Embed Size (px)
Citation preview

www.thelancet.com
Reprint
Open Access article
Copyright 2020 ELSEVIER LIMITED, 125 London Wall, London EC2Y 5AS, UK.
Secukinumab versus adalimumab for treatment of active psoriatic arthritis (EXCEED): a double-blind, parallel-group, randomised, active-controlled, phase 3b trialIain B McInnes, Frank Behrens, Philip J Mease, Arthur Kavanaugh, Christopher Ritchlin, Peter Nash, Jordi Gratacós Masmitja, Philippe Goupille, Tatiana Korotaeva, Alice B Gottlieb, Ruvie Martin, Kevin Ding, Pascale Pellet, Shephard Mpofu, Luminita Pricop, on behalf of EXCEED Study GroupLancet 2020; 395: 1496–505
See www.thelancet.com for WebExtra content Version verified by CrossMark

Elsevier España, S.L.U.(A member of Elsevier)
Josep Tarradellas, 20-30, 1ª pl.08029 Barcelona
Tel. 93 2000711Fax 93 2091136
© 2020 Elsevier Ltd. All rights reserved. This journal and the indi-vidual contributions contained in it are protected under copyright by Elsevier Ltd, and the following terms and conditions apply to their use. The Lancet is a trade mark of Elsevier Limited.Publication information The Lancet (ISSN 0140-6736) is published weekly by Elsevier (The Boulevard, Langford Lane, Kidlington, Oxford, OX5 1GB). Periodicals Postage Paid at Rahway, NJ, USA. POSTMASTER: send address corrections to The Lancet, c/o Mercury International, 365 Blair Road, Avenel, NJ 07001, USA.Photocopying Single photocopies of single articles may be made for personal use as allowed by national copyright laws. Permission of the Publisher and payment of a fee is required for all other photocopying, including multiple or systematic copying, copying for advertising or promotional purposes, resale, and all forms of document delivery. Special rates are available for educational institutions that wish to make photocopies for non-profit educational classroom use.
Permissions may be sought directly from Elsevier Global Rights Department, The Boulevard, Langford Lane, Kidlington, Oxford,
OX5 1GB, UK; tel: +1 215 239 3804 or +44 (0)1865 843 830, fax: +44 (0)1865 853 333, email [email protected].
In the USA, users may clear permissions and make payments through the Copyright Clearance Center, Inc, 222 Rosewood Drive, Danvers, MA 01923, USA; tel: +1 (978) 7508400, fax: +1 (978) 646 8600.
Other countries may have a local reprographic rights agency for payments.
Derivative works Subscribers may reproduce tables of contents or prepare lists of articles including abstracts for internal circulation within their institutions. Permission of the Publisher is required for resale or distribution outside the institution.
Permission of the Publisher is required for all other derivative works, including compilations and translations.
Electronic storage or usage Permission of the Publisher is required to store or use electronically any material contained in this journal, including any article or part of an article.
Except as outlined above, no part of this publication may be reproduced,
stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without prior written permission of the Publisher.
Address permissions requests to: Elsevier Health Sciences Rights Department, at the mail, fax, and e-mail addresses noted above.
Notice Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds or experiments described herein. Because of rapid advances in the medical sciences, in particular, independent verification of diagnoses and drug dosages should be made. To the fullest extent of the law, no responsibility is assumed by Elsevier for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
The views expressed in this journal are not necessarily those of the Editor, the International Advisory Board, or Elsevier Ltd.
Account Manager Joan Gomà
T: +34 932000711 [email protected]
The Lancet is a weekly subscription journal. For further
information on how to subscribe please contact our
Subscription Department T: +44 (0) 1865 843077 F: +44 (0) 1865 843970
(North America) T: +1 (800) 462 6198 F: +1 (800) 327 9021
Printed by

Articles
1496 www.thelancet.com Vol 395 May 9, 2020
Secukinumab versus adalimumab for treatment of active psoriatic arthritis (EXCEED): a double-blind, parallel-group, randomised, active-controlled, phase 3b trialIain B McInnes, Frank Behrens, Philip J Mease, Arthur Kavanaugh, Christopher Ritchlin, Peter Nash, Jordi Gratacós Masmitja, Philippe Goupille, Tatiana Korotaeva, Alice B Gottlieb, Ruvie Martin, Kevin Ding, Pascale Pellet, Shephard Mpofu, Luminita Pricop, on behalf of EXCEED Study Group
SummaryBackground Head-to-head trials in psoriatic arthritis are helpful in guiding clinical decision making. The EXCEED study evaluated the efficacy and safety of secukinumab versus adalimumab as first-line biological monotherapy for 52 weeks in patients with active psoriatic arthritis, with a musculoskeletal primary endpoint of American College of Rheumatology (ACR) 20 response.
Methods This parallel-group, double-blind, active-controlled, phase-3b, multicentre (168 sites in 26 countries) trial enrolled patients aged at least 18 years with active psoriatic arthritis. Eligible patients were randomly assigned (1:1) by means of interactive response technology to receive secukinumab or adalimumab. Patients, investigators, site personnel, and those doing the assessments (except independent study drug administrators) were masked to study assignment. 300 mg secukinumab was administered subcutaneously at baseline, weeks 1, 2, 3, and 4, and then every 4 weeks until week 48 as a pre-filled syringe. Adalimumab was administered every 2 weeks from baseline until week 50 as 40 mg per 0·4 mL citrate free subcutaneous injection. The primary outcome was the proportion of patients with at least 20% improvement in the ACR response criteria (ACR20) at week 52. Patients were analysed according to the treatment to which they were randomly assigned. Safety analyses included all safety data reported up to and including the week 52 visit for each patient who received at least one dose of study drug. The trial is registered at ClinicalTrials.gov, NCT02745080.
Findings Between April 3, 2017 and Aug 23, 2018, we randomly assigned 853 patients to receive secukinumab (n=426) or adalimumab (n=427). 709 (83%) of 853 patients completed week 52 of the study, of whom 691 (81%) received the last study treatment at week 50. 61 (14%) of 426 patients in the secukinumab group discontinued treatment by week 52 versus 101 (24%) of 427 patients in the adalimumab group. The primary endpoint of superiority of secukinumab versus adalimumab for ACR20 response at week 52 was not met. 67% of patients in the secukinumab group achieved an ACR20 response at week 52 versus 62% of patients in the adalimumab group (OR 1·30, 95% CI 0·98–1·72; p=0·0719). The safety profiles of secukinumab and adalimumab were consistent with previous reports. Seven (2%) of 426 patients in the secukinumab group and six (1%) of 427 patients in the adalimumab group had serious infections. One death was reported in the secukinumab group due to colon cancer and was assessed as not related to the study drug by the investigator.
Interpretation Secukinumab did not meet statistical significance for superiority versus adalimumab in the primary endpoint of ACR20 response at week 52. However, secukinumab was associated with a higher treatment retention rate than adalimumab. This study provides comparative data on two biological agents with different mechanisms of action, which could help guide clinical decision making in the management of patients with psoriatic arthritis.
Funding Novartis Pharma.
Copyright © 2020 Elsevier Ltd. All rights reserved.
IntroductionPsoriatic arthritis is clinically heterogeneous, comprising musculoskeletal and dermatological manifestations that might involve arthritis, spondylitis, enthesitis, dactylitis, and psoriasis of skin and nails, and is associated with impaired physical function and poor quality of life.1 Non-steroidal anti-inflammatory drugs (NSAIDs) are typically the first choice in treating psoriatic arthritis symptoms, but have associated safety issues of cardio-vascular risk and gastrointestinal toxicity; therefore,
physicians initiate conventional synthetic disease-modi-fying anti-rheumatic drugs (csDMARDs), preferably methotrexate, early in patients with poor prognostic factors and relevant skin involvement to modify under-lying musculoskeletal and skin inflammation.2,3
Several biological disease modifying anti-rheumatic drugs (bDMARDs) targeting inflammatory cytokines are recommended for patients with psoriatic arthritis with inadequate response to csDMARDs.3,4 Adalimumab, a human monoclonal antibody against tumour necrosis
Lancet 2020; 395: 1496–505
See Comment page 1463
Institute of Infection, Immunity and Inflammation, College of Medical, Veterinary
and Life Sciences, University of Glasgow, Glasgow, UK
(I B McInnes FRCP); Rheumatology University
Hospital and Fraunhofer Institute for Molecular Biology
and Applied Ecology, Branch for Translational Medicine and Pharmacology and Fraunhofer
Cluster of Excellence for Immune-Mediated Diseases,
Goethe University, Frankfurt, Germany (F Behrens MD); Swedish Medical Centre,
Providence St Joseph Health and University of Washington,
Seattle, WA, USA (P J Mease MD); Rheumatology, Allergy, Immunology Division,
University of California San Diego, School of Medicine,
La Jolla, CA, USA (A Kavanaugh MD); Allergy,
Immunology and Rheumatology Division, University of Rochester,
Rochester, NY, USA (C Ritchlin MD); Department of
Medicine, Griffith University, Brisbane, QLD, Australia
(P Nash FRACP); Rheumatology Department, University
Hospital Parc Taulí, Sabadell, Universitat Autònoma de
Barcelona, Spain (J G Masmitja PhD); Department
of Rheumatology and INSERM-CIC1415, University
Hospital of Tours, EA 7501 GICC, University of
Tours, Tours, France (P Goupille MD); Research
Institute of Rheumatology n.a. V A Nasonova, Moscow, Russia (T Korotaeva PhD); Department
of Dermatology, Icahn School of Medicine at Mount Sinai,
New York, NY, USA (A B Gottlieb PhD); Novartis
Pharmaceuticals, East Hanover, NJ, USA (R Martin PhD,
K Ding MSc, L Pricop MD); and Novartis Pharma, Basel,

Articles
www.thelancet.com Vol 395 May 9, 2020 1497
Switzerland (P Pellet PhD, S Mpofu FRCP)
Correspondence to: Dr Iain B McInnes, Institute of Infection, Immunity and Inflammation, College of Medical, Veterinary and Life Sciences, University of Glasgow, Scotland, UK [email protected]
factor (TNF), is widely used as a first line bDMARD in the treatment of patients with psoriatic arthritis as mono-therapy or an add-on to methotrexate.5 Secukinumab, a human monoclonal antibody that directly inhibits IL-17A, has shown substantial improvement in the key clinical domains of psoriatic arthritis, including signs and symp-toms, radiographic progression, physical functioning, and quality of life.6–8 In the treatment of patients with moderate to severe psoriasis and plaque psoriasis, secukinumab has shown greater efficacy versus a TNF inhibitor (etanercept) and an IL-12/23 inhibitor (ustekinumab).9–11
Both adalimumab and secukinumab are approved for treatment of patients with active psoriatic arthritis with or without the use of concomitant methotrexate.5,6,12 More than 40% of patients treated with methotrexate discon-tinue treatment or are non-compliant because of poor tolerability or toxicity, or cannot receive methotrexate because of liver abnormalities related to psoriatic arthritis or concomitant alcohol abuse.13–15 The European League Against Rheumatism (EULAR) and Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) recommendations differ. EULAR proposes a treatment algorithm, whereas GRAPPA proposes an evidence-based clinical domain approach that includes biologicals with novel mechanisms of action.3,16 However, there is a paucity of trials to determine which biological treatment should be the initial treatment in patients with psoriatic arthritis upon csDMARD failure or intolerance.
The advent of biological therapies with selective mecha-nisms of action that are approved and widely used in clinical practice has prompted indirect comparison approaches to guide therapy, but these comparisons have metho dological limitations.17
Head-to-head trials have shown that IL-17A inhibitors have higher efficacy in treatment of patients with moderate to severe psoriasis and on the skin manifes-tations of patients with psoriatic arthritis. However, comparative data are lacking on the efficacy of these drugs on musculo skeletal manifestations of psoriatic arthritis and are urgently required. The aim of the EXCEED study was to investigate whether secukinumab 300 mg monotherapy was superior to adalimumab 40 mg monotherapy as first-line bDMARD treatment, thus testing the musculoskeletal endpoint of the American College of Rheumatology (ACR) 20 response as the primary objective in a fully blinded manner. Safety of secukinumab and adalimumab was also assessed.
MethodsStudy design and participantsEXCEED is a randomised, double-blind, active-controlled, phase-3b, multicentre (168 sites in 26 countries; appendix p 19), parallel-group, 52-week study that evaluated secukinumab monotherapy and adalimumab mono-therapy in patients with active psoriatic arthritis who were naive to biological therapy for psoriatic arthritis and
Research in context
Evidence before this studyMany patients with psoriatic arthritis who have active psoriasis and musculoskeletal symptoms show inadequate clinical responses to conventional synthetic disease-modifying antirheumatic agents (csDMARDs), including methotrexate, in all manifestations of psoriatic arthritis, including arthritis, spondylitis, enthesitis, dactylitis, and psoriasis. Several biological disease-modifying anti-rheumatic drugs (bDMARDs) that target different inflammatory cytokines are recommended for patients with psoriatic arthritis with inadequate response to csDMARDs. Adalimumab, a human monoclonal antibody against tumour necrosis factor (TNF), is widely used as a first-line bDMARD in the treatment of patients with psoriatic arthritis in monotherapy or in combination with methotrexate. We searched PubMed using the terms “psoriatic arthritis”, “biologic”, and “head-to-head” for English language articles published from inception up to Jan 13, 2020, with no limitation or restriction for year of publication or article type. The search results yielded 30 articles, of which nine used matching adjusted indirect comparisons to compare two biologicals, 20 were review articles, and one was a head-to-head comparison of two biologicals in psoriatic arthritis. However, matching adjusted indirect comparisons have an inherent limitation of the methodology used and might lead to different conclusions; therefore, prospective head-to-head trials in psoriatic arthritis are needed to help guide physicians in
clinical decision making. A 2020 head-to-head, open label, 24-week trial compared the efficacy and safety of two biologicals—adalimumab and ixekizumab (an IL-17A inhibitor)—in psoriatic arthritis and supported that ixekizumab was superior to adalimumab in achieving combined American College of Rheumatology 50 (ACR50) and Psoriasis Area and Severity Index 100 responses at week 24.
Added value of this studyTo our knowledge, EXCEED is the first fully blinded head-to-head trial to evaluate the efficacy and safety of secukinumab (an IL-17A inhibitor) versus adalimumab (an anti-TNF agent) as first-line biological monotherapy in patients with active psoriatic arthritis with a musculoskeletal primary endpoint of ACR20 at week 52. The efficacy data in this study suggest that secukinumab was at least as efficacious as adalimumab in improving musculoskeletal endpoints, provided better responses on skin endpoints, and had a higher retention rate at week 52. No new safety signals were reported for secukinumab and adalimumab.
Implications of all the available evidenceThis study presents a considerable volume of comparative efficacy and safety data on two biologicals with different mechanisms of action in the treatment of patients with psoriatic arthritis.
See Online for appendix
Articles
1498 www.thelancet.com Vol 395 May 9, 2020
psoriasis, and who were intolerant or had an inadequate response to csDMARDs.
Patients fulfilling all the following criteria were included in the study: aged at least 18 years of age, fulfilled the Classification Criteria for Psoriatic Arthritis,18 had active psoriatic arthritis (defined as ≥3 swollen joints and ≥3 tender joints), had active plaque psoriasis with at least one plaque of at least 2 cm diameter or nail changes consistent with psoriasis or documented history of plaque psoriasis, were naive to treatment with biologicals, had previously been treated with csDMARDs (including but not limited to methotrexate) with an inadequate response or had stopped treatment due to safety or tolerability problems, and had a previous inadequate response to NSAIDs for at least 4 weeks before randomisation.
Patients had to stop any csDMARD, including metho-trexate, before randomisation, with a washout period of 4 weeks for all csDMARDs or 8 weeks for leflunomide. Patients who were receiving concomitant corticosteroids were required to be on a stable dose of 10 mg/day or less of prednisone or equivalent for at least 2 weeks before randomisation and remain on a stable dose up to week 52 (appendix p 13).
Key exclusion criteria were pregnancy, evidence of ongoing infection or malignancy, previous exposure to any biologicals or opioids, ongoing use of oral or topical retinoids, photochemotherapy, phototherapy, or topical skin treatment. For detailed information on the exclusion criteria, please refer to the appendix (p 14).
All clinical studies were done in compliance with the Declaration of Helsinki, International Council for Harmonization Guidelines for Good Clinical Practice, and local country regulations. All patients provided written informed consent to participate in the respective studies. The institutional review board at each participating centre approved the protocol.
Randomisation and maskingAfter a screening period of up to 8 weeks, eligible patients were randomly assigned (1:1) by means of interactive response technology to receive secukinumab or adalim-umab. The interactive response technology assigned a randomisation number to the patient (randomisation block size was 4), which linked the patient to a treatment group and specified a unique medication number. The randomisation scheme for patients was reviewed and approved by a member of the Novartis randomisation office.
To maintain allocation concealment, all groups received placebo injections to ensure a consistent number of injections at each visit. Study treatments were admin-istered by suitably qualified independent study drug administrators, who were not masked and had no responsibility for any aspect of patient assessment or follow-up. Before administration of study treatment, unmasked site personnel were required to use physical barriers (curtains, blindfolds, or similar measures) to prevent patients from seeing their study treatment to preserve the masking. Patients, investigators, site personnel, and those performing the assessments (except independent study drug administrators) were masked to the study assignment (appendix p 16).
ProceduresSecukinumab 300 mg was administered at baseline, weeks 1, 2, 3, and 4, and then every 4 weeks until week 48. Adalimumab 40 mg was administered every 2 weeks from baseline until week 50 (appendix p 19). Secukinumab was administered with a pre-filled syringe and adalim-umab as 40 mg in 0·4 mL citrate free subcutaneous injection. Additional information about the assessments undertaken during the trial is provided in the appendix (p 17). Key efficacy (assessed by primary endpoint, key secondary endpoints, and other relevant exploratory endpoints), safety, and tolerability (assessed by adverse events, laboratory values, injection site reaction, and immunogenicity) assessments were done at screening, baseline, week 2, week 4, and every 4 weeks until week 52 (primary endpoint). 337 (40%) of 853 patients had at least one protocol deviation in the study, of whom
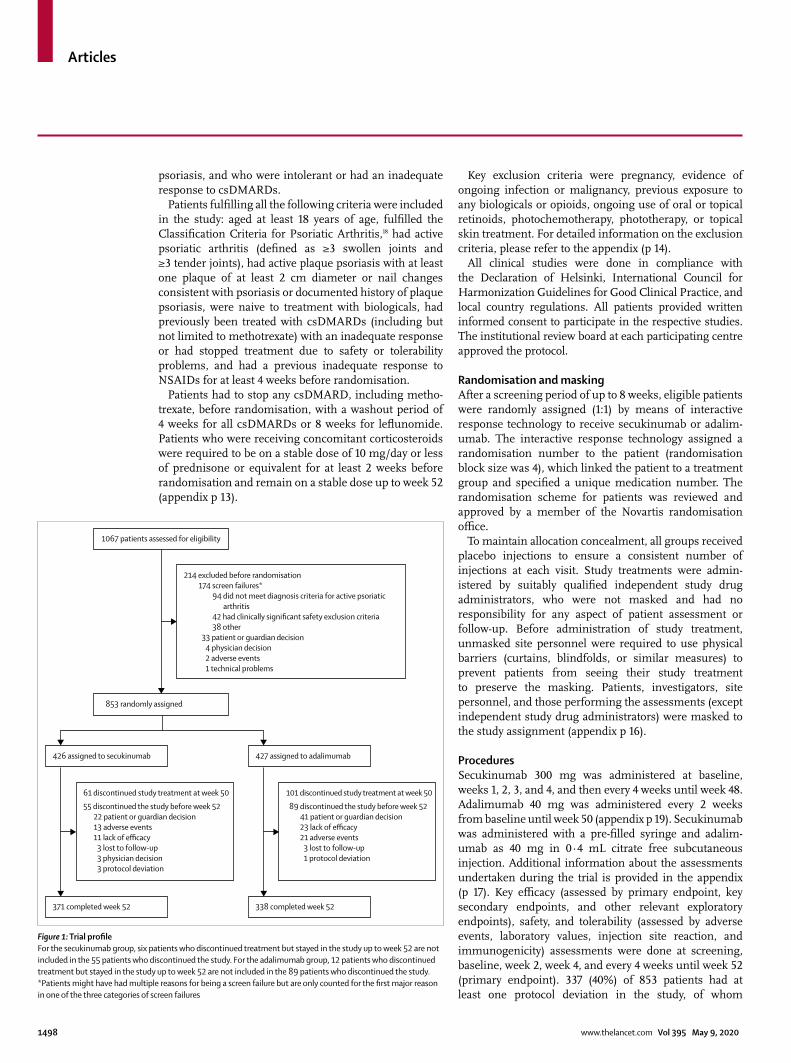
Figure 1: Trial profileFor the secukinumab group, six patients who discontinued treatment but stayed in the study up to week 52 are not included in the 55 patients who discontinued the study. For the adalimumab group, 12 patients who discontinued treatment but stayed in the study up to week 52 are not included in the 89 patients who discontinued the study. *Patients might have had multiple reasons for being a screen failure but are only counted for the first major reason in one of the three categories of screen failures
426 assigned to secukinumab
371 completed week 52
61 discontinued study treatment at week 50
55 discontinued the study before week 5222 patient or guardian decision13 adverse events11 lack of efficacy
3 lost to follow-up3 physician decision3 protocol deviation
214 excluded before randomisation174 screen failures*
94 did not meet diagnosis criteria for active psoriaticarthritis
42 had clinically significant safety exclusion criteria38 other
33 patient or guardian decision4 physician decision2 adverse events1 technical problems
427 assigned to adalimumab
1067 patients assessed for eligibility
853 randomly assigned
338 completed week 52
101 discontinued study treatment at week 50
89 discontinued the study before week 5241 patient or guardian decision23 lack of efficacy21 adverse events
3 lost to follow-up1 protocol deviation
Articles
www.thelancet.com Vol 395 May 9, 2020 1499
172 (40%) of 426 were in the secukinumab group and 165 (39%) of 427 were in the adalimumab group. Major reasons for protocol deviations were use of prohibited concomitant medi cation and other deviations from Good Clinical Practice guidelines. Other reasons for protocol deviations included unmet selection criteria and treatment deviation. For further details of protocol deviations, see the appendix (p 24).
OutcomesThe primary outcome was the proportion of patients with at least 20% improvement in the ACR response criteria (ACR20) at week 52. Key secondary endpoints in order of the statistical hierarchy were Psoriasis Area and Severity Index (PASI) 90 response, ACR50 response, mean change from baseline in Health Assessment Questionnaire-Disability Index (HAQ-DI) score, and resolution of enthesitis (based on Leeds Enthesitis Index [LEI] criteria) at week 52.
Prespecified exploratory endpoints assessed at week 52 were clinically relevant musculoskeletal and skin endpoints, which included the proportion of patients achieving a combined ACR50 and PASI 100 response, PASI 75 or 100 response, absolute PASI score of 3 or less, ACR70 response, psoriatic arthritis response criteria response, resolution of dactylitis, resolution of enthesitis (based on Spondyloarthritis Research Consortium of Canada [SPARCC] criteria), proportion of patients achieving Psoriatic Arthritis Disease Activity Score (PASDAS) low disease activity and remission, Disease Activity in Psoriatic Arthritis (DAPSA) low disease activity and remission, minimal disease activity, and very low disease activity response and quality-of-life questionnaires (HAQ-DI). Additional prespecified efficacy analyses in the subset of patients with psoriasis with body surface area greater than 10% or PASI of at least 10 were also done.
Safety analyses included all safety data reported up to and including the week 52 visit for each patient who received at least one dose of study drug. MedDRA version 22.0 was used for reporting adverse events.
Statistical analysisThe study was powered based on the planned analysis of patients achieving an ACR20 response at week 52. An ACR20 response rate of 50% for the TNF inhibitor-naive population without methotrexate use (monotherapy) was assumed for adalimumab based on observed week 48 response rate reported in a previous study.19 The response to secukinumab was estimated to be 62% based on ACR20 response in the TNF inhibitor-naive monotherapy population from phase 3 studies.6 With 425 patients per treatment group, we anticipated that there would be approximately 94% power to detect a treatment difference of around 12% (odds ratio [OR] 1·63) in ACR20 response rates at two-sided α=0·05 between secukinumab and adalimumab in the evaluation of the primary efficacy hypothesis at week 52.
Secukinumab 300 mg (n=426)
Adalimumab 40 mg (n=427)
Total (n=853)
Age (years) 48·5 (12·38) 49·5 (12·44) 49·0 (12·41)
Sex
Male 208 (49%) 229 (54%) 437 (51%)
Female 218 (51%) 198 (46%) 416 (49%)
Weight (kg) 83·5 (19·12) 84·1 (18·33) 83·8 (18·72)
Body-mass index (kg/m²) 28·8 (6·03) 28·9 (5·55) 28·8 (5·79)
Race
White 402 (94%) 391 (92%) 793 (93%)
Asian 16 (4%) 20 (5%) 36 (4%)
Other or unknown 8 (2%) 16 (4%) 24 (3%)
No smoking status at baseline 333 (78%) 351 (82%) 684 (80%)
Systemic glucocorticoids use at randomisation 61 (14%) 58 (14%) 119 (14%)
Time since first diagnosis of psoriatic arthritis (years)
5·1 (7·60) 5·7 (7·29) 5·4 (7·45)
Baseline PASI score 10·6 (9·00) 10·0 (8·15) 10·3 (8·60)
Patients with psoriasis (BSA ≥3%) 215 (50%) 202 (47%) 417 (49%)
Patients with psoriasis (BSA >10% or PASI ≥10) 110 (26%) 101 (24%) 211 (25%)
Adjusted tender joint total score for psoriatic arthritis (78 joints)
19·4 (13·86) 20·6 (14·81) 20·0 (14·35)
Adjusted swollen joint total score for psoriatic arthritis (76 joints)
9·7 (7·30) 10·2 (7·86) 10·0 (7·58)
Patient’s global assessment (0–100) 64·0 (19·67) 61·9 (20·75) 62·9 (20·23)
Physician’s global assessment (0–100) 60·0 (17·12) 61·4 (15·92) 60·7 (16·54)
Psoriatic arthritis pain (0–100) 58·6 (23·49) 57·9 (22·42) 58·3 (22·95)
Health Assessment Questionnaire-Disability Index 1·3 (0·64) 1·2 (0·64) 1·3 (0·64)
CRP ≥10 mg/L 131 (31%) 128 (30%) 259 (30%)
Disease Activity Score 28-CRP 4·7 (1·00) 4·7 (0·94) 4·7 (0·97)
Presence of enthesitis (Leeds Enthesitis Index) 234 (55%) 264 (62%) 498 (58%)
Presence of enthesitis (Spondyloarthritis Research Consortium of Canada)
301 (71%) 330 (77%) 631 (74%)
Presence of dactylitis 130 (31%) 137 (32%) 267 (31%)
Data are mean (SD) or n (%). BSA=body surface area. CRP=C-reactive protein. PASI=Psoriasis Area Severity Index.
Table 1: Baseline and disease characteristics of patients
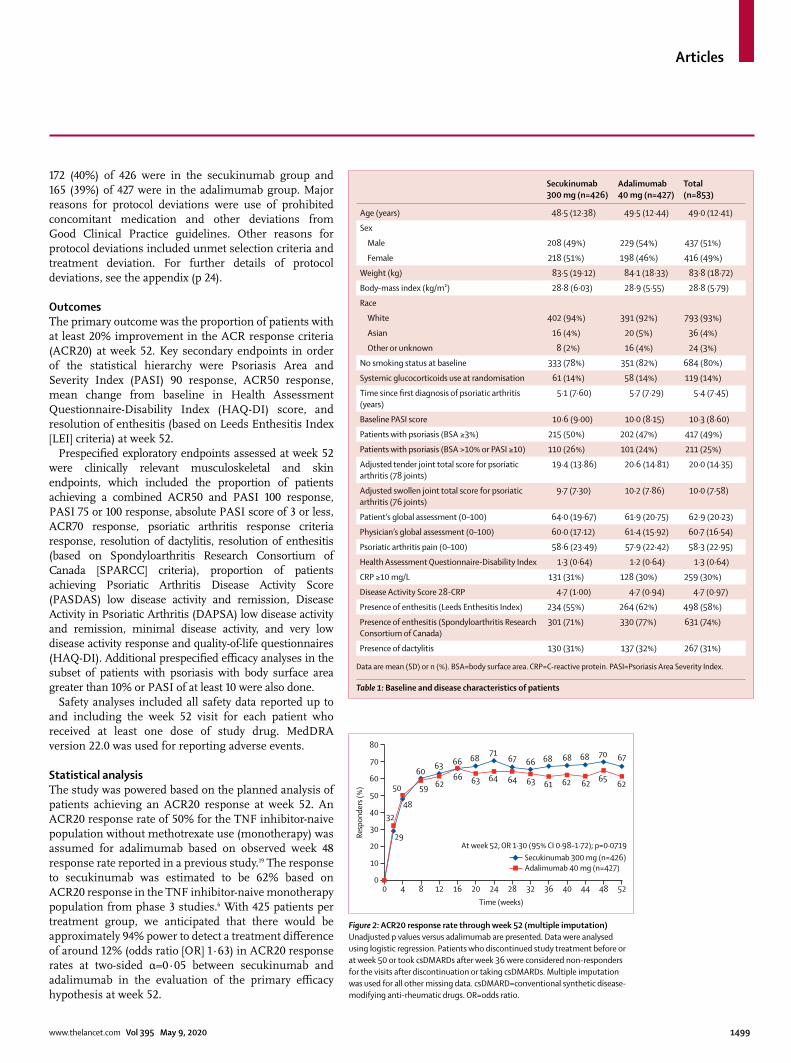
Figure 2: ACR20 response rate through week 52 (multiple imputation)Unadjusted p values versus adalimumab are presented. Data were analysed using logistic regression. Patients who discontinued study treatment before or at week 50 or took csDMARDs after week 36 were considered non-responders for the visits after discontinuation or taking csDMARDs. Multiple imputation was used for all other missing data. csDMARD=conventional synthetic disease-modifying anti-rheumatic drugs. OR=odds ratio.
0 4 8 12 16 20 24 28 32 36 40 44 48 520
10
20
30
40
50
60
70
80
Resp
onde
rs (%
)
Time (weeks)
29
48
6063 66 68
7167 66 68 68 68 70 67
32
50 59 6266 63 64 64 63 61 62 62 65
62
At week 52, OR 1·30 (95% CI 0·98–1·72); p=0·0719Secukinumab 300 mg (n=426)Adalimumab 40 mg (n=427)
Articles
1500 www.thelancet.com Vol 395 May 9, 2020
The full analysis set used for efficacy analysis comprised all patients who were randomly assigned to study treatment. As per the intention-to-treat principle, patients were analysed according to the treatment to which they were randomly assigned. Psoriasis-related endpoints used the psoriasis subset, which included all patients in the full analysis set who had at least 3% of their body surface area affected by psoriasis at baseline. Enthesitis-related endpoints used the enthesitis subset, which included all patients in the full analysis set who had enthesitis based on LEI (as a key secondary endpoint) and based on SPARCC criteria (as an exploratory endpoint) at baseline.
We used a sequential hierarchical testing method to maintain the familywise type 1 error rate at 5% across the primary and ranked secondary endpoints. If the primary efficacy analysis was significant, secondary analyses were planned to be completed in the following sequence: ACR20, PASI 90, ACR50, HAQ-DI, and resolution of enthesitis. The inferential testing procedure only con-tinued if the previous test was rejected at the two-sided 5% level. Subgroup analysis was tested independently from the hierarchical testing strategy.
The primary efficacy endpoint was defined as meeting the following three conditions: achieving an ACR20 response, with no permanent study treatment (secukinumab or adalimumab) discontinuation before or at week 50 (the last dosing visit), and no concomitant use of csDMARDs (including methotrexate) after week 36 (regardless of the time initiation of csDMARDs). A patient meeting all these conditions was regarded as a responder, otherwise they were considered non-responders. All secondary and exploratory binary end-points were defined in the same way as the primary endpoint.
For analyses of binary endpoints, we computed ORs, 95% CIs, and p values for comparisons of secukinumab versus adalimumab from a logistic regression model, with treatment as a factor and baseline weight as a covariate.
For the primary endpoint and other binary endpoints, if a patient discontinued study treatment prematurely or took csDMARDs after week 36 they were considered a non-responder. If a patient neither discontinued study treatment prematurely nor took csDMARDs after week 36 but had all or some components missing that precluded the calculation of ACR20 response (eg, missed visits, electronic device malfunction, or site error), then missing data for these components were handled by multiple imputation. This method imputes missing data based on a patient’s own observed data and observed data from similar patients in similar conditions. As a sensi tivity analysis, non-responder imputation was specified to assess the effect of missing data. Non-responder impu-tation is a highly conservative method that assumes non-response for all missing data.
We evaluated between-group differences in continuous endpoints using a mixed-effect model repeated measures
Secukinumab 300 mg
Adalimumab 40 mg
Odds ratio (95% CI)
p value (unadjusted)*
Primary endpoint
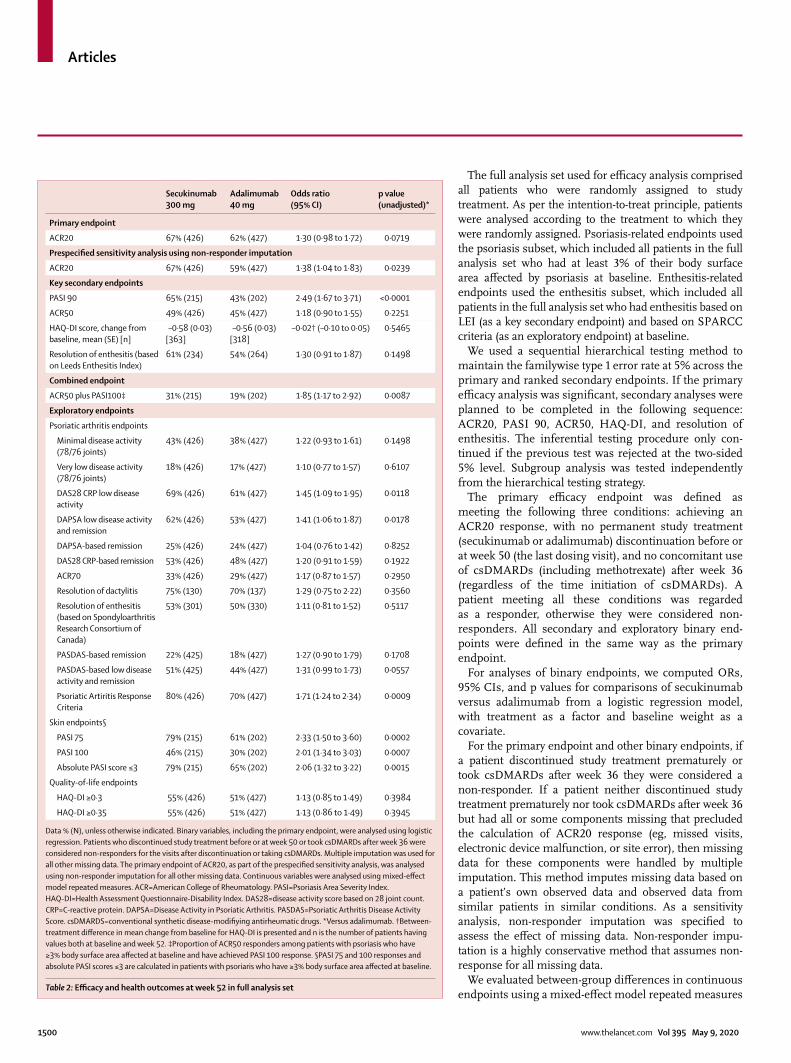
ACR20 67% (426) 62% (427) 1·30 (0·98 to 1·72) 0·0719
Prespecified sensitivity analysis using non-responder imputation
ACR20 67% (426) 59% (427) 1·38 (1·04 to 1·83) 0·0239
Key secondary endpoints
PASI 90 65% (215) 43% (202) 2·49 (1·67 to 3·71) <0·0001
ACR50 49% (426) 45% (427) 1·18 (0·90 to 1·55) 0·2251
HAQ-DI score, change from baseline, mean (SE) [n]
–0·58 (0·03) [363]
–0·56 (0·03) [318]
–0·02† (–0·10 to 0·05) 0·5465
Resolution of enthesitis (based on Leeds Enthesitis Index)
61% (234) 54% (264) 1·30 (0·91 to 1·87) 0·1498
Combined endpoint
ACR50 plus PASI100‡ 31% (215) 19% (202) 1·85 (1·17 to 2·92) 0·0087
Exploratory endpoints
Psoriatic arthritis endpoints
Minimal disease activity (78/76 joints)
43% (426) 38% (427) 1·22 (0·93 to 1·61) 0·1498
Very low disease activity (78/76 joints)
18% (426) 17% (427) 1·10 (0·77 to 1·57) 0·6107
DAS28 CRP low disease activity
69% (426) 61% (427) 1·45 (1·09 to 1·95) 0·0118
DAPSA low disease activity and remission
62% (426) 53% (427) 1·41 (1·06 to 1·87) 0·0178
DAPSA-based remission 25% (426) 24% (427) 1·04 (0·76 to 1·42) 0·8252
DAS28 CRP-based remission 53% (426) 48% (427) 1·20 (0·91 to 1·59) 0·1922
ACR70 33% (426) 29% (427) 1·17 (0·87 to 1·57) 0·2950
Resolution of dactylitis 75% (130) 70% (137) 1·29 (0·75 to 2·22) 0·3560
Resolution of enthesitis (based on Spondyloarthritis Research Consortium of Canada)
53% (301) 50% (330) 1·11 (0·81 to 1·52) 0·5117
PASDAS-based remission 22% (425) 18% (427) 1·27 (0·90 to 1·79) 0·1708
PASDAS-based low disease activity and remission
51% (425) 44% (427) 1·31 (0·99 to 1·73) 0·0557
Psoriatic Artiritis Response Criteria
80% (426) 70% (427) 1·71 (1·24 to 2·34) 0·0009
Skin endpoints§
PASI 75 79% (215) 61% (202) 2·33 (1·50 to 3·60) 0·0002
PASI 100 46% (215) 30% (202) 2·01 (1·34 to 3·03) 0·0007
Absolute PASI score ≤3 79% (215) 65% (202) 2·06 (1·32 to 3·22) 0·0015
Quality-of-life endpoints
HAQ-DI ≥0·3 55% (426) 51% (427) 1·13 (0·85 to 1·49) 0·3984
HAQ-DI ≥0·35 55% (426) 51% (427) 1·13 (0·86 to 1·49) 0·3945
Data % (N), unless otherwise indicated. Binary variables, including the primary endpoint, were analysed using logistic regression. Patients who discontinued study treatment before or at week 50 or took csDMARDs after week 36 were considered non-responders for the visits after discontinuation or taking csDMARDs. Multiple imputation was used for all other missing data. The primary endpoint of ACR20, as part of the prespecified sensitivity analysis, was analysed using non-responder imputation for all other missing data. Continuous variables were analysed using mixed-effect model repeated measures. ACR=American College of Rheumatology. PASI=Psoriasis Area Severity Index. HAQ-DI=Health Assessment Questionnaire-Disability Index. DAS28=disease activity score based on 28 joint count. CRP=C-reactive protein. DAPSA=Disease Activity in Psoriatic Arthritis. PASDAS=Psoriatic Arthritis Disease Activity Score. csDMARDS=conventional synthetic disease-modifiying antirheumatic drugs. *Versus adalimumab. †Between-treatment difference in mean change from baseline for HAQ-DI is presented and n is the number of patients having values both at baseline and week 52. ‡Proportion of ACR50 responders among patients with psoriasis who have ≥3% body surface area affected at baseline and have achieved PASI 100 response. §PASI 75 and 100 responses and absolute PASI scores ≤3 are calculated in patients with psoriaris who have ≥3% body surface area affected at baseline.
Table 2: Efficacy and health outcomes at week 52 in full analysis set
Articles
www.thelancet.com Vol 395 May 9, 2020 1501
approach, with missing data assumed to be missing at random. Treatment and assessment visit were included in the model as factors. Weight and baseline values of the endpoints were included in the model as continuous covariates. Treatment by analysis visit and baseline score by analysis visit were interaction terms, and an unstructured covariance structure was assumed.
For continuous efficacy endpoints, data for patients who discontinued study treatment before week 50 or took csDMARDs after week 36 were set to missing for the visits after discontinuation or taking csDMARDs.
Safety endpoints were assessed for all patients who received at least one dose of study drug and were summarised descriptively for data reported up to and including each patient’s week 52 visit at the time of the week 52 database lock (Oct 21, 2019).
Analyses were done with SAS version 9.4. The trial is registered at ClinicalTrials.gov, NCT02745080.
Role of the funding sourceThe study was designed by the funder, Novartis, in collaboration with the authors. Data were collected in accordance with Good Clinical Practice guidelines by the study investigators and were analysed by the funder. All authors contributed to interpretation of the data and had access to the full datasets. Statistical analyses were done by statisticians employed by the funder and were reviewed by all authors. Agreements between the funder and the inves tigators included provisions relating to confidentiality of the study data. Writing support for the manuscript was provided by a medical writer from Novartis, India, and funded by the funder. All authors vouch for the accuracy and completeness of the data and analyses, as well as for the fidelity of this report to the trial protocol, which is available from the funder. All authors had the final responsibility for the decision to submit the manuscript for publication.
ResultsBetween April 3, 2017, and Aug 23, 2018, we randomly assigned 853 patients to receive secukinumab (n=426) or adalimumab (n=427). 709 (83%) of 853 patients completed week 52 of the study (figure 1), of whom 691 (81%) received the last study treatment at week 50 (appendix p 20). 61 (14%) of 426 patients in the secukinumab group discontinued treatment by week 52 versus 101 (24%) of 427 patients in the adalimumab group. Major reasons for disconti nuation of treatment were adverse events (15 [4%] of 426 patients in the secukinumab group vs 30 [7%] of 427 patients in the adalimumab group), lack of efficacy (15 [4%] of 426 patients in the secukinumab group vs 32 [7%] of 427 patients in the adalimumab group), and patient or guardian decision (23 [5%] of 426 patients in the secukinumab group vs 35 [8%] of 427 patients in the adalimumab group). A Kaplan-Meier curve for time to study treatment discontinuation is shown in the appendix (p 21), indicating a higher proportion of patients
being retained for a longer duration on secukinumab versus adalimumab until the last dosing visit at week 50 (p=0·0005).
Baseline demographics and disease characteristics were similar across the secukinumab and adalimumab groups, except for the proportion of female patients and patients with enthesitis as defined by LEI (table 1).
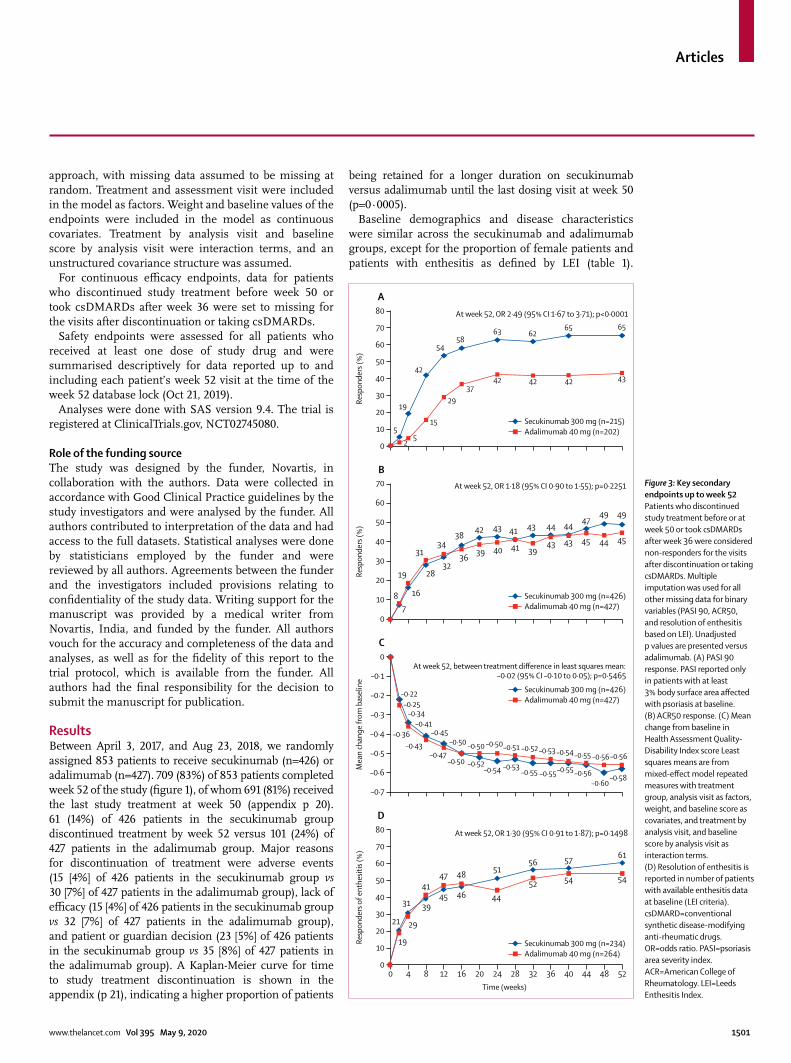
Figure 3: Key secondary endpoints up to week 52Patients who discontinued study treatment before or at week 50 or took csDMARDs after week 36 were considered non-responders for the visits after discontinuation or taking csDMARDs. Multiple imputation was used for all other missing data for binary variables (PASI 90, ACR50, and resolution of enthesitis based on LEI). Unadjusted p values are presented versus adalimumab. (A) PASI 90 response. PASI reported only in patients with at least 3% body surface area affected with psoriasis at baseline. (B) ACR50 response. (C) Mean change from baseline in Health Assessment Quality-Disability Index score Least squares means are from mixed-effect model repeated measures with treatment group, analysis visit as factors, weight, and baseline score as covariates, and treatment by analysis visit, and baseline score by analysis visit as interaction terms. (D) Resolution of enthesitis is reported in number of patients with available enthesitis data at baseline (LEI criteria). csDMARD=conventional synthetic disease-modifying anti-rheumatic drugs. OR=odds ratio. PASI=psoriasis area severity index. ACR=American College of Rheumatology. LEI=Leeds Enthesitis Index.
0 4 8 12 16 20 24 28 32 36 40 44 48 520
10
20
30
40
50
60
70
80
D
Resp
onde
rs o
f ent
hesit
is (%
)
–0·7
–0·6
–0·5
–0·4
–0·3
–0·2
–0·1
0
C
Mea
n ch
ange
from
bas
elin
e
0
10
20
30
40
50
60
70B
Resp
onde
rs (%
)
0
10
20
30
40
50
60
70
80
A
Resp
onde
rs (%
)
Time (weeks)
Secukinumab 300 mg (n=215)Adalimumab 40 mg (n=202)
Secukinumab 300 mg (n=426)Adalimumab 40 mg (n=427)
Secukinumab 300 mg (n=426)Adalimumab 40 mg (n=427)
Secukinumab 300 mg (n=234)Adalimumab 40 mg (n=264)
5
19
42
5458
63 6265 65
25
15
2937
42 42 42 43
At week 52, OR 2·49 (95% CI 1·67 to 3·71); p<0·0001
7
16
2832
3842 43 41 43 44 44
4749 49
8
19
3134
36 39 40 41 3943 43 45 44 45
At week 52, OR 1·18 (95% CI 0·90 to 1·55); p=0·2251
–0·22
–0·34–0·41
–0·45–0·50 –0·50 –0·50
–0·53–0·55 –0·55–0·55 –0·56
–0·60
–0·56
–0·25
–0·36–0·43
–0·47–0·50 –0·52
–0·54
–0·51 –0·52 –0·53 –0·54 –0·55 –0·56
–0·58
At week 52, between treatment difference in least squares mean: –0·02 (95% CI –0·10 to 0·05); p=0·5465
21
31 3945 46
5156 57
61
19
29
4147 48
44
52 54 54
At week 52, OR 1·30 (95% CI 0·91 to 1·87); p=0·1498
Articles
1502 www.thelancet.com Vol 395 May 9, 2020
357 (84%) of 426 patients in the secukinumab group and 371 (87%) of 427 patients in the adalimumab group were previously exposed to methotrexate.
The primary endpoint of superiority of secukinumab versus adalimumab for ACR20 response at week 52 was not met. 67% of patients in the secukinumab group has an ACR20 response at week 52 versus 62% in the adalimumab group (OR 1·30, 95% CI 0·98–1·72; p=0·0719; figure 2, table 2). Three patients in the secukinumab group and ten patients in adalimumab group with partial or all missing values of the ACR components at baseline or week 52 (not because of treatment or study discontinuation) had values imputed
using multiple imputation. In the prespecified sensiti-vity analysis using non-responder imputation, these 13 patients were imputed as non-responders and ACR20 response at week 52 was reported in 285 (67%) of 426 patients in the secukinumab group and 254 (59%) of 427 patients in the adalimumab group (OR 1·38, 95% CI 1·04–1·83; p=0·0239; table 2).
As the superiority of secukinumab versus adalimumab was not established for the primary endpoint, key secondary endpoints in the hierarchy were not formally tested for statistical significance. Therefore, we present unadjusted p values (without adjusting for multiplicity) and ORs with 95% CIs for key secondary endpoints (table 2; figure 3).
In prespecified exploratory analyses, a higher propor-tion of patients in the secukinumab group versus the adalimumab group achieved combined joint and skin response (simultaneous ACR50 and PASI 100 response), specific skin outcomes (PASI 75 response, PASI 100 response, absolute PASI score ≤3), low disease activity score (disease activity score based on 28 joint count C-reactive protein low disease activity, DAPSA-based low disease and remission, PASDAS-based low disease activity and remission, and Psoriatic Arthritis Response Criteria responses (table 2).
Overall, 211 (25%) of 853 patients had psoriasis with body surface area greater than 10% or PASI of at least 10. In this subset of patients, ACR20 and PASI 90 responses with secukinumab versus adalimumab were seen in 76% versus 68% of patients and 69% versus 42% of patients, respectively. The data for efficacy outcomes reported in this subset of patients were consistent with the overall study population (appendix p 22).
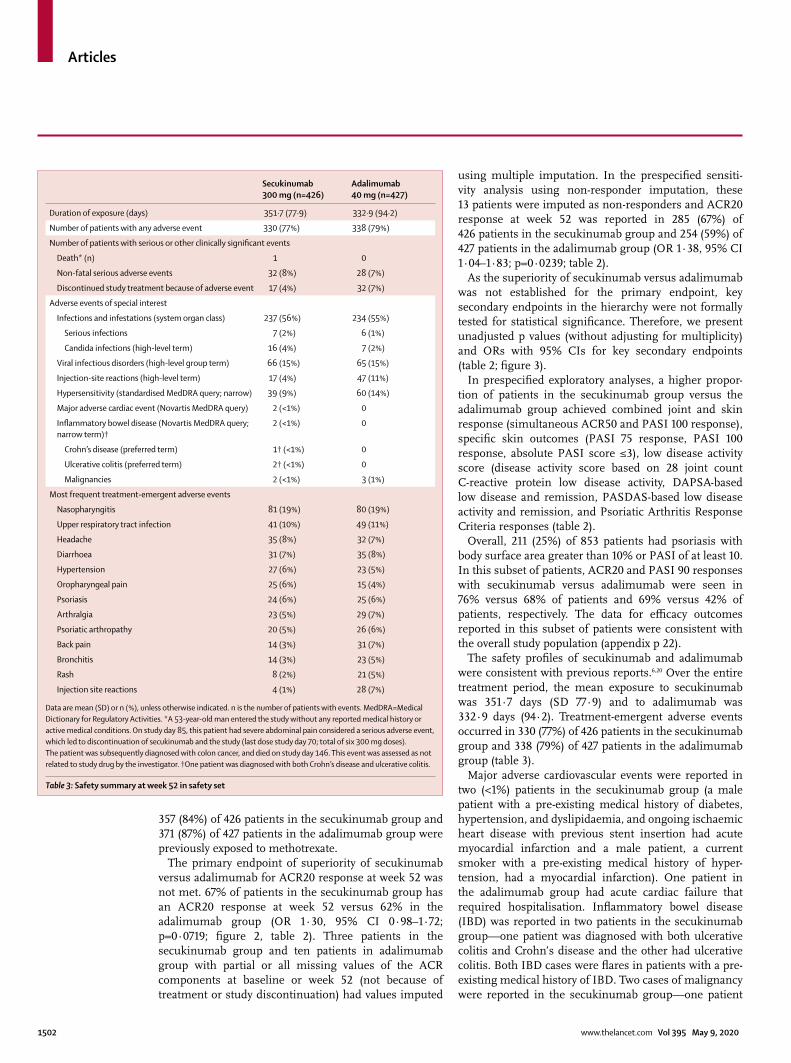
The safety profiles of secukinumab and adalimumab were consistent with previous reports.6,20 Over the entire treatment period, the mean exposure to secukinumab was 351·7 days (SD 77·9) and to adalimumab was 332·9 days (94·2). Treatment-emergent adverse events occurred in 330 (77%) of 426 patients in the secukinumab group and 338 (79%) of 427 patients in the adalimumab group (table 3).
Major adverse cardiovascular events were reported in two (<1%) patients in the secukinumab group (a male patient with a pre-existing medical history of diabetes, hypertension, and dyslipidaemia, and ongoing ischaemic heart disease with previous stent insertion had acute myocardial infarction and a male patient, a current smoker with a pre-existing medical history of hyper-tension, had a myocardial infarction). One patient in the adalimumab group had acute cardiac failure that required hospitalisation. Inflammatory bowel disease (IBD) was reported in two patients in the secukinumab group—one patient was diagnosed with both ulcerative colitis and Crohn’s disease and the other had ulcerative colitis. Both IBD cases were flares in patients with a pre-existing medical history of IBD. Two cases of malignancy were reported in the secukinumab group—one patient
Secukinumab 300 mg (n=426)
Adalimumab 40 mg (n=427)
Duration of exposure (days) 351·7 (77·9) 332·9 (94·2)
Number of patients with any adverse event 330 (77%) 338 (79%)
Number of patients with serious or other clinically significant events
Death* (n) 1 0
Non-fatal serious adverse events 32 (8%) 28 (7%)
Discontinued study treatment because of adverse event 17 (4%) 32 (7%)
Adverse events of special interest
Infections and infestations (system organ class) 237 (56%) 234 (55%)
Serious infections 7 (2%) 6 (1%)
Candida infections (high-level term) 16 (4%) 7 (2%)
Viral infectious disorders (high-level group term) 66 (15%) 65 (15%)
Injection-site reactions (high-level term) 17 (4%) 47 (11%)
Hypersensitivity (standardised MedDRA query; narrow) 39 (9%) 60 (14%)
Major adverse cardiac event (Novartis MedDRA query) 2 (<1%) 0
Inflammatory bowel disease (Novartis MedDRA query; narrow term)†
2 (<1%) 0
Crohn’s disease (preferred term) 1† (<1%) 0
Ulcerative colitis (preferred term) 2† (<1%) 0
Malignancies 2 (<1%) 3 (1%)
Most frequent treatment-emergent adverse events
Nasopharyngitis 81 (19%) 80 (19%)
Upper respiratory tract infection 41 (10%) 49 (11%)
Headache 35 (8%) 32 (7%)
Diarrhoea 31 (7%) 35 (8%)
Hypertension 27 (6%) 23 (5%)
Oropharyngeal pain 25 (6%) 15 (4%)
Psoriasis 24 (6%) 25 (6%)
Arthralgia 23 (5%) 29 (7%)
Psoriatic arthropathy 20 (5%) 26 (6%)
Back pain 14 (3%) 31 (7%)
Bronchitis 14 (3%) 23 (5%)
Rash 8 (2%) 21 (5%)
Injection site reactions 4 (1%) 28 (7%)
Data are mean (SD) or n (%), unless otherwise indicated. n is the number of patients with events. MedDRA=Medical Dictionary for Regulatory Activities. *A 53-year-old man entered the study without any reported medical history or active medical conditions. On study day 85, this patient had severe abdominal pain considered a serious adverse event, which led to discontinuation of secukinumab and the study (last dose study day 70; total of six 300 mg doses). The patient was subsequently diagnosed with colon cancer, and died on study day 146. This event was assessed as not related to study drug by the investigator. †One patient was diagnosed with both Crohn’s disease and ulcerative colitis.
Table 3: Safety summary at week 52 in safety set

Articles
www.thelancet.com Vol 395 May 9, 2020 1503
had colon cancer (day 85) and the other was diagnosed with plasma cell myeloma (day 201). Three cases of malignancy were reported in the adalim umab group, a synovial sarcoma (day 361), intraductal papillary carcinoma of the pancreas (day 85), and non-Hodgkin lymphoma (day 222). All cases of malignancy led to treatment discontinuation.
One death was reported in the secukinumab group. The patient had severe abdominal pain and discontinued the study on day 85 after receiving six doses of secukinumab. The patient died after study discontinuation on day 146 due to colon cancer assessed as not related to study drug by the investigator.
DiscussionWith increased availability of approved medicines that have distinct mechanisms of action, head-to-head trials can be useful to help guide clinical decision making in the management of psoriatic arthritis after csDMARD (including methotrexate) failure, intolerance, or contra-indication.3,21 To our knowledge, EXCEED is the first head-to-head, double-blind, randomised trial to compare secukinumab and adalimumab, and tested a musculo-skeletal primary endpoint of ACR20 response in psoriatic arthritis. This trial addresses an important gap in knowledge that informs the initiation of biological treatment in patients with psoriatic arthritis in the context of biological monotherapy. Pooled FUTURE 2–5 studies show that secukinumab 300 mg provides greater efficacy than does secukinumab 150 mg or placebo and long-term maintenance of response in biological-naive patients irrespective of concomitant methotrexate use; hence, we used secukinumab 300 mg in this study.22 The results of the pre-specified sensitivity analysis also showed higher ACR20 response rates at week 52 versus adalimumab.
Baseline demographics and disease characteristics were generally similar between the secukinumab group and adalimumab group; however, the proportion of female patients was higher in the secukinumab group than in the adalimumab group. Several reports have shown that female patients have lower treatment response rates in psoriatic arthritis than do male patients.23
It is becoming increasingly clear that different tissue compartments in psoriatic arthritis might not be driven by identical pathogenetic pathways. A cutaneous psoriasis study showed superiority of IL-17A inhibition with secukinumab compared with etanercept, a TNF inhibitor, in a head-to-head trial.9
A 2020 open-label, head-to-head study of the IL-17A inhibitor ixekizumab versus adalimumab reported that ixekizumab was superior in achievement of simultaneous improvement of joint and skin disease (combined ACR50 and PASI 100 response) in patients with psoriatic arthritis and inadequate response to csDMARDs.24 The current study has several important elements. It was fully blinded, minimising the potential bias and effect of knowledge of treatment allocation on reporting of outcomes. The study
included patients who more closely reflect patients with psoriatic arthritis who visit the rheumatology clinic, as the patients predominantly had articulatar symptoms. We investigated biological monotherapy, representing a common, clinically relevant scenario given either primary methotrexate intolerance or prevalence of metabolic syndrome and hepatosteatosis in psoriatic arthritis, both of which pose challenges for the use of methotrexate.13–15 Importantly, we evaluated musculoskeletal disease as the primary outcome, thereby removing the influence of cutaneous responses on interpretation of the results. Moreover, our primary outcome directly addresses a key research question in psoriatic arthritis management, namely whether IL-17A or TNF inhibition confer musculoskeletal advantage. However, we recognise that improvements in both musculoskeletal and skin manifestations are considered essential for optimising overall quality of life in psoriatic arthritis.25 Notably, secukinumab also showed a higher combined ACR50 and PASI 100 response, PASI 75 response, and PASI 100 responses compared with adalimumab in the current study. Overall, the data suggest that IL-17A inhibitors could offer a more robust proposition to manage the entirety of the clinical manifestations of patients with psoriatic arthritis.
EULAR recommends a treat-to-target approach for patients with psoriatic arthritis for achieving low disease activity or remission as an important goal of treatment, which has been shown to improve physician-reported and patient-reported outcomes in those with recent onset of psoriatic arthritis.26 The heterogeneous manifestations of psoriatic arthritis are captured in several composite definitions that encompass clin-ically important aspects, such as synovitis, psoriasis, enthesitis, pain, patient-assessed global disease activity, and physical function. One such composite definition, DAPSA, primarily focuses on peripheral arthritis, and does not include other psoriatic arthritis manifestations such as psoriasis, axial disease, nail disease, dactylitis, or enthesitis.27 Secukinumab showed numerically higher efficacy compared with adalimumab across musculoskeletal endpoints and composite indices including DAPSA low disease activity, PASDAS low disease activity, minimal disease activity, and Psoriatic Arthritis Response Criteria response. A higher propor-tion of patients treated with secukinumab versus adalimumab achieved the stringent outcome of DAPSA low disease activity and remission, suggesting that improvements with secukinumab were driven primarily by musculoskeletal outcomes.
There were fewer overall discontinuations with secukinumab compared with adalimumab during the study. Higher proportions of patients discontinued adalimumab because of loss of efficacy, adverse events, and acute injection site reactions. Injection site reactions (including injection site pain) were higher with citrate-free adalimumab formulation, as shown in previous

Articles
1504 www.thelancet.com Vol 395 May 9, 2020
studies in other indications.28 The rates of IBD and candidiasis reported in this study for secukinumab were consistent with previously reported data for IL-17A inhibitors.24,29 Overall, the safety profiles of both bDMARDs were consistent with those published in previous studies.6,20,29,30
Management of psoriatic arthritis in the clinical setting should be targeted at the disease domains (peripheral arthritis, axial disease, dactylitis, enthesitis, skin psoriasis, and nail psoriasis) that are active in, and important to, individual patients. Although there is evidence suggesting that IL-17A, IL-12/23p40, and IL-23p19 inhibitors have high efficacy in plaque psoriasis, the current study provides evidence for efficacy in musculoskeletal disease.
The monotherapy design of this study might limit the generalisation of its findings to the entire population, as concomitant methotrexate is widely used in psoriatic arthritis. Another limitation of this study is the lack of comparative data on inhibition of radiographic progres-sion. Given the different treatment discontinuation rates between secukinumab and adalimumab, the underlying assumption behind the mixed model repeated measures (ie, missing at random) warrants further investigation. The influence of sex on efficacy of treatment also needs further analysis.
In conclusion, secukinumab did not meet statistical significance for superiority versus adalimumab in the primary endpoint of ACR20 response at week 52. However, secukinumab was associated with a higher treatment retention rate than was adalimumab and provided numerically higher clinical responses across musculoskeletal endpoints, skin endpoints, and com-posite indices at week 52. The safety profiles of secukinumab and adalimumab were consistent with previous reports. This study presents a considerable volume of comparative efficacy and safety data on two biological agents with different mechanisms of action in the treatment of patients with psoriatic arthritis.ContributorsAll authors meet the International Committee of Medical Journal Editors criteria for authorship for this Article, take responsibility for the integrity of the work as a whole, were involved in drafting and critical review of the manuscript, and approved the final version for submission. All authors agree to be accountable for all aspects of the work and attest to the accuracy and integrity of the work. SM, LP, IBM, PJM, AK, CR, and PN designed and conceived the study. FB, PN, JGM, PG, TK, and ABG interpreted the data. PP and KD acquired and analysed the data. RM analysed the data.
Declaration of interestsIBM declares research grants, consultation fees, or speaker honoraria from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Janssen, Lilly, Novartis, Pfizer, and UCB. FB declares research grants from Pfizer, Janssen, Chugai, Celgene, and Roche; consultation fees from Pfizer, AbbVie, Sanofi, Lilly, Novartis, Genzyme, Boehringer, Janssen, Merck Sharp & Dohme, Celgene, Roche, and Chugai; and investigator fees from Lilly. PJM reports grants or research support from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Galapagos, Genentech, Gilead, Janssen, Lilly, Merck, Novartis, Pfizer, SUN Pharma, and UCB; consultancy for AbbVie, Amgen, Bristol-Myers Squibb, Boehringer Ingelheim, Galapagos, Celgene, Genentech, Gilead, Janssen, Lilly, Novartis, Pfizer, SUN Pharma, and UCB; and speakers bureau fees
from AbbVie, Amgen, Genentech, Janssen, Lilly, Merck, Novartis, Pfizer, and UCB. AK reports consultancy fees and grants or research support from AbbVie, Amgen, Celgene, Eli Lilly, Janssen, Novartis, and UCB. CR reports research grants from AbbVie, Amgen, and UCB and consultancy for AbbVie, Amgen, UCB, Novartis, Pfizer, Lilly, Janssen, and Bristol-Myers Squibb. PN reports research grants for clinical trials and honoraria for lectures and advice from Novartis, Abbvie, Roche, Pfizer, Bristol-Myers Squibb, Janssen, Celgene, UCB, Lilly, Merck Sharp & Dohme, Sanofi, and Gilead. JGM reports research grants, consultation fees, or speaker honoraria from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Janssen, Lilly, Novartis, and Pfizer. PG reports research grants, consultation fees, or speaker honoraria from AbbVie, Amgen, Biogen, Bristol-Myers Squibb, Celgene, Chugai, Janssen, Lilly, Medac, Merck Sharp & Dohme, Nordic Pharma, Novartis, Pfizer, Sanofi, and UCB. TK reports research grants, consultation fees, or speaker honoraria from AbbVie, Bristol-Myers Squibb, Janssen, Lilly, Novartis, Pfizer, BIOCAD, and UCB. ABG reports research grants from Janssen, Incyte, Novartis, XBiotech, UCB, and Boerhinger Ingelheim, and consulting fees from Janssen, Incyte, Novartis, XBiotech, UCB, Boerhinger Ingelheim, Celgene, Beiesdorf, Bristol-Myers Squibb, Abbvie, Lilly, SUN Pharma, and Avotres Therapeutics. RM, PP, SM, and LP are shareholders and employees of Novartis. KD is an employee of Novartis.
Data sharingThe datasets generated and analysed during the current study are not publicly available. Novartis is committed to sharing access to patient-level data and supporting clinical documents from eligible studies with qualified external researchers. These requests are reviewed and approved based on scientific merit. All data provided are anonymised to respect the privacy of patients who have participated in the trial, in line with applicable laws and regulations. The data can be requested from the corresponding author of the manuscript. The protocol can be made available on request by contacting the corresponding author.
AcknowledgmentsWe thank the patients who participated in this study and the study investigators for their contributions. Suchita Dubey (Novartis) provided medical writing support and John Gallagher (Novartis) provided medical and editorial guidance. The study was funded by Novartis Pharma in accordance with Good Publication Practice guidelines. Patient consent was not required for the publication.
References1 Coates LC, Helliwell PS. Psoriatic arthritis: state of the art review.
Clin Med (Lond) 2017; 17: 65–70.2 Crofford LJ. Use of NSAIDs in treating patients with arthritis.
Arthritis Res Ther 2013; 15 (suppl 3): S2.3 Coates LC, Gossec L, Ramiro S, et al. New GRAPPA and EULAR
recommendations for the management of psoriatic arthritis. Rheumatology (Oxford) 2017; 56: 1251–53.
4 Coates LC, Kavanaugh A, Mease PJ, et al. Group for Research and Assessment of Psoriasis and Psoriatic Arthritis 2015 treatment recommendations for psoriatic arthritis. Arthritis Rheumatol 2016; 68: 1060–71.
5 Mease PJ, Gladman DD, Ritchlin CT, et al. Adalimumab for the treatment of patients with moderately to severely active psoriatic arthritis: results of a double-blind, randomized, placebo-controlled trial. Arthritis Rheum 2005; 52: 3279–89.
6 McInnes IB, Mease PJ, Kirkham B, et al. Secukinumab, a human anti-interleukin-17A monoclonal antibody, in patients with psoriatic arthritis (FUTURE 2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2015; 386: 1137–46.
7 van der Heijde D, Mease PJ, Landewe RBM, et al. Secukinumab provides sustained low rates of radiographic progression in psoriatic arthritis: 52-week results from a phase 3 study, FUTURE 5. Rheumatology (Oxford) 2019; published online Oct 5. DOI:10.1093/rheumatology/kez420.
8 Mease PJ, McInnes IB, Kirkham B, et al. Secukinumab inhibition of interleukin-17A in patients with psoriatic arthritis. N Engl J Med 2015; 373: 1329–39.
9 Langley RG, Elewski BE, Lebwohl M, et al. Secukinumab in plaque psoriasis—results of two phase 3 trials. N Engl J Med 2014; 371: 326–38
Articles
www.thelancet.com Vol 395 May 9, 2020 1505
10 Bagel J, Nia J, Hashim PW, et al. Secukinumab is superior to ustekinumab in clearing skin in patients with moderate to severe plaque psoriasis (16-week CLARITY results). Dermatol Ther (Heidelb) 2018; 8: 571–79.
11 Thaçi D, Blauvelt A, Reich K, et al. Secukinumab is superior to ustekinumab in clearing skin of subjects with moderate to severe plaque psoriasis: CLEAR, a randomized controlled trial. J Am Acad Dermatol 2015; 73: 400–09.
12 Behrens F, Koehm M, Arndt U, et al. Does concomitant methotrexate with adalimumab influence treatment outcomes in patients with psoriatic arthritis? Data from a large observational study. J Rheumatol 2015; 42: 632–39.
13 Pakchotanon R, Ye Y, Cook RJ, Chandran V, Gladman DD. Liver abnormalities in patients with psoriatic arthritis. J Rheumatol 2019; published online Oct 15. DOI:10.3899/jrheum.181312.
14 Kingsley GH, Kowalczyk A, Taylor H, et al. A randomized placebo-controlled trial of methotrexate in psoriatic arthritis. Rheumatology (Oxford) 2012; 51: 1368–77.
15 Nikiphorou E, Negoescu A, Fitzpatrick JD, et al. Indispensable or intolerable? Methotrexate in patients with rheumatoid and psoriatic arthritis: a retrospective review of discontinuation rates from a large UK cohort. Clin Rheumatol 2014; 33: 609–14.
16 Ritchlin CT, Krueger JG. New therapies for psoriasis and psoriatic arthritis. Curr Opin Rheumatol 2016; 28: 204–10.
17 Nash P, McInnes IB, Mease PJ, et al. Secukinumab versus adalimumab for psoriatic arthritis: comparative effectiveness up to 48 weeks using a matching-adjusted indirect comparison. Rheumatol Ther 2018; 5: 99–122.
18 Taylor W, Gladman D, Helliwell P, Marchesoni A, Mease P, Mielants H. Classification criteria for psoriatic arthritis: development of new criteria from a large international study. Arthritis Rheum 2006; 54: 2665–73.
19 Gladman DD, Mease PJ, Ritchlin CT, et al. Adalimumab for long-term treatment of psoriatic arthritis: forty-eight week data from the adalimumab effectiveness in psoriatic arthritis trial. Arthritis Rheum 2007; 56: 476–88.
20 Mease PJ, Ory P, Sharp JT, et al. Adalimumab for long-term treatment of psoriatic arthritis: 2-year data from the adalimumab effectiveness in psoriatic arthritis trial (ADEPT). Ann Rheum Dis 2009; 68: 702–09.
21 Gossec L, Smolen JS, Ramiro S, et al. European League Against Rheumatism (EULAR) recommendations for the management of psoriatic arthritis with pharmacological therapies: 2015 update. Ann Rheum Dis 2016; 75: 499–510.
22 Kirkham B, Mease PJ, Nash P, et al. AB0945 Secukinumab efficacy in patients with active psoriatic arthritis: pooled analysis of four phase 3 trials by prior anti-TNF therapy and concomitant methotrexate use. Ann Rheum Dis 2018; 77 (suppl 2): 1597–98.
23 Højgaard P, Ballegaard C, Cordtz R, et al. Gender differences in biologic treatment outcomes-a study of 1750 patients with psoriatic arthritis using Danish Health Care Registers. Rheumatology (Oxford) 2018; 57: 1651–60
24 Mease PJ, Smolen JS, Behrens F, et al. A head-to-head comparison of the efficacy and safety of ixekizumab and adalimumab in biological-naïve patients with active psoriatic arthritis: 24-week results of a randomised, open-label, blinded-assessor trial. Ann Rheum Dis 2020; 79: 123–31.
25 Kavanaugh A, Gottlieb A, Morita A, et al. The contribution of joint and skin improvements to the health-related quality of life of patients with psoriatic arthritis: a post hoc analysis of two randomised controlled studies. Ann Rheum Dis 2019; 78: 1215–19.
26 Smolen JS, Schöls M, Braun J, et al. Treating axial spondyloarthritis and peripheral spondyloarthritis, especially psoriatic arthritis, to target: 2017 update of recommendations by an international task force. Ann Rheum Dis 2018; 77: 3–17.
27 Smolen JS, Schoels M, Aletaha D. Disease activity and response assessment in psoriatic arthritis using the disease activity index for psoriatic arthritis (DAPSA). A brief review. Clin Exp Rheumatol 2015; 33 (suppl 93): S48–50.
28 Keystone EC, Kavanaugh AF, Sharp JT, et al. Radiographic, clinical, and functional outcomes of treatment with adalimumab (a human anti-tumor necrosis factor monoclonal antibody) in patients with active rheumatoid arthritis receiving concomitant methotrexate therapy: a randomized, placebo-controlled, 52-week trial. Arthritis Rheum 2004; 50: 1400–11.
29 Deodhar A, Mease PJ, McInnes IB, et al. Long-term safety of secukinumab in patients with moderate-to-severe plaque psoriasis, psoriatic arthritis, and ankylosing spondylitis: integrated pooled clinical trial and post-marketing surveillance data. Arthritis Res Ther 2019; 21: 111
30 Mease P, van der Heijde D, Landewé R, et al. Secukinumab improves active psoriatic arthritis symptoms and inhibits radiographic progression: primary results from the randomised, double-blind, phase III FUTURE 5 study. Ann Rheum Dis 2018; 77: 890–97.
Supplementary appendixThis appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors.
This online publication has been corrected. The corrected version first appeared at thelancet.com on May 28, 2020.
Supplement to: McInnes IB, Behrens F, Mease PJ, et al. Secukinumab versus adalimumab for treatment of active psoriatic arthritis (EXCEED): a double-blind, parallel-group, randomised, active-controlled, phase 3b trial. Lancet 2020; 395: 1496–505.
1
APPENDIX
Secukinumab versus Adalimumab Comparison for the Treatment of Active Psoriatic Arthritis (EXCEED): A
Randomised, Double-blind, Active-controlled Phase 3b Trial
Iain B McInnes1*, Frank Behrens2, Philip J Mease3, Arthur Kavanaugh4, Christopher Ritchlin5, Peter Nash6, Jordi
Gratacós Masmitja7, Philippe Goupille8, Tatiana Korotaeva9, Alice B Gottlieb10, Ruvie Martin11, Kevin Ding12,
Pascale Pellet13, Shephard Mpofu14, and Luminita Pricop15 on behalf of EXCEED Study
1University of Glasgow, Glasgow, United Kingdom 2Rheumatology University Hospital and Fraunhofer Institute for Molecular Biology and Applied Ecology IME,
Branch for Translational Medicine and Pharmacology TMP and Fraunhofer Cluster of Excellence for Immune-
Mediated Diseases CIMD, Goethe University, Frankfurt, Germany 3Swedish Medical Centre/Providence St. Joseph Health and University of Washington, Seattle, United States 4Rheumatology, Allergy, Immunology Division, University of California, San Diego, School of Medicine, La Jolla,
United States, La Jolla, United States 5Allergy/Immunology and Rheumatology Division, University of Rochester, Rochester, United States 6Department of Medicine, Griffith University, Brisbane, Australia 7Rheumatology Department, University Hospital Parc Taulí, Sabadell, UAB, Spain 8Department of Rheumatology and INSERM-CIC1415, University hospital of Tours, EA 7501 GICC, University of
Tours, Tours, France 9Research Institute of Rheumatology n.a. V.A. Nasonova, Moscow, Russia 10Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, United States 11Novartis Pharmaceuticals Corporation, East Hanover, United States 12Novartis Pharmaceuticals Corporation, East Hanover, United States 13Novartis Pharma AG, Basel, Switzerland
14Novartis Pharma AG, Basel, Switzerland 15Novartis Pharmaceuticals Corporation, East Hanover, United States
Corresponding author: Dr. (Prof.) Iain B McInnes
Director
Institute of Infection, Immunity and Inflammation
College of Medical, Veterinary and Life Sciences
University of Glasgow
Scotland, United Kingdom
Tel: + +44 141 330 8412
E-mail: [email protected]
2
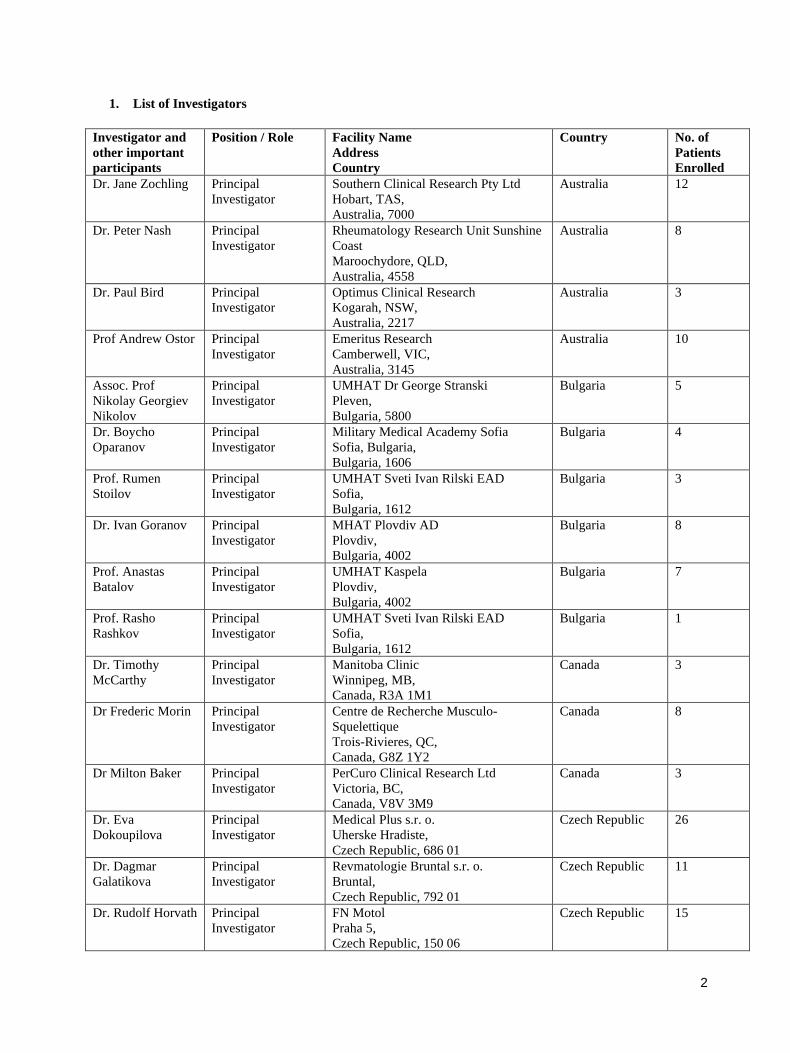
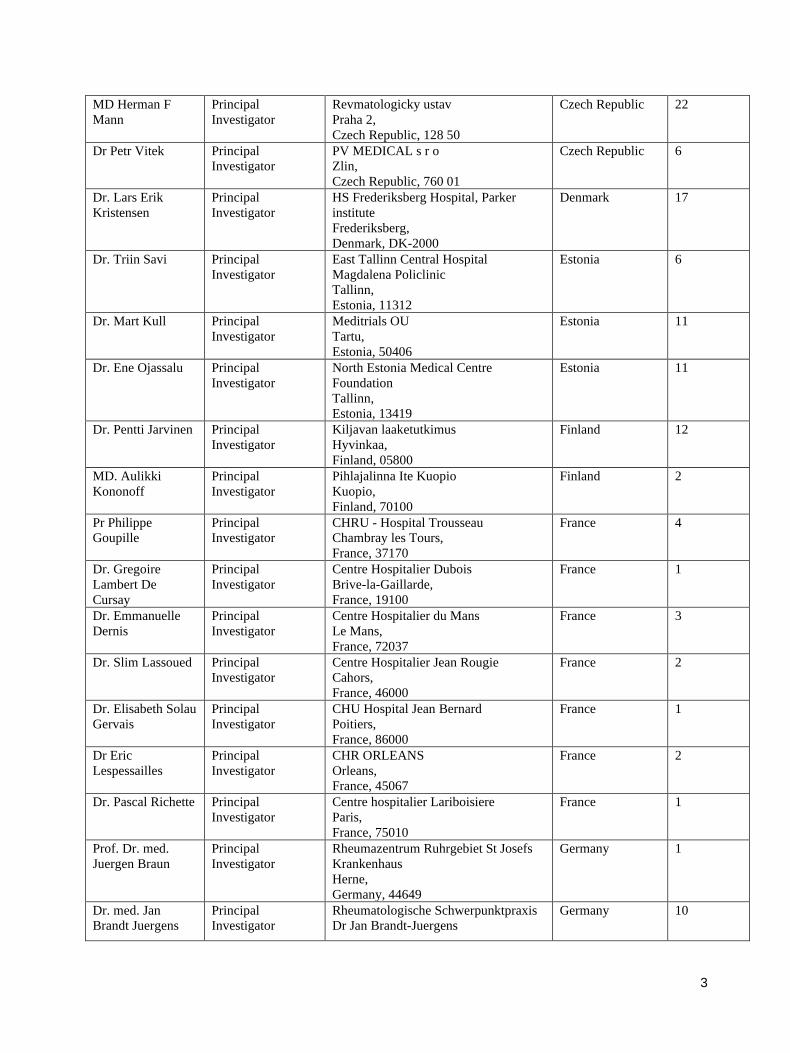
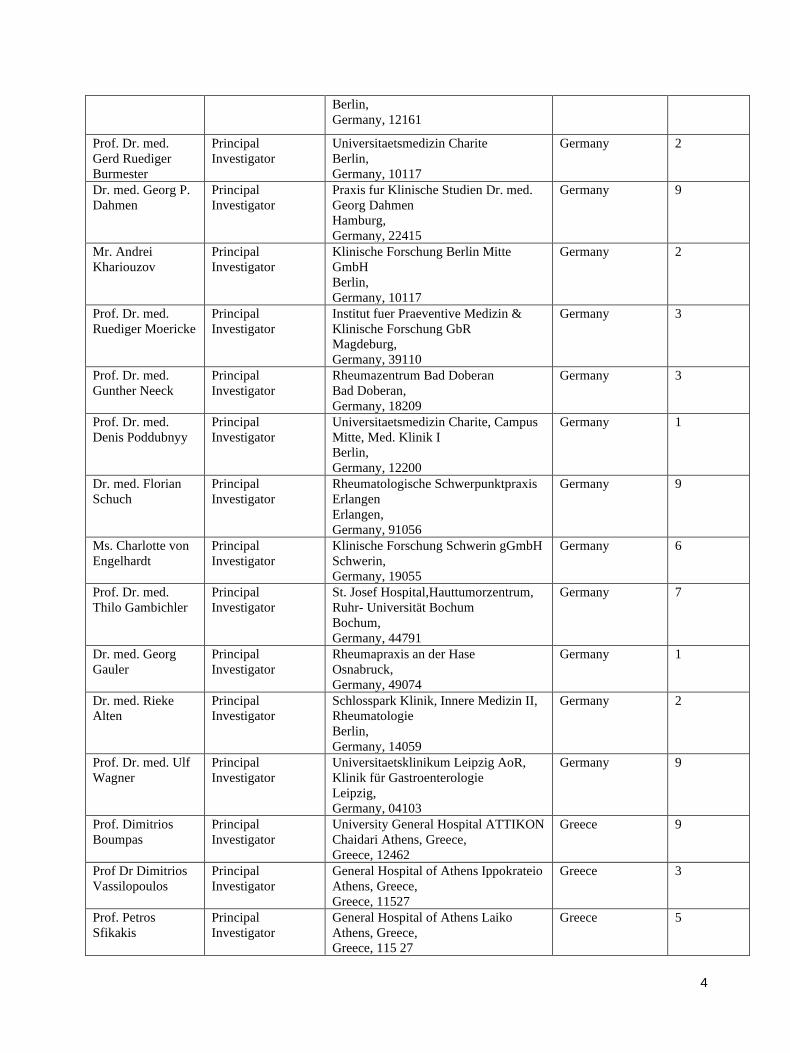
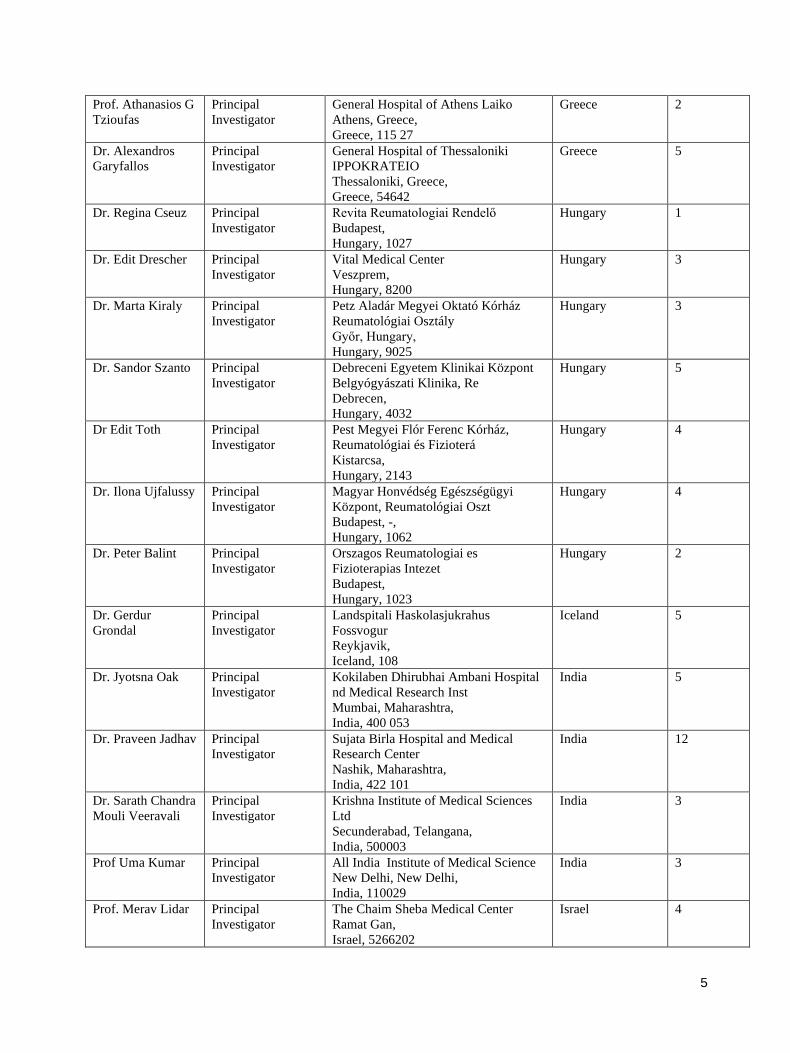
1. List of Investigators
Investigator and
other important
participants
Position / Role Facility Name
Address
Country
Country No. of
Patients
Enrolled
Dr. Jane Zochling Principal
Investigator
Southern Clinical Research Pty Ltd
Hobart, TAS,
Australia, 7000
Australia 12
Dr. Peter Nash Principal
Investigator
Rheumatology Research Unit Sunshine
Coast
Maroochydore, QLD,
Australia, 4558
Australia 8
Dr. Paul Bird Principal
Investigator
Optimus Clinical Research
Kogarah, NSW,
Australia, 2217
Australia 3
Prof Andrew Ostor Principal
Investigator
Emeritus Research
Camberwell, VIC,
Australia, 3145
Australia 10
Assoc. Prof
Nikolay Georgiev
Nikolov
Principal
Investigator
UMHAT Dr George Stranski
Pleven,
Bulgaria, 5800
Bulgaria 5
Dr. Boycho
Oparanov
Principal
Investigator
Military Medical Academy Sofia
Sofia, Bulgaria,
Bulgaria, 1606
Bulgaria 4
Prof. Rumen
Stoilov
Principal
Investigator
UMHAT Sveti Ivan Rilski EAD
Sofia,
Bulgaria, 1612
Bulgaria 3
Dr. Ivan Goranov Principal
Investigator
MHAT Plovdiv AD
Plovdiv,
Bulgaria, 4002
Bulgaria 8
Prof. Anastas
Batalov
Principal
Investigator
UMHAT Kaspela
Plovdiv,
Bulgaria, 4002
Bulgaria 7
Prof. Rasho
Rashkov
Principal
Investigator
UMHAT Sveti Ivan Rilski EAD
Sofia,
Bulgaria, 1612
Bulgaria 1
Dr. Timothy
McCarthy
Principal
Investigator
Manitoba Clinic
Winnipeg, MB,
Canada, R3A 1M1
Canada 3
Dr Frederic Morin Principal
Investigator
Centre de Recherche Musculo-
Squelettique
Trois-Rivieres, QC,
Canada, G8Z 1Y2
Canada 8
Dr Milton Baker Principal
Investigator
PerCuro Clinical Research Ltd
Victoria, BC,
Canada, V8V 3M9
Canada 3
Dr. Eva
Dokoupilova
Principal
Investigator
Medical Plus s.r. o.
Uherske Hradiste,
Czech Republic, 686 01
Czech Republic 26
Dr. Dagmar
Galatikova
Principal
Investigator
Revmatologie Bruntal s.r. o.
Bruntal,
Czech Republic, 792 01
Czech Republic 11
Dr. Rudolf Horvath Principal
Investigator
FN Motol
Praha 5,
Czech Republic, 150 06
Czech Republic 15
3
MD Herman F
Mann
Principal
Investigator
Revmatologicky ustav
Praha 2,
Czech Republic, 128 50
Czech Republic 22
Dr Petr Vitek Principal
Investigator
PV MEDICAL s r o
Zlin,
Czech Republic, 760 01
Czech Republic 6
Dr. Lars Erik
Kristensen
Principal
Investigator
HS Frederiksberg Hospital, Parker
institute
Frederiksberg,
Denmark, DK-2000
Denmark 17
Dr. Triin Savi Principal
Investigator
East Tallinn Central Hospital
Magdalena Policlinic
Tallinn,
Estonia, 11312
Estonia 6
Dr. Mart Kull Principal
Investigator
Meditrials OU
Tartu,
Estonia, 50406
Estonia 11
Dr. Ene Ojassalu Principal
Investigator
North Estonia Medical Centre
Foundation
Tallinn,
Estonia, 13419
Estonia 11
Dr. Pentti Jarvinen Principal
Investigator
Kiljavan laaketutkimus
Hyvinkaa,
Finland, 05800
Finland 12
MD. Aulikki
Kononoff
Principal
Investigator
Pihlajalinna Ite Kuopio
Kuopio,
Finland, 70100
Finland 2
Pr Philippe
Goupille
Principal
Investigator
CHRU - Hospital Trousseau
Chambray les Tours,
France, 37170
France 4
Dr. Gregoire
Lambert De
Cursay
Principal
Investigator
Centre Hospitalier Dubois
Brive-la-Gaillarde,
France, 19100
France 1
Dr. Emmanuelle
Dernis
Principal
Investigator
Centre Hospitalier du Mans
Le Mans,
France, 72037
France 3
Dr. Slim Lassoued Principal
Investigator
Centre Hospitalier Jean Rougie
Cahors,
France, 46000
France 2
Dr. Elisabeth Solau
Gervais
Principal
Investigator
CHU Hospital Jean Bernard
Poitiers,
France, 86000
France 1
Dr Eric
Lespessailles
Principal
Investigator
CHR ORLEANS
Orleans,
France, 45067
France 2
Dr. Pascal Richette Principal
Investigator
Centre hospitalier Lariboisiere
Paris,
France, 75010
France 1
Prof. Dr. med.
Juergen Braun
Principal
Investigator
Rheumazentrum Ruhrgebiet St Josefs
Krankenhaus
Herne,
Germany, 44649
Germany 1
Dr. med. Jan
Brandt Juergens
Principal
Investigator
Rheumatologische Schwerpunktpraxis
Dr Jan Brandt-Juergens
Germany 10
4
Berlin,
Germany, 12161
Prof. Dr. med.
Gerd Ruediger
Burmester
Principal
Investigator
Universitaetsmedizin Charite
Berlin,
Germany, 10117
Germany 2
Dr. med. Georg P.
Dahmen
Principal
Investigator
Praxis fur Klinische Studien Dr. med.
Georg Dahmen
Hamburg,
Germany, 22415
Germany 9
Mr. Andrei
Khariouzov
Principal
Investigator
Klinische Forschung Berlin Mitte
GmbH
Berlin,
Germany, 10117
Germany 2
Prof. Dr. med.
Ruediger Moericke
Principal
Investigator
Institut fuer Praeventive Medizin &
Klinische Forschung GbR
Magdeburg,
Germany, 39110
Germany 3
Prof. Dr. med.
Gunther Neeck
Principal
Investigator
Rheumazentrum Bad Doberan
Bad Doberan,
Germany, 18209
Germany 3
Prof. Dr. med.
Denis Poddubnyy
Principal
Investigator
Universitaetsmedizin Charite, Campus
Mitte, Med. Klinik I
Berlin,
Germany, 12200
Germany 1
Dr. med. Florian
Schuch
Principal
Investigator
Rheumatologische Schwerpunktpraxis
Erlangen
Erlangen,
Germany, 91056
Germany 9
Ms. Charlotte von
Engelhardt
Principal
Investigator
Klinische Forschung Schwerin gGmbH
Schwerin,
Germany, 19055
Germany 6
Prof. Dr. med.
Thilo Gambichler
Principal
Investigator
St. Josef Hospital,Hauttumorzentrum,
Ruhr- Universität Bochum
Bochum,
Germany, 44791
Germany 7
Dr. med. Georg
Gauler
Principal
Investigator
Rheumapraxis an der Hase
Osnabruck,
Germany, 49074
Germany 1
Dr. med. Rieke
Alten
Principal
Investigator
Schlosspark Klinik, Innere Medizin II,
Rheumatologie
Berlin,
Germany, 14059
Germany 2
Prof. Dr. med. Ulf
Wagner
Principal
Investigator
Universitaetsklinikum Leipzig AoR,
Klinik für Gastroenterologie
Leipzig,
Germany, 04103
Germany 9
Prof. Dimitrios
Boumpas
Principal
Investigator
University General Hospital ATTIKON
Chaidari Athens, Greece,
Greece, 12462
Greece 9
Prof Dr Dimitrios
Vassilopoulos
Principal
Investigator
General Hospital of Athens Ippokrateio
Athens, Greece,
Greece, 11527
Greece 3
Prof. Petros
Sfikakis
Principal
Investigator
General Hospital of Athens Laiko
Athens, Greece,
Greece, 115 27
Greece 5
5
Prof. Athanasios G
Tzioufas
Principal
Investigator
General Hospital of Athens Laiko
Athens, Greece,
Greece, 115 27
Greece 2
Dr. Alexandros
Garyfallos
Principal
Investigator
General Hospital of Thessaloniki
IPPOKRATEIO
Thessaloniki, Greece,
Greece, 54642
Greece 5
Dr. Regina Cseuz Principal
Investigator
Revita Reumatologiai Rendelő
Budapest,
Hungary, 1027
Hungary 1
Dr. Edit Drescher Principal
Investigator
Vital Medical Center
Veszprem,
Hungary, 8200
Hungary 3
Dr. Marta Kiraly Principal
Investigator
Petz Aladár Megyei Oktató Kórház
Reumatológiai Osztály
Győr, Hungary,
Hungary, 9025
Hungary 3
Dr. Sandor Szanto Principal
Investigator
Debreceni Egyetem Klinikai Központ
Belgyógyászati Klinika, Re
Debrecen,
Hungary, 4032
Hungary 5
Dr Edit Toth Principal
Investigator
Pest Megyei Flór Ferenc Kórház,
Reumatológiai és Fizioterá
Kistarcsa,
Hungary, 2143
Hungary 4
Dr. Ilona Ujfalussy Principal
Investigator
Magyar Honvédség Egészségügyi
Központ, Reumatológiai Oszt
Budapest, -,
Hungary, 1062
Hungary 4
Dr. Peter Balint Principal
Investigator
Orszagos Reumatologiai es
Fizioterapias Intezet
Budapest,
Hungary, 1023
Hungary 2
Dr. Gerdur
Grondal
Principal
Investigator
Landspitali Haskolasjukrahus
Fossvogur
Reykjavik,
Iceland, 108
Iceland 5
Dr. Jyotsna Oak Principal
Investigator
Kokilaben Dhirubhai Ambani Hospital
nd Medical Research Inst
Mumbai, Maharashtra,
India, 400 053
India 5
Dr. Praveen Jadhav Principal
Investigator
Sujata Birla Hospital and Medical
Research Center
Nashik, Maharashtra,
India, 422 101
India 12
Dr. Sarath Chandra
Mouli Veeravali
Principal
Investigator
Krishna Institute of Medical Sciences
Ltd
Secunderabad, Telangana,
India, 500003
India 3
Prof Uma Kumar Principal
Investigator
All India Institute of Medical Science
New Delhi, New Delhi,
India, 110029
India 3
Prof. Merav Lidar Principal
Investigator
The Chaim Sheba Medical Center
Ramat Gan,
Israel, 5266202
Israel 4
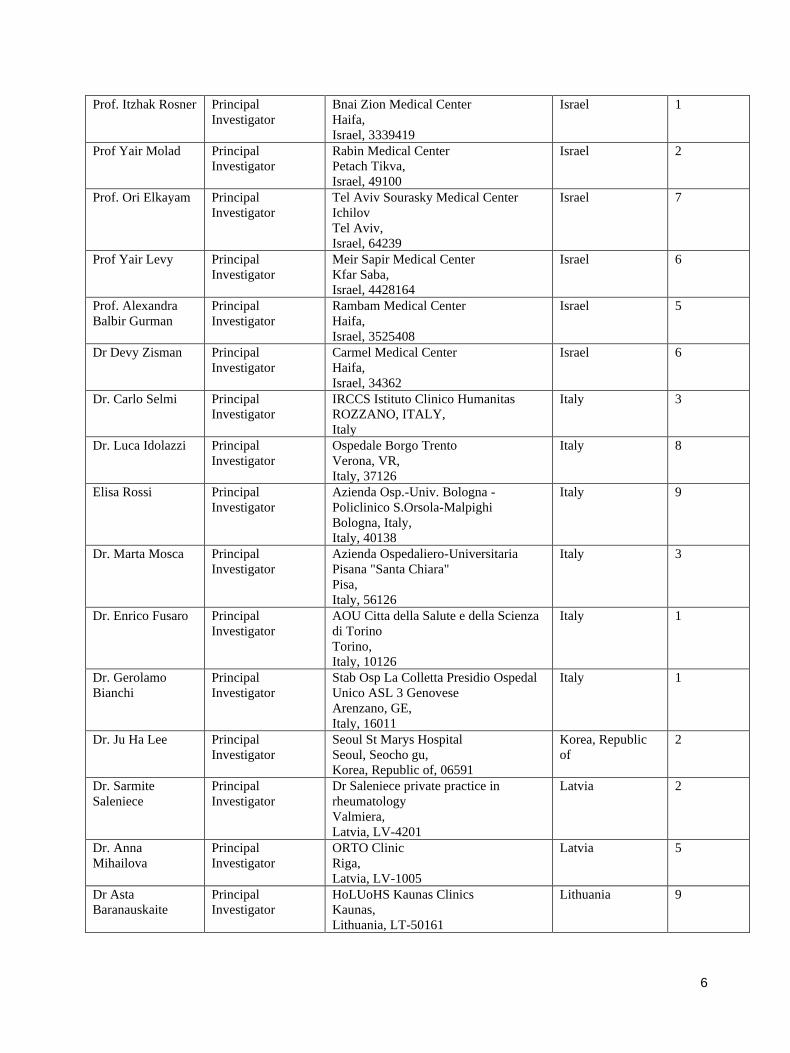
6
Prof. Itzhak Rosner Principal
Investigator
Bnai Zion Medical Center
Haifa,
Israel, 3339419
Israel 1
Prof Yair Molad Principal
Investigator
Rabin Medical Center
Petach Tikva,
Israel, 49100
Israel 2
Prof. Ori Elkayam Principal
Investigator
Tel Aviv Sourasky Medical Center
Ichilov
Tel Aviv,
Israel, 64239
Israel 7
Prof Yair Levy Principal
Investigator
Meir Sapir Medical Center
Kfar Saba,
Israel, 4428164
Israel 6
Prof. Alexandra
Balbir Gurman
Principal
Investigator
Rambam Medical Center
Haifa,
Israel, 3525408
Israel 5
Dr Devy Zisman Principal
Investigator
Carmel Medical Center
Haifa,
Israel, 34362
Israel 6
Dr. Carlo Selmi Principal
Investigator
IRCCS Istituto Clinico Humanitas
ROZZANO, ITALY,
Italy
Italy 3
Dr. Luca Idolazzi Principal
Investigator
Ospedale Borgo Trento
Verona, VR,
Italy, 37126
Italy 8
Elisa Rossi Principal
Investigator
Azienda Osp.-Univ. Bologna -
Policlinico S.Orsola-Malpighi
Bologna, Italy,
Italy, 40138
Italy 9
Dr. Marta Mosca Principal
Investigator
Azienda Ospedaliero-Universitaria
Pisana "Santa Chiara"
Pisa,
Italy, 56126
Italy 3
Dr. Enrico Fusaro Principal
Investigator
AOU Citta della Salute e della Scienza
di Torino
Torino,
Italy, 10126
Italy 1
Dr. Gerolamo
Bianchi
Principal
Investigator
Stab Osp La Colletta Presidio Ospedal
Unico ASL 3 Genovese
Arenzano, GE,
Italy, 16011
Italy 1
Dr. Ju Ha Lee Principal
Investigator
Seoul St Marys Hospital
Seoul, Seocho gu,
Korea, Republic of, 06591
Korea, Republic
of
2
Dr. Sarmite
Saleniece
Principal
Investigator
Dr Saleniece private practice in
rheumatology
Valmiera,
Latvia, LV-4201
Latvia 2
Dr. Anna
Mihailova
Principal
Investigator
ORTO Clinic
Riga,
Latvia, LV-1005
Latvia 5
Dr Asta
Baranauskaite
Principal
Investigator
HoLUoHS Kaunas Clinics
Kaunas,
Lithuania, LT-50161
Lithuania 9
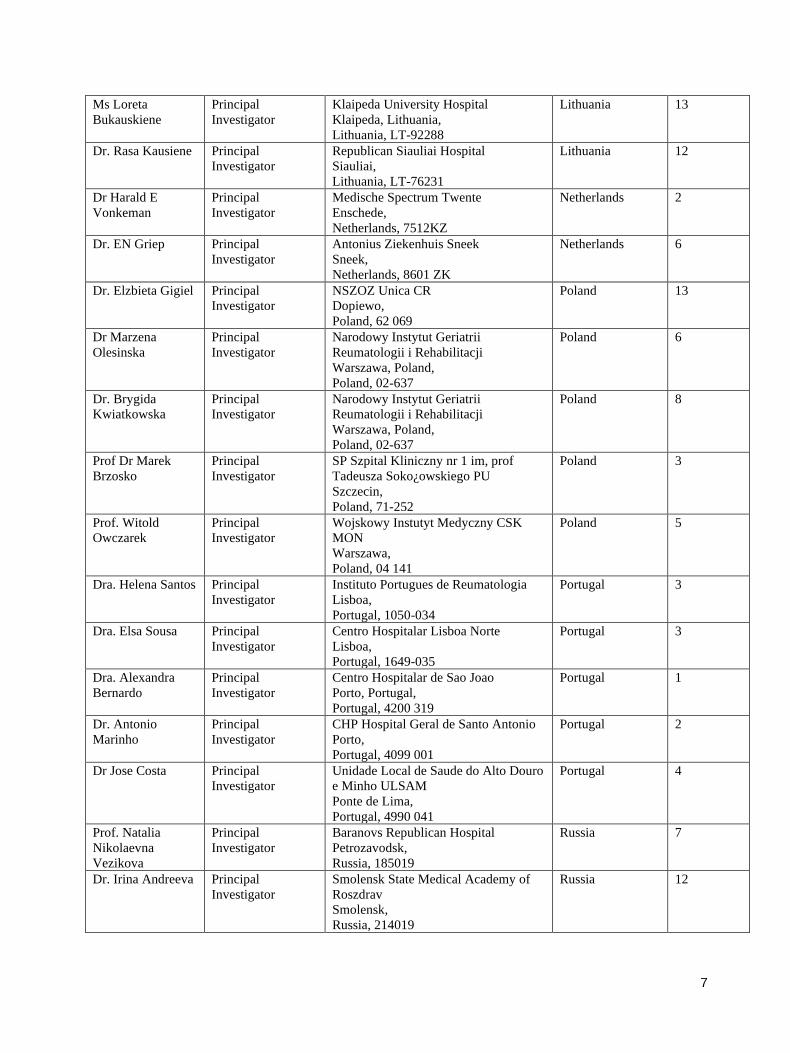
7
Ms Loreta
Bukauskiene
Principal
Investigator
Klaipeda University Hospital
Klaipeda, Lithuania,
Lithuania, LT-92288
Lithuania 13
Dr. Rasa Kausiene Principal
Investigator
Republican Siauliai Hospital
Siauliai,
Lithuania, LT-76231
Lithuania 12
Dr Harald E
Vonkeman
Principal
Investigator
Medische Spectrum Twente
Enschede,
Netherlands, 7512KZ
Netherlands 2
Dr. EN Griep Principal
Investigator
Antonius Ziekenhuis Sneek
Sneek,
Netherlands, 8601 ZK
Netherlands 6
Dr. Elzbieta Gigiel Principal
Investigator
NSZOZ Unica CR
Dopiewo,
Poland, 62 069
Poland 13
Dr Marzena
Olesinska
Principal
Investigator
Narodowy Instytut Geriatrii
Reumatologii i Rehabilitacji
Warszawa, Poland,
Poland, 02-637
Poland 6
Dr. Brygida
Kwiatkowska
Principal
Investigator
Narodowy Instytut Geriatrii
Reumatologii i Rehabilitacji
Warszawa, Poland,
Poland, 02-637
Poland 8
Prof Dr Marek
Brzosko
Principal
Investigator
SP Szpital Kliniczny nr 1 im, prof
Tadeusza Soko¿owskiego PU
Szczecin,
Poland, 71-252
Poland 3
Prof. Witold
Owczarek
Principal
Investigator
Wojskowy Instutyt Medyczny CSK
MON
Warszawa,
Poland, 04 141
Poland 5
Dra. Helena Santos Principal
Investigator
Instituto Portugues de Reumatologia
Lisboa,
Portugal, 1050-034
Portugal 3
Dra. Elsa Sousa Principal
Investigator
Centro Hospitalar Lisboa Norte
Lisboa,
Portugal, 1649-035
Portugal 3
Dra. Alexandra
Bernardo
Principal
Investigator
Centro Hospitalar de Sao Joao
Porto, Portugal,
Portugal, 4200 319
Portugal 1
Dr. Antonio
Marinho
Principal
Investigator
CHP Hospital Geral de Santo Antonio
Porto,
Portugal, 4099 001
Portugal 2
Dr Jose Costa Principal
Investigator
Unidade Local de Saude do Alto Douro
e Minho ULSAM
Ponte de Lima,
Portugal, 4990 041
Portugal 4
Prof. Natalia
Nikolaevna
Vezikova
Principal
Investigator
Baranovs Republican Hospital
Petrozavodsk,
Russia, 185019
Russia 7
Dr. Irina Andreeva Principal
Investigator
Smolensk State Medical Academy of
Roszdrav
Smolensk,
Russia, 214019
Russia 12
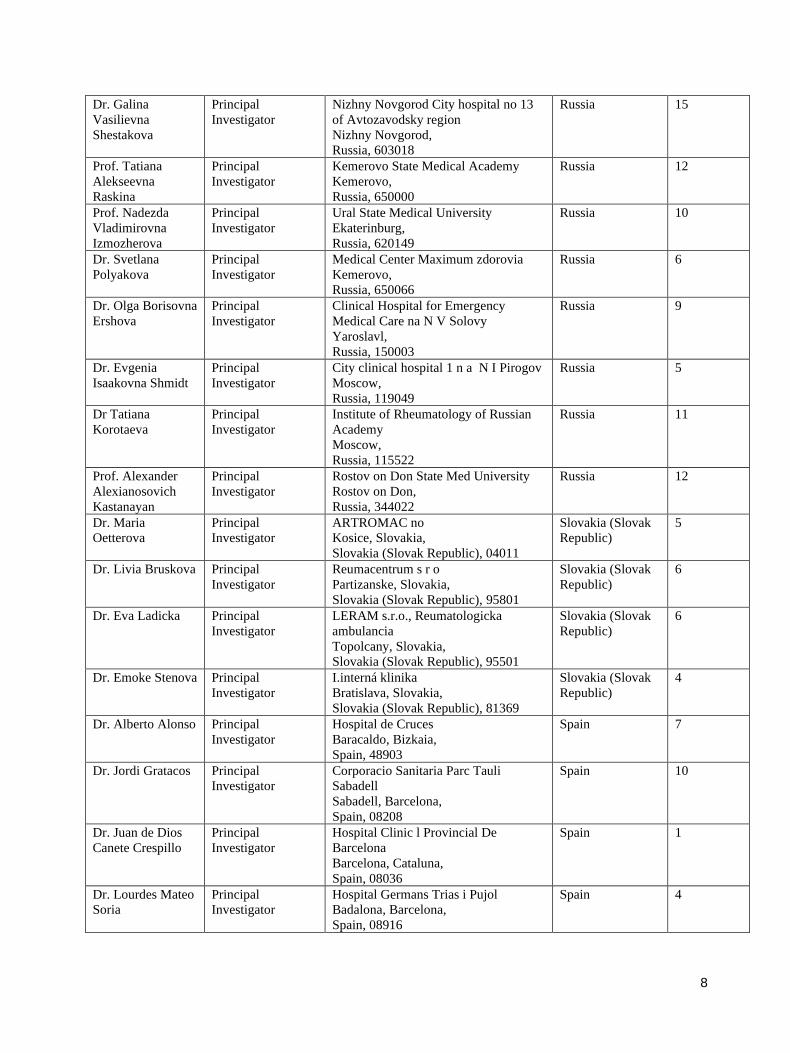
8
Dr. Galina
Vasilievna
Shestakova
Principal
Investigator
Nizhny Novgorod City hospital no 13
of Avtozavodsky region
Nizhny Novgorod,
Russia, 603018
Russia 15
Prof. Tatiana
Alekseevna
Raskina
Principal
Investigator
Kemerovo State Medical Academy
Kemerovo,
Russia, 650000
Russia 12
Prof. Nadezda
Vladimirovna
Izmozherova
Principal
Investigator
Ural State Medical University
Ekaterinburg,
Russia, 620149
Russia 10
Dr. Svetlana
Polyakova
Principal
Investigator
Medical Center Maximum zdorovia
Kemerovo,
Russia, 650066
Russia 6
Dr. Olga Borisovna
Ershova
Principal
Investigator
Clinical Hospital for Emergency
Medical Care na N V Solovy
Yaroslavl,
Russia, 150003
Russia 9
Dr. Evgenia
Isaakovna Shmidt
Principal
Investigator
City clinical hospital 1 n a N I Pirogov
Moscow,
Russia, 119049
Russia 5
Dr Tatiana
Korotaeva
Principal
Investigator
Institute of Rheumatology of Russian
Academy
Moscow,
Russia, 115522
Russia 11
Prof. Alexander
Alexianosovich
Kastanayan
Principal
Investigator
Rostov on Don State Med University
Rostov on Don,
Russia, 344022
Russia 12
Dr. Maria
Oetterova
Principal
Investigator
ARTROMAC no
Kosice, Slovakia,
Slovakia (Slovak Republic), 04011
Slovakia (Slovak
Republic)
5
Dr. Livia Bruskova Principal
Investigator
Reumacentrum s r o
Partizanske, Slovakia,
Slovakia (Slovak Republic), 95801
Slovakia (Slovak
Republic)
6
Dr. Eva Ladicka Principal
Investigator
LERAM s.r.o., Reumatologicka
ambulancia
Topolcany, Slovakia,
Slovakia (Slovak Republic), 95501
Slovakia (Slovak
Republic)
6
Dr. Emoke Stenova Principal
Investigator
I.interná klinika
Bratislava, Slovakia,
Slovakia (Slovak Republic), 81369
Slovakia (Slovak
Republic)
4
Dr. Alberto Alonso Principal
Investigator
Hospital de Cruces
Baracaldo, Bizkaia,
Spain, 48903
Spain 7
Dr. Jordi Gratacos Principal
Investigator
Corporacio Sanitaria Parc Tauli
Sabadell
Sabadell, Barcelona,
Spain, 08208
Spain 10
Dr. Juan de Dios
Canete Crespillo
Principal
Investigator
Hospital Clinic l Provincial De
Barcelona
Barcelona, Cataluna,
Spain, 08036
Spain 1
Dr. Lourdes Mateo
Soria
Principal
Investigator
Hospital Germans Trias i Pujol
Badalona, Barcelona,
Spain, 08916
Spain 4
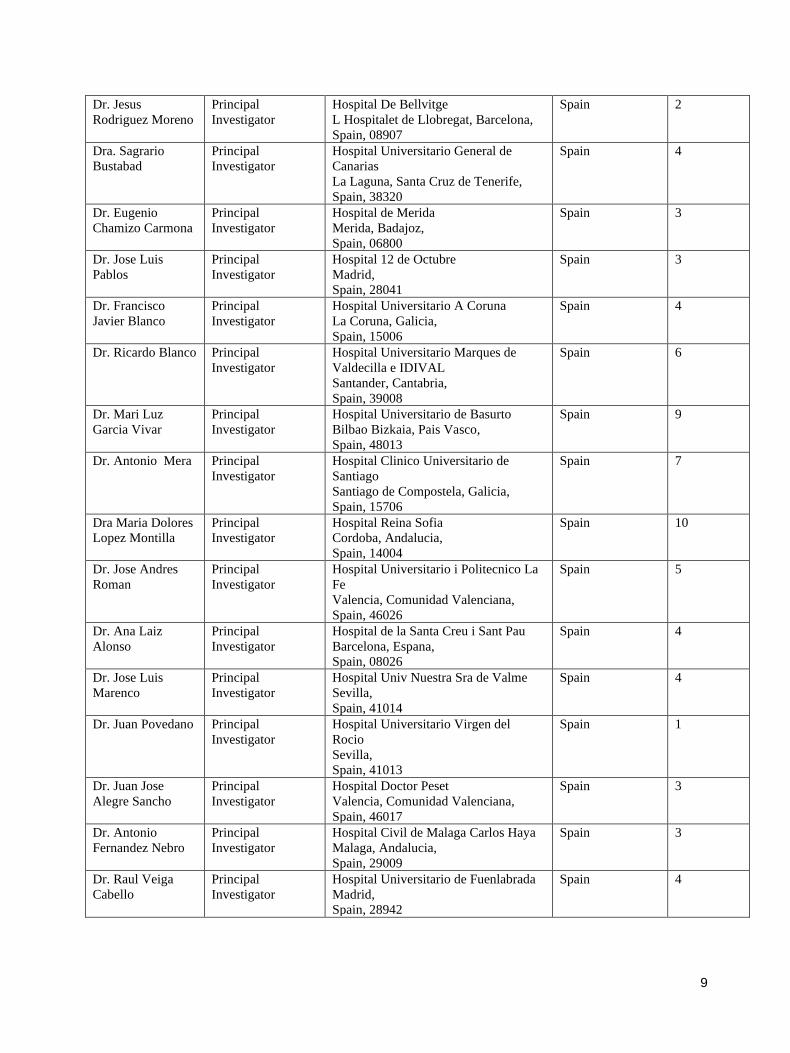
9
Dr. Jesus
Rodriguez Moreno
Principal
Investigator
Hospital De Bellvitge
L Hospitalet de Llobregat, Barcelona,
Spain, 08907
Spain 2
Dra. Sagrario
Bustabad
Principal
Investigator
Hospital Universitario General de
Canarias
La Laguna, Santa Cruz de Tenerife,
Spain, 38320
Spain 4
Dr. Eugenio
Chamizo Carmona
Principal
Investigator
Hospital de Merida
Merida, Badajoz,
Spain, 06800
Spain 3
Dr. Jose Luis
Pablos
Principal
Investigator
Hospital 12 de Octubre
Madrid,
Spain, 28041
Spain 3
Dr. Francisco
Javier Blanco
Principal
Investigator
Hospital Universitario A Coruna
La Coruna, Galicia,
Spain, 15006
Spain 4
Dr. Ricardo Blanco Principal
Investigator
Hospital Universitario Marques de
Valdecilla e IDIVAL
Santander, Cantabria,
Spain, 39008
Spain 6
Dr. Mari Luz
Garcia Vivar
Principal
Investigator
Hospital Universitario de Basurto
Bilbao Bizkaia, Pais Vasco,
Spain, 48013
Spain 9
Dr. Antonio Mera Principal
Investigator
Hospital Clinico Universitario de
Santiago
Santiago de Compostela, Galicia,
Spain, 15706
Spain 7
Dra Maria Dolores
Lopez Montilla
Principal
Investigator
Hospital Reina Sofia
Cordoba, Andalucia,
Spain, 14004
Spain 10
Dr. Jose Andres
Roman
Principal
Investigator
Hospital Universitario i Politecnico La
Fe
Valencia, Comunidad Valenciana,
Spain, 46026
Spain 5
Dr. Ana Laiz
Alonso
Principal
Investigator
Hospital de la Santa Creu i Sant Pau
Barcelona, Espana,
Spain, 08026
Spain 4
Dr. Jose Luis
Marenco
Principal
Investigator
Hospital Univ Nuestra Sra de Valme
Sevilla,
Spain, 41014
Spain 4
Dr. Juan Povedano Principal
Investigator
Hospital Universitario Virgen del
Rocio
Sevilla,
Spain, 41013
Spain 1
Dr. Juan Jose
Alegre Sancho
Principal
Investigator
Hospital Doctor Peset
Valencia, Comunidad Valenciana,
Spain, 46017
Spain 3
Dr. Antonio
Fernandez Nebro
Principal
Investigator
Hospital Civil de Malaga Carlos Haya
Malaga, Andalucia,
Spain, 29009
Spain 3
Dr. Raul Veiga
Cabello
Principal
Investigator
Hospital Universitario de Fuenlabrada
Madrid,
Spain, 28942
Spain 4
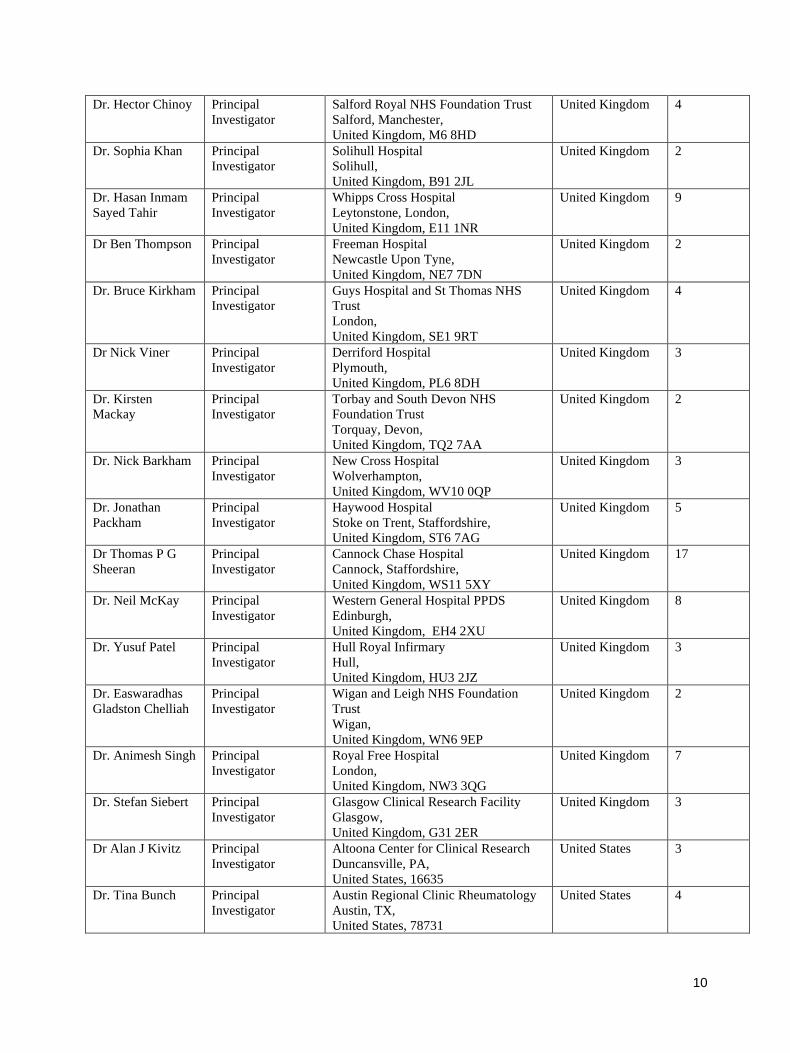
10
Dr. Hector Chinoy Principal
Investigator
Salford Royal NHS Foundation Trust
Salford, Manchester,
United Kingdom, M6 8HD
United Kingdom 4
Dr. Sophia Khan Principal
Investigator
Solihull Hospital
Solihull,
United Kingdom, B91 2JL
United Kingdom 2
Dr. Hasan Inmam
Sayed Tahir
Principal
Investigator
Whipps Cross Hospital
Leytonstone, London,
United Kingdom, E11 1NR
United Kingdom 9
Dr Ben Thompson Principal
Investigator
Freeman Hospital
Newcastle Upon Tyne,
United Kingdom, NE7 7DN
United Kingdom 2
Dr. Bruce Kirkham Principal
Investigator
Guys Hospital and St Thomas NHS
Trust
London,
United Kingdom, SE1 9RT
United Kingdom 4
Dr Nick Viner Principal
Investigator
Derriford Hospital
Plymouth,
United Kingdom, PL6 8DH
United Kingdom 3
Dr. Kirsten
Mackay
Principal
Investigator
Torbay and South Devon NHS
Foundation Trust
Torquay, Devon,
United Kingdom, TQ2 7AA
United Kingdom 2
Dr. Nick Barkham Principal
Investigator
New Cross Hospital
Wolverhampton,
United Kingdom, WV10 0QP
United Kingdom 3
Dr. Jonathan
Packham
Principal
Investigator
Haywood Hospital
Stoke on Trent, Staffordshire,
United Kingdom, ST6 7AG
United Kingdom 5
Dr Thomas P G
Sheeran
Principal
Investigator
Cannock Chase Hospital
Cannock, Staffordshire,
United Kingdom, WS11 5XY
United Kingdom 17
Dr. Neil McKay Principal
Investigator
Western General Hospital PPDS
Edinburgh,
United Kingdom, EH4 2XU
United Kingdom 8
Dr. Yusuf Patel Principal
Investigator
Hull Royal Infirmary
Hull,
United Kingdom, HU3 2JZ
United Kingdom 3
Dr. Easwaradhas
Gladston Chelliah
Principal
Investigator
Wigan and Leigh NHS Foundation
Trust
Wigan,
United Kingdom, WN6 9EP
United Kingdom 2
Dr. Animesh Singh Principal
Investigator
Royal Free Hospital
London,
United Kingdom, NW3 3QG
United Kingdom 7
Dr. Stefan Siebert Principal
Investigator
Glasgow Clinical Research Facility
Glasgow,
United Kingdom, G31 2ER
United Kingdom 3
Dr Alan J Kivitz Principal
Investigator
Altoona Center for Clinical Research
Duncansville, PA,
United States, 16635
United States 3
Dr. Tina Bunch Principal
Investigator
Austin Regional Clinic Rheumatology
Austin, TX,
United States, 78731
United States 4
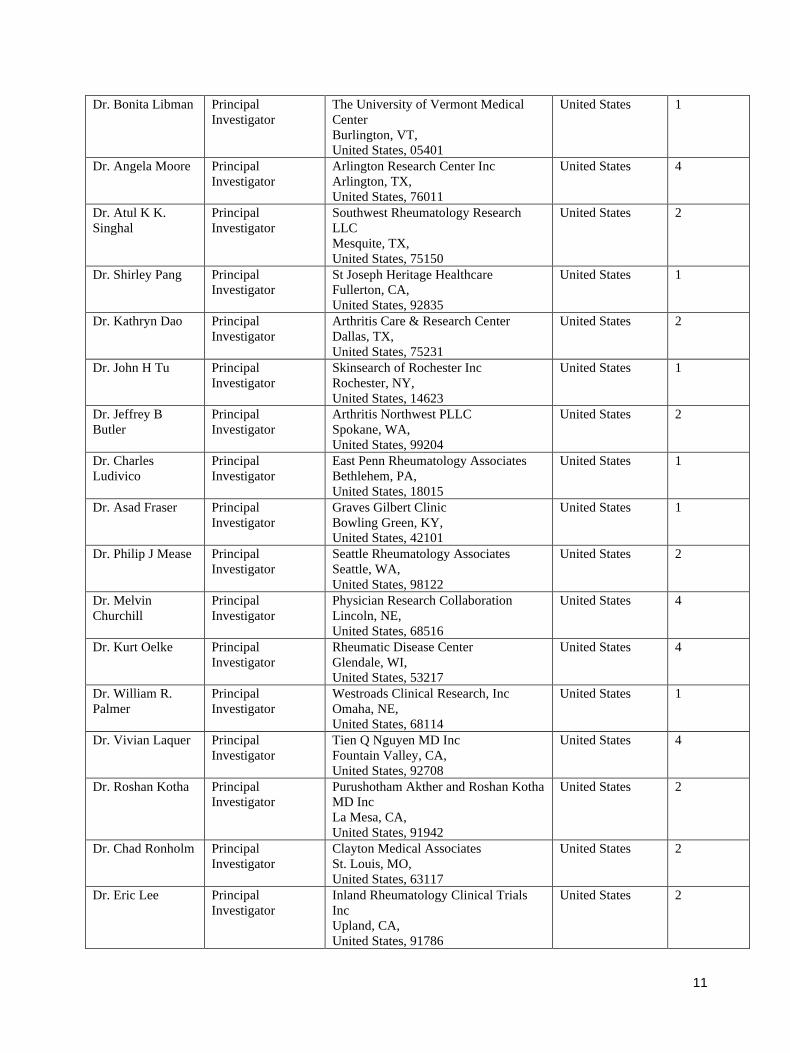
11
Dr. Bonita Libman Principal
Investigator
The University of Vermont Medical
Center
Burlington, VT,
United States, 05401
United States 1
Dr. Angela Moore Principal
Investigator
Arlington Research Center Inc
Arlington, TX,
United States, 76011
United States 4
Dr. Atul K K.
Singhal
Principal
Investigator
Southwest Rheumatology Research
LLC
Mesquite, TX,
United States, 75150
United States 2
Dr. Shirley Pang Principal
Investigator
St Joseph Heritage Healthcare
Fullerton, CA,
United States, 92835
United States 1
Dr. Kathryn Dao Principal
Investigator
Arthritis Care & Research Center
Dallas, TX,
United States, 75231
United States 2
Dr. John H Tu Principal
Investigator
Skinsearch of Rochester Inc
Rochester, NY,
United States, 14623
United States 1
Dr. Jeffrey B
Butler
Principal
Investigator
Arthritis Northwest PLLC
Spokane, WA,
United States, 99204
United States 2
Dr. Charles
Ludivico
Principal
Investigator
East Penn Rheumatology Associates
Bethlehem, PA,
United States, 18015
United States 1
Dr. Asad Fraser Principal
Investigator
Graves Gilbert Clinic
Bowling Green, KY,
United States, 42101
United States 1
Dr. Philip J Mease Principal
Investigator
Seattle Rheumatology Associates
Seattle, WA,
United States, 98122
United States 2
Dr. Melvin
Churchill
Principal
Investigator
Physician Research Collaboration
Lincoln, NE,
United States, 68516
United States 4
Dr. Kurt Oelke Principal
Investigator
Rheumatic Disease Center
Glendale, WI,
United States, 53217
United States 4
Dr. William R.
Palmer
Principal
Investigator
Westroads Clinical Research, Inc
Omaha, NE,
United States, 68114
United States 1
Dr. Vivian Laquer Principal
Investigator
Tien Q Nguyen MD Inc
Fountain Valley, CA,
United States, 92708
United States 4
Dr. Roshan Kotha Principal
Investigator
Purushotham Akther and Roshan Kotha
MD Inc
La Mesa, CA,
United States, 91942
United States 2
Dr. Chad Ronholm Principal
Investigator
Clayton Medical Associates
St. Louis, MO,
United States, 63117
United States 2
Dr. Eric Lee Principal
Investigator
Inland Rheumatology Clinical Trials
Inc
Upland, CA,
United States, 91786
United States 2
12
2. Changes to the Study Protocol
Important changes to the study protocol after commencement of the trial (no patients were randomised at this stage)
included: inclusion of additional follow-up visit, update in wording of exclusion criteria per guidelines for
contraception use after the last dose of study treatment for women of childbearing potential, extension of the
interruption requirement if the patient received a live vaccine underwent an update (to extend the recommended time
before starting a new biologic as elimination of adalimumab may take up to 4 months).
Amendment 2 happened to clarify the estimand to align with the study objectives, which were comparing efficacy of
secukinumab monotherapy with adalimumab monotherapy. Non-parametric regression1 model was not essential to
the final analysis but could be performed and sensitivity analyses was to be conducted to examine the effect of taking
concomitant treatment of methotrexate (MTX) and/or other conventional synthetic disease modifying antirheumatic
drugs (csDMARDs) along with study drug.
None of the changes were made due to safety concerns, had an impact on the conduct of the trial, or altered the
treatment of study patients. The changes occurred while the sponsor remained blinded to study data.
3. Patient Inclusion Exclusion Criteria
Inclusion criteria
Patients eligible for inclusion in this study had to fulfill all of the following criteria:
• Male or non-pregnant, non-lactating female patients at least 18 years of age.
• Diagnosis of psoriatic arthritis (PsA) as classified by ClASsification of Psoriatic ARthritis (CASPAR)
criteria2 and with symptoms for at least 6 months and with active PsA at baseline defined as ≥3 tender joints
out of 78 and ≥3 swollen joints out of 76 (dactylitis of a digit, counts as one joint each).
• Rheumatoid factor (RF) and anti-cyclic citrullinated peptide (CCP) antibodies negative at screening.
• Diagnosis of active plaque psoriasis, with at least one psoriatic plaque of ≥2 cm diameter or nail changes
consistent with psoriasis or documented history of plaque psoriasis.
• Patients with PsA who took non-steroidal anti-inflammatory drugs (NSAIDs) for at least 4 weeks prior to
randomization with inadequate control of symptoms or at least one dose if stopped due to intolerance to
NSAIDs.
• Patients who regularly received NSAIDs as part of their PsA therapy were required to be on a stable dose for
at least 2 weeks before study randomization and remained on a stable dose up to Week 52.
• Patients who received corticosteroids were required to be on a stable dose of ≤10 mg/day prednisone or
equivalent for at least 2 weeks before randomization and remained on a stable dose up to Week 52.
• Patients who were previously treated with a csDMARD, including but not limited to MTX, with an
inadequate response to therapy, or had stopped treatment due to safety/tolerability problems after at least one
administration of the csDMARD.
13
• Patients who received a csDMARD were allowed to enter the study only after csDMARD discontinuation
and appropriate wash-out e.g. 4 weeks prior to randomization visit except for leflunomide, which had to be
discontinued for 8 weeks prior to randomization unless a cholestyramine wash-out was performed.
Exclusion criteria
Patients fulfilling any of the following criteria were not eligible for inclusion in this study.
• Pregnant or nursing (lactating) women, where pregnancy was defined as the state of a female after conception
and until the termination of gestation, confirmed by a positive human chorionic gonadotropin (hCG)
laboratory test.
• Women of childbearing potential, defined as all women physiologically capable of becoming pregnant,
unless they were using effective methods of contraception during dosing of study treatment and minimum 16
weeks or longer if local label required it after the last dose (e.g. 20 weeks for secukinumab, 5 months for
adalimumab in Europe). Effective contraception methods included:
o Total abstinence (when this is in line with the preferred and usual lifestyle of the patient. Periodic
abstinence (e.g., calendar, ovulation, symptothermal, post-ovulation methods) and withdrawal were
not acceptable methods of contraception.
o Female sterilization (had surgical bilateral oophorectomy with or without hysterectomy), total
hysterectomy or tubal ligation at least six weeks before taking investigational drug. In case of
oophorectomy alone, only when the reproductive status of the woman had been confirmed by follow
up hormone level assessment.
o Male sterilization (at least 6 months prior to screening); for female patients on the study, the
vasectomized male partner should be the sole partner for that subject.
o Barrier methods of contraception: Condom or Occlusive cap (diaphragm or cervical/vault caps).
o Use of oral, (estrogen and progesterone), injected or implanted hormonal methods of contraception
or other forms of hormonal contraception that had comparable efficacy (failure rate <1%), for
example hormone vaginal ring or transdermal hormone contraception or placement of an
intrauterine device (IUD) or intrauterine system (IUS). In case of use of oral contraception, women
who had been stable on the same pill for a minimum of 3 months before taking investigational drug.
Women were considered post-menopausal and not of child bearing potential if they had at least 12 months of natural
(spontaneous) amenorrhea with an appropriate clinical profile (e.g. age appropriate, history of vasomotor symptoms)
or had surgical bilateral oophorectomy (with or without hysterectomy), total hysterectomy or tubal ligation at least six
weeks ago. In the case of oophorectomy alone, only when the reproductive status of the woman had been confirmed
by follow up hormone level assessment was she considered not of childbearing potential.
• Chest X-ray or chest magnetic resonance imaging (MRI) with evidence of ongoing infectious or malignant
process obtained within 3 months prior to screening and evaluated by a qualified physician.
• Previous exposure to any biologic drugs for PsA and PSO, including but not limited to TNFα inhibitors,
secukinumab or other biologic drugs targeting IL-17 or IL-17 receptor.
14
• Patients who received high-potency opioid analgesics, including but not limited to, methadone,
hydromorphone, and morphine.
• Ongoing use of prohibited psoriasis treatments/medications (e.g., topical corticosteroids or ultraviolet (UV)
therapy at randomisation). The following wash out periods need to be observed:
o Oral or topical retinoids: 4 weeks.
o Photochemotherapy (e.g., PUVA): 4 weeks.
o Phototherapy (UVA or UVB): 2 weeks.
o Topical skin treatments (except in face, eyes, scalp and genital area during screening; only
corticosteroids with mild to moderate potency): 2 weeks.
• Previous treatment with any cell-depleting therapies, including but not limited to anti-CD20 or investigational
agents (e.g., alemtuzumab (Campath®), anti-CD4, anti-CD5, anti-CD3, and anti-CD19).
• Use of other investigational drugs within 5 half-lives of enrollment, or within 30 days until the expected
pharmacodynamic effect had returned to baseline, whichever is longer.
• History of hypersensitivity to any of the study drugs or excipients or to drugs of similar chemical classes.
• Any intramuscular or intravenous corticosteroid treatment within 4 weeks before randomization.
• Any therapy by intra-articular injections (e.g., corticosteroid) within 4 weeks before randomization.
• Active ongoing inflammatory diseases other than PsA that had confound the evaluation of the benefit of
secukinumab therapy.
• Underlying metabolic, hematologic, renal, hepatic, pulmonary, neurologic, endocrine, cardiac, infectious or
gastrointestinal conditions which in the opinion of the investigator immunocompromised the patient and/or
placed the patient at unacceptable risk for participation in an immunomodulatory therapy.
• Significant medical problems or diseases, including but not limited to the following: uncontrolled
hypertension (≥160/95 mmHg), congestive heart failure (New York Heart Association status of class III or
IV) and uncontrolled diabetes.
• History of clinically significant liver disease or liver injury as indicated by abnormal liver function tests
(LFTs) such as aspartate aminotransferase/serum glutamic oxaloacetic transaminase (AST/SGOT), alanine
aminotransferase/ serum glutamic pyruvictransaminase (ALT/SGPT), alkaline phosphatase or serum
bilirubin. The investigator was guided by the following criteria:
o Any single parameter not exceeding 2 x upper limit of normal (ULN). A single parameter elevated
up to and including 2 x ULN was re-checked once more as soon as possible and in all cases, at least
prior to enrollment/randomization, to rule out any possible lab error.
o If the total bilirubin concentration was increased above 2 x ULN, total bilirubin was differentiated
into the direct and indirect reacting bilirubin.
• History of renal trauma, glomerulonephritis, or patients with one kidney only, or a serum creatinine level
exceeding 1.5 mg/dL (132.6 μmol/L).
• Screening total white blood cell (WBC) count <3,000/μL, or platelets <100,000/μL or neutrophils <1,500/μL
or hemoglobin <8.5 g/dL (85 g/L).
15
• Active systemic infections during the last two weeks (exception: common cold) prior to randomization.
• History of ongoing, chronic or recurrent infectious disease or evidence of tuberculosis infection as defined
by either a positive purified protein derivative (PPD) skin test (the size of induration was measured after 48-
72 hours, and a positive result was defined as an induration of ≥ 5mm or according to local
practice/guidelines), or a positive QuantiFERON TB-Gold test. Patients with a positive test were to
participate in the study if further work up (according to local practice/guidelines) established conclusively
that the patient has no evidence of active tuberculosis. If presence of latent tuberculosis was established then
treatment according to local country guidelines were initiated prior to enrollment.
• Known infection with human immunodeficiency virus (HIV), hepatitis B or hepatitis C at screening or
randomization.
• History of lymphoproliferative disease or any known malignancy or history of malignancy of any organ
system within the past 5 years (except for basal cell carcinoma or actinic keratoses that had been treated with
no evidence of recurrence in the past 3 months, carcinoma in situ of the cervix or non-invasive malignant
colon polyps that had been removed).
• Current severe progressive or uncontrolled disease, which in the judgment of the clinical investigator
rendered the patient unsuitable for the trial.
• Inability or unwillingness to undergo repeated venipuncture (e.g., because of poor tolerability or lack of
access to veins).
• Any medical or psychiatric condition, which in the investigator’s opinion precluded the patient from adhering
to the protocol or completing the study per protocol.
• Donation or loss of 400 mL or more of blood within 8 weeks before randomisation.
• History or evidence of ongoing alcohol or drug abuse, within the last six months before randomisation.
• Plans for administration of live vaccines during the study period or within 6 weeks preceding randomisation.
4. Randomisation and blinding
At baseline, all eligible patients were randomised via interactive response technology (IRT) to one of the two treatment
groups: (secukinumab 300 mg s.c. or adalimumab 40 mg s.c.). A designated Site-staff member other than the
investigator or study staff involved in safety and efficacy assessments or eCRF completion contacted IRT after
confirming that the patient fulfilled all the inclusion/exclusion criteria. The IRT assigned a randomisation number to
the patient, which was used to link the patient to a treatment arm and specified a unique medication number for the
first package of investigational treatment to be dispensed to the patient. The randomisation number was not to be
communicated to the investigator or study site staff involved in the conduct of efficacy assessments.
This was a double-blind randomised treatment trial. Patients, investigators, site personnel, and persons performing the
assessments (except for those described below) remained blinded to treatment assignment from the time of
randomisation until the database lock and analyses were completed, using the following methods: Randomisation data
are kept strictly confidential until the time of unblinding and were not be accessible by anyone else involved in the
study with the exception of the bioanalyst. Investigational treatment was to be dispensed by an unblinded pharmacist
(or other unblinded qualified site personnel) who was independent of those involved in the assessment of study
16
patients. In addition, the unblinded pharmacist (or other unblinded qualified site personnel) stored study medication
and kept medication records containing unblinded information in a separate area to which blinded staff did not have
access.
Study treatment was administered by “independent study drug administrator”- an unblinded suitably qualified
individual (nurse, physician, or other unblinded qualified site personnel) who was not responsible for any aspect of
patient assessment or follow-up. “Independent study drug administrator” could be the same person dispensing the
drug if suitably qualified to perform both activities. Prior to the administration, the unblinded site personnel put in
place suitable methods, e.g physical barriers such as curtains, blindfolds, or similar as agreed with the patient and
available to prevent patient seeing the appearance of their study treatment. The individual administering study
treatment and all study patients were advised to refrain from making any comments to study staff or to other patients
regarding the appearance of study treatments.
5. Outcomes
The efficacy outcome measures used in this study are standard measures used across all PsA trials:
• American College of Rheumatology (ACR) 20, 50 and 70 responses
• Swollen Joint Count (SJC)/Tender Joint Count (TJC)
• Patient’s global assessment of disease activity (VAS)
• Physician’s global assessment of disease activity (VAS)
• Patient’s assessment of PsA pain intensity (VAS)
• Health Assessment Questionnaire – Disability Index (HAQ-DI©)
• high sensitivity C-Reactive Protein (hsCRP) and Erythrocyte Sedimentation Rate (ESR)
• Psoriatic arthritis response criteria (PsARC) response
• Disease Activity Score (DAS28) and EULAR response criteria
• Psoriatic Arthritis Disease Activity Score (PASDAS)
• Patient’s global assessment of psoriasis and arthritis disease activity (VAS)
• Leeds Dactylitis Index (LDI)
• Leeds Enthesitis Index (LEI)
• Spondyloarthritis Research Consortium of Canada (SPARCC) index
• Psoriasis Area and Severity Index (PASI)
• Modified Composite Psoriatic Disease Activity Index (mCPDAI)
Safety Outcomes
Evaluation of adverse events/serious adverse events
• Physical examination
• Vital signs
• Height and weight
• QuantiFERON TB-Gold test or PPD skin test
17
• Electrocardiogram
• Local tolerability (injection site reactions)
• Laboratory evaluations (hematology, clinical chemistry, lipids)
• Pregnancy and assessment of fertility
• Tolerability of study treatment
• Immunogenicity
References.
1. Koch GG, Tangen CM, Jung JW, et al. Issues for covariance analysis of dichotomous and ordered categorical
data from randomized clinical trials and non-parametric strategies for addressing them. Stat Med 1998; 17:
1863-92.
2. Taylor W, Gladman D, Helliwell P, et al. Classification criteria for psoriatic arthritis: development of new
criteria from a large international study. Arthritis Rheum 2006; 54(8): 2665-73.
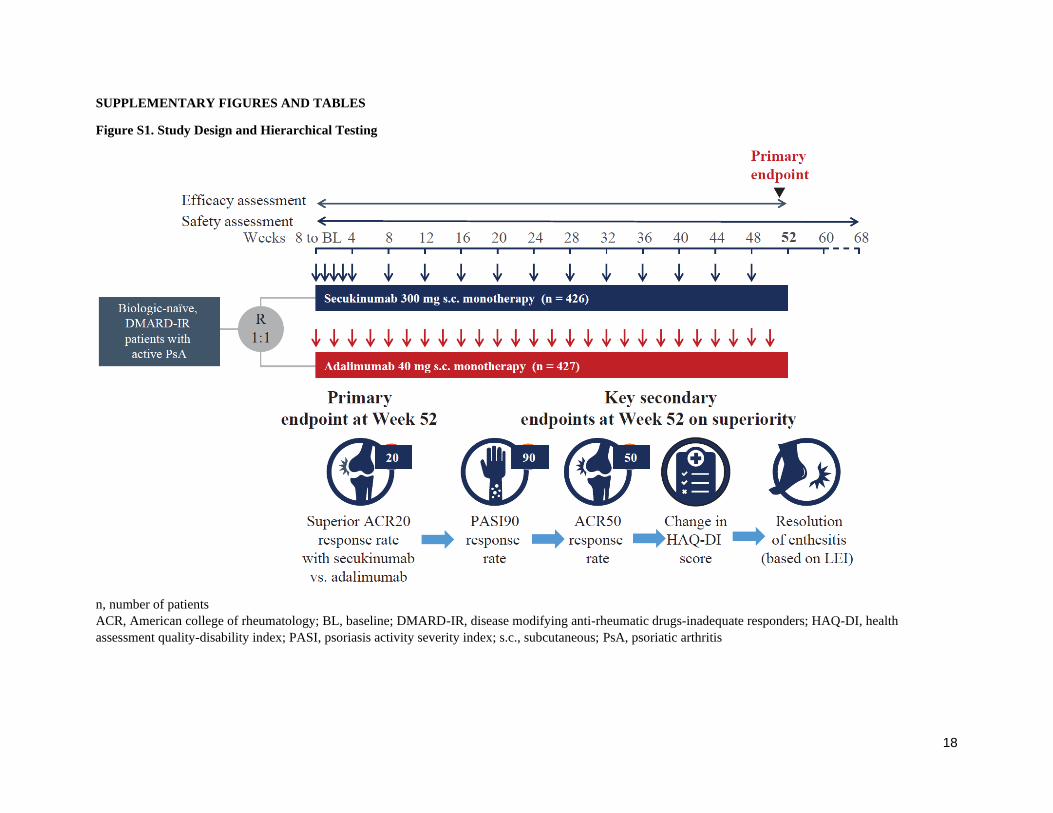
18
SUPPLEMENTARY FIGURES AND TABLES
Figure S1. Study Design and Hierarchical Testing
n, number of patients
ACR, American college of rheumatology; BL, baseline; DMARD-IR, disease modifying anti-rheumatic drugs-inadequate responders; HAQ-DI, health
assessment quality-disability index; PASI, psoriasis activity severity index; s.c., subcutaneous; PsA, psoriatic arthritis
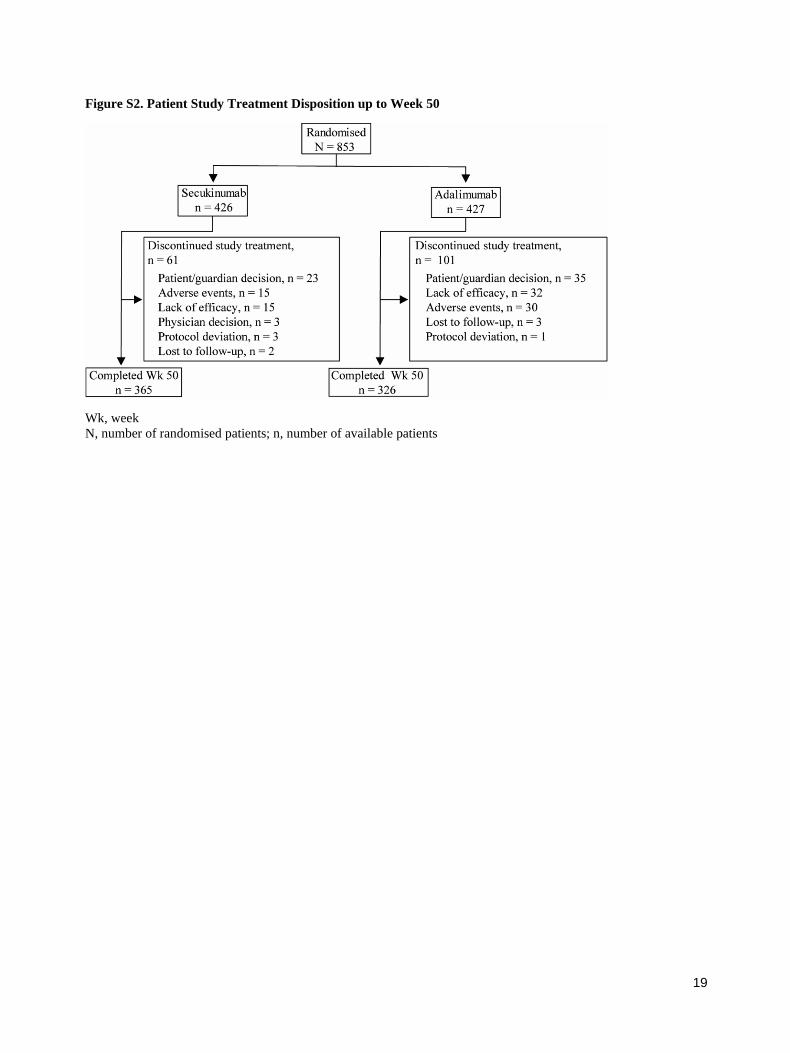
19
Figure S2. Patient Study Treatment Disposition up to Week 50
Wk, week
N, number of randomised patients; n, number of available patients
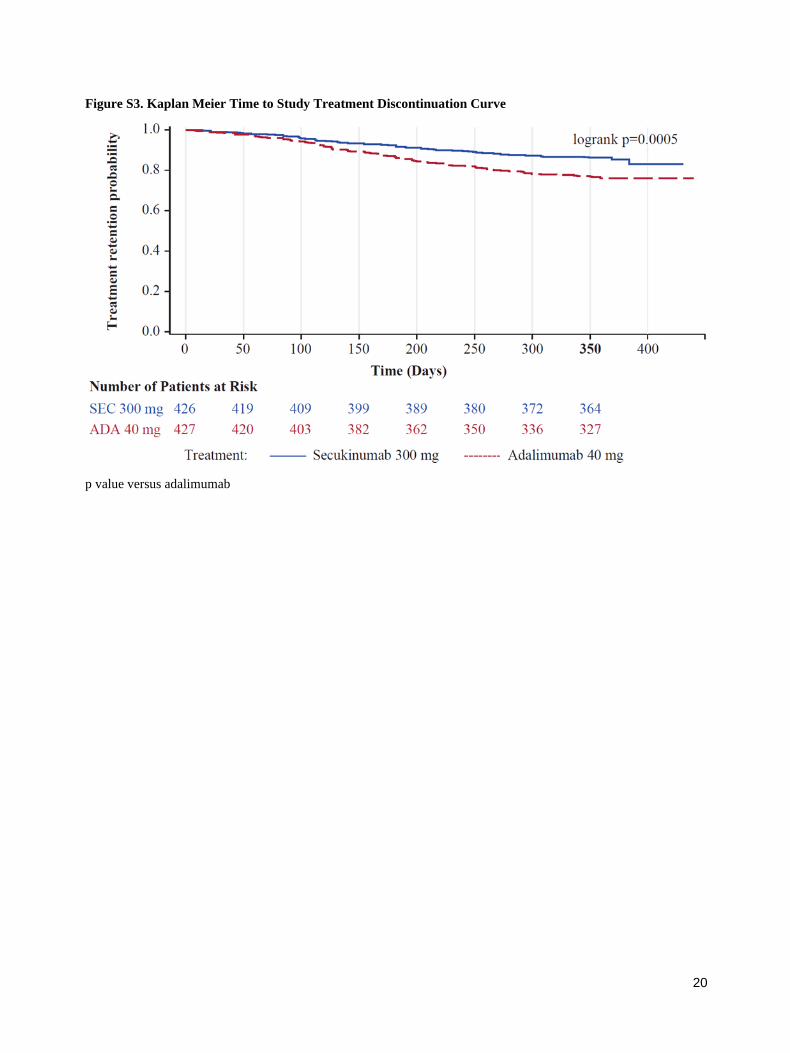
20
Figure S3. Kaplan Meier Time to Study Treatment Discontinuation Curve
p value versus adalimumab
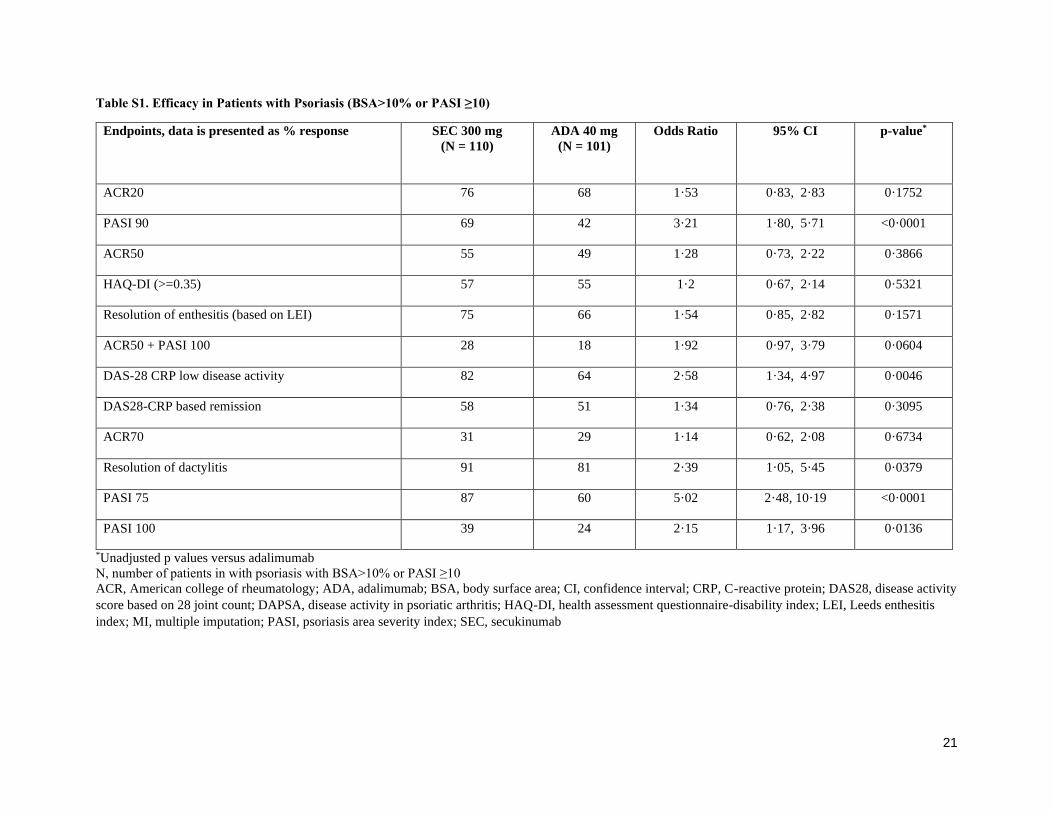
21
Table S1. Efficacy in Patients with Psoriasis (BSA>10% or PASI ≥10)
Endpoints, data is presented as % response SEC 300 mg
(N = 110)
ADA 40 mg
(N = 101)
Odds Ratio 95% CI p-value*
ACR20 76 68 1·53 0·83, 2·83 0·1752
PASI 90 69 42 3·21 1·80, 5·71 <0·0001
ACR50 55 49 1·28 0·73, 2·22 0·3866
HAQ-DI (>=0.35) 57 55 1·2 0·67, 2·14 0·5321
Resolution of enthesitis (based on LEI) 75 66 1·54 0·85, 2·82 0·1571
ACR50 + PASI 100 28 18 1·92 0·97, 3·79 0·0604
DAS-28 CRP low disease activity 82 64 2·58 1·34, 4·97 0·0046
DAS28-CRP based remission 58 51 1·34 0·76, 2·38 0·3095
ACR70 31 29 1·14 0·62, 2·08 0·6734
Resolution of dactylitis 91 81 2·39 1·05, 5·45 0·0379
PASI 75 87 60 5·02 2·48, 10·19 <0·0001
PASI 100 39 24 2·15 1·17, 3·96 0·0136
*Unadjusted p values versus adalimumab
N, number of patients in with psoriasis with BSA>10% or PASI ≥10
ACR, American college of rheumatology; ADA, adalimumab; BSA, body surface area; CI, confidence interval; CRP, C-reactive protein; DAS28, disease activity
score based on 28 joint count; DAPSA, disease activity in psoriatic arthritis; HAQ-DI, health assessment questionnaire-disability index; LEI, Leeds enthesitis
index; MI, multiple imputation; PASI, psoriasis area severity index; SEC, secukinumab
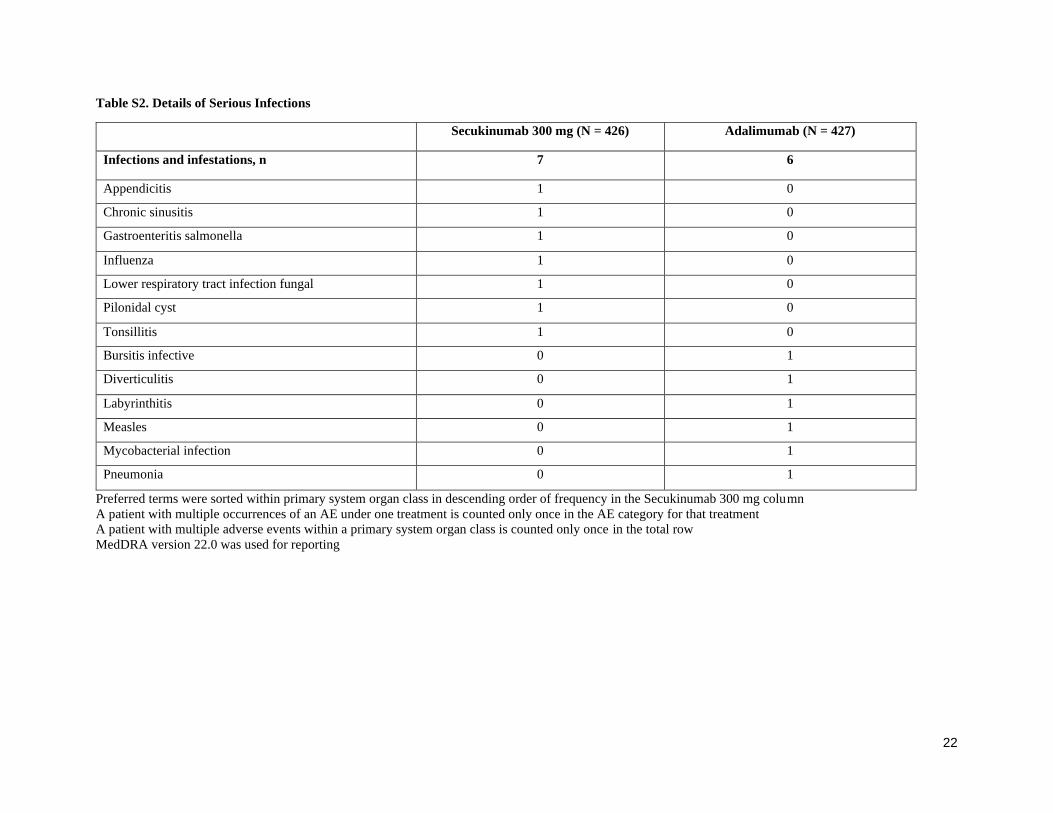
22
Table S2. Details of Serious Infections
Secukinumab 300 mg (N = 426) Adalimumab (N = 427)
Infections and infestations, n 7 6
Appendicitis 1 0
Chronic sinusitis 1 0
Gastroenteritis salmonella 1 0
Influenza 1 0
Lower respiratory tract infection fungal 1 0
Pilonidal cyst 1 0
Tonsillitis 1 0
Bursitis infective 0 1
Diverticulitis 0 1
Labyrinthitis 0 1
Measles 0 1
Mycobacterial infection 0 1
Pneumonia 0 1
Preferred terms were sorted within primary system organ class in descending order of frequency in the Secukinumab 300 mg column
A patient with multiple occurrences of an AE under one treatment is counted only once in the AE category for that treatment
A patient with multiple adverse events within a primary system organ class is counted only once in the total row
MedDRA version 22.0 was used for reporting
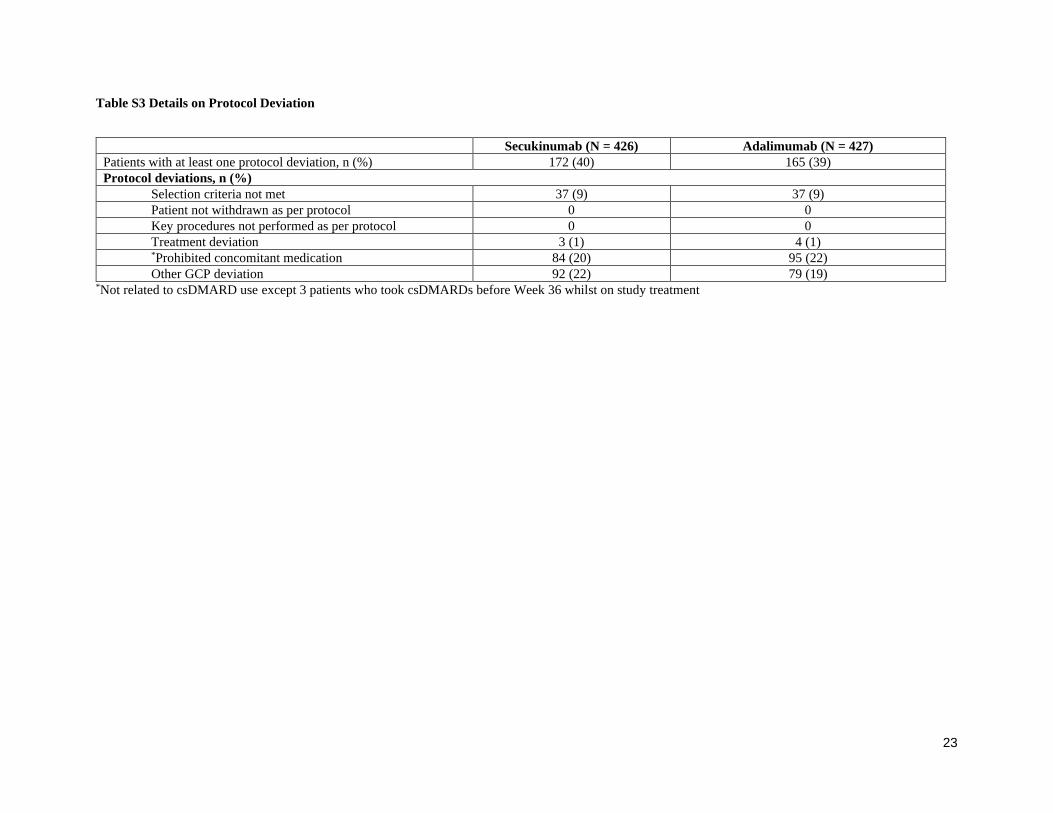
23
Table S3 Details on Protocol Deviation
Secukinumab (N = 426) Adalimumab (N = 427)
Patients with at least one protocol deviation, n (%) 172 (40) 165 (39)
Protocol deviations, n (%)
Selection criteria not met 37 (9) 37 (9)
Patient not withdrawn as per protocol 0 0
Key procedures not performed as per protocol 0 0
Treatment deviation 3 (1) 4 (1) *Prohibited concomitant medication 84 (20) 95 (22)
Other GCP deviation 92 (22) 79 (19) *Not related to csDMARD use except 3 patients who took csDMARDs before Week 36 whilst on study treatment
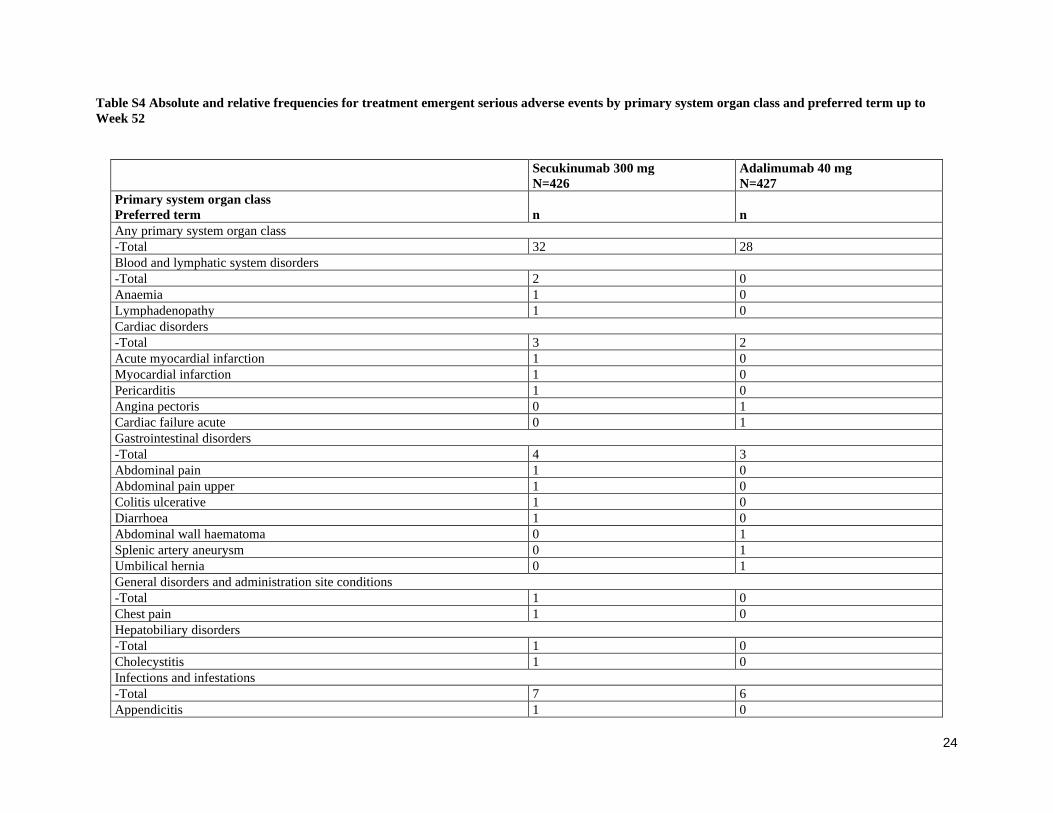
24
Table S4 Absolute and relative frequencies for treatment emergent serious adverse events by primary system organ class and preferred term up to
Week 52
Secukinumab 300 mg
N=426
Adalimumab 40 mg
N=427
Primary system organ class
Preferred term n n
Any primary system organ class
-Total 32 28
Blood and lymphatic system disorders
-Total 2 0
Anaemia 1 0
Lymphadenopathy 1 0
Cardiac disorders
-Total 3 2
Acute myocardial infarction 1 0
Myocardial infarction 1 0
Pericarditis 1 0
Angina pectoris 0 1
Cardiac failure acute 0 1
Gastrointestinal disorders
-Total 4 3
Abdominal pain 1 0
Abdominal pain upper 1 0
Colitis ulcerative 1 0
Diarrhoea 1 0
Abdominal wall haematoma 0 1
Splenic artery aneurysm 0 1
Umbilical hernia 0 1
General disorders and administration site conditions
-Total 1 0
Chest pain 1 0
Hepatobiliary disorders
-Total 1 0
Cholecystitis 1 0
Infections and infestations
-Total 7 6
Appendicitis 1 0
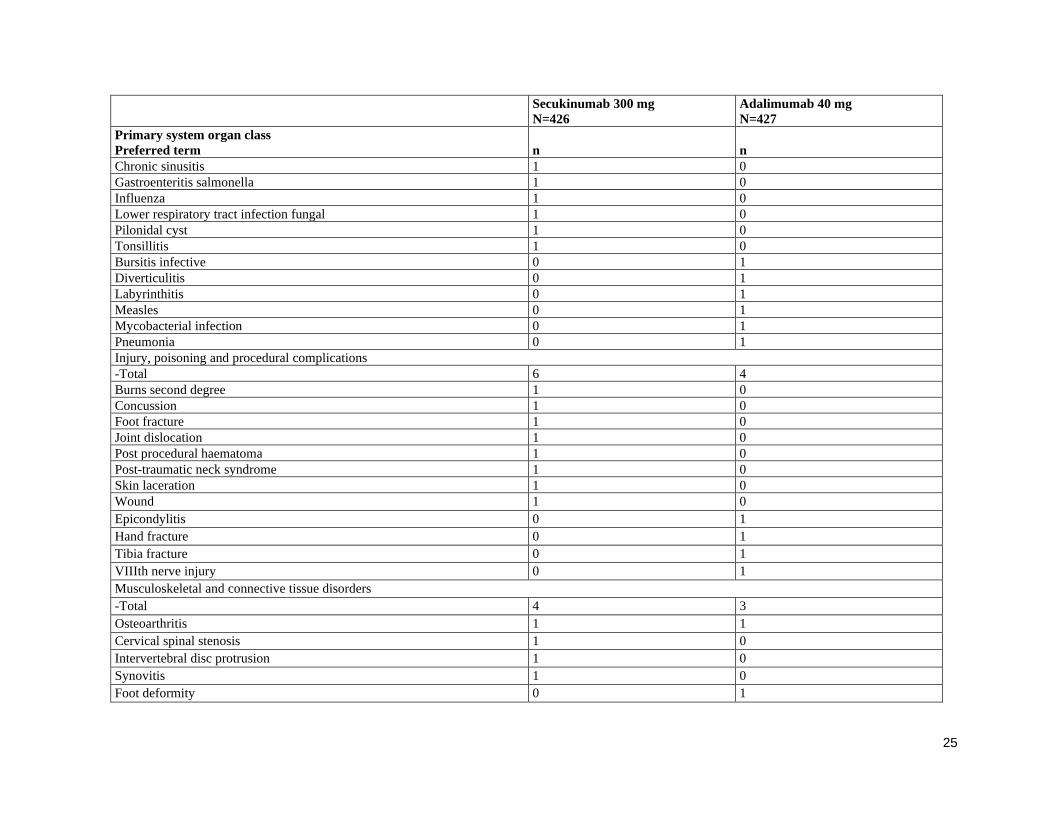
25
Secukinumab 300 mg
N=426
Adalimumab 40 mg
N=427
Primary system organ class
Preferred term n n
Chronic sinusitis 1 0
Gastroenteritis salmonella 1 0
Influenza 1 0
Lower respiratory tract infection fungal 1 0
Pilonidal cyst 1 0
Tonsillitis 1 0
Bursitis infective 0 1
Diverticulitis 0 1
Labyrinthitis 0 1
Measles 0 1
Mycobacterial infection 0 1
Pneumonia 0 1
Injury, poisoning and procedural complications
-Total 6 4
Burns second degree 1 0
Concussion 1 0
Foot fracture 1 0
Joint dislocation 1 0
Post procedural haematoma 1 0
Post-traumatic neck syndrome 1 0
Skin laceration 1 0
Wound 1 0
Epicondylitis 0 1
Hand fracture 0 1
Tibia fracture 0 1
VIIIth nerve injury 0 1
Musculoskeletal and connective tissue disorders
-Total 4 3
Osteoarthritis 1 1
Cervical spinal stenosis 1 0
Intervertebral disc protrusion 1 0
Synovitis 1 0
Foot deformity 0 1
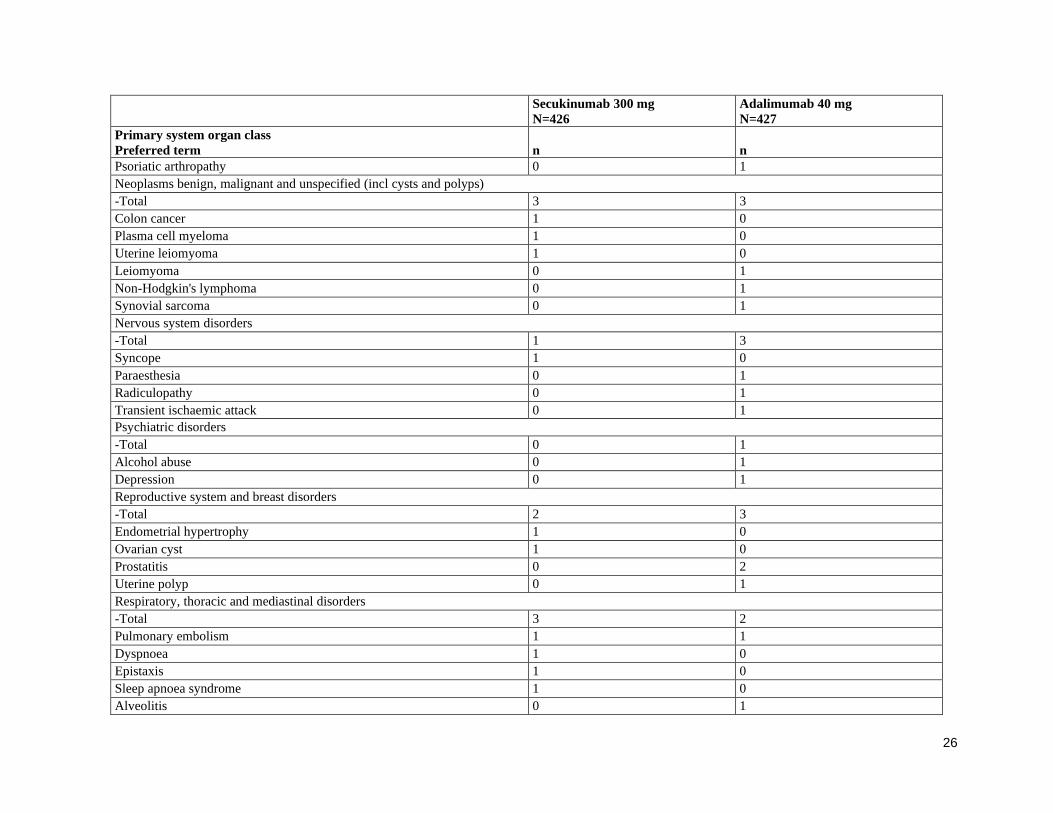
26
Secukinumab 300 mg
N=426
Adalimumab 40 mg
N=427
Primary system organ class
Preferred term n n
Psoriatic arthropathy 0 1
Neoplasms benign, malignant and unspecified (incl cysts and polyps)
-Total 3 3
Colon cancer 1 0
Plasma cell myeloma 1 0
Uterine leiomyoma 1 0
Leiomyoma 0 1
Non-Hodgkin's lymphoma 0 1
Synovial sarcoma 0 1
Nervous system disorders
-Total 1 3
Syncope 1 0
Paraesthesia 0 1
Radiculopathy 0 1
Transient ischaemic attack 0 1
Psychiatric disorders
-Total 0 1
Alcohol abuse 0 1
Depression 0 1
Reproductive system and breast disorders
-Total 2 3
Endometrial hypertrophy 1 0
Ovarian cyst 1 0
Prostatitis 0 2
Uterine polyp 0 1
Respiratory, thoracic and mediastinal disorders
-Total 3 2
Pulmonary embolism 1 1
Dyspnoea 1 0
Epistaxis 1 0
Sleep apnoea syndrome 1 0
Alveolitis 0 1
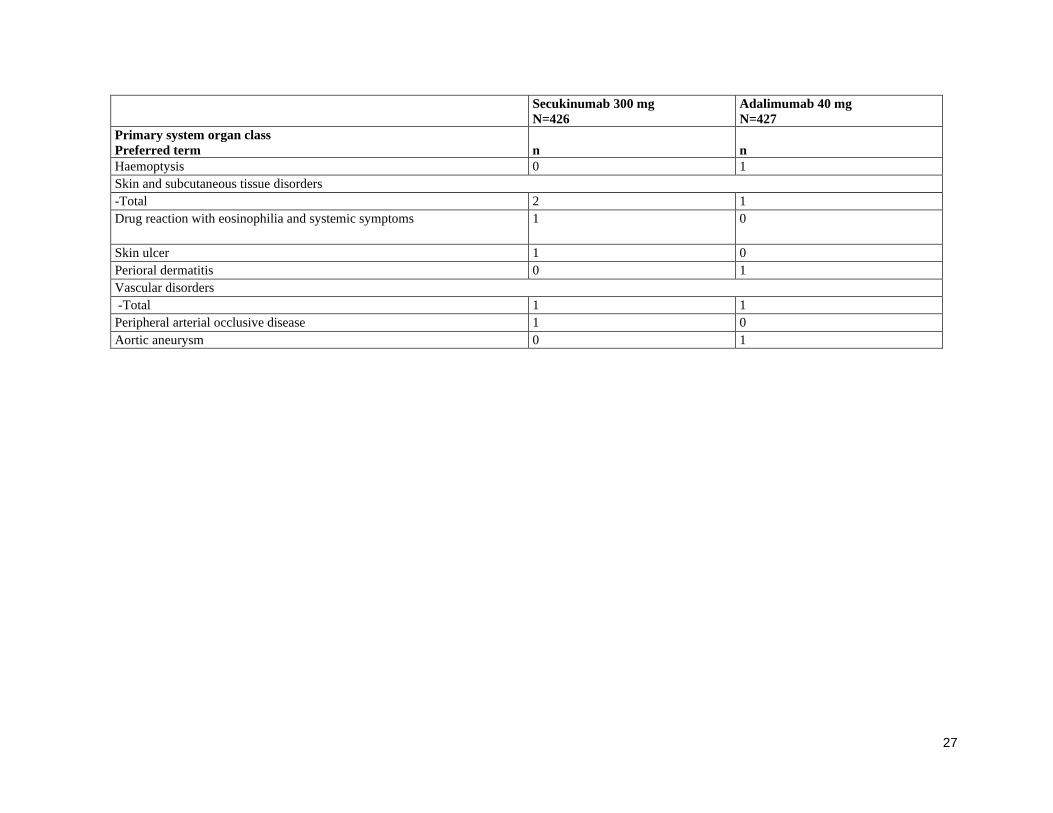
27
Secukinumab 300 mg
N=426
Adalimumab 40 mg
N=427
Primary system organ class
Preferred term n n
Haemoptysis 0 1
Skin and subcutaneous tissue disorders
-Total 2 1
Drug reaction with eosinophilia and systemic symptoms 1 0
Skin ulcer 1 0
Perioral dermatitis 0 1
Vascular disorders
-Total 1 1
Peripheral arterial occlusive disease 1 0
Aortic aneurysm 0 1
www.thelancet.com
This e-print is distributed with the support of Novartis
eNP4: March 2020/B12003808039





























