QLQ C-30, EORTC QTQ-H-N35 and Kiel Questionnaire. Otolaryngology Polish, 55(3),287–292.
Wnuk, M. (2006). Involvement in self-help groups and the quality of life among al-cohol dependent persons: Meaning in life’s mediating role. Alkoholizm I Narko-mania, 19, 357–368.
Wnuk, M. (2008). Comparison of existential and religious-spiritual aspects amongstudents and alcohol dependent persons. Roczniki Psychologiczne, 11, 175–189.
Wronska, I. (2003). The quality of women’s life after mastectomy in Poland. HealthCare Women International, 24(10), 900–909.
Young, K. W. (2006). Social support and life satisfaction. International Journal ofPsychosocial Rehabilitation, 10(2), 155–164.
Dow
nloa
ded
by [
Ms
Patr
icia
Fob
air]
at 1
2:43
24
Aug
ust 2
012





























