Embed Size (px)
Citation preview

Ultrasound in Med. & Biol., Vol. 41, No. 1, pp. 187–196, 2015Copyright � 2015 World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/$ - see front matter
/j.ultrasmedbio.2014.08.018
http://dx.doi.org/10.1016d Original Contribution
SHAKEN AND STIRRED: MECHANISMS OF ULTRASOUND-ENHANCEDTHROMBOLYSIS
KENNETH B. BADER,* MATTHEW J. GRUBER,y and CHRISTY K. HOLLAND*y
*Division of Cardiovascular Health and Disease, Department of Internal Medicine, University of Cincinnati, Cincinnati, Ohio,USA; and yBiomedical Engineering Program, University of Cincinnati, Cincinnati, Ohio, USA
(Received 24 April 2014; revised 5 August 2014; in final form 22 August 2014)
AWay, Cbader@
Abstract—The use of ultrasound and microbubbles as an effective adjuvant to thrombolytics has been reportedin vitro, ex vivo and in vivo. However, the specific mechanisms underlying ultrasound-enhanced thrombolysishave yet to be elucidated. We present visual observations illustrating two mechanisms of ultrasound-enhancedthrombolysis: acoustic cavitation and radiation force. An in vitro flow model was developed to observe humanwhole blood clots exposed to human fresh-frozen plasma, recombinant tissue-type plasminogen activator (0,0.32, 1.58 or 3.15 mg/mL) and the ultrasound contrast agent Definity (2 mL/mL). Intermittent, continuous-waveultrasound (120 kHz, 0.44 MPa peak-to-peak pressure) was used to insonify the perfusate. Ultraharmonic emis-sions indicative of stable cavitation were monitored with a passive cavitation detector. The clot was observedwith an inverted microscope, and images were recorded with a charge-coupled device camera. The images werepost-processed to determine the time-dependent clot diameter and root-mean-square velocity of the clot position.Clot lysis occurred preferentially surrounding large, resonant-sized bubbles undergoing stable oscillations. Ultra-harmonic emissions from stable cavitation were found to correlate with the lytic rate. Clots were observed to trans-late synchronously with the initiation and cessation of the ultrasound exposure. The root-mean-square velocity ofthe clot correlated with the lytic rate. These data provide visual documentation of stable cavitation activity andradiation force during sub-megahertz sonothrombolysis. The observations of this study suggest that the processof clot lysis is complex, and both stable cavitation and radiation force aremechanistically responsible for this bene-ficial bio-effect in this in vitromodel. (E-mail: [email protected]) � 2015World Federation for Ultrasoundin Medicine & Biology.
Key Words: Acute ischemic stroke, Ultrasound, Ultrasound contrast agents, Acoustic cavitation.
INTRODUCTION
Stroke is currently the fourth leading cause of death in theUnited States (Go et al. 2013). At present, the only throm-bolytic therapy that is approved by the U.S. Food andDrug Administration for the treatment of ischemic strokeis recombinant tissue-type plasminogen activator (rt-PA).However, this potent thrombolytic is administered in only1.5% of cases (Go et al. 2013) because of potentialbleeding complications and strict contraindicationcriteria (Turi et al. 1993). Adjuvant therapies that lowerthe dose of rt-PA or increase efficacy would representan important breakthrough. Ultrasound-enhanced throm-bolysis (UET) has exhibited the potential for both.
ddress correspondence to: Kenneth B. Bader, 231 Albert SabinVC 3933, Cincinnati, OH 45267-0586, USA. E-mail: kenneth.uc.edu
187
The efficacy of UET has been demonstrated in vitro(Cheng et al. 2005; Datta et al. 2008; Prokop et al. 2007)and in clinical trials (Alexandrov et al. 2004; Molina et al.2009), but the specific mechanisms underlying UET haveyet to be elucidated. Enhancement of thrombolysis isthought to be primarily mechanical in nature (Blincet al. 1993; Francis et al. 1992; Shaw et al. 2007).Acoustic streaming, generated by absorption of theultrasonic energy (Nyborg 1953), increases penetrationof rt-PA into the clot (Francis et al. 1995) or radiationforce displaces the clot (Devcic-Kuhar et al. 2002).Acoustic cavitation, or the nucleation and generation ofbubble activity by an acoustic source (Apfel 1981), hasbeen found to enhance thrombolytic efficacy (Everbachand Francis 2000). Acoustic emissions from stable cavi-tation, characterized by gentle non-linear oscillations ofthe bubbles (Flynn 1964), have previously been corre-lated with the enhancement of rt-PA thrombolysis(Datta et al. 2008; Prokop et al. 2007). These stable

188 Ultrasound in Medicine and Biology Volume 41, Number 1, 2015
bubbles are known to induce small-scale streaming,termed microstreaming (Elder 1959), which is thoughtto facilitate increased penetration of rt-PA into thethrombus (Datta et al. 2008). Additionally, microstream-ing is thought to remove fibrin degradation products,which increases the availability of plasminogen bindingsites for rt-PA (Sutton et al. 2013).
Previous studies did not, however, provide real-timemeasurement of the lytic rate, which would enable iden-tification of the mechanisms underlying thrombolyticenhancement. To overcome this difficulty, Cheng et al.(2005) developed an in vitro model to observe thrombol-ysis in real time. This model was extended by Gruberet al. (2014) to include fluid flow past the clot, a poten-tially important aspect of the lytic rate (Bajd and Ser�sa2012), to allow replenishment of cavitation nuclei(Hitchcock et al. 2011). The ability to detect bubble activ-ity optically and track the movement of the clot hasrecently been integrated into this measurement system,to probe the relationship between lytic rate, cavitationand clot movement.
METHODS
Preparation of human fresh-frozen plasma andrecombinant tissue-type plasminogen activator
Human fresh-frozen plasma (hFFP) was procuredfrom a blood bank (Hoxworth Blood Center, Cincinnati,OH, USA). Thirty-milliliter aliquots of the hFFP werethawed for each experiment and allowed to reach atmo-spheric gas equilibrium at 37�C in an open containerfor 2 h. Recombinant tissue-type plasminogen activator(rt-PA) was obtained from the manufacturer (Activase,Genentech, San Francisco, CA, USA) as lyophilized po-wer. Each vial was mixed with sterile water to a concen-tration of 1 mg/mL as per manufacturer instructions,aliquoted into 1.0-mL centrifuge tubes and stored at280�C. The enzymatic activity of rt-PA is stable over aperiod of 7 y using this protocol (Shaw et al. 2009b).
Preparation of blood clotsHuman whole blood clots were manufactured
around silk sutures according to a protocol developedby Shaw et al. (2008). After local institutional reviewboard approval and written informed consent, venous hu-man whole blood was drawn from a pool of five healthyvolunteers. Aliquots of 500 mL were transferred to sterileglass tubes containing borosilicate glass micropipets(1.12-mm inner diameter, World Precision Instruments,Sarasota, FL, USA), pre-threaded with 7-O silk sutures(Ethicon Industries, Cornelia, GA, USA). The bloodwas allowed to clot around the silk suture at 37�C for3 h. After clot formation, the tubes were stored at 5�Cfor a minimum of 3 d to allow for maximal clot retraction
(Shaw et al. 2009a), lytic resistance and stability (Shawet al. 2006). Before each measurement, the micropipetwas removed to produce a cylindrical clot adherent tothe suture. The initial clot (550 6 43 mm) was smallerthan the middle cerebral artery (2.4–4.6 mm) (Ng et al.2007; Saqqur et al. 2007), the site of occlusion for themajority of ischemic strokes (Gibo et al. 1981). However,the clot is comparable in size to intracerebral perforatingbranches of the middle cerebral artery (80–840 mm)(Marinkovic et al. 1985), which are highly vulnerableto occlusion.
Preparations of ultrasound contrast agentsVials ofDefinity (perflutren lipidmicrospheres; Lan-
theus Medical Imaging, North Billerica, MA, USA), mi-crobubbles consisting of octofluoropropaneencapsulated by a lipid shell monolayer, were activatedaccording to the manufacturer’s instructions. Vials werestored at 5�C until needed. The vials were allowed towarm to room temperature (20�C–24�C) for 1 h beforeactivation by shaking for 45 s using a Vial-Mix (LantheusMedical Imaging). The agent was diluted to a final con-centration of 2 mL/mL (13 104 particles/mL). This num-ber density is consistent with the manufacturer’srecommended dose (Lantheus Medical Imaging) for leftventricular opacification.
In vitro flow phantomThe in vitro flowmodel based on Cheng et al. (2005)
and Gruber et al. (2014) used to quantify thrombolyticefficacy and bubble activity is depicted in Figure 1. Anacrylic tank (16 3 33 3 9 cm) was filled with approxi-mately 3 L of degassed (20 6 5% dissolved oxygen),reverse-osmosis water heated to 37.36 0.3�C. The waterwas filtered (0.2 mm), and the gas content and temperaturewere maintained throughout the experiment with acustom-built recirculation system. The walls of the tankwere lined with a 1-cm-thick acoustic absorber (AptflexF48, Precision Acoustics, Dorchester, Dorset, UK).
The flow channel consisted of low-density polyeth-ylene tubing (inner diameter 1.6 mm, outer diameter3.2 mm; Part 1 J-109-10, Freelin Wade, McMinnville,OR, USA) to direct the perfusate from a reservoir to aglass micropipet (2.15-mm inner diameter, 0.3-mm wallthickness; Part 5-000-2200, Drummond Scientific, Broo-mall, PA, USA). A clot was mounted along the centralaxis of the micropipet by snuggly fitting the suture atthe ends of the micropipet with latex tubing. The micro-pipet was positioned over a microscope slide (Fisher-brand 12-550 C, Fisher Scientific, Pittsburg, PA, USA)in the bottom of the tank to allow imaging of the clotwith an inverted microscope (IX71, Olympus, CenterValley, PA, USA). The focal area of the objective (UP-lanFLN 10 3 , 10-mm working distance, Olympus)

Fig. 1. Experimental setup for observation of ultrasound-enhanced thrombolysis. CCD 5 charge-coupled device,
PCD 5 passive cavitation detector.
US-enhanced thrombolysis d K. B. BADER et al. 189
was approximately 1200 3 900 mm. Images werecaptured with a charge-coupled device camera (Retiga-2000 R, Q Imaging, Surrey, BC, Canada) at the rate of2.33 Hz. Flowwas maintained at 0.65 mL/min with a pro-grammable syringe pump (Model 44, Harvard Apparatus,South Natick, MA, USA) in continuous withdrawalmode. This flow rate is in the range of physiologic flowrates measured in the occluded middle cerebral arteryduring ischemic stroke (Alexandrov et al. 2010).
Clot diameter and positionImages of the clots were used to determine the lytic
rate (Cheng et al. 2005). The Sobel approximation(Gonzalez and Woods 2002) was used to determine thespatial gradient of each gray-scale image. The clot edgeswere determined by determined with an edge-detectionroutine according toMeunier et al. (2007). The clot diam-eter for a given frame, d, was defined as the average dis-tance between detected edges for each pixel row of theimage (600 rows total, 900-mm total length) minus thediameter of the suture (956 15 mm) (Shaw et al. 2009a).
The lytic rate was defined as the ratio of the changein clot diameter, Dd, to the change in time, Dt, as
Dd
Dt5
1
t22t1
dðt2Þ2dðt1Þdðt0Þ
(1)
where dðtÞ is the clot diameter at time t, the subscriptsindicate initial (1) and final (2) time points over whichthe lytic rate was calculated and dðt0Þ indicates the clotdiameter at time t5 0. The position of the clot for a givenframe was defined as the average location of the center ofthe clot determined over the entire length of the clot in theimage. Movement of the clot was quantified by the root-mean-square (RMS) velocity of the clot position, vRMS, as
vRMS 5
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi1
t22t1
ð t2
t1
dt
�xðt2Þ2xðt1Þ
t22t1
�2s
(2)
where xðtÞ denotes the position of the clot at time, t, andthe subscripts indicate initial (1) and final (2) time pointsover which the RMS velocity is being calculated.
Ultrasound exposure and cavitation detectionA custom-designed transducer (H160, Sonic Con-
cepts, Woodburn, WA, USA) was used to insonate theclot and perfusate. The unfocused transducer element(30-mm-diameter aperture) was excited at its resonantfrequency of 120 kHz with a function generator (33250A, Agilent Technologies, Santa Clara, CA, USA) and po-wer amplifier (1040 L, ENI, Rochester, NY, USA). Acustom-built impedance matching network (Sonic Con-cepts) maximized power transfer to the transducer. Theacoustic field was measured along the clot with a 0.5-mm hydrophone (TC 4038, Teledyne Reson Inc. Goleta,CA, USA) mounted on a computer-controlled three-axispositioner (NF-90, Velmex, Bloomfield, NY, USA).
Ultraharmonic (UH) emissions, a key acoustic signa-ture of stable cavitation (Datta et al. 2008; Hitchcock et al.2011), and broadband emissions, characteristic of inertialcavitation (Datta et al. 2008), were monitored with a pas-sive cavitation detector (PCD) aligned confocal with theclot. The PCD, a 19-mm-diameter circular single-element, long-focus 2.25-MHz transducer (595516 C,Picker Roentgen GmbH, Espelkamp, Germany), has pre-viously been used to detect cavitation at 120 kHz (Dattaet al. 2008; Hitchcock et al. 2011). The signal receivedfrom the PCD was filtered by a 10-MHz low-pass filter(J73 E, TTE, Los Angeles, CA, USA) to halt noise fromradiofrequency interference, and amplified with a wide-band low-noise amplifier (CLC100, Cadeka Microcir-cuits, Loveland, CO, USA). The signal was digitized(10-ms duration, 31.25-MHz sampling frequency), andthe power spectrum computed in MATLAB (The Math-Works, Natick, MA, USA). Ultraharmonic bands(Hitchcock et al. 2011) of the power spectrum between250 kHz and 1 MHz were summed over a 2-kHz band-width centered around the UH band. Broadband emissionsin the received signal were summed in 4-kHz bandscentered at each UH band610 kHz and630 kHz. TheseUH and broadband bands were found to have a signal-to-noise ratios greater than 3 dB (Gruber et al. 2014).
An intermittent ultrasound exposure scheme wasused as described by Hitchcock et al. (2011). A peak-to-peak pressure of 0.44 MPa and insonation period of50 s were found to maximize UH emissions and minimizebroadband emissions, indicative of inertial cavitation(Datta et al. 2006), over the 30-min treatment duration.The insonation period was followed by a 30-s quiescentperiod to allow a fresh influx of Definity to fill the micro-pipet. The optimized insonation period and quiescentperiod were repeated in succession for the duration ofthe 30-min treatment.
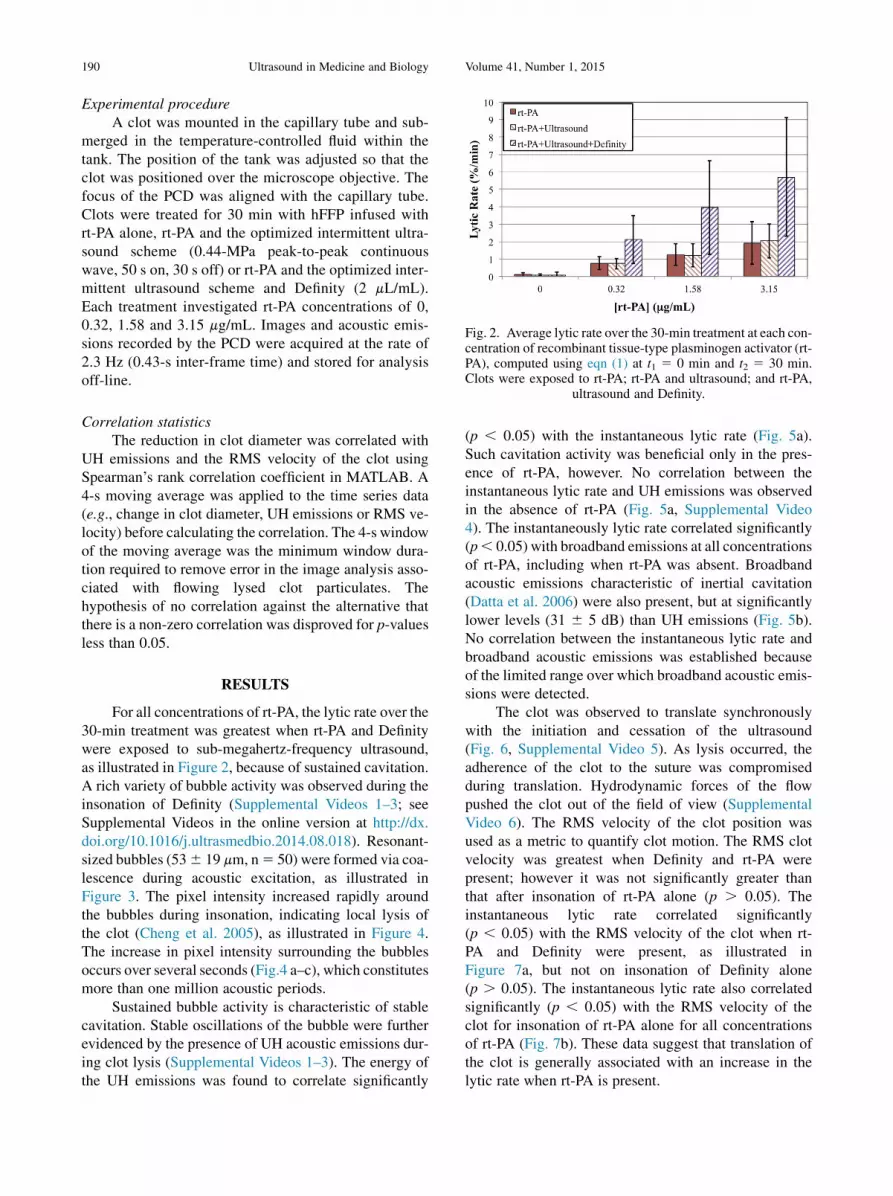
Fig. 2. Average lytic rate over the 30-min treatment at each con-centration of recombinant tissue-type plasminogen activator (rt-PA), computed using eqn (1) at t1 5 0 min and t2 5 30 min.Clots were exposed to rt-PA; rt-PA and ultrasound; and rt-PA,
190 Ultrasound in Medicine and Biology Volume 41, Number 1, 2015
Experimental procedureA clot was mounted in the capillary tube and sub-
merged in the temperature-controlled fluid within thetank. The position of the tank was adjusted so that theclot was positioned over the microscope objective. Thefocus of the PCD was aligned with the capillary tube.Clots were treated for 30 min with hFFP infused withrt-PA alone, rt-PA and the optimized intermittent ultra-sound scheme (0.44-MPa peak-to-peak continuouswave, 50 s on, 30 s off) or rt-PA and the optimized inter-mittent ultrasound scheme and Definity (2 mL/mL).Each treatment investigated rt-PA concentrations of 0,0.32, 1.58 and 3.15 mg/mL. Images and acoustic emis-sions recorded by the PCD were acquired at the rate of2.3 Hz (0.43-s inter-frame time) and stored for analysisoff-line.
ultrasound and Definity.
Correlation statisticsThe reduction in clot diameter was correlated with
UH emissions and the RMS velocity of the clot usingSpearman’s rank correlation coefficient in MATLAB. A4-s moving average was applied to the time series data(e.g., change in clot diameter, UH emissions or RMS ve-locity) before calculating the correlation. The 4-s windowof the moving average was the minimum window dura-tion required to remove error in the image analysis asso-ciated with flowing lysed clot particulates. Thehypothesis of no correlation against the alternative thatthere is a non-zero correlation was disproved for p-valuesless than 0.05.
RESULTS
For all concentrations of rt-PA, the lytic rate over the30-min treatment was greatest when rt-PA and Definitywere exposed to sub-megahertz-frequency ultrasound,as illustrated in Figure 2, because of sustained cavitation.A rich variety of bubble activity was observed during theinsonation of Definity (Supplemental Videos 1–3; seeSupplemental Videos in the online version at http://dx.doi.org/10.1016/j.ultrasmedbio.2014.08.018). Resonant-sized bubbles (536 19 mm, n5 50) were formed via coa-lescence during acoustic excitation, as illustrated inFigure 3. The pixel intensity increased rapidly aroundthe bubbles during insonation, indicating local lysis ofthe clot (Cheng et al. 2005), as illustrated in Figure 4.The increase in pixel intensity surrounding the bubblesoccurs over several seconds (Fig.4 a–c), which constitutesmore than one million acoustic periods.
Sustained bubble activity is characteristic of stablecavitation. Stable oscillations of the bubble were furtherevidenced by the presence of UH acoustic emissions dur-ing clot lysis (Supplemental Videos 1–3). The energy ofthe UH emissions was found to correlate significantly
(p , 0.05) with the instantaneous lytic rate (Fig. 5a).Such cavitation activity was beneficial only in the pres-ence of rt-PA, however. No correlation between theinstantaneous lytic rate and UH emissions was observedin the absence of rt-PA (Fig. 5a, Supplemental Video4). The instantaneously lytic rate correlated significantly(p, 0.05) with broadband emissions at all concentrationsof rt-PA, including when rt-PA was absent. Broadbandacoustic emissions characteristic of inertial cavitation(Datta et al. 2006) were also present, but at significantlylower levels (31 6 5 dB) than UH emissions (Fig. 5b).No correlation between the instantaneous lytic rate andbroadband acoustic emissions was established becauseof the limited range over which broadband acoustic emis-sions were detected.
The clot was observed to translate synchronouslywith the initiation and cessation of the ultrasound(Fig. 6, Supplemental Video 5). As lysis occurred, theadherence of the clot to the suture was compromisedduring translation. Hydrodynamic forces of the flowpushed the clot out of the field of view (SupplementalVideo 6). The RMS velocity of the clot position wasused as a metric to quantify clot motion. The RMS clotvelocity was greatest when Definity and rt-PA werepresent; however it was not significantly greater thanthat after insonation of rt-PA alone (p . 0.05). Theinstantaneous lytic rate correlated significantly(p , 0.05) with the RMS velocity of the clot when rt-PA and Definity were present, as illustrated inFigure 7a, but not on insonation of Definity alone(p . 0.05). The instantaneous lytic rate also correlatedsignificantly (p , 0.05) with the RMS velocity of theclot for insonation of rt-PA alone for all concentrationsof rt-PA (Fig. 7b). These data suggest that translation ofthe clot is generally associated with an increase in thelytic rate when rt-PA is present.

Fig. 3. Coalescence and translation of bubbles. (a) Before insonation, three bubbles are visible on the clot. (b) The threebubbles coalesce within 400 ms after ultrasound exposure. (c) The resultant bubble translates after remaining stationaryfor 3.5 s. The surrounding fluid contains recombinant tissue-type plasminogen activator (0.32 mg/mL), and Definity (2 mL/mL). The bubble appears distorted because of the long exposure time of the camera (16 ms) compared with the acoustic
period (8.33 ms). Bar in (a) 5 100 mm.
US-enhanced thrombolysis d K. B. BADER et al. 191
DISCUSSION
An in vitro flow model that allows both qualitativeobservations and real-time quantitative assessment ofthe lytic rate was developed for investigating UETmech-anisms. Two primary observations were noted in the re-sults of this study. First, clot lysis was found to occurpreferentially surrounding large, resonant-sized micro-bubbles undergoing stable oscillations. UH emissionsfrom these stable oscillations correlated with the instan-taneous lytic rate (Fig. 5a). Previous studies had docu-mented microbubble interactions with clots (Acconciaet al. 2013; Chen et al. 2013), but had not correlatedthe instantaneous lytic rate with microbubble activity.Furthermore, these studies focused primarily oninertial cavitation, whereas the present study focusedon promoting sustained stable cavitation. Other studiesmonitored the instantaneous lytic rate while insonatingrt-PA (Cheng et al. 2005) or rt-PA and microbubbles(Petit et al. 2012), but did not monitor cavitation emis-sions. Datta et al. (2006) established a correlationbetween thrombolytic efficacy and the total dose ofUH emissions over a 30-min treatment period in vitro,but lacked the ability to track the instantaneous lyticrate. The results of this study suggest that the correlation
between UH emissions and thrombolytic efficacyextends to time scales on the order of hundreds of milli-seconds. Thus, UH emissions can be used as a real-timemetric of sonothrombolytic efficacy.
The second observation of this study is that clotstranslate synchronously with the initiation and cessionof the ultrasound exposure. The RMS velocity of theclot correlates with the lytic rate (Fig. 7). Previous studiesdocumented the displacement of clots under ultrasoundexcitation (Wright et al. 2012), but did not assess throm-bolytic efficacy. A correlation was previously establishedbetween insonation parameters that promote radiationforce and thrombolytic efficacy (Francis et al. 1995;Frenkel et al. 2006; Lauer et al. 1992), but the means toquantify clot translation was lacking.
During insonation, a wide variety of microbubbleactivities were observed. Microbubbles were observedto coalesce during acoustic excitation (Fig. 3a, b), result-ing in large, resonant-sized microbubbles (53 6 19 mm).The formation of resonant-sized microbubbles via sec-ondary Bjerknes forces (Leighton 1995) has beenobserved previously (Postema et al. 2004). Microbubblestypically persisted on the clot longer than 100 s (Fig. 3),which was greater than either the insonation period (50 s)or the quiescent period (30 s). There was no discernable

Fig. 4. Increase in pixel intensity surrounding stable oscillations of acoustically activated bubble. Lysis occurs over a longtime scale compared with the acoustic period (interframe time5 1.7 s, acoustic period5 8.33 ms). The effluent surround-ing the clot is human fresh-frozen plasma, recombinant tissue-type plasminogen activator (1.58 mg/mL) and Definity(2 mL/mL). The ultrasound (120 kHz, 0.44 MPa continuous wave) is on in (a–c). The bubble appears distorted because
of the long exposure time of the camera (16 ms) compared with the acoustic period (8.33 ms).
192 Ultrasound in Medicine and Biology Volume 41, Number 1, 2015
change in the size of the persistent microbubbles, sug-gesting the presence of a stabilizing shell to overcomesurface tension (Neppiras 1980). The persistence of themicrobubbles resulted in continual lysis during insona-tion, as evident in Supplemental Videos 1–3. This sug-gests that sustained microbubble activity, a hallmark ofstable cavitation, aids in the enhancement of thrombo-lytic efficacy for these ultrasound parameters.
The significant correlation between instantaneousUH emissions and thrombolytic efficacy and lytic ratecould have a profound influence on the insonationschemes used in future UET studies. The fixed insonifica-tion and quiescent periods used in this study did not opti-mize the well-known stochastic nature of cavitation (Holtet al. 1994; Lauterborn and Holzfuss 1991). In addition,the flow rate must be known to determine the quiescentperiod. Flow rates in highly ischemic middle cerebralarteries can vary between 0 and 15 cm/s (Alexandrovet al. 2010), but can be as high as 50 cm/s without anocclusion (Reinhard 2005). Thus, the cavitation optimi-zation routine could be made more robust by real-timefeedback to assess the amount of cavitation activity andthe presence of cavitation nuclei. Such feedback couldensure the presence of a target instantaneous UH energyand, therefore, maximum lytic rate.
In addition to bubble activity, the clot was seen totranslate with the initiation and cessation of the ultra-sound (Fig. 6, Supplemental Video 5). Wright et al.(2012) and Frenkel et al. (2006) observed similar transla-tion of whole blood clots, although with focused ultra-sound pulses at 1.5 and 1.0 MHz, respectively, and notin the presence of ultrasound contrast agents. Translationof the clot is most likely due to acoustic radiation force(Nyborg 1953). The acoustic radiation force (FRAD) canbe written in terms of the time-averaged intensity of theultrasound field (I), acoustic absorption (a) and soundspeed (c) (Nyborg 1965):
FRAD 52aI
c(3)
In the case of fluids, the acoustic radiation force gen-erates acoustic streaming (Lighthill 1978), whereas intissues, it causes tissue displacement (Palmeri andNightingale 2011). The sound speeds of plasma andhuman whole blood clots are similar: 1540 m/s (Calor-Filho and Machado 2006) and 1600 m/s (Nahirnyaket al. 2006), respectively. However, the sound absorptionin human whole blood clots is two orders of magnitudelarger than that in plasma (Calor-Filho and Machado2006; Nahirnyak et al. 2006). Thus, displacement of the

Fig. 5. (a) Absolute lytic rate (��Dd=Dt��) as a function of the ul-
traharmonic (UH) energy at each concentration of recombinanttissue-type plasminogen activator (rt-PA). The lytic rate wascomputed using eqn (1), with t2 – t1 5 0.43 s, the interframetime of the clot images. Error bars represent standard deviationsof the lytic rate over a 0.05-mV2 range of UH energies. The lyticrate significantly correlates (p, 0.05) with the UH energy whenrt-PA is present. (b) Absolute lytic rate (
��Dd=Dt��) as a functionof UH and broadband energy at an rt-PA concentration of3.15 mg/mL. The lytic rate was computed using eqn (1), witht2 – t1 5 0.43 s, the interframe time of the clot images. Errorbars represent standard deviations of the lytic rate over a 0.03-
mV2 range of UH energies.
Fig. 6. Clot position as a function of time. The clot position was0 mm at time 0 min. The clot was exposed to 0.32 mg/mL recom-binant tissue-type plasminogen activator, sub-megahertz-frequency ultrasound and 2 mL/mL Definity. Positive positionvalues indicate movement along the direction of propagationof the ultrasound (i.e., away from the transducer).
US 5 ultrasound.
US-enhanced thrombolysis d K. B. BADER et al. 193
clot by acoustic radiation force should dominate overacoustic streaming. In addition, any adherent orembedded microbubbles (Acconcia et al. 2013) wouldincrease the force (Commander and Prosperetti 1989;Nyborg 1965). However, no significant increase wasobserved in the RMS velocity of the clot duringinsonation of Definity and rt-PA in comparison to rt-PAalone. The instantaneous lytic rate was found to correlatesignificantly with the RMS velocity of the clot (p, 0.05).
It is unknown whether clot translation would occurin vivo, or if this motion is specific to the in vitro throm-bolysis model used in these studies. Regardless, the cor-relation between the instantaneous lytic rate and RMSvelocity of the clot suggests translation of the clot couldbe associated with an increase in the lytic rate whenrt-PA is present.
No correlation between the instantaneous lytic rateand UH energy or clot translation in the presence of Def-inity was observed with these sub-megahertz -frequency,low-amplitude (,0.5 MPa peak to peak) acoustic excita-tions. The lack of ultrasound-mediated thrombolysis inthe absence of rt-PA has previously been observed(Frenkel et al. 2006; Holland et al. 2008; Petit et al.2012). Other types of ultrasound exposures with higheramplitudes, such as histotripsy (Maxwell et al. 2009)and high-intensity focused ultrasound (Borrelli et al.2012; Chuang et al. 2010; Rosenschein et al. 2000;Westermark et al. 1999), have been found to causeappreciable lysis without a thrombolytic drug. Thesetypes of ultrasound exposures rely on the mechanicalcollapse of inertial cavitation to initiate lysis (Maxwellet al. 2011). The ultrasound scheme employed here, incontrast, relies on the gentle oscillations of stable cavita-tion to enhance the penetration of the thrombolytic intothe clot and the removal of fibrin degradation products(Datta et al. 2008). No definitive correlation could beestablished between the instantaneous lytic rate andbroadband acoustic emissions from inertial cavitation.Note, however, that the insonation scheme used in thisstudy minimized inertial cavitation and promoted persis-tent stable cavitation. Such a correlation between the

Fig. 7. Absolute lytic rate (��Dd=Dt��) as a function of the root-
mean-square (RMS) velocity of the clot at each concentrationof recombinant tissue-type plasminogen activator (rt-PA). Thelytic rate was computed using eqn (1), with t2 – t1 5 0.43 s,the interframe time of the clot images. Similarly, the RMS ve-locity of the clot was computed using eqn (2), with t2 –t1 5 0.43 s. The Error bars represent standard deviations ofthe lytic rate over a 0.41 mm/s range of RMS velocities. (a) In-sonation of rt-PA and Definity. The lytic rate significantly corre-lates (p , 0.05) with the RMS velocity when rt-PA is present.(b) Insonation of rt-PA alone. The lytic rate significantly corre-lates (p , 0.05) with the RMS velocity at all concentrations of
rt-PA.
194 Ultrasound in Medicine and Biology Volume 41, Number 1, 2015
instantaneous lytic rate and inertial cavitation may existfor higher-amplitude schemes well above the inertialcavitation threshold, such as histotripsy.
There are several aspects of this in vitro study thatlimit the applicability of these findings in vivo. Clearlythe composition of the thrombus in the brain duringischemic stroke does not include a silk suture, and thepresence of the suture could potentially alter the clotmorphology during formation in vitro. The tethered
suture does not translate during pulsed insonation inthe in vitro model. Minimal cavitation activity was de-tected in the absence of Definity, and lysis was notobserved to occur preferentially around the suture.Thus, the contribution from the suture to clot lysis isprobably minimal. This in vitro study does not addressthe potential for embolization of the observedresonant-sized microbubbles, which may occur in vivo(Muth and Shank 2000). The low flow rate consideredin this model was fixed, and neglects the contributionof increased flow rates as the clot lyses. The additionalshear stresses associated with increased flow rates, aswould occur in vivo, have previously been reported toincrease the lytic rate (Bajd et al. 2010). The acousticperiod of 8.33 ms was much shorter than either the framerate (2.33 Hz, or 0.42-s period) or the shutter speed(16 ms) of the charge-coupled device camera. Conse-quently, any motion acting on this time scale could notbe resolved. This limitation could be overcome withhigh-speed photography studies at frame rates greaterthan the acoustic period (Bouakaz et al. 2005).
CONCLUSIONS
The observations presented here suggest that theprocess of clot lysis during sub-megahertz -frequencyUET is complex, with a combination of mechanismscontributing to this beneficial bio-effect. The mechanicalagitation of clots from ultrasound exposure was sustainedover several hundred thousand acoustic cycles. However,the correlation between the lytic rate and UH emissions ortranslation of the clot indicate these mechanisms actnearly instantaneously to enhance thrombolysis.
Acknowledgments—The authors thank Dr. George J. Shaw and Dr. JasonM. Meunier for their help in human blood for the production of clots.The authors also thank members of the Image-Guided Ultrasound Lab-oratories, especially Dr. Guillaume Bouchoux, for their helpful discus-sions during preparation of this article.—This work was supported bya grant from the National Institutes of Health (R01 NS047603).
SUPPLEMENTARY DATASupplementary data related to this article can be found online at
http://dx.doi.org/10.1016/j.ultrasmedbio.2014.08.018.
REFERENCES
Acconcia C, Leung BYC, Hynynen K, Goertz DE. Interactions betweenultrasound stimulated microbubbles and fibrin clots. Appl Phys Lett2013;103:053701.
Alexandrov AV, Molina CA, Grotta JC, Garami Z, Ford SR,Alvarez-Sabin J, Montaner J, Saqqur M, Demchuk AM,Moy�e LA. Ultrasound-enhanced systemic thrombolysis for acuteischemic stroke. N Engl J Med 2004;351:2170–2178.
Alexandrov AV, Tsivgoulis G, Rubiera M, Vadikolias K, Stamboulis E,Molina CA, Alexandrov AW, for the TUCSON Investigators. End-diastolic velocity increase predicts recanalization and neurologicimprovement in patients with ischemic stroke with proximal arterialocclusions receiving reperfusion therapies. Stroke 2010;41:948–952.

US-enhanced thrombolysis d K. B. BADER et al. 195
Apfel RE. Acoustic cavitation. In: Edmonds PD, (ed). Methods in exper-imental physics. New York: Academic Press; 1981. p. 355–411.
Bajd F, Ser�sa I. A concept of thrombolysis as a corrosion–erosion pro-cess verified by optical microscopy. Microcirculation 2012;19:632–641.
Bajd F, Vidmar J, Blinc A, Ser�sa I. Microscopic clot fragment evidenceof biochemo-mechanical degradation effects in thrombolysis.Thromb Res 2010;126:137–143.
Blinc A, Francis CW, Trudnowski JL, Carstensen EL. Characterizationof ultrasound-potentiated fibrinolysis in vitro. Blood 1993;81:2636–2643.
Borrelli MJ, O’Brien WD, Hamilton E, Oelze ML, Wu J, Bernock LJ,Tung S, Rokadia H, Culp WC. Influences of microbubble diameterand ultrasonic parameters on in vitro sonothrombolysis efficacy.J Vasc Interv Radiol 2012;23:1677–1684.e1.
Bouakaz A, Versluis M, de Jong N. High-speed optical observations ofcontrast agent destruction. Ultrasound Med Biol 2005;31:391–399.
Calor-Filho MM, Machado JC. Measurement of the ultrasonic attenua-tion coefficient of human blood plasma during clotting in the fre-quency range of 8 to 22 MHz. Ultrasound Med Biol 2006;32:1055–1064.
Chen X, Leeman JE, Wang J, Pacella JJ, Villanueva FS. New insightsinto mechanisms of sonothrombolysis using ultra-high-speed imag-ing. Ultrasound Med Biol 2013;40:258–262.
Cheng JY, Shaw GJ, Holland CK. In vitro microscopic imaging ofenhanced thrombolysis with 120-kHz ultrasound in a human clotmodel. Acoust Res Lett Online 2005;6:25.
Chuang YH, Cheng PW, Chen SC, Ruan JL, Li PC. Effects ofultrasound-induced inertial cavitation on enzymatic thrombolysis.Ultrason Imaging 2010;32:81–90.
Commander KW, Prosperetti A. Linear pressure waves in bubbly liq-uids: Comparison between theory and experiments. J Acoust SocAm 1989;85:1–15.
Datta S, Coussios CC, Ammi AY, Mast TD, de Courten-Myers GM,Holland CK. Ultrasound-enhanced thrombolysis using Definity�as a cavitation nucleation agent. Ultrasound Med Biol 2008;34:1421–1433.
Datta S, Coussios CC, McAdory LE, Tan J, Porter T, DeCourten-Myers G, Holland CK. Correlation of cavitation with ultra-sound enhancement of thrombolysis. Ultrasound Med Biol 2006;32:1257–1267.
Devcic-Kuhar B, Pfaffenberger S, Grschl M, Kollmann C, Benes E,Gottsauner-Wolf M. In vitro thrombolysis enhanced by standingand travelling ultrasound wave fields. Ultrasound Med Biol 2002;28:1181–1187.
Elder SA. Cavitation microstreaming. JAcoust Soc Am 1959;31:54–64.Everbach EC, Francis CW. Cavitational mechanisms in ultrasound-
accelerated thrombolysis at 1 MHz. Ultrasound Med Biol 2000;26:1153–1160.
Flynn HG. Physics of acoustic cavitation in liquids. In: MasonWP, (ed).Physical acoustics. New York: Academic Press; 1964. p. 58–172.
Francis CW, Blinc A, Lee S, Cox C. Ultrasound accelerates transport ofrecombinant tissue plasminogen activator into clots. UltrasoundMed Biol 1995;21:419–424.
Francis CW, Onundarson PT, Carstensen EL, Blinc A, Meltzer RS,Schwarz K, Marder VJ. Enhancement of fibrinolysis in vitro by ul-trasound. J Clin Invest 1992;90:2063.
Frenkel V, Oberoi J, Stone MJ, Park M, Deng C, Wood BJ, Neeman Z,Horne M III, Li KC. Pulsed high-intensity focused ultrasound en-hances thrombolysis in an in vitro model. Radiology 2006;239:86–93.
Gibo H, Carver CC, Rhoton AL Jr, Lenkey C, Mitchell RJ. Microsur-gical anatomy of the middle cerebral artery. J Neurosurgery 1981;54:151–169.
Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, BordenWB,Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ,Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD,Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD,Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK,Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP,Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND,Woo D, Turner MB, on behalf of the American Heart Association
Statistics Committee and Stroke Statistics Subcommittee. HeartDisease and Stroke Statistics—2013 update: A report from theAmerican Heart Association. Circulation 2013;127:e6–e245.
Gonzalez RC, Woods RE. Digital image processing. 2nd ed. Upper Sad-dle River, NJ: Prentice-Hall; 2002.
Gruber MJ, Bader KB, Holland CK. Cavitation thresholds of contrastagents in an in vitro human clot model exposed to 120-kHz ultra-sound. J Acoust Soc Am 2014;135:646–653.
Hitchcock KE, Ivancevich NM, Haworth KJ, Stamper DNC, Vela DC,Sutton JT, Pyne-Geithman GJ, Holland CK. Ultrasound-enhancedrt-PA thrombolysis in an ex vivo porcine carotid artery model. Ultra-sound Med Biol 2011;37:1240–1251.
Holland CK, Vaidya SS, Datta S, Coussios CC, Shaw GJ. Ultrasound-enhanced tissue plasminogen activator thrombolysis in an in vitroporcine clot model. Thromb Res 2008;121:663–673.
Holt RG, Gaitan DF, Atchley AA, Holzfuss J. Chaotic sonolumines-cence. Phys Rev Lett 1994;72:1376.
Lauer CG, Burge R, Tang DB, Bass BG, Gomez ER, Alving BM. Effectof ultrasound on tissue-type plasminogen activator-induced throm-bolysis. Circulation 1992;86:1257–1264.
Lauterborn W, Holzfuss J. Acoustic chaos. Int J Bifurcat Chaos 1991;1:13–26.
Leighton TG. Bubble population phenomena in acoustic cavitation.Ultrason Sonochem 1995;2:S123–S136.
Lighthill SJ. Acoustic streaming. J Sound Vib 1978;61:391–418.Marinkovic SV, Milisavljevic MM, Kovacevic MS, Stevic ZD. Perfo-
rating branches of the middle cerebral artery: Microanatomy andclinical significance of their intracerebral segments. Stroke 1985;16:1022–1029.
Maxwell AD, Cain CA, Duryea AP, Yuan L, Gurm HS, Xu Z. Noninva-sive thrombolysis using pulse cavitation therapy—Histotripsy.Ultrasound Med Biol 2009;35:1982–1994.
Maxwell AD, Owens G, Gurm HS, Ives K, Myers DD Jr, Xu Z. Nonin-vasive treatment of deep venous thrombosis using pulsed ultrasoundcavitation therapy (histotripsy) in a porcine model. J Vasc IntervRadiol 2011;22:369–377.
Meunier JM, Holland CK, Lindsell CJ, Shaw GJ. Duty cycle depen-dence of ultrasound enhanced thrombolysis in a human clot model.Ultrasound Med Biol 2007;33:576.
Molina CA, Barreto AD, Tsivgoulis G, Sierzenski P, Malkoff MD,Rubiera M, Gonzales N, Mikulik R, Pate G, Ostrem J. TranscranialUltrasound in Clinical Sonothrombolysis (TUCSON) trial. AnnNeurol 2009;66:28–38.
Muth CM, Shank ES. Gas embolism. N Engl J Med 2000;342:476–482.Nahirnyak VM, Yoon SW, Holland CK. Acousto-mechanical and ther-
mal properties of clotted blood. J Acoust Soc Am 2006;119:3766.Neppiras EA. Acoustic cavitation. Phys Rep 1980;61:159–251.Ng YS, Stein J, Ning M, Black-Schaffer RM. Comparison of clinical
characteristics and functional outcomes of ischemic stroke indifferent vascular territories. Stroke 2007;38:2309–2314.
Nyborg WL. Acoustic streaming due to attenuated plane waves.J Acoust Soc Am 1953;25:68.
Nyborg WL. Acoustic streaming. In: Mason WP, (ed). Physical acous-tics. Waltham, MA: Academic Press; 1965. p. 265–331.
Palmeri ML, Nightingale KR. Acoustic radiation force-based elasticityimaging methods. Interface Focus 2011;1:553–564.
Petit B, Gaud E, Colevret D, Arditi M, Yan F, Tranquart F, All�emann E.In vitro sonothrombolysis of human blood clots with BR38 micro-bubbles. Ultrasound Med Biol 2012;38:1222–1233.
Postema M, Marmottant P, Lanc�ee CT, Hilgenfeldt S, de Jong N. Ultra-sound-induced microbubble coalescence. Ultrasound Med Biol2004;30:1337–1344.
Prokop AF, Soltani A, Roy RA. Cavitational mechanisms in ultrasound-accelerated fibrinolysis. Ultrasound Med Biol 2007;33:924–933.
Reinhard M. Dynamic cerebral autoregulation in acute ischemic strokeassessed from spontaneous blood pressure fluctuations. Stroke 2005;36:1684–1689.
Rosenschein U, Furman V, Kerner E, Fabian I, Bernheim J, Eshel Y.Ultrasound imaging-guided noninvasive ultrasound thrombolysis:Preclinical results. Circulation 2000;102:238–245.
Saqqur M, Uchino K, Demchuk AM, Molina CA, Garami Z, Calleja S,Akhtar N, Orouk FO, Salam A, Shuaib A, Alexandrov AV, for

196 Ultrasound in Medicine and Biology Volume 41, Number 1, 2015
CLOTBUST Investigators. Site of arterial occlusion identified bytranscranial Doppler predicts the response to intravenous thrombol-ysis for stroke. Stroke 2007;38:948–954.
ShawGJ, Bavani N, Dhamija A, Lindsell CJ. Effect of mild hypothermiaon the thrombolytic efficacy of 120 kHz ultrasound enhanced throm-bolysis in an in vitro human clot model. Thromb Res 2006;117:603–608.
Shaw GJ, Dhamija A, Bavani N, Wagner KR, Holland CK. Arrheniustemperature dependence of in vitro tissue plasminogen activatorthrombolysis. Phys Med Biol 2007;52:2953–2967.
Shaw GJ, Meunier JM, Huang SL, Lindsell CJ, McPherson DD,Holland CK. Ultrasound-enhanced thrombolysis with tPA-loadedechogenic liposomes. Thromb Res 2009a;124:306–310.
Shaw GJ, Meunier JM, Lindsell CJ, Holland CK. Tissue plasminogenactivator concentration dependence of 120 kHz ultrasound-enhanced thrombolysis. Ultrasound Med Biol 2008;34:1783–1792.
Shaw GJ, Sperling M, Meunier JM. Long-term stability of recombi-nant tissue plasminogen activator at 280 C. BMC Res Notes2009b;2:117.
Sutton JT, Haworth KJ, Pyne-Geithman G, Holland CK. Ultrasound-mediated drug delivery for cardiovascular disease. Expert OpinDrug Deliv 2013;10:573–592.
Turi ZG, Goldberg S, LittleJohn JK, VanderArk C, Shadoff N,Karlsberg R, Williams J, Butman S, Stadius ML, Wise K. Dose-related efficacy and bleeding complications of double-chain tissueplasminogen activator in acute myocardial infarction. Am J Cardiol1993;71:1009–1014.
Westermark S, Wiksell H, Elmqvist H, Hultenby K, Berglund H. Effectof externally applied focused acoustic energy on clot disruptionin vitro. Clin Sci 1999;97:67–71.
Wright CC, Hynynen K, Goertz DE. Pulsed focused ultrasound-induceddisplacements in confined in vitro blood clots. IEEE Trans BiomedEng 2012;59:842–851.





























