Embed Size (px)
Citation preview

Risk factors for suicide attempts in patients with alcoholdependence or abuse and a history of depressive symptoms:A subgroup analysis from the WHO/ISBRA studydar_089 64..74
ÖZGÜR YALDIZLI1, HANS CHRISTIAN KUHL1, MARC GRAF1, GERHARD A. WIESBECK1 &FRIEDRICH M. WURST1,2
1Psychiatric University Clinics, Basel, Switzerland, and 2Department of Psychiatry and Psychotherapy/AddictionMedicine, Paracelsus Medical University, Salzburg, Austria
AbstractIntroduction and Aims. Alcoholism, depression and suicide attempts (SA) are strongly interrelated.The aims wereto determine risk factors and develop a prognostic predictor model for SA in a subgroup of patients with a historyof alcohol dependence or abuse and depressive symptoms. Design and Methods. A subgroup analysis from the dataof the World Health Organisation (WHO)/the International Society for Biomedical Research on Alcoholism(ISBRA)-collaborative study on biological state and trait marker of alcohol use and dependence, an internationalmulti-centre study with a cross-sectional design, based on a standardised questionnaire. We analysed from 1314variables 43 factors—including demographic characteristics, dependence variables, comorbid disorders, personalitytrait markers and family history—that were supposed to be most predictive for SA according to the literature.Correlation analyses by the c2-test and Mann–Whitney U-test were performed to obtain statistical meaningfulparameters for logistic regression analysis. Results. Of the 1863 persons included in theWHO/ISBRA study, 292 hadboth a history of depressive symptoms and alcohol dependence or abuse and were included in the subgroup analysis.In the logistic regression analysis, drinking status, depressive symptoms, adverse drinking experiences during alcoholconsumption, bad experiences from drug abuse and antidepressant therapy were found to be independent risk factorsfor SA. Positive family history of alcoholism was a model-improving co-factor. This predictive model explainsapproximately 60% of the variance (Nagelkerkes’ square). Discussion and Conclusions. This prognostic modelderived from data of theWHO/ISBRA collaborative study shows important risk factors for SA in patients with historyof alcohol abuse or dependence and depressive symptoms. [Yaldizli Ö, Kuhl HC, Graf M,Wiesbeck GA,Wurst FM.Risk factors for suicide attempts in patients with alcohol dependence or abuse and a history of depressive symptoms:A subgroup analysis from the WHO/ISBRA study. Drug Alcohol Rev 2010;29:64–74]
Key words: suicide, suicidal behaviour, prognostic predictor model, alcoholism, depression.
Introduction
Suicide is a serious public health problem. In 2000,suicide was the 13th leading cause of death worldwide[1] and with 10.7 completed suicides for every 100 000people, the 11th cause of death in the United States [2].According to World Health Organisation (WHO) esti-mates worldwide approximately one million people diefrom suicide annually, and 10 to 20 times more peopleattempted suicide [3]. Subjects with a previous suicide
attempt (SA) have a more than 20-fold higher risk for asubsequent completed suicide, independent of the psy-chopathology [4–9]. Referring to underlying condi-tions, mood disorders, alcoholism and personalitydisorders are the three most important risk factors forcompleted suicide [10–15]. Approximately 60% of sui-cides occur during a phase of a mood disorder. Lifetimemortality due to suicide in major depression is esti-mated from 2% to 15% depending on severity andinpatient status [16]. According to a study on 4000
This study used data from the WHO/ISBRA study on biological state and trait markers of alcohol use and dependence.Özgür Yaldizli MD, Hans Christian Kuhl MSc, Marc Graf MD, Gerhard A. Wiesbeck MD, Professor, Friedrich M. Wurst MD, Professor.Correspondence to Dr ÖzgürYaldizli, Cantonal Hospital St. Gallen, 9007 St. Gallen, Switzerland.Tel: +41 76 201 53 07; Fax: +41 71 494 28 95;E-mail: [email protected]
Received 11 April 2008; accepted for publication 7 March 2009.
Drug and Alcohol Review (January 2010), 29, 64–74DOI: 10.1111/j.1465-3362.2009.00089.x
© 2009 Australasian Professional Society on Alcohol and other Drugs

patients, there is a 26-fold higher risk of death bysuicide in patients with depression [17]. Inskip et al.found in a meta-analysis a lifetime mortality due tosuicide of 6% in patients with affective disorders [18].
In industrialised countries, 90% of people consumealcohol at some time of their lives and approximately athird develop alcohol-related problems [15]. The life-time risk for alcohol abuse or dependence is 15–20% inmen and 8–15% in women [19]. Lifetime mortality dueto suicide in alcoholism has been reported to be 2–15%[18,20], Roy et al. (1986) found even, 18%. The moresevere the alcoholism is, the higher is the risk forsuicidal behaviour. Alcohol-dependent patients havea 60–120 times greater suicide risk than a non-psychiatric ill population [20–22]. There is good evi-dence for an additive interaction between depressionand alcoholism regarding risk of suicidal ideation, SAand completed suicides [23–28]: depressed subjectswith a history of alcoholism significantly more oftenhave suicidal ideations as compared with depressed sub-jects without alcohol-related problems in the past [29].
Although there are many studies trying to assess riskfactors for SA, suicidal behaviour remains complex. Inthe last decades, many epidemiological studies havebeen conducted regarding general disease-independentrisk factors for suicide: male sex, being separated ordivorced, less educational attainment and unemploy-ment were found to be such general risk factors forsuicide [8,12,13,30–35]. Regarding alcohol-dependentpatients, similar characteristics have been reported[25,27,36–38]. Among alcohol-dependent patients,additional substance-abuse associated factors wererelated to suicidal behaviour. Among these were earlyonset of alcohol-related problems, higher maximumquantities of drinking, histories of treatment for sub-stance use disorders, acute alcohol intoxication[26,27,36,39]. Furthermore, aggressive and impulsivepersonality traits and psychological distress are impor-tant proximal risk factors for suicide in patients withalcohol-related problems [39].
The objective was to determine risk factors for SAand develop a prognostic model in patients with ahistory of alcohol dependence or abuse and depressivesymptoms for at least 2 weeks from data, generated bythe WHO/the International Society for BiomedicalResearch on Alcoholism (ISBRA) Study on State andTrait Markers for Alcohol Use and Dependence.
Methods
The WHO/ISBRA Study on State and Trait Markers ofAlcohol Use and Dependence was a multinationalinvestigation, recruiting subjects in Australia (Sydney),Brazil (Sao Paulo), Canada (Montreal), Finland(Helsinki) and Japan (Sapporo). Details of this cross-
sectional study, the diagnostic tool and the characteris-tics of the participants have been described by Glanzet al. in 2002 [40]. Subjects were recruited after writteninformed consent. A total of 1863 men and womenwere included. Among these, 439 were not consumingalcohol (23.6%), 722 were light to moderate alcoholconsumers (<210 g ethanol per week) (38.8%), 349heavy alcohol consumers (>210 g ethanol per week)(18.7%) and 353 were patients with alcohol-relatedproblems in treatment (18.9%). During the interview,all subjects were in good mental and physical healthverified by both interview and physical examination. Allparticipants were evaluated face to face by trained inter-viewers with the WHO/ISBRA Interview Schedule, astructured questionnaire. Before being applied to thisstudy the interview had been tested and revised tooptimise its reliability [40].The questionnaire containedinformation about recruitment setting, backgroundcharacteristics, alcohol and drug use, lifetime and past30 days occurrence of medical conditions as well as onfamily history. From the 1314 variables, generated bythe interviewed data, we chose 43 factors (includingdemographic characteristics, dependency variables, sec-ondary disorders, personality trait markers and charac-teristics of the family history in patients with a history ofalcohol abuse or dependency and depressive symptomsfor at least 2 weeks) which are considered to be mostpredictive for a SA according to the literature.
Statistical analysis
We used spss 13 (SPSS Inc., Chicago, IL, USA) forstatistical analysis. In a first step, we correlated these 43factors with SA in a univariate analysis by the c2-testand Mann–Whitney U-test to obtain statistical mean-ingful parameters for the regression analysis. We usedstepwise backward logistic regression analysis to evalu-ate the association between SA (dependent variable)and all statistical meaningful parameters (independentvariables). Sensitivity and specifity of the logisticregression model are illustrated by using receiver oper-ated characteristics (ROC) [41].
Results
Of the 1863 persons included in the WHO/ISBRAstudy, 292 had both a history of depressive symptomsand alcohol dependence or abuse and therefore wereincluded in the subgroup analysis (Figure 1).They weredivided in two subgroups: with and without a history ofSA. One hundred and four of these 292 patients(35.6%) [50 women (48.1%) and 54 men (51.9%)]had at least one SA whereas 186 patients (63.7%) [71women (38.2%) and 115 men (61.8%)] neverattempted suicide (Figure 1).
Risk factors of suicide in alcoholics 65
© 2009 Australasian Professional Society on Alcohol and other Drugs

General characteristics
Patients with and without SA did not differ significantlyin mean age (Mann–Whitney U-test score = 9640;P = 0.96), sex (P = 0.1), religion (P = 0.45), race(P = 0.85), marital status (P = 0.73), educationalattainment (P = 0.16) or living area (P = 0.35)(Table 1).
Dependence variables
The categories according to the drinking status were: (i)light to moderate drinkers (<210 g ethanol per week;n = 68, 23.3%); (ii) heavy alcohol consumers (>210 gethanol per week; n = 85, 29.1%); and (iii) patients whowere currently in alcohol treatment (137 patients,46.9%). Patients, currently in alcohol treatment, hadhigh significantly more SA in their case history (53.3%)than heavy drinkers (27.1%) and heavy drinkers hadsignificantly more SA (27.1%) than light-to-moderatedrinkers (11.8%) (P < 0.001). Patients with SA startedto consume alcohol earlier than those without SA
(Mann–Whitney U-test score = 7970; P = 0.01).SA correlated significantly with lifetime abuse formarijuana (P = 0.05), lifetime abuse for cocaine(P = 0.001), drinking experiences during alcohol intake(P < 0.001), including flush or blush (P = 0.01), hives(P = 0.05), sleepiness (P = 0.003), being sick in thestomach (P < 0.001), palpitations (P = 0.001), head-ache (P < 0.001) and bad experiences from drug use(P = 0.002). Smoking status (P = 0.2) or bad effectsafter ceasing alcohol drinking that lasted for at least aday (or less than a day when the subject drank to avoidor relieve the symptoms) did not correlate significantlywith SA (Table 2).
Depressive symptoms
Patients with a major depression (according to the diag-nostic criteria of DSM IV) had significantly more oftenSA than patients without (P < 0.001). Eleven out of 13depressive symptoms, including crying a lot, loss ofinterest, weight changes, sleep disturbances, restless-ness, feeling of low energy, sense of worthlessness orguilt, loss of concentration, hopelessness, suicideideation, delusions or hallucinations, correlated sig-nificantly or highly significantly with SA with thehighest odds ratio for suicidal ideations [OR = 33.1(11.7–93.8)]. Irritability and depressive symptoms inthe morning (P = 0.31) did not correlate with SA.Antidepressant treatment, including antidepressantdrugs, sedative drugs, tranquilliser or electro-convulsivetherapy, correlated highly significantly with SA with thehighest odds ratio for the use of antidepressant drugs[P < 0.001; OR = 2.88 (1.72–4.80)] (Table 3).
Personality traits
With regard to personality traits, the occurrence ofdisciplinary problems before the age of 15 years,including to play hooky, to be suspended from lessons,to run away from home, to tell lies, to steal things, todamage property, to fight physically, to use weapons, tohurt persons on purpose, to injure animals, to start fire,to be arrested or could have been arrested and thediagnosis of a conduct disorder according to the diag-nostic criteria of DSM IV, did not correlate significantlywith SA. In contrast, the occurrence of any antisocialbehaviour, including not working when expected towork, being absent from work, quitting job, travellingaround, having no regular place to live, telling lies,failing to pay bills, stealing things, damaging property,injuring another person, using a weapon in fights, toscam, not offering medical care to children, dependingon friends for care of children, being unfaithful topartner, being arrested or having been arrested after theage of 15 (P = 0.006) and the diagnosis of an antisocial
Figure 1. Home-cities and selection of patients for subgroupanalysis. (*: incomplete data).
66 Ö.Yaldizli et al.
© 2009 Australasian Professional Society on Alcohol and other Drugs

personality disorder according to the diagnostic criteriaof DSM IV (P = 0.002), correlated significantly withSA (Table 1).
Family history
Alcoholism in parents and full brothers or sisters incontrast to depression was significantly associated withSA (P = 0.005; c2 = 7.86) (Table 1).
Logistic regression and ROC curve analysis
Data from 285 of 292 patients were complete and wereincluded in the logistic regression analysis (Table 4).According to this analysis, seven variables remainedsignificant in predicting SA: drinking status of thepatients (P = 0.02), drinking experiences like being sickin the stomach (P = 0.02) or palpitations (P = 0.04),
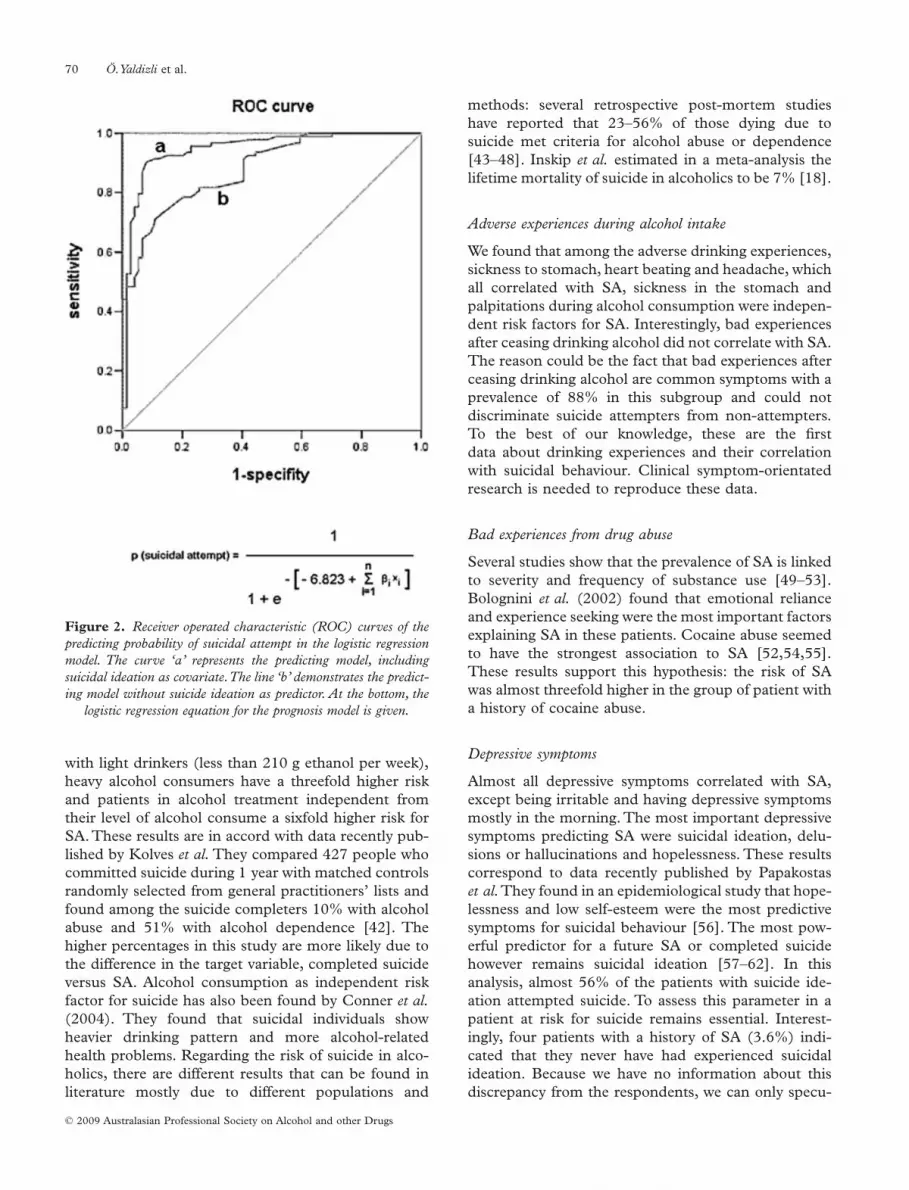
bad experiences from drug use generally (P = 0.02),delusions or hallucinations during depressive episode(P = 0.003), suicide ideation (P < 0.001) and any formof antidepressant treatment (P = 0.006). A positivefamily history for alcoholism was not an independentsignificant predictor for SA but seemed to be a model-improving factor (Table 3). The prognostic modelexplains approximately 60% of the variance of thedependent variable SA (Nagelkerkes’ square). Theanalysis showed the predominant role of suicidal ide-ation as predictor variable. Patients with alcohol depen-dence or abuse and a history of at least a brief episodeof depressive symptoms had an approximately 42-foldhigher risk of SA if they have suicidal ideations com-pared with those without. The relative impact of sui-cidal ideation as a risk factor for SA is illustrated by theROC-curve comparison in Figure 2. By adding suicidalideation to the logistic regression model, the area under
Table 1. Correlation analysis of general parameters, personality traits and characteristics of the family history with suicide attempt
Parameters
Suicide attempt
Odds ratio PNo Yes
Mean age � SD 37.36 � 11.13 37.34 � 11.21 0.96Sex (%) Female 71 (58.7) 50 (51.3) 0.1
Male 115 (68) 54 (32)Religion (%) Moslem, Christian, Jewish,
Protestant156 (62.9) 92 (37.1) 0.45
Other Religion 19 (67.9) 9 (32.1)No Religion 11 (78.6) 3 (21.4)
Race (%) White 154 (63.6) 88 (36.4) 0.85Black 16 (64) 9 (36)Others 16 (69.6) 7 (30.4)
Marital status (%) Married or similarrelationship
52 (65.8) 27 (34.2) 0.73
Separated, divorced orwidowed
51 (60.7) 33 (39.3)
Never married 82 (65.6) 43 (34.4)Educational attainment (%) Did not complete high
school54 (58.7) 38 (41.3) 0.36
High school 38 (63.3) 22 (36.7)College or post-graduate 93 (67.9) 44 (32.1)
Living area (%) Other 28 (59.6) 19 (40.4) 0.33Inner city 90 (62.1) 55 (37.9)Suburban city 68 (70.1) 29 (29.9)
Disciplinary problems beforethe age of 15 (%)
No 41 (61.2) 26 (38.8) 0.58Yes 144 (64.9) 78 (35.1)
Conduct disorder DSM IV(%)
No 171 (62.9) 101 (37.1) 0.08Yes 15 (83.3) 3 (16.7)
Antisocial behaviour after theage of 15 (%)
No 49 (79) 13 (21) 2.50 (1.29–4.88) <0.01Yes 137 (60.1) 91 (39.9)
Antisocial personality disorderDSM IV (%)
No 125 (71) 51 (29) 2.13 (1.30–3.48) <0.01Yes 61 (53.5) 53 (46.5)
Close relatives everdepression (%)
No 85 (66.9) 42 (33.1) 0.38Yes 101 (62) 62 (38)
Close relatives everalcoholism (%)
No 70 (72.2) 27 (27.8) 1.72 (1.01–2.92) 0.04Yes 116 (60.1) 77 (39.9)
Risk factors of suicide in alcoholics 67
© 2009 Australasian Professional Society on Alcohol and other Drugs

the curve (AUC) is 0.91 instead of 0.81.The regressionequation can quantify the individual risk of SA(Figure 2). According to this equation, a patient cur-rently in alcohol treatment with a history of depressivesymptoms longer than 2 weeks, having had bad expe-riences from drug abuse and suicidal ideation has therisk of having had SA of 38%.
Discussion
The major finding of this study is that drinking status,adverse experiences during drinking, bad experiencesfrom drug abuse, depressive symptoms and antidepres-sant treatment are independent risk factors for SA. Apositive family history for alcoholism is not a significantindependent factor for SA, but improves the prognosticmodel. The prognostic model explains approximately60% of the variance of SA.The most important predic-tor for SA, with an odds ratio of approximately 42, wassuicidal ideation.
The initial purpose of the multinational WHO/ISBRA study was to investigate biological state and trait
markers of alcohol use and dependence [40].The 1863recruited subjects were not representative for thegeneral population regarding alcohol consumption.Because depression and alcoholism are important riskfactors for SA and common comorbid conditions, thisstatistical analysis focused on the subgroup of patientswith a history of alcohol abuse or dependence anddepressive symptoms for at least 2 weeks. Regardinggeneral parameters, this subgroup population was rela-tively homogenous. Suicide attempters and non-attempters did not differ significantly in age, sex,marital status, education or living areas.
Drinking status
Results of the present study regarding correlationsbetween drinking status and suicidal behaviour are inaccordance with previous studies. In this study, 35.6%of the patients with alcohol abuse or dependency and53.3% of the patients currently in alcohol treatmenthad at least one SA in their lives. The severity of alco-holism is an independent risk factor for SA: compared
Table 2. Correlation analysis of dependence parameters with suicide attempt
Parameters
Suicide attempt
Odds ratio PNo Yes
Age began regularly drinking 17.97 � 5.03 16.85 � 4.42 0.01Drinking status (%) Light 60 (88.2) 8 (11.8) 0.000
Heavy 62 (72.9) 23 (27.1)Currently inalcohol treatment
64 (56.7) 73 (53.3)
Any adverse drinking experiences (%) No 141 (71.6) 56 (28.4) 2.69 (1.61–4.48) 0.000Yes 45 (48.4) 48 (51.6)
Drinking exp.: flush, blush (%) No 157 (67.7) 75 (32.2) 2.09 (1.17–3.75) 0.01Yes 29 (50) 29 (50)
Drinking exp.: hives (%) No 183 (65.1) 98 (34.9) 3.74 (0.92–15.26) 0.05Yes 3 (33.3) 6 (66.7)
Drinking exp.: sleepy (%) No 167 (67.6) 80 (32.4) 2.64 (1.37–5.09) 0.003Yes 19 (44.2) 24 (55.8)
Drinking exp.: sickness (%) No 180 (67.7) 86 (32.3) 6.28 (2.41–16.38) 0.000Yes 6 (25) 18 (75)
Drinking exp.: heart beating (%) No 171 (67.6) 82 (32.4) 3.06 (1.51–6.20) 0.001Yes 15 (40.5) 22 (59.5)
Drinking exp.: headache (%) No 180 (67.2) 88 (32.8) 5.46 (2.06–14.42) <0.001Yes 6 (27.3) 16 (72.7)
Bad effects after stop drinking (%) No 24 (68.6) 11 (31.4) 0.56Yes 162 (63.5) 93 (36.5)
Smoking (%) Non-smok. 16 (72.7) 6 (27.3) 0.20Ex-smok. 27 (75) 9 (25)Current smok. 143 (61.6) 89 (38.4)
Ever had bad exp. from drug use (%) No 124 (71.3) 50 (28.7) 2.16 (1.32–3.53) <0.01Yes 62 (53.4) 54 (46.6)
Lifetime abuse for marijuana (%) No 166 (66.4) 84 (33.6) 1.98 (1.0–3.87) 0.05Yes 20 (50) 20 (50)
Lifetime abuse for cocaine (%) No 164 (68.3) 76 (31.7) 2.75 (1.48–5.11) 0.001Yes 22 (44) 28 (56)
68 Ö.Yaldizli et al.
© 2009 Australasian Professional Society on Alcohol and other Drugs

Table 3. Correlation analysis of depression parameters with suicide attempt
Parameters
Suicide attempt
Odds ratio PNo Yes
DSM IV major depression (%) No 55 (88.7) 7 (11.3) 5.82 (2.54–13.33) 0.000Yes 131 (57.5) 97 (42.5)
Being irritable (%) No 67 (67) 33 (33) 0.461Yes 119 (62.6) 71 (37.4)
Cried a lot (%) No 79 (79.8) 20 (20.2) 3.10 (1.76–5.47) 0.000Yes 107 (56) 84 (44)
Loss of interest (%) No 36 (76.6) 11 (23.4) 2.03 (0.99–4.18) 0.05Yes 150 (61.7) 93 (38.3)
Weight change (%) No 88 (76.5) 27 (23.5) 2.56 (1.52–4.33) 0.000Yes 98 (56) 77 (44)
Sleep change (%) No 45 (78.9) 12 (21.1) 2.45 (1.23–4.87) 0.009Yes 141 (60.5) 92 (39.5)
Restless (%) No 81 (72.3) 31 (27.7) 1.82 (1.09–3.03) 0.02Yes 105 (59) 73 (41)
Tired, low energy (%) No 66 (75.9) 21 (24.1) 2.17 (1.24–3.83) 0.006Yes 120 (59.1) 83 (40.9)
Mostly in morning (%) No 108 (66.7) 54 (33.3) 0.31Yes 78 (60.9) 50 (39.1)
Worthless/Guilty (%) No 53 (77.9) 15 (22.1) 2.36 (1.26–4.45) 0.007Yes 133 (59.9) 89 (40.1)
Loss of concentration (%) No 62 (82.7) 13 (17.3) 3.5 (1.82–6.75) 0.000Yes 124 (57.7) 91 (42.3)
Hopelessness (%) No 61 (84.7) 11 (15.3) 4.13 (2.06–8.27) 0.000Yes 125 (57.3) 93 (42.7)
Suicide ideation (%) No 106 (96.4) 4 (3.6) 33.13 (11.7–93.78) 0.000Yes 80 (44.4) 100 (55.6)
Delusions/Hallucinations (%) No 154 (72) 60 (28) 3.53 (2.05–6.08) 0.000Yes 32 (42.1) 44 (57.9)
Any antidepressant treatment No 89 (74.8) 30 (25.2) 2.34 (1.40–3.90) 0.001Yes 94 (56) 74 (44)
Antidepressant drugs (%) No 142 (72.1) 55 (27.9) 2.88 (1.72–4.80) 0.000Yes 44 (47.3) 49 (52.7)
Table 4. Logistic regression analysis of factors associated with suicide attempt
Regressionscoefficient bi
Standarderror Wald df Sig. Exp (b)
95% Confidenceinterval
1. Drinking statusLight drinker 12.48 2 0.002Heavy drinker 1.091 (b1) 0.547 4.00 1 0.046 2.98 1.02 8.70Currently in alcohol treatment 1.759 (b2) 0.507 12.04 1 0.001 5.81 2.15 15.67
2. Drinking experience: sick to stomach 1.713 (b3) 0.731 5.49 1 0.019 5.55 1.32 23.263. Drinking experience: hearts beats hardly 1.178 (b4) 0.580 4.13 1 0.042 3.25 1.04 10.124. Ever had bad experience from drug use 0.841 (b5) 0.359 5.50 1 0.019 2.32 1.15 4.685. Suicidal ideation 3.735 (b6) 0.602 38.54 1 0.000 41.88 12.88 136.166. Delusions during depressive episode 1.252 (b7) 0.427 8.59 1 0.003 3.50 1.51 8.087. Any treatment during depressive episode 1.044 (b8) 0.379 7.58 1 0.006 2.84 1.35 5.988. Close relatives alcoholism 0.701 (b9) 0.376 3.48 1 0.062 2.02 0.97 4.21
constant -6.823 (b0) 0.898 57.68 1 0.000 0.001
Risk factors of suicide in alcoholics 69
© 2009 Australasian Professional Society on Alcohol and other Drugs
with light drinkers (less than 210 g ethanol per week),heavy alcohol consumers have a threefold higher riskand patients in alcohol treatment independent fromtheir level of alcohol consume a sixfold higher risk forSA.These results are in accord with data recently pub-lished by Kolves et al. They compared 427 people whocommitted suicide during 1 year with matched controlsrandomly selected from general practitioners’ lists andfound among the suicide completers 10% with alcoholabuse and 51% with alcohol dependence [42]. Thehigher percentages in this study are more likely due tothe difference in the target variable, completed suicideversus SA. Alcohol consumption as independent riskfactor for suicide has also been found by Conner et al.(2004). They found that suicidal individuals showheavier drinking pattern and more alcohol-relatedhealth problems. Regarding the risk of suicide in alco-holics, there are different results that can be found inliterature mostly due to different populations and
methods: several retrospective post-mortem studieshave reported that 23–56% of those dying due tosuicide met criteria for alcohol abuse or dependence[43–48]. Inskip et al. estimated in a meta-analysis thelifetime mortality of suicide in alcoholics to be 7% [18].
Adverse experiences during alcohol intake
We found that among the adverse drinking experiences,sickness to stomach, heart beating and headache, whichall correlated with SA, sickness in the stomach andpalpitations during alcohol consumption were indepen-dent risk factors for SA. Interestingly, bad experiencesafter ceasing drinking alcohol did not correlate with SA.The reason could be the fact that bad experiences afterceasing drinking alcohol are common symptoms with aprevalence of 88% in this subgroup and could notdiscriminate suicide attempters from non-attempters.To the best of our knowledge, these are the firstdata about drinking experiences and their correlationwith suicidal behaviour. Clinical symptom-orientatedresearch is needed to reproduce these data.
Bad experiences from drug abuse
Several studies show that the prevalence of SA is linkedto severity and frequency of substance use [49–53].Bolognini et al. (2002) found that emotional relianceand experience seeking were the most important factorsexplaining SA in these patients. Cocaine abuse seemedto have the strongest association to SA [52,54,55].These results support this hypothesis: the risk of SAwas almost threefold higher in the group of patient witha history of cocaine abuse.
Depressive symptoms
Almost all depressive symptoms correlated with SA,except being irritable and having depressive symptomsmostly in the morning. The most important depressivesymptoms predicting SA were suicidal ideation, delu-sions or hallucinations and hopelessness. These resultscorrespond to data recently published by Papakostaset al.They found in an epidemiological study that hope-lessness and low self-esteem were the most predictivesymptoms for suicidal behaviour [56]. The most pow-erful predictor for a future SA or completed suicidehowever remains suicidal ideation [57–62]. In thisanalysis, almost 56% of the patients with suicide ide-ation attempted suicide. To assess this parameter in apatient at risk for suicide remains essential. Interest-ingly, four patients with a history of SA (3.6%) indi-cated that they never have had experienced suicidalideation. Because we have no information about thisdiscrepancy from the respondents, we can only specu-
Figure 2. Receiver operated characteristic (ROC) curves of thepredicting probability of suicidal attempt in the logistic regressionmodel. The curve ‘a’ represents the predicting model, includingsuicidal ideation as covariate.The line ‘b’ demonstrates the predict-ing model without suicide ideation as predictor. At the bottom, the
logistic regression equation for the prognosis model is given.
70 Ö.Yaldizli et al.
© 2009 Australasian Professional Society on Alcohol and other Drugs

late about the true reason. One explanation could bethe low stability and reliability of self-reports in subjectswith SA [63].
Antidepressant treatment
Not only depressive symptoms but also the use of anti-depressants seemed to be an independent risk factor forSA. In this analysis, 53% of all patients receiving anti-depressants indicated SA versus 28% of all patientswho never used antidepressants. The relationshipbetween antidepressant medication use and suicidalbehaviour is controversial. There is an ethical concernto perform randomised, controlled trials evaluating thesafety and efficacy of antidepressant medication indepressed patients at risk of suicide. Large epidemio-logic studies in Europe suggest that a decrease insuicide rate correlates with an increased use of antide-pressants in Europe [64–68], USA [69] and Australia[70], but there are contradictory data published as well:in Japan, the suicide rates have risen despite or becauseof increasing use of selective serotonin reuptake inhibi-tors (SSRI) [71] and in Iceland there was no significantchange in suicide rates despite a fourfold increase inantidepressant prescriptions. Recent studies suggestthat it is not the prescription of antidepressants thatcorrelates with suicidal behaviour but the quality oflocal health care. According to an analysis of theNational Vital Statistics from the Centers for DiseaseControl and Prevention, the positive correlationbetween tricyclic antidepressant prescription andsuicide rate arose rather from the limited access toquality mental health than from the prescription ofantidepressants. In contrast, increases in prescriptionsfor SSRI or other new-generation non-SSRI are asso-ciated in the same study with a lower suicide rate. Inthis subgroup analysis, there were no local differencesin the use of antidepressants. Simon et al. did not findan increase in suicide after starting treatment withnewer antidepressants in a population-based study of65 103 patients [72].
Family history
A positive family history for alcoholism is correlatedclosely significantly with SA, but was not an indepen-dent risk factor for SA in this subgroup. This resultcorresponds to data published by Hesselbrock et al.They found also that alcoholic suicide attempterstended to have a parental history of alcoholism [27].
Limitations of the study
The main limitation of this study is methodical. Thedesign was cross-sectional. All data were subjective and
interviewed retrospectively. It is known from data fromChristl et al. that approximately one-third of all base-line suicide attempters did not report their SA again inan assessment 4 years later [63]. This work was a sub-group analysis of patients who were not representativefor the population. Subjects with SA without havingdepressive symptoms were excluded from this analysis.This is however a rather unimportant limitationbecause it is known that only 8% of all suicide attempt-ers answered negatively in depression-related gate ques-tions of suicide surveys [63]. We could not analyseproximal risk factors, for example, alcohol consump-tion during SA. It is known that alcohol consumptiondecreases voluntary control and is strongly associatedwith suicide ideation in women even when they are lightdrinkers [73–75]. In this analysis, there were no dataavailable covering the time-point of SA. Personalitytraits, including aggressiveness and impulsivity, werenot investigated in the study.There were no data aboutaggression scores or impulsivity indices in this analysis,but the data showed that antisocial behaviour occurringafter the age of 15 was more relevant for suicidal behav-iour than in childhood, suggesting that only persistentbehaviour abnormalities are relevant for suicidal behav-iour. We did not find a positive correlation betweensmoking and SA.This could be a data pool related biasbecause 92.5% of the patients were smokers.There areseveral prospective studies suggesting a significantdose-dependent relationship irrespective of the level ofviolence used [76–82].
Despite these disadvantages, we could include ameaningful number of patients in this subgroup analy-sis.These results were controlled for general character-istics like age, sex, religion, race, marital status,educational attainment and living area. Higher age[2,83], male sex [2,84–86], marital isolation [87], inter-personal difficulties in relationships [87], white race[84,88], living in socioeconomic deprived areas[89,90], less education [85,91,92] are described as riskfactors for SA in the literature.
Conclusions
In conclusion, we provide evidence to the relationshipbetween alcohol consumption, depressive symptoms,previous use of drugs and SA. This corresponds withresults published recently by Black et al. investigating262 alcoholics. They also performed a logistic regres-sion analysis and found that the extent of alcohol con-sumption, previous alcohol treatment, previous use ofother drugs and a high Hamilton score for depressionwere the most relevant predictors for suicidal behaviour[26]. To the best of our knowledge, this is the firstpublication describing adverse experiences duringalcohol consume as risk factors for suicidal behaviour.
Risk factors of suicide in alcoholics 71
© 2009 Australasian Professional Society on Alcohol and other Drugs
Furthermore, the prognostic model explains approxi-mately 60% of the variance of SA and the regressionsequation can quantify the individual risk of SA.
Acknowledgements [Acknowledgements addedafter online publication, 28 August 2009]
We would like to express our gratitude to Boris Taba-koff, Global Study Director of theWHO/ISBRA Study,Denver, for pre-review of this manuscript. The projectrelied on the dedication of staff at every clinical andassay center and at the sample and data processingcenters.TheWHO/ISBRA study on biological state andtrait markers of alcohol use and dependence investiga-tors are: K. M. Conigrave, M. Dongier, H. Edenberg,C. J. P. Eriksson, M. L. O. S. Formigoni, B. F. Grant, A.Helander, P. L. Hoffman, K. Kiianmaa, T. Koyama, L.Legault,T-K Li, M. Monteiro,T. Methuen,T. Saito, M.Salaspuro, J. B. Saunders, B. Tabakoff, S. Tufik, J. B.Whitfield, F. M.Wurst.We are, in addition, indebted tothe subjects who participated in the study.
References
[1] Krug EG, Mercy JA, Dahlberg LL, et al. The world reporton violence and health. Lancet 2002;360:1083–8.
[2] Minino AM, Arias E, Kochanek KD, et al. Deaths: finaldata for 2000. Natl Vital Stat Rep 2002;50:1–119.
[3] World Health Organisation. The world health report 2004.Changing history. Geneva: World Health Organisation,2004.
[4] Hawton K, Fagg J. Suicide, and other causes of death, fol-lowing attempted suicide. Br J Psychiatry 1988;152:359–66.
[5] Rosenberg ML, Davidson LE, Smith JC, et al. Operationalcriteria for the determination of suicide. J Forensic Sci1988;33:1445–56.
[6] Schmidtke A. Perspective: suicide in Europe. Suicide LifeThreat Behav 1997;27:127–36.
[7] Isometsa ET, Lonnqvist JK. Suicide attempts precedingcompleted suicide. Br J Psychiatry 1998;173:531–5.
[8] Rossow I, Romelsjo A, Leifman H. Alcohol abuse and sui-cidal behaviour in young and middle aged men: differenti-ating between attempted and completed suicide. Addiction1999;94:1199–207.
[9] Dhossche DM, Meloukheia AM, Chakravorty S. The asso-ciation of suicide attempts and comorbid depression andsubstance abuse in psychiatric consultation patients. GenHosp Psychiatry 2000;22:281–8.
[10] Brent DA, Perper JA, Goldstein CE, et al. Risk factors foradolescent suicide. A comparison of adolescent suicidevictims with suicidal inpatients. Arch Gen Psychiatry 1988;45:581–8.
[11] Beautrais AL, Joyce PR, Mulder RT, et al. Prevalence andcomorbidity of mental disorders in persons making serioussuicide attempts: a case-control study. Am J Psychiatry1996;153:1009–14.
[12] Kessler RC, Borges G, Walters EE. Prevalence of and riskfactors for lifetime suicide attempts in the National Comor-bidity Survey. Arch Gen Psychiatry 1999;56:617–26.
[13] Dieserud G, Loeb M, Ekeberg O. Suicidal behavior in themunicipality of Baerum, Norway: a 12-year prospective
study of parasuicide and suicide. Suicide Life Threat Behav2000;30:61–73.
[14] Kelly TM, Soloff PH, Lynch KG, et al. Recent life events,social adjustment, and suicide attempts in patients withmajor depression and borderline personality disorder. J Per-sonal Disord 2000;14:316–26.
[15] Sher L. Preventing suicide. QJM 2004;97:677–80.[16] Bostwick JM, Pankratz VS. Affective disorders and suicide
risk: a reexamination. Am J Psychiatry 2000;157:1925–32.
[17] Newman SC, Bland RC. Suicide risk varies by subtype ofaffective disorder. Acta Psychiatr Scand 1991;83:420–6.
[18] Inskip HM, Harris EC, Barraclough B. Lifetime risk ofsuicide for affective disorder, alcoholism and schizophrenia.Br J Psychiatry 1998;172:35–7.
[19] Sher L. Depression and alcoholism. QJM 2004;97:237–40.[20] Murphy GE, Wetzel RD. The lifetime risk of suicide in
alcoholism. Arch Gen Psychiatry 1990;47:383–92.[21] Cornelius JR, Salloum IM, Day NL, et al. Patterns of sui-
cidality and alcohol use in alcoholics with major depression.Alcohol Clin Exp Res 1996;20:1451–5.
[22] Sher L, Zalsman G. Alcohol and adolescent suicide. Int JAdolesc Med Health 2005;17:197–203.
[23] Berglund M. Suicide in alcoholism. A prospective study of88 suicides: I. The multidimensional diagnosis at firstadmission. Arch Gen Psychiatry 1984;41:888–91.
[24] Martin RL, Cloninger CR, Guze SB. Alcohol misuse anddepression in women criminals. J Stud Alcohol 1985;46:65–71.
[25] Whitters AC, Cadoret RJ, Widmer RB. Factors associatedwith suicide attempts in alcohol abusers. J Affect Disord1985;9:19–23.
[26] Black DW, Yates W, Petty F, et al. Suicidal behavior inalcoholic males. Compr Psychiatry 1986;27:227–33.
[27] Hesselbrock M, Hesselbrock V, Syzmanski K, et al. Suicideattempts and alcoholism. J Stud Alcohol 1988;49:436–42.
[28] Cornelius JR, Salloum IM, Mezzich J, et al. Disproportion-ate suicidality in patients with comorbid major depressionand alcoholism. Am J Psychiatry 1995;152:358–64.
[29] Sher L, Oquendo MA, Galfalvy HC, et al. The relationshipof aggression to suicidal behavior in depressed patientswith a history of alcoholism. Addict Behav 2005;30:1144–53.
[30] Platt S. Clinical and social characteristics of male parasui-cides: variation by employment status and duration ofunemployment. Acta Psychiatr Scand 1986;74:24–31.
[31] Sorenson SB, Golding JM. Suicide ideation and attempts inHispanics and non-Hispanic whites: demographic and psy-chiatric disorder issues. Suicide LifeThreat Behav 1988;18:205–18.
[32] Petronis KR, Samuels JF, Moscicki EK, et al. An epidemio-logic investigation of potential risk factors for suicideattempts. Soc Psychiatry Psychiatr Epidemiol 1990;25:193–9.
[33] Hawton K, Fagg J, Simkin S, et al. The epidemiology ofattempted suicide in the Oxford area, England (1989–1992). Crisis 1994;15:123–35.
[34] Schmidtke A, Bille-Brahe U, DeLeo D, et al. Attemptedsuicide in Europe: rates, trends and sociodemographic char-acteristics of suicide attempters during the period 1989–1992. Results of the WHO/EURO Multicentre Study onParasuicide. Acta Psychiatr Scand 1996;93:327–38.
[35] Welch SS. A review of the literature on the epidemiologyof parasuicide in the general population. Psychiatr Serv2001;52:368–75.
72 Ö.Yaldizli et al.
© 2009 Australasian Professional Society on Alcohol and other Drugs

[36] Schuckit MA. Primary men alcoholics with histories ofsuicide attempts. J Stud Alcohol 1986;47:78–81.
[37] Windle M. Characteristics of alcoholics who attemptedsuicide: co-occurring disorders and personality differenceswith a sample of male Vietnam era veterans. J Stud Alcohol1994;55:571–7.
[38] Driessen M, Veltrup C, Weber J, et al. Psychiatricco-morbidity, suicidal behaviour and suicidal ideation inalcoholics seeking treatment. Addiction 1998;93:889–94.
[39] Hufford MR. Alcohol and suicidal behavior. Clin PsycholRev 2001;21:797–811.
[40] Glanz J, Grant B, Monteiro M, et al. WHO/ISBRA Studyon State and Trait Markers of Alcohol Use and Depen-dence: analysis of demographic, behavioral, physiologic,and drinking variables that contribute to dependence andseeking treatment. International Society on BiomedicalResearch on Alcoholism. Alcohol Clin Exp Res 2002;26:1047–61.
[41] McFall RM, Treat TA. Quantifying the information value ofclinical assessments with signal detection theory. Annu RevPsychol 1999;50:215–41.
[42] Kolves K, Varnik A, Tooding LM, et al. The role of alcoholin suicide: a case-control psychological autopsy study.Psychol Med 2006;36:923–30.
[43] Henriksson MM, Aro HM, Marttunen MJ, et al. Mentaldisorders and comorbidity in suicide. Am J Psychiatry1993;150:935–40.
[44] Lesage AD, Boyer R, Grunberg F, et al. Suicide and mentaldisorders: a case-control study of young men. Am J Psy-chiatry 1994;151:1063–8.
[45] Cheng AT. Mental illness and suicide. A case-control studyin east Taiwan. Arch Gen Psychiatry 1995;52:594–603.
[46] Conwell Y, Duberstein PR, Cox C, et al. Relationships ofage and axis I diagnoses in victims of completed suicide: apsychological autopsy study. Am J Psychiatry 1996;153:1001–8.
[47] Foster T, Gillespie K, McClelland R, et al. Risk factors forsuicide independent of DSM-III-R Axis I disorder. Case-control psychological autopsy study in Northern Ireland. BrJ Psychiatry 1999;175:175–9.
[48] Vijayakumar L, Rajkumar S. Are risk factors for suicideuniversal? A case-control study in India. Acta PsychiatrScand 1999;99:407–11.
[49] Fowler RC, Rich CL, Young D. San Diego Suicide Study.II. Substance abuse in young cases. Arch Gen Psychiatry1986;43:962–5.
[50] Marzuk PM, Tardiff K, Leon AC, et al. Prevalence ofcocaine use among residents of New York City who com-mitted suicide during a one-year period. Am J Psychiatry1992;149:371–5.
[51] Rich CL, Dhossche DM, Ghani S, et al. Suicide methodsand presence of intoxicating abusable substances: someclinical and public health implications. Ann Clin Psychiatry1998;10:169–75.
[52] Garlow SJ. Age, gender, and ethnicity differences in pat-terns of cocaine and ethanol use preceding suicide. Am JPsychiatry 2002;159:615–19.
[53] Garlow SJ, Purselle D, D’Orio B. Cocaine use disorders andsuicidal ideation. Drug Alcohol Depend 2003;70:101–4.
[54] Burge V, Felts M, Chenier T, et al. Drug use, sexual activ-ity, and suicidal behavior in U.S. high school students. J SchHealth 1995;65:222–7.
[55] Cornelius JR, Thase ME, Salloum IM, et al. Cocaine useassociated with increased suicidal behavior in depressedalcoholics. Addict Behav 1998;23:119–21.
[56] Papakostas GI, Petersen T, Pava J, et al. Hopelessness andsuicidal ideation in outpatients with treatment-resistantdepression: prevalence and impact on treatment outcome.J Nerv Ment Dis 2003;191:444–9.
[57] Robins E, Gassner S, Kayes J, et al. The communication ofsuicidal intent: a study of 134 consecutive cases of success-ful (completed) suicide. Am J Psychiatry 1959;115:724–33.
[58] Barraclough B, Bunch J, Nelson B, et al. A hundred cases ofsuicide: clinical aspects. Br J Psychiatry 1974;125:355–73.
[59] Avery D, Winokur G. Suicide, attempted suicide, andrelapse rates in depression. Arch Gen Psychiatry 1978;35:749–53.
[60] Leon AC, Friedman RA, Sweeney JA, et al. Statistical issuesin the identification of risk factors for suicidal behavior: theapplication of survival analysis. Psychiatry Res 1990;31:99–108.
[61] Diekstra RF. The epidemiology of suicide and parasuicide.Acta Psychiatr Scand Suppl 1993;371:9–20.
[62] Brown GK, Beck AT, Steer RA, et al. Risk factors forsuicide in psychiatric outpatients: a 20-year prospectivestudy. J Consult Clin Psychol 2000;68:371–7.
[63] Christl B, Wittchen HU, Pfister H, et al. The accuracy ofprevalence estimations for suicide attempts. How reliably doadolescents and young adults report their suicide attempts?Arch Suicide Res 2006;10:253–63.
[64] Isacsson G, Bergman U, Rich CL. Epidemiological datasuggest antidepressants reduce suicide risk among depres-sives. J Affect Disord 1996;41:1–8.
[65] Ohberg A, Vuori E, Klaukka T, et al. Antidepressants andsuicide mortality. J Affect Disord 1998;50:225–33.
[66] Rihmer Z, Rutz W, Pihlgren H, et al. Decreasing tendencyof seasonality in suicide may indicate lowering rate ofdepressive suicides in the population. Psychiatry Res1998;81:233–40.
[67] Rich CL. Relationship between antidepressant treatmentand suicide. J Clin Psychiatry 1999;60:340.
[68] Markowitz JC. Antidepressants and suicide risk. Br J Psy-chiatry 2001;178:477.
[69] Olfson M, Shaffer D, Marcus SC, et al. Relationshipbetween antidepressant medication treatment and suicidein adolescents. Arch Gen Psychiatry 2003;60:978–82.
[70] Hall WD, Mant A, Mitchell PB, et al. Association betweenantidepressant prescribing and suicide in Australia, 1991–2000: trend analysis. BMJ 2003;326:1008.
[71] Takahashi Y. Amidst a sudden increase of suicide. In:Takahashi Y, ed. Suicide in Japan. Tokyo, Japan, 2003:1–12.
[72] Simon GE, Savarino J, Operskalski B, et al. Suicide riskduring antidepressant treatment. Am J Psychiatry 2006;163:41–7.
[73] Powell KE, Kresnow MJ, Mercy JA, et al. Alcohol con-sumption and nearly lethal suicide attempts. Suicide LifeThreat Behav 2001;32:30–41.
[74] Conner KR, Li Y, Meldrum S, et al. The role of drinking insuicidal ideation: analyses of Project MATCH data. J StudAlcohol 2003;64:402–8.
[75] Cherpitel CJ, Borges GL, Wilcox HC. Acute alcohol useand suicidal behavior: a review of the literature. AlcoholClin Exp Res 2004;28:18S–28S.
[76] Hemenway D, Solnick SJ, Colditz GA. Smoking and suicideamong nurses. Am J Public Health 1993;83:249–51.
[77] Tverdal A, Thelle D, Stensvold I, et al. Mortality in relationto smoking history: 13 years’ follow-up of 68 000 Norwe-gian men and women 35–49 years. J Clin Epidemiol 1993;46:475–87.
Risk factors of suicide in alcoholics 73
© 2009 Australasian Professional Society on Alcohol and other Drugs

[78] Doll R, Peto R, Wheatley K, et al. Mortality in relation tosmoking: 40 years’ observations on male British doctors.BMJ 1994;309:901–11.
[79] Paffenbarger RS Jr, Lee IM, Leung R. Physical activity andpersonal characteristics associated with depression andsuicide in American college men. Acta Psychiatr ScandSuppl 1994;377:16–22.
[80] Rantakallio P, Laara E, Koiranen M. A 28 year follow up ofmortality among women who smoked during pregnancy.BMJ 1995;311:477–80.
[81] Angst J, Clayton PJ. Personality, smoking and suicide: aprospective study. J Affect Disord 1998;51:55–62.
[82] Tanskanen A, Tuomilehto J, Viinamaki H, et al. Smokingand the risk of suicide. Acta Psychiatr Scand 2000;101:243–5.
[83] Carney SS, Rich CL, Burke PA, et al. Suicide over 60: theSan Diego study. J Am Geriatr Soc 1994;42:174–80.
[84] Conwell Y, Brent D. Suicide and aging. I: patterns of psy-chiatric diagnosis. Int Psychogeriatr 1995;7:149–64.
[85] Grabbe L, Demi A, Camann MA, et al. The health status ofelderly persons in the last year of life: a comparison ofdeaths by suicide, injury, and natural causes. Am J PublicHealth 1997;87:434–7.
[86] Preuss UW, Schuckit MA, Smith TL, et al. Predictors andcorrelates of suicide attempts over 5 years in 1237 alcohol-dependent men and women. Am J Psychiatry 2003;160:56–63.
[87] Duberstein PR, Conwell Y, Conner KR, et al. Poor socialintegration and suicide: fact or artifact? A case-controlstudy. Psychol Med 2004;34:1331–7.
[88] Castle K, Duberstein PR, Meldrum S, et al. Risk factors forsuicide in blacks and whites: an analysis of data from the1993 National Mortality Followback Survey. Am J Psychia-try 2004;161:452–8.
[89] McLoone P, Boddy FA. Deprivation and mortality in Scot-land, 1981 and 1991. BMJ 1994;309:1465–70.
[90] Gunnell D, Bennewith O, Peters TJ, et al. Do patients whoself-harm consult their general practitioner soon after hos-pital discharge? A cohort study. Soc Psychiatry PsychiatrEpidemiol 2002;37:599–602.
[91] Hem E, Haldorsen T, Aasland OG, et al. Suicide amongphysicians. Am J Psychiatry 2005;162:2199–200.
[92] Tran Thi Thanh H, Tran TN, Jiang GX, et al. Life timesuicidal thoughts in an urban community in Hanoi,Vietnam. BMC Public Health 2006;6:76.
74 Ö.Yaldizli et al.
© 2009 Australasian Professional Society on Alcohol and other Drugs





























