Embed Size (px)
Citation preview
Specialty Mental Health Services
Clinical and Documentation
Practice Guidelines
This Manual is made available to the public and providers. The manual addresses the
documentation standards for all Specialty Mental Health Services except Psychiatric
Inpatient, PHF and Nursing Facility Services and can be referred to and downloaded at
www.placer.ca.gov

3-28-2019 FINAL Page 2 of 244
All service providers within the Placer County Mental Health Services system shall
follow the Clinical Record Documentation Standards Policy. This includes providers
employed by PCSOC and all contracted providers. Service providers may develop
additional policies in order to adapt these standards to their specific needs. If variance
from this policy is needed, approval must be obtained from the Quality Assurance
Program Manager.
This Specialty Mental Health Documentation Manual contains information about basic
required chart management, informing materials, and the minimum requirements for
clinical documentation. Most requirements are for all types of providers, as indicated;
differences and exceptions for certain types of providers are so noted.
This guide is in compliance with the following Federal and California statutes:
• Federal Social Security Act XIX
• Code of Federal Regulations (CFR) – Health Insurance Portability and
Accountability
Act of 1996 (HIPAA, Title II)
• California Welfare & Institutions (W&I) Code, Section
• California Code of Regulations (CCR), Title 9
In the spirit of ensuring the highest quality service to our consumers, the PCSOC is
committed to working towards completion of goals relating to service delivery,
accessibility to Mental Health services, quality services provided as measured by client
satisfaction, and appropriately coordinating with other providers and professionals
when necessary. We do this through incorporating Wellness and Recovery and belief in
Resiliency into all work with consumers.
We welcome your feedback, concerns and questions. FAQ’s will be updated regularly on
the SOC Managed Care Intranet. If you find things in this manual are not clear, or look
for things in the manual and are unable to find them, please let us know. Please contact
the Quality Management office with your input and questions.
Thank you,
The Quality Management staff
DOCUMENTATION MANUAL POLICY STATEMENT
3-28-2019 FINAL Page 3 of 244
TABLE OF CONTENTS
CHAPTER ONE _____________________________________________________________________________________ 8
INTRODUCTION ____________________________________________________________________________________ 8 Source OF CHART Document Guidance ____________________________________________________________________ 8 The Role of the MHP Compliance Program ________________________________________________________________ 9 Why Do We Have This Manual? ____________________________________________________________________________ 9 Support to the Direct Service Providers _________________________________________________________________ 10 Compliance ________________________________________________________________________________________________ 11
Compliance is accomplished by: _______________________________________________________________________ 11 Utilization Review _________________________________________________________________________________________ 12 Quality Management ______________________________________________________________________________________ 14
Definition Of Commonly Used Terms _________________________________________________________ 15 A Word about Terminology: ___________________________________________________________________________ 15 Medi-Cal Medical Necessity ____________________________________________________________________________ 15 Important Area of Life Functioning include: __________________________________________________________ 15 Specialty Mental Health Services ______________________________________________________________________ 15 Long Term Care Beneficiary ___________________________________________________________________________ 16 EPSDT ___________________________________________________________________________________________________ 16 Types of Providers ______________________________________________________________________________________ 17 Master Contract Providers (Claims submitted DIRECTLY THROUGH AVATAR EHR) _____________ 17 Organization and Symbols _____________________________________________________________________________ 17
CHAPTER TWO ___________________________________________________________________________________ 19
SERVICE DELIVERY PHILOSOPHY _____________________________________________________________ 19 Cultural Competency ______________________________________________________________________________________ 19 Care/Service Coordination Overview ____________________________________________________________________ 19 Trauma Informed Care and Service Delivery ____________________________________________________________ 20
Adopting a Trauma Informed Care approach as service providers involves: ______________________ 21
Emphasis On Person Centered, Integrated Care Focusing On Wellness, Recovery, And
Resiliency _________________________________________________________________________________________ 23 SAMHSA Definition Of Wellness And Recovery ______________________________________________________ 23 Wellness and Recovery In Documentation ___________________________________________________________ 24 Recovery Oriented Practices VS. Non Recovery Oriented Practices ________________________________ 25
RECOVERY-ORIENTED PRACTICE _____________________________________________________________ 25
NON-RECOVERY PRACTICE ____________________________________________________________________ 25
Figure 2.1 Diagram of Recovery Oriented Services __________________________________________________ 26 Eight Milestones to Recovery __________________________________________________________________________ 27
Person Centered Planning ________________________________________________________________________________ 27 What Is It? _______________________________________________________________________________________________ 27 Why Use It? ______________________________________________________________________________________________ 27
Family Center Care ______________________________________________________________________________ 29
Resiliency __________________________________________________________________________________________________ 29 Family Inclusion ___________________________________________________________________________________________ 30
3-28-2019 FINAL Page 4 of 244
Co-Occurring Competency ______________________________________________________________________ 30 THE EXPECTATION _______________________________________________________________________________________ 31 DEFINITIONS ______________________________________________________________________________________________ 32
Figure 2.2 Stages of Change Cycle _____________________________________________________________________ 33 DETAILS ON STAGES OF CHANGE _______________________________________________________________________ 34
CHAPTER THREE _________________________________________________________________________________ 36
INFORMED Decision Making AND INFORMING MATERIALS _______________________________ 36 Consent for Treatment-Adults ____________________________________________________________________________ 37 Minor Consent _____________________________________________________________________________________________ 37 Emancipated Minors include: ____________________________________________________________________________ 40 Psychotropic Medication Consents for Wards of the Juvenile Court __________________________________ 42 Medication Consent _______________________________________________________________________________________ 42 Confidentiality and Authorization To Exchange Protected Health Information ______________________ 42 Revoking an Authorization to Use, Exchange, and/or Disclose Information __________________________ 43
Special Considerations for minors _____________________________________________________________________ 44 Limits of Confidentiality __________________________________________________________________________________ 44
Informing Materials _____________________________________________________________________________ 45
CHAPTER FOUR __________________________________________________________________________________ 47
DELIEVERY OF SERVICES-REFERRALS, OPENINGS AND CLOSING ________________________ 47
Admission and Opening an Umbrella Episode __________________________________________________________ 47 Care Coordination-Timelines for Admission _________________________________________________________ 48 Annual Renewal Of Services ___________________________________________________________________________ 49 Care Coordination-Transfer of Services _______________________________________________________________ 50 Uniformed Method of Determining the Ability to Pay (UMDAP) ____________________________________ 52
CHAPTER FIVE____________________________________________________________________________________ 53
SCOPE OF PRACTICE AND CREDENTIALING __________________________________________________ 53 BACKGROUND ON SCOPE OF PRACTICE ________________________________________________________________ 54 Background On Credentialing ____________________________________________________________________________ 55
Licensed Professional of the Healing Arts (LPHA) (Physician/Non Physician) ____________________ 55 Licensed Practitioner of Healing Arts-Waivered/Registered _______________________________________ 56 Student LPHA ___________________________________________________________________________________________ 57 Mental Health Rehabilitation Specialist (MHRS) as defined in CCR, Title 9. ________________________ 57 Mental Health Workers (“Other Qualified Provider”) ________________________________________________ 58 Peer Advocate Staff-I/II within Mental Health _______________________________________________________ 59 INSIGHTS FROM DHCS” MHSUDS INFORMATION NOTICE #17-040 _______________________________ 59
CHAPTER SIX _____________________________________________________________________________________ 64
MEDICAL NECESSITY ____________________________________________________________________________ 64
MEDICAL NECESSITY IN CONCEPT ______________________________________________________________________ 64 MEDICAL NECESSITY CRITERIA _________________________________________________________________________ 65
Criteria One: Diagnostic Criteria ______________________________________________________________________ 66 INCLUDED ICD -10-CM DIAGNOSIS FOR SPECIALTY MENTAL HEALTH SERVICES (ADULTS AND
CHILDREN) ______________________________________________________________________________________________ 67 CRITERIA TWO: RESULTING IMPAIRMENT CRITERIA _________________________________________________ 69 Criteria Three: Intervention Related Criteria (Must have all 3) _______________________________________ 70
3-28-2019 FINAL Page 5 of 244
The Golden Thread of Medical Necessity ________________________________________________________________ 70 NOTICE OF ADVERSE BENEFICIARY DETERMINATION ____________________________________________ 72
CHAPTER SEVEN _________________________________________________________________________________ 74
ASSESSMENTS ____________________________________________________________________________________ 74 Building a Foundation_____________________________________________________________________________________ 74
Flow of Client Information in developing the assessment ___________________________________________ 75 Conducting Assessments _______________________________________________________________________________ 75 Client Assessment ______________________________________________________________________________________ 76 Elements of an Assessment ____________________________________________________________________________ 76 Clinical Summary: ______________________________________________________________________________________ 84 Elements of Clinical Summary _________________________________________________________________________ 86
Special Consideration _____________________________________________________________________________________ 87
ASSESSMENT TIMELINE: ________________________________________________________________________ 87
Initial Assessment _________________________________________________________________________________________ 87 Updated Assessments _____________________________________________________________________________________ 87
Billing and Code Requirements ________________________________________________________________ 88
Level of Care Tools- Assessment/Evaluation ________________________________________________ 89 The Child Assessment of Needs and Strengths (CANS) _________________________________________________ 89 The Level of Care Utilization Scale (LOCUS) For Adults ________________________________________________ 90
CANS and LOCUS ________________________________________________________________________________________ 90
CHAPTER EIGHT _________________________________________________________________________________ 92
UNIFIED SERVICE PLANS/TREATMENT PLANS ______________________________________________ 92 Understanding the purpose of the Treatment Plan _____________________________________________________ 92 Developing Client/Family Centered Unified Service Plans _____________________________________________ 93 COLLABORATION AND UNIFIED SERVICE PLANS COMPONENTS ____________________________________ 93
Service Strategies: ______________________________________________________________________________________ 93 Ethnic Specific Service Strategy: _______________________________________________________________________ 93 Psycho-educational: ____________________________________________________________________________________ 93 Peer/Family Delivered: ________________________________________________________________________________ 94 Family Support: _________________________________________________________________________________________ 94 Age Specific Service Strategy __________________________________________________________________________ 94 Integrated Services for MH and the Aging: ___________________________________________________________ 94 Integrated Services for MH and the Developmental Disability: _____________________________________ 94 Delivered in partnership with health care: ___________________________________________________________ 94 Delivered in partnership with Substance Use Services: _____________________________________________ 94 Delivered in partnership with Law Enforcement: ____________________________________________________ 94 Delivered in partnership with Social Services: _______________________________________________________ 94
ASSESS THE CLIENT'S STAGE OF CHANGE. _____________________________________________________________ 94 Set realistic goals _______________________________________________________________________________________ 95
Unified Service Plans/Treatment Plan Basics: __________________________________________________________ 95 TRAITS OF EFFECTIVE CLIENT TREATMENT PLANS: _______________________________________________ 96
ELEMENTS OF A TREATMENT PLAN ____________________________________________________________________ 96 Client Strengths _________________________________________________________________________________________ 98 Life Goals/Aspirations (In client’s own words) ______________________________________________________ 99 Clinical Treatment GOALS (Hopes and Desired outcomes) _________________________________________ 100
3-28-2019 FINAL Page 6 of 244
Challenges/Recovery Barriers/Problem. ____________________________________________________________ 101 ACTION STEP (OBJECTIVE) ___________________________________________________________________________ 101
INTERVENTION(S)-THE SERVICES THAT STAFF WILL PROVIDE ________________________ 103
Treatment Plan Timelines _______________________________________________________________________________ 107 Initial USP/Treatment Plan ___________________________________________________________________________ 107 Renewals _______________________________________________________________________________________________ 108 Client participation and Signatures on Treatment Plans:___________________________________________ 108 Minor (17 and Under) and Conserved Clients: ______________________________________________________ 109 Examples of Treatment planning DOCUMENTATION When client did not sign plan. ____________ 109 Offering copy of treatment plan: ______________________________________________________________________ 110 Staff Approval-Licensed/non licensed staff signing treatment plans: _____________________________ 110
CHAPTER NINE _________________________________________________________________________________ 114
SPECIALTY MENTAL HEALTH SERVICES _____________________________________________________ 114
Rehabilitative Mental Health Services _______________________________________________________ 115 Assessment _______________________________________________________________________________________________ 116 Plan Development ________________________________________________________________________________________ 116 Collateral __________________________________________________________________________________________________ 117 Rehabilitation _____________________________________________________________________________________________ 118 Therapy ___________________________________________________________________________________________________ 118 Crisis Intervention Services _____________________________________________________________________________ 119
Crisis Intervention Special Billing Rules _____________________________________________________________ 119 Crisis Intervention Special Documentation Requirements & Billing Rules ________________________ 120
TARGETED CASE MANAGEMENT _______________________________________________________________________ 125
CHAPTER TEN __________________________________________________________________________________ 129
PATHWAYS to MENTAL HEALTH SERVICES –CORE PRACTICE MODEL __________________________ 129
Intensive Care Coordination (ICC) SERVICE Definition _______________________________________________ 129 ICC Service Components ______________________________________________________________________________ 130 Claiming for Multiple Staff ____________________________________________________________________________ 131 The CFT FACILITATOR SERVES as the single point of accountability to: _________________________ 131 Intensive Home Based Services (IHBS) Service Definition:_________________________________________ 132 Service Components/Activities _______________________________________________________________________ 132 Service Lockouts for IHBS _____________________________________________________________________________ 133
Therapeutic Behavioral Services (TBS) _________________________________________________________________ 133 TBS Service Definition _________________________________________________________________________________ 133 TBS Intervention Definition ___________________________________________________________________________ 134 TBS Collateral Service Definition _____________________________________________________________________ 134 TBS Client Assessment Requirements ________________________________________________________________ 134 TBS Client Plan Requirements ________________________________________________________________________ 135 TBS Client Plan Reviews _______________________________________________________________________________ 136 TBS Client Progress Notes _____________________________________________________________________________ 136 TBS Service Restrictions ______________________________________________________________________________ 137
CHAPTER ELEVEN _____________________________________________________________________________ 139
Medication Support Services __________________________________________________________________ 139 Medication Support Services Scope of Practice ________________________________________________________ 140
3-28-2019 FINAL Page 7 of 244
Medication Consent Requirements: __________________________________________________________ 140 Medication Support Services General Billing Rules ____________________________________________________ 141 Progress Notes ____________________________________________________________________________________________ 141 Non-Medication Support Billing _________________________________________________________________________ 141 Urgent Meds Guidelines __________________________________________________________________________________ 143 Urgent Meds Guidelines __________________________________________________________________________________ 144
Medicare Evaluation and Management Services ____________________________________________ 146
CHAPTER TWELVE ______________________________________________________________________________ 164
DOCUMENTATION ________________________________________________________________________________ 164
GENERAL PRINCIPLES OF DOCUMENTATION: ________________________________________________________ 165
STYLES of DOCUMENTATION- Progress Notes _____________________________________________ 173 Progress Note Formats/Templates _____________________________________________________________________ 174
BIRP and IGBIRP _______________________________________________________________________________________ 175 IGBIRP NOTES ___________________________________________________________________________________________ 177
APPENDICES ____________________________________________________________________________________ 230
APPENDIX F ______________________________________________________________________________________ 230
Appendix G _______________________________________________________________________________________ 239
APPENDIX H______________________________________________________________________________________ 240
APPENDIX I_______________________________________________________________________________________ 242 DSM-5 Tools ______________________________________________________________________________________________ 243
3-28-2019 FINAL Page 8 of 244
CHAPTER ONE
INTRODUCTION
SOURCE OF CHART DOCUMENT GUIDANCE
The Placer/Sierra Mental Health Plan, Specialty Mental Health Services are funded
through Medi-Cal and County General Fund. To claim for Medi-Cal reimbursement of
qualifying services, counties must meet contractual requirements between the
California State Department of health Care Services (DHCS) and the Placer County
Health and Human Services. This contract is known at the Mental Health Plan Contract
(MHP contract) and it conforms to the state regulations that implement Specialty Mental
Health Services (CCR Title 9, Chapter 11) to Medi-Cal beneficiaries.
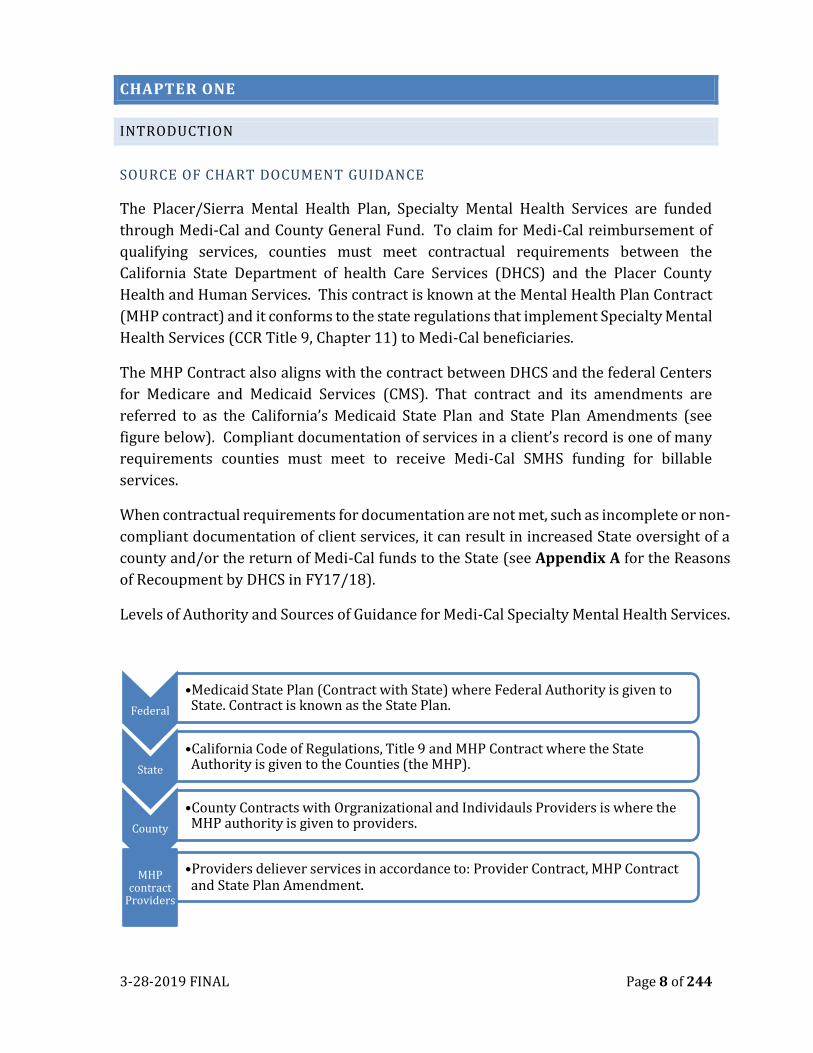
The MHP Contract also aligns with the contract between DHCS and the federal Centers
for Medicare and Medicaid Services (CMS). That contract and its amendments are
referred to as the California’s Medicaid State Plan and State Plan Amendments (see
figure below). Compliant documentation of services in a client’s record is one of many
requirements counties must meet to receive Medi-Cal SMHS funding for billable
services.
When contractual requirements for documentation are not met, such as incomplete or non-
compliant documentation of client services, it can result in increased State oversight of a
county and/or the return of Medi-Cal funds to the State (see Appendix A for the Reasons
of Recoupment by DHCS in FY17/18).
Levels of Authority and Sources of Guidance for Medi-Cal Specialty Mental Health Services.
Federal
•Medicaid State Plan (Contract with State) where Federal Authority is given to State. Contract is known as the State Plan.
State
•California Code of Regulations, Title 9 and MHP Contract where the State Authority is given to the Counties (the MHP).
County
•County Contracts with Orgranizational and Individauls Providers is where the MHP authority is given to providers.
MHP contract
Providers
•Providers deliever services in accordance to: Provider Contract, MHP Contract and State Plan Amendment.
3-28-2019 FINAL Page 9 of 244
THE ROLE OF THE MHP COMPLIANCE PROGRAM
The MHP Compliance Program is responsible for monitoring local compliance with
Medi-Cal SMHS requirements and promoting complaint client medical record keeping
in partnership with MHP network.
The Placer/Sierra MHP Clinical Documentation Manual is a resource developed by to
support behavioral health providers in meeting documentation compliance standards.
This manual includes client service documentation requirements for the following
services:
1. Rehabilitative Mental Health Services including:
• Outpatient Mental Health Services
• Medication Support Services
• Evaluation & Management Services
• Day Treatment Intensive
• Day Rehabilitation
• Crisis Intervention
• Crisis Stabilization
• Specialty Mental Health Services in Adult Residential Treatment
• Psychiatric Health Facility Services
2. Targeted Case Management
3. Intensive Case Coordination, Intensive Home-Based Services & Therapeutic
Foster Care
4. Therapeutic Behavioral Services
Compliant documentation is more than just a contractual requirement or the subject of
a triennial audit; it’s an important record of an individual’s behavioral health journey.
Whether a provider has worked in the behavioral health system for many years or just
started a career at a community clinic, reviewing this manual and visiting the Placer
County website for documentation updates and tools are both essential parts of good
clinical practice.
WHY DO WE HAVE THIS MANUAL?
Placer County Adult and Children’s Systems of Care (SOC) is a county mental health
organization (also referred to as a Mental Health Plan) that provides services to the
community and then seeks reimbursement from state and federal funding sources.
There are many rules associated with billing the state and federal government, thus the
need for this documentation guide. In general, good ethical standards meet nearly all of
the requirements. At times, there is a need to provide some guidance and clarity so staff
can efficiently and effectively document for the services they provide. Although some
3-28-2019 FINAL Page 10 of 244
clients receive services that are funded through grants, as a policy we do not reduce or
alter documentation standards based of the client’s funding source.
This manual defines key concepts, explains documentation
requirements per state laws and regulations, and provides clear
instructions and guidance on how to correctly document the various
types of Specialty Mental Health Services provided to clients. All
Services providers strive to provide high quality care to their clients
and documentation that is accurate, comprehensive and timely plays a crucial part in
the process of delivering excellent care. All Documentation must follow a logical flow
and be interconnected. To illustrate this concept, Figure 1.1. depicts the “Golden
Thread”. The Golden Thread demonstrates the flow of documentation that captures the
progression of services provided to the client and contributes to a comprehensive
record of care that is error free and ready for treatment use and billing.
SUPPORT TO THE DIRECT SERVICE PROVIDERS
The development and utility of a practice manual is supported throughout systems,
including the Code of Federal Regulations (Title 42, Chapter IV, Subchapter C, Part
438.236 The Practice Standards Manual is intended to support the following uses and
associated users:
Applications:
• Auditing and Documentation Compliance
• Clinical Supervision, Staff Coaching
• Professional Development and Training
• Consumer (Counsel Council)
Comprehensive Clinical
Assessment
Personalized Unified
Service Plan
Progress Notes outlining progress toward goals
Figure 1.1
3-28-2019 FINAL Page 11 of 244
• On boarding of New Hires
• Performance =Management/Quality Improvement
• System design
With this in mind, the following SOC and Contracted Community based agency
references should be informed by these clinical practices:
• SOC MH Policies and Procedures
• Documentation Practices/Standards
• Employee Performance evaluations
• Clinical Review
• Utilization Review
• Provider Contracts
• Supervisor Tools
• Training Programs
COMPLIANCE
Placer County’s MHP has adopted a Compliance Plan to express our commitment to
providing high quality health care services in compliance with all applicable federal,
state and local rules and regulations based on guidance and standards established by
the Office of Inspector General, U.S. Department of Health and Human Services. The
intent of the compliance plan is to prevent fraud and abuse at all levels. The compliance
plan particularly supports the integrity of all health data submissions, as evidenced by
accuracy, reliability, validity, and timeliness. The plan applies to staff, volunteers,
trainees, and contractors working in county owned or operated sites. A key component
of the Compliance Plan is the assurance that all of services submitted for reimbursement
are based on accurate, complete, and timely documentation. It is the personal
responsibility of every provider to submit a complete and accurate record of the services
they provide, and to document services in compliance with all applicable laws and
regulations.
COMPLIANCE IS ACCOMPLISHED BY:
• Adherence to legal, ethical, code of conduct and best-practice standards for
billing and documentation.
• Participation by all providers in proactive training and quality improvement
processes.
• Providers working within their professional scope of practice.
• Having a compliance Plan to ensure that there is accountability for all
Placer/Sierra MHP, Community Programs activities and functions. This includes
the accuracy of progress note documentation by defined practitioners who will
3-28-2019 FINAL Page 12 of 244
select correct procedure codes and service location to support the
documentation of services provided.
To ensure compliance, all services, and the charting of all services,
must observe the following overriding rules:
• All services shall be documented in a timely manner.
• A late entry must clearly be identified in the documentation.
• All notes must be signed (wet or electronically) by services provider, and include
discipline, License or with job classification.
• All services shall be based on a current assessment and updated in accordance to
service program requirements.
• All charts must contain an assessment, and when applicable, updated
assessments.
• Services provided without a current assessment and treatment plan may be at
risk of disallowance.
• All services shall be based on a current treatment/service treatment plan (except
when conditions occur, as identified in DHCS MHSUDS Information Notice #17-040-
in appendix B. Prior to the client plan being approved, or when there is a “gap”
in approved client plans, the following SMHS and service activities are
reimbursable:
o Assessment
o Plan Development
o Crisis Intervention
o Crisis Stabilization
o Medication Support Services (for assessment, evaluation, or plan
development; or if there is an urgent need, which must be documented)
o Targeted Case Management and Intensive Care Coordination (ICC) (for
assessment plan development, and referral/linkage to help a beneficiary
obtain needed services including medical, alcohol and drug treatment,
social, and educational services)
• Services shall be provided within the staff person’s scope of practice as specified
in this manual.
• Progress notes should reflect actual duration of the intervention, e.g. 23 minutes,
no rounding up.
UTILIZATION REVIEW
This guide reflects the current requirements for direct services reimbursed by Medi-
Cal Specialty Mental Health Services, California Code of Regulations (CCR, Title 9,
3-28-2019 FINAL Page 13 of 244
Division 1) and serves as the basis for all documentation and claiming in County
Behavioral Health, regardless of payer source. All staff, whether directly operated by
the County or Contracted Community “Providers” are expected to abide by the
information found in this guide.
Quality Improvement may issue updates and/or clarifications to information found in
this manual via Newsletters, Policy Clarification Memos, PCSOC Behavioral Health
Managed Care Network website at https://www.placer.ca.gov/6019/Behavioral-
Health-Quality-Management and/or other acceptable modes of communication. The
updates and/or clarifications are considered to be official PCSOC requirements and will
be incorporated into this guide as appropriate.
State regulations and Behavioral Health policies specify that beneficiary health records,
regardless of format (electronic or print) go through the utilization review (UR) process.
The UR process is meant to ensure the following: all planned clinical services are
appropriate to address the client’s mental health needs; comply with all State, Federal
and Behavioral Health regulations; and maintain the integrity of the client’s health
records in accordance with documentation standards.
We have established a Utilization Review process with an aim to review 10% or
minimum of ten (10), whichever is greater, of all MHP behavioral health records per
calendar year. The Quality Improvement (QI) team oversees the UR processes. The UR
process includes licensed staff members from the QI Team (QI Reviewers) and
Supervisors (Reviewer). The roles of these reviewers are critical as they provide clinical
oversight and function as a “check and balance” system.
All Reviewers are responsible to ensure the following is met: All services meet medical
necessity standards; planned services benefit the client by significantly diminishing the
impairment, or preventing significant deterioration in an important area of life
functioning; all documents are completed within established the MHP Behavioral Health
standards; and review that treatment planning is co - authored with individual/family
and written in a manner that is easily understood by the individual/family.
Supervisors/Reviewers utilize the “Mental Health Chart Review Tool” located in
appendix C when performing internal MHP mental health chart reviews.
Representatives from the SOC Quality Management team utilize the “2017 Provider Audit
Tool” located in appendix D to conduct reviews of contracted Organizational and
Individual providers. The most significant difference between the two review tools is
that although the UR tool and Clinical Supervisory tool are used to review medical
necessity and quality of care, the Clinical Supervisory tool allows for the direct
supervisor to provide real-time feedback to the supervisee.
3-28-2019 FINAL Page 14 of 244
We recognize the importance in providing information about review findings to staff.
Some common methods for providing feedback include:
1) The Supervisor reviewing the chart may provide direct feedback to the staff
member as an opportunity for further coaching and support.
2) The Quality Management team member sends reports to Program Managers and
Supervisors that indicate the clinical records that were reviewed, whether or not
corrections are required, and whether or not the corrections have been verified
(for County internal staff, the staff member also receives a copy).
3) The Quality Improvement team provides SOC Directors, Program Managers and
Supervisors and Organizational providers’ direct feedback regarding any
identified program trends.
4) Information from utilization reviews is used to review overall program or system
trends when considering performance improvement projects.
5) Quarterly reports summarizing UR activities are shared and discussed during the
quarterly SOC QI meeting.
6) UR findings are taken into consideration when exploring training needs of
County and Organizational Provider’s staff members along with the individual
network providers.
QUALITY MANAGEMENT
Quality Management is comprised of two very distinct components: Quality Assurance
and Quality Improvement. Quality Assurance is a systematic, ongoing process that is
designed to assess and evaluate the quality and appropriateness of services, to resolve
identified problems, to identify gaps in service, to promote opportunities to improve
business practices and service delivery and overall organizational performance
The Quality Improvement Program provides a formal process to objectively and
systematically monitor and evaluate the quality, appropriateness, efficiency, safety, and
effectiveness of care and services utilizing a multidimensional approach. This approach
enables Placer County Systems of Care, to focus on opportunities for improving
operational processes, as well as health outcomes and satisfactions of service recipients
and providers. Quality Improvement promotes the accountability of all employees and
contracted organizations for the quality of care and services provided to our recipients.
The goals of the SOC Quality Improvement is to:
Provide timely access to high quality care for all recipients, through a cost
effective, safe service delivery system that objectively and systematically
monitors and evaluates the quality and appropriateness of mental health and
substance use services; pursue opportunities to improve health, service and
safety and resolve identified problems in a timely manner.

3-28-2019 FINAL Page 15 of 244
Scope of Quality Improvement Program:
The Quality Improvement Program provides for review and evaluation of all
aspects of mental health and substance use services, encompassing both clinical
care and services provided to external and internal service recipients. All
departments/programs and staff members participate in the quality
improvement of services delivered by the MHP.
DEFINITION OF COMMONLY USED TERMS
A WORD ABOUT TERMINOLOGY: PCSOC providers and administrative offices have
the intention to be inclusive in the language used to refer to beneficiaries of the Mental
Health Plan (e.g., consumers, clients, families, children, youth, transition-age youth, etc.).
Depending on the language used, it is possible that some beneficiaries could feel
excluded or secondary in importance. While it is the goal of PCSOC to honor each
individual’s desire to be identified as they wish, this Section of the Quality Assurance
Manual is bound by regulatory language that uses “beneficiary” and “client” in reference
to documentation standards. Therefore, in the interest of clarity, inclusion, and
consistency with regulatory language, all beneficiaries will be referred to as “clients”.
MEDI-CAL MEDICAL NECESSITY
Medical necessity is a term used by certain third party payers that encompasses
criteria they feel are essential for reimbursement of services. If all the criteria
making up medical necessity are not met, a payer will refuse or deny payment.
While the wording of definitions vary slightly among payer sources, their intent is
generally the same and compliance with one will often merit compliance with
another. The Medi-Cal Medical Necessity criteria have three components-
Diagnosis, impairment, and interventions. These are detailed within this manual
along with additional comments regarding EPSDT (Early Periodic Screening,
Diagnosis, & Treatment) medical necessity criteria.
IMPORTANT AREA OF LIFE FUNCTIONING INCLUDE:
When exploring Medical Necessity, staff must identify how an individual’s
symptoms of their Mental illness has a negative impact in one or more of the
following areas of their Life: Living arrangement/Housing, Activities of daily
living, Primary Support Group, Education/Employment, Financial or Economic
Issues, Access to Health Care Services, Social/Relationship,
Environment/Community or School Situations.
SPECIALTY MENTAL HEALTH SERVICES
3-28-2019 FINAL Page 16 of 244
This is the broad umbrella of Medi-Cal services directed at the mental health
needs of Medi-Cal beneficiaries. Specialty Mental Health Services include the
smaller umbrella of Mental Health Services.
• Mental Health Services: Assessment, Plan Development, Psychotherapy,
Rehabilitation, and Collateral.
• Medication Support
• Case Management/Brokerage
• Psychiatrist & Psychologist Services
• EPSDT Supplemental Specialty Mental Health Services
• Day Treatment Intensive & Day Treatment Rehabilitation
• Crisis Intervention
• Crisis Stabilization
• Adult Residential Treatment Services & Crisis Residential Treatment
Services
• Psychiatric Inpatient Hospital Services, Psychiatric Health Facility
Services (PHF), and Psychiatric Nursing Facility Services (Mental
Health Rehabilitation Centers [MHRC’s] follow the documentation
standards established in the California Code of Regulations, Title 9;
Chapter 3.5: Section 786.15.)
Definitions of the outpatient services listed above included in Chapter 8 of this
manual.
LONG TERM CARE BENEFICIARY
A beneficiary who receives case management and/or multidisciplinary mental
health services, for a period of 365 days or more. Case Management is defined as
a system in which long term, high cost, and high-risk and/or complex beneficiary
mental health needs are identified; monitored; and addressed, in order to
maximize the mental health status of the beneficiary, utilizing available resources
and multidisciplinary mental health providers.
EPSDT
The Early and Periodic Screening, Diagnosis, and Treatment program (EPSDT)
was first implemented by the former California State Department of Mental Health
(DMH) in Fiscal Year 1995-96. EPSDT differs from the CCR, Title 9, Chapter 11,
Section 1830.205(a)(1)(A-R) for Medical Necessity by permitting a broader
definition and inclusion of diagnosed mental illness that is not limited to targeted
population criteria established in the Welfare and Institution Code §5600.3 for
Seriously Emotionally Disturbed children and adolescents.
3-28-2019 FINAL Page 17 of 244
TYPES OF PROVIDERS
The type of provider contract determines the documentation standards and
method of claiming for reimbursement of services. Each provider’s contract
specifies which specialty mental health services they may claim; not all provider
contracts authorize claiming for all possible services. Providers may only provide
and bill services within their scope of practice.
MASTER CONTRACT PROVIDERS (CLAIMS SUBMITTED DIRECTLY THROUGH
AVATAR EHR)
The following are provider subtypes that are considered Master MHP/DHCS
Contract Providers:
• County-operated service providers of outpatient services (includes PCSOC -
identified Brief Service Programs, e.g., Crisis, Assessment Only).
• Organizational providers of outpatient services (CBO’s).
• Full Service Partnerships (FSP’s) Organizational Providers.
ORGANIZATION AND SYMBOLS
This manual is organized into color-coded sections and clickable links to help you
navigate it with as much ease as possible. This manual contains many links connecting
you to either online resources or to other parts of the document. If ANY Word or phrase
is underlined, this means that it can be clicked on for instant access to another part of
the manual; these are called “Section Shortcuts.” The following symbols and graphics are
used to help bring clarity and simplicity to the manual as a whole:
Reminders of areas to pay attention
Areas within the manual are identified as “important”.
Pay close attention to this area as these are identified as Compliance
areas and will result in disallowances if this area is not adhered to.
3-28-2019 FINAL Page 18 of 244
This symbol represents Quality Improvement-a way to improve the
documentation or the services being rendered.
The Golden Thread symbol is inserted in select areas of the manual to
remind the provider of the importance of documenting the common
thread that links the assessment, treatment plans, interventions and
progress notes together.
KEY POINTS contain summary highlights from the chapter.
• This manual defines key concepts, explains documentation requirements per state laws and regulations, and provides clear instructions and guidance on how to correctly document the various types of Specialty Mental Health Services provided to clients.
• The intention of this manual is to provide documentation standards; and quick references to recording clinical documentations within the AVATAR system.
• This guide reflects the current requirements for direct services reimbursed by Medi-Cal Specialty Mental Health Services, California Code of Regulations (CCR, Title 9, Division 1) and serves as the basis for all documentation and claiming within County Behavioral Health, regardless of payer source.
• State regulations and Behavioral Health policies specify that beneficiary health records, regardless of format (electronic or print) go through the utilization review (UR) process.
• The UR process is meant to ensure the following: all planned clinical services are appropriate to address the client’s mental health needs; comply with all State, Federal and Behavioral Health regulations; and maintain the integrity of the client’s health records in accordance with documentation standards.
• The Golden Thread demonstrates the flow of documentation that captures the progression of services provided to the client and contributes to a comprehensive record of care that is error free and ready for treatment use and billing.
• All Services providers strive to provide high quality care to their clients and documentation that is accurate, comprehensive and timely plays a crucial part in the process of delivering excellent care.
• Ensuring quality services and compliance with regulatory requirements is EVERYONES duty.
3-28-2019 FINAL Page 19 of 244
CHAPTER TWO
SERVICE DELIVERY PHILOSOPHY
CULTURAL COMPETENCY
Health care professionals agree on the importance of capturing the impact that beliefs,
culture and language can have on attitudes and access to mental health care. That is why
the MHP adheres to principles that demonstrate our commitment to cultural
competence across all spectrums of care, including documentation practices and
standards. As such, all cultural, racial, linguistic, religious/spiritual, physical
abilities/challenges, sexual orientation, socioeconomic and other relevant factors
affecting service delivery must be documented in the intake and clinical assessment
process.
The inclusion of cultural perspectives and factors are critical so that perceived problems
or issues are identified and placed in the appropriate cultural context.
For all clinical assessments, professionals will document evidence of:
• A discussion and exploration of culturally significant topics with the client
and/or significant support persons.
• An exploration and discussion of relevant cultural issues that may pertain to the
presenting mental health problem and which can be used in the development of
a culturally appropriate treatment plan.
• Linguistic accommodations made either through a bilingual certified staff or
interpreter service.
Moreover, treatment planning efforts must take into account any cultural
considerations and how they may influence progress towards goals. By understanding
and embracing a client’s cultural background, professionals are able to provide effective,
personalized assessment and treatment strategies that elaborate on the client’s natural
resources and strengths.
CARE/SERVICE COORDINATION OVERVIEW
The MHP uses a Care/Service Coordination (Coordinator) model for its delivery of
services to the individual/family in an effort to support the individual/family’s recovery.
The Coordinator plays an integral part of the treatment team in supporting the
client/family’s access to medically necessary services and avoids duplication of services
by working in conjunction with other staff and Providers to support client/family’s
recovery. It is important to point out that it is not the Coordinator’s sole responsible for
the direct delivery of all mental health services to the client; instead the Coordinator is
3-28-2019 FINAL Page 20 of 244
responsible for coordinating care among service providers to meet the mental health
needs of the client/family. Further, the Coordinator is responsible to ongoing
assessment of the client’s mental health needs and medical necessity.
As noted above, there may be a variety of service providers involved in the delivery of
services. For this reason we have included a “Supporting Staff” form in AVATAR which
is used to communicate which staff is supporting the client’s recovery. Once a
Supporting Staff member has been added, the designated client will display on the “my
clients” widget for the given Supporting Staff member. This option, in no way, waives
client’s confidentiality. Thus, we must all continue to adhere to all policies regarding
confidentiality of client information.
As the Care/Service Coordinator you are responsible for maintaining communication
and collaboration with treatment providers as well as maintain the accuracy and
integrity of the medical record by adhering to documentation standards and timelines.
The Coordinator role also includes reviewing and approving medically necessary
services to be included on the client’s treatment plan as well as denying those services
that are deemed not medically necessary. When services are denied or modifications to
the services are made, the Coordinator is responsible for communication of these needs
with other staff and/or service providers.
The Care/Service Coordinator is responsible for ensuring the assessments/treatment
plans are completed and for removing any additional “support staff” members from the
supporting staff list once the support person is no longer a part of the client’s treatment
team.
TRAUMA INFORMED CARE AND SERVICE DELIVERY
Traumatic events happen to all people at all ages and across all socio-economic strata in
our society. These events can cause terror, intense fear, horror, helplessness and
physical stress reactions. Sometimes the impact of these events does not simply go away
when they are over. Instead, some traumatic events are profound experiences that can
change the way children, adolescents and adults see themselves and the world.
Sometimes the impact of the trauma is not felt until weeks, months or even years after
the traumatic event.
Psychological trauma is a major public health issue affecting the health of people,
families and communities across Canada. Trauma places an enormous burden on every
health care and human service system. Trauma is not only a mental health issue, but it
also belongs to every health sector, including primary/ physical, mental and spiritual
health. Given the enormous influence that trauma has on health outcomes, it is
important that every health care and human services provider has a basic
3-28-2019 FINAL Page 21 of 244
understanding of trauma, can recognize the symptoms of trauma, and appreciates the
role they play in supporting recovery. Health care, human services and, most
importantly, the people who receive these services benefit from trauma informed
approaches.
Trauma Informed Care is an approach that embraces and understanding of trauma at
every step of service delivery; Trauma informed care is an approach that is incorporated
into the structure of a variety of practices, which are aimed to provide services in ways
that are appropriate and welcoming for those who may have been affected by trauma.
While the effects of trauma frequently have an impact on services and organizations,
trauma often goes undetected. Thus, interfering with their recovery and healing,
individuals may be re-traumatized by the services, and organizations that they interact
with.
The effects of trauma have serious health outcomes for individuals, families and
communities, and services must recognize the role they play in creating supportive and
welcoming environments. As there are many different types of trauma affecting people
of all ages, and across all socioeconomic backgrounds in society, a trauma informed care
approach should be an essential component for all services and organizations.
As research has indicated the experiences of trauma in early childhood trauma are
different from trauma experienced later on in life, trauma informed care takes into
account age-appropriate service delivery. For mothers, these services may include
dealing with major depression and Post Traumatic Stress Disorder (PTSD). For children,
services should include therapy or supportive services to address their learning and
emotional needs, a safe and supportive environment, and the presence of continuous
and nurturing caregivers.
Furthermore, case management services case should address both individual, short-
term needs along with the long-term needs of clients. Some examples of short term
needs include: income, education, and employment, whereas long-term needs may
involve addressing histories of trauma, health/ mental health, and emotional difficulties.
ADOPTING A TRAUMA INFORMED CARE APPROACH AS SERVICE PROVIDERS
INVOLVES:
1. Understanding trauma and stress (Trauma Competence): Without
understanding trauma, we are more like to adopt behaviors and beliefs that are
negative.
• Trauma-We understand that trauma is common, but experienced
uniquely due to its many variations in form and impact.
3-28-2019 FINAL Page 22 of 244
• Stress-We understand that optimal levels of positive stress can be healthy,
but that chronic or extreme stress has damaging effects.
• Reactions -We understand that many trauma reactions are adoptive, but
that some resulting behaviors and beliefs may impeded recovery and
wellness.
• Recovery-We understand that trauma can be overcome and unhealthy.
However, when we understand trauma and stress we can act
compassionately, and take well-informed steps toward wellness.
2. Compassion and dependability (Trustworthiness): Trauma is overwhelming
and can leave us feeling isolated or betrayed, which may make it difficult to trust
others and receive support. However, when we experience compassionate and
dependable relationships, we reestablish trusting connections with others that
foster mutual wellness.
• Compassion-We strive to act compassionately across our interactions
with others through the genuine expression of concern and support.
• Relationships-We value and seek to develop secure and dependable
relationships characterized by mutual respect and attunement.
• Communication- We promote dependability and create trust by
communication in ways that are clear, inclusive, and useful to others.
3. Safety and stability (Physical and Emotional Safety): Trauma unpredictably
violates our physical, social, and emotional safety resulting in a sense of threat
and need to manage risks. Increasing stability in our daily lives and having these
core safety needs meet can minimize our stress reactions and allow us to focus
our resources on wellness.
• Stability-We minimize unnecessary changes and, when changes are
necessary, provide sufficient notice and preparation.
• Physical-We create environments that are physically safe, accessible,
clean and comfortable.
• Social/Emotional-We maintain health interpersonal boundaries and
mange conflict appropriately in our relationship with others.
4. Collaboration and empowerment (Empowerment, Choice and
Collaboration): Trauma involves a loss of power and control that makes us feel
helpless. However, when we are prepared for and given real opportunities to
make choices for our care, and ourselves we feel empowered and can promote
our own wellness.
• Empowerment-We recognize the value of personal agency and
understand how it supports recovery and overall wellness.
3-28-2019 FINAL Page 23 of 244
• Preparation-We proactively provide information and support the
development of skills that are necessary for the effective empowerment
of others.
• Opportunities-We regularly offer others opportunities to make decisions
and choices that have a meaningful impact on their lives.
5. Cultural humility and Responsiveness: We come from diverse social and
cultural groups that may experience and react to trauma differently. When we
are open to understanding these differences and respond to them sensitively we
make each other feel understood and wellness is enhanced.
• Differences-We demonstrate knowledge of how specific social and
cultural groups may experience, react to, and recover from trauma
differently.
• Humility-We are proactive in respectfully seeking information and
learning about differences between social and cultural groups.
• Responsiveness-We have and can easily access support and resources
from sensitively meeting the unique social and cultural needs of others.
6. Resiliency and recovery (Commitment to Trauma Informed Care): Trauma
can have a long-lasting and broad impact on our lives that may create a feeling of
hopelessness. Yet, when we focus on our strengths and clear steps we can take
toward wellness we are more likely to be resilient and recover.
• Path-We recognizes the value of instilling hope by seeking to develop a
clear path towards wellness that addresses stress and trauma.
• Strengths-We proactively identify and apply strengths to promote
wellness and growth, rather than focusing singularly on symptom
reductions.
• Practices-We are aware of and have access to effective treatments, skills,
and personal practices that support recovery and resilience.
EMPHASIS ON PERSON CENTERED, INTEGRATED CARE FOCUSING ON
WELLNESS, RECOVERY, AND RESILIENCY
To provide mental health services and supports in Placer County that are person-
centered, safe, effective, efficient, timely and equitable, that are supported by friends and
community, that promote wellness and recovery, and that fully incorporate shared
decision making between consumers, family members and providers.
SAMHSA DEFINITION OF WELLNESS AND RECOVERY
3-28-2019 FINAL Page 24 of 244
The Federal Substance Abuse and Mental Health Services Administration (SAMHSA)
recently released their official working definition of recovery: A process of change
through which individuals improve their health and wellness, live a self-directed life,
and strive to reach their full potential. SAMHSA has also delineated four major
dimensions that support a life in recovery:
• Health: overcoming or managing one’s
disease(s) as well as living in a
physically and emotionally healthy
way.
• Home: a stable and safe place to live.
• Purpose: meaningful daily activities,
such as a job, school, volunteerism,
family caretaking, or creative
endeavors, and the independence,
income and resources to participate in
society.
• Community: relationships and social networks that provide support, friendship,
love, and hope.
WELLNESS AND RECOVERY IN DOCUMENTATION
We want all Mental Health Plan staff to emphasize a focus on the wellness and recovery
of the clients you serve in your documentation. We recommend that services and
documentation focus on:
• Ensuring that all services are based on a shared belief, between Provider and the
individual seeking treatment, that greater mental health wellness can be
achieved.
• Achieving the goals and aspirations of the individual as they relate to the client’s
mental health wellness and recovery.
• Involving the client and families in the planning and implementation of
treatment.
• Client self-determination and informed decision-making.
• Achieving specific objectives to support the individual in accomplishing his/her
desired goals.
• Identifying and encouraging the use of strengths that assist individuals to
overcome challenges and barriers to greater wellness.
• Documenting services that are funded under the authority of Short Doyle Medi-
Cal (SD/MC) in a manner that meets Medi-Cal documentation requirements.
3-28-2019 FINAL Page 25 of 244
• Ensure that services and documentation are based on hope and a shared belief,
between Provider and the individual seeking treatment, that greater mental
health wellness can be achieved
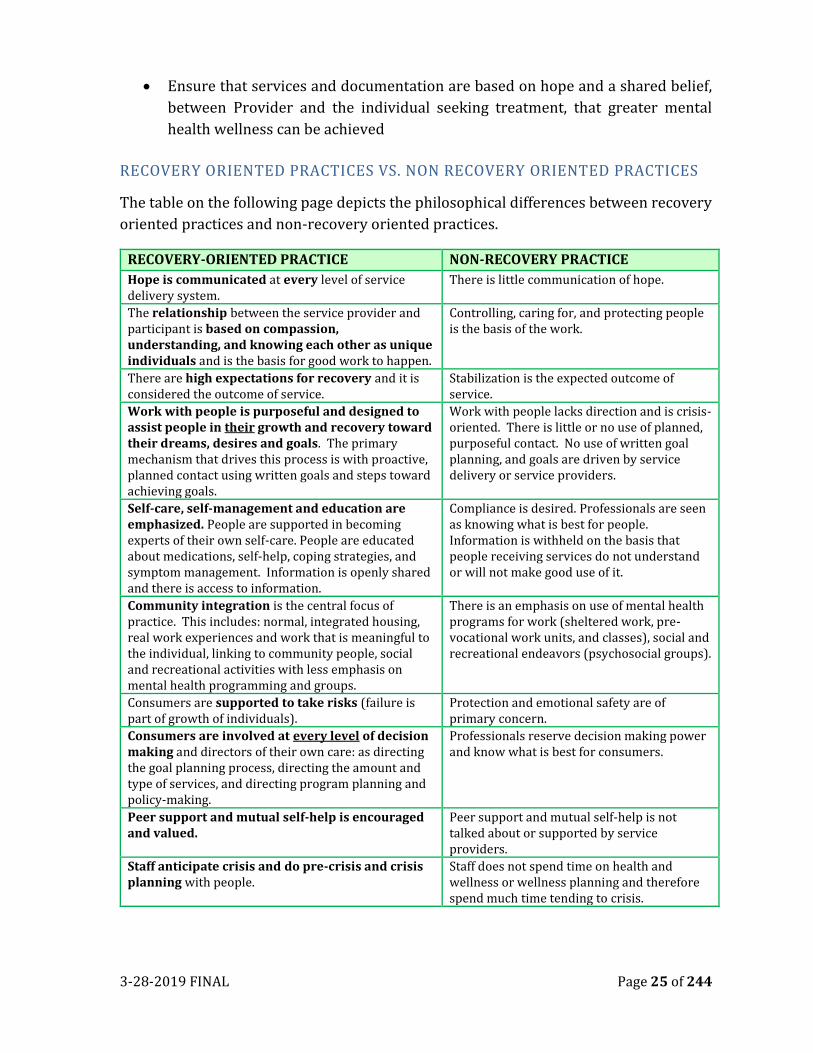
RECOVERY ORIENTED PRACTICES VS. NON RECOVERY ORIENTED PRACTICES
The table on the following page depicts the philosophical differences between recovery
oriented practices and non-recovery oriented practices.
RECOVERY-ORIENTED PRACTICE NON-RECOVERY PRACTICE
Hope is communicated at every level of service delivery system.
There is little communication of hope.
The relationship between the service provider and participant is based on compassion, understanding, and knowing each other as unique individuals and is the basis for good work to happen.
Controlling, caring for, and protecting people is the basis of the work.
There are high expectations for recovery and it is considered the outcome of service.
Stabilization is the expected outcome of service.
Work with people is purposeful and designed to assist people in their growth and recovery toward their dreams, desires and goals. The primary mechanism that drives this process is with proactive, planned contact using written goals and steps toward achieving goals.
Work with people lacks direction and is crisis-oriented. There is little or no use of planned, purposeful contact. No use of written goal planning, and goals are driven by service delivery or service providers.
Self-care, self-management and education are emphasized. People are supported in becoming experts of their own self-care. People are educated about medications, self-help, coping strategies, and symptom management. Information is openly shared and there is access to information.
Compliance is desired. Professionals are seen as knowing what is best for people. Information is withheld on the basis that people receiving services do not understand or will not make good use of it.
Community integration is the central focus of practice. This includes: normal, integrated housing, real work experiences and work that is meaningful to the individual, linking to community people, social and recreational activities with less emphasis on mental health programming and groups.
There is an emphasis on use of mental health programs for work (sheltered work, pre-vocational work units, and classes), social and recreational endeavors (psychosocial groups).
Consumers are supported to take risks (failure is part of growth of individuals).
Protection and emotional safety are of primary concern.
Consumers are involved at every level of decision making and directors of their own care: as directing the goal planning process, directing the amount and type of services, and directing program planning and policy-making.
Professionals reserve decision making power and know what is best for consumers.
Peer support and mutual self-help is encouraged and valued.
Peer support and mutual self-help is not talked about or supported by service providers.
Staff anticipate crisis and do pre-crisis and crisis planning with people.
Staff does not spend time on health and wellness or wellness planning and therefore spend much time tending to crisis.
3-28-2019 FINAL Page 26 of 244
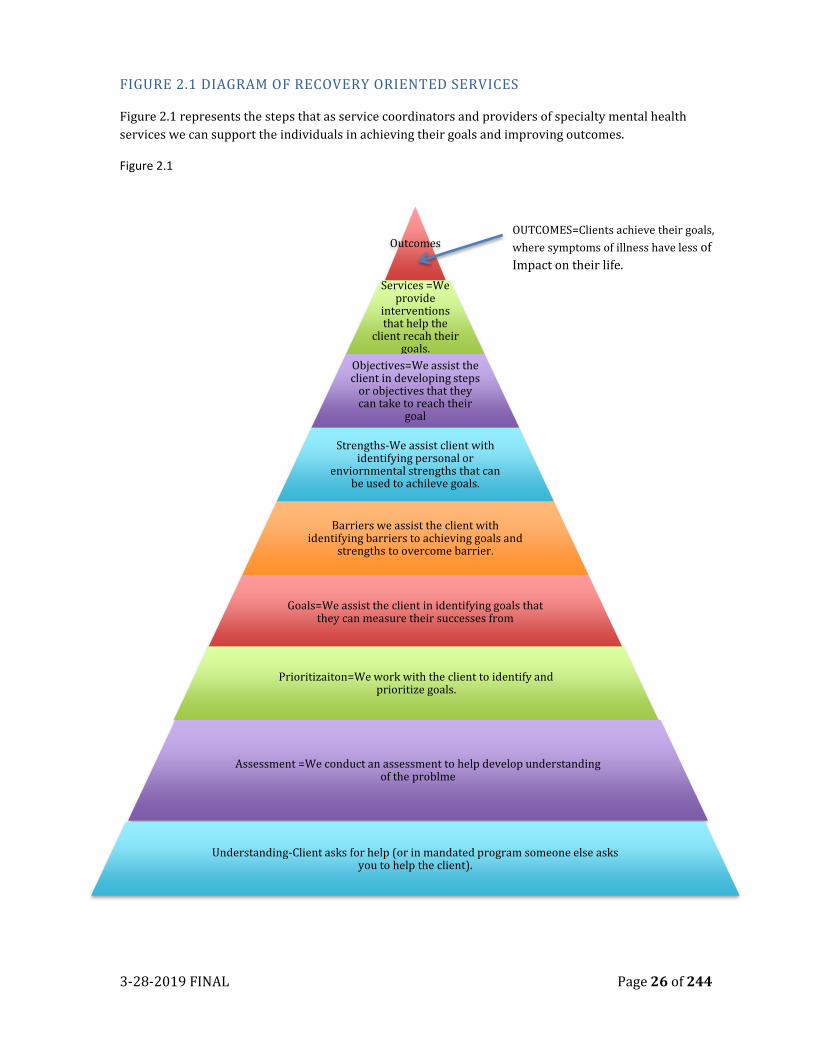
FIGURE 2.1 DIAGRAM OF RECOVERY ORIENTED SERVICES
Figure 2.1 represents the steps that as service coordinators and providers of specialty mental health
services we can support the individuals in achieving their goals and improving outcomes.
Figure 2.1
Outcomes
Services =We provide
interventions that help the
client recah their goals.
Objectives=We assist the client in developing steps
or objectives that they can take to reach their
goal
Strengths-We assist client with identifying personal or
enviornmental strengths that can be used to achileve goals.
Barriers we assist the client with identifying barriers to achieving goals and
strengths to overcome barrier.
Goals=We assist the client in identifying goals that they can measure their successes from
Prioritizaiton=We work with the client to identify and prioritize goals.
Assessment =We conduct an assessment to help develop understanding of the problme
Understanding-Client asks for help (or in mandated program someone else asks you to help the client).
OUTCOMES=Clients achieve their goals,
where symptoms of illness have less of
Impact on their life.
3-28-2019 FINAL Page 27 of 244
EIGHT MILESTONES TO RECOVERY
R I begin to recognize my inner distress but may be unable to identify what it is.
E I begin to examine my distress with the help of others.
C I choose to believe that hope exists.
O I start overcoming symptoms that keep me from examining what is important to me.
V I voluntarily take some action toward recovery.
E I start to enjoy the benefits of mutual recovery.
R I am responsible for my own recovery.
Y Yes, I am helping others strengthen my recovery.
PERSON CENTERED PLANNING
Person and family centered treatment planning is a collaborative process where clients
have control over their services, including the amount, duration and scope of services,
and participate in the development of treatment goals and services provided, to the
greatest extent possible.
Effective person-centered care planning strengthens the voice of the individual, builds
resiliency, and fosters recovery. It is important to note that while person-centered
planning is respectful and responsive to the needs of the individual, it also occurs within
the professional responsibilities of providers and care teams.
WHAT IS IT?
It’s an approach to assessment and service planning which:
• Person Centered Planning is respectful and responsive to the cultural and
linguistic and other social and environmental needs of the individual.
• Emphasizes the uniqueness of each person and his/her right to self-
determination.
• Is based on principles of wellness, recovery, and hope.
• Seeks to discover strengths that each person/family possesses that will help
them in their journey.
WHY USE IT?
3-28-2019 FINAL Page 28 of 244
Too often assessment and service planning are not fully inclusive of the client/family.
Helping professionals may make the mistake of:
• Assuming to know what is best for the client.
• Not sharing the assessment/diagnosis results.
• Not communicating and making shared decisions.
• Dismissing the individual’s preferences and goals.
• Fostering dependency rather than self-reliance and recovery.
• Why are these things a mistake? It invalidates the client’s experience, damages
the relationship, and decreases the chances of a positive outcome of the
treatment process.
• Use of a person centered approach has been shown to improve treatment
outcome for clients
WORKING FROM A PERSON CENTERED APPROACH
• Providers view the relationship with the individual/family as a partnership that
supports the person’s hopes, dreams and goals.
• The process is dynamic and changes based on the person’s/family’s wishes and
needs, not on some predetermined outcome such as medication compliance,
abstinence or “stability”
PERSON CENTERED PLANNING-ENGAGEMENT
• Person centered assessment and planning include the client/family as a team
members. In fact, they are the most important team members.
• The person centered service plan is a shared vision between the client and the
provider.
• The person centered helping professional thinks and speaks in strengths-based
and recovery language.
• Provider and client work together to identify barriers and roadblocks to
reaching goals. These are considered to be things standing in the way rather
than as pathology.
“As Clinicians and helpers our job is not to judge who
will and who will not recover. Our job is to establish
strong, supportive relationships in order to maximize
the chance of recovery”. People need to have the
“dignity to risk” and the “right to fail”. -Patricia
Deegan

3-28-2019 FINAL Page 29 of 244
FAMILY CENTER CARE
When serving children, the MHP strive to be a family-driven system of care that fosters
resiliency. The chart below demonstrates some differences between “traditional care”
and “client/family-driven care” services.
TRADITIONAL CARE CLIENT/FAMILY CENTER CARE
Practitioner based Client/Family Directed Problem Based Strength based
Professional Dominance Skill Acquisition Cure and/or Amelioration Quality of Life Dependence Empowerment Reactive Preventative and/or Wellness Professional Supports Natural Supports
RESILIENCY
Resilience refers to the personal qualities of optimism and hope, personal traits of
effective problem solving skills that lead individuals to live, work and learn with a sense
of mastery and competence. Research has shown that resilience is fostered by positive
experiences in childhood at home, in school and in the community. When children
encounter negative experiences at home, at school and in the community, mental health
treatments, which may teach good problem solving skills, optimism, and hope that may
help build and enhance resiliency in children (California Family Partnership Association,
March 2005).
1. Families and youth are given accurate, understandable, and complete
information necessary to set goals and to make choices for improved planning
for individual children and their families.
2. Families and youth, providers and administrators embrace the concept of
sharing decision-making and responsibility for outcomes with providers.
3. Families and youth are organized to collectively use their knowledge and skills
as a force for systems transformation.
4. Families and family-run organizations engage in peer support activities to reduce isolation, gather and disseminate accurate information, and strengthen the family voice.
5. Families and family-run organizations provide direction for decisions that impact funding for services, treatments, and supports.
6. Providers take the initiative to change practice from provider-driven to family-driven.
7. Administrators allocate practitioner, training, support and resources to make family-driven practice work at the point where services and supports are delivered to children, youth, and families.
3-28-2019 FINAL Page 30 of 244
8. Community attitude change efforts focus on removing barriers and discrimination created by stigma.
9. Communities embrace, value, and celebrate the diverse cultures of their children, youth, and families.
10. Everyone who connects with children, youth, and families continually advances their own cultural and linguistic responsiveness as the population served changes.
FAMILY INCLUSION
The MHP is committed to the fullest possible involvement of consumers/clients and
family members in planning, developing, providing and evaluating services for
consumers/clients of all ages through engaging and building partnership with
consumers/clients and their families to promote recovery while respecting strengths
and choices. The purpose of this policy is to outline and provide guidance to staff
members on how to encourage clients to involve family in their treatment and recovery
process while adhering to all federal, state, and local laws pertaining to confidentiality.
Within this guidance, the term “family” is used broadly and can include relatives, friends,
partners, recovery support people, significant others, etc. with the purpose of:
• Encouraging behavioral health staff, including contractors, to work inclusively
with families in the care, treatment and support of their family member who is
recovering from mental health or substance use problem;
• Promoting active, culturally responsive partnership with the family, the
consumer/client and the clinical staff; and
• Promoting the inclusion of culturally and linguistically competent family
member participation in Systems of Care (SOC) design, operations and
governance.
The MHP Family Information Form in accordance to AB1424 provides a means for
family members or support persons to communicate about their relative/loved one’s
(i.e. consumer/client) mental health history and requires that all staff making decisions
about involuntary treatment consider information supplied by family members. The
Mental Health Family Information form has been made available to the public at the
following location:
http://www.placer.ca.gov/departments/hhs/adult/mentalhealthservices
CO-OCCURRING COMPETENCY
The mission of the placer county’s adult and children’s systems of care, known as
systems of care (SOC) is to oversee, through the safe at home framework, the
development, transformation, implementation, evaluation, and improvement of a
welcoming, accessible, culturally competent, integrated, continuous and comprehensive

3-28-2019 FINAL Page 31 of 244
system of care. This system of care is for individuals and families with needs including
for substance abuse and/or mental health intervention, prevention, treatment and
recovery services. Based on the SOCs awareness that among the individuals and families
served, complex co-occurring needs are the expectation rather than an exception.
Clients may present in any behavioral health setting with any combination of mental
health and substance use symptoms or disorders. Further, the mental health disorders
may or may not be substance-induced, and the mental health and substance use
conditions may be active or in remission. For individuals and families with co-occurring
conditions and other complex needs, the provision of integrated services matched to the
multiple needs of the individual and/or family is an evidence-based practice.
All substance abuse and mental health providers will gladly welcome children,
adolescents, adults, aging adults, and their families, regardless of race, gender, ethnicity,
religion and/or sexual preference, seeking substance and/or mental health services. All
individuals will be treated with respect and understanding and will be welcomed into
our system of care. Necessary interviews, screening and assessment will be conducted
in order to determine services needed. Individuals will be linked and/or referred based
on their unique needs, regardless of the door through which they enter the system.
Families include biological families, current caregivers, and others viewed as significant
in the life of the client.
THE EXPECTATION
It is believed that co-occurring psychiatric and substance
problems are frequently present but not always recognized.
During every phase of treatment/recovery, clients will be
offered individualized screening and assessment, case
management, treatment, and referral. The department of
children & families in collaboration with the community
network of providers, stakeholders and community
representatives has adopted a best practices model called
Comprehensive Continuous Integrated System of Care
(CICSC) which espouses an integrated clinical treatment and
recovery philosophy that makes sense from the perspective
of both the mental health system of care and the substance
abuse treatment/ recovery system.
As noted in the literature, welcoming is only one component
of the CCISC, but it represents an important strategic
starting place to initiate a more comprehensive system
change process that applies not only to clients but to their families. The success of this
This expectation must be
incorporated in a
WELCOMING Manner into
All Clinical Contract, to
promote ACCESS to CARE
AND accurate identification
When substance disorder
and psychiatric disorder co-
exist, each disorder should
be considered primary, and
integrated dual primary
treatment is recommended,
where each disorder
receives appropriately
intensive diagnosis-specific
treatment
3-28-2019 FINAL Page 32 of 244
concept depends on staff “engaging in care” with an individual in need of assistance even
if they cannot immediately be served by that program. Communicating a sincere desire
to engage the client as soon as possible as well as to welcome that person into the system
as a whole (Minkoff & Cline, 2004).
The MHP Services consistently assesses and treats co-occurring disorders (including
substance abuse/dependency, trauma related, and developmental disorders). The
presence of a co-occurring substance abuse/dependence disorder will not, in and
of itself, trigger disallowance of specialty mental health Medi-Cal claiming. All
diagnoses for mental illness and substance abuse/dependence shall be documented in
the PCSOC chart when criteria are present.
DEFINITIONS
CO-OCCURRING DISORDER: Youth, adults and older adults are considered to have a co-
occurring disorder when they exhibit the co-occurrence of mental health and substance
misuse, whether or not they have already been diagnosed. Co-occurring disorders vary
according to severity, duration, recurrence, and degree of impairment in functioning.
CO-OCCURRING FAMILIES: Families in which the identified child has an emotional
disturbance and a significant family member or caregiver has a substance use issue.
Note: Integrated services and documentation apply to co-occurring families as well as
to co-occurring individuals receiving adult and child mental health service funding.
However, clinicians need to use care when documenting these issues in the child’s chart.
C0-OCCURRING TREATMENT PLANNING/SERVICE DELIVERY
Treatment and Recovery Plans for clients and families (of children) with co-occurring
disorders shall address both mental health and substance use issues. The goals for each
issue will be tailored to the client’s readiness to address that issue, with the
understanding that the client or family member may have a different level of readiness
to address each issue.
CO-OCCURING PROGRESS NOTES:
Mental Health progress notes shall document ongoing assessment and monitoring of co-
occurring substance use issues. These notes shall focus on how substance use may be
exacerbating mental health issues or impeding recovery from a mental illness, and how
integrated interventions will promote mental health recovery.
STAGES of CHANGE
Mental health treatment will look different based on the client’s stage of change. For
example, if a client is experiencing symptoms of depression and they are in a pre-
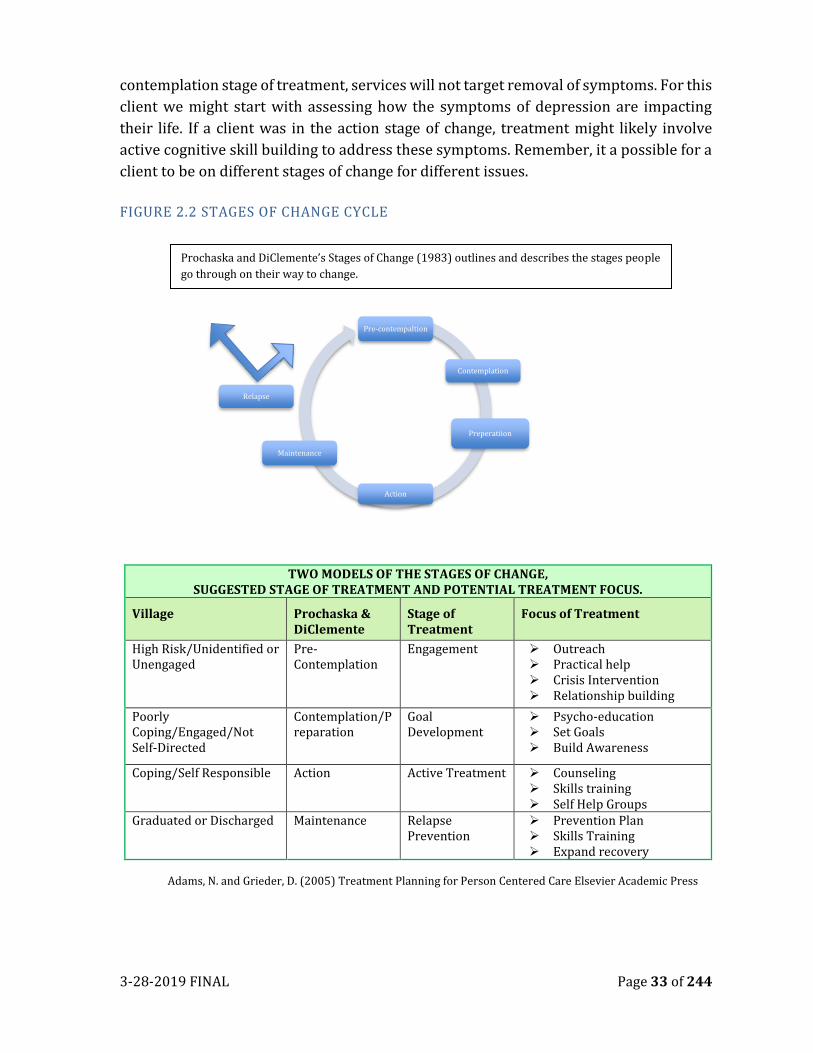
3-28-2019 FINAL Page 33 of 244
contemplation stage of treatment, services will not target removal of symptoms. For this
client we might start with assessing how the symptoms of depression are impacting
their life. If a client was in the action stage of change, treatment might likely involve
active cognitive skill building to address these symptoms. Remember, it a possible for a
client to be on different stages of change for different issues.
FIGURE 2.2 STAGES OF CHANGE CYCLE
TWO MODELS OF THE STAGES OF CHANGE, SUGGESTED STAGE OF TREATMENT AND POTENTIAL TREATMENT FOCUS.
Village Prochaska & DiClemente
Stage of Treatment
Focus of Treatment
High Risk/Unidentified or Unengaged
Pre-Contemplation
Engagement ➢ Outreach ➢ Practical help ➢ Crisis Intervention ➢ Relationship building
Poorly Coping/Engaged/Not Self-Directed
Contemplation/Preparation
Goal Development
➢ Psycho-education ➢ Set Goals ➢ Build Awareness
Coping/Self Responsible Action Active Treatment ➢ Counseling ➢ Skills training ➢ Self Help Groups
Graduated or Discharged Maintenance Relapse Prevention
➢ Prevention Plan ➢ Skills Training ➢ Expand recovery
Adams, N. and Grieder, D. (2005) Treatment Planning for Person Centered Care Elsevier Academic Press
Pre-contempaltion
Contemplation
Preperatiion
Action
Maintenance
Relapse
Prochaska and DiClemente’s Stages of Change (1983) outlines and describes the stages people
go through on their way to change.
3-28-2019 FINAL Page 34 of 244
DETAILS ON STAGES OF CHANGE
Pre-contemplation is the stage in which there is no intention to change behavior in the
foreseeable future. Most individuals in this stage are unaware or under-aware of their
problems. Families, friends, neighbors, or employees, however, are often well aware that
the person is struggling. When people in the Pre-contemplation stage present for
service, they often do so because of pressure from others.
Contemplation is the stage in which people are aware that a problem exists and are
seriously thinking about overcoming it but have not yet made a commitment to take
action. Individuals can remain stuck in the contemplation stage for long periods.
Individuals in the contemplation stage would be endorsing such items as, "I have a
problem and I really think I should work on it" and "I've been thinking that I might want
to change something about myself."
Preparation is a stage that combines intention and behavioral criteria. Individuals in
this stage are intending to take action in the next month and have unsuccessfully taken
action in the past year.
Action is the stage in which individuals modify their behavior, experiences, and
environment in order to overcome their problems. Action involves the most overt
behavioral changes and requires considerable commitment of time and energy.
Modifications of the problem behavior made in the action stage tend to be most visible
and receive the greatest external recognition. Individuals are classified in the action
stage if they have successfully altered the dysfunctional behavior for a period from 1 day
to 6 months. Individuals in the action stage endorse statements like, "I am really working
hard to change" and "Anyone can talk about changing; I am actually doing something
about it."
Maintenance is the stage in which people work to prevent relapse and consolidate the
gains attained during action. Being able to remain free of the problem behavior and to
consistently engage in a new incompatible behavior for more than 6 months are the
criteria for considering someone to be in the maintenance stage. Individuals in the
maintenance stage might say, "I may need a boost right now to help me maintain the
changes I've already made" and "I'm here to prevent myself from having a relapse of my
problem."
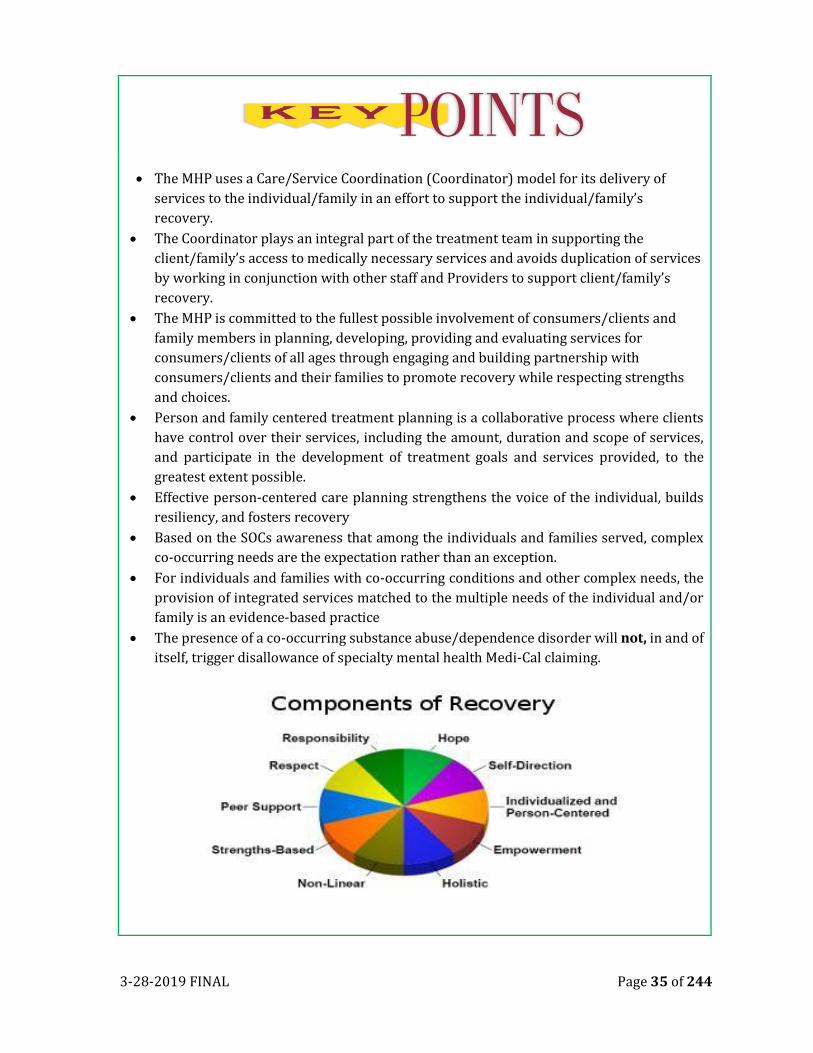
3-28-2019 FINAL Page 35 of 244
• The MHP uses a Care/Service Coordination (Coordinator) model for its delivery of
services to the individual/family in an effort to support the individual/family’s
recovery.
• The Coordinator plays an integral part of the treatment team in supporting the
client/family’s access to medically necessary services and avoids duplication of services
by working in conjunction with other staff and Providers to support client/family’s
recovery.
• The MHP is committed to the fullest possible involvement of consumers/clients and
family members in planning, developing, providing and evaluating services for
consumers/clients of all ages through engaging and building partnership with
consumers/clients and their families to promote recovery while respecting strengths
and choices.
• Person and family centered treatment planning is a collaborative process where clients
have control over their services, including the amount, duration and scope of services,
and participate in the development of treatment goals and services provided, to the
greatest extent possible.
• Effective person-centered care planning strengthens the voice of the individual, builds
resiliency, and fosters recovery
• Based on the SOCs awareness that among the individuals and families served, complex
co-occurring needs are the expectation rather than an exception.
• For individuals and families with co-occurring conditions and other complex needs, the
provision of integrated services matched to the multiple needs of the individual and/or
family is an evidence-based practice
• The presence of a co-occurring substance abuse/dependence disorder will not, in and of
itself, trigger disallowance of specialty mental health Medi-Cal claiming.
3-28-2019 FINAL Page 36 of 244
CHAPTER THREE
INFORMED DECISION MAKING AND INFORMING MATERIALS
Informed Decision Making
We strive to provide excellent quality care to every individual who receives services
from the Placer/Sierra MHP. We aim to involve the individual and/or the family in
treatment in order to provide services that are meaningful to them and help them thrive.
We must include the individual/family in the treatment process at the onset of services.
It is our responsibility to ensure that every individual and/or family is treated with
respect and that every person is informed about what services are offered from MHP as
well as provide information on treatment options in the community in a way that helps
support the client in making an informed decision about whether the services offered
through the MHP are right for them or for their child.
Clients should be given the necessary information and opportunity to exercise the
degree of control they choose over health care decisions that affect them. The system
should be able to accommodate differences in client preferences and encourage shared
decision making.
Adults, including those receiving mental health services, have the right
to give or refuse consent to medical, diagnostic or treatment procedures.
California Health and Safety Code § 7185.5(a) states that "the legislature
finds that adult persons have the fundamental right to control the
decisions relating to the rendering of their own medical care..." California Code of
Regulations, Title22 § 70707(b)(6) provides that a patient has a right to "participate
actively in decisions regarding medical care. To the extent permitted by law, this includes
the right to refuse treatment."
The range of services provided shall be discussed prior to admission
with the prospective client or an authorized representative so that the
program's services are clearly understood. Behavioral Health has an
obligation to inform clients of the risks and benefits of treatment. At the onset of
services, we must ensure that clients understand the content of not only the Informed
Consent form but of all the onset of services documentation prior to the client agreeing
to services and signing these forms. This includes ensuring that minors who are able to
consent for their own services without a parent are fully educated about the similarities
and differences in the types of services they can receive. In addition, although we do not
need to have clients re-sign Informed Consent forms when they transfer from program-
to- program, it is important we inform them of the specific risks and benefits of each
3-28-2019 FINAL Page 37 of 244
particular services when they initially transfer.
An important part of informed concept is the person’s capacity to
consent. A person is deemed to have legal capacity to consent to
treatment if he/she has the ability to understand the nature and
consequences of the proposed health care, including its significant benefits, risks and
alternatives (including doing nothing), and can make and communicate a health care
decision. A person's lack of mental capacity to consent to medical care may be temporary
or it may be permanent, and the provider should determine capacity on a case-by-case
basis whenever consent is sought. For example, a client who is clearly under the
influence of drugs or alcohol may lack capacity temporarily, but could provide consent
at a later time, when not so impaired. If you have any questions regarding a beneficiary’s
ability to consent, please consult with your supervisor and Quality Improvement.
In the MHP behavioral health system, all medical records are maintained through a
hybrid model, including hard copy charts and the use of an Electronic Health Record
(EHR). The hybrid model holds all information pertinent to the individuals/family
treatment including mental health, and substance abuse services provided through
county or contracted providers. All staff must inform, educate and obtain consent
regarding the sharing of client information, prior to any disclosure of information. In
summary, all MHP staff are expected to discuss issues related to individual’s treatment
along with the risks and benefits associated with these treatments in order to support
the individual/family in making an informed decision about their treatment. Equally as
important is to have ongoing communication with every individual/family about the
treatment process and discharge planning.
CONSENT FOR TREATMENT-ADULTS
The Consent of Outpatient Treatment Form explains certain
conditions of treatment, including circumstances under which
confidential information may be disclosed without the client’s
consent. The client or responsible guardian, conservator, etc. should sign the form
before the client receives professional services, if at all possible, or as soon as possible
thereafter.
MINOR CONSENT
The information below is a brief summary of minor consent.
Please refer to Minor Consent policy. This section provides
guidance regarding consent for health care services for minors
receiving services from Placer County Systems of Care. The term health care and
medical care include assessment, care, services or referral for treatment for general
medical conditions, mental health issues, and alcohol and other drug treatment. As an

3-28-2019 FINAL Page 38 of 244
adult clients consenting for their own services, parents or minors who can consent for
their own services have the fundamental right to consent to, or refuse medical
treatment.
Generally speaking, minors need the consent of their parents to receive mental health
services unless the minor has the right to consent to care under minor consent laws (see
Circumstances that Allow for Minor to Consent to Their Own Services). Only one parent
is necessary to provide consent unless we are aware of evidence that the other parent
has objected. Adoptive parents have the same rights to consent as natural parents.
In the case of divorced parents, the right to consent rests with the parent who has legal
custody. If the parents have “joint legal custody” usually either parent can consent to the
treatment unless the court has required both parents to consent. In most situations, we
can presume that either parent can consent unless there is evidence to contrary. Some
teams prefer to obtain consent from both parents. This is not a legal requirement but
this is acceptable within MHP as long as it does not pose a significant detriment or cause
harmful delay to the treatment of the client.
A parent or guardian who has the legal authority to consent to care for the minor child
has the right to delegate this authority to other third parties (aged 18 and older). For
example, the parent may delegate authority to consent to medical care to the school, to
a coach, to a step-parent, or to a baby-sitter who is temporarily caring for the child while
the parent is away or at work. A copy of the written delegation of authority should be
scanned into the Electronic Medical Records.
In some cases, a “surrogate parent” is raising a minor child. If this adult is a qualified
relative (often the grandparent, or an aunt or uncle, or older sibling) who has stepped
into the role of parent because the biological parents are no longer willing or able to care
for the child, he or she should fill out the Caregiver's Affidavit form which is used widely
throughout California.
These so called Caregivers who have "unofficially" undertaken the care of the child are
authorized by law to consent to most medical and mental health care and to enroll these
children in school. Once they have completed the Caregiver's Affidavit form (which is
then scanned into the Electronic Medical Records) they may consent to medical or
mental health care for the minor child; however, if the parent(s) returns, the
"caregiver's" authority is ended, and once again the parent has authority to consent to
or refuse care for the child. A Caregiver’s Affidavit does not have to be “renewed” and
can remain in effect until the parent returns, or until the child turns 18.
The court has the power to authorize medical and mental health treatment for
abandoned minors and for minors who are dependents or wards of the court (for
example, kids in foster care or juvenile hall). Furthermore, the court may order that
3-28-2019 FINAL Page 39 of 244
other individuals be given the power to authorize such medical and mental health
treatment as may appear necessary, if the parents are unable or unwilling to consent. In
some circumstances a court order is not necessary. For example, under certain
circumstances, a police officer can consent to medically necessary care for a minor who
is in "temporary custody."
In situations where an adult other than the parent or guardian is providing consent,
(unless it is an emergency) care must be taken to establish their legal authority to
consent to care before treatment begins. Often this requires identification of the child's
status as well as the ability or inclination of the natural parents to provide consent. A
copy of The Court Order delegating this authority (to a Foster Parent, for example)
should be scanned into the Electronic Medical Records before care is provided. For those
treatments for which a minor can legally provide his or her own consent, no court order
or other authorization is necessary when treating a dependent or ward.
In rare situations a court may summarily grant consent to medical or mental health
treatment upon verified application of a minor aged 16 or older who resides in California
if consent for medical care would ordinarily be required of the parent or guardian, but
the minor has no parent or guardian available to give the consent. A copy of the court
order should be obtained and scanned in the minor’s Electronic Medical Record before
treatment is provided pursuant to the order.
Consent from the parent is not required if the minor is involuntarily held for a 72 hour
assessment and treatment pursuant to Welfare and Institutions 324 Code 5585.2 or
5150 et seq.
Circumstances that Allow for Minor to Consent to Their Own Services Minors generally
need a parent to consent to healthcare services because minors suffer automatic legal
incapacity due to their young age. However, there are certain minors who can consent
for their own services. These minors are:
A. Minors who are treated as "adults" under the law for purposes of medical
consent. These are:
a. Emancipated minors b. Self-sufficient minors
B. Minors seeking sensitive services
These minors do not suffer automatic legal incapacity due to their young age but must
still display legal capacity. As with adults, legal capacity to consent to services indicate
an ability to understand the nature and consequences of the proposed health care,
including its significant benefits, risks, and alternatives; make a health care decision; and
communicate this health care decision.
3-28-2019 FINAL Page 40 of 244
EMANCIPATED MINORS INCLUDE:
A. Minors 14 and older who have been emancipated by court order;
B. Minors who are serving in the active US military forces; and
C. Minors who married or who have been married
Before providing services to these minors, we should obtain a copy of their
emancipation card or court order, a copy of their military ID card, or a copy of their
wedding certificate and scan these documents into their Electronic Medical Records.
Self-sufficient minors are defined by law as minors aged 15 and older who are living
separate and apart from their parents and who are also managing their own financial
affairs regardless of their source of income. Even though self-sufficient minors can
consent to outpatient mental health services such as therapy, rehabilitative counseling,
and case management, the law is not clear whether or not self-sufficient minors can
consent to psychotropic medication treatment. Please consult with your supervisor and
Quality Improvement if psychotropic medication treatment is part of the services being
sought by a self-sufficient minor.
Minors seeking certain sensitive services may be legally authorized to provide their own
consent to those services. The minor also controls whether or not the parent will have
access to records generated as a result of receiving those services. When minor consent
applies, sensitive services should not be provided over the minor's objection. In other
words, even if the parent provides consent, non-consent by the qualified minor presents
ethical issues and provision of care should be delayed until consultation using the chain
of command can be obtained on a case by case basis.
Minors 12 or older may consent to medical care and counseling related to the diagnosis
and treatment of a drug or alcohol related problem. Since the law deems such minors
to be legally competent to consent to such care, parents, or guardians have no legal
authority to demand drug testing for their minor children who are 12 or older. The law
requires providers to involve the patient or legal guardian in the care, unless to do so
would be inappropriate. The decision and reasons to involve or not involve, the
parent/legal guardian needs to be recorded within the electronic records, as well as the
staff efforts to involve them.
There are two separate California laws that permit minors 12 and older to consent to
outpatient mental health counseling services. The first is Family Code 6924(b). It states
that minors 12 and older may consent to mental health treatment or counseling on an
3-28-2019 FINAL Page 41 of 244
outpatient basis (and also, to residential shelter services), if both of the following
requirements are satisfied:
1. The minor, in the opinion of the attending professional person, is mature enough
to participate intelligently in the outpatient services or residential shelter
services, and
2. The minor would either present a danger of serious physical or mental harm to
self or to others without the mental health treatment or counseling or residential
shelter services, or is the alleged victim of incest or child abuse.
The second, more recent law is found at Health and Safety Code section 124260. It
removes the requirement that the provider must first determine that the minor 12 and
older be “at risk” before services can be provided. Instead, the provider need only
determine that the minor, in the opinion of the attending professional person, is mature
enough to participate intelligently in the outpatient mental health services. The
attending professional person should clearly chart that any required “qualifying”
criteria have been met if services are provided pursuant to either of these provisions of
the law.
When outpatient mental health care or residential shelter services are provided, the
laws state that it shall include the involvement of the minor's parent or guardian unless,
in the opinion of the professional person who is treating or counseling the minor, the
involvement would be inappropriate. The professional person must state in the
Electronic Medical Record whether and when the person attempted to contact the
minor's parent or guardian, and whether the attempt to contact was successful or
unsuccessful, or the reason why, in the professional person's opinion, it would be
inappropriate to contact the minor's parent or guardian. (Note: If outpatient mental
health services are provided pursuant to Health and Safety Code 124260, the law states
that the decision to involve, or not involve, the parents shall be made in collaboration
with the minor patient.).
It needs to be reiterated that even though a minor 12 or over can provide their own
consent for sensitive services related to substance abuse and mental health, mental
capacity to provide consent and informed consent is still required. If a minor who
otherwise qualifies for minor consent lacks mental capacity, and insists that there not
be parental involvement, staff should consult with their supervisor and Quality
Improvement so that appropriate steps may be taken.
Note: Psychotropic medication treatment is not one of the sensitive
services that a minor can consent for. Parent/guardian consent is
required if psychotropic medications are prescribed. Parent/guardian
consent is also needed if voluntary inpatient mental health facility services are provided.

3-28-2019 FINAL Page 42 of 244
Further, the minor consent laws do not authorize a minor to consent to convulsive
therapy or psychosurgery.
PSYCHOTROPIC MEDICATION CONSENTS FOR WARDS OF THE JUVENILE COURT
Forms JV-220 through JV-223:
The JV court forms do not include all of the required components for informed consent
to medication(s); specifically, the court forms do not include information on the method
of administration (oral or injection) or additional side effects if the child were to take
the medication for more than three months. The method of administration for each
medication must be documented in the medical record. The side effects (if the child
were to take the medication for more than three months) may be documented in the
beneficiary’s medical record or may be included in written information about the
medication which is provided to the beneficiary or the beneficiary’s legal representative.
In addition, the client’s and/or the client’s legal representative’s signature is required to
be on the medication consent form.
MEDICATION CONSENT
A Medication Consent form must be obtained for every new medication or an increase
in dose not included in previous consent. A note indicating discussion about
medications and side effects doesn’t replace the signed form. It is good practice to
document a discussion about risks of not taking as prescribed, what side effects for client
to be aware of, and other education about risks and benefits of taking or not taking the
recommended medication. As discussed under minor consent, a parent or guardian
must sign a consent for a minor for psychotropic medications. For adult clients receiving
mental health under the Lanterman-Petris-Short Act (LPS) Conservatorship, the
Conservator must consent for psychiatric medications prior to administration of
medications. The MD/NP is responsible for providing information to client about the
specific medications, preferably in written form. The provision of this information
should be documented within the Medication Support Services note.
CONFIDENTIALITY AND AUTHORIZATION TO EXCHANGE PROTECTED HEALTH
INFORMATION
The confidentiality of medical, psychiatric, and substance abuse information is
protected by State and Federal statutes, rules and regulations. The statues, rules, and
regulations require that we protect the client’s personal health information (PHI) and
that we obtain informed consent from the client in order to disclose any PHI
information, prior to doing so, except under specific conditions as indicated by the laws.
3-28-2019 FINAL Page 43 of 244
Only staff members who are directly involved in the client’s treatment may access the
health record for treatment purposes. It is never okay for staff members to access a
client’s health record to satisfy a curiosity for their own purpose, even when the client
is related to the staff member.
The electronic medical record stores information on who has accessed the medical
record as part of the audit trail. The audit record is necessary to make efforts to
safeguard the client’s confidentiality as well as to provide an “account of disclosure” if
requested by the client or legal entities via subpoena.
We recognize that there may be times when you access a client’s health record in error.
As an example, you may have incorrectly entered the client’s medical record number
and opened a client’s chart before realizing your error. When a client record is accessed
in error, it is important to complete the “Accidental/Incorrect Client Access” form in
AVATAR. This form will record the error in accessing the client’s health record should a
reason ever need to be given to the client or legal entities.
All information and records obtained in the course of providing services shall be
confidential.40 A client or authorized representative who consents to release of any
and/or specific information about their health record must read and sign the
“Authorization to Use, Exchange, and/or Disclosure of Confidential Behavioral
Health Information” previously referred to as “Release of Information.” The
Authorization, once signed, may be valid for a designated period of time or on an event.
The client, or authorized representative must state who the information may be released
to, the purpose for which the information may be used, what specific information may
be released, and when the authorization will expire. A client may decide to revoke the
Authorization, at any time and may do so by submitting the request verbally or in
writing to any staff member.
The Authorization will at that time be revoked, making it invalid. If the client, at a later
time, decides to reactivate the Authorization, a new Authorization must be completed as
indicated above.
Note: Any subpoenas or requests for medical records should be directed
to the Medical Records office or specific contract provider.
REVOKING AN AUTHORIZATION TO USE, EXCHANGE, AND/OR DISCLOSE
INFORMATION
A client may withdraw consent or REVOKE a previously signed Authorization at any
time during their course of treatment (CCR, Title 9, Section 854). In the event the client
asks to revoke a release of information, the behavioral health staff must complete the
“revoke” section of the release of information form, being careful to enter a reason for
3-28-2019 FINAL Page 44 of 244
revoke and notifying necessary team members of this request. For Authorizations
completed on paper, you must print the Authorization, write “revoke” across the page
and scan back into the EMR in the appropriate section.
SPECIAL CONSIDERATIONS FOR MINORS
• For minors who are eleven (11) years or younger, the authorized representative
may authorize the release of information.
• For minors who are treated as "adults" under the law for purposes of medical
consent (emancipated and self-sufficient minors) and minors seeking sensitive
services for which they are qualified to provide their own consent under the law,
the minor must authorize the release of information even to their own parents
or guardians.
The client is in control of their health information. A client has a right to
view the information in their medical record, but must complete the
designated request of information document (a verbal release of records
will NOT be accepted).
LIMITS OF CONFIDENTIALITY
It is the policy of the SOC that all MH Providers adhere to State confidentiality, privacy
and security laws wand the Health Insurance Portability and Accountability Act of 1996
(HIPAA), and to apply those laws and regulations which provide the greatest degree of
protection and autonomy for clients, within the scope of providing care, treatment, and
business. In cases of perceived conflict among laws and/or regulations, the general
rule is that precedence is given to the law and/or rule which provide the client with the
greatest protection of client privacy or autonomy.
However, with regard to specific disclosures, if the disclosure is required by law
(whether State or Federal); the disclosure is permitted without constituting a violation
of law. Many staff of the MHP are required to share limited confidential information
when required to do so as a Mandated Reporter for Child and Dependent Adult/Elderly
Abuse. lt is the policy of the MHP that any staff member, including child care custodian,
elder/dependent adult care custodians, medical practitioners, and non-medical
practitioners have the legal duty to report any incident of suspected child abuse or
elder/dependent adult abuse that he or she has knowledge of or reasonably suspects
when acting in their professional capacity or within the scope of their employment.
3-28-2019 FINAL Page 45 of 244
Under the Duty to Warn and Protect third Parties in response to a client threat (Tarosoff-
Ewing), the MHP must take actions to warn and protect reasonably identifiable potential
victims of an MHP client, consistent with State law.
Clients/guardians must be made aware of the limits of confidentiality
when beginning services and when clinically appropriate throughout
their course of services.
INFORMING MATERIALS
Under CCR, Title 9, Chapter 11, the Local Mental Health Plan and its network providers
are required to provide beneficiaries with a booklet and provider list up on request and
when a beneficiary first receives a specialty mental health service.
The MHP has developed user friendly Medi-Cal beneficiary materials that are provide a
general understanding of services offered. All Medical Beneficiaries materials are
required to be posted in prominent locations where Medi-Cal beneficiaries obtain
outpatient specialty mental health services, which includes the waiting areas of County
operated, contracted organizational and individual network providers’ place of service.
The MHP has made an effort to ensure that the cultural and linguistic needs of the
diverse populations throughout the MHP (are met) by developing Medi-Cal beneficiary
materials in the MHP Threshold Language of Spanish and in the sixteen Prominent
language within the State.
The Medi-Cal beneficiary /Informing materials include:
• Beneficiary Guide to Medi-Cal Mental Health Services: Booklet informs Medi-
Cal Beneficiaries on how to access and obtain routine and emergency specialty
mental health services.
• Grievance Procedures: Pamphlet describes the informal and formal process for
filing a grievance.
• Beneficiary Grievance Form: Forms provide Medi-Cal beneficiaries the
opportunity to register written dissatisfaction about any aspect of the services
offered by the MHP.
• Beneficiary Poster: A poster designed to provide Medi-Cal beneficiaries simple
and user friending information while upholding Title 9, CCR. All MHP service
locations should post the beneficiary poster in prominent locations and/or
waiting areas where Medi-Cal beneficiaries obtain outpatient specialty mental
health services.

3-28-2019 FINAL Page 46 of 244
• It is our responsibility to ensure that every individual and/or family is treated with
respect and that every person is informed about what services are offered from MHP
as well as provide information on treatment options in the community in a way that
helps support the client in making an informed decision about whether the services
offered through the MHP are right for them or for their child.
• Consent for Treatment: Direct Services staff must ensure that they have received the
proper consent to treat, regardless if the client is a voluntary adult, a conserved adult,
and emancipated youth, a youth over the age of 12 or a child. Medication Consents
must be obtained for all MHP Prescribed medications.
• Limits of Confidentiality: When beginning services, and when otherwise indicated,
clients should be informed of the limits of confidentiality. Without a release of
information or client consent, the disclosure is required by law (whether State or
Federal); the disclosure is permitted without constituting a violation of law. C
• Family Inclusion (AB1424): The SOC encourage family participation in the
treatment/recovery process. The family inclusion form allows family members to
provide information even when there are no releases of information provided. SOC
staff members may always receive information, but cannot respond or acknowledge
the person receives services without a release on file.
• Revoking Releases of information: A client may withdraw consent or REVOKE a
previously signed Authorization at any time during their course of treatment (CCR,
Title 9, and Section 854). In the event the client asks to revoke a release of information,
the behavioral health staff must complete the “revoke” section of the release of
information form, being careful to enter a reason for revoke and notifying necessary
team members of this request
• Medi-Cal informing Materials: Under CCR, Title 9, Chapter 11, the Local Mental
Health Plan and its network providers are required to provide beneficiaries with a
booklet and provider list up on request and when a beneficiary first receives a
specialty mental health service.
3-28-2019 FINAL Page 47 of 244
CHAPTER FOUR
DELIEVERY OF SERVICES-REFERRALS, OPENINGS AND CLOSING
ADMISSION AND OPENING AN UMBRELLA EPISODE
The MHP receives referrals from a variety of resources. Referrals for services may be
by self-referral, mental health unit, Community Providers, from other counties, or the
larger community. Placer/Sierra MHP Mental Health services are voluntary. All
individuals who seek behavioral health services from MHP are entitled to receive, at
minimum, an assessment to determine their need and whether MHP services might
meet those needs or whether a referral is warranted to better serve the
individual/family.
In order for MHP to begin the process for determination of the needs of the individual
who is requesting services, we must first begin with establishing a clinical (electronic or
hard copy) health record. The intention with establishing a health record for the
individual is that it will create a unique record of the individual’s request for services,
the outcome of the request, as well as provide information on MHP’s responsiveness to
the request for services. The initiation of a health record does not, in any way, guarantee
the person will receive all or some of their mental health services from MHP. It means
the individual/family has requested mental health services and we are responding to
the request.
All MHP direct service staff are expected to discuss important issues related to
treatment options along with the risks and benefits in order to support the
individual/family in making an informed decision about their treatment. At the onset of
services, the service coordinator/case manager is expected to discuss, provide or offer
the following documents to the individual or family:
FOR ALL INDIVIDUALS REQUESTING
SERVICES
ONLY WHEN APPLICABLE
3-28-2019 FINAL Page 48 of 244
• Informed consent
• Notice of Privacy Practices
• Limitations of Confidentiality
Acknowledgement
• Consumer Rights (aka. Patients’
Rights)
• MHP Problem Resolution
• Guide to Medi-Cal Mental Health
Services
• Minor Consent
• Authorization to use, exchange, and/or
disclosure of confidential behavioral health
information (as indicated)
• Authorization to use, exchange, and/or
disclosure of confidential behavioral health
information for Multi-Disciplinary teams (when
applicable)
• Notification of Unlicensed Clinician (when
applicable)
During the period of assessment for determination of the individual’s mental health
needs and the development of a course of treatment, specific service codes are
permissible for documenting services rendered.
CARE COORDINATION-TIMELINES FOR ADMISSION
The Service Coordinator (aka Case Manager, Practitioner, and Clinician) is responsible
for ensuring timeliness of service delivery. Meaning, the Coordinator is responsible for
making sure that all forms are completed within the designated timelines. The following
forms need to be completed at the start of an initial assessment/intake or for episodes
where the client was previously closed for services for 365 days or longer:
• Onset (Initial Request) of Services
o Informed Consent
o Notice of Privacy Practices
o Consumer Rights
o MHP Problem Resolution
o Authorization for use, exchange, and/or disclosure of confidential
behavioral health information within the Systems of Care.
o Authorization to bill private insurance or Medicare
o Offer a copy of “Guide to Medi-Cal Mental Health Services”
o Minor Consent, if applicable
o Release of Information for the authorization to use, exchange, and/or
disclosure of confidential behavioral health information (as indicated)
• Biopsychosocial Assessment (aka Placer Combined Assessment)
• Diagnosis (DSM-5 AND ICD-10 code set)
• Child Assessment of Needs and Strengths (CANS) or Level of Care Utilization
System (LOCUS)
• Unified Services Plan ( County Treatment Plan)-(finalized)
• Evidence of participation in the development of the Unified Service
Plan/Treatment Plan (usually demonstrated through client signature).
• UMDAP-Uniform Method of Determining the Ability to Pay
3-28-2019 FINAL Page 49 of 244
The health record must meet timeliness standards in order to comply
with claiming (billing) regulations and avoid disallowances. The client
record must meet the above compliance requirements for billing. In the
event that the client record is “out of compliance”, claiming for services is generally not
allowed. Please refer to appendix B -DHCS MHSUDS Information Notice #17-040 pages
12-14 for further guidance.
In order to comply with claiming (billing), the health record must include an admission
diagnosis prior to claiming any service. The diagnosis (DSM 5 criteria and ICD 10 code
set) is informed by the assessment. Additionally, the health record must also include
both the Psychosocial Assessment (finalized) and 2) Unified Service/Treatment Plan
(finalized), prior to claiming for services. For claiming purposes, the service may be
claimed when a diagnosis, assessment, and treatment plan have been completed and
finalized. In the event the chart is out of compliance, claiming for services will not be
allowed and services will automatically be moved to a non-billable service code and the
progress note will continue to remain as part of the health record. In order to meet
documentation expectation standards, all applicable documents listed above must be
completed (as applicable).
Please note: During the period of assessment for determination of the
individual’s mental health needs and the development of a course of
treatment, specific service codes are permissible for documenting services
rendered (please refer to appendix B for further guidance).
ANNUAL RENEWAL OF SERVICES
On an annual basis, the Coordinator is responsible for the annual evaluation of the
individual’s needs, which include the evaluation for medical necessity, renewal of
services, maintaining the accuracy of the health record, and ensure all necessary
documents are completed in a timely manner. Of note is that many of the documents
previously completed at onset of services do not need to be collected again during the
annual review/renewal of services, with the exception of the Releases of Information,
authorizing the Use, Exchanges, and/or Disclosure of Confidential Behavioral Health
Information that have expired and Medication Consents (medical staff only). It is,
however, good practice to review the limits of confidentiality and risks and benefits with
the individual as often as clinically relevant.
The Coordinator is responsible to ensure the completion of the following forms, which
may be completed up to 30 days prior to the end of the current authorization (end
date of approved unified service/treatment plan):
• Update Client Data
• Annual Plan Bundle:
3-28-2019 FINAL Page 50 of 244
o Client Relationships
o Mental Status
o Psychosocial Assessment
o Child Assessment of Needs and Strengths (CANS) or Level of Care
Utilization Scale (LOCUS)
o Diagnosis DSM 5 AND ICD10 code set (make sure to select “update”
option)
o Unified Service/Treatment Plan
o Evidence of participation of involvement/participation in the
development of the unified service/treatment plan (i.e. signature) must
be documented every time information on the treatment plan is added or
updated.
o Releases of Information: Authorization to use, exchange, and/or
disclosure of confidential behavioral health information (as indicated-if
expired)
o Special Considerations (if applicable)
o Unlicensed Clinician form (at the start of services provided by an
unlicensed, but licensed eligible clinician)
• UMDAP: Uniform Method to Determine Ability to Pay: All Adult Clients must
complete an UMDAP when beginning services and annually thereafter to
determine if the client will have a co-payment for services.
Please Note: information gathered for completion of UMDAP should be
collected for present timeframe moving forward. Meaning there is no need
to complete UMDAP information for years in which the individual was
closed to prior episodes.
CARE COORDINATION-TRANSFER OF SERVICES
Transfer of services means that the responsibility of providing services to an
individual/family has been transferred to a different Service Program/Provider.
If the services are transferred from one MHP program to another MHP program (with
no break or closure of services in the process of transfer), most onset of services
documentation do not need to be completed again, with the exception of the
Authorization for Use, Exchanges, and/or Disclosure of Confidential Behavioral Health
Information that have expired and Medication Consents (medical staff only). As always,
it is good practice to review the limits of confidentiality and risks and benefits with the
individual for the services they will receive as often as clinically relevant.
The receiving SOC MH program takes on the Care Coordination responsibilities and
should do the following as soon as possible:
3-28-2019 FINAL Page 51 of 244
• Discuss risks and benefits of their particular program services with the
individual/family and ensure that the individual/family clearly understand these
risks and benefits before beginning services.
• The individual’s informed consent should then be documented clearly in a
progress note in their health record.
• Admission form (if applicable).
• Admission Part 2 (Bundle) form which includes the Client and Services
Information (CSI).
• Diagnosis DSM 5 AND ICD10 code set (must be completed before claiming any
service)
• Client Service Coordinator/Practitioner form.
• Bio-Psychosocial Assessment, if applicable-update if there is significant clinical
data not included in the latest version of the assessment.
• Mental Status Exam, if applicable Unified Service/Treatment Plan (must update
with current provider and treatment goals.
The health record must meet timeliness standards in order to comply with
claiming (billing) regulations and avoid disallowances. The client record
must meet the above compliance requirements for billing. In the event
that the client record is “out of compliance”, claiming for services is not
allowed.
In order to comply with claiming (billing), the health record must include an admission
diagnosis prior to claiming any service. The diagnosis (DSM 5 criteria and ICD 10 code
set) is informed by assessment. Additionally, the health record must also include 1)
Psychosocial Assessment (finalized) and 2) Treatment Plan (finalized), prior to claiming
for services. For claiming purposes, the service may be claimed when a diagnosis,
assessment, and treatment plan have been completed and finalized. In the event the
chart is out of compliance, claiming for services will not be allowed and services will
automatically be moved to a non-billable service code and the progress note will
continue to remain as part of the health record. In order to meet documentation
expectation standards, all applicable documents listed above must be completed (as
applicable).
During the period of assessment for determination of the individual’s mental health
needs and the development of a course of treatment, specific service codes are
permissible for documenting services rendered.
Note: Please extend a level of professionalism when transferring services to
another program by ensuring the integrity of the client record is up to date.
In the event the client’s annual plan renewal is due at the time of the transfer,

3-28-2019 FINAL Page 52 of 244
the receiving program should complete all annual renewal of services documents.
UNIFORMED METHOD OF DETERMINING THE ABILITY TO PAY (UMDAP)
The Placer County System of Care uses the Uniformed Method of Determining the Ability
to Pay (UMDAP) as a sliding scale of liabilities based on clients and/or financially
responsible parties’ ability to pay for the cost of mental health services provided. The
UMDAP establishes a process for collecting client’s financial information, billing clients
for their financial liability, and/or collecting payment for services. This information is
used to assess client/family’s and/or the financially responsible party’s annual liability.
The client/financial responsible party are responsible for payment of actual cost of care,
inclusive of all other resources such as Medi-Cal and third party payers, up to their
annual liability. The UMDAP information is obtained during the intake progress and is
renewed, at least, on an annual basis.
3-28-2019 FINAL Page 53 of 244
• The MHP receives referrals from a variety of resources. Referrals for services may be by
self-referral, mental health unit, Community Providers, from other counties, or the larger
community
• All MHP direct service staff are expected to discuss important issues related to treatment
options along with the risks and benefits in order to support the individual/family in
making an informed decision about their treatment.
• Forms need to be completed at the start of an initial assessment/intake or for episodes
where the client was previously closed for services for 365 days or longer
• In order to comply with claiming (billing), the health record must include an admission
diagnosis prior to claiming any service.
• The health record must meet timeliness standards in order to comply with claiming
(billing) regulations and avoid disallowances.
• Please refer to Appendix B DHCS MHSUDS Information Notice #17-040 pages 12-14 for
further guidance on what services may be billed prior to assessment and treatment
planning.
• On an annual basis, the Coordinator is responsible for the annual evaluation of the
individual’s needs, which include the evaluation for medical necessity, renewal of
services, maintaining the accuracy of the health record, and ensure all necessary
documents are completed in a timely manner
• If the services are transferred from one MHP program to another MHP program (with
no break or closure of services in the process of transfer), most onset of services
documentation do not need to be completed again, with the exception of the
Authorization for Use, Exchanges, and/or Disclosure of Confidential Behavioral Health
Information that have expired and Medication Consents (medical staff only).
• It is good practice to review the limits of confidentiality and risks and benefits with the
individual for the services they will receive as often as clinically relevant.
CHAPTER FIVE
SCOPE OF PRACTICE AND CREDENTIALING
Since 1993, California has implemented its Medicaid-funded Specialty Mental Health
Services (also known as Medi-Cal SMHS) program through the “Rehabilitation Services
Option” rather than the “Clinic Services Option.”
The switch from “Clinic” to “Rehabilitation” allowed California to broaden the array of
services, provider types and service settings. The table below compares the two models
across domains (with bold/italicized print to highlight key differences).
Domain Clinic Services Option Rehabilitation Service Option
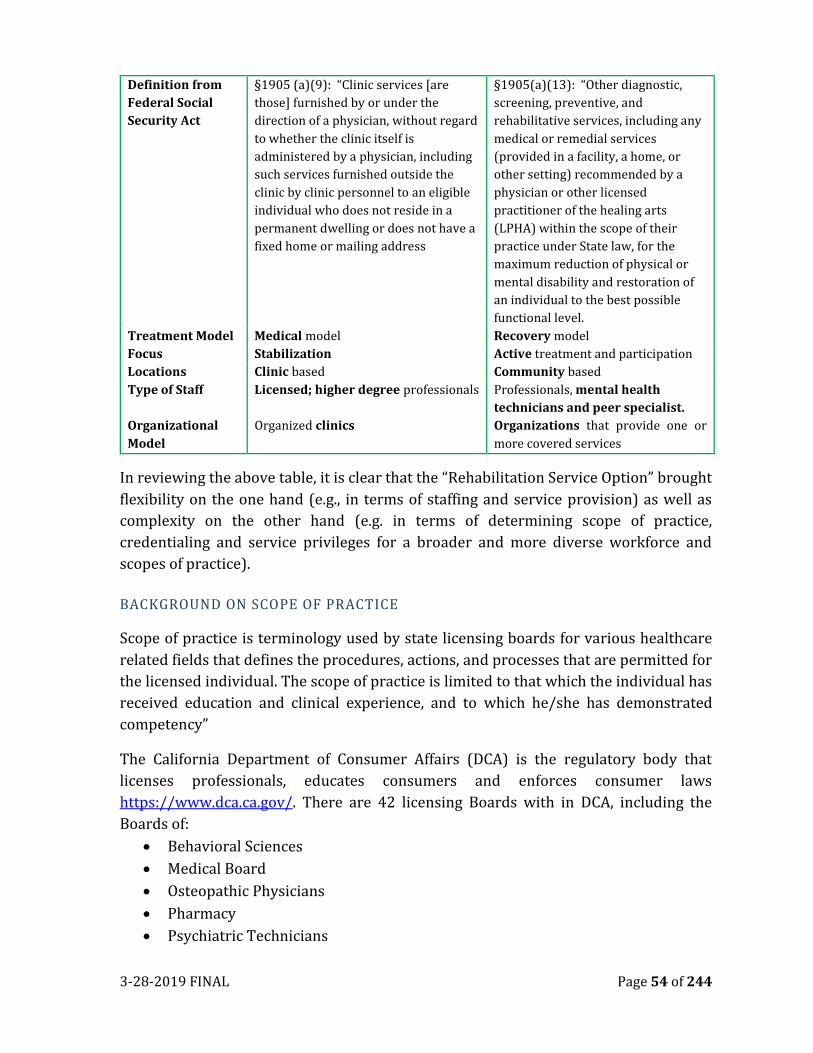
3-28-2019 FINAL Page 54 of 244
Definition from
Federal Social
Security Act
§1905 (a)(9): “Clinic services [are
those] furnished by or under the
direction of a physician, without regard
to whether the clinic itself is
administered by a physician, including
such services furnished outside the
clinic by clinic personnel to an eligible
individual who does not reside in a
permanent dwelling or does not have a
fixed home or mailing address
§1905(a)(13): “Other diagnostic,
screening, preventive, and
rehabilitative services, including any
medical or remedial services
(provided in a facility, a home, or
other setting) recommended by a
physician or other licensed
practitioner of the healing arts
(LPHA) within the scope of their
practice under State law, for the
maximum reduction of physical or
mental disability and restoration of
an individual to the best possible
functional level.
Treatment Model Medical model Recovery model
Focus Stabilization Active treatment and participation
Locations Clinic based Community based
Type of Staff Licensed; higher degree professionals Professionals, mental health
technicians and peer specialist.
Organizational
Model
Organized clinics Organizations that provide one or
more covered services
In reviewing the above table, it is clear that the “Rehabilitation Service Option” brought
flexibility on the one hand (e.g., in terms of staffing and service provision) as well as
complexity on the other hand (e.g. in terms of determining scope of practice,
credentialing and service privileges for a broader and more diverse workforce and
scopes of practice).
BACKGROUND ON SCOPE OF PRACTICE
Scope of practice is terminology used by state licensing boards for various healthcare
related fields that defines the procedures, actions, and processes that are permitted for
the licensed individual. The scope of practice is limited to that which the individual has
received education and clinical experience, and to which he/she has demonstrated
competency”
The California Department of Consumer Affairs (DCA) is the regulatory body that
licenses professionals, educates consumers and enforces consumer laws
https://www.dca.ca.gov/. There are 42 licensing Boards with in DCA, including the
Boards of:
• Behavioral Sciences
• Medical Board
• Osteopathic Physicians
• Pharmacy
• Psychiatric Technicians
3-28-2019 FINAL Page 55 of 244
• Psychology
• Registered Nursing
California’s laws (statutes) are grouped by issues/topics (codes) and the laws that govern health
care services and professional licensure can be found in Business & Professions Code, Health &
Safety Code, Insurance Code, Welfare & Institutions Code, etc.
(http://leginfo.legislature.ca.gov/faces/codes.xhtml)
BACKGROUND ON CREDENTIALING
When a mental health provider joins the network of a managed care organization, such
as the MHP, the provider receives privileges to provide and bill for services. This
privilege is based on an analysis and review of the provider’s license, education, scope
of practice and health care laws. This analysis and review of a provider’s documentation
is called credentialing.
The MHP Credentialing process is completed by the SOC Quality Management Program.
The SOC QM Program is also responsible to publish and update the “Service and Staff
Billing Matrix” (included at the end of this chapter). This Matrix shows the services that
individual providers are allowed (or privileged) to provide, given the credentialing
process (review of material, scope of practice and health care laws).
Note: A Staff member’s Professional classification will NOT match their
licensure/registration/certification nor job classification. A program may
have two people in the same job classification who receive different
classifications as classifications are determined by various combinations of
education and experience.
The Service and Staff Billing Privileges Matrix identified six categories of credentialed
staff. The following pages focus on these categories:
LICENSED PROFESSIONAL OF THE HEALING ARTS (LPHA) (PHYSICIAN/NON
PHYSICIAN)
An LPHA is an individual who can function as "Head of Service" on the agency
application and possesses a valid California License in one of the following professional
categories:
a. Psychiatrist, Medical Doctor, Psychiatric Resident (Licensed or Unlicensed)*
b. Licensed Clinical Psychologist (PsyD, Ph.D, LCP)
c. Licensed Clinical Social Worker (LCSW)
d. Licensed Marriage and Family Therapist (LMFT)
e. Licensed Professional Clinical Counselor I (LPCC)
f. Licensed Professional Clinical Counselor II (LPCC)**

3-28-2019 FINAL Page 56 of 244
g. Registered Nurse, Nurse Practitioner, Nurse Practitioner Intern (RN, NP, NPI)
h. Physician Assistant (PA)
i. Licensed Vocational Nurse (LVN)***
j. Licensed Psychiatric Technician (LPT)***
*Physicians are a sub-category of the LPHA definition and must be licensed, registered,
certified, or recognized under California State scope of practice statutes. Physicians shall
provide services within their individual scope of practice.
**The Licensed Professional Clinical Counselor II classified as an LPHA must verify
completion of additional training and education of six semester units or nine quarter
units specifically focused on the theory and application of marriage and family therapy
or a named specialization or emphasis are on the qualifying degree in marriage and
family therapy, marital and family therapy, marriage, family and child counseling; or
couple and family therapy. In addition, submit proof on no less than 500 hours of
documented supervised experience working directly with couples, families, or children
and a minimum of six hours of continuing education specific to marriage and family
therapy, completed in each licensed renewal cycle. Business and Professions Code 4999.
***LVN and LPT must meet specific criteria in order to be “Head of Service”
LICENSED PRACTITIONER OF HEALING ARTS-WAIVERED/REGISTERED
A “waivered” individual may function as an LPHA with the exception of “Head of
Service”. A Licensed Waivered LPHA is either (1) an individual who has been “waivered”
by the County and has a Master’s Degree and who is registered with a licensing board as
either an Associate/Registered Clinical Social Worker, Associate/Registered Marriage
and Family Therapist, Associate/Registered Professional Clinical Counselor, Registered
Psychologist (RPS) or a Registered Psychological Assistant (PSB) or (2) is an individual
who has a PhD, is registered with the Board of Psychology and is granted a waivered by
the State Department of Health Care Services, exception is UCD Interns/Fellow (See
Business and Professions Code Section 2909).
Note: Registered Psychologist/Psychological Assistants are waivered by DMH, as per DMH Letter
10-03. Submit the required form and information to the COUNTY Quality Improvement
Coordinator. Submit a copy of a diploma, or transcripts showing at least 48 semester/trimester or
72 quarter units of graduate coursework completed, not including thesis, internship or
dissertation; and a resume · Psychologists/ Social Workers / Marriage Family Therapists who are
licensed in another state, must be waivered by DMH as per DMH Letter 10-03. Submit the required
form and information to the COUNTY Quality Improvement Coordinator. Submit a copy of: a letter
from the appropriate licensing board which states that the applicant has sufficient experience to
3-28-2019 FINAL Page 57 of 244
gain admission to the licensing examination and a copy of applicant’s registration with their
respective California licensing board.
Non-Waivered psychologist, Social Worker or Marriage and Family Therapist may not claim for
services as an LPHA until they receive waiver recognition from the State Department of Health
Services. · DMH/DHCS waivers are non-transferable from one California County to another.
STUDENT LPHA
A student trainee may function as an LPHA throughout the placement time period with
appropriate co-signatures and is one of the following: (1) “Post Graduate Student”
participating in a field trainee placement while enrolled in an accredited PhD
Psychology program or (2) “Master’s Level Student” participating in a field trainee
placement program while enrolled in an accredited Masters of Social Work (MSW) or
Masters of Arts(MA) /Masters of Science (MS) Copy of current, valid registration issued
by the Board of Behavioral Science (BBS).
MENTAL HEALTH REHABILITATION SPECIALIST (MHRS) AS DEFINED IN CCR,
TITLE 9.
An MHRS is an individual who meets one of the following requirements:
• Master’s Degree or Ph.D. and two years of full time/equivalent (FTE) direct care
experience in a mental health setting.
• Bachelor’s Degree and 4 years FTE direct care experience in a mental health
setting
• Associate Arts Degree and six years of FTE direct care experience in a mental
health setting. At least two of the six years must be post AA experience in a mental
health setting.
FTE experience may be direct services providing in a mental health setting in the field
of:
• Physical Restoration
• Psychology
• Social Adjustment
• Vocation Adjustment
• Criminal Justice
• Substance Use
• Adjunctive Therapies
3-28-2019 FINAL Page 58 of 244
Despite their range of privileges, remember that MHRS Staff cannot work
independently; they ARE NOT permitted to complete some elements of the assessment
and they MUST obtain the signature of a LPHA or Waivered/Registered LPHA to finalize
Assessment and Client/Treatment Plan documents.
MENTAL HEALTH WORKERS (“OTHER QUALIFIED PROVIDER”)
California’s Medicaid State Plan defines another category of provider in the Specialty
Mental Health Services Program under “Other Qualified Provider.”
An individual at least 18 years of age with a high school diploma or equivalent degree
determined to be qualified to provide the services by the county mental health
department (SPA #12-025; “Qualification of Providers”).
Within the SOC, “Other Qualified Provider” category has been operationalized as a
“Mental Health Worker” (MHW) who receives training and works closely under the
direction of an MHRS, LPHA, or Waivered/Registered LPHA. The services rendered by
a staff Member who is credentialed as a MHW is more narrow and may require a co-
signature. An individual may qualify as an MHW as follows:
1. MHW III
An individual with at least four (4) years of full-time/equivalent (FTE) direct care
experience in the mental health, substance use or related field. Up to two years
(2) years of education in a mental health or related field can substitute for years
of experience. [As of this time, this is not a classification used by the MHP]
a. Four years of FTE direct care experience in a mental health related field
providing mental health services.
Or
b. Two years of FTE direct care experience in a mental health related field
providing mental health services; and two (2) years of education (60
semester or 90 quarter units) with a minimum of 12 semester (18
quarter) units in a mental health related subject area such as child
development, social work, human behavior, rehabilitation, psychology, or
alcohol and drug counseling.
Or
c. Two years of FTE experience in the mental health related field providing
direct mental health services; and a certificate of completion from the
County Core Skills Training.
2. MHW-II
3-28-2019 FINAL Page 59 of 244
An individual who has at least two (2) years but less than four (4) years of full-
time/equivalent (FTE) experience in a mental health related field providing
direct mental health services. There is no educational requirement.
3. MHW-I
An individual who has less than two (2) years of FTE in a mental health related
field providing direct mental health services. There is no educational
requirement.
PEER ADVOCATE STAFF-I/II WITHIN MENTAL HEALTH
A person maybe credentialed as Peer Advocate
I/II. To meet this classification, the individual is
someone who acknowledges having either direct
lived experience or having a loved one with direct
experience in receiving mental health service, and
some experience related to the position being
applied for. A Peer Advocate II is someone who
acknowledges having either direct lived
experience or having a loved one with direct
experience in receiving mental health service, and
preferred to have one year of experience working
within the mental health or related field.
INSIGHTS FROM DHCS” MHSUDS INFORMATION NOTICE #17-040
Major clarifications were issued by DHCS in August 2017 through Information Notice
#17-040 (appendix B) regarding scope of practice and the services, activities and
functions that are restricted in the SMHS program. All of the following are based on the
staff member’s scope of practice, requirement for direction by an LPHA, Co-signatures,
etc.
Assessment:
1. Diagnosis, Mental Status Exam, Relevant Conditions (Functional Impairments),
Psychosocial Factors and Medication History: These sections of the assessment
are restricted to the LPHA, Waivered/Licensed LPHA and Graduate Students
Enrolled in School.
Based on their privileges, other staff could contribute to the assessment
through the collection of historic information (e.g. mental health and medical
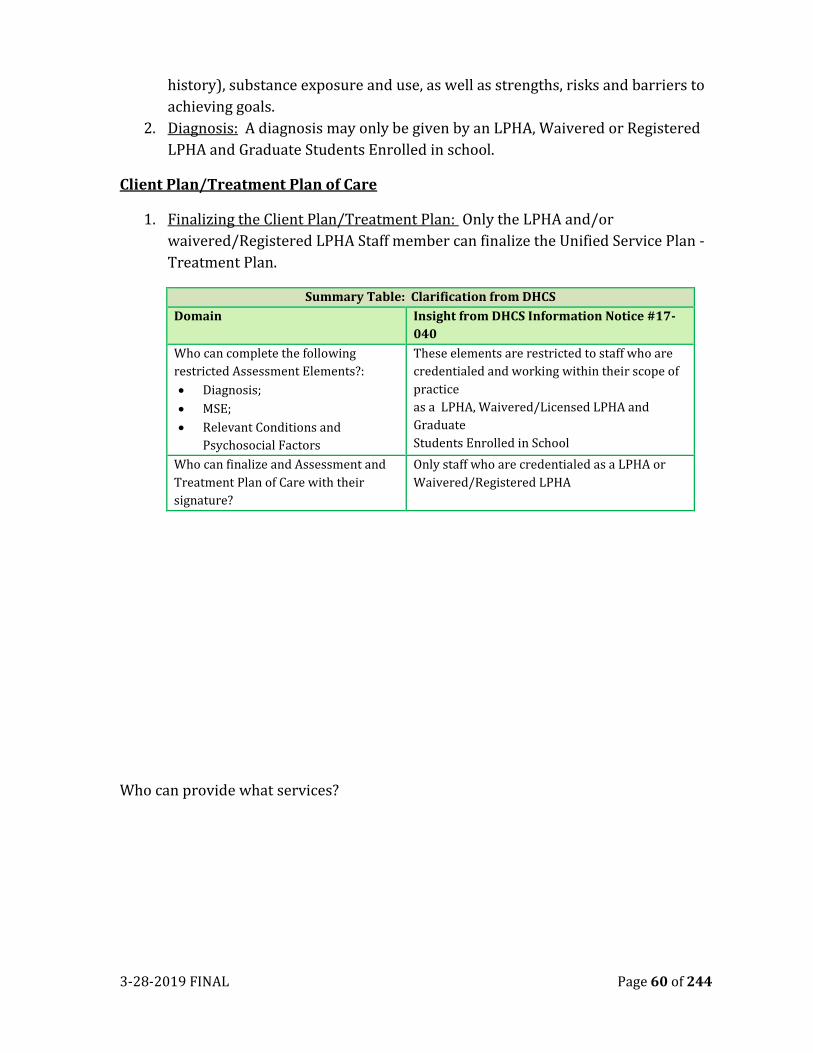
3-28-2019 FINAL Page 60 of 244
history), substance exposure and use, as well as strengths, risks and barriers to
achieving goals.
2. Diagnosis: A diagnosis may only be given by an LPHA, Waivered or Registered
LPHA and Graduate Students Enrolled in school.
Client Plan/Treatment Plan of Care
1. Finalizing the Client Plan/Treatment Plan: Only the LPHA and/or
waivered/Registered LPHA Staff member can finalize the Unified Service Plan -
Treatment Plan.
Summary Table: Clarification from DHCS
Domain Insight from DHCS Information Notice #17-
040
Who can complete the following
restricted Assessment Elements?:
• Diagnosis;
• MSE;
• Relevant Conditions and
Psychosocial Factors
These elements are restricted to staff who are
credentialed and working within their scope of
practice
as a LPHA, Waivered/Licensed LPHA and
Graduate
Students Enrolled in School
Who can finalize and Assessment and
Treatment Plan of Care with their
signature?
Only staff who are credentialed as a LPHA or
Waivered/Registered LPHA
Who can provide what services?
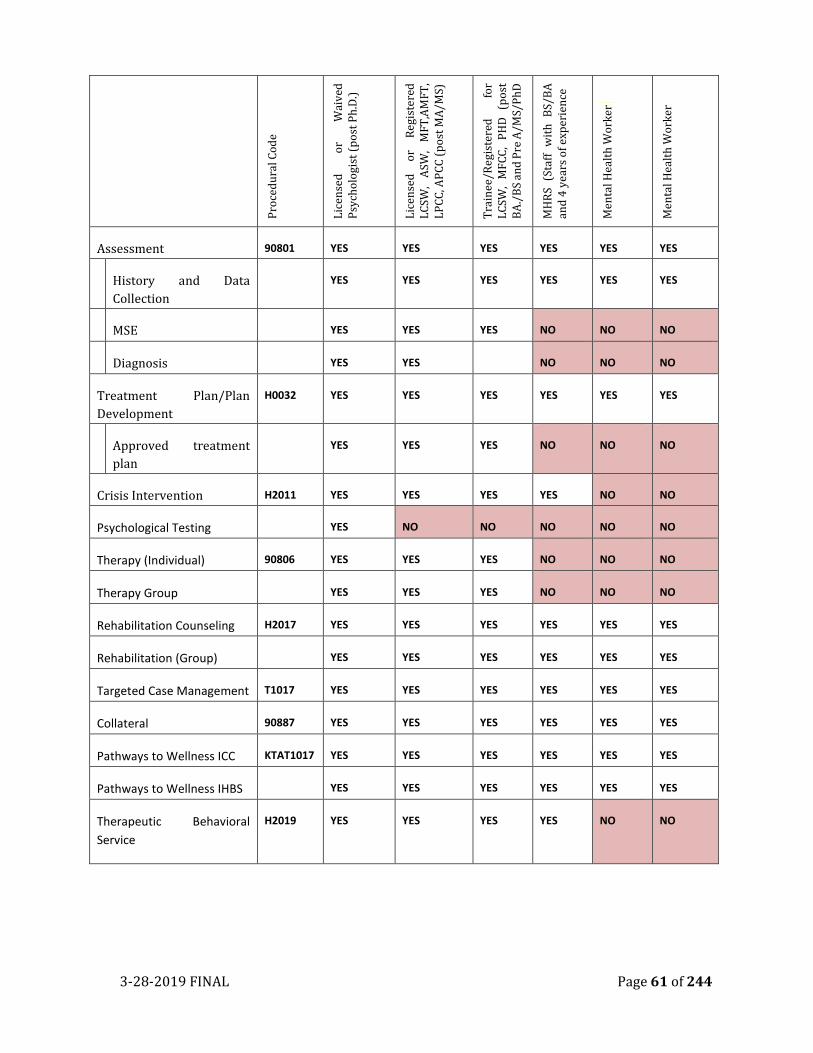
3-28-2019 FINAL Page 61 of 244
Pro
ced
ura
l Co
de
Lic
ense
d
or
Wai
ved
P
sych
olo
gist
(p
ost
Ph
.D.)
Lic
ense
d
or
Reg
iste
red
L
CSW
, A
SW,
MF
T,A
MF
T,
LP
CC
, AP
CC
(p
ost
MA
/MS)
Tra
inee
/Reg
iste
red
fo
r L
CSW
, M
FC
C,
PH
D
(po
st
BA
./B
S an
d P
re A
/MS/
Ph
D
MH
RS
(Sta
ff
wit
h
BS/
BA
an
d 4
yea
rs o
f ex
per
ien
ce
Men
tal H
ealt
h W
ork
er
Men
tal H
ealt
h W
ork
er
Assessment 90801 YES YES YES YES YES YES
History and Data
Collection
YES YES YES YES YES YES
MSE YES YES YES NO NO NO
Diagnosis YES YES NO NO NO
Treatment Plan/Plan
Development
H0032 YES YES YES YES YES YES
Approved treatment
plan
YES YES YES NO NO NO
Crisis Intervention H2011 YES YES YES YES NO NO
Psychological Testing YES NO NO NO NO NO
Therapy (Individual) 90806 YES YES YES NO NO NO
Therapy Group YES YES YES NO NO NO
Rehabilitation Counseling H2017 YES YES YES YES YES YES
Rehabilitation (Group) YES YES YES YES YES YES
Targeted Case Management T1017 YES YES YES YES YES YES
Collateral 90887 YES YES YES YES YES YES
Pathways to Wellness ICC KTAT1017 YES YES YES YES YES YES
Pathways to Wellness IHBS YES YES YES YES YES YES
Therapeutic Behavioral
Service
H2019 YES YES YES YES NO NO
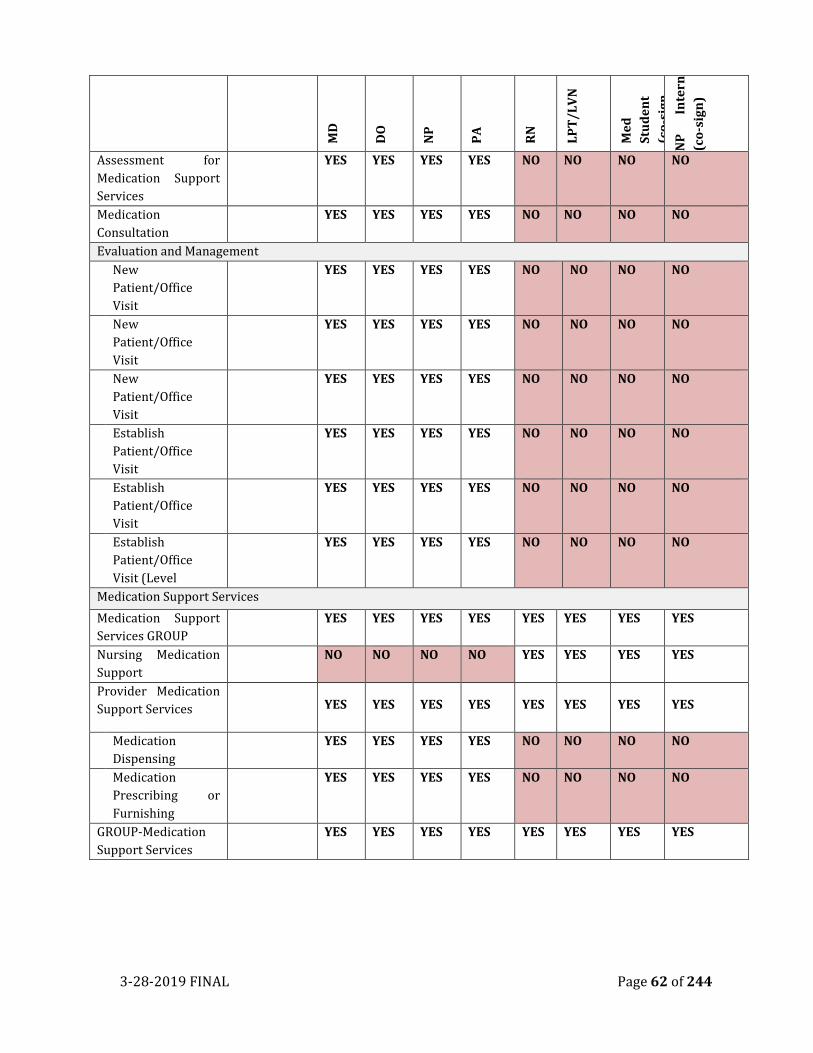
3-28-2019 FINAL Page 62 of 244
MD
DO
NP
PA
RN
LP
T/
LV
N
Me
d
Stu
de
nt
(co
-sig
n
by
MD
)
NP
In
tern
(co
-sig
n)
Assessment for
Medication Support
Services
YES YES YES YES NO NO NO NO
Medication
Consultation
YES YES YES YES NO NO NO NO
Evaluation and Management
New
Patient/Office
Visit
YES YES YES YES NO NO NO NO
New
Patient/Office
Visit
YES YES YES YES NO NO NO NO
New
Patient/Office
Visit
YES YES YES YES NO NO NO NO
Establish
Patient/Office
Visit
YES YES YES YES NO NO NO NO
Establish
Patient/Office
Visit
YES YES YES YES NO NO NO NO
Establish
Patient/Office
Visit (Level
YES YES YES YES NO NO NO NO
Medication Support Services
Medication Support
Services GROUP
YES YES YES YES YES YES YES YES
Nursing Medication
Support
NO NO NO NO YES YES YES YES
Provider Medication
Support Services YES YES YES YES YES YES YES YES
Medication
Dispensing
YES YES YES YES NO NO NO NO
Medication
Prescribing or
Furnishing
YES YES YES YES NO NO NO NO
GROUP-Medication
Support Services
YES YES YES YES YES YES YES YES
3-28-2019 FINAL Page 63 of 244
• The States Medicaid “ Rehabilitation Service Option” brought flexibility on the one
hand (e.g., in terms of staffing and service provision) as well as complexity on the other
hand (e.g. in terms of determining scope of practice, credentialing and service
privileges for a broader and more diverse workforce and scopes of practice).
• Scope of practice is terminology used by state licensing boards for various healthcare
related fields that defines the procedures, actions, and processes that are permitted
for the licensed individual
• The scope of practice is limited to that which the individual has received education and
clinical experience, and to which he/she has demonstrated competency”
• As a mental health provider within a managed care organization, such as the MHP, the
individual provider receives privileges through the credentialing process to provide
and bill for services. This privilege is based on an analysis and review of the provider’s
license, education, scope of practice and health care laws
• A Staff member’s Professional classification will NOT match their
licensure/registration/certification nor job classification. A program may have two
people in the same job classification who receive different classifications as
classifications are determined by various combinations of education and experience.
• Despite their range of privileges, remember that MHRS Staff cannot work
independently; they ARE NOT permitted to complete some elements of the assessment
and they MUST obtain the signature of a LPHA or Waivered/Registered LPHA to
finalize Assessment and Client/Treatment Plan documents.
• California’s Medicaid State Plan defines another category of provider in the Specialty
Mental Health Services Program under “Other Qualified Provider.”
• Within the SOC, “Other Qualified Provider” category has been operationalized as a
“Mental Health Worker” (MHW) who receives training and works closely under the
direction of an MHRS, LPHA, or Waivered/Registered LPHA. The services rendered by
a staff Member who is credentialed as a MHW is more narrow and may require a co-
signature.
3-28-2019 FINAL Page 64 of 244
CHAPTER SIX
MEDICAL NECESSITY
MEDICAL NECESSITY IN CONCEPT
In 2012, the Institute of Medicine (IOM) convened a group of experts to identify the
common elements of medical necessity reflected across payer sources (IOM, 2012). The
expert panel described the following general elements:
• Prudent provider with authority: to be medically necessary, the
service/procedure is recommended by an eligible provider acting with
practicality, wisdom and judiciousness;
• Medical/Rehabilitative purpose: to be medically necessary, the purpose of the
service/procedure is to treat a condition (medical condition; functional
condition);
• Scope: to be medically necessary, the type, frequency, extent, site and duration
of the service/procedure should be clinically appropriate;
• Evidence: to be medically necessary, the service/procedure should be in
accordance with generally accepted standards of practice (e.g., scientific
evidence, professional standards, expert opinion);
• Value: to be medically necessary, the service/procedure should be cost-
effective—that does not mean it must be the “least costly,” but rather, not more
expensive than other acceptable/effective treatments;
• Not Primarily for Convenience: to be medically necessary, the
service/procedure should not be primarily for (a) the convenience of the client
or provider or (b) the economic benefit of the health plan/purchaser;
• Individualized: medical necessity must refer to what is medically necessary for
a particular client and thus, requires an individual assessment (vs. a general
determination of what works in the ordinary case).
The above list is not exhaustive—for rehabilitative and recovery services in particular, experts
emphasize the client’s understanding and ability to use and improve with services:
• Appropriately signed treatment plan: to be medically necessary, a service
must have been ordered and provided though a current and appropriately signed
treatment plan;
• Client’s willingness to participate and client’s ability to benefit: to be
medically necessary, the client must be willing to participate in the treatment.
Additionally, the client must have the cognitive ability to benefit from the service
3-28-2019 FINAL Page 65 of 244
• Active treatment plan and sufficient intensity of treatment: to be medically
necessary, there must be an active treatment plan and services are at a sufficient
intensity and duration, given generally accepted standards of practice.
You may be surprised to know that “medical necessity” is not defined in the Federal
Medicaid statute—each State develops their own definition. The key exception here is
Medicaid’s EPSDT benefit (Early and Periodic Screening, Diagnosis, and Treatment) for
children under the age of 21 years. Under EPSDT, Medicaid programs must cover
“necessary health care, diagnostic services, treatment and other measures...to correct or
ameliorate defects and physical and mental illnesses and conditions” (IOM, 2012).
In contrast to Medicaid, the authorizing legislation for Medicare actually specifies the
definition of “medically necessary” services—CMS also includes the term in their glossary:
Notwithstanding any other provisions of this file, no payment may be made under Part A or
Part B for any expenses incurred for items or services, which are not reasonable and
necessary for the diagnosis or treatment of illness or injury or to improve the functioning of
a malformed body member [Social Security Act § 1862 (42 U.S.C. 1395y)].
Services or supplies that: are proper and needed for the diagnosis or treatment
of your medical condition, are provided for the diagnosis, direct care, and treatment of
your medical condition, meet the standards of good medical practice in the local area, and
aren’t mainly for the convenience of you or your doctor
(https://www.cms.gov/apps/glossary)
Medical Necessity is the key element of good clinical documentation as this justifies why
we are providing services to the client. If there is no medical necessity clearly noted
within an assessment, or an annual update of client information, then all services for
that reporting period could be subject to disallowance during an audit. Likewise, each
claimed service provided to a client should be medically necessary and the progress note
should reflect this. In order to best support your clinical work and reduce audit
disallowances, we have included the following formula from California Code of
Regulations, Title 9, as to how Medical Necessity is determined.
MEDICAL NECESSITY CRITERIA
To be eligible for Medi-Cal reimbursement for Outpatient/Specialty Mental Health
Services, a service must meet all three criteria for medical necessity: Diagnostic,
Impairment and Intervention criteria. The following table can be used as quick guide
to the Medical Necessity Criteria. Each criteria of Medical Necessity will be explained
following the table.
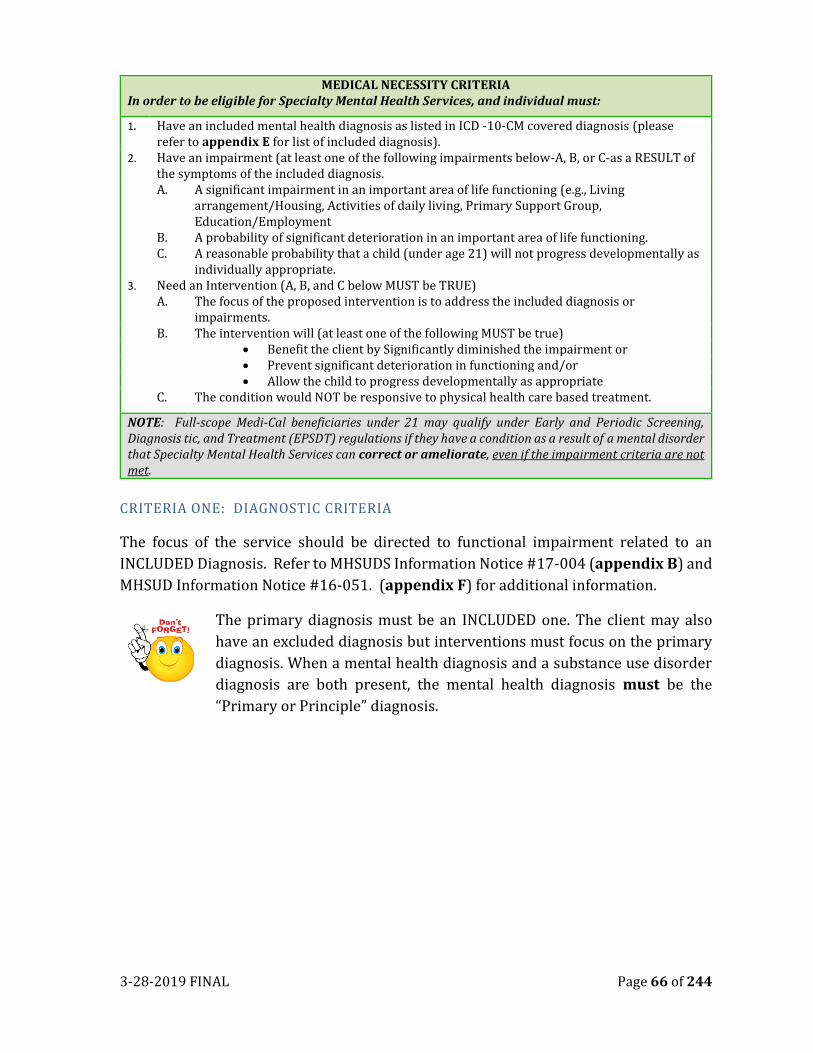
3-28-2019 FINAL Page 66 of 244
MEDICAL NECESSITY CRITERIA In order to be eligible for Specialty Mental Health Services, and individual must:
1. Have an included mental health diagnosis as listed in ICD -10-CM covered diagnosis (please refer to appendix E for list of included diagnosis).
2. Have an impairment (at least one of the following impairments below-A, B, or C-as a RESULT of the symptoms of the included diagnosis.
A. A significant impairment in an important area of life functioning (e.g., Living arrangement/Housing, Activities of daily living, Primary Support Group, Education/Employment
B. A probability of significant deterioration in an important area of life functioning. C. A reasonable probability that a child (under age 21) will not progress developmentally as
individually appropriate. 3. Need an Intervention (A, B, and C below MUST be TRUE) A. The focus of the proposed intervention is to address the included diagnosis or
impairments. B. The intervention will (at least one of the following MUST be true)
• Benefit the client by Significantly diminished the impairment or • Prevent significant deterioration in functioning and/or • Allow the child to progress developmentally as appropriate C. The condition would NOT be responsive to physical health care based treatment.
NOTE: Full-scope Medi-Cal beneficiaries under 21 may qualify under Early and Periodic Screening, Diagnosis tic, and Treatment (EPSDT) regulations if they have a condition as a result of a mental disorder that Specialty Mental Health Services can correct or ameliorate, even if the impairment criteria are not met.
CRITERIA ONE: DIAGNOSTIC CRITERIA
The focus of the service should be directed to functional impairment related to an
INCLUDED Diagnosis. Refer to MHSUDS Information Notice #17-004 (appendix B) and
MHSUD Information Notice #16-051. (appendix F) for additional information.
The primary diagnosis must be an INCLUDED one. The client may also
have an excluded diagnosis but interventions must focus on the primary
diagnosis. When a mental health diagnosis and a substance use disorder
diagnosis are both present, the mental health diagnosis must be the
“Primary or Principle” diagnosis.
3-28-2019 FINAL Page 67 of 244
INCLUDED DIAGNOSES EXCLUDED DIAGNOSES
(CANNOT be primary but may be secondary diagnosis)
• Pervasive Developmental Disorders, excluding
Autistic Disorder
• Attention Deficit Disorder and Disruptive
Behavior Disorders
• Feeding and Eating Disorders of Infancy and
Early Childhood
• Elimination Disorders
• Other Disorders of Infancy, Childhood, or
Adolescence
• Schizophrenia & Other Psychotic Disorders Mood
Disorders Anxiety Disorders
• Somatoform Disorders
• Factitious Disorders
• Paraphilia’s
• Gender Identity Disorder
• Eating Disorders
• Impulse-Control Disorders Not Elsewhere
Classified
• Adjustment Disorders
• Personality Disorders, excluding Antisocial
Personality Disorder Medication-Induced
Movement Disorders
• “Deferred” or “by history” diagnoses (except can be used
as opening diagnosis)
• Stand Alone “Rule Out” diagnosis
• Provisional Diagnoses
• “Z” Codes
• Intellectual Disability (mental retardation)
• Motor Skills Disorder
• Communication Disorders
• Autistic Disorder (Other Pervasive Developmental
Disorders are included)
• Tic Disorders
• Delirium, Dementia, and Amnestic and Other Cognitive
Disorders
• Mental Disorders Due to a General Medical Condition
• Substance-Related Disorders
• Sexual Disorders
• Sleep Disorders
• Antisocial Personality Disorder
• Other Conditions that May Be a Focus of Clinical Attention
• 799.9 Deferred diagnosis • V71.09 No Diagnosis
A primary, provisional, deferred, or rule-out diagnosis MUST be confirmed
or changed within 6 months of case opening
A client may receive services for an included diagnosis when an excluded diagnosis is
also present Clients may receive services if they have an excluded diagnosis as long as
an included diagnosis is also present and the included diagnosis is the primary focus of
treatment.
• Practitioners are expected to include any substance related diagnosis (as a
secondary diagnosis) when warranted.
• The presence of a non-eligible diagnosis does not impact the ability to provide
treatment as long as there is a primary eligible diagnosis that is the focus of
treatment.
• Practitioners are expected to include any substance diagnosis when warranted.
INCLUDED ICD -10-CM DIAGNOSIS FOR SPECIALTY MENTAL HEALTH SERVICES
(ADULTS AND CHILDREN)
All MHSUDS claims with a Date of Service on or after October 1, 2015 must include the
appropriate ICD 10 code set. The diagnostic formulation is based on the client’s current
and historical assessment, where information of onset symptoms, and level of
functioning are determined. The accuracy of the diagnosis is important because it
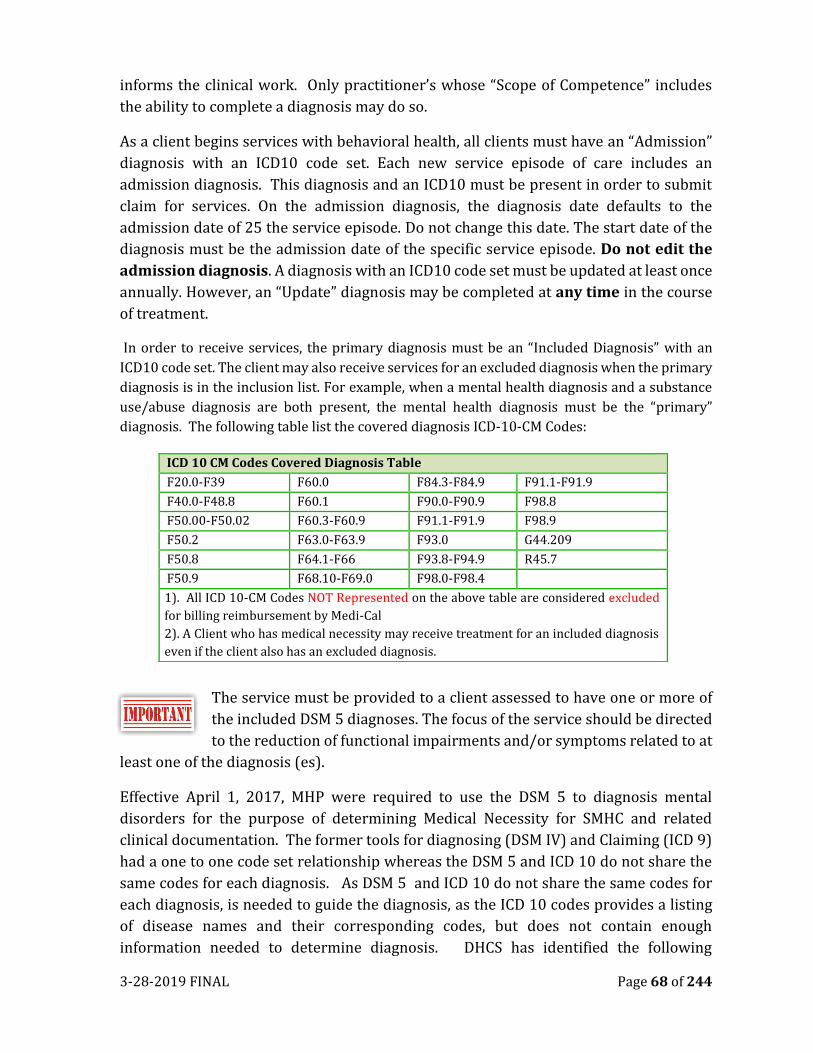
3-28-2019 FINAL Page 68 of 244
informs the clinical work. Only practitioner’s whose “Scope of Competence” includes
the ability to complete a diagnosis may do so.
As a client begins services with behavioral health, all clients must have an “Admission”
diagnosis with an ICD10 code set. Each new service episode of care includes an
admission diagnosis. This diagnosis and an ICD10 must be present in order to submit
claim for services. On the admission diagnosis, the diagnosis date defaults to the
admission date of 25 the service episode. Do not change this date. The start date of the
diagnosis must be the admission date of the specific service episode. Do not edit the
admission diagnosis. A diagnosis with an ICD10 code set must be updated at least once
annually. However, an “Update” diagnosis may be completed at any time in the course
of treatment.
In order to receive services, the primary diagnosis must be an “Included Diagnosis” with an
ICD10 code set. The client may also receive services for an excluded diagnosis when the primary
diagnosis is in the inclusion list. For example, when a mental health diagnosis and a substance
use/abuse diagnosis are both present, the mental health diagnosis must be the “primary”
diagnosis. The following table list the covered diagnosis ICD-10-CM Codes:
The service must be provided to a client assessed to have one or more of
the included DSM 5 diagnoses. The focus of the service should be directed
to the reduction of functional impairments and/or symptoms related to at
least one of the diagnosis (es).
Effective April 1, 2017, MHP were required to use the DSM 5 to diagnosis mental
disorders for the purpose of determining Medical Necessity for SMHC and related
clinical documentation. The former tools for diagnosing (DSM IV) and Claiming (ICD 9)
had a one to one code set relationship whereas the DSM 5 and ICD 10 do not share the
same codes for each diagnosis. As DSM 5 and ICD 10 do not share the same codes for
each diagnosis, is needed to guide the diagnosis, as the ICD 10 codes provides a listing
of disease names and their corresponding codes, but does not contain enough
information needed to determine diagnosis. DHCS has identified the following
ICD 10 CM Codes Covered Diagnosis Table
F20.0-F39 F60.0 F84.3-F84.9 F91.1-F91.9
F40.0-F48.8 F60.1 F90.0-F90.9 F98.8
F50.00-F50.02 F60.3-F60.9 F91.1-F91.9 F98.9
F50.2 F63.0-F63.9 F93.0 G44.209
F50.8 F64.1-F66 F93.8-F94.9 R45.7
F50.9 F68.10-F69.0 F98.0-F98.4
1). All ICD 10-CM Codes NOT Represented on the above table are considered excluded
for billing reimbursement by Medi-Cal
2). A Client who has medical necessity may receive treatment for an included diagnosis
even if the client also has an excluded diagnosis.
3-28-2019 FINAL Page 69 of 244
Crosswalk as a guide to specialty mental health services. The Complete DSM 5 to ICD
10 CM Cross Walk of Diagnosis for Specialty Mental Health Services are included in
appendix E
Guidance in using the above Cross Walk is included in the DHCS MHSUD
Information Notice 16-051. This Information notice is included in appendix
D.
CRITERIA TWO: RESULTING IMPAIRMENT CRITERIA
The second element required to determine medical necessity is the presence
of a “functional impairment” as a result of the symptoms associated with an
included diagnosis. The resulting impairment must be in an important area
of life functioning. During the assessment process, the clinician should identify the
client’s areas of life functioning, which are impacted by their behavioral health.
The client must have at least one of the following as a result of the mental disorder(s):
1. A significant impairment in an important area of life functioning, or
2. A probability of significant deterioration in an important area of life functioning,
or
3. Children also qualify if there is a probability the child will not progress
developmentally as individually appropriate.
4. Children covered under EPSDT quality if they have a mental disorder that can be
corrected or ameliorated through the provision of Specialty Mental Health
Services.
Important areas of Life Functioning include:
The areas identified below provides a snapshot of the domains included in “an important
area of life functioning” in the provision of SMHS.
• Problems with primary group • Problems related to social
environment • Education Problems • Occupational Problems • Housing Problems • Safety Issues
• Economic Problems • Problems with access to healthcare services • Problems related to interactions with legal
system/criminal system • Other psychological or environmental
problems.
Medical Necessity is established through the Assessment and Client Plan
Process. Diagnosis and identification of the Client’s functional
impairments further strengthen and reaffirm the need for behavioral
health services that support the client/family’s road to recovery.
3-28-2019 FINAL Page 70 of 244
Additional Information for EPSDT Clients who not meet Medical-Necessity:
Clients who are under the age of 21 who do not meet SMHS medical
necessity functional impairment and the intervention criteria described in
CCR Title 9, §1830.205 may still qualify when all of the following criteria
are met (CCR, Title 9, §1830.210): All of the following are met:
a. The requirement of governing EPSDT Supplement services, or for
targeted case management services (Source: 22 CCR §51340(e) (3))
governing EPSDT services (Source: 22 CCR §51340), or for targeted case
management services (Source: 22 CCR §51351);
b. The services that a client will be linked to is medically necessary for the
client (Source: 9 CCR §1830.205) or 22 CCR §5134 (e)(3); and (c) the
requirements of that the services (Source: 22 CCR §51340 (f))) to which
access is to be gained through case management is medically necessary
for the EPSDT eligible client and the EPSDT eligible client has a medical or
mental health condition or diagnosis.
CRITERIA THREE: INTERVENTION RELATED CRITERIA (MUST HAVE ALL 3)
1. The focus of the proposed intervention is to address the condition identified in
impairment criteria B above, and
2. It is expected the proposed intervention will benefit the client by significantly
diminishing the impairment, or preventing significant deterioration in an
important areas of life functioning; and/or for children it is probable the child
will be enabled to progress developmentally as individually appropriate (or if
covered by EPSDT, the identified condition can be corrected or ameliorated), and
3. The condition would not be responsive to physical health care based treatment
Please see the chapter of Unified Service Plans/Treatment Plans for
additional information on the use of Interventions.
All Mental Health Services are provided based on medical necessity
criteria, in accordance with an individualized Unified
Services/Treatment Plan that is approved and authorized according to
DHCS requirements.
THE GOLDEN THREAD OF MEDICAL NECESSITY
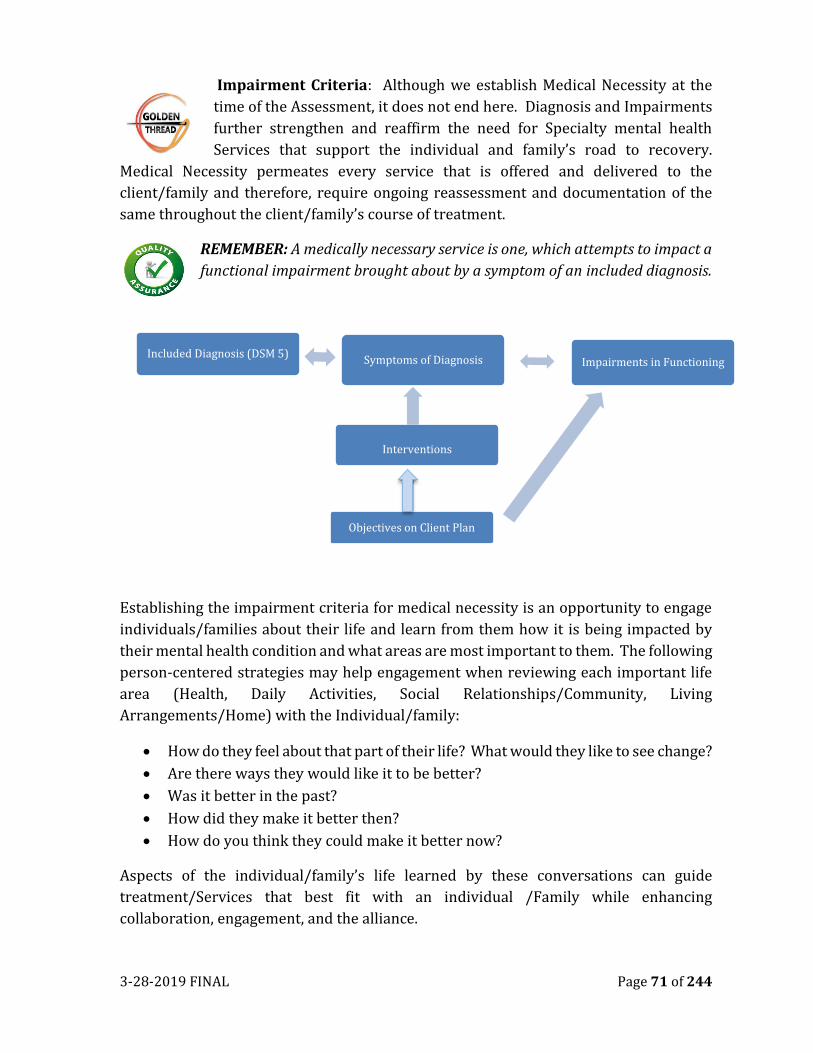
3-28-2019 FINAL Page 71 of 244
Impairment Criteria: Although we establish Medical Necessity at the
time of the Assessment, it does not end here. Diagnosis and Impairments
further strengthen and reaffirm the need for Specialty mental health
Services that support the individual and family’s road to recovery.
Medical Necessity permeates every service that is offered and delivered to the
client/family and therefore, require ongoing reassessment and documentation of the
same throughout the client/family’s course of treatment.
REMEMBER: A medically necessary service is one, which attempts to impact a
functional impairment brought about by a symptom of an included diagnosis.
Establishing the impairment criteria for medical necessity is an opportunity to engage
individuals/families about their life and learn from them how it is being impacted by
their mental health condition and what areas are most important to them. The following
person-centered strategies may help engagement when reviewing each important life
area (Health, Daily Activities, Social Relationships/Community, Living
Arrangements/Home) with the Individual/family:
• How do they feel about that part of their life? What would they like to see change?
• Are there ways they would like it to be better?
• Was it better in the past?
• How did they make it better then?
• How do you think they could make it better now?
Aspects of the individual/family’s life learned by these conversations can guide
treatment/Services that best fit with an individual /Family while enhancing
collaboration, engagement, and the alliance.
Included Diagnosis (DSM 5)Symptoms of Diagnosis Impairments in Functioning
Interventions
Objectives on Client Plan

3-28-2019 FINAL Page 72 of 244
Effective 1/1/14 The three Managed Care Plans (MCP) in Placer County-
California Health and Wellness, Anthem and Kaiser started providing
mental health services to Medi-Cal beneficiaries whose mental health
disorder results in a mild to moderate distress or behavioral impairments. Beneficiaries
with mild to moderate impairments do not meet medical necessity criteria for Specialty
Mental Health Services provided by the Placer/Sierra Counties Mental Health Plan
(MHP).
When a Medi-Cal beneficiary is found not to meet Medical Necessity
criteria, a Notice of Adverse Benefit Determination (NOABD) formerly
known as a Notice of Action (NOA) must be issued and mailed to the
individual by the clinician.
NOTICE OF ADVERSE BENEFICIARY DETERMINATION as a result of Assessment
and Medical Necessity:
In July 1, 2017, the Notice of Action was changed to Notice of Adverse Benefit
Determination (NOABD) No changes were made to its purpose or use. A Denial Notice
NOABD is entered when it is determined that a client is not eligible for services or there
has been an alteration in the services provided. Before completing a NOABD, a MHP
provider should consult with their supervisor. For further explanation please refer to
Notice of Adverse Benefit Determination (NOABD) policy and procedure RE-210.
Documentation for Medical Necessity.
3-28-2019 FINAL Page 73 of 244
It is important to understand that while documentation rules include specific points at which medical
necessity must be verified, these are not the only points at which the medical necessity criteria must
be met. Every claimed (progress note) service must meet the test and “Stand alone” for
documentation of medical necessity: i.e. the service must be directed toward an included diagnosis,
and the impairments that are a result of the diagnosis have interventions aimed at maintaining,
reducing, or minimizing the effect of the diagnostic symptoms or impairments on a client’s life. Each
time a service is claimed, the staff person who delivered the service and submitted the claim is
saying that he/she belies that the services met all medical necessity criteria. Examples:
Treatment plans: Should be unique and are mean to be updated annually or more frequently as the
client either makes progress, or his/her needs or goals change. The interventions should change as
well. Treatment plans remaining the same each year can potentially be viewed as if our services are
either not helping or that we are not in tune to the client’s unique goals
Assessment/Medical Necessity Determination/Mental Status Exams: Client’s not only age each
year but will have more likely made some life changes, having at least some symptom differences, and
have a response to our treatment that can be accurately captured in an updated assessment. It
should be updated and include a summary of the client’s care and services over the past year.
Documents that are capturing the client’s current functioning such as the Mental Status Exam, should
not be exactly as the year prior as well. It would be expected that at least some changes are present
due to the need for treatment.
Progress notes: each time a client comes in for a service, each progress note should “stand alone”
and include the client’s unique presentation and response to our intervention in each session. Notes
that are exactly the same each week or have very little variance are not only subject to disallowance,
but can indicate a quality of care concern, or be viewed as fraud or abuse
3-28-2019 FINAL Page 74 of 244
CHAPTER SEVEN
ASSESSMENTS
BUILDING A FOUNDATION
The psychosocial assessment provides the foundation for the delivery of services and
establishes the need for mental health services to address impairments in the client’s
life domains. Among many things, a well-written assessment explores areas of need as
well as strengths; it provides an opportunity to capture the essence of the individual;
what is important to this individual, to his/her family, how culture factors in, how the
individual sees themselves in relation to others/family/peers, clearly outlines mental
health history and how mental health impacts their overall functioning, explores their
past successes and shortcomings; and offers an opportunity to explore what meaningful
goals they may have. Remember, it is extremely important to take the time to clearly
document the information. Oftentimes, the treatment team may need to rely on the
information in the psychosocial assessment when determining the next steps for the
individual/family.
The assessment consists of the Psychosocial Assessment and the Mental Status Exam
(MSE). The MSE is an important part of the comprehensive clinical assessment process.
It is a way of documenting observations on the client’s state of mind for a particular
point in time. The psychosocial assessment is designed to provide a comprehensive
clinical picture of the client to establish medical necessity, to help treatment teams and
clients define goals and objectives, and to fulfill State and Federal requirements. The
information contained in the MSE, along with biological and historical information
obtained through the assessment process informs the diagnosis.
One section that is often not fully explored is the strengths section on the assessment.
You may want to pay special attention to the strengths section as this may help with
identifying areas that can later be used for treatment planning. When looking at
strengths, look beyond the traditional strengths. Strengths can include:
• Abilities and accomplishments
• Interests and aspirations
• Risk and Protective Factors
• Recovery resources and Developmental assets (such as a support team or WRAP
plan)
• Unique individual attributes
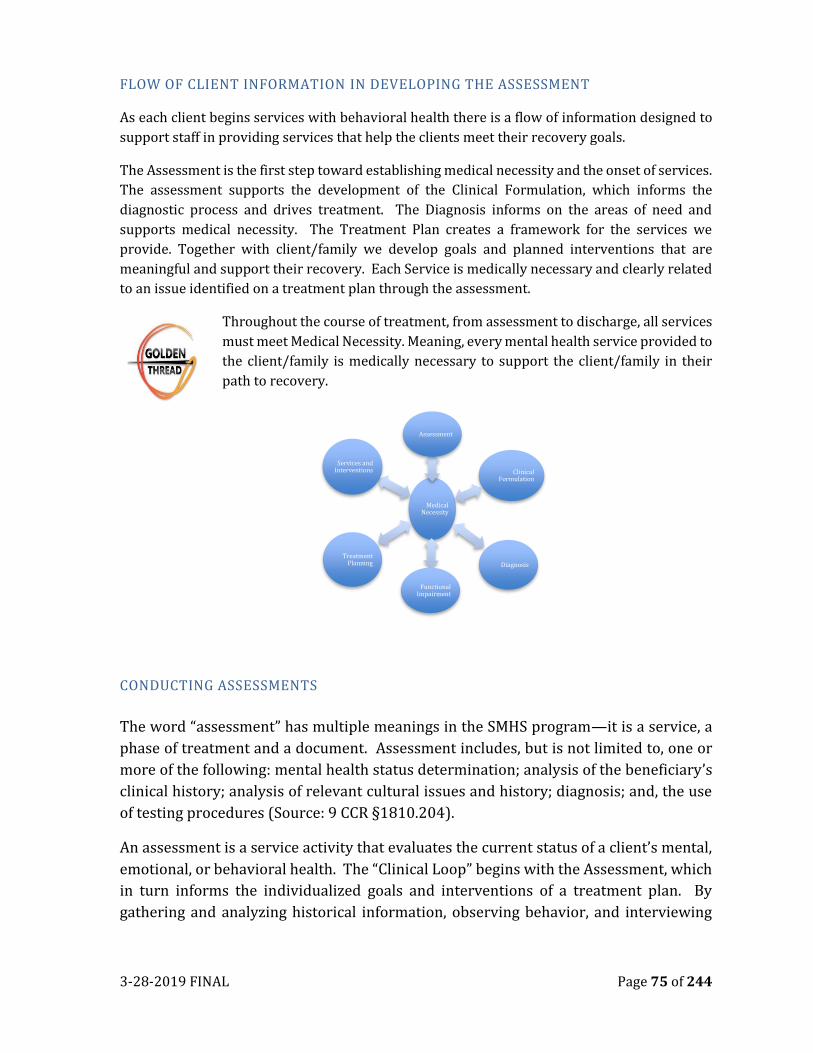
3-28-2019 FINAL Page 75 of 244
FLOW OF CLIENT INFORMATION IN DEVELOPING THE ASSESSMENT
As each client begins services with behavioral health there is a flow of information designed to
support staff in providing services that help the clients meet their recovery goals.
The Assessment is the first step toward establishing medical necessity and the onset of services.
The assessment supports the development of the Clinical Formulation, which informs the
diagnostic process and drives treatment. The Diagnosis informs on the areas of need and
supports medical necessity. The Treatment Plan creates a framework for the services we
provide. Together with client/family we develop goals and planned interventions that are
meaningful and support their recovery. Each Service is medically necessary and clearly related
to an issue identified on a treatment plan through the assessment.
Throughout the course of treatment, from assessment to discharge, all services
must meet Medical Necessity. Meaning, every mental health service provided to
the client/family is medically necessary to support the client/family in their
path to recovery.
CONDUCTING ASSESSMENTS
The word “assessment” has multiple meanings in the SMHS program—it is a service, a
phase of treatment and a document. Assessment includes, but is not limited to, one or
more of the following: mental health status determination; analysis of the beneficiary’s
clinical history; analysis of relevant cultural issues and history; diagnosis; and, the use
of testing procedures (Source: 9 CCR §1810.204).
An assessment is a service activity that evaluates the current status of a client’s mental,
emotional, or behavioral health. The “Clinical Loop” begins with the Assessment, which
in turn informs the individualized goals and interventions of a treatment plan. By
gathering and analyzing historical information, observing behavior, and interviewing
Medical Necessity
Assessment
Clinical Formulation
Diagnosis
Functional Impairment
Treatment Planning
Services and Interventions
3-28-2019 FINAL Page 76 of 244
the individual, and their significant others, a clinician can formulate a comprehensive
view of an individual’s strengths, and needs.
Information gathered in the assessment includes, but is not limited to, the following:
mental health status determination, client’s clinical history, cultural identity and
history; client’s strengths and resources; developmental history; diagnosis; and
use of testing procedures.
Most assessment activities must be conducted face-to-face with the individual. Best
practices indicate that conducting face-to-face assessments supports a more detailed,
comprehensive and meaningful assessment. Examples include a Mental Status
Examination and behavioral observation to formulate initial diagnostic impressions.
Other assessment activities may be performed either face-to-face or by telephone, and
may involve family members or other significant parties without the client. For example,
sensitive family and developmental history may be better collected in a separate
session with the parent of a young child rather than with the child present.
If the purpose of the contact is to gather information for an intake
assessment-the service is coded as an ASSESSMENT
Limits of confidentiality, risks/benefits of treatment and MHP
policies pertaining to standards of care must be explained before
commencing the assessment process. Repeat as necessary to ensure that
all parties involved in treatment understand the issues involved. Signature(s) on the
Consent for Treatment form must be obtained to document that the client/Legally
Responsible Person understands and agrees to participate in treatment.
CLIENT ASSESSMENT
DHCS defines some requirements for the assessment and allows the County Mental
Health Plan (MHP) to define other requirements. For timeliness and frequency of the
assessment, DHCS expects the initial assessments required within the first 60
calendar days of Episode Opening and a new assessment is completed as needed, based
on the changes in the client’ status/condition, medical/clinical change, and/or a change
in diagnosis. For regular ongoing reassessments for ongoing services, DHCS requires the
MHP to establish frequency timelines (Source: MHP Contract).
ELEMENTS OF AN ASSESSMENT
DHCS requires that every SMHS assessment document/form contain 11 required elements. When an assessment is correctly and completely filled out, the 11 required elements capture the information needed to identify medical necessity and the client’s mental health needs. The 11 required elements from DHCS are:
3-28-2019 FINAL Page 77 of 244
1. Presenting Problem: Describe the client’s presenting complaint and history. You must include the current level of functioning and symptoms. Also address any relevant family history and current family information.
2. Relevant Mental Health Conditions and psychosocial factors: Describe the factors that affect the client’s physical health and mental health including, as applicable; living situation, daily activities, social support, cultural and linguistic factors, and history of trauma or exposure to trauma.
3. Mental Health History: Describe the client’s prior treatment, including providers, therapeutic modality (e.g., medications, psychosocial treatments) and response, and inpatient admissions. If possible, include information from other sources of clinical data such as previous mental health records and relevant psychological testing or consultation reports.
4. Medical History: Describe the relevant physical health conditions reported by the beneficiary or a significant support person. Include name and address of current source of medical treatment. For children and adolescents the history must include prenatal and perinatal events and relevant/significant developmental history. If possible, include other medical information from medical records or relevant consultation reports.
5. Medications: Information about medications the beneficiary has received, or is receiving, to treat mental health and medical conditions, including duration of medical treatment. The assessment must include documentation of the absence or presence of allergies or adverse reactions to medications and documentation of an informed consent for medications.
6. Substance Exposure/Substance Use: Past and present use of tobacco, alcohol, caffeine, CAM (complementary and alternative medications) and over-the-counter drugs, and illicit drugs.
7. Client Strengths: Documentation of the beneficiary’s strengths in achieving client plan goals related to the beneficiary’s mental health needs and functional impairments as a result of the mental health diagnosis.
8. Risks: Situations that present a risk to the beneficiary and/or others, including past or current trauma.
DHCS MHSUDS Info Notice #17-040included the following as possible areas of risk: History of Danger to Self (DTS) or Danger to Others (DTO); Previous inpatient hospitalizations for DTS or DTO; Prior suicide attempts; Lack of family or other support systems; Arrest history, if any; Probation status; History of alcohol/drug abuse; History of trauma or victimization; History of self-harm behaviors (e.g., cutting); History of assaultive behavior; Physical impairments (e.g., limited vision, deaf, wheelchair bound) which make the beneficiary vulnerable to others; and, Psychological or intellectual vulnerabilities (e.g., intellectual disability (low IQ), traumatic brain injury, dependent personality).
3-28-2019 FINAL Page 78 of 244
9. A mental status examination: A mental status examination. 10. A Complete Diagnosis: A diagnosis from the current ICD-code must be
documented, consistent with the presenting problems, history, mental status examination and/or other clinical data; including any current medical diagnoses.
11. Additional clarifying formulation information, as needed: Additional clarifying formulation (clinical/diagnostic formulation) information, as needed.
Integrated Assessment: The Placer County AVATAR Bio-psychosocial Assessment is
an enhance assessment, capturing more than the eleven elements listed above. This
assessment is used for multiple programs including Mental Health, Substance Use
Treatment, Whole Person Care, Etc. Staff members completed the AVATAR Combined
Assessment must complete all elements of the assessment. If an assessment element is
not applicable, the staff must indicate N/A in the client record when cleaning the
assessment.
The following grid breaks down the various components of an assessment along with
brief descriptions and documentation examples. All areas are required for an
assessment to be considered complete as mandated by the County’s Mental Health Plan
(MHP).
Note: The information in the “Area” column reflects the layout of Placer
County Combined Assessment within the AVATAR electronic Health
Record. Additionally, the grid does not capture all components of an
assessment and instead focuses on areas that need further clarification or
are commonly documented incorrectly. The California Code of Regulations notes items
that MUST be included in an assessment. These areas are bolded below.
Area Information to include/Description Example
Presenting
Problem
Describe the reason(s) for assess the
individual at this time. What is the current
situation requiring assistance? What
stressors are affecting the individual?
Describe the problem(s) the individual is
experiencing. Include:
• Identifying information,
• Criteria to justify DSM dx including
symptoms behavior, impairments in
functioning, duration, frequency, and
severity.
• Impact on life/behavior leading to
the client seeking services,
• Cultural explanation of problem,
illness in client’s own words
Demetri is a 36 year old Ukrainian, married male.
He has experienced two inpatient psychiatric
hospitalizations as DS within the last 60 days.
(These are his only hospitalizations).
Demetri reports that he is seeking services as a
condition of his employment. He reports that he is
having problems at work, is unable to concentrate
or finish task, has thoughts of self-harm but is “too
chicken” to go through with it. Believes his family
will be better off without him. ”She will be able to
move on and find someone who can be there for
her and the kids”. Hygiene and grooming are poor.
Reports to having no appetite and has lost 40 lbs.
in last 3 months.
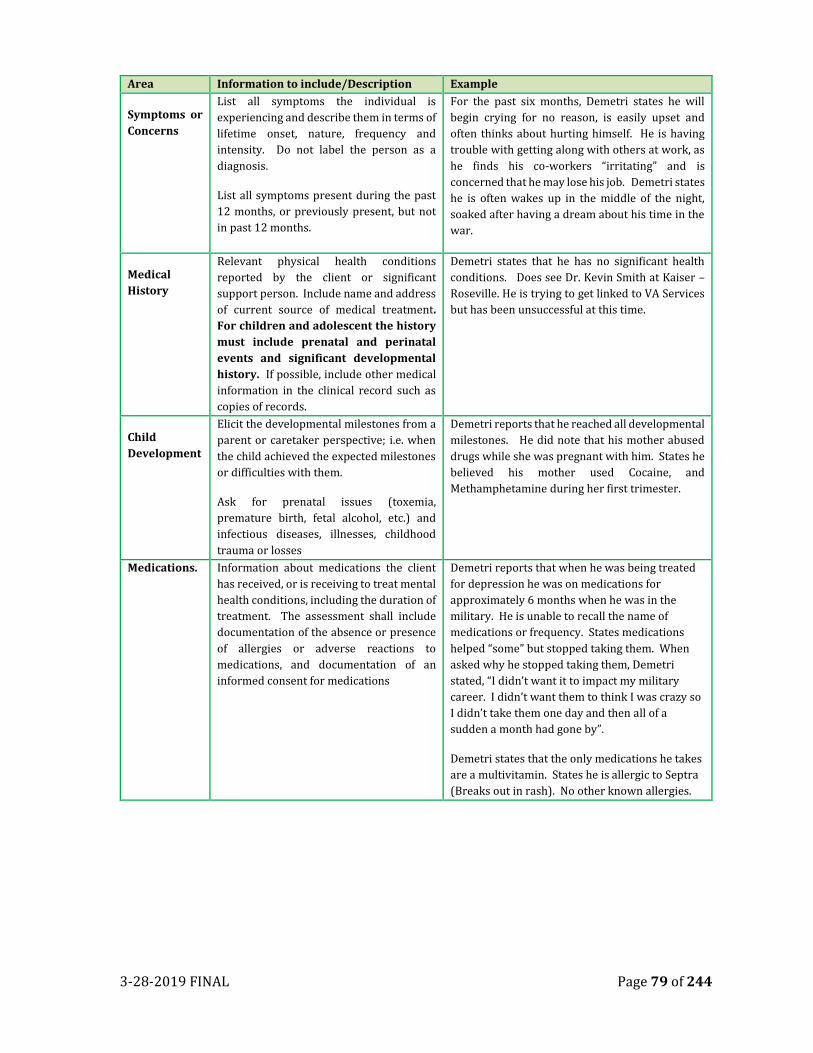
3-28-2019 FINAL Page 79 of 244
Area Information to include/Description Example
Symptoms or
Concerns
List all symptoms the individual is
experiencing and describe them in terms of
lifetime onset, nature, frequency and
intensity. Do not label the person as a
diagnosis.
List all symptoms present during the past
12 months, or previously present, but not
in past 12 months.
For the past six months, Demetri states he will
begin crying for no reason, is easily upset and
often thinks about hurting himself. He is having
trouble with getting along with others at work, as
he finds his co-workers “irritating” and is
concerned that he may lose his job. Demetri states
he is often wakes up in the middle of the night,
soaked after having a dream about his time in the
war.
Medical
History
Relevant physical health conditions
reported by the client or significant
support person. Include name and address
of current source of medical treatment.
For children and adolescent the history
must include prenatal and perinatal
events and significant developmental
history. If possible, include other medical
information in the clinical record such as
copies of records.
Demetri states that he has no significant health
conditions. Does see Dr. Kevin Smith at Kaiser –
Roseville. He is trying to get linked to VA Services
but has been unsuccessful at this time.
Child
Development
Elicit the developmental milestones from a
parent or caretaker perspective; i.e. when
the child achieved the expected milestones
or difficulties with them.
Ask for prenatal issues (toxemia,
premature birth, fetal alcohol, etc.) and
infectious diseases, illnesses, childhood
trauma or losses
Demetri reports that he reached all developmental
milestones. He did note that his mother abused
drugs while she was pregnant with him. States he
believed his mother used Cocaine, and
Methamphetamine during her first trimester.
Medications. Information about medications the client
has received, or is receiving to treat mental
health conditions, including the duration of
treatment. The assessment shall include
documentation of the absence or presence
of allergies or adverse reactions to
medications, and documentation of an
informed consent for medications
Demetri reports that when he was being treated
for depression he was on medications for
approximately 6 months when he was in the
military. He is unable to recall the name of
medications or frequency. States medications
helped “some” but stopped taking them. When
asked why he stopped taking them, Demetri
stated, “I didn’t want it to impact my military
career. I didn’t want them to think I was crazy so
I didn’t take them one day and then all of a
sudden a month had gone by”.
Demetri states that the only medications he takes
are a multivitamin. States he is allergic to Septra
(Breaks out in rash). No other known allergies.
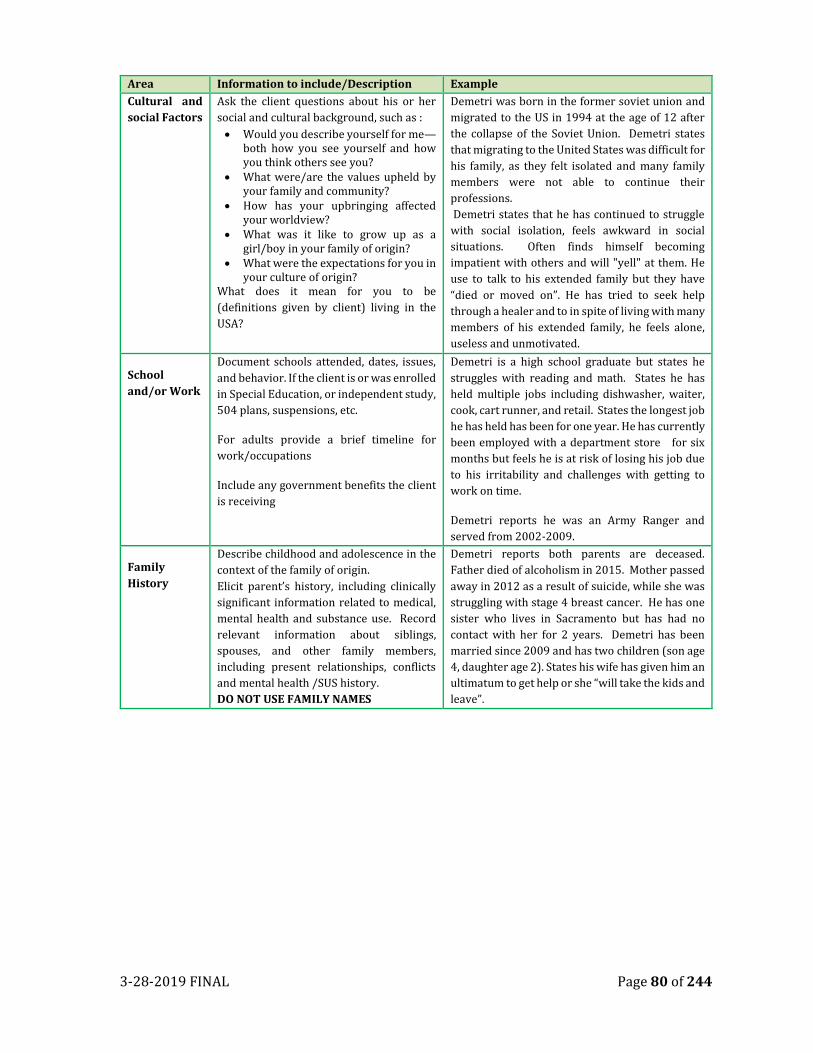
3-28-2019 FINAL Page 80 of 244
Area Information to include/Description Example
Cultural and
social Factors
Ask the client questions about his or her
social and cultural background, such as :
• Would you describe yourself for me—both how you see yourself and how you think others see you?
• What were/are the values upheld by your family and community?
• How has your upbringing affected your worldview?
• What was it like to grow up as a girl/boy in your family of origin?
• What were the expectations for you in your culture of origin?
What does it mean for you to be
(definitions given by client) living in the
USA?
Demetri was born in the former soviet union and
migrated to the US in 1994 at the age of 12 after
the collapse of the Soviet Union. Demetri states
that migrating to the United States was difficult for
his family, as they felt isolated and many family
members were not able to continue their
professions.
Demetri states that he has continued to struggle
with social isolation, feels awkward in social
situations. Often finds himself becoming
impatient with others and will "yell" at them. He
use to talk to his extended family but they have
“died or moved on”. He has tried to seek help
through a healer and to in spite of living with many
members of his extended family, he feels alone,
useless and unmotivated.
School
and/or Work
Document schools attended, dates, issues,
and behavior. If the client is or was enrolled
in Special Education, or independent study,
504 plans, suspensions, etc.
For adults provide a brief timeline for
work/occupations
Include any government benefits the client
is receiving
Demetri is a high school graduate but states he
struggles with reading and math. States he has
held multiple jobs including dishwasher, waiter,
cook, cart runner, and retail. States the longest job
he has held has been for one year. He has currently
been employed with a department store for six
months but feels he is at risk of losing his job due
to his irritability and challenges with getting to
work on time.
Demetri reports he was an Army Ranger and
served from 2002-2009.
Family
History
Describe childhood and adolescence in the
context of the family of origin.
Elicit parent’s history, including clinically
significant information related to medical,
mental health and substance use. Record
relevant information about siblings,
spouses, and other family members,
including present relationships, conflicts
and mental health /SUS history.
DO NOT USE FAMILY NAMES
Demetri reports both parents are deceased.
Father died of alcoholism in 2015. Mother passed
away in 2012 as a result of suicide, while she was
struggling with stage 4 breast cancer. He has one
sister who lives in Sacramento but has had no
contact with her for 2 years. Demetri has been
married since 2009 and has two children (son age
4, daughter age 2). States his wife has given him an
ultimatum to get help or she “will take the kids and
leave”.
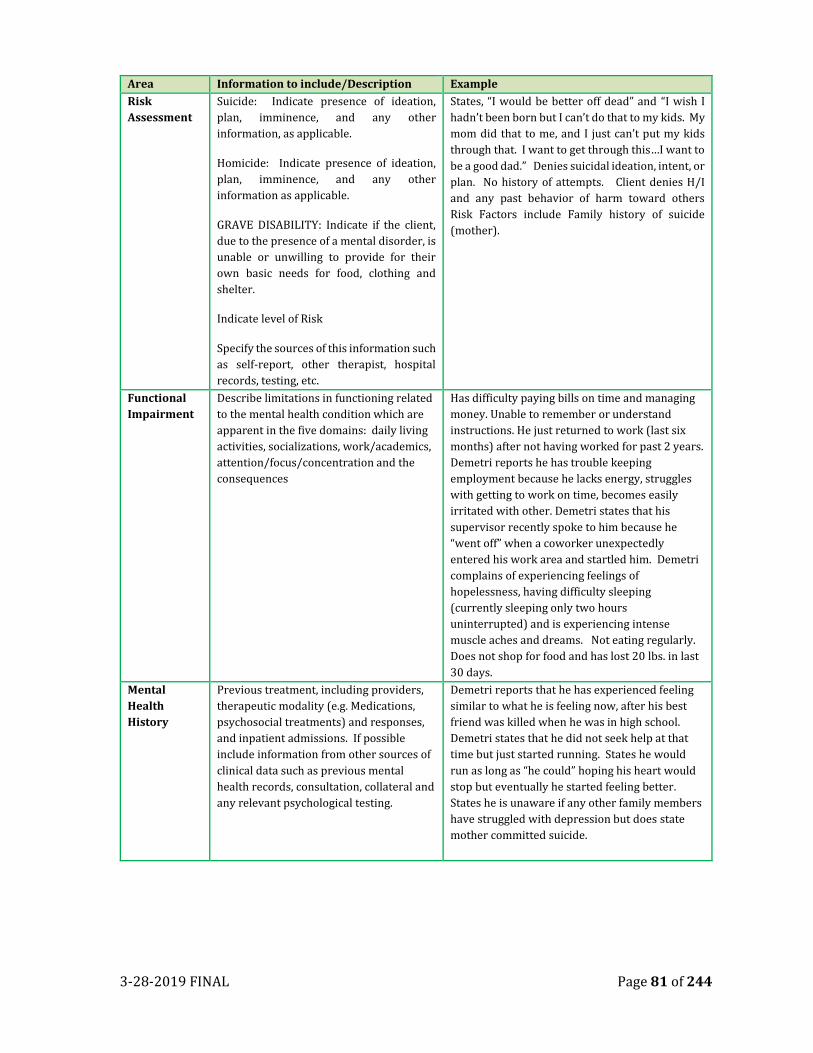
3-28-2019 FINAL Page 81 of 244
Area Information to include/Description Example
Risk
Assessment
Suicide: Indicate presence of ideation,
plan, imminence, and any other
information, as applicable.
Homicide: Indicate presence of ideation,
plan, imminence, and any other
information as applicable.
GRAVE DISABILITY: Indicate if the client,
due to the presence of a mental disorder, is
unable or unwilling to provide for their
own basic needs for food, clothing and
shelter.
Indicate level of Risk
Specify the sources of this information such
as self-report, other therapist, hospital
records, testing, etc.
States, “I would be better off dead” and “I wish I
hadn’t been born but I can’t do that to my kids. My
mom did that to me, and I just can’t put my kids
through that. I want to get through this…I want to
be a good dad.” Denies suicidal ideation, intent, or
plan. No history of attempts. Client denies H/I
and any past behavior of harm toward others
Risk Factors include Family history of suicide
(mother).
Functional
Impairment
Describe limitations in functioning related
to the mental health condition which are
apparent in the five domains: daily living
activities, socializations, work/academics,
attention/focus/concentration and the
consequences
Has difficulty paying bills on time and managing
money. Unable to remember or understand
instructions. He just returned to work (last six
months) after not having worked for past 2 years.
Demetri reports he has trouble keeping
employment because he lacks energy, struggles
with getting to work on time, becomes easily
irritated with other. Demetri states that his
supervisor recently spoke to him because he
“went off” when a coworker unexpectedly
entered his work area and startled him. Demetri
complains of experiencing feelings of
hopelessness, having difficulty sleeping
(currently sleeping only two hours
uninterrupted) and is experiencing intense
muscle aches and dreams. Not eating regularly.
Does not shop for food and has lost 20 lbs. in last
30 days.
Mental
Health
History
Previous treatment, including providers,
therapeutic modality (e.g. Medications,
psychosocial treatments) and responses,
and inpatient admissions. If possible
include information from other sources of
clinical data such as previous mental
health records, consultation, collateral and
any relevant psychological testing.
Demetri reports that he has experienced feeling
similar to what he is feeling now, after his best
friend was killed when he was in high school.
Demetri states that he did not seek help at that
time but just started running. States he would
run as long as “he could” hoping his heart would
stop but eventually he started feeling better.
States he is unaware if any other family members
have struggled with depression but does state
mother committed suicide.
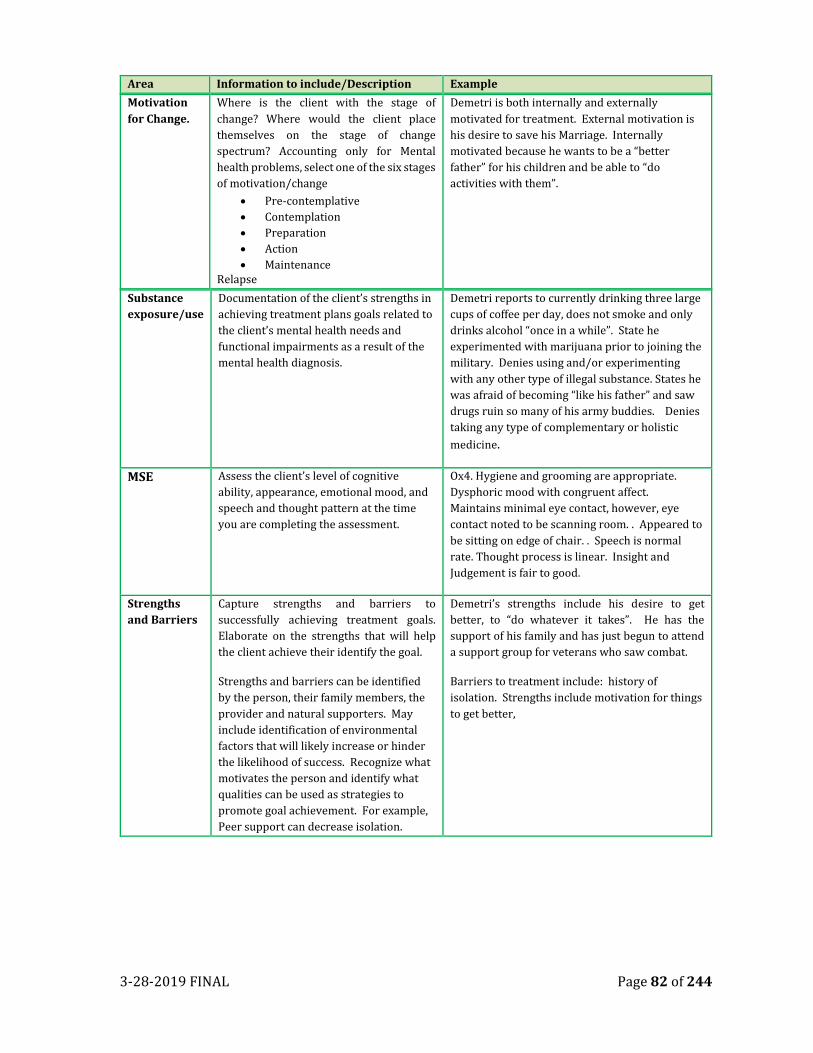
3-28-2019 FINAL Page 82 of 244
Area Information to include/Description Example
Motivation
for Change. Where is the client with the stage of
change? Where would the client place
themselves on the stage of change
spectrum? Accounting only for Mental
health problems, select one of the six stages
of motivation/change
• Pre-contemplative
• Contemplation
• Preparation
• Action
• Maintenance Relapse
Demetri is both internally and externally
motivated for treatment. External motivation is
his desire to save his Marriage. Internally
motivated because he wants to be a “better
father” for his children and be able to “do
activities with them”.
Substance
exposure/use
Documentation of the client’s strengths in
achieving treatment plans goals related to
the client’s mental health needs and
functional impairments as a result of the
mental health diagnosis.
Demetri reports to currently drinking three large
cups of coffee per day, does not smoke and only
drinks alcohol “once in a while”. State he
experimented with marijuana prior to joining the
military. Denies using and/or experimenting
with any other type of illegal substance. States he
was afraid of becoming “like his father” and saw
drugs ruin so many of his army buddies. Denies
taking any type of complementary or holistic
medicine.
MSE Assess the client’s level of cognitive
ability, appearance, emotional mood, and
speech and thought pattern at the time
you are completing the assessment.
Ox4. Hygiene and grooming are appropriate.
Dysphoric mood with congruent affect.
Maintains minimal eye contact, however, eye
contact noted to be scanning room. . Appeared to
be sitting on edge of chair. . Speech is normal
rate. Thought process is linear. Insight and
Judgement is fair to good.
Strengths
and Barriers Capture strengths and barriers to
successfully achieving treatment goals.
Elaborate on the strengths that will help
the client achieve their identify the goal.
Strengths and barriers can be identified
by the person, their family members, the
provider and natural supporters. May
include identification of environmental
factors that will likely increase or hinder
the likelihood of success. Recognize what
motivates the person and identify what
qualities can be used as strategies to
promote goal achievement. For example,
Peer support can decrease isolation.
Demetri’s strengths include his desire to get
better, to “do whatever it takes”. He has the
support of his family and has just begun to attend
a support group for veterans who saw combat.
Barriers to treatment include: history of
isolation. Strengths include motivation for things
to get better,
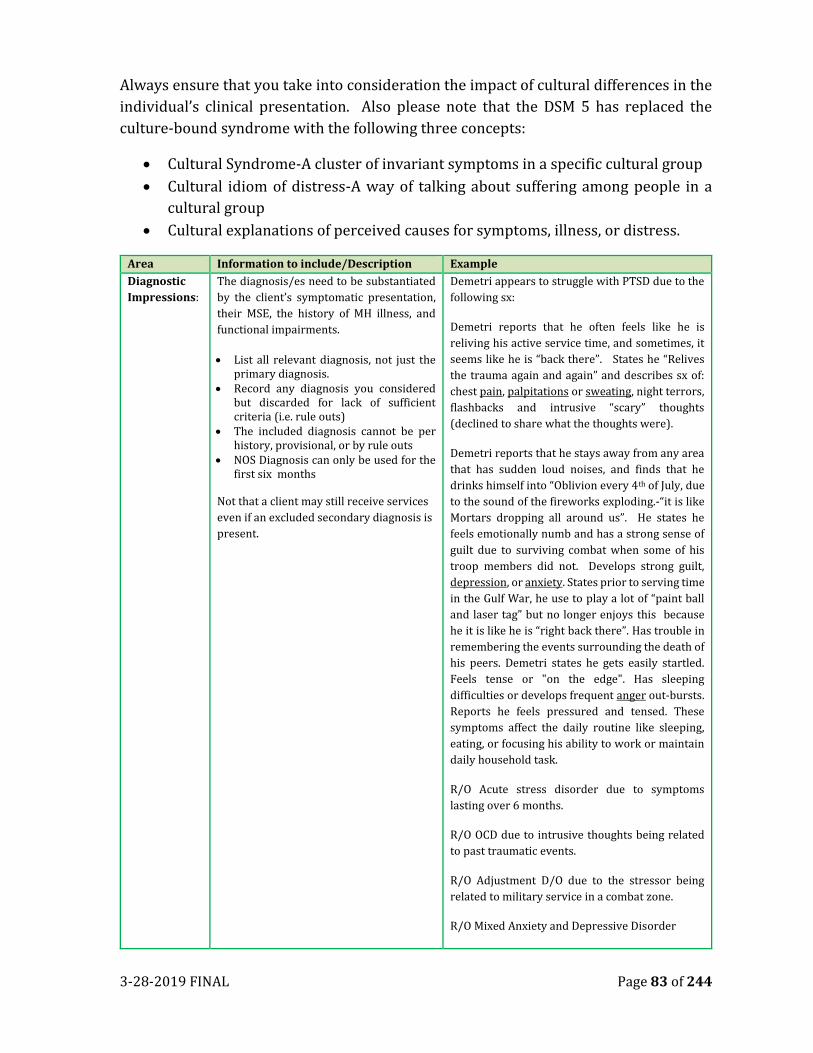
3-28-2019 FINAL Page 83 of 244
Always ensure that you take into consideration the impact of cultural differences in the
individual’s clinical presentation. Also please note that the DSM 5 has replaced the
culture-bound syndrome with the following three concepts:
• Cultural Syndrome-A cluster of invariant symptoms in a specific cultural group
• Cultural idiom of distress-A way of talking about suffering among people in a
cultural group
• Cultural explanations of perceived causes for symptoms, illness, or distress.
Area Information to include/Description Example
Diagnostic
Impressions: The diagnosis/es need to be substantiated
by the client’s symptomatic presentation,
their MSE, the history of MH illness, and
functional impairments.
• List all relevant diagnosis, not just the primary diagnosis.
• Record any diagnosis you considered but discarded for lack of sufficient criteria (i.e. rule outs)
• The included diagnosis cannot be per history, provisional, or by rule outs
• NOS Diagnosis can only be used for the first six months
Not that a client may still receive services
even if an excluded secondary diagnosis is
present.
Demetri appears to struggle with PTSD due to the
following sx:
Demetri reports that he often feels like he is
reliving his active service time, and sometimes, it
seems like he is “back there”. States he “Relives
the trauma again and again” and describes sx of:
chest pain, palpitations or sweating, night terrors,
flashbacks and intrusive “scary” thoughts
(declined to share what the thoughts were).
Demetri reports that he stays away from any area
that has sudden loud noises, and finds that he
drinks himself into “Oblivion every 4th of July, due
to the sound of the fireworks exploding.-“it is like
Mortars dropping all around us”. He states he
feels emotionally numb and has a strong sense of
guilt due to surviving combat when some of his
troop members did not. Develops strong guilt,
depression, or anxiety. States prior to serving time
in the Gulf War, he use to play a lot of “paint ball
and laser tag” but no longer enjoys this because
he it is like he is “right back there”. Has trouble in
remembering the events surrounding the death of
his peers. Demetri states he gets easily startled.
Feels tense or "on the edge". Has sleeping
difficulties or develops frequent anger out-bursts.
Reports he feels pressured and tensed. These
symptoms affect the daily routine like sleeping,
eating, or focusing his ability to work or maintain
daily household task.
R/O Acute stress disorder due to symptoms
lasting over 6 months.
R/O OCD due to intrusive thoughts being related
to past traumatic events.
R/O Adjustment D/O due to the stressor being
related to military service in a combat zone.
R/O Mixed Anxiety and Depressive Disorder
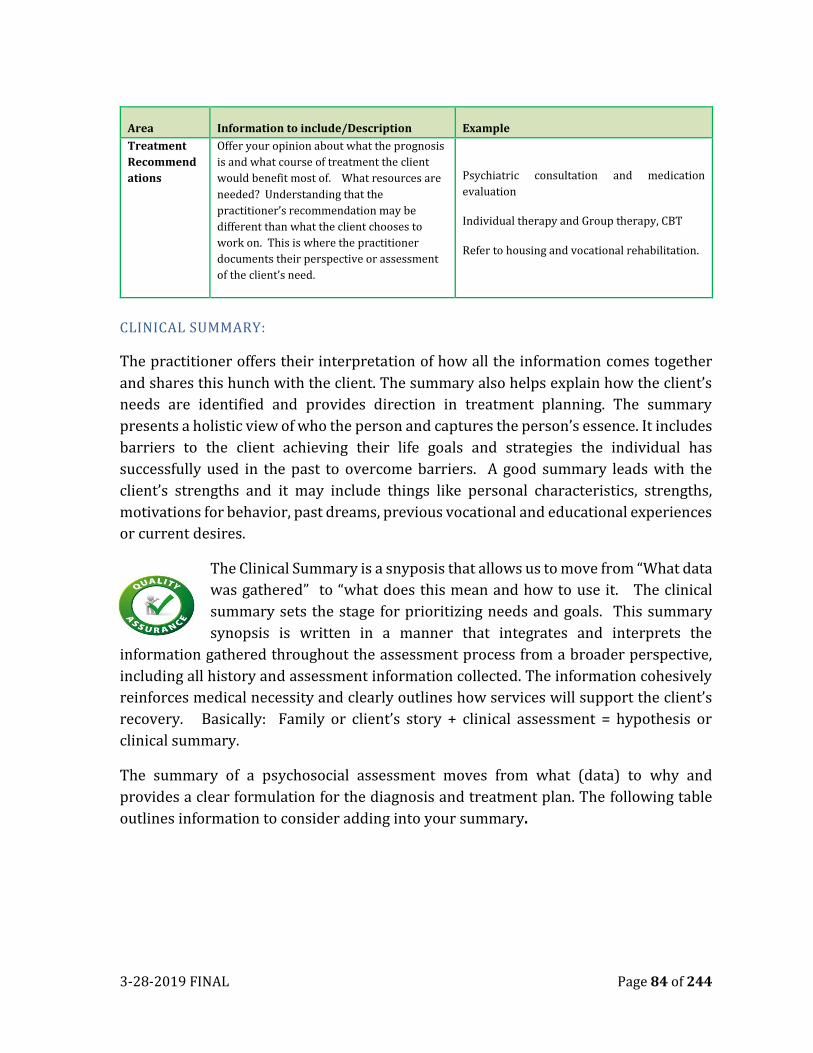
3-28-2019 FINAL Page 84 of 244
Area Information to include/Description Example
Treatment
Recommend
ations
Offer your opinion about what the prognosis
is and what course of treatment the client
would benefit most of. What resources are
needed? Understanding that the
practitioner’s recommendation may be
different than what the client chooses to
work on. This is where the practitioner
documents their perspective or assessment
of the client’s need.
Psychiatric consultation and medication
evaluation
Individual therapy and Group therapy, CBT
Refer to housing and vocational rehabilitation.
CLINICAL SUMMARY:
The practitioner offers their interpretation of how all the information comes together
and shares this hunch with the client. The summary also helps explain how the client’s
needs are identified and provides direction in treatment planning. The summary
presents a holistic view of who the person and captures the person’s essence. It includes
barriers to the client achieving their life goals and strategies the individual has
successfully used in the past to overcome barriers. A good summary leads with the
client’s strengths and it may include things like personal characteristics, strengths,
motivations for behavior, past dreams, previous vocational and educational experiences
or current desires.
The Clinical Summary is a snyposis that allows us to move from “What data
was gathered” to “what does this mean and how to use it. The clinical
summary sets the stage for prioritizing needs and goals. This summary
synopsis is written in a manner that integrates and interprets the
information gathered throughout the assessment process from a broader perspective,
including all history and assessment information collected. The information cohesively
reinforces medical necessity and clearly outlines how services will support the client’s
recovery. Basically: Family or client’s story + clinical assessment = hypothesis or
clinical summary.
The summary of a psychosocial assessment moves from what (data) to why and
provides a clear formulation for the diagnosis and treatment plan. The following table
outlines information to consider adding into your summary.
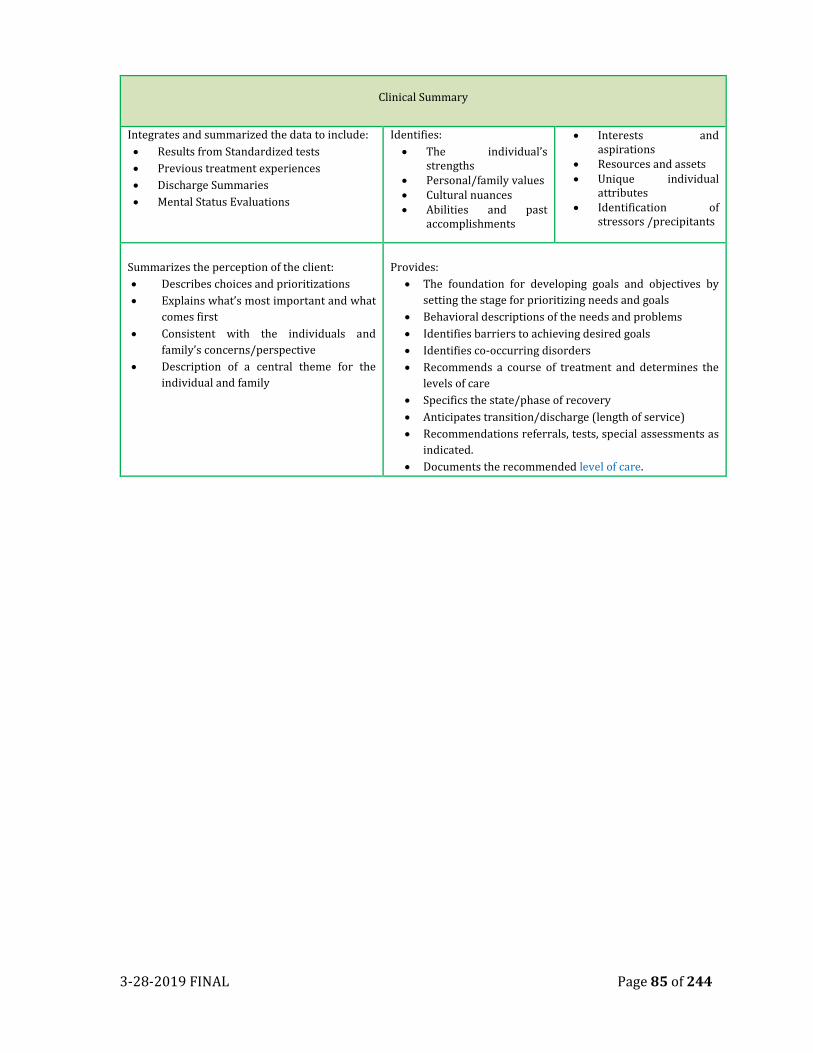
3-28-2019 FINAL Page 85 of 244
Clinical Summary
Integrates and summarized the data to include:
• Results from Standardized tests
• Previous treatment experiences
• Discharge Summaries
• Mental Status Evaluations
Identifies:
• The individual’s strengths
• Personal/family values • Cultural nuances • Abilities and past
accomplishments
• Interests and aspirations
• Resources and assets • Unique individual
attributes • Identification of
stressors /precipitants
Summarizes the perception of the client:
• Describes choices and prioritizations
• Explains what’s most important and what
comes first
• Consistent with the individuals and
family’s concerns/perspective
• Description of a central theme for the
individual and family
Provides:
• The foundation for developing goals and objectives by
setting the stage for prioritizing needs and goals
• Behavioral descriptions of the needs and problems
• Identifies barriers to achieving desired goals
• Identifies co-occurring disorders
• Recommends a course of treatment and determines the
levels of care
• Specifics the state/phase of recovery
• Anticipates transition/discharge (length of service)
• Recommendations referrals, tests, special assessments as
indicated.
• Documents the recommended level of care.
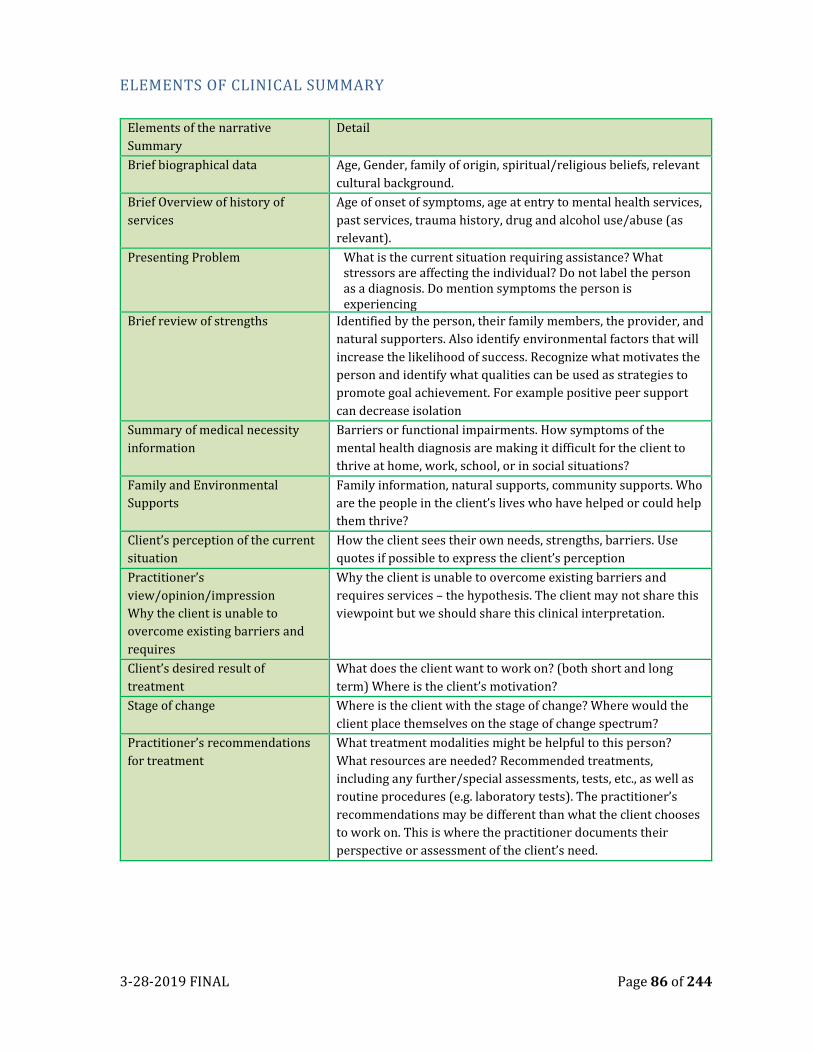
3-28-2019 FINAL Page 86 of 244
ELEMENTS OF CLINICAL SUMMARY
Elements of the narrative
Summary
Detail
Brief biographical data Age, Gender, family of origin, spiritual/religious beliefs, relevant
cultural background.
Brief Overview of history of
services
Age of onset of symptoms, age at entry to mental health services,
past services, trauma history, drug and alcohol use/abuse (as
relevant).
Presenting Problem What is the current situation requiring assistance? What stressors are affecting the individual? Do not label the person as a diagnosis. Do mention symptoms the person is experiencing
Brief review of strengths Identified by the person, their family members, the provider, and
natural supporters. Also identify environmental factors that will
increase the likelihood of success. Recognize what motivates the
person and identify what qualities can be used as strategies to
promote goal achievement. For example positive peer support
can decrease isolation
Summary of medical necessity
information
Barriers or functional impairments. How symptoms of the
mental health diagnosis are making it difficult for the client to
thrive at home, work, school, or in social situations?
Family and Environmental
Supports
Family information, natural supports, community supports. Who
are the people in the client’s lives who have helped or could help
them thrive?
Client’s perception of the current
situation
How the client sees their own needs, strengths, barriers. Use
quotes if possible to express the client’s perception
Practitioner’s
view/opinion/impression
Why the client is unable to
overcome existing barriers and
requires
Why the client is unable to overcome existing barriers and
requires services – the hypothesis. The client may not share this
viewpoint but we should share this clinical interpretation.
Client’s desired result of
treatment
What does the client want to work on? (both short and long
term) Where is the client’s motivation?
Stage of change Where is the client with the stage of change? Where would the
client place themselves on the stage of change spectrum?
Practitioner’s recommendations
for treatment
What treatment modalities might be helpful to this person?
What resources are needed? Recommended treatments,
including any further/special assessments, tests, etc., as well as
routine procedures (e.g. laboratory tests). The practitioner’s
recommendations may be different than what the client chooses
to work on. This is where the practitioner documents their
perspective or assessment of the client’s need.
3-28-2019 FINAL Page 87 of 244
SPECIAL CONSIDERATION
During the course of assessment and treatment, there may be information shared
and/or observed by the practitioner that is deemed pertinent for all staff to be informed
of in order to safely engage the client in services.
The “Special Considerations” form is used to communicate to the treatment team any
special circumstances related to client’s treatment. The special consideration form will
allow the practitioner to include information regarding an active “Safety Plan” as well as
other considerations.
The Safety Plan section shall be used to communicate the active safety plan that is in
place to help support the client’s needs. The safety plan section will display at the top of
the “client notifications” (green widget) section of the client chart overview. The safety
plan will provide an opportunity to the treatment team to quickly view and understand
the client’s active safety plan and provide information on how to best support the client
during this time. The form will allow the practitioner to enter a start and end date for
the safety plan; only one “active” safety plan at a time is permitted.
ASSESSMENT TIMELINE:
Initial Assessment
The initial mental health assessment is required for all clients meeting medical necessity
who are not currently opened or are new to the outpatient mental health system (or are
returning after being discharged from all clinic (outpatient) services for more than 30
days). This assessment shall be completed within 60 calendar days of the client’s
signature on the consent to treatment form or that of the legal guardian or adult.
Assessments are considered “approved” only when signed by an LPHA and finalized in
the HER (the date of validation appears by the LPHA staff signature).
UPDATED ASSESSMENTS
An assessment is updated under two circumstances:
1) Whenever clinically indicated, such as following a significant life event that
potentially changes the client’s mental status, diagnosis or treatment direction,
or any other major life stressor, or
2) According to guidelines identified with the MHP policies and procedures.
An updated assessment must be completed on or before within the guidelines identified
within the MHP policies and procedures. Updated assessments are required to be
comprehensive and complete, and must clearly state why the client continues to
require services in the presenting problem section of the assessment and in the
3-28-2019 FINAL Page 88 of 244
medical necessity determination form (i.e. this is what establishes continued medical
necessity). Updated assessments must clearly state why the client continues to require
services and contain a summary of the treatment provided in the past year and the
response to that treatment. Explain what might happen/what are the risk should the
client no longer be eligible for specialty mental health services.
In other words, the updated assessment must stand-alone and not simply be the same
as the initial assessment or initial medical necessity determination form. When
completing an updated or annual assessment the clinician must complete a new form.
• The updated assessment must contain a summary of the treatment provided in the past year and the response to that treatment in the mental health treatment section of the assessment
• The information required for the assessment will be re-evaluated no less
frequently than every 12 months for children/youth and every 24 months for
adult client who continues to receive specialty mental health services during
those 12 months.
• The information from the previous psychosocial will “flow forward” when writing an updated assessment. However, the practitioner is expected to ensure the updated assessment accurately reflects the client’s current needs and establishes medical necessity. For clinical reasons, the information of the previously entered and Recommendations sections do not flow forward.
BILLING AND CODE REQUIREMENTS
If more than one assessment service is billed, the reason for each subsequent
assessment service must be clearly explain in the progress note for each service. The
number of assessment sessions and total time for the assessment must be reasonable
and supported by the documentation contained within the progress notes.
If a therapist sees a client on Thursday and finished the paperwork on Monday (when
client is not present), the time spent on the paperwork is added to Thursday’s
assessment and billed as one bundled service. The write up/documentation is an
important part of the assessment process, but it is not a separate service.
It is understood that if a practitioner completes their documentation late, this could
appear as if the practitioner provided over 8 hours of service in a given day.
3-28-2019 FINAL Page 89 of 244
LEVEL OF CARE TOOLS- ASSESSMENT/EVALUATION
The Placer County Children’s System of Car utilized the Child Assessment of Needs and
Strengths (CANS) and the Placer County SMART Outcome Tools. The SMART Outcomes
Tool was developed by Placer County’s Children’ System of Care and has been used to
track Child/Youth outcomes for over 15 years. The Child and Adolescent Needs and
Strengths (CANS) is a multi-purpose tool developed for children’s services to support
decision making, including level of care and service planning, to facilitate quality
improvement initiatives, and to allow for the monitoring of outcomes of services.
THE CHILD ASSESSMENT OF NEEDS AND STRENGTHS (CANS)
The CANS is an assessment tool that incorporates the principles of resiliency. These
principles are in keeping with the Integrated Division of Children’s System of Care
(CSOC) principles and Mental Health Services Act (MHSA) essential elements. The CSOC
chose to implement the CANS as part of the assessment and treatment planning within
the Children’s MH Programs in 2013 to aid in assessment and treatment planning, and
in the evaluation of client, agency and system level outcomes. The CANS will be
implemented within the CSOC Child Welfare Programs when DHCS guidance is given.
The CANS gathers information on clients’ and caregivers’ needs and strengths. Strengths
are areas of a child’s life where he or she is doing well or has an interest or ability. Needs
are areas where a child requires help or serious intervention. Service providers in
Alameda County use an assessment process to get to know the child and families with
whom they work and to understand their strengths and needs.
Helpful Hints with Documenting Medical Necessity within the Assessment
When you are completing the assessment, it is important to ensure that you
have documented all of the symptoms to justify the client’s diagnosis. Please
review this prior to submitting for approval.
After you have ensured that all symptoms are documented, you will link the
client’s presenting symptoms to their presenting impairment. This is a crucial
element of The Golden Thread and must be completed. In other words, why
has the client sought treatment (symptoms), and what areas of life are their
symptoms affecting (impairment)?
Please refer to appendix G for examples.
3-28-2019 FINAL Page 90 of 244
THE LEVEL OF CARE UTILIZATION SCALE (LOCUS) FOR ADULTS
The LOCUS has multiples uses including accessing the immediate service needs, to assist
with planning for resource needs over time, as in assessing service requirements
defined by populations and to monitor changes in status or placement at different points
within the treatment service timelines. The LOCUS determines six levels of care in the
service continuum, each level has a variety and frequency of services. Scoring the LOCUS
includes evaluating the six subcomponents: 1) Risk of Harm; 2) Functional Status; 3)
Medical, Addictive and Psychiatric Co-Morbidity; 4) Recovery Environment; 5)
Treatment and Recovery History; and 6) Engagement and Recovery Status. Additional
information pertaining the scoring of the LOCUS will be available to ASOC Staff members
through the E-learning process.
CANS AND LOCUS
Both the CANS and LOCUS are multi-purpose communication tools developed to support
decision making, including level of care and service planning that allow for the
monitoring of outcomes and goal attainment. These tools allow for effective
communication with the client/family/support groups to accurate represent the shared
vision of the individuals receiving services. It is important to consider the scoring of
these tools when collaborating with the client/family in the development of their
treatment goals
The CANS and LOCUS can help providers decide which of a client’s needs are the most
important to address in a treatment plan and identify strengths. By working with the
client and family closely during the assessment process and talking together about the
MH providers can develop a treatment plan that addresses a child’s strengths and needs
while building strong engagement. These ratings help the provider understand where
intensive or immediate action is most needed, and also where a child has strengths that
could be a major part of the treatment plan. Of course, ratings do not tell the whole story
of a client’s strengths and needs. Each domain and subsection is merely the output of a
comprehensive assessment process and is documented alongside narratives where a
provider can give more information about that area of life. The provider can note
questions that need to be explored further, or areas where people involved with the
child have different ideas.
3-28-2019 FINAL Page 91 of 244
WHEN TO COMPLETE THE LEVEL OF CARE TOOLS
TOOL AGE FREQUENCY
CANS clients under 21 years Upon initial assessment and at least every 3 months
LOCUS clients 18 and above Upon initial assessment, and anytime a change in status
occurs (decrease or increase level of service is being
considered). Must be completed at least annually
• The updated assessment must contain a summary of the treatment provided in the past year,
and the responses to that treatment in the mental health treatment history section of the
assessment.
• The information required for the assessment will be re-evaluated no less frequently than every
12 months for children/youth and every 24 months for adult client who continues to receive
specialty mental health services during those 12 months.
• The assessment anniversary is one year from the first day of the last assessment. For example,
if the assessment is completed on August 15, 2016, the reassessment should be completed by
August 14, 2017 for youth and August 14, 2018 for an Adult.
• Remember Medical Necessity can be met when ongoing services may prevent the reoccurrence
of a significant impairment (i.e. hospitalization).
• Clients who are discharged from all open programs and return for services within 30 days or
less can be reopened without having to re-do all the opening paperwork. Consents, assessments,
treatment plans, etc. can be defaulted from a previous program as long as the information is
sufficient and was completed within the past year.
• You will need to be able to justify why treatment shall continue. Example:
If a client had received individual therapy each week for a year, but had not made significant
progress, why would we continue this service with the same frequency and duration?
3-28-2019 FINAL Page 92 of 244
CHAPTER EIGHT
UNIFIED SERVICE PLANS/TREATMENT PLANS
UNDERSTANDING THE PURPOSE OF THE TREATMENT PLAN
A treatment plan is a document, co-created by the client and the
provider, which outlines the steps needed to achieve particular
goals or outcomes based on the information contained in the
psychosocial assessment and informed by the diagnosis.
The Placer/Sierra MHP is committed to providing client-centered care. This
commitment is shown when our mental health practitioners engage clients in the
development of a meaningful treatment plan. The treatment plan is the primary way we
empower the client/family to develop a plan to achieve their recovery and resiliency
goals. Placer County strives to develop treatment plans that serve as unified service
plans, where all service providers can co-create treatment goals with the client /family
to help them achieve their goals. This model helps the client understand who is
providing what services and more specifically, what the expectations are from everyone.
This understanding extends to writing treatment plans in the client’s primary/preferred
language alongside the English version. In addition, the treatment planning process
supports clients in understanding what they can expect from the behavioral health
services we provide and their own role in their recovery.
A treatment plan should be like a roadmap to success. We join with our clients to develop
an understanding of where they are and where they want to arrive. Then we plot out a
map of how we, as mental health providers, can help them reach their goals. The
treatment plan was recognized as the core to clients reaching their recovery goals by the
Presidents New Freedom Commission who noted: Achieving the promise: Transforming
Mental Health Care in America (The President’s New Freedom Commission on Mental
Health. http://store.samhas.gov/product/SMA03-3831 10.28.17).
“An individualized plan of care will give consumers, families of children with
serious emotional disturbances, clinicians, and other providers a valid
opportunity to construct and maintain meaningful, productive, and healing
relationships. Opportunities for updates —based on changing needs across the
stages of life and the requirement to review treatment plans regularly —will be
an integral part of the approach. The plan of care will be at the core of the
consumer-centered, recovery-oriented mental health system. The plan will
include treatment, supports, and other assistance to enable consumers to better
integrate into their communities; it will allow consumers to realize improved
mental health and quality of life.”
Note: the terms Service
Plan, Treatment plan are
used interchangeably
throughout this chapter.
3-28-2019 FINAL Page 93 of 244
DEVELOPING CLIENT/FAMILY CENTERED UNIFIED SERVICE PLANS
The development of the treatment plan is an interactive process between the client and
the treatment team designed to establish the client’s goals, to develop a set of objectives
to help realize the treatment goals, and to reach agreement on the types of services
provided through the MHP. The Treatment plan is a primary way of involving clients in
their own mental health treatment and recovery.
As you start to develop a treatment plan, don’t focus on what is a problem, goal,
objective, or intervention. Start first with why are we treatment planning? Although we
find the fiscal consequences of audit exceptions when we don’t have a treatment plan
quite motivating –our real reason for completing a treatment plan is the opportunity to
develop a shared vision of success with our clients and their families. At least once a
year we have the chance to join with our clients to ask the following questions. Why are
you here, what do you want, and how can we help you get it? If we find ourselves unable
to ask or answer these questions then we need to look closely at medical necessity –are
the services we are providing necessary for this client? Are the services helping to
reduce risk and improve functioning? All services need to be medically necessary and
must be treating symptoms of an included diagnosis. It is the responsibility of the Care
Coordinator to work with the client and any providers to ensure that the client receives
agreed upon services that will help reduce the barriers/impairments resulting from
their mental health condition. Remember, without the opportunity to develop a
meaningful treatment plan, we lack a measurement to define the success our clients
deserve.
COLLABORATION AND UNIFIED SERVICE PL ANS COMPONENTS
When developing a unified services plan with a client or client and support system, it is
important for the coordinator to explore available natural supports including cultural,
peer, family, etc. that can be included within the USP to assist the client on their road to
recovery. When developing a collaborative (“Unified”) treatment plans, the following
components should be reviewed with the client for possible inclusion:
SERVICE STRATEGIES: Broad categories describing underlying concepts or fundamental
approaches by the various teams within SOC.
ETHNIC SPECIFIC SERVICE STRATEGY: Culturally appropriate services tailored to persons
of diverse cultures. Can include ethnic specific strategies and practices such as
traditional practitioners, natural healing, and recognized community ceremonies.
PSYCHO-EDUCATIONAL: Services providing education regarding diagnosis, assessment,
medication, supports, and treatments and development/identification of tracking and
coping with symptomology to reduce the impact on a significant area of life.
3-28-2019 FINAL Page 94 of 244
PEER/FAMILY DELIVERED: Services provided by individuals with lived experience who
are employees of the MHP or contractor.
FAMILY SUPPORT: Services provided to family members in support of the client
AGE SPECIFIC SERVICE STRATEGY: Age appropriate services tailored to specific age
groups. These services should promote a wellness philosophy including concepts or
recovery and resiliency
INTEGRATED SERVICES FOR MH AND THE AGING: Services integrated or coordinated with
issues related to aging, including co-location, or collaboration with providers and sites
offering aging services.
INTEGRATED SERVICES FOR MH AND THE DEVELOPMENTAL DISABILITY: Services
integrated or coordinated with services for developmental disability, including -
location, or collaboration with providers and sites offering services for developmental
disability.
DELIVERED IN PARTNERSHIP WITH HEALTH CARE: Services integrated or coordinated
with physical health care, including co-location or collaboration with providers and sites
offering physical health care.
DELIVERED IN PARTNERSHIP WITH SUBSTANCE USE SERVICES: Services integrated or
coordinated with substance use services, including co-location or collaboration with
providers and sites offering substance use services.
DELIVERED IN PARTNERSHIP WITH LAW ENFORCEMENT: Services integrated or
coordinated with law enforcement, probation, or courts (e.g., MH Court, AOT) to provide
an alternative to incarceration.
DELIVERED IN PARTNERSHIP WITH SOCIAL SERVICES: Services integrated or coordinated
with social services, including co-location or collaboration with providers and sites
offering social services.
ASSESS THE CLIENT'S STAGE OF CHANGE.
As you begin treatment planning, it is important to consider the client’s stage of change.
The treatment plan should be reflective of the client’s current stage of change or
willingness for change. Even for those individuals who are referred and/or “mandated”
to treatment or when their illness acts as a barrier to insight, we must include them in
the treatment planning process. Treatment planning does not work when we are not
willing to work alongside the client on the development of goals that are meaningful to
them.
3-28-2019 FINAL Page 95 of 244
Probably the most obvious and direct implication of the research evidence is the need
to assess the stage of a client's readiness for change and to tailor therapeutic
relationships and interventions accordingly. Beware of treating all clients as though they
are in action. Professionals frequently design excellent action-oriented treatments, but
then are disappointed when only a small percentage of clients remain in therapy or
treatment. The vast majority of clients are not in the action stage. Aggregating across
studies and populations, we estimate that 10% to 20% are prepared for action,
approximately 30% to 40% are in the contemplation stage, and 50% to 60% in the Pre-
contemplation stage. Thus, those professionals with only action-oriented programs are
likely to under serve or “misserve” the majority of their target population.
SET REALISTIC GOALS
Move one stage at a time. A reasonable expectation for many clients is to set initial goals,
such as progressing from Pre-contemplation to Contemplation. Such progress means
that clients are changing. We view change as a process that unfolds over time, through a
series of stages. Helping clients break out of the stuck phase of Pre-contemplation is a
therapeutic success, since it about doubles the chances that clients will take effective
action within the next 6 months. If we can help them progress two stages with brief
therapy, we triple to quadruple the chances they will take effective action.
UNIFIED SERVICE PLANS/TREATMENT PLAN BASICS:
1. The USP/Treatment Plan is an agreement between the client and the clinician that states which mental health problem(s) will be the focus of treatment. The Treatment Plan consists of specific goals, objectives, and the treatment interventions that will be provided (See “Signatures” at the end of this section).
2. There needs to be a clear connection and flow from the DSM 5 diagnosis and functional impairments in the assessment to the problem, goal, objectives, and interventions in the USP/treatment plan
3. A client receiving both general mental health and medication support services will have an “integrated treatment plan.” Integrated plans include both general mental health interventions and medication interventions. If the client is receiving integrated treatment the LPHA is encouraged to coordinate care with the psychiatrist or prescriber as needed to provide continuity of care and inform the treatment planning process.
4. The USP/Treatment Plan is only valid from the date in which the LPHA has signed the plan. In the event of a new diagnosis, a new USP/treatment plan may be needed if clinically appropriate. Please consult with your clinical supervisor if needed.
5. All planned services (except TBS, which has its own plan) must have plans using the USP/Treatment plan. Occasionally, unplanned services do not require a USP/Treatment plan but documentation must support Medical Necessity for their position (i.e. Crisis Intervention).
3-28-2019 FINAL Page 96 of 244
TRAITS OF EFFECTIVE CLIENT TREATMENT PLANS:
• Culturally Relevant: The plan should take into account cultural issues to arrive at a
meaningful understanding of the client’s worldview. These considerations should
include but not be limited to ethnicity; but are expanded to include any other types of
culture that the client might identify with (i.e. Veterans, homeless, LGBTQ, or may include
family of origin, traditions and holidays, religion/spirituality, education, work ethics, etc.
• Client Centered: The plan should be written in a way that is culturally sensitive and
personally relevant. The plan is developed in partnership with the client and uses
language that is understandable and acceptable. Both the client and provider agree on
the conditions that indicate when a goal is met
• Flexible: Capable of being change
• Supportive: of the client’s need, taking into account the appropriate level of care and
length of treatment
• Reality Based: reflects “where the client is at”. For example, if the client is in the early
stages of change, the objectives should be reasonable and consistent with the client’s
willingness and ability to accomplish them.
• Realistic: objectives are achievable, observable, and measurable (and includes
Baselines).
• Strength Based: Identifies strengths of the individual and utilized the client’s strengths
to reduce barriers. The plan focuses on the person’s competencies as well as what the
person needs to do to overcome impairments.
• Simple: Clients, family and staff can understand them. The plan is written in plain, non-
technical language.
• Useful: Objectives provide clear indicators of progress
• Identify clinical responsibilities; staff know what they should do, with whom and how
often.
• Identify the type and frequency of interventions (i.e. methods, approach with duration
and frequency).
• Is integrated and facilitates interdisciplinary collaboration when others.
ELEMENTS OF A TREATMENT PLAN
DHCS requires that 10 elements appear in every Client Plan document. These 10
requirements are enumerated in the contract between DHCS and the MHP (for TBS
specific client plan requirements please refer TBS Section). The following grid breaks
down the various components of the treatment plan along with brief descriptions and
documentation examples. All areas are required for a USP/treatment plan to be
considered complete as mandated by the MHP. Note: The information in the “Area”
column reflects the components of the tx plan but does not reflect the layout of the
Client’s unified service plan/ treatment plan. The following components will be
explained further in this chapter.
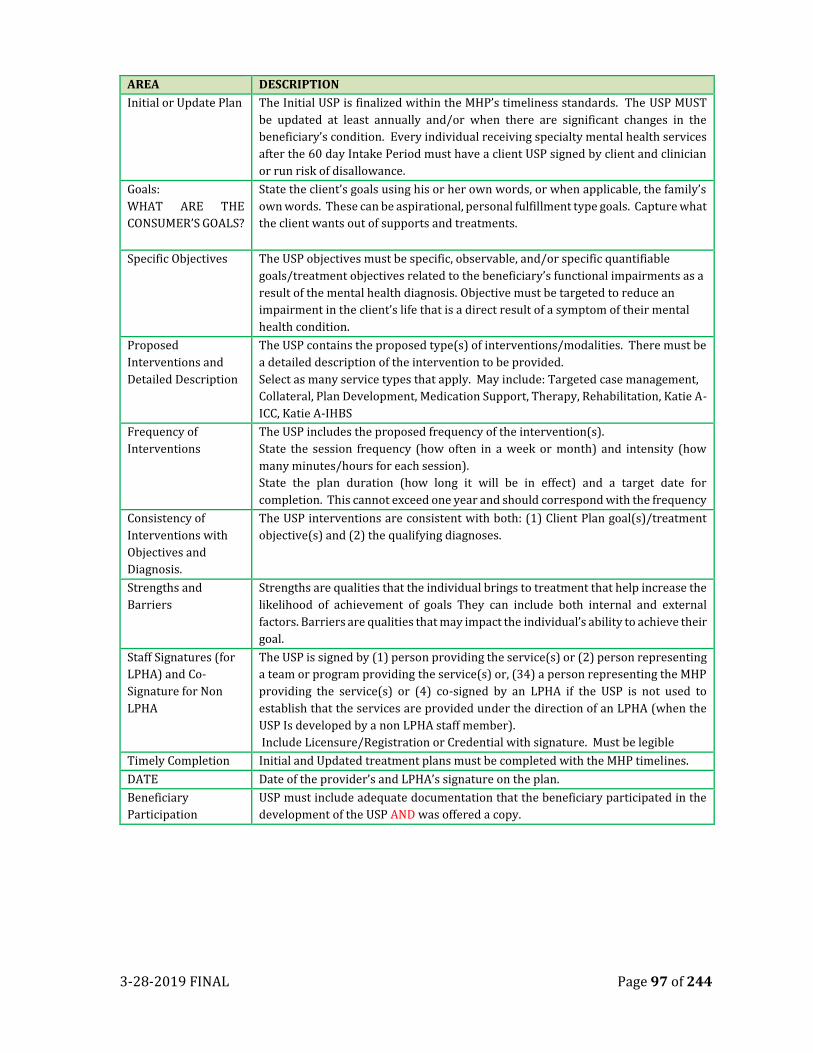
3-28-2019 FINAL Page 97 of 244
AREA DESCRIPTION
Initial or Update Plan The Initial USP is finalized within the MHP’s timeliness standards. The USP MUST
be updated at least annually and/or when there are significant changes in the
beneficiary’s condition. Every individual receiving specialty mental health services
after the 60 day Intake Period must have a client USP signed by client and clinician
or run risk of disallowance.
Goals:
WHAT ARE THE
CONSUMER’S GOALS?
State the client’s goals using his or her own words, or when applicable, the family’s
own words. These can be aspirational, personal fulfillment type goals. Capture what
the client wants out of supports and treatments.
Specific Objectives The USP objectives must be specific, observable, and/or specific quantifiable
goals/treatment objectives related to the beneficiary’s functional impairments as a
result of the mental health diagnosis. Objective must be targeted to reduce an
impairment in the client’s life that is a direct result of a symptom of their mental
health condition.
Proposed
Interventions and
Detailed Description
The USP contains the proposed type(s) of interventions/modalities. There must be
a detailed description of the intervention to be provided.
Select as many service types that apply. May include: Targeted case management,
Collateral, Plan Development, Medication Support, Therapy, Rehabilitation, Katie A-
ICC, Katie A-IHBS
Frequency of
Interventions
The USP includes the proposed frequency of the intervention(s).
State the session frequency (how often in a week or month) and intensity (how
many minutes/hours for each session).
State the plan duration (how long it will be in effect) and a target date for
completion. This cannot exceed one year and should correspond with the frequency
Consistency of
Interventions with
Objectives and
Diagnosis.
The USP interventions are consistent with both: (1) Client Plan goal(s)/treatment
objective(s) and (2) the qualifying diagnoses.
Strengths and
Barriers
Strengths are qualities that the individual brings to treatment that help increase the
likelihood of achievement of goals They can include both internal and external
factors. Barriers are qualities that may impact the individual’s ability to achieve their
goal.
Staff Signatures (for
LPHA) and Co-
Signature for Non
LPHA
The USP is signed by (1) person providing the service(s) or (2) person representing
a team or program providing the service(s) or, (34) a person representing the MHP
providing the service(s) or (4) co-signed by an LPHA if the USP is not used to
establish that the services are provided under the direction of an LPHA (when the
USP Is developed by a non LPHA staff member).
Include Licensure/Registration or Credential with signature. Must be legible
Timely Completion Initial and Updated treatment plans must be completed with the MHP timelines.
DATE Date of the provider’s and LPHA’s signature on the plan.
Beneficiary
Participation
USP must include adequate documentation that the beneficiary participated in the
development of the USP AND was offered a copy.
3-28-2019 FINAL Page 98 of 244
CLIENT STRENGTHS
Strengths are qualities that clients brings to treatment that help increase the likelihood
of achievement of goals. Clients strengths are be internal and external factors that
should be identified in and emphasized as helpful to the treatment process. Examples
include: Community supports, family/relationships, work, etc. Maybe unique to racial,
ethnic, linguistic and culture (including lesbian, gay, bisexual, and transgender)
communities. Some examples are:
• Client/Family’s best qualities
• Strategies already utilized to help (What worked in the past)
• Competencies/accomplishments interests and activities, i.e. sports, art identified
by the consumer, and/or provider.
• Motivation for change
• Employed/engaged in volunteer work
• Has skills/competencies: vocation, relational, transportation savvy, activities of
daily living
• Intelligent, artistic, musical, good at sports
• Has knowledge about their illness
• Values medication as a recovery tool
• Has a spiritual program/connected to a church
• Good physical health
• Adaptive coping skills/help seeking behavior
• Capable of living independently.
When considering strengths, it is beneficial to explore different areas. Examples may
ben and individuals’ most significant or most valued accomplishment, what motivates
them? Educational achievement, ways of relaxing and having fun, ways of calming down
when upset, preferred living environment, personal heroes, most meaningful
compliment ever received, etc.
It is important to take the time to acknowledge the values of the individual’s existing
relationships and connections. If it is the individual’s preference, significant effort
should be made to include these “natural supports” and unpaid participants as they
often have critical input and support to offer to the treatment team. Treatment should
complement NOT interfere with, what people are already doing to keep themselves well.
Strengths should be utilized in every part of the treatment process.
• Strengths identified in the assessment process
• Set objectives to build on strengths in the USP

3-28-2019 FINAL Page 99 of 244
• The progress notes help us show how our interventions help build up the
strengths of that help individuals thrive.
LIFE GOALS/ASPIRATIONS (IN CLIENT’S OWN WORDS)
Currently, not all providers under the MHP include “Life Goals” as part of the treatment
plan, however, coordinators should be aware of the client’s life goals and assist identify
the mental health reasons that are impact the client from obtaining their life goal and
work on steps to reduce the mental health barriers.
Example:
• When Suzy’s coordinator inquires as to what she would like to achieve during the
coming year, Suzy states that she would like to become a contestant on American
Idol.
• The coordinator respectfully acknowledges Suzy’s goal and inquires as to what
steps she would have to take to become a contestant and what has prevented her
from following through on these steps.
• Through a series of open ended questioning, the coordinator and Suzy may
decide that Suzy first needs to be able to work on her anxiety, her depression, or
not responding loudly to her voices. These areas become the goal for mental
health services.
For providers who include Life Goals on their treatment plan. This statement is
generally located at the beginning of the treatment plan and it is intended to be a space
where the client’s goals are freely stated. This space may indicate the client’s desired
outcome of successful treatment. This is the reason the client is seeking treatment.
Overall goals are broad life goals, such as returning to work or graduating from high
school. The overall goal is meant to be a global objective that reflects the client’s intent
and interests. The overall goal should be clear to the client and the treatment team, and
it should reflect the client’s preferences and strengths. These goals have a special place
in a system committed to recovery and resiliency–they should speak to the client’s
ability to manage or recover from his/her illness and achieve major developmental
milestones.
A Life goal should be stated in the client’s and/or family’s own words. For example:
• “I want a job”
• “I want to go back to school”
• “I want to live in my own apartment”
• “I want some friends”
• “I want to be an actor”
3-28-2019 FINAL Page 100 of 244
A goal should be a shared vision of success. Goals express the hopes and dreams of the
client. Goals identify the hoped-for destination be arrived at through the services
provided. Examples of Person centered goals are:
• Ideally expressed in the words of the individual, their family and/or other
supportive individuals.
• Easily understandable in the client’s preferred language
• Appropriate to the person’s culture; reflects values, traditions, identify, etc.
• Written in a positive manner
• Consistent with abilities/strengths, preferences, and needs
• Embody Hope/Alternative to current circumstances.
Reminder: treatment plans written in both, English and the client/family’s
preferred language, support the client’s increase understanding of treatment
and encourage participation goal attainment.
CLINICAL TREATMENT GOALS (HOPES AND DESIRED OUTCOMES)
The clinical treatment goal must relate to the client’s desired outcome of successful
treatment. What is the reason the client is seeking services? The overall goals should
be clear to the client and the treatment team, and should reflect the client’s desired
outcome and strengths. These goals should speak to the client’s ability to manage or
recover from this/her mental health condition and achieve major developmental
milestones.
The clinical treatment goals must be “specific, observable or measurable” and stated in
terms of the specific impairment identified in the assessment, diagnosis, and clinical
formulation of Medical Necessity. The goal is the development of new skills/behaviors
and the reduction, stabilization or removal of the barrier/problem. Individual goals are
generally related to important areas of functioning affected by the client’s mental health
condition, such as living situation, daily activities, school, work, social support, legal
issues, safety, physical health, substance abuse, and psychiatric symptoms. The
assessment must clearly document how a particular goal reflects the client’s mental
health condition.
Goals build upon the strengths, preferences, and needs of the client. Goals should
embody hope. Practitioners need to be mindful that identifying a goal to a practitioner
can be frightening to a client, child or family. Sharing one’s aspirations with another can
make people feel vulnerable. A practitioner may help the client start thinking about their
goals by asking the “Miracle Question” —If you woke up tomorrow and all was well,
what would that look like?
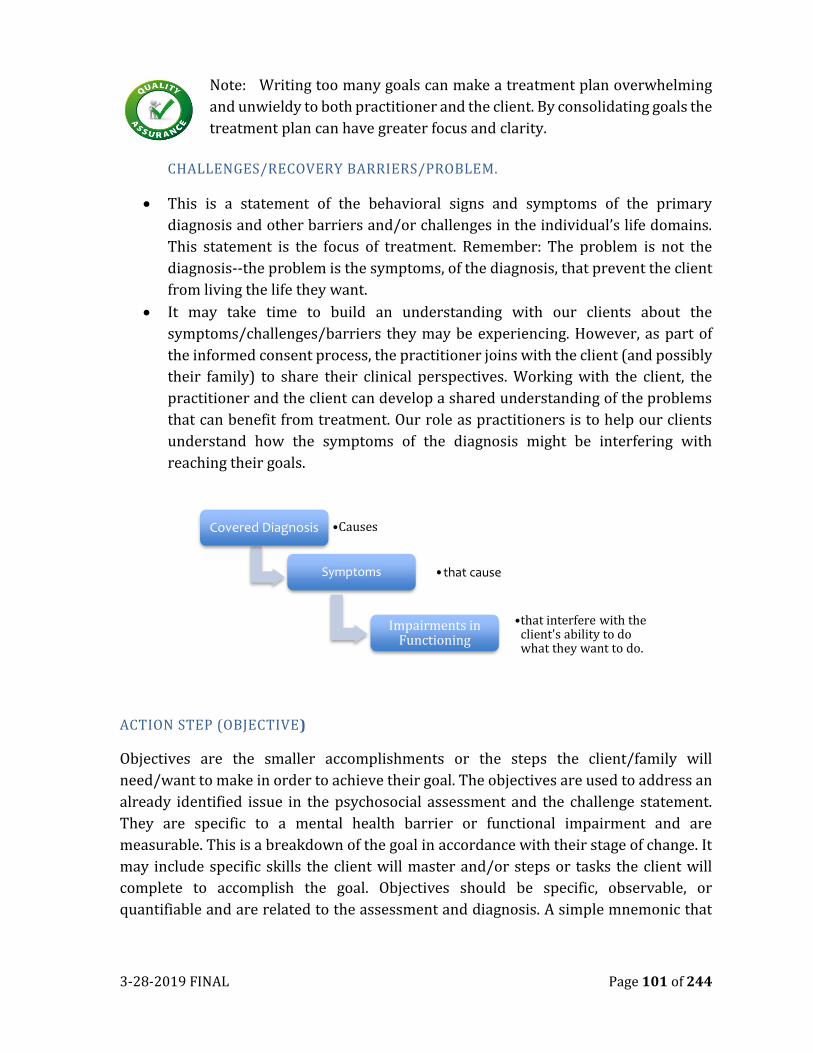
3-28-2019 FINAL Page 101 of 244
Note: Writing too many goals can make a treatment plan overwhelming
and unwieldy to both practitioner and the client. By consolidating goals the
treatment plan can have greater focus and clarity.
CHALLENGES/RECOVERY BARRIERS/PROBLEM.
• This is a statement of the behavioral signs and symptoms of the primary
diagnosis and other barriers and/or challenges in the individual’s life domains.
This statement is the focus of treatment. Remember: The problem is not the
diagnosis--the problem is the symptoms, of the diagnosis, that prevent the client
from living the life they want.
• It may take time to build an understanding with our clients about the
symptoms/challenges/barriers they may be experiencing. However, as part of
the informed consent process, the practitioner joins with the client (and possibly
their family) to share their clinical perspectives. Working with the client, the
practitioner and the client can develop a shared understanding of the problems
that can benefit from treatment. Our role as practitioners is to help our clients
understand how the symptoms of the diagnosis might be interfering with
reaching their goals.
ACTION STEP (OBJECTIVE)
Objectives are the smaller accomplishments or the steps the client/family will
need/want to make in order to achieve their goal. The objectives are used to address an
already identified issue in the psychosocial assessment and the challenge statement.
They are specific to a mental health barrier or functional impairment and are
measurable. This is a breakdown of the goal in accordance with their stage of change. It
may include specific skills the client will master and/or steps or tasks the client will
complete to accomplish the goal. Objectives should be specific, observable, or
quantifiable and are related to the assessment and diagnosis. A simple mnemonic that
Covered Diagnosis •Causes
Symptoms •that cause
Impairments in Functioning
•that interfere with the client's ability to do what they want to do.
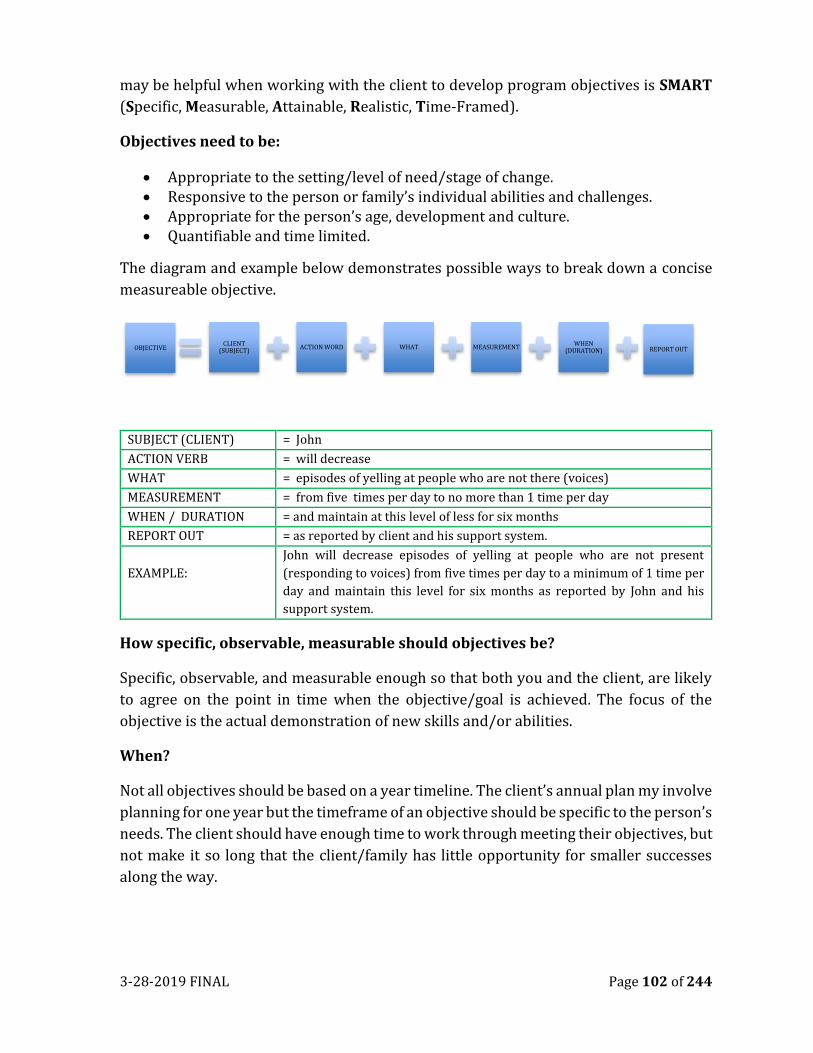
3-28-2019 FINAL Page 102 of 244
may be helpful when working with the client to develop program objectives is SMART
(Specific, Measurable, Attainable, Realistic, Time-Framed).
Objectives need to be:
• Appropriate to the setting/level of need/stage of change. • Responsive to the person or family’s individual abilities and challenges. • Appropriate for the person’s age, development and culture. • Quantifiable and time limited.
The diagram and example below demonstrates possible ways to break down a concise
measureable objective.
SUBJECT (CLIENT) = John
ACTION VERB = will decrease
WHAT = episodes of yelling at people who are not there (voices)
MEASUREMENT = from five times per day to no more than 1 time per day
WHEN / DURATION = and maintain at this level of less for six months
REPORT OUT = as reported by client and his support system.
EXAMPLE:
John will decrease episodes of yelling at people who are not present
(responding to voices) from five times per day to a minimum of 1 time per
day and maintain this level for six months as reported by John and his
support system.
How specific, observable, measurable should objectives be?
Specific, observable, and measurable enough so that both you and the client, are likely
to agree on the point in time when the objective/goal is achieved. The focus of the
objective is the actual demonstration of new skills and/or abilities.
When?
Not all objectives should be based on a year timeline. The client’s annual plan my involve
planning for one year but the timeframe of an objective should be specific to the person’s
needs. The client should have enough time to work through meeting their objectives, but
not make it so long that the client/family has little opportunity for smaller successes
along the way.
OBJECTIVECLIENT
(SUBJECT)ACTION WORD WHAT MEASUREMENT
WHEN (DURATION) REPORT OUT
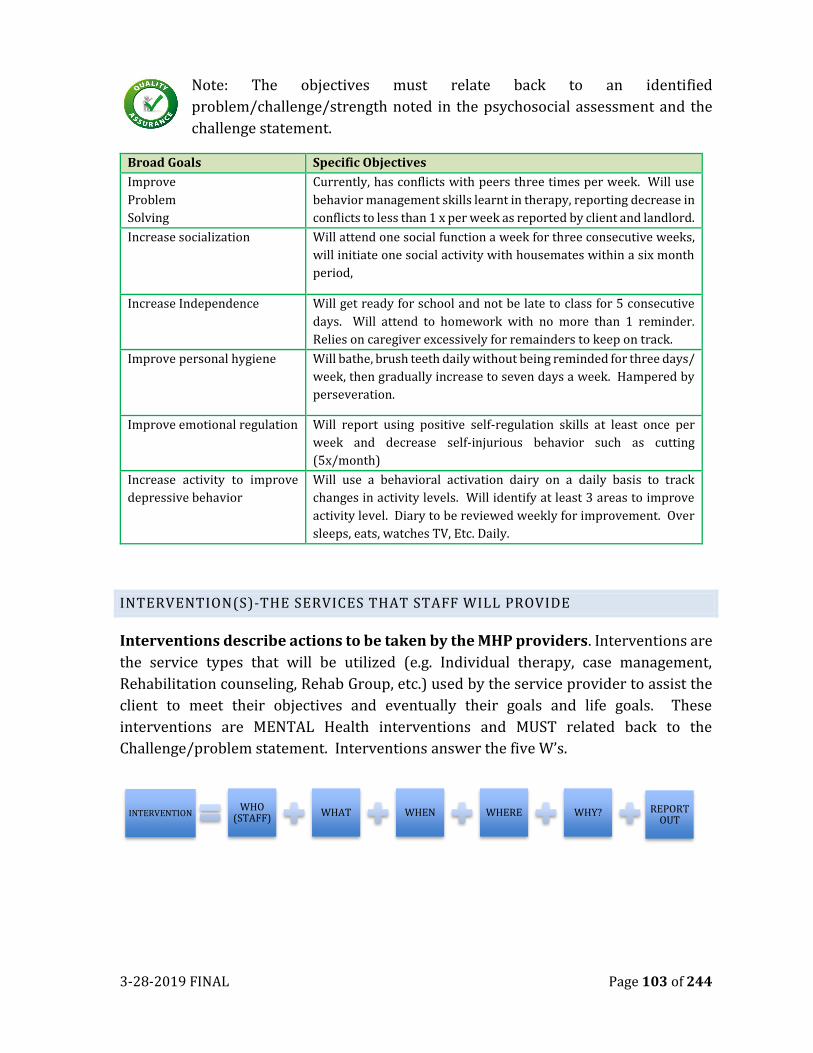
3-28-2019 FINAL Page 103 of 244
Note: The objectives must relate back to an identified
problem/challenge/strength noted in the psychosocial assessment and the
challenge statement.
Broad Goals Specific Objectives
Improve
Problem
Solving
Currently, has conflicts with peers three times per week. Will use
behavior management skills learnt in therapy, reporting decrease in
conflicts to less than 1 x per week as reported by client and landlord.
Increase socialization Will attend one social function a week for three consecutive weeks,
will initiate one social activity with housemates within a six month
period,
Increase Independence
Will get ready for school and not be late to class for 5 consecutive
days. Will attend to homework with no more than 1 reminder.
Relies on caregiver excessively for remainders to keep on track.
Improve personal hygiene Will bathe, brush teeth daily without being reminded for three days/
week, then gradually increase to seven days a week. Hampered by
perseveration.
Improve emotional regulation Will report using positive self-regulation skills at least once per
week and decrease self-injurious behavior such as cutting
(5x/month)
Increase activity to improve
depressive behavior
Will use a behavioral activation dairy on a daily basis to track
changes in activity levels. Will identify at least 3 areas to improve
activity level. Diary to be reviewed weekly for improvement. Over
sleeps, eats, watches TV, Etc. Daily.
INTERVENTION(S)-THE SERVICES THAT STAFF WILL PROVIDE
Interventions describe actions to be taken by the MHP providers. Interventions are
the service types that will be utilized (e.g. Individual therapy, case management,
Rehabilitation counseling, Rehab Group, etc.) used by the service provider to assist the
client to meet their objectives and eventually their goals and life goals. These
interventions are MENTAL Health interventions and MUST related back to the
Challenge/problem statement. Interventions answer the five W’s.
INTERVENTIONWHO
(STAFF) WHAT WHEN WHERE WHY? REPORT
OUT
3-28-2019 FINAL Page 104 of 244
THE FIVE W’S OF INTERVENTIONS
WHO = clinical discipline of practitioner (e.g. Service coordinator, clinician, MHW, MHRS)
WHAT = Modality/Service provided
WHEN = Frequency, Intensity and duration
WHERE = Location
WHY = purpose, intent, impact
Interventions should be clearly expressed for planned services such as “bi-weekly
individuals CBT therapy for 60 minutes to improve reality testing “or “weekly individual
rehabilitation counseling for 45 minutes focusing on interpersonal sill building or
“biweekly case management for 30 minutes to evaluate progress in treatment program.”
Every planned intervention including Case Management must be listed on the
treatment plan of the service WILL Be Disallowed. An intervention added during the
course of treatment must be written and dated on the plan with a appropriate signatures
as an updated or addendum.
The interventions are why we receive reimbursement from Medi-Cal. All proposed
interventions must meet the medical necessity criteria-meaning the “proposed
interventions will benefit the client by significantly diminishing the impairment, or
preventing significant deterioration in an important area of life functioning; and/or for
children, it is probable the child will be enabled to progress developmentally as
individually appropriate; or if covered by EPSDT, the identified condition can be
corrected or ameliorated.” Additionally, interventions define the concrete
strategies/actions that will be utilized to assist the client/family in meeting the
objectives.
Keep in mind that you can have multiple interventions (different service
types) for the same problem/goal/objective cluster. Service types often
include: medication services, group counseling, individual counseling, case
management, and for the full service partnership clients, intensive case
management. Each intervention needs to be specific and non-duplicative.
Duration of Intervention: Usually this will be 12 months but may also be 3, 6, or 9
months if appropriate. When writing the duration, consider matching this to the
frequency (i.e. reduce episodes from anger outburst from 3 x per day to 1 x per week
and maintain at this level or lower for 52 weeks). The table on the following page
provide examples of unacceptable and acceptable documented interventions as well as
the “why”.
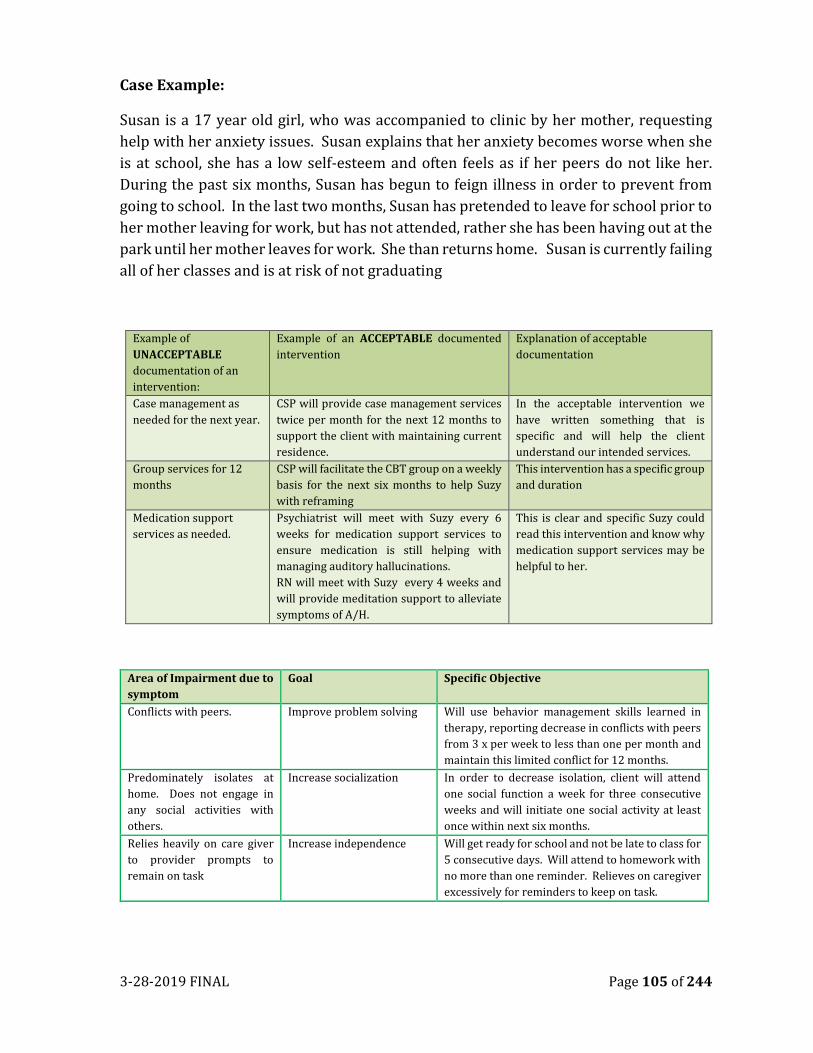
3-28-2019 FINAL Page 105 of 244
Case Example:
Susan is a 17 year old girl, who was accompanied to clinic by her mother, requesting
help with her anxiety issues. Susan explains that her anxiety becomes worse when she
is at school, she has a low self-esteem and often feels as if her peers do not like her.
During the past six months, Susan has begun to feign illness in order to prevent from
going to school. In the last two months, Susan has pretended to leave for school prior to
her mother leaving for work, but has not attended, rather she has been having out at the
park until her mother leaves for work. She than returns home. Susan is currently failing
all of her classes and is at risk of not graduating
Example of
UNACCEPTABLE
documentation of an
intervention:
Example of an ACCEPTABLE documented
intervention
Explanation of acceptable
documentation
Case management as
needed for the next year.
CSP will provide case management services
twice per month for the next 12 months to
support the client with maintaining current
residence.
In the acceptable intervention we
have written something that is
specific and will help the client
understand our intended services.
Group services for 12
months
CSP will facilitate the CBT group on a weekly
basis for the next six months to help Suzy
with reframing
This intervention has a specific group
and duration
Medication support
services as needed.
Psychiatrist will meet with Suzy every 6
weeks for medication support services to
ensure medication is still helping with
managing auditory hallucinations.
RN will meet with Suzy every 4 weeks and
will provide meditation support to alleviate
symptoms of A/H.
This is clear and specific Suzy could
read this intervention and know why
medication support services may be
helpful to her.
Area of Impairment due to
symptom
Goal Specific Objective
Conflicts with peers. Improve problem solving Will use behavior management skills learned in
therapy, reporting decrease in conflicts with peers
from 3 x per week to less than one per month and
maintain this limited conflict for 12 months.
Predominately isolates at
home. Does not engage in
any social activities with
others.
Increase socialization In order to decrease isolation, client will attend
one social function a week for three consecutive
weeks and will initiate one social activity at least
once within next six months.
Relies heavily on care giver
to provider prompts to
remain on task
Increase independence Will get ready for school and not be late to class for
5 consecutive days. Will attend to homework with
no more than one reminder. Relieves on caregiver
excessively for reminders to keep on task.
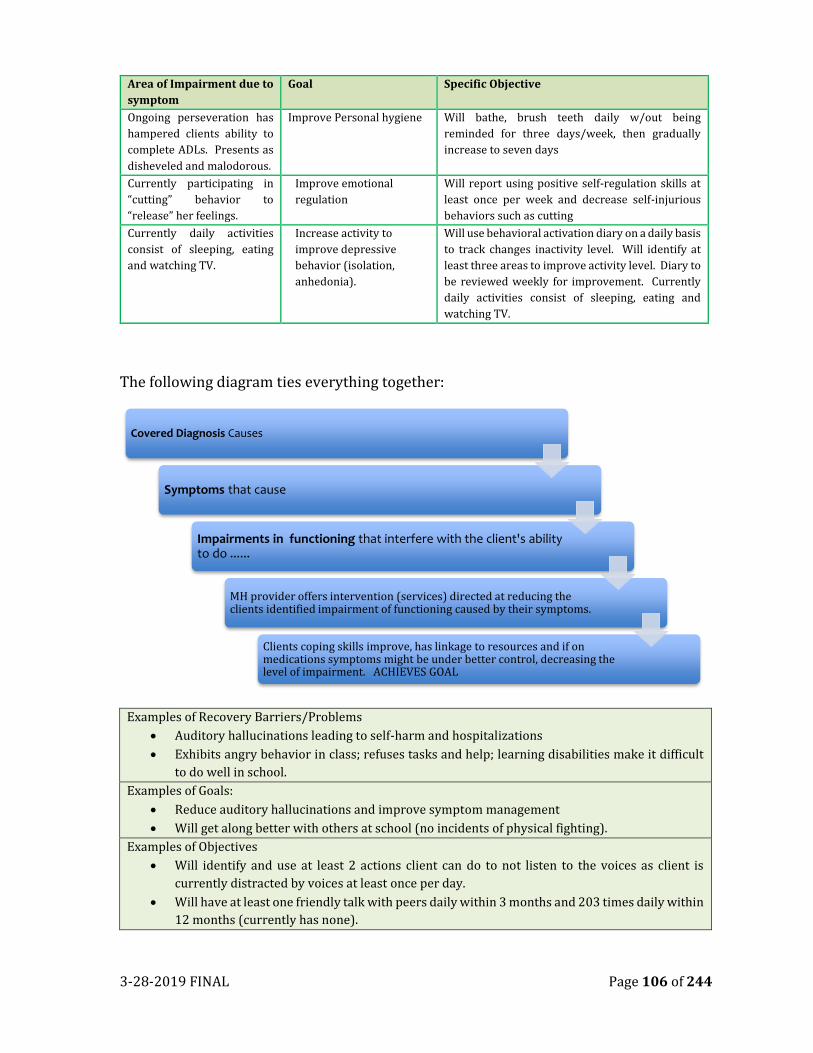
3-28-2019 FINAL Page 106 of 244
Area of Impairment due to
symptom
Goal Specific Objective
Ongoing perseveration has
hampered clients ability to
complete ADLs. Presents as
disheveled and malodorous.
Improve Personal hygiene Will bathe, brush teeth daily w/out being
reminded for three days/week, then gradually
increase to seven days
Currently participating in
“cutting” behavior to
“release” her feelings.
Improve emotional
regulation
Will report using positive self-regulation skills at
least once per week and decrease self-injurious
behaviors such as cutting
Currently daily activities
consist of sleeping, eating
and watching TV.
Increase activity to
improve depressive
behavior (isolation,
anhedonia).
Will use behavioral activation diary on a daily basis
to track changes inactivity level. Will identify at
least three areas to improve activity level. Diary to
be reviewed weekly for improvement. Currently
daily activities consist of sleeping, eating and
watching TV.
The following diagram ties everything together:
Examples of Recovery Barriers/Problems
• Auditory hallucinations leading to self-harm and hospitalizations
• Exhibits angry behavior in class; refuses tasks and help; learning disabilities make it difficult
to do well in school.
Examples of Goals:
• Reduce auditory hallucinations and improve symptom management
• Will get along better with others at school (no incidents of physical fighting).
Examples of Objectives
• Will identify and use at least 2 actions client can do to not listen to the voices as client is
currently distracted by voices at least once per day.
• Will have at least one friendly talk with peers daily within 3 months and 203 times daily within
12 months (currently has none).
Covered Diagnosis Causes
Symptoms that cause
Impairments in functioning that interfere with the client's ability to do ......
MH provider offers intervention (services) directed at reducing the clients identified impairment of functioning caused by their symptoms.
Clients coping skills improve, has linkage to resources and if on medications symptoms might be under better control, decreasing the level of impairment. ACHIEVES GOAL
3-28-2019 FINAL Page 107 of 244
Examples of Interventions:
• Rehabilitation counseling to support ADL’s weekly for 45 minutes
• Case management services monthly for 30 minutes to monitor progress toward treatment
progress
• Individual therapy using CBT 1x week for 40minutes to decrease paranoia.
• Individual with Family using Brief Strategic Therapy bi-weekly for 50 minutes
TREATMENT PLAN TIMELINES
Unified Service Plans/Treatment plans drive services. In exceptional circumstances, if a
service (other than Assessment, Crisis Intervention, and/or Plan Development) is
provided during the intake period, before completion of the USP, it must be documented
to demonstrate the Medical Necessity for that service. That is: 1) the Diagnosis Sheet,
must include, a covered diagnosis (even if provisional), and the gathered assessment
information, to date, should be sufficient to support that Diagnosis; 2) the impairments
must be adequately described (in the progress note), and be significant, to justify the
service before intake completion; 3) the planned intervention will address the
impairment condition (documented in the progress note); and 4) the client had input
into the provision of the intervention and was in agreement with its provision
(documented in the progress note).
BEST PRACTICE: Good clinical practice includes completion of assessment and client
planning as soon as possible, so service providers are urged to write complete unified
service plans/tx plans as soon as possible. The USP/Tx plan must be reviewed and
updated every six months for children/youth, and annually for adults. It is an
expectation that the USP/Tx plan will also be updated when events that are “clinically
significant” occur.
As clients achieves their particular goals or is no longer interested in working on a
particular goal, it is the responsibility of each program to close out the program’s
treatment goals by entering the date the goal was closed and/or completed on the
treatment plan.
The completion of the Treatment Plan is subject to the specific deadlines and signature
requirements as described below:
INITIAL USP/TREATMENT PLAN
An initial treatment plan can occur in tow primary instances: New to services or
Transferring to a new program.
3-28-2019 FINAL Page 108 of 244
1. New to Services: The initial Treatment plan shall be completed within 60 days of the clients entry to a program. This deadline applies to clients who are New to the MHP or are re-entering services after being previously discharged.
2. Transfer: For existing clients who enter a new program or if the client transfers to a different program, the plan if still appropriate can be “pulled forward” and utilized in the new service program. When pulling a document forward, the person pulling it forward will attest that they have pulled it forward and not made any changes. In order to bill for services in a new service program, each client must have a valid treatment plan within the treatment goal/
RENEWALS
Each Treatment Plan can be authorized for up to six months for CSOC and one year for
ASOC, however, many clients achieve goals prior to a year, and plans shall be updated
prior to a year based on goal achievement. Additionally, treatment plans must be
updated whenever clinically indicated, such as following a significant life event that
potentially changes the client’s mental status, diagnosis or treatment direction or any
other major life stressors.
Updated- used when the existing treatment plan continues to meet the client’s needs,
and only a minor revision to reflect new goals or interventions is necessary, or when a
client is transferred to another program/service provider. Choosing Update does not
change the treatment plan anniversary date. Additionally, if the treatment plan
anniversary date passes and the treatment plan was not renewed, the option to revise
will no longer be available.
CLIENT PARTICIPATION AND SIGNATURES ON TREATMENT PLANS:
Best practices support coordinators to seek the client’s signatures on treatment plans. The client
and/or parent/guardian are expected to sign the plan. The Public Guardian’s signature is
required for all LPS Conserved Clients. Other types of Conservators are required to sign
treatment plans as well. However, regulations allow for periods when the client does not sign
the treatment plan, and only requires that the MHP document the client’s participation in the
development of their treatment plan (and their agreement). At a minimum, client participation
is documented by obtaining either a client signature or documenting the reason why the client
signature was not obtained.
A client’s participation and agreement to treatment plan can be demonstrated through the
following ways:
1. Signature on treatment plan
2. Through documenting participation and agreement in non-signature explanation
area.
3.
3-28-2019 FINAL Page 109 of 244
MINOR (17 AND UNDER) AND CONSERVED CLIENTS:
If the client is a minor or conserved under LPS, a parent or legally responsible person must sign
the USP/Treatment Plan on behalf of the client. Checking the box that a client or legally
responsible person has signed the plan should be used only when the signature has been
obtained and not when the plan is to obtain the signature.
The parent or legally responsible person’s signature must be obtained prior to delivering
ongoing services for all minors and for all LPS Conservatees (except minor consent services). If
the parent or legally responsible person participates in the development of the USP/Treatment
plan, document agreement and participation, and then ask he/she to sign the USP/treatment
plan. Document attempts to obtain signature. Do NOT finalized the USP/Treatment plan until
an electronic or hard copy signature is obtained.
DHCS MHSUDS Information Notice #17-040 excerpt:
Each time a beneficiary’s signature or the signature of the beneficiary’s legal
representative is required on a client plan or an updated client plan “and the
beneficiary refuses or is unavailable for signature, the client plan (or updated
plan) shall include a written explanation of the refusal or unavailability”. The
written explanation may be on the plan itself or within the progress note.
Although not required, it is best practice to made additional attempts to obtain
the beneficiary’s signature and document the attempts in the client record. (MHP
Contract: Cal. Code Regulations, Title9, §1810.440 (c)(2)(B)).
EXAMPLES OF TREATMENT PLANNING DOCUMENTATION WHEN CLIENT DID NOT
SIGN PLAN.
1. Writer called client to discuss progress toward treatment goals. Client
acknowledged that he made some progress toward the goal to reduce responding
to internal stimuli and would like to continue to work on this goal. John agrees
to modify goal to: Reduce episodes of outward responding to internal stimuli for
2 x per day to 1 x per day and maintain for 365 days.
2. Writer spoke to client and reviewed progress toward treatment goals. Client
agreed to modify goals as indicated on treatment plans. Writer and client will
monitor progress toward achieving these goals throughout the year and modify
as needed.
3. Writer met with client at clinic and reviewed treatment goals. Discussed progress
toward goals and made decision to modify goals for upcoming year. Client unable
to sign as he had to leave to catch bus. Writer and client will continue to monitor
progress toward achieving the new goals and update or modify as needed.
4. Client verbally accepts services but declines to sign due to X. (document a specific
and valid explanation for this choice.

3-28-2019 FINAL Page 110 of 244
Remember: To not only document the reason on the treatment plan but
also within the plan development note!
OFFERING COPY OF TREATMENT PLAN:
Remember to offer/provide the client/parent/guardian a copy of the plan. Giving a copy
of the plan to the client/family member is an important acknowledgment of their
participation in its development and of the practitioner’s commitment to involving our
clients. Remember, treatment plans must be co-created and whenever possible written
in English followed by the client/family’s primary/preferred language in order to
encourage goal attainment.
STAFF APPROVAL-LICENSED/NON LICENSED STAFF SIGNING TREATMENT PLANS:
If the staff developing the treatment plan is not an approved staff (LPHA) the staff
member must forward the USP/treatment plan to an LPHA who will review, and
approve USP/Treatment plan thus authorizing services. This is demonstrated by the
LPHA signature and date of signature on the USP/Treatment plan. LPHAs include:
Licensed physician, Registered Nurse Practitioner, Licensed/ Waived clinical
psychologist, Licensed/Registered Clinical Social worker, Licensed//Registered
Marriage and Family Therapist, and Licensed/Registered Professional Clinical
Counselor
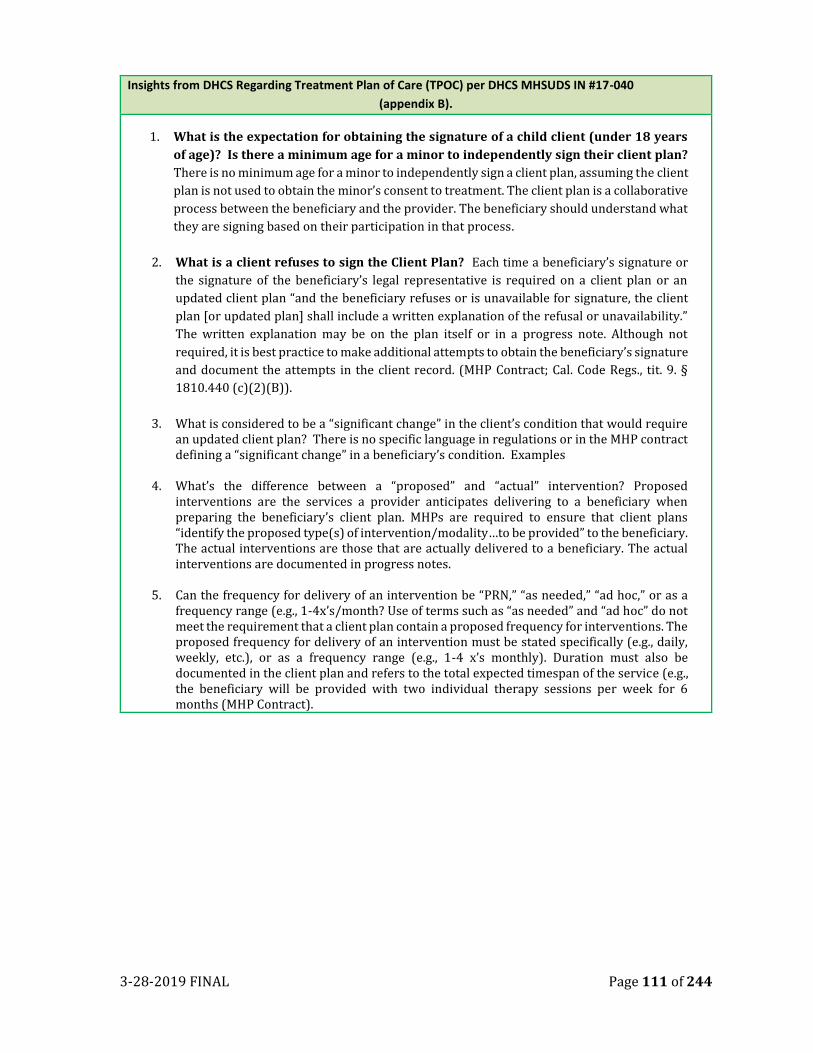
3-28-2019 FINAL Page 111 of 244
Insights from DHCS Regarding Treatment Plan of Care (TPOC) per DHCS MHSUDS IN #17-040
(appendix B).
1. What is the expectation for obtaining the signature of a child client (under 18 years
of age)? Is there a minimum age for a minor to independently sign their client plan?
There is no minimum age for a minor to independently sign a client plan, assuming the client
plan is not used to obtain the minor’s consent to treatment. The client plan is a collaborative
process between the beneficiary and the provider. The beneficiary should understand what
they are signing based on their participation in that process.
2. What is a client refuses to sign the Client Plan? Each time a beneficiary’s signature or
the signature of the beneficiary’s legal representative is required on a client plan or an
updated client plan “and the beneficiary refuses or is unavailable for signature, the client
plan [or updated plan] shall include a written explanation of the refusal or unavailability.”
The written explanation may be on the plan itself or in a progress note. Although not
required, it is best practice to make additional attempts to obtain the beneficiary’s signature
and document the attempts in the client record. (MHP Contract; Cal. Code Regs., tit. 9. §
1810.440 (c)(2)(B)).
3. What is considered to be a “significant change” in the client’s condition that would require an updated client plan? There is no specific language in regulations or in the MHP contract defining a “significant change” in a beneficiary’s condition. Examples
4. What’s the difference between a “proposed” and “actual” intervention? Proposed interventions are the services a provider anticipates delivering to a beneficiary when preparing the beneficiary’s client plan. MHPs are required to ensure that client plans “identify the proposed type(s) of intervention/modality…to be provided” to the beneficiary. The actual interventions are those that are actually delivered to a beneficiary. The actual interventions are documented in progress notes.
5. Can the frequency for delivery of an intervention be “PRN,” “as needed,” “ad hoc,” or as a frequency range (e.g., 1-4x’s/month? Use of terms such as “as needed” and “ad hoc” do not meet the requirement that a client plan contain a proposed frequency for interventions. The proposed frequency for delivery of an intervention must be stated specifically (e.g., daily, weekly, etc.), or as a frequency range (e.g., 1-4 x’s monthly). Duration must also be documented in the client plan and refers to the total expected timespan of the service (e.g., the beneficiary will be provided with two individual therapy sessions per week for 6 months (MHP Contract).
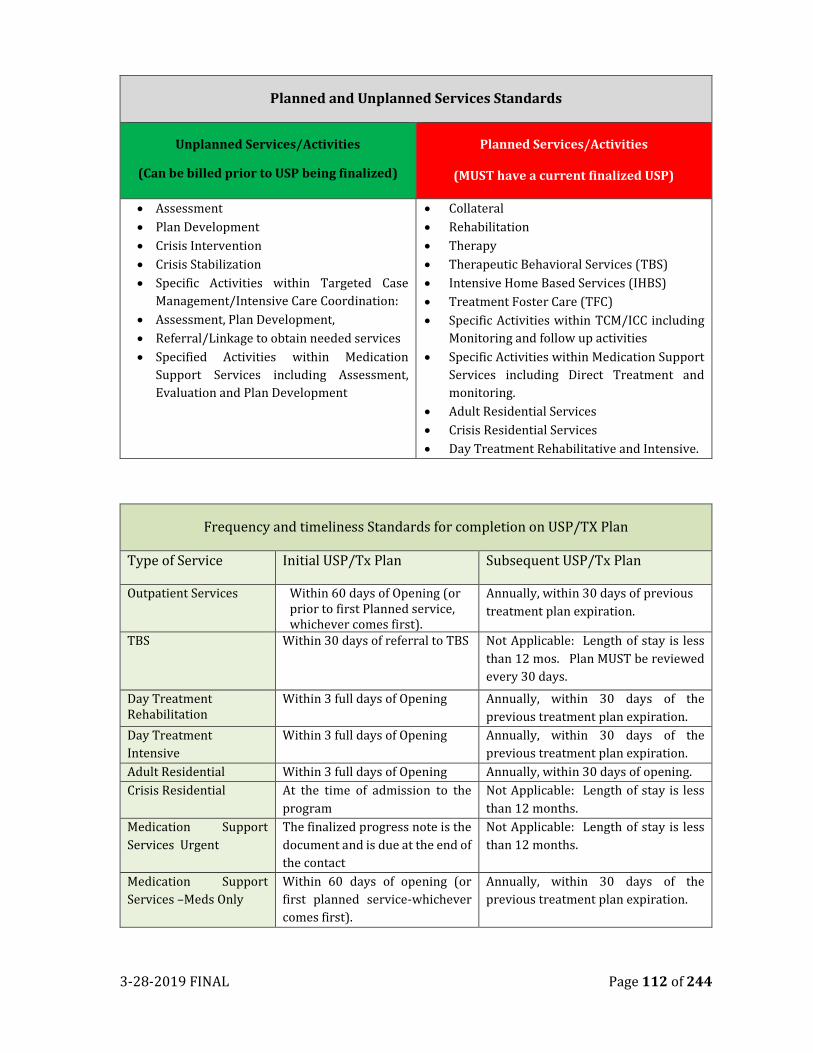
3-28-2019 FINAL Page 112 of 244
Planned and Unplanned Services Standards
Unplanned Services/Activities
(Can be billed prior to USP being finalized)
Planned Services/Activities
(MUST have a current finalized USP)
• Assessment
• Plan Development
• Crisis Intervention
• Crisis Stabilization
• Specific Activities within Targeted Case
Management/Intensive Care Coordination:
• Assessment, Plan Development,
• Referral/Linkage to obtain needed services
• Specified Activities within Medication
Support Services including Assessment,
Evaluation and Plan Development
• Collateral
• Rehabilitation
• Therapy
• Therapeutic Behavioral Services (TBS)
• Intensive Home Based Services (IHBS)
• Treatment Foster Care (TFC)
• Specific Activities within TCM/ICC including
Monitoring and follow up activities
• Specific Activities within Medication Support
Services including Direct Treatment and
monitoring.
• Adult Residential Services
• Crisis Residential Services
• Day Treatment Rehabilitative and Intensive.
Frequency and timeliness Standards for completion on USP/TX Plan
Type of Service Initial USP/Tx Plan Subsequent USP/Tx Plan
Outpatient Services Within 60 days of Opening (or prior to first Planned service, whichever comes first).
Annually, within 30 days of previous
treatment plan expiration.
TBS Within 30 days of referral to TBS Not Applicable: Length of stay is less
than 12 mos. Plan MUST be reviewed
every 30 days.
Day Treatment Rehabilitation
Within 3 full days of Opening Annually, within 30 days of the
previous treatment plan expiration.
Day Treatment
Intensive
Within 3 full days of Opening Annually, within 30 days of the
previous treatment plan expiration.
Adult Residential Within 3 full days of Opening Annually, within 30 days of opening.
Crisis Residential At the time of admission to the
program
Not Applicable: Length of stay is less
than 12 months.
Medication Support
Services Urgent
The finalized progress note is the
document and is due at the end of
the contact
Not Applicable: Length of stay is less
than 12 months.
Medication Support
Services –Meds Only
Within 60 days of opening (or
first planned service-whichever
comes first).
Annually, within 30 days of the
previous treatment plan expiration.
3-28-2019 FINAL Page 113 of 244
• Without developing client friendly treatment plans, research shows we fail to retain
consumers who feel they have not developed a shared vision of success with their
practitioner (Shared Decision Making in Public Mental Health Care: Perspectives from
Consumers Living with Severe Mental Illness. Psychiatric Rehabilitation Journal Issue Volume
34, Number 1/Summer 2010).
Goals: (at least two) –The removal of reduction of the Problem:
Goals address the problem. The goals include the development of new skills/behaviors and the
reduction, stabilization or removal of the barrier or problem. Individual goals address the barriers
that prevent clients from reaching overall goals. Individual goals should be related to important
areas of functioning affected by the client’s mental health condition, such as living situation, daily
activities, school, work, social support, legal issues, safety, physical health, substance abuse, and
psychiatric symptoms. Goals MUST be related to the assessment, diagnosis, and formulation.
Objectives (at least two)-What the client will do
This is a breakdown of the goals. It may include specific skills client will master and /or steps or
tasks the client will complete to accomplish the goals. Objectives should be specific observable,
quantifiable with baselines and are related to the assessment and diagnosis. A simply mnemonic that
may be helpful when working with the clients to develop program objectives is SMART (Simple,
Measureable, Accurate, Realistic and Time-bound).
Example: Client will (ACTION VERB-reduce/Increase/maintain) (WHAT-symptom of Mental
Illness) from (current level) times per (day, week, month) to (desired level) times per
(day, week, month) for duration (365 days, 52 weeks, 12 months) as evidenced by (REPORT OUT-
self report, collateral report, treatment team report).
Interventions: (The Service the Staff will provide).
These are ALL of the service types that will utilized (e.g. individual therapy, case management
rehabilitation,). Interventions describe the actions to be taken by the MHP providers to assist the
client in achieving their goals. These are NOT interactions taken by the client.
Frequency: How often will each individual Intervention (service) will be provided
Duration Of Intervention: Usually this will be 12 months but may be 3, 6, or 9 months if appropriate. Should
be correspond to frequency. If frequency is weekly than duration will be for X number of weeks.
3-28-2019 FINAL Page 114 of 244
CHAPTER NINE
SPECIALTY MENTAL HEALTH SERVICES
Services provided by the MHP are designed to improve behavioral health outcomes for
clients and families with mental illness and/or co-occurring disorders. These services
are based on the needs, strengths and choices of the individual client/family and involve
clients and families in planning and implementing treatment. Services are based on the
client’s/family’s recovery goals concerning his/her own life, functional impairment(s),
symptoms, disabilities, strengths, life conditions, cultural background, spirituality and
rehabilitation readiness. Services are focused on achieving specific objectives to support
the individual in accomplishing his/her desired goals.
Mental Health Services are those individual, group, or family therapies and
interventions that are designed to reduce mental health conditions and/or facilitate
improvement or maintenance of functioning consistent with the goals of learning,
development, independent living and enhanced self-sufficiency. Services are directed
toward achieving the client/family’s goals and must be consistent with the current
Client Treatment Plan.
Specialty Mental Health Services may be provided face-to-face or by telephone with the
client, their family, or significant support persons and anywhere in the community
(Source: 9 CCR §1840.324). There are seven (7) categories of Specialty Mental Health
Services (SMHS)). Outpatient (non-hospital) providers generally use three of those
categories: Rehabilitative Mental Health Services, Targeted Case Management, and
EPSDT Supplemental SMHC (CCR, Title 9, Section 1810.217).
1. Rehabilitative Mental Health Services includes the following
a. Mental Health Services
i. Assessment
ii. Plan Development
iii. Collateral
iv. Rehabilitation*
v. Therapy
b. Medication Support Services
c. Day Treatment Intensive
d. Day Treatment Rehabilitation
e. Crisis Intervention
f. Crisis Stabilization
g. Adult Residential Treatment Services
h. Crisis Residential Treatment Services
3-28-2019 FINAL Page 115 of 244
2. Psychiatric Inpatient Hospital Services
3. Targeted Case Management
4. Psychiatrist/Provider Medication Support Services
5. Psychologist Services
6. EPSDT Supplemental SMHS
a. Therapeutic Behavioral Services (TBS)
b. Intensive Care Coordination (ICC)
c. Intensive Home Based Services (IHBS)
d. Therapeutic Foster Care (TFC)
REHABILITATIVE MENTAL HEALTH SERVICES
Rehabilitative Mental Health Services are services recommended by a physician or other LPHA within the scope of their practice under state law both to reduce mental disorders and emotional disturbances, and to restore, improve, and/or maintain a client’s level of functioning.”
CCR, Title 9,
Section
1810.227
“Mental Health Services” means individual or group therapies and interventions that
are designed to provide reduction of mental disability and restoration, improvement
or maintenance of functioning consistent with the goals of learning, development,
independent living and enhanced self-sufficiency and that are not provided as a
component of adult residential services, crisis residential treatment services, crisis
intervention, crisis stabilization, day rehabilitation, or day treatment intensive.
Service activities may include but are not limited to assessment, plan development,
therapy, rehabilitation and collateral.
California
State Plan
Amendment
(SPA) 12-025
“Mental Health Services” are individual, group or family-based interventions that are
designed to provide reduction of the beneficiary' s mental or emotional disability,
restoration, improvement and/or preservation of individual and community
functioning, and continued ability to remain in the community consistent with the
goals of recovery, resiliency, learning, development, independent living and
enhanced self-sufficiency and that are not provided as a component of adult
residential services, crisis residential treatment services, crisis intervention, crisis
stabilization, day rehabilitation, or day treatment intensive.
Mental health services may be provided face-to-face, by telephone or by telemedicine
with the beneficiary or significant support person(s) and may be provided anywhere
in the community.
This service includes one or more of the following service components: (1)
Assessment; (2) Plan Development; (3) Therapy; (4) Rehabilitation; and (5)
Collateral.
Mental Health Services may be provided face-to-face or by telephone with the client,
their family, or significant support persons and anywhere in the community (Source: 9
CCR §1840.324).
3-28-2019 FINAL Page 116 of 244
ASSESSMENT
Assessment services must be provided within a clinician’s scope of practice—see the Service
and Staff Billing Privilege Matrix to identify the types of credentialed staff who may provide
assessment services.
CCR, Title 9,
Section
1810.204
“Assessment” means a service activity designed to evaluate the current status of a
beneficiary’s mental, emotional, or behavioral health. Assessment includes but is not
limited to one or more of the following: mental status determination, analysis of the
beneficiary’s clinical history; analysis of relevant cultural issues and history;
diagnosis; and the use of testing procedures.
State Plan
Amendment
(SPA) 12-025
"Assessment" means a service activity designed to evaluate the current status of a
beneficiary's mental, emotional, or behavioral health. Assessment includes one or
more of the following: mental status determination, analysis of the beneficiary's
clinical history, analysis of relevant biopsychosocial and cultural issues and history,
diagnosis, and the use of testing procedures.
PLAN DEVELOPMENT
Plan Development services must be provided within a clinician’s scope of practice—see the Service and Staff Billing Privilege Matrix to identify the types of credentialed staff who may provide plan development services.
CCR, Title 9,
Section
1810.232
“Plan Development” means a service activity that consists of development of client
plans, approval of client plans, and/or monitoring of a beneficiary’s progress.
State Plan
Amendment
(SPA) 12-025
"Plan Development" means a service activity that consists of one or more of the
following: development of client plans, approval of client plans and/or monitoring of
a beneficiary's progress.
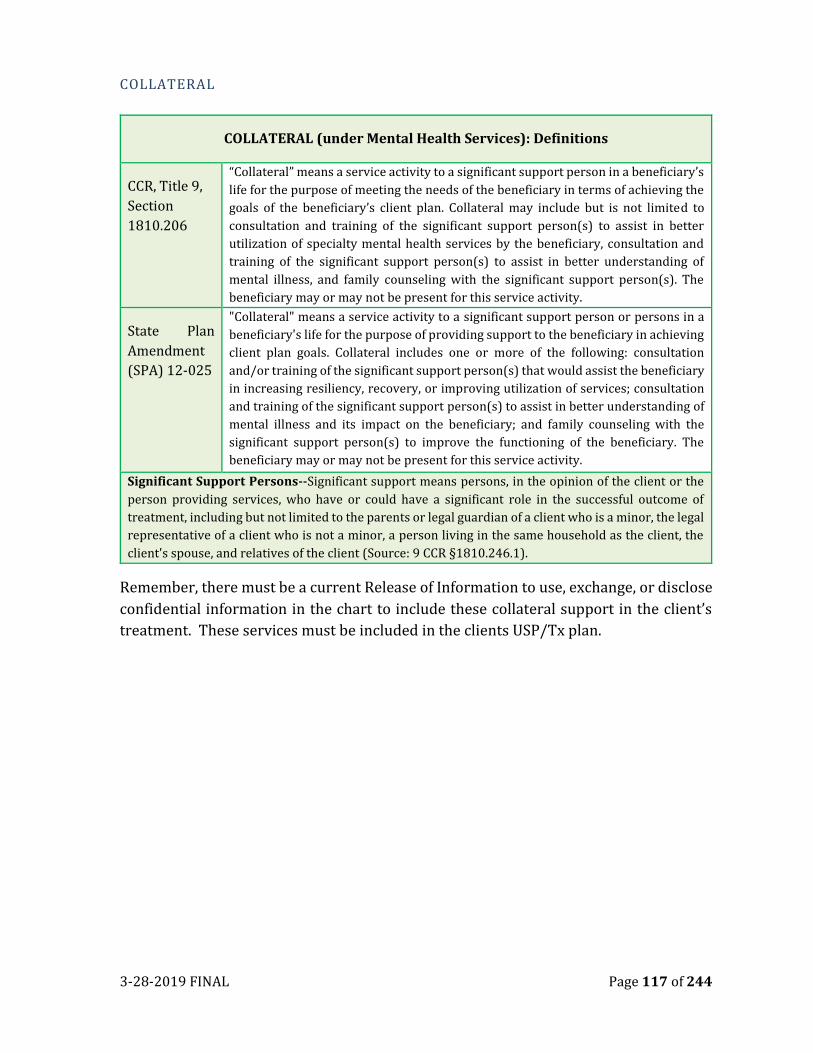
3-28-2019 FINAL Page 117 of 244
COLLATERAL
COLLATERAL (under Mental Health Services): Definitions
CCR, Title 9,
Section
1810.206
“Collateral” means a service activity to a significant support person in a beneficiary’s
life for the purpose of meeting the needs of the beneficiary in terms of achieving the
goals of the beneficiary’s client plan. Collateral may include but is not limited to
consultation and training of the significant support person(s) to assist in better
utilization of specialty mental health services by the beneficiary, consultation and
training of the significant support person(s) to assist in better understanding of
mental illness, and family counseling with the significant support person(s). The
beneficiary may or may not be present for this service activity.
State Plan
Amendment
(SPA) 12-025
"Collateral" means a service activity to a significant support person or persons in a
beneficiary's life for the purpose of providing support to the beneficiary in achieving
client plan goals. Collateral includes one or more of the following: consultation
and/or training of the significant support person(s) that would assist the beneficiary
in increasing resiliency, recovery, or improving utilization of services; consultation
and training of the significant support person(s) to assist in better understanding of
mental illness and its impact on the beneficiary; and family counseling with the
significant support person(s) to improve the functioning of the beneficiary. The
beneficiary may or may not be present for this service activity.
Significant Support Persons--Significant support means persons, in the opinion of the client or the
person providing services, who have or could have a significant role in the successful outcome of
treatment, including but not limited to the parents or legal guardian of a client who is a minor, the legal
representative of a client who is not a minor, a person living in the same household as the client, the
client's spouse, and relatives of the client (Source: 9 CCR §1810.246.1).
Remember, there must be a current Release of Information to use, exchange, or disclose
confidential information in the chart to include these collateral support in the client’s
treatment. These services must be included in the clients USP/Tx plan.
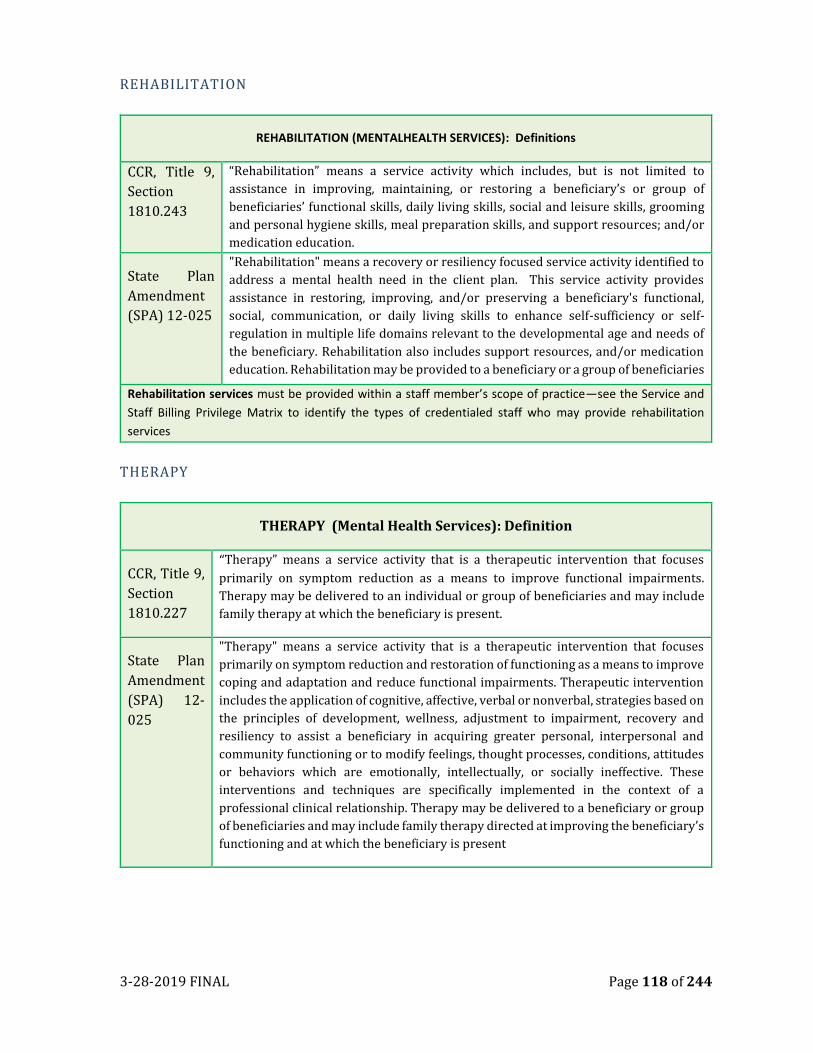
3-28-2019 FINAL Page 118 of 244
REHABILITATION
REHABILITATION (MENTALHEALTH SERVICES): Definitions
CCR, Title 9,
Section
1810.243
“Rehabilitation” means a service activity which includes, but is not limited to
assistance in improving, maintaining, or restoring a beneficiary’s or group of
beneficiaries’ functional skills, daily living skills, social and leisure skills, grooming
and personal hygiene skills, meal preparation skills, and support resources; and/or
medication education.
State Plan
Amendment
(SPA) 12-025
"Rehabilitation" means a recovery or resiliency focused service activity identified to
address a mental health need in the client plan. This service activity provides
assistance in restoring, improving, and/or preserving a beneficiary's functional,
social, communication, or daily living skills to enhance self-sufficiency or self-
regulation in multiple life domains relevant to the developmental age and needs of
the beneficiary. Rehabilitation also includes support resources, and/or medication
education. Rehabilitation may be provided to a beneficiary or a group of beneficiaries
Rehabilitation services must be provided within a staff member’s scope of practice—see the Service and
Staff Billing Privilege Matrix to identify the types of credentialed staff who may provide rehabilitation
services
THERAPY
THERAPY (Mental Health Services): Definition
CCR, Title 9,
Section
1810.227
“Therapy” means a service activity that is a therapeutic intervention that focuses
primarily on symptom reduction as a means to improve functional impairments.
Therapy may be delivered to an individual or group of beneficiaries and may include
family therapy at which the beneficiary is present.
State Plan
Amendment
(SPA) 12-
025
"Therapy" means a service activity that is a therapeutic intervention that focuses
primarily on symptom reduction and restoration of functioning as a means to improve
coping and adaptation and reduce functional impairments. Therapeutic intervention
includes the application of cognitive, affective, verbal or nonverbal, strategies based on
the principles of development, wellness, adjustment to impairment, recovery and
resiliency to assist a beneficiary in acquiring greater personal, interpersonal and
community functioning or to modify feelings, thought processes, conditions, attitudes
or behaviors which are emotionally, intellectually, or socially ineffective. These
interventions and techniques are specifically implemented in the context of a
professional clinical relationship. Therapy may be delivered to a beneficiary or group
of beneficiaries and may include family therapy directed at improving the beneficiary’s
functioning and at which the beneficiary is present
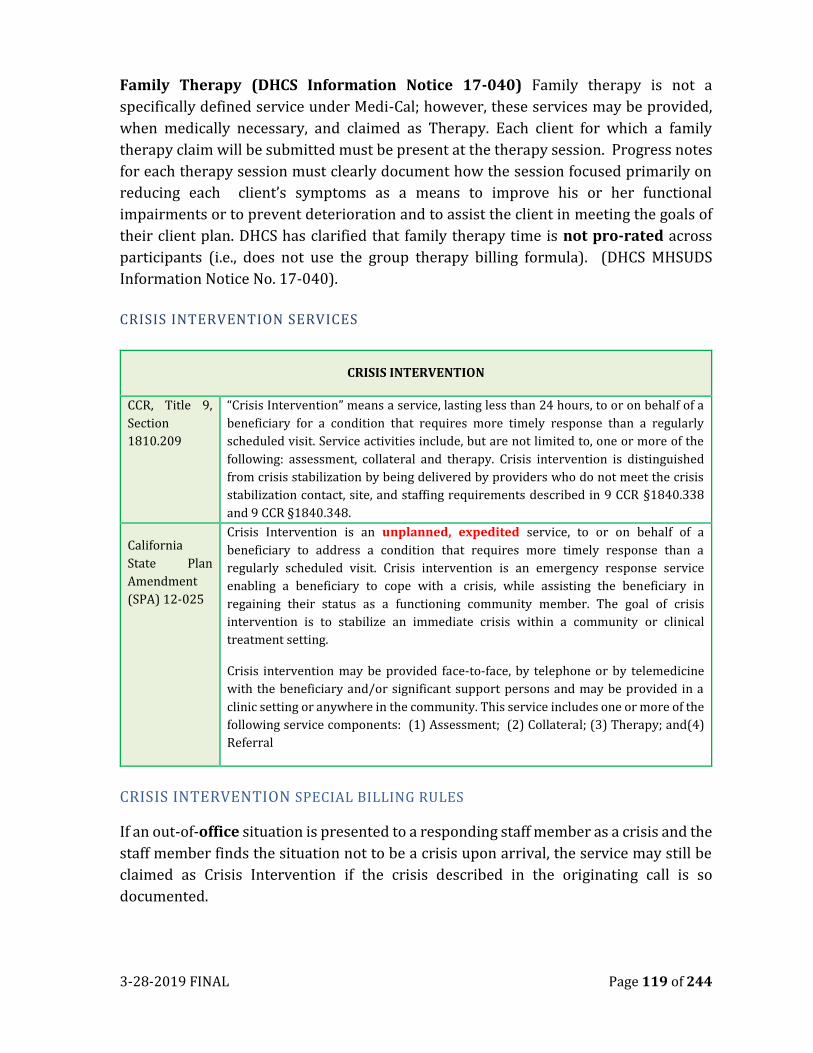
3-28-2019 FINAL Page 119 of 244
Family Therapy (DHCS Information Notice 17-040) Family therapy is not a
specifically defined service under Medi-Cal; however, these services may be provided,
when medically necessary, and claimed as Therapy. Each client for which a family
therapy claim will be submitted must be present at the therapy session. Progress notes
for each therapy session must clearly document how the session focused primarily on
reducing each client’s symptoms as a means to improve his or her functional
impairments or to prevent deterioration and to assist the client in meeting the goals of
their client plan. DHCS has clarified that family therapy time is not pro-rated across
participants (i.e., does not use the group therapy billing formula). (DHCS MHSUDS
Information Notice No. 17-040).
CRISIS INTERVENTION SERVICES
CRISIS INTERVENTION
CCR, Title 9,
Section
1810.209
“Crisis Intervention” means a service, lasting less than 24 hours, to or on behalf of a
beneficiary for a condition that requires more timely response than a regularly
scheduled visit. Service activities include, but are not limited to, one or more of the
following: assessment, collateral and therapy. Crisis intervention is distinguished
from crisis stabilization by being delivered by providers who do not meet the crisis
stabilization contact, site, and staffing requirements described in 9 CCR §1840.338
and 9 CCR §1840.348.
California
State Plan
Amendment
(SPA) 12-025
Crisis Intervention is an unplanned, expedited service, to or on behalf of a
beneficiary to address a condition that requires more timely response than a
regularly scheduled visit. Crisis intervention is an emergency response service
enabling a beneficiary to cope with a crisis, while assisting the beneficiary in
regaining their status as a functioning community member. The goal of crisis
intervention is to stabilize an immediate crisis within a community or clinical
treatment setting.
Crisis intervention may be provided face-to-face, by telephone or by telemedicine
with the beneficiary and/or significant support persons and may be provided in a
clinic setting or anywhere in the community. This service includes one or more of the
following service components: (1) Assessment; (2) Collateral; (3) Therapy; and(4)
Referral
CRISIS INTERVENTION SPECIAL BILLING RULES
If an out-of-office situation is presented to a responding staff member as a crisis and the
staff member finds the situation not to be a crisis upon arrival, the service may still be
claimed as Crisis Intervention if the crisis described in the originating call is so
documented.
3-28-2019 FINAL Page 120 of 244
CRISIS INTERVENTION SPECIAL DOCUMENTATION REQUIREMENTS & BILLING
RULES
In addition to all applicable documentation requirements in this manual, the acuity of
the client or situation which jeopardizes the client’s ability to maintain community
functioning must be clearly documented. Crisis Intervention Progress Notes describle:
The immediate emergency requirement crisis response
• Collateral information obtained (include relationship to client)
• Interventions utilized to stabilize the crisis
• Safety Plan developed (if applicable)
• The Client’s response and the outcomes
• Follow up plan and recommendations
Examples of Crisis Intervention Activities
• Client in crisis-assess mental status and current needs related to immediate crisis
• Danger to self and others-assessed/provided immediate therapeutic responses
to stabilize crisis.
• Gravely disabled client/Current danger to self –provided therapeutic responses
to stabilize crisis.
• Client was an imminent danger to self/others-was having a sever reaction to
current stressors.
Note: Crisis Intervention progress notes may not always link to the client’s treatment
plan and the provider may also provide TCM to link client to other resources once the
crisis situation has been stabilized, such as a Crisis Residential Program.
Critical Considerations when documenting Crisis Intervention and other supportive
services:
Some basic information to include in Crisis Intervention (H2011) note:
• How did the client get to the ER
• Who asked you to evaluate
• Who did you gather collateral information from (include first name, relationship and time)
• If on a hold, who did you consult with to lift hold
• If you are doing a reassessment, state why.
Documentation time:
The documentation time, should reflect the time you are writing the note. Do not put 15 minutes if you
only have three lines. You cannot bill a client because you are a slow typist.
3-28-2019 FINAL Page 121 of 244
The amount of time, completing the documentation, should be included in the services time as you
should be writing this as you interview the client
Service Time:
• Service time should reflect the exact time of providing a service. When you enter 60 minutes,
120 minutes, 15 minutes, this is a red flag for auditors. Not all crisis evaluations are 120
minutes. Each client is different.
• If you spend 68 minutes with the client, this is the amount of services time.
• 4 hours for a crisis eval is not okay. You may be providing multiple services during this time
and will need to capture each service separately.
• You should NEVER bill more than the time you work. This is fraud.
Client Current Functioning/Progress Note:
State reason why you are assessing the client such as: (put this as an opening to the Client Current
Functioning).
• Client residing in ICU at SRMC post possible suicide attempt (Overdosed on 3/3/14). Writer
requested to see client for MH evaluation to determine if client meets criteria for involuntary
inpatient psychiatric treatment per W&I 5150.
• Client brought to SAF for MH crisis evaluation. Currently on a W&I 5150 from Auburn PD as
Danger to self and Grave Disability.
• Writer requested by SAF to completed MH Crisis Evaluation after client self-presented to SAF
complaining of sx of severed depression, including poor sleep, feeling hopeless/helpless and
experiencing an increase in S/I.
Interventions:
• Writer provided reflective listening, asked open ended questions and provided supportive feedback
to assist with establishing therapeutic rapport and completing PC MH Crisis Evaluation form.
• Writer spoke to collateral contacts (parent, husband, and spouse) to assist with obtaining
collateral information.
• Writer provided some reality orientation and cognitive reframing. Completed Suicide risk
assessment.
• Writer consulted with PC MH on-call psychiatrist, Dr. Smith regarding status of evaluation. Dr.
Smith request (writer release client from hold/writer continues to keep client on involuntary hold
and seek placement/obtain more collateral information/request that ER order additional labs,
request to speak to an ER physician, etc…..).
Client Response:
• Client was responsive to feedback
• Client remained delusional as evidenced by (insisting he is “Sherlock Holmes” / that he is “David
the Archangel” and his mission is to inform the world that “Armageddon has begun”.
3-28-2019 FINAL Page 122 of 244
• Client reports he/she has a history of bipolar disorder and has been off medications x
weeks/months.
• Client became increasingly agitated (as evidenced by pacing/raising voice, clenching fist/yelling)
at writer/ or when writer attempted to challenge clients beliefs that he was Sherlock Holmes
Plan:
• Client meets criteria for involuntary tx per W&I 5150 as DS, DO and GD. Writer will begin to
seek placement for inpatient treatment.
• Client, at this time, does not meet criteria for inpatient treatment.
Example of a Targeted case management:
Scenario 1:
Client was determined to meet criteria for involuntary hold upon completion of mental health crisis
evaluation (please refer to documentation/form for additional information). Writer contacted Sierra Vista
Hospital and spoke with Joe Schmoe to determine/inquire if a male/female bed was available.
Male/Female bed is available. Writer presented client’s case to Joe Schmoe and faxed copies of 5150 and
crisis evaluation for review. Received/Made follow up call to Joe Schmoe who stated client is accepted.
Writer completed paperwork for transfer and informed client that they will be transferred to Sierra Vista
Hospital for ongoing services.
Scenario 2:
Client was determined to meet criteria for involuntary hold upon completion of mental health crisis
evaluation (please refer to documentation/form for additional information). Writer contacted Sierra Vista
Hospital and spoke with Joe Schmoe to determine/inquire if a male/female bed was available.
Male/Female bed is not available. Writer contacted Heritage Oaks hospital and spoke to Barbie Brown to
inquire about bed status. Informed that potential discharges to do and requested to present client’s case
and faxed copies of 5150 and crisis evaluation for review. Made follow up call to Barbie Brown who stated
client is not accepted at this time, as receiving psychiatrist has expressed concerns regarding labs and
asked for more current labs. Writer spoke to Dr. Jones in the ER and provided information abut Heritage
Oaks hospital requesting newer labs. Upon receipt of lab result, writer contacted Henry Ford at Heritage
Oaks to inform him that new lab results were obtained. Upon acceptance at Heritage Oaks, Writer
completed paperwork for transfer and informed client that they will be transferred to Heritage Oaks for
ongoing services.
Scenario 3:
Upon completion of Crisis Intervention evaluation, client was determined not to meet criteria for
involuntary treatment. Writer met with client to explore/discuss community resource available for client.
Client and writer discussed writer assisting client with referrals and linkage to AA/NA, welcome
center/Cirby Club House/Housing/Legal Aid/Veterans Services/Placer County Veterans officer to assist
with _(fill in area) _. Writer provided client phone numbers. Provided client with information on the
community groups for developing a Wellness Recovery Action Plan Client informed that Placer County
follow up services will be contacting him to offer further assistance with linking to services/resources.
Client thanked writer for assistance and states that he will follow up with referrals. .
Scenario 4:
3-28-2019 FINAL Page 123 of 244
Client’s presentation remains the same since Crisis Evaluation completed. Client is currently in the ER
waiting for placement in an inpatient psychiatric facility. Writer received call from Telecare PHF and may
be accepted there. Telecare is requesting additional information. Writer spoke to Telecare staff to assist
with linking client to their inpatient program. Received request for additional information, writer obtained
this information from client and ER nursing staff. Information was faxed to Telecare. Client informed of
status update
Do not document such statements as:
• Client is throwing a tantrum
• She is obviously impaired
• Client has excellent insurance.
• Client is delusional
• He claims a history of self-harm and suicidal ideations but received no treatment for any injury,
and repeatedly denies any actual intent to kill himself or desire to die.
• Client and boyfriend signed safety plan.
Things to do:
• Identify symptoms not just diagnosis
• Describe the behaviors you are seeing (why do you think someone is internally preoccupied).
Follow Up:
Called several psychiatric facilities, none had an adolescent female bed available.
H0032 Plan Development
Safety planning should be a part of the crisis evaluation as you want to ensure client has a good safety
plan before you make determination about to involuntarily detain or not.
Other plans: Discharge plan. Be specific in the documentation of your progress note such as:
Plan: Client will contact Sacramento County Adult access team at 916-xxx-xxxx and request services or
walk in to Sacramento County Mental Health Treatment Center. If client begins to feel increasing suicidal,
client will go to emergency room and request assistance.
Post Crisis Discharge Plan:
Writer met with Client after determining client did not meet criteria for involuntary detention per W&I
5150 upon completion of Mental Health Crisis Evaluation. Writer assisted client with developing a post
crisis plan. With support from this writer, client identified the following plan:
(1) Return home with family,
(2) contact insurance to request additional services,
3-28-2019 FINAL Page 124 of 244
(3) Contact Therapist , primary care, etc.
(4) Call Adult Intake and request evaluation,
(5) Contact CSOC to request assistance for Children (who are current stressors for client),
(6) Attend Alcohol and Drug Screening clinic on
(7) Develop a WRAP plan
(8) Attend Support Group (NAMI, ALANON, etc).
(9) Contact Placer County 24/7 crisis line, Friend ship line,
Provide Contact Information and Time line for completing each element of the plan.
Sample Note:
System of Care Progress Note
Billing Formula: Minutes of service:_75
Documentation Time: 20
Travel Time: 0
Total Time: 95
Service Provided: Crisis Intervention Location: Health Care/Primary Care/ER
Client’s Current Functioning/Progress:
This is a 43 year old single caucsain male who was self presented to the SRMC requesting medications
for severe migrains. Mental health contracted for psychiatric evaluation by SRMC due to client
presenting as delusional and agitated. Client appears stated age and was insistent of wearing dark
glasses throughout interview. Client stated he needed to wear the dark glasses due to severe
migrains. Client also states that he has been "injecting medications" to manage the level of pain.
Client would not state where or how he was obtaining the medications. Client appeared to become
more and more agitated (as evidenced by tone of voice) during interview when discussing the
"Donuts on Wheels" and "Mr. Jolly Rogers". Client lives with Sister and provided writer with a release
of information to contact sister. Collateral contact made with David (brother ) who stated that her
brother has been seeing receiving mental health services from Dr. Jones at the Outclient Clinic in
Roseville and has been diagnosed with schizoaffective disorder. Client’s brother reports that client
will routinely focuses his agitation on "donuts on wheels and Mr. Jolly Rogers" as client had his
driver's license permanently revoked 18 years ago. Per brotherr, "Wheels on Donuts" represents law
enforcement and "Mr. Rogers " represents a person at DMV who processed paperwork (not person's
real name and has since retired from DMV). Client does expreience chronic pain from migraines and
a "botched surgery". Client would not share where he obtains his pain medications, stating that "you
will ruin it and I won't be able to get my meds anymore.” Per brother, client at baseline presents with
3-28-2019 FINAL Page 125 of 244
pressured and tangential speech, thought process focused on getting car and licensed back. No
history of self harm, or harm towards other.
Current Intervention: Writer provided reflective listening, some cognitive reframming, explored
protective factors and collateral contacts and completed mental health crisis evaluation.
Client’s Response: lient stated that he would not hurt himself orothers as that is a "sin" and he wants
to see his mother (in heaven) when he dies. Client apologetic for "causeing all these problems" and
states he is feeling better now that he has some medicaiton for his migrains. Client's brother contacted
and agree's that client may return home.
Follow Up and/or Referrals Made: Client stated that he would not hurt himself orothers as that
is a "sin" and he wants to see his mother (in heaven) when he dies. Client apologetic for "causeing all
these problems" and states he is feeling better now that he has some medicaiton for his migrains.
Client's sister contacted and agree's that client may return home.
Florence Nightingale, RN, LPHA 03/28/16
TARGETED CASE MANAGEMENT
Targeted Case Management Definitions.
CCR, Title 9,
Section
1810.209
“Targeted Case Management” means services that assist a beneficiary to access needed
medical, educational, social, prevocational, vocational, rehabilitative, or other
community services. The service activities may include, but are not limited to,
communication, coordination, and referral; monitoring service delivery to ensure
beneficiary access to service and the service delivery system; monitoring of the
beneficiary’s progress; placement services; and plan development
3-28-2019 FINAL Page 126 of 244
Targeted Case Management Definitions (continued)
State Plan
Amendment
Targeted Case Management (TCM) means services that assist a beneficiary to access
needed medical, alcohol and drug treatment, educational, social, prevocational,
vocational, rehabilitative, or other community services. The service activities include
(dependent upon the practitioner’s judgment regarding the activities needed to assess
and/or treat the beneficiary): communication, coordination, and referral; monitoring
service delivery to ensure beneficiary access to service and the service delivery
system; monitoring of the beneficiary's progress; placement services; and plan
development:
TCM may be provided face-to-face, by telephone, or by telemedicine with the
beneficiary or significant support person and may be provided anywhere in the
community. TCM contacts with significant support persons may include helping the
eligible beneficiary access services, identifying needs and supports to assist the eligible
beneficiary in obtaining services, providing case managers with useful feedback, and
alerting case managers to changes in the eligible beneficiary's needs (42 CFR
440.169(e)).
TCM includes the following assistance:
1. Comprehensive assessment and periodic reassessment of the individual needs to
determine the need for establishment or continuation of TCM services to access
any medical, education, social, or other services. These assessment activities
include:
• Taking client history;
• Identifying the individual’s needs and completing related documentation,
reviewing all available medical, psychosocial, and other records, and
gathering information from other sources such as family members, medical
providers, social workers, and educators (if necessary) to form a complete
assessment of the individual; and
• Assessing support network availability, adequacy of living arrangements,
financial status, employment status, and potential and training needs.
Assessments are conducted one an annual basis or at a shorter interval as
appropriate.
2. Development and periodic Revision of a USP/tx plan that is:
• Based on the information collected through the assessment;
• Specifies the goals , treatment, service activities, and assistance to address
the negotiated objectives of the plan and the medical, social, educational, and
other services needed by the individuals; • Includes activities such as ensuring the active participation of the eligible
individual, and working with the individual (or the individual's authorized
health care decision maker) and others to develop those goals;
• Identifies a course of action to respond to the assessed needs of the eligible
individuals; and
• Develops a transition plan with a beneficiary has achieved the goals of their
USP.
3-28-2019 FINAL Page 127 of 244
Targeted Case Management Definitions (continued)
3. Referral and Related Activities:
• To help an eligible individual obtain needed services including activities that
help link an individual with medical, substance use treatment, social,
educational providers or other programs and services that are capable of
providing needed services, such as making referrals to providers for need
services and scheduling appointments for the individual;
• To intervene with the client/others at the onset of a crisis to provide assistance
in problem resolution and to coordinate or arrange for the provision of other
needed services;
• To identify, assess, and mobilize resources to meet the client’s needs. Services
would typically include consultation and intervention on behalf of the client
with Social Security, schools, social services and health departments, and other
community agencies, as appropriate; and
• Placement coordination services when necessary to address the identified
mental health condition, including assessing the adequacy and
appropriateness of the client’s living arrangements when needed. Services
would typically include locating and coordinating the resources necessary to
facilitate a successful and appropriate placement in the least restrictive setting
and consulting, as requires with the care provider
4. Monitoring and Follow Up Activities
• Activities and contacts that are necessary to ensure the Client Plan is
implemented and adequately addresses the individual's needs, and which
may be with the individual, family members, providers, or other entities or
individuals and conducted as frequently as necessary, and including at least
one annual monitoring, to determine whether the following conditions are
met: (1) Services are being furnished in accordance with the individual's
Client Plan; (2) Services in the Client Plan are adequate; and (3) There are
changes in the needs or status of the individual, and if so, making necessary
adjustments in the Client Plan and service arrangements with providers.
Activities to monitor, support, and assist the client on a regular basis in developing or
maintaining the skills needed to implement and achieve the goals of the Client Plan.
Services would typically include support in the use of psychiatric, medical, educational,
socialization, rehabilitation, and other social services. Monitoring and update of the
Client Plan is conducted on an annual basis or at a shorter interval as appropriate
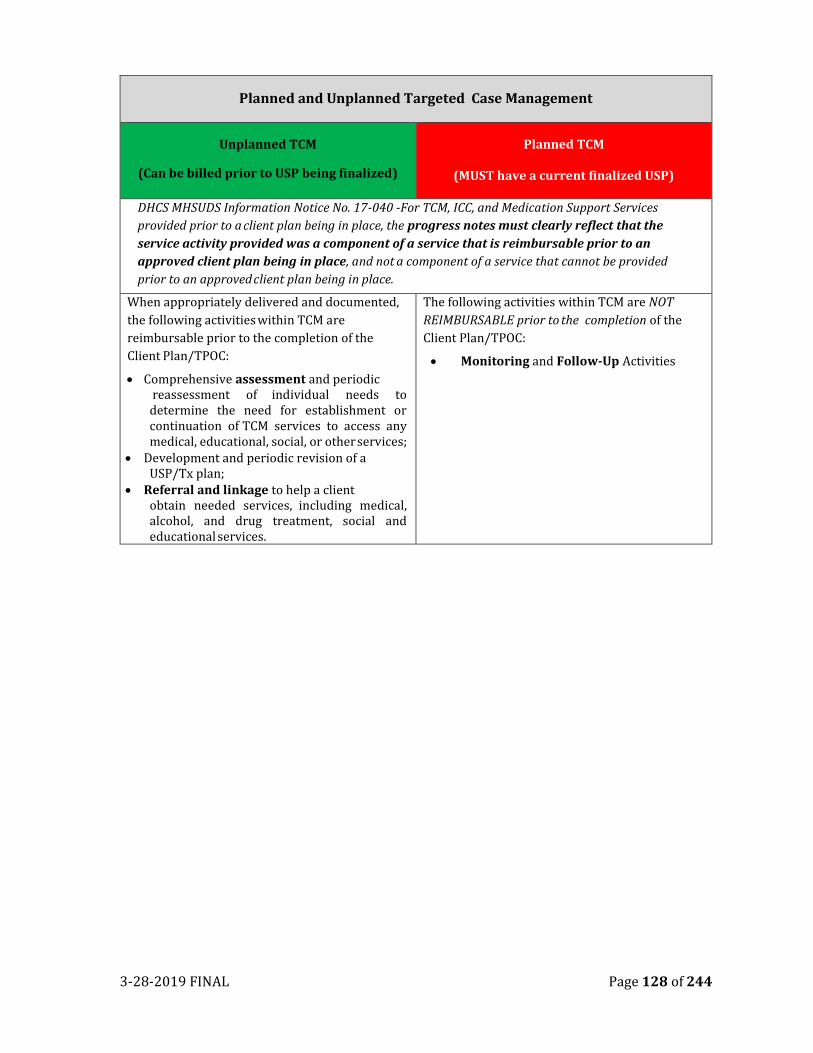
3-28-2019 FINAL Page 128 of 244
Planned and Unplanned Targeted Case Management
Unplanned TCM
(Can be billed prior to USP being finalized)
Planned TCM
(MUST have a current finalized USP)
DHCS MHSUDS Information Notice No. 17-040 -For TCM, ICC, and Medication Support Services
provided prior to a client plan being in place, the progress notes must clearly reflect that the
service activity provided was a component of a service that is reimbursable prior to an
approved client plan being in place, and not a component of a service that cannot be provided
prior to an approved client plan being in place.
When appropriately delivered and documented,
the following activities within TCM are
reimbursable prior to the completion of the
Client Plan/TPOC:
• Comprehensive assessment and periodic reassessment of individual needs to determine the need for establishment or continuation of TCM services to access any medical, educational, social, or other services;
• Development and periodic revision of a USP/Tx plan;
• Referral and linkage to help a client obtain needed services, including medical, alcohol, and drug treatment, social and educational services.
The following activities within TCM are NOT
REIMBURSABLE prior to the completion of the
Client Plan/TPOC:
• Monitoring and Follow-Up Activities
3-28-2019 FINAL Page 129 of 244
CHAPTER TEN
PATHWAYS TO MENTAL HEALTH SERVICES –CORE PRACTICE MODEL
Intensive Care Coordination (ICC) and Intensive Home Based Services (IHBS) are a part
of a mental health treatment plan, developed by the clinician and the Child, Family and
Team. ICC and IHBS can be provided for youth who meet the following criteria:
1. Age 21 or under
2. Eligible for Full Scope Medi-cal
3. Meets medical necessity criteria
4. In need of intensive mental health services
INTENSIVE CARE COORDINATION (ICC) SERVICE DEFINITION
Intensive Care Coordination (ICC) is a targeted case management service that facilitates
assessment of, care planning for and coordination of services, including urgent services
for beneficiaries with intensive needs. Clients NEED NOT be a member of the Katie A.
class to receive ICC. ICC services are intended to link clients to services provided by
other child serving systems, to facilitate teaming, and to coordinate mental health care.
If a client is involved in two or more child serving systems, ICC is used to facilitate cross-
system communication and planning.
ICC is intended to link beneficiaries to services provided by other child-serving systems,
to facilitate teaming, and to coordinate mental health care. ICC services are similar to,
but more intense than, Targeted Case Management. ICC service components/activities
include: assessing; service planning and implementation; monitoring and adapting; and
transition. ICC differs in that it is integrated into the Child and Family Team (CFT)
process, and it typically requires more active participation by the ICC Provider in order
to ensure that the needs of the client are appropriately and effectively met.
Although there may be more than one mental health providers participating on a Child
and Family Team (CFT), the CFT is also comprised of the child or youth and family and
all of the ancillary individuals who are working with them to address the child or youth’s
needs and strengths, and focuses on issues such as successful treatment of the child or
youth’s mental health needs and achieving goals in other child-serving systems in which
the child or youth is involved. Youth who are not involved with other child-serving
systems may have smaller teams to include supportive individuals identified by the youth
and family, rather than system involved professionals. As the youth continues in services,
their strengths and needs will change, and inclusion of individuals in the Child and
Family team should be re-evaluated. Team composition should always be guided by the
families input.
3-28-2019 FINAL Page 130 of 244
ICC SERVICE COMPONENTS
While the key service components of ICC are similar to TCM, ICC differs in that it is
integrated into the CFT process, and it typically requires more active participation by
the ICC provider in order to ensure that the needs of the client are appropriately and
effectively met. As such the ICC service components include the following:
1. Comprehensive Assessment and Periodic Reassessment:
These assessment activities are different from the clinical assessment to
establish medical necessity for specialty mental health services but must align
with the mental health client plan. Information gathering and assessing needs
is the practice of gathering and evaluating information about the client and
family which includes gathering and assessing strengths, as well as assessing
the underlying needs. Assessing also includes determining the capability,
willingness, and availability of resources for achieving safety, permanence, and
well-being of clients.
2. Development and Periodic Revision of the Plan
Planning within the Core Practice Model (CPM) is a dynamic and interactive
process that addresses the goals and objectives necessary to assure that clients
are safe, live in permanent loving families and achieve well-being. This process
is built on an expectation that the planning process and resulting plans reflect
the client’s and family’s own goals and preferences and that they have access to
necessary services and resources that meet their needs.
3. The ICC coordinator is responsible for working within the CFT to ensure that plans
from any of the system partners (child welfare, education, juvenile probation, etc.)
are integrated to comprehensively address the identified goals and objectives and
that the activities of all parties involved with service to the client and/or family are
coordinated to support and ensure successful and enduring change.
4. Referral, Monitoring and Follow-Up Activities
Monitoring and adapting is the practice of evaluating the effectiveness of the
plan, assessing circumstances and resources, and reworking the plan as
needed. The CFT is also responsible for reassessing the needs, applying
knowledge gained through ongoing assessments, and adapting the plan to
address the changing needs of the client and family in a timely manner.
Intervention strategies should be monitored on a frequent basis so that
modifications to the plan can be made based on results, incorporating
approaches that work and refining those that do not.
3-28-2019 FINAL Page 131 of 244
5. Transition
When the client has achieved the goals of his/her client plan, developing a
transition plan for the client and family to foster long term stability including
the effective use of natural supports and community resources.
CLAIMING FOR MULTIPLE STAFF
When multiple staff are claiming for ICC services, the following requirements must be
met:
1. Each staff may claim to ICC for time at the CFT meeting clearly linked to the
mental health client plan goals and/or the information gleaned during the
meeting that contributed to the formulation of the mental health client plan or
revisions.
2. Medi-Cal reimbursement must be based on staff time, including the length of
the meeting, plus any documentation and travel time (e.g., a single staff member
who participates in the CFT meeting cannot claim for more time than was
provided).
3. Progress notes must include evidence of incorporation of Core Practice Model
(CPM) elements described in the CPM Guide. Please see Reference G for
examples of ICC progress notes.
THE CFT FACILITATOR SERVES AS THE SINGLE POINT OF ACCOUNTABILITY TO:
• Ensure that medically necessary services are accessed, coordinated and
delivered in a strength-based, individualized, family/youth driven and
culturally and linguistically relevant manner and that services and supports
are guided by the needs of the child or youth;
• Ensure that plans are integrated with the multiple CSOC partners (child
welfare, education, juvenile probation, etc.) to comprehensively address the
identified goals and objectives and that the activities of all parties involved
with service to the client and/or family are coordinated to support and
ensure successful and enduring change.
• Facilitate a collaborative relationship among the child or youth, his/her family
and involved child-serving systems;
• Support the parent/caregiver in meeting their child or youth’s needs;
• Help establish the Child and Family Team (CFT) and provide ongoing support;
• Organize and match care across providers and child serving systems to allow
the child or youth to be served in their home community.
3-28-2019 FINAL Page 132 of 244
Placer County CSOC and partner agency staff shall be responsible for the convening
and facilitation of the Child and Family team meeting. See below to determine which
staff shall be the lead. Staff shall:
• Discuss Team composition with the youth and family
• Convene the CFT
• Facilitate the CFT – with the entire team; See CFT Meeting Format
o Identify strengths and needs of the child, and the family
o Develop the Treatment goals
o Develop the plan to allow the youth to achieve the treatment goals
Note: The formal treatment plan document may be created outside of the
meeting, using the information and agreements developed by the team
INTENSIVE HOME BASED SERVICES (IHBS) SERVICE DEFINITION:
Intensive Home Based Services (IHBS) are mental health rehabilitation services
provided to Medi-Cal clients as medically necessary. IHBS are individualized, strength-
based interventions designed to ameliorate mental health conditions that interfere with
a client’s functioning and are aimed at helping the client build skills necessary for
successful functioning in the home and community and improving the client’s family
ability to help the client successfully function in the home and community.
SERVICE COMPONENTS/ACTIVITIES
Service activities may include, but are not limited to:
Medically necessary, skills-based interventions for the remediation of behaviors or
improvement of symptoms, including but not limited to the implementation of a
positive behavioral plan and/or modeling interventions for the client’s family and/or
significant others to assist them in implementing the strategies;
1. Development of functional skills to improve self-care, self-regulation, or other
functional impairments by intervening to decrease or replace non- functional
behavior that interferes with daily living tasks or the avoidance of exploitation by
others;
2. Development of skills or replacement behaviors that allow the client to fully
participate in the Child and Family Team (CFT) and service plans, including, but
not limited to, the plan and/or child welfare service plan;
3. Improvement of self-management of symptoms, including self-administration of
medications as appropriate;
3-28-2019 FINAL Page 133 of 244
4. Education of the client and/or their family or caregiver(s) about, and how to
manage the client’s mental health disorder or symptoms;
5. Support of the development, maintenance and use of social networks including
the use of natural and community resources;
6. Support to address behaviors that interfere with the achievement of a stable and
permanent family life;
7. Support to address behaviors that interfere with seeking and maintaining a job;
8. Support to address behaviors that interfere with a client’s success in achieving
educational objectives in an academic program in the community;
9. Support to address behaviors that interfere with transitional independent living
objectives such as seeking and maintaining housing and living independently.
SERVICE LOCKOUTS FOR IHBS
Mental health services (including IHBS) are not reimbursable when provided by day
treatment intensive or day rehabilitation staff during the same time period that day
treatment intensive or day rehabilitation services are being provided. Authorization is
required for mental health services if these services are provided on the same day that
day treatment intensive or day rehabilitation services are provided.
Certain services may be part of the child’s or youth’s course of treatment, but may not
be provided during the same hours of the day that IHBS services are being provided to
the child or youth. These services include:
• Day Treatment Rehabilitative or Day Treatment Intensive,
• Group Therapy, and
• Therapeutic Behavioral Services (TBS)
THERAPEUTIC BEHAVIORAL SERVICES (TBS)
TBS SERVICE DEFINITION
Therapeutic Behavioral Services, or TBS, is a one-to-one behavioral mental health
service available to children and youth with serious emotional challenges who are
under 21 years old and who are eligible for a full array of Medi-Cal benefits without
restrictions or limitations (full scope Medi-Cal). TBS can help children/youth and
parents/caregivers, foster parents, group home staff, and school staff learn new
ways of reducing and managing challenging behaviors, as well as strategies and
skills to increase the kinds of behavior that will allow children and youth to be
successful in their current environment. TBS is designed to help children and youth
and parents and caregivers (when available) manage these behaviors utilizing
short-term, measurable goals based on the needs of the child and youth and their
family.
3-28-2019 FINAL Page 134 of 244
TBS can be provided anywhere in the community: at home, school, other places
such as after-school programs and organized recreation programs except during
Medi-Cal service lockouts.
As an EPSDT Supplemental Specialty Mental Health Service (CCR, Title 9,
§1810.215), TBS is not a stand-alone service; it is a short-term, supplemental
specialty mental health service for clients that meet medical necessity criteria and
defined class criteria:
• Child or youth is placed in a group home facility (RCL 12 or above) or in a
locked treatment facility for the treatment of mental health needs or child
or youth is being considered by DPH for a placement in a facility described
above;
• Child or youth has undergone at least one emergency psychiatric
hospitalization related to his/her current presenting mental health
diagnosis within the preceding 24 months;
• Child or youth has previously received TBS while a member of the certified
class or child or youth is at risk of psychiatric hospitalization.
TBS INTERVENTION DEFINITION
A TBS intervention is defined as an individualized one-to-one behavioral assistance
intervention to accomplish outcomes specifically outlined in a written TBS treatment
plan.
TBS COLLATERAL SERVICE DEFINITION
A TBS collateral service activity is an activity provided to significant support persons
in a client’s life rather than to the client. Progress notes must clearly indicate the
overall goal of the collateral service activities to help improve, maintain, and restore
the client’s mental health status through interaction with the significant support
person.
TBS CLIENT ASSESSMENT REQUIREMENTS
A TBS client assessment may be made as part of an overall assessment for specialty
mental health services or may be a separate document specifically establishing
whether TBS is needed. A TBS client assessment must be completed within 30 days
or less of a referrals
In addition to minimum assessment items for Specialty Mental Health Services,
TBS client assessments must document:
1. Medical necessity criteria specifically for TBS;
2. Client is a full-scope Medi-Cal client under 21 years;
3-28-2019 FINAL Page 135 of 244
3. Client is a member of the certified class, receiving specialty mental health
services, and has specific behaviors that require TBS;
4. Client has specific targeted behaviors that jeopardize continuation of a
residential placement, put the client at risk for psychiatric hospitalization, or
the specific behaviors that are expected to interfere with a plan to transition
to a lower level of residential placement;
5. Clinical information that demonstrates TBS is necessary to sustain a
residential placement or successfully transition to a lower level of
residential placement and that TBS can be expected to provide a level of
intervention necessary to stabilize the client in the existing placement;
6. Observable and measurable changes and indicate when TBS services have
been successful and could be reduced or ended; and
7. Identification of skills and positive adaptive behaviors that the client uses
to manage the problem behavior and/or uses other circumstances that
could replace the specified problem behaviors.
TBS CLIENT PLAN REQUIREMENTS
TBS client plans of care must be completed within 30 days or less of a referral for
services. TBS plans of care can be a separate plan of care or part of a more
comprehensive plan but must document all of the following:
1. The targeted behaviors that jeopardize a client’s placement or transition to
lower level of care;
2. Plan goals;
3. Benchmarks (the objectives to be met as the client progresses toward plan
goals;
4. A specific plan of intervention for each of the targeted behaviors or
symptoms identified in the assessment and the client plan developed with
the family/caregiver (if available and appropriate), a specific description of
the changes in the behaviors that the interventions are intended to produce
including the estimated time frame for these changes, and a specific way to
measure the effectiveness of the intervention at regular intervals and
documentation of refining the intervention plan when the original
interventions are not achieving expected results;
5. Transition plan that describes the method the treatment team will use to
decide how and when TBS will be decreased and ultimately discontinued
including assisting parents/caregivers/school personnel with skills and
strategies to provide continuity of care when TBS is discontinued;
3-28-2019 FINAL Page 136 of 244
6. For transition age youth, a plan for transition to adult services when the
client is no longer eligible (21 years and older) and will need continued
services;
7. Signature of the clinician that developed the care plan or is providing the
service(s) and/or a clinician representing the MHP.
TBS CLIENT PLAN REVIEWS
All TBS USP/Tx plans must be reviewed every 30 days to ensure that TBS continues
to be effective for the client in making progress toward the specified measurable
outcomes in the client’s TBS plan.
TBS CLIENT PROGRESS NOTES
TBS progress notes must clearly document the specific behaviors that threaten the
stability of a current placement or interfere with the transition to a lower level of
residential placement and which are the result of the covered mental health
diagnosis and the interventions provide to address those behaviors and symptoms.
All notes must clearly, concisely, succinctly and legibly include all of the following:
1. Date service was provided;
2. Start time of the service (required for TBS only)
3. Key clinical decisions and interventions that are directed to the TBS goals of
the client:
a. That are consistent with interventions reflected in the TBS client plan;
b. Document how interventions changed or eliminated client targeted
behaviors and increased adaptive behaviors (were not provided solely for
the convenience of the family or other caregivers, a physician, a teacher,
or staff);
c. Focus on identified target behaviors;
d. Client response and receptivity to interventions; and
e. Address conditions that are not part of the identified client’s mental
health condition; Signature of the staff providing the service including
their clinical licensure, professional degree and job title;
4. A corresponding note for every TBS service contact including, but not limited
to, direct one-to-one TBS service, TBS assessment and/or reassessment, TBS
collateral contact, and TBS Plan of Care/USP/TxPlan or its documented
review and updates.
All TBS progress notes must include a comprehensive summary covering the time TBS
services were provided but do not need to document every minute of service time.
3-28-2019 FINAL Page 137 of 244
TBS SERVICE RESTRICTIONS
TBS is not billable when:
1. Services are solely:
a. For the convenience of the family or other caregivers, physician, or teacher;
b. To provide supervision or to assure compliance with terms and conditions
of probation;
c. To ensure a child or youth’s physical safety or the safety of others (e.g.,
suicide watch); or
d. To address behaviors that are not a result of a child or youth’s mental health
condition;
2. A child or youth can sustain non-impulsive self-directed behavior, handle
themselves appropriately in social situations with peers, and appropriately
handle transitions during the day;
3. A child or youth will never be able to sustain non-impulsive self-directed
behavior and engage in appropriate community activities without full-time
supervision;
4. On-call time for the staff person providing TBS (note, this is different from “non-
treatment” time with staff who are physically “present and available” to provide
intervention – only the time spent actually providing the intervention is a
billable expense);
5. The TBS staff provides services to a different child or youth during the time
period authorized for TBS;
6. Transporting a child or youth (accompanying a child or youth who is being
transported may be reimbursable, depending on the specific, documented,
circumstances);
7. TBS supplants a child or youth’s other mental health services provided by other
mental health staff.
8. Services are solely:
• For the convenience of the family or other caregivers, physician, or
teacher;
• To provide supervision or to assure compliance with terms and
conditions of probation;
• To ensure a child or youth’s physical safety or the safety of others
(e.g., suicide watch); or
3-28-2019 FINAL Page 138 of 244
• To address behaviors that are not a result of a child or youth’s
mental health condition;
9. A child or youth can sustain non-impulsive self-directed behavior, handle
themselves appropriately in social situations with peers, and appropriately
handle transitions during the day;
10. A child or youth will never be able to sustain non-impulsive self-directed
behavior and engage in appropriate community activities without full-time
supervision;
11. On-call time for the staff person providing TBS (note, this is different from “non-
treatment” time with staff who are physically “present and available” to provide
intervention – only the time spent actually providing the intervention is a
billable expense);
12. The TBS staff provides services to a different child or youth during the time
period authorized for TBS;
13. Transporting a child or youth (accompanying a child or youth who is being
transported may be reimbursable, depending on the specific, documented,
circumstances);
TBS supplants a child or youth’s other mental health services provided by other mental
health staff
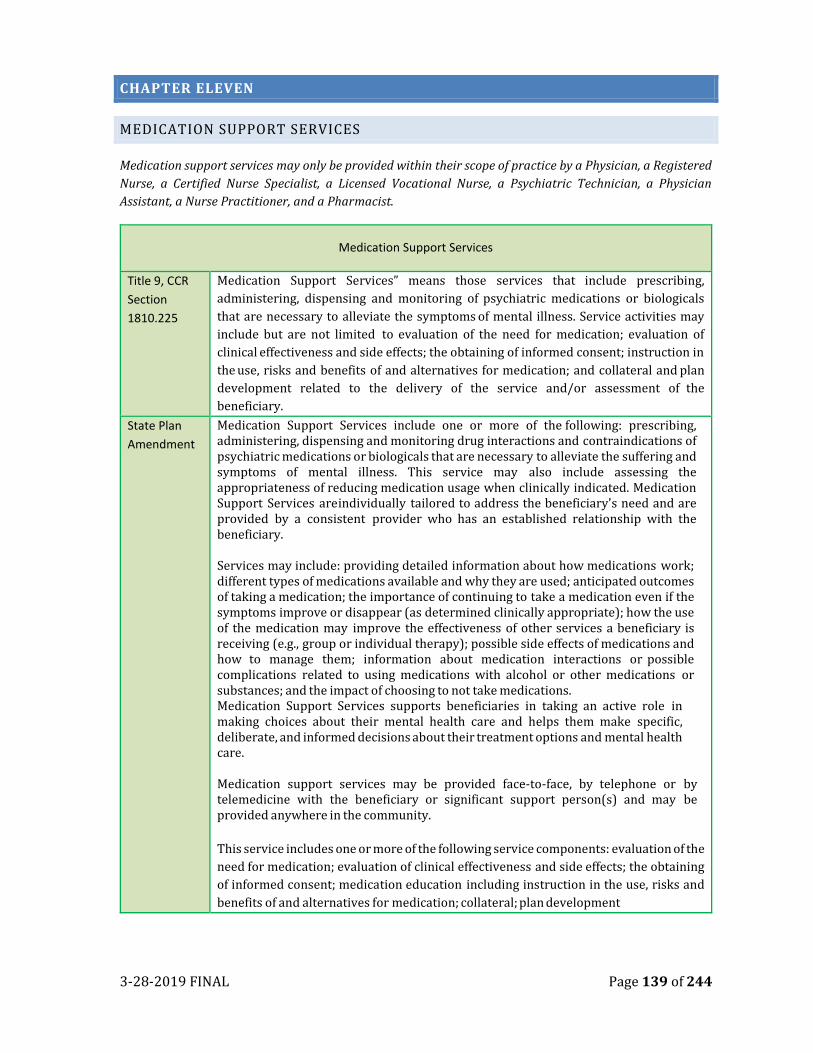
3-28-2019 FINAL Page 139 of 244
CHAPTER ELEVEN
MEDICATION SUPPORT SERVICES
Medication support services may only be provided within their scope of practice by a Physician, a Registered
Nurse, a Certified Nurse Specialist, a Licensed Vocational Nurse, a Psychiatric Technician, a Physician
Assistant, a Nurse Practitioner, and a Pharmacist.
Medication Support Services
Title 9, CCR
Section
1810.225
Medication Support Services” means those services that include prescribing,
administering, dispensing and monitoring of psychiatric medications or biologicals
that are necessary to alleviate the symptoms of mental illness. Service activities may
include but are not limited to evaluation of the need for medication; evaluation of
clinical effectiveness and side effects; the obtaining of informed consent; instruction in
the use, risks and benefits of and alternatives for medication; and collateral and plan
development related to the delivery of the service and/or assessment of the
beneficiary.
State Plan
Amendment
Medication Support Services include one or more of the following: prescribing, administering, dispensing and monitoring drug interactions and contraindications of psychiatric medications or biologicals that are necessary to alleviate the suffering and symptoms of mental illness. This service may also include assessing the appropriateness of reducing medication usage when clinically indicated. Medication Support Services are individually tailored to address the beneficiary's need and are provided by a consistent provider who has an established relationship with the beneficiary. Services may include: providing detailed information about how medications work; different types of medications available and why they are used; anticipated outcomes of taking a medication; the importance of continuing to take a medication even if the symptoms improve or disappear (as determined clinically appropriate); how the use of the medication may improve the effectiveness of other services a beneficiary is receiving (e.g., group or individual therapy); possible side effects of medications and how to manage them; information about medication interactions or possible complications related to using medications with alcohol or other medications or substances; and the impact of choosing to not take medications. Medication Support Services supports beneficiaries in taking an active role in making choices about their mental health care and helps them make specific, deliberate, and informed decisions about their treatment options and mental health care. Medication support services may be provided face-to-face, by telephone or by telemedicine with the beneficiary or significant support person(s) and may be provided anywhere in the community.
This service includes one or more of the following service components: evaluation of the
need for medication; evaluation of clinical effectiveness and side effects; the obtaining
of informed consent; medication education including instruction in the use, risks and
benefits of and alternatives for medication; collateral; plan development
3-28-2019 FINAL Page 140 of 244
MEDICATION SUPPORT SERVICES SCOPE OF PRACTICE
Consistent with scope of practice, Medication Support Services may be provided
by the following staff:
1. Licensed Physician (MD/DO); 2. Certified Nurse Practitioner (NP); 3. Registered Nurse (RN); 4. Certified Nurse Specialist (CNS); 5. Licensed Vocational Nurse (LVN); 6. Licensed Psychiatric Technician (LPT); 7. Licensed Pharmacist (PharmD, RPh).
MEDICATION CONSENT REQUIREMENTS:
Medication Support Services prescribers must obtain and retain a current written medication consent form signed by the client or legal representative (e.g. parent or caregiver) agreeing to treatment with each prescribed medication. A new consent form must be completed and signed for each new medication prescribed Psychiatric medication consent forms must contain the following elements to be considered compliant with Medi-Cal requirements, all of which must be discussed with the client and/or parent/caregiver:
1. What condition or diagnoses the client has that medications are prescribed to address;
2. Which symptoms the medication(s) should reduce and how likely the medication(s) will work;
3. What are the chances of getting better without taking the medication(s); 4. Reasonable options or alternatives to taking the medication(s); 5. Name, dosage, dosage range, frequency, route of administration and duration of
each prescribed medication; 6. Common side effects of the medication(s), including possible additional side
effects which may occur beyond three months or long-term; 7. If antipsychotic medications are prescribed, notice that antipsychotic
medications may cause additional side effects for some persons, including persistent involuntary movements which are potentially irreversible, and may continue after the antipsychotic medication has been stopped; and
8. Any special instructions you should know about taking the medication(s).
All client medication consent forms must include:
1. Date of service; 2. Signature of person providing the service (or electronic equivalent); 3. Person’s type of professional degree AND licensure OR job title (see
examples below); 4. The date the documentation was entered into the medical record; and
3-28-2019 FINAL Page 141 of 244
5. Client or legal representative’s signature and date signed.
Examples for signing with “persons’ type of professional degree AND licensure OR job title:”
• Psychiatrist: signature, MD, psychiatrist • Nurse Practitioner: signature, MSN, NP • Pharmacist: signature, PharmD, clinical pharmacist
Note that “type of professional degree” is defined as your educational degree, not board
certification and “licensure” is defined as the type of your license, not the license number.
MEDICATION SUPPORT SERVICES GENERAL BILLING RULES
The following general billing rules apply to Medication Support Services:
PROGRESS NOTES
The client’s progress notes should include the evaluation of the client’s signs and
symptoms, the client’s compliance with the medication, the response to medication,
consideration of drug interactions, adverse drug effects when applicable, and any
changes in dose and medication(s) prescribed, when
NON-MEDICATION SUPPORT BILLING
When providing a service that is not primarily medication support, medication support
staff must use the relevant service code billing associated with the service provided
(e.g. case management, therapy, collateral, etc.).
PHONE CONTACT
In contrast to Medicare, for Medi-Cal billing, Medication Support Services allows
services provided by phone contact or non-face to face. “Units of time may be billed
regardless of whether there is face-to-face or phone contact with the beneficiary.”
Multiple Providers
When Medication Support Services are provided to a client by a physician and nurse
concurrently, the time of both staff should be claimed. If both staff provide the same
services, then one note may be written that covers both staff and one claim submitted
that includes the time of both staff. If two staff provide different services during the
contact with the client (e.g. a medical doctor writes the prescription and a nurse gives
an injection), two notes should be written with each staff submitting his or her own
claim with his or her own time.
Medication Administration: For medication administration, the progress note needs to include:
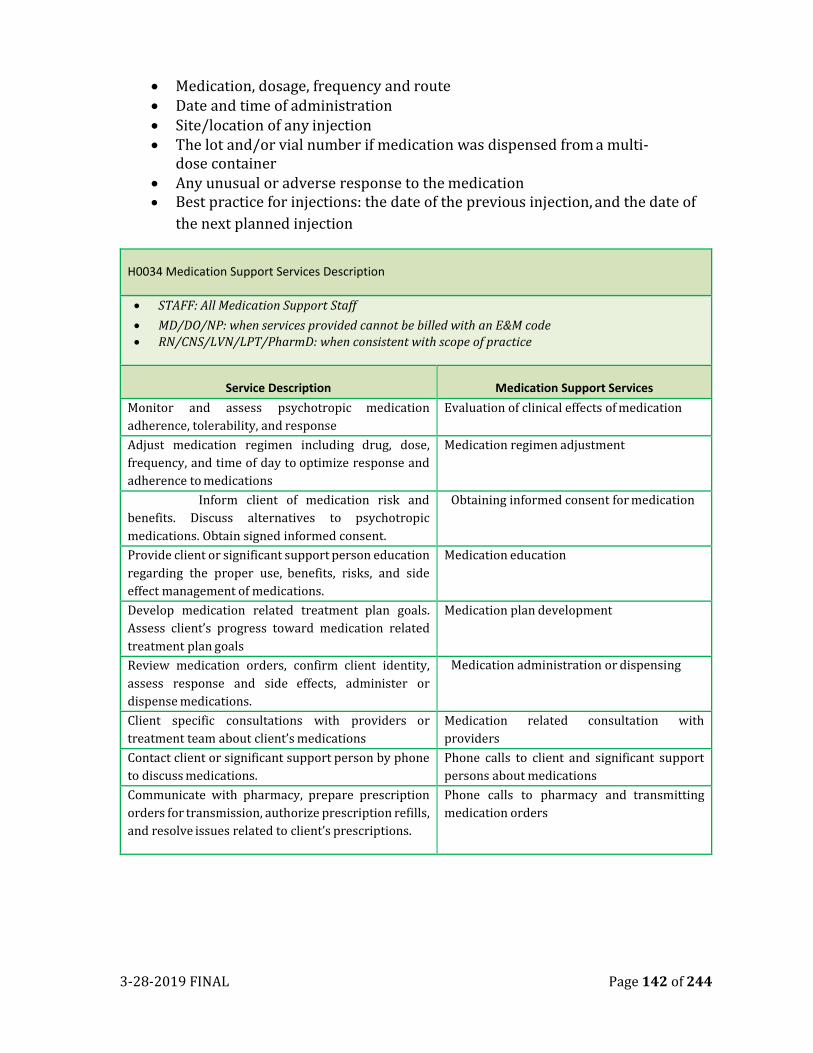
3-28-2019 FINAL Page 142 of 244
• Medication, dosage, frequency and route • Date and time of administration • Site/location of any injection • The lot and/or vial number if medication was dispensed from a multi-
dose container • Any unusual or adverse response to the medication • Best practice for injections: the date of the previous injection, and the date of
the next planned injection
H0034 Medication Support Services Description
• STAFF: All Medication Support Staff
• MD/DO/NP: when services provided cannot be billed with an E&M code • RN/CNS/LVN/LPT/PharmD: when consistent with scope of practice
Service Description Medication Support Services
Monitor and assess psychotropic medication
adherence, tolerability, and response
Evaluation of clinical effects of medication
Adjust medication regimen including drug, dose,
frequency, and time of day to optimize response and
adherence to medications
Medication regimen adjustment
Inform client of medication risk and
benefits. Discuss alternatives to psychotropic
medications. Obtain signed informed consent.
Obtaining informed consent for medication
Provide client or significant support person education
regarding the proper use, benefits, risks, and side
effect management of medications.
Medication education
Develop medication related treatment plan goals.
Assess client’s progress toward medication related
treatment plan goals
Medication plan development
Review medication orders, confirm client identity,
assess response and side effects, administer or
dispense medications.
Medication administration or dispensing
Client specific consultations with providers or
treatment team about client’s medications
Medication related consultation with
providers
Contact client or significant support person by phone
to discuss medications.
Phone calls to client and significant support
persons about medications
Communicate with pharmacy, prepare prescription
orders for transmission, authorize prescription refills,
and resolve issues related to client’s prescriptions.
Phone calls to pharmacy and transmitting
medication orders
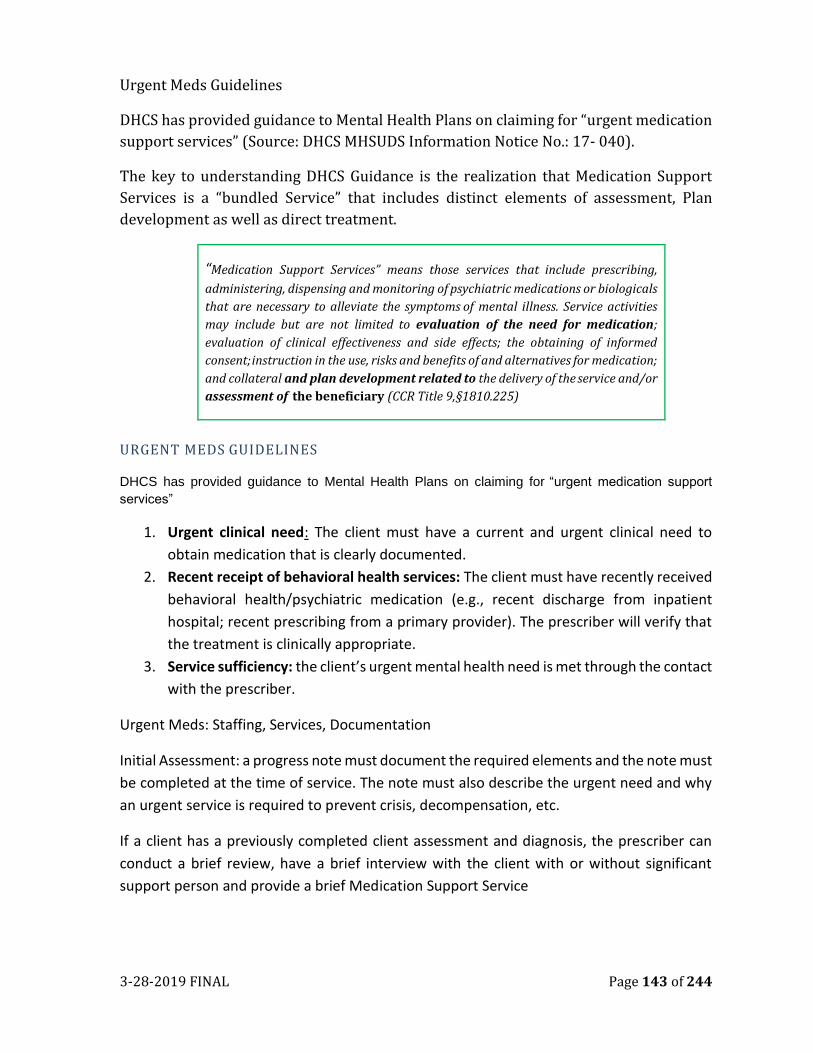
3-28-2019 FINAL Page 143 of 244
Urgent Meds Guidelines
DHCS has provided guidance to Mental Health Plans on claiming for “urgent medication
support services” (Source: DHCS MHSUDS Information Notice No.: 17- 040).
The key to understanding DHCS Guidance is the realization that Medication Support
Services is a “bundled Service” that includes distinct elements of assessment, Plan
development as well as direct treatment.
“Medication Support Services” means those services that include prescribing,
administering, dispensing and monitoring of psychiatric medications or biologicals
that are necessary to alleviate the symptoms of mental illness. Service activities
may include but are not limited to evaluation of the need for medication;
evaluation of clinical effectiveness and side effects; the obtaining of informed
consent; instruction in the use, risks and benefits of and alternatives for medication;
and collateral and plan development related to the delivery of the service and/or
assessment of the beneficiary (CCR Title 9, §1810.225)
URGENT MEDS GUIDELINES
DHCS has provided guidance to Mental Health Plans on claiming for “urgent medication support
services”
1. Urgent clinical need: The client must have a current and urgent clinical need to
obtain medication that is clearly documented.
2. Recent receipt of behavioral health services: The client must have recently received
behavioral health/psychiatric medication (e.g., recent discharge from inpatient
hospital; recent prescribing from a primary provider). The prescriber will verify that
the treatment is clinically appropriate.
3. Service sufficiency: the client’s urgent mental health need is met through the contact
with the prescriber.
Urgent Meds: Staffing, Services, Documentation
Initial Assessment: a progress note must document the required elements and the note must
be completed at the time of service. The note must also describe the urgent need and why
an urgent service is required to prevent crisis, decompensation, etc.
If a client has a previously completed client assessment and diagnosis, the prescriber can
conduct a brief review, have a brief interview with the client with or without significant
support person and provide a brief Medication Support Service
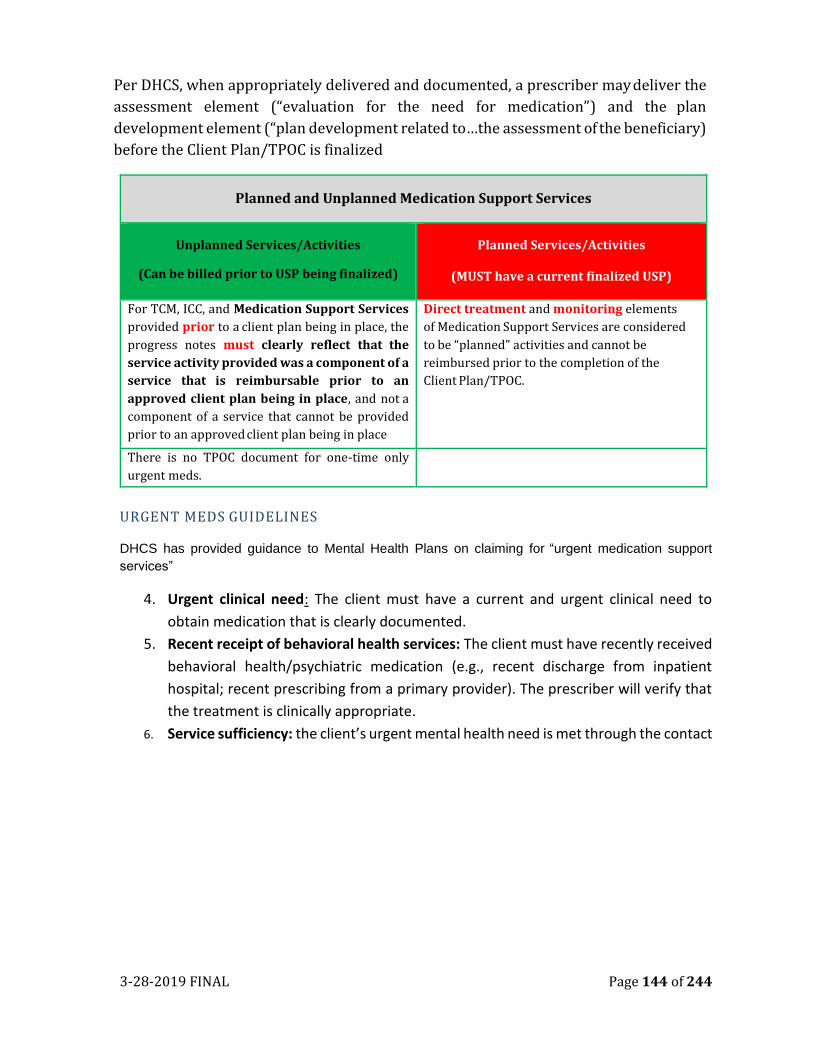
3-28-2019 FINAL Page 144 of 244
Per DHCS, when appropriately delivered and documented, a prescriber may deliver the
assessment element (“evaluation for the need for medication”) and the plan
development element (“plan development related to…the assessment of the beneficiary)
before the Client Plan/TPOC is finalized
Planned and Unplanned Medication Support Services
Unplanned Services/Activities
(Can be billed prior to USP being finalized)
Planned Services/Activities
(MUST have a current finalized USP)
For TCM, ICC, and Medication Support Services
provided prior to a client plan being in place, the
progress notes must clearly reflect that the
service activity provided was a component of a
service that is reimbursable prior to an
approved client plan being in place, and not a
component of a service that cannot be provided
prior to an approved client plan being in place
Direct treatment and monitoring elements
of Medication Support Services are considered
t o b e “pla n ne d ” activities and cannot be
reimbursed prior to the completion of the
Client Plan/TPOC.
There is no TPOC document for one-time only
urgent meds.
URGENT MEDS GUIDELINES
DHCS has provided guidance to Mental Health Plans on claiming for “urgent medication support
services”
4. Urgent clinical need: The client must have a current and urgent clinical need to
obtain medication that is clearly documented.
5. Recent receipt of behavioral health services: The client must have recently received
behavioral health/psychiatric medication (e.g., recent discharge from inpatient
hospital; recent prescribing from a primary provider). The prescriber will verify that
the treatment is clinically appropriate.
6. Service sufficiency: the client’s urgent mental health need is met through the contact
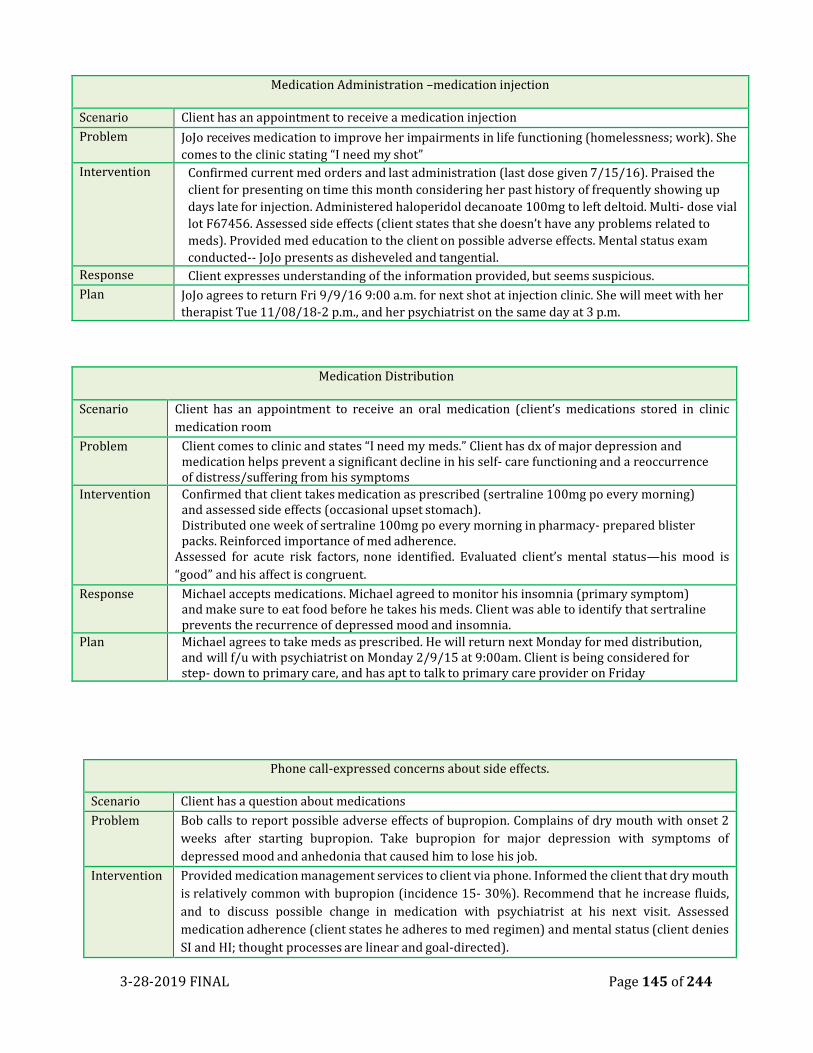
3-28-2019 FINAL Page 145 of 244
Medication Administration –medication injection
Scenario Client has an appointment to receive a medication injection
Problem JoJo receives medication to improve her impairments in life functioning (homelessness; work). She
comes to the clinic stating “I need my shot”
Intervention Confirmed current med orders and last administration (last dose given 7/15/16). Praised the
client for presenting on time this month considering her past history of frequently showing up
days late for injection. Administered haloperidol decanoate 100mg to left deltoid. Multi- dose vial
lot F67456. Assessed side effects (client states that she doesn’t have any problems related to
meds). Provided med education to the client on possible adverse effects. Mental status exam
conducted-- JoJo presents as disheveled and tangential.
Response Client expresses understanding of the information provided, but seems suspicious.
Plan JoJo agrees to return Fri 9/9/16 9:00 a.m. for next shot at injection clinic. She will meet with her
therapist Tue 11/08/18-2 p.m., and her psychiatrist on the same day at 3 p.m.
Medication Distribution
Scenario Client has an appointment to receive an oral medication (client’s medications stored in clinic
medication room
Problem Client comes to clinic and states “I need my meds.” Client has dx of major depression and medication helps prevent a significant decline in his self- care functioning and a reoccurrence of distress/suffering from his symptoms
Intervention Confirmed that client takes medication as prescribed (sertraline 100mg po every morning) and assessed side effects (occasional upset stomach). Distributed one week of sertraline 100mg po every morning in pharmacy- prepared blister packs. Reinforced importance of med adherence.
Assessed for acute risk factors, none identified. Evaluated client’s mental status—his mood is
“good” and his affect is congruent.
Response Michael accepts medications. Michael agreed to monitor his insomnia (primary symptom) and make sure to eat food before he takes his meds. Client was able to identify that sertraline prevents the recurrence of depressed mood and insomnia.
Plan Michael agrees to take meds as prescribed. He will return next Monday for med distribution, and will f/u with psychiatrist on Monday 2/9/15 at 9:00am. Client is being considered for step- down to primary care, and has apt to talk to primary care provider on Friday
Phone call-expressed concerns about side effects.
Scenario Client has a question about medications
Problem Bob calls to report possible adverse effects of bupropion. Complains of dry mouth with onset 2
weeks after starting bupropion. Take bupropion for major depression with symptoms of
depressed mood and anhedonia that caused him to lose his job.
Intervention Provided medication management services to client via phone. Informed the client that dry mouth
is relatively common with bupropion (incidence 15- 30%). Recommend that he increase fluids,
and to discuss possible change in medication with psychiatrist at his next visit. Assessed
medication adherence (client states he adheres to med regimen) and mental status (client denies
SI and HI; thought processes are linear and goal-directed).
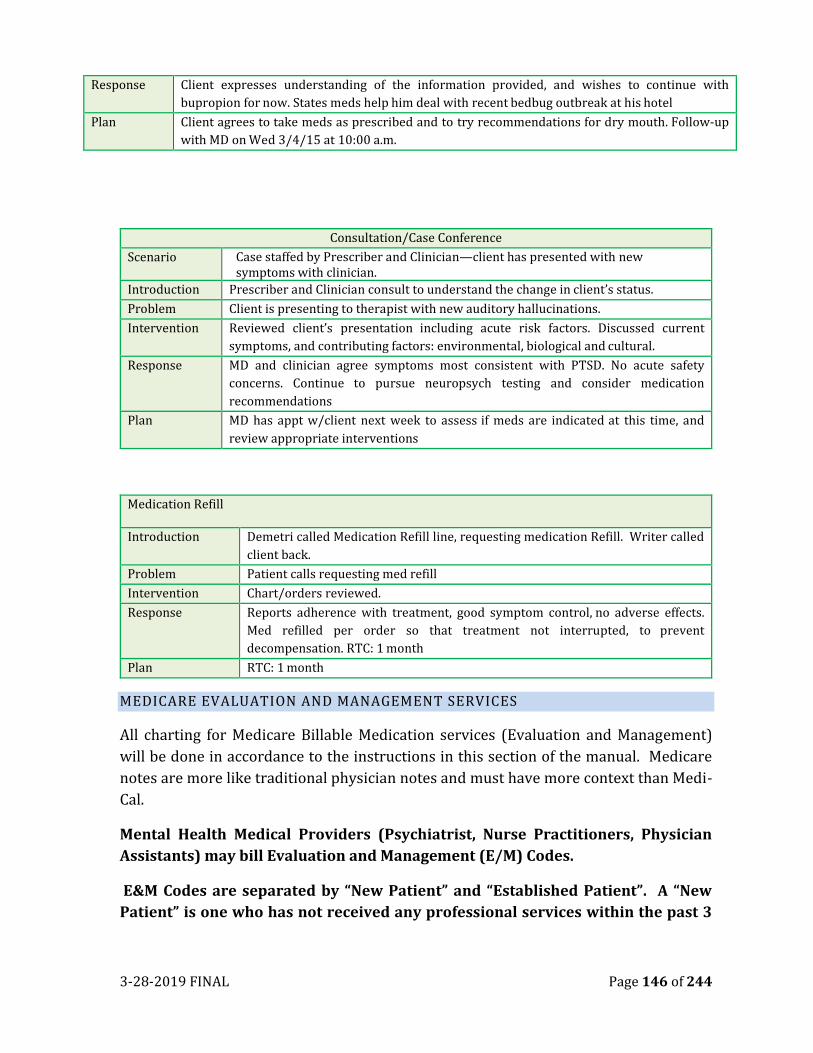
3-28-2019 FINAL Page 146 of 244
Response Client expresses understanding of the information provided, and wishes to continue with
bupropion for now. States meds help him deal with recent bedbug outbreak at his hotel
Plan Client agrees to take meds as prescribed and to try recommendations for dry mouth. Follow-up
with MD on Wed 3/4/15 at 10:00 a.m.
Consultation/Case Conference
Scenario Case staffed by Prescriber and Clinician—client has presented with new symptoms with clinician.
Introduction Prescriber and Clinician consult to understand the change in client’s status.
Problem Client is presenting to therapist with new auditory hallucinations.
Intervention Reviewed client’s presentation including acute risk factors. Discussed current
symptoms, and contributing factors: environmental, biological and cultural.
Response MD and clinician agree symptoms most consistent with PTSD. No acute safety
concerns. Continue to pursue neuropsych testing and consider medication
recommendations
Plan MD has appt w/client next week to assess if meds are indicated at this time, and
review appropriate interventions
Medication Refill
Introduction Demetri called Medication Refill line, requesting medication Refill. Writer called
client back.
Problem Patient calls requesting med refill
Intervention Chart/orders reviewed.
Response Reports adherence with treatment, good symptom control, no adverse effects.
Med refilled per order so that treatment not interrupted, to prevent
decompensation. RTC: 1 month
Plan RTC: 1 month
MEDICARE EVALUATION AND MANAGEMENT SERVICES
All charting for Medicare Billable Medication services (Evaluation and Management)
will be done in accordance to the instructions in this section of the manual. Medicare
notes are more like traditional physician notes and must have more context than Medi-
Cal.
Mental Health Medical Providers (Psychiatrist, Nurse Practitioners, Physician
Assistants) may bill Evaluation and Management (E/M) Codes.
E&M Codes are separated by “New Patient” and “Established Patient”. A “New
Patient” is one who has not received any professional services within the past 3
3-28-2019 FINAL Page 147 of 244
years from the medical provider or another medical provider of the same
specialty or subspecialty.
Evaluation and Management (E&M) Services Overview:
Evaluation and Management (E&M) service billing codes are used by medical doctors
and nurse practitioners to bill for medication management services when they are
evaluating a client face-to-face to inform progress toward a client’s treatment plan of
care goals.
General Principles of E&M Medical Record Documentation:
While E/M services vary in several ways, such as the nature and amount of physician
work required, these general principles help to ensure that the Medical Record
documentation for all E/M services is appropriate:
1. The Medical Record is complete and legible
2. The documentation of each patient encounter should include:
• Reason for the encounter and relevant history, physical examination
findings,
• and prior diagnostic test results
• Assessment, clinical impression, or diagnosis
• Medical plan of care
• Date and legible identity of the observer
3. If the rationale for ordering diagnostic and other ancillary services is not
documented, it should be easily inferred.
4. Past and present diagnoses should be accessible to the treating and/or consulting
Physician.
5. Appropriate health risk factors should be identified.
6. The patient’s progress, response to and changes in treatment, and revision of
diagnosis should be documented.
7. The diagnosis and treatment codes reported on the health insurance claim form
or billing statement should be supported by documentation in the medical r
E&M Service Billing Rules:
In general, the more complex a client visit, the higher the level billed within the
appropriate category. To bill E&M services, services provided must meet the definition
of the E&M billing level (E&M Billing Code Selection Decision Making Process), be
documented in the client record, and reflect the services provided.
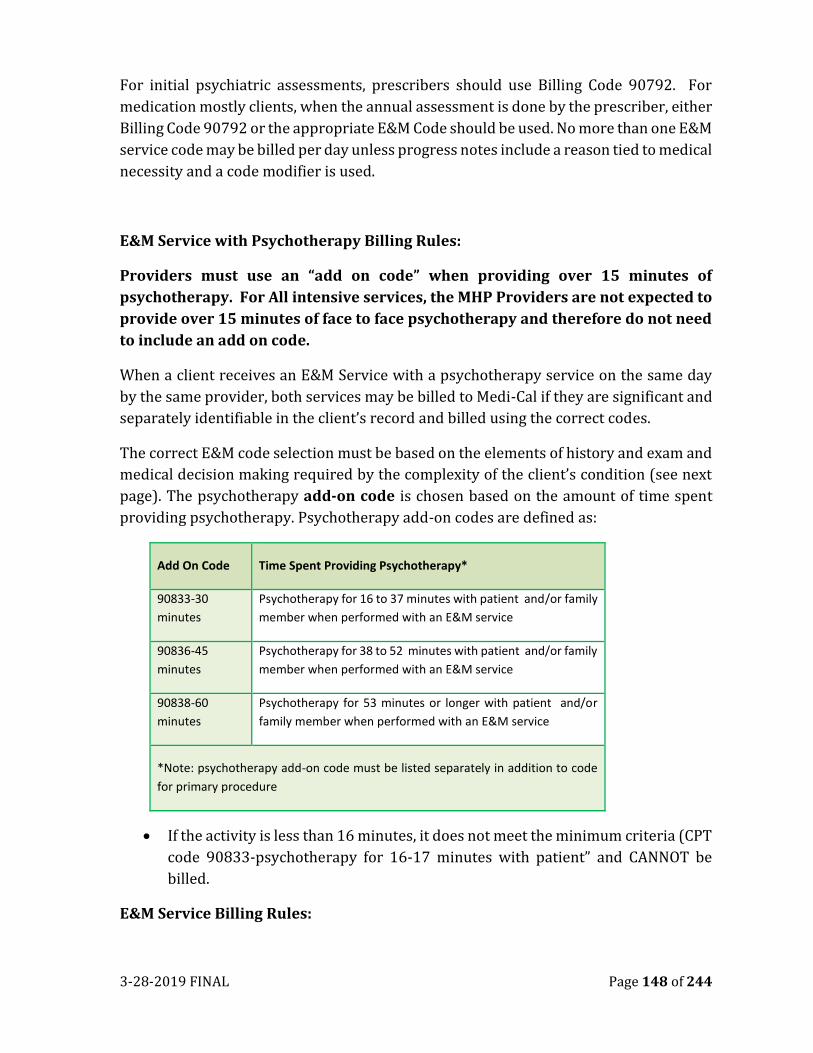
3-28-2019 FINAL Page 148 of 244
For initial psychiatric assessments, prescribers should use Billing Code 90792. For
medication mostly clients, when the annual assessment is done by the prescriber, either
Billing Code 90792 or the appropriate E&M Code should be used. No more than one E&M
service code may be billed per day unless progress notes include a reason tied to medical
necessity and a code modifier is used.
E&M Service with Psychotherapy Billing Rules:
Providers must use an “add on code” when providing over 15 minutes of
psychotherapy. For All intensive services, the MHP Providers are not expected to
provide over 15 minutes of face to face psychotherapy and therefore do not need
to include an add on code.
When a client receives an E&M Service with a psychotherapy service on the same day
by the same provider, both services may be billed to Medi-Cal if they are significant and
separately identifiable in the client’s record and billed using the correct codes.
The correct E&M code selection must be based on the elements of history and exam and
medical decision making required by the complexity of the client’s condition (see next
page). The psychotherapy add-on code is chosen based on the amount of time spent
providing psychotherapy. Psychotherapy add-on codes are defined as:
Add On Code Time Spent Providing Psychotherapy*
90833-30
minutes
Psychotherapy for 16 to 37 minutes with patient and/or family
member when performed with an E&M service
90836-45
minutes
Psychotherapy for 38 to 52 minutes with patient and/or family
member when performed with an E&M service
90838-60
minutes
Psychotherapy for 53 minutes or longer with patient and/or
family member when performed with an E&M service
*Note: psychotherapy add-on code must be listed separately in addition to code
for primary procedure
• If the activity is less than 16 minutes, it does not meet the minimum criteria (CPT
code 90833-psychotherapy for 16-17 minutes with patient” and CANNOT be
billed.
E&M Service Billing Rules:
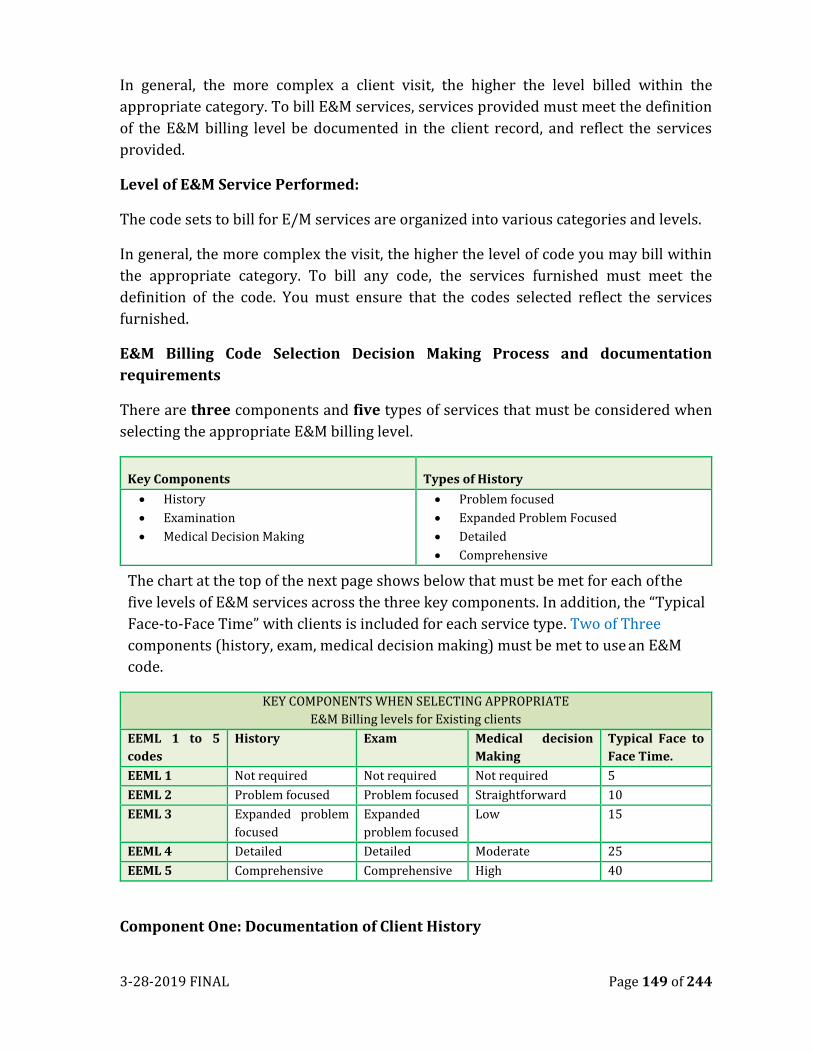
3-28-2019 FINAL Page 149 of 244
In general, the more complex a client visit, the higher the level billed within the
appropriate category. To bill E&M services, services provided must meet the definition
of the E&M billing level be documented in the client record, and reflect the services
provided.
Level of E&M Service Performed:
The code sets to bill for E/M services are organized into various categories and levels.
In general, the more complex the visit, the higher the level of code you may bill within
the appropriate category. To bill any code, the services furnished must meet the
definition of the code. You must ensure that the codes selected reflect the services
furnished.
E&M Billing Code Selection Decision Making Process and documentation
requirements
There are three components and five types of services that must be considered when
selecting the appropriate E&M billing level.
Key Components Types of History
• History
• Examination
• Medical Decision Making
• Problem focused
• Expanded Problem Focused
• Detailed
• Comprehensive
The chart at the top of the next page shows below that must be met for each of the
five levels of E&M services across the three key components. In addition, the “Typical
Face-to-Face Time” with clients is included for each service type. Two of Three
components (history, exam, medical decision making) must be met to use an E&M
code.
KEY COMPONENTS WHEN SELECTING APPROPRIATE
E&M Billing levels for Existing clients
EEML 1 to 5
codes
History Exam Medical decision
Making
Typical Face to
Face Time.
EEML 1 Not required Not required Not required 5
EEML 2 Problem focused Problem focused Straightforward 10
EEML 3 Expanded problem
focused
Expanded
problem focused
Low 15
EEML 4 Detailed Detailed Moderate 25
EEML 5 Comprehensive Comprehensive High 40
Component One: Documentation of Client History
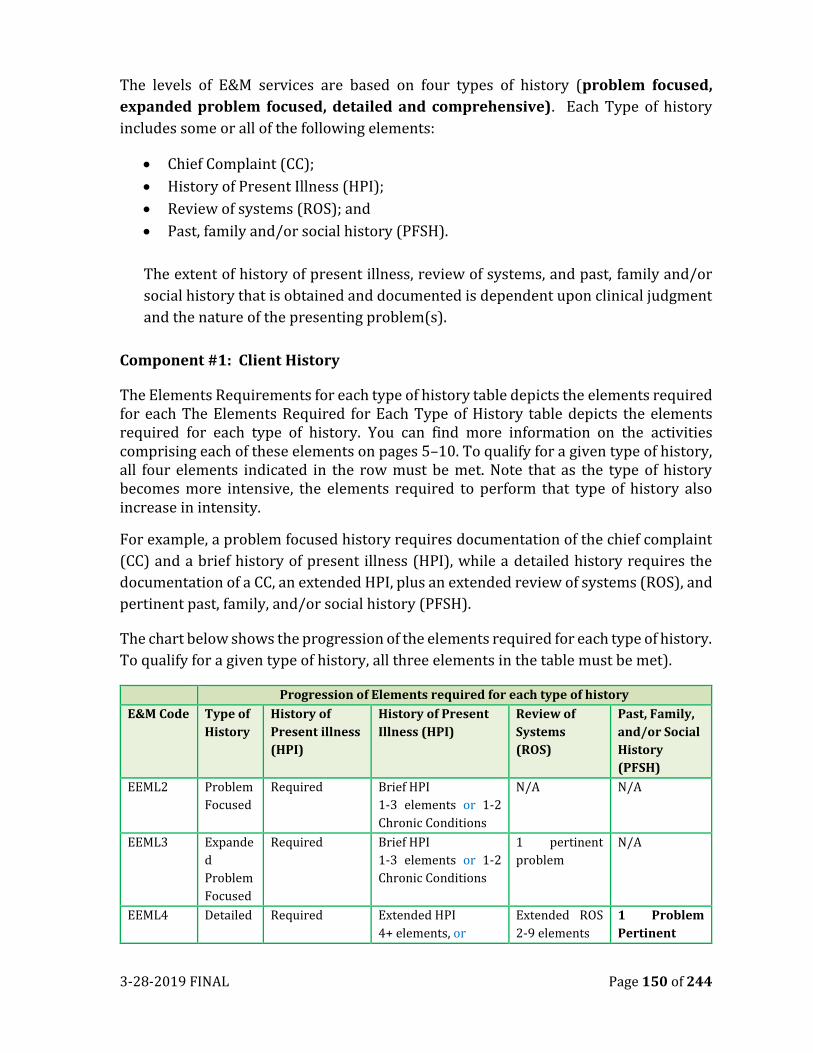
3-28-2019 FINAL Page 150 of 244
The levels of E&M services are based on four types of history (problem focused,
expanded problem focused, detailed and comprehensive). Each Type of history
includes some or all of the following elements:
• Chief Complaint (CC);
• History of Present Illness (HPI);
• Review of systems (ROS); and
• Past, family and/or social history (PFSH).
The extent of history of present illness, review of systems, and past, family and/or
social history that is obtained and documented is dependent upon clinical judgment
and the nature of the presenting problem(s).
Component #1: Client History
The Elements Requirements for each type of history table depicts the elements required for each The Elements Required for Each Type of History table depicts the elements required for each type of history. You can find more information on the activities comprising each of these elements on pages 5–10. To qualify for a given type of history, all four elements indicated in the row must be met. Note that as the type of history becomes more intensive, the elements required to perform that type of history also increase in intensity.
For example, a problem focused history requires documentation of the chief complaint
(CC) and a brief history of present illness (HPI), while a detailed history requires the
documentation of a CC, an extended HPI, plus an extended review of systems (ROS), and
pertinent past, family, and/or social history (PFSH).
The chart below shows the progression of the elements required for each type of history.
To qualify for a given type of history, all three elements in the table must be met).
Progression of Elements required for each type of history
E&M Code Type of
History
History of
Present illness
(HPI)
History of Present
Illness (HPI)
Review of
Systems
(ROS)
Past, Family,
and/or Social
History
(PFSH)
EEML2 Problem
Focused
Required Brief HPI
1-3 elements or 1-2
Chronic Conditions
N/A N/A
EEML3 Expande
d
Problem
Focused
Required Brief HPI
1-3 elements or 1-2
Chronic Conditions
1 pertinent
problem
N/A
EEML4 Detailed Required Extended HPI
4+ elements, or
Extended ROS
2-9 elements
1 Problem
Pertinent
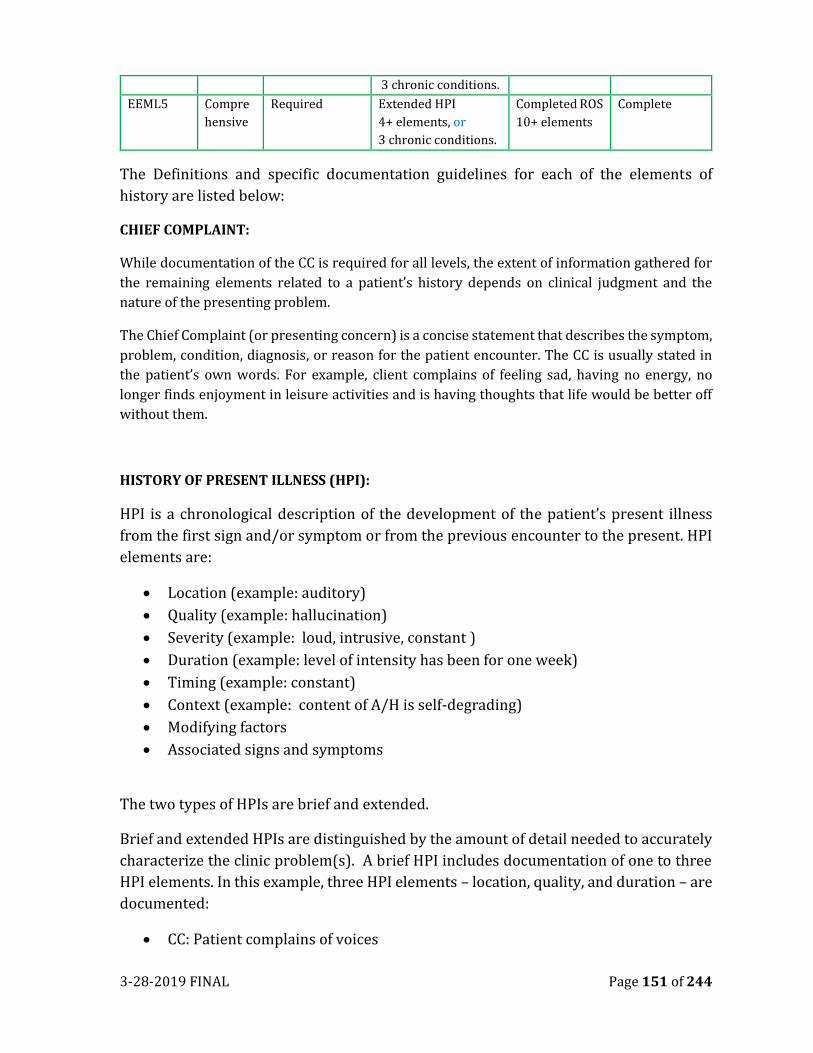
3-28-2019 FINAL Page 151 of 244
3 chronic conditions.
EEML5 Compre
hensive
Required Extended HPI
4+ elements, or
3 chronic conditions.
Completed ROS
10+ elements
Complete
The Definitions and specific documentation guidelines for each of the elements of
history are listed below:
CHIEF COMPLAINT:
While documentation of the CC is required for all levels, the extent of information gathered for
the remaining elements related to a patient’s history depends on clinical judgment and the
nature of the presenting problem.
The Chief Complaint (or presenting concern) is a concise statement that describes the symptom,
problem, condition, diagnosis, or reason for the patient encounter. The CC is usually stated in
the patient’s own words. For example, client complains of feeling sad, having no energy, no
longer finds enjoyment in leisure activities and is having thoughts that life would be better off
without them.
HISTORY OF PRESENT ILLNESS (HPI):
HPI is a chronological description of the development of the patient’s present illness
from the first sign and/or symptom or from the previous encounter to the present. HPI
elements are:
• Location (example: auditory)
• Quality (example: hallucination)
• Severity (example: loud, intrusive, constant )
• Duration (example: level of intensity has been for one week)
• Timing (example: constant)
• Context (example: content of A/H is self-degrading)
• Modifying factors
• Associated signs and symptoms
The two types of HPIs are brief and extended.
Brief and extended HPIs are distinguished by the amount of detail needed to accurately
characterize the clinic problem(s). A brief HPI includes documentation of one to three
HPI elements. In this example, three HPI elements – location, quality, and duration – are
documented:
• CC: Patient complains of voices
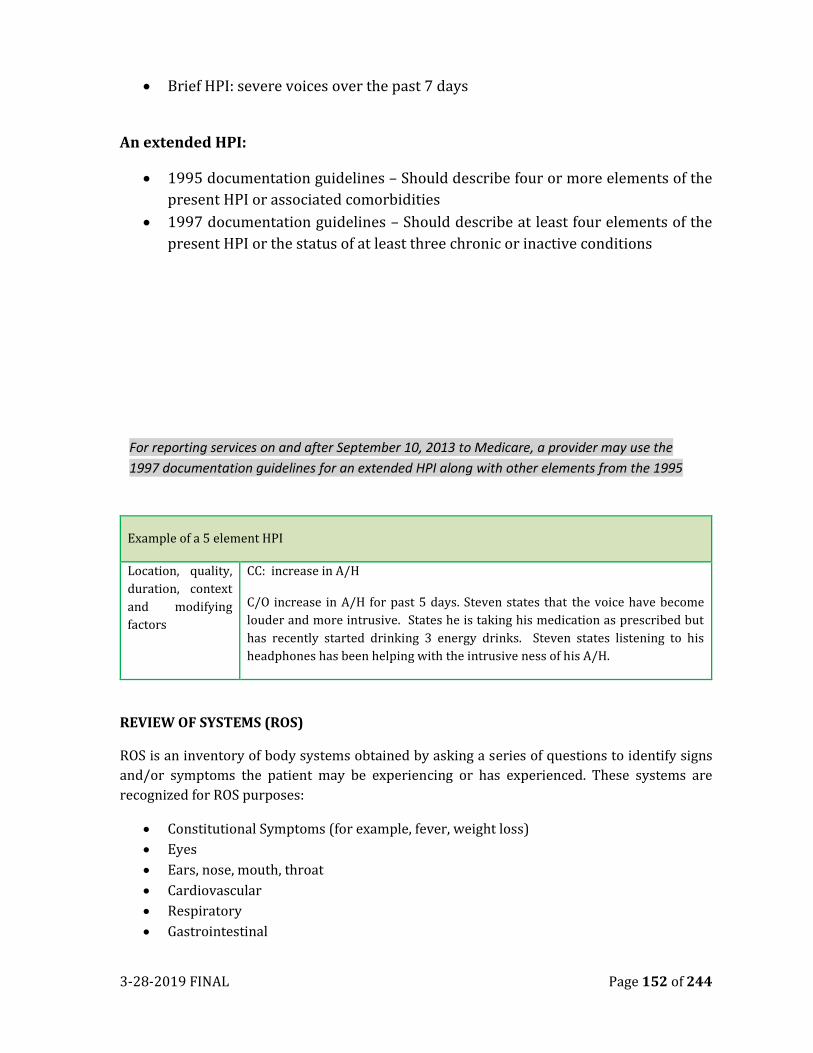
3-28-2019 FINAL Page 152 of 244
• Brief HPI: severe voices over the past 7 days
An extended HPI:
• 1995 documentation guidelines – Should describe four or more elements of the
present HPI or associated comorbidities
• 1997 documentation guidelines – Should describe at least four elements of the
present HPI or the status of at least three chronic or inactive conditions
Example of a 5 element HPI
Location, quality,
duration, context
and modifying
factors
CC: increase in A/H
C/O increase in A/H for past 5 days. Steven states that the voice have become
louder and more intrusive. States he is taking his medication as prescribed but
has recently started drinking 3 energy drinks. Steven states listening to his
headphones has been helping with the intrusive ness of his A/H.
REVIEW OF SYSTEMS (ROS)
ROS is an inventory of body systems obtained by asking a series of questions to identify signs
and/or symptoms the patient may be experiencing or has experienced. These systems are
recognized for ROS purposes:
• Constitutional Symptoms (for example, fever, weight loss)
• Eyes
• Ears, nose, mouth, throat
• Cardiovascular
• Respiratory
• Gastrointestinal
For reporting services on and after September 10, 2013 to Medicare, a provider may use the
1997 documentation guidelines for an extended HPI along with other elements from the 1995
documentation guidelines to document E/M Services.
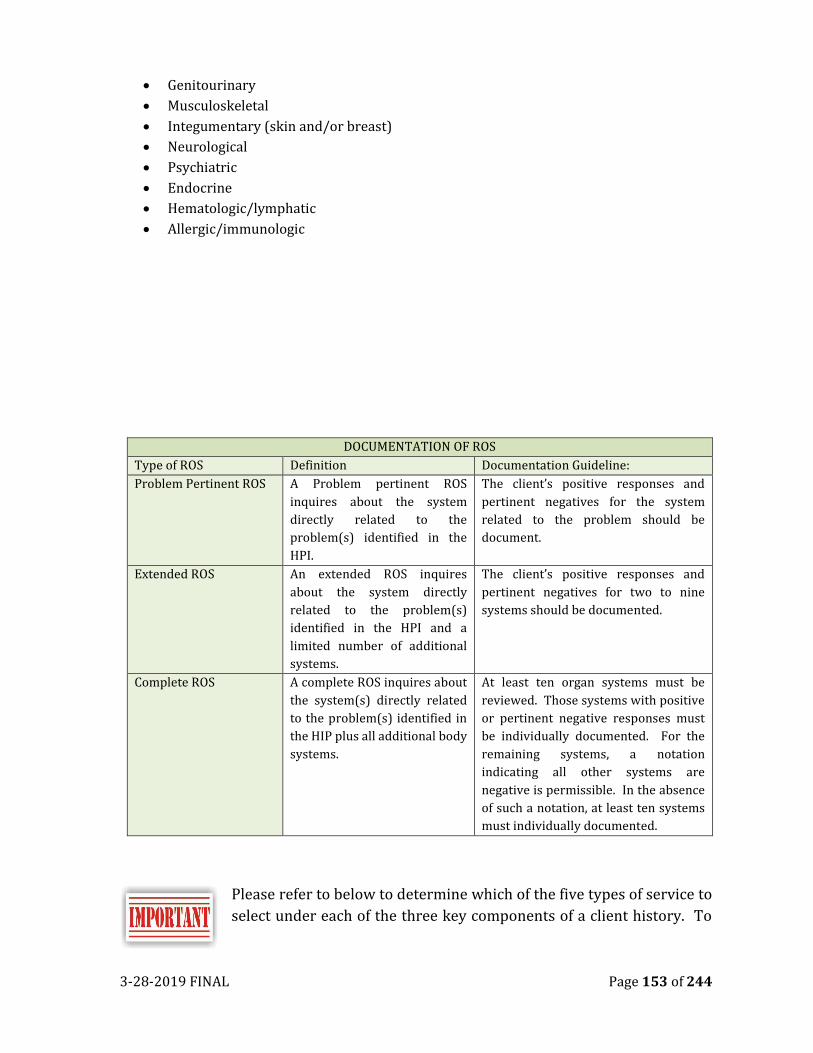
3-28-2019 FINAL Page 153 of 244
• Genitourinary
• Musculoskeletal
• Integumentary (skin and/or breast)
• Neurological
• Psychiatric
• Endocrine
• Hematologic/lymphatic
• Allergic/immunologic
DOCUMENTATION OF ROS
Type of ROS Definition Documentation Guideline:
Problem Pertinent ROS A Problem pertinent ROS
inquires about the system
directly related to the
problem(s) identified in the
HPI.
The client’s positive responses and
pertinent negatives for the system
related to the problem should be
document.
Extended ROS An extended ROS inquires
about the system directly
related to the problem(s)
identified in the HPI and a
limited number of additional
systems.
The client’s positive responses and
pertinent negatives for two to nine
systems should be documented.
Complete ROS A complete ROS inquires about
the system(s) directly related
to the problem(s) identified in
the HIP plus all additional body
systems.
At least ten organ systems must be
reviewed. Those systems with positive
or pertinent negative responses must
be individually documented. For the
remaining systems, a notation
indicating all other systems are
negative is permissible. In the absence
of such a notation, at least ten systems
must individually documented.
Please refer to below to determine which of the five types of service to
select under each of the three key components of a client history. To
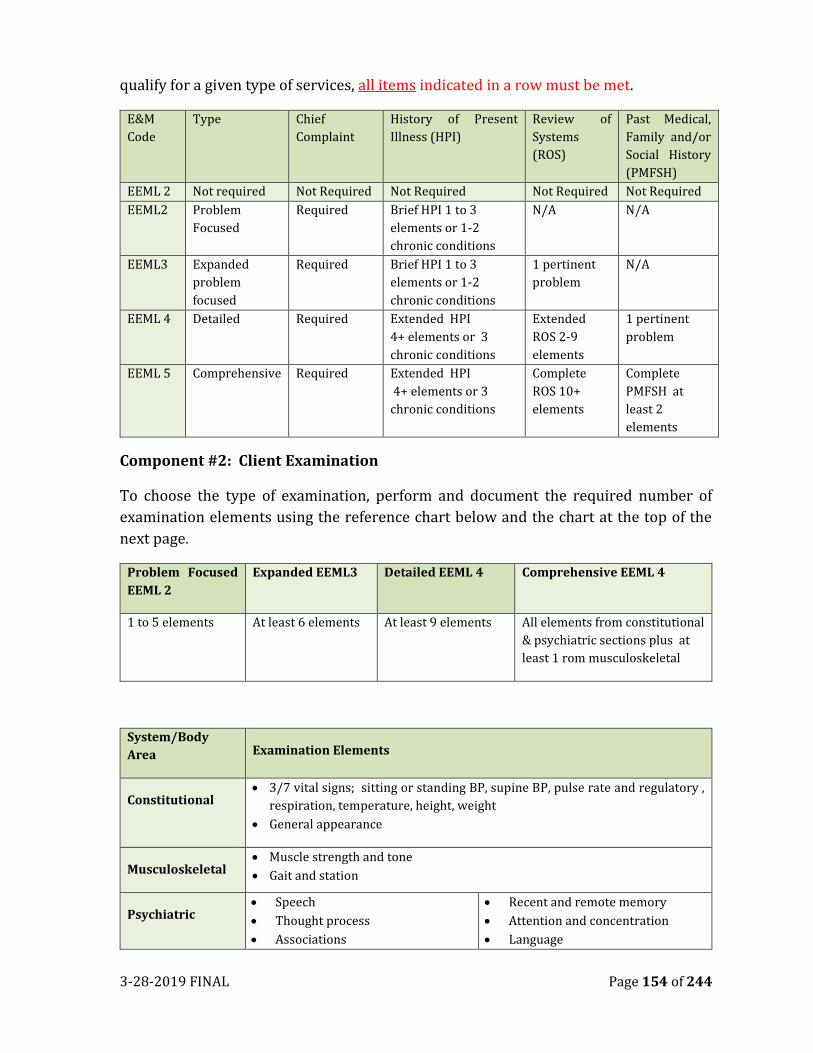
3-28-2019 FINAL Page 154 of 244
qualify for a given type of services, all items indicated in a row must be met.
E&M
Code
Type Chief
Complaint
History of Present
Illness (HPI)
Review of
Systems
(ROS)
Past Medical,
Family and/or
Social History
(PMFSH)
EEML 2 Not required Not Required Not Required Not Required Not Required
EEML2 Problem
Focused
Required Brief HPI 1 to 3
elements or 1-2
chronic conditions
N/A N/A
EEML3 Expanded
problem
focused
Required Brief HPI 1 to 3
elements or 1-2
chronic conditions
1 pertinent
problem
N/A
EEML 4 Detailed Required Extended HPI
4+ elements or 3
chronic conditions
Extended
ROS 2-9
elements
1 pertinent
problem
EEML 5 Comprehensive Required Extended HPI
4+ elements or 3
chronic conditions
Complete
ROS 10+
elements
Complete
PMFSH at
least 2
elements
Component #2: Client Examination
To choose the type of examination, perform and document the required number of
examination elements using the reference chart below and the chart at the top of the
next page.
Problem Focused
EEML 2
Expanded EEML3 Detailed EEML 4 Comprehensive EEML 4
1 to 5 elements At least 6 elements At least 9 elements All elements from constitutional
& psychiatric sections plus at
least 1 rom musculoskeletal
System/Body
Area Examination Elements
Constitutional • 3/7 vital signs; sitting or standing BP, supine BP, pulse rate and regulatory ,
respiration, temperature, height, weight
• General appearance
Musculoskeletal • Muscle strength and tone
• Gait and station
Psychiatric • Speech
• Thought process
• Associations
• Recent and remote memory
• Attention and concentration
• Language
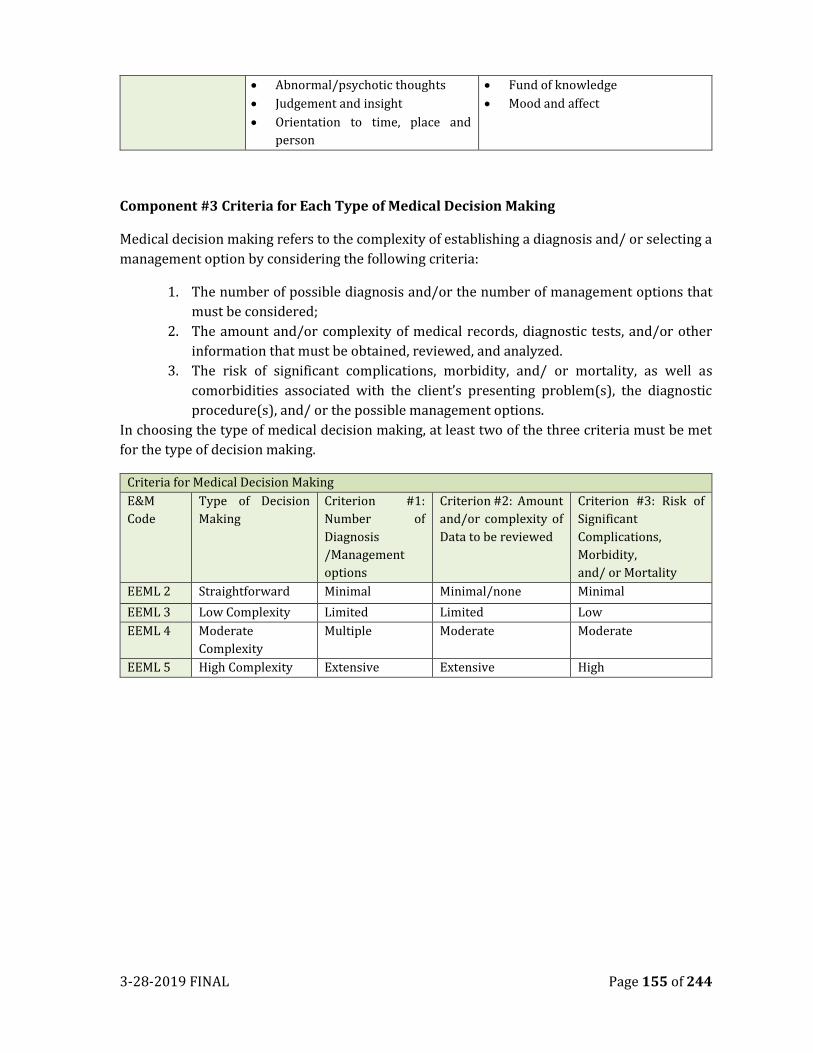
3-28-2019 FINAL Page 155 of 244
• Abnormal/psychotic thoughts
• Judgement and insight
• Orientation to time, place and
person
• Fund of knowledge
• Mood and affect
Component #3 Criteria for Each Type of Medical Decision Making
Medical decision making refers to the complexity of establishing a diagnosis and/ or selecting a
management option by considering the following criteria:
1. The number of possible diagnosis and/or the number of management options that
must be considered;
2. The amount and/or complexity of medical records, diagnostic tests, and/or other
information that must be obtained, reviewed, and analyzed.
3. The risk of significant complications, morbidity, and/ or mortality, as well as
comorbidities associated with the client’s presenting problem(s), the diagnostic
procedure(s), and/ or the possible management options.
In choosing the type of medical decision making, at least two of the three criteria must be met
for the type of decision making.
Criteria for Medical Decision Making
E&M
Code
Type of Decision
Making
Criterion #1:
Number of
Diagnosis
/Management
options
Criterion #2: Amount
and/or complexity of
Data to be reviewed
Criterion #3: Risk of
Significant
Complications,
Morbidity,
and/ or Mortality
EEML 2 Straightforward Minimal Minimal/none Minimal
EEML 3 Low Complexity Limited Limited Low
EEML 4 Moderate
Complexity
Multiple Moderate Moderate
EEML 5 High Complexity Extensive Extensive High
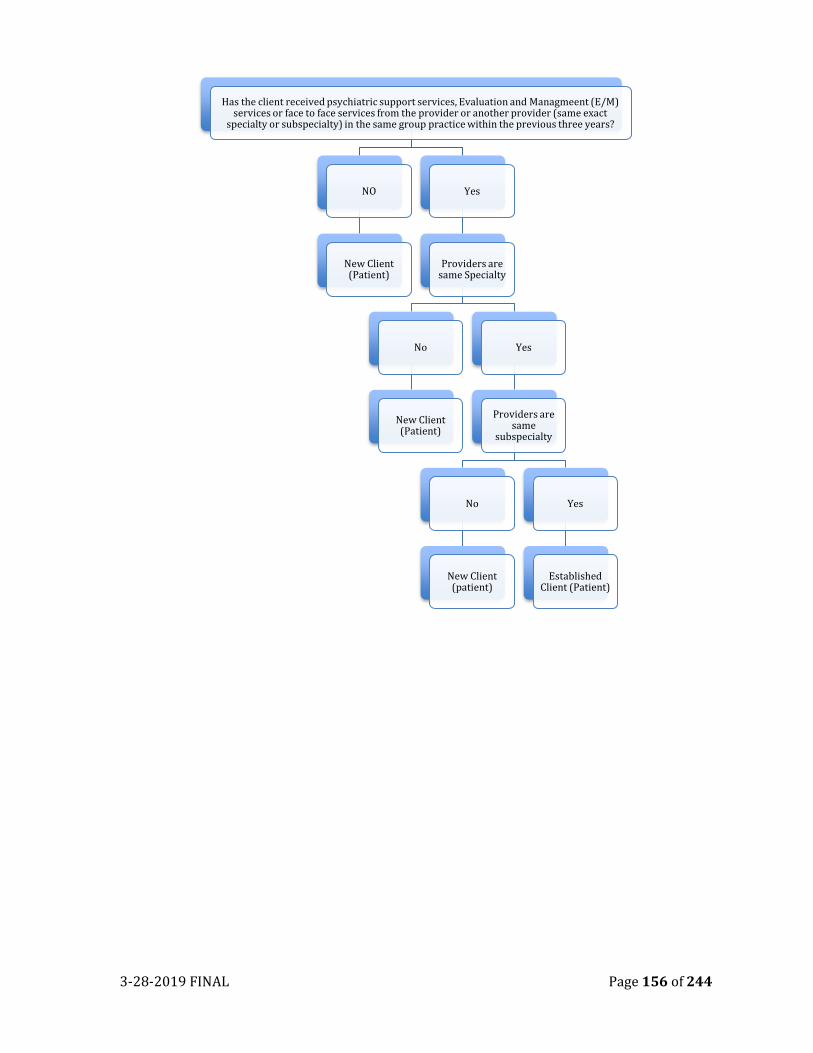
3-28-2019 FINAL Page 156 of 244
Has the client received psychiatric support services, Evaluation and Managmeent (E/M) services or face to face services from the provider or another provider (same exact
specialty or subspecialty) in the same group practice within the previous three years?
NO
New Client (Patient)
Yes
Providers are same Specialty
No
New Client (Patient)
Yes
Providers are same
subspecialty
No
New Client (patient)
Yes
Established Client (Patient)
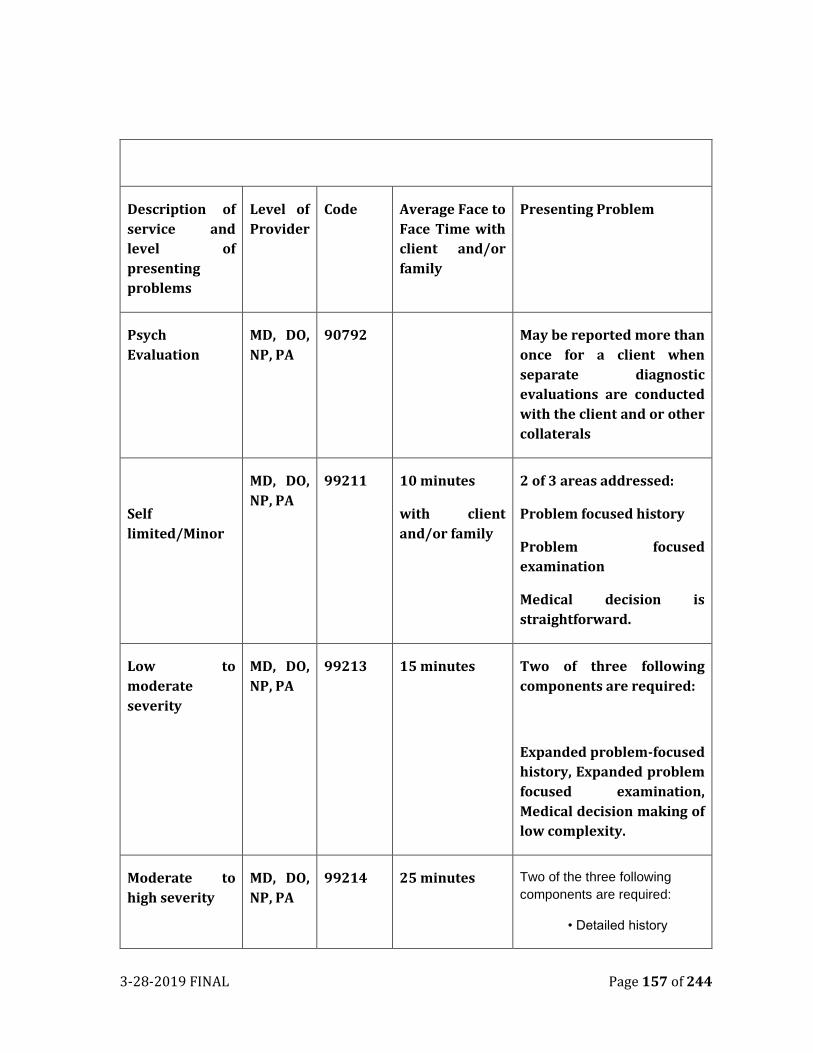
3-28-2019 FINAL Page 157 of 244
Description of
service and
level of
presenting
problems
Level of
Provider
Code Average Face to
Face Time with
client and/or
family
Presenting Problem
Psych
Evaluation
MD, DO,
NP, PA
90792 May be reported more than
once for a client when
separate diagnostic
evaluations are conducted
with the client and or other
collaterals
Self
limited/Minor
MD, DO,
NP, PA
99211 10 minutes
with client
and/or family
2 of 3 areas addressed:
Problem focused history
Problem focused
examination
Medical decision is
straightforward.
Low to
moderate
severity
MD, DO,
NP, PA
99213 15 minutes Two of three following
components are required:
Expanded problem-focused
history, Expanded problem
focused examination,
Medical decision making of
low complexity.
Moderate to
high severity
MD, DO,
NP, PA
99214 25 minutes Two of the three following
components are required:
• Detailed history
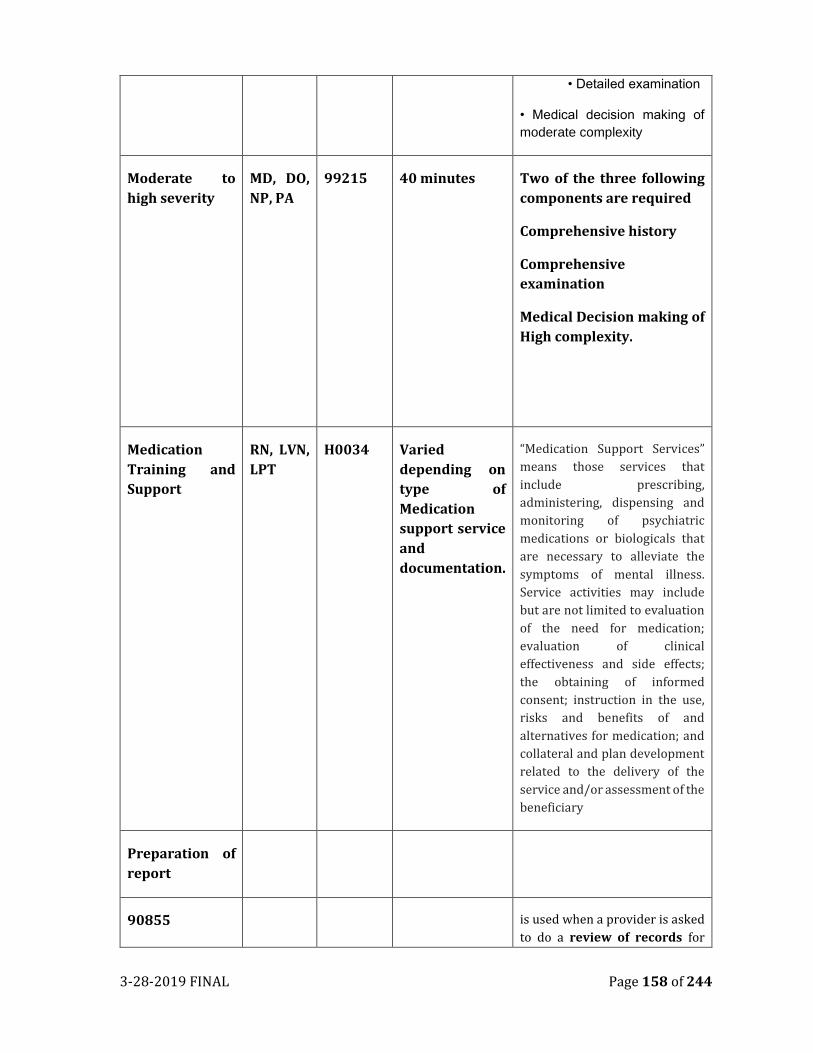
3-28-2019 FINAL Page 158 of 244
• Detailed examination
• Medical decision making of
moderate complexity
Moderate to
high severity
MD, DO,
NP, PA
99215 40 minutes Two of the three following
components are required
Comprehensive history
Comprehensive
examination
Medical Decision making of
High complexity.
Medication
Training and
Support
RN, LVN,
LPT
H0034 Varied
depending on
type of
Medication
support service
and
documentation.
“Medication Support Services”
means those services that
include prescribing,
administering, dispensing and
monitoring of psychiatric
medications or biologicals that
are necessary to alleviate the
symptoms of mental illness.
Service activities may include
but are not limited to evaluation
of the need for medication;
evaluation of clinical
effectiveness and side effects;
the obtaining of informed
consent; instruction in the use,
risks and benefits of and
alternatives for medication; and
collateral and plan development
related to the delivery of the
service and/or assessment of the
beneficiary
Preparation of
report
90855 is used when a provider is asked
to do a review of records for
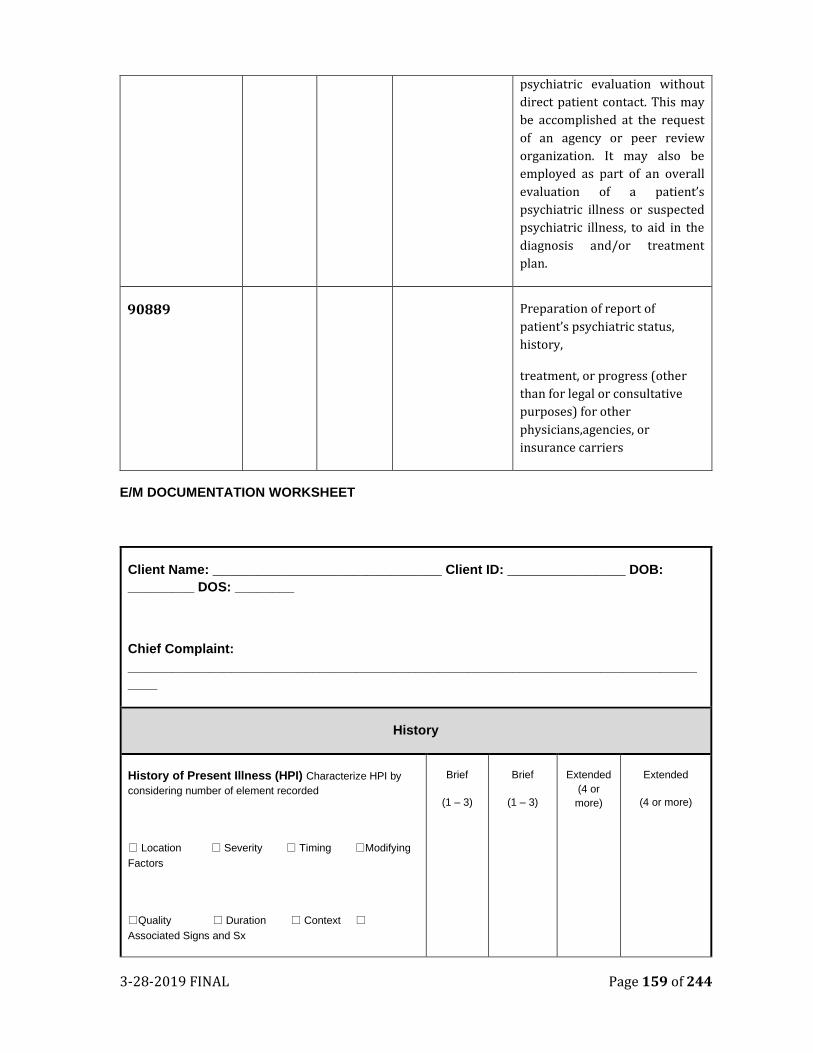
3-28-2019 FINAL Page 159 of 244
psychiatric evaluation without
direct patient contact. This may
be accomplished at the request
of an agency or peer review
organization. It may also be
employed as part of an overall
evaluation of a patient’s
psychiatric illness or suspected
psychiatric illness, to aid in the
diagnosis and/or treatment
plan.
90889 Preparation of report of
patient’s psychiatric status,
history,
treatment, or progress (other
than for legal or consultative
purposes) for other
physicians,agencies, or
insurance carriers
E/M DOCUMENTATION WORKSHEET
Client Name: _______________________________ Client ID: ________________ DOB:
_________ DOS: ________
Chief Complaint:
_____________________________________________________________________________
____
History
History of Present Illness (HPI) Characterize HPI by
considering number of element recorded
Location Severity Timing Modifying
Factors
Quality Duration Context
Associated Signs and Sx
Brief
(1 – 3)
Brief
(1 – 3)
Extended
(4 or
more)
Extended
(4 or more)
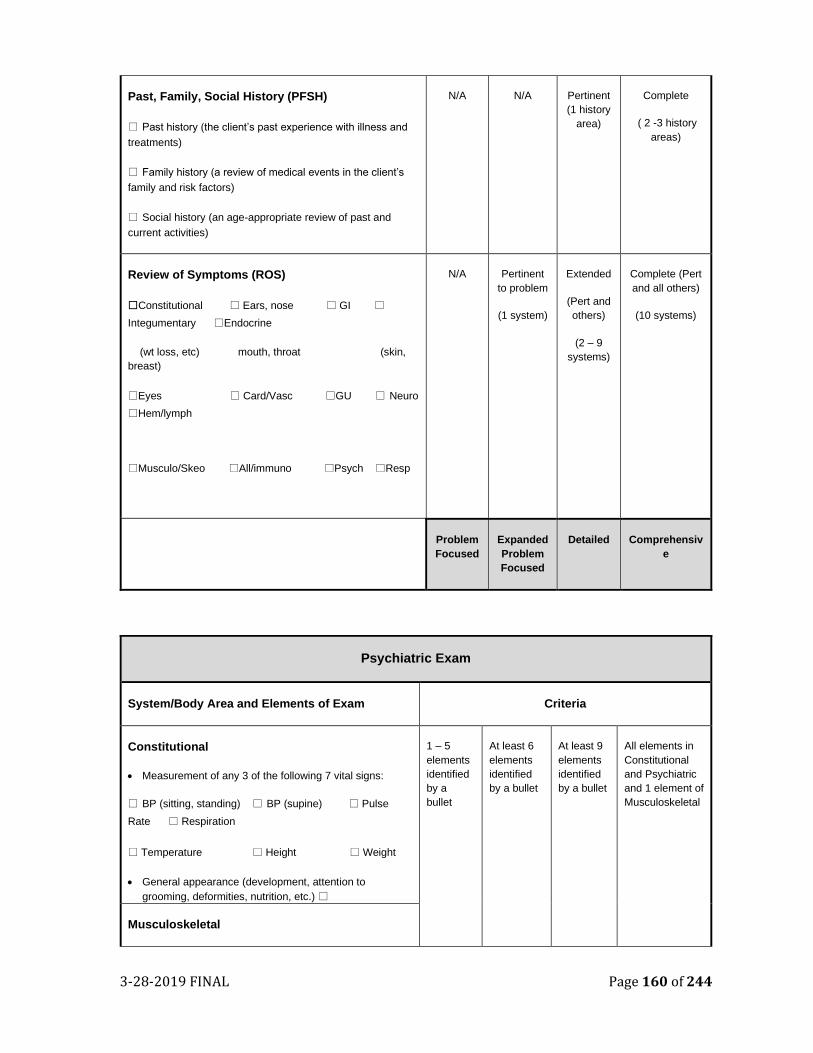
3-28-2019 FINAL Page 160 of 244
Past, Family, Social History (PFSH)
Past history (the client’s past experience with illness and
treatments)
Family history (a review of medical events in the client’s
family and risk factors)
Social history (an age-appropriate review of past and
current activities)
N/A N/A Pertinent
(1 history
area)
Complete
( 2 -3 history
areas)
Review of Symptoms (ROS)
Constitutional Ears, nose GI
Integumentary Endocrine
(wt loss, etc) mouth, throat (skin,
breast)
Eyes Card/Vasc GU Neuro
Hem/lymph
Musculo/Skeo All/immuno Psych Resp
N/A Pertinent
to problem
(1 system)
Extended
(Pert and
others)
(2 – 9
systems)
Complete (Pert
and all others)
(10 systems)
Problem
Focused
Expanded
Problem
Focused
Detailed Comprehensiv
e
Psychiatric Exam
System/Body Area and Elements of Exam Criteria
Constitutional
• Measurement of any 3 of the following 7 vital signs:
BP (sitting, standing) BP (supine) Pulse
Rate Respiration
Temperature Height Weight
• General appearance (development, attention to
grooming, deformities, nutrition, etc.)
1 – 5
elements
identified
by a
bullet
At least 6
elements
identified
by a bullet
At least 9
elements
identified
by a bullet
All elements in
Constitutional
and Psychiatric
and 1 element of
Musculoskeletal
Musculoskeletal
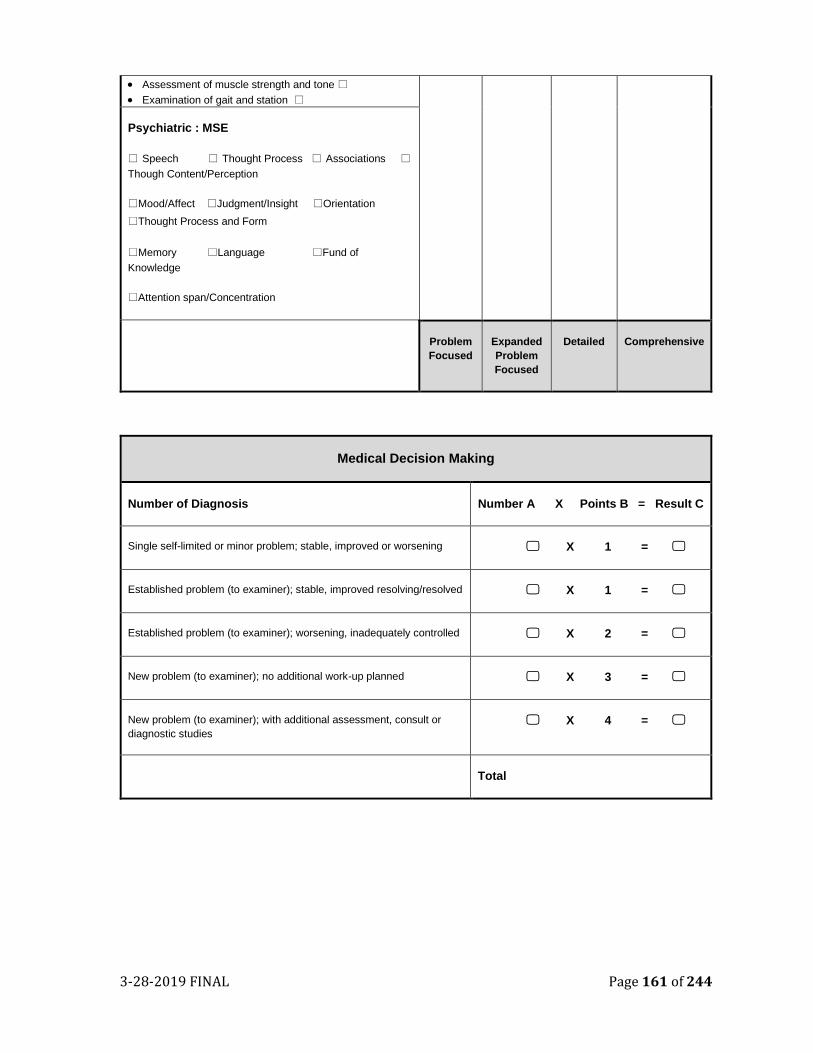
3-28-2019 FINAL Page 161 of 244
• Assessment of muscle strength and tone
• Examination of gait and station
Psychiatric : MSE
Speech Thought Process Associations Though Content/Perception
Mood/Affect Judgment/Insight Orientation
Thought Process and Form
Memory Language Fund of
Knowledge
Attention span/Concentration
Problem
Focused
Expanded
Problem
Focused
Detailed Comprehensive
Medical Decision Making
Number of Diagnosis Number A X Points B = Result C
Single self-limited or minor problem; stable, improved or worsening X 1 =
Established problem (to examiner); stable, improved resolving/resolved X 1 =
Established problem (to examiner); worsening, inadequately controlled X 2 =
New problem (to examiner); no additional work-up planned X 3 =
New problem (to examiner); with additional assessment, consult or
diagnostic studies
X 4 =
Total
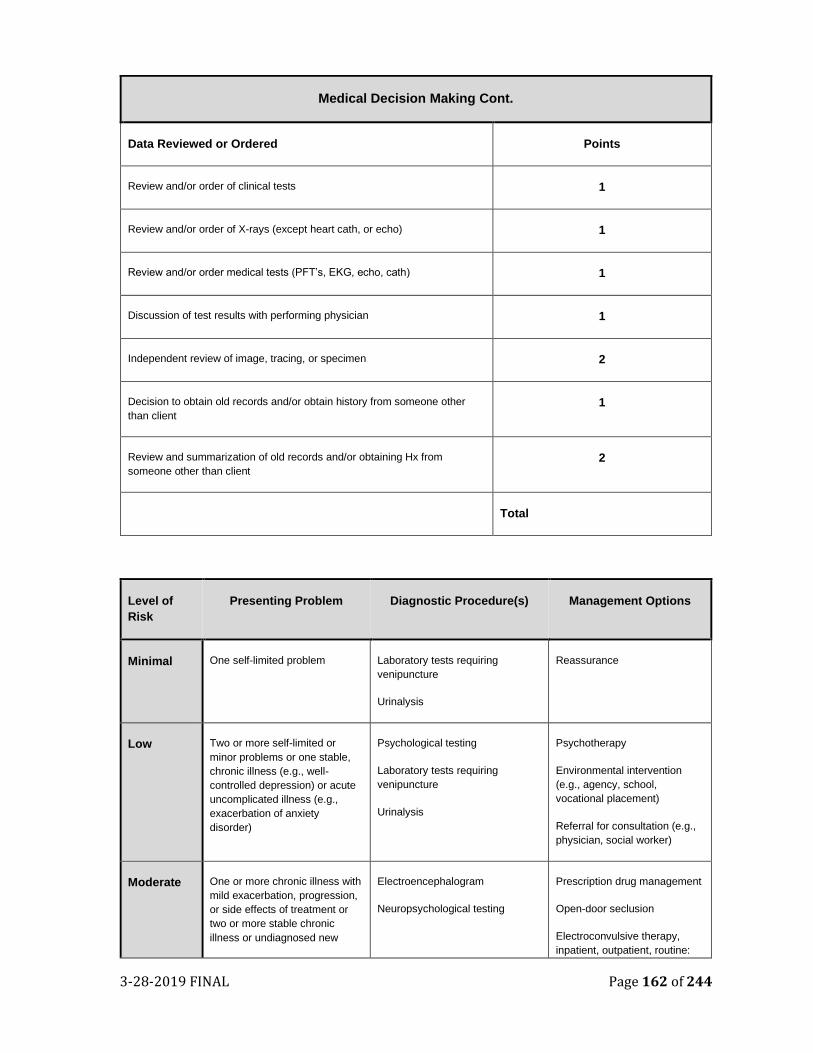
3-28-2019 FINAL Page 162 of 244
Medical Decision Making Cont.
Data Reviewed or Ordered Points
Review and/or order of clinical tests 1
Review and/or order of X-rays (except heart cath, or echo) 1
Review and/or order medical tests (PFT’s, EKG, echo, cath) 1
Discussion of test results with performing physician 1
Independent review of image, tracing, or specimen 2
Decision to obtain old records and/or obtain history from someone other
than client
1
Review and summarization of old records and/or obtaining Hx from
someone other than client
2
Total
Level of
Risk
Presenting Problem Diagnostic Procedure(s) Management Options
Minimal One self-limited problem Laboratory tests requiring
venipuncture
Urinalysis
Reassurance
Low Two or more self-limited or
minor problems or one stable,
chronic illness (e.g., well-
controlled depression) or acute
uncomplicated illness (e.g.,
exacerbation of anxiety
disorder)
Psychological testing
Laboratory tests requiring
venipuncture
Urinalysis
Psychotherapy
Environmental intervention
(e.g., agency, school,
vocational placement)
Referral for consultation (e.g.,
physician, social worker)
Moderate One or more chronic illness with
mild exacerbation, progression,
or side effects of treatment or
two or more stable chronic
illness or undiagnosed new
Electroencephalogram
Neuropsychological testing
Prescription drug management
Open-door seclusion
Electroconvulsive therapy,
inpatient, outpatient, routine:
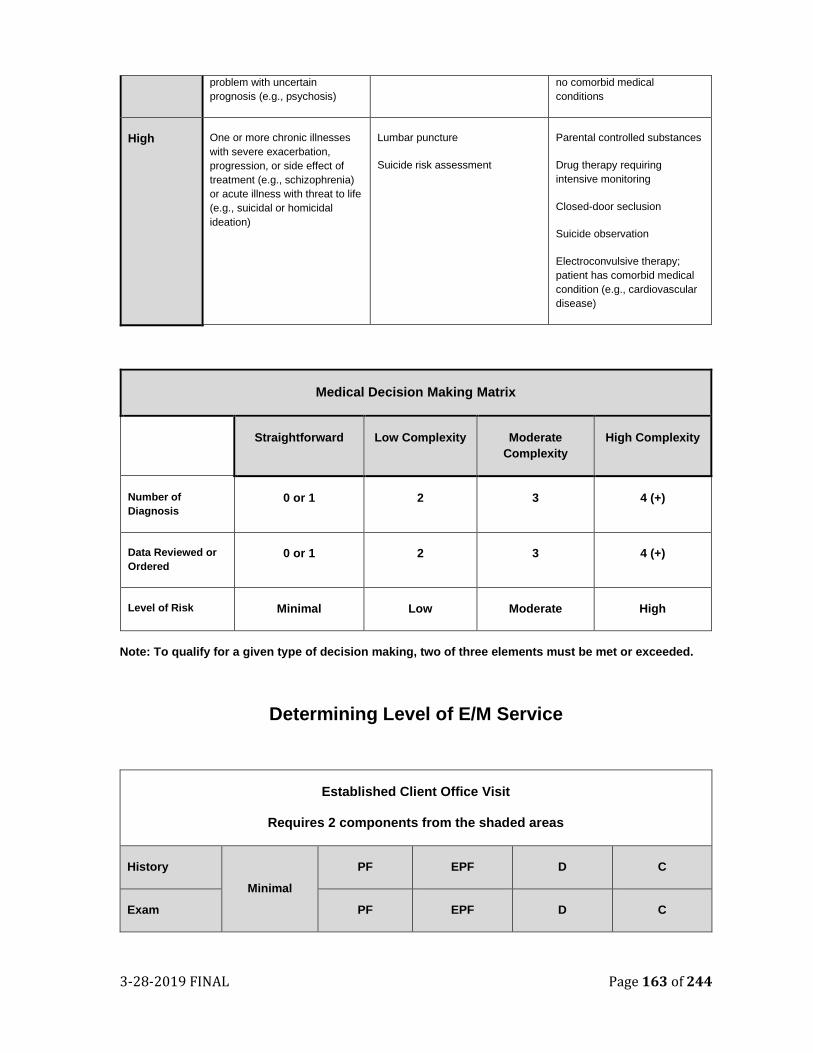
3-28-2019 FINAL Page 163 of 244
problem with uncertain
prognosis (e.g., psychosis)
no comorbid medical
conditions
High One or more chronic illnesses
with severe exacerbation,
progression, or side effect of
treatment (e.g., schizophrenia)
or acute illness with threat to life
(e.g., suicidal or homicidal
ideation)
Lumbar puncture
Suicide risk assessment
Parental controlled substances
Drug therapy requiring
intensive monitoring
Closed-door seclusion
Suicide observation
Electroconvulsive therapy;
patient has comorbid medical
condition (e.g., cardiovascular
disease)
Medical Decision Making Matrix
Straightforward Low Complexity Moderate
Complexity
High Complexity
Number of
Diagnosis
0 or 1 2 3 4 (+)
Data Reviewed or
Ordered
0 or 1 2 3 4 (+)
Level of Risk Minimal Low Moderate High
Note: To qualify for a given type of decision making, two of three elements must be met or exceeded.
Determining Level of E/M Service
Established Client Office Visit
Requires 2 components from the shaded areas
History
Minimal
PF EPF D C
Exam PF EPF D C
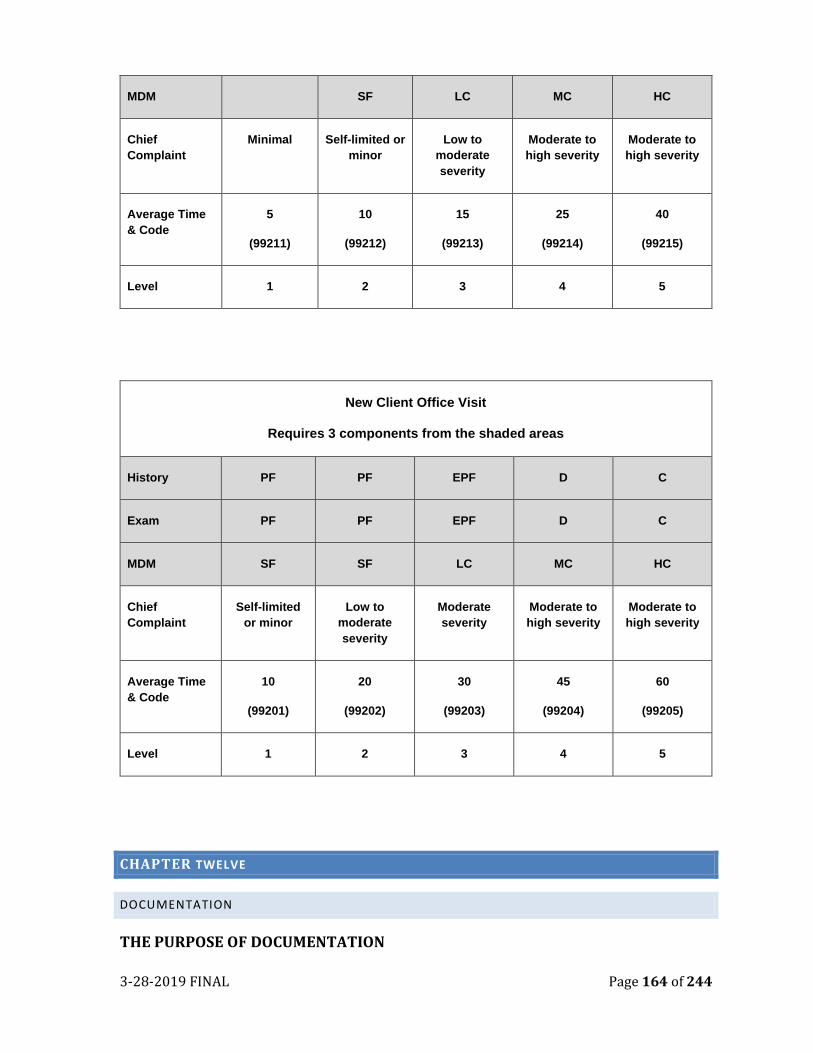
3-28-2019 FINAL Page 164 of 244
MDM SF LC MC HC
Chief
Complaint
Minimal Self-limited or
minor
Low to
moderate
severity
Moderate to
high severity
Moderate to
high severity
Average Time
& Code
5
(99211)
10
(99212)
15
(99213)
25
(99214)
40
(99215)
Level 1 2 3 4 5
New Client Office Visit
Requires 3 components from the shaded areas
History PF PF EPF D C
Exam PF PF EPF D C
MDM SF SF LC MC HC
Chief
Complaint
Self-limited
or minor
Low to
moderate
severity
Moderate
severity
Moderate to
high severity
Moderate to
high severity
Average Time
& Code
10
(99201)
20
(99202)
30
(99203)
45
(99204)
60
(99205)
Level 1 2 3 4 5
CHAPTER TWELVE
DOCUMENTATION
THE PURPOSE OF DOCUMENTATION
3-28-2019 FINAL Page 165 of 244
The Placer County MHP establishes documentation
standards in order to help realize a core value of our
system: commitment to clinical and service excellence.
The importance of maintaining a comprehensive,
detailed and uniform clinical record and
documentation system cannot be overemphasized. The
clinical record stores the information concerning the
client and his/her care. The content of the clinical
record is developed as a result of the interaction of the
mental health care team which uses it as a
communication tool.
To be complete, the clinical record must contain
sufficient information to identify the client clearly,
support the diagnosis, justify treatment, and record
observations, plans, outcomes and interventions as
well as the client’s response to treatment. It is
necessary that there be prompt recording of observation, treatment and care by all who
contribute to the care of a client.
Establishing uniform standards for the clinical record facilitates access to necessary
client documentation and simplifies review of records. The clinical record is potentially
one of the most important and persuasive items of evidence available counteracting a
client’s allegations of medical negligence and can protect us from risk in legal
proceedings. In addition, accurate, complete documentation helps us to comply with all
legal requirements when we claim for services and enables professionals to discharge
their legal and ethical duties.
GENERAL PRINCIPLES OF DOCUMENTATION:
For the purposes of these documentation standards, charts containing documentation
of mental health services are referred to as Clinical Records or Records.
Until the MHP has adopted an Electronic Health Record (EHR) within the county owned and operated clinics, MHP continues to operate a hybrid model of clinical records. Some providers continue to use paper-based documents, while others have fully transitions into an EHR and others operate a hybrid model.
1. All CBOs who currently utilize EHR must adhere to MHP’s memo, regarding EHR and electronic signature, dated.
2. All Providers must use MHP pre-approved forms. Contract providers who utilize an electronic health record system for documentation must incorporate all MHP required documentation elements identified in MHP’s memo regarding EHR and electronic signature, dated
Confidentiality: Do not write another client’s name in the client’s chart. If another client must be identified in the record, do not identify the client by name, rather use MR number or do not identify the other client as a mental health client. Names of family members/support persons should be recorded only when needed to complete intake registration and financial documentation. Otherwise, refer to the relationship-mother, father, friend, etc. You may use first name or initials for clarifications.
3-28-2019 FINAL Page 166 of 244
3. Required clinical documents include a completed Assessment, Unified Service Plan (Treatment Plan), and on-going progress notes. Remember that the medical records, both paper and electronic, are legal documents.
4. Services can only be entered for billing if there is a corresponding progress note. 5. All services shall be provided by staff within the scope of practice of the
individual delivering the service. Clinicians will follow specific scope of practice requirements as determined by the applicable license regulations of their governing board.
6. Each progress note should provide enough detail so that auditors and other service providers can easily ascertain the service provided, the client’s current status, and needs without having to refer to previous progress notes. Each progress note must stand “alone”.
7. Each progress note must show that the service was “medically necessary”. 8. Progress notes should clearly indicate the type of service provided and how the
service is medically necessary to address an identified area of impairment, and the progress (or lack of progress) in treatment.
9. Clinicians should document how the intervention provided relates to the clinical goals written in the treatment plan, addresses behavioral issues and/or link to the mental health condition. Remember a “medically necessary service” is one which attempts to improve a functional impairment impacted by a symptom of the client’s mental health diagnosis.
10. Until the MHP contracted services have adopted Electronic Health Record (EHR) MHP continues to operate a hybrid model of records. Regardless if a provider has adopted an EHR or continues to use a “hard copy” clinical record, the provider is required to ensure that all documentation forms contain all the necessary elements to submit for reimbursement.
11. It is crucial that the staff providing the service records the correct procedure code for the service provided and that the documentation supports and substantiates this service. In order for the MHP to receive the correct reimbursement for services provided, clinical staff must ensure that they choose the correct procedure code.
Understanding the difference between Nonbillable and X CODES
Documenting the services that you provide to your clients is an integral part of the service itself. Not only is it required for purposes of reimbursement, but it should provide a clear and concise record of your encounters with your clients. There is a distinction between activities that are NEVER claimable to Medi-Cal (“non billable code”), and services that are eligible to be billed to Medi-Cal but for some reason, that cannot be billed (such as a client receiving a specific service in a lock out location).
Some service codes are not billable to the State. Non-billable and non-billable
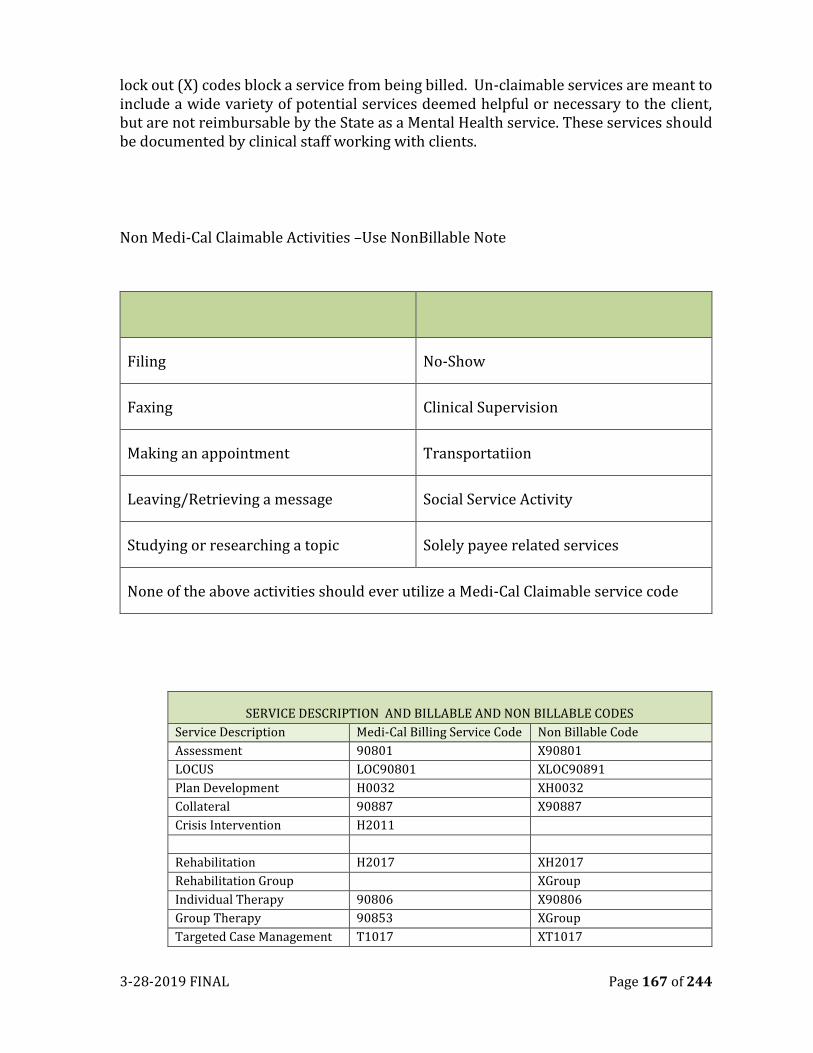
3-28-2019 FINAL Page 167 of 244
lock out (X) codes block a service from being billed. Un-claimable services are meant to include a wide variety of potential services deemed helpful or necessary to the client, but are not reimbursable by the State as a Mental Health service. These services should be documented by clinical staff working with clients.
Non Medi-Cal Claimable Activities –Use NonBillable Note
Filing No-Show
Faxing Clinical Supervision
Making an appointment Transportatiion
Leaving/Retrieving a message Social Service Activity
Studying or researching a topic Solely payee related services
None of the above activities should ever utilize a Medi-Cal Claimable service code
SERVICE DESCRIPTION AND BILLABLE AND NON BILLABLE CODES
Service Description Medi-Cal Billing Service Code Non Billable Code
Assessment 90801 X90801
LOCUS LOC90801 XLOC90891
Plan Development H0032 XH0032
Collateral 90887 X90887
Crisis Intervention H2011
Rehabilitation H2017 XH2017
Rehabilitation Group XGroup
Individual Therapy 90806 X90806
Group Therapy 90853 XGroup
Targeted Case Management T1017 XT1017
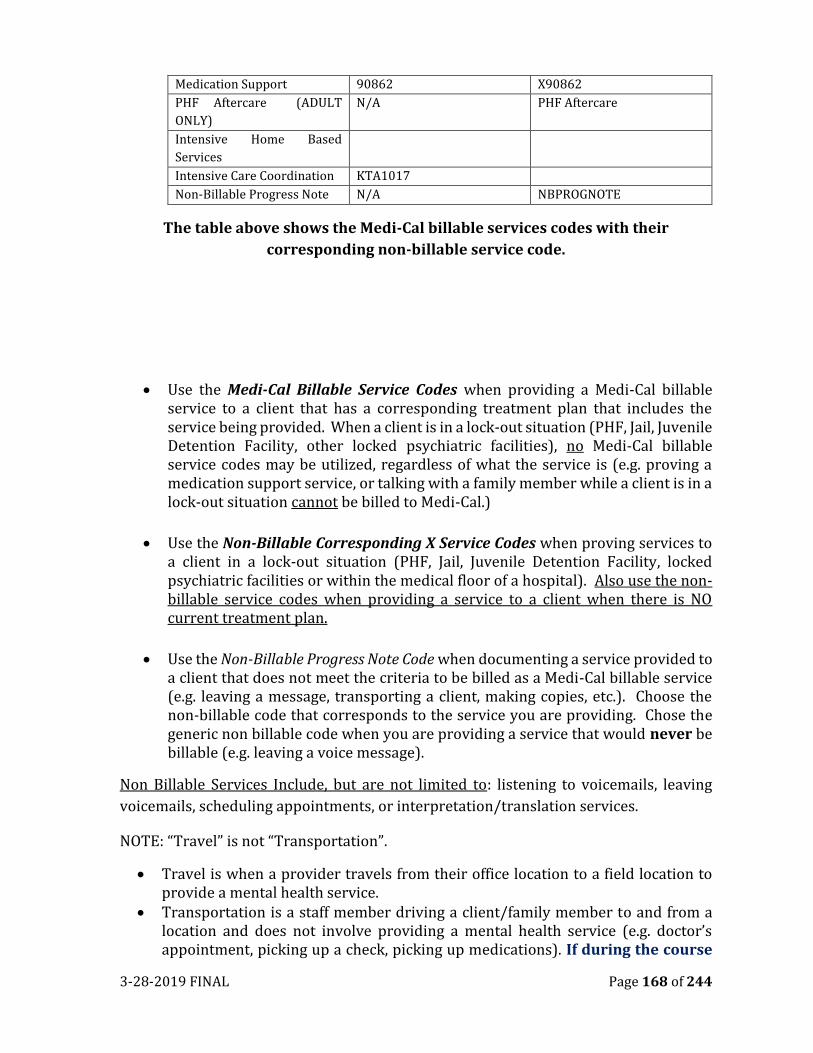
3-28-2019 FINAL Page 168 of 244
Medication Support 90862 X90862
PHF Aftercare (ADULT
ONLY)
N/A PHF Aftercare
Intensive Home Based
Services
Intensive Care Coordination KTA1017
Non-Billable Progress Note N/A NBPROGNOTE
The table above shows the Medi-Cal billable services codes with their
corresponding non-billable service code.
• Use the Medi-Cal Billable Service Codes when providing a Medi-Cal billable service to a client that has a corresponding treatment plan that includes the service being provided. When a client is in a lock-out situation (PHF, Jail, Juvenile Detention Facility, other locked psychiatric facilities), no Medi-Cal billable service codes may be utilized, regardless of what the service is (e.g. proving a medication support service, or talking with a family member while a client is in a lock-out situation cannot be billed to Medi-Cal.)
• Use the Non-Billable Corresponding X Service Codes when proving services to a client in a lock-out situation (PHF, Jail, Juvenile Detention Facility, locked psychiatric facilities or within the medical floor of a hospital). Also use the non-billable service codes when providing a service to a client when there is NO current treatment plan.
• Use the Non-Billable Progress Note Code when documenting a service provided to a client that does not meet the criteria to be billed as a Medi-Cal billable service (e.g. leaving a message, transporting a client, making copies, etc.). Choose the non-billable code that corresponds to the service you are providing. Chose the generic non billable code when you are providing a service that would never be billable (e.g. leaving a voice message).
Non Billable Services Include, but are not limited to: listening to voicemails, leaving
voicemails, scheduling appointments, or interpretation/translation services.
NOTE: “Travel” is not “Transportation”.
• Travel is when a provider travels from their office location to a field location to provide a mental health service.
• Transportation is a staff member driving a client/family member to and from a location and does not involve providing a mental health service (e.g. doctor’s appointment, picking up a check, picking up medications). If during the course
3-28-2019 FINAL Page 169 of 244
of transporting the client a mental health service is provided, then the time spent providing the mental health service during transportation can be claimed.
• Total time billed should be documented on each progress note. Total time billed includes time spent providing services to the client (i.e. on the phone, face to face, in the field, etc.), documentation time (up to a maximum of 10-15 minutes, and travel time (to and from work site) if applicable. • Please remember to bill for “Actual” time spent providing a service to the
client
• Do not bill “blocks of time” (e.g. an hour for a weekly individual therapy
session).
• Each service contact is documented din a progress note and documentation
must be completed in a timely manner. A progress note is completed for each
service contact, except for Psychiatric Emergency Services (Crisis Evaluation
suffices), Crisis Residential Services and Day Treatment Services.
1. Progress Note Timeline: Progress notes must be completed in a timely
manner according to the following guidelines:
• Every effort should be made to complete progress notes on the same day
of the service
• Individual and Group Notes must be finalized within 5 business days from
the delivery of the service.
• After 5 business days, the clinician shall write “late Entry” at the beginning
of the note.
• For group notes billing, staff must detail the purpose of the group and individualize the note for each client in the group which documents how the client participated in and benefited from the group as well as their individual response to the interventions provided during the group
• If the supervisor is not available, the providing staff must coordinate with the program director or other designated supervisors for reviewing notes and other clinical documents for co-signature.
2. Documentation must be readable and legible (including author’s name and
licensure). Ensure that the spell check function is turned on. Spell check
before finalizing the document.
3. The use of abbreviations in clinical documentation must be consistent with
approved MHP abbreviations for approved abbreviations.
4. Restriction of Client Information: Adverse Incidents, Unusual Occurrences,
Utilization Review recommendations or forms and audit sheets would never
be scanned into the electronic health record, or filed within the paper record
or billed.
5. Copy and Paste: Do not copy and paste notes into a client’s medical record.
3-28-2019 FINAL Page 170 of 244
Each notes needs to be specific to the service provide. If using a MHP
template that brings forward text from the previous note, the narrative must
be changed to reflect the current service being documented. Progress notes
that are submitted which appear to be worded exactly like, or too similar to,
previous entries may be assumed to be pasted, i.e., containing inaccurate,
outdated, or false information, therefore claiming associated with these notes
could be considered fraudulent.
6. Every page must have some form of client identification (name or
identification number, etc.).
7. Correcting errors: Do not use correction tape/fluid, scribble over, etc. Instead,
draw a single line through the error & initial, and then enter correct material.
8. Only original authors may make alterations.
9. Reviewers or supervisors may not edit original authors but may supply an
addendum with dated signature.
MEDI-CAL REIMBURSEMENT RULES
Key Points Applicable to One or More Mode of Services
• These rules apply to Mental Health Services, Medication Support Services, Crisis
Intervention and Targeted Case Management:
• The exact number of minutes used by persons providing a reimbursable service
shall be reported and billed. In no case shall more than 60 units of time be
reported or claimed for any one person during a one hour period. In no case shall
the units of time reported or claimed for any one person exceed the hours
worked [CCR Title 9, § 1840.316 (b)(1)].
• A service is an individual service when one client is present or represented for
the service and is a group when more than one client is present or represented
at the same time for a service.
• When a person provides services to, or on behalf of, more than one client at the
same time, the person’s time must be prorated to each client. When more than
one person provides a service to more than one client at the same time, the time
utilized by all those providing the services shall be added together to yield the
total claimable services. The total time claimed shall not exceed the total time
utilized for claimable services [CCR, Title 9, § 1840.316(b)(2)].
• The time required for documentation and travel is reimbursable when the
documentation or travel is a component of a reimbursable service activity,
whether or not documentation time is on the same day as the reimbursable
service activity [CCR, Title 9, § 1840.316(b)(3)].
3-28-2019 FINAL Page 171 of 244
• Every claim must be supported by a note that must be present in the clinical
record prior to the submission of the claim (DHCS Contract, Exhibit A,
Attachment 1, Appendix C).
Services shall be provided within the staff person’s scope of practice (CCR Title 9,
§1840.314) and his/her employer’s job description/responsibility. The local mental
health director shall be responsible for assuring that services provided are
commensurate with the professionalism and experience of the staff utilized.
The time required for documentation and travel must be linked to the delivery of the
reimbursable service [CCR, Title 9, § 1840.316(a)(3)].
Non Medi-Cal Reimbursement Services
These rules apply to all Mental Health Services:
• Mental Health Services are not reimbursable on days when Crisis Residential
Treatment Services, Inpatient Services, or Psychiatric Health or Nursing Facilities
are reimbursed, except on the day of admission to either service [CCR, Title 9,
§1840.36 (a)]
• Mental Health Services are not reimbursed when provided by Day Rehabilitation or Day Treatment Intensive Staff during the same time period that Day Rehabilitation or Day Treatment Intensive Services are being provided [CCR Title 9, §1840.36 (b)]
• Crisis Stabilization is a packaged program and no other specialty mental health services are reimbursed during the same period this service is reimbursed except for Targeted Case Management [CCR Title 9, §1840.369 (b)].
• Mental Health Services are not reimbursable when provided in a jail or prison setting [CCR, Title 22, § 50273 (a)(1-8)].
• Mental Health Services are not reimbursable when provided to persons aged 22 through 64 who are residents of an Institution for Mental Disease (IMD) [CCR Title 9, §1840.312(g). An IMD is defined as a hospital nursing facility, or other institution that has minimally more than 16 beds and is primarily engaged in providing diagnosis, treatment or care of persons with mental illness, including medical attention, and related services (CCR, Title 9, §1810.222.1); [ Title 42, CFR§435.1009(b)(2)]. As such, a free standing Psychiatric Hospital or a state Hospital qualifies as an IMD.
• A client under 21 years of age resides in an IMD other than a Psychiatric Health
Facility (PHF) that is a hospital or an acute psychiatric hospital, except if the
client under 21 years of age was receiving such services prior to his/her 21st
birthday. If this client continues without interruption to require and receive such
services, the eligibility for Federal Financial Participation (FFP) dollars continues
to the date he/she no longer requires such services, or if earlier, to his/her 22nd
birthday.

3-28-2019 FINAL Page 172 of 244
• Services of clerical support personnel are not reimbursable [CCR Title 9, §1830.205(b)(3). While it may be appropriate at times to record in the clinical record activities or observation of these personnel, their cost is included in the overhead rates, for which the Department receives a percent of Medi-Cal reimbursement, so these services should not be separately claimed.
• Supervision time is not reimbursable. Supervision focuses on the supervisee’s clinical/educational growth (as when meeting to monitor his/her caseload or his/her understanding of the therapeutic process) and is NOT reimbursable time. Supervision time required by the System of Care or State Licensing boards always falls within this definition and thus, is never reimbursable.
• Personal care services performed for the client are not reimbursable These would include examples such as grooming, personal hygiene, assisting with medication child or respite care, housekeeping and the preparation of meals
• Conservatorship investigations are not reimbursable.
Signatures:
Clinical staff signature is a required part of most clinical documents. At this time, MHP
does not have an Uniformed EHR within the county owned and operated clinics,
therefore, requires either a “wet signatures” or an “electronic” on all Assessments,
Annual Updates, Unified Services Plans and Progress Notes. At minimum the signatures
must include first initial of first name, full last name, and date.
Each signature must include licensure and/or designation (e.g. M.D., N.P., Ph.D, LCSW,
MFT, LPCC, ASW, MFTI, LPCCI, MHRS, etc.)
Co-Signatures:
Co-Signatures for staff may be required for several reasons. The State Department of
Health Care Services (DHCS) requires that some documents, e.g., client plans, be
approved by a Licensed Practitioner of the Healing Arts (LPHA). Additionally, MHP
policy requires that some documents be reviewed and co-signed by a supervisor as part
of the authorization process. Also, some staff are required to have progress notes co-
signed for a specific or indefinite periods. One example with new or reassigned staff,
supervisors may requires note to be co-signed as part of the oversight when onboarding
new staff members. Other co-signature requirements may be assigned for purposes of
quality assurance and/or compliance. Staff should consult with their supervisor for
additional specifics and refer to PCSOC MHP Guidelines for Scope of Practice
Service Time: This is the specific start time when staff begins working with a client,
collateral or case management contact in person or via telephone. This must be
documented to the minute. (For instance, an individual session time begins at 2:03 p.m.
The Clinician would document 2:03 p.m. in the “start time”).
3-28-2019 FINAL Page 173 of 244
Travel Time: If traveling to provide services to a client, travel time can be billed. If t
raveling outside of the county, please document how much time was spent in travel. The
time spent traveling from home to an appointment or from an appointment to home is
not billable
Documentation Time: The actual time it takes to document the service provided. The
length and substance of the progress note should justify the length of the
documentation. If the service provider does not have strong typing skills, the entire time
it takes to submit the note cannot be billed.
Total Time: This includes the time it takes for providing the services, documenting the
services and the travel time added together. You will note that throughout the guide, this
is included in the example progress notes, however in AVATAR, this will be completed
in the “Minutes billed” section.
STYLES OF DOCUMENTATION- PROGRESS NOTES
The progress Note is used to record any service being rendered to or on behalf of a client
(billable or non-billable). When staff write submit a billable progress note a bill is submitted
to Medi-Cal, for reimbursement. It is imperative that all MHP progress notes are accurate,
factual and follow the guidelines for reimbursement, including correct location,
treatment code, and time of services being rendered under the direction of an approved
and current treatment plan. This is an aspect of compliance, and compliance is the
responsibility of ALL employees.
What makes a good progress note?
A good progress note accurately represents the services provided. Each progress note
needs to justify the service provided, must be medically necessary.
1. The focus of the proposed intervention is to address the condition identified in
the impairment criteria related to the “included diagnosis”, and
2. It is expected the proposed intervention will benefit the consumer by
significantly diminishing the impairment or preventing significant deterioration
in an important area of life functioning. Check how the proposed intervention
helps the client improve or maintaining his/her functioning in important areas
of life.
Progress notes are used to inform other clinical staff about the client’s treatment, to
document and claim for services, and to provide a legal record. Clients/family members
may read progress notes. Use your judgment about what to include. Aim for clarity and
brevity when writing notes. Lengthy narrative notes are discouraged.
3-28-2019 FINAL Page 174 of 244
Clear and concise documentation is crucial to client care. Progress notes are used, not
only to claim for services, but to document the client/family’s course and progress in
treatment. Progress notes should clearly indicate the type of service provided and how
the service is medically necessary to address an identified area of impairment, and the
progress (or lack of progress) in treatment.
In order to meet regulatory and compliance standards, progress notes:
1. Must be related to the client’s progress in treatment 2. Must provide timely documentation of relevant aspects of client care 3. Must document:
a. Client Encounters b. Interventions c. Follow up care d. Clinical decisions e. Client’s response to interventions f. New assessment information g. Referrals to community responses h. Signature of the person providing the service, including professional
degree, licensure or job title i. Date services were provided j. Location where services were provided k. If service is provided in a language other than English, state the language
used. If an interpreter is used, include the name of the interpreter in the progress note.
4. Progress notes are the method by which other treatment team members or other reviewers (such as the State, Federal or contracted reviewers) are able to determine Medical Necessity and level of care/treatment for the client.
5. The client’s presenting signs, symptoms or other clinical problems should be clearly described in order to support the need for the service.
6. Each progress note must have components that show what has been done to help a client reach their goal or objective.
7. If two practitioners are providing a service to a client together, each person’s role and participation in the intervention needs to be clearly documented
Progress Notes should be written as if an attorney and/or client/family
member will be reading it. You should be able to explain or defend every
statement.
PROGRESS NOTE FORMATS/TEMPLATES
Placer County Quality Improvement Unit has not adopted a standardized method of
documenting a progress note for mental health clinicians, psychologists, and mental
health specialists. The findings from Medi-Cal audits since that time were considered
3-28-2019 FINAL Page 175 of 244
and a solution created to reduce disallowances and increase consistency within the
Mental Health System as a whole. There are many methods for writing case notes.
Included within this manual are four examples (BIRP< IGBIRP, PIRP and SOAP) used in
behavioral health programs.
BIRP AND IGBIRP
The BIRP and IGBIRP models for progress notation may not be “the best thing since
sliced bread”, but in the auditing world it comes pretty close. In the past, there had been
wide variation in documentation practices from provider to provider, or even from one
program to another within the same agency.
BIRP NOTES
B= Behavior I= Interventional R=Response P=Plan
Behavior/Presenting Problem:
Subjective data about the client: What are the client’s observations, thought, encouraged
to use direct quotes. Objective data about the client: What does the service coordinator
observe during the session? (Affect, Mood, appearance).
Identify the location of the service to justify travel time and indicate the type of service
provided (i.e., “This writer provided an individual therapy session at Bart Simpson High
School.”) Refer to both the long-term presenting problems and client’s current
presentation to document why the service is medically necessary:
• Do not repetitively restate the same Behavior/Presenting Problem from note to note.
• Provide a description of the long-term presenting problem as well as the client’s presentation on the day of treatment (the current presentation will differ from session to session).
• Do not cut and paste using the same “B” for every session.
Interventions:
What goals and objectives where addressed in this session? Was homework done? Housing
application? What are the methods you used to address the goals and objectives, what are
your observations, clients statements?
Use verbs to capture what you did in the session to address the treatment plan goals.
Indicate the therapeutic modality from which the intervention came: i.e. cognitive
behavioral, client-centered, etc. Examples of verbs to be used when identify
interventions include:
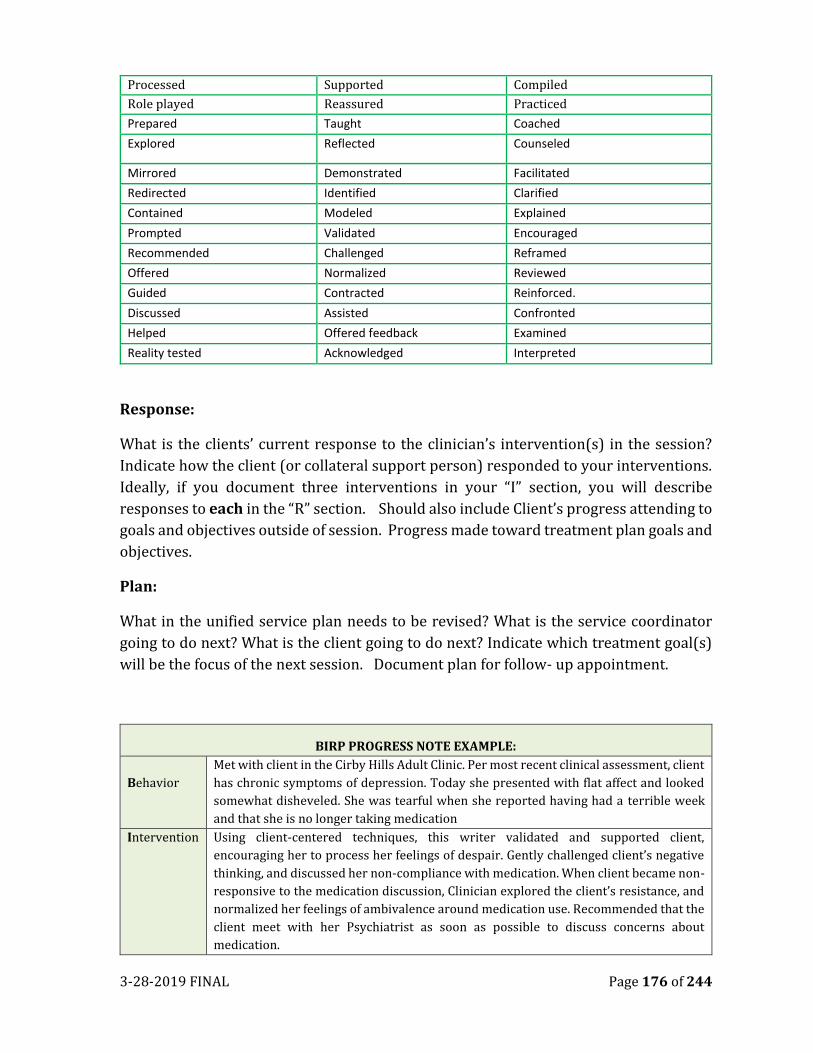
3-28-2019 FINAL Page 176 of 244
Processed Supported Compiled
Role played Reassured Practiced
Prepared Taught Coached
Explored Reflected Counseled
Mirrored Demonstrated Facilitated
Redirected Identified Clarified
Contained Modeled Explained
Prompted Validated Encouraged
Recommended Challenged Reframed
Offered Normalized Reviewed
Guided Contracted Reinforced.
Discussed Assisted Confronted
Helped Offered feedback Examined
Reality tested Acknowledged Interpreted
Response:
What is the clients’ current response to the clinician’s intervention(s) in the session?
Indicate how the client (or collateral support person) responded to your interventions.
Ideally, if you document three interventions in your “I” section, you will describe
responses to each in the “R” section. Should also include Client’s progress attending to
goals and objectives outside of session. Progress made toward treatment plan goals and
objectives.
Plan:
What in the unified service plan needs to be revised? What is the service coordinator
going to do next? What is the client going to do next? Indicate which treatment goal(s)
will be the focus of the next session. Document plan for follow- up appointment.
BIRP PROGRESS NOTE EXAMPLE:
Behavior
Met with client in the Cirby Hills Adult Clinic. Per most recent clinical assessment, client
has chronic symptoms of depression. Today she presented with flat affect and looked
somewhat disheveled. She was tearful when she reported having had a terrible week
and that she is no longer taking medication
Intervention Using client-centered techniques, this writer validated and supported client,
encouraging her to process her feelings of despair. Gently challenged client’s negative
thinking, and discussed her non-compliance with medication. When client became non-
responsive to the medication discussion, Clinician explored the client’s resistance, and
normalized her feelings of ambivalence around medication use. Recommended that the
client meet with her Psychiatrist as soon as possible to discuss concerns about
medication.
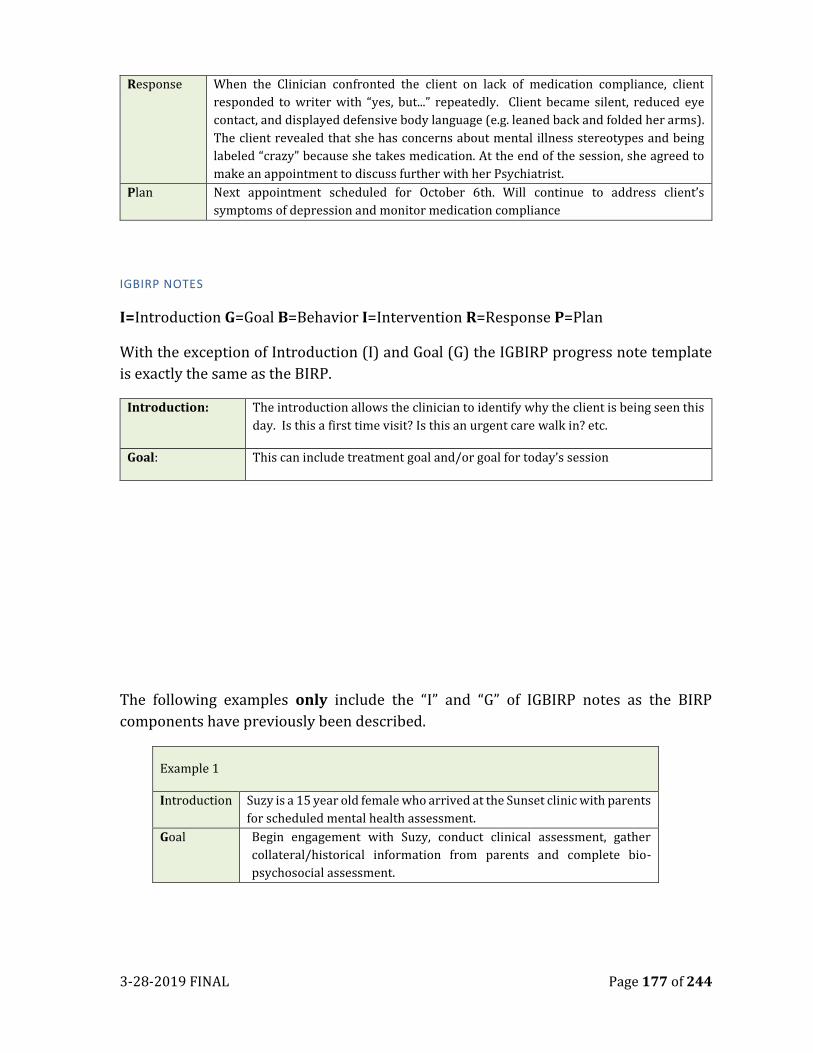
3-28-2019 FINAL Page 177 of 244
Response When the Clinician confronted the client on lack of medication compliance, client
responded to writer with “yes, but...” repeatedly. Client became silent, reduced eye
contact, and displayed defensive body language (e.g. leaned back and folded her arms).
The client revealed that she has concerns about mental illness stereotypes and being
labeled “crazy” because she takes medication. At the end of the session, she agreed to
make an appointment to discuss further with her Psychiatrist.
Plan Next appointment scheduled for October 6th. Will continue to address client’s
symptoms of depression and monitor medication compliance
IGBIRP NOTES
I=Introduction G=Goal B=Behavior I=Intervention R=Response P=Plan
With the exception of Introduction (I) and Goal (G) the IGBIRP progress note template
is exactly the same as the BIRP.
Introduction: The introduction allows the clinician to identify why the client is being seen this
day. Is this a first time visit? Is this an urgent care walk in? etc.
Goal: This can include treatment goal and/or goal for today’s session
The following examples only include the “I” and “G” of IGBIRP notes as the BIRP
components have previously been described.
Example 1
Introduction Suzy is a 15 year old female who arrived at the Sunset clinic with parents
for scheduled mental health assessment.
Goal Begin engagement with Suzy, conduct clinical assessment, gather
collateral/historical information from parents and complete bio-
psychosocial assessment.
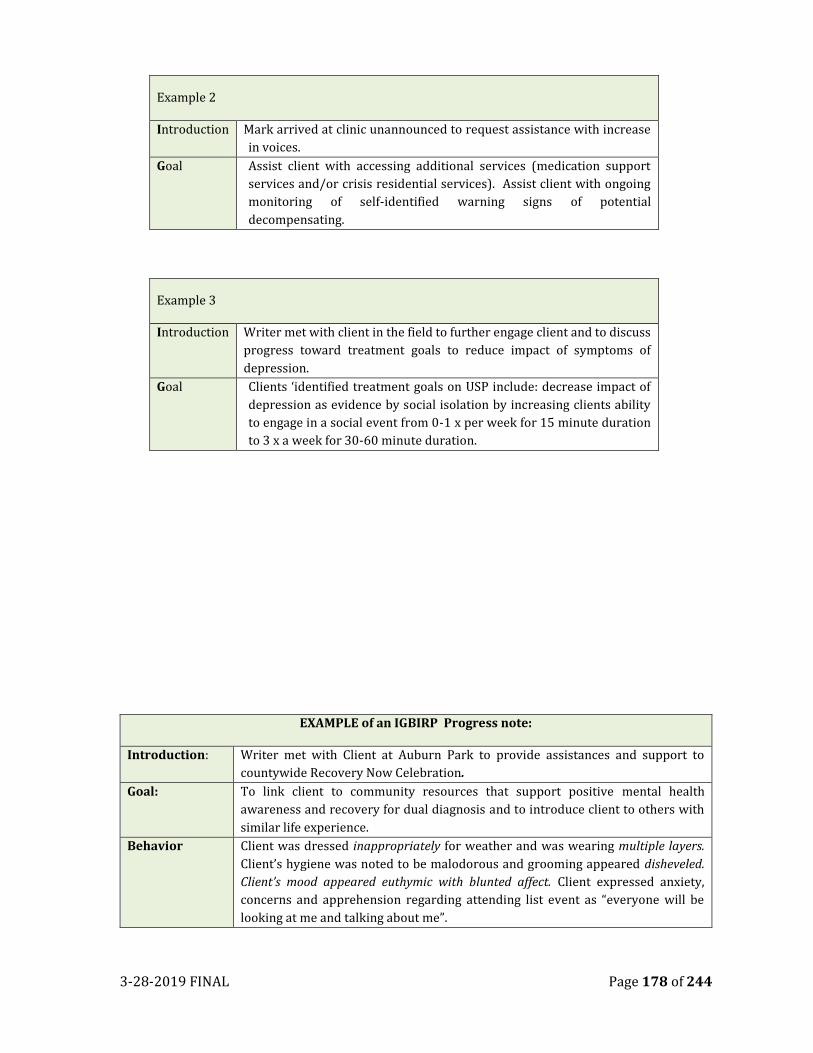
3-28-2019 FINAL Page 178 of 244
Example 2
Introduction Mark arrived at clinic unannounced to request assistance with increase
in voices.
Goal Assist client with accessing additional services (medication support
services and/or crisis residential services). Assist client with ongoing
monitoring of self-identified warning signs of potential
decompensating.
Example 3
Introduction Writer met with client in the field to further engage client and to discuss
progress toward treatment goals to reduce impact of symptoms of
depression.
Goal Clients ‘identified treatment goals on USP include: decrease impact of
depression as evidence by social isolation by increasing clients ability
to engage in a social event from 0-1 x per week for 15 minute duration
to 3 x a week for 30-60 minute duration.
EXAMPLE of an IGBIRP Progress note:
Introduction: Writer met with Client at Auburn Park to provide assistances and support to
countywide Recovery Now Celebration.
Goal: To link client to community resources that support positive mental health
awareness and recovery for dual diagnosis and to introduce client to others with
similar life experience.
Behavior Client was dressed inappropriately for weather and was wearing multiple layers.
Client’s hygiene was noted to be malodorous and grooming appeared disheveled.
Client’s mood appeared euthymic with blunted affect. Client expressed anxiety,
concerns and apprehension regarding attending list event as “everyone will be
looking at me and talking about me”.
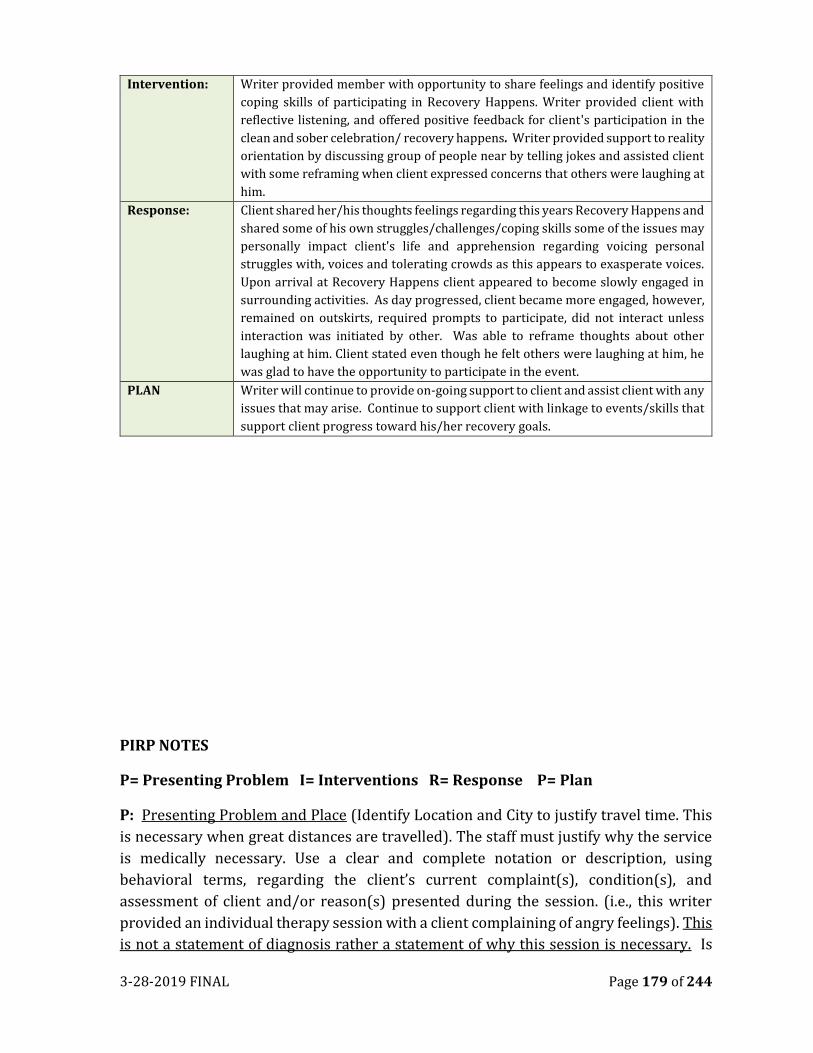
3-28-2019 FINAL Page 179 of 244
Intervention: Writer provided member with opportunity to share feelings and identify positive
coping skills of participating in Recovery Happens. Writer provided client with
reflective listening, and offered positive feedback for client's participation in the
clean and sober celebration/ recovery happens. Writer provided support to reality
orientation by discussing group of people near by telling jokes and assisted client
with some reframing when client expressed concerns that others were laughing at
him.
Response: Client shared her/his thoughts feelings regarding this years Recovery Happens and
shared some of his own struggles/challenges/coping skills some of the issues may
personally impact client's life and apprehension regarding voicing personal
struggles with, voices and tolerating crowds as this appears to exasperate voices.
Upon arrival at Recovery Happens client appeared to become slowly engaged in
surrounding activities. As day progressed, client became more engaged, however,
remained on outskirts, required prompts to participate, did not interact unless
interaction was initiated by other. Was able to reframe thoughts about other
laughing at him. Client stated even though he felt others were laughing at him, he
was glad to have the opportunity to participate in the event.
PLAN Writer will continue to provide on-going support to client and assist client with any
issues that may arise. Continue to support client with linkage to events/skills that
support client progress toward his/her recovery goals.
PIRP NOTES
P= Presenting Problem I= Interventions R= Response P= Plan
P: Presenting Problem and Place (Identify Location and City to justify travel time. This
is necessary when great distances are travelled). The staff must justify why the service
is medically necessary. Use a clear and complete notation or description, using
behavioral terms, regarding the client’s current complaint(s), condition(s), and
assessment of client and/or reason(s) presented during the session. (i.e., this writer
provided an individual therapy session with a client complaining of angry feelings). This
is not a statement of diagnosis rather a statement of why this session is necessary. Is
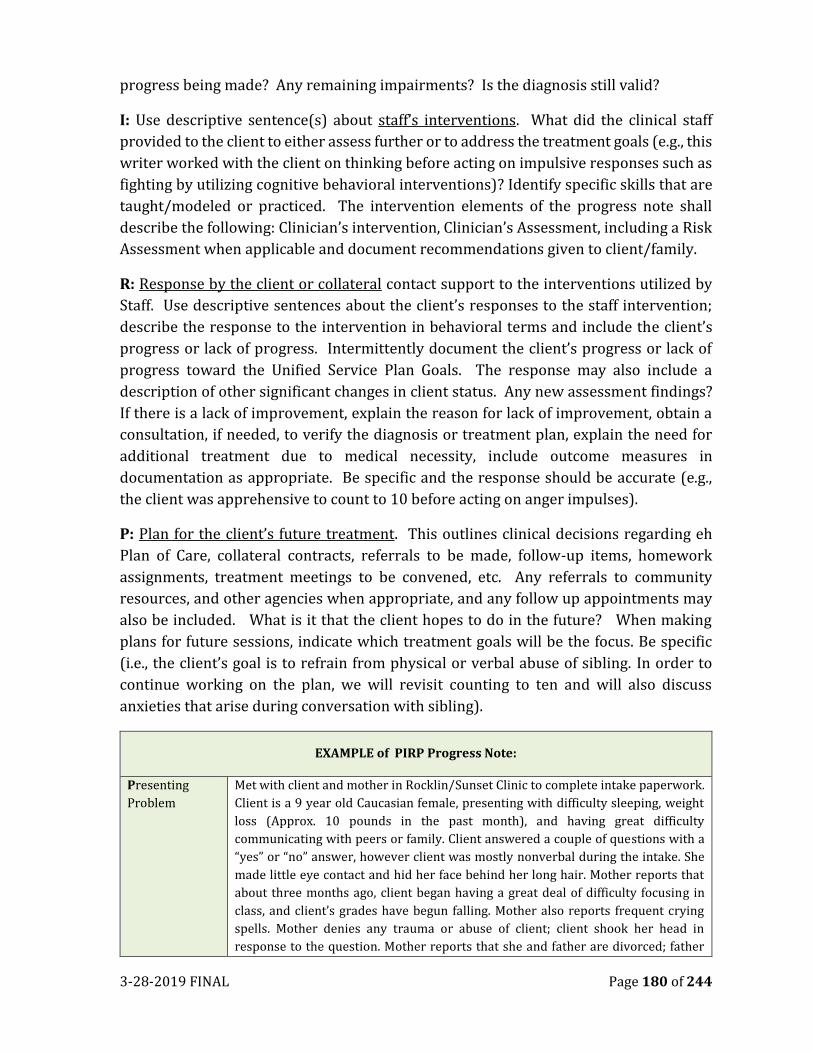
3-28-2019 FINAL Page 180 of 244
progress being made? Any remaining impairments? Is the diagnosis still valid?
I: Use descriptive sentence(s) about staff’s interventions. What did the clinical staff
provided to the client to either assess further or to address the treatment goals (e.g., this
writer worked with the client on thinking before acting on impulsive responses such as
fighting by utilizing cognitive behavioral interventions)? Identify specific skills that are
taught/modeled or practiced. The intervention elements of the progress note shall
describe the following: Clinician’s intervention, Clinician’s Assessment, including a Risk
Assessment when applicable and document recommendations given to client/family.
R: Response by the client or collateral contact support to the interventions utilized by
Staff. Use descriptive sentences about the client’s responses to the staff intervention;
describe the response to the intervention in behavioral terms and include the client’s
progress or lack of progress. Intermittently document the client’s progress or lack of
progress toward the Unified Service Plan Goals. The response may also include a
description of other significant changes in client status. Any new assessment findings?
If there is a lack of improvement, explain the reason for lack of improvement, obtain a
consultation, if needed, to verify the diagnosis or treatment plan, explain the need for
additional treatment due to medical necessity, include outcome measures in
documentation as appropriate. Be specific and the response should be accurate (e.g.,
the client was apprehensive to count to 10 before acting on anger impulses).
P: Plan for the client’s future treatment. This outlines clinical decisions regarding eh
Plan of Care, collateral contracts, referrals to be made, follow-up items, homework
assignments, treatment meetings to be convened, etc. Any referrals to community
resources, and other agencies when appropriate, and any follow up appointments may
also be included. What is it that the client hopes to do in the future? When making
plans for future sessions, indicate which treatment goals will be the focus. Be specific
(i.e., the client’s goal is to refrain from physical or verbal abuse of sibling. In order to
continue working on the plan, we will revisit counting to ten and will also discuss
anxieties that arise during conversation with sibling).
EXAMPLE of PIRP Progress Note:
Presenting
Problem
Met with client and mother in Rocklin/Sunset Clinic to complete intake paperwork.
Client is a 9 year old Caucasian female, presenting with difficulty sleeping, weight
loss (Approx. 10 pounds in the past month), and having great difficulty
communicating with peers or family. Client answered a couple of questions with a
“yes” or “no” answer, however client was mostly nonverbal during the intake. She
made little eye contact and hid her face behind her long hair. Mother reports that
about three months ago, client began having a great deal of difficulty focusing in
class, and client’s grades have begun falling. Mother also reports frequent crying
spells. Mother denies any trauma or abuse of client; client shook her head in
response to the question. Mother reports that she and father are divorced; father
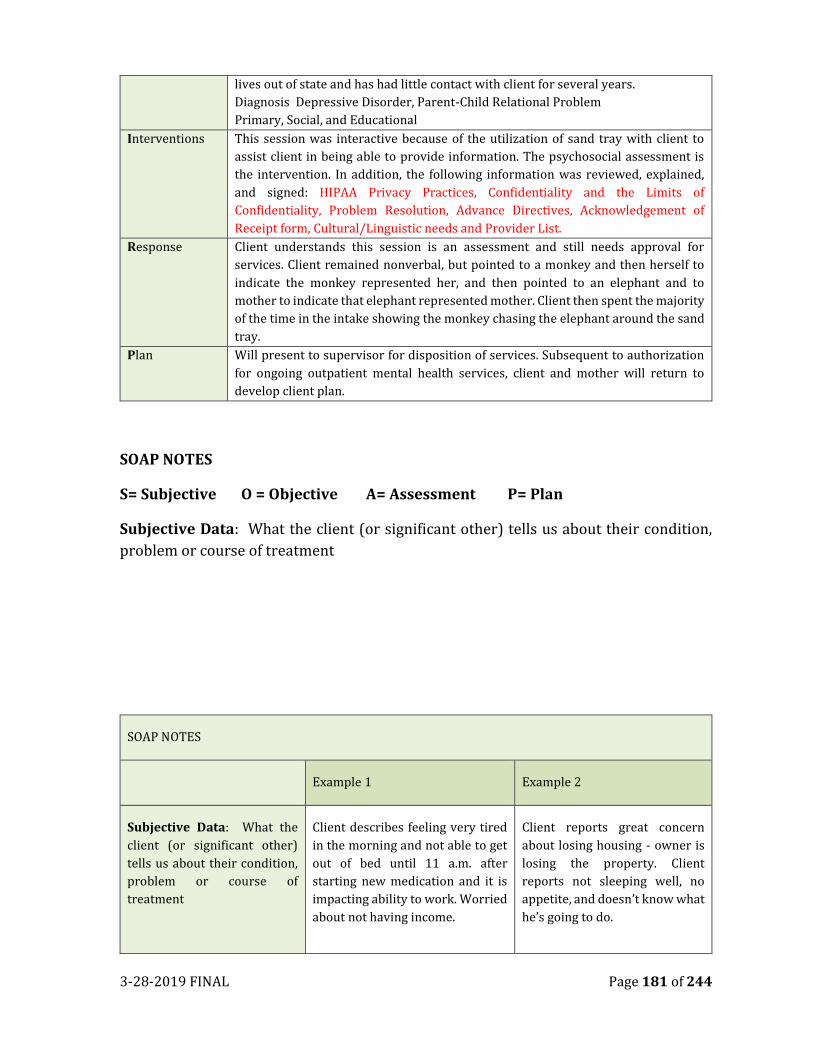
3-28-2019 FINAL Page 181 of 244
lives out of state and has had little contact with client for several years.
Diagnosis Depressive Disorder, Parent-Child Relational Problem
Primary, Social, and Educational
Interventions This session was interactive because of the utilization of sand tray with client to
assist client in being able to provide information. The psychosocial assessment is
the intervention. In addition, the following information was reviewed, explained,
and signed: HIPAA Privacy Practices, Confidentiality and the Limits of
Confidentiality, Problem Resolution, Advance Directives, Acknowledgement of
Receipt form, Cultural/Linguistic needs and Provider List.
Response Client understands this session is an assessment and still needs approval for
services. Client remained nonverbal, but pointed to a monkey and then herself to
indicate the monkey represented her, and then pointed to an elephant and to
mother to indicate that elephant represented mother. Client then spent the majority
of the time in the intake showing the monkey chasing the elephant around the sand
tray.
Plan Will present to supervisor for disposition of services. Subsequent to authorization
for ongoing outpatient mental health services, client and mother will return to
develop client plan.
SOAP NOTES
S= Subjective O = Objective A= Assessment P= Plan
Subjective Data: What the client (or significant other) tells us about their condition,
problem or course of treatment
SOAP NOTES
Example 1 Example 2
Subjective Data: What the
client (or significant other)
tells us about their condition,
problem or course of
treatment
Client describes feeling very tired
in the morning and not able to get
out of bed until 11 a.m. after
starting new medication and it is
impacting ability to work. Worried
about not having income.
Client reports great concern
about losing housing - owner is
losing the property. Client
reports not sleeping well, no
appetite, and doesn’t know what
he’s going to do.
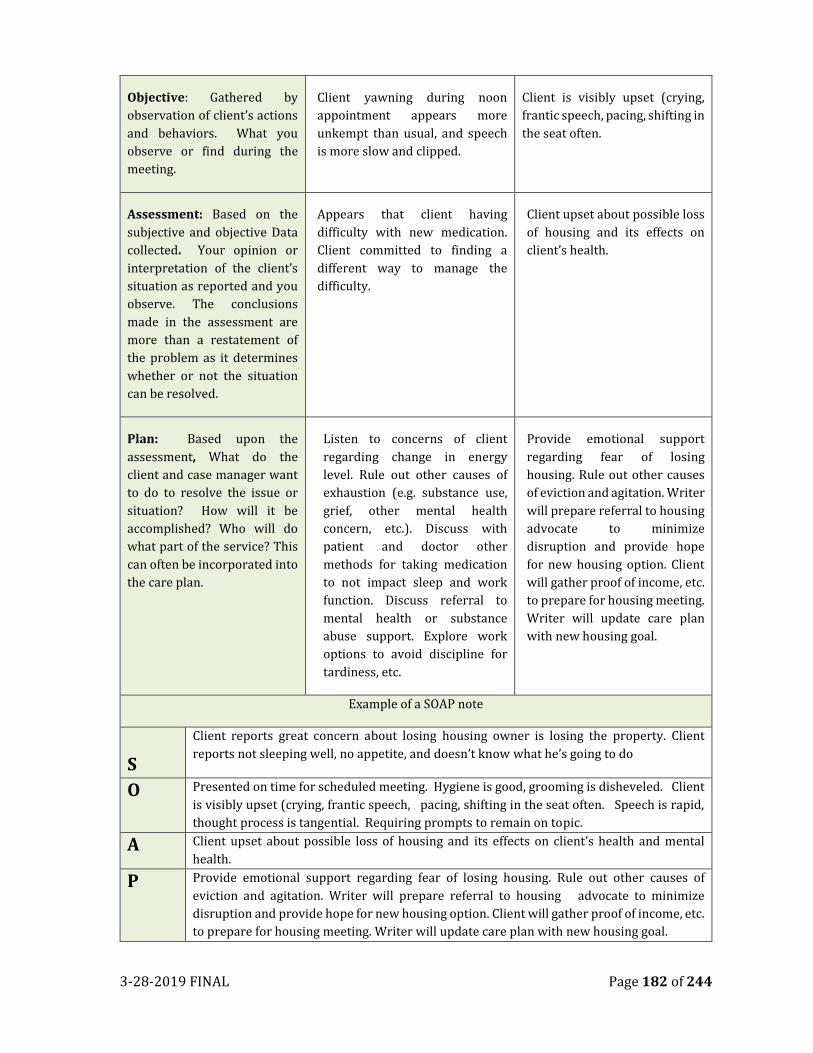
3-28-2019 FINAL Page 182 of 244
Objective: Gathered by
observation of client’s actions
and behaviors. What you
observe or find during the
meeting.
Client yawning during noon
appointment appears more
unkempt than usual, and speech
is more slow and clipped.
Client is visibly upset (crying,
frantic speech, pacing, shifting in
the seat often.
Assessment: Based on the
subjective and objective Data
collected. Your opinion or
interpretation of the client’s
situation as reported and you
observe. The conclusions
made in the assessment are
more than a restatement of
the problem as it determines
whether or not the situation
can be resolved.
Appears that client having
difficulty with new medication.
Client committed to finding a
different way to manage the
difficulty.
Client upset about possible loss
of housing and its effects on
client’s health.
Plan: Based upon the
assessment, What do the
client and case manager want
to do to resolve the issue or
situation? How will it be
accomplished? Who will do
what part of the service? This
can often be incorporated into
the care plan.
Listen to concerns of client
regarding change in energy
level. Rule out other causes of
exhaustion (e.g. substance use,
grief, other mental health
concern, etc.). Discuss with
patient and doctor other
methods for taking medication
to not impact sleep and work
function. Discuss referral to
mental health or substance
abuse support. Explore work
options to avoid discipline for
tardiness, etc.
Provide emotional support
regarding fear of losing
housing. Rule out other causes
of eviction and agitation. Writer
will prepare referral to housing
advocate to minimize
disruption and provide hope
for new housing option. Client
will gather proof of income, etc.
to prepare for housing meeting.
Writer will update care plan
with new housing goal.
Example of a SOAP note
S
Client reports great concern about losing housing owner is losing the property. Client
reports not sleeping well, no appetite, and doesn’t know what he’s going to do
O Presented on time for scheduled meeting. Hygiene is good, grooming is disheveled. Client
is visibly upset (crying, frantic speech, pacing, shifting in the seat often. Speech is rapid,
thought process is tangential. Requiring prompts to remain on topic.
A Client upset about possible loss of housing and its effects on client’s health and mental
health.
P Provide emotional support regarding fear of losing housing. Rule out other causes of
eviction and agitation. Writer will prepare referral to housing advocate to minimize
disruption and provide hope for new housing option. Client will gather proof of income, etc.
to prepare for housing meeting. Writer will update care plan with new housing goal.
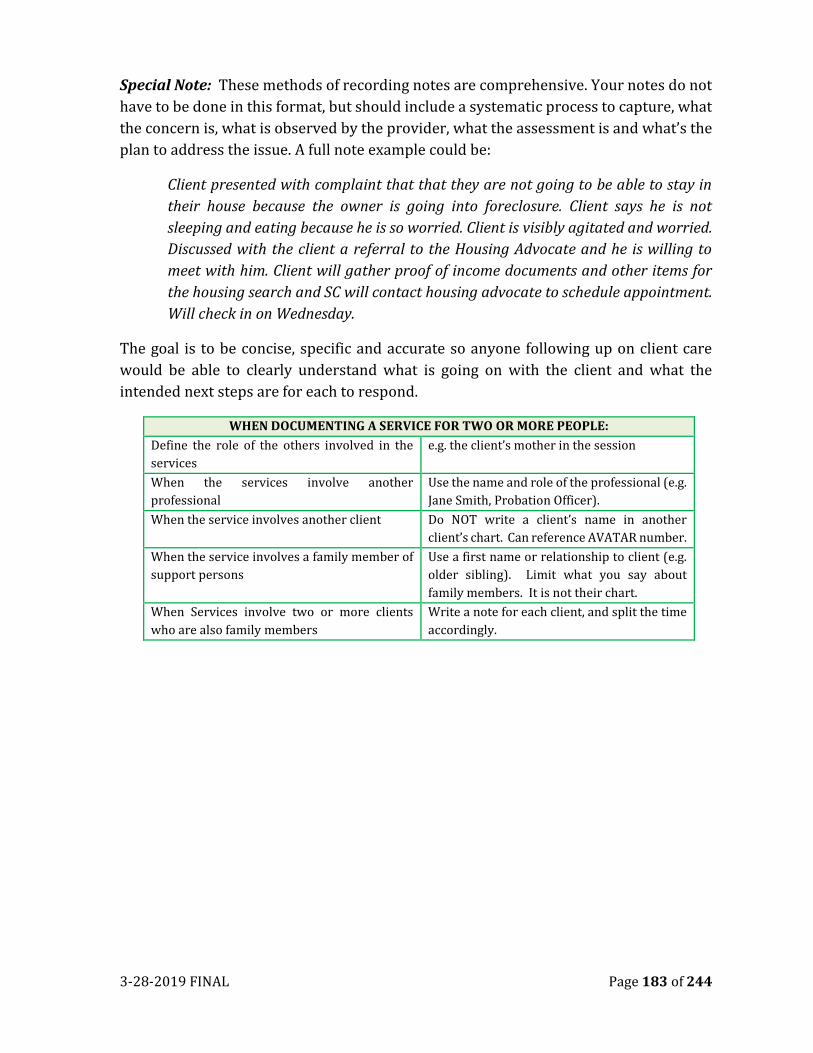
3-28-2019 FINAL Page 183 of 244
Special Note: These methods of recording notes are comprehensive. Your notes do not
have to be done in this format, but should include a systematic process to capture, what
the concern is, what is observed by the provider, what the assessment is and what’s the
plan to address the issue. A full note example could be:
Client presented with complaint that that they are not going to be able to stay in
their house because the owner is going into foreclosure. Client says he is not
sleeping and eating because he is so worried. Client is visibly agitated and worried.
Discussed with the client a referral to the Housing Advocate and he is willing to
meet with him. Client will gather proof of income documents and other items for
the housing search and SC will contact housing advocate to schedule appointment.
Will check in on Wednesday.
The goal is to be concise, specific and accurate so anyone following up on client care
would be able to clearly understand what is going on with the client and what the
intended next steps are for each to respond.
WHEN DOCUMENTING A SERVICE FOR TWO OR MORE PEOPLE:
Define the role of the others involved in the
services
e.g. the client’s mother in the session
When the services involve another
professional
Use the name and role of the professional (e.g.
Jane Smith, Probation Officer).
When the service involves another client Do NOT write a client’s name in another
client’s chart. Can reference AVATAR number.
When the service involves a family member of
support persons
Use a first name or relationship to client (e.g.
older sibling). Limit what you say about
family members. It is not their chart.
When Services involve two or more clients
who are also family members
Write a note for each client, and split the time
accordingly.
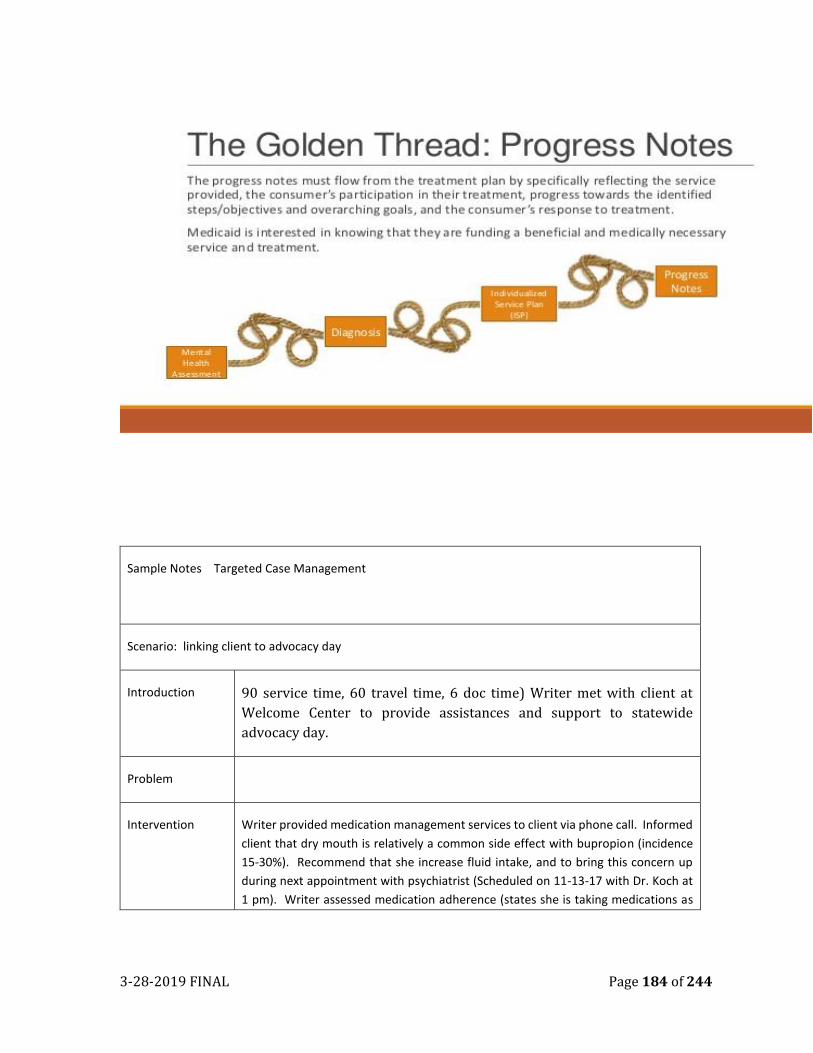
3-28-2019 FINAL Page 184 of 244
Sample Notes Targeted Case Management
Scenario: linking client to advocacy day
Introduction 90 service time, 60 travel time, 6 doc time) Writer met with client at
Welcome Center to provide assistances and support to statewide
advocacy day.
Problem
Intervention Writer provided medication management services to client via phone call. Informed
client that dry mouth is relatively a common side effect with bupropion (incidence
15-30%). Recommend that she increase fluid intake, and to bring this concern up
during next appointment with psychiatrist (Scheduled on 11-13-17 with Dr. Koch at
1 pm). Writer assessed medication adherence (states she is taking medications as
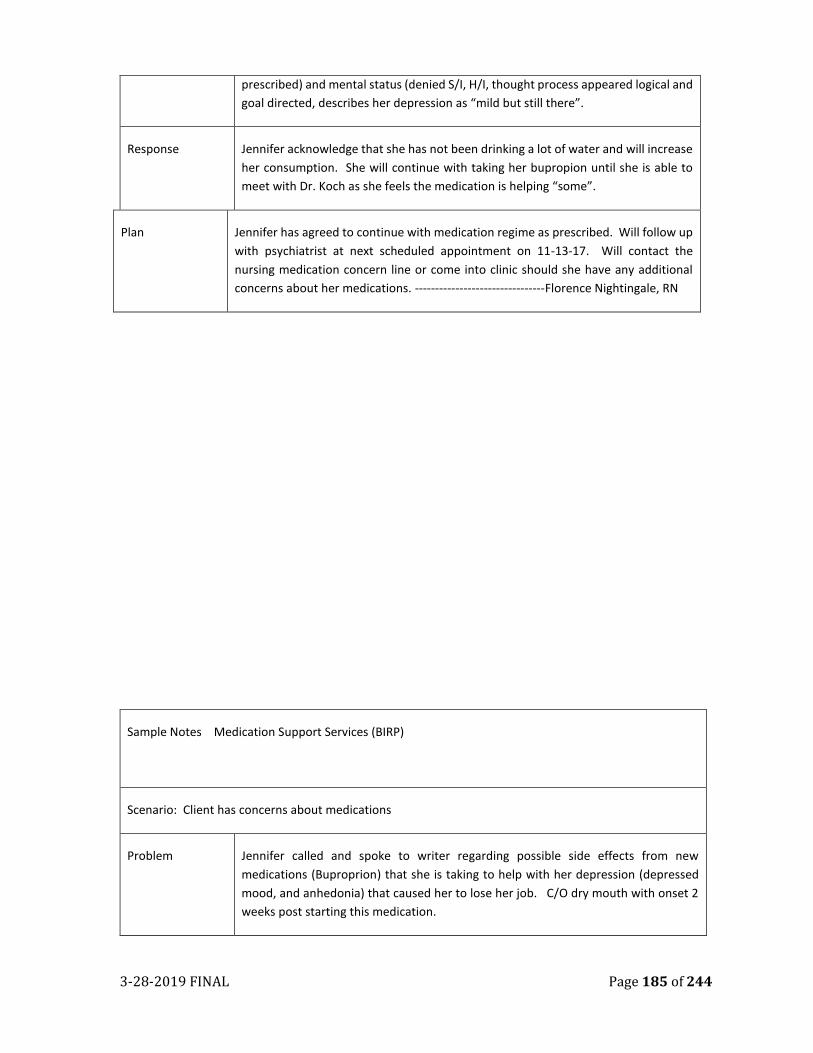
3-28-2019 FINAL Page 185 of 244
prescribed) and mental status (denied S/I, H/I, thought process appeared logical and
goal directed, describes her depression as “mild but still there”.
Response Jennifer acknowledge that she has not been drinking a lot of water and will increase
her consumption. She will continue with taking her bupropion until she is able to
meet with Dr. Koch as she feels the medication is helping “some”.
Plan Jennifer has agreed to continue with medication regime as prescribed. Will follow up
with psychiatrist at next scheduled appointment on 11-13-17. Will contact the
nursing medication concern line or come into clinic should she have any additional
concerns about her medications. --------------------------------Florence Nightingale, RN
Sample Notes Medication Support Services (BIRP)
Scenario: Client has concerns about medications
Problem Jennifer called and spoke to writer regarding possible side effects from new
medications (Buproprion) that she is taking to help with her depression (depressed
mood, and anhedonia) that caused her to lose her job. C/O dry mouth with onset 2
weeks post starting this medication.
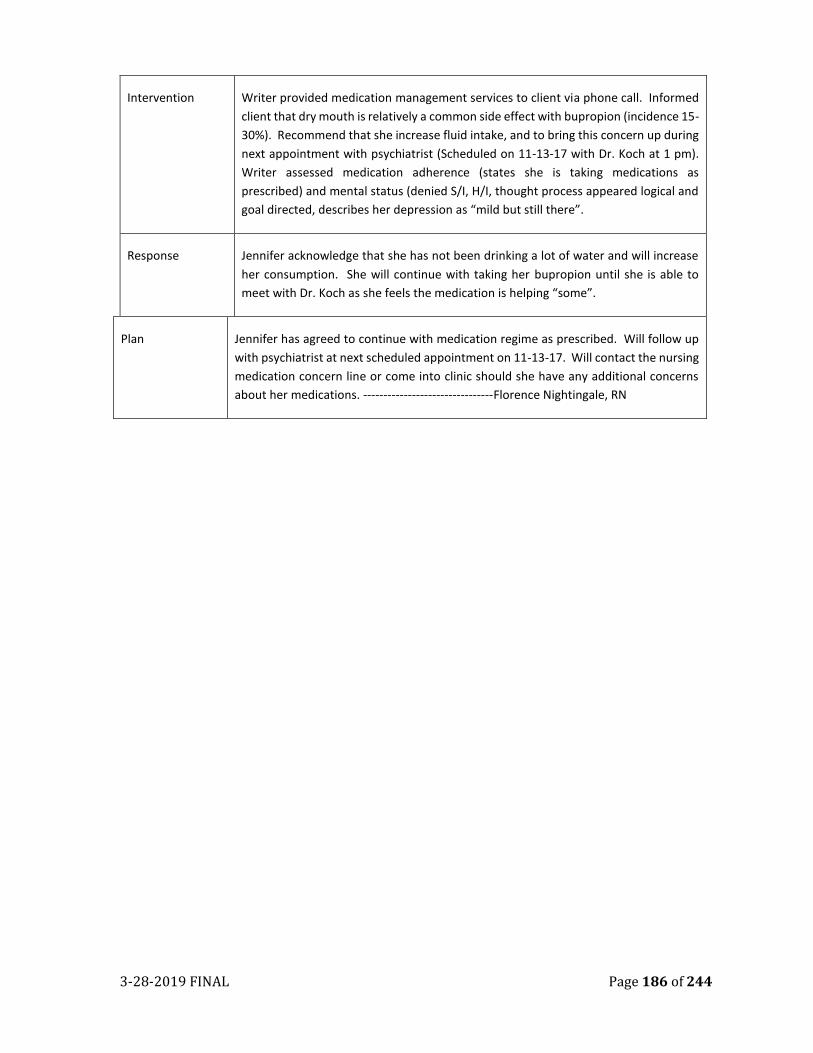
3-28-2019 FINAL Page 186 of 244
Intervention Writer provided medication management services to client via phone call. Informed
client that dry mouth is relatively a common side effect with bupropion (incidence 15-
30%). Recommend that she increase fluid intake, and to bring this concern up during
next appointment with psychiatrist (Scheduled on 11-13-17 with Dr. Koch at 1 pm).
Writer assessed medication adherence (states she is taking medications as
prescribed) and mental status (denied S/I, H/I, thought process appeared logical and
goal directed, describes her depression as “mild but still there”.
Response Jennifer acknowledge that she has not been drinking a lot of water and will increase
her consumption. She will continue with taking her bupropion until she is able to
meet with Dr. Koch as she feels the medication is helping “some”.
Plan Jennifer has agreed to continue with medication regime as prescribed. Will follow up
with psychiatrist at next scheduled appointment on 11-13-17. Will contact the nursing
medication concern line or come into clinic should she have any additional concerns
about her medications. --------------------------------Florence Nightingale, RN
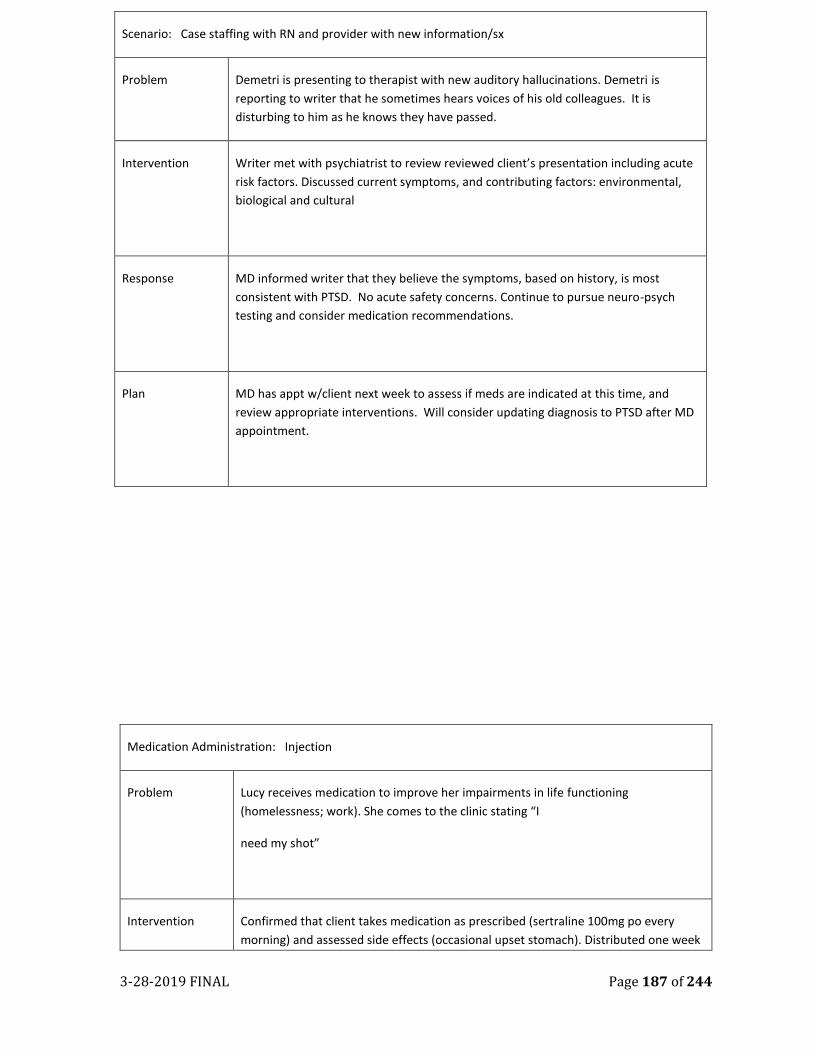
3-28-2019 FINAL Page 187 of 244
Medication Administration: Injection
Problem Lucy receives medication to improve her impairments in life functioning
(homelessness; work). She comes to the clinic stating “I
need my shot”
Intervention Confirmed that client takes medication as prescribed (sertraline 100mg po every
morning) and assessed side effects (occasional upset stomach). Distributed one week
Scenario: Case staffing with RN and provider with new information/sx
Problem Demetri is presenting to therapist with new auditory hallucinations. Demetri is
reporting to writer that he sometimes hears voices of his old colleagues. It is
disturbing to him as he knows they have passed.
Intervention Writer met with psychiatrist to review reviewed client’s presentation including acute
risk factors. Discussed current symptoms, and contributing factors: environmental,
biological and cultural
Response MD informed writer that they believe the symptoms, based on history, is most
consistent with PTSD. No acute safety concerns. Continue to pursue neuro-psych
testing and consider medication recommendations.
Plan MD has appt w/client next week to assess if meds are indicated at this time, and
review appropriate interventions. Will consider updating diagnosis to PTSD after MD
appointment.
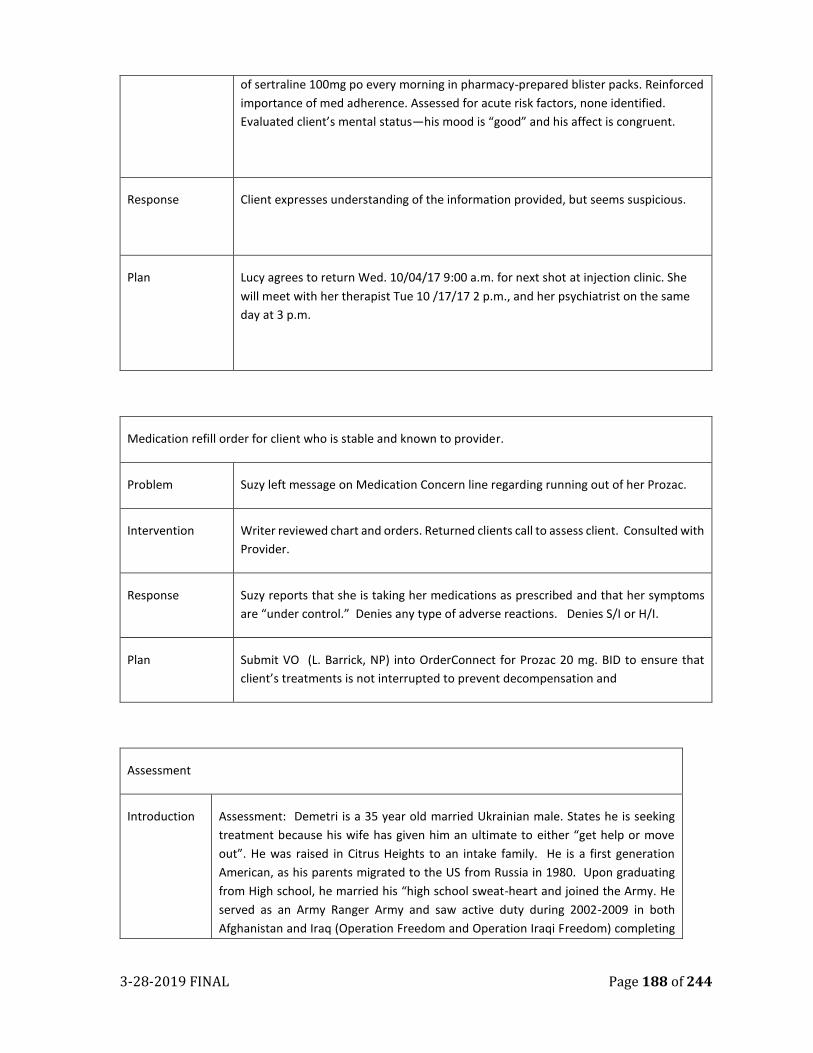
3-28-2019 FINAL Page 188 of 244
of sertraline 100mg po every morning in pharmacy-prepared blister packs. Reinforced
importance of med adherence. Assessed for acute risk factors, none identified.
Evaluated client’s mental status—his mood is “good” and his affect is congruent.
Response Client expresses understanding of the information provided, but seems suspicious.
Plan Lucy agrees to return Wed. 10/04/17 9:00 a.m. for next shot at injection clinic. She
will meet with her therapist Tue 10 /17/17 2 p.m., and her psychiatrist on the same
day at 3 p.m.
Medication refill order for client who is stable and known to provider.
Problem Suzy left message on Medication Concern line regarding running out of her Prozac.
Intervention Writer reviewed chart and orders. Returned clients call to assess client. Consulted with
Provider.
Response Suzy reports that she is taking her medications as prescribed and that her symptoms
are “under control.” Denies any type of adverse reactions. Denies S/I or H/I.
Plan Submit VO (L. Barrick, NP) into OrderConnect for Prozac 20 mg. BID to ensure that
client’s treatments is not interrupted to prevent decompensation and
Assessment
Introduction Assessment: Demetri is a 35 year old married Ukrainian male. States he is seeking
treatment because his wife has given him an ultimate to either “get help or move
out”. He was raised in Citrus Heights to an intake family. He is a first generation
American, as his parents migrated to the US from Russia in 1980. Upon graduating
from High school, he married his “high school sweat-heart and joined the Army. He
served as an Army Ranger Army and saw active duty during 2002-2009 in both
Afghanistan and Iraq (Operation Freedom and Operation Iraqi Freedom) completing
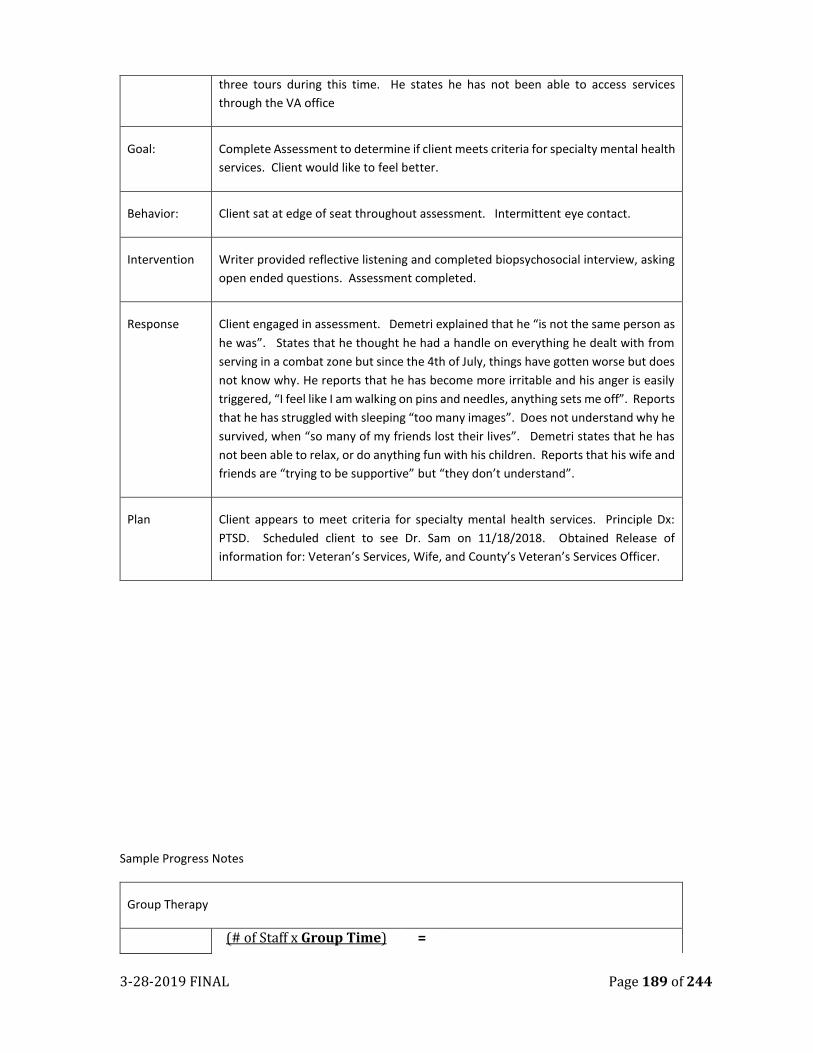
3-28-2019 FINAL Page 189 of 244
three tours during this time. He states he has not been able to access services
through the VA office
Goal: Complete Assessment to determine if client meets criteria for specialty mental health
services. Client would like to feel better.
Behavior: Client sat at edge of seat throughout assessment. Intermittent eye contact.
Intervention Writer provided reflective listening and completed biopsychosocial interview, asking
open ended questions. Assessment completed.
Response Client engaged in assessment. Demetri explained that he “is not the same person as
he was”. States that he thought he had a handle on everything he dealt with from
serving in a combat zone but since the 4th of July, things have gotten worse but does
not know why. He reports that he has become more irritable and his anger is easily
triggered, “I feel like I am walking on pins and needles, anything sets me off”. Reports
that he has struggled with sleeping “too many images”. Does not understand why he
survived, when “so many of my friends lost their lives”. Demetri states that he has
not been able to relax, or do anything fun with his children. Reports that his wife and
friends are “trying to be supportive” but “they don’t understand”.
Plan Client appears to meet criteria for specialty mental health services. Principle Dx:
PTSD. Scheduled client to see Dr. Sam on 11/18/2018. Obtained Release of
information for: Veteran’s Services, Wife, and County’s Veteran’s Services Officer.
Sample Progress Notes
Group Therapy
(# of Staff x Group Time) =
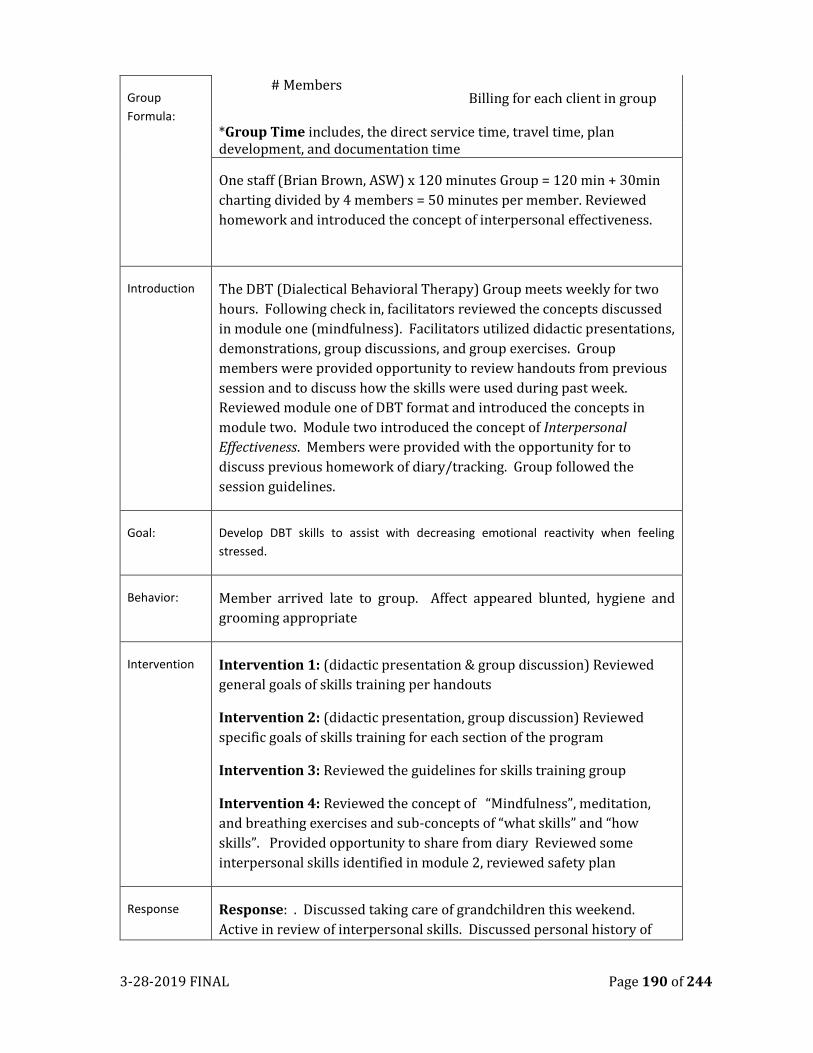
3-28-2019 FINAL Page 190 of 244
Group
Formula:
# Members Billing for each client in group
*Group Time includes, the direct service time, travel time, plan development, and documentation time
One staff (Brian Brown, ASW) x 120 minutes Group = 120 min + 30min
charting divided by 4 members = 50 minutes per member. Reviewed
homework and introduced the concept of interpersonal effectiveness.
Introduction The DBT (Dialectical Behavioral Therapy) Group meets weekly for two
hours. Following check in, facilitators reviewed the concepts discussed
in module one (mindfulness). Facilitators utilized didactic presentations,
demonstrations, group discussions, and group exercises. Group
members were provided opportunity to review handouts from previous
session and to discuss how the skills were used during past week.
Reviewed module one of DBT format and introduced the concepts in
module two. Module two introduced the concept of Interpersonal
Effectiveness. Members were provided with the opportunity for to
discuss previous homework of diary/tracking. Group followed the
session guidelines.
Goal: Develop DBT skills to assist with decreasing emotional reactivity when feeling
stressed.
Behavior: Member arrived late to group. Affect appeared blunted, hygiene and
grooming appropriate
Intervention Intervention 1: (didactic presentation & group discussion) Reviewed
general goals of skills training per handouts
Intervention 2: (didactic presentation, group discussion) Reviewed
specific goals of skills training for each section of the program
Intervention 3: Reviewed the guidelines for skills training group
Intervention 4: Reviewed the concept of “Mindfulness”, meditation,
and breathing exercises and sub-concepts of “what skills” and “how
skills”. Provided opportunity to share from diary Reviewed some
interpersonal skills identified in module 2, reviewed safety plan
Response Response: . Discussed taking care of grandchildren this weekend.
Active in review of interpersonal skills. Discussed personal history of
3-28-2019 FINAL Page 191 of 244
abuse when group member’s began reviewing healthy/unhealthy
boundaries. Became tearful when other member’s shared their stories.
Able to identify plans/skills to keep self safe and encouraged to continue
to work with Clinician to further process this self-disclosure. .
Plan
Appendix A
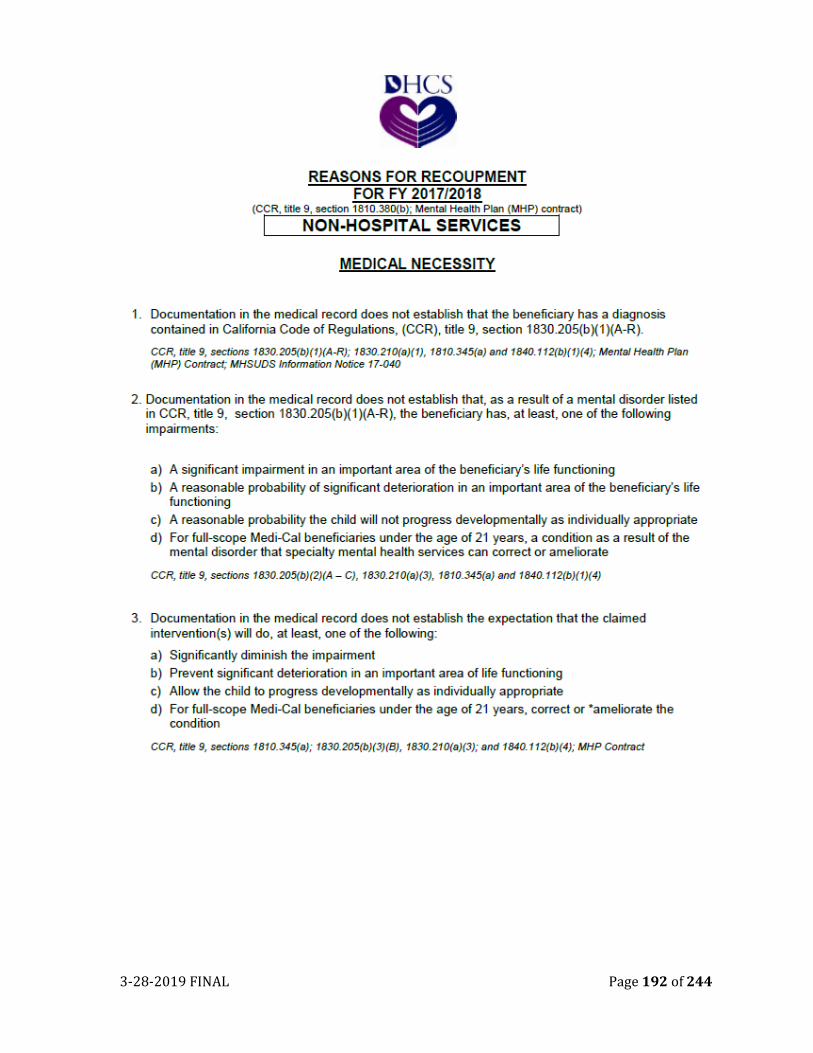
3-28-2019 FINAL Page 192 of 244
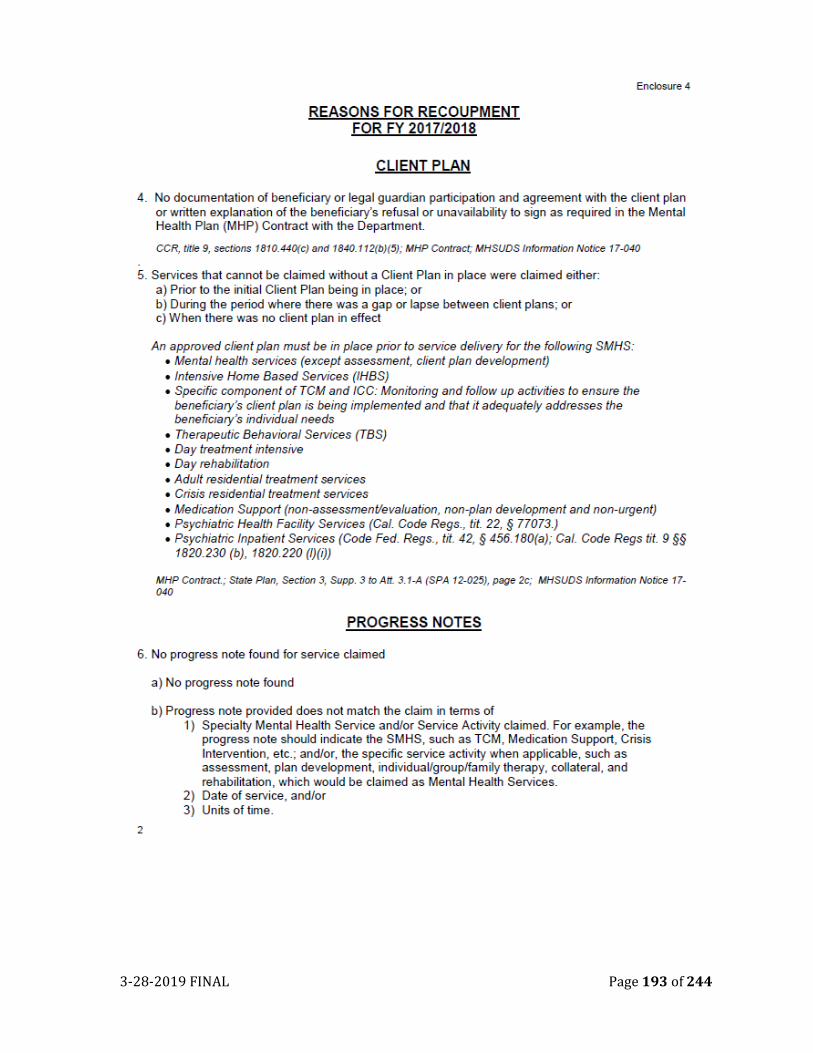
3-28-2019 FINAL Page 193 of 244
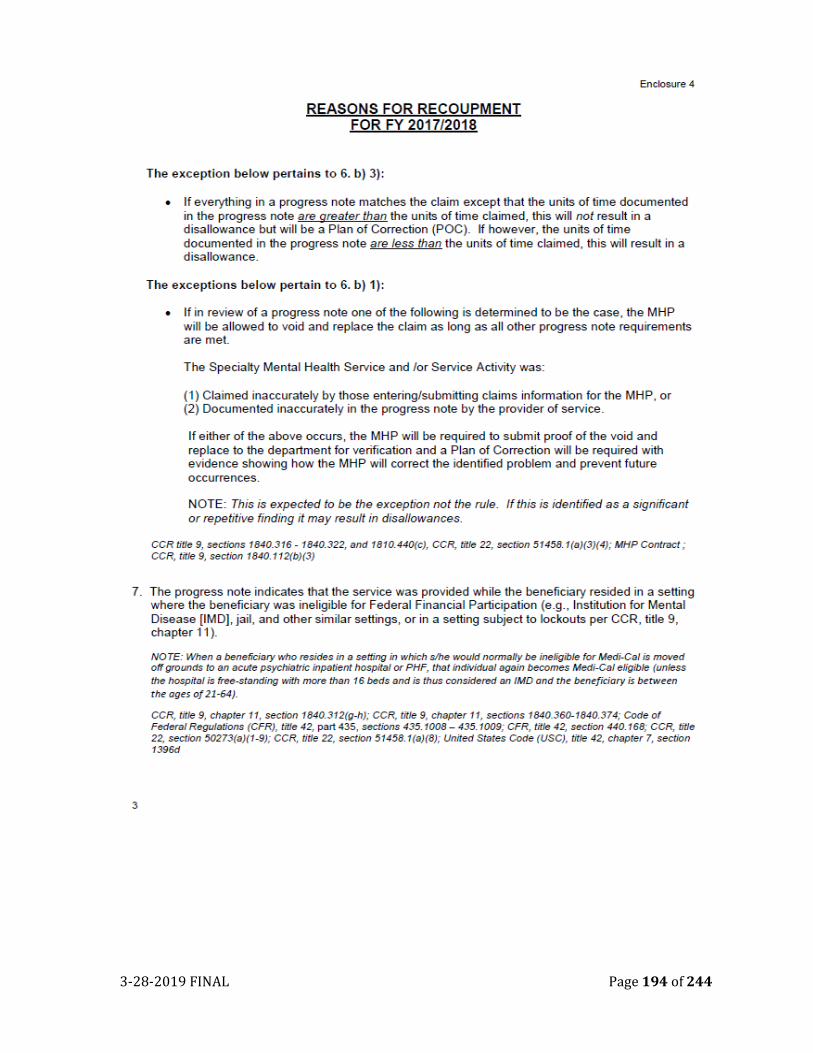
3-28-2019 FINAL Page 194 of 244
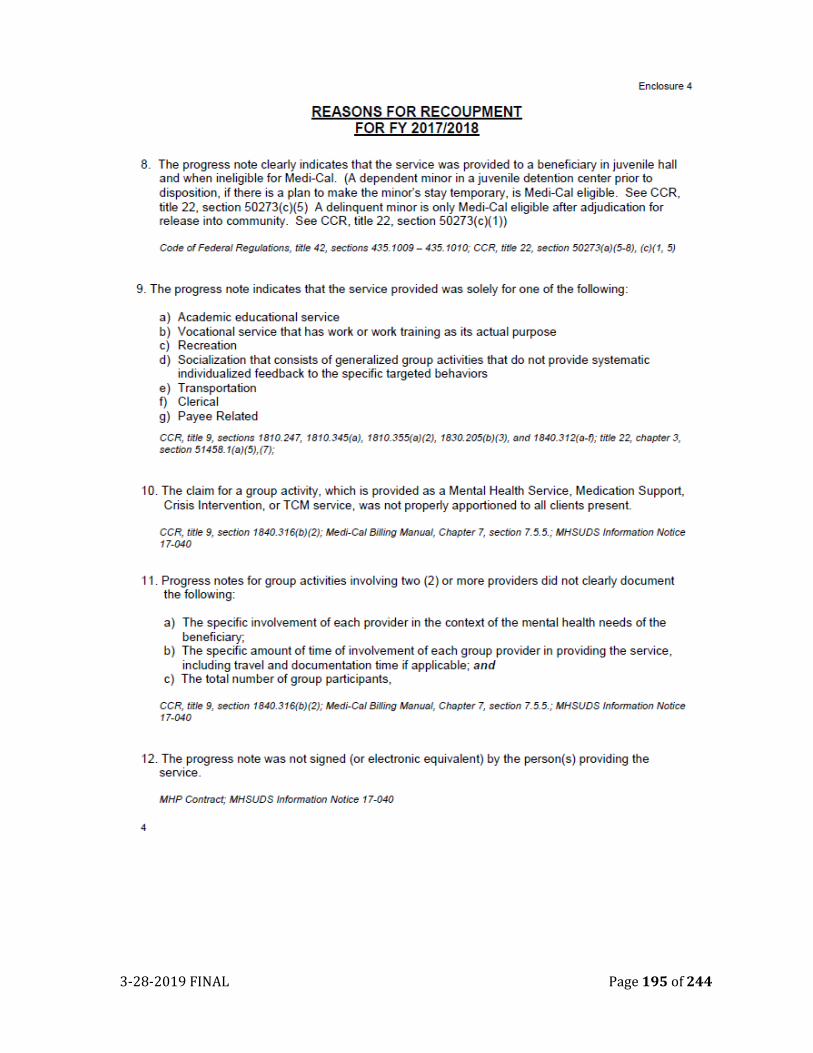
3-28-2019 FINAL Page 195 of 244
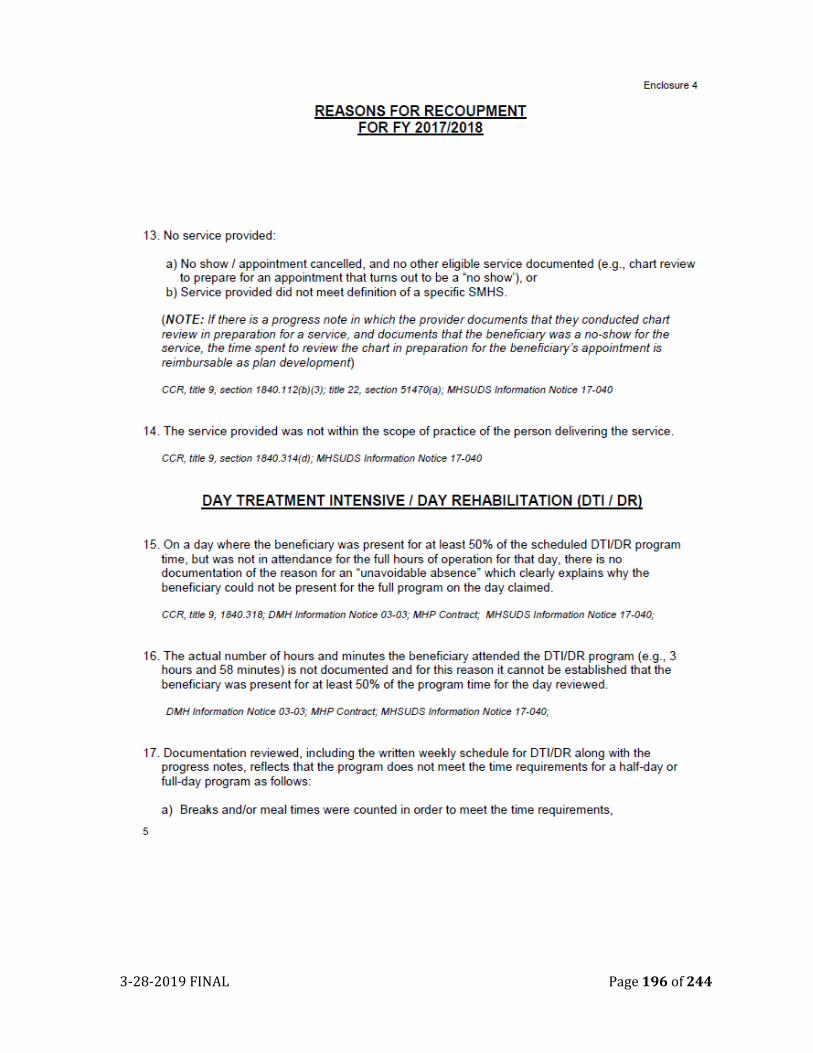
3-28-2019 FINAL Page 196 of 244
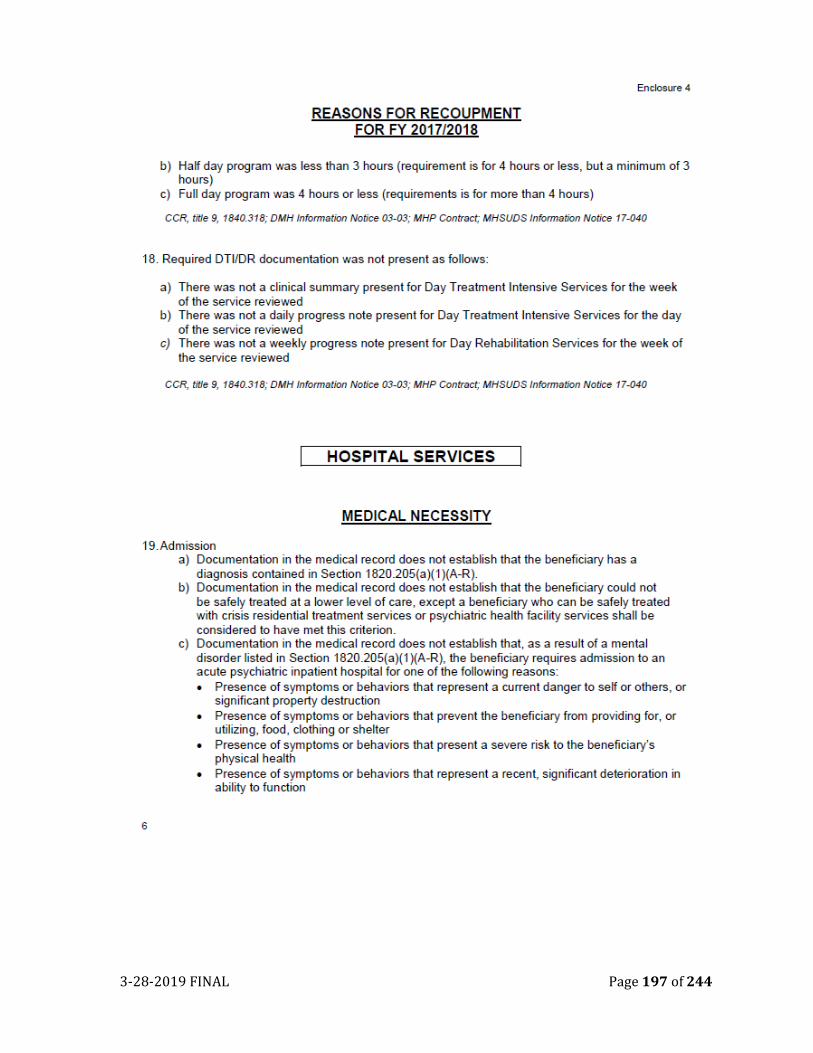
3-28-2019 FINAL Page 197 of 244
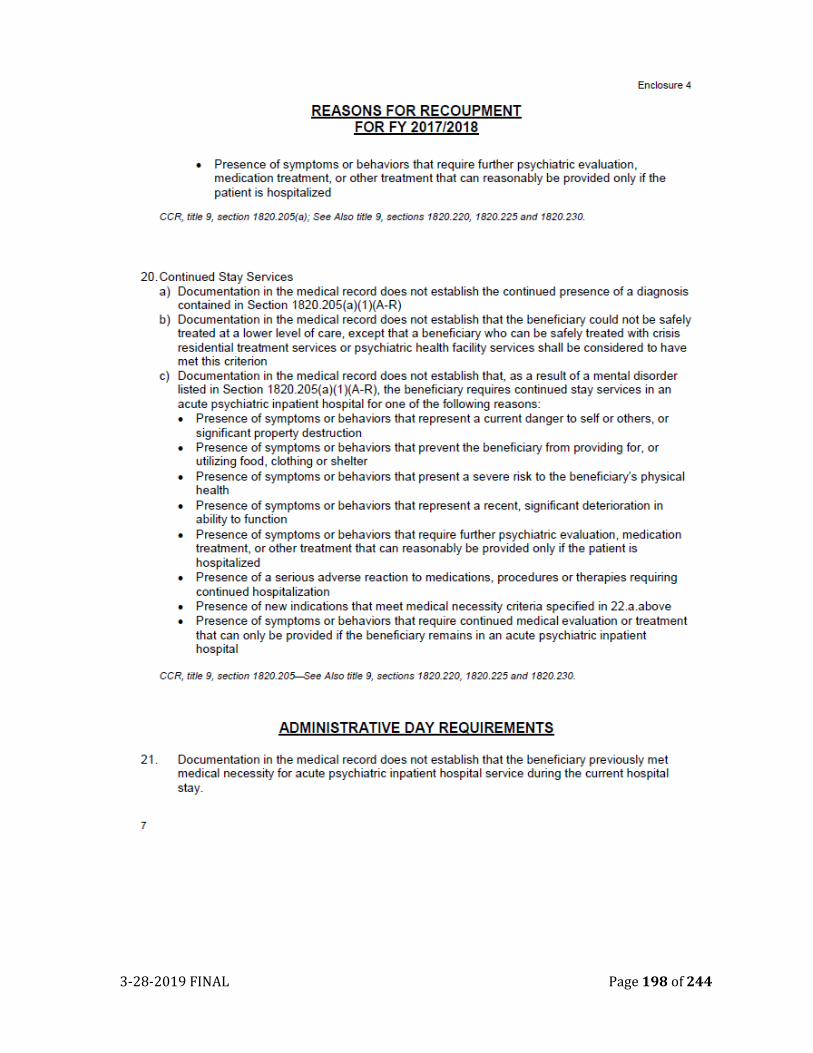
3-28-2019 FINAL Page 198 of 244
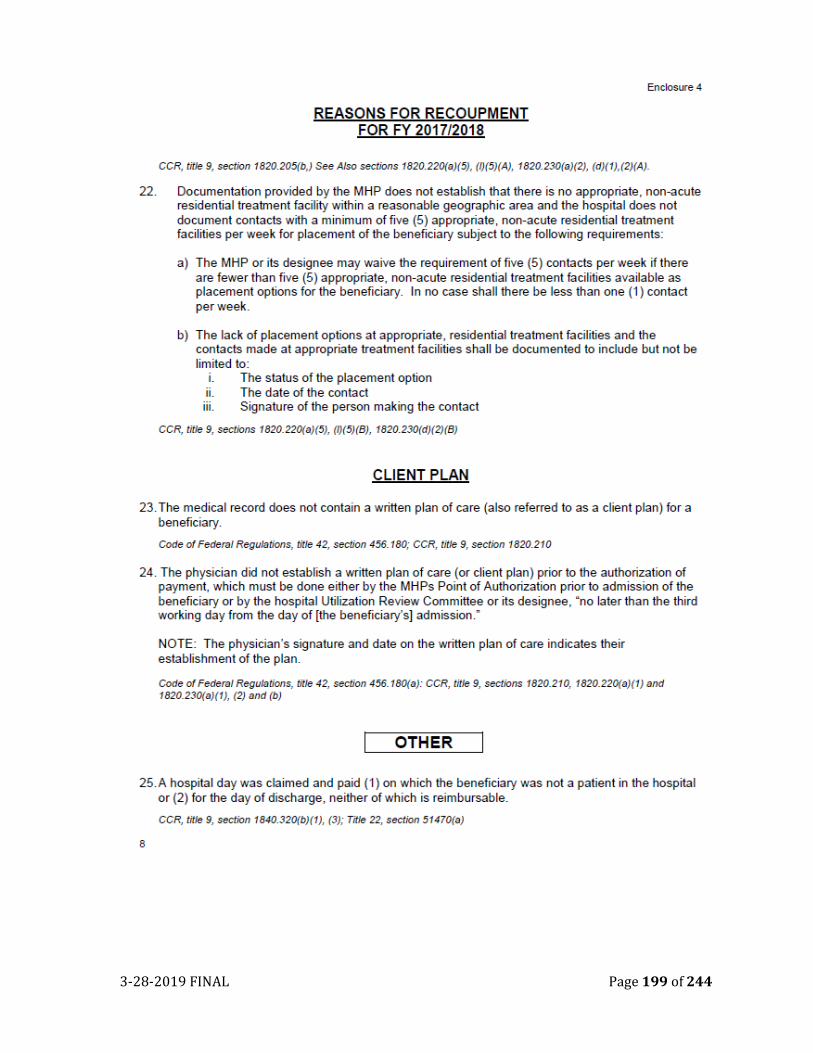
3-28-2019 FINAL Page 199 of 244
3-28-2019 FINAL Page 200 of 244
Appendix B
3-28-2019 FINAL Page 201 of 244
3-28-2019 FINAL Page 202 of 244
3-28-2019 FINAL Page 203 of 244
3-28-2019 FINAL Page 204 of 244
3-28-2019 FINAL Page 205 of 244
3-28-2019 FINAL Page 206 of 244
3-28-2019 FINAL Page 207 of 244
3-28-2019 FINAL Page 208 of 244
3-28-2019 FINAL Page 209 of 244
3-28-2019 FINAL Page 210 of 244
3-28-2019 FINAL Page 211 of 244
3-28-2019 FINAL Page 212 of 244
3-28-2019 FINAL Page 213 of 244
3-28-2019 FINAL Page 214 of 244
3-28-2019 FINAL Page 215 of 244
3-28-2019 FINAL Page 216 of 244
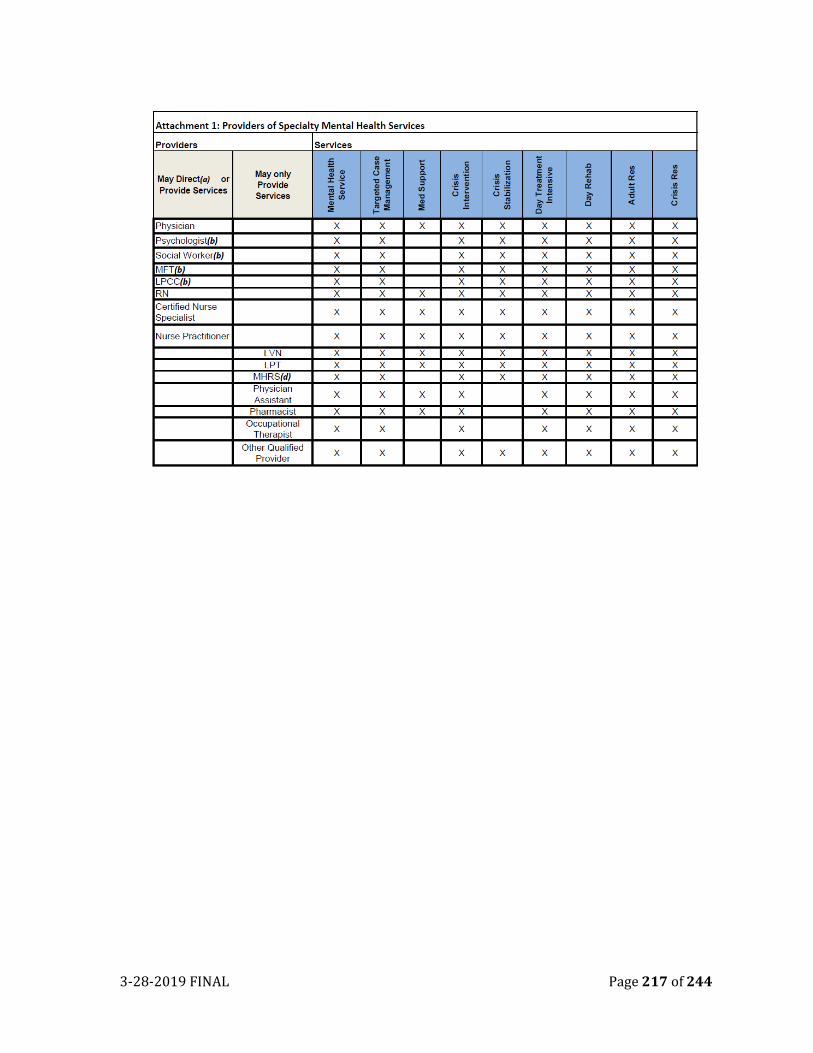
3-28-2019 FINAL Page 217 of 244
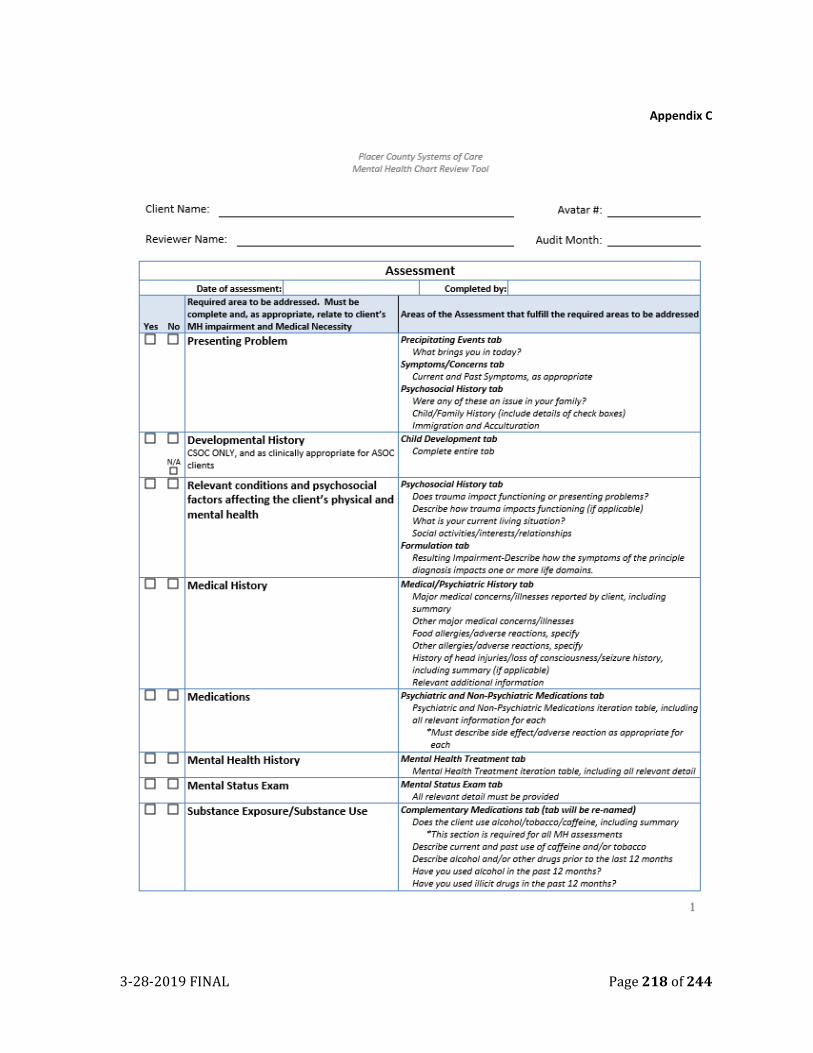
3-28-2019 FINAL Page 218 of 244
Appendix C
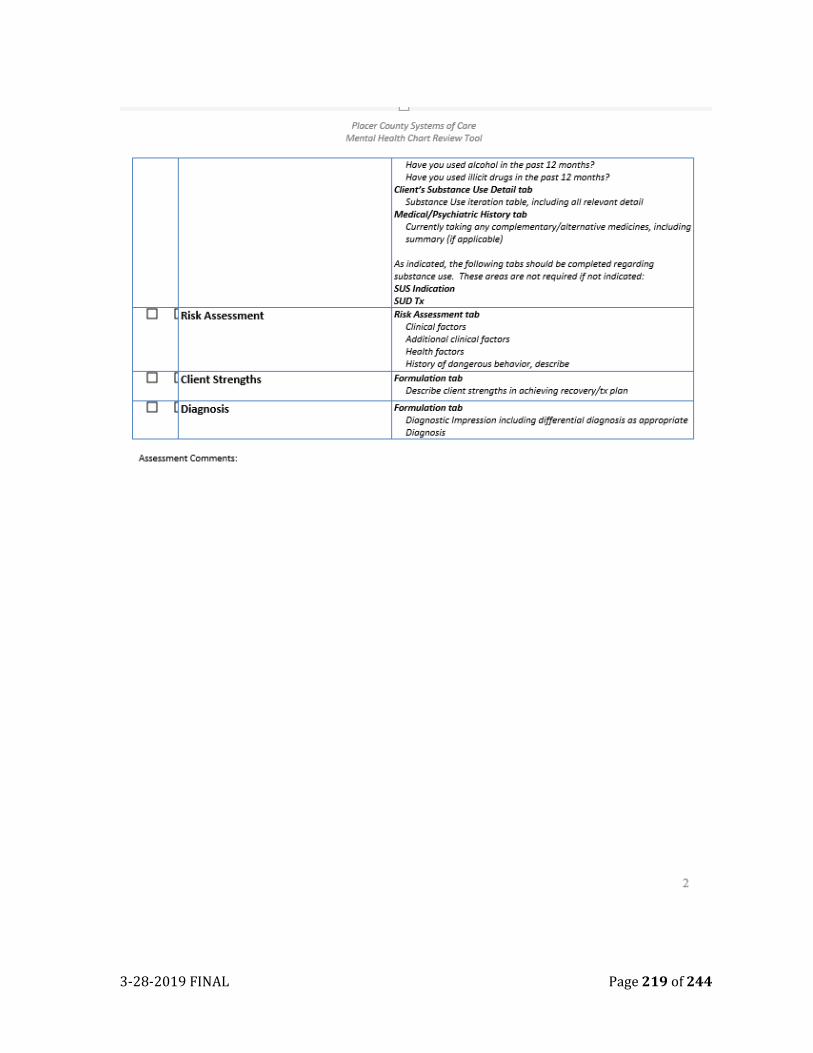
3-28-2019 FINAL Page 219 of 244
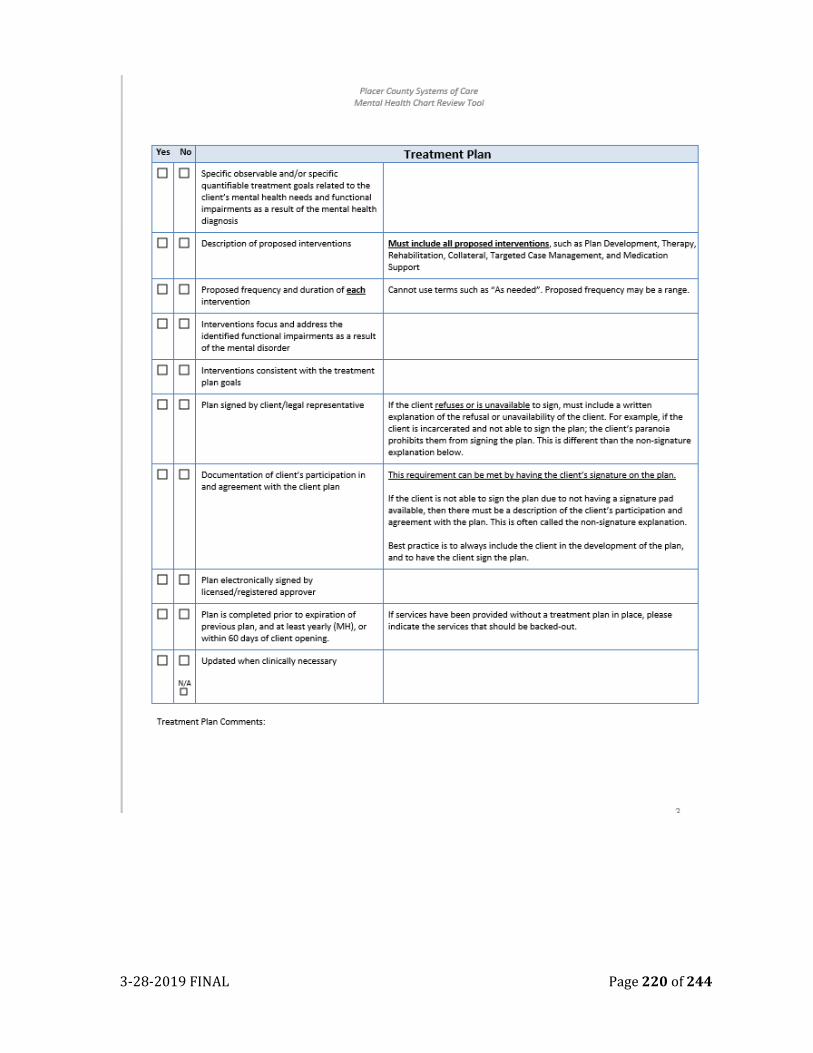
3-28-2019 FINAL Page 220 of 244
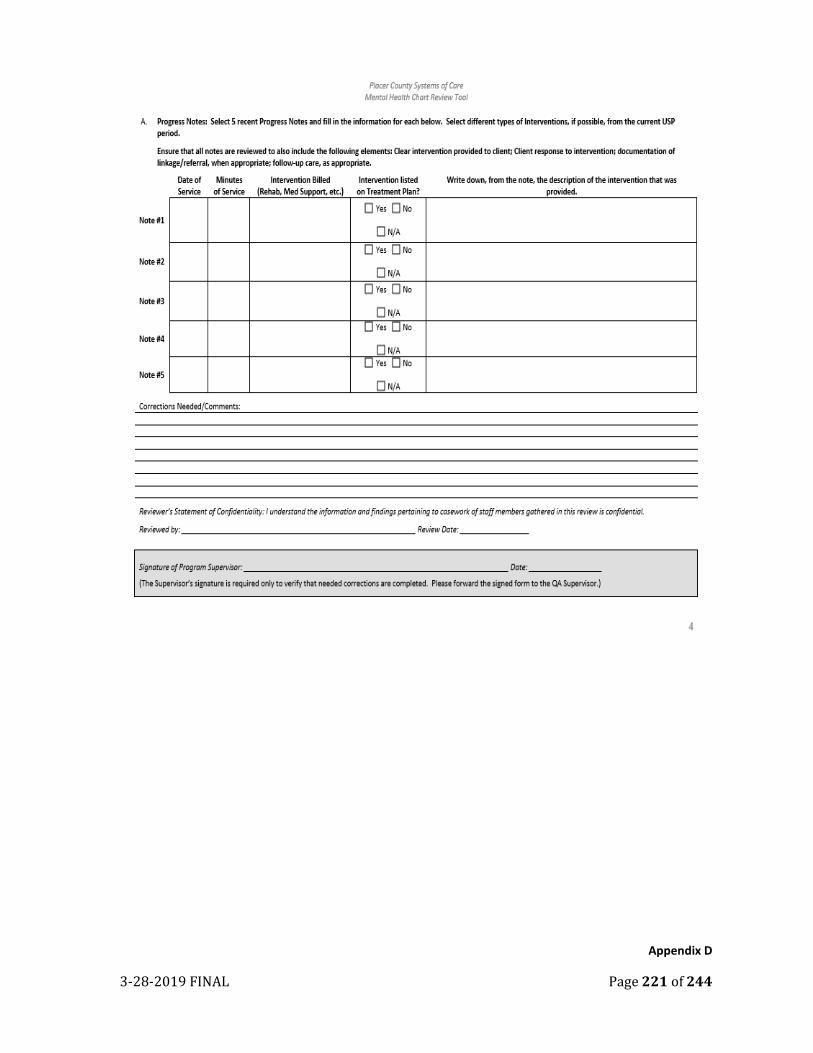
3-28-2019 FINAL Page 221 of 244
Appendix D
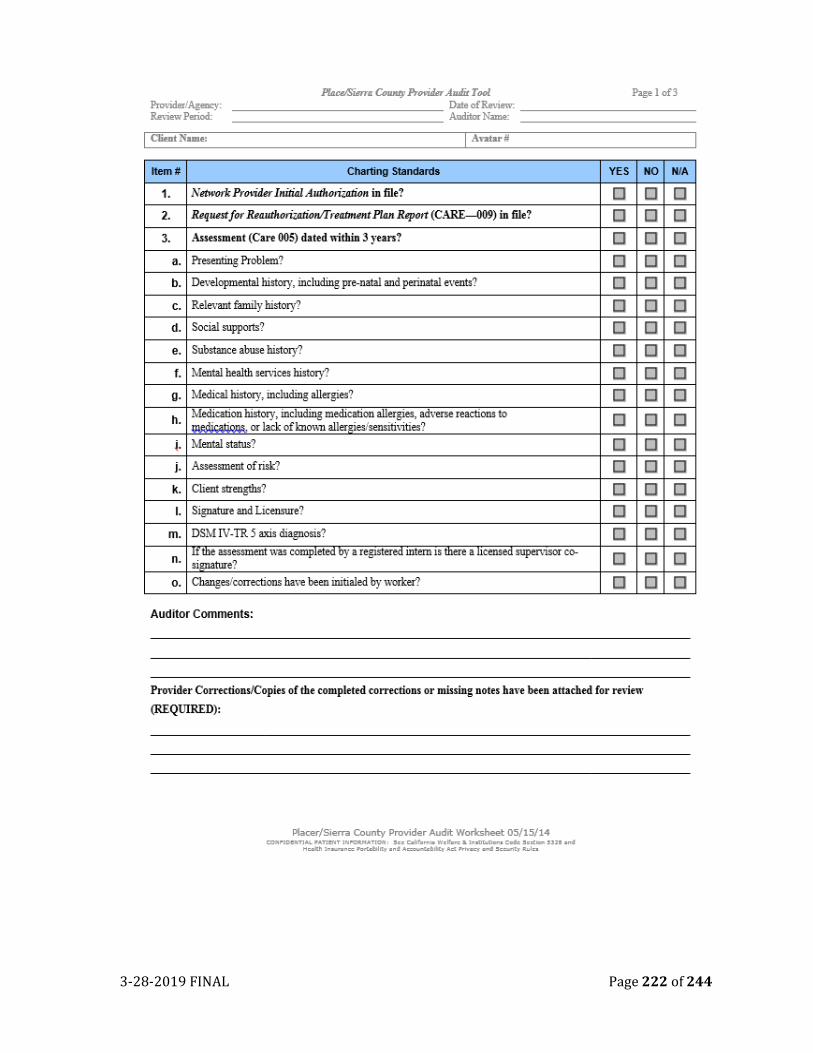
3-28-2019 FINAL Page 222 of 244
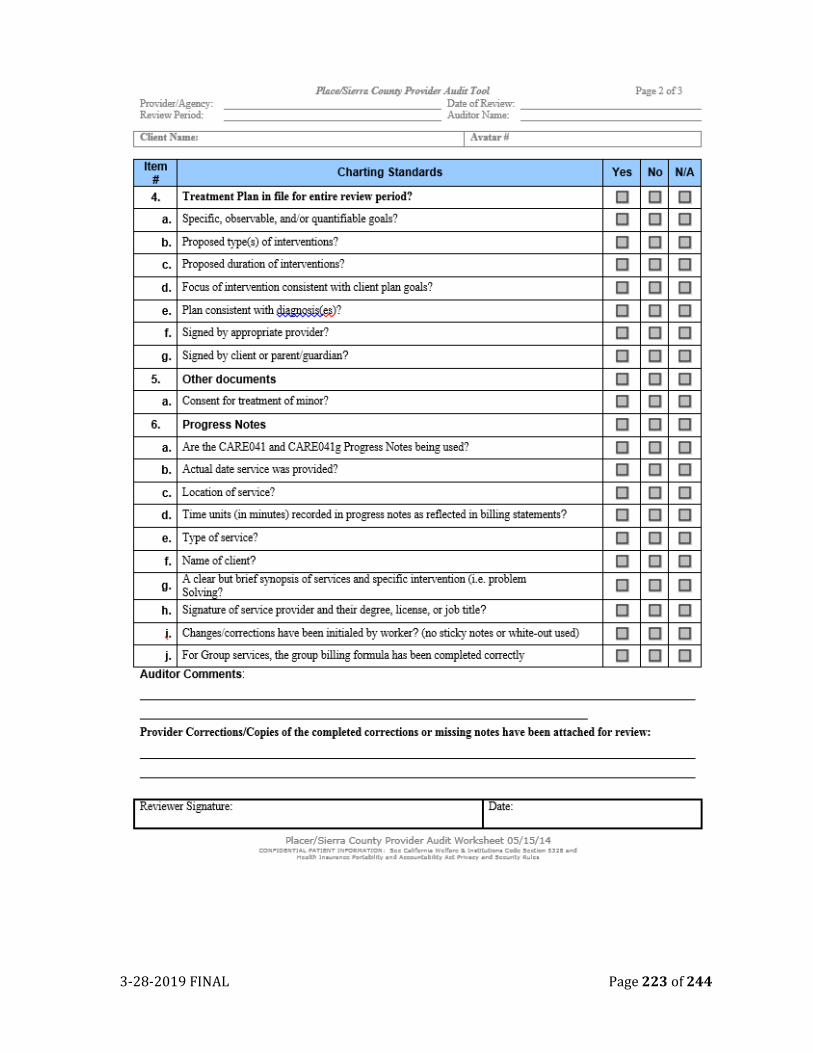
3-28-2019 FINAL Page 223 of 244
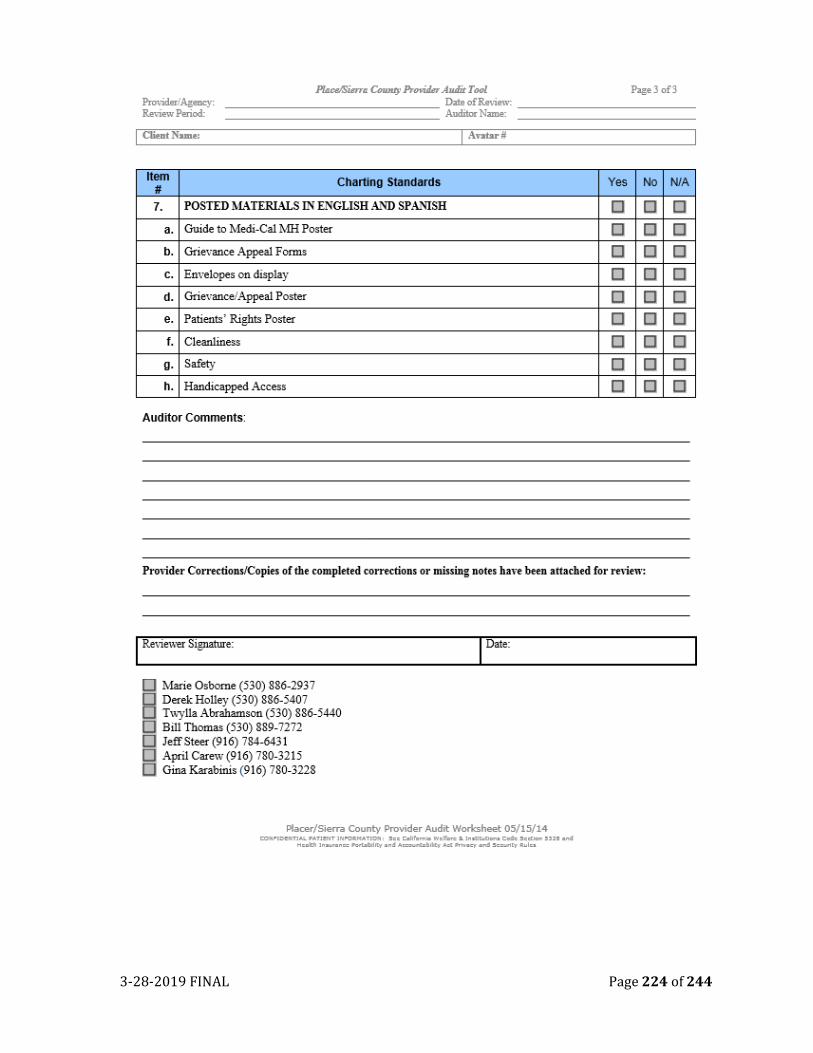
3-28-2019 FINAL Page 224 of 244
3-28-2019 FINAL Page 225 of 244
Appendix E
3-28-2019 FINAL Page 226 of 244
3-28-2019 FINAL Page 227 of 244
3-28-2019 FINAL Page 228 of 244
3-28-2019 FINAL Page 229 of 244
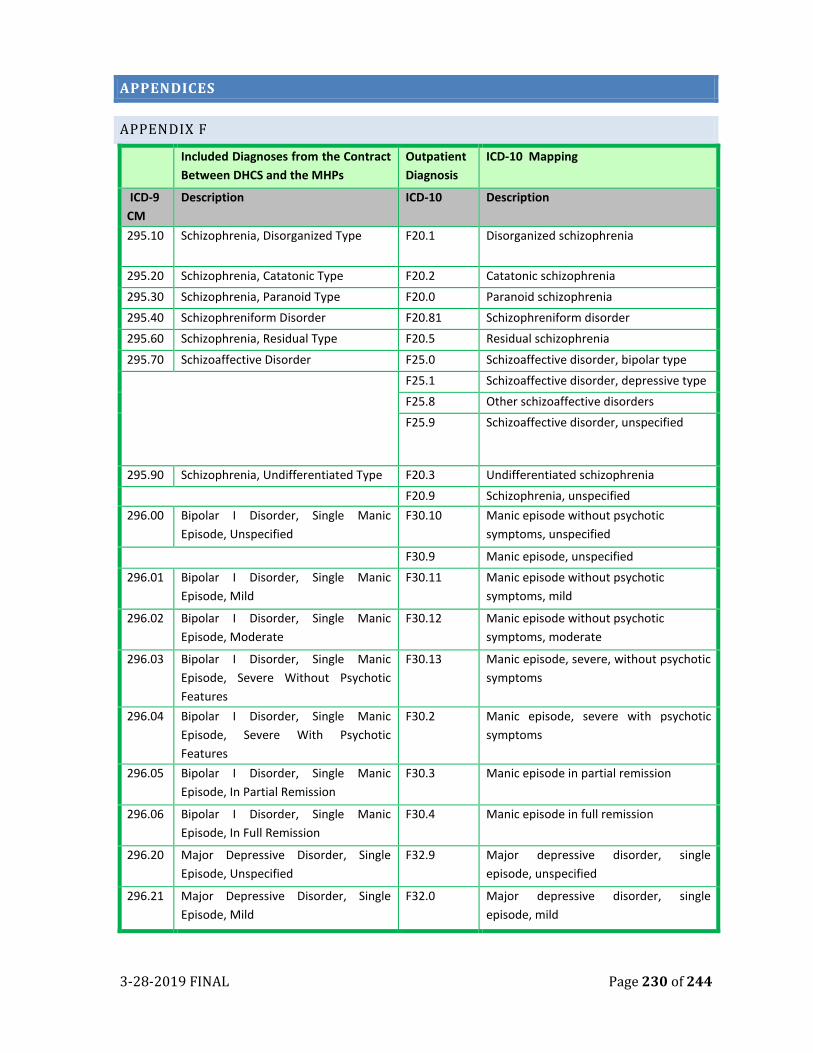
3-28-2019 FINAL Page 230 of 244
APPENDICES
APPENDIX F
Included Diagnoses from the Contract
Between DHCS and the MHPs
Outpatient
Diagnosis
ICD-10 Mapping
ICD-9
CM
Description ICD-10 Description
295.10 Schizophrenia, Disorganized Type F20.1 Disorganized schizophrenia
295.20 Schizophrenia, Catatonic Type F20.2 Catatonic schizophrenia
295.30 Schizophrenia, Paranoid Type F20.0 Paranoid schizophrenia
295.40 Schizophreniform Disorder F20.81 Schizophreniform disorder
295.60 Schizophrenia, Residual Type F20.5 Residual schizophrenia
295.70 Schizoaffective Disorder F25.0 Schizoaffective disorder, bipolar type
F25.1 Schizoaffective disorder, depressive type
F25.8 Other schizoaffective disorders
F25.9 Schizoaffective disorder, unspecified
295.90 Schizophrenia, Undifferentiated Type F20.3 Undifferentiated schizophrenia
F20.9 Schizophrenia, unspecified
296.00 Bipolar I Disorder, Single Manic
Episode, Unspecified
F30.10 Manic episode without psychotic
symptoms, unspecified
F30.9 Manic episode, unspecified
296.01 Bipolar I Disorder, Single Manic
Episode, Mild
F30.11 Manic episode without psychotic
symptoms, mild
296.02 Bipolar I Disorder, Single Manic
Episode, Moderate
F30.12 Manic episode without psychotic
symptoms, moderate
296.03 Bipolar I Disorder, Single Manic
Episode, Severe Without Psychotic
Features
F30.13 Manic episode, severe, without psychotic
symptoms
296.04 Bipolar I Disorder, Single Manic
Episode, Severe With Psychotic
Features
F30.2 Manic episode, severe with psychotic
symptoms
296.05 Bipolar I Disorder, Single Manic
Episode, In Partial Remission
F30.3 Manic episode in partial remission
296.06 Bipolar I Disorder, Single Manic
Episode, In Full Remission
F30.4 Manic episode in full remission
296.20 Major Depressive Disorder, Single
Episode, Unspecified
F32.9 Major depressive disorder, single
episode, unspecified
296.21 Major Depressive Disorder, Single
Episode, Mild
F32.0 Major depressive disorder, single
episode, mild
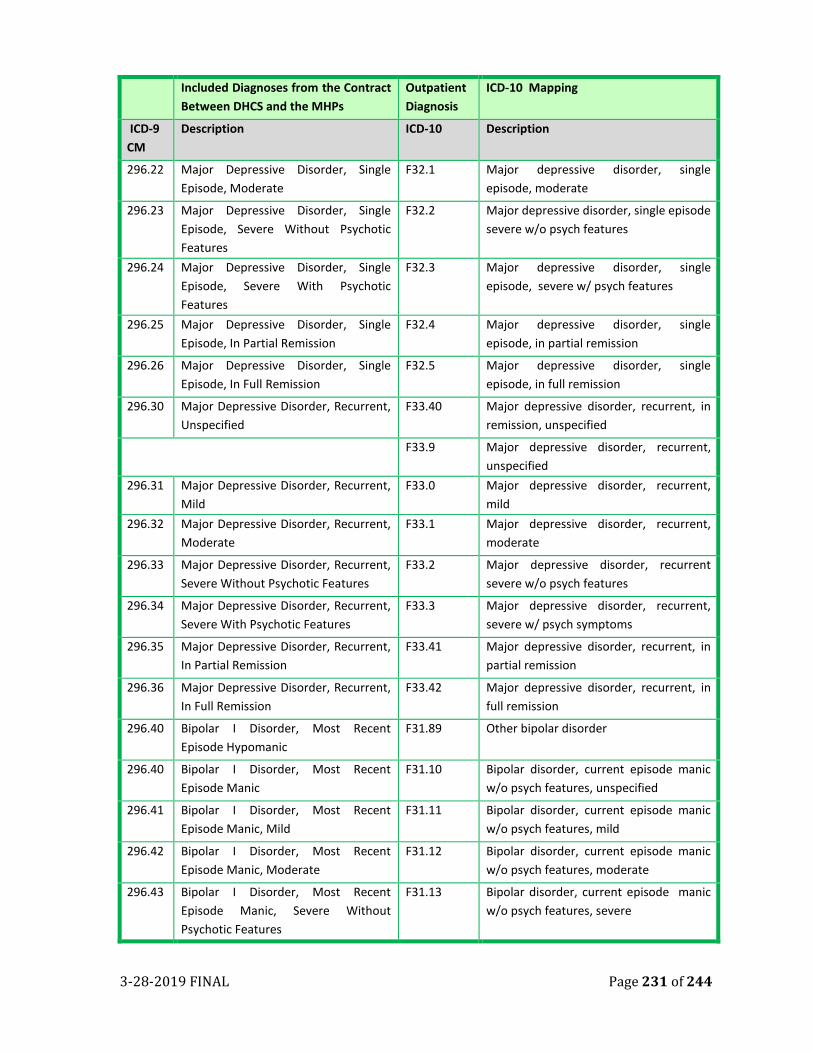
3-28-2019 FINAL Page 231 of 244
Included Diagnoses from the Contract
Between DHCS and the MHPs
Outpatient
Diagnosis
ICD-10 Mapping
ICD-9
CM
Description ICD-10 Description
296.22 Major Depressive Disorder, Single
Episode, Moderate
F32.1 Major depressive disorder, single
episode, moderate
296.23 Major Depressive Disorder, Single
Episode, Severe Without Psychotic
Features
F32.2 Major depressive disorder, single episode
severe w/o psych features
296.24 Major Depressive Disorder, Single
Episode, Severe With Psychotic
Features
F32.3 Major depressive disorder, single
episode, severe w/ psych features
296.25 Major Depressive Disorder, Single
Episode, In Partial Remission
F32.4 Major depressive disorder, single
episode, in partial remission
296.26 Major Depressive Disorder, Single
Episode, In Full Remission
F32.5 Major depressive disorder, single
episode, in full remission
296.30 Major Depressive Disorder, Recurrent,
Unspecified
F33.40 Major depressive disorder, recurrent, in
remission, unspecified
F33.9 Major depressive disorder, recurrent,
unspecified
296.31 Major Depressive Disorder, Recurrent,
Mild
F33.0 Major depressive disorder, recurrent,
mild
296.32 Major Depressive Disorder, Recurrent,
Moderate
F33.1 Major depressive disorder, recurrent,
moderate
296.33 Major Depressive Disorder, Recurrent,
Severe Without Psychotic Features
F33.2 Major depressive disorder, recurrent
severe w/o psych features
296.34 Major Depressive Disorder, Recurrent,
Severe With Psychotic Features
F33.3 Major depressive disorder, recurrent,
severe w/ psych symptoms
296.35 Major Depressive Disorder, Recurrent,
In Partial Remission
F33.41 Major depressive disorder, recurrent, in
partial remission
296.36 Major Depressive Disorder, Recurrent,
In Full Remission
F33.42 Major depressive disorder, recurrent, in
full remission
296.40 Bipolar I Disorder, Most Recent
Episode Hypomanic
F31.89 Other bipolar disorder
296.40 Bipolar I Disorder, Most Recent
Episode Manic
F31.10 Bipolar disorder, current episode manic
w/o psych features, unspecified
296.41 Bipolar I Disorder, Most Recent
Episode Manic, Mild
F31.11 Bipolar disorder, current episode manic
w/o psych features, mild
296.42 Bipolar I Disorder, Most Recent
Episode Manic, Moderate
F31.12 Bipolar disorder, current episode manic
w/o psych features, moderate
296.43 Bipolar I Disorder, Most Recent
Episode Manic, Severe Without
Psychotic Features
F31.13 Bipolar disorder, current episode manic
w/o psych features, severe
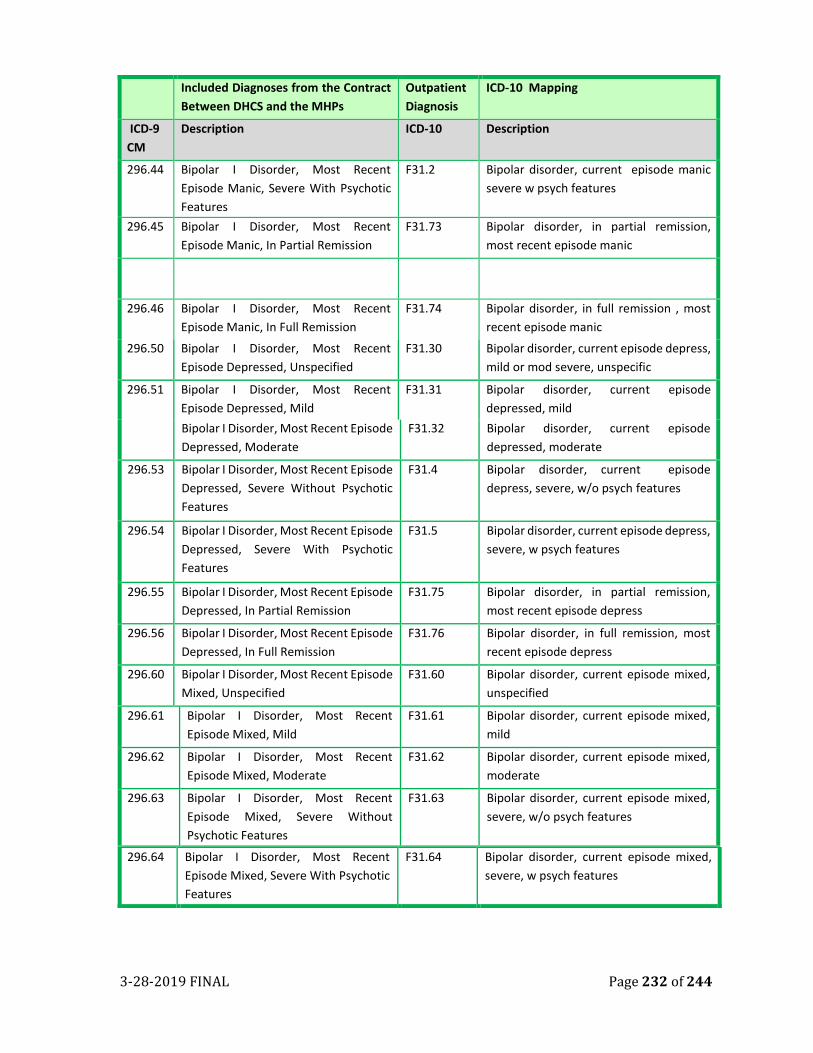
3-28-2019 FINAL Page 232 of 244
Included Diagnoses from the Contract
Between DHCS and the MHPs
Outpatient
Diagnosis
ICD-10 Mapping
ICD-9
CM
Description ICD-10 Description
296.44 Bipolar I Disorder, Most Recent
Episode Manic, Severe With Psychotic
Features
F31.2 Bipolar disorder, current episode manic
severe w psych features
296.45 Bipolar I Disorder, Most Recent
Episode Manic, In Partial Remission
F31.73 Bipolar disorder, in partial remission,
most recent episode manic
296.46 Bipolar I Disorder, Most Recent
Episode Manic, In Full Remission
F31.74 Bipolar disorder, in full remission , most
recent episode manic
296.50 Bipolar I Disorder, Most Recent
Episode Depressed, Unspecified
F31.30 Bipolar disorder, current episode depress,
mild or mod severe, unspecific
296.51 Bipolar I Disorder, Most Recent
Episode Depressed, Mild
F31.31 Bipolar disorder, current episode
depressed, mild
Bipolar I Disorder, Most Recent Episode
Depressed, Moderate
F31.32 Bipolar disorder, current episode
depressed, moderate
296.53 Bipolar I Disorder, Most Recent Episode
Depressed, Severe Without Psychotic
Features
F31.4 Bipolar disorder, current episode
depress, severe, w/o psych features
296.54 Bipolar I Disorder, Most Recent Episode
Depressed, Severe With Psychotic
Features
F31.5 Bipolar disorder, current episode depress,
severe, w psych features
296.55 Bipolar I Disorder, Most Recent Episode
Depressed, In Partial Remission
F31.75 Bipolar disorder, in partial remission,
most recent episode depress
296.56 Bipolar I Disorder, Most Recent Episode
Depressed, In Full Remission
F31.76 Bipolar disorder, in full remission, most
recent episode depress
296.60 Bipolar I Disorder, Most Recent Episode
Mixed, Unspecified
F31.60 Bipolar disorder, current episode mixed,
unspecified
296.61 Bipolar I Disorder, Most Recent
Episode Mixed, Mild
F31.61 Bipolar disorder, current episode mixed,
mild
296.62 Bipolar I Disorder, Most Recent
Episode Mixed, Moderate
F31.62 Bipolar disorder, current episode mixed,
moderate
296.63 Bipolar I Disorder, Most Recent
Episode Mixed, Severe Without
Psychotic Features
F31.63 Bipolar disorder, current episode mixed,
severe, w/o psych features
296.64 Bipolar I Disorder, Most Recent
Episode Mixed, Severe With Psychotic
Features
F31.64 Bipolar disorder, current episode mixed,
severe, w psych features
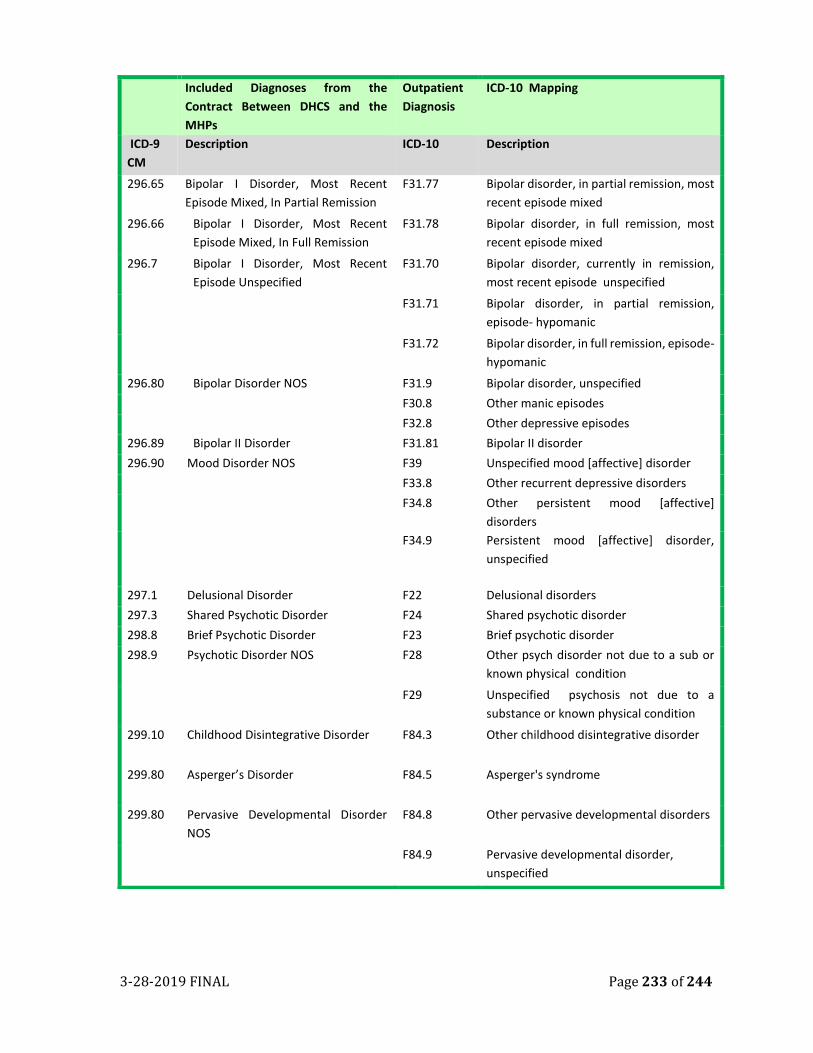
3-28-2019 FINAL Page 233 of 244
Included Diagnoses from the
Contract Between DHCS and the
MHPs
Outpatient
Diagnosis
ICD-10 Mapping
ICD-9
CM
Description ICD-10 Description
296.65 Bipolar I Disorder, Most Recent
Episode Mixed, In Partial Remission
F31.77 Bipolar disorder, in partial remission, most
recent episode mixed
296.66 Bipolar I Disorder, Most Recent
Episode Mixed, In Full Remission
F31.78 Bipolar disorder, in full remission, most
recent episode mixed
296.7 Bipolar I Disorder, Most Recent
Episode Unspecified
F31.70 Bipolar disorder, currently in remission,
most recent episode unspecified
F31.71 Bipolar disorder, in partial remission,
episode- hypomanic
F31.72 Bipolar disorder, in full remission, episode-
hypomanic
296.80 Bipolar Disorder NOS F31.9 Bipolar disorder, unspecified
F30.8 Other manic episodes
F32.8 Other depressive episodes
296.89 Bipolar II Disorder F31.81 Bipolar II disorder
296.90 Mood Disorder NOS F39 Unspecified mood [affective] disorder
F33.8 Other recurrent depressive disorders
F34.8 Other persistent mood [affective]
disorders
F34.9 Persistent mood [affective] disorder,
unspecified
297.1 Delusional Disorder F22 Delusional disorders
297.3 Shared Psychotic Disorder F24 Shared psychotic disorder
298.8 Brief Psychotic Disorder F23 Brief psychotic disorder
298.9 Psychotic Disorder NOS F28 Other psych disorder not due to a sub or
known physical condition
F29 Unspecified psychosis not due to a
substance or known physical condition
299.10 Childhood Disintegrative Disorder F84.3 Other childhood disintegrative disorder
299.80 Asperger’s Disorder F84.5 Asperger's syndrome
299.80 Pervasive Developmental Disorder
NOS
F84.8 Other pervasive developmental disorders
F84.9 Pervasive developmental disorder,
unspecified
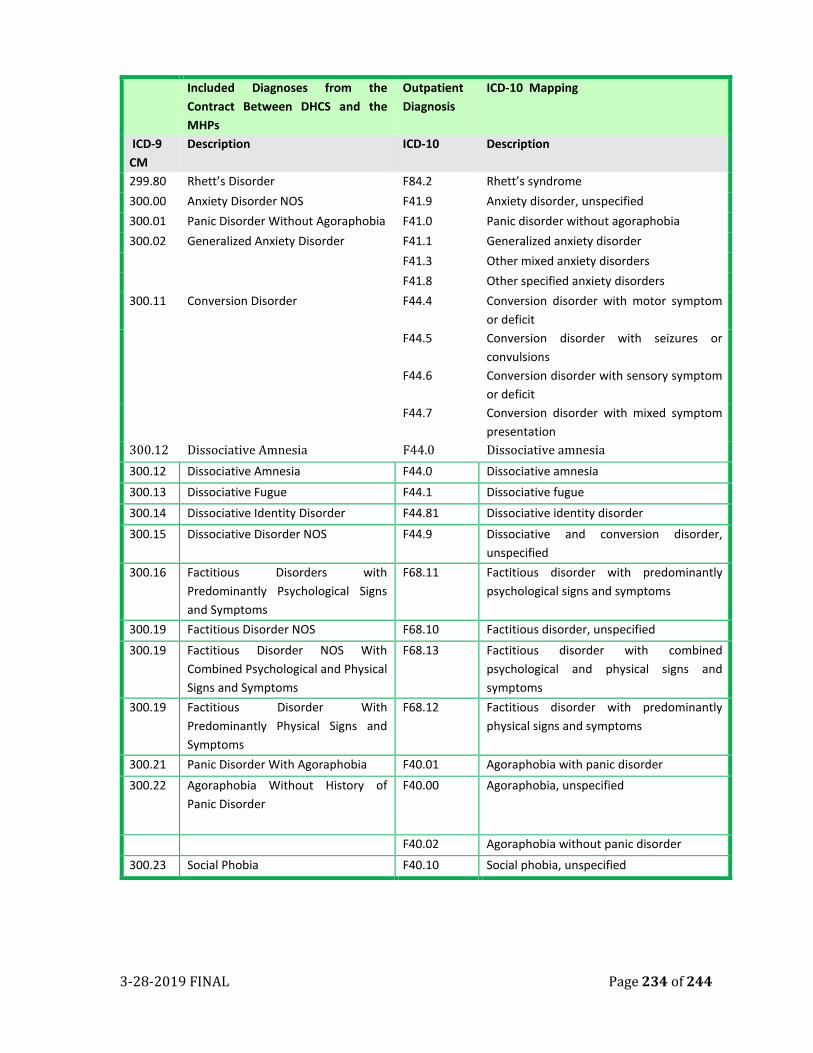
3-28-2019 FINAL Page 234 of 244
Included Diagnoses from the
Contract Between DHCS and the
MHPs
Outpatient
Diagnosis
ICD-10 Mapping
ICD-9
CM
Description ICD-10 Description
299.80 Rhett’s Disorder F84.2 Rhett’s syndrome
300.00 Anxiety Disorder NOS F41.9 Anxiety disorder, unspecified
300.01 Panic Disorder Without Agoraphobia F41.0 Panic disorder without agoraphobia
300.02 Generalized Anxiety Disorder F41.1 Generalized anxiety disorder
F41.3 Other mixed anxiety disorders
F41.8 Other specified anxiety disorders
300.11 Conversion Disorder F44.4 Conversion disorder with motor symptom
or deficit
F44.5 Conversion disorder with seizures or
convulsions
F44.6 Conversion disorder with sensory symptom
or deficit
F44.7 Conversion disorder with mixed symptom
presentation
300.12 Dissociative Amnesia F44.0 Dissociative amnesia
300.12 Dissociative Amnesia F44.0 Dissociative amnesia
300.13 Dissociative Fugue F44.1 Dissociative fugue
300.14 Dissociative Identity Disorder F44.81 Dissociative identity disorder
300.15 Dissociative Disorder NOS F44.9 Dissociative and conversion disorder,
unspecified
300.16 Factitious Disorders with
Predominantly Psychological Signs
and Symptoms
F68.11 Factitious disorder with predominantly
psychological signs and symptoms
300.19 Factitious Disorder NOS F68.10 Factitious disorder, unspecified
300.19 Factitious Disorder NOS With
Combined Psychological and Physical
Signs and Symptoms
F68.13 Factitious disorder with combined
psychological and physical signs and
symptoms
300.19 Factitious Disorder With
Predominantly Physical Signs and
Symptoms
F68.12 Factitious disorder with predominantly
physical signs and symptoms
300.21 Panic Disorder With Agoraphobia F40.01 Agoraphobia with panic disorder
300.22 Agoraphobia Without History of
Panic Disorder
F40.00 Agoraphobia, unspecified
F40.02 Agoraphobia without panic disorder
300.23 Social Phobia F40.10 Social phobia, unspecified
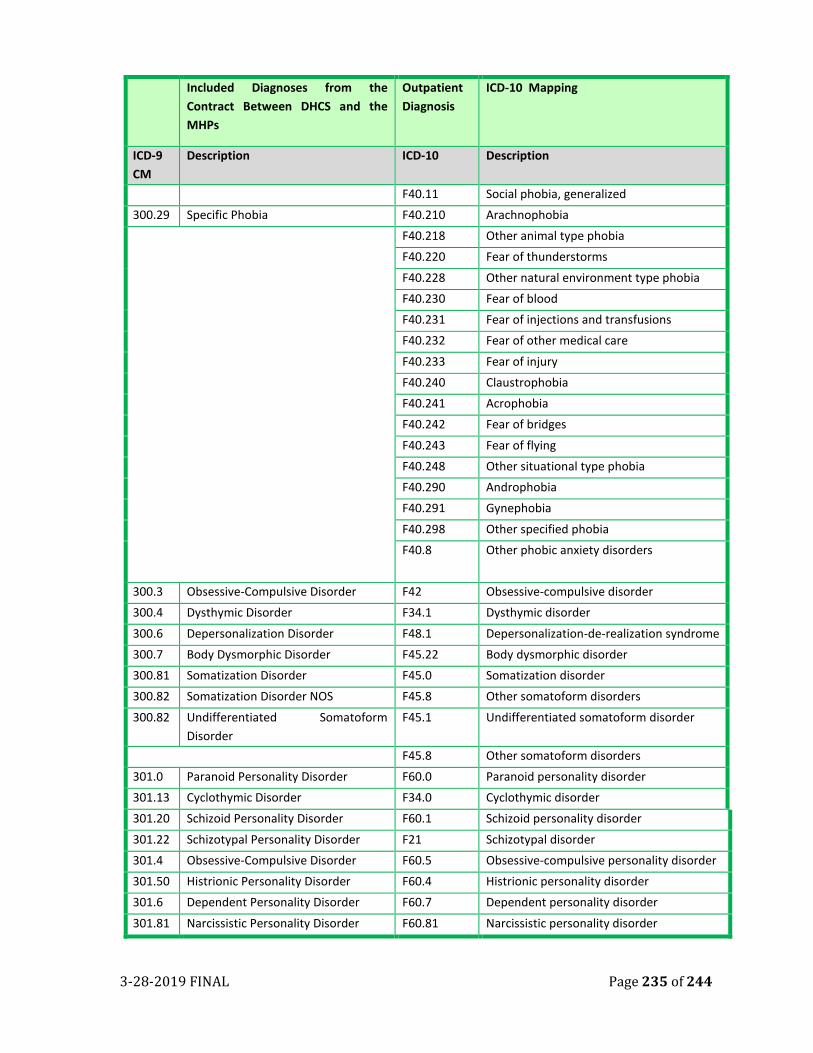
3-28-2019 FINAL Page 235 of 244
Included Diagnoses from the
Contract Between DHCS and the
MHPs
Outpatient
Diagnosis
ICD-10 Mapping
ICD-9
CM
Description ICD-10 Description
F40.11 Social phobia, generalized
300.29 Specific Phobia F40.210 Arachnophobia
F40.218 Other animal type phobia
F40.220 Fear of thunderstorms
F40.228 Other natural environment type phobia
F40.230 Fear of blood
F40.231 Fear of injections and transfusions
F40.232 Fear of other medical care
F40.233 Fear of injury
F40.240 Claustrophobia
F40.241 Acrophobia
F40.242 Fear of bridges
F40.243 Fear of flying
F40.248 Other situational type phobia
F40.290 Androphobia
F40.291 Gynephobia
F40.298 Other specified phobia
F40.8 Other phobic anxiety disorders
300.3 Obsessive-Compulsive Disorder F42 Obsessive-compulsive disorder
300.4 Dysthymic Disorder F34.1 Dysthymic disorder
300.6 Depersonalization Disorder F48.1 Depersonalization-de-realization syndrome
300.7 Body Dysmorphic Disorder F45.22 Body dysmorphic disorder
300.81 Somatization Disorder F45.0 Somatization disorder
300.82 Somatization Disorder NOS F45.8 Other somatoform disorders
300.82 Undifferentiated Somatoform
Disorder
F45.1 Undifferentiated somatoform disorder
F45.8 Other somatoform disorders
301.0 Paranoid Personality Disorder F60.0 Paranoid personality disorder
301.13 Cyclothymic Disorder F34.0 Cyclothymic disorder
301.20 Schizoid Personality Disorder F60.1 Schizoid personality disorder
301.22 Schizotypal Personality Disorder F21 Schizotypal disorder
301.4 Obsessive-Compulsive Disorder F60.5 Obsessive-compulsive personality disorder
301.50 Histrionic Personality Disorder F60.4 Histrionic personality disorder
301.6 Dependent Personality Disorder F60.7 Dependent personality disorder
301.81 Narcissistic Personality Disorder F60.81 Narcissistic personality disorder
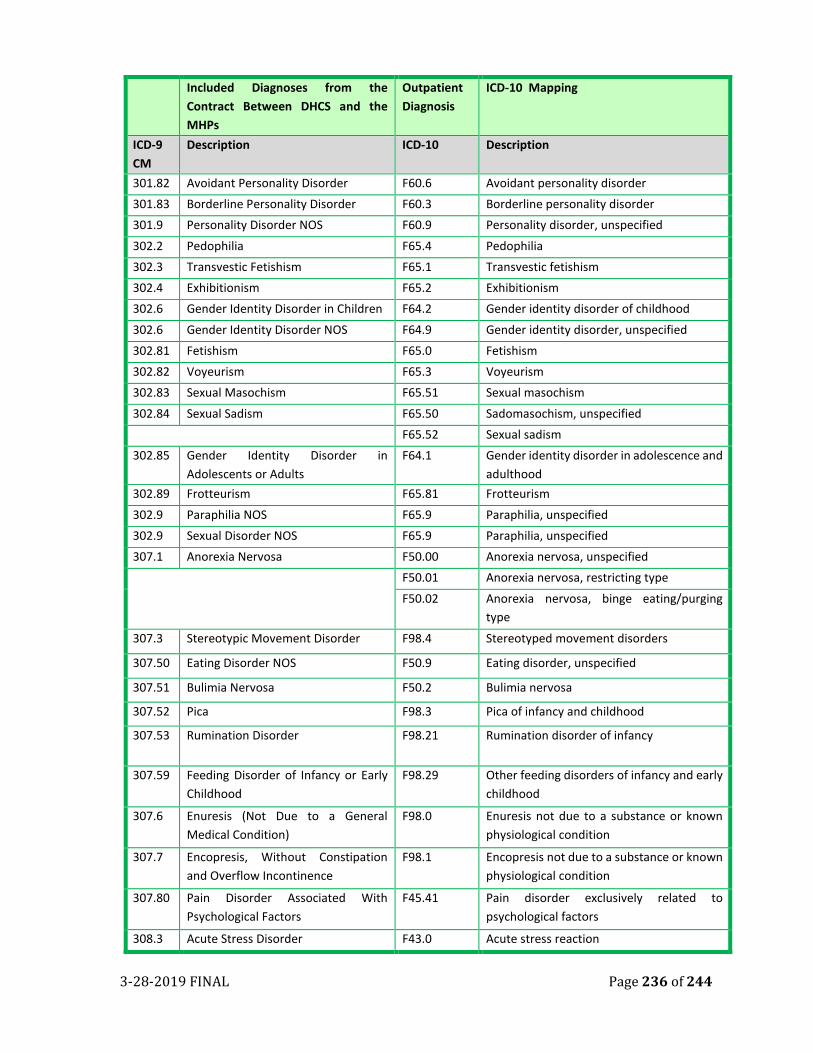
3-28-2019 FINAL Page 236 of 244
Included Diagnoses from the
Contract Between DHCS and the
MHPs
Outpatient
Diagnosis
ICD-10 Mapping
ICD-9
CM
Description ICD-10 Description
301.82 Avoidant Personality Disorder F60.6 Avoidant personality disorder
301.83 Borderline Personality Disorder F60.3 Borderline personality disorder
301.9 Personality Disorder NOS F60.9 Personality disorder, unspecified
302.2 Pedophilia F65.4 Pedophilia
302.3 Transvestic Fetishism F65.1 Transvestic fetishism
302.4 Exhibitionism F65.2 Exhibitionism
302.6 Gender Identity Disorder in Children F64.2 Gender identity disorder of childhood
302.6 Gender Identity Disorder NOS F64.9 Gender identity disorder, unspecified
302.81 Fetishism F65.0 Fetishism
302.82 Voyeurism F65.3 Voyeurism
302.83 Sexual Masochism F65.51 Sexual masochism
302.84 Sexual Sadism F65.50 Sadomasochism, unspecified
F65.52 Sexual sadism
302.85 Gender Identity Disorder in
Adolescents or Adults
F64.1 Gender identity disorder in adolescence and
adulthood
302.89 Frotteurism F65.81 Frotteurism
302.9 Paraphilia NOS F65.9 Paraphilia, unspecified
302.9 Sexual Disorder NOS F65.9 Paraphilia, unspecified
307.1 Anorexia Nervosa F50.00 Anorexia nervosa, unspecified
F50.01 Anorexia nervosa, restricting type
F50.02 Anorexia nervosa, binge eating/purging
type
307.3 Stereotypic Movement Disorder F98.4 Stereotyped movement disorders
307.50 Eating Disorder NOS F50.9 Eating disorder, unspecified
307.51 Bulimia Nervosa F50.2 Bulimia nervosa
307.52 Pica F98.3 Pica of infancy and childhood
307.53 Rumination Disorder F98.21 Rumination disorder of infancy
307.59 Feeding Disorder of Infancy or Early
Childhood
F98.29 Other feeding disorders of infancy and early
childhood
307.6 Enuresis (Not Due to a General
Medical Condition)
F98.0 Enuresis not due to a substance or known
physiological condition
307.7 Encopresis, Without Constipation
and Overflow Incontinence
F98.1 Encopresis not due to a substance or known
physiological condition
307.80 Pain Disorder Associated With
Psychological Factors
F45.41 Pain disorder exclusively related to
psychological factors
308.3 Acute Stress Disorder F43.0 Acute stress reaction
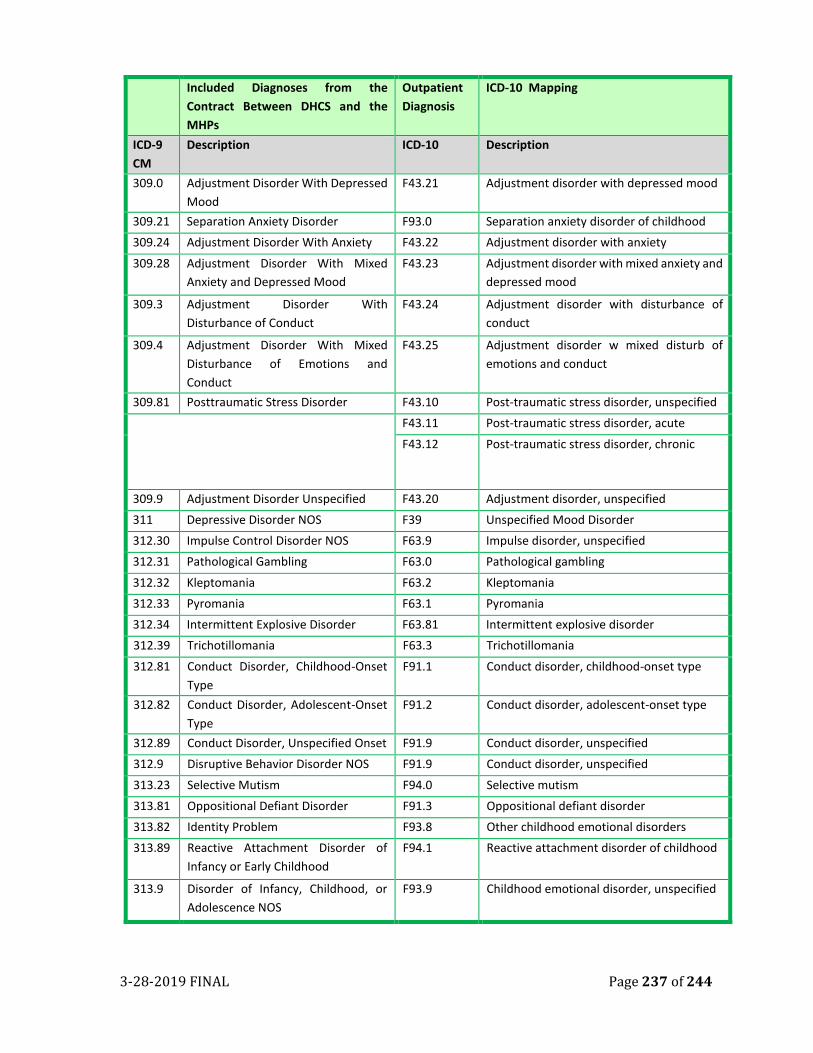
3-28-2019 FINAL Page 237 of 244
Included Diagnoses from the
Contract Between DHCS and the
MHPs
Outpatient
Diagnosis
ICD-10 Mapping
ICD-9
CM
Description ICD-10 Description
309.0 Adjustment Disorder With Depressed
Mood
F43.21 Adjustment disorder with depressed mood
309.21 Separation Anxiety Disorder F93.0 Separation anxiety disorder of childhood
309.24 Adjustment Disorder With Anxiety F43.22 Adjustment disorder with anxiety
309.28 Adjustment Disorder With Mixed
Anxiety and Depressed Mood
F43.23 Adjustment disorder with mixed anxiety and
depressed mood
309.3 Adjustment Disorder With
Disturbance of Conduct
F43.24 Adjustment disorder with disturbance of
conduct
309.4 Adjustment Disorder With Mixed
Disturbance of Emotions and
Conduct
F43.25 Adjustment disorder w mixed disturb of
emotions and conduct
309.81 Posttraumatic Stress Disorder F43.10 Post-traumatic stress disorder, unspecified
F43.11 Post-traumatic stress disorder, acute
F43.12 Post-traumatic stress disorder, chronic
309.9 Adjustment Disorder Unspecified F43.20 Adjustment disorder, unspecified
311 Depressive Disorder NOS F39 Unspecified Mood Disorder
312.30 Impulse Control Disorder NOS F63.9 Impulse disorder, unspecified
312.31 Pathological Gambling F63.0 Pathological gambling
312.32 Kleptomania F63.2 Kleptomania
312.33 Pyromania F63.1 Pyromania
312.34 Intermittent Explosive Disorder F63.81 Intermittent explosive disorder
312.39 Trichotillomania F63.3 Trichotillomania
312.81 Conduct Disorder, Childhood-Onset
Type
F91.1 Conduct disorder, childhood-onset type
312.82 Conduct Disorder, Adolescent-Onset
Type
F91.2 Conduct disorder, adolescent-onset type
312.89 Conduct Disorder, Unspecified Onset F91.9 Conduct disorder, unspecified
312.9 Disruptive Behavior Disorder NOS F91.9 Conduct disorder, unspecified
313.23 Selective Mutism F94.0 Selective mutism
313.81 Oppositional Defiant Disorder F91.3 Oppositional defiant disorder
313.82 Identity Problem F93.8 Other childhood emotional disorders
313.89 Reactive Attachment Disorder of
Infancy or Early Childhood
F94.1 Reactive attachment disorder of childhood
313.9 Disorder of Infancy, Childhood, or
Adolescence NOS
F93.9 Childhood emotional disorder, unspecified
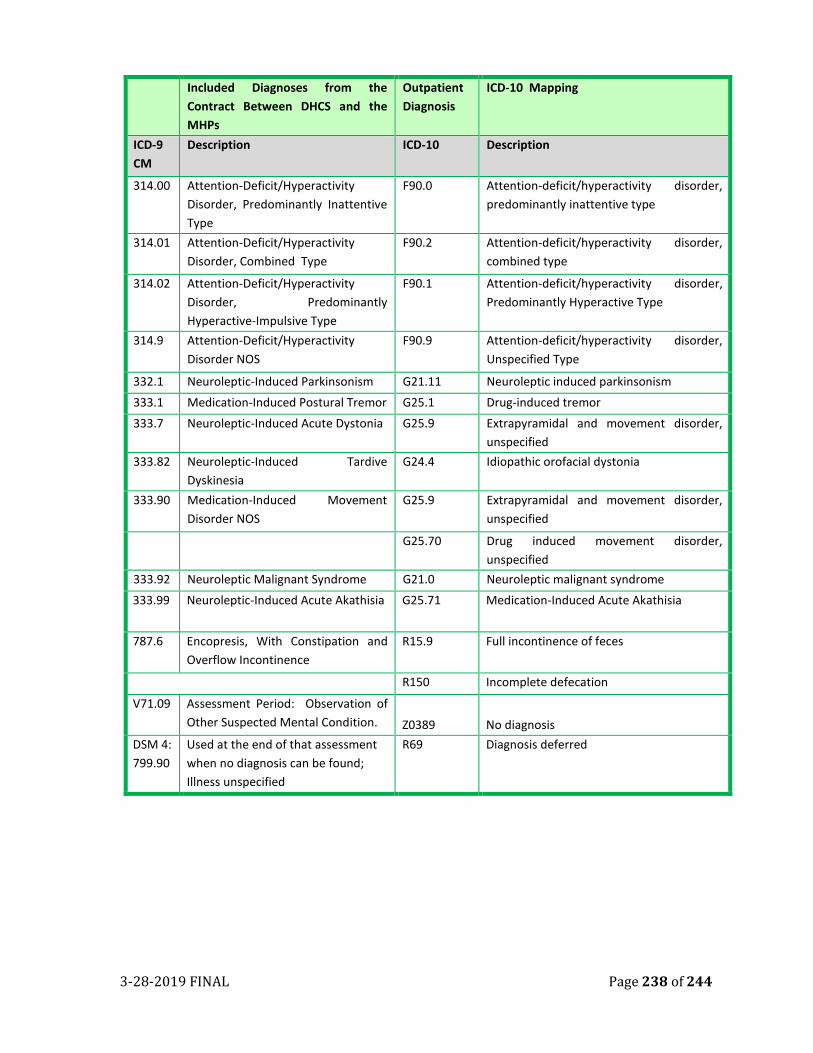
3-28-2019 FINAL Page 238 of 244
Included Diagnoses from the
Contract Between DHCS and the
MHPs
Outpatient
Diagnosis
ICD-10 Mapping
ICD-9
CM
Description ICD-10 Description
314.00 Attention-Deficit/Hyperactivity
Disorder, Predominantly Inattentive
Type
F90.0 Attention-deficit/hyperactivity disorder,
predominantly inattentive type
314.01 Attention-Deficit/Hyperactivity
Disorder, Combined Type
F90.2 Attention-deficit/hyperactivity disorder,
combined type
314.02 Attention-Deficit/Hyperactivity
Disorder, Predominantly
Hyperactive-Impulsive Type
F90.1 Attention-deficit/hyperactivity disorder,
Predominantly Hyperactive Type
314.9 Attention-Deficit/Hyperactivity
Disorder NOS
F90.9 Attention-deficit/hyperactivity disorder,
Unspecified Type
332.1 Neuroleptic-Induced Parkinsonism G21.11 Neuroleptic induced parkinsonism
333.1 Medication-Induced Postural Tremor G25.1 Drug-induced tremor
333.7 Neuroleptic-Induced Acute Dystonia G25.9 Extrapyramidal and movement disorder,
unspecified
333.82 Neuroleptic-Induced Tardive
Dyskinesia
G24.4 Idiopathic orofacial dystonia
333.90 Medication-Induced Movement
Disorder NOS
G25.9 Extrapyramidal and movement disorder,
unspecified
G25.70 Drug induced movement disorder,
unspecified
333.92 Neuroleptic Malignant Syndrome G21.0 Neuroleptic malignant syndrome
333.99 Neuroleptic-Induced Acute Akathisia G25.71 Medication-Induced Acute Akathisia
787.6 Encopresis, With Constipation and
Overflow Incontinence
R15.9 Full incontinence of feces
R150 Incomplete defecation
V71.09 Assessment Period: Observation of
Other Suspected Mental Condition. Z0389 No diagnosis
DSM 4:
799.90
Used at the end of that assessment
when no diagnosis can be found;
Illness unspecified
R69 Diagnosis deferred
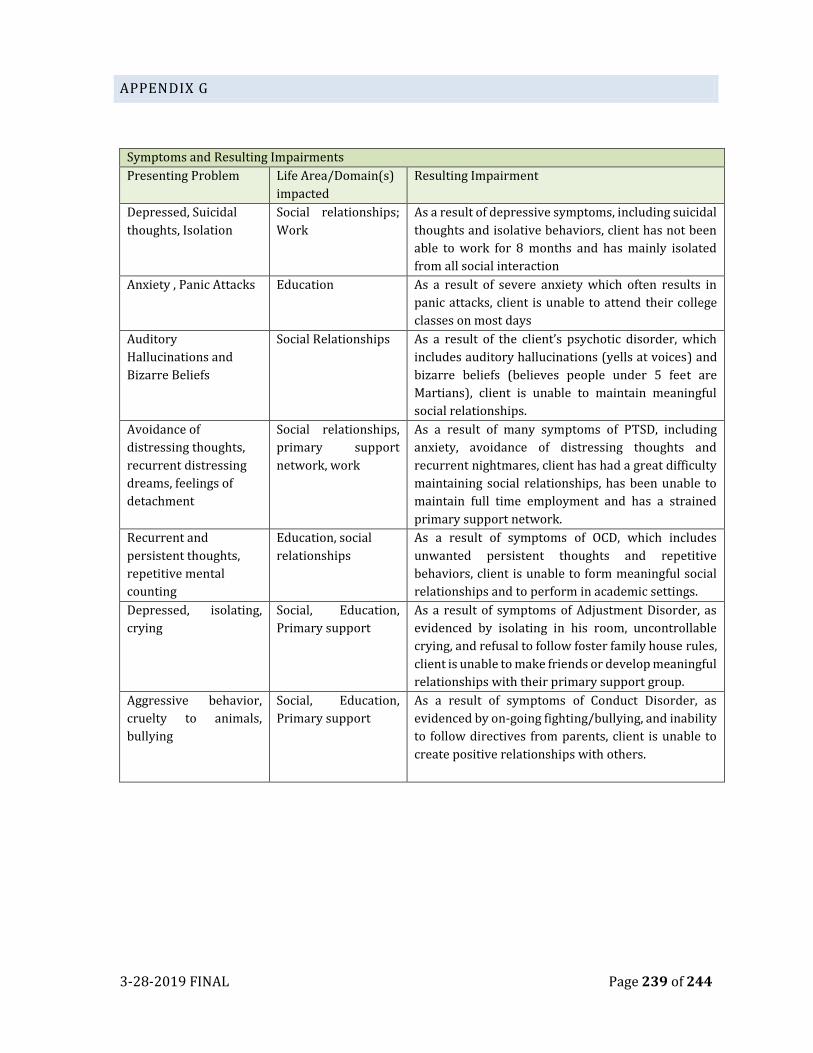
3-28-2019 FINAL Page 239 of 244
APPENDIX G
Symptoms and Resulting Impairments
Presenting Problem Life Area/Domain(s)
impacted
Resulting Impairment
Depressed, Suicidal
thoughts, Isolation
Social relationships;
Work
As a result of depressive symptoms, including suicidal
thoughts and isolative behaviors, client has not been
able to work for 8 months and has mainly isolated
from all social interaction
Anxiety , Panic Attacks Education As a result of severe anxiety which often results in
panic attacks, client is unable to attend their college
classes on most days
Auditory
Hallucinations and
Bizarre Beliefs
Social Relationships As a result of the client’s psychotic disorder, which
includes auditory hallucinations (yells at voices) and
bizarre beliefs (believes people under 5 feet are
Martians), client is unable to maintain meaningful
social relationships.
Avoidance of
distressing thoughts,
recurrent distressing
dreams, feelings of
detachment
Social relationships,
primary support
network, work
As a result of many symptoms of PTSD, including
anxiety, avoidance of distressing thoughts and
recurrent nightmares, client has had a great difficulty
maintaining social relationships, has been unable to
maintain full time employment and has a strained
primary support network.
Recurrent and
persistent thoughts,
repetitive mental
counting
Education, social
relationships
As a result of symptoms of OCD, which includes
unwanted persistent thoughts and repetitive
behaviors, client is unable to form meaningful social
relationships and to perform in academic settings.
Depressed, isolating,
crying
Social, Education,
Primary support
As a result of symptoms of Adjustment Disorder, as
evidenced by isolating in his room, uncontrollable
crying, and refusal to follow foster family house rules,
client is unable to make friends or develop meaningful
relationships with their primary support group.
Aggressive behavior,
cruelty to animals,
bullying
Social, Education,
Primary support
As a result of symptoms of Conduct Disorder, as
evidenced by on-going fighting/bullying, and inability
to follow directives from parents, client is unable to
create positive relationships with others.

3-28-2019 FINAL Page 240 of 244
APPENDIX H
SAMPLE PROGRESS NOTES CO-OCCURING
Introduction Client arrived at clinic for unscheduled appointment. Client presents with depressed
mood and congruent affect. Little eye contact. Hygiene is poor, grooming is disheveled.
Goal Reduce level of depression as evidenced by reducing periods of feeling hopeless/helpless
and crying spells from 5 x per day to 1 x per seven days and maintain reduction x 365
days.
Behavior Client expressing feelings of guilt and hopelessness. Client states that he is no longer
“clean and sober”, sharing that he has been drinking alcohol and smoking marijuana for
the last month. Last drank and used marijuana 3 days ago. Client states that he stopped
attending his support groups due as his depression worsen. Client states that he began
drinking alcohol again to alleviate the “pain”. Client states that he is feeling unsafe and
has been experiencing an increase in suicidal thoughts since his relapse. Client also
reports that he finds himself feeling “hopeless and crying for no reason” on a daily basis
during the last two. When asked about how he would hurt himself, client responded that
he thought about obtaining a gun as it “would be quick”. Currently does not have access
to a weapon. No other Suicidal plans identified.
Intervention Writer provided client with reflective listening and cognitive reframing. Reviewed clients
WRAP plan and relapse prevention plan. Assisted client with identifying new warning
signs of depression and linking how level of depression is increase with substance misuse.
Completed suicide assessment. Currently, client does not meet criteria for a W&I 5150.
Provided positive feedback for client having three days of being clean and sober and for
seeking additional supports to assist with managing increase levels of depression.
Reviewed resources for ongoing substance use treatment.
Response Client acknowledge increase in suicidal thoughts, acknowledges how depression and
misuse of substances “go hand in hand” and how he “needs to monitor” both to support
his own recovery. Requesting assistance with linking to ongoing Substance use services.
Client states that he will begin developing a WRAP plan that addresses both MH and
Substance misuse. Client stated that he stopped tracking his early warning sign of
isolation and negative self-talk which leads to his feeling hopeless/helpless.
Plan Writer will assist client with obtaining admission to Crisis Residential and will assist
client with obtaining substance uses services
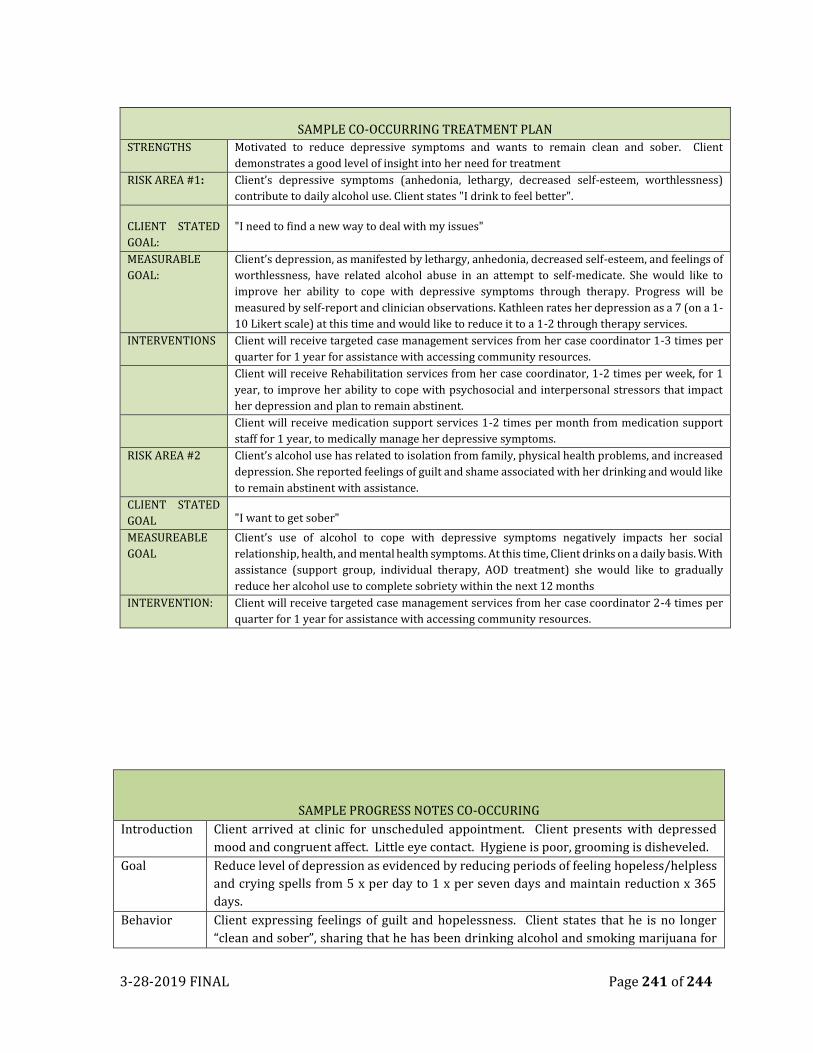
3-28-2019 FINAL Page 241 of 244
SAMPLE CO-OCCURRING TREATMENT PLAN
STRENGTHS Motivated to reduce depressive symptoms and wants to remain clean and sober. Client
demonstrates a good level of insight into her need for treatment
RISK AREA #1: Client’s depressive symptoms (anhedonia, lethargy, decreased self-esteem, worthlessness)
contribute to daily alcohol use. Client states "I drink to feel better".
CLIENT STATED
GOAL:
"I need to find a new way to deal with my issues"
MEASURABLE
GOAL:
Client’s depression, as manifested by lethargy, anhedonia, decreased self-esteem, and feelings of
worthlessness, have related alcohol abuse in an attempt to self-medicate. She would like to
improve her ability to cope with depressive symptoms through therapy. Progress will be
measured by self-report and clinician observations. Kathleen rates her depression as a 7 (on a 1-
10 Likert scale) at this time and would like to reduce it to a 1-2 through therapy services.
INTERVENTIONS Client will receive targeted case management services from her case coordinator 1-3 times per
quarter for 1 year for assistance with accessing community resources.
Client will receive Rehabilitation services from her case coordinator, 1-2 times per week, for 1
year, to improve her ability to cope with psychosocial and interpersonal stressors that impact
her depression and plan to remain abstinent.
Client will receive medication support services 1-2 times per month from medication support
staff for 1 year, to medically manage her depressive symptoms.
RISK AREA #2 Client’s alcohol use has related to isolation from family, physical health problems, and increased
depression. She reported feelings of guilt and shame associated with her drinking and would like
to remain abstinent with assistance.
CLIENT STATED
GOAL "I want to get sober"
MEASUREABLE
GOAL
Client’s use of alcohol to cope with depressive symptoms negatively impacts her social
relationship, health, and mental health symptoms. At this time, Client drinks on a daily basis. With
assistance (support group, individual therapy, AOD treatment) she would like to gradually
reduce her alcohol use to complete sobriety within the next 12 months
INTERVENTION: Client will receive targeted case management services from her case coordinator 2-4 times per
quarter for 1 year for assistance with accessing community resources.
SAMPLE PROGRESS NOTES CO-OCCURING
Introduction Client arrived at clinic for unscheduled appointment. Client presents with depressed
mood and congruent affect. Little eye contact. Hygiene is poor, grooming is disheveled.
Goal Reduce level of depression as evidenced by reducing periods of feeling hopeless/helpless
and crying spells from 5 x per day to 1 x per seven days and maintain reduction x 365
days.
Behavior Client expressing feelings of guilt and hopelessness. Client states that he is no longer
“clean and sober”, sharing that he has been drinking alcohol and smoking marijuana for
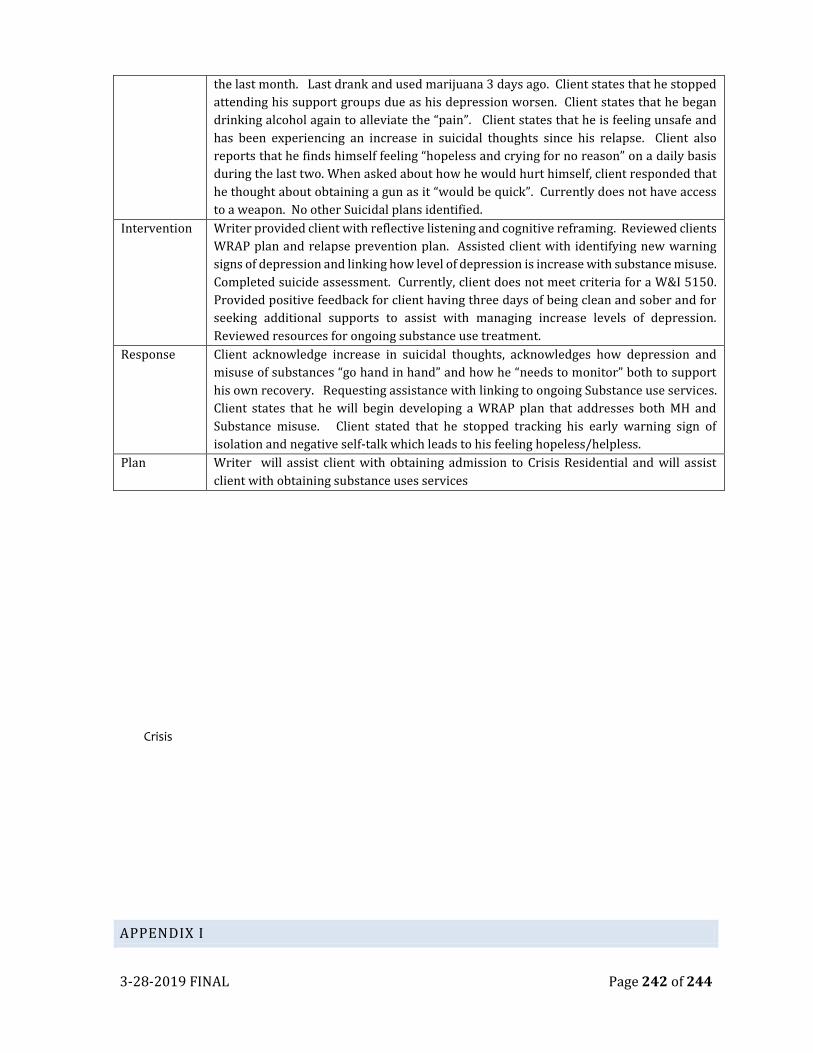
3-28-2019 FINAL Page 242 of 244
the last month. Last drank and used marijuana 3 days ago. Client states that he stopped
attending his support groups due as his depression worsen. Client states that he began
drinking alcohol again to alleviate the “pain”. Client states that he is feeling unsafe and
has been experiencing an increase in suicidal thoughts since his relapse. Client also
reports that he finds himself feeling “hopeless and crying for no reason” on a daily basis
during the last two. When asked about how he would hurt himself, client responded that
he thought about obtaining a gun as it “would be quick”. Currently does not have access
to a weapon. No other Suicidal plans identified.
Intervention Writer provided client with reflective listening and cognitive reframing. Reviewed clients
WRAP plan and relapse prevention plan. Assisted client with identifying new warning
signs of depression and linking how level of depression is increase with substance misuse.
Completed suicide assessment. Currently, client does not meet criteria for a W&I 5150.
Provided positive feedback for client having three days of being clean and sober and for
seeking additional supports to assist with managing increase levels of depression.
Reviewed resources for ongoing substance use treatment.
Response Client acknowledge increase in suicidal thoughts, acknowledges how depression and
misuse of substances “go hand in hand” and how he “needs to monitor” both to support
his own recovery. Requesting assistance with linking to ongoing Substance use services.
Client states that he will begin developing a WRAP plan that addresses both MH and
Substance misuse. Client stated that he stopped tracking his early warning sign of
isolation and negative self-talk which leads to his feeling hopeless/helpless.
Plan Writer will assist client with obtaining admission to Crisis Residential and will assist
client with obtaining substance uses services
Crisis
APPENDIX I
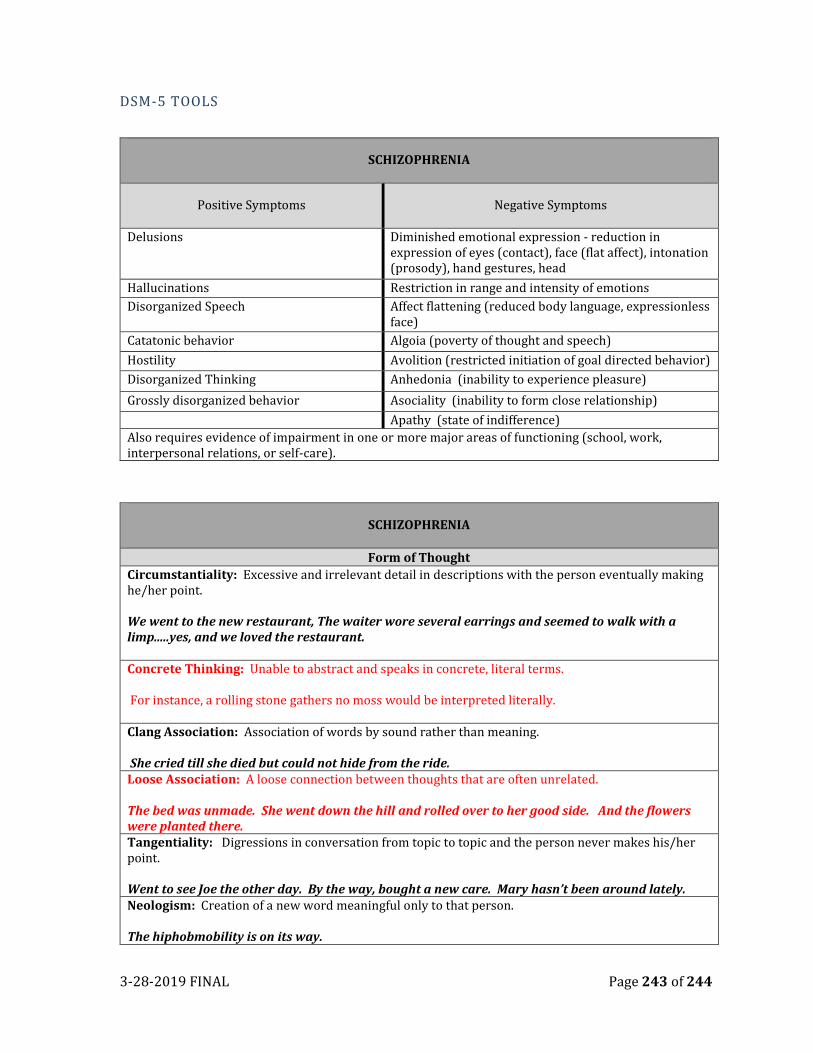
3-28-2019 FINAL Page 243 of 244
DSM-5 TOOLS
SCHIZOPHRENIA
Positive Symptoms Negative Symptoms
Delusions
Diminished emotional expression - reduction in expression of eyes (contact), face (flat affect), intonation (prosody), hand gestures, head
Hallucinations Restriction in range and intensity of emotions
Disorganized Speech Affect flattening (reduced body language, expressionless face)
Catatonic behavior Algoia (poverty of thought and speech)
Hostility Avolition (restricted initiation of goal directed behavior)
Disorganized Thinking Anhedonia (inability to experience pleasure)
Grossly disorganized behavior Asociality (inability to form close relationship)
Apathy (state of indifference)
Also requires evidence of impairment in one or more major areas of functioning (school, work, interpersonal relations, or self-care).
SCHIZOPHRENIA
Form of Thought
Circumstantiality: Excessive and irrelevant detail in descriptions with the person eventually making he/her point. We went to the new restaurant, The waiter wore several earrings and seemed to walk with a limp.....yes, and we loved the restaurant. Concrete Thinking: Unable to abstract and speaks in concrete, literal terms. For instance, a rolling stone gathers no moss would be interpreted literally. Clang Association: Association of words by sound rather than meaning. She cried till she died but could not hide from the ride. Loose Association: A loose connection between thoughts that are often unrelated. The bed was unmade. She went down the hill and rolled over to her good side. And the flowers were planted there. Tangentiality: Digressions in conversation from topic to topic and the person never makes his/her point. Went to see Joe the other day. By the way, bought a new care. Mary hasn’t been around lately. Neologism: Creation of a new word meaningful only to that person. The hiphobmobility is on its way.
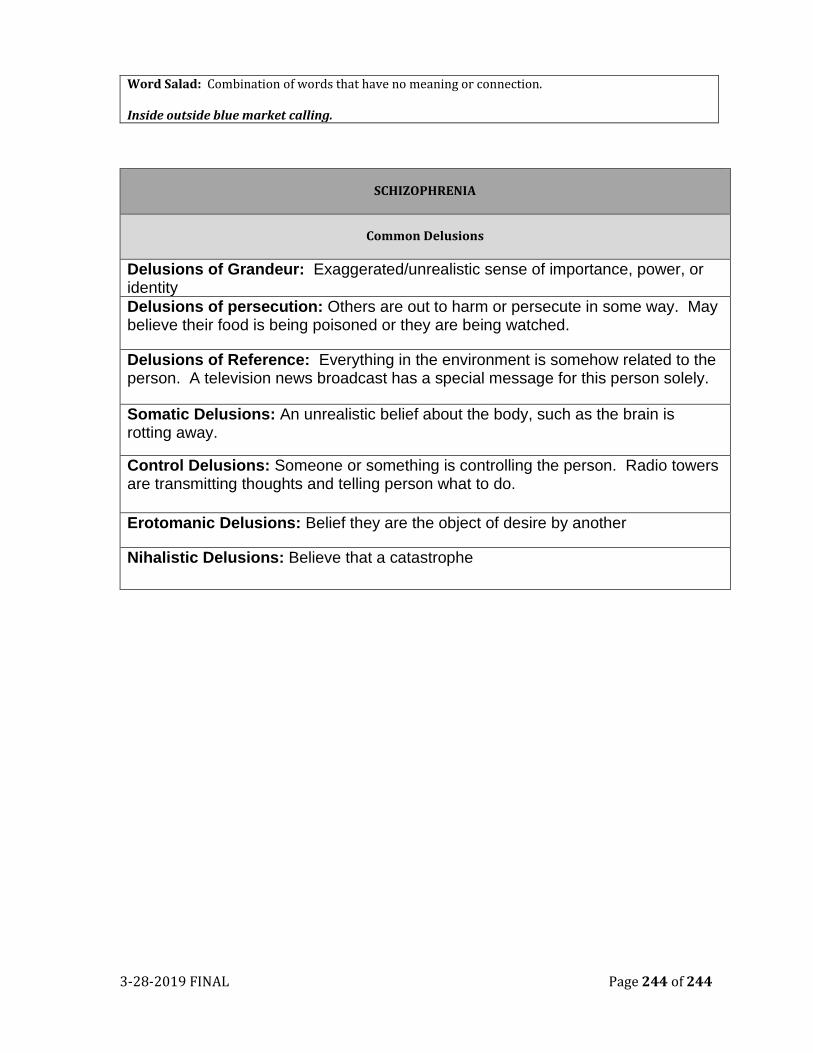
3-28-2019 FINAL Page 244 of 244
Word Salad: Combination of words that have no meaning or connection. Inside outside blue market calling.
SCHIZOPHRENIA
Common Delusions
Delusions of Grandeur: Exaggerated/unrealistic sense of importance, power, or identity
Delusions of persecution: Others are out to harm or persecute in some way. May believe their food is being poisoned or they are being watched.
Delusions of Reference: Everything in the environment is somehow related to the person. A television news broadcast has a special message for this person solely.
Somatic Delusions: An unrealistic belief about the body, such as the brain is rotting away.
Control Delusions: Someone or something is controlling the person. Radio towers are transmitting thoughts and telling person what to do.
Erotomanic Delusions: Belief they are the object of desire by another
Nihalistic Delusions: Believe that a catastrophe





























