Embed Size (px)
Citation preview

Skeletal Radiol (2004) 33:63–79DOI 10.1007/s00256-003-0680-7 R E V I E W A R T I C L E
K. FinlayM. FerriL. Friedman
Ultrasound of the elbow
Received: 14 June 2002Revised: 15 June 2003Accepted: 16 June 2003Published online: 9 January 2004� ISS 2004
K. Finlay · L. Friedman ())McMaster University Departmentof Diagnostic Imaging,Hamilton Health Sciences,Henderson Hospital,711 Concession Street E., Hamilton,Ontario, L8V 1C3, Canadae-mail: [email protected].: +1-905-5274322 ext 42261Fax: +1-905-5752660
M. FerriMcMaster University Departmentof Diagnostic Imaging,McMaster University Medical Centre,1200 Main Street W., Hamilton, Ontario,L8N 3Z5, Canada
Abstract The elbow is an importantsynovial hinge joint of the upperextremity. This joint represents acommon site of musculoskeletalsymptomatology, affecting all agegroups. The advantages of ultrasoundimaging of the elbow include easyavailability, multiplanar capabilityand the ability to assess structuresdynamically. Patient symptomatolo-gy and site of maximal tendernesscan be directly correlated with im-aging findings. Comparison is easilymade with the contralateral side.Particular strengths include the abil-ity to assess para-articular structures,such as regional tendons and liga-ments, in addition to assessment ofjoint effusions, loose bodies and
regional bursae. With operator expe-rience and excellent technique, ultra-sound is a valuable imaging tool forassessment of disorders of the elbowjoint.
Keywords Ultrasound · Elbow ·Tendons · Effusions · Bursitis
Introduction
Ultrasound has emerged as a useful imaging modality forthe diagnosis of joint and soft tissue pathology. The elbowjoint is easily amenable to ultrasound examination, due toits superficial position. Soft tissue elbow pathology iscommon, including para-articular conditions such asepicondylitis, tendon and ligament abnormalities. Thesecan be confused clinically with other diagnoses. Ultra-sound is able to demonstrate the fibrillar microanatomy oftendons, ligaments and muscles, enhancing its diagnosticcapability. Bursal distension and joint effusions are alsoimportant to recognize and easily assessed. Ultrasoundserves as both a strong diagnostic tool and an aid forintervention.
The development of extended field-of-view imagingfurther enhances the ability of ultrasound to image and
document findings [1]. This is often very useful fordemonstrating findings for referring clinicians. It assiststhem in appreciating the extent of pathology andrelationship to adjacent anatomical structures and planes,as is the case with MRI. Limitations of musculoskeletalultrasound include operator-dependence, a long learningcurve and the need for high-resolution ultrasound equip-ment. Operator experience and technology requirementsare important for performing excellent high-qualitystudies. Examinations should be performed with high-resolution, multi-frequency linear transducers.
A complete and successful sonographic examinationrequires an adequate understanding of the anatomy andfunction of the regional soft tissue and bony structures ofthe elbow. It is also important to recognize commondisease patterns and mechanisms of injury, in order toenhance diagnosis. The purpose of this article is to outline

64
the scanning technique for the evaluation of the elbowjoint. The normal ultrasound anatomy of the elbow andsurrounding structures will be illustrated. In addition, thesonographic appearance of common disorders involvingthe elbow and regional structures will be presented in asystematic fashion, with respect to each anatomicalstructure examined.
Technique and pathology
The elbow joint ultrasound examination is performingusing multifrequency linear 10–12 MHz transducers. Onoccasion, particularly when evaluating the ulnar nerve, a10–12 MHz hockey-stick or small footprint probe provesuseful. More recent transducer technology advances,specifically the development of multifrequency trans-ducers, have allowed greater tissue characterizationthrough a process referred to as tissue harmonics. Thistechnology exploits the characteristic resonant frequencyof tissues that fall within the range of diagnosticultrasound. The authors prefer to use a large amount ofgel for superficial structures; however, a standoff padmay be utilized.
Examinations are often tailored to the site of thepatient’s symptomatology, as well as the suspectedanatomical structure involved. It is therefore useful todivide the ultrasound study into anterior, medial, lateraland posterior examinations.
Anterior elbow
Elbow joint
To examine the anterior aspect of the elbow joint, thepatient is positioned sitting, facing the examiner, with thearm extended comfortably on a bedside table or stretcher[2, 3]. Techniques have also been described with thepatient positioned supine [4]. An intimate knowledge ofnormal anatomy is essential to the elbow joint evaluation(Figs. 1, 2). Beginning in the transverse plane (Fig. 3A),the distal humeral cartilage is assessed for smoothnessand uniformity (Fig. 3B). To assess adequately for thepresence of joint effusion and intra-articular bodies, thejoint should be examined in both the longitudinal andtransverse planes. Normally, the anterior fat pad ishyperechoic [5]. In the setting of a joint effusion, thefat pad is displaced anteriorly.
The lateral radiocapitellar joint (Fig. 4) and medialtrochlea-ulnar joint (Fig. 5) are assessed in the longitu-dinal view. Normally, hypoechoic cartilage covers thearticular surfaces. The anterior joint capsule appears as athin hyperechoic line overlying the cartilage, with anadjacent thin layer of joint fluid [6]. The brachialis
muscle lies immediately anterior to the joint capsulemedially and brachioradialis muscle laterally.
The radial neck and annular recess are assessed in thelongitudinal and transverse planes. The coronoid fossa isalso examined in both planes. It is often useful to supinateand pronate the forearm, to assist in the detection of loosebodies in these regions [7].
Fig. 1 Anterior view of the elbow joint
Fig. 2 Cross-sectional view of the elbow joint

65
Joint pathology
Effusions
Elbow joint effusions are easily detected by ultrasoundand may be medial or lateral, free-flowing or loculated.The normal elbow fat pads lie between the fibrous capsuleand the synovial lining, with the posterior fat pat in theolecranon fossa larger than the anterior fat pad in thecoronoid fossa. The joint capsule is easily identifiedposteriorly, lying deep to the triceps tendon and super-ficial to the posterior fat pad. The capsule appears as alinear transverse echogenic structure, with normal thick-ness in the adult population approaching 2 mm [6]. Itrepresents a relatively lax or weak fibrous capsule that isreinforced laterally by the collateral ligaments. Effusion
results in the displacement or elevation of both theanterior and posterior fat pads and distension of the jointcapsule [8, 9] (Fig. 6). This displacement is equivalent tothe sail sign seen on plain radiographs. Ultrasound is veryuseful for distinguishing extra-articular soft tissue swell-ing from joint disease [10, 11].
Positioning of the elbow can change the distribution ofjoint fluid. Sonography is more sensitive for diagnosingjoint fluid with the elbow flexed; however, the fluid isbetter identified posteriorly rather than anteriorly. In thisflexed position, 1–3 ml of joint fluid can be identified,compared with the 5–10 ml required for identification of aposterior fat pad on plain films [8]. Anteriorly, ultrasoundis less sensitive than MRI for detecting small jointeffusions [8]. When examining joints with ultrasound, it isimportant to distinguish hypoechoic fluid from hypo-
Fig. 4A, B Anterior elbow. A Transducer position for longitudinalanterior imaging of the radiocapitellar joint. B Correspondingextended field-of-view image demonstrating the radial fossa
(arrow), capitellum (C) and radial head (R). The brachioradialismuscle (BR) is seen anteriorly
Fig. 3A, B Anterior elbow. ATransducer position for trans-verse anterior imaging of thedistal humerus. B Correspond-ing transverse ultrasound im-age, demonstrating the humeralcapitellum (HC) and humeraltrochlea (HT). Note the bonyarticular cortex (arrow), normalhypoechoic cartilage (star) andoverlying brachialis muscle (Br)

66
echoic cartilage. Once fluid has been identified, ultra-sound can easily guide joint aspiration [12].
Simple effusions are usually anechoic and suggest anacute process. Infection, hemarthrosis and trauma canresult in complex fluid with increased echogenicity.Debris is often related to small loose bodies, inflamma-tory or hemorrhagic material. Septic arthritis must berecognized early, in order to avoid aggressive, irreversibleloss of joint function, with ultrasound serving as avaluable imaging tool for diagnosis of joint fluid andassistance in joint aspiration [13, 14]. Absence of a jointeffusion can spare the patient unnecessary needle aspira-tion.
Synovial thickening can be distinguished from jointfluid with the aid of graded compression. Synovialthickening and nodularity can be visualized by ultra-sound, with power Doppler flow present in acute inflam-matory processes [15, 16, 17, 18]. Pannus or thickenedsynovium demonstrates decreased echogenicity comparedwith adjacent soft tissues [2, 15, 16]. Capsular thickeningmay also indicate synovitis [19].
Distal biceps tendon
The distal portion of the biceps tendon is assessed in boththe longitudinal (Fig. 7A) and transverse planes. It can beidentified traversing superficial to the brachialis muscle.Adequate evaluation of the biceps tendon is challenging,as the tendon takes a deep oblique course towards itsinsertion on the radial tuberosity (Fig. 7B). In addition,the tendon fans out distally, with a very flat configurationat the point of attachment to the radial tuberosity. It is
Fig. 6 Joint effusion. Transverse (top) and longitudinal images(bottom) demonstrate hypoechoic fluid (arrow) distending theelbow joint anteriorly, consistent with a joint effusion. HC humeralcapitellum, HT humeral trochlea, RH radial head. Note thedisplaced anterior joint capsule (small arrow)
Fig. 5A, B Anterior elbow. A Transducer position for longitudinalanterior imaging of the medial joint. B Corresponding extendedfield-of-view image demonstrating the coronoid fossa (arrow),
trochlea (T), and coronoid process (CP) of the ulna. The brachialis(Br) muscle is seen anteriorly

67
therefore useful to place the forearm in maximalsupination in order to evaluate the distal course of thebiceps tendon as it inserts onto the tuberosity of theradius [20].
Distal biceps tendon rupture
The ability to assess tendons is a particular strength ofultrasound, as it is able to clearly visualize and evaluatethe fibrillar echotexture of normal tendons. Ultrasound isparticularly good for assessing degree of tendon retraction[15, 21].
Normally, the distal biceps tendon is formed approx-imately 7 cm above the elbow joint. Distal ruptures,common in weightlifters, consist of avulsion of the tendonfrom the site of attachment on the radial tuberosity. Theclassic clinical history consists of sudden anterior painand a popping or tearing sensation, experienced during alifting maneuver. Complete rupture of the tendon oftenoccurs as a single traumatic injury, with forced extensionagainst an elbow positioned in mid-flexion. Clinicallythere is often a palpable defect in the antecubital fossa,proximal soft tissue mass and difficulty with flexion andsupination.
On ultrasound, complete tears present as a hypoechoicgap between the proximal retracted tendon fragment andthe radial tuberosity. Hematoma can be seen distally,identified as variable amounts of fluid in the gap (Fig. 8).Most tears have associated tendon retraction, makingthem easier to recognize than those not associated withretraction (Fig. 9). While retracted complete tears can beobvious clinically, ultrasound is a useful imaging modal-ity for identifying non-retracted or partial-thickness tears[20, 22]. Partial-thickness tears may present with abnor-mal undulation of the tendon fibers, without retraction.These findings have significant implications for clinicalmanagement, as partial tears are treated conservatively
Fig. 7A, B Anterior elbow. A Transducer position for longitudinalassessment of the distal biceps tendon. B Corresponding imageillustrating the steep oblique course of the tendon (arrow) at its
point of insertion onto the radial tuberosity (RT). P proximal, Ddistal
Fig. 8 Torn distal biceps tendon. Hematoma fills the course of thetendon, with a retracted distal biceps tendon tear (arrow, rightimage). Compare this with the course of the normal tendon (arrow,left image). A complete tear was confirmed at surgery (arrow,lower image). RT radial tuberosity, P proximal, D distal

68
whereas full-thickness tears need acute surgical interven-tion.
Medial elbow
The flexor tendon
To examine the medial aspect of the elbow, the patient ispositioned with the elbow in extension and the forearmfully supinated (Fig. 10A). Longitudinal images of themedial epicondyle and common flexor origin are obtained(Fig. 10B). Typically, the common flexor tendon appearsas a hyperechoic “beak” or triangle. The medial commonflexor origin is normally broader than the lateral commonextensor origin. Assessment of thickening, calcifications
and local tenderness is made. Comparison between thetwo elbows is frequently warranted, in order to appreciatesubtle differences.
Medial epicondylitis and tears
Medial epicondylitis is commonly referred to as “golfer’selbow”.
With epicondylitis, the tendon often appears thick andheterogeneous on ultrasound, with focal hypoechoicareas. It is extremely useful to compare findings withthose of the unaffected contralateral elbow. The findingmay be discrete, or the tendon may be diffusely affected[23]. In the chronic phase, calcifications can be identified[15, 23, 24]. Partial- or full-thickness tears can occur withchronic tendinosis or may be unrelated, secondary to anacute traumatic episode (Fig. 11).
Ulnar (medial) collateral ligament
The ulnar collateral ligament is composed of threecomponents: anterior, posterior and oblique bands [25](Fig. 12). The anterior band is strong and cord-like andbecomes taut with elbow extension. It is located betweenthe anteroinferior aspect of the medial epicondyle and themargin of the medial coronoid process. It plays animportant role in stability with valgus stress, particularlywhen the elbow is extended [21, 26]. Conversely, theposterior band is weak, fan-like and becomes taut uponelbow flexion. It extends between the posteroinferiormedial epicondyle and the medial olecranon margin. Theoblique fibers serve to deepen the socket for the trochlearprocess of the humerus, and play a minimal role in elbowjoint stabilization [25, 27].
Ultrasound examination is usually confined to theanterior band, this being the most important functionallyand the most readily visible. It normally appears as a
Fig. 10A, B Medial elbow. ALongitudinal transducer posi-tion and B corresponding ultra-sound image for evaluation ofthe common flexor tendon ori-gin. The tendon demonstrates acompact fibrillar appearance(arrow). ME medial epicondyle,CP coronoid process
Fig. 9 Torn distal biceps tendon. Longitudinal ultrasound image(right), demonstrates a torn distal biceps tendon, with retractedproximal end (large arrow) and distal end (small arrow). Thecorresponding MR image (left) obtained shortly after the ultrasoundconcurs with the ultrasound finding, demonstrating a torn distalbiceps tendon (arrow). P proximal, D distal

69
hyperechoic, fibrillar structure, arising from the distalulna, inserting onto the medial epicondyle [28] (Fig. 13).
Ulnar (medial) collateral ligament tears
Tears occur with abnormal valgus stress at the elbow andmay also be associated with avulsion injuries in younger
patients. Tears are often sports-related [29]. Sonograph-ically, they present as partial or complete disruption ofthe normal ligamentous fibers (Fig. 14). Imagingassessment is important, as arthroscopy is limited in itsability to visualize this structure. Partial tears are treated
Fig. 12 Medial view of the elbow joint, demonstrating theorientation of the ulnar (medial) collateral ligament
Fig. 13 Ulnar (medial) collat-eral ligament. The normal ap-pearance of this ligament isindicated with an arrow, bridg-ing between the medial epicon-dyle (ME) and the ulnarcoronoid process (CP)
Fig. 11 Acute complete traumatic tear of the common flexortendon. Both the longitudinal (middle) and transverse images(right) demonstrate disruption of the normal common flexor
tendon. Compare these with the normal appearance of the commonflexor tendon on the contralateral side (left). ME medial epicondyle
Fig. 14 Torn anterior band of the ulnar (medial) collateralligament. An oblique longitudinal image of the medial elbow (leftimage) demonstrates disruption of normal fibers, indicating a tear(arrow). Compare this with the normal appearance of the anteriorband, ulnar collateral ligament (arrow, right image). ME medialepicondyle, CP coronoid process

70
conservatively while full-thickness tears may requireearly surgical intervention, particularly if the tear affectsfunction, as is the case with athletes. If the tear iscomplete and does not affect function, complete tearsmay be treated conservatively. With chronic injuries,secondary to repetitive microtrauma, the ligament maydegenerate, demonstrating thickening, calcifications,hypoechoic areas and tears [30]. Dynamic assessmentwith ultrasound at rest and with valgus stress has beenadvocated for assessment of ligament integrity or laxity[28, 30, 31].
Epitrochlear lymph node enlargement
Regional lymph node enlargement can present clinicallyas a palpable soft tissue nodule or mass. Ultrasoundreveals the typical appearance of lymph nodes as a solid“kidney-bean”-shaped structure, with a central echogenicnotch (Fig. 15). Lymphatic drainage of the forearm islimited to the medial epitrochlear nodes. Nodal enlarge-ment can present as a tender, discrete palpable mass at themedial aspect of the elbow joint [16, 32]. These nodes areclassically involved with cat-scratch disease.
Lateral elbow
Common extensor tendon
To examine the lateral aspect of the elbow, the patient ispositioned with the elbow flexed, forearm extended andpalm down or halfway between supination and pronation(Fig. 16A). The lateral epicondyle and common extensororigin are examined in the longitudinal plane. Thecommon extensor origin has a uniform hyperechoictriangular configuration and can be seen traversing thelateral aspect of the radiocapitellar joint (Fig. 16B). Thesuperficial tendon consists of tendon fibers from theextensor carpi radialis brevis, extensor digitorum, exten-sor digiti minimi and extensor carpi ulnaris. The deepfibers are predominantly formed by the extensor radialisbrevis. At the level of the lateral epicondyle, these fibersblend together to form the common extensor tendonorigin.
Fig. 15 Epitrochlear lymph node. The patient was referred with apalpable nodule at the medial aspect of the elbow joint. Ultrasoundimage reveals the typical appearance of a lymph node with ahypoechoic “kidney-bean”-shaped structure (large arrow) andechogenic fatty hilum (small arrow)
Fig. 16A, B Lateral elbow. A Longitudinal transducer position for evaluation of the common extensor tendon origin. B Correspondinglongitudinal ultrasound image demonstrating the tendon (arrow) at the level of the lateral epicondyle (LE). RH radial head

71
Lateral epicondylitis and tears
The most common soft tissue abnormality affecting theelbow joint is lateral epicondylitis. This is commonlyknown as “tennis elbow”, and is thought to be secondaryto chronic repetitive stress. It is often a self-limitedcondition, diagnosed on clinical examination. Frequentlythis responds to conservative treatment and does notrequire imaging for diagnosis [33]. In persistent cases, orpatients being considered for surgical therapy, ultrasoundcan prove a valuable imaging modality for confirmationof diagnosis, and assessment of severity and extent ofinvolvement [23].
With epicondylitis, often the tendon origin appearsthick and hypoechoic on ultrasound [34] (Fig. 17). Thefinding may be discrete, or the tendon may be diffuselyaffected [23]. Acutely, one may also see increased powerDoppler flow with soft tissue inflammation [18](Fig. 18). Deep tendon fiber injury at the commonextensor origin has been reported as more common thanmiddle or superficial fiber changes [23]. Hypoechoiclinear changes or clefts within the substance of thetendon are thought to represent partial-thickness tears(Fig. 19), with complete disruption representing full-thickness defects [23]. These tears are often identified intendons with diffuse changes of tendinopathy. Tears areimportant to identify, as they are less likely to respond toconservative therapy, often requiring surgical consulta-tion. Chronic epicondylitis or tendon injury is associatedwith tendon thickening and calcification [15, 24]. Occa-sionally cortical irregularity or spur formation may beidentified on the epicondyle [23]. It is important not to
confuse the hypoechoic affect created by anisotropy withtendinosis or a partial tear. With anisotropy, the hypo-echoic area fills in by angling the transducer perpendic-ular to the tendon fibers (Fig. 20), whereas true pathologyremains hypoechoic.
Fig. 17 Lateral epicondylitis, focal. Longitudinal extended field-of-view image of the common extensor tendon (bottom) demon-strates abnormal focal swelling and hypoechogenicity (arrow).Compare this with the echogenic fibrillar pattern of the normaltendon (top, arrow). LE lateral epicondyle, RH radial head, CEcommon extensor tendon
Fig. 18 Lateral epicondylitis, diffuse. Abnormal common extensortendon (left image), demonstrating extensive tendon thickening andhypoechoic change (arrow). This is associated with abnormalincreased power Doppler flow (arrow, right image). LE lateralepicondyle, RH radial head, P proximal, D distal
Fig. 19 Partial-thickness tear, common extensor tendon. Longitu-dinal image (top) demonstrates a small hypoechoic area centrallywithin the tendon (arrow), consistent with a small partial-thicknesstear. Note the hyperemia with power Doppler assessment. Follow-up ultrasound examination (bottom) shows progression of the tear(arrow). LE lateral epicondyle, RH radial head

72
Posterior elbow
Triceps tendon and olecranon fossa
The patient is positioned with the elbow flexed at 90� andthe forearm fully pronated (Fig. 21A). In the longitudinalprojection, the distal triceps tendon can be followed to itsinsertion on the proximal aspect of the olecranon
(Fig. 21B). To examine the olecranon fossa properly,both longitudinal and transverse views are required(Fig. 22A). The fossa is normally filled with echogenicfat (Fig. 22B). This region can also be assessed for thepresence of loose bodies or effusion. Dynamic assessmentcan supplement the posterior elbow examination, partic-ularly in the setting of suspected ulnar nerve dislocationor snapping triceps syndrome [35]. To perform this, thetriceps tendon and ulnar nerve are evaluated for locationand appearance during varying degrees of flexion andextension.
Joint aspiration is best performed at the elbow jointwith a posterior approach [12]. Aside from the tricepstendon, the olecranon fossa has no additional importantneurovascular structures present, minimizing the risk ofcomplications.
Triceps tendon tear
Triceps tendon tears are uncommon. They may beassociated with avulsion fractures of the olecranonprocess, and are usually caused by excess stress on thecontracted muscle. Tears may be partial or complete.Causes include direct trauma, systemic diseases, steroidtherapy, renal disease and olecranon bursitis. On ultra-sound, disruption of the normal tendon appearance is seen(Fig. 23). An associated avulsion fracture may also beidentified by ultrasound [36]. As this injury is usuallyevident clinically, the role of ultrasound is to determinethe extent of the tear and assess the degree of retraction, ifany. Longitudinal scanning during flexion and extensionis extremely helpful in helping in distinguishing a partial
Fig. 21A, B Posterior elbow. A Patient position (left) and probeorientation (right) for longitudinal posterior elbow joint evaluation.B Corresponding sagittal extended field-of-view image shows the
olecranon fossa (arrow). Note the triceps muscle and tendon (TR)inserting onto the olecranon (O)
Fig. 20 Anisotropy. Longitudinal image of the common extensortendon showing an apparent hypoechoic area (arrowhead, topimage) due to anisotropy, corrected by angling the transducerperpendicular to the tendon surface (arrowhead, bottom image) LElateral epicondyle, RH radial head

73
tear, where residual fibers remain intact, from a non-retracted rupture, where all the fibers are torn.
Ulnar nerve
The ulnar nerve can be identified within the medialolecranon groove. To image the nerve, the transducer isbridged from the olecranon to medial epicondyle(Figs. 24). On transverse imaging, normal nerves appearas oval or round hypoechoic structures, interspersed bymultiple, discrete, slightly echogenic foci [37]. Theechogenic foci represent the nerve fascicles in cross-section. The ulnar nerve is normally of uniform thicknessand typically measures approximately 2 mm by 3 mm, in
the posterior aspect of the fossa [38]. Comparison withthe contralateral side is often useful in cases of suspectedtendon enlargement or atrophy. If subluxation or dislo-cation is suspected, dynamic examination with flexionand extension should be performed [35]. In these differentpositions, the location of the ulnar nerve relative to themedial epicondyle can be assessed and dynamicallyevaluated. Dislocation is confirmed when the ulnar nerveis documented lying over the apex of the medialepicondyle, with the elbow in flexion [35].
It is important to mention that the ulnar nerve can justas easily be imaged medially with the elbow extended orsemi -flexed and the forearm supinated. Longitudinally,the ulnar nerve appears as a cord-like hypoechoicstructure, with parallel hyperechoic linear structures
Fig. 23 Torn triceps tendon.Longitudinal ultrasounddemonstrates complete disrup-tion of the normal triceps ten-don (left) with the position ofthe proximal retracted tendonmarked by an arrow. Comparethis with the normal appearanceof the triceps tendon (arrow,middle) and corresponding sag-ittal MR image (arrow, right),showing a tear in the longitudi-nal plane, with a retractedproximal tendon (arrow). Oolecranon, P proximal, D distal
Fig. 22A, B Posterior elbow. AProbe position for evaluation ofthe posterior elbow joint. BCorresponding transverse imageof the olecranon fossa (arrow).M medial, L lateral
74
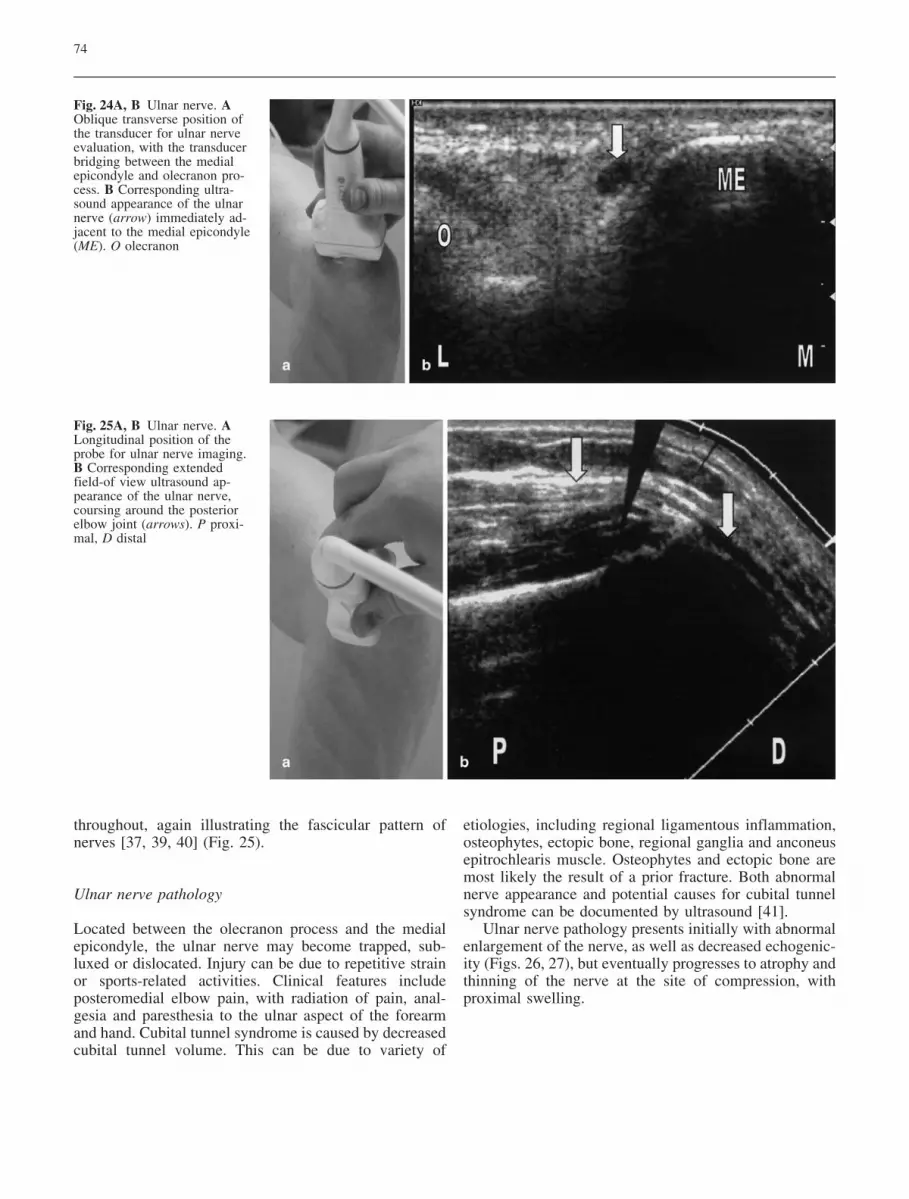
throughout, again illustrating the fascicular pattern ofnerves [37, 39, 40] (Fig. 25).
Ulnar nerve pathology
Located between the olecranon process and the medialepicondyle, the ulnar nerve may become trapped, sub-luxed or dislocated. Injury can be due to repetitive strainor sports-related activities. Clinical features includeposteromedial elbow pain, with radiation of pain, anal-gesia and paresthesia to the ulnar aspect of the forearmand hand. Cubital tunnel syndrome is caused by decreasedcubital tunnel volume. This can be due to variety of
etiologies, including regional ligamentous inflammation,osteophytes, ectopic bone, regional ganglia and anconeusepitrochlearis muscle. Osteophytes and ectopic bone aremost likely the result of a prior fracture. Both abnormalnerve appearance and potential causes for cubital tunnelsyndrome can be documented by ultrasound [41].
Ulnar nerve pathology presents initially with abnormalenlargement of the nerve, as well as decreased echogenic-ity (Figs. 26, 27), but eventually progresses to atrophy andthinning of the nerve at the site of compression, withproximal swelling.
Fig. 25A, B Ulnar nerve. ALongitudinal position of theprobe for ulnar nerve imaging.B Corresponding extendedfield-of view ultrasound ap-pearance of the ulnar nerve,coursing around the posteriorelbow joint (arrows). P proxi-mal, D distal
Fig. 24A, B Ulnar nerve. AOblique transverse position ofthe transducer for ulnar nerveevaluation, with the transducerbridging between the medialepicondyle and olecranon pro-cess. B Corresponding ultra-sound appearance of the ulnarnerve (arrow) immediately ad-jacent to the medial epicondyle(ME). O olecranon

75
Olecranon bursitis
Bursae are flattened potential spaces that are lined bysynovial cells, often present between a tendon andunderlying bone, or within superficial soft tissues. Theymay contain fluid and may or may not communicate withthe adjacent joint. On ultrasound, bursae appear ashypoechoic clefts in the soft tissue, often bounded by ahyperechoic periphery. Synovial thickening and prolifer-ation can be observed, particularly in rheumatoid arthritisand other chronic inflammatory conditions. Long-stand-ing effusions result in fibrous adhesions or debris.Echogenic material identified within bursae may indicateinflammatory, hemorrhagic or infectious etiologies. Theappearance on ultrasound alone cannot distinguish infect-ed from non-infected bursal fluid collections. Clinicaldifferentiation between bursitis and tendon pathology isoften difficult; however, these two entities are easilydifferentiated by ultrasound examination. There are bothsuperficial and deep bursae present around the elbow[42].
Olecranon bursitis is a common superficial bursitis,which may result from direct trauma, repetitive stress andor friction [42] (Fig. 28). It is often painless, unless thesynovium is inflamed. Olecranon bursitis changes onultrasound consist of fluid distension of the bursa. Withactive inflammatory change, power Doppler assessmentmay demonstrate increased flow within the bursal lining[18]. Infection and arthropathies such as rheumatoidarthritis, crystal deposition diseases (calcium pyrophos-phate depositional disease, hydroxyapatite deposition,gout), and pigmented villonodular synovitis are alsopossible etiologies. Ultrasound is helpful for distinguish-ing between bursal distension and chronic fibrosis of theoverlying soft tissues.
Fig. 27 Ulnar nerve enlargement. Transverse ultrasound shows anabnormal enlarged ulnar nerve (arrow, right), with the correspond-ing normal ulnar nerve (arrow, left). O olecranon, ME medialepicondyle
Fig. 26 Ulnar neuropathy.Longitudinal ultrasounddemonstrates abnormal fusi-form enlargement of the ulnarnerve (arrow, left). Comparethis with the corresponding im-age of the normal ulnar nerve(arrow, right) P proximal, Ddistal
Fig. 28 Olecranon bursitis. Longitudinal ultrasound image (upper,left) demonstrates abnormal fluid within the olecranon bursa(arrow). Increased power Doppler flow is present surrounding thebursa on the transverse (upper right) and longitudinal images(lower left). Ultrasound findings underlie a clinically palpable areaof tender swelling over the posterior elbow (arrow, lower right). Oolecranon

76
Miscellaneous
Intra-articular bodies
The elbow is a common joint affected by intra-articularbodies. Patients may present with limited flexion orextension, intermittent locking or pain. These bodies canbe identified by ultrasound, and are often found in thesynovial recesses. This includes the radial neck recess,coronoid fossa and olecranon fossa. Less commonly, theymay be located within the lateral and medial recesses.They may be loose, trapped in synovial folds or adherentto the synovial lining. On ultrasound they appear as focalhyperechoic foci, if calcified, which are separate fromadjacent bony structures (Fig. 29). They may be sur-rounded by joint fluid [43]. Real-time imaging maydemonstrate movement of these bodies. Intra-articularbodies can be difficult to identify with plain films and, ifnon-calcified, can prove difficult to visualize with cross-sectional imaging such as CT or MRI, in the absence ofjoint fluid or arthrographic injection. Intra-articularinjection with saline has been reported to increase thedetection of intra-articular bodies of the elbow onultrasound [43, 44].
Fig. 30 Synovial osteochon-dromatosis. Transverse (right)and longitudinal images (left) ofthe olecranon fossa demonstratemultiple hyperechoic nodularintra-articular bodies (arrow)filling the joint space, biopsy-proven as synovial osteochon-dromatosis
Fig. 29 Loose bodies. Longitudinal (left) and transverse (right)images of the olecranon fossa (OF) demonstrate an echogenic loosebody separate from the underlying bone (arrows)
Fig. 31 Radial head fracture. Longitudinal ultrasound image of theradial head (right) demonstrates disruption of the normal smootharticular surface, with a small bony fragment present (arrow). Theinitial radiograph at the time of injury was reported as showing a
joint effusion but no definitive fracture. Fracture was confirmedwith a repeat radiograph taken at the time of the ultrasoundexamination (left) C capitellum, RH radial head

77
In acute injury, the intra-articular bodies are oftenosteochondral fragments. In the setting of chronic jointpathology, they are thought to be secondary to osteoar-throsis, chronic repetitive trauma and, more rarely,synovial osteochondromatosis (Fig. 30).
Fig. 32 Radial neck fracture. Longitudinal ultrasound image of theradial neck demonstrates subtle disruption of the smooth radialneck contour (arrow, top left), compared with normal (top right).While radiographs remain inconclusive (lower left), CT withsagittal reformatting confirms the presence of a subtle fracture(arrow, bottom right). C capitellum, R radial head
Fig. 33 Accessory ossicle. The ultrasound image must be corre-lated with the plain film findings, in order to avoid mistakingaccessory ossicles. The longitudinal image at the level of the medialjoint space demonstrates a small separate bone lesion (arrow, right)identified as an accessory ossicle with plain film correlation(arrow, left)
Fig. 34 Hardware complication. Radiograph (top left) demonstratesa portion of surgical staple positioned in soft tissue, rather than theolecranon process. Ultrasound, performed to assess the integrity ofthe triceps tendon, demonstrates the staple lying beyond theolecranon process, within the soft tissues (arrow, bottom left). Thehead of the screw projecting beyond the periosteal margin can alsobe identified on ultrasound (arrow, bottom right), and correlateswith frontal radiography (arrow, top right). Care must be taken notto misdiagnose these as a fracture fragments or loose bodies
Fig. 35 Tubercular infection of the elbow. Frontal view of thedistal humerus (top left) demonstrates diffuse periosteal reaction, aswell as a more focal area of lucency involving the metaphysis(arrow). Axial T1-fat-suppressed post-gadolinium MR image (topright) demonstrates extensive, diffuse enhancement of the synovi-um, as well as enhancement within the intercondylar portion of thehumerus (stars). Transverse and longitudinal US images (bottomleft and right) clearly demonstrate an abnormal hypoechoicappearance within the joint capsule (arrows), proven to representextensive caseous material on biopsy. Images courtesy of Dr. M.Azouz, Montreal Children’s Hospital, Canada

78
References
1. Barberie JE, Wong AD, CooperbergPL, Carson BW. Extended field-of-view sonography in musculoskeletaldisorders. AJR Am J Roentgenol 1998;171:751–757.
2. Martinoli C, Bianchi S, Giovagnorio F,Pugliese F. Ultrasound of the elbow.Skeletal Radiol 2001; 30:605–614.
3. Martinoli C, Bianchi S, Zamorani MP,Zunzunegui JL, Derchi LE. Ultrasoundof the elbow. Eur J Ultrasound 2001;14:21–27.
4. Barr LL, Babcock DS. Sonography ofthe normal elbow. AJR Am J Roent-genol 1991; 157:793–798.
5. Miles KA, Lamont AC. Ultrasonicdemonstration of the elbow fat pads.Clin Radiol 1989; 40:602–604.
6. Hogan MJ, Rupich RC, Bruder JB, BarrLL. Age-related variability in elbowjoint capsule thickness in asymptomaticchildren and adults. J Ultrasound Med1994; 13:211–213.
7. Bianchi S, Martinoli C. Detection ofloose bodies in joints. Radiol ClinNorth Am 1999; 37:679–690.
8. De Maeseneer M, Jacobson JA, Jao-visidha S, et al. Elbow effusions:distribution of joint fluid with flexionand extension and imaging implica-tions. Invest Radiol 1998; 33:117–125.
9. Koski JM. Ultrasonography of the el-bow joint. Rheumatol Int 1990; 10:91–94.
10. Markowitz RI, Davidson RS, Harty MP,Bellah RD, Hubbard AM, RosenbergHK. Sonography of the elbow in infantsand children. AJR Am J Roentgenol1992; 159:829–833.
11. Loyer EM, Dubrow RA, David CL,Coan JD, Eftekhari F. Imaging ofsuperficial soft-tissue infections: sono-graphic findings in cases of cellulitisand abscess. AJR Am J Roentgenol1996; 166:149–152.
12. Fessell DP, Jacobson JA, Craig J, et al.Using sonography to reveal and aspiratejoint effusions. AJR Am J Roentgenol2000; 174:1353–1362.
13. Lim-Dunham JE, Ben-Ami TE, Yousef-zadeh DK. Septic arthritis of the elbowin children: the role of sonography.Pediatr Radiol 1995; 25:556–559.
14. Bureau NJ, Chhem RK, Cardinal E.Musculoskeletal infections: US mani-festations. Radiographics 1999;19:1585–1592.
15. van Holsbeeck MT, Introcaso JH.Musculoskeletal ultrasound, 2nd edn. StLouis: Mosby-Year Book, 2001.
Occult fractures
Injuries to the skeletally immature elbow often present adiagnostic challenge. This is particularly true with non-ossified epiphyses, as the utility of plain film radiographyis limited. Ultrasound has a diagnostic advantage overplain radiographs, due to its ability to visualize cartilage[10, 45, 46]. Ultrasound can also supplement injury
assessment, by documenting the degree of stability. Thiscan be accomplished with manipulation of the elbowjoint, under sedation or stress testing in the operatingroom [45]. Subtle buckle fractures can be identified byultrasound. The site of injury may be identified withcareful attention to associated subperiosteal hematoma oroverlying soft tissue swelling [19]. Sonography has alsobeen explored as an imaging tool for assessment ofosteochondritis dissecans of the humeral capitellum, aswell as medial epicondyle avulsion injuries [47, 48, 49].
In all age groups, elbow ultrasound has potential fordiagnosing occult fractures unrecognized by plain filmassessment [3]. Radial head fractures are common, andmay be incidentally detected in patients with undiagnosedelbow pain and normal plain radiographs (Figs. 31, 32).The presence of a joint effusion or hemarthrosis isstrongly suggestive of a fracture. Care must be taken toavoid the misdiagnosis of accessory ossicles or intra-articular bodies as avulsion fractures (Fig. 33). Compli-cations of orthopedic procedures can also be assessed orrecognized with ultrasound examination (Fig. 34).
Ultrasound-guided aspiration and biopsy
With its portability, excellent soft tissue imaging, and thefact that it is usually readily available, ultrasoundprovides an economical and accurate method of aspiratinga joint, or obtaining a tissue sample of an intra-articular orjuxta-articular mass (Figs. 35, 36). Ultrasound is able toguide the needle to the most appropriate fluid collectionor safest site for biopsy, by directing the needle awayfrom vessels and nerves under real time.
Fig. 36 Osteogenic sarcoma. Ultrasound in the longitudinal planewas used to guide the biopsy needle posteriorly into the olecranonfossa, at the site of posterior exophytic extension of the tumour(arrow, left). The corresponding spin echo T1-weighted longitudi-nal MR image (right) also demonstrates the soft tissue mass(arrow). H humerus, O olecranon

79
16. Chhem RK, Cardinal E, eds. Guidelinesand gamuts in musculoskeletal ultra-sound. New York: Wiley, 1999.
17. Breidahl WH, Newman JS, TaljanovicMS, Adler RJ. Power Doppler sonog-raphy in the assessment of musculo-skeletal fluid collections. AJR Am JRoentgenol 1996; 166:1443–1446.
18. Newman JS, Adler RS, Bude RO,Rubin JM. Detection of soft-tissue hy-peremia: value of power Doppler so-nography. AJR Am J Roentgenol 1994;163:385–389.
19. Barr LL. Elbow. Clin Diagn Ultrasound1995; 30:135–149.
20. Miller TT, Adler RS. Sonography oftears of the distal biceps tendon. AJRAm J Roentgenol 2000; 175:1081–1086.
21. Potter HG. Imaging of posttraumaticand soft tissue dysfunction of the elbow.Clin Orthop 2000; 370:9-18.
22. Lozano V, Alonso P. Sonographic de-tection of the distal biceps tendonrupture. J Ultrasound Med 1995;14:389–391.
23. Connell D, Burke F, Coombs P, et al.Sonographic examination of lateralepicondylitis. AJR Am J Roentgenol2001; 176:777–782.
24. Lin J, Jacobson JA, Fessell DP, Wead-ock WJ, Hayes CW. An illustratedtutorial of musculoskeletal sonography.2. Upper extremity. AJR Am J Roent-genol 2000; 175:1071–1079.
25. Agur AMR, Grant JC, Lee MJ. Grant’satlas of anatomy. Baltimore: Lippincott,Williams & Wilkins, 1999.
26. Daniels DL, Mallisee TA, Erickson SJ,Boynton MD, Carrera GF. The elbowjoint: osseous and ligamentous struc-tures. Radiographics 1998; 18:229–236.
27. Morrey BF. Anatomy of the elbowjoint. In: Morrey BF, ed. The elbow andits disorders, 2nd edn. Philadelphia:Saunders, 1993:16–52.
28. Ward SI, Teefey SA, Paletta GA Jr, etal. Sonography of the medial collateralligament of the elbow: a study ofcadavers and healthy adult male vol-unteers. AJR Am J Roentgenol 2003;180:389–394.
29. Gaary EA, Potter HG, Altchek DW.Medial elbow pain in the throwingathlete: MR imaging evaluation. AJRAm J Roentgenol 1997; 168:795–800.
30. Nazarian LN, McShane JM, CiccotteMG, O’Kane PL, Harwood MI. Dy-namic US of the anterior band of theulnar collateral ligament of the elbow inasymptomatic major league baseballpitchers. Radiology 2003; 227: 149–154.
31. De Smet AA, Winter TC, Best TM,Bernhardt DT. Dynamic sonographywith valgus stress to assess elbow ulnarcollateral ligament injury in baseballplayers. Skeletal Radiol 2002; 31:671–676.
32. Barr LL, Kirks DR. Ultrasonography ofacute epitrochlear lymphadenitis. Pe-diatr Radiol 1993; 23:72–73.
33. Sevier TL, Wilson JK. Treating lateralepicondylitis. Sports Med 1999;28:375–380.
34. Miller TT, Shapiro MA, Schultz E,Kalish PE. Comparison of sonographyand MRI for diagnosing epicondylitis. JClin Ultrasound 2002; 30:193–202.
35. Jacobson JA, Jebson PJL, Jeffers AW,Fessell DP, Hayes CW. Ulnar nervedislocation and snapping triceps syn-drome: diagnosis with dynamic sonog-raphy—report of three cases. Radiology2001; 220:601–605.
36. Kaempffe FA, Lerner RM. Ultrasounddiagnosis of triceps tendon rupture. ClinOrthop 1996; 332:138–142.
37. Fornage BD. Peripheral nerves of theextremities: imaging with US. Radiol-ogy 1988; 167:179–182.
38. Okamoto M, Abe M, Shirai H, Ueda N.Morphology and dynamics of the ulnarnerve in the cubital tunnel: observationby ultrasonography. J Hand Surg [Br]2000; 25:85–89.
39. Loewy J. Sonoanatomy of the median,ulnar and radial nerves. Can AssocRadiol J 2002; 53:33–38.
40. Silvestri E, Marinoli C, Derchi LE,Bertolotto M, Chiaramondia M,Rosenberg I. Echotexture of peripheralnerves: correlation between US andhistologic findings and criteria to dif-ferentiate tendons. Radiology 1995;197:291–296.
41. Okamoto M, Abe M, Shirai H, Ueda N.Diagnostic ultrasonography of the ulnarnerve in cubital tunnel syndrome. JHand Surg [Br] 2000; 25:499–502.
42. Steiner E, Steinbach LS, SchnarkowskiP, Tirman PFJ, Benant HK. Ganglia andcysts around joints. Radiol Clin NorthAm 1996; 34:395–425.
43. Frankel DA, Bargiela A, Bouffard JA,Craig JG, Shirazi KK, van HolsbeeckMT. Synovial joints: evaluation ofintraarticular bodies with US. Radiolo-gy 1998; 206:41–44.
44. Miller JH, Beggs, I. Detection of intra-articular bodies of the elbow with salinearthrosonography. Clin Radiol 2000;56:231–234.
45. Davidson RS, Markowitz RI, DormansJ, Drummond DS. Ultrasonographicevaluation of the elbow in infants andyoung children after suspected trauma. JBone Joint Surg 1994; 76:1804–1813.
46. Lazar RD, Waters PM, Jaramillo D.The use of ultrasonography in thediagnosis of occult fracture of the radialneck. J Bone Joint Surg 1998; 9:1361–1364.
47. May DA, Disler DG, Jones EA, PearceDA. Using sonography to diagnose anunossified medial epicondyle avulsionin a child. AJR Am J Roentgenol 2000;174:1115–1117.
48. Takahara M, Ogino T, Tsuchida H,Takagi M, Kashiwa H, Nambu T.Sonographic assessment of osteochon-dritis dissecans of the humeral capitel-lum. AJR Am J Roentgenol 2000;174:411–415.
49. Takahara M, Shundo M, Kondo M,Suzuki K, Nambu T, Ogino T. Earlydetection of osteochondritis dissecansof the capitellum in young baseballplayers. J Bone Joint Surg Am 1998;80:892–897.





























