Embed Size (px)
Citation preview

VOL. 94-B, No. 1, JANUARY 2012 1
SPECIALTY UPDATE: UPPER LIMB
Frozen shoulder
C. M. Robinson,K. T. M Seah,Y. H. Chee,P. Hindle,I. R. Murray
From Edinburgh Shoulder Clinic, Edinburgh, United Kingdom
C. M. Robinson, BMedSci, FRCSEd, Consultant Orthopaedic Surgeon K. T. M Seah, BMedSci, MChB, Foundation Doctor P. Hindle, MRCSEng, Specialty TraineeEdinburgh Shoulder Clinic, Royal Infirmary of Edinburgh, Old Dalkeith Road, Edinburgh EH16 4SA, UK.
Y. H. Chee, FRCSEd, Trauma FellowRoyal Liverpool University Hospital, Prescot Street, Liverpool, Merseyside L7 8XP, UK.
I. R. Murray, BMedSci, MRCSEd, DipSEM, Clinical LecturerScottish Centre for Regenerative Medicine, The University of Edinburgh, 5 Little France Drive, Edinburgh EH16 4UU, UK.
Correspondence should be sent to Mr C. M. Robinson; e-mail: [email protected]
©2012 British Editorial Society of Bone and Joint Surgerydoi:10.1302/0301-620X.94B1. 27093 $2.00
J Bone Joint Surg Br 2012;94-B:1–9.
Frozen shoulder is commonly encountered in general orthopaedic practice. It may arise spontaneously without an obvious predisposing cause, or be associated with a variety of local or systemic disorders. Diagnosis is based upon the recognition of the characteristic features of the pain, and selective limitation of passive external rotation. The macroscopic and histological features of the capsular contracture are well-defined, but the underlying pathological processes remain poorly understood. It may cause protracted disability, and imposes a considerable burden on health service resources. Most patients are still managed by physiotherapy in primary care, and only the more refractory cases are referred for specialist intervention. Targeted therapy is not possible and treatment remains predominantly symptomatic. However, over the last ten years, more active interventions that may shorten the clinical course, such as capsular distension arthrography and arthroscopic capsular release, have become more popular.
This review describes the clinical and pathological features of frozen shoulder. We also outline the current treatment options, review the published results and present our own treatment algorithm.
Definitions and terminologyMany patients present with painful shoulderconditions that produce apparent ‘stiffness’ byrestricting active movement, either through paininhibition (antalgic shoulder) or muscle weak-ness (such as a rotator cuff tear or deltoid pare-sis). In contrast, patients who have a frozenshoulder have characteristic features of thepainful selective restriction of certain active andpassive movements of the shoulder, in the pres-ence of normal radiographs. Unfortunately,patients in each of these two categories tend tobe considered together under an inclusive clini-cal umbrella, leading to misdiagnosis andinappropriate treatment. The reasons for thisare twofold: first, the terms in common usage,such as frozen shoulder, adhesive capsulitis andpericapsulitis, are either non-specific or inaccu-rate, and therefore can be misused by cliniciansand patients. Secondly, although identificationof the syndrome rests on the recognition ofcharacteristic clinical features, clearly defineddiagnostic criteria are lacking. The need forstandardisation in diagnosis has recently beenemphasised and a system of terminology andclassification based on consensus would beadvantageous.1 In this review, we use the termfrozen shoulder, as it is the most commonly usedand avoids the ambiguities associated with
terms that attempt to describe the underlyingpathology.
Many conditions are associated with frozenshoulder, but these should be classified intosub-groups only where there is a known differ-ence in prognosis, or modification of treatmentis required (Fig. 1). The largest single group ofpatients have no detectable underlying causefor their symptoms (primary idiopathic frozenshoulder). The substantial group of patientswith diabetes mellitus are considered as a sep-arate group (secondary diabetic frozen shoul-der), since their disease course is usually moresevere and protracted.2 A wide variety of othersystemic conditions are associated with frozenshoulder, but most are uncommon and do notaffect prognosis or treatment.3,4 They aretherefore not considered under separate cate-gories. Patients who have a clear primarypathology in the shoulder with secondary painand stiffness (secondary frozen shoulder) areconsidered as a separate group, since theyoften have a poorer prognosis, and mayrequire treatment of their underlying primaryshoulder condition. This heterogeneous groupof patients cause the greatest difficulty in diag-nosis, since it is increasingly recognised thatthey may have pain and stiffness from both theprimary condition and the secondary capsular

2 C. M. ROBINSON, K. T. M SEAH, Y. H. CHEE, P. HINDLE, I. R. MURRAY
THE JOURNAL OF BONE AND JOINT SURGERY
contracture. A final complex group of patients have frozenshoulder associated with stroke and other neuromusculardisorders affecting the upper limb. These patients have painand stiffness that is multifactorial and associated with mus-cle spasticity as well as contracture. They are usually man-aged with supportive physiotherapy and are not consideredin detail in this review.
EpidemiologyDespite the lack of strict diagnostic criteria and hence theplausible over-diagnosis, frozen shoulder is estimated toaffect 2% of the general population,5 with a cumulativeincidence of 2.4 per 1000 person-years.6 It is rare before theage of 40, with a peak incidence between 40 and 60 and isunusual in patients over 70 years (except secondary trau-matic frozen shoulder) and in manual workers. It affectswomen slightly more often than men.7-9 The economicimpact of the condition is underscored by its predilectionfor adults of working age (8.2% for men and 10.1% forwomen).10 Recurrence in the same shoulder is rare, but upto 20% of patients develop similar problems in the other
shoulder.8,9 Bilateral simultaneous involvement occurs in14% of patients, and 80% will experience a recurrence ofsymptoms within five years.11 There is a two- to threefoldincreased risk in twins, suggesting a genetic component,12
but there is no known racial predisposition. Diabetes mellitus is the condition most commonly associ-
ated with frozen shoulder. The combined prevalence of adiabetic predisposition and frozen shoulder is estimated tobe as high as 71.5%.13 Approximately half of these patientshave been diagnosed previously with either Type I or II dia-betes, and the remainder have pre-diabetes with an abnor-mal fasting blood glucose or glucose tolerance test.13
Diabetics have a 10% to 20% lifetime risk of developing afrozen shoulder,14-16 with a 4% point prevalence,17 and atwo to four times greater risk than the general population.13
PathoanatomyThe shoulder is the most unconstrained and mobile articu-lation of the appendicular skeleton. The balance betweeninstability and stiffness is therefore largely maintained bythe static and dynamic soft-tissue stabilisers. Loss of both
NoPain:
•• Present for more than one month•
Consider:No
Yes
Pattern of stiffness
Muscle weakness:• Rotator cuff tear• Deltoid paresis• Others
Systemic diseases:IdiopathicTraumaticNon-traumatic
Yes
Clinical staging:
Constant, severe burning generalised shoulder pain
Night pain regularly disturbing sleep
Active and passive ROM restricted
Prominent loss of external rotationwith normal radiographs?
Mild = ER ≥ 45°Moderate = ER between 11° and 45°Severe = ER ≤ 10°
Assess for associated shoulder disorderScreen for diabetes mellitus/other systemic conditions
Secondary frozen shoulder
A. Shoulder soft-tissue injury/dislocation without fracture/cuff injuryB. Rotator cuff tear/greatertuberosity fractureC. FNOH treated non-operatively: I. with no malunion ii. with malunionD. FNOH treated operatively: i. ORIF ii. Arthroplasty
A. Rotator cufftears/impingementB. Biceps tendinopathyC. Calcific tendonitisD. Early OA
A. Thyroid diseaseB. HyperlipidaemiaC. HypoadrenalismD. COPDE. Osteopenia/reduced BMD Miscellaneous conditions:A. Ipsilateral distal limb injuryB. Dupuytren’s/Peyronie’s diseaseC. Ischaemic heart diseaseD. Cardiac, head/neck surgeryE. HyperkyphosisF. Medications
Diabetic frozen shoulderPrimary frozen shoulder
“Antalgic” shoulder
OA (global DROM) Locked posterior dislocationMuscular contracture“Atypical” frozen shoulder
Suspected frozen shoulder
Active restrictedPassivepreserved
Other causes of pain/stiffness andconsider “red flags” (infection/tumour):Atypical pain distributionSystemic features/weight lossLocal tenderness swelling
Fig. 1
An algorithm for the investigation and treatment of frozen shoulder (ROM, range of movement; ER, external rotation; FNOH, fractured neck ofhumerus; COPD, chronic obstructive pulmonary disease; OA, osteoarthritis; DROM, decreased range of motion; ORIF, open reduction and internal fix-ation; BMD, bone mineral density).

FROZEN SHOULDER 3
VOL. 94-B, No. 1, JANUARY 2012
active and passive movement can be produced by loss of thenormal congruity of the articulation (such as in a chronicdislocation), increased constraint from bony overgrowth(such as that produced by osteophytes), or contracture ofthe dynamic muscular stabilisers. However, the most com-mon cause of painful restriction of movement is an idio-pathic frozen shoulder, which is characterised by aninflammatory contracture of the capsule and ligaments,which reduces the available intra-articular volume, limitingglenohumeral movement. Macroscopically, the capsule hasa glassy appearance with acute vasculitis, inflammationand thickening, progressing to a more indolent fibroticappearance with time (Fig. 2).
Cadaveric studies have demonstrated predictable pat-terns of limited movement produced by plication of differ-ent parts of the capsule.18 The selective restriction ofexternal rotation characteristic of frozen shoulder syn-drome is produced by anterosuperior capsular tightening,which particularly affects external rotation of the adductedarm, and anteroinferior tightening, which reduces externalrotation in abduction. Clinical and MRI studies corrobo-rate these findings, confirming that the structures primarilyinvolved are the rotator interval (which comprises the supe-rior glenohumeral ligament), the rotator interval capsule,and the coracohumeral ligament,19-21 and the anterior cap-sule and the inferior glenohumeral ligament. Postero-superior capsular tightening limits internal rotation, andmay be present in more severe forms. In frozen shouldersecondary to trauma or previous surgery for instability,
there may also be stiffness due to extrinsic contracture ofthe rotator cuff (especially subscapularis) and obliterationof the normal subdeltoid tissue planes. This may be due tosoft-tissue trauma, or post-operative scarring.
Histological and biochemical pathwaysA variety of immunological, biomechanical, inflammatoryand endocrine abnormalities have been described inpatients with idiopathic frozen shoulder, but the basicpathogenesis remains poorly understood. Much work hasbeen done to characterise the microscopic pathology andthere is evidence of both inflammatory and fibrotic pro-cesses.22,23 However, no model completely explains why thestiffness tends to resolve, or why a disparate group of otherco-morbidities predispose to its development.
Characteristically, pain precedes stiffness, which suggestsan evolution from inflammation to fibrosis. Histologicalevidence of both chronic inflammatory cell infiltrate andfibrosis have been found in rotator interval biopsies ofpatients undergoing arthroscopic release.9 However, thesefindings have been observed in more severe forms of thecondition and may not apply to the early phases. The path-ological appearances have been likened to those ofDupuytren’s disease, with a fibrous contracture of the cora-cohumeral ligament and the surrounding tissues of the rota-tor interval, which is composed of a dense matrix of maturetype-III collagen containing fibroblasts and myofibro-blasts.23,24 The compact arrangement of capsular collagenfibres causes the limitation of movement.25,26 A proposedmechanism highlights the role of cytokines and growth fac-tors, leading to the accumulation and propagation of fibro-blasts, which produce excess Type III collagen.27 Thecytokine response may also initiate angiogenesis within thecapsule, producing the typical arthroscopic appearances ofnew blood vessels on the capsular surface.28,29
Collagen remodelling is currently being studied in order toelucidate a possible treatment. Local metalloproteinasesdegrade the connective tissue matrix and can be inhibited byspecific tissue metalloproteinase inhibitors, other cytokinesand growth factors. Frozen shoulder can be induced byadministering a synthetic metalloproteinase inhibitor, sug-gesting that a decrease in metalloproteinases: metallopro-teinase inhibitors ratio affects collagen turnover.30 Capsulartissues from patients with frozen shoulder have also beenfound to have increased mRNA for metalloproteinases, aswell as a natural metalloproteinase inhibitor.27
In patients with diabetes mellitus and other systemic dis-orders, microvascular disease may cause abnormal collagenrepair, which could then predispose to frozen shoulder. Thepain may also be neurogenic, as there are similarities withType 1 complex regional pain syndrome. In both condi-tions, there is sympathetic autonomic hyperactivity, periph-eral alpha-adrenoreceptor hyper-responsiveness, abnormaldorsal root reflexes, central nervous hypersensitivity, andsensory nerve degeneration.31 In addition, both conditionsare more common after trauma to the shoulder, and are
Fig. 2
The arthroscopic appearances of primary frozen shoulder. The gleno-humeral joint is viewed from a posterior portal and the characteristicappearance of scarring in the rotator interval is shown.

4 C. M. ROBINSON, K. T. M SEAH, Y. H. CHEE, P. HINDLE, I. R. MURRAY
THE JOURNAL OF BONE AND JOINT SURGERY
associated with diabetes, thyroid disease and dyslipidae-mia. However, it is over-simplistic to consider frozen shoul-der as a form of complex regional pain syndrome. Otherneuropathic mechanisms, including suprascapular nervecompression, have been considered.32 Although evidencesuggests an association between these neuropathic and vas-cular conditions, there is no convincing single pathophysio-logical pathway that fully explains the pathology of frozenshoulder.
Natural historyMany studies suggest that frozen shoulder is a benign con-dition, with most cases recovering within two years.33-36
However, it is now accepted that up to 40% of patients mayexperience persistent symptoms.37 In the most comprehen-sive study of the natural history, 50% of patients still hadmild pain after seven years, and 60% had persistent stiff-ness.24 It is estimated that approximately 7% to 15% havesome degree of permanent loss of movement, though fewhave persistent functional disability.38
Clinical assessmentFrozen shoulder is a clinical diagnosis; the history andphysical examination are therefore crucial. It is essential toconfirm the characteristic features of the condition, gradeits severity and exclude other contributory systemic or localcauses which may require laboratory investigations, radio-graphs and specialist imaging.History. The pain is characteristically severe, felt diffuselyaround the shoulder girdle, with a deep-seated burningquality. It should have been present for more than onemonth to exclude other transient causes of shoulder pain.Intense night pain disturbing sleep is invariably presentand is a key diagnostic feature (Fig. 1), as is impairment ofmost normal daily activities.39,40 Pain from the acromio-clavicular joint is common, presumably because therestricted glenohumeral movement increases the stress onthis joint. Primary frozen shoulder is traditionally dividedinto three consecutive stages35,41: ‘freezing’ with acutepain and stiffness, ‘frozen’ with established stiffness andreduced pain and ‘thawing’ with the return of movement.However, clear stages of development are often difficult todefine, or may be absent.Clinical examination. The clinical diagnosis rests on con-firming the characteristic pattern of limitation of bothactive and passive ranges of glenohumeral movement. Typ-ically, there is pronounced and selective loss of passiveexternal rotation, both with the arm in neutral and inabduction, which may not reach 90°. There is also somelimitation of flexion and internal rotation. Since the assess-ment of pain is subjective and the limitation of externalrotation is an objective and constant feature, we grade theclinical severity on external rotation (Fig. 1).
The pattern of stiffness helps to determine the anatomi-cal structures most involved. Contracture of the rotatorinterval produces anterosuperior tightness and limits
external rotation with the arm adducted, whereasanteroinferior contracture of the capsule and inferiorglenohumeral ligament limits external rotation in abduc-tion. Posterior capsular contracture limits adduction andinternal rotation, and extra-articular contractures produceglobal stiffness. Intra-articular local anaesthetic injectionmay improve pain, but loss of passive movement remains.Scapulothoracic movement may also be limited, withsecondary pseudowinging.
Shoulder girdle wasting may be present in protractedcases. The presence of swelling or erythema should suggestthe possibility of infection or tumour. Specific clinical testsof the biceps tendon and tests for rotator cuff and acromio-clavicular joint dysfunction and instability should be per-formed to exclude secondary causes.42-45
Investigation. There are no laboratory tests or radiologicalmarkers for frozen shoulder. Conventional radiographs areusually performed to assess for causes of secondary frozenshoulder syndrome, such as a bone tumour, acute calcificdeposits or fracture (if there is a recent history of trauma).Specialist imaging (ultrasound or magnetic resonancearthrography) may be useful if rotator cuff pathology, or aradiologically occult fracture of the greater tuberosity issuspected.46 Blood glucose levels should be checked toexclude diabetes. Other haematological or biochemicaltests may be ordered, if other endocrine or rheumatologicalabnormalities are suspected.Differential diagnosis. Selective loss of external rotation isassociated with only two other commonly encounteredshoulder pathologies: locked posterior dislocation andosteoarthritis. Both of these can usually be excluded withconventional radiographs. Features of frozen shoulder arecommonly present in patients with calcific tendonitis, frac-tures of the proximal humerus (especially those of thegreater tuberosity), tears of the rotator cuff and early osteo-arthritis of the glenohumeral joint (Table I). These pathol-ogies can usually be detected using conventionalradiographs and ultrasound examination. It may be diffi-cult to determine whether the clinical features are due to theprimary condition, or a secondary frozen shoulder. Othersecondary causes are rare, but indicators such as weightloss, systemic upset, shoulder swelling and bony tendernessshould raise the possibility of infection or tumour, andprompt urgent investigation.47,48
TreatmentThe goal of treatment is to relieve pain, restore movementand regain function of the shoulder. Treatment should beindividualised and based on the severity and chronicity ofsymptoms. A multidisciplinary approach is preferable, andmost patients can be managed non-operatively in a primarycare setting with the expectation of a good outcome. Thereare many alternative forms of treatment for this condition,but evidence of their efficacy is not well-established fromclinical trials,1 and it is unclear if several interventions usedin combination are better.

FROZEN SHOULDER 5
VOL. 94-B, No. 1, JANUARY 2012
Physiotherapy. An initial six- to 12-week therapeutic trial ofphysiotherapy is typically prescribed early, to try to preventfurther limitation of movement, and later to re-establishmovement. Passive mobilisation and capsular stretching iscommonly used. However, this may be counter-productive inthe painful acute inflammatory phase, where analgesia andactivity modification may be more appropriate. Use of oralnon-steroidal anti-inflammatory drugs and local heat/coldtreatment may help to increase movement and reduceinflammation. The physiotherapist plays a major role insupervising the exercise programme, explaining the timecourse to resolution of symptoms, and encouraging a pro-gramme of home exercises.
Despite its ubiquity, the use of physiotherapy alone is notsupported by higher level studies, although several lowerlevel studies report a benefit. A recent Cochrane review49
concluded that the existing literature was insufficient toprove that physiotherapy alone was beneficial, with twosmall clinical trials50,51 concluding that physiotherapy alonedid not offer any benefit when compared with no-treatmentcontrols. A further study52 found little difference in outcome,regardless of the physiotherapy technique used.
Other interventions have included ultrasound, acupunc-ture, bipolar interferential current, transcutaneous electro-magnetic stimulation, laser and pulsed electromagneticfield therapy. None of these have been subjected to prospec-tive comparative studies and their value remains uncertain.Post-surgical and post-traumatic secondary frozen shoulderis more refractory to physiotherapy, and a more interven-tional approach tends to be adopted at an earlier stage.Steroid therapy. Steroid therapy is commonly prescribedboth orally, and by intra-articular injection, despite a lackof good evidence that it helps. Since this treatment is oftenused as an adjunct to physiotherapy, it is often difficult toseparate the relative effects of each.53 A recent Cochranereview looked at the evidence in favour of oral steroids.54
The available trials suggest that they improve pain, stiffnessand disability scores compared with controls, but this effectis not constant, and may not be sustained in the longer-term. Studies have also noted a rebound when thetreatment is stopped53 and any benefits have to be balancedagainst the potential systemic side-effects.
Although some studies have shown improvement withintra-articular steroid injection,55 others have found thatthis produces little benefit.56,57 A recent meta-analysisshowed little evidence of benefit from steroid injection.58
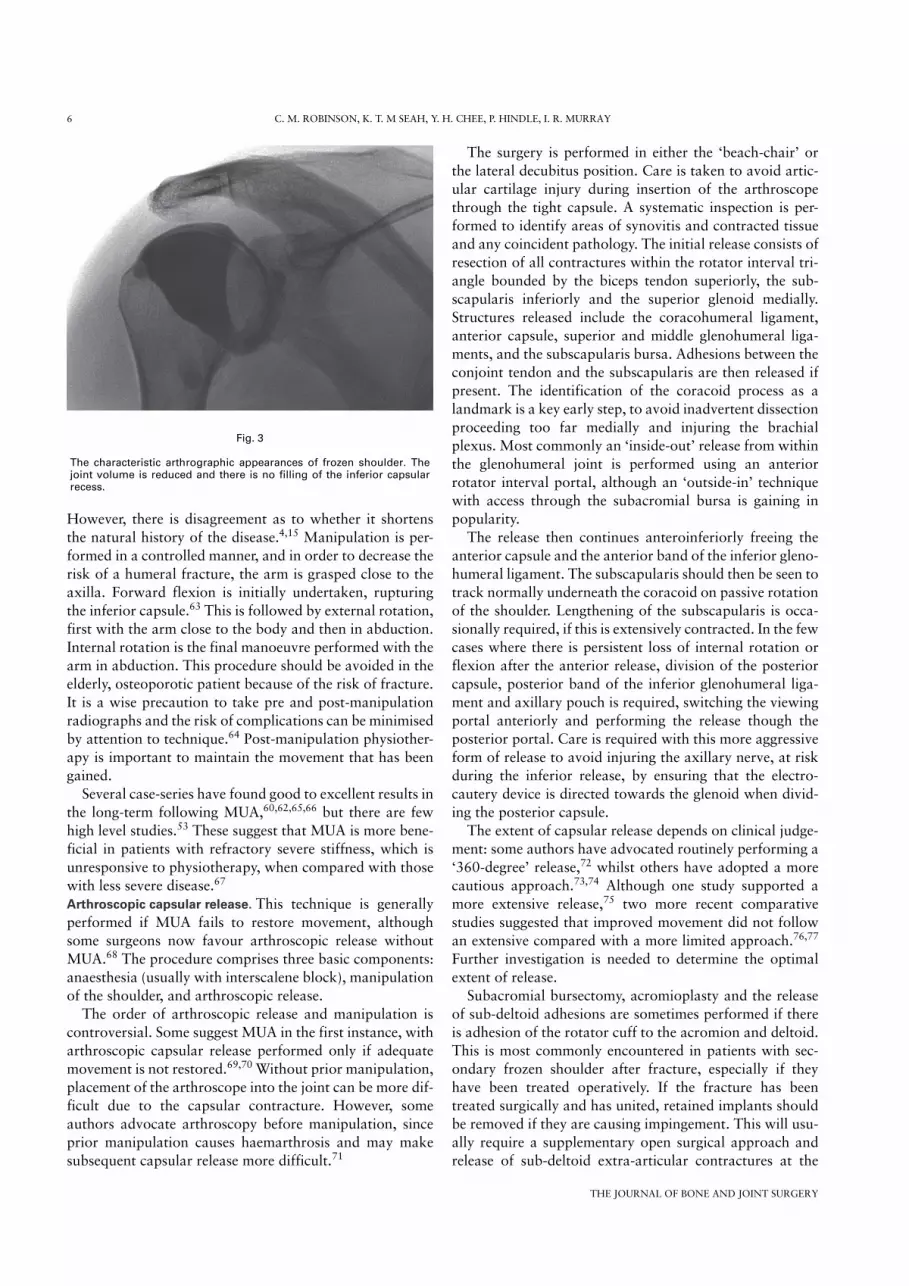
Like oral steroids, they appear to provide earlier relief frompain, when compared with placebo, but whether this is sus-tained in the long term is unknown. Distension arthrography. This local anaesthetic has theadvantage of producing rapid improvement in movement,without recourse to a more interventional surgical proce-dure. Under fluoroscopic control, an arthrogram is initiallyperformed to exclude a rotator cuff tear. The diagnosis offrozen shoulder is supported by the characteristic arthro-graphic appearance of a contracted capsule (Fig. 3). Sterilewater is then injected under pressure sufficient to cause cap-sular rupture (evidenced by a decrease in the pressure nec-essary to continue injection). An intra-articular injection ofsteroid is usually given at the end of the procedure, but rup-ture of the contracted capsule is the probable cause ofsymptomatic relief.59 Intensive physiotherapy should beginimmediately after the procedure to retain the improvedrange of movement achieved.
It is not possible to draw firm conclusions about the effi-cacy of the technique, due to the small number of studiesavailable. It is the authors’ experience that the technique isvery successful in the treatment of primary frozen shoulder,but less effective in secondary frozen shoulder after fracture,either treated non-operatively, or by open reduction andinternal fixation. This is probably because the limitation ofmovement in these patients is produced by a combination ofcapsular contractures and extra-articular adhesions.
Data from a small placebo-controlled trial suggested thatarthrographic distension provides significant short-term ben-efit, which is maintained in the medium term.53 A secondtrial showed similar improvements when distension wascompared with physiotherapy alone.57 Further comparativestudies are required to evaluate the efficacy of this technique.Manipulation under anaesthesia. Manipulation under anaes-thesia (MUA) has been used extensively if physiotherapy fails.It has been successfully used alone or combined with a steroidinjection or with an arthroscopic capsular release,37,60-62 andusually results in a rapid return of movement of the shoulder.
Table I. Differential diagnoses of primary frozen shoulder
Differential diagnosis Signs and symptoms
Calcific tendonitis* Painful arc; characteristic radiological appearancesRotator cuff tears* Selective pattern of rotator cuff weakness on testingRotator cuff impingement Positive impingement signs on testingGlenohumeral arthritis* Generalised pain and crepitus on movement of glenohumeral jointAcromioclavicular arthritis* Localised tenderness and restricted cross-body adductionCervical spine pathology Neck stiffness; upper limb neurologyGlenohumeral instability Recurrent dislocation; apprehensionProximal humeral fracture* History of trauma; localised tenderness and bruisingTumour/infection Red flags of fever, weight loss, other systemic signsParsonage-Turner syndrome Sudden pain; marked muscle weakness and wasting
* indicates conditions that often have a concomitant element of secondary frozen shoulder
6 C. M. ROBINSON, K. T. M SEAH, Y. H. CHEE, P. HINDLE, I. R. MURRAY
THE JOURNAL OF BONE AND JOINT SURGERY
However, there is disagreement as to whether it shortensthe natural history of the disease.4,15 Manipulation is per-formed in a controlled manner, and in order to decrease therisk of a humeral fracture, the arm is grasped close to theaxilla. Forward flexion is initially undertaken, rupturingthe inferior capsule.63 This is followed by external rotation,first with the arm close to the body and then in abduction.Internal rotation is the final manoeuvre performed with thearm in abduction. This procedure should be avoided in theelderly, osteoporotic patient because of the risk of fracture.It is a wise precaution to take pre and post-manipulationradiographs and the risk of complications can be minimisedby attention to technique.64 Post-manipulation physiother-apy is important to maintain the movement that has beengained.
Several case-series have found good to excellent results inthe long-term following MUA,60,62,65,66 but there are fewhigh level studies.53 These suggest that MUA is more bene-ficial in patients with refractory severe stiffness, which isunresponsive to physiotherapy, when compared with thosewith less severe disease.67
Arthroscopic capsular release. This technique is generallyperformed if MUA fails to restore movement, althoughsome surgeons now favour arthroscopic release withoutMUA.68 The procedure comprises three basic components:anaesthesia (usually with interscalene block), manipulationof the shoulder, and arthroscopic release.
The order of arthroscopic release and manipulation iscontroversial. Some suggest MUA in the first instance, witharthroscopic capsular release performed only if adequatemovement is not restored.69,70 Without prior manipulation,placement of the arthroscope into the joint can be more dif-ficult due to the capsular contracture. However, someauthors advocate arthroscopy before manipulation, sinceprior manipulation causes haemarthrosis and may makesubsequent capsular release more difficult.71
The surgery is performed in either the ‘beach-chair’ orthe lateral decubitus position. Care is taken to avoid artic-ular cartilage injury during insertion of the arthroscopethrough the tight capsule. A systematic inspection is per-formed to identify areas of synovitis and contracted tissueand any coincident pathology. The initial release consists ofresection of all contractures within the rotator interval tri-angle bounded by the biceps tendon superiorly, the sub-scapularis inferiorly and the superior glenoid medially.Structures released include the coracohumeral ligament,anterior capsule, superior and middle glenohumeral liga-ments, and the subscapularis bursa. Adhesions between theconjoint tendon and the subscapularis are then released ifpresent. The identification of the coracoid process as alandmark is a key early step, to avoid inadvertent dissectionproceeding too far medially and injuring the brachialplexus. Most commonly an ‘inside-out’ release from withinthe glenohumeral joint is performed using an anteriorrotator interval portal, although an ‘outside-in’ techniquewith access through the subacromial bursa is gaining inpopularity.
The release then continues anteroinferiorly freeing theanterior capsule and the anterior band of the inferior gleno-humeral ligament. The subscapularis should then be seen totrack normally underneath the coracoid on passive rotationof the shoulder. Lengthening of the subscapularis is occa-sionally required, if this is extensively contracted. In the fewcases where there is persistent loss of internal rotation orflexion after the anterior release, division of the posteriorcapsule, posterior band of the inferior glenohumeral liga-ment and axillary pouch is required, switching the viewingportal anteriorly and performing the release though theposterior portal. Care is required with this more aggressiveform of release to avoid injuring the axillary nerve, at riskduring the inferior release, by ensuring that the electro-cautery device is directed towards the glenoid when divid-ing the posterior capsule.
The extent of capsular release depends on clinical judge-ment: some authors have advocated routinely performing a‘360-degree’ release,72 whilst others have adopted a morecautious approach.73,74 Although one study supported amore extensive release,75 two more recent comparativestudies suggested that improved movement did not followan extensive compared with a more limited approach.76,77
Further investigation is needed to determine the optimalextent of release.
Subacromial bursectomy, acromioplasty and the releaseof sub-deltoid adhesions are sometimes performed if thereis adhesion of the rotator cuff to the acromion and deltoid.This is most commonly encountered in patients with sec-ondary frozen shoulder after fracture, especially if theyhave been treated operatively. If the fracture has beentreated surgically and has united, retained implants shouldbe removed if they are causing impingement. This will usu-ally require a supplementary open surgical approach andrelease of sub-deltoid extra-articular contractures at the
Fig. 3
The characteristic arthrographic appearances of frozen shoulder. Thejoint volume is reduced and there is no filling of the inferior capsularrecess.

FROZEN SHOULDER 7
VOL. 94-B, No. 1, JANUARY 2012
same time. If the frozen shoulder is secondary to calcifictendonitis, the deposit is usually excised from within thesubacromial bursa at the time of release. If there is an asso-ciated rotator cuff tear, it would be typical practice to per-form a release to re-establish movement before proceedingto rotator cuff repair.
Intensive rehabilitation should begin immediately post-operatively with daily stretching exercises. Continuouspassive motion machines may also be useful to maintainmovement. Adequate analgesia in the early post-operativeperiod is therefore important and this may be administeredvia an indwelling interscalene catheter for several dayspost-operatively. Patients are made aware that pain maynot subside for up to six weeks and some residual loss ofmovement is to be expected.
High-level comparative studies of arthroscopic releaseare lacking, though in a quasi-randomised study arthro-scopic release was compared with manipulation in patients
with refractory frozen shoulder.78 Similar movement wasachieved, but there was greater pain relief and functionalimprovement in the arthroscopic group.Open surgical release. Open release of contracture was orig-inally described by Codman33 and other authors later rec-ommended and described various open techniques.20,79
Current indications include previous failed arthroscopicrelease, no improvement after six months of home exercise,and frozen shoulder secondary to fracture or previous sur-gery.80 Dense adhesions and scarring following soft-tissueinjury and haemorrhage can make closed manipulation orattempted arthroscopic release particularly difficult and therisk of injury is high. An open procedure therefore allowsdirect visualisation of structures undergoing release andlengthening, removal of retained implants and excision ofheterotopic ossification or bony spurs.81 Disadvantagesinclude the risk of disruption of the lengthened subscapula-ris tendon and its repair, and the greater post-operative pain
MUA
A/P capsule tightAnterior capsule tight
Operative procedure
No response
No responseNo response
Clinical improvement
No response
Diagnosis of frozen shoulder
6- to 12-week trial of physiotherapy
Diabetic frozen shoulder Primary frozen shoulder
Continued maintenancephysiotherapy
Secondary frozen shoulder
Simultaneous treatment of underlying cause
Arthroscopic arthrolysis
Rotator interval/anteriorcapsular release only
360° release
Intensive post-operative physiotherapy
Distension arthrography + intensive physiotherapy
Fig. 4
A suggested treatment protocol for frozen shoulder (MUA, manipulation under anaesthetic; A/P, anterior and posterior).

8 C. M. ROBINSON, K. T. M SEAH, Y. H. CHEE, P. HINDLE, I. R. MURRAY
THE JOURNAL OF BONE AND JOINT SURGERY
and limitation of movement, compared with arthroscopicrelease.
A deltopectoral approach is used and subdeltoid adhe-sions are released after careful identification and protectionof the axillary nerve. The rotator interval is next identifiedand opened along the line of the superior aspect of the sub-scapularis tendon. The coracohumeral ligament and rota-tor interval capsule are excised, and the subscapularistendon can be z-lengthened if contracted. Further release ofthe inferior and posterior capsule can be performed ifabduction and internal rotation are still limited. Secondaryfrozen shoulder after non-operative treatment of a proxi-mal humeral fracture may be due to both capsular contrac-ture and malunion or nonunion of the fracture. In thissituation, capsular release may need to be combined withcorrection of any deformity of the humeral head.
Summary of treatmentMost patients with primary frozen shoulder are best ini-tially treated symptomatically with pain modification andsupportive physiotherapy. Steroid injection is a usefuladjunctive primary care treatment. Increasingly distensionarthrography is being advocated at an earlier stage in thosepatients who fail to respond to this ‘first-line’ treatment.Manipulation under anaesthesia supplemented with openor arthroscopic capsular release is useful in the minority ofpatients with frozen shoulder syndrome who are refractoryto these measures. Those with frozen shoulder secondary tostructural abnormalities within the shoulder usually requireadditional treatment of the underlying pathology, in addi-tion to treatment of the frozen shoulder. Further compara-tive clinical studies are required to evaluate the efficacy ofthe various methods of treatment. However, a suggestedalgorithm for treatment currently used by the authors isshown in Figure 4.
Supplementary materialTables detailing studies investigating treatments forfrozen shoulder: i) physical therapies, ii) steroid
treatment, iii) arthrographic distension, iv) manipulationunder anaesthesia, v) arthroscopic release, and vi) open sur-gical release, are available with the electronic version of thispaper on our website www.jbjs.org.uk
No benefits in any form have been received or will be received from a commer-cial party related directly or indirectly to the subject of this article.
References1. Rookmoneea M, Dennis L, Brealey S, et al. The effectiveness of interventions in
the management of patients with primary frozen shoulder. J Bone Joint Surg [Br]2010;92-B:1267–1272.
2. Griggs SM, Ahn A, Green A. Idiopathic adhesive capsulitis: a prospective func-tional outcome study of nonoperative treatment. J Bone Joint Surg [Am] 2000;82-A:1398–1407.
3. Chambler AF, Carr AJ. The role of surgery in frozen shoulder. J Bone Joint Surg [Br]2003;85-B:789–795.
4. Murnaghan JP. Frozen shoulder. In: Rockwood CA Jr, Matsen FA, eds. The shoulder.Philadelphia: WB Saunders, 1990:837.
5. Shah N, Lewis M. Shoulder adhesive capsulitis: systematic review of randomisedtrials using multiple corticosteroid injections. Br J Gen Pract 2007;57:662–667.
6. van der Windt DA, Koes BW, de Jong BA, Bouter LM. Shoulder disorders in gen-eral practice: incidence, patient characteristics, and management. Ann Rheum Dis1995;54:959–964.
7. Wright V, Haq AM. Periarthritis of the shoulder. I: aetiological considerations withparticular reference to personality factors. Ann Rheum Dis 1976;35:213–219.
8. Rizk TE, Pinals RS. Frozen shoulder. Semin Arthritis Rheum 1982;11:440–452.9. Hand GC, Athanasou NA, Matthews T, Carr AJ. The pathology of frozen shoulder.
J Bone Joint Surg [Br] 2007;89-B:928–932.10. Walker-Bone K, Palmer KT, Reading I, Coggon D, Cooper C. Prevalence and
impact of musculoskeletal disorders of the upper limb in the general population.Arthritis Rheum 2004;51:642–651.
11. Zuckerman JD, Cuomo FC. Frozen shoulder. In: Matsen FA 3rd, Fu FH, Hawkins RJ,eds. The shoulder: a balance of mobility and stability. Rosemont: American Academyof Orthopaedic Surgery 1993:253-67.
12. Hakim AJ, Cherkas LF, Spector TD, MacGregor AJ. Genetic associationsbetween frozen shoulder and tennis elbow: a female twin study. Rheumatology(Oxford) 2003;42:739–742.
13. Tighe CB, Oakley WS Jr. The prevalence of a diabetic condition and adhesive cap-sulitis of the shoulder. South Med J 2008;101:591–595.
14. Anton HA. Frozen shoulder. Can Fam Physician 1993;39:1773–1778.15. Lundberg BJ. The frozen shoulder: clinical and radiographical observations: the
effect of manipulation under general anesthesia: structure and glycosaminoglycancontent of the joint capsule: local bone metabolism. Acta Orthop Scand Suppl1969;119:1–59.
16. Bridgman JF. Periarthritis of the shoulder and diabetes mellitus. Ann Rheum Dis1972;31:69–71.
17. Thomas SJ, McDougall C, Brown ID, et al. Prevalence of symptoms and signs ofshoulder problems in people with diabetes mellitus. J Shoulder Elbow Surg2007;16:748–751.
18. Gerber C, Werner CM, Macy JC, Jacob HA, Nyffeler RW. Effect of selective cap-sulorrhaphy on the passive range of motion of the glenohumeral joint. J Bone JointSurg [Am] 2003;85-A:48–55.
19. Jost B, Koch PP, Gerber C. Anatomy and functional aspects of the rotator interval.J Shoulder Elbow Surg 2000;9:336–341.
20. Ozaki J, Nakagawa Y, Sakurai G, Tamai S. Recalcitrant chronic adhesive capsu-litis of the shoulder: role of contracture of the coracohumeral ligament and rotatorinterval in pathogenesis and treatment. J Bone Joint Surg [Am] 1989;71-A:1511–1515.
21. Mengiardi B, Pfirrmann CW, Gerber C, Hodler J, Zanetti M. Frozen shoulder:MR arthrographic findings. Radiology 2004;233:486–492.
22. Bulgen DY, Binder A, Hazleman BL, Park JR. Immunological studies in frozenshoulder. J Rheumatol 1982;9:893–898.
23. Bunker TD, Anthony PP. The pathology of frozen shoulder: a Dupuytren-like dis-ease. J Bone Joint Surg [Br] 1995;77-B:677–683.
24. Shaffer B, Tibone JE, Kerlan RK. Frozen shoulder: a long-term follow-up. J BoneJoint Surg [Am] 1992;74-A:738–746.
25. Schollmeier G, Uhthoff HK, Sarkar K, Fukuhara K. Effects of immobilization onthe capsule of the canine glenohumeral joint: a structural functional study. ClinOrthop 1994;304:37–42.
26. Kilian O, Pfeil U, Wenisch S, et al. Enhanced alpha 1(I) mRNA expression in frozenshoulder and dupuytren tissue. Eur J Med Res 2007;12:585–590.
27. Bunker TD, Reilly J, Baird KS, Hamblen DL. Expression of growth factors,cytokines and matrix metalloproteinases in frozen shoulder. J Bone Joint Surg [Br]2000;82-B:768–773.
28. Wiley AM. Arthroscopic appearance of frozen shoulder. Arthroscopy 1991;7:138–143.
29. Uitvlugt G, Detrisac DA, Johnson LL, Austin MD, Johnson C. Arthroscopicobservations before and after manipulation of frozen shoulder. Arthroscopy1993;9:181–185.
30. Hutchinson JW, Tierney GM, Parsons SL, Davis TR. Dupuytren's disease andfrozen shoulder induced by treatment with a matrix metalloproteinase inhibitor. JBone Joint Surg [Br] 1998;80-B:907–908.
31. Muller LP, Rittmeister M, John J, Happ J, Kerschbaumer F. Frozen shoulder: analgoneurodystrophic process? Acta Orthop Belg 1998;64:434–440.
32. Wassef MR. Suprascapular nerve block: a new approach for the management of fro-zen shoulder. Anaesthesia 1992;47:120–124.
33. Codman EA. The shoulder: rupture of the supraspinatus tendon and other lesions inor about the subacromial bursa. Boston: Thomas Todd Co., 1934.
34. Grey RG. The natural history of "idiopathic" frozen shoulder. J Bone Joint Surg [Am]1978;60-A:564.
35. Reeves B. The natural history of the frozen shoulder syndrome. Scand J Rheumatol1975;4:193–196.
36. Miller MD, Wirth MA, Rockwood CA Jr. Thawing the frozen shoulder: the"patient" patient. Orthopedics 1996;19:849–853.
37. Hazleman BL. The painful stiff shoulder. Rheumatol Phys Med 1972;11:413–421.38. Binder AI, Bulgen DY, Hazleman BL, Roberts S. Frozen shoulder: a long-term pro-
spective study. Ann Rheum Dis 1984;43:361–364.39. Neviaser RJ, Neviaser TJ. The frozen shoulder: diagnosis and management. Clin
Orthop 1987;223:59–64.

FROZEN SHOULDER 9
VOL. 94-B, No. 1, JANUARY 2012
40. Nicholson GP. Arthroscopic capsular release for stiff shoulders: effect of etiologyon outcomes. Arthroscopy 2003;19:40–49.
41. Hannafin JA, Chiaia TA. Adhesive capsulitis: a treatment approach. Clin Orthop2000;372:95–109.
42. McFarland EG, Selhi HS, Keyurapan E. Clinical evaluation of impingement: whatto do and what works. Instr Course Lect 2006;55:3–16.
43. Chen AL, Rokito AS, Zuckerman JD. The role of the acromioclavicular joint inimpingement syndrome. Clin Sports Med 2003;22:343–357.
44. Ahrens PM, Boileau P. The long head of biceps and associated tendinopathy. JBone Joint Surg [Br] 2007;89-B:1001–1009.
45. Johnson SM, Robinson CM. Shoulder instability in patients with joint hyperlaxity.J Bone Joint Surg [Am] 2010;92-A:1545–1557.
46. Patten RM, Mack LA, Wang KY, Lingel J. Nondisplaced fractures of the greatertuberosity of the humerus: sonographic detection. Radiology 1992;182:201–204.
47. Robinson D, Halperin N, Agar G, Alk D, Rami K. Shoulder girdle neoplasms mim-icking frozen shoulder syndrome. J Shoulder Elbow Surg 2003;12:451–455.
48. Sano H, Hatori M, Mineta M, Hosaka M, Itoi E. Tumors masked as frozen shoul-ders: a retrospective analysis. J Shoulder Elbow Surg 2010;19:262–266.
49. Green S, Buchbinder R, Hetrick S. Physiotherapy interventions for shoulder pain.Cochrane Database Syst Rev 2003;2:CD004258.
50. Carette S, Moffet H, Tardif J, et al. Intraarticular corticosteroids, supervised phys-iotherapy, or a combination of the two in the treatment of adhesive capsulitis of theshoulder: a placebo-controlled trial. Arthritis Rheum 2003;48:829–838.
51. Bulgen DY, Binder AI, Hazleman BL, Dutton J, Roberts S. Frozen shoulder: pro-spective clinical study with an evaluation of three treatment regimens. Ann RheumDis 1984;43:353–360.
52. Vermeulen HM, Rozing PM, Obermann WR, le Cessie S, Vliet Vlieland TP.Comparison of high-grade and low-grade mobilization techniques in the managementof adhesive capsulitis of the shoulder: randomized controlled trial. Phys Ther2006;86:355–368.
53. Buchbinder R, Hoving JL, Green S, Hall S, Forbes A, Nash P. Short course pred-nisolone for adhesive capsulitis (frozen shoulder or stiff painful shoulder): a ran-domised, double blind, placebo controlled trial. Ann Rheum Dis 2004;63:1460–1469.
54. Buchbinder R, Green S, Youd JM, Johnston RV. Oral steroids for adhesive cap-sulitis. Cochrane Database Syst Rev 2006;4:CD006189.
55. Hollingworth GR, Ellis RM, Hattersley TS. Comparison of injection techniques forshoulder pain: results of a double blind, randomised study. Br Med J (Clin Res Ed)1983;287:1339–1341.
56. Buchbinder R, Green S. Effect of arthrographic shoulder joint distension withsaline and corticosteroid for adhesive capsulitis. Br J Sports Med 2004;38:384–385.
57. Khan AA, Mowla A, Shakoor MA, Rahman MR. Arthrographic distension of theshoulder joint in the management of frozen shoulder. Mymensingh Med J2005;14:67–70.
58. Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain.Cochrane Database Syst Rev 2003;1:CD004016.
59. Rizk TE, Gavant ML, Pinals RS. Treatment of adhesive capsulitis (frozen shoulder)with arthrographic capsular distension and rupture. Arch Phys Med Rehabil1994;75:803–807.
60. Hill JJ Jr, Bogumill H. Manipulation in the treatment of frozen shoulder. Orthope-dics 1988;11:1255–1260.
61. Berghs BM, Sole-Molins X, Bunker TD. Arthroscopic release of adhesive capsu-litis. J Shoulder Elbow Surg 2004;13:180–185.
62. Thomas WJ, Jenkins EF, Owen JM, et al. Treatment of frozen shoulder by manip-ulation under anaesthetic and injection: Does the timing of treatment affect the out-come? J Bone Joint Surg [Br] 2011;93-B:1377–1381.
63. Neviaser RJ. Painful conditions affecting the shoulder. Clin Orthop 1983;173:63–69.64. Farrell CM, Sperling JW, Cofield RH. Manipulation for frozen shoulder: long-term
results. J Shoulder Elbow Surg 2005;14:480–484.65. Haggart GE, Dignam RJ, Sullivan TS. Management of the frozen shoulder. J Am
Med Assoc 1956;161:1219–1222.66. Harmon PH. Methods and results in the treatment of 2,580 painful shoulders, with
special reference to calcific tendinitis and the frozen shoulder. Am J Surg1958;95:527–544.
67. Iannotti JP. Manipulation under anesthesia did not enhance the benefit conferred byhome exercises for frozen shoulder. J Bone Joint Surg [Am] 2008;90-A:1792.
68. Ogilvie-Harris DJ, Biggs DJ, Fitsialos DP, MacKay M. The resistant frozenshoulder: manipulation versus arthroscopic release. Clin Orthop 1995;319:238–248.
69. Rill BK, Fleckenstein CM, Levy MS, Nagesh V, Hasan SS. Predictors of outcomeafter nonoperative and operative treatment of adhesive capsulitis. Am J Sports Med2011;39:567–574.
70. Cuomo F, Holloway G. Diagnosis and management of the stiff shoulder. In: IannottiJP, Williams GR, eds. Disorders of the shoulder: diagnosis and management. Philadel-phia: Lippincott, Williams & Wilkins, 2007:541-59.
71. Tomlinson D, Hannafin J. Arthroscopic treatment of shoulder stiffness and calcifictendinitis of the rotator cuff. In: Rockwood CA Jr, Matsen FA 3rd, eds. The shoulder.Philadelphia: Elsevier Health Sciences, 2009:993-1002.
72. Jerosch J. 360 degrees arthroscopic capsular release in patients with adhesive cap-sulitis of the glenohumeral joint: indication, surgical technique, results. Knee SurgSports Traumatol Arthrosc 2001;9:178–186.
73. Harryman DT 2nd. Shoulders: frozen and stiff. Instr Course Lect 1993;42:247–257.74. Warner JJ, Allen A, Marks PH, Wong P. Arthroscopic release for chronic, refrac-
tory adhesive capsulitis of the shoulder. J Bone Joint Surg [Am] 1996;78-A:1808–1816.
75. Diwan DB, Murrell GA. An evaluation of the effects of the extent of capsularrelease and of postoperative therapy on the temporal outcomes of adhesive capsuli-tis. Arthroscopy 2005;21:1105–1113.
76. Snow M, Boutros I, Funk L. Posterior arthroscopic capsular release in frozen shoul-der. Arthroscopy 2009;25:19–23.
77. Chen J, Chen S, Li Y, Hua Y, Li H. Is the extended release of the inferior gleno-humeral ligament necessary for frozen shoulder? Arthroscopy 2010;26:529–535.
78. Ogilvie-Harris DJ, Biggs DJ, Fitsialos DP, MacKay M. The resistant frozenshoulder: manipulation versus arthroscopic release. Clin Orthop 1995;319:238–248.
79. Omari A, Bunker TD. Open surgical release for frozen shoulder: surgical findingsand results of the release. J Shoulder Elbow Surg 2001;10:353–357.
80. Harryman DT, Lazarus MD. The stiff shoulder. In: Rockwood CA Jr, Matsen FA 3rd,eds. The shoulder. Philadelphia: WB Saunders, 2003:1121–72.
81. Kieras DM, Matsen FA 3rd. Open release in the management of refractory frozenshoulder. Orthop Trans 1991;15:801–802.



![[Efficacy of a manual treatment method according to the fascial distortion model in the management of contracted (\"frozen\") shoulder]](https://img.pdfslide.net/doc/110x75/634e5ec16b2f6dfefb0ad832/efficacy-of-a-manual-treatment-method-according-to-the-fascial-distortion-model.jpg)

























