Embed Size (px)
Citation preview
Psychotherapy Volume 24/Fall 1987/Number 3
SOME GENDER EFFECTS IN A BRIEF PSYCHOTHERAPY
ENRICO E. JONES JANICE L. KRUPNICK PATRICIA K. KERIGUniversity of California, Berkeley
Two studies investigated the influenceof therapist gender as well as patientage and pretreatment distress level onprocess and outcome in a brief 12-session psychodynamic psychotherapy.Pre- and posttherapy assessmentsdisclosed that patients treated byfemale therapists experienced moresymptomatic improvement and reportedmore satisfaction with treatment thanthose treated by male therapists.However, patient age accounted fortwice, and patient pretreatment level ofdisturbance more than three times, theoutcome variance contributed bygender. In Study 2 female therapistswere judged to arouse less negativeaffect in women patients and to arousefewer interpersonal difficulties.
There has been a good deal of discussion con-cerning the role of gender in psychotherapy. Theemergence of gender as a theme in both clinicaland research literatures is in part a reflection ofcontemporary social issues, but the fact that therecipients of treatment in mental health settingsare more likely to be women, while the providersare more often men (Brodsky & Hare-Mustin,1980) has given rise to some uncertainty aboutthe effectiveness of this common gender matchin promoting change and psychological well-beingin women clients. Much of the debate revolvesaround the concern that male therapists may serve
Grateful acknowledgment is extended to Mardi J. Horowitzand his colleagues at the Center for the Study of Neuroses,Langley Porter Institute, University of California, San Franciscofor granting access to the Center's data archive.
Reprints may be ordered from Enrico E. Jones, PsychologyDepartment, University of California, Berkeley, CA 94720.
as agents of social control, encouraging womento adjust to a status quo that inhibits personalgrowth and adjustment (Chesler, 1972), and theapprehension that male therapists may influencewomen clients to accept traditional roles, em-phasizing dependence and a primary orientationtoward the family. It has also been suggested thatwomen fare better in psychotherapy with womenpractitioners because of their presumed superiorityin effectively understanding and empathizing withwomen's experience, and assumed lesser tendencyto sex-role stereotype (Rice & Rice, 1973).
These assertions, however, rest more on the-oretical assumptions or ideological biases than onclinical observation and empirical evidence. Someresearch suggests that therapists in general (Brov-erman et al., 1970), and perhaps male therapistsin particular (Maslin & Davis, 1975), hold differentstandards of ideal behavior and emotional healthfor men and women, but is is not clear that suchviews affect psychotherapy to any great extent.While acknowledging that some mental health-care providers may well share the sex-role stereo-types of their lay contemporaries, Whitley (1979)notes that there is little evidence to suggest thatsuch thinking affects professional judgments ortreatment goals. It is quite possible that cliniciansadhere more to therapeutic norms that stress de-velopment of the patient's personal values, talents,and autonomy than to social biases and genderstereotypes. An overview of the literature on sex-role bias and stereotyping leaves us not only un-certain whether bias against women patients ac-tually exists but also whether this presumptivebias is more pronounced among male cliniciansand, if so, how it might translate into unhelpfultherapeutic behavior in psychotherapy.
These important ambiguities derive in part fromthe fact that analogue studies comprise most ofthe research in this area. Frequently these studiesinvolve single interviews employing subjects drawnfrom college populations; or, they are investigationsof therapists' attitudes and expectations that rely,for example, on ratings of hypothetical case de-
336

Gender Effects in Brief Therapy
scriptions. There is some question about how ef-fectively these sorts of studies capture meaningfuldimensions of psychotherapy; they may in facthave only a tenuous relationship to practice. Inthis area of investigation, naturalistic designs thatreflect psychotherapy as it is actually conductedare clearly superior (Maffeo, 1979). Still, studiesof gender in actual treatment situations have sim-ilarly failed to yield unambiguous findings; thosethat have attempted to use gender as a variableto predict therapy outcome have been sparse, andtheir results equivocal. Even reviewers of thisliterature have arrived at different positions, withLuborsky et al. (1971) concluding that superioroutcomes may be achieved when patient and ther-apist are matched according to gender, while Melt-zoff & Kornreich (1970) and Garfield (1978) werepersuaded that the evidence shows no clear re-lationship between gender and outcome. However,these and other reviewers (e.g., Orlinsky andHoward, 1980) are united in their criticism ofboth the limited quantity and questionable qualityof existing studies. Among the method problemsthat have been identified as contributing to a lackof clarity are the failure of most investigators toemploy control groups, the use of small samplesdrawn from varied populations, and the lack ofrandom assignment.
These prevailing conditions have sustained theimpression that gender in and of itself is not apowerful or consistent predictor of outcome. Thenature of existing research notwithstanding, how-ever, this should come as no great surprise inlight of psychotherapy research's consistent failureto establish a definitive relationship between anysingle therapist characteristic, ranging from ex-perience level to personality type, and treatmentoutcome (Parloff et al., 1978). The psychotherapysituation is obviously influenced by many forces;and these multiple variables interact with eachother and can contribute to individual changethrough divergent modes of causality (Meehl,1978). There are serious difficulties inherent inattempting to assess the influence of these variablesin isolation from each other; a single dimensionwithin the therapy situation would have a robusteffect indeed to be able to demonstrate a consistentrelationship to outcome.
In fact, the most convincing studies of genderin psychotherapy demonstrate interaction effects.For example, both Cartwright & Lerner (1963)and Kirshner et al. (1978) found that therapistlevel of experience interacts with gender in influ-
encing outcome. Similarly, while Orlinsky &Howard (1976, 1980) found no main effects as afunction of therapist-patient gender match, theydiscovered significant interactions when certainantecedent patient characteristics, such as age,marital status, and diagnosis were considered,showing that therapy experience for younger, un-married and depressed women was more satisfyingand supportive with women therapists. Jones &Zoppel (1982) conducted two related studies withrelatively large samples of therapists and patientsdemonstrating that female therapists rated theirclients, and particularly their women clients, ashaving shown greater improvement than did maletherapists; moreover, former clients, regardlessof gender, agreed in retrospective reports of theirexperience of treatment process that women ther-apists were more effective in terms of the actualbehavior that constitutes psychological interven-tion. Nevertheless, generalizations from thesefindings are probably limited by the type of therapy,its length and frequency (average of once a weekfor about 35 weeks), and the nature of the sample,which was, like the Orlinsky & Howard study,comprised of predominantly young, single patients.It is possible that these findings will not generalizeto other forms of psychotherapy, such as cognitivetherapies, with their greater emphasis on problemsolving rather than interpersonal issues, or forpsychoanalysis, with its intensive focus ontherapist-patient relationship issues. What isneeded is a replication of these potentially importantfindings on other samples, and with other formsof therapy, and in a manner that allows the detectionof other treatment variables that may interact tocontribute to a gender effect. The two studiespresented here address some of these deficienciesby examining gender in a broader, multidimen-sional framework. Study 1 attempts to replicatethe finding of gender effects in psychotherapy bydetermining whether women patients achieve su-perior outcomes when treated by female, ratherthan male, therapists in a particular treatment mo-dality: a brief (12-session) psychodynamic therapy.In addition, and perhaps even more important, itinquires how other patient characteristics, spe-cifically patient age and pretreatment psychologicalstatus, may influence treatment outcomes relativeto therapist gender. In Study 2, psychotherapyprocess is explored in a subset of the treatmentsfor which outcomes were investigated in an effortto understand how these patient characteristicsinfluence therapeutic processes.
337
E. E. Jones et al.
Study 1
Method
Procedures
Data for the study were obtained from the ar-chives of the Center for the Study of Neuroses,a clinical research project within the Universityof California, San Francisco, department of psy-chiatry. The center is a clinic specializing in thetreatment of individuals who have experienced astressful life event, specifically a personal loss orinjury, and who are suffering from a posttraumaticstress reaction. Although most patients were re-ferred by mental health professionals or physicians,some were self-referred, having learned about thecenter through articles in local media. Individualsaccepted for treatment must have experienced sometraumatic life event involving loss within the pre-ceding year. The loss could have been of anotherperson, a job, a home, a body part, or an aspectof the self, for example, a diminution of self-esteem due to a perceived, if not actual, loss.Most commonly, individuals sought help followingthe death of a loved one or after personal injurydue to accidents or violence. In addition, theymust have suffered from symptoms characteristicof a stress-response syndrome, such as insomnia,nightmares, or intrusive ideas, images, or feelingsrelated to the traumatic event. Signs of avoidance,such as excessive "busyness" or conscious attemptsto avoid reminders of the event, also indicatedpresence of the syndrome. Those accepted fortreatment were assessed as functioning at a neuroticto borderline level; they met the DSM-III criteriafor posttraumatic stress disorder or adjustmentdisorder, and most qualified as well for additionalanxiety or affective disorder diagnoses. Excludedand referred elsewhere were those with a historyof psychiatric hospitalization, persons with severe,longstanding character problems, and those witha life-style of traumatic life events.
After initial evaluation, patients were randomlyassigned to therapists for a 12-session treatmentcourse. Patients and therapists completed an ex-tensive battery of assessment instruments pre- andposttherapy and all therapy sessions were audio-taped. Four months after termination, patients wereseen in follow-up interviews conducted by thesame independent clinical evaluator who ini-tially interviewed the patient before treatment.The evaluators, which included both men andwomen, were blind as to the identity of the ther-
apists and to the responses of therapists and patientson outcome instruments. Since the data were ob-tained from the archives months, and in someinstances, years after they were collected, eval-uators obviously had no knowledge of the aimsof these studies.
Patient Sample
The patient sample for Study 1 consisted of 60cases, all women, selected from the archives. Halfof these patients had been treated by female ther-apists, while the other half had been treated bymale therapists. Individual cases were selected onthe basis of completeness of the record; for ex-ample, only patients who completed the recom-mended course of 12-session therapy were includedin the sample, and cases which contained an excessof missing assessment data were excluded in favorof other cases treated by the same therapist whichwere more complete. Although it would have beenpreferable to include male patients in the study,they were not, simply because there were notenough cases available to comprise a sufficientlylarge male sample. The disproportionate numberof women patients treated at the clinic is consistentwith the greater numbers of women generally seenin outpatient psychotherapy.
The 60 women who ultimately comprised thesample ranged in age from 20 to 67, with a meanage of 39 (SD = 13.1). The age distribution oftherapy samples is frequently badly skewed towardyounger ages; this was not the case in the presentpopulation, which had a median age of 35 years.Thirty percent (N = 18) of the sample had neverbeen married, 28% (N = 17) were widowed, 20%(AT = 12) were married, 17% (N = 10) weredivorced, and 5% (N = 3) were separated fromtheir spouses. The vast majority (75%) had ex-perienced a bereavement, 25 (42%) of these fol-lowing the death of a parent, 17 (28%) after thedeath of a husband, and 3 (5%) after the deathof a son, friend, or student. Robbery or assaultwas the precipitating stress for 10% (N = 6) ofthe sample; 2 (3%) of the women came in followinga rape; 3 (5%) had undergone mastectomy; theremaining 4 (7%) came in after abortion, threatof cancer, fire, or car accident. Ninety percentwere white; all had at least some high schooleducation, with 62% (N = 37) having completedcollege; occupations included sales, clerical, ortechnical positions as well as homemakers andprofessionals. The sample probably reflects verywell the demographic characteristics of patients
338
Gender Effects in Brief Therapy
commonly seen in outpatient psychotherapy.
Therapist Sample
The 25 therapists in the sample, 11 women and14 men, had been trained in the psychodynamicmodel and considered it to be their primary the-oretical orientation. Although their training hadinitially focused on the practice of longer-termtherapy, they had since acquired additional trainingand experience in short-term dynamic treatment.In addition, each therapist received an initial ori-entation to time-limited dynamic psychotherapywith persons suffering from posttraumatic stressdisorders. This model, derived from that of Malan(1976) and Mann (1973), includes strategies forworking with stress-related symptomatology aswell as specific techniques for patients with dif-ferent defensive styles. A manual outlines theprescribed treatment model (Horowitz et al.,1984a), and frequent presentation of cases in theclinic aided therapists in adhering to the recom-mended pattern of treatment. The theoreticalframework common to the therapists as well astraining in the application to a particular therapeuticmodel resulted, we believe, in fairly standardizedtreatments.
Since therapist experience level has been foundto interact with therapist gender in influencingoutcomes, male and female therapists were matchedto the extent possible in experience as well as interms of the professional discipline (source oftraining) they represented. The male therapistsample of 14 therapists ranged from 3 to 20 yearsof experience; this group included 7 third-yearpsychiatric residents, 4 Ph.D. psychologists with1 to 2 years of postgraduate experience, and 3psychiatrists, one with 6 years of psychotherapyexperience and two with psychoanalytic trainingand roughly 20 years of experience. The femalesample of 11 therapists also ranged from 3 to 20years of experience, and included 3 third-yearpsychiatric residents, 2 fifth-year Doctor of MentalHealth trainees, 3 Ph.D. psychologists with 1 to3 years of postgraduate experience, one psychiatristwith 20 years of experience, and two psychiatricsocial workers with 5 and 8 years of experience,respectively. Although a relatively close matchbetween male and female therapists was achieved,male therapists nevertheless had a slight edge inexperience level.
Instruments
Patient Ratings. The Brief Symptom Inventory
(BSI), completed by patients at initial evaluation,termination, and follow-up, is a brief form of theSCL-90-R, a self-report symptom inventory con-structed to assess the psychological and symptomstatus of psychiatric patients, and which has beenused successfully in a wide variety of settings andapplications. The BSI comprises 53 items; eachitem is rated on a 5-point scale of distress (0-4)ranging from "not at all" to "extremely." Itemswere selected to best reflect the nine primarysymptom dimensions of its parent instrument, theSCL-90-R: somatization, obsessive-compulsive,interpersonal sensitivity, depression, anxiety,hostility, phobic anxiety, paranoid ideation, andpsychoticism. A Global Severity Index combinesinformation on the numbers of symptoms and theintensity of experienced stress. Extensive normativedata for the BSI are available, and both test-retestand internal consistency reliabilities have beenshown to be very good for the primary symptomdimensions. Furthermore, correlations with thecomparable dimensions of the SCL-90-R are high,and high convergence between BSI scales andlike dimensions of the MMPI provide good evi-dence of convergent validity (Derogatis & Mel-isaratos, 1983).
The Impact of Event Scale (IES), also a patientself-report, is designed to tap the dimensions ofsymptomatology that are more specific to stressresponses. This 16-item scale was constructed todetect the presence of a posttraumatic stress dis-order, a relatively new diagnostic category in DSM-III, which designates a characteristic set of psy-chological symptomatology in response to trau-matic life events. The IES can be anchored toany specific life event and assesses two of theessential psychological experiences associated withstress disorders: "intrusion" (intrusively experi-enced ideas, images, feelings, and bad dreams)and "avoidance" (consciously recognized avoidanceof certain ideas, feelings, or situations). The itemsin this instrument were derived from interviewswith nonpatient subjects who had been exposedto stressful films in experimental studies as wellas from the responses of a sample of patients.The scale has been subjected to a series of reliabilityand validity studies, and has been demonstratedto be sensitive to changes in the degree of severityof distress in psychotherapy patient samples (Zil-berg et al., 1979). The instrument was completedby patients at initial evaluation, termination, andfollow-up.
The Client Satisfaction Questionnaire (CSQ) is
339

E. E. Jones et al.
a simple, 8-item scale constructed to assess patients'general satisfaction with services, usable in a widevariety of settings. Although this self-report mea-sure yields a single score assessing the client'ssatisfaction with services, it allows respondentsto differentiate their expressions of satisfactionalong several dimensions. Examples of items are:"Have our services helped you deal more effectivelywith your problems?" and "If you were to seekhelp again, would you come back to our program?"Each item is rated on a 4-point scale. In a seriesof validation studies (Larsen et al., 1979), ther-apists' estimates of how satisfied they believedtheir patients to be with their therapy correlated.56 with actual patient ratings on the CSQ. Furtherevidence of concurrent validity is the relationshipbetween patient ratings of therapy gains or globalimprovement, based on responses to SCL-90 items,and the CSQ (r = .53); a positive association wassimilarly demonstrated between therapist ratingsof patient improvement on the Brief PsychiatricRating Scale and CSQ scores. The CSQ was ad-ministered to patients at the follow-up evaluation.
Therapist and Clinical Evaluator Ratings. TheStress Response Rating Scale (SRRS) is the cli-nician's measure for rating the patient's responseto a stressful life event. Designed to parallel thepatient-rated Impact of Event Scale, the SRRSaims to identify and rate the intensity of patients'psychological experience consistent with the stressresponse syndrome, for example, rumination orpreoccupation with the stress event, bad dreams,intrusive images, and the like. Operational defi-nitions of each item are provided for the observer.Instructions call for the rater to "judge the degreeto which these signs and symptoms describe theperson within the last seven days only"; items arescored on a 4-point scale. Although the SRRSwas originally constructed to yield two scores,one for 'intrusion' and another for 'avoidance,'pilot work revealed difficulties with the avoidancesubscale. The interrater reliability coefficient forthe 'intrusion' subscale was .87, and the alphacoefficient estimating internal consistency was .86,while for the 'avoidance' subscale these coefficientswere .60 and .54, respectively (Weiss et al., 1984).Only the 'intrusion' items were therefore used inthe present study. Therapists completed the SRRSafter the initial therapy hour and at termination;the clinical evaluator completed the scale at thepretherapy and follow-up interviews.
A modified version of the Brief Psychiatric Rat-ing Scale (Overall & Gorham, 1962) was also
completed by the clinical evaluator at pretherapyand follow-up, and by therapists after the firsthour and at termination. The measure consists of16 categories of observable signs and symptoms,each rated on a 7-point scale. Eight of the original16 items were eliminated because they were ap-plicable to psychotic conditions and hence notrelevant to the patient population under study; inturn, eight additional items of other conditionsmore specific to our concerns were added, includingitems for conceptual inhibition, conceptualswitching, intrusive representations, conceptualdistortions, conceptual disorganization, unusualthought content, emotional numbness, and emo-tional pangs.
Results
Analysis of Covariance
Pre/postassessment data were analyzed by meansof analyses of covariance (ANCOVA) with re-peated measures. A covariance strategy was chosenbecause in comparisons of psychotherapies, randomassignment does not necessarily guarantee equiv-alent groups, and covarying pretreatment distresslevel controls for the problem of initial level effectson change. In this sample of 60 women patients,follow-up assessment data could not be obtainedfor 15 subjects. In order to determine whetherthere might be significant differences between pa-tients for whom follow-up data were obtained andthose for whom they were not available, Mestswere conducted on all outcome variables betweenthe two groups on both pre- and posttherapy scores.No differences emerged between the two patientgroups, and they were closely comparable in termsof distress and symptom level at both pre- andposttherapy. Since the two groups did not differin any important respect, the group mean at follow-up on outcome scales was substituted for thosecases for which follow-up data were missing.
A repeated-measures ANCOVA conducted forthe intrusion and avoidance scales of the impactof event measure failed to reveal any gender effectson outcome, though patients reported significantimprovement pre- to posttherapy on intrusivesymptomatology (F(l,56) = 10.05, p < .01) andnear-significant improvement (F(l,56) = 3.65,p < .06) in avoidant symptoms. Patients did notreport any important changes in level of adjustmentfrom termination to follow-up. Responses to theClient Satisfaction Scale obtained at follow-updemonstrated significant differences, all favoring
340
Gender Effects in Brief Therapy
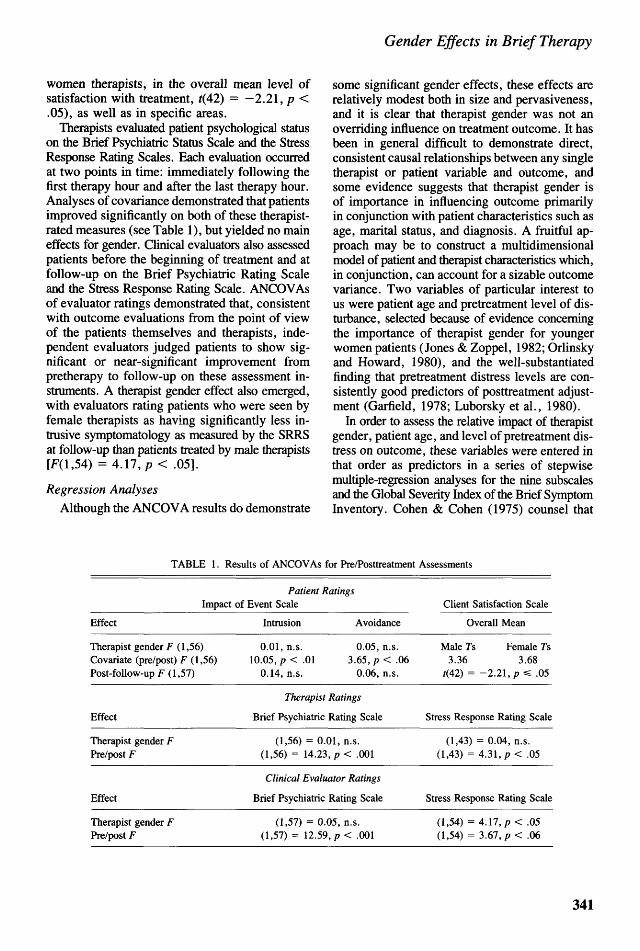
women therapists, in the overall mean level ofsatisfaction with treatment, f(42) = — 2.21, p <.05), as well as in specific areas.
Therapists evaluated patient psychological statuson the Brief Psychiatric Status Scale and the StressResponse Rating Scales. Each evaluation occurredat two points in time: immediately following thefirst therapy hour and after the last therapy hour.Analyses of covariance demonstrated that patientsimproved significantly on both of these therapist-rated measures (see Table 1), but yielded no maineffects for gender. Clinical evaluators also assessedpatients before the beginning of treatment and atfollow-up on the Brief Psychiatric Rating Scaleand the Stress Response Rating Scale. ANCOVAsof evaluator ratings demonstrated that, consistentwith outcome evaluations from the point of viewof the patients themselves and therapists, inde-pendent evaluators judged patients to show sig-nificant or near-significant improvement frompretherapy to follow-up on these assessment in-struments. A therapist gender effect also emerged,with evaluators rating patients who were seen byfemale therapists as having significantly less in-trusive symptomatology as measured by the SRRSat follow-up than patients treated by male therapists[F(l,54) = 4.17,p < .05].
Regression Analyses
Although the ANCOVA results do demonstrate
some significant gender effects, these effects arerelatively modest both in size and pervasiveness,and it is clear that therapist gender was not anoverriding influence on treatment outcome. It hasbeen in general difficult to demonstrate direct,consistent causal relationships between any singletherapist or patient variable and outcome, andsome evidence suggests that therapist gender isof importance in influencing outcome primarilyin conjunction with patient characteristics such asage, marital status, and diagnosis. A fruitful ap-proach may be to construct a multidimensionalmodel of patient and therapist characteristics which,in conjunction, can account for a sizable outcomevariance. Two variables of particular interest tous were patient age and pretreatment level of dis-turbance, selected because of evidence concerningthe importance of therapist gender for youngerwomen patients (Jones & Zoppel, 1982; Orlinskyand Howard, 1980), and the well-substantiatedfinding that pretreatment distress levels are con-sistently good predictors of posttreatment adjust-ment (Garfield, 1978; Luborsky et al., 1980).
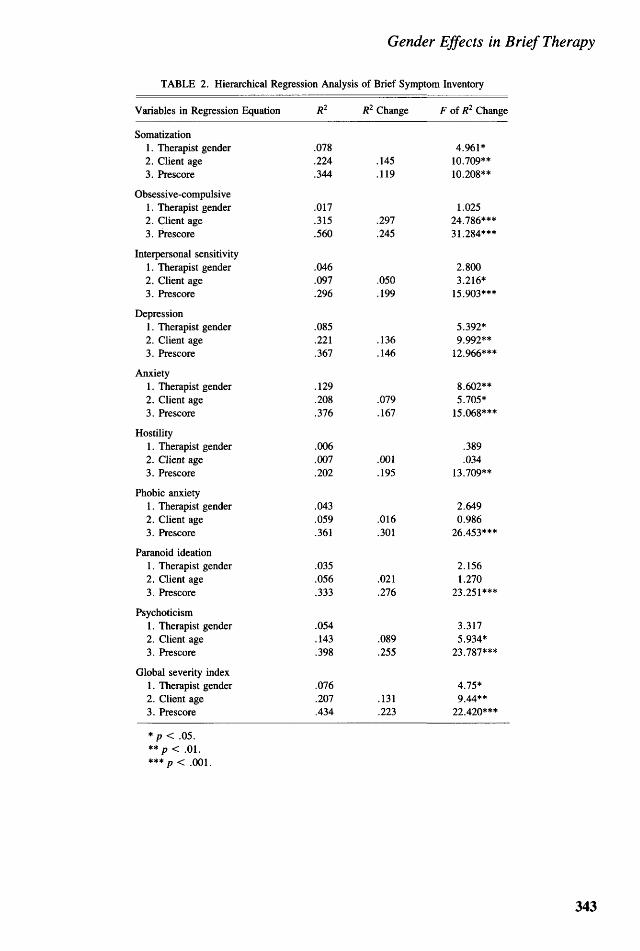
In order to assess the relative impact of therapistgender, patient age, and level of pretreatment dis-tress on outcome, these variables were entered inthat order as predictors in a series of stepwisemultiple-regression analyses for the nine subscalesand the Global Severity Index of the Brief SymptomInventory. Cohen & Cohen (1975) counsel that
TABLE 1. Results of ANCOVAs for Pre/Posttreatment Assessments
Patient RatingsImpact of Event Scale
Effect
Therapist gender F (1,56)Covariate (pre/post) F (1,56)Post-follow-up F (1,57)
Effect
Therapist gender FPre/post F
Effect
Therapist gender FPre/post F
Intrusion Avoidance
0.01, n.s. 0.05, n.s.10.05, p< .01 3.65, p < .06
0.14, n.s. 0.06, n.s.
Therapist Ratings
Brief Psychiatric Rating Scale
(1,56) = 0.01, n.s.(1,56) = 14.23, p< .001
Clinical Evaluator Ratings
Brief Psychiatric Rating Scale
(1,57) = 0.05, n.s.(1,57) = 12.59, p< .001
Client Satisfaction Scale
Overall Mean
Male 7s Female Ts3.36 3.68
/(42) = - 2 . 2 1 , p =£ .05
Stress Response Rating Scale
(1,43) = 0.04, n.s.(1,43) = 4.31, p< .05
Stress Response Rating Scale
(1,54) = 4.17, p < .05(1,54) = 3.67, p< .06
341

E. E. Jones et al.
the sequence in which variables are entered intoa regression equation be determined by the purposeand logic of the research. Since the ANCOVAsdemonstrate that pretherapy distress levels con-tribute a great deal to posttreatment variance, en-tering prescore first in the multiple regression wouldnot only fail to contribute much of further interest,but it would also reduce the amount of varianceavailable substantially, thereby sharply decreasingthe chance of demonstrating an effect other thanthat of pretreatment distress levels. Results of theregression analyses demonstrated that all threevariables—therapist gender, patient age, and pre-treatment symptom level—accounted for a sig-nificant portion of the outcome variance on mostof the nine subscales as well as on the GSI (seeTable 2). The regression analyses permitted thecalculation of the relative influence of each ofthese factors on outcome, allowing another per-spective on the influence of gender. In combination,these three variables accounted for .42 of the var-iance in outcome (as measured by the Global Se-verity Index), with pretreatment symptom scoreaccounting for .22 of the variance, patient ageaccounting for . 13, and therapist gender accountingfor .08. While therapist gender did contribute asignificant portion of the variance, it was clearlynot the single, or most important, contributingfactor. Significant differences between male- andfemale-treated patient groups emerged on measuresof somatization (F of R2 change = 4.96, p <.05); depression (F of R2 change = 5.39, p <.05); anxiety (F of R2 change = 8.60, p < .01);and on the GSI (F of R2 change = 4.75, p <.05). All findings were consistently in the direc-tion of better outcomes for the women patientswho were treated by female rather than male thera-pists. Interaction terms for therapist gender andpatient age (F of/?2 change = 1.45, n.s.), therapistgender and pretreatment disturbance level (F ofR2 change = 1.30, n.s.), and patient age anddistress level (F of/?2 change = 1.84, n.s.) failedto yield significant effects.
Study 2
Method
Patients and Therapists
Patients for the study comprised a subset of the60 women selected for Study 1 from the dataarchives. The reduction in sample size was ne-
cessitated by the fact that audio tapes of therapysessions for some patients were either unavailableor of very poor quality. A total of 40 femalepatients were included, 20 of whom had been seenby male therapists and 20 by female therapists.The sample ranged in age from 21 to 67, with amean age of 40 years. As in Study 1, the majoritywere college educated and were employed asprofessionals or as office workers; only four werehomemakers. In the group treated by male ther-apists, 3 had never married, 4 were married orliving with someone, 6 were divorced, and 7 werewidowed. Among those treated by female ther-apists, 7 had never married, 6 were married orliving with someone, 1 was separated, and 6 werewidowed. Seventy percent (28) were suffering abereavement, almost half (43%) of them becauseof the death of a parent, and another third as aresult of the death of a spouse; the remainder hadexperienced a traumaic event. Of the 20 therapistswho treated the patients in this sample, 12 weremale and 8 were female. The male and femaletherapists were again matched closely in experiencelevel and professional status. In each group, oneof the therapists had 11 or more years of experience,three had 6 to 10 years of experience, and eightof the male therapists and four of the female ther-apists had 3 to 6 years of experience.
The 12-session therapy was specifically tailoredfor the treatment of stress syndromes, focusingon the experience of loss and its meaning, andattempting to facilitate a normal grieving process.Highlights of this approach included willingnessto give information concerning stress-response re-actions when helpful in alleviating patients' fears,a focus on the therapeutic relationship and itstermination in order to assist the patient in con-fronting this reexperience of loss, early interpre-tation of transference reactions, and the creationof a supportive environment in which the patientwas given permission to "dose" her feelings ratherthan being stripped of defenses. The therapist wasalso encouraged to discuss with the patient newplans and decisions, and to help the patient practicethese on a trial-and-error basis. Therapists werecautioned to be aware of countertransference feel-ings, especially discomfort with the patient's angerregarding termination. This approach differed,then, from a generic psychodynamic model in itsemphasis on focusing the therapy, confrontingtermination, addressing reality issues, and in par-ticular in directing interpretations to the link be-
342
Gender Effects in Brief Therapy
TABLE 2. Hierarchical Regression Analysis of Brief Symptom Inventory
Variables in Regression Equation
Somatization1. Therapist gender2. Client age3. Prescore
Obsessive-compulsive1. Therapist gender2. Client age3. Prescore
Interpersonal sensitivity1. Therapist gender2. Client age3. Prescore
Depression1. Therapist gender2. Client age3. Prescore
Anxiety1. Therapist gender2. Client age3. Prescore
Hostility1. Therapist gender2. Client age3. Prescore
Phobic anxiety1. Therapist gender2. Client age3. Prescore
Paranoid ideation1. Therapist gender2. Client age3. Prescore
Psychoticism1. Therapist gender2. Client age3. Prescore
Global severity index1. Therapist gender2. Client age3. Prescore
R2
.078
.224
.344
.017
.315
.560
.046
.097
.296
.085
.221
.367
.129
.208
.376
.006
.007
.202
.043
.059
.361
.035
.056
.333
.054
.143
.398
.076
.207
.434
R2 Change
.145
.119
.297
.245
.050
.199
.136
.146
.079
.167
.001
.195
.016
.301
.021
.276
.089
.255
.131
.223
F of R2 Change
4.961*10.709**10.208**
1.02524.786***31.284***
2.8003.216*
15.903***
5.392*9.992**
12.966***
8.602**5.705*
15.068***
.389
.03413.709**
2.6490.986
26.453***
2.1561.270
23.251***
3.3175.934*
23.787***
4.75*9 44**
22.420***
*p< .05.** p < .01.*** p < .001.
343
E. E. Jones et al.
tween transference reactions and conflicts relatedto the stress event.
The Psychotherapy Process Q-Sort
Study 2 employed a 100-item psychotherapyprocess Q-sort, the purpose of which is to providea basic language for the description and classi-fication of therapy process. The use of the standardlanguage and rating procedure provided by theQ-sort supplies the means for systematically char-acterizing a wide range of patient—therapist inter-actions. Most research in psychotherapy processhas taken a variable-centered approach (e.g., ex-periencing, therapeutic alliance). However, muchthinking about psychotherapy has assumed a per-son-centered approach, where the emphasis hasbeen not on separately considered variables butrather on a closer understanding of individuals.The variable-centered approach has a normativeframe of reference; that is, a case is rated on aparticular variable (e.g., empathy) in relation toa specified referent. The Q-sort procedure is an"ipsative" one, in which variables in the Q-setare ordered or scaled relative to each other, withthe specific case as the frame of reference (Block,1961). This procedure allows the complex de-scription of individual cases in the manner of aclinical formulation.
An advantage of the Q-sort, then, is that it ismulti- rather than unidimensional. Instead ofmeasuring one state or feeling of relatedness, theQ-sort describes the elements which might comprisean effective relationship as well as the eventswhich might accompany or evoke it. Psychotherapyprocess obviously involves the interaction of mul-tiple influences; what is needed is a measure ofsufficient complexity to adequately reflect thephenomenon it is attempting to assess, one thatcan tap configurations or patterns or interrela-tionships in process. The Q-method holds an ad-ditional advantage over process measures whichinvolve multiple ratings on conventional scalesthat do not require a rank ordering or discriminationamong variables. Such scales are susceptible toa common response bias in which judges tend togroup together all favorable and all unfavorableitems without making distinctions among them.The Q-method requires judges to sort the itemsinto a normal distribution consisting of nine cat-egories, with 1 representing 'least characteristic'of the hour, 5 neutral or irrelevant, and 9 'mostcharacteristic' The fixed distribution of the Q-sort ensures multiple discriminations among items,
reducing the 'halo effect.' Moreover, it minimizesthe possibility of judges making statements aboutthe process material that are very general by al-lowing greater salience to important features aboutthe material. When multiple ratings using con-ventional scales are employed, there is a strongtendency to rate what is very generally true aboutthe segment of process under observation. Thisvery likely explains why such measures usuallyfactor analyze into global or general dimensions(see Hartley and Strupp, 1983) that fail to genuinelyfurther our understanding of process.
The Q-sort comprises three types of items: 1)items describing patient attitude and behavior orexperience; 2) items reflecting the therapist's ac-tions and attitudes; and 3) items attempting tocapture the nature of the interaction in the dyador the climate or atmosphere of the encounter. Alarge pool of potential Q-sort items was createdby conducting an exhaustive search of extant psy-chotherapy process measures and selecting itemsfrom them, and by constructing items in discussionsinvolving research-oriented clinicians. From theseefforts emerged a pool of more than 500 items;100 items that appeared to provide broad coverageof therapy process, and which seemed to haveleast redundancy, were then selected. Each itemwas individually discussed with respect to its clar-ity, importance for psychotherapy, and its impli-cations for the sufficiency of the total Q-deck.Items were rewritten for conciseness, or amplifiedand unrequired jargon and multiply understoodlanguage were eliminated. An item was excludedor retained as a function of its additive informationvalue as well as its general relevance in describingpsychotherapy process. As a next step, the itemswere rewritten, as far as possible, in a theoreticallyneutral form. While built on general assumptionsabout psychotherapy as an interpersonal process,the items themselves are not committed to a specialtheoretical viewpoint, so that the formulations de-rived from the Q-items are compatible with anyof several viewpoints about psychotherapy process.
The question which then arose was whether theinitial set of 100 items were sufficient in themselvesor in combinations to encompass the varieties ofpsychotherapeutic process. In order to test thelimits of the capabilities of the item set, pilotratings were conducted on video tapes and audiotapes of psychotherapies representing a wide rangeof theoretical orientations, including client-cen-tered, Gestalt, rational-emotive, psychodynamic,and cognitive-behavioral. Whenever it was con-
344

Gender Effects in Brief Therapy
sidered that a gap or inadequacy existed in theQ-set, or whenever some facet of therapy processjudged to be important proved not to be capturedor expressed by an existing item or some con-junction of items, then item revisions were made,or appropriate items were written and added tothe Q-set.
A substantially altered set of items emergedfrom the first pilot phase. The next step was totest the second version of the Q-set, now improvedin terms of its effectiveness, for its psychometricproperties. In a second pilot test, the Q-set wasapplied to the transcripts of the audio tapes oftherapy hours. Independent ratings were made bytwo judges, and interrater reliability was calculatedusing the Pearson product-moment correlationcoefficient. Reliabilities, which ranged from .71to .89, were considered very adequate. Dispersionsfor each item were calculated in order to finditems showing little variation over a wide rangeof subjects (and therapy hours). Such items con-veyed little differential information, and wereeliminated. A second psychometric considerationaffecting the revision of the Q-deck was the extentof correlation existing among items. An item co-variance matrix was computed to determine ifexcessive redundancy was present. Items that werenot useful discriminators were either eliminatedor restated in an effort to enhance their potentialfor genuine variance; items demonstrating lowinterrater reliability were also eliminated.
This entire process was conducted several times.In one pilot, the existing version of the Q-sortwas applied to the transcripts of the therapy hoursof two treatment cases, one highly successful andone unsuccessful. Sixty-six of the one hundreditems differentiated the good and poor outcomecases. Repeated piloting as well as the experimentaldata presented below provide evidence for the Q-sort's construct validity. Factorial validity in theQ-sort is irrelevant, since items are constructedto be maximally independent; indeed, a factoranalysis, including various rotational possibilities,revealed an absence of factor structure, highlydesirable from the standpoint of Q-methodology.A coding manual details instructions for Q-sorting,and provides the items and their definitions alongwith examples in order to minimize potentiallyvarying interpretations of the items (Jones, 1985).
An important feature of the Q-method is theunit of information that forms the basis for judg-ment. Almost all process rating scales employ asunits for measurement 4- to 16-minute segments
of therapy hours, requiring judgments based onrelatively brief impressions. The psychotherapyprocess Q-sort requires a record of an entire hour.This procedure allows judges to approach theirtask in a manner in which theorists, clinicians,and patients experience as important—the grad-ual unfolding of the meaning of events within thewhole of the therapy hour.
Q-sort ratings were obtained for the fifth hourof each case. The fifth hour was chosen as onewhich would be representative (cf., Sloane et al.,1975), and which for this sample would not yetbe dominated by discussion of termination. Audiotapes were first transcribed roughly by the supportstaff at the archives. A second step in the tran-scription process required research assistants tore-listen to the recordings and make additions andcorrections to the first transcription draft, followinga set of guidelines developed by a member of theresearch team to ensure description of pauses,sighs, rustling noises in the background, and otheraudible aspects of the conversation that mightotherwise be lost. The use of typed transcriptsalso had the advantage of leaving judges blind asto the gender of the therapists being rated. Fivejudges were used in all, three women and twomen; all had been members of the research teamfor at least five months and had been trained inthe use of the Q-sort. Pairs of judges who hadrated the same hour met periodically to comparetheir ratings and "calibrate" their use of the Q-sort; three judges rated each of the transcripts.
Results
Gender and Therapy Process
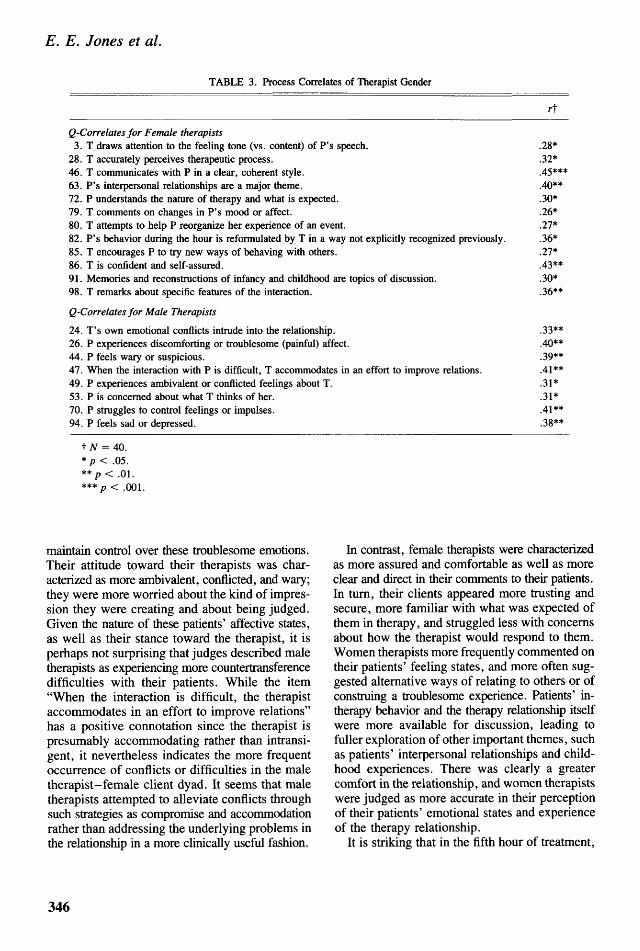
Interrater reliabilities were calculated for eachset of raters, using the Pearson product-momentcorrelation coefficient corrected with the Spearman-Brown formula. Interrater reliability ranged from.63 to .90, with the median reliability attaining.86. Q-item means were correlated with therapistgender; 20 items achieved significant correlations(see Table 3).
These items allow a revealing look into dif-ferences in the nature of treatment process withmen and women therapists among these womenpatients. Particularly noteworthy is that patientsof male therapists were described as generallyexperiencing more negative affect, for example,sadness, depression, or other discomforting orpainful feelings, and as struggling to manage or
345
E. E. Jones et al.
TABLE 3. Process Correlates of Therapist Gender
Q-Correlates for Male Therapists
24. T's own emotional conflicts intrude into the relationship.26. P experiences discomforting or troublesome (painful) affect.44. P feels wary or suspicious.47. When the interaction with P is difficult, T accommodates in an effort to improve relations.49. P experiences ambivalent or conflicted feelings about T.53. P is concerned about what T thinks of her.70. P struggles to control feelings or impulses.94. P feels sad or depressed.
rt
Q-Correlates for Female therapists3. T draws attention to the feeling tone (vs. content) of P's speech.
28. T accurately perceives therapeutic process.46. T communicates with P in a clear, coherent style.63. P's interpersonal relationships are a major theme.72. P understands the nature of therapy and what is expected.79. T comments on changes in P's mood or affect.80. T attempts to help P reorganize her experience of an event.82. P's behavior during the hour is reformulated by T in a way not explicitly recognized previously.85. T encourages P to try new ways of behaving with others.86. T is confident and self-assured.91. Memories and reconstructions of infancy and childhood are topics of discussion.98. T remarks about specific features of the interaction.
.28*
.32*
.45***
.40**
.30*
.26*
.27*
.36*
.27*
.43**
.30*
.36**
.33**
.40**
.39**
.41**
.31*
.31*
.41**
.38**
t N = 40.* p < .05.** p < .01.*** p < .001.
maintain control over these troublesome emotions.Their attitude toward their therapists was char-acterized as more ambivalent, conflicted, and wary;they were more worried about the kind of impres-sion they were creating and about being judged.Given the nature of these patients' affective states,as well as their stance toward the therapist, it isperhaps not surprising that judges described maletherapists as experiencing more countertransferencedifficulties with their patients. While the item"When the interaction is difficult, the therapistaccommodates in an effort to improve relations"has a positive connotation since the therapist ispresumably accommodating rather than intransi-gent, it nevertheless indicates the more frequentoccurrence of conflicts or difficulties in the maletherapist-female client dyad. It seems that maletherapists attempted to alleviate conflicts throughsuch strategies as compromise and accommodationrather than addressing the underlying problems inthe relationship in a more clinically useful fashion.
In contrast, female therapists were characterizedas more assured and comfortable as well as moreclear and direct in their comments to their patients.In turn, their clients appeared more trusting andsecure, more familiar with what was expected ofthem in therapy, and struggled less with concernsabout how the therapist would respond to them.Women therapists more frequently commented ontheir patients' feeling states, and more often sug-gested alternative ways of relating to others or ofconstruing a troublesome experience. Patients' in-therapy behavior and the therapy relationship itselfwere more available for discussion, leading tofuller exploration of other important themes, suchas patients' interpersonal relationships and child-hood experiences. There was clearly a greatercomfort in the relationship, and women therapistswere judged as more accurate in their perceptionof their patients' emotional states and experienceof the therapy relationship.
It is striking that in the fifth hour of treatment,
346

Gender Effects in Brief Therapy
patients of male therapists were observably moredepressed and emotionally distraught. While pa-tients (randomly) assigned to male therapists didnot differ significantly in mean level of pathologyat pretreatment from those assigned to femaletherapists, an examination of raw data plots ofpretreatment pathology scores did show that themale therapist group included the four or fivemost disturbed patients in the sample, and thatmean pathology scores tended to average somewhatlower for the female therapist-treated group. Still,it is unlikely that these statistically insignificantdifferences can account entirely for the variabilityin patient experience across therapist group, par-ticularly in light of the dissimilar constellation ofQ-descriptors of treatment process that emergedfor more severely disturbed patients in a separateanalysis (see below). More likely, the data suggestthat the concerns for which these mostly bereavedwomen had entered therapy were not being assuccessfully addressed in treatments conductedby male therapists, an interpretation supported bythe significant posttherapy differences in im-provement of depression scores across therapistgender found in Study 1.
Process Correlates of Patient Age
In the analyses of treatment outcomes presentedin Study 1, increasing patient age predicted lesspositive outcomes. In order to investigate howthe age variable might influence therapy process,scores for each Q-item were correlated with patient
age (range: 21 to 67). Thirteen items achievedsignificant correlations (see Table 4). The contentof the items suggests that a problematic and lessproductive interaction more commonly charac-terized treatment among older patients. The olderpatient appeared to have sought a more dependentrelationship with the therapist; she more frequentlyconveyed feeling misunderstood, while at the sametime she appeared to comprehend less readily thetherapist's comments and observations and moreoften disagreed with or ignored the therapist'ssuggestions and interpretations. The older patientwas characterized as more defended, less frequentlyexpressing deeply felt emotion and less readilyexpressing angry or antagonistic feelings. This isparticularly noteworthy in light of the fact thatby far the majority of the older patients in thissample were bereaved widows for whom mourningand the working through of feelings of grief andloss might be considered particularly important.In a finding that extends an emerging and clinicallyintelligible picture, these patients were also de-scribed as less likely to bring up problems ormaterial that might be significant for the therapy,more often talking of matters that were somehowunrelated or removed from issues of presumedcentral concern. There was, perhaps also as aconsequence, less emphasis on intrapsychic themesand more discussion of particular activities or tasksfor the patient to attempt outside of treatment inan effort to improve her life.
The descriptors of therapist behavior reflect the
TABLE 4. Process Correlates of Patient Age
Q-Item rt
2. T draws attention to P's nonverbal behavior. .30*5. P has difficulty understanding T's comments. .32*6. T is sensitive to P's feelings; attuned to P; empathic. —.39**8. P is concerned or conflicted about her dependency on T (vs. comfortable with, or wanted dependency). - .26*
14. P does not feel understood by T. .29*18. T conveys a sense of nonjudgmental acceptance. - .34*24. T's own emotional conflicts intrude into the relationship. .33*38. There is discussion of specific activities or tasks for P to attempt outside of session. .33*42. P rejects (vs. accepts) T's comments and observations. .28*56. P discusses experiences as if distant from her feelings. .37**62. T identifies a recurrent theme in P's experience or conduct. .41**84. P expresses angry or aggressive feelings. - . 3 1 *88. P brings up significant issues and material. - . 3 1 *
t W = 40.* p < .05.**p < .01.
347

E. E. Jones et al.
reciprocal nature of the stance assumed by therapistsin relation to the difficulties posed by the olderpatient. Therapists were less able to be attunedto and empathic with these patients, and less ableto communicate a sensitivity to their feelings andexperience. Similarly, they were less likely toconvey a sense of nonjudgmental acceptance,finding it more difficult to refrain from subtlenegative judgments of the patient. In a clearlyrelated finding, therapists' own emotional responsesto the patients were more likely to intrude in in-effective or inappropriate ways. Possibly in anattempt to discover a vehicle for promoting greaterself-reflection in the patient, the therapist morefrequently drew attention to the patient's nonverbalcommunications, such as facial expressions andbody posture. Perhaps because these patients hadless access to their feeling states, therapists moreoften confined themselves to pointing out recurrentpatterns in their life experience or behavior. Q-cerrelates of patient age provide some importantinsights concerning how increasing age may in-fluence process in a way that tends to lead to lessbeneficial outcomes.
Process Correlates of Patient DisturbanceLevel
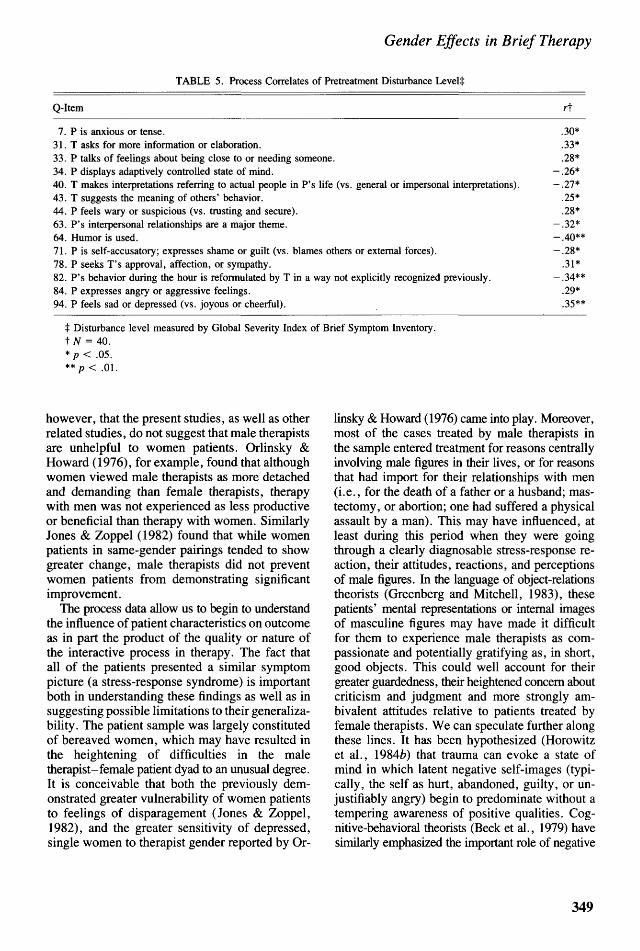
Study 1, in finding that patient disturbance levelwas a primary predictor of improvement in treat-ment, replicates the results of several other majorinvestigations. In order to identify what distin-guished the nature of therapy process with moreseverely disturbed individuals in this sample, Q-values were correlated with patients' scores onthe Global Severity Index of the Brief SymptomInventory. Fourteen items correlated significantlywith pretreatment level of disturbance (Table 5).In the fifth treatment hour, these patients weredescribed as displaying more anxiety and tenseness,as feeling more depressed and melancholy, andas more likely to express resentment, anger, orbitterness; they were also more likely to appearwary, distrustful, or suspicious of the therapist;therefore, the emotional tone of these hours wereparticularly humorless and somber. These patientsalso appeared to be more needy, frequently talkingabout being, or wanting to be, close or intimatewith someone in their lives. The fact that theywere more likely to behave in a manner apparentlydesigned to gain the therapist's attention, approval,or sympathy may well be an expression of thisemotional state in the therapy relationship. Themore disturbed patient was also less likely to display
"working states," that is, they were less able todemonstrate adaptive control by having access to,or the willingness to work on, problematic themeswithout feeling overwhelmed by negative affect.This difficulty may be related to raters' impressionsthat these patients, more than the less disturbed,tended to externalize, blaming others or chanceevents for their difficulties.
The emerging picture suggests that the moretroubled among this bereaved population werepowerfully threatened by negative affect, whichmay in turn have restricted therapists' range ofpotential interventions. Perhaps in an attempt towork effectively with these more difficult patients,therapists more actively elicited information byasking exploratory questions or pressing for moreelaboration and detail about the patient's conditionand life circumstances. Therapists were much lesslikely to comment on and reformulate the in-therapybehavior of these patients, and problems in inter-personal relationships were less likely to be dis-cussed as carrying potential intrapsychic meaningsbut rather as emerging from real external circum-stances.
DiscussionThese two studies demonstrate that therapist
gender influenced both the process and outcomeof a brief, psychodynamically oriented therapyfor posttraumatic stress disorders. Patients treatedby female therapists reported more symptomaticimprovement (Brief Symptom Inventory) and sat-isfaction with treatment (Client SatisfactionQuestionnaire) than in those seen by male ther-apists. Independent clinical evaluators assessedthose patients seen by female therapists as havingimproved more at follow-up in terms of the ame-lioration of intrusive thoughts and feelings aboutthe stressful life event that they had experienced(Stress Response Rating Scale). The magnitudeand pervasiveness of therapist gender effects onoutcome was, however, modest; patient age ac-counted for twice and patient pre-treatment levelof disturbance more than three times the outcomevariance contributed by gender. Nevertheless, thesefindings confirm and replicate those of Jones &Zoppel's (1982) earlier investigation of time-un-limited dynamic psychotherapies. The presentreplication is all the more persuasive in that itinvolved a different therapy modality (a 12-sessionbrief therapy), conducted on a demographicallydifferent patient population, diagnosed as sufferingfrom a specific disorder. It should be emphasized,
348
Gender Effects in Brief Therapy
TABLE 5. Process Correlates of Pretreatment Disturbance Levelt
Q-Item rt
7. P is anxious or tense. .30*31. T asks for more information or elaboration. .33*33. P talks of feelings about being close to or needing someone. .28*34. P displays adaptively controlled state of mind. —.26*40. T makes interpretations referring to actual people in P's life (vs. general or impersonal interpretations). - .27*43. T suggests the meaning of others' behavior. .25*44. P feels wary or suspicious (vs. trusting and secure). .28*63. P's interpersonal relationships are a major theme. - .32*64. Humor is used. - .40**71. P is self-accusatory; expresses shame or guilt (vs. blames others or external forces). —.28*78. P seeks T's approval, affection, or sympathy. .31*82. P's behavior during the hour is reformulated by T in a way not explicitly recognized previously. - .34**84. P expresses angry or aggressive feelings. .29*94. P feels sad or depressed (vs. joyous or cheerful). .35**
t Disturbance level measured by Global Severity Index of Brief Symptom Inventory.t N = 40.* p < .05.** p < .01.
however, that the present studies, as well as otherrelated studies, do not suggest that male therapistsare unhelpful to women patients. Orlinsky &Howard (1976), for example, found that althoughwomen viewed male therapists as more detachedand demanding than female therapists, therapywith men was not experienced as less productiveor beneficial than therapy with women. SimilarlyJones & Zoppel (1982) found that while womenpatients in same-gender pairings tended to showgreater change, male therapists did not preventwomen patients from demonstrating significantimprovement.
The process data allow us to begin to understandthe influence of patient characteristics on outcomeas in part the product of the quality or nature ofthe interactive process in therapy. The fact thatall of the patients presented a similar symptompicture (a stress-response syndrome) is importantboth in understanding these findings as well as insuggesting possible limitations to their generaliza-bility. The patient sample was largely constitutedof bereaved women, which may have resulted inthe heightening of difficulties in the maletherapist-female patient dyad to an unusual degree.It is conceivable that both the previously dem-onstrated greater vulnerability of women patientsto feelings of disparagement (Jones & Zoppel,1982), and the greater sensitivity of depressed,single women to therapist gender reported by Or-
linsky & Howard (1976) came into play. Moreover,most of the cases treated by male therapists inthe sample entered treatment for reasons centrallyinvolving male figures in their lives, or for reasonsthat had import for their relationships with men(i.e., for the death of a father or a husband; mas-tectomy, or abortion; one had suffered a physicalassault by a man). This may have influenced, atleast during this period when they were goingthrough a clearly diagnosable stress-response re-action, their attitudes, reactions, and perceptionsof male figures. In the language of object-relationstheorists (Greenberg and Mitchell, 1983), thesepatients' mental representations or internal imagesof masculine figures may have made it difficultfor them to experience male therapists as com-passionate and potentially gratifying as, in short,good objects. This could well account for theirgreater guardedness, their heightened concern aboutcriticism and judgment and more strongly am-bivalent attitudes relative to patients treated byfemale therapists. We can speculate further alongthese lines. It has been hypothesized (Horowitzet al., 19842?) that trauma can evoke a state ofmind in which latent negative self-images (typi-cally, the self as hurt, abandoned, guilty, or un-justifiably angry) begin to predominate without atempering awareness of positive qualities. Cog-nitive-behavioral theorists (Beck et al., 1979) havesimilarly emphasized the important role of negative
349

E. E. Jones et al.
self-images or self-valuations in depression. Ifindividuals' experience of who they are is closelyaligned with inner representations of others, thesepatients' relatively more positive images of womentherapists as good objects may have aided in thesuppression of negative self-images and the al-leviation of associated painful affect.
Examination of the Q-items that failed to dif-ferentiate therapies conducted by male and femaletherapists are also revealing. Specifically, our datado not support the notion that what occurs intherapy is simply a recapitulation of stereotypicsex-role dynamics between males and females.Female therapists were not described as beingsignificantly more sensitive, supportive, or re-assuring, as adopting, in other words, a "nurturant"stance. Nor were male therapists rated as signif-icantly more aloof, controlling, impatient, con-descending, status conscious, in pursuit of insightor, in other words, as more impassively "analyt-ical." Similarly, female patients did not behavein a more sex-role-stereotyped fashion with maletherapists and were not described as more depen-dent, seductive, inadequate, shy and embarrassed,or passive with male therapists. It would seemthat, as Kirshner et al. (1978) have stated, genderplays as diverse and complex a role in psycho-therapy as in other domains of life.
Psychotherapists do not need to be convincedof their central importance in bringing treatmentsto successful conclusion. Despite this certainty,studies of therapy process generally have founda relatively weak association between therapistvariables, (e.g., actions or therapist-offered re-lationship qualities) and treatment outcomes(Hartley & Strupp, 1983; Luborsky et al., 1980).Such patient variables as depth of experiencing,involvement, and motivational level have beenshown to be far stronger predictors. Our studiesbring new information to this unsatisfactory stateof affairs, providing suggestive evidence that boththerapist and patient behaviors and attitudes interactto produce outcomes of varying levels of success.Although our interpretation of process differencesacross therapist gender emphasizes patients' ca-pacity to experience therapists as helpful ratherthan therapist variables, it implies an interactionalview of process. The patient's fundamental stanceor posture limits or extends the therapist's fieldof possible interventions. It is true that the dataare open to other explanations: for example, it isnot entirely certain whether more positive statesof mind among the patients of female therapists
allowed more effective intervention, or whetherfemale therapists' skill promoted greater emotionalcomfort in their patients. Still, either of these inter-pretations rest on an interactional perspective. Q-correlates of patient age leave less uncertaintyabout whether therapists' responses are at least inpart determined by patient characteristics and be-havior. Older patients' relative difficulty in gainingaccess to their emotional experience, their tendencyto reject or fail to understand therapist's commentsand observations, the fact that they were less likelyto bring up important issues as well as their wishfor a dependent relationship all very likely con-tributed to therapists' difficulty in effectively em-pathizing and in assuming a nonjudgmental attitude.
An unanticipated finding that emerged from ourdata is the important predictive role played bypatient age, which accounted for almost twice asmuch outcome variance (13 percent) as therapistgender. The possible influence of patient age ontherapeutic outcome has long been a topic of clinicalinterest. In contrast to the clear findings of thepresent study, previous investigations of this patientvariable have generally yielded inconsistent results.While Luborsky et al. (1971) conclude on thebasis of their review of research that youngerpatients have a greater capacity for change, Garfield(1978) raises a question about the quality andgeneralizability of these studies. He argues thata serious problem arises from the considerablevariation in the manner in which "older age" and"younger age" are denned, pointing out that incontrast to a variable like patient sex, where allstudies use the same critieria and where it is possibleto objectively classify subjects into dichotomouscategories, patient age cannot be easily bifurcatedbecause age, unlike gender, is a continuous ratherthan dichotomous variable. As a result, arbitrarydecisions must be made by the individual inves-tigator about how to operationally define "older"and "younger." Since all investigators do not definethese categories in like manner, cutoff points di-viding samples by age vary across studies, and ithas therefore not been possible to draw meaningfulconclusions about patient age and outcome. An-other way of viewing this problem is that it stemsfrom an overreliance on analysis of covariancedesigns in psychotherapy research. In many in-stances in which patient or therapist characteristics,including age, are investigated, a superior strategylies in regression models, which allow the treatmentof continuous variables as such.
The felicitous influence of youth on psycho-
350

Gender Effects in Brief Therapy
therapy has been discussed most often in the contextof the presumed greater flexibility and malleabilityof character structure in the younger patient. Recentinvestigations have shown that psychotherapy canbe beneficial to older adults (Gallagher & Thomp-son, 1982). Nevertheless, our data suggest thatthere is in fact some validity to the belief thatincreasing age can have a negative effect on therapyoutcome. It is possible that at base, older individualsretain a capacity for change, but require muchmore time to do so. It should also be noted thatthe majority of older patients in this sample werebereaved, suffering from profound grief reactionsto the loss of a spouse. It is not difficult to imaginethat the loss of perhaps the most important intimaterelationship in an individual's life, one that fre-quently spanned decades, might require more than12 therapy sessions to work through successfully.
The present studies begin to elucidate the in-fluence of therapist gender relative to pretreatmentpsychological status as well as patient age. Ourresults place the effect of the gender variable inperspective by assessing its relative contributionto outcome in comparison with these other patientcharacteristics. Patient pretherapy level of distresswas clearly the factor most predictive of outcome.This finding is wholly consistent with those of anumber of major psychotherapy outcome studies,including the Chicago Counseling Center Psy-chotherapy Study (Fiske et al., 1964), the Men-ninger Study (Kernberg et al., 1964) and the PennPsychotherapy Study (Luborsky et al., 1980). In-deed, our findings concur with the conclusion ofimportant reviews of factors influencing psycho-therapy outcome (e.g., Garfield, 1978; Luborskyet al., 1971) that the single best predictor of post-therapy adjustment is patients' initial adequacyof personality functioning. The role of gender andother patient variables in psychotherapy need tobe conceptualized within a multidimensionalframework that can more adequately account forthe interactive and divergent effects of multiplepatient characteristics on the change process.
ReferencesBECK, A. T., RUSH, J. A., SHAW, B. F. & EMERY, G. (1979).
Cognitive Therapy of Depression. New York: Guilford Press.BLOCK, J. (1961). The Q-Sort Method in Personality Assessment
and Research. Springfield, 111.: Charles C. Thomas.BRODSKY, A. & HARE-MUSTIN, R. (1980). Psychotherapy and
woman: Priorities for research. In A. Brodsky and R. Hare-Mustin (Eds.), Women and Psychotherapy. New York:Guilford Press.
BROVERMAN, I., BROVERMAN, D., CLARKSON, F., ROSENK-
RANTZ, P. & VOGEL, S. (1970). Sex-role stereotypes and
clinical judgments of mental health. Journal of Consultingand Clinical Psychology, 34, 1-7.
CARTWRIGHT, R. & LERNER, B. (1963). Empathy, need tochange, and improvement with psychotherapy. Journal ofConsulting Psychology, 27, 138-144.
CHESLER, P. (1972). Women and Madness. New York: Dou-bleday.
COHEN, J. & COHEN, P. (1975). Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences. Hillsdale,N.J.: Lawrence Erlbaum.
DEROGATIS, L. & MEUSARATOS, N. (1983). The brief symptominventory: An introductory report. Psychological Medicine,13, 595-605.
FISKE, D., CARTWRIGHT, D. & KIRTNER, W. (1964). Arepsychotherapeutic changes predictable? Journal of AbnormalSocial Psychology, 69, 413-426.
GALLAGHER, D. & THOMPSON, L. (1982). Differential effec-tiveness of psychotherapies for the treatment of major de-pressive disorder in older adult patients. Psychotherapy:Theory Research, and Practice, 19, 482-490.
GARFIELD, S. (1978). Research on client variables in psycho-therapy. In S. Garfield and A. Bergin (Eds.), Handbookof Psychotherapy and Behavior Change: An EmpiricalAnalysis (2nd ed.). New York: John Wiley.
GREENBERG, J. R. & MITCHELL, S. A. (1983). Object Relationsin Psychoanalytic Theory. Cambridge, Mass.: HarvardUniversity Press.
HARTLEY, D. E. & STRUPP, H. H. (1983). The therapeuticalliance: Its relationship to outcome in brief psychotherapy.In J. Masling (Ed.), Empirical Studies of PsychoanalyticTheories, Vol. 1. Hillsdale, N.J.: Lawrence Erlbaum.
HOROWITZ, M., MARMAR, C , KRUPNICK, J., WILNER, N.,KALTREIDER, N. & WALLERSTEIN, R. (1984a). PersonalityStyles and Brief Psychotherapy. New York: Basic Books.
HOROWITZ, M. J., MARMAR, C , WEISS, D. S., DEWITT,K. N. & ROSENBAUM, R. (19846). Brief psychotherapy ofbereavement reactions. Archives of General Psychiatry, 41,438-448.
JONES, E. E. & ZOPPEL, C. (1982). Impact of client andtherapist gender on psychotherapy process and outcome.Journal of Consulting and Clinical Psychology, 50, 259-272.
JONES, E. E. (1985). Manual for the psychotherapy processQ-sort. Unpublished manuscript, University of California,Berkeley.
KERNBERG, O., BURSTEIN, E., COYNE, L., APPLEBAUM, A.,HORWITZ, L. & NOTH, H. (1972). Psychotherapy and psy-choanalysis: Final report of the Menninger Foundation'sPsychotherapy Research Project. Bulletin of the MenningerFoundation's Psychotherapy Research Project, 36, 1-278.
KIRSHNER, L., GENACK, A. & HAUSER, S. (1978). Effects ofgender on short-term psychotherapy. Psychotherapy: Theory,Research and Practice, 15, 158-167.
LARSEN, D., ATTKISSON, C. & HARGREAVES, W. (1979). As-sessment of client/patient satisfaction: Development of ageneral scale. Evaluation and Program Planning, 2, 197-207.
LUBORSKY, L., CHANDLER, M., AUERBACH, A., COHEN, J. &BACHRACH, H. (1971). Factors influencing the outcome ofpsychotherapy: A review of quantitative research. Psycho-logical Bulletin, 75, 145-184.
LUBORSKY, L., MINTZ, J., AUERBACH, A., CHRISTOPH, P.,BACHRACH, H., TODD, T., JOHNSON, M., COHEN, M. &O'BRIEN, E. P. (1980). Predicting the outcome of psycho-therapy: Findings of the Penn Psychotherapy Project. Archives
351
E. E. Jones et al.
of General Psychiatry, 37, 471-481.MAFFEO, P. (1979). Thoughts on Strieker's "Implications of
research for psychotherapeutic treatment of women." Amer-ican Psychologist, 34, 690-695.
MALAN, D. (1976). Towards the Validation of Dynamic Psy-chotherapy: A Replication. New York: Plenum MedicalBooks.
MANN, J. (1973). Time-Limited Psychotherapy. Caqmbridge:Harvard University Press.
MASLIN, A. & DAVIS, J. (1975). Sex-role stereotyping as afactor in mental health standards among counselors-in train-ing. Journal of Counseling Psychology, 22, 87-91.
MEEHL, P. (1978). Theoretical risks and tabular asterisks: SirKarl, Sir Ronald and the slow progress of soft psychology.Journal of Consulting and Clinical Psychology, 46, 806-834.
MELTZOFF, J. & KORNREICH, M. (1970). Research in Psy-chotherapy. New York: Atherton.
ORLINSKY, D. & HOWARD, K. (1976). The effects of sex oftherapist on the therapeutic experiences of women. Psy-chotherapy: Theory, Research and Practice, 13, 82-88.
ORLINSKY, D. & HOWARD, K. (1980). Gender and psycho-therapeutic outcome. In A. Brodsky and R. Hare-Mustin(Eds.), Women and Psychotherapy. New York: GuilfordPress.
OVERALL, J., & GORHAM, D. (1962). The Brief PsychiatricRating Scale. Psychological Reports, 10, 799.
PARLOFF, M., WASKOW, I., & WOLFE, B. (1980). Researchon therapist variables in relation to process and outcome.In S. Garfield and A. Bergin (Eds.), Handbook of Psycho-therapy and Behavior Change (2nd ed.). New York: JohnWiley.
RICE, J. & RICE, D. (1973). Implications of the Women'sLiberation Movement for psychotherapy. American Journalof Psychiatry, 130, 191-199.
SLOANE, R. B., STAPLES, F. R., CRISTOL, A. H., YORKSTON,N. J. & WHIPPLE, K. (1975). Psychotherapy versus BehaviorTherapy. Cambridge: Harvard University Press.
WEISS, D., WILNER, N. & HOROWITZ, M. (1984). The stressresponse rating scale: A clinician's measure for rating theresponse to serious life events. British Journal of ClinicalPsychology, 23, 202-215.
WHITLEY, B. E. (1979). Sex roles and psychotherapy: A currentappraisal, Psychological Bulletin, 86, 1309-1321.
ZILBERG, N., WEISS, D. & HOROWITZ, M. (1982). Impact ofevent scale: A cross-validation study and some empiricalevidence supporting a conceptual model of stress responsesyndromes. Journal of Consulting and Clinical Psychology,50, 407-414.
352



























![Psychotherapie [Psychotherapy]](https://img.pdfslide.net/doc/110x75/6324779548d448ffa0072963/psychotherapie-psychotherapy.jpg)

