Embed Size (px)
Citation preview
Caspian Journal of
Dental Research
Original Article
Reliability and validity of the persian version of the General Oral Health Assessment Index (GOHAI)
Mina Motallebnejad (DDS)
1, Kataayoun Mottaghi (DDS)2, Shervin Mehdizade (DDS)
3, Farshid
Alaeddini (PhD)4, Ali Bijani (MD)
5
1. Associate Professor, Cellular & Molecular Biology Research Center, Department of Oral Medicine, Faculty of Dentistry, Babol
University of Medical Sciences, Babol-Iran.
2. General Dentist.
3. Assistant Professor, Department of Prosthodontics, Faculty of Dentistry, Babol University of Medical Sciences, Babol-Iran.
4. Scholar, Health Research and Development Institute, Tehran-Iran.
5. General Practitioner, Social Determinants of Health Research Center, Babol University of Medical Sciences, Babol-Iran.
Corresponding Author: Mina Motallebnejad, Faculty of Dentistry, Babol University of Medical Sciences, Babol- Iran.
Email: [email protected] Tel: +981113230831
Abstract
Introduction: As the oral health related quality of life has been important in many dental patients
GOHAI is an acceptable tool, preparing its Persian version can be useful in oral health research
among Persian populations. The aim of this study was to evaluate the reliability and validity of the
Persian version of General Oral Health Assessment Index (GOHAI).
Methods: Translation was performed using the forward-backward process. The final Persian
version was then tested through an interview and test-retest to evaluate its comprehensibility and
reliability. A sample of 150 subjects (20-65 years old) was requested to answer the GOHAI items
prior to a clinical examination.
Data on the subjects’ socio-demographic characteristics and self-rating report of oral health,
general health and dental care needs were recorded. Internal consistency was calculated by
Cronbach’s α. Interview and test-retest reliability was evaluated by weighted kappa. Concurrent
validity was assessed by comparing GOHAI scores and self-rated measures of oral health, general
health and perceived dental care needs. Discriminant validity was tested by comparing GOHAI
scores with clinical oral condition.
Results: The mean GOHAI score was 46.78±7.85. Cronbach’s α (0.78) showed a high internal
consistency and homogeneity between items. Weighted kappa coefficient for the interview varied
from 0.60 to 0.96 and was between 0.33 and 0.64 for test-retest. Bland-Altman plot displayed a
good agreement between the two GOHAI scores for both the interview and test-retest. There was
no significant relationship between GOHAI scores and self-rating oral health (p=0.090), but there
was a relationship between self-rating general health and mean GOHAI scores (p=0.047). Also,
the low GOHAI scores were associated with the perceived dental care needs (p=0.001). There was
an opposite correlation between GOHAI scores and caries and missing teeth (p<0.0001).
Conclusions: The Persian version of the GOHAI exhibits acceptable reliability and validity, so it
can be used widely throughout the Persian communities.
Keywords: GOHAI, Persian, Quality of life, Questionnaire
[ D
OI:
10.
2208
8/cj
dr.2
.1.8
]
[ D
OR
: 20.
1001
.1.2
2519
890.
2013
.2.1
.4.7
]
[ D
ownl
oade
d fr
om c
jdr.
ir o
n 20
22-0
2-12
]
1 / 10
Caspian J Dent Res - March 2013, 2(1): 8-17
Validation of persian GOHAI version
9
GOHAI)پرسشنامه )پايايي و روايي نسخه فارسي
چكيذه
امزيسٌ کیفیت سوذگی يابستٍ بٍ سالمت دَان در بیماران دوذاوپششکی ي پششکی اَمیت يیژٌ ای داشتٍ :مقذمه
فارسیتًاوذ در جًامع باشذ. لذا تُیٍ وسخٍ فارسی آن می مًرد قبًل می GOHAIي در ایه سمیىٍ پزشسىامٍ
GOHAI َذف ایه مطالعٍ بزرسی ريایی ي پایایی وسخٍ فارسی پزسشىامٍ تفادٌ قزار گیزد.اس مًردسبان
.است
تزجمٍ پزسشىامٍ اوجام شذ. وسخٍ وُایی forward-backward با استفادٌ اس ريش :مواد و روش ها
افزاد وفز 150ارسیابی گزدیذ. test-retest ي پایایی تًسط مصاحبٍ ي comprehensibilityجُت بزرسی
اطالعات مزبًط بٍ مشخصات فزدی .سالٍ قبل اس معایىٍ دَان پزسشىامٍ وُایی را تکمیل کزدوذ 65تا 20
با internal consistency.سالمت دَان خًد ثبت شذ اقتصادی ي وظزات افزاد اس سالمت عمًمی ي
Weighted)با ضزیب کاپا test-retest استفادٌ اس ضزیب آلفا کزيوباخ محاسبٍ گزدیذ. پایایی مصاحبٍ ي
Kappa) تعییه گزدیذ. ريایی Concurrent ٌاس طزیق مقایسٍ ومز GOHAI ي وظزات افزاد اس سالمت
اس طزیق مقایسٍ Discriminant عمًمی ي سالمت دَان ي ویاسَای درماوی دوذاوپششکی محاسبٍ شذ. ريایی
.شذ با يضعیت سالمت دَان )معایىات بالیىی( محاسبٍ GOHAI ومزٌ
دَىذٌ وشان 78/0بًد ضزیب آلفای کزيوباخ معادل GOHAI 87/64± 85/7 میاوگیه ومزٌ يافته ها:
internal consistency ي homogeneity بیه مًارد بًد.
متغیز بًد. 64/0تا 33/0اس test-retest ي بزای 96/0تا 6/0بزای مصاحبٍ اس Weighted ضزیب کاپا
وشان داد ارتباط معىی test-retest در مصاحبٍ GOHAI خًبی بیه ومزٌتًافق Bland-Altmanاما
يلی ارتباط بیه ومزٌ (p =0.090)وظز بیماران اس سالمت دَان يجًد وذاشت ي GOHAI داری بیه ومزٌ
GOHAI ي وظز بیمار وسبت بٍ سالمت عمًمی يجًد داشت(p=0.047 ) َمچىیه ومزات کم GOHAI
ي دوذان َای کشیذٌ GOHAI ارتباط معکًس بیه ومزٌ p)=(0.001وی در ارتباط بًدبا ویاسَای درمان دوذا
>p) (0.0001شذٌ ي پًسیذٌ يجًد داشت
تُیٍ شذٌ ريایی ي پایایی قابل قبًلی داشتٍ ي می تًان اس آن در GOHAIوسخٍ فارسی :نتيجه گيري
.زدجمعیت فارسی سبان جُت بزرسی َای بُذاشتی ي سالمت دَان استفادٌ ک
، فارسی، کیفیت سوذگی، پزسشىامGOHAIٍ :واژگان کليذي
[ D
OI:
10.
2208
8/cj
dr.2
.1.8
]
[ D
OR
: 20.
1001
.1.2
2519
890.
2013
.2.1
.4.7
]
[ D
ownl
oade
d fr
om c
jdr.
ir o
n 20
22-0
2-12
]
2 / 10

Caspian J Dent Res -March 2013; 2(1): 8-17
Motallebnejad M, et al.
10
Introduction
Recently, the definition of (oral) health has shifted
to address more than the absence of physical disease.
The new definition defines health as an individual's
perception of his health in the context of physical,
psychological and social well-being (1).The disease-
based approach is the traditional way to measure oral
health. Oral disease has been assessed by objective and
quantitative indicators (2).
Oral disease prevalence has been studied in
different samples of adults, but less is known about
how the disease and symptoms affect adults' daily
activities and quality of life (2). Therefore, oral
epidemiology uses multidimensional constructs known
as socio-dental indicators or oral health–related quality
of life measures (OHRQoL), which refer to the extent
to which oral disorders disrupt an individual’s normal
functioning and result in major behavior chang (3, 4).
To date, OHRQoL has become an important tool
for assessing the impact of a range of oral and
systemic conditions on an individual’s quality of life
and well-being (5- 10). The outcomes of clinical care,
such as the efficiency of treatment interventions, are
also important (11, 12).
Several measures have been developed that have
the potential to be used this way (4). The Geriatric Oral
Health Assessment Index (GOHAI) is a questionnaire
designed to assess the impact of oral conditions on the
quality of life (QoL) of the elderly population. GOHAI
has also been referred to as the General Oral Health
Assessment Index (13).
The original GOHAI has 12 negatively and
positively worded items assessing three dimensions of
OHRQoL: 1) physical function, representing the
pattern of eating, speech and swallowing; 2) pain or
discomfort, representing the use of medications to
relieve pain or discomfort in the mouth; 3)
psychosocial function, representing the worry or
concern about oral health, dissatisfaction with
appearance, self-consciousness about oral health and
avoidance of social contacts because of oral problems
(13).
GOHAI has also been found to be a remarkable
predictor of self-rated dental appearance in aged people
(14). In comparison with other self-reported measures
of oral health, GOHAI has been found to be sensitive
to dental treatment needs (15, 16). Although GOHAI
has been translated into several languages and tested
for its validity and reliability (1, 2, 16-23), a Persian
version is not yet available. The purpose of this study
was to develop a Persian version of the GOHAI, to
make the obligatory cultural and ethnical adaptation
and to evaluate its reliability, validity and internal
consistency for use among the Persian people.
Methods
English version of the GOHAI: The English
GOHAI has 12 items in three hypothetical dimensions:
physical function, psychosocial function and pain
and/or discomfort. For each of the 12 items, the
participants were asked if they have always, often,
sometimes, seldom or never experienced any of those
problems in the previous 3 months.
The questions were sometimes worded in a
positive manner and sometimes in a negative manner to
force respondents to consider their answer. The
responses were scored on a scale ranging from 1 to 5
(1=never; 2=seldom; 3=sometimes; 4=often;
5=always).
When the data were interred into a database, the
responses were recoded, if necessary, so that responses
indicating good conditions and no problems carried the
highest scores. Thus, the scale score was a sum of
values; a low value indicated an oral health problem. A
summary score (Add-GOHAI) ranging from 12 to 60
was calculated for each subject, with a higher score
indicating better oral health.
The translation process and the pilot study: The
proposal of this study was approved by the Research
Committee and the Ethics Committee of Babol
University of Medical Sciences. The written informed
consent was taken from each participant. The GOHAI
was translated into Persian.
The process involved translating from English to
Persian by two bilingual people whose first language
was Persian and then a backward translation from
Persian to English by two bilingual people whose first
language was English.
Once the translation was complete, comparisons
between the original English, the back-translated
version and the Persian version were drafted and
revised by two professional translators and scrutinized
for changes in sense.
The final Persian version was then tested on a
sample of adults (n=40). The volunteers first answered
the 12 questions from the final Persian version on their
own; then, they were asked the same questions in an
[ D
OI:
10.
2208
8/cj
dr.2
.1.8
]
[ D
OR
: 20.
1001
.1.2
2519
890.
2013
.2.1
.4.7
]
[ D
ownl
oade
d fr
om c
jdr.
ir o
n 20
22-0
2-12
]
3 / 10
Caspian J Dent Res - March 2013, 2(1): 8-17
Validation of persian GOHAI version
11
interview. The interviewers probed the answers to
ascertain the meaning equivalent to the original and
recoded the volunteers' comments and any difficulty
that they encountered.
The comprehensibility of the translated version
was assessed, and only minor changes were made to
make the questionnaire more understandable. To
evaluate test-retest reliability, the GOHAI was re-
administered after one week.
Main study
Sample size: The sample size calculation was
based on the test-retest reliability, which was measured
by the intraclass correlation (r). To be acceptable, the
questionnaire had to have an r=0.8 and an r≥0.7; thus,
H0: P0=0.7 and H1: P1=0.8. A two-sided test
suggested by Atieh et al, (14) was used. With β=0.2
(80% power) and α=0.05, a sample size of 150 subjects
was required.
Data collection: The final Persian version of the
GOHAI was administered to 150 Persian adults (20–65
years old) attending Ayatollah Rohani Hospital from
September 2009 to February 2010. The data came from
a self-administered questionnaire followed by a clinical
oral examination performed by a single dentist. In
addition to the GOHAI items, the questionnaire
included socio-demographic data such as age, gender,
educational level and employment. The subjects were
also asked about the use of removable prostheses, self-
rated oral and general health and dental treatment
needs.
All oral examinations were performed the same
day the questionnaire was administered, in either a
dental or medical examination room using portable
lamps and disposable instruments. The oral status
examination based on 28 teeth involved recording the
number of missing teeth, DMFT, root DFT, pathologic
tooth mobility and the Oral Hygiene Index-Simplified
(OHI-S).
Data analysis: The analysis of the study was
carried out using STATA V 10 and SPSS 17.0 for
Windows (SPSS 17.0, SPSS Inc. Chicago, IL, USA).
The mean Persian GOHAI scores were calculated for
the demographic variables using the independent t-test
and ANOVA.The GOHAI was computed by adding the
score of the 12 items; the final values ranged from 12
to 60.
The original scores were kept for three items—
―able to swallow comfortably‖, ―able to eat without
discomfort‖ and ―pleased with look of teeth‖—and
reversed for the remaining nine items, such that a
higher score was associated with a more positive oral
health. The test-interview and test-retest reliabilities
were assessed by paired t-test, the Spearman
correlation coefficient and weighted kappa values. A
Bland–Altman plot was also used to describe the
agreement between the two GOHAI scores taken from
the same participants on two separate occasions.
The internal consistency of the GOHAI was
assessed by the standardized Cronbach's alpha (the
reliability coefficient), the alpha if the item was deleted
and the inter-item and inter-table correlation
coefficients.
Concurrent validity was assessed by examining the
relation between the GOHAI scores and the global oral
health rating questions. It was hypothesized that the
subjects reporting functional problems, pain or
discomfort or psychosocial impacts would have a low
GOHAI score and would be more likely to report
dissatisfaction with their oral health, more likely to
report their oral health as fair or poor and more likely
to report a self-perceived need for dental care. The
discriminant validity was tested by comparing the
individuals’ item responses and GOHAI scores with
their objectively evaluated dental condition.
Results
For the test-interview, the mean GOHAI score was
50.37–51.1, (p=0.009), and for the test-retest, the mean
GOHAI score was 51.28–51.05 (p=0.776) (table 1).
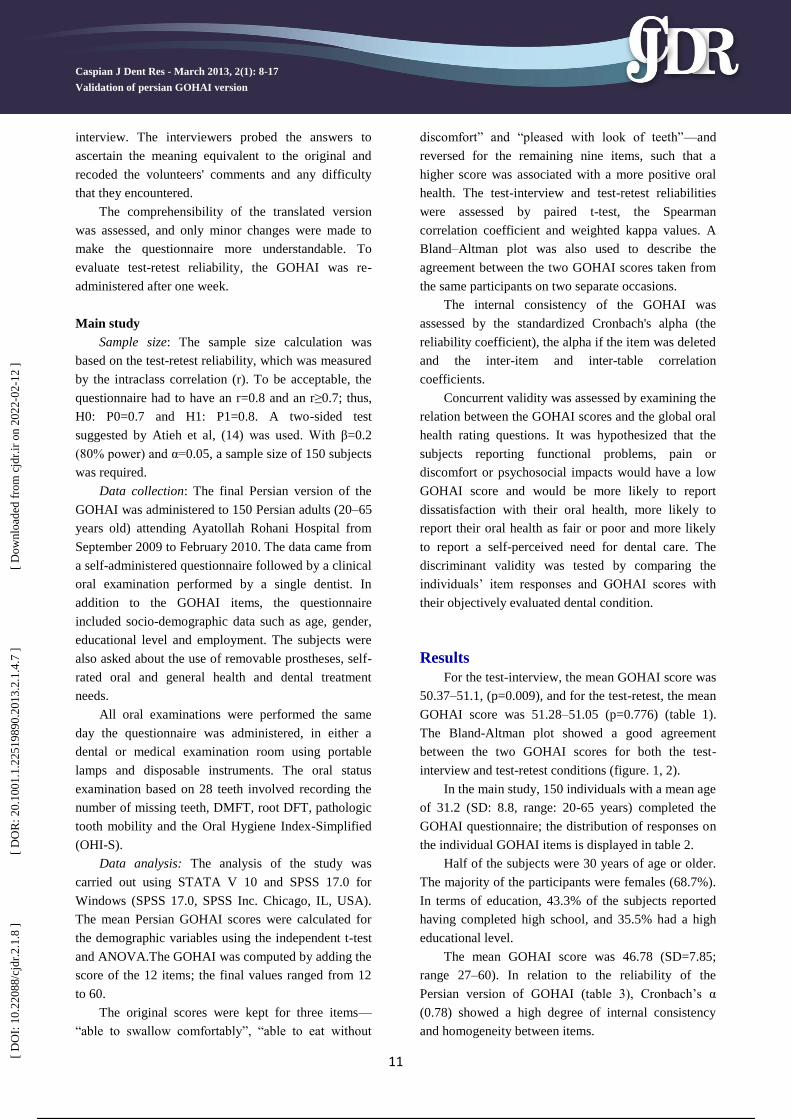
The Bland-Altman plot showed a good agreement
between the two GOHAI scores for both the test-
interview and test-retest conditions (figure. 1, 2).
In the main study, 150 individuals with a mean age
of 31.2 (SD: 8.8, range: 20-65 years) completed the
GOHAI questionnaire; the distribution of responses on
the individual GOHAI items is displayed in table 2.
Half of the subjects were 30 years of age or older.
The majority of the participants were females (68.7%).
In terms of education, 43.3% of the subjects reported
having completed high school, and 35.5% had a high
educational level.
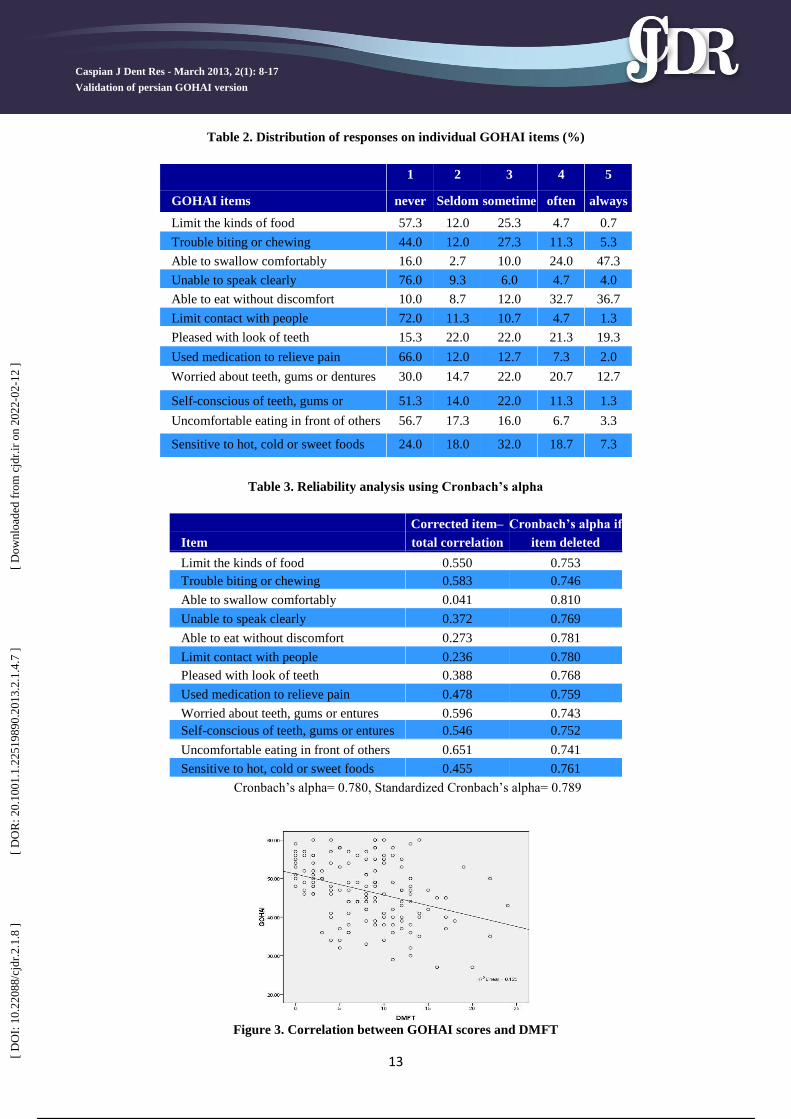
The mean GOHAI score was 46.78 (SD=7.85;
range 27–60). In relation to the reliability of the
Persian version of GOHAI (table 3), Cronbach’s α
(0.78) showed a high degree of internal consistency
and homogeneity between items.
[ D
OI:
10.
2208
8/cj
dr.2
.1.8
]
[ D
OR
: 20.
1001
.1.2
2519
890.
2013
.2.1
.4.7
]
[ D
ownl
oade
d fr
om c
jdr.
ir o
n 20
22-0
2-12
]
4 / 10
Caspian J Dent Res -March 2013; 2(1): 8-17
Motallebnejad M, et al.
12
Figure 1. Bland-Altman plot (test-interview)
Figure 2. Bland-Altman plot (test-retest)
Table 1. Test-interview & test-retest correlation for the Persian GOHAI items
Item Weighted
kappa
Spearman’s
rank
correlation
coefficient
Weighted
kappa
Spearman’s
rank
correlation
coefficient
Limit the kinds of food 0.783 0.876 0.353 0.445
Trouble biting or chewing 0.829 0.585 0.525 0.709
Able to swallow comfortably 0.868 0.904 0.509 0.571
Unable to speak clearly 0.825 0.866 0.463 0.516
Able to eat without discomfort 0.600 0.620 0.592 0.637
Limit contact with people 0.884 0.954 0.425 0.498
Pleased with look of teeth 0.842 0.827 0.508 0.559
Used medication to relieve pain 0.798 0.872 0.329 0.430
Worried about teeth, gums or dentures 0.888 0.956 0.424 0.519
Self-conscious of teeth, gums or
dentures 0.751 0.775 0.638 0.763
Uncomfortable eating in front of others 0.749 0.865 0.590 0.635
Sensitive to hot, cold or sweet foods 0.958 0.980 0.447 0.552
Total – 0.971 – 0.779
Kappa<0.40 (poor agreement), 0.41–0.60 (moderate agreement), 0.61–0.80 (good agreement),>0.80 (very good agreement)
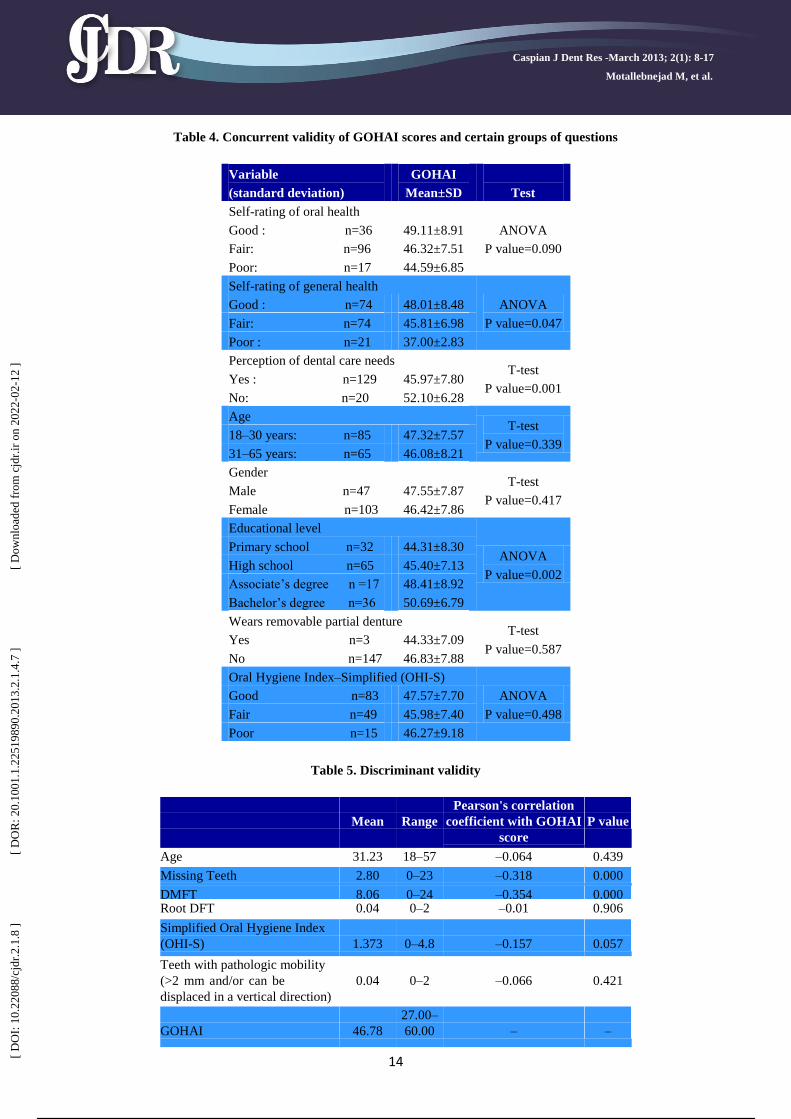
There was no significant relationship between
mean GOHAI score and the subject’s age, gender, use
of removable partial dentures or Oral Hygiene Index–
Simplified (OHI-S), although the subjects with a good
OHI-S had a higher GOHAI score than those who had
a fair or poor OHI-S. The individuals with a low level
of education had lower GOHAI scores compared with
the well-educated respondents (table 4). In relation to
the concurrent validity (table 4), the subjects with a
higher mean GOHAI score were more satisfied with
their oral and general health, whereas, low GOHAI
scores were associated with self-perceived fair or poor
oral health, self-perceived fair or poor general health, a
low level of satisfaction with oral health and with the
self-perception of dental needs. In relation to the
discriminant validity (table 5), the respondents with
higher GOHAI scores were associated with a lower
number of carious and missing teeth (figure. 3), a
better OHI-S score and fewer pathologically mobile
teeth.
[ D
OI:
10.
2208
8/cj
dr.2
.1.8
]
[ D
OR
: 20.
1001
.1.2
2519
890.
2013
.2.1
.4.7
]
[ D
ownl
oade
d fr
om c
jdr.
ir o
n 20
22-0
2-12
]
5 / 10
Caspian J Dent Res - March 2013, 2(1): 8-17
Validation of persian GOHAI version
13
Table 2. Distribution of responses on individual GOHAI items (%)
GOHAI items
1
never
2
Seldom
3
sometime
s
4
often
5
always
Limit the kinds of food 57.3 12.0 25.3 4.7 0.7
Trouble biting or chewing 44.0 12.0 27.3 11.3 5.3
Able to swallow comfortably 16.0 2.7 10.0 24.0 47.3
Unable to speak clearly 76.0 9.3 6.0 4.7 4.0
Able to eat without discomfort 10.0 8.7 12.0 32.7 36.7
Limit contact with people 72.0 11.3 10.7 4.7 1.3
Pleased with look of teeth 15.3 22.0 22.0 21.3 19.3
Used medication to relieve pain 66.0 12.0 12.7 7.3 2.0
Worried about teeth, gums or dentures 30.0 14.7 22.0 20.7 12.7
Self-conscious of teeth, gums or
dentures
51.3 14.0 22.0 11.3 1.3
Uncomfortable eating in front of others 56.7 17.3 16.0 6.7 3.3
Sensitive to hot, cold or sweet foods 24.0 18.0 32.0 18.7 7.3
Table 3. Reliability analysis using Cronbach’s alpha
Item
Corrected item–
total correlation
Cronbach’s alpha if
item deleted
Limit the kinds of food 0.550 0.753
Trouble biting or chewing 0.583 0.746
Able to swallow comfortably 0.041 0.810
Unable to speak clearly 0.372 0.769
Able to eat without discomfort 0.273 0.781
Limit contact with people 0.236 0.780
Pleased with look of teeth 0.388 0.768
Used medication to relieve pain 0.478 0.759
Worried about teeth, gums or entures 0.596 0.743
Self-conscious of teeth, gums or entures 0.546 0.752
Uncomfortable eating in front of others 0.651 0.741
Sensitive to hot, cold or sweet foods 0.455 0.761
Cronbach’s alpha= 0.780, Standardized Cronbach’s alpha= 0.789
Figure 3. Correlation between GOHAI scores and DMFT
[ D
OI:
10.
2208
8/cj
dr.2
.1.8
]
[ D
OR
: 20.
1001
.1.2
2519
890.
2013
.2.1
.4.7
]
[ D
ownl
oade
d fr
om c
jdr.
ir o
n 20
22-0
2-12
]
6 / 10
Caspian J Dent Res -March 2013; 2(1): 8-17
Motallebnejad M, et al.
14
Table 4. Concurrent validity of GOHAI scores and certain groups of questions
Variable
(standard deviation)
GOHAI
Mean±SD
Test
Self-rating of oral health
ANOVA
P value=0.090
Good : n=36 49.11±8.91
Fair: n=96 46.32±7.51
Poor: n=17 44.59±6.85
Self-rating of general health
ANOVA
P value=0.047
Good : n=74 48.01±8.48
Fair: n=74 45.81±6.98
Poor : n=21 37.00±2.83
Perception of dental care needs T-test
P value=0.001 Yes : n=129 45.97±7.80
No: n=20 52.10±6.28
Age T-test
P value=0.339 18–30 years: n=85 47.32±7.57
31–65 years: n=65 46.08±8.21
Gender T-test
P value=0.417 Male n=47 47.55±7.87
Female n=103 46.42±7.86
Educational level
ANOVA
P value=0.002
Primary school n=32 44.31±8.30
High school n=65 45.40±7.13
Associate’s degree n =17 48.41±8.92
Bachelor’s degree n=36 50.69±6.79
Wears removable partial denture T-test
P value=0.587 Yes n=3 44.33±7.09
No n=147 46.83±7.88
Oral Hygiene Index–Simplified (OHI-S)
ANOVA
P value=0.498
Good n=83 47.57±7.70
Fair n=49 45.98±7.40
Poor n=15 46.27±9.18
Table 5. Discriminant validity
Mean
Range
Pearson's correlation
coefficient with GOHAI
score
P value
Age 31.23 18–57 –0.064 0.439
Missing Teeth 2.80 0–23 –0.318 0.000
DMFT 8.06 0–24 –0.354 0.000 Root DFT 0.04 0–2 –0.01 0.906
Simplified Oral Hygiene Index
(OHI-S)
1.373
0–4.8
–0.157
0.057
Teeth with pathologic mobility
(>2 mm and/or can be
displaced in a vertical direction)
0.04
0–2
–0.066
0.421
GOHAI
46.78
27.00–
60.00
–
–
[ D
OI:
10.
2208
8/cj
dr.2
.1.8
]
[ D
OR
: 20.
1001
.1.2
2519
890.
2013
.2.1
.4.7
]
[ D
ownl
oade
d fr
om c
jdr.
ir o
n 20
22-0
2-12
]
7 / 10
Caspian J Dent Res - March 2013, 2(1): 8-17
Validation of persian GOHAI version
15
Discussion
The GOHAI was originally presented and
evaluated for assessing oral health–related quality of
life in middle-aged and well-educated Americans, but
subsequent studies showed that it could also be
successfully used in less-educated young people (2).
Cultural and language differences, which can even
occur in one country, make validity assessment more
complicated.
People with different cultural backgrounds may
respond differently to GOHAI items. For instance,
being edentulous (missing teeth) may have different
levels of importance in various cultures. As a result,
people's quality of life given the same oral conditions
may be evaluated differently.
Therefore, it is important that the GOHAI be
tested in diverse populations in terms of culture,
language and geography. In this study, the first step
consisted of using a standardized translation process.
Translation and back-translation were performed to
ensure the accuracy and interpretability of the
questions, and this led to the creation of a Persian
version with pleasing psychometric properties. The
assessment of certain social and demographic
characteristics, including age and gender, did not
indicate significant differences in the mean GOHAI
scores for these parameters.
The concurrent validity of the Persian version of
the GOHAI was tested and confirmed; there was a
meaningful relationship between individuals' self-
report of general health and dental care needs with
GOHAI scores.
In addition, people with a good self-impression of
their oral health received higher mean GOHAI scores
compared with those with moderate to poor self-
impressions, and all of these cases display high
concurrent validity with the Persian version of the
GOHAI.
The clinical indicators studied in the discriminant
validity assessment had been used in other studies as
well (2, 19, 21 and 24).
Because the GOHAI has not been specifically
proposed as a predictor of clinical indices, it should be
used as a complement to clinical and objective
assessments. Some articles have shown reasonable
correlation between the GOHAI and clinical
observations (2, 19, 24), whereas others have
mentioned the weak correlation between them (25). In
the present study, the correlation was significant
between the clinical indicators such as DMFT and the
number of missing teeth.
For loose teeth, a weak relationship with the
GOHAI score was observed. However, in the study by
Atieh et al, who provided the Arabic version of the
GOHAI, the clinical index revealed the strongest
relationship with the GOHAI score (21); the cause of
this difference could be potentially explained by the
mean age group studied, which was 71.20 (age range:
60–90) years in the Arab studies and 31.2 (age range:
18–65) years in our study.
All assessment instruments should possess the
quality of repeatability at different times. In this case,
the same results at two different time points for a
patient would indicate that the patient’s situation had
not changed. The findings demonstrated that the
questions on the Persian version of the GOHAI have
good internal consistency (Cronbach's alpha
coefficient=0.78). This value did not become
significantly larger by eliminating any of the questions,
except question 3 (ability to swallow comfortably),
which showed less internal consistency, suggesting
poor compatibility with other GOHAI questions. The
Cronbach's alpha coefficient would increase if question
3 was deleted.
The question is primarily designed to evaluate the
people with dry mouth problems. Dry mouth is much
more common in the elderly, and thus, the incidence of
swallowing difficulties is more prevalent in middle-
aged people than in younger people (2). It would
probably be better if the GOHAI scoring did not
include this question or if the response was fully
reversed.
The result of the test-retest was acceptable in this
study, and the weighted kappa values were satisfactory
for the GOHAI questions. Only two questions
(numbers 1 and 8) did not have desirable weighted
kappa values. This was a problem for questions 3 and 5
in the French version and for questions 4 and 10 in the
Chinese version of the GOHAI, illustrating that these
questions were not easily understood in these
languages (2, 17).
A Bland-Altman plot indicated an acceptable
result, and the 95% of differences in the questions,
both for the test-interview and the test–retest cases,
were within the limits of agreement.
As conclusion, the Persian version of the GOHAI
exhibited acceptable reliability and validity. This
instrument can be applied to evaluate OHRQoL in
[ D
OI:
10.
2208
8/cj
dr.2
.1.8
]
[ D
OR
: 20.
1001
.1.2
2519
890.
2013
.2.1
.4.7
]
[ D
ownl
oade
d fr
om c
jdr.
ir o
n 20
22-0
2-12
]
8 / 10

Caspian J Dent Res -March 2013; 2(1): 8-17
Motallebnejad M, et al.
16
cross-sectional and longitudinal studies of different age
groups.
This version may be better tested for different oral
and systemic conditions and disorders to evaluate the
validity in future studies.
Acknowledgments
We sincerely thank the UCLA for providing the
original version and scoring system of GOHAI. Special
appreciation to Dr. Jenabian N for her critical advice in
translating the questionnaire.
Funding: This project was approved and financially
supported by the Vice-Chancellery for Research &
Technology of Babol University of Medical Sciences
Conflict of interest: There was no conflict of interest.
References
1. Hassel AJ, Rolko C, Koke U, Leisen J, Rammelsberg
P. A German version of the GOHAI. Community
Dent Oral Epidemiol 2008; 36: 34-42.
2. Tubert-Jeannin S, Riordan PJ, Morel-Papernot A,
Porcheray S, Saby-Collet S. Validation of an oral
health quality of life index (GOHAI) in France.
Community Dent Oral Epidemiol 2003; 31: 275-84.
3. Locker D. Measuring oral health: a conceptual
framework. Community Dent Health 1988; 5: 3-18.
4. Sheiham A, Cushing AM, Maizels JE. The social
impacts of dental disease. In: Slade GD, editor:
Measuring oral health and quality of life. Chapel
Hill, NC: University of North Carolina; 1997.p. 47-56.
5. Gift HC, Atchison KA, Dayton CM. Conceptualising
oral health and oral health-related quality of life.
Soc Sci Med 1997; 44: 601-8.
6. Shyama M, Honkala S, Al-Mutawa SA, Honkala E.
Oral Health-Related Quality of Life among Parents
and Teachers of Disabled Schoolchildren in
Kuwait.Med Princ Pract 2013 ; 22: 285-90.
7. Ribeiro GR, Costa JL, Ambrosano GM, Garcia RC.
Oral health of the elderly with Alzheimer's
disease.Oral Surg Oral Med Oral Pathol Oral
Radiol 2012; 114: 338-43.
8. Li Z, Zhu L, Sha Y. [Effects of periodontal health
and related factors on the oral health-related quality
of life in type 2 diabetic patients with chronic
periodontitis]. Hua Xi Kou Qiang Yi Xue Za
Zhi 2011;29:379-83. [In Chinese]
9. Deshmukh SP, Radke UM. Translation and
validation of the Hindi version of the Geriatric Oral
Health Assessment Index. Gerodontology 2012; 29:
e1052-8.
10. A-Dan W, Jun-Qi L. Factors associated with the
oral health-related quality of life in elderly persons
in dental clinic: validation of a Mandarin
Chinese version of GOHAI. Gerodontology 2011;
28: 184-91.
11. Allen PF, McMillan AS, Locker D. An assessment
of sensitivity to change of the oral health impact
profile in a clinical trial. Community Dent Oral
Epidemiol 2001; 29: 175-82.
12. Albaker AM. The oral health-related quality of life
in edentulous patients treated with Conventional
complete dentures. Gerodontology 2013; 30:61-6..
13. Atchison KA. The General Oral Health Assessment
Index. In: Slade G, editor: Measuring oral health
and quality of life. Chapel Hill, NC: University of
North Carolina; 1997.p. 79-80.
14. Matthias RE, Atchison KA, Schweitzer SO, Lubben
JE, Mayer-Oakes A, De Jong F. Comparisons
between dentist rating and self-ratings of dental
appearance in an elderly population. Spec Care
Dentist 1993; 13: 53-60.
15. Dolan TA. The sensitivity of the Geriatric Oral
Health Assessment Index to dental care. J Dent
Educ 1997; 67: 37-46.
16. El Osta N, Tubert-Jeannin S, Hennequin M, Bou
Abboud Naaman N, El Osta L, Geahchan N.
Comparison of the OHIP-14 and GOHAI as
measures of oral health among elderly in Lebanon.
Health Qual Life Outcomes 2012; 10:131.
17. Wong MC, Liu JK, Lo EC. Translation and
validation of the Chinese version of GOHAI. J
Public Health Dent 2002; 62: 78-83.
18. Hagglin C, Berggren U, Lundgren J. A Swedish
version of the GOHAI index. Psychometric
properties and validation. Swed Dent J 2005; 29:
113-24.
19. Othman WN, Muttalib KA, Bakri R, Doss JG,
Jaafar N, Salleh NC, Chen S. Validation of the
Geriatric Oral Health Assessment Index (GOHAI)
in Malay language. J Public Health Dent 2006; 66:
199-204.
20. Naito M, Suzukamo Y, Nakayama T, Hamajima N,
Fukuhara S. Linguistic adaptation and validation of
the General Oral Health Assessment Index
[ D
OI:
10.
2208
8/cj
dr.2
.1.8
]
[ D
OR
: 20.
1001
.1.2
2519
890.
2013
.2.1
.4.7
]
[ D
ownl
oade
d fr
om c
jdr.
ir o
n 20
22-0
2-12
]
9 / 10

Caspian J Dent Res - March 2013, 2(1): 8-17
Validation of persian GOHAI version
17
(GOHAI) in an elderly Japanese Population. J
Public Health Dent 2006; 66: 273-5.
21. Atieh MA. Arabic version of the Geriatric Oral
Health Assessment Index.Gerodontology 2008; 25:
34-41.
22. Daradkeh SH, Khader YS. Translation and
validation of the Arabic version of the Geriatric
Oral Health Assessment Index (GOHAI). J Oral Sci
2008; 50: 453-9.
23. Ergül S, Akar GC. Reliability and validity of the
Geriatric Oral Health Assessment Index in Turkey.
J Gerontol Nurs 2008; 34: 33-9.
24. Atchison K, Dolan TA. Development of the
Geriatric Oral Health Assessment Index. J Dent
Educ 1990; 54: 680-7.
25. Locker D, Matear D, Stephens M, Lawrence H,
Payne B. Comparison of the GOHAI and OHIP-14
as measures of the oral health-related quality of life
of the elderly. Community Dent Oral Epidemiol
2001; 29: 373-81.
[ D
OI:
10.
2208
8/cj
dr.2
.1.8
]
[ D
OR
: 20.
1001
.1.2
2519
890.
2013
.2.1
.4.7
]
[ D
ownl
oade
d fr
om c
jdr.
ir o
n 20
22-0
2-12
]
Powered by TCPDF (www.tcpdf.org)
10 / 10





























![[Validity and reliability of the nursing organizational health questionnaire]](https://img.pdfslide.net/doc/110x75/635c7354095e4caf22053c1f/validity-and-reliability-of-the-nursing-organizational-health-questionnaire.jpg)