Embed Size (px)
Citation preview

JOURNAL OF BONE AND MINERAL RESEARCH Volume 4, Number 3, 1989 Mary Ann Liebert, Inc., Publishers
Skeletal Disease in Primary Hyperparathyroidism
SHONNI J . SILVERBERG, ELIZABETH SHANE, LUZ DE LA CRUZ, DAVID W. DEMPSTER, FRIEDA FELDMAN, DAVID SELDIN, THOMAS P. JACOBS, ETHEL S. SIRIS,
MAUREEN CAFFERTY, MAY V. PARISIEN, ROBERT LINDSAY, THOMAS L. CLEMENS, and JOHN P. BILEZIKIAN
ABSTRACT
Most patients with primary hyperparathyroidism in the 1980s do not have evidence of bone disease when they are evaluated by conventional radiography. We sought to determine whether skeletal involvement can be appreciated when more sensitive techniques, such as bone densitometry and bone biopsy, are utilized. We investigated 52 patients with primary hyperparathyroidism. They had mild hypercalcemia, 2.8 f 0.03 mmol/liter (11.1 f 0.1 mg/dl), low normal phosphorus, 0.9 f 0.03 mmol/liter (2.8 f 0.1 mg/dl), and no symptoms or specific radiological signs of skeletal involvement.
The greatest reduction in bone mineral density was found at the site of predominantly cortical bone, the radius (0.54 f 0.1 g/cm; 79 f 2% of expected), whereas the site of predominantly cancellous bone, the lumbar spine (1.07 f 0.03 g/cm2), was normal (95 f 3% of expected). The site of mixed composition, the femoral neck (0.78 f 0.14 g/cm2), gave an intermediate value (89 f 2% of expected). Preferential involve- ment of cortical bone with apparent preservation of cancellous bone in primary hyperparathyroidism was confirmed by percutaneous bone biopsy. Over 80% of patients had a mean cortical width below the expected mean, whereas cancellous bone volume in over 80% of patients was above the expected mean. The results in- dicate that the majority of patients with asymptomatic primary hyperparathyroidism have evidence by bone densitometry and bone biopsy for cortical bone disease. The results also indicate that the mild hyperparathy- roid state may be protective of cancellous bone. The therapeutic implications of these observations await further longitudinal experience with this study population.
INTRODUCTION
N AN EARLIER ERA, primary hyperparathyroidism was I often accompanied by radiographically evident bone dis- ease. Specific signs, such as subperiosteal bone resorption, brown tumors, osteitis fibrosa cystica generalisata, or non- specific osteopenia were relatively common. (',') The degree of hypercalcemia reflected the severity of skeletal involve- ment.
As the multichannel autoanalyzer became widely used in clinical medicine, primary hyperparathyroidism presented more commonly as a disorder of mild hypercalcemia and infrequent apparent skeletal involvement. ( 3 , 4 ) Questions
arose quite naturally from the new clinical profile of pri- mary hyperparathyroidism as to the advisability of surgery in these patient^.'^.^' The argument was made that these patients might be better managed conservatively when there was no evidence for target organ involvement. On the other hand, nagging doubts as t o the possible existence of a hyperparathyroid process in bone, not readily appar- ent by routine skeletal radiographs, introduced a thera- peutic dilemma. Was it advisable to recommend parathy- roidectomy for patients with so-called asymptomatic hyperparathyroidism?
In the 1980s a new set of tools became available for the assessment of metabolic bone diseases. Foremost among
-
Departments of Medicine, Neurology, Pathology, Pharmacology, and Radiology, College of Physicians and Surgeons, Columbia University, New York, NY, and Helen Hayes Hospital, West Haverstraw, NY.
283

284 SILVERBERG ET AL.
these are noninvasive measurement of bone mineral den- sity and the quantitative histomorphometric analysis of the percutaneous bone biopsy specimen. With these two tech- niques, it is possible to evaluate bone in such disorders as primary hyperparathyroidism with sensitivity and specific- ity that are far superior to conventional radiography.
As part of a long-term study of primary hyperparathy- roidism, we have initiated a set of investigations designed to determine the presence, extent, and distribution of para- thyroid bone disease among patients seen today with pri- mary hyperparathyroidism. As we enter a third generation of observations to be made on this classical metabolic bone disease, more complete information on this issue should help with formulation of appropriate diagnostic and thera- peutic plans for patients. In this study, we provide evi- dence for the existence of significant bone involvement among a cohort of patients with mild primary hyperpara- thyroidism whose routine radiographs show no specific signs of the disease.
METHODS
Fifty-two patients with primary hyperparathyroidism were enrolled in the study. The diagnosis of primary hy- perparathyroidism was based upon clinical and laboratory criteria including persistent hypercalcemia, in the absence of any other cause, and elevated parathyroid hormone levels. In 15 patients, the diagnosis of primary hyper- parathyroidism was surgically confirmed at neck explora-
tion with removal of a single parathyroid adenoma in all cases.
Serum concentrations of total calcium, phosphorus, alkaline phosphatase, and albumin were determined by automated techniques (Technicon Instruments, Tarry- town, NY). Parathyroid hormone concentration was deter- mined by three different assays: two radioimmunoassays with specificities for the amino-terminal or midregion of the parathyroid hormone m01ecule~'~~~ and an immunora- diometric assay for intact parathyroid hormone. (') 25-Hydroxyvitamin D and 1,25-dihydroxyvitarnin D were fractionated from serum extracts by Sep-Pak chromatog- raphy. ( l o ) 25-Hydroxyvitamin D was then quantitated by competitive protein binding assay, and 1,25-dihydroxyvita- min D was measured by a radioreceptor assay. ( l o . l L ) Uri- nary calcium was determined by atomic absorption spec- trophotometry; urinary phosphorus by the method of Gindler and Ishizaki(L2); urinary cyclic AMP by radioim- munoassay('31; and hydroxyproline excretion by the method of Kivirikko et The normal ranges for these determinations are shown in Table 1.
Bone mineral density was determined by single-photon absorptiometry of the distal third of the nondominant ra- dius (SP 2: Lunar Radiation Corporation) and by dual- photon absorptiometry of the femoral neck and the L2-L4 regions of the lumbar spine (DP 3: Lunar Radiation Cor- poration). The precision of the single- and dual-photon measurements were 1.9 and 3.8%, respectively, with a co- efficient of variation of 5%.(15' For both machines, the data obtained on the study population were evaluated in comparison to age, sex, and race-matched control sub- jects.'L6-18) In addition, the results were analyzed by com-
TABLE 1. BIOCHEMICAL INDICES IN 52 PATIENTS WITH PRIMARY HYPERPARATHYROIDISM
Indices Mean f SEM Normal range
Serum Calcium Phosphorus Albumin Alkaline phosphatase
Midmolecule-PTH
25-Hydroxyvitamin D 1,25-Dihydroxyvitamin D
N-PTH
IRMA-PTH
Urine Calcium Phosphorus Cyclic AMP Hydroxyproline
2.8 f 0.03 mmol/liter 0.9 f 0.03 mmol/liter 44 f 1 g/liter
114 f 6 IU/liter 36 f 3 pg/ml
835 f 110 pg/ml 126 f 9 pg/ml 20 + 2 ng/ml 54 f 3 pg/ml
263 f 20 mg/g Cr
475 * 45 nmol/mmol Cr 25 * 1.5 mmol/day
41.2 f 3.6mg/day
2.2-2.7 0.8-1.5 35-50 80-110 8-24
50-330 10-65 9-52
15-60
< 250
441 + 124 < 40 mg/day

PRIMARY HY PERPARATHY ROIDlSM 285
80
paring deviation from expected at an individual site to de- viation from expected at other sites in the same subject. This kind of analysis permitted conclusions to be reached about relative involvement of bone at differing sites inde- pendent of the particular set of normals used to evaluate the data.
To date, percutaneous transiliac crest bone biopsy has been performed on 20 patients. The specimen of bone, ob- tained according to well-established technique, was fixed in 70% ethanol, dehydrated, and embedded in methyl methacrylate as previously described.(z01 Sections (7 pm) were cut with a Reichert-Jung microtome and stained with eriochrome cyanin R and Goldner's tri- chrome.'" ** ) Histomorphometric parameters were quanti- tated using a Zeiss integrating eyepiece and an eyepiece mi- crometer. A full report of the complete static and dynamic histomorphometric analysis is beyond the scope of the questions addressed in this paper. Cancellous bone volume was calculated as the fraction of a given volume of bone tissue consisting of mineralized and unmineralized cancel- lous bone. Mean cortical width was measured at seven equidistant sites along the length of each cortex. The eye- piece micrometer was oriented perpendicular to the sub- periosteal surface, and the distance t o the endosteal sur- face was recorded. Areas where cortical trabeculation con- fused the exact location of the endosteal margin were avoided. This index could not be determined on one pa- tient because of irregular insertions of aponeurotic fibers. The data were compared to an established set of normative age- and sex-matched control values.(23 24)
All results are expressed as the mean f the standard error of the mean (SEM) for each index. The data were analyzed by analysis of variance, post hoc Newman-Keuls multiple comparison test, and/or unpaired Student's t-tests when appropriate. Correlation coefficients were deter- mined by linear regression analysis. The general clinical and biochemical characteristics of the entire study popula- tion ( n = 52) were indistinguishable from those of the two smaller groups that had complete densitometry (vertebral spine, femoral neck, and radius; n = 31) or percutaneous bone biopsy ( n = 20). Moreover, the two subgroups were not significantly different from each other in any respect. This study was performed in the Center for Clinical Re- search of the Columbia-Presbyterian Medical Center. It was approved by the Institutional Review Board of the CPMC. All subjects gave their written, informed consent.
-
RESULTS Pa tien t characteristics
The majority of patients were in their middle years (fe- males: 58 * 2 years; males 55 f 3 years). The oldest pa- tient was 77; the youngest was 26. There were 36 women and 16 men. Thirty-three of the women were postmenopau- sal, but none was receiving estrogen therapy. Mean serum calcium, 2.8 * 0.03 mmol/liter (11.1 f 0.1 mg/dl), and mean serum phosphorus, 0.9 + 0.03 mmol/liter (2.8 *
0.1 mg/dl), were typical of patients with primary hyper- parathyroidism (Table 1). In only 11 patients (21%) was the serum phosphorus below normal. The mean serum alkaline phosphatase was slightly above normal, 114 f 6 IU/liter.
Parathyroid hormone levels were elevated by all three assays; for the N-terminal radioimmunoassay, 36 * 3 pg/ ml (N-PTH, nl: 8-24); midregion radioimmunoassay, 835 + 110 pg/ml (midmolecule PTH, nl: 50-330); immunora- diometric assay, 126 * 9 pg/ml (IRMA-PTH, nl: 10-65). Although all three assays for parathyroid hormone are clearly of diagnostic usefulness, their relative utility is more apparent when they awre compared to each other (Fig. 1). The midregion radioimmunoassay and the immu- noradiometric assay are both highly sensitive and showed frank elevations in 94 and 96% of patients, respectively. In contrast, only 79% of the patients had frank elevations by the N-terminal radioimmunoassay. 25-Hydroxyvitamin D levels were normal in all but one patient. The mean value was 20 * 2 ng/ml (nl: 9-52 ng/ml). In contrast, the mean 1,25-dihydroxyvitamin D level, 54 * 3 pg/ml, was in the upper range of normal (15-60 pg/ml). A total of 18 pa- tients (35%) had elevated levels of the active vitamin D metabolite. For both 25-hydroxyvitamin D and 1,25-dihy- droxyvitamin D, the distribution of values about the mean is best described as unimodal.
The mean urinary calcium excreion, determined by three separate 24 h urine collections, was 263 * 20 mg per 24 h. The value for mean was 320 f 33 (nl, < 300); for women, 237 * 23 (nl, < 250). Urinary phosphorus was 25 * 1.4
280 : 30001 '
I I I -
- E . D
60- 210- . i
40- F 140- I
P 20- I']
I .i' 70
l - l U
PTH BY IRMA MID-MOLECLLE 0
N-TERMINAL Pin PTH
FIG. 1. Parathyroid hormone concentrations in primary hyperparathyroidism as measured in three different assays. Radioimmunoassays with specificities for N-terminal and midmolecular aspects of parathyroid hormone and the im- munoradiometric assay were used on identical serum sam- ples. For each assay, rectangular area is the normal range. Also shown in each panel is the mean f SEM for the values.

286 SILVERBERG ET AL.
mmol/day (779 f 45 mg); hydroxyproline excretion was in the upper range of normal, 41 f 4 mg/day. Cyclic AMP was 475 f 45 nmol/mmol Cr (4.2 * 0.4 nmol/g Cr; nl: 3.9 f 1.1).
The study group was similar to others that have been de- scribed recently in other respects as well. The hypercal- cemia in most patients (> 90%) was mild (within 1 mg/dl above normal). A total of 10 patients had a history of nephrolithiasis, and only 1 patient had a neuromuscular syndrome consistent with the classic description of this organ system in primary hyperparathyroidism.'25' Radio- graphs of the hands, skull, pelvis, and spine were evalu- ated for the presence of specific changes of primary hyper- parathyroidism. In no patient were any signs seen (e.g., os- teitis fibrosa cystica, brown tumors, or subperiosteal bone resorption).
Bone mineral measurement A major subset of this population, 31 patients, had com-
plete densitometric studies of three skeletal sites that corre- spond principally to cortical bone (diaphyseal radius), can- cellous bone (lumbar spine), or a combination of both (femoral neck). At the lumbar spine, the average bone mineral density was 1.07 f 0.03 g/cm2, which is within 5% of the expected mean for sex, age, and race-matched subjects (Table 2). At the femoral neck, the hyperparathy- roid population began to diverge from normal with a mean value of 0.78 f 0.14 g/cm2, 89 * 2% of the expected value. The radius showed the greatest difference from nor- mal. Mean bone mineral density at this site was 0.54 * 0.10 g/cm, only 79 f 2% of the expected mean. When data from all three sites were subjected to analysis of vari- ance using the post hoc Newman-Keuls multiple compari- son test, the three sites were significantly different from each other in terms of the extent of their divergence from their expected value (p = O.OOO1; Fig. 2).
These results were also analyzed in view of the observa- tion that sites comprised primarily of cortical bone are most frequently affected by the hyperparathyroid state.
One might expect that the percentage of individuals show- ing a reduction in bone mineral density of the radius should be significantly greater than the percentage of indi- viduals showing a reduction in bone mineral density of the lumbar spine. At a site of mixed composition, the femoral neck, the percentage of individuals showing a reduction in bone mineral density would be expected to fall between those at the radius and the lumbar spine. As shown in Table 2, the results were consistent with preferential in- volvement of cortical bone in primary hyperparathyroid- ism. Bone mineral density of the lumbar spine was below 80% of the expected value in only 13% of patients. At the femoral neck, the percentage of patients with values below 80% of expected almost doubled to 23%. The radius was most extensively involved: 58% of patients had values be- low 80% of the expected value. Preferential reduction of cortical bone mineral density in primary hyperparathyroid- ism also held true when men and women were examined separately. Premenopausal women were similar to post- menopausal women in this regard, although the number of
'""1 * r I'
0 LUMBAR
0 FEMORAL = RADIUS
FIG. 2. Bone densitometry in primary hyperparathyroid- ism. Three different sites-radius, femoral neck, and lum- bar spine - are shown in comparison to expected values for age-, sex-, and ethnicity-matched normal subjects, Diver- gence from expected values is different at each site (p = 0.0001).
TABLE 2. BONE DENSITOMETRY IN PRIMARY HYPERPARATHYROIDISM
~ ~ ~~~
Mean * SEM 1.07 I 0.03 0.78 f 0.14 0.54 f 0.10 Male ( n = 11) 1.09 f 0.05 0.82 f 0.05 0.61 f 0.03 Female ( n = 20) 1.05 f 0.04 0.76 f 0.03 0.51 f 0.02
<80% of age and sex- matched control 13% 23 Vo 58%
PRIMARY HYPERPARATHYROIDISM 287
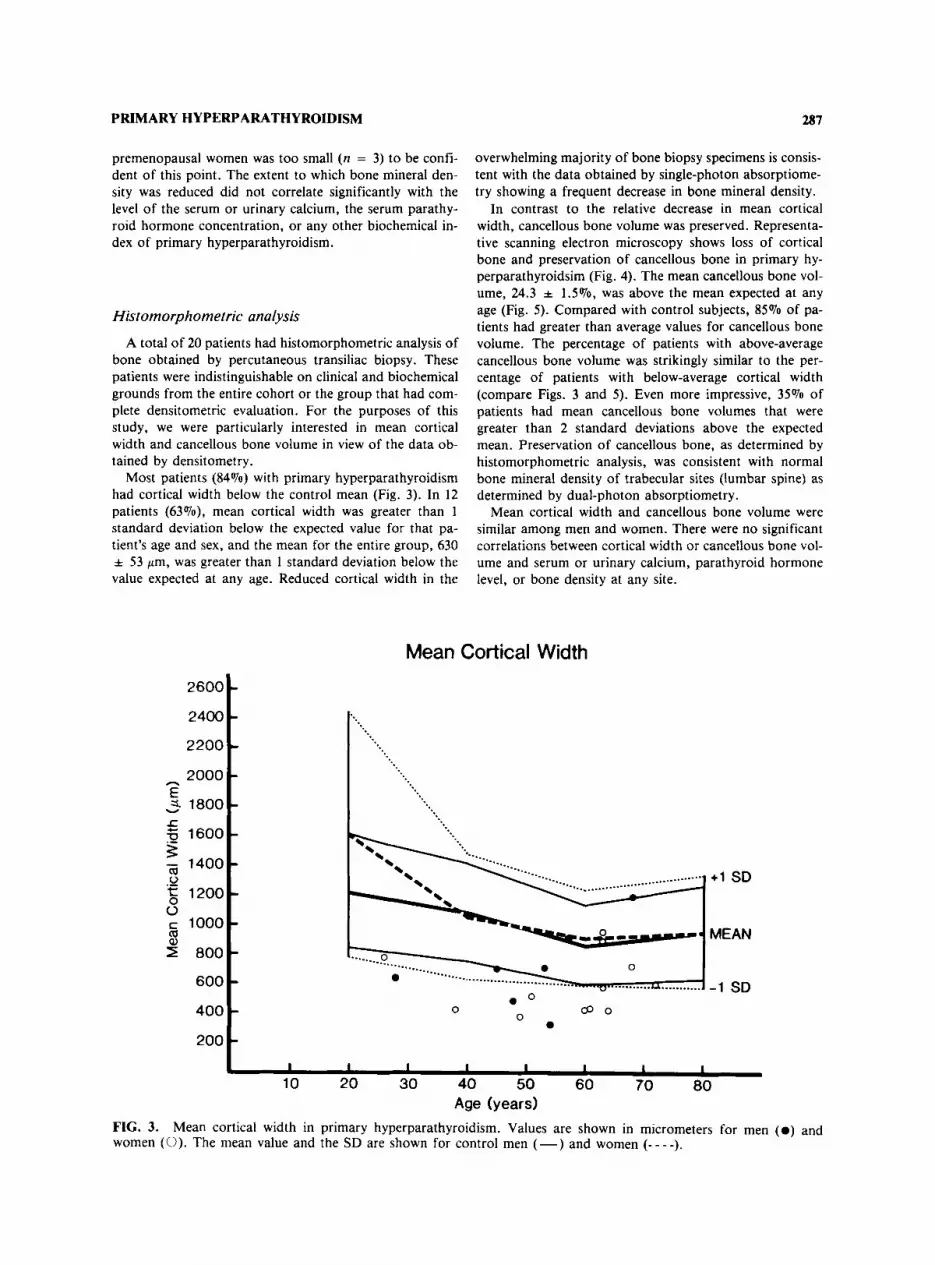
premenopausal women was too small (n = 3) to be confi- dent of this point. The extent to which bone mineral den- sity was reduced did not correlate significantly with the level of the serum or urinary calcium, the serum parathy- roid hormone concentration, or any other biochemical in- dex of primary hyperparathyroidism.
Histomorphometric analysis A total of 20 patients had histomorphometric analysis of
bone obtained by percutaneous transiliac biopsy. These patients were indistinguishable on clinical and biochemical grounds from the entire cohort or the group that had com- plete densitometric evaluation. For the purposes of this study, we were particularly interested in mean cortical width and cancellous bone volume in view of the data ob- tained by densitometry.
Most patients (84%) with primary hyperparathyroidism had cortical width below the control mean (Fig. 3). In 12 patients (63070), mean cortical width was greater than 1 standard deviation below the expected value for that pa- tient's age and sex, and the mean for the entire group, 630 f 53 pm, was greater than 1 standard deviation below the value expected at any age. Reduced cortical width in the
overwhelming majority of bone biopsy specimens is consis- tent with the data obtained by single-photon absorptiome- try showing a frequent decrease in bone mineral density.
In contrast to the relative decrease in mean cortical width, cancellous bone volume was preserved. Representa- tive scanning electron microscopy shows loss of cortical bone and preservation of cancellous bone in primary hy- perparathyroidsim (Fig. 4). The mean cancellous bone vol- ume, 24.3 * 1.5%, was above the mean expected at any age (Fig. 5). Compared with control subjects, 85% of pa- tients had greater than average values for cancellous bone volume. The percentage of patients with above-average cancellous bone volume was strikingly similar to the per- centage of patients with below-average cortical width (compare Figs. 3 and 5). Even more impressive, 35% of patients had mean cancellous bone volumes that were greater than 2 standard deviations above the expected mean. Preservation of cancellous bone, as determined by histomorphometric analysis, was consistent with normal bone mineral density of trabecular sites (lumbar spine) as determined by dual-photon absorptiometry.
Mean cortical width and cancellous bone volume were similar among men and women. There were no significant correlations between cortical width or cancellous bone vol- ume and serum or urinary calcium, parathyroid hormone level, or bone density a t any site.
Mean Cortical Width
2600
2400
2200
2000 E v =L 1800
1600
h
3
5 1200
9 800
- 1400 m 0 .-
0 c 1000 m
600
400
200
-..._. 0
........... u........... 0 ..--... e u
0 8 0 0
0
+1 SD
MEAN
-1 SD
I I I I I I 1 I
10 20 30 40 50 60 70 80 Age (years)
Mean cortical width in primary hyperparathyroidism. Values are shown in micrometers for men ( 0 ) and FIG. 3. women (0). The mean value and the SD are shown for control men (-) and women (- - - -).

288 SILVERBERG ET AL.
FIG. 4. Scanning electron micrographs of bone biopsy specimens from normal (a) and hyperparathyoid (b) subjects. Each micrograph is shown at the same magnification, x45. The field width is 2.4 mm in each case. Loss of cortical thickness (C) with preservation of trabecular plates (P) can be seen in the hyperparathyroid subject (b).

PRIMARY HYPERPARATHYROIDISM
Cancellous Bone Volume
0
289
Age (Years)
FIG. 5. men ( 0 ) and women (0). The mean value and the SD are shown for control men (-) and women (----).
Cancellous bone volume in primary hyperparathyroidism. Values are expressed as percentage (see Methods) for
DISCUSSION
The results provide information about the presence of hyperparathyroid bone disease among patients with modern- day primary hyperparathyroidism. This area of inquiry is important because most patients with primary hyperpara- thyroidism d o not show bone involvement by conventional radiography. The acknowledged insensitivity of skeletal ra- diographs in detection of parathyroid bone disease, com- bined with the clinical presentation of mild hypercalcemia in the vast majority of patients with primary hyperparathy- roidism, has raised doubts about whether skeletal involve- ment would be appreciated when more sensitive techniques became available. With newer tools, densitometry and his- tomorphometric analysis of the percutaneous bone biopsy, the results indicate that the majority of patients with asymptomatic primary hyperparathyroidism d o have evi- dence for hyperparathyroid bone disease.
Densitometry and histomorphometric analysis both show preferential involvement of cortical bone in primary hyperparathyroidism. The findings are compatible with the known physiological actions of parathyroid hormone on cortical bone as opposed to cancellous bone. Using x-ray spectrophotometry, Dalen and Hjern observed a decrease in bone mineral content at the radius but not a t the fem- oral neck, humeral head, or third lumbar With single-photon absorptiometry of the distal radius and computed tomography of the lumbar spine, Pozzi-Mucelli et al. reported greater demineralization at the A
summary of many studies employing single-photon ab- sorptiometry to assess bone mineral density of the radius confirms reductions at this site in primary hyperparathy- roidism. Two reports, however, have suggested that cancellous bone, in contrast to cortical bone, is reduced preferentially in primary hyperparathyroidism. In the re- port of Seeman et some patients may have had co- existing osteoporosis; three patients had vertebral crush fractures. Moreover, the patients included in that study were unselected and evaluated retrospectively. In the study by Hesp et a1.,(341 assessment of both cortical and cancel- lous bone was made at one site. A derived mathematical calculation was required to factor the component at the ra- dius due to cortical bone (75%) versus that due to cancel- lous bone (25%). The authors chose not to examine two different sites more representative of cortical (radius) or cancellous (lumbar spine) bone. Their results thus cannot be directly compared to those of the current study.
Histological examination of bone in primary hyperpara- thyroidism has concentrated on the bone remodeling pro- cess per se,'35-39) but there has been relatively little atten- tion given to the effects of the hyperparathyroid state on cortical versus cancellous elements. Most reports, how- ever, that have measured cancellous bone volume confirm its preservation in primary hyperparathyroidism. (35.36.38.401 Extremely little information is available about cortical width in bone biopsy specimens from patients with pri- mary hyperparathyroidism. Preliminary data from Parfitt et al. have suggested that in primary hyperparathyroidism,

SILVERBERG ET AL. 290
osteoclast resorptive activity is increased on the endocorti- cal, but not on the trabecular surfaces of bone.(4L) If con- firmed, this observation would provide an interesting cellu- lar mechanism for our observation of preferential cortical bone involvement in primary hyperparathyroidism. It is also possible that the endocortical surface of bone grad- ually becomes “trabecularized,” with maintenance of total bone volume at the expense of the cortical elements.
The results show widespread evidence for excessive para- thyroid hormone action on bone in patients with asympto- matic primary hyperparathyroidism. They confirm earlier findings of Riggs et al., who, using an older microradio- graphic technique, reported increased bone resorption rate on biopsy in patients with primary hyperparathyroidism, including a subset of patients with mild hypercalcemia. 14‘)
Our results, however, raise questions about the signifi- cance of observations that can be gleaned only by sophisti- cated technologies. It could be argued that evidence for parathyroid hormone action on bone is not unexpected in this disease and that it does not in itself indicate any reason for reclassifying patients who were previously thought to be asymptomatic. On the other hand, the pervasiveness of skeletal involvement among this cohort of patients must be duly noted.
The last implication of this study pertains to postmeno- pausal women with primary hyperparathyroidism. It has been reasoned that primary hyperparathyroidism in post- menopausal women may place them at additional risk for the development of osteoporosis. ( 4 3 1 Certainly, in those patients with obvious bone disease by skeletal radiography, this argument is reasonable. However, the population de- scribed in this report shows relative preservation of cancel- lous bone, the component of bone that is predominantly affected in postmenopausal osteoporosis. It is conceivable that the increased level of parathyroid hormone in these patients is actually helping to preserve cancellous bone. In this regard, treatment of osteoporosis with low-dose para- thyroid hormone has led to an increase in cancellous bone mass. ( 4 4 , 4 5 ) Furthermore, postmenopausal women who de- velop primary hyperparathyroidism and are treated with estrogens show no change in cancellous bone but an in- crease in cortical b ~ n e . ‘ ~ ’ , ~ ~ ) Obviously, definitive conclu- sions regarding the relative risk or protection of the trabec- ular skeleton in the postmenopausal woman with asymto- matic primary hyperparathyroidism cannot be reached until further information is available.
The data from this study suggest that aggressive therapy of primary hyperparathyroidism should not be undertaken solely for the purpose of preventing osteoporosis. On the other hand, the possibility does exist that enhanced corti- cal bone loss in primary hyperparathyroidism may contrib- ute to an increase in fracture incidence at the radius or at the femoral neck, a site of mixed cortical and cancellous bone. The overall therapeutic implications of widespread skeletal involvement of cortical bone in patients with mild primary hyperparathyroidism must, however, await the re- sults of ongoing careful longitudinal follow-up of these in- dividuals.
ACKNOWLEDGMENTS
We are indebted to the following individuals for their help in this project: Drs. P. Alderson, P. Esser, and S. Turken, Mr. D. McMahon, Ms. A. Dixon, and Ms. D. Slonim. Supported, in part, by AM 32333, AR 36446, AR 35647, DK 01836, and RR 00645 from the National Insti- tutes of Health.
REFERENCES
1 . Albright F, Reifenstein EC 1948 The Parathyroid Glands and Metabolic Bone Disease. Williams & Wilkins, Baltimore.
2. Pugh DG 1951 Subperiosteal resorption of bone. Am J Ro- entg 66:577-581.
3. Heath H, Hodgson SF, Kennedy MA 1980 Primary hyper- parathyroidism: Incidence, morbidity and economic impact in a community. N Engl J Med 302:189-193.
4. Mundy GR, Cove DH, Fisken R, Sommers S, Heath DA 1980 Primary hyperparathyroidism: Changes in the pattern of clinical presentation. Lancet 1:1317-1320.
5. Scholz DA, Purnell DC 1981 Asymptomatic primary hyper- parathyroidism: 10 year study. Mayo Clin Proc 56:473-478.
6 . Vant Hoff W, Ballardie FW, Bicknell EJ 1983 Primary hy- perparathyroidism: The case for medical management. Br Med J 287:1605-1608.
7. Cholst IN, Steinberg SF, Tropper PJ, Fox HE, Segre GV, Bilezikian J P 1984 The influence of hyperrnagnesernia on se- rum calcium and PTH levels in human subjects. N Engl J Med 310:1221- 1225.
8. Mallette LE, Tuma SN, Berger RE, Kirkland JL 1982 RIA for the middle region of human parathyroid hormone. J Clin Endocrinol Metab 54:1017-1024.
9. Nussbaum SR, Zahradnik RJ, Lavigne JR, et al. 1987 Highly sensitive two-site IRMA of parathyrin and its clinical utility in evaluating patients with hypercalcemia. Clin Chem 33:
10. Reinhardt TA, Horst RL, Orf JW, Hollis BW 1984 A micro- assay for 1,25-dihydroxyvitamin D not requiring high-perfor- mance liquid chromatography: Application to clinical stud- ies. J Clin Endocrinol. Metab 58:91-98.
11. Preece MA, O’Riordan JLH, Lawson DEM, Kodicek E 1974 An assay for 2.5-hydroxycholecalciferol and 25-hydroxyergo- calciferol in serum. Clin Chim Acta 54:235-242.
12. Gindler EM, lshizaki RT 1969 Rapid semimicrocolorimetric determination of phosphorus in serum and nonionic surfac- tants. Clin Chem 15807.
13. Steiner AL, Parker CW, Kipnis DM 1972 Radioimmunoas- say for cyclic nucleotides. J Biol Chem 247:1106-1112.
14. Kivirikko Kl, Laitinen 0, Prockop DJ 1967 Modification of a specific assay for hydroxyproline in urine. Anal Biochem
15. Wahner HW, Dunn WL, Mazess RE, Towsley M, Lindsay R, Markhard L, Dempster D 1985 Dual photon Gd-153 ab- sorptiometry of bone. Radiology 156:203-206.
16. Mazess RV (ed) 1974 Bone mineral content in normal white women. International Conference on Bone Mineral Measure- ment. DHEW publication NlH 75-683.
1364- 1367.
19:249-255.

PRIMARY HYPERPARATHYROIDISM 291
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31 .
32.
33.
Mazess RV, Barden HS, Ettinger M, Johnston C, Dosuinui B, Baran D, Powell M, Notelovitz M 1987 Spine and femur density using DPA in US white women. Bone Min 2211- 219. Luckey MM, Meier DE, Mandeli J , Goldsmith S 1987 Axial and appendicular bone density in healthy white and black women. J Bone Min Res Z:(suppl 1):abstract 327. Recker RR 1983 Bone ~ ~ s I o m o ~ ~ h o m e t r y Techniques and Interpretation. CRC Press, Boca Raton, FL. Dempster DW, Shane E, Horbert W, Lindsay R 1986 A sim- ple method for correlative light and scanning electron mi- croscopy of human iliac crest bone biopsies. J Bone Min Res 1: 15-21. Matrajit H , Hioco D 1966 Solochrome cyanine/R as an indi- cator dye of bone morphology. Stain Techno1 41:97-100. Goldner J 1937 A modification of the Masson trichrome technique for routine laboratory purposes. Am J Pathol 14:
Courpran P , Meunier P , Bressot C, Giroux AM 1977 Amount of bone in iliac crest biopsy: Significance of the tra- becular bone volume. In Meunier P (ed) Second Interna- tional Workshop on Bone Histomorphometry. Societe de la Nouvelle Imprimarie Fournie, Toulouse, pp. 39-53. Melsen F, Melsen B, Mosekilde L, Bergmann S 1978 Histo- morphometric analysis of normal bone from iliac crest bi- opsy. Acta Pathol Microbiol Scand A86:70-81. Patten BM, Bilezikian J P , Mallette LE, Prince A, Engel WK, Aurbach CiD 1974 The neuromuscular disease of hyper- parathyroidism. Ann Intern Med 80:182-193. Dalen N, Hjern B 1974 Bone mineral content in patients with primary hyperparathyroidism without radiological evidence of skeletal changes. Acta Endocrinol (Copenh) 75:297-304. Pozzi-Mucelli RS. Kanter AS, Genant HK, Cann CE, Ettin- ger B, Kolb FO 1983 Quantitative bone mineral analyses in primary hyperparathyroidism. J Comput Assist Tomogr 7: 555. Mautalen C , Reyes HR, Ghiringhelli G , Fromm G 1986 Cor- tical bone mineral content in primary hyperparathyroidism. Acta Endocrinol (Copenh) 111:494-497. Leppla DC, Snyder W, Pak CYC 1982 Sequential changes in bone density before and after parathyroidectomy in primary hyperparathyroidism. Invest Radio1 17:604-606. Fuss M, Gillet C , Simon J , Vandewalle JC, Schoutens A, Bergmann P 1983 Bone mineral content in idiopathic renal stone disease and in primary hyperparathyroidism. Eur Urol
Pak CYC, Kaplan R, Notz C, Stewart A, Bone H, Browne R 1975 Photon absorptiometric analysis of bone density in pri- mary hyperparathyroidism. Lancet 1:7-8. Horowitz M, Wishart J , Need AG, Morris H, Philcox, J . Nordin C 1987 'Treatment of postmenopausal hyperparathy- roidism with norethindrome. Arch Intern Med 147:681-685. Seeman E, Wahner HW, Offord KP, Kumar R, Johnson WJ, Riggs BL 1982 Differential effects of endocrine dysfunc-
237-243.
9~32-34.
tion on the axial and appendicular skeleton. J Clin Invest 69:
34. Hesp R, Tellez M, Davidson L, Elton A, Reeve J 1987 Tra- becular and cortical bone in the radii of women with para- thyroid adenomata. Bone Min 2:301-3 10.
35. Eriksen EF, Mosekilde L, Melsen F 1986 Trabecular bone re- modelling and balance in primary hyperparathyroidism. Bone 7:213-221.
36. Tam CS, Bayley A, Cross EG, Murray TM, Harrison J E 1982 Increased bone apposition in primary hyperparathy- roidism. Metabolism 31:759-765.
37. Delmas PD, Meunier P, Faysse E, Saubier EC 1986 Bone histomorphometry and BGP in the diagnosis of primary hy- perparathyroidism. World J Surg 10572-577.
38. Charhon SA, Edouard CM, Arlot ME, Meunier PJ 1982 Ef- fect of PTH on remodeling of iliac trabecular bone packets in patients with primary hyperparathyroidism. Clin Orthop
39. Meunier PJ , Vignon G , Bernard J, Edouard C, Courpron D 1973 Quantitative bone histology in the diagnosis of hyper- parathyroid states. In Frame B, Parfitt AM, Duncan H (eds) Clinical Aspects of Metabolic Bone Disease. Exerpta Medica, Amsterdam.
40. Marcus R, Madrig P, Crim M, Pont A, Kosek J 1984 Conju- gated estrogens in the treatment of postmenopausal women with hyperparathyroidism. Ann Intern Med 100:633-640.
41. Parfitt AM, Kleerekoper M, Rao D, Stanciu J, Villanueva AR 1987 Cellular mechanisms of cortical thinning in primary hyperparathyroidism. J Bone Min Res Z(suppl 1):abstract 384.
42. Riggs BL, Kelly PJ , Jowsey J , Keating FR 1965 Skeletal al- terations in hyperparathyroidism. J Clin Endocrinol 25:777- 783.
43. Hodgson SF, Heath H 1981 Asymptomatic primary hyper- parathyroidism: Treat or follow? Mayo Clin Proc 56521- 523.
44. Reeve J, Meunier PJ , Parsons JA, et al. 1987 Anabolic ef- fect of human PTH on trabecular bone in involutional osteo- porosis. Br Med J 280:1340-1344.
45. Slovik DM, Rosenthal DC, Coppelt SH, et a1 1986 Restora- tion of spinal bone in osteoporotic men by treatment with human PTH (1-34) and 1,25-dihydroxyvitamin D. J Bone Min Res 1:377-382.
1302-1309.
162255-263.
Address reprint requests to: Dr. John P. Bilezikian
Department of Medicine 9-410 College of Physicians and Surgeons
630 W. 168th Street New York, NY I0032
Received for publication October 12, 1988; in revised form De- cember 24, 1988; accepted December 26, 1988.





























