Embed Size (px)
Citation preview

JHT READ FOR CREDIT #021
Reprint of Imaging of the Elbow: A Review ofImaging Findings in Acute and Chronic
Traumatic Disorders of the Elbow
SCIENTIFIC/CLINICAL ARTICLES
Matthew A. Frick, MDDepartment of RadiologyDivision of Musculoskeletal ImagingMayo Clinic and FoundationRochester, Minnesota
Traumatic injuries to the elbow are frequent inpatients of all ages but are particularly common inyoung children and adolescents engaged in normalplay and athletic competition. The elbow may sustaininjury because of direct trauma or secondary to trans-mission of forces occurring during a fall on an out-stretched hand. While acute traumatic injuries tothe elbow also occur with some frequency in mid-dle-aged and older individuals, injuries related tochronic repetitive stress are more prevalent in theseage groups. Radiographs have long been the hall-mark of elbow imaging, particularly in the settingof trauma, and continue to be the initial imagingstudy of choice. Many patients, however, may needadvanced cross-sectional imaging either at presenta-tion or during the course of their treatment andfollow-up.1 Owing to its superior soft tissueresolution, magnetic resonance imaging (MRI) hasgreatly enhanced our understanding of elbow pathol-ogy and has become the imaging study of choice to
No extramural funding was provided for this work.
This article is a reprint of Imaging of the Elbow: A Review ofImaging Findings in Acute and Chronic Traumatic Disorders ofthe Elbow. Journal of Hand Therapy. April/June 2006;19(2):98–113.
Correspondence and reprint requests to Matthew A. Frick, MD,Department of Radiology, Division of Musculoskeletal Imaging,Mayo Clinic and Foundation, 200 First Street SW, Rochester, MN55905; e-mail: <[email protected]>.
doi:10.1197/j.jht.2007.02.001
Refers to doi:10.1197/j.jht.2006.02.007
186 JOURNAL OF HAND THERAPY
ABSTRACT: Traumatic injuries of the elbow are frequent in pa-tients of all ages but are particularly common in young childrenand adolescents engaged in normal play and athletic competition.Injury may result primarily due to direct trauma or may be second-ary to transmission of forces through the elbow following a fall on anoutstretched hand. In middle-aged and older individuals, chronicrepetitive injuries tend to predominate. In all patients, radiographsremain the initial imaging study of choice. Many patients, however,may need advanced cross-sectional imaging (i.e. MRI, CT, or ultra-sound) either at presentation or during the course of their treatmentand follow-up. This article reviews the imaging appearance of com-mon acute and chronic traumatic disorders of the elbow.
J HAND THER. 2007;20:186–201.
evaluate the complex normal and injured anatomyof the elbow.2–8 Recent advances in scanner technol-ogy have brought computed tomography (CT) tothe fore in trauma imaging. In particular, two- andthree-dimensional high-resolution CT images of com-plex fractures are of particular benefit to the orthope-dic surgeon in preoperative decision making andplanning. CT and magnetic resonance arthrographyare additional diagnostic tools that have been shownto be very sensitive for evaluating injuries to the artic-ular surfaces of the elbow.9 This article reviews elbowanatomy and emphasizes the use of radiography,MRI, and CT in the evaluation and diagnosis of elbowpathology commonly encountered in the setting ofboth acute and chronic trauma. Several investigatorshave recently discussed the use of ultrasound forevaluation of the painful or traumatized elbow.10–13
This modality is not used with great frequency atour institution and will not be discussed further.
ANATOMY
The elbow is a complex joint comprising threebones (distal humerus, proximal radius, and proxi-mal ulna) with three distinct synovial articulations:the radiocapitellar joint, the ulnotrochlear joint,and the proximal radioulnar joint enclosed within acommon capsule. The ulnotrochlear and radiocapi-tellar joints are hinge-type articulations allowing

flexion and extension over an arc of approximately150�. The biceps, brachioradialis, and brachialis arethe primary flexors of the elbow. The triceps is theprincipal extensor muscle of the elbow. The proximalradioulnar joint, along with the distal radioulnarjoint at the wrist, allows for an approximately 90� arcof supination and pronation through the forearm.The collateral ligaments at the medial and lateralaspects of the elbow provide varus and valgusstability at the elbow joint. The medial, or ulnar, col-lateral ligament (MCL) provides the primary re-straint to valgus stress and is composed of threedistinct bundles: anterior, posterior, and transverse(Figure 1). The latter two bundles are often not welldepicted at MRI and are of less clinical importancethan the anterior bundle, which is consistently wellseen both at MRI and ultrasound. The lateral, or
FIGURE 1. Illustration of the medial aspect of the elbowdemonstrating the three distinct bands of the ulnar or me-dial collateral ligament. The anterior bundle, composed ofanterior and posterior bands (not shown), is the most im-portant restraint to valgus stress on the elbow.
radial, collateral (LCL) and the lateral ulnar collateral(LUCL) ligaments are the primary restraint to varusstress at the elbow (Figure 2). The annular and acces-sory annular ligaments are additional lateral struc-tures that primarily confer stability of the proximalradioulnar articulation. It is also important that onebe familiar with common normal variants of elbowanatomy when contemplating the clinical signifi-cance of findings encountered on imagingstudies.14,15
OSSEOUS INJURIES
Radiography is the initial imaging study of choicein all patients presenting with elbow trauma andshould be the initial imaging study in all patients
FIGURE 2. Illustration of the lateral aspect of the elbowdemonstrating the components of the radial or lateral col-lateral ligament and the lateral ulnar collateral ligament,which arises on the lateral epicondyle and forms a slingfor the proximal radius before inserting on the supinatorcrest of the proximal ulna.
FIGURE 3. Anteroposterior (A) and lateral (B) radiographs of a normal elbow demonstrate the normal articulations of theelbow: the ulnotrochlear, radiocapitellar, and the proximal radioulnar joints.
April–June 2007 187

presenting with nonspecific elbow pain. The routinetrauma elbow series at our institution consistsof standard anteroposterior and lateral views(Figure 3) and two oblique views obtained in inter-nal and external rotation. While all images shouldbe closely examined for evidence of a fracture,which is usually readily apparent, the lateral viewshould be thoroughly evaluated for the presence of
FIGURE 4. Lateral radiograph of the elbow demonstratesa small effusion demonstrated by the presence of the ‘‘pos-terior fat pad sign’’ (arrow). Note also the presence of anondisplaced supracondylar fracture of the distal humerus.
188 JOURNAL OF HAND THERAPY
an elbow effusion, which may be the only radio-graphic sign of an underlying fracture or serioussoft tissue injury.16 A small anterior fat pad is nor-mally seen just anterior to the distal humerus onthe lateral view; in the presence of an effusion, thisis often exaggerated and simulates the shape of asail, the so-called sail sign. The posterior fat pad isnot normally visible on the lateral radiograph andonly becomes visible in the presence of an effusion,the so-called posterior fat pad sign (Figure 4). Inchildren, the presence of an effusion often heraldsthe presence of a supracondylar fracture of thedistal humerus, while in adult patients, an effusionmay be the only radiographic clue to an intra-articular fracture of the radial head (Figure 5).Important radiographic osseous landmarks to con-sider are the anterior humeral line and the radio-capitellar line. On a properly positioned lateralradiograph of the elbow, a line drawn tangentiallyto the anterior cortex of the humerus should passthrough the middle third of the capitellum, while aline drawn along the long axis of the radius shouldbisect the capitellum (Figure 6). Disruption of theanterior humeral line may be seen in posteriorly dis-placed or angulated supracondylar fractures of thedistal humerus. These injuries typically occur inchildren following a fall on an outstretched hand.The radiocapitellar relationship should be main-tained on all views of the elbow. Disruption of theradiocapitellar line is most commonly seen in thesetting of elbow dislocation (Figure 7). Posterior el-bow dislocations far outnumber anterior disloca-tions and are often associated with underlyingfractures, particularly fractures of the coronoid pro-cess. Fractures of the coronoid process may be diffi-cult to detect radiographically but are well depicted
FIGURE 5. Anteroposterior and lateral radiographs of the right elbow demonstrate a nondisplaced intra-articular fractureof the radial head.

FIGURE 6. Lateral view of the elbow demonstrating the normal anterior humeral line (A) and the radiocapitellar line (B). Aline drawn parallel to the long axis of the radius should bisect the capitellum on all views.
at CT, particularly on two- or three-dimensionalreformatted images (Figure 8).
LIGAMENTOUS INJURIES
The collateral ligaments are the primary stabi-lizers of the elbow and are commonly injured in thesetting of both acute and chronic, or repetitive,trauma. The literature is replete with investigationsdemonstrating the utility and accuracy of MRI forthe evaluation of ligamentous injuries about theelbow.3,7,8,17 As discussed previously, the medialcollateral ligament confers stability at the medial as-pect of the elbow in the face of valgus stress. In thisrespect, the anterior bundle of the medial collateralligament is of greatest clinical importance. The ante-rior bundle arises from the medial epicondyle and
FIGURE 7. Lateral radiograph of the elbow demonstratesposterior dislocation of the radius and ulna relative to thedistal humerus.
inserts onto the sublime tubercle of the proximalulna. This structure, as is true of all ligaments,should image as a uniformly dark structure on allMRI sequences. Injuries to the medial collateralligament may be associated with injuries to thecommon flexor tendon origin and occur most com-monly in participants of athletic activities that placevalgus stress on the elbow. The medial collateralligament may be damaged but intact (i.e., sprained),or may be partially or completely torn (Figure 9).Increased T2 signal intensity within a thickened orattenuated MCL, without disruption of the fibers,constitutes evidence of a sprain. If some or all ofthe fibers are disrupted, the injury is classified asa partial or a complete tear, respectively. Whilethe ulnar collateral ligament (UCL) may avulse ei-ther proximally or distally, disruptions of the mid-substance of the ligament account for a majorityof traumatic injuries.
The lateral, or radial, collateral ligament complexcomprises the radial collateral ligament (RCL) andthe LUCL and provides the primary restraint tovarus stress at the elbow. Both of these structuresare routinely visualized at MRI. The lateral collat-eral ligament arises more posteriorly on the lateralepicondyle and acts as a sling, passing posteriorto the radial head to insert onto the supinator crestof the proximal ulna (Figure 10). The RCL arisesfrom the anterior aspect of the lateral epicondyleand inserts onto the fibers of the annular ligamentstabilizing the radial head. The lateral collateral lig-ament complex is injured less frequently than themedial, or ulnar, collateral ligament, and injuryusually occurs in the setting of chronic repetitivevarus stress due to either athletic competition(e.g., ‘‘tennis elbow’’) or occupation-related activi-ties. As with the MCL, either component of the lat-eral collateral ligament complex may be sprained
April–June 2007 189

FIGURE 8. Sagittal two-dimensional reformatted (A) and three-dimensional reconstructed (B) computed tomography im-ages of the elbow demonstrate a minimally displaced intra-articular fracture of the coronoid process of the proximal ulna(arrows).
(Figure 11) or partially or completely torn. In con-trast to the MCL where midsubstance tears aremost common, tears of the lateral collateral liga-ment most commonly occur near the humeral ori-gin (Figure 12), with tears of the midsubstancebeing relatively rare. These injuries are often seenin association with injury to the common extensortendon origin on the lateral epicondyle (Figures12 and 13). When seen in the setting of lateral epi-condylitis, MRI will often demonstrate increased T2signal intensity within the adjacent bone marrowconsistent with edema.
190 JOURNAL OF HAND THERAPY
MUSCLE AND TENDON INJURIES
The muscular anatomy of the elbow is complex,and the appearance and orientation of these mus-cles may vary depending on the positioning of theelbow at the time of imaging, i.e., flexion versusextension and pronation versus supination. A com-partmental approach is valuable in evaluating themusculature of the elbow. The primary anteriormuscles are the biceps and the brachialis. Thebiceps tendon, which should appear uniformlyblack (low signal intensity) on all imaging
FIGURE 9. Coronal proton-density (A) and fat-saturated T2-weighted (B) images of the elbow demonstrate complete dis-ruption of the medial collateral ligament (arrows). Images also demonstrate partial tearing of the common flexor origin.
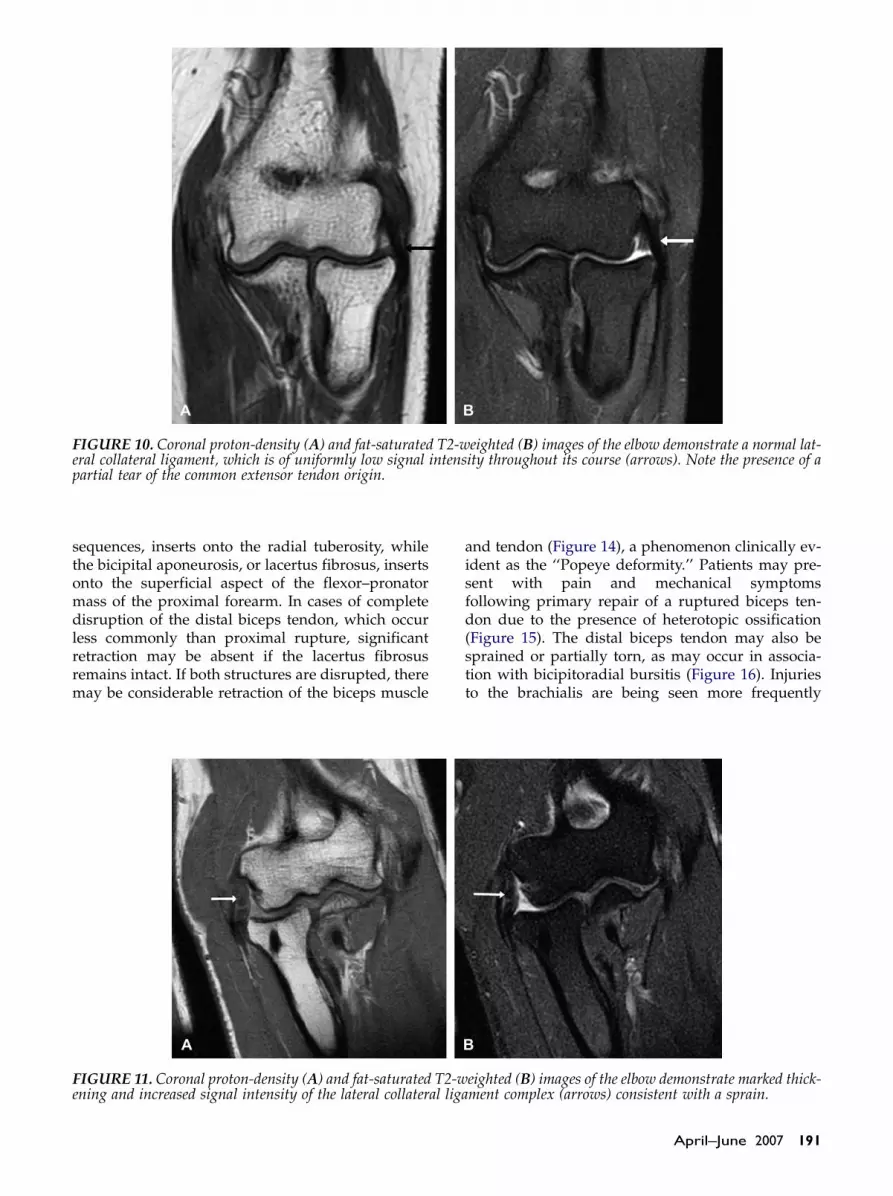
FIGURE 10. Coronal proton-density (A) and fat-saturated T2-weighted (B) images of the elbow demonstrate a normal lat-eral collateral ligament, which is of uniformly low signal intensity throughout its course (arrows). Note the presence of apartial tear of the common extensor tendon origin.
sequences, inserts onto the radial tuberosity, whilethe bicipital aponeurosis, or lacertus fibrosus, insertsonto the superficial aspect of the flexor–pronatormass of the proximal forearm. In cases of completedisruption of the distal biceps tendon, which occurless commonly than proximal rupture, significantretraction may be absent if the lacertus fibrosusremains intact. If both structures are disrupted, theremay be considerable retraction of the biceps muscle
and tendon (Figure 14), a phenomenon clinically ev-ident as the ‘‘Popeye deformity.’’ Patients may pre-sent with pain and mechanical symptomsfollowing primary repair of a ruptured biceps ten-don due to the presence of heterotopic ossification(Figure 15). The distal biceps tendon may also besprained or partially torn, as may occur in associa-tion with bicipitoradial bursitis (Figure 16). Injuriesto the brachialis are being seen more frequently
FIGURE 11. Coronal proton-density (A) and fat-saturated T2-weighted (B) images of the elbow demonstrate marked thick-ening and increased signal intensity of the lateral collateral ligament complex (arrows) consistent with a sprain.
April–June 2007 191

FIGURE 12. Coronal proton-density (A) and fat-saturated T2-weighted (B) images of the elbow demonstrate a high-gradepartial thickness tear of the lateral collateral ligament. Note also the near complete tear of the common extensor tendonorigin (arrows).
due to the continued rise in popularity of competi-tive and recreational rock climbing (‘‘climber’selbow’’).
Muscles of the posterior compartment include thetriceps and anconeus. The triceps, which is theprimary extensor muscle of the elbow, inserts ontothe proximal aspect of the olecranon. The triceps ten-don normally demonstrates striated increased T2 sig-nal intensity parallel to the long axis of the tendonthat should not be mistaken for a sprain or partial
192 JOURNAL OF HAND THERAPY
tear. True disruptions, partial or complete, of thetriceps tendon and musculotendinous junction areexceedingly rare but may occur (Figure 17). Thetriceps tendon may be secondarily damaged bynearby inflammatory changes in the setting of olecra-non bursitis in patients with poorly controlled orlong-standing gouty arthritis.
The lateral compartment muscles include theextensors of the hand and wrist arising as thecommon extensor origin on the lateral epicondyle
FIGURE 13. Coronal proton-density (A) and fat-saturated T2-weighted (B) images of the elbow demonstrate a completetear of the lateral collateral ligament. Note also the near complete tear of the common extensor tendon origin (arrows).

FIGURE 14. Axial proton-density (A), fat-saturated T2-weighted (B), and sagittal fat-saturated T2-weighted (C, D)images demonstrate complete disruption of the distal biceps tendon and aponeurosis with proximal retraction of the freeedge of the tendon.
(Figure 18) and the supinator and brachioradialismuscles. Chronic, repetitive microtrauma is themost common cause of injury to the commonextensor origin, referred to clinically as ‘‘lateral epi-condylitis,’’ or ‘‘tennis elbow,’’ owing to the highfrequency of this injury among tennis players.Similar to the injuries seen in the deeper collateralligaments, the tendon of the common extensor ori-gin may be sprained (i.e., tendinosis or tendinop-athy), or may be partially or completely torn. Likethe other ligaments and tendons about the elbow,
FIGURE 15. Lateral radiograph of the elbow demonstratessignificant heterotopic ossification adjacent to the radialtuberosity. Notice the soft tissue anchors in the radialtuberosity from prior repair of a ruptured biceps tendon.
=
April–June 2007 193

FIGURE 16. Axial proton-density (A), axial fat-saturated T2-weighted (B), and sagittal fat-saturated T2-weighted (C)images demonstrate an enlarged, fluid-filled bicipitoradial bursa consistent with bursitis. Note the low signal intensitybiceps tendon passing through the bursa (black arrow in B).
the common extensor tendon should appearuniformly dark on all MRI sequences. Abnormalincreased T2 signal intensity with thickening orattenuation of the tendon fibers constitutes evidenceof a sprain or tendinopathy, while partial or com-plete disruption of the tendon fibers constitutesevidence of a tear (Figures 11–13).
The medial compartment muscles include thepronator teres and the flexors of the hand and wristarising as the common flexor tendon on the medialepicondyle (Figure 19). Repetitive stress injuries ofthe tendon origins of the medial muscle group arereferred to clinically as ‘‘medial epicondylitis’’ andmay be seen in throwing athletes (‘‘Little leaguer’selbow’’), golfers (golfer’s elbow), or tennis players(‘‘medial tennis elbow’’). Injuries range from tendin-opathy to partial and complete disruptions of thecommon flexor tendon origin, and the appearance
194 JOURNAL OF HAND THERAPY
of these injuries on MRI (Figure 20) is similar to thosepreviously described at the lateral aspect of theelbow.
INJURIES TO THE ARTICULARSURFACE
While traumatic injury may precipitate degenera-tive arthritis in the elbow with subsequent irregular-ity of the articular surface, several other diseaseprocesses may also cause such irregularities andwill be discussed briefly. The most common diseaseentity to affect the articular surfaces of the elbow isprobably age-related degenerative osteoarthritis. Theradiographic hallmarks of osteoarthritis in the elbow,or any joint, are joint space narrowing, subchondral
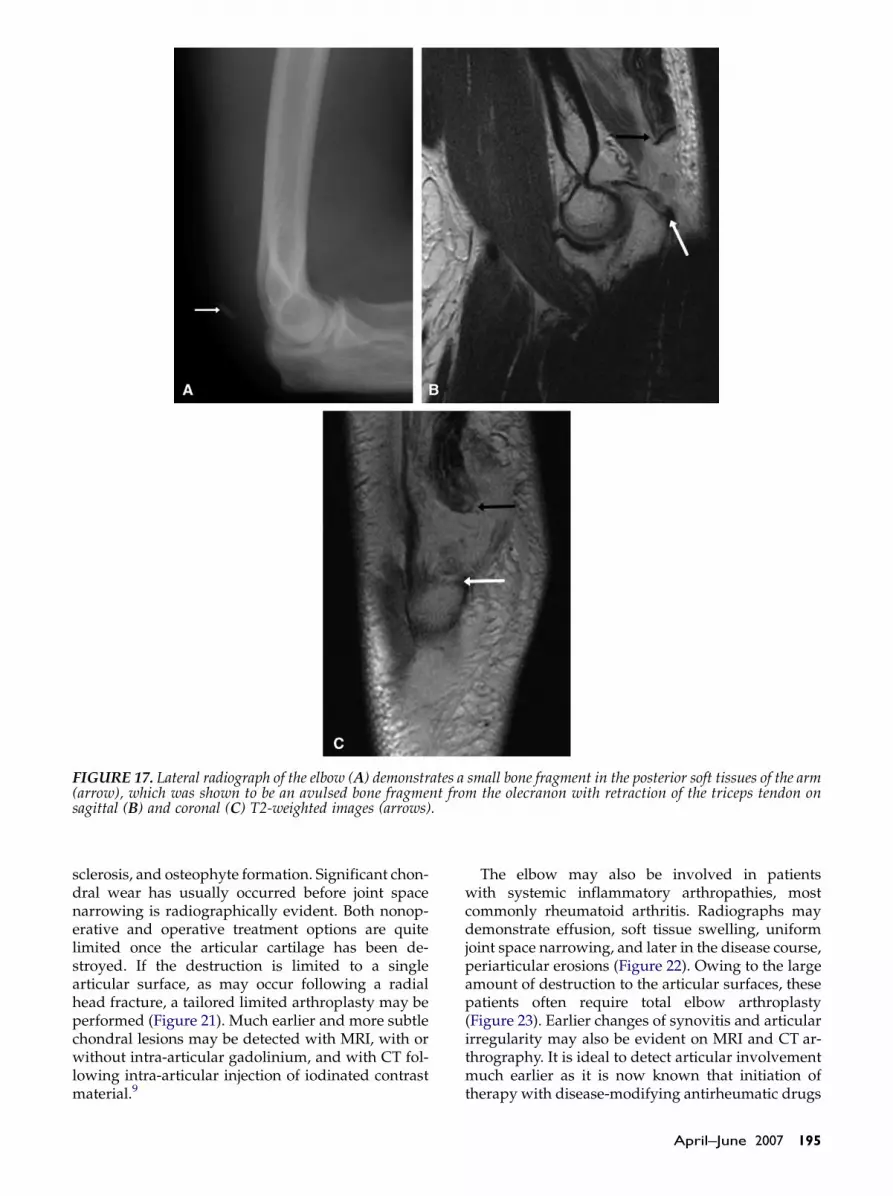
FIGURE 17. Lateral radiograph of the elbow (A) demonstrates a small bone fragment in the posterior soft tissues of the arm(arrow), which was shown to be an avulsed bone fragment from the olecranon with retraction of the triceps tendon onsagittal (B) and coronal (C) T2-weighted images (arrows).
sclerosis, and osteophyte formation. Significant chon-dral wear has usually occurred before joint spacenarrowing is radiographically evident. Both nonop-erative and operative treatment options are quitelimited once the articular cartilage has been de-stroyed. If the destruction is limited to a singlearticular surface, as may occur following a radialhead fracture, a tailored limited arthroplasty may beperformed (Figure 21). Much earlier and more subtlechondral lesions may be detected with MRI, with orwithout intra-articular gadolinium, and with CT fol-lowing intra-articular injection of iodinated contrastmaterial.9
The elbow may also be involved in patientswith systemic inflammatory arthropathies, mostcommonly rheumatoid arthritis. Radiographs maydemonstrate effusion, soft tissue swelling, uniformjoint space narrowing, and later in the disease course,periarticular erosions (Figure 22). Owing to the largeamount of destruction to the articular surfaces, thesepatients often require total elbow arthroplasty(Figure 23). Earlier changes of synovitis and articularirregularity may also be evident on MRI and CT ar-thrography. It is ideal to detect articular involvementmuch earlier as it is now known that initiation oftherapy with disease-modifying antirheumatic drugs
April–June 2007 195

within the first several months of involvement has asignificant effect on long-term outcomes. MRI mayalso be used to monitor effects of therapy. The ‘‘rheu-matoid variants,’’ or seronegative spondyloarthropa-thies (e.g., psoriasis, Reiter’s disease, ankylosing
FIGURE 18. Illustration demonstrating the origin of thecommon extensor tendon on the lateral epicondyle of thedistal humerus.
196 JOURNAL OF HAND THERAPY
spondylitis), are less common causes of inflamma-tory arthropathy at the elbow. Eventually, secondarydegenerative arthritis may develop, which maymask some of the signs of prior erosive damage.Chondrocalcinosis of the elbow may also be
FIGURE 19. Illustration demonstrating the origin of thecommon flexor tendon on the medial epicondyle of thedistal humerus.
FIGURE 20. Coronal proton-density (A) and fat-saturated T2-weighted (B) images of the elbow demonstrate a high-gradepartial thickness tear of the common flexor tendon at its origin on the medial epicondyle.

FIGURE 21. Anteroposterior (A) and lateral (B) radiographs of the left elbow demonstrate a well-seated radial headendoprosthesis in a patient who had previously sustained an intra-articular fracture of the radial head.
radiographically evident. While this finding has beendescribed in association with several disorders, mostoften calcium pyrophosphate deposition disease, or‘‘pseudogout,’’ in our experience this finding isseen most commonly in the setting of degenerativeosteoarthritis.
Synovial chondromatosis and pigmented villo-nodular synovitis (PVNS) are less common synovialprocesses that may manifest in the elbow. Synovialchondromatosis represents synovial metaplasia
producing multiple small cartilaginous or osteocar-tilaginous intra-articular loose bodies that areusually similar in size and when calcified, radio-graphically evident. MRI demonstrates several smallloose bodies with low T1 and T2 signal intensities inthe setting of a high T2 signal intensity effusion.PVNS also demonstrates intra-articular loose bodiesthat demonstrate low signal intensity on standardspin-echo and fast spin-echo T1- and T2-weightedsequences, and characteristic ‘‘blooming’’ artifact
FIGURE 22. Anteroposterior (A) and lateral (B) radiographs of the right elbow demonstrate advanced changes of rheuma-toid arthritis with relatively uniform loss of joint space and prominent periarticular erosive changes (arrow).
April–June 2007 197

FIGURE 23. Anteroposterior (A) and lateral (B) radiographs of the right elbow demonstrate a well-seated total elbowarthroplasty in the patient whose radiographs are shown in Figure 22.
on gradient echo imaging owing to the presence ofhemosiderin (i.e., ‘‘pigmented’’) deposits withinthe bodies.
Osteochondritis dissecans and Panner’s diseasetypically involve the capitellum in younger childrenand adolescents. Osteochondritis dissecans primarilyoccurs in adolescents and likely occurs secondary tocompromise of the tenuous blood supply to thecapitellum that may occur in the setting of repetitivetrauma, as may be seen in the dominant arm inthrowing athletes. While the irregularity of the cap-itellum is usually radiographically evident, MRIplays an essential role in determining the stabilityof the osteochondral fragment. The presence of a high
FIGURE 24. Axial proton-density image of the elbowdemonstrates a normal appearing ulnar nerve within thecubital tunnel (arrow). The retinaculum is formed by aportion of the flexor carpi ulnaris muscle.
198 JOURNAL OF HAND THERAPY
T2 signal intensity (equal to or greater than fluid)surrounding the entire osteochondral fragment sug-gests instability and is an indication for operativestabilization. Panner’s disease, which typically in-volves children aged less than 10 years, may beradiographically evident but at MRI demonstrateslow T1 and increased T2 signal intensity throughoutthe entire capitellum. Panner’s disease, in contrast toosteochondritis dissecans, typically heals with nopersistent deformity of the capitellar articularsurface.
NEUROPATHIES
The radial, median, and ulnar nerves all traversethe elbow joint en route to the hand and are subject toboth direct trauma and injury secondary to masseffect or entrapment neuropathy. Enlargement andindistinctness of a nerve with increased T2 signalintensity constitute the MRI findings of neuropathy.Innervated muscles affected by the damaged nervewill demonstrate increased T2 signal intensity in theacute and subacute periods, with eventual atrophyand fatty replacement of the muscle fibers in the morechronic setting. The ulnar nerve, owing to its rela-tively superficial location within the cubital tunnel(Figure 24), is the most frequently injured nerve in theelbow and is the most common neuropathy about the
FIGURE 25. Axial proton-density (PD) (A, B), axial fat-saturated T2-weighted (C, D), coronal PD (E), and coronalfat-saturated T2-weighted images of the elbow demonstratesurgical release of the retinaculum with transposition ofthe ulnar nerve (arrows).
<

April–June 2007 199

elbow. The ulnar nerve lies deep in the retinaculum ofthe cubital tunnel, which is formed by a portion of theflexor carpi ulnaris muscle and should be sur-rounded by a collar of fat. Multiple disease processescan narrow or ‘‘entrap’’ the ulnar nerve within therelatively limited confines of the cubital tunnel in-cluding osteophytes, masses (e.g., ganglion cystsand tumors), accessory muscle, or an abnormallythickened retinaculum. In the latter case, a releaseand transposition of the ulnar nerve from the cubitaltunnel may be undertaken (Figure 25). Radial andmedian neuropathies due to elbow pathology areless commonly encountered but have been describedin the literature.18–20
REFERENCES
1. Fritz RC, Breidahl WH. Radiographic and special studies:recent advances in imaging of the elbow. Clin Sports Med.2004;23:567–80, ix.
2. Sofka CM, Potter HG. Imaging of elbow injuries in the childand adult athlete. Radiol Clin North Am. 2002;40:251–65.
3. Thornton R, Riley GM, Steinbach LS. Magnetic resonanceimaging of sports injuries of the elbow. Top Magn ResonImaging. 2003;14:69–86.
4. Kaplan LJ, Potter HG. MR imaging of ligament injuries to theelbow. Magn Reson Imaging Clin N Am. 2004;12:221–32, v–vi.
5. Chung CB, Chew FS, Steinbach L. MR imaging of tendonabnormalities of the elbow. Magn Reson Imaging Clin N Am.2004;12:233–45, vi.
6. Kijowski R, Tuite M, Sanford M. Magnetic resonance imagingof the elbow. Part I: normal anatomy, imaging technique, andosseous abnormalities. Skeletal Radiol. 2004;33:685–97.
200 JOURNAL OF HAND THERAPY
7. Kijowski R, Tuite M, Sanford M. Magnetic resonance imagingof the elbow. Part II: abnormalities of the ligaments, tendons,and nerves. Skeletal Radiol. 2005;34:1–18.
8. Chung CB, Stanley AJ, Gentili A. Magnetic resonance imagingof elbow instability. Semin Musculoskelet Radiol. 2005;9:67–76.
9. Waldt S, Bruegel M, Ganter K, et al. Comparison of multisliceCT arthrography and MR arthrography for the detection ofarticular cartilage lesions of the elbow. Eur Radiol. 2005;15:784–91.
10. Finlay K, Ferri M, Friedman L. Ultrasound of the elbow.Skeletal Radiol. 2004;33:63–79.
11. Miller TT, Shapiro MA, Schultz E, Kalish PE. Comparison ofsonography and MRI for diagnosing epicondylitis. J ClinUltrasound. 2002;30:193–202.
12. Miller TT, Adler RS, Friedman L. Sonography of injury ofthe ulnar collateral ligament of the elbow—initial experience.Skeletal Radiol. 2004;33:386–91.
13. Wakefield RJ, Brown A, O’Connor P, et al. Rheumatologicalultrasound. Rheumatology (Oxford). 2003;42:1001.
14. Fowler KA, Chung CB. Normal MR imaging anatomy ofthe elbow. Magn Reson Imaging Clin N Am. 2004;12:191–206, v.
15. Rosenberg ZS, Bencardino J, Beltran J. MRI of normal variantsand interpretation pitfalls of the elbow. Semin MusculoskeletRadiol. 1998;2:141–55.
16. O’Dwyer H, O’Sullivan P, Fitzgerald D, Lee MJ, McGrath F,Logan PM. The fat pad sign following elbow trauma in adults:its usefulness and reliability in suspecting occult fracture.J Comput Assist Tomogr. 2004;28:562–5.
17. Potter HG, Ho ST, Altchek DW. Magnetic resonance imagingof the elbow. Semin Musculoskelet Radiol. 2004;8:5–16.
18. Rosenberg ZS, Bencardino J, Beltran J. MR features of nervedisorders at the elbow. Magn Reson Imaging Clin N Am.1997;5:545–65.
19. Dogan BE, Sahin G, Yagmurlu B, Erden I. Neuroarthropathy ofthe extremities: magnetic resonance imaging features. CurrProbl Diagn Radiol. 2003;32:227–32.
20. Bordalo-Rodrigues M, Rosenberg ZS. MR imaging of entrap-ment neuropathies at the elbow. Magn Reson Imaging Clin NAm. 2004;12:247–63, vi.

JHT Read for CreditQuiz: Article #021
Record your answers on the Return Answer Formfound on the tear-out coupon at the back of this is-sue. There is only one best answer for eachquestion.
#1. The following can be said about imaging of theelbow:a. MRI has excellent potential for further devel-
opment, but radiographs will remain thegold standard throughout the current decade
b. historically radiographs have been the hall-mark, but MRI is becoming the study of choice
c. CT scans are far superior to radiographs andMRI studies
d. imaging is not a primary tool in the diagnosisof elbow problems
#2. Upon presentation to the emergency room, theinitial imaging study to evaluate nonspecific el-bow pain should be:a. MRIb. CT scansc. ultrasoundd. radiographs
#3. The presence of raised fat pads (e.g., sail sign orposterior fat pad sign) suggests:a. morbid obesityb. skeletal immaturityc. effusion in the jointd. osteoporosis
#4. The important medial and lateral collateral liga-ments are best imaged with:a. radiographsb. MRIc. CT scansd. ultrasound
#5. The diagnosis of osteoporosis is routinely madewith the aid of:a. radiographsb. MRIc. CT scansd. ultrasound
When submitting to the HTCC for recertification,please batch your JHT RFC certificates in groupsof three or more to get full credit.
April–June 2007 201





























